
GPU Implementation of Stokes Equation with Strongly Variable Coefficients

ARTICLE IN PRESS+ModelEPIRES-3950; No. of Pages 10
Epilepsy Research (2008) xxx, xxx—xxx
journa l homepage: www.e lsev ier .com/ locate /ep i lepsyres
Strongly lateralized activation in language fMRI ofatypical dominant patients—–Implications forpresurgical work-up
Jorg Wellmera,∗, Bernd Webera,c, Susanne Weisa,1, Peter Klavera,2,Horst Urbachb, Jurgen Reuld,3, Guillen Fernandeza,e, Christian E. Elgera
a Department of Epileptology, University of Bonn, Sigmund-Freud-Str. 25, D-53105 Bonn, Germanyb Department of Radiology, University of Bonn, Sigmund-Freud-Str. 25, D-53105 Bonn, Germanyc Department of NeuroCognition, Life&Brain Center, Sigmund-Freud-Str. 25, D-53105 Bonn, Germanyd Department of Diagnostic and Therapeutic Neuroradiology, Medical Center Bonn, Spessartstraße 9, D-53119 Bonn, Germanye F.C. Donders Center for Cognitive Neuroimaging and Department of Neurology, Radboud University,PO Box 9109, NL-6500 HB Nijmegen, The Netherlands
Received 6 June 2007; received in revised form 30 November 2007; accepted 10 March 2008
KEYWORDSFunctional magneticresonance imaging;Languagelateralization;Epilepsy surgery;Wada-test
SummaryPurpose: Functional magnetic resonance imaging (fMRI) is being used increasingly for lan-guage dominance assessment in the presurgical work-up of patients with pharmacoresistantepilepsy. However, the interpretation of bilateral fMRI-activation patterns is difficult. Variousstudies propose fMRI-lateralization index (LI) thresholds between ±0.1 and ±0.5 for discrimi-nation of atypical from typical dominant patients. This study examines if these thresholds allowidentifying atypical dominant patients with sufficient safety for presurgical settings.Methods: 65 patients had a tight comparison, fully controlled semantic decision fMRI-task and
a Wada-test for language lateralization. According to Wada-test, 22 were atypical languagedominant. In the remaining, Wada-test results were compatible with unilateral left dominance.Please cite this article in press as: Wellmer, J., et al., Strongly lateralized activation in language fMRI of atypical dominantpatients—–Implications for presurgical work-up, Epilepsy Res. (2008), doi:10.1016/j.eplepsyres.2008.03.005
We determined fMRI-LI for two frontal and one temporo-parietal functionally defined, protocol-specific volume of interest (VOI), and for the least lateralized of these VOIs (‘‘low-VOI’’) in eachpatient.Results: We find large intra-individual LI differences between functionally defined VOIs irrespec-tive of underlying type of language dominance (mean LI difference 0.33 ± 0.35, range 0—1.6;
∗ Corresponding author. Tel.: +49 228 287 14778; fax: +49 228 287 19351.E-mail addresses: [email protected] (J. Wellmer), [email protected] (B. Weber), [email protected] (S. Weis),
[email protected] (P. Klaver), [email protected] (H. Urbach), [email protected] (J. Reul),[email protected] (G. Fernandez), [email protected] (C.E. Elger).
1 Current address: Department of Neurological Neuropsychology, University Hospital RWTH, Pauwellstr. 30, D-52074 Aachen, Germany.2 Current address: Department of Psychology and Children’s Hospital Zurich, Steinwiessr. 75, CH-8032 Zurich, Switzerland.3 Current address: Klinik fur Diagnostische und Interventionelle Neuroradiologie KKH Siegen, Weidenauer Str. 76, 57076 Siegen, Germany.
0920-1211/$ — see front matter © 2008 Elsevier B.V. All rights reserved.doi:10.1016/j.eplepsyres.2008.03.005

ARTICLE IN PRESS+ModelEPIRES-3950; No. of Pages 10
2 J. Wellmer et al.
15% of patients have inter-VOI-LI differences >1.0). Across atypical dominant patients fMRI-LI inthe Broca’s and temporo-parietal VOI range from −1 to +1, in the ‘‘remaining frontal’’ VOI from−0.93 to 1. The highest low-VOI-LI detected in atypical dominant patients is 0.84.Conclusions: Large intra-individual inter-VOI-LI differences and strongly lateralized fMRI-activation in patients with Wada-test proven atypical dominance question the value of theproposed fMRI-thresholds for presurgical language lateralization. Future studies have to developstrategies allowing the reliable identification of atypical dominance with fMRI. The low-VOI
s reserved.
