Supplemental Nutrition Assistance Program - Hunger ...
147
Supplemental Nutrition A ssistance P rogram in New York State An Eligibility Prescreening Guide October 2015 edition
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Supplemental Nutrition Assistance Program - Hunger ...
Supplemental NutritionAssistance Programin New York State
An Eligibility Prescreening GuideOctober 2015 edition

Supplemental NutritionAssistance Programin New York State
An Eligibility Prescreening GuideOctober 2015 edition
For questions or comments related to this guide, please contact the SNAP Technical Assistance Specialist at 518-436-8757 ext 126.
14 Computer Drive East • Albany, NY 12205 • 518-436-8757 • HungerSolutionsNY.org

1
TABLE OF CONTENTS
INTRODUCTION………………………………………………………………………………………………………………… 4 THE APPLICATION PROCESS………………………………………………………………………………………………. 5 The Application Form…………………………………………………………………………………………………….. 5 NYS “myBenefits” Screening Tool and “myBenefits” Online SNAP Application……………. 6 Accessing the Application……………………………………………………………………………………………… 6 Filing the Application……………………………………………………………………………………………………. 7 Applying for SNAP When Not Applying for Cash Assistance Benefits…………………………... 8 Timeliness……………………………………………………………………………………………………………………… 8 SNAP Expedited Service………………………………………………………………………………………………. 10 THE SNAP INTERVIEW…………………………………………………………………………………………………….. 12 Phone Interviews……………………..…………………………………………………………………………………. 12 Authorized Representatives……………………………………………………………………………………..... 13 Notice of Missed Interview Rules at Application………………………………………………………… 13 VERIFICATION AND DOCUMENTATION………………………………………………………………………….. 15 Collateral Contacts……………………………………………………………………………………………………… 15 Computer Matches for Verification……………………………………………………………………………. 16 Necessary Verification………………………………………………………………………………………………… 16 Verification of Questionable Information………………………………………………………………….. 18 Front End Detection Systems……………………………………………………………………………………... 19
Social Security Numbers…………………………………………………………………………………………….. 19 Households With Undocumented Non-Citizens…………………………………………………………. 20 People Who Do Not Speak English……………………………………………………………………………… 20 Accommodating Persons With Disabilities………………………………………………………………... 20 Notification of Acceptance or Denial…………………………………………………………………………. 21 STATUS-BASED LIMITATIONS………………………………………………………………………………………… 22 Students…………………………………………………………………………………………………………………….. 22 Strikers………………………………………………………………………………………………………………………. 24 Non-Citizen Eligibility……………………………………………………………………………………………….. 24 Fleeing Felons and Probation Officers……………………………………………………………………….. 26 WORK REQUIREMENTS………………………………………………………………………………………………….. 27 Voluntary Quit……………………………………………………………………………………………………………. 28 Able-Bodied Adults Without Dependents (ABAWDs)………………………………………………… 28 Work Sanctions, Internal Program Violations……………………………………………………………. 29 HOUSEHOLD COMPOSITION…………………………………………………………………………………………. 30 Special Rules for Homeless Youth, Foster Care Children, and Boarders….………………… 30 Special Rules for Severely Disabled People Living With Others………………………………… 31 EXPANDED CATEGORICAL ELIGIBILITY………………………………………………………………………..... 32 Households with Dependent Care Costs…………………………………………………………………… 32 Households that ARE NOT Categorically Eligible………………………………………………………. 33 CALCULATING A BUDGET………………………………………………………………………………………………. 35 Overview of Budgeting……………………………………………………………………………………………… 35 Household Information……………………………………………………………………………………………… 36
2
Using the SNAP Budget Worksheet……………………………………………………………………………. 36 BUDGET WORKSHEET……………………………………………………………………………………………………. 39 Income……………………………………………………………………………………………………………………….. 39 Deductions…………………………………………………………………………………………………………………. 40 Shelter Expenses………………………………………………………………………………………………………… 42 Excess Shelter Deduction……………………………………………………………………………………………. 44 Calculating the Excess Shelter Deduction…………………………………………………………………… 44 Calculating the SNAP Benefit Allotment…………………………………………………………………….. 44 ADVANCED BUDGETING…………………………………………………………………………………………………. 46 Income of Ineligible Household Members………………………………………………………………..... 46 Budgeting for Non-Citizens…………………………………………………………………………………………. 46 Budgeting Shelter Costs for Homeless People.……………………………………………………………. 47 Budgeting Rules for Other Groups………………………………………………………………………………. 48 Self-Employment Income……………………………………………………………………………………………. 48 Military Families………………………………………………………………………………………………………….. 50 KEEPING AND USING BENEFITS……………………………………………………………………………………….. 52 Using SNAP Benefits…………………………………………………………………………………………………… 52 Eligible Food Items………………………………………………………………………………………………………. 53 SNAP Monthly Benefits Issuance Schedule………………………………………………………………….. 54 Recertification and Reporting Requirements………………………………………………………………. 54 Telephone Recertification……………………………………………………………………………………………. 55 Changes Between Certification Periods………………………………………………………………………. 55 Case Reactivation Waiver……………………………………………………………………………………………. 56 Emergency Food Replacement……………………………………………………………………………………. 58 Disaster SNAP……………………………………………………………………………………………………………… 59 Transitional Benefits…………………………………………………………………………………………………… 59 New York State Nutrition Improvement Project – NYSNIP…………………………………………. 60

3
LIST OF APPENDICES
APPENDIX A: COMMON ACRONYMS
APPENDIX B: ORGANIZATIONAL CHART OF SNAP
APPENDIX C: “HOW TO” SHEET FOR ORDERING SNAP APPLICATIONS & OTDA ORDER FORM 876 EL APPENDIX D: SNAP APPLICATION FORM (LDSS-4826) & “HOW TO COMPLETE” BOOKLET (LDSS-4826A)
APPENDIX E: SNAP APPLICATION EXPEDITED PROCESSING SUMMARY SHEET (LDSS-3938)
APPENDIX F: DOCUMENTATION REQUIREMENTS CHECKLIST (LDSS-2642)
APPENDIX G: TA/SNAP DOCUMENTATION/VERIFICATION DESK GUIDE (LDSS-3666)
APPENDIX H: NON-CITIZEN ELIGIBILITY CHART (LDSS-4579)
APPENDIX I: WORK RULES DESK GUIDE
APPENDIX J: CATEGORICAL ELIGIBILITY DESK GUIDE
APPENDIX K: BUDGET WORKSHEET
APPENDIX L: CHECKLIST FOR STUDENT ELIGIBILITY
APPENDIX M: HOUSEHOLD COMPESITION DESKGUIDE (LDSS 4314)
APPENDIX N: AUTHORIZED REPRESENTATIVE REQUEST FORM (LDSS 4942)
APPENDIX O: REQUEST FOR REPLACEMENT SNAP (LDSS 2291)
APPENDIX P: CHANGE REPORT FORM (LDSS 3151)

4
INTRODUCTION
This Supplemental Nutrition Assistance Program (SNAP) prescreening guide is designed for human service agencies, advocates, and volunteers working with low-income households who wish to:
(1) Determine which households may qualify for SNAP benefits as well as theirestimated SNAP benefit allotment;
(2) Assist potentially eligible households through the SNAP application process; and
(3) Assist current SNAP participants in the recertification process.
This guide only briefly addresses SNAP work rules. The New York State Temporary Assistance and SNAP Employment Policy Manual provides a comprehensive explanation of SNAP’s employment and training requirements. It focuses on the application process and establishing eligibility. Hunger Solutions New York encourages advocates to try to resolve problems by communicating with local SNAP offices.
About the Supplemental Nutrition Assistance Program (SNAP) (12-ADM-07; Appendix B)
Governor Cuomo signed into law a bill to change the name of New York State's Food Stamp Program to the national name of "Supplemental Nutrition Assistance Program" (SNAP) in June of 2012. SNAP, the new name for the Food Stamp Program, is a state-administered federal nutrition assistance program. Federal law governs the criteria for eligibility and levels of benefits. Each state is responsible for determining and documenting eligibility, issuing benefits, and maintaining records.
The United States Department of Agriculture (USDA) administers the program at the national level. In New York State, the Office of Temporary and Disability Assistance (OTDA) oversees the local administration of SNAP. Most administrative functions are delegated to counties through local departments of social services (LDSS). In New York City, the Human Resources Administration (HRA) administers SNAP (Appendix B: Organizational Chart). Please note that throughout this guide, LDSS is also referred to as the “local office” and “SNAP office,” as applicants and offices use these terms interchangeably.
New York State policy is explained in detail in the Supplemental Nutrition Assistance Program Sourcebook (SNAPSB). The sourcebook includes New York State’s instructions to the local districts on the administration of SNAP. The sourcebook is essential to anyone working with SNAP in New York State.
Throughout this guide, various headings will refer back to the specific section of the SNAPSB. Recent policy changes issued through administrative directives (ADMs), informational letters (INFs), local commissioner memoranda (LCMs), and General Information Messages (GIS) can be found at OTDA’s website.
Please note that this guide is updated annually to reflect the October 1 SNAP standards/ deductions/adjustments, as well as policy changes that occurred throughout the year. This version of the guide is valid from October 1, 2015 through September 30, 2016, but does not take into account any policy changes that have been instituted after September 2015. Hunger Solutions New York provides SNAP Policy Updates (on our website) that highlight new policy changes or clarifications provided to SNAP offices throughout the year.

5
THE APPLICATION PROCESS
(SNAPSB Section 3 & 4; 10-INF-22) The application process begins with getting an application, filling it out, and submitting (filing) the application to the local department of social services office (LDSS) or the Human Resources Administration (HRA) in New York City. The applicant must then:
• Be interviewed - this must be scheduled for a specific day and at a specific time or be done at the time the application is submitted.
• Provide information about the circumstances of those applying, and • Provide verification of the criteria necessary to determine eligibility.
The application process is paperwork intensive and can be complicated— but, getting SNAP benefits can make the difference between going hungry and having food on the table.
The Application Form (SNAPSB Section 3: p. 6, Section 4: p. 17; 03-ADM-03; 10-INF-22; 12-INF-12 Appendix C and D) Applicants apply for SNAP by filing an application form. Anyone can get an application form online or by contacting any SNAP office. If an individual goes to the SNAP office and asks for an application, the office must give them one. If a person asks a SNAP office to mail an application form, the office must mail it that same day. Many human service agencies keep a supply of SNAP applications on hand. New York State has two application forms:
• 6-page simplified SNAP application—a SNAP-only application (Appendix D) • 16-page common application form—also known as the joint application—used by
anyone who wishes to apply for multiple assistance programs Previously, all applications contained the OTDA “Helping Hands” brochure to confer ‘categorical eligibility’ for SNAP benefits (12-INF-12 and Appendix J). However, the brochure is no longer required to be included in application packets. The Helping Hands brochure information is incorporated as an addition to the client approval notices provided at application and recertification. Households applying for multiple assistance programs (Temporary Assistance (TANF), SNAP, Medicaid, and/or child care assistance) should utilize the joint application form. Anyone applying for TANF is also considered to be a SNAP applicant, even though eligibility guidelines and definitions of household composition vary. There are boxes on the form where the applicant can check off the programs for which they want to apply. If the applicant is found eligible for SNAP but not TANF, the SNAP application should be accepted and opened as a SNAP-only case. In most districts, the case will be transferred to an “NPA (non-public assistance)” SNAP unit or office.
Please see Appendix C for simple “How To” instructions for Community Agencies wanting to order SNAP applications and other brochures from OTDA. This appendix also includes the necessary order form.

6
Anyone has a right to submit an application to any SNAP office in NYS and that office must forward the application to the correct SNAP office based on the applicant’s county of residence. However, this is not always a smooth process. Therefore, it is best to be clear about a county’s SNAP application procedures and direct applicants to the SNAP office in their county of residence. For a listing of all local county departments of social services in NYS, go to: http://otda.ny.gov/workingfamilies/dss.asp or call the toll-free hotline at 1-800-342-3009. NYS “myBenefits” Screening Tool and “myBenefits” Online SNAP Application “myBenefits” is an online tool available to all NYS residents to connect with benefits, services, and work supports. myBenefits is a single portal of NYS programs and benefits. It allows individuals and families to learn about and apply for an array of programs customized to fit their unique circumstances. Applicants follow basic instructions to answer a simple set of online questions. Applicant information will stay private and secure. To use myBenefits, go to: http://www.mybenefits.ny.gov. Currently, myBenefits covers the following benefit programs:
• Child and Dependent Care Tax Credit • Child Health Plus • Earned Income Tax Credit • EPIC • Family Health Plus • Healthy New York • HEAP • Medicaid • Noncustodial Parent Tax Credit
• Nutrition Education • Prescription Saver • School Meals • SNAP • Summer Meal Program • Temporary Assistance • Veteran Affairs • WIC • Programs continue to be added
Remember that Nutrition Outreach and Education Program (NOEP) Coordinators can provide an in-depth SNAP prescreening and also help potentially eligible families through the SNAP application process. For local NOEP contact information, please visit www.FoodHelpNY.org. Accessing the Application (10-INF-22) When distributing or accepting an application for SNAP, the SNAP/HRA office must follow federal and state regulations that require:
A. All people must be allowed to receive an application and/or apply for SNAP benefits at any time during the regular business hours of the local office.
B. SNAP offices must NOT establish any of the following:
o Periodic daily quotas on application submissions;

7
o Limits on application pickup or submission times during normal office business hours;
o Limits on daily submissions based on the number of available interview slots; or
o Zip code or alphabetic restrictions that limit when a person may request or submit an application during a local district’s business hours.
C. A household’s right to apply and be interviewed for SNAP must not be denied
or limited due to: o National origin; o Citizenship status of any member of the household; or o For any other reason.
D. All people applying for SNAP, including those submitting applications by mail,
shall: o Have an interview scheduled on a specific day and at a specific time if
they are not interviewed on the same day they apply. o Receive expedited benefits no later than five days following the date of the
application. • This means that the LDSS/HRA office must schedule the interview
in a timeframe that is consistent with the five-day rule. Filing the Application (SNAPSB Section 4: pp. 3, 9, 19, 27; 13-INF-05) Applicants should turn in a completed application form right away. The form does not have to be completely filled out to be turned in, but it is best to provide as much information as possible when submitting a SNAP application. To be submitted and accepted as an “identifiable application” the application must include at minimum the applicant’s name, address, signatures, and the date. Applications can be turned in:
• by mail • in person • by a third party (friend, relative, or
community agency representative) • by fax, or • completed online
Some SNAP offices may have trouble with mailed/faxed applications, either because they do not understand that they must accept applications by mail/fax or simply due to logistical problems. Mediating on behalf of SNAP applicants with those SNAP offices that will not accept applications by mail/fax may result in better access for future SNAP applicants in that county. HRA in NYC has a Mail-In Application and Referral Unit (MARU). MARU allows households citywide to request a SNAP application package by mail by calling the city’s 311 information line. MARU applications can then be returned by mail to the HRA MARU
The date the application is turned in is called the filing date. The filing date is very important because, if approved, SNAP benefits are issued based on the filing date, not the date the application is approved.

8
Center by using MARU Business Reply Envelopes (form #W90A). Community-based organizations assisting households with SNAP applications can also use MARU Business Reply Envelopes (form #W90A). NYC HRA implemented a fax system for their new Mail-In Application and Referral Unit (MARU). Applicants do not have to wait for a caseworker to see them before they turn in their applications at their county SNAP Office. They can drop off (file) the application and come back for the interview at a later date. Applicants will have to provide more information during the interview (see page 12 for more information on interviews). All SNAP offices must post the LDSS-4995 “Right to File” poster in their reception areas. This poster provides information concerning the rights of individuals to file a SNAP application.
Applying for SNAP When Not Applying for Cash Assistance Benefits (SNAPSB Section 4: pg. 3, 12) If a SNAP applicant submits a joint application for TA and SNAP and is determined not eligible for TANF, the LDSS must continue to process their SNAP eligibility based on the original joint application. The applicant cannot be made to submit a new application. This should not cause any delay in processing the SNAP application. Timeliness (14-INF-16; SNAPSB Section 3: pg. 4; Section 4: pp. 9, 20-23) Once the SNAP office receives an application, it has no more than 30 days to act on the application and issue SNAP benefits if the household is eligible. The SNAP office must make a timely decision on the SNAP application. Delays are usually the result of problems with obtaining documentation, although they are sometimes caused by administrative or workload problems within the SNAP office. SNAP offices must give applicants at least 10 days to submit all the necessary documentation. If the applicant is having difficulty securing the required documents, the SNAP office must assist them in obtaining the verification. If the SNAP office does not make a decision on an application within the normal 30 days, we recommend contacting a SNAP supervisor or manager to discuss the situation.
Note: If everyone in a household is applying for or receiving Supplemental Security Income (SSI) benefits, which are administered by the Social Security Administration (SSA), the household can file their SNAP application at SSA. An SSA representative will forward the SNAP application to the proper SNAP office for processing. Single SSI live-alone recipients are now automatically enrolled in SNAP through a special project called the New York State Nutrition Improvement Project (NYSNIP); see page 60 for more information.

9
Delays Caused By the Applicant(s) If the applicant does not turn in the required documents within the time period allotted by the SNAP office, and does not have good reason, the SNAP application can be denied. Applicants who submit any missing documents within the initial 30-day application period, and who are otherwise found eligible for SNAP, must have their case opened and be provided SNAP benefits back to the application date. No new application is required. Similarly, if the applicant submits the missing documents after the initial 30-day period, but within 60 days of the application date, the SNAP office must open the case, but benefits will not be provided back to the date of application; instead the case will be opened as of the month following the application month (the second 30-day period). Applicants wishing to submit any missing documents later than 60 days after their initial application date must file a new SNAP application. Delays Caused By the SNAP Office If the applicant has submitted all of their documents and is eligible for SNAP, but the SNAP office hasn’t provided the applicant with SNAP benefits within the allotted 30 days, then the SNAP office must provide SNAP benefits back to the day the application was first handed in. This is true even if the LDSS does not decide on the application until more than 60 days after it was submitted. When a household submits a SNAP application that has not been processed within the 30 day time period and the delay is caused by the SNAP office, the household will receive a notice that the SNAP application is “pending”. This is an effort to keep the applicant informed; however the application will be completed as timely as possible and SNAP
TIMELINESS: PROMPT ACTION TIME FRAMES
ACTION TIME FRAME
Providing application forms to households Same day the request is received
Accepting an identifiable application Same day as received
Expedited service screening Same day that an application is received
Application interview As soon as possible after receipt of an application
(Households eligible for expedited service should be interviewed within 5 days of their application date.)
Application processing/eligibility determination and issuance of benefits
As soon as possible and always within 30 days of application

10
benefits will be provided back to the day the application was submitted. SNAP application processing time is mandated by federal regulations and should be adhered to by SNAP offices. SNAP Expedited Service (05-ADM-13; 12-INF-06; SNAPSB Section 4: pg. 24-25; Section 5: pp. 128, 133-136; Section 15: pp. 316-317; Section 20: pg. 381; Appendix E) People with very low income and few resources may qualify for “expedited service” under the federal rules and regulations for the program. Everyone who applies for SNAP must be screened for eligibility for expedited service on the day they apply. New York has a standard screening form for this (LDSS-3938). Some SNAP offices may not always screen for expedited service when they should. Therefore, SNAP applicants should always ask to be screened for expedited service. People eligible for expedited service will get their SNAP benefits within 5 calendar days of the filing date. Many districts, including HRA, have a practice of making benefits available on the day of application. Expedited SNAP benefits is not a separate program, but instead a right to get SNAP more quickly. For those meeting the expedited criteria, this service is provided while the ongoing SNAP application is being processed. An applicant is still eligible to apply for and receive expedited service, even if they have an authorized representative, such as a friend or relative, apply for them. They may also have a phone interview or an interview in their home if they are unable to get to the LDSS office.
ELIGIBILITY FOR EXPEDITED SNAP BENEFITS
A household is eligible for expedited service if: 1. Their liquid resources (cash or readily available savings) do not exceed $100 and they
have received less than $150 in gross income during the calendar month in which they are applying for SNAP; OR
2. The household’s shelter costs for the month – rent or mortgage, plus utility expenses (the Standard Utility Allowance) – are greater than the combination of the household’s liquid resources and gross income for the calendar month in which they are applying; OR
3. They are a migrant or seasonal farm worker household who have liquid resources of $100 or less and meet SNAP requirements for being destitute.
After determining that a household meets any one of the above three conditions, the SNAP office must interview the household and obtain proof of the applicant’s identity so that expedited benefits can be issued. No other verification is required for expedited SNAP purposes. Identity can be verified through either:
• a driver's license • a voter registration card OR

11
• any other document that proves the applicant’s identity.
If the applicant does not have any ID, the SNAP office must try to call someone (such as a friend, a relative, or a worker at a shelter or other agency) to verify their identity. The SNAP office should attempt to obtain as much verification as possible during the interview. Expedited processing should not be delayed due to a lack of verification (other than identity) if it is likely that the other verification cannot be obtained within the 5 day time frame. The SNAP office should use the information submitted on the application for expedited budgeting purposes even if this information has not been verified. If no verification of identity is possible, then benefits cannot be issued. If the applicant qualifies for expedited service, they must get their SNAP benefits within 5 calendar days. For example, if a person applies on a Monday and qualifies for expedited service, the SNAP office must provide SNAP benefits by the following Saturday. Even if the office is closed on Saturday, it must get the EBT (Electronic Benefit Transfer) card to the family and have the benefits authorized by Saturday. The SNAP office must also assess whether the applicant has ever received expedited SNAP benefits in the past. Families who received expedited SNAP benefits the last time they applied but were not certified for ongoing benefits (because they didn’t follow through with the verification process) have to meet certain additional criteria the next time they apply in order to receive expedited SNAP benefits. In order to be processed for expedited benefits, these applicants must submit either:
• the missing verification from their last application OR • all verification required with their new application*
Once the applicant has submitted all the necessary documents and is found eligible, the SNAP office must provide SNAP benefits within the expedited time frame (5 days). The SNAP office must give the household at least 10 days to gather paperwork for ongoing benefits.
∗Technically, these households are not eligible for expedited SNAP benefits under federal rules. However, if they submit all their current verification, New York State’s policy as outlined in 05 ADM-13 directs local districts to issue ongoing SNAP benefits using the expedited time frame of 5 days, rather than making the household wait up to 30 days.

12
THE SNAP INTERVIEW (GIS 06 TA/DC 010; GIS 08 TA/DC018; SNAPSB Section 4: pp. 5, 11;
Appendix N) All SNAP applicants must be interviewed either in person or over the phone. Applicants can be interviewed at the time of application submission or at a later date. Applicants are always able to have an in-person interview when requested and they can bring anyone they want with them, including legal representation. Applicants are scheduled for an interview as quickly as possible. Applicants eligible for expedited processing must be interviewed within 5 days of submitting the application. The SNAP worker will cover the following in the interview:
• review application, • clarify any incomplete or confusing information, • ask additional questions as needed, and • provide a list of any missing documentation and give the applicant at least 10 days
to turn in the needed information.
Phone Interviews (07-ADM-10; 08-INF-07; LDSS 4921) Many SNAP applicants will automatically be granted a phone interview, as opposed to having an in-office interview. The phone interviews are helpful to applicants because they do not need to go to the SNAP office in person. This is especially helpful for working families and people with disabilities. Phone interviews are granted for:
Working Families: Any non-temporary assistance SNAP applicants get an automatic phone interview when one of the following conditions is met:
1. One adult on the application is working 30 hours or more per week or earning an average of at least the federal minimum wage ($7.25/hour) multiplied by 30 hours per week. Ultimately, the adult on the application would need to average $217.50 gross per week.
2. Two adults on the application are each working 20 hours per week or earning at least the federal minimum wage ($7.25/hour) multiplied by 20 hours per week. In this instance each adult would need to be earning $145 gross per week, for a total of $290 per week.
Application Submission Type: Submitting an electronic application (ex. myBenefits or AccessNYC) results in an automatic phone interview. In addition, in NYC only, when applicants apply using the Mail-In Application and Referral Unit system (MARU), they are automatically scheduled a phone interview. This process allows NYC residents to apply by mail or fax at some community agencies, or by using the 311 system.

13
Others By Request: Many other applicants can request a phone interview on a case-by-case basis. Applicants demonstrating a hardship are welcome to request a phone interview. Hardships can include transportation difficulties, illness, prolonged severe weather, care of a household member, or work hours that conflict with the SNAP office hours. Disabled/Senior Applicants: When an application is submitted by a household comprised of all elderly and/or disabled adults with no earned income, then special rules can apply. If these types of applicants request to forego the in-office interview, they can be granted a telephone interview or the SNAP office can send a worker to the home for the interview. All home visits are required to be scheduled in advance; the worker cannot show up without notice. Authorized Representatives (Appendix N) SNAP applicants can appoint an “authorized representative” who can apply on their behalf, including attending the interview and using the EBT card to make purchases if approved.
• The authorized representative can be a friend, a relative, someone who works for an agency, or anyone else the applicant chooses.
• This person cannot be part of the applicant’s household, but must be able to provide the SNAP office all the information it needs to determine eligibility, including the household’s documentation.
• If an applicant wants someone to act as an authorized representative, an adult member of the household must provide a written notice to the SNAP office giving the person permission to act as their authorized representative. It is recommended to use the OTDA form (LDSS 4942).
• The SNAP office cannot force an applicant to use an authorized representative. OTDA form LDSS-4942:
• Is specifically for households wishing to designate an authorized representative • Is available in both English and Spanish • Cannot be required by the LDSS, but it is recommended • Is developed for use with the new electronic application, but is available statewide
for use with any applicant household
A copy of the form is provided in Appendix N. Notice of Missed Interview Rules at Application (GIS 08TA/DC018) SNAP offices must comply with the federal regulations for sending a Notice of Missed Interview (NOMI) during the SNAP application and recertification process.

14
NYS policy reminds SNAP offices that they must follow these regulations during the application process:
1. If the SNAP office cannot interview the household on the day it is submitting the application, then the SNAP office must provide a date and time for the interview.
2. For new applicants that have missed their interview, the SNAP office must mail a “Notice of Missed Interview” letter (NOMI). This required notice informs the household that it is now the household’s responsibility to reschedule the eligibility interview.
3. If the new SNAP applicant fails to appear for the scheduled interview AND does not contact the local district upon receiving the NOMI, the district will deny the case for failure to comply with the eligibility interview requirement. The SNAP office must allow 30 days from the filing date before sending this denial notice. (The SNAP office will send the household two notices: 1. the NOMI and 2. denial letter.)
4. The SNAP office must reschedule the eligibility interview for all applicants that respond to the missed interview notice.

15
VERIFICATION AND DOCUMENTATION (SNAPSB Section 5: pp. 114-127; 12-INF-06; Appendix F and Appendix G)
All eligibility criteria must be verified before the worker can determine that the household is eligible to receive a SNAP benefit. The SNAP office gains verification from documents, usually provided by the applicant(s), “collateral contacts” (people outside the applying household that the worker contacts), home visits, and computer matches. Every piece of information that is used to determine eligibility and a budget must be verified. Even if the worker is sure the information is true, s/he still must have some kind of verification for the file. If the applicant has receipts for their rent or mortgage payments, telephone and utility bills, and child care expenses, as well as pay stubs and verification of identity and address, they should bring these documents to the interview. For SNAP program purposes, any reasonable form of documentation must be accepted and the acceptable verification shall not be limited to any single type of document. The documentation requirements checklist (LDSS-2642 – see Appendix F) includes each eligibility criterion and acceptable forms of verification. One document may serve as verification for more than one eligibility criterion. If an applicant has tried to get a form of documentation and is unable to, then the caseworker is obligated to assist, including paying necessary fees. If the needed documentation is simply unavailable, the worker must find some other way to verify the eligibility criteria. Collateral contacts are almost always possible; even identity can be verified this way. Collateral Contacts (SNAPSB Section 5: pp. 121-122; 12-INF-06) When documentation is unavailable, the SNAP office will use a collateral contact. Collateral contacts are a substitute for written verification. The SNAP office calls the collateral contact directly for information to support what the household has reported. The worker is responsible for obtaining the information from the acceptable collateral contacts that have been provided by the applicant. The SNAP office can get information in writing, over the telephone, or in person. If the SNAP office wants to call someone, it should ask the applicant whom it could contact. If the applicant does not give the SNAP office an acceptable contact person, the SNAP office will identify a person to contact.
Case example: A birth certificate can serve as verification of identity, date of birth, and citizenship. OTDA has issued a desk guide (Appendix G: LDSS-3666) highlighting different forms of acceptable Primary and Secondary verification; however, SNAP does not differentiate between Primary and Secondary verification.
A collateral contact is a verbal confirmation of a household’s circumstances by a person outside the applicant’s household. For example, the SNAP office might call the landlord or neighbors to confirm the applicant’s address and household.
16
When the SNAP office makes collateral contact it is inadvertently letting that person know that the applicant household is applying for some type of benefit. In order to approach a collateral contact, the SNAP office must get the applicant’s permission to disclose household information. If the family does not want a person selected by the SNAP office contacted, they should be given the chance to verify information in some other way, or to withdraw their application. The SNAP office should only call collateral contacts when other verification is unavailable or inadequate. The SNAP office should conduct a home visit only if it cannot verify household eligibility criteria through documentation or collateral contacts. Home visits are to be used on a case-by-case basis where the supplied documentation is insufficient. Applicants do not have to let workers visit their homes, but the LDSS can deny the application if it cannot verify the household’s eligibility. Computer Matches for Verification (12-INF-06)
• The SNAP office can get information from computer systems of other public benefit programs, the Internal Revenue Service (IRS), the Social Security Administration (SSA), some banks, the NYS Department of Motor Vehicles, tax collectors, or other agencies and organizations.
• The SNAP office may want information from these agencies’ computers because they have records about people’s wages, their benefit checks, their addresses, and sometimes other things that affect whether they qualify for SNAP.
• The SNAP office usually will not tell the applicant when it is checking information in this way. If the SNAP office gets information from computer records that affects the SNAP case, it will usually either contact the household to verify the information or refer the case to an internal investigation unit.
Necessary Verification (SNAPSB Section 5:pp. 114-117; 12-INF-06, GIS 13 TA/DC043) SNAP rules require that the SNAP worker get proof of the following:
1. Identity of applicant. If an authorized representative applies for an applicant, the SNAP office must verify both the identity of the authorized representative and the head of the household. Identity is the only necessary verification for households eligible for expedited processing.
2. Household size. Verification can be obtained from a collateral contact such as a landlord statement or other readily available documentation. For example: driver’s license, work ID, school district report, housing authority section 8, ID for health benefits or other assistance programs, wage stubs, or any other documents which can be used to establish identity.
3. Age. The household must provide the date of birth for all applying household members. The household has until the next recertification to provide verification of the date of birth. Examples of verification of date of birth include birth certificates, marriage certificates, and school records or the SSN validation.

17
4. Citizenship status (also referred to as Alien Status by OTDA) of anyone in the household who is applying for SNAP and who is not a U.S. citizen. The SNAP office will verify the claimed legal status and any immigration documents submitted with the U.S. Citizenship and Immigration Services (USCIS, formerly known as INS or the Immigration and Naturalization Service). The SNAP office will only verify USCIS status for those household members who submit proof of their immigration status. Any non-citizen household members who do not submit proof of their immigration status (such as undocumented non-citizens) will be excluded from the household for SNAP purposes, but the rest of the household can still receive SNAP benefits.
5. Social security numbers (SSNs) of everyone in the household. In New York State, eligibility workers verify SSNs directly with the Social Security Administration (SSA). Therefore, individuals do not have to provide proof of their SSN unless the number they provide to the SNAP office does not match the SSA’s records or cannot be verified. Household members who do not already have a SSN (or do not know their SSN) must apply for a number before they can start receiving SNAP benefits, unless they have good cause for not applying. Failure or refusal to apply will mean that person is excluded from the household for SNAP purposes. That person will be treated as an ineligible non-citizen for budgeting purposes.
6. Income and resources.
7. Residence in the county. Residence is verified at a household level. The SNAP office does not have to verify where the applicant lives if it is not reasonably possible to get verification. For example: if the applicant recently moved to the area, is homeless, or is a migrant farm worker and cannot get verification easily. Homeless SNAP applicants do not need a permanent address to apply. They are specifically exempt from the residency verification. Homeless applicants can use the address of an authorized representative, a community organization (ex: shelter, soup kitchen), or the local SNAP office as an acceptable mailing address. See GIS 13TA/DC043 for more information on documentation requirements for homeless youth.
Note: If verification of an item used only for budgeting a deduction (#’s 7-10 above) is not available, the case can still be opened and budgeted without the deduction; however, the household may get a smaller benefit than it would have if the item had been verified.
The following documents are used for budgeting ONLY:
8. Shelter and utility costs. 9. Childcare and child support costs being deducted in the budgeting process. 10. Medical expenses for elderly and disabled applicants. 11. Disability if the applicant wants to use the special budgeting rules applicable
to disabled people or needs to be exempted from work activities.
18
Case Example: If the household does not have verification of child care costs, the budget can be calculated without the child care deduction. When the household provides documentation for the child care expense, they might get an increase based on the new budget with the deduction.
When the verification is provided, the worker will re-budget and may increase the amount of SNAP benefits the household receives. The four items outlined in the above boxed list of necessary verification are used for budgeting purposes only, not eligibility determinations. The SNAP office cannot limit which forms of necessary verification it will accept, and must accept anything listed on the documentation checklist. Also, any other form of credible documentation should be accepted. As a practical matter, it is easiest to get an application accepted promptly if the usual forms of documentation are provided. The SNAP office should only ask a household to verify their present circumstances. They should only use verification to assess if the household is currently eligible.
Verification of Questionable Information (SNAPSB Section 5: pp. 119-120; 12-INF-06) The SNAP office will also ask for verification of any information that it finds questionable. These requests, and the guidelines upon which they are based, must not discriminate based on race, religion, ethnic background, or national origin. The applicant(s) should be ready to verify as many facts as possible. If there is anything unusual about the household’s circumstances, the applicant should try to explain it completely in the initial interview, rather than hope the worker will not notice. When SNAP workers ask for more information, they should give the applicant a written notice listing what information they need, along with the date by which the household should provide the information. The following items shall only be verified if questionable:
• Citizenship; • Household composition, and; • Whether members of the household purchase and prepare meals together or
separately.
Important Note About Verification: If an applicant cannot provide verification of an eligibility criterion, the SNAP office has an obligation to assist. This includes paying fees when necessary. SNAP offices can sometimes obtain copies of official documents, like birth certificates, without paying a fee. However, if a fee is required, the SNAP office must either pay it or find another way to verify the eligibility criterion.
To be considered questionable, the information on the application must be inconsistent with statements made by the applicant, inconsistent with other information on the application or previous applications, or inconsistent with information received by the worker.

19
Front End Detection Systems (05-ADM-08) The Front End Detection System (FEDS) program is an anti-fraud measure allowed by New York State. FEDS conducts investigations of applications that appear to have questionable circumstances. For cash assistance purposes, all counties are required to operate a FEDS program. However, it is optional for SNAP-only cases. New York City does not have a SNAP-only FEDS plan; about two-thirds of counties throughout the state do. All local FEDS plans must be approved by OTDA. Caseworkers may only refer those cases which meet specific criteria spelled out in the county’s FEDS plan, and only after the household has first been given an opportunity to explain their situation. Typically, a FEDS referral results in an LDSS/HRA investigator visiting the applicant at their home, or asking the household to appear for an in-office interview. However, for SNAP purposes there is no obligation on the part of the household to meet with the investigator. A SNAP application cannot be denied due to a household’s failure to attend a FEDS interview. In this situation, the investigator should continue without the household’s cooperation and forward his/her report to the eligibility worker. The worker will then consider the information in the FEDS report before making a final decision on the household’s application. FEDS should not delay the normal application process. Social Security Numbers (SNAPSB Section 5: pp. 95-97) Every person in a household applying for SNAP must provide the SNAP office with his or her social security number (SSN). If a household member does not have a SSN, they must apply for one before they can receive SNAP benefits unless they have "good cause.” If an applicant applies for a SSN, the receipt from the SSA showing that they have applied for the SSN satisfies the requirement. Applicants who do not give the SNAP office their SSN or provide proof that they have applied for one, or who do not have good cause for not applying for a SSN, cannot receive SNAP benefits. However, the rest of the household members can proceed with the application without that household member. The excluded household member will be treated as an ineligible non-citizen for budgeting purposes. As soon as the household member qualifies (i.e. provides proof they have applied for a SSN), they will be added as a member of that SNAP case.
05-ADM-08 lists the type of criteria—called “indicators”—that can trigger a FEDS referral.
“Good cause” means that they have tried to apply for a social security number but cannot get it yet. For example, they may have good cause if the social security office will not take the application because they are waiting for a replacement copy of a lost birth certificate.

20
Households With Undocumented Non-Citizens (03-INF-14; SNAPSB Section 5: pp. 69 - 89) Non-citizens who cannot verify their immigration status (often referred to as “undocumented”) are not eligible for SNAP benefits. When a household contains a member who cannot provide immigration verification, the SNAP office must continue to process the application for the remaining household members. The SNAP office is not to report anyone to United States Citizenship and Immigration Services (USCIS). The SNAP office can report a non-citizen to OTDA if presented with proof that the person is illegally in the country (deportation orders). A threat by the SNAP office to contact USCIS to verify immigration status is a violation of the non-citizen’s civil rights. If the ineligible non-citizen is someone who would otherwise have to be part of the SNAP household (for example, the parent of minor children in the household), his/her income must be reported because a pro-rata portion will count in determining the amount of SNAP benefits for which the rest of the family is eligible. More information on budgeting for this type of household can be found in the Advanced Budgeting section of this guide. People Who Do Not Speak English (06-ADM-05) People who do not speak English or have limited English proficiency (LEP) often have an especially difficult time navigating the SNAP application process. They cannot, and should not, be denied access to SNAP because of LEP issues. In New York State, the SNAP application form is available in English, Spanish, Arabic, Chinese, Haitian Creole, Korean, and Russian. SNAP offices should have applications on hand in all seven languages. SNAP offices must have an “Interpreter Services” poster in their waiting areas. This poster has information in many different languages about the availability of translation services to any individuals who need them. Additionally, SNAP offices must provide a translator or interpreter to any applicant who needs one. If the SNAP office does not have an interpreter or bilingual worker on staff, they should make other arrangements to provide translation services. Households can bring their own interpreter, but only if they wish to do so. New York City has special requirements to ensure that LEP households have access to translation services, as part of a class action lawsuit settlement, Ramirez v. Giuliani. Accommodating Persons With Disabilities (06-ADM-05; GIS 15 TA/DC023) SNAP is subject to the Americans with Disabilities Act (ADA) of 1990 and the Rehabilitation Act (RA) of 1973, which protect people who have a physical or mental disability. The ADA and the RA are not limited to people who are "disabled" under SNAP regulations. Therefore, the SNAP office must provide the accommodations required by these laws, even if the applicant is not considered disabled for SNAP purposes. OTDA
21
issued a comprehensive policy directive (06-ADM-05) clarifying local districts’ obligations to provide equal access to persons with disabilities. In an effort to remain compliant with ADA standards, SNAP offices will be required to offer SNAP notices and materials in alternate formats including large print, braille, audio recordings, and data CDs upon request. This policy will be effective throughout all of New York State by June, 2016. Notification of Acceptance or Denial (SNAPSB Section 8; 14-INF-16) Whether a SNAP application is accepted or denied, the SNAP office must send a notice telling the applicant its decision within 30 calendar days of the application filing date.
If the SNAP office decides that applicant qualifies for SNAP, the notice of acceptance must: ● State how much the household’s SNAP benefit will be, and
● Include the start and end dates of the certification period.
If the SNAP office denies the application, this notice of denial must explain the reason for the denial. All notices must include the following information:
• Phone number of the SNAP office • The name of someone at the SNAP office the applicant can call with questions, if
possible • Information about the right to a fair hearing • How to get free legal aid
New York State uses an automated computer notice system for most notices. These computer-generated notices are very long and include a lot of information. The notices provide a lot of information about how the budget was calculated, so if there are any mistakes, these can be identified and mediated on with the SNAP office. The regular SNAP application processing time is 30 days from receipt of application, however there are times when an application cannot be processed within that time frame. When the application is delayed beyond 30 days and the fault lies with the SNAP office, the SNAP office has the responsibility of notifying applicants about the delay. A notice will be sent to applicants whose applications have not been processed within 30 days due to the fault of the SNAP office. A “Notice of Pending Application” will be created and sent to inform applicants that there has been a delay in application processing and that the application is still pending. Applications cannot be denied when the pending application is beyond 30 days and it is due to the fault of the SNAP office.

22
STATUS-BASED LIMITATIONS Special rules limit the eligibility of certain groups of people. The main groups are: students, people on strike, non-citizens, and employable adults (work rules are covered in the next section). When dealing with a household that contains a person with a status-based limitation, it is important to evaluate each individual's eligibility, since some people in a household might be eligible, even if others are not. For example, a citizen child would still be eligible even if his/her non-citizen parent were not eligible. Special budgeting rules also apply in these cases. Students (SNAPSB Section 5: pp. 91-92; 09-ADM-08; 11-INF-06; 12-INF-14; Appendix L) STUDENT: A student is any person who is:
• 18 through 49 years of age • Physically and mentally fit • Enrolled at least half time in an institution of higher education
Definition of INSTITUTION OF HIGHER EDUCATION - Any institution at the post-high school level which normally requires a high school diploma or equivalency certificate for enrollment, including, but not limited to:
• Colleges • Universities • Business schools • Vocational schools • Trade or technical schools • Correspondence schools • On-line courses, and • Colleges or universities that offer degree programs regardless of whether a high
school diploma is required Students enrolled at least half time in higher education cannot get SNAP unless they meet at least one of the following exceptions:
• Employed an average of 20 hours a week or more • If self-employed, be working an average of 20 hours a week and make an average
income equal to the federal minimum wage multiplied by 20 hours • Participating in work study, even if it is less than 20 hours a week • 17 years old or younger • 50 years old or older • Physically or mentally unable to work (see work rules) • TANF recipient (complying with the TANF work rules) • A single parent enrolled full time who is responsible for the care of child under the
age of 12 • Primary caretaker of a household member who is under age 6 or is incapacitated • Primary caretaker of a household member between the ages of 6 and 11, if no
adequate childcare is available that would make it possible to work and go to school
Students receiving 50% or more of their meals from a college meal plan cannot get SNAP, as they are considered to be living in an institution.

23
• Required to attend school by the SNAP employment and training program, or a similar program operated by a state or local government (This includes students receiving UIB.)
Students who do not meet one of these exceptions are excluded from the SNAP household and neither the income nor the resources of the ineligible student will be used in determining eligibility for the rest of the household. However, if the student makes any cash contributions to the remaining members of the household, this will count as income. The rest of the household members may still be eligible. For help in determining if a student meets any of these exceptions, see the Student Eligibility Checklist provided in this guide under Appendix L. Continuing Eligibility of Students Eligible students remain eligible between school breaks (vacations, summer, etc.) unless the student graduates, is suspended or expelled, drops out, or does not intend to register for the next school term (excluding summer semesters). Ineligible students remain ineligible between school breaks (vacations, summer, etc.), unless the student graduates, is suspended or expelled, drops out, or does not intend to register for the next school term (excluding summer semesters). Students who have work study lose their SNAP eligibility between semesters (if the break is a full month or longer) and in summer months unless the work study continues or they fit into another exemption. Example: If a student who participated in work study during the school year got a regular job during the semester breaks/summer months working an average of 20 hours a week, they would remain eligible for SNAP. Students Receiving Unemployment Insurance Benefits (UIB) (12-INF-14) A student who is receiving UIB and who is enrolled at least half time in an institution of higher education is considered to be an eligible student for SNAP purposes if they meet the following:
• Participate in one of the following UIB Educational Programs: o “599” Education Training Programs o Workforce Investment Act (WIA) o Trade Act Programs
• Enrolled in school through one of the following programs: o SNAP Employment and Training Program o Safety Net Assistance employment program activity
These students fall under the current student exemption that states, “Required to attend school by the SNAP Employment and Training Program, or a similar program operated by a state or local government.”
24
Students enrolled in the above programs do not need to meet any additional student work requirements or fit into any additional student exemptions in order to participate in SNAP. Strikers (SNAPSB Section 5: pg. 131) If the primary wage earner of a household is participating in a job action (on strike, a walk-out, etc.), the striker and the whole household are ineligible for SNAP unless they were eligible for benefits before the strike began. Thus, the striker’s income before the strike will be budgeted and applied to the entire household as if s/he were still working. In this case, other household members cannot simply exclude the striker to establish a separate case. A household cannot get more SNAP benefits because its income goes down during the strike. If the striker leaves the household, the remaining household members become eligible again. The following people are NOT considered to be strikers:
• People who have been locked out • People out of work because of someone else’s strike • People in a different bargaining unit who are afraid to cross a picket line • People exempt from work registration (other than those exempt because they are
working) • Strikers who have been permanently replaced
Non-Citizen Eligibility (GIS 10 TA/DC005; 03-INF-14; Appendix H) Among the most complicated rules in SNAP are those applied to non-citizens. Although this is commonly referred to as immigrant eligibility, it is important to remember that it applies only to non-citizens who are legally present in the country. Naturalized citizens (immigrants who become citizens) receive the same benefits as all other citizens. Undocumented non-citizens – those who cannot prove that they are legally present in this country – are never eligible for SNAP. The desk guide prepared by OTDA (see Appendix H) is very helpful – it lists the categories of non-citizens who are eligible for SNAP (as well as cash assistance and Medicaid) along with what documents can be used to verify status.
CITIZEN: A person (other than a child of a foreign diplomat) who is born in: • One of the 50 states • District of Columbia • Puerto Rico • Guam • U.S. Virgin Islands • Northern Mariana Islands who
has not renounced or otherwise lost his or her citizenship

25
The guiding principle is that in order for a non-citizen to be able to receive SNAP, the non-citizen must:
1. Have “qualified non-citizen” status AND 2. Meet a condition that allows qualified non-citizens to get SNAP.
Qualified Alien Status: Remember all non-citizens must meet one criterion from each list. Which non-citizens have qualified alien status?
• Lawful permanent residents (LPRs or “green card” holders)
• Refugees • Asylees • Persons whose deportation or
removal has been withheld • Persons paroled for at least 1 year • Cuban Haitian entrants • Amerasian immigrants
• North American Indians born in Canada
• Certain Hmong or Highland Laotian non-citizens
• Conditional entrants • Certain domestic violence
survivors
Which qualified non-citizens can get SNAP?
• Children under 18 with qualified alien status
• Disabled individuals with qualified alien status
• Adults who have held qualified alien status for at least 5 years
• Refugees (now includes Afghan and Iraqi Special Immigrants)
• Asylees • Persons whose deportation or removal
has been withheld • Cuban Haitian entrants • Amerasian immigrants • LPRs with substantial work history in the
U.S. (“40 quarters” test) • LPRs on active military duty or with
honorable discharge status, as well as their spouses and children under 18
Qualified non-citizens who came to the U.S. for humanitarian reasons – including refugees, asylees, and those with withholding of deportation – continue to be eligible for SNAP benefits even if they adjust their status to LPR. See Appendix H for further clarification on non-citizen status.
40 Quarters Test LPRs that can be credited with 40 qualifying quarters of work history are qualified to receive SNAP. One quarter is the equivalent of a 3-month period; therefore roughly 10 years of work equals 40 quarters. To count as a qualifying quarter, a worker must have earned a minimum salary during that quarter. Quarters of work history can be shared with some family members. Quarters earned during a marriage can be shared between spouses, even if separated or deceased (but not if divorced), and between parents and their children (for quarters worked before the child’s 18th birthday, including quarters worked before the child was born). The SNAP office will get the Social Security records of any worker’s quarters claimed by an applicant.

26
Ineligible Non-Citizens Households containing ineligible non-citizens can still get SNAP if someone in the household is an eligible non-citizen or a U.S. citizen. Even undocumented parents can apply for SNAP on behalf of their citizen children.
There is an immigration reporting requirement in the SNAP Law that makes some families with undocumented members reluctant to apply. The law requires the state SNAP agency to report “aliens it knows to be unlawfully present” to USCIS. However, SNAP offices in NYS have been instructed to report only those individuals who present evidence of a USCIS determination that they are not here lawfully.
Practically speaking, this means the SNAP office has no duty to report someone unless the person shows the SNAP office that s/he has a final Order of Deportation or has submitted falsified immigration documents. It is also important to note that the SNAP office is not to make the report directly to USCIS, but is simply required to give the name of the person with the Order of Deportation to OTDA.
USCIS has made it clear that receiving SNAP benefits does not make a person a public charge. Households with non-citizens should be reassured that if they receive SNAP benefits the non-citizen member should be able to adjust their status (apply for permanent residence or citizenship).
To view the USCIS Public Charge Fact Sheet visit http://www.uscis.gov/
Although the law has been very favorably interpreted concerning how SNAP households with non-citizen members should be treated, no one can ever guarantee that proper procedures will always be followed. It cannot be stressed highly enough, though, that LDSS employees only have authorization to report the names and addresses of non-citizens who have final deportation orders and those with falsified immigration documents. However, even in these circumstances, any reporting would be made to OTDA, not to USCIS. There is no authority for SNAP workers to contact Immigration directly except to verify immigration documents that are presented by the applicant to support the applicant's eligibility for benefits. If an eligibility worker threatens to report a non-citizen member of an applicant household to USCIS in order to get them to withdraw their application, this is a violation of the Civil Rights Law and should be brought to the attention of the supervisor, the Commissioner, or OTDA.
Fleeing Felons and Probation Violators (GIS 10 TA/DC026)
People who have felony warrants pending against them (fleeing felons), and people in violation of probation may be identified by computer matches and denied SNAP. However, in all these cases, other household members may continue to be eligible for SNAP and special budgeting rules apply.
OTDA clarified with SNAP offices that they must NOT discontinue SNAP benefits for anyone with a warrant based on an alleged probation or parole violation. These types of warrants do not constitute a determination of a violation but, instead, are allegations of a violation.

