
The distal semimembranosus complex: normal MR anatomy, variants, biomechanics and pathology
11
Received: 5 November 2002 Revised: 20 February 2003 Accepted: 21 February 2003 Published online: 24 May 2003 © ISS 2003 J. Mota Department of Radiology, Instituto Clinica Corachan, Barcelona, Spain L. Beltran New York Medical College, Valhalla, New York, USA M. Sundaram Department of Radiology, Mayo Clinic, Rochester, Minnesota, USA Abstract Objective: To describe the normal MR anatomy and variations of the distal semimembranosus tendinous arms and the posterior oblique ligament as seen in the three orthogonal planes, to review the biomechanics of this complex and to illustrate pathologic examples. Results and conclusion: The distal semimembranosus tendon divides into five tendinous arms named the anterior, direct, capsular, inferior and the oblique popliteal ligament. These arms intertwine with the branches of the posterior oblique ligament in the posterior medial aspect of the knee, providing sta- bility. This tendon-ligamentous com- plex also acts synergistically with the popliteus muscle and actively pulls the posterior horn of the medial meniscus during knee flexion. Patho- logic conditions involving this com- plex include complete and partial tears, insertional tendinosis, avulsion fractures and bursitis. Keywords Knee · MRI · Normal anatomy · Semimembranosus tendon · Tendon tear Skeletal Radiol (2003) 32:435–445 DOI 10.1007/s00256-003-0641-1 REVIEW ARTICLE Javier Beltran Amir Matityahu Ki Hwang Marlena Jbara Ron Maimon Mario Padron Javier Mota Luis Beltran Murali Sundaram The distal semimembranosus complex: normal MR anatomy, variants, biomechanics and pathology Introduction The semimembranosus muscle is one of the hamstring muscles, along with the semitendinosus and biceps fem- oris. They originate in a conjoined tendon in the posterolat- eral aspect of the ischial tuberosity. Distally, the hamstrings cross the knee joint and have a complex insertion in the proximal tibia and meniscocapsular structures of the knee. The primary function of the hamstrings is knee flexion; however, the intricate distal insertions of the semimem- branosus in the posteromedial aspect of the knee and bi- ceps femoris in the posterolateral aspect of the knee allow these two muscles to become very important stabilizing structures during knee flexion. This function is achieved through the relationships between the tendinous insertions and the adjacent menisci, joint capsule and ligaments. The purpose of this article is to review the normal anatomy and variants of the distal semimembranosus tendon and the ad- jacent structures (the distal semimembranosus complex), as well as the biomechanics and pathology of this complex structure. Emphasis is placed on the MR imaging depiction of the normal anatomy and pathologic findings. Normal anatomy and variants The distal semimembranosus tendon divides into five ten- dinous branches or arms at approximately the level of the joint line: (1) the anterior or tibial arm, (2) the direct arm, (3) the inferior or popliteal arm, (4) the capsular arm and (5) the oblique popliteal ligament (OPL) (Fig. 1) [1, 2, 3, 4, 5, 6]. J. Beltran ( ✉ ) · M. Jbara · R. Maimon Department of Radiology, Maimonides Medical Center, 4802 Tenth Avenue, Brooklyn, NY 11219, USA e-mail: [email protected] Tel.: +1-718-2837277 Fax: +1-718-6358411 A. Matityahu · K. Hwang Department of Orthopedic Surgery, Maimonides Medical Center, Brooklyn, New York, USA M. Padron Department of Radiology, Clinica CEMTRO, Madrid, Spain
Transcript of The distal semimembranosus complex: normal MR anatomy, variants, biomechanics and pathology

Received: 5 November 2002Revised: 20 February 2003Accepted: 21 February 2003Published online: 24 May 2003© ISS 2003
J. MotaDepartment of Radiology,Instituto Clinica Corachan,Barcelona, Spain
L. BeltranNew York Medical College,Valhalla, New York, USA
M. SundaramDepartment of Radiology,Mayo Clinic,Rochester, Minnesota, USA
Abstract Objective: To describe thenormal MR anatomy and variationsof the distal semimembranosus tendinous arms and the posterioroblique ligament as seen in the threeorthogonal planes, to review the biomechanics of this complex and to illustrate pathologic examples. Results and conclusion: The distal
semimembranosus tendon divides into five tendinous arms named theanterior, direct, capsular, inferior and the oblique popliteal ligament.These arms intertwine with thebranches of the posterior oblique ligament in the posterior medial aspect of the knee, providing sta-bility. This tendon-ligamentous com-plex also acts synergistically withthe popliteus muscle and activelypulls the posterior horn of the medialmeniscus during knee flexion. Patho-logic conditions involving this com-plex include complete and partialtears, insertional tendinosis, avulsionfractures and bursitis.
Keywords Knee · MRI · Normalanatomy · Semimembranosus tendon · Tendon tear
Skeletal Radiol (2003) 32:435–445DOI 10.1007/s00256-003-0641-1 R E V I E W A RT I C L E
Javier BeltranAmir MatityahuKi HwangMarlena JbaraRon MaimonMario PadronJavier MotaLuis BeltranMurali Sundaram
The distal semimembranosus complex: normal MR anatomy, variants, biomechanicsand pathology
Introduction
The semimembranosus muscle is one of the hamstringmuscles, along with the semitendinosus and biceps fem-oris. They originate in a conjoined tendon in the posterolat-eral aspect of the ischial tuberosity. Distally, the hamstringscross the knee joint and have a complex insertion in theproximal tibia and meniscocapsular structures of the knee.The primary function of the hamstrings is knee flexion;however, the intricate distal insertions of the semimem-branosus in the posteromedial aspect of the knee and bi-ceps femoris in the posterolateral aspect of the knee allowthese two muscles to become very important stabilizingstructures during knee flexion. This function is achievedthrough the relationships between the tendinous insertionsand the adjacent menisci, joint capsule and ligaments. The
purpose of this article is to review the normal anatomy andvariants of the distal semimembranosus tendon and the ad-jacent structures (the distal semimembranosus complex),as well as the biomechanics and pathology of this complexstructure. Emphasis is placed on the MR imaging depictionof the normal anatomy and pathologic findings.
Normal anatomy and variants
The distal semimembranosus tendon divides into five ten-dinous branches or arms at approximately the level of thejoint line: (1) the anterior or tibial arm, (2) the direct arm,(3) the inferior or popliteal arm, (4) the capsular arm and(5) the oblique popliteal ligament (OPL) (Fig. 1) [1, 2, 3,4, 5, 6].