I
ApLepbafdbapisrml2
tatifeB2oaiec
uaorlelptanIet
fe(vat2abaocfaJcfs2flfic
ifdf±SadbtmdvWsp
thresholds actually solve the problem of bilateral fMRI-activations in clinical routine, i.e. if they allow detecting
approach may be useful.© 2008 Elsevier B.V. All right
ntroduction
typical cerebral language organization is a well-describedhenomenon in epilepsy patients (Kurthen et al., 1994;oring et al., 1990; Saltzman-Benaiah et al., 2003; Webert al., 2006b). Language organization can be rather com-lex. It can comprise various degrees of contributions ofoth hemispheres to intact language use including dissoci-ted representations of expressive and receptive languageunctions between both hemispheres. Also partial redun-ancy of language functions in both hemispheres haseen described (Kurthen et al., 1994; Helmstaedter etl., 1997). In the presurgical work-up of patients withharmacoresistant epilepsies the existence of atypical dom-nance is clinically relevant. This accounts not only forurgery close to typically eloquent cortex. Risks for neu-opsychological deficits after epilepsy surgery (in particularesio-temporal surgery and callosotomy) rely on the under-
ying language dominance, too (for review see Helmstaedter,004)
Traditionally, language lateralization was performed withhe Wada-test (or intracarotid amobarbital procedure; Wadand Rasmussen, 1960). Yet, numerous studies published overhe last decades suggest that functional magnetic resonancemaging (fMRI) may be capable of replacing the Wada-testor the determination of language lateralization (Desmondt al., 1995; Binder et al., 1996; Hertz-Pannier et al., 1997;enson et al., 1999; Fernandez et al., 2001; Spreer et al.,002). Compared with the Wada-test, fMRI offers a numberf advantages. It is non-invasive, which entails the virtualbsence of morbidity risk. It is easily accessible. Its setups comparatively simple. fMRI requires less staff and timeffort than the Wada-test. Additionally, fMRI produces lowerosts than the traditional Wada-test (Medina et al., 2004).
However, the results of recent studies question thencritical replacement of the Wada-test by fMRI. The over-ll concordance between fMRI and IAP is estimated to benly ∼90% (Detre, 2004), and recent studies show even moreelevant discrepancies between fMRI- and Wada-test-basedanguage lateralization on the single subject level (Lehericyt al., 2000; Woermann et al., 2003). A particular prob-em with fMRI lies in the mode of interpretation of bilateralatterns of BOLD activation. While the Wada-test is an inac-ivating method blocking the function of one hemisphere
Please cite this article in press as: Wellmer, J., et al., Strongly lapatients—–Implications for presurgical work-up, Epilepsy Res. (
nd allowing testing the functional reserve capacity of theon-anesthetized hemisphere, fMRI is an activation method.f fMRI shows bilateral activation this does not necessarilymbody a bilateral distribution of language-essential cor-ex. Bilateral activation patterns can, for example, result
apnaa
rom the detection of language-associated but not language-ssential cortex contralateral to the dominant hemisphereDesmond and Chen, 2002). Even when using optimized acti-ation protocols aiming to subtract any unspecific neuronalctivation from the contrast between the active and con-rol condition (Binder et al., 1999; Hund-Georgiadis et al.,001), it cannot be excluded that parts of the active cortexre not essential for intact language use. Further reasons forilateral distribution of BOLD activation can be an unfavor-ble scanner signal-to-noise ratio, the sub-optimal settingf statistical thresholds set to discriminate voxels which areonsidered activated during the language-condition of theMRI-protocol from voxels considered non-active (Desmondnd Chen, 2002; Loring et al., 2002; Rutten et al., 2002;ansen et al., 2006) and the renunciation of anatomi-ally or functionally defined volumes of interest (VOIs),or which a lateralization index (LI) between both hemi-pheres is determined (Rutten et al., 2002; Spreer et al.,002). On the individual patient level the cause of bilateralMRI-activation is mostly a matter of uncertainty. Mistakinganguage-associated cortex or artificially highlighted areasor language-essential cortex, however, can have relevantmpact on the surgical strategies and the postoperative out-ome (Desmond and Chen, 2002; Loring et al., 2002).