27
WORK REQUIREMENTS (NYS Temporary Assistance and SNAP Employment Manual, Section 3; Appendix I; GIS 12
TA/DC035) SNAP has an employment and training component. Unless they are exempt, adults must participate in some type of work or training activity to receive SNAP. However, there are many people who are exempt and have no further obligation to participate in work activities. A SNAP participant is exempt if he or she is: • under 16 • 60 and over • age 16 or 17 and not the head of the
household • attending school, training, or college on
at least a half-time basis Note: College students between the ages of 18 and 49 must meet the student eligibility criteria listed on pp. 22-24.
• working at least 30 hours/week or earning weekly pay of at least 30 times the hourly federal minimum wage
• a migrant or seasonal farm worker under contract to begin work within the next 30 days
• meeting TANF work requirements • receiving unemployment benefits • participating in a drug or alcohol
treatment program • taking care of a child under 6 or an
incapacitated person • jointly applying for SNAP and SSI and
awaiting an SSI eligibility determination • physically or mentally unable to work
(less documentation is required than for being disabled - generally doctor’s or other health care provider certification is sufficient)
In NYC the following exempts an individual from the work rules: • Pregnancy • Participating in a refugee training program at least half time
Anyone who is not exempt must comply with the SNAP office’s work requirements once they are receiving SNAP. This usually involves attending an evaluation appointment with an employment office at the SNAP office, providing information about education and work history, and then participating in an assigned work program. Work programs typically include workfare, job search, “job clubs,” GED programs, and, occasionally, training or other educational activities. If the local district does not assign a work activity, the participant is still eligible to receive SNAP. Individuals who must comply with work requirements cannot be required by their SNAP office to spend more than 120 hours per month participating in employment and training activities. This includes:
• job search • classes • work programs • workfare • paid work
• any work the individual is doing for something other than money (such as work they do in exchange for free housing or free meals)

28
Workfare cannot exceed the value of the SNAP (and cash assistance for people receiving both) divided by the minimum wage.
If a participant fails to comply with work requirements, voluntarily quits a job without good cause, or fails to meet cash assistance work requirements, they can be “sanctioned,” or made ineligible to participate for a period of time. The sanction disqualifies only the individual, not the whole household. If there are other people in the household who are still eligible, the SNAP case will stay open and the sanctioned person should request to be restored to the case at the end of the sanction period. If there are no other eligible participating household members, the sanctioned person will have to reapply for benefits the month before the sanction ends in order to receive SNAP benefits again. Voluntary Quit (NYS Temporary Assistance and SNAP Employment Manual, Section 13; Appendix I) The “voluntary quit” rule is an attempt to prevent people from deliberately making themselves poor so they can get SNAP. The rule disqualifies such people from receiving SNAP for a specified length of time (called a sanction period) of two months or longer. In reality, this usually arises when someone quits their job for some other reason, such as a decision to relocate, and immediately applies for SNAP. This rule should not be a major problem, although SNAP offices frequently question the reasons for leaving a job. All the applicant has to show is that there was some valid reason for leaving the job. This will prove “good cause” for leaving the job and satisfy the rule. Applicants who were fired did not quit for SNAP purposes -- it does not matter why they were fired. The NYS Temporary Assistance and SNAP Employment Policy Manual states that “provoked discharge” termination situations in which an employee causes him/herself to be fired are not subject to a voluntary quit disqualification. The voluntary quit rule is frequently misapplied because the cash assistance program rule is different. Those without a valid reason for quitting their job may or may not be subject to a voluntary quit sanction. It is important to remember that there are many people who are exempt from the voluntary quit rule. See the SNAP Work Rules Desk Guide (Appendix I) for further details on the voluntary quit rules. Able-Bodied Adults Without Dependents (ABAWDs) (NYS Temporary Assistance and SNAP Employment Policy Manual, Section 3; Appendix I; 14-52-ELI) Many unemployed adults without children – called Able-Bodied Adults Without Dependents (ABAWDs) – may have to meet a time limit requirement as well as the “regular” SNAP employment and training rules. The general rule is that ABAWDs can receive SNAP for only three months in three years, unless they meet certain work-related criteria. USDA has provided NYS with a waiver of the ABAWD requirements until December
An ABAWD is a person between 18 and 49 years old who is not disabled and who lives in a SNAP household without any children under 18.

29
31st, 2015. USDA granted waivers to states based on their eligibility for extended unemployment benefits. Through December 2015, no county in New York State is applying ABAWD requirements. Beginning on January 1, 2016, many counties in New York will need to re-instate the ABAWD time limits. Local Districts will be made aware of the policy changes and will be notified if they meet a waiver or if they will need to begin evaluating SNAP applicants/participants using ABAWD rules. Hunger Solutions New York will provide additional information on the re-instatement of the time limits in NYS as policy information from OTDA is released. Please check our website for policy updates and new resources, and to register for upcoming webinars. Work Sanctions, Intentional Program Violations (14-ADM-06; GIS 13 TA/DC048; GIS 13 TA/DC005; GIS 12 TA/DC035) People who do not comply with work requirements, or who are found to have committed an Intentional Program Violation (IPV), will be removed from the household SNAP case for a period of time specified by the SNAP office. The SNAP Work Rules Desk Guide (Appendix I) has a summary of SNAP employment and training rules.

30
HOUSEHOLD COMPOSITION (SNAPSB Section 5: pp. 48-52; Appendix M, LDSS-4314; 08-ADM-04)
A SNAP household is defined as:
• People who live together and • Purchase and prepare meals together
Why is household composition important when prescreening for SNAP eligibility?
• Individuals included in a SNAP household must have their income included when determining eligibility and calculating the budget.
Some people are “mandatory” household members. This means that if they are living in the same house, they MUST BE INCLUDED IN THE SNAP HOUSEHOLD, EVEN IF THEY ARE NOT PURCHASING AND PREPARING MEALS TOGETHER. Mandatory household members include:
• Spouses; • Parents (natural, adoptive or step-parent) and
their children under 22; AND • Children under 18 under parental control of a
person other than a parent. (See chart on next page for additional details.)
Other people can apply for SNAP as their own household, as long as they are purchasing and preparing their meals separately. See the Household Composition Guide on the next page for a step-by-step guide to determining household composition. Special Rules for Homeless Youth, Foster Care Children, and Boarders SNAP regulations do not have an age requirement in most cases for homeless youth. Any homeless youth under the age of 22 can apply for SNAP as long as they are not residing with their parents and are not under “parental control” of another person. They do not need to be included in a parent’s SNAP case unless they live together. A homeless individual must apply as a household with the other people that they are living with, if they regularly buy and prepare food together. See GIS 13TA/DC043 for more information. Boarders and foster care children may be either included in or excluded from the SNAP household of the landlord or foster parents at the household’s option. It is important to note that foster care income (in excess of allowable, verified, reimbursable expenses) is counted as unearned income when the foster child is included in the SNAP household. If a foster care child is not included in the SNAP household, then the foster care income is exempt. Adopted children must be included in the SNAP household and adoption subsidies (in excess of allowable, verified, reimbursable expenses) are counted as unearned income. See income chart on pg. 37 of this guide.
If a person living in the same house or apartment with an applicant is not a member of the applicant’s SNAP household, that person’s income and resources are completely ignored. On the other hand, people who are not living together are not part of the same SNAP household, even if they are married or have other legal relationships to each other.
31
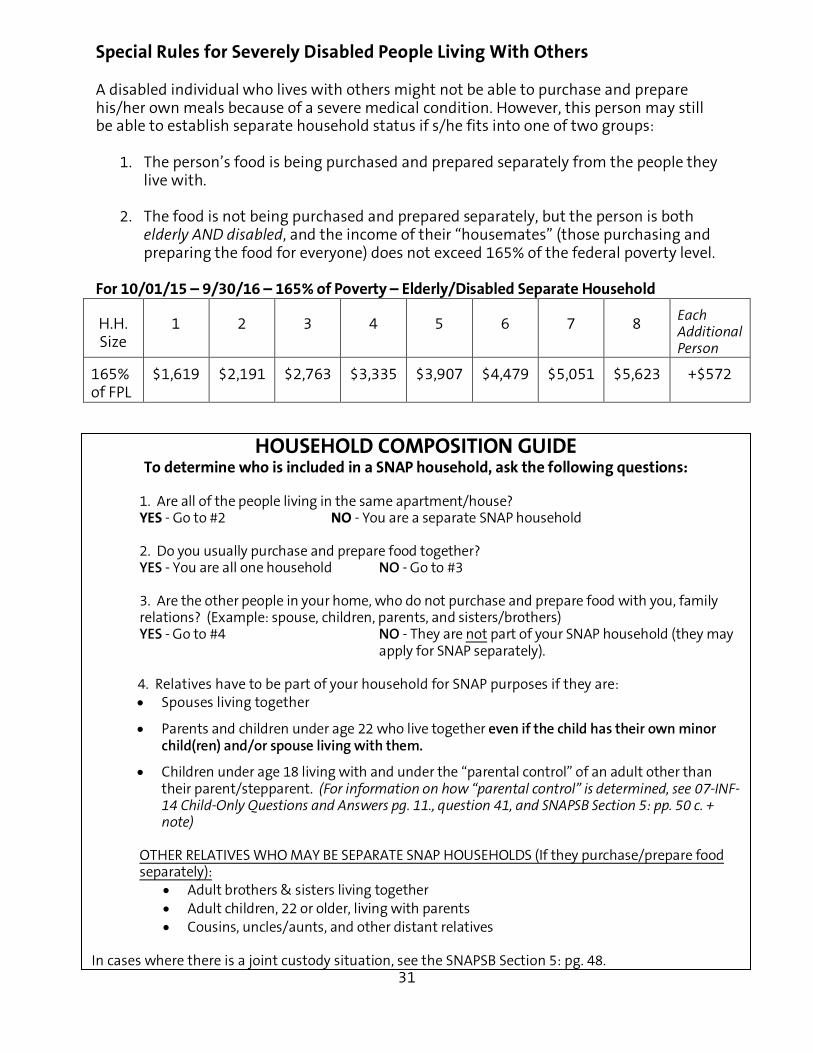
Special Rules for Severely Disabled People Living With Others A disabled individual who lives with others might not be able to purchase and prepare his/her own meals because of a severe medical condition. However, this person may still be able to establish separate household status if s/he fits into one of two groups:
1. The person’s food is being purchased and prepared separately from the people they live with.
2. The food is not being purchased and prepared separately, but the person is both
elderly AND disabled, and the income of their “housemates” (those purchasing and preparing the food for everyone) does not exceed 165% of the federal poverty level.
For 10/01/15 – 9/30/16 – 165% of Poverty – Elderly/Disabled Separate Household
H.H. Size
1 2 3 4 5 6 7 8 Each Additional Person
165% of FPL
$1,619 $2,191 $2,763 $3,335 $3,907 $4,479 $5,051 $5,623 +$572
HOUSEHOLD COMPOSITION GUIDE To determine who is included in a SNAP household, ask the following questions:
1. Are all of the people living in the same apartment/house?
YES - Go to #2 NO - You are a separate SNAP household
2. Do you usually purchase and prepare food together? YES - You are all one household NO - Go to #3
3. Are the other people in your home, who do not purchase and prepare food with you, family relations? (Example: spouse, children, parents, and sisters/brothers) YES - Go to #4 NO - They are not part of your SNAP household (they may
apply for SNAP separately).
4. Relatives have to be part of your household for SNAP purposes if they are: • Spouses living together
• Parents and children under age 22 who live together even if the child has their own minor child(ren) and/or spouse living with them.
• Children under age 18 living with and under the “parental control” of an adult other than their parent/stepparent. (For information on how “parental control” is determined, see 07-INF-14 Child-Only Questions and Answers pg. 11., question 41, and SNAPSB Section 5: pp. 50 c. + note)
OTHER RELATIVES WHO MAY BE SEPARATE SNAP HOUSEHOLDS (If they purchase/prepare food separately):
• Adult brothers & sisters living together • Adult children, 22 or older, living with parents • Cousins, uncles/aunts, and other distant relatives
In cases where there is a joint custody situation, see the SNAPSB Section 5: pg. 48.

32
EXPANDED CATEGORICAL ELIGIBILITY/RESOURCES (SNAPSB Section 16; 07-ADM-09; 09-ADM-06; 10-INF-07; GIS 12 TA/DC001;
Appendix J) Expanded categorical eligibility is granted to most households applying for SNAP. Households granted categorical eligibility will be budgeted differently. These families:
• Do not need to pass a resource test • Do not need to pass a net income test, and • May be able to use higher income levels for eligibility, depending on the household
type: o Households with an elderly and/or disabled member – 200% for Gross
Income Test (GIT) o Households with dependents care costs – 200% for GIT o All other households – 130% for GIT
Poverty Guidelines Chart
Households with Dependent Care Costs: Households with out-of-pocket dependent care costs, which are categorically eligible for SNAP, can use 200% of poverty when testing gross income. Households are eligible to deduct out-of-pocket daycare expenses when all adult members are:
• Working or needing daycare to continue work • Looking for work • Attending employment training programs (not limited to FSET, UIB job
search…), or • Pursuing education that is preparatory to employment
This language can be found in the SNAPSB Section 11: Standards and Deductions pg. 251.
Family Size 130% of Poverty Monthly Income
Oct. 1, 2015 – Sept. 30, 2016
200% of Poverty Monthly Income
Oct. 1, 2015 – Sept. 30, 2016
1 $1,276 $1,962
2 $1,726 $2,655
3 $2,177 $3,348
4 $2,628 $4,042
5 $3,078 $4,735
6 $3,529 $5,428
7 $3,980 $6,122
8 $4,430 $6,815
Each Additional Person
+ $451 + $693

33
Households That ARE NOT Categorically Eligible: Most households which are income eligible for SNAP are also categorically eligible. However, there are still a small number of households which cannot be considered categorically eligible and must have their resources and net income considered as part of the application process. These include:
1. Households with members who have been disqualified from SNAP due to an IPV or other sanction.
2. Households with an elderly or disabled member whose gross income is above 200% of poverty per household size.
These households may still qualify under regular SNAP rules:
• Resources would need to be considered. • Gross income must be at or below 130% of poverty for household size if no one is
elderly /disabled. • Net income must be at or below 100% of poverty for household size. • Households with an elderly/disabled member do not need to meet a GIT. Net
income would need to fall at or below 100% of poverty. Appendix J of this guide is the “Expanded Categorical Eligibility Desk Guide” which aids in determining whether a household is categorically eligible for SNAP. What resources count if a household is not categorically eligible?
Households which are not categorically eligible have a $2,250 resource limit if no one is elderly or disabled, and $3,250 if there is an elderly or disabled household member.
Resources are everything owned by the people in the household. This includes cash, bank accounts, stocks and bonds, lump sum payments received, and real estate. Things the household has on hand, but does not own, do not count.
Any resource owned by a non-categorically eligible household counts toward the household’s resource limit, unless it is exempt. There are many exemptions from the resource rules. The most common exemptions are:
• One licensed vehicle for each adult household member (Additional licensed vehicles used by children under 18 to attend school, training, or work are also exempt.)
• One house (if the household lives in it) • Life insurance • One burial plot per person • Earned Income Tax Credits (EITCs) • Inaccessible resources
For a complete list of exempt resources, see SNAPSB Section 17. Remember, resources are not counted at all if the household is categorically eligible.

34
“Tax Preferred” Retirement Accounts such as Keogh Plans, IRAs, Simplified Employer Plans, Profit Sharing Plans, and Cash Balance Plans are excluded from countable resources for any household subject to the resource limits. “Tax Preferred” educational accounts such as 529s and Coverdell educational savings accounts are also excluded from countable resources for any household subject to the resource limits. See OTDA’s 08-ADM-09 for more information.

35
CALCULATING A BUDGET (SNAPSB Sections 11, 12 & 13; GIS 14 TA/DC011, 018, 023, 033; Appendix K)
Overview of Budgeting SNAP budgeting is complicated when compared to budgeting for other means- tested programs. This is the result of an effort to carefully target the benefits to the neediest households. This section is intended to guide advocates through the process of estimating the SNAP benefit for which a household might be eligible. If it appears that the household may be eligible for benefits, the household should be referred to their Local Department of Social Services (LDSS) to apply for SNAP. The line numbers in the following narrative correspond to the budget worksheet in Appendix K. The SNAP budgeting section explains how to determine an estimated SNAP budget using the attached worksheet (Appendix K). Please note that Hunger Solutions New York’s web site has SNAP Budget Estimator Tools that can be downloaded for use. Unlike the paper budget worksheet, these tools do some of the math for you. There are several determinations that must be made in the SNAP budgeting process before a budget can be calculated:
1. Determine which household members are eligible for SNAP benefits and are applying together.
2. Add up all income from earned and unearned sources to determine the household’s gross income.
3. Determine if the household is categorically eligible, and if so, which gross income test must be applied.
4. Test the income against the correct percent of poverty for household size. If the household is below the income listed you can start the budgeting process.
All budget calculations should be considered estimates. Many factors can affect each aspect of the budget, and there are an equal number of opportunities for inaccuracies. In particular, reported income used in the calculation may change or may be the applicant’s own estimate. Therefore, it is important to emphasize to the applicant that you are providing them with an estimate of the SNAP benefits for which the household may be eligible. If the allotment ultimately granted by the SNAP office is significantly different, the applicant or advocate should read the budget explanation in the notice carefully to determine where the difference occurred. If the SNAP office has made an error, it should be corrected.
36
Household Information To accurately calculate the household’s SNAP budget, you will need the following household information:
• Household composition • Age of household members • Disability status of household
members • Amount and source of income • Daycare costs
• Child support paid • Medical expenses for elderly or
disabled household members • Shelter costs • Type of shelter • Utility costs
For SNAP purposes,
• “Elderly” means 60 or older. • “Disabled” means receiving a federally related disability benefit such as:
o Supplemental Security Income (SSI) o Social Security Disability (SSD) o Disability-related Medicaid o VA Disability 100%
For details see the SNAP Sourcebook Section 5, pp. 56-67. Using the SNAP Budget Worksheet Earned vs. Unearned Income (SNAPSB Section 13) It is important to know whether income is earned or unearned, since a 20% deduction from the earned income will be taken on Line 6. This deduction makes a big difference in the final SNAP allotment amount. If income is incorrectly classified, the resulting budget will be wrong. Income of Non-Household Members (SNAPSB Section 13: pg. 272) The income of people who are not part of the SNAP household does not count. However, the income of people in the household who are not included in the household because they are ineligible for SNAP, may count. Income of ineligible students does not count, while the income of sanctioned individuals is counted. Income of ineligible non-citizen household members is prorated. See the Advanced Budgeting chapter for more details.

37
These are some of the most common sources of income -- this list is NOT exhaustive:
* See 08-ADM-04 for more information on what an allowable, verified, reimbursable expense (things that do not count as income) is for adopted and foster children included in the SNAP household.
** Social Security beneficiaries and SSI recipients with a my Social Security account can go online and easily view, print,
or save an official benefit verification letter instantly. Individuals 18 and older can sign up for a my Social Security account at www.socialsecurity.gov/myaccount. For more information see GIS 13 TA/DC010.
Earned Income
Unearned Income
• Gross wages from work (including income from part time work of high school/GED students who are age 18 or over)
• Self-employment earnings (minus the cost of doing business)
• Gross income from rental property (minus the cost of doing business) in which a household member is engaged in management for at least 20 hours a week
• Payments from boarders/lodgers (excluding related costs incurred)
• Youth Opportunity Program payments
• Earnings from the Workforce Investment Act (WIA) for household members over 18 (if under 19, the earnings are not counted)
• Training allowances, to the extent they are not a reimbursement from the TA or SNAP
• VISTA income (however, if the household was on SNAP or TA when they entered VISTA, then the VISTA income is not counted
• Wages earned by a household member that are garnished or diverted by an employer (except court-ordered child support)
• Adoption subsidy*
• Alimony payments
• Annuities
• Any portion of Veterans Administration scholarships for general living expenses (the remainder is excluded) – all other higher education scholarships, loans, and grants are excluded including work study income
• Child support payments received (including any TA “pass-through”)
• FEMA payments to homeless in absence of major disaster
• Foster care subsidy if child is included in the household*
• Monies and dividends paid from trusts, interest, and royalties
• Pensions
• Short-term disability payments
• Social security retirement, survivors’ benefits, SSI, SSD**
• Strike benefits
• Temporary assistance payments (TANF)
• Veterans’ benefits including VA Aid and Assistance (14-INF-10)
• Worker's compensation and unemployment benefits
• Any other direct money payment that represents a gain or benefit not falling under an exemption

38
WHAT DOES NOT COUNT AS INCOME FOR SNAP?
(These are some common sources NOT countable as income -- this list is NOT exhaustive)
• Allowances, earnings, or payments to Workforce Investment Act program participants • Annual school and daycare clothing allowances, regardless of method of payment • Child support collected and not passed through to household by Child Support • Cost of producing self-employment income • Earned Income Tax Credits (EITC) and all other tax credits -- Federal and State (13-ADM-02) • Earnings from On the Job Training (OJT) training if under 19 years old • Earnings of child under 18 who attends high school or GED • Educational loans, grants, scholarships for tuition, and mandatory fees (except portion of Veterans
Administration scholarships earmarked for general living expenses – these are treated as unearned income)
• Home Energy Assistance Program (HEAP) payments • H.U.D. housing subsidies (e.g., Section 8 vouchers, Housing Authority unit subsidies) • Housing provided to employee by employer • Income from reverse mortgages (unless there is a cash-out option) • Income of persons who are not members of the SNAP household • Income Tax refunds, rebates, and credits – Federal and State (GIS 14 TA/DC044) • Income under Title V of the Older Americans Act • Individual Development Account (IDA) contributions • In-kind income (things of value that are not cash) • Insurance policy dividends • Interest from funeral agreements or funds • Irregular or infrequent income less than $20 per month • Legally obligated child support paid on behalf of child(ren) not living in the household
• Loans (including educational) • Lump sum or one-time payments • Military combat pay • Monies for care and maintenance of third-party beneficiary who is not in the household • National Community Services Act income (AmeriCorps) • Non-cash benefits from other federal programs such as WIC or School Meals • Payments made on behalf of a household member to a third party (vendor payment) (except
payments made as part of a cash assistance grant, including Jiggetts payments) • Payments specifically exempted by federal law (i.e. to Hmong refugees, Aleuts, World War II-
related payments, etc.) • Payments to relocate • Payments to volunteers under Title II of the Domestic Volunteers Services Act (i.e., RSVP, Foster
Grandparents, Senior Companion, and senior health aide programs) • Private charity income under $300 in three months • Public Assistance Restaurant Allowances by voucher or direct to vendor • Reimbursements for other-than-normal non-living expenses, e.g. medical, special work clothes, car
use for work • Reimbursements for training-related expenses • SSI PASS account income • Work study income funded through the Higher Education Act • VISTA income, but only if the household had been on TA or SNAP when they entered VISTA (05-
ADM-14)

39
BUDGET WORKSHEET (See Appendix K; GIS 13 TA/DC038)
Income (SNAPSB Section 12 & 13; 02 ADM 07) SNAP defines one month as 4.33 weeks. Calculate monthly income as follows:
- If income is received weekly, multiply by 4.33 (e.g., work income, UIB) - If income is received every other week, multiply by 2.17 - If income is received twice per month, multiply by 2 (work income, PA)
Line 1. Gross monthly earned income – Gross monthly income is your income from earned sources before any deductions, such as taxes, FICA, health benefits, or union dues are taken out. All the income received by every member of the SNAP household counts, unless it is specifically exempt. This includes the income of children, unless the child is under 18 AND a student. Only earned income goes on Line 1. Line 2. Gross monthly unearned income – Monthly unearned income is the total household income from unearned sources. Line 3. Gross income -- Add Lines 1 and 2. This is the household’s monthly gross income, earned and unearned combined. Line 4. Child support paid – Enter the amount of any legally obligated child support paid by a household member. Legally obligated health insurance payments for children and court-ordered arrears can be included. Use the same methodology described in the earned income section (Line 1) to convert weekly payments into a monthly total. (02 ADM 07) Line 5. Adjusted gross income -- Subtract Line 4 from Line 3. This is the household’s countable monthly gross income. The Maximum Gross Monthly Income limit is set at:
• 200% of the federal poverty level for households with elderly or disabled members, or who pay out-of-pocket daycare expenses, or
• 130% of the federal poverty level for all other households. • Households without an elderly or disabled member whose adjusted gross income
exceeds the correct GIT are NOT eligible for SNAP. • Households with at least one elderly (age 60+) or disabled member who exceeds
200% GIT, or who are not categorically eligible, do not have to meet a GIT. Do not apply this limit to these households; continue with the budgeting process.

40
Household Size and Gross Monthly Maximum Incomes (October 1, 2015 - September 30, 2016):
H.H. Size 1 2 3 4 5 6 7 8 Each
Additional Person
130% of FPL
$1,276 $1,726 $2,177 $2,682 $3,078 $3,529 $3,980 $4,430 +$451
200% of FPL
$1,962 $2,655 $3,348 $4,042 $4,735 $5,428 $6,122 $6,815 +$693
Deductions (SNAPSB Section 12)
Line 6. Earned Income Deduction – Multiply Line 1 (earned income) x .2. The earned income expense deduction is twenty percent (20%) of the gross wages, salary, or self-employment income.
Line 7. Standard Deduction – Enter amount from chart below.
Standard Deduction Amounts (October 1, 2015 - September 30, 2016):
Household size 1-3 people 4 people 5 people 6 or more people
$155 $168 $197 $226 Line 8. Child/Dependent Care – The actual cost for care of each child/dependent household member due to work (including households looking for work or attending employment and training programs) or school responsibilities can be deducted. This deduction can be applied to the care of a disabled adult household member if necessary. (08-ADM-09)
Line 9. Homeless Household Shelter Deduction – SNAP households that have no fixed and permanent address can take a deduction of $143 per household, in lieu of actual shelter costs. See the section on Advanced Budgeting for more information. Line 10. Medical Expense Deductions for Elderly and Disabled applicants only – All non-reimbursable medical expenses incurred by elderly or disabled household members can be deducted, except for the first $35/mo. This includes cost of transportation to medical appointments, over the counter medications purchased pursuant to the instructions of a medical professional, prescriptions not covered by insurance, and co-pays. Unpaid medical bills can be included. Medical expenses of other household members cannot be included. For more details about what types of medical expenses can be included as deductions, see the worksheet on the next page.

41
SNAP MEDICAL EXPENSE DEDUCTION WORKSHEET
SNAP law permits people who are elderly (age 60+) or disabled to deduct from their income all out-of- pocket medical costs greater than $35 per month – the first $35 is not deductible. Below: Enter monthly estimated, anticipated non-reimbursable out-of-pocket medical expenses
for each household member who is elderly (60+) or medically disabled. $ Medical and dental care, including psychotherapy and rehabilitation services. $ Hospitalization or outpatient treatments, nursing care, and nursing home care. $ Prescription drugs, over-the-counter medications approved by a licensed
practitioner, costs of medical supplies, sickroom, or other prescribed equipment. Unfortunately, the costs of special diets are not allowed as a medical deduction.
$ Health and hospital insurance policy premiums, including Medicare, Medicaid
and private medical insurance premiums, co-payments, and deductibility. This includes, but is not limited to, "spend-down" expenses incurred by Medicaid recipients.
$ Payments to maintain an attendant, home health aid, child care service, or
housekeeper necessary due to age or illness (includes reasonable cost of food eaten in the home by caretaker).
$ Costs of transportation and lodging to obtain medical treatment and services.
Households who drive their own vehicle should use the IRS medical mileage rate - currently 23 cents per mile. The SNAP office is encouraged to use the LDSS mileage reimbursement rate set for county employees, but only if it is higher than the IRS rate above.
$ Medical supplies and equipment, including eyeglasses, dentures,
hearing aids, and prosthetics. $ Cost of securing & maintaining a seeing eye, hearing, or service dog
(including food costs for dog). $ Unpaid medical bills. ══════════════════════════════════════════════════════════════ $ Subtract $35 = $ Monthly Medical Expense Deduction

42
Line 11. Add Lines 6 through 10 to determine the total non-shelter deduction. Line 12. Subtract Line 11 (deductions) from Line 5 (adjusted gross monthly income) to get the money assumed to be available for shelter costs and food. Shelter Expenses (SNAPSB Section 12; GIS 14 TA/DC 018; GIS 14 TA/DC023) Line 13. Actual Rent or Mortgage – this is the actual monthly rent or mortgage payment incurred by the household for the home in which it lives. If the household has multiple mortgages, or other loans for which the home was used as collateral, such as home equity loans, they can all be included. Clarification has been made by OTDA stating that homes that are in foreclosure and households facing eviction proceedings continue to have an allowable shelter deduction as long as the cost is incurred. Mortgage costs, homeowners insurance, property taxes, and rent remain as allowable shelter expenses even if they are not being paid, including during foreclosure and eviction processes. If there are non-household members living with the SNAP household, use the share of the rent or mortgage actually paid by the SNAP household. Do not include the non-household member’s share. For example, if two families share a house and each family pays half the rent, the applying household can only deduct their half of the rent as a shelter cost. Some households take in roomers to help cover their rent or mortgage expense. Local districts should generally treat these situations as “shared living” arrangements, meaning that the roomer’s share of rent would not count as income to the household – even if the roomer is paying his share of the rent or mortgage directly to the household. However, the roomer’s share of rent would not be included in the household’s shelter deduction. (SNAPSB Section 5, p. 52,55) Line 14. Standard Utility Allowance (SUA) SNAP households living in New York may receive one of three possible Standard Utility Allowances (SUA) depending on their type of housing and where they live in NYS. In all cases the standardized allowance is used, rather than the household’s actual utility expense – even if the household’s actual expenses are higher than the standard. The SUA is never prorated. Households in shared living situations and households with ineligible members can still receive a full (non-prorated) SUA. Using the wrong SUA can result in dramatically miscalculating a household’s benefits. LEVEL 1. Combined Heat, Utility, and Phone Allowance. Anyone who pays his or her own heating or cooling costs or owns their own home is eligible for the Level 1 deduction. Anyone in receipt of a $21 or more Home Energy Assistance Program (HEAP) benefit in the month of application or in the immediately preceding 12 months is also eligible for the Level 1 SUA deduction. Previously, “potential eligibility” for HEAP allowed for an automatic Level 1 SUA. Households that are potentially eligible for HEAP will no longer be credited with a Level 1

43
SUA until they are in actual receipt of at least a $21 HEAP payment. See GIS 14 TA/DC023 for more information. The following SNAP households are ineligible to receive the Level 1 SUA:
• Households that are renting that are not paying a heating/cooling cost separate from their rent and have not received a HEAP benefit of $21 or more in the month of application or in the preceding 12 months
• Households that are living in a shared living situation in which no adult in any SNAP household in the domicile has received a HEAP benefit of $21 or more in the month of application or in the preceding 12 months
• Un-domiciled (households getting the homeless deduction (Line 9) – they’re not eligible for a SUA)
• Households in domestic violence or homeless shelters (they get Level 3) LEVEL 2. Combined Utility and Phone Allowance. Any household that is not eligible for Level 1, but can show some non-heat utility cost (like electricity not used for heating, water, sewage or trash collection) is eligible for Level 2. LEVEL 3. Phone Allowance Only. This is for households that have no other utility costs, but do have a telephone. This allowance is automatically provided to households not eligible for Levels 1 or 2 (except for homeless households receiving the standard homeless deduction – they cannot receive a separate SUA).
Line 15. Other Shelter Expenses – Other expenses related to shelter can be deducted here. This includes taxes, homeowners insurance, and condo fees. (You should use a standard figure of 55% of the homeowners’ insurance premium, unless you can determine the portion of the premium cost attributable to insurance on structure of the home.) Routine home maintenance cannot be deducted, and repairs can be deducted only if the damage was the result of a disaster (such as fire or flood). Line 16. Total Shelter Costs – Add Lines 13, 14, and 15 to get the total shelter cost.
Standard Utility Allowances for NYS (Effective 10/1/15)
Level 1 Level 2 New York City $768 $304 Nassau & Suffolk Counties $716 $281 Rest of State $636 $257 Level 3 (Telephone SUA for all counties) -- $33

44
Excess Shelter Deduction
The concept of “excess shelter costs” is unique to SNAP. It assumes that certain percentages of the household’s income should be allocated to pay shelter costs. Households with particularly high shelter costs relative to their income (excess shelter costs) are assumed to not have as much money left for food, and so are allowed to deduct the “excess” portion of their shelter costs. However, the amount of excess shelter cost that can be deducted is capped at $504. This “excess shelter cap” does not apply to households with an elderly or disabled member. Any household including an elderly or disabled person can deduct the entire excess shelter cost. This is a very important difference, which results in significantly higher benefit amounts for most households categorized as elderly or disabled.
Calculating the Excess Shelter Deduction Line 17. Divide Line 12 (income available after other deductions) by 2. Half of the income left after the other deductions is considered to be theoretically available to cover housing costs. Line 17a. Calculate the Excess Shelter Deduction. Subtract Line 17 (total shelter cost) from Line 16 (amount theoretically available for housing). The result is the excess shelter cost. If it is a negative number, enter zero here. For elderly/disabled households, enter the actual amount on Line 17a. For all other households, if Line 17a exceeds $504, enter $504 (the amount of the Excess Shelter Cap); otherwise enter the actual amount. Calculating the SNAP Benefit Allotment Line 18. Net SNAP Income – Subtract Line 17a (excess shelter deduction) from Line 12 (income after other deductions). Categorically eligible households do not have to pass the net income test although you still input the income information and continue through the budget worksheet process. Although the net income test doesn’t apply to categorically eligible households, not all categorically eligible households will be able to receive SNAP. See Line 21 below for more information. For households who are not categorically eligible for SNAP, the net income amount must be under 100% of poverty in order for the household to be SNAP eligible. If this amount is over 100% of poverty, the remainder of the calculation will result in an allotment of zero. If the amount is a negative number, the net SNAP income is $0.

45
Household Size and Net Monthly Maximum Incomes (October 1, 2015 - September 30, 2016)
These income limits do not apply to categorically eligible households
Line 19. Thrifty Food Plan Amount (Maximum SNAP Allotment for HH size) – The maximum benefit allotment is based on the Thrifty Food Plan, a theoretical idea of the costs of feeding a household. Determine the maximum allotment for the eligible household members by looking at the correct chart below. Enter the maximum allotment on this line. Do not include ineligible members, such as ineligible aliens or sanctioned household members.
Maximum SNAP (Thrifty Food Plan) ALLOTMENTS by Household Size (October 1, 2015 - September 30, 2016):
H.H. Size 1 2 3 4 5 6 7 8 Each
Additional Person
Maximum Allotment
$194 $357 $511 $649 $771 $925 $1,022 $1,169 +$146
Line 20. SNAP Budget Income – Multiply Line 18 (Net Income) x .3 – Thirty percent of the household’s net income is assumed to be available for food purchases, and is deducted from the maximum SNAP allotment. Line 21. Estimated SNAP Benefit – Subtract Line 20 (30% of net income) from Line 19 (maximum allotment) – This is the estimated SNAP benefit for the household. The minimum SNAP benefit issued to all eligible one- and two-person households is $16 through September 30, 2016. If the estimated SNAP benefit for a one- and two-person household falls between $1-15, the household should be eligible for $16 per month through September 30, 2016. If the estimated benefit is zero or a negative number:
• One-and two-person households will get the $16 minimum benefit. • Households of 3 or more will not be eligible for any SNAP benefits.
H.H. Size 1 2 3 4 5 6 7 8 Each Additional
Person
100% of FPL
$981 $1,328 $1,675 $2,021 $2,368 $2,715 $3,061 $3,408 +$347

46
ADVANCED BUDGETING
Income of Ineligible Household Members Some members of a household may be ineligible for SNAP because of their immigration status, sanctions relating to previous participation in the program, or because they are students or participating in a job action. In most cases, though, some or all of the income of household members ineligible for SNAP is counted in the SNAP budgeting process. Hunger Solutions New York has SNAP Benefit Estimator tools available for download on our website. These tools are designed to help estimate the SNAP allotment for households with ineligible members. Unlike the paper budget worksheet (found in Appendix K of this guide), these tools do the math for you, including prorating for ineligible members. Budgeting for Non-Citizens (SNAPSB Section 13: pp. 267 - 271; 03-INF-14) Budgeting income for households with ineligible non-citizen member(s):
The income of people ineligible due to immigration status is prorated proportionate to the number of people being included in the SNAP case. Thus, if there are three people in the household and two are eligible to receive SNAP, two-thirds of the ineligible person’s income would count as income for the SNAP household. Thus, to determine the amount of income to be budgeted:
1. Divide the income by the number of people in the household. 2. Multiply the result by the number of people in the SNAP case.
(see the formula below)
The result is budgeted as income to the SNAP household, with earned income receiving the earned income deduction.
However, if an eligible household member earns the household’s income, the full amount is budgeted. There is no prorating to allow for the presence of the ineligible household members. Resources of ineligible non-citizens are counted in their entirety – not prorated. If a sponsored non-citizen is eligible for SNAP, the income of a non-household member who sponsored a non-citizen may be counted. This “sponsor deeming” applies only to sponsor agreements entered into since December 1997.

47
Very few non-citizens should be subject to sponsor deeming. Sponsor deeming does not apply to:
• Refugees • Asylees • People with deportation withheld • LPRs with 40 qualifying quarters, or • LPRs who are indigent (whose gross income, including any income provided by the
sponsor, is below 130% of the federal poverty level) Additionally, sponsor deeming does not apply if:
• The sponsor is a part of the SNAP household • The sponsor is ineligible for SNAP based on immigration status, or • The sponsored non-citizen is a battered spouse or dependent
In addition to the sponsor deeming requirement, there is also a “sponsor liability” rule for non-citizens whose sponsors entered into a sponsor agreement since December 1997. Under the sponsor liability rule, the sponsor may be held liable for – and asked to repay – the value of any SNAP benefits issued to the sponsored non-citizen. However, in New York State, even though the LDSS may request reimbursement from sponsors, OTDA has indicated that no legal action will be pursued against sponsors for repayment. Deductions for Households with Ineligible Non-Citizens The shelter and dependent care expenses billed to or paid by the ineligible household member are prorated in the same manner as income. The amount of actual expenses paid by the eligible household members can be deducted. The household receives a full standard utility allowance (SUA). Budgeting Shelter Costs for Homeless People Homeless Shelter Deduction The Homeless Shelter Deduction can be applied to families who are not living in a shelter or receiving free shelter for the entire month. These households are assumed to be incurring a shelter cost and the applicant does not need to prove actual shelter expense to receive this deduction. If the Homeless Shelter Deduction is used in budgeting, the household is not eligible to receive a SUA of any level. However, if actual shelter costs can be verified and they are more than the standard Homeless Shelter Deduction ($143), then the regular shelter deduction will be used. Regular Shelter Deduction If the family is incurring any actual shelter costs which they can document (ex: paying to stay with family/friends) and these expenses are greater than the Homeless Shelter Deduction ($143), then the actual shelter costs will be deducted. Another example would be a homeless household that is living in their car and making a car payment. If the car payment is more than the standard Homeless Shelter Deduction ($143), then this would

48
be considered the household’s actual shelter deduction. When using a regular shelter deduction, families and individuals would be eligible for at least a Level 3 SUA ($33), possibly more depending on what their financial contributions to the dwelling are. Other Deductions Child support can be deducted, as well as medical deductions for elderly/disabled households and daycare costs for most families. Budgeting Rules for Other Groups Sanctioned People The full income of a person sanctioned due to work rule violations or disqualified due to IPV is budgeted, and all deductions may be taken. Therefore, the budget is calculated as if the sanctioned person were participating, except that the household size is reduced in determining income eligibility and SNAP allotment amounts. Resources of sanctioned people are counted in their entirety. Students Ineligible students are invisible to the SNAP case. Their income and resources do not count. Self-Employment Income (SNAPSB Section 13 pp. 282-285) What is Self-Employment Income? Self-Employment Income is the income received from a self-employment enterprise. Some examples of self-employment enterprises include:
• Payments from rental income o Managed 20 hours or more each week counted as earned income o Managed less than 20 hours a week counted as unearned income
• In-home daycare provider • Running own business
For most self-employment households this income is meant to support them throughout the year. In this case you would:
• Average the income over a 12-month period o even if the income is received during a shorter period of time, and/or o if the household receives income from additional sources.
For some self-employment households this income only represents a portion of their yearly income. In this case you would:
• Average the income over the time period it is intended to cover.
Example: If a person runs an ice cream stand each summer, but has a regular job during the rest of the year, the income from the ice cream stand can be averaged over the months that it is in operation.

49
Determining Gross Monthly Self-Employment Income (Line 1 of budget worksheet):
1. Add the total amount of self-employment income (including the full amount of capital gains).
2. Subtract the cost of producing the self-employment income. 3. Divide the self-employment income by 12 or by the number of months the income
is intended to cover. 4. The resulting figure is the household’s GROSS monthly self- employment income. 5. Continue through the rest of SNAP budgeting process.
What is a Capital Gain? For SNAP purposes, a capital gain is a profit that results from the sale of capital goods, equipment, or property. This is calculated by comparing the sales price to the cost. If the sales price is greater, there is a gain. If the costs are greater, there is a loss. The cost includes, but is not limited to:
• Property • Purchase commission • Improvements, or • Sales expenses (broker's fees and commissions)
The full amount of the capital gain, if any, is counted as income for SNAP purposes.
Allowable Adjustments from Income for Self-Employment Households The allowable cost of producing the self-employment income includes, but is not limited to, the identifiable costs of:
• Labor • Stock • Raw material • Payments on the principal of the purchase price of income-producing real estate
and capital assets • Equipment and machinery • Other durable goods • Interest paid to purchase income-producing property • Insurance premiums • Taxes paid on income-producing property.
In-home child care providers can exclude:
• A standard deduction of $5.00 per day per child in care (not including their own children), or
• The amount they receive from the Child and Adult Care Food Program (CACFP) • Without documenting the specific costs of doing business, or • They can verify actual costs if they exceed the $5 standard expense

50
Applicants/recipients residing in income-producing multi-unit property can exclude:
• The portion of the building expenses that are related to the cost of producing the self-employment income which includes:
o mortgage o interest o property taxes
o heating o utilities o insurance
• The portion of the building costs which are for the applicants’/recipients’ own living unit may not be excluded from the gross self-employment income, but are allowed as shelter deductions in the regular budgeting process.
Non-Allowable Adjustments for Self-Employment Households The following items are not allowable costs of producing the self-employment income:
• Net losses from previous years • Federal, state, and local income taxes • Money set aside for retirement purposes • Other work-related personal expenses (such as transportation to and from work) • Depreciation • Garnishments
To calculate a household’s monthly self-employment income, add the gross self-employment income (including capital gains) and then subtract out the cost of producing the self-employment income. The resulting figure is the household’s net monthly self-employment income. (Note: The household is still entitled to the 20% earned income deduction during the net income test.)
Net Monthly Self-Employment Income
=
Sum of gross self-employment income
–
Cost of producing self-employment income
There are special rules for self-employed farmers. See the SNAPSB Section 13, pp. 286-295 for details on countable vs. excludable income and additional allowable business costs for farmers. Military Families Figuring out what military pay and allowance must be counted as income for SNAP for families with members in the armed forces can be difficult. Here are examples of situations and how military pay and allowances are counted in SNAP budgeting: 1. When the service member lives with the rest of the family
• Count all military pay as income for SNAP purposes.

51
• Count the living allowances that military personnel get in addition to their base pay. There are two allowances:
o BAS (Basic Allowance for Subsistence). This pays for meals for a military person living off-post, and for the meals for the dependents of a military person.
o BAH (Basic Allowance for Housing). This allowance replaces the older BAQ (Basic Allowance for Quarters) and the VHA (Variable Housing Allowance). The BAH is a single payment that varies by locality and is based on local costs for civilians at similar pay levels.
• Some military personnel living on-post get free housing. Free housing is an in-kind benefit that is not counted as income because the Food Stamp Act of 1977 excluded “any gain or benefit which is not in the form of money payable directly to a household…”
2. When the service member is deployed away from the family • Count only the money that is available to the family. Do not count money that the
service member keeps. • Do not count the portion of the family’s income that is hazardous duty pay.
3. When the service member’s family also receives nutrition assistance from the
Department of Defense (DoD) • The family may be eligible for both the DoD’s program and regular SNAP benefits. • Families receiving both benefits will have to count the DoD assistance as income
when computing the family’s SNAP benefit.

52
KEEPING AND USING BENEFITS Using SNAP Benefits (EBT Brochure LDSS-5004; 13-INF-03; GIS 15TA/DC030) New York State uses an Electronic Benefits Transfer (EBT) system to issue SNAP benefits, TANF benefits, and Medicaid health insurance. SNAP participants use their EBT cards in the machines at checkout counters, just like debit and credit cards.
To use the SNAP benefits on the EBT card, SNAP recipients shop and take their purchases to the cash register. They swipe the card through the machine and enter their Personal Identification Number (PIN). The system will take the amount spent on food purchases out of the SNAP account. It is also possible to pay only a portion of the bill from the SNAP account and pay the remainder with cash. The machine will ask how much the participant wants to pay from their EBT SNAP account, and the participant can enter any amount up to the amount of benefits that are available in their account. The grocery store receipt will tell them how much is left. Any non-SNAP-eligible purchases can be paid for with cash. If the participant has a cash assistance account, the non-food purchases can be paid directly from the cash account by swiping the card again. Food and non-food purchases do not have to be separated at the checkout counter.
For people receiving cash assistance (TANF), some stores will give cash back from the cash account. TANF participants can also use their EBT card to get cash from Automated Teller Machines (ATMs). SNAP households can never get cash, as their SNAP benefits are only to be spent on food items at approved retailers. If the amount entered for the EBT payment is more than the amount available, the machine will reject the entire transaction. In that case, the participant should check the balance. This is done right at the cash register. Once the customer knows how much is available and enters that amount, the machine will accept the transaction, even if it is less than the amount of the purchase. The customer can then pay the balance with cash. At no point should SNAP recipients be charged a fee for using their SNAP benefits for food purchases. Unspent SNAP balances stay in the account for 365 days. The only time benefits should be expunged (removed from the account by the LDSS) earlier than 365 days is in certain NYSNIP cases, when a new NYSNIP participant has not accessed any SNAP benefits within the first 90 days of case opening—in these cases, the benefits are expunged after the first 90 days (See pg. 61 for more details about NYSNIP). SNAP participants can check their account balances at any time by calling the customer service number at 1-888-328-6399 (listed on the back of the EBT card) or by visiting https://www.mybenefits.ny.gov/ and logging into their account. Many larger stores also have machines available at the customer service desk where participants can check their balances before shopping. OTDA offers a household informational brochure (LDSS-5004) entitled Electronic Benefits Transfer (EBT) – How To Use Your Benefit Card To Get SNAP and/or Cash Benefits, which is
53
provided to households as an insert with their SNAP approval notice. The brochure includes a fairly detailed section on how to prevent theft of benefits (someone improperly gaining access to your account) AND what to do if theft of benefits occurs. SNAP offices and HRA centers must provide a photo on the Common Benefit Identification Card (CBIC), or EBT card, of any Non-Temporary Assistance (NTA) SNAP head of household upon their request. Individuals who have difficulty accessing their EBT benefits, such as the homebound, can choose someone to be their authorized representative. The authorized representative should be a person that the household trusts, such as a home attendant or family member. Once appointed by the household, the authorized representative can get a separate benefit ID card and PIN, and use these to do grocery shopping for the SNAP household. SNAP recipients who have requested and used more than 4 EBT cards in a 12-month period will receive a letter from NYS. This letter is mandated by USDA under new fraud prevention rules. While NYS understands that some SNAP recipients need further information on using an EBT card, the letter does warn cardholders that misuse of EBT cards and SNAP benefits will result in a program violation that is subject to various penalties and sanctions. The letter also states that if the recipient continues to request new EBT cards they can be referred to the local SNAP Program Integrity Unit for possible investigation. Under this policy OTDA will continue to monitor EBT card requests of current SNAP recipients and their benefit redemption history going forward. Eligible Food Items SNAP benefits can be used to buy almost all foods, as well as seeds and plants that produce food for a household to eat. Households CANNOT buy the following items with SNAP benefits:
• Beer, wine, or liquor • Cigarettes or tobacco • Non-food items like toiletries, pet foods, or household supplies • Vitamins and medicines • Ready-to-eat hot foods • Prepared cold foods which will be eaten in the store (prepared cold foods to be
eaten at home are allowed) For a complete listing of SNAP eligible food items from USDA/FNS visit: http://www.fns.usda.gov/snap/eligible-food-items

54
SNAP Monthly Benefits Issuance Schedule Benefits are generally made available over the first 9-14 days of every month, based on the last digit of the client’s case number. For all counties, except the 5 boroughs of NYC:
Case Number Ends In: Benefits Available On:
0 or 1 1st of the month 2 2nd of the month 3 3rd of the month 4 4th of the month 5 5th of the month 6 6th of the month 7 7th of the month 8 8th of the month 9 9th of the month
For NYC cases, benefit postings are spread out over 10 different days that are not Sundays or holidays, during the first two weeks of the month. The actual dates change from one month to the next, so NYC publishes a six-month schedule showing the exact availability dates. To view the current NYC schedule, go to: http://www.fns.usda.gov/sites/default/files/NYC_Issuance_Schedule.pdf. This schedule is based on the last digit of the case number. Find the digit in the first column of the schedule. This row lists the monthly deposit dates for benefits over the six-month period. SNAP deposits are made during the A Cycle of each month. Recertification and Reporting Requirements (SNAPSB Sections 6 and 14; 04-INF-25; 07-ADM-05; 08 ADM 09; GIS 08 TA/DC018; 11-INF-07; 13-ADM-04) A household is only authorized to be eligible for SNAP benefits for a specified, limited period of time, called the certification period. At the end of that period, the SNAP case is automatically closed unless the LDSS/case examiner enters a new certification period. The certification period can be any period up to 12 months and sometimes longer:
• Most households with income: 12-month certification period • Households with income that changes frequently: 6-month certification period • Households with no income, homebound individuals, group home residents
receiving SSI/SSD, and people that are homeless: 12-month certification period • Households where all members are a senior or disabled and with no earned
income: 24-month certification period • NYS Nutrition Improvement Project (NYSNIP) households: SSI recipients with live-
alone status who receive SNAP automatically: 48-month certification period

55
Before the end of the certification period, the household will receive a notice asking them to come in for a recertification interview. If they do not come in for this interview, the case will close at the end of the certification period. At the recertification interview, the participant will be asked to bring in documentation of information that changes, such as income and housing costs. Telephone Recertification During the recertification process, existing SNAP participants will need to complete an additional interview. The purpose of the interview is the same as for new applicants, in addition to checking to make sure that no changes have occurred since the last application. SNAP offices can choose to have telephone interviews with current SNAP recipients; however, participants can always request to have the interview in person. The interview time is included with the recertification packet; however, the SNAP office may attempt to call up to four times before the interview date. If a household does not submit the recertification packet, the SNAP participant will not receive the interview. The SNAP office will not contact a household or go through with the scheduled interview if the household has not sent in their signed recertification form. It is very important that households return their completed recertification application as soon as possible. If the household sends in their recertification form, but the district cannot reach them for their interview, a “notice of missed interview” will be mailed. This notice advises the household to contact the local SNAP office immediately to reschedule their interview if they wish to have their recertification application processed. See Notice of Missed Interview on page 13 of this guide. Changes Between Certification Periods (11-INF-07; Appendix P) Besides certification periods (the specified period of time that a household is determined eligible for SNAP benefits), SNAP households must also follow complicated reporting rules. Any failure to report information when it is required may result in an overpayment, and the SNAP office will try to get the overpaid amount back, either by “recouping” it from future benefits, or through a “claims” process. This can result in the overpaid amount being taken from tax refunds. Households with Six-Month Reporting Rules The only thing these households must report during the six-month period is:
• Change in income that causes the household to be over 130% of the Federal Poverty Level. If this happens, they must report it immediately.
• ABAWDs who are subject to the ABAWD rules must also report if their work hours fall below 80 hours per month.

