
Sulfur mustard and respiratory diseases
15
688 Contents 1. Introduction ........................................................................................................................................................................ 689 2. Clinical study of patients with pulmonary diseases after sulfur mustard exposure....................................................... 689 2.1. Symptoms and pathological changes of the lung at early stages after HD exposure ............................................ 689 2.2. Symptoms, pathological and functional changes of the lung at late stages after HD exposure ........................... 690 2.2.1. Victims from World War I ................................................................................................................................. 690 2.2.2. Victims from Iran–Iraq War ............................................................................................................................. 690 2.3. Victims from occupational or accidental exposure of HD ....................................................................................... 691 2.4. Linkage of the early and late toxic effects of HD ....................................................................................................... 691 2.5. Sulfur mustard exposure and lung cancer ................................................................................................................ 692 3. Molecules involved in HD-induced pathophysiological changes in the respiratory system in the human ................ 692 4. Experimental study of HD-induced pulmonary diseases in the animal models .......................................................... 693 5. Mechanism of HD-induced damages in the respiratory system and the respectively therapeutic targets for effectively controlling these damages in animal models and patients exposed to mustard ........................................ 694 5.1. HD-induced acute damages ...................................................................................................................................... 694 REVIEW ARTICLE Sulfur mustard and respiratory diseases Feng Ru Tang 1,2 and Weng Keong Loke 3 1 Temasek Laboratories, 2 Department of Anatomy, National University of Singapore, Singapore, and 3 Defense Medical and Environmental Research Institute, DSO National Laboratories, Singapore Abstract Victims exposed to sulfur mustard (HD) in World War I and Iran–Iraq war, and those suffered occupational or accidental exposure have endured discomfort in the respiratory system at early stages after exposure, and marked general physical deterioration at late stages due to pulmonary fibrosis, bronchiolitis obliterans or lung cancer. At molecule levels, significant changes of cytokines and chemokines in bronchoalveolar lavage and serum, and of selectins (in particular sE-selectin) and soluble Fas ligand in the serum have been reported in recent studies of patients exposed to HD in Iran–Iraq war, suggesting that these molecules may be associated with the pathophysiological development of pulmonary diseases. Experimental studies in rodents have revealed that reactive oxygen and nitrogen species, their product peroxynitrite (ONOO − ), nitric oxide synthase, glutathione, poly (adenosine diphosphate-ribose) polymerase, activating protein-1 signaling pathway are promising drug targets for preventing HD-induced toxicity, whereas N-acetyl cysteine, tocopherols, melatonin, aprotinin and many other molecules have been proved to be effective in prevention of HD-induced damage to the respiratory system in different animal models. In this paper, we will systemically review clinical and pathophysiological changes of respiratory system in victims exposed to HD in the last century, update clinicians and researchers on the mechanism of HD-induced acute and chronic lung damages, and on the relevant drug targets for future development of antidotes for HD. Further research directions will also be proposed. Keywords: Sulfur mustard, pulmonary diseases, World War I, Iran–Iraq war, molecular mechanism, drug targets Address for Correspondence: Feng Ru Tang, Temasek Laboratories, National University of Singapore 5A, Engineering Drive 1, Singapore 117411, Singapore. Tel: (65) 66011094. Fax: (65) 68726840. E-mail: [email protected]; Weng Keong Loke, Defense Medical and Environmental Research Institute, DSO National Laboratories, 20 Science Park Drive, Singapore 118230, Singapore. E-mail: [email protected] (Received 19 March 2012; revised 22 May 2012; accepted 27 May 2012) Critical Reviews in Toxicology, 2012; 42(8): 688–702 © 2012 Informa Healthcare USA, Inc. ISSN 1040-8444 print/ISSN 1547-6898 online DOI: 10.3109/10408444.2012.698405 Critical Reviews in Toxicology Downloaded from informahealthcare.com by NATIONAL UNIVERSITY OF SINGAPORE on 08/17/12 For personal use only.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Sulfur mustard and respiratory diseases

688
Contents
1. Introduction ........................................................................................................................................................................ 6892. Clinical study of patients with pulmonary diseases after sulfur mustard exposure ....................................................... 689
2.1. Symptoms and pathological changes of the lung at early stages after HD exposure ............................................ 689 2.2. Symptoms, pathological and functional changes of the lung at late stages after HD exposure ........................... 690
2.2.1. Victims from World War I ................................................................................................................................. 690 2.2.2. Victims from Iran–Iraq War ............................................................................................................................. 690
2.3. Victims from occupational or accidental exposure of HD ....................................................................................... 691 2.4. Linkage of the early and late toxic effects of HD ....................................................................................................... 691 2.5. Sulfur mustard exposure and lung cancer ................................................................................................................ 692
3. Molecules involved in HD-induced pathophysiological changes in the respiratory system in the human ................ 6924. Experimental study of HD-induced pulmonary diseases in the animal models .......................................................... 6935. Mechanism of HD-induced damages in the respiratory system and the respectively therapeutic targets for
effectively controlling these damages in animal models and patients exposed to mustard ........................................ 694 5.1. HD-induced acute damages ...................................................................................................................................... 694
REVIEW ARTICLE
Sulfur mustard and respiratory diseases
Feng Ru Tang1,2 and Weng Keong Loke3
1Temasek Laboratories, 2Department of Anatomy, National University of Singapore, Singapore, and 3Defense Medical and Environmental Research Institute, DSO National Laboratories, Singapore
AbstractVictims exposed to sulfur mustard (HD) in World War I and Iran–Iraq war, and those suffered occupational or accidental exposure have endured discomfort in the respiratory system at early stages after exposure, and marked general physical deterioration at late stages due to pulmonary fibrosis, bronchiolitis obliterans or lung cancer. At molecule levels, significant changes of cytokines and chemokines in bronchoalveolar lavage and serum, and of selectins (in particular sE-selectin) and soluble Fas ligand in the serum have been reported in recent studies of patients exposed to HD in Iran–Iraq war, suggesting that these molecules may be associated with the pathophysiological development of pulmonary diseases. Experimental studies in rodents have revealed that reactive oxygen and nitrogen species, their product peroxynitrite (ONOO−), nitric oxide synthase, glutathione, poly (adenosine diphosphate-ribose) polymerase, activating protein-1 signaling pathway are promising drug targets for preventing HD-induced toxicity, whereas N-acetyl cysteine, tocopherols, melatonin, aprotinin and many other molecules have been proved to be effective in prevention of HD-induced damage to the respiratory system in different animal models. In this paper, we will systemically review clinical and pathophysiological changes of respiratory system in victims exposed to HD in the last century, update clinicians and researchers on the mechanism of HD-induced acute and chronic lung damages, and on the relevant drug targets for future development of antidotes for HD. Further research directions will also be proposed.Keywords: Sulfur mustard, pulmonary diseases, World War I, Iran–Iraq war, molecular mechanism, drug targets
Address for Correspondence: Feng Ru Tang, Temasek Laboratories, National University of Singapore 5A, Engineering Drive 1, Singapore 117411, Singapore. Tel: (65) 66011094. Fax: (65) 68726840. E-mail: [email protected]; Weng Keong Loke, Defense Medical and Environmental Research Institute, DSO National Laboratories, 20 Science Park Drive, Singapore 118230, Singapore. E-mail: [email protected]
(Received 19 March 2012; revised 22 May 2012; accepted 27 May 2012)
Critical Reviews in Toxicology, 2012; 42(8): 688–702© 2012 Informa Healthcare USA, Inc.ISSN 1040-8444 print/ISSN 1547-6898 onlineDOI: 10.3109/10408444.2012.698405
Critical Reviews in Toxicology
42
8
688
702
Mar192012
May222012
May272012
1040-8444
1547-6898
© 2012 Informa Healthcare USA, Inc.
10.3109/10408444.2012.698405
2012
HD and respiratory diseases
F. R. Tang and W. K. Loke
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

HD and respiratory diseases 689
© 2012 Informa Healthcare USA, Inc.
1. Introduction
Sulfur mustard bis(dichloroethyl) sulfide (HD) with the
formula of (ClCH2CH
2)
2S
(MW 159.08) and other names as Iprit, Kampfstoff ‘Lost,’ Lost, Mustard gas, Senfgas, Yellow Cross Liquid, Yperite, Distilled Mustard, or Mustard T-mixture, is a synthetic substance prepared by treating ethylene with sulfur chlo-ride [SCl
2 + 2 C
2H
4 → (ClCH
2CH
2)
2S](Depretz method)
or by treating 2, 2′-dihydroxyethyl sulfide with HCl gas [(HO-CH
2CH
2)
2S + 2HCl → (Cl-CH
2CH
2)
2S + 2H
2O]
(Meyer method).It is a viscous liquid at normal temperatures, color-
less if pure (but normally ranges from pale yellow to dark brown), with slight garlic or horseradish type odor. The pure compound has a melting point of 14°C (57°F) and decomposes before boiling at 218°C (424.4°F). Mustard gas is not very soluble in water but is very soluble in fat, contributing to its rapid absorption into the skin. It was synthesized by German chemists, Despretz in 1822 and Niemann and Guthrie in 1860 (Guthrie, 1860; Niemann, 1860). The synthesis of mustard gas was first reported by Victor Meyer in 1886.
HD was first used as a chemical-warfare agent during World War I (WWI), and subsequent in Ethiopia dur-ing 1936 by Italy. It was extensively produced by Britain, Canada, France, Germany, Hungary, Italy, Japan, the Netherlands, Poland, South Africa, the USA and the Union of Soviet Socialist Republics during WWII, but was used only by Japan in China. It is a chemical weapon agent that is stockpiled, by far the largest quantity – on the order of hundreds of thousands of tons overall. It was used by Egypt in Yemeni civil war of the mid-1960s and by Iraq during and post the Iran–Iraq war (1980–1988) in the Iraqi Kurdish village of Halabja (Leikin and McFee, 2007).
2. Clinical study of patients with pulmonary diseases after sulfur mustard exposure
2.1. Symptoms and pathological changes of the lung at early stages after HD exposureDepending on the inhaled amount, the early toxic effects on respiratory system include pain or discomfort in the nose and pharynx with increased nasal secre-tions, sneezing, and sore throat, which usually develop 2–16 h after exposure. Rhinorrhea is often profuse and epistaxis may occur. Larger amounts of vapor cause laryngeal injury (aphonia or husky voice) and damage to upper medium-sized airways (tracheobronchitis), which is usually manifested by a nonproductive hacking cough (Warthin et al., 1918; Sidell, 1990; Du, 2003). In a
study of 62 cases of lethal gassing with HD, Koch (1921) reported that 11 heavily HD-exposed soldiers died dur-ing the first 3 days of exposure, 51 died within 2 weeks, seven of all cases that survived the first 2 weeks showed lung abscesses, and lung gangrene was observed in three of 62 cases. Pathological study showed a collapsed right lung caused by pseudomembranous obstruction of the right main stem bronchus in one case. In general, four phases of the pathological changes i.e. catarrhal, pseudomembranous laryngotracheitis, pseudomem-branous bronchitis and bronchopneumonia, lung abscess and gangrene occurred in the respiratory sys-tem (Koch, 1921).
Exposure to a very large amount of vapor also dam-aged the terminal airways, causing severe cough, dys-pnea, hemorrhage into the alveoli and purulent sputum (Balali-Mood and Navaeian, 1986; Willems, 1989). Necrosis of the mucosa with associated inflammation in severe cases led to the formation of a diphtheritic-like membrane which obstructed the airway or broke off to obstruct lower airways (Freitag et al., 1991). Respiratory distress syndrome might be present at later stage, as seen in Iranian victims suffered multi-system organ failure (Balali-Mood and Navaeian, 1986; Balali et al., 1986). Infection of the respiratory tract was a common compli-cation, usually developed 36–48 h after exposure which might result in bronchopneumonia and death between the second day and the fourth week after exposure (Easton et al., 1988; Papirmeister et al., 1991). Victims recovered in 1–2 months after exposure, particularly for those with secondary infections and necrotic broncho-pneumonia. In cases with severe lung complications requiring artificial ventilation, prognosis was very poor (Papirmeister et al., 1991).
