Systematic review of retention of pediatric patients on HIV treatment in low and middle-income...
10
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. Systematic review of retention of pediatric patients on HIV treatment in low and middle-income countries 2008–2013 Matthew P. Fox a,b,c and Sydney Rosen a,c Objectives: There are several published systematic reviews of adult retention in care after antiretroviral therapy (ART) initiation among adults, but limited information on pediatric retention. Design: Systematic review of pediatric retention on ART in low and middle-income countries during 2008–2013. Methods: We estimated all-cause attrition (death and loss to follow-up) and retention for pediatric patients receiving first-line ART in routine settings. We searched PubMed, Embase, Cochrane Register, and ISI Web of Science (January 2008–December 2013) and abstracts from AIDS and IAS (2008–2013). We estimated mean retention across cohorts using simple averages; interpolated any time period not reported to, up to the last period reported; summarized total retention in the population using Kaplan – Meier survival curves; and compared pediatric to adult retention. Results: We found 39 reports of retention in 45 patient cohorts and 55 904 patients in 23 countries. Among them, 37% of patients not retained in care were known to have died and 63% were lost to follow-up. Unweighted averages of reported retention were 85, 81, and 81% at 12, 24, and 36 months after ART initiation. From life-table analysis, we estimated retention at 12, 24, and 36 months at 88, 72, and 67%. We estimated 36- month retention at 66% in Africa and 74% in Asia. Conclusion: Pediatric ART retention was similar to that among adults. There were limited data from Asia, only one study from Latin America and the Caribbean, and no data from Eastern Europe, Central Asia, or the Middle East. ß 2015 Wolters Kluwer Health, Inc. All rights reserved. AIDS 2015, 29:000–000 Keywords: antiretroviral therapy, attrition, HIV, loss to follow-up, low and middle-income countries, meta-analysis, pediatric, retention, systematic review Introduction While the success of programs for prevention of mother- to-child transmission of HIV has meant that fewer children are being infected over time, a substantial number of children are still being born infected or are infected after birth through breastfeeding. The WHO estimates that under 300000 children were newly infected with HIV in 2012, down from a high of over 500 000 in the early 2000 [1]. With current treatment guidelines recommending earlier treatment for HIV-infected children [2], substantial resources will continue to be needed to be invested in pediatric HIV care and treatment programs over the coming decades. For children who initiate antiretroviral therapy (ART), treatment has been demonstrated to be highly effective, with substantially increased survival, in particular, when treatment is started early [3–6]. Retention in HIV care both before and after treatment initiation has received a great deal of attention in recent a Center for Global Health & Development, Boston University, b Department of Epidemiology, Boston University School of Public Health, Boston, Massachusetts, USA, and c Health Economics and Epidemiology Research Office, Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand. Correspondence to Matthew Fox, Crosstown Center, 3rd Floor, 801 Massachusetts Ave, Boston, MA 02118, USA. Tel: +1 617 414 1270; e-mail: [email protected] Received: 19 June 2014; revised: 28 November 2014; accepted: 3 December 2014. DOI:10.1097/QAD.0000000000000559 ISSN 0269-9370 Copyright Q 2015 Wolters Kluwer Health, Inc. All rights reserved. 1
Transcript of Systematic review of retention of pediatric patients on HIV treatment in low and middle-income...

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
Systematic review of retention of pediatric patients onHIV treatment in low and middle-income countries
2008–2013
Matthew P. Foxa,b,c and Sydney Rosena,c
Objectives: There are several published systematic reviews of adult retention in careafter antiretroviral therapy (ART) initiation among adults, but limited information onpediatric retention.
Design: Systematic review of pediatric retention on ART in low and middle-incomecountries during 2008–2013.
Methods: We estimated all-cause attrition (death and loss to follow-up) and retentionfor pediatric patients receiving first-line ART in routine settings. We searched PubMed,Embase, Cochrane Register, and ISI Web of Science (January 2008–December 2013)and abstracts from AIDS and IAS (2008–2013). We estimated mean retention acrosscohorts using simple averages; interpolated any time period not reported to, up to thelast period reported; summarized total retention in the population using Kaplan–Meiersurvival curves; and compared pediatric to adult retention.
Results: We found 39 reports of retention in 45 patient cohorts and 55 904 patients in23 countries. Among them, 37% of patients not retained in care were known to havedied and 63% were lost to follow-up. Unweighted averages of reported retention were85, 81, and 81% at 12, 24, and 36 months after ART initiation. From life-table analysis,we estimated retention at 12, 24, and 36 months at 88, 72, and 67%. We estimated 36-month retention at 66% in Africa and 74% in Asia.
Conclusion: Pediatric ART retention was similar to that among adults. There werelimited data from Asia, only one study from Latin America and the Caribbean, and nodata from Eastern Europe, Central Asia, or the Middle East.
! 2015 Wolters Kluwer Health, Inc. All rights reserved.
AIDS 2015, 29:000–000
Keywords: antiretroviral therapy, attrition, HIV, loss to follow-up, low andmiddle-income countries, meta-analysis, pediatric, retention, systematic review
Introduction
While the success of programs for prevention of mother-to-child transmission of HIV has meant that fewer childrenare being infected over time, a substantial number ofchildren are still being born infected or are infected afterbirth through breastfeeding. The WHO estimates thatunder 300 000 children were newly infected with HIV in2012, down from a high of over 500 000 in the early 2000[1]. With current treatment guidelines recommending
earlier treatment for HIV-infected children [2], substantialresources will continue to be needed to be invested inpediatric HIV care and treatment programs over thecoming decades. For children who initiate antiretroviraltherapy (ART), treatment has been demonstrated to behighly effective, with substantially increased survival, inparticular, when treatment is started early [3–6].
Retention in HIV care both before and after treatmentinitiation has received a great deal of attention in recent
aCenter for Global Health & Development, Boston University, bDepartment of Epidemiology, Boston University School of PublicHealth, Boston, Massachusetts, USA, and cHealth Economics and Epidemiology Research Office, Department of InternalMedicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand.Correspondence to Matthew Fox, Crosstown Center, 3rd Floor, 801 Massachusetts Ave, Boston, MA 02118, USA.Tel: +1 617 414 1270; e-mail: [email protected]: 19 June 2014; revised: 28 November 2014; accepted: 3 December 2014.
