
Technology-based cognitive training and rehabilitation ...
19
RESEARCH ARTICLE Open Access Technology-based cognitive training and rehabilitation interventions for individuals with mild cognitive impairment: a systematic review Shaoqing Ge 1* , Zheng Zhu 2,3 , Bei Wu 4,5 and Eleanor S. McConnell 1,6 Abstract Background: Individuals with mild cognitive impairment (MCI) are at heightened risk of developing dementia. Rapid advances in computing technology have enabled researchers to conduct cognitive training and rehabilitation interventions with the assistance of technology. This systematic review aims to evaluate the effects of technology- based cognitive training or rehabilitation interventions to improve cognitive function among individuals with MCI. Methods: We conducted a systematic review using the following criteria: individuals with MCI, empirical studies, and evaluated a technology-based cognitive training or rehabilitation intervention. Twenty-six articles met the criteria. Results: Studies were characterized by considerable variation in study design, intervention content, and technologies applied. The major types of technologies applied included computerized software, tablets, gaming consoles, and virtual reality. Use of technology to adjust the difficulties of tasks based on participants’ performance was an important feature. Technology-based cognitive training and rehabilitation interventions had significant effect on global cognitive function in 8 out of 22 studies; 8 out of 18 studies found positive effects on attention, 9 out of 16 studies on executive function, and 16 out of 19 studies on memory. Some cognitive interventions improved non-cognitive symptoms such as anxiety, depression, and ADLs. Conclusion: Technology-based cognitive training and rehabilitation interventions show promise, but the findings were inconsistent due to the variations in study design. Future studies should consider using more consistent methodologies. Appropriate control groups should be designed to understand the additional benefits of cognitive training and rehabilitation delivered with the assistance of technology. Keywords: Technology, Cognition, Cognitive training, Cognitive rehabilitation, Systematic review Background Due to the aging of the world’ s population, the number of people who live with dementia is projected to triple to 131 million by the year 2050 [1, 2]. Development of preventative strategies for individuals at higher risk of developing dementia is an international priority [3, 4]. Mild cognitive impairment (MCI) is regarded as an intermediate stage between normal cognition and dementia [5, 6]. Individuals with MCI usually suffer with significant cognitive complaints, yet do not exhibit the functional impairments required for a diagnosis of dementia. These people typically have a faster rate of progression to dementia than those without MCI [5], but the cognitive decline among MCI subjects has the potential of being improved [7, 8]. Previous systematic reviews of cognitive intervention studies, both cognitive training and cognitive rehabilitation, have demonstrated promising effects on improving cognitive function among subjects with MCI [3, 7, 9, 10]. Recently, rapid advances in computing technology have enabled researchers to conduct cognitive training and rehabilitation interventions with the assistance of * Correspondence: [email protected] 1 Duke University School of Nursing, 307 Trent Drive, Durham, NC, USA Full list of author information is available at the end of the article © The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. Ge et al. BMC Geriatrics (2018) 18:213 https://doi.org/10.1186/s12877-018-0893-1
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Technology-based cognitive training and rehabilitation ...
RESEARCH ARTICLE Open Access
Technology-based cognitive training andrehabilitation interventions for individualswith mild cognitive impairment: asystematic reviewShaoqing Ge1* , Zheng Zhu2,3, Bei Wu4,5 and Eleanor S. McConnell1,6
Abstract
Background: Individuals with mild cognitive impairment (MCI) are at heightened risk of developing dementia.Rapid advances in computing technology have enabled researchers to conduct cognitive training and rehabilitationinterventions with the assistance of technology. This systematic review aims to evaluate the effects of technology-based cognitive training or rehabilitation interventions to improve cognitive function among individuals with MCI.
Methods: We conducted a systematic review using the following criteria: individuals with MCI, empirical studies,and evaluated a technology-based cognitive training or rehabilitation intervention. Twenty-six articles met the criteria.
Results: Studies were characterized by considerable variation in study design, intervention content, and technologiesapplied. The major types of technologies applied included computerized software, tablets, gaming consoles, and virtualreality. Use of technology to adjust the difficulties of tasks based on participants’ performance was an importantfeature. Technology-based cognitive training and rehabilitation interventions had significant effect on global cognitivefunction in 8 out of 22 studies; 8 out of 18 studies found positive effects on attention, 9 out of 16 studies on executivefunction, and 16 out of 19 studies on memory. Some cognitive interventions improved non-cognitive symptoms suchas anxiety, depression, and ADLs.
Conclusion: Technology-based cognitive training and rehabilitation interventions show promise, but the findings wereinconsistent due to the variations in study design. Future studies should consider using more consistentmethodologies. Appropriate control groups should be designed to understand the additional benefits of cognitivetraining and rehabilitation delivered with the assistance of technology.
Keywords: Technology, Cognition, Cognitive training, Cognitive rehabilitation, Systematic review
BackgroundDue to the aging of the world’s population, the numberof people who live with dementia is projected to triple to131 million by the year 2050 [1, 2]. Development ofpreventative strategies for individuals at higher risk ofdeveloping dementia is an international priority [3, 4].Mild cognitive impairment (MCI) is regarded as anintermediate stage between normal cognition anddementia [5, 6]. Individuals with MCI usually suffer with
significant cognitive complaints, yet do not exhibit thefunctional impairments required for a diagnosis ofdementia. These people typically have a faster rate ofprogression to dementia than those without MCI [5],but the cognitive decline among MCI subjects has thepotential of being improved [7, 8]. Previous systematicreviews of cognitive intervention studies, both cognitivetraining and cognitive rehabilitation, have demonstratedpromising effects on improving cognitive functionamong subjects with MCI [3, 7, 9, 10].Recently, rapid advances in computing technology
have enabled researchers to conduct cognitive trainingand rehabilitation interventions with the assistance of
* Correspondence: [email protected] University School of Nursing, 307 Trent Drive, Durham, NC, USAFull list of author information is available at the end of the article
© The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Ge et al. BMC Geriatrics (2018) 18:213 https://doi.org/10.1186/s12877-018-0893-1

technology. A variety of technologies, including virtualreality (VR), interactive video gaming, and mobile tech-nology, have been used to implement cognitive trainingand rehabilitation programs. Potential advantages tousing technology-based interventions include enhancedaccessibility and cost-effectiveness, providing a user ex-perience that is immersive and comprehensive, as wellas providing adaptive responses based on individualperformance. Many computerized cognitive interventionprograms are easily accessed through a computer ortablet, and the technology can objectively collect dataduring the intervention to provide real-time feedback toparticipants or therapists. Importantly, interventionsdelivered using technology have shown better effectscompared to traditional cognitive training and rehabilita-tion programs in improving cognitive function andquality of life [11–13]. The reasons for this superiorityare not well-understood but could be related to the us-ability and motivational factors related to the real-timeinteraction and feedback received from the training sys-tem [13].Three recent reviews of cognitive training and rehabili-
tation for use with individuals with MCI and dementiasuggest that technology holds promise to improve bothcognitive and non-cognitive outcomes [14–16]. The re-views conducted by Coyle, et al. [15] and Chandler, et al.[14] were limited by accessing articles from only twodatabases, and did not comprehensively cover availabletechnologies. Hill, et al. [16] limited their review topapers published until July 2016 and included only olderadults aged 60 and above. More technology-based inter-vention studies have been conducted since then, andonly including studies with older adults 60 and abovecould limit the scope of the review given that adults candevelop early-onset MCI in their 40s [17]. Therefore, thepurpose of this review is to 1) capture more studiesusing technology-based cognitive interventions by con-ducting a more comprehensive search using additionaldatabases 2) understand the effect of technology-basedcognitive interventions on improving abilities among indi-viduals with MCI; and 3) examine the effects of multi-modal technology-based interventions and their potentialsuperiority compared to single component interventions.
MethodsSearch strategyPRISMA guidelines were followed for conducting thissystematic review [18]. Based on the research aims andkey words, an experienced librarian searched five data-bases: PubMed (Medline), PsychoINFO (EBSCOhost),CINAHL (EBSCOhost), Embase, and Cochrane Library(Wiley). The search strategy used a combination ofsubject headings and key words for these main concepts:technology, MCI, training, and rehabilitation. The full
search strategy is available in Additional file 1. Theliterature search was limited to empirical studies amonghuman subjects. We did not set boundaries on age sinceMCI can occur among middle aged to older adults. Theliterature search was completed on December 1, 2017.
Inclusion and exclusion of publicationsTwo authors (SG and ESM) independently reviewed thelist of articles found in the literature search. Inclusioncriteria were: 1) participants were diagnosed with MCI;2) a technology-based cognitive training or rehabilitationintervention was evaluated; and 3) an empirical studywas conducted. Exclusion criteria were: 1) the effect ofthe intervention on MCI participants could not beextracted from effects among healthy or dementia par-ticipants, and 2) the publication was not in English.Titles were first reviewed for obvious exclusions. Then,
for those retained from the first-round title screening,abstracts were screened. A third-round of full-textscreening was then conducted. Any uncertainties ordiscrepancies between the two authors (SG and ESM)were discussed and resolved.
Quality assessmentThe quality of studies identified as relevant was assessedby two independent reviewers (SG and ZZ) using theJoanna Briggs Institute (JBI) critical appraisal checklistfor randomized controlled trials (RCT) and JBI checklistfor quasi-experimental studies [19]. Any disagreementsthat arose were resolved through discussion, or with athird reviewer (BW). The studies were generally meth-odologically sound with some variations in quality acrossstudies (see Additional file 1: Table S2 and S3).
Data extraction and synthesisTwo reviewers (SG and ZZ) independently extractedinformation from each article into the Tables 1 and 2.Disagreements on data extraction were resolved byconsensus with the assistance of a third author. Ameta-analysis of the 26 articles was inappropriate due tothe large variability between the study designs, interven-tion contents, outcomes measured, and populationsamples across different studies [20, 21]. We selectivelycalculated effect sizes for a pair of studies that used thesame intervention materials [22, 23]. All data syntheseswere conducted by using Revman 5.3 [24]. The forestplot is presented in Additional file 1: Figure S1.
ResultsBased on the strategy and criteria described above, 26 of411 studies identified were deemed eligible for review.The PRISMA flowchart in Fig. 1 presents the decisionpathway for final inclusion of studies.