In a case report of a patient accidently exposed to splashed HD (abandoned by Japanese in China–Japanese War in WWII) with 95% skin burning in Qi Qi Ha Er city in Hei Long Jiang Province, China on August 4, 2003 (HD exposure accident in Qi Qi Ha Er city), Du (2003) described severe pharyngeal pain, badly cough, husky voice and sputum with blood 2 h after exposure. Subsequent changes at 17 days after HD exposure in respiratory system included dyspnea, respiratory dis-tress, heavy bloody sputum and rhonchi. X-ray study showed atelectasis in the upper half of right lung, and shadows in both left and right lungs. Tracheoscope examination indicated edema, false membrane forma-tion and sloughing off, spillover of bloody sputum from the openings of bronchi. The patient died of respiratory failure on the same day. Necropsy study demonstrated inflammation and necrosis in the trachea and bronchi, false membrane consisting of necrotic tissue, fibrin and
5.2. HD-induced chronic damages ................................................................................................................................... 6966. Conclusions ......................................................................................................................................................................... 6977. Future studies ...................................................................................................................................................................... 698Acknowledgements ................................................................................................................................................................ 698
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

690 F. R. Tang and W. K. Loke
Critical Reviews in Toxicology
inflammatory exudate, edema and narrowing of bronchi, fibrosis of left and right lungs (Du, 2003).
2.2. Symptoms, pathological and functional changes of the lung at late stages after HD exposure2.2.1. Victims from World War IIn 2000 U.S. servicemen exposed to HD in WWI, 30% victims suffered bronchitis, characterized by prolonged expiration and coarse moist rales, and 22% had chara-cteristics associated with emphysema, including a rigid chest, limited diaphragm movement, and impaired expansion (Berghoff, 1919). Of 83 British pensioners with recognized disability due to HD poisoning, the principal symptom was shortness of breath. Persistent cough, expectoration, and chest tightness were also frequent. Physical examination indicated that 26% pensioners had signs of ‘emphysema,’ while another 20% had some definite signs of bronchitis (Sandall, 1922). Hankins and Klotz (1922) observed the common symptoms of shortness of breath, cough, expectoration, and asthma in 166 sanatorium patients exposed to HD. X-ray examination suggested chronic peribronchitis which might be due to a permanent thickening of the bronchial mucous membrane. Gilchrist and Matz (1933) examined 89 living and 53 deceased cases from 1016 U.S. servicemen exposed to HD, and reported that 27 of the 89 men 9–10 years after gassing had chronic bronchitis, emphysema, and bronchial asthma. In a group of 1267 war pensioners suffered from HD poisoning, 80% of them had chronic bronchitis. It suggested that British soldiers exposed to HD also had a higher incidence of chronic bronchitis than the general population (Case and Lea, 1955). Furthermore, lung cancer was also reported in those WWI veterans (Case and Lea, 1955; Beebe, 1960; Norman, 1975; Aasted et al., 1987).
2.2.2. Victims from Iran–Iraq WarIn 61 victims exposed to HD during Iran–Iraq War, all of them had cough, 75% patients had sputum, and 62% experienced shortness of breath (Hosseini et al., 1989). Chronic bronchitis and recurrent pneumonia occurred in the victims 2 years after the exposure (Somani and Babu, 1989). Autopsy of bronchus from a victim died 8 days after HD exposure demonstrated a large piece of mucous membrane blocking a bronchus and severe pseudomembranous inflammation of the trachea and the bronchi (Eisenmenger et al., 1991). A triad of cough, expectoration and dyspnea was diagnosed in more than 80% of Iranian veterans 3 years after the initial expo-sure (Afshinniaz and Ghanei, 1996). Hemoptysis, chest tightness, pain, and nocturnal dyspnea were also fre-quent symptoms. Clinical findings included generalized wheezing, crackles, decreased lung sounds, clubbing and cyanosis (Balali-Mood, 1986). Pulmonary function testing revealed more obstructive patterns than restric-tion. About half of these obstructive spirometric results were reversible in response to inhaled bronchodilators. Forced vital capacity (FVC), forced expiratory volume in
1s (FEV1), and FEV1/FVC (FEV1%), a calculated ratio used in the diagnosis of obstructive and restrictive lung disease, which represented the proportion of the FVC exhaled in the first second, were significantly lower in HD intoxicated veterans in comparison to healthy non-exposed people as well as to those chemical-warfare survivors who used a gas mask at the time of attack (Afshinniaz and Ghanei, 1966). In a group of 197 Iranian veterans 10 years after a single heavy exposure to HD, delayed destructive pulmonary squeal such as chronic bronchitis (58%), asthma (10%), bronchiectasis (8%), large airway narrowing (9%) and pulmonary fibrosis (12%) were diagnosed (Emad and Rezaian, 1997). By 16–20 years after exposure, much more percentage of patients developed chronic obstructive pulmonary dis-ease (35%), bronchiectasis (32.5%) and asthma (25%). It suggested a deterioration of lung diseases. Large airway narrowing (15%), pulmonary fibrosis (7.5%), and simple chronic bronchitis (5%) were also observed in some vic-tims (Hefazi et al., 2005). Khateri et al. (2003) reported that 42.5% of their cohort of 34,000 patients suffered from lung lesions in an obstructive pattern, i.e. decreases in the FVC, FEV1, and in the ratio of FEV1/FVC. Chest X-ray showed increased bronchovascular markings, hyperinflation, bronchiectasis, pneumonic infiltration and radiologic evidence of pulmonary hypertension (Bijani and Moghadamnia, 2002; Bagheri et al., 2003; Balali-Mood et al., 2005).
In a case report of a 5-year-old Kurdish boy exposed to HD and developed severe respiratory symptoms with a chemical pneumonia in the acute phase, Dompeling et al. (2004) observed that his FEV1 as measured in pul-monary function tests (PFTs) deteriorated over time and his PFTs over a 10-year period postexposure showed severe air trapping. The lung function abnormalities were not reversed by treatment with corticosteroids or bronchodilators. Infectious exacerbations of the boy’s lung disease occurred. High-resolution computed tomography (HRCT) scan showed multiple bronchiecta-sis. Pathological study of an open lung biopsy indicated a ‘chronic bronchiolitis.’ Direct toxic effects of HD could also lead to tracheobronchial stenosis with different degrees of involvement ranging from diffuse tracheal stenosis to stenosis of the isolated left main bronchus or glottic and subglottic stenosis 15 years after exposure (Ghanei et al., 2004a). The demonstration of bronchi-ectasis, mosaic parenchymal attenuation, irregular and dilated major airways, bronchial wall thickening, and interlobular septal wall thickening by HRCT suggested the occurrence of bronchiolitis obliterans (BO) (Ghanei et al., 2004b,c).
In 23 patients 14 years after exposure to HD, cough, dyspnea, and/or feeling of tight in the chest were observed in all of them (Beheshti et al., 2006). HRCT showed a significant air trapping, and PFT indicated a marked increase of residual volume. The most common inflammatory cells in bronchoalveolar lavage (BAL) fluid were neutrophils (88%). Biopsy demonstrated
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

HD and respiratory diseases 691
© 2012 Informa Healthcare USA, Inc.
11 cases of airway epithelial injury and nine cases of organizing pneumonia (OP) or bronchiolitis obliterans OP (BOOP). A retrospective cohort study on patients with mild, moderate, and severe initial symptoms of HD exposure indicated that the ‘mild’ group had no early symptom at the time of exposure, the ‘moderate’ group had early symptoms after exposure but patients were not hospitalized for treatment, and the ‘severe’ group had early symptoms and patients were hospitalized accordingly. PFT and HRCT showed that the severe and moderate groups had a similar frequency of obstructive pattern, whereas only one patient in the mild group had this pattern. Air trapping was similar between groups. Moderate and severe exposure to HD caused an equal risk of late pulmonary complication, while mild exposure had less risk. Combined HRCT scanning, BAL and open lung biopsies revealed asthma, emphysema, chronic bronchitis, pulmonary fibrosis, and bronchiolitis, and the major one was BO which involved a chronic scarring process affecting primarily the bronchioles. In addition to lower airway disease, the direct effect of HD on the upper airways led to damage to the trachea and bronchi. Scarring, fibrosis and mucociliary malfunction could then lead to stenosis of the bronchi and trachea (Ghanei et al., 2008a).
Kehe et al. (2009) recently reported hoarseness and a sore throat in 12 Iranian exposed to HD. The most affected patients were not able to swallow. Edema was observed among a large fraction of patients, whereas inflammation or obliterative necrosis occurred less frequently. Significant lung symptoms such as cough-ing (92%), sputum (67%) or even bloody sputum devel-oped. The blood gases were altered in 67% of all patients with alcalosis (33%), hypoxia (50%) or acidosis (17%). However, there was no significant difference of the aver-age number of red blood cells, white blood cells (WBCs) such as neutrophils, lymphocytes and hemoglobin from victims compared to the controls, but the average num-ber of red blood cells and hemoglobin were increased compared with data from 5 years ago (Ghanei, 2004). Atypical lymphocytes in their peripheral blood smears were found in 20 cases (from 318 victims). In a compre-hensive cohort study undertaken on a HD-exposed pop-ulation in Sardasht-Iran, named as Sardasht-Iran Cohort Study (SICS), Pourfarzam et al. (2009a) reported that dys-pnea was the most common symptom. Chronic cough, cough severity, sputum, hemoptysis, dyspnea, pattern and severity of dyspnea, and chest pain were statisti-cally significantly different between the two subgroups of hospitalized and nonhospitalized groups based on the severity of the injuries indicated by hospitalization a few days following exposure. Wheezing was the most common pulmonary finding. There was also a statisti-cally significant difference in the auscultation of wheez-ing and rhonchi between the hospitalized and control groups. Hematological study revealed that the hospi-talized group had significantly higher numbers of red blood cells than not hospitalized and the control groups.
The exposed group had significantly higher hematocrit and mean corpuscular volume than the control group. Exposure group had significantly lower numbers of platelet count, WBC and polymorphonuclear leukocytes than the control group but from clinical viewpoint this difference was not valuable. Furthermore, the number of lymph cells in the exposed group was significantly more than the control group (Shams et al., 2009). It sug-gested the probability of severe damage to bone marrow and predisposing to infection in other organs (especially lung) due to exposure to HD. In victims from Iran–Iraq War, the diagnosis of pulmonary fibrosis, OP or BOOP, which was not reported in those from WWI, might be due to the advancement of diagnostic technology instead of the differences in HD toxicity.
2.3. Victims from occupational or accident exposure of HDEpidemiologic studies on occupational exposure to HD in British and Japanese munitions factories showed that workers exposed to mustard agents developed chronic nonmalignant respiratory symptoms (Nishimoto et al., 1970; Manning et al., 1981; Easton et al., 1988). Furthermore, lung cancer was also reported in those workers in sulfur mustard production plant (Wada et al., 1968; Nishimoto et al., 1970, 1983, 1987; Manning et al., 1981; Tokuoka et al., 1986; Easton et al., 1988; Takeshima et al., 1994) and in fishermen exposed to mustard (Assennato et al., 1997). Of 44 patients (aged from 8 to 55 years old male (39) and female (5)) suffered from HD exposure in Qi Qi Ha Er city, 15 of them had respiratory symptoms with latency ranged from 2 to 11.4 h depend-ing on the ways of exposure. The symptoms of patients ranged from pharyngeal pain, cough, bloody purulent sputum, to fever and dyspnea (Sun et al., 2003a).
