Supporting Pregnant Women with Substance Use Disorders
53
Me and My Baby: Supporting Pregnant Women with Substance Use Disorders Principal Authors: Melissa T. Foss, Karen M. Foss, Denise F. Clarke
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Supporting Pregnant Women with Substance Use Disorders
Me and My Baby: Supporting Pregnant Women with Substance Use Disorders
Principal Authors: Melissa T. Foss, Karen M. Foss, Denise F. Clarke
1
Me and My Baby: Supporting Pregnant Women with
Substance Use Disorders Lead Author: Melissa T. Foss Supporting Authors: Karen M. Foss, Denise F. Clarke Contributing Authors/Consultants: Laureen McPeak, RN BScN Kathy Pincombe, BScPharm Clarissa Chow, PharmD Kim Chapman, BScPharm APA Dr. Matthew Simmonds, MD FRCPC Maternal Medication Use and Neonatal Abstinence (MMUNA) Collaborative: Karen Foss, RN PhD, Project Lead Neonatal Nurse Practitioner, Women’s & Child Health Grey Nuns Community Hospital, Covenant Health Denise Clarke, RN MN, Project Lead Neonatal Nurse Practitioner Northern Alberta Neonatal Intensive Care Program, Alberta Health Services Women’s & Child Health, Covenant Health Stephanie Haire, MSW RSW, Project Coordinator Social Worker, Women’s & Child Health Grey Nuns Community Hospital, Covenant Health Dr. Kathy Cardinal, BSc MD CCFP, Lead Project Physician Physician, Grey Nuns Community Hospital, Covenant Health Physician, Woodcroft Community Perinatal Program, Alberta Health Services Physician, Millwoods Maternity Care Clinic Dr. Paul Byrne, MB ChB BAO FRCPC FAAP, Consulting Neonatologist Medical Director Grey Nuns Community Hospital NICU Staff Neonatologist, Stollery Children’s Hospital Clinical Professor, Faculty of Medicine and Dentistry, University of Alberta Dr. Matt Hicks, MD PhD FRCPC, Consulting Neonatologist Neonatologist and Developmental Pediatrician Assistant Professor, Department of Pediatrics Faculty of Medicine and Dentistry, University of Alberta Gail Cameron, RN BScN Senior Director, Operations Women’s & Child Health, Covenant Health Grey Nuns Community Hospital Social Work Team Angelica Allende, MSW (Equiv.) RSW Jody Cook, BSW RSW Lynn Lyskoski, BSW RSW Brandy Zakal, Administrative Support
2
[Foreword]
“When we do the best we can, we never know what miracle is wrought in our life, or in the life of another”
Albert Einstein
I congratulate Melissa Foss and her co-authors on the completion of this booklet, entitled Me and My Baby: Supporting Pregnant Women with Substance Use Disorders. In this comprehensive review two main themes emerge. First, there is increased substance use globally, including among women of child bearing age. Second, there is a pervasive need for information sharing with health care professionals and community providers interconnecting with these women and their babies. This education resource addresses a current noticeable gap in knowledge for many health care providers, and showcases the MMUNA Team’s commitment to advancing understanding for these vulnerable women and their babies. The MMUNA Team’s ongoing education efforts, with the aim of changing practice in the acute management of pregnant women with substance use disorders and their babies at risk for Neonatal Abstinence Syndrome, exemplifies how one group can enact small changes to have a positive impact in the caring landscape. These efforts align with Covenant Health’s value of achieving the best possible health outcomes, including enabling those with substance use disorders to live and participate in programs with dignity and hope. Gail Cameron Senior Director, Operations Women’s & Child Health Covenant Health
3
Table of ContentsIntroduction …………………………………………………………………………………4
Substance Use Disorders and Pregnancy……………………………………………………7
Harm Reduction…………………………………………………………………………….10
Trauma Informed Care……………………………………………………………………...15
Opioid Replacement Therapy……………………………………………………………….18
The Dynamics of Acute Pain Management…………………………………………………23
Neonatal Abstinence Syndrome…………………………………………………………….28
Transitioning from Hospital to Home………………………………………………………37
Appendix A: Substance and Withdrawal Effects…………………………………………...46
Appendix B: Finnegan Neonatal Abstinence Scoring Tool………………………………...47
Appendix C: NAS Medication Management Plan………………………………………….48
Maternal Medication Use and Neonatal Abstinence (MMUNA) Collaboration Maternal and Neonatal Programs, Grey Nuns Community Hospital, Covenant Health 1100 Youville Drive West Edmonton, Alberta T6L 5X8
© Covenant Health 2017 Disclaimer The opinions reflected in this report do not necessarily reflect those of Covenant Health. Acknowledgements The MMUNA Collaboration acknowledges the project funding contributions provided by the Alberta Government. Photo credits front cover and inside back cover to Lisa Lacroix. Author Contact [email protected]

4
Introduction Substance use is a common problem and is a growing concern worldwide. In Canada alone, nearly five million people use illegal drugs, more than six million are addicted to cigarettes, and about two million abuse alcohol (Canada Drug Rehab, 2014). According to Teen Challenge Canada (2015), in Canada the average age drug use begins is 15.7 years and approximately 47, 000 deaths are linked to substance abuse each year. A review of various studies was done by Single et al. (1999) to summarize morbidity and mortality related to substance use. They found that in 1992, approximately 6700 Canadians lost their lives from alcohol abuse, just over 33000 tobacco-related deaths occurred and around 700 illicit drug-related deaths occurred. The majority of alcohol-related deaths were from impaired driving motor vehicle collisions, though liver cirrhosis and alcohol-related suicides were also reported, especially involving relatively young people. Tobacco-related deaths included lung cancer, causing the most deaths, ischemic heart disease, and chronic obstructive pulmonary disease. An estimated 66% percent of these deaths occurred in men. Of the illicit drug related deaths, 87% of these mortalities occurred in men with suicide accounting for a large proportion. Opiate poisoning, cocaine poisoning, and AIDS related deaths were also reported. These fatalities, though much fewer in number, typically involved much younger victims in comparison to those caused by alcohol or tobacco. In a study carried out in the state of New York by Kandel and Logan (1984), patterns of substance use were observed in a cohort of male and female grade 10 and 11 students through to the age of 24.7 years. This interview-based study found that the highest risk for initiation of cigarette, alcohol and marijuana use is before the age of 20, while for illicit drugs, excluding cocaine, the age of initiation is 21 years. Participants that did not experiment with these substances by these ages were unlikely to do so at later ages; however, it is known that initiation of prescribed psychoactive drug use usually occurs later in life and would not have been captured in this study. Interestingly, between the ages of 20-21 there was a steep decline in marijuana and alcohol use, in contrast to cigarette use, which began to increase during this
“Addiction begins with the hope that something ‘out there’ can instantly fill up the emptiness inside.” – Jean Kilbourne

5
period. Overall, it has been found that men typically have higher use rates than women for all substances except for prescribed psychoactives (Kandel & Logan, 1984). A later study by Anthony et al. (1994), involving secondary analysis of the National Comorbidity Survey (NCS) of drug dependence in an American nationally representative population, examined alcohol, tobacco, controlled substances and inhalant dependencies. Results of this analysis indicated that in people aged 15-54 approximately 24% had a history of tobacco use, about 14% had a dependence on alcohol, and nearly 8% had a dependence on inhalants or controlled drugs. A later analysis of this same data by Wagner and Anthony (2002) explored age-specific risks of drug initiation to substance dependence. They found that the highest rate of alcohol and marijuana use occurred in 18 year olds, while cocaine initiation was estimated to occur more frequently in 20 years old. Participants who were at risk for meeting the criteria to be considered to have clinical dependence syndrome for alcohol and marijuana peaked at 17-18 years old, as opposed to the mean cocaine clinical dependence syndrome at 23-35 years old. After ten years from the first use, about 8% of marijuana users were considered dependent on the substance, and approximately 12-13% of alcohol users were found to be dependent. An estimated 5-6% of cocaine users became dependent on the drug within one year of initiation and after ten years of continued use approximately 15-16% met the criteria for cocaine dependence. In Canada, as a whole, a 2011 Health Canada survey on drug and alcohol use reported that among women of child bearing age (15 years and older), nearly 77% admitted to alcohol consumption, nearly 11% admitted to cannabis use and approximately 2% reported illicit drug use (Health Canada, 2011 results retrieved 2015). In a more recent Health Canada survey, in 2013 psychoactive pharmaceutical use (opioid pain relievers, stimulants, tranquilizers/ sedatives) among Canadians aged 15 years and older was reported in 22% of those surveyed (6.4 million), and prevalence continued to be higher in females than in males (Health Canada, 2013 results retrieved 2015). Of the three categories of psychoactive drugs surveyed in 2013, opioid pain relievers were the most commonly used, reported by one in seven Canadians aged 15 years and older, 2% of which reported abuse of these substances.
References
Anthony, J., Warner, L., & Kessler, R. (1994). Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: Basic findings from the National Comorbidity Survey. Experimental Clinical Psychopharmacology, 2(3), 244-268. Canada Drug Rehab. (2014). Drug and alcohol addiction in Canada. Retrieved from http://www.canadarehab.ca/drug_addictions_canada.html Health Canada. (2014). Canadian Alcohol and Drug Use Monitoring Survey (CADUMS): Summary of results for 2011/2012/2014. Retrieved from http://www.hc-sc.gc.ca/hc-ps/drugs-drogues/cadums-esccad-eng.php Health Canada. (2015). Canadian Tobacco, Alcohol and Drugs Survey (CTADS). Summary of Results for 2013. Ottawa: Office of Research and Surveillance, Controlled Substances and Tobacco Directorate. Retrieved from http://healthycanadians.gc.ca/science-research-sciences-recherches/data-donnes/ctads-ectad/summary/sommaire-2013-eng.php Kandel, D., & Logan, J. (1984). Patterns of drug use from adolescence to young adulthood: I. Periods of risk for initiation, continued use, and discontinuation. American Journal of Public Health, 74(7), 660-666.

6
Single, E., Robson, L., Rehm, J., & Xi, X. (1999). Morbidity and mortality attributable to alcohol, tobacco, and illicit drug use in Canada. American Journal of Public Health, 89(3), 385-390. Teen Challenge. (2015). Canadian drug crisis. Retrieved from http://www.teenchallenge.ca/get-help/canadian-drug-crisis Wagner, F., & Anthony, J. (2002). From first drug use to drug dependence: Developmental periods of risk for dependence upon marijuana, cocaine, and alcohol. Neuropsychopharmacology, 26, 479-488.
7
Substance Use Disorders and Pregnancy In Canada, between 1994 and 1996, approximately 6 to 10% of pregnant women used substances, and of the women who admitted to and named the illicit drugs they used, marijuana was the most common at 77% (Elliott et al., 2004). In Alberta specifically, in 2006 2.3% of women reported using illicit substances while pregnant, also with marijuana being the most commonly used substance (Porath-Waller, 2009). McVay (2015) summarizes more recent statistics relating to substance use and pregnancy. In the years 2011-2012 approximately 5% of pregnant American women aged 15 to 44 used substances during pregnancy. Among these same pregnant American women, nearly 9% used alcohol during their pregnancy. The effects of drug and alcohol use during pregnancy vary according to the substance used. Refer to Finnegan (2013) and Wong et al. (2011) for a summary of the maternal consequences of antenatal substance use. The problem of substance use during pregnancy continues to be a global health issue. The incidence of heroin and other opiate addiction in pregnancy has been steadily increasing in Canada. In 2011, 18% of pregnant women used opiates (CIHI in Finnegan, 2013), though this percentage is climbing. In Ontario, for example, about 30% of pregnant women use opioids (Spurr, 2016). Prescription opioid use during pregnancy is reaching concerning levels, in part due to the widespread increase in the number of opioid prescriptions dispensed to all Canadians (Canadian Centre on Substance Abuse, 2015; Gomez et al., 2014; Volkow, 2014), and has a parallel association with the rise in heroin use (Muhuri et al., 2013; Volkow, 2016). Non-medical use of prescription opioids is a growing problem worldwide and especially in Canada where, in 2011, it has the highest consumption of oxycodone in the world (International Narcotics Control Board, 2013). According to Muhuri et al. (2013), on behalf of the American federal agency Substance Abuse and Mental Health Services Administration (SAMHSA), the strongest risk factor for heroin use is opioid addiction. The Centers for Disease Control and Prevention (2015) states that heroin use has more than doubled in adults aged 18-25 in the last decade. Heroin use among pregnant women, in particular, has seen a dramatic increase in comparison to men.
“[In 2011], at least 1,057 babies were born in Canada with NAS, an 18-per-cent increase over the year before according to the Canadian Institute for Health Information.” – Anna Mehler Paperny

8
The social response to substance use during pregnancy varies. In some US states pregnant women testing positive for drug use are punished through incarceration, and have a high chance of having their children removed from their care (Miller, 2015; Miranda et al., 2015). Some states are even testing all pregnant women for opiate use, not just those deemed to be a high risk based on their background. In Canada these controversial criminalization laws dictating incarceration have not been explored; a pregnant woman cannot be mandated by a court order to attend addiction treatment (CanFASD Research Network’s Action Team, 2014). Further, tendencies towards apprehension of children of substance using women are changing as substance use disorders are fast becoming recognized as an illness reaching pandemic proportions (CanFASD Research Network’s Action Team, 2013; Drabble & Poole, 2011; Finnegan, 2013; Nathoo et al., 2013; Poole & Isaac, 2001). As such, North American movements in various regions are calling for social reform in approaches to and management of substance use disorders during pregnancy, one of which is harm reduction.
References
Canadian Centre on Substance Abuse. (2015). Canadian drug summary. Prescription opioids. Retrieved from http://www.ccsa.ca/Resource%20Library/CCSA-Canadian-Drug-Summary-Prescription-Opioids-2015-en.pdf CanFASD Research Network’s Action Team on Prevention from a Women’s Health Determinants Perspective. (2013). Supporting pregnant and parenting women who use substances. What communities are doing to help. Vancouver: Canada FASD Research Network. Retrieved from http://www.canfasd.ca/wp-content/uploads/2013/02/ What_Communities_Are_Doing_to_Help_February_7_2013.pdf CanFASD Research Network’s Action Team on Prevention from a Women’s Health Determinants Perspective. (2014). Substance use during pregnancy. An overview of key Canadian policy and practice areas. Vancouver: Canada FASD Research Network. Retrieved from http://bccewh.bc.ca/wpcontent/uploads/2014/09/ Canadian.Policy-on.Subst-Use-+-Preg.Sept-2-2014web.pdf Centers for Disease Control and Prevention. (2015). Today’s heroin epidemic. Retrieved from www.cdc.gov/vitalsigns/heroin/ Drabble, L., & Poole, N. (2011). Collaboration between addiction treatment and child welfare fields: Opportunities in a Canadian context. Journal of Social Work Practice in the Addictions, 11(2), 124-149. Elliott, M., Cunliffe, P., Demianczuk, N., & Robertson, C. (2004). Frequency of newborn behaviours associated with neonatal abstinence syndrome: A hospital-based study. Journal of Obstetrics & Gynaecology of Canada, 26(1), 25-34. Finnegan, L. (2013). Licit and illicit drug use during pregnancy: Maternal, neonatal and early childhood consequences. Ottawa: Canadian Centre on Substance Abuse. Gomez, T., Mamdani, M., Paterson, J., et al. (2014). Trends in high-dose opioid prescribing in Canada. Canadian Family Physician, 60, 826-832. International Narcotics Control Board. (2013). Narcotic drugs technical report: Estimated world requirements of 2013 – statistics for 2011. New York: United Nations. McVay, D. (2015). Common sense for drug policy. Drug War Facts (6th ed.). Retrieved from http:www.drugwarfacts.org Miller, A. (2015). Using the “War on Drugs” to arrest pregnant women. Retrieved from www.politicalresearch.org
9
Miranda, L., Dixon, V., & Reyes, C. (2015). How states handle drug use during pregnancy. Retrieved from https://projects.propublica.org/graphics/maternity-drug-policies-by-state Muhuri, P. Gfroener, J., & Davies, M. (2013). Association of nonmedical pain relievers and initiation of heroin use in the United States. CBHSQ Data Review August 2013. Substance Abuse and Mental Health Services Administration [SAMHSA]. Retrieved from http://www.samhsa.gov/data/ Nathoo, .T, Poole, N., Bryans, M., et al. (2013). Voices from the community: Developing effective community programs to support pregnant and early parenting women who use alcohol and other substances. First Peoples Child & Family Review, 8(1), 94-107. Poole, N., & Isaac, B. (2001). Apprehensions: Barriers to treatment for substance using mothers. Vancouver: BC Centre of Excellence for Women’s Health. Porath-Waller, A. (2009). Clearing the smoke on cannabis: Chronic use and cognitive functioning and mental health. Ottawa: Canadian Centre on Substance Abuse. Spurr, B. (2016). Pregnancy ‘addiction problem’ hits Thunder Bay area. Thestar.com. Retrieved from https://www.thestar.com/news/canada/2016/03/07/pregnancy-addiction-problem-hits-thunder-bay-area.html Volkow, N., Senate Caucus on International Narcotics Control. (2014). America’s addiction to opioids: Heroin and prescription drug abuse. Bethseda, MD: National Institute of Drug Abuse. Retrieved from www.drugabuse.gov/about/nida/legislative-activities/testimony-to-congress/2016/americas-addiction-to-opioids-heroin-prescription-drug-abuse Volkow, N. (2016). Opioids in pregnancy. British Medical Journal, 352, i19. http://dx.doi.org/10.1136/bmj.i19 Wong, S., Ordean, A., & Kahan, M. (2011). Substance use in pregnancy. SOGC Clinical Practice Guideline. Journal of Obstetrics & Gynaecology of Canada, 33(4), 367-384.