J. Beltran (✉) · M. Jbara · R. MaimonDepartment of Radiology,Maimonides Medical Center,4802 Tenth Avenue, Brooklyn, NY 11219, USAe-mail: [email protected].: +1-718-2837277Fax: +1-718-6358411
A. Matityahu · K. HwangDepartment of Orthopedic Surgery,Maimonides Medical Center,Brooklyn, New York, USA
M. PadronDepartment of Radiology,Clinica CEMTRO,Madrid, Spain
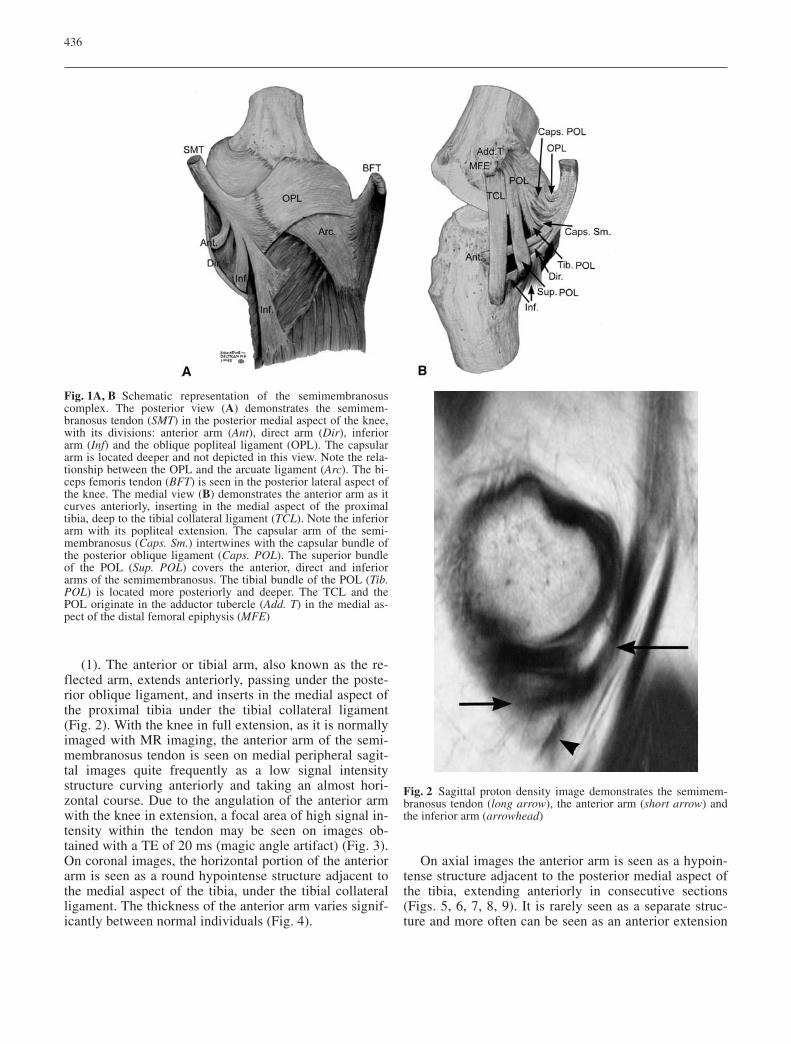
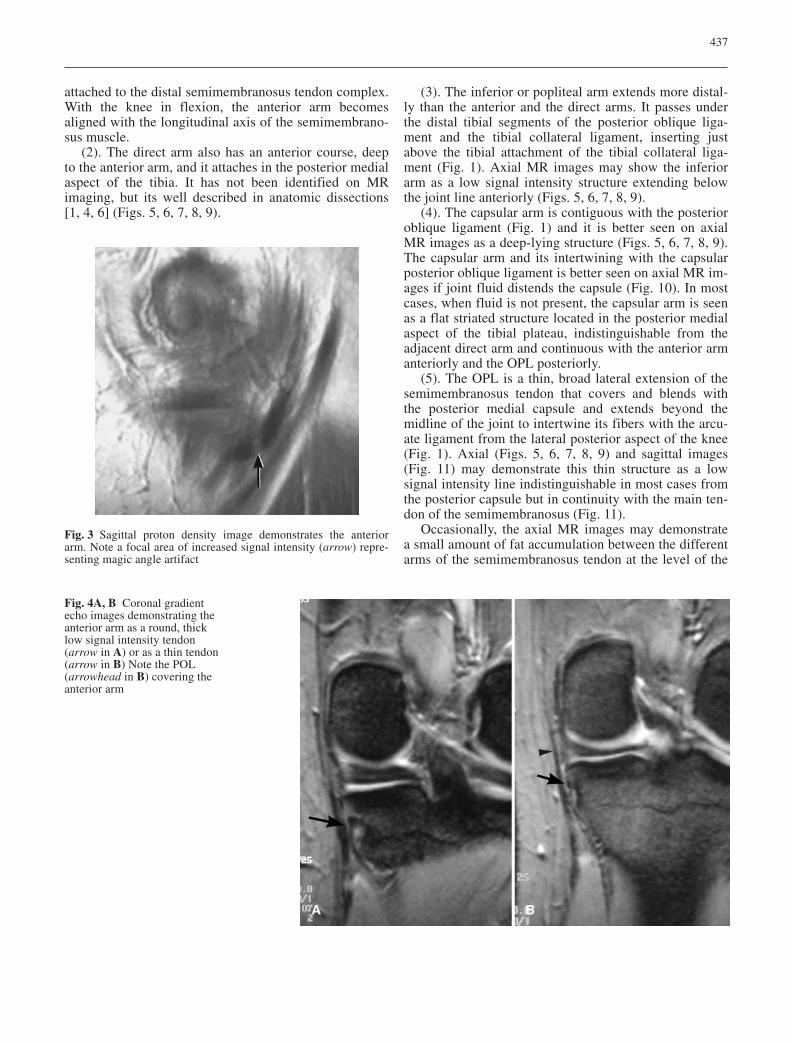
(1). The anterior or tibial arm, also known as the re-flected arm, extends anteriorly, passing under the poste-rior oblique ligament, and inserts in the medial aspect ofthe proximal tibia under the tibial collateral ligament(Fig. 2). With the knee in full extension, as it is normallyimaged with MR imaging, the anterior arm of the semi-membranosus tendon is seen on medial peripheral sagit-tal images quite frequently as a low signal intensitystructure curving anteriorly and taking an almost hori-zontal course. Due to the angulation of the anterior armwith the knee in extension, a focal area of high signal in-tensity within the tendon may be seen on images ob-tained with a TE of 20 ms (magic angle artifact) (Fig. 3).On coronal images, the horizontal portion of the anteriorarm is seen as a round hypointense structure adjacent tothe medial aspect of the tibia, under the tibial collateralligament. The thickness of the anterior arm varies signif-icantly between normal individuals (Fig. 4).