2.4. Linkage of the early and late toxic effects of HDIn previous study of the progressive toxic effects of HD poisoning at the early (1 week after exposure) and late (2 years after exposure) stages of exposure in 77 chemical-warfare victims, no significant change in eye lesion and decreased dermal complications were reported, whereas respiratory complications generally deteriorated over the years (Shirazi and Balali-Mood, 1988). Aghanouri et al. (2004) observed that inflammation and fibrotic processes in lung tissue of HD-exposed patients might be progressive. It was consistent with report from Hefazi et al. (2005) who observed that airway hypersensitivity, manifested as typical attacks of breathlessness, wheezing and nocturnal cough, as well as a reversible obstructive pattern on PFTs occurred between 4 weeks and 20 years after sulfur mustard inhalation with the increased severity and frequency of bronchiectatic lesions over the long-term follow-ups (Hefazi et al., 2005). These lesions usually began bilaterally in the lower lobes and then progressed toward the middle lobe and the lingula. In severe cases with extensive bronchiectatic lesions, pulmonary hypertension and ultimately cor pulmonale might occur (Emad and Rezaian,
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

692 F. R. Tang and W. K. Loke
Critical Reviews in Toxicology
1997; Bagheri et al., 2003; Ghanei et al., 2004c; Hefazi et al., 2005). Ghanei et al. (2003) reported that subclinical exposure to sulfur mustard could be responsible for the occurrence of delayed respiratory complications such as bronchiectasis and BO, as victims with respiratory disorders at late stages had no acute signs and symptoms at the time of exposure (Ghanei et al., 2004c). Late onset pulmonary fibrosis was observed in several Iranian veterans with combat exposure to HD (Bijani and Moghadamnia, 2002; Bagheri et al., 2003; Aghanouri et al., 2004; Balali-Mood et al., 2005). Analysis of BAL fluid from patients with mustard gas inhalation showed that patients with an ongoing local inflammatory process of the lower respiratory tract might develop pulmonary fibrosis years after initial exposure (Emad and Rezaian, 1999). Follow-up study of 12 patients with respiratory symptoms after HD exposure in Qi Qi Ha Er city demonstrated a significant improvement of the symptoms, suggesting that early treatment might prevent or cure HD-induced subsequent damage to respiratory system (Sun et al., 2003b).
2.5. Sulfur mustard exposure and lung cancerEarly study by comparing the mortality of WWI American veterans gassed with HD suggests that the causal rela-tion between HD exposure and lung cancer was weak or equivocal (Case and Lea, 1955; Beebe, 1960). Similar conclusion was made in a study of 7151 WWI veterans by Norman (1975) who reported the mortality of 2.5%, 1.8% and 1.9% for those died of lung cancer after the mustard gas, the pneumonia group and the controls respectively. It suggested that the dose of mustard gas might not be so high to produce a carcinogenic effect. Manning et al. (1981) provided evidence that exposure to HD led to a sig-nificant risk of laryngeal cancer. However, Yamakido et al. (1996) reported that 8.3% of 1632 male Japanese worked in poison gas factories (from 1927–1945) suffered malig-nant tumors. The pathological study indicated that 51% cases were squamous cell carcinoma, 33% undifferenti-ated carcinoma, and 15% adenocarcinoma. Squamous cell carcinoma often occurred in the paranasal sinus, tongue, pharynx, and larynx, whereas undifferentiated carcinoma and squamous cell carcinoma in the trachea and central portion of bronchi. This was also supported by the data from Yamada’s group (Yamada et al., 1953, 1957, 1961; Yamada, 1963). Pathological study form Nishimoto et al. (1987) showed that lung cancer from Japanese mus-tard gas workers was a central pulmonary carcinoma, and was distributed from the upper airway to the hilar region. Squamous cell carcinoma and undifferentiated carcinoma predominated, whereas adenocarcinoma and other types were rare. In a study of 3354 (95%) indi-viduals employed in the manufacture of mustard gas in Cheshire during the WWII, it was found that a highly sig-nificant number of workers died of cancers of the respira-tory system compared with national death rates (Easton et al., 1988). In 20 Iranian male lung cancer patients with single high-dose HD exposures during the Iran–Iraq War, Hosseini-Khalili et al. (2009) reported that the most
frequently occurring type of lung cancer was adenocarci-noma (45%), followed by squamous cell carcinoma (20%) and small cell carcinoma (15%). This was not in agree-ment with previous studies by Nishimoto et al. (1987) and Yamakido et al. (1996). In addition, a single case of muco-epidermal lung cancer was observed in a 33-year-old indi-vidual. They also observed an overall younger age of cancer onset in HD victims, and suggested that a single exposure might increase the risk of lung cancer development. It was supported by a recent study showing that exposure to HD gas accelerated the age at risk of developing lung cancer in former poisonous gas factory workers (Doi et al., 2011). However, similar findings were not made in Iranian patients exposed to mustard gas during the Iran–Iraq War (Emad and Rezaian, 1997; Ghanei et al., 2008a,b). Ghanei et al. (2008b) could not observe differences between the low- and high-dose groups, and suggested that effects of HD were not solely dependent on the severity of exposure.
3. Molecules involved in HD-induced pathological changes in the respiratory system in patients after its exposure
Recent studies from Iranian war victims suffered from chronic effects of HD have suggested a significant linkage between the progress of respiratory diseases and cytokine/chemokine expression. In a study of 126 war veterans with lung disease, Aghanouri et al. (2004) reported a significant increase in transforming growth factor (TGF)-β1 levels in BAL fluid between the case and control group without lung diseases, suggesting that inflammation and fibrotic processes in lung tissue of patients exposed to HD were progressive and interferon-γ (IFN-γ) might be a useful drug to treat this group of patients as it could reduce TGF-β expression and fibrosis (Ziesche et al., 1999). Compared to the control group, significant increases in interleukin (IL)-1β, IL-5, IL-6, IL-8, IL-12, TGF-β, tumor necrosis factor (TNF)-α, Regulated upon Activation Normal T-cell Expressed and Secreted (RANTES), eotaxin, monocyte chemotactic protein-1 (MCP-1), macrophage inflammatory protein-1α (MIP-1α), and MIP-1β, insulin-like growth factor-1 (IGF-1), and epidermal growth factor (EGF) granulocyte-macrophage colony stimulating pulmonary fibrosis (GM-CSF) and granulocyte-colony stimulating factor (G-CSF) levels in BAL were observed in victims exposed to HD (Emad and Emad, 2007a,b,c,d,e). Clinically, these patients suffered eosinophilic and neutrophil’s alveolitis. It suggested that cytokine and chemokines might be associated with the development of alveolitis and fibrosis in the victims. In SICS of a group of people 20 years after HD exposure, increased serum levels of soluble Fas ligand (sFasL), MCP-1, decreased IL-1α, IL-1β, interleukin-1 receptor antagonist (IL-1RA), TNF, IL-8 and RANTES have been reported (Ghazanfari et al., 2009a,b; Yaraee et al., 2009a). There was a significant negative correlation between sFasL and the WBC count in the HD-exposed cohort, suggesting that elevated serum levels of sFasL might be
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

HD and respiratory diseases 693
© 2012 Informa Healthcare USA, Inc.
associated with progression of pulmonary diseases in the HD-exposed subjects. Interestingly, the same research group also showed a positive relationship between a high physical activity and the levels of anti-inflammatory cytokine IL-10. It suggested that active lifestyles might help to improve the symptoms for those HD-exposed subjects with various inflammatory complications (Ghazanfari et al., 2009c). SICS further indicated no significant association between the serum levels of IL-8 and pulmonary symptoms (chronic cough, sputum, hemoptysis, and dyspnea), breath sounds (crackles, rales, and wheezing) as well as spirometry parameters. However, IL-6 was associated with wheezing, and C reactive protein was associated with wheezing and rales in HD-exposed group. It suggested that the serum levels of these inflammatory mediators probably did not have any major role in pathogenesis and persistence of pulmonary complications and did not reflect the degree of severity of pulmonary involvement following HD exposure (Pourfarzam et al., 2009b). However, there were positive correlations between circulating levels of GM-CSF with IL-1α, IL-1β, TNF-α and IL-6, but not with IL-8. Furthermore, the serum levels of GM-CSF had no association with clinical complications (Amiri et al., 2009). The selectins (L, P and E, or sL-selectin, sP-selectin and sE-selectin) are carbohydrate-binding membrane glycoproteins acting as adhesion molecules involved in the development of different inflammatory reactions. In HD-exposed group, sL-selectin and sP-selectin in the serum were significantly lower than the control group. However, sE-selectin was significantly increased in the exposed group compared to the control. As sL-selectin was positively correlated with the percentage of polymorphonuclear cells and negatively with the percentage of lymphocytes, and there was a significant correlation between the count of platelets and sP-selectin in both the control and exposed groups, the change in the pattern of selectins in the HD-exposed group indicated suppressed acute inflammatory condition in which new remodeling of cytokine expression might play a more crucial role in the immune-regulation (Yaraee et al., 2009b).
In vitro exposure of human bronchial (BEAS-2B) and alveolar (A549) cells to the nitrogen mustard derivative melphalan demonstrates that alkylating compounds not only caused cell death of lung epithelial cells but also activated stress-associated mitogen-activated pro-tein kinase (MAPK) signal transduction pathways and induced expression of mediators known to participate in the recruitment of inflammatory cells such as TNF and intercellular adhesion molecule-1 (Osterlund et al., 2005). Exposure of differentiated human respira-tory epithelial cells in air-liquid interface to nitrogen mustard also induced secretion of chemokines and pro-inflammatory cytokines including TNF-α, IL-1 α, IL-1β, IL-6, IL-8, RANTES, MCP-1, IP-10, G-CSF, GM-CSF and IL-15 (Karacsonyi et al., 2009). The in vitro model imi-tated some characteristics of the above in vivo studies
and it suggested that this model might be used for further study of mechanism of HD induced acute toxicity to the respiratory system.
4. Experimental study of HD-induced respiratory diseases in the animal models
Experimental studies in animal models of respiratory tox-icity after HD exposure have been done since WWI. In the rabbit model, severe damage in the upper respiratory tract, including the nasal passages, pharynx, larynx, trachea, and bronchi after inhalation of HD was reported. The damage was exposure concentration-dependent with the high-est levels of exposure causing necrosis of the epithelium, infiltration of WBCs, and the formation of diphtheritic-like pseudomembranes (Warthin and Weller, 1919). Similar damage was also found in dog model by Winternitz (1919) who showed necrotizing pneumonia in those died two to ten days following exposure, and ulceration or constriction of the trachea in those sacrificed at later times. Subsequent studies in strain A mice (a strain with an extremely high genetic susceptibility for development of pulmonary ade-nomas) indicated carcinogenic effect of HD and nitrogen mustard in lung (Heston, 1950, 1953a,b). In A/J mice, intra-peritoneal injection of uracil mustard increased the inci-dence and average number of pulmonary tumors (Abell et al., 1965). Changes in the upper respiratory airways after HD exposure also occurred in the rat model (Szarejko, 1974). In the adult rat lung organ cultures, Sawyer et al. (1995) observed that the structural changes in the lung tissue after HD exposure paralleled the toxicity measured biochemically, and were also similar to the damage found in animals and man exposed to HD in vivo. In guinea pigs intoxicated with HD intratracheally (0.3 mg/kg), Calvet et al. (1994) reported the increment of respiratory system resistance and microvascular permeability, columnar cell shedding all along the tracheal epithelium, broncho-constriction, and peribronchial edema 5 h after exposure. At 14 days, the tracheal epithelium was disorganized and atrophic. Airway hyper-reactivity to aerosolized substance P and histamine occurred, suggesting that HD-induced lesions of the tracheal epithelium might account for the airway hyper-responsiveness. In male hairless guinea pigs treated with HD by the respiratory route, Langenberg et al. (1998) showed that the respiratory toxicity of HD appeared to be local, rather than systemic. Pretreatment of hairless guinea pigs with the potential scavengers N-acetyl cyste-ine (NAC) or cysteine isopropyl ester did not significantly increase the LCt50-value for nose--only exposure to HD vapor. When investigating the acute effects of HD on air-way, lung, and surface tension of BAL fluid in guinea pigs following intratracheal (i.t.) exposure to an aerosolized solution of HD in saline, van Helden et al. (2004) observed two clinically relevant symptoms, i.e. asthma-like symp-toms reflected by an early bronchoconstriction and ‘late asthmatic responses,’ and acute respiratory distress syn-drome-like symptoms (pulmonary edema and damage to the lung surfactant). The respiratory minute volume was
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

694 F. R. Tang and W. K. Loke
Critical Reviews in Toxicology
enhanced. Histochemical study showed inflammation and severe epithelial injury in the upper respiratory system, whereas the lungs were homogeneously affected. The sur-face tension of BAL fluid derived at 24 h after HD exposure was much higher than that of unexposed control animals, indicating that the lung surfactant was altered, and exog-enous surfactant should be used for treatment.