To overcome the problem how to classify patients withntermediate fMRI-LI, many groups propose the use ofMRI-lateralization index thresholds between +1 and −1 toiscriminate unilateral from bilateral dominant patients inMRI. Liegeois et al. (2004) use a lateralization index of0.1. Springer et al. (1999), Szaflarski et al. (2002), and
abbah et al. (2003) use ±0.2, Sabsevitz et al. (2003) ±0.25,nd Adcock et al. (2003) use ±0.265. Lehericy et al. (2000)efined LI between 0.5 and 1 to represent strong, and an LIetween 0.25 and 0.5 to represent weak language lateraliza-ion. However, these studies predominantly targeted on theatch of fMRI and Wada-tests on the group level or on theistribution of language dominance patterns in function ofarious biographical factors or the side of the seizure focus.ith exception of the study of Sabsevitz et al. (2003) the
tudies do not address the problem of language dominancerediction on the single case level.
The current study sets out to examine if the proposed
teralized activation in language fMRI of atypical dominant2008), doi:10.1016/j.eplepsyres.2008.03.005
typical language dominance in individual patients. Weerform an analysis of fMRI-LI found in atypical domi-ant patients. The fMRI-protocol applied in this study issemantic decision task which reliably activates frontal
nd temporo-parietal cortex (Fernandez et al., 2003). To

ARTICLE IN+ModelEPIRES-3950; No. of Pages 10
Strongly lateralized activation in language fMRI of atypical domi
Table 1 Biographical data of the examined patients
Number of patients 65M/F 35/30Age at examination 35.9 (S.D. 11.3; 13—63)Age at onset 13.8 (S.D. 9.1; 1—43)
Handedness (Edinburgh handedness inventory)Right 40 (61.5%)Ambidextrous 21 (32.3%)Left 4 (6.2%)
Lesion sideLeft 47 (72.3%)
afcctctHpbtwlaslplrsilo
f
TtdWiisuiitwT(sr
Sas63(me
uTtfmpaW‘rt
Right 14 (21.5%)Bilateral 1 (1.5%)
exclude any uncontrollable compliance effects which couldquestion the results of the language lateralization we applya tight comparison task (Donaldson and Buckner, 2001) withactive control condition and continuous performance con-trol. Since there is ongoing discussion about the applicationof different volumes of interest for fMRI-LI determinationwe analyze the impact of the choice of different VOIs forthe identification of patients with atypical language domi-nance. LIs are primarily determined for three functionallydetermined VOIs. However, in case of large intra-individualLI differences it might remain unclear which of the VOIsfinally stands for the individual degree of language later-alization. We therefore also evaluate if referral to the leastlateralized of all individual VOIs can increase the sensitivityof fMRI for atypical language dominance patterns in practicalroutine.
Materials and methods
Patients
Between April 2000 and March 2005, 832 patients underwent presur-gical evaluation at our institution. 65 of them had both, a Wada-testand fMRI for language lateralization. These 65 are subject tothis study. Indications for language lateralization were intendedresection close to possibly eloquent cortex; intended callosotomy;discrepancy of neuropsychological and clinical (in particular semio-logical) estimations of language lateralization. In 22 of 65 patientsWada-tests proved the existence of atypical language dominance.In 43 patients Wada-test results were compatible with unilateralleft language dominance. All except nine of the patients had onlyunilateral Wada-tests. Therefore, below the Wada-procedure andits mode of interpretation are described in detail.
Biographical data of the patients are given in Table 1.