On axial images the anterior arm is seen as a hypoin-tense structure adjacent to the posterior medial aspect ofthe tibia, extending anteriorly in consecutive sections(Figs. 5, 6, 7, 8, 9). It is rarely seen as a separate struc-ture and more often can be seen as an anterior extension
436
Fig. 1A, B Schematic representation of the semimembranosuscomplex. The posterior view (A) demonstrates the semimem-branosus tendon (SMT) in the posterior medial aspect of the knee,with its divisions: anterior arm (Ant), direct arm (Dir), inferiorarm (Inf) and the oblique popliteal ligament (OPL). The capsulararm is located deeper and not depicted in this view. Note the rela-tionship between the OPL and the arcuate ligament (Arc). The bi-ceps femoris tendon (BFT) is seen in the posterior lateral aspect ofthe knee. The medial view (B) demonstrates the anterior arm as itcurves anteriorly, inserting in the medial aspect of the proximaltibia, deep to the tibial collateral ligament (TCL). Note the inferiorarm with its popliteal extension. The capsular arm of the semi-membranosus (Caps. Sm.) intertwines with the capsular bundle ofthe posterior oblique ligament (Caps. POL). The superior bundleof the POL (Sup. POL) covers the anterior, direct and inferiorarms of the semimembranosus. The tibial bundle of the POL (Tib.POL) is located more posteriorly and deeper. The TCL and thePOL originate in the adductor tubercle (Add. T) in the medial as-pect of the distal femoral epiphysis (MFE)
Fig. 2 Sagittal proton density image demonstrates the semimem-branosus tendon (long arrow), the anterior arm (short arrow) andthe inferior arm (arrowhead)
attached to the distal semimembranosus tendon complex.With the knee in flexion, the anterior arm becomesaligned with the longitudinal axis of the semimembrano-sus muscle.
(2). The direct arm also has an anterior course, deepto the anterior arm, and it attaches in the posterior medialaspect of the tibia. It has not been identified on MR imaging, but its well described in anatomic dissections[1, 4, 6] (Figs. 5, 6, 7, 8, 9).
(3). The inferior or popliteal arm extends more distal-ly than the anterior and the direct arms. It passes underthe distal tibial segments of the posterior oblique liga-ment and the tibial collateral ligament, inserting justabove the tibial attachment of the tibial collateral liga-ment (Fig. 1). Axial MR images may show the inferiorarm as a low signal intensity structure extending belowthe joint line anteriorly (Figs. 5, 6, 7, 8, 9).
(4). The capsular arm is contiguous with the posterioroblique ligament (Fig. 1) and it is better seen on axialMR images as a deep-lying structure (Figs. 5, 6, 7, 8, 9).The capsular arm and its intertwining with the capsularposterior oblique ligament is better seen on axial MR im-ages if joint fluid distends the capsule (Fig. 10). In mostcases, when fluid is not present, the capsular arm is seenas a flat striated structure located in the posterior medialaspect of the tibial plateau, indistinguishable from theadjacent direct arm and continuous with the anterior armanteriorly and the OPL posteriorly.
(5). The OPL is a thin, broad lateral extension of thesemimembranosus tendon that covers and blends withthe posterior medial capsule and extends beyond themidline of the joint to intertwine its fibers with the arcu-ate ligament from the lateral posterior aspect of the knee(Fig. 1). Axial (Figs. 5, 6, 7, 8, 9) and sagittal images(Fig. 11) may demonstrate this thin structure as a lowsignal intensity line indistinguishable in most cases fromthe posterior capsule but in continuity with the main ten-don of the semimembranosus (Fig. 11).
Occasionally, the axial MR images may demonstratea small amount of fat accumulation between the differentarms of the semimembranosus tendon at the level of the
437
Fig. 3 Sagittal proton density image demonstrates the anteriorarm. Note a focal area of increased signal intensity (arrow) repre-senting magic angle artifact
Fig. 4A, B Coronal gradientecho images demonstrating theanterior arm as a round, thicklow signal intensity tendon (arrow in A) or as a thin tendon(arrow in B) Note the POL (arrowhead in B) covering theanterior arm
joint line (Fig. 12). This should not be interpreted as tendon degeneration or tear and it represents a normalvariant.
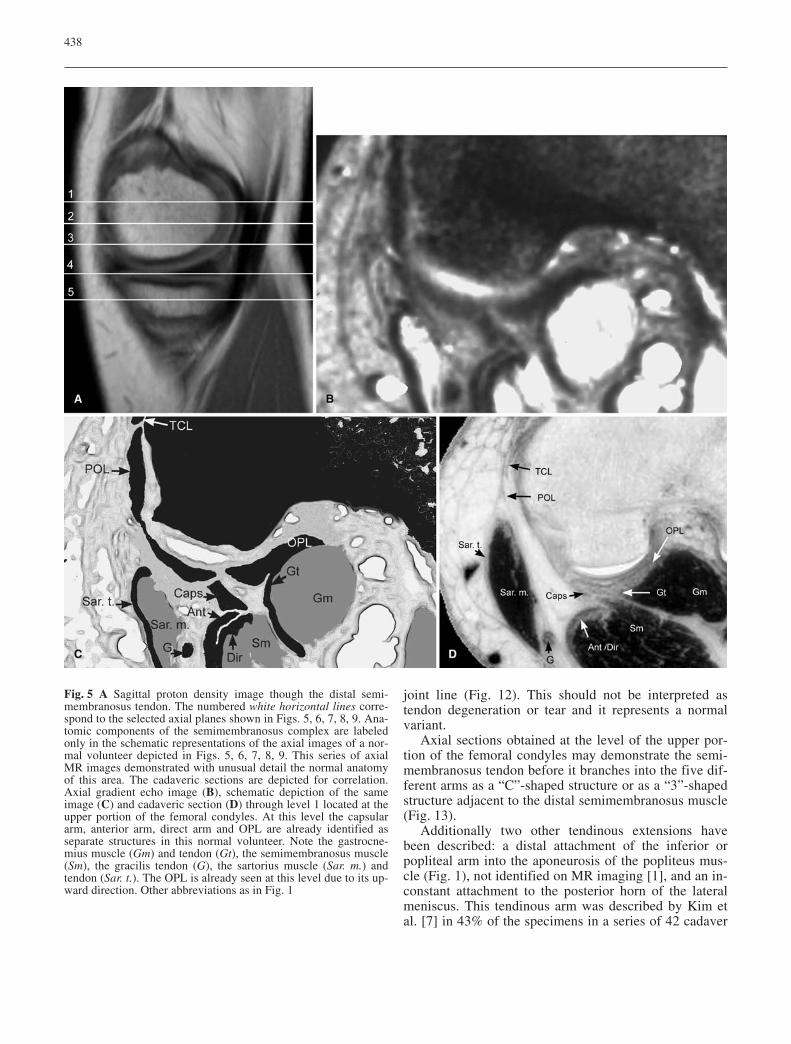
Axial sections obtained at the level of the upper por-tion of the femoral condyles may demonstrate the semi-membranosus tendon before it branches into the five dif-ferent arms as a “C”-shaped structure or as a “3”-shapedstructure adjacent to the distal semimembranosus muscle(Fig. 13).