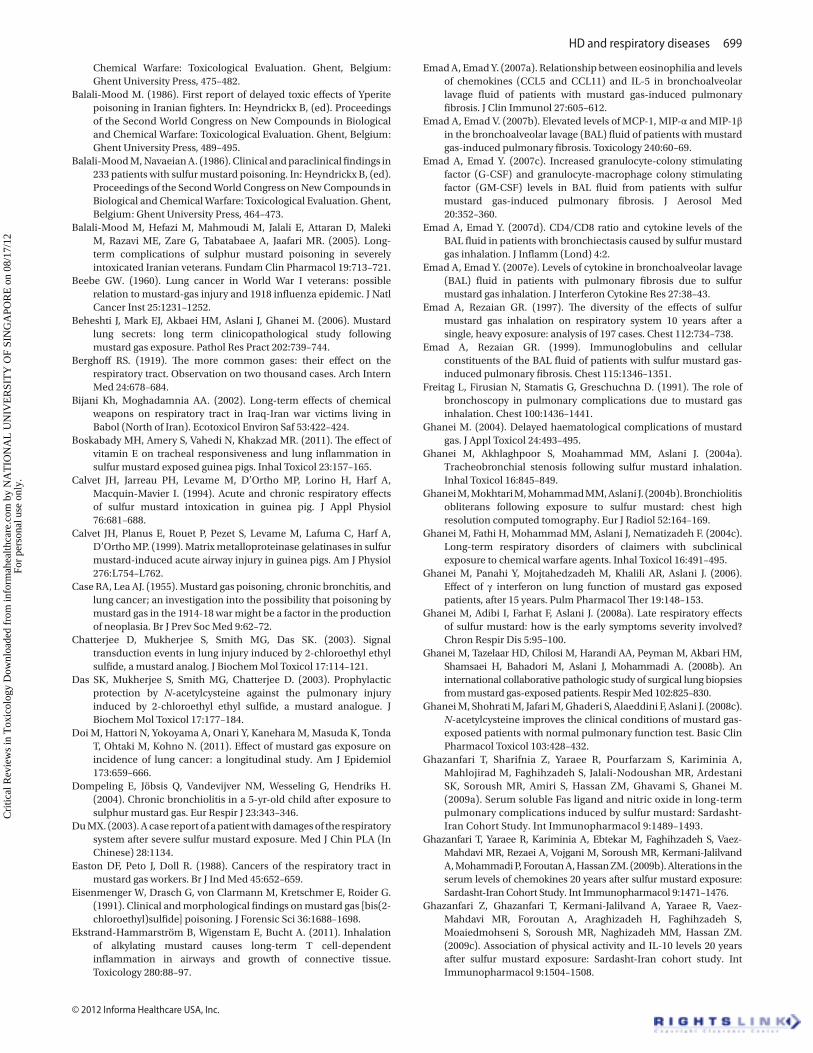
In guinea pigs exposed (head only) to various concentrations of HD vapor in individual plethysmography, clinical symptoms such as erythematic and swelling nose with extensive mucous secretion (with or without bleeding) occurred as early as at 3 h postexposure. At 6 h postexposure, most of the guinea pigs had breathing difficulties, rhonchi and dyspnea. The symptoms peaked at 48 h and were still observed 8 days after treatment with deaths of a few animals. A spontaneous healing with recovery of respiratory parameters and normal weight gain occurred within 2 weeks after HD challenging (Allon et al., 2009). Histopathological evaluation of lungs and trachea in the surviving guinea pigs at 4 weeks postexposure revealed a dose-dependent residual injury in both lung and trachea expressed by abnormal recovery of the tracheal epithelium concomitant with a dose-dependent increase in cellular volume in the lungs. These abnormal epithelial regeneration and lung remodeling were accompanied with significant changes in protein, lactic dehydrogenase activity, differential cell count and glutathione levels in the BAL. All these changes were similar to human casualties exposed to HD. Weber et al. (2010) recently established excellent inhalation exposure systems for the development of rodent models of HD-induced pulmonary injury, and demonstrated significant pulmonary injury when a higher dose of HD (180 mg/m3) was used. They have also clearly demonstrated that nose-only exposure caused extensive nasal injury, but lung injury was absent or minimal. The latter was consistent with our study in the rat model of intranasal administration of HD. In our recent study in the rat model of intratracheal spray of nebulized HD, we observed progressively pathological changes in the trachea and bronchi which included loss of epithelial cells, hemorrhage, false membrane formation (including fibrin, necrotic cell debris, neutrophil and macrophage infiltration) (Figure 1). Pathological changes in the lung, such as edema, neutrophil and macrophage infiltration, perivascular lymphocyte aggregation were observed in a minority of rats at different time points after HD challenging (Figure 2). Our study suggested that the rat model of intratracheal administration of nebulized HD might be a good model for the injury of the trachea and bronchi, but not an adequate lung injury model suggested by Weber et al. (2010). Delivery of HD vapor through a custom built intubation exposure system made by Weber et al. (2010) may be a better approach to mimic pulmonary injury in human, and this model may be a good model for further elucidating the mechanism of HD-induced pathogenesis and for development of novel therapeutic approaches to treat lung injury.
5. Mechanism of HD-induced damages in the respiratory system and the respectively therapeutic targets for effectively controlling these damages in animal models and patients exposed to mustard
5.1. HD-induced acute damagesThe mechanism of HD-induced acute and chronic dam-ages to the respiratory system is still not clear. Early in vitro studies on rabbit tracheal primary cultures (Giuliani et al., 1997) or a human bronchial epithelial cell line (Rappeneau et al., 1999) indicated that oxidative stress might be involved in nitrogen mustard-induced epithe-lial cell damage at acute stage after its exposure. In in vivo model, mustard gas exposure decreased the overall activ-ity of superoxide dismutase (SOD) at 7 days after exposure. The activity of SOD-1 (35%) was significantly increased, SOD-3 was decreased (62%), whereas SOD-2 remained the same between the control and experimental groups (Mukhopadhyay et al., 2006). Yaren et al. (2007) showed dramatically increased levels of the lipid peroxidation end product malondialdehyde, inducible nitric oxide synthetase (iNOS) activation and urine nitrite-nitrate values, suggesting that lung toxicity of nitrogen mustard might be mediated by nitric oxide and peroxynitrite in rats. In other words, mustard induced both oxidative and nitrosative stress. In the elegant review paper, Korkmaz et al. (2006) proposed that the pathogenesis of mustard toxicity might go through three steps: (i) mustard bond target cell surface receptor, (ii) it activated intracellular reactive oxygen species (ROS) and reactive nitrogen spe-cies (RNS) leading to peroxynitrite (ONOO−) production, and (iii) the increased ONOO− level damaged organic molecules leading to poly (adenosine diphosphate-ribose) polymerase (PARP) activation. Therefore, multi-ple therapies by a combination of cell membrane receptor blockers, antioxidants, NOS inhibitors, peroxynitrite scavengers, and PARP inhibitors may be a promising approach to effectively control mustard-induced acute damage to the respiratory system. It was supported by the fact that melatonin, a potent antioxidant molecule, acted as an iNOS inhibitor and a peroxynitrite scaven-ger, restored the selected oxidative and nitrosative stress markers in a dose-dependent manner (Topal et al., 2005 ; Ucar et al., 2007; Korkmaz et al., 2008a; Laskin et al., 2010), and suggested that melatonin might be one of ideal can-didate antidotes to effectively prevent HD-induce acute damage to the respiratory system. Antioxidant liposome significantly counteracts the 2-chloroethyl ethyl sulfide (CEES)-induced activation of activating protein-1 (AP-1) transcription factors and corresponding increase in the protein levels of Fos, activating transcription factor and Jun family members. It also blocks the CEES-induced increase in the protein levels of cyclin D1, a cell cycle protein and proliferating cell nuclear antigen, a cell differentiation marker. Furthermore, it protects lung against CEES-induced inflammation and infiltration of neutrophils, eosinophils and erythrocytes in the alveolar
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

HD and respiratory diseases 695
© 2012 Informa Healthcare USA, Inc.
space and blocks the CEES-induced activation of IL-6, IL-1β, and serum accelerator factor-1 (SAF-1)/Myc-associated zinc finger protein (MAZ), i.e. SAF-1/MAZ (Mukhopadhyay et al., 2009, 2010). It may therefore be a candidate drug to prevent HD-induced lung damage, and such a protective effect is mediated via controlling MAPK/AP-1 signaling.
Glutathione (GSH) is the major nonprotein thiol that can protect cells from damage due to electrophilic alkylating agents (such as HD) by forming conjugates with the agent. Gross et al. (1993) demonstrated that pretreatment of peripheral blood lymphocytes for 48 h with NAC, which elevates intracellular GSH levels to 122% of control, appeared to partially protect these in vitro cells from the cytotoxic effects of HD (at 10 mM), suggesting that augmentation of intracellular levels of GSH might provide partial protection against cytotoxicity of HD. Atkins et al. (2000) indicated that pretreatment with NAC acted through
two different pathways to minimize endothelial injury by HD, i.e. enhancing GSH synthesis and suppressing HD-induced activation of the nuclear transcription factor NF-κB. Das et al. (2003) and before McClintock et al. (2006) McClintock et al. (2006) showed that CEES-induced injury of rat lungs could be substantially diminished by the presence of reducing agents such as NAC, GSH, or resveratrol, or antioxidant enzymes pegylated (PEG)-catalase, PEG-SOD, and their combination delivered via liposomes. NAC also helped to prevent CEES toxicity in LPS-treated macrophages (Paromov et al., 2008). Further study suggested that antioxidant liposomes containing both NAC and vitamin E were an effective antidote against CEES-induced lung injury (Mukherjee et al., 2009).
Matrix metalloproteinase (MMP) gelatinases of both inflammatory and epithelial cell origins may be involved in epithelial cell detachment in HD respiratory intoxication (Calvet et al., 1999). Treatment with the MMP-inhibitor
Figure 1. H & E staining shows a transverse section of a normal bronchus from a control rat (A, Epi: epithelial cells; double arrow: a cartilage cell), and those abnormal ones from experimental rats at different time points after intratracheal spray of sulfur mustard (HD) (C–I). At day 1 (B, C; arrowhead: neutrophil) and day 3 (D, E; arrowhead: neutrophil; arrows: macrophages) epithelial cells almost disappear. In the lumen of the bronchus, false membrane (stars) which includes fibrin, infiltrated neutrophil and macrophage, and necrotic cell debris is formed. At day 7 (F, G), there is a sloughing off of false membrane. At 14 days after HD exposure (H, I), basal cells cover the surface of the lumen. Scale bar = 50 µm in A applies to Figure 1C, E, G, I and Figure 2B–F; Scale bar = 100 µm in B applies to Figure 1D, F, H, and Figure 2A.
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

696 F. R. Tang and W. K. Loke
Critical Reviews in Toxicology
Figure 2. H & E staining shows the histology of a normal left lung from a control rat (A) and those from experimental rats at different time points after intratracheal spray of HD. At 1 day (B), 3 (C), 7 (D) and 14 (E, F) days after HD exposure, edema (asterisks in B and D), reactive macrophage (arrows in B, C, D and F) and neutrophil (arrowheads B and D) infiltration are observed in a few rats. Lymphocyte (arrowheads in E) infiltration around blood vessels (BV in E) in the lung also occurs.
doxycycline attenuated lung injury (Guignabert et al., 2005). Recent study has also shown increased expres-sion of connective tissue growth factor and MMP-9, mediators regulating extracellular matrix turnover, following exposure of rats to nitrogen mustard (Sunil et al., 2011a). It suggests that MMP may be a very impor-tant molecule involved in HD-induced acute lung injury, a candidate drug target for prevention of HD-induced acute lung damages.