DOI:10.1097/QAD.0000000000000559
ISSN 0269-9370 Copyright Q 2015 Wolters Kluwer Health, Inc. All rights reserved. 1
Karla Ojeda
Karla Ojeda
Karla Ojeda

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
years [1]. For ART programs to achieve long-termsuccess, both mortality and loss to follow-up, for anyreason, must be minimized. In two reviews of retention incare of adult patients in sub-Saharan Africa, conducted in2007 [7] and 2010 [8], we found that overall retention incare at 24 months averaged 60–75% up to 2009. Thesereviews excluded children for two main reasons: wesuspected that factors influencing retention in pediatrictreatment programs differ from those affecting adultretention; and, more practically, few reports on pediatricretention had been published at the time of those reviews.
Realization that retention in adult treatment programswas poorer than expected led many researchers toinvestigate pediatric retention as well. The result has beena small flurry of papers published since 2008 that considerthis issue amongst children. With data now available, weconducted a systematic review of retention in pediatricART programs in all low and middle-income countries(LMICs) to help policy makers and program managersmake informed decisions about pediatric treatmentprogram design and resource allocation, and provideother researchers with estimates of pediatric retentionthat were drawn upon all available data.
Methods
We conducted this analysis of pediatric ARTretention as acomponent of a broader systematic review of retention inall populations in LMICs. As with our previous reviews,we sought to estimate attrition (defined as death and lossto follow-up) and retention for patients receiving first-line ART in routine service delivery settings World Bankdefined LMICs. For this analysis, we included any cohortswhere the reported mean or median age was below18 years. When possible, we excluded transfers to othertreatment sites from both the numerator and denominatorof our estimates, as the outcomes of patients who transfercare are unknown. Patients who stopped treatment butremained in care were counted as retained.
We included observational studies describing retention inHIV treatment programs published in 2008 or later. Weincluded cohorts receiving standard first-line ART at anytype or level of facility that followed prevailing nationaltreatment guidelines. We excluded clinical trials, inter-vention evaluations, and studies that provided care thatpatients would not have received under usual care. Weincluded standard-of-care arms from studies evaluatinginterventions in nonrandomized trials.
When multiple reports described a single cohort ofpatients, we chose the one with the most complete dataand/or the longest duration of follow-up. If a reportprovided data on multiple cohorts, we included it only ifthe data could be stratified by country and there was noother report of any of the cohorts individually. If such a
report disaggregated the data by cohort, only cohorts thatwere also reported in other sources were excluded,whereas the remaining cohorts were included. Werequired the report follow patients from ART initiationto a mean or median of 6 full months of follow-up.Studies had to report or provide enough information toestimate all-cause attrition (death and loss to follow-up)for one or more of the following endpoints: 6, 12, or 18months, or a later 12-month interval after treatmentinitiation. We placed no restrictions on how a cohortassessed mortality among patients lost.
To identify studies, we searched PubMed, Embase, theCochrane Register, and ISI Web of Science from 1January 2008 to 28 July 2013. We searched conferenceabstracts from AIDS and IAS conferences from 2008 to2013. We did not search the Conference on Retrovirusesand Opportunistic Infections as its website archives wereunavailable. We did not review data from prior to 2007 asso much has changed in the care and treatment ofpediatric HIV patients since then that we believed thedata would not be relevant to current policy debates onhow to address retention in care.
Within each index, we combined ‘antiretroviral’ and anyof ‘Africa’/’Asia’/’Central America’/‘Mexico’/’SouthAmerica’/’Middle East’/’Eastern Europe’/’CaribbeanRegion’, with any of the following: ‘retention’/’attri-tion’/’adherence’/‘mortality’/’loss to follow-up’/’effi-cacy’/or ‘evaluation’. Conference abstracts weresearched using ‘attrition,’ ‘retention’, or ‘loss to follow-up’.
We then conducted three secondary searches. First, tocapture journals that are not MeSH-indexed, we searchedagain in PubMed, substituting region names withindividual country names for all LMICs for which wedid not initially include at least two adult or pediatriccohorts. Second, we searched the PubMed to determineif any conference abstracts identified in the primary searchhad been published as full-text articles. Finally, werepeated each search in PubMed for the period from 1August 2013 to 9 January 2014, when the database for thesearch was closed.
M.F. supervised the search that was performed by twograduate research assistants, as well as determination ofeligibility. After excluding those whose titles were notrelevant, abstracts were read to determine eligibility. Full-text articles were then reviewed to confirm eligibility.S.R. confirmed the eligibility of sources for inclusion,and uncertainties were resolved through consensus ofboth authors.
Statistical analysisWe defined retention in care as follows: for cohortsreporting retention to a particular time point (either as aproportion or Kaplan–Meier estimate), retention at eachpoint was defined as the cohort’s report of all cause
2 AIDS 2015, Vol 00 No 00

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
retention; for cohorts that did not report retention atspecific time points, but provided data on the number ofpatients lost and who died, we defined retention as theproportion alive and in care and assigned this estimate tothe time closest to the median follow-up. We acceptedeach report’s own definition of loss to follow-up.
For analysis, countries were grouped into four regions:Africa (including North Africa); Asia (including Pacificisland states and the Middle East); Europe and CentralAsia (ECA); and Latin America and the Caribbean (LAC)(including South and Central America and Caribbeanisland states).
Analysis of retention proportions as reportedWe estimated mean retention across cohorts using simpleaverages unweighted by sample size. As each cohortreported to different time periods, we also interpolatedany time period not reported to, up to the last time periodreported. For example, if a cohort reported 12 and24-month retention, we interpolated 6 and 18-monthretention, assuming a linear decline between the twopoints. To look for potential reporting bias, we plottedthe mean values of retention over time by period reportedto, weighted by its sample size. This allowed us to assesswhether cohorts reporting to longer time periods weremore likely to report higher retention at earlier timeperiods than cohorts that reported to shorter timeperiods. We also conducted a linear regression ofretention at 12 and 24 months by cohort level factors,but as no important or significant associations wereidentified, we do not present these results.
Meta-analysis of retention ratesTo synthesize the data, we conducted a meta-analysisstratified by last time period reported to. We plotted eachretention estimate and its 95% confidence interval (CI) in aforest plot and combined estimates using a random-effectsregression with a Freeman and Tukey arcsine transform-ation [9]. We then created a patient-level dataset for eachstudy with all attrition occurring at the time periodattrition was reported. We then summarized total retentionusing Kaplan–Meier survival curves and estimatedretention at each time period using life-table analysis.We do not report CIs for this specific set of estimates as thesample size creates misleadingly narrow intervals.