56
Reporting Rules for Households with Certification Periods Longer than Six Months: • These households will receive a change report form to be filled out at the six-
month point of their SNAP certification. • The change report form is mailed at the end of the fifth month of certification. • The household should complete the form and return it to the LDSS in order to
continue receiving benefits. • These households must do the following under reporting rules:
o Return the 6-month reporter. o Report any change in household income above 130% of poverty, and o Report a drop in ABAWD work hours (below 80).
Households with certification periods of six months or more do not have to report any other changes in circumstances until their next SNAP recertification interview. Households that are 10 Day Reporters Some households cannot take advantage of the generous six-month reporting rules. Instead, these households are required to report almost all changes in household information within the 10th day of the month following the month of the change. Ten Day reporting households include:
• Unearned income households in which all the adults are elderly or disabled • Group home residents receiving SSI/SSD • Households with no income • Migrant workers • Homeless households • Households with a certification period of less than 4 months
Even these households do not have to report certain changes in between certification periods. For example, it is not necessary for elderly households to inform the SNAP office when their Social Security benefits increase each January, so long as the increase is less than $50 per month. It is best to check reporting rules for specifics on what must be reported by when and by which households. A helpful source of information is 04-INF-25. Case Reactivation Waiver (13-ADM-04) A new waiver now allows SNAP offices and HRA centers to reinstate SNAP benefits during the certification period for households that re-establish their eligibility. Households can do this by reporting and verifying any change in circumstances, or complying with an unfulfilled program requirement within 30 days of the date their SNAP case was closed.

57
These households are not required to file a new SNAP application, or to complete an eligibility interview. A common situation where case reactivation will be used is when a household’s SNAP case has been closed for failure to submit or complete a periodic report, but the household provides the needed information after the SNAP case has been closed.
How Households Can Be Reinstated Under the Case Reactivation Waiver
Affected households must do the following within 30 days of their case closing:
1. Report and verify all changes in circumstances that have occurred 2. Provide any outstanding information that may be missing 3. Continue to be eligible for SNAP benefits, and 4. For households in Upstate Counties: The household should have at least 3 full
months remaining in their certification period following the date of fulfilling all the above requirements for reactivation. For Households in NYC: The household should have at least 4 full months remaining in their certification period following the date of fulfilling all the above requirements for reactivation.
These timeframes are necessary due to the requirements districts must follow for generating timely recertification notices and scheduling and completing recertification interviews.
OTDA reserves the right to permit exceptions to this last requirement and permit reactivation during the last 3 or 4 months of the certification period if the case circumstances merit the exception.
When the Case Reactivation Waiver Cannot Be Used Case reactivations are not re-applications for SNAP. Therefore:
• Consideration for expedited processing is not part of the reactivation process.
• Households that provide missing information or comply with eligibility requirements 30 days or more after their SNAP certification end date must file a new SNAP application.

58
This waiver does not apply to households that have not complied with SNAP E&T activities resulting in their SNAP case closing:
• An individual whose SNAP case has been closed because of a SNAP E&T sanction must serve the minimum durational sanction in addition to complying with the SNAP E&T requirements as assigned by the SNAP office or HRA Center, unless the individual documents that they have become exempt from SNAP work requirements.
Emergency Food Replacement (11 GIS TA/DC018 & 21; 06 GIS TA/DC 018; 08 GIS TA/DC 031; Appendix O) SNAP has special rules to help households which experience food loss due to an emergency. SNAP recipients who experience a household misfortune which causes their food to spoil or be destroyed can receive a SNAP replacement benefit. The loss of food can be due to a situation that affects large areas, such as a storm or a flood, or can be specific to a single household, such as a fire. The amount of the replacement benefit cannot be higher than the household’s usual monthly allotment. Examples of Household Misfortune
• Extended power outage (4 hours or more) • A flood • Fire • An equipment failure (refrigerator/freezer) • Failure to pay a utility bill
Under the regular SNAP regulations, it is always possible for SNAP recipients who lose food in a “household misfortune” to obtain replacement benefits if the household:
• Reports the loss within 10 days of the misfortune either verbally (by phone or in person) or in writing to their SNAP office, AND
• Returns a signed and completed LDSS Form 2291(Appendix O) within 10 days of the date of the reported loss to the SNAP office, either by mail or in person.
Other Things to Note:
• The SNAP office should always issue replacement benefits if a household requests a replacement and has experienced a power outage/shutoff of 4 hours or longer.
• SNAP offices are advised not to require the household to bring in spoiled food as verification of need, as this is inappropriate for reasons of both health and administrative impracticality.
• A household may not be denied replacement SNAP benefits if it has applied for replacement issuances in the past.

59
• The SNAP office may use available information to confirm or deny the accuracy of the statement attesting to the household misfortune.
Disaster SNAP (USDA D-SNAP Guide) In the event of a large-scale disaster, states may request permission from USDA to operate a Disaster SNAP program (D-SNAP). The D-SNAP program has special income rules and a very simple application process. It provides benefits quickly to households which would not ordinarily qualify for SNAP benefits, but which suddenly need food assistance due to the disaster situation. D-SNAP may also include special provisions for existing recipients. The largest D-SNAP to date was implemented after Hurricane Katrina. New York State has operated D-SNAP programs in the following counties since 2001:
• Fall of 2001 – in New York City, after the World Trade Center attacks • Summer of 2006 – in 12 upstate counties, in response to severe flooding • Summer of 2011 – in 16 upstate counties, in response to Hurricane Irene and
Tropical Storm Lee • Fall of 2012 – in Westchester County and in 10 full and 2 partial zip codes in NYC, in
response to Super Storm Sandy For more detailed information about Disaster SNAP benefits, consult “An Advocate’s Guide to the Disaster Food Stamp Program,” issued by the Food Research and Action Center (FRAC). This document can be found here: http://frac.org/wp-content/uploads/2009/09/dfspguide06.pdf. Transitional Benefits (02 ADM-07; 09-ADM-22) Most households who leave TANF are now automatically eligible for transitional SNAP benefits. New York’s transitional SNAP is called the Transitional Benefits Alternative (TBA). TBA was implemented to provide a critical work support to newly employed households. However, TBA is available to other households who leave TANF, so long as the reason for the case closing does not involve a SNAP violation. New York does not provide TBA benefits to households who miss their TANF/SNAP recertification interview. At the time the TANF case is closed, if a household is eligible for TBA, the caseworker will authorize TBA for 5 months – even if a household had less than 5 months left in its SNAP certification period. The TBA benefit is frozen at the SNAP benefit level issued prior to the Family Assistance case closing, but the Family Assistance is no longer counted as income. There is no income “cap” for TBA; even households with gross incomes above 130% of poverty are eligible. The household is not obligated to report any change in income, resources, or household composition during the TBA period. Before the TBA period expires, households are sent a

60
recertification notice to allow them to certify for ongoing SNAP benefits. To “unfreeze” the SNAP benefits during the 5-month TBA period – for example, if a household’s income dramatically decreases or a new member joins the household – the household would have to undergo an early recertification. Temporary assistance households without children who leave Safety Net Assistance (SNA) cannot get TBA benefits, but they may be eligible for regular SNAP benefits. SNAP households (with children) who leave TANF or SNA are eligible for TBA. For more information on this policy change see 09-ADM-22. New York State Nutrition Improvement Project – NYSNIP (04 LCM-13; GIS 12TA/DC019; GIS 13 TA/DC030) In recent years, USDA has encouraged states to develop combined application projects (CAPs) to make it easier for elderly and disabled recipients of Supplemental Security Income (SSI) to receive SNAP. OTDA operates a CAP called the New York State Nutrition Improvement Project (NYSNIP), which automatically enrolls single SSI live-alone recipients into SNAP. No separate SNAP application, no interview, and no separate verification are needed. Who can participate? NYSNIP is available only to SSI live-alone recipients – those classified as “living alone” by SSA (i.e. - live by themselves and pay their own food, shelter, and clothing expenses). This code, called an “A/A,” designates a federal SSI living code of ‘A’ and a State Supplement code of ‘A.’ SSA sets these codes, not the SNAP office/HRA center. Only SSA can code SSI recipients as live-alones. The SNAP office/HRA center uses data matching to find eligible NYSNIP participants each month from the list of newly approved SSI recipients in NYS. SSI couples and recipients in other living arrangement categories cannot participate in NYSNIP, but they can receive SNAP through the regular application process. SSI live-alone applicants will not get SNAP benefits through NYSNIP; only if/when they become SSI recipients will their NYSNIP benefits start. Unlike Medicaid or SSI, there is no retroactive NYSNIP eligibility. NYSNIP benefits start the first or second month after the first ongoing SSI check is issued.

61
NYSNIP eligibility rules for 18- to 21-year-old SSI recipients coded A/A by SSA: SSI participants age 18-21 who live with their parents can be coded (A/A) designating them as an SSI live-alone. This is true even if they reside with their parents, as long as they are paying their parents for living at home. These SSI recipients:
• Can participate in NYSNIP as a separate SNAP household even if they live with their parent(s), as long as the parents are not in receipt of SNAP benefits.
• If both the parents and the 18-21 year-old SSI live-alone are either current SNAP participants or are applying for SNAP, then this family must apply together as one household under regular non-NYSNIP SNAP eligibility rules.
NYSNIP eligibility rules for adult SSI recipients coded A/A by SSA who are living with their 18- to 21-year-old children: SSI participants who live with their 18- to 21-year-old children can be coded (A/A) designating them as an SSI live alone. These SSI recipients:
• Can participate in NYSNIP as a separate SNAP household even if they live with their children who are ages 18-21,
• As long as the 18- to 21-year-old child(ren) is not applying or currently receiving SNAP benefits.
• If both the adult SSI recipient and their children ages 18-21 are either participating in or apply for SNAP, then this family must apply together as one household under regular non-NYSNIP SNAP eligibility rules.
What are the benefit amounts and certification periods? NYSNIP has standardized SNAP benefits; the SNAP budget is not individualized. The benefit standards consider four factors: cost of shelter, eligibility for the heating/cooling standard utility allowance, presence of other income, and geographic location. A chart listing the NYSNIP benefit allotments can be found at HungerSolutionsNY.org in the News and Resources section. One of the guiding principles behind NYSNIP is that participants should get the same or more SNAP benefits than they would ordinarily receive through the regular SNAP application process. Anyone who would receive a lower amount should be able to “opt out” of NYSNIP and enter the regular SNAP application process if they wish. Some SNAP recipients will be eligible for a higher SNAP allotment if they opt out of NYSNIP. This is because those households with high shelter costs (more than$246) who did not receive a HEAP benefit of $21 and are not paying for heating/cooling costs will be receiving a minimum benefit of $26 or $17 through NYSNIP. Actual shelter costs may exceed $246 in the regular SNAP budgeting process and because NYSNIP is a standardized benefit, the costs are not budgeted in the same way. It is important to verify whether NYSNIP is the most advantageous way for households to access SNAP benefits. New SNAP recipients under NYSNIP will initially receive the minimum benefit level of $16. However, by filling out and returning a short form (LDSS-4841) included with their NYSNIP opening notice (includes questions about shelter and utility costs), benefits may be adjusted up to the maximum SNAP benefit level – as high as $194.

62
New NYSNIP participants must access their SNAP account within 90 days of the case opening. If redemption of SNAP benefits does not occur within 60 days, OTDA sends a reminder notice urging the individual to use their SNAP benefits within the next month. The reminder has a list of community agencies that NYSNIP recipients can call for assistance. At the end of the 90 days, if the person still has not accessed any SNAP benefits, OTDA closes the NYSNIP case. This individual has to go through the regular SNAP application process if s/he wants to rejoin NYSNIP or to participate in the regular SNAP application process. The certification period under NYSNIP lasts up to 4 years, with a short mail-in questionnaire required at the midway point. Recipients MUST return this questionnaire – called an “interim report” (LDSS-4836) – in order to continue receiving SNAP for the remaining 2-year period. Participants who lose SSI live-alone status will be taken out of NYSNIP; however, they can still receive regular SNAP benefits, if eligible. NYSNIP benefit allotments will change on October 1, 2015. NYSNIP recipients who do not pay separately for heating or cooling costs and have not received a HEAP benefit of $21 or more in the last twelve months or in the current month will receive a shelter code type 96 or 97 (no SUA) and will see their SNAP benefit decrease substantially. This is a result of the federal changes to the farm bill. Budgets may need to be looked at closely to see if the person would benefit from using regular SNAP rules or if NYSNIP enrollment is more beneficial. Some households may receive a higher benefit amount by switching to the regular SNAP program because their actual shelter costs are higher than the capped amount of $246 allowed in the NYSNIP matrix. Medical bills are also not counted in the NYSNIP matrix. NYSNIP recipients who see a decrease in their SNAP benefits can ask the SNAP office to do a comparison budget to help them determine whether they will receive a higher SNAP benefit by using regular SNAP rules or if NYSNIP enrollment is more beneficial. The SNAP office should then give these NYSNIP recipients the opportunity to opt out of NYSNIP. If a person decides to opt out of NYSNIP, they will no longer be eligible for the 48-month certification period. A new application does not need to be submitted for people that transition from NYSNIP to the regular SNAP program. New SSI live-alone recipients not already in receipt of SNAP are placed into NYSNIP at the minimum benefit level. Included with their opening notice is the shelter questionnaire (the “NYSNIP Food Stamp Case Information Collection Sheet” (LDSS-4841)). Once the local SNAP office receives the person’s completed shelter questionnaire, the SNAP benefits can be adjusted to take into account the person’s shelter and utility expenses. Any new NYSNIP participant who fails to access their SNAP account within 60 days will get the reminder notice mentioned above, and have an additional 30 days to access their benefits. The NYSNIP notices contain a lot of information which may be overwhelming to many SSI recipients. Community agencies and advocacy groups working with the elderly and disabled can help new NYSNIP participants understand what the program is all about, assist in completing the shelter & utility questionnaire, and encourage people to use their

63
SNAP benefits. Ongoing recipients may need help completing the interim mailer and returning it to their local SNAP office.
NYSNIP BENEFITS MATRIX BY SHELTER TYPES
10/01/15 - 09/30/16
High shelter = More than $246/month Low shelter = Less than or equal to $246/month SUA = Eligible for Level 1 (heating/cooling) SUA *SUA/$21 HEAP = Eligible for Level 1 (heating/cooling) SUA **No SUA = Not eligible for Level 1 (heating/cooling) SUA No Shelter/ SUA = no information on households shelter costs or heating/cooling expenses For more information on changes to the NYSNIP program and for any updates to the current NYSNIP benefit matrix, see the News and Resources section at HungerSolutionsNY.org.
HOUSEHOLD MONTHLY FOOD STAMP BENEFIT AMOUNT New York City Nassau/Suffolk Upstate
Shelter Type 94 (High Shelter/SUA)
SSI Only Other Income
$194 $194
$194 $194
$194 $194
Shelter Type 95 (Low Shelter/SUA)
SSI Only Other Income
$194 $189
$183 $174
$159 $150
Shelter Type 96 (High Shelter/ SUA/$21 HEAP)
SSI Only Other Income
$194 $194
$194 $194
$194 $194
Shelter Type 96 (High Shelter/No SUA)
SSI Only Other Income
$26 $17
$26 $17
$26 $17
Shelter Type 97 (Low Shelter/ SUA/$21 HEAP)
SSI Only Other Income
$194 $189
$183 $174
$159 $150
Shelter Type 97 (Low Shelter/No SUA)
SSI Only Other Income
$16 $16
$16 $16
$16 $16
Shelter Type 98 (No Shelter or SUA Data)
SSI Only Other Income
$16 $16
$16 $16
$16 $16
Appendix A –
Common Acronyms
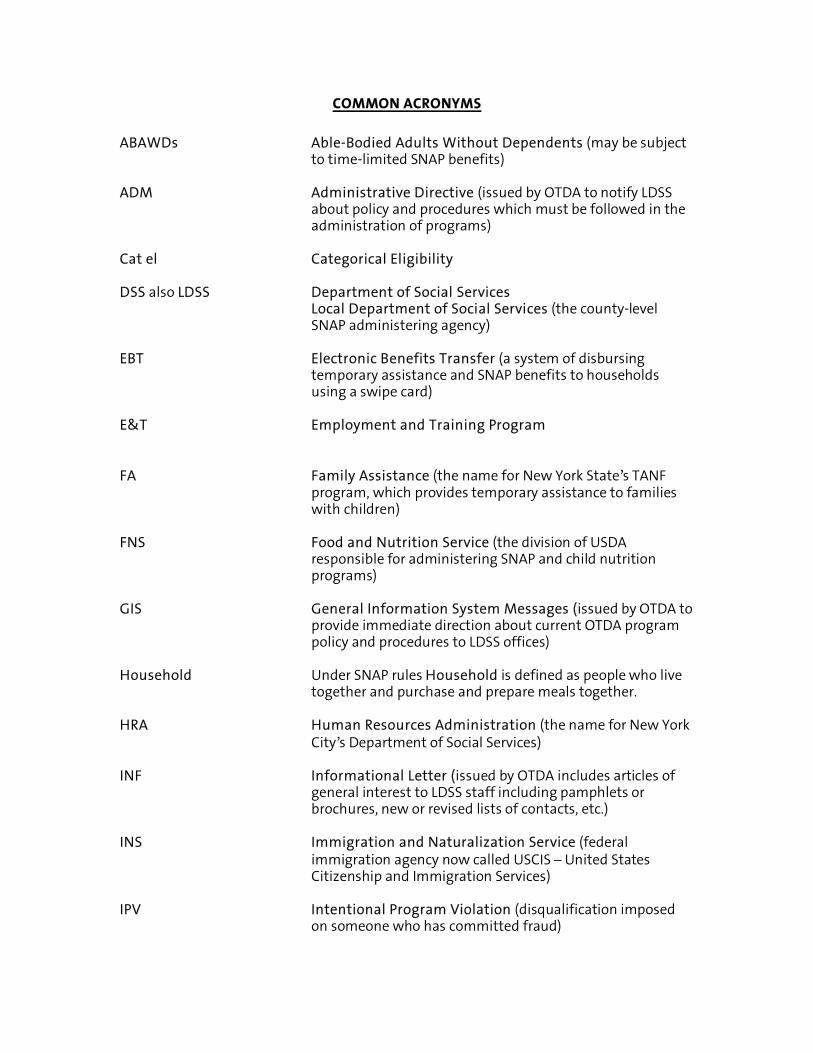
COMMON ACRONYMS
ABAWDs Able-Bodied Adults Without Dependents (may be subject
to time-limited SNAP benefits) ADM Administrative Directive (issued by OTDA to notify LDSS
about policy and procedures which must be followed in the administration of programs)
Cat el Categorical Eligibility DSS also LDSS Department of Social Services
Local Department of Social Services (the county-level SNAP administering agency)
EBT Electronic Benefits Transfer (a system of disbursing
temporary assistance and SNAP benefits to households using a swipe card)
E&T Employment and Training Program FA Family Assistance (the name for New York State’s TANF
program, which provides temporary assistance to families with children)
FNS Food and Nutrition Service (the division of USDA
responsible for administering SNAP and child nutrition programs)
GIS General Information System Messages (issued by OTDA to
provide immediate direction about current OTDA program policy and procedures to LDSS offices)
Household Under SNAP rules Household is defined as people who live
together and purchase and prepare meals together. HRA Human Resources Administration (the name for New York
City’s Department of Social Services) INF Informational Letter (issued by OTDA includes articles of
general interest to LDSS staff including pamphlets or brochures, new or revised lists of contacts, etc.)
INS Immigration and Naturalization Service (federal
immigration agency now called USCIS – United States Citizenship and Immigration Services)
IPV Intentional Program Violation (disqualification imposed
on someone who has committed fraud)

LDSS Local Department of Social Services (the county- level SNAP administering agency)
LPR Lawful (or Legal) Permanent Resident (also known as “green card” holder)
MA Medicaid MARU Mail-In Application Referral Unit- (HRA initiative that
encourages households to apply for SNAP through mail or fax) NTA/NPA Non-Temporary Assistance/Non-Public Assistance (household in which no one receives temporary assistance) NOMI Notice of Missed Interview NYSNIP New York State Nutrition Improvement Project (program which provides automatic SNAP benefits to SSI
live-alone recipients) OTDA also NYSOTDA Office of Temporary and Disability Assistance (the state
agency responsible for administering SNAP in New York State)
SN or SNA Safety Net Assistance (the state’s temporary assistance
program for households without children and households who have exceeded the 5 year TANF time limit)
SNAP Supplemental Nutrition Assistance Program (the new
name for the Food Stamp Program) SNAPSB Supplemental Nutrition Assistance Program Source Book
(New York State administrative policy manual) SSA Social Security Administration SSD or SSDIB Social Security Disability Insurance Benefits SSI Supplemental Security Income (cash assistance program
for low-income elderly [65+] and disabled individuals – is administered by SSA)
SSN Social Security Number SUA Standard Utility Allowance TA Temporary Assistance (generic term for SNA and TANF --
also known as “cash assistance,” “public assistance” or “welfare”)

TANF Temporary Assistance for Needy Families (the temporary assistance program for families with children, also known in New York State as Family Assistance)
TBA Transitional Benefits Alternative (the name for New York State’s transitional SNAP for people leaving TANF) UIB Unemployment Insurance Benefits USCIS United States Citizenship and Immigration Services (the
federal immigration agency formerly known as INS – Immigration and Naturalization Service)
USDA United States Department of Agriculture (administers
SNAP on the federal level) WFSNAPI Working Families Supplemental Nutrition Assistance
Program Initiative (simplifies application process for working families who qualify)

Appendix B –
SNAP Organizational Chart

Prep
ared
by
Hu
nge
r Sol
uti
ons
New
Yor
k U
pdat
ed S
epte
mbe
r 201
5
Org
aniz
atio
nal
Str
uct
ure
of
the
Sup
ple
men
tal N
utr
itio
n A
ssis
tan
ce P
rogr
am
Un
ited
Sta
tes
Dep
artm
ent
of
Ag
ricu
ltu
re
(USD
A)
Fede
ral a
gen
cy re
spon
sibl
e fo
r adm
inis
trat
ion
of t
he S
upp
lem
enta
l Nu
trit
ion
Ass
ista
nce
Pro
gram
(SN
AP)
.
Issu
es S
NA
P re
gula
tion
s an
d po
licie
s. M
onit
ors
stat
e ag
ency
per
form
ance
.
Off
ice
of
Tem
po
rary
an
d D
isab
ilit
y A
ssis
tan
ce (
OTD
A)
Resp
onsi
ble
for a
dmin
iste
ring
SN
AP,
the
new
nam
e fo
r th
e Fo
od S
tam
p Pr
ogra
m (F
SP) i
n N
ew Y
ork
Stat
e.
Is
sues
sta
te re
gula
tion
s, p
olic
y di
rect
ives
and
tra
ins
and
mon
itor
s Lo
cal D
epar
tmen
ts o
f Soc
ial S
ervi
ces.
Resp
onsi
ble
for a
dmin
istr
atio
n o
f sta
te S
NA
P Em
ploy
men
t &
Tra
inin
g Pl
an a
nd
ABA
WD
pol
icie
s.
Loca
l Dep
artm
ent
of S
ocia
l Ser
vice
s (L
DSS
) or
Hu
man
Res
ourc
e A
dm
inis
trat
ion
(H
RA
) In
NYC
Cou
nty
gov
ernm
ent a
gen
cy d
eter
min
es S
NA
P el
igib
ility
an
d is
sues
ben
efit
s to
elig
ible
h
ouse
hol
ds.
H
ouse
hold
s ap
ply
for S
NA
P th
rou
gh t
hei
r LD
SS/H
RA.
Un
ited
Sta
tes
Co
ng
ress
Con
gres
s au
thor
izes
th
e Su
pple
men
tal N
utr
itio
n A
ssis
tan
ce P
rogr
am th
roug
h th
e Fa
rm B
ill e
very
five
yea
rs

Appendix C –
“How To” Sheet for ordering SNAP application and
OTDA Form 876 EL

Prepared by Hunger Solutions New York SNAP Prescreening Guide September 2015
ORDERING BLANK SNAP APPLICATIONS FROM OTDA
Hard copies of SNAP applications and other related publications from OTDA are available free of charge. To order copies of these documents in large quantities follow the following steps.
Order OTDA Publications:
To order OTDA Publications, visit http://otda.ny.gov/programs/publications/order/ or fill out OTDA Form 876 and mail the completed form to the below address. Please allow 3 weeks for processing of order. Form 867 can be found on the next page of this guide. NYS Office of Temporary and Disability Assistance Document Services PO Box 1990 Albany, NY 12201 Fax: 518-402-0084 Email: [email protected] This information can be found at http://otda.ny.gov/programs/publications/order/
1. Instructions for filling out the form: For SNAP only applications use document number 4826 For Document Title: use “SNAP Benefits
Application/Recertification” Make sure to specify language(s) you would like:
• English • Spanish • Arabic • Chinese
• Haitian-Creole • Korean • Russian
2. Things to know about ordering applications:
Request for the same items are limited to twice per year Remember to order a sufficient supply at least two months in
advance.

OTDA-876 (Rev. 7/09) REQUEST FOR FORMS OR PUBLICATIONS
Submit Request To: NYS Office of Temporary and Disability Assistance Document Services P.O. Box 1990 Albany, N.Y. 12201
Deliver Supply To: (Complete Address)
We recommend that you establish a re-order point to insure sufficient quantities are on hand to meet your needs. Please order documents in numerical sequence and allow 3 weeks for processing
and shipping of your order. FORM NUMBER FORM TITLE QUANTITY
REQUESTEDQUANTITY SHIPPED
Agency Submitting Request:
Name of Person Submitting Request:
Phone Number
Date Submitted
E-mail Address: Shaded areas to be completed by Document Services staff Cost Center Code Date Filled Filled By
Sent VIA: UPS Truck Other

Appendix D –
SNAP APPLICATION
FORM and “How to Complete” Booklet
(LDSS-4826; LDSS-4826A)

LDSS
-482
6A (R
ev. 8
/12)
N
EW Y
OR
K ST
ATE
OFF
ICE
OF
TEM
POR
ARY
AND
DIS
ABIL
ITY
ASS
ISTA
NC
E
HO
W T
O C
OM
PLET
E TH
E SU
PPLE
MEN
TAL
NU
TRIT
ION
ASS
ISTA
NC
E PR
OG
RAM
(SN
AP)
A
PPLI
CA
TIO
N/R
ECER
TIFI
CA
TIO
N A
ND
APP
LIC
AN
T/R
ECIP
IEN
T R
IGH
TS A
ND
RES
PON
SIB
ILIT
IES
FOR
SN
AP
SN
AP
is
th
e n
ew
nam
e f
or
the F
oo
d S
tam
p P
rog
ram
Use
Th
is F
orm
If
Ap
ply
ing
Fo
r S
NA
P O
nly
If yo
u ar
e on
ly a
pply
ing
for
SNAP
you
can
use
this
sho
rter
appl
icat
ion.
If y
ou w
ould
like
to a
pply
for
othe
r be
nefit
s su
ch a
s Te
mpo
rary
Ass
ista
nce,
C
hild
Car
e A
ssis
tanc
e, H
ome
Ener
gy A
ssis
tanc
e or
Med
icai
d pl
ease
ask
for a
diff
eren
t app
licat
ion.
T
his
app
lica
tion
ca
n o
nly
be u
sed t
o a
pp
ly f
or
SN
AP
Be
ne
fits
.
Wh
en
Yo
u A
re A
pp
lyin
g F
or
SN
AP
Yo
u ca
n fil
e an
app
licat
ion
the
sam
e da
y yo
u re
ceiv
e it.
If y
ou a
re e
ligib
le, b
enef
its w
ill be
pro
vide
d ba
ck to
the
filin
g da
te o
f you
r app
licat
ion.
You
can
file
your
app
licat
ion
befo
re y
ou h
ave
an in
terv
iew
.
We
mus
t acc
ept y
our a
pplic
atio
n if,
at a
min
imum
, it c
onta
ins
your
nam
e, a
ddre
ss (i
f you
hav
e on
e), a
nd a
sig
natu
re. T
his
info
rmat
ion
will
esta
blis
h yo
ur a
pplic
atio
n fil
ing
date
. How
ever
, the
app
licat
ion
proc
ess
incl
udin
g th
e in
terv
iew
and
a s
igna
ture
on
page
5 o
f the
app
licat
ion/
rece
rtific
atio
n m
ust b
e co
mpl
eted
for u
s to
det
erm
ine
your
elig
ibilit
y.
Yo
u ca
n ap
ply
for
and
get
SNAP
for
elig
ible
hou
seho
ld m
embe
r(s)
eve
n if
you
or s
ome
othe
r m
embe
rs o
f yo
ur h
ouse
hold
are
not
elig
ible
for
be
nefit
s be
caus
e of
imm
igra
tion
stat
us. F
or e
xam
ple,
inel
igib
le a
lien
pare
nts
can
appl
y fo
r SN
AP fo
r th
eir
child
ren
and
rece
ive
bene
fits
for
thei
r el
igib
le c
hild
ren.
You
can
still
appl
y an
d be
elig
ible
for S
NAP
eve
n if
you
have
reac
hed
your
Tem
pora
ry A
ssis
tanc
e tim
e lim
its.
Ne
ed
SN
AP
Ben
efi
ts R
igh
t A
wa
y?
Yo
u M
ay
Be
Eli
gib
le F
or
Ex
ped
ited
Pro
ce
ss
ing
Of
Yo
ur
SN
AP
Ap
pli
ca
tio
n.
If yo
ur h
ouse
hold
has
littl
e or
no
inco
me
or li
quid
res
ourc
es, o
r if
your
ren
t and
util
ity e
xpen
ses
are
mor
e th
an y
our
inco
me
and
liqui
d re
sour
ces,
or
you
are
a m
igra
nt o
r sea
sona
l far
m w
orke
r with
littl
e or
no
inco
me
or re
sour
ces
whe
n yo
u ap
ply,
you
may
be
qual
ified
to re
ceiv
e SN
AP b
enef
its w
ithin
5
cale
ndar
day
s af
ter t
he d
ate
that
you
app
ly. Y
our w
orke
r will
alw
ays
revi
ew y
our c
ircum
stan
ces
to s
ee if
you
are
qua
lifie
d fo
r exp
edite
d pr
oces
sing
of
you
r SN
AP a
pplic
atio
n. A
pro
cess
is in
pla
ce to
issu
e SN
AP b
enef
its to
all
elig
ible
hou
seho
lds
who
mee
t the
sta
ndar
ds fo
r exp
edite
d se
rvic
e.
Wh
ere
Yo
u C
an
Ap
ply
Fo
r S
NA
P B
en
efi
ts
If yo
u liv
e ou
tsid
e of
New
Yor
k C
ity, c
all o
r vis
it th
e so
cial
ser
vice
s di
stric
t in
the
coun
ty w
here
you
live
and
ask
for a
n ap
plic
atio
n pa
ckag
e. Y
ou c
an
get t
he a
ddre
ss a
nd p
hone
num
ber b
y ca
lling
toll
free
l-800
-342
-300
9, o
r app
ly o
n-lin
e at
myB
enef
its.n
y.go
v.
If yo
u liv
e in
New
Yor
k C
ity a
nd y
ou a
re n
ot a
lso
appl
ying
for T
empo
rary
Ass
ista
nce,
cal
l or v
isit
any
SNA
P O
ffice
and
ask
for a
n ap
plic
atio
n pa
ckag
e.
You
can
get t
he a
ddre
ss a
nd p
hone
num
ber b
y ca
lling
1-71
8-55
7-13
99 o
r tol
l fre
e l-8
00-3
42-3
009,
or a
pply
on-
line
at m
yBen
efits
.ny.
gov.
H
av
ing
Pro
ble
ms
Co
min
g T
o U
s F
or
A S
NA
P A
pp
oin
tmen
t?
If it
is d
iffic
ult f
or y
ou to
com
e in
for
a SN
AP a
pplic
atio
n ap
poin
tmen
t (re
ason
s m
ay in
clud
e em
ploy
men
t, he
alth
issu
es, t
rans
porta
tion
or c
hild
car
e pr
oble
ms)
, you
may
hav
e so
meo
ne e
lse
appl
y fo
r you
, or y
ou m
ay a
pply
on-
line
at m
yBen
efits
.ny.
gov.
You
als
o ca
n m
ail u
s yo
ur a
pplic
atio
n or
dro
p it
off a
nd, i
n so
me
circ
umst
ance
s; w
e ca
n in
terv
iew
you
by
tele
phon
e.
Plea
se c
onta
ct th
e so
cial
ser
vice
s di
stric
t if y
ou h
ave
any
ques
tions
, to
see
if yo
u ar
e el
igib
le fo
r a te
leph
one
inte
rvie
w, o
r if
yo
u n
ee
d t
o r
es
ch
ed
ule
a
n i
nte
rvie
w.

LDSS
-482
6A (R
ev. 8
/12)
P
age
2
INST
RU
CTI
ON
S O
N H
OW
TO
CO
MPL
ETE
THE
SNA
P A
PPLI
CA
TIO
N/R
ECER
TIFI
CA
TIO
N
Ple
ase
PRIN
T cl
early
in b
lue
or b
lack
ink.
D
o N
OT
prin
t in
the
shad
ed a
reas
. B
e su
re to
com
plet
e ea
ch s
ectio
n.
If y
ou
are
ap
ply
ing a
s s
om
eo
ne
’s r
ep
resen
tative
, p
lea
se
info
rma
tio
n a
bou
t th
at p
ers
on,
no
t yo
urs
elf.
SEC
TIO
N 1
: APP
LIC
AN
T IN
FOR
MA
TIO
N
NA
ME:
PR
INT
your
lega
l nam
e in
clud
ing
your
firs
t nam
e, m
iddl
e in
itial
and
last
nam
e.
TELE
PHO
NE
NU
MB
ER: P
RIN
T yo
ur h
ome
phon
e nu
mbe
r. O
THER
PH
ON
E: P
RIN
T an
othe
r pho
ne n
umbe
r whe
re y
ou c
an b
e re
ache
d, if
you
hav
e on
e.
RES
IDEN
CE
AD
DR
ESS:
PR
INT
the
stre
et, a
venu
e, ro
ad, e
tc.,
whe
re y
ou n
ow li
ve. P
RIN
T th
e ci
ty y
ou li
ve in
. PR
INT
your
zip
cod
e.
MAI
LIN
G A
DD
RES
S: P
RIN
T yo
ur m
ailin
g ad
dres
s if
it is
diff
eren
t fro
m y
our r
esid
ence
. O
THER
NA
ME:
PR
INT
any
mai
den
nam
es, n
ames
from
a p
revi
ous
mar
riage
, or o
ther
nam
es th
at a
ny p
erso
n lis
ted
has
or n
ow u
ses.
C
heck
() w
heth
er y
ou a
re a
pply
ing
or re
certi
fyin
g fo
r SN
AP
. C
heck
() i
f you
wis
h to
rece
ive
notic
es in
Spa
nish
and
Eng
lish
or ju
st E
nglis
h.
SEC
TIO
N 2
: S
ign
your
nam
e an
d da
te, O
NLY
if y
ou w
ant t
o su
bmit
your
app
licat
ion
with
out c
ompl
etin
g th
e ne
xt p
age
at th
is ti
me.
You
mus
t co
mpl
ete
the
appl
icat
ion
and
sign
on
page
5 fo
r us
to d
eter
min
e yo
ur e
ligib
ility.
SE
CTI
ON
3: H
OU
SEH
OLD
MEM
BER
S IN
FOR
MA
TIO
N:
LIST
TH
E N
AM
ES O
F EV
ERYO
NE
WH
O L
IVES
WIT
H Y
OU
, EVE
N IF
TH
EY A
RE
NO
T A
PPLY
ING
WIT
H Y
OU
. PR
INT
your
full
nam
e fir
st. T
hen
PRIN
T th
e na
mes
of t
he o
ther
peo
ple
who
live
with
you
: PR
INT
the
da
te o
f b
irth
, S
ocia
l S
ecu
rity
Num
be
r (if
the
ind
ivid
ua
l d
oe
s n
ot
ha
ve
a S
SN
, ente
r “n
on
e”)
, m
arita
l sta
tus a
nd
se
x f
or
eac
h pe
rson
ap
plyi
ng.
Che
ck (
) Yes
or N
o to
tell
us w
ho is
app
lyin
g.
For e
ach
pers
on in
the
hous
ehol
d, P
RIN
T ho
w th
ey a
re re
late
d to
you
(for
exa
mpl
e: w
ife, s
on, f
riend
, etc
.).
Che
ck (
) Yes
if th
at p
erso
n bu
ys a
nd/o
r pre
pare
s fo
od w
ith y
ou.
Che
ck (
) Yes
or N
o to
indi
cate
if e
ach
pers
on a
pply
ing
is H
ispa
nic
or L
atin
o.
Ent
er Y
(Yes
) or N
(No)
for e
ach
race
*.
Rac
e/E
thni
c co
des:
I – N
ativ
e A
mer
ican
or A
lask
an N
ativ
e, A
– A
sian
, B –
Bla
ck o
r Afri
can
Am
eric
an, P
– N
ativ
e H
awai
ian
or P
acifi
c Is
land
er,
W –
Whi
te
U –
Unk
now
n (M
A O
NL
Y)
*The
se a
nsw
ers
are
optio
nal b
ut, i
f not
com
plet
ed, t
he in
terv
iew
er m
ay h
ave
to r
ecor
d th
em b
y ob
serv
atio
n. T
his
info
rmat
ion
will
not a
ffect
yo
ur e
ligib
ility
.

LDSS
-482
6A (R
ev. 8
/12)
P
age
3
SEC
TIO
N 4
: Ans
wer
all
ques
tions
in s
ectio
n 4.
Fill
in n
ames
of i
ndiv
idua
ls w
ho a
re n
ot U
.S. c
itize
ns.
SEC
TIO
N 5
: IN
CO
ME:
Lis
t all
your
inco
me
and
the
inco
me
of e
very
one
livin
g w
ith y
ou. P
RIN
T th
e na
me
of th
e pe
rson
rece
ivin
g th
e in
com
e,
the
sour
ce o
f inc
ome
and
how
ofte
n it
is re
ceiv
ed. I
ncom
e ca
n in
clud
e: R
egul
ar jo
b (w
ages
), in
com
e be
fore
stri
ke, o
n-th
e-jo
b-tra
inin
g, m
ilitar
y re
serv
es,
natio
nal g
uard
, w
ork
stud
y, a
limon
y, c
hild
sup
port,
edu
catio
nal a
ssis
tanc
e (g
rant
s, s
chol
arsh
ips,
etc
.), f
riend
s or
rel
ativ
es (
othe
r th
an lo
ans)
, tem
pora
ry a
ssis
tanc
e, p
ensi
ons
or r
etire
men
t, S
uppl
emen
tal S
ecur
ity In
com
e (S
SI),
Soc
ial S
ecur
ity b
enef
its, v
eter
ans
bene
fits,
u
nem
plo
ym
en
t b
enefits
, w
ork
er’s c
om
pen
sa
tio
n,
ba
bysittin
g,
taxi d
rivin
g,
cle
an
ing h
om
es o
r o
the
r b
uild
ings,
farm
ing/r
an
ch
ing, i
ncom
e fro
m a
ro
omer
, inc
ome
from
a b
oard
er o
r arts
and
cra
fts.
NO
TE
: Fos
ter C
are
Pay
men
ts a
nd S
NA
P –
You
may
cho
ose
to in
clud
e th
e fo
ster
car
e ch
ild o
r adu
lt in
the
SN
AP
hou
seho
ld. I
f you
do,
any
as
soci
ated
fost
er c
are
paym
ents
will
be c
ount
ed a
s in
com
e. A
ll ot
her i
ncom
e or
reso
urce
s of
the
fost
er c
are
child
als
o w
ill be
cou
nted
. If
you
have
any
que
stio
ns a
bout
this
, mak
e su
re to
ask
you
r wor
ker.
Be
sure
to a
nsw
er a
ll ot
her q
uest
ions
in s
ectio
n 5.
SE
CTI
ON
6:
RES
OU
RC
ES:
Res
ourc
es d
o no
t af
fect
the
elig
ibilit
y of
mos
t ho
useh
olds
app
lyin
g fo
r S
NA
P. H
owev
er,
som
e re
sour
ce
info
rmat
ion
is u
sed
to d
eter
min
e if
you
qual
ify fo
r exp
edite
d pr
oces
sing
of y
our a
pplic
atio
n.
Ans
wer
all
the
ques
tions
in S
ectio
n 6
for y
ours
elf a
nd e
very
one
who
is a
pply
ing
for S
NA
P. L
ist t
he d
olla
r ($)
am
ount
or v
alue
and
the
nam
e of
th
e pe
rson
who
has
the
reso
urce
. Be
sure
to li
st a
ny jo
int h
oldi
ngs.
Res
ourc
es m
ay in
clud
e an
y of
the
follo
win
g: c
ash
on h
and,
cas
h he
ld
by o
ther
s, c
heck
ing
or s
avin
gs a
ccou
nt,
savi
ngs
bond
s, i
ndiv
idua
l re
tirem
ent
acco
unt,
pens
ion
plan
, in
divi
dual
dev
elop
men
t ac
coun
t, st
ocks
/bon
ds, m
utua
l fun
ds, t
rust
fund
, mon
ey m
arke
t cer
tific
ates
, bui
ldin
gs, l
and,
rent
al p
rope
rty, v
acat
ion
or re
crea
tiona
l pro
perty
or h
ouse
ot
her t
han
hom
e.
SEC
TIO
N 7
: LIV
ING
AR
RA
NG
EMEN
TS A
ND
EXP
ENSE
S:
PR
INT
the
amou
nt y
ou p
ay fo
r re
nt, m
ortg
age,
roo
m a
nd b
oard
or
othe
r ho
usin
g. L
ist t
he d
olla
r ($
) am
ount
that
you
pay
for
your
pro
perty
ta
xe
s a
nd h
om
eo
wn
er’s in
su
ran
ce
(in
clu
din
g fire
in
su
ran
ce
).
If yo
u pa
y fo
r you
r hea
t sep
arat
ely,
che
ck (
) wha
t typ
e of
hea
t you
hav
e.
A
lso,
indi
cate
if:
yo
u pa
y fo
r ot
her
utilit
ies
sepa
rate
ly fr
om y
our
rent
/mor
tgag
e, h
ave
tele
phon
e co
sts
or a
ir co
nditi
onin
g co
sts
and
if yo
u do
, w
ho p
ays
the
sepa
rate
exp
ense
?
anyo
ne p
ays
cour
t-ord
ered
chi
ld s
uppo
rt an
d if
so, w
ho, h
ow m
uch
and
the
frequ
ency
of p
aym
ents
?
anyo
ne a
pply
ing
has
any
med
ical
bills
suc
h as
in-h
ome
nurs
ing
serv
ice,
den
ture
s, h
earin
g ai
d, e
yegl
asse
s, s
eein
g ey
e do
g or
ser
vice
an
imal
, he
alth
insu
ranc
e an
d m
edic
al p
aym
ents
, ho
spita
l or
nurs
ing
care
, m
edic
al o
r de
ntal
ser
vice
s, p
resc
riptio
n dr
ugs
or m
edic
al
trans
porta
tion?
anyo
ne in
you
r hou
seho
ld is
on
Med
icai
d, w
ith a
spe
ndow
n an
d if
so, w
ho a
nd h
ow m
uch?
anyo
ne in
you
r hou
seho
ld is
enr
olle
d in
sch
ool o
r in
a tra
inin
g pr
ogra
m a
nd if
so,
who
and
whe
re?
Be
sure
to a
nsw
er a
ll ot
her q
uest
ions
in s
ectio
n 7.