Wada-test procedure
The applied Wada-test protocol verifies the integrity of series repe-tition, comprehension of spoken commands and questions, motorresponses to verbal body commands, naming of pictorially pre-sented objects, repetition of sentences or proverbs, reading aloud,
Please cite this article in press as: Wellmer, J., et al., Strongly lapatients—–Implications for presurgical work-up, Epilepsy Res. (2
and spontaneous speech. However, since about 1999, at our cen-ter hypothesis-led unilateral Wada-test on the side of intendedsurgery is the standard procedure and bilateral Wada-tests are per-formed only under special circumstances (Wellmer et al., 2005).In contrast to bilateral Wada-tests, unilateral Wada-tests do not
admii
PRESSnant patients—–Implications for presurgical work-up 3
llow for the estimation of a Wada-test LI for the tested languageunctions but for the determination of the hemispheric languageapacity (HLC) contralateral to the anesthetization. HLC can beategorized as complete, incomplete, or insufficient, depending onhe degree of expressive and receptive language functions whichan be observed during the Wada-test (Wellmer et al., 2005). Forhose patients showing a complete left HLC or insufficient rightLC, typical left language dominance is likely, although the rarehenomena of positive or negative bilaterality cannot completelye ruled out in this constellation (for details on this nomencla-ure see Kurthen et al., 1994; Wellmer et al., 2005). For patientsith complete or incomplete right, or incomplete or insufficient
eft HLC, atypical dominance is evident. From the 22 patients withtypical language dominance, 13 patients had unilateral left Wadahowing incomplete or complete right HLC, 3 patients with uni-ateral right Wada had incomplete or insufficient left HLC, and 6atients with bilateral Wada showed bilateral or unilateral rightanguage representation. In the 43 patients in which Wada-testesults are compatible with the assumption of typical left hemi-pheric language dominance, 33 had unilateral left Wada showingnsufficient right HLC, 7 had unilateral right Wada showing completeeft HLC, and 3 had bilateral Wada showing unilateral left languagerganization.
MRI-protocol
he applied fMRI-protocol consists of a visually presented seman-ic task with continuous performance control which is described inetail in earlier studies of our group (Fernandez et al., 2001, 2003;eber et al., 2006a,b). While undergoing fMRI, the patient is placed
n a supine position inside the scanner with the head stabilizedn an individually moulded vacuum cushion. The patient comparesimultaneously presented item pairs which are either word pairs ornpronounceable letter-string pairs of 5—11 letters. The patient isnstructed to press a button if she/he recognizes word pairs withdentical or highly similar meanings (synonyms) or identical let-er strings, and not to press the button in case of non-synonymord pairs or letter strings in which one consonant is different.he semantic and control conditions alternate every six-item pairsevery 25 s). The task is comprised of 15 blocks of word and letter-tring pairs each. Matching and non-matching items (50% each) areandomly intermixed in the blocks.
The functional and anatomical data sets were acquired in a 1.5 Tcanner (Siemens Symphony, Erlangen, Germany). For the fMRI, wecquired 248 T2*-weighted, gradient-echo EPI-scans with 16 axiallices (slice thickness: 6 mm; interslice gap: 0.6 mm; matrix size:4 × 64; field of view: 220 mm; echo time: 50 ms; repetition time:.125 s). For the structural MRI, a T1-weighted 3D-FLASH sequencenumber of slices: 120; slice thickness: 1.5 mm (no interslice gap);atrix size: 256 × 256; field of view: 230 mm; echo time: 4 ms; rep-
tition time: 11 ms) was acquired.The MRI data were analyzed using SPM99 (www.fil.ion.ucl.ac.
k/spm) (for processing details see Fernandez et al., 2001, 2003).o increase the functional specificity of the fMRI, we calculatedhe lateralization indices for three functionally defined VOIs: arontal inferior VOI comprising Broca’s area (including parts of Brod-ann areas 44, 45, 46, and 47: ‘‘Broca’s’’), an area combiningrefrontal activations outside Broca’s (‘‘remaining prefrontal’’),nd a temporo-parietal VOI showing a good overlap with theernicke-area (including parts of Brodmann areas 22, 39, and 40:
‘temporo-parietal’’) (Fig. 1). These VOIs proved intra-individuallyeliable language lateralization (Fernandez et al., 2003). For iden-ification of voxels activated during the semantic condition, we
teralized activation in language fMRI of atypical dominant008), doi:10.1016/j.eplepsyres.2008.03.005
pplied individual thresholds to the t-test-maps of each patientefined as 50% of a mean maximum t-value, which is defined as theean of those 5% of voxels showing the highest level of activation
n each VOI of both hemispheres. To derive weighted lateralizationndices for each VOI, we performed an automated quantification