Sensitivity analysisWe then plotted mean retention by last time periodreported to assess whether cohorts reporting to longer timeperiods were more likely to report higher retention atearlier time periods than cohorts that reported to shortertime periods. To suggest upper and lower bounds on trueretention rates given the varying time periods reported to,we conducted a sensitivity analysis to consider the best andworst-case scenarios for retention. In the best-casescenario, we assume all no additional attrition from thelast period reported to through 60 months. In the worst-
case scenario, we assumed retention continued along thesame linear trend to what was observed between baselineand the last time period reported to.
Results
Our primary search for the overall review (all popu-lations) identified 3517 potentially relevant articles and6846 abstract citations. Our secondary search added 1236more citations. Of these, 39 sources met the inclusioncriteria for this analysis of pediatric retention (30 articles,9 abstracts) (Appendix 1, http://links.lww.com/QAD/A624). The citations reported on 55 904 patients enrolledin 45 separate cohorts, as described in Table 1. Thevarious definitions used by each cohort are provided inAppendix 2 (http://links.lww.com/QAD/A624).
The eligible studies came from 23 countries in three ofthe four regions: 17 from Africa (37 cohorts), 5 fromSouthern and Eastern Asia (7 cohorts), and 1 from LatinAmerica and the Caribbean (LAC) (1 cohort). No studywas reported from Europe or Central Asia, so this regionwill not be included in further analysis. Because we onlyfound one cohort from Latin America and the Caribbean,disaggregation by region will include only Africa andAsia. Most cohorts (82%) were from Africa. WithinAfrica, 32% of the cohorts, and just over one quarter of allcohorts in the review, were from South Africa. Thedistribution of individual patient numbers was not quiteas skewed: South Africa contributed just over 13 000patients, or 27% of the total from Africa, but Kenya andMozambique were also well represented, with 8000–9000 patients (17–19%) each. In Asia, two cohorts eachwere identified from Thailand and Vietnam, withThailand contributing half of all participants from Asia.
The average patient age was 5.2 years at ART initiation.There was no evidence of a trend toward starting ART atyounger ages over calendar time; average age at initiationwas between 5 and 8 years in every year from 2002 to2009. The average CD4þ percentage at initiation was12.7%. About half of the patients were female, withalmost no variation by region. Most (60%) cohortsreported to less than 2 years after ART initiation (n¼ 24).
Retention on antiretroviral therapyTable 2 details the proportion of patients who died orwere lost to follow-up from each cohort by the end of thatcohort’s follow-up period. For cohorts that reported bothdeaths and losses to follow-up (n¼ 34), a simple average(not weighted by cohort size) of 37% of all patients notretained in care were known to have died, whereas theremaining 63% were lost to follow-up.
Retention in care at each time period reported to, bycountry, is presented in Table 3, and Appendix 3 (http://links.lww.com/QAD/A624) illustrates retention rates
Review of pediatric antiretroviral therapy retention Fox and Rosen 3

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
and 95% CIs at 12, 24, and 36 months using forest plots.Simple average retention over time for select time pointsis plotted in Appendix 4 (http://links.lww.com/QAD/A624). Simple average retention rates with no interp-olation of missing values across all regions averaged 85% at12 months, 81% at 24 months, and 81% at 36 months.Because different cohorts reported to different timeperiods, however, retention can increase over time ashappens at months 12 and 24 for Asian cohorts. Reportedretention rates were higher at later time periods in Asiacompared to Africa.
To assess publication bias, we plotted weighted averageattrition rates stratified by last time point reported to.As Appendix 5 (http://links.lww.com/QAD/A624)shows, studies with shorter periods of follow-up alsoreported higher attrition at any given time point than didstudies with longer follow-up. Studies reporting onlyto 12 months, for example, retained an average of 85%of their patients at 12 months, whereas those reportingto 36 months retained an average of 90% of their patientsat 12 months, suggesting that actual retention at latertime points would be lower than the averages shown, had
4 AIDS 2015, Vol 00 No 00
Table 1. Characteristics of cohorts included in the review by regionM.
Study code Reference
Yearof
reportFacilities
(n) Sector
Yearsof
cohortenrollment
Patientsstartedon ART
(n)
Medianage
(years)Female
(%)
Medianstarting
CD4þ cellcount
(cells/ml)MedianCD4þ%