Ge et al. BMC Geriatrics (2018) 18:213 Page 2 of 19

Table
1Samplecharacteristic
ofinclud
edstud
ies
Firstauthor
Year
ofpu
blication
Locatio
nSetting/context
Samplesize
aAge
b(year)
MCIC
riteria
Baselinecogn
itive
characteristic
b
Cipriani,2006[29]
2006
Italy
Dayho
spital
10(AD)+
10(M
CI)
70.6
Not
specified
MMSE:28.0
Rozzini,2007
[40]
2007
Italy
Med
icalcenters
5963–78
Petersen
criteria
MMSE:IG1:26.4
IG2:26.0CG
:26.8
Talassi,2007
[36]
2007
Italy
Com
mun
ity-dwelling
37(M
CI)+29(AD)
IG:76.2CG
:76.1
Not
specified
MMSE:IG:27.5
CG:26.9
Barnes,2009[22]
2009
US
Med
icalcenters
47IG:74.1CG
:74.8
IWGcriteria
BRAN
S:IG:85.2
CG:87.8
Finn
,2011[25]
2011
Australia
Med
icalcenter
27IG:69.00
CG:76.38
IWGcriteria
MMSE:IG:28.5
CG:27.5
Rosen,2011
[23]
2011
US
Com
mun
ity-dwelling
12IG:70.67
CG:78.00
IWGcriteria
MMSE:IG:29.33
CG:27.83
Gagno
n,2012
[43]
2012
Canada
Med
icalcenters
24IG:68.42
CG:67.00
Petersen
criteria
MMSE:IG:27.83
CG:28.08
Herrera,2012[42]
2012
France
Med
icalcenter
22IG:75.09
CG:78.18
Petersen
criteria
MMSE:IG:27.36
CG:27.18
Man,2012[13]
2012
Hon
gKo
ngCom
mun
ityservicesetting
44IG:80.30
CG:80.28
Petersen
criteria
MMSE:IG:21.05
CG:23.00
Gon
zalez-Palau,2014
[33]
2014
Spain
Com
mun
itycenters
39(HE)+11(M
CI)
74.60
Petersen
criteria
MEC
35:29.61
Han,2014[30]
2014
Korea
Med
icalcenter
1072.1
IWGcriteria
MMSE:26.7
Hug
hes,2014
[45]
2014
US
Com
mun
itysetting
20IG:78.5CG
:76.2
MYH
ATCog
nitive
Classificatio
nMMSE:IG:27.2
CG:27.1
Fiataron
eSing
h,2014
[26]
2014
Australia
Com
mun
ity-dwelling
100
70.1
Petersen
criteria
ADAS-Cog:IG1:8.79
IG2:8.29
IG3:8.02
CG:8.09
Manera,2015
[32]
2015
France
Med
icalCen
terandresearch
unit
9(MCI)+12(AD)
75.8
NationalInstituteon
Aging
andAlzhe
imer
Associatio
ngrou
pclinicalcriteria
MMSE:27.2
Styliadis,2015
[34]
2015
Greece
Med
icalfacility
70IG1:71.21IG2:70.42IG3:72.71
CG1:71.07CG
2:67.64
Petersen
criteria
MMSE:IG1:25.85
IG2:26.21IG3:25.14
CG1:26.21CG
2:25
Barban,2016[39]
2016
Italy,G
reece,
Norway
andSpain
Med
icalcenters
114(HE)+
106(MCI)+81(AD)
IG:74.4CG
:72.9
Petersen
criteria
MMSE:IG:27.3
CG:28.1
Goo
ding
,2016[35]
2016
US
Med
icalcenter
7475.59
Petersen
criteria
mMMSE:IG1:51.25
IG2:50.29CG
:50.39
Heyer,2016[28]
2016
US
Com
mun
ity-dwelling
68IG:75.1CG
:75.2
IWGcriteria
MMSE:26
Klados,2016[37]
2016
Greece
Not
specified
50IG:69.60
CG:67.92
Petersen
criteria
MMSE:IG:26.04
CG:25.64
Ge et al. BMC Geriatrics (2018) 18:213 Page 3 of 19

Table
1Samplecharacteristic
ofinclud
edstud
ies(Con
tinued)
Firstauthor
Year
ofpu
blication
Locatio
nSetting/context
Samplesize
aAge
b(year)
MCIC
riteria
Baselinecogn
itive
characteristic
b
Lin,2016
[44]
2016
US
Com
mun
ity-dwelling
24IG:72.9CG
:73.1
Albertcriteria
MoC
A:IG:24.4
CG:25.6
Verm
eij,2016
[31]
2016
Nethe
rland
sCom
mun
itysetting
25(HE)+22(M
CI)
68.4
Petersen
criteria
MMSE
>27.1
Not
specified
Bahar-Fuchs,2017
[27]
2017
Australia
Com
mun
ity-dwelling
9(MCI)+
11(M
rNPS)+
25(M
CI+MrNPS)
74.8
NationalInstituteon
Aging
andAlzhe
imer
Associatio
ngrou
pclinicalcriteria
GDS:2.9
Delbroe
k,2017
[47]
2017
Belgium
Reside
ntialcarecenter
20IG:86.9CG
:87.5
Not
specified
Moca:IG:17.5
CG:16.3
Hagovská,2017
[12]
2017
Slovakia
Outpatient
psychiatric
clinics
60IG:67.8CG
:68.2
Albertcriteria
MMSE:IG:25.6
CG:24.9
Mansbach,2017
[38]
2017
US
Com
mun
ity-dwelling
3878.08c
Petersen
criteria
BCAT
c :IG:38.65
CG:35.72
Savulich,
2017
[41]
2017
UK
Research
andmed
icalcenter
42IG:75.2CG
:76.9
Albertcriteria
MMSE:IG:26.6
CG:26.8
IGInterven
tiongrou
p,CG
Con
trol
grou
pa HEHealth
yelde
rlywith
nohistoryof
neurolog
ical
orpsychiatric
deficits,M
rNPS
Moo
d-relatedne
urop
sychiatric
symptom
sbDataon
lyinclud
edelde
rlywith
MCI
c Dem
ograph
icda
tainclud
edbo
thMCIa
ndAD
Ge et al. BMC Geriatrics (2018) 18:213 Page 4 of 19
Table
2Overview
ofinclud
edstud
ies
Firstauthor
andyear
Stud
yde
sign
Interven
tionand
Techno
logy
Con
trol
Techno
logy
descrip
tion
Sessions/
Duration
Follow-up
Cog
nitiveou
tcom
emeasures
Other
outcom
emeasures
Keyfinding
s
Cipriani,
2006
[29]
Pre-
post
stud
y
Com
puter
based-Cog
nitive
Rehabilitation
(cb-CR)
prog
rams
NA
TNPsoftw
are:de
livers
individu
alized
cogn
itive
rehabilitationexercisesin
thefollowingcogn
itive
domains:atten
tion,
mem
ory,pe
rcep
tion,
visuospatialcog
nitio
n,lang
uage
,and
non-verbal
intellige
nce
2*16
*13–
45min
sessions
for
8weeks
3mon
ths
MMSE
Atten
tion:Visualsearch;
Executivefunctio
n:Trail
MakingtestAandB;
BehavioralMem
ory:
RBMT;Psycho
motor
learning
:digitsymbo
ltest;Verbalfluen
cy:
phon
emicandsemantic
verbalfluen
cy
Dep
ression(GDS);
Anxiety:STA
I-X1,STAI-
X2;A
DL:AADL;QOL:SF-
12
MCI:O
nlysign
ificantly
improved
inmem
ory
(RBM
T)
Rozzini,
2007
[40]
RCT
TNP+ChEIs
CG1:ChEIs
CG2:No
treatm
ent
TNPSoftw
are
20*1h/
session,five
days/w
eek
forfour
weeks
1yr
MMSE
Mem
ory:Shortstory
recall;Executivefunctio
n:Rey’sfig
urecopy
and
recall,Raven’scolored
matrices;Verbalfluen
cy:
Letter
verbalfluen
cy,
Semantic
verbalfluen
cy
Moo
d:de
pression
:GDS;
anxiety,apathy
Behavioraldisturbances:
NPI
Activities
ofdaily
living:
BADL
IG:significant
improvem
entin
mem
ory,
abstract
reason
ing,
and
depression
CG1:no
improvem
ents
onanycogn
ition
but
bene
fitin
depression
CG2:no
improvem
entin
anyou
tcom
emeasures
Talassi,
2007
[36]
CCT
TNP+OT+BT
PR+OT+BT
TNPSoftw
are
30–45min/
session,
4days/w
eek
for3weeks
Interven
-tio
nen
dMMSE
Working
mem
ory:
forw
ardandbackward
digitspan;Executive
functio
n:Rey’sfig
ure
copy;Verbalfluen
cy:
phon
emicandsemantic
verbalfluen
cy;C
DT;
Episod
icMem
ory:
episod
icmem
orysubset
ofRBMT;Verbalfluen
cy:
Phon
emicandsemantic
verbalfluen
cy;A
tten
tion:
visualsearch,p
rocessing
speed:
digitsymbo
ltest
Moo
d:de
pression
GDS;
anxiety(Stai-Y1,Stai-Y2;
ADL:BA
DL,IADL,PPT;
MCI
subjectsin
IGim
proved
inexecutive
functio
n,visuospatial
mem
ory,anxiety,
depression
,and
PPTbu
tno
tIADL
MCI
subjectsin
CG:no
improvem
ents
Barnes,
2009
[22]
RCT
cb-CT
Passive
compu
ter
activities
Com
puter-based
cogn
itive
training
softwarede
velope
dby
PositScienceCorpo
ratio
n(San
Francisco,CA),
involvingsevenexercises
includ
ingprim
aryand
working
auditory
mem
ory
tasksto
improve
processing
speedand
accuracy
intheauditory
cortex
IG:100
min/
dayfivedays/
weekfor
6weeks
CG:
90min/day,
5days/w
eek
for6weeks
Interven
-tio
nen
dGlobalcog
nitivefunctio
n:RBANStotalscore,5
RBANSinde
xscore
Mem
ory:CVLT-II
Lang
uage
:COWAT,BN
TExecutivefunctio
n:CaliforniaTrailM
aking
Test
Atten
tion:DesignFluency
test;W
orking
mem
ory:
SpatialSpantest
Moo
d:de
pression
(GDS)
IGshow
edgreater
improvem
enton
RBANS
totalscoresbu
tno
sign
ificant
betw
een
grou
pdifference.
Effect
sizesforverbal
learning
andmem
ory
measurestend
edto
favor
IG.
Effectsizes
forlangu
age
andvisuospatialfun
ction
measurestend
edto
favor
CG(con
trolgrou
p).
Ge et al. BMC Geriatrics (2018) 18:213 Page 5 of 19

Table
2Overview
ofinclud
edstud
ies(Con
tinued)
Firstauthor
andyear
Stud
yde
sign
Interven
tionand
Techno
logy
Con
trol
Techno
logy
descrip
tion
Sessions/
Duration
Follow-up
Cog
nitiveou
tcom
emeasures
Other
outcom
emeasures
Keyfinding
s
Finn
,2011
[25]
RCT
Com
puterized
Cog
nitiveTraining
Package
Nointerven
tion
Lumosity
softwareon
acompu
tercontains
four
orfivecogn
itive
exercise
that
targeted
four
cogn
itive
domains
30sessions,
4–5sessions/
week
Interven
-tio
nen
dExecutivefunctio
n:IED;
Atten
tion:RVP
Subjectivemem
ory
impairm
ent:MFQ
Visualmem
ory:PA
L
Moo
d:Dep
ression
Anxiety
andStress
Scale
IGhadsign
ificant
improvem
entin
visual
attentionbu
tno
tprocessing
speed,
visual
mem
ory,no
rmoo
d
Rosen,
2011
[23]
RCT
cb-CT
listening
toaudiobo
oks,
readingon
line
newspapers,and
playinga
visuospatial
oriented
compu
tergame
Com
puter-based
cogn
itive
training
softwarede
velope
dby
PositScienceCorpo
ratio
n
IG:24
sessions,100
mins/day,
5days/w
eek
CG:24
sessions,
90min/day,
5days/w
eek
Interven
-tio
nen
dGlobalcog
nitivefunctio
n:RBANS
Neuroim
aging:
fMRI
Not
specified
IG>CG:improvem
entin
verbalmem
oryandleft
hipp
ocam
palactivation
CG:d
eclined
inVM
Gagno
n,2012
[43]
RCT
Com
puter-basedVP
AC:C
ompu
ter-
basedFP
Com
puter-baseddivide
dattentiondu
al-tasktrain-
ing:
VP:p
erform
ingbo
thtasksconcurrentlyand
varyingallocatio
nprior-
ities
across
theseriesof
blocks,feedb
acks
arepro-
vide
d;FP:perform
both
tasksconcurrentlyandto
allocate
50/50attentional
resourcesto
each
task,no
feed
backsprovided
6*1h/
session,3
times/w
eek
fortw
oweeks
Interven
-tio
nen
dAtten
tion:du
altask
(digit
span
task,visuald
etectio
ntask);Executivesubtestof
TEA
Atten
tion:TrailM
aking
TestA;Executivefunctio
n:TrailM
akingTestB;
QOL:Well-Being
Scale
Divided
attention:
Divided
Atten
tion
Questionn
aire
VPshow
edsign
ificant
advantageover
FPin
improvingaccuracy
and
reactio
ntim
eFP
andVP
both
prod
uced
improvem
entson
focusedattention,speed
ofprocessing
,and
switching
abilities
Noreliableadvantagefor
VPover
FP
Herrera,
2012
[42]
RCT
Com
puter–b
ased
Mem
oryand
attentiontraining
Stim
ulating
Cog
nitive
activities
Com
puter-based
cogn
itive
training
that
involved
amem
orytask
andan
attentiontask
24*60
min/
session
twice/week
for12
weeks.
6mon
ths
MMSE-recall;Mem
ory:
theforw
ardand
backwarddigitspan
test,
BEM-144
12-w
ord-listre-
call,the16-item
freeand
cued
reminding
test,sub
-scorerecallof
theMMSE,
visualrecogn
ition
subtest
from
theDoo
rsand
Peop
lemem
orybattery,
theDMS48test;executive
functio
n:Rey–Osterrieth
Com
plex
Figu
rerecalltest
N/A
Sign
ificant
improvem
ent
inmem
ory,bo
thep
isod
icrecallandrecogn
ition
Man,2012
[13]
CCT
VR-based
mem
ory
training
prog
ram
Therapist-led
prog
ram
VR:p
articipantsuseeither
thejoystickor
the
directionbu
tton
sof
the
keyboard
tocontrolthe
navigatio
nactio
nand
give
respon
sesto
amem
orytask
10sessions,
30min/
session2–3
times/w
eek
Interven
-tio
nen
dMem
ory:MMQ;Episodic
Mem
ory:FO
ME
ADL:LawtonIADL
VR:significant
improvem
entin
total
encoding
,totalrecall,
delayedrecallandMMQ-
strategy
Therapist-led:
sign
ificant
improvem
entin
total
recall,de
layedrecalland
MMQ-con
tentmen
t
Ge et al. BMC Geriatrics (2018) 18:213 Page 6 of 19
Table
2Overview
ofinclud
edstud
ies(Con
tinued)
Firstauthor
andyear
Stud
yde
sign
Interven
tionand
Techno
logy
Con
trol
Techno
logy
descrip
tion
Sessions/
Duration
Follow-up
Cog
nitiveou
tcom
emeasures
Other
outcom
emeasures
Keyfinding
s
VR>therapistin
improvingob
jective
mem
ory;Therapist>VR
insubjectivemem
ory
Gon
zalez-
Palau,2014
[33]
Pre-
post
stud
y
LLM
includ
edCTC
andPTC
NA
CTC
:Gradior
Softw
are:a
multi-do
maincogn
itive
training
prog
ram
includ
-ingattention,pe
rcep
tion,
episod
icmem
oryand
working
mem
orytasks.