ARTICLE IN PRESS+ModelEPIRES-3950; No. of Pages 10
4 J. Wellmer et al.
Figure 1 Protocol-specific volumes of interest (VOIs) depicted on a left hemisphere of a three-dimensional surface rendering ofa etrict rasth
of
L
whv
Dl
Tbetlafhtaal−
tftllV
e
bLtd
R
DV
Dttgso0UltplVlat
normalized brain. The VOIs are derived from statistical paramhat are activated in response to a semantic decision in contemispheric VOIs are mirrored from the left hemisphere.
f the sum of t-values of supra-threshold voxels according to theollowing equation:
I =∑
VXL − ∑
VXR∑
VXL +
∑V
XR
here V is the set of activated voxels, XL the t-value of leftemispheric voxels, and XR is the t-value of right hemisphericoxels.
etermination of individual degrees of languageateralization via fMRI
he evaluation of the individual degree of language lateralization isased on the LI determination in the above-mentioned VOIs. How-ver, LI may differ between VOIs. In this case it is not clear which ofhe three VOIs finally stands for the degree of individual languageateralization. As pointed out in the Introduction we also performn analysis of the individual low-VOI. The low-VOI is determined asollows: if all three VOIs lateralize language functions to the sameemisphere the low-VOI-LI is defined as the value of the LI closesto 0. In case of positive and negative LI within one patient (dissoci-ted LI), the low-VOI-LI is defined as 0. This circumvents classifyingpatient strongly lateralized if the following exemplary constel-
ation occurs: Broca’s 0.9, remaining frontal 0.8, temporo-parietal0.7.
To test to what extent the choice of VOIs affects the classifica-ion of patients as having more or less strongly lateralized languageunctions we perform an analysis of the frequency distribution ofhe respective LI over the whole patient group. Also on the group
Please cite this article in press as: Wellmer, J., et al., Strongly lapatients—–Implications for presurgical work-up, Epilepsy Res. (
evel we assess the fraction of patients that would be classified uni-ateral or atypical language dominant in dependence of the selectedOIs and of various LI thresholds.
On the individual patient level, we analyze the fMRI-LI differ-nces between the VOIs and thereby test if the LI in one VOI can
Ir
Tt
maps of healthy right-handed subjects and represent volumesto a letter-matching task (Fernandez et al., 2001). The right
e predicted from other VOIs. Finally, based on the range of fMRI-I found in the different VOIs we explore the possibility to predicthe result of a Wada-test from language dominance assessment inifferent VOIs.
esults
egrees of language lateralization over differentOIs on the group level
etermination of the frequency distribution shows that inhe Broca’s, remaining frontal and temporo-parietal VOIhere is a predominance of strongly left lateralized lan-uage functions (Fig. 2A—C). On the group level, no VOIhowed significantly less language lateralization than thethers (Broca’s: mean LI 0.54 ± 0.57; remaining frontal:.53 ± 0.57; temporo-parietal: 0.53 ± 0.57; Mann—Whitney-test: n.s.). However, in the low-VOI fMRI-LIs are more
eveled over the whole spectrum of LI (Fig. 2D, note thathe frequency peak at 0 derives from the classification ofatients with dissociated LI as 0). As a consequence of theower frequency of strong language lateralization in the low-OI the number of patients that would be classified typical
eft dominant at various low-VOI-LI thresholds between 1nd 0 is lower than at identical thresholds but in any of thehree functionally defined VOIs (Fig. 3).