10
Harm Reduction Harm reduction, rooted in an HIV and overdose epidemic of the late twentieth century, opposes the traditional approach to dealing with substance use disorders: The War on Drugs (Marlatt, 1996). The 1994 Drug Control Strategy (Office of National Drug Control Policy, 1994) outlined goals for dealing with drug usage in the United States. The ultimate goals outlined by this national office emphasized the idea of use reduction. Drawing from European success in achieving a middle ground approach to the HIV epidemic, American public health responses to this “no-use” message focused on shifting the prevailing mindset to harm reduction drug policy instead: “The principal goal for drug policy should instead be to reduce the harms to society arising from the production, consumption and control of drugs. Total harm (to users and the rest of society) can be expressed as the product of total use and the average harm per unit of use and thus can be lowered by reducing either component” (Marlatt, 1996, page, 779). Though proponents of harm reduction strategies do recognize withdrawing use of substances to complete abstinence as an ideal outcome, this philosophy is tolerant of changes that diminish harm (Barnaby et al., 2010). Canada, as well, has adopted harm reduction practices to address similar critical public health issues. For example, a discussion guide for the BC Centre of Excellence (Poole, Urquhart & Talbott, 2010), focusing on HIV/AIDS in an impoverished Vancouver community, indicates that as a result of various integrated community-based harm reduction programs fewer women are using drugs and, of those who do, fewer are injecting them.
Harm Reduction in Pregnancy A woman’s pregnancy is seen as an optimal time to provide support in enhancing her health, as well as an opportunity to diminish or stop substance abuse, as she may be motivated by the potential adverse effects on her child (Canada Northwest FASD Research Network Action Team, 2010; Nathoo et al., 2015). The main goal of harm reduction when aiding pregnant women is to help them set practical and intermediate steps towards a healthier lifestyle and a safer use of substances, rather than withdrawing to complete abstinence (Poole & Urquhart, 2010). The mother’s needs, such as housing and nutrition, must be cared for in order to
“I see harm reduction as a way of engaging people as part of that path to recovery.” – Paul R. Ehrlich
11
achieve this goal, as well as caring for other harm factors such as violence and trauma, previous criminalizations, sex work, and HIV risk to improve the health of herself and her baby during her pregnancy (Poole, Urquhart & Talbot, 2010). Even so, it is important to recognize that “while women are typically motivated to reduce their substance use during pregnancy women who are in abusive relationships may not be able to do so” (CanFASD Research Network’s Action Team, 2013, p.4). Safer and reduced substance use is known to improve the nutrition of both the mother and baby, as well as result in less preterm births and fewer low birth weight babies (Goler et al., 2008; Marshall et al., 2005; Wodinski et al., 2013). These improved pregnancy outcomes translate to shorter birth hospitalizations and higher rates of babies going home with their mothers (Motz et al., 2006; Poole, 2000; Wodinski et al., 2013). Harm reduction in pregnancy may also positively impact breastfeeding, maternal attachment, and enhance the early development of the baby (Motz et al., 2006; Niccols, Milligan, Smith et al., 2012; Niccols, Milligan, Sword et al., 2012; Poole, 2000). Similarly, harm reduction is economically beneficial. In Alberta from 2008 to 2011, nearly 400 women were involved with Parent-Child Assistance Programs, for example, which yielded in the prevention of approximately 31 children being born with Fetal Alcohol Spectrum Disorder (Thanh et al., 2014). In this three year period, this Parent-Child Assistance Program resulted in cost savings of about $22 million.
Harm Reduction Strategies There are many evidence-based harm reduction strategies that caregivers may use to attend to the needs of pregnant women. Housing is a large concern and is often disregarded in relation to harm reduction. Instability in housing is associated with reduced physical and mental health, insignificant education, lack of employment, and traumatic histories (Barnaby et al., 2010; Elifson et al., 2007; Freund & Hawkins, 2004; Poole, Urquhart & Talbot, 2010). Women with a lack of stable housing are also at high risk for experiencing violence, including unwanted sexual encounters (Barnaby et al., 2010; Finnegan, 2013; Khandor & Mason, 2007; Poole, 2000). Sheway, a Vancouver-based substance abuse program, has shown that even small amounts of financial support may aid mothers in obtaining sufficient housing to reduce the harms they are subject to while homeless, and in turn possibly helping them to maintain custody of their children (Salmon, 2010). Education about safer drug use is another highly important harm reduction strategy. For example, programs exist that aid in the distribution of clean needles and other supplies to prevent the spread of infections and ensure that women understand that they should not share any materials related to preparing, injecting or inhaling drugs (Nathoo et al., 2015). The first North American government approved supervised injection facility (SIF) was opened in Vancouver in 2003 (Nathoo et al., 2015; Wong et al., 2011). The opening of the SIF occurred in response to a call for action by drug user groups desiring change in relation to the detrimental health concerns of injection drugs (Tyndall et al., 2005). In the first 14 months of operation of this facility there were 4764 individuals registered into the SIF database. This program was not only successful in attracting a vast amount of drug users, but also improved drug overdose outcomes: of the 273 witnessed overdoses there were no fatalities. Also, as a result of potentially being the only point of contact for health related services for many of these drug users, over 2000 individuals were referred for counseling and addiction services. In a later mathematical modelling study aimed at the analysis of cost-benefit and cost-

12
effectiveness, Andresen & Boyd (2009) found that 35 cases of HIV and 3 deaths were prevented on average each year from SIF, which had a societal benefit in excess of $6 million annually even after program costs were taken into account. Therefore, SIFs have proven to be an effective and efficient use of health care resources (Andresen & Boyd, 2009). Another harm reduction approach is improving the relationships between the caregivers and pregnant women so that they feel physically and emotionally safe when accessing health services. A study that has been carried out in Vancouver’s Downtown Eastside suggests that street-involved women are discouraged from accessing health and social services programs for fear of exposure to violence and policing in the areas where these services are located (Shannon, 2005). Many women avoid seeking care when pregnant while using substances because they fear that Child Protective Services will apprehend their babies (Cormier et al., 2004). However, it is suggested that if the mother has health and social supports in place to help her care for her baby and aid in managing her substance use disorder, there is decreased likelihood of apprehension occurring (Maternity Centre, 2013; Poole & Isaac, 2001). Ultimately, the goal of health and social support is to have the babies remain in the care of their mothers or other family in the same home if it is safe to do so. Therefore, for improved harm reduction programming to occur, health and social services must interact to create an atmosphere that is both safe and that the mothers are willing to attend. This includes comprehensive and accessible programs addressing violence and sexual assault prevention, addiction services, support for residential school survivors and Sexually Transmitted Infection prevention and management (Poole, Urquhart & Talbot, 2010). The 1998 two phase cross-site study entitled Women, Co-occurring Disorders and Violence Study (Substance Abuse and Mental Health Services Administration, no date) examined integrated service models in nine US sites. The key aim of the models in this study were to reduce the stress experienced by mothers accessing these services, especially for those with complex psychosocial and physical needs. This study found that women with multiple health and social issues reduced their dependence on drugs, experienced fewer symptoms of trauma, and demonstrated increased mental health as a result of integrated care (Cocozza et al., 2005; Cusack, 2008). These integrated service models are seen as the ideal since they are cost friendly and ultimately the caregivers are trauma informed (BC Centre of Excellence for Women’s Health, 2009).
References
Andresen, M., & Boyd, N. (2009). A cost-benefit and cost-effectiveness analysis of Vancouver’s supervised injection facility. International Journal on Drug Policy, 21(1), 70-76. Barnaby, L., Penn, R., & Erickson, P. (2010). Drugs, homelessness & health: Homeless youth speak out about harm reduction. Toronto: Shout Clinic Harm Reduction Report. BC Centre of Excellence for Women’s Health. (2009). Trauma-informed approaches in addictions treatment. Gendering the National Framework series (Vol. 1). Vancouver: Author. Canada Northwest FASD Research Network Action Team on Prevention from a Women’s Health Determinants Perspective. (2010). Taking a relational approach: The impotence of timely and supportive connections for women. Retrieved from http://www.canfasd.ca/wpcontent/uploads/2013/02/RelationalApproach_March_2010.pdf
13
CanFASD Research Network’s Action Team on Prevention from a Women’s Health Determinants Perspective. (2013). Supporting pregnant and parenting women who use substances. What communities are doing to help. Vancouver: Canada FASD Research Network. Retrieved from http://www.canfasd.ca/wp-content/uploads/2013/02/ What_Communities_Are_Doing_to_Help_February_7_2013.pdf Cocozza, J, Jackson, E., Henningan, K., et al. (2005). Outcomes for women with co-occurring disorders and trauma: Program-level effects. Journal of Substance Abuse Treatment, 28(2), 109-119.
Cormier, R., Dell, C., & Poole, N. (2004). Women and substance use problems. Women’s health surveillance report. BioMedical Central Women’s Health, 4(Suppl 1), S1-S8. http://dx.doi.org/10.1186/1472-6874-4-S1-S8
Cusack, K., Morrissey, J.,& Ellis, A. (2008) Targeting trauma-related interventions and improving outcomes for women with co-occurring disorders. Administration & Policy in Mental Health & Mental Health Services Research, 35(3), 147-158. Elifson, K., Sterk, C., & Theall, K. (2007). Safe living: The impact of unstable housing conditions on HIV risk reduction among female drug users. AIDS and Behavior, 11(6 Suppl), 45-55. Finnegan, L. (2013). Licit and illicit drug use during pregnancy: Maternal, neonatal and early childhood consequences. Ottawa: Canadian Centre on Substance Abuse. Freund, P., & Hawkins, D. (2004). What street people reported about service access and drug treatment. Journal of Health & Social Policy, 18(3), 87-93. Goler, N., Armstrong, M., Taillac, C., & Osejo, V. (2008). Substance abuse treatment linked with prenatal visits improves perinatal outcomes: A new standard. Journal of Perinatalogy, 28(9), 597-603. Khandor, E., & Mason, K. (2007). The street health report. Toronto: Street Health. Marlatt, L. (1996). Harm reduction: Come as you are. Addictive Behaviors, 21(6), 779-788. Marshall, S., Charles, G., Hare, J., et al. (2005). Sheway’s services for substance using pregnant and parenting women: Evaluating the outcomes for infants. Canadian Journal of Community Mental Health, 24(1), 19-33. Maternity Centre. (2013). Healthy outcomes for you and your baby. Thunder Bay Regional Health Sciences Centre. Retrieved from http://www.tbdhu.com/sites/default/files/files/ resource/201603/Neonatal% 20Abstinence%20Syndrome%20Pamphlet%202013.pdf Motz, M., Leslie, M., Pepler, D., et al. (2006). Breaking the cycle: Measures of progress 1995-2005. Journal of FAS International, Special Supplement, 4, e22. Retrieved from http://www.motherisk.org/JFAS_documents/ BTC_JFAS_ReportFINAL.pdf Nathoo, T., Marcellus, L., Bryans, M., et al. (2015). Harm reduction and pregnancy: Community-based approaches to prenatal substance use in Western Canada. Victoria and Vancouver: University of Victoria School of Nursing and BC Centre of Excellence for Women’s Health. Niccols, A., Milligan, K., Smith, A., et al. (2012). Integrated programs for mothers with substance abuse issues and their children: A systematic review of studies reporting on child outcomes. Child Abuse & Neglect, 36(4), 308-322.
Niccols, A., Milligan, K., Sword, W., et al. (2012). Integrated programs for mothers with substance abuse issues: A systematic review of studies reporting on parenting outcomes. Harm Reduction Journal, 19(9), 14. http://dx.doi.org/ 10.1186/1477-7517-9-14
Office of National Drug Control Policy. (1994). National drug control strategy. Reclaiming our communities from drugs and violence. Washington, DC: Author.
14
Poole, N. (2000). Evaluation report of the Sheway project for high-risk pregnant and parenting women. Vancouver: BC Centre of Excellence for Women’s Health. Poole, N., & Isaac, B. (2001). Apprehensions: Barriers to treatment for substance using mothers. Vancouver: BC Centre of Excellence for Women’s Health. Poole, N., & Urquhart, C. (2010). Mothering and substance use: Approaches to prevention, harm reduction and treatment. Gendering the National Framework Series (Vol. 3). Vancouver: BC Centre of Excellence for Women’s Health. Poole, N., Urquhart, C., & Talbot, C. (2010). Women-centered harm reduction. Gendering the National Framework Series (Vol.4). Vancouver: BC Centre of Excellence for Women’s Health. Salmon, A. (2010). The impact of MEIA-funded support on Sheway clients. Presentation at Network Action Team on FASD Prevention Biannual Meeting. Victoria: BC Centre of Excellence for Women’s Health. Shannon, K. (2005). Access and utilization of HIV treatment and services among women sex workers in Vancouver’s downtown eastside. Journal of Urban Health, 82(3), 488-497. Substance Abuse and Mental Health Services Administration (no date). Women, co-occurring disorders & violence study. Program Summary. Substance Abuse and Mental Health Services Administration. Retrieved from http://www.wcdvs.com/pdfs/ ProgramSummary.pdf Thanh, N., Jonsson, E., Moffat, J., et al. (2014). An economic evaluation of the parent-child assistance program for preventing Fetal Alcohol Spectrum Disorder in Alberta, Canada. Administration and Policy in Mental Health and Mental Health Services Research, 42(1), 10-18. Tyndall, M., Kerr, T., Zhang, R., et al. (2005). Attendance, drug use patterns, and referrals made from North America’s first supervised injection facility. Drug and Alcohol Dependence 83(3), 193-198. Wodinski, L., Wanke, M., & Khan, F. (2013). Impact evaluation of the H.E.R. pregnancy program – final summary report. Edmonton: Charis Management Consulting for the Alberta Centre for Child, Family and Community Research. Wong, S., Ordean, A., & Kahan, M. (2011). Substance use in pregnancy. SOGC Clinical Practice Guideline. Journal of Obstetrics & Gynaecology of Canada, 33(4), 367-384.
15
Trauma Informed Care Trauma Informed Care involves recognizing trauma, coming to an understanding of the effects it has on women, and responding appropriately in a non-judgmental way. Service providers should be knowledgeable of the traumatic experiences women may have dealt with and recognize the possible impact it has had on their choices, and then incorporate this knowledge into the services being provided (BC Centre of Excellence for Women’s Health, 2009; Poole, Urquhart & Talbott, 2010). This knowledge-based service is highly dependent on the idea that the behaviors women display are merely a means of coping with previous distressing events (BC Centre of Excellence for Women’s Health, 2010). Ideally, the mindsets of caregivers shift from a negative outlook to an understanding: “Disorders become responses, and symptoms become adaptations” (Haskell, 2003, p. 20 as quoted in BC Centre of Excellence for Women’s Health, 2009, p.4). Even so, it is important to note that being trauma informed does not mean knowing the specific details of each woman’s personal story, but rather having an encompassing knowledge that each woman may have a traumatic history and to be conscientious of it (BC Centre of Excellence for Women’s Health, 2009). Nearly 2/3 of women that have issues with substance abuse admit to having a pre-existing mental health condition, such as depression or Post Traumatic Stress Disorder (PTSD) (Logan et al., 2002). Trauma is also connected to other health issues, including sleep disorders and cardiovascular problems (Haskell, 2003; National Institute on Alcohol Abuse and Alcoholism, 1999; Poole & Dell, 2005), and women have been found to be twice as likely as men to acquire PTSD after suffering a trauma (Norris et al., 2002). The extent of the symptoms experienced by women may last up to four times longer as those faced by men (Norris et al., 2002). Many women with mental health and substance use disorders admit to previously having been subject to physical or sexual abuse, demonstrating a relationship between trauma and substance use (BC Centre of Excellence for Women’s Health, 2009). Increasingly, it has been shown that many women with mental health issues have substance use disorders, and often these affected women in turn have a history of trauma (Fallot & Harris, 2004; Larkin et al., 2014; Wolf et al., 2015).
“Improving the system of care for girls and women requires a paradigm shift from ‘what is wrong with her?’ to ‘what happened to her?’“ -BC Centre of Excellence for Women’s Health, 2009, page 8
16
Traumatic experiences in childhood, also known as adverse childhood events (ACEs), are largely determinant of a woman’s physical and mental health throughout the remainder of her life (Masterson, 2014). These ACEs may include different forms of abuse such as psychological, physical and sexual, as well as emotional and physical neglect (Center for the Developing Child at Harvard University, 2016). When threatened, their bodies prepare them to respond through a life-saving fight or flight response, but continuous activation of this mechanism can have a “wear and tear effect” (Center for the Developing Child at Harvard University, 2016, p. 13). The number of ACEs an individual experiences is not only associated with risk for premature death (Brown et al., 2009), but also is directly correlated with the likelihood of substance abuse later in life: a child who experiences five or more ACEs is seven to ten times more likely to report illicit drug use problems, addiction to illicit drugs and injection drug use (Dube et al., 2003). However, positive early experiences and the early development of adaptive skills, through the reliable presence of at least one supportive relationship and multiple opportunities to develop effective coping skills, help build a foundation for strengthening the individual’s capacity to thrive in the face of significant adversity (Center on the Developing Child at Harvard University, 2016; National Scientific Council of the Developing Child, 2015).