LDSS
-482
6A (R
ev. 8
/12)
P
age
4
SEC
TIO
N 8
: LEG
AL S
TATE
MEN
TS:
Rea
d th
is s
ectio
n ca
refu
lly o
r hav
e so
meo
ne re
ad it
to y
ou.
For
Life
line,
SN
AP a
pplic
ants
/reci
pien
ts m
ust
chec
k (
) th
e bo
x if
you
do
no
t au
thor
ize
the
NYS
Offi
ce o
f Te
mpo
rary
and
Dis
abilit
y A
ssis
tanc
e to
pos
sibl
y di
sclo
se y
our n
ame
and
addr
ess
to y
our
tele
phon
e se
rvic
e pr
ovid
er. Y
our
tele
phon
e se
rvic
e pr
ovid
er m
ay o
r m
ay
not u
se th
is in
form
atio
n to
enr
oll y
ou in
thei
r Life
line
Ser
vice
for a
dis
coun
ted
tele
phon
e ra
te. L
ifelin
e is
the
low
est r
ate
avai
labl
e fo
r bas
ic
tele
phon
e se
rvic
e fro
m te
leph
one
serv
ice
prov
ider
s.
No
te:
NY
Sta
te L
aw p
rovi
des
for f
ine
or ja
il, o
r bot
h, fo
r a p
erso
n fo
und
guilt
y of
obt
aini
ng S
NA
P b
y hi
ding
the
fact
s or
not
tellin
g th
e tru
th.
SEC
TIO
N 9
: SN
AP A
UTH
OR
IZED
REP
RES
ENTA
TIVE
: If
you
wan
t som
eone
from
out
side
you
r ho
useh
old
to g
et th
e S
NA
P b
enef
its o
r to
bu
y th
e fo
od fo
r you
, PR
INT
thei
r nam
e, a
ddre
ss a
nd p
hone
num
ber.
SEC
TIO
N 1
0: S
IGN
ATU
RES
: S
ign
your
nam
e. If
you
are
an
Auth
oriz
ed R
epre
sent
ativ
e, b
oth
you
and
the
head
of h
ouse
hold
mus
t sig
n an
d da
te th
e si
gnat
ure
sect
ions
on
page
5 o
f the
App
licat
ion/
Rec
ertif
icat
ion.
W
hen
an A
utho
rized
Rep
rese
ntat
ive
is a
pply
ing
on b
ehal
f of a
SN
AP
Hou
seho
ld th
at d
oes
not r
esid
e in
an
inst
itutio
n, b
oth
the
Aut
horiz
ed
Rep
rese
ntat
ive
and
the
Hea
d of
Hou
seho
ld o
r ano
ther
resp
onsi
ble
adul
t mem
ber o
f the
hou
seho
ld m
ust s
ign
and
date
the
sign
atur
e se
ctio
ns
on P
age
5 of
the
App
licat
ion/
Rec
ertif
icat
ion.
SE
CTI
ON
11:
AD
DIT
ION
AL
INFO
RM
ATI
ON
: U
se th
is s
ectio
n to
let u
s kn
ow a
dditi
onal
info
rmat
ion
that
you
thin
k w
e m
ight
nee
d to
kno
w.
SEC
TIO
N 1
2: C
ON
SEN
T TO
WIT
HD
RAW
: If
you
dec
ide
you
no lo
nger
wis
h to
app
ly fo
r S
NA
P, s
ign
your
nam
e an
d en
ter
date
. You
may
re
appl
y at
any
tim
e.
No
te:
The
last
pag
e of
this
app
licat
ion
is a
n ap
plic
atio
n to
reg
iste
r to
vot
e. If
you
wou
ld li
ke h
elp
fillin
g ou
t the
vot
er r
egis
trat
ion
appl
icat
ion
form
, ask
you
r w
orke
r. A
pply
ing
or d
eclin
ing
to r
egis
ter
to v
ote
will
not
affe
ct y
our
elig
ibili
ty o
r th
e am
ount
of
assi
stan
ce th
at y
ou w
ill b
e gi
ven
by th
is a
genc
y.
Info
rmat
ion
from
you
r ap
plic
atio
n an
d in
terv
iew
will
be
ente
red
and
stor
ed in
the
Wel
fare
Man
agem
ent
Sys
tem
(W
MS
), a
stat
ewid
e co
mpu
ter
syst
em.
This
sys
tem
is u
sed
to im
prov
e th
e m
anag
emen
t of
Soc
ial
Ser
vice
s P
rogr
ams
and
to d
eter
fra
ud.
LDSS
-482
6A (R
ev. 8
/12)
P
age
5
R
EAD
TH
E IM
POR
TAN
T IN
FOR
MA
TIO
N B
ELO
W
APP
LIC
AN
T/R
ECIP
IEN
T R
IGH
TS A
ND
RES
PON
SIB
ILIT
IES
FOR
SN
AP
A
dditi
onal
info
rmat
ion
rega
rdin
g yo
ur ri
ghts
and
resp
onsi
bilit
ies
is c
onta
ined
in th
e C
lient
Info
rmat
ion
Boo
ks (L
DSS
-414
8A; L
DSS
-41
48B
and
LD
SS-4
148C
). T
hese
boo
ks c
an b
e ob
tain
ed a
t you
r soc
ial s
ervi
ces
dist
rict.
AS
AN
AP
PL
ICA
NT
/RE
CIP
IEN
T O
F S
NA
P Y
OU
HA
VE
RIG
HT
S:
TO
HA
VE
AN
IN
TE
RV
IEW
:
Th
e in
terv
iew
mus
t be
sche
dule
d as
pro
mpt
ly a
s po
ssib
le in
ord
er to
det
erm
ine
elig
ibilit
y an
d to
issu
e be
nefit
s w
ithin
30
days
of a
pplic
atio
n fil
ing.
You
may
brin
g so
meo
ne to
you
r int
ervi
ew to
inte
rpre
t for
you
. If y
ou n
eed
an in
terp
rete
r, th
e ag
ency
will
arra
nge
for o
ne. Y
ou c
anno
t be
deni
ed
acce
ss to
ser
vice
s be
caus
e yo
u ar
e no
t flu
ent i
n En
glis
h or
hea
ring
or s
peec
h im
paire
d.
Soci
al S
ervi
ces
dist
ricts
may
util
ize
the
TTY/
TTD
rela
y sy
stem
s to
gai
n ac
cess
to s
ervi
ces
for H
earin
g or
spe
ech
impa
ired
appl
ican
ts/re
cipi
ents
. If
you
have
any
spe
cial
nee
ds y
ou c
an re
ques
t spe
cial
acc
omm
odat
ions
from
you
r soc
ial s
ervi
ces
dist
rict.
If
you
have
a d
isab
ility,
you
hav
e th
e sa
me
right
to a
cces
s an
d be
inte
rvie
wed
for S
NAP
as
som
eone
who
doe
s no
t hav
e a
disa
bilit
y.
Yo
u m
ust b
e to
ld, w
ithin
30
days
of t
he d
ate
you
turn
ed in
(file
d) y
our
Appl
icat
ion
for
SNAP
, if y
our
Appl
icat
ion
is a
ppro
ved
or d
enie
d. I
f you
are
el
igib
le fo
r exp
edite
d pr
oces
sing
you
mus
t be
told
with
in 5
day
s af
ter t
he d
ate
you
turn
ed in
(file
d) y
our A
pplic
atio
n if
you
are
qual
ified
for S
NAP
.
You
may
requ
est t
hat t
he in
-offi
ce in
terv
iew
be
wai
ved
in h
ards
hip
situ
atio
ns. H
ards
hip
gene
rally
incl
udes
, but
is n
ot li
mite
d to
, illn
ess,
tra
nspo
rtatio
n di
fficu
lties
, car
e of
a h
ouse
hold
mem
ber,
hard
ship
due
to re
side
ncy
in a
rura
l are
a, p
rolo
nged
sev
ere
wea
ther
, or w
ork
or tr
aini
ng
hou
rs t
hat p
reve
nt yo
u f
rom
com
ing
in
during
th
e s
ocia
l se
rvic
es d
istr
ict’s o
ffic
e h
ours
. Th
e in
-offi
ce in
terv
iew
will
be
wai
ved,
at y
our r
eque
st, i
f al
l the
adu
lt m
embe
rs o
f you
r hou
seho
ld a
re e
lder
ly o
r dis
able
d w
ith n
o ea
rned
inco
me.
The
age
ncy
may
wai
ve th
e in
-offi
ce in
terv
iew
in
favo
r of a
tele
phon
e in
terv
iew
or s
ched
uled
hom
e vi
sit.
In-p
erso
n in
terv
iew
s m
ay b
e sc
hedu
led
in a
dvan
ce a
t any
mut
ually
acc
epta
ble
loca
tion
incl
udin
g a
ho
useh
old
’s r
esid
en
ce.
G
et a
writ
ten
notic
e te
lling
you
if yo
ur a
pplic
atio
n fo
r SN
AP is
app
rove
d or
den
ied:
--
I
f you
r App
licat
ion
is a
ppro
ved,
this
not
ice
will
tell
you
the
amou
nt o
f SN
AP b
enef
its y
ou w
ill ge
t;
--
If
your
App
licat
ion
is d
enie
d, th
is n
otic
e w
ill te
ll yo
u w
hy a
nd w
hat y
ou s
houl
d do
if y
ou d
isag
ree
or d
o no
t und
erst
and
this
dec
isio
n.
TO A
CO
NFE
REN
CE
AN
D/O
R F
AIR
HEA
RIN
G
If yo
u th
ink
any
deci
sion
abo
ut y
our c
ase
is w
rong
, or y
ou d
o no
t und
erst
and
any
deci
sion
, tal
k to
you
r wor
ker r
ight
aw
ay.
If yo
u st
ill di
sagr
ee o
r do
not
unde
rsta
nd, y
ou h
ave
the
right
to a
Con
fere
nce
and/
or a
Fai
r Hea
ring.
C
ON
FER
ENC
E - A
Con
fere
nce
is w
hen
you
mee
t with
som
eone
oth
er th
an th
e pe
rson
who
mad
e th
e de
cisi
on a
bout
you
r cas
e. A
t the
Con
fere
nce
this
per
son
will
revi
ew th
at d
ecis
ion.
Som
etim
es a
Con
fere
nce
is th
e fa
stes
t way
to s
olve
any
pro
blem
s yo
u m
ay h
ave.
We
enco
urag
e yo
u to
ask
for
one
even
if y
ou h
ave
requ
este
d a
Fair
Hea
ring.
H
owev
er, C
onfe
renc
es a
re v
olun
tary
, and
you
can
requ
est a
Fai
r Hea
ring
even
if y
ou d
o no
t re
ques
t a C
onfe
renc
e. T
o as
k fo
r a C
onfe
renc
e, c
all o
r writ
e yo
ur s
ocia
l ser
vice
s di
stric
t. A
CO
NFE
REN
CE
IS N
OT
A FA
IR H
EAR
ING
. If y
ou a
re to
ld th
at y
our c
ase
is b
eing
clo
sed,
or t
hat y
our S
NAP
ben
efits
or o
ther
hel
p yo
u ar
e ge
tting
w
ill ch
ange
, and
the
prob
lem
is n
ot s
ettle
d th
roug
h a
Con
fere
nce,
you
mus
t ask
for a
Fai
r Hea
ring
to k
eep
your
SN
AP b
enef
its o
r oth
er h
elp
you
are
getti
ng fr
om b
eing
sto
pped
or c
hang
ed.
Yo
ur
tim
e t
o r
eq
uest
a f
air h
earin
g a
nd
yo
ur
rig
ht to
“a
id to c
ontin
ue
” w
ill n
ot
be e
xte
nd
ed
by r
eq
uestin
g o
r ha
ving
a c
onfe
renc
e.
NO
TE:
A re
ques
t for
a C
onfe
renc
e is
not
a re
ques
t for
a F
air H
earin
g. If
you
wan
t a F
air H
earin
g, y
ou m
ust r
eque
st o
ne.

LDSS
-482
6A (R
ev. 8
/12)
P
age
6
REA
D T
HE
IMPO
RTA
NT
INFO
RM
ATI
ON
BEL
OW
(cont’d)
FA
IR H
EAR
ING
- A
Fair
Hea
ring
is a
cha
nce
for y
ou to
tell
an A
dmin
istra
tive
Law
Jud
ge fr
om th
e N
ew Y
ork
Stat
e O
ffice
of T
empo
rary
and
Dis
abili
ty
Assi
stan
ce w
hy y
ou th
ink
the
deci
sion
abo
ut y
our c
ase
was
wro
ng. T
he S
tate
will
then
issu
e a
writ
ten
deci
sion
whi
ch w
ill st
ate
whe
ther
the
soci
al
serv
ices
dis
tric
t’s d
ecis
ion
was
righ
t or w
rong
. The
writ
ten
deci
sion
may
ord
er th
e so
cial
ser
vice
s di
stric
t to
corr
ect y
our c
ase.
At
a F
air H
earin
g yo
u w
ill h
ave
a ch
ance
to e
xpla
in w
hy y
ou th
ink
the
deci
sion
is w
rong
.
TIM
E LI
MIT
S TO
ASK
FO
R A
FAI
R H
EAR
ING
- If
you
wan
t to
ask
for a
Fai
r Hea
ring
for S
NAP
, cal
l rig
ht a
way
bec
ause
ther
e ar
e tim
e lim
its. I
f you
w
ait t
oo lo
ng, y
ou m
ay n
ot b
e ab
le to
get
a F
air H
earin
g.
NO
TE:
If yo
ur s
ituat
ion
is v
ery
serio
us, t
he N
ew Y
ork
Stat
e O
ffice
of T
empo
rary
and
Dis
abilit
y As
sist
ance
will
set u
p a
Fair
Hea
ring
for y
ou a
s so
on a
s po
ssib
le. W
hen
you
call
or w
rite
for a
Fai
r Hea
ring,
be
sure
to e
xpla
in th
at y
our s
ituat
ion
is v
ery
serio
us.
If
you
do g
et a
not
ice
abou
t you
r cas
e an
d yo
u w
ant t
o as
k fo
r a F
air H
earin
g, th
e no
tice
will
tell
you
how
muc
h tim
e yo
u ha
ve to
ask
for t
he F
air
Hea
ring.
Be
sure
to re
ad a
ll of
the
notic
e ca
refu
lly.
If yo
ur n
otic
e te
lls y
ou th
at y
our S
NAP
ben
efits
hav
e be
en d
enie
d, w
ill b
e st
oppe
d or
will
be
redu
ced,
you
may
ask
for a
Fai
r Hea
ring
with
in
90 d
ays
from
the
date
of t
he n
otic
e. Y
ou m
ay a
sk fo
r a F
air H
earin
g if
you
thin
k yo
u ar
e no
t get
ting
enou
gh S
NA
P be
nefit
s at
any
time
with
in
the
cert
ifica
tion
perio
d.
If yo
u do
not
get
a n
otic
e ab
out y
our c
ase,
and
you
r ben
efits
are
den
ied,
sto
pped
or r
educ
ed y
ou c
an a
lso
ask
for a
Fai
r Hea
ring.
H
OW
TO
AS
K F
OR
A F
AIR
HE
AR
ING
If
you
do g
et a
not
ice
abou
t you
r cas
e an
d yo
u w
ant t
o as
k fo
r a F
air H
earin
g, th
e no
tice
will
tell
you
how
. Be
sure
to re
ad a
ll of
the
notic
e ca
refu
lly.
If yo
u ge
t a n
otic
e te
lling
you
that
you
r ben
efits
will
be s
topp
ed o
r red
uced
, and
you
ask
for a
Fai
r Hea
ring
befo
re th
e ef
fect
ive
date
on
your
not
ice,
yo
ur m
oney
or o
ther
hel
p w
ill, in
mos
t ins
tanc
es, s
tay
the
sam
e ("
aid
cont
inui
ng")
unt
il th
e Fa
ir H
earin
g de
cisi
on is
mad
e. If
the
notic
e w
as n
ot s
ent
befo
re th
e ef
fect
ive
date
, and
you
ask
for a
Fai
r Hea
ring
with
in 1
0 da
ys o
f the
pos
tmar
k da
te o
f the
not
ice,
you
als
o ha
ve th
e rig
ht to
hav
e yo
ur m
oney
or
oth
er h
elp
stay
the
sam
e ("
aid
cont
inui
ng")
unt
il th
e Fa
ir H
earin
g de
cisi
on is
mad
e.
How
ever
, if y
ou d
o ge
t "ai
d co
ntin
uing
" an
d yo
u lo
se th
e Fa
ir H
earin
g, y
ou w
ill ha
ve to
pay
bac
k an
y be
ne
fits
th
at yo
u r
ece
ive
d a
s “
aid
co
ntin
uin
g”
whi
le w
aitin
g fo
r the
Fai
r Hea
ring
deci
sion
.
If yo
u do
not
wan
t the
mon
ey o
r oth
er h
elp
you
have
bee
n ge
tting
to s
tay
the
sam
e un
til th
e Fa
ir H
earin
g de
cisi
on is
mad
e, y
ou m
ust t
ell t
his
to th
e N
ew Y
ork
Stat
e O
ffice
of T
empo
rary
and
Dis
abilit
y As
sist
ance
whe
n yo
u ca
ll or
writ
e fo
r a F
air H
earin
g.
If yo
u do
not
get
a n
otic
e ab
out y
our c
ase,
and
you
r ben
efits
are
sto
pped
or r
educ
ed, y
ou c
an s
till a
sk fo
r a F
air H
earin
g. A
t the
sam
e tim
e th
at y
ou
ask
for a
Fai
r Hea
ring,
you
can
ask
that
you
r mon
ey o
r oth
er h
elp
be re
stor
ed ("
aid
cont
inui
ng")
.

LDSS
-482
6A (R
ev. 8
/12)
P
age
7
R
EAD
TH
E IM
POR
TAN
T IN
FOR
MA
TIO
N B
ELO
W (c
ont’d)
WH
AT
YOU
SH
OU
LD D
O F
OR
A F
AIR
HEA
RIN
G
The
New
Yor
k St
ate
Offi
ce o
f Tem
pora
ry a
nd D
isab
ility
Assi
stan
ce w
ill se
nd y
ou a
not
ice,
whi
ch te
lls y
ou w
hen
and
whe
re th
e Fa
ir H
earin
g w
ill be
he
ld.
To h
elp
you
get r
eady
for t
he F
air H
earin
g, y
ou h
ave
the
right
to lo
ok a
t you
r cas
e re
cord
and
get
free
cop
ies
of th
e fo
rms
and
pape
rs w
hich
will
be
give
n to
the
Adm
inis
trativ
e La
w J
udge
at t
he F
air H
earin
g. Y
ou c
an a
lso
get f
ree
copi
es o
f any
oth
er p
aper
s in
you
r cas
e re
cord
whi
ch y
ou th
ink
you
may
nee
d fo
r the
Fai
r Hea
ring.
Usu
ally
, you
can
get
thes
e pa
pers
bef
ore
the
hear
ing
or a
t the
hea
ring
at th
e la
test
. If
you
ask
for a
ny p
aper
s, a
nd th
e so
cial
ser
vice
s di
stric
t doe
s no
t giv
e th
em to
you
bef
ore
or a
t the
hea
ring,
you
sho
uld
tell
the
Adm
inis
trativ
e La
w J
udge
abo
ut it
. Yo
u ca
n br
ing
a la
wye
r, a
rela
tive
or a
frie
nd to
the
Fair
Hea
ring
to h
elp
you
expl
ain
why
you
thin
k a
deci
sion
abo
ut y
our c
ase
is w
rong
. If y
ou c
anno
t go
to th
e Fa
ir H
earin
g, y
ou c
an s
end
som
eone
els
e in
you
r pla
ce. I
f you
are
sen
ding
som
eone
who
is n
ot a
law
yer t
o th
e Fa
ir H
earin
g, y
ou s
houl
d gi
ve
this
per
son
a le
tter t
o gi
ve to
the
Adm
inis
trativ
e La
w J
udge
. Thi
s le
tter s
houl
d te
ll th
e Ju
dge
that
this
per
son
is ta
king
you
r pla
ce.
To h
elp
you
expl
ain
at th
e Fa
ir H
earin
g w
hy y
ou th
ink
the
deci
sion
is w
rong
, you
sho
uld
also
brin
g an
y w
itnes
ses
who
can
hel
p yo
u an
d an
y in
form
atio
n yo
u ha
ve s
uch
as:
Pay
stub
s
Bill
s
R
ecei
pts
Le
ases
Do
cto
r’s S
tate
me
nts
So
meo
ne fr
om th
e so
cial
ser
vice
s di
stric
t will
also
be
at th
e Fa
ir H
earin
g to
exp
lain
the
deci
sion
abo
ut y
our c
ase.
You
or y
our r
epre
sent
ativ
e w
ill be
ab
le to
que
stio
n th
is p
erso
n an
d pr
esen
t you
r sid
e of
the
case
. You
or y
our r
epre
sent
ativ
e w
ill al
so b
e ab
le to
que
stio
n an
y w
itnes
ses
who
you
brin
g to
he
lp y
ou.
If
you
thin
k yo
u ne
ed a
law
yer t
o he
lp y
ou w
ith y
our F
air H
earin
g, y
ou m
ay b
e ab
le to
get
a la
wye
r at n
o co
st to
you
by
calli
ng y
our l
ocal
Leg
al A
id o
r Le
gal S
ervi
ces
Offi
ce. F
or th
e na
mes
of o
ther
law
yers
, cal
l you
r loc
al B
ar A
ssoc
iatio
n.
NO
TE:
If yo
u as
k, y
ou w
ill be
abl
e to
get
bac
k th
e m
oney
you
had
to p
ay fo
r pub
lic tr
ansp
orta
tion,
chi
ld c
are
and
othe
r nec
essa
ry e
xpen
ses
to
go to
the
fair
hear
ing.
If n
o pu
blic
tran
spor
tatio
n is
ava
ilabl
e, y
ou m
ay b
e ab
le to
get
bac
k th
e m
oney
you
had
to p
ay fo
r ano
ther
type
of
trans
porta
tion.
If y
ou a
re u
nabl
e to
use
pub
lic tr
ansp
orta
tion
beca
use
of a
med
ical
pro
blem
, you
may
be
able
to g
et b
ack
the
mon
ey y
ou
had
to p
ay fo
r ano
ther
type
of t
rans
porta
tion.
How
ever
, you
may
be
aske
d to
pro
vide
med
ical
ver
ifica
tion.
If yo
u liv
e an
ywhe
re in
New
Yor
k St
ate,
you
may
requ
est a
Fai
r Hea
ring
by te
leph
one,
fax,
onl
ine,
or b
y w
ritin
g to
th
e ad
dres
s be
low
.
Tele
phon
e: S
tate
wid
e to
ll fre
e re
ques
t num
ber i
s 80
0-34
2-33
34.
Plea
se h
ave
the
notic
e, if
any
, with
you
whe
n yo
u ca
ll.
Fax:
you
r Fai
r Hea
ring
Req
uest
to:
518-
473-
6735
O
nlin
e: C
ompl
ete
onlin
e re
ques
t for
m a
t http
://w
ww
.otd
a.st
ate.
ny.u
s.us
/oah
/form
s.as
p

LDSS
-482
6A (R
ev. 8
/12)
P
age
8
REA
D T
HE
IMPO
RTA
NT
INFO
RM
ATI
ON
BEL
OW
(cont’d)
In
writ
ing:
For
not
ices
, fill
in th
e su
pplie
d sp
ace
and
send
a c
opy
of th
e no
tice,
or w
rite
to:
Fa
ir H
earin
g Se
ctio
n N
YS O
ffice
of T
empo
rary
and
Dis
abili
ty A
ssis
tanc
e Fa
ir H
earin
gs
P.
O. B
ox 1
930
Alb
any,
New
Yor
k 12
201-
1930
P
lease
ke
ep
a c
opy o
f a
ny n
otice f
or
yo
urs
elf
If yo
u liv
e in
New
Yor
k C
ity y
ou m
ay a
lso
mak
e yo
ur re
ques
t in
pers
on b
y w
alki
ng in
to th
e of
fice
liste
d be
low
. W
alk-
In (N
ew Y
ork
City
Onl
y)
Brin
g a
copy
of t
he n
otic
e, o
r ask
for a
hea
ring
on a
mat
ter n
ot b
ased
on
a no
tice,
to:
O
ffice
of A
dmin
istr
ativ
e H
earin
gs
Offi
ce o
f Tem
pora
ry &
Dis
abili
ty A
ssis
tanc
e
14 B
oeru
m P
lace
B
rook
lyn,
New
Yor
k
NO
TE:
For N
ew Y
ork
City
em
erge
ncy
fair
hear
ings
onl
y – C
all 8
00-2
05-0
110.
Do
not u
se th
is te
leph
one
num
ber f
or a
nyth
ing
exce
pt
emer
genc
ies.
Req
uest
s th
at d
o no
t inv
olve
em
erge
ncie
s w
ill no
t be
take
n at
this
num
ber.
TO
LO
OK
AT
YO
UR
CA
SE
AN
D C
OM
PU
TE
R R
EC
OR
DS
: O
nce
you
appl
y fo
r SN
AP o
r oth
er h
elp,
cas
e re
cord
s an
d co
mpu
ter r
ecor
ds a
re k
ept a
bout
you
r cas
e. U
sual
ly, y
ou h
ave
the
right
to lo
ok a
t tho
se re
cord
s.
How
ever
, you
may
not
be
able
to lo
ok a
t all
of th
e re
cord
s. Y
our w
orke
r can
exp
lain
the
rule
s to
you
.
Whe
n yo
u w
rite
for c
opie
s of
you
r com
pute
r rec
ords
, the
Per
sona
l Priv
acy
Prot
ectio
n La
w re
quire
s th
at N
ew Y
ork
Stat
e ag
enci
es, s
end
you
your
reco
rds;
or
tell
you
why
they
will
not g
ive
you
your
reco
rds;
or
tell
you
they
hav
e yo
ur re
ques
t and
they
will
det
erm
ine
if yo
u ar
e al
low
ed to
get
you
r rec
ords
with
in
five
wor
king
day
s of
whe
n th
ey g
et y
our r
eque
st le
tter.
R
EG
AR
DIN
G E
MP
LO
YM
EN
T:
If yo
u do
not
agr
ee th
at y
ou a
re a
ble
to w
ork,
you
sho
uld
notif
y th
e so
cial
ser
vice
s di
stric
t tha
t you
bel
ieve
you
sho
uld
be e
xem
pt fr
om p
artic
ipat
ion
in
wor
k ac
tiviti
es.
You
will
be n
otifi
ed o
f the
soc
ial s
ervi
ces
dis
tric
t’s d
eter
min
atio
n re
gard
ing
your
cla
im.
If th
e so
cial
ser
vice
s di
stric
t dis
agre
es w
ith y
ou,
you
may
requ
est a
fair
hear
ing
to te
ll an
Adm
inis
trativ
e La
w J
udge
why
you
thin
k yo
u ar
e no
t abl
e to
wor
k.
If yo
u ar
e re
quire
d to
par
ticip
ate
in S
NAP
wor
k ac
tiviti
es, y
ou m
ay b
e ab
le to
get
hel
p pa
ying
for c
erta
in w
ork-
rela
ted
expe
nses
. Yo
u al
so m
ay b
e ab
le
to re
ceiv
e as
sist
ance
with
chi
ld c
are
cost
s.
IF Y
OU
AR
E SU
SPEC
TED
OF
FRAU
D
If yo
u fin
d ou
t tha
t you
are
bei
ng in
vest
igat
ed b
ecau
se y
our w
orke
r thi
nks
you
did
not t
ell t
he tr
uth
abou
t you
r cas
e, y
ou s
houl
d ta
lk to
a la
wye
r. If
you
are
char
ged
with
wel
fare
frau
d in
crim
inal
cou
rt, th
e co
urt w
ill, if
you
are
elig
ible
, ass
ign
a la
wye
r to
repr
esen
t you
at n
o co
st.

LDSS
-482
6A (R
ev. 8
/12)
P
age
9
REA
D T
HE
IMPO
RTA
NT
INFO
RM
ATI
ON
BEL
OW
(cont’d)
AS
AN
AP
PL
ICA
NT
/RE
CIP
IEN
T O
F S
NA
P Y
OU
HA
VE
SE
VE
RA
L R
ES
PO
NS
IBIL
ITIE
S:
EM
PL
OY
ME
NT
RE
SP
ON
SIB
ILIT
IES
FO
R S
NA
P R
EC
IPIE
NT
S:
Unl
ess
you
are
exem
pt fr
om w
ork
requ
irem
ents
as
an a
pplic
ant f
or o
r rec
ipie
nt o
f SN
AP y
ou m
ust c
ompl
y w
ith c
erta
in ru
les,
incl
udin
g pa
rtici
patio
n in
w
ork
activ
ities
and
acc
eptin
g a
job.
You
r wor
ker w
ill ex
plai
n th
ese
rule
s.
If
you
do n
ot c
ompl
y w
ith th
e w
ork
requ
irem
ents
, you
may
lose
you
r SN
AP
bene
fits.
Th
ere
are
seve
ral e
xem
ptio
ns fr
om p
artic
ipat
ion
in S
NAP
wor
k re
quire
men
ts.
Ask
your
wor
ker i
f you
qua
lify
for o
ne o
f the
exe
mpt
ions
. Yo
u m
ay b
e re
quire
d to
pro
vide
doc
umen
tatio
n to
sup
port
your
cla
im.
If yo
u ar
e no
t exe
mpt
from
par
ticip
atio
n in
wor
k ac
tiviti
es a
nd d
o no
t com
ply
with
the
wor
k re
quire
men
ts, y
ou m
ay lo
se y
our S
NAP
ben
efits
. The
leng
th
of ti
me
you
will
lose
you
r ben
efits
dep
ends
on
the
num
ber o
f tim
es y
ou h
ave
faile
d to
com
ply.
AD
DIT
ION
AL
RE
SP
ON
SIB
ILIT
IES
AN
D R
EQ
UIR
EM
EN
TS
FO
R S
NA
P R
EC
IPIE
NT
S W
HO
AR
E A
BL
E-B
OD
IED
AD
UL
TS
WIT
HO
UT
DE
PE
ND
EN
TS
(A
BA
WD
S)
If yo
u ar
e an
abl
e-bo
died
wor
k re
gist
rant
, you
may
als
o be
req
uire
d to
mee
t add
ition
al S
NAP
elig
ibilit
y re
quire
men
ts.
Your
wor
ker
will
expl
ain
thes
e re
quire
men
ts a
nd th
e ex
empt
ions
from
the
requ
irem
ents
.
If yo
u ar
e a
wor
k re
gist
rant
and
not
exe
mpt
, you
will
only
be
elig
ible
to r
ecei
ve S
NA
P be
nefit
s fo
r th
ree
mon
ths
in e
very
36
mon
ths
unle
ss y
ou a
re
mee
ting
the
addi
tiona
l req
uire
men
ts.
If
you
wan
t to
cont
inue
to re
ceiv
e SN
AP b
enef
its b
eyon
d th
e th
ree
mon
th li
mit,
you
sho
uld
ask
your
wor
ker f
or a
qua
lifyi
ng w
ork
or tr
aini
ng o
ppor
tuni
ty.
If
you
lose
you
r el
igib
ility
for
SNAP
bec
ause
you
did
not
mee
t the
add
ition
al r
equi
rem
ent f
or th
ree
or m
ore
mon
ths
durin
g w
hich
you
rec
eive
d S
NAP
be
nefit
s, y
ou m
ay b
e ab
le to
re-e
stab
lish
your
elig
ibilit
y in
sev
eral
diff
eren
t way
s. Y
our w
orke
r will
expl
ain
how
to d
o th
is.
RES
PON
SIB
ILIT
Y TO
RES
CH
EDU
LE A
MIS
SED
INTE
RVI
EW:
As a
n Ap
plic
ant/R
ecip
ient
of S
NAP
, you
hav
e th
e re
spon
sibi
lity
of re
sche
dulin
g a
mis
sed
inte
rvie
w b
efor
e th
e 30
th d
ay a
fter t
he d
ate
you
appl
ied
to a
void
lo
sing
SN
AP.
RES
PON
SIB
ILIT
Y TO
PR
OVI
DE
PRO
OF
W
hen
you
are
appl
ying
for
or g
ettin
g he
lp, y
ou w
ill be
ask
ed to
pro
vide
pro
of o
f cer
tain
thin
gs. Y
our
wor
ker
will
tell
you
whi
ch o
f the
se th
ings
you
mus
t pr
ove.
Not
all
of th
ese
thin
gs a
re re
quire
d fo
r eve
ry p
rogr
am.
You
may
hav
e to
pro
ve s
ome
thin
gs fo
r one
pro
gram
and
not
for a
noth
er.
If yo
u br
ing
proo
f with
you
whe
n yo
u fir
st c
ome
in to
app
ly fo
r ass
ista
nce,
you
may
be
able
to g
et h
elp
soon
er.
If yo
u dr
op d
ocum
enta
tion
off a
t the
soc
ial s
ervi
ces
dist
rict,
you
shou
ld a
sk fo
r a re
ceip
t to
prov
e w
hat d
ocum
enta
tion
you
left.
The
rece
ipt s
houl
d ha
ve
your
nam
e, th
e sp
ecifi
c do
cum
enta
tion
that
you
dro
pped
off,
the
time,
dat
e, d
istri
ct n
ame
and
the
nam
e of
the
soci
al s
ervi
ces
wor
ker w
ho p
rovi
ded
the
rece
ipt.

LDSS
-482
6A (R
ev. 8
/12)
P
age
10
REA
D T
HE
IMPO
RTA
NT
INFO
RM
ATI
ON
BEL
OW
(cont’d)
If yo
u ca
nnot
get
the
proo
f you
nee
d, a
sk y
our w
orke
r to
help
you
. If
the
soci
al s
ervi
ces
dist
rict a
lread
y ha
s pr
oof o
f the
thin
gs th
at d
o no
t cha
nge,
suc
h as
yo
ur s
ocia
l sec
urity
num
ber,
you
do n
ot n
eed
to p
rove
them
aga
in.
If yo
ur w
orke
r tel
ls y
ou th
at y
ou n
eed
addi
tiona
l pap
ers
and
info
rmat
ion
to fi
nd o
ut if
you
can
get
hel
p, y
ou m
ust p
rovi
de th
at p
roof
. If
you
cann
ot g
et th
ese
pape
rs a
nd in
form
atio
n, y
our w
orke
r mus
t try
to h
elp
you.
N
ON
-CIT
IZE
N E
LIG
IBIL
ITY
IN
FO
RM
AT
ION
M
any
non-
citiz
ens
are
qual
ified
alie
ns w
ho a
re e
ligib
le fo
r SN
AP. E
ven
if yo
u ar
e no
t, yo
ur c
hild
ren
may
be
elig
ible
. SN
AP s
houl
d no
t affe
ct y
our
imm
igra
tion
stat
us w
ith re
spec
t to
any
USC
IS d
ecis
ion
rega
rdin
g yo
ur im
mig
ratio
n m
atte
r.
Yo
u m
ay b
e el
igib
le fo
r SN
AP if
you
are
a U
nite
d St
ates
(U.S
.) ci
tizen
, a
non-
citiz
en U
.S. n
atio
nal (
peop
le b
orn
in A
mer
ican
Sam
oa o
r Sw
ain
Isla
nd),
or
a qu
alifi
ed a
lien.
A q
ualif
ied
alie
n fo
r SN
AP e
ligib
ility
is:
1.
An
Am
eric
an In
dian
bor
n in
Can
ada
with
at l
east
50
per c
entu
m o
f blo
od o
f the
Am
eric
an In
dian
race
und
er s
ectio
n 28
9 of
the
Imm
igra
tion
and
Nat
iona
lity
Act (
INA)
, or
2.
A m
embe
r of a
n In
dian
trib
e th
at is
a fe
dera
lly re
cogn
ized
Indi
an tr
ibe
(25
U.S
.C. (
450b
(e)),
or
3.
An a
lien
adm
itted
as
a H
mon
g or
Hig
hlan
d La
otia
n, in
clud
ing
spou
se a
nd d
epen
dent
chi
ld, o
r 4.
A
refu
gee
adm
itted
und
er s
ectio
n 20
7 of
the
INA,
or
5.
An
alie
n gr
ante
d as
ylum
und
er s
ectio
n 20
8 of
the
INA,
or
6.
An a
lien
who
se d
epor
tatio
n ha
s be
en w
ithhe
ld u
nder
sec
tion
234(
h) o
f the
INA
as in
effe
ct p
rior t
o Ap
ril 1
, 199
7, o
r rem
oval
with
held
und
er
sect
ion
241(
b)(3
) of t
he IN
A, o
r 7.
An
alie
n ad
mitt
ed a
s a
Cub
an o
r Hai
tian
entra
nt, o
r
8.
An a
lien
who
is a
vic
tim o
f tra
ffick
ing
unde
r sec
tion
103(
8) o
f the
Tra
ffick
ing
Vict
ims
Prot
ectio
n A
ct, o
r
9.
An a
lien
who
is o
n ac
tive
duty
in th
e U
.S. a
rmed
forc
es o
r, an
hon
orab
ly d
isch
arge
d v
eter
an, t
heir
spou
se a
nd d
epen
dent
chi
ldre
n, a
nd th
e un
-rem
arrie
d su
rviv
ing
spou
se a
nd u
nmar
ried
depe
nden
t chi
ldre
n of
an
activ
e du
ty m
embe
r or v
eter
an w
ho h
as d
ied,
or
10.
An a
lien
adm
itted
as
an A
mer
iasi
an, o
r 11
. An
alie
n la
wfu
lly a
dmitt
ed fo
r per
man
ent r
esid
ence
und
er th
e IN
A a
nd w
ho h
as 5
yea
rs in
sta
tus,
or
12.
An a
lien
paro
led
unde
r sec
tion
212(
d)(5
) of t
he IN
A fo
r at l
east
1 y
ear a
nd w
ho h
as 5
yea
rs in
sta
tus,
or
13.
An a
lien
or p
aren
t or c
hild
of a
n al
ien
who
has
bee
n ba
ttere
d or
sub
ject
ed to
ext
rem
e cr
uelty
in th
e U
.S. b
y a
fam
ily m
embe
r and
ent
ered
th
e U
.S. b
efor
e 8/
22/9
6 or
has
5 y
ears
in s
tatu
s, o
r
14.
Alie
ns a
lso
may
be
elig
ible
for S
NAP
if:
They
are
law
fully
adm
itted
for p
erm
anen
t res
iden
ce a
nd h
ave
earn
ed, o
r can
be
cred
ited
with
40
quar
ters
of w
ork;
They
are
in
a qu
alifi
ed s
tatu
s lis
ted
abov
e an
d re
ceiv
e ce
rtain
dis
abilit
y or
blin
dnes
s be
nefit
s;
Th
ey a
re in
a q
ualif
ied
stat
us li
sted
abo
ve a
nd a
re u
nder
18
year
s ol
d;
Th
ey a
re la
wfu
lly in
the
U.S
. on
Augu
st 2
2, 1
996
and
are
now
blin
d or
dis
able
d, o
ld, o
r was
bor
n on
or b
efor
e A
ugus
t 22,
193
1.
NEW
YO
RK
STA
TE O
FFIC
E O
F TE
MP
OR
AR
Y A
ND
DIS
AB
ILIT
Y A
SS
ISTA
NC
E
SUPP
LEM
ENTA
L N
UTR
ITIO
N A
SSIS
TAN
CE
PRO
GR
AM
(S
NA
P) A
PPLI
CA
TIO
N/R
ECER
TIFI
CAT
ION
SN
AP
is
th
e n
ew
nam
e f
or
the
Fo
od
Sta
mp
Pro
gra
m
Use
th
is f
orm
if
Ap
ply
ing
Fo
r S
NA
P O
nly
If yo
u ar
e on
ly a
pply
ing
for
SNAP
you
can
use
this
sho
rter a
pplic
atio
n. If
you
wou
ld li
ke to
app
ly fo
r oth
er b
enef
its s
uch
as T
empo
rary
Ass
ista
nce,
C
hild
Car
e A
ssis
tanc
e, H
ome
Ener
gy A
ssis
tanc
e or
Med
icai
d pl
ease
ask
for a
diff
eren
t app
licat
ion.
T
his
app
lica
tion
ca
n o
nly
be u
sed t
o a
pp
ly fo
r S
NA
P.
Wh
en
Yo
u A
re A
pp
lyin
g F
or
SN
AP
Yo
u ca
n fil
e an
app
licat
ion
the
sam
e da
y yo
u re
ceiv
e it.
If y
ou a
re e
ligib
le, b
enef
its w
ill be
pro
vide
d ba
ck to
the
filin
g da
te o
f you
r app
licat
ion.
You
can
file
your
app
licat
ion
befo
re y
ou h
ave
an in
terv
iew
.
We
mus
t ac
cept
you
r ap
plic
atio
n if,
at
a m
inim
um,
it co
ntai
ns y
our
nam
e, a
ddre
ss (
if yo
u ha
ve o
ne),
and
a si
gnat
ure.
Thi
s in
form
atio
n w
ill es
tabl
ish
your
ap
plic
atio
n fil
ing
date
. How
ever
, the
app
licat
ion
proc
ess,
incl
udin
g th
e in
terv
iew
and
a s
igna
ture
on
page
5 o
f the
app
licat
ion/
rece
rtific
atio
n m
ust b
e co
mpl
eted
fo
r us
to d
eter
min
e yo
ur e
ligib
ility.
You
can
appl
y fo
r and
get
SN
AP
for e
ligib
le h
ouse
hold
mem
ber(
s) e
ven
if yo
u or
som
e ot
her m
embe
rs o
f you
r hou
seho
ld a
re n
ot e
ligib
le fo
r ben
efits
bec
ause
of
imm
igra
tion
stat
us. F
or e
xam
ple,
inel
igib
le a
lien
pare
nts
can
appl
y fo
r SN
AP
for t
heir
child
ren
and
rece
ive
bene
fits
for t
heir
elig
ible
chi
ldre
n.
Yo
u ca
n st
ill ap
ply
and
be e
ligib
le fo
r SN
AP
even
if y
ou h
ave
reac
hed
your
Tem
pora
ry A
ssis
tanc
e tim
e lim
its.
Ne
ed
SN
AP
Ben
efi
ts R
igh
t A
wa
y?
Yo
u M
ay
Be
Eli
gib
le F
or
Ex
ped
ited
Pro
ces
sin
g o
f y
ou
r S
NA
P A
pp
lic
ati
on
. If
your
hou
seho
ld h
as li
ttle
or n
o in
com
e or
liqu
id re
sour
ces,
or i
f you
r ren
t and
util
ity e
xpen
ses
are
mor
e th
an y
our i
ncom
e an
d liq
uid
reso
urce
s, o
r yo
u ar
e a
mig
rant
or
seas
onal
farm
wor
ker
with
littl
e or
no
inco
me
or r
esou
rces
whe
n yo
u ap
ply,
you
may
be
qual
ified
to r
ecei
ve S
NAP
with
in 5
ca
lend
ar d
ays
afte
r the
dat
e th
at y
ou a
pply
. You
r wor
ker w
ill al
way
s re
view
you
r circ
umst
ance
s to
see
if y
ou a
re q
ualif
ied
for e
xped
ited
proc
essi
ng
of y
our S
NAP
app
licat
ion.
A p
roce
ss is
in p
lace
to is
sue
SNAP
ben
efits
to a
ll el
igib
le h
ouse
hold
s w
ho m
eet t
he s
tand
ards
for e
xped
ited
serv
ice.
W
he
re Y
ou
Can
Ap
ply
Fo
r S
NA
P
If yo
u liv
e ou
tsid
e of
New
Yor
k C
ity, c
all o
r vis
it th
e so
cial
ser
vice
s di
stric
t in
the
coun
ty w
here
you
live
and
ask
for a
n ap
plic
atio
n pa
ckag
e. Y
ou c
an
get t
he a
ddre
ss a
nd p
hone
num
ber b
y ca
lling
toll
free
1-80
0-34
2-30
09, o
r app
ly o
n-lin
e at
myB
enef
its.n
y.go
v.
If yo
u liv
e in
New
Yor
k C
ity a
nd y
ou a
re n
ot a
lso
appl
ying
for
Tem
pora
ry A
ssis
tanc
e, c
all o
r vi
sit
any
SNA
P O
ffice
and
ask
for
an
appl
icat
ion
pack
age.
Yo
u ca
n ge
t th
e ad
dres
s an
d ph
one
num
ber
by
calli
ng
1-71
8-55
7-13
99
or
toll
free
1-80
0-34
2-30
09,
or
appl
y on
-line
at
m
yBen
efits
.ny.
gov.
H
av
ing
Pro
ble
ms
Co
min
g T
o U
s F
or
A S
NA
P A
pp
oin
tmen
t?
If it
is d
iffic
ult f
or y
ou to
com
e in
for a
SN
AP a
pplic
atio
n ap
poin
tmen
t (re
ason
s m
ay in
clud
e em
ploy
men
t, he
alth
issu
es, t
rans
porta
tion
or c
hild
car
e pr
oble
ms)
, you
may
hav
e so
meo
ne e
lse
appl
y fo
r you
, or y
ou m
ay a
pply
on-
line
at m
yBen
efits
.ny.
gov.
You
als
o ca
n m
ail u
s yo
ur a
pplic
atio
n or
dro
p it
off a
nd, i
n so
me
circ
umst
ance
s; w
e ca
n in
terv
iew
you
by
tele
phon
e.
Pl
ease
con
tact
you
r soc
ial s
ervi
ces
dist
rict i
f you
hav
e an
y qu
estio
ns, t
o se
e if
you
are
elig
ible
for a
tele
phon
e in
terv
iew
, or
if y
ou
need
t
o r
es
ch
ed
ule
an
in
terv
iew
.