AfricaBotswana 1 Gomilla [10] 2011 1 2008–2009 38 4 60%Cote d’Ivoire 1 Auld [11] 2011 29 2004–2008 2110 46% 11%DRC 1 Edmonds et al. [12] 2011 2 2004–2010 619 6 53% 15%Ethiopia 1 Asfawesen et al. [13] 2011 1 Public 2005–2008 188 6 51% 236Ethiopia 2 Koye et al. [14] 2012 1 Public 2006–2011 549 6 48%Ethiopia 3 Hagstromer et al. [15] 2013 6 Public 2007–2012 974Gambia 1 Okomo et al. [16] 2012 1 Public 2004–2009 70 5 48% 390 13%Kenya 1 McNairy et al. [17] 2013 69 2005–2011 5710 5 50% 222 16%Kenya 2 Nyandiko et al. [18] 2013 65 Public 2001–2009 3255 5 49% 18%Kenya 3 Sivapalasingam et al. [19] 2014 NGO 2005–2008 130 5 46%Lesotho 1 Cohen [20] 2009 15 Public 2006–2008 283Malawi 1 Ardura Garcia [21] 2012 1 2006–2010 985Malawi 2 Weigel et al. [22] 2010 1 Public 2001–2006 497 8 49%Mali 1 Germanaud et al. [23] 2010 2 2006–2007 105 3 46% 491Mozambique 1 Fenner et al. [24] 2010 1 Public 1999– 854 1 49% 12%Mozambique 2 McNairy et al. [17] 2013 31 2005–2011 7226 5 53% 265 15%Nigeria 1 Omoni et al. [25] 2013 2 2008–2009 150Rwanda 1 Tene et al. [26] 2013 39 Public, private 2004–2010 2035 6 48%Rwanda 2 van Griensven et al. [27] 2008 2 Public 2003–2007 315 7 50% 14%South Africa 1 Kaplan [28] 2009 1 Public 2002–2008 140 312South Africa 2 Sengayi et al. [29] 2013 1 Public 2004–2011 4470 4 49% 15%South Africa 3 Chhagan et al. [30] 2012 1 Public 2006–2009 151 5 49% 13%South Africa 4 Colvin[31] 2009 3 Public 2001–2007 583 3 48%South Africa 5 Barth et al. [32] 2011 1 NGO 2003–2007 101 5 57% 244 11%South Africa 6 Janssen et al. [33] 2010 19 Public 2004–2008 477 6 48% 433 17%South Africa 7 Zanoni et al. [34] 2011 1 Semi-private 2003–2008 537 6 51% 226South Africa 8a Fenner et al. [24] 2010 1 Public 1999– 560 4 48% 13%South Africa 8b Fenner et al. [24] 2010 1 Public 1999– 764 8 51% 11%South Africa 8c Fenner et al. [24] 2010 1 Public 1999– 1125 3 48% 12%South Africa 9 Meyer-Rath et al. [35] 2013 2 Public 2008–2011 288 5 13%South Africa 10 Fatti et al. [36] 2014 - Public 2004–2010 3871 6 50% – 12%Tanzania 1 McNairy et al. [17] 2013 50 - 2005–2011 2606 5 51% –265 15%Tanzania 2 Mwiru et al. [37] 2013 1 NGO 2004–2010 3144 – 50% – –Uganda 1 Kiboneka et al. [38] 2008 10 Public 2008 770 9 54% 12 –Zambia 1 Scott et al. [39] 2013 6 Public, private, NGO 2006–2011 1334 4 - – 14%Zambia 2 Sikazwe [40] 2011 1 Public 2004–2010 163 5 50% – –Zimbabwe 1 Fenner et al. [24] 2010 1 Private 1999– 699 2 49% – 15%
AsiaCambodia 1 Isaakidis et al. [41] 2010 2 Public 2003–2007 673 6 48% 190 11%China 1 Zhao et al. [42] 2013 Public 2005–2010 1818 6 43% 9%India 1 Rajasekaran et al. [43] 2009 1 Public 2004–2006 295 8 44%Thailand 1 Collins et al. [44] 2010 40 Public 1999–2009 597 7 53% 165 7%Thailand 2 McConnell et al. [45] 2010 380 Public 2000–2005 3409 7 53% 104 5%Vietnam 1 Duong[46] 2010 4 Public 2005–2008 789 - - – –Vietnam 2 Lu [47] 2010 2 Public 2006–2008 252 3 45% – 11%
LACBrazil 1 Souza et al. [48] 2011 1 Public 1987–2007 195 3 52%
ART, antiretroviral therapy; LAC, Latin America and the Caribbean.

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
all studies followed their cohorts to those later timepoints.
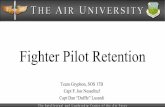
Meta-analysis of antiretroviral therapy retentionTo pool the data from all time points, we plotted Kaplan–Meier survival curves using the interpolated data by agegroup and region, as shown in Fig. 1a–c. We regard theseas our most accurate estimates of retention, as they takeinto account the different time periods that studiesreported to. Using life-table analysis, we estimate that 1,
2, and 3-year retention rates at 88, 72, and 67%,respectively, similar to what we observed in adults, forwhom our estimates for the same time periods were 83,74, and 68%, respectively [49]. Estimates for the pediatriccohorts did vary by region, with 3-year retentionaveraging 74% in Asia and 66% in Africa.
Sensitivity analysisBecause of the potential for publication bias identifiedabove, simple averages at each time point may
Review of pediatric antiretroviral therapy retention Fox and Rosen 5
Table 2. Median follow-up and rates of patient attrition, as reported, from antiretroviral therapy programs.
Study code
Medianfollow-up(months)
Died(A)
Lost tofollow-up
(B)
Total attritionfrom ART
(C)a
Totalretained
(D)
Transferredcare(E)
Total retainedat original site
(F)
AfricaBotswana 1 12.0 0.0% 2.6% 2.6% 97.4% – 97.4%Cote d’Ivoire 1 – – – – – – –DRC 1 36.9 8.2% 7.9% 16.2% 83.8% – 83.8%Ethiopia 1 24.0 7.2% 3.3% 10.6% 89.4% 4.3% 85.2%Ethiopia 2 22.0 9.0% 7.0% 16.0% 84.0% 16.8% 67.3%Ethiopia 3 34.2 3.6% 21.5% 25.2% 74.8% 15.2% 59.6%Gambia 1 18.2 11.6% 17.4% 29.0% 71.0% 1.4% 69.6%Kenya 1 19.6 – – – – – –Kenya 2 21.6 2.7% 17.4% 20.1% 79.9% – 79.9%Kenya 3 11.8 8.9% 22.0% 30.9% 69.1% 5.4% 63.7%Lesotho 1 12.0 4.9% 2.1% 7.1% 92.9% – 92.9%Malawi 1 24.4 1.8% 20.4% 22.2% 77.8% 4.3% 73.4%Malawi 2 23.4 5.8% 38.8% 44.6% 55.4% 27.4% 28.0%Mali 1 6.0 9.0% 20.0% 29.0% 71.0% 4.8% 66.2%Mozambique 1 8.7 26.0% 14.8% 40.9% 59.1% 45.6% 13.6%Mozambique 2 19.6 – – – – – –Nigeria 1 12.0 2.7% 7.4% 10.1% 89.9% 1.3% 88.5%Rwanda 1 31.2 6.8% 2.6% 9.3% 90.7% 21.5% 69.2%Rwanda 2 24.0 2.8% 4.2% 7.0% 93.0% 9.5% 83.5%South Africa 1 – – – – – – –South Africa 2 18.5 3.6% 17.1% 20.7% 79.3% 11.1% 68.2%South Africa 3 24.0 4.3% 9.3% 13.6% 86.4% 7.3% 79.1%South Africa 4 – – – – – –South Africa 5 31.0 – – 26.1% 73.9% 8.9% 65.0%South Africa 6 18.4 6.9% 3.9% 10.8% 89.2% 2.5% 86.7%South Africa 7 22.0 10.1% 3.9% 14.0% 86.0% 13.4% 72.6%South Africa 8a 24.3 2.2% 7.3% 9.5% 90.5% 9.8% 80.7%South Africa 8b 12.1 4.9% 16.4% 21.4% 78.6% 22.8% 55.9%South Africa 8c 24.4 1.3% 14.0% 15.3% 84.7% 1.5% 83.2%South Africa 9 24.0 4.2% 13.5% 17.7% 82.3% 0.0% 82.3%South Africa 10 24.0 3.0% 5.0% 8.0% 92.0% – 92.0%Tanzania 1 19.6 – – – – – –Tanzania 2 17.2 8.5% – 8.5% 91.5% – 91.5%Uganda 1 12.4 2.3% 0.0% 2.3% 97.7% – 97.7%Zambia 1 12.0 – – – – – –Zambia 2 – – – – – – –Zimbabwe 1 18.9 15.8% 8.0% 23.8% 76.2% 39.2% 37.0%
AsiaChina 1 24.4 5.1% 10.6% 89.4% –India 1 10.0 8.1% 11.9% 88.1% –Thailand 1 53.0 7.0% 15.1% 84.9% –Thailand 2 20.4 8.9% 19.1% 80.9% –Vietnam 1 – – – – 3.7%Vietnam 2 15.0 11.5% 17.3% 82.7%
LACb
Brazil 1 58.8 – 47.7% 52.3% 12.0%Simple averages 21.8 6.7% 10.4% 17.8% 82.2% 11.9% 74.3%Weighted averages 21.2 5.9% 11.0% 16.2% 83.8% 14.6% 69.2%
ART, antiretroviral therapy; LAC, Latin America and the Caribbean.aCalculations: C¼AþB; D¼1#C; F¼D# E.bThe data could not be determined from the report.