References BC Centre of Excellence for Women’s Health. (2009). Trauma-informed approaches in addictions treatment. Gendering the National Framework series (Vol. 1). Vancouver: Author. BC Centre of Excellence for Women’s Health. (2010). Girl-centred approaches to prevention, harm reduction and treatment. Gendering the National Framework series (Vol. 2). Vancouver: Author. Brown, D., Anda, R., Tiemeier, H., et al. (2009). Adverse childhood experiences and the risk of premature mortality. American Journal of Prevention Medicine, 37(5), 389-396. Center on the Developing Child at Harvard University. (2016). From best practices to breakthrough impacts: A science-based approach to building a more promising future for young children and families. Retrieved from http://www.developingchild.harvard.edu Dube, S., Felliti, V., Dong, M., et al. (2003). Childhood abuse, neglect, and household dysfunction and the risk of illicit drug use: The adverse childhood experiences study. Pediatrics, 111(3), 564-572. Fallot, R., & Harris, M. (2004). Integrated service teams for women survivors with alcohol and other drug problems and co-occurring mental disorders. In B. Veysey and C. Clark (Eds.) Responding to Physical and Sexual Abuse in Women with Alcohol and Other Drug and Mental Disorders. Binghampton, New York: Haworth Press. Haskell, L. (2003). First stage trauma treatment: A guide for mental health professionals working with women. Toronto: Centre for Addiction and Mental Health Larkin, H., Felitti, V., & Anda, R. (2014). Social work and adverse childhood experiences research: Implications for practice and health policy. Social Work in Public Health, 29, 1-16. Logan, T., Walker, R., Cole, J., & Leukefeld, C. (2002). Victimization and substance abuse among women: Contributing factors, interventions and implications. Review of General Psychology, 6(4), 325-397. Masterson, T. (2014). Trauma informed neonatal care. Alberta Neonatal Nurses Association (ANNA) Conference. Edmonton: ANNA.
17
National Institute on Alcohol Abuse and Alcoholism. (1999). Are women more vulnerable to alcohol’s effects? Alcohol Alert, No. 46. Retrieved from http://pubs.niaaa.nih.gov/publications/aa46.htm National Scientific Council of the Developing Child. (2015). Supportive relationships and active skill-building strengthen the foundations of resilience: Working paper no. 13. Retrieved from http://www.developingchild. harvard.edu Norris, F., Foster, J., & Weisshaar, D. (2002). The epidemiology of sex differences in PTSD across developmental, societal, and research contexts. In R. Kimerling, P. Ouimette, and J. Wolfe (Eds.) Gender and PTSD (pp. 207-231). New York: Guilford. Poole, N., & Dell, C. (2005). Girls, women and substance use. Vancouver: BC Centre of Excellence for Women’s Health. Poole, N., Urquhart, C., & Talbot, C. (2010). Women-centered harm reduction. Gendering the National Framework Series (Vol.4). Vancouver: BC Centre of Excellence for Women’s Health. Wolf, M., Nochajski, T., & Farrell, M. (2015). The effects of childhood sexual abuse and other trauma on drug court participants. Journal of Social Work Practice in the Addictions, 15(1), 44-65.
18
Opioid Replacement Therapy In Canada there are several policies and practices that contribute to effective supportive care for pregnant women with SUD (CanFASD Research Network’s Action Team, 2013). Among these social supports is access to addiction treatment programs where pregnant women are seen as a priority. In-utero opiate exposure produces the most dramatic effects on the infant (Ashraf, 2014) including low birth weight, prematurity and intrauterine growth restriction (Schempf, 2007). While Methadone has been the mainstay of Opioid Replacement Therapy (ORT) for pregnant women in Canada, Buprenorphine is emerging as a comparably safe treatment option. The maternal and fetal benefits of participating in a structured opioid replacement program, without doubt outweigh no therapy (Kraft & van den Anker, 2012); however, to date, the long term effects of in-utero exposure to ORT on infant development, while thought to be safe on the basis of limited outcome data, remain unclear (Finnegan, 2013; Jansson et al., 2011; Kraft & van den Anker, 2012; Sanchez et al., 2008). Objectives of ORT include preventing opioid withdrawal, providing comfortable induction onto the medication, and blocking the euphoric effects of illicit opioids while attenuating the motivation to use them (Jones, Martin, Heil et al., 2008).
Methadone Treatment Methadone Maintenance Treatment (MMT) is substitution-based therapy meant to allow women to improve their physical and mental functioning (Murphy-Oikonen et al., 2012). This therapy is a common consideration for women with SUD during pregnancy to decrease their dependency on opioids (Wong et al., 2011). Methadone is an opioid agonist that has many benefits during pregnancy, such as enhanced prenatal care, longer gestation, and an increased chance of the mother maintaining custody after being discharged from the birth hospitalization. Other maternal social and harm reduction benefits of MMT include healthier lifestyle and diminished cravings for licit and illicit opiate substances (Winklbaur et al., 2008). Although infants whose mothers use methadone tend to have a lower birth weight, length, and head circumference in comparison to non-exposed babies, studies have shown that by twelve months of age exposed babies catch up to a normal size (Hunt et al., 2008; Vance et al., 1997). In neonates, maternal MMT has been shown to be effective in decreasing the severity of Neonatal Abstinence Syndrome (NAS) as well as length of birth hospitalization (Murphy-Oikonen et al., 2012).
“The mentality and behavior of drug addicts and alcoholics is wholly irrational until you understand they are completely powerless over their addiction and unless they have structured help, they have no hope.”
– Russell Brand
19
Methadone is administered daily by physicians and pharmacists which provides regular opportunities to interact with the mother and assess how she is doing (Dow et al., 2012). This contact also increases women’s ability to access social and health services including prenatal care, addiction treatment services, and other support services. To receive methadone in Alberta, women must visit an Initiating Physician for evaluation and decision-making about whether or not MMT is a suitable treatment option (College of Physicians & Surgeons of Alberta [CPSA], 2014). In order to be considered eligible for MMT women must have a diagnosis of an Opioid Dependence Disorder. The Initiating Physician will then make sure the patient understands any risks involved and the daily MMT program requirements, such as frequent physician visits and witnessed ingestions daily, as well as discussing all other available treatment options. Detoxification is one treatment option that may be considered however, risk of relapse is higher in pregnant women with this treatment modality and the risk of adverse fetal/infant outcomes is increased (Dashe et al., 1998; Kraft & van den Anker, 2012). When prescribing methadone, a physician is expected to encourage the patient to take part in other services, such as addiction counseling, to ensure optimal results (CPSA, 2014). The Alberta Methadone and Maintenance Treatment Standards and Guidelines for Dependence (CPSA, 2014) is meant to guide practitioners in the safe use of methadone for treating opioid dependent patients. For example, a major safety risk of MMT is the long half-life and rapid absorption rate of the drug, giving it the ability to accumulate and lead to sedation, respiratory depression, or death (McCarthy et al., 2005). According to the Alberta practice guideline, the starting dose of methadone is less than 30 mg daily depending on the risk factors involved for the patient, as overdose resulting in possible death is most likely to occur in the first two weeks of treatment initiation. In the stabilization phase, the Initiating Physician is encouraged to avoid increasing the dose by more than 10 mg per dose every 5-7 days, and if a dose is missed, future doses must be managed carefully as built up tolerance can easily be lost resulting in unexpected overdoses. Once a patient has been stabilized on methadone, she visits a Maintaining Physician who manages MMT as part of her general primary care. The most ideal dose of methadone the patient will receive conceivably minimizes withdrawal symptoms and reduces cravings for 24 hours without causing significant side effects. It is anticipated that this dose is reached by 2-8 weeks after initiating methadone, though it is recommended that the patient show stability with a constant dose for three months before being transferred to the Maintaining Physician. In Edmonton there are three methadone clinics: Panorama Medical Clinic, Metro City Medical Clinic, and Alberta Health Services Opioid Dependency Program. A woman who is pregnant and requesting MMT is given priority for entering a program over other candidates. Since pregnancy increases methadone metabolism, higher dosages or split doses are typically required, and to maintain stability the dosage must often be altered throughout the pregnancy (Bogen et al., 2013; Jarvis et al., 1999; McCarthy et al., 2005; McCarthy et al., 2015; Patrick et al., 2012). In the postpartum period, as drug utilization changes after delivery, women on MMT must be observed for signs of methadone overdose, such as increased drowsiness (CPSA, 2014; McCarthy et al., 2005).

20
Buprenorphine Treatment1 Buprenorphine Maintenance Treatment (BMT) is a newer option for treating opioid dependency in pregnant women. Both the American and Canadian College/Society of Obstetricians and Gynecologists recognize buprenorphine as an appropriate alternative to MMT in these women. Like methadone, buprenorphine use in pregnancy increases the likelihood of the mother receiving regular prenatal care and maintaining custody after birth (Finnegan, 2013). Recent studies show that infants whose mothers use buprenorphine compared to methadone in pregnancy are of longer gestation, increased birth weight, and larger head circumference (Jones et al., 2010). Exact benefits of these findings are yet to be determined due to the lack of long-term neurodevelopmental outcome data. Buprenorphine availability in Canada is limited. If a woman, who is maintained on buprenorphine-naloxone (Suboxone) for opioid dependency, becomes pregnant, her prescribing physician will switch her to the single agent buprenorphine (Subutex) as naloxone use in pregnancy is not well studied (Wong et al., 2011). Buprenorphine is a special access medication that requires informed consent and patient specific application to be approved and stock obtained through Health Canada (Dow et al., 2012; Wong et al., 2011). The medication is dispensed directly by the physician at the physician’s office to the specific patient. There is no involvement by a community pharmacy/pharmacist. The patient’s physician will provide medication supply as daily, weekly, or monthly depending on how stable she is. Due to the complicated nature of supplying buprenorphine, the pregnant woman would ideally bring her own supply to use when she is admitted into hospital for her baby’s birth. Buprenorphine has a unique pharmacological and pharmacokinetic profile that creates both pros and cons with use in opioid dependency. It acts on two different opioid receptors in the body, one as a partial agonist and the other as a weak antagonist (Hilton, 2012; Mattick et al., 2008/2014). Due to the differing receptor actions, buprenorphine’s opioid agonist effect is limited at higher doses (Hall et al., 2015; Wong et al., 2011). This limited agonist effect leads to a lower risk of overdose and abuse potential (Walsh et al., 1995). The maximum daily dose of buprenorphine is 32 mg per day, which may not be sufficient in all women for maintenance treatment (NICE, 2007). Because of the ceiling effect and maximum dosing, some studies have shown an increase in patient dropout rate when compared to methadone due to the dissatisfaction with the drug (Jones et al., 2010). Buprenorphine has poor oral bioavailability therefore is supplied as a sublingual tablet. This poor oral bioavailability makes it safe to use when breast-feeding as it is unlikely that significant absorption will occur from the intake of breast milk (Lindemalm et al., 2009). The long half-life of the medication allows for daily administration however, elimination may be enhanced during pregnancy therefore twice daily dosing can be used if necessary (Jones, Martin, Heil et al., 2008). The daily dosage should be reassessed postpartum. Lastly, when compared with methadone, buprenorphine has significantly fewer drug interactions allowing for minimal prescribing restrictions when needing other medications. An exciting benefit of using BMT is the evolving evidence suggesting less severe neonatal withdrawal for the infants. The poor bioavailability, lower trans-placental passage, and higher affinity to bind to the opioid receptor, but less intrinsic activity than methadone, may all contribute to this evidence (Hilton, 2012). The Maternal Opioid Treatment: Human
1AuthoredbyKathyPincombe,Pharmacist,GreyNunsCommunityHospital

21
Experimental Research (MOTHER) trial (Jones et al., 2010), the largest study comparing methadone versus buprenorphine use in pregnant women, revealed that buprenorphine treatment resulted in lower doses of morphine for treatment of NAS, shorter duration of treatment for NAS, and shorter neonatal hospital stays. The time to initiation of treatment was longer in the buprenorphine group compared to the methadone group, which was approximately 60 hours versus 35 hours respectively. Withdrawal symptoms also differed between the two groups. Buprenorphine exposed infants demonstrated higher nasal stuffiness, sneezing, and loose stools, while the methadone exposed infants demonstrated more tremors and hyperactive symptoms. The use of buprenorphine in pregnancy will likely become more popular as more data on pregnancy and infant neurological outcomes becomes available.
References Ashraf, H. (2014). Neonatal abstinence syndrome. Retrieved from http://emedicine.medscape. com/article/978763-overview#a6 Bogen, D., Perel, J., Helsel, J., et al. (2013). Pharmacologic evidence to support clinical decision making for peripartum methadone treatment. Psychopharmacology, 225(2), 441–451. CanFASD Research Network’s Action Team on Prevention from a Women’s Health Determinants Perspective. (2013). Supporting pregnant and parenting women who use substances. What communities are doing to help. Vancouver: Canada FASD Research Network. Retrieved from http://www.canfasd.ca/wpcontent/ uploads/2013/02/What_ Communities_Are_Doing_to_Help_February_7_2013.pdf College of Physicians & Surgeons of Alberta. (2014). Alberta methadone maintenance treatment. Standards and guidelines for dependence. Edmonton: Author. Dashe, J., Jackson, G., Olscher, D., et al. (1998). Opioid detoxification in pregnancy. Obstetrics & Gynecololgy, 92, 854–858. Dow, K., Ordean, A., Murphy-Oikonen, J., et al. (2012). Neonatal abstinence syndrome clinical practice guidelines for Ontario. Journal of Population Therapeutics and Clinical Pharmacology, 19(3), e488-e506. Finnegan, L. (2013). Licit and illicit drug use during pregnancy: Maternal, neonatal and early childhood consequences. Ottawa: Canadian Centre on Substance Abuse.
Hall, E., Wexelblatt, S., Crowley, M., et al. (2015). Implementation of a neonatal abstinence syndrome weaning protocol: A multicenter cohort study. Pediatrics, 136(4), e803-e810. http://dx.doi.org/10.1542/peds.2015-1141
Hilton, T. (2012). Breastfeeding considerations of opioid dependent mothers and infants. MCN: The American Journal of Maternal Child Nursing, 37(4), 236-240. Hunt, R., Tzioumi, D., Collins, E., & Jeffery, H. (2008). Adverse neurodevelopmental outcome of infants exposed to opiate in-utero. Early Human Development, 84, 29–35. Jansson, L., Dipietro, J., Velez, M., et al. (2011). Fetal neurobehavioral effects of exposure to methadone or buprenorphine. Neurotoxicology and Teratology, 33, 240–243. Jarvis, M., Wu-Pong, S., Kniseley, J., et al. (1999). Alterations in methadone metabolism during late pregnancy. Journal of Addiction Disease, 18(4), 51–61. Jones, H., Kaltenbach, K., Heil, S., et al. (2010). Neonatal abstinence syndrome after methadone or buprenorphine exposure. New England Journal of Medicine, 363, 2320-2331.
22
Jones, H., Martin, P., Heil, S., et al. (2008). Treatment of opioid dependent pregnant women: Clinical and research issues. Journal of Substance Abuse & Treatment, 35(3), 245-250. Kraft, W., & van den Anker, J. (2012). Pharmacologic management of the opioid neonatal abstinence syndrome. Pediatric Clinics of North America, 59(5), 1147-1165. Lindemalm, S., Nydert, P., Svensson, J., et al. (2009). Transfer of buprenorphine into breast milk and calculation of infant drug dose. Journal of Human Lactation, 25(2), 199–205.
Mattick, R., Kimber, J., Breen, C., & Davoli, M. (2008/2014). Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence (Review). Cochrane Database of Systematic Reviews, Issue 2, Art. No.: CD002207. http://dx.doi.org/10.1002/14651858.CD002207
McCarthy, J., Leamon, M., Parr, M., et al. (2005). High-dose methadone maintenance in pregnancy: Maternal and neonatal outcomes. American Journal of Obstetrics & Gynecology, 193, 606–610. McCarthy, J., Leamon, M., Willits, N., & Salo, R. (2015). The effect of methadone dose regimen on neonatal abstinence syndrome. Journal of Addiction Medicine, 9(2), 105-110. Murphy-Oikonen, J., Montelpare, W., Bertoldo, L., et al. (2012). The impact of a clinical practice guideline on infants with neonatal abstinence syndrome. British Journal of Midwifery, 20(7), 493-501. National Institute for Health and Clinical Excellence (NICE). (2007). Methadone and buprenorphine for the management of opioid dependence. Retrieved from https://www.nice.org.uk/guidance/ta114 Patrick, S., Schumacher, R., Benneyworth, B., et al. (2012). Neonatal abstinence syndrome and associated health care expenditures: United States 2000-2009. Journal of the American Medical Association, 307(18), 1934–1940. Sanchez, E., Bigbee, J., Fobbs, W., et al. (2008). Opioid addition and pregnancy: Perinatal exposure to buprenorphine affects myelination in the developing brain. Glia,56, 1017–1027. Schempf, A. (2007). Illicit drug use and neonatal outcomes: A critical review. Obstetrical & Gynecological Survey, 62(11), 749–757. Vance, J., Chant, D., Tudehope, D., et al. (1997). Infants born to narcotic dependent mothers: Physical growth patterns in the first 12 months of life. Journal of Paediatrics and Child Health, 33, 504–508. Walsh, S., Preston, K., Bigelow, G., & Stitzer, M. (1995). Acute administration of buprenorphine in humans: Partial agonist and blockade effects. Journal of Pharmacological Experimental Therapy, 274, 361-372. Winklbaur, B., Kopf, N., Ebner, N. et al. (2008). Treating pregnant women dependent on opioids is not the same as treating pregnancy and opioid dependence: A knowledge synthesis for better treatment for women and neonates. Addiction, 103, 1429–1440. Wong, S., Ordean, A., & Kahan, M. (2011). Substance use in pregnancy. SOGC Clinical Practice Guideline. Journal of Obstetrics & Gynaecology of Canada, 33(4), 367-384.
23
The Dynamics of Acute Pain Management Pain is the most commonly experienced symptom in adults (Parsons, 2015). This condition, also known as nociception, occurs in up to 60% of adults (Marshall & Jackson, 2011; Parsons, 2015) and is commonly defined as the process of communication between the site of tissue damage/injury and the central nervous system (Prince, 2011). Two types of pain exist: chronic (does not settle as injury recovers, prevents normal functioning and lasts more than 3 months) and acute (from an injury or surgery that diminishes/disappears as the injury recovers) (Parsons, 2015).