LDSS
-482
6 (R
ev.8
/12)
Pa
ge 1
N
EW Y
OR
K S
TATE
OFF
ICE
OF
TEM
PO
RA
RY
AN
D D
ISA
BIL
ITY
AS
SIS
TAN
CE
SN
AP
APP
LIC
ATI
ON
/ R
ECER
TIFI
CA
TIO
N
App
licat
ion
Dat
e In
terv
iew
Dat
e C
ente
r/O
ffice
U
nit
Wor
ker
Cas
e T
ype
Cas
e N
umbe
r R
egis
try
Num
ber
Ver
sion
L
ifelin
e
A
pply
Rec
ertif
y
Lan
g
Nam
e: _
____
____
____
____
____
____
Tel
epho
ne N
umbe
r: __
____
____
____
___O
ther
pho
ne w
here
you
can
be
reac
hed:
___
____
____
__
Res
iden
ce A
ddre
ss: _
____
____
____
____
____
____
____
Apt
.# _
___
City
___
____
____
____
____
, NY
Zip
Cod
e __
____
____
____
__
Mai
ling
Add
ress
(if d
iffer
ent)
____
____
____
____
____
___
Apt.#
___
_ C
ity _
____
____
____
____
__, N
Y Z
ip C
ode
____
____
____
____
O
ther
Nam
e: _
____
____
____
____
_ A
re Y
ou:
App
lyin
g o
r
Rec
ertif
ying
Do
you
wan
t to
rece
ive
notic
es in
:
Spa
nish
an
d E
nglis
h o
r
Eng
lish
On
ly
We
mus
t acc
ept y
our a
pplic
atio
n if,
at a
min
imum
, it c
onta
ins
you
r nam
e,
addr
ess
(if y
ou h
ave
one)
, and
sig
natu
re in
this
box
.
AP
PLI
CA
NT/
RE
PR
ESE
NTA
TIV
E S
IGN
ATU
RE
D
ATE
SIG
NE
D
Lis
t eve
ryon
e w
ho li
ves
with
you
eve
n if
they
are
not
app
lyin
g. L
ist y
ours
elf f
irst.
L N
Firs
t Nam
e M
I La
st N
ame
Soc
ial S
ecur
ity N
umbe
r (S
SN
) of a
pply
ing
mem
ber
(If
none, w
rite
“N
ON
E”)
D
ate
of B
irth
Mar
ital
Sta
tus
Sex
M
or
F
Is th
is
pers
on
appl
ying
? R
elat
ions
hip
to y
ou
Do
you
buy
and/
or
pre
pare
food
w
ith th
is
pers
on?
His
pani
c or
La
tino?
Ent
er Y
(Yes
) or N
(No)
for
each
race
*
Yes
N
o Ye
s N
o Ye
s N
o I
A
B
P W
U
1
se
lf
2
3
4
5
6
7
8
*Rac
e/E
thni
c C
odes
: I –
Nat
ive
Am
eric
an o
r A
lask
an N
ativ
e, A
- A
sian
, B
– B
lack
or
Afr
ican
Am
eric
an,
P –
Nat
ive
Haw
aiia
n or
Pac
ific
Isla
nder
, W
– W
hite
, U
– U
nkno
wn
(MA
On
ly)
Are
you
and
is e
very
one
livin
g w
ith y
ou a
US
citi
zen?
□
Yes
No
If
No,
who
is n
ot a
citi
zen?
Has
a c
ourt
issu
ed a
war
rant
bec
ause
it fo
und
that
you
or
anyo
ne li
ving
with
you
is fl
eein
g to
avo
id p
rose
cutio
n, c
usto
dy o
r co
nfin
emen
t for
a fe
lony
or
an a
ttem
pted
felo
ny?
Y
es
No
Are
you
or
is a
nyon
e liv
ing
with
you
in v
iola
tion
of p
roba
tion
or p
arol
e ac
cord
ing
to a
cou
rt?
Yes
N
o H
ave
you
or h
as a
nyon
e liv
ing
with
you
eve
r be
en d
isqu
alifi
ed fr
om r
ecei
ving
SN
AP
bec
ause
of f
rau
d or
inte
ntio
nal p
rogr
am v
iola
tion?
Yes
N
o
Are
you
or
is a
nyon
e in
you
r ho
useh
old
appl
ying
for
or r
ecei
ving
SN
AP
or
Tem
pora
ry A
ssis
tanc
e in
ano
ther
pla
ce?
Y
es
No
Are
you
or
is a
nyon
e liv
ing
with
you
blin
d, d
isab
led
or p
regn
ant?
Yes
No
If
Yes
, who
Are
you
or
is a
nyon
e liv
ing
with
you
a v
eter
an?
Y
es
No
If
Yes
, who
Do
you
or d
oes
anyo
ne li
ve in
a d
rug
or a
lcoh
ol tr
eatm
ent c
ente
r, S
tate
-cer
tifie
d gr
oup
livin
g fa
cilit
y or
Sta
te-c
ertif
ied
supe
rvis
ed/s
uppo
rtiv
e ap
artm
ent?
Y
es
No
If yo
u ar
e re
cert
ifyin
g fo
r S
NA
P, l
ist o
n th
e P
age
6 w
hat h
as c
hang
ed s
ince
you
r la
st a
pplic
atio
n or
rec
ertif
icat
ion
(suc
h as
mov
ed, h
ad
a ba
by, s
omeo
ne m
oved
in o
r ou
t of
you
r ho
useh
old)
. Y
ou
ma
y u
se
th
e p
ag
e 6
if
yo
u n
ee
d m
ore
ro
om
or
the
re is
oth
er
info
rma
tio
n t
ha
t y
ou
th
ink
we m
igh
t n
ee
d.
Go
to
Pa
ge
2

LDSS
-482
6 (R
ev.8
/12)
Pa
ge 2
IN
CO
ME
List
AL
L y
our i
ncom
e an
d th
e in
com
e of
any
one
livin
g w
ith y
ou. T
his
incl
udes
, but
is n
ot li
mite
d to
wag
es, i
ncom
e fr
om s
elf-e
mpl
oym
ent
(for e
xam
ple:
bab
ysitt
ing,
cle
anin
g, in
com
e fr
om a
room
er o
r boa
rder
) chi
ld s
uppo
rt, p
ensi
ons,
vet
eran
s be
nefit
s, d
isab
ility
, soc
ial
secu
rity
or S
SI, g
rant
for s
chol
arsh
ips
for r
ent o
r foo
d, T
empo
rary
Ass
ista
nce,
and
inco
me
from
frie
nds
or re
lativ
es.
Nam
e of
Per
son
Rec
eivi
ng In
com
e S
ourc
e of
Inco
me
H
ours
Wor
ked
Per
Mon
th
How
Ofte
n is
it R
ecei
ved?
(f
or
exa
mp
le,
we
ekly
, b
i-w
ee
kly
, m
on
thly
)
Gro
ss A
mou
nt R
ecei
ved
Bef
ore
Ded
uctio
ns
Do
you
or d
oes
anyo
ne li
ving
with
you
hav
e ch
ild/d
epen
dent
car
e co
sts
rela
ted
to e
mpl
oym
ent o
r tr
aini
ng?
Y
es
No
If Y
es, w
ho
.
A
mou
nt p
aid
$ __
____
____
__.
How
ofte
n pa
id (
e.g.
, wee
kly,
mon
thly
) __
____
____
____
____
____
___.
Hav
e yo
u or
has
any
one
livin
g w
ith y
ou c
hang
ed o
r qu
it jo
bs o
r re
duce
d an
y fo
rm o
f inc
ome
in th
e la
st 3
0 da
ys –
incl
udin
g re
duce
d w
ork
hour
s or
inco
me?
Y
es
No
Do
you
or d
oes
anyo
ne li
ving
with
you
hav
e an
y po
tent
ial i
ncom
e th
at h
as n
ot y
et b
een
rece
ived
?
Yes
No
If Y
es, e
xpla
in o
n P
age
6.
Do
you
or d
oes
anyo
ne li
ving
with
you
rec
eive
a P
erso
nal N
eeds
Allo
wan
ce (
PN
A)
or a
Mea
l Allo
wan
ce?
Y
es
No
If Y
es, w
ho
.
Hav
e yo
u or
has
any
one
in y
our
hous
ehol
d se
t asi
de a
ny in
com
e un
der
“PA
SS
: Pla
n T
o A
chie
ve S
elf S
uppo
rt”
appr
oved
by
the
Soc
ial S
ecur
ity A
dmin
istr
atio
n?
Yes
No
If Y
es, w
ho
.
Are
you
or
is a
nyon
e liv
ing
with
you
par
ticip
atin
g in
a s
trik
e?
Yes
No
If Y
es, w
ho
.
RE
SO
UR
CE
S
Res
ourc
es d
o no
t affe
ct th
e el
igib
ility
of m
ost h
ouse
hold
s ap
plyi
ng fo
r S
NA
P. H
owev
er, s
ome
reso
urce
info
rmat
ion
is u
sed
to d
eter
min
e if
you
qual
ify fo
r ex
pedi
ted
proc
essi
ng o
f you
r ap
plic
atio
n.
How
muc
h m
oney
doe
s ev
eryo
ne in
you
r ho
useh
old
have
? (F
or e
xam
ple,
on
your
per
son;
in y
our
hom
e, in
che
ckin
g an
d sa
ving
s ac
coun
ts, o
r ot
her
loca
tions
, inc
ludi
ng
join
tly h
eld
acco
unts
)
$_
____
____
____
_ B
elon
gs to
.
Oth
er fi
nanc
ial a
sset
s? (
For
exa
mpl
e, s
tock
s, b
onds
, ret
irem
ent a
ccou
nts,
sav
ings
bon
ds, m
utua
l fun
ds, I
RA
s, tr
ust f
unds
, mon
ey m
arke
t cer
tific
ates
)
Yes
N
o
If
Yes
, am
ount
$__
____
____
____
_ T
ype
____
____
____
____
____
____
____
____
Ow
ner
____
____
____
____
____
____
____
____
_.
How
man
y ca
rs, t
ruck
s or
oth
er v
ehic
les
do y
ou o
r an
yone
in y
our
hous
ehol
d ha
ve?
___
#1
Yea
r __
___
Mak
e __
____
____
____
____
____
_ M
odel
___
____
____
____
____
____
_ O
wne
r __
____
____
____
____
____
___
___
#2
Yea
r __
___
Mak
e __
____
____
____
____
____
_ M
odel
___
____
____
____
____
____
_ O
wne
r __
____
____
____
____
____
___
Do
you
or a
nyon
e ap
plyi
ng o
wn
any
prop
erty
incl
udin
g yo
ur o
wn
hom
e?
Yes
No
if y
es, l
ist p
rope
rty_
____
____
____
____
____
____
Ow
ner
____
____
____
____
____
Has
any
one
appl
ying
sol
d, g
iven
aw
ay o
r tr
ansf
erre
d ca
sh o
r pr
oper
ty in
the
last
thre
e m
onth
s to
qua
lify
for
SN
AP
?
Yes
No
LIV
ING
AR
RA
NG
EM
EN
TS
AN
D E
XP
EN
SE
S
Che
ck a
ll th
e de
scrip
tions
that
app
ly to
you
r ho
useh
old:
O
wn
hom
e or
pay
ing
for
hom
e
Ren
ting
M
igra
nt/s
easo
nal f
arm
wor
ker
N
o pe
rman
ent r
esid
ence
Liv
e w
ith r
elat
ives
or
frie
nds
List
exp
ense
s:
Mon
thly
ren
t or
mor
tgag
e pa
ymen
t $ _
____
____
____
Tax
on
hom
e pe
r ye
ar $
___
____
____
_ In
sura
nce
on h
ome
per
year
$ _
____
____
____
.
Pay
sep
arat
ely
for
Hea
t?
Yes
No
If y
es, s
peci
fy ty
pe o
f hea
ting:
G
as
Ele
ctric
O
il
Woo
d
Coa
l
Pro
pane
O
ther
(lis
t) _
____
____
____
____
H
eat C
o. N
ame
____
____
____
____
____
____
___
H
eat C
o. A
cct.
No.
___
____
____
____
____
____
____
___
Yo
u m
ay u
se
th
e p
ag
e 6
if
yo
u n
ee
d m
ore
ro
om
or
the
re is
oth
er
info
rma
tio
n t
ha
t y
ou
th
ink
we m
igh
t n
ee
d.
Go
to
Pa
ge
3

LDSS
-482
6 (R
ev.8
/12)
Pa
ge 3
LIV
ING
AR
RA
NG
EM
EN
TS
AN
D E
XP
EN
SE
S (
Co
nt’
d)
Pay
for
air
cond
ition
ing,
eith
er in
you
r el
ectr
ic b
ill o
r as
a s
epar
ate
fee?
Y
es
No
Pay
sep
arat
ely
for
utili
ties
(oth
er th
an h
eatin
g/co
olin
g)?
Y
es
No
(for
exa
mpl
e, li
ghts
, coo
king
gas
, was
her/
drye
r fe
es, g
arba
ge/tr
ash,
wat
er, i
nitia
l ins
talla
tion
of u
tiliti
es).
Doe
s an
yone
els
e pa
y an
y of
thes
e ex
pens
es fo
r yo
u (s
ome
exam
ples
are
Sec
tion
8 or
oth
er s
ubsi
dy p
rogr
am)?
Yes
N
o I
f yes
, who
pay
s w
hat?
___
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
_ .
Do
you
or d
oes
anyo
ne li
ving
with
you
pay
cou
rt-o
rder
ed c
hild
sup
port
?
Yes
No
If y
es, w
ho _
____
____
____
____
____
____
____
____
____
N
ame(
s) o
f chi
ld(r
en)
supp
ort i
s be
ing
paid
for
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
___
____
____
____
___
P
aym
ent a
mou
nt $
____
____
____
___
Fre
quen
cy o
f pay
men
ts (
for
exam
ple,
wee
kly,
bi-w
eekl
y, m
onth
ly)
____
____
____
___
Are
you
, and
/or
anyo
ne li
ving
with
you
, blin
d/di
sabl
ed o
r at
leas
t age
60?
If s
o, d
oes
such
per
son
have
med
ical
bill
s?
Yes
N
o I
f yes
, lis
t on
the
page
6 w
hat t
hey
are
for,
how
muc
h an
d w
ho is
res
pons
ible
for
paym
ent.
Are
you
, and
/or
anyo
ne li
ving
with
you
, on
Med
icai
d w
ith a
spe
ndow
n?
Yes
N
o If
yes
, who
___
____
____
____
____
____
___
Am
ount
$ _
____
____
____
____
____
Are
you
, and
/or
anyo
ne li
ving
with
you
(16
yea
rs o
ld o
r ol
der)
enr
olle
d in
sch
ool o
r tr
aini
ng?
Y
es
No
If y
es, w
ho _
____
____
____
____
_ w
here
___
____
____
____
__
Yo
u m
ay u
se
th
e p
ag
e 6
if
yo
u n
ee
d m
ore
ro
om
or
the
re is
oth
er
info
rma
tio
n t
ha
t y
ou
th
ink
we m
igh
t n
ee
d.
REA
D T
HE
IMPO
RTA
NT
INFO
RM
ATI
ON
BEL
OW
SN
AP P
ENAL
TY W
AR
NIN
G –
Any
info
rmat
ion
you
prov
ide
in c
onne
ctio
n w
ith y
our
appl
icat
ion
for
SNAP
will
be
subj
ect t
o ve
rific
atio
n by
Fed
eral
, Sta
te a
nd
loca
l offi
cial
s. If
any
info
rmat
ion
is in
corre
ct, y
ou m
ay b
e de
nied
SN
AP
. You
may
be
subj
ect t
o cr
imin
al p
rose
cutio
n fo
r kno
win
gly
prov
idin
g in
corre
ct in
form
atio
n.
You
will
nev
er b
e ab
le to
get
SN
AP
aga
in if
you
are
foun
d gu
ilty
in a
cou
rt of
law
for t
he s
econ
d tim
e of
buy
ing
or s
ellin
g co
ntro
lled
subs
tanc
es (i
llega
l dru
gs o
r ce
rta
in d
rugs f
or
whic
h a
do
cto
r’s p
rescrip
tio
n i
s r
eq
uir
ed)
in e
xcha
nge
for S
NAP
; or
foun
d gu
ilty
in a
cou
rt of
law
of s
ellin
g or
get
ting
firea
rms,
am
mun
ition
or
expl
osiv
es in
exc
hang
e fo
r SN
AP
; or
foun
d gu
ilty
in a
cou
rt of
traf
ficki
ng in
SN
AP w
orth
$50
0 or
mor
e. T
raffi
ckin
g in
clud
es th
e ille
gal u
se, t
rans
fer,
acqu
isiti
on,
alte
ratio
n or
pos
sess
ion
of S
NA
P, a
utho
rizat
ion
card
s or
acc
ess
devi
ces;
or f
ound
gui
lty o
f com
mitt
ing
a th
ird In
tent
iona
l Pro
gram
Vio
latio
n (IP
V).
You
will
not
be
able
to g
et S
NAP
for t
wo
year
s if
you
are
foun
d gu
ilty
in a
cou
rt of
law
for t
he fi
rst t
ime
of b
uyin
g or
sel
ling
cont
rolle
d su
bsta
nces
(ille
gal d
rugs
or
ce
rta
in d
rug
s fo
r w
hic
h a
do
cto
r’s p
rescrip
tio
n is r
equ
ire
d)
in e
xch
ang
e fo
r SN
AP
.
If yo
u ha
ve c
omm
itted
you
r:
Firs
t IP
V, y
ou w
ill n
ot b
e ab
le to
get
SN
AP fo
r one
yea
r.
Sec
ond
IPV
, you
will
not
be
able
to g
et S
NAP
for t
wo
year
s.
A c
ourt
coul
d al
so b
ar y
ou fr
om re
ceiv
ing
SNAP
for a
n ad
ditio
nal 1
8 m
onth
s. If
you
mak
e a
fals
e st
atem
ent a
bout
who
you
are
or w
here
you
live
in o
rder
to g
et
mul
tiple
SN
AP b
enef
its, y
ou w
ill n
ot b
e ab
le to
get
SN
AP fo
r ten
yea
rs (o
r per
man
ently
if th
is is
the
third
IPV
).
You
may
be
foun
d gu
ilty
of a
n IP
V if
you
mak
e a
fals
e or
mis
lead
ing
stat
emen
t, or
mis
repr
esen
t, co
ncea
l or w
ithho
ld fa
cts;
or
com
mit
any
act t
hat c
onst
itute
s a
viol
atio
n of
Fed
eral
or S
tate
law
for t
he p
urpo
se o
f usi
ng, p
rese
ntin
g, tr
ansf
errin
g, a
cqui
ring,
rece
ivin
g, p
osse
ssin
g or
traf
ficki
ng o
f SN
AP
ben
efits
, aut
horiz
atio
n ca
rds
or re
usab
le d
ocum
ents
use
d as
par
t of t
he E
lect
roni
c B
enef
it Tr
ansf
er (E
BT)
sys
tem
.
You
coul
d al
so b
e fin
ed u
p to
$25
0,00
0, s
ent t
o ja
il fo
r up
to 2
0 ye
ars,
or b
oth.
A
nyon
e w
ho is
flee
ing
to a
void
pro
secu
tion,
cus
tody
or c
onfin
emen
t for
a fe
lony
, or w
ho is
vio
latin
g a
cond
ition
of p
roba
tion
or p
arol
e, is
not
elig
ible
to re
ceiv
e S
NAP
. If
you
get
mor
e SN
AP b
enef
its t
han
you
shou
ld h
ave
(ove
rpay
men
t), y
ou m
ust
pay
them
bac
k. I
f yo
ur c
ase
is a
ctiv
e, w
e w
ill t
ake
back
the
am
ount
of
the
over
paym
ent f
rom
futu
re S
NAP
ben
efits
that
you
get
. If y
our c
ase
is c
lose
d, y
ou m
ay p
ay b
ack
the
over
paym
ent t
hrou
gh a
ny u
nuse
d S
NAP
ben
efits
rem
aini
ng
in y
our a
ccou
nt, o
r you
may
pay
cas
h.

LDSS
-482
6 (R
ev.8
/12)
Pa
ge 4
R
EAD
TH
E IM
POR
TAN
T IN
FOR
MA
TIO
N B
ELO
W (c
ont’d)
If yo
u ha
ve a
n ov
erpa
ymen
t tha
t is
not p
aid
back
, it w
ill b
e re
ferre
d fo
r col
lect
ion
in a
num
ber o
f way
s, in
clud
ing
auto
mat
ed c
olle
ctio
n by
the
fede
ral g
over
nmen
t. Fe
dera
l ben
efits
(su
ch a
s S
ocia
l Sec
urity
) an
d ta
x re
fund
s th
at y
ou a
re e
ntitl
ed to
rec
eive
may
be
take
n to
pay
bac
k th
e ov
erpa
ymen
t. Th
e de
bt w
ill al
so b
e su
bjec
t to
proc
essi
ng c
harg
es.
Any
exp
unge
d SN
AP b
enef
its w
ill b
e pu
t tow
ards
you
r ove
rpay
men
t. If
you
appl
y fo
r SN
AP
agai
n, a
nd h
ave
not r
epai
d th
e am
ount
you
ow
e, y
our S
NA
P be
nefit
s w
ill b
e re
duce
d if
you
begi
n to
get
them
aga
in. Y
ou w
ill b
e no
tifie
d, a
t tha
t tim
e, o
f the
am
ount
of r
educ
ed b
enef
its y
ou w
ill g
et.
CO
NSE
NT
– I
unde
rsta
nd th
at b
y si
gnin
g th
is a
pplic
atio
n fo
rm I
agre
e to
any
inve
stig
atio
n m
ade
by th
e N
ew Y
ork
Sta
te O
ffice
of
Tem
pora
ry a
nd D
isab
ility
A
ssis
tanc
e or
my
loca
l soc
ial s
ervi
ces
dist
rict t
o ve
rify
or c
onfir
m th
e in
form
atio
n I h
ave
give
n or
any
oth
er in
vest
igat
ion
mad
e by
them
in c
onne
ctio
n w
ith m
y re
ques
t fo
r SN
AP.
If ad
ditio
nal i
nfor
mat
ion
is r
eque
sted
, I
will
pro
vide
it.
I w
ill a
lso
coop
erat
e w
ith S
tate
and
Fed
eral
per
sonn
el in
a S
NAP
Qua
lity
Con
trol
Rev
iew
.
CO
NSE
NT
FOR
REL
EASE
OF
CO
NFI
DEN
TIA
L U
NEM
PLO
YMEN
T IN
SUR
ANC
E (U
I) IN
FOR
MAT
ION
– I
auth
oriz
e th
e N
ew Y
ork
Sta
te D
epar
tmen
t of L
abor
(D
OL)
to re
leas
e an
y co
nfid
entia
l inf
orm
atio
n, m
aint
aine
d by
DO
L fo
r U
nem
ploy
men
t Ins
uran
ce (U
I) pu
rpos
es, t
o th
e N
ew Y
ork
Sta
te O
ffice
of T
empo
rary
and
D
isab
ility
Ass
ista
nce
(OTD
A).
This
inf
orm
atio
n in
clud
es U
I be
nefit
cla
ims
and
wag
e re
cord
s. I
und
erst
and
that
OTD
A,
alon
g w
ith S
tate
and
loc
al a
genc
y em
ploy
ees
wor
king
in lo
cal s
ocia
l ser
vice
s di
stric
t offi
ces,
will
use
the
UI i
nfor
mat
ion
for e
stab
lishi
ng o
r ver
ifyin
g el
igib
ility
for,
and
the
amou
nt o
f, TA
, MA
, or F
S be
nefit
s ap
plie
d fo
r in
this
app
licat
ion
and
for i
nves
tigat
ions
to d
eter
min
e w
heth
er I
rece
ived
ben
efits
to w
hich
I w
as n
ot e
ntitl
ed.
SUA
(STA
ND
ARD
UTI
LITY
ALL
OW
AN
CE)
IN
FOR
MAT
ION
– I
und
erst
and
that
SN
AP r
ecip
ient
s ar
e ca
tego
rical
ly i
ncom
e el
igib
le f
or t
he H
ome
Ener
gy
Ass
ista
nce
Pro
gram
(HEA
P).
If I a
m n
ot in
clud
ed in
the
annu
al a
utom
atic
HE
AP p
aym
ent p
roce
ss fo
r cer
tain
SN
AP r
ecip
ient
s, m
y ho
useh
old
inte
nds
to a
pply
fo
r a H
EAP
ben
efit
with
in th
e ne
xt 1
2 m
onth
s. If
I de
cide
not
to a
pply
for H
EAP
with
in th
e ne
xt 1
2 m
onth
s, I
will
let m
y w
orke
r kno
w.
TELE
PHO
NE
ALL
OW
ANC
E IN
FOR
MA
TIO
N –
I un
ders
tand
that
SN
AP
reci
pien
ts a
re e
ligib
le fo
r a te
leph
one
allo
wan
ce if
they
pay
to u
se a
hom
e ph
one,
cel
l ph
one,
pho
ne, p
hone
cal
ling
card
or c
oin
oper
ated
pay
pho
ne. I
f I d
o no
t hav
e an
y co
st to
mak
e ph
one
calls
, I w
ill le
t my
wor
ker k
now
.
CH
ANG
ES –
I ag
ree
to in
form
the
agen
cy p
rom
ptly
of a
ny c
hang
e in
my
need
s, in
com
e, p
rope
rty, l
ivin
g ar
rang
emen
t, pr
egna
ncy
stat
us o
r add
ress
to th
e be
st
of m
y kn
owle
dge
or b
elie
f in
acco
rdan
ce w
ith m
y re
porti
ng re
quire
men
ts.
REQ
UIR
EMEN
T TO
REP
OR
T/VE
RIF
Y H
OU
SEH
OLD
EXP
ENSE
S –
I un
ders
tand
that
my
hous
ehol
d m
ust r
epor
t chi
ld c
are
and
utili
ty e
xpen
ses
in o
rder
to g
et
a SN
AP d
educ
tion
for
thes
e ex
pens
es.
I fu
rther
und
erst
and
that
my
hous
ehol
d m
ust
repo
rt an
d ve
rify
rent
/mor
tgag
e pa
ymen
ts,
prop
erty
tax
es,
insu
ranc
e,
med
ical
exp
ense
s an
d ch
ild s
uppo
rt pa
id t
o a
non-
hous
ehol
d m
embe
r in
ord
er t
o ge
t a
SNAP
ded
uctio
n fo
r th
ese
expe
nses
. I
unde
rsta
nd t
hat
failu
re t
o re
port/
verif
y th
e ab
ove
expe
nses
will
be
seen
as
a st
atem
ent b
y m
y ho
useh
old
that
I/w
e do
not
wan
t to
rece
ive
a de
duct
ion
for
thos
e un
repo
rted/
unve
rifie
d ex
pens
es. A
ded
uctio
n fo
r th
ese
expe
nses
may
mak
e m
e el
igib
le f
or S
NA
P or
may
incr
ease
my
SNA
P be
nefit
s. I
und
erst
and
that
I m
ay r
epor
t/ver
ify t
hese
ex
pens
es a
t any
tim
e in
the
futu
re. T
his
dedu
ctio
n w
ould
then
be
appl
ied
to th
e ca
lcul
atio
n of
SN
AP in
futu
re m
onth
s in
acc
orda
nce
with
the
rule
s fo
r ch
ange
re
porti
ng a
nd p
roce
ssin
g ch
ange
s.
PRIV
ACY
AC
T ST
ATE
MEN
T –
CO
LLEC
TIO
N A
ND
USE
OF
SOC
IAL
SEC
UR
ITY
NU
MB
ER (S
SN) –
Th
e c
olle
ctio
n o
f S
SN
’s is a
uth
orize
d f
or
ea
ch
ho
use
hold
m
embe
r w
ith r
espe
ct t
o S
NAP
pur
suan
t to
the
Foo
d S
tam
p Ac
t of
197
7 (a
s am
ende
d, 7
US
Cod
e 20
11-2
036)
. Th
e in
form
atio
n w
e co
llect
will
be
used
to
dete
rmin
e w
heth
er y
our
hous
ehol
d is
elig
ible
or
cont
inue
s to
be
elig
ible
for b
enef
its. W
e w
ill v
erify
this
info
rmat
ion
thro
ugh
com
pute
r mat
chin
g pr
ogra
ms.
Thi
s in
form
atio
n w
ill a
lso
be u
sed
to m
onito
r co
mpl
ianc
e w
ith p
rogr
am r
egul
atio
ns a
nd fo
r pr
ogra
m m
anag
emen
t. Th
e in
form
atio
n w
ill b
e us
ed to
che
ck id
entit
y, to
ve
rify
earn
ed a
nd u
near
ned
inco
me,
and
to d
eter
min
e if
appl
ican
ts o
r rec
ipie
nts
can
rece
ive
mon
ey o
r oth
er h
elp.
The
info
rmat
ion
may
be
disc
lose
d to
Sta
te a
nd
Fede
ral a
genc
ies
for o
ffici
al e
xam
inat
ion
and
to la
w e
nfor
cem
ent o
ffici
als
for t
he p
urpo
se o
f app
rehe
ndin
g pe
rson
s fle
eing
to a
void
the
law
.
If yo
u or
any
one
appl
ying
/rece
rtify
ing
does
not
hav
e an
SSN
, a S
SN m
ust b
e ap
plie
d fo
r at t
he S
ocia
l Sec
urity
Age
ncy.

LDSS
-482
6 (R
ev.8
/12)
Pa
ge 5
R
EAD
TH
E IM
POR
TAN
T IN
FOR
MAT
ION
BEL
OW
(cont’d)
CIT
IZEN
SHIP
/IMM
IGR
ATIO
N S
TATU
S– I
sw
ear
and/
or a
ffirm
und
er p
enal
ty o
f pe
rjury
tha
t th
e in
form
atio
n I
have
pro
vide
d ab
out
the
citiz
ensh
ip a
nd
imm
igra
tion
stat
us o
f m
y se
lf an
d ev
eryo
ne li
ving
with
me
is t
rue
and
corre
ct.
I un
ders
tand
tha
t an
y in
form
atio
n I p
rovi
de t
o ve
rify
the
imm
igra
tion
stat
us o
f an
yone
app
lyin
g fo
r SN
AP m
ay b
e ch
ecke
d fo
r aut
hent
icity
with
the
Uni
ted
Stat
es C
itize
nshi
p an
d Im
mig
ratio
n Se
rvic
es.
Fo
r S
NA
P, c
itize
nshi
p m
ust b
e do
cum
ente
d on
ly if
que
stio
nabl
e.
NO
N-D
ISC
RIM
INAT
ION
NO
TIC
E –
In
acco
rdan
ce w
ith F
eder
al L
aw a
nd U
.S.
Dep
artm
ent
of A
gric
ultu
re (
USD
A)
polic
y, t
his
inst
itutio
n is
pro
hibi
ted
from
di
scrim
inat
ing
on th
e ba
sis
of ra
ce, c
olor
, nat
iona
l orig
in, s
ex, a
ge, r
elig
ion,
pol
itica
l bel
ief,
or d
isab
ility
. To
file
a co
mpl
aint
of d
iscr
imin
atio
n w
rite
US
DA
, Dire
ctor
, O
ffice
of
Civ
il R
ight
s, R
oom
326
-W, W
hitte
n B
uild
ing,
140
0 In
depe
nden
ce A
venu
e, S
.W.,
Was
hing
ton,
D.C
. 20
250-
9410
or
call
(202
) 72
0-59
64 (
voic
e an
d TD
D).
USD
A is
an
equa
l opp
ortu
nity
pro
vide
r and
em
ploy
er.
LIFE
LIN
E: F
or a
pplic
ants
/reci
pien
ts o
f SN
AP:
Th
e O
ffice
of T
empo
rary
and
Dis
abili
ty A
ssis
tanc
e m
ay o
r m
ay n
ot r
elea
se y
our
nam
e an
d ad
dres
s to
you
r te
leph
one
serv
ice
prov
ider
. You
r tel
epho
ne s
ervi
ce p
rovi
der m
ay o
r may
not
use
this
info
rmat
ion
to e
nrol
l you
in th
eir L
ifelin
e S
ervi
ce fo
r a d
isco
unte
d te
leph
one
rate
.
If
you
do
no
t wan
t thi
s in
form
atio
n re
leas
ed, c
heck
this
box
You
may
con
tact
you
r tel
epho
ne s
ervi
ce p
rovi
der d
irect
ly fo
r enr
ollm
ent i
n th
e di
scou
nted
rate
Life
line
Serv
ice.
Med
icai
d-on
ly a
pplic
ants
/reci
pien
ts m
ust c
onta
ct th
eir t
elep
hone
ser
vice
pro
vide
r dire
ctly
for e
nrol
lmen
t in
the
disc
ount
ed ra
te L
ifelin
e S
ervi
ce.
AUTH
OR
IZED
REP
RES
ENTA
TIVE
– Y
ou c
an a
utho
rize
som
eone
who
kno
ws
your
hou
seho
ld c
ircum
stan
ces
to a
pply
for
SN
AP
for
you
. Yo
u ca
n al
so
auth
oriz
e so
meo
ne o
utsi
de y
our h
ouse
hold
to g
et S
NAP
ben
efits
for y
ou a
nd to
use
them
to b
uy fo
od fo
r you
. If y
ou w
ould
like
to a
utho
rize
som
eone
, you
mus
t do
so
in w
ritin
g. Y
ou m
ay d
o so
by
prin
ting
the
pe
rso
n’s
nam
e,
ad
dre
ss a
nd
ph
one
num
ber b
elow
. W
hen
an A
utho
rized
Rep
rese
ntat
ive
is a
pply
ing
on b
ehal
f of
a S
NAP
Hou
seho
ld th
at d
oes
not r
esid
e in
an
inst
itutio
n, b
oth
the
Aut
horiz
ed R
epre
sent
ativ
e an
d th
e S
NAP
Hea
d of
Hou
seho
ld o
r ot
her
resp
onsi
ble
adul
t m
embe
r of t
he h
ouse
hold
mus
t sig
n an
d da
te th
e si
gnat
ure
sect
ions
at t
he b
otto
m o
f thi
s pa
ge.
IF Y
OU
WO
ULD
LIK
E TO
AU
THO
RIZ
E SO
MEO
NE,
PR
INT
TH
E P
ER
SO
N’S
NAM
E, A
DD
RES
S A
ND
TEL
EPH
ON
E N
UM
BER
, AN
D S
IGN
BEL
OW
. N
ame
____
____
____
____
____
____
Add
ress
___
____
____
____
____
____
____
____
____
____
____
____
____
_ P
hone
___
____
____
____
C
ERTI
FIC
ATI
ON
: I s
wea
r and
/or a
ffirm
und
er th
e pe
nalti
es o
f per
jury
that
the
info
rmat
ion
I hav
e gi
ven
or w
ill g
ive
to th
e lo
cal
Soci
al S
ervi
ces
dist
rict i
s co
rrec
t. Y
our s
igna
ture
is re
quire
d be
low
to c
ompl
ete
the
appl
icat
ion
proc
ess.
A
PPLI
CA
NT
SIG
NA
TUR
E
X
DA
TE S
IGN
ED
Aut
horiz
ed R
epre
sent
ativ
e S
IGN
ATU
RE
X
DA
TE S
IGN
ED
IF Y
OU
HEL
PED
CO
MPL
ETE
THIS
APP
LIC
ATI
ON
/ R
ECER
TIFI
CA
TIO
N F
OR
SO
MEO
NE
ELSE
, PR
INT
YOU
R N
AM
E A
ND
AD
DR
ESS
HER
E. Y
OU
MA
Y A
LSO
VO
LUN
TAR
ILY
PRIN
T YO
UR
TEL
EPH
ON
E N
UM
BER
. N
ame
____
____
____
____
____
____
Add
ress
___
____
____
____
____
____
____
____
____
____
____
____
____
_ P
hone
___
____
____
____

LDSS
-482
6 (R
ev.8
/12)
Pa
ge 6
Use
this
are
a f
or
addit
ional
info
rmati
on:
Who
: _______________
_________________________E
xpla
nati
on:
Who
: _______________
_________________________E
xpla
nati
on:
Who
: _______________
_________________________E
xpla
nati
on:
I C
ON
SEN
T TO
WIT
HD
RA
W M
Y A
PPLI
CA
TIO
N/R
ECER
TIFI
CA
TIO
N. I
und
erst
and
that
I m
ay re
appl
y at
any
tim
e.
SIG
NA
TUR
E
DA
TE
For
Agen
cy U
se O
nly
Elig
ibilit
y D
eter
min
ed b
y __
____
____
____
____
____
____
____
____
____
____
____
____
____
____
__
Dat
e __
____
____
____
____
_
Sig
natu
re o
f Per
son
Who
Obt
aine
d E
ligib
ility
Info
rmat
ion:
___
____
____
____
____
____
____
____
____
____
_ D
ate
____
____
____
___
Em
ploy
ed b
y:
Soc
ial S
ervi
ces
Dis
trict
Pro
vide
r Age
ncy
(Spec
ify)
__________
__
________________
__________________________________________________________
Rea
son
____
_/__
___/
____
__
With
draw
al
Den
ial
Rec
ert.
Clo
sing
Elig
ibilit
y A
ppro
ved
by _
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
_ D
ate
____
____
____
____
__
SN
AP
Aut
horiz
atio
n Pe
riod:
Fro
m _
____
____
____
____
____
_ To
___
____
____
____
____
___
IN
-PER
SON
INTE
RVI
EW
T
ELEP
HO
NE
INTE
RVI
EW
Com
men
ts:

1
2
Will you be 18 years old on or before election day? Yes □ No □
If you answered NO, do not complete this form unless you will be 18 by the end of the year.
For Board use only!
3
4
5 Address where you get your mail (if different from above) P.O. Box, star route, etc. Post Office Zip Code
6 Date of Birth
7 Sex (circle)
M F
8 Home Tel. Number (optional)
The last year you voted Your Address was (give house number, street and city)
In county/state Under the Name (if different from your name now)
NYS Agency-Based Voter Registration Form
(If you check yes, please complete VOTER REGISTRATION APPLICATION at bottom of page)
“If you are not registered to vote where you live now, would you like to apply to register here today?”
□ YES
□ NO because I choose not to register OR
□ I am already registered at my current address OR
□ I asked for and received a mail registration form.
If you do not check any box, you will be considered to have
decided not to register to vote at this time.
_____/______/______
(Signature) (Date)
(Please Print Name)
Important! Applying to register or declining to register to vote will not affect the amount of assistance that you will be provided by this agency. If you would like help filling out the voter registration application form, we will help you. The decision whether to seek or accept help is yours. You may fill out the application form in private. Información en español: si le interesa obtener este formulario en español, llame al 1-800-367-8683
□ Yes, I need an application for an Absentee Ballot Please print or type in blue or black ink □ Yes, I would like to be an Election Day worker
9
ID Number—Check the applicable box and provide your number:
□ New York DMV number __ __ __ __ __ __ __ __ __ If you do not have a New York DMV number, please provide:
□ Last four digits of your Social Security Number __ __ __ __ □ I do not have a New York Driver’s license number
12
AFFIDAVIT: I swear or affirm that I am a citizen of the United States. I will have lived in the county, city or village for at least 30 days before the election. I will meet all requirements to register to vote in New York State. This is my signature or mark on the line below. The above information is true, I understand that if it is not true, I can be convicted and fined up to $5,000 and/or jailed for up to four years.
(Signature or Mark in Ink) (Date)
→
NVRA-05 (01/2011) VOTER REGISTRATION APPLICATION (instructions on back)
(Optional) Register to donate your organs and tissues Last Name First Name Middle Initial Suffix Address Apt Number Zip Code City Birth Date Sex □ M □ F Eye Color Height Ft. In.
By signing below, you certify that you are:
18 years of age or older
Consent to donate all of your organs and
tissues for transplantation, research, or both;
Authorizing the Board of Elections to provide your name and identifying
information to DOH for enrollment in the Registry;
And authorizing DOH to allow access to this information to federally
regulated organ procurement organizations and NYS-licensed tissue and eye banks and hospitals upon your death.
Sign Date
11
Choose a party -- Check one box only □ Democratic Party □ Republican Party □ Conservative Party □ Working Families Party □ Independence Party □ Green Party □ Other (write in)
□ I do not wish to enroll in a party
Are you a U. S. citizen?
Yes □ No □
If you answered NO, do not complete this form.
Last Name First Name Middle Initial Suffix
Address where you live (do not give P.O. address) Apt. No. City/Town/Village Zip Code County
10

Qualifications for Registration You Can Use This Form To:
register to vote in New York State; change your name and/or address, if there is a change since you last voted; enroll in a political party or change your enrollment.
To Register You Must: be a U.S. citizen; be 18 years old by December 31 of the year in which you file this form (note: You must be 18 years old by the date of the general, primary, or other election in which you want to vote.); be a resident of the County, or of the City of New York at least 30 days before an election; not be in jail or on parole for a felony conviction; and not claim the right to vote elsewhere.
Important! If you believe that someone has interfered with your right to register or to decline to register to vote, your right to privacy in deciding whether to register or in applying to register to vote, or your right to choose your own political party or other political preference, you may file a complaint with:
New York State Board of Elections, 40 Steuben Street, Albany, New York 12207-2109 Telephone: 1-800-469-6872;
TDD/TTY users contact the New York State Relay at 711; or visit our web site - www.elections.state.ny.us
Your decision to register will remain confidential and will be used only for voter registration purposes. Anyone not choosing to register to vote and/or information regarding the office to which the application was submitted will remain confidential, to be used only for voter regis-tration purposes.
Verifying your identity We will try to check your identity before Election Day, through the DMV number (driver’s license number or non-driver ID number), or the last four digits of your social security number, which you will fill in Box 9. If you do not have a DMV or Social Security number, you may use a valid photo ID, a current utility bill, bank statement, pay-check, government check or some other government document that shows your name and address. You may include a copy of one of those types of ID with this form. If we are unable to verify your identity before Election Day, you will be asked for ID when you vote for the first time.
To complete this form:
It is a crime to procure a false registration or to furnish false information to the Board of Elections.
Box 9: You must make one selection. For questions refer to Verifying your identity above.
Box 10: If you have never voted before, write “None”. If you can’t remember when you last voted, put a question mark (?). If you voted before under a different name, put down that name. If not, write “Same”.
Box 11: Check one box only. To vote in a primary election, you must be enrolled in one of these listed parties — Except the Independence Party, which permits non-enrolled voters to participate in certain primary elections.
Appendix E –
SNAP Application
Expedited Processing Summary Sheet
(LDSS-3938)

LDSS-3938 NYC (Rev. 9/14) NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE DATE
APPLICATION FILED
MONTH DAY YEAR
SUPPLEMENTAL NUTRITION ASSISTANCE PROGRAM (SNAP)
APPLICATION EXPEDITED PROCESSING SUMMARY SHEET
CASE NAME CASE NUMBER SCREENED BY DATE OF
SCREENING
MONTH DAY YEAR
INSTRUCTIONS FOR COMPLETING THIS FORM
1. Screen all applicants for expedited application processing and Working Families Supplemental Nutrition Program Initiative (WFSNAPI), on the day of application.
2. State results of screening in Part Four; and if qualified for expedited application processing, conduct a Full Eligibility Interview and complete Part Five within five calendar days of application.
3. If Full Eligibility Interview determines Household eligible for SNAP benefits:
Make benefits available to client within five calendar days after the date of application.
Send/Provide client with the CNS “Approval Notice” or manual “Action Taken Notice” within five calendar days after the application date.
Follow-up on all pended verification before issuance of on-going benefits beyond the initial expedited issuance period.
PART ONE – CHECK YES OR NO
IS THE HOUSEHOLD ALREADY RECEIVING SNAP BENEFITS THIS MONTH?
NOTE: IF “YES” IS CHECKED, BUT HOUSEHOLD ENTERED A DOMESTIC VIOLENCE SHELTER DURING THE MONTH OF APPLICATION, CONTINUE WITH PART TWO.
YES - IF YES, HOUSEHOLD DOES
NOT QUALIFY FOR EXPEDITED PROCESSING COMPLETE PART FOUR
NO - IF NO, CONTINUE
WITH PART TWO
PART TWO – CHECK YES OR NO
** In determining GROSS INCOME, exclude non-countable income such as child support payments made to a person outside the household.
SECTION
A
CHECK YES OR NO
DOES THE HOUSEHOLD HAVE $100 OR LESS IN CASH, SAVINGS OR OTHER LIQUID RESOURCES, AND
YES – IF YES, HOUSEHOLD
QUALIFIES FOR EXPEDITED PROCESSING.
COMPLETE PART FOUR
NO – IF NO, CONTINUE
WITH SECTION B.
HAS THE HOUSEHOLD RECEIVED OR DOES IT EXPECT TO
RECEIVE LESS THAN $150 GROSS INCOME ** DURING THE
MONTH OF APPLICATION?
SECTION
B
ARE HOUSEHOLD’S TOTAL GROSS INCOME ** DURING MONTH OF APPLICATION PLUS THE HOUSEHOLD’S LIQUID RESOURCES LESS THAN THEIR MONTHLY RENT/MORTGAGE PLUS UTILITY EXPENSES?
YES
IF YES, HOUSEHOLD QUALIFIES FOR EXPEDITED PROCESSING. COMPLETE PART FOUR
NO
IF NO, HOUSEHOLD DOES NOT QUALIFY FOR EXPEDITED PROCESSING UNLESS QUALIFIED UNDER PART THREE.
GO TO PART THREE IF A MIGRANT/SEASONAL FARMWORKER OTHERWISE, COMPLETE PART FOUR
Rent/Mortgage: $ _____________ Income: $_____________
*Heat/AC: ______________Resources: ____________
*Utilities: ______________
*Telephone: ______________
*Homeless Shelter Deduction _______________
Total Expenses: $ ______________ Totals: _____________
* Use HT/AC Standard Utility Allowance (SUA) only if household incurs costs or received HEAP greater than $20 during the month of application or within the previous 12 months of application. ** Use the Homeless Shelter Deduction for “undomiciled” households who do no reside in a homeless shelter.
PART THREE – MIGRANT/SEASONAL FARM WORKER HOUSEHOLDS ONLY - CHECK YES OR NO
A. IS THIS A HOUSEHOLD WITH NO MORE THAN $100 IN LIQUID RESOURCES?
AND
YES NO – IF NO, HOUSEHOLD DOES NOT QUALIFY
FOR EXPEDITED PROCESSING. COMPLETE PART FOUR
B. THE ONLY INCOME FOR THE MONTH OF APPLICATION:
(1) WAS TERMINATED BEFORE APPLICATION?
OR
(2) IS NEW, AND NO MORE THAN $25 GROSS INCOME WILL BE RECEIVED WITHIN TEN DAYS AFTER APPLICATION
YES
YES
NO CONTINUE WITH B2
NO
IF YES TO QUESTION A, AND YES TO EITHER QUESTION B1 OR QUESTION B2, HOUSEHOLD QUALIFIES FOR EXPEDITED PROCESSING,
IF NO TO BOTH B1 & B2 HH DOES NOT QUALIFY, COMPLETE PART FOUR IN EITHER SITUATION
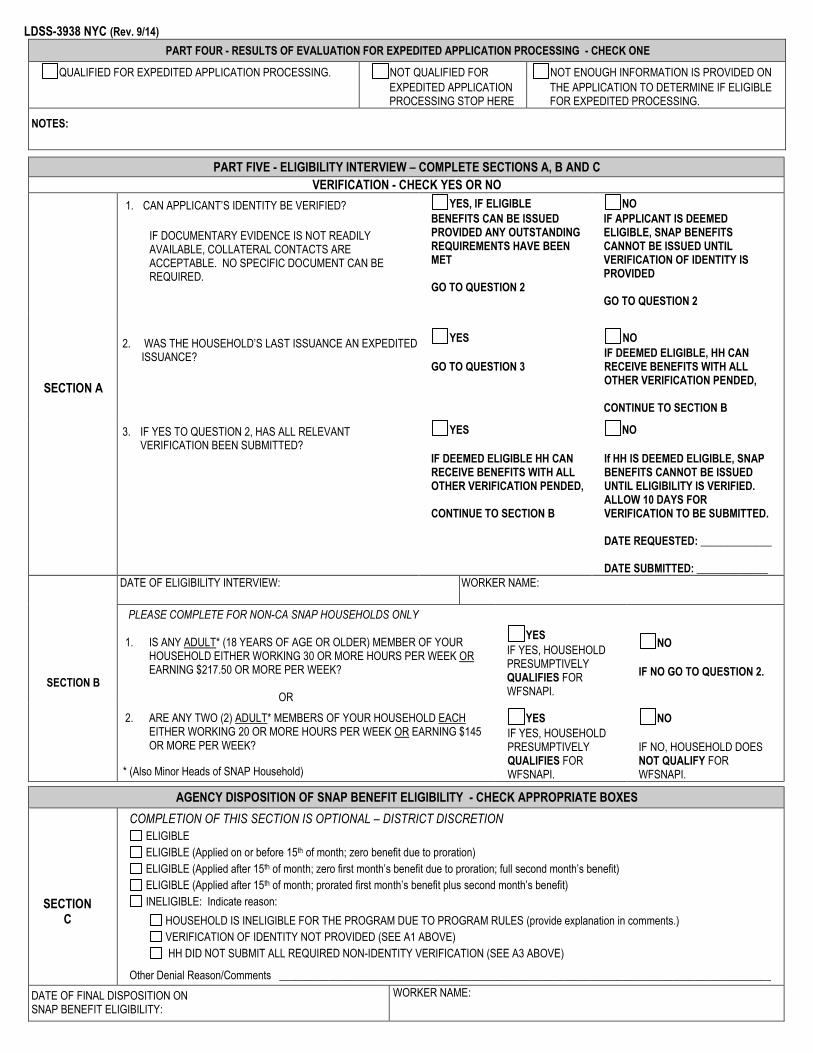
LDSS-3938 NYC (Rev. 9/14)
PART FOUR - RESULTS OF EVALUATION FOR EXPEDITED APPLICATION PROCESSING - CHECK ONE
QUALIFIED FOR EXPEDITED APPLICATION PROCESSING. NOT QUALIFIED FOR
EXPEDITED APPLICATION PROCESSING STOP HERE
NOT ENOUGH INFORMATION IS PROVIDED ON
THE APPLICATION TO DETERMINE IF ELIGIBLE FOR EXPEDITED PROCESSING.
NOTES:
PART FIVE - ELIGIBILITY INTERVIEW – COMPLETE SECTIONS A, B AND C
VERIFICATION - CHECK YES OR NO
SECTION A
1. CAN APPLICANT’S IDENTITY BE VERIFIED?
IF DOCUMENTARY EVIDENCE IS NOT READILY AVAILABLE, COLLATERAL CONTACTS ARE ACCEPTABLE. NO SPECIFIC DOCUMENT CAN BE REQUIRED.
YES, IF ELIGIBLE
BENEFITS CAN BE ISSUED PROVIDED ANY OUTSTANDING REQUIREMENTS HAVE BEEN MET GO TO QUESTION 2
NO
IF APPLICANT IS DEEMED ELIGIBLE, SNAP BENEFITS CANNOT BE ISSUED UNTIL VERIFICATION OF IDENTITY IS PROVIDED GO TO QUESTION 2
2. WAS THE HOUSEHOLD’S LAST ISSUANCE AN EXPEDITED ISSUANCE?
YES
GO TO QUESTION 3
NO
IF DEEMED ELIGIBLE, HH CAN RECEIVE BENEFITS WITH ALL OTHER VERIFICATION PENDED, CONTINUE TO SECTION B
3. IF YES TO QUESTION 2, HAS ALL RELEVANT VERIFICATION BEEN SUBMITTED?
YES
IF DEEMED ELIGIBLE HH CAN RECEIVE BENEFITS WITH ALL OTHER VERIFICATION PENDED, CONTINUE TO SECTION B
NO
If HH IS DEEMED ELIGIBLE, SNAP BENEFITS CANNOT BE ISSUED UNTIL ELIGIBILITY IS VERIFIED. ALLOW 10 DAYS FOR VERIFICATION TO BE SUBMITTED. DATE REQUESTED: _____________ DATE SUBMITTED: _____________
SECTION B
DATE OF ELIGIBILITY INTERVIEW: WORKER NAME:
PLEASE COMPLETE FOR NON-CA SNAP HOUSEHOLDS ONLY
1. IS ANY ADULT* (18 YEARS OF AGE OR OLDER) MEMBER OF YOUR HOUSEHOLD EITHER WORKING 30 OR MORE HOURS PER WEEK OR EARNING $217.50 OR MORE PER WEEK?
OR
YES
IF YES, HOUSEHOLD PRESUMPTIVELY QUALIFIES FOR WFSNAPI.
NO
IF NO GO TO QUESTION 2.
2. ARE ANY TWO (2) ADULT* MEMBERS OF YOUR HOUSEHOLD EACH EITHER WORKING 20 OR MORE HOURS PER WEEK OR EARNING $145 OR MORE PER WEEK?
* (Also Minor Heads of SNAP Household)
YES
IF YES, HOUSEHOLD PRESUMPTIVELY QUALIFIES FOR WFSNAPI.
NO
IF NO, HOUSEHOLD DOES NOT QUALIFY FOR WFSNAPI.
AGENCY DISPOSITION OF SNAP BENEFIT ELIGIBILITY - CHECK APPROPRIATE BOXES
SECTION
C
COMPLETION OF THIS SECTION IS OPTIONAL – DISTRICT DISCRETION
ELIGIBLE
ELIGIBLE (Applied on or before 15th of month; zero benefit due to proration)
ELIGIBLE (Applied after 15th of month; zero first month’s benefit due to proration; full second month’s benefit)
ELIGIBLE (Applied after 15th of month; prorated first month’s benefit plus second month’s benefit)
INELIGIBLE: Indicate reason:
HOUSEHOLD IS INELIGIBLE FOR THE PROGRAM DUE TO PROGRAM RULES (provide explanation in comments.)
VERIFICATION OF IDENTITY NOT PROVIDED (SEE A1 ABOVE)
HH DID NOT SUBMIT ALL REQUIRED NON-IDENTITY VERIFICATION (SEE A3 ABOVE)
Other Denial Reason/Comments __________________________________________________________________________________________
DATE OF FINAL DISPOSITION ON SNAP BENEFIT ELIGIBILITY:
WORKER NAME:

LDSS-3938 (Rev. 9/14)
NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE
DATE APPLICATION
FILED
MONTH DAY YEAR
SUPPLEMENTAL NUTRITION ASSISTANCE PROGRAM (SNAP) APPLICATION EXPEDITED PROCESSING SUMMARY SHEET
CASE NAME CASE NUMBER SCREENED BY DATE OF
SCREENING
MONTH DAY YEAR
INSTRUCTIONS FOR COMPLETING THIS FORM
1. Screen all applicants for expedited application processing Working Families SNAP Initiative (WFSNAPI), on the day of application.
2. State results of screening in Part Four; and if qualified for expedited application processing, conduct a Full Eligibility Interview and complete Part Five within five calendar days of application.
3. If Full Eligibility Interview determines Household eligible for SNAP benefits:
Make benefits available to client within five calendar days after the date of application
Send/Provide client with the CNS “Approval Notice” or manual “Action Taken Notice” within five calendar days after the application date
Follow-up on all pended verification before issuance of on-going benefits beyond the initial expedited issuance period
PART ONE – CHECK YES OR NO
IS THE HOUSEHOLD ALREADY RECEIVING SNAP BENEFITS THIS MONTH?
NOTE: IF “YES” IS CHECKED, BUT HOUSEHOLD ENTERED A DOMESTIC VIOLENCE SHELTER DURING THE MONTH OF APPLICATION, CONTINUE WITH PART TWO.
YES - IF YES, HOUSEHOLD DOES
NOT QUALIFY FOR EXPEDITED PROCESSING COMPLETE PART FOUR
NO - IF NO, CONTINUE
WITH PART TWO
PART TWO – CHECK YES OR NO
** In determining GROSS INCOME, exclude non-countable income such as child support payments made to a person outside the household.
SECTION
A
CHECK YES OR NO
DOES THE HOUSEHOLD HAVE $100 OR LESS IN CASH, SAVINGS OR OTHER LIQUID RESOURCES, AND
YES – IF YES, HOUSEHOLD
QUALIFIES FOR EXPEDITED PROCESSING.
COMPLETE PART FOUR
NO – IF NO, CONTINUE
WITH SECTION B.
HAS THE HOUSEHOLD RECEIVED OR DOES IT EXPECT TO
RECEIVE LESS THAN $150 GROSS INCOME ** DURING THE
MONTH OF APPLICATION?
SECTION
B
ARE HOUSEHOLD’S TOTAL GROSS INCOME ** DURING MONTH OF APPLICATION PLUS THE HOUSEHOLD’S LIQUID RESOURCES LESS THAN THEIR MONTHLY RENT/MORTGAGE PLUS UTILITY EXPENSES?
YES
IF YES, HOUSEHOLD QUALIFIES FOR EXPEDITED PROCESSING. COMPLETE PART FOUR
NO
IF NO, HOUSEHOLD DOES NOT QUALIFY FOR EXPEDITED PROCESSING UNLESS QUALIFIED UNDER PART THREE.
GO TO PART THREE IF A MIGRANT/SEASONAL FARMWORKER OTHERWISE, COMPLETE PART FOUR
Rent/Mortgage: $ _____________ Income: $_____________
*Heat/AC: ______________Resources: ____________
*Utilities: ______________
*Telephone: ______________
*Homeless Shelter Deduction ______________
Total Expenses: $______________ Totals: ______________
* Use HT/AC Standard Utility Allowance (SUA) only if household incurs costs or received HEAP greater than $20 during the month of application or within the previous 12 months of application. ** Use the Homeless Shelter Deduction for “undomiciled” households who do not reside in a homeless shelter.
PART THREE – MIGRANT/SEASONAL FARM WORKER HOUSEHOLDS ONLY - CHECK YES OR NO
A. IS THIS A HOUSEHOLD WITH NO MORE THAN $100 IN LIQUID RESOURCES?
AND
YES NO – IF NO, HOUSEHOLD DOES NOT QUALIFY
FOR EXPEDITED PROCESSING. COMPLETE PART FOUR
B. THE ONLY INCOME FOR THE MONTH OF APPLICATION:
(1) WAS TERMINATED BEFORE APPLICATION?
OR
(2) IS NEW, AND NO MORE THAN $25 GROSS INCOME WILL BE RECEIVED WITHIN TEN DAYS AFTER APPLICATION
YES
YES
NO CONTINUE WITH B2
NO
IF YES TO QUESTION A, AND YES TO EITHER QUESTION B1 OR QUESTION B2, HOUSEHOLD QUALIFIES FOR EXPEDITED PROCESSING,
IF NO TO BOTH B1 & B2 HH DOES NOT QUALIFY, COMPLETE PART FOUR IN EITHER SITUATION