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
overestimate true retention in care. We thus alsoundertook a sensitivity analysis in which we modeledexpected attrition under best-case and worst-casescenarios, and a midpoint scenario as the average ofthe two (Fig. 2). As we also see with adults, there is littlevariation among the three scenarios up to 24 months onART. By 36 months, the difference widens, and itcontinues to expand for the duration of the periodanalyzed. The midpoint estimate of retention at36 months is 71%. The worst and best-case estimatesat the same time point are 66 and 77%, respectively. Theseestimates are slightly higher than those for adults, forwhom we estimated midpoint, worst, and best-caseretention at 36 months of 67, 62, and 72%, respectively.
Discussion
The review of retention in care among pediatric patientsincluded 55 904 patients from 45 cohorts in 23 LMICsbetween 2008 and 2013. It found that average retentionin care across all the cohorts, using life-table analysis (ourbest estimate of overall programmatic retention), was 88,72, and 67% at 12, 24, and 36 months after ARTinitiation. In a sensitivity analysis that estimated the bestand worst-case scenarios for long-term outcomes,36-month retention did not vary dramatically, rangingfrom 66% in the worst case to 77% in the best case. Wedid find some variation in retention across regions, with
36-month retention estimated by life-table analysis inAsia at 74% and only 66% in Africa.
There are no other reviews with which to compare ourfindings, but pooled pediatric cohorts from Africa andAsia have been published. In 2008, the KIDS ART-LINCcohort reported outcomes from a pooled cohort ofroughly 2400 children in sub-Saharan Africa whoinitiated ART in 2006 or earlier. They found that2-year mortality and loss to follow-up was 6.9 and 10.3%respectively, summing to 2-year retention of 83%, whichis somewhat better than our estimate of 72% at 24 monthsfor African cohorts. Whether this difference reflects aworsening of retention over calendar time or is merely anartifact of the specific cohorts included in our review andin the pooled KIDS ART-LINC cohort is unclear. ForAsia, in contrast, the TREAT Asia Pediatric HIVObservational Database – a pooled cohort of 1655children in seven Asian countries – reported 5% mortalityand 4% loss to follow-up, or 91% retention at 12 monthsafter initiation [3], in which case we estimated 97% forAsian cohorts. In both the TREAT Asia study and ourreview, however, attrition increased substantially in lateryears, with TREAT Asia reporting retention of 68% at5 years after initiation, which is nearly identical to ourlife-table estimate of 67% at 5 years.
Retention rates for children appear very similar to thosefound in our recent review of adults in LMICs over the
6 AIDS 2015, Vol 00 No 00
Table 3. Summary of retention at specified time points after antiretroviral therapy initiation by country.
Country
Months on antiretroviral therapy
6 12 18 24 36 48 60
AfricaBotswana 97%Cote d’Ivoire 84% 79% 77% 73%DRC 84%Ethiopia 92% 90% 89% 75% 71%Gambia 71%Kenya 78% 79%Lesotho 93%Malawi 67%Mali 71%Mozambique 59% 71% 62%Nigeria 90%Rwanda 95% 93%South Africa 82% 89% 86% 85% 87%Tanzania 75% 67% 33%Uganda 98%Zambia 90% 81% 76% 74% 68%Zimbabwe 76%
AsiaCambodia 93% 91%China 89%India 88%Thailand 81% 85%Vietnam 84%
LACBrazil 52%Total 81% 85% 79% 81% 81% 74% 61%
ART, antiretroviral therapy; LAC, Latin America and the Caribbean.

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
same time, among whom retention averaged 83, 74, and68% at 12, 24, and 36 months, respectively [49]. Unlikefor adults, however, we could not accurately estimateretention beyond 36 months due to the limited samplesize. We identified only seven reports in this review thatpresented retention beyond 36 months, and only about10 000 patients still in care beyond 36 months. Amongadults, attrition is generally high in the first 1–2 years aftertreatment initiation; then it slows dramatically. Here, wesee that same high rate of early attrition, but trends in lateryears, are unclear. Both our review and the TREAT Asiastudy described above found continuing high rates ofattrition in later years, whereas the KIDS ART-LINCcohort saw attrition fall dramatically from year 1 to year 2.Future research should aim for more long-term reportson pediatric outcomes, to help guide allocation ofresources toward the time when retention support isneeded most.
The reports included in this review were publishedbetween 2008 and 2013. Because of delays in publication,
the data generally reflect cohorts that began enrolling inor after 2004 and ended in or before 2009. These data canthus serve as a baseline against which future research canmeasure the impact of changes in guidelines for care ofpediatric patients. For example, in this review, the medianage at initiation of therapy was 5 years. In 2010, theWHO, acting on the results of the CHER trial [50], calledfor immediate initiation of treatment as soon as HIV wasdetected in pediatric patients [2]. It will be important toexamine in future reviews if the median age at initiationdrops as more countries enact this recommendation. Ourreview identified significant gaps in the literature aboutretention in care for pediatric patients. We identified only39 studies eligible for inclusion, covering just 23countries of the nearly 140 that fall into the low ormiddle-income categories. As with adults, we identifiedno study that met our inclusion criteria from the MiddleEast, Central Asia, or Eastern Europe, and only one fromLatin America and the Caribbean. In addition, most ofthe cohorts in our review stopped enrolling in or before2010. Recent investment in early infant diagnosis and
Review of pediatric antiretroviral therapy retention Fox and Rosen 7
1.00
0.75
0.50
Attr
ition
0.25
0.00
0
(a) All pediatric patients
6 12 18 24 36
Months
48 60
0 mos 12 mos 24 mos 36 mos 48 mos 60 mos
55,904 54,547 41,441 9005 8340 3733
1
N
Retention 0.8849 0.7219 0.6686 0.6564 0.4515
1.00
0.75
0.50
Attr
ition
0.25
0.00
0
(c) Asia
6 12 18 24 36
Months
48 60
0 mos 12 mos 24 mos 36 mos 48 mos 60 mos
7833 6497 3088 1270 1209 507
1
N
Retention 0.9721 0.7768 0.7395 0.6658 0.6658
1.00
0.75
0.50
Attr
ition
0.25
0.00
0
(b) Africa
6 12 18 24 36
Months
48 60
0 mos 12 mos 24 mos 36 mos 48 mos 60 mos
47,876 46,519 38,158 7540 6936 3031
1
N
Retention 0.8707 0.7128 0.6557 0.6530 0.4388
Fig. 1. (a–c) Kaplan–Meir curves of time to attrition for all adults and stratified by region. (!) Kaplan–Meir data use interpolatedestimates.

