Greater Nutrition Knowledge Is Associated with Lower 1-Year Postpartum Weight Retention in...
9
RESEARCH Current Research Influence of Nutrition Attitudes and Motivators for Eating on Postpartum Weight Status in Low-Income New Mothers HENRY NUSS, PhD; KRISTINE CLARKE, PhD, MPH, RD; DEBORAH KLOHE-LEHMAN, PhD, RD; JEANNE FREELAND-GRAVES, PhD, RD ABSTRACT Objective The purpose of this study was to identify atti- tudes about nutrition and their influence on weight sta- tus in low-income mothers in the first year postpartum. Design Nutrition attitudes were assessed at 1.5, 6, and 12 months postpartum. Body weight was measured at each time point and height at 1.5 months to calculate body mass index. Nutrition attitudes at each time were com- pared with demographic variables and weight status. Subjects Subjects were 340 non-Hispanic white (31.3%), non-Hispanic black (25.1%), and Hispanic (43.7%) new mothers (mean age22.4 years) located in central Texas. Criteria for participation included good health at delivery and low income (185% federal poverty guideline). Statistical analyses 2 tests were used to compare demo- graphic groups to categorical variables. Multivariate analysis of variance was done to investigate the effect of demographic variables on instrument subscale scores. A repeated-measures analysis of variance was used to iden- tify significant changes over time. Results Obese women had higher barriers to healthful eating subscale means at 1 year compared with normal and overweight subjects at 1.5 and 6 months, and had more barriers than overweight participants at 12 months. Obese individuals also had higher emotional eating sub- scale scores than did overweight women at 1.5 months and both normal and overweight subjects at 12 months. Conclusions Women who were obese at 1 year postpartum were more likely to perceive more barriers to healthful eating and respond more to emotional cues to eat. Health professionals could emphasize potential changes and dif- ficulties often faced in postpartum and identify tech- niques to overcome these obstacles to healthful eating. J Am Diet Assoc. 2006;106:1774-1782. T he United States is experiencing an epidemic of obesity. In adults, the incidence has increased from 22.5% in 1994 to 30.6% in 2002 (1-3). Women seem to be at a greater risk than men, particularly those of low socioeconomic status, Hispanic and non- Hispanic black ethnicity (3-5), and childbearing age (3,6,7). For many women, weight retained after preg- nancy may be a substantial factor in the development of overweight and obesity in later life (8-10). This arti- cle will explore whether attitudes about nutrition and motivators for eating were related to weight status in the first year postpartum. This topic has received little attention, particularly in low-income populations. The only studies of attitudes re- lated to nutrition in postpartum have focused on those related to eating disorder pathology (11-13). In 1996 Stein and Fairburn (13) administered the Eating Disor- der Examination (14) to 97 women of varied socioeco- nomic levels in the United Kingdom to document con- cerns about eating, weight, and body shape. These concerns increased during the first 3 months after child- birth and stabilized during the next 3 months. Although Eating Disorder Examination scores were not compared with weight, the inclusion of weight as a covariate in the analysis mitigated changes in Eating Disorder Examina- tion scores, implying an association. In 1999, Baker and colleagues (12) used the Eating Attitudes Test (15) to discern attitudes such as preoccupation with shape and fattening foods, binge and purging behaviors, and self- control. The sample consisted of 90 pregnant women who were primarily non-Hispanic white, married, and middle class. Concerns about weight and shape increased from pregnancy to postpartum, and weight/shape satisfaction was negatively associated with body mass index (BMI) at 4 months postpartum. In 2000 Carter and colleagues (11) also used the Eating Attitudes Test to determine relation- ships with BMI and symptoms of depression and anxiety during postpartum. In 64 primarily non-Hispanic white, married, middle-class women at 14 months postpartum, eating attitudes were associated with depression and H. Nuss has graduated with a PhD in Nutritional Sci- ences from the University of Texas at Austin; at the time of the study, he was a doctoral candidate in Nutritional Sciences, University of Texas at Austin. K. Clarke is an assistant professor, Division of Nutrition, University of Utah, Salt Lake City; at the time of the study, she was a postdoctoral fellow, Department of Pediatrics, Center for Pediatric Nutrition Research, Salt Lake City, UT. D. Klohe-Lehman is the State Marketing Coordinator for Nutrition, Texas Department of Agriculture, Austin. J. Freeland-Graves is professor and head, Nutritional Sci- ences, The Bess Heflin Centennial, Austin, TX. Address correspondence to: Jeanne Freeland-Graves, PhD, RD, The Bess Heflin Centennial, Professor and Head, Nutritional Sciences, 1 University Station, A2700, Austin, TX 78712. E-mail: [email protected] Copyright © 2006 by the American Dietetic Association. 0002-8223/06/10611-0011$32.00/0 doi: 10.1016/j.jada.2006.08.016 1774 Journal of the AMERICAN DIETETIC ASSOCIATION © 2006 by the American Dietetic Association
Transcript of Greater Nutrition Knowledge Is Associated with Lower 1-Year Postpartum Weight Retention in...

C
IfLH
AOttDmtmpSnmCaSgadrtReamOsa
HeoSaUpPKNFe
PHA
A
1
RESEARCH
urrent Research
nfluence of Nutrition Attitudes and Motivatorsor Eating on Postpartum Weight Status inow-Income New Mothers
ENRY NUSS, PhD; KRISTINE CLARKE, PhD, MPH, RD; DEBORAH KLOHE-LEHMAN, PhD, RD; JEANNE FREELAND-GRAVES, PhD, RD
CwepfinJ
TstH(nocmt
llrSdnccbEwatcdfcwcpw4asdm
BSTRACTbjective The purpose of this study was to identify atti-udes about nutrition and their influence on weight sta-us in low-income mothers in the first year postpartum.esign Nutrition attitudes were assessed at 1.5, 6, and 12onths postpartum. Body weight was measured at each
ime point and height at 1.5 months to calculate bodyass index. Nutrition attitudes at each time were com-
ared with demographic variables and weight status.ubjects Subjects were 340 non-Hispanic white (31.3%),on-Hispanic black (25.1%), and Hispanic (43.7%) newothers (mean age�22.4 years) located in central Texas.riteria for participation included good health at deliverynd low income (�185% federal poverty guideline).tatistical analyses �2 tests were used to compare demo-raphic groups to categorical variables. Multivariatenalysis of variance was done to investigate the effect ofemographic variables on instrument subscale scores. Aepeated-measures analysis of variance was used to iden-ify significant changes over time.esults Obese women had higher barriers to healthfulating subscale means at 1 year compared with normalnd overweight subjects at 1.5 and 6 months, and hadore barriers than overweight participants at 12 months.bese individuals also had higher emotional eating sub-
cale scores than did overweight women at 1.5 monthsnd both normal and overweight subjects at 12 months.