Additionally two other tendinous extensions havebeen described: a distal attachment of the inferior orpopliteal arm into the aponeurosis of the popliteus mus-cle (Fig. 1), not identified on MR imaging [1], and an in-constant attachment to the posterior horn of the lateralmeniscus. This tendinous arm was described by Kim etal. [7] in 43% of the specimens in a series of 42 cadaver
438
Fig. 5 A Sagittal proton density image though the distal semi-membranosus tendon. The numbered white horizontal lines corre-spond to the selected axial planes shown in Figs. 5, 6, 7, 8, 9. Ana-tomic components of the semimembranosus complex are labeledonly in the schematic representations of the axial images of a nor-mal volunteer depicted in Figs. 5, 6, 7, 8, 9. This series of axialMR images demonstrated with unusual detail the normal anatomyof this area. The cadaveric sections are depicted for correlation.Axial gradient echo image (B), schematic depiction of the sameimage (C) and cadaveric section (D) through level 1 located at theupper portion of the femoral condyles. At this level the capsulararm, anterior arm, direct arm and OPL are already identified asseparate structures in this normal volunteer. Note the gastrocne-mius muscle (Gm) and tendon (Gt), the semimembranosus muscle(Sm), the gracilis tendon (G), the sartorius muscle (Sar. m.) andtendon (Sar. t.). The OPL is already seen at this level due to its up-ward direction. Other abbreviations as in Fig. 1
knees, as a thin structure crossing the joint horizontallyand dorsal to the posterior cruciate ligament.
The different tendinous arms of the semimembrano-sus complex are intimately related to the posterioroblique ligament and the arcuate ligament. In order tounderstand the biomechanics of the knee it is importantto review these relationships. The superficial fibers ofthe tibial collateral ligament extend from the medial
femoral condyle to the proximal medial tibia, over theanterior and direct arms of the semimembranosus, buttheir fibers are not intertwined. However, the fibers ofthe posterior oblique ligament merge with the tendinousarms of the semimembranosus. The posterior oblique ligament or ligament of Winslow [1] originates in the adductor tubercle of the femur. Hughston [2, 6, 8] de-scribed three bundles of the posterior oblique ligament:
439
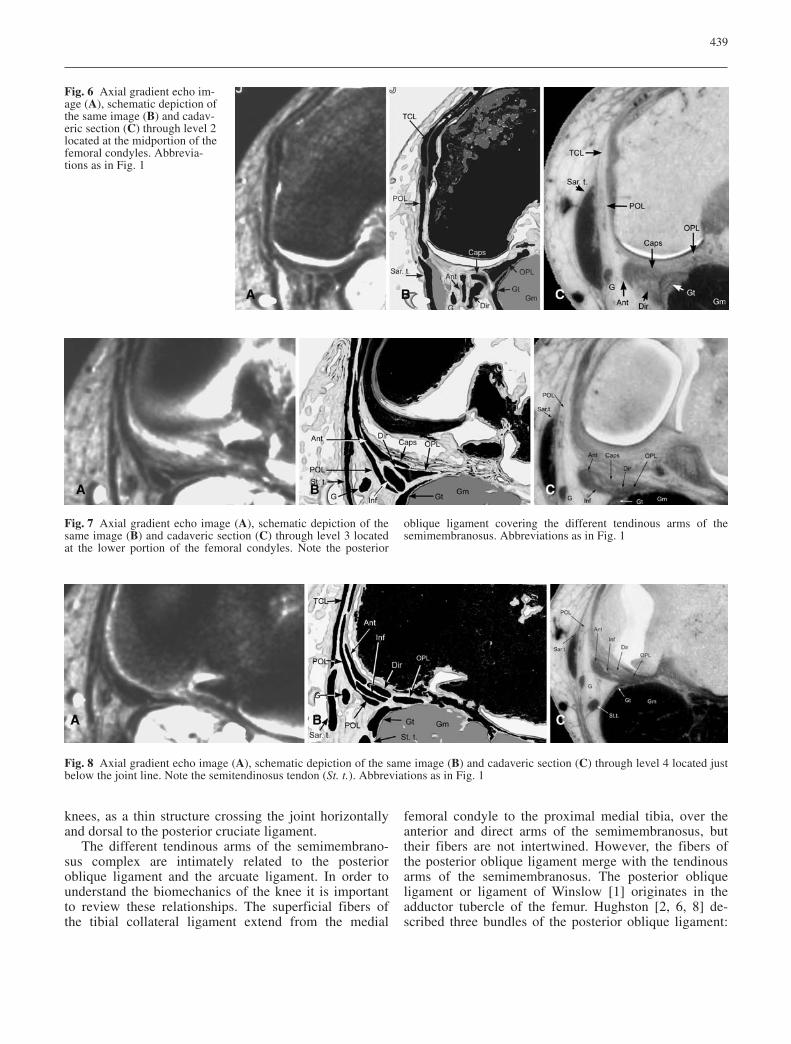
Fig. 6 Axial gradient echo im-age (A), schematic depiction ofthe same image (B) and cadav-eric section (C) through level 2located at the midportion of thefemoral condyles. Abbrevia-tions as in Fig. 1
Fig. 7 Axial gradient echo image (A), schematic depiction of thesame image (B) and cadaveric section (C) through level 3 locatedat the lower portion of the femoral condyles. Note the posterior
oblique ligament covering the different tendinous arms of thesemimembranosus. Abbreviations as in Fig. 1
Fig. 8 Axial gradient echo image (A), schematic depiction of the same image (B) and cadaveric section (C) through level 4 located justbelow the joint line. Note the semitendinosus tendon (St. t.). Abbreviations as in Fig. 1
the superficial, the tibial and the capsular arms. The su-perficial arm passes distally over the anterior arm of thesemimembranosus tendon and attaches in the fascial tis-sue of the pes anserinus (Fig. 1). The tibial arm of theposterior oblique ligament is deeper and passes beneaththe anterior arm of the semimembranosus and attachessolidly to the posterior medial aspect of the tibia and tothe posterior horn of the medial meniscus (Fig. 1). Thecapsular arm of the posterior oblique ligament mergeswith the OPL and the capsular arm of the semimem-branosus tendon, over the posterior aspect of the capsulecovering the medial femoral condyle posteriorly (Fig. 1),and these then course together towards the posterior lat-
eral aspect of the knee. This capsular arm has bony anattachment in the posterior intercondylar rim of the later-al femoral condyle, according to Hughston [2, 6, 8].
Between the posterior margin of the superficial fibersof the tibial collateral ligament and the anterior marginof the superficial arm of the posterior oblique ligamentthere is a small gap occupied by synovial and fascial tis-sue (Fig. 1). This space is palpable clinically and demon-strable at surgery, and constitutes an important landmarkfor posteromedial arthrotomy [2, 6, 8, 9].
On MR imaging, the posterior oblique ligament can beseen on axial (Figs. 5, 6, 7, 8, 9) and coronal (Fig. 4) im-ages as a low signal intensity linear structure located pos-terior to the superficial fibers of the tibial collateral liga-ment. The three arms described by Hughston cannot beclearly distinguished with MR imaging, but is importantto appreciate their relationship with the semimembranosustendon insertions in order to comprehend the biomechan-ics of the knee joint during flexion, as described below.
The arcuate ligament originates in the head of the fib-ula and extends proximally in a fan-like shape over thebelly of the popliteus muscle and the posterior aspect ofthe lateral femoral condyle, merging with the fibers ofthe OPL (Fig. 1).
