the child with deficit - MCH Library
155
the child with centtal system nefvous deficit F. 39 U L96s 9680 .-_tist. I Col ].ect ion :ument Number 1035 Providedby the Maternal and Child Health Library, Georgetown University
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of the child with deficit - MCH Library

the child with
centtal
system
nefvous
deficit
F . 3 9U
L 9 6 s9 6 8 0
.-_t ist.
I C o l ] . e c t i o n
:ument Number 1035
Provided by the Maternal and Child Health Library, Georgetown University
:,-.
' :
cHrrDREh{'s BUREAU PUBIICATION NUMBER 432-L965
. . : . . : , . . , . . . . .
Provided by the Maternal and Child Health Library, Georgetown University

the child with
central nervous
system deficit
. f .fePoft or tv/o symposlums
U.S. DEPAI{TIVIENT OF l{EALTlt. EDLTCATION, AND WELFAREWF,LFARE ADMINISTRATION . Children's Bureau r 1965
For sale by the Superintendent of Documents. Lr.S. Government Prhting omce
Washington, D.C.,n402 - Price 75 cents
Provided by the Maternal and Child Health Library, Georgetown University

foreword
Treatment procedures for children with central nervous system deficits have been in a
state of transition in recent years. Aware of this fact, the Division of Physical Therapy,
School of AIIied Medical Professions of the Unir,'ersity of Pennsylvania, the Journal of the
American Physical Therapy Association and the Children's Bureau of the Department of
Health, Education, and Welfare staged two symposiums during the latter part of 1964 to
consider the changing and growing knowledge in the treatment of these children.The sponsors of these symposiums, which were held at the University of Pennsylvania
at Philadelphia, Pa., believed that an approach in depth to the basic problem would assist
in clarifying and identifying the direction treatment should take for children with central
nervous system deficits.The program for the two S-day sessions was designed to integrate concepts and knowl-
edge in present-day scientific studies of the child before and after birth with respect to
eti;logic;I factors and developmental and growth patterns together with the anatomical,physiological, and pathological evidence related to them.
Around 200 qualified physical therapists from over the country attended one or the
other of the two symposiums. To be eligible, they were either engaged in the care of, or
in teaching programs related to, the child with disorders of the central nervotls system.Originally, the speeches given before the two symposinms were published in the Joun-
NAL oF THE AMERT61N Pnysrcer, THpnepy Assocr.trrow. The Children's Bureau recogniz-ing that the information from these sessions would be of value to specialists in other fieldsas well as those in physical therapv who work with children with central ner\:ous systemdeficits, has gathered this material together in this publication. The Bureau rvishes to thankthe Journal of the Amer ican Physical Therapy Association for graciously giving the Bureaupermission to do so.
K.U^,6,YKATHERINE B, OETTINGERChief, Children's BureauWELFARE ADMINISTRATION
Provided by the Maternal and Child Health Library, Georgetown University_
contents
The Child With Central Nervous System Deficit,: The Scope of theProblem-Alice D. Chenoweth, \'I.D-- - 1
The Dual Sensory Role of \"{uscle Spindles-Earl Eldred, \'{.D- 8
Basic \{echanisms of \{otor Learning-Jennifer S. Buchv'ald, Ph. D - - - 32
Postural Integration at Spinal Levels-Earl Eldred, N'I.D- - - - 50
Predisposing Genetic and \{etabolic Factors to Developlnental Defectsof the Central Nerr-otts System-Allen S. Goldman, N{.D----- 63
Perinatal Problems and the Central Nerr.'ous System-Virginia Apgar,N { . D _ _ _ _ _ - 7 5
Attitudinat Reflexes-'lhomas E. Twitchell, N .D- 77
Normal Nlotor Development-Thomas E. Twitchell, \ '{.D--- 85
Variations and Abnormalities of \'{otor Development-Thomas E.' l 'wi tchel l , NI.D- 90
Some Considerations of \4uscle Actir.' ity-H. D. Bouman, NII.D-----.,- 97
The Plasticity of the Nerr.otts Systern of Early Childhood-G. \{iltonShy, N'{.D- 103
I,Iental Retardation and the Child With Central Nervous SystemDeficit-\Iary D. Ames, \{.D-
tr'actors Contributing tci a Successful Patient Evaluation-IsadoreBrown, \ { .S , - - - 114
A Pattern for Eralutrtion in the Assessrnent of \'Iotor Performance-Shir ley Stockmeyer, \ I .A---- - 119
Specific Tests and Evaluation Tools for the Child \\'ith Central NervousSystem Deficit-Sarah Semans, \'LA 122
A Cerebral Palsy Assessment Chart: Instrtictions for Administration ofthe Test Sarah Semans, \LA., Rosalvn Phillips, B'A., \(adelineRomanol i , R.N., Ruth \ I i l ler,8.S., and \ Iary Ski l len, B.A--- l2g
Some Considerations of the Physiology of Sensation-H. D. Bouman,r , I .D__- 135
Proprioceptive, Yestibular, and Cerebellar \ Iechanisms in the Control
of tr{ovement-Stella Y. Botellio, \I.D
1 1 0
140
Provided by the Maternal and Child Health Library, Georgetown University

Nervous System DeficitTHE SCOPE OF THE PHOBLEM
The Child with Central
ALICE D. CHENOWETH. M.D.
Tlr rs a privilege for The Children's
Bureau to participate with the University of Penn-sylvania and the JounNer- of the American Phys-ical Therapy Association in making this Sympo-sium possible.
An excellent faculty has been chosen to presentnew knowledge from many fields of research. Wehope that there will be ample opportunity to ex-change experiences and that this conference will beproductive of new ideas and new approaches to thevery complex problems presented by the child withcentral nervous system deficit.
The "scope" of the problem can best be defined
Adapted from a paper given at the Symposium on TheChild with Central Nervous System Deficit, September28-October 2, 1964, The University of Pennsylvania,Philadelohia.
Dr. Chenoweth is Chief, Program Services Branch, Divi-sion of Health Services, The Children's Bureau, WelfareAdministration, Department of Health, Education, andWelfare, Washington, D.C. 20201.
by using examples of conditions encountered bystaff members of The Children's Bureau Depart-ment of Health Services.
MAGNITUDE AND COMPLEXITYOF CENTRAL NERVOUS SYSTEMDEFICIT DISEASES
The problem is of great magnitude and com-plexity. Central nervous system deficits of child-hood represent a multiplicity of clinical conditions.Many are incapacitating in the extreme. Many areobscure because scientific knowledge of them ismeager. Many do not as yet lend themselves tosuccessful correction. In many the underlyingmaturational arrest cannot be effectively overcome.Many are lifelong. Some are progresslve. Ma.Pyare especially grave not only because of the result-ing physical handicap, but because of associated
Provided by the Maternal and Child Health Library, Georgetown University

sensory, perceptual, emotional, or intellectual rm-pairments. Both mental retardation, which resultsfrom biological or organic defect, and mental re-tardation, which has no known or identifiable phys-ical cause, belong to the general classification ofcentral nervous system deficit disease.
If one wished to interpret the subject of thisSymposium very broadly, one might even includemental illness, i.e., the psychoneurotic and person-ality disorders which are another huge, complex,ill-defined group of diseases.
Many neurological conditions have inherentlyserious effects not only on the individual, but alsoon rhe family aod society as well. Central nervoussystem disease may be accompanied by emotional,social, and economic consequences which are ashandicapping as the physical defects. By andlarge the services needed by persons with centra,lnervous system deficits are expensive services.
Neurological conditions are also important be-cause of their sheer numbers and because as agroup they appear to be increasing. There arenotable exceptions, however, especially among in-fectious diseases which are followed by neurologi-cal sequelae, for example, poliomyelitis.
Po l iomye l i i i s
In the United States only sixty-four cases of par-alytic poliomyelitis of all ages had been reportedto the Public Health Service through September12. 1964. a sribstantial reduction over the sameperiod in 1963, when the number had reached229.1
For a given disease, the numbers of childrenreceiving services through state crippled chil-dren's agencies do not reffect either incidence orprevalence since budgets, resources, and adminis-trative policy determine what conditions a givenstate agency wil l accept. Nevertheless, numbetsof children cared for '.rnder crippled children's pro-grams reflect unmistakable trends when reviewedat intervals of ten or more years. In 1962, thelatest year for which crippled children's statisticsare presently available, 488 patients u'ith acutepoliomyelitis were given care under official crippledchildren's programs; this is more than twice thenumber of paralytic cases vrhich occurred in allages in the U.S.A. in 1963. The states st i l l report22.412 cases of late effects of pol iomyeli t is ontheir crippled children's rosters.2
Tubercu los is
Great str"ides have been made in reducing tuber-culosis n.reningitis, as well as a number of othermeningit ides.
Aithough not the subject of this Sym-posirim, another manifestation of tuberculosisshowed a marked reduction between the years 1950and 1952 in crippled children's progiams, overrvhich period there was a 61 per cent decrease inchildren with "tuberculosis of bone and ioint." :
)
Congen i ia l Ma l fo rmai ions
Unfortunately, many other conditions whichproduce or are associated with neurological damagehave not been brought under control and may beincreasing. An example of such conditions iscongenital malformations of the ientral nervoussystem. According to Mclntosh's classification ofcongenital malformations by organ systems, thecentral nervous system ranks third among the sys-tems which contributed the iargest numbers of in-fants born with defects.3 Malformations of themusculoskeletal system and the skin were morenumerous.
In the Mclntosh study which followed up 5,964pregnancies, the incidence of defects of the centralnervous systenl was 1.3 per cent of total births,7.2 per cent of stillbirths, 6.1 per cent of neonataldeaths, and l.i per cent of live-born infants whosurvived the neonatal period. Though malforma-tions of the musculoskeletal system and of the skinare more numerous than those of the central nerv-ous system, they are not as lethal. Nearly 30per cent \29.7% ) of the latter had died (in-cluding stillbirths) by the end of a year in contrastto L2.3 per cent deaths in infants with defects ofmusculoskeletal system and only 2.2 per centdeaths in infants with defects of skin. Nearlyone-fourth (24.6Vo ) of central nervous systemanomalies were not suspected or noted till infantswere examined at twelve months. Anencephaly,hydrocephaiy, and meningomyelocele and menin-goencephalocele accounted for nearly four-fifthsof the defects in the stillbirths and neonatal deathsin the Mclntosh study.
In the crippled chiidren's program nurnbers ofchi ldren with spina bif ida and meningocele in-creased from 1,708 in 19,s0 to 3,728 in 1962, arise of 1 i8 per cent.e
Whether or not there is an absolute increase inihe incidence of congenital malformations, it isprobabll' true that more babies with congenitaldefects are surviving because of life-saving surgeryand other improvements in therapy, including anti-biotics. At the present time nearly 30 per centof the children being cared for by official crippledchildren's agencies have congenital malformations.Children with all forms of congenital malformationunder the crippled children's program increased152 per cent between 1950 and 1962; one of thelargest increases rr.'as in congenital heart dlsease("congenital malformation of the circulatory sys-tem"), an increase of 932 per ceni during the sarneperiod of time.2
'Ihis remarkabie increase in
nnmber of children with congenital heart disease inonly thirteen years does not necessarily reflect ahigher inci<lence of congenitai heart disease, butrather is indicative of trvo important developmenis:effective therapy anci tire avaiiability of services ina1l state crippled chiirlren's programs. Cerebralvascular accidents are usually associated with theelderly, but rarely they oct:ur in children, for ex-
Provided by the Maternal and Child Health Library, Georgetown University
I

ample, in children with congenital heart disease orcerebral palsy.
Prematuri ty
Another condition associated with a relativelyhigh incidence of neurological damage and mentalretardation is prematurity, "low birth weight." In-fants in the U.S.A. weighing 2,500 gms. or less in-creased from 7.5 per cent in 1950-1951 to 8 percent in 1962.a Though a rise of 0.5 per centseems small, 0.5 per cent of 4 million live birthswhich occur annually in this country means 20,000additional low-weight infants each year. In thenonwhite infants the increase in prematurity waseven greater for it rose from 10.7 per cent in 1951to 13.1 per cent in 196C.a At the sarne t ime ahigher percentage of babies in the lcwer birth-weight range ( i .e., under 1.500 gms.) now surviveand tbese infants contribute more than their pro-portionate share to the number who are neuro-logically damaged and mentally retarded.
It has long been known that low-birth-weight in-fants have an increased mortality risk and that thisrisk is inversely proportional to birth weight, butno controlled longitudinal study had been donewhich clarified the outlook for infants who lived.Such an anterospective study is continuing underthe direction of Dr. Paul Harper at the Johns Hop-kins School of Hygiene and Public Health, one ofthe special projects supported by The Children'sBurearr. Started in 1952, follow-up examinationshave been done on prematures and matched full-term controls at forty weeks of age, at three tofive years, at six to seven years, arrd at eight to nineyears. The low-weight infants as a group werefound to be handicapped as compared with thefull-term controls on all criteria which werestudied.s These criteria included intellectual andneurological status, vision, sphincter control andmaturity of speech. Lubchenco found a 68 percent incidence of neurological damage, mentalretardation, and eye defects in her ten-year fol-low-up study of infants weighing 1,500 gms. andbelow at the University of Colorado6; many ofthe mothers of Lubchenco's infants had compli-cated pregnancies. These studies and others likethem leave little doubt that there is a high incr-dence of residual handicaps in small prematureinfants (possibly in about 50Vo of babies under1 , 5 0 0 g m s . ) .
Accidents
The death toll from accidents continued to risein 1963. Motor vehicle accidents are the majorcause of death for all ages from five to thirty-four.They cause 15 per cent of deaths at ages onethrough fourteen; 37 per cent of deaths at agesfifteen through twenty-four years. Motor vehicleaccident death rates increased by 4 per cent be-t w e e n 1 9 6 2 a n d 1 9 6 3 . ;
There are over 500 nonfatal injuries for every
accidental death. Though the precise dimensionsof neurological damage to children from accidentsis not known, some insight into the seriousness ofaccident sequelae can be gained by the followingfacts.
In one study of children's accidents, the headand brain were found to be injured in 30 per centof those hospitalized.8 Two per cent of residentsof institutions for the mentally retarded are thereas a result of an accident. Onethird of these per-sons are children under fifteen. Each year Iper cent of first admissions to institutions for merr-tally retarded are adrnitted because of an accident.Sixty-eight per cent of these first admissions arechildren under fifteen years of age.s
Epi lepsyBecause of social stigma associated wittr epilepsy,
the size of this problem has been harder to ascer-tain than for nearly any other handicapping con-dition. The experience of official crippled chil-dren's programs is that when a service is offeredfor convulsive disorders many affected childrenwhose condition was unknown previously come toIight. Though advances in the therapy of con-vulsive disorders are not as dramatic as oDen-heart surgery for congenital heart disease, tbe avail-ability of new drugs which control seizures inabout 85 per cent of epileptic patients s has givenimpetus to the develcpment of programs for thesechildren. Between 1950 and 1962 the number ofchildren with epilepsy increased nearly ten times;thirty states accepted such children in 1962.2
Neurometabo l ic D isorders o f Ch i idhood
Recently advances in biochemistry, which areat least as great as in any other branch of medicine,have raised the hope of detecting and at somefuture time of treating a large number of diseasesknown by the generic term, inborn errors of me-tabolisn.r. Approximately twenty-eight of thesediseases known in 1963 are associated with mentalretardation.lo Usually in these diseases the motheris able to protect the fetus from brain damagewhich may result from chemical toxtns in utero.Consequently, theoretically, if a disease such asphenylketonuria (PKU) is detected early and iftreatment is begun and continued until there is nolonger danger of damage to the brain, mental re-tardation will be averted. Though the incidencecf each separate inborn error of metabolism isusually small, in the aggregate they add up to aproblem of considerable magnitude.
The neurometabolic disorder with which TheChildren's Bureau has had most experience isPKU. When both a screening test to identifyaffected infants and a dietary treatment becameavailable, The Children's Bureau's Technical Ad-visory Committee on Clinical Programs for MentalRetardation was asked to recommend next steps.Specifically, they were asked whether knowledge of
Provided by the Maternal and Child Health Library, Georgetown University
PKU was sufficient to have practical applicationas a public health program. They recommendedthat affected infants be identified and broughtunder treatment at as early an age as possible, andthat Children's Bureau funds be used to pay forthe low phenylalanine diet for those infants andchildren whose families could not afford it. TheGeneral Counsel of the Department of Health,Education, and Welfare ruled that this specialdiet was "therapy" and not "food." The reasona legal opinion was sought was because welfarefunds are appropriated for food whereas Chil-dren's Bureau health funds can be used for drugs,biologics, a variety of appliances, prostheses, hear-ing aids, eyeglasses, braces, and so on.
At the beginning of the PKU screening programonly urine tests were available. Because of thelow yield of positive tests in mass screening pro-grams, some states concentrated on so.called"high-risk" groups, such as siblings of knowncases, and children in clinics and institutions forthe mentally retarded, special education classes,and epilepsy clinics where a higher incidence ofaffected children would be found than in the gen-eral population.
The difficulty of reaching infants after they leavethe newborn nursery and the very real possibilityof damage to the infant's brain before the urinetest becomes positive led to a search for a methodof screening which would be simple, yet effectivein locating affected babies within the few days theyare in the hospital of their birth.
Because the Guthrie "inhibition assay" bac-terial test, which requires only a few drops ofblood from the newborn, gave promise of meelingthese criteria, The Children's Bureau supported afield trial of this test as a routine screening pro-cedure for early detection of PKU. Twenty-ninestate health departments and 505 hospitals co-op-erated in the testing of 404,568 newborn infants.Thirty-seven confirmed cases were found, an in-cidence among this population of I to 10,347.11
It appears from this field trial that it is feasibleto test newborn infants for PKU while they arestill in the hospital. Similar screening tests usingdried spots of blood collected on filter paper arebeing tried for other inborn errors of metabolism-galactosemia, maple syrup urine disease, histi-dinemia. At the same time research is continuingin an attempt to find a multiple screening testwhich will be positive when any one of a numberof these diseases is present.
p6u1 5f3fgs-Massachusetts. Rhode Island. Lou-isiana, and New York-have passed mandatorylegislation requiring screening of newborn infantsfor PKU; Oregon and Illinois have passed per-missive legislation. Eight states report that in 90per cent or more of their hospitals newborns arenow being screened for PKU; in three states, thenewborns in 50-90 per cent of the hospitals; inthirty-four states, the newborns in less than 50
4
per cent of the hospitals. In only six states wereno hospitals screening newborn infants for PKU.12Screening, however, is only the first step along along hard road to salvage these children and pre-vent mental retardation. The diagnosis must firstbe confirmed. There are many dietary problems.There is need for biochemical monitoring to keepthe blood phenylalanine at a safe level (the child'srequirement for phenylalanine is constantly chang-ing because of his growth needs). There is needfor genetic counseling of the family backed up byappropriate laboratory studies.
Menial Retardation
A development which has helped to get PKUchildren under therapy is that by 1960 most ofthe states had developed multidiscipline clinics formentally retarded children under their maternaland child health program and the services of theseclinics were available for instituting and regulatingdiet therapy. Nearly 500 children with PKU wereknown to mental retardation clinics and maternaland child health and crippled children's programsduring the period 1957-1961, a Children's Bureaustudy revealed;212 of these children were underthe dietary supervision of mental retardation clinicsin January 1962.13 A protocol to evaluate theresults of therapy on the mental development ofchildren with PKU supervised by mental retarda-tion clinics is being developed at the present timeby members of The Children's Bureau TechnicalAdvisory Committee on Clinical Programs.
There are now 110 special clinics for mentallyretarded children, eighty of which are supportedin full or part by Children's Bureau funds. In1962 approximately 25,000 children and theirfamilies received services through the special clin-ics for mentally retarded children supported bymaternal and child health programs. Yet the needis not being met because the waiting list in clinicscontinues to mount.
In the clinics reporting to The Children's Bureauin 1962, approximately 75 per cent of the childrenunder six years of age were found to have a va-riety of handicapping conditions in addition totheir mental retardation. Because of these dis-abilities the services of state crippled children'sagencies have been needed to supplement theservices of the mental retardation clinic.
Also crippled children's agencies are increasinglymaking their services available to institutions forthe mentally retarded. Serviceq designed to in-crease mobility and self-care activities are beingdeveloped for the severely mentally and physicallyhandicapped.
Though the author was unable to find substanti-ating statistics, it is commonly reported that thecharacteristics of the population of institutions forthe mentally retarded have been changing notice-ably in recent years. As community services de-velop, borderline retarded persons are not being
Provided by the Maternallnd Child Health Libiary, Georgetown University:

institutionalized; on the other hand, there has beena marked increase in the numbers of severely men-tally and physically handicapped infants andchildren, i.e., of "bed" patients,
Brain Damage
"Brain damage" or "mild brain damage" is alabel which is being assigned to more and morechildren, particularly educationally difficult chil-dren. There is much dissatisfaction with the name,partly because it implies a knowledge of etiologywhich does not exist. Nevertheless, the childrenwho are being included have many clinical char-acteristics ia ssrnrnen-hyperactivity, distractibil-ity, perceptual and learning difficulties. The num-ber seems to be increasing either because ofimproved diagnostic skill or because, perhaps,medical science has done its work "too well" inkeeping more of such children alive.
The term "brain damage" suggests a lesion whichcan be demonstrated by the pathologist, eithergrossly or microscopically. Many factors influ-ence the developing nervous system of the fetusand child and biochemical factors are among themost important. A striking example of the effectof chemicals on the mind can be demonstrated bythe infant with PKU if one contrasts the markedchange in his behavior prior to treatment with thatafter therapy has been instituted.
A recent British article reports the case of apsychiatric patient who had cyclic swings of moodfrom hyperactive manic state to depressed lethargicstate. Water and salt retention were marked dur-ing the inactive phase, the reverse during the hyper-active periods.la
Much has been written about the effect on thebrain of an insufficiency of such an essential ele-ment as oxygen. The problem of anoxia will bediscussed during this Symposium. The damagecaused by an excess of oxygen administered to thepremature in-fant is well known. Recent researchsuggests that it may be possible to prevent themental retardation associated with hypoglycemiaif newborn infants are given injections of glu-cose.
Cerebral Palsy
One of the oldest diagnoses for which crippledchildren's agencies accepted responsibility is cere-bral palsy. Since the crippled children's programin the beginning was chiefly orthopedic and plas-tic. one can assume that these cases were treatedorthopedically on the basis that motor abnormal-ities were their outstanding and most obvious fea-ture. Though neuromotor disability may appearto be the most important one, many of these chil-dren have multiple handicaps, and in the long runthe associated visual, hearing, speech, perceptual,behavioral, and emotional handicaps can affect theeventual achievement and potential of the indi-vidual more than his abnormal motor functionins.
There is a general awareness at the present timethat cerebral palsy is a multifaceted neurologicalproblem to which many disciplines can make a sig-nificant contribution.
It is not known if the incidence of cerebralpalsy is increasing. Crippled ctrildren's statisticswould suggest that it is. Between 1950 and 1962the number of children with cerebral palsy beingcared for under the state crippled children's pro-grams increased more than 61 per cent; the case-load grew from 19,334 to 31,225.2
Two observations of the Health Services staffmay be of interest:
1. Infants with cerebral palsy are being diag-nosed and referred for treatment at an earlier agewhen therapy is more effective and when measurescan be taken to prevent contractures and otherdisability secondary to the initial condition.
2. On the negative side, some states report theyare losing their cerebral palsy patients in theirmiddle adolescent years. One state crippled chil-dren's agency has a staff member investigating thisproblem and hopes as a result to provide a moreadequate program for the teenager with cerebralpalsy.
Deafness and lmpairmenf of HearingThe number of children with hearing loss in
crippled children's programs increased by 160 percent from 1950 through 1962.2 Two developmentsin this program are closely related to centralnervous system deficit. One is the greater compe-tency of specialists who make more discrete diag-nosis of hearing difficulties because of perceptualor central nervous system deficits in children. Theother is the interest of some maternal and childhealth programs in testing the eight-month-old in-fant's response to sound stimuli. Developed by theCo-operative Study which is supported by the Na-tional Institute of Neurological Disease and Blind-ness, the test is not so much a screening test forhearing loss as for mental or neurological diffi-culties, since four out of five infants who failthe test have the latter in contrast to only one infive whose failure is due to hearing impairment.
The Mul t ip le Handicapped Chi ldAll of the central nervous system problems we
have been discussing are complex. Because chil-dren do not fall into neat categories, some stateshave developed services for children with multiplehandicaps. Though excellent services for a childwith a single diagnosis may exist, the child withmultiple problems is likely to get lost among amaze of specialized clinics and between numerousscattered appointments, especially if considerableperiods of time elapse between appointments. Per-haps the most serious lack is that of a medical,or at least some professional, person to followthe child to insure that reports and recommenda-tions are correlated and that Darents and child are
Provided by the Maternal and Child Health Library, Georgetown University

helped to work out a practical plan to follow inthe treatment of the child.
Services for the multiply handicapped are basi-cally built around a specialized clinical team in amedical center. The nucleus of this core staffvaries, but usually consists of a pediatrician, oftenwith training in neurology, a clinical psychologist,a medical social worker, a pediatric nurse, in someclinics a speech therapist, a nutritionist, or one ofthe several other disciplines. Many medical spe-cialists are available for consultation and if appro-priate may be present at the evaluation conferenceof any given child. Representatives from otherdisciplines such as dentists, audiologists, physicaltherapists, occupational therapists may also becalled on to contribute.
In addition to the purposes of providing athorough evaluation of the handicapped child andhis family, and of making a unified treatment planfor the child, a very important by-product of theteam evaluation conference is the professionalgiowth of the members of the team in understand-ing their own and their colleagues' roles and intheir own continuing education. Such care asdescribed is child-centered rather than condition-centered. It is "comprehensive" care. Good qual-ity team care not only attracts patients and pro-vides a favorable setting for clinical research butis an excellent laboratory for training of profes-sional persons in concepts of multidisciplinarycare.
An advisory committee has recornmended toThe Children's Bureau that the multidisciplinarydiagnostic, evaluation, treatment, and follow-upclinics supported by the Bureau be utilized to agreater extent than at present for training of pro-fessional teams.
A New York State Committee on Medical Edu-cation in a report to the Governor (1963) haspointed out some inadequacies in medical educa-tion as follows:
The characteristics of comprehensive medicalcare do not exist, by and large, in the teachinghospitals of today. . . . Clinical services usuallyare conducted in the isolated framework of theprevailing specialties with the result that teamwork among specialists is frequently lacking. . . .Continuity and coordination of services are lostfor both the patient and the students as thepatient is referled from specialty clinic to spe-cialty clinic, from the inpatient to the outpatientservice, from the outpatient service to the home,and as students and staff rotate in their assign-ments, from specialty to specialty or service toservice. While professional students (medical,nurse, and other) receive their basic training inthe same institution, they are often, in fact,isolated from each other. . . Strange as it mayseem the professional student is often isolatedfrom the social and historical forces responsiblefor the role he will assume as a practicing pro-fessional.ls
6
IMPACT OF THE HANDICAPPED CHILDON THE FAMILY
Albert J. Solnit has written an excellent articleon the subject of the impact on the family of hav-ing a defective or handicapped child, "Mourningand the Birth of a Defective Child."16 During prag-nancy the mother wishes for a perfect child, yet
fears she will have a damaged one. When her fearsare a reality, she mourns for her "dream" childwho is a composite of her loved ones (mother, hus-band, father, siblings). This grieving process re-quires time and passes through many phases-initially the mother feels numbness and disbelief.Parents have described this period as living in anightmare, with only the hope that they wouldawaken and find that they had had a bad dream.Parents are often critical of their physiciansbecause of what they were not told-perhapstheir physician is sure he has explained tothem, but they could not comprehend. Parentshave said their doctor told them "in a coldway." Usually this means that rather thanbeing cold the doctor himself was very emotion-ally involved because he felt helpless and de-pressed.lT
Not only the physician but also the nursesand other professional persons who are in contactwith the parents are upset when a deformed childis born. This anxiety and depression is trans-mitted to the mother. The staff often wishes to"protect" the mother and not show her her de-formed baby, thus making it difficult or even im-possible for the mother to start dealing with reality.If she is shown her baby by a member of the staff
who displays revulsion for the baby, the mothersenses this rejection. This reaction from a profes-
sional person is difficult for the mother since shehas a right to expect acceptance of her baby as heis and also encouragement and moral support.ls
One of the outstanding pediatricians in the Los
Angeles amputee project will fly any place in Cali-
fornia to see the parents of a newly born congenitalamputee. Not that he will fit a prosthesis then,
but he knows the child and parents will be better
able to accept the prosthesis when the proper time
comes, if he has given them help at this critical
time. In other words, as professional health work-
ers, we should recognize that the birth of a de-
formed, abnormal baby is a crisis situation, which
requires immediate and skillful management.
There is a natural tendency for parents (or
mother especially), because of their sorrow andguilt, to dedicate themselves to the child and do
everything for him, often to the neglect of other
members of the family. This is detrimental to the
defective child too since he should develop as
much independence as possible. At the other ex-
treme is the reaction of some parents of intolerance
and rejection of the child.Parents should be helped to understand that they
Provided by the Maternal and Child Health Library, Georgetown University

are not alone with their problem and that the pro-fessional persons who help them are standing readyto give them encouragement and support.
SUMMARY
The problem of the child with central nervoussystem deficit is an intricate one. It is of greatmagnitude and probably is increasing. It has manyramifications and in its consequences it reachesfar beyond the affected child to his family and intohis community. Many facets of the problem havescarcely begun to be understood. The means ofprevention are often not known. The complexityof the problem makes it one of the most challengingproblems confronting the health worker today. Itis our hope that this Symposoum will result in someprogress toward reaching our goal of a brighterfuture for the neurologicaliy handicapped child.
REFER EN CES
1. Morbidity and Mortality Weekly Report. Prepared byCoirmunicable Disease Center, Publ ic Heal th Service,U.S. Department of Health, Education, and Welfare,Vol . 13, No. 37, September 18, 1964. Washington, D.C.:U.S. Government Printing Omce.
2.Crippled Children's Program-Statistical Highlights1962. Children's Bureau Statistical Series No. 74.Washington, D.C.: U.S. Government Printing Office.
3. Mclntosh, R. , et a l . : The incidence of congeni ta l mal-formations: a study of 5,964 pregnancies, Pediatrics,l 4 : 505 , November 1954 .
4. Hunt, E. P., and Goldstein, S. M.: Trends in Infant andChildhood Mortality, 1961. Children's Bureau Sta-tistical Series No. 76. Washington, D.C.: U.S. Gov-ernment Printing Office.
5.Harper, Paul , et a l . : Neurological and inte l lectualstatus of prematures at three to five years of age, J.Pediat , 55:679. December 1959.
6.Lubchenco, L. O., et al.: Development of prematureinfants of low birth weights: evaluation at ten years ofage, Amer. J. Dis. Child., 102:752, November 1961.
7. Accidental Death and Injury Statistics, Public HealthService, Division of Accident Prevention, Public HealthService Publ icat ion 1111. Washington, D.C.: U.S.Government Printing Office.
8. Patients in Mental Institutions 1962-Part I, PublicInstitutions for the Mentally Retarded. Prepared bythe National Institute of Mental Health. Public HealthService Publication No. 1143. Washington, D.C.: U.S.Government Printing Office.
9. Livingston, S.: What hope for the child with epilepsy?,Children, 12:9, January-February 1965.
10. Mental Retardation, Its Biological Factors-HopeThrough Research, prepared by National Institute ofNeurological Diseases and Blindness. Public HealthService Publication No. 1152, Health Information SeriesNo. 114. Washington, D.C.: U.S. Government Print-ins Office.
11. Guthrie, R., and Whitney, S.: Phenylketonuria-Detec-tion in the Newborn Infant as a Routine Hospital Pro-cedure. Children's Bureau Publication No. 419, 1964.Washington, D.C.: U.S. Government Printing Office.
12. PKU Blood Screening in Flospitals-Summary of Re-plies to Query by Children's Bureau, September 30,1964. Washington, D.C.: U.S. Government PrintingOffice.
13. An Inventory of Children With Phenylketonuria. Chil-dren's Bureau Study, 1962. Washington, D.C.: U.S.Government Printing Office.
14.Jenner, F. A.: Biochemical Aspects of Disorders ofMood in Neurometabolic Disorders in Childhood. Pro-ceedings of a Symposium held at Sheffield, England,May 1963. Edited by K. S. Holt and J. Milner. Edin-burgh and London: E. & S. Livingstone Ltd., 1964.
15. Education for the Health Professions-A Compre-hensive Plan for Comprehensive Care to Meet NewYork's Needs in an Age of Change. A Report to theGovernor and the Board of Regents from the NewYork State Committee on Medical Education. June1 963 .
16. Solnit, A. J.: Mourning and the birth of a defectivechi ld, Psychoanal . Stud. Chi ld, 16:523, 1961.
l7.Parmelee, A. J. , Jr . : The doctor and the handicappedchi ld, Chi ldren, 9:189, September-October 1962.
18. Gurney, W.: Parents of chi ldren wi th congeni ta l ampu-tat ion, Chi ldren, 5:95, May-June 1958.
Provided by the Maternal and Child Health Library, Georgetown University

.THE DUAL SEIVSORY
ORIGIN OF THE IDEA THAT SPINDLES ARESENSORY ORGANS
Some of the earliest descriptions of spindles notedthat the encapsulated bundle of muscle fibers waswrapped in a profuse tangle of nerve terminals.Despite limitations of teasing and improvised dark-field techniques then in use, a "most beautiful andelaborate structure" was seen in which "very finenerve-fibres divide into branches as they passparallel to the muscular fibre; and transversebranches can be seen crossing the fibre at short
ROLEOF MIJSCLE SPI]VDLES
EARL ELDRED, M.D.
Adapted from a paper presented at the Symposium onThe Child with Central Nervous System Deficit, Septem-ber 28-October 2, 1964, The University of Pennsylvania,Philadelphia.
The author is a member of the Department of Anatomy,Center for the Health Sciences, University of California,Los Angeles, 90024.
+ In order not to encumber the bibliography, referencesto older articles have been omitted. They may be foundin the Bibliography on Muscle Receptors I and rnMatthews' comprehensive review.2
8
intervals" (Beale, 1862).* A sensory role for the"Weismann bundles" of contractile flbers was notsuggested, although Sir Charles Bell's concept of amuscle sense was known. Because spindles werefirst noted in growing muscles and have smallfibers with a profusion of central nuclei resemblingthose in a developing muscle fiber, the thoughtunderstandably arose that these "Muskelknospen"(muscle buds) were sources of myogenesis, andthat the "nerve tufts" represented multiplicationof innervation paralleling the divison in musclefibers.
The demonstration in chronic deafferented frogpreparations that muscle nerves contain sensoryfibers and the advent of specific neurologic stain-ing methods led to deeper appreciation of theneural composition of muscle spindles, and in1884 Mays hesitantly suggested that they mightbe sensory organs. Kerschner, in an 1888 articleprophetically entitled "Ein besonderes Muskelsys-tem im willkiirlichen Muskel," compared endings
Provided by the Maternal and Child Health Library, Georgetown University

of muscle spindles with those of "Golgi tendonspindles" and gave other arguments that causedhim to conclude that spindles were complicatedsensory organs. In the same year Cajal accuratelyfigured the appearance of methylene-blue-stainedspindle endings and correctly surmised their sen-sory function, but his paper written in Spanish andappearing in the first issue of his own journal wassubsequently little quoted. Descriptions or nota-tions of spindles by two dozen other authors ap-peared between 1878 and 1892,1 of which themost far-reaching in its consequences to laterthought was the claim by Ruffini that at least twotypes of sensory endings were discernible in mam-malian spindles.3
As Kerschner argued, appearances strongly sug-gest that the intricate nerve endings in spindles aresensory, but rigid proof of this requires demonstra-tion that the endings remain intact after the ventralspinal roots are cut and motor terminals within themuscles degenerate. Cattaneo narrowly missedthis research coup when he showed that tendonorgans in dogs remained intact after motor rootsection, but that they degenerated if the dorsalroots were cut. Onanoff in 1890, also workingwith dogs, found that section of either dorsal orventral roots resulted in some degenerative changein spindle innervation and logically concluded thatthe spindle was a sense organ under'motor control.His brief report, though published in the well-establ ished "Comptes Rendus," was apparentlyoverlooked by Sherrington, who four years laterin his masterful presentation of the results of selec-tive root sectioning gave the accepted proof of thesensory nature of spindles.a The quantitative im-portance of sensory return from muscle. moreover.was shown by the fact that one-third to one-halfof the axons in demotored muscle nerves were in-tact. Some of these axons were the largest to befound in peripheral nerves.
Ruff ini in his later papers,s'6 thoroughly con-vinced now of the sensory function of spindles bySherrington's proof, reasserted his belief that thespindle was not a simple sensor l ike Pacini 's cor-puscle or Golgi 's tendon organ, but had at least twodistinct forms of sensory terminals. These he hadalready termed annulospiral and flower-wreath or-spray endings from their appearance in gold-stained spindles in cat muscles.3 The annulospiral(AS) endings were prominent, spiral ing, bandlikewrappings located midway along the length of thespindle (Fig. 2). Flower-spray (FS) terminalswere variously foliate, clawlike, or spirilliformwrappings. Some spindles of small size had nosecondary ending and only the single AS ending.Most, however, had FS endings on one or bothpoles distal to the equatorial zone occupied bythe AS winding.
That two endings of such morphological dist inc-t ion must monitor two modali t ies of sensory st imuliseems axiomatic. I t is the objective of this paper
to review what is known of these sensory modalitiesand the structural adaptation of the spindle forthis dual role.
THE EVIDENCE FOR A DUAL SENSORY
I N N E R V A T I O N
l . T e r m i n a l s
The significance of Ruffini's distinction of ASand FS configurations in unspecified [sic] musclesof the cat depends upon whether these representtruly separate categories, and whether the distinc-tion holds for other muscles and animals. Criti-cism has been raised that the irregular pattern ofstained patches joined by faint filaments in Ruffini'sillustrations of the FS ending indicate incompletefixation and that the entire outline of the endingis not seen. Electronmicroscopy reveals thatsmaller sensory branches may in places be sealedover by the gutters of intrafusal fiber cytoplasm inwhich the endings l ie.7 and this might lead topatchy access of the metallic stain to the terminal.In any case, numerous observers, using light mi-croscopy with a variety of staining methods, haverecognized that sensory endings distal to the mainAS wrappings may also have spiral windings ora stem with multiple side branches that clasp theunderlying intrafusal (IF) fibers, and that onlythose endings at more distal sites along the axialbundle present the classical FS configuration.Moreover, variations occur from muscle to muscleand between species. For these reasons, and be-cause the terms correlate logically with embryo-logical t ime of appearance, dominance in posit ion,persistence in simplified spindles, and size of affer-ent axon, the alternative terms "primary" and"secondary" endings proposed by Ruffini for theAS and FS endings are in increasing use.*
The most productive workers in this field, D.Barker,s I . A. Boyd,e and S. Cooper, lo seem ingeneral agreement on the organization of spindlesensory endings into two categories upon criterianot alone of form, but the number of endingspresent in a given spindle, relative position alongits length, relation to the several IF fibers, andsize of axon (Fig. 3). Primary endings are lo-cated at the equator where branch coils of thetotal ending wrap about each of the IF fibers.Every spindle has one and only one such primaryending and afferent axon. Secondary endings, incontrast, may be absent in spindles of small size,but most units have one to a total of five secondaryendings arrayed in successive zones lying to eitherside of the equator. Branches of these endings arelargely confined to the smaller IF fibers. Eachsecondary ending has its own axon, althoughbranches of the same axon may perhaps supplyendings in nearby spindles.l2 As mentioned al-ready, the size and form of these two types of
* Convenience for abbreviation, however, causes thepresent author to retain the more picturesque names.
Provided by the Maternal and Child Health Library, Georgetown University

rl..-i
fjq
;:H
; i l* i t i
>* -F { :il. L,i - * ' .
ri'!.' :rar . #{ *};{,: t{,f f i -
L'"
i,
{_
f . {
41
h . t rs* '{ft
*l, *-
i { d l l. xus -l* 4 iijg 6i {riI.r.t f* :"Fk ' *d *
J
F - { u i- N
6 < Hi d p . :X l * t LL ) XY * )
x.*
{*rX,;uj
i.:!..
J_.]Lrit
L}
rii:-
{F*F&ff,*
4;1'
ot nxu
<.
a , :z t Is'< L na )
3*J ;
.t-
It."- l-:.
t_r iI4 : ,* - l
1--.'" !.'
10
\ : : ,1
u
r*
Provided by the Maternal and Child Health Library, Georgetown University

<(<
FlG. 1. A c0nception of the mammalian muscle spindle.The sensory organ is seen to l ie in an interfascicularcleft , paral lel to the extrafusal f ibers, and, as is often thecase, near to an intramuscular nerve and artery. Theprominent lamellar capsule encloses a large space whichin this drawing is exaggerated in relat ion to spindlelength but not to f iber cross-sectional sizes. The intra-capsular f luid has a mucopolysaccharid consti tueni andis presumably viscous. An axial bundle of six special izedstr iated muscle f ibers traverses the space anci two f ibersare indicated as extending beyond the capsule. Theselarger "percapsular f ibers" are somewhat smaller incross section than the extrafusal f ibers, but are two tothree t imes larger than the " intracapsular f ibers." Threesensory axons approach the polynucleated central zones ofthe f ibers and lead to primary (annulospiral) and sec-ondary (f loweFspray) endings. Branches of the primaryending wrap individual ly about large and small intra-fusal f ibers; the secondary ending is largely restr ictedto the small f ibers. A trunk of f ine motor axons aD-proaches one pole of the axial bundle. Drawing by Dr.C. F. Bridgman, Department of Anatomy, Universi iy ofCali fornia at Los Angeles.
endings vary considerably, even between the twoor three secondary endings that may be lined upalong one pole of the spindle.e Despite this inter-gradation, the modern histologists and many of theearlier observers accept the idea that primary andsecondary endings fall into separbte categories anddo not represent extremes of a single population.
2. AxonsAxons observed within the capsule 5 or in intra-
muscular nerves close to spindles 8'e are larger forthe primary than the secondary endings (Fig. a).Individual axons generally cannot be followed intothe nerve trunk to the muscle, but with physio-logical techniques slow and fast conducting fiberscan be identified among units giving typical spindleresponses. Conduction rates collected from a num-ber of such spindle units fall into two distinctgroups with the separation point at 72 ntm./sec.73Calculation of axon diameters from conductionrates (rate in meters/sec. is six times the diameter
FlG. 2. Ruff ini 's pen-and-inkdepict ion of the two typesof sensory endings found ingold chloride-stained spindlesin cat muscles with his alter-native terms. The uooer draw-ing shows three axons enteringfrom the left to supply spiralterminals wrappeci individual lyabout the three or four intra-fusal f ibers, which, incident-ally, ate not represented ashaving the nuclear aggrega-t ions that would be expectedat this equatorial level. End-ings in the lower f igure prob-ably include the motor end-plate terminals as well as thesensory terminal. Ruff ini de-scribed the secondary endingas having "various kinds ofrounded, bif id, tr iangular, leaf-l ike varicosit ies seeming al-ways disposed in such a wayas to recal l the arrangementof a festoon.wreath of flow-ers." (Adapted from Ruff ini .6)
; *-:*"*\,.. "\*-
*,w**ffipt
ANNULOSPIRAL OR PRIMARY ENDING
FLOWER.SPRAY OR SENSORY ENDING
? 8 0 - 2 8 0 0 - 6 6 - 2
Provided by the Maternal and Child Health Library, Georgetown University
l 1

SENS ORY
BAG FIBERS ]
cHArN FTBERS )
Io AXON
tr AXON
SECONDARYENDING
FlG. 3. Current concept of the sensory innervati0n of the mammalian muscle spindle. In upper sketch a single axon isseen t0 branch dichotomously to supply annulospiral c0i ls of various sizes, each wrapped ar0und an individual intrafusal ( lF)f iber. The axon belongs t0 the la subgroup of f iber sizes and is among the largest found in sensory nerves. The secondaryendings, less regular in form and sometimes having a f lower-spray appearance, are found poleward from the AS wrappings.They are distr ibuted chief ly to the smaller lF f ibers. Intermediate-size axons of group l l classif icat ion supply the secondaryendings. There may be several of these axons and endings, or in some spindles no secondary endings. Insert to r ight is avariat ion of the above scheme based up0n a specimen reconstruction by Barker and Cope.t ' The distr ibution of the la axonis confined to the large lF f ibers, the left-hand group l l f iber to the smaller lF f ibers, while the group l l axon to the r ightis intermediate in size and distr ibutional pattern. ( lnsert adapted from Barker and Cope.1')
in micra) indicates that the spindle afferents fallnicely into the faster group I (12-20p) and grouplI (4-12p) axon size categories recognizable inthe afferent histogram.la Relation oi this break-down of fiber size in nerve trunks to the size ofsensory axons seen at the spindle has led to theconclusion that primary endings are connected togroup I axons and secondary endings to the slowergroup II fibers.
3. Patterns of Discharge
Progress in analysis of the spindle mechanismclearly illustrates the dependence of biological un-derstanding upon technological advance. UntilAdrian ln 1927 applied a three-valve amplifier andelectrometer oscillograph to the study of sensorydischarges in frog muscle nerve, no material contri-bution to knowledge of the intrinsic physiology ofthe spindle organ was made. The effects of affer-ent inflow from muscle on its reflex behavior hadbeen abundantly explored and the myogenic sourceof the stretch reflex confirmed, but there werecontrary speculations as to whether the discharge
t 2
from spindles 15 or tendon organs 16 was responst-ble. This point was cleared up when BryanMatthews, by monitoring activity of single units,demonstrated the well-known differentiation indischarge pattern of these afferents.17-1e All affer-ents showed accelerated and usually sustaineddischarge with passive stretch (Fig. 5). During ac-tive contraction, however, the discharge of Mat-thews' "type A afferent" decelerated (Fig. 6),even to the point of completely pausing i f themuscle were allowed to shorten, whereas "type Bunits" accelerated. Since spindles l ie in paral lelwith contracting muscle fascicles and the tendonorgans in series (Fig. 7), it was inferred that typeA responses must be characteristic of spindle end-ings and the B responses of tendon organs (TO's).The degree of stretch required to cause the TO's todischarge was greater than that for spindle affer-ents. Matthews also recognized two subtypes ofspindle afferents. One of these, presenting gen-erally smaller axon potentials, in his experiencehad a lower threshold to stretch than units withlarger potentials, and this led him to the opinion
PRIMARY ENDING
Provided by the Maternal and Child Health Library, Georgetown University
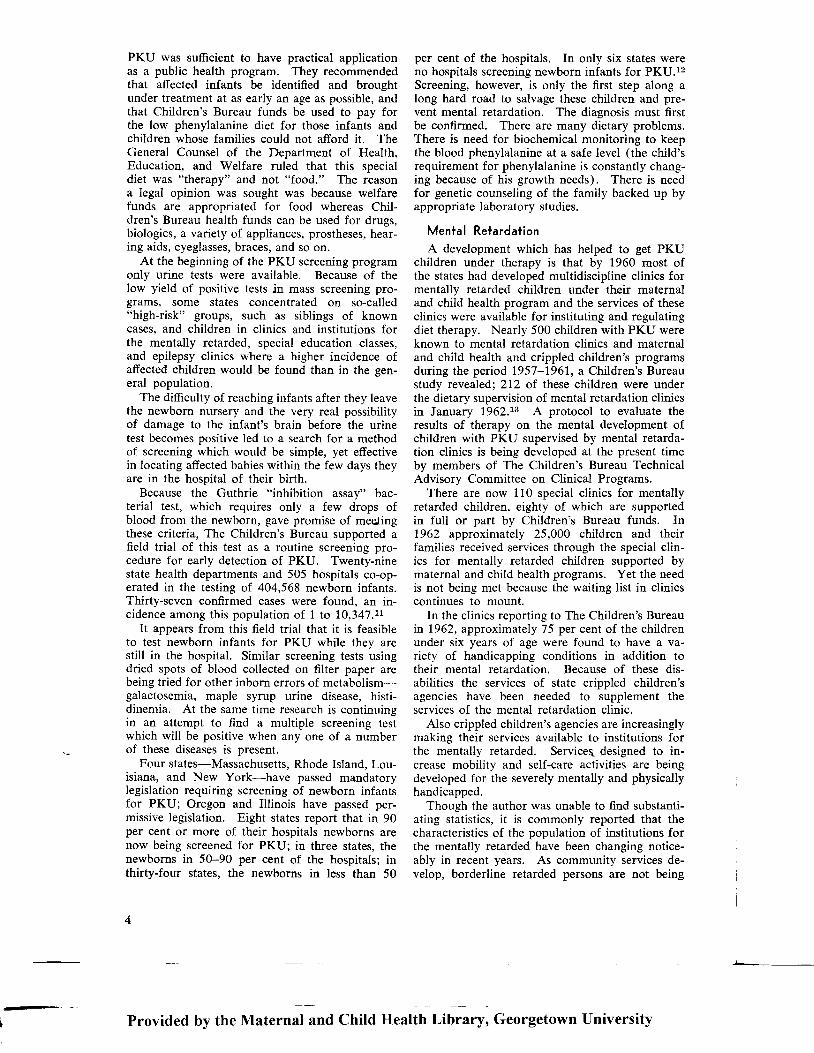
H I S T O G R A M O F A F F E R E N T A X O N S
N 4 E A S U R E D O N E m mF R O I ' , 4 S P I N D L E S
S E C O N D A R Y E N D I N G S( G R O U P I I F I B E R S }
PRIMARYE N D I N G S
l G R O U P I o )\ F I B E R S /
zX
u
EUo
3z
AXON DIAIVETERS
FlG. 4. Bimodal but overlapping distr ibution 0f axons t0the two types of sensory endings as measured at a distanceof 1 mm. from sDindles in the tenuissimus muscle of thecat. More numerous secondary endings were innervatedby f ibers having dianreters chief ly between 4 and g micra.Primary endings led to axons in the range from g t0 19micra. In further course of the axons centralward themuscle afferents probably increase in diameter so that theminimum separating the two groups of f ibers approaches72 p, the separation point between group I and l l sensoryaxon sizes in the dorsal root. (Adapted from B0yd.,)
that the FS afferents were probably responsible forexcitation of the exquisitely sensitive stretch reflex.Since opinion now holds the AS ending responsibleinstead, each of the three major sensory terminalsof muscle has been thought at one lime or anotherto mediate the stretch reflex!
Difference in relation of spindle and tendonorgan to extrafusal muscle fibers leads to contrastin their discharge behavior; difference in relationof the two spindle sensory terminals to the intra-fusal fibers probably is the cause of contrast in
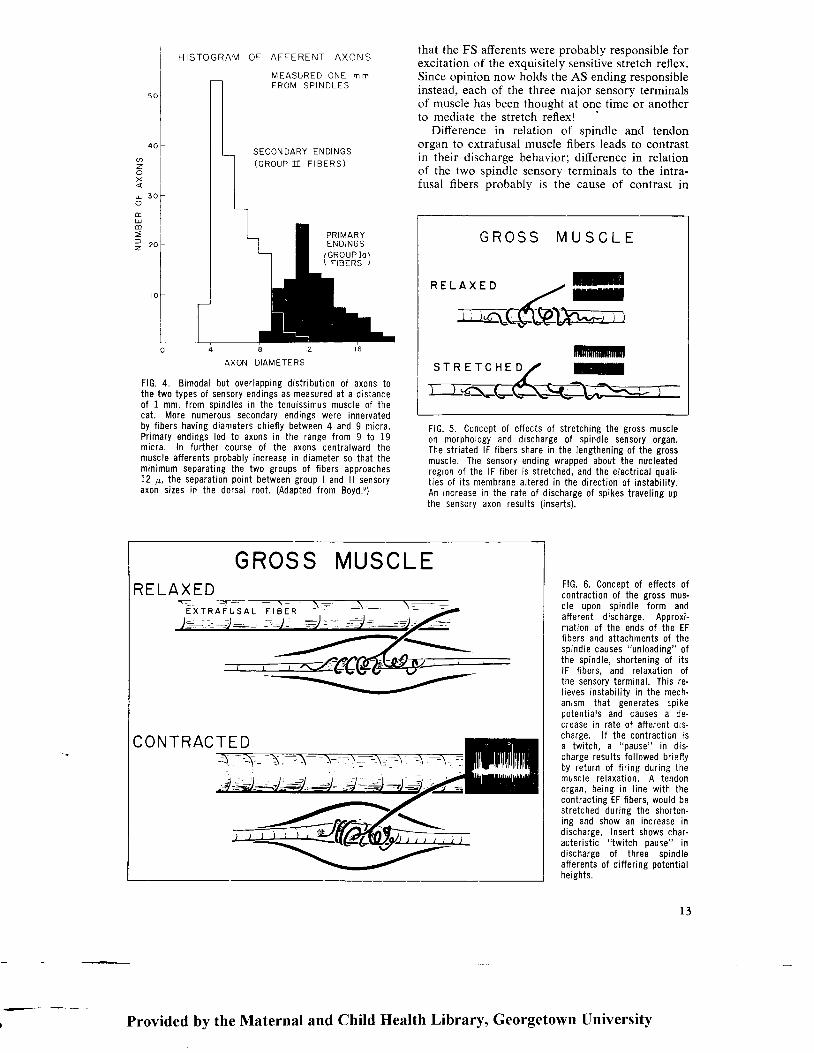
GROSS MUSCLE
S T R E T C H E DmnmmlU
R E L A X E D
FlG. 5. C0ncept of effects of stretching the gross muscleon morphology and discharge of spindle sensory organ.The str iated lF f ibers share in the lengthening of the grossmuscle. The sensory ending wrapped about the nucleatedregion of the lF f iber is stretched, and the electr ical qual i-t ies of i ts membrane altered in the direct ion of instabi l i ty.An increase in the rate of discharge of spikes travel ing upthe sensory axon results ( inserts).
FlG. 6. Conceot of effects ofcontract ion of the gross mus-cle upon spindle form andafferent d ischarge. Approxi-mat ion of the ends of the EFf ibers and at tachments of thespindle causes "unloading" ofthe spindle, shortening of i tslF f ibers, and re laxat ion ofthe sensory terminal . This re-l ieves instabi l i ty in the mech-anrsm that generates spikeDotent ia ls and causes a de-crease in rate of af fergnt drs-charge. l f the contract ion isa twi tch. a "Dause" in d is-charge resul ts fo l lowed br ief lyby return of f i r ing dur ing themuscle re laxat ion. A tendonorgan, being in l ine wi th thecontract ing EF f ibers, would bestretched dur ing the shoi ten-ing and show an increase indischarge. Insert shows char-acter is t ic " twi tch oause" indischarge of three spindleafferents of differing potentialheights.
GROSSRELAX ED
MUSC L E
CONTRACTED
E X T R A F U S A L F I B E R
Provided by the Maternal and Child Health Library, Georgetown University
L3

FlG. 7. Fundamental dif ferencein relat ions of spindles andtendon organs (T0) to extra-fusal muscle f ibers. The T0,attached at one end to theaponeurosis and receiving in-sertions of extrafusal (EF)f ibers at the other, is " inseries" with these contracti lef ibers. The spindle l ies be-tween and in the same orien-tat ion as the EF f ibers, thatis , i t i s " in para l le l " w i ththem. This contrast was notful ly appreciated by earlyworkers as Sherrington andothers gave prominence indescript ions of spindle dis-tr ibution to their occurrencein the neighborhood of ten-d o n s a n d a p o n e u r o s e s ,whereas in fact spindleschief ly l ie central within themass of muscle f ibers.s
their responses. Annulospiral endings chiefly wrapabout the nonstriated, nucleated zone of IF fibers,which presumably is not contractile and may pre-sent less viscose resistance than the striated fibrillarstructure underlying the FS endings. Also thesecondary endings lie only on shorter IF fibers,most of which insert into the spindle capsule, sothat the endings would be affected by musclestretch only if this first lengthened the capsule;the major AS wrappings clasp the longer IF fibers,which pass beyond the capsule and must be directlystretched through their attachments to tendon andendomysium. As expected, the stretch needed forprimary afferents to assume a steady discharge isless than that of flower-spray units. Mean thresh-olds for units in soleus muscles, identified bytwitch response and axonal conduction rate, wasfor AS endings 3 gms., FS units 19, and TO'sover 100 gms.13 This general order of sensitivityhas been confirmed by other authors,2l-24 althoughit is said that in the tibialis anterior and extensordigitorum longus FS afferents have a lower thresh-old than AS endings.2s The differences in thresholdof spindle afferents mentioned above seem smallfor a muscle capable of exerting kilograms of ten-sion, but appear more significant if consideredrelative to muscie length, since at low tensions ex-tensive change in length is associated with smallalteration in tension.
Comparisons of the relation of frequency to
muscle length revealed little difference in summa-rized data from populations of the two types ofspindle endings 23 or randomly sampled units.24However, in an exacting experiment in which thedischarge from secondary and primary afferentsof the same tenuissimus spindle unit were mon-itored, secondary afferents exhibited greater
changes in discharge per unit stretch once theywere brought to flre (Fig. 8). If generally ap-plicable, this would imply that at greater degrees
r4
of passive stretch the FS discharge gained relativelyin volume and reflex influence.
AS and FS afferents are similar in their capa-bility for maintaining an afferent discharge forhours, that is, they both are "slow adapting."Tokizane and Eldred noted. however. that the end-
A F F E R E N T U N I T S F R O MS I N G L E O E - E F F E R E N T E D S P I N D L EI N T E N U I S S I M U S
G R O U P I F I E E R \
l O 4 m / s e c \ .
o 3 0 'zl
U
L - - o
cRoup n rreen--r ' i
[ , I A X I I V U MP H Y S l O L O G I C A L
L E N G T F I
. ^ 3 5 m / s e c :l u - o
O m m 5 r 0 1 5LENGTHE N ING
FlG. 8. Comparison of discharge rates at increasing musclelengths of group I and group l l afferent f ibers from a single-spindle in the cat 's tenuissimus muscle. Ventral roots sup-plying the muscle were cut. Afferents were thought toarise from the same sDindle because both were sensit iveto probing 0f essential ly the same site on this very tenuousmuscle. Conduction rates well above and below the valueof 70 m/sec. mark the one unit as an annulospiral (AS)afferent and the other f iber as a f lower-spray (FS) unit . Dis-charge of the FS ending had a higher threshold for onsetf ir ing, but thereafter gained relat ive to the AS unit. (Adaptedfrom Bessou and Laoorte.P)
T E NDONORGAN,INSERIES
MUSCLESPINDL E ,IN
PARAL LEL\> EXT RAFU SA L5\ TIBERS
Provided by the Maternal and Child Health Library, Georgetown University

ings differed prominently in their sensitivity tophasic stretch as evidenced by several character-istics in discharge behavior (Fig. 9)21:
1 The discharge of AS endings rose abruptlywith sudden extension of the muscle and then fellmore gradually to a tonic level of discharge ap-propriate to the new length. The discharge ofsecondary endings exhibited little of this over-shoot effect.
2. AS units were more prone than FS units toshow an "early discharge" preceding the character-istic pause in firing during a twitch of the muscle.
3. AS units displayed bursts of excessive dis-charge upon the return of firing during musclerelaxation, and these were frequently followed bya secondary pause in discharge. The discharge ofsecondary endings, in contrast, resumed essentially
the control rate of discharge upon re-extension ofthe muscle.
4. A long pause in discharge after release ofpassive muscle stretch 1e was characteristic of ASafferents, but scarcely evident for FS units.
5. Even during steady stretch th"e greater phasicsensitivity of the AS afferents was probably re-flected in the wider variability in interspike inter-vals of the discharge (Fig. 10).21
The greater phasic sensitivity of primary endingsrelative to secondary endings has since been studiedin detail under varying rates and degrees of linearand alternating stretch.2s' 24 2()-3o These find-ings show that AS endings exhibit the charac-teristics of both slow and rapid adapting receptors,whereas the secondary ending behaves as a re-ceptor of little adaptation. It is speculated that
. . \ 5 O g m s n l 2 O g m s
P R I M A R Y E N D I N G 9 O m / s e cr I ) l
4 0 m , z s e c
mS E C O N D A R Y E N D I N G
L l r l j r I I I l l
P R I M A R Y E N D I N G K C t L f 1
S E C O N D A R Y E N D I N G
POST-STRETCH PAUSE
o . 5 s e c .
FlG. 9. Comparisons in discharge patterns of a primary gas-trocnemius afferent conducting at 90 m/sec., and a secondaryun i t ,40 m/sec . , under p rocedures favor ing phas ic change.The rows of traces at the top show discharges during non-isometric twitches of the muscle under several loads. Dis-charge of the primary ending shows a burst of acceleratedactivi ty during the relaxation phase, and at the lesser loadsa secondary pause in f ir ing. These features are absent orfeeble in traces from the secondary ending. The "earlydischarge," several closely grouped spikes appearing beforethe primary pause in spindle discharge and seen in the 200
gm. twitch response of the primary ending, is more prominentin AS units. The Iower four l ines of continuous record showresponses to maintained stretch of the primary ending aboveand the secondary below the basel ine. 0nset of the passivestretch induced a greaier overshoot in afferent discharge ofthe primary afferent, and after release a long pause in dis-charge ensued before a stable rate of discharge was re-establ ished. These several indices show that the AS endinghas greater sensit ivi ty to phasic change than AS afferents.(From presentation by Tokizane and EIdred. '1)
Provided by the Maternal and Child Health Library, Georgetown University
I 5