Substance Use Disorders and Pain Management Subjective perceptions of SUD are commonly hampered by a societal view of substance dependence as a moral/criminal issue (Grant et al., 2007). People with SUD are often seen as “bad” people undeserving of respect or compassion: they “did this to themselves” and have to “earn” their pain medications. Yet, society does not seem to carry that same bias toward other lifestyle–related diseases, such as coronary artery disease, emphysema, Type II diabetes, and obesity. Patients are sensitive to the bias about SUD and fear that their pain needs will not be acknowledged (Mehta & Langford, 2006). Added to this bias are hospital safe guards, for example, against high dose opioid, which creates delays in drug release from pharmacy (Grant et al., 2007). According to Action on Addiction (2013), two key barriers to safe and effective pain management for recovering and current users have been identified, both of which relate to interactions between patients and care providers. First, there is stigma associated with the substance dependent identity (Oliver et al., 2012). These individuals often “live by [their] wits”, have a history of difficulty with authority structures and may have “difficulty trusting anyone” (Action on Addiction, 2013, p. 26). Internalized stigma, fear of pain and fear of withdrawal means that they are concerned they will be pre-judged and not believed when they are in pain. As a result their behavior may at times be demanding (Action on Addiction, 2013). Second, the knowledge, skills and attitudes of care providers may hinder caregiver-patient relationships and trust (Oliver et al., 2012). It is important to achieve balance amongst skepticism, appreciation of structure (rules and mutual expectations) and an empathetic stance towards distressed patients.
No one is immune from addiction; it afflicts people of all ages, races, classes, and professions. – Patrick J. Kennedy
24
In principle and in practice it is important to err on the side of over treating the occasional drug seeker than under treating the patient in pain (Buckley & Ibrahim, 2014; Roberts, 2008). The key challenges of pain management within a background of SUD include improving communication, strengthening evidence, and challenging negative stereotypes and attitudes (Buckley & Ibrahim, 2014). Common misconceptions about opioid dependency and pain management centre on various competing concerns. The first concern is about opioid analgesia triggering relapse with re-exposure, despite there being no high grade evidence that this occurs (Parsons, 2015; Roberts, 2008). This lack of evidence is compounded by other physical and emotional stressors which may actually be the triggers for cravings (Action on Addiction, 2013; Prince, 2011), defined as neuroplastic changes that occur that are not fully reversible even after several years of abstinence (Action on Addiction, 2013). While it is surmised that exposure to the former drug of choice may trigger relapse and prior opioid dependency elevates risk of relapse, there are no reliable data to estimate risk (Parsons, 2015). Anecdotal and observational studies suggest the risk of relapse is low (Action in Addiction, 2013). Second, the patient may have legitimate anxiety about pain being undertreated if adequate analgesia is not provided (Buckley & Ibrahim, 2014). As mentioned, misconceptions exist that treating the pain with opioid analgesia will cause relapse. However, the opposite is true: inadequate pain relief is more likely to trigger relapse (Action in Addiction, 2013; Grant et al., 2007). In other words, relapse is more likely to occur if pain goes untreated and patients are left to manage their own pain by self-medicating through illicit means (Parsons, 2015). Third, there is concern about the high doses of opioids that some patients with a history of opioid dependency require. This need for higher analgesic doses is actually due to increased tolerance, and not addiction (Grant et al., 2007). Fourth, caregivers may be concerned about the medical side effects of opioids and maintenance opioid replacement therapy, such as an increased risk of respiratory depression. However, the effects of tolerance secondary to long-term opioid use minimize this risk (Grant et al., 2007; Prince, 2011). These competing concerns call for robust multidisciplinary management of pain in patents with a history of past or current opioid dependency. Ideally, comprehensive history taking of what patients are actually taking versus what is prescribed should occur because if they are not part of a supervised consumption scheme they may not have been taking the full prescribed dose. When hospitalized the patient will get their full prescribed dose which may lead to over-sedation, unconsciousness, and respiratory depression, or the opposite, withdrawal, if the prescribed dose is too low (Parsons, 2015). Other agents that impact seriously patient safety are the concurrent use of benzodiazepines and/or alcohol. It is also important to have developed an individualized care plan as some patients may not want their pain treated by opioids. In these situations it is important in communicating with the patient to come up with a plan that includes use of non-opioids and/or less reinforcing opioids that are stopped as quickly as possible (Action in Addiction, 2013; Best Practice Advocacy Centre New Zealand, 2014; Mehta & Langford, 2006).
General Principles of Acute Pain Management International human rights law indicates that no one in pain should be denied adequate analgesia (Green et al., 2006; Parsons, 2015). The challenge for health care providers is balancing this right against the possibility of misuse, especially when prescribing opioids (Parsons, 2015). Opioid dependency augments the experience of pain, which leads to decreased pain tolerance (Prince, 2011). Acute pain management and provision of analgesia
25
follows the same principles for all patients regardless of their substance use history: pain is subjective in nature; self-reporting is the gold standard; and caregivers assume their patients’ pain reports are true unless there is factual evidence to believe otherwise (Grant et al., 2007; Huxtable et al., 2011; Prater et al., 2002; Roberts, 2008). It is important to reassure patients explicitly that their dependency history will not be a stigma or an obstacle to their pain relief (Mehta & Langford, 2006). Antenatally, discuss pain management goals and options with each pregnant woman with the aims of getting an accurate pre-hospitalization assessment of substance usage, keeping in mind that illicit drugs are manufactured differently from mainstream medication production. Remember that opioid using patients often are inaccurate about drug use and that the patient may be a poor historian (Buckley & Ibrahim, 2014; Mehta & Langford, 2006). As an example, opioid rotation, non-selective NSAIDs, epidural or local anaesthesia with added systemic analgesia are viable options for pain management (Jones, Martin, Heil et al., 2008; Prince, 2011). For intrapartum pain management higher doses of opioids may be required as tolerance counterbalances any analgesic effect. Of note, there is no cross-tolerance between opioids and most other substances of abuse (alcohol, benzodiazepines, cannabis, cocaine, amphetamines) therefore, patients using these substances usually only require conventional doses of opioids (Roberts, 2008). In the postpartum period accept that there is “no right answer” in recommendations for pain management in relation to patients with SUD (Action on Addiction, 2013). If an opioid is chosen for pain management it is recommended to select a drug and administration route with lower reinforcing properties, such as Morphine in oral instead of parenteral form (Roberts, 2008). It is important to emphasize that complete absence of pain postpartum may not be a realistic goal but decreased pain to optimize day to day functioning is likely attainable (Prince, 2011). If the patient is consistently reporting high pain scores a good way to assess pain is to look for impaired function (Grant et al., 2007; Marshall & Jackson, 2011), such as limited mobility and difficulty participating in the treatment plan including performing self-care and baby care. For pain that increases or fails to decline consider intrapartum/post partum complications or Opioid-Induced Hyperalgesia (OIH) (Huxtable et al., 2011; Prince, 2011). High doses of opioids can cause OIH, described as neuroplastic changes in the nervous system leading to increased pain sensitivity from opioid administration, as opposed to tolerance which leads to decreased sensitivity to opioids (Marshall & Jackson, 2001; Parsons, 2015). Management of OIH involves decreasing opioid dose, opioid rotation, and optimizing non-opioid analgesics (Parsons, 2015).
Acute Pain Management and Opioid Replacement Therapy During labor, delivery and the postpartum period the opioid replacement agent (methadone, buprenorphine) is continued (Jones, Martin, Heil et al., 2008). If the woman is NPO methadone should still be administered or replaced with other agents to prevent withdrawal (Buckley & Ibrahim, 2014; Prince, 2011; Roberts, 2008). (See sidebar). Buprenorphine patients, on the other hand, will experience minimal withdrawal with short-term interruptions; even so, the emerging trend is to continue to administer it to optimize maintenance of pain control (Jones, Martin & Heil et al., 2008; Roberts, 2008).

26
In addition to continuing a patient’s ORT, it is recommended that a multimodal approach to acute pain management be adopted by using various agents at different sites of the pain pathway. Different options include local or regional anaesthesia, patient controlled analgesia (PCA),
non-selective NSAIDs, acetaminophen, and opioid rotation (Huxtable et al., 2011; Jones, Martin, Heil et al., 2008; Marshall & Jackson, 2011; Neil, 2012). Post-operative epidural alone, without continuing the ORT, is not advisable as the patient may withdraw due to lack of provision of systematic opioids (Prince, 2011). Further, methadone and buprenorphine maintenance are inadequate for pain relief. Doses prescribed are not usually in the range to provide effective analgesia. These agents would need to be given every 6-8 hours instead, especially in the case of buprenorphine to displace it from the mu-opioid receptors (Jones, Martin, Heil et al., 2008; Parsons, 2015). For pain management, significantly higher doses of opioids may be required as tolerance counterbalances and may nullify any analgesic effect (Parsons, 2015). Consensus dictates the use of the pre-existing maintenance ORT and an additional opioid (Jones, Martin, Heil et al., 2008; Roberts, 2008). Methadone patients often require 2-3 times more opioid than the opioid naïve; it is suggested to initially provide doses 50-100% greater than usual (Roberts, 2008). In one report, women on methadone required near 70% more analgesia following a caesarean section, especially in the first 24 hours post-op in comparison to their opioid naïve counterparts (Jones, Martin, Heil et al., 2008; Prince, 2011). Buprenorphine is a partial opioid agonist that antagonizes the effects of additional illicit or therapeutic opioids (Mehta & Langford, 2006). It has a high receptor affinity and supplemental opioids given in standard doses do not displace it from mu-opioid receptors, making pain management with conventional opioid doses challenging (Jones, Martin, Heil et al., 2008; Mehta & Langford, 2006). Further, buprenorphine disassociates from mu-opioid receptors very slowly, reducing access of drugs like morphine to the receptor (Roberts, 2008). One suggestion, for example, is to provide an intravenous form of opioid that binds strongly to mu-opioid receptors, such as fentanyl and sufentanil (Prince, 2011). Buprenorphine may inhibit opioid analgesia up to 12 hours from the last administered dose of this agent, though this is not as likely to occur with the transdermal patch (Roberts, 2008). In the case of analgesia interference it is suggested to maximize non-opioid medications, such as acetaminophen and NSAIDs (Roberts, 2008). While pain assessment remains fundamental in the management of acute pain in intrapartum and postpartum periods, it is equally important to assess for signs of withdrawal (Neil, 2012). Prevention of withdrawal can be accomplished through opioid rotation since different opioids act to different degrees on various opioid receptors, are metabolized differently and there is incomplete cross-tolerance (Mehta & Langford, 2006, Parsons, 2015).
IV Morphine Conversion if No Oral Intake or Vomiting 1mg oral methadone = 4mg oral morphine 3mg oral morphine = 1mg IV morphine Eg. 30mg oral methadone à 120 mg oral morphine, 120mg oral morphine à 40 mg IV morphine
27
References Action on Addiction. (2013). The management of pain in people with a past or current history of addiction. Salisbury, Wiltshire: Author. Best Practice Advocacy Centre New Zealand. (2014). Identifying and managing addiction to opioids. Best Practice Journal, 64, 16-25. Buckley, N., & Ibrahim, M. (2014). Brief review: Obstetric care and perioperative analgesic management of the addicted patient. Canadian Journal of Anesthesia, 61, 154-163. Grant, M., Cordts, G., & Doberman, D. (2007). Acute pain management in hospitalized patients with current opioid abuse. Topics in Advanced Practice Nursing Journal, 7(1). Retrieved from http://www.medscape. com/viewarticle/557043 Green, C., Todd, K., Lebovits, A., & Framcis, M. (2006). Disparities in pain: Ethical issues. Pain Medicine, 7, 530-533. Huxtable, C., Roberts, L., Somogyi, A., & Macintyre, P. (2011). Acute pain management in opioid-tolerant patients: A growing challenge. Anaesthesia and Intensive Care, 39(5), 804-823. Jones, H., Martin, P., Heil, S., et al. (2008). Treatment of opioid dependent pregnant women: Clinical and research issues. Journal of Substance Abuse & Treatment, 35(3), 245-250. Marshall, S., & Jackson, M. (2011). Acute pain management for opioid tolerant patients. Updates in Anaesthesia, 35, 35-39. Retrieved from http://e-safe-anaesthesia.org/e_library/10/Acute_pain_management_for_opioid_ tolerant_patients_Update_20.pdf Mehta, V., & Langford, R. (2006). Acute pain management for opioid dependent patients. Anaesthesia, 61, 269-276. Neil, M. (2012). Peri-operative management of patients on strong opioids. Anaesthesia Tutorial of the Week 260. Retrieved from file:///C:/data/Downloads/260%20Perioperative%20Management%20of%20Patients% 20on%20Strong%20Opioids.pdf Oliver, J., Coggins, C., Compton, P., et al. (2012). American Society for Pain Management nursing position statement: Pain management in patients with substance abuse disorders. Pain Management Nursing, 13(3), 169-183. Parsons, G. (2015). Pain management in patients with a substance use disorder. Pharmaceutical Journal. Retrieved from http://www.pharmaceutical-journal.com/ learning/pain-management-in-patients-with-a-substance-use-disorder/ 20069490.article Prater, C., Zylstra, R., & Miller, K. (2002). Successful pain management for the recovering addicted patient. Journal of Clinical Psychiatry, 4(4), 125-131. Prince V. (2011). Pain management in patients with substance-use disorders. In Chronic Illnesses I, II, and III – PSAP-VII, Book 5. Lenexa, KS: American College of Clinical Pharmacology. Retrieved from https://www.accp.com/docs/bookstore/psap/ p7b05.sample03.pdf Roberts, L. (2008). Managing acute pain in patients with an opioid abuse or dependence disorder. Australian Prescriber, 31(5), 133-135.
28
Neonatal Abstinence Syndrome Neonatal Abstinence Syndrome (NAS) is described as the signs and symptoms displayed by a neonate experiencing withdrawal after in-utero substance exposure (Elliott et al., 2004; Jansson & Velez, 2012; Lall, 2008). The rate of NAS is increasing; it occurs in 55-94% of neonates exposed to opiates in-utero (American Academy of Pediatrics [AAP] Committee on Drugs, 1998), and for all substances represents 27 cases per 1000 NICU admissions (Tolia et al., 2015), or 3.39 cases per 1000 hospital births per year in the United States (Patrick et al., 2012). Similarly, in Canada three of every 1000 babies born from 2009-2010 had a diagnosis of NAS (Finnegan, 2013), with an average length of hospitalization ranging from 13-19 days (Canadian Institute of Health Information, 2012; Johnson, Greenough & Gerada, 2003; Ordean et al., 2015; Patrick et al., 2012). This prolonged hospitalization for treatment of NAS results in hospital charges amounting to at least five times those of healthy newborns (Patrick et al., 2012; Patrick, Davis, Lehman, & Cooper, 2015; Tolia et al., 2015). Hospitalization costs for NAS-related admissions are reported to have increased from $39,400 to $53,400 USD per case (Patrick et al., 2012).
The symptoms of NAS generally relate to neurological, gastrointestinal, and respiratory disturbances; however, some babies may not exhibit overt signs of NAS and their withdrawal may go unnoticed (Dow et al., 2012; Elliott et al., 2004; Jansson & Velez, 2012; Kraft & van den Anker, 2012; Lall, 2008; Logan et al., 2013; Orlando, 2014; Seligman et al., 2008). The substance and amount used by the pregnant woman determines the severity of the withdrawal effects experienced by the baby, as well as the onset and duration of symptoms (Dryden et al., 2009; Dysart et al., 2007; Jansson et al., 2009; Lim et al., 2009; Tierney, 2013) (See Appendix A). The varied onset of infant withdrawal symptoms is highly dependent on the half-life of the substance used: a substance with a longer half-life, such as methadone, results in a later onset of withdrawal, whereas a substance with a shorter half-life, such as heroin, results in earlier onset of withdrawal behaviors (Jansson et al., 2009; Johnson, Greenough & Gerada, 2003; Lall, 2008).
“No one else will ever know the strength of my love for you. After all, you’re the only one who knows the sound of my heart from the inside.”