440
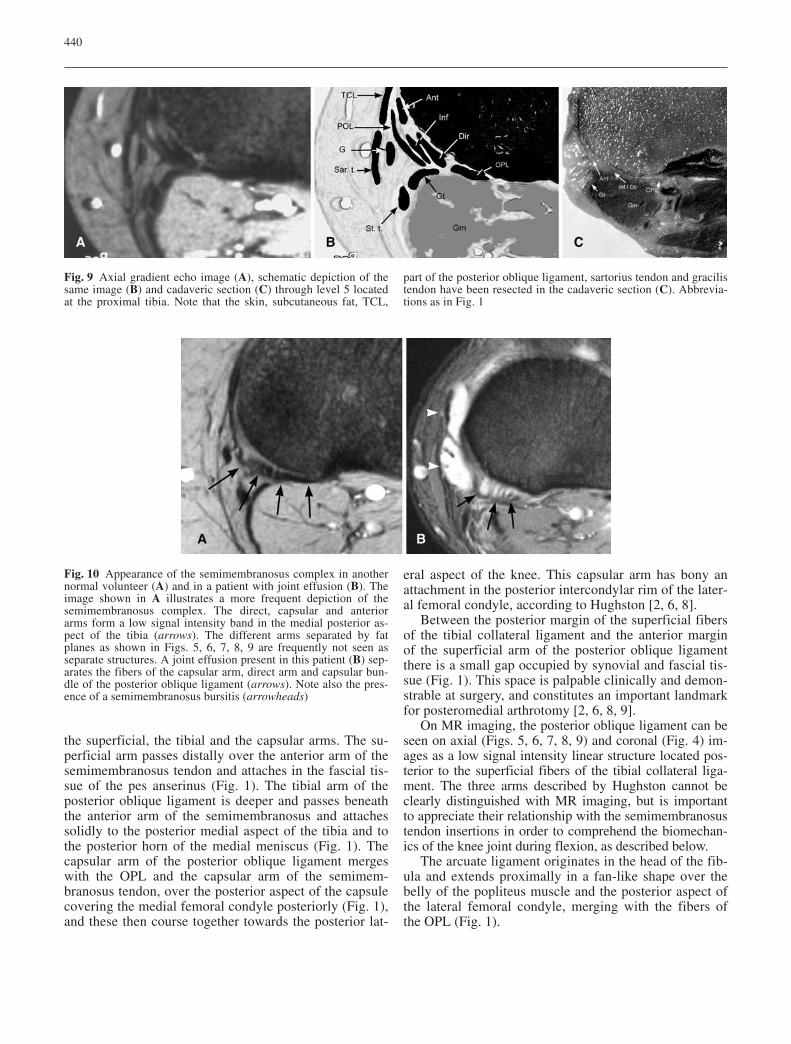
Fig. 9 Axial gradient echo image (A), schematic depiction of thesame image (B) and cadaveric section (C) through level 5 locatedat the proximal tibia. Note that the skin, subcutaneous fat, TCL,
part of the posterior oblique ligament, sartorius tendon and gracilistendon have been resected in the cadaveric section (C). Abbrevia-tions as in Fig. 1
Fig. 10 Appearance of the semimembranosus complex in anothernormal volunteer (A) and in a patient with joint effusion (B). Theimage shown in A illustrates a more frequent depiction of thesemimembranosus complex. The direct, capsular and anteriorarms form a low signal intensity band in the medial posterior as-pect of the tibia (arrows). The different arms separated by fatplanes as shown in Figs. 5, 6, 7, 8, 9 are frequently not seen asseparate structures. A joint effusion present in this patient (B) sep-arates the fibers of the capsular arm, direct arm and capsular bun-dle of the posterior oblique ligament (arrows). Note also the pres-ence of a semimembranosus bursitis (arrowheads)
Biomechanics
The stability of the knee is dependent on the integrity ofthe anatomic structures including the capsule, ligaments,tendons and menisci. The semimembranosus complexhas several functions. First, it stabilizes the posteriorcapsule through the OPL. Second, it acts synergisticallywith the popliteus muscle through the fibrous extensiontowards this muscle. Third, it actively pulls the posteriorhorn of the medial meniscus, protecting it from beingcrushed between the medial femoral condyle and the
posterior medial tibial plateau during knee flexion [2, 6,8, 9, 10, 11]. This function is achieved through its capsu-lar arm and the relationships between the posterioroblique ligament and the semimembranosus complex.Emphasizing this function of the semimembranosuscomplex, Hughston [2, 6, 8] states that when performingarthrotomy for posterior medial meniscal tears, he fre-quently found tears or laxity of the posterior oblique lig-ament.
Additionally, the semimembranosus complex contrib-utes to the stability of the posterior medial aspect of thejoint through its intertwining with the posterior obliqueligament. On knee flexion during running, cutting andpivoting, the capsular arm of the semimembranosus ac-tively tightens the posterior oblique ligament providingdynamic stability. The anterior arm provides stability ofthe flexed knee that is sustaining lateral rotational forces.
Furthermore, the tendinous insertion of the semimem-branosus complex into the posterior horn of the lateralmeniscus described by Kim et al. [7] provides an ele-ment of posterior traction over the posterior horn of thelateral meniscus, along with the structures forming thestabilizing mechanism of the posterolateral aspect of theknee.
One can appreciate better the complexity of the bio-mechanical functions of the semimembranosus complexby conceptualizing the different structures as a suctioncup placed over the posterior medial aspect of the kneeas seen from inside of the joint with the knee in flexion(Fig. 14A).