Changes of cytokines and chemokines have been reported in HD respiratory intoxication models. High levels of TNF-α were induced in guinea pigs exposed to CEES intratracheally, which activated both acid and neutral sphingomyelinases, resulting in high accumulation of ceramides, a second messenger involved in cell apoptosis (Chatterjee et al., 2003). TNF-α also activated MAPKs/AP-1 signaling pathway and cell proliferation (Mukhopadhyay et al., 2008). In the mouse CEES model, Sunil et al. (2011b) observed reduced expression of oxidative stress markers in mice lacking the p55 receptor for TNF-α (TNFR1−/−), suggesting that signaling via TNFR1 was key to CEES-induced injury, oxidative stress and inflammation, and targeting on TNF-α signaling pathway may be useful in mitigating lung injury, inflammation and functional alterations induced by vesicants. In the rat HD-induced lung injury model, significant increase in the total protein (TP), in the cytokines IL-1α and IL-13 has been observed in lung lavage fluid, and protease inhibitors aprotinin and ilomastat could reduce the increment of those proteins
(Anderson et al., 2009), and therefore, they may be used to control HD-induced acute lung damage. In in vitro model, nitrogen mustard, a HD functional analog, induced secretion of chemokines and proinflammatory cytokines including TNF-α, IL-1α, IL-1β, IL-6, IL-8, RANTES, MCP-1, IP-10, G-CSF, GM-CSF and IL-15 (Karacsonyi et al., 2009). Dermal exposure of HD to euthymic hairless guinea pigs could also induce strongly up-regulated expression of proinflammatory cytokines (TNF-α, IFN-γ) and chemokines (IL-8) in the lung (Mishra et al., 2010). Lung exposure of the nitrogen mustard melphalan induced an early burst of the proinflammatory cytokines IL-1β, IL-6 and IL-23 in airways, followed by extensive infiltration of neutrophils in the lung tissue and airways within 24 h (Ekstrand-Hammarström et al., 2011). A higher IL-4 in serum is also demonstrated in guinea pigs 14 days postexposure (Boskabady et al., 2011). These studies suggest that proinflammatory cytokines or chemokines may be potential drug targets for prevention of HD-induced acute damage to the respiratory system.
Other treatments such as Nigella sativa (Hossein et al., 2008), dexamethasone, vitamin E (Wigenstam et al., 2009) have also been reported to be effective to protect against HD-induced lung injury in different ani-mal models.
5.2. HD-induced chronic damagesSo far, the mechanism of delayed damage of respiratory system after a single exposure of HD still remains unknown. HD has a short half-life of 19–24 min in
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

HD and respiratory diseases 697
© 2012 Informa Healthcare USA, Inc.
normal saline and 30–60 min in the blood (Hambrook et al., 1993). Its metabolites are usually cleared from the body within a few weeks after exposure, and therefore, may not be related to the chronic damages and clinical symptoms (Somani and Babu, 1989). However, as mentioned above, at acute stages, mustard exposure may activate intracellular ROS and RNS leading to peroxynitrite (ONOO−) production, and the increased ONOO− level may cause acute lung damage (Korkmaz et al., 2006). If the damage is limited and reversible, the lung architecture may restore to normal within a few days. If it is intense to overwhelm the repair and regenerative abilities of lung, it may cause apoptotic cell death and chronic pathological changes such as pulmonary fibrosis. Furthermore, neutrophils alveolitis, presence of eosinophils, and higher concentrations of CCL5, CCL11, IL-5, IL-8, MCP-1, MIP-1α, MIP-1β, G-CSF, GM-CSF, TGF-β in BAL fluid were also associated with the development of fibrosis in HD victims. These chemokines, cytokines and growth factor may contribute to the recruitment of neutrophils and eosinophils in the lung, and may be therapeutic targets for prevention of progressive pulmonary fibrosis at chronic stages (Aghanouri et al., 2004; Emad and Emad, 2007a,b,c). Sulfur mustard and nitrogen mustard are two alkylating agents, and they have a similar ability to alkylate DNA. These two alkylating agents induced apoptosis which was evidenced by DNA ladder and by 4′,6-diamidino-2-phenylindole (DAPI) DAPI staining (Korkmaz et al., 2008a). Korkmaz et al. (2008b,c) recently demonstrated that single nitrogen mustard injection induced severe lung toxicity with strong interstitial and alveolar edema, hemorrhage, emphysematous changes as well as mild inflammatory cell infiltration and septal thickening. When nitrogen mustard was injected with histone deacetylase inhibitor Trichostatine A, interstitial and alveolar edema, hemorrhage and inflammatory cell infiltration were reduced significantly. However, combined administration of DNA methyl transferase inhibitor decitabine with nitrogen mustard exacerbated lung damage. Histone deacetylase and DNA methyl transferase have been known to be involved in histone modifications and DNA methylation respectively, whereas epigenetic regulation of gene expression involves histone modifications and DNA methylation (Miremadi et al., 2007). The findings from Korkmaz et al. (2008b,c) therefore suggest that nitrogen mustard itself and/or its intracellular metabolites may perturb the epigenetic environment of the affected cell in lung tissue, and this may be a possible explanation of HD-induced delayed toxicity. In other words, epigenetic mechanism may be involved in delayed mustard toxicity to the respiratory system. In this case, histone deacetylase and DNA methyl transferase may be new potential targets for development of epigenetic drugs to prevent HD-induced delayed toxicity to the respiratory system. In a recent study of 208 Kurdish patients suffered a high exposure to mustard gas with clinical symptoms such as erythema,
edema, vesiculation, scaling, ulceration, or crusting, Hosseini-Khalili et al. (2008) reported that angiotensin-converting enzyme (ACE) genotype influenced the severity of the late respiratory complications of mustard exposure with the D-allele polymorphism might be associated with a higher percentage of forced expiratory volume over 1 s predicted many years after exposure. Combined with previous studies showing the association of ACE D-allele polymorphism with the severity of other pulmonary diseases (Kanazawa et al., 2000; Schurmann, 2003; Hotta et al., 2004), it suggests that ACE may be another new therapeutic target for controlling HD-induced delayed lung damage. In HD gas-exposed patients with bronchiolitis, a 6-month treatment with IFNγ-1b plus a low-dose of prednisolone was associated with the improvement of lung function, suggesting that IFNγ-1b might be a candidate drug to control mustard-induced bronchiolitis (Panahi et al., 2005; Ghanei et al., 2006). On the other hand, a 4-month administration of NAC could improve clinical conditions and spirometric findings in mustard exposed in BO syndrome classes 1 and 2 (Ghanei et al., 2008c; Shohrati et al., 2008).
In skin exposure model, HD led to immune activa-tion, infiltration of T cells into the HD-exposed skin, delayed-type hypersensitivity response, and molecular imprints of inflammation in tissues distal from the site of HD exposure, it suggested that immunological responses might contribute to the delayed or chronic HD toxicity to the skin (Mishra et al., 2010). Whether similar immuno-logical responses are involved in chronic HD toxicity to respiratory system after single HD exposure remains to be further studied. In the rat, mouse and monkey mod-els, Mishra et al. (2012) recently found that IL-17 might be involved in HD-induced lung fibrosis across the mam-malian species and be a potential target for therapeutic interventions. Further study in HD gas-exposed patients is still needed to clarify whether results from animal models are applicable to human.
6. Conclusions
Clinical studies of combatants exposed to sulfur mustard in WWI and Iran–Iraq war and civilians working in poison gas factory, or accidently exposed to leaked HD have consistently shown both acute and chronic respiratory symptoms. The variations of symptoms, pathological changes, functional parameters reported from different groups may be due to, the ways of HD exposure, the amounts of inhaled HD gas, different treatments at the early stages after exposure, and diagnostic techniques. Chronic respiratory failure and cancers are main causes for those died of HD exposure. In BAL, there are significant increases in CCL5, CCL11, IL-1β, IL-5, IL-6, IL-8, IL-12, TGF-β, TNF-α, RANTES, eotaxin, MCP-1, MIP-1α, and MIP-1β, IGF-1, and EGF granulocyte-macrophage colony stimulating pulmonary fibrosis (GM-CSF) and granulocyte-colony stimulating factor (G-CSF) in victims 20 years after HD exposure in Iran–Iraq war. These changes
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

698 F. R. Tang and W. K. Loke
Critical Reviews in Toxicology
may be involved in bronchiectasis, pulmonary fibrosis and other pathological changes by the recruitment of eosinophils cells, neutrophils, monocytes in the lung. In the serum of these victims, significant changes of different cytokines (decreased IL-1α, IL-1β, IL-1RA, TNF, increased IL-10), chemokines (increased MCP-1, decreased IL-8 and RANTES), selectins (reduced sL- and sP-selectin, increased sE-selecrin) and sFasL (increased in the exposed group with pulmonary problems) are also observed. These changes may not be associated with pathophysiological changes of respiratory system. However, up-regulation of sFasL in those with respiratory problems may be related to the progression of pulmonary diseases.
In different animal models of HD inhalation, increased cytokines such as IL-1β, IL-4, IL-6, IL-8, IL-23, TNF-α (Malaviya et al., 2010; Mishra et al., 2010; Boskabady et al., 2011; Ekstrand-Hammarström et al., 2011), and che-mokines such as MCP-1 (Sunil et al., 2011b) have been reported in the lung tissue or BAL at acute stages after HD exposure. HD also activates intracellular ROS and RNS leading to peroxynitrite (ONOO−) production. Glutathione, MMP, p55 receptor for TNF-α are also very important mol-ecules involved in HD-induced acute damages to respira-tory system. Therapeutic approaches by targeting on these molecules using melatonin, NAC, antioxidant liposomes containing both NAC and vitamin E have been effective. It strongly suggests that ROS and RNS play very impor-tant roles in mustard-induced pulmonary diseases, and they may be promising therapeutic target for controlling pulmonary diseases at both acute and chronic stages. At chronic stage, epigenetic aberrations, ACE D-allele poly-morphism may be related to SM-induced delayed toxicity, and histone deacetylase and DNA methyl transferase may be potential targets for epigenetic drug development, and Trichostatine A may be one of candidate drugs for treating delayed pulmonary injury.
7. Future studies
Recent studies in victims survived Iran–Iraq war have established significant linkages between BAL cytokines, chemokines, selectins (in particular sE-selectin), sFasL and the development of pulmonary diseases 20 years after exposure to HD. Therapies targeting on these molecules at late stages are expected to be symptomatic as HD-induced damages are not reversible. Systemic study of the roles of these molecules at acute or early stages after HD exposure in the rodent models in general, and focusing on a few very effective ones in large animal models (such as like mon-key, pig or other species) in particular, may provide more significant evidences for the development of antidotes for HD. It may also provide more clues for understanding the mechanism of the development of chronic pulmonary dis-eases after HD-induced acute lung damage.
Experimental studies in rodents have revealed sev-eral promising drug targets including glutathione, reactive oxygen and nitrogen species, nitric oxide
synthase, PARP, AP-1 signaling pathway for preven-tion of HD-induced acute damages. Melatonin, NAC, doxycycline, tocopherols, aprotinin and other candidate drugs have been proved to be effective in prevention of HD-induced damage. Further study of these promising candidate drug targets or trial of candidate drugs in large animals such as monkey or pig may provide evidence for the possible translational use of the drugs as antidotes to control HD-induced lung injury to the human being.
Acknowledgements
We thank Chang May Ling Joyce, Sew Wen Hui Tracey and Seow Josefina for preparation of the rat model of intratracheal spray of sulfur mustard for pathological study of the lung.
Declaration of interest
The author’s affiliation is as shown on the cover page. The authors have sole responsibility for the writing and content of the paper. The paper was prepared during the normal course of our employment and, thus, the costs were borne by our employer.