. Nuss has graduated with a PhD in Nutritional Sci-nces from the University of Texas at Austin; at the timef the study, he was a doctoral candidate in Nutritionalciences, University of Texas at Austin. K. Clarke is anssistant professor, Division of Nutrition, University oftah, Salt Lake City; at the time of the study, she was aostdoctoral fellow, Department of Pediatrics, Center forediatric Nutrition Research, Salt Lake City, UT. D.lohe-Lehman is the State Marketing Coordinator forutrition, Texas Department of Agriculture, Austin. J.reeland-Graves is professor and head, Nutritional Sci-nces, The Bess Heflin Centennial, Austin, TX.
Address correspondence to: Jeanne Freeland-Graves,hD, RD, The Bess Heflin Centennial, Professor andead, Nutritional Sciences, 1 University Station, A2700,ustin, TX 78712. E-mail: [email protected] © 2006 by the American Dietetic
ssociation.0002-8223/06/10611-0011$32.00/0
edoi: 10.1016/j.jada.2006.08.016
774 Journal of the AMERICAN DIETETIC ASSOCIATION
onclusions Women who were obese at 1 year postpartumere more likely to perceive more barriers to healthful
ating and respond more to emotional cues to eat. Healthrofessionals could emphasize potential changes and dif-culties often faced in postpartum and identify tech-iques to overcome these obstacles to healthful eating.Am Diet Assoc. 2006;106:1774-1782.
he United States is experiencing an epidemic ofobesity. In adults, the incidence has increasedfrom 22.5% in 1994 to 30.6% in 2002 (1-3). Women
eem to be at a greater risk than men, particularlyhose of low socioeconomic status, Hispanic and non-ispanic black ethnicity (3-5), and childbearing age
3,6,7). For many women, weight retained after preg-ancy may be a substantial factor in the developmentf overweight and obesity in later life (8-10). This arti-le will explore whether attitudes about nutrition andotivators for eating were related to weight status in
he first year postpartum.This topic has received little attention, particularly in
ow-income populations. The only studies of attitudes re-ated to nutrition in postpartum have focused on thoseelated to eating disorder pathology (11-13). In 1996tein and Fairburn (13) administered the Eating Disor-er Examination (14) to 97 women of varied socioeco-omic levels in the United Kingdom to document con-erns about eating, weight, and body shape. Theseoncerns increased during the first 3 months after child-irth and stabilized during the next 3 months. Althoughating Disorder Examination scores were not comparedith weight, the inclusion of weight as a covariate in thenalysis mitigated changes in Eating Disorder Examina-ion scores, implying an association. In 1999, Baker andolleagues (12) used the Eating Attitudes Test (15) toiscern attitudes such as preoccupation with shape andattening foods, binge and purging behaviors, and self-ontrol. The sample consisted of 90 pregnant women whoere primarily non-Hispanic white, married, and middle
lass. Concerns about weight and shape increased fromregnancy to postpartum, and weight/shape satisfactionas negatively associated with body mass index (BMI) atmonths postpartum. In 2000 Carter and colleagues (11)lso used the Eating Attitudes Test to determine relation-hips with BMI and symptoms of depression and anxietyuring postpartum. In 64 primarily non-Hispanic white,arried, middle-class women at 14 months postpartum,
ating attitudes were associated with depression and
© 2006 by the American Dietetic Association

aed
jtaitpsbHvotinPwT(
sfiwnafaiotda
MEIelwsTw
hrbcpaAew
SAsdw
caidyapppeg
NA1wptvmoisck�c
slh“
nxiety, but not with BMI. Collectively, these studiesxplain attitudes in postpartum related only to eatingisorders.Motivators for eating, such as emotional cues (anger,
oy, fear, depression) and physiological cues (hunger,aste), have been studied extensively in non-postpartum,dult populations (16-34). Research about emotional eat-ng, or eating in response to an emotional cue, has shownhat subjects eat more under an emotional influence,articularly during negative emotions such as anger oradness (17,19-23). Furthermore, emotional eating haseen associated with increased weight status (18,24-26).unger (27-31) and taste (32-34) are indeed strong moti-
ators for eating, yet only hunger seems to be related tobesity (28-30,32). Two recent studies measured suscep-ibility to hunger (food consumption in response to feel-ngs of hunger) via the Three Factor Eating Question-aire (35). In a sample of 244 men and 325 women,rovencher and colleagues (29) found that obese subjectsere more susceptible to hunger than nonobese subjects.his finding was also reported by Boschi and colleagues
31) in a sample of 93 women.The goal of the present study was to identify and mea-
ure nutrition attitudes and motivators of eating in therst year postpartum and to assess relationships witheight status. These concepts will be measured via aewly validated instrument that determines attitudesnd barriers about healthful eating as well as motivatorsor eating. Low-income and minority women were chosens subjects for this study because they represent a signif-cant segment of the US population who are overweightr obese. A secondary purpose was to compare associa-ions of nutrition attitudes and motivators for eating withemographic and anthropometric data to discern subjectst risk for obesity.