The dynamic synergy of the semimembranosus com-plex and the biceps femoris also provides controlled stability of the flexed knee during internal and external
441
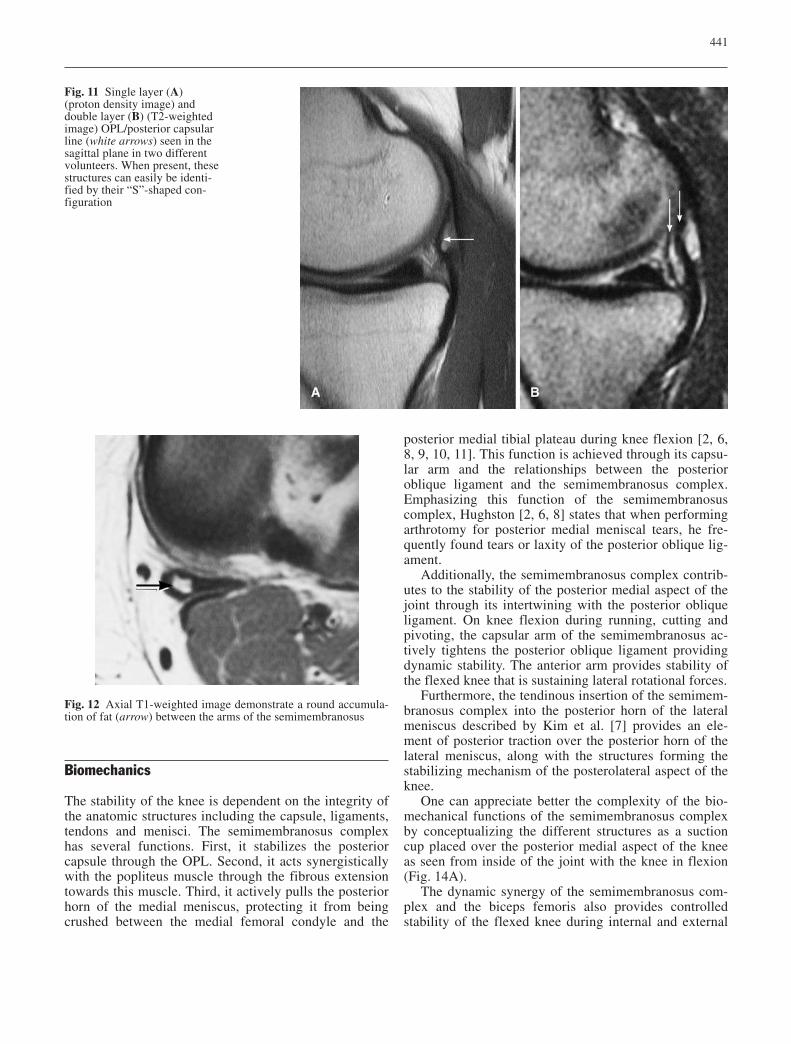
Fig. 11 Single layer (A) (proton density image) anddouble layer (B) (T2-weightedimage) OPL/posterior capsularline (white arrows) seen in thesagittal plane in two differentvolunteers. When present, thesestructures can easily be identi-fied by their “S”-shaped con-figuration
Fig. 12 Axial T1-weighted image demonstrate a round accumula-tion of fat (arrow) between the arms of the semimembranosus
442
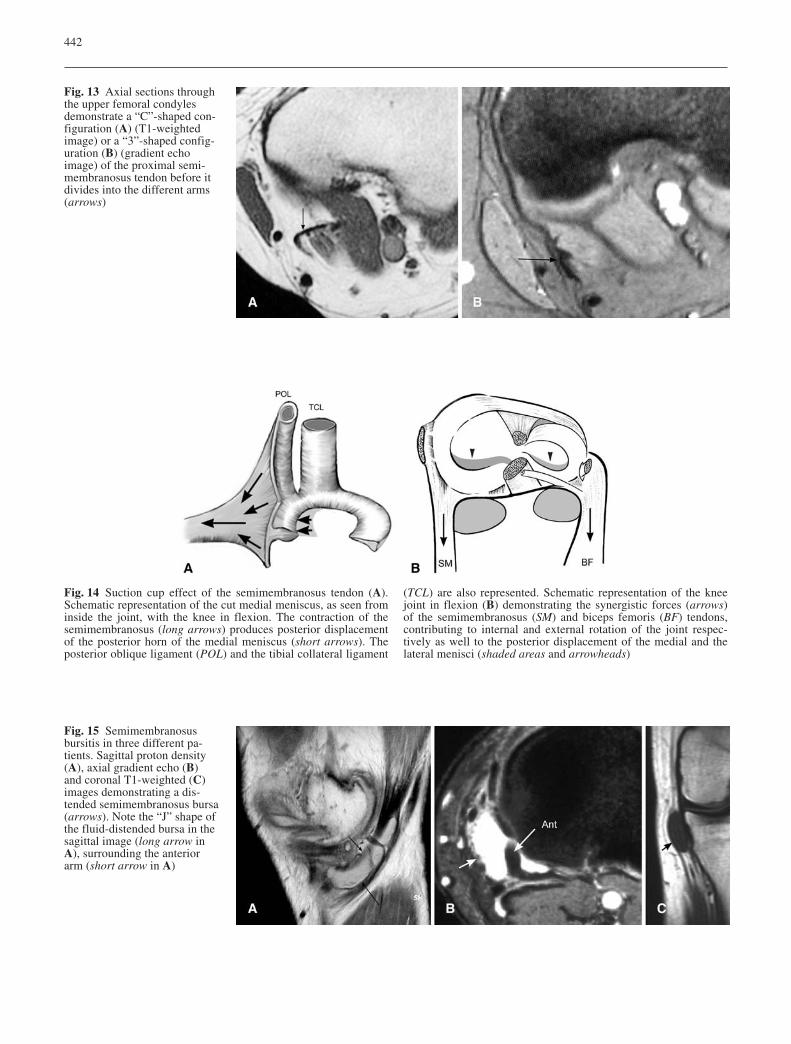
Fig. 13 Axial sections throughthe upper femoral condylesdemonstrate a “C”-shaped con-figuration (A) (T1-weightedimage) or a “3”-shaped config-uration (B) (gradient echo image) of the proximal semi-membranosus tendon before itdivides into the different arms(arrows)
Fig. 14 Suction cup effect of the semimembranosus tendon (A).Schematic representation of the cut medial meniscus, as seen frominside the joint, with the knee in flexion. The contraction of thesemimembranosus (long arrows) produces posterior displacementof the posterior horn of the medial meniscus (short arrows). Theposterior oblique ligament (POL) and the tibial collateral ligament
(TCL) are also represented. Schematic representation of the kneejoint in flexion (B) demonstrating the synergistic forces (arrows)of the semimembranosus (SM) and biceps femoris (BF) tendons,contributing to internal and external rotation of the joint respec-tively as well to the posterior displacement of the medial and thelateral menisci (shaded areas and arrowheads)
Fig. 15 Semimembranosusbursitis in three different pa-tients. Sagittal proton density(A), axial gradient echo (B)and coronal T1-weighted (C)images demonstrating a dis-tended semimembranosus bursa(arrows). Note the “J” shape ofthe fluid-distended bursa in thesagittal image (long arrow inA), surrounding the anteriorarm (short arrow in A)
rotation, in addition to pulling the posterior horns of themedial and lateral menisci. Conceptualization of thesemimembranosus and biceps femoris complexes ashorse reins attached to the medial and lateral aspects ofthe capsule aids understanding of these functions(Fig. 14B).
Two synovial-lined bursae are associated with the dis-tal semimembranosus tendon. The better-known is thegastrocnemius-semimembranosus bursa, located betweenthe medial gastrocnemius tendon and the semimem-branosus tendon, above its division into the various armsdescribed above. This bursa, when distended by fluid, is also known as a popliteal or Baker cyst. The gastroc-nemius-semimembranosus bursa communicates with theknee joint in a very high percentage of cases [12]. A sec-ond synovial bursa is present between the anterior arm ofthe semimembranosus complex and the tibial collateralligament. This bursa is located more medially than thegastrocnemius-semimembranosus bursa and more proxi-mally than the pes anserinus bursa [13]. When distendedby fluid, the semimembranosus bursa has a “J”-shapedappearance on sagittal MR images (Fig. 15). On axialand coronal images it is seen as a fluid collection extend-ing anteriorly, in the medial aspect of the knee adjacentto the proximal divisions of the semimembranosus ten-don (Fig. 15).