4 5 G m s 5OO msec
O Grns
S EQU E NCE OF INTERVALS
roo
@J
EtrJFz
l-rJ)<o-aE.LdFz.
u_oazoF
Elo
200
r5of
47 Gms
145
2to
FlG. 10. Contrast in regulari ty of interspike intervals in dis.charge from a deafferented gastrocnemius secondary afferent( left column) and primary afferent (r ight). A record similar tothe samples at the top was projected to permit measurementof each interval, and these durations then plotted along the
the phasic component of the AS discharge be-havior arises in just those spirals of the total ASterminal that clasp the nuclear-bag region of theIF fibers. If this region is less viscose than thestriated poles, it would temporarily undergo excesslengthening with rapid loading, only to subse-quently shorten as the viscose resistance of thestr iated pole gave way under the stress.:r ' le ' 31
4. Central Connecl ions
Differences in central distr ibution of spindleaxons strengthen the argument that there are twobasic types of sensory innervation. All spindleafferents. of course. have cell bodies in dorsalroot ganglia or the mesencephalic nucleus of thefi f th nerve. With degeneration techniques, axons,tentatively identified as primary afferents by theirunsurpassed large size, have been traced histolog-ically to synaptic junctions directly on fifth nervemotoneurons.s2 This monosynaptic l inkage by
r6
ordinate to form one of the curves at the bottom. Curveswere constructed under several loads applied t0 the muscle.The greater variabi l i ty in intervals of discharge from the pri .mary ending is evident both in the sample records and the de-rived curves. (From presentation by Tokizane and Eldred.,1)
larger muscle afferents has also been abundantlydemonstrated through careful timing of motoneu-ron responses as monitored from their axons inventral roots or cel l bodies in the cord. Moreover.selective adequate activation of large afferentsfrom spindles or tendon organs by minute phasicpul ls on muscle in lax or contracted states, re-spectively, demonstrated that spindle afferents,and not TO's, produced the monosynaptic re-sponse.!e None of these experimental approachesrevealed direct connection by group II afferents.The two spindle afferents also dif fer in the topo-graphical patterning of potential changes they in-duce in areas of the dorsal horn and intermediatenuclei of the spinal gray matter,;J;r and in theirrelat ive contr ibutions to spinocerebellar path-ways .2e
Difference in distribution of afferents impliesdist inct ion in ref lex effect and. indeed. there is asharp but poorly understood difference in the re-
Provided by the Maternal and Child Health Library, Georgetown University
5OO m sec

sponse to st imulat ion of secondary and primaryspindle afferents. The latter through their mono-synaptic connections on motoneurons give r ise tothe myotatic reflexes, which are characterized bystrong faci l i tat ion of homonymous motoneurons.weaker faci l i tat ion of synergists, and concurrentindirect inhibit ion of antagonist motoneurons (Fig.1 I ). Group I afferents in muscles of one func-t ional type, e.9., extensors, faci l i tate extension andlessen action in the antagonist flexors, while thosein the opposing flexors do the opposite to yield a"double reciprocal innervation." The reaction fromstimulation of group II afferents, as achieved bydifferential stimulation of axons in peripheralnerves, is not doubly reciprocal, for these afferentsin both major muscle groups facilitate flexor con-tract ion (Fig. 12). This contrast in ref lex effect,perhaps more than any other feature, demonstratesthe signif icance of the dual dif ferentiat ion amongspindle afferents.
EVIDENCE FOR TWO TYPES OFINTRAFUSAL FIBERS
In Weismann's 1861 descript ion of the frog spin-dle, an eight-fold range in cross-sectional diametersof muscle fibers within a spindle was noted. Heused the term "mother fibers" to distinguish thelarge units from the "daughter fibers" and to indi-cate their supposed relationship in myogenesis.Beale disagreed with Weismann and Kcilliker "thatthe flne muscle fibers result from longitudinal split-t ing of wider f ibers," and with this a controversystarted that was st i l l the subject of warm debatenearly a century later.sa It is now generally agreed,however, that in the grown animal the larger fibersof spindles are entirely separate units, and thatthe smaller IF fibers similarly are discrete, thoughoccasionally small fibers may branch. In retro-spect, many indications for the existence of twotypes of IF fibers are to be found in older liter-ature. The statement, for example, that "musclefibers, generally two, sometimes three in number,enter the spindle at one pole and pass through tothe opposite pole; at the equatorial region thesemuscle f ibers undergo division" (Batten, 1898)might be interpreted as indicating the presence offibers of differing length and attachment. Thewide range in size of IF f ibers as seen in spindlecross sections is commented upon or incidentallyillustrated by a number of authors. One recentphotograph of a human lumbrical muscle spindle,for instance, shows two fibers that have areas fourand seven times as great as any of the three smallfibers.35 This is extreme and in most muscle, theratio is only two or three to one (Fig. 13 ) .Cuajunco, from measurements on a small sampleof pig and human IF fibers, was prompted to clas-sify them into "large, small and intermediate" cate-gories, the last group containing less numerous,transitional forms.s{i' 37 However. iustification and
ANNULOSPIRALIN EXTENSOR
GROUP IoFIBER
FACILITATIONOFEXTENSORS
INHIB IT IONOFFLEXORS
FlG. 11. Reflex effects of st imulat ion of group Ia f ibers,that is, AS axons, in the vastus intermedius muscle. Str0ngfaci l i tat ion of the same muscle and weaker faci l i tat ion ofsynergist ic extensors at the same and nearby loints occurs.C0ncurrently, the antagonist f lexors are inhibited.
FLOWER -SPRAYIN EXTENSOR
GROUP IFIBER
INHIBITION
OFEXTENSORS
FACILITATIONO FFLEXORS
FIG. 12. Ef fects of f lower-spray ending discharge in theknee extensor. Inhib i t ion of the same muscle and synergistsdeveloDs wi th faci l i tat ion 0f f lexors. FS af ferents in f lexormusc les a l so f ac i l i t a t e f l e x i on .
Provided by the Maternal and Child Health Library, Georgetown University
t 7

li:l:: . : . : . : .
l : : i l : : :
i i i : ; : t :i ; l ; i ; i ;
i ; : : : : : :
iiiiiiii; i ; l ; i ; i
: i : i : i : i
i : : : : : : :. : . : . : - :
i:i:i:ii. : . : . :. : . : . :
, : ' i ' :
aE.trJml!
LoE l0LrJm
lz.
20
LARGESMALL
DIAMETER OF F BERS
FlG. 13. Cross section of individual spindle and histogram made of populat ion of gastrocnemius intrafusal f ibers to showseparation of lF f ibers into two groups upon basis of size. The section and measurements were taken just distal t0 thenucleated regions of the f ibers. Two large "nuclear-bag f ibers" and f ive small diameter "nuclear chain f ibers" are seen inthe center 0f the intracapsular space. The smaller number of large f ibers as compared to small ones is ref lected in thehistogram also. An arteriole and bundle oi axons are embedded in the r ight side of the capsule.
criteria for his categories are not clear from thestatistical data furnished, and more important,Cuajunco, who has been the foremost student ofspindle development, considered these types tobe merely "different stages in the development of[spindle] muscle fibers." This view was shared byone recent worker.38
Clear enunciations of the concept that theremight be two distinct morphological types of IFfibers were advanced at about the same time byI. A. Boyd,3e Cooper and Daniel,e0 and L.Walker.al The latter presented histograms ofcross-sectional sizes of IF fibers from a populationof spindles in the dog's sphincter ani muscle, whichdemonstrated that the IF fibers fell into two fairlydistinct groups, rather than at the poles of a uni-modal distr ibution curve (Fig. 13).e' 34' 42 The
1 8
other authors stressed the conformation of thenucleated region, and Boyd designated two typesof fibers, "nuclear-bag" and "nuclear-chain IFfibers," from a difference in arrangement of thenuclei. These terms have wide acceptance, butmore recently attention has been directed to yetanother structural feature that may bear significantfunctional consequence and the terms "percap-sular fiber" for longer IF fibers and "intracap-sular" for the shorter fibers have been suggestedfrom the relationship of these flber types to thespindle capsule.a3 Whatever terminology is se-Iected, the assignment of a given IF fiber to oneof the types should rest upon a triad of criteria(Fig. la): (1) the form of the central nuclearaggregate, (2) the flber length and attachmentwithin or beyond the capsule, and (3) the cross-
Provided by the Maternal and Child Health Library, Georgetown University

sectional size of the motor pole. Other character-istics such as appearance of myofibrillar fields incross sections, or length of myonieres seem tobe too variable for effective use, although elec-tronmicrography may yet reveal some fine cyto-logical differentiation (Fig. 8 in Merrillees).aaThe value of respective criteria varies with differentmuscles. In spindles of the pig biceps brachiimuscle, all IF fibers have several nuclei on cross-sectional view. that is, a bag conformation.sG Thesame is true in human lumbrical muscles 10 andseveral rabbit muscles.45, 46 At the other extreme,human extraocular muscle IF fibers rarely displaya nuclear-bag conformation.aT Intrafusal fibers insome small rnuscles of the foot are not distinguish-able on the basis of cross-sectional size, but arein others.e' 48 Furthermore, as Cuajunco pointedout, in a population of fibers there are transitionalforms.sa' 36' 42 Fibers of unquestioned nuclear-bagconformation within one encapsulated region mayeven change to a chain form within an adjacenttandem-linked spindle.s, ra Despite these de-tractions from credibility of the concept, it appears
that at least five investigative groups recognizethe,existence of two more-or-less distinct histo-logical types of IF fibers in mammalian spin-d les .8 , e , 10 , 41 , 48
Monitoring of electromyographic potentials inthe vicinity of a spindle,4e or observation ofchanges in a spindle's afferent discharge followingstimulation of its motor fibers,22 have failed toprovide evidence of contractions in IF flbers otherthan the propagated twitch contractions seen inboth fast and slow mammalian extrafusal muscle.Upon direct visual observation of IF fiber con-tractions in the cat tenuissimus preparation, fastand slow contractions can be discerned,sO but thisobservation does not necessarily indicate the pres-ence of metabolically different contractile mecha-nisms, since differences in visible deformation of thespindle following motor axon stimulation couldarise if some IF fibers inserted into a resistantspindle capsule, while others passed freely beyondthe capsule.
Indirect evidence suggests a dif ferential chemicalsusceptibi l i ty of the two types of IF f ibers. The
BAG
FtBERSTf f i
FlG. 14. Concept of the di f ferent iat ion of mammalran lF f ibers i ; r to two basic types. Each spin,J le has typical ly two f iberswhich are large in d iameter, re lat ively long, and are dist inguished by the presence at their midlength of a i iuster-of vesicularnuc le i . 0 The same sp ind le has t h ree o r mo re sma l l e r f i be r s w i t h cen t ra l nuc le i a r r ayed s i ng le - f ; l e as i n a cha in . These"nuclear-chain f ibers" do n0t usual ly reach beyond the l imi ts of the capsuie as do the "nuClear-bag f ibers, , , but rather in-sert into the capsule wai l and at tendant connect ive t issue. The terms "percapsular" and " intracapiular . f ibers" have oeensuggested to stress th is d i f ference in insert ion, which may be s igni f icant te funct icns of the two tyoes of f iber. lB Brarchingof the srnal ler f ibers may occur, but is not common. The insert , based ui . rcn a spindie studieC by Barker and Cole. ,1 r j is-p lays more real is t ical ly the dist r ibut ion of nucle i . ( lnsert adapted f rorn Barker and Cope.11)
TRAFUSAL
CAPSULE
cHArN FTBERS j
FIBER
Provided by the Maternal and Child Health Library, Georgetown University
19

agent acetylcholine, its homologues like succinyl-choline, and anticholinesterases cause strong ac-celeration of spindle afferent discharge. This effectapparently results from contracture induced bythe drug in IF fibers, rather than any direct actionon the sensory endings.sl The acceleratory effectupon AS discharge is far greater than on FS dis-charge.52-51 This suggests that nuclear-bag IFfibers are distorted more by the drug action thanchain fibers, since both endings wrap about chainfibers and would be affected by these fibers more orless equally, whereas the bag fiber supports onlythe AS ending.
THE EVIDENCE FOR A DUALFUSIMOTOR INNERVATION
l. Motor EndplatesRecognition of a cross-striated, myofibrillar
structure in IF fibers resembling closely that inextrafusal (EF) fibers suggested to the earliestobservers that IF fibers should also have an efferentinnervation, and indeed, the "nerve tufts" to spin-dles were thought to be entirely motor. Para-doxically, the motor endplates were not identifieduntil descriptions by Cajal and Kerschner appearedin 1888. Their efforts to interpret spindles with
intact innervation were hindered by the complexityof terminals in an end organ which may have as
many as twenty-six entering axons,1o and theirviews did not go unchallenged. Ruffini, for exam-ple, thought the "plate endings" were a third type
of spindle sensory receptor, a view he again
stressed 5 after Sherrington failed to find degen-
erated endplates in spindles following ventral root
section nor even significant change in the IF fibers
themselves.a Sherrington pointed out that this
latter finding did not prove the absence of motorinnervation of IF fibers, but only the independenceof these fibers from trophic efferent influence. As
late as 1927 authots who had made intensivestudies of developing spindles 36 and of deaffer-
ented material 55 had difficulty identifying motor
endplates in spindles. Cipol lone, however, hadgiven direct proof of IF motor innervation by his
demonstration of degenerated plaques upon thesefibers one week after temporarily compressing the
rabbit 's abdominal aorta to bring about necrosis of
anterior horn cells. Later authors supported this
observation from rhizotomized preparations, andcollateral evidence that the IF plaques are motor
came from the demonstration that they appear
later during embryonic development than sensoryendings.3? Basic phylet ic dif ferences in motor in-
nervation were recognized, a participation by the
sympathetic system excluded. and the mult iple in-
nervation of individual IF fibers and multisegmen-
tal supply of the axial bundle were demonstrated.
Amid all these discoveries, the impression that
spindles had a single system of efferent innervation
persisted. For example, Barker's authoritat ive
20
1948 review and description based upon a detailedserial reconstruction of neural-stained sections ofthe rabbit spindle mentions only the presence ofthe miniature plaques of Ruffini.ai
Attempts to uncover a dual fusimotor mecha-nism in the spindle seem to have followed the dem-
onstration in frog muscle of a distinction i;etween"tonic" and "twitch" extrafusal fibers.56 TwitchEF fibers were found to respond to single indirectstimuli by propagation of a wave of excitation overthe membrane surface and an attendant total,brisk contraction; axonal stimulation of slow, tonicfibers caused local, nonpropagated depolarizationand associated contractions slowly developed onlyafter repetitive stimulation. Motor endings onthese two types of EF fibers were morphologicallydistinct. This plan of organization was found to
extend to the frog spindle where IF fibers were
separable into two types which in reaction re-
sembled the EF slow and fast fibers, and further-more, were innervated by branches of the axonsto these two EF types.i'6 Two types of IF motorending were demonstrated ;7 and it appeared prob-
able that each was restricted to one type of IF
fiber. In mammals, fibers with nonpropagated ex-citation have not been demonstrated in skeletalmuscle, but the distinction of "slow or red" and"fast or pale" motor units, sometimes within thesame muscle, is well recognized. Thus in analogywith the paral lel dist inct ion among EF and IFf ibers in the frog, the mammalian spindle might be
expected to have two types of contractile fiber and
motor innervation.Recently, two configurations of motor terminals
on mammalian IF f ibers have been dist inguished by
several authors, who do not agree, however, upon
the distr ibution of these terminals. Boyd stoutly
maintains that each type of motor ending is re-
stricted to one type of muscle fiber.e His "nuclear-
bag intrafusal fibers" are supplied, generally at
both motor poles, with one or a few endplates not
dissimilar except in size to those on extrafusal
muscle (Fig. 15). These are the motor terminals
of older descript ions. The other endings are re-
str icted to chain f ibers and appear in deafferentedpreparations as beaded f i laments and networks
coursing longitudinal ly on the juxtanuclear port ions
of the IF f ibers. Barker and his co-workers also
dist inguish somewhat comparable types of end-
ings.s They bel ieve, however, that neither motor
ending is restr icted as to the type of IF f iber i t
innervates and some IF f ibers carry both kinds of
motor terminals. Contr ibuting to this divergence
in opinion is choice of technique, for although both
investigative groups have used several staining
techniques, Boyd prefers gold-impregnated prepa-
rat ions of teased total spindles, whereas Barkerand his co-workers have principal ly based their
conclusions on painstaking reconstruction of si lverstained serial sections. Cooper and Daniel, who
are the only other investigators intensively ap-
Provided by the Maternal and Child Health Library, Georgetown University

AXON
i rHREET, axorus
7, axoru
D rHnrr (raxo
( END-PLATE ON CHAIN F IBER
FlG. 15. The fusimotor innervation of a spindle as conceived by L A. Boyd.e The large "nuclear-bag f ibers" are innervatedexclusively by several "gamma efferents" that lead to small but otherwise fair ly typical motor endplates scattered along bothstr iated poles of the f iber. The more numerous "nuclear-chain f ibers" receive somewhat smaller g?mff iar f ibers" whichend in "narrow, elongated, del icate structures l inked by very f ine axon branches and frequently arranged in a row end toend. ." (Based upon figures by Boyd.0)
THRE E 4 'AXONSI
plying several histological techniques to the studyof spindle structure, tentatively recognize motorendings of two types,1O which seem to be restrictedto innervation of specific IF fibers. Codrs, with theintravital methylene-blue technique, distinguishedtwo patterns of motor ending but did not assignthem to fiber types.58
Additional evidence for two forms of IF motorendings derives from the staining of spindles forcholinesterase, an enzyme that is concentrated atmotor endplates. Codrs, using this technique onintact spindles, noted discrete concentrations thatresembled extrafusal endplates and originatedfrom medium-sized axons, as well as zones of "ex-tended and loose arborizations" lying just distalto the central nucleated regions and arising fromsmall nerve fibers.58 He did not determine whetherboth types lie on a single IF fiber. Since the zoneof diffuse staining coincided more or less with thedistribution of the flower-spray endings, CoErs, inearlier publications appearing before the possibilityof a dual motor innervation had been raised, ques-tioned whether flower-spray terminals had beenmisinterpreted and were, in fact, motor endings.Hess, simplifying interpretation through use ofchronic deafferented preparations, has also shownthe persistence of a secondary zone of "diffusemultiterminal endings" lying between the scatteringof "discrete motor endplates" and the unstained
n,END-PLATE ON BAG FIBER
equatorial region but did not relate these endingsto specific types of IF fibers.5e Kupfer from ob-servations on human extraocular muscle spindlesrecognized that the smaller IF fibers displayeddiscrete loci scattered along the motor poles, whilethe "medium sized" IF fibers had both the smallscattered loci and other more typical motor end-plates.6o His view of the innervation pattern isthus intermediate between those of Barker andBoyd. It should be pointed out that with thecholinesterase staining procedure carried out onfixed histological material, definition of very fineloci of activity may be blurred. Staining andmicrochemical analysis of unfixed muscle demon-strates that the IF fibers themselves have an activitythree times that of extrafusal tissue, introducingfurther difficulty in interpretation.6l Nevertheless,the histochemical evidence strongly suggests thepresence of two different motor endings, both ofcholinergic type; it does not contribute much tothe problem of the distribution of these endings tointrafusal fiber types.
2. Efferent Axon Sizes
The smaller size of IF fibers and fewer numbersof these fibers per "motor unit" as compared toextrafusal fibers suggest that fusimotor axons tospindles should lie toward the small end of thespectrum of motor axon sizes. It could be argued,
2L
Provided by the Maternal and Child Health Library, Georgetown University

GASTROCN EMH ISTOG RAM
IUS NERVE
2 0 0
aEIJcDlr-
tL
EUJm
lz
t 5 0
r 0 0
5 0
4 8 1 2 1 6
AXON D IAMETER
FlG. 16. Separation of gastrocnemius muscle nerve f ibers into two categories by measurement of diameters. Photograph atleft i l lustrates appearance ot osmic.acid-stained myelin sheaths of.axons that are measured to construct distr ibutional graphs
relat ing number oi a*ons to their diameter. The histogram reveals a separation into small- and large-size groups. (Histo-gram adapted from Rexed and Therman.6')
on the other hand, that timing requirements ofspindle function which dictate that AS afferentshave the largest sensory axons in peripheral nervescould also require rapid-transit motor control. Theappearance of axons as they enter the spindle isnot fully helpful in answering this question, sinceaxons to extrafusal muscle branch so profusely thatterminal twigs are equal or smaller in diameterthan axons entering spindles.8 Nevertheless, in his-tological accounts the motor innervation of spin-dles is generally ascribed to small myelinated fibers'The existence of a distinct group of small calibersomatic efferents (Fig. 16) was pointed out byEccles and Sherrington, though surprisingly theydid not ascribe any of them to IF innervation.G3Raising the strength of stimulation to a musclenerve to add these smaller fibers to the excitation of
22
large axons did not contribute to further increase in
tension, leading to the conclusion that the smallaxons did not innervate extrafusal motor units.64The direct demonstration of the innervation ofspildles by small efferents and their capability for
modifying the afferent discharge was given by
Leksell using differential blocking techniques on
whole nerves,65 and by Kuffier, Hunt, and Quilliamthrough stimulation of isolated motor axons of
measured conduction rate.66 In both methods ex-
amination was made for changes in afferent dis-
charge to reveal effects on the spindles. Axons
innervating IF fibers were found to conduct at
rates less than 55 meters/sec. This places them
among fibers causing the delayed "gamma" hump
in the neurogram recorded along a muscle nerve
trunk distant to a point of st imulat ion (Fig. 17).
Provided by the Maternat and Child Health Library, Georgetown University-
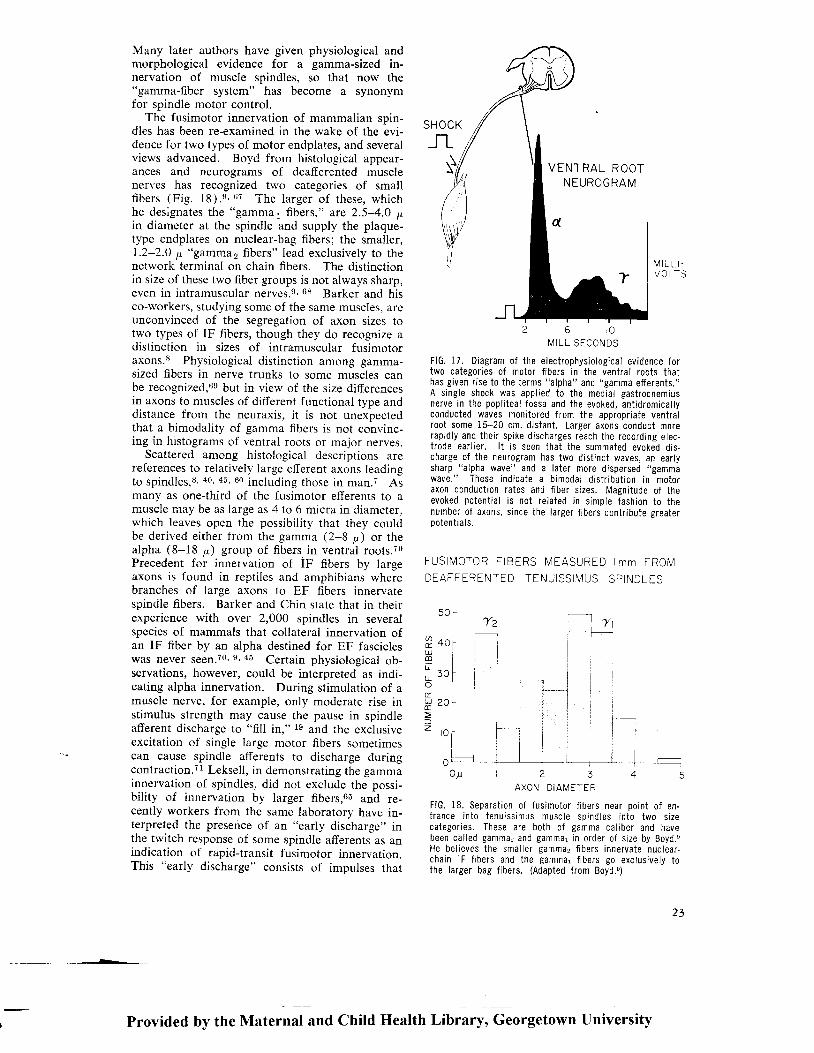
Many lerter authors have given physiological andmorphological evidence for a gamma-sized in-nervation of muscle spindles, so that now the"gamma-fiber system" has become a synonymfor spindle motor control,
'fhe fusimotor innervation of mammalian soin-
dlcs has been re-examined in the wake of the Lvi-dence for two types of motor endplates, and severalviews advanced. BoyC from histological appear-ances and neurograms of deafferented musclenerves has recognized two categories of smallf ibers (Fig. 18).s' er The larger of these, whichhe designates the "gamma, fibers," arc 2.5-4.0 p.in diameter at the spindle and supply the plaque-type endplates on nuclear-bag fibers; the smaller,1.2-2.0 pr. "gamma2 fibers" lead exclusively to thenetwork terminal on chain fibers. The distinctionin size of these two fiber groups is not always sharp,even in intramusculal 1s1yss.e, 68 Barker and hisco-workers, studying some of the same muscles, areunconvinced of the segregation of axon sizes totwo types of IF fibers, though they do recognize adistinction in sizes of intramuscular fusimotoraxons.E Physiological distinction among gamma-sized fibers in nerve trunks to some muscles canbe recognized,6e but in view of the size differencesin axons to muscles of different functional tvoe anddistance from the neuraxis, it is not unexbectedthat a bimodality of gamma fibers is not convinc-ing in hrstograms of ventral roots or major nerves.
Scattered among histological descriptions arereferences to relatively large efferent axons leadingto spindles,s' 40' 45, 60 including those in man.7 Asmany as one-third of the fusimotor efferents to amuscle may be as large as 4 to 6 micra in diameter.which leaves open the possibility that they couldbe derived either from the gamma (2-8 p) or thealpha (8-18 p) Broup of f ibers in ventral roots.?0Precedent for innervation of IF f ibers by largeaxons is found in reptiles and amphibians wherebranches of large axons to EF fibers innervatespindle fibers. Barker and Chin state that in theirexperience with over 2,000 spindles in severalspecies of mammals that collateral innervation ofan IF fiber by an alpha destined for EF fascicleswas never seen.To' e' 45 Certain physiological ob-servations, however, could be interpreted as indi-cating alpha innervation. During stimulation of amuscle nerve, for example, only moderate rise instimulus strength may cause the pause in spindleafferent discharge to "fill in," ts uo{ the exclusiveexcitation of single large motor fibers sometimescan cause spindle afferents to discharge duringcontraction.Tl Leksell, in demonstrating the gammainnervation of spindles, did not exclude the possi-bility of innervation by larger fibers,6r and re-cently workers from the same laboratory have in-terpreted the presence of an "early discharge" inthe twitch response of some spindle afferents as anindication of rapid-transit fusimotor innervation.This "early discharge" consists of impulses that
I \ 4 I LL ISECONDS
FlG. 17. Diagram of the electrophysio logical evidence fortwo categor ies of motor f ibers in the ventra l roots thathas given r ise to the terms "alpha" and "gamma ef ferents."A s ingle sh0ck was appl ied to the medial gastrocnemiusnerve in the popl i teal fossa and the evoked, ant idromical lyconducted waves moni tcred f rom the appropr ia ie ventra lroot some 15-20 cm. d istant . Larger axons conduct morerapidly and their spike discharges reach the recording elec-t rode ear l ier . l t is seen that the summated evoked dis-charge of the neurogram has two dist inct waves, an ear lysharp "a lpha wave" and a later more dispersed "gammawave." These indicaie a b imodal d ist r ibut i0n in motorax0n c0nductaon rates and f iber s izes. Magni tude of theevoked potent ia l is not re lated in s imple fashion to thenumber of axons, s ince the larger f ibers contr ibute greaterpotent i a ls .
FUSIN /0TOR F iBERS MEASURED lmm FROMDEAFFERENTED TENUISSIMUS SPINDLES
l \ 4 t LL t -VOLTS
5 0 rT2
4 0 f
i i3 0 [
i
'ilt-I
O y t 2 3 4AXON D IAMETER
F lG .18 . Sepa ra t i on o f f us imo to r f i be r s nea r po in t o f en -t r ance i n t 0 t enu i ss imus musc le sp ind les i n t o two s i zecategor ies. These are both of gamma cal iber and havebeen cal led S?mma: and gammar in order of s ize by Boyd.nHe bel ieves the smal ler gamma, f ibers innervate nuclear-chain lF f ibers and the gammar f ibers go exctusively tothe larger bag f ibers. (Adapted f rom Boyd.0)
TIU)tu.lmL.
L
t
(!
lz
VENTRAL ROOTNEUROGRAM
Provided by the Maternal and Child Health Library, Georgetown University
23

arise before the characteristic pause in afferentfiring that accompanies active shortening of a
muscle (Fig. 9). I t may appear whether the con-traction is induced by nerve stimulation at anintensity just sufficient to excite alpha fibers,72 73
local reflex elicitation,Ts or supraspinal stimula-tion.Ta The early discharge could have severalcauses among the temporally and spatially com-plex events that occur in contraction of a totalmuscle,7l but these are excluded in those instancesin which early effects on spindle discharge were
obtained without detectable change in tension at
the tendon.?3 This indication that some large fibersinnervate spindles exclusively is opposed to otherevidence that all alpha efferents set up twitch-typecontractions in EF motor units.71 Alpha f iber in-nervation also seems to have been demonstratedin a study of temporal relations of the effect onan isolated afferent unit from stimulation of singleefferent fibers in the lumbrical muscle.?5 In eval-uation of this physiological evidence, it must beremembered that occasionally extrafusal fibersmay terminate on the capsule, pass through it,
or even undergo transition to IF fibers.8' 10' 31i' '1:r' 48
However, the short-delay spindle effects were seenwith too many afterent units to admit this explana-t ion.75
In an early brief report of a study of histogramsand neurograms of the deafferented tenuissimusnerve, Boyd recognized "beta," as well as alphaand gamma efferent categories.T6 In his mono-graph 8 the term "beta" is not used, being replacedapparently by his "gamma"' designation. How-ever, recently the term "beta fibers" has been re-
introduced for relatively fast conducting spindleefferents in analogy to a "beta" ( i .e., slow-conduct-ing) innervation in some mammalian muscle.77Thus there are current claims for alpha, beta,gammal, and gamma2 categories of fusimotorfibers! This plethora arises from methodologicaldifferences in measurement of conduction rates bythe several authors, expected variation in the motoraxon sizes characteristic of various muscles, andchoice of terms. It should not obscure the factthat all authors recognized fusimotor fibers oftwo different sizes.
3 . ln ie r re la t ion o f Dua l Mo ior andSensory Innervafions
The role of fusimotor innervation is enhance-ment of sensit ivi ty of the afferent terminals (Fig.
I 9 ) .air, ?8-to Intraf usal fibers are too small andfew to make any detectable contribution tomuscle tension even under generalized excitationinduced, for example, by st imulat ion of faci l i tatoryareas in the ret icular formation.8l Decelerationof discharge from secondary endings could con-ceivably occur, since these l ie along str iated por-tions of the IF fibers where contraction might re-lease them from stress. Inhibit ion, of dif ferentmechanism, is a prominent feature of stretch re-
24
ceptor organization in the crustacean. However,most observations indicate that FS terminals in themammalian spindle are made more responsive byincreased fusimotor activity. Slight lowering ofstatic sensitivity of AS endings with fusimotorstimulation has been described.6E, 7e
Information on spindle organization suggeststhat the dual fusimotor innervation could serve todifferentially affect the two types of sensory end-ings. If one type of fusimotor innervation is re-stricted, as Boyd believes, to chain IF fibers, theactivity of FS endings which are almost entirelyrestricted to these fibers could be enhanced with-out effect on the AS endings. Discharge of ASendings on the other hand would be presumablysubject. to change regardless of pattern of motorinnervation of IF fibers, since branches of eachAS terminal typically wrap about all IT fibers.
Qualitative differences in AS discharge could stillresult from changes in the balance of fusimotoractivation to bag and chain fibers, if phasic sensi-t ivi ty of the AS ending depended on those spiralson the nuclear regions of bag fibers and the staticsensitivity arose chiefly from wrappings aboutchain fibers. Peter Matthews has brought forthmuch evidence that such qualitative differentia-tion in sensory effect of fusimotor activity doesoccur.?e, t0 Some isolated ventral root fibers, the"dynamic fibers," when stimulated caused in-creased sensitivity of an AS ending to phasic aswell as tonic stretch (Fig. 20). Other fusimoto-neurons, the "static fibers," increased sensitivity ofthe same afferent only to static stretch. Thus thedual motor innervation had qualitatively differenteffects on a single sensory ending. Stimulation ofstatic fusimotor fibers, as expected, may affect theresponse of FS endings to static stretch, whereasstimulat ion of dynamic f ibers is without effect.6E
THE CHOICE IN INTRAMUSCULARVARIABLES
The duality in IF fiber, efferent and afferentneural organization, and the dichotomy in reflexeffects of the afferent discharge are comprehensiveargument that the mammalian spindle fulf i l ls twodist inct sensory roles. The question then fol lows:What variables in intramuscular status are moni-tored? There are several to consider.
l . Tens ion
If rate of spindle discharge is plotted againstmuscle tension the curve approaches a plateau athigher tensions, but i f the rate is plotted againstlength the curve is nearly l inear.8:r Spindle dis-charge, then, becomes progressively less sensit iveas an indicator of tension at greater degrees ofstretch, but continues to have unchanged effect ive-ness in gauging length. Moreover, spindles may beincapable of rel iably monitoring tension in a con-tract ing muscle. A r ise of one ki logram in tension
---Provided by the Maternal and Child Health Library, Georgetown University

INTRAFUSAL FIBER
CONTRACTE
FIG 19. The prevai l ing, but unproven, concept 0f ihe ef fect of gamma ef ferent exci tat ion of lF f iber contract ion on the ASsensory terminal . Contract i le shortening of the str iated poles of the lF f iber st retches the nonstr iated, and presumably non-c0ntract i le, nucleated zone of the f iber. Sens0ry terminals wrapped ab0ut th is zone are stretched and their d ischarge in-creased. The fusimotor exci tat ion places the spindle terminal under "b ias" and increases i ts sensi t iv i ty to i ts adequate srrm-ulus, the stretch of neighbor ing extrafusal muscle.
at the tendon, for example, wi l l be associated withan increase in spindle f ir ing i f i t is induced bypassive pul l on the muscle, but could accompanydiminution in firing if the tension rise results frorncontracti le shortening. Tendon organs, on the otherhand, are in series between muscle and tendon inboth situations. Their rates of discharge in thestat ic state show in general a l inear correlat ionu' i th tension developed, reacting in this respect l ikeRuffini receptors of joints.sr
2 . S ta t i c Length
The prevai l ing concept of spindle functionholds that they gauge muscle length or, moreexactly, the length of those neighboring extrafusalfascicles which the spindle bridges. Both the dis-charge of secondary endings and the stat ic com-ponent of primary ending discharge exhibit the lowralues of adaptation required for continued sig-
nal l ing of stat ionary length. Attachments of spin-dles are suited to this purpose for motor poles ofthe longer IF fibers are fixed to endomysial or ten-dinous t issue. In muscles structured so that fas-cicles are a centimeter or less in length, spindlesmay bridge the entire distance between tendons oforigin and insert ion,as while in thicker muscles af i f th or more of the spindles may be l inked intandem,8':0 perhaps to give better representationof total EF fascicle length. Secondary endings arepredominantly associated with shorter IF f ibers,most of which insert into the spindle capsule,a3and could not gauge length unless the capsule it-self lengthened during muscle stretch. As passiveendings, they would be less suited than primaryendings for signal l ing length of the muscle, forsecondary endings often require some musclelengthening to attain a steady discharge. Thismay not be a physiological limitation, however,
E
Provided by the Ntaternal and Child Health Library, Georgetown University
25

since spindles in the intact animal are probablyunder tonic-fusimotor-induced bias which rendersthe endings more sensit ive (Fig. 21). In anyevent, it does appear that the levels of tonic dis-charge of both secondary and primary endings inthe passive state show an approximate linear cor-relat ion with gross muscle length.2? 24
3. Change in Length
An ending whose discharge correlates truly toabsolute muscle length under all conditions caneffectively signal changing length only if the periodof change is long relative to duration of interspikeintervals of the discharge. To illustrate, if thestable rate of receptor discharge at an initial lengthwere 20 pulses/sec, and at a greater length 30, andthe length changed over a period of 1 sec., the rateof length increase would be signal led by 10 or 11progressively shortening interpulse intervals. This
would perhaps be acceptable coding to permit ap-propriate reflex response to the lengthening (notjust the new static length). If the movement werefaster and lasted only 0.1 sec., at most only twointervals would be affected and reflex correctionmight not be appropriate to the violent movement.An ending in which the level of discharge was re-lated to velocity or acceleration of lengthening canrnore closely report the changing status and give
opportunity for reflex reaction. The primary
spindle ending through its "dynamic component" in
stretch sensitivity answers this requirement'24 In
reflex fusimotor control over the muscle, whether
in simple correction of errors in length under a
changing load or in "leading" the muscle to a new
state of contraction and length, absolute registra-
tion of length might not give the best functional
result. To make a comparison with servomecha-nisms, exaggeration in afferent signals during
PRIMARY AFFERENT D ISCHARGEDURING LENGTHENING
NO ST IMULATION
/t\STIM ULATIONOF DYNAM ICFUSIMOTOR F IBER
STIMULATIONOF STATICFUSIMOTOR F IBER
a+.-g*--
2 0 0
r o o
O / s e c .
M U S C L E5 I K E . I U r l i,'-S O L F U S
FlG. 20. Ef fect of fus imotor innervat ion on response pat tern
of a spindle af ferent to phasic stretch of the muscle. Thepr imary af ferent was isolated f rom a Corsal root leading f romthe cat 's leg, denervated except f0r tne soleus muscle. In-terspike intervais of d ischarge of th is af ferent are inverselyrelated to the heights of the response curves, that is , thehigher the resp0nse curve the greater the rate 0f d ischarge.From the ventra l root of the same segment, two ef ferentf i lannents l .vere isolated which upon repet i t ive st imulat ioncaused an increase in d ischarge of the s0leus uni t wi th0utinducing concomitant extrafusal contract ion. The muscle wassubjected to rapid stretch as indicated by the length t race atthe lower r ight . In the absence of ef ferent st imulat ion a r ise
26
in af ferent d ischarge occurred Cur ing the actual lengtheni ' lgand th is was fo l lowed by a s l ighi ly decaying plateau of ac 'celerated discharge at the new length (uppermost recorc, 'St imulat ion of one of the fusimotor f ibers, indicated by thehor jzontal bar beneath the record (second record), caused animmediate increase in basel ine rate of the spindle d ischargeand a great ly enhanced acceleratory response to ihe stretchwhen subsequent ly appl ied. Because of ih is ef fect on phasicsensi t rv i ty of the af ferent uni t , P. Matthews designaied th isef ferent uni t a "dynamic fusimotor f iber." The second or"stat ic fusimotor f iber" under s imi lar st imulat ion caused ar ise in basel ine discharge rate, but no increase in responseto the stretch (third record). (Adapted from Matthews'@)
Provided by the Maternal and Child Health Library, Georgetown University

MEDIAL GAST ROCNEMlUSINTACT
,aI
280UJfotrJE.t!
75"
DE-EFFERENTEt
40
/sec
U
2
go"
DORSIFLEXION
--: -r -75
t900
DORSIF LE X ION
1450 75"
f t145"
)
J
'/'./
,a-' /'lh'L =
a'--/--a
FlG. 21. Effect of " intrafusal bias" on rate of afferent dis.charge from spindles. One hindleg of a cat under l ight bar-biturate anesthesia was de.efferented to el iminate the tonicfusimotor discharge to spindles; ventral roots in the otherleg were intact. Both sides were denervated except for themedial gastrocnemius muscle, and ref lex contractions wereavoided by cutting the appropriate dorsal roots. The legswere f ixed in an automatic device that f lexed both anklesover the physiological range in 45 sec., thus stretching thegastrocnemius muscle. Spike discharges of spindle afferent
change in length over those appropriate to theabsolute lengths may serve to prevent oscillationswhich can develop in a simpler system having a flatresponse to "errors" in length.
Primary endings have also a "static component"in discharge behavior so that dynamic responses tochange in muscle length superimpose upon a levelof tonic discharge, rather than arise abruptly fromsilence in the way a Pacinian corpuscle responds.This slow adaptation component would permit theending to serve also as an indicator of static musclelength, though in this use interpretation of lengthfrom discharge rates would be misleading duringactual lengthening because of the added and pre-dominant rate changes arising from excitation of
units were monitored from dorsal roots, rates counted atseveral stages of f lexion and these plotted. Each sol id l inecurve represents the discharge rate of an individual soindreafferent and the dashed heavy l ine an approximate mean forthe family of curves. Al l units with intact fusimotor innerva-t ion discharged at the minimum extension of the muscle, butover 0ne-third of ihe demotored units were si lent. At sreaterextensions, rates on the intact side greai ly exceeded thoseon the de-efferented side. (From unpublished data by H. yel lrnand E. Eldred.)
the dynamic sensit ivi ty of the ending. An alterna-tive purpose, which relates again to function of theAS ending as a sensor of rate of length change, isthat the static sensitivity furnishes an elevated levelof discharge which can be either lowered or ele-vated by length changes. Thus the ending isalways ready to signal shortening of the muscle, aswell as lengthening. The fact that tonic levels ofprimary-ending discharge happen to show goodlinear correlation with muscle length may be anincidental consequence to the necessary struc-tural provision that IF fibers have fixed intramus-cular attachments in order to participate in thephasic length changes.
To summarize, the concept of the spindle as a
l Provided by the Maternal and Child Health Library, Georgetown University
27

dual gauge of muscular length would hold that ( 1)the registration of static muscular length would beserved by the secondary endings which have littledynamic sensitivity and could thus reliably indi-cate mean muscular length, even during movement,and (2) the primary endings signal rate of lengthchange.
4. Pressure
One functional characteristic of the flower-sprayafferents appears peculiar, if they, indeed, func-tion to gauge static muscle length and thereby pre-sumably play a part in governing contractile status.The pattern of reflex effect, homonymous inhibi-tion from endings in extensor muscles and homon-ymous facilitation from endings in flexor muscles,is not meaningful to the interpretation of myotaticmechanisms of whole muscles. I t should be con-sidered whether the FS endings may monitor yetanother variable in muscle status and serve someother pattern of reflex activity. Intramuscular pres-sure is one such variable.
The pressure within a muscle rises with pas-sive stretch, but is increased far more by activecontraction. The fluid-filled, fusiform capsule ofa spindle resembles a double-ended squeeze bulb,suggesting that this organ serves to register thesepressure changes. Electronmicroscope views ofthe capsule where it narrows down to form a collarabout the longer IF fibers show several regularr idges ( in frogs) which may be a gasket arrange-ment to prevent f luid escape (Fig. 22)'85 Direct,
solid contact by neighboring extrafusal fibers re-sulting in a vector of force directed normal to the
spindle axis is indicated by histological reconstruc-t ions, which show neighboring extrafusal warped
out of a straight-line course by the equatorialswelling of the spindle capsule.a3 Pressure gra-
dients directed poleward from the equator. such as
might develop during contraction of neighboringEF fascicles, could express intracapsular fluid to-ward the poles, increasing the over-al l length of the
capsule (Fig. 23). Shorter IF f ibers which insert
into the capsule would then be stretched and theirneural wrappings excited. These chiefly are the FS
endings, although AS endings would be affected in
the degree that their minor spirals clasp smaller IF
fibers. The capsttlar collar might slide freely along
the longer IF fibers, so that these would not be
affected by changes in capsule length per se. In
order for deformation to result from direct con-
tact pressure, intrafascicular tissue fluid surround-ing the poles of the capsule must be able to escape
through the intercel lular spaces along l ines of pres-
sure gradients. A contraction of the total muscle
with uniform rise in pressure throughout the
muscle could not lead to spindle deformation any
more than does increasing water pressllre actlng on
a ful l milk can sinking to the bottom of the sea'
Thus, afferent acceleration induced by the hypo'
thetical pressure mechanism could occur only in
subtotal, or topographical ly local ized, contractions.
This suggests that FS endings mediate reflexes re-
str icted to local areas or individual motor units of
FlG. 22. Drawing made from electronmicroscopic appearance of the relat ion of the capsule to an intrasufal { iber in an am-pr, i l i in .Jinor..-where the capsule "col lar" approache_s the lFf iber, several r idges, seen in cross secti0n on this l0ngitudinal
i i .*,-proi. . t t0 contact the surface of the lF f iber. These r idges possibly prevent escape of intracapsular f luid. (From
manusi:r ipt in preparation by U. Karlsson and E. Andersson-Cedergren ^')
2 8
I NT R ACAPSU L ARSPACE CAPSULE WALL
RIDGES INSIDE COLLAROF CAPSULE
J
a
Provided by the Maternal and Child Health Library, Georgetown University

In l rocopsulorI n f r o fuso l f i be r s
Perc opsu lor
the muscle, and thereby regulate the balance incontractile activity within the population of motorunits. It would follow that summed stimulationof all FS afferents in a muscle nerve gave a con,fusing picture of the reflex significance of FSendings. This argument, it should be recognized,is speculative and goes far beyond demonstratedproor.
CONCLUSION
This article cannot consider the large body of in-formation available on organization of myogenicreflexes, except to point out that many finer attri-
FlG. 23. Schematic diagram ofa mechanism in the musclespindle for transducing altera-t ions in intramuscular pres-sure into changes in sensorydischarge. (From Bridgman andEld red. '3)
butes of sensitivity, restraint, and co-ordinationwhich distinguish the activity of muscle must bederived from the feedback of data on moment-ro-moment status of the muscle. The three majorafferents transduce and transmit this data. Oneof these, the tendon organs, has no demonstratedmotor control and the measure it gives of statictension, and probably rate of tension change, bearsinvariable relation solely to the conditions of themuscle itself. The other two receDtors are moreadvanced in design in that their gain or sensitivityis susceptible to modulation by central influences.These sensors do not give absolute measure oflength or any other quality of the muscle, but only
zoo_
5
( J t
- Q <
5U Ct)' C l
v
Yt ,r--
oJ
(
\ t 4Q
Jo > r
3;qA
tq
to
Provided by the Maternal and Child Health Library, Georgetown University

a measure under a particular set of central and ex-ternal circumstances.
There is abundant indication that this modula-tion is not locked in step with central influence onthe alpha motor system, as occurs, for example, inthe frog muscle where branches of axons to EFflbers innervate also IF fibers. It is likely thatindependence in control, comparable to that be-tween mammalian alpha and fusimotor innerva-tion, exists also for the two types of fusimotorcontrol. Since the reflex effects of AS and FSdischarge on alpha motoneuron differ, it followsthat alpha output to the muscle is modifiable bytwo systems of central control additional to thosedirectly affecting the alpha motoneuron itself. Theinduced modifications in alpha activity must takethe form of changes in spatial and temporal char-acteristics of alpha unit activation. Ultimate un-derstanding of the composition of movement, then,must take into account the interplay by triplesensory influence, a dual motor-sensory modula-tion, and the reaction of the alpha motoneuron"final common pathwaY."
REFERENCEs
1.Eldred, E., Gadbois, L., Sweeney, S., agd.Yellin, H.:A Bibliogr'aphy on Muscle Receptors:.Their Jvlorphol-ogy, Pat-hology and Intrinsic Physiology. Riverside,California: Bibliographic Associates, Inc., 1965.
2. Matthews, P. B. C.: Muscle spindles and their motorcontrol, Physiol. Rev., 44:219-288, 1964.
3. Ruffini, A.: Sur la terrninaison nervelse dans lesfaisceaux musculaires et sur leur signification physi-o logique, Arch. I ta l . Bio l . , 18:106-114, 1893.
4. Sherrington, C. S.: On the anatomical constitution ofnerves of skeletal muscles; with remarks on recurrentfibres in the ventral spinal nerve-root, J. Physiol. (Lon-don), l'7 :217-258, 1894.
5.Ruffini, A.: Observations on sensory nerve-endings involuntary muscles. Brain, 20:368-374, 1891.
6.Ruffini, A.: On the minute anatomy of the neuro-muscular spindles of the cat, and on their physiologicals igni f icance, J. Physio l . (London), 23:190-207, 1898.
7.Gruner, J-E.: La structure fine du fuseau neuromus-cula i re humain, Rev. Neurol . (Par is) , 104:490-507,1961 .
8. Barker. D.: The structure and distribution of musclereceptors. In Barker, D., ed.: Symposium on MuscleReceptors. Hong Kong: Hong Kong Unirersity Press,1.962, pp. 227-240.
9.Bovd. I. A.: The structure and innervation of thenu6lelr bag muscle fibre system and the nuclear chainmuscle fibre system in mammalian muscle spindles,Phil. Trans. Roy. Soc. (London), 245:87-736,1962.
10. Cooper, S., and Daniel, P. M.: Muscle spindles in man;theii morphology in the lumbricals and the deepmuscles of the neck, Brain, 86:563-586, 1963.
I 1. Barker. D., and Cope, M.: The innervation of individualmuscie fibers. In Barker, D. ed.: Sy,nposiurn on MuscleReceptors. Hong Kong: Hong Kong University Press,i962. pp. 263-269.
12.Wohlfurt, G., and Henriksson, K. G.: Obsenations onthe distribution, number and innervation of Golgimusculo-tendinous organs, Acta Anat. (Basel), 4l:192-204, 7960.
i 3. Hunt. C. C.: Relation of function to diameter inafferent fibers of muscle nerves, J. Gen, Physiol.,3 8 : 1 1 7 - 1 3 1 , 1 9 5 4 .
14. Llovd. D. P. C., and Chang, H-T.: Afferent fibers hmuicli: nerves, J. Neurophysiol., lll.199-2O7, 1948.
30
15.Fulton. J. F.. and Pi-Suffer, J.: A note concerning theo.oUaUt" function of varibus afferent end-organs inikeleta l muscle, Amer. J. Phvsio l . , 83:554-561, 1928.
l6.Bvrnes. C. M.: A contribution to the pathology ofpiralysis agitans, Arch. Neurol. Psychiat., 1'5:407443,1926.
17. Matthews, B. H. C.: The response of a single endorgan, J. Physiol. (London), 71':64-710, 1937.
18. Matthews. B. H. C' : The response of e muscle spindledur ins act ive contract ion of a muscle, J ' Physio l .(London ) , 7 2 :153-17 4, 1931.
19.Matthews, B. H. C.: Nerve endings in,-mammalianmuscle, J. Physio l . (London),78:1-53, 1933.
20. Swett. J.. and Eldred, E.: Distribution and numbersof strbtch receptors in mediai gastrocnemius and soleusmuscles of the cat, Anat. Rec., l3'1 :453460, 1960.
21. Eldred, E., and Tokizane, T.: Two patterns of.afferentdischarge from muscle spindles, Amer. J. Physiol. 183:K l ) 1 0 < <
22. Bessou, P. and Laporte, Y.: Responses from primaryand secondary endings of the same neuromuscularspindle of the tenuissimus muscle of the cat. In Barker,D., ed.: Symposium on Muscle Receptors. Hong Kong:Hong Kong University Press, 1962, pp. 105-119.
23. Harvey, R. J., and Matthews, P. B. C.: The responseof de-efferented muscle spindle endings in the cat'ssoleus to slow extension of the muscle, J. Physiol (Lon-don), 157:37G-392, 1967.
24. Renkin, B., and Vallbo, A. B.: Simultaneous responsesof groups I and II cat muscle spindle afferents to musclepos-itiod and movement, Neirrophysiol., 27:42945O,7964.
25. Fehr, H-U.: Aktivitiit der Muskelspindel-Endigungender Fasergluppen I A und II als Funktion der Muskele-longation, Helv. Physiol. Pharmacol. Acta, 20:163-l'12,1962.
26. Bianconi, R., and Van der Meulen, J. P.: The responseto vibratjon of the end organs of mammalian musclespindles, J. Neurophysiol., 26:177-190, 1963.
21.Granit, R., and Van der Meulen, J. P.: The pauseduring contraction in the discharge of the spindleaflerents from primary end organs in cat extensormuscles, Acta Physiol. Scand., 55: 231-244,1962.
28. Ishikawa, K., Ott, K., Stuart, D. G., and Eldred, E.:Muscle responses to sinusoidal stretch, Physiologist,7 : 1 6 4 , 1 9 6 4 .
29.Lundberg, A., and Winsbury, G.: Selective adequateactivation of large afferents from muscle spindles andGolgi tendon organs, Acta Physio l . Scand.,49:155-164,1 960.
30. Matthews, . P. B. C.: The response of de-efferentedmuscle spindle receptors to stretching at differentveloci t ies, J. Physio l . (London), 168:660-678, 1963.
31. Lippold, O. C. J., Nicholls, J. G., and Redfearn, .T.W. T.: Electrical and mechanical factors in the adapta-tion of a mammalian muscle spindle, J. Physiol. (Lon-don), 153 :209-217, 7960.
32.Szent6gothai, J.: Anatomical considerations of mono-synaptic reflex arcs, J. Neurophysiol., ll:445454,1948.
33.Eccles, J. C.: Central connections of muscle afferentfibres. In Barter, D., ed.: Symposium on Muscle Re-ceptors. Hong Kong: Hong Kong University Press,1962 , pp . 81 -101 .
34. Barker, D., and Gidumal, J. L.: The morphology ofintrafusal muscle fibres in the cat, J. Physiol. (Lon-don ) , 157 :513 -528 , 1961 .
35. Winckter, G.: Caracteristiques morphologiques de I'in-nervation des muscles stries, Rev, Otoneuroophtal.,23:7-9, 1961.
36.Cuajunco, F.: Embryology of the neuromuscularspindle, Contr. Embryol. Carneg. lnst., 19:.45-72,7927.
37.Cuajunco, F.: Development of the neuromuscularspindle in human fetuses, Contr. Embryol, Carneg.Inst . . 25 :95-128. 1940.
38. Latyshev, V. A.: New formation process in skeletalmusculature of man and mammals. Intern. Abstr. Biol.Sc i . , 11 :163 , 1958 .
Provided by the Maternal and Child Health Library, Georgetown University
39.Boyd, I. A.: The innervation of mammalian neuro-muscular spindles, J. Physiol. (London), 140:14-15P,19s6.
40. Cooper, S., and Daniel, P. M.: Human muscle spindles,J. Physio l . (London), 133:1-3P, 1956.
4l.Walker, L. 8., Jr.: Diameter spectrum of intrafusalmuscle fibers in muscle spindles of the dog, Anat. Rec.,1 3 0 : 3 8 5 . 1 9 5 8 .
42. Swett, J. E'., and Eldred, E.: Comparisons in structureof stretch receptors in medial gastrocnemius and soleusmuscles of the cat, Anat. Rec., 137:461473, 1960.
43. Bridgman, C. F., and Eldred, E.: Hypothesis for apressure-sensitive mechanism in muscle spindles, Sci-ence, 743:481482, 1964.
44.Merrillees,' N. C. R.: The fine structure of musclespindles in the lumbrical muscles of the rat, J. Biophys.Biochem. Cytol., 7:725-742, 1960.
45. Barker, D.: The innervation of the muscle spindle,Quart . J . Micr . Sci . , 89:148- i86, 1948.
46.Barker, D., and Hunt, J. P.: Mammalian intrafusalmuscle fibres, Nature, 203:1193, 7964.
47. Cooper, S., Daniel, P. M., and Whitteridge, D.: Musclespindles and other sensory endings in the extrinsic eyemuscles: The physiology and anatomy of these re-ceptors and of their connexions with the brain stem,B ra in . 78 :564 -583 . 1955 .
48. Bridgman, C. F., Eldred, E., and Eldred, B.: Distribu-tion and structure of muscle spindles in the extensordigitorum brevis of the cat, Anat. Rec., 143:219-227,1962.
49.Eyzaguirre, C.: The electrical activity of mammalianintrafusal fibers, J. Physiol. (London), 150:169-185,1960.
50. Boyd, L A.: Simple and compound mammalian musclespindles, J. Physiol. (London), I45:4546, 1958.
51.Smith, C. M., and Eldred, E. : Mode of act ion ofsuccinylcholine on sensory endings of mammalianmuscle spindles, J. Pharmacol. Exp. Ther., 131:237-242, 1.961..
52.\'erhey, B. A., and Voorhoeve, P. E.: Activation ofgroup IA and group II muscle spindle afferents bysuccinylcholine and other cholinergic drugs, ActaPhysiol. Pharmacol. Neerl., 12:23-29, 1963.
53. Albuquerque, X.: Personal communication.
54. Smith, C.: Personal communication.
-55. Hines, M.: Nerve and muscle, Quart. Rev. Biol.,2:149-180, 7927.
56, Eyzaguirre, C.: Motor regulation of the yertebratespindle. In Barker, D., ed.: Symposium on MuscleReceptors. Hong Kong: Hong Kong University Press,1962, pp. 155-166.
57. Gray, E. G.: The spindle and extrafusal innervation ofa frog rnuscle, Proc. Roy. Soc. [Biol.], 146:416430,1957.
58. Co6rs, C.: Histochemical identification of motor nerveendings in muscle spindles, In Barker, D., ed.: Sym-posium on Muscle Receptors. Hong Kong: Hong HongUniversity Press, 1962, pp. 221-226.
59. Hess, Arthur: Two kinds of motor nerve endings onmammalian intrafusal fibers revealed by the cholines-t e rase t echn ique . Ana t . Rec . . 139 :173 -117 , 1961 .
60. Kupfer, C.: Motor innervation of extraocular muscle,J. Physiol. (London), 753:522*526, 1960.
61.Giacomini, E., and Holmstedt, B.: Cholinesterase inmuscles: A histochemical and microgasometric study.Acta Pharmacol. (Kobenhavn), 17:94-105, 1960.
62. Rexed, B., and Therman, P.-O.: Calibre spectra ofmotor and sensory nerve fibres to flexor and extensormuscle, J. Neurophysio l . , 11:133-139, 1948.
63.Ecc1es, J. C., and Sherrington, C. S.: Numbers andcontraction values of individual motor-units examinedin some muscles of the limb, Proc. Roy. Soc. [Biol.],106 :32G-357 .1930 .
64.O'Leary, J., Heinbecker, P., and Bishop, G. H.: Analy-sis of function of a nerve to a muscle, Amer. J. Physiol.,1 1 0 : 6 3 6 - 6 5 8 , 1 9 3 5 .
65.Leksell, L.: The action potential and excitatory effectsof the small ventral root fibres to skeletal muscle, ActaPhysio l . Scand., 10, Suppl . 31:1-84, 1945.
66. Kuffer, S. W., Hunt, C. C., and Quilliam, J. P.: Func-tion of medullated small-nerve fibers in mammalianventral roots: Efferent muscle spindle innervation, J.Neurophysiol., 14 :29-54, 1,951.
67.Boyd, I . A. , and Davey, M. R.: The groups of or ig inin the nerves to skeletal muscle of the gammar andgammae fusimotor fibres present, close to-and within,mammalian muscle spindles. In Barker, David, ed.:Symposium on Muscle Receptors. Hong Kong: HongKong University Press, 1962, pp. 191-198.
68.Appe1berg, 8., Bessou, P., and Laporte, Y.: Effectsof dynamic and static fusimotor fibres on the responsesof primary and secondary endings belonging io thesame spindle (to be published).
69. Boyd, I. A., and Eccles. J. C.: Fast- and slow-conduct-ing small motor fibres in nerves to mammalian skeletalmuscle, J. Physio l . (London), 165:29-30P, 1963.
70. Barker, D., and Chin, N. K.: Efferent innervation ofmammalian muscle spindles, Nature, 190:461463, 1961.
71.Hunt, C. C., and Kuffier, S. W.: Stretch receptor dis-c.harges_ _during,muscle,contraction, J. Physioi. (Lon-don ) , 113 :298 -315 , 1951 .
72.Gtaniq R., Pompeiano, O., and Waltman, B.: Theearly discharge of mammalian muscle spindles at onsetof contraction, J. Physiol. (London)-, 74j:399418,1 959.
73. Rutledge, L. T., and Haase, J.: Flexor muscle spindlesand reflex firing of early discharging units, J. Neuro-physiol., 24:182-192, 7961.
74.Granit, R., Pompeiano, O., and Waltman, B.; Fastsupraspinal control of mammalian muscle spindles:extra- and intrafusal co-activat.ion, J. Physiol. (Lon-don ) , 147 :385 -398 , 1959 .
75. Bessou, P., Emonet-Denand, F., and Laporte, Y.: Oc-currence of intrafusal muscle libre innervation bvbranches of slow alpha motor fibres in the cat, Naturd,1 9 8 : 5 9 4 - 5 9 5 , 1 9 6 3 .
76.Boyd, I. A., and Davey, M. R.: 6-efferent fibres innerves to mammalian skeletai muscle, J. Physiol. (Lon-don), 149 :28-29P, 1959.
77. Kidd, G. L.: Excitation of primary muscle spindle end-ings by B-axon stimulation, Nature, 203:1248-7251,1964.
78. Granit, R., and Henatsch, H. D.: Gamma control ofdynamic properties of muscle spindles, J. Neurophysiol.,19 :35G366 , 1956 .
79.Jansen, J. K. S., and Matthews, P. B. C.: The effectsof fusimotor activity on the siatic responsiveness ofpr imary and secondary endings of muscle spindles inthe decerebrate cat , Acta Physio l . Scand., 55;376-386,1962_
80.Jansen, J. K. S. , and Matthews, P. B. C. : The centra lcontrol of the dynamic response of muscle spindle re-ceptors. J. Physiol. (London), 16l:35'7-378, 7962.
81. Eldred, E., and Fujimori, B.: Relations of the reticularformation to muscle spindle activation, In Jasper, H.H., ed.: Reticular Formation of the Brain. Boston:Little, Brown & Co., 1958, pp. 275-283.
82. Matthews, P. B. C.: The differentiation of two typesof fusimotor fibre by their effects on the dynamic re-sponses of muscle spindle priru1y endings, Quart. J,Exp. Physiol., 47:324-333, 1962.
83.Eldred, E., Granit, R., and Merton, P. A.: Supra-spinal control of the muscle spindles and its signifi-cance, J. Physiol. (London), 722:498-523, 1953.
84.Eklund, G., and Skoglund, S.: On the speci-ficity ofthe Ruffinilike joint receptors, Acta Phyisol. Scand.,49 :184 -191 , 1960 .
85.Karlsson, Ulf, and Andersson-Cedergren, E.: Satellitecells of the frog muscle spindle as revealed by electron-microscopy (in preparation).
E
Provided by the Maternal and Child Health Library, Georgetown University
3r

