Studies on a novel combination polymer system: in vitro erosion prevention and promotion of fluoride...
8
journal of dentistry 38, S3 (2010) S4–S11 available at www.sciencedirect.com journal homepage: www.intl.elsevierhealth.com/journals/jden Studies on a novel combination polymer system: in vitro erosion prevention and promotion of fluoride uptake in human enamel Louise H. Gracia a , Alan Brown b , Gareth D. Rees c , Christabel E. Fowler a, * a GlaxoSmithKline Consumer Healthcare, Weybridge, Surrey, UK b CERAM Surface and Materials Analysis, Penkhull, Stoke-on-Trent, UK c Genesis Oral Bioscience, Regents Mews, Horley, Surrey, UK article info Keywords: Human enamel Erosion Mouthrinse Fluoride Profilometry Dynamic secondary ion mass spectrometry DSIMS abstract Objectives: Firstly, determine the effect of pre-treating sound human enamel with a hydrosoluble combination polymer system (TriHydra™) comprising 0.20% carboxymethylcellulose, 0.010% xanthan gum and 0.75% copovidone, alone or in combination with fluoride, on in vitro erosion by citric acid. Secondly, investigate the effect of the polymers on fluoride uptake by incipient erosive lesions. Methods: Study 1: Sound enamel specimens were treated (60 s, 20ºC, 150 rpm) with either (i) deionised water, (ii) polymers in deionised water, (iii) 300 mg/L fluoride or (iv) polymers in 300 mg/L fluoride. Specimen groups (n = 5) were then immersed in 1.0% citric acid (pH 3.8, 300 s, 20ºC, 50 rpm) and non-contact profilometry was used to determine surface roughness (Sa) and bulk tissue loss. Study 2: Incipient erosive lesions were similarly treated with (i)-(iv). Dynamic Secondary Ion Mass Spectrometry (DSIMS) was then used to determine the fluoride depth-distribution. Results: Study 1: Mean±SD Sa and erosion depths for treatment groups (i)−(iv) were a 657±243, b 358±50, c 206±72, d 79±16 nm and a 19.73±8.70, b 2.52±1.34, b 0.49±0.34 and b 0.31±0.21 mm respectively (matching superscripts denote statistically equivalent groups). Study 2: Lesions treated with (iii) and (iv) exhibited similar fluoride penetration depths (~60 mm). Mean fluoride intensity ratios based on F/(F+P) at 1 mm for treatment groups (i)−(iv) were a 0.010±0.004, a 0.011±0.004, b 0.803±0.148 and c 0.994±0.004 respectively. Conclusions: The combination polymer system exhibited anti-erosion efficacy in its own right. The polymer/fluoride admixture statistically significantly reduced Sa, however suppression of bulk tissue loss was not statistically significantly different versus either treatment alone. The presence of polymer appears to promote fluoride uptake by erosive lesions most noticeably in the first 6 mm. © 2010 Elsevier Ltd. All rights reserved. 1. Introduction Erosive wear is a multifactorial process that, in vivo, involves erosion in combination with either abrasion or *Corresponding author. Dr Christabel Fowler, GlaxoSmith- Kline Consumer Healthcare, Weybridge, Surrey KT13 0DE, UK. Tel.: +44 1932 822000; fax: +44 1932 822100. E-mail address: [email protected] (C.E. Fowler). attrition, or a combination of both. 1−4 These processes are of chemical and physical, but not microbiological, origin and do not involve dental plaque. 3,4 This is one of a number of key features distinguishing erosion and erosive wear from dental caries. Erosion is primarily a surface chemical dissolution phenomenon characterised by top-down demineralisation, whilst the latter involves sub-surface demineralisation. 4 The two types of incipi- 0300-5712/$ – see front matter © 2010 Elsevier Ltd. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Studies on a novel combination polymer system: in vitro erosion prevention and promotion of fluoride...
journal of dentistry 38, S3 (2010) S4–S11
avai lab le at www.sc iencedi rect .com
journal homepage: www.intl.elsevierhealth.com/journals/jden
Studies on a novel combination polymer system: in vitroerosion prevention and promotion of fluoride uptake inhuman enamel
Louise H. Graciaa, Alan Brownb, Gareth D. Reesc, Christabel E. Fowlera, *a GlaxoSmithKline Consumer Healthcare, Weybridge, Surrey, UKb CERAM Surface and Materials Analysis, Penkhull, Stoke-on-Trent, UKc Genesis Oral Bioscience, Regents Mews, Horley, Surrey, UK
article info
Keywords:Human enamelErosionMouthrinseFluorideProfilometryDynamic secondary ion mass
spectrometryDSIMS
abstract
Objectives: Firstly, determine the effect of pre-treating sound human enamelwith a hydrosoluble combination polymer system (TriHydra™) comprising 0.20%carboxymethylcellulose, 0.010% xanthan gum and 0.75% copovidone, alone or incombination with fluoride, on in vitro erosion by citric acid. Secondly, investigatethe effect of the polymers on fluoride uptake by incipient erosive lesions. Methods:Study 1: Sound enamel specimens were treated (60 s, 20ºC, 150 rpm) with either(i) deionised water, (ii) polymers in deionised water, (iii) 300mg/L fluoride or(iv) polymers in 300mg/L fluoride. Specimen groups (n=5) were then immersed in1.0% citric acid (pH3.8, 300 s, 20ºC, 50 rpm) and non-contact profilometry was usedto determine surface roughness (Sa) and bulk tissue loss. Study 2: Incipient erosivelesions were similarly treated with (i)-(iv). Dynamic Secondary Ion Mass Spectrometry(DSIMS) was then used to determine the fluoride depth-distribution. Results: Study 1:Mean±SD Sa and erosion depths for treatment groups (i)−(iv) were a657±243, b358±50,c206±72, d79±16nm and a19.73±8.70, b2.52±1.34, b0.49±0.34 and b0.31±0.21mmrespectively (matching superscripts denote statistically equivalent groups). Study 2:Lesions treated with (iii) and (iv) exhibited similar fluoride penetration depths(~60mm). Mean fluoride intensity ratios based on F/(F+P) at 1mm for treatment groups(i)−(iv) were a0.010±0.004, a0.011±0.004, b0.803±0.148 and c0.994±0.004 respectively.Conclusions: The combination polymer system exhibited anti-erosion efficacy inits own right. The polymer/fluoride admixture statistically significantly reduced Sa,however suppression of bulk tissue loss was not statistically significantly differentversus either treatment alone. The presence of polymer appears to promote fluorideuptake by erosive lesions most noticeably in the first 6mm.