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
treatment has likely reduced the average age of ARTinitiation among pediatric patients and may also affectretention in care. More studies from more countries,longer follow-up, and more recent data are needed toimprove the validity and precision of estimates.
Unlike for adult attrition, when a substantial body ofwork has demonstrated that many patients who are lostfollow-up have either died or sought care at otherfacilities [51–54], very little empirical work has beendone to investigate the true outcomes of pediatric patientswho are lost follow-up. Studies tracing lost pediatricpatients are needed to determine this. As such, thefindings of any individual study included in the review arelikely upper bounds on attrition, as some patients may beself-transfers (sometimes referred to as ‘silent transfers’)and would have been excluded from the analysis had wehad more accurate data. Still, the high rate of attritionseen in pediatric cohorts is concerning given thatpediatric disease progression tends to occur faster thanfor adults in the absence of treatment and therefore likelymeans that the distribution of mortality among those lostmay be higher than in adults. Interventions to reduceattrition from pediatric care are urgently needed. As such,the findings of any individual study included in thereview are likely upper bounds on loss to follow-up, assome patients may be self-transfers (sometimes referred toas ‘silent transfers’) and would have been excluded fromthe analysis had we had more accurate data. At the sametime, they are likely lower bounds on mortality, as somepatients who are recorded as lost to follow-up would havebeen recorded as deaths had we had more accurate data. Inthe absence of treatment, disease progression tends to occurmore rapidly in children than adults, suggesting that thedistribution of mortality among lost pediatric patients may
be higher than in adults. Interventions to reduce attritionfrom pediatric care are urgently needed, as are studies thattrace the true outcomes of lost pediatric patients.
In addition to the limited geographic coverage and smallsample sizes of the studies included, this review has severallimitations that should be kept in mind when interpretingthe results. First, as for adults, we do find evidence ofpublication bias that may influence our results. Studies inour review which report to shorter time periods (e.g. 12months) show worse retention at that time period than dostudies that report retention at the same time period butthen continue to follow patients for longer durations. Thissuggests that if studies that only report to shorter timeperiods were to report to longer time periods, overallattrition at later time periods would be lower than what wereport. Second, meta-analyses like ours are susceptible tothe influence of large cohorts. In this review, while therewere no extremely large cohorts, we included severalcohorts of over 5000 patients each, representing more than10% of the entire study population. These studies can haveundue influence on overall study results. We also note thatour analysis excluded patients who transferred out of care.Transferring could be seen as a competing risk for attrition,and our estimates may have differed if transfer wasconsidered a competing risk. The studies did not containsufficient data on time to transfer to allow us to do thisanalysis, however. In addition, we did not have sufficientdata to comment on whether the procedures used toprepare patients for ART influenced retention. Futurestudies should be encouraged to provide this informationto allow assessment of its impact. Also, the studies reviewedeach reported to differing time points and used differentdefinition of loss to follow-up. Definitions of loss that usethe date of dataset closure give patients time to become lost,
8 AIDS 2015, Vol 00 No 00
100%
90%
80%
70%
60%
50%
% r
etai
ned
40%
30%
20%
10%
0%0 6 12 18
Months
24 36 48 60
Best case
Mid point
Worst case
Fig. 2. Sensitivity analysis, best case, worst case, and midpoint case scenarios.

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
but then return to care. This can artificially inflate retentionestimates. Also we did not extract data in duplicate. Thiscould have led to missing studies that could have beenrelevant. Finally, like with adults, mortality in observationalcohorts is frequently under-reported and appears as lost tofollow-up. Our results cannot accurately distinguishbetween patients who are lost and those who died, thoughthis does not affect our primary outcome of total attritionfrom death or loss to follow up.
In conclusion, we found in this review, of roughly 56 000pediatric HIV treatment patients from 23 LMICs, thatretention in care was 88, 72, and 67% in the 12, 24, and 36months, respectively, after ART initiation. Future effortsto estimate changes in retention over time would benefitfrom more cohorts that are representative of pediatrictreatment populations throughout LMICs and longerduration of follow-up for existing and new cohorts.
Acknowledgements
Author contributions: M.F. supervised the primary searchand S.R. conducted the secondary searches. M.F. andS.R. conducted the primary analyses. M.F. drafted theinitial manuscript and S.R. reviewed and edited it.
Funding: WHO, National Institutes of Health(K01AI083097), US Agency for International Develop-ment (AID 674-A-12-00029).
Conflicts of interestNone declared.
References
1. World Health Organization. Global update on HIV treatment2013: results, impact and opportunities. Geneva: World HealthOrganization; 2013.
2. World Health Organization (WHO). Antiretroviral therapy forHIV infection in infants and children: towards universal access.Recommendations for a public health approach. 2010 revision.Geneva: World Health Organization; 2010.
3. Hansudewechakul R, Sirisanthana V, Kurniati N, Puthanakit T,Lumbiganon P, Saphonn V, et al. Antiretroviral therapy out-comes of HIV-infected children in the TREAT Asia pediatricHIV observational database. J Acquir Immune Defic Syndr2010; 55:503–509.
4. Kabue MM, Buck WC, Wanless SR, Cox CM, McCollum ED,Caviness A C, et al. Mortality and clinical outcomes in HIV-infected children on antiretroviral therapy in Malawi, Lesotho,and Swaziland. Pediatrics 2012; 130:e591–e599.
5. Raguenaud M-E, Isaakidis P, Zachariah R, Te V, Soeung S, AkaoK, et al. Excellent outcomes among HIVR children on ART, butunacceptably high pre-ART mortality and losses to follow-up: acohort study from Cambodia. BMC Pediatr 2009; 9:54.