ETHODSxperimental Designnitially, a scale of nutrition attitudes and motivators forating was developed and validated in a sample of 134ow-income women at 1.5 months postpartum. Validityas established using principal component factor analy-
is (36) and reliability was determined via Cronbach �.he validated scale was tested in a second group of 206omen at 1.5, 6, and 12 months postpartum (Table 1).Body weights were measured at each time point, and
eight was measured at 1.5 months. All participants wereecruited in the hospital the day of or day after givingirth to a healthy newborn. At the hospital, data wereollected on sociodemographic variables (age, ethnicity,arity, education, marital status) and pregnancy vari-bles (prepregnancy weight and gestational weight gain).t each time point, nutrition attitudes and motivators forating were compared with demographic variables andeight status.
ubjectsconvenience sample was derived from the first 340
ubjects of a larger observational study of new mothersuring the first year postpartum (37). Each participant
as informed about the nature of the study and signed a TN
onsent form approved by the Institutional Review Boardt The University of Texas at Austin. Criteria for partic-pation were: good health at delivery (no complicationsuring pregnancy or childbirth and no current illness); 18ears of age or older; parity of 3 or more; ability to speaknd read English; a healthy child at birth without com-lications; low income (�185% the federal guideline foroverty); and self-identified as non-Hispanic white, His-anic, or non-Hispanic black. All subjects were eligible fornrollment in the Special Supplemental Nutrition Pro-ram for Women, Infants, and Children.
utrition Attitudes Scale73-item questionnaire (Likert scale ranging from
�strongly disagree/never to 7�strongly agree/always)as constructed (based on concepts from the medical andsychosocial research literature) to assess nutrition atti-udes. A panel of nutrition experts reviewed the initialersion of the instrument for face validity, and the instru-ent then was revised and pilot-tested in the first group
f postpartum women. Data reduction was performed bytem and factor analyses (Principal Components Analy-is) to determine construct validity. Items were reverse-oded as needed. Criteria for item inclusion included: aurtosis ratio �1, item-to-total correlation of �0.30, an�.60, factor loading of �0.40, and loading on only oneomponent.A Scree plot was also used to determine the final in-
trument of 21 items contained in four distinct factors,abeled as “healthful eating,” “perceived barriers toealthful eating,” “emotionally influenced eating,” andsensory/physiological motivators for eating” (Table 2).
Table 1. Demographic characteristics of low-income new mothers(n�206)
Characteristics n %a
Age (y)18-20 73 35.421-24 86 41.7�24 47 22.8
EthnicityNon-Hispanic white 63 30.6Non-Hispanic black 57 27.7Hispanic 86 41.7
Parity1 78 37.92 78 37.93 50 24.3
EducationNo/some high school 83 40.6High school graduate 79 38.7Some college/college graduate 42 20.6
Marital statusSingle, not living with partner 81 39.5Married, living with partnerb 124 60.5
aPercentages are row percentages.bCohabitation with a partner was included as married.
he first factor, healthful eating, consisted of question-
ovember 2006 ● Journal of the AMERICAN DIETETIC ASSOCIATION 1775

nsbstmcftsi
sf.pwscwmi
aprdrymI
WPPnSm(kom
for ea
1
aire items related to various aspects of healthful eating,uch as choosing low-fat foods, using nutrition labels, andeing concerned with the nutritional content of foods. Theecond factor, perceived barriers to healthful eating, con-ained items associated with obstacles to adopting oraintaining a healthful diet. These barriers included:
hanging eating habits, work, and unappetizing low-fatoods. Emotionally influenced eating related to how emo-ional states influenced eating behavior. The last factor,ensory/physiological motivators for eating, containedtems related to taste, hunger, and cravings.
To determine the internal reliability of the four sub-cales, Cronbach � (38) for the factors were .84 for health-ul eating, .77 for perceived barriers to eating healthfully,79 for emotionally influenced eating, and .65 for sensory/hysiological motivators for eating. Mean subscale scoresere obtained and used for the results presented in this
tudy. Scores ranged from 1 to 7; higher subscales indi-ated that a participant felt that the construct in questionas more of a factor in their lives, whereas a lower scoreeant it was not relevant or lacked significance to the
Table 2. Factor loadings of the Nutrition Attitudes and Motivators fo
FactorsFactor 1Healthful eati
Healthful eatingChoosing low-fat foods is important to me nowa 0.809My diet as being low-fatb 0.750I enjoy low-fat foodsb 0.739I use nutrition labels to help me select foodsb 0.732Eating a healthful diet is important to me nowa 0.703I consider the Food Guide Pyramid in choosing
my dietb 0.674My diet as being healthfulb 0.645I am very concerned with the nutritional content
of foodsa 0.622Nutritionc 0.457
Barriers to healthful eatingd
Too much effort 0.108Don’t want to change my eating habits 0.081Must please family 0.032Work �0.034Nutrition is too confusing to me 0.181Low-fat foods are unappetizing �0.202
Emotionally influenced eatinge
When I am depressed, I eat more junk food �0.025When I am stressed/anxious, I tend to eat more 0.128When I am angry, I tend to eat more 0.019
Sensory/physiological motivators for eatingf
Taste �0.014Hunger/satiety 0.196Cravings �0.014
aResponse options range from 1 (strongly disagree) through 7 (strongly agree).bResponse options range from 1 (never) through 7 (always).cPreceded with: “How important is each of the following in determining your motivationdPreceded with: “Currently, what prevents you from eating as healthy as you want to eeResponse options range from 1 (strongly disagree) to 7 (strongly agree).fPreceded with: “How important is each of the following in determining your motivation
ndividual.
776 November 2006 Volume 106 Number 11
Five Likert-type items (1�disagree to 7�stronglygree) that did not factor into one of the subscales also areresented in survey form because of their interest toesearchers. These included: (a) “How important is bore-om in determining your motivation for eating?”; “Cur-ently, what prevents you from eating as healthfully asou want to?”; (b) cost; (c) time; (d) “My family would helpe if I chose to lose weight”; and (e) “I am confident thatwill return to my prepregnancy weight.”
eight, Height, and Lactation Statusrepregnancy weight was self-reported at recruitment.ostpartum weights were measured at each visit to theearest 0.1 kg on a calibrated digital scale (Fairbankscales, Model No. HS100, Kansas City, MO). Height waseasured (to the nearest 0.1 cm) using a stadiometer
Perspective Enterprises, Portage, MI). BMI calculated asg/m2. Normal weight was defined as BMI less than 25;verweight as BMI 25 to 29.9, and obese as BMI of 30 orore.
ing Questionnaire administered to low-income new mothers
Factor 4Factor 2 Factor 3 Sensory/physiologicalPerceived barriers Emotional eating motivators for eating
0.081 �0.026 0.1230.042 0.085 �0.098
�0.005 �0.166 �0.1570.177 0.052 0.002
�0.041 0.075 0.168
0.081 0.104 0.045�0.137 0.061 �0.098
0.004 �0.036 0.077�0.126 �0.106 �0.120
0.726 �0.063 0.1780.703 0.190 �0.0180.659 0.098 �0.1390.638 0.212 0.0050.621 0.068 �0.0650.500 0.031 0.139
0.096 0.807 0.0530.152 0.793 �0.0450.064 0.680 �0.202
0.162 0.072 0.771�0.031 �0.100 0.765
0.162 0.072 0.530
ting?” Response options range from 1 (least important) to 7 (very important).esponse options range from 1 (no influence) through 7 (influences a lot).