LDSS-3938 (Rev. 9/14)
PART FOUR - RESULTS OF EVALUATION FOR EXPEDITED APPLICATION PROCESSING - CHECK ONE
QUALIFIED FOR EXPEDITED APPLICATION PROCESSING. NOT QUALIFIED FOR
EXPEDITED APPLICATION PROCESSING STOP HERE
NOT ENOUGH INFORMATION IS
PROVIDED ON THE APPLICATION TO DETERMINE IF ELIGIBLE FOR EXPEDITED PROCESSING.
NOTES:
PART FIVE - ELIGIBILITY INTERVIEW – COMPLETE SECTIONS A
VERIFICATION - CHECK YES OR NO
SECTION A
1. CAN APPLICANT’S IDENTITY BE VERIFIED?
IF DOCUMENTARY EVIDENCE IS NOT READILY AVAILABLE, COLLATERAL CONTACTS ARE ACCEPTABLE. NO SPECIFIC DOCUMENT CAN BE REQUIRED.
YES, IF ELIGIBLE
BENEFITS CAN BE ISSUED PROVIDED ANY OUTSTANDING REQUIREMENTS HAVE BEEN MET GO TO QUESTION 2
NO
IF APPLICANT IS DEEMED ELIGIBLE, SNAP BENEFITS CANNOT BE ISSUED UNTIL VERIFICATION OF IDENTITY IS PROVIDED GO TO QUESTION 2
2. WAS THE HOUSEHOLD’S LAST ISSUANCE AN EXPEDITED ISSUANCE?
YES
GO TO QUESTION 3
NO
IF DEEMED ELIGIBLE, HH CAN RECEIVE BENEFITS WITH ALL OTHER VERIFICATION PENDED, CONTINUE TO SECTION B
3. IF YES TO QUESTION 2, HAS ALL RELEVANT VERIFICATION BEEN SUBMITTED?
YES
IF DEEMED ELIGIBLE HH CAN RECEIVE BENEFITS WITH ALL OTHER VERIFICATION PENDED, CONTINUE TO SECTION B
NO
If HH IS DEEMED ELIGIBLE, SNAP BENEFITS CANNOT BE ISSUED UNTIL ELIGIBILITY IS VERIFIED. ALLOW 10 DAYS FOR VERIFICATION TO BE SUBMITTED. DATE REQUESTED: _____________ DATE SUBMITTED: _____________
WORKING FAMILIES SUPPLEMENTAL NUTRITION ASSISTANCE PROGRAM INITIATIVE
SECTION B
PLEASE COMPLETE FOR NON-TA SNAP HOUSEHOLDS ONLY
1. IS ANY ADULT* (18 YEARS OF AGE OR OLDER) MEMBER OF YOUR YES – IF YES, HOUSEHOLD NO – IF NO, GO TO
HOUSEHOLD EITHER WORKING 30 OR MORE HOURS PER WEEK PRESUMPTIVELY QUALIFIES QUESTION 2 OR EARNING $217.50 OR MORE PER WEEK? FOR WFSNAPI
OR
2. ARE ANY TWO (2) ADULT* MEMBERS OF YOUR HOUSEHOLD EACH YES – IF YES, HOUSEHOLD NO – IF NO,
EITHER WORKING 20 OR MORE HOURS PER WEEK OR EARNING PRESUMPTIVELY QUALIFIES HOUSEHOLD DOES $145 OR MORE PER WEEK? FOR WFSNAPI NOT QUALIFY FOR WFSNAP
DATE ELIGIBILITY INTERVIEW:
WORKER NAME:

Appendix F –
Documentation Requirements Checklist
(LDSS-2642)


Appendix G –
SNAP Documentation Verification Desk Guide (LDSS-3666)

LD
SS-3
666
(Rev
.8/1
2) F
RO
NT
NEW
YO
RK
STA
TE O
FFIC
E O
F TE
MP
OR
AR
Y A
ND
DIS
AB
ILIT
Y A
SS
ISTA
NC
E
TA/S
UPP
LEM
ENTA
L N
UTR
ITIO
N A
SSIS
TAN
CE
PRO
GR
AM
(SN
AP)
DO
CU
MEN
TATI
ON
/VER
IFIC
ATI
ON
DES
K G
UID
E TA
SN
AP
ELIG
IBIL
ITY
FAC
TOR
PR
IMA
RY
SEC
ON
DA
RY
TA
SN
AP
ELIG
IBIL
ITY
FAC
TOR
PR
IMA
RY
M
M
Id
entit
y
Pho
to I.
D.
Drive
r’s L
ice
nse
US
Pas
spor
t N
atur
aliz
atio
n C
ertif
icat
e H
osp
ita
l/D
octo
r’s R
eco
rds
Ado
ptio
n P
aper
s Fo
r SN
AP – Id
entit
y is
onl
y m
anda
tory
for t
he p
erso
n m
akin
g th
e ap
plic
atio
n.
Sta
tem
ent f
rom
Ano
ther
Per
son
Soc
ial S
ecur
ity N
umbe
r B
irth/
Bapt
ism
al C
ertif
icat
e S
OLQ
Fo
r SN
AP
- In
the
case
of a
n au
thor
ized
re
pres
enta
tive,
bot
h th
e au
th re
p an
d ap
plic
ant m
ust v
erify
Iden
tity.
M
N
A
bsen
t Par
ent
Info
rmat
ion
Pay
Stu
bs
Tax
Ret
urns
S
ocia
l Sec
urity
or V
A R
ecor
ds
Une
mpl
oym
ent (
UIB
) Boo
k ID
Car
ds (H
ealth
Insu
ranc
e)
Drive
r’s L
ice
nse o
r R
egis
tration
M
N
M
arita
l Sta
tus
Mar
riage
/Dea
th C
ertif
icat
es
Sep
arat
ion
Agr
eem
ent
Div
orce
Dec
ree
Soc
ial S
ecur
ity R
ecor
ds
VA
Rec
ords
Sta
tem
ent f
rom
Cle
rgy
Cen
sus
Rec
ords
N
ewsp
aper
Not
ice
Sta
tem
ent f
rom
Ano
ther
Per
son
M
M *
Soci
al S
ecur
ity
Num
ber
Soc
ial S
ecur
ity C
ard
Offi
cial
Cor
resp
onde
nce
from
SS
A Fo
r TA
and
SN
AP,
pro
vide
d or
app
ly fo
r # a
t ce
rtific
atio
n; m
ust v
erify
at f
irst r
ecer
tific
atio
n un
less
va
lidat
ed b
y W
MS
SO
LQ
M
M *
Res
iden
ce
Sta
tem
ent f
rom
Lan
dlor
d C
urre
nt R
ent R
ecei
pt o
r Lea
se
Mor
tgag
e R
ecor
ds
For S
NA
P- R
esid
ence
is
verif
ied
at a
hou
seho
ld le
vel
Sta
tem
ent f
rom
Ano
ther
Per
son
Cur
rent
Mai
l S
choo
l Rec
ords
Fu
el/U
tility
bill
M
M
Q
M
Citi
zens
hip
Alie
n St
atus
Birt
h/Ba
ptis
mal
Cer
tific
ate
H
ospi
tal R
ecor
ds
US
Pas
spor
t M
ilitar
y S
ervi
ce R
ecor
ds
Nat
ural
izat
ion
Cer
tific
ate
US
CIS
Doc
umen
tatio
n Ev
iden
ce o
f Con
tinuo
us U
S R
esid
ence
sin
ce P
rior t
o 1/
1/72
Fo
r TA
and
SN
AP,
alie
n st
atus
is v
erifi
ed o
n an
in
divi
dual
bas
is
For S
NA
P O
nly,
citi
zens
hip
is v
erifi
ed o
nly
if qu
estio
nabl
e
M
M *
Hou
seho
ld
Com
posi
tion/
Size
Sta
tem
ent f
rom
N
on-r
elat
ive
Land
lord
Fo
r SN
AP –
hou
seho
ld s
ize
mus
t be
verif
ied.
Thi
s ca
n be
do
ne th
roug
h co
llate
ral
cont
acts
or r
eadi
ly a
vaila
ble
docu
men
ts w
hich
can
be
used
to
est
ablis
h Id
entit
y.
Sta
tem
ent f
rom
Oth
er P
erso
ns
M
M *
Earn
ed In
com
e
Cur
rent
Wag
e St
ubs
and
Stat
emen
t of T
ips
Pay
Env
elop
es
Con
tact
with
Em
ploy
er
Bus
ines
s R
ecor
ds
Rec
ords
and
Rel
ated
Mat
eria
ls C
once
rnin
g S
elf-
Em
ploy
men
t Ear
ning
s an
d E
xpen
ses
Cur
rent
Inco
me
Tax
Ret
urn
Sta
tem
ent f
rom
Roo
mer
, Boa
rder
, Ten
ant
Inco
me
Tax
Rec
ords
M
M *
Age
Birt
h C
ertif
icat
e B
aptis
mal
Cer
tific
ate
Hos
pita
l Rec
ords
A
dopt
ion
Rec
ords
N
atur
aliz
atio
n C
ertif
icat
e D
rive
r’s L
ice
nse
For S
NA
P O
nly,
DO
B c
an b
e V
erifi
ed a
t Rec
ertif
icat
ion
Insu
ranc
e Po
licy
Cen
sus
Rec
ords
S
choo
l Rec
ords
S
tate
men
t fro
m A
noth
er P
erso
n P
hysi
cian
Sta
tem
ent
Offi
cial
Cor
resp
onde
nce
from
SSA
M
M *
Une
arne
d In
com
e
Sta
tem
ent f
rom
Fam
ily C
ourt
Sta
tem
ent f
rom
Per
son
Pay
ing
S
tate
men
t fro
m S
choo
l S
tate
men
t fro
m B
ank
or C
redi
t Uni
on
Sta
tem
ent f
rom
Bro
ker/A
gent
S
uppo
rt C
heck
stu
bs
Cur
rent
Aw
ard
Cer
tific
ate
Cur
rent
Ben
efit
Che
ck
Offi
cial
Cor
resp
onde
nce
with
NY
S D
ept.
of L
abor
O
ffici
al C
orre
spon
denc
e fro
m S
SA
Offi
cial
Cor
resp
onde
nce
from
VA
Offi
cial
Cor
resp
onde
nce
from
sou
rce
of in
com
e A
war
d Le
tter
M
N
A
bsen
t Par
ent
Dea
th C
ertif
icat
e S
urv
ivo
r’s B
en
efits
H
ospi
tal R
ecor
ds
VA
or M
ilitar
y R
ecor
ds
Div
orce
Pap
ers
Pro
of o
f Rem
arria
ge
New
spap
er N
otic
e In
sura
nce
Com
pany
Rec
ords
In
stitu
tiona
l Rec
ords
A
genc
y C
ase
Rec
ords
and
B
uria
l Pay
men
t Lin
es
Sta
tem
ent f
rom
a N
on-R
elat
ive
LE
GE
ND
: M
=
Man
dato
ry D
ocum
enta
tion/
Verif
icat
ion
requ
ired
for C
ertif
icat
ion
Q =
Ver
ifica
tion
is O
nly
Nec
essa
ry if
Que
stio
nabl
e N
=
No
Doc
umen
tatio
n/Ve
rific
atio
n re
quire
d O
=
Opt
iona
l Doc
umen
tatio
n/V
erifi
catio
n (m
ay b
e ne
cess
ary
for T
A a
nd/o
r SN
AP
elig
ibilit
y or
ben
efit
amou
nt.)
* =
Ver
ifica
tion
can
be p
ende
d un
der S
NA
P E
xped
ited
Pro
cess
ing

L
DSS
-366
6 (R
ev. 8
/12)
REV
ER
SE
NEW
YO
RK
STA
TE O
FFIC
E O
F TE
MP
OR
AR
Y A
ND
DIS
AB
ILIT
Y A
SS
ISTA
NC
E
TA/S
UPP
LEM
ENTA
L N
UTR
ITIO
N A
SSIS
TAN
CE
PRO
GR
AM
(SN
AP)
DO
CU
MEN
TATI
ON
/VER
IFIC
ATI
ON
DES
K A
ID
TA
SNA
P EL
IGIB
ILIT
Y FA
CTO
R
PRIM
AR
Y
EXPE
NSE
S TH
AT
MA
Y A
FFEC
T EL
IGIB
ILIT
Y O
R B
ENEF
IT A
MO
UN
T
M
M *
Res
ourc
es
Sta
tem
ent f
rom
hou
seho
ld
Sta
tem
ent f
rom
nur
sing
hom
e C
urre
nt b
ank
reco
rds
Cur
rent
cre
dit u
nion
reco
rds
Sto
ck c
ertif
icat
e B
onds
S
tate
men
t fro
m fi
nanc
ial i
nstit
utio
n
Insu
ranc
e po
licy
Sta
tem
ent f
rom
insu
ranc
e co
mpa
ny
Bur
ial a
gree
men
t B
uria
l plo
t dee
d S
tate
men
t fro
m fu
nera
l dire
ctor
Ref
und
or E
ITC
che
ck
Sta
tem
ent f
rom
tax
offic
e
Dee
d S
tate
men
t fro
m re
al e
stat
e br
oker
A
ppra
isal
/est
imat
e of
cur
rent
val
ue b
y br
oker
Ti
tle o
f ow
ners
hip
Reg
istra
tion
(old
er m
odel
s)
App
rais
al o
f cur
rent
val
ue b
y de
aler
Fi
nanc
ing
data
Sta
tem
ent f
rom
sou
rce
of p
aym
ent
TA
SNA
P EL
IGIB
ILIT
Y FA
CTO
R
PRIM
AR
Y
O
O
*
She
lter
Expe
nses
Cur
rent
rent
rece
ipt
Cur
rent
leas
e M
ortg
age
book
/reco
rds
Pro
perty
and
sch
ool t
ax re
cord
s La
ndlo
rd s
tate
men
t S
ewer
and
wat
er b
ills
Hom
eow
ner’s insura
nce re
cord
s Fu
el b
ills
Non
-hea
ting
utilit
y bi
lls
Tel
epho
ne b
ills
O
O
*
Med
ical
Bill
s
Cop
ies
of m
edic
al b
ills (p
aid
and
unpa
id)
Pro
vide
r Sta
tem
ent o
f Hea
lth In
sura
nce
prem
ium
s M
edic
are
Pre
scrip
tion
Dru
g C
ard
For S
NAP
, for
A/D
indi
vidu
als
only
O
O
*
Unp
aid
Bill
s R
ent,
Util
ity
Cop
y of
eac
h bi
ll sh
owin
g am
ount
ow
ed, p
erio
d of
se
rvic
es a
nd p
rovi
der
O
O
*
Oth
er E
xpen
ses
Dep
ende
nt C
are
Cos
t
Cou
rt or
der
Sta
tem
ent f
rom
day
car
e ce
nter
or o
ther
chi
ld c
are
prov
ider
S
tate
men
t fro
m a
ide
or a
ttend
ant
Can
celle
d ch
ecks
or r
ecei
pts
M
O
*
Hea
lth
Insu
ranc
e
Insu
ranc
e po
licy
Insu
ranc
e ca
rd
Sta
tem
ent f
rom
pro
vide
r of c
over
age
Med
icar
e ca
rd
M
O
*
Dis
able
d/
Inca
paci
tate
d/
Preg
nant
Sta
tem
ent f
rom
med
ical
pro
fess
iona
l ver
ifyin
g pr
egna
ncy
and
expe
cted
dat
e of
birt
h S
tate
men
t fro
m m
edic
al p
rofe
ssio
nal
Pro
of o
f SSA
or S
SI b
enef
its fo
r dis
abilit
y or
blin
dnes
s
M
M
*
Able
-Bod
ied
Adul
t W
ithou
t D
epen
dent
s (A
BAW
D) E
ligib
ility
For
non-
wai
ver
area
s an
d no
n-ex
clud
ed
ABA
WD
in
divi
dual
s P
roof
of w
orki
ng a
nd/o
r w
ork
prog
ram
par
ticip
atio
n fo
r at
leas
t 80
hour
s pe
r mon
th
Che
ck T
ime
Lim
it Tr
acki
ng M
enu
(#17
on
WM
S m
enu)
fo
r 3
or m
ore
mon
ths
of F
S r
ecei
pt in
pas
t 36
mon
ths
with
out m
eetin
g AB
AWD
wor
k re
quire
men
t
M
O
*
Ref
erra
l S
tate
men
t fro
m p
rovi
der o
f tre
atm
ent
Sta
tem
ent f
rom
em
ploy
men
t ser
vice
*L
EG
EN
D: M
=
Man
dato
ry D
ocum
enta
tion/
Verif
icat
ion
requ
ired
for C
ertif
icat
ion
N
=
No
Doc
umen
tatio
n/V
erifi
catio
n re
quire
d O
=
Opt
iona
l D
ocum
enta
tion/
Ver
ifica
tion
(may
be
nece
ssar
y fo
r TA
an
d/or
SN
AP
elig
ibili
ty o
r ben
efit
amou
nt.)
Q
= V
erifi
catio
n is
onl
y ne
cess
ary
if qu
estio
nabl
e *
= V
erifi
catio
n ca
n be
pen
ded
unde
r SN
AP
Exp
edite
d P
roce
ssin
g O
O
*
Scho
ol
Atte
ndan
ce
Sch
ool r
ecor
ds (
curre
nt re
port
card
) S
tate
men
t fro
m s
choo
l Fo
r SN
AP, a
ffect
s w
ork
regi
stra
tion
and
earn
ings
of
child
ren
unde
r 18

Appendix H –
Non-Citizen Eligibility Chart (LDSS-4579)

LDSS
-457
9 (R
ev. 8
/12)
A
LIEN
ELI
GIB
ILIT
Y D
ESK
AID
Pa
ge 1
Des
crip
tion
of S
tatu
s W
MS/
AC
I C
ode
Com
mon
Doc
umen
tatio
n
Rel
evan
t D
ate
for
Elig
ibili
ty
M
edic
aid
1
Fam
ily
Assi
stan
ce
Safe
ty N
et
Assi
stan
ce
Supp
lem
enta
l Nut
ritio
n As
sist
ance
Pro
gram
(S
NAP
) Ben
efits
Ref
ugee
s R
I-94:
sta
mped “
Adm
itte
d u
nder
Sectio
n 2
07
of
the I
NA
,” “
Refu
gee,”
“R
E1, R
E2,
RE
3,
RE
4”
or
I-5
51: s
tam
ped “R
8-6
, RE
5, R
E6,
RE
7, R
E8
or
RE
9”
or
I-571
: Ref
ugee
Tra
vel D
ocum
ent
or
I-688
B:
Empl
oym
ent A
utho
rizat
ion
Doc
umen
t annota
ted w
ith “
8 C
.F.R
. § 2
74a.
12(a
) (3
)”
or
I-7
66:
Empl
oym
ent A
utho
rizat
ion
Doc
umen
t annota
ted “
a3”
Entr
y
Yes
Cub
an/H
aitia
n En
tran
ts
H
I-94:
sta
mped “
Cuban/H
aitia
n E
ntr
ant
(sta
tus
pendin
g),
” “S
ectio
n 2
12(d
) (5
) of th
e I
NA
,” “
Fo
rm
I-589 f
iled,”
or
“CU
6,”
or
CU
7”
or
I-9
4 st
amp
show
ing
paro
le u
nder
Sec
tion
212(
d)(5
) of I
NA
or s
tam
p sh
owin
g pa
role
in U
S
on o
r afte
r 10/
10/8
0 an
d re
ason
able
evi
denc
e th
at p
arol
ee h
as b
een
a N
atio
nal (
citiz
en) o
f C
uba
or H
aiti2
or
I-551
: sta
mp
ed “
CU
6,
CU
7,
or
CH
6”
or
Tem
pora
ry I-
551
stam
p in
fore
ign
pass
port.
or
US
CIS
not
ice
or le
tter i
ndic
atin
g on
goin
g ex
clus
ion
or d
epor
tatio
n pr
ocee
ding
s
Stat
us
Gra
nted
Asyl
ees
A
I-94:
sta
mped “
Gra
nte
d a
sylu
m u
nder
Sectio
n
208 o
f th
e I
NA
” or
I-5
51: S
tam
ped “
AS
1,A
S2, A
S3, A
S6, A
S7,
or
AS
8”
or
I-688
B:
Empl
oym
ent A
utho
rizat
ion
Car
d annota
ted w
ith “
8 C
.F.R
. § 2
74a.
12(a
)(5)”
or
I-7
66:
Empl
oym
ent A
utho
rizat
ion
Doc
umen
t annota
ted “
(a5)
” or
G
rant
lette
r fro
m U
SC
IS A
sylu
m O
ffice
or
O
rder
of a
n im
mig
ratio
n ju
dge
gran
ting
asyl
um.
1 REM
IND
ER: F
or M
edic
aid,
und
ocum
ente
d al
iens
and
tem
pora
ry n
on-im
mig
rant
s m
ay re
ceiv
e co
vera
ge fo
r car
e an
d se
rvic
es n
eces
sary
for t
he tr
eatm
ent o
f em
erg
en
cy m
edic
al c
ondi
tions
on
ly, n
ot in
clud
ing
care
and
ser
vice
s re
late
d to
an
orga
n tr
ansp
lant
pro
cedu
re, i
f oth
erw
ise
elig
ible
. Pr
egna
nt w
omen
may
be
prov
ided
Med
icai
d at
an
y t
ime w
ithou
t reg
ard
to a
lien
stat
us, i
f ot
herw
ise
elig
ible
. Chi
ldre
n m
ay b
e pr
ovid
ed m
edic
al a
ssis
tanc
e w
ithou
t reg
ard
to im
mig
ratio
n st
atus
und
er C
hild
Hea
lth P
lus
(CH
Plu
s) p
rogr
am.
2 EXC
EPTI
ON
: Th
is g
uide
line
does
not
app
ly w
hen
the
indi
vidu
al w
as p
arol
ed s
olel
y to
test
ify a
s a
witn
ess
in a
judi
cial
, adm
inis
trat
ive
or le
gisl
ativ
e pr
ocee
ding
or w
hen
the
paro
lee
is in
lega
l cu
stod
y pe
ndin
g cr
imin
al p
rose
cutio
n.
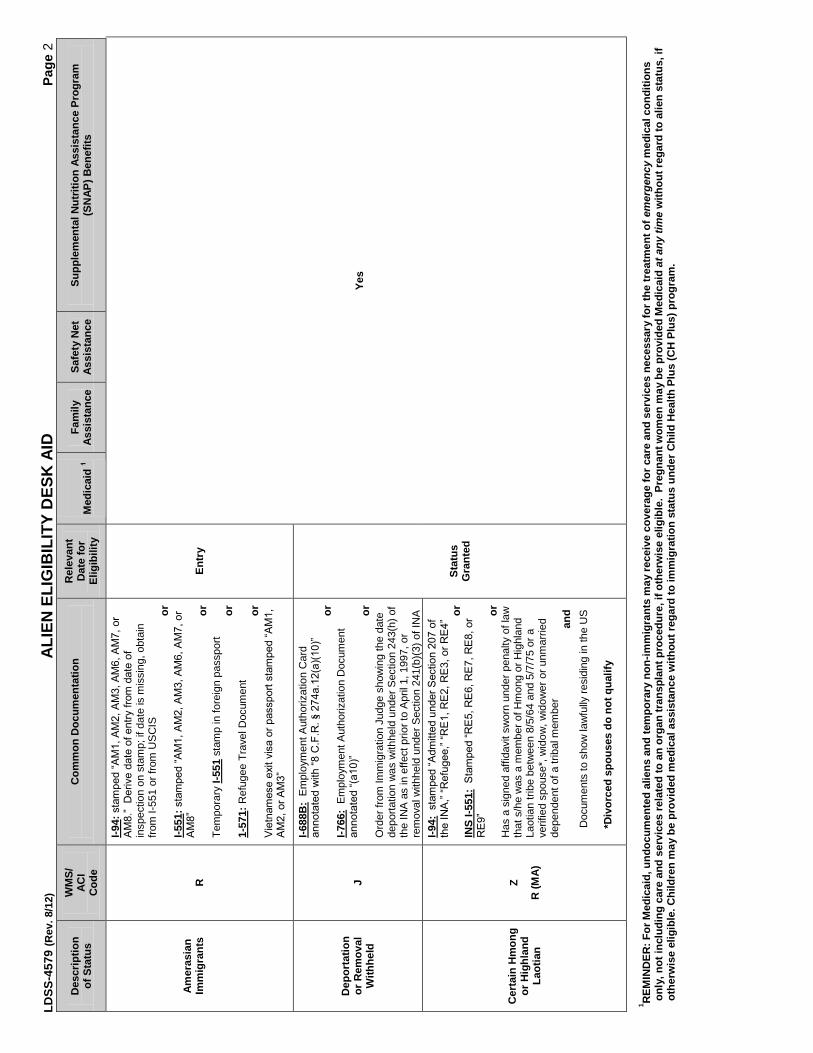
LDSS
-457
9 (R
ev. 8
/12)
A
LIEN
ELI
GIB
ILIT
Y D
ESK
AID
Pa
ge 2
Des
crip
tion
of S
tatu
s W
MS/
AC
I C
ode
Com
mon
Doc
umen
tatio
n
Rel
evan
t D
ate
for
Elig
ibili
ty
M
edic
aid
1
Fam
ily
Assi
stan
ce
Safe
ty N
et
Assi
stan
ce
Supp
lem
enta
l Nut
ritio
n As
sist
ance
Pro
gram
(S
NAP
) Ben
efits
Amer
asia
n Im
mig
rant
s
R
I-94:
sta
mped “
AM
1, A
M2, A
M3, A
M6,
AM
7,
or
AM
8.”
D
erive d
ate
of entr
y f
rom
date
of
insp
ectio
n on
sta
mp;
if d
ate
is m
issi
ng, o
btai
n fro
m I-
551
or fr
om U
SC
IS
or
I-5
51: s
tam
ped “
AM
1, A
M2, A
M3, A
M6,
AM
7, or
AM
8”
or
Tem
pora
ry I-
551
stam
p in
fore
ign
pass
port
or
1-57
1: R
efug
ee T
rave
l Doc
umen
t
or
Vie
tnam
ese e
xit v
isa o
r passport
sta
mped “
AM
1,
AM
2,
or
AM
3”
Entr
y
Yes
Dep
orta
tion
or R
emov
al
With
held
J
I-688
B:
Empl
oym
ent A
utho
rizat
ion
Car
d annota
ted w
ith “
8 C
.F.R
. §
274a.1
2(a
)(10)”
or
I-7
66:
Empl
oym
ent A
utho
rizat
ion
Doc
umen
t annota
ted “
(a10)”
or
O
rder
from
Imm
igra
tion
Judg
e sh
owin
g th
e da
te
depo
rtatio
n w
as w
ithhe
ld u
nder
Sec
tion
243(
h) o
f th
e IN
A a
s in
effe
ct p
rior t
o A
pril
1, 1
997,
or
rem
oval
with
held
und
er S
ectio
n 24
1(b)
(3) o
f IN
A
Stat
us
Gra
nted
Cer
tain
Hm
ong
or H
ighl
and
Laot
ian
Z
R (M
A)
I-94:
sta
mped “
Adm
itte
d u
nder
Sectio
n 2
07 o
f th
e I
NA
,” “
Refu
gee,”
“R
E1, R
E2,
RE
3,
or
RE
4”
or
INS
I-551
: S
tam
ped “
RE
5, R
E6, R
E7,
RE
8, or
RE
9”
or
Has
a s
igne
d af
fidav
it sw
orn
unde
r pen
alty
of l
aw
that
s/h
e w
as a
mem
ber o
f Hm
ong
or H
ighl
and
Laot
ian
tribe
bet
wee
n 8/
5/64
and
5/7
/75
or a
ve
rifie
d sp
ouse
*, w
idow
, wid
ower
or u
nmar
ried
depe
nden
t of a
trib
al m
embe
r a
nd
Doc
umen
ts to
sho
w la
wfu
lly re
sidi
ng in
the
US
*Div
orce
d sp
ouse
s do
not
qua
lify
1 R
EMIN
DER
: For
Med
icai
d, u
ndoc
umen
ted
alie
ns a
nd te
mpo
rary
non
-imm
igra
nts
may
rece
ive
cove
rage
for c
are
and
serv
ices
nec
essa
ry fo
r the
trea
tmen
t of e
merg
en
cy m
edic
al c
ondi
tions
on
ly, n
ot in
clud
ing
care
and
ser
vice
s re
late
d to
an
orga
n tr
ansp
lant
pro
cedu
re, i
f oth
erw
ise
elig
ible
. Pr
egna
nt w
omen
may
be
prov
ided
Med
icai
d at
an
y t
ime w
ithou
t reg
ard
to a
lien
stat
us, i
f ot
herw
ise
elig
ible
. Chi
ldre
n m
ay b
e pr
ovid
ed m
edic
al a
ssis
tanc
e w
ithou
t reg
ard
to im
mig
ratio
n st
atus
und
er C
hild
Hea
lth P
lus
(CH
Plu
s) p
rogr
am.

LDSS
-457
9 (R
ev. 8
/12)
A
LIEN
ELI
GIB
ILIT
Y D
ESK
AID
Pa
ge 3
D
escr
iptio
n of
Sta
tus
WM
S/
ACI
Cod
e C
omm
on D
ocum
enta
tion
R
elev
ant
Dat
e fo
r El
igib
ility
Med
icai
d 1
Fam
ily A
ssis
tanc
e Sa
fety
Net
As
sist
ance
SN
AP
Ben
efits
* La
wfu
lly A
dmitt
ed
For P
erm
anen
t R
esid
ence
(LPR
) with
40
Qua
lifyi
ng Q
uart
ers
S
I-551
: (P
erm
anen
t Res
iden
t Car
d)
or
Tem
pora
ry I-
551
stam
p in
fore
ign
pass
port
or
on I-
94
or
I-327
: (R
e-en
try P
erm
it)
or
I-1
81:
Mem
oran
dum
of C
reat
ion
of L
awfu
l P
erm
anen
t Res
iden
ce w
ith a
ppro
val s
tam
p
and
Proo
f of q
ualif
ying
qua
rter
s
Ente
red
Bef
ore
8/22
/96
Yes
Ente
red
On/
Afte
r 08
/22/
96
Yes
Yes,
afte
r 5 y
ears
in U
S in
a
qual
ified
sta
tus
Ye
s
Law
fully
Adm
itted
For
Pe
rman
ent R
esid
ence
(L
PR) w
ithou
t 40
Q
ualif
ying
Qua
rter
s K
I-551
: (P
erm
anen
t Res
iden
t Car
d)
or
Tem
pora
ry I-
551
stam
p in
fore
ign
pass
port
or
on I-
94.
or
I-327
(Re-
entry
Per
mit)
or
I-1
81:
Mem
oran
dum
of C
reat
ion
of L
awfu
l P
erm
anen
t Res
iden
ce w
ith a
ppro
val s
tam
p
Ente
red
Bef
ore
8-22
-96
Ye
s Ye
s
Yes
if:
In
a q
ualif
ied
stat
us
and
in re
ceip
t of
cert
ain
disa
bilit
y be
nefit
s
[7 U
SC 2
012(
r)]
or
Af
ter f
ive
year
s in
US
in
a qu
alifi
ed s
tatu
s
o
r
In a
qua
lifie
d st
atus
and
un
der a
ge 1
8
Ente
red
On
or
Afte
r 08
/22/
96
Yes
Yes,
afte
r 5 y
ears
in U
S in
a
qual
ified
sta
tus
Yes
Vete
ran,
spo
use,
un
mar
ried
surv
ivin
g sp
ouse
and
unm
arrie
d de
pend
ent c
hild
of a
U
.S. v
eter
an w
ho
fulfi
lled
min
imum
ac
tive
duty
re
quire
men
t (2
year
s)
V
A D
isch
arge
Cer
tific
ate
(For
m D
D-2
14) t
hat
sta
tes “
Honora
ble
.” A
chara
cte
r of dis
charg
e
“Under
Honora
ble
Conditio
ns”
is n
ot
an
“Honora
ble
Dis
charg
e”
for
these p
urp
oses.
Nar
rativ
e R
easo
n fo
r Sep
arat
ion
bloc
k m
ust
not s
tate
that
dis
char
ge w
as fo
r rea
son
of
“alie
nage”
or
lack o
f U
.S. citi
zens
hip.
Stat
us
Gra
nted
Ye
s
Activ
e M
ilita
ry:
Activ
e du
ty o
r a m
embe
r of
the
Arm
ed F
orce
s on
fu
ll-tim
e du
ty in
the
Arm
y, N
avy,
Air
Forc
e,
Mar
ine
Cor
ps o
r Coa
st
Gua
rd, s
pous
e an
d ch
ildre
n
M
Mili
tary
Iden
tific
atio
n C
ard
(DD
For
m 2
) (Ac
tive)
th
at li
sts
an e
xpira
tion
date
of m
ore
than
one
ye
ar fr
om th
e da
te o
f det
erm
inat
ion.
If I
D c
ard
is d
ue to
exp
ire w
ithin
one
yea
r fro
m th
e da
te
of d
eter
min
atio
n, u
se a
cop
y of
cur
rent
milit
ary
orde
rs.
Stat
us
Gra
nted
Ye
s
Con
ditio
nal E
ntra
nt
(sta
tus
gran
ted
to
refu
gees
bef
ore
1980
) F
I-94
with
sta
mp
show
ing
adm
itted
und
er
Sec
tion
203(
a)(7
) of I
NA
or
I-6
88B
(Em
ploy
men
t Aut
horiz
atio
n C
ard)
annota
ted “
274a
.12(a
)(3)”
or
I-7
66 (E
mpl
oym
ent A
utho
rizat
ion
Doc
umen
t) an
nota
ted
“(A1)
” or “
(A3)
”
Entr
y Ye
s
*No
quar
ters
ear
ned
afte
r 12/
31/9
6 m
ay b
e co
unte
d in
whi
ch a
n al
ien
has
rece
ived
a F
eder
al m
eans
-test
ed p
ublic
ben
efit
(FA,
SSI
, SN
AP o
r Med
icai
d.)
1 REM
IND
ER: F
or M
edic
aid,
und
ocum
ente
d al
iens
and
tem
pora
ry n
on-im
mig
rant
s m
ay re
ceiv
e co
vera
ge fo
r car
e an
d se
rvic
es n
eces
sary
for t
he tr
eatm
ent o
f em
erg
en
cy m
edic
al c
ondi
tions
on
ly, n
ot in
clud
ing
care
and
ser
vice
s re
late
d to
an
orga
n tr
ansp
lant
pro
cedu
re, i
f oth
erw
ise
elig
ible
. Pr
egna
nt w
omen
may
be
prov
ided
Med
icai
d at
an
y t
ime w
ithou
t reg
ard
alie
n st
atus
, if
othe
rwis
e el
igib
le.
Chi
ldre
n m
ay b
e pr
ovid
ed m
edic
al a
ssis
tanc
e w
ithou
t reg
ard
to im
mig
ratio
n st
atus
und
er C
hild
Hea
lth P
lus
(CH
Plu
s) p
rogr
am.
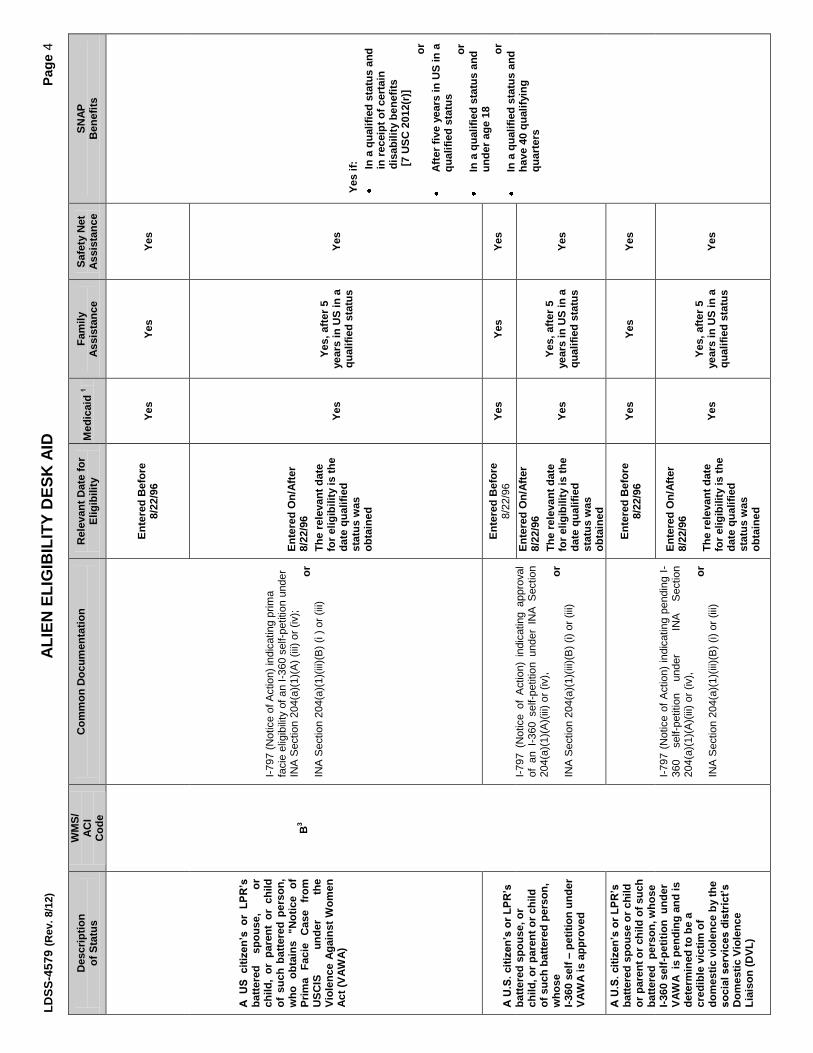
LDSS
-457
9 (R
ev. 8
/12)
A
LIEN
ELI
GIB
ILIT
Y D
ESK
AID
Pa
ge 4
Des
crip
tion
of S
tatu
s W
MS/
AC
I C
ode
Com
mon
Doc
umen
tatio
n
Rel
evan
t Dat
e fo
r El
igib
ility
M
edic
aid
1
Fam
ily
Assi
stan
ce
Safe
ty N
et
Assi
stan
ce
SNAP
B
enef
its
A U
S cit
izen
’s o
r L
PR
’s
batte
red
spou
se,
or
ch
ild,
or p
aren
t or
chi
ld
of s
uch
batte
red
pers
on,
who
obt
ains
"N
otic
e of
Pr
ima
Faci
e C
ase
from
U
SCIS
un
der
the
Viol
ence
Aga
inst
Wom
en
Act (
VAW
A)
B3
I-797
(Not
ice
of A
ctio
n) in
dica
ting
prim
a fa
cie
elig
ibilit
y of
an
I-360
sel
f-pet
ition
und
er
INA
Sec
tion
204(
a)(1
)(A) (
iii) o
r (iv
);
or
IN
A S
ectio
n 20
4(a)
(1)(i
ii)(B
) (i )
or (
iii)
Ente
red
Bef
ore
8/22
/96
Yes
Yes
Yes
Y
es if
:
In a
qua
lifie
d st
atus
and
in
rece
ipt o
f cer
tain
di
sabi
lity
bene
fits
[7 U
SC 2
012(
r)]
o
r
Afte
r fiv
e ye
ars
in U
S in
a
qual
ified
sta
tus
or
In
a q
ualif
ied
stat
us a
nd
unde
r age
18
or
In
a q
ualif
ied
stat
us a
nd
have
40
qual
ifyin
g qu
arte
rs
Ente
red
On/
Afte
r 8/
22/9
6
The
rele
vant
dat
e
for e
ligib
ility
is th
e da
te q
ualif
ied
stat
us w
as
obta
ined
Yes
Yes,
afte
r 5
year
s in
US
in a
qu
alifi
ed s
tatu
s Ye
s
A U
.S.
cit
izen
’s o
r L
PR
’s
batte
red
spou
se, o
r ch
ild, o
r par
ent o
r chi
ld
of s
uch
batte
red
pers
on,
who
se
I-360
sel
f – p
etiti
on u
nder
VA
WA
is a
ppro
ved
I-797
(N
otic
e of
Act
ion)
ind
icat
ing
appr
oval
of
an
I-360
sel
f-pet
ition
und
er I
NA
Sec
tion
204(
a)(1
)(A)(i
ii) o
r (iv
),
or
INA
Sec
tion
204(
a)(1
)(iii)
(B) (
i) or
(iii)
Ente
red
Bef
ore
8/22
/96
Yes
Yes
Yes
Ente
red
On/
Afte
r 8/
22/9
6 Th
e re
leva
nt d
ate
fo
r elig
ibili
ty is
the
date
qua
lifie
d st
atus
was
ob
tain
ed
Yes
Yes,
afte
r 5
year
s in
US
in a
qu
alifi
ed s
tatu
s Ye
s
A U
.S.
cit
izen
’s o
r L
PR
’s
batte
red
spou
se o
r chi
ld
or p
aren
t or c
hild
of s
uch
batte
red
per
son,
who
se
I-360
sel
f-pet
ition
und
er
VAW
A is
pen
ding
and
is
dete
rmin
ed to
be
a cr
edib
le v
ictim
of
dom
estic
vio
lenc
e by
the
so
cia
l serv
ices d
istr
ict’
s
Dom
estic
Vio
lenc
e Li
aiso
n (D
VL)
I-797
(N
otic
e of
Act
ion)
indi
catin
g pe
ndin
g I-
360
self-
petit
ion
unde
r
INA
S
ectio
n 20
4(a)
(1)(A
)(iii)
or (
iv),
or
IN
A S
ectio
n 20
4(a)
(1)(i
ii)(B
) (i)
or (i
ii)
En
tere
d B
efor
e 8/
22/9
6
Yes
Yes
Yes
Ente
red
On/
Afte
r 8/
22/9
6 Th
e re
leva
nt d
ate
fo
r elig
ibili
ty is
the
date
qua
lifie
d st
atus
was
ob
tain
ed
Yes
Yes,
afte
r 5
year
s in
US
in a
qu
alifi
ed s
tatu
s Ye
s

LDSS
-457
9 (R
ev. 8
/12)
A
LIEN
ELI
GIB
ILIT
Y D
ESK
AID
Pa
ge 5
D
escr
iptio
n of
Sta
tus
WM
S/
ACI
Cod
e C
omm
on D
ocum
enta
tion
R
elev
ant D
ate
for
Elig
ibili
ty
Med
icai
d 1
Fam
ily
Assi
stan
ce
Safe
ty N
et
Assi
stan
ce
SNAP
B
enef
its
An
alie
n de
term
ined
to
be a
cre
dibl
e vi
ctim
of
dom
estic
vio
lenc
e by
the
so
cia
l serv
ices d
istr
ict’
s
DVL
with
a p
endi
ng o
r ap
prov
ed I-
130
petit
ion
I-797
(N
otic
e of
Act
ion)
ind
icat
ing
appr
oval
or
pen
ding
I-13
0 vi
sa p
etiti
on u
nder
Sec
tion
201(
b) o
f the
INA
(spo
use
or c
hild
of a
U.S
. ci
tizen
) or
Sec
tion
203(
a)(2
)(A)
(spo
use
or
child
of a
per
man
ent l
egal
resi
dent
);
or
I-94
code
d K
3, K
4, V
1, V
2 or
CR
-1-7
and
a
pend
ing
or a
ppro
ved
I-13
0;
or
Any
oth
er U
SC
IS d
ocum
ent i
ndic
atin
g th
e al
ien
has
a K
or V
vis
a an
d a
pend
ing
or
appr
oved
I-13
0;
or
I-688
B o
r I-7
66 (
Empl
oym
ent
Aut
horiz
atio
n D
ocum
ents
) ann
otat
ed (a
)(9) o
r (a)
(15)
Ente
red
Bef
ore
8/22
/96
Ye
s Ye
s Ye
s
Ente
red
On/
Afte
r 8/
22/9
6 Th
e re
leva
nt d
ate
fo
r elig
ibili
ty is
the
date
qua
lifie
d st
atus
was
ob
tain
ed
Yes
Yes,
afte
r 5
year
s in
US
in a
qu
alifi
ed s
tatu
s Ye
s
An a
pplic
atio
n fo
r VAW
A ca
ncel
latio
n of
rem
oval
or
sus
pens
ion
of
depo
rtat
ion
has
been
gr
ante
d or
is p
endi
ng
and
the
imm
igra
tion
cour
t fin
ds th
at a
pplic
ant
has
a pr
ima
faci
e ca
se
for t
his
relie
f
B3
(Co
nt’
d.)
Ord
er
from
th
e E
xecu
tive
Offi
ce
of
Imm
igra
tion
Rev
iew
(E
OIR
) un
der
INA
24
0A(b
) or
if
the
appl
icat
ion
is
pend
ing
docu
men
tatio
n th
at t
he c
ourt
finds
tha
t th
e applic
ant
has a “p
rim
a fa
cie
case”
for
this
re
lief
Ente
red
Bef
ore
8/22
/96
Yes
Yes
Yes
Yes,
If:
In
a q
ualif
ied
stat
us a
nd
in re
ceip
t of c
erta
in
disa
bilit
y be
nefit
s
[7 U
SC 2
012(
r)]
or
Af
ter f
ive
year
s in
US
in
qual
ified
sta
tus
o
r
In a
qua
lifie
d st
atus
and
un
der a
ge 1
8
or
In
a q
ualif
ied
stat
us a
nd
have
40
qual
ifyin
g qu
arte
rs
Ente
red
On/
Afte
r 8/
22/9
6 Th
e re
leva
nt d
ate
fo
r elig
ibili
ty is
the
date
qua
lifie
d st
atus
was
ob
tain
ed
Yes,
afte
r 5
year
s in
US
in a
qu
alifi
ed s
tatu
s
Yes

LDSS
-457
9 (R
ev. 8
/12)
A
LIEN
ELI
GIB
ILIT
Y D
ESK
AID
Pa
ge 6
D
escr
iptio
n of
Sta
tus
WM
S/
ACI
Cod
e C
omm
on D
ocum
enta
tion
R
elev
ant D
ate
for
Elig
ibili
ty
Med
icai
d 1
Fam
ily
Assi
stan
ce
Safe
ty N
et
Assi
stan
ce
SNAP
B
enef
its
Vict
im o
f Hum
an
Traf
ficki
ng
D
(Ups
tate
)
R (N
YC)
Cer
tific
atio
n D
ocum
ent (
for a
dults
) or
Elig
ibilit
y Le
tter (
for c
hild
ren)
from
the
Offi
ce
of R
efug
ee R
eset
tlem
ent (
OR
R);
Mus
t cal
l 1-
866-
401-
5510
for v
erifi
catio
n
o
r I-9
4 C
oded
T1,
T2,
T3,
T4
or T
5 st
atin
g ad
mis
sion
und
er S
ectio
n 21
2(d)
(5) o
f the
IN
A if
sta
tus
gran
ted
for a
t lea
st o
ne y
ear
Entr
y4 Ye
s
Paro
lee
(for a
t lea
st o
ne
year
) (N
on-c
itize
ns w
ho
have
bee
n al
low
ed to
co
me
into
the
U.S
. for
hu
man
itaria
n or
pub
lic
inte
rest
reas
ons)
G
I-94
with
ann
ota
tio
n
“Paro
led
purs
uant
to
Sectio
n 2
12(d
)(5)”
or
“paro
le”
or
“PIP
” w
ith
date
of
en
try
and
date
of
ex
pira
tion
indi
catin
g on
e ye
ar
or
I-688
B
annota
ted
“8
CF
R
Sectio
n
274a
12(a
)(4)
or
274(a
) 12(c
)(11)”
or
I-766
an
nota
ted
“C11”
or
A4,
and
I-
94 in
dica
ting
adm
itted
for a
t lea
st o
ne y
ear
Ente
red
befo
re
8/22
/96
Yes
Yes,
If:
In
a q
ualif
ied
stat
us a
nd
in re
ceip
t of c
erta
in
disa
bilit
y be
nefit
s
[7 U
SC 2
012(
r)]
or
Af
ter f
ive
year
s in
US
in
qual
ified
sta
tus
o
r
In
a q
ualif
ied
stat
us a
nd
unde
r age
18
or
In
a q
ualif
ied
stat
us a
nd
have
40
qual
ifyin
g qu
arte
rs
Ente
red
on o
r afte
r 8/
22/9
6 Ye
s
Yes,
afte
r 5
year
s in
US
in a
qu
alifi
ed s
tatu
s
Yes
Paro
lee
(for l
ess
than
on
e ye
ar)
T
I-94
with a
nnota
tio
n “
Paro
led p
urs
uant
to
Sec
tion
212(
d)(5
)” or
“paro
le”
or
“PIP
”
or
I-688
B c
oded
274
a.12
(a)(4
) or 2
74a1
2(c)
(1
1)
or
I-766
cod
ed A
4 or
C11
NA
Ye
s N
o Ye
s N
o
Nor
th A
mer
ican
Indi
an
born
in C
anad
a
To b
e de
term
ined
(P
A)
C
(MA)
I-551
: (P
erm
anen
t Res
iden
t Car
d): s
tam
ped
“S1-3
” , t
empo
rary
I-55
1 st
amp
in a
C
anad
ian
pass
port
or
I-94:
sta
mped “
S1
-3”
or
Trib
al d
ocum
ent c
ertif
ying
at l
east
50%
Am
eric
an In
dian
blo
od, a
s re
quire
d by
S
ectio
n 28
9 of
the
INA
or d
ocum
ente
d m
embe
r of a
fede
rally
reco
gniz
ed tr
ibe
an
d
S
choo
l rec
ords
,
o
r
A b
irth
or b
aptis
mal
cer
tific
ate
issu
ed o
n a
rese
rvat
ion,
or
O
ther
sat
isfa
ctor
y ev
iden
ce o
f birt
h in
C
anad
a
NA
Ye
s
1 R
EMIN
DER
: For
Med
icai
d. u
ndoc
umen
ted
alie
ns a
nd te
mpo
rary
non
-imm
igra
nts
may
rece
ive
cove
rage
for c
are
and
serv
ices
nec
essa
ry fo
r the
trea
tmen
t of e
merg
en
cy m
edic
al c
ondi
tions
onl
y,
not
incl
udin
g ca
re a
nd s
ervi
ces
rela
ted
to a
n or
gan
tran
spla
nt p
roce
dure
, if
othe
rwis
e el
igib
le.
Pre
gnan
t w
omen
may
be
prov
ided
Med
icai
d at
an
y t
ime w
ithou
t re
gard
to
alie
n st
atus
, if
othe
rwis
e el
igib
le. C
hild
ren
may
be
prov
ided
med
ical
ass
ista
nce
with
out r
egar
d to
imm
igra
tion
stat
us u
nder
Chi
ld H
ealth
Plu
s (C
H P
lus)
pro
gram
.
4 Fo
r a V
ictim
of H
uman
Tra
ffick
ing,
EN
TRY
mea
ns th
e da
te o
f Cer
tific
atio
n by
the
Offi
ce o
f Ref
ugee
Res
ettle
men
t (O
RR
) – S
ee 0
3 AD
M-1
.