Pathology
Lesions of the semimembranosus complex can be divid-ed into complete tears, myotendinous injuries, avulsioninjuries, partial tears involving one or more of the tendi-nous components and insertional tendinosis. Completetears of the semimembranosus tendon are very unusual.Varela et al. [14] reported two cases of a middle-aged anelderly woman respectively without a history of strenu-ous exercise. Alioto et al. [15] reported a case of a com-plete rupture of the semimembranosus tendon in a pro-
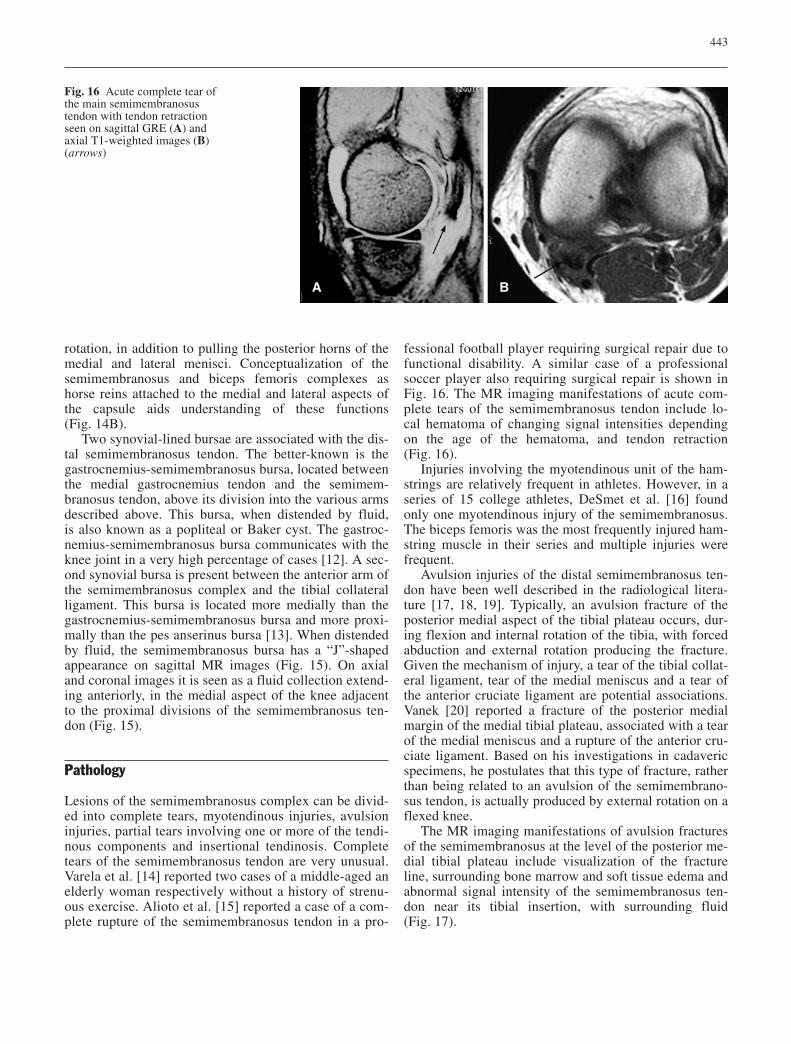
fessional football player requiring surgical repair due tofunctional disability. A similar case of a professionalsoccer player also requiring surgical repair is shown inFig. 16. The MR imaging manifestations of acute com-plete tears of the semimembranosus tendon include lo-cal hematoma of changing signal intensities dependingon the age of the hematoma, and tendon retraction(Fig. 16).
Injuries involving the myotendinous unit of the ham-strings are relatively frequent in athletes. However, in aseries of 15 college athletes, DeSmet et al. [16] foundonly one myotendinous injury of the semimembranosus.The biceps femoris was the most frequently injured ham-string muscle in their series and multiple injuries werefrequent.
Avulsion injuries of the distal semimembranosus ten-don have been well described in the radiological litera-ture [17, 18, 19]. Typically, an avulsion fracture of theposterior medial aspect of the tibial plateau occurs, dur-ing flexion and internal rotation of the tibia, with forcedabduction and external rotation producing the fracture.Given the mechanism of injury, a tear of the tibial collat-eral ligament, tear of the medial meniscus and a tear ofthe anterior cruciate ligament are potential associations.Vanek [20] reported a fracture of the posterior medialmargin of the medial tibial plateau, associated with a tearof the medial meniscus and a rupture of the anterior cru-ciate ligament. Based on his investigations in cadavericspecimens, he postulates that this type of fracture, ratherthan being related to an avulsion of the semimembrano-sus tendon, is actually produced by external rotation on aflexed knee.
The MR imaging manifestations of avulsion fracturesof the semimembranosus at the level of the posterior me-dial tibial plateau include visualization of the fractureline, surrounding bone marrow and soft tissue edema andabnormal signal intensity of the semimembranosus ten-don near its tibial insertion, with surrounding fluid(Fig. 17).
443
Fig. 16 Acute complete tear ofthe main semimembranosustendon with tendon retractionseen on sagittal GRE (A) andaxial T1-weighted images (B)(arrows)
Partial tears of the semimembranosus complex and itsassociated structures, including the posterior oblique liga-ment, are not described in the radiological literature, butare emphasized by Hughston et al. [2, 6, 8] in the orthope-dic literature. These authors stress the association of acutetears of the tibial collateral ligament with tears of the pos-terior oblique ligament, the semimembranosus complex(avulsion fractures or partial tears) and anterior cruciateligament tears. In a series of 41 cases undergoing surgicalrepair of acutely torn medial ligaments, six had eitheravulsion or partial tears of the semimembranosus [8].
The partially torn semimembranosus and/or posterioroblique ligament can be diagnosed with MR imaging bymeans of detecting abnormal signal intensity of thesestructures in the posterior medial corner of the knee orlack of visualization of the anterior arm of the semimem-branosus in the coronal images (Fig. 18).
Insertional tendinosis is seen in association withchronic, repetitive injuries and stress of the tibial inser-tion of the semimembranosus, resulting in irregularityand cystic changes at the level of the posterior medialtibia (Fig. 19).