Principles
offeed
back
anddifficulty
adaptatio
nareused
PTC:FFA
:aninno
vative,
low-costgameplatform
.Workou
rintensity
grad-
ually
increases
CTC
:40/
session,three
times/w
eek
for12
weeks
PTC:one
-ho
ursession
ofFFA,three
times/w
eek
for12
weeks
Interven
-tio
nen
dGlobalcog
nitivefunctio
n:TheMiniExamen
Cog
nitivo(M
EC35)
Mem
ory:LogicalM
emory
subtestsof
theWMSIII
Atten
tion:TheColor
Trail
Test1and2
Verballearning
and
mem
ory:HVLT-R
Moo
d:de
pression
(GDS)
ForMCIsub
jects:
Sign
ificant
improvem
ent
inglob
alcogn
itive
functio
n,verbal
mem
ory,ep
isod
icmem
ory,andde
crease
insymptom
sof
depression
.
Han,2014
[30]
Pre-
post
stud
y
Ubiqu
itous
Spaced
Retrieval-b
ased
Mem
oryAdvance-
men
tandRehabili-
tatio
nTraining
USM
ART
Prog
ram
NA
USM
ART
prog
ram
appon
IPad
24face-to-
face
sessions
Interven
-tio
nen
dCERAD-K-N
includ
ing:
verbalfluen
cy:the
Categ
oricalFluencytest,
theMod
ified
BNT;MMSE;
mem
ory:WLM
T,WLRT,
theWordListRecogn
ition
Test,C
RT;visuo
spatial:
Con
structionalP
raxisTest;
Atten
tion:TrailM
aking
TestA;executivefunctio
n:TrailM
akingTestB
N/A
Sign
ificantlyim
proved
onlyin
mem
ory(W
LMT);
numbe
rof
training
sessions
correlated
with
WLM
Tscores
Hug
hes,
2014
[45]
RCT
Interactivevide
ogames
(Wii)
Health
yaging
education
prog
ram
Nintend
oWiigaming
consoleforinteractive
vide
ogaming(bow
ling,
golf,tenn
is,and
baseball)
24*90
min,
1session/
weekfor
24weeks
1year
Globalcog
nitio
n:CAMCI;
Processing
speed/
Atten
tion:Tracking
A;
Executivefunctio
n:Tracking
B;Subjective
cogn
itive
ability
Moo
d/socialfunctio
ning
:CSRQ-25;
ADL:TIADL
IG:N
osign
ificant
improvem
entin
anyof
theou
tcom
emeasures.
Med
ium
effect
size
estim
ates
werefoun
dfor
glob
alcogn
ition
,subjectivecogn
ition
,executivefunctio
n,and
gaitspeed
Fiataron
eSing
h,2014
[26]
RCT
IG1:CT+Sham
exercise
IG2:PRT+Sham
cogn
itive
interven
tion
IG3:CT+PRT
Sham
exercise
+Sham
cogn
itive
interven
tion
COGPA
CKprog
ram:
compu
ter-basedmulti-
mod
alandmulti-do
main
exercisestargetingmem
-ory,executivefunctio
n,attention,andspeedof
inform
ationprocessing
,includ
ing14
prog
ressively
moredifficultexercises
CG:60min
IG:75min
PRT/CT
grou
ps,
100min
combine
d2–3days/
weekfor
6mon
ths
18mon
ths
Globalcog
nitio
n:ADAS-
Cog
ExecutiveFunctio
n:WAIS-
III;Verbalfluen
cy:C
OWAT,
anim
alnaming;
Mem
ory:
BVRT-R,aud
itory
Logical
Mem
oryIand
II,subsets
ofWMS-III,ListLearning
subsectio
nof
ADAS-Cog
;Atten
tion:SD
MT
ADL:B-IADL
CTpreven
tedmem
ory
declineon
lyup
until
6mon
ths
PRTim
proved
glob
aland
executivefunctio
nun
til18
mon
ths;PRTwas
better
than
CT+PRTin
improvingglob
aland
executivefunctio
n
Ge et al. BMC Geriatrics (2018) 18:213 Page 7 of 19
Table
2Overview
ofinclud
edstud
ies(Con
tinued)
Firstauthor
andyear
Stud
yde
sign
Interven
tionand
Techno
logy
Con
trol
Techno
logy
descrip
tion
Sessions/
Duration
Follow-up
Cog
nitiveou
tcom
emeasures
Other
outcom
emeasures
Keyfinding
s
Manera,
2015
[32]
Pre-
post
Stud
y
‘Kitche
nand
Coo
king
’Gam
eNA
Com
puterized
Kitche
nandCoo
king
’serious
gamewhich
challeng
esattention,executive
functio
n,andpraxis
4weeks
Interven
-tio
nen
dAtten
tion:TrailM
aking
TestA
VisualMem
ory:theVisual
Associatio
nTest
Executivefunctio
n:the
VictoriaStroop
Test
ADL:IADL,ADL
Sign
ificant
improvem
ent
inexecutivefunctio
n.Im
provem
entin
MCI>
AD.Lon
gertim
eplayed
correlated
with
better
executivefunctio
n
Styliadis,
2015
[34]
CCT
IG1:Long
-Lastin
gMem
ories(LLM
)Interven
tion:com-
bine
dcogn
itive
training
(CT)
and
physicaltraining
(PT)
IG2:CTalon
eIG3:PT
alon
e
CG1:Active
Con
trol
(AC)
(docum
entaries
view
ing)
CG2:Passive
Con
trol
LLM
training
system
CT
andPT
asfollows:CT:
Greek
adaptatio
nof
Brain
FitnessSoftware:6self-
pacedexercisesfocused
oncatego
ries:Atten
tion
andAud
itory
Processing
Speed.
PT:FFA
gameplatform
incorporatingNintend
oWIIbalancegames
8weeks
LLM
grou
p:Upto
10h/
week
PTgrou
p:Up
to5h/week
CTgrou
p:Up
to5h/week
ACgrou
p:Up
to5h/week
Interven
-tio
nen
dElectroe
ncep
halogram
(EEG
)measuresof
Cortical
activity
forde
lta,the
ta,
beta
1andbe
ta2band
s
N/A
Asign
ificant
training
effect
was
iden
tifiedin
theLLM
grou
prevealed
byEEGmeasuresbu
tno
training
effectson
the
MMSE
Barban,
2016
[39]
RCT
Process-based-
Cog
nitiveTraining
(pb-CT
)plus
reminiscence
therapy(RT)+rest
Reminiscence
therapy(RT)+
pb-CT
SOCIABLEsoftwareon
atouchscreen
compu
ter
containing
27games
design
edto
improve
functio
nin
7cogn
itive
domains:atten
tion,
executivefunctio
n,mem
ory,logical
reason
ing,
orientation,
lang
uage
,and
constructio
nalP
raxis
24*1h
treatm
ent
sessions,2
sessions/
weekfora
abou
t3mon
ths
Interven
-tio
nen
dMMSE
Mem
ory:RA
VLT;Executive
functio
n:Rey–Osterreith
Com
plex
Figu
reTest,
Phon
olog
icalVerbal
FluencyTest;Executive
functio
n:TrailM
akingTest
IADL
pb-CT:Sign
ificant
training
effectson
mem
oryin
MCI
subjectsandtheeffect
was
maintaine
dafter
reminiscencepe
riod;
Sign
ificant
training
effect
onMMSE
was
not
maintaine
ddu
ring
reminiscencepe
riod;
Med
ium
effect
sizes
Goo
ding
,2016
[35]
CCT
IG1:Com
puter
basedCog
nitive
Training
(cb-CT)
IG2:Cog
nitive
VitalityTraining
(CVT:cb-CT+
Neuropsycho
logical
andEducationalA
p-proach
toRemed
i-ation(NEA
R)
ActiveCon
trol
Group
(ACG)
cb-CT:BrainFitness:
repe
ated
drill-and
-practiceexercisesinvolv-
ingmem
ory,attention,
andexecutivefunctio
nswith
indo
main-specific
training
mod
ules
that
allow
foradaptivetrain-
ingwith
titrateddifficulty
levels.
SameCTexercises
delivered
with
ina
framew
orkthat
allowsfor
person
alization,individu
alcontrol,and
contextualizationof
exercises
30*60
min/
session,
twice/week
for16
weeks
4mon
ths
Intellectualfun
ctioning
:WRA
T-3;mMMSE;Verbal
learning
andMem
ory:the
BSRT,the
WMS-RLM
IandIIsubtests
Visuallearning
and
mem
ory:theWMS-RVis-
ualR
eprodu
ctions
(VR)
IandIIsubtests
Moo
d:de
pression
(BDI-II)
CVT
andcb-CTgrou
pshadim
provem
entsin
glo-
balcog
nitio
n,verbal
learning
,and
verbal
mem
ory;CVT
andcb-CT
hadsign
ificantlygreater
improvem
entsthan
ACG
inglob
alcogn
ition
,verbal
mem
ory,andverbal
learning
;Nosign
ificant
differencebe
tweencb-CT
andCVT;Large
stmoo
dim
provem
entin
CVT,sig-
nificantdifferencebe
-tw
eenCVT
andACGbu
tno
tbe
tweenCVT
andcb-
CT
Ge et al. BMC Geriatrics (2018) 18:213 Page 8 of 19
Table
2Overview
ofinclud
edstud
ies(Con
tinued)
Firstauthor
andyear
Stud
yde
sign
Interven
tionand
Techno
logy
Con
trol
Techno
logy
descrip
tion
Sessions/
Duration
Follow-up
Cog
nitiveou
tcom
emeasures
Other
outcom
emeasures
Keyfinding
s
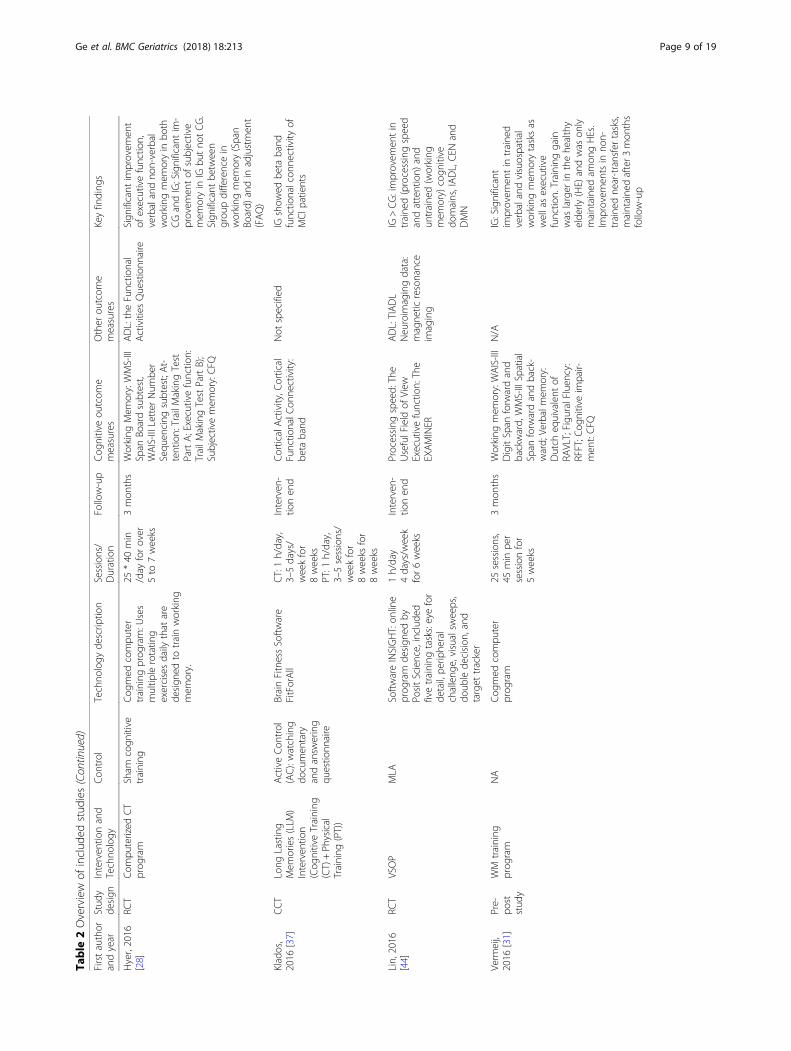
Hyer,2016
[28]
RCT
Com
puterized
CT
prog
ram
Sham
cogn
itive
training
Cog
med
compu
ter
training
prog
ram:U
ses
multip
lerotatin
gexercisesdaily
that
are
design
edto
trainworking
mem
ory.