ting?” Response options range from 1 (least important) to 7 (very important).
r Eat
ng
for eaat?” R
Lactation status was estimated by a lactation score

acbVfip9f
ST2Dadcsrsdavs(ihtmTcca
RDTniwogsc((ffiAlmw
WTB2sg1a
(wsmkBwNwHH
gngn1i
ioprhH(dcmPl
WMmocH(hy2g3thtctmd(
l2Tptan(P
ssessed at 1.5, 6, and 12 months postpartum. The scoreonsisted of 1�not lactating/bottle feeding only, 2�com-ination breast/bottle feeding, and 3�breastfeeding only.alues from each time point were summed to yield thenal score. A sum score of 3 (lowest) indicated that aarticipant did not lactate at all, whereas a sum score of(highest) meant that the subject breastfed exclusively
or the first year.
TATISTICAL ANALYSIShe Statistical Package for Social Sciences (version 11.5,002, SPSS, Chicago, IL) was used for data analysis.ata were entered into SPSS and checked for normalitynd accuracy. Means and frequencies were computed asescriptive statistics for demographic variables, weightategories, instrument subscale scores, and survey re-ponses. Pearson correlations were used to determineelationships between demographic variables, subscale,urvey scores, and weight status. �2 tests were used toetermine differences between groups on categorical vari-bles. Multivariate analysis of variance was used to in-estigate the effect of demographic variables on all sub-cale scores. A repeated measures analysis of variancevia the general linear model procedure) was used todentify significant changes in responses over time. Postoc (Tukey’s significant difference test) and pairwise mul-iple comparisons (Bonferroni test) were used to compareean scores of demographic and weight status groups.he McNemar test was used to identify significanthanges in response to individual survey items. Statisti-al significance was set at a P value of less than 0.05 forll tests.
ESULTSemographicshe profile of the subjects is shown in Table 1. There wereo differences in demographic variables between the val-
dation and attitudes assessment groups. The mean ageas 22.2�0.4 and 22.5�0.3 years (mean�standard errorf the mean) for the validation and attitudes assessmentroups, respectively. Hispanics accounted for 44% of bothamples, and were nearly twice as likely to have notompleted high school (60%) than non-Hispanic whites33%), and more than double that of non-Hispanic blacks27%) (�2�40.6, df�4, P�0.05). Approximately threeourths of both samples had one or two children. Only onefth of all women had attended or graduated from college.pproximately two thirds of all women were married or
iving with a partner. Non-Hispanic black women wereore likely to be single (67%) than non-Hispanic whiteomen (39%) and Hispanic women (30%).
eight Status and Lactationhe mean (�standard error of the mean) prepregnancyMI for both the validation and study populations were5.8�0.31 and 25.4�0.40, respectively, and did not differignificantly between samples. Also, gestational weightains did not vary significantly (15.3�7.1 kg and6.3�2.1 kg, respectively). Within the study population,
ge had a significant influence on prepregnancy BMI hN
F�3.9, P�0.05), as the youngest subjects had lowereights. At 1 year postpartum, the mean BMI in the
tudy populations increased to 28�0.5 (P�0.05), with aean weight gain of 6.0�0.6 kg (range of �14.0 kg to 42.4
g) from prepregnancy. Approximately 40% had a normalMI (n�83), whereas more than one fourth were over-eight (n�55) and the remaining 33% were obese (n�68).early two thirds of the sample had modest or severeeight gain; 35.9% (n�74) gained 7 kg or more. Non-ispanic white women had lower BMIs (26�0.9) thanispanic women (29�0.8) (P�0.05).Those who had completed some college or were college
raduates had lower BMIs (25�1.0) than those who didot complete high school (28�0.7, not significant), or whoraduated from high school (29�0.9, P�0.05); this wasot affected by age or lactation score. Weight retention atyear postpartum did not differ according to demograph-
cs or BMI.The mean lactation score for the study population dur-
ng 12 months postpartum was 4.0�0.11, as the majorityf women (61.2%) did not lactate during any of the timeoints assessed (no lactation�score of 3; higher scoreepresents more lactation). Non-Hispanic white womenad a higher mean lactation score (4.2�0.12) than non-ispanic blacks (3.5�0.14, P�0.05) and Hispanics
3.3�0.13, P�0.05) at 12 months. Lactation score did notiffer by other demographic groups, but was negativelyorrelated to BMI at 1.5 months (r��0.21, P�0.05), 6onths (r��0.21, P�0.05), and 12 months (r��0.21,�0.05). Thus, mothers who breastfed more often had
ower BMIs.
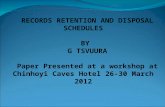
eight Status, Demographics, and Attitude Subscalesean scores on the instrument subscales at 1.5, 6, and 12onths are illustrated in the Figure. With a mean value
f 3.7�0.08 at 1.5 months, healthful eating did nothange over time within the entire study population.owever, there was a significant association with age
F�4.9, P�0.05), as women older than 24 years hadigher scores at 1.5 months than those 20 years orounger (4.0�0.19 vs 3.4�0.12, P�0.05), and both those0 years or younger and those in the 21- to 24-year ageroups at 6 months (3.9�0.19 vs 3.2�0.14, P�0.05, and.9�0.19 vs 3.6�0.11, P�0.05, respectively). Similarly,hose with the most education had scores that wereigher than all other groups at every measurement in-erval (F�12.6, P�0.05). Lactation score was positivelyorrelated with healthful eating at 1.5 months postpar-um (r�0.22, P�0.05), 6 months (r�0.18, P�0.05), and 12onths postpartum (r�0.15, P�0.05). Healthful eating
id not differ according to BMI at 1 year postpartumTable 3).