© 2010 Elsevier Ltd. All rights reserved.
1. Introduction
Erosive wear is a multifactorial process that, in vivo,involves erosion in combination with either abrasion or
*Corresponding author. Dr Christabel Fowler, GlaxoSmith-Kline Consumer Healthcare, Weybridge, Surrey KT13 0DE,UK. Tel.: +44 1932 822000; fax: +44 1932 822100.E-mail address: [email protected] (C.E. Fowler).
attrition, or a combination of both. 1−4 These processesare of chemical and physical, but not microbiological,origin and do not involve dental plaque. 3,4 This is oneof a number of key features distinguishing erosion anderosive wear from dental caries. Erosion is primarily asurface chemical dissolution phenomenon characterisedby top-down demineralisation, whilst the latter involvessub-surface demineralisation. 4 The two types of incipi-
0300-5712/$ – see front matter © 2010 Elsevier Ltd. All rights reserved.

Journal of Dentistry 38, S3 (2010) S4–S11 S5
ent lesion can be differentiated in vitro using a techniquesuch as transverse microradiography (TMR) which willshow a mineralised front in the case of the carieslesion. 5
The prophylaxis and treatment of dental caries hasrightly been a major and important focus of dentalresearch for over fifty years. The introduction andnow almost ubiquitous availability of fluoride beingthe principal driver for the observed decline in cariesincidence. 6 However there is growing evidence thatthe last 10−15 years have seen an increase in theprevalence of erosion and erosive wear. 7 With improvedself-awareness and general improvements in healthcare,individuals are keeping their dentition for longer. Studiesreporting erosion and erosive wear in adolescents arethus concerning, 8−10 albeit there is significant variabilityin the reported incidence, 6,11 and few longitudinal epi-demiological studies. 12−14 Agreement within the researchcommunity regarding choice of clinical indices and studydesign would further understanding of the contributingaetiologies and true extent and severity of the prob-lem. 4,6,15 To date, excluding intrinsic sources of acidassociated with voluntary or involuntary regurgitation,the primary aetiological factors correlated with erosionand erosive wear are gender, socioeconomic status anddietary acid intake. 8−14 Chemical and biological factorsthat are known to be important include pH, titratableacidity and substantivity of the erosive challenge, as wellas saliva flow rate, buffering capacity and the presenceof enamel-binding pellicle proteins. 16,17
In vivo, the salivary pellicle provides a physicalbarrier that confers a degree of protection against anerosive challenge, however the pellicle is susceptible todesorption under acid conditions, and newly formedpellicle is believed to be less effective at mitigatingthe damaging effects of an erosive challenge on theunderlying hard tissue. 18 This may in part explainwhy subjects with higher frequency and total intakeof dietary acid exhibit a higher incidence of dentalerosion. As with caries, fluoride has been shown to beeffective in vitro and in situ at inhibiting dietary acid-mediated erosion of dental hard tissues as well aspromoting repair of demineralised incipient erosivelesions. 19−30 Fluoride has also been shown to reduceerosive wear both in enamel and dentine. 20,21 Themechanism of action of fluoride is similar in bothcases, that is to suppress acid demineralisation andpromote remineralisation through formation of less acid-soluble fluoridated mineral phases. However, a typicalerosive challenge is at least an order of magnitudemore severe than that posed by plaque acid, andconsequently higher fluoride levels are recommended forthe management of dental erosion. 31 As fluoride levelsin conventional delivery formats available to the public,such as dentifrices and rinses, are controlled throughthe relevant monograph, there is considerable interest
in potentiating fluoride efficacy, adopting regimes andidentifying anti-erosion technologies that may act inconcert with existing fluoride technologies.A variety of analytical techniques have been used to
study hard tissue erosion in vitro that include nanoin-dentation, microindentation, microradiography and 3Dnon-contact profilometry. 32 All the aforementionedtechniques have advantages as well as disadvantagesas some are destructive whilst others are not, andmany provide only an indirect measure of the extent ofsubstrate mineralisation. The major drawback, however,is that none of the techniques are element specific.Consequently, and despite fluoride being the mostwidely studied active in these systems, the measurementendpoints tell us little concerning the fate of fluorideitself. Fluoride incorporation onto and into enamelsurfaces has been studied using X-ray photoelectronspectroscopy (XPS), 33,34 however the detection sensitivityis poor and the depth profiling rate slow. Secondaryion mass spectrometry (SIMS) is an alternative element-specific technique whose superior sensitivity to XPShas been exploited in the determination of elementaldistributions in biominerals. 35,36 The technique providesdetailed compositional analysis of materials on adepth scale ranging from nanometers to several hundredmicrons in depth profiling mode with sensitivity inthe ppm–ppb region for all elements. Additionally, inimaging mode, SIMS provides elemental maps withlateral resolution on the sub-micron scale.The primary aim of the present study was to evaluate
a trademarked hydrosoluble combination triple polymersystem (Tri-Hydra™) comprising 0.20% carboxymethyl-cellulose (CMC), 0.010% xanthan gum and 0.75% copovi-done as a fluoride-compatible anti-erosion agent. Thecombination polymer system was originally developedfor its utility as a film-forming oral lubricant inmouthrinses designed to prevent and/or relieve symp-toms associated with xerostomia. 37 The combinationpolymer system has been evaluated alone and as anadmixture with sodium fluoride in a single-treatmentenamel erosion demineralisation model. A secondaryaim of the study is to employ SIMS to investigatethe effect of the combination polymer system onfluoride uptake by incipient erosive lesions preparedfrom polished human enamel.