– Kristen Proby, Fight With Me
29
Generally accepted ways to support the baby during withdrawal include noise and light reduction, swaddling, and non-nutritive sucking (Alberta Safe Babies Development Committee, 2012; AAP Committee on Drugs, 1998; Bagley et al., 2014; Balain & Johnson, 2014; D’Apolito & Hepworth, 2001; Dow et al., 2012; Weiner & Finnegan, 2010). Also, when holding infants with alcohol withdrawal, for example, they should be held vertically with their face outwards, and to avoid sleep disruptions, care and treatment should be carried out in clusters (Alberta Safe Babies Development Committee, 2012). Small regular feedings may be most effective in treating gastrointestinal upset noted during acute withdrawal (Alberta Safe Babies Development Committee, 2012; D’Apolito & Hepworth, 2001; Pediatric Interim Care Centre, no date; Sublett, 2013). Other recognized intervention strategies to minimize NAS include rooming-in, breast-feeding and pharmacologic treatment. Rooming-In is the practice of keeping the mother and her newborn together in the same room directly following the birth and afterwards, as opposed to the historical care model of admitting babies of mothers with SUD to the neonatal intensive care unit (NICU) immediately or soon after birth (Abrahams et al., 2007; Sublett, 2013). In this rooming-in model mothers are taught how to hold and cuddle their babies to settle them, and are encouraged to provide skin-to-skin care as much as possible (Abrahams et al., 2007; Abrahams et al., 2010). During a series of studies on rooming-in carried out by Ronald R. Abrahams and colleagues at the BC Women’s Hospital in Vancouver, it was found that this care model had positive effects for the baby. More specifically, rooming-in care decreased the need for treatments for NAS, such as morphine administration to the baby (Abrahams et al., 2007; Abrahams et al., 2010; Hodgson & Abrahams, 2012). Further, babies exhibited less severe and shorter withdrawal symptoms (Hodgson & Abrahams, 2012). Overall, there was a decrease in NICU admissions, a decrease in the length of birth hospitalizations for the babies, and an increase in the chance of the mother maintaining custody of her baby after discharge. Rooming-in practice also encouraged mothers to breastfeed their babies. Rooming-in promotes continuous contact between the mother and her baby. Skin-to-skin care in particular has also been shown to have positive effects for the mother: reduced parental anxiety, improved maternal-infant bonding and increased confidence for parenting (Cattaneo et al., 1998; Hiles, 2011; Ibe et al., 2004; Phillips, 2013). For the baby, skin-to-skin care results in temperature stabilization, improved sleep patterns, decreased crying, reduced incidence of infection, better weight gain and respiratory stability (Conde-Aqudelo & Diaz-Rossello, 2014). In terms of breastfeeding, skin-to-skin care results in increased milk production, longer duration of breastfeeding, and more regular initiation of breastfeeding (Hake-Brooks & Anderson, 2008; Phillips, 2013). Breastfeeding is recommended by the World Health Organization (WHO) for at least 6 months after birth to ensure ideal health and growth of the baby (World Health Organization, 2011). There is a concern however, with mothers with SUD and the perceived consequences breastfeeding will have on their babies (Jansson et al., 2008). The apprehension is that the contents of the maternal milk will cause sedation of the baby and possibly other health diminishing effects (Lefevre & Allegaert, 2015). However, this apprehension is unfounded because breastmilk concentrations of maternally ingested substances are typically low (Academy of Breastfeeding Medicine, 2009; Bogen et al., 2011; Ilett et al., 2012; Jansson et al., 2007; Lindemalm et al., 2009; McCarthy et al., 2005; Pritham, 2013; Reece-Stremtan et
30
al., 2015; Sublett, 2013). Further, observational studies have found that there are positive effects for substance using mothers who breastfeed their babies, though it has not been determined if there are other factors leading to these effects (Abdel-Latif et al., 2006; Lefevre & Allegaert, 2015; Oei & Lui, 2007). Nonetheless, several studies indicate that symptoms of NAS are less severe and there is less need for pharmacological treatment in the in-utero exposed infants who breastfeed (Bagley et al., 2014; Balain & Johnson, 2014; Kocherlakota, 2014; Lefevre & Allegaert, 2015; Mozurkewich & Rayburn, 2014; Sutter et al., 2014; Welle-Strand et al., 2013). In one study, there was a decrease in incidence of infants with NAS when comparing formula feeding to breastfeeding, 80% and 50% respectively (Welle-Strand et al., 2013). Likewise, the duration of treatment for NAS decreased from 48.9 days in non-breastfed infants to 31 days in breastfed infants. The milk of a mother on opioid replacement therapy does not cause adverse effects on the baby, as long as the mother does not have contractile viruses such as HIV (Lefevre & Allegaert, 2015). Regardless, the mother should talk to her health care provider if she is using other substances to confirm that breastfeeding is safe. Abdel-Latif and colleague’s (2006) often-cited study compared breastfed and formula-fed infants of a sample of Australian drug dependent mothers to determine the effects these drugs had on the frequency and severity of NAS experienced. The study included 85 breastfed infants and 105 formula-fed infants. Using the Finnegan scoring system, infants were treated with medication if their score was greater than or equal to 8 two consecutive times. In the first nine days of the life, the breastfed group had significantly lower Finnegan scores, required less pharmacological treatment, and withdrawal effects were delayed. The need for pharmacological treatment for withdrawal in particular decreased from 79% to 52.9% in breastfed infants. Though this study is limited by small sample size, the authors suggest that drug dependent mothers could breastfeed to decrease the severity and chance of their infant experiencing NAS. A United Kingdom based study showed that near 46% of infants born to women taking methadone needed pharmacologic treatment for NAS (Dryden et al., 2009). However, when these women breastfed their babies for more than 72 hours the odds that their babies needed treatment for NAS was decreased by half. Withdrawal symptoms exhibited by the baby may hinder establishment of successful breastfeeding (Hilton, 2012). Further, history of childhood trauma commonly results in long-term effects on women that may decrease their willingness to breastfeed (Prentice et al., 2002). Women who have experienced abuse as children have an increased chance of experiencing abuse in current relationships and are more likely to have unplanned pregnancies (BC Centre of Excellence for Women’s Health, 2010; Prentice et al., 2002). These factors, along with low financial stability and education, often result in a decreased likeliness to breastfeed (Prentice et al., 2002). Likewise, women who have been sexually abused commonly develop mental health disabilities in their adult life, such as depression, leading them to feel discomfort when performing parenting tasks including bathing and breastfeeding (Barnaby et al., 2010). Prentice et al. (2002) explored the relationship between the willingness to breastfeed and previous experiences of childhood sexual abuse. They conducted a retrospective secondary analysis of data collected from the Commonwealth Survey of Parents with Young Children in Ann Arber, Michigan during 1995. The original study involved telephone interviews with 2017 parents with children younger than three years of age. Drawing from this sample, the
31
responses of 1220 biological mothers were evaluated for the secondary analysis. Of this group of mothers, 7% reported having been sexually abused as children. The mothers were also asked whether or not they breastfed their children. Other factors that were considered in determining the relationship between childhood sexual abuse and breastfeeding included marital status, education, race, ethnicity, maternal age, prenatal care insurance coverage, mode of delivery, attendance at childbirth classes and encouragement to breastfeed by doctors. However, only variables that were found to be significant in the results were considered and therefore prenatal care insurance coverage and mode of delivery were excluded. Unexpectedly, it was found that a greater proportion of women who were sexually abused initiated breastfeeding (77%), as opposed to women who initiated breastfeeding and did not admit to a sexually abusive history (65%). The researchers hypothesize that the women in this study who have self-identified a childhood replete with sexual abuse may have a heightened concern about their own parenting. For example, these women were more likely to attend parenting classes and were more likely to provide comfort for their children at the start of crying. Overall, they found that women who experienced childhood sexual abuse were 2.6 times more likely to initiate breastfeeding. Even so, in keeping with trauma-informed care, sensitivity from health care providers in relation to breastfeeding is highly important in all women with SUD and mental health concerns. Pharmacologic approaches are considered a final resort for treatment of infants with NAS, and instead an attempt should be made to manage withdrawal with non-pharmacological interventions such as rooming-in and skin-to-skin care (Abrahams et al., 2007; Abrahams et al., 2010; Dow et al., 2012). As many as 80% of infants exposed to maternal opioids in-utero require pharmacologic intervention (Greenough & Kassim, 2005; Logan et al., 2013). Consensus amongst various experts indicates that the medication/s used to treat NAS should match the agent/s causing the withdrawal (AAP Committee on Drugs, 1998; Hudak & Tan, 2012). Neonatal abstinence secondary to maternal opioid use is often treated with morphine (Dow et al., 2012; Kraft & van den Anker, 2012; Osborn et al., 2010; Tolia et al., 2015). Methadone is considered less suitable to manage withdrawal in infants because it has a long half-life, increasing risk of overdose and death (College of Physicians & Surgeons of Alberta, 2014). Intractable withdrawal in newborns that is not well managed with morphine may require adjunct therapy, for example with Phenobarbital (Bio et al., 2011; Sublett, 2013) or Clonidine (Bio et al., 2011; Esmaeli et al., 2010; Kraft & van den Aknker, 2012). More recently, single therapy treatment with Clonidine has been explored, though its effectiveness in this capacity remains unclear (Bada et al., 2015). Poly drug exposures, particularly with benzodiazepines, increase risk for both severity and duration of NAS (Bass, 2015; Kaltenbach et al., 2012; Ordean et al., 2015; Wachman et al., 2011). Maternal non-opioid poly drug use may be managed with Phenobarbital (Agthe et al., 2009; Finnegan, 2013). Of note, neonatal withdrawal from maternal Selective Serotonin Reuptake Inhibitors (SSRIs), alcohol, marijuana and tobacco use is self-limiting and pharmacologic treatment of the withdrawal is not recommended (Ashraf, 2014; Bass, 2015; Hudak & Tan, 2012; Kraft & van den Anker, 2012). Mainstream infant management during pharmacotherapy involves using a modified version of the Finnegan Neonatal Abstinence Scoring System (Bagley et al., 2014; O’Grady et al., 2009; Sarkar & Donn, 2006). (See Appendix B). Pharmacologic treatment is initiated when is a total score of 8 or greater on three consecutive scorings, or the average of any three consecutive scores is 8 or greater, and total score of 12 or greater on two consecutive scorings, or the

32
average of any two consecutive scores is 12 or greater. A caveat of this scoring tool is that it has been validated in term neonates with in-utero exposure to opioids and other illicit drugs. It has not been validated for use in preterm neonates or those exposed to other substances, such as tobacco, alcohol and SSRIs. Further, a current limitation of NAS scoring practices in general is that they are not universal. A survey-based study of 17 neonatal units in the United Kingdom illuminated inconsistencies in NAS scoring practices, as well as in identifying and managing the symptoms (Nandakumar & Sankar, 2006). This study also highlighted the lack of reliable information and evidence to help practitioners determine the best regimen to treat NAS. Infants requiring initiation of pharmacologic treatment should be considered for admission to the NICU for monitoring while they begin treatment (Dow et al., 2012; Kraft & van den Anker, 2012). During the initiation phase of neonatal pharmacologic treatment for NAS, or until the medication dose is reduced, babies should be considered for monitoring using a cardio-respiratory monitor (Kandall et al., 1993). Once pharmacotherapy has been started, infants are watched carefully for signs of toxicity or central nervous system depression. The signs and symptoms that suggest central nervous system depression include drowsiness, decreased respiratory drive, and decreased tone (Chow & Gideon, 2015). If signs of toxicity occur, dose adjustments are required; the goal of treatment is to make the infant as comfortable as possible and to ensure proper feeding and development while minimizing the risk for toxicity (Kraft & van den Anker, 2012). In Edmonton, stabilized infants requiring pharmacologic management to treat NAS may be sent home for continued detoxification in the community. See Appendix C for a suggested medication management plan.
References
Abdel-Latif, M., Pinner, J., Clews, S., et al. (2006). Effects of breast milk on the severity and outcome of neonatal abstinence syndrome among infants of drug-dependent mothers. Pediatrics, 117(6), e1163-e1169. http://dx.doi.org/ 10.1542/peds.2005-1561
Abrahams, R., Kelly, S., Payne, S., et al. (2007). Rooming-in compared with standard care for newborns of mothers using methadone or heroin. Canadian Family Physician, 53, 1722-1730. Abrahams, R., MacKay-Dunn, M., Nevmerjitskaia, V., et al. (2010). An evaluation of rooming-in among substance-exposed newborns in British Columbia. Journal of Obstetrics & Gynaecololgy of Canada, 32(9), 866-871. Academy of Breastfeeding Medicine Protocol Committee. (2009). ABM clinical protocol #21: Guidelines for breastfeeding and the drug-dependent woman. Breastfeeding Medicine, 4(4), 225-228.
Agthe, A., Kim, G., Mathias, K. et al. (2009). Clonidine as an adjunct therapy to opioids for neonatal abstinence syndrome: A randomized, controlled trial. Pediatrics, 123, e849-e856. http://dx.doi.org/10.1542/peds.2008-0978
Alberta Safe Babies Development Committee. (2012). Baby steps: Caring for babies with prenatal substance exposure. Alberta Version. Edmonton: Ministry of Human Services, Government of Alberta. American Academy of Pediatrics Committee on Drugs. (1998). Neonatal drug withdrawal. Pediatrics, 101(6), 1079-1088.
33
Ashraf, H. (2014). Neonatal abstinence syndrome. Retrieved from http://emedicine.medscape.com/ article/978763-overview#a6
Bada, H., Sithisarn, T., Gibson, J., et al. (2015). Morphine versus clonidine for neonatal abstinence syndrome. Pediatrics, 135(2), e383-e391. http://dx.doi.org/10.1542/peds.2014-2377
Bagley, S., Wachman, E., & Brogly, S. (2014). Review of the assessment and management of neonatal abstinence syndrome. Addiction Science & Clinical Practice, 9, 19. Balain, M., & Johnson, K. (2014). Neonatal abstinence syndrome: The role of breastfeeding. Infant, 10(1), 9-13. Barnaby, L., Penn, R., & Erickson, P. (2010). Drugs, homelessness & health: Homeless youth speak out about harm reduction. Toronto: Shout Clinic Harm Reduction Report. Bass, P. (2015). Neonatal abstinence syndrome. Special report. Modern Medicine Network. Retrieved from www.modernmedicine.com/taxonomy/term/5519 BC Centre of Excellence for Women’s Health. (2010). Girl-centred approaches to prevention, harm reduction and treatment. Gendering the National Framework series (Vol. 2). Vancouver: Author. Bio L., Siu A., & Poon C. (2011). Update on the pharmacologic management of neonatal abstinence syndrome. Journal of Perinatology, 31, 692–701. Bogen, D., Perel, J., Helsel, J., et al. (2011). Estimated infant exposure to enantiomer-specific methadone levels in breastmilk. Breastfeeding Medicine, 6(6), 377-385. Canadian Institute of Health Information. (2012). CIHI Annual Report. (2011-2012 Data). Retrieved from https://secure.cihi.ca//free_products/AnnualReport2012-ENweb.pdf Cattaneo, A., Davanzo, R., Worku, B., et al. (1998). Kangaroo mother care for low birthweight infants: A randomized controlled trial in different settings. Acta Paediatrica, 87, 976–985. Chow, C., & Gideon, K. (2015). Sedating drugs and breastfeeding. Canadian Family Physician. 61(3), 241-243. College of Physicians & Surgeons of Alberta. (2014). Alberta methadone maintenance treatment. Standards and guidelines for dependence. Edmonton: College of Physicians & Surgeons of Alberta.
Conde-Agudelo, A., & Díaz-Rossello, J. (2014). Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane Database Systematic Reviews, 4(4): CD002771. http://dx.doi.org/10.1002/14651858.CD002771.pub4
D’Apolito, K., & Hepworth, J. (2001). Prominence of withdrawal symptoms in polydrug-exposed infants. Journal of Perinatal and Neonatal Nursing, 14(4), 46-60. Dow, K., Ordean, A., Murphy-Oikonen, J., et al. (2012). Neonatal abstinence syndrome clinical practice guidelines for Ontario. Journal of Population Therapeutics and Clinical Pharmacology, 19(3), e488-e506. Dryden, C. , Young, D., Hepburn, M., & Mactier, H. (2009). Maternal methadone use in pregnancy: Factors associated with the development of neonatal abstinence syndrome and implications for healthcare resources. BJOG: An International Journal of Obstetrics and Gynaecology, 116(5), 665-671. Dysart, K., Hsieh,H., Kaltenbach, K., & Greenspan, J. (2007). Sequela of preterm versus term infants born to mothers on a methadone maintenance program: Differential course of neonatal abstinence syndrome. Journal of Perinatal Medicine, 35(4), 344-346.
34
Elliott, M., Cunliffe, P., Demianczuk, N., & Robertson, C. (2004). Frequency of newborn behaviours associated with neonatal abstinence syndrome: A hospital-based study. Journal of Obstetrics & Gynaecology of Canada, 26(1), 25-34. Esmaeili, A., Keinhorst, A., Schuster, T., et al. (2010). Treatment of neonatal abstinence syndrome with clonidine and chloral hydrate. Acta Paediatrica, 99, 209-214. Finnegan, L. (2013). Licit and illicit drug use during pregnancy: Maternal, neonatal and early childhood consequences. Ottawa: Canadian Centre on Substance Abuse. Greenough, A., & Kassim, Z. (2005). Effects of substance abuse during pregnancy. The Journal of the Royal Society for the Promotion of Health, 125(5), 212-214. Hake-Brooks, S., & Anderson, G. (2008). Kangaroo care and breastfeeding of mother-preterm infant dyads 0-18 months: A randomized, controlled trial. Neonatal Network, 27(3), 151–159. Hiles M. (2011). Conference Abstracts: An Evidence based intervention for promoting sleep in infants experiencing neonatal abstinence syndrome (NAS) due to maternal methadone use [Abstract]. Clinical Nurse Specialist, 25(3), 153–158. Hilton, T. (2012). Breastfeeding considerations of opioid dependent mothers and infants. MCN: The American Journal of Maternal Child Nursing, 37(4), 236-240. Hodgson, Z., & Abrahams, R. (2012). A rooming-in program to mitigate the need to treat for opiate withdrawal in the newborn. Journal of Obstetrics & Gynaecology of Canada, 34(5), 475-481.