The barrier to healthful eating subscale score was at itsowest point during early postpartum, with a mean of.9�0.08 at 1.5 months postpartum for the entire sample.his was significantly less when compared with 6 monthsostpartum (3.3�0.08, P�0.05) and 12 months postpar-um (3.3�.09, P�0.05). Although there was no effect ofny of the demographic variables, lactation score wasegatively correlated with barriers at all time pointsr��0.14, P�0.05, r��0.21, P�0.05, and r��0.14,�0.05, respectively). Women who were obese at 1 year
ad higher barrier subscale means than did normal andovember 2006 ● Journal of the AMERICAN DIETETIC ASSOCIATION 1777

ovptoPsa
lc(twggaPsPs2nl
oca
itmWtwmrp
hboCn
NMmst6ept(
Flc
(p
1
verweight subjects at 1.5 months postpartum (3.3�0.16s 2.9�0.12 and 2.5�0.13, respectively) and 6 monthsostpartum (3.6�0.14 vs 3.2�0.12 and 3.1�0.16, respec-ively), and greater scores than overweight participantsnly at 12 months (3.5�0.16 vs 3.0�0.19) (F�6.1,�0.05). Controlling for lactation score eliminated thetatistical significance between normal and obese woment 1.5 and 6 months.The emotional eating subscale mean was also at its
owest value in early postpartum (2.6�0.11), and in-reased at 6 months (3.2�0.12, P�0.05) and 12 months3.1�0.12, P�0.05). Age had a significant effect on emo-ional eating (F�5.5, P�0.05), because mean scores foromen older than 24 years were greater than all otherroups at 1.5 months, and higher than the youngestroup at 1 year postpartum. At 1.5 months, weight statuslso significantly affected emotional eating (F�4.3,�0.05), as obese individuals had higher mean subscalecores than overweight women (3.0�0.21 vs. 2.4�0.18,�0.05), and greater than both normal and overweightubjects at 12 months (3.7�0.26 vs 2.8�0.16 and.8�0.21, respectively, P�0.05). This relationship wasot affected by controlling for demographic variables or
actation.The sensory/physiological subscale was higher than
ther subscales at each time point (P�0.05) and in-reased from baseline (4.6�0.11) at 6 months (5.1�0.09)
igure. Mean (�standard error of the mean) values of nutrition attitow-fat foods, using labels, concerned with nutritional content of foodEmotional states influenced eating behavior. dSensory/physiological mrange: 1�lowest to 7�highest) indicate a greater contribution of subscostpartum (P�0.05).
nd 12 months (5.3�0.09) (P�0.05). Within the subscale t
778 November 2006 Volume 106 Number 11
tself, at 12 months normal-weight women believed thathe influences of hunger/satiety were more importantotivations for eating than overweight/obese women did.omen with a parity of three had lower mean values on
he sensory/physiological subscale than single-infantomen, and lower than those with a parity of two at 6onths only (F�6.6, P�0.05). Lactation was positively
elated to the sensory/physiological subscale only in earlyostpartum (r�0.23, P�0.05).Women with a normal BMI at 1 year postpartum had
igher sensory subscale scores than overweight women atoth 1.5 and 6 months postpartum, and higher than bothverweight and obese women at 12 months (Table 3).ontrolling for parity, education, and lactation scores hado influence.
utrition Attitude Surveyothers agreed least with the question “Was boredom aotivation for eating?” Scores for this item increased
ignificantly as postpartum time progressed. Similarly,he percentage of subjects who reported cost (42.4% vs1%, P�0.05) and time as (50% vs 60.4%, P�0.05) barri-rs to healthful eating increased from 1.5 to 6 monthsostpartum, respectively. Cost was a greater barrier tohe obese women than to overweight women after 1 year4.3�0.21 vs 3.5�0.29, P�0.05, respectively). More than
ubscale scores during the first year postpartum (n�206). aChoosingstacles that prevent the adoption or maintenance of a healthful diet.tors for eating, such as taste, hunger, and cravings. eHigher scoresa greater motivator for eating. �Significantly different from 1.5 months
ude ss. bOb
otivaale as
hree fourths of the women (77.6%) believed that “My

fe(wm1wf
DLswwrOaafitttwAjn
dMsaeppt
wwoTerdisi
rbafwtm
we(hjuhwp
ncttcamwroos
eyciprasmc
amily would help me if I chose to lose weight” duringarly postpartum; this percentage decreased to 67.5%P�0.05) at 6 months. The same pattern was observedith the statement “I am confident that I will return toy prepregnancy weight,” with 84.5% agreeing to this at
.5 months vs 73.8% at 6 months (P�0.05). Normal-eight women had significantly higher scores (P�0.05)
or this item than the obese women at all time points.
ISCUSSIONow-income women who were obese at 1 year postpartumeemed to be emotional eaters, as compared with thoseith normal weights. Obese women reported eating morehen they were depressed, stressed/anxious, or angry,
egardless of age, parity, ethnicity, or lactation score.ther studies measuring emotional eating in postpartumre lacking, but Elfhag and colleagues (16) found thatdult women of low socioeconomic status experienced dif-culties in coping with stressors and irregular meal pat-erns. However, this study did not differentiate accordingo body weights. Other research also has shown a nega-ive association between emotional eating and healthfuleight status (17,18,24-26). For example, Geliebter andversa (17) observed that normal or underweight sub-
ects ate less than overweight adult men and women with
Table 3. Nutrition Attitudes subscales of questionnaire given tolow-income new mothers over the first postpartum year accordingto BMIa groupsb
Nutritionattitudesubscales
Months Postpartum
1.5 6 12
4™™™™™™™™™™™ meanc�SDd ™™™™™™™™™™™3Healthful
eatingNormal 3.6�1.1 3.5�1.2 3.4�1.0Overweight 3.7�1.2 3.6�1.2 3.6�1.3Obese 3.7�1.1 3.6�1.3 3.6�1.2BarriersNormal 2.9�1.1y 3.2�1.1y 3.4�1.2Overweight 2.5�1.0y 3.1�1.2y 3.0�1.4y
Obese 3.3�1.3z 3.6�1.2z 3.5�1.3z
EmotionalNormal 2.6�1.5 3.0�1.6 2.9�1.5y
Overweight 2.4�1.4y 3.2�1.7 2.8�1.6y
Obese 3.0�1.7z 3.5�1.9 3.7�2.1z
SensoryNormal 4.9�1.4y 5.5�1.3y 5.7�1.1y
Overweight 4.1�1.5z 4.7�1.4z 4.9�1.3z
Obese 4.5�1.7 5.1�1.4 5.1�1.5z
aBMI�body mass index. Normal�BMI �24.9, overweight�BMI 25–29.9, obese�BMI�30.bNormal: n�83; overweight: n�55; obese: n�68.cValues represent the relative influence of a subscale on a mother’s motivation to eat(range of 1�lowest to 7�highest).dSD�standard deviation.xyzWithin subscales within columns, means with different superscripts are significantlydifferent.
egative emotions (sad, bored, angry, frustrated, tired, p
N
epressed, frightened, under pressure). In addition,acht (18) found a positive correlation between weight
tatus and greater anger, fear, and sadness. The associ-tion to weight status is not surprising because emotionalaters often overindulge with energy-dense, nutrient-oor foods (19). Collectively, these studies support theresent findings that obese subjects ate more in responseo emotional cues.