2. Materials and methods
2.1. Materials
Citric acid monohydrate, sodium fluoride, sodium hy-droxide and thymol were obtained from Sigma-Aldrich(Poole, Dorset, UK). Carboxymethylcellulose (Blanose®
7H3SXF) was supplied by Hercules (Wilmington, DE, USA),xanthan gum (Keltrol-F) was supplied by NutrasweetKelco Co. (Chicago, IL, USA) and copovidone (Plasdone®
S-630) obtained from ISP (Tadworth, Surrey, UK). Stycast

S6 Journal of Dentistry 38, S3 (2010) S4–S11
acrylic resin was obtained from Hitek Electronic Materi-als (Scunthorpe, Lincolnshire, UK).
2.2. Preparation of enamel specimens
Extracted human molars and premolars were storedin an aqueous solution of saturated thymol for up to2 weeks after removal of the roots and pulp. Priorto use, teeth were thoroughly rinsed and visuallyexamined for evidence of damage, decay and whitespot lesions. Sound enamel sections were cut fromthe buccal and lingual sides of the teeth using aMicroslice 2 diamond wire saw supplied by MetalsResearch (Cambridge, Cambridgeshire, UK) fitted withan annular saw, grit size 280, supplied by Ultratec(Santa Ana, CA, USA). The sections were mounted inacrylic resin and cured overnight, then polished flatusing 1200 and 2400 grit silicon carbide paper. Whererequired, artificial incipient erosive lesions were createdby immersing the sound enamel specimens into 1.0%citric acid solution pH3.8 (300 s, 20ºC, 50 rpm). Enamelspecimens were stored enamel side up in a humidifiedsealed container at 4ºC.
2.3. Surface roughness and bulk tissue loss
An ADE PhaseShift MicroXAM white light interferometer(ADE Phase Shift Inc., Tucson, AZ, USA) was usedto interrogate surface topography. This non-contacttechnique allows surface roughness parameters to bedetermined on the nanometer scale, and allows thecalculation of bulk tissue loss following an erosivechallenge. 38 Multiple scans (n=3) were acquired foreach specimen within the erosion window created usingan acid-resistant tape. Two scan areas were employed(200mm×160mm and 100mm×80mm) in order to ensurecalculated values of the mean surface roughness (Sa)were representative. Bulk tissue loss was calculatedfrom the step height difference between the exposedand unexposed enamel surface following removal ofthe tape.
2.4. Dynamic secondary ion mass spectrometry (DSIMS)analysis and fluoride quantification
Fluoride uptake by enamel erosive lesions was deter-mined by DSIMS depth profiling and cross-sectionalimaging using a Cameca ims 4f instrument (Cameca,Paris, France). Specimens were sputter-coated with goldto prevent excessive charging, and depth profile analysisperformed using a 12.5 keV O− primary ion beam withbeam current of ~100nA into an area of 150 mm×150mm,detecting negatively charged secondary ions with anextraction field of −2.25 keV. The sputtered craterdepths were measured using white light interferometry,facilitating calibration of the depth profile x-axis (time)to depth (in microns). Following depth profile analysis,
specimens were cross-sectioned to expose the centralplane (surface to bulk) of the enamel. After polishingthe cut surface to remove the smear layer, sections weregold-coated prior to SIMS imaging analysis using a 15keVO+
2 primary ion beam (~1nA). Images were acquired fromareas of typically 200 mm× 200mm and 70mm× 70mmrespectively. Negative secondary ion detection was usedwith an extraction field of −4.5 keV and a normal-incidence electron gun for charge compensation. Theintensity of the ionised phosphorus signal was usedto normalise the data, thereby allowing comparison ofthe relative fluoride concentration at a given depthvia the mean fluoride intensity ratio (F/F+P) for eachtreatment group.