25*40
min
/day
forover
5to
7weeks
3mon
ths
Working
Mem
ory:WMS-III
Span
Boardsubtest,
WAIS-IIILetterNum
ber
Sequ
encing
subtest;At-
tention:TrailM
akingTest
PartA;Executivefunctio
n:TrailM
akingTestPartB);
Subjectivemem
ory:CFQ
ADL:theFunctio
nal
Activities
Questionn
aire
Sign
ificant
improvem
ent
ofexecutivefunctio
n,verbalandno
n-verbal
working
mem
oryin
both
CGandIG;Significantim
-provem
entof
subjective
mem
oryin
IGbu
tno
tCG.
Sign
ificant
betw
een
grou
pdifferencein
working
mem
ory(Span
Board)
andin
adjustmen
t(FAQ)
Klados,
2016
[37]
CCT
Long
Lasting
Mem
ories(LLM
)Interven
tion
(Cog
nitiveTraining
(CT)+Ph
ysical
Training
(PT))
ActiveCon
trol
(AC):watching
documen
tary
andansw
ering
questio
nnaire
BrainFitnessSoftw
are
FitForAll
CT:1h/day,
3–5days/
weekfor
8weeks
PT:1
h/day,
3–5sessions/
weekfor
8weeks
for
8weeks
Interven
-tio
nen
dCorticalActivity,C
ortical
Functio
nalC
onne
ctivity:
beta
band
Not
specified
IGshow
edbe
taband
functio
nalcon
nectivity
ofMCI
patients
Lin,2016
[44]
RCT
VSOP
MLA
Softw
areINSIGHT:on
line
prog
ram
design
edby
PositScience,includ
edfivetraining
tasks:eyefor
detail,pe
riphe
ral
challeng
e,visualsw
eeps,
doub
lede
cision
,and
target
tracker
1h/day
4days/w
eek
for6weeks
Interven
-tio
nen
dProcessing
speed:
The
UsefulField
ofView
Executivefunctio
n:The
EXAMINER
ADL:TIADL
Neuroim
agingdata:
magne
ticresonance
imaging
IG>CG:improvem
entin
traine
d(processingspeed
andattention)
and
untraine
d(working
mem
ory)cogn
itive
domains,IADL,CEN
and
DMN
Verm
eij,
2016
[31]
Pre-
post
stud
y
WM
training
prog
ram
NA
Cog
med
compu
ter
prog
ram
25sessions,
45min
per
sessionfor
5weeks
3mon
ths
Working
mem
ory:WAIS-III
DigitSpan
forw
ardand
backward,
WMS-IIISpatial
Span
forw
ardandback-
ward;
Verbalmem
ory:
Dutch
equivalent
ofRA
VLT;Figu
ralFluen
cy:
RFFT;C
ognitiveim
pair-
men
t:CFQ
N/A
IG:Significant
improvem
entin
traine
dverbalandvisuospatial
working
mem
orytasksas
wellasexecutive
functio
n.Training
gain
was
larger
inthehe
althy
elde
rly(HE)
andwas
only
maintaine
dam
ongHEs.
Improvem
entsin
non-
traine
dne
ar-transfertasks,
maintaine
dafter3
mon
ths
follow-up
Ge et al. BMC Geriatrics (2018) 18:213 Page 9 of 19
Table
2Overview
ofinclud
edstud
ies(Con
tinued)
Firstauthor
andyear
Stud
yde
sign
Interven
tionand
Techno
logy
Con
trol
Techno
logy
descrip
tion
Sessions/
Duration
Follow-up
Cog
nitiveou
tcom
emeasures
Other
outcom
emeasures
Keyfinding
s
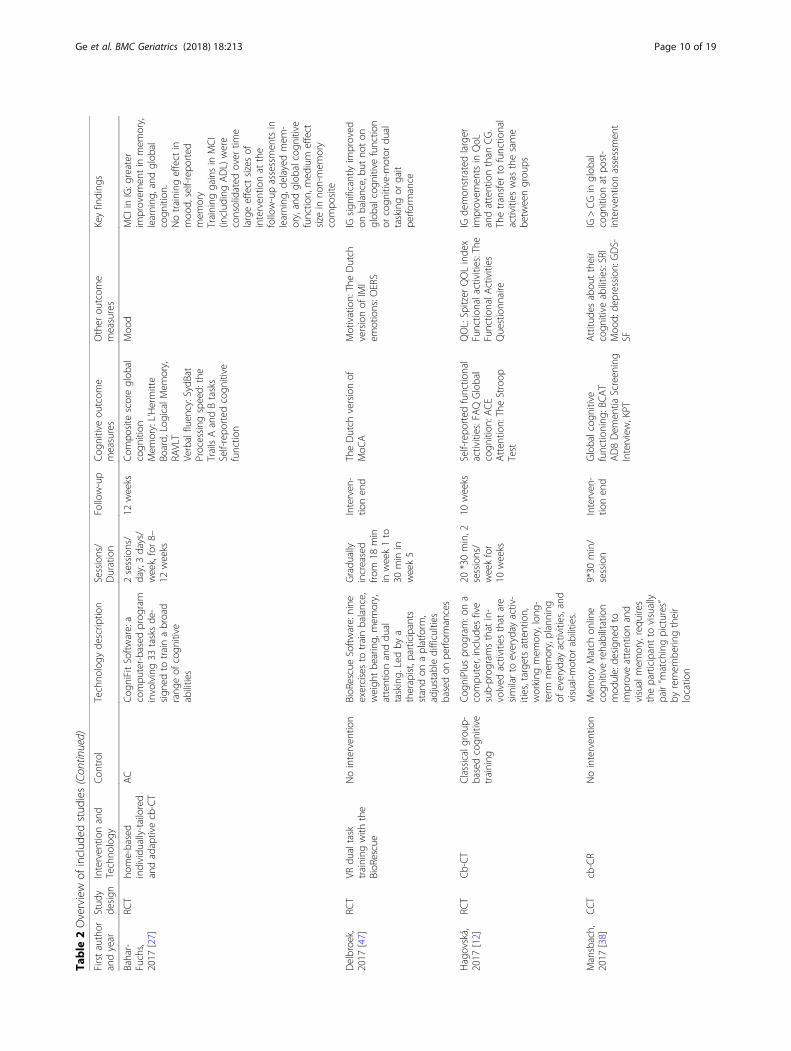
Bahar-
Fuchs,
2017
[27]
RCT
home-based
individu
ally-tailored
andadaptivecb-CT
AC
Cog
niFitSoftw
are:a
compu
ter-basedprog
ram
involving33
tasksde
-sign
edto
trainabroad
rang
eof
cogn
itive
abilities
2sessions/
day,3days/
week,for8–
12weeks
12weeks
Com
posite
scoreglob
alcogn
ition
Mem
ory:L’Hermitte
Board,
LogicalM
emory,
RAVLT
Verbalfluen
cy:SydBat
Processing
speed:
the
TrailsAandBtasks
Self-repo
rted
cogn
itive
functio
n
Moo
dMCI
inIG:g
reater
improvem
entin
mem
ory,
learning
,and
glob
alcogn
ition
.Notraining
effect
inmoo
d,self-repo
rted
mem
ory
Training
gainsin
MCI
(includ
ingADL)
were
consolidated
over
time
largeeffect
sizesof
interven
tionat
the
follow-upassessmen
tsin
learning
,delayed
mem
-ory,andglob
alcogn
itive
functio
n,med
ium
effect
size
inno
n-mem
ory
compo
site
Delbroe
k,2017
[47]
RCT
VRdu
altask
training
with
the
BioR
escue
Nointerven
tion
BioR
escueSoftw
are:nine
exercisesto
trainbalance,
weigh
tbe
aring,
mem
ory,
attentionanddu
altasking.
Ledby
atherapist,participants
standon
aplatform
,adjustabledifficulties
basedon
perfo
rmances
Gradu
ally
increased
from
18min
inweek1to
30min
inweek5
Interven
-tio
nen
dTheDutch
versionof
MoC
AMotivation:TheDutch
versionof
IMI
emotions:O
ERS
IGsign
ificantlyim
proved
onbalance,bu
tno
ton
glob
alcogn
itive
functio
nor
cogn
itive-m
otor
dual
taskingor
gait
perfo
rmance
Hagovská,
2017
[12]
RCT
Cb-CT
Classicalgrou
p-basedcogn
itive
training
Cog
niPlus
prog
ram:ona
compu
ter,includ
esfive
sub-prog
ramsthat
in-
volved
activities
that
are
similarto
everyday
activ-
ities,targe
tsattention,
working
mem
ory,long
-term
mem
ory,planning
ofeveryday
activities,and
visual-m
otor
abilities.
20*30min,2
sessions/
weekfor
10weeks
10weeks
Self-repo
rted
functio
nal
activities:FAQGlobal
cogn
ition
:ACE
Atten
tion:TheStroop
Test
QOL:Spitzer
QOLinde
xFunctio
nalactivities:The
Functio
nalA
ctivities
Questionn
aire
IGde
mon
stratedlarger
improvem
entsin
QoL
andattentionthan
CG.
Thetransfer
tofunctio
nal
activities
was
thesame
betw
eengrou
ps
Mansbach,
2017
[38]
CCT
cb-CR
Nointerven
tion
Mem
oryMatch
online
cogn
itive
rehabilitation
mod
ule:de
sign
edto
improveattentionand
visualmem
ory,requ
ires
theparticipantto
visually
pair“m
atchingpictures”
byremem
berin
gtheir
locatio
n
9*30
min/
session
Interven
-tio
nen
dGlobalcog
nitive
functio
ning
:BCAT
AD8Dem
entia
Screen
ing
Interview,KPT
Attitu
desabou
ttheir
cogn
itive
abilities:SRI
Moo
d:de
pression
:GDS-
SF
IG>CGin
glob
alcogn
ition
atpo
st-
interven
tionassessmen
t
Ge et al. BMC Geriatrics (2018) 18:213 Page 10 of 19
Table
2Overview
ofinclud
edstud
ies(Con
tinued)
Firstauthor
andyear
Stud
yde
sign
Interven
tionand
Techno
logy
Con
trol
Techno
logy
descrip
tion
Sessions/
Duration
Follow-up
Cog
nitiveou
tcom
emeasures
Other
outcom
emeasures
Keyfinding
s
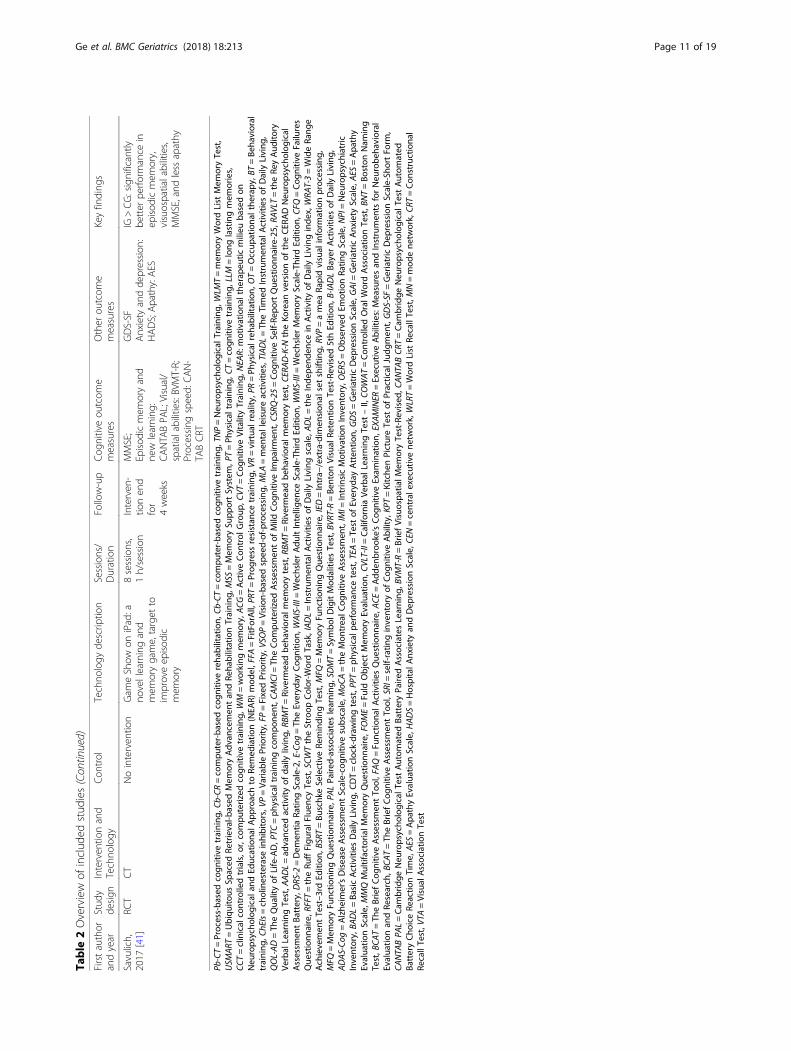
Savulich,
2017
[41]
RCT
CT
Nointerven
tion
Gam
eShow
oniPad:a
novellearningand
mem
orygame,target
toim
proveep
isod
icmem
ory
8sessions,
1h/session
Interven
-tio
nen
dfor
4weeks
MMSE;
Episod
icmem
oryand
new
learning
:CANTA
BPA
L;Visual/
spatialabilities:BVMT-R;
Processing
speed:
CAN-
TABCRT
GDS-SF
Anxiety
andde
pression
:HADS;Apathy:AES
IG>CG:significantly
better
perfo
rmance
inep
isod
icmem
ory,
visuospatialabilities,
MMSE,and
less
apathy
Pb-CT=Process-ba
sedcogn
itive
training
,Cb-CR
=compu
ter-ba
sedcogn
itive
reha
bilitation,
Cb-CT=compu
ter-ba
sedcogn
itive
training
,TNP=Neu
ropsycho
logicalT
raining,
WLM
T=mem
oryWordList
Mem
oryTest,
USM
ART
=Ubiqu
itous
Spaced
Retrieval-b
ased
Mem
oryAdv
ancemen
tan
dRe
habilitationTraining
,MSS
=Mem
orySu
pportSystem
,PT=Ph
ysical
training
,CT=cogn
itive
training
,LLM
=long
lastingmem
ories,
CCT=clinical
controlledtrials,o
r,compu
terized
cogn
itive
training
,WM=working
mem
ory,ACG
=ActiveCon
trol
Group
,CVT
=Cog
nitiv
eVitalityTraining
,NEA
R:motivationa
lthe
rape
uticmilieu
basedon
Neu
ropsycho
logicala
ndEd
ucationa
lApp
roachto
Remed
iatio