In contrast, compared with overweight or obese women,omen who had healthful weights at 1 year postpartumere more concerned with sensory/physiological aspects
f foods, such as taste, hunger/satiety, and cravings.aste is believed to be the most important motivator forating (32-34), more so for women than men (34). Theelationship of taste to eating may be particularly trueuring lactation, when an enhanced uptake of prolactinn the brain (39) increases appetite, making the tasteense more acute. However, lactation had no discernablenfluence in this study.
Increased taste sensitivity, as determined by a positiveesponse to the bitter-tasting 6-n-propylthiouracil, haseen observed in women with lower BMIs (40) and indults with a diminished preference for sweet and high-at foods (41). Although sensitivity to 6-n-propylthiouracilas not measured in the present study, these observa-
ions support the finding that taste was the strongestotivator for eating among women with normal BMIs.Compared with overweight/obese women, normal-eight women indicated that hunger had a greater influ-
nce on eating. In contrast, Provencher and colleagues29) found that obese subjects ate more in response tounger than nonobese subjects. The quantity that sub-
ects from the present study ate in response to hunger isncertain. Others have not found an association betweenunger and weight status in women (31) or men andomen (18), but these studies were not conducted inostpartum.Scores on healthful eating subscales in this study did
ot vary during the first year after childbirth. This lack ofhange was unexpected, as one might anticipate womeno become more health-conscious as they became accus-omed to their new role as mothers. However, Devine andolleagues (42) also did not observe changes in attitudesbout diet, exercise, and weight from prepregnancy to 8onths postpartum in well-educated, non-Hispanic whiteomen. Thus, health may not be a focus for new mothers,
egardless of socioeconomic status. Presumably, this lackf emphasis on health may be due to competing demandsf time, physiological changes, altered finances, or re-tructuring of social life.A healthful diet was more important to older, more
ducated participants as compared to those who wereounger and less educated. The interaction of age, edu-ation, and healthful attitudes about nutrition has beendentified by several investigators (34,43-46). For exam-le, Satia and colleagues (46) found that personal healthelated to dietary behavior was less important in middle-ged vs older non-Hispanic whites. In a larger nationaltudy of US adults, Glanz and colleagues (34) also docu-ented that nutrition was of greater interest as age in-
reased.Barriers to healthful eating increased significantly as
ostpartum progressed, and were quite prevalent in this
ovember 2006 ● Journal of the AMERICAN DIETETIC ASSOCIATION 1779

skcwdi5aetoef
atnfirssltafictmmhmbs
puAftIotnlafitp
p
potrw
CWlrwwEem
owtmcat
tcapc
TUB
R
1
ample of obese women of different ethnicities. To ournowledge, the present study is the first to measure thisharacteristic in the first year postpartum in low-incomeomen. However, barriers to healthful eating have beenocumented by others (47-51) in US minority and low-ncome populations. Common barriers included time (47-1), cost (48-51), lack of understanding or informationbout nutrition (knowledge) (48-50), taste and prefer-nces of “healthy” foods vs high-fat foods (47,48,50,51). Inhe present study, cost, time, and a lack of understandingf nutrition also were significant barriers to healthfulating, and their influences became more pronouncedrom early to mid- and late postpartum.
Early identification of women whoeat in response to emotional cues
could be part of an effective strategyto minimize weight retention during
postpartum.
The instrument developed for this research seems to bereliable measure of nutrition attitudes in this popula-
ion of low-income new mothers from three different eth-ic groups. As assessed using Cronbach �, three of theour subscales (healthful eating, barriers to healthful eat-ng, and emotional eating) had good internal consistencyeliability (��.70) (38). The sensory/physiological sub-cale was slightly less (��.65), presumably due to themall number of items that was significant in the factoroading. Nonetheless, this construct was the most impor-ant for the new mothers in this study. In 1989, Andersonnd Shepherd (52) developed an instrument that identi-ed attitudes and beliefs pertaining to healthful foodhoices in pregnant and postnatal women. Their popula-ion differed in that they were British, predominatelyarried, and of mixed social class. In their study, theajority of women indicated positive intentions towardealthful eating. Although behavioral intent was noteasured in the present study, subjects did not appear to
e motivated to eat healthfully, as indicated by the lowubscale scores throughout the first year postpartum.Other studies of attitudes related to nutrition in post-
artum have focused on eating disorder pathologies inpper- (12) and mixed-income (11,13) populations.mong high-income women, Baker and colleagues (12)
ound that attitudes related to unhealthful eating prac-ices increased from pregnancy to 4 months postpartum.n the mixed-income population, Stein and Fairburn (13)bserved that attitudes related to eating disorders fluc-uated greatly during the first 6 months postpartum, witho differences between social classes. Carter and col-
eagues (11) disclosed that attitudes related to body shapend pathological avoidance of fattening foods increasedrom 4 to 14 months postpartum, with no influence fromncome. In the present study of low-income women, atti-udes about healthful eating remained unchanged inostpartum.One limitation of this study was the self-report of
repregnancy weights. Measured body weights would be
780 November 2006 Volume 106 Number 11
referable, but self-reported weights have been used inther previous investigations of pregnant and postpar-um populations (9,53,54). Studies have found that self-eported weights of adults corresponded closely to actualeights (55,56).