444
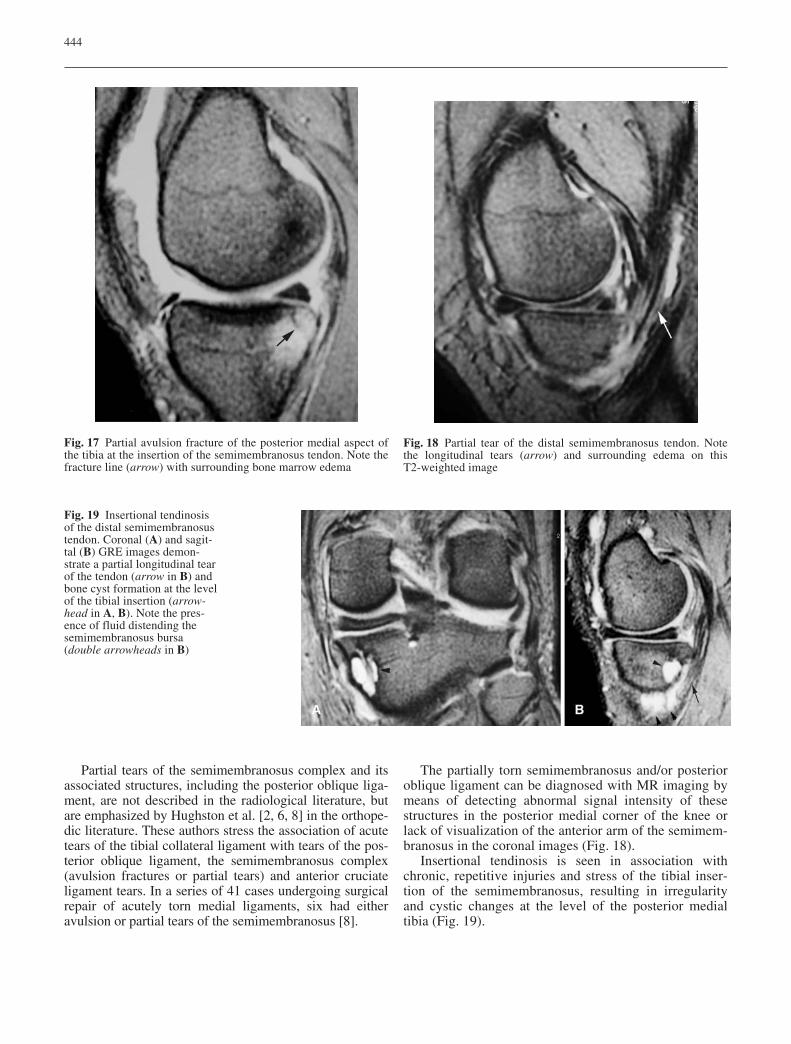
Fig. 17 Partial avulsion fracture of the posterior medial aspect ofthe tibia at the insertion of the semimembranosus tendon. Note thefracture line (arrow) with surrounding bone marrow edema
Fig. 18 Partial tear of the distal semimembranosus tendon. Notethe longitudinal tears (arrow) and surrounding edema on this T2-weighted image
Fig. 19 Insertional tendinosisof the distal semimembranosustendon. Coronal (A) and sagit-tal (B) GRE images demon-strate a partial longitudinal tearof the tendon (arrow in B) andbone cyst formation at the levelof the tibial insertion (arrow-head in A, B). Note the pres-ence of fluid distending thesemimembranosus bursa (double arrowheads in B)

Finally, the semimembranosus bursa can become in-flamed (semimembranosus bursitis) and distended byfluid (Fig. 15) or in rare cases it can rupture either due totrauma [21] or as a complication of arthroscopic surgery[22].
In conclusion, the distal semimembranosus tendinousinsertions and its relationships with the posterior medial
capsule, medial meniscus and posterior oblique ligamentare important structures contributing to the stability ofthe posterior medial corner of the knee. MR imaging canidentify several of these complex anatomic structures.The radiologist should be aware of the MR imagingmanifestations of the variety of lesions involving thisimportant complex.
445
References
1. Kaplan EB. Some aspects of functionalanatomy of the human knee joint. ClinOrthop 1962; 23:18–29.
2. Hughston JC, Eilers AF. The role ofthe posterior oblique ligament in repairs of acute medial (collateral)ligament tears of the knee. J Bone
Joint Surg Am 1973; 55:923–940.3. Hassine D, Rougereau G, Feron JM,
Henry-Feugeas MC, Fabre V, et al. MRimaging of posteromedial and postero-lateral stabilizers of the knee: anatomicbasis and patterns of lesions in knee injuries. Surg Radiol Anat 1994;16:293–301.
4. Loredo R, Hodler J, Pedowitz R, Yeh LR, Trudell D, Resnick D. Posteromedial corner of the knee: MR imaging with gross anatomic correlation. Skeletal Radiol 1999;28:305–311.
5. Warren LF, Marshall JL. The support-ing structures and layers on the medialside of the knee: an anatomical analy-sis. J Bone Joint Surg Am 1979;61:56–62.
6. Hughston JC. Knee ligaments. Injuryand repair. St Louis: Mosby,1993:3–70.
7. Kim YC, Yoo WK, Chung IH, Seo JS,Tanaka S. Tendinous insertion of semi-membranosus muscle into the lateralmeniscus. Surg Radiol Anat 1997;19:365–369.
8. Hughston JC. The importance of theposterior oblique ligament in repairs ofacute tears of the medial ligaments inknees with and without an associatedrupture of the anterior cruciate liga-ment. J Bone Joint Surg Am 1994;76:1328–1344.
9. Brantigan OC, Voshell AF. The tibialcollateral ligament: its function, itsbursae, and its relation to the medialmeniscus. J Bone Joint Surg 1943;25:121–131.
10. Brantigan OC, Voshell AF. The me-chanics of the ligaments and menisci ofthe knee joint. J Bone Joint Surg 1941;23:44–66.
11. Renstrom P, Johnson RJ. Anatomy andbiomechanics of the menisci. ClinSports Med 1990; 9:523–538.
12. Torreggiani WC, Al-Ismail K, MunkPL, Roche C, Keogh C, Nicolau S,Marchinkow LP. The imaging spec-trum of Baker’s (popliteal) cysts. Clin Radiol 2002; 57:681–691.
13. Rothstein CP, Laorr A, Helms CA, Tirman P. Semimembranosus-tibialcollateral ligament bursitis: MR find-ings. AJR Am J Roentgenol 1996;166:875–877.
14. Varela JR, Rodriguez E, Soler R,Gonzalez J, Pombo S. Complete rupture of the distal semimembranosustendon with secondary hamstring muscles atrophy: MR findings in twocases. Skeletal Radiol 2000;29:362–364.
15. Alioto RJ, Browne JE, Barnthouse CD,Scott AR. Complete rupture of the distal semimembranosus complex in aprofessional athlete. Clin Orthop RelRes 1997; 336:162–165.
16. DeSmet AA, Best TM. MR imaging ofthe distribution and location of acutehamstring injuries in athletes. AJR AmJ Roentgenol 2000; 174:393–399.
17. Yao L, Lee JK. Avulsion of the posteromedial tibial plateau by thesemimembranosus tendon: diagnosiswith MR imaging. Radiology 1989;172:513–514.
18. Chan KK, Resnick D, Goodwin D,Seeger LL. Posteromedial tibial plateauinjury including avulsion fracture ofthe semimembranosus tendon insertionsite: ancillary sign of anterior cruciateligament tear at MR imaging. Radiology 1999; 211:754–758.
19. Bencardino JT, Rosenberg ZS, BrownR, Hassakhani A, Lustrin E, Beltran J.Traumatic musculotendinous injuriesof the knee: diagnosis with MR imaging. RadioGraphics 2000;20:S103-S120.
20. Vanek J. Posteromedial fracture of thetibial plateau is not an avulsion injury.A case report and experimental study. J Bone Joint Surg 1994; 76:290–292.
21. Andersen-Ranberg F, Hejgaard N.Ruptured semimembranosus bursa: anunusual complication following sportsinjury of the knee. J Sports Med 1986;20:23–24.
22. Bunker TD, Thomas E. Ruptured semi-membranosus bursa: a complication ofarthroscopy. A short case report. Injury1983; 15:182–183.




