ReferencesAasted A, Darre E, Wulf HC. (1987). Mustard gas: clinical, toxicological,
and mutagenic aspects based on modern experience. Ann Plast Surg 19:330–333.
Abell CW, Falk HL, Shimkin MB, Weisburger EK, Weisburger JH, Gubareff N. (1965). Uracil mustard: a potent inducer of lung tumors in mice. Science 147:1443–1445.
Afshinniaz F, Ghanei M. (1966). Relationship of the chronic respiratory symptoms with spirometric and laboratory parameters. Isfahan, Iran: Isfahan University of Medical Sciences, Dissertation.
Aghanouri R, Ghanei M, Aslani J, Keivani-Amine H, Rastegar F, Karkhane A. (2004). Fibrogenic cytokine levels in bronchoalveolar lavage aspirates 15 years after exposure to sulfur mustard. Am J Physiol Lung Cell Mol Physiol 287:L1160–L1164.
Allon N, Amir A, Manisterski E, Rabinovitz I, Dachir S, Kadar T. (2009). Inhalation exposure to sulfur mustard in the guinea pig model: clinical, biochemical and histopathological characterization of respiratory injuries. Toxicol Appl Pharmacol 241:154–162.
Amiri S, Ghazanfari T, Yaraee R, Salimi H, Ebtekar M, Shams J, Ghasemi H, Pourfarzam S, Moin A, Sharifnia Z, Soroush MR, Faghihzadeh S, Hassan ZM. (2009). Serum levels of GM-CSF 20 years after sulfur mustard exposure: Sardasht-Iran Cohort Study. Int Immunopharmacol 9:1499–1503.
Anderson DR, Taylor SL, Fetterer DP, Holmes WW. (2009). Evaluation of protease inhibitors and an antioxidant for treatment of sulfur mustard-induced toxic lung injury. Toxicology 263:41–46.
Assennato G, Ambrosi F, Sivo D. (1997). Possible long-term effects on the respiratory system of exposure to yperite of fishermen. Med Lav 88:148–154.
Atkins KB, Lodhi IJ, Hurley LL, Hinshaw DB. (2000). N-acetylcysteine and endothelial cell injury by sulfur mustard. J Appl Toxicol 20 Suppl 1:S125–S128.
Bagheri MH, Hosseini SK, Mostafavi SH, Alavi SA. (2003). High-resolution CT in chronic pulmonary changes after mustard gas exposure. Acta Radiol 44:241–245.
Balali M, Farhoodi M, Panjvani, FK. (1986). Report of three fatal cases of war gas poisoning. In: Heyndrickx B, (ed). Proceedings of the Second World Congress on New Compounds in Biological and
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.
HD and respiratory diseases 699
© 2012 Informa Healthcare USA, Inc.
Chemical Warfare: Toxicological Evaluation. Ghent, Belgium: Ghent University Press, 475–482.
Balali-Mood M. (1986). First report of delayed toxic effects of Yperite poisoning in Iranian fighters. In: Heyndrickx B, (ed). Proceedings of the Second World Congress on New Compounds in Biological and Chemical Warfare: Toxicological Evaluation. Ghent, Belgium: Ghent University Press, 489–495.
Balali-Mood M, Navaeian A. (1986). Clinical and paraclinical findings in 233 patients with sulfur mustard poisoning. In: Heyndrickx B, (ed). Proceedings of the Second World Congress on New Compounds in Biological and Chemical Warfare: Toxicological Evaluation. Ghent, Belgium: Ghent University Press, 464–473.
Balali-Mood M, Hefazi M, Mahmoudi M, Jalali E, Attaran D, Maleki M, Razavi ME, Zare G, Tabatabaee A, Jaafari MR. (2005). Long-term complications of sulphur mustard poisoning in severely intoxicated Iranian veterans. Fundam Clin Pharmacol 19:713–721.
Beebe GW. (1960). Lung cancer in World War I veterans: possible relation to mustard-gas injury and 1918 influenza epidemic. J Natl Cancer Inst 25:1231–1252.
Beheshti J, Mark EJ, Akbaei HM, Aslani J, Ghanei M. (2006). Mustard lung secrets: long term clinicopathological study following mustard gas exposure. Pathol Res Pract 202:739–744.
Berghoff RS. (1919). The more common gases: their effect on the respiratory tract. Observation on two thousand cases. Arch Intern Med 24:678–684.
Bijani Kh, Moghadamnia AA. (2002). Long-term effects of chemical weapons on respiratory tract in Iraq-Iran war victims living in Babol (North of Iran). Ecotoxicol Environ Saf 53:422–424.
Boskabady MH, Amery S, Vahedi N, Khakzad MR. (2011). The effect of vitamin E on tracheal responsiveness and lung inflammation in sulfur mustard exposed guinea pigs. Inhal Toxicol 23:157–165.
Calvet JH, Jarreau PH, Levame M, D’Ortho MP, Lorino H, Harf A, Macquin-Mavier I. (1994). Acute and chronic respiratory effects of sulfur mustard intoxication in guinea pig. J Appl Physiol 76:681–688.
Calvet JH, Planus E, Rouet P, Pezet S, Levame M, Lafuma C, Harf A, D’Ortho MP. (1999). Matrix metalloproteinase gelatinases in sulfur mustard-induced acute airway injury in guinea pigs. Am J Physiol 276:L754–L762.
Case RA, Lea AJ. (1955). Mustard gas poisoning, chronic bronchitis, and lung cancer; an investigation into the possibility that poisoning by mustard gas in the 1914-18 war might be a factor in the production of neoplasia. Br J Prev Soc Med 9:62–72.
Chatterjee D, Mukherjee S, Smith MG, Das SK. (2003). Signal transduction events in lung injury induced by 2-chloroethyl ethyl sulfide, a mustard analog. J Biochem Mol Toxicol 17:114–121.
Das SK, Mukherjee S, Smith MG, Chatterjee D. (2003). Prophylactic protection by N-acetylcysteine against the pulmonary injury induced by 2-chloroethyl ethyl sulfide, a mustard analogue. J Biochem Mol Toxicol 17:177–184.
Doi M, Hattori N, Yokoyama A, Onari Y, Kanehara M, Masuda K, Tonda T, Ohtaki M, Kohno N. (2011). Effect of mustard gas exposure on incidence of lung cancer: a longitudinal study. Am J Epidemiol 173:659–666.
Dompeling E, Jöbsis Q, Vandevijver NM, Wesseling G, Hendriks H. (2004). Chronic bronchiolitis in a 5-yr-old child after exposure to sulphur mustard gas. Eur Respir J 23:343–346.
Du MX. (2003). A case report of a patient with damages of the respiratory system after severe sulfur mustard exposure. Med J Chin PLA (In Chinese) 28:1134.
Easton DF, Peto J, Doll R. (1988). Cancers of the respiratory tract in mustard gas workers. Br J Ind Med 45:652–659.
Eisenmenger W, Drasch G, von Clarmann M, Kretschmer E, Roider G. (1991). Clinical and morphological findings on mustard gas [bis(2-chloroethyl)sulfide] poisoning. J Forensic Sci 36:1688–1698.
Ekstrand-Hammarström B, Wigenstam E, Bucht A. (2011). Inhalation of alkylating mustard causes long-term T cell-dependent inflammation in airways and growth of connective tissue. Toxicology 280:88–97.
Emad A, Emad Y. (2007a). Relationship between eosinophilia and levels of chemokines (CCL5 and CCL11) and IL-5 in bronchoalveolar lavage fluid of patients with mustard gas-induced pulmonary fibrosis. J Clin Immunol 27:605–612.
Emad A, Emad V. (2007b). Elevated levels of MCP-1, MIP-α and MIP-1β in the bronchoalveolar lavage (BAL) fluid of patients with mustard gas-induced pulmonary fibrosis. Toxicology 240:60–69.
Emad A, Emad Y. (2007c). Increased granulocyte-colony stimulating factor (G-CSF) and granulocyte-macrophage colony stimulating factor (GM-CSF) levels in BAL fluid from patients with sulfur mustard gas-induced pulmonary fibrosis. J Aerosol Med 20:352–360.
Emad A, Emad Y. (2007d). CD4/CD8 ratio and cytokine levels of the BAL fluid in patients with bronchiectasis caused by sulfur mustard gas inhalation. J Inflamm (Lond) 4:2.
Emad A, Emad Y. (2007e). Levels of cytokine in bronchoalveolar lavage (BAL) fluid in patients with pulmonary fibrosis due to sulfur mustard gas inhalation. J Interferon Cytokine Res 27:38–43.
Emad A, Rezaian GR. (1997). The diversity of the effects of sulfur mustard gas inhalation on respiratory system 10 years after a single, heavy exposure: analysis of 197 cases. Chest 112:734–738.
Emad A, Rezaian GR. (1999). Immunoglobulins and cellular constituents of the BAL fluid of patients with sulfur mustard gas-induced pulmonary fibrosis. Chest 115:1346–1351.
Freitag L, Firusian N, Stamatis G, Greschuchna D. (1991). The role of bronchoscopy in pulmonary complications due to mustard gas inhalation. Chest 100:1436–1441.
Ghanei M. (2004). Delayed haematological complications of mustard gas. J Appl Toxicol 24:493–495.
Ghanei M, Akhlaghpoor S, Moahammad MM, Aslani J. (2004a). Tracheobronchial stenosis following sulfur mustard inhalation. Inhal Toxicol 16:845–849.
Ghanei M, Mokhtari M, Mohammad MM, Aslani J. (2004b). Bronchiolitis obliterans following exposure to sulfur mustard: chest high resolution computed tomography. Eur J Radiol 52:164–169.
Ghanei M, Fathi H, Mohammad MM, Aslani J, Nematizadeh F. (2004c). Long-term respiratory disorders of claimers with subclinical exposure to chemical warfare agents. Inhal Toxicol 16:491–495.
Ghanei M, Panahi Y, Mojtahedzadeh M, Khalili AR, Aslani J. (2006). Effect of γ interferon on lung function of mustard gas exposed patients, after 15 years. Pulm Pharmacol Ther 19:148–153.
Ghanei M, Adibi I, Farhat F, Aslani J. (2008a). Late respiratory effects of sulfur mustard: how is the early symptoms severity involved? Chron Respir Dis 5:95–100.
Ghanei M, Tazelaar HD, Chilosi M, Harandi AA, Peyman M, Akbari HM, Shamsaei H, Bahadori M, Aslani J, Mohammadi A. (2008b). An international collaborative pathologic study of surgical lung biopsies from mustard gas-exposed patients. Respir Med 102:825–830.
Ghanei M, Shohrati M, Jafari M, Ghaderi S, Alaeddini F, Aslani J. (2008c). N-acetylcysteine improves the clinical conditions of mustard gas-exposed patients with normal pulmonary function test. Basic Clin Pharmacol Toxicol 103:428–432.
Ghazanfari T, Sharifnia Z, Yaraee R, Pourfarzam S, Kariminia A, Mahlojirad M, Faghihzadeh S, Jalali-Nodoushan MR, Ardestani SK, Soroush MR, Amiri S, Hassan ZM, Ghavami S, Ghanei M. (2009a). Serum soluble Fas ligand and nitric oxide in long-term pulmonary complications induced by sulfur mustard: Sardasht-Iran Cohort Study. Int Immunopharmacol 9:1489–1493.
Ghazanfari T, Yaraee R, Kariminia A, Ebtekar M, Faghihzadeh S, Vaez-Mahdavi MR, Rezaei A, Vojgani M, Soroush MR, Kermani-Jalilvand A, Mohammadi P, Foroutan A, Hassan ZM. (2009b). Alterations in the serum levels of chemokines 20 years after sulfur mustard exposure: Sardasht-Iran Cohort Study. Int Immunopharmacol 9:1471–1476.
Ghazanfari Z, Ghazanfari T, Kermani-Jalilvand A, Yaraee R, Vaez-Mahdavi MR, Foroutan A, Araghizadeh H, Faghihzadeh S, Moaiedmohseni S, Soroush MR, Naghizadeh MM, Hassan ZM. (2009c). Association of physical activity and IL-10 levels 20 years after sulfur mustard exposure: Sardasht-Iran cohort study. Int Immunopharmacol 9:1504–1508.