ONCLUSIONSomen who were obese at 1 year postpartum were more
ikely than normal and overweight subjects to eat inesponse to emotional cues. These results are consistentith other studies measuring emotional eating andeight status in non-postpartum, adult populations.arly identification of women who eat in response tomotional cues could be part of an effective strategy toinimize weight retention during postpartum.Compared with those with healthful BMIs, among the
verweight and obese subjects in this study, sensory aspectsere not as important in the decision to eat. It is plausible
hat strong emotional influences in postpartum may haveitigated the influence of sensory aspects of eating in this
ohort. Learning skills to cope with emotional stressorsfter childbirth could permit new mothers to respond moreo the internal physiological cues that impact eating.
The increase in barriers to healthful eating as postpar-um progressed is not surprising because lifestylehanges so abruptly during this time. Health profession-ls should discuss changes and difficulties often faced inostpartum and identify potential techniques to over-ome these obstacles to healthful eating.
his study was supported by grant NIHRO1N04679 andTA 00-377 from the Higher Education Coordinatingoard, The University of Texas System.
eferences1. Flegal KM, Carroll MD, Kuczmarski RJ, Johnson CL.
Overweight and obesity in the United States: Preva-lence and trends, 1960-1994. Int J Obes Relat MetabDisord. 1998;22:39-47.
2. Must A, Spadano J, Coakley EH, Field AE, Colditz G,Dietz WH. The disease burden associated with over-weight and obesity. JAMA. 1999;282:1523-1529.
3. Hedley AA, Ogden CL, Johnson CL, Carroll MD, Cur-tin LR, Flegal KM. Prevalence of overweight andobesity among US children, adolescents, and adults,1999-2002. JAMA. 2004;291:2847-2850.
4. Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vini-cor F, Bales VS, Marks JS. Prevalence of obesity,diabetes, and obesity-related health risk factors,2001. JAMA. 2003;289:76-79.
5. Kristal AR, Shattuck AL, Patterson RE. Differencesin fat-related dietary patterns between blacks, His-panics, and white women: Results from the Women’sHealth Trial Feasibility Study in Minority Popula-tions. Public Health Nutr. 1999;2:253-262.
6. Rooney BL, Schauberger CW. Excess pregnancyweight gain and long-term obesity: One decade later.Obstet Gynecol. 2002;100:245-252.
7. Healthy People 2010 Web site. Leading Health Indica-tors. Available at: http://www.healthypeople.gov/document/html/uih/uih_bw/uih_4.htm#overandobese.
Accessed April 1, 2005.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
8. Linne Y, Dye L, Barkeling B, Rossner S. Long-termweight development in women: A 15-year follow-up ofthe effects of pregnancy. Obes Res. 2004;12:1166-1178.
9. Lederman SA, Alfasi G, Deckelbaum RJ. Pregnancy-associated obesity in black women in New York City.Matern Child Health J. 2002;6:37-42.
0. Gunderson EP, Abrams B, Selvin S. The relativeimportance of gestational gain and maternal charac-teristics associated with the risk of becoming over-weight after pregnancy. Int J Obes Relat Metab Dis-ord. 2000;12:1660-1668.
1. Carter AS, Baker CW, Brownell KD. Body mass in-dex, eating attitudes, and symptoms of depressionand anxiety in pregnancy and the postpartum period.Psychosom Med. 2000;62:264-270.
2. Baker CW, Carter AS, Cohen LR, Brownell KD. Eat-ing attitudes and behaviors in pregnancy and post-partum: Global stability versus specific transitions.Ann Behav Med. 1999;21:143-148.
3. Stein A, Fairburn CG. Eating habits and attitudes inthe postpartum period. Psychosom Med. 1996;58:321-325.
4. Fairburn CG, Cooper Z. The interview schedule of theeating disorder examination. In: Fairburn CG, Wil-son GT, eds. Binge Eating: Nature, Assessment andTreating, 12th ed. New York, NY: Guilford Press;1993:317-357.
5. Garner DM, Garfinkel PE. The Eating AttitudesTest: An index of the symptoms of anorexia nervosa.Psychol Med. 1979;9:273-279.
6. Elfhag K, Carlsson AM, Rossner S. Subgrouping inobesity based on Rorschach personality characteris-tics. Scand J Psychol. 2003;44:399-407.
7. Geliebter A, Aversa A. Emotional eating in over-weight, normal weight, and underweight individuals.Eat Behav. 2003;3:341-347.
8. Macht M. Characteristics of eating in anger, fear,sadness and joy. Appetite. 1999;33:129-139.
9. de Lauzon B, Romon M, Deschamps V, Lafay L, Bo-rys JM, Karlsson J, Ducimetiere P, Charles MA;Fleurbaix Laventie Ville Sante Study Group. TheThree-Factor Eating Questionnaire-R18 is able todistinguish among different eating patterns in a gen-eral population. J Nutr. 2004;134:2372-2380.
0. van Strien T, Ouwens MA. Counterregulation in fe-male obese emotional eaters: Schachter, Goldman,and Gordon’s (1968) test of psychosomatic theory re-visited. Eat Behav. 2003;3:329-340.
1. Hargreaves MK, Schlundt DG, Buchowski MS. Con-textual factors influencing the eating behaviours ofAfrican American women: A focus group investiga-tion. Ethn Health. 2002;7:133-147.
2. Macht M, Simons G. Emotions and eating in every-day life. Appetite. 2000;35:65-71.
3. Popkess-Vawter S, Brandau C, Straub J. Triggers ofovereating and related intervention strategies forwomen who weight cycle. Appl Nurs Res. 1998;11:69-76.
4. Fassino S, Leombruni P, Piero A, Abbate-Daga G,Giacomo Rovera G. Mood, eating attitudes, and angerin obese women with and without Binge Eating Dis-order. J Psychosom Res. 2003;54:559-566.
5. Popkess-Vawter S, Gerkovich MM, Wendel S. Reli-
N
ability and validity of the Overeating Tension Scale.J Nurs Meas. 2000;8:145-160.
6. Cox DN, van Galen M, Hedderley D, Perry L, MoorePB, Mela DJ. Sensory and hedonic judgments of com-mon foods by lean consumers and consumers withobesity. Obes Res. 1998;6:438-447.
7. Cornier MA, Grunwald GK, Johnson SL, BessesenDH. Effects of short-term overfeeding on hunger, sa-tiety, and energy intake in thin and reduced-obeseindividuals. Appetite. 2004;43:253-259.