6. Matida LH, Ramos AN, Heukelbach J, Hearst N. Continuingimprovement in survival for children with acquired immuno-deficiency syndrome in Brazil. Pediatr Infect Dis J 2009;28:920–922.
7. Rosen S, Fox MP, Gill CJ. Patient retention in antiretroviraltherapy programs in sub-Saharan Africa: a systematic review.PLoS Med 2007; 4:e298.
8. Fox MP, Rosen S. Patient retention in antiretroviral therapyprograms up to three years on treatment in sub-Saharan Africa,2007-2009: systematic review. Trop Med Int Heal 2010; 15(Suppl 1):1–15.
9. Freeman M, Tukey J. Transformations related to the angular andthe square root. Ann Inst Stat Math 1950; 21:607–611.
10. Fox MP, Rosen S. Retention of adult patients on antiretroviraltherapy in low-and middle- income countries: systematic review2008–2013. Boston: Center for Global Health & Development;2014.
11. Violari A, Cotton MF, Gibb DM, Babiker AG, Steyn J, Madhi SA,et al. Early antiretroviral therapy and mortality among HIV-infected infants. N Engl J Med ; 359:2233–2244.
12. Geng EH, Emenyonu N, Bwana MB, Glidden DV, Martin JN.Sampling-based approach to determining outcomes of patientslost to follow-up in antiretroviral therapy scale-up programs inAfrica. J Am Med Assoc 2008; 300:506–507.
13. Egger M, Spycher BD, Sidle J, Weigel R, Geng EH, Fox MP, et al.Correcting mortality for loss to follow-up: a nomogram appliedto antiretroviral treatment programmes in sub-Saharan Africa.PLoS Med 2011; 8:e1000390.
14. Brinkhof MWG, Spycher BD, Yiannoutsos C, Weigel R, WoodR, Messou E, et al. Adjusting mortality for loss to follow-up:analysis of five ART programmes in sub-Saharan Africa. PLoSOne 2010; 5:e14149.
15. Fox MP, Brennan A, Maskew M, MacPhail P, Sanne I. Using vitalregistration data to update mortality among patients lost tofollow-up from ART programmes: evidence from the ThembaLethu Clinic, South Africa. Trop Med Int Health 2010; 15:405–413.
16. Gomilla A. Antiretroviral therapy (ART) in children less than 24months of age at the Botswana Baylor Children’s Clinical Centreof Excellence (COE) in Gaborone, Botswana: characteristics atinitiation and outcomes after 52 weeks of ART. 6th IAS Conf HIVPathog Treat; Abstract MOPE235, Rome, 17–20 July 2011.
17. Auld AF. Predictors of treatment outcomes among children initia-ting antiretroviral therapy in Cote d’Ivoire during 2004–2008. 6thIAS Conf HIV Pathog Treat; MOPE242, Rome, 17–20 July 2011.
18. Edmonds A, Yotebieng M, Lusiama J, Matumona Y, Kitetele F,Napravnik S, et al. The effect of highly active antiretroviraltherapy on the survival of HIV-infected children in a resource-deprived setting: a cohort study. PLoS Med 2011; 8:e1001044.
19. Asfawesen GY, Solomie J, Bisirat T, Berhanu GM, Mebratu B,Rahlenbeck S. Outcome in a paediatric cohort receiving ART inAddis Abeba, Ethiopia. Acta Paediatr 2011; 100:1164–1167.
20. Koye DN, Ayele TA, Zeleke BM. Predictors of mortality amongchildren on antiretroviral therapy at a referral hospital, North-west Ethiopia: a retrospective follow up study. BMC Pediatr2012; 12:161.
21. Hagstromer O, Lundstedt L, Balcha TT, Bjorkman P. Decen-tralised paediatric HIV care in Ethiopia: a comparison betweenoutcomes of patients managed in health centres and in ahospital clinic. Glob Health Action 2013; 6:22274.
22. Okomo U, Togun T, Oko F, Peterson K, Townend J, Peterson I,et al. Treatment outcomes among HIV-1 and HIV-2 infectedchildren initiating antiretroviral therapy in a concentrated lowprevalence setting in West Africa. BMC Pediatr 2012; 12:95.
23. Mcnairy ML, Lamb MR, Carter RJ, Fayorsey R, Tene G, MutabaziV, et al. Retention of HIV-infected children on antiretroviraltreatment in HIV care and treatment programs in Kenya,Mozambique, Rwanda, and Tanzania. J Acquir Immune DeficSyndr 2013; 62:17–19.
24. Nyandiko W, Vreeman R, Liu H, Shangani S, Sang E, Ayaya S,et al. Nonadherence to clinic appointments among HIV-in-fected children in an ambulatory care program in WesternKenya. J Acquir Immune Defic Syndr 2013; 63:49–55.
25. Sivapalasingam S, Mendillo M, Ahmed A, Mwamzuka M, SaidS, Marshed F, et al. The importance of caregivers in the out-come of pediatric HIV management, Mombasa, Kenya. AIDSCare 2013; 00:1–9.
26. Cohen R. Nurse-driven, community-supported HIV/AIDS careand treatment: 2 year antiretroviral treatment outcomes from aprimary care level programme in rural Lesotho. 5th IAS Conf HIVPathog Treat; Abstract MOAD102, Cape Town, 19–22 July 2009.
27. Ardura Garcia C. Risk factors and true outcomes of children lost tofollow-up from antiretroviral therapy in Lilongwe, Malawi. 19thInt AIDS Conf; Abstract WEAE0203, Washington, 22–27 July2012.
Review of pediatric antiretroviral therapy retention Fox and Rosen 9

Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
CE: Namrta; AIDS-D-14-00672; Total nos of Pages: 10;
AIDS-D-14-00672
28. Weigel R, Phiri S, Chiputula F, Gumulira J, Brinkhof M, GsponerT, et al. Growth response to antiretroviral treatment in HIV-infected children: a cohort study from Lilongwe, Malawi. TropMed Int Health 2010; 15:934–944.
29. Germanaud D, Derache A, Traore M, Madec Y, Toure S, DickoF, et al. Level of viral load and antiretroviral resistance after 6months of nonnucleoside reverse transcriptase inhibitor first-line treatment in HIV-1-infected children in Mali. J AntimicrobChemother 2010; 65:118–124.
30. Fenner L, Brinkhof MWG, Keiser O, Weigel R, Cornell M,Moultrie H, et al. Early mortality and loss to follow-up inHIV-infected children starting antiretroviral therapy in South-ern Africa. J Acquir Immune Defic Syndr 2010; 54:524–532.