LDSS
-457
9 (R
ev. 8
/12)
A
LIEN
ELI
GIB
ILIT
Y D
ESK
AID
Pa
ge 7
D
escr
iptio
n of
Sta
tus
WM
S/
ACI
Cod
e C
omm
on D
ocum
enta
tion
R
elev
ant D
ate
for
Elig
ibili
ty
M
edic
aid
1
Fa
mily
Ass
ista
nce
Safe
ty N
et
Assi
stan
ce
SNAP
B
enef
its
Mem
ber o
f fed
eral
ly
reco
gniz
ed tr
ibe
born
ou
tsid
e U
.S.
To b
e de
term
ined
(P
A)
C (M
A)
Mem
bers
hip
card
or o
ther
trib
al
docu
men
t dem
onst
ratin
g m
embe
rshi
p in
a fe
dera
lly
reco
gniz
ed In
dian
trib
e un
der
Sec
tion
4(e)
of t
he In
dian
Sel
f-D
eter
min
atio
n an
d E
duca
tion
Ass
ista
nce
Act
NA
Ye
s
PRU
CO
L (n
ot in
any
of
abov
e st
atus
es)
O (P
A &
M
A)
See
GIS
07
TA/D
C00
1 S
ee O
MM
04
AD
M-7
AN
D
07 O
HIP
INF-
2 N
A
Yes5
No5
Yes5
No
Und
ocum
ente
d im
mig
rant
s or
non
-im
mig
rant
s (a
liens
w
ith a
tem
pora
ry
imm
igra
tion
stat
us)
E
NA
Tr
eatm
ent o
f em
erge
ncy
med
ical
con
ditio
n on
ly1
No
1 R
EMIN
DER
: For
Med
icai
d, u
ndoc
umen
ted
alie
ns a
nd te
mpo
rary
non
-imm
igra
nts
may
rece
ive
cove
rage
for c
are
and
serv
ices
nec
essa
ry fo
r the
trea
tmen
t of e
mer
genc
y m
edic
al c
ondi
tions
on
ly, n
ot in
clud
ing
care
and
ser
vice
s re
late
d to
an
orga
n tr
ansp
lant
pro
cedu
re, i
f oth
erw
ise
elig
ible
. Pr
egna
nt w
omen
may
be
prov
ided
Med
icai
d at
any
tim
e w
ithou
t reg
ard
to a
lien
stat
us, i
f ot
herw
ise
elig
ible
. C
hild
ren
may
be
prov
ided
med
ical
ass
ista
nce
with
out r
egar
d to
imm
igra
tion
stat
us u
nder
Chi
ld H
ealth
Plu
s (C
H P
lus)
pro
gram
. 5
PRU
CO
L re
fers
to a
liens
who
are
per
man
ently
resi
ding
in th
e U
S un
der C
olor
of L
aw.
OT
DA
’s a
nd
the
Dep
art
men
t o
f H
ealt
h’s
(D
OH
) in
terp
reta
tio
n o
f P
RU
CO
L i
s d
iffe
ren
t. A
des
crip
tion
of
TA P
RU
CO
L ca
n be
foun
d in
GIS
07
TA/D
C00
1. A
des
crip
tion
of M
A PR
UC
OL
can
be fo
und
in O
MM
04
ADM
-7 a
nd 0
7 O
HIP
INF-
2.
U
nite
d St
ates
Citi
zens
hip
and
Imm
igra
tion
Serv
ices
(USC
IS –
For
mer
ly IN
S) D
ocum
ents
I-9
4
Arr
ival
/Dep
artu
re R
ecor
d I-5
71
Ref
ugee
Tra
vel D
ocum
ent
I-130
P
etiti
on fo
r an
Alie
n R
elat
ive
I-688
Te
mpo
rary
Res
iden
t Car
d
I-181
M
emor
andu
m o
f C
reat
ion
of R
ecor
d of
Law
ful P
erm
anen
t Res
iden
ce
I-688
A E
mpl
oym
ent A
utho
rizat
ion
For L
egal
izat
ion
App
lican
ts
I-327
R
eent
ry P
erm
it of
Per
man
ent R
esid
ents
I-6
88B
Em
ploy
men
t Aut
horiz
atio
n C
ard
I-360
S
peci
al Im
mig
rant
Pet
ition
I-7
66
Em
ploy
men
t Aut
horiz
atio
n C
ard
I-485
A
pplic
atio
n to
Reg
iste
r Per
man
ent R
esid
ence
or t
o A
djus
t Sta
tus
I-7
97
Not
ice
of A
ctio
n (1
-797
C c
urre
nt v
ersi
on)
I-551
L
eg
al P
erm
an
en
t R
esid
en
t C
ard
, R
esid
ent
Alie
n C
ard
or
“gre
en
ca
rd”
Foot
note
s fo
r Pag
es 4
and
Pag
e 5
3 Th
ere
are
four
requ
irem
ents
for q
ualif
ied
batte
red
alie
n st
atus
:
1.
Be
a cr
edib
le v
ictim
of b
atte
ry o
r ext
rem
e cr
uelty
; an
d
2.
Hav
e ap
prop
riate
imm
igra
tion
docu
men
tatio
n;
a
nd
3.
Be
able
to s
how
a s
ubst
antia
l con
nect
ion
betw
een
the
need
for b
enef
its a
nd th
e ba
ttery
or e
xtre
me
crue
lty;
and
4.
N
o lo
nger
resi
de in
the
sam
e ho
useh
old
as th
e ab
user
.

Appendix I – Work Rules Desk Guide
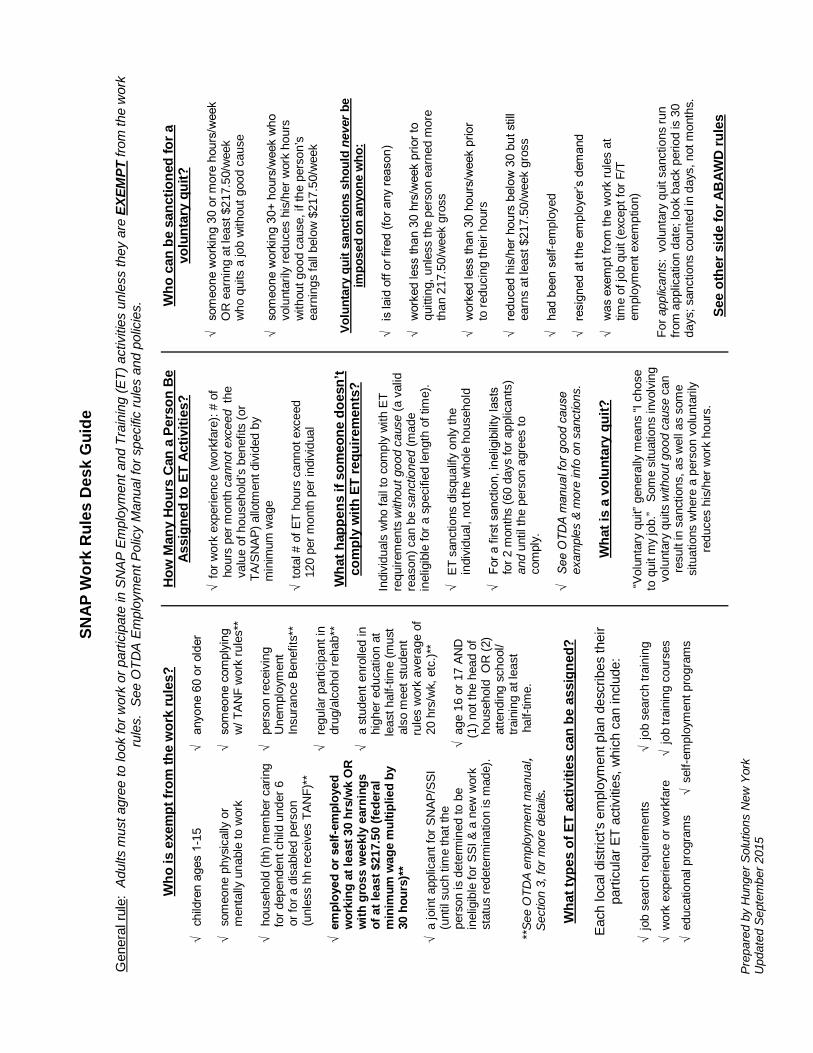
Prep
ared
by
Hun
ger S
olut
ions
New
Yor
k U
pdat
ed S
epte
mbe
r 201
5
SNA
P W
ork
Rul
es D
esk
Gui
de
Gen
eral
rule
: A
dults
mus
t agr
ee to
look
for w
ork
or p
artic
ipat
e in
SN
AP
Em
ploy
men
t and
Tra
inin
g (E
T) a
ctiv
ities
unl
ess
they
are
EXE
MPT
from
the
wor
k ru
les.
See
OTD
A E
mpl
oym
ent P
olic
y M
anua
l for
spe
cific
rule
s an
d po
licie
s.
W
ho is
exe
mpt
from
the
wor
k ru
les?
√ c
hild
ren
ages
1-1
5
√ a
nyon
e 60
or o
lder
√
som
eone
phy
sica
lly o
r
√ s
omeo
ne c
ompl
ying
men
tally
una
ble
to w
ork
w
/ TAN
F w
ork
rule
s**
√ h
ouse
hold
(hh)
mem
ber c
arin
g
√ p
erso
n re
ceiv
ing
fo
r dep
ende
nt c
hild
und
er 6
Une
mpl
oym
ent
o
r for
a d
isab
led
pers
on
Ins
uran
ce B
enef
its**
(un
less
hh
rece
ives
TAN
F)**
√
reg
ular
par
ticip
ant i
n √
em
ploy
ed o
r sel
f-em
ploy
ed
dr
ug/a
lcoh
ol re
hab*
*
wor
king
at l
east
30
hrs/
wk
OR
with
gro
ss w
eekl
y ea
rnin
gs
√ a
stu
dent
enr
olle
d in
o
f at l
east
$21
7.50
(fed
eral
hig
her e
duca
tion
at
m
inim
um w
age
mul
tiplie
d by
le
ast h
alf-t
ime
(mus
t
30
hour
s)**
als
o m
eet s
tude
nt
ru
les
wor
k av
erag
e of
√
a jo
int a
pplic
ant f
or S
NAP
/SSI
20
hrs/
wk,
etc
.)**
(u
ntil
such
tim
e th
at th
e
p
erso
n is
det
erm
ined
to b
e √
age
16
or 1
7 AN
D
inel
igib
le fo
r SSI
& a
new
wor
k
(
1) n
ot th
e he
ad o
f
sta
tus
rede
term
inat
ion
is m
ade)
.
hou
seho
ld O
R (2
)
a
ttend
ing
scho
ol/
t
rain
ing
at le
ast
**Se
e O
TDA
empl
oym
ent m
anua
l,
h
alf-t
ime.
Sec
tion
3, fo
r mor
e de
tails
.
Wha
t typ
es o
f ET
activ
ities
can
be
assi
gned
?
Eac
h lo
cal d
istri
ct’s
em
ploy
men
t pla
n de
scrib
es th
eir
parti
cula
r ET
activ
ities
, whi
ch c
an in
clud
e:
√
job
sear
ch re
quire
men
ts
√ jo
b se
arch
trai
ning
√ w
ork
expe
rienc
e or
wor
kfar
e
√
job
train
ing
cour
ses
√ e
duca
tiona
l pro
gram
s
√ s
elf-e
mpl
oym
ent p
rogr
ams
How
Man
y Ho
urs
Can
a P
erso
n B
e As
sign
ed to
ET
Activ
ities
?
√ fo
r wor
k ex
perie
nce
(wor
kfar
e): #
of
h
ours
per
mon
th c
anno
t exc
eed
the
val
ue o
f hou
seho
ld’s
ben
efits
(or
TA
/SN
AP) a
llotm
ent d
ivid
ed b
y
m
inim
um w
age
√
tota
l # o
f ET
hour
s ca
nnot
exc
eed
1
20 p
er m
onth
per
indi
vidu
al
W
hat h
appe
ns if
som
eone
doe
sn’t
com
ply
with
ET
requ
irem
ents
?
Indi
vidu
als
who
fail
to c
ompl
y w
ith E
T re
quire
men
ts w
ithou
t goo
d ca
use
(a v
alid
re
ason
) can
be
sanc
tione
d (m
ade
inel
igib
le fo
r a s
peci
fied
leng
th o
f tim
e).
√
ET
sanc
tions
dis
qual
ify o
nly
the
ind
ivid
ual,
not t
he w
hole
hou
seho
ld
√ F
or a
firs
t san
ctio
n, in
elig
ibilit
y la
sts
f
or 2
mon
ths
(60
days
for a
pplic
ants
)
and
unt
il th
e pe
rson
agr
ees
to
c
ompl
y.
√ S
ee O
TDA
man
ual f
or g
ood
caus
e
e
xam
ples
& m
ore
info
on
sanc
tions
.
Wha
t is
a vo
lunt
ary
quit?
“V
olun
tary
qui
t” ge
nera
lly m
eans
“I c
hose
to
qui
t my
job.
” S
ome
situ
atio
ns in
volv
ing
volu
ntar
y qu
its w
ithou
t goo
d ca
use
can
resu
lt in
san
ctio
ns, a
s w
ell a
s so
me
situ
atio
ns w
here
a p
erso
n vo
lunt
arily
re
duce
s hi
s/he
r wor
k ho
urs.
Who
can
be
sanc
tione
d fo
r a
volu
ntar
y qu
it?
√
som
eone
wor
king
30
or m
ore
hour
s/w
eek
OR
ear
ning
at l
east
$21
7.50
/wee
k
who
qui
ts a
job
with
out g
ood
caus
e
√ s
omeo
ne w
orki
ng 3
0+ h
ours
/wee
k w
ho
v
olun
taril
y re
duce
s hi
s/he
r wor
k ho
urs
w
ithou
t goo
d ca
use,
if th
e pe
rson
’s
e
arni
ngs
fall
belo
w $
217.
50/w
eek
Volu
ntar
y qu
it sa
nctio
ns s
houl
d ne
ver b
e im
pose
d on
any
one
who
:
√ i
s la
id o
ff or
fire
d (fo
r any
reas
on)
√ w
orke
d le
ss th
an 3
0 hr
s/w
eek
prio
r to
q
uitti
ng, u
nles
s th
e pe
rson
ear
ned
mor
e
tha
n 21
7.50
/wee
k gr
oss
√
wor
ked
less
than
30
hour
s/w
eek
prio
r
to
redu
cing
thei
r hou
rs
√ r
educ
ed h
is/h
er h
ours
bel
ow 3
0 bu
t stil
l
ear
ns a
t lea
st $
217.
50/w
eek
gros
s
√ h
ad b
een
self-
empl
oyed
√
res
igne
d at
the
empl
oyer
’s d
eman
d √
was
exe
mpt
from
the
wor
k ru
les
at
t
ime
of jo
b qu
it (e
xcep
t for
F/T
em
ploy
men
t exe
mpt
ion)
Fo
r app
lican
ts:
volu
ntar
y qu
it sa
nctio
ns ru
n fro
m a
pplic
atio
n da
te; l
ook
back
per
iod
is 3
0 da
ys; s
anct
ions
cou
nted
in d
ays,
not
mon
ths.
See
othe
r sid
e fo
r AB
AWD
rule
s

Prep
ared
by
Hun
ger S
olut
ions
New
Yor
k U
pdat
ed S
epte
mbe
r 201
5
Able
-Bod
ied
Adul
ts W
ithou
t Dep
ende
nts
(AB
AWD
s)
C
urre
ntly
all
dist
ricts
, inc
ludi
ng N
YC, h
ave
wai
ved
the
AB
AWD
requ
irem
ents
unt
il af
ter D
ecem
ber 3
1, 2
015.
B
egin
ning
Jan
uary
1st
, 201
6 m
any
coun
ties
will
nee
d to
re
inst
ate
the
time
limits
for m
any
child
less
, une
mpl
oyed
ad
ults
. AB
AWD
= a
ge 1
8-49
no c
hild
und
er 1
8 in
SN
AP h
ouse
hold
not d
isab
led
no
t pre
gnan
t
not e
xem
pt fr
om w
ork
rule
s
ABAW
Ds
can
only
get
SN
AP fo
r 3 m
onth
s in
a 3
6-m
onth
per
iod
unle
ss th
ey a
re:
√ w
orki
ng 8
0 ho
urs/
mon
th o
r mor
e; o
r √
in
wor
k pr
ogra
m fo
r 20
hour
s/w
eek;
or
√ c
ompl
ying
with
wor
kfar
e; o
r √
loc
al d
istri
ct a
ccep
ted
wai
ver*
*; or
√
dis
trict
gra
nts
indi
vidu
al e
xem
ptio
n.**
**
NYS
Offi
ce o
f Tem
pora
ry a
nd D
isab
ility
Assi
stan
ce
rele
ases
an
annu
al li
stin
g of
dis
trict
s pr
ovid
ing
wai
vers
a
nd/o
r ind
ivid
ual e
xem
ptio
ns.
The
NYS
OTD
A Em
ploy
men
t Pol
icy
Man
ual is
acc
essi
ble
onlin
e at
:
http
://ot
da.n
y.go
v/re
sour
ces/
empl
oym
ent-m
anua
l/em
ploy
men
tman
ual.p
df
Hun
ger S
olut
ions
New
Yor
k w
ill pr
ovid
e ad
ditio
nal in
form
atio
n on
the
re-
inst
atem
ent o
f the
tim
e lim
its in
NYS
as
polic
y in
form
atio
n fro
m O
TDA
is re
leas
ed.
Plea
se c
heck
our
web
site
for p
olic
y up
date
s, n
ew re
sour
ces
and
to re
gist
er fo
r up
com
ing
web
inar
s

Appendix J –
Categorical Eligibility Desk Guide

Hunger Solutions New York,
September 2015
Expanded Categorical Eligibility Desk Guide:
Hh WITH a senior or disabled member
Hh WITH a senior or
disabled member
which does not pass
the 200% GIT
Hh WITH Dependent
Care Costs
All other Households
If Hh Passes following
Gross Income Test *
200%
N/A
200%
130%
Are they Categorically Eligible for
SNAP
YES
NO
YES
YES
Must meet resource limit
NO YES NO NO
Must meet 100% Net
Income Test
NO YES NO NO
Note: if someone in the household has been disqualified from SNAP due to an intentional program violation or
other sanction, the household is not categorically eligible for SNAP and must instead be evaluated under regular
SNAP eligibility rules.
*Court ordered child support paid by a household member is always deducted from the household’s gross income
before applying the gross income test.
Poverty Guidelines Chart
Family Size 130% of Poverty Monthly Income
Oct. 1, 2015 – Sept. 30 2016
200% of Poverty Monthly Income
Oct. 1, 2015 – Sept. 30, 2016
1 $1,276 $1,962 2 $1,726 $2,655 3 $2,177 $3,348 4 $2,628 $4,042 5 $3,078 $4,735 6 $3,529 $5,428 7 $3,980 $6,122 8 $4,430 $6,815
Each Additional Person
+ $451 + $693

Hunger Solutions New York,
September 2015
Determining a Household’s Categorical Eligibility for SNAP
No Yes No Yes
No Yes No Yes
* Court ordered child support paid by a household member is always deducted from the household’s gross income before applying the
gross income test.
** Households that are not categorically eligible can still qualify for SNAP, but they must be evaluated under regular SNAP rules.
*** Senior and Disabled households that do not pass the 200% GIT may still be eligible for SNAP. See last box above.
NOT Categorically
Eligible**
Is any member of the household a senior or person with disabilities?
OR
Does the Household pay any out-of-pocket dependent care costs?
Is any member of
the household
currently
disqualified from
FSP due to an
Intentional Program
Violation (IPV) or
sanction?
Do not consider
Household’s Resources
Do not apply
Net Income Test
NOT Eligible for
SNAP
NOT Categorically
Eligible**
***Senior/Disabled Hh
See last box in last
column
Is the household’s gross monthly income at or
below the 130% Federal Poverty Level?*
Is the household’s gross monthly income at or
below the 200% Federal Poverty Level?*
Categorically
Eligible
Is any member of
the household
currently
disqualified from
FSP due to an
Intentional Program
Violation (IPV) or
sanction?
Categorically
Eligible
NOT Categorically
Eligible**
Do not consider
Household’s Resources
Do not apply
Net Income Test
Resource Limit
required
Net Income Test
required
***ONLY
For senior/disabled Hh Resource Limit
required
Net Income Test
required
Yes No

Appendix K –
Budget Worksheet

Supplemental Nutrition Assistance Program Budget Worksheet Effective 10/1/15 through 9/30/16
INCOME 1 Gross Monthly Earned Income ____________________
2 Monthly Unearned Income ____________________
3 Gross Income (Line 1 + Line 2) ____________________
4 Child support paid ____________________
5 Adjusted Gross income (Line 3 - Line 4) ____________________ (cannot exceed 130% Gross Income Limit
UNLESS there is an elderly/disabled person or household incurs dependent care costs then use 200%Gross Income Limit)
DEDUCTIONS 6 Earned Income deduction (Line 1 x 20%) ____________________
7 Standard deduction (see chart) ____________________
8 Dependent care (use actual costs) ____________________
9 Homeless deduction ($143) ____________________
10 Medical expenses over $35/month* ____________________
11 Total deductions (Add Lines 6 thru 10) ____________________
12 Adjusted Income (Line 5 – Line 11) ____________________ If the amount is a negative number, enter $0
SHELTER 13 Rent/Mortgage ____________________ EXPENSES
14 Standard utility allowance (SUA) ____________________
15 Other shelter (taxes, etc.) ____________________
16 Total shelter expenses (13+14+15) ____________________
EXCESS 17 Divide line 12 (adjusted income) by 2 ____________________ SHELTER DEDUCTION 17a Shelter Excess (Line 16- Line 17): ____________________
If the amount is greater than $504 enter $504 on 17a -- UNLESS there is an elderly/disabled household member (in which case enter the full amount). If the amount is a negative number, enter $0.
CALCULATING 18 Net Income (Line 12 - Line 17a) ____________________ THE BENEFIT cannot exceed Net Income Limit unless categorically eligible ALLOTMENT (negative number = $0 net income) 19 Thrifty Food Plan amount ____________________
20 Net Income (Line 18) multiplied by 30% ____________________
21 Estimated Benefit (Line 19 - Line 20)** & *** ____________________
*Medical deduction available ONLY to elderly/disabled household members
**ALL 1-2 person households, who pass the net income test or who are categorically eligible, automatically receive a minimum $16 allotment, even if Line 21 is less than $16. ***Categorically eligible households with 3 or more members who yield a zero or negative monthly SNAP benefit (line 21) will NOT be eligible for SNAP.

2
Poverty Guidelines Chart
165% of poverty is used for severely disabled and elderly people who live with others and are unable to purchase and prepare their own food. See page 33 of the Prescreening Guide for more information:
Each Additional H.H. Size 1 2 3 4 5 6 7 8 Person
165% of FPL $1,619 $2,191 $2,763 $3,335 $3,907 $4,479 $5,051 $5,623 +$572
Standard Deduction Amounts
(October 1, 2015 - September 30, 2016):
Household size 1-3 people 4 people 5 people 6 or more people $155 $168 $197 $226
Standard Utility Allowances for NYS (Oct. 1, 2015 - Sept. 30, 2016)
Level 1 Level 2 Level 3 (telephone) New York City $768 $304 $33 Nassau & Suffolk Counties $716 $281 $33 Rest of State $636 $257 $33
MAXIMUM SNAP (Thrifty Food Plan) ALLOTMENTS, by household size
For each
H.H. Size 1 2 3 4 5 6 7 8 Additional Person Maximum $194 $357 $511 $649 $771 $925 $1,022 $1,169 + $146 Allotment
Family Size
130% of Poverty Monthly GROSS Income
10/1/15– 9/30/16
200% of Poverty Monthly GROSS
Income 10/1/15 – 9/30/16
100% of Poverty Monthly NET Income
10/1/15 – 9/30/16
1 $1,276 $1,962 $981 2 $1,726 $2,655 $1,328 3 $2,177 $3,348 $1,675 4 $2,628 $4,042 $2,021 5 $3,078 $4,735 $2,368 6 $3,529 $5,428 $2,715 7 $3,980 $6,122 $3,061 8 $4,430 $6,815 $3,408
Each Additional
Person
+ $451 + $693 + $347

Appendix L –
Checklist for Student Eligibility

Prepared by Hunger Solutions New York Updated September 2015
Checklist for Student SNAP Eligibility Step 1. Establish applicant’s status as a student:
______ The applicant is enrolled in higher education institution that normally requires a high school diploma or equivalency certificate for enrollment. This includes (but is not limited to) colleges*, universities*, correspondence school or online courses, vocational and trade/technical schools at the post-high school level. * Colleges or Universities that offer degree programs regardless of whether a high school diploma is required are also considered Institutions of Higher Education. ______The applicant is enrolled at least half-time (using the school’s definition of half- time). For applicants applying between semesters: ______ The applicant intends to register for the next school term. If checked ‘YES’ to ALL of the above, the applicant is considered a student and the student rule applies - proceed to Step 2. If checked ‘NO’ to ANY ONE of the above, the applicant is NOT considered a student and the student rules do not apply (continue to screen applicant under regular SNAP rules). Step 2. Is the student enrolled in a college meal plan?
______The student receives 50% or more of their meals from a college meal plan. If checked ‘YES’ to above, the student is NOT eligible for SNAP as he/she is considered to be defined as living in an institution. If checked ‘NO’, continue to Step 3. If the student meets ANY ONE of the exemptions below, the student is eligible for SNAP and can be included in the SNAP household. The income of the student will be used in determining eligibility for the household. Step 3. Does the student meet ANY of the following exemptions?
Individual Characteristics ______ 17 years of age and under or 50 years of age and over. ______ Mentally or physically unfit under ET or ABAWD rules to work. ______ Primary caretaker for a household member who is under 6 or is incapacitated. ______ Primary caretaker for a household member between the ages of 6 and 11, if no
adequate child care is available that would make it possible to work and go to school**.
______ Is a single parent enrolled full-time who is responsible for the care of a child under 12. Student Is Working ______ Works an average of 20 hours per week. ______ Is self-employed an average of 20 hours/week and receives average weekly earnings at least equal to the federal minimum wage multiplied by 20 hours.
______ Participates in work-study (even if it is less than 20 hours/week). Student Participates in a Qualifying Government Program ______ Is a TANF recipient (and is complying with the TANF work rules). ______ Is required to attend school by the SNAP employment and training program, or a similar program operated by a state or local government. ______ Student is attending school through unemployment (Department of Labor). For additional information on Student Eligibility consult Hunger Solutions New York's SNAP Eligibility Guide, under status-based limitations.

Appendix M –
Household Composition Desk Guide (LDSS 4314)

LDSS
-431
4 (R
ev. 8
/12)
SUPP
LEM
ENTA
L N
UTR
ITIO
N A
SSIS
TAN
CE
PRO
GR
AM
(SN
AP)
BEN
EFIT
S H
OU
SEH
OLD
CO
MPO
SITI
ON
DES
K G
UID
E A
ll pe
rson
s, e
ven
if th
ey a
re m
embe
rs o
f diff
eren
t fam
ilies,
who
cus
tom
arily
pur
chas
e an
d pr
epar
e m
eals
toge
ther
are
to b
e co
nsid
ered
m
embe
rs o
f the
sam
e S
NA
P b
enef
its h
ouse
hold
.
REL
ATI
ON
SHIP
S:
SIT
UA
TIO
N R
ES
UL
T
Spou
ses
Livi
ng T
oget
her
Mus
t alw
ays
be c
onsi
dere
d as
a s
ingl
e ho
useh
old.
Pare
nts
and
thei
r Chi
ldre
n, 2
1 Ye
ars
of A
ge o
r You
nger
, Li
ving
Tog
ethe
r (In
clud
es S
tepc
hild
ren)
rega
rdle
ss o
f w
heth
er th
e ch
ildre
n ha
ve a
spo
use
or c
hild
ren
of th
eir
own.
Mus
t be
cons
ider
ed a
s a
sing
le h
ouse
hold
.
Chi
ldre
n U
nder
18
(Exc
ept F
oste
r Chi
ldre
n)
Und
er th
e Pa
rent
al C
ontro
l of a
n Ad
ult H
ouse
hold
Mem
ber
Who Is N
ot th
e C
hild
ren’s
Pare
nt or
Ste
ppare
nt.
Mus
t be
cons
ider
ed a
s a
sing
le h
ouse
hold
.
(Rem
ind
er:
A c
hild
und
er 1
8 liv
ing
with
thei
r spo
use
or c
hild
is n
ot c
onsi
dere
d un
der p
aren
tal
cont
rol.)
NO
TE:
Ther
e is
no
age
requ
irem
ent f
or a
n in
divi
dual
not
und
er p
aren
tal c
ontro
l to
rece
ive
SNAP
ben
efits
.
CIR
CU
MST
AN
CES
CA
USI
NG
INEL
IGIB
ILIT
Y:
SIT
UA
TIO
N R
ES
UL
T
Res
iden
t of I
nstit
utio
n In
elig
ible
unl
ess
a re
side
nt o
f a:
Dru
g/al
coho
l Tre
atm
ent f
acilit
y S
ubsi
dize
d ho
usin
g fo
r the
eld
erly
S
helte
r for
the
hom
eles
s
Cer
tain
gro
up li
ving
arr
ange
men
t S
helte
r for
bat
tere
d w
omen
and
chi
ldre
n
Inel
igib
le S
tude
nt
Non
-hou
seho
ld m
embe
r. (In
com
e an
d re
sour
ces
are
excl
uded
. The
hou
seho
ld c
an c
laim
th
eir p
rora
ted
shar
e of
exp
ense
s.)
Wor
k R
ules
San
ctio
ned
or In
tent
iona
l Pro
gram
Vi
olat
ion
Dis
qual
ified
Ex
clud
ed h
ouse
hold
mem
ber.
(Inco
me
and
reso
urce
s ar
e co
unte
d in
thei
r ent
irety
. The
ho
useh
old
can
clai
m fu
ll ex
pens
es.)
Any
indi
vidu
al w
ho is
inel
igib
le to
get
a S
ocia
l Se
curit
y N
umbe
r, or
any
indi
vidu
al w
ho if
una
ble
to
prov
ide
a S
SN, f
ails
to a
pply
for a
SS
N o
r ref
uses
to c
oope
rate
with
reso
lvin
g a
SSN
va
lidat
ion
disc
repa
ncy.
Excl
uded
hou
seho
ld m
embe
r. (In
com
e is
pro
rate
d; re
sour
ces
are
coun
ted
in th
eir e
ntire
ty.
Expe
nses
pai
d by
or b
illed
to th
e ex
clud
ed p
erso
n ar
e pr
orat
ed.
An in
divi
dual
who
fails
to p
rovi
de o
r app
ly fo
r a S
ocia
l Se
curit
y N
umbe
r (SS
N),
or a
ny in
divi
dual
who
if
unab
le to
pro
vide
a S
SN, f
ails
to a
pply
for a
SSN
Excl
uded
hou
seho
ld m
embe
r. (I
ncom
e is
pro
rate
d; re
sour
ces
are
coun
ted
in th
eir e
ntire
ty.
Expe
nses
pai
d by
or b
illed
to th
e ex
clud
ed p
erso
n ar
e pr
orat
ed.)
App
lyin
g fo
r or p
rovi
ding
th
e SS
N im
med
iate
ly b
rings
the
excl
uded
indi
vidu
al in
to c
ompl
ianc
e.
A ho
useh
old
that
fails
to o
r ref
uses
to c
oope
rate
in
the
SSN
val
idat
ion
proc
ess.
Th
e SN
AP c
ase
is c
lose
d.

LDSS
-431
4 (R
ev. 8
/12)
SUPP
LEM
ENTA
L N
UTR
ITIO
N A
SSIS
TAN
CE
PRO
GR
AM
(SN
AP)
BEN
EFIT
S H
OU
SEH
OLD
CO
MPO
SITI
ON
DES
K G
UID
E P
erso
ns re
sidi
ng to
geth
er w
ho d
o no
t mee
t any
of t
he p
revi
ous
defin
ition
s m
ay b
e se
para
te h
ouse
hold
s if
they
pur
chas
e an
d pr
epar
e fo
od
sepa
rate
ly fr
om th
e ot
her p
erso
ns.
SPEC
IAL
LIVI
NG
AR
RA
NG
EMEN
T:
SIT
UA
TIO
N R
ES
UL
T
Boar
der (
Roo
m a
nd M
eals
) N
ot a
par
t of t
he h
ouse
hold
, but
may
be
cons
ider
ed to
be
a m
embe
r of a
hou
seho
ld a
t the
h
ou
seh
old
’s r
eq
uest.
May
nev
er b
e a
sepa
rate
hou
seho
ld. T
he fo
llow
ing
can
neve
r be
cons
ider
ed b
oard
ers:
Pare
nts
and
child
ren,
age
21
and
youn
ger w
ho li
ve to
geth
er.
A
spou
se o
f a m
embe
r of t
he h
ouse
hold
.
Chi
ldre
n un
der 1
8 ye
ars
of a
ge w
ho a
re u
nder
the
pare
ntal
con
trol o
f an
adul
t m
embe
r of t
he h
ouse
hold
incl
udin
g a
sibl
ing.
Roo
mer
(Roo
m, N
o M
eals
) N
ot c
onsi
dere
d pa
rt of
hou
seho
ld, b
ut m
ay a
pply
as
a se
para
te h
ouse
hold
.
Shar
ed L
ivin
g (P
ays
a Sh
are
of S
helte
r Exp
ense
s)
Not
con
side
red
part
of h
ouse
hold
, but
may
app
ly a
s a
sepa
rate
hou
seho
ld.
Elde
rly In
divi
dual
s an
d th
eir S
pous
es
Sepa
rate
hou
seho
ld s
tatu
s m
ay b
e gr
ante
d to
thos
e el
derly
indi
vidu
als
and
thei
r spo
use
who
can
not p
urch
ase
and
prep
are
thei
r ow
n m
eals
bec
ause
they
suf
fer f
rom
cer
tain
di
sabi
litie
s, e
ven
if th
ey a
re li
ving
and
eat
ing
with
oth
ers,
if th
ey m
eet c
erta
in c
ondi
tions
.*
Fost
er C
hild
ren
It is t
he h
ou
seh
old
’s d
ecis
ion t
o inclu
de
or
exclu
de
fost
er c
hild
ren
as h
ouse
hold
mem
bers
. If
incl
uded
, tho
se fo
ster
car
e pa
ymen
ts th
at c
anno
t be
excl
uded
as
verif
ied
reim
burs
emen
ts
are
coun
ted
as in
com
e. I
f exc
lude
d, th
e fo
ster
car
e pa
ymen
ts a
re n
ot c
ount
ed a
s in
com
e.
*ALL
OF
THE
FOLL
OW
ING
CO
ND
ITIO
NS
MU
ST B
E M
ET:
Th
e in
divi
dual
mus
t be
60 y
ears
of a
ge o
r old
er; a
nd
Th
e in
divi
dual
mus
t suf
fer f
rom
a d
isab
ility
cons
ider
ed p
erm
anen
t und
er th
e S
ocia
l Sec
urity
Act
or f
rom
a n
on-d
isea
se re
late
d, s
ever
e, p
erm
anen
t dis
abilit
y an
d be
una
ble
to p
urch
ase
and
prep
are
mea
ls; a
nd
Th
e gr
oss
inco
me
of th
e ot
hers
with
who
m th
e in
divi
dual
resi
des
(exc
ludi
ng th
e in
com
e of
the
indi
vidu
al a
nd th
e sp
ouse
) can
not e
xcee
d 16
5% o
f the
pov
erty
le
vel.
STU
DEN
TS:
In o
rder
to p
artic
ipat
e in
the
SNAP
Pro
gram
, a s
tude
nt w
ho is
enr
olle
d at
leas
t hal
f-tim
e in
an
inst
itutio
n of
hig
her e
duca
tion
and
is a
t lea
st 1
8 ye
ars
old
but l
ess
than
50
year
s ol
d an
d is
not
dis
able
d m
ust m
eet o
ne o
f the
follo
win
g cr
iteria
:
Be
rece
ivin
g Fa
mily
Ass
ista
nce
or F
eder
ally
fund
ed S
afet
y N
et A
ssis
tanc
e Be
nefit
s.
Pr
ovid
e m
ore
than
hal
f the
phy
sica
l car
e fo
r a c
hild
und
er 6
or a
n in
capa
cita
ted
pers
on.
Be
enr
olle
d fu
ll tim
e an
d be
a s
ingl
e pa
rent
resp
onsi
ble
for t
he c
are
of a
chi
ld u
nder
12.
Prov
ide
mor
e th
an h
alf t
he c
are
of a
chi
ld u
nder
12
and
not h
ave
adeq
uate
chi
ld c
are
to w
ork
and
go to
sch
ool.
Be
par
ticip
atin
g du
ring
the
scho
ol y
ear i
n a
Sta
te o
r Fed
eral
ly fi
nanc
ed w
ork
stud
y pr
ogra
m fu
nded
und
er T
itle
IV-C
.
Be e
mpl
oyed
for a
n av
erag
e of
20
hour
s pe
r wee
k an
d be
pai
d. I
f sel
f em
ploy
ed, m
ust b
e w
orki
ng a
n av
erag
e of
20
hour
s pe
r wee
k an
d ea
rn a
n am
ount
equ
al
to th
e Fe
dera
l min
imum
wag
e x
20 h
ours
.
Was
pla
ced
in s
choo
l thr
ough
WFA
, SN
APE&
T, S
afet
y N
et E
mpl
oym
ent A
ctiv
ity w
hich
is c
ompa
rabl
e to
a S
NAP
E&T
act
iviti
es o
r DO
L.

Appendix N –
Authorized Representative Request Form
(LDSS-4942)
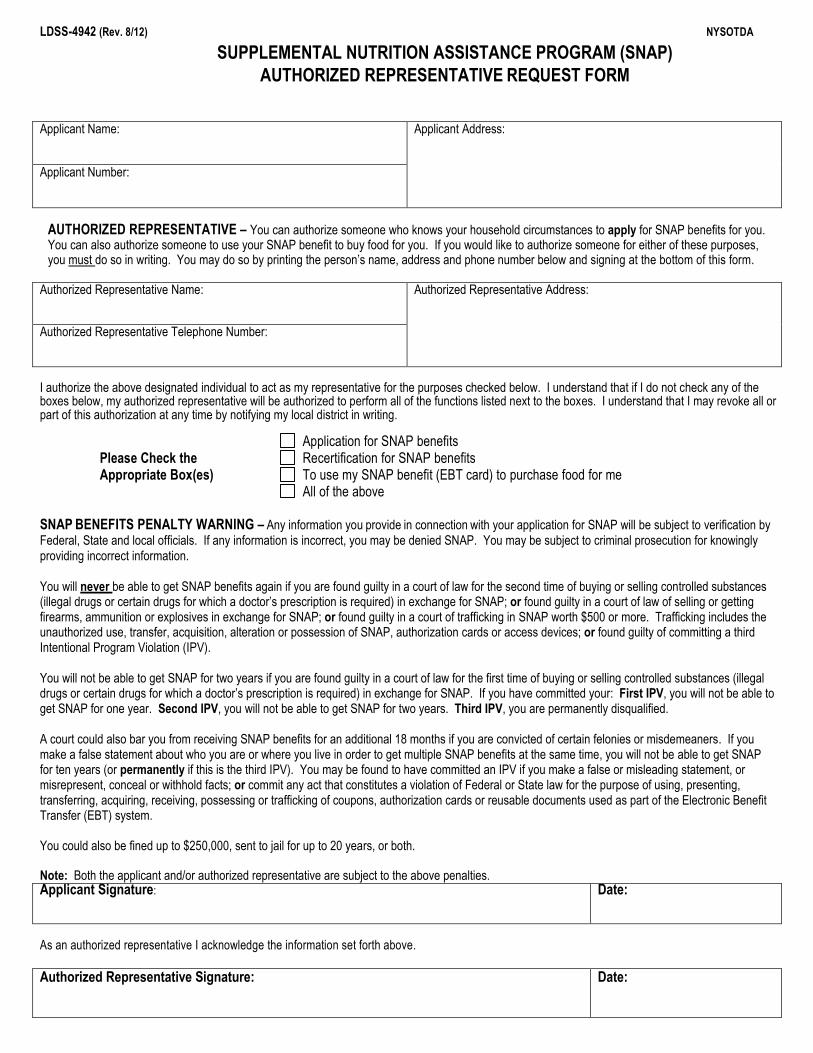
LDSS-4942 (Rev. 8/12) NYSOTDA
SUPPLEMENTAL NUTRITION ASSISTANCE PROGRAM (SNAP)
AUTHORIZED REPRESENTATIVE REQUEST FORM
Applicant Name:
Applicant Address:
Applicant Number:
AUTHORIZED REPRESENTATIVE – You can authorize someone who knows your household circumstances to apply for SNAP benefits for you. You can also authorize someone to use your SNAP benefit to buy food for you. If you would like to authorize someone for either of these purposes, you must do so in writing. You may do so by printing the person’s name, address and phone number below and signing at the bottom of this form.
Authorized Representative Name:
Authorized Representative Address:
Authorized Representative Telephone Number: I authorize the above designated individual to act as my representative for the purposes checked below. I understand that if I do not check any of the boxes below, my authorized representative will be authorized to perform all of the functions listed next to the boxes. I understand that I may revoke all or part of this authorization at any time by notifying my local district in writing.
Application for SNAP benefits Please Check the Recertification for SNAP benefits Appropriate Box(es) To use my SNAP benefit (EBT card) to purchase food for me All of the above
SNAP BENEFITS PENALTY WARNING – Any information you provide in connection with your application for SNAP will be subject to verification by Federal, State and local officials. If any information is incorrect, you may be denied SNAP. You may be subject to criminal prosecution for knowingly providing incorrect information. You will never be able to get SNAP benefits again if you are found guilty in a court of law for the second time of buying or selling controlled substances (illegal drugs or certain drugs for which a doctor’s prescription is required) in exchange for SNAP; or found guilty in a court of law of selling or getting firearms, ammunition or explosives in exchange for SNAP; or found guilty in a court of trafficking in SNAP worth $500 or more. Trafficking includes the unauthorized use, transfer, acquisition, alteration or possession of SNAP, authorization cards or access devices; or found guilty of committing a third Intentional Program Violation (IPV). You will not be able to get SNAP for two years if you are found guilty in a court of law for the first time of buying or selling controlled substances (illegal drugs or certain drugs for which a doctor’s prescription is required) in exchange for SNAP. If you have committed your: First IPV, you will not be able to get SNAP for one year. Second IPV, you will not be able to get SNAP for two years. Third IPV, you are permanently disqualified. A court could also bar you from receiving SNAP benefits for an additional 18 months if you are convicted of certain felonies or misdemeaners. If you make a false statement about who you are or where you live in order to get multiple SNAP benefits at the same time, you will not be able to get SNAP for ten years (or permanently if this is the third IPV). You may be found to have committed an IPV if you make a false or misleading statement, or misrepresent, conceal or withhold facts; or commit any act that constitutes a violation of Federal or State law for the purpose of using, presenting, transferring, acquiring, receiving, possessing or trafficking of coupons, authorization cards or reusable documents used as part of the Electronic Benefit Transfer (EBT) system.
You could also be fined up to $250,000, sent to jail for up to 20 years, or both.
Note: Both the applicant and/or authorized representative are subject to the above penalties. Applicant Signature: Date:
As an authorized representative I acknowledge the information set forth above.
Authorized Representative Signature: Date:

LDSS-4942 SP (3/09) NYSOTDA
PROGRAMA DE CUPONES PARA ALIMENTOS FORMULARIO DE PETICIÓN DE REPRESENTANTE AUTORIZADO
Nombre del Solicitante: Domicilio del Solicitante: Número de Teléfono del Solicitante:
REPRESENTANTE AUTORIZADO: usted puede autorizar a alguien familiarizado con las circunstancias de su hogar para que solicite los beneficios de cupones para alimentos (FS) por usted. Usted también puede autorizar a otra persona a utilizar sus beneficios de cupones para alimentos para que dicha persona compre los alimentos por usted. Si desea autorizar a otra persona para que realice uno de esos propósitos, debe hacerlo por escrito. También puede hacerlo escribiendo, a continuación, el nombre, domicilio y número de teléfono de dicha persona y firmando al pie de este formulario.
Nombre de Representante Autorizado:
Domicilio del Representante Autorizado:
Número de Teléfono de Representante Autorizado:
Autorizo a la persona arriba mencionada a que actúe en mi representación para el propósito marcado a continuación. Entiendo que si no marco ninguno de los casilleros a continuación, mi representante autorizado estará autorizado a realizar todas las funciones listadas en los casilleros. Entiendo que puedo revocar parcial o enteramente esta autorización cuando lo decida notificando al respecto y por escrito, al distrito local.
Solicitar los beneficios de Cupones para Alimentos Favor de marcar el / los Revalidar los beneficios de Cupones para Alimentos
casillero(s) apropiados Usar mi Beneficio de Cupones para Alimentos (Tarjeta EBT) para comprar los alimentos por mí.
Todas las anteriores ADVERTENCIA SOBRE SANCIONES RELACIONADAS CON EL PROGRAMA DE CUPONES PARA ALIMENTOS (FS): toda información que brinde en relación con su solicitud para recibir los cupones para alimentos estará sujeta a la verificación por autoridades federales, estatales y locales. De encontrarse información inexacta, se le podrán denegar los cupones. Se le someterá a enjuiciamientos penales por proporcionar, a sabiendas, información incorrecta.
Nunca más podrá obtener beneficios de cupones para alimentos (FS) si se le declara culpable por segunda vez en un tribunal de justicia de comprar o vender sustancias controladas (drogas ilegales o drogas para las cuales se requiere receta médica) a cambio de cupones; o si se le declara culpable en un tribunal de justicia de vender u obtener armas de fuego, municiones o explosivos a cambio de cupones; o si se le declara culpable en un tribunal de justicia de traficar cupones para alimentos por un valor de $500 o más. El tráfico incluye el uso no autorizado la transferencia, la adquisición, la manipulación o la posesión de cupones para alimentos, tarjetas de autorización o elementos de acceso; o si es declarado culpable de cometer la tercera Violación Intencional al Programa (IPV).
No podrá recibir cupones para alimentos durante dos años si se le declara culpable, por primera vez, en un tribunal de justicia de comprar o vender sustancias controladas (drogas ilegales o determinadas drogas que sólo se pueden comprar con receta médica) a cambio de cupones para alimentos. Si ha cometido su: Primera Violación Intencional al Programa, no podrá recibir los cupones para alimentos por un periodo de un año. Segunda Violación Intencional al Programa, no podrá recibir los cupones por un periodo de dos años. Tercera Violación Intencional al Programa, se le negarán permanentemente.
Además, el juez puede prohibirle de recibir los beneficios de Cupones para Alimentos por unos 18 meses adicionales si se le declara culpable de ciertos delitos graves o delitos menores. Si hace una declaración falsa sobre su identidad o domicilio a fin de recibir beneficios múltiples de cupones a la misma vez, no podrá recibir cupones durante un periodo de diez años (o en forma permanente si ésta es su tercera violación intencional al programa). Se le puede declarar culpable de haber perpetrado una violación intencional si presta testimonio falso o engañoso, o hace representaciones falsas, oculta o retiene datos; o comete un acto que constituya una violación de la ley federal o estatal con el propósito de usar, presentar, transferir, adquirir, recibir, poseer o traficar cupones, tarjetas de autorización o documentos reusables pertenecientes al sistema de Transferencia Electrónica de Beneficios (EBT).
Se le puede imponer una multa de hasta $250,000, una pena de prisión de hasta 20 años, o ambas sanciones.
Nota: tanto el solicitante como el representante autorizado estarán sujetos a las sanciones anteriores. Firma del Solicitante: Fecha:
Como representante autorizado, doy fe de lo anterior.
Firma del Representante Autorizado: Fecha:

Appendix O –
Replacement SNAP Benefits Request Form (LDSS-2291)
& Hunger Solutions New York Client-Friendly Cover Sheet

LDSS-2291 (Rev.8/14)
REQUEST FOR REPLACEMENT OF FOOD PURCHASED WITH SUPPLEMENTAL NUTRITION ASSISTANCE PROGRAM (SNAP) BENEFITS
NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE
CASE NAME
COUNTY
CASE NUMBER
SSN DATE OF BIRTH
ADDRESS (including house and Apt number)
CITY STATE ZIP PHONE NUMBER
I ________________________________________, am the head of household or an adult household member for the above named case and wish to report the following to the agency representative: My household experienced a loss in the amount of $ _______________________ of food purchased with Supplemental Nutrition Assistance Program (SNAP) benefits, destroyed as a result of:
A power outage A flood A fire Other disaster Describe: ______________________________________________________________________
Worker Comments: _________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Client Comments: _________________________________________________________________________________
_________________________________________________________________________________________________
CERTIFICATION DO NOT SIGN UNTIL YOU HAVE READ AND UNDERSTAND THE STATEMENTS BELOW
I am aware that offering a false instrument for filing as described in Article 175 of the Penal Law is a crime that may have a maximum penalty of four (4) year’s imprisonment. If I do so, I will be subject to prosecution under the Civil and Criminal Laws of the United States and New York State and under the regulations of the New York State Office of Temporary and Disability Assistance.
I understand I have a right to a fair hearing to contest the denial or delay of a replacement issuance for my household. Replacements would not be issued pending the fair hearing decision.
I understand that if I do not sign and return this statement to the agency within ten (10) days of the date the loss was reported, the agency will not replace the SNAP benefits.
Signature
Date
*Please return this completed form to your local County Social Service Department (SSD) or for NYC residents visit the HRA website
for a list of the local center closest to you.