BASIC MECHANISMSOF MOTOR LEARNING
JENNIFER S. BUCHWALD, Ph.D.
]\TL \ o H U M A N B E I N c k n o w s a
more relentless enemy than motor nerve cellswhich have been wrongly trained early in life.Such a man may be worth a mil l ion, but thebad grammar will continue to flow automatically
lrom the motor mechanism of speech, and to'mortily him in good society. Rightly tained
nerve cells occupy a position .analo,go.us t,o Ihatol a trusty servant, who, wi lhout being lookeda'lter, attends to all the wearying details olhousekeeping, leaving the mistress lree to enter-tain her lriends and to develop her higherpowers.T
Before embarking upon a discussion of mechan-
isms basic to motor learning, we should clearly
dif ferentiate between a learned motor response and
a motor reflex.
Adapted from a paper presented at the -Symp-osium onrrre Cfiia wittr Cenirai Nelvous System-Deficit, Septemberia-Oi i ; -b. . i . Deq, The Univers i tv of Pennsvlvania, Phi l -adelohia.--ffi""iutttor
is Assistant Professor of Pediatrics' Depart-.n* i -o]-F.a;utr ics, School of Medic ine, and Brain Re-.Jiiitt- tnitii,ii", University of California, Los Angeles,90024.
32
In its simplest form, tlte molor reflex requires
only an afferent fiber synaptically connected to a
motoneuron. With adequate st imulat ion of the
afferent fiber, as '*'ith muscle stretch, the moto-
neuron will discharge. While motor reflexes are
usually far more complex than this with many
interneuronal synaptic connections intervening be-
tween the afferent input and the efferent response'
the important point is that the st imulus has im-mediate signif icance and can el ici t a response the
first t ime i t is presented. One steps on a tack and
immediately withdraws his foot.In contrast, a learned motor response develops
only i f an init ial ly neutral st imulus becomes cap-
able of discharging the motoneurons. One learns
to step on the brake when driving a car i f he
sees a red l ight. Thus, a st imulus which init ial ly
Droduces no efferent activation acquires this ca-
pacity. How such "motor learning" occurs is one
of the prevai l ing mysteries of experimental investi-gation. This discussion wil l indicate, in a very
general way, some of the structures and mechan-
isms within the central nervous system which are
Provided by the Maternal and Child Health Library, Georgetown University
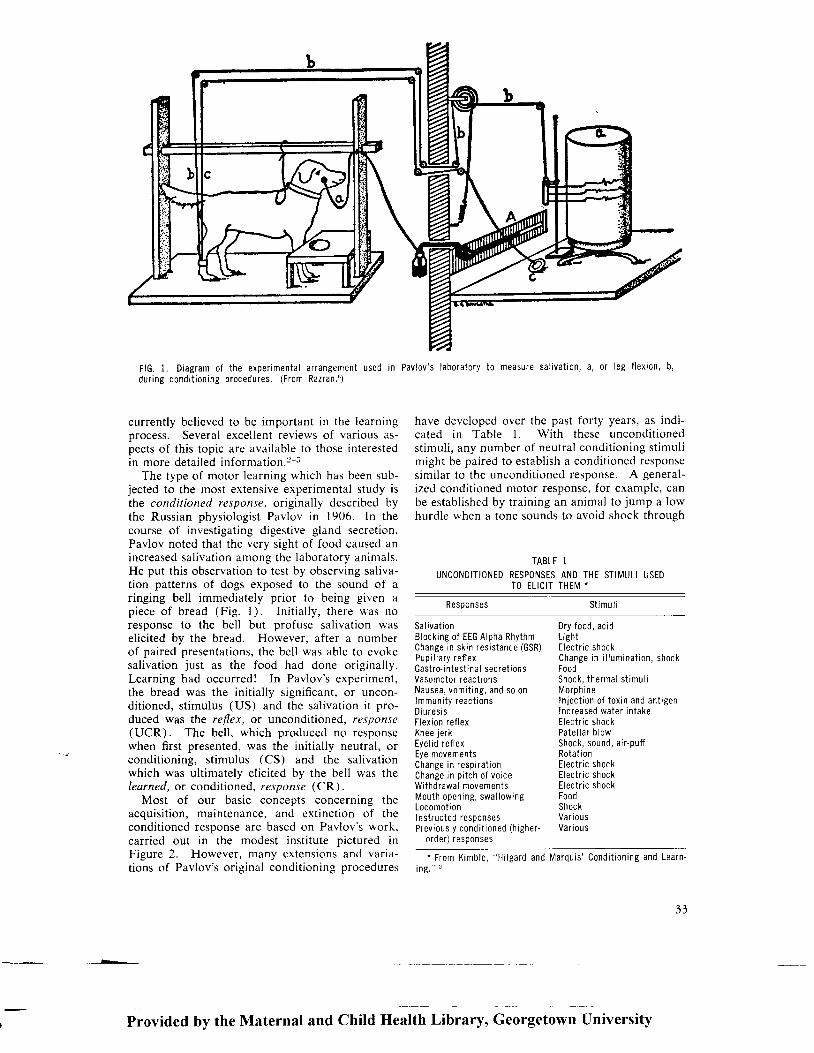
F lG .1 . D iag ram o f t he expe r imen ta l a r rangemen t used i n Pav lov ' s l abo ra to r y t o measu re sa l i va t i on , a , o r I eg f l ex i on , b ,du r i ng cond i t i on i ng p rocedu res . (F rom Raz ran . " )
currently bel ieved to be important in the learningprocess. Several excel lent reviews of various as-pects of this topic are avai lable to those interestedin more detai led information.2 5
The type of motor learning which has been sub-jected to the most extensive experimental study isthe conditioned response, originally described bythe Russian physiologist Pavlov in 1906. In thecourse of investigating digestive gland secretion,Pavlov noted that the very sight of food caused anincreased sal ivat ion among the laboratory animals.He put this observation to test by observing sal iva-tion patterns of dogs exposed to the sound of aringing bel l immediately prior to being given apiece of bread (Fig. 1). Init ial ly, there '*as noresponse to the bel l but profuse sal ivat ion uasel ici ted by the bread. However, after a numberof paired presentations, the bel l was able to evokesalivation just as the food had done original ly.Learning had occurred! In Pavlov's experiment,the bread was the init ial ly signif icant, or uncon-dit ioned, st imulus (US) and the sal ivat ion i t pro-duced was tbe reflex, or unconditioned, response(UCR). The bel l , which produced no responsewhen first presented, was the initially neutral, orcondit ioning, st imulus (CS) and the sal ivat ionwhich was ult imately el ici ted by the bel l was thelearned, or condit ioned, response (CR).
Most of our basic concepts concerning theacquisit ion, maintenance, and extinct ion of theconditioned response are based on Pavlov's work,carr ied out in the modest inst i tute pictured inFigure 2. However, many extensions and varia-t ions of Pavlov's original condit ioning procedures
have developed over the past forty years, as indi-cated in Table 1. With these uncondit ionedstimuli , any number of neutral condit ioning st imulimight be paired to establ ish a condit ioned responsesimilar to the uncondit ioned response. A general-ized conditioned motor response, for example, canbe establ ished by training an animal to jump a lowhurdle *'hen a tone sounds to avoid shock through
TABLE 1UNCONDITIONED RESPONSES AND THE STIMULI USED
TO ELICIT THEIV *
Responses St imu l i
Sa I ivat ionBlocking of EEG Alpha RhythmChange in skin resistance (GSR)Pup i l l a r y r e f l exGastro- intest inal secret ionsVasomotor react ionsNausea , vom i t i ng , and so onlmmun i t y r eac t i onsD iu resi sFlexion ref lexKnee jerkEyel id ref lexEye movementsChange i n r esp i r a t i onChange in p i tch of voiceWithdrawal movementsMou th open ing , swa l l ow ingLocomot i onInstructed responsesPrev ious l y cond i t i oned (h i ghe r -
orderJ resp0nses
Dry food, acidLightElectr ic shockChange i n i l l um ina t i on , shockFoodShock , t he rma l s t imu l iMorph in eIn ject ion of toxin and ant igenIncreased water intakeElectr ic shockPa te l l a r b l owShock, sound, a i r -puf fRotat ionElectr ic shockElectr ic shockE lec t r i c shockFoodShoc kVa r i ousVar i ou s
" F rom K imb le , "H i l ga rd and lMa rqu i s ' Cond i t i 0n i ng and Lea rn 'ing." z
Provided by the Maternal and Child Health Library, Georgetown University
3 3

FlG. 2. The special laboratory bui l t for the study of con-dit ioned ref lexes, Inst i tute of Experimental Medicine, Petro-grad. (From Pavl0v, translated by Anrep.?)
the cage floor grids (Fig. 3) or, if a more restrictedmotor response is desired, the animal can be taughtto flex one leg when a light flashes to avoid ashock to the paw or to press a lever when apatterned figure is presented and thereby obtain afood reward.
As a model, the conditioned response has seriousshortcomings, for learning is not simply a stimulus-
response situation. With the same amount oftraining (stimulus), some individuals may per-form far better than others (response) because ofnumerous variables such as motivation, past ex-perience, inherent capacity. Likewise, in the labo-ratory the rate at which motor responses areacquired varies considerably, depending upon theparticular learning situation and the type of animalbeing trained. Typically, however, there is reten-tion of conditioned learning from one trainingsession to the next so that the number of responsesper session increases with the number of trainingsessions until the new response is consistentlyelicited by the CS (Fig. a). Because of this pre-dictable development and maintenance of a re-sponse which can be observed behaviorally, theconditioned response remains the most practicaltype of motor learning to investigate experi-mentally.
BRAIN MECHANISMS
The classical concept of brain mechanismsessential for conditioned learning was based uponthe views of Pavlov who believed that the cerebralcortex should be regarded as the essential organfor the establishment and maintenance of con-ditioned reflexes.? Pavlov's conclusions were, inturn, based upon the failure of Zeliony in l9l2 toestablish conditioned iesponses in dogs after re-
ff"r
J-- t r r r { t - {
c.*A
FlG. 3. Training technique for establ ishing a general ized motor response. Shock through the f loor grids on one side of thehurdle (US) causes the cat to jump to the other side. l f a tone (CS) precedes the shock for several tr ials, the cat quicklyfearns to jump the hurdle at the onset of the tone and thereby escape the subsequent shock. (From Neff,8)
34
Provided by the Maternal and Child Health Library, Georgetown University

roo
90
80
70
60
30
40
30
20
to
o
tv,-ocoUGclU-IEct-C'a,Eo
o2U=<tuc
Fz(tG,
E, 2 3 4
fOURTHS TO CRIIERIONOF EXTINCTION
€LEVENTHS TO CR|TERTot.| 0F ACourStTrOrl
FlG. 4. Average performancecurves showing an increasingtransfer of learning during ac-quisit ion of a condit ioned f lex-ion response in dogs fromone group of tr ials to the next(open circles) and an increas-ing transfer of inhibit ion dur-ing extinct ion of the sameresponse (sol id circles). (FromBrogden.,)
FlG. 5. Di f fuse condi t ioned re-sponses establ ished in com-pletely decort icated dog. Thetonal CS, presented at (1) ,e l ;c i ts a condi t ioned bi lateralh indleg f lex ion which becomesmaximal at (3) ; on the nextt r ia l , CS presentat ion (4) pro-duces not only b i lateral f lex ionof the hindlegs but f lex ion ofthe r ight foreleg as wel l (5) .(From Girden, Mett ler , F inch,and Cul ler .u)
Provided by the Maternal and Child Health Library, Georgetown University
3 5

reErsr;THALAMUS
F lG . 6 . S imp l i f i ed ana tom ica lp l an o f t he neu ra l connec t i onsinvo l ved i n l ea rn i ng . The c l as -s ical af ferent systems dissem-inate informat ion about cur-rent environmental events tothe cortex and to the ret icularformat ion. Ef ferent sensorytracts or ig inat ing f rom theselat ter st ructures terminate inthe af ferent nucle i and even inthe sense organs themselves.The l imb i c -m idb ra i n c i r cu i t ,which star ts in, and dist r ib-utes to, the ret icular sub-stance, br ings the phyloge-net ical ly o ldest parts of thecort ical mant le, as wel l asthe hypothalamus, into func-t ional contact wi th the restof the brain structures. (FromGalambos and Morgan. ' )
moval of the cerebral cortex.lo Twenty yearslater, after Pavlov had developed his theory ofcortical dominance in conditioned learning,Zeliony repeated his original experiments.ll Incontrast to the previous results, the decorticatedogs in this study acquired conditioned responses.The degree of decortication was not known, how-ever, as the animals were not sacrificed.
Soon after this report from Russia, Girden andhis associates in the United States repeated the ex-periment on dogs and removed essentially all ofthe cerebral cortex.12 In these animals, condi-tioned flexion responses were readily established tosuch diverse conditioning stimuli as sound, touch,
>>FlG. 7. Examples of the electroencephalogram, or slowwave electr ical act ivi ty of the brain, recorded from thecerebral cortex of a number of dif ferent sDecies. (FromBrazier.u) | | S r c o n d I
36
TARGETSNOOCRINE
GUINEA-P IO :
M O N K E Y :
+
Provided by the Maternal and Child Health Library, Georgetown University

and temperature. However, the conditioned re-sponses tended to be diffuse and bilateral (Fig. 5).
Thus, it was concluded that generalized motorresponses could be learned in the absence of thecerebral cortex but a deflnite, localized response!such as conditioned flexion of just one leg, wastoo complex a behavioral pattern for the decorti-cate animal. A few years later, however, Bromileysucceeded in establishing conditioned flexion re-sponses confined to the hindleg in decorticate dogs,thereby proving that the cerebral cortex was notnecessary for even such discrete motor learning.13Failure of the earlier group to reach the same con-
clusion might have resulted from their trainingprocedure in which the US was applied to bothhindlegs where it elicited a diffuse unconditionedresponse. Bromiley's findings have been confirmedand extended so that today the Pavlovian conceptof cerebral dominance has been modified. Whilethe cerebral cortex is considered imoortant in facil-itating motor learning, it is not essential for the de-velopment of simple conditioned responses.
With the cortex no longer established as theneuronal origin of the learning process, experi-mental investigation has enthusiastically plungeddeeper into the brain. From the overwhelming
FlG. 8. Spike discharge of asingle audi tory nerve cel l inthe cochlear nucleus. Thefrequency of neuronal d is-charge increases as the in-tensi ty of a 2,600 cps tone be-comes progressively greater .(From Galambos and Davis. 'o)
illliltll mnilil ilt!|iln iiilintruryilroruiliiiiltli ililtimFF FrfltFliilit m!ilililllFltil
t25
2600.
Ncrvc rcsponlc59irt%.c.
r00 90df bclr 2v trom orcrtlrlor
50
25
i l0
rorutruruillttttillFtl nmililF ; lr?tr1F iFrrFf lltT'liilrtil?
tro ilsllfl tlillJqruu Htllruflll|llltlFll||'Fl'0tt t|ilrPiinfll'l rtFitrFF tfft Fllfiiltnr
il8tlul HI{II!,4 tllttuC[trn ddltutllu-5".- '
Provided by the Maternal and Child Health Library, Georgetown University
37

mass of experimental data which is being produced
by these studies, one possible synthesis suggests that
three major neuronal systems are primarily in-
volved in learning: a
1. The classical afierent pathway to specific
thalamic nuclei and to corresponding cortical pro-jection areas, modulated by descending efferent
control arising from cortical and subcortical re-gions and making synaptic connections with the
ascending pathways at all levels including the first
sensory relay. This system provides the nervous
system with information about the external en-vironment.
2. The reticular or nonspecific ascending path-way receivrng collaterals from specific sensorytracts and passing to the cortex by way of the intra-laminar and midline thalamic nuclei. This systemsubserves arousal and alerting functions'
3. The limbic-midbrain circuit in which activityarising in the midbrain passes to the hippocampus,amygdala, hypothalamus, septal nuclei and thenback to the midbrain reticular formation. This sys-tem is responsible for motivational factors.
The interplay of these anatomical-physiologicalcircuits (Fig. 6) probably provides the informa-tional, alerting, and motivational components inthe iearning process. In general, observations madewith chronically implanted electrodes have sup-ported the idea that early in the course of con-ditioning reticular and limbic systems are in-volved. In later stages, activity in the reticularand limbic systems disappears and activation of
F lG.9 . Absence o f cond i t ionedmotor learn ing in chron ica l lYspinal ized adult dogs. UPPergraph shows the f lexion (sol idl ine) and extension (dottedl ine) responses el ici ted by theCS over 1 ,000 t ra in ing t r ia ls .In the bottom graph both typesof responses are summed overthe same training period. Themovements in al l three plotssuggest only random activi tyand indicate no progressivedeveloDment of a condit ionedresponse. (From Kellogg,Deese, Pronko, and Feinberg.z)
the midline thalamic nuclei and neocortical areas
develops.
As the present electrophysiological era con-tinues to blossom, new techniques are constantlyincreasing our knowledge of where, in what se-quence, and how changes in neuronal activity de-
velop during the learning process. Physiologists,pharmacologists, neurochemists, experimental psy-
chologists are collaborating in experimental in-vestigations to an ever increasing degree. Electri-cal changes in brain activity, recorded throughindwelling electrodes, are analyzed in the formof slow-wave electroencephalograms (Fig. 7) orin the discharge patterns of single nerve cells (Fig.
8 ). Simultaneously, chemical changes in neuronalactivity can be examined by the use of cannulaechronically implanted in the brain through which
samples may be removed for analysis or minuteinjections made. Although such techniques as
these are providing an ever more penetrating view
of brain function during learning, investigators are
not yet able to locate the primary neuronal sites
of altered excitability nor to determine the way inwhich these primary excitability changes areproduced.
SPINAL MECHANISMS
In discussing basic mechanisms of motor learn-ing, we must remember that a great portion of thecentral nervous system dangles below the brain in
38
- ALL 0065 - FLEX\ON ANO EXT€A'SIONg
E,,Oat{
.'o,.J
taoto
3 4 5HUNOFIEDS OF
6 7rRULS
<n
9 a ou\ . ! l 2
$ato
3 4 5 6 7HUNMEOS OF TRIALS
ALL N6S - FLEXPN EUE EXTENS|ON
Provided by the Maternal and Child Health Library, Georgetown University

intimate contact with the peripheral environment.While the contributions of cortical and subcorticalsystems are undoubtedly of extreme significance,the role of the spinal cord must also be considered.In such invertebrate forms as planaria, wherecephalization is rudimentary, various kinds ofmotor learning have been demonstrated.lG'17Whether, in mammals, the brain is essential to thelearning process would depend upon the capacityof the spinal cord, divorced from the brain, tomediate the development of a learned response.
The possibility of establishing conditioned re-sponses in the mammalian spinal cord isolatedfrom higher centers was first suggested by thework of Shurrager and his associates in the1940's.18 21 In these experiments on acute spinaldogs, a pressure stimulus to the tip of the tail (CS)was followed each time by an electric shock to onehindpaw (US). No conditioned response involv-ing movement of the limb was observed but a smalltwitch at one end of the exposed semitendinosusmuscle developed in response to the pressure stim-ulation of the tail. These results suggested that aconditioned motor response had been established inthe isolated spinal cord.
In an effort to confirm these findings, Kelloggand his co-workers attempted to train chronicspinal dogs to perform a conditioned hindlegflexion response but were completely unsuccessful(Fig. 9).22 Kellogg's group attributed Shurrager'sresults to sensitization of the semitendinosus mus-cles as a result of the extensive surgery necessaryfor their exposure and to the insufficient criteriautilized in classifying the contractions observed asconditioned responses. It was suggested that thesemitendinosus contractions were more likely avariation of the unconditioned reflex response orof a generalized startle response.2s
Subsequently, Shurrager and his student Dyk-man also turned to chronic spinal preparations bututilized kittens instead of adult animals. In thesestudies, the spinal animals were prepared witn alow thoracic section of the cord two days to eightweeks after birth and none was more than fourmonths old at the termination of the experiment.Although the hindquarters did not co-ordinate withthe forequarters, hindleg walking movements wereobserved to develop which were discrete enoughto permit the animal to step up and over obstruct-ing objects (Fig. l0). Moreover, in a single seriesof hindleg movements one animal was reportedable to propel itself 15 or more feet across thelaboratory floor, The authors concluded thatamong the ten animals in which these walkingmovements were studied, performance was best inthe kittens youngest at time of spinal transectionand, in this subgroup, best in the kittens that hadreceived the most physical therapy, i.e., stimula-tion of the hindquarters by electrical shock andmassage.2a The extent to which walking is con-sidered a reflex rather than a learned resDonse
would limit the extrapolation of this study to exem-plify learning in the spinal animal.
In a second study, the acquisition of a condi-tioned flexion response was studied in fifteenchronic kittens, spinalized two to qighty-four daysafter birth, and one puppy.25 The CS was a softbrush stroke to the hindleg or tail and the US wasa shock to the hindleg. In twelve of the kittensand in the puppy a conditioned flexion was estab-lished (Fig. 11). It was shown that a carry-overor retention of learning occurred from one trainingsession to the next, as in true conditioning, so thatwith each successive session more conditioned re-sponses were made. During extinction, in whichthe US is withheld and the conditioned responsenormally disappears, the spinal preparations againshowed a carry-over from one session to the nextso that the number of the conditioned responsesper session became progressively less (Fig. 12).Dykman and Shurrager concluded that the spinalcord, isolated either acutely or chronically fromhigher centers, had the capacity to mediate motorlearning. They further believed that this capacitywas, to an important extent, a function of age sothat the younger the animal at the time of spinalcord transection the more easily motor learning inthe isolated cord could proceed.
Unfortunately, the work of Dykman and Shur-rager has never been repeated. The only re-lated study during the past decade reported no re-tention of conditioned motor learning when adultcats were trained, spinalized, and then resubjectedto the preoperative training situation.26 In ourown laboratory we have initiated a study on chron-ically spinalized kittens utilizing the same ages forspinal transection and the same training proce-dures as those employed by Dykman and Shur-rager. Hopefully, such an investigation will fur-ther illuminate the unresolved question of whetherthe isolated spinal cord can provide the necessaryneuronal components for the development of alearned motor response.
In considering factors operating to facilitate thelearning process, not only must we think of the in-herent capacity of the spinal cord to learn butalso of the role of segmental afferent inflow re-ceived at spinal levels but influencing both brainand spinal cord function. The significance to motorlearning of information coming in over the spinaldorsal roots concerning location and sensation ofthe innervated somatic parts has been studied incats, dogs, and monkeys during several types oftraining procedures.
The development of a localized conditionedmovement, i.e., a conditioned flexion of the cat'shindleg, was found to require intact afferent inner-vation of the hindlimb musculature.2z In thisstudy, the lumbar dorsal roots were unilaterallysectioned and subsequently the animals weretrained in a procedure which combined tone (CS)with shock delivered through the central stump of
Provided by the Maternal and Child Health Library, Georgetown University
39

one of the sectioned dorsal roots (US). While aconsistent reflex flexion could be elicited by thedorsal root stimulus, the deafferented leg did notrespond to the CS.
In contrast, the contralateral leg with intactafferent innervation responded with a flexion tothe US and after several training sessions beganto respond with a conditioned flexion to the CS(Figs. 13, l4). If instead of total deafferentation,a fragment of afferent inflow was left intact on theoperated side, the partially innervated muscleswere found to develop a conditioned responsealthough completely deafferented muscles did not(F ' i g . 15 ) .
In a more diffuse type of motor learning, such asa conditioned scratch response, this local afferentinput does not seem to be so essential. In exten-sively deafferented hindlimbs, conditioned scratchresponses could be developed or, if the responseswere first established, they could be maintainedafter the deaffet"o1s1iorr.28' 20 Such a response asthis involves motor nuclei over an extensive portionof the neuraxis with some muscles activated todirect the head and make postural adjustments
4a
l '-l : , 't .
ij'.,
while others move the hindleg. Thus, it might beanticipated that interruption of local afferent in-flow from one portion of the body would havelittle effect. In general, the more widely distrib-uted the sensbry cues which trigger or support areflex action, the less effect deletion of one portionof the sensory inflow will have on the reflex.
Species difference must also be considered, how-ever, for even specific, localized movements havebeen shown to develop in the absence of sensoryinflow in dogs and monkeys. Dogs with one hind-leg totally deafferented could be trained to flexthat limb to attain a food reward or to avoid ashock.3O Similarly, monkeys with one forearmdeafferented could be trained to flex the deaf-ferented arm in order to prevent a shock to thecontralateral arm.'31 If the conditioned flexion re-sponse were first established and then the perform-ing limb deafferented, the response disappeared butcould be re-established with retraining.'rz
In all motor learning, the overt response is aproduct of local sensory inflow and descending in-fluences from the brain. The preceding data indi-cate that the relative dependence upon these
i ,
i,til* :.r riii i
l i i
::.'::i,
FlG. 10. Walking movements displayed by kittens following spinal cord transections at lower thoracic levels. (From Shurragerand Dykman.z4)
Provided by the Maternal and Child Health Library, Georgetown University

FlG. 11 . Acqu is i t ion o f con-dit ioned responses in threegroups of chronical lY sPinaFized kit tens. In the f irst group,the CS (a l ight brush stroke)was aoolied to the tai l andpaired with the US (electr icalshock) appl ied to the r ight leg.The development of a r ightleg f lexion to the brush strokeis indicated by the uppercurve (sol id circles). Eachpoint on this and subsequentcurves reDresents mean num'ber of condit ioned responsesin seven consecutive trainingsessions of fortY tr ials each.In a second group of animals,the CS was applied to the tai l ,the US to the left leg, and aleft leg condit ioned f lexionwas establ ished as indicatedby the middle curve (opencircles). In a third group ofanimals, the CS was applied tothe contralateral leg and theUS to the r ight leg. The lowercurve (sol id squares) indicatesthe appearance of a r ight legcondi t ioned f lex ion. (From Dykman and Shurrager.e5)
3 5
3 0o
ot
R t c H T L E G ( T A | L )
L E F T L E G ( T A I L )
R I G H T L E G ( C O N T R A -
LATERAL )U''
u25zor , 2 0U
f f rsz
=rozo()
3
3 4 5C O N D I T I O N I N G S E S S I O N S
a
o
t
RrGHT LEC (TAIL)
LEFT LEC (TAIL)
RIGHT I-FG(CONTRALATERAL)
. 2 5aQz
a 2 0bl
L1
3 t tt-
z( . ) l 0
FlG. 12. Extinct ion of condit ioned responses in three groups of chronical ly spinal ized kit tens. Designation of groups the sameas in the preceding f igure. Condit ioned responses in al l groups pro8ressively decreased with increasing numbers of ext inc-t ion sessions (ordinltei during which the CS was presented without the US. (From Dykman and Shurrager.s)
Provided by the Maternal and Child Health Library, Georgetown University
4 r

ac)oF
alrlazoo-QlrJE.
FE.t!
C - C
INTACT . ^_"/ 'L E G \
c cy\" /., " / \ /
'";"'^.-
.{,
Ia
R E S P O N S ET O
U J
-rNl-/ti l t
UFLEXION
rh,f(
5 t o t 5
FlG. 13. Condit ioned f lexion responses in intact and deafferented hindl imbs of a chronical ly trained cat. Each point label led"C" represents the percentage 0f overt aondit ioned responses made during f i f ty tr ials of successive training sessions. (FromBuchwald, Standish, and Eldred., i)
FlG.14. Electromyographic responses recorded during the training sequence of Figure 12. 0nset of the total CS producesmarked EMG activation in the "hamstring" muscles with intact innervation but no response in the deafferented muscle.Both muscles subsequently respond t0 the US.
42
E MG RESPONSES
INTACTHhttllttV'tr"r|$(trtul'r't
I
t
DEAFFERENTEDwlnN#)ttttlll|Nl
fcT-lUsI
l-aI sEc .
Provided by the Maternal and Child Health Library, Georgetown University

CAT 38
HAMSTRI i lG EMG
aL)
oF
aUJazoLal!E
F(rUJ
o
, "- -- .
il -i:Ec-
[il
c
III
' , \ lI ,
. r /
r r c
c
H A M S T R I N G E M C
FfG. 15. Development of condit ioned responses in the cat 's part ial ly deafferented hindleg with dorsal roots 14, 6,7,51,2sectioned but dorsal root L5 intact. The condit ioned f lexion response is associated with increased electromyographic ac-t ivi ty in the part ial ly innervated "hamstring" muscles (upper left). Section of the i l iopsoas muscle does not not abol ish theovert condit ioned response which continues to occur concurrently with the "hamstring" EMG discharge ( lower r ight). (FromBuchwald, Standish, and Eldred. '7)
G o m m oL l r e r e n l
FlG. 16 . Gamma and a lphamotoneuron activi ty recordedfrom a f ine lumbar ventral rootf i lament. The gamma moto-neuron characterist ical ly dis-charges tonical ly with f luctua.t ions in i ts pattern of dis-charge ref lect ing i ts extremesensit ivi ty to changing levelsof excitabi l i ty in other parts ofthe nervous system. The lowamplitude spike potential ofthe gamma unit may be con-trasted with the larger, phasicspikes characterist ic of theless sensit ive alpha motoneu-rons. Here, the alpha moto-neuron discharge is producedby squeezing the hindpaw.
? 8 0 - 2 8 0 0 - 6 6 - {
Provided by the Maternal and Child Health iib.u.y, Georgetown University
43

Tr io l
T r io I
T r io l
T r io I iltilFlG. 17. Development of condit ioned discharge in a tonical ly discharging gamma motoneuron. The CS, a three-second dura-t ion tone, was paired with O.$second shock to the ipsi lateral hindpaw, US, as indicated by the l ine diagrams below thetraces. Intertr ial interval 3 minutes. Condit ioning was not apparent on the f irst to fourth tr ials (A), but condit ioned accelera-t ion of the tonic gamma unit was seen in the f i f th tr ial (B) and became marked on the sixth (C). Addit ional spike of moderateheight giving condit ioned responses in C and D may also be that of a gamma f iber. By comparison, potentials of alpha f iberselicited by pinching the toe extended off the oscilloscope face (insert to right). (From Buchwald and Eldred.&)
projections depends upon the type of tesponse andthe species considered. Local sensory iniow isso important to the development of restricted con-ditioned movements in the cat that its deletion pre-vents this type of motor learning. On the otherhand, in species with greater cerebral develop-ment, specific movements may be lost followingdeletion of local sensory inflow but these can bere-established. This suggests that sufficient facili-tation is provided by additional descending in-fluences from the brain to compensate for localsensory loss in these higher forms.
FEEDBACK MECHANISMSInvestigations of efferent control over sensory
input have shown that changing excitability levelsof the central nervous system can markedly alterthe sensitivity of such peripheral receptors as theretina, cochlea, or muscle spindle and subse-quently their discharge back into the central nerv-
44
ous system.33 Of these feedback circuits, thegamma motoneuron-muscle spindle loop has beenmost extensively investigated and the relationshipof this system to motor learning seems an impor-tant one.
The gamma motoneuron system is extremelysensitive to descending influences from the brainas well as to stimuli coming in from the peripheryover the dorsal roots. When such influences pro-duce a discharge of the gamma motoneurons, thesmall intrafusal fibers of the muscle spindle con-tract although there is no concomitant change ingross muscle tension. As a result of the intrafusalcontractions, the terminal endings of the spindleproprioceptive fibers attached to the intrafusalmuscles are stretched and depolarized. Increasedproprioceptive discharge from the muscle spindlesis thus produced which may, in turn, facilitateneuronal discharge both at segmental and supra-segmental levels.
In several types of reflexes and during stimula-
Provided by the Maternal and Child Health Library, Georgetown University
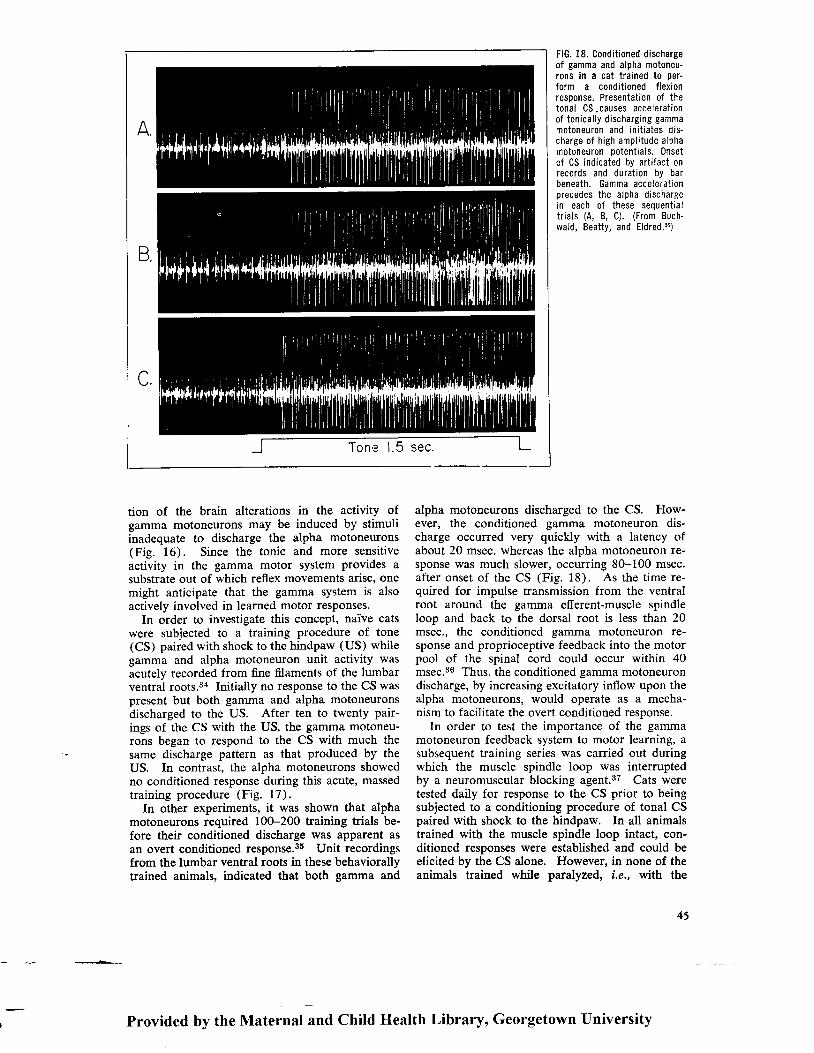
Tone 1.5 sec.
tion of the brain alterations in the activity ofgamma motoneurons may be induced by stimuliinadequate to discharge the alpha motoneurons(Fig. 16). Since the tonic and more sensitiveactivity in the gamma motor system provides asubstrate out of which reflex movements arise, onemight anticipate that the gamma system is alsoactively involved in learned motor responses.
In order to investigate this concept, naive catswere subjected to a training procedure of tone(CS) paired with shock to the hindpaw (US) whilegamma and alpha motoneuron unit activity wasacutely recorded from fine filaments of the lumbarventral roots.3a Initially no response to the CS waspresent but both gamma and alpha motoneuronsdischarged to the US. After ten to twenty pair-ings of the CS with the US, the gamma motoneu-rons began to respond to the CS with much thesame discharge pattern as that produced by theUS. In contrast, the alpha motoneurons showedno conditioned response during this acute, massedtraining procedure (Fig. 17).
In other experiments, it was shown that alphamotoneurons required 100-200 training trials be-fore their conditioned discharge was apparent asan overt conditioned response.ss Unit recordingsfrom the lumbar ventral roots in these behaviorallytrained animals, indicated that both gamma and
FlG. 18. Condit ioned dischargeof gamma and alpha motoneu-rons in a cat trained to Der-form a conditioned flexionresoonse. Presentation of thetonal CS,causes accelerat ionof tonical ly discharging gammamotoneuron and init iates dis-charge of high ampli tude alphamotoneuron Dotentials. 0nsetof CS indicated by art i fact onrecords and duration by barbeneath. Gamma accelerat ionprecedes the alpha dischargein each of these seouentialir ials (A, B, C). (From Buch-wald, Beatty, and Eldred.s)
alpha motoneurons discharged to the CS. How-ever, the conditioned gamma motoneuron dis-charge occurred very quickly with a latency ofabout 20 msec. whereas the alpha motoneuron re-sponse was much slower, occurring 8G-100 msec.after onset of the CS (Fig. 18). As the time re-quired for impulse transmission from the ventralroot around the gamma efferent-muscle spindleloop and back to the dorsal root is less than 20msec., the conditioned gamma motoneuron re-sponse and proprioceptive feedback into the motorpool of the spinal cord could occur within 40msec.36 Thus, the conditioned gamma motoneurondischarge, by increasing excitatory inflow upon thealpha motoneurons, would operate as a mecha-nism to facilitate the overt conditioned response.
In order to test the importance of the gammamotoneuron feedback system to motor learning, asubsequent training series was carried out duringwhich the muscle spindle loop was interruptedby a neuromuscular blocking agent.37 Cats weretested daily for response to the CS prior to beingsubjected to a conditioning procedure of tonal CSpaired with shock to the hindpaw. In all animalstrained with the muscle spindle loop intact, con-ditioned responses were established and could beelicited by the CS alone. However, in none of theanimals trained while paralyzed, i.e., with the
45
Provided by the tVtaternal and Child Health Library, Georgetown University
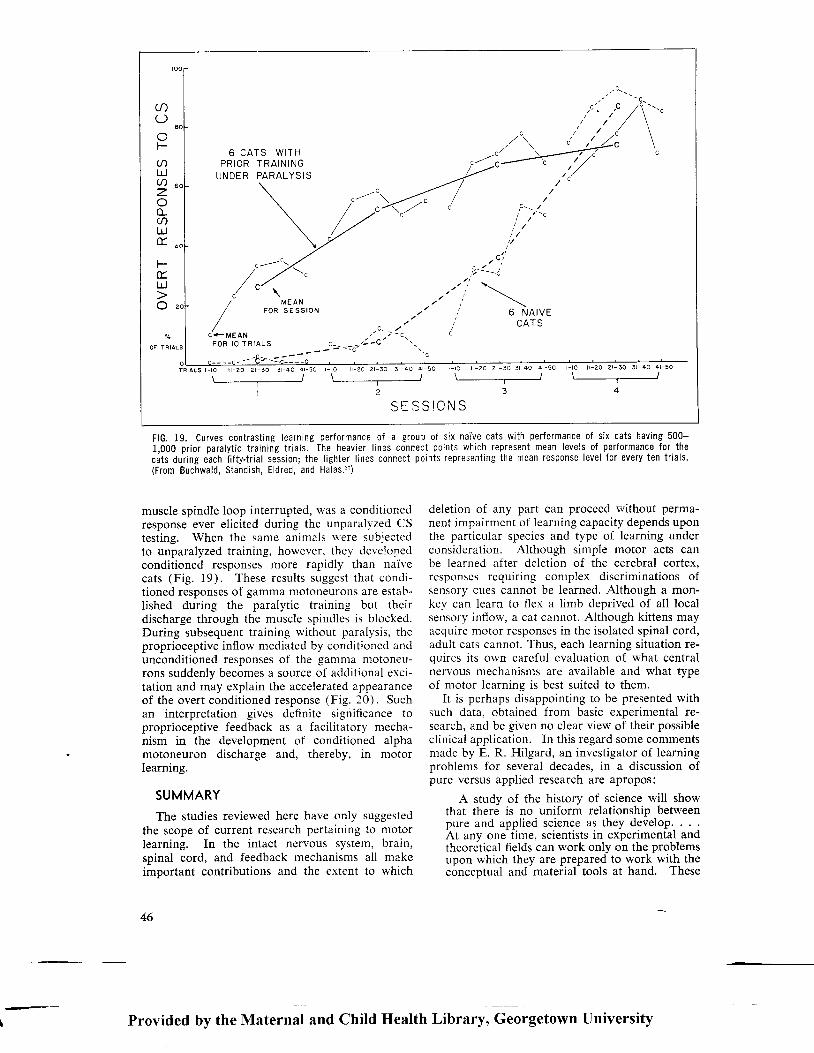
c '
O
F
LrJU)z
U)L!t
E.L.J
6 C A T S W I T HP R I O R T R A I N I N G
UNDER PARALYSIS
M E A NF O R S E S S I O N
C + M E A NF O R I O T R I A L S
T R T A L S l - t O | - 2 0 2 r - 3 0 3 l - 4 0 4 l - 5 0
r /--.--_-r-l-l
, c - -
r - l o r - 2 0 2 r - 3 0 3 - 4 0 4 l - 5 0
z
t - r o i l - 2 0 2 r - 3 0 3 r - 4 0 4 l - 5 0\ /"-_-
OF TRIALS
SISS IC i ' JS
e )Bi-.."/ , / \
9 r - 1r - c
a',1
, r ; ' - - i
\6 N A I V E
CATS
i - t o r L - 2 0 2 - 3 0 3 r - 4 0 4 l - 5 0\ /- - - - - - - - - - - - - - - -
J
FlG. 19. Curves contrasting Iearning performance 0f a group of six naive cats with performance of six cats having 500-1,000 prior paralyt ic training tr ials. The heavier l ines c0nnect points which represent mean levels of performance for thecats during each f i f tytr ial session; the l ighter l ines connect points representrng the mean response level for every ten tr ials.(From Buchwald, Standish, Eldred, and Halas.3')
muscle spindle loop interrupted, was a conditionedresponse ever elicited during the unparalyzed CStesting. When the same animals \\'ere subjectedto unparalyzed training, however, they develooedconditioned responses more rapidly than naivecats (Fig. 19). These results suggest that condi-tioned responses of gamma motoneurons are estab-lished during the paralytic training but theirdischarge through the muscle spindles is blocked.During subsequent training without paralysis, theproprioceptive inflow mediated by conditioned andunconditioned responses of the gamma motoneu-rons suddenly becomes a source of addit ional erci-tation and may explain the accelerated appearanceof the overt condit ioned response (Fig. 20). Suchan interpretation gives definite significance toproprioceptive feedback as a facilitatory mecha-nism in the development of conditioned alphamotoneuron discharge and, thereby, in motorlearning.
SUMMARY
The studies reviewed here have only suggestedthe scope of current research pertaining to motorlearning. In the intact nervous system, brain,spinal cord, and feedback mechanisms all makeimportant contributions and the extent to which
46
deletion of any part can proceed l'rithout perma-nent impairment of learning capacity depends uponthe particular species and type of learning underconsideration. Although simple motor acts canbe learned after deletion of the cerebral cortex,responses requiring complex discriminations ofsensory cues cannot be learned. Although a mon-key can learn to flex a limb deprived of all localsensory inflow, a cat cannot. Although kittens mayacquire motor responses in the isolated spinal cord,adult cats cannot. Thus, each learning situation re-quires its own careful evaluation of what centralnervous mechanisms are available and what typeof motor learning is best suited to them.
It is perhaps disappointing to be presented withsuch data, obtained from basic experimental re-search, and be given no clear view of their possibleclinical application. In this regard some commentsmade by E. R. Hilgard, an investigator of learningproblems for several decades, in a discussion ofpure versus applied research are apropos:
A study of the history of science will showthat there is no uniform relationship betweenpure and applieci science as they develop. . . .ht unv o.r.^iime. scientists in exberimental andtheoretical fields can work only on the problemsupon which they are prepared to work with theconceptual and material tools at hand. These
-Provided by the Maternal and Child Health Library, Georgetown University

TRAINING DURING
CSPASSIVE FLEX IONON L IMB RECEPTORS
US
PARALYSIS
FlG. 20. Diagram of an alphamotoneuron, discharge ofwhich causes contraction ofthe f lexor muscle, during earlyand late paralyt ic training andduring sybsequent trainingwithout paralysis. Excitatorybarrages which result fromCSUS presentations during theprogressive stages of trainingare shown by the numbered3r'fowS: L Direct stimulationof sensory fibers by the US.l l . Discharge of tendon, ioint,skin, and muscle receptorswith passive or active flexormovements accompanying theUS. l l l . Downward discharge ofsupraspinal centers respond-ing to the CS. lV. Discharge ofgamma motoneuron-mediated-proprioceptive feedback in re-sponse to the US. V. Dischargeof gamma motoneuron-medi-ated-proprioceptive feedbackin response to the CS. (FromBuchwald, Standish, Eldred,and Halas.tr)
STIM.F I B E R S
NO DISCHARGE
TO CS
SUBSEQUENT TRAININGWITHOUT PARALYSIS
CS
N O D I S C H A R G E
TO CSU51 \ cororrrorueoI I t DTSCHARGE
OISCHARGE
TO CS{
OVERT CR
DIRECT
Provided by the Maternal and Child Health Library, Georgetown University
47

\ )'r.7,$
' \ \\'::a}\- /-
may or may not be appropriate to the practicalproblem calling for solution. . . . Children mayhave rickets because at the time nothing isknown about vitamins, and patients may die be-cause a new curative drug has not yet emergedfrom the laboratory. . . . Because scientists haveto develop appropriate methods and conceptsbefore their iesults can become efficient regu-lators of practice, their concerns for a t ime mayappear to be remote from practical affairs, andsome of their disputes will seem to be quibblesover dist inct ions that do not matter. Al l thissuggests the need for patience and tolerancetoward experimentation.
If in the end a principle has to be experi-mented upon at the point of appl icat ion, i tmight be asked, why do laboratory research atal l? I f what we do with animals has to be re-peated with chi ldren, why not work with chi l-dren in the f irst place? There are several an-swers. For one thing, we do some things withanimals which we cannot do with chi ldren. Foranother thing, we make many false starts in thelaboratory, and i t would be wasteful to subjectschool children to all the things we try in thelaboratory. Again, in the laboratory we areable to control conditions as we are not able tocontrol them in the school. A principle oncediscovered in a better control led situation can beval idated in a less-well-control led one. Eventhough the sole aim of learning experimentationwere practical, it might prove economical to
48
-*,.L"-
FlG. 21. The basic research worker.
work in the laboratory in order to find the leadsworth test ing in practice.3s
In closing, consider the sequence presented inFigure 21 . The basic research worker (A)journeys quietly to his laboratory. He is quicklycaught in confl ict, however. On the one hand,he is besieged by urgent cl inical problems (B) formeans of ut i l iz ing his experimental data. At thesame t ime, he is pul led in the opposite direct ionby the mult i tudinous problems of basic researchsti l l to be solved (C). In the case i l lustrated, thescientist has successful ly been able to stretch tothe requirements of both the cl inic and the lab-oratory.
REFE REN CES
1. Hal leck, R. P. : The Educat ion of the Central NervousSystem. New York: The Macmi l lan Company, 1897,p. vr l l .
2. Kimble, G. A. : Hi lgard and Marquis 'Condi t ioning andLearning. New York: Appleton-Century-Crof ts, Inc. ,1 9 6 1 , p . 5 1 .
3. Morrel l , F. : Electrophysio logical contr ibut ions to theneural basis of learning, Physiol. Rev., 4l:443-494,1 9 6 1 .
4.Galambos, R. , and Morgan, C. T. : The neural basisof learning. In Fie ld, J. , ed. : The Handbook of Physi-o logy. Sect ion I . Neurophysio logy, Vol . I I I . Wash-ington, D.C. : American Physio logical Society, 1960,pp. l47l-1499.
5.John, E. R. : High nervous funct ions: brain funct ionsand learning, Ann. Rev. Physio l . , 23:451484, 1961.
6. Razran, G. H. S. : The law of ef fect or the law of
Provided by the Nlaternal and Child Health Library, Georgetown University

qualitative conditioning, Psychol. F.ev., 46:445463,1939.
7.Pavlov, I. P.: Conditioned Reflexes an Investigationof the Physiological Activity of the Cerebral Cortex(G. V. Anrep, ed.). New York: Dover Publications,1960.
8. Neff, W. D.: Discriminatory capacity of differentdivisions of the auditory system. In Brazier, M. A. B.,ed.: Brain and Behavior. Madison, New Jersey: Mad-ison Pr int ing Co., 1961, p. 206.
9. Brogden, W. J.: Acquisition and extinction of a con-ditioned avoidance response in dogs, J. Comp. Physiol.Psychol., 42:296-3O2, 1949.
10.Zeliony, G. P.: Effects de I'ablation des hemispherescerebraux, Rev. Med. (Par is) , 46:191-214, 1929.
1 1. Poltyrev, S. S., and 7,eliony, G. P. : Grosshirnrindeund Assoziat ions-funkt ion, Z. Bio l . , 90:157-160, 1930.
12.Girden, E. , Mett ler , F. A. , F inch, G., and Cul ler , E. :Conditioned responses in a decorticate dog to acoustic,thermal, and tactile stimulation, J. Comp. Physiol.Psychol . , 21:367-385, 1936.
13. Bromiley, R. B.: Conditioned responses in a dog afterremoval of neocortex, J. Comp. Physio l . Psychol . ,41:102-1 10, 1948.
14.Brazter , M. A. B. : The Electr ical Act iv i ty of the Nerv-ous System. New York: The Macmillan Company,1958 . o . 196 .
15. Galambos, R. , and Davis, H. : The response of s ingleauditory nerve fibers to acoustic stimulation, J. Neuro-physio l . , 6:39-57, 1943.
16.Thompson, R. , and McConnel l , J . V. : Classical con-ditioning in the planarian, Dugesia Sorotocephala,J. Comp. Physio l . Psychol . , 48:65-68, 1955.
17.Halas, E. S. , James, R. L, , and Knutson, C. S. : Anattempt at classical conditioning in the planarian, J.Comp. Physiol. Psychol., 55:969-971, 1962.
18.Shurrager, P. S. , and Cul ler , E. : Condi t ioning in thespinal dog. J. Exp. Psychol . , 26:133-159. 1940.
19. Shurrager, P. S. , and Cul ler , E. : Condi t ioned ext inct ionof a reflex in the spinal dog, J. Exp. Psychol., 28:287-3 0 3 . 1 9 4 1 .
20. Shurrager, P. S., and Shurrager, H. C.: Converting aspinal CR into a reflex, J. Exp, Psychol.,29:217-224,1941.
2l.Shurrager, P. S., and Shurrager, H. C.: The rate oflearning measured at a single synapse, J. Exp. Psychol.,36:347-354, 7946.
22. Kellogg, W. N., Deese, J., Pronko, N. H., and Feinberg,M.: An attempt to condition the chronic spinal dog,J. Exp. Psychol., 37:99-117, 7947.
23.Kellogg, W. N.: Is "spinal conditioning" conditioning?Reply to "a comment," J. Exp. Psychol., 37:263-265,1947.
24. Shurrager, P. S., and Dykman, R. A.: Walking spinalcarnivores, J. Comp. Physiol. Psychol., 44:252-262,1 9 5 1 .
25.Dykman, R. A. , and Shurrager, P. ,S. : Successive andmaintained conditioning in spinal carnivores, J, Comp.Physiol. Psychol., 49:27-35, 1956.
26. Forbes, A., and Mahan, C.: Attempts to train the spinalcord, J. Comp. Physiol. Psychol., 56:36-40, 1963.
27.Buchwald, J. S. , Standish, M., and Eldred, E. : Ef fectof deafferentation upon acquisition of a conditionedflexion response in the cat, Exp. Neurol:, 9:372-385,1964.
28. Gorska, T., and Jankowska, E.: Instrumental condi-tioned reflexes of the deafierented limb in cats andrats, Bul l . Acad. Pol . Sci . [Bio l . ] ,7:16l-164,1959.
29. Jankowska. E.: Instrumental scratch reflex of the de-afferented limb in cats and rats, Acta Biol. Exp.(Warsz.) , 19 :233-247, 1959.
30. Gorska, T., and Jankowska, E.: The effect of deafferen-tation on instrumental (Type II) conditioned reflexes indogs, Acta Biol. Exp. (Warsz.), 21:219-234, 1961.
31. Knapp, H. D. , Taub, E. , and Berman, A. J. : Ef fect ofdeafferentation on a conditioned avoidance response,Science. 128 :842-843. 1958.
32.Knapp, H. D. , Taub, 8. , and Berman, A. J. : Move-ments in monkeys with deafferented forelimbs, Exp.Neu ro l . , 7 : 305 -315 , 1963 .
33.Granit, R.: Receptors and Sensory Perception, NewHaven, Connecticut: Yale University Press, 1955.
34. Buchwald, J. S., and Eldred, E.: Conditioned responsesin the gamma efferent system, J. Nerv. Ment. Dis.,132:746-152, 7961.
35. Buchwald, J. S., Beatty, D., and Eldred, E.: Condi-tioned responses of gamma and alpha motoneurons inthe cat trained to conditioned avoidance, Exp. Neurol.,4 : 9 1 - 1 0 5 , 1 9 6 1 .
36. Kuffier, S. W., Hunt, C. C., and Quilliam, J. P.: Func-tion of medullated smali-nerve fibers in mammalianventral roots: efferent muscle spindle innervation, J.Neurophysiol., 14 :2O-54, 1951.
37. Buchwald. J. S., Standish, M., Eldred, E., and Halas,E. S.: Contribution of muscle spindle circuits to learn-ing as suggested by training under Flaxedil, Electro-enceph. Clin. Neurophysiol., 76:582-594, 1964.
38. Hilgard, E. R.: Theories of Learning. New York: Ap-pleton-Century-Crofts, Inc., 1956, pp. 488-490.
- L
Provided by the Maternal and Child Health Library, Georgetown University
49

Posfurol lntegrotionof Spinol Levels
EARL ELDRED, M.D.
O u* **o*rrocr of motor func-tion is growing at an accelerating, even over-whelming rate (Fig. l) . In just that small partof this subject field treating of the morphology andintrinsic physiology of muscle receptors at least268 reports appeared in the last five years, com-pared to 198 and 88 in the preceding five-yearperiods.l Obviously, in a paper with as broada title as this one, only eclective illustration ofthe subject matter can be attempted.
SEGMENTAL ORGANIZATION ASA COMPLEX OF FIXED REFLEXES
Sherrington's statement that "the unit reaction innervous integration is the reflex" 2 has become thecentral tenet of our understanding of motor co-ordination. Archetype of reflexes is the stretch re-sponse, in which receptor cells, the annulospiral
Adapted from a paper presented at the Symposium onThe Child with Central Nervous System Deficit, September28-October 2, 1964, at The University of Pennsylvania,Philadelphia.
The duthor is Professor of Anatomy, Department ofAnatomy and Brain Research Institute, University of Cali-fornia, Los Angeles, 90024.
50
afferents of muscle spindles, directly contact thealpha motoneuron effector (Fig. 2). A variety ofother receptive cells establish connections with thesame motoneuron, but always through interme-diary neurons. Even the spindle flower-spray end-ings, which lie alongside of the annulospiral ter-minais and frequently resemble them, shun directcontact with motoneurons.
The interneurons greatly enrich flexibility inintegration of nervous activity. Picture for a mo-ment the limitations imposed by a neural organi-zation in which afferents were linked to motoneu-rons solely by direct synaptic connection. Thefinal common path would still be responsive tostretch receptors of its own muscle and synergists.Other receptors in joints, skin, and muscle of thelimb, if they were to have reflex meaning, mustalso have footholds on the motoneuron membrane.The number of such contacts the membrane sur-face could support is limited, necessitating multi-plication of motoneurons and afferent axons. Theneuron membrane would be a field for competitiveinteraction by a constellation of afferent pathwaysthat might in one behavioral situation lead tofunctional outcome, but be disruptive in others.
Provided by the Maternal and Child Health Library, Georgetown University

E
c
E
U
r
EUo
E
f
z
<-<<((FlG. 1. Numbers of publications by five-year periods inthe subiect field of nrorphology, pathology, and intrinsicphysiology of muscle receptors, based upon a compre.hensive bibliographic search of the literature.l Centralreflex effects of afferent discharge and closely relatedmaterial on joint receptors are not includdd. lt is seenthat investigative interest in this field, which had a flurryof activity in the late eighteen hundreds and hesitatingprogress over the next several decades, has recently ex-oloded. The number of authors increased to 225 in thelast f ive-year period from earlier totals of 137 and 52, sug.gesting that future multiplication in productivity is to beexDected.
Sensory stimulation might easily arise in whichantagonist muscles were coactivated, yielding ageneral arousal of muscle action rather than di-rected action. To provide for reciprocal innerva-tion, duplication of sensory afferents would benecessary, since the branches of one sensory alionwould probably be incapable of facilitating at onemotoneuron and inhibiting at others. The tem-poral course of reflex events would be stereotyped.as it would be limited by response characteristicsof the sensory ending and the motoneuron.
This caricature of neural organization drawsattention to the vital contributions interneuronsmake to integration. They ( 1) provide forwidened and economical central distribution ofsensory input, (2) give multiple opportunity for
FlG. 2. organization of astretch ref lex as exempli f iedby the "jaw jerk." Afferentimpulses init iated by plenti fulspindles in jaw muscles travelcentralward to establ ish directsynaptic connection with rno-toneurons resoonsible for con-tract ion of the same muscle.The fact that cel l bodies ofthe annulosoiral axons in thissDecial instance are locatedwithin the neuraxis, ratherthan in a peripheral ganglion,does not alter the basic sim-pl ici ty of the stretch ref lex.The masseter and temporal ismuscles part icipate in thetonic contractions found gen-eral ly among antigravity mus-c Ies.
MESENCEPHALICNUCLEUSOFTJAW
RE FLEX
MOTONUCLEUS
MASSETER MUSCLESPINDLE ANNULOSPIRAL ENDING
5r
Provided by the Maternal and Child Health Library, Ceorgetown University
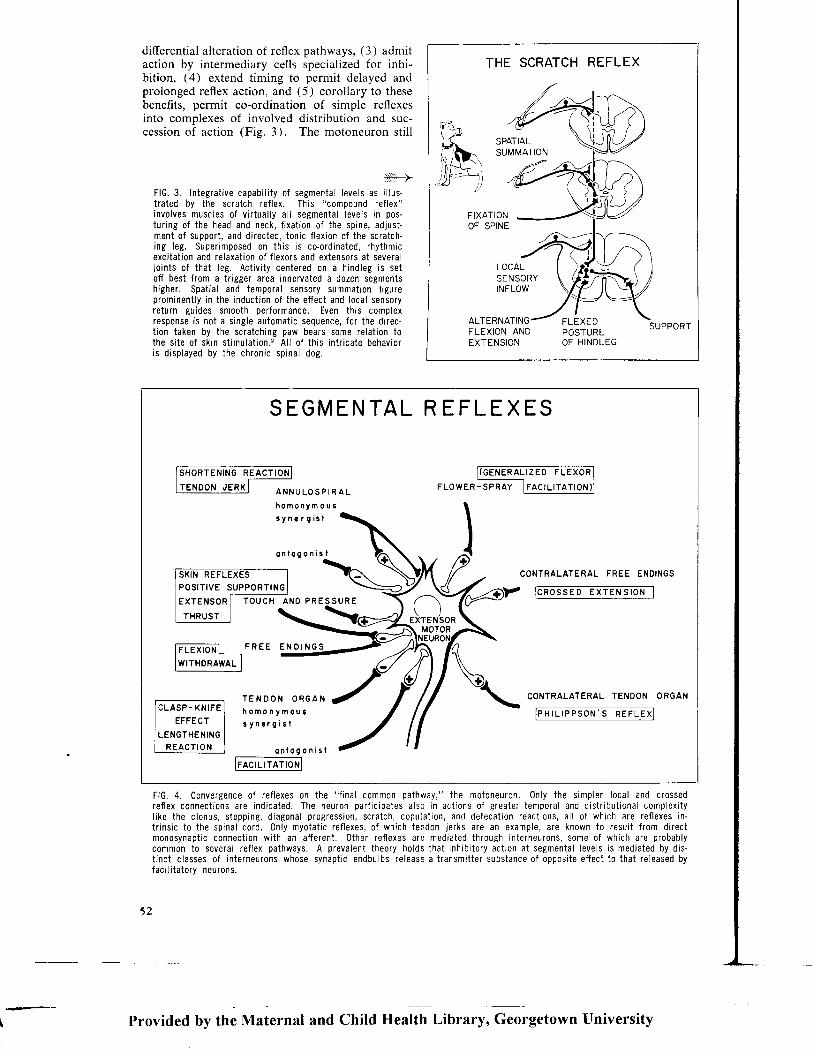
differential alteration of reflex pathways, (3) admitaction by intermediary cells specialized for inhi-bition, (4) extend timing to permit delayed andprolonged reflex action, and (5) corollary to thesebenefits, permit co-ordination of simple reflexesinto complexes of involved distribution and suc-cession of action (Fig. 3). The motoneuron sti l l
>->FlG. 3. Integrat ive capabi l i ty 0f segmental levels as i l lus"t rated by the scratch ref lex. This "compound ref lex"involves muscles of v i r tual ly a l l segmental levels in pos-tur ing of the head and neck, f ixat ion of the spine, adjust-ment of support , and di rected, tonic f lex ion of the scratch-ing leg. Super imposed on th is is co-ordinated, rhythmicexci tat ion and re laxat ion of f lexors and extensors at severaljo ints of that leg. Act iv i ty centered on a hindleg is setof f best f rom a t r igger area innervated a dozen segmentshigher. Spat ia l and temporal sens0ry summati0n f igureprominent ly in the induct ion of the ef fect and local sensoryreturn guides smooth performance. Even th is complexresponse is not a s ingle automat ic sequence, for the di rec-t ion taken by the scratching paw bears some relat ion tothe s i te of sk in st imulat ion. ' Al l of th is int r icate behavioris d isplayed by the chronic spinal dog.
FlG. 4. Convergence of ref lexes on the " f inal common pathway," the motoneuron. 0nly the s impler l0cal and crossedref lex connect ions are indicated. The neuron part ic ipates also in act ions of greater temporal and dist r ibut ional complexi tyl ike the c lonus, stepping, d iagonal progression, scratch, copulat ion, and defecat ion react ions, a l l of which are re{ lexes in-t r ins ic to the spinal c0rd. 0nly myotat ic ref lexes, of which terdon Jerks are an example, are known to resul t f rom directmonosynapt ic connect ion wi th an af ferent . Other ref lexes are mediated through interneurons, some of which are probablycomm0n to several ref lex pathways. A prevalent theory holds that inhib i tory act i0n at segmental levels is mediated by dis-t inct c lasses of interneurons whose svnaot ic endbulbs re lease a t ransmit ter substance of opposi te ef fect to that re leased bvfaci l i tatory neurons.
52
THE SCRATCH REFLEX
SPATIALSUMMATION
FIXATIONOF SPINE
LOCALSENSORYINFLOW
ALTERNAT FLEXEDPOSTUREOF H INDLEG
SUPPORTFLEXION ANDEXTENSION
SEGMENTAL R EFLEXES
troRrEr,xNG-nEacno[|I T E N D O N J E R K I A N N U L O S P I R A L FLOW
n 0 m o n y m o u s
3 y n € r 9 r s l
o n l o g o n i s f
C O N T R A L A T E R A L F R E E E N D I N G S
P R E SUR EI C R O S S E D E X T E N S I O N I
F L E X I o N L - F R E E E N o I N G
lwrrHoRAWAL I
T E N D O N O R G A Nh o m o n y m o u ts y n . r g i s l
CONTRALATERAL TENDON ORGAN
IFHTLTFPsoJ I - JREFLT I I
o n l o g o n i s l
tF crLrrArfcNl
Provided by the Maternal and Child Health Library, Georgetown University

b-1 1 '
J l "
- l - - ' l I
+lt | i l r , l . . i lt l*** ll
r l li - r ' r r l r rs i l' t i r r . r r , rs l l
t t l{rrt{rJl{Jt |l
I | [ t ,
- 1 | l ' I
- l t
o
I *,.**I , , ,*-I -.**.l-Il_l-\ * ' rr-
| - r ' | '
lr-r 96 g
J\AA/\AIVWIAA
50 cylsec
remains a final stage in integration where contri-butions from annulospiral afferents and a varietyof facilitatory and inhibitory interneurons areweighed to give graded output (Fig. a).
Integration at segmental levels is not restrictedto the spinal cord. Spindles in muscles, unlikemost other receptors, have an efferent controlthat alters sensitivity of the sensory organ to itsadequate stimulus. Terminal wrappings in theseorgans, then, are sites for integration of data onmuscle status and levels of central activity. Thefusimotor control is not a generalized arousalmechanism whereby all spindles are affectedequally, but is topographically specific (Fig. 5).Patterns of reflex spindle activation in most in-stances are similar to those of the alpha motoneu-rons, but the sensitivities of these two motor sys-tems differ importantly. The external loopthrough spindles is activated at lower thresholdsand earlier in time than are the alpha motoneuronsmediating contractions (Fig. 6). Such change inspindle motor activity may trigger a chain ofevents: the increase in fusimotor discharge in-creases sensitivity of phasic and tonic componentsof spindle discharge; the increased sensory dis-charge facilitates firing of motoneurons to the same
FlG. 5. Patterns of change ingamma motoneuron responsesas affected by skin stimula-t ion. Pinching the toe.pads inthis spinal cat caused thesmall spike discharge moni-tored from a branch of themedial gastrocnemius nerve(sweep records from abovedownward under a) to es-sential ly disappear for theduration of the st imulus (barto right of sweep records).The myograph trace (verticall ine labeled "M") revealed nochange in muscle tension.Stimulat ion over the heel orcalf in contrast caused ac-celerated f ir ing of the smallunit ( traces under b). Addi-t ional ly, a tal l spike potentialappeared in the three latersweeo records. These repre-sent the f ir ing of an alphamotoneuron. The delay inalpha discharge, ref lected alsoin the myograph deflect ions,(to le{t of sweep traces)compared to the early ac-celerat ion of the gamma unitis characterist ic of the rela-t ive sensit ivi ty in ref lexthreshold of these two typesof motoneurons. (From Eldredand Hagbarth 3).
muscle; shortening of the gross muscle may result,releasing spindles from stretch and reducing theirdischarge; finally, at some shorter length a newequilibrium is reached between muscular length,spindle discharge, and alpha motoneuron activity.This concept of initiation of motor action by anadjustable sensor of "error in length" has beenlikened to engineering servomechanisms.
FLEXIBILITY INREFLEX ORGANIZATION
Spinal organization as outlined above has aflexibility limited only by the number of "reflexunits" and the combinations they may form. Eachreflex has its specifc input terminals, pathwaythrough the cord neuropil, and final outlet. Wheretwo reflexes compete, the outcome is foreseeable,given sufficient data on strength of respective stim-uli and constants of the reflex pathways. Thismosaic of reflexes, of course, may be intrudedupon by supraspinal influence. In addition, otherfactors of purely segmental origin seem to play apart. The spinalized rat, for instance, respondsto light tapping of skin at the root of the tail bya reflex electromyographic activation of tail mus-
Provided by the Maternal and Child Health iib.u.y, Georgetown University
5 3