2.5. Effect of a combination polymer system on enamelerosion
The anti-erosion efficacy of a hydrosoluble combinationpolymer system comprising 0.20% CMC, 0.010% xanthangum and 0.75% w/w copovidone was investigatedin vitro in the presence and absence of fluoride. Twentysound polished enamel specimens were randomlyassigned to one of four treatment groups. Specifically,(i) deionised (DI) water, (ii) combination polymer systemin DI water, (iii) 300mg/L fluoride and (iv) a 300mg/Lfluoride solution containing the combination polymersystem. Following treatment (60 s, 20ºC, 150 rpm), spec-imens were rinsed with DI water, then immersed in1.0% citric acid (pH3.8, 20ºC, 50 rpm), rinsed againand analysed by non-contact profilometry to determineSa and bulk tissue loss. The pH of all treatment solutionsfell in the range 6.5−7.0.
2.6. The effect of the combination polymer system on fluorideuptake by incipient enamel erosive lesions
Twenty enamel specimens, each containing an incipienterosive lesion, were randomly assigned to one of thefour treatment groups (n=5) detailed in section 2.5.Following treatment (60 s, 20ºC, 150 rpm), specimens wererinsed with DI water, then analysed by DSIMS. Depthprofiling mode was used initially to determine therelative fluoride concentration in the first few micronsof the surface. Specimens were subsequently verticallysectioned through the lesion and fluoride distributionmapped to a depth of 170 mm.
2.7. Statistical analyses
Means and standard deviation (SD) were calculated for Saand erosion depth for each treatment group. Analysis ofvariance (ANOVA) and post hoc Student–Newman–Keulswere used to compare between-treatment statisticaldifferences for each endpoint. Significance levels (p) wereset at 0.05.
Journal of Dentistry 38, S3 (2010) S4–S11 S7
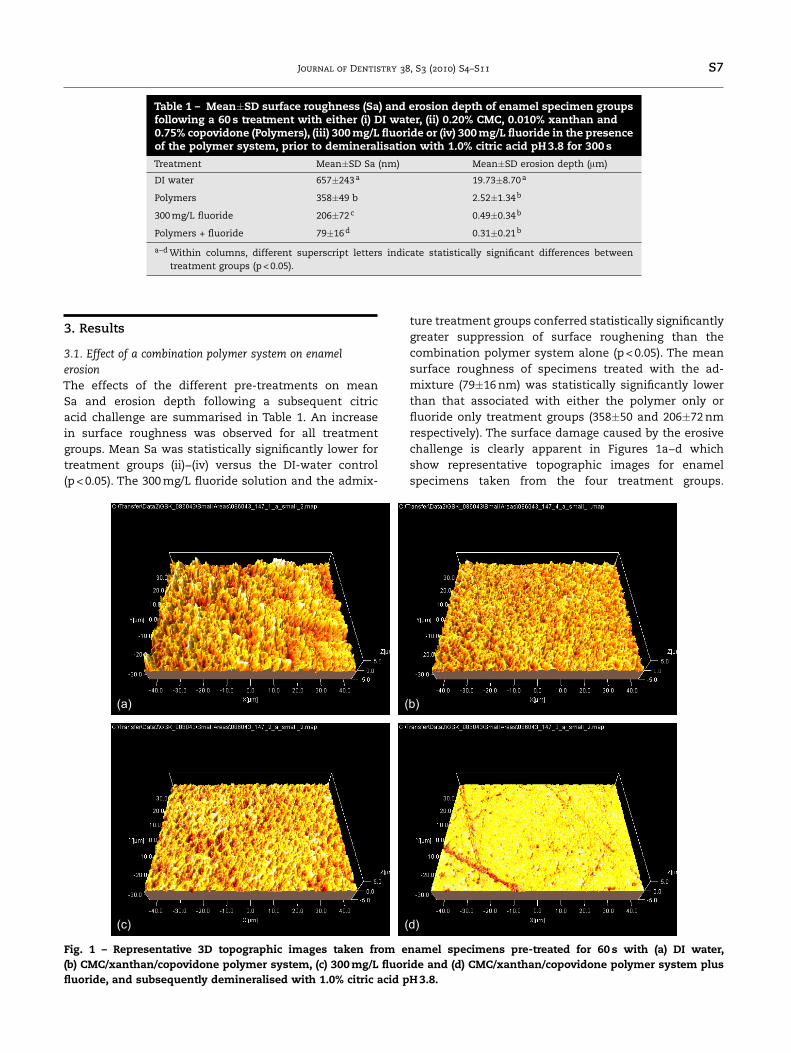
Table 1 – Mean±SD surface roughness (Sa) and erosion depth of enamel specimen groupsfollowing a 60s treatment with either (i) DI water, (ii) 0.20% CMC, 0.010% xanthan and0.75% copovidone (Polymers), (iii) 300mg/L fluoride or (iv) 300mg/L fluoride in the presenceof the polymer system, prior to demineralisation with 1.0% citric acid pH3.8 for 300s
Treatment Mean±SD Sa (nm) Mean±SD erosion depth (mm)
DI water 657±243a 19.73±8.70a
Polymers 358±49 b 2.52±1.34b
300mg/L fluoride 206±72c 0.49±0.34b
Polymers + fluoride 79±16d 0.31±0.21b
a−dWithin columns, different superscript letters indicate statistically significant differences betweentreatment groups (p< 0.05).