Hudak, M., & Tan, R. (2012). Neonatal drug withdrawal. Pediatrics, 129(2), e540-e560. http://dx.doi.org/10.1542/2012-3212
Ibe, O., Austin, T., Sullivan, K., et al. (2004). A comparison of kangaroo mother care and conventional incubator care for thermal regulation of infants < 2000 g in Nigeria using continuous ambulatory temperature monitoring. Annals of Tropical Paediatrics, 24(3), 245–251. Ilett, K., Hackett, L., Gower, S., et al. (2012). Estimated dose exposure of the neonate to buprenorphine and its metabolite norbuprenorphine via breastmilk during maternal buprenorphine substitution treatment. Breastfeeding Medicine, 7, 269-274. Jansson, L., Choo, .R, Harrow, C., et al. (2007). Concentrations of methadone in breast milk and plasma in the immediate perinatal period. Journal of Human Lactation, 23(2), 184–190. Jansson, L., Choo, R,. Velez, M., et al. (2008). Methadone maintenance and breastfeeding in the neonatal period. Pediatrics, 121, 106–114. Jansson, L., & Velez, M. (2012). Neonatal abstinence syndrome. Current Opinion in Pediatrics, 24(2), 252-258. Jansson, L., Velez, M., & Harrow, C. (2009). The opioid exposed newborn: Assessment and pharmacologic management. Journal of Opioid Management, 5(1), 47-55. Johnson, K., Greenough, A., & Gerada, C. (2003). Maternal drug use and length of neonatal unit stay. Addiction, 98(6), 785–789. Kaltenbach, K., Holbrook, A., Coyle, M., et al. (2012). Predicting treatment for neonatal abstinence syndrome in infants born to women maintained on opioid agonist medication. Addiction, 107(Suppl 1), 45–52. Kandall, S., Gaines, J., Habel, L., et al. (1993). Relationship of maternal substance abuse to subsequent sudden infant death syndrome in offspring. Journal of Pediatrics, 123(1), 120–126.
35
Kocherlakota, P. (2014). Neonatal abstinence syndrome. Pediatrics, 134, e547-e561. http://dx.doi.org/10.1542/peds.2013-3524
Kraft, W., & van den Anker, J. (2012). Pharmacologic management of the opioid neonatal abstinence syndrome. Pediatric Clinics of North America, 59(5), 1147-1165. Lall, A. (2008). Neonatal abstinence syndrome. British Journal of Midwifery, 16(4), 220-223. Lefevere, J., & Allegaert, K. (2015). Question: Is breastfeeding useful in the management of neonatal abstinence syndrome? Archives of Diseases in Childhood, 100(4), 414-415.
Lim, S., Prasad, M., Samuels, P., et al. (2009). High-dose methadone in pregnant women and its effect on duration of neonatal abstinence syndrome. American Journal of Obstetrics & Gynecolology, 200(1), 70.e1-5. http://dx.doi.org/10.1016/j.ajog.2008.08.041
Lindemalm, S., Nydert, P., Svensson, J., et al. (2009). Transfer of buprenorphine into breast milk and calculation of infant drug dose. Journal of Human Lactation, 25(2), 199–205. Logan, B., Brown, M., & Hayes, M. (2013). Neonatal abstinence syndrome: Treatment and pediatric outcomes. Clinical Obstetrics and Gynecology, 56(1), 186-192. McCarthy, J., Leamon, M., Parr, M., et al. (2005). High-dose methadone maintenance in pregnancy: Maternal and neonatal outcomes. American Journal of Obstetrics & Gynecology, 193, 606–610. Mozurkewich, E., & Rayburn, W. (2014). Buprenorphine and methadone for opioid addiction during pregnancy. Obstetrics & Gynecology Clinics of North America, 41, 241-253.
Nandakumar, N., & Sankar, V. (2006). What is the best evidence based management of neonatal abstinence syndrome? Archives of Disease in Childhood. Fetal and Neonatal Edition. 91(6), F463. http://dx.doi.org/10.1136/adc.2006.095166
Oei, J., & Lui K. (2007). Management of the newborn infant affected by maternal opiates and other drugs of dependency. Journal of Paediatric Child Health, 43, 9-18.
O’Grady, M., Hopewell, J., & White, M. (2009). Management of neonatal abstinence syndrome: A national survey and review of practice. Archives of Disease in Childhood. Fetal and Neonatal Edition, 94(4), F249-F252. http://dx.doi.org/ 10.1136/adc.2008.152769
Ordean, A., Kahan, M., Graves, L., et al. (2015). Obstetrical and neonatal outcomes of methadone-maintained pregnant women: A Canadian multisite cohort study. Journal of Obstetrics and Gynecology Canada, 37(3), 252-257. Orlando, S. (2014). An overview of clinical tools used to assess neonatal abstinence syndrome. The Journal of Perinatal & Neonatal Nursing, 28(3), 212-219.
Osborn, D., Jeffery, H., & Cole, M. (2010). Opiate treatment for opiate withdrawal in newborn infants. Cochrane Database of Systematic Reviews, Issue 10 Article No. CD002059. http://dx.doi.org/10.1002/14651858.CD002059.pub3
Patrick, S., Davis, M., Lehman, C., & Cooper, W. (2015). Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009 to 2012. Journal of Perinatology, 35, 650-655. Patrick, S., Schumacher, R., Benneyworth, B., et al. (2012). Neonatal abstinence syndrome and associated health care expenditures: United States 2000-2009. Journal of the American Medical Association, 307(18), 1934–1940. Pediatric Interim Care Center. (no date). Therapeutic handling. Retrieved from http://picc.net/handling.html

36
Phillips, R. (2013). Uninterrupted skin-to-skin contact immediately after birth. Newborn and Infant Nursing Reviews (NAINR), 13(2), 67-72. Prentice, J., Lu, M., Lange, L., & Halfon, N. (2002). The association between reported childhood sexual abuse and breastfeeding initiation. Journal of Human Lactation, 18(3), 219-226. Pritham, U. (2013). Breastfeeding promotion for management of neonatal abstinence syndrome. Journal of Obstetric, Gynecologic & Neonatal Nursing, 42(5), 517-526. Reece-Stremtan, S., Marinelli, K, & Academy of Breastfeeding Medicine. (2015). ABM Clinical Protocol #21: Guidelines for breastfeeding and substance use or substance use disorder, revised 2015. Breastfeeding Medicine, 10(3), 135-141. Sarkar, S., & Donn, S. (2006). Management of neonatal abstinence syndrome in neonatal intensive care units: A national survey. Journal of Perinatology, 26(1), 15-17.
Seligman, N., Salva, N., Hayes, E., et al. (2008). Predicting length of treatment for neonatal abstinence syndrome in methadone-exposed neonates. American Journal of Obstetrics & Gynecology, 199, 396.e1-396.e7. http://dx.doi.org/10.1016/j.ajog.2008.06.088
Sublett, J. (2013). Neonatal abstinence syndrome: Therapeutic interventions. MCN, The American Journal of Maternal/Child Nursing, 38(2), 102-107. Sutter, M., Leeman, L., & His, A. (2014). Neonatal opioid withdrawal syndrome. Obstetrics & Gynecology Clinics of North America, 41, 317-334. Tierney, S. (2013). Identifying neonatal abstinence syndrome (NAS) and treatment guidelines. Iowa City, IA: University of Iowa Children’s Hospital. Tolia, V., Patrick, S., Bennett, M., et al. (2015). Increasing incidence of the neonatal abstinence syndrome in US neonatal units. New England Journal of Medicine, 372(22), 2118-2126. Wachman, E., Newby, P., Vreeland, J., et al. (2011). The relationship between maternal opioid agonists and psychiatric medications on length of hospitalization for neonatal abstinence syndrome. Journal of Addiction Medicine, 5(4), 293–299. Weiner, S., & Finnegan, L. (2010). Drug withdrawal in the neonate. In G. Merenstein & S. Gardner (Eds.) Handbook of Neonatal Intensive Care (6th ed.). St. Louis, MO: Mosby. Welle-Strand, G., Skurtveit, S., Jansson, L., et al. (2013). Breastfeeding reduces the need for withdrawal treatment in opioid-exposed infants. Acta Paediatrica, 102, 1060-1066. World Health Organization (WHO). (2011). Exclusive breastfeeding for six months best for babies everywhere. Statement. Geneva: Author. Retrieved from http://www.who.int/mediacentre/news/statements/ 2011/breastfeeding_20110115/en/
37
Transitioning from Hospital to Home
Safety at Home The way babies sleep is highly important in ensuring they do not succumb to sudden death, either from Sudden Infant Death Syndrome (SIDS) or Sudden Unexpected Infant Death (SUID). Sudden Infant Death Syndrome is the number one cause of death for babies 28 days to one year of age in developed countries (American Academy of Pediatrics [AAP] Policy Statement; 2011; AAP Technical Report, 2011) and is commonly defined as the unexplained death of an infant, even after a complete death scene investigation, thorough infant history and autopsy are done (Willinger et al., 1991). Sudden Unexpected Infant Death, in comparison, describes any sudden and unexpected deaths occurring during infancy, whether explained or unexplained, and includes SIDS (AAP Technical Report, 2011). As well, infant deaths of this nature may be attributed to suffocation, asphyxia, entrapment, infection, ingestions, metabolic diseases and trauma (AAP Policy Statement, 2011). In Canada, in 2004 SIDS accounted for 5% of all infant deaths up to one year of age and 17.2% of postneonatal deaths (28 days to one year of age) (Public Health Agency [PHA] of Canada, 2008; Trifunov, 2009). Commonly, SIDS peaks between 1 to 4 months of life, with fewer deaths occurring beyond 6 months (AAP Technical Report, 2011; Blair et al., 2006; Leach et al., 1999; PHA of Canada, 2008). Characteristics placing infants at higher risk for SIDS include being born male, preterm, or low birth weight (Blair & Fleming, 2002; Blair et al., 2006; Leach et al., 1999; PHA of Canada, 2008). Understanding of modifiable risk factors for SIDS is increasing. Overall, the risk of dying from SIDS is decreasing, mainly due to success in identifying and increasing awareness of modifiable risk factors (Trifunov, 2009). Evidence exists about specific modifiable risk factors: infants sleeping in a prone or side-lying position (even for infants that regurgitate), young maternal age less than 20 years, low socioeconomic status, low birth weight, maternal smoking, consciousness-depressing drug or alcohol use in either parent, and bed sharing (PHA of Canada, 2008; Trifunov, 2009). Attention to infant sleep position, in particular, has been found to reduce the rate of SIDS. Epidemiologic studies carried out in the 1980s and 1990s
“Don’t judge me by my past. I’m not in the past anymore. Accept me for who I am today.”
– Anonymous
38
observing sleep positions in infants found that there was a reduced incidence of SIDS for babies who slept on their back (AAP Technical Report, 2011; Kattwinkel et al., 1992; Kattwinkel et al., 2000). After which, “Back to Sleep” public health campaigns in many countries, including Canada and the United States, resulted in an appreciable 50-90% decrease in incidence of SIDS (AAP, 2005). Even so, the rate of deaths from other adverse sleeping situations is increasing (Shapiro-Mendoza et al., 2009) due to unintentional suffocation, entrapment and strangulation deaths in bed (Centers for Disease Control in Trifunov, 2009). Infant deaths of this nature result from suffocation by soft bedding, pillows or waterbed mattresses, overlaying (rolling on top of or against an infant while sleeping), wedging and entrapment of the infant between two objects, such as between the bed and a wall, and strangulation by asphyxiation (PHA of Canada, 2012; Trifunov, 2006). Bed sharing with either a care giver or sibling has been a recent topic for debate in both professional and lay communities (Trifunov, 2006; Trifunov, 2009). Bed sharing is defined as a sleeping arrangement in which the infant shares the same sleep surface with another person (Canadian Paediatric Society [CPS], 2004; Trifunov, 2006). This sleeping situation creates additional risk factors that are known to contribute to unintentional suffocation, entrapment and strangulation deaths (Centers for Disease Control and Ottawa Public Health in Trifunov 2009). Adult beds and other sleep surfaces, including sofas, arm chairs and futons, are not safe for use by infants. Room sharing, on the other hand, is being endorsed as a protective and safer option. This sleeping environment supports the infant being taken to the parental bed for breastfeeding or comforting but returned to the crib/cot, that is free of objects such as stuffed toys, bumper pads, pillows and quilts/comforters, in the parents’ room and within their reach (CPS, 2004; Trifunov, 2006). Room sharing is a breastfeeding responsive option whereby the mother can alert her support person/s that infant feeding is occurring with the aim of preventing her from falling asleep and ensuring that the infant is returned to the crib/cot (Ottawa Public Health in Trifunov, 2009). Unintentional smothering and falls can also happen during skin-to-skin care. For this reason, the mother and other caregivers should always ensure the front of the infant’s face is not completely pressed up against their skin and that they remain awake and attentive to infant positioning at all times (Wallace, 2014). Choosing to bed share when safer options are available is a multifactorial issue (Trifunov, 2009). “Many factors influence choices families make regarding sleeping arrangements for infants and include a combination of parental values, socioeconomic factors, and cultural diversity” (Trifunov, 2006, p. 4). Unanimously though, the following recommendations are being communicated globally: the back to sleep position for infant sleep during the first year of life, even with gastroesophageal reflux, and pre-terms starting at 32 weeks gestation (AAP, 2008); a smoke free environment; and not placing on sofas, chairs, waterbeds or cushions even when sleeping with someone (AAP Committee on Fetus and Newborn, 2008; Calgary Health Region in Trifunov, 2009; CPS, 2004). Additionally, car seats and infant carriers must not replace the crib/cot as a sleep surface (CPS, 2004). Cigarette smoking is the second most commonly accepted modifiable risk factor for SIDS (Kemp et al., 2000; Trifunov, 2009), especially during pregnancy, as well as in the infant’s postnatal environment (AAP Technical Report, 2011; McGarvey et al., 2006; Moon et al., 2007; Ostfeld et al., 2006; Vennemann et al., 2007). It is estimated that one third of SIDS
39
deaths could be prevented if all maternal smoking during pregnancy were eliminated (Dietz et al., 2010). From a harm reduction perspective, meant to reduce the risk exposure without expecting the activity to stop completely (Trifunov, 2009), women who reduce the amount of cigarettes smoked during pregnancy can reduce the risk of SIDS for their infants, and women who stop smoking altogether can further reduce the risk (Blair et al., 1996; Mitchell et al., 1992; Vennemann et al., 2005). In the postnatal period the risk of SIDS increases with level of exposure (Blair et al., 1996; Carpenter et al., 2004). Further, when there is antenatal and postnatal exposure to smoking, the risk of SIDS is even higher in a bed sharing sleep environment (CPS 2004; Horsley et al., 2007; McGarvey et al., 2006; Moon et al., 2007; Ostfeld et al., 2006; Vennemann et al., 2007). Less is known about the infant effects of exposure to third hand cigarette smoke (AAP Technical Report, 2011).
Community Programs and Support Programs that shift attention to the underlying cause of why pregnant women use substances and that involve the entire community in finding solutions have been shown to be the most successful (CanFASD Research Network’s Action Team, 2013). Even so, it remains a challenge to implement broad systemic responses in a manner that links prevention, enforcement, harm reduction and treatment strategies (Cormier et al., 2004). Early engagement in support services for pregnant women with SUD is highly important to ensure optimal outcomes for both the mother and the baby. The more frequent the prenatal visits, the more likely there will be a reduction in the frequency and quantity of substance use (Canada Northwest FASD Research Network Action Team, 2010). This reduction in drug use, in turn, reduces the substance exposure to the baby. Pregnancy is often seen as an opportune time for service providers to support women in improving their health (Canada Northwest FASD Research Network Action Team, 2010). Care must not only focus on the health of the baby, but also make the mother feel as though her health is important too. Fetus-centered care gives women the impression that their health only matters when they are pregnant (Armstrong, 2003); a woman’s perceptions of her caregiver’s concern with her well-being is closely associated with improved engagement and increased length of stay in various treatment settings (Comfort et al., 2000; Grella et al., 2000; O’Connor & Whaley, 2007; Payne, 2007; Tait, 2000; Watkins & Chovanec, 2006; Wisdom et al., 2009). To encourage engagement in community programs, services must be respectful and non-judgmental, as well as being able to deliver care in a timely manner (Canada Northwest FASD Research Network Action Team, 2010; Kasarabada et al., 2002; Leslie & Roberts, 2004; O’Connor & Whaley, 2007; Parkes et al., 2008; Poole & Isaac, 2001; Tait, 2003; Watkins & Chovanec, 2006). Likewise, women will be more likely to connect with staff whom they share similar characteristics to such as language, ethnicity, culture or age (Canada Northwest FASD Research Network Action Team, 2010). Together, these practices may motivate women to return for future health care and possibly make positive changes in their lives. There is not just one uniform approach to community support programs across Canada. Some provinces, such as Ontario and British Columbia, have more comprehensive integrated programs for women with SUD than others. For example, New Choices in Hamilton, Ontario is an integrated treatment program for pregnant and parenting women with SUD (Sword et al., 2004). This program combines many services, such as addiction counseling, nutrition
40
counseling, parenting education and peer support, as well as links to prenatal services, family physicians and a perinatal home visiting program.