n(NEA
R)mod
el,FFA
=FitForAll,PR
T=Prog
ress
resistan
cetraining
,VR=virtua
lreality,PR
=Ph
ysical
reha
bilitation,
OT=Occup
ationa
lthe
rapy
,BT=Be
havioral
training
,ChEIs=cholinesterase
inhibitors,V
P=Va
riablePriority,FP
=FixedPriority,VSOP=Vision
-based
speed-of-processing,
MLA
=men
talleisure
activ
ities,TIADL=Th
eTimed
Instrumen
talA
ctivities
ofDaily
Living
,QOL-AD=Th
eQua
lityof
Life-AD,P
TC=ph
ysical
training
compo
nent,C
AMCI=Th
eCom
puterized
Assessm
entof
Mild
Cog
nitiv
eIm
pairm
ent,CS
RQ-25=Cog
nitiv
eSelf-Re
portQue
stionn
aire-25,
RAVLT=theRe
yAud
itory
Verbal
Learning
Test,A
ADL=ad
vanced
activ
ityof
daily
living,
RBMT=Riverm
eadbe
havioral
mem
orytest,R
BMT=Riverm
eadbe
havioral
mem
orytest,C
ERAD-K-N
theKo
rean
versionof
theCER
ADNeu
ropsycho
logical
Assessm
entBa
ttery,DRS-2
=Dem
entia
Ratin
gScale-2,
E-Co
g=Th
eEveryd
ayCog
nitio
n,WAIS-III=
WechslerAdu
ltIntellige
nceScale-Th
irdEd
ition
,WMS-III=WechslerMem
oryScale-Th
irdEd
ition
,CFQ
=Cog
nitiv
eFailures
Que
stionn
aire,R
FFT=theRu
ffFigu
ralF
luen
cyTest,SCW
TtheStroop
Color-W
ordTask,IADL=Instrumen
talA
ctivities
ofDaily
Living
scale,
ADL=theInde
pend
ence
inActivity
ofDaily
Living
inde
x,WRA
T-3=WideRa
nge
Achievemen
tTest–3
rdEd
ition
,BSRT=Bu
schk
eSelectiveRe
minding
Test,M
FQ=Mem
oryFu
nctio
ning
Que
stionn
aire,IED
=Intra−
/extra-dim
ension
alsetshifting,
RVP=amea
Rapidvisual
inform
ationprocessing
,MFQ
=Mem
oryFu
nctio
ning
Que
stionn
aire,P
ALPa
ired-associates
learning
,SDMT=Symbo
lDigitMod
alities
Test,B
VRT-R=Be
nton
Visual
RetentionTest-Revised
5thEd
ition
,B-IA
DLBa
yerActivities
ofDaily
Living
,ADAS-Co
g=Alzhe
imer’sDisease
Assessm
entScale-cogn
itive
subscale,M
oCA=theMon
trealC
ognitiv
eAssessm
ent,IMI=
IntrinsicMotivationInventory,OERS=ObservedEm
otionRa
tingScale,
NPI=Neu
ropsychiatric
Inventory,BA
DL=Ba
sicActivities
Daily
Living
,CDT=clock-draw
ingtest,P
PT=ph
ysical
performan
cetest,TEA
=Test
ofEveryd
ayAtten
tion,
GDS=GeriatricDep
ressionScale,
GAI=
GeriatricAnx
iety
Scale,
AES
=Apa
thy
Evalua
tionScale,
MMQMultifactoria
lMem
oryQue
stionn
aire,FOME=Fu
ldObjectMem
oryEvalua
tion,
CVLT-II=Califo
rnia
Verbal
Learning
Test
–II,CO
WAT=Con
trolledOralW
ordAssociatio
nTest,B
NT=Bo
ston
Nam
ing
Test,B
CAT=Th
eBriefCog
nitiv
eAssessm
entTo
ol,FAQ=Fu
nctio
nalA
ctivities
Que
stionn
aire,A
CE=Add
enbroo
ke’sCog
nitiv
eExam
ination,
EXAMINER
=ExecutiveAbilities:Measuresan
dInstrumen
tsforNeu
robe
havioral
Evalua
tionan
dRe
search,B
CAT=Th
eBriefCog
nitiv
eAssessm
entTo
ol,SRI=self-ratin
ginventoryof
Cog
nitiv
eAbility,KP
T=Kitche
nPictureTest
ofPractical
Judg
men
t,GDS-SF
=GeriatricDep
ressionScale-Sh
ortFo
rm,
CANTA
BPA
L=Cam
bridge
Neu
ropsycho
logicalT
estAutom
ated
BatteryPa
iredAssociatesLearning
,BVM
T-R=BriefVisuospa
tialM
emoryTest-Revised
,CANTA
BCR
T=Cam
bridge
Neu
ropsycho
logicalT
estAutom
ated
BatteryCho
iceRe
actio
nTime,AES
=Apa
thyEvalua
tionScale,
HADS=HospitalA
nxiety
andDep
ressionScale,
CEN=centrale
xecutiv
ene
twork,WLRT=WordList
RecallTest,M
N=mod
ene
twork,CR
T=Con
structiona
lRe
callTest,V
TA=Visual
Associatio
nTest
Ge et al. BMC Geriatrics (2018) 18:213 Page 11 of 19

Quality of the studiesAdditional file 1: Tables S2 and S3 summarize thequality assessment of the 26 eligible studies using the JBIcriteria, which included both randomized controlledtrials and quasi-experimental studies. Of these, 15 wererandomized controlled trials (Table 2), 6 were controlledclinical trials, 5 were pretest-posttest studies (Table 2).Among the RCT studies, only four articles [12, 25–27]
reported the procedure for randomization. Two studiesallocated the participants by utilizing computer-generatedrandom numbers [26, 27], while the other two studies[12, 25] randomized participants by having an independ-ent person use sealed envelopes. The remaining 11 articlesdid not report the randomization procedure used for allo-cating participants. Only three studies [26–28] reportedthat they were double-blinded sham-control trials.In the quasi-experimental studies, five studies [29–33]
utilized pretest-posttest design. The conveniencesamples and limited sample sizes (n = 10; n = 10; n = 22;n = 9; n = 11) restricted their generalizability. Six studiesutilized a controlled clinical trial design [13, 34–38]. Allthe studies lacked external validity due to use of
convenience samples or sampling methods that were notclearly described. Quasi-experimental studies whichlacked randomization also were limited by a potentialallocation bias.
Sample characteristics of the included studiesThe sample and design characteristics of each study aresummarized in Table 1. More than 40% of the includedstudies were published from 2016 to 2017 (n = 11).Studies were conducted in different countries: UnitedStates (n = 7), Italy (n = 3), Australia (n = 3), France (n = 2),Greece (n = 2), Canada (n = 1), Hong Kong (n = 1), UnitedKingdom (n = 1), Belgium (n = 1), Slavonia (n = 1), Spain(n = 1), South Korea (n = 1), and Netherlands (n = 1). Onlyone study [39] reported recruitment across multiplecountries.The total number of the participants with MCI included
in this systematic review was 1040. Seven studies includedboth participants living with MCI and those with othercognitive statuses (either individuals who were cognitivelynormal or individuals who had dementia), and reportedintervention effects for groups of MCI individuals. The
Fig. 1 PRISMA Flow Chart
Ge et al. BMC Geriatrics (2018) 18:213 Page 12 of 19

mean age ranged from 67.8 and 87.5. All but three studiesreported the criteria used to diagnose MCI. Petersoncriteria were used in 12 studies, International WorkingGroup (IWG) criteria were used in five studies, Albertcriteria were used in three studies, National Institute onAging and Alzheimer Association workgroup clinicalcriteria were used in two studies, and Monongahela-Youghiogheny Healthy Aging Team (MYHAT) CognitiveClassification criteria were used in one study.
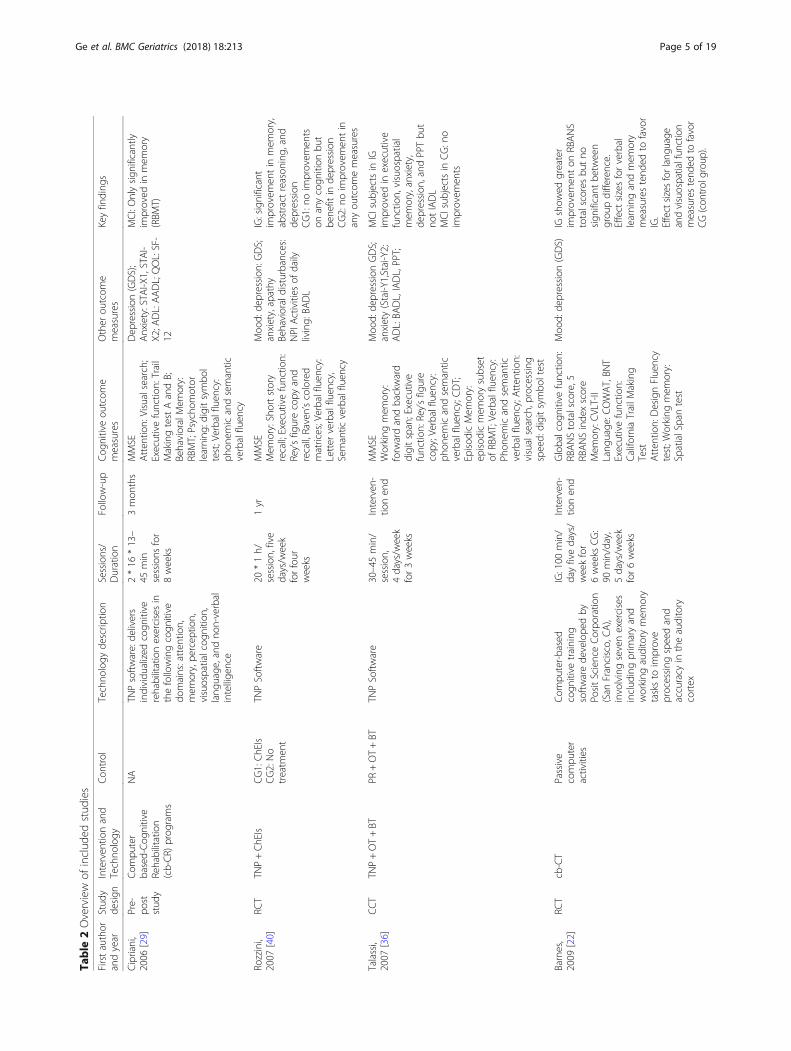
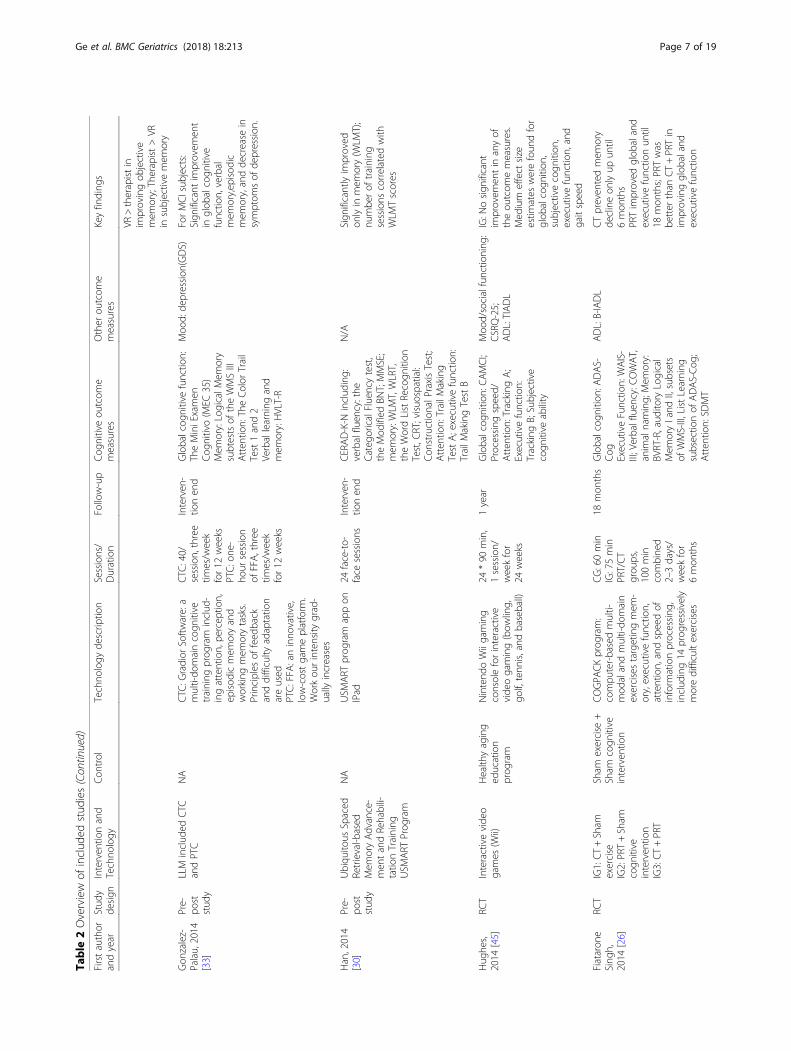
Characteristics of interventionsSingle-component interventionsThe majority of the studies (n = 18, or 69%) involvedsingle-component technology-based cognitive interven-tions (Table 2). Characteristics of the interventionsvaried widely. Seventeen different interventions wereutilized in the cognitive training programs studied (seedetails in Table 2).