M E D I A L G A S T R O C N E M I U S
E X T E N S O R O I G I T O R U M L ,
B L A D O E R P R E S S U R ECAL IBRAT ION IOO MM
H z o
D U R I N G
INJ ECTION
4 0 c c I N 5 0
D U R I N G
WITH DRAWAL
30 cc OUT
M E D I A L
GASTROCNEMIUS
4 0 c c E 6 a a
E X T E N S O R
DIGITORUM
FlG. 6. Difference in effect on f lexor and extensor spindle circuits induced by distending the bladder of a spinal cat. Waterat body temperature was injected in the quanti t ies indicated and the pressure (smooth trace) monitored by a f luid pressuretransducer. An extensor afferent unit from the gastrocnemius, identi f ied as a spindle by i ts twitch response (bottom record),shows above the basel ine of the spiked trace. Discharge of an extensor digitorum longus (EDL) unit appears below the base-l ine. This muscle is physiglogical ly a f lexor. During inject ion (second record) the rate of discharge of the EDL afferent in'creased strongly compar;d to the control rate (upper str ip), but the gastrocnemius unit showed l i t t le change. This viscero-somatic ref lei bf the fusimotor system would presumably faci l i tate overt contraction by the alpha motoneurons of the samemuscle i f dorsal roots at that segmental level had not been severed. Specif ical ly in ref lex patterns of fusimotor ref lexes andthe lower threshold of these compared to alpha motoneurone effects are evident. (From Abdullah and Eldred.a)
F lG.7 . Reproduc ib i l i tY o f re 'f lex electromyograph activa't ion o f ta i l musc les in chron icspinal rat. Each uPward stePrepresents a posit ive responseto a taD over the skin at thebase of the tai l . The responseswere reDeatable over a num'ber of tr ials, but eventual ly be-came "habituated." New st inn-ul i of a pinch or tapping overa dif ferent skin site caused thereflex to return or be "disin-hibited." (Adapted from Pros-ser and Hunter.s)
S P I N A L R A T
S T I M U L U S : T A P O N T A I -
R E S P O N S E : T A I L M U S C L EE M G A C T I V A T I O N D I S I N H I B I T I O N
U'lrlcDz
@lrJtr
H A B I T U A T I ' ' \ \
BtTlON ----- \ , !D t S t N H t B t T t 0 N - = - - _ \ 1 _
HABlruAr I oN ----liv\\- P lxcH/ / | \onrcrr,rar-
/ ( Pos l r l oN
/ N E w P o S r T r 0 NI ON TAIL
2 ' R E S T
S T I M U L A T I O N S
t4
Provided by the Maternal and Child Health Library, Georgetown University

cles (Fig. 7). This response, as expected in a setinput-output relationship, is stereotyped and maybe elicited repeatedly. However, after severaldozen trials, the response begins progressively todecli:re in amplitude and eventually ceases; it hasbecome "habituated." This is not fatigue, as stim-ulation of a second area on the tail will cause acti-vation at the original site of response and, more-over, may induce a "disinhibition" or transitoryreturn of reflex elicitation from the original stim-ulus locus. These habituation effects are probablynot dependent upon change mediated through thefusimotor system, since diminution in alpha re-sponse can occur in spinal anirr,als totally para-lyzed to break feedback through the spindle loop(Fig. 8). Increase in excitability with repetitiveuse of a reflex pathway is a capability of segmentalorganization, as well as is decrease.6 Thesechanges, as witnessed in acute preparations, areof short duration, but trace effects of a habitua-tion procedure can persist hours or days to build upalteration in reflex behavior comparable to those
ordinarily associated with learning processes (Fig.e) .
The mechanisms of synaptic connection andneuronal excitability responsible for such changein reflex outcome are not known, but they mustsatisfy criteria of being lasting in duration, addi-tive, and, for the examples given, subject to changewith repetitive use of the particular reflex pathwayunder observation. The effects of use on synapticlinkage have been studied extensively in the stretchreflex itself, where monosynaptic connection andthe feasibility of selective stimulation of afferentsmake quantitative analysis possible. Repetitive useof this reflex pathway, as simulated by applyinga series of stimuli at intervals to a muscle nerve andmonitoring of the synchronized lesponses inventral roots, reveals no lasting effect. Intensi-fication of use by tetanic stimuiation is moreeffective, for after a brief conditioning period oftetanic stimulation, responses to individual teststimuli may be enhanced for minutes (Fig. 10,right column). Far more effective in altering total
2ACONTROL STtMULATtON.6mo STIMULATION S
TRIAL I
ozOLdaqo
EI!o_ lo
at!a)f&
+ l 5 s e c .@ { . € - a a o a a a o a a o a a a e
I y | 9 l g
TRIALS AT 15 SECONDS
[ . 2 m v
O . 5 s e c .
FlG. 8. Habi tuat ion in response of motoneuron in acutely spinal ized cat . The motor uni t was is0lated in the L6 ventra l rootof a paralyzed cat in which the cord had been t ransected at a low thoracic level several hours ear l ier . The uni t gave phasicresponses to touch and 0.5 second t ra ins of s ixty cycles per second st imul i appl ied to the hindpaw (Tr ia l 1) , but-showed rrointer t r ia l tonic d ischarge. Repet i t ion of st imulus t ra ins at f i f teen-sec0nd intervals resul ted in progressivJ decl ine of re-sponse as seen in records of t r ia ls ten and twenty and in the curve showing as a running average of three the numbers ofpotent ia ls appear ing wi th in 0.5 sec. af ter cessat ion of st imulatron. (From J. S. Buchwald, E. S. Hl las, and S. Schramm.6)
Provided by the Maternal and Child Health Library, Georgetown University
55

HABITUATTON PROCEDURE TO 25 CMz AREA OF oNE FLANK (lOTdoy)
RUBBING
CONTROLLEVEL
80lrJaz8.0U'UJE
b40
F( / ,20z1rlFzo
7 0 90
CHLORPROMAZINE
FlG. 9. Habituation of a scratch ref lex in chronic spinal cat as induced by ten minutes dai ly massage of the 25 cm. skin areaused for test el ici tat ion of the ref lex. A decl ine in response intensit ies, indicated in arbitrary values along ordinate, oc-curred over several days fol lowing onset of the habituation regime (black bars). Administrat ion of chlorpromazine on twooccasions resulted in ieturn of the scratch ref lex. (Adapted from Fig. 1, Kozak and Westerman.T 0nly data from I to 12and 60 to 100 days represented. Curves are those drawn by original authors.)
accumulated volume of traffic over this reflex path-way are operative procedures. Chronic deaffer-entation of a segment, as expected from the hy-pothesis that synaptic transmission is facilitatedby use, is marked by diminution of monosynapticresponse (Fig. 10). Moreover, reflexes of intactspinal segments adjacent to those with severedroots are enhanced. These intact segments pre-sumably relate to muscles which have been put togreater reflex use through assuming a share of theworkload of deafferented muscles. An even sim-pler method of reducing use of the stretch reflexpathway should be tenotomy, since reduction instretch-responsive afferent discharge of only theoperated muscle should occur. Actually, afferentactivity, at least several weeks after tenotomy, issaid to be greater from the operated muscle thanthe opposite intact one.e This would explain whymonosynaptic reflexes at this period are also en-hanced.
The preparations just cited had quantitativechange in use of the stretch reflex pathway. Moresubtle experiments directed to qualitative altera-tion in afferent influx have been made in kittensby cross-uniting muscle nerves to two antagonistsor between muscles of a synergist pair, so that the
56
central stump of one muscle was joined to thedistal stub of the second, and vice versa.1o Eachmotor nucleus was then subject during its develop-ment to a new set of afferent influences, and themuscles conversely governed by strange efferents.This procedure could cause complex central effectsarising not only from the obvious exchange ofinitially different afferent inflows, but from second-ary changes that develop in the muscles them-selves. As is well known. "red" or "tonic" musclehas a slower twitch contraction than "pale" or"phasic" muscle, a difference that is present ondirect stimulation and arises in the contractilemechanism itself. At birth, all muscles yield con-tractions of slow time course. Only after thesecond week does the speed of contraction of thecat's gastrocnemius outstrip that of its soleus syner-gist, and by the second month the full contrastof the adult state is attained.ll If nerves to thesoleus and gastrocnemius are cross-united in kit-tens, differentiation of the two muscles is reversedso that the soleus twitch becomes faster than thatof the gastrocnemius. There is evidentially atrophic or inductive influence transmitted ortho-dromically along the motor axons. Evidence fora comparable influence exerted orthodromically
Provided by the Maternal and Child Health Library, Georgetown University

Le,z ,+Sr DR 's . r ; DAys
I N T A C T S I D E
I 6 0 0 0 P U L S E S
)A T 4 0 0 / S E C
o ' l l "
S T I M U L U S :Lz + St DR's
R E S P O N S E :G A S T R O C -N E M I U S N t ' t
m s e c s\ \ L \ L \ \ \ \ \ \ L \
FlG. 10. The effect 0n the monosynaptic response of l0ng-term disuse attained by deafferentat ion. Sensory roots 16, 17,and S1 were cut distal to the dorsal root ganglion, thus Ieaving the central stubs of these roots viable. Forty days latertests were made alternately on operated and intact sides for responses in the gastrocnemius nerve to single-shock st imuliappl ied to the L7 and S1 dorsal roots. Response height over the disused monosynaptic pathway was 0ne-fourth that 0n theintact side (top pair of traces). Individual responses fol lowing tetanization were enhanced on both sides, but st i l l had rela-t ively less ampli tude on the deafferented side. Enhancement fol lowing tetanization was greatly prolonged on the deafferentedside. (Adapted from J. C. Eccles and Mclntyre.s)
along sensory axons is less obvious. However, in-tracellular microelectrode recording of thestrength of reflex connections made by a motonu-cleus subjected to cross union reveals a patternunusual for that motonucleus, but expected for thefoster muscle to which i t has been united.l l I tmust be stressed that the detected differences aresmall, even though the procedure was performedon young animals which should have greater ca-pacity for plastic change.
INHIBITORY MECHANISMSIN SEGMENTAL INHIBIT ION
Widespread change in reflex behavior can resultfrom tipping the balance between descending tonicinfluences over flexors and extensors. The exag-geration of antigravity activity in the decerebrateanimal is a prime illustration. In part, this
change in ref lex response arises from augmentationof faci l i tatory inf luence. for act ivi ty over spindleloops is greatly increased in decerebrate prepara-t ions with resultant faci l i tat ion of extensor neu-rons.12 But also, the shif t in behavior stemsfrom a change in the tonic level of descending in-hibitory activi ty. In the decerebrate animal, forexample, ref lexes evoked by st imulat ion of groupII and III afferent fibers of skin and muscle arediff icult to detect (Fig. 11). In spinal animalsthe same reflex pathways are hyperactive. Evi-dental ly cutt ing the descending pathways removespowerful tonic inhibit ion of interneurons mediat ingthese reflexes.
The i l lustrat ions given earl ier of behavioral"habituation" and "disinhibit ion" in spinal animalssuggest that levels of tonic inhibit ion can undergomodiflcation at purely segmental levels. Asso-ciation of known neurophysiological inhibitory
Provided by the Maternal and Child Health Library, Georgetown University
5 7

BEFORE SPINALTRANSE CT ION
AFTER DECEREBRATE
IJ'q
zo(L(nIJE
Lo
IJo=L-)
IJ
:F
JLtJ(r
t 4 0
t o o
t 4 0
t o o
I
"" ' l ', , \t \
i \ ., i..r
3,0 x
TESTING
t 8 0
1 4 0
I
, i t . r
\TESTINGI5 X THRESHOLD
too
t l, , \t \t \
m s e c l o 2 0T I M E A F T E R P O T E N T I A T I O N
CONDIT IONING
FlG. 11. Contrast in effects on f lexor monosynaptic responsein decerebrate state (sol id curves 0n graphs) and after spinaltransection (dashed curves) of a condit ioning st imulus to anextensor muscle nerve. The ventral root monosynaptic re-sponse was el ici ted by single shock st imulat ion of the biceps-semitendinosus (BST) nerve. Condit ioning st imuli to the nerveof antagonist gastrocnemius (G) muscle were at three levelsof intensity:1.6 t imes threshold, at which strength grouplb f ibers from tendon organs should be activated, as well as
mechanisms with these phenomena of diminishingbehavioral response is not possible at present, butinhibitory mechanisms intrinsic to spinal levels,nevertheless, may be mentioned. These can bebroadly classified into those dependent upon ( I )afferent inflow, (2) efferent outflow, and (.3),possibly, activity autochthonous to the cord. Prob-ably all afferent fibers, in addition to causing facil-itation of appropriate motonuclei, make other con-nections of inhibitory effect. Tendon organssuppress activity of homonymous muscles, annul-ospiral afferents suppress antagonists, touch recep-
5 8
the la f ibers from spindles; 3.0 t imes, or suff iciently strongto evoke discharges in group l l f ibers; and 15 t imes threshold,for st imulat ion of group l l l afferents also, In the decerebratestate, scarcely any effect of the condit ioning st imulus at any0f these strengths was n0ticeable, but after spinal izat ion eachgroup of afferents made a dist inct faci l i tatory contr ibution tothe f lexor monosynaptic response. (Adapted from R. M. Ecclesand A. Lundberg.a)
tors on the shin inhibit contractions in the calf,and so on. Since many endings are capable ofsustained flring, they presumably give rise to acontinuing hail of inhibition. If increase in useleads to facilitated transmission between neurons,repeated exercise of one reflex pathway and itsresultant facilitation should be paralleled by aug-mentation of inhibition over opposing reflexes.Such inhibitory effect on interfering backgroundactivity should cause the primary reflex to standout in progressively greater relief; or contrariwise,habituation could arise if incidental activation of
Provided by'the N{aternal and Child Health Librar,v, G.org.rornn University

other sensory afferents, not conducive to the pri-mary response, led to the gradual bui ld-up of anopposing inhibition.
Inhibitory activity dependent upon motor gut-flow is illustrated by the phenomenon of "recurrentinhibition." If a single shock is applied to a musclenerve, motoneurons of other muscles not includedin the antidromic stimulation are inhibited, asjudged by their ventral root or intracellular re-sponses to appropriate sensory stimulation. Thevolley ascending the motor axons presumably alsotravels up the collateral branches of these axonswhich arise close to the cell body and are directedrecurrently within the ventral horn. These re-current coilaterals are postulated to synapse oninhibitory interneurons named "Renshaw cells"after the discoverer of this inhibition. The Ren-shaw cells, according to this hypothesis, are chem-ical transducers which produce inhibitory effects attheir widespread connections with homonymousand other motonuclei. This inhibition, like thatdeveloped in response to afferent volleys, lasts buta few milliseconds under customary conditions oftesting. Whether under prolonged activity of thisrecurrent inhibitory pathway trace effects may per-sist, comparable to those ascribed to the mono-synaptic reflex pathway, is unknown.
A third type of segmental inhibition exists whichis perhaps independent of both afferent andefferent flow. Schiff, working with frogs, andSherrington in the cat noted that decerebraterigidity of forelimbs underwent marked augmenta-tion subsequent to section of the thoracic cord.This "Schiff-Sherrington effect" was interpretedas a release of brachial motoneurons from sup-pressive action by the lower spinal cord. Thephenomenon is demonstrable in the cat deprivedof afferent activation at lumbosacral levels,la sothat the suppressive influence must arise eitherfrom activity descending from supraspinal struc-tures to be reflected upward from lumbosacralIevels, or more simply, is generated within thelumbosacral cord itself. In this respect, it is ofbasic interest to note that the spinal cord isolatedcompletely from descending and afferent impulsessupports some neural activity.l5, 16 Presence ofan inhibition generated tonically in the cord wouldadd new dimension for flexibility in spinal organ-ization, since reflex alteration could arise fromprogressive retraction of ongoing inhibition, as wellas facilitation of the reflex path.
The existence of tonic inhibition over motoroutflow confined entirely to segmental levels hasbeen demonstrated. As mentioned earlier, asingle volley applied to a motor nerve results inwidespread recurrent inhibition of motoneurons.If, however, a stimulus is applied to the appropri-ate muscle nerve, the excitability of some moto-neurons may be found to be increased instead(Figs. 12, 13). This has been interpreted as a re-
? 8 0 - 2 8 0 0 - 6 6 - 5
moval of the suppression of motoneurons tonicallyimposed by "Renshaw cells," an inhibition of inhib.itory cells! u' 18 The severe impairment of in-terneural activity occurring after an episode ofanoxia of the cord results in exaggerated motoneu-ron excitability which may have a.similar explana-tion in the lifting of tonic background inhibi-t ion.1e
The relay of afferent activity to ascending sen-sory tracts is also subject to descending inhibitoryinfluence,20 furnishing in the intact animal a fur-ther mechanism by which motor activity pre-sumably could be modified. Evidence for asupraspinally controlled filtering of ascending sen-sory information, for example, is seen in thereduction of evoked waves in spinothalamic tractssubsequent to stimulation of the inhibitory retic-ular formation. The evoked waves are augmentedafter transection of the spinal cord, demonstratingthe tonic nature of the suppressive influence (Fig.14 ) .
The relation of these several types of segmentaland descending inhibition to one another is poorlyunderstood and some of the phenomena may rep-resent different facets of the same mechanism.The descending influence that dampens reflex path-ways of group II and III afferents, for example,could be that which affects ascending sensoryrelay. In any case, an active role of tonic inhib-itory mechanisms in integration at segmentallevels seems assured. Plastic change in reflexeffect may conceivably arise from accumulativeincrease or decrease in this tonic inhibition. Theability of some drugs with prominent effect oninterneurons to cause behavioral "disinhibition"of a habituated response, for example, might be soexplained (Fig. 9). Even the speciously simplediminution in reflex transmission resultins fromdisuse might not depend entirely on the dirict lossof facilitation over the reflex pathway, but ariseas well from the active development of intribitionover that pathway. It has been suggested, forinstance, that the loss of tonic electromyographicactivity in the soleus consequent to reduction ofafferent inflow by tenotomy may in part be due toinhibition of the myotatic reflex pathway, sinceunder anesthesia electromyographic activation re-turns.21
CONCLUSION
Most of what has been said here is evident inFigure 15. In the dog segmental reflexes intheir simplest form are operating to hold his bellyin and trunk up. Undoubtedly other more com-plicated but local pathways are also activated byreceptors in the paw to yield positive support.Rearing the head has stretched vertebro-occiDitaljoint receptors, initiating a statokinetic rifl"xwhich spreads over two dozen segments to intensifyprotrusion of the forelegs, but softens the stance
Provided by the Maternal and Child Health finrary, Ceorgetown University
59

ICROELECTRODEPICK- UP OF
TESTVOLLEY
I"'CONDITIONINGVOTLEY lOmV
GASTROCNEMIUS-SOLEUS
| , 2 0 m s e c s-CONDITIONING
VOLLEY
MOTONEURONtr
TEST
DEEP PERONEALMOTONEURON
. g 4 - o
VOLLEY
FlG. 12. A demonstrat ion of the presence of tonic inhibit ionof motor act ivi ty in a spinal animal. The excitabi l i ty of twodeep peroneal motoneurons was gaged by the ampli tude ofshif ts in membrane potential m0nitored intracel lularly duringa shock aDDlied to the dorsal root. Deflect ions upward 0nthe curves represent increased excitabi l i ty tending to bringthe motoneuron t0 i ts f i r ing thresh0ld. These "excitatorypostsynaptic potentisls" (EPSPs) seen during the control periodare represented for each neuron by a curve marked by f i l led
c i rc les . The open c i rc les ou t l ine responses 0b ta ined to thesame test st imulus after appl icat ion of a single "condit ioningvol ley" antidromical ly to the nerve of the antagonist gastro-cnemius-soleus nerve. Fol lowing a 1 msec. delay, the curvesfor each neuron diverge by a small amount, that is, the moto-neurons are driven by the test st imulus closer to the thresh-old for f i r ing. This indicates that in the control period thetwo f lexor muscles must have been under tonic inhibit i0n.(Adapted from Wilson and Burgess.u)
>>FlG. 13. The mechanism postulated " t0 under ly the phe-n0menon of " recurrent faci l i tat ion" i l lustrated in Figure 12.The motoneuron is thought to be tonical ly subject e i therdirect ly , or thr0ugh at tenuat ion of impinging faci l i tatoryact iv i ty , to an inhib i t ion by some interneurons (b lack 'bodied neurons wi th t r iangles indicat ing inhib i tory syn'apses). These interneurons in turn are subject to suppres-s ion by other inhib i tory cel ls , inc luding perhaps theRenshaw cel ls (whi te-bodied cel l wi th t r iangle inhib i torysynapse). Thus there may ar ise an inhib i t ion of ongoinginh ib i t i on , a " d i s i nh ib i t i on . " I n " r ecu r ren t f ac i l i t a t i 0n , "the Renshaw cel ls are exci ted by recurrent c0l laterals ofaxons belonging to motoneurons of appropr iate musclegroups. Some af ferent modal i t ies have also been demon-strated to inhib i t Renshaw cel ls . '8
60
I L J I
STI i / U L US
TESTR ESPON S E
C O N D I T I O N I N GSTIN4 U LUS
Provided by the Maternal and Child Health Library, Georgetown University

S T I M U L U S : L 7 D R
R E S P O N S E : V E N T R A L C O L U M N
BEFOR E AFTE R
CHLORALOSE
5 msec
BE FORE AFTER I h r
CORDTRANSECTION
5 m s e c
FlG.14. Demonst ra t ion o f ton ic descend ing inh ib i to ry in -f luence over afferent relay at segmental levels. The L7 DRin the two curarized preparations represented by upper andlower rows of traces was sttmulated with single shocks(small art i facts to left in records). Rec0rdings were madefor relayed discharges in sensory tracts located in the ventralcolumn of the cord. In the unanesthetized cat yielding thetop two traces, no relayed wave was detectable in the con-
posteriorly. Vestibular organs are largely re-sponsible for the stretch reflex tone in the fustplace, just as the behavioral "orientation reaction"to the sausages overhead was responsible for thehead-rearing that modified the standing porse.The sausages have been the cause of even moreintense, generalized motor tone, for obviously theanimal's reticular formation is thoroughly acti-vated. The cat, who by his raised hair appearsto view the situation somewhat differently, re-minds us of a factor not considered before.Endocrine secretions affect not only metabolismof the muscle contractile process, but have moresubtle influences on the central neural processes aswell.
Fortunately, the intact dog does not have to passthrough such a conscious analysis of his actions oreven wait out a sequential play of them, forthese processes are going on simultaneously, co-
t ro l per iod ("before") . Af ter g iv ing chloralose, an anesthet icwhich may act speci f ical ly on inhib i tory mechanisms, a markedevoked wave was recorded ( to r ight) . In the second prepara-t ion, tota l t ransect i0n of the cord caused comparable markedenhancement of the wave 0f response. These f indings areinterpreted to indicate that the re lay 0f sensory act iv i ty toascending pathways was under tonic descending inhib i t ion.(Adapted f rom Hagbarth and Kerr .4)
F r G . 1 5 .(Adapted
Thefrom
integral result ofRushworth.2)
postural mechanisms.
Provided by the Maternal and Child Health Library, Georgetown University
6r
ordinately, and with final purpose. A11 eventuallyis segmental postural preparedness for that onevolitional discharge that will trigger the morephasic final common pathways into firing and thedog to jump-but this is no longer posture!
REFERENCES
1. Eidred, E., Gadbois, L., Sweeney, S., and Yellin, H.:A Bibliography on Muscle Receptors; their Morphol-ogy, Pathology and Intrinsic Physiology. In Press.
2. Sherrington, C. S.: The Integrative Action of the Nerv-ous System. New Haven, Connecticut: Yale UniversityPress, 1906.
3.Eldred, E., and Hagbarth, K-E.: Facilitation and in-hibition of gamma efferents by stimulation of certainskin areas, J. Neurophysiol., 1.7:59-65, 1954.
4. Abdullah, A., and Eldred, E.: Activity in gamma effer-ent circuits induced by distension of the bladder, J,Neuropath. Exp. Neurol . , 18:590-596, 1959.
5. Prosser, C. L. , and Hunter, W. S. : The ext inct ion ofstartle responses and spinal reflexes in the white rat,Amer. J. Physio l . , 117:609-618, 1936.
6. Buchwald, J. S., Halas, E. S., and Schramm, S.: Pro-gressive changes in efferent unit responses to repeatedcutaneous stimulation in spinal cats, J. Neurophysiol.,ln Dress.
1.Ko2ak, W., and Westerman, R. A.: Longlasring re-rers ib le change in the ref lex responses
-of chionic
spinal cats to touch, heat, and cold, Nature, 193:ljl-773. 7962.
8.Eccles, J. C., and Mclntyre, A. K.: The effects of dis-g9e pd of activity on mammalian spinal reflexes, J.
- Physiol. (London), 121:492-516, 1953.9. Kozak, W., and Westerman, R. A.-: Plastic changes
ot spinal monosynaptic responses from tenotomizedmuscles in cats, Nature, 789 753-755, 1961.
10. Eccles, J. C., Eccles, R. M., Shealy, C. N., and Willis,W. D.: Experiments utilizing monosynaptic excitatoryaction on motoneurons for testing hypotheses relatingto specificity of neuronal connections, J. Neurophysiol.,25:559-58O, 7962.
ll.Eccles, J. C.: Plasticity at the simplest levels of thenervous system. In Culbertson, J. T,, ed.: The Cen-tennial Lectures, Commemorating the One-HundredthAnniversary of E. R. Souibb & Sons. New York: G. P.Putnam's Sons, 1959, plp. Ztl-ZZ+.
12. Eldred, E., Granit, R., and Merton, P. A.: Supraspinalcontrol of the muscle spindles and its significance, J.Physiol. (London), 1.221498-523, 1953.
i3.Eccles, R. M., and Lundberg, A.: Significance ofsupraspinal control of reflex actions by impulses inmuscle afferents, Experientia, 14:197-232, 1958.
14. Ruch, T. C.: Evidence of the nonsegmental character ofspinal reflexes from an analysis of the cephalad effectsof spinal transection, Amer. J. Physiol., 114:456-467,193 5 .
15. Lindsley, D., and Eldred, E.: Spontaneous activity ingamma ef lerents of a deaf ferented spinal cord segment,P roc . Soc . Exp . B io l . Med . , 103 :413 -415 , 1960 .
-
l6.Voorhoeve, P. E.: Autochthonous activity of fusimotorneurones in the cat, Acta Physiol. Pharmacol. Neerl.,9 : 1 -43 , 1960 .
17. Wilson, J., and Burgess, P. R.: Disinhibition in the cat. spinal cord, J. Neurophysio l . , 25:3924O4, 1962.lS.Wi lson, J. , Talbot , W. H., and Kato, M.: Inhib i tory
ggnyglgenqe upon Renshaw cells, J. Neurophysiol.,2 '7:1063-1079. 1964.
19. Gelfan, S., and Tarlov, I. M.: Altered neuron pooula-tion in T 7 segment of dogs with experimentai irind-
- llmb rigidity, Amer. J. phyiiol., 205t06-216, 1963.20. Hagbarth, K-E., and Kerr, D. I. B.: Central influences
ggr_spiqql afferent conduction, J. Neurophysiol., 77 :295-307. 1954.
21 . Vrbova, G. : C_hangqs in the motor reflexes produced bytenoromy. J. Physiol. (London), j66:241-250. 1963.
22. Rushworth, G.: On postural anit righting refleies, Cere-b ra l Pa l sy Bu l l . . 3 : 5J5 -543 , 1961 . -
*
62
Provided by the Maternal and Child Health Library, Georgetown University

PREDISPOSING GENETICAND METABOLICFACTORSto Developmentol Defects of the Centrol Nervous Sysfem
ALLEN S. GOLDMAN, M.D.
T7A.Nowr-rocE oF THE factors giv-
ing rise to developmental defects of the centralnervous system is quite limited. However, theinformation available does permit spelling out afew principles which may be of preventive signifi-cance. Remarks will be confined to available dataconcerning human development and will includeanimal data only to illustrate or elaborate theprinciples. The central nervous system is particu-larly vulnerable to malformation by malformingagents or "teratogens." The principles, however,apply to human fetal malformation in general.
STRUCTURAL MALFORMATIONS
Genetic FaciorsBefore considering the first principle, that the
kind of fetal effect an agent produces is dependent
Adapted from a paper presented at the Symposium onThe Child with Central Nervous System Deficit, Septem-ber 28-October 2, 1964, at The University of Pennsylvania,Philadelphia.
The author is Associate in Pediatrics, University ofPennsylvania School of Medicine, Philadelphia.
upon the time of its action during development,it may be of value to review briefly some geneticsand the period of development in which eithergenetic or metabolic factors may lead to malforma-tion. Meiosis is the process of chromosomal divi-sion which occurs only in the development of theegg or sperm. As is shown in Figure 1, the num-ber of chromosomes in each egg or sperm is re-duced in two consecutive divisions from 46 to 23so that the union of egg and sperm at fertilizationrestores the number of 46. All other chromosomaldivisions during the life of the individual aremitotic in which the number 46 is reduplicated foreach daughter cell, as illustrated in Figure 2.
Figure 3 shows the development of a human egg(in the present discussion destined to become achild with central nervous system defect) in theovary of his mother, while she, herself, is a fetus.At this developmental stage all the mother's eggswill start the flrst chromosomal division of meiosisand stop midway during this division until themother is mature and just about to conceive.lFigure 4 shows the shedding of the egg from the
Provided by the Maternal and Child Health Library, Georgetown University
63

MEto$ts
Provided by the Maternal and Chitd Health Library, Georgetown University

MITOSIS
FlG. 2. Normal mitosis.
ovary to the tube. This process of ovulationstimulates the egg to continue its first meioticdivision where it left off many years earlier. Aftersuch a long delay it should not be surprising thatabnormalities in this chromosomal division mavoccur. Figure 5 illustrates fertilization of the eggby the father's sperm twenty-four to thirty-slihours after ovulation whereupon the second mei-otic division is completed. From this point in
development all further chromosomal divisions aremitotic. Figure 6 shows the multicellular eggmaking-its way down the tube. Figure 7 depictsthe implantation of the early embryo in the ut6rus.Implantation occurs in the human around theninth day of pregnancy. Differentiation of theembryo proceeds in this site until the eighth orninth week of pregnancy, at which time almost allcentral nervous system structures and other organs
Provided by the Maternal and Child Health Library, Georgetown University
6 5

FlG. 3. Development of the human egg. Maternal feta l ovary.
6
Provided by the Maternal and Child Health Library, Georgetown University

i i , , . ,r t '
Provided by the Maternal and Child Health Library, Georgetown University
FlG. 5. Fert i l izat ion.
FlG. 6. Cleavage
67
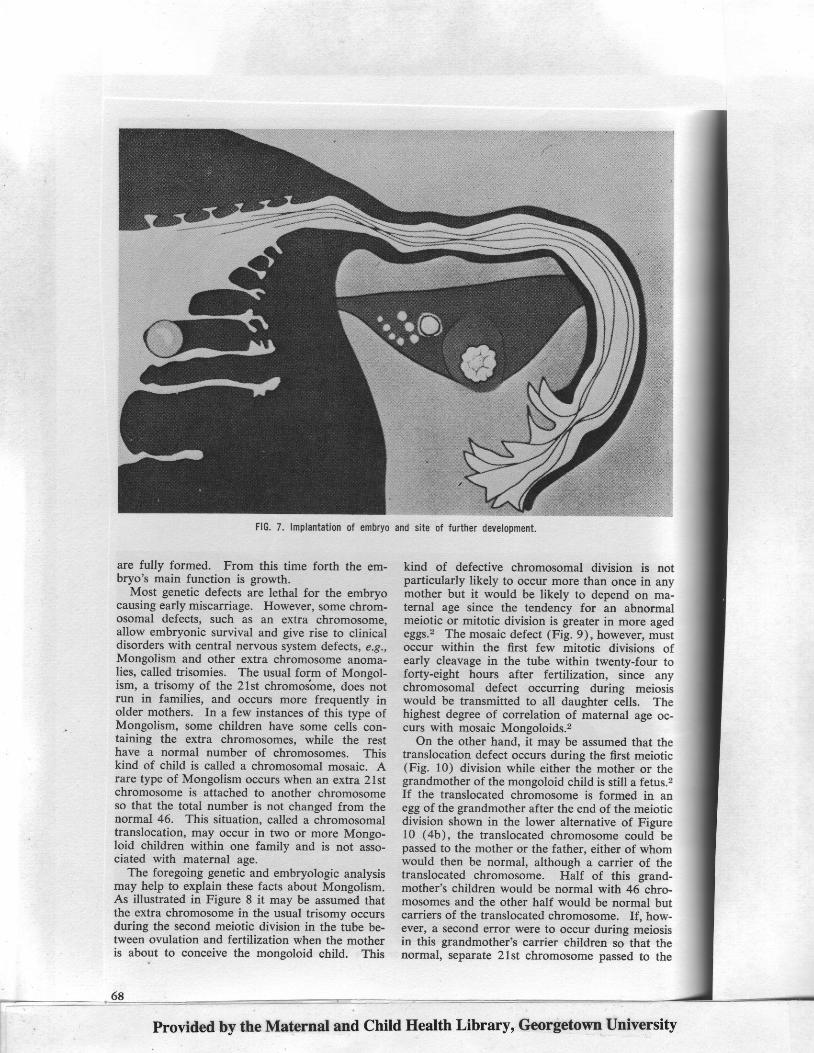
FlG. 7. lmplantat ion of embryo and site of further development.
are fully formed. From this time forth the em-bryo's main function is growth.
Most genetic defects are lethal for the embryocausing early miscarriage. However, some chrom-osomal defects, such as an extra chromosome,allow embryonic survival and give rise to clinicaldisorders with central nervous system defects, e.g.,Mongolism and other extra chromosome anoma-lies, called trisomies. The usual form of Moneol-ism, a trisomy of the 21st chromoiome, doesiotrun in families, and occurs more frequently inolder mothers. In a few instances of this type ofMongolism, some children have some cells con-taining the extra chromosomes, while the resthave a normal number of chromosomes. Thiskind of child is called a chromosomal mosaic. Arare type of Mongolism occurs when an extra 21stchromosome is attached to another chromosomeso that the total number is not changed from thenormal 46. This situation, called a chromosomaltranslocation, may occur in two or more Mongo-loid children within one family and is not asso-ciated with maternal age.
The foregoing genetic and embryologic analysismay help to explain these facts about Mongolism.As illustrated in Figure 8 it may be assumed thatthe extra chromosome in the usual trisomy occursduring the second meiotic division in the tube be-tween ovulation and fertilization when the motheris about to conceive the mongoloid child. This
kind of defective chromosomal division is notparticularly likely to occur more than once in anymother but it would be likely to depend on ma-ternal age since the tendency for an abnormalmeiotic or mitotic division is greater in more agedeggs.2 The mosaic defect (Fig. 9), however, mustoccur within the first few mitotic divisions ofearly cleavage in the tube within twenty-four toforty-eight hours after fertilization, since anychromosomal defect occurring during meiosiswould be transmitted to all daughter cells. Thehighest degree of correlation of maternal age oc-curs with mosaic Mongoloids.2
On the other hand, it may be assumed that thetranslocation defect occurs during the first meiotic(Fig. 10) division while either the mother or thegrandmother of the mongoloid child is still a fetus.2If the translocated chromosome is formed in anegg of the grandmother after the end of the meioticdivision shown in the lower alternative of Figure10 (4b), the translocated chromosome could bepassed to the mother or the father, either of whomwould then be normal, although a carrier of thetranslocated chromosome. Half of this grand-mother's children would be normal with 46 chro-mosomes and the other half would be normal butcarriers of the translocated chromosome. If, how-ever, a second error were to occur during meiosisin this grandmother's carrier children so that thenormal, separate 21st chromosome passed to the
68
Provided by the Maternal and Child Health Library, Georgetown University

]$ONGOLOID TRISOMY
FlG. 8. Possible mechanism of origin of mongoloid tr isomy.
Provided by the Maternal and Child Health Library, Georgetown University
69

MONGOLOID MOSAIC
FlG. 9. Possible mechanism
egg or sperm along with the 21st chromosome at-tached on the translocated chromosome as in theother alternative in Figure 10 (4a) , a 2l trisomywould result upon fertilization. The other egg orsperm missing the 21st chromosome would pre-sumably not survive after fertilization. Since thismother or father is a carrier of the translocatedchromosome, a mongoloid could be conceivedmore than once in this marriage. Further, sincethis defect occurs in fetal life the clinical svndrome
70
of origin of mosaic mongoloid.
would occur independent of maternal age. Thecauses of these chromosomal defects are notknown, but this consideration points to the factthat whatever genetic or possibly environmentalfactors may be operative they produce their effectseither in the ovary while the mother or grand-mother is a fetus or in the ovum within two tothree days after ovulation. It may be that meta-bolic or environmental factors may operate dur-ing this period to produce chromosomal defects.
Provided by the Maternal and Child Health Library, Georgetown University

MONGOLOID TRANSLOCATION
ei?her @a
or 0nFlG. 10. Possib le mechanism of or ig inof mongoloid t ranslocat ion.
in the father, and maturation of the egg as de-scribed before. The kind of effect produced by avariety of agents (mostly contraceptives in ani-mals) during this period most frequently is deathof the sperm or eggs or embryonic death leadingto early abortion. Recently, two reports have ap-peared of birth of a defective child, whose fatheronly had taken Thalidomide @ before conception.BFurther, malformed rabbit fetuses have been pro-duced by giving Thalidomide @ only to theirfathers prior to conception.a These observations
Metabolic Faclors
Figure 11 illustrates the role of metabolic factorsand the principle that the kind of fetal effect de-pends on the period of development in whichthey act. The figure schematically presents a sum-mary of agents, possible fetal effects, and possiblematernal factors which may influence the degreeand nature of fetal effects. The time scale is con-tracted toward the end for graphic representation.The earliest period depicted is that of maturationof the sperm, occurring in two- to four-week cycles
Provided by the Maternal and Child Health Library, Georgetown University
7r

E F F E C T S O F M A T E R N A L M E T A B O L I C F A C T O R S O N H U M A N D E V E L O P M E N T
have stimulated interest in this period as a criticalone for long-term effects on further development.
The next period depicted in Figure 1 1, the weekfollowing conception during which the egg travelsdown the tube, has been thought to be a relativelyinsensitive period to metabolic malforming in-fluences primarily because of the failure of mostexperimental agents to affect embryonic develop-ment when administered to pregnant females dur-ing this time. However, the recent production ofmalformations both by maternal administration ofActinomycin D during this period i and by directintratubal administrat ion of otherwise nonterato-genic agents 6 shows that this period is also acri t ical one.
The next period shown, that of embryonic dif-ferentiat ion, occurs between one and eight to nineweeks of pregnancy. I t is one in which metabolicfactors may produce prematurity, abortion, ormalformation. The t iming of this sensit ive periodfor malforming influences is particularly unfortun-nate because i t occurs before many women areaware that they are pregnant. The avai lablehuman data indicate that teratogenic metabolicinf luences may be radiat ion (roentgenograms), vi-ral infect ion by Gernran measles, hornrones, anddrugs or chemical agents. Most studies show that
1 )
BIR|}I UCTATION
infection with German measles during the first twomonths of pregnancy may result in cardiac defectsand cataracts, which may be considered true mal-formations.T However, when contracted betweenthe second to fourth months, German measles mayproduce primarily central nervous system damagewith or without deafness. This damage result ingat a later embryonic stage should be regarded moreas tissue injury rather than malformation much inthe same way as may result from any postnatalencephali t is.
Drugs. Maternal administration of somesteroid sex hormones as well as some cases oftumors secreting these hormones during this periodoccasional ly produce masculinization of femalechi ldren.8 The drugs known to produce humanmalformations fal l into two types: ( 1 ) thosegiven to mothers for anticancer treatment prior toplanned therapeutic abort ions, and (2) those im-plicated by certain malformations resulting in chil-dren of mothers known retrospectively to havetaken them during this period.e The f irst group in-cludes anticancer drugs, Aminopterin @, Amethop-terin @, Chlorambucil @, and Myleran @, primarily.
The administrat ion of Aminopterin @ in the f irsttr imestcr to pregnant women, for whom latersurgical intervention was planned, has led to
EI'IBRYOi{IC FETAL GRCIi,TH
DIFFERENTIATION
F lG .11 . Me tabo l i c f ac to r s and c r i t i ca l De r i ods o f human deve loomen t .
PRGTSS
OCCENES
Fert iLlzat lon Inplantat ion
DRLGS
Hduones Contra-cept ives
Abort i -facients
E s t r o q e n G e m dneasl-es
ruogest lnsAminopte!LnAnethopter inMylerancarbon Monqide
Thal idoidc
? Tolbut i l ide? Podophyl l ln
T e t r a c y c l i n e s I . V . F l u i
Q u i n i n e P i t l e s s i n
A n t i c G g u l a n t s s a l i c y l a t e
ler ids vi tein K
Goitrogens NaphthalenCemn neasleF cangl ionic
ReserpineMorPhine- -
Alcohol
AmmoniwLntoraoe
, e t c .3 1 @ k e ! s
edat ivese t c .
A n t i b i o t i c !Itren o lph -
t h a l e i nSedat ives
ruSIBL8
EFFECTS
Twinn
D€ath
P!@a-
t u i t y
1 9
lbo!t ion
Prenaturity
Death-- abortl,on
MALFORY,ATIOIT
Prenatur i ty
Abort ion
Organ DsageFetal Morbidi ty
veonatal
"orbidi ty
fnfantM o l b i d i t y
MATERMT
FACToRS
A9e
?
S e a s o nMet abo I iEnot ion s
NeuralEnd@!inS t a t e s
m
Nut ! i t i ,onMate!naI Di.sease
crddtngS @ i a l C l a s sGeog!aphySeason
Matelna1 Disease
?
Provided by the Maternal and Child Health Library, Georgetown University

either lethal or teratogenic effects in their fetuses.There have been reported several cases of mal-formed children born to mothers after this com-pound or related ones were administered to induceabortions. One case of a baby with multiple severedefects was born of a mother treated with thecancerocidal drug Myleran @, and a recent reporthas shown that two pregnant mothers treated withChlorambucil @ during the first trimester have de-livered malformed children. However, no abnor-malities were found in one ten-year follow-up studyof the children of pregnant women who weretreated with other cancerocidal drugs such as
6-mercaptopurine, triethylene melamine, or Ure-thane @ for leukemia or Hodgkin's disease. Since
the recent events involving Thalidomide @ havebeen well publicized, only the principle that this
agent demonstrates will be mentioned. Most drugswhich malform the fetus, such as anticancer drugs,also produce some side effects which may lead tomaternal illness but the Thalidomide @ experienceshows that the fetus may be greatly malformedby an agent which produces little or no adverseeffect on the mother. This second principle furthercomplicates medical detection of malformingagenrs.
The next period, that of fetal growth, is one inwhich metabolic factors may produce prematurity,abortion, and organ or tissue injury rather thanmalformation. Maternal medication with quinineused long ago sometimes produced nerve deafnessin both children and their mothers.e Tetracyclineadministered during this period is deposited in fetalbones where they persist to inhibit markedly fetaland neonatal bone growth.to At this time maternaltreatment with antithyroid drugs, propyl-thiouracil,and so on may produce goiter in the child.3Teridax @ was used about a decade ago for thevisualization of the gall bladder. The use of thisdye in pregnant mothers during this period gave
rise to a benign elevation of protein-bound iodinefrom the normal newborn level of 4-5 mg' per
cent to 4,000-5,000 per cent.11 Since the adminis-tration of this dye may have been up to as muchas two years prior to the conception of the affectedchild, the third principle to be described is: Thetime of action of any agent may long postdate thetime of i ts administrat ion.
Figure 6 also gives a list of agents which mayproduce transient central nervous system defects inthe newborn child when administered to themother just before birth or during the often-over-looked period of breast feeding 11 though thesewill not be discussed here.
The maternal factors e, 12-15 which may influ-ence susceptibility to malformation by metabolicagents have been implicated by several suggestivestudies on human and animal malformations.
Nutrition. The experimental production of con-genital malformations by maternal deficiencies orexcesses of a variety of vitamins or fasting at
produces is dependent upon the time of its
action during development.
2. The fetus may be greatly mallormed
by an agent which produces little or no
adverse efiect on the mother.
3. The time ol action of any agent may
long postdate the time of its administra-
tion,
i q. The unborn child, especialty in theii.i ea4y phase of its development, should not
ii t, considered as beyond being damaged
i within the salety ol his mother's womb.
Itra..a,oorrrr,oaraa.a,o.raaa,orrlr:iirrlilli:ffir:tr:*rr:i!:llrtrlr]frrr:tirtlffi
specific periods has raised the possibility thatnausea, vomiting, or lack of food may be terato-genic in pregnant women. Although some have re-ported higher anomaly rates in Germany and Italyduring and after World War II than in the previousperiod and in children born of Jewish women inconcentration camps, most workers believe thatthe effects of severe malnutrition seen in animaloffspring are unlikely to occur in man. An in-stance of malformation in human offspring as aresult of a specific kind of malnutrition in pregnantwomen is that of endemic congenital cretinismcharacterized by goiter, dwarfism, deafness, skele-tal deformities, and mental defect resulting frommaternal iodine deficiency.
Maternal Disease States. Many reports haveshown a higher incidence of malformations in chil-dren born of diabetic mothers, of mothers with sev-eral febrile illnesses, and of mothers with toxemiaof pregnancy. These factors, however, are not wellunderstood.
Emotional Stress. The ancient belief that ma-ternal psychogenic factors such as fright, shock, orstress may lead to malformations had been largelydiscounted in this century. However, in the lastfew years, several animal investigations have sug-gested a renewed look at this question in light ofdisturbed maternal endocrine or autonomic func-t ions. Electr ic st imuli to the maternal hypothala-
I:;:::::t::::
Provided by the Maternal and Child Health iib.u.y, Georgetown University
73

mus in rabbits and high levels of noise producedaround pregnant rats at critical periods led to mal-formations. Our own work has shown that theproduction of anomalies in rats by salicylate poi-soning is enhanced by maternal immobilization,crowding or isolation to the degree that anomaliesare produced by low, otherwise nonteratogenicdoses of sal icylate in immobil ized animals (" immo-bilization effect"). That this "immobilizationeffect" can be prevented by a sedative, sodiumpentobarbital, or a tranquilizer, chlorpromazine,suggests that the maternal central nervous systemmay be involved in this production of anomaliesin rats.
Social Class. A markedly higher incidence ofcentral nervous system anomalies and mental de-ficiency has been reported to occur in the lowersocial classes in studies of Phi ladelphia, New York,England, and Japan. The reasons for this associa-tion are not clear but probably include environ-mental or possibly genetic factors.
Geography and Season. The incidence of anen-cephaly varies among certain Europeans andAfrican natives. There are geographic differencesin the rates of spina bifida between the North andSouth of the United States and in cleft palate be-tween Hawaii and Wisconsin or New Jersey.Higher levels of background radioactivity havebeen observed in areas having the higher fre-quencies of anomalies such as, in the South-western United States and in certain areas of NewYork. Seasonal variation in rates of congenitalmalformations has been found in studies of Bir-mingham, England, Japan, Canada, and Ohio. Thereasons for these associations, again, are obscure.
FUNCTIONAL MALFORMATIONS
The last kind of effect that metabolic factors mayproduce on the unborn child is that of retardedor defective postnatal behavior u'ithout obviousanatomic defect. There is precious little hu-man data on this subject, but some excit ing sug-gestions are apparent in some recent animalexperimentation. It has been shown that X-irradia-tion of pregnant rats gives rise to apparentl.vnormal offspring which cannot solve maze prob-lems that their nonirradiated controls can.16 Fur-thermore, pregnant animals given usual therapeuticdoses of tranquilizers during any trimester haveoffspring with increased seizure susceptibility, anddecreased activity and emotionality over controlsup to two years postnatal. lT The last point whichhas many interesting implications is the observa-tion that when pregnant mice are crowded togetherthroughout gestation their offspring show markedlydepressed exploratory behavior and problem solv-ing compared to the control offspring.ls Theseanimal experiments clearly suggest that a child'spostnatal central nervous system function can bealtered by prenatal environmental influences.
74
The last principle to be mentioned, if not ap-parent from the above discussion, is accentuatedby some studies,le, 20 showing that pregnantmothers take an average of four drugs during thefirst trimester of pregnancy. Thg principle is thatthe unborn child especially in the early phase of itsdevelopment should not be considered as beyondbeing damaged within the safety of his mother'swomb. Rather he should be considered as vulner-able and in our present state of knowledge, womenin the child-bearing age would be reasonably cau-tioned against self-medication and take drugs un-der a physician's care.
REFERENC ES
l. Ohno. S., and Makino, S.: Female germ cells of man'Exp. Cel l Res. , 24:106, 1961.
2. Hamerton. John L.. ed.: Chromosomes in Mediclne.Medical Advisory
.Committee of National Spastics
Committee, Little Club Clinics in Medicine, No. 5.3.Edi tor ia l , The drugged sperm, Br i t . Med' J. , 1:1063'
1964.4. Lutwak-Mann, C.: Observations of progeny of Thali-
domide-treated male rabbi ts, Br i t . Med. J. , 1:1090'1964.
5.Wilson, J. G.: Reported at Teratology Workshop,1 963.
6. Lutwak-Mann, C., and Hay, M. F.: Effect on-the earlyembryo of alent3 administered to the mother, Brit'Med. J. . 2:944. 1.962.
7. Manson, M. M., Logan, W. P. D. , and Loy, R. M.:Rubella and other virus infections during pregnancy,Reports on Public Health and Medical Subjects, Min-istry of Health #101, London, 1960.
8. Grumbach, M. M., and DuCharme, J. R.: The effectsof androgens on fetal sexual development, Fertil.S t e r i l . . 1 1 : 1 7 0 . 1 9 6 0 .
9. Nishimura, H.: Chemistry and Prevention of Congen-ital Anomalies. Springfield, Illinois: Charles C Thomas,1964.
10. Cohlan, S. Q., Bevelander, G., and Tiamsic, T':Growth inhibition of prematutes receiving tetracycline:A clinical and laboratory investigation of tetracycline-induced bone fluorescence, Amer. J. Dis. Child., 105:4 5 3 , 1 9 6 3 .
1l.Lucey, J. F.: Hazards to the newborn infant fromdrugs administered to the mother, Pediat. Clin. N.A m e r . . 8 : 4 1 3 . 1 9 6 1 .
12. Goldman, A. S., and Yakovac, W. C.: Salicylate inloxi-cation and congenital anomalies, Arch. Envir. Health(Chicago), 8:648, 1964.
13. Goldman, A. S., and Yakovac, W. C.: The enhance-ment of salicylate teratogenicity by maternal immobili-zation in the rat, J. Pharmacol. Exp. Ther., 142:351,I 963 .
14. Goldman, A. S., and Yakovac, W. C.: Prevention ofsalicylate teratogenicity in immobilized rats by certaincentral nervous system depressants, Proc. Soc. Exp.B io l . Med . . 115 :693 . 1964 .
15. Desmond, M. M., Franklin, R. R., Blattner, R. J., andHill, R. M.: The relation of maternal disease to {etaland neonatal morbidity and mortality, Pediat. Clin.N. Amer. , 8:421, 1961.
16. Hicks, S. P.: Radiation as an experimental tool inmammalian developmental neurology, Physiol. Rev.,38 :337 , 19 , s8 .
17. Werboff, J., and Havlena, J.: Postnatal behavioraleffects of tranquilizers administered to the gravid rat,Exp. Neurol., 6:263, 1962.
18. Keeley, K.: Prenatal influence on behavior of oflspringof crowded mice, Science, 135:44,1962.
19. Mellin, G. W.: Fetal life study. A prospective epi-demiologic study of prenatal influences on fetal de-velopmenr, Bull. Soc. Roy. Belg. Gynec. Obstet., 33(Spec . ) : 79 , 1963 .
20. t r4cKay, R. .J. , and Lucey, J. F. : Neonatology, NewEng . J . Med . , 27O:1231 , 1964 .
Provided by the Maternal and Child Health Library, Georgetown University

Perinatal Problems and theCentral Nervous System
VIRGINIA APGAR, M.D.
1-Iur, ueNv REvIEws on the sub-
ject of perinatal problems and the central nervoussystem, in general, show that ccmplicated deliv-eries are followed by a decrease, in varying de-grees, in mental function of the child.
The problems of antepartal factors leading toasphyxia have been discussed elsewhere.l' ? Dur-ing labor and delivery the three factors present inalmost every birth are ( 1) compression of theumbilical cord between the baby's head or bodyand the unyielding maternal bony pelvis, (2) thestrong contractions of the uterus in the final stagesof expulsion of the infant, which prevents normalplacental transfer of oxygen, carbon dioxide, andother metabolic substances, and (3) the separationof part or all of the placenta from the uterus asthe child is born. These are expected situationsin normal births. If labor proceeds normally, anddelivery is expeditious, a normal fetus becomes anequally healthy infant. The short period of "nor-mal" asphyxia is not permanently injurious.
Numerous obstetric and anesthetic complica-tions may act singly or in combination to prolong
the period of birth asphyxia. Relative dispropor-tion in the size of the baby and the size and shape
of the mother's pelvis, an unusual presenting part
Adapted from a paper presented at the Symposium onThe Child with Ceritrll Nervous System Deficit, Septem-ber 28-October 2, 1964, The University of Pennsylvania,Philadelohia.
The duthor is Director, Division of Congenital Mal-formations, Department of Research. The National Foun-dation, 80d Secbnd Avenue, New York, New York 10017.
? 8 0 2 3 0 0 6 6 - 6
such as an arm and shoulder, or brow, an abnormalimplantation site of the placenta, an unusual reac-tion to an oxytocic induction of labor, the breechpresentation of a large baby with an unmoldedhead are examples of obstetric difficulties. Hypo-tensive reactions to the use of regional anestheticagents, convulsive reactions, too generous doses ofsedative and analgesic agents, too deep planes ofanesthesia during delivery contribute to newbornasphyxia.
The final outlook for infants born with drug oranesthetic depression, when treated promptly, ismuch better than that resulting from obstetricdifficulties.
Three relatively new studies are pertinent tothis problem. Two relate to investigations inmonkeys, and one in human infants.
In pathological studies of the brains of monkeyssubjected to mechanical birth asphyxia, Windlefound that, contrary to previous interpretations ofhuman infant brain lesions, hemorrhage was not ausual finding.3 Necrosis and atrophy of the cen-tral nervous system were common, but were notaccompanied by hemorrhagic lesions.
Mechanical asphyxia in monkeys could and didresult in a cerebral palsy-type syndrome. Babymonkeys, delivered under local anesthesia, wereintentionally prevented from breathing directlyafter birth, by covering their heads with a saline-filled rubber condom. The rubber was drawntightly over the nose and mouth. The period ofasphyxia averaged ten minutes, to allow for cer-
Provided by the Maternallnd Child Health Library, Georgetown University
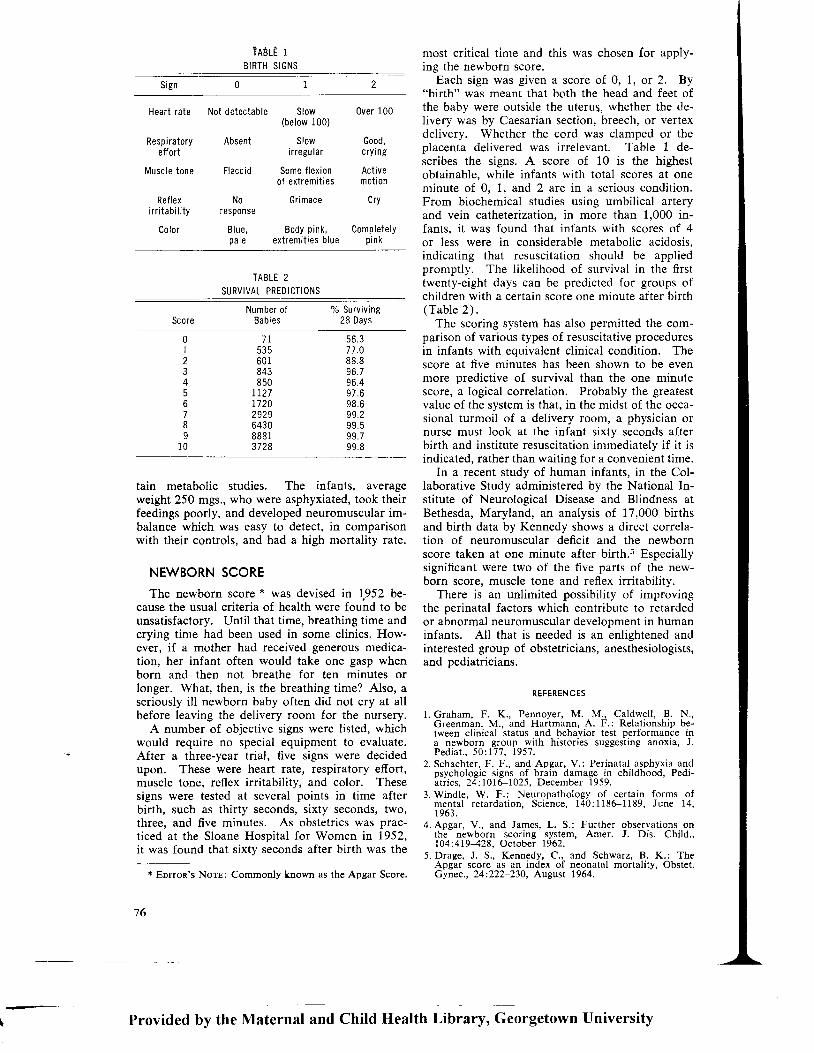
tain metabolic studies. The infants, averageweight 250 mgs., who were asphyxiated, took theirfeedings poorly, and developed neuromuscular im-balance which was easy to detect, in comparisonwith their controls, and had a high mortality rate.
NEWBORN SCORE
The newborn score * was devised in 1,952 be-cause the usual criteria of health were found to beunsatisfactory. Until that time, breathing time andcrying time had been used in some clinics. How-ever, if a mother had received generous medica-tion, her infant often would take one gasp whenborn and then not breathe for ten minutes orlonger. What, then, is the breathing time? Also, aseriously ill newborn baby often did not cry at allbefore leaving the delivery room for the nursery.
A number of objective signs were listed, whichwould require no special equipment to evaluate.After a three-year trial, five signs were decidedupon. These were heart rate, respiratory effort,muscle tone, reflex irritability, and color. Thesesigns were tested at several points in time afterbirth, such as thirty seconds, sixty seconds, two,three, and five minutes. As obstetrics was prac-ticed at the Sloane Hospital for Women in 1952,it was found that sixty seconds after birth was the
* Eorron's Norr: Commonly known as the Apgar Score
rnost critical time and this was chosen for apply-ing the newborn score.
Each sign was given a score of 0, 1, or 2. By"birth" was meant that both the head and feet ofthe baby were outside the uterus, whether the de-livery was by Caesarian section, breech, or vertexdelivery. Whether the cord was clamped or theplacenta delivered was irrelevant. Table 1 de-scribes the signs. A score of 10 is the highestobtainable, while infants with total scores at oneminute of 0. 1. and 2 arc in a serious condition.From biochemical studies using umbilical arteryand vein catheterization, in more than 1,000 in-fants, it was found that infants with scores of 4or less were in considerable metabolic acidosis,indicating that resuscitation should be appliedpromptly. The likelihood of survival in the firsttwenty-eight days can be predicted for groups ofchildren with a certain score one minute after birth(Table 2) .
The scoring system has also permitted the com-parison of various types of resuscitative proceduresin infants with equivalent clinical condition. Thescore at five minutes has been shown to be evenmore predictive of survival than the one minutescore, a logical correlation. Probably the greatestvalue of the system is that, in the midst of the occa-sional turmoil of a delivery room, a physician ornurse must look at the infant sixty seconds afterbirth and institute resuscitation immediately if it isindicated, rather than waiting for a convenient time.
In a recent study of human infants, in the Col-laborative Study administered by the National In-stitute of Neurological Disease and Blindness atBethesda, Maryland, an analysis of 17,000 birthsand birth data by Kennedy shows a direct correla-tion of neuromuscular deficit and the newbornscore taken at one minute after birth.s Especiallysignificant were two of the five parts of the new-born score, muscle tone and reflex irritability.
There is an unlimited possibility of improvingthe perinatal factors which contribute to retardedor abnormal neuromuscular development in humaninfants. All that is needed is an enlightened andinterested group of obstetricians, anesthesiologists,and pediatricians.
RE FEREN CES
1. Graham, F. K., Pennoyer, M. M., Caldwell, B. N',Greenman, M.. and Hartmann, A. F.: Relationship be-tween clinical status and behavior test performance ina newborn group with histories suggesting anoxia, J.P e d i a t . . 5 0 : 1 7 7 . 1 9 5 7 .
2. Schachter, F. F., and Apgar, V.: Perinatal asphyxia andpsychologic signs of brain damage in childhood, Pedi-atr ics. 24: 1016-1025. December 1959.
3.Windle, W. F.: Neuropathology of certain forms ofmental retardat ion, Science, 140:1186-1189, June 14,1963.
4.Apgar, V. , and James, L. S. : Further observat ions onthe newborn scoring system, Amer. J. Dis. Child.,104:419428, October 1962.
5. Drage, J. S., Kennedy, C., and Schwarz, B. K.: TheApgar score as an index of neonatal mortality, Obstet.Gynec., 24:222-230, August 1964.
TnBlf iBIRTH S IGNS
Sign
Heart rate Not detectable
Respiratory Absenteffort
l \4uscle tone Flaccid
Reflex Noirr i tabi l i ty response
Color B lue ,pa le
Slow(below 100)
Slowi r regu lar
Some f lex ionof extremit ies
Grimace
Body pink,extremit ies b lue
0ver 100
Good,c r y rng
Act ivemot ion
cry
Com p lete lyp i nk
TABLE 2SURVIVAL PREDICTIONS
Number ofBabi es
% Surviv ing28 Days
0123456789
1 0
56.377.088.896.796.4v / . b98.699.299.599.799.8
7 7535601843850
7127172029296430888r3728
76
Provided by the Maternal and Child Health Library, Georgetown University

ATTITUDINALREF'LEXES
THOMAS E. TWITCHELL. M.D.
'T.IHe ettituolNAl or postural re-
flexes 1 a are those reactions which automaticallyprovide for maintenance of an upright position ofan animal in relation to its environment.
A classification of these reactions with examplesof each together with their principal sites of inte-gration in the central nervous system is shownin Table l .
This paper will consider the subject of atti-tudinal reflexes from a broader viewpoint. Clas-sically, attitudinal reflexes' being concerned pri-marily with posture involve extensor mechanisms.Because flexion reactions and their relationship tothese extension reactions become extremely im-portant,5, 6 this discussion will include both flexorand extensor reactions.
Adaoted from a paper presented at the Symposiumon Tha Child with Central Nervous Svstem Deficit, Sep-tember 28-October 2, 1964, at The University of Pennsyl-vania, Philadelphia.
Fr6m the Department of Neurology, Tufts Unive-rsitySchool of Mediiine and the Boston Floating Hospital forInfants and Children and the Department of Psychology,Massachusetts Institute of Technology.
Aided by PHS Research Grant NB02193 frory the Na-tional Ins[itute of Neurological Diseases and Blindness,U.S. Public Health Service, and by a grant from the JohnA. Hartford Foundation.
Generally, discussions of reflex function areover anatomized. That is, reflexes are treated interms of their relationships to certain specific ana-tomical levels of the nervous system without indi-cating how they are interrelated (integrated).
Therefore, the various attitudinal reflexes andother mechanisms will be discussed in terms oftheir lowest level substrata, showing how these be-come elaborated at a higher level. Such a conceptis important in consideration of normal and ab-normal motor function, for studies have indicatedan intimate relationship between so-called reflexand voluntary motor activity. For example, aware-ness of this interrelationship was sharpened someyears ago in our study of recovering hemiplegia inman which revealed that the course of such re-covery showed a regular sequence of reflexchanges, each associated with a corresponding in-crease in the ability for willed movement.T It waspointed out that the initial overactive propriocep-tive responses (spasticity) did not constitute asimple entity but that these proprioceptive re-sponses were modified and conditioned by otherfactors such as stretch on associated muscles,tonic neck reflexes, body-on-body righting reflexes,
Provided by the Maternal and Child Health Library, Georgetown University
77