LDSS-2291 SP (Rev.8/14)
PETICIÓN DE REEMPLAZO DE ALIMENTOS ADQUIRIDOS CON EL SUBSIDIO DEL PROGRAMA DE ASISTENCIA NUTRICIONAL SUPLEMENTARIA (SNAP)
NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE
CASO A NOMBRE DE:
CONDADO
Nº DE CASO
Nº DE SEGURO SOCIAL FECHA DE
NACIMIENTO
DIRECCIÓN (incluya el Nº de la casa o del apartamento)
CIUDAD ESTADO CÓDIGO
POSTAL Nº DE TELÉFONO
I ________________________________________, siendo el jefe del hogar o integrante adulto del hogar correspondiente al caso mencionado arriba, deseo informar lo siguiente al representante de la agencia: Mi hogar sufrió una desgracia debido a:
Una interrupción del servicio eléctrico Una inundación Un incendio Otro desastre Describa: ________________________________________________________________
Como resultado se dañaron los alimentos comprados con el subsidio del Programa de Asistencia Nutricional Suplementaria (SNAP) por un valor de $ _______________________ Comentarios del trabajador(a) social: _________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________
Comentarios del cliente: ____________________________________________________________________________
______________________________________________________________________________________________
CERTIFICACIÓN NO FIRME HASTA QUE HAYA LEIDO Y COMPRENDIDO LAS DECLARACIONES SIGUIENTES
Estoy consciente que el proveer un instrumento falso para ser archivado en mi caso, tal como lo describe el Artículo 175 de la Ley Penal, es un delito que puede acarrear una pena máxima de cuatro (4) años en prisión. Si lo hago, estaré sujeto(a) a enjuiciamiento bajo las Leyes Civiles y Penales de Estados Unidos y del Estado de Nueva York como también bajo las regulaciones de la Oficina de Asistencia Temporal y Asistencia para Incapacitados del Estado de Nueva York.
Comprendo que tengo el derecho a una audiencia imparcial para cuestionar la negación o el retraso de la emisión de reemplazo de beneficios para mi hogar. Los reemplazos no se emitirán si la decisión de la audiencia imparcial está pendiente.
Comprendo que si yo no firmo y devuelvo esta declaración a la agencia dentro de diez (10) días a partir de la fecha en que se informó la pérdida de mi subsidio SNAP, la agencia no reemplazará mi subsidio SNAP.
*Sírvase regresar este formulario completamente rellenado al departamento local de servicios sociales de su condado (SSD). Para los residentes de
la Ciudad de Nueva York, sírvanse ingresar a la página web de HRA para ver la lista de los centros locales más cercanos a su domicilio.
Firma
fecha

Have you lost food because of an emergency?Do you buy groceries with SNAP? You may be able to get some of your SNAP dollars added back to your EBT card.
WHAT YOU NEED TO KNOW:• If you receive SNAP benefits and you have lost food due to a household
misfortune, you can request replacement SNAP benefits
• The loss can be due to a situation that affects large areas, such as a storm or a flood, or can be specific to a single household, such as a fire
• Household misfortunes can include: Storms Equipment failure (refrigerator or freezer) Flooding Extended power outages Fire Failure to pay a utility bill Note: power must be out for 4 hours or more to be eligible for SNAP replacement
WHAT YOU NEED TO DO:• Fill out and submit a replacement form to your local SNAP/HRA office
within 10 days of the loss. You can do this by mail or in person.
• If you are unable to submit the form within 10 days, call the SNAP/HRA office immediately to verbally report the loss. You will then have 10 days to return the form after you report.
• Your local Nutrition Outreach and Education Program (NOEP) Coordinator can help you report the loss and submit the form. They can also help you obtain the form in other languages if necessary. NOEP Coordinators are community partners who can help with any questions you may have about SNAP. It’s free and confidential.
To find your local NOEP Coordinator, visit FoodHelpNY.org. If there is not a NOEP Coordinator in your county, call to find your local SNAP/HRA office: Outside New York City, dial 800-342-3009 In New York City, dial 311
HungerSolutionsNY.org • FoodHelpNY.org • SummerMealsNY.org • SchoolMealsHubNY.org • AfterschoolMealsNY.org
Prepared by Hunger Solutions New York with support from NYSOTDA, USDA/FNS, FRAC, Walmart Foundation, Share Our Strength, and MAZON: A Jewish Response to Hunger. This institution is an equal opportunity provider.

Appendix P –
Change Report Form (LDSS - 3151)

LDSS-3151 (Rev. 8/12) PAGE 1
NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE CASE NUMBER
SUPPLEMENTAL NUTRITION ASSISTANCE PROGRAM (SNAP) CHANGE REPORT FORM
(Please Print Clearly)
YOU MUST REPORT ANY CHANGES IN YOUR CIRCUMSTANCES DATE: _________________
ACCORDING TO THE RULES LISTED BELOW. COMPLETE THIS FORM AND MAIL TO:
TO:
ADDRESS:
LOCAL DISTRICT NAME, ADDRESS AND TELEPHONE NUMBER:
YOUR RESPONSIBILITY TO REPORT CHANGES
Please read the questions and rules carefully. If you fail to report any changes that you are required to report under the rules, we may have to establish a claim for overpayment of Supplemental Nutrition Assistance Program (SNAP) benefits and collect the amount of the overpayment from you.
The changes that you MUST report are explained below. You may still voluntarily report any change about your SNAP household and, if this change will increase your benefit level and you verify this change, we will increase your benefit. ARE YOU A “SIMPLIFIED REPORTER” (6 MONTH) OR A “CHANGE REPORTER”? YOU MAY ANSWER THESE QUESTIONS TO FIND OUT WHETHER YOU ARE A “SIMPLIFIED REPORTER” OR A “CHANGE REPORTER”.
1. Do you receive transitional SNAP benefits (TBA)?
YES – Go To “TBA” on page 3 (Skip questions 2 through 8)
NO – Go To Question #2, below
2. Do you receive New York State Nutrition Improvement Project (NYSNIP) benefits?
YES – Go To “NYSNIP” on page 3 (Skip questions 3 through 8)
NO – Go To Question #3, below
3. Are you certified for SNAP benefits for three months or less at a time?
YES –Go To “Change Reporting” on
page 2 (Skip questions 4 through 8) NO – Go To Question #4, below
4. Does anyone in your household have earned income that is being counted in your SNAP benefit amount?
YES –Go To “Simplified Reporting”
on page 2 (Skip questions 5 through 8)
NO – Go To Question #5, below
5. Are all of the adults (18 or older) in your household either permanently disabled or 60 or older?
YES –Go To “Change Reporting” on
page 2 (Skip questions 6 through 8) NO – Go To Question #6, below
6. Does your household receive $0 income (including $0 Temporary Assistance)
YES –Go To “Change Reporting” on
page 2 (Skip questions 7 and 8) NO – Go To Question #7, below
7. Are you without shelter (undomiciled) or a migrant/seasonal farmworker?
YES – Go To “Change Reporting”
on page 2 (Skip question 8) NO – Go To #8, below
8. You answered “NO” to all 7 questions
above Go To “Simplified Reporting” on the
top of page 2

PAGE 2 LDSS-3151 (Rev. 8/12)
SIMPLIFIED REPORTING RULES: As a SNAP household under the “Simplified Reporting” rules, you are only required to report
changes at the time of your next recertification, except for the following three situations:
1. If your household’s gross monthly income exceeds 130% of the poverty level, you MUST report this monthly amount to your social services district by telephone, in writing, or in person within 10 days after the end of the calendar month in which you exceed the 130% level. Gross income is the amount of income before taxes and other deductions are taken out, not the amount you receive when you cash your check. We must use the gross income in figuring your eligibility for SNAP benefits. Your worker will explain what 130% of the poverty level means for a family of your size. Any other kind of income that you receive besides earnings must be added to your gross earned income to know if you are over 130% of the poverty level. Examples of other sources of income that count include child support you receive, Unemployment Insurance, Temporary Assistance (TA) payments, Workers Compensation, Social Security Benefits, Supplemental Security Income (SSI) and private disability payments.
If you fail to report that your gross income is above 130% of the poverty level in any calendar month, all benefits received after that month may be considered an overpayment. This is true even if your gross income falls below the 130% poverty level in a future month.
2. If your household’s certification period is longer than 6 months: At a six-month checkpoint into your certification period, you will receive a report form that you MUST return within ten days after you receive the form. If your household has any of the changes listed below, you MUST report them on the report form that is sent to you at the six-month checkpoint. List of Changes you must report at the six-month checkpoint:
Changes in any source of income for anyone in your household Changes in your household’s total earned income when it goes up or down by more than $100 a month Changes in your household’s total unearned income from a public source such as Social Security Benefits or
Unemployment Insurance Benefits when it goes up or down by more than $50 a month Changes in your household’s total unearned income from a private source such as Child Support Payments or Private
Disability Insurance when it goes up or down by more than $100 a month Changes in the amount of court ordered child support you pay to a child outside of your SNAP household Changes in who lives with you If you move, your new address and your new rent or mortgage costs, heat costs and utility costs A new or different car, or other vehicle Increases in your household’s cash, stocks, bonds, money in the bank or savings institution if the total cash and
savings of all household members now amounts to more than $2000 (more than $3250 if anyone in your household is disabled or 60 years old or older)
Any changes in your household that would result in a penalty as described on page 6
3. If anyone in your SNAP household is an Able-Bodied Adult Without Dependents (“ABAWD”), you MUST tell us if their work hours go below 80 hours a month within 10 days after the end of that month.
CHANGE REPORTING RULES: As a SNAP household under the “Change Reporting” rules, you MUST report the following changes within 10 days after the end of the month in which the change happened:
Changes in any source of income for anyone in your household Changes in your household’s total earned income when it goes up or down by more than $100 a month Changes in your household’s total unearned income from a public source such as Social Security Benefits or
Unemployment Insurance Benefits when it goes up or down by more than $50 a month Changes in your household’s total unearned income from a private source such as Child Support Payments or Private
Disability Insurance when it goes up or down by more than $100 a month Changes in the amount of court ordered child support you pay to a child outside of your SNAP household Changes in who lives with you If you move, your new address and your new rent or mortgage costs, heat costs and utility costs A new or different car, or other vehicle Increases in your household’s cash, stocks, bonds, money in the bank or savings institution if the total cash and savings
of all household members now amounts to more than $2000 for a household without an elderly or permanently disabled household member or $3250 for a household with an elderly or permanently disabled household member.
If anyone in your SNAP household is an Able-Bodied Adult Without Dependents (“ABAWD”), you must tell us if their work hours go below 80 hours a month within 10 days after the end of that month
Any changes in your household that would result in a penalty as described on page 6

LDSS-3151 (Rev. 8/12) PAGE 3
TBA CHANGE REPORTING for household in receipt of transitional benefits: Transitional SNAP benefits can continue for up to five months after your Temporary Assistance case closes. You are not required to report changes during the transition period. If you have changes that may increase your benefits you
can contact your worker to file an early recertification application at any time during your transitional period to receive the increase. The increase cannot be done until a signed recertification application is filed, and the entire recertification process is completed.
You must recertify near the end of your transitional period to see if you can continue to receive SNAP benefits after your transitional period ends. We will send you a notice reminding you of this recertification requirement. If you do not recertify, we will not send you any other notice and must close your SNAP case.
NYSNIP CHANGE REPORTING for participants in NYSNIP: You will receive a contact letter 24 months after you begin participation in NYSNIP that you must complete and return. You are not required to report changes during your certification period other than the 24-month contact letter. You may
voluntarily report increases in your medical expenses, rent or utility costs, or decreases in your income. If you report and verify these changes, you may be eligible for more SNAP benefits. You are not required to, but should report your new address if you move, so that you continue to receive any notices we send to you.
Medical Expenses: You are not required to report changes in your medical expenses during your certification period. However, you may voluntarily report changes in your medical expenses for household members that are:
- 60 years old or older - getting veterans’ disability benefits - disabled spouses or children of a deceased veteran - getting government disability retirement benefits - getting Supplemental Security Income (SSI) - getting Railroad Retirement disability benefits - getting Social Security Disability payments - getting disability-based medical assistance
If you report and verify an increase in your medical expenses, you may be eligible for more SNAP benefits. Changes in medical expenses must be reported at your next recertification.
Temporary Assistance (TA) Reporting Rules: The rules listed above apply only to SNAP. If you also receive TA, you are still required to report changes for TA within 10 days of the change, on periodic report mailers, TA Eligibility Questionnaires and at recertification.
When to use this form:
This form may be used to report any required or voluntary changes. You can also use this form to report changes in the cost of caring for children or disabled adults, or changes in shelter costs even if you haven’t moved. If these expenses go up you may be eligible for more SNAP benefits.
If proof of the changes you are reporting is available, please include it with this form. This will help make sure that you get the correct amount of SNAP benefits. Reported changes must be verified before we can increase your benefits.
This form should be mailed or brought to the agency listed above. If for some reason you can’t mail or bring in this form, you can report the changes by calling us at the telephone number listed on Page 1.
If you no longer want to receive SNAP benefits, sign here to withdraw from participation in SNAP. Your SNAP benefits will stop. You have the right to contest this withdrawal if you feel that you were given incorrect or incomplete information about your eligibility for SNAP benefits by requesting a Fair Hearing within 90 days. You may re-apply for SNAP benefits at any time after your withdrawal.
X
IF YOU WITHHOLD INFORMATION ABOUT CHANGES IN YOUR HOUSEHOLD THAT YOU ARE REQUIRED TO REPORT, YOU WILL OWE US THE VALUE OF ANY EXTRA SNAP BENEFITS YOU RECEIVE AS A RESULT. IF YOU INTENTIONALLY WITHHOLD INFORMATION WHEN YOU ARE REQUIRED TO REPORT IT, YOU MAY ALSO BE DISQUALIFIED FROM SNAP AND COULD BE SUBJECT TO CRIMINAL PROSECUTION (SEE ATTACHED “SNAP PENALTY WARNING” ON PAGE 6).

PAGE 4 LDSS-3151 (Rev. 8/12)
Use the Form Below to Report Changes CHANGE IN INCOME OR SOURCE OF INCOME – If you are a Simplified Reporter, your reporting rules are explained beginning on Page 2. If you are a Change Reporter, your reporting rules are also explained on Page 2.
NAME OF PERSON RECEIVING INCOME SOURCE OF INCOME NEW AMOUNT HOW OFTEN RECEIVED
1. $
2. $
3. $
CHANGE IN HOUSEHOLD - List below all new members to your household including newborn children. Also list members who have moved in or out or have died.
NAME AGE RELATIONSHIP CHANGE (CHECK ONE) DATE INCOME AMOUNT SOURCE
1. CAME INTO HOUSEHOLD
LEFT HOUSEHOLD $
2. CAME INTO HOUSEHOLD
LEFT HOUSEHOLD $
3. CAME INTO HOUSEHOLD
LEFT HOUSEHOLD $
4. CAME INTO HOUSEHOLD
LEFT HOUSEHOLD $
CHANGE OF ADDRESS NEW MAILING ADDRESS CITY STATE ZIP CODE
IF YOU DON’T HAVE A STREET ADDRESS, GIVE DIRECTIONS TO YOUR HOME (if you are homeless, leave blank) TELEPHONE NUMBER WHERE YOU CAN BE REACHED
( ) AREA CODE
CHANGE IN HOUSING COSTS - If you have moved, you must list your new costs below. Even if you have not moved, you can use this section to tell us that your rent, mortgage payment or other costs have changed.
Are you a roomer or boarder? YES NO If Yes, are meals INCLUDED NOT INCLUDED RENT YES NO IF YES, GIVE MONTHLY AMOUNT CHANGE (CHECK ONE)
Do you pay rent? $ Same More Less Do you pay for the following separate from your rent? YES NO
Heat and/or air conditioning Utilities (electricity, cooking gas, etc.) Telephone
MORTGAGE PAYMENT YES NO IF YES, GIVE MONTHLY AMOUNT CHANGE (CHECK ONE)
Do you have a mortgage payment? $ Same More Less Do you pay for the following separate from your mortgage: YES NO IF YES, GIVE MONTHLY AMOUNT CHANGE (CHECK ONE)
Property taxes $ Same More Less House Insurance $ Same More Less Heat and/or air conditioning Utilities (electricity, cooking gas, etc.) Telephone
Are you living in section 8 or other subsidized housing? YES NO Are you living in public housing? YES NO

LDSS-3151 (Rev. 8/12) PAGE 5
CHANGE IN NUMBER OF CARS OR VEHICLES - Has anyone in your household purchased, sold or traded a car, truck, boat, camper, motorcycle or other vehicle since the last time you told us about vehicles?
MAKE MODEL YEAR IF SOLD, AMOUNT RECEIVED
1. $
2. $
3. $
CHANGE IN SAVINGS - List the total amount of money that the members of your household now have. Include cash, savings accounts, checking accounts, stocks, bonds or other investments. You must tell us if your household savings have increased to more than $2,000 (more than $3,250 if anyone in your household is 60 years old or older or been determined to be disabled).
$
CHANGE IN CHILD CARE, DEPENDENT CARE COSTS OR THE AMOUNT OF CHILD SUPPORT PAID - Have your child care or dependent care costs changed? If so, you may be eligible for more SNAP benefits.
CHANGE (CHECK ONE) FOR WHOM? WHOM DO YOU PAY? NEW AMOUNT HOW OFTEN DO YOU PAY?
1. NO LONGER HAVE COST HAVE COST
$
2. NO LONGER HAVE COST HAVE COST
$
3. NO LONGER HAVE COST HAVE COST
$
CHANGE IN MEDICAL COSTS (Doctors, Dentists, Hospitals, Prescriptions, etc.) – You are only required to report changes in your medical expenses at recertification. However, you may voluntarily report changes in your medical expenses at any time for household members who are:
60 years old or older disabled spouse or children of a deceased veteran getting Supplemental Security Income (SSI) getting Social Security Disability payments getting veterans’ disability benefits getting government disability retirement benefits getting Railroad Retirement disability benefits getting disability-based medical assistance
If you report and verify an increase in your medical expenses, you may be eligible for more SNAP benefits.
NAME TYPE OF COST AMOUNT HOW OFTEN IS EACH PAYMENT DUE?
$
$
$
$
DO YOU EXPECT THE CHANGES YOU HAVE REPORTED TO CONTINUE NEXT MONTH? YES NO
If “NO”explain:
CHECK HERE IF YOU HAVE NO CHANGES TO REPORT ABOUT YOUR SNAP HOUSEHOLD NO CHANGES
BE SURE TO READ AND SIGN PAGE 6
PAGE 6 LDSS-3151 (Rev. 8/12)
CHANGE OF BENEFITS We will use your answers on this form to see if your household’s benefits will change. Before we change your benefits, we will send you a notice explaining what will happen. If you don’t agree with our decision, you have the right to a fair hearing to challenge our decision.
SUPPLEMENTAL NUTRITION ASSISTANCE PROGRAM (SNAP) BENEFITS PENALTY WARNING
Any information you provide in connection with your application for SNAP benefits will be subject to verification by Federal, State and local officials. If any information is incorrect, you may be denied SNAP. You may be subject to criminal prosecution for knowingly providing incorrect information.
You will never be able to get SNAP again if you are:
Found guilty in a court of law for the second time of buying or selling controlled substances (illegal drugs or certain drugs for which a doctor’s prescription is required) in exchange for SNAP: or
Found guilty in a court of law of selling or obtaining firearms, ammunition or explosives in exchange for SNAP; or
Found guilty in a court of law of trafficking in SNAP worth $500 or more. Trafficking includes the illegal use, transfer, acquisition, alteration or possession of SNAP, authorization cards or access devices; or
Found guilty in a court of law of committing a third Intentional Program Violation (IPV).
You will not be able to get SNAP for two years if you are found guilty in a court of law for the first time of buying or selling controlled substances (illegal drugs or certain drugs for which a doctor’s prescription is required) in exchange for SNAP.
If you have committed your:
First IPV, you will not be able to get SNAP for one year.
Second IPV, you will not be able to get SNAP for two years.
A court could also bar you from receiving SNAP benefits for an additional 18 months.
If you make a false statement about who you are or where you live in order to get multiple SNAP, you will not be able to get SNAP for ten years (or permanently if this is the third IPV).
You may be found guilty of an Intentional Program Violation if you:
Make a false or misleading statement, or misrepresent, conceal or withhold facts; or
Commit any act that constitutes a violation of Federal or State law for the purpose of using, presenting, transferring, acquiring, receiving, possessing or trafficking of SNAP benefits, authorization cards or reusable documents used as part of the Electronic Benefit Transfer (EBT) system.
You could also be fined up to $250,000, sent to jail for up to 20 years, or both. CERTIFICATION
I understand the penalty for hiding or giving false information. I also understand I will owe the value of any extra SNAP benefits I receive because I don’t fully report changes in my household. I agree to prove any changes reported if necessary. The answers on this form are correct and complete to the best of my knowledge. I understand that my signature authorizes federal, state and local officials to contact other persons or organizations to verify the information I have provided. SIGNATURE
X
DATE

LDSS-3151-SP (Rev. 8/12) PÁGINA 1
NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE CASO NÚMERO PROGRAMA DE ASISTENCIA NUTRICIONAL
SUPLEMENTARIA (SNAP) FORMULARIO DE INFORME DE CAMBIOS
(Favor de escribir en letra de molde legible)
SE LE EXIGE INFORMAR TODO CAMBIO EN LA SITUACIÓN DE SU HOGAR FECHA: SEGÚN LAS REGLAS A CONTINUACIÓN: LLENE ESTE FORMULARIO Y ENVÍELO POR CORREO A:
SR.(A): NOMBRE, DIRECCIÓN Y NÚMERO TELEFÓNICO DEL DISTRITO LOCAL:
DOMICILIO:
RESPONSABILIDAD DE INFORMAR CAMBIOS
Lea las preguntas y reglas con atención. Si usted no informa un cambio que está obligado a informar, de acuerdo con las reglas establecidas, es posible que tengamos que iniciar un reclamo por pago excesivo de Asistencia Nutricional Suplementaria (SNAP – por sus siglas en inglés) y cobrarle dicho monto.
Los cambios que ESTÁ OBLIGADO a informar se explican a continuación. Usted puede informar, voluntariamente, todo cambio en la composición del grupo familiar que recibe SNAP. Si el cambio a reportar tendría como resultado un aumento en la cantidad de beneficios que recibe, una vez usted presente comprobantes de dicho cambio, aumentaremos la cantidad de beneficios que recibe.
¿PRESENTA USTED UN REPORTE «CADA SEIS MESES» O SÓLO CADA VEZ QUE HAY CAMBIOS A REPORTAR «REPORTE DE CAMBIOS»? CONTESTE LAS SIGUIENTES PREGUNTAS PARA DETERMINAR SI DEBE INFORMAR CADA SEIS MESES O A MEDIDA QUE SE DAN LOS CAMBIOS.
1. ¿Recibe usted beneficios Transitorios de SNAP (TBA)?
SÍ – Vaya a la sección de beneficios transitorios «TBA» en la página 3 (Salte las preguntas 2 a 8)
NO – Vaya a la pregunta #2, a continuación
2. ¿Recibe beneficios del Proyecto de Mejora Nutricional del Estado de Nueva York (New York State Nutritional Improvement Project -NYSNIP-)?
SÍ – Vaya a «NYSNIP» en la página 3 (Salte las preguntas 3 a 8)
NO – Vaya a la pregunta #3, a continuación
3. ¿Se le ha aprobado para recibir SNAP por un periodo de tres meses a la vez o por menos tiempo?
SÍ –Vaya a «Reporte de cambios» en la página 2 (Salte las preguntas 4 a 8)
NO – Vaya a la pregunta #4, a continuación
4. ¿Algún miembro de familia tiene ingresos trabajados que se toman en cuenta al hacer el cálculo de la cantidad de beneficios SNAP que recibe?
SÍ –Vaya a «Reporte de seis meses» en la página 2 (Salte las preguntas 5 a 8)
NO – Vaya a la pregunta #5, a continuación
5. ¿Hay adultos (de 18 años o mayor) en el hogar que estén incapacitados o que tengan 60 años de edad o más?
SÍ –Vaya a «Reporte de cambios» en la página 2 (Salte las preguntas 6 a 8)
NO – Vaya a la pregunta #6, a continuación
6. ¿Recibe su hogar $0 ingresos (incluyendo $0 en Asistencia Temporal)?
SÍ –Vaya a «Reporte de cambios» en la página 2 (Salte las preguntas 7 y 8)
NO – Vaya a la pregunta #7, a continuación
7. ¿No tiene usted vivienda (domicilio fijo) o es trabajador agrícola migratorio o temporal?
SÍ – Vaya a «Reporte de cambios» en la página 2 (Salte la pregunta 8)
NO – Vaya a pregunta #8, a continuación
8. ¿Contestó «No» a las 7 preguntas anteriores?
Vaya a «Reporte de seis meses» al principio de la página 2

FORMULARIO DE INFORME DE CAMBIOS PÁGINA 2 LDSS-3151-SP (Rev. 8/12)
REGLAS DEL REPORTE DE LOS SEIS MESES
Como hogar beneficiario de SNAP, según las las reglas de «Informe de Cambios de Seis Meses», usted solamente tiene que informar cambios en la próxima revalidación, excepto en las tres situaciones siguientes:
1. Si el ingreso bruto mensual del hogar sobrepasa por un 130 % el índice nacional de pobreza, DEBE reportar esa cantidad mensual al distrito de servicios sociales, ya sea, por teléfono, por escrito o en persona, dentro de los 10 días de finalizado el mes calendario en el que el ingreso sobrepasa por un 130 %. El ingreso bruto es la cantidad de ingresos antes de descontar impuestos y otras deducciones, y no la cantidad que usted recibe cuando cobra su cheque. Al calcular la cantidad del subsidio SNAP que usted recibirá, usamos el monto del ingreso bruto. La persona a cargo de su caso le explicará qué significa el 130 % del índice nacional de pobreza para una familia con el número de miembros en el hogar como la suya. Todo otro tipo de ingreso que usted reciba, además de los ingresos trabajados, deben agregarse a su ingreso bruto ganado para determinar si usted sobrepasa el 130 % del índice nacional de pobreza. Ejemplos de otros tipos de ingresos que se toman en cuenta son: pagos de Sustento de Menores, Seguro de Desempleo, pagos de Asistencia Temporal (TA), pagos por Compensación Laboral, Seguro Social, Seguridad de Ingreso Suplementario (SSI) o beneficios privados por incapacidad.
Si usted no nos informa que sus ingresos brutos sobrepasan el 130 % del índice nacional de pobreza en un determinado mes calendario; todos los beneficios recibidos después de ese mes se podrían considerar como pagos excesivos. Esto aplica aun cuando su ingreso bruto sea menos del 130 % del índice nacional de pobreza en un mes futuro.
2. Cuando el período de certificación de su hogar dura más de 6 meses: en la fecha de la revisión de los seis meses de su período de certificación, recibirá un formulario de informe que DEBE devolver dentro de los diez días de recibirlo. Si en su hogar se han producido algunos de los cambios que se mencionan a continuación, usted DEBE informarlos en el formulario que se le envía a la fecha de revisión de los seis meses.
Lista de cambios que debe informar en la revisión de los seis meses:
Cambios en cualquier fuente de ingresos de cualquier miembro de su hogar
Cambios en el total de ingresos trabajados de su hogar cuando este total aumenta o disminuye por más de $100 al mes
Cambios en el total de ingresos no trabajados de su hogar provenientes de fondos públicos, tales como beneficios de Seguro Social o beneficios del Seguro de Desempleo (UIB), cuando este total aumenta o disminuye por más de $50 al mes
Cambios en el total de ingresos no trabajados de su hogar provenientes de fondos privados, tales como pagos de Sustento de Menores o pagos del seguro privado por incapacidad, cuando este total aumenta o disminuye por más de $100 al mes
Cambios en los pagos por orden judicial de Sustento para Menores para un(a) niño(a) que no sea miembro del hogar beneficiario de SNAP.
Cambio en a quiénes viven con usted
Si se muda, su nueva domicilio, o los nuevos montos de alquiler o hipoteca, gastos de calefacción y servicios públicos
Un automóvil nuevo o diferente, u otro vehículo
Aumento en la cantidad de dinero en efectivo, acciones, bonos, dinero en el banco o instituciones de ahorro cuando la cantidad total en efectivo y en ahorros de todos los miembros del hogar es más de $2000 (o más de $3250 si algún miembro del hogar está incapacitado(a) o tiene 60 años de edad o más)
Todo cambio, en la circunstancias de su hogar, que pudiese resultar en una sanción, tal como se explica en la página 6. 3. Si un integrante del grupo familiar que recibe SNAP es un Adulto Habilitado para Trabajar sin Dependientes (Able-Bodied Adult
Without Dependents - ABAWD), usted DEBE informarnos si esa persona trabajó menos de 80 horas al mes. Debe reportarlo dentro de los diez días de finalizado el mes en que se dio ese cambio.
REGLAS SOBRE INFORME DE CAMBIOS
Según las reglas de «Informe de Cambios», un hogar que reciba SNAP DEBE reportar los siguientes cambios dentro de los 10 días de ocurrido:
Cambios en la fuente de ingresos de miembros del hogar.
Cambios en el total de ingresos trabajados del hogar cuando este total aumenta o disminuye por más de $100 al mes
Cambios en el total de ingresos no trabajados del hogar provenientes de fondos públicos, tales como beneficios de Seguro Social o beneficios del Seguro de Desempleo (UIB), cuando este total aumenta o disminuye por más de $50 al mes.
Cambios en el total de ingresos no trabajados del hogar provenientes de fondos privados, tales como pagos de Sustento de Menores o pagos del seguro privado por incapacidad, cuando este total aumenta o disminuye por más de $100 al mes.
Cambios en los pagos por orden judicial de Sustento de Menores de un(a) niño(a) que no sea miembro del hogar beneficiario de SNAP.
Cambios en cuanto quiénes viven con usted.
Si se muda, su nuevo domicilio, o los nuevos montos de alquiler, hipoteca; gastos de calefacción y servicios públicos.
Un automóvil nuevo o diferente, u otro vehículo.
Aumento en la cantidad de dinero en efectivo, acciones, bonos, dinero en el banco o instituciones de ahorro, cuando la cantidad total en efectivo y en ahorros de todos los miembros del hogar es más de $2000, si en el hogar no hay miembros de edad avanzada, o con una incapacidad permanente; o más de $3250 si en el hogar hay miembros de edad avanzada o con una incapacidad permanente.
Si un integrante del hogar beneficiario de SNAP es un Adulto Habilitado para Trabajar sin Dependientes (Able Bodied Adults Without Dependents- ABAWD), usted DEBE informarnos si esa persona trabajó menos de 80 horas al mes; debe informar este cambio dentro de los diez días de finalizado el mes en en el que se dio el cambio.
Todo cambio, en las circunstancias de su hogar, que pudiese resultar en una sanción, tal como se explica en la página 6.

FORMULARIO DE INFORME DE CAMBIOS PÁGINA 3 LDSS-3151-SP (Rev. 8/12)
INFORME DE CAMBIOS – Hogares que reciben beneficios transitorios (TBA): Puede continuar recibiendo los beneficios transitorios de SNAP por un período de hasta cinco meses
después de que se cierra su caso de Asistencia Temporal. No se le requiere reportar cambios durante el período de transición. Si ciertos cambios tuviesen como
resultado un aumento en sus beneficios; para recibir el aumento, comuníquese con la persona a cargo de su caso y solicite una solicitud temprana de revalidación; esto puede hacerlo en cualquier momento durante el período de transición. No se le puede aprobar el aumento hasta que no presente una solicitud firmada de revalidación y pase por todo el proceso de revalidación.
Se le exige presentar una revalidación próximo a la fecha de vencimiento de su período de transición para determinar si puede continuar recibiendo el subsidio SNAP una vez finalizado el período de transición. Le enviaremos un aviso recordándole este requisito de revalidación. Si usted no presenta una revalidación, no le enviaremos ningún otro aviso y nos veremos obligados a cerrar su caso de SNAP.
REPORTE DE CAMBIOS - Participantes del Proyecto de Mejora Nutricional del Estado de Nueva York - NYSNIP:
24 meses después de empezar a participar en el proyecto NYSNIP, recibirá una carta que debe rellenar y devolver.
Aparte de la carta que usted recibe a los 24 meses, no se le requiere reportar ningún cambio durante el período de revalidación. Puede, voluntariamente, reportar aumentos en gastos médicos, alquiler o servicios públicos o disminución de ingresos. Si usted reporta y comprueba esos cambios, es posible que reciba un aumento en la cantidad del subsidio SNAP que recibe. No es obligatorio, pero le sugerimos que si se muda nos informe de su nuevo domicilio, de manera que pueda seguir recibiendo los avisos que le enviamos.
Gastos médicos: no tiene que reportar cambios en sus gastos médicos durante el período de certificación. Sin embargo, puede, voluntariamente, informar cambios en los gastos médicos que incurran los miembros del hogar que:
- tengan 60 años de edad o más - reciban subvención por incapacidad para veteranos - sean cónyuges incapacitados o hijos incapacitados de un veterano fallecido
- pensión gubernamental de jubilación por incapacidad
- reciban Seguridad de Ingreso Suplementario (SSI) - pensión de jubilación ferroviaria por incapacidad - reciban pagos del Seguro Social por Incapacidad - asistencia médica por incapacidad
Si usted reporta y demuestra el aumento en sus gastos médicos, es posible que reciba un aumento en el subsidio SNAP. Los cambios en los gastos médicos deben reportarse en su próxima cita de revalidación.
Asistencia Temporal (TA) - Reglas sobre informe de cambios: las reglas anteriores aplican sólo al programa de SNAP. Si usted también recibe Asistencia Temporal (TA), igualmente se le requiere reportar cambios relacionados al programa de TA dentro de los 10 días de haberse producido el cambio, en las comunicaciones periódicas de reporte, en los cuestionarios para determinar si satisface los requisitos para recibir TA y durante la revalidación.
¿Cuándo debe usar este formulario?
Puede usar este formulario para informar cambios obligatorios o voluntarios. También, puede utilizar este formulario para informar cambios en el costo de cuidado de niños o adultos incapacitados, o cambios en los costos de vivienda, aunque no se haya mudado. De haber un aumento en estos gastos, usted podría recibir un aumento en el subsidio SNAP.
Si tiene comprobantes de los cambios que está reportando, favor de adjuntarlos a este formulario para asegurarnos que recibe la cantidad correcta de SNAP. Debemos verificar los cambios que reporta antes de aumentarle el monto del subsidio SNAP.
Este formulario debe enviarlo por correo o traerlo a la agencia mencionada arriba. Si por algún motivo no puede enviarlo por correo o entregarlo en persona, reporte los cambios por teléfono al número que aparece en la página 1.
Si ya no desea recibir el subsidio SNAP, firme quí y le retiraremos del programa. De esta manera dichos beneficios cesarán. Ya no recibirá el subsidio SNAP. Tiene derecho a oponerse a este retiro y solicitar una audiencia imparcial dentro de los próximos 90 días si considera que se le proporcionó información incorrecta o incompleta sobre los requisitos del programa de SNAP. Puede volver a solicitar el subsidio SNAP cuando usted lo desee aunque se haya retirado antes.
X
SI USTED NO REPORTA LOS CAMBIOS QUE ESTÁ OBLIGADO A REPORTAR, NOS ADEUDARÁ EL VALOR DEL SUBSIDIO ADICIONAL DE SNAP QUE RECIBIÓ COMO RESULTADO DE NO REPORTAR DICHOS CAMBIOS. SI USTED, A SABIENDAS, RETIENE INFORMACIÓN QUE ESTÁ OBLIGADO A REPORTAR, SE LE PUEDE ELIMINAR DEL PROGRAMA SNAP Y SOMETER A UN JUICIO EN LO PENAL (CONSULTE EL TEMA ADJUNTO TITULADO «ADVERTENCIA SOBRE LAS SANCIONES RELACIONADAS CON EL PROGRAMA DE ASISTENCIA NUTRICIONAL SUPLEMENTARIA - SNAP» EN LA PÁGINA 6).

FORMULARIO DE INFORME DE CAMBIOS PÁGINA 4 LDSS-3151-SP (Rev. 8/12)
Use el formulario a continuación para informar cambios CAMBIO EN INGRESOS O FUENTE DE INGRESOS – Si se reporte cada seis meses, las reglas pertinentes a dichos cambios las encuentra en la página 2. Y si reporta cambios según se dan, o reporte por cambios, las reglas las encuentra también en la página 2.
NOMBRE DE LA PERSONA QUE RECIBE EL INGRESO
FUENTE DE INGRESO NUEVA CANTIDAD ¿CON QUÉ FRECUENCIA LO RECIBE?
1. $
2. $
3. $
CAMBIOS EN EL HOGAR: Incluya todos los nuevos miembros del hogar, incluyendo recién nacidos. También incluya a miembros que se hayan incorporado o retirado del hogar o que hayan fallecido.
NOMBRE EDAD PARENTESCO CAMBIO (MARQUE UNO) FECHA
CANTIDAD DEL INGRESO
FUENTE
1.
LLEGÓ AL HOGAR SE FUE DEL HOGAR
$
2.
LLEGÓ AL HOGAR SE FUE DEL HOGAR
$
3.
LLEGÓ AL HOGAR SE FUE DEL HOGAR
$
4.
LLEGÓ AL HOGAR SE FUE DEL HOGAR
$
CAMBIO DE DOMICILIO NUEVA DIRECCIÓN DE CORREO CIUDAD ESTADO CÓDIGO POSTAL
SI SU DOMICILIO NO INCLUYE EL NOMBRE DE LA CALLE, PROPORCIONE INSTRUCCIONES PARA LLEGAR A SU CASA (si está desamparado(a), deje este espacio en blanco)
No. DE TELÉFONO DONDE SE LE PUEDE LLAMAR Código de área
( ) CAMBIOS EN LOS COSTOS DE VIVIENDA: Si se ha mudado, se le exige indicar abajo sus nuevos gastos. Aunque no se haya mudado, puede usar esta sección para indicar cambios en su alquiler, pagos de hipoteca u otros gastos.
¿Es usted pensionista o renta una habitación?
SÍ NO Si contesta Sí, las comidas ESTÁN INCLUIDAS NO ESTÁN INCLUIDAS
ALQUILER/RENTA SÍ NO
¿SÍ? INDIQUE CANTIDAD
MENSUAL CAMBIO (MARQUE UNO)
¿Paga usted por el alquiler/renta? $ Igual Más Menos ¿Paga los siguientes gastos por separado del alquiler/renta? SÍ NO
Calefacción y/o aire acondicionado $
Servicios públicos (electricidad, gas para cocinar, etc.) $
Teléfono $
PAGO DE HIPOTECA SÍ NO ¿SÍ? INDIQUE CANTIDAD MENSUAL CAMBIO (MARQUE UNO)
¿Paga usted una cuota de hipoteca? $ Igual Más
Menos ¿Paga los siguientes gastos por separado de la hipoteca?
Sí NO ¿SÍ? INDIQUE CANTIDAD MENSUAL CAMBIO (MARQUE UNO)
Impuesto sobre la propiedad $ Igual Más Menos
Seguro de vivienda $ Igual Más Menos
Calefacción y/o aire acondicionado
Servicios públicos (electricidad, gas para cocinar, etc.)
Teléfono
¿Vive usted en una vivienda de la «Sección 8» u otra vivienda subsidiada? SÍ NO ¿Vive usted en una vivienda pública? SÍ NO

FORMULARIO DE INFORME DE CAMBIOS PÁGINA 5 LDSS-3151-SP (Rev. 8/12)
CAMBIOS EN LA CANTIDAD DE AUTOMÓVILES O VEHÍCULOS: ¿Algún miembro de su hogar compró, vendió o intercambió un automóvil, camión, barco, casa rodante, motocicleta u otro vehículo desde la última vez que nos informó acerca de sus vehículos?
MARCA MODELO AÑO SI LO VENDIÓ, CANTIDAD RECIBIDA
1. $
2. $
3. $
CAMBIOS EN LOS AHORROS: Incluya el total de dinero que los miembros de su hogar tienen actualmente. Incluya dinero en efectivo, cuentas de ahorro, cuentas corrientes, acciones, bonos u otras inversiones. Se le exige informarnos si los ahorros de su hogar han aumentado a más de $2,000 (o más de $3250 si un miembro del hogar tiene 60 años de edad o más, o es una persona incapacitada).
$
CAMBIOS EN EL CUIDADO DE NIÑOS, GASTOS POR EL CUIDADO DE DEPENDIENTES O EN LA CANTIDAD PAGADA DE SUSTENTO DE MENORES: ¿Han habido cambios en los gastos de cuidado de niños o el cuidado de dependientes? De ser así, podría recibir un aumento en el subsidio SNAP.
CAMBIO (MARQUE UNO)
¿PARA QUIÉN? ¿A QUIÉN LE PAGA UD.?
NUEVA CANTIDAD
FRECUENCIA DEL PAGO
1. YA NO TIENE EL GASTO TIENE EL GASTO
$
2. YA NO TIENE EL GASTO TIENE EL GASTO
$
3. YA NO TIENE EL GASTO TIENE EL GASTO
$
CAMBIOS EN GASTOS MÉDICOS (médicos, dentistas, hospitales, recetas médicas, etc.) – Sólo se le requiere informar los cambios en gastos médicos al momento de la revalidación. Sin embargo, cuando lo desee, puede voluntariamente reportar los gastos médicos de miembros del hogar que:
tengan 60 años de edad o más
sean cónyuges incapacitados(as) o hijos/hijas de un veterano fallecido
reciban Seguridad de Ingreso Suplementario (SSI)
reciban beneficios del Seguro Social por Incapacidad
reciban beneficios por incapacidad para veteranos
reciban beneficios gubernamentales de jubilación por incapacidad
reciban beneficios ferroviarios de jubilación por incapacidad
reciban asistencia médica por incapacidad
Si usted reporta y demuestra el aumento en gastos médicos, podría recibir un aumento en el subsidio SNAP.
NOMBRE TIPO DE GASTO CANTIDAD ¿CON QUÉ FRECUENCIA HACE ESTE PAGO?
$
$
$
$
¿CREE QUE LOS CAMBIOS QUE HA REPORTADO SE REPETIRÁN EL PRÓXIMO MES? SÍ NO
Si contesta «NO», explique la razón:
MARQUE ESTA CASILLA SI NO TIENE CAMBIOS QUE REPORTAR SOBRE EL HOGAR QUE RECIBE SNAP
NO HAY CAMBIOS
ASEGÚRESE DE LEER Y FIRMAR LA PÁGINA 6

FORMULARIO DE INFORME DE CAMBIOS PÁGINA 6 LDSS-3151-SP (Rev. 8/12)
CAMBIO DE BENEFICIOS La información que usted proporcione en este formulario se usará para determinar si se modificarán sus beneficios. Si se modifican, se le enviará un aviso explicándole lo que sucederá antes de realizar el cambio. Si no está de acuerdo con nuestra determinación, tiene el derecho a solicitar una audiencia imparcial para interponerse a nuestra decisión.
ADVERTENCIA SOBRE SANCIONES RELACIONADAS CON EL PROGRAMA DE ASISTENCIA NUTRICIONAL SUPLEMENTARIA - SNAP
La información que usted brinde en relación con su solicitud de SNAP estará sujeta a verificación por autoridades federales, estatales y locales. Se le podrá negar el subsidio SNAP si nos percatamos que proporcionó información inexacta. Se le podrá someter a un proceso en lo penal por suministrar, a sabiendas, información inexacta.
Usted nunca más podrá volver a recibir el subsidio SNAP si:
Un tribunal de justicia lo/la declara culpable por segunda vez de comprar o vender sustancias controladas (drogas ilegales o drogas para las cuales se requiere una receta médica) a cambio de SNAP: o
Un tribunal de justicia lo/la declara culpable de vender u obtener armas de fuego, municiones o explosivos a cambio de SNAP; o
Un tribunal de justicia lo/la declara culpable de traficar cupones por un valor de $500 ó más. El tráfico incluye el uso, la transferencia, la adquisición, alteración o la posesión ilegal de fondos SNAP, tarjetas de autorización o elementos de acceso; o
Un tribunal de justicia lo/la declara culpable de cometer una tercera Violación Intencional del Programa
Usted no podrá recibir SNAP durante dos años si un tribunal de justicia lo/la declara culpable por primera vez de comprar o vender sustancias controladas (drogas ilegales o drogas para las cuales se requiere una receta médica) a cambio de SNAP. Por la:
Primera Violación Intencional del Programa (IPV), usted no podrá recibir SNAP por un año.
Segunda Violación Intencional del Programa (IPV), usted no podrá recibir SNAP por dos años.
Además, una orden judicial podrá prohibirle recibir SNAP por un período adicional de 18 meses.
Si hace una declaración falsa sobre su identidad o sobre su domicilio con el propósito de recibir múltiples subsidios de SNAP, se le prohibirá recibir SNAP por diez años (o de forma permanente si ésta fuese la tercera violación que usted comete).
Se le puede declarar culpable de una violación intencional del programa (IPV) si usted:
Hace una declaración falsa, engañosa o una representación falsa, oculta o retiene hechos; o
Comete un acto que constituya violación de una ley federal o estatal con el objeto de usar, presentar, transferir, adquirir, recibir, poseer o traficar fondos de SNAP, tarjetas de autorización o documentos reutilizables del sistema de Transferencia Electrónica de Beneficios (EBT).
Además, se puede imponer una multa de hasta $250,000 o pena de prisión de hasta 20 años, o ambas. CERTIFICACIÓN
Comprendo la naturaleza del castigo que se impone por ocultar o suministrar información falsa. También, comprendo que adeudaré el valor de todo monto adicional que reciba de SNAP como resultado de no informar todos los cambios que ocurran en mi grupo familiar. Acepto comprobar los cambios, si fuese necesario. Las respuestas en este formulario son exactas y completas según mi leal saber y entender. Entiendo que mi firma en este documento autoriza a las autoridades federales, estatales y locales a comunicarse con personas u organizaciones con el fin de verificar la información que he proporcionado.
FIRMA X
FECHA
14 Computer Drive East • Albany, NY 12205 • 518-436-8757
FoodHelpNY.orgSummerMealsNY.org
SchoolMealsHubNY.orgA�erschoolMealsNY.org
H un gerSolut ion sNY.org