Multimodal interventionsEight studies utilized multimodal interventions (Table 2).One approach was cognitive training combined withdifferent types of therapies [35, 36, 39, 40]; anotherapproach was cognitive training combined with physicaltraining [26, 33, 34, 37].
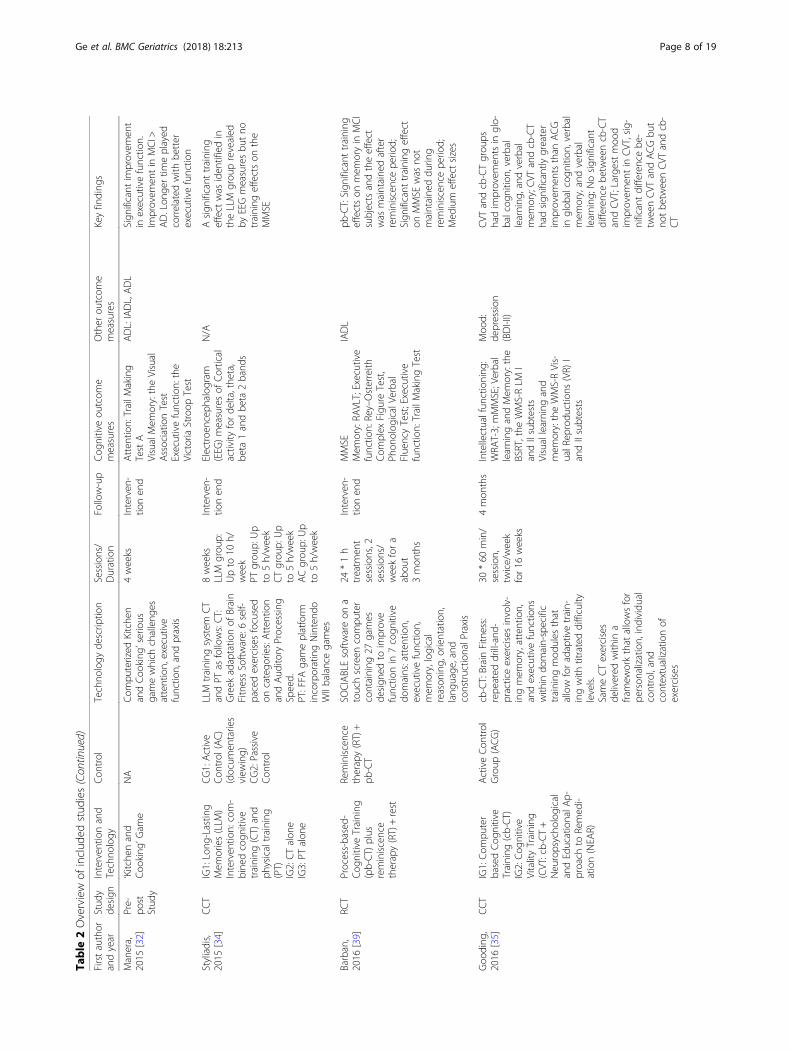
Cognitive training plus therapy Four studies combinedthe technology-based cognitive training with othertherapies as intervention, specifically reminiscence ther-apy [39], Neuropsychological and Educational Approachto Remediation (NEAR) [35], occupational therapy [36],and medications (cholinesterase inhibitors (ChEIs)) [40].Two types of software were involved in the cognitiveintervention component, including SOCIABLE [39], andNeuroPsychological Training (TNP) [36, 40]. The train-ing sessions lasted for a minimum of 3 weeks [36] to amaximum of 16 weeks [35].
Cognitive training combined with physical trainingFour studies examined the combined effects oftechnology-based cognitive and physical training. Twostudies used the Long-Lasting Memories (LLM) interven-tion to provide integrated cognitive and physical training[34, 37], and the physical component was delivered usingthe FitForAll platform. Gonzalez-Palau, et al. [33] alsoused the FitForAll platform to provide physical training,but used Gradior program to deliver the cognitivetraining. Singh and colleagues used Pneumatic resistancemachines (Keiser Sports Health Equipment, Ltd) toprovide progressive resistance training [26]. The length ofthese physical trainings lasted from 6 weeks [34] to6 months [26].
Overview of technologiesThe studies reviewed used the following types oftechnologies: traditional keyboard computers (n = 16),touch screen computers (n = 4), gaming consoles or plat-forms (n = 5), and tablets (n = 3). Gonzalez-Palau, et al.[33] and Styliadis [34] used both computer and gamingplatforms in their interventions. Since 2014, technologiesthat are more interactive and immersive (virtual reality,gaming console, exergaming platform) have been intro-duced in cognitive intervention studies.Compared to traditional therapist-led or pen and
paper cognitive interventions, technologies are “smarter”in tracking participants’ performances and adjusting theintervention difficulty. By applying technologies as adelivery method, researchers were able to record theparticipants’ performance throughout the interventionprocess. Thirteen studies tracked participants’ perform-ance as one of the outcome variables. Twelve studiesused intervention programs that could adjust the inter-vention difficulties to keep challenging the participants’abilities, as well as avoid distressing them with too manytraining failures.
Effects of interventionsCognitive outcomesGlobal cognitive function Twenty-two studies assessedthe effects of the interventions on global cognitivefunction (Table 2). Various instruments were used,including MMSE, Repeatable Battery for Assessment ofNeuropsychological Status (RBANS), ComputerizedAssessment of Mild Cognitive Impairment (CAMCI),Alzheimer’s Disease Assessment scale-cognitive subscale(ADAS-Cog), Brief Cognitive Assessment Tool (BCAT),Addenbrooke’s Cognitive Examination (ACE), MontrealCognitive Assessment (MoCA), Spanish version MMSE(MEC35), and composite score from measured cognitivedomains.Out of the 22 studies, eight studies found their inter-
vention significantly improved global cognitive functionamong individuals with MCI. These studies useddifferent cognitive interventions, all but one [20] ofthem were interventions targeting multiple cognitivedomains. Five studies used an active control group, andthree of them found a significant between-groupdifference in global cognition improvement. Barban, etal. [39] reported a significant treatment effect of a com-puterized multi-domain process-based cognitive train-ing combined with reminiscence therapy in MMSEmean scores (Cohen’s d = 0.44). Gonzalez-Palau, et al.[33] reported a significant improvement in globalcognitive function (MEC35) among MCI individualswho went through a multi-domain cognitive trainingprogram including both cognitive and physical trainingcomponents. Gooding, et al. [35] compared the
Ge et al. BMC Geriatrics (2018) 18:213 Page 13 of 19

computerized cognitive training and cognitive vitalitytraining to an active control group, and reported sig-nificantly larger improvements in both interventiongroups than the active control group in mMMSE meanscore [F (2, 71) = 11.56, p < 0.001, η2p ¼ 0.25] with a
medium effect size (Cohen’s d = 0.30 – 0.53). However,this training effect was not maintained at 3-monthfollow-up. Bahar-Fuchs, et al. [27] reported a signifi-cantly greater improvement in global cognition com-posite score in the training group than the activecontrol with a large effect size (Cohen’s d = 0.80). Onthe other hand, Barnes, et al. [22] found significantRBANS total score improvement in the interventiongroup after an auditory processing speed and accuracytraining, but the between-group difference comparedto the active controls was not significant (SD = 0.33).All the other three studies that did not use an activecontrol found significant between-group differences inchanges in global cognitive function [26, 38, 41].Two studies that compared the computer-based cogni-
tive training with listening to audio books, reading on-line newspapers, and playing a visuospatially-orientedcomputer game met the requirement for meta-analysis[22, 23]. The design of study, content of intervention,duration and length of follow-up were similar. A totalof 59 individuals were included in the meta-analysis.In Additional file 1: Figure S1, the pool weightedstandard mean difference score of RBANS total scorewas 1.62 (95% CI: -1.63 - 4.87). This result indicatedthat there was no significant difference in the effect-iveness for computer-based cognitive training in im-proving RBANS total score for individuals with MCIafter intervention.
Attention and working memory Eighteen studiesassessed the effects of technology-based cognitive train-ing or rehabilitative programs on attention/workingmemory, which are required for storage of new infor-mation. The most commonly used measures were thedigit span test. Other measures included the spatialspan test, Trail Making Test A and B, visual search,spanboard, dual task (digit span task + visual detec-tion task), subscale of Addenbrooke’s Cognitive Exam-ination, and Symbol Digit Modalities Test (SDMT).Out of 18 studies, eight studies reported significant
improvement in attention/working memory. Two studiescompared computerized training programs (CogmedSoftware) with no intervention or a sham cognitiveintervention [28, 31]. Significant improvements on span-board (p = .01) [28], digit span (p < .01) [31], and spatialspan (p < .05) [31] performance were observed at a3-month follow-up in the intervention group. Other inter-ventions included memory and attention training, variable
priority training, and vision-based speed-of-processingtraining. Significant improvements were found in digit spanforward ability (η2p= .14, p < .05) [42], accuracy (p = 0.001),
reaction time (p < .01) [43], spatial span (p = .003) [22] andworking memory (η2p = .28, p = .01) [44]. However, three
other studies that measured attention using digit span didnot report significant results [23, 33, 36].In terms of technologies used among the eight studies,
all of them applied computerized programs to deliverthe interventions. Specifically, they all used a keyboard,not a touch screen, to record the test responses.
Executive function Sixteen studies assessed the effectof technology-based cognitive intervention on executivefunction. Among them, six studies used the TrailMaking Task B, six studies used the phonemic and se-mantic fluency test, four studies used the Rey-OsterreithComplex Figure Test. Other measures included: WAISMatrices, Ruff Figural Fluency Test, Test of EverydayAttention (TEA), the intra−/extra-dimensional setshifting, and Executive Abilities: Measures and Instru-ments for Neurobehavioral Evaluation and Research(EXAMINER).Out of the 16 studies, nine studies reported significant
improvement in executive function [22, 26–28, 31, 32,36, 40, 44]. The interventions used in these studies in-cluded both multi-domain cognitive training, specifictraining tasks, and gaming. The length of interventionsranged from 3 [36] to 24 weeks [26]. Interestingly, threestudies used TNP software as an intervention compo-nent [29, 36, 40]; although the intervention lengthvaried, two out of the three studies found significant im-provement in executive function but used different mea-sures [36, 40]. Talassi [36] found that TNP integratedwith occupational therapy and behavioral therapy had asignificant improvement in the Rey-Osterreith ComplexFigure Test. Rozzini and Costardi [40] found that MCIindividuals receiving cognitive training and ChEIsreported significant improvements in Ravens ColouredProgressive Matrices post-intervention (p < 0.02). Thisbeneficial effect was not found when using TNP only[29]. However, both Talassi [36] and Rozzini [40] failedto report an effect size for their intervention effect.Other studies that demonstrated significant improve-ments in executive function varied greatly in terms ofsample size, intervention content, total interventiontime, and executive function measures.