TABLE 1
CLASSIFICATION OF ATTITUDINAL REFLEXES
l . Local stat ic react ions involve one part of the body suchas a l imb .
A. Stretch ref lex- integrated at spinal cord level .The basic p0stural react ion by which passive
stretch of a muscle ref lex ly induces c0ntract i0n inthat same muscle, thus counteract ing the stretchupon i t .
B. Posi t ive support ing react ion-bulbospinal level .Passive dors i f lex ion of foot causes leg to extend
strongly; the extension may be faci l i tated by con-tact st imulat ion of the sole of the foot .
l l . Segmental stat ic react i0ns involve whole segments ofthe body.
A. Crossed extension ref lex-spinal cord level .Ref lexly induced f lex ion of one leg causes exten-
s ion of the opposi te leg.
l l l . General stat ic react i0ns- involv ing var ious segmentsof the body.
A. Tonic neck ref lexes-(high cerv ical cord) (Fig. 1) .Movement of the head in re lat ion to the body
al ters the posture of the l imbs. Asymmetr ical tonicneck ref lexes are those in which the l imbs on theside toward which the face is turned ( face l imbs)extend and the l imbs on the s ide away f rom whichthe face is turned (occiput l imbs) f lex as the head isturned t0 one s ide. When the face turns to the op-posi te s ide, the posture of the l imbs is reversed.Symmetr ical tonic neck ref lexes are those in whichventrof lex ion of the head causes f lex ion of upperl imbs and extension and adduct ion of lower l imbs,and dors i f lex ion of the head causes extension andadduct ion 0f upper and f lex ion of lower l imbs.
B. Tonic labyr inth ine ref lexes-medul la (Fig. 2) .The posi t ion of the head (and consequen|y of the
labyr inths) in space determines l rmb posture.Thus , w i t h t he an ima l he ld i n t he suD ine Dos i t i on
(and the head, c0nsequent ly, fac ing upwards), thel imbs ex tend . When t he an ima l i s he ld i n t he p ronep0si t ion ( face downwards), the l imbs f lex. In man.however, wi th neurological d isease, the exact oppo-si te may occur so that a f lex ion posture oredomi-nates wi th the pat ient in the supine, and extensionwith the pat ient in the prone posi t i0n or wi th thehead facing downwards. (Magnus and Rademaker
also observed a s imi lar pat tern in some 0f theiranimal preparat ions, but the nature of these di f -ferences has not been elucidated. : , 3)
lV. Right ing ref lexes (pons and midbrain) (Fig. 3) .
A. Labyr inth ine r ight ing ref lexeslmpulses ar is ing in the otol i ths of the labyr inth
cause the head to be maintained in the DroDer re-lat ion to the environment even when other channelsof sensory inf0rmat i0n ( for example, v is i0n and c0n.tact) are excluded.
B. Body r ight ing ref lexes act ing on the headAsymmetr ic contact of the body wi th a support ing
surface when the animal l ies 0n i ts s ide providess t imu lus f o r a mechan i sm caus ing t he head t o r o -t a te i n t o t he ho r i zon ta l p l ane .
C. Neck r ight ing ref lexesThrough ref lexes ar is ing in the neck muscles, the
body or ients into proper re lat ion wi th the head whenthe head i s t u rned .
D, Body r ight ing ref lexes act ing on the bodyAsymmetr ic contact wi th the body when the an.
imal is ly ing on i ts s ide causes the body to r ighti tsel f .
V. Postural react ions drpending on cerebral cor tex
A. 0pt ical r ight ing ref lexesBy means of v is ion, the animal can or ient i tsel f to
the environment when the other sens0rv channelsare excluded.
8. Hopping react ionsPassive displacement of the standing animal in
the hor izontal p lane causes correct ion movements 0ff lex ion and extension or abduct ion and adduct ion ofthe l imbs to restore the center of gravi ty.
C . P lac i ng reac t i onsV l sua l p l ac i ng reac t i ons occu r as an an ima l i s
brought, for example, to the edge of a table. Thel imbs are extended in ant ic ipat ion of c0ntact wi ththe t ab le .
Contact p lacing react ions are el ic i ted in thebl indfolded animal . The l ightest touch then of thehand or foot wi th an object causes an immediateor ientat ion to and placing on the object .
and later by certain contactual stimulation. Vol-untary movement itself occurred as a further facil-itation of the available responses at each stage ofrecovery. It was pointed out then that voluntarymovement was not a simple entity but from itsfirst appearance took the form of conditionedproprioceptive and contactual responses.
A detailed analysis of the basic mechanisms ofcertain of the reflexes will not be given, but thispaper will attempt to relate the particular be-
78
havior to that of the organism as a whole.Although the integrative aspect of our approach
has been stressed here, it will be necessary for con-venience to discuss the reactions in terms of theirintegration at various anatomical levels of the cen-tral nervous system. How reactions at higher levelsevolve out of those at lower levels will be indi-cated; repeated reference will be made to the lowerlevel reactions in order to show this interrelation-ship.
Provided by the Maternal and Child Health Library, Georgetown University

FlG. 1. Tonic neck ref lexes.Symmetr ical (upper f igures)and Asymmetr ical ( lower f ig-u res) .
Provided by the Maternal and Child Health Library, Georgetown University

FlG. 2. Tonic labyrinthine ref lexes. (Note that in man these postures may be reversed; see text.)
SPINAL CORD 8_10
Immediately after transection of the spinal cord,there is a profound depression of all reflex andvoluntary activity below the level of the transec-
80
tion. This depression is known as "spinal shock."The first reflexes to recover after a period of spinalshock are the flexor reflexes elicited by nociceptive(noxious) stimulus. The posture of the limbs atthis stage assumes an intermittent flexion as the
Provided by the Maternal and Child Health Library, Georgetown University

k:\tt<' 'k ilL A B Y R I N T H I N ER I G H T I N GAnimol ups ide-down,but heod r igh ts
Heod poss ive ly r igh ted ,body f o l lows
B O D Y R I G H T I N GO N H E A DAssymet r ic contoc tto body,h e o d r i g h t s
BODY ON BODYAssymetr ic conioct to body,body r igh ts
O P T I C A L R I G H T I N GA n i m o l u p s i d e - d o w n ,r i g h t s b y v i s i o n
-d"\I -1 BLINDFOLDED&'r
*(.Fi"
\ ' - ' T LABYRINTHEcToM l zED
F lG . 3 . R igh t i ng re l l exes .
Provided by the Maternal and Child Healttr iibrary, Georgetown University
8 1

after discharge of the flexor reflexes increases.Eventually the limb opposite to that in which
flexion has been reflexly induced extends, indi-cating the appearance of the crossed extension re-fex. Flexion after discharge now diminishes andan intermittent extension posture of the limb en-sues. With the appearance of extension reflexes,increased resistance to passive flexion of the limbscan be detected indicating recovery of the stretcltreflex, a proprioceptive reaction. With the re-covery of the stretch reflex, a knee jerk may beobtained. In the dog, with spinal transection, thestretch reflex may be sufficiently strong to supportthe hind quarters if he is propped up, but he soonsags to the floor for the reflex is not sufficientlystrong to maintain standing of long duration.
The proprioceptive stretch reflexes may be modi-fied by certain forms of contractual stimulation ofthe skin. Thus contact st imulat ion of the bal l ofthe foot in a flexed limb leads to a transient strongextension of the leg, the extensor thrust. Contactwith the rump induces extension of the lowerlimbs. Pressure on a foot pad increases extensionand the so-called reflexes of ipsilateral extensionmay be obtained from stimulat ion of the skin ofthe foot or of the lateral thigh. I f the animal islaid on i ts side, the lower l imbs may f lex brief ly.However, throughout this period of recoverv ofstretch reflexes and extensor reflexes, the flexor re-flex remains prepotent, and mixed undifferentiatedstimuli will cause a flexor reflex.
As Denny-Brown has pointed out, the spinalmechanism itself provides al l the elements oi thepostural responses,e but their integration with thewhole of the organism is lacking.
B R A I N S T E M 3 , 1 1 - 1 {
If the neuraxis is transectioned anyvhere at alevel between the red nucleus in the midbrain andthe vestibular nuclei in the medulla. there imme-diately ensues the phenomenon of decerebraterigidity with st i f f extension of al l l imbs, andmarked enhancement of the stretch ref lexes. Thisphenomenon contrasts with the spinal state in sev-eral respects. Thus, although f l ixor ref lexes pre-dominate in the spinal srate, extensor ref lexes arepredominant when the transection is at brain stemlevel. Secondly, nociceptive st imulat ion has thegreatest affect and is prepotent in the spinal prepa-rat ion while proprioceptive st imulat ion is of greatestimportance at the brain stem level. Decerebraterigidity is related to disequil ibr ium between pro-prioceptive faci l i tatory and inhibitory effects ir is-ing in the l imbs and the basic phenomenon resultsfrom an enhancement of the proprioceptive posr-t ive support ing reaction. At the decerebrate level.tonic neck reflexes and tonic laby,rinthine reflexesmay be easily demonstrated and these reactionscan alter the basic posture of the l imbs.
Decerebrate rigidity itself is a transient state and,
82
after a number of days, certain important changesoccur. It is instructive to compare the effect of thetransection of the brain stem at various levels inorder to learn more about the mechanisms forposture and movement. Thus the behavior of ananimal with transection at the anterior pons, knownas a pontine preparation, will be compared withthat in which the section is somewhat below thered nucleus ( low mesencephalic preparation), andflnally with an animal with section through therostral midbrain slightly above the red nucleus(high mesencephalic or subthalamic preparation).Following transection at any of these levels, theanimal initially reveals decerebrate rigidity. Thisstate, hou'ever, eventually subsides as the animalis laid on a supporting surface, rigidity again re-appearing i f the animal is l i f ted in the air. At thistime various other alterations in behavior occur.
A . Pont ine PreDdra t ion 11- -11
The pontine cat will remain quietly on its sideunless st imulated. At seven to ten days, handlingof the animal or nociceptive st imulat ion inducesrighting of the head. In seventeen days, the samekind of st imulat ion causes r ighting of the shouldersand head. The animal will never step or walk,although while on i ts side running movements mayeventually occur following nociceptive stimula-t ion. Hopping reactions and placing reactions(fol lowing intense contact st imulat ion of a largersurface area of the limb) are poorly executed.
When this animal is placed on i ts side, a par-t icular posture ensues which is not just pecul iarfor the pontine preparation but occurs in al l of thebrain stem preparations to be described. This con-sists of extension of the under-lying l imbs andflexion of the upper-lying limbs. Acute flexionof the wrist is particularly common in the upper-lying arm in the pontine monkey. This posture isbasic to the bod_v-righting reflex acting on the body,and later we shal l see how it is ut i l ized in the mes-encephalic preparations to enable effective rightingof the whole animal.
After several days, i f one pul ls on the upper-lying f lexed l imb so as to stretch the shoulder ad-ductors, f lexion at al l joints is intensif ied. Thusa fleror synergy is induced by a proprioceptivestimulus. The reaction is cal led the tract ion re-sponse. In the primate and in man, f lexion of thefingers occurs as part of this flexor synergy. Withinseveral da.vs fol lowing the appearance of this re-sponse to a proprioceptive st imulus, contact st im-ulat ion to the palm of the hand also produces thereaction. The tract ion response can be faci l i tatedor depressed by other postural reactions such as thetonic neck reflex and body-on-body righting reflex,being faci l i tated by those reactions which induceflexion of the limb and depressed by those whichinduce extension. Thus in an asymmetric tonicneck ref lex the tract ion response is enhanced inthe flexed "occiput" limb and diminished in the
Provided by the Maternal and Child Health Library, Georgetown University

extended "face" limb. When the animal is lyingon its side, the traction response is facilitated inthe upperJying flexed limb and depressed in theunder-lying extended limb.
B. Low Mesencephal ic Preparat ion 11
After the period of decerebrate rigidity has sub-sided, this animal assumes the posture of extensionof underJying limbs and flexion of upper-lyinglimbs when lying on its side. In two weeks, how-ever, it will right itself to a crouching position fol-lowing moderate stimulus, for example, a gentleslap. The cat rights itself by adaptation of thisbasic posture. Thus the claws of the flexed upper-lying limbs are dug into the floor, while the ex-tended lower-lying limbs are used as fulcra onwhich to pivot the body. Much later the animalwill right itself spontaneously without having to bestimulated. It will even walk eventually followinga strong stimulus.
C. High Mesencephal ic Preparat ion e '11
After a short period of decerebrate rigidity, inthree to four days, this animal (the cat) followinga mild stimulus will right to a crouch, In sixdays, it reveals spontaneous crawling or sitting and,following a light stimulus, will walk. Within oneweek, it will immediately right itself and within twoweeks, it will walk spontaneouslY.
These brain stem preparations reveal a numberof interesting and instructive features. First, thespinal proprioceptive stretch reflexes are enhancedat this level. Secondly, contact stimulation tothe body assumes greater importance in modifyingthese proprioceptive reactions in the form of body-on-body and body-on-head righting reflexes' How-ever, one should recall that these mechanisms hadtheir substrata at a spinal level and that variousforms of contact stimulation even at this levelcaused some modification of proprioceptive reac-tions. Thirdly, at the brain stem ievel, from thebody-on-body righting reflex, the traction responseis evolved. This reaction is of considerable im-portance as the physiological substrate for spon-taneous prehension in the lower primates and inma'a (vide infra). At this level the traction re-sponse is itself facilitated by contact stimulationof the palm of the hand. Lastly, at successivelyhigher levels of brain stem transection the rightingreflexes gain increasing kinetic effectiveness.
Thus, although some elements of body contactrighting reflexes were present in the spinal prepara-tion, they become wholly evident only at the pon-tine level. However, at this level, righting reflexeswere still quite ineffective and primarily evidentonly in a rather tonic asymmetry of limb posturewhen the animal lay on its side, although somerighting of head and shoulders could be effectedwith a strong stimulus. At higher levels of thebrain stem, righting reactions became increasingly
effective and required less intense stimuli so thatin the high mesencephalic (subthalamic) prepara-tion, eventually even spontaneous righting, stand-ing, and walking occurred.
A few further remarks concerning the tractionresponse which is integrated at'the brain stemIevel would be apropos at this point. The tractionresponse appears to be the basic mechanism forprehension in the primate. Indeed following re-moval of an entire cerebral hemisphere in themonkey, the traction response can be adapted toenable crude prehension, and to permit him tograsp the wire of his cage in order to climb. Pre-vious studies have indicated that in man there re-sides in the traction response the basic mechanismfor Ciscrete isolated maneuvers of the fingers.7 Thedifficulty, however, is in initiating these move-ments or giving them kinetic effectiveness. Inman, this generally requires the contribution ofother reactions integrated at still higher levels.
CORTICAL AND SUBCORTICALL E V E L S 1 , 3 , e
At the high brain stem or subthalamic level,mechanisms for righting, standing, and progressionhave been laid down. At cortical and subcorticallevels, reactions enabling projected movements ofthe limbs in space and greater dexterity and pre-cision of gait and station are integrated.
The next stage in the elaboration of the appa-ratus serving as substrata for spontaneous prehen-sion occurs at a subcortical level (the exact regionis not known) in the form of a grasp reflex.
In this reaction a contact stimulus moving dis-tally along the medial aspect of the palm elicitsa sudden flexion and adduction of the fingers(catching phase) which flexion can then be pro-longed by tract ion on the f ingers (holding phase).The grasp reflex is not associated with synergisticflexion at other joints of the upper extremity nor isit influenced by other postural reactions such asneck, labyrinthine, and righting reflexes.
At the cortical level, an even more complexform of automatic grasping response is integrated.This is the instinctive grasp reaction which com-prises a series of light palpating movements, ori-entation to and eventual grasping of an objectfollowing a light contact stimulus to the hand ora visual stimulus in the field of the same side.
With elaboration of the grasp reflex and the con-tactual instinctive grasp reaction, more dexterousfinger movements can occur together with preciseprojected movements of the limb in space. Insome way these reactions appear to facilitate themechanism for finger movement inherent in thetraction response.
The instinctive grasp reactions are balanced outat the cortical level with the avoiding responses.The avoiding responses occur as wide abductionand dorsiflexion of fingers and toes associated
__-.\-. -
Provided by the Maternal and Child Health Library, Georgetown University
83

with flexion withdrawal of the extremity. They
too may occur following a light contact stimulus
or visual stimulus in the field of the same side.
These reactions are integrated in relatively re-
stricted regions of the cerebral cortex. Thus'
automatic grasping reactions are integrated in the
rolandic and parietal cortex while avoiding re-sponses are integrated in the cingulate gyrus andparts of frontal and temporal lobes.
Since these reactions are balanced otl t or eqtl i -l ibrated, a cort ical lesion af{ect ing the region forintegration of one of these reactions wil l abol ishthat reaction and enhance the opposite. Thus alesion of cingulate cortex wil l impair avoidingresponses and cause exaggeration of grasping re-sponses in the opposite l imbs. A lesion of parietalcortex, on the other hand, wi l l abol ish graspingreactions and intensify avoiding responses. Thisis known as transcort ical release.
With elaboration of the cort ical contact reactionsthe overactivi ty of proprioceptive ref lexes so char-acterist ic of lower Ievel transection is dampened.
Following a lesion of the cerebral cortex, how-ever, proprioceptive reactions and other lower levelpostural mechanisms are heightened. This is knownas subcor t i ca l re lease.
Therefore, the effect of a cort ical lesion is two-fold, producing both transcort ical and subcort icalrelease. For example, a lesion of the rolandiccortex results in transcortical release in the formof sl ight exaggeration of the avoiding response,and subcort ical release in the form of spastici ty.
Further reactions elaborated at the cortical leveland important in gait and stat ion are the hoppingreactions and placing reactions. Hopping reactions.though present at brain stem levels. are more pre-cise and effective at cortical levels. An awkwardform of contact placing could be obtained in thebrain stem preparation but coarse contact over awide area of l imb surface was necessarv to el ici ti t . At the cort ical level. contact placing requiresonly the l ightest touch to any part of the foot ofthe animal for i ts el ici tat ion.
RECAPITULATION
At the spinal level, more or less stereotyped re-
actions consist ing of rather gross f lexion and ex-
tension are formed. Flexion reactions predom-
inate. At the brain stem level extensor reactionsassume a greater role and the segmental spinalstretch ref lex is intensif ied. Neck and labyrinthinereflexes dominate at lower brain stem levels whileat higher brain stem and subthalamic levels therighting reflexes are further elaborated. Here theproprioceptive extensor reactions are modif ied bycontact from body surface. However, these are
not wholly new reactions for their substrata were
seen at spinal level. Proprioceptive reactions are
dampened with the appearance of a grasp ref lex.
At the cort ical level the oroprioceptive reactions
I, 8 4
are completely dominated by exteroceptive reac-t ions.
Throughout the ascendancy of the neuraxis, re-actions show less stereotypy and a more completerelation of the organism with the environment be-comes possible. At ascending brain stem levels,tonic spinal and brain stem reactions are givenincreasing kinetic effectiveness. It is only at thecortical level, however, that true projected reac-t ions emerge.
Stimulus at lower levels is of a more coarseform. At higher levels it becomes more discrim-inating and with this increasing discrimination ofst imulus is an increasing elaboration of response.Throughout, however, there is a clear-cut rela-t ionship of the various st imulus and responsemechanisms. The crude nociceptive flexor reac-t ion at spinal level may be related to the moreprecise avoiding response to contactual st imulus atcort ical and subcort ical levels. At the spinallevel, effects of contact st imulat ion on proprio-ceptive reactions were minimal. They become in-creasingly effect ive upon proximal l imb segmentsand trunk at brain stem level while at cortical levelsthe effect is st i l l more discrete on distal l imb seg-ments. Thus, wholly new and dist inct reactionsare not added at successively higher levels of thenervous system. but more primit ive reactions be-come modif ied and elaborated as the st imulus fortheir response becomes more discriminating.
REFE R ENCES
1.Ful ton, John F. : Physio logy of the Nervous System.New York: Oxford University Press, 1949.
2. Magnus, R.: Kcirperstellung. Berlin: J. Springer, 1924.3. Rademaker, G. G. J. : Das Stehen. Ber l in: J . Spr inger,
1 9 3 1 .4. Rushworth, Geoffrey: On postural and righting re-
f lexes, Cereb. Palsy Bul l . , 3:535-543, 1961.5.Twitchel l , Thomas E.: Normal motor development, J.
Amer. Phys. Ther. Ass. , 45:419-423, May 1965.
6. Twitchel l . Thomas E.: Var iat ions and abnormal i t ies . inmotor development, J. Amer. Phys. Ther. Ass. , 45:424-430 , May 1965 .
T.Twitchel l , Thomas E.: The restorat ion of motor re-covery fo l lowing hemiplegia in man, Brain, 74:443-4 8 0 , 1 9 5 1 .
8. Creed, R. S. , Denny-Brown, D., Eccles, J. C. , L iddel l ,E. G. T. , and Sherr ington, C. S. : Ref lex Act iv i ty of theSpinal Cord. London: Oxford Univers i ty Press, 1932.
9.Denny-Brown, D.: Motor mechanisms- introduct ion:the general principles of motor integration. In Field,John, Magoun, H. W., and Hal l , Victor E. , eds: Hand-book of Physiology-Neurophysiology, Volume II.Washington: American Physio logical Society, 1960.
10. Sherr ington, Sir Char les: The Integrat ive Act ion of theNervous System. New Haven, Connect icut : Yale Uni-vers i ty Press, 1947.
11. Bard, Phi l ip, and Macht, Mart in B. : The behavjorchronically decerebrate cats. In Wolstenholme, G.W., and O'Connor, C. M., eds. : Neurological BasisBehavior . Boston: L i t t le Brown & Co., 1958.
12. Denny-Brown, D.: The midbrain and motor integration,Proc. Roy. Soc. Med., 55:527-538, 1962.
13.Twitchel l , Thomas E.: The nature of motor recoveryfollowing hemispherectomy in the monkey, Neurology(Minneap.) , 12:295, 1962.
14. Twitchel l , Thomas E.: Unpubl ished observat ions.
ofE.of
Provided by the Maternal and Child Health Library, Georgetown University
NORMAL MOTORDEVELOPMENT
THOMAS E. TWITCHELL, M.D.
/-\(-/un sruores have indicated that
evolving voluntary movement in the human infanthas a reflex substrata.l Many of these reflexes havetheir origin in fetal life and we may gain furtherunderstanding of the principles of maturation ofbehavior in the infant by first examining some ofthe fetal reactions el ici ted in the l iving humanfetus by stimulating various body parts with a fineh a i r . 2 ' 3
The receptive field for stimulation alters withmaturation of the fetus. The earliest fetal re-sponses can be obtained at seven-and-a-half weeksof fetal age. At this time the perioral region isstimulus sensitive. The receptive field spreads tothe alae of the nose and the chin bv eieht to nine-
Adapted from a paper presented at the Symposium onThe Child with Central Nervous System Deficit, Sep-tember 28-October 2, 1964, at The University of Pennsyl-vania, Philadeiphia.
From the Department of Neurology, Tufts UniversitySchool of Medicine and the Boston Floating Hospital forInfants and Children, and the Department of Psychology,Massachusetts Institute of Technology.
Aided by PHS Research Grant N802076 from the Na-tional Institutes of Neurological Diseases and Blindness,U.S. Public Health Service, and by a grant from the JohnA. Harrford Foundation.
and-a-half weeks. At ten to ten-and-a-half weeksthe eyelids and palms of the hand are stimulussensitive. At ten-and-a-half to eleven weeks thesoles of the feet can be stimulated. At eleven-and-a-half weeks the entire face except the peripheryis receptive as well as the upper chest. The thighsand the legs become sensitive at eleven to twelveweeks and at thirteen weeks the remaining chestarea. At fourteen weeks the tongue, the back, andside of the trunk are stimulus sensitive, and atfifteen weeks is added the abdomen, at seventeenweeks, the buttocks, and at thirty-two weeks, theinside of the thigh.
The responses obtained in the fetus at differentages are presented in Table 1.
Several features should be emphasized here be-fore going on to a discussion of development ofmotor function in the infant. First, more general-ized and less differentiated reactions involving thehead and trunk develop prior to more localizedreactions. Secondly, of these generalized reac-tions, avoiding or withdrawal responses developinitially and remain prepotent over groping orpursuit (turning toward) reactions.
Provided by the Maternal and Chitd Health Library, Georgetown University
85

::Ll;tt:nt:ninrlltt!:{ ::r!: t.:n.!tl!!i;!:*.ll:l tll:{.}:nlt:{.iilll!lli!}i!ilttll
Age(in weeks) Stimu lus
TABLE 1
FETAL RESPONSE AT DIFFERENT AGES 2, 3
Gen era I izedResponse
0pen ing mouth
Rotation awayDorsif lexion (extension of head)
Lips close and with repeated st imu'lus , swa l low ing
Face turns away alone without trunkmovementRetractionProtrusion of upPer l iPProtrusion of lower l iPProtrusion and PursingSuc kin gAud ib le suck ingTongue l i cks lower l ipFace turns toward st imulus withouttrunk movement. Rooting, inst inct ivesucking responses
are previous studies which indicated that partingof the lips and retraction of tongue are analogousto avoiding responses of the extremities, whilepursing of lips and protraction of tongue areanalogous to the grasping responses.a
Another interesting reaction is observed ateleven-and-a-half weeks when stimulation of themidline of the face induces dorsiflexion of thehead. I ts probable relat ionship to a similar reac-t ion in the neonate wil l be discussed later.
The spread of the receptive field in the fetusdeserves comment. Note that it begins with avery small receptive field around the second andthird division of the fifth cranial nerve, graduallyinvolves ali three divisions of the fifth nerve, andthen gradually spreads down the trunk beginningwith the ventral surface.
We have not commented on reactions involving
91/z
l 0Vz
I 1
Lower l i p
Per i o ra I
L ips
7Y2 Per ioral
8t /z Per ioral
91/z Per ioral
Contralateral f lex ion of neck and uppert r un k .
Contralateral f lex ion of neck and t runkal0ng wi th contra lateral rotat ion of pel-v is and retract ion of shoulders.
Same general ized react ion but rumprotat ion more pronounced.
Same general ized response and rotat ionof face away.
C0ntralateral response modi f ied by ex-tension of the t runk al ternat ing wi thf lex ion.Extension of t runk increasing but notreplacing lateral f lex ion. Face maynow turn toward the st imulus associ-ated wi th t runk movement.
l \4arked extensi0n of neck and t runk.
Var iety of responses-f lex ion and ex-tension, uni lateral 0r contra lateralturning, and so on. Stereotypy disap-pea n ng.
I IY2 L i ps
Side of face
M id l i ne o f f ace
I2-12Y2 FaceL ips or tongueor both
Perio ra I
:: l
ttl
ti
IIix
T J
Ir:
i;::i:::::l:{
73Y2-74 Lips
Tonguel7 Upper l ip20 Lower l ip22 L ips24 Mouth29 L ips33 Lower l ip40 L|PS
(n ewborn)
i:ii:
In terms of local reactions, again several fea-
tures are noteworthy. First, head turning evolves
out of a more generalized response involving head
and trunk. However, when movement of the head
dissociated from that of the trunk first appears, it
occurs as a turning away from the stimulus'
Movements involving lips and tongue are par-
ticularly interesting' The first local response of
the mouth is one of opening of the mouth. The
first reaction of the tongue is one of retraction of
tongue. A protrusion of the upper lip appears
before protrusion of lower lip and before pursing
of the l ips. Both of these responses appear before
any sucking response. A late response is licking
of the lower lip by the tonque, and of course the
more highly integrated and elaborate rooting re-
sponses finally appear only in the full-term infant.
Of significance to this sequence of development
86
Provided by the Maternal and Child Health Library, Ceo.geto*n University

the hands or the feet in that it has been difficultto relate fetal responses with those in the newbornand young infant. It would appear that the fetalresponses are related to the traction response andavoiding reaction.
To recapitulate, fetal responses begin as rathergeneralized responses in which avoiding or with-drawal predominates. The earliest local responsesare those of lips and tongue in which again thosereactions analogous to avoiding responses occurinitially to be followed later by reactions whichstudies have shown to be related to grasping re-sponses.
RESPONSES OFTHE HUMAN INFANT
In the neonate, in addit ion to al l of the reac-tions of lips and tongue that occur in the fetus,one can elicit the "rooting reactions" which takethe form of a kind of "pursuit reaction" followingstimulat ion of the l ips.
The posture of the newborn infant in the supineconsists of external rotation of shoulders andhips, some abduction of the shoulders and hips,and flexion of elbows and knees. The fingersgenerally remain flexed around a flexed thumb butdo extend occasionally. This resting posture isonly slightly altered in the normal infant by thetonic neck reflex, and any effect is more apparentin lower extremities than upper. The restingposture is, however, markedly altered by a kineticlabyrinthine reaction, the Moro reflex. This re-action is best elicited by allowing the head to movequickly backwards and consists of wide abductionand extension of upper and sometimes lower ex-tremit ies. I t may be fol lowed b! adduction of theextremit ies to the midl ine.
When the baby is placed in the prone posit ion,righting of the head is common. This is relatedto a body righting reflex acting on the head inwhich the adequate stimulus is contact with theupper chest. ( In this regard, i t is interesting torecall the dorsiflexion of the head from midlinestimulation of the face in the fetus, this fetal reac-tion perhaps representing a premature form ofthis righting reflex. ) Labyrinthine righting re-flexes are not present in the newborn.
The true grasp reflex is not present in theneonate but the tract ion response is easi ly obtained.Increased resistence to passive movement is pres-ent in flexors and adductors of upper and lowerextremit ies and this is more prominent proximallythan distally. The posture of the fingers and toesmay be easi ly altered by el ici tat ion of the avoid-ing response which is facile in the newborn. Con-sequently, a l ight tact i le st imulus to any part ofthe hand or foot will cause a dorsiflexion and ab-duction of fingers or toes. Further discussion ofthe responses of the hands and feet will be deferredto a separate section later.
The newborn has a proprioceptive positive sup-port ing reaction and when placed in the uprightposit ion wil l "stand" for a few seconds. The posi-t ive support ing reaction here involves not only thelower extremities but the whole trunk and neck,and the infant frequently takes a lhort-lived opis-thotonic posture. The neonate also has a primi-tive stepping response. This stepping is charac-terized by overflexion of hips and knees andfrequently by overextension of ankles, and overad-duction of the legs producing therefore a "scissorgait."
Throughout early infancy, certain changes inposture and substrata for locomotion occur.s Inthe prone posit ion, the abi l i ty to elevate the headincreases so that not only the head but the uppertrunk is lifted off a supporting surface. Alongwith this the infant gradually gets up more on hiselbows and then on to his hands with elaborationof posit ive support ing reactions in the upper ex-tremities. The ability to sit is related to extensionof the receptive field for positive supporting reac-tion to the buttock areas. Prior to the ability ofspontaneous sit t ing, i f one holds the infant in thesit t ing posit ion and t i l ts him to one side or an-other, certain abduction and adduction reactionsof the legs occur which are no doubt importantin maintaining sit t ing balance. These reactionsresult from asyn.rmetric contact with the buttocks.More facile righting of the head and head controlobtains as the labyrinthine r ighting ref lexes de-velop along with the body on head r ighting re-flexes.
The abi l i ty to stand and walk fol lows upon mod-ification of the positive supporting reactions, anddevelopment of hopping reactions, contact placingreactions, and the inst inct ive grasp response of thefeet. The hopping reactions and contact placingreactions have been described in the previouspaper.{ i The true contact placing reactions whichdevelop in the infant prior to spontaneous stand-ing and walking are far more elaborate and dex-terous reactions than the crude placing reactionsin the neonate. In the older infant, the l ightesttouch of a table edge to any part of the foot causesimmediate adjustment of the foot to the table edgeand appropriate placing on the table. Inst inct ivegrasping responses of the feet are del icate orient-ing reactions of the foot as i f to prehend st imu-lat ing objects. Al l of these reactions probablycontr ibute to the del icate alterat ions of Dosturaladjustment in the legs which enable standing withm i n i m a l m u s c u l a r a c r i v i t y .
GRASPING AUTOMATISMSAND THEIR RELATIONTO VOLUNTARY PREHENSION 1
Before considering the automatic grasping re-sponses of infants, it is necessary to comment onthe avoiding reactions. In the newborn, these are
87
, Provided by the Maternal and Child Health Libraryo Georgetown University

the only reactions which can be obtained by con-tact stimulus to the hand or foot alone. They be-come somewhat more facile in the first months oflife and remain facile throughout infancy and earlychildhood. The avoiding responses contaminatevoluntary activity even at five and six years of ageas evidenced by the overabduction and exagger-ated dorsiflexion of the hand as it approaches toprehend an object.
In the neonate, the traction response can be ob-tained by pulling on the arm so as to stretch theshoulder adductor muscles (Fig. 1). This inducesa strong synergistic flexion at all joints. The trac-tion response itself can be facilitated by contactstimulation of the hand at around one month ofage. At one to two months of age, contact stimu-lation between the thumb and index finger causesan adduction and flexion of these segments indi-cating the earliest phase of the development ofthe true grasp reflex.
By three to four months of age, the true graspreflex has developed so that a distally moving con-tact s'timulus to the medial part of the palm of thehand wil l produce a f lexion and adduction of thefingers which may be sustained when they are
pulled on (Fig. 1). When the grasp reflex is fullydeveloped, the traction response and its componentflexor synergy can no longer be obtained. Follow-ing development of the grasp reflex, the infantbegins to reach for things and utilizes a crudepalmar grasp.
The grasp reflex itself becomes altered at aroundfour to five months of age so that a contact stim-ulus to the medial side of the hand causes somesupination of the hand. This orienting responseheralds the beginning evolution of the instinctivegrasp reaction. This supination is soon followedby groping or palpating after a retreating stimulus.By eight to ten months of age, the hand not onlygropes after a contact stimulus but adjusts to itand grasps it, documenting full development of theinstinctive grasp reaction (Fig. 1).
As the instinctive grasp reaction is emerging, itbecomes possible to fractionate the grasp reflex.By this we mean that contact stimulus l imited tothe flexor surface of one digit alone will enableflexion of that digit alone without inducing flexionin all the digits together. When the grasp reflexcan be entirely fractionated and when the instinc-tive grasp reaction has developed completely, a
HOLDS RATTLE BRIEFLY P A L M A R G R A S P
T R A C T I O N R E S P O N S E
A t b i r t h
G R A S P R E F L E X
2 Io 4 months
I N S T I N C T I V E G R A S PR E A C T I O N
5 to lO months
P I N C E R G R I P
FlG. 1. Reiat ion of automat ic grasping react ions ( lower f igures) to devel0pment 0f ev0lv ing forms 0f voluntary grasp (upperf igures). (Voluntary grasp occurs at some t ime af ter appearance of automat ic react ion.)
88
Provided by the Maternal and Child Health Library, Georgetown University

true pincer grasp with opposit ion of thumb andindex f inger characterizes the "voltrntary" pre-hension of the infant. Fol lowing development ofthe inst inct ive grasp reaction, true projected move-ment of the limb in space is acquired. Even withdevelopment of the instinctive grasp reaction,however, the avoiding response contaminates ac-t ivi ty again as evidenced by the marked dorsif lexionand abduction of the hand as the hand approachesan object.
THE PLANTAR RESPONSE IN INFANTS I
A brief note is required concerning the plantarresponse in the normal infant. This response hasbeen a source of controversy for years. Textbooksgenerally state that the plantar response in thenewborn consists of dorsiflexion of the great toe(Babinski sign) and that i t may remain so fromsix months to three years. On the other hand,some investigators have stated that the normalplantar response is a flexor response in the new-born .
The author is convinced that this dilemma hasarisen from a failure to realize that the plantarresponse is not a simple reflex but is a compositcof four different reactions, two of which causedorsiflexion of the toes and two of which causeplantar f lexion. Al l of these reactions have theirspecific receptive fields and their particttlar ade-quate st imuli .
Thus in the neonate. dorsif lexion of the toes canbe easi ly obtained as a part of the contact avoidingresponse of the feet. I t may also be obtained asa fragment of the nociceptive f lexor ref lex identicalto the spinal flexor reflex described elsewhere.G(The f lexor ref lex, however, is more easi ly el ici tedand more stereotyped in a premature infant.)
On the other hand in the neonate, plantar f lexionof the toes can be obtained as a part of the pro-prioceptive posit ive support ing reaction el ici tedby pushing on the bal l of the foot so as to dorsif lexthe fcot. The plantar f lexion of the toes then maybe associated with extension of the entire leg.
By several months of age, however, certain
changes have occurred in these responses. Thr.rs
the nociceptive flexor reflex in the older infant is
identical to the response in the adult, where nox-
ious st imulat ion of the dorsum or bal l of the footwill cause plantar flexion, with dorsiflexion occur-r ing only with nociceptive st imulat ion of the bal l
of the toes. The avoiding response in the infant ofseveral months of age has i ts receptive f ield pri-
mari ly on the dorsttm of the foot and the lateralborder of the foot. At several months of age, the
true grasp reflex of the foot identical in nature to
that in the hand has also developed so that a dis-tal ly moving contact st imulus to the medial part
of the sole wil l cause plantar f lexion and adduction
of the toes.Thus the plantar response is real ly a composite
of four different reactions-the flexor reflex, theavoiding response, the proprioceptive posit ive sup-port ing reaction, and the grasp ref lex of the foot,each reaction having its specific adequate stimnlusand receptive field.
The difficulty which has arisen.orrer the plantarresponse of the infant is related to the usual un-dif ferentiated form of st imulus used to el ici t theresponse. Consequently, an object dragged alongthe sole may combine quali t ies of nociceptive,contact, and proprioceptive st imulus and the reac-t ion obtained wil l depend on the relat ive prepon-derance of st imulus effect. In l ike manner, thepart of the sole st imulated can detern.r ine to an.rarked degree the kind of response elicited sothat st imulat ion of the lateral border of the footis more likely to elicit dorsiflexion responses whilest imulat ion of the medial side of the foot wi l lel ici t plantar f lexion responses.
RECAPITULATION
In the fetus the contact responses are general-ized reactions of neck and trunk in which avoidingmovements appear first and remain prepotent. Thefirst localized responses appear in the lips andtongue where reactions analogous to avoiding re-sponses develop prior to those analogous to grasp-ing reactions.
The newborn infant is dominated by proprio-ceptive reflexes and avoiding reactions except inthe oral region where reactions analogous to grop-ing responses are highly developed.
With maturation of righting reflexes, furtherabi l i t l ' for voluntary activi ty is acquired, enablingrollin-e, sitting, creeping and crawling, and eventu-a l l y s tand ing and wa lk ing .
Development of contact reactions in the handof the infant is similar to development of reactionsof the l ips in the fetus. Avoiding reactions ap-pear f irst and remain dominant. With the matura-t ion of increasingly complex automatic graspingresponses, there is a corresponding development ofmore precise and dexterous prehension and pro-ject ion of the hand in space.
RE FE R ENC E5
1. Twitchel l , Thomas E.: The automat ic grasping responsesof infants, Neuropsychologia ( to be publ ished).
2. Hooker, Davenport: The Prenatal Origin of Behalior.Lawrence: University of Kansas Press, 1952.
3. Humphrey, Tryphena: Some correlat ions between theappearance of human fetal reflexes and the developmentof the nervous system. In Purpura, D. P. , and Schade,J. P. , eds. : Progress in Brain Research, Volume IV.Amsterdam: Elsevier Publishing Co., 1964.
4. Twitchell, Thomas E.: On the motor deficit in congenitalbilateral athetosis, J. Nerv. Ment. Dis., 129:705-132,1 959 .
5. Peiper, Albrecht: Die Eigenart der Kindlichen Hirntii-t igkei t . Leipzig: Georg Thieme, 1956.
6. Twitchell, Thomas E.: Attitudinal reflexes, J. Amer.Phys . The r . Ass . , 45 :411 -418 , May 1965 .
T.Twitchel l , Thomas E.: The nature of the plantar re-sponse in infancy, Program of the American Academyof Neurology, 1961, p. 35.
Provided by the Maternal and Child Health Library, Georgetown University
89

Voriofions ondAbnormolifiesof Motor Development
THOMAS E. TWITCHELL, M.D.
VARIATIONS IN MOTOR DEVELOPMENTUNRELATED TO CENTRAL NERVOUSSYSTEM PATHOLOGY
Some variations in motor development occurwhich are not the result of pathology of the cen-tral nervous system. First, there are certain varia-tions in the timing of motor development whichare related to the t ime of gestat ion. Therefore,infants born prematurely may reveal an apparent
Adapted from a paper presented at the Symposium onThe Child with Central Nervous System Deficit, Sep-tember 28-October 2, 1964, at The University of Pennsyl-vania, Philadelphia.
Fr6m the Department of Neurology, Tufts UniversitySchool of Medicine and the Boston Floating Hospital forInfants and Children, and the Department of Psychology,Massachusetts Institute of Technology.
Aided by PHS Research Grant NB 02076 from the Na-tional lnstitute of Neurological Diseases and Blindness,U.S. Public Health Service, and by a grant from the JohnA. Hartford Foundation.
90
retardation of motor development but go throughthe regular sequences of motor development. Onthe other hand, infants born of gestation of overforty weeks in length (but who do not reveal the
syndrome of postmaturi ty) may appear to be pre-
cocious in motor development. The reflex sub-strata for spontaneous motor function, describedin another paper, may appear somewhat later thanexpected in the premature infant while they appearearlier than expected in the infant born somewhatpostmaturely.l It is to be noted that we are notreferring to those premature infants who have aninfanti le spastic diplegia.
There is also evidence that development ofmotor function may be altered by various degreesof environmental enrichment or deprivation. Thus,the instinctive sucking response has a low thresh-old at the time of birth, and if lhe infant is imme-diately al lowed to suck, the threshold remains atthis level. However, if sucking is delayed for a
Provided by the Maternal and Child Health Library, Georgetown University

day or two, the threshold for this response rises;i t then requires several days for the thresholi l toreturn to its optimal level. In like manner, infantswho sleep in the prone position customarily de-velop sitting, standing, and walking more rapidlythan those who sleep in the supine position. Thisdifference appears to be related to more constantstimulation of righting reflexes arising from bodycontact in the prone position. A similar situationoccurs in those infants whose mothers customarily"play with them" by "standing" them on their lapsduring periods of wakefulness thus restimulatingthe positive supporting reactions. These infantsbegin to stand and walk earlier than those who arenot provided with this kind of st imulat ion. Re-cent animal studies of Held and Hein indicated theimportance of environmental stimulation in devel-opment of sensory-motor r6sponses even at a re-flexive level.2 The recent studies of White havealso conclusively demonstrated that environmentalenrichment may hasten spontaneous prehension inthe developing infant by six weeks.3
Another cause of abnormality in motor develop-ment is disease of the muscles. Consequently,spontaneous motor development may appear moreslowly in the infant with a benign congenital hypo-tonia or congenital myopathy. Detailed studiesof the reflex mechanisms in these infants indicatethat central nervous system maturation is proceed-ing at the normal rate in that the reflex substratafor "voluntary" movements for the given chrono-logical age are present. They cannot be utilizedbecause of weakness of musculature.
THE RELATIONSHIP OF NORMAL ANDABNORMAL MOTOR DEVELOPMENT
There is no clear-cut dividing l ine betweennormal and abnormal motor development; just asintellectual capacity shades off from the "normal"range to the subnormal so does normal motorfunction shade off into the abnormal. Experiencewith a large number of patients with cerebral palsyindicates that there are quantitative variationsranging from the most severely involved to thoseminimally involved. From the author's studies, ithas been clear that those with "minimal degrees" ofcerebral palsy represent the link between normaland abnormal motor function. Indeed, the physio-logical basis for mild motor defect in the clumsychild is identical to that found in cerebral palsyalthough of lesser degree.
Another link between the normal and abnormalare those children whose motor development pro-ceeds through the same sequence as the normalinfant but is stretched out over a five- or six-yearperiod. At three years of age these children mayreveal features of cerebral palsy such as spasticity,increased reflexes, inability to stand without as-sistance, a "scissor gait," and overextension ofankles when assisted in walking. Several years
? 8 0 - 2 8 0 0 - 6 6 - ?
later a number of these children can walk andperform reasonably well . Although clumsy at thatt ime, they show no spastici ty, or ref lex changes,and walk withor-rt the overadduction characteristicof the "scissor gait ." In a sense, the patient withcerebral palsy represents a still nlore profoundphysiological defect in sensory-motor maturationor integration with a hypertrophy of various in-fanti le ref lexes. Physiological ly, many of the ab-normal motor reactions in the patient with cerebralpalsy are identical in nature to similar reactionsof the normal infant.
THE INFANTILE CEREBRAL PALSIES
Before discussing the nature of the motor defectin cerebral palsy, several points are worth empha-sizing.
First, these conditions are not static, and for aclear understanding of the phenomena, one mustconsider the patient from a chronological or de-velopmental view. Thus, the patient with a spasticquadriplegia or with double athetosis may revealdifferences in motor deficit over a period of yearsfor these patients show some evidence of neuralmaturation just as the normal infant and chi ld.In some patients, this is quite remarkable so thatthey n.ray eventually learn to stand and walk andto care for themselves without the benefit of anykind of formal therapy. On the other hand, thedeficit may be so severe that any maturation orimprovement can be measured over a l i fet ime onlyby sophist icated neurological techniques.
Secondly, from the neurophl 'siological view, theseparation of patients into various categories-such as spastici ty, r igidity, athetosis, tremor-is wholly artificial. The various arguments for thisview have been presented elsewhere and fa1l be-yond the scope of this paper.a Nevertheless, i tmay be stated at this point that regardless of arbi-trary classif icat ion, the physiological substrata forspastici ty, for example, can be demonstrated in al lpatients, and that the physiological substrata forsuch phenomena as athetosis can be demonstratedin al l patients. Str ict adherence to the variousclassifications of cerebral palsy are artificial andbased on unphysiological tenets.5
The Resting Posiure
The resting posture of the patient with infanti lecerebral palsy is unique and occurs only in patientswith encephalopathies of congenital or early ac-quired onset. This posture is identical with thatof the normal infant in the supine posit ion andconsists of some external rotation and abductionof the shoulders, flexion of elbows, and generallyflexion or extension of fingers. The lower ex-tremities reveal external rotation and abductionof hips, and flexion of knees, or may be relativelymore extended (Fig. 1).
This posture may be altered by several reflexes.
91
Provided by the Maternal and Child Health Library, Georgetown University

F lG . 1 . Res t i ng pos tu re o ffour-year-old chi ld wi th spast icquadr ip legia and athetosis.
It is frequentll' altered by the tonic neck reflexes.and the effect is more easi ly demonstrated i f thepatient himself moves his head rather than i f the
examiner moves it passivel1".Tonic lab-vrinthine reflexes can also efiect the
resting posture in patients with cerebral pals-v.Thus i f the patient is held in the air in the supincposit ion, he maintains a relat ively f lexed posturcof the l imbs as described above. However, i f heis held in the air in the prone posit ion, the l imbsmay extend and adduct strongly. In some patientsthe flexed infantiie posture of the upper limbs maypersist even in an upright posit ion. but r ' r ' i l l change
92
to extension i f the patient bends his head forwardwith his face down.
The resting posture mav also be altered in somepatients b1 a kinetic labyrinthine ref lex identicalto the Moro ref lex of infants. Thr-rs, i f the patientis quickl l ' t i l ted backward, the upper extremit iesabduct and extend widely.
When some patients are laid on their sides theunder-lying l imbs may extend and the upper-lyinglimbs flex, as a bodv-on-body righting reflex.
In man-v patients these reactions may not be ofsufflcient intensity to cause an actual change inlimb posture. The overactivity of these reflexes
Provided by the Maternal and Child Health Library, Georgetown University

may then be manifest only in terms of increasingor decreasing the resistance to passive movementin the limbs.
The Defici t in Prehension
Patients with infantile cerebral palsy frequentlyhave extraordinary dilliculty in use of the upperlimbs and the hand for prehension of an object.Indeed all movement appears to be biased towardflexion and the ability to project the limb in spaceis seriously hampered and is even impossible forsome patients. The major difficulty is related tothe exaggeration of the avoiding responses.s'6 I fthe patient is able to project the hand toward anobject, the hand reaches ataxically with fingerswidely abducted and dorsiflexed (Fig. 2). Thehand may touch an object and quickly withdraw asthe contact avoiding response is elicited, or the pa-tient may palpate an object for several secondsonly to have the hand withdrawn because of theoveractive avoiding response. If the patient cangrasp the object, the increased avoiding responsemay contribute to weakness of grip.6
Visual avoiding responses may also contributeto the motor defect, In some patients, the visualavoiding response is so striking'as to cause the
head and eyes to deviate away from any objectwhich enters the opposite visual field. In mostpatients the effect is not so profound. Yet, alarge number of these patients do exhibit a curiousinattentiveness in regard to the object to begrasped. They frequently do not,appear to lookat the object. This may be related to a less pro-nounced exaggeration of the visual avoiding re-sponse.
Further defects in projection of the limbs maybe related to unintegrated tonic neck or laby-rinthine reflexes. Consequently, because of per-sistent tonic labyrinthine reflexes, for example, thelimbs may remain in the flexed posture describedin the section above. Or because of the difficulty inprojecting the limbs, many patients attempt tobend the head forward to get closer to the objectsought. When neck reflexes are exaggerated, thisventroflexion of the head may only increase flexronof the arms through operation of the symmetricaltonic neck reflex.
Further difficulty may be encountered once anobject is grasped because of exaggeration of thetraction response.s'e This reaction may lead tosynergistic flexion of the upper extremity at alljoints. Particularly devastating to power of grip
FlG.2. Ef fect of exaggeratedavoiding response on handfunct ion. Pat ient 's hand hasjust touched object to begrasped, but hand wi thdrawsbecause of avoid ing response.Note posture of f lexed wr istand extended and abducteddigi ts .
Provided by the Maternal and Child Health Library, Georgetown University
93

is the synergist ic f lexion of the wrist which imposesa mechanical disadvantage on the f inger f lexorsand may diminish the strength of grip by 50 percent or more.6
The Defec f in S i t f ing and S iand ing
Various dif f icult ies in sit t ing or: standing may berelated to fai lure in development of the r ightingreflexes and support ing reactions which form thebasis for these acts, or may on the other hand alsoresult from exaggeration of these same reactions.Thus, poor head control may result from a defectof the labyrinthine r ighting ref lexes or from adefect of the body r ighting ref lexes acting on thehead determined from contact with the tnrnk orbuttocks. Diff iculty in sit t ing or standing mayresult from a faulty development of the bodyrighting reflex acting on the body or again fromthe posit ive support ing response either from but-tock contact or contact with the soles. On theother hand, sit t ing or standing may be virtual lyabolished by marked intensif icat ion of these re-sponses, in which contact with the soles or thebuttocks may cause extreme hyperextension and anopisthotonic posture which makes i t impossiblefor the patient to sit or stand.
Marked exaggeration of the kinetic labyrinthinereflex described above can impair si t t ing and stand-ing because a sudden wide extension and abductionof the upper, lower, or both extremities may throwthe patient off balance.
Inability to stand may also be related to exagger-ation of the avoiding responses of the feet. Ifthese are markedly exaggerated, any slight contactof the foot with the floor can cause the legs towithdraw immediately. On the other hand, i f theavoiding responses are not this exaggerated, weak-ness of extension of the legs and tendency towardflexed posture can result.
The Defec t in Ga i i 7
A common gait disorder in patients with cerebralpalsy is the "scissor gait" in which one leg adductsover the other as steps are taken. This gait iscommonly explained as result ing from spastici ty.of the adductor muscles of the hip. Such a hy-pothesis is untenable, however, in that a numberof patients who do "scissor" have no spastici ty ofthe hip adductor muscles, while some patients whodo not "scissor" have considerable adductor sDas-t ici ty. Although the complete story is not as yerunraveled in regard to this phenomenon, severalmechanisms for scissoring have been identified.
Overadduction of the legs is probably relatedprimarily to reactions arising from contact of thesoles with the f loor. In some patients i t can clearlybe shown that certain contact reactions of the feetcause the overadduction. In others, the reactionsmay result from an imbalance of certain adductorreactions that are normally conditioned or alteredby the contact placing reactions which are so
94
poorly developed in patients with cerebral palsy.On the other hand. the overadduction in some
patients is clearly related either to tonic neck ortonic labyrinthine reflexes. As pointed out pre-viously, tonic neck or labyrinthine reflexes whichcause extension of limbs also c'ause adduction oflimbs. Consequently, some patients with poorhead control reveal a "scissor gait" because ofstimulation of both tonic neck and labyrinthinereflexes as the head hangs ventroflexed. In thesepatients, i f the head can be held in a straight posi-t ion, "scissoring" does not occur.
Another common defect of gait is overextensionof the ankles and indeed some overextension oflegs. This can be traced to exaggeration of theproprioceptive or contact positive supporting re-actrons.
Although less frequently recognized, exaggeratedavoiding reactions of the feet also produce a com-mon defect of gait. This is an overflexion of thehips and knees so that the feet tend to lift too highfrom the floor and are not advanced far enough.
In most patients, some combination of theseeffects occurs so that exaggerated avoiding re-sponses cause too much flexion at the hips or knees,while exaggerated positive supporting reactions atthe same time cause an overextension of theankles.
Defects in Speech 8
As stated previously, the motor defect in cerebralpalsy is closely related to exaggeration of avoidingresponses. In the oropharyngeal region, the ana-logues of the avoiding reactions of the hands andfeet are those of parting of the lips, retraction oftongue, and velopharyngeal opening. Conse-quently, the patient with cerebral palsy usually hasdifficulty pursing his lips, protruding his tongue,or effecting velopharynleal closure. Linguadentalsounds are difficult because he cannot protrude histongue. Labial sounds are difficult because he isunable to purse his l ips well , and the stop con-sonants are difficult because of the difficultv invelopharyngeal closure.
Invo lun ia ry Movements
The common form of "involuntary movement"in patients with cerebral palsy is athetosis. Athe-tosis is essential ly an instabi l i ty of posture, and ismost prominent in the hands, next most frequentin l ips and tongue, and least of al l in the feet. Inthe hand it consists of periodic swings from flexionto extension of the fingers. Athetotic movementsof the face occur as pursing-parting of the lips, orprotraction-retraction of the tongue. In the feetit consists of alternating flexion and extension ofthe toes. In the upper and lower extremit ies, al-ternating pronation and supination of the handsand feet often accompany the flexion and extensionof the digits.
The physiological basis for athetosis is generally
Provided by the Maternal and Child Health Library, Georgetown University

a conflict between the avoiding response (inducingdorsiflexion and abduction of fingers or toes andpronation of hands or feet) and the grasp reflex(inducing flexion and adduction of fingers or toesand supination of hands or feet).5 Thus, athe-tosis can occasionally be induced reflexly byevoking simultaneously a grasp reflex and an avoid-ing response. On the other hand, athetosis mayalso occur as a conflict between the avoiding re-sponse of the hand and the traction response. Inthe face athetosis results from a conflict betweenthose reactions determining pursing and parting oflips and protraction and retraction of tongue.
Coarse ballistic-type movements may occur atproximal limb segments particularly in the upperextremity. Although the exact nature of this maynot be determined in all patients. we have beenable to show clearly that in some patients, thiscoarse tremor results from a conflict betweentonic labyrinthine and tonic neck refiexes and isconsequently closely related to posit ion of the headin relation to the body and environment.
Pos fura l Abnormal i ies and Deformi t ies
Various abnormalities of posture eventuailybecoming fixed deformities from myostatic con-tracture may occur in patients with cerebral palsy.The physiological basis for many of these relativelyfixed postures can be shown to result from con-flicting reflex mechanisms. Thus tonic persistenceof a labyrinthine reflex may cause a fixed postureof the upper extremit ies in the infanti le posit ionas described above.
Exaggerated and unbalanced neck or rightingreflexes may cause asymmetries of posture leadingto f lexion of one l imb and extension of the other.
A common deformity is f lexion contracture ofhips and knees. Although in some patients thisappears to result from exaggeration of stat iclabyrinthine reflexes, in which instance the patienthas been kept in a supine position thus accentu-ating the flexion posture, the deformity is mostoften related to exaggerated avoiding responses ofthe lower extremit ies leading to a f lexion posture.
Tonic persistence of the tract ion response mayproduce marked flexion of the upper extremitywith part icularly marked f lexion of the wrist.
At distal l imb segments, relat ively unopposedexaggeration of avoiding response, traction re-sponse, or grasp reflex in the upper extremifi', orof posit ive support ing response in the lower ex-tremity may lead to deformit ies. Thus, tonic per-sistence of the avoiding response produces the well-known athetoid or choreic hand, with f lexion ofwrist and dorsiflexion and abduction of fingers.Certain degrees of pronation of the hand may alsooccur with this. Tonic persistence of tract ion re-sponse or grasp reflex may lead to fixed flexion off ingers. In the lower extremity, tonic persistenceof the posit ive support ing reaction may lead tomarked extension of the ankle with shortening of
the heel cord while tonic persistence of the avoid-ing response leads to marked eversion of the foot.Indeed the tendency for the foot of the patientwith cerebral palsy to pronate or evert is clearlyrelated to the avoiding response a4d many patientswho show rather a neutral position of the foot innon-weight-bearing condit ions show marked ever-sion when contact is made with the f loor. Inmany patients, however, although one reflex mayoverpower another, these reflexes are most oftenin disequil ibr ium so that grotesque postures occur.For example, proximal l in.rb posit ion may be de-termined by one mechanism and distal deformitvby another.
Resistance lo Passive Movement
Spastici ty in the patient with cerebral palsy oftentakes a dif ferent distr ibution from that of the adultwith disease of the central nervous s\,stem acor-r iredlater in l i fe.e Spastici ty in cerebrai palsy is mostprominent in proximal l imb segments and usuallydistr ibuted in f lexors and adductors. Spastici ty inpatients with cerebral palsy is not always associ-ated with increased deep tendon ref lexes nor is i talways associated with the extensor plantar re-sponse or Babinski sign. The phenomenon ofspastici ty is altered markedly by neck, labyrinthine,and r ighting ref lexes. In double athetosis spas-t ici ty is said to be absent. We have not found thel imbs of any of these patients to be wholly f laccid,however, and indeed have invariably detected someexaggeration of postural reflexes suggesting thatpresence or absence of "spastici ty" here is more amatter of degree than of kind.
Not al l the increased resistance to passive move-ment in cerebral pals-v, however. is spastici ty. Thus,frequently, a kind ol intense resistance can be de-tected when one n.ranipulates the l imb by the handor the foot. This resistance is related to eitherexaggeration of avoiding response or grasp ref lexso that contact with the hand or foot inducesthese reactions which then resist the examiner'sattempt to manipulate the l imb. When the l intbis manipulated from a more proxintal l imb seg-n-rent, these reactions are not induced and con-sequentlv this kind of increased resistance is notobtained. This is the nature of the so-cal ledtension athetosis of Phelps which dif fers onlv indegree f ronr h is r ron tens ion a the tos is .
The so-cal led variable r igidity of Coll is is clearlythe result of unbalanced neck, labvrinthine. andrighting ref lexes.
THE NATURE OF THE MOTOR DISORDERAND IMPLICATIONS FCR THERAPYIn tbe above sections i t has been pointed out
how exaggeration of certain ph1'siological reac-t ions can contr ibute to the defect in motor func-t ion in a patient with cerebral palsy. This wouldindicate that the defect in motor function is not
Provided by the Maternal and Child Health Library, Georgetown University
9 t

the result of st i f fness induced by spastici ty or ofinterference by an "involuntary movement" on avoluntary movement. Rather the defect in volun-tary movement and the defect in reflex mecha-nisms have a common basis. The common ingredi-ent is a defect in sensory-motor integration withconflict between hypertrophied infantile reflexes.
Although in the preceding sections it has beenshown how exaggeration of isolated reflex mech-anisms contributes to the motor defect, the prob-lem in the individual patient is much more com-plex. In general, the defect of voluntary move-ment of any kind results not from exaggeration ofone reaction of the motor mechanism but ratherfrom exaggeration of several all of which are inmutual confl ict. Thr"rs in some patients, the un-raveling of the physiology behind the motor defectmay be difficult.
Nevertheless, with this kind of analysis i t be-comes clear that the classif icat ions in general useare wholly art i f ic ial from the physiological view.We would urge that more attention be paid to thephysiological basis for the motor defici t in eachindividual Datient so that treatment could be ori-
ented to that individual patient rather than to somearbitrary grouping.
REFERENCES
l.Twitchell. Thomas E.: Normal motor development, J'Amer. Phys. Ther. Ass. , 45:419423, May 1965'
2. Held. R. . and Hein. A. : M-ovement-produced. st imula-t ion in the development ot v lsual ly gulded benavlor .J. Comp. Physiol.-Psychol., 56:872-876, 1963.
l . Whi te. b. L. : The development of percept ion dur ingthe f i rs t s ix months of l i fe. Read at American Asso-clition for the Advancement of Science meeting inCleveland, Ohio, December 30, 1963.
4.Twitchell, Thomas E.: The spectrum of rhe inJantilecerebral
'palsies, a neurophysiologic analysis (to be
publ ished).S.1witchell, Thomas E.: On the motor deficit-in con-
genital bilateral athetosis, J. Nerv. Ment. Dis., 129:1 0 5 - 1 3 2 , 1 9 5 9 .
6.Twitchell. Thomas E.: The grasping deficit in infantilespastic hemiparesis, Neurology (Minneap.), 8:13-21'1958 .
?.Twitchell, Thomas E.: The nature of the gait disorderin infant i le cerebral palsy, Cl in. Orthop. 36:111-117'1964.
8. Clement, Mary, and Twitchell, Thomas.E.:-Dysarthriain cerebial paisy, J. Speech Hearing Dis., 24:-118-1'22'I 959 .
g.Twitchell, Thomas E.: The clinical differentiation anCnhvsio logical nature of increased resistance to passivei nouemen t . Ce rcb . Pa l sy Bu l l . , 3 : 110 -116 , 1961 .
96
Provided by the Maternal and Child Health Library, Georgetown University

Some Considerationsof Muscle Activity
H. D. BOUMAN. M.D.
Huto* MovEMENT is the resultof interaction and co-ordination of several ele-ments such as muscle, nerve, the central nervoussystem, and the sense organs that are responsiblefor the control of muscle function. The most ele-mentary item is the muscle fiber with its innervat-ing nerve fiber. The nerve impulse con.ring downthe nerve fiber is the final path that activatesmuscle function and the information which it trans-mits must therefore contain all the necessary datawhich will allow the individual muscle fiber to co-ordinate its function with the others in the samemuscle and with other synergistic and antagonisticmuscles.
The nerve impulse activates the muscles throughtwo time delays. The first one is the well-knownneuromuscular junction which is a chemical trans-mission mechanism with acetylchol ine as the trans-mitter. There is then a second delay which occursbetween the excitation of the muscle and its actual
Adapted from a paper presented at the Symposiumon The Child with Central Nervous System Deficit, Sep-tember 28-October 2, 1964, at the University of Pennsyl-vania, Phi ladelphia.
Dr. Bouman is Chairman, Department of Physical Med-icine and Rehabilitation, University of Cincinnati Collegeof Medic ine. Cincinnat i . Ohio 45219.
contraction. This is the so-called excitation con-traction coupling with which we have become fa-miliar very largely through the work of Sandow.lIt is of considerable physiological importance eventhough no pathology of this transmission is knownat the present time. There are, however, diseaseswhich f ind their origin in malfunction of the neuro-muscular junction, specif ical ly myasthenia gravis.
Several individual muscle f ibers, al l innervatedby one nerve fiber, form the motor unit. The all-or-none response of the individual muscle fiber andof the individual nerve fiber results in an all-or-none response of the motor unit. There is amechanical result of stimulation and an electricalresult, the action potential or electromyogram(EMG). The normal motor unit is spread out.A potential of 50 microvolts means thatlhe needleis within /z millimeter of the electrode. The workof Buchthal with fourteen lead electrodes showsthat the motor unit is 5 to 10 mil l imeters in di-ameter and varies by a factor of 3 to 5.2 Thismeasurement of the size of the motor unit canactually be used in diagnostic procedures. Forinstance, in the myopathies the territory of themotor unit is sometimes reduced by as much as
Provided by the Maternal and Child Health Library, Georgetown University
97
--