8. Dykes J, Brunner EJ, Martikainen PT, Wardle J.Socioeconomic gradient in body size and obesityamong women: The role of dietary restraint, disinhi-bition and hunger in the Whitehall II study. Int JObes Relat Metab Disord. 2004;28:262-268.
9. Provencher V, Drapeau V, Tremblay A, Despres JP,Lemieux S. Eating behaviors and indexes of bodycomposition in men and women from the Quebecfamily study. Obes Res. 2003;11:783-792.
0. Fedoroff IC, Polivy J, Herman CP. The effect of pre-exposure to food cues on the eating behavior of re-strained and unrestrained eaters. Appetite. 1997;28:33-47.
1. Boschi V, Iorio D, Margiotta N, D’Orsi P, Falconi C.The three-factor eating questionnaire in the evalua-tion of eating behaviour in subjects seeking partici-pation in a dietotherapy programme. Ann NutrMetab. 2001;45:72-77.
2. Cox DN, Perry L, Moore PB, Vallis L, Mela DJ. Sen-sory and hedonic associations with macronutrientand energy intakes of lean and obese consumers. IntJ Obes Relat Metab Disord. 1999;23:403-410.
3. Snoek HM, Huntjens L, Van Gemert LJ, De Graaf C,Weenen H. Sensory-specific satiety in obese and nor-mal-weight women. Am J Clin Nutr. 2004;80:823-831.
4. Glanz K, Basil M, Maibach E, Goldberg J, Snyder D.Why Americans eat what they do: Taste, nutrition,cost, convenience, and weight control concerns as in-fluences on food consumption. J Am Diet Assoc. 1998;98:1118-1126.
5. Stunkard AJ, Messick S. The three-factor eatingquestionnaire to measure dietary restraint, disinhi-bition, and hunger. J Psychosom Res. 1985;29:71-83.
6. Waltz CF, Strickland OL, Lenz ER. Measurement inNursing Research. 2nd ed. Philadelphia PA: FADavis Co; 1991.
7. Walker LO, Freeland-Graves JH, Milani T, Hanss-Nuss H, George G, Sterling BS, Kim M, TimmermanGM, Wilkinson S, Arheart KL, Stuifbergen A. Weightand behavioral and psychosocial factors among eth-nically diverse, low-income women after childbirth: I.Methods and context. Women Health. 2004;40:1-17.
8. Nunnally JC. Psychometric Theory. 2nd ed. NewYork, NY: McGraw-Hill; 1978.
9. Grattan DR, Pi XJ, Andrews ZB, Augustine RA,Kokay IC, Summerfield MR, Todd B, Bunn SJ. Pro-lactin receptors in the brain during pregnancy andlactation: Implications for behavior. Horm Behav.2001;40:115-124.
0. Tepper BJ, Ullrich NV. Influence of genetic taste sen-
sitivity to 6-n-propylthiouracil (PROP), dietary re-ovember 2006 ● Journal of the AMERICAN DIETETIC ASSOCIATION 1781

4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
1
straint and disinhibition on body mass index in middle-aged women. Physiol Behav. 2002;75:305-312.
1. Duffy VB, Bartoshuk LM. Food acceptance and ge-netic variation in taste. J Am Diet Assoc. 2000;100:647-655.
2. Devine CM, Bove CF, Olson CM. Continuity andchange in women’s weight orientations and lifestylepractices through pregnancy and the postpartum pe-riod: The influence of life course trajectories and tran-sitional events. Soc Sci Med. 2000;50:567-582.
3. Stafleu A, Van Staveren WA, De Graaf C, Burema J,Hautvast JG. Nutrition knowledge and attitudes to-wards high-fat foods and low-fat alternatives in threegenerations of women. Eur J Clin Nutr. 1996;50:33-41.
4. McArthur L, Chamberlain V, Howard AB. Behaviors,attitudes, and knowledge of low-income consumersregarding nutrition labels. J Health Care Poor Un-derserved. 2001;12:415-428.
5. Glanz K, Kristal AR, Sorensen G, Palombo R, Hei-mendinger J, Probart C. Development and validationof measures of psychosocial factors influencing fat-and fiber-related dietary behavior. Prev Med. 1993;22:373-387.
6. Satia JA, Kristal AR, Curry S, Trudeau E. Motiva-tions for healthy dietary change. Public Health Nutr.2001;4:953-959.
7. Chatterjee N, Blakely DE, Barton C. Perspectives onobesity and barriers to control from workers at acommunity center serving low-income Hispanic chil-dren and families. J Community Health Nurs. 2005;22:23-36.
8. Kieffer EC, Willis SK, Odoms-Young AM, GuzmanJR, Allen AJ, Two Feathers J, Loveluck J. Reducing
disparities in diabetes among African-American and782 November 2006 Volume 106 Number 11
Latino residents of Detroit: The essential role of com-munity planning focus groups. Ethn Dis. 2004;14:S27-S37.
9. James DC. Factors influencing food choices, dietaryintake, and nutrition-related attitudes among Afri-can Americans: Application of a culturally sensitivemodel. Ethn Health. 2004;9:349-367.
0. Eikenberry N, Smith C. Healthful eating: Percep-tions, motivations, barriers, and promoters in low-income Minnesota communities. J Am Diet Assoc.2004;104:1158-1161.
1. Palmeri D, Auld GW, Taylor T, Kendall P, AndersonJ. Multiple perspectives on nutrition education needsof low-income Hispanics. J Community Health. 1998;23:301-316.
2. Anderson AS, Shepherd R. Beliefs and attitudes to-wards “healthier eating” among women attendingmaternity hospital. J Nutr Educ. 1989;21:208-213.
3. Kac G, Benicio MH, Velasquez-Melendez G, ValenteJG, Struchiner CJ. Breastfeeding and postpartumweight retention in a cohort of Brazilian women.Am J Clin Nutr. 2004;79:487-493.
4. Linne Y, Rossner S. Interrelationships betweenweight development and weight retention in subse-quent pregnancies: The SPAWN study. Acta ObstetGynecol Scand. 2003;82:318-325.
5. Gunderson EP, Abrams B, Selvin S. Does the patternof postpartum weight change differ according to pre-gravid body size? Int J Obes Relat Metab Disord.2001;25:853-862.
6. Stewart AW, Jackson RT, Ford MA, Beaglehole R.Underestimation of relative weight by use of self-reported height and weight. Am J Epidemiol. 1987;
125:122-126.