3. Results
3.1. Effect of a combination polymer system on enamelerosionThe effects of the different pre-treatments on meanSa and erosion depth following a subsequent citricacid challenge are summarised in Table 1. An increasein surface roughness was observed for all treatmentgroups. Mean Sa was statistically significantly lower fortreatment groups (ii)−(iv) versus the DI-water control(p< 0.05). The 300mg/L fluoride solution and the admix-
ture treatment groups conferred statistically significantlygreater suppression of surface roughening than thecombination polymer system alone (p< 0.05). The meansurface roughness of specimens treated with the ad-mixture (79±16nm) was statistically significantly lowerthan that associated with either the polymer only orfluoride only treatment groups (358±50 and 206±72nmrespectively). The surface damage caused by the erosivechallenge is clearly apparent in Figures 1a−d whichshow representative topographic images for enamelspecimens taken from the four treatment groups.
(a)
(c)
(b)
(d)
Fig. 1 – Representative 3D topographic images taken from enamel specimens pre-treated for 60 s with (a) DI water,(b) CMC/xanthan/copovidone polymer system, (c) 300mg/L fluoride and (d) CMC/xanthan/copovidone polymer system plusfluoride, and subsequently demineralised with 1.0% citric acid pH3.8.
S8 Journal of Dentistry 38, S3 (2010) S4–S11
(a) (b)
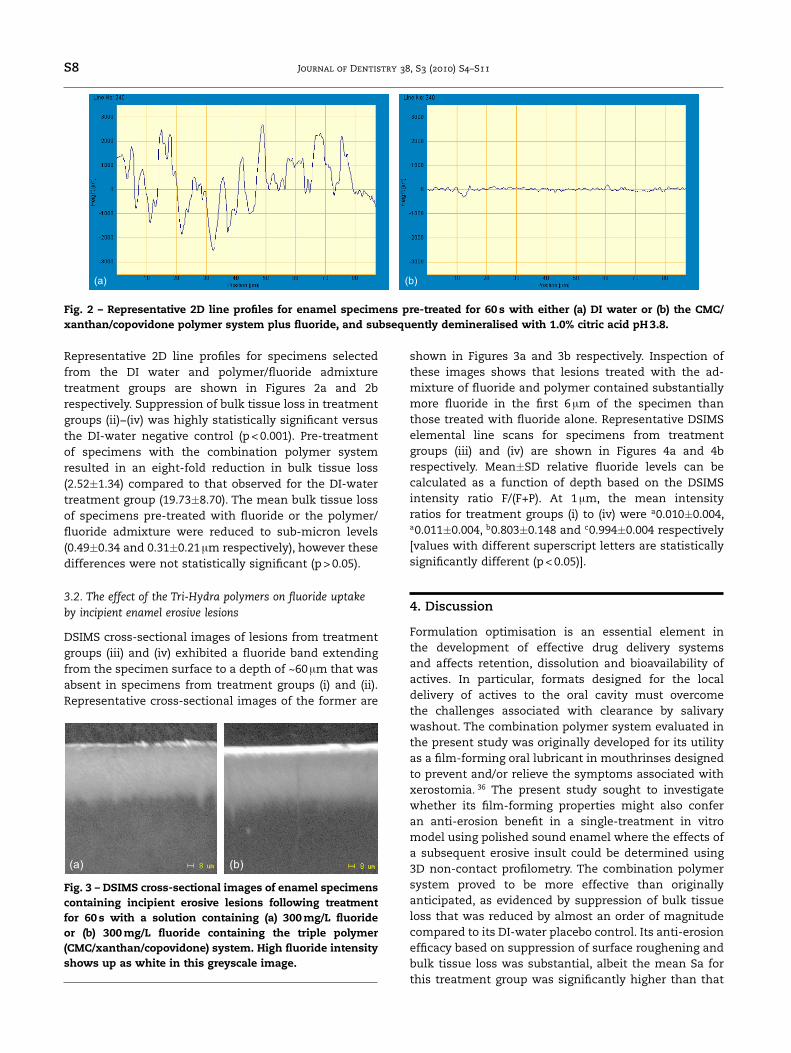
Fig. 2 – Representative 2D line profiles for enamel specimens pre-treated for 60 s with either (a) DI water or (b) the CMC/xanthan/copovidone polymer system plus fluoride, and subsequently demineralised with 1.0% citric acid pH3.8.
Representative 2D line profiles for specimens selectedfrom the DI water and polymer/fluoride admixturetreatment groups are shown in Figures 2a and 2brespectively. Suppression of bulk tissue loss in treatmentgroups (ii)−(iv) was highly statistically significant versusthe DI-water negative control (p< 0.001). Pre-treatmentof specimens with the combination polymer systemresulted in an eight-fold reduction in bulk tissue loss(2.52±1.34) compared to that observed for the DI-watertreatment group (19.73±8.70). The mean bulk tissue lossof specimens pre-treated with fluoride or the polymer/fluoride admixture were reduced to sub-micron levels(0.49±0.34 and 0.31±0.21mm respectively), however thesedifferences were not statistically significant (p> 0.05).
3.2. The effect of the Tri-Hydra polymers on fluoride uptakeby incipient enamel erosive lesions
DSIMS cross-sectional images of lesions from treatmentgroups (iii) and (iv) exhibited a fluoride band extendingfrom the specimen surface to a depth of ~60mm that wasabsent in specimens from treatment groups (i) and (ii).Representative cross-sectional images of the former are
(a) (b)
Fig. 3 – DSIMS cross-sectional images of enamel specimenscontaining incipient erosive lesions following treatmentfor 60 s with a solution containing (a) 300mg/L fluorideor (b) 300mg/L fluoride containing the triple polymer(CMC/xanthan/copovidone) system. High fluoride intensityshows up as white in this greyscale image.