30 per cent in diameter and 50 per cent in area'
The motor unit potential is the sum of the poten-
tial of several fibers that form the motor unit' If
as in myopathy some of the fibers are inactive, the
motor unit potential becomes either shorter or
polyphasic. Ho*euer, in maximal contraction the
hberi stiii form a normal interference pattern, in
contrast with neuropathy where entire motor units
disappear and an interference pattern does not
alwil's develop. It should be reaiized that such
EMG findings are the most common findings but
many exceptions occur'The duration of the motor unit potential is found
to be about flve times that of the individual muscle
fiber potential. Buchthal found, by means of mul-
tiple simultaneous recording, that some fibers. are
five to seven milliseconds displaced in time':r It
was originally thought that these are conduction
delays but this is probably not correct' Most likely
there are differences in end-plate zone delays'
Again in myopathies the slow beginnings and. end-
ings are not detectable and the unit potential is
shorter.
ELECTROMYOGRAPHY
Electromyographic recordings are important in
myotonia because after act ivi ty or contraction or
teianic stimulation there is considerable continued
activity in the myotonic muscle. This usually
lasts a few seconds but can last as long as thirty
seconds. Mechanical tapping can produce i t '
Final ly there is a type of electr ical act ivi ty which
starts at about 100 or 150 spikes per second and
then decreases. This is the so-called "dive bomber"
rhythm which can be obtained in rest and some-
times even with surface leads. The duration of
the individual potentials is about two to four milli-
seconds. I t i i interesting to note that this deals
with the activation of spontaneous activity by
mechanical or electrical stimulation' In other
words this expresses an overexcitability of the mus-
cle which is triggered off by this stimulus'
I t should be clearly real ized that every elec-
trical potential that is recorded from the muscle in
the electromyogram is the result of muscular activ-
ity. The fibrillation potential therefore is the
result of spontaneous activity of individual muscle
f ibers, while the fasciculat ion potential and the
other potentials described in myotonia are the re-
sult of spontaneous activi ty of entire motor units'
I t is interesting to compare the independent act ivi ty
of individual muscle fibers and individual motor
units. Heat enhances f lbr i l lat ion while ' cool ing
enhances motor act ivi ty. In some diseases me-
chanical stimulation is particularly effective in
precipitat ing automatic act ivi ty such as in poly-
myosit is in which f ibr i l lat ion potentials occur on
needle insert ion together with a reduction in
motor unit terr i tory. I t should be noted in
passing that there are also diseases which produce
98
a decrease in spontaneous activity or in which
spontaneous activity (such as flbrillation) cannotbi obtained in spite of complete paralysis. An ex-arnple of this is found in familial periodic paralysis'To summarize then from clinical data' there is animportant physiological fact, hamely that spon-taneous activity can occur both in individual fibers(which then is recognized as fibrillation potentials)and in motor unit potentials such as seen in myo-tonia. The reason to emphasize these points isthat for instance in myopathy and particularly inmuscular dystrophy the finding of fibrillation po-tentials has lead to widespread speculation as towhether there is a neuropathy superimposed on themyopathY.
Spontaneous activity can occur following physio-logiial changes such as low potassium content, andit ian be started by more or less physiological stim-uli such as mechanical stimulation, a strong con-traction, or electrical stimulation. It can involveindividual muscle fibers (fibrillation), or it caninvolve a few fibers of a motor unit on mechanicalstimulation such as seen in polymyositis or inlarger groups such as seen in the myotonic diseases.
Dumoulin has recently suggested the clinicaluse of electrical stimulation to start fibrillation indenervated muscles.a It is well known that de-nervated muscles do not always show fibrillationpotentials and Dumoulins suggests that electricalstimulation can be used to obtain automatic ac-tivity of these fibers and therefore fibrillation po-tentials. Much clinical evaluation will have to bedone to establish the value of Dumoulins' methodof recognition of denervation.
NERVE CONDUCTION VELOCITY
Mention should be made of the recent use of
electromyography in the measurement of con-
duction velociiy. This has been used to assist in
detection of such disorders as carpal tunnel syn-drome in which a compression of the nerve is
reported to slow down the conduction rate, pos-
sibly as a result of minor demyelinization.5 It is
also used widely in evaluating peripheral neuritis'Conduction velocity is quite closely related to thediameter of the nerve and some physiologists areskeptical of the validity of these measurements'Recently Gassel pointed out the sources of errorin motor nerve conduction velocity studies, be-cause potentials can be, and often are, recordedfrom muscles that are different from the musclesthat one thinks one is recording from.6 There arethree major sources of error: (1) abnormal in-nervation, (2) recording from adjacent muscles viaconduction of the electricity through the tissuesfrom one muscle to another, or in other words,current leakage, and (3) stimulation of additionalnerves. The dangers in this procedure are par-ticularly severe because conduction velocity mustbe done by supramaximal stimuli which increases
Provided by the Maternal and Child Health Library, Georgetown University

the problem of current leakage to other muscles.Even with good technique Gassel reports differ-ences of almost 2 meters per second to a maximumof 7Vz meters per second.6
In concluding the comments on clinical blec-tromyography, a word of general warning is pos-sibly in order. Electromyography is basically aphysiological procedure which expresses activityof muscle fibers. It shares the disadvantage ofevery other laboratory procedure, namely that itcan be given a significance way out of proportionto its value. It is no more than one method of in-vestigation in an entire clinical diagnostic contin-uum. Because i t produces visible excursions andso-called accurate data (conduction velocity) itsometimes impresses the younger members of theprofession as having an absolute value which itdoes not really have. In rare instances doeselectromyography actually make a diagnosis butin many instances i t is a valuable contr ibutionto the diagnosis.
RELATIONSHIP BETWEENINNERVATION AND CONTRACTION
There are, however. additional ways in whichelectromyography can be useful. They need to bediscussed. One of these has been pointed out in apaper by Poudrier and Knowlton.T In the muscleitself one can separate the excitatory phenomenafrom the contractile phenomena. They are sep-arated by the excitation-contraction couplingmechanism and a small time delay. The electro-myogram is a membrane phenomenon and iscoupled with the excitatory phenomena. Knowltonand Poudrier have, therefore, compared the actionpotential with the mechanical contraction as ameans of identifying which part of the change inmuscle force is a result of changes in excitabilityand which part is a result of changes in contracta-bility in human subjects. They recorded the actionpotentials with surface electrodes (one on themotor point and one on the tendon) and at thesame time recorded the mechanical contractionof the muscle. The results showed that in manysubjects the ratio between the force produced andthe voltage is a constant. They suggest that thismeasures the relationship between the amount ofinnervation activating the muscle and the amountof contraction resulting.
Obviously this is a concept of considerable im-portance, particularly since Knowlton and Pou-drier could demonstrate that the innervation-con-traction relationship is a reliable indicator of unitstrength of the muscle. For instance, ttrey showthat when fatigue sets in, with maximal effort thereis a decrease in the muscular response but no de-crease in excitation (as expressed by the aciionpotential voltage). This is a fascinating findingbecause most investigators would have assumedthat neuromuscular fatigue takes place primarily
at the neuromuscular junction. It shouid be re-membered that both the action potential and thecontraction are beyond the neuromuscular junc-
tion and the conclusion that can be suggested fromthese experiments is that fatigue has indeed a mus-cular factor, assuming that a maltimum effort isexerted. If, on the other hand, the patient doesnot exert a maximal effort, force and voltagechange in the same way so that the ratio of forceto voltage remains constant. Whether this methodcan be cl inical ly useful to check i f a patient per-forms a maximal effort, or if it could contributeto recognit ion of malingering, should be studied.
In maximal isometric contractions of the bicepsbrachii muscle, Knowlton and Poudrier found adrop in contraction with an increase in voltage ifmeasurements were carried to failure of contrac-tion. This indicates that the cause of such fatigueis attributable to the contractile mechanism of themuscle i tself whi le actual ly the central nervoussystem tries to compensate by an increase in in-nervation. It is well known that a maxirnal con-traction can cut oII circulation almost completelyin animal muscles. The question arises as towhether in strong isometric contractions reductionof vascular supply could be responsible for thestrong reduction in muscular strength r,l'ithout thereduction in innervation.
Another question that Knowlton and Poudriervery logically raise is whether this method can beused to analyze training and particularly can itanswer the question as to which training proce-dures are effective because of changes in the mus-cle contractability and which are effective becauseof changes in innervation. Their results with iso-metric exercise as a training procedure appear tobe of the order of magnitude of Hislop's data s
(namely about 12 ro 2OVa increase) rather thanthose of Liberson e and Rose 10 which are wellover 100 per cent.
Another point that Poudrier and Knowlton in-vestigated in this initial study was the question ofendurance. Some subjects trained with exercisesto increase endurance showed that contractility-endurance actually dropped while the innervation-endurance increased. This method of analysisallows an evaluation of the two peripheral aspectsof training, namely, how much of a certain type oftraining is the result of increased activity from thecentral nervous system and how much is the re-sult of actual training of the muscle itself. It isobvious that these results, if extended, open an en-tirely new field of the study of muscle function inman, the evaluation of training programs, and pos-sibly even re-education methods. These resultsmay aiso explain why in myopathies the excursionsof the electromyogram are higher than that innormal muscle for the same load. It may be thatin the myopathies the contractile mechanism is dis-eased and the central nervous system compensatesby a relative increase in innervation.
Provided by the Maternal and Child Health Library, Georgetown University
99

TROPHIC INNERVATION OF MUSCLE
Another point in the physiology of periphera!
nerve and muscle on which much investigation has
been done recently is trophic innervation. Cli-
nicians are famil iar with the pol iomyeli t is patientwith zero function and normal muscle size and thepatient with severely atrophied muscle and almost
normal function. Recently a great deal of physio-
logical evidence has become available showing that
we are indeed dealing with physiologically different
mechanisms (Gutmann).11'1:r There is evidence for
the existence of separate motor and trophic inner-
vation of muscle. However both types of inner-
vation would have to be transmitted by the motornerve.
Three physiological phenomena relating to
trophic innervation have been studied. One is the
sensitization of the muscle to acetylcholine. Thesecond is the development of fibrillation potentials
or independent activity of muscle fibers. The third
is the lengthening and change of the electr ical con-
stants of excitabilit)', such as the strength-durationcurve, chronaxie, and others. Al l of these have
been known as effects of denervation. What is
new in the present concept is the suggestion that
these changes are not the result of the same mech-
anism as the disappearance of contractility. The
reasons for this concept are basically twofold.
First, disuse atrophy does not produce trophic
changes, and, second, the t iming (part icularly on
the reinnervation of muscle) of the disappearance
of the so-called trophic abnormalities and the re-
turn of motor function is quite different. The
trophic functions return before motor function
occurs.
This concept of the double innervation of mus-
cles through the motor flbers is of such importancethat sonle specific evidences for it should be men-tioned. One is the experiment by Katz and Miledi
on sartorius muscle fibers which have a double rn-
nervation.l:l When they cut one nerve branch,
the muscle fibers remained active yet at the de;
nervated end-plates there was an oversensitivity to
acetylcholine. Reinnervation reduces the over-sensitivity long before nerve conduction leading to
contraction occurred. Thesleff has shown that the
oversensitivity to acetylcholine in the center of the
fiber is accompanied by a positive action potential
and an increase in membrane impedence. Thishypopolarization followed by depolarization is an
ideal predisposition for the formation of automaticspikes as shown by several experiments.la Theseexperiments may provide an explanation of the
mechanism by which fibrillation actually develops'
It is now well known that transmission of an im-pulse from the nerve to the muscle occurs in thepresence of acetylcholine. The normal nerve at
rest produces small quantities of acetylcholine into
the muscle and, when excitation across the neuro-
muscular junction occurs, these bursts suddenly
loo
synchronize and produce enough acetylcholine to
fire the muscle action potential. It would therefore
be logical to suggest that maintenance of trophic
innervation of muscle would be dependent on a
constant acetylcholine supply from the nerve to
the muscle. However, curare eliminates the effect
of acetylcholine on muscle contraction but does
not interfere with the trophic innervation of mus-
cle. This phenomenon is rather important evi-
dence for the fact that there are two independentmechanisms of contractile and trophic innervation.
Little is known about the possible second mech-
anism of nerve conduction for trophic innervation.Weiss showed years ago that a substance movesthrough the nerve fiber from the central part to
the periphery,15, 16 and the question has been raisedwhether this central conduction in the nerve fiber
could be responsible for the so-called trophicinnervation.
SYNCHRONIZATION OF MOTOR UNITS
On repetitive stimulation the individual muscleflbers form a tetanic response and finally the in-dividual motor units of the muscle together formthe observed muscular contraction. Man is ca-pable of very fine adjustment of his voluntarymuscle function in spite of the fact that the indi-vidual motor unit follows the all-or-none law.This is done in three ways. The first is by increasein the number of firing motor units. The secondis by increased frequency of firing. The third(which is often forgotten) is by sudden synchroni-zation of motor units. When all the motor unitsare firing at maximum frequency (as shown bythe constancy of the integrated action potential),the muscle still has the possibility of increasedfunction by synchronization.li This is of courseone of the reasons why sudden movements can ex-ert a far larger force than a maintained contraction.Evidence of the use of this synchronization to in-crease muscle output is seen in some chronic dis-eases. The French have drawn attention to thefact that in old poliomyelitis patients, sometimesa very high degree of synchronized action poten-tials can be found which are still existent manyyears after the disease.ls Possibly one explanationof this phenomenon is that the central nervouss)'stem overcompensates for the lack of availablemotor units by using the available ones more effec-tively by synchronization.
SENSE ORGANS
The muscle and its nerve are part of a reflexarc the simplest form of which is the monosynapticreflex arc in which impulses travel through thespinal cord with only one synapse on the anteriorhorn cell. This was reported for the first time byRenshaw ts and Lloyd 20 almost twenty-five yearsago. Equally well-known are the multineuron re-flex arcs and the reflex pathways up and down the
- .Provided by the Maternal and Child Ilealth Library, Georgetown University

spinal cord. Sense organs for this ref lex systemare essential ly of three types: the Golgi organs inthe tendons, the muscle spindles, and sense organsin the joints.
The Golgi organ as a sense organ is in serieswith the muscle fibers. It is located in the tendonand when the muscle is stretched, the organ isexcited; when the muscle contracts, the tendon isalso stretched and therefore the organ is again ex-cited. Of fundamental importance to understand-ing the function of the muscle spindle is that this isa separate muscle f iber with sense organs, whichruns paral lel to the active muscle f ibers. I f themuscle is stretched, the spindle organ is stretchedin the same way as the muscle fibers are stretched.However, when the muscle i tself contracts thespindle organ relaxes. We are therefore dealingwith a double sensory mechanism and Granit andhis school have shown that these organs have dif-ferent functions.!] Basical ly the Golgi organ in-hibits the agonist and faci l i tates the antagonist andthe spindle organ does the opposite.
An equally important point is that the spindlehas a contracti le mechanism and that b,v contract-ing independently from the muscle it can, as itwere, prestretch its own sense organs. The totalsensory excitation of the sense organ then becomesthe difference between the contraction of the mus-cle fibers themselves and those of the spindle fibers.The muscle therefore has the possibility to setthe sensitivity of its own sense organs in the spin-dles by producing a contraction of the spindlemuscle fibers. This has been referred to as thecentrifugal innervation of a sense organ. Thespindle organs have their own innervation in thegamma nerve fibers. We are therefore dealingwith a double system of innervation: the alphamotor system and the gamma motor s1'stem whichare closely coupled but which nevertheless can, andsometimes do, become quite independent to thedetriment of good muscle function. Such inde-pendence appears to be particularly detrimental tomuscular co-ordination.
Muscle spindle physiology is a large and activefield of research. There is, however, some evi-dence from the work on muscle physiology thatappears to have clinical importance. The firstpoint relates to the tonic neck reflexes. When thesensory roots are cut, tonic neck reflexes disap-pear even though the actual motor innervation ofthe muscle remains intact. Granit has recordednot only the motor function but also the functionof the muscle spindles.21 In his experiments itbecame obvious that even when the actual reflexno longer occurs after the sensory roots have beencut, the spindles themselves are still as active asbefore. What this means clinically is that activitl'can occur in the spindles which are part of themuscle without any visible muscular activity, andthe question immediately arises whether trainingand learning can occur in this spindle system with-
out visible muscular contraction. The experimentsof Buchwald showing that condit ioning can occurin the spindle system are of course of fundamentalimportance in this respect.22' 23 In fact, gammaconditioning can precede and contribute to the de-velopment of an alpha conditioned rtsponse. Theseexperiments are therefore of major importance inthe development of concepts of muscle re-educa-t ion and training.
Differences in Aci ivi ty and Response
Of considerable importance also, is that Granitand his co-workers have been able to show a defi-nite dif ference in gamma activi ty and spindle ac-t ivi ty between so-cal led phasic and tonic muscles.:aThere is also a difference between the stretch re-sponse of small motor neurons and large motorneurons before and after activation of the gammafibers. Small motor neurons are under consider-ably more spindle control than the large ones.Small motor neurons innervate mostly the tonicmuscles and the larger ones the phasic muscles.Eccles and his co-workers have shown that thereare phasic motor neurons and tonic motor neu-rons.r; Among the phasic muscles and motorneurons are those of the gastrocnemius. Amongthe tonic ones are those of the soleus. The motorneurons are smaller; they have more postsynapticpotentials;they have more synaptic receptivi ty; theyhave more positive afterpotential and more post-tetanic potentiat ion. The tonic muscles appear tohave very strong spindle control and also have verystrong inhibition from recurrent collaterals so thatthey are able to fire continuously at a iow rate.If this were not so, they would run wild. In otherwords, this is a needed negative feedback system.
It is possible to gradually el iminate the effect ofthe gamma efferents on the tension stretch curve lndecerebrate animals by cocaine blocks.:6 In theseexperiments the curve remains the same in slopebut moves to the r ight. In other words the spindlehas set the level at which the tension stretch dia-gram occurs and, by an adjustment in the spindlebias, a tonic muscle can hold tension at differentlengths. Again it is found that this system is farmore developed in tonic muscles than in phasicmuscles.
Granit points out that this appears to be evidenceof a fundamental arrangement.:7 Eccles has per-formed experiments in young kittens in which themuscles are undifferentiated.?8' 2e He crossed thenerves between a slow and a fast muscle (thesoleus and the flexor digitorum longus). Afterthe kittens grew up, the soleus became a fastmuscle and the flexor became a slow muscle. Inother words the difference between tonic andphasic muscles is not just in the musculatrlre butis in the central nervous system. Recently Koc-zocik-Przedpelska has shown that regeneration inthe central nervous system on crossed nerve ex-periments occurs in three phases and also that con-
Provided by the Maternal and Child Health Library, Georgetown University
1 0 1

tralateral extremities are influenced during thisprocess.30 In the clinical evaluation of muscletraining and muscle re-education, we have not paidadequate attention to these differences. In fact,it would be fair to say that it would be a fertilefleld for research in the field of physical therapy toevaluate whether these differences can be foundin human patients. Any physiologist with clinicalexperience has become extremely aware of thedifficulty of transferring animal experimental datato man. Physiology has the advantage in that anexperiment can be set up at will. The clinic hasthe advantage of having far more detailed lesionsand far more variety of lesions than the averagephysiologist can produce, and it is in this field thatgood clinical observation by research-minded phys-ical therapists can be of much value.
Cor t i ca l Innerva t ion o f Musc le Sp ind les
Of considerable importance to our understand-ing of the fundamentals of human movement is theouestion of the cortical innervation of the musclespindles. Mortimer and Akert have shown that cor-tical activation of the spindles indeed exists and thatthis often precedes the start of the voluntary move-ment.31 Moreover they have shown that there aregamma motor centers as there are alpha motorcenters. Akert comes to the conclusion that onepossible mechanism of initiation of movement isthat the cortex fust activates the spindles and thatthe afferent spindle impulses reaching the spinalcord would then collaborate with and facilitate cor-tical impulses going to the alpha motor neuronsand that together they would activate the musclefiber. It seems certain that this is not the onlymechanism for motor activation and that indeedthe possibility of direct cortical activation of thealpha motor neurons leading to voluntary con-traction does exist. Akert has shown that thealternate double mechanism through the interme-diate of the muscle spindles is a valid alternative.
Very little is known at present about clinical dis-turbances of the co-ordination and co-operationbetween the alpha system and the gamma systemand the so-called alpha-gamma linkage.az In animalexperiments it is possible to disrupt this linkage invarious degrees and sometimes severe inco-ordina-t ion results. Whether the inco-ordination result ingfrom a disturbance of the alpha-gamma linkage canbe recognized as a clinical entity is again a prob-lem that is open to further research.
Cruz and Hufschmidt have shown evidence inunanesthetized rabbits of afferent inflow fromGolgi receptors to the contralateral side 33 whichobviously relates closely to the work of Hellebrandtand others in crossed exercises.3a
SUMMARY
Several aspects of the physiology of peripheralmuscle which are of importance to physical therapy
ro2
are reviewed. Nerve activates muscle throughtwo time delays. Electromyography is a tool ofconsiderable present importance and great futurepotential, but its interpretation requires more crit-ical evaluation than is commonly used. The rela-tionship between innervation and contraction andthe problem of trophic innervation are activephysiological research fields with clinical implica-tions. The synchronization and co-ordination ofperipheral motor units and their relation to thegamma system are discussed. Fundamental differ-ences between the innervation of phasic and tonicmuscles are becoming apparent. Clinical studiesof disturbances of the alpha-gamma linkage andits relations to contralateral innervation are needed.
REFERENCES
1 . Sandow. A . : Amer . J . Phvs . Med . , 31 :103 -125 ' l 95Z '2. Buchthal . F. . Erminio, F. , and Rosenfalck, P. : Acta
Phvsio l . Scand., 45:72-87' 1959.3.Bu;hthal. F., Guld, C., and Rosenfalck, P.: Acta
Phvsio l . Scand.. 39:83-1A4, 1957.4- Dumoulin. J.: La Stimulo D6tection par Courants de
Longe Dur66. Paris: Librairie Maloine' -1963'S. rUiyii, R. F., and Denny-Brown, D': Neurology' 14:
714 -726 .7964 .6. Gassel , M. M.: Neurology. 14:825-836' 1964' . -i.F""ariei, C., and Knowfton, G' C.: Amer. J. Phys.
Med . . 43 :109 -1 16 , 1964 .SHis lo i , H. J. : J . Amer. Phys. Ther. Ass. , 43:21-38,
1963:9. Liberson, W. T.: In Licht, Sidney, ed.:- Tlerapeutic
Exercise.-New Haven: Elizabeth Licht, Publisher' 1961'lO.Rose. D. L., Radzyminski, S. F., and Beatty, R. R.:
Arch. Phys. Med., 38:157-164, 1957.11. Gutmann. E. : Amer. J. Phvs' Med., 42:187-191' 1963.12. Gutmarur, E., and Hnik, P, eds.: The.Effect-of Use
and Disise on Neuromuscular Functions. Prague:Czechoslovak Academy of Sciences, 1963.
13. Katz, B. , and Mi ledi , R. : J . Physio l . (London), 155:399415, 1961.
14. Thesleff, S.: Physiol. Rev., 40:734-752, 1960'15. Weiss, P.: Arcli. Surg. (Chicago), 46:525-547,-1943.16.Weiss, P. , and Davis, H. : J . Neurophysio l . ,6:269-286'
1943.17.Stetson, R. H. , and Bouman, H. D. : Arch. N66r l .
Physion. , 20 :117 -254, 1935.18. Drimoulin, J.. and Augremanne, Ch.: Pr6cis d' 6lectro-
myographie. Paris: Librairie Maloine, 1959.19. Renshaw, B. : J . Neurophysio l . , 3:373-386,1940.20. L loyd, D. P. C. : J . Neurophysio l ,6:11l-120,1941-21. Granii. R. Receptors and Sensorv Perception. New
Haven: Yale University Press, 1955.22. Buchwald, J. S., and Eldred, E.: J. Nerv. Ment. Dis.,
132:146-1.52. 1961.23.Buchwald, J. S. , Beatty, D. , and Eldred, E. : Exp.
Neurol., 6:524-537, 1962.24.Grani t , R. , Henatch, H. T. , and Steg, G.: Acta
Physio l . Scand., 37: l l4-126, 1956.25. Ect les, J. C. , Eic les, R. M., Shealv, C M., and Wi l l is ,
W. D.: J . Neurophysio l . , 25:559-580, 1962.26. Matthews, P. B. C.: J. Physiol., 141:547-564, 1959.27. Granit, R. In Rodahl, Kaare, and Horvath, Steven {.,
eds.: Muscle as a Tissue. New York: McGraw-Hill,1962. pp. 790-210.
28.Bul ler , 'A. J. , Eccles, J. C. , and Eccles, R. M.: J.Physio l . (London), 150:399-416, 1960'
29.Bul ler , A. J. , Eccles, J. C. , and Eccles, R' M.: J .Physio l . (London), 750:417439, 1960.
30. Koczocik-Przedpelska, J.: Amer. J. Phys. Med., 43:146-156,1964.
31. Mort imer, E. M., and Akert , K. : Amer. J. Phys' Med.,40:228-248, 1961.
32. Granit, R. In Barker, David, ed.: Symposium onMuscle Receptors. Hong Kong: Hong Kong Uni-versity Press, 1962, pp. 1-12.
33.Cruz, J., and Hufschmidt, H. J.: Pfliigers Arch. ges.Physiol., 27 5 :l2l-133, 1962.
34. Hellebrandt, F. A., Houtz, S. J., and Partridge, M, J.:Amer. J. Phys Med, 36:196-211,, 1957.
II Provided by the Maternal and Child Health Library, Georgetown University

The Plosticityof the Nervous Sysfemof Eorly Childhood
G. MILTON SHY. M.D.
'rIne cr,Nrnel NERvous system of
the human may be looked upon in i ts simplestterms as a telephone switchboard or computerwhich may receive a message from any part of theenvironment, correlate internal ly, code, and emitan objective response of the individual to that en-vironmental st imulus. In addit ion, the brain iscapable of independent correlations based uponpast memory experiences and init iates upon i tsown ideation certain responses to the environmentnot of neccssity dependent upon a recent signalfrom that environment. Through the -vears, thenervous system has laid dorvn a system of patternresponse to this environment. 81' the ninth to
Adapted from a paper presented at the Symposium onThe Chiki with Central Nervous System Deficit, September28-October 2, 1964, at the University of Pennsylvania,Philadelohia.
Dr. S[y is Chairman and Professor of Neurology, Schoolof Medicine and Graduate School of Medicine, TheUnivers i ty of Pennsylvania.
tenth year this pattern response has been com-pleted. Deviat ions of the pattern response of theadult from injurl ' to the nervous s1'stem might,therefore. be anticipated i f such an injury occttrredduring the period of growth of this computermechanism. That this is indeed true may be seenin the response of the plast ic nervous s1'stem ofearl1' chi ldhood to disease {
BRAIN GROWTH AND SKULL GROWTH
The skul l is shaped largely by the internalgrowth of the central nervous system. The con-verse is not true unless patl.rology affects the skulibones themselves. Thus. the usual cause ofmicrocephaly is an arrested brain growth. Sincethe bones of the skul l do not fuse unti l the ninthand tenth 1'ear of age, at the completion of braingrorvth i t is expected that anything rvhich displacestissue within the skull which ordinarily would
Provided by the Maternal and Child Healtnlibrary, Geo.getown University
103
I

lead to all signs of increased intracranial pressure
in the adult wi l l instead in the chi ld merely lead to
enlargement of the head by separation of the
sutures. This is true in the hydrocephalic child
as against the hydrocephalic adult. T'his is also
true of tumors in chi ldren since the sutures may
separate and the response of nervous t issue to
pressure from ingrowing lesions may be markedly
delayed in chi ldhood cr may not be apparent on
roentgenographs as increased pressure or as pa-
pi l ledema and vomit ing, al l of which are cardinal
signs of expanding intracranial lesions. The con-
verse of this, of course, is also true, i 'e., a prema-
ture closing of the bones of the skul l cal led cranio-
stenosis wil l cause increased intracranial presstlre
because the brain wil l continue to grow and the
skul l can no longer accomnrodate i t and this can
be catacl l 's6ic to the chi ld indeed
The growth of the extremit ies is also control ledlargely by the brain. The shortening of a l imb ofless than 2 inches in the presence of a centralnervous system lesion indicates that such a lesionwas dependent upon some type of abnormali tybefore tlie second year of age. Beyond this age
some shortening may occur but more commonlythere is a wasting of the extremity in i ts bulkrather than i ts length.
The effects of the central nervous system andthe peripheral nervous system upon motor functionis one of the keystones upon which al l neurologyis laid. Two types of abnormali t ies have beennoted classical l ,v, those of the upper motor neuronand those of the lower lnotor neuron. Thus, thecentral nervous s) 'stem in i ts response to the st ir l t-ulus from its environment when pathological l l 'al tered in the so-cal led upper motor neuron s)s-tem usuall-v has i ts disorder manifested in the fol-lowing wavs: First, there is an increase in tone ofthe involvcd extrenri t ies. Second. the ref lexes arecommonly inc reased. Th i rd , un less the les ion l iesin the parietal lobe wasting is uncomnton. Whensuch wasting does occur i t does not f i t any givenn lyo tonre . Fasc icu la t ions ( the spontanecus d is -charge of muscle f ibers to lesions of the n'rotorun i t ) a re no t seen nor a re f ib r i l i a t ions ( the spon-taneolrs discharge of single m',rscle f ibers). Thelower motor nerlron lesion on the contrar.v is ustt-al l .v accompanied b.v nrarked wasting. decreasedre f lexes . fasc icu la t ions . and f ib r i l l a t ions . Un l ikethe adult. the af l l icted l imb of a chi lcl n' i th anupper nrotor neLlron lesion freqtrentl l ' . later in l i fe,is the object of involuntar.v movements sttch aschorea and athetosis.
The co-ordination of such extrerr i t ies is largely
under the cont ro l o f two sys ten ls . pos i t i ve sensc
and the cerebellum. It is of interest in the chi ld
that cerebellar lesions (acute or chronic) wi l l fre-
quently, i f al leviated, leave no residual effect.
Many cases of complete agenesis of the cerebellumhave been found at post mortem in which no
s)'mptomatology has been seen. The majori ty of
I M
neoplasms in childhood are found in the posterior
fossa; one of the most common of these is the
astrocytoma of the cerebellum. Complete re-
moval of a cerebellar astrocytoma in a child with
characteristic symptoms of inco-ordination on the
ip'silateral side will usually,'if successful, result
in a completely normal limb within two to three
years. This is not possible in the adult.
The time of life in which speech becomes cen-
tered in what is commonly termed the dominant
hemisphere is still uncertain. However, it is com-
mon linowledge that lesions in the dominant hem-
isphere in children may frequently have complete
or partial compensation by the other hemisphere
and speech patterns will still be normal or at least
part ial ly acquired, which again is impossible in
ihe adult. The same is true of lesions involving
discriminative sensation which appears to be a
function largety of the cortical gray mantle. The
adult with a major lesion in the parietal lobe has
severe incapacitation of the extremity of the op-
posite side because of his inability to discriminate
what is in the aflicted extremity. Children fre-
quently may have major lesions in the parietal
lobe with minimal sensory deficits. On the other
hand, the autonomic nervous system is a very old
phylogenetic system; it is extremely poor in myelin
and it is well developed in early life. Disorders
of the autonomic function in childhood, therefore,are common.
There is no obvious center for intelligence. In-
telligence appears to be that response of neuronal
networks to total environmental stimulation re-
ceived throughout l i fe. Testing of intel l igence in
early chi ldhood depends mostly on motor ski l ls and
involvement of the motor system or i ts functions
wil l be ref lected in intel l igence whereas abstract
thought and ideation cannot be tested at this age.
Therefore, the majori ty of motor- impaired chi l-
dren wil l be recorded as intel lectual ly deficient
when indeed they may not be. I t is dangerous
indeed to make a record assessment of intel l igencebefore the eighth or ninth year of age. A record
of mental retardation in a chi ld should not pre-
clude obvious retraining of the chi ld in his dai l ,v
activi t ies unti l accurate assessment of intel l igencecan be ob ta ined la te r in l i fe .
There are many disorders that affect vision in
chi ldren. On the other hand, the chi ld not re-
sponding normally to his environment may appear
to be bl ind when he is not. Visual izat ion of the
fundi of a chi ld under six months of age normall l
ref lects a white optic nerve which in the adultrvould be cal led oPtic atroPhY.
The temperature centers in the diencephalon
are not normally co-ordinated unti l the f i f th or
sixth year of age. Thus, the chi ld with an in-
fection may have much higher fevers than will an
adult with the same infection. Such high temper-
atures in turn affect growing neurons which re-
spond to such injury by spontaneously discharging
--Provided by the Maternal and Child Health Library, Georgetown University

with the external manifestat ion of seizures. This
does not of necessity mean that the chi ld is a
seizure patient.
Keeping in mind, therefore, the remarkableplastici ty as well as certain l imitat ions of the chi ld's
nervous system, the main part of this presentation
wil l deal with certain common remedial and non-
remediable disorders acquired in childhood. To
entirely cover the nervous system of chi ldhood
and its disorders would require a monograph ofthousands of pages. There wil l be no attempt,therefore, in this discourse to do such but ratherto use certain common disorders as examples ofthe chi ld's response to disease of the nervous sys-tem. An occasional rare disorder wil l also beincluded merely as an example of how the centralnervous system and the peripheral nervous systenrfunction when one or more of i ts cel lular elementsis being altered.
COMMON EXAMPLES OF REMEDIABLEDTSoRDERS ACQUIRED lN CHILDHCOD
The Suppurative and Infective Disorders
Fot practical purposes, the brain, its covering,
and the skull may be considered as contiguous ele-
ments into which infective bacteria may enter
either by the blood stream or directly from the ex-
ternal environment by contiguous routes such as
ear infection, nasal infection, and infections on
and about the face. When such an infection comes
to lie within the membranes of the pia and arach-
noid linings of the brain, it is normally termed a
meningit is. I t is a rare meningit is, however, that
is limited to such coverings of the brain and almost
all such disorders have as one of their concomitantmanifestations an acute cerebritis of the under-lying brain substance. Thus, a middle ear abscessmay penetrate and give an epidural infection, sub-dural infection, a meningitis, a brain abscess, orinfection into one of the venous sinuses drainingthe involved hemisphere of that side.
The most common conditions affecting suchstructures in childhood are meningococcal menin-gitis, pneumococcal meningitis, Escherichia colimeningitis, influenzal meningitis, tuberculous men-ingitis, and occasionally fungus meningitis. Thetype of pathogen usually is related to the patient'sage and unfortunately the symptomatology is like-wise related.
The most common pathogen of the first sixmonths of life is the Escherichia coli in which theinfection commonly enters by way of the umbilicalcord. The child under six months of age does nothave the reflexes maintained or developed to dem-onstrate the usual picture of a meningitis. Thus,nuchal rigidity and reflexes dependent upon irrita-tion of spinal membranes are not obtained at thisage. The child usually has a severe fever, dehydra-tion, and, not of necessity, signs of increased intra-
cranial pressure. The fontanels may be sunken. Asa result, the diagnosis is commonly missed unti llater in the course of the disease at which t imepus in the spinal fluid is found and large subduraland arachnoid empyemas are noted. The result isthat the chi ld usually dies.
Between the ages of two and nine years influ-enzal meningitis from the Hemophilus influenzaorganism is probably the most common cause ofcentral nervous system infection. Approximately60 per cent of these chi ldren may be saved i f theinfection is detected early and appropriate anti-biot ic therapy inst i tuted.
Third in order would be the meningococcalmeningitis of which 90 per cent of affiicted pa-t ients may be saved with the proper antibiot ictreatment with penici l l in and the sulfonamides.
As recently as ten years ago 90 per cent of chil-dren with tuberculous meningitis succumbed to thisinfection. At the present time an equal numbermay be saved by a prolonged treatment programlasting one to two years with trsoniazid, pata-Am-ino salicylic acid preparations, and streptomycin.Such children, however, commonly have as re-sidual effects the thickening of the membranes inthe spinal cord and the base of the brain withcranial nerve palsies and occasional involvementof long tracts of the spinal cord with hemiparesisor diplegia. These children, during the period ofintense treatment, need almost constant physicaltherapy to prevent contractures, reduce spasticity,and prevent decubiti. The sequelae of the menin-gococcal or the meningitic syndromes commonlyare those of delayed hydrocephalus (with a block-age of the normal passage of spinal fluid from thebase of the brain over the convexities) and di-plegia (from adhesive arachnoiditis in the spinalcord). Numerous cranial nerves may also bein.rolved. It is axiomatic, particplarly in the men-ingococcal and pneumococcal group, that thelength of time lvithout diagnosis is directly pro-portionate to the number of sequelae. Thus, assoon as the diagnosis is suspected, the doctor him-self should do the appropriate examination of thespinal fluid and institute immediate therapy with-out waiting for laboratory results.
Brain Abscess. Not uncommonly contiguous orhematogenous infection may go directly into thehemisphere and cause a cerebritis which ultimatelyresults in a brain abscess. All brain abscesses arepreceded by cerebritis in which an acutely ill pa-tient frequently is comatose with localizing symp-tomatology to the side involved. The most com-mon sources of brain abscess in childhood areinfections in the middle eai and frontal sinuses.Once again, treatment may be curative. Thetreatment most likely to succeed in this particulartime is a combination of antibiotics and completeremoval of the abscess with its membranes.Should this be impossible, an external drainage ofthe abscess and placement of radiopaque material
r05
Provided by the Maternal and Child Health Library, Georgetown University

into the abscess to follow its migration to the sur-face is the next treatment of choice.
Usually confused with such an abscess, however,is the lateral sinus thrombosis picture of a middleear infection. The infection involves the lateralsinus and then proceeds into the superior longi-tudinal sinus to give an acute picture of increasedintracranial pressure, usually bilateral 6th nervepalsies which have no localizing significance, andusually a retention of awareness of the environmentin contradistinction to the abscess with which acerebritis is associated. The presence of increasedintracranial pressure, the retention of awarenessof environment, and bilateral 6th nerve palsies inthe presence of an infected right ear is almostpathognomonic of this syndrome. The treatmentinvolves reduction of intracranial pressure which
may be done safely by lumbar puncture in contra-distinction to the abscess in which lumbar puncture
is dangerous. Thus, the differential diagnosis be-comes important. Accompanying this reductionin pressure should be a combined approach with amastoidectomy by the otolaryngologist and tyingoff of the lateral sinus by the neurosurgeon. Thisprevenis hematogenous abscess spread throughoutthe lungs. If such patients may be broughtthrough the acute phase by such therapy and sup-portive physical therapy, the patient will respondand develop as a perfectly normal individual.
Sydenham's Chorea and Guillain-Barr6 Syn-dromes. In light of present advances in immu-nology, it is of interest to note the response of thecentral nervous system to infections by what ispossibly an autoimmune reaction. Although seenrarely these days, perhaps the most common typeof this particular involvement is Sydenham'schorea. This is acute involuntary phasic move-ment of the extremities as a result of involvernentof the brain in rheumatic fever. Exacerbation ofthis syndrome may occur in the female duringpregnancy which is called chorea gravidarumwhich may be so severe as to threaten the birth
of the child. The treatment of choice lies in un-
derstanding the theory that such choreiform move-
ments are dependent upon spontaneous seizure foci
and dependent upon scar tissue as well as upon im-
munological responses of the brain to streptococcalinfections. The treatment of choice is Dilantin@which is remarkably effective in the majority of
such children. Such chorea may last when closely
searched for as long as four years after the initia-
tion of sy.mptomatologY.The physical therapist may aid such a patient
to handle his extremities so as to prevent the in-
voluntary movements from injuring him and toguide him in taking care of daily activities, such as
eating, by fixation of the larger muscle groups'
Similar in nature and life-threatening is a dis-
order termed the Guillain-Barr6 syndrome in
which usually an upper respiratory infection and
ascending paralysis occurs. The pathology is
l06
found largely in the root entry zone; the spinalfluid albumen is raised but the cell count remainsnormal. The ascent of this to respiratory centersmay occur in as short a time as four hours and sucha patient is always a neurological emergency. Ifone may sustain the patient by way of respiratorycare, oxygen, and prevention of subsequent throm-bophlebitis, gastrointestinal ulcerations, pulmonaryemboli, and atelectasis, one will have a well pa-tient. During this entire period of time passive
movement of extremities is extremely importantto prevent thrombophlebitis within the extremitiesand to prevent contractures. With total care onemay anticipate that 80 per cent of such patientswill have complete recovery or have less than a10 per cent deficit.
Of the viral infections of the central nervoussystem, the most common are the eastern andwestern equinae encephalitides and poliomyelitis.The common residua of the encephalitis group isdementia, upper motor neuron involvement ofthe extremities, and occasionally later involuntarymovements particularly in the western equinegroup. A picture, not unlike Parkinson's disease,may result. Here again, a period of unconscious-ness may occur during which physical therapy isimportant to prevent contractures, thrombophle-bitis, and so on. In the eastern equine groupapproximately 60 per cent of such patients willdie and of those who recover, over 40 per centwill have some type of sequelae which will needphysical therapy. Poliomyelitis is too well knownto spend much time on it; fortunately, with thenew vaccines it is expected to be seen but rarelyin the future. The relief of spasm, the preventionof contracture, the re-education of other musclegroups to take over affiicted muscle groups is well-known. Of interest miglit be the warning sign ina patient with beginning poliomyelitis, as towhether paralysis can be expected, fasciculations,absence of a reflex, persistent tenderness, aud adromedary-type fever pattern all indicate an emi-nent paresis of an extremity. Certain key signsmay be evident as to the recovery of such an ex-tremity: partial paresis as against total paresis ofthe involved part is a good sign. Early recoveryof the deep tendon reflexes is a good prognosticvariant. Improvement may be expected up totwo years from the initial paresis.
Tumors of the Central Nervous System
Which Are Remediab le in Chi ldhood
Brain Tumors, The primary tumors of the cen-tral nert'ous system in childhood differ from thosein the adult in that 80 per cent of tumors arisingfrom brain substance itself arise in the posteriorfossa, i.e., the cerebellum or brain stem of thechild whereas in the adult 80 per cent arise fromthe cerebral hemispheres. The reason for this isunknown at this time.
The most common tumors above the tentorium
Provided by the Maternal and Child Health Library, Georgetown University

in the child do not occur within the cerebral hemi-spheres, but are tumors of the pituitary gland.
Of the tumors of the posterior fossa, the twomost common are the medulloblastoma and theastrocytoma. An astrocytoma commonly affectsthe cerebellar hemisphere. This causes ataxia ofthe extremities on the ipsilateral side along withsigns of intracranial pressure or diastasis of thecranial sutures.
The most common manifestation of the pituitarytumor is impairment of vision by way of visualfields with a bitemporal hemianopsia.
The most common manifestation of the medullo-blastoma is that of balance. A large medulloblas-toma may be present in the vermis of the cerebel-lum with little or no ataxia of the extremities. Theproper diagnosis will be missed unless the childis made to walk during examination; this will re-veal a balance problem commonly called trunkalataxia as against extremity ataxia of the astrocy-toma of the lateral hemisphere. The medulloblas-toma is extremely difficult to remove. It is, how-ever, radiosensitive. Such children may live formany years and need physical therapy.
The astrocytoma, if well out in the hemisphere,may be completely removed. If the latter is thecase, then all signs of ataxia of that involved ex-tremity or of the involved side of the body maywithin a period of eleven months or so completelydisappear and it would be difficult to tell that thechild ever had a brain tumor. During the periodof recovery, physical therapy is of extreme im-portance, particularly for exercise to aid the childin the difficult period of transition from abnormalto normal.
A pituitary tumor may be almost entirely re-moved. Although there is a 40 per cent or greaterchance of recurrence, there still is a good chanceof complete cure. Such tumors are commonlytreated by either radiation or surgery, and usuallythe extent of involvement of the visual field is thecommon parameter upon which decision is made.Adequate visualization of the tumor by pneumo-encephalographic studies is also necessary becausethe tumor may appear larger than can be con-templated by examination of the visual fieldsalone.
Spinal Cord Tumor. Tumors of the spinal cordare common in childhood, the most frequent beingthe ependymoma. The most common site of thistumor is at the distal end of the spinal cord, inthe filum terminale. Long-term relief may be ex-pected if adequate surgical removal is ,attemptedearly. A child with an ependymoma usually hasinitial complaints of pain in the lower extremities,weakness within muscles innervated by the lowerlumbar and sacral roots, and difficulty in urina-tion. Frequently the tumor involves the conusmedullaris in which case the child may have a per-manent paraplegia. It is possible to remove atumor of the conus medullaris. but the child will
7 8 0 - 2 8 0 0 - 6 6 . 8
require extensive rehabilitation. The majority ofsuch patients seem to have a lower motor neuronlesion because of the location of the tumor.Ependymomas higher in the cord may present thesymptoms of an upper motor neuron lesion andsuch a diagnosis must be kept in mind in a childwho has any lesion involving the cord, be it tumor,trauma, or infection. Based upon studies of post-traumatic paraplegia patients in World War II,the child should be able to be taught to walk againas long as that lesion is below T1 and is nonprogres-sive. The other tumors of childhood almost uni-versally are progressive and nonoperative and willbe discussed later.
TraumaTraumatic lesions affecting the central nervous
system in childhood are extremely common andconstitute one of the largest groups seen by theneurologist. The amount of sequelae is usuallydependent upon the period of unconsciousness andthe amount of retrograde amnesia. Prolongedperiods of unconsciousness (several days) usuallyare followed by midbrain findings indicating thatthe reticular formation has been involved in thelesion. These are most commonly seen in basilarskull fractures. The patient should be searchedfor ecchymoses behind the ear. Inquiry may alsobe followed by dural tears, spinal fluid leaks, andsubsequent meningitis. The brain signs commonlyfollowing prolonged unconsciousness are: externalocular palsies, varying degrees of spasticity, andalmost always ataxia and nystagmus.
Children also may have subdural hematomaswhich differ from the adult in their location. Thecommon si-te of a subdural hematoma in earlychildhood is beneath the temporal lobe, not overthe convexity. The diagnosis may be ascertainedby roentgenograms of the skull on the involvedside within a few months after the initial lesion;the middle fossa will be enlarged. Removal of thesubdural hematoma will result in a good prognosisprovided the brain can once again re-expand.
Common among childhood traumas are fallingor diving accidents where paraplegias which areusually permaDent may occur, but improvementmay be expected up until one year after the initialinjury. Bladder care, rectal care, prevention ofsecondary infections, spasticity, and the teaching ofthe patient to walk again are necessary for long-term care.
Genef ica l ly Determined Disorders
Phakomatoses constitute interesting chapters inthemselves. These are genetically determined andhence always occur in childhood. They are fivein number, all of which have skin lesions as wellas central nervous system lesions and may also in-volve the other organs of the body.
The most common is probably von Reckling-hausen's disease, also known as neurofibromatosis.
Provided by the Maternal and Child Health Library, Georgetown University
107
This particular disease is accompanied by skin
neurofibromas, neurofibromas of peripheral nerves
or crania'l nerves, as well as abnormalities of the
skin such as lipomas, caf6-aulait spots, and sha-green patches. In addition, retinal lesions such asdri-isen may occur which when found around the
optic nerve may mimic papilledema. A1l types oftumors of the central nervous system may occurwith this particular syndrome such as meningi-omas, ependymomas, and gliomas. In addition,about 10 per cent of the patients have pheochro-mocytomas of the adrenal gland.
Ataxia telangiectasia is a newly describedphakomatosis in which telangiectasia may occurin certain areas of the skin and is accompaniedby a picture of cerebellar ataxia and rectlrrentsinopulmonary infect ion. This is a chronic i l l -ness and about 25 per cent of the children haveinvoluntary movements such as athetosis as well.Here therapeutic exercise is of great importanceas the intellect may be the last to fail.
Tuberous sclerosis is another phakomatosis inwhich an abnormality of the skin of the face,adenoma sebaceum, may occur; tumors of theheart may be found, and in addition so-calledtubers or glial pseudotumors of the brain are foundwhich are commonly calcified and which giverise to seizures and mental deficiency. Such pa-tients usually live a normal life span.
Von Hippel-Lindau's disease is multiple he-mangioblastomas of the retina, cerebellum, andspinal cord, associated with polycystic disease ofthe kidney or pancreas. The disease may last all thepatient's life or if the tumors grow rapidly in theposterior fossa they may cause an early demise.Frequently associated with this disease is poly-cythemia because such tumors may contain eryth-ropoietins, the substances responsible for red cellmaturation.
Finally, the Sturge-Weber-Dimitri syndrome of a
cavernous angioma of the face associated withtelangiectasia over the occipital lobes is not un-common. The patient may develop seizures ormental retardation or hemiplegia or all three'
These five constitute the phakomatoses. Withthe exception of ataxia telangiectasia, the phako-
matoses are slowly progressive and not necessarilyinconsistent with normal life. Patients with thesediseases frequently are dependent on the physicaltherapist to aid them in carrying on normal lifefunctions.
Of interest recently is the delineation of enzy-matic defects as the cause of cerebral disease'These are many in origin, a few of which will bedescribed here. Thus, galactosemia is a defect inthe enzyme galactose-1-phosphate-uridyl trans-ferase and may be manifest by cerebral diplegia,mental deficiency, and cataracts. This disease maybe arrested early in its development, if it is recog-nized, by eliminating galactose from the diet untilthe brain has reached full maturation after which
108
the main danger is over. The same is true ofphenylketonuria, a disorder of tyrosine metabo-lism. Failure of tyrosine metabolism decreases
the total melanin content in the hair, iris, and skin,
hence, the usual patient is blond, blue-eyed, maybe mentally defective, and may have cerebraldiplegia. The disease is readily recognized by the
addition of ferric chloride to the urine, a positive
test being the appearance of a dark green color.
Of more recent interest is the Guthrie test forphenylalanine in the urine using bacillus subtilis.This allows recognition of the disease in the firsttwo weeks of life. Early detection is necessarybecause i f phenylalanine-restr icted diets are im-posed, the patient may expect a relat ively non-progressive disorder.
Hepatolenticular degeneration (Wilson's dis-
ease) is a hereditary abnormality of coppermetabolism in which excess copper is absorbedfrom the intestines. In addition, there is an ab-sence of the plasma protein ceruloplasmin (a cop-per-containing alpha globulin) and excess copperis excreted in the urine and stored in such tissuesas brain, liver, and kidney. Pathological changesin the basal ganglia and other areas of the brain areresponsible for involuntary tremor and spasticity'A greenish-ycllow pigment surrounding the cornea(Kayser-Fleischer ring) is characteristic, The useof chelating agents has been useful in the retardingor stopping of this disorder, the most common ofwhich is penicillamine.
Hartnup's disease is a disorder in which there
is a cerebellar ataxia and a rash upon the skin not
unlike pellagra. It is an abnormality of tryptophan
metabolism in which there is an excretion of ab-
normal indoles in the urine. To date, this diseaseis not reversible.
Common Progressive Disorders
This leads to examples of some of the commonprogressive disorders of the central nervous system
of childhood. Since many of these are slowly pro-gressive, it is dependent upon the allied medicalprofessions to keep these patients ambulatory as
long as possible.Often the most distressing are the diffuse demye-
linating disorders of the brain which have recentlybeen chemically broken down into three cate-gories. One is sudanophilic leukodystrophies' In-cluded in this group is so-called Schilder's disease(Schilder's dif fuse sclerosis). This chi ld exhibitsmonoparesis or hemiparesis followed by visual andspeech difficulties and ultimately quadriplegia,cortical blindness, and dysphasia. The metachro-matic leukoencephalopathies are characterized by
an ataxic gait and later hypotonia and muscularatrophy. Both of these disorders usually go frombeginning to end in one to two years, althoughthe metachromatic form may take considerablylonger. Finally is the form described by Krabbe(globoid cell leukodystrophy) in which multinu'
Provided by the Maternal and Child Health Library, Georgetown University

cleated cells are found in the central nervous sys-tem. This again progresses rapidly in a period ofone to two years from beginning to end. Themajori ty of these disorders, as in metachromaticIeukodystrophy and Krabbe's, exist under six yearsof age. As far as the Schilder's form, half existunder the age of twenty-one and half over.
The second large group of abnormalities ofprogressive nature in childhood are the lipidoses.These constitute amaurotic familial idiocy in whichgangliosides are stored in membranous tissue inthe neurons of the brain and in which there appearsto be an abnormality in the formation of certainl ipids or their destruction. Intensive research isbeing done on these at present, and there is hopefor the ult imate del ineation of the enzvmatic ab-normali ty. Gaucher's disease (cerebroside l ipi-dosis) may also affect the central nervous systemin infancy and in this there is an abnormali ty ofcerebrosides. Niemann-Pick's disease (sphingo-myelin lipidosis) affects the central nervous sys-tem, liver, spleen, and erythropoietic system.Sphingomyelin is present in increased quanti t ies.All of these may be gradually progressive over aperiod of from one to seven years. To keep suchsmall patients ambulatory during this period oftime is indeed difficult.
The next large group of progressive disordersof the central nervous system in childhood wouldbe the encephalic tumors arising from the brainstructure itself as well as metastatic carcinoma fromadrenal glands and leukemia affecting the centralnervous system, all of which have a poor prog-nosis. Retinoblastomas are commonly progressiveunless diagnosed early in which case only the nu-cleation of the eye will help and even then 80 percent will ultimately involve the rest of the neuralaxis.
Progressive, intermittent disorders, the classicalform of which is multiple sclerosis, also require theaid of physical therapy. Multiple sclerosis con-stitutes one of the most common neurological dis-eases, the pathology of which is dependent upondestruction of myelin within the central nervoussystem, including the brain, cerebral hemispheres,and spinal cord. It is relatively unknown in theperipheral nervous system, i.e., where the oligo-dendroglia end. Twenty-five per cent of such pa-tients may only have one episode of abnormalityand nothing else the rest of their lives. Another25 per cent are relentlessly progressive and the
remaining 50 per cent appear to have spontaneousremissions and exacerbations. Thus, multiplesclerosis gets its name from the fact that the lesionsare multiple in time and in place in the centralnervous system. If one cannot .fulfill these twocriteria one should question the diagnosis. Mul-tiple sclerosis is a disease of young people; theaverage longevity of all types of cases combinedis about twenty-two years. The most commonlesions affect the optic nerve or nerves to the eyemuscles with either transitory retrobulbar neuritisand blindness which will almost always clear upor external ocular palsies which also most com-monly clear. Lesions which do not commonlyclear are those effecting the spinal cord and cere-bellar pathways with spasticity and signs of uppermotor neuron syndrome and ataxia. In these par-ticular cases which constitute the majority of caseswith multiple sclerosis, the physical therapist is ofextreme value. The etiology of this disease isnot known. A similar picture may occur in al ler-gic encephalomyelitis ind in c.ituin nutritionaldisorders of the central nervous system in bothman and animals. There is a suggestion that vas-cular abnormalities may play a role in this dis-order.
Among the intermittent disorders are certainintermittent disorders of the muscle such as myo-globinuria, megaconial myopathy, and familialperiodic paralysis.
SUMMARY
Some of the more common neurological dis-orders which may affect the central nervous systemhave been presented. In these the neurologist isextremely dependent on the physical therapist foraid. The plasticity of the central nervous systemof childhood tends to make such disorders appearclinically different from those of the adult. Onthe other hand, such a plasticity may frequentlybe rewarding for the physical therapist workingwith a child in contradistinction to the one work-ing with the adult.
SELECTED EIELIOERAPHY
1. lg{9r_F. R.: Diseases of the Nervous_ Sy_stem in Infancy,Childhood,. and _ Adoleslence, Fourth Edition. Sprjng-field, Illinois: Charles C Thomas, 1960.
2.Korey, S., Pope, A., and Rubins, 8., eds.: tlltra_structure and Metabolism of the Nervoui System, Balti_more: Williams and Wilkins Company. 1962.
- - _ L
-
ru)
Provided by the Maternal and Child Health Library, Georgetown University

MENTALRETARDATIONand the Child with Central Nervous System Deficit
MARY D. AMES, M.D.
TI N aNerYzrNG every child with
neurological or special sensory deficit, the questionof mental ability will be raised. Between 3 and 4per cent of all children born in the United Stateswill, at some time in their lives, be classed as men-tally handicapped; thus about 120,000 born eachyear will be so affiicted.l A secure diagnosis isdifficult and often impossible to make before thechild reaches the age of eight or nine years andhas also been exposed to several years of school-ing. However, the father and mother will want toknow as soon as possible whether their child isabnormal. Not to recognize the intellectual short-comings of a child before he reaches school ageplaces on the youngster a great burden which canlead to a serious psychological disturbance.
The doctor is usually the first to be suspiciousof a child's deviation from the normal. His first
Adapted from a paper presented at the Symposiumon Tlie Child with eential Nervous System Deficit.September 28-October 2, 1964, at The University ofPeirnsylvania, Philadelphia.
Dr.' Ames is Co-ordinator of Rehabilitation Servicesat The Children's Hospital of Philadelphia, Philadelphia,Pennsylvania.
1 1 0
awareness of mental reta-rdation may be aroused
by failure of the newborn to nurse, cry, or ex-
hibit normal reflexes. Between the ages of two to
four months, an infant should gain some aware-
ness of persons and nearby objects, and, if not,
the physician should suspect some degree of re-
tarded mental development or sensory impairment'Later signs, such as failure to sit, walk, talk, orto advance in school work, make the diagnosis
easier.2Walter H. Ehlers, in his study on the maternal
perceptions of retardation of the moderately and
severely retarded child, concludes that, in respectto the severely mentaily retarded child, the motherrecognizes the atypical condition of behavior of
the mentally retarded child, but in most cases re-
lates it to a physical rather than a mental condi-tion.3 If a pediatrician or family physician has not
brought the slowness of the child to the attention
of the parents, the parents will often seek help
from orthopedists, because "the child has some-thing wrong with his back" (because he does notsit), or because "he has something the matter with
his legs" (because he does not walk). Sometimes
Provided by the Maternal and Child Health Library, Georgetown University

the child does not sit or walk because he doeshave something wrong with his back or with hislegs, but usually it is the result of an over-all slow-ness, and the child will, in most cases. slowlv de-velop these motor abil it ies.
When the delay in motor development resultsfrom neurological deficits and the term "cerebralpalsy" is used in describing the condition with theparents, the optimistic outlook of the 1940's andearly 1950's with respect to mental capacity of thechild with cerebral palsy is immediately assumedby the parents and all their efforts are thereafterdirected to the motor development.
THE PHYSICAL THERAPIST'SRESPONSIBILITY
In either case, the physical therapist has an im-portant role in the management of the child withmental retardation. Children who have slow motordevelopment without any positive neurologicalfindings can profit from a program of "develop-mental guidance." Definite program plans aregiven to the mother for teaching the child to holdhis head, to balance himself in sitting, to crawl,and so on. This may not hasten the actual ac-complishment of these milestones but it does:
i. Offer the child positive attention from hismother, and
2. Give the mother actual insight into the slow-ness of her child's development.
In addition, the parents "are doing something"so that in answer to the "advice" of neighbors andrelatives, the parents are not idle. The use ofthis method for children who are not so severelyretarded that they will not learn to walk on theirown permits the mothers to develop a gradualrealization that their child is "totally slow." Dur-ing this time of gradual acceptance, a definitecause for the slowness is sought but, in most cases,is not found.
Children with motor disabilities in connectionwith mental retardation have always been caredfor by physical therapists. However, it appearsunfair that the physical therapist should handlethis most complicated problem alone. As hasbeen asked, "When do we recommend discontinu-ing of therapy in the cerebral palsied"; the answer,of course, is that therapy never stops because thechild always has problems. Physical therapy, how-ever, should be discontinued intermittently in orderto permit other areas to develop and also to deter-mine whether there will be retrogression or pro-gression lvithout treatment. What is meant, how-ever, is that the child should be in a comprehensiveprogram so that he will not be fragmented but willbecome a total person.
At the Children's Hospital of Philadelphia thechild receives physical therapy, play therapy,speech therapy, and educational therapy. Becausewalking precedes talking in the course of human
events, the phvsical therapist obviously is amongthe first to see the child in an evaluation of hisdisabilities. The audiologist gets into the picturevery early in the evaluation because deafness isone of the common complicationg of central nerv-ous system deficit, and hearing aides are put onthese children as early as the deficit is discovered.Other modalities are used very early because, aswith normal children, disabled children should bestimulated in general, rather than in particular.
The goal of the program at Children's Hospitalof Philadelphia is to evaluate the youngsters fre-quently and to plan a continuing program forthem. fhe program is planned until they reachsix years because by this age other facilities areavailable. In Philadelphia children whose intelli-gence quotients are as high as 50 are taken into apublic school for the physically handicapped forkindergarten at age five.
The United Cerebral Palsy Associationof Philadelphia has a Children's Opportunity Cen-ter which accepts children at four years who donot reach the mental development required by thepublic school. By the time they are taken inChildren's Opportunity Center, the motor develop-ment has probably progressed as far as it can withthe mental disability.
Children with hydrocephalus (there are a largenumber of these youngsters, particularly in con-junction with myelomeningocele since the Holtervalve was developed at Children's Hospital ofPhiladelphia) have varying degrees of mental dis-ability. The program is started for these young-sters as early as possible-shortly after birth. Thephysical therapist enters the program immediatelyand at five days of age begins a "swaddling" pro-gram to prevent contractures of the lower ex-tremities.
DEFINITION AND CAUSES OF MENTALRETARDATION
Having discussed mental retardation in relationto disabilities, it might be well to ask what ismeant by mental retardation. The National Asso-ciation for Retarded Children defines it as a condi-tion in which intelligence is prevented from attain-ing full development, limiting the victim's abilityto learn and to put learning to use. The NationalInstitute of Nervous Disease and Blindness callsit a manifestation of disease or dysfunction of thebrain. Personally, the author prefers the U.S.Children's Bureau definit ion of impaired or incom-plete mental development. At any age an accidentto the brain or an inflammation or contagious dis-ease can cause damage which results in mentaldisability but most causes are connected with pre-,peri-, and postnatal factors.
In recent years there has been a wider aware-ness of the importance of possible causes of mentalretardation in certain prenatal conditions, espe-
Provided by the Maternal and Child Health Library, Georgetown University