Memory Nineteen studies assessed memory. Sixteen outof the 19 studies found a significant effect on memory.The measures of memory varied greatly. Major measuresincluded the Wechsler Memory Scale (WMS) and ReyAuditory Verbal Learning Test (RAVLT). Four studies
Ge et al. BMC Geriatrics (2018) 18:213 Page 14 of 19
used the WMS-III and three out of the four studiesfound significant improvements in memory after inter-vention. The intervention used in the three studies in-cluded Cogmed computer program [31], Game show oniPad [41], and LLM including both cognitive and physicaltraining components [33]. The intervention period rangedfrom 5 to 12 weeks and significant improvement in mem-ory was reserved until end of the three months’ follow-up[31]. The other study used GOPACK multi-domain cogni-tive training program to conduct a 6-month interventionbut did not find a significant improvement in memorymeasured by subsets of WMS-III [26]. Three studies usedRAVLT to measure verbal memory and all of them foundsignificant benefit of the cognitive interventions beingused [27, 31, 39]. The interventions included SOCIABLE,Cogmed, and CogniFit software programs, with the inter-vention lengths ranged from 5 to 12 weeks and follow-upperiod up to 3 months [27, 31]. Among the three trainingsoftware programs, Cogmed targeted on working memory,while the other two targeted on multiple cognitivedomains.Other studies that studied memory as an outcome
variable each used various measures including the12-word-list recall test from the BEM-144 memory bat-tery, the 16-item free and cued reminding test, BuschkeSelective Reminding Test, Hopkins Verbal LearningTest, Auditory Logical Memory, Short story recall,WMS-R Visual Reproductions I and II subtests, Patternrecognition memory, Benton Visual Retention Test,short story recall, Rivermead behavioral memory test,and Brief Visuospatial Memory Test-Revised. The inter-ventions of these studies lasted for 3 [36] to 16 weeks[35] with the follow-up time up to 6 months. All butone [32] of these studies demonstrated significantimprovements in memory. Manera et al. [32] found the4-week “kitchen and cooking game” intervention had nosignificant effect on improving memory.In terms of technologies, all but two studies used
computer to deliver the interventions and usedkeyboard to collect the data. Only two studies usediPad [41] and VR technology [38] to deliver theirmemory training programs.
Non-cognitive outcomesMood Nine studies assessed depression. The mostcommonly used measures were Geriatric DepressionScale (GDS) and its short form GDS-SF [22, 29, 33,36, 38, 40, 41], other inventory used included Beck’sDepression Inventory [35] and Depression Anxietyand Stress Scale [25]. Four studies reported significantreduction of depression among individuals with MCI[33, 35, 36, 40]. None of these studies reported effectsizes for their interventions reducing depression. Two
out of these four studies used a multimodal interven-tion that also integrated physical trainings [33, 36].Five studies assessed anxiety [25, 29, 36, 40, 41]. The
most often used measure was the State Trait AnxietyInventory (STAI) [29, 36] used in two studies. Only onestudy showed a significant reduction in anxiety for indi-viduals with MCI. Talassi used a multimodal interven-tion including cognition, behavioral, and occupationaltraining compared to its control group that had phys-ical rehabilitation, occupational, and behavioral train-ing, and found that the intervention group hadsignificant decrease in anxiety but not the controlgroup participants [36].
ADL Eleven studies assessed ADL as a secondary out-come. The Basic Advanced and Instrumental Activitiesof Daily Living scales were used in 5 studies [29, 36, 40,44, 45]. Other measures included the Functional Activ-ities Questionnaire [28], B-IADL scale [26], and HKLawton IADL [13]. Two out of nine studies reported astatistically significant improvement in ADL [27, 44].However, only one study found a significantbetween-group difference with a small to medium effectsize (η2 = 0.21) [44].
Quality of life Three studies assessed quality of life [12,29, 43]. Measures included SF-12 [29], Well-Being Scale[43] and Spitzer-QOL [12]. Only one study reportedsignificant results. Hagovská, et al. [12] found thattechnology-based cognitive training produced a largerimprovement in QoL than classical group-based cogni-tive training with a medium effect size (r = 0.69).
DiscussionIn the past decade, technology-based cognitive interven-tions have gained increased research interest worldwide.Almost half (42%) of the studies reviewed were pub-lished in 2016 and 2017, suggesting the growth in theimportance of technology-based interventions. The vastmajority of the studies were conducted in developedcountries, which may be associated with the limitedavailability of and familiarity with technology amongolder adults in lower income countries.The types of technology used varied across studies and
included computers, tablets, VR, and gaming consoles.Computers were the most widely used technology with77% using computers to assist delivery of cognitive inter-ventions. The majority utilized commercially availablesoftware or programs, with only nine of the studies usedtraining programs developed by the study researchersfor the specific study purpose. Therapists or coacheswere used to teach, assist, or even supervise the use oftechnologies along the intervention process. In nearlyhalf of studies (n = 12) therapists provided instructions
Ge et al. BMC Geriatrics (2018) 18:213 Page 15 of 19
at the beginning of the intervention, or provided helpthroughout the intervention. All but two studies wereconducted using only one type of technology, so no con-clusions can be drawn regarding the effect of differenttypes of technology on intervention results. Comparingeffects of technology across studies was not possible dueto the variability among interventions. With the rapiddevelopment of technologies, we can anticipate newtypes of technologies being utilized to assist cognitivetraining and rehabilitation interventions in the future.Overall, technology-based cognitive training and
rehabilitation have demonstrated promising beneficialeffects on various domains of cognition with moderate tolarge effect sizes. Most studies (e.g., [28, 31, 44]) assessedparticipants on different cognitive domains that were notlimited to the trained task, but also in other non-trainedtasks and other cognitive domains, suggesting a transfer-able beneficial effect of cognitive training and rehabilita-tion. For example, Hyer, et al. [28] found that workingmemory training also improved executive function amongtrained MCI participants, and the impact was preserveduntil the end of the 3-month follow-up. This transferabil-ity is consistent with previous systematic reviews [14, 15].However, the training gain and transferability of the train-ing gain varied by intervention (e.g., [22]) and deliverymethod (e.g., [13]). Therefore, future studies are stillneeded to understand which intervention would benefitvarious cognitive domains most efficiently.Only one study included in this review examined
whether applying technology as the delivery methodwould have a stronger effect on the intervention out-comes, in comparison to the use of a traditional manualdelivery. Man, et al. [13] compared the training effect of amemory training program delivered with a non-immersiveVR-based system versus with color-print images thatmatched the VR images. This study found that the VRgroup showed greater improvement in objective mem-ory but the non-VR group reported greater content-ment with memory performance, highlighting thepotential importance of receiving verbal and emo-tional support from training therapists on improvingparticipants’ satisfaction with their memory perform-ance. This study shows that depending on the out-comes that an intervention targets, technology-basedand manual trainings may have their own strengthsand weaknesses. No conclusions can be made whetherone type of intervention is generally more effectivethan the other.The effect of the same technology-based cognitive
intervention seems to vary between groups with differentlevel of cognitive decline. Some but still limited evidencesuggested that participants without cognitive impair-ment seem to obtain a larger cognitive improvementfrom technology-based cognitive interventions than
those with MCI. Vermeij, et al. [31] found that healthyparticipants had a larger gain in both trained workingmemory tasks and untrained executive function tasksthan those with cognitive impairment. However, thefindings are not conclusive. Barban, et al. [39] found thatprocess-based cognitive training improved verbal mem-ory among MCI participants and improved executivefunction among healthy participants. On the other hand,participants with MCI seem to gain a larger cognitivebenefit than those with Alzheimer’s disease (AD).Cipriani, et al. [29] fount that the TNP program signifi-cantly improved memory and global cognition amongparticipants with MCI, but only improved memoryamong those with AD. Similarly, Manera, et al. [32]found that the serious cooking game significantly im-proved executive function among participants with MCIbut not those with AD.Measures of physical function and mood were used in
most studies, but unfortunately most of these wereused to ensure non-biased randomization assignmentat baseline rather than as outcome measures, so wehave limited understanding of the effects oftechnology-based cognitive interventions on these out-comes. Nine studies evaluated mood (e.g., depression,anxiety) as an outcome, and eleven studies includedADL as an outcome variable. Among these, four studiesfound technology-based cognitive interventions hadbeneficial effect on mood and two studies found benefi-cial effect on functional activity. Technology-based cog-nitive training studies included in this review may havelimited impact on mood and functional activity.Two studies of technology-based cognitive training
and one study of technology-based cognitive rehabilita-tion examined the effect of their interventions on qualityof life [12, 29, 43]. However, only one of the four studiesreported significant result. Hagovská, et al. [12] foundthat technology-based cognitive training produced alarger improvement in QoL than classical group-basedcognitive training. This lack of effect of cognitive inter-vention on QoL is consistent with previous systematicreview on the efficacy of cognitive interventions on QoL[14]. However, each study used a different QoL instru-ments, and various research designs (e.g., types of inter-ventions, lengths of follow-up, and types of controlgroups). Given the limited number of studies conducted,future studies using comparable designs are still neededto further understand the effectiveness of the interven-tion on quality of life.A previous systematic review suggested that multimodal
cognitive inventions were a promising research area [15].In our review, we found eight studies that applied multi-modal interventions combining technology-based cogni-tive training and physical exercise or other therapeuticmethods. We expected to see the findings of these studies
Ge et al. BMC Geriatrics (2018) 18:213 Page 16 of 19

would provide support for speculation that multimodalcognitive interventions would produce a greater impacton improving cognitive function as well as mood andfunctional abilities. However, the eight reviewed articlesprovided insufficient evidence to support this conjecture.Five out of the eight studies were not designed to comparethe efficacy of multimodal cognitive intervention com-pared to cognitive intervention alone [33, 34, 36, 37, 39],and it was difficult to draw any conclusions from theremaining three studies remained due to the great vari-ability in the designs across studies. According to onestudy, customized technology-based cognitive trainingproduced additional benefit, and technology-based cogni-tive intervention plus ChEIs was superior to ChEIsalone [35]. Interestingly, Fiatarone-Singh, et al. [26]found that progressive resistance training producedmore improvement in executive function and globalcognition than both cognitive training and multimodalintervention including cognitive training and progres-sive resistance training. Findings from this study sug-gest that physical exercise may particularly benefitexecutive function, but that implementing multimodalcognitive and physical interventions may be toochallenging for people with MCI. Previous systematicreview on the efficacy of combined cognitive andexercise intervention in older adults with and withoutcognitive impairment did not find sufficient evidenceto confirm the beneficial effect among older adultswith cognitive impairment [46]. Taken together, morestudies are needed to understand the advantages of amultimodal cognitive intervention in individuals withMCI. Future studies should design appropriate controlgroups to understand the additional value producedby a multimodal cognitive intervention than a singlemodel intervention. Additionally, researchers shouldalso bear in mind the possibility that older adults withMCI may not be able to manage the cognitive chal-lenge associated with multimodal interventions.The studies reviewed generally had small sample sizes,
ranged widely from 10 [13] to 301 participants [39]. Theaverage sample size across studies was 54; 39% of thestudies had sample sizes of less than 30. The small sam-ple sizes may be related to the complicated diagnosticcriteria of MCI, the ethical challenges of conductingintervention studies in older adults with MCI, and thelimited availability of some technology-based cognitiveintervention programs. More importantly, potentialbeneficial effects of an intervention could be diminisheddue to a small sample size.The measures applied varied greatly across studies,
which created challenges in the comparison andgeneralizability of the study findings. Future studiesshould consider using measures that have been shown tohave good validity and reliability as well as have been
frequently used among the MCI population (e.g., CES-D,MMSE, QOL-AD, etc.). Neuroimaging techniques haveemerged to be more widely used to obtain information onhow technology-based cognitive interventions wouldaffect neural connectivity [37], activation [23], and brainatrophy [31].We conducted a comprehensive search of literature on
the topic area using five major databases. However, thissystematic review should be considered in light of itslimitations. We only reviewed articles in Englishlanguage. There may be other relevant studies that werepublished in other languages. We also need to be awarethat technology is developing rapidly so that promisingtechnology-based cognitive training and rehabilitationprograms may exist that have not yet been publisheddue to concerns about protecting participants.
ConclusionThe findings from this systematic review suggest thattechnology-based cognitive training and rehabilitationprograms show promise for improving cognitive function,with some interventions showing moderate to large effectsizes. Computers, tablets, gaming consoles and platforms,and VR systems were the common types of technologiesused. Both general and domain-specific cognitive traininghave led to improved cognition, primarily in memory, butwith some evidence that executive function may also bepositively affected. Studies that examined the impact ofcognitive training on improving mood and functional abil-ities, have generated less convincing evidence. Multimodalintervention programs integrated technology-basedcognitive intervention and other therapies have producedinconsistent findings on the superiority over only applyingtechnology-based single model cognitive intervention.Overall, technology-based cognitive training and rehabili-tation are promising intervention methods to improvecognitive function. Future studies should put effort to clar-ify whether the added benefits of implementing multi-modal interventions exist, and carefully consider thepotential extra burden caused to individuals with MCI.Additionally, future studies should aim to lessen the vari-abilities in intervention design and measures applied.