Edmonton has several programs that operate to target at-risk pregnant women2. To date, many of these programs have varied public and private funding sources and often operate in isolation. Affordable and suitable housing programs, for instance, are lacking. However, efforts are underway to establish connections amongst the various publicly and privately funded programs. For example, for the first time in Edmonton, a community of practice group, made up of hospital and community-based professionals with a common interest in improving access to programs for women with SUD and family integrated management of NAS, has been formed. While still in its infancy, efforts such as this serve to enhance communication between hospital to home, as well as amongst various social service agencies, including Children and Family Services, for pregnant women with SUD and their babies. Addiction Recovery and Community Health (ARCH) program offers a consult service for inpatients and emergency department patients at the Royal Alexandra Hospital. The program was launched in July 2014. ARCH is a team consisting of a social worker, a dietician, a nurse practitioner and a physician that is available to see patients on weekdays during the hours of 8:00am to 4:00pm. The physician may also be able to see patients off hours including weekends and holidays during the hours of 8:00am to 9:00pm for urgent medical consults. To be able to qualify for a referral to ARCH from the emergency department women must have any of the following: regular or escalating substance use problems, substance use during pregnancy, multiple social risk factors, regular drug use related infections, or substance use and multiple medical morbidities. More information can be found at: https://www.acfp.ca/wp-content/uploads/2015/03/1_ARCH_Poster.pdf Catholic Social Services reaches out to 60,000 people of all faiths and cultures each year, providing services based on the Catholic social teachings of social justice, human dignity, and the common good. In terms of substance use specifically, Catholic Social Services helps people during recovery and re-entry into the community, such as those released from a correctional facility. Programs include counseling for families and individuals, open adoption and kinship programs, training and mentorship for parents in need, support for children and families affected by Fetal Alcohol Spectrum Disorder, and support for ‘at risk’ youth and children affected by sexual exploitation. More information can be found at: http://www.catholicsocialservices.ab.ca/ Community Perinatal Program (CPP) is a multidisciplinary program designed to provide maternity care to women who are unable to regularly access perinatal health services due to challenges with the social determinants of health. Examples include: poverty, isolation, substance use, language and cultural barriers, or complex life issues. In addition to providing maternity care, the community health nurses and family physicians on the team ensure the women are connected to resources that may help improve their pregnancy and parenting outcomes: housing, food, substance abuse counseling, dental care, home visitation, etc. Physicians and nurses at CPP support harm reduction and embrace trauma informed care. Healthy, Empowered and Resilient (H.E.R) Program provides professional and peer support to pregnant or parenting women who are at risk. This program is located in inner city 2AuthoredbyLaureenMcPeak,ProgramManager,MaternalChildHealth,PublicHealthEdmontonZone
41
Edmonton and the ultimate goal is to support street involved women through access to basic screening level healthcare services throughout their pregnancy. As well, the staff addresses issues such as addiction, poverty, and family violence. http://alberta.ca/release.cfm?xID=3661947077475-AB7B-D87A-56CF6820FB632D11 provides more information on the program. Healthy Beginnings Postpartum Program is available for parents of babies less than 2 months old. Registered Nurses are able to help with breastfeeding, counseling, providing knowledge on baby care, and provide support and referrals to healthcare providers or other resources as needed. This program has four required contact points
1. Initial phone call – day of discharge 2. Initial Home Visit – day after discharge 3. Routine 3-5 day phone or home visit 4. Routine 10-14 day phone, clinic visit or home visit
Information can be found at: http://www.albertahealthservices.ca/services.asp?pid=service&rid=5808, including the addresses of the various locations in Edmonton and their contact information. Health for Two, offered by Alberta Health Services, provides information, nutrition and support programs for women who are pregnant. It is accessible through health centres in Edmonton and surrounding areas (St. Albert, Leduc County, Fort Saskatchewan, Parkland County, and Strathcona County). Health for Two is available to women who have low incomes, poor nutrition, smoking, drug and alcohol habits, issues due to language barriers, cultural problems or who are in violent relationships. These women are supported throughout their pregnancy and during their delivery up until their child is two months old by a team of care providers. This team includes child development workers, outreach workers, registered nurses, social workers, and youth workers. http://www.albertahealthservices.ca/services.asp?pid=service&rid=5807 provides information on the numerous locations as well as their addresses and contact information. First Steps with Catholic Social Services is a free program that offers mentorship to women for up to three years who have a high risk of giving birth to a child with NAS. First Steps applies to mothers who are currently pregnant or have an infant up to six months of age and who have used substances during their pregnancy. These women aspire to make a positive change in their life to better the life of their child, however, they lack connections to other community services. First steps is located on Jasper Avenue and more information can be found at: http://www.catholicsocialservices.ab.ca/CSSFindServicesbyLocation/default.aspx?id=143, as well as the address and contact info. Metro City Medical Clinic This is one of three methadone clinics in Edmonton. Contact information can be found at: http://www.cpsa.ca/physician-prescribing-practices/methadone-program/methadone-clinics-alberta/ http://www.opiateaddictionresource.com/treatment/methadone_clinic_directory/ab_clinics provides address information.
42
Opioid Dependency Program (ODP) provides many services such as: personalized medical and substance use assessments for opioid dependent clients, methadone maintenance treatment with long-term support, counseling services, referral to other addiction treatment services, coordinated access to methadone for clients through community pharmacies, and consultations to pharmacists and family physicians, as well as screening for HIV and hepatitis. This program is available to pregnant women who are 18 years of age or older, or women who have HIV/AIDS and is accessible by a health care professional or self-referral. Fees accompanying the ODP are dispensing fees that are payable to the patient’s assigned pharmacy and coverage may occur through the client’s health plan. This program is located near Edmonton’s city centre and can be contacted through telephone by 780-422-1302. More information about the program can be accessed at: http://www.albertahealthservices.ca/services.asp?pid=saf&rid=1046543 Panorama Medical Clinic is located on 10106 111 Ave and currently has four physicians that see patients for Opioid Replacement Therapy two days a week. This clinic gets its referrals from word of mouth, physician referral and walk-ins. Each patient must have an active Alberta Health Care number, live in the Edmonton area and be abusing opioids on a daily basis to be accepted into the program. Once accepted, the patients need to see the prescribing physician once a week and the pharmacy located in the same building as the clinic for witnessed daily ingestions. After a period of stability with clean drug screens the patient may be permitted to carry multiple doses and have the prescription transferred to a pharmacy of their choice. Streetworks Needle Exchange is a service that provides a free service for clean needles. The purpose of this program is for injection drug users throughout Edmonton to dispose of their dirty needles in exchange for clean needles to prevent the spread of diseases and life-threatening infections. The contact number is 780-990-6641 and can be reached Tuesday through Friday from 8:30pm to 12:00am and on weekends from 8:30am to 12:30pm. A mobile van then comes to the location requested and delivers clean needles. More information can be found at http://www.albertahealthservices.ca/services.asp?pid=saf&rid=1078493
References American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome. (2005). The changing concept of sudden infant death syndrome: Diagnostic coding shifts, controversies regarding the sleeping environment, and new variables to consider in reducing risk. Policy Statement. Pediatrics, 116, 1245-1255. American Academy of Pediatrics Committee on Fetus and Newborn. (2008). Hospital discharge of the high-risk neonate. Pediatrics, 122(5), 1119–1126
American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome. (2011). SIDS and other sleep-related infant deaths: Expansion of recommendations for a safe infant sleeping environment. Policy Statement. Pediatrics, 128(5), 1030-1039. http://dx.doi.org/10.1542/peds.2011-2284
American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome. (2011). SIDS and other sleep-related infant deaths: Expansion of recommendations for a safe infant sleeping environment. Technical Report. Pediatrics, 128(5), e1341-e1367. http://dx.doi.org/10.1542/peds.2011-2285
Armstrong, E. (2003). Conceiving risk, bearing responsibility. Fetal alcohol syndrome and the diagnosis of moral disorder. Baltimore, Maryland: John Hopkins University Press.
43
Blair, P., & Fleming, P. (2002). Epidemiological investigation of sudden infant death syndrome in infants: Recommendations for future studies. Child: Care, Health & Development. 28, 49-54. Blair, P., Fleming, P., Bensley, D., et al. (1996). Smoking and sudden infant death syndrome: Results from 1993-1995 case-control study for confidential inquiry into stillbirths and deaths in infancy. British Medical Journal, 313, 195-198. Blair, P., Sidebotham, P., Berry, P., et al. (2006). Major epidemiological changes in sudden infant death syndrome: A 20 year population-based study in the UK. Lancet, 367, 314-319. Canada Northwest FASD Research Network Action Team on Prevention from a Women’s Health Determinants Perspective. (2010). Taking a relational approach: The importance of timely and supportive connections for women. Retrieved from http://www.canfasd.ca/wpcontent/uploads/2013/02/RelationalApproach_March_2010.pdf Canadian Paediatric Society. (2004). Recommendations for safe sleeping environments for infants and children. Position Statement (CP 2004-02). Paediatric Child Health, 9(9), 659-663. CanFASD Research Network’s Action Team on Prevention from a Women’s Health Determinants Perspective. (2013). Supporting pregnant and parenting women who use substances. What communities are doing to help. Vancouver: Canada FASD Research Network. Retrieved from http://www.canfasd.ca/wpcontent/uploads/ 2013/02/What_ Communities_Are_Doing_to_Help_February_7_2013.pdf Carpenter, R., Irgens, L., Blair, P., et al. (2004). Sudden unexplained infant death in 20 regions in Europe: Case-control study. Lancet, 363, 185-191. Comfort, M., Loverro, J. & Kaltenbach, K. (2000). A search for strategies to engage women in substance abuse treatment. Social Work and Health Care, 31(4), 59-70.
Cormier, R., Dell, C., & Poole, N. (2004). Women and substance use problems. Women’s health surveillance report. BioMedical Central Women’s Health, 4(Suppl 1), S1-S8. http://dx.doi.org/10.1186/1472-6874-4-S1-S8
Dietz, P., England, L., Shapiro-Mendoza, C., et al. (2010). Infant morbidity and mortality attributable to prenatal smoking in the US. American Journal of Prevention Medicine, 39(1), 45–52. Grella, C., Joshi, V., & Hser, Y. (2000). Program variation in treatment outcomes among women in residential drug treatment. Evaluation Review, 24(4), 364-383. Horsley, T., Clifford, T., Barrowman, N., et al. (2007). Benefits and harms associated with the practice of bed sharing. A systematic review. Archives of Pediatric and Adolescent Medicine, 161, 237-245. Kasarabada, N., Hser, Y., Boles, S. & Huang, Y. (2002). Do patients’ perceptions of their counselors influence outcomes of drug treatment? Journal of Substance Abuse Treatment, 23(4), 327-334. Kattwinkel., J., Brooks, J., & Myerberg, D. (1992). Positioning and SIDS. American Academy of Pediatrics Task Force on Infant Positioning and SIDS. Pediatrics, 89, 1120-1126. Kattwinkel, J., Brooks, J., Keenan, M., & Malloy, M. (2000). Changing concepts of sudden infant death syndrome: Implications for infant sleeping environment and sleep position. Pediatrics, 105(3), 650-656. Kemp, J., Unger, B., Wilkins, D., et al. (2000). Unsafe sleep practices and an analysis of bedsharing among infants dying suddenly and unexpectedly: Results of a four-year, population-based, death-scene investigation study of sudden infant death syndrome and related deaths. Pediatrics, 106(3), e41. Retrieved from http://www.pediatrics.org/cgi/ content/full/106/3/e41.full Leach, C., Blair, P., Fleming, P., et al. (1999). Epidemiology of SIDS and explained sudden infant deaths. Pediatrics, 104, e43. Retrieved from http://pediatrics.aappublications.org/ content/pediatrics/104/4/e43.full.html
44
Leslie, M. & Roberts, G. (2004). Nurturing change: Working effectively with high risk women and affected children to prevent and reduce harms associated with FASD. Ottawa: Mothercraft Press. McGarvey, C., McDonnell, M., Hamilton, K., et al. (2006). Bed sharing and sudden infant death syndrome: Irish case-control study. Journal of Paediatrics and Child Health, 11, Supplement A, 19A-21A. Mitchell, E., Taylor, B., Ford, R., et al. (1992). Four modifiable and other major risk factors for cot death: The New Zealand study. Journal of Paediatric Child Health, 28, Supplement 1, S3-8. Moon, R., Horne, R., & Hauck, F. (2007). Sudden infant death syndrome. Lancet, 370, 1578-1587. O’Connor, M., & Whaley, S. (2007). Brief intervention for alcohol use by pregnant women. American Journal of Public Health, 97(2), 252-258. Ostfeld, B., Perl, H., Esposito, L., et al. (2006). Sleep environment, positional, lifestyles, demographic characteristics associated with bed sharing in sudden infant death syndrome cases: A population-based study. Pediatrics, 118, 2051-2059. Parkes, T., Poole, N., Salmon, A., et al. (2008). Double exposure: A better practices review on alcohol interventions during pregnancy. Vancouver: BC Centre of Excellence for Women’s Health. Payne, S. (2007). In-Hospital Stabilization of Pregnant Women Who Use Drugs. In N. Poole and L. Greaves (Eds.) Highs and lows: Canadian perspectives on women and substance use (pp. 249-255). Toronto: Centre for Addiction and Mental Health. Poole, N., & Isaac, B. (2001). Apprehensions: Barriers to treatment for substance using mothers. Vancouver: BC Centre of Excellence for Women’s Health. Public Health Agency of Canada. (2008). Canadian perinatal health report. Ottawa: Author. Public Health Agency of Canada. (2012). Preventing sudden infant deaths in Canada. Joint statement on safe sleep. Retrieved from http://www.phac-aspc.gc.ca/hp-ps/dca-dea/stages-etapes/childhood-enfance_0-2/sids/jss-ec. Shapiro-Mendoza, C., Kimball, M.,Tomashek, K., et al. (2009). US infant mortality trends attributable to accidental suffocation and strangulation in bed from 1984 through 2004: Are rates increasing? Pediatrics, 123(2), 533. Sword, W., Niccols, A., & Fan, A. (2004). “New Choices” for women with addictions: Perceptions of program participants. BMC Public Health, 4(10), 1-11. Available: http://www.biomedcentral.com/1471-2458/4/10. Tait, C. (2000). A study of the service needs of pregnant addicted women in Manitoba. Winnipeg: Prairie Women’s Health Centre of Excellence. Tait, C. (2003). Fetal alcohol syndrome among Canadian aboriginal people in Canada: Review and analysis of the intergenerational links to residential schools. Ottawa: Aboriginal Healing Foundation. Trifunov, W. (2006). Examining the evidence regarding infant sleeping practices and sudden infant death syndrome. Calgary: Regional Infant Sleep Committee. Trifunov, W. (2009). The practice of bed sharing: A systematic literature and policy review. Ottawa: Public Health Agency of Canada. Vennemann, M., Findeisen, M., Butterfab-Bahloul, T., et al. (2005). Modifiable risk factors for SIDS in Germany: Results of GeSID. Acta Paediatrica, 94, 655-660.
45
Vennemann, M., Bajanowski, T., Butterfab-Bahloul, T., et al. (2007). Do risk factors differ between explained sudden unexpected death in infancy and sudden infant death syndrome? Archives of Diseases in Childhood. 92, 133-136. Wallace, S. (2014). Balancing family bonding with newborn safety. Pennsylvania Patient Safety Authority, 11(3), 102-108. Watkins, M. & Chovanec, D. (2006). Women working toward their goals through AADAC Enhanced Services for Women (ESW). Edmonton: AADAC. Willinger, M., James, L., & Catz, C. (1991). Defining the sudden infant death syndrome (SIDS): Deliberations of an expert panel convened by the National Institute of Child Health and Human Development. Pediatric Pathology, 11(5), 677-684. Wisdom, J., Hoffman, K., Rechberger, E., et al. (2009). Women-focused treatment agencies and process improvement: Strategies to increase client engagement. Women & Therapy, 32(1), 69-87.