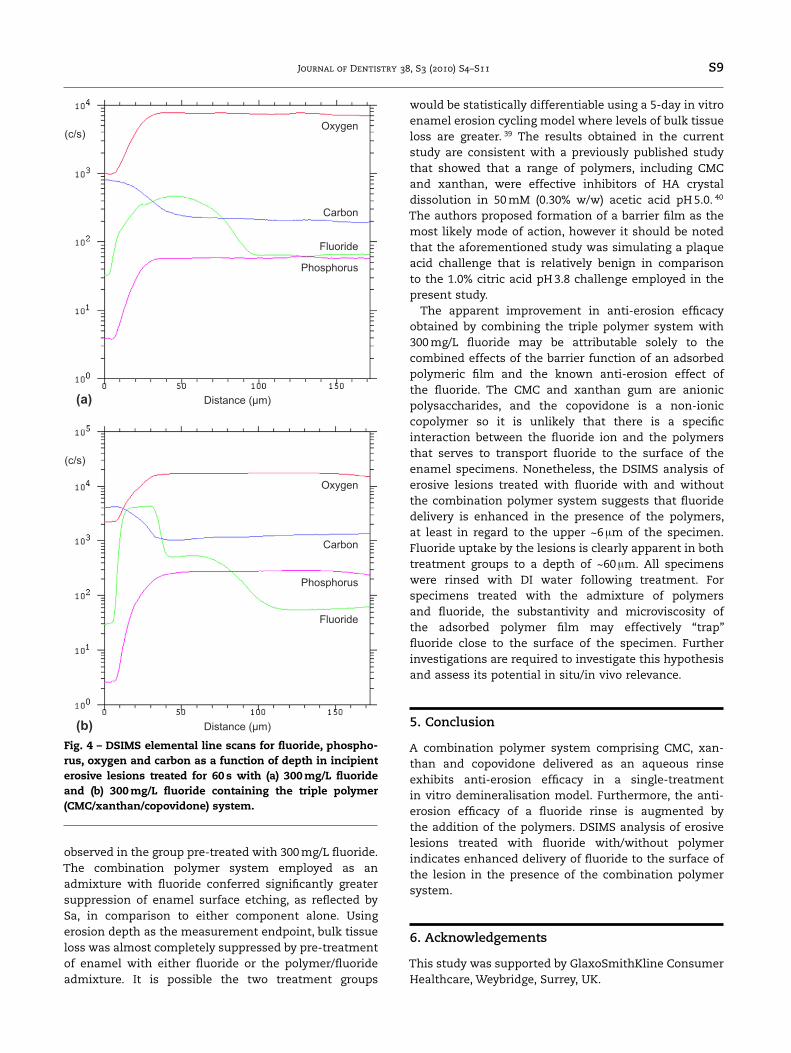
shown in Figures 3a and 3b respectively. Inspection ofthese images shows that lesions treated with the ad-mixture of fluoride and polymer contained substantiallymore fluoride in the first 6mm of the specimen thanthose treated with fluoride alone. Representative DSIMSelemental line scans for specimens from treatmentgroups (iii) and (iv) are shown in Figures 4a and 4brespectively. Mean±SD relative fluoride levels can becalculated as a function of depth based on the DSIMSintensity ratio F/(F+P). At 1 mm, the mean intensityratios for treatment groups (i) to (iv) were a0.010±0.004,a0.011±0.004, b0.803±0.148 and c0.994±0.004 respectively[values with different superscript letters are statisticallysignificantly different (p< 0.05)].
4. Discussion
Formulation optimisation is an essential element inthe development of effective drug delivery systemsand affects retention, dissolution and bioavailability ofactives. In particular, formats designed for the localdelivery of actives to the oral cavity must overcomethe challenges associated with clearance by salivarywashout. The combination polymer system evaluated inthe present study was originally developed for its utilityas a film-forming oral lubricant in mouthrinses designedto prevent and/or relieve the symptoms associated withxerostomia. 36 The present study sought to investigatewhether its film-forming properties might also conferan anti-erosion benefit in a single-treatment in vitromodel using polished sound enamel where the effects ofa subsequent erosive insult could be determined using3D non-contact profilometry. The combination polymersystem proved to be more effective than originallyanticipated, as evidenced by suppression of bulk tissueloss that was reduced by almost an order of magnitudecompared to its DI-water placebo control. Its anti-erosionefficacy based on suppression of surface roughening andbulk tissue loss was substantial, albeit the mean Sa forthis treatment group was significantly higher than that
Journal of Dentistry 38, S3 (2010) S4–S11 S9
Distance (μm)
Oxygen
Oxygen
Carbon
Carbon
Fluoride
Fluoride
Phosphorus
Phosphorus
Distance (μm)
(c/s)
(c/s)
(a)
(b)
Fig. 4 – DSIMS elemental line scans for fluoride, phospho-rus, oxygen and carbon as a function of depth in incipienterosive lesions treated for 60 s with (a) 300mg/L fluorideand (b) 300mg/L fluoride containing the triple polymer(CMC/xanthan/copovidone) system.