Additional file
Additional file 1: Table S1. Searching Strategy. Table S2. Results ofquality assessment based on JBI critical appraisal checklist for randomizedcontrolled trials*. Table S3. Results of quality assessment based on JBIcritical appraisal checklist for quasi-experimental studies*. Figure S1.Forest plot - RBANS score (computer-based intervention VS. Control).(DOCX 34 kb)
AbbreviationsACE: Addenbrooke’s Cognitive Examination; AD: Alzheimer’s disease; ADAS-Cog: Alzheimer’s Disease Assessment scale-cognitive subscale; BCAT: Brief
Ge et al. BMC Geriatrics (2018) 18:213 Page 17 of 19
Cognitive Assessment Tool; CAMCI: Computerized Assessment of MildCognitive Impairment; ChEIs: cholinesterase inhibitors; GDS: GeriatricDepression Scale; GDS-SF: Geriatric Depression Scale short form;IWG: International Working Group; JBI: Joanna Briggs Institute; LLM: Long-Lasting Memories; MMSE: Mini-mental state examination; MoCA: MontrealCognitive Assessment; MYHAT: Monongahela-Youghiogheny Healthy AgingTeam; NEAR: Neuropsychological and Educational Approach to Remediation;RAVLT: Rey Auditory Verbal Learning Test; RBANS: Repeatable Battery forAssessment of Neuropsychological Status; RCT: randomized controlled trial;SDMT: Symbol Digit Modalities Test; STAI: State Trait Anxiety Inventory;TEA: Test of Everyday Attention; TNP: Neuropsychological Training; VR: virtualreality; WMS: Wechsler Memory Scale
Availability of data and materialsAll data generated or analysed during this study are included in thispublished article [and its supplementary information files].
Authors’ contributionsSG designed and conducted the study, abstracted data, interpreted theresults, and played a major role in writing the manuscript. ZZ providedmethodological support, helped abstracted data, appraised quality, andhelped wrote a certain section of the manuscript. BW helped conceive thestudy and edited the manuscript. ESM helped conceive the study, screenedcitations and full-text articles, and edited the manuscript. All authors readand approved the final manuscript.
Ethics approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Duke University School of Nursing, 307 Trent Drive, Durham, NC, USA.2Fudan University School of Nursing, Shanghai, China. 3Fudan UniversityCenter for Evidence-Based Nursing, a Joanna Briggs Institute Center ofExcellence, Shanghai, China. 4New York University Rory Meyers College ofNursing, New York, NY, USA. 5Hartford Institute for Geriatric Nursing, NewYork University, New York, NY, USA. 6Geriatric Research, Education andClinical Center (GRECC) of the Department of Veterans Affairs Medical Center,Durham, NC, USA.
Received: 1 June 2018 Accepted: 27 August 2018
References1. Alzheimer's Disease International: World Alzheimer Report 2016. In.; 2016.2. Prince M, Guerchet M, Prina M. The epidemiology and impact of dementia:
current state and future trends. Geneva: World Health Organization; 2015.3. Gates NJ, Sachdev PS, Singh MAF, Valenzuela M. Cognitive and memory
training in adults at risk of dementia: a systematic review. BMC Geriatr.2011;11(1):55.
4. The White House Office of the Press Secretary: FACT SHEET: the whitehouse conference on Aging 2015. In.; 2015.
5. Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med.2004;256(3):183–94.
6. Feldman HH, Jacova C. Mild cognitive impairment. Am J Geriatr Psychiatry.2005;13(8):645–55.
7. Jean L, Bergeron M-È, Thivierge S, Simard M. Cognitive interventionprograms for individuals with mild cognitive impairment: systematic reviewof the literature. Am J Geriatr Psychiatry. 2010;18(4):281–96.
8. Zheng G, Xia R, Zhou W, Tao J, Chen L. Aerobic exercise amelioratescognitive function in older adults with mild cognitive impairment: a
systematic review and meta-analysis of randomised controlled trials.Br J Sports Med. 2016;50(23):1443.
9. Belleville S. Cognitive training for persons with mild cognitive impairment.Int Psychogeriatr. 2008;20(1):57–66.
10. Reijnders J, van Heugten C, van Boxtel M. Cognitive interventions in healthyolder adults and people with mild cognitive impairment: a systematicreview. Ageing Res Rev. 2013;12(1):263–75.
11. Faucounau V, Wu Y-H, Boulay M, De Rotrou J, Rigaud A-S. Cognitiveintervention programmes on patients affected by mild cognitiveimpairment: a promising intervention tool for MCI? J Nutr Health Aging.2010;14(1):31–5.
12. Hagovská M, Dzvoník O, Olekszyová Z. Comparison of two cognitivetraining programs with effects on functional activities and quality of life. ResGerontol Nurs. 2017;10:172–80.
13. Man D, Chung J, Lee G: Evaluation of a virtual reality-based memorytraining programme for Hong Kong Chinese older adults with questionabledementia: a pilot study. 2012.
14. Chandler MJ, Parks AC, Marsiske M, Rotblatt LJ, Smith GE. Everyday impactof cognitive interventions in mild cognitive impairment: a systematic reviewand meta-analysis. Neuropsychol Rev. 2016;26(3):225–51.
15. Coyle H, Traynor V, Solowij N. Computerized and virtual reality cognitivetraining for individuals at high risk of cognitive decline: systematic review ofthe literature. Am J Geriatr Psychiatr. 2015;23(4):335–59.
16. Hill NT, Mowszowski L, Naismith SL, Chadwick VL, Valenzuela M, Lampit A.Computerized cognitive training in older adults with mild cognitiveimpairment or dementia: a systematic review and meta-analysis.Am J Psychiatr. 2017;174(4):329–40.
17. Visser PJ, Kester A, Jolles J, Verhey F. Ten-year risk of dementia in subjectswith mild cognitive impairment. Neurology. 2006;67(7):1201–7.
18. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reportingitems for systematic reviews and meta-analyses: the PRISMA statement.PLoS Med. 2009;6(7):e1000097.
19. Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp L: Chapter 3: Systematicreviews of effectiveness. In: Joanna Briggs Institute Reviewer's Manual TheJoanna Briggs Institute, 2017. Edited by Aromataris E, Munn Z; 2017.
20. Nordmann AJ, Kasenda B, Briel M. Meta-analyses: what they can and cannotdo. Swiss Med Wkly. 2012;142:w13518.
21. Greco T, Zangrillo A, Biondi-Zoccai G, Landoni G. Meta-analysis: pitfalls andhints. Heart, lung and vessels. 2013;5(4):219.
22. Barnes DE, Yaffe K, Belfor N, Jagust WJ, DeCarli C, Reed BR, et al.Computer-based cognitive training for mild cognitive impairment:results from a pilot randomized, controlled trial. Alzheimer Dis AssocDisord. 2009;23:205–10.
23. Rosen AC, Sugiura L, Kramer JH, Whitfield-Gabrieli S, Gabrieli JD. Cognitivetraining changes hippocampal function in mild cognitive impairment: apilot study, vol. 2; 2011. p. 617–25.
24. RevMan. Copenhagen: the Nordic Cochrane Centre, the Cochranecollaboration. 5.3 ed; 2014.
25. Finn M, McDonald S. Computerised cognitive training for older personswith mild cognitive impairment: a pilot study using a randomisedcontrolled trial design. Brain Impairment. 2011;12(3):187–99.
26. Fiatarone Singh MA, Gates N, Saigal N, Wilson GC, Meiklejohn J, Brodaty H,et al. The study of mental and resistance training (SMART) study—resistancetraining and/or cognitive training in mild cognitive impairment: arandomized, double-blind, double-sham controlled trial. J Am Med DirAssoc. 2014;15(12):873–80.
27. Bahar-Fuchs A, Webb S, Bartsch L, Clare L, Rebok G, Cherbuin N, et al.Tailored and adaptive computerized cognitive training in older adults at riskfor dementia: a randomized controlled trial. J Alzheimers Dis.2017;60(3):889–911.
28. Hyer L, Scott C, Atkinson MM, Mullen CM, Lee A, Johnson A, et al. Cognitivetraining program to improve working memory in older adults with MCI.Clinical Gerontologist: The Journal of Aging and Mental Health.2016;39(5):410–27.
29. Cipriani G, Bianchetti A, Trabucchi M. Outcomes of a computer-basedcognitive rehabilitation program on Alzheimer's disease patients comparedwith those on patients affected by mild cognitive impairment. Archives ofGerontology & Geriatrics. 2006;43(3):327–35.
30. Han JW, Oh K, Yoo S, Kim E, Ahn KH, Son YJ, et al. Development of theubiquitous spaced retrieval-based memory advancement and rehabilitationtraining program. Psychiatry investigation. 2014;11(1):52–8.
Ge et al. BMC Geriatrics (2018) 18:213 Page 18 of 19
31. Vermeij A, Claassen JA, Dautzenberg PL, Kessels RP. Transfer andmaintenance effects of online working-memory training in normal ageing andmild cognitive impairment. Neuropsychol Rehabil. 2016;26(5–6):783–809.
32. Manera V, Petit PD, Derreumaux A, Orvieto I, Romagnoli M, Lyttle G, et al.‘Kitchen and cooking,’ a serious game for mild cognitive impairment andAlzheimer’s disease: a pilot study. Front Aging Neurosci. 2015;7:24.
33. Gonzalez-Palau F, Franco M, Bamidis P, Losada R, Parra E, Papageorgiou SG,et al. The effects of a computer-based cognitive and physical trainingprogram in a healthy and mildly cognitive impaired aging sample.Aging Ment Health. 2014;18(7):838–46.
34. Styliadis C, Kartsidis P, Paraskevopoulos E, Ioannides AA, Bamidis PD.Neuroplastic effects of combined computerized physical and cognitivetraining in elderly individuals at risk for dementia: an eLORETA controlledstudy on resting states. Neural plasticity. 2015;2015:172192.
35. Gooding AL, Choi J, Fiszdon JM, Wilkins K, Kirwin PD, van Dyck CH, et al.Comparing three methods of computerised cognitive training for olderadults with subclinical cognitive decline. Neuropsychol Rehabil.2016;26(5/6):810–21.
36. Talassi E, Guerreschi M, Feriani M, Fedi V, Bianchetti A, Trabucchi M.Effectiveness of a cognitive rehabilitation program in mild dementia (MD)and mild cognitive impairment (MCI): a case control study. Arch GerontolGeriatr. 2007;44:391–9.
37. Klados MA, Styliadis C, Frantzidis CA, Paraskevopoulos E, Bamidis PD. Beta-band functional connectivity is reorganized in mild cognitive impairmentafter combined computerized physical and cognitive training. FrontNeurosci. 2016;10:55.
38. Mansbach WE, Mace RA, Clark KM. The efficacy of a computer-assistedcognitive rehabilitation program for patients with mild cognitive deficits: apilot study. Exp Aging Res. 2017;43:94–104.
39. Barban F, Annicchiarico R, Pantelopoulos S, Federici A, Perri R, Fadda L, et al.Protecting cognition from aging and Alzheimer's disease: a computerizedcognitive training combined with reminiscence therapy. Int J GeriatrPsychiatry. 2016;31(4):340–8.
40. Rozzini L, Costardi D, Chilovi BV, Franzoni S, Trabucchi M, Padovani A.Efficacy of cognitive rehabilitation in patients with mild cognitiveimpairment treated with cholinesterase inhibitors. International Journal ofGeriatric Psychiatry: A journal of the psychiatry of late life and alliedsciences. 2007;22(4):356–60.
41. Savulich G, Piercy T, Fox C, Suckling J, Rowe JB, O'Brien JT, et al. Cognitivetraining using a novel memory game on an iPad in patients with amnesticmild cognitive impairment (aMCI). Int J Neuropsychopharmacol.2017;20:624–33.
42. Herrera C, Chambon C, Michel BF, Paban V, Alescio-Lautier B. Positive effectsof computer-based cognitive training in adults with mild cognitiveimpairment. Neuropsychologia. 2012;50(8):1871–81.
43. Gagnon LG, Belleville S. Training of attentional control in mild cognitiveimpairment with executive deficits: results from a double-blind randomisedcontrolled study. Neuropsychol Rehabil. 2012;22(6):809–35.
44. Lin F, Heffner KL, Ren P, Tivarus ME, Brasch J, Chen DG, et al. Cognitive andneural effects of vision-based speed-of-processing training in older adultswith amnestic mild cognitive impairment: a pilot study. J Am Geriatr Soc.2016;64:1293–8.
45. Hughes TF, Flatt JD, Fu B, Butters MA, Chang CCH, Ganguli M. Interactivevideo gaming compared with health education in older adults with mildcognitive impairment: a feasibility study. Int J Geriatr Psychiatry.2014;29(9):890–8.
46. Law LL, Barnett F, Yau MK, Gray MA. Effects of combined cognitive andexercise interventions on cognition in older adults with and withoutcognitive impairment: a systematic review. Ageing Res Rev. 2014;15:61–75.
47. Delbroek T, Vermeylen W, Spildooren J. The effect of cognitive-motor dualtask training with the biorescue force platform on cognition, balance anddual task performance in institutionalized older adults: a randomizedcontrolled trial. Journal of physical therapy science. 2017;29(7):1137–43.
Ge et al. BMC Geriatrics (2018) 18:213 Page 19 of 19




