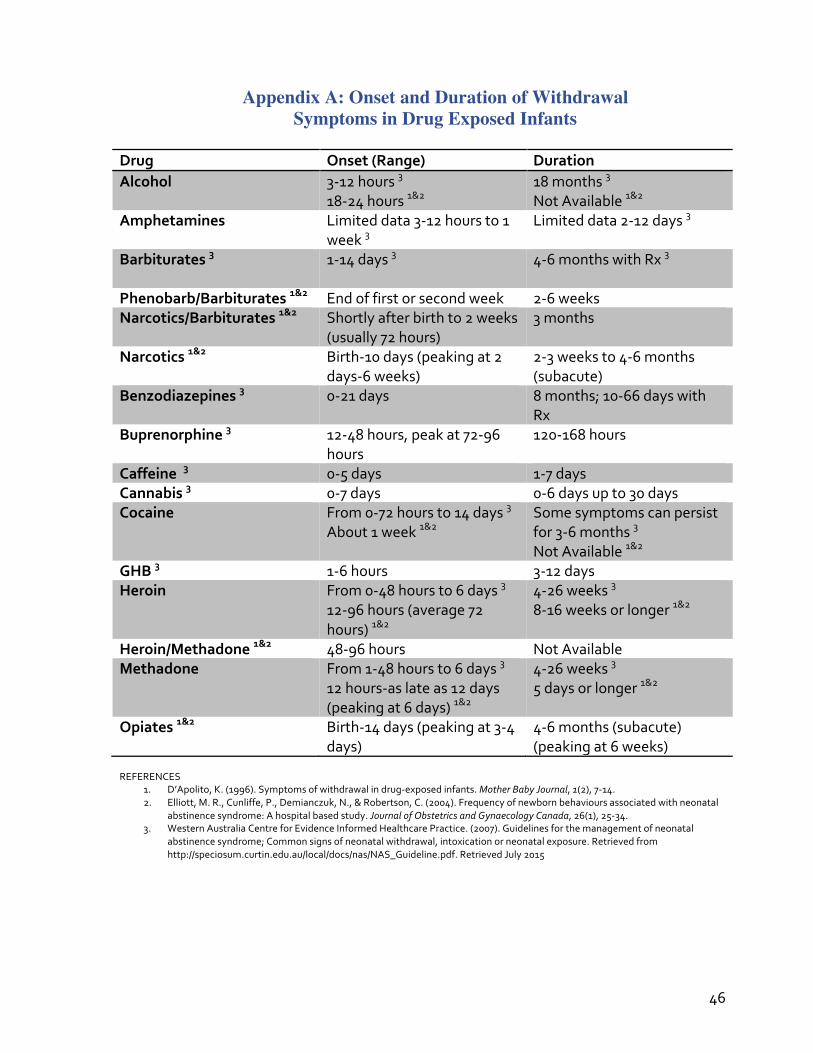
46
Appendix A: Onset and Duration of Withdrawal Symptoms in Drug Exposed Infants
Drug Onset(Range) DurationAlcohol 3-12hours3
18-24hours1&218months3NotAvailable1&2
Amphetamines Limiteddata3-12hoursto1week3
Limiteddata2-12days3
Barbiturates3 1-14days3
4-6monthswithRx3
Phenobarb/Barbiturates1&2 Endoffirstorsecondweek 2-6weeksNarcotics/Barbiturates1&2 Shortlyafterbirthto2weeks
(usually72hours)3months
Narcotics1&2 Birth-10days(peakingat2days-6weeks)
2-3weeksto4-6months(subacute)
Benzodiazepines3 0-21days 8months;10-66dayswithRx
Buprenorphine3 12-48hours,peakat72-96hours
120-168hours
Caffeine3 0-5days 1-7daysCannabis3 0-7days 0-6daysupto30daysCocaine From0-72hoursto14days3
About1week1&2Somesymptomscanpersistfor3-6months3NotAvailable1&2
GHB3 1-6hours 3-12daysHeroin From0-48hoursto6days3
12-96hours(average72hours)1&2
4-26weeks38-16weeksorlonger1&2
Heroin/Methadone1&2 48-96hours NotAvailableMethadone From1-48hoursto6days3
12hours-aslateas12days(peakingat6days)1&2
4-26weeks35daysorlonger1&2
Opiates1&2 Birth-14days(peakingat3-4days)
4-6months(subacute)(peakingat6weeks)
REFERENCES
1. D’Apolito,K.(1996).Symptomsofwithdrawalindrug-exposedinfants.MotherBabyJournal,1(2),7-14.2. Elliott,M.R.,Cunliffe,P.,Demianczuk,N.,&Robertson,C.(2004).Frequencyofnewbornbehavioursassociatedwithneonatal
abstinencesyndrome:Ahospitalbasedstudy.JournalofObstetricsandGynaecologyCanada,26(1),25-34.3. WesternAustraliaCentreforEvidenceInformedHealthcarePractice.(2007).Guidelinesforthemanagementofneonatal
abstinencesyndrome;Commonsignsofneonatalwithdrawal,intoxicationorneonatalexposure.Retrievedfromhttp://speciosum.curtin.edu.au/local/docs/nas/NAS_Guideline.pdf.RetrievedJuly2015
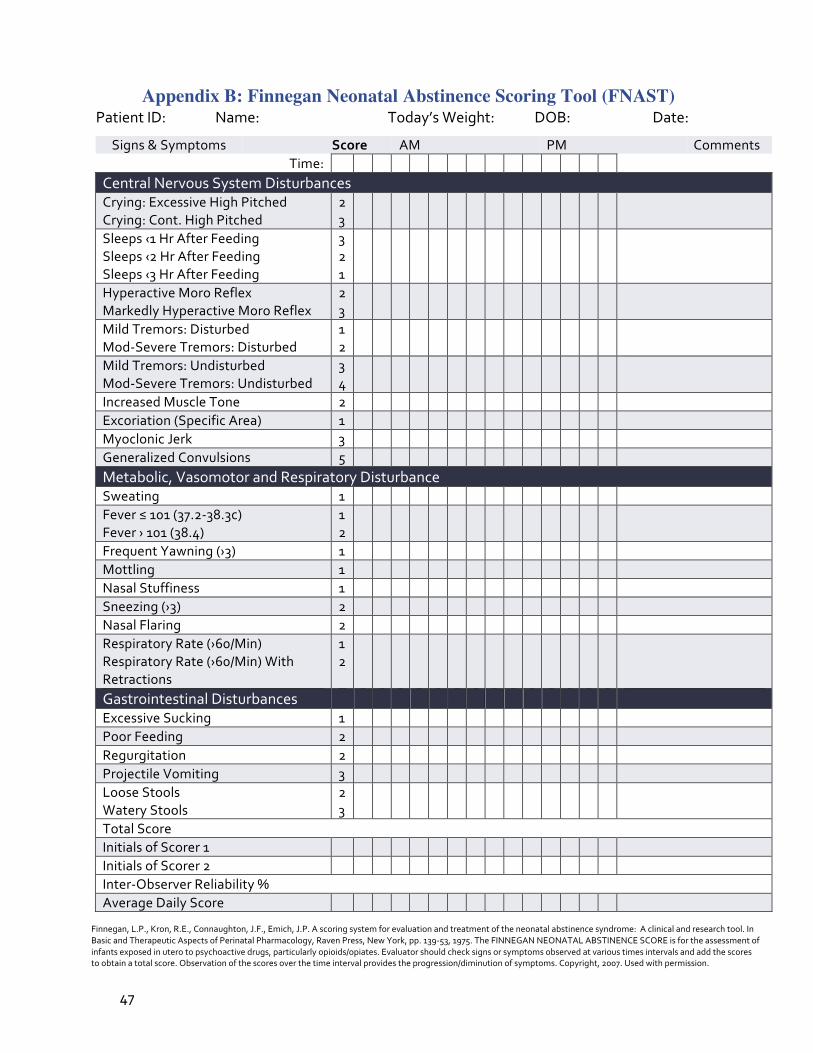
47
Appendix B: Finnegan Neonatal Abstinence Scoring Tool (FNAST) PatientID: Name: Today’sWeight: DOB: Date:
Finnegan,L.P.,Kron,R.E.,Connaughton,J.F.,Emich,J.P.Ascoringsystemforevaluationandtreatmentoftheneonatalabstinencesyndrome:Aclinicalandresearchtool.InBasicandTherapeuticAspectsofPerinatalPharmacology,RavenPress,NewYork,pp.139-53,1975.TheFINNEGANNEONATALABSTINENCESCOREisfortheassessmentofinfantsexposedinuterotopsychoactivedrugs,particularlyopioids/opiates.Evaluatorshouldchecksignsorsymptomsobservedatvarioustimesintervalsandaddthescorestoobtainatotalscore.Observationofthescoresoverthetimeintervalprovidestheprogression/diminutionofsymptoms.Copyright,2007.Usedwithpermission.
Signs&Symptoms Score AM PM CommentsTime:
CentralNervousSystemDisturbancesCrying:ExcessiveHighPitchedCrying:Cont.HighPitched
23
Sleeps‹1HrAfterFeedingSleeps‹2HrAfterFeedingSleeps‹3HrAfterFeeding
321
HyperactiveMoroReflexMarkedlyHyperactiveMoroReflex
23
MildTremors:DisturbedMod-SevereTremors:Disturbed
12
MildTremors:UndisturbedMod-SevereTremors:Undisturbed
34
IncreasedMuscleTone 2
Excoriation(SpecificArea) 1
MyoclonicJerk 3
GeneralizedConvulsions 5
Metabolic,VasomotorandRespiratoryDisturbanceSweating 1
Fever≤101(37.2-38.3c)Fever›101(38.4)
12
FrequentYawning(›3) 1
Mottling 1
NasalStuffiness 1
Sneezing(›3) 2
NasalFlaring 2
RespiratoryRate(›60/Min)RespiratoryRate(›60/Min)WithRetractions
12
GastrointestinalDisturbances
ExcessiveSucking 1
PoorFeeding 2
Regurgitation 2
ProjectileVomiting 3
LooseStoolsWateryStools
23
TotalScoreInitialsofScorer1
InitialsofScorer2
Inter-ObserverReliability%AverageDailyScore
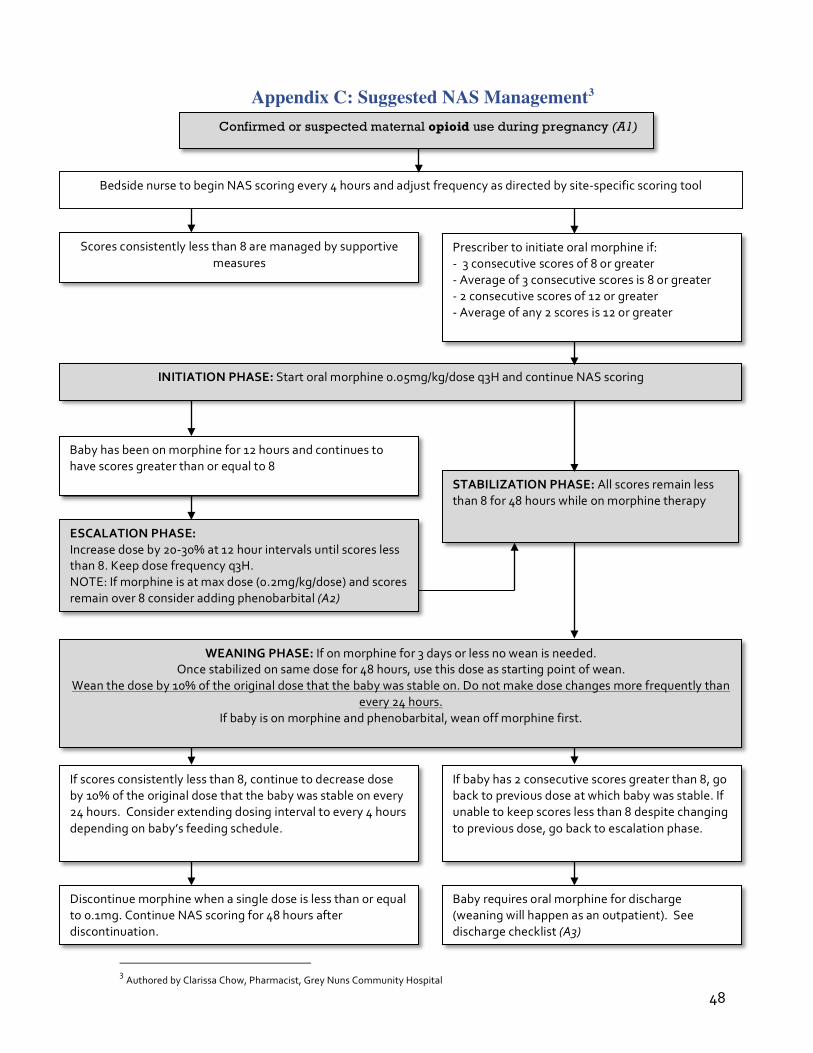
48
Appendix C: Suggested NAS Management3
3AuthoredbyClarissaChow,Pharmacist,GreyNunsCommunityHospital
Confirmed or suspected maternal opioid use during pregnancy (A1)
Scoresconsistentlylessthan8aremanagedbysupportivemeasures
BedsidenursetobeginNASscoringevery4hoursandadjustfrequencyasdirectedbysite-specificscoringtool
Prescribertoinitiateoralmorphineif:-3consecutivescoresof8orgreater-Averageof3consecutivescoresis8orgreater-2consecutivescoresof12orgreater-Averageofany2scoresis12orgreater
INITIATIONPHASE:Startoralmorphine0.05mg/kg/doseq3HandcontinueNASscoring
Babyhasbeenonmorphinefor12hoursandcontinuestohavescoresgreaterthanorequalto8
WEANINGPHASE:Ifonmorphinefor3daysorlessnoweanisneeded.Oncestabilizedonsamedosefor48hours,usethisdoseasstartingpointofwean.
Weanthedoseby10%oftheoriginaldosethatthebabywasstableon.Donotmakedosechangesmorefrequentlythanevery24hours.
Ifbabyisonmorphineandphenobarbital,weanoffmorphinefirst.
ESCALATIONPHASE:Increasedoseby20-30%at12hourintervalsuntilscoreslessthan8.Keepdosefrequencyq3H.NOTE:Ifmorphineisatmaxdose(0.2mg/kg/dose)andscoresremainover8consideraddingphenobarbital(A2)
STABILIZATIONPHASE:Allscoresremainlessthan8for48hourswhileonmorphinetherapy
Discontinuemorphinewhenasingledoseislessthanorequalto0.1mg.ContinueNASscoringfor48hoursafterdiscontinuation.
Ifbabyhas2consecutivescoresgreaterthan8,gobacktopreviousdoseatwhichbabywasstable.Ifunabletokeepscoreslessthan8despitechangingtopreviousdose,gobacktoescalationphase.
Ifscoresconsistentlylessthan8,continuetodecreasedoseby10%oftheoriginaldosethatthebabywasstableonevery24hours.Considerextendingdosingintervaltoevery4hoursdependingonbaby’sfeedingschedule.
Babyrequiresoralmorphinefordischarge(weaningwillhappenasanoutpatient).Seedischargechecklist(A3)
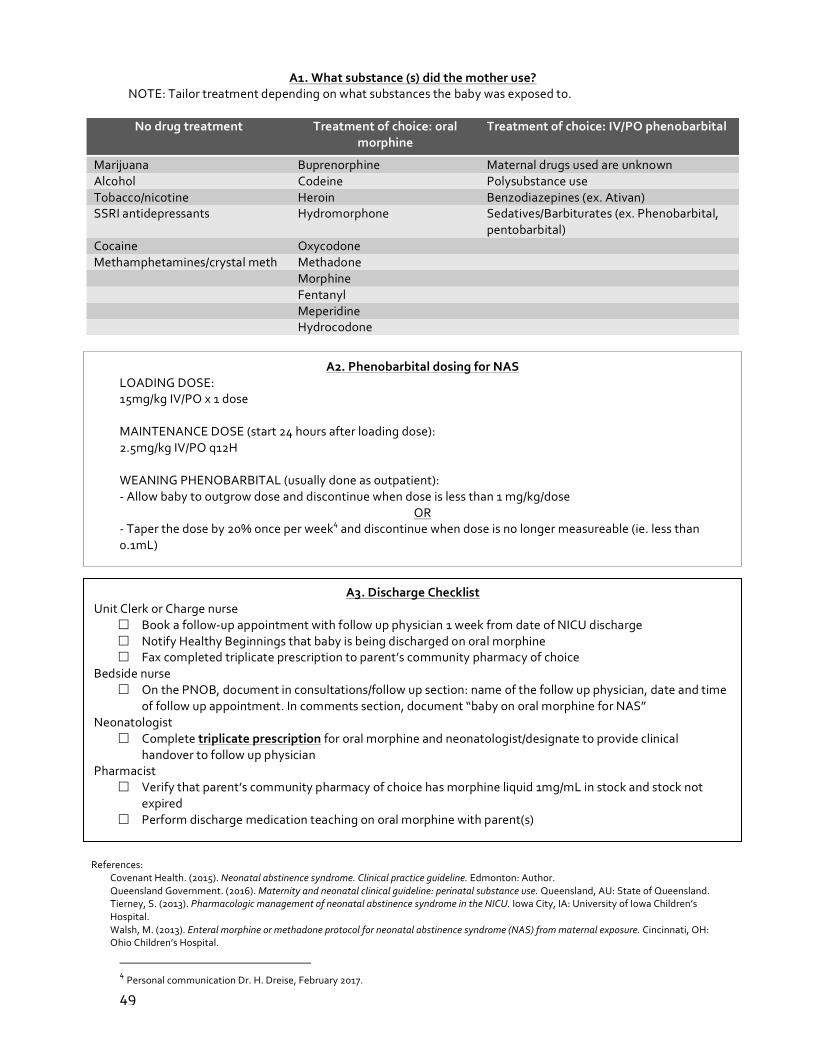
49
A2.PhenobarbitaldosingforNASLOADINGDOSE:15mg/kgIV/POx1doseMAINTENANCEDOSE(start24hoursafterloadingdose):2.5mg/kgIV/POq12HWEANINGPHENOBARBITAL(usuallydoneasoutpatient):-Allowbabytooutgrowdoseanddiscontinuewhendoseislessthan1mg/kg/dose
OR-Taperthedoseby20%onceperweek4anddiscontinuewhendoseisnolongermeasureable(ie.lessthan0.1mL)
References:CovenantHealth.(2015).Neonatalabstinencesyndrome.Clinicalpracticeguideline.Edmonton:Author.QueenslandGovernment.(2016).Maternityandneonatalclinicalguideline:perinatalsubstanceuse.Queensland,AU:StateofQueensland.Tierney,S.(2013).PharmacologicmanagementofneonatalabstinencesyndromeintheNICU.IowaCity,IA:UniversityofIowaChildren’sHospital.Walsh,M.(2013).Enteralmorphineormethadoneprotocolforneonatalabstinencesyndrome(NAS)frommaternalexposure.Cincinnati,OH:OhioChildren’sHospital.
4PersonalcommunicationDr.H.Dreise,February2017.
A1.Whatsubstance(s)didthemotheruse?NOTE:Tailortreatmentdependingonwhatsubstancesthebabywasexposedto.
Nodrugtreatment Treatmentofchoice:oralmorphine
Treatmentofchoice:IV/POphenobarbital
Marijuana Buprenorphine MaternaldrugsusedareunknownAlcohol Codeine PolysubstanceuseTobacco/nicotine Heroin Benzodiazepines(ex.Ativan)SSRIantidepressants Hydromorphone Sedatives/Barbiturates(ex.Phenobarbital,
pentobarbital)Cocaine Oxycodone Methamphetamines/crystalmeth Methadone
Morphine Fentanyl Meperidine Hydrocodone
A3.DischargeChecklistUnitClerkorChargenurse
£ Bookafollow-upappointmentwithfollowupphysician1weekfromdateofNICUdischarge£ NotifyHealthyBeginningsthatbabyisbeingdischargedonoralmorphine£ Faxcompletedtriplicateprescriptiontoparent’scommunitypharmacyofchoice
Bedsidenurse£ OnthePNOB,documentinconsultations/followupsection:nameofthefollowupphysician,dateandtime
offollowupappointment.Incommentssection,document“babyonoralmorphineforNAS”Neonatologist
£ Completetriplicateprescriptionfororalmorphineandneonatologist/designatetoprovideclinicalhandovertofollowupphysician
Pharmacist£ Verifythatparent’scommunitypharmacyofchoicehasmorphineliquid1mg/mLinstockandstocknot
expired£ Performdischargemedicationteachingonoralmorphinewithparent(s)

50
NOTES
51
Learn from yesterday. Live for today. Hope for tomorrow. – ALBERT EINSTEIN

52