observed in the group pre-treated with 300mg/L fluoride.The combination polymer system employed as anadmixture with fluoride conferred significantly greatersuppression of enamel surface etching, as reflected bySa, in comparison to either component alone. Usingerosion depth as the measurement endpoint, bulk tissueloss was almost completely suppressed by pre-treatmentof enamel with either fluoride or the polymer/fluorideadmixture. It is possible the two treatment groups
would be statistically differentiable using a 5-day in vitroenamel erosion cycling model where levels of bulk tissueloss are greater. 39 The results obtained in the currentstudy are consistent with a previously published studythat showed that a range of polymers, including CMCand xanthan, were effective inhibitors of HA crystaldissolution in 50mM (0.30% w/w) acetic acid pH5.0. 40
The authors proposed formation of a barrier film as themost likely mode of action, however it should be notedthat the aforementioned study was simulating a plaqueacid challenge that is relatively benign in comparisonto the 1.0% citric acid pH3.8 challenge employed in thepresent study.The apparent improvement in anti-erosion efficacy
obtained by combining the triple polymer system with300mg/L fluoride may be attributable solely to thecombined effects of the barrier function of an adsorbedpolymeric film and the known anti-erosion effect ofthe fluoride. The CMC and xanthan gum are anionicpolysaccharides, and the copovidone is a non-ioniccopolymer so it is unlikely that there is a specificinteraction between the fluoride ion and the polymersthat serves to transport fluoride to the surface of theenamel specimens. Nonetheless, the DSIMS analysis oferosive lesions treated with fluoride with and withoutthe combination polymer system suggests that fluoridedelivery is enhanced in the presence of the polymers,at least in regard to the upper ~6 mm of the specimen.Fluoride uptake by the lesions is clearly apparent in bothtreatment groups to a depth of ~60 mm. All specimenswere rinsed with DI water following treatment. Forspecimens treated with the admixture of polymersand fluoride, the substantivity and microviscosity ofthe adsorbed polymer film may effectively “trap”fluoride close to the surface of the specimen. Furtherinvestigations are required to investigate this hypothesisand assess its potential in situ/in vivo relevance.
5. Conclusion
A combination polymer system comprising CMC, xan-than and copovidone delivered as an aqueous rinseexhibits anti-erosion efficacy in a single-treatmentin vitro demineralisation model. Furthermore, the anti-erosion efficacy of a fluoride rinse is augmented bythe addition of the polymers. DSIMS analysis of erosivelesions treated with fluoride with/without polymerindicates enhanced delivery of fluoride to the surface ofthe lesion in the presence of the combination polymersystem.
6. Acknowledgements
This study was supported by GlaxoSmithKline ConsumerHealthcare, Weybridge, Surrey, UK.
S10 Journal of Dentistry 38, S3 (2010) S4–S11
7. Conflict of interest statement
LHG and CEF are employees of GlaxoSmithKline Con-sumer Healthcare; GDR was an employee of GSK atthe time this research was conducted. Subsequent tothis study, GDR received compensation from GSK forconsulting and scientific writing services in his newrole as Director of Genesis Oral Bioscience. AB is anemployee of CERAM Surface and Materials Analysis andwas engaged by GSK to undertake profilometric andDSIMS analysis of pre-coded specimens supplied by thestudy sponsor.
References
1. Milosevic A. Tooth wear: An etiological and diagnosticproblem. European Journal of Prosthodontic and RestorativeDentistry 1993;1:173−8.
2. Smith BG, Robb ND. The prevalence of tooth-wear in1007 dental patients. Journal of Oral Rehabilitation 1996;23:232−9.
3. Bartlett DW. The role of erosion in tooth wear:aetiology, prevention and management. InternationalDental Journal 2005;55:277−84.
4. Barbour ME, Rees GD. The role of erosion, abrasion andattrition in tooth wear. Journal of Clinical Dentistry 2006;17:88−94.
5. Elton V, Cooper L, Higham SM, Pender N. Validationof enamel erosion in vitro. Journal of Dentistry2009;37:336−41.
6. Reich E. Trends in caries and periodontal healthepidemiology in Europe. International Dental Journal2001;51:392−8.
7. Jaeggi T, Lussi A. Prevalence, incidence and distributionof erosion. Monographs in Oral Science 2006;20:44−65.
8. Al-Dlaigan YH, Shaw L, Smith A. Dental erosion in agroup of British 14-year-old school children. Part I:Prevalence and influence of differing socioeconomicbackgrounds. British Dental Journal 2001;190:145−9.
9. Al-Dlaigan YH, Shaw L, Smith A. Dental erosion in agroup of British 14-year-old school children. Part II:Influence of dietary intake. British Dental Journal2001;190:258−61.
10. Bardsley PF, Taylor S, Milosevic A. Epidemiologicalstudies of tooth wear and dental erosion in 14-year old children in North West England. Part 1:The relationship with water fluoridation and socialdeprivation. British Dental Journal 2004;197:413−6.
11. Linnett V; Seow WK. Dental erosion in children: aliterature review. Pediatric Dentistry 2001;23:37−43.
12. Lussi A, Schaffner M. Progression of and risk factors fordental erosion and wedge-shaped defects over a 6-yearperiod. Caries Research 2000;34:182−7.
13. Dugmore CR, Rock WP. The progression of tootherosion in a cohort of adolescents of mixed ethnicity.International Journal of Paediatric Dentistry 2003;13:295–303.
14. El Aidi H, Bronkhorst EM, Huysmans MC, Truin GJ.Dynamics of tooth erosion in adolescents: a 3-yearlongitudinal study. Journal of Dentistry 2010;38:131−7.
15. Fares J, Shirodaria S, Chiu K, Ahmad N, Sherrif M,Bartlett D. A new index of tooth wear. Reproducibilityand application to a sample of 18- to 30-year-olduniversity students. Caries Research 2009;43:119−25.