31. Omoni AO, Christian PS, Sadoh WE, Okechukwu A, Olateju E,Omoigberale A, et al. Immunologic outcomes of antiretroviraltherapy among HIV-infected Nigerian children and its associa-tion with early infant feeding and nutritional status at treat-ment initiation. Pediatr Infect Dis J 2013; 32:e291–e297.
32. Tene G, Lahuerta M, Teasdale C, Mugisha V, Kayonde L,Muhayimpundu R, et al. High retention among HIV-infectedchildren in Rwanda during scale-up and decentralization ofHIV care and treatment programs to. Pediatr Infect Dis J 2013;32:e341–e347.
33. Van Griensven J, De Naeyer L, Uwera J, Asiimwe A, Gazille C,Reid T. Success with antiretroviral treatment for children inKigali, Rwanda: experience with health center/nurse-basedcare. BMC Pediatr 2008; 8:39.
34. Kaplan R. Long term programmatic outcomes for adults andchildren at a primary healthcare antiretroviral clinic in SouthAfrica. 5th IAS Conf HIV Pathog Treat; Abstract MOAD105,Cape Town, 19–22 July 2009.
35. Sengayi M, Dwane N, Marinda E, Sipambo N, Fairlie L, MoultrieH. Predictors of loss to follow-up among children in the firstand second years of antiretroviral treatment in Johannesburg,South Africa. Glob Health Action 2013; 6:19248.
36. Chhagan MK, Kauchali S, Van den Broeck J. Clinical andcontextual determinants of anthropometric failure at baselineand longitudinal improvements after starting antiretroviraltreatment among South African children. Trop Med Int Heal2012; 17:1092–1099.
37. Colvin CJ. Paediatric outcomes after five years on ART inKhayelitsha Township, South Africa. 5th IAS Conf HIV PathogTreat; Abstract CDB109, Cape Town, 19–22 July 2009.
38. Barth RE, Tempelman HA, Smelt E, Wensing AMJ, Hoepelman AI,Geelen SP. Long-term outcome of children receiving antiretro-viral treatment in rural South Africa: substantial virologic failureon firstline treatment. Pediatr Infect Dis J 2011; 30:52–56.
39. Janssen N, Ndirangu J, Newell M-L, Bland RM. Successfulpaediatric HIV treatment in rural primary care in Africa. ArchDis Child 2010; 95:414–421.
40. Zanoni BC, Phungula T, Zanoni HM, France H, Feeney ME. Riskfactors associated with increased mortality among HIV in-fected children initiating antiretroviral therapy (ART) in SouthAfrica. PLoS One 2011; 6:e22706.
41. Meyer-Rath G, Brennan A, Long L, Ndibongo B, Technau K,Moultrie H, et al. Cost and outcomes of paediatric antiretro-viral treatment in South Africa. AIDS 2013; 27:243–250.
42. Fatti G, Shaikh N, Eley B, Grimwood A. Improved virologicalsuppression in children on antiretroviral treatment receivingcommunity-based adherence support: a multicentre cohortstudy from South Africa. AIDS Care 2014; 26:448–453.
43. Mwiru RS, Spiegelman D, Duggan C, Seage GR, Semu H,Chalamilla G, et al. Nutritional status and other baselinepredictors of mortality among HIV-infected children initiatingantiretroviral therapy in Tanzania. J Int Assoc Provid AIDS Care2013(Published Online First: 8 October; doi: 10.1177/2325957413500852).
44. Kiboneka A, Wangisi J, Nabiryo C, Tembe J, Kusemererwa S,Olupot-Olupot P, et al. Clinical and immunological outcomesof a national paediatric cohort receiving combination antire-troviral therapy in Uganda. AIDS 2008; 22:2493–2499.
45. Scott C, Iyer H, Bwalya DL, McCoy K, Meyer-Rath G, Moyo C,et al. Retention in care and outpatient costs for childrenreceiving antiretroviral therapy in zambia: a retrospectivecohort analysis. PLoS One 2013; 8:e67910.
46. Sikazwe I. Clinical outcomes and factors contributing to loss tofollow-up of paediatric patients on ART in rural Zambia: retro-spective cohort study 2004-2010. 6th IAS Conf HIV PathogTreat, Abstract CDD081, Rome, 17–20 July 2011.
47. Isaakidis P, Raguenaud M-E, Te V, Tray CS, Akao K, Kumar V,et al. High survival and treatment success sustained after twoand three years of first-line ART for children in Cambodia. J IntAIDS Soc 2010; 13:11.
48. Zhao Y, Li C, Sun X, Mu W, McGoogan JM, He Y, et al. Mortalityand treatment outcomes of China’s National Pediatricantiretroviral therapy program. Clin Infect Dis 2013; 56:735–744.
49. Rajasekaran S, Jeyaseelan L, Ravichandran N, Gomathi C, TharaF, Chandrasekar C. Efficacy of antiretroviral therapy programin children in India: prognostic factors and survival analysis. JTrop Pediatr 2009; 55:225–232.
50. Collins IJ, Jourdain G, Hansudewechakul R, Kanjanavanit S,Hongsiriwon S, Ngampiyasakul C, et al. Long-term survival ofHIV-infected children receiving antiretroviral therapy in Thai-land: a 5-year observational cohort study. Clin Infect Dis 2010;51:1449–1457.
51. McConnell MS, Chasombat S, Siangphoe U, Yuktanont P,Lolekha R, Pattarapayoon N, et al. National program scale-up and patient outcomes in a pediatric antiretroviral treatmentprogram Thailand. J Acquir Immune Defic Syndr 2010; 54:423–429.
52. Duong B. Application of ART cohort analysis and HIV drugresistance early warning indicators as tools to monitor HIV/AIDScare and treatment program in Viet Nam. AIDS 2010 – XVIII IntAIDS Conf; Abstract CDC0508, Vienna, 18–23 July 2010.
53. Lu D. First-line antiretroviral therapy in HIV-infected children inVietnam: a 12-month outcome analysis. AIDS 2010 – XVIII IntAIDS Conf; Abstract THPE0178, Vienna, 18–23 July 2010.
54. Souza ES, dos Santos NR, Valentini SZ, da Silva GA, FigueiroaJN, Falbo AR. Predictors of long-term antiretroviral therapyeffectiveness among Brazilian HIV-1-infected children in ahybrid scenario: what really matters? J Trop Pediatr 2011;57:197–203.
10 AIDS 2015, Vol 00 No 00