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

700 F. R. Tang and W. K. Loke
Critical Reviews in Toxicology
Gilchrist HL, Matz PB. (1933). The residual effects of warfare gases. Washington, DC: U.S. Government Printing Office.
Giuliani I, Baeza-Squiban A, Marano F. (1997). Early cytotoxic effects of mechlorethamine, a nitrogen mustard, on mammalian airway epithelium. Toxicol In Vitro 11:695–702.
Gross CL, Innace JK, Hovatter RC, Meier HL, Smith WJ. (1993). Biochemical manipulation of intracellular glutathione levels influences cytotoxicity to isolated human lymphocytes by sulfur mustard. Cell Biol Toxicol 9:259–267.
Guignabert C, Taysse L, Calvet JH, Planus E, Delamanche S, Galiacy S, d’Ortho MP. (2005). Effect of doxycycline on sulfur mustard-induced respiratory lesions in guinea pigs. Am J Physiol Lung Cell Mol Physiol 289:L67–L74.
Guthrie F. (1860). Ueber einige Derivate der Kohlenwasserstoffe CnHn. Ann Chem Pharm 113:266–288.
Hambrook JL, Howells DJ, Schock C. (1993). Biological fate of sulphur mustard (1,1′-thiobis(2-chloroethane)): uptake, distribution and retention of 35S in skin and in blood after cutaneous application of 35S-sulphur mustard in rat and comparison with human blood in vitro. Xenobiotica 23:537–561.
Hankins JL, Klotz, WC. (1922). Permanent pulmonary effects of gas in warfare. Am Rev Tubercul 6:571–574.
Hefazi M, Attaran D, Mahmoudi M, Balali-Mood M. (2005). Late respiratory complications of mustard gas poisoning in Iranian veterans. Inhal Toxicol 17:587–592.
Heston WE. (1950). Carcinogenic action of the mustards. J Natl Cancer Inst 11:415–423.
Heston WE. (1953a). Occurrence of tumors in mice injected subcutaneously with sulfur mustard and nitrogen mustard. J Natl Cancer Inst 14:131–140.
Heston WE. (1953b). Pulmonary tumors in strain A mice exposed to mustard gas. Proc Soc Exp Biol Med 82:457–460.
Hossein BM, Nasim V, Sediqa A. (2008). The protective effect of Nigella sativa on lung injury of sulfur mustard-exposed Guinea pigs. Exp Lung Res 34:183–194.
Hosseini K, Moradi A, Mansouri A, Vesssal K. (1989). Pulmonary manifestations of mustard gas injury: a review of 16 cases. IJMS 14:20–26.
Hosseini-Khalili AR, Thompson J, Kehoe A, Hopkinson NS, Khoshbaten A, Soroush MR, Humphries SE, Montgomery H, Ghanei M. (2008). Angiotensin-converting enzyme genotype and late respiratory complications of mustard gas exposure. BMC Pulm Med 8:15.
Hosseini-Khalili A, Haines DD, Modirian E, Soroush M, Khateri S, Joshi R, Zendehdel K, Ghanei M, Giardina C. (2009). Mustard gas exposure and carcinogenesis of lung. Mutat Res 678:1–6.
Hotta J, Hanaoka M, Droma Y, Katsuyama Y, Ota M, Kobayashi T. (2004). Polymorphisms of renin-angiotensin system genes with high-altitude pulmonary edema in Japanese subjects. Chest 126:825–830.
Kanazawa H, Okamoto T, Hirata K, Yoshikawa J. (2000). Deletion polymorphisms in the angiotensin converting enzyme gene are associated with pulmonary hypertension evoked by exercise challenge in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 162:1235–1238.
Karacsonyi C, Shanmugam N, Kagan E. (2009). A clinically relevant in vitro model for evaluating the effects of aerosolized vesicants. Toxicol Lett 185:38–44.
Kehe K, Thiermann H, Balszuweit F, Eyer F, Steinritz D, Zilker T. (2009). Acute effects of sulfur mustard injury–Munich experiences. Toxicology 263:3–8.
Khateri S, Ghanei M, Keshavarz S, Soroush M, Haines D. (2003). Incidence of lung, eye, and skin lesions as late complications in 34,000 Iranians with wartime exposure to mustard agent. J Occup Environ Med 45:1136–1143.
Koch WD. (1921). Direkte Kriegserkrankungen durch Einwirkung chemischer Mittel. In: Aschoff L, ed. Handbuch der ärztlichen Erfahrungen im Weltkriege 1914/1918 Band VIII. Pathologische Anatomie. Germany: J.A. Barth Leipzig, 526–536.
Korkmaz A, Yaren H, Topal T, Oter S. (2006). Molecular targets against mustard toxicity: implication of cell surface receptors, peroxynitrite production, and PARP activation. Arch Toxicol 80:662–670.
Korkmaz A, Kunak ZI, Paredes SD, Yaren H, Tan DX, Reiter RJ. (2008a). The use of melatonin to combat mustard toxicity. REVIEW. Neuro Endocrinol Lett 29:614–619.
Korkmaz A, Tan DX, Reiter RJ. (2008b). Acute and delayed sulfur mustard toxicity; novel mechanisms and future studies. Interdiscip Toxicol 1:22–26.
Korkmaz A, Yaren H, Kunak ZI, Uysal B, Kurt B, Topal T, Kenar L, Ucar E, Oter S. (2008c). Epigenetic perturbations in the pathogenesis of mustard toxicity; hypothesis and preliminary results. Interdiscip Toxicol 1:236–241.
Langenberg JP, van der Schans GP, Spruit HE, Kuijpers WC, Mars-Groenendijk RH, van Dijk-Knijnenburg HC, Trap HC, van Helden HP, Benschop HP. (1998). Toxicokinetics of sulfur mustard and its DNA-adducts in the hairless guinea pig. Drug Chem Toxicol 21 Suppl 1:131–147.
Laskin JD, Black AT, Jan YH, Sinko PJ, Heindel ND, Sunil V, Heck DE, Laskin DL. (2010). Oxidants and antioxidants in sulfur mustard-induced injury. Ann N Y Acad Sci 1203:92–100.
Leikin JB, McFee RB. (2007). Handbook of Nulcear, Biological and Chemical Agent Exposures. FL, USA: CRC Press, Taylor & Francis Group, 334–341.
Malaviya R, Sunil VR, Cervelli J, Anderson DR, Holmes WW, Conti ML, Gordon RE, Laskin JD, Laskin DL. (2010). Inflammatory effects of inhaled sulfur mustard in rat lung. Toxicol Appl Pharmacol 248: 89–99.
Manning KP, Skegg DC, Stell PM, Doll R. (1981). Cancer of the larynx and other occupational hazards of mustard gas workers. Clin Otolaryngol Allied Sci 6:165–170.
McClintock SD, Hoesel LM, Das SK, Till GO, Neff T, Kunkel RG, Smith MG, Ward PA. (2006). Attenuation of half sulfur mustard gas-induced acute lung injury in rats. J Appl Toxicol 26:126–131.
Miremadi A, Oestergaard MZ, Pharoah PD, Caldas C. (2007). Cancer genetics of epigenetic genes. Hum Mol Genet 16 Spec No 1:R28–R49.
Mishra NC, Rir-sima-ah J, March T, Weber W, Benson J, Jaramillo R, Seagrave JC, Schultz G, Grotendorst G, Sopori M. (2010). Sulfur mustard induces immune sensitization in hairless guinea pigs. Int Immunopharmacol 10:193–199.
Mishra NC, Rir-sima-ah J, Grotendorst GR, Langley RJ, Singh SP, Gundavarapu S, Weber WM, Pena-Philippides JC, Duncan MR, Sopori ML. (2012). Inhalation of sulfur mustard causes long-term T cell-dependent inflammation: possible role of Th17 cells in chronic lung pathology. Int Immunopharmacol 13:101–108.
Mukherjee S, Stone WL, Yang H, Smith MG, Das SK. (2009). Protection of half sulfur mustard gas-induced lung injury in guinea pigs by antioxidant liposomes. J Biochem Mol Toxicol 23:143–153.
Mukhopadhyay S, Rajaratnam V, Mukherjee S, Smith M, Das SK. (2006). Modulation of the expression of superoxide dismutase gene in lung injury by 2-chloroethyl ethyl sulfide, a mustard analog. J Biochem Mol Toxicol 20:142–149.
Mukhopadhyay S, Mukherjee S, Smith M, Das SK. (2008). Activation of MAPK/AP-1 signaling pathway in lung injury induced by 2-chloroethyl ethyl sulfide, a mustard gas analog. Toxicol Lett 181:112–117.
Mukhopadhyay S, Mukherjee S, Stone WL, Smith M, Das SK. (2009). Role of MAPK/AP-1 signaling pathway in the protection of CEES-induced lung injury by antioxidant liposome. Toxicology 261:143–151.
Mukhopadhyay S, Mukherjee S, Ray BK, Ray A, Stone WL, Das SK. (2010). Antioxidant liposomes protect against CEES-induced lung injury by decreasing SAF-1/MAZ-mediated inflammation in the guinea pig lung. J Biochem Mol Toxicol 24:187–194.
Niemann A. (1860). Ueber die Einwirkung des braunen Chlorschwefels auf Elaylgas. Ann Chem Pharm 113:288–292.
Nishimoto Y, Burrows B, Miyanishi M, Katsuta S, Shigenobu T, Kettel LJ. (1970). Chronic obstructive lung disease in Japanese poison gas workers. Am Rev Respir Dis 102:173–179.
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.
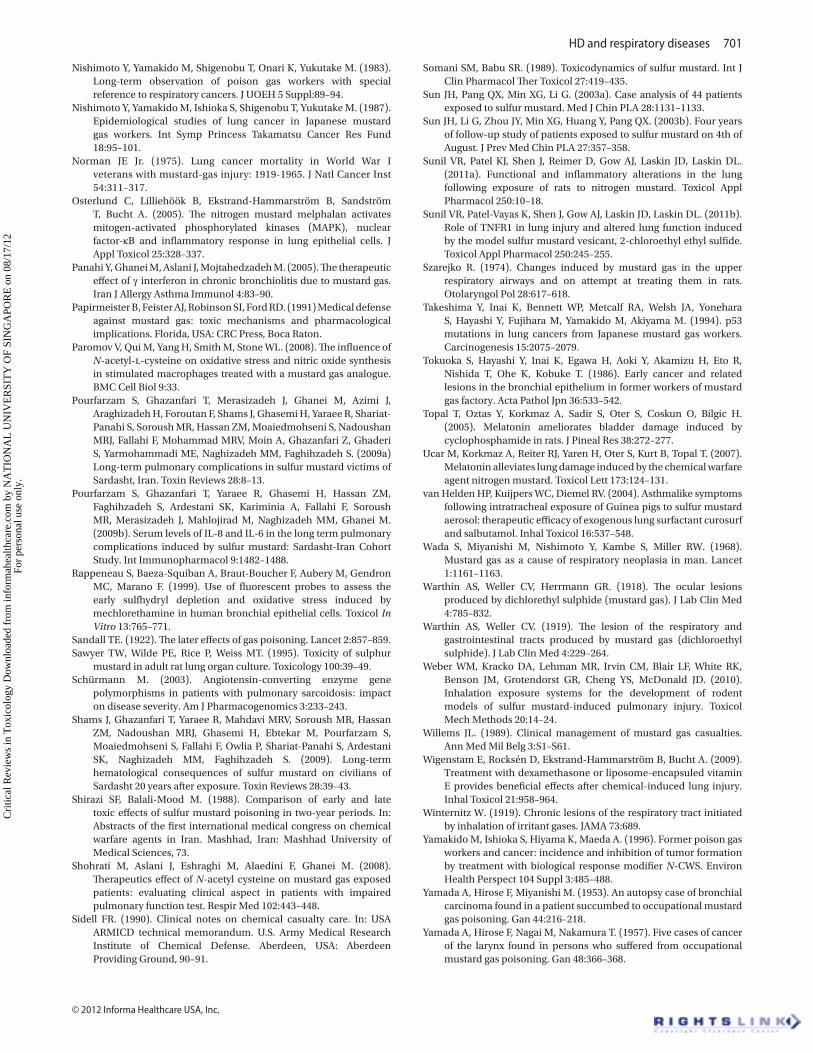
HD and respiratory diseases 701
© 2012 Informa Healthcare USA, Inc.