16. Lussi A, Jaeggi T, Zero D. The role of diet inthe aetiology of dental erosion. Caries Research2004;38:33−44.
17. Zero DT, Lussi A. Erosion − chemical and biologicalfactors of importance to the dental practitioner.International Dental Journal 2005;55:285−90.
18. Amaechi BT, Higham SM, Edgar WM, Milosevic A.Thickness of acquired salivary pellicle as a determinantof the sites of dental erosion. Journal of Dental Research1999;78:1821−8.
19. Sorvari R, Meurman JH, Alakuijala P, Frank RM. Effectof fluoride varnish and solution on enamel erosionin vitro. Caries Research 1994;28:227−32.
20. Bartlett DW, Smith BG, Wilson RF. Comparison of theeffect of fluoride and non-fluoride toothpaste on toothwear in vitro and the influence of enamel fluorideconcentration and hardness of enamel. British DentalJournal 1994;176:346−8.
21. Attin T, Zirkel C, Hellwig E. Brushing abrasion of erodeddentin after application of sodium fluoride solutions.Caries Research 1998;32:344−50.
22. Ganss C, Klimek J, Schaffer U, Spall T. Effectiveness oftwo fluoridation measures on erosion progression inhuman enamel and dentine in vitro. Caries Research2001;35:325−30.
23. van Rijkom H, Ruben J, Vieira A, Huysmans MC,Truin GJ, Mulder J. Erosion-inhibiting effect of sodiumfluoride and titanium tetrafluoride treatment in vitro.European Journal of Oral Science 2003;111:253−7.
24. Hughes JA, West NX, Addy M. The protective effect offluoride treatments against enamel erosion in vitro.Journal of Oral Rehabilitation 2004;31:357−63.
25. Fowler CE, Willson R, Rees GD. In vitro microhardnessstudies on a new anti-erosion, desensitizing toothpaste.Journal of Clinical Dentistry 2006;17:100−5.
26. Fowler CE, Brown A, Gracia L, Edwards MI, Rees GD.Inhibition of enamel erosion and promotion of lesionrehardening by fluoride: a white light interferometryand microindentation study. Journal of Clinical Dentistry2009;20:178−85.
27. Ganss C, Klimek J, Brune V, Schurmann A. Effects oftwo fluoridation measures on erosion progression inhuman enamel and dentine in situ. Caries Research2004;38:561−6.
28. Zero DT, Hara AT, Kelly SA, Gonzalez-Cabezas C,Eckert GJ, Barlow AP, Mason SC. Evaluation of adesensitizing test dentifrice using an in situ erosionremineralization model. Journal of Clinical Dentistry2006;17:107−12.
29. Barlow AP, Sufi F, Mason SC. Evaluation of differentfluoridated dentifrice formulations using an in situremineralization model. Journal of Clinical Dentistry2009;20:192−8.
30. Hara AT, Kelly SA, Gonzalez-Cabezas C, Eckert GJ,Barlow AP, Mason SC, Zero DT. Influence of fluorideavailability of dentifrices on eroded enamelremineralization in situ. Caries Research 2009;43:57−63.
31. Magalhaes AC, Wiegand A, Rios D, Honorio HM,Buzalaf MA. Insights into preventive measuresfor dental erosion. Journal of Applied Oral Science2009;17:75−86.

Journal of Dentistry 38, S3 (2010) S4–S11 S11
32. Barbour ME, Rees JS. The laboratory assessmentof enamel erosion: a review. Journal of Dentistry2004;32:591–602.
33. Hercules DM, Craig NL. Composition of fluoridateddental enamel studied by X-ray photoelectronspectroscopy (ESCA). Journal of Dental Research1976;55:829−35.
34. Vyas HA, Damle SG. Fluoride profiles of enamelfollowing topical application of neutral and acidulatedNaF solution using X-ray photoelectron spectroscopy(ESCA) − An in vitro study. Journal of Indian Society ofPedodontics and Preventive Dentistry 1994;12:35−7.
35. Derand T, Lodding A, Petersson LG. Effect of topicalF− solutions on caries-like lesions in root surfaces.Caries Research 1989;23:135−40.
36. Petersson LG, Lodding A, Hakeberg M, Koch G. Fluorineprofiles in human enamel after in vitro treatment withdentifrices of different compositions and acidities.Swedish Dental Journal 1989;13:177−83.
37. Corcoran RA, Stovell AG, Urquhart D, Chui T,Richardson M. Evaluation of a combined polymersystem for use in relieving the symptoms ofxerostomia. Journal of Clinical Dentistry 2006;17:34−8.
38. Fowler CE, Brown A, Gracia L, Edwards MI, Rees GD.Fluoride penetration from toothpastes into incipientenamel erosive lesions investigated using DynamicSecondary Ion Mass Spectrometry. Journal of ClinicalDentistry 2009;20:186−91.
39. Venasakulchai A, Williams NA, Gracia LH, Rees GD.A comparative evaluation of fluoridated andnon-fluoridated mouthrinses using a 5-daycycling enamel erosion model. Journal of Dentistry2010;38(Suppl 3):S21−9.
40. Van der Reijden WA, Buijs MJ, Damen JJ, Veerman EC,ten Cate JM, Nieuw Amerongen AV. Influence ofpolymers for use in saliva substitutes on de- andremineralization of enamel in vitro. Caries Research1997;31:216−23.