" - " . l ' t r
FlG. 1. Photograph shows how mater ia ls at hand can be used to maintain good posi t ion for s leeping. A diaper is wrapped f romumbi l icus to ankles. An A.shaped pad between the lower extremit ies is cut to determine the amount of h ip abduct ion. l tis made of scraps of upholstery foam rubber covered wi th p last ic and wrapped in a d iaper. Safety p ins hold the diaper andpad f i rmly in p lace so that the chi ld can move about, but the wrapping can be removed easi ly . Hightopped shoes help to con-tro l foot posi t ion.
cially those occurring during the first trimester ofpregnancy. Inadequate maternal diet, viral dis-eases such as German measles, and exposure toX-radiation are in this category.
Mental deficiency may also be traced to heredi-tary conditions associated with phenylketonuriaand galactosemia. These so-called inborn errorsof metabolism, however, are responsible for re-tardation in only a small percentage of mentallyhandicapped children. However, if the conditionis diagnosed at birth or a few days later, themental handicap may be prevented.
In phenylketonuria the enzymatic deficit in-volves failure in the hydroxylation of phenylalanineto tyrosine. This results in accumulation ofphenylalanine in the body fluids which, after de-amination, is excreted in the urine as phenylpy-ruvic acid. There seems to be a direct correlationbetween the amount of phenylalanine ingested andphenylpyruvic acid excreted. Therefore, treat-ment consists of early detection of the disorder andthen elimination of phenylalanine from the diet.About 80 per cent of these patients are blond andblue-eyed, often with some eczema. Their urinehas a characteristic musty odor attributable to thederivatives of phenylalanine. The presence ofphenylpyruvic acid in the urine is easily detectedby dropping eight to ten drops of a 10 per centferric chloride solution on the wet diaper. A greendiscoloration indicates a positive test. The diag-nosis is confirmed by increased blood phenylala-nine levels.
t t 2
Galactosemia is responsible for retardation ofgrowth and development and wide spread t issueinjury. Galactose is not ingested in free formbut with glucose is the result of intestinal hy-drolysis of the lactose of milk and milk products.Galactose must be converted into glucose to beutilized and this occurs in the liver. The deficiencyof the enzyme phosphor-galactose uridyl trans-ferase which catalyzes the first of three metabolicsteps is the inborn error of metabolism. The clin-ical findings are apparently the result of the dele-terious effect of galactose 1-phosphate on cellularmetabolism. The severe form of the disease may be-gin during the first few weeks of life with vomit-ing and other feeding difficulties and weight loss.There is a progressive hepatic damage and deathoccurs from infection or severe hepatic failure.In some infants the disease is milder and is identi-fied by presence of by hepatomegaly and cataracts.A significant mental retardation is present and,with cirrhosis of the liver and cataracts, is irrevers-ible.
Some hereditary diseases are not reversible but,through early diagnosis, can be handled better'
Mongolism, congenital hypothyroidism, and gar-goylism are causes of mental retardation and be-cause the children have common physical char-acteristics, they must be differentiated.
Mongolism can be suspected in the deliveryroom and chromosome examination is diagnostic.
Cretinism, or congenital hypothyroidism, mustbe considered in any case of retarded growth or
Provided by the Maternal and Child Health Library, Georgetown University

mental development. A low protein-bound iodineand a low radio-iodine uptake are diagnostic.
Gargoylism resembles the two above but an en-larged spleen and l iver, skeletal changes, dwarf-ism, and opaque cornea help to dif ferentiate i t .This disorder is the result of a metabolic defectwhich affects the skeletal. as well as soft. t issue.There is an accumulation of an abnormal inter-cellular fluid which is thought to be a mucopoly-saccharide. I t is genetical ly determined, mostcases result ing from a single recessive gene.
Injuries at birth may cause mental handicapand even when a chi ld has passed the neonatalperiod and is regarded as normal, retardation mayresult from encephali t is and meningit is, poisoningby heavy metals, vascular accidents, and skul l frac-tures.a
The invasion of the brain by viruses or bacteriamay result in damage to the intellect in varyingdegrees, depending on the age of the child. How-ever, early diagnosis of bacterial infection andprompt institution of specific therapy can, in manycases, prevent permanent cerebral damage. Pre-vious cerebral viral infections, with the exceptionof rabies, have no specific treatment. Secondaryencephalitides occur as an aftermath of varioussystemic viral diseases and occasional ly have beenreported following the use of vaccines, both at-tenuated and dead. The encephalitis followingrubeola now is disappearing with the eradicationof the disease fol lowing the advent of the vaccines.Roseola and rubel la are mild diseases but whenthe secondary encephalitis does occur, it is verysevere and may lead to death. The encephalopathyaccompanying roseola appears to be rather dif-ferent from other diffuse inflammatory cerebral dis-eases in that it tends to leave behind it focal per-manent residua, such as hemiplegias combined withmore or less severe diffuse cerebral damage.
On the other hand, presence of physical handi-caps may lead to an underestimation of the mentalcapacity of a child. Unrecognized deafness, par-ticularly partial deafness, will affect the child'slinguistic abilities, an important measure of mentaldevelopment in children over one year of age.Blindness, although more easily recognized thandeafness, disrupts normal development in the childand sometimes produces an appearance of mentalretardation. Also emotional disturbances are aotto create the impression of mental deficiency.Autism, for example, is characterized by a power-ful desire for solitude, by poor linguistic achieve-ments, and by inability to relate to other persons.Rather than being an expression of mental defi-ciency in the child, it may be a manifestation ofemotional disturbance.
MEASURING DEFICIENCIES
Intelligence tests presently in use measure cer-tain functions of the chi ld based on experience. I t
has been found that chi ldren with motor disabi l-i t ies, in addit ion to mental retardation. have a l im-ited environmental experience. Because it is toodifficult to take the child on an outing, either heis left at home with a babysitter
"or no one goes.At a large long-term orthopedic hospital standardintel l igence tests have been given chi ldren whowere thought by the personnel to have averageintelligence, only to find the results to be disap-point ingly low. As a test of the tests, so to speak,new questions regarding the experiences around thehospital-such as who goes to physical therapymore often, pol iomyeli t is patients or patients withLegg-Perthes disease; or who stays in the hospitalthe longest; or who is operated on most frequently-are much more pert inent questions than whichgoes faster, a car or a train. Also in the youngerchild, intelligence tests are based on motor per-formance and in so many handicapped youngstersthere are hand disabilities and language disabilityso that the child fails both the performance andthe verbal expression. The score would be unre-liable if they were the only measure of the child'smental capacity. The hospital, therefore, relies oninterpretation of results of a developmental exam-ination which is designed to measure the chi ld'sadaptive behavior, as well as his motor and socialbehavior. The psychologists interested in thisfield are devising more valid tests which needneither verbal nor motor performance to measuremental capacity.
CONCLUSION
The physical therapist has a real stake in aidingin the evaluation and planning of program manage-ment for children who are developmentally slow onthe basis of mental retardation, with or withoutconcomitant motor disabilities. With a positiveprogram, it is hoped that these children can bespared to some extent the additional handicap ofemotional overlay produced by anxious parents.The over-all purpose of any such program, in addi-t ion to the early detection of the chi ld who is devi-ating from normal growth and development, is thediagnosis and evaluation of his abilities and theplanning of a well-integrated program so that hecan achieve his optimal place in society.
RE FERENCES
1. Duhl,_ L. Jr:. The normal development of the mentallyretarded chi ld, Amer. J. Menr. Def. , 62:585. 1958.
-
2.Watson, E. H. : Counsel ing parents of mental ly de-f ic ient chi ldren, Pediarr ics, 22:401. 1958.
3. Ehlers, Walter H.: The moderately and severelv re-tarded chi ld. maternal percept ions bf retardar ion andsubsequent. seeking and using services rendered bya community agency, Amer. J. Ment. Def . . 68:660. 1964.
4. I ,esser. A. J. : New program for mental ly re iardedch i l d ren . Amer . J . Pub l i c Hea l t h , 48 :9 . 1958 .
SELECTED B IBL IOGRAPHY
1. Nelson,_ W. E.: Textbook of Pediatrics, Eighth Editron.Phi ladelphia: W. B. Saunders Co., 1964, pp. i132.
-Provided by the Maternal and Child Health Library, Georgetown University
Lr3

Factors Contributingto a SuccessfulPatient Evaluation
ISADORE BROWN, M.S.
DI)EFoRE DrscussrNc factors that
contribute to successful patient evaluation, thepurpose or use of evaluative measures must beconsidered. Evaluative information is commonlyused in three areas: as a diagnostic aid, in plan-ning the treatment program, and to evaluate theeffectiveness of the treatment program.
USES OF EVALUATIVE INFORMATION
As a diagnostic aid the information collectedduring an evaluative procedure is relatively clearcut. Information .gained by the physical therapist
Adapted from a paper presented at the Symposium onThe Chi ld wi th Cenrral Nervous Sysrem Def ic i i . Seoiem-ber,28-October 2, 1964, at the Univers i ry of pennsylvania,rn l laoelDnra-
Miss Brown is Chief Physical Therapist, St. Anthony'sHospital, Denver. Colorado.
Lt4
is rarely definitive in and of itself, but added toother flndings, it serves to reinforce or cast doubton a diagnosis, leading to further investigation.
With re-evaluation one can say of a patient "he'simproved," "he's the same," or "he has regressed."Such evaluation goes to problems if improvementis too readily accepted as the result of effectivetreatment, or lack of improvement as the resultof ineffective treatment.
This potential problem might be illustrated bythe story of a small garrison town in England. Avisitor to the town was impressed with the firingof cannons on the sfroke of five o'clock eachevening. He inquired of the officer of the garrisonhow he could be sure of the time. The officerreplied, "This town is famous for its- clockmaker.Each morning on my way to the garrison I setmy watch by the clock in the clockmaker's shop."
Provided by the fUate.nallnd Child ffeattfi finrary, Georgetown University

This sounded reasonable. But the visitor aSkedthe clockmaker how he ascertained the correcttime. His reply was, "This town has a famousgarrison that fires cannons each afternoon at thestroke of five. Each afternoon when the cannonsfire, I set all my clocks and therefore am sure ofthe correct time." 1
Evaluation and improvement may be operatingin a similar circle. In the vast problem of thebrain-damaged child, if evaluation has been toorestricted, improvement may be likewise restricted,and. when considered in relation to the total child(that is, the child as a part of society), wouldnot show notable improvement. In some instances,it may serve only to increase his frustration andsense of deficit.
Of the uses of the evaluative information, plan-ning an efiective treatment program presents thegreatest challenge. If one could resolve all theproblems in this area, the potential problems ofevaluation might also be reduced.
The use of evaluative measures in programplanning is of interest to both classroom instruc-tors and clinicians. What should be taueht? Whatshou ld be and is be ing used? Phys ica i therap is tscommonly comment, with special reference to thetime involved in giving the manual muscle test,"Evaluaticn takes more time than it is worth."This might be true for the manual muscle test, butthe test was not designed for brain-damaged chil-dren.
Or the physical therapist may complain, "Thetreatment load is so heavy we just don't have timeto evaluate." Is this statement justified? Indi-vidual centers have made useful adaptations offunctional or activities of daily iiving tests, andthere is an increasing trend to use adaptations ofthe motor maturation scales, primarily patternedafter those of Gesell.
Much of the physical therapist's time is spenton what the child can or cannot do, with a mini-mum of information given in the evaluative recordsas to why he cannot accomplish the activity. Con-tinued or increased effort toward understandingthe mechanisms behind the response will hopefullyfill the gaps in knowledge and thus provide betteranswers to the problems existing in the clinrc,namely planning a successful treatment program.
SOURCES OF NECESSARYINFORMATION
Sources from which information can be gainedmust be considered. First, there is the child. Hemay not, by spoken word, tell much, but he hotdsa wealth of information that can be obtained byvarious means. The family or medical records orboth can yield pre-, peri-, and postnatal history.The family can also provide much informationregarding the social history of the child. Theremay be community sources, such as nursery schoolsor public schools. And, of course, there are the
many medical and allied medical specialties fromwhich information can be obtained.
Knowledge of Normal Developmenf
Basic to any evaluation is knowledge of therange of normal development. Recognition ofthe abnormal becomes relatively easy when thelimits of normalcy are well understood. Thisknowledge should go beyond the well-known de-velopmental scales. If one wishes to restrict hisview to motor maturation, even this can be con-sidered in terms of experiences necessary to thcmaturation of the child.
A few of these necessary experiences include:exercise-the experience, learning, or develop-ment that comes from movement; exploration olthe environment-exploring with senses such assight, hearing, and touch as weil as getting fromplace to place which extends the environment;development of communication skills-not neces-sarily talking, but some method of give and take;affiliation with social collectives-the family, theneighborhood group, or a special club whichaffords necessary experiences for maturation. Mat-uration carries with it increasing responsibility.One would not be disturbed if the three-year-oldchild was not independent in dressing, but hewould expect it of a seven-year-old.
Treatment, thcugh related to the child's func-tioning, often focuses sharply on a specificmalfunction and fails to take into account theconsequences and implications of the child'sfunctioning or his ability to obtain necessaryexperiences for maturation or the extent to whichtreatment will influence this ability. The childwho has been taught to walk with crutches orbraces is not necessarily insured of the increasedexperience that comes with the increasing re-sponsibilities of growing up. The parent may findit easier to continue doing things for the childand may exclude him from family chores andduties. The teacher may hesitate to give thischild tasks that the average chiid can handle withease. If full restoration cannot be achievedthrough attention to a specific function, then otherfactors must be considered for successful results-
The fact that the child cannot sit does not initself explain why he cannot do this. Normal func-tion is much more than muscles or muscle groupsfunctioning in response to direct command, al-though some treatment goals and approaches con-sider only this narrow view.
Divergent Opinions. Divergent opinions exist asto what constitutes a developmental sequence, butthis is not sufficient reason to ignore the area andwait for the answers.
One extreme view is that of the innate, geneti-cally determined nature of performance and de-velopment, with acceptance of some plasticity inthe maturing central nervous system. The op-posite extreme is the learned aspect of behavior,
Provided by the Maternal and Chitd Health Library, Georgetown University
rt5

although the learning process and potential are notyet understood. Common ground seems to l ie inthe interdependency of varied sensory input. Theconcept of the central nervous system functioningas an active, dynamic system rather than the pas-sive receiver of sensory information with a pureconductive system leading to action can find aplace in all approaches. The final common path-way probably will lie somewhere between the twoextremes. For example, Weizsaecher believesthat disturbances of function are not positively
analyzable entities but are merely abstractions.They are qualitatively different from the averageand are not derivable by meie subtraction orel imination of a functional component from a totalperformance complex. Anatomical lesions changethe entire character of a performance rather thanisolating and eliminating pre-existing fractions offunction.2
In ie rac t ion o{ Var ious D isc ip l ines
Specialized training may sensitize the exam-iner's perception of certain areas of function,but often at the cost of inattention to other
areas of functioning. I f one asked a parent,
sibl ing, neighbor, teacher, or the various medical
and al l ied special ists to describe a chi ld, theirdescriptions would be quite different. The differ-ences would reflect different relationships with thechild, the different contexts in which they see thechild, and differences in their training and back-ground.
Recorded measurements reflect the bias of theexaminer. A person may miss malfunction insome area i f he makes no demands that bring outthat aspect of function. This should present noproblem since each specialist can do a better evalu-ation in his respective area. By sharing informa-t ion, a more accurate view of the total chi ld canbe derived. Apparently, however, there is somebreakdown in this system because of the continuedstress placed on looking at the "total" child.
How can this be resolved? First, there shouldbe no fear of overlapping or duplication of effort.In the evaluation of human behavior the examinerbecomes part of the stimulus or the stimulus situ-ation and may, therefore, have an effect on theresponse given or observed. A better total pic-ture may be gained from a composite of manyexaminers, even when exploring the same generalarea. One may profess, "but think of the t ime."This will take time. But a u'eek, a month, eventwo months or longer in the life of the individualis not great if a better treatment program can bedevised. This, in fact, would seem more justified
than the rtrshing in to treat an obvious defect forsix months or a year only to learn that the treat-ment did not reach the basis of the problem.
Take, for example, a child who was a problemto his kindergarten teacher. He dropped thingsoften, seemed somewhat clumsy, and showed
1 1 6
marked changes in temperament. A parent-teacherconference brought out that he had developed a"little" slowly and had always been somewhatclumsy. The parents agreed to take him to theirphysician for an examination. When a motorevaluation showed the child fo be borderlineaverage for his age group, physical therapy wasprescribed with activities directed toward increas-ing co-ordination. At the end of the academicyear no apparent improvement was observed andthe school situation remained unchanged. Theschool authorities recommended a psychologicalevaluation before permitting the boy to enter thefirst grade. These tests and further investigationwith the family and physician resulted in placingthe chi ld in special classes, and physical therapywas discontinued. By the end of the fol lowingyear the apparent motor problem had disappearedand his school record was much irnproved.
Fami ly Recogn i t ion
An evaluation often is started and its directionoften is influenced by a problem that bothers theparents. Motor function and perfornrance levelare commonly early malfunctions that come tothe notice and therefore the concern of the parent.They, however, may be secondary to, or compen-sation for, other forms of malfunction. In theabsence of total evaluation cl inics, a chi ld may beseen only by the physical therapist and the physi-c ian .
Psycho log ica l Tes ts
The physical therapist should be famil iar withpsychological tests such as the Goodenough Drawa Man. Bender-Gestalt , or Figure Assembly tests.Without trying to interpret the results of thesetests, the physical therapist should be able torecognize defici t so that he understands when acomplete psychological evaluation may be indi-cated. He should also constantly be alert to be-havioral characterist ics of the brain-injured patient,such as hyperkinesis, short-attention span, or dis-tractability, that might better be evaluated by thepsychologist than by any form of motor functiontest. Actual ly, the chi ld's evaluation should alwaysgo beyond motor function since other factors per-tain to treatment goals and kind of treatment.But all have read reports of ps.vchoiogists andwondered how such reports harl bearing on treat-ment planning.
Free Observai ion
The evaluation should include free observation.The report of the astute observer may be of nruchgreater value than results of a poor test si tuation.Such observation can be made within the evalua-tion environment, but preferably without thechi ld's awareness that the observations are beingmade. Watch the chi ld on a mat. on the f loor. orat piay in the room. It can be done while talking
.-Provided by the Maternal and Child Health Library, Georgetown University

to the parent, for in this situation the child issecure because his parent is there, but at the sametime the parent is busy and is not giving "helpful"reminders to the chi ld. Hopeful ly, this free ob-servation can be extended to include the childwith other chi ldren and with sibl ings.
Correctly, the information recorded from ob-servation would relate to the examiner's area ofspecial ized training. The ski l l of observationcannot be replaced by any amount of ski l l in per-forming a test. Observation should be an impor-tant part of any contact with the chi ld.
Deve lopmenfa l H is to ry
Detailed developnrental history is essential. Thisarea is open to wide variation u'hen obtainedsolely through recal l of the parent. A parentmay not remember correctly or at all. He n"raybe hesitant to admit that something had been ir-regular for some time before he sought profes-sional assistance for the chi ld. Therefore, dupl i-cation of effort in this area results in a more ac-curate history. Careful ly documented pre-, peri-,and postnatal history wil l provide valuable cluesabout the nature and cause of problem. Cautronmust be used against too quickly saying that ananswer has been found. There can be severe dis-tort ion of normal brain configuration withoutfunctionai impairment. At the same t ime, largeor small injuries to the brain of the fetus andneonate may lead to later problems. Performancemay be within normal l imits and the malfunctionmay not be apparent unti l the chi ld is severalyears of age.
The status of the chi ld at the t ime of evaluationwil l be recorded by many discipl ines. This isnecessary to get all aspects of development. Thephysical therapist should accept and make use ofthis duplication rather than being restricted to hisown favorite method or skilled area of assessment.Hopefully, from this pool he can learn "why" thechild cannot perform rather than just that hecannot. The pediatr ic neurologist commonly re-cords the presence or absence of tonic reflexactivi ty. This informaton can be repeated andextended-how it may be reflected in the child'sinability to roll over, sit up, and so forth. If thepsychological evaluation shou's severe perceptualdefici t , can this be carr ied through to the settrngof treatment goals or the area in which the treat-ment is given?
Fami ly Reac i ion
Family reaction to the chi ld's disabi l i ty is alsoan important area of information. The recordshould include the reaction of each parent and ofthe sibl ings, when feasible. Where does the chi ldwith the handicap f i t in the family? What plansdoes the family have for the child? Does thisplace a hardship on other chi ldren? Is the family"child-directed" or is the child another member
of the family? These questions are properly theconcern of the medical social worker, but eachdiscipline should be alert to conflict between re-actions expressed and those reported by others.Assistance or support for the family may be avital part of the treatment prograrir and may meanthe difference between successful and unsuccessfultreatment.
Environmental Factors
Somewhere the contribution of environmentalfactors must be considered. The normal child hasa large adaptive capacity so that he shows adequatedevelopment in a wide variety of environments.The handicapped chi ld may show a reduction inthis adaptive capacity so that the environmentswithin which he can effectively develop may berestricted considerably.
The immediate family, the neighborhood, theschool system, and the community may contributeto environmental restrictions. Is the child cul-turally deprived as well as physically handicapped?The family and the community may need guidanceso that the child with a handicap may be acceptedand his progress-even though something less thannormal--viewed vrith a realistic attitude.
SUMMARY
Evaluation or assessment will be adequate andsuccessful only if the information obtained is usedto improve treatment. This cannot be done bykeeping the chi ld divided into units. The physicaltherapist must seek more information and makebetter use of all information available. Treatmentcan be successful only when the child is consideredas an individual, as a member of a family, andas a member of society, with no one area beingindependent of the others or taking precedenceover another.
The detection of malfunction should not stopu'hen it is identified, but should reach to the vari-ous contributing factors. Neuroanatomical, neu-rophysiological, psychosocial, psychophysiological,and environmental factors all should be considered.
RE FEREN CE5
1.Birch, Herbert G., ed. : Brain Damage in Chi ldren-The Biological and Social Aspects. Baltimore: Wil-liams and Wilkins Company, 1964.
2. Schlesinger, Benno: Higher Cerebral Functions andTheir Clinical Disorders. New York: Grune and Strat-ton, 1962, p. 358.
SELECTED B IBL IOGRAPHY
l.Caldwell, E. M.: Some aspects of teaching brain-in-jured children, Physiotherapy, 49:149-152, 1963.
2. Escardo, F., and De Coriat, Lydia F.: Development ofpostural and tonic patterns in the newborn infant, Pe-d i a t . C I i n . N . A m e r . , 7 : 5 l l - 5 2 5 , I 9 6 0 .
3. Francis-Wi l l jams, J. : Diagnosing brain damage iny9u1e^qh-ii{req with thq Bender Gestalt test, Develop.Med . Ch i l d Neu ro l . , 5 : 291 -294 , 1963 .
4.Gesell, A., and Amatruda, C.: Developmental Diag-nosis, Normal and Abnormal Child Development. Chn-ical Methods and Pediatric Applications.
-New york:
Paul B. Floeber, Inc., 1947.
tr7
Provided by the Maternal and Child Health Library, Georgetown University

5.Gibson, E. J., and Walk, R. D.: The visual cliff, Sci'Amer. , 202:64- '1 l , 1960.
6 . Jaynes , Ju l i an : lmp r i n t i ng : The i n t e rac t i on o f - l ea rnedand innr le behavior : I -development and general tzat lon.
J. Comp. Physiol. Psychol., 49:201-206, 1956; Il-thec r i t i ca l be r i od , 50 :6 -10 ' 1957 .
7.Jones. j . David: Problems in evaluat ing centra l ner-'uou. iyst"- funcl ion in chi ldren, N. Carol ina Med. J. '
2 4 : 5 5 0 - 5 5 4 , 1 9 6 3 .8. Paine, Richmond S.: Neurological examinat ion of in-
fants and children, Pediat. Clin. N' Amer., 7:4'71-510,1 960.
9. Palani . Paul E. , and MacKei th, R. C. : Neurological ex-amination of the newborn according to the work ofAndr6-Thomas, Cereb. Palsy Bul l . , 2:2-50, 1960. - .
10. Pascal , G. R. , and Jenkins, W.. O.: -Systemat ic O^bser-vat ions of Gross Human Behavior . New York: Grunea n d S t r a t t o n , 1 9 6 l .
11 .Rub in , G . , and Sm i th , Ka r l U ' : . Lea rn i ng and . i n t e -sral ion of component movements in a pat tern ol mo-i i on . J . Exn . Ps i cho l . , 44 :301 -305 ' 1952
12. S; ; t bdpr iu j t ion. A Svmposium held at Harvard- MeOi iat Sihool . Cambridge,-Massachusetts: HarvardUnivers i ty Press, 1961.
r : .S- i t t r . - ( . U. . ind Smith, W. M.: Percept ion andMot ion. Phi ladelphia: W' B. Saunders Company,1962.
1a.Soel t . D. K. : The condi t ioning of the human fetusin utero, J. Exp. Psychol . , 38:33-8-346' 1948' -
15. Wapner, S. , and Werner, H. : Exper iments o l senory-" t , i " i " 'h" ta
' th iory of percept ion:
- V-Effect . of . bodv
iiiiur on the kinestbdtic perception of verticality, J'Exp. Psychol., 44:126-131, 1952.
te. wi iora ' . A. T. : Ageing and Human Ski l l ' New York:Ox fo rd Un i ve rs i tY P ress , 1958 '
l ? . Werne r . H . . and Wapne r , S . : Toward a gene ra t t heo ryo f pe rcep t i on . Psychb l . Rev . , 59 :124 -338 ' 1952 .
t 1 8
Provided by the Maternal and Child Health Library, Georgetown University

A PATTERNFOR EVALTJATIONin the Assessment of Motor Performance
SHIRLEY STOCKMEYER, M.A.
T" "*o."rs
which is carried outin the development of an evaluation device hasbeen called the evaluation paradigm or the eval-uation pattern.l Those who are interested in theassessment of the child with central nervous sys-tem deficit may have a number of reasons for de-veloping an evaluation device, and, therefore,should concern themselves with the evaluation pat-tern in its entirety. Available tests may not supplyspecific information which is needed, or the prob-lem to be evaluated may be unique and require anunusual test procedure. Problems which appearto be concerned only with the actual test formor with only one step in the process of evaluationmay be more readily resolved in relation to theentire process of developing an evaluation device.
STEPS OF THE EVALUATION PROCESS
The five steps of the evaluation pattern whichare followed in the development and use of anevaluation device are:
Adapted from a paper presented at the Symposium onthe Child with Central Nervous System Deficit, September28-October 2, 1964, at The Univers.ity of Pennsylvania,Philadelphia.
Miss Stockmeyer is an Assistant Professor in the Schoolof Physical Therapy, Medical College of Virginia, Rich-mono.
1. Determine goals toward which the child isto work.
2. Define standards which will tell when thechild has achieved each goal.
3. Organize the criteria (standards) into ameasuring device.
4. Administer the test in order to make an ap-praisal of the child's performance.
5. Utilize the information eained from the eval-uation process.
De iermine Goa ls
The goals or objectives represent those thingswhich are of value for the child to achieve. Nor-mal functioning would be a valuable goal orachievement. The goa.l is something toward whichthe child works, not necessarily the thing he isexpected to achieve completely. It may seemhighly unrealistic and unwise to set "normal func-tioning" as a goal for a severely handicapped child.Therefore, it is necessary to question, "Should thegoal be essentially abnormal or artificial, or shouldtreatment proceed along the steps toward nor-malcy, trying to approach the goal as nearly as pos-sible?" If normalcy is of indisputable value, it isworthwhile working toward that goal, even withoutreaching it completely. Test procedures which use
Provided by the Maternal and Child Health Library, Georgetown University
r r9

normal steps in motor development as test items velop and administer. It is easy to administer and
fall into the category of evaluation devices which score.set normalcy as a goal without expecting to reach 3.It is reliable. It can be administered by sev-
it 100 per cent. Such test items point to the de- eral examiners or by one examiner repeatedly with
sired direction of progress. consistency in the results. This assumes that in thetest-retest interim there is no change in the variable
Define Standards being measured.
Standards ultimately become the performance 4. It is valid. The test actually measures that
items to be tested in the evaluation procedure. The which it purports to measure. If this is to be a test
standards may be known as criteria, signs, or evi- of motor activity then it is important to avoid
dence which indicate to the examiner that the complex instructions to the child which would tend
child has achieved the goal, is working toward the to measure verbal comprehension rather than
goal, or has accomplished some of the steps which motor skills, and would therefore alter the test
are the groundwork for achieving the goal. Cri- validity'
teria may be formulated by asking the question, There are many appropriate ways to organize
"What activities must the child perform before it the performance items so that the test results yield
can be said that he has reached the goal?" If a score or tabulation of results. The simplest
normal functioning serves as the source for the method would be to indicate rvhether or not thegoals, then the thoroughness and relevance of the child was able to accomplish the performance item
criteria depend on a knowledge of the components or criterion by checking "yes" or "no" in a col-
of a completed motor activity as well as a detailed umnar table. A quantitative score could be ob-
knowledge of the steps which go into a normal tained by determining the percentage of criteria or
child's learning of a certain motor activity. performance items achieved'
A specific example of a goal and some criteriawhich relate to that objective may serve as a guide:
Goer: The child should possess the proximalstability necessary for a normal walking pattern.
CntreRre: (Note: These are but a few of thecriteria which would be included in a completedevaluation device.)
1. In the prone position with the trunk in fullextension the chi ld can hold his extremit ies upagainst gravity using the proximal extensor mus-cles in their shortened range. (This response isotherwise known as the pivot prone, the grossextension pattern, and the Symmetrical ChainReflex in the Abdominal Posit ion.2)
2. In standing (holding on with hands) thechild is able to lower and raise his body wei-ehtin a bouncing type of motion.
3. He is able to maintain the semisquat posi-t ion independently.
4. He is able to use his lower extremit ies topush to standing from squat without using hishands to pull up.
Organ ize the Cr i ie r ia
This is the procedure of constructing the actualtest form for scoring the child's performance. Thistest will be referred to as a measuring device. Thequalities of a measuring device must be carefullyconsidered in test construction, but because of theircomplex nature it is not possible to deal with themin detail in this paper. There are four character-istics of a good measuring device 3:
l.It is objective. The items which comprise thedevice have the same meaning to all who willbe administering the test or using the results.
2. It is practical. In terms of cost, time, andtraining of the examiners it is inexpensive to de-
t20
If it is desirable to indicate the quality of theperformance, a scale of descriptive characteristicsor categories can be used to indicate such thingsas: "Init iates activi ty-cannot complete i t ," "min-imal assistance needed," "no assistance needed,but awkward," "speed and accuracy normal."
The spaces opposite each criterion can bechecked or numbered according to the number ofthe test, i .e., 7 for ini t ial test, 2 for f i rst retest, 3for second retest; or the box may be filled in whenthe i tem has been accomplished at that level. Dif-ferent colors or direct ions of hash marks can beused to indicate results of re-examinations.
Giving consideration to the importance of thetemporal sequence of motor learning, an assess-ment form could be planned which would com-pare the speed of motor learning of the handi-capped chi ld with that of the normal chi ld. Atable could be constn-rcted to indicate the chrono-logical age of the child at the time he has achievedperformance of the test items. Performance itemsshould be arranged in the normal sequence ofmotor learning. This profile of the individual hand-icapped chitd would then be compared to theprofile of normal children.
A total measuring device could easily containten goals each with ten or twenty cri teria. Insuch a case the total number of criteria or per-formance items could be as many as two hundred.If this were found to be unwieldy, the criteriacould be condensed in several ways. Followingtrial runs of administering the test, those criteriawhich give the best indication of whether the childmeets the goal can be chosen as being representa-tive of all the criteria for the one goal. The word-ing of the criteria can be reduced to a few keywords whose extended meaning is readily under-stood by those who will administer the test or use
Provided by the Maternal and Child Health Library, Georgetown University

the evaluation results. Also, the examiner willfind that some performance items can be combinedbecause the child in his activitv works toward bothin a single response,
Administer TeslIf the previous steps have been followed dili-
gently the process of administering the test shouldadvance with little difficulty. It is necessary tohave a specific set of instructions for administeringthe test. Such instructions, if understandable anduncomplicated, will increase the reliability of thetest because all examiners will interpret and carryout their duties in the same way.
Util ize lnformationThere are four possible uses for the information
gained from the evaluation device. The clinicalphysical therapist is mainly concerned with the firsttwo uses.
1. To plan a treatment program.2. To identify areas of progress or the lack of
progress.3. To identify or rule out the existence of a
specific problem.4. To provide diagnostic information.The fifth step in the evaluation pattern, utili-
zation of test results, should not be left until last inthe planning of an evaluation device. The way inwhich the test data are to be used should be deier_mined before any other step is taken. This prede-termination will avoid the collection of superfluousinformation and will assure that all neceisary in_formation is obtained. Unfortunately evaluationdevices are often developed with little thought
given to the use of their results. The decision onwhat to do with evaluation findings is often de-layed until after the information has been col-lected. It appears to be a great waste of time andeffort to perform extensive tests just in the nameof being thorough unless all the information gainedfrom the evaluation is to be utilized. A discussionof how to utilize the data from the evaluation de-vice will not be included in this paper. Such apresentation would have to be preceded by exten-sive coverage of the principles and objectives oftreatment and related progress.
Once the evaluation pattern has been completedand the information from the test utilized, thewhole pattern begins again. The evaluation pat-tern is a cycle, an ongoing process. As test dataare utilized, the goals are reviewed to determinetheir value and appropriateness. New or additionalperformance items may have to be added. Weakareas of the test become obvious when they donot yield the information needed to plan a treat-ment program or judge progress. Revisions in thetest items provide new ideas for treatment pro-cedures, lead to an understanding of how welltreatment goals are being met, and indicate areaswhere there is a need to strengthen the treatmentprogram.
REFERENCES1, Husted, F. L.: Implementation of the evaluation Dara-
digm and recapitulation. In Evaluation in phvsicalTherapy Educat ion-1963 APTA-VRA Inst i tute papers.New Yo rk : APTA , 1964 , pp .27 -28 .
2. Peiper, Albrecht: Cerebral Function in Infancy andChildhood. New York: Consultants Bureau. 1963. pp.182 - l 87 .
3. Mi l ler , George E. . et a l . : Teaching and Learnine inMedical School. Cambridge: Harvaid University piess,1961, pp. 205-206.
l2l
Provided by the Maternal and Child Health Library, Georgetown University

SPECIFIC TESTS AND
SARAH SEMANS, M.A.
WHAT SHOULD BE ASSESSED?
To keep in focus the most important aspects ofthe problems to be assessed in the child with cen-tral nervous s)'stem deficit, i t is well to keep in minda broad view of the child's difficulty and its signifi-cance for him. A disorder in the brain may pre-sent a wiile variety of behavioral difficulties. Achild with such disorder has-in fact, has hadfrom birth-problems of coping with his environ-ment and interacting with it. Physical therapistsmust find out how they best can help him to func-tion to the fullest extent of his potential, be it greator small.
EVALIJATION TOOLS
f or the Child with Centrol Nervous System Deficit
Adapted from a paper presented at the Symposium onThe Child with Central Nervous System Deficit, Sep-tember 28-October 2, 1964, at The University of Penn-sylvania, Philadelphia.
The author is Assistant Professor, Division of PhysicalTherapy, Stanford University School of Medicine, PeloAlto. California.
t2z
His problem has many aspects, some of whichcan be dealt r ' , i th more effectively b1' other special-is:s. Certain aspecis, however, ciln be moste5ecl ive ly l randleJ by phl 's ica l therapists . A r ig iddivision of labor between therapists is unwise. De-pending upon individual training and competence,the traditional roles of the physical, occupational,and speech therapist may overlap. Most physicaltherapists, however, will be chiefly concerned withthe basic gross motor adaptations of the child tohis environment. All specialists are concerned withmaturation and learning.
Effort may be required to focus on those aspectsof motor behavior which are of most concern andwhich must be evaluated. Because the distal partsof the child are most visible and because thephysical therapist's training conditions him tolook at muscles and joints, it is sometimes diffcultto observe total patterns of motor behavior. It isimportant to learn to look at Patterns of posture
Provided by the Maternal and Child Health Library, Georgetown University

and movement in relation to central nervous sys-
tem deficit in order to explore ways of alteringsuch patterns in useful directions by stressing oneor another pattern of input. To form an idea ofthe chi ld's potential. the ph1'sicai therapist needs to
assess the extent and severity of the handicapcoupled with the learning already accomplished.It is also necessary to know how well the child is
responding to physical therapy procedures and hisrate of progress.
A battery of tests is required, including motor
ability, perceptual and intellectual status, and,
when appropriate, prevocational and vocational
aptitude. The present discussion will be concernedwith assessment in the motor sphere. However'increasing recognition of the role of perception in
learning should alert us to the need for testing in
this area. Attention is called to the PerceptualMotor Test Battery prepared h 1964 by Dr. JeanAyers.l It includes twenty-five tests, some of whichare standardized psychological tests and some
originally designed. In the book PsychologicalEvaluation ol the Cerebral Palsied Person by Allenand Jefferson available tests are reviewed for in-
tellectual, personality, and vocational assessment.2Within the motor sphere three main areas are to
be investigated: (l) developmental, (2) patho-
logical, (3) adaptive.
DEVELOPMENTAL TESTS
Oue aspect of developmental evaluation has
been very well worked out; that is, determination
of the level of operation of the child or the mile-
stones reached, based on the developmental scales
of Gese11.3 This information will be of value in
several ways:1. It will indicate where to start and what to
strive for next in working with the child.
2. Translated to the parents, it will help them in
understanding the child's limitations-what can
and cannot be expected of him; it will establish
agreement on the next step as immediate goal and
it may help them in planning for the future.
3. Since there is usually a spread in level of
achievement in dif ferent areas-more advance in
some areas than others-it will indicate where to
go trouble-shooting to find what is causing the de-
tuy. For instance, one may find a total flexion
pattern in the arms interfering with development
of prehension, or a persistent Moro reflex inter-
fering with sitting balance. If one can remove the
delaying factors, the child can develop on a broad
front.4. By charting successive examinations on a
graph, the rate and general trend of development
can be ascertained.Although Gesell's norms and the developmental
scales are standardized, the majority of tests de-
rived from them for evaluation of the child with
neurological deficit are not standardized' Relia-
i 8 0 - 2 8 0 0 - 6 6 - 9
bility studies are lacking; instructions for adminis-tration of test items and criteria for successfulaccomplishment are not always clear or are lack-ing. Footh and Kogan, having noted such inade-quacies, have overcome them il their GeneralMotor Development Test.4 The instructions andcriteria for each item are quite clear, and their re-liability in scoring is excellent.
In other tests reviewed, some items selected arenot valid for cerebral-palsied children and in sometests, significant items are not included' For ex-ample, the item "takes full (or partial) supportwhen placed on the feet" may not be valid forsuch children because the test procedure is likelyto elicit pathological rigidity in the legs rather thanshowing the normal accretion of support tonus inthe limbs which the test is intended to indicate.Tests of eye control and the breakdown in variouslevels of prehension are sometimes lacking.
The Developmental Screening Instrument of Dr.Hilda Knoblock has clear and specific instructionsand sufficient detail.s The test items are groupedin five categories: adaptive, gross motor, finemotor, language, and personal-social. This divisionhas the virtue of indicating the specific area of re-tardation. For instance, a child might have well-co-ordinated, discrete flnger movements (fine mo-tion) and yet not know how to use them for auseful purpose (adaptive).
Dr. Margaret Jones' Appraisal ol Progress in theCerebral Palsied Child has similar categories basedon Gesell's norms, but is less detailed and lacksspecific instructions.G The graphic summaries withthese tests compare rates of physical growth anddevelopment in each area.
The Doman-Delacato Developmental Profile hasthe virtue of being brief-on one page-and in-cludes a graphic summary.T A numerical scoreis derived frcm six categories at seven develop-mental stages. The categories are mobility, lan-guage, and manual, visual, auditory, and tactilecompetence. Instruction manuals are availablefor the mobility and language categories. Thevalidity of the sample of mobility test items mightbe questioned because reciprocal organization andcerebral dominance are emphasized to the exclu-sion of some other aspects of motor developmentwhich may be of equal importance.
Another published developmental scale, theBlum-Fieldsteel Developmental Charts, includes atest for motor activities and a test for functionalactivit ies with a cumulative record for each'8 Itis well set up to show rate of developrnent but itis impractical for any except the most mildly in-volved children since the early level items withwhich the physical therapist would be concernedover long periods are crowded together in thebottom of the record. Also, finer gradations oflevels during the first eighteen months are needed.
The Motor Age Test of Johnson, Zuck, and Win-gate is objective, reproducible by difterent testers,
r23
Provided by the Maternal and Child Health Library, Georgetown University

and gives a separate numerical score for: upperand lower extremities.e Although useful for mildlyinvolved children, it lacks discriminating items atthe lower developmental levels.
Ingram, Withers, and Speltz 10 developed a sim-ilar test based on the Gesell developmental sched-ule and modification of the Johnson, Zuck, andWingate tests. It ranges from four weeks to fiveyears and yields a motor quotient and a socialquotient.
The Dallas Motor Development Test is pre-dominantly one of motor development of the trunkand extremeties as a whole.11 It is geared towardthe lower developmental levels and extendsthrough the six-year age level. It has been used on2,500 children over a ten-year period, but hasnot been tested for relilbility, and criteria forsome of the test items are not clear.
A Code Method for Evaluating Function inCerebral Palsy developed at the Detroit Ortho-pedic Clinic is not strictly a developmental test.l2There are four charts of function in speech, handfacility, balance and locomotion, and maturity.The test items are grouped according to develop-mental sequence in each. Some items are derivedfrom Gesell's developmental schedules and someare from other sources. "The combined chartswill convey a profile of the functional activity levelof the child, expressed in a numerical code." Theinstructional manual and charts are well set upand the test items clearly described.
A number of other institutions have developedtheir own tests based on Gesell's developmentalschedules.
A good standardized test form based on Gesell'snorms should be available for physical therapists.It should have the majority of items from theperiod of birth to eighteen months, since this isthe period of basic motor development. Itemsshould be carefully selected and described. Acompanion test for finer skills should also includevery early items such as visual control, but shouldextend into later chronological age periods, Ques-tions arise, such as should one person administerall categories of the development test in a com-bined form? Should the physical therapist betrained to do this? Or, should each of the differentcategories be tested separately by a differentspecialist?
Although it is of great interest and will undoubt-edly be worth while to try to correlate 'behavior
patterns with specific brain mechanisms, presentknowledge of central nervous system integrationdoes not warrant the assignment of specific be-havioral patterns to certain geographic levels ofthe brain in tests of this kind.
Mechanisms of Development
Missing in the type of developmental test de-scribed above, based on the achievement of mile-stones, is information about the developmental
r24
processes themselves which bring about theachievement of these milestones. The lack oftests in this area reflects the meager informationwhich has been available concerning these impor-tant neurophysiological processes. These includethose well-organized, mostly subcortical and auto-matic mechanisms which pattern most of the earlybehavior as well as the adult posture and movementpatterns which are not consciously directed. Theyhave been described as orientation or righting re-actions, equilibrium reactions, reactions to pro-gressive movements, approach and avoidanceresponses, defense and attack, other bodily expres-sions of emotion, and the somatic componentsof vegetative functions, e.g., sucking, licking, spit-ting, chewing, defecating. (A number of thesemechanisms are described in papers by Twitchellin this is5us.r3' u)
As Andr6-Thomas points out, such responses arelike reflexes but more complex and inconstant andtheir appearance depends upon the general state.l5Although inborn, relatively few of these responsesare present at birth but emerge in an organizedsequence first in primitive form and graduallymodified to the mature form.
Upright walking movements, for example, gothrough several stages. After inhibition of pri-mary walking ("reflex stepping"), the hips flexin weight bearing and the feet drag if propelledalong; then, an extensor phase begins, at first in-termittent when the child beats or stamps a footand bounces; gradually he begins to make stepsagain if pulled along, jerky and unpatterned, toestouching first.15 Further progress awaits equilib-rium, which, having gone through several stagesin horizontal and sitting positions, is developed instanding by cruising laterally. The mechanismsof cruising (variously calied "stembein," "d'arc-boutement," "protective extension," "propping,"and "hopping" reactions) must be assessed. Thissame cruising pattern is then used in the child'sfirst independent locomotion forward as a toddlerwith wide abduction of arms and legs, exaggeratedlifting of legs, and lateral shift. Similar walkingprogressions of the arms precede those of the legs.Propping reactions of the arms develop in threerecognized stages: in front at six-seven months,laterally at eight months, and posteriorly at ten-twelve months.15
It is even more important to assess mechanismsunderlying the progressive development of pre-hension (see pages 419423).16
Several aspects of the evolution of movementmust be mentioned:
1. The progressive selectivity of movement fromproximal to distal segments.
2. Co-ordination of comPensatory trunk balancereactions with prehension, each assisting the other,e.g., leaning forward with reaching up.
3. Equilibrium reactions of arms and legs which
Provided by the Vfate.nal and Child HealthiiUrary, Georgetown University

combine with compensatory trunk reactions tosecure sitting and standing.
4. Achievement of manipulative skills by co-ordination of the segregated wrist and fingermovements with developing visual and tactile per-ception.
These and other components of co-ordinatingmechanisms should be included in testing the un-derlying mechanisms of sensory-motor develop-ment. An increasing number of sources of infor-mation on mechanisms of development are avail-able.15, 17-23
Equi l ibr ium React ions
Detailed studies of the equilibrium reactions 2-1-26had not been utilized to any great extent nor theirvalue appreciated until they were brought to ourattention by the Bobaths.2T Rademaker and Zadorstudied in detail with cinematographic records thepatterns of these responses in animals and man,their maturation in the human infant from briefbeginnings at four to six months to the mature formsat about six years.2a,2r They also studied theeffects on the equilibrium reactions of lesions ofdifferent parts of the central nervous system.Rademaker had found the receptors for equilib-rium reactions to be the labyrinths and the limbproprioceptors. The brain stem from the 8th nerveto thalamus was required but not the cerebellumnor the striatum, nor was the cortex requiredfor those in horizontal positions. The cortex isrequired for these responses in the upright posi-tions in man. The responses are all present.butexaggerated and poorly controlled in cerebellarataxia. In athetoid children, the equilibrium re-sponses are lively but often distorted.
Testing of these basic mechanisms of developingequilibrium would appear to be of particular im-portance to the physical therapist for treatmentplanning. In the manual on Reflex Testing Meth-ods by Mary Fiorentino some of these reactionsare included as well as some of the righting reac-tions.28
In a recent study by Ruth Ladue at StanfordUniversity, a group of supposedly normal childrenbetween six and eight years were given, as part ofa more extensive evaluation, some of these equi-librium tests.2e A few of these children stillshowed the transitional form of the reactions char-acteristic of the three- and four-year levels. Thisentire test which included the later stages of grossmotor development and elements of motor functionwas designed to test minimal cerebral dysfunction.
PATHOLOGICAL ASPECTS
As often pointed out, evaluation of the childwith neurological deficit should include not onlywhat he can do but how he does it. The develop-mental activities and their underlying mechanismsjust discussed, as well as activity of a more voli-
tional or planned nature, are distorted, delayed, orblocked completely by the effects of the brain in-jury or defect. Assessment of the child shouldindicate in some way the nature and extent of theinterference. Tonic brainstem and spinal reflexesmay be released by lesions of thosb higher centerswhich normally reorganize them. These preventselectivity of movement and adaptation of postureas the Bobaths have shown.27 As Denny-Brownhas pointed out, the abnormal motor manifesta-tions resulting from brain injury are expressions ofdisequilibrium of conflicting elements of behaviorat various levels of integration.so One or theother type of primitive conflicting responses(avoidance or reaching out) may dominate, orthey may fluctuate from one to the other withoutbeing resolved, as observed in athetoid and dys-tonic postures and movements. A distinctionshould be made if possible between the franklypathological posture and movement responses andthose of a normal but immature nervous systemwhich may resemble them. This requires clinicaljudgment based on familiarity with normal infants.
Tests for some of these abnormal postural re-flexes are illustrated in Fiorentino's manual.28Others can be found among the tests used in neu-rological examinations of infants. Another way ofassessing abnormality is illustrated in the CerebralPalsy Assessment Chart for Basic Motor Controltests reported here (pages 463468) which wasconstructed to indicate degree of freedom fromthese abnormal influences.31
The state of muscle tone is recorded routinelyin neurological examinations. The French neu-rologists consider several aspects of tone. Andr6-Thomas 15 dist inguishes three components: (1)consistency, tested by palpation, (2) extensibility,tested by range of muscular lengthening, and (3)passivit6, tested by resistance to passive stretching.Tardieu in the French manual on Cerebral Palsy,I.M.C., has a range-of-motion chart in which thesecomponents of tone are recorded.32 The samemanual contains an interesting code method ofassessing the various aspects of athetosis.
ADAPTIVE ASPECTS
Functional activities or achievement tests havelong been used in evaluating children with cerebralpalsy. Most institutions have evolved a suitabletest of act ivi t ies of dai ly l iv ing, many adapted fromthe original test by Brown.33 Tests which blockin successful achievements with color are easy tosee at a glance and are favored by therapists andchildren. Such tests are often joint projects ofphysical and occupational therapists. As bracingand special equipment are becoming less frequentlyused in training programs, items such as gettingin and out of braces and managing special equip-ment are being deleted. Wheel chair managementand use of crutches in postsurgical cases should
Provided by the Maternal and Child Health Library, Georgetown University
r2t

be included where appropriate. It is importantto continue testing competence in everyday activi-t ies.
THE ASSESSMENT CHARTOF MOTOR ABILITIES
The Assessment Chart of Motor Abilities is in-tended as one of a battery of tests.31 It is con-cerned with basic postural controls which underliefunctional activities. It contains prerequisites forarm use, moving about, control of body segmentsrelative to gravity, getting up and down, and thestance phase of walking. Movement proceeds fromposture which is not static but variable with themovement it supports.
A series of test postures adapted from thoseoriginally developed by the Bobaths are utilized.3aEach of the test postures constitutes a patterned,measured input stimulus which is applied, and theresponse is graded with reference to that of anormal child. The test is operational in that spe-cific behavioral responses are utilized to revealpresence of or freedom from the pathologicalprocesses which would interfere with their ac-complishment. Thus, freedom from hypertonusis measured by the ability to be placed and remainin a position which is the reverse of the tonic pat-tern. The full range of motion demanded alsoindicates presence or absence of adaptive shorten-ing. If the test posture cannot be attained initially,maneuvers to release tension are used to determinewhether the limitation is a result of hypertonus orcontracture. Tardieu found in his joint range teststhat such maneuvers were as effective as curarein difterentiating these limiting factors.32
Lack of sufficient tone or flaccidity is indicatedby failure to maintain the required antigravity posi-tions.
To grade the quality of active movement, thechild is asked to assume the test posture inde-pendently, and is graded 3, 4, or 5 according tothe manner of accomplishment. Thus, the in-fluence upon movement of dyskinesia and fluctu-ating tone, as in conflicting athetoid postures,would be indicated by the grade. Minor statesof spastic hypertonus which slow movement ornecessitate effort are also indicated by less thannormal grade even if the test item is accomplished.
The individual items are designed to show de-gree of freedom from the abnormal posture andmovement patterns which would prevent or distortassumptions of the test postures. The items aregrouped in supine, prone, sitting, kneeling, andstanding postures.
Aspects of the child's problem which are meas-ured include:
1. Automatic postural adjustment to the im-posed position.
2. Inhibition or control over abnormal posturalreflexes.
126
3. Limitations of range of movement.4. Capacity for motor learning (reproducing
the postural pattern).5. Readiness for specific developmental activi-
t ies.6. Rate of progress.
Development of the Assessment Chart
The Assessment Chart of Motor Abilities wasdeveloped by a group of physical and occupationaltherapists in Northern California-supervisors instate and county programs for physically handi-capped children and physical therapy school in-structors. Two motivating factors underlay theproject. First was the need to replace the out-moded "Basic Motor Abilities Test" in current usein the school program. This test was consideredunsatisfactory because its construction was basedon inadequate understanding of the neurophysi-ology involved. The second motive grew out ofthe Bobaths' visit to the United States and theircourse at Stanford University in 1958. The course,under the joint auspices of Stanford Universityand the State Crippled Children's Services, wassponsored by The Children's Bureau which re-quested a follow-up evaluation of the treatmentmethods introduced. Such an evaluation seemeda reasonable request at the time; a committee wasestablished for this purpose and proceeded tosearch for a suitable instrument for evaluating theresults of treatment. Several alternative test formswere oonsidered.
The need for determining developmental statusof the child was recognized, but a developmentaltest alone failed to indicate the pathological aspectsof the child's motor behavior and the subsequentchanges in respect to such abnormal influences.Qualitative testing of posture and movement re-sponses at each deveiopmental level proved toocumbersome. A modified form of Bobaths' As-sessment Chart was finally chosen as being mostsuitable.34
The grading system was changed from six tofive grades, some items were eliminated, and thewording of other items was changed to make thetest items as objective as possible and to increasethe reliability of the test as a whole.
Revisions were made following each of severalfield trials. With forty-six examiners, there was6l per cent agreement on a choice of six grades(0-5); 85 per cent agreed within one grade, 96per cent within two grades, and 99 per cent withinthree grades. This agreement among examinerswas comparable to that among those giving manualmuscle tests for poliomyelitis during the Salk vac-cine field trials 35 and was considered adequate forthe purpose.
A further study of the test was made to comparethe test scores to scores on a developmental testgiven the same group of children and also to relatethe test scores to certain functional activities.s6
Provided by the Maternal and Child Health Library, Georgetown University

Comparison of test scores on tlte Assessment
Chart with those on the Dallas DevelopmentalTest showed a coefficient of correlation of .87' Inrelating the assessment scores to specific activities,it was found that early activities such as prone
support on forearms with trunk extension and facevertical and secure sitting could be predictecl withinnarrow limits. Independent walking, however,showed a wide spread of scores, which may resultfrom the grading system which indicates quali tyof the performance.
In revising the Assessment Chart, a number ofthe original test items were omitted because ofdifficulty in applf ing the grading system to them.These were "moving" tests. mostly automatic in
nature involving righting and equilibrium re-
sponses, Since these developmental mechanismsare important to assess both for treatment plan-
ning and recording progress, a supplement to thepresent test is being developecl in which such auto-
matic responses can be checked plus or minus.In addition to protective and equilibrium reactionsof trunk and l imbs, patterns of turning over, get-
ting up, and reciprclcal organization in locomotioncan be included.
The Assessment Chart has proved useful inanalysis of the chi ld's motor problem, in guiding
treatment, and in checking progress' The nu-
merical score in the form of a motor quotient can
be used in a graph along with the results of othertypes of tests to give an over-all picture of progress.
The original purpose of evaluating a new system
of treatment turned out to be impractical and in-
val id. First, the training of physical therapists in
the special skills involved time off for special train-
ing. Then, orientat ion of the treatment "team" ( in-
cluding parent training) was necessary for con-
sistency of approach. Difficulties arose in a public
school program. Since many of the programs
were orthopedically oriented, it was difficult tofind a group of children who could be followed forseveral years without the complication of bracingor surgery. Since public school physical therapistsdo not go into the homes and parents could not bepresent for treatment, and since it is generallyagreed that the skill of the parent in handling thechild and other outside activities have a muchgreater influence on the child than the half-hourperiods with the physical therapist, this variableseemed uncontrollable.
Finally, and most important, the various "sys-
tems" of treatment which are neurologically ori-ented have much in common and utilize many ofthe same principles and procedures. A goodphysical therapist who understands the motor prob-
lem probably would use similar procedures to at-tack the same problem regardless of the system inwhich he was trained. It is quite possible that twophysical therapists following one system mightvary in their approach to the child as much astwo trained in different systems. These many un-
controlled variables make it useless to attempt to
compare one person's "system" of procedures with
another's system.However, it might be worth while to compare
the effectiveness of specific proaedures, e'g., to
combat the problem of hip flexion and internal ro-
tation in diplegia. Or one might cornpare the re-
sults of teaching a patient to walk with braces and
crutches with the standard methods used for lower
motor neuron disorders and of teaching a patient
a developmental program emphasizing facilitation
of righting and equilibrium reactions or reciprocalpatterning. One could compare in a state mentalhospital the advantages of an S.O.S. (Stimulatron
of Senses) program over one of routine nursingcare. In a day-care center, one could assess the
value of a developmental program in comparisonto one purely diversional. With a large group ofhemiplegic children, the relative effectiveness oftactile stimulation with prehensile activities and aprogram emphasizing the postural supportive func-
tion of the arm might be compared. One rnightdetermine whether the improvement in a programof motor co-ordination would be reflected in theschool work or social adjustment of children with"minimal brain damage." Many other pressingproblems will occur to those working with childrenwith neurological deficit for which the effectivenessof suggested procedures or types of managementcan be evaluated with appropriate testing instru-ments.
SUMMARY
Some specific tests to determine how well thechild with neurological deficit can interact with hisenvironment in the motor sphere have been re-viewed. These included assessment of the develop-mental, pathological, and adaptive aspects of hisproblem. A standardized developmental test with
emphasis on the early stages is needed. Furtherwork is needed to devise tests of the inborn, auto-matic mechanisms underlying motor adjustment tothe environment. Possible uses of evaluation toolsin determining effectiveness of specific proceduresand types of management were discussed.
REFERENC E5
1. Ayres. A. J.: Perceptual Motor Test Battery. In AyresS6ace Test. Los Angeles: Western Psychological Serv-ices, 1962.
2.Allen. R. M., and Jefferson, T. W.: PsychologicalEvaluation of the Cerebral Palsied Person. Spring-field, Illinois: Charles C Thomas, 1962.
3.Gesel l . A. . and Amatruda, C. : Developmental Diag-nosis. New York: Paul B. Hoeber, 1947.
4.Footh, W. K. , and Kogan, K. L. : Measur ing theeffectiveness of physical therapy in the treatment ofcerebral palsy, J. Amer. Phys. Ther. Ass., 43l.867-873, December 1963.
5. Knoblock, H.: Developmental Screening Instrument.Columbus, Ohio: Child Development Service, TheChildren's Hospital, 1963. (Mimeographed.)
6. Jones, M. H.: Appraisal of progress in the cerebralpalsied child. In Proceedings, Fourth Symposium on
r27
Provided by the Maternal and Child Health Library, beorgetown University

Cerebral Palsy by the Research Council' UnitedCerebral Palsy Association, Inc., New York Aqq{grnyof Medicine, November 15: 1952. Pamphlet publishedand distributed by United Cerebral Palsy Associationof Los Angeles County.
7. Doman. G. J.. Delacato, C. H., and Doman, R. J.:The Doman-Delacato Developmental Profile; andDoman. G. J.. and Moran, P.: The Doman-MoranGraphii Summary. Philadelphia: The Institutes for theAchievement of Human Potential, 1964.
8. Blum. L. H.. and Fieldsteel. N. D.: Blum-FieldsteelDevelopmental Charts. New York: World Book Com-pany, 1952.
g.Johnson, M. K. , Zuck, F. N. , and Wingate, K. : Themotor age test: Measurement of motor handicap inchildren with neuromuscular disorders such as cerebralpalsy, J. Bone Joint Surg. (Amer.) 33:693-707, July1 9 5 1 .
10. Ingram, A. J., Withers, E., and Speltz, E-: Role ofintensive physical and occupational therapy in the treat-ment of cerebral palsy: Testing and results, Arch.Phys. Med., 4O:429438, October 1959.
1 1. Dallas Society for Crippled Children: The Dallaslr4otor Development Test. 1963. (Mimeographed.)
12. Anderson, R. , Bargowski , E. , and Blodgett , w. H. : ACode Method for Evaluating Function in CerebralPalsy. Detroit: Detroit Orthopaedic Clinic, 1961.
13. Twitchell, Thomas E.: Attitudinal reflexes, J. Amer.Phys. Ther. Ass. , 45:411-418, May 1965.
14. Twitchell, Thomas E.: Variations and abnormalities ofmotor development, J. Amer. Phys. Ther. Ass., 45:42,t-430, May 1965.
' I5. Andr6-Thomas, Chesni , Y. , and Saint-Anne Dargassies,S.: The Neurological Examination of the Infant. LittleClub Clinics in Developmental Medicine, No. 1.London: National Spastics Society, 1960.
16. Twitchell, Thomas E.: Normal motor development, J.Amer. Phys. Ther. Ass., 45:419423, May 1965.
lT.Peiper, A.: Cerebral Function in Infancy and Child-hood. New York: Consultants Bureau, 1963.
18. Twitchell, Thomas E.: On the motor deficit in congen-ital bilateral athetosis. J. Nerv. Ment. Dis.. 129:I05-132, August 1959.
19. Paine, Richmond S.: The immediate value of neonatalneurological examination. In Child Neurology andCerebral Palsy. Little Club Clinics in DevelopmentalMedicine, No. 2. London: National Spastics Society,7962, pp. 62-68.
20. Illingworth, R. S.: An Introduction to DevelopmentalAssessment in the First Year. Little Club Clinics in De-velopmental Medicine, No. 3. London: National Spas-tics Society, 1962.
21. Prechtl, H., and Beintema, D.: The Neurological Ex-
amination of the Full-Term Infant. Little Club Clinicsin Developmental Medicine, No. 12. London: TheSnastics Sbcietv Medical Education and InformationUnit. Witiiam Heinemann Medical Books, Ltd., 1964.
22. Films: Neurological Examination of the Newborn In-fant and Neurological Examinatio4 of the 1-year-old In-fant. Narrated by Richmond S. Paine' Available onloan from United Cerebral Palsy Association, Inc,,321 East 44th Street, New York, New York 10036.
23. Film: Neurological Examination of Infants' Paul Ell-wood. 28 minutes, sound. Available on loan fromKenny Rehabilitation Institute, Minneapolis 4, Minne-sota.
24. Rademaker, G. G. J.: Reactions ! abyrinthiques etEqui l ibre. Par is: Masson et Cie. , 1935.
25.Zador, J.: Les Reactions d'Equilibre Chez I'Homme.Par is: Masson et Cie. , 1938.
26.Weisz, S.: Studies in equilibrium reactions, J' Nerv.Men t . D i s . , 88 :150 -162 , 1938 .
27. Bobath, B.: A study of abnormal postural reflex ac-tivity in patients with lesions of the central nervoussystem, Physiotherapy, 40:259-267, 295-300, 326-334,368-373, September, October, November, December1954.
28. Fiorentino, M. R.: Reflex Testing Methods for lvalu-ating C.N.S. Development. Springfield, Illinois: CharlesC Thomas, 1963.
29. Ladue, R. A.: Evaluation of basic motor abilities forpatients with neuromuscular dysfunciion, unpublishedMaster's thesis, Stanford University.
30. Denny-Brown, D.: The Basal Ganglia and Their Re-lation to Disorders of Movement. New York: OxfordUniversity Press, 1962.
31. Semans, Sarah, et. al.: A cerebral palsy assessmentchart, J. Amer. Phys. Ther. Ass., 45:463468, May 1965.
32.Tardieu, G.: Bilan et caracteres distinctifs des diversesraideurs d'origine cerebrale. Les Feuillets de l'InfirmiteMotrice Cerebrale, Volume II. Paris: Association Na-tionale des Infirmes Moteurs-Cerebraux.
33.Brown, M. E.: Daily activity inventories of cerebralpalsy children in experimental classes, Phys. Ther. Rev.,30:415421, October 1950.
34. Bobath. K.: The long-term results of treatment. InChild Neurology and Cerebral Palsy. Little ClubClinics in Developmental Medicine, No. 2. London:National Spastics Society, 1960.
35. Lilienfeld, A. M., Jacobs, M., and Willis, M.: A studyof the reproducibility of muscle testing and certainother aspects of muscle scoring, Phys. Ther. Rev., 34:279-289, June 1954.
36. Mosser, D. A.: An evaluative study of a cerebral palsyassessment chart, unpublished Master's thesis, StanfordUniversity.
t2a
Provided by the Maternal and Child Health Library, Georgetown University