Nishimoto Y, Yamakido M, Shigenobu T, Onari K, Yukutake M. (1983). Long-term observation of poison gas workers with special reference to respiratory cancers. J UOEH 5 Suppl:89–94.
Nishimoto Y, Yamakido M, Ishioka S, Shigenobu T, Yukutake M. (1987). Epidemiological studies of lung cancer in Japanese mustard gas workers. Int Symp Princess Takamatsu Cancer Res Fund 18:95–101.
Norman JE Jr. (1975). Lung cancer mortality in World War I veterans with mustard-gas injury: 1919-1965. J Natl Cancer Inst 54:311–317.
Osterlund C, Lilliehöök B, Ekstrand-Hammarström B, Sandström T, Bucht A. (2005). The nitrogen mustard melphalan activates mitogen-activated phosphorylated kinases (MAPK), nuclear factor-κB and inflammatory response in lung epithelial cells. J Appl Toxicol 25:328–337.
Panahi Y, Ghanei M, Aslani J, Mojtahedzadeh M. (2005). The therapeutic effect of γ interferon in chronic bronchiolitis due to mustard gas. Iran J Allergy Asthma Immunol 4:83–90.
Papirmeister B, Feister AJ, Robinson SI, Ford RD. (1991) Medical defense against mustard gas: toxic mechanisms and pharmacological implications. Florida, USA: CRC Press, Boca Raton.
Paromov V, Qui M, Yang H, Smith M, Stone WL. (2008). The influence of N-acetyl-l-cysteine on oxidative stress and nitric oxide synthesis in stimulated macrophages treated with a mustard gas analogue. BMC Cell Biol 9:33.
Pourfarzam S, Ghazanfari T, Merasizadeh J, Ghanei M, Azimi J, Araghizadeh H, Foroutan F, Shams J, Ghasemi H, Yaraee R, Shariat-Panahi S, Soroush MR, Hassan ZM, Moaiedmohseni S, Nadoushan MRJ, Fallahi F, Mohammad MRV, Moin A, Ghazanfari Z, Ghaderi S, Yarmohammadi ME, Naghizadeh MM, Faghihzadeh S. (2009a) Long-term pulmonary complications in sulfur mustard victims of Sardasht, Iran. Toxin Reviews 28:8–13.
Pourfarzam S, Ghazanfari T, Yaraee R, Ghasemi H, Hassan ZM, Faghihzadeh S, Ardestani SK, Kariminia A, Fallahi F, Soroush MR, Merasizadeh J, Mahlojirad M, Naghizadeh MM, Ghanei M. (2009b). Serum levels of IL-8 and IL-6 in the long term pulmonary complications induced by sulfur mustard: Sardasht-Iran Cohort Study. Int Immunopharmacol 9:1482–1488.
Rappeneau S, Baeza-Squiban A, Braut-Boucher F, Aubery M, Gendron MC, Marano F. (1999). Use of fluorescent probes to assess the early sulfhydryl depletion and oxidative stress induced by mechlorethamine in human bronchial epithelial cells. Toxicol In Vitro 13:765–771.
Sandall TE. (1922). The later effects of gas poisoning. Lancet 2:857–859.Sawyer TW, Wilde PE, Rice P, Weiss MT. (1995). Toxicity of sulphur
mustard in adult rat lung organ culture. Toxicology 100:39–49.Schürmann M. (2003). Angiotensin-converting enzyme gene
polymorphisms in patients with pulmonary sarcoidosis: impact on disease severity. Am J Pharmacogenomics 3:233–243.
Shams J, Ghazanfari T, Yaraee R, Mahdavi MRV, Soroush MR, Hassan ZM, Nadoushan MRJ, Ghasemi H, Ebtekar M, Pourfarzam S, Moaiedmohseni S, Fallahi F, Owlia P, Shariat-Panahi S, Ardestani SK, Naghizadeh MM, Faghihzadeh S. (2009). Long-term hematological consequences of sulfur mustard on civilians of Sardasht 20 years after exposure. Toxin Reviews 28:39–43.
Shirazi SF, Balali-Mood M. (1988). Comparison of early and late toxic effects of sulfur mustard poisoning in two-year periods. In: Abstracts of the first international medical congress on chemical warfare agents in Iran. Mashhad, Iran: Mashhad University of Medical Sciences, 73.
Shohrati M, Aslani J, Eshraghi M, Alaedini F, Ghanei M. (2008). Therapeutics effect of N-acetyl cysteine on mustard gas exposed patients: evaluating clinical aspect in patients with impaired pulmonary function test. Respir Med 102:443–448.
Sidell FR. (1990). Clinical notes on chemical casualty care. In: USA ARMICD technical memorandum. U.S. Army Medical Research Institute of Chemical Defense. Aberdeen, USA: Aberdeen Providing Ground, 90–91.
Somani SM, Babu SR. (1989). Toxicodynamics of sulfur mustard. Int J Clin Pharmacol Ther Toxicol 27:419–435.
Sun JH, Pang QX, Min XG, Li G. (2003a). Case analysis of 44 patients exposed to sulfur mustard. Med J Chin PLA 28:1131–1133.
Sun JH, Li G, Zhou JY, Min XG, Huang Y, Pang QX. (2003b). Four years of follow-up study of patients exposed to sulfur mustard on 4th of August. J Prev Med Chin PLA 27:357–358.
Sunil VR, Patel KJ, Shen J, Reimer D, Gow AJ, Laskin JD, Laskin DL. (2011a). Functional and inflammatory alterations in the lung following exposure of rats to nitrogen mustard. Toxicol Appl Pharmacol 250:10–18.
Sunil VR, Patel-Vayas K, Shen J, Gow AJ, Laskin JD, Laskin DL. (2011b). Role of TNFR1 in lung injury and altered lung function induced by the model sulfur mustard vesicant, 2-chloroethyl ethyl sulfide. Toxicol Appl Pharmacol 250:245–255.
Szarejko R. (1974). Changes induced by mustard gas in the upper respiratory airways and on attempt at treating them in rats. Otolaryngol Pol 28:617–618.
Takeshima Y, Inai K, Bennett WP, Metcalf RA, Welsh JA, Yonehara S, Hayashi Y, Fujihara M, Yamakido M, Akiyama M. (1994). p53 mutations in lung cancers from Japanese mustard gas workers. Carcinogenesis 15:2075–2079.
Tokuoka S, Hayashi Y, Inai K, Egawa H, Aoki Y, Akamizu H, Eto R, Nishida T, Ohe K, Kobuke T. (1986). Early cancer and related lesions in the bronchial epithelium in former workers of mustard gas factory. Acta Pathol Jpn 36:533–542.
Topal T, Oztas Y, Korkmaz A, Sadir S, Oter S, Coskun O, Bilgic H. (2005). Melatonin ameliorates bladder damage induced by cyclophosphamide in rats. J Pineal Res 38:272–277.
Ucar M, Korkmaz A, Reiter RJ, Yaren H, Oter S, Kurt B, Topal T. (2007). Melatonin alleviates lung damage induced by the chemical warfare agent nitrogen mustard. Toxicol Lett 173:124–131.
van Helden HP, Kuijpers WC, Diemel RV. (2004). Asthmalike symptoms following intratracheal exposure of Guinea pigs to sulfur mustard aerosol: therapeutic efficacy of exogenous lung surfactant curosurf and salbutamol. Inhal Toxicol 16:537–548.
Wada S, Miyanishi M, Nishimoto Y, Kambe S, Miller RW. (1968). Mustard gas as a cause of respiratory neoplasia in man. Lancet 1:1161–1163.
Warthin AS, Weller CV, Herrmann GR. (1918). The ocular lesions produced by dichlorethyl sulphide (mustard gas). J Lab Clin Med 4:785–832.
Warthin AS, Weller CV. (1919). The lesion of the respiratory and gastrointestinal tracts produced by mustard gas (dichloroethyl sulphide). J Lab Clin Med 4:229–264.
Weber WM, Kracko DA, Lehman MR, Irvin CM, Blair LF, White RK, Benson JM, Grotendorst GR, Cheng YS, McDonald JD. (2010). Inhalation exposure systems for the development of rodent models of sulfur mustard-induced pulmonary injury. Toxicol Mech Methods 20:14–24.
Willems JL. (1989). Clinical management of mustard gas casualties. Ann Med Mil Belg 3:S1–S61.
Wigenstam E, Rocksén D, Ekstrand-Hammarström B, Bucht A. (2009). Treatment with dexamethasone or liposome-encapsuled vitamin E provides beneficial effects after chemical-induced lung injury. Inhal Toxicol 21:958–964.
Winternitz W. (1919). Chronic lesions of the respiratory tract initiated by inhalation of irritant gases. JAMA 73:689.
Yamakido M, Ishioka S, Hiyama K, Maeda A. (1996). Former poison gas workers and cancer: incidence and inhibition of tumor formation by treatment with biological response modifier N-CWS. Environ Health Perspect 104 Suppl 3:485–488.
Yamada A, Hirose F, Miyanishi M. (1953). An autopsy case of bronchial carcinoma found in a patient succumbed to occupational mustard gas poisoning. Gan 44:216–218.
Yamada A, Hirose F, Nagai M, Nakamura T. (1957). Five cases of cancer of the larynx found in persons who suffered from occupational mustard gas poisoning. Gan 48:366–368.
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.

702 F. R. Tang and W. K. Loke
Critical Reviews in Toxicology
Yamada A, Tamura H, Harada Y. (1961). Case of carcinoma of the hypopharynx developing in a male following prolonged occupational exposure to mustard gas. Gencho Hiroshima Igaku 9:1427–1432.
Yamada A. (1963). On the late injuries following occupational inhalation of mustard gas, with special references to carcinoma of the respiratory tract. Acta Pathol Jpn 13:131–155.
Yaraee R, Ghazanfari T, Ebtekar M, Ardestani SK, Rezaei A, Kariminia A, Faghihzadeh S, Mostafaie A, Vaez-Mahdavi MR, Mahmoudi M, Naghizadeh MM, Soroush MR, Hassan ZM. (2009a). Alterations in serum levels of inflammatory cytokines (TNF, IL-1α, IL-1β and IL-1Ra) 20 years after sulfur mustard exposure: Sardasht-Iran cohort study. Int Immunopharmacol 9:1466–1470.
Yaraee R, Ghazanfari T, Faghihzadeh S, Mostafaie A, Soroush MR, Inai K, Foroutan A, Shams J, Naghizadeh MM, Hassan ZM. (2009b). Alterations in the serum levels of soluble L, P and E-selectin 20 years after sulfur mustard exposure: Sardasht-Iran Cohort Study. Int Immunopharmacol 9:1477–1481.
Yaren H, Mollaoglu H, Kurt B, Korkmaz A, Oter S, Topal T, Karayilanoglu T. (2007). Lung toxicity of nitrogen mustard may be mediated by nitric oxide and peroxynitrite in rats. Res Vet Sci 83:116–122.
Ziesche R, Hofbauer E, Wittmann K, Petkov V, Block LH. (1999). A preliminary study of long-term treatment with interferon γ-1b and low-dose prednisolone in patients with idiopathic pulmonary fibrosis. N Engl J Med 341:1264–1269.
Cri
tical
Rev
iew
s in
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
NA
TIO
NA
L U
NIV
ER
SIT
Y O
F SI
NG
APO
RE
on
08/1
7/12
For
pers
onal
use
onl
y.




