A Cerebral PalsyAssessment ChartInstructions for Administrotion of the Test
SARAH SEMANS, M.A., ROSALYN PHILLIPS. 8.A.. MADELINE ROMANOLI, R.N..
RUTH MILLER, B.S. and MARY SKILLEN, B.A.
SOURCE AND BASIS OF SELECTION OFTEST ITEMSThe test items were selected and adapted from
the Asssesment Chart developed by Karel Bobath'
M.D., and Berta Bobath, F'C.S.P.1 The general
arrangement follows that of the original tests.
The decision to use the series of test postures
for assessment of motor ability was based on thefollowing considerations. Movements, whichevolve into functional activities, can serve no prac-tical purpose unless they can be supported andcontrolled by the appropriate postures whichrender them effective. Lacking their underlyingpostural control, attempted movements are hap-hazard and cannot be sustained to reach their goal'Well-defined postural patterns appear in an orderlysequence as the child develops' By selectingcharacteristic postural patterns simple enough foraccurate observation, the assessment can be reason-ably objective. The progress sequence from hori-
From the Division of Physical Therapy, Stanford Uni-versitv School of Medicine, Palo Alto, California, and-theoioiitment of Public Heilth, Bureau of Crippled Chil-dren's Services, State of California. Berkeley'
Provided by the Maternal and Child Health Library, Georgetown University
129

TABLE 1
CEREBRAL PALSY ASSESSMENT CHARTBASIC MOTOR CONTROL
Supine1. Hips and knees ful ly f lexed,
a r m s c r o s s e d , p a l m s o nshou lders.
2. Hips and knees ful ly f texed.(a) Extend r ight leg.(b) Extend left leg.
6. (a) Flex r ight knee, hips ex-tended.
(b) Flex left knee, hips ex-tended.
7. Trunk supported on forearms,upper trunk extended, facevert ica l .
8. Trunk supported on hands withelbows and hiDs extended.
Sitting erect9. Soles of feet together, hips
f lexed and external ly rotatedto a t leas t 45 ' .
10. Knees extended and legs ab-duc ted ; h ips 90 ' -100" .
r30
Test Postures and Movements
3. Head raised.
4. Arms extended beside head.Raise head in midDosi t ion.
ll-
5. Arms extendedpalms down. _:.ll
Provided by the Maternal and Child Health Library, Georgetown University

TABLE 1-Continued
CEREBRAL PALSY ASSESSMENT CHARTBASIC MOTOR CONTROL
Diagnosi Birthdate
Kneeling ! n=-.--_12. Back and neck straight (not 11 vj /L^
hyperextended). | - /n(a) Weight on knees. |
'-{----\(b) Weight on hands. | -4 \<'
13. Side sit t ing, upper trunk erect,arms relaxed:(a) 0n r ight hip.(b) 0n left hip.
D
Test Postures and Movements
1i . Legs hanging over edge ofta b le.(a) Extend r ight knee.(b) Extend lef t knee.
14. Knee l ing upr igh t , h ips ex .tended, head in midposit ion,arms at sides.
15. (a) Hal f kneel ing: weight onr ight knee.
(b) Hal f kneel ing: weight onlef t knee.
Squatt ing16. Heels down, toes not clawed,
knees point ing in same direc-t ion as toes, hips ful ly f lexed,head in l ine with trunk.
Standing and components ofwalking17. Standing, correct al ignment.
?!)
18. Pelvis and trunk al igned overforward leg. Eoth knees ex-tended.(a) Right leg forward.(b) Left leg forward.
19. Bear weight on one leg inm idstanc e.(a) Shi f t weight over r ight leg.(b) Shi f t weight over lef t leg.
2 0 . H e e r s t r i k e . R e a r r e g e x t e n d e d | O I R l n l l t Iand externally rotated, heel I A I l l Idown. Both knees st ra ight : | / ) l ] - l - ] l l - l( a ) R i s h t h e e r s t r i k e . | / l l L | l l L . I l l l I(b) Left heer strike. | ,/ J I I l l I l l I
Provided by the Maternal and Child Health Library, Georgetown University
r31

zontal to upright postures indicates how far thechild has come in his development of postur4l con-trol.
Information Yielded
by the Test
In cerebral palsy, the state of muscle tone andabnormal patterns of movement interfere with theorderly sequence of motor development. The testpostures selected show the nature and extent of thisinterference. Ability to sustain a test posture notpreviously possible indicates a freedom from thatpathological state which had prevented its achieve-ment. The significance of such newly gained free-dom is that it makes possible the learning of newskills. For example, when a child achieves posturalsupport on the arms, indicating a freedom from hy-pertonus of the flexor muScles, he can learn handskills which persistent flexion would not have per-mitted. Thus, the various items representing basicpostural controls which underlie support and align-ment of the body with respect to gravity, hand use,and locomotion indicate whether or not there issufficient freedom from pathological influences todevelop useful skills in each of these areas. Inthe early tests, attention is focused on control ofproximal parts; in later tests, greater individuationand segregation from the total limb synergies isrequired.
By noting limitations in range of motion whichprevent passive positioning in the test postures,the assessment can also serve as a range-of-motiontest.
Ease and quality of movement are indicated bythe numerical grade for the active movement whenthe child is asked to assume the test position.
Since each of the test items has some develop-mental significance and since total scores werefound to correlate closely with developmental testscores, the assessment yields information regard-ing developmental status of the child.
The init ial test serves as a guide in planningtreatment procedures by indicating areas of neededemphasis. Increase in total score may representthe effects of maturation. or treatment. or a com-bination of both factors. Changes in either a nega-tive or positive direction in specific areas mayreflect the relative effectiveness of treatment.
Exp lanat ion
of Tesfing Procedures
Throughout the test ing, the therapist should in-sure maximal freedom from emotional and phys-ical tension through proper handling. In all tests,the therapist should first place the child in thetest position. Physical manipulation to reducetension should be used if this factor interferes withplacement. If the therapist is unable to place thepatient, inability to relax tension or the presenceof contractures or structural deviations are indi-cated. Secondly, after being placed, the child
r32
is asked to stay in the test position. As a thirdstep, he is asked to move into the test position in-dependently.
Grading ThroughUse of a Key
A grading system with values from 0 to 5 is usedas follows:
0-Cannot be placed in test posture.l-Can be placed in test posture, but the posi-
tion cannot be held.Z-Can hold test posture momentarily after be-
ing placed.3-Can assume an approximate test posture un-
aided, in any manner.4-Can assume and sustain test posture in a
near normal manner (note any abnormal detail).5-Normal.
Interpretation of Useof Key in Grading
Grades 0 to 2 indicate the severity of the handi-cap as tested by resistance to passive motion, bylimitation of joint range, or by ability to maintainposture. These are static tests. Grades 3 to 5indicate the quality of movement when performedactivefy by the patient. Grades 3 to 5 would notbe given when grades I and 2 cannot be attained.
If for any reason the child cannot be placed, heis given a grade of 0 and a note is made to explain,under appropriate nelvrenr column, why, e.9., achild with an elbow flexion contracture, eventhough he can assume a posture normally exceptfor the use of the elbow, would be graded 0 onall test postures requiring complete elbow exten-sion.
For a grade ol 2, it is only necessary to main-tain the test posture momentarily. This indicatessome control over the disabling factors.
For grades ol 3 to 5, it is important that thechild understands what is expected of him whenhe is asked to move into the test position. Properplacing will usually be sufficient, but visual cuessuch as a demonstration by the therapist or the useof dolls or stick figures or assistance given pre-ceding the test may be helpful.
Grade 4 requires the child to assume and sas-tain the test position, but allows for slight ab-normality of movement, or a lack of a very fewdegrees from the test posture into which he couldbe placed passively. For example, a spastic childmay not be able to achieve the same degree ofextension of the thoracic spine in the sitting posi-tion as he could in the supine or prone positions,or he may have slower than normal movement; theathetoid child may perform the complete move-ment, except for tension or extraneous movementin some distal part.
To obtain a grade ol 5, each test should be ex-actly as indicated.
Provided by the Maternal and Child Health Libraryo Georgetown University

In judging whether a movement is normal, thefollowing qualities should be considered: normalmovement-smooth, easy, free, and in the lineof movement; abnormal movement-jerky, trem-orous, sluggish, labored, or deviating from theline of movement.
Tesfing HemiplegiaIn hemiplegia, the primary consideration should
be that of evaluating the aflected side.
SPECIFIC INSTRUCTIONS FOR
ADMINISTERING THE TEST ITEMS
Each item in the test represents a necessary pos-tural control for various functional activities' Forinstance, the arm position in Test 1 is a prerequisitefor engaging the hands in front of the body andfor later self-help activities. Other test positionswill be recognized as stages of postural controlpreparatory to creeping, sitting, standing, andwalking. It is helpful to keep in mind the func-tional significance of each test while administeringit in order to observe the most critical aspectscontributing to the test score. The followinggroups are arranged in the approximate order ofnormal developmental sequence.
SuPine
Test I
Purpose. To test freedom from extensor hyper-tonus in the supine position. Emphasis in this testis on proximal joints.
Bring knees, one after the other, to chest withenough external rotation at hips to point kneestoward axillae. This is needed to get completeflexion; if not attained, there is probably not fullrange of hip flexion. Steady knees in position withyour body while placing child's arms as follows:Pull arms forward at shoulders, abducting thescapulae, and fold across chest so that open palmscup shoulders; arms should be up, away from chestwall; head should remain in a neutral position;feet should be relaxed in plantar flexion, If childassumes position except for dorsiflexed feet or in-completely relaxed hands, grade 4 should be given'
Test 2Purpose. To test ability to flex or extend one leg
at a time through full range.Starting with hips and knees fully flexed, arms
across chest or relaxed at side, bring right legdown to table in an extended position, avoidinginternal rotation. Back should not arch' Returnto starting position and repeat with left leg.
Test 3
Purpose. To test ability to raise head'Placl in a symmetrical supine position with legs
extended and arms at sides' Raise head by flexing
at the atlanto-occipital joint and in the cervicalspine. The shoulders remain relaxed. If the childcin raise the head but protracts the shoulder, agrade of 3 is given.
Prone
Tesi 4Purpose. To test freedom from flexor hyper-
tonus in prone position.Place prone, lift under shoulder to free arm;
place arms overhead one after the other, elbowsind wrists extended, palms down, legs extendedand relaxed. Head is raised in midposition. Re-olace arms below shoulder level before asking childio -ou. into test position.
Test 5Purpose. To test freedom of arms and shoulders
from flexor hypertonus in prone position.Place prone, arms beside body, palms down.
To extricate arms from under the body, lift theshoulder and externally rotate arm. Place handsout a short distance from the body so that armsare not pressed against the thorax. To assume posi-tion actively, start with arms at shoulder level orabove. Note any change of tension resulting fromturning head from one side to the other.
Test 5Purpose. To test selective control of hip and
knee.Place prone, arms relaxed beside head or at
sides. Flex right knee to 90 degrees withoutflexion at hip. The foot should not dorsiflex;other leg should remain relaxed. Repeat with leftleg. For grade 4 or 5, there should be no appreci-able motion in the hip.
Test 7Purpose. To test postural control in spinal ex-
tension.This is important for beginning locomotion
(crawling), erect sitting, and beginning use ofhands. Place prone, extend thoracic spine, andplace arms one after the other in at least 90 de-grees shoulder flexion and slight abduction, sup-ported on forearms. Head is raised with facevertical. Arms point straight ahead and handsare oPen.
Tesf 8Purpose. To test ability to support weight on
extended arms.Start from test position 7. Lift child's head
giving gentle traction on cervical spine so thatsupport is on extended arms and heel of openhand; entire spine and hips are fully extended.Alternate method: Lift under shoulders or underchest. This position is often difficult to attain butis necessary for creeping.
Provided by the Maternal and Child Health Library, Georgetown University
133

Sill ing Erect
Test 9Purpose. To test control of hips in flexion, ab-
duction. and external rotation.Place in erect sitting position with legs abducted,
flexed, and externally rotated to at least 45 de-grees; soles of feet together, arms relaxed. Forgrades 3 to 5, start in any sitting position on flatsurface.
Tesi l0Purpose. To test erect sitting with legs straight.Place in erect sitting position with thighs ab-
ducted without internal rotation, and with kneesextended; ansle at hip should be 90 to 100 degrees,arms relaxed.
Test | |Purpose. To test selective control of hip and
knee.Place in erect sitting position, angle at hip 90
to 100 degrees, legs hanging vertically. Extendknee fully without further extension of hip. Otherleg and arms should remain relaxed. (a) Rightknee extended: (b) left knee extended.
Kneel ing
Test | 2Purpose. To test weight-bearing and balance
control on knees and heels of open hands.Start in four-point kneeling, back and neck
straight (not hyperextended). legs paral lel, el-bows extended, hands point ing forward. (a)Weight predominantly on knees; (b) weight pre-dominantly on hands.
Tesi | 3
Purpose. To test ability of trunk to adapt togravitational changes.
Place in side sit t ing from four-point or uprightkneeling by lowering the hips to one side of feet.Head and upper trunk should be erect; arms free.(a) On r ight hip; (b) on left hip.
Test l4Purpose. To test anterior-posterior control of
pelvis and trunk on thighs.Place in upright kneeling posit ion, hips ex-
tended, legs paral lel, trunk and head erect, headin midposit ion, arms relaxed.
Tesi | 5
Purpose. To test control of rotation at hip.Place in half-kneeling position from upright
kneeling. The other foot is placed on floor infront and to the side for adequate supporting base.Hip, knee, and ankle of forward leg at 90 degrees,toes not clawed. Pelvis and trunk face forward.knee slightly outward.
r34
Squotling
Test l6Purpose. To test control of extensor spasticity.Place from squat sitting, i.e., legsand hips fully
flexed and outwardly rotated, feet flat on floor, toesnot clawed, knees pointing in same direction astoes, arms forward for balance. Shift weight for-ward over feet into squatting position. Older childcan be placed from a low stool. It is easier to as-sume this position if the legs are spread wide apart.
Standing ond Componenfs of Wolking
Test I 7Purpose. To test normal distribution of tone in
standing.Place in standing position with body segments
in normal alignment with relation to the line ofgravity in midcoronal and midsagittal planes, i.e.,weight evenly distributed over both feet, legs inmidposition of rotation, and so on. Points of con-trol might be the hip of one side and the knee ofopposite side, or hip and opposite arm. A liftmay be used to equalize leg length.
Tesf | 8Purpose. To test the ability to shift weight for-
ward onto stance leg with rear leg extended readyfor push off.
Place in forward step position. Shift weightover forward leg with trunk, pelvis, thigh, and legcorrectlv aligned over foot. Rear leg shouid beextended, outwardly rotated at hip, and restingon the normal roll-off point (the head of the firstmetatarsal) ; arms should be relaxed. For grades2 to 5, the therapist may steady child by holdingone hand.
Test l9Purpose. To test the ability to support the body
over one leg (absence of Trendelenberg sign).From a symmetrical standing position, shift
weight laterally over one leg and lift the other freeof the floor, as for the swing phase of walking.Trunk should remain erect. For grades 2 to 5,therapist may steady child by holding one hand.
Tesf 20Purpose. To test heel strike.One foot is advanced in dorsiflexion and heel
placed on the floor. Weight is supported mainlyon rear leg, hip extended, both knees straight.Ankles remain at approximately 90 degrees. Armsshould be relaxed. For grades 2 to 5, therapistmay steady child by holding one hand.
REFE RENCE
1. Bobath, K.: The long-term results of treatment. InChild Neurology and Cerebral Palsy. Little Club Clinicsin Developmental Medicine, No. 2. London; NationalSpastics Society, 1960.
Provided by the Maternal and Child Health Library, Georgetown University

Some Considerations of thePhysiology of Sensation
H. D. BOUMAN, M.D.
DATA TRANSMISSION FROMSENSE ORGANS
Basically the sense organs are transducers whichtransform environmental information impulsesinto nerve impulses for transmission to the centralnervous system. Quite elaborate mechanisms aresometimes necessary for adequate stimulation ofthe sense organ, such as is the situation in the eyeand in the ear. It is interesting to note, however,that if one considers other sense organs, such asthe skin and particularly the proprioceptive or-gans, in their entirety as one sense organ they.arein effect almost as complicated as the eye and theear. The mechanisms by which the sense organstransmit a large and varied amount of informationto the central nervous system are fundamentallysimple. It is not possible to vary the size of the
Adapted from a paper presented at the Symposium onThe Child with Central Nervous System Deficit, Septem-ber 28-October 2, 1964, at the University of Pennsylvania,Philadelphia.
The author is Professor and Chairman, Department ofPhysical Medicine and Rehabilitation, University of Cin-cinnati, College of Medicine, Cincinnati, Ohio.
individual nerve impulse. Only the frequency ofthe impulse, the number of active fibers and theirspatial localization can be varied.
One of the basic characteristics of sense organphysiology is the Weber-Fechner Law which statesthat the intensity of a sensation varies by a seriesof equal increments as the strength of the stimulusis increased geometrically; in other words, a cer-tain step increase in sensation is proportional toa percentage increase in the stimulus. It is ex-pressed thus:
S e n s a t i o n - K l o g I * C
This results in a logarithmic relationship be-tween the stimulus and the sensation. In manysense organs the relationship between the fre-quency of impulses in the nerve and the intensityof the stimulus is also a logarithmic one. Thisleads to the important conclusion that such afundamental property of sensation as the Weber-Fechner Law is actually determined by the peri-pheral sense organs rather than by the centralnervous system. Examples of this can be foundin the sense organs of the muscle I and in the eye 2
Provided by the Maternal and Chitd Health Library, Georgetown University
r35

of animals u'hich have a relatively simple nervoussystem. Moreover, in many sense organs slowpotentials develop and the relationship betweenimpulse frequency in the nerve and these slowpotentials is linear.s'a Therefore the logarithmicrelation is found between the stimulus and thelocal activity in the sense organ itself, at leastin rather gross simplification.
ADAPTATION OF SENSE ORGANS
One of the best-known phenomena of senseorgans is that of adaptation.5 It is the reason whywe do not feel our clothes. It is also the reasonwhy we can look at a busy street scene and theconstant flow of faces without getting too excitedand nevertheless be immediately alerted when afresh stimulus (such as a sudden disturbance) oc-curs. Again it is physiologically possible to demon-strate that this phenomenon is already expressedin the nerve impulses passing from the sense or-gans. If a stimulus is maintained, the frequencyof impulses decreases and this is adaptation. Thisphenomenon is often called accommodation andshould not be confused with the accommodation ofnerve described by A. V. Hill.6 The latter is aproperty of the nerve fiber; the mechanism dis-cussed here as adaptation is located in the senseorgan. Examples of this adaptation are found inthe eye, in the ear, and in most of the senseorgans in the skin, particularly those for the senseof touch. It is possible to adapt a sense organ socompletely that it never fires an impulse, re-empha-sizing the fact that the adaptation or accommoda-tion of the sense organ is entirely independent ofthe accommodation mechanism in the nerve fiber.There are some notable exceptions to this adapta-tion process in the form of sense organ nervefibers which can keep on firing for a long time atvery high frequency.
THE OFF-EFFECT
Another basic physiological phenomenon foundin sense organs is the so-called off-effect. Thishas been described particularly in the eye. Hart-line and his co-workers have demonstrated thatwhen the retina of the eye is illuminated there arecertain receptors that start firing at the beginningof the illumination but there are also receptorswhich will fire only when the light is turned off.?Finally there is a third group of receptors whichproduce nerve impulses both at the start and atthe end of the light stimulus. The eye receptorstransmit to the central nervous system informationwhen the light stimulus starts and also when thelight stimulus is terminated or diminished. Sinceadaptation exists, if the central nervous systemwere informed only of the beginning of the lightstimulus, this information would gradually dis-appear. Failure to transmit information concern-
r36
ing the termination of the light stimulus wouldresult in faulty vision. This "off-phenomenon" isa function of the receptor organ and is by nomeans limited to the eye. It is found in the acous-tical system and in connection.with the sensoryimpulses arising in the muscle sense organs.Sherrington described a phenomenon which hecalled rebound, which is essentially the equivalentfor the muscle sense organs of the off-effect whichhas been studied so extensively in the eye.8 Evi-dence has been presented that an off-effect occursin the muscle spindles.
POI NT-TO-POI NT CONN ECTIONBETWEEN SENSE ORGANS AND THECENTRAL NERVOUS SYSTEM
Considerable work has been done on the factthat there appears to be a close anatomical rela-tionship between some sense organs and the areaof the cerebral cortex in which an organ is repre-sented. The older physiologists have grown upwith the idea that the retina has such a very exactprojection. The belief seems to persist that inthe sensory area related to the skin there is almosta point{o-point localization of the skin. We areall familiar with touch points, cold points, and hotpoints.
In recent years it has become clear that thissituation is not as simple as once believed. Thelocalization of the retina projection in the cortexis probably not as exact as it once was thoughtto be. Evidence is being brought forward to showthat sensation received from the skin can dependas much on the area stimulaied as on the repre-sentation of individual sensory spots. Studies ofthe effects of one area of stimulation on anothershow remarkable interaction. Certain sensationsare very difficult to localize at all and frequentlysuch localization is faulty. A classical exampleof this is pain, particularly pain from the internalorgans. The clinician talks about referred painby which he means pain felt in an organ or sitedifferent from the diseased one in which the stim-ulus supposedly originates. It is becoming in-creasingly clear that muscular pain can be referred.Another classical example is itching which canbe widely spread and can be caused by impulsesin other areas. This is one of the reasons whyit is not easy to explain the physiologic mechanismof pain which is associated with severe muscularspasm.
SPECIFIC RESPONSE OFINDIVIDUAL SENSE ORGANS
One of the basic laws of sense organ physiologyis the law of specific energies which says in effectthat a particular sense organ will transmit only oneparticular sensation. For instance, the eye whenstimulated in any way with any type of stimulus
Provided by the Maternal and Child Health Library, Georgetown University

will produce only light sensations. The internalear when stimulated with any type of stimulus willgive only auditory sensations. Similarly in theskin certain spots on the skin when stimulated byany type of stimulus will give only touch sensa-tions or heat sensations or cold sensations. Thespecific sensation is independent of the type ofstimulus. Electrical stimulation of the eye for in-stance will produce visual effects; electrical stimu-lation of an individual touch recepter or cold re-ceptor will produce a sensation of touch or cold.This is one of the classical hypotheses of senseorgan physiology and has been demonstrated ina wide range of experiments. This basic principlehas been questioned in recent research. In experi-ments on the preputium Bazett found that therewere seven different types of sensory organs, butthat with the best available techniques he couldfind only four different sensations.e
Extensive work has been done on the separationof touch and pressure receptors, yet the differencebetween these two sensations is not very marked.In recent years the work of Weddel,lo Seegrev,llRitchie,9 and others has reactivated this prob-lem. Itching on the other hand seems to bea distinct sensation and it is difficult if not imoos-sible to find special receptors for itching. Somenerve fibers are particularly sensitive to heat andother studies have revealed that in nerve fiberswithout sense organs the sensitivity to heat or colddepends to a certain extent on the diameter ofthe nerve fiber.l3 The skin of the outer ear seemsto have the same sensations as the rest of the skinbut it has remarkably few specific sensory nerveendings, certainly fewer than would be expectedon the basis of the number of sensations elicitedthere and on the basis of our knowledge of specificend organs for certain sensations. The facialpit organ of the rattlesnake is particularly sensi-tive to infrared but also to touch, two sensationswhich normally require separate sense organs. Zot-terman has shown that special sensations can betransmitted by different combinations of smallfibers in a narrow bundle.ra
There are important sensations and sensory ex-periences for which no specific end organs areknown. The most outstanding of course are thesensations aroused during the sexual act. Thisis obviously not meant to imply that the sexualsensations do not find their origin in stimulationof certain areas. The point made is that thereseem to be no specific sensory organs which areresponsible for this sensation.
It should be made clear that these examplesof nonconformity with the law of specific energyare still the exception rather than the rule. Infact in recent years vibration receptors have beenstudied and identified by Hun1.rs,10 However, thefact that such exceptions can be found is somewhatastonishing to many physiologists.
Closely related to the problem of specific re-
sponse of individual sense organs is the fact thatsome sense organs have only a limited range intheir particular sensation. This again is a generalphenomenon. It has been demonstrated in coldreceptors in which case different cold receptorshave their optimum response at different tempera-tures.17 This phenomenon is of particular impor-tance because a similar thing occurs in the jointreceptors where it is found that each receptorfunctions over a specific but limited range. Anumber of receptors, therefore, are activated dur-ing the total range of motion of a joint. Finally,paradoxical reactions do occur as in the case wherea cold receptor fust shows a decreasing responsewith an increase in temperature and then whenthe temperature is further increased the cold re-ceptor shows a paradoxical increase in activity.
PERIPHERAL FIELDSAND CONNECTIONS TO THECENTRAL NERVOUS SYSTEM
Cold and heat are generally conducted by smallnerve fibers with a conduction velocity of lessthan 2 meters per second. The fast initial painis conducted by larger fibers with a conductionvelocity of 15 to 20 meters per second and theslow burning or secondary pain is conducted bymore slowly conducting fibers. Tactile responsesare conducted by fibers with widely different con-duction velocities varying between 90 meters persecond and 2 meters per second. The specific en-ergies of the end organs are expressed to a certainextent in the velocity and also in the diameterof the conducting nerve fibers.
The peripheral fields of individual receptors alloverlap.l8 They vary in size and the total image ofsensation is the result of impulses from these over-lapping areas. This is again a basic physiologicalprinciple and is of considerable importance in thefield of muscle function where sensory impulsesfrom different muscle fibers overlap. Many of themodern techniques of exercise depend on thisoverlap which can come from adjacent synergisticmuscles and from antagonistic muscles, resultingin a complex pattern of facilitation and inhibitionon which ultimately co-ordinated movement de-pends. It is, however, important to realize thatthis overlap of receptor fields is not specific formuscle sense organs, but is a basic principle ofsense organ physiology. Certain skin areas haveinhibitory or excitatory effects on muscles, de-pending upon the location of both the muscle andthe skin areas.le Generally spreading fields forpressure sensation are small, nociceptive fields aresomewhat larger and can be as large as 5 by 9centimeters. Sensory areas can deliver not onlyspecific and localized information but also generalinformation to the central nervous system.
The integration of different sensory activities
Provided by the Maternal and Child ffealttt Library, Georgetown University
t37

is not limited to one side of the body, again theretina being a classical example. Sensory stimulifrom the skin are integrated between the rightside and left side of the body. There is probablyno area where this is more important than in theimpulses arising from muscles and joints whereactivity on the one side of the body can produceresults on the other side.2o This phenomenon canbe used for therapeutic purposes in such proce-dures as cross-exercise and other neuromuscularfacilitation procedures.
SPONTANEOUSACTIVITYOF THE SENSE ORGANS
Many sense organs show spontaneous activityeven without exteroceptive stimuli reaching them.The classical example is found in the retina. Whenthe eyes are closed or a person is in a dark room,impulses are transmitted over the optic nerve.The individual sees a faint light. The first physio-logical evidence of this was found in 1927 whenAdrian recorded the rest activity in the optic nerveof the eel.21 23 Important is the fact that similarevidence has been found in the muscle spindle.There is evidence that such spontaneous activity istransmitted to the ventral horn ce11.2a This con-tinuous flow of impulses from the sense organ with-out specific activity of that sense organ temptsone to use the expression "sensory tonus."
Magoun and his colleagues have shown that inthe medulla oblongata there is an area (the retic-ular substance) which has a general excitatoryfunction on the central nervous system.25 Quiteliterally one might say that this reticular substance(which has other functions also) keeps us awake.Relays from the reticular system go to the cortexand it receives a large number of impulses fromdifferent afferent areas (somatic, auditory, andvisual). The spontaneous activity of the senseorgans plays an important role in providing thismedullary center with a continuous influx of im-pulses. Actually this phenomenon has been knownfor some time even though it could neither be ex-plained nor could its full significance be realized.In 1877, Strumpell discussed a patient in whom allsense organs except one ear and one eye had be-come inoperative. Eliminating stimuli from thiseye and ear caused the patient to fall asleep im-mediatelY.26' 27
Another important result of the spontaneousactivity of the sense organs is that inhibition be-comes an entity of its own. Obviously withoutspontaneous activity inhibition could occur onlyif specific activity were present. However, if thesense organs fire continuously, inhibition can occurwithout such specific functional activity of thesense organ. Examples of this are found in manysense organs. It permits a response to direction offlow in some flow-sensitive organs in lower ani-
138
mals.28 In some sense organs this spontaneous flowis of particular importance, for instance in thesemicircular canals and in the carotid sinus.
CENTRIFUGAL CONTROL "OF THE SENSE ORGANS
The centrifugal control of sense organs has beenknown for a long time and such control is some-times located in the accessory parts of the highersense organs. For instance, the contraction of thepupil of the eye is a protection against excessivelight and occurs as a result of excessive light stim-ulation. It is a centrifugal reaction from thecentral nervous system by which the latter protectsthe eye against too much light. There is evidenceof the existence of centrifugal fibers going to theear and it has been found that the dorsal cochlearnucleus can be inhibited by impulses from theskin and by visual and olfactory stimuli. There is,however, also evidence of direct centrifugal inhib-itory effects on the sense organ itself (as Granitshowed with the retina 2e) as a result of stimula-tion of the reticular substance. The centrifugaleffects on the sense organ itself are nowhere moreimportant than in the muscle. It is a well-knownfact that the magnitude of the response of thesensory fibers from the muscle spindle is undercontrol of centrifugal impulses coming from thecentral nervous system 30 which adjust the musclespindle itself. Here is probably the most importantcase of centrifugal adjustment of the response andsensitivity of a sensory end organ. Added to thisshould be the effect of presynaptic inhibition ofafferent somatosensory fibers by higher levels.This would mean that a feedback mechanism ex-ists both on the sensory and on the motor sideof the neuromuscular reflex arc (Andersen, Car-penter, Lundberg).31-34
SUMMARY
It should be realized, the proprioceptive system,viewed as a unit, is a sense organ of considerablecomplexity. Evidence has been discussed that sug-gests that fundamental laws of sense organ physi-ology apply to the proprioceptive system as wellas to other more conventional sense organs, suchas the eye and the ear. Understanding the sensoryaspects of the functioning of the neuromuscularsystem and knowledge of the fundamental laws ofsense organ physiology are important'
REFERENCES
1. Matthews, B. H. C.: J. Physiol. (London), 77:64-110,1 9 3 1 .
2. Hartline. H. K.. and Graham, C. H.: J. Cell. Comp.Phvsio l . . | :271 -295. 1932.
3. Kaiz, B.: J. Physiol. (London), 111:261-282' 195O.4. Frcihlich, F. W.: Grundziige einer Lehre vom Licht und
Farbensinn. Jena: Fischer, 1921.5. Adrian, E. D.: The Basis of Sensalion. London: Chris-
t oohe rs .1928 .6. Hi l l , A. V. : Proc. Roy. Soc. Bio l . , 119;305-355, 1935-
1936.
Provided by the Maternal and Chitd Health Library, Georgetown University
7. Granit, R.: Sensory Mechanisms of the Retina. NervYork: Oxford University Press, 1947.
8. Sherrington, C. S.: The Integrative Action of the Nerv-ous System. New Haven, Connecticut: Yale UniversityPress, 1906.
g.Bazett, H. C., McGlone, B., Williams, R. G., and Luf-kin, H. M.: Arch. Neurol. Psych., 27:489-51'1, 1932.
l0.Weddel, G., Palmer, E., and Taylor, D.: The signifi-cance of the peripheral anatornical arrangements of thenerves which serve pain and itch. In Wolstenholme,G. E. W., and O'Connor, M., eds.: Pain and Itch,Nervous Mechanisms. Boston: Little. Brown and Com-pany, 1959, pp. 3-12.
11. Seegrev, K. K.: Sechenov. Physiol. J. USSR, 44:97-1.00,1958 .
12. Douglas, W. W., and Ritchie, J. M.: The sensory func-tion of the nonmyelinated afferent nerve fibers fromthe skin. In Wolstenholme, G. E. W., and O'Connor,M.. eds.: Pain and Itch, Nervous Mechanisms. Boston:Little, Brown and Company, 1959, pp. 2640.
13. Douglas, W. W., Ritchie, J. M., and Straub, R. W.: J.Physiol. (London), 150:266-283, 7960.
l4.Zotterman, Y.: Thermal sensations. In Handbook ofPhysiology, Section I, Volume I. Baltimore: Williamsand Wi lk ins, 1959, pp. 431-458.
15.Hunt, C. C. , and Mclntyre, A. K. : J . Physio l . (Lon-d o n ) . 1 5 3 : 7 4 - 8 7 . 1 9 6 0 .
16 .Hun t , C . C . : J . Phys io l . ( London ) ,155 :175 -186 , 1961 .17.Hensel , H. , and Zot terman, Y. : Acta Physio l . Scand.,
23 :291 -319 ,1951 .18.Hunt, C. C. , and Mclntyre, A. K. : J . Physio l . (Lon-
don), 153 : 88-1 12, 1960.
19. Hagbarth, K. E. : Acta Physio l . Scand., 26:Supp1. 94,1952.
2}.Cruz, I . , and Hufschmidt , H. J. : Arch. Ges. Physio l . ,275:12l-133, 1962.
21. Adrian, E. D., and Matthews, R.: J. Physiol. (London),63:381414. 1927.
22. Adrian, E. D., and Matthews, R.: f. Physiol. (London),64:279-301, 1927.
23. Adrian, E. D., and Matthews, R.: J. Physiol. (London),65:273-298, 1928.
24.Eldred, E. , Grani t , R. , and Merton, P. A. : J . Physio l .(London), 122:498-523, 1953.
25. Starz l , T. E. , Taylor , C. W., and Magoun, H. W.: J.Neurophysiol., 14:479-496, 1951.
26. Striimpell, A.: Pfliiger. Arch. Ges. Physiol., 15:573-574,1871.
27.Chang, H. T. : Res. Publ . Ass. Nerv. Ment. Dis. ,39:430453. t952.
28.Sand, A. : Proc. Roy. Soc. Bio l ,123:472495,7937.29,Granit, R.: Receptors and Sensory Perception. New
Haven, Connecticut: Yale University Press, 1955, pp.105-107.
30 .Ma t t hews , B . H . C . : J . Phys io l . ( London ) ,78 :1 -33 ,1 9 3 3 .
31. Andersen, P. , Eccles, J. C. , and Sears, T. A. ; Nature,194:140-741,1962.
32. Andersen, P., Eccles, J. C., and Schmidt, R. F.: Nature,194:741,-'743, 1962.
33. Carpenter, D. , Lundberg, A. , and Norrsel l , U. : Ex-per ient ia, 18 :337, 1962.
34. Lundberg, A. and Vyklicky, L.: Experientia, 1.9:247-248, 1962.
? 8 0 - 2 8 0 0 - 6 6 - 1 0
Provided by the Maternal and Child Health Library, Georgetown University
139

Proprioceptive,Vestibular, and CerebellarMechanismsIN THE CONTROL OF MOVEMENT
STELLA Y. BOTELHO, M.D.
r}.[nrqurNrr,v rHE TERMS proprio-
ception, sense of position, and kinesthesia are usedas synonyms. Sir Julian Huxley recently pointedout the great need to verbalize the sense which isknown as kinesthesia. In other words, we ought toknow how a craftsman uses his hands, how asinger uses her larynx, how an ambidexterous per-son uses his hands simultaneously. Once we candescribe and define these things, we can devisedefinitive tests.
Adapted from a paper presented at the Symposium onThe Child with Ceniral Neivous System Defiiit. September28-October 2,1964, at the University of Pennsylvania, phil-adelnhia.
D;. Botelho is Associate Professor in the Departmcntof Physiology, Division of Graduate Medicine, School ofMedicine, Univcrsity of Pennsylvania, Philadelphia 19104.
140
First, a brief review is necessary of the pathwaysfor the somesthetic sensations, the sensations neces-sary for kinesthesia. Somesthetic sensation for thebody is that sensation which is perceived whenimpulses reach the postcentral gyrus of the parietallobe of the cerebral cortex. These sometheticimpulses originate from receptors in the skin, inthe muscles, in the joints, and in the viscera. InFigure 1 the skin and muscle and joint receptorsare shown diagramatically, though the visceralreceptors are not shown. Thus, free nerve end-ings are the receptors for pain; Vater-Paciniancorpuscles are the receptors for cutaneous pressure;Meissner corpuscles are the receptors for cutaneoustemperature; hair endings are the receptors forcutaneous light touch; and the proprioceptors, the
Provided by the Maternal and Child Health Library, Georgetown University

SOMESTHETIC SYSTEM
POST. CENTRAL
PARIETAI,C O R T E X
R N A L C A P S U L E
V E N T R A L . L A T E R A LN U C L E U S
M E S E N C E P H A L O N
L O W E R M E D U L L A
L A T E R A LS P I N O T H A L A M I C
T R A C T
D O R S A LR O O T
C E R V I C A L C O R D
P € R I P H E R A L N E R V E
aNTERtOR HORiI
VENTRAL ROOI
V E N T R A LS P I N O T { I A L A M I CT R A C T
FlG. 1. Somesthetic System.
Provided by the Maternal and Child Health Library, Georgetown University
t4r

muscle spindles, joint receptors, and Golgi tendonorgans are the receptors for deep sensibility. Thecutaneous receptors for pain and temperature giverise to impulses which travel in the lateral spino-thalamic tract; the cutaneous receptors for pressureand touch give rise to impulses which travel in theventral spinothalamic tract; and proprioceptorsgive rise to impulses which travel in the dorsalcolumns, the columns of Goll and Burdach. Theimpulses in these spinal tracts reach the ventrallateral thalamic nucleus and ultimately the post-central gyrus of the parietal lobe of the cerebralcortex.
THE ROLE OF PROPRIOCEPTORS
The proprioceptors are those receptors whichare found in muscles and in joints, and the sensa-tion arising from stimulation of these receptorsmay be called myesthesia or bathesthesia (bathyes-thesia) or deep sensibility.
Kinesthesia is that sensation which has to dowith muscular motion, muscular weight, or mus-cular position, and the kinesthetic sensation is thatwhich indicates how much or how fast a muscleis moving. Thus the perception of movement,the perception of weight, and the perception ofposition are known as kinesthesia, which is de-pendent not only upon the proprioceptors, whichare located in the muscle and in the joints, butalso upon cutaneous sensations and visceral sen-sations. Kinesthetic sensation can be subdividedinto (1) a kinetic sense. i.e., a sensation of activeor passive movement or an awareness of motion,and (2) a static sense or the sense of position, i.e.,the awareness of position of the body or any of itsparts in space. Thus kinesthesia and the subdi-visions of kinesthesia, the kinetic sense and thesense of position, are dependent not only uponproprioceptors located in the muscles, tendons,and joints, but also upon cutaneous sensations andupon visceral sensations. These two portions ofkinesthetic sensation, i.e., the kinetic sense andthe sense of position, are most frequently testedtogether although there may be circumstanceswhere there is loss of static sense or sense of posi-tion with retention of the kinetic sense or sensa-tion of movement.
The proprioceptors signal information about thetension and length of a muscle, the position of ajoint, and the acceleration or deceleration of ajoint. It becomes apparent therefore that althoughsense of position and proprioception are frequentlyused synonymously, the two are not necessarily thesame. Sense of position is part of the kinestheticsensation, and proprioception is that sensationwhich arises from muscles and joints. Kinestheticsensation comes not only from proprioceptive re-ceptors but also from cutaneous receptors. Oneof the places where this is best shown is in theextraocular muscles. Here electromyographic evi-
r42
dence of muscle spindle activity can be detected.Thus when a muscle is stretched it will contractand its antagonist muscle will relax; this is evidencettrat there is proprioception. However, if oneblocks sensation from the cornea, which is com-parable to cutaneous sensation, and if one blocksvision, the subject is unable to tell where his eyeis pointing, indicating that he has lost the sense ofpositicn, although proprioceptive reflexes are in-tact. Thus, proprioception can be present whenthe sense of position is lost.
There are very few truly objective methods fordetermining sensory deficit with respect to senseof position. One objective method is to detectevoked potentials on the electroencephalogram.Thus when the fingers or the toes are stimulatedelectrically, an evoked potential from the cerebralcortex can be recorded through the skin in anawake individual. If electrodes are placed overthe hand or foot area of the postcentral gyrus ofthe parietal lobe, there may be no evoked po-tential or an abnormal evoked potential whenthere is loss of the joint position sense, althougha normal cortical evoked potential can be de-tected upon electrical stimulation of the fingers ortoes or afferent nerves from the fingers or toes.Here then is objective evidence that there is lossof joint position sense, when there is no loss ofpain, temperature, or light touch.
What is the importance of the sensory input?Consider, for example, the congenitally deaf per-son who does not have an auditory input and isalso a mute individual, unless he is trained to talkby some other sensory input; or the visually de-prived animal which does not learn normal be-havior patterns that are dependent upon visualguides. Thus motor expression is dependent upona sensory input.
Two other types of experiments which demon-strate the importance of sensory inputs are pro-longed isolation and prolonged immobilizationexperiments. During prolonged isolation or sen-sory deprivation experiments, when subjects areplaced in rooms where they are deprived of asmany sensory inputs as possible, they may becomedisoriented. In prolonged immobilization, or motordeprivation experiments, the element of sensorydeprivation may also be present. Both sensorydeprivation and motor deprivation may lead toimpaired motor function. Indeed, motor functionmay also be impaired if, despite a normal amountof sensory input, the sensory input is deranged intime. Thus an abnormal sensory feedback mayimpair motor function. As an example, if as aperson speaks a loud speaker were to play thespeaker's voice back to him slightly delayed, hewould find that he would be unable to speak in anyunderstandable way. Thus not only must therebe a sufficient amount of sensory input, theremust be a correct time sequence or a correct feed-back in order to have efficient motor function.
Provided by the Maternal and Child Health Library, Georgetown University

THE VESTIBULAR SYSTEM ANDVESTIBULAR MECHANISMS
Thc function of the vestibular system is to signalthe position or movement of the head; the re-ceptors for this system are the labyrinths, whichare located in the inner ear. In signaling the posi-tion and movement of the head, these receptorsset up reflexes which involve the neck, the trunk,and the limb muscles to maintain Dosture or equi-l ibrium. In addition, in signaling i lre position andmovement of the head, the vestibular receptorsalso set up reflexes which involve the eye musclesin order to keep images on the retina. There are,of course, other receptors which do the samethings. Thus the proprioceptors in the musclesand the joints; the cutaneous and visceral recep-tors; and the visual receptors, the eyes, can alsosignal the position and movement of the head. Thesignals from the eye are particularly important inman. Thus, in any chronic condition involvingthe vestibular system, man can compensate quitewell, for he is less dependent upon an intact vestib-ular system than are subhuman animals.
Figure 2 shows the essential parts of the ves-tibular system, including the receptors, which arein the inner ear, the labyrinths, consisting of thesuperior, lateral, and posterior semicircular canals,and the otolithic structures, the maculae of thesaccule and utricle. When these vestibular re-ceptors are stimulated appropriately, impulsestravel through the vestibular nerve to the brainstem and to the four vestibular nuclei in the brainstem: the superior (Bechterew's), medial (Schwal-be's), lateral (Deiter's), and spinal or inferior(Roller's) vestibular nuclei. The vestibular nucleicontain cells which, when stimulated, will sendascending impulses to the motor nuclei of theextraocular muscles, to the reticular formation, tothe cerebellum, and ultimately to the cerebral cor-tex. In addition, cells in the vestibular nuciei willsend descending impulses to motor nerve cells forthe neck muscles and for the limb muscles. therebvproducing limb and neck movements.
The actual receptors in the three semicircularcanals are structures which are the cristae of theampullae. Each crista consists of a gelatinousmaterial into which hairs project. When the en-dolymphatic fluid in the canal moves, it bendsthis gelatinous structure which in turn producesmovement of the hairs. Movement of the hairsgenerates impulses along the nerve fibers whichmake up the vestibular nerve. In the utricle andsaccule, the receptors are otoliths or otoconia,which are calcified particles, that rest upon gela-tinous material, into which hairs project. Whenthe otoconia become depressed or raised, the gela-tinous material becomes squeezed or expanded,causing the hairs in the gelatinous material to bend.Movement of the hairs will produce impulses inthe nerve endinss which surround the hairs. These
impulses then travel in the vestibular nerve fibersto the vestibular nuclei,
The saccule and utricle with their maculae con-taining otolithic organs respond to changes in theforce of gravity, vibration, and linear accelerationor linear deceleration, whereas'the semicircularcanals with their ampullary cristae respond tochanges in angular acceleration and angular de-celeration, which occur with rotational movements.There are many examples of postural reflexes,which result from stimulation of the labyrinths.Thus, the gravitational force acting upon theutricle and saccule is altered when the head isturned from side to side or when it is tilted up orback.
These maneuvers may produce characteristicpositions of the limbs in decerebrate preparations,such that the limbs toward which the chin isturned extend and the opposite limbs flex; ordorsiflexion of the neck will produce reflex ex-tension of both upper and lower extremities; orwhen the neck is ventroflexed, there is reflex flexionof both upper and lower extremities. However, itis important to remember that in turning or tiltingthe head it is almost impossible to stimulate theutricle and saccule without also stimulating theproprioceptors of the neck. In animals these toniclabyrinthine reflexes, uncontaminated by tonicneck reflexes, have been studied when the dorsalroots of the upper cervical segments of the spinalcotd, i.e,, the sensory nerves from the neck mus-cles. are severed.
The otoliths are also stimulated when one tiltsa subject on a tilt table, particularly if the neckis prevented from moving. Thus, when the in-dividual is tilted in this fashion, the utricle andsaccule send impulses to the vestibular nuclei,which result in flexion of the limbs in the uoperposition and extension of the limbs in the lowerposition. For example, if the subject is tilted sothat the left arm and leg are up, they will flexwhile the right arm and leg, the down limbs, willextend.
The otoliths are also stimulated when, in movingalong the horizontal or vertical, there is a suddenstop or sudden start, i.e., a sudden linear decelera-tion or linear acceleration such as occurs withmoving vehicles. Such stimulation of the utricleand saccule will produce contraction of the appro-priate muscles to maintain the individual in theupright position. On the other hand, when an in-dividual is rotated, as on a human centrifuge, notonly are the otolithic organs subjected to abnormalgravitational forces, which result from centripetalforces, but the semicircular canals are stimulatedby changing angular accelerations and decelera-tions. For example, when an individual is rotatedin a human centrifuge at a speed which involvesa force about equal to I g, he may have theillusion that he is tilting backwards about 45 de-grees. If the angular acceleration is then increased
Provided by the Maternal and Child Health Library, Georgetown Universify
143

tTO NUCLET OFEXTRAOCULAR MUSCLES,coRtEx
SUP VESTIBULARNUCLEUS
MED. VESTIBULARNU CLE US
UPPER MEDULLA
A TVESTIBULARN U C L E U S
SPINAL WSTIEULAR
NUCLEUS
V E S T I E U LGANGLION
SPINAL ACC€ VEST IEUL A R
L A I E R A L Y E S T I B U L A R
N U ' L E U S
SPINAL TRACT
M E O I A L L O N G I T U O I N I
F A S C I C U L U S
c€RvrcAL coRo
VESTIBULAR NUCLEI
FlG. 2, Vestibular l{uclei.
r44
Provided by the Maternal and Child Health Library, Georgetown University

to about 1.5 g, he may feel that he is motionlessand resting on his back while the walls of the roomappear to be moving around him. These illusionsresult from stimulation of the semicircular canalsby angular accelerations and decelerations.
Tests of Vestibular FunctionIt is extremely difficult to test otolithic function.
It is, however, easier to test semicircular canal func-tion, either by rotating the individual in a Baranychair or by flushing the ear with hot or cold water.In both of these tests (the rotation and calorictests) for semicircular canal function, movementof the endolymphatic fluid is produced and thedirection of eye movement, falling and pastpoint-ing, are observed.
Vestibular DysfunctionWhat are the disturbances which indicate ves-
tibular dysfunction? One disturbance related tothe vestibular system is the fatigue associated withlong, uninterrupted journeys in moving vehicles.This fatigue results not from the motion per sebut rather from the fact that the various musclesof the body are continuously contracting uponsignals from the vestibular receptors, which aresubjected to linear accelerations and decelerations,and changes in gravitational forces and vibrations.This is not motion sickness, for motion sickness,which is another disturbance related to the vestib-ular system, results not from the motion per sebut because there is a conflict of informationoriginating from the labyrinths and that originatingfrom the eye. Thus the various forms of motionsickness (car sickness, air sickness, sea sickness,space sickness) with their attendant nausea, vomit-ing, dizziness, headache, and so forth result fromconflicting sensory inputs. Suppression of in-formation from one sensory input may cure thistype of sickness.
Another disturbance obviously related to ves-tibular function is disequilibrium, manifested byunsteadiness or staggering. In lower animals ifthe labyrinth is destroyed, the animal will fall tothe side opposite the lesion or will circle or deviateto the side of the lesion. In man if there is achronic labyrinthine disorder, there may be a gooddeal of compensation with little unsteadiness untilthe individual is blindfolded. If there is an acutedysfunction, such as in M6ni6re's disease or anacute labyrinthitis, the individual may suddenlycollapse or may feel that he has been suddenlythrown and there would be unsteadiness or stag-gering which would be particularly related to sud-den movements of the head.
Nystagmus. Another abnormality related tovestibular dysfunction is nystagmus. Nystagmusoccurs when the eye moves slowly in one directionand quickly moves back in the other direction.This normally occurs in order to keep the imageon the retina as the head turns. If one labvrinth
is destroyed there may be a marked nystagmus withthe slow phase to the side which is destroyed andthe rapid phase to the uninvolved side. If onehas a hyperirritable labyrinth, e.g., an early uni-lateral labyrinthitis, then the nystagmus is suchthat the slow phase will be in the direction of theuninvolved side and the rapid phase will be in thedirection of the involved side. Many disoroers,of course, may start as a hyperirritable type oflabyrinthine disorder; then as the labyrinth isdestroyed there would be a hypoirritable or de-structive type.
Vertigo. In addition to disequilibrium and ny-stagmus, labyrinthine dysfunctions may be accom-panied by vertigo. Vertigo may be of the typewhere the individual feels that he is rotating inthe room while the objects and the room itself arestationary. This would be a subjective or subjectvertigo. On the other hand the individual may feelthat he is stationary and the room or objects inthe room are moving around him, and this is anobjective vertigo, i.e., the objects are moving. Bothtypes of vertigo are subjective sensations for theindividual says either he is moving around orthe objects in the room are moving around. Invertigo there must be the elernent of motion orfeeling of movement. This is different from dizzi-ness. Many people incorrectly use dizziness andvertigo as synonymous terms. Dizziness is anyfaintness or lightheadedness, or drunkenness with-out the element of movement. Disturbances ofthe labyrinth are associated with true subjectiveor objective vertigo. Frequently, of course, thevertigo is accompanied by nausea and vomiting.This is most likely because there are centers inthe brain stem for nausea and vomiting close tothe vestibular nuclei.
Problems in Space Ftight. Finally, there areproblems which are related to space travel whichare associated with the vestibular system. Onecan actually detach the otoliths with a sufficientlygreat centrifugal force. In blasting off, linearaccelerations up to 20,000 miles per hour may beproduced and this may be sufficient to "blast off,'the otoliths as well. There may be diftculties inaccelerating or decelerating related to the factthat the force of gravity now may be greater, e.g.,ten times the normal force of gravity (10 s).Under such circumstances a limb which weighs apound in water or 10 pounds in air would nowweigh 100 pounds. Such a limb would be ex-tremely diffcult to lift, so that the individual sub-jected to a force of 10 g would be unable tolift his limb and therefore there would have to becompensatory mechanisms for him to push buttonsand pull switches. Another difficulty associatedwith space travel relative to the vestibular ap-paratus is the weightless state itself. An individualis used to impulses from the proprioceptors at Ig for given types of movement. In the weightlessstate he no longer has gravitational forces to give
Provided by the Maternal and Child Health Library, Georgetown University
145

AFFERENT PATHWAYS OF CEREBELLUM
F R O M C E R E B R A L C O R T E X
CONJUNCTIVUM
L A B Y R I N T H S
PRIMARY
F I S S U R E
VESTIBIJLAR N
A GANGUON
U P P E RM E OIJLL A
L DORSAL SPINOCERESELLAR TR
LEFT INF. OLIVE
L O W E R M E O U L L AS C I C U L U S C U N E A T U S
C E R V I C A L C O R O
VESTIAULAR NUCLEi
F lG .3 . A f f e ren t pa thways o f t he ce rebe l l um .
146
-Provided by the Maternal and Child Health Library, Georgetown University

INATE TR.
GI.OBOSE NUCLEUS OF RUSSELL
EMBOLIFORM NUCLEUS
DENTATENUCLEU F'ASTIGIALNUCLEUS
BRACHIUM CONJIJNCTIVUM FASTIGO-BULBAR TR.
RETICULARFORMATION
MEDULLA
LEFT R I G H T
CEREBELLUMEFFERENT PATHWAYS
F lG .4 . E f f e ren t pa thways f r 0m the ce rebe l l um
Provided by the Maternal and Child Health Library, Georgetown University
r47

him cues about his environment. He may there-fore run into difficulties by undercompensating orovercompensating in making movements.
CEREBELLAR MECHANISMS
The cerebellum is an organ the discussion of
which is frequently slighted in physiology courses.This may be because cerebellar disorders are notcommon, although many of these disorders maybe congenital. Furthermore, man can compensaterather well for chronic cerebellar disorders.
Because the cerebellum apparently has no rolein sensory perception, it is not a sensory organ inthe sense that if it is destroyed, awareness or per-ception are lost. Perhaps tests of sensory percep-t ion are not adequate, because patients with uni-lateral cerebellar lesions may be able to detectnormal small differences in weight with the in-volved hand but, nevertheless, may state that ob-jects feel heavier in the involved hand than in theuninvolved hand. So although the cerebellum issaid to have no function related to sensory percep-tion, this may be because of inability to test ade-quately these functions.
In terms of motor function the cerebellum isan organ which co-ordinates or integrates, but itdoes not initiate movement. In this age of com-puters, the cerebellum may be considered as acomparator, a system which compares the inputfrom the cerebral cortex with impulses arising fromthe periphery , i.e., from the muscles themselves.
The cerebellum therefore compares impulsesfrom the cerebral cortex with a sensory feedbackfrom the muscles. Having compared the twoinputs, it corrects any differences between the two,thereby correcting any errors between what thecerebral cortex wants the muscles to do and whatthe muscles are actually doing. Essentially thecircuit to the cerebellum consists of ( 1 ) afferentfibers which go, for the most part, to (2) thecerebellar cortex where the Purkinje cells in thecerebellar cortex give rise to impulses which im-pinge upon (3) the cerebellar nuclear cells, fromwhich originate the majority of the (4) efferentfibers from the cerebellum.
Afierent Paihways to the Cerebellum
Figure 3 is a diagram of the afferent pathu'aysto the cerebellum. Thus, there are pathways forproprioception, for touch, for pain, and for tem-perature from the spinal cord to the cerebellumand there are afferent pathways from the vestibularnuclei to the cerebellum. Anatomically one candemonstrate fibers to the cerebellum from thelabyrinths, so that there are labyrinthine impulses,the majority of which go to the cerebellar cortexalthough a small number may go directly to thefastigial nucleus; from proprioceptive receptors;and fronr cutaneous receDtors.
r48
The anatomical afferent pathways to the cere-bellum include the fibers of the vestibular nerve,
the dorsal columns, and the ventral and dorsalspinal cerebellar tracts, which carry respectivelyimpulses from the labyrinths, from the proprio-
ceptors, and from cutaneous'receptors. Thereare in addition functional pathways, i.e., althoughan anatomical pathway may not be demonstrable,a functional pathway can be demonstrated bystimulating a region in the periphery and recordingan evoked potential from the cerebellum. Thesefunctional afferent pathways to the cerebellum in-clude a visual pathway such that when the eye isstimulated an evoked potential can be recordedfrom the cerebellum; an auditory pathway suchthat stimulation of the cochlea in the ear producesan evoked potential in the cerebellum; a pathwayfrom the brain stem reticular formation, stimula-tion of which will produce a cerebellar evokedpotential; and a pathway from the cerebral cortexsince stimulation of the cerebral cortex may pro-duce a cerebellar evoked potential.
Efferent Pathways {rom the Cerebellum
Figure 4 is a diagram of the efterent fibers themajority of which originate from cells in the cere-bellar nuclei, i.e., tbe dentate, the emboliform,the globose, and the fastigial. The medial fastigialnucleus for the most part has to do with equi-librium whereas the lateral dentate nucleus hasto do with voluntary movement. The efferentfibers from these cerebellar nuclei go to the rednucleus, to the brainstem reticular formation inthe medulla, and to the cerebral cortex.
The efferent fibers from the cerebellum includea few fibers which go from the cerebellar cortexdirectly to the vestibular nuclei but the majorityof the efferents arise from the cerebellar nuclei.These efferent fibers carry impulses to the thalamusand basal ganglia, the red nucleus, and the reticularformation. In addition there are functional effer-ent pathways from the cerebellum to the cerebralcortex. Thus the cerebellum not only receivesimpulses from a variety of peripheral receptorsand from the cerebral cortex, but it also sends im-pulses to the cerebral cortex and to those portionsof the nervous system which have to do with mod-ifying cortically induced, reflex and voluntarymovement.
The origin of the major port ion of the cerebellarefferent impulses is the cerebellar cortex, which iscomposed of three major lobes: the flocculonodu-lar lobe or archicerebellum, the anterior lobe orpaleocerebellum, and the posterior lobe or neo-cerebellum. In general, the posterior lobe is con-cerned with voluntary movement; the anterior lobewith spinal and postural reflexes; and the floccu-lonodular lobe with vestibular reflexes. The cere-bellar cortex is also divided into midline structures(including the l ingula, port ions of the lobuluscentral is and culmen of the anterior lobc: Dort ions
Provided by the Maternal and Child Health Library, Ceorgetown University

of the lobulus simplex, the declive, tuber, pyramis,and uvula of the posterior lobe; and the nodulusof the flocculonodular lobe) and lateral structures(the intermediate portions of the anterior lobe andthe hemispheral portions of the posterior lobe).
Cerebellar DysfuncfionAbnormalities of the cerebellum include disequi-
librium, which would be particularly evident withdisorders of the flocculonodular lobe since thislobe has to do with vestibular functions. Particu-larly associated with dysfunction of the anteriorlobe would be abnormalities of spinal and posturalreflexes, which might be manifested by hypotonia,pendular reflexes, and abnormal gait. Dysfunctionof the major portions of the posterior lobe are as-sociated with abnormal voluntary movement pat-terns, i.e., ataxia. Ataxic phenomena includeintention tremor, which is an exaggeration of thenormal hunting maneuver, which occurs at theend of a movement; dysmetria evidenced by ina-bility to estimate distances in the absence of visualcues such that there may be undershooting (hypo-metria) or overshooting (hypermetria); decom-position of movement as evidenced by the inabilityto perform rapidly alternating movements, such asalternate supination and pronation (adiadokoki-nesis or dysdiadokokinesis) or indeed inability toperform smooth co-ordinated movements, includ-ing walking. Since much of the compensation forchronic cerebellar disorders is through visual cues,it is not unexpected that signs of cerebellar func-tion become more marked when the individual isblindfolded.
Although in general, flocculonodular lobe dys-function is associated with disequilibrium, anteriorlobe dysfunction with abnormal spinal and posturalreflexes, and posterior lobe dysfunction with ab-normal voluntary movements, it is of some interestthat dysfunction of certain midline structures,such as the lingula of the anterior lobe and theuvula of the posterior lobe, result in disequilibrium;dysfunction of other midline structures, such asthe lobulus centralis and culmen of the anteriorlobe and the uvula and pyramis of the posteriorlobe, results in abnormal spinal reflexes: and dvs-function of sti l l other miil ine structures of tteposterior lobe, such as the declive and tuber, re-sults in ataxia.
Three conditions, which have been described inpatients with cerebellar lesions are: (1) instabil ityof the involved limb, e.g., the patient may not usehis involved arm to support himself when he sitsupon the examining table; (2) trunkal ata.ria,where the patient is unable to walk or stand be-
cause the trunk muscles do not stabilize him inthe upright position, yet he can make appropriatewalking movements when he is lying down; and(3) "cerebellar fits," in which there is suddenopisthotonus with the limbs in a posture similarto that which occurs with fast running. "Cere-bellar seizures" of this type may occur in childrenwith cerebellar tumors. The belief that "cerebellarfits" result from an increase in intracerebral pres-sure, which produces a transient decerebration,probably results from the fact that there is nogood evidence that the cerebellum can initiatemovement. It is unlikely that the characteristicposture during the "cerebellar fits" results fromabnormal stimulation of cerebellar cells by thetumor, for stimulation of the cerebellum does notproduce muscular contraction although cerebellarstimulation may modify voluntary contraction andcortically or reflexly induced movement.
SUMMARY
The function and dysfunction of proprioceptive,vestibular, and cerebellar mechanisms have beendescribed. Appropriate anatomical and functionalpathways have also been presented.
SELECTED BIBLIOERAPHY
l.Arnhoff, F. N., Leon, H. V., and Brownfield, C. A.:Sensory deprivation: its effect upon human learning,Science. 138:899. 1962.
2. Brindley, G., and Merton, P. A.: The absence of po-sition sense in the human eye, J. Physiol. (London),1 5 3 : 1 2 7 - 1 3 0 , 1 9 6 0 .
3. Brodal, A., Pompeiano, O., and Walberg, F.: The Ves-tibular Nuclei and Their Connections: Anatomy andFunctional Correlations. Edinburgh: Oliver and Boyd,1962.
4. Brookhart. J. M.: The cerebellum. In Field. J.. Ma-goun, H. W., and Hall, V. E., eds.: Handbook ofPhysiology, Section 1. Neurophysiology, II. Baltimore:Waverly Press, Inc., 1960, pp. 1245-1280.
5. De Jong, R. N.: The Neurologic Examination. NewYork: Paul B. Hoeber. Inc.. 1958.
6.Ford, F. R.: Diseases of the Nervous System in In-fancy, Childhood, and Adolescence. Springfield, Illi-nois: Charles C Thomas. 1960.
7. Haldane, J. B. S.: Biological possibilities for the humanspecies in the next ten thousand years. In Wolsten-holme, G., ed.: Man and His Future. Boston: Little,Brown & Co.. 1963.
8. Halliday, A. M., and Wakefield, G. S.: Cerebral evokedpotentials in patients with dissociated sensory loss, J.Neurol. Neurosurg. Psychiat., 26:2lI-219, 1963.
9. Ruch, T. C., Patton, H. D., Woodbury, J. W., andTowe, A. L.: Neurophysiology. Philadelphia: W. B.Saunders Company, 1962.
10.Sears, M. L. , Teasdal l , R. D. , and Stone, H. H. :Strelch effects in human extraocular muscles. Bull.Johns Hopkins Hosp., 104:174-178, 1959.
ll.Walsh, E. G.: Physiology of the Nervous System.London: Longmans, Green & Co.. 1957.
12. Zubek. J. P. , and Wi lgosh, L. : Prolonged immobi l iza-tion of the body: changes in performance and in theelectroencephalogram, Science, 140:306-308, 1963.
r L ' . S . C O V E R N " U E N T P R I N T 1 N G O F F I C E : 1 9 6 6 0 - ? 8 0 - 2 8 0
Provided by the Maternal and Child Health Library, Georgetown University
149

CHILDREN'S BUREAU PUBLICATION NUMBER 432_196'
U.S. DEPARTMENT OFHEALTH, EDUCATION, AND \TELFARE
W'ELFARE ADMINISTRATION^-.E Children's Bureau-
Provided by the Maternal and Child Health Library, Georgetown University