teralized activation in language fMRI of atypical dominant2008), doi:10.1016/j.eplepsyres.2008.03.005
ntra-individual differences between Broca’s,emaining frontal and temporo-parietal fMRI-LI
he tendency for weaker lateralization of language func-ions in the low-VOI as compared to the Broca’s, remaining
Please cite this article in press as: Wellmer, J., et al., Strongly lapatients—–Implications for presurgical work-up, Epilepsy Res. (2
ARTICLE IN PRESS+ModelEPIRES-3950; No. of Pages 10
Strongly lateralized activation in language fMRI of atypical dominant patients—–Implications for presurgical work-up 5
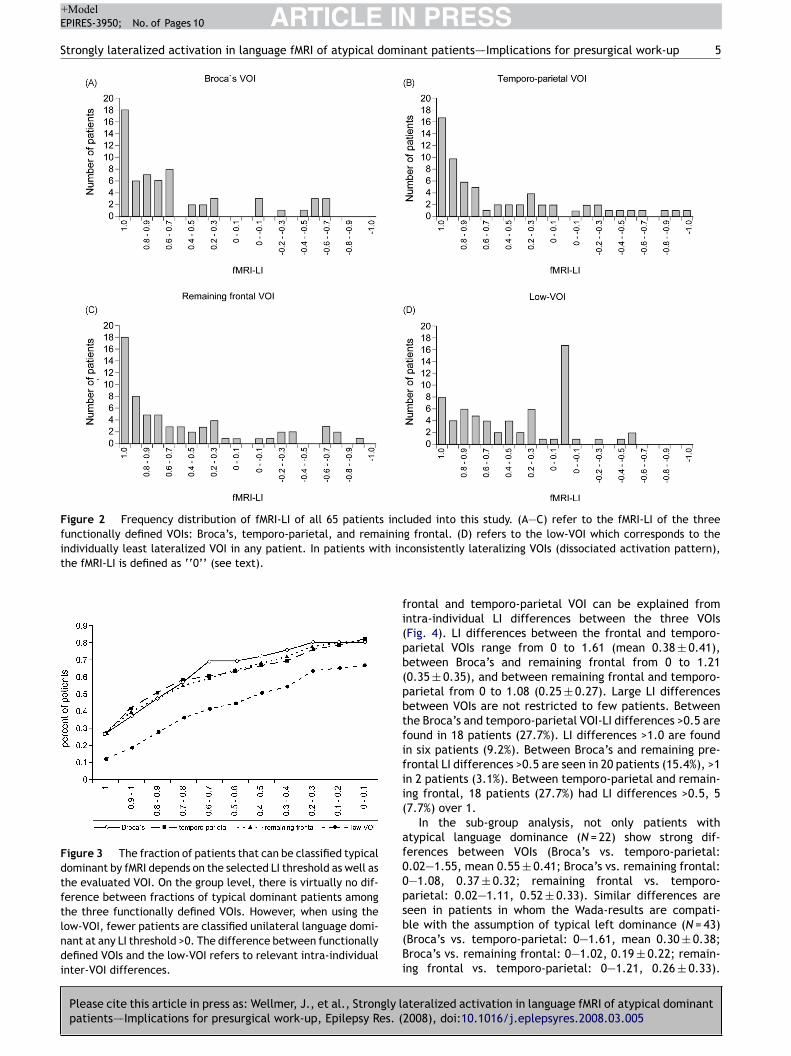
Figure 2 Frequency distribution of fMRI-LI of all 65 patients included into this study. (A—C) refer to the fMRI-LI of the threefunctionally defined VOIs: Broca’s, temporo-parietal, and remaininindividually least lateralized VOI in any patient. In patients with inthe fMRI-LI is defined as ‘‘0’’ (see text).
Figure 3 The fraction of patients that can be classified typicaldominant by fMRI depends on the selected LI threshold as well asthe evaluated VOI. On the group level, there is virtually no dif-ference between fractions of typical dominant patients amongthe three functionally defined VOIs. However, when using thelow-VOI, fewer patients are classified unilateral language domi-nant at any LI threshold >0. The difference between functionallydefined VOIs and the low-VOI refers to relevant intra-individualinter-VOI differences.
fi(pb(pbtfifii(
af00psb(Bi
g frontal. (D) refers to the low-VOI which corresponds to theconsistently lateralizing VOIs (dissociated activation pattern),
rontal and temporo-parietal VOI can be explained fromntra-individual LI differences between the three VOIsFig. 4). LI differences between the frontal and temporo-arietal VOIs range from 0 to 1.61 (mean 0.38 ± 0.41),etween Broca’s and remaining frontal from 0 to 1.210.35 ± 0.35), and between remaining frontal and temporo-arietal from 0 to 1.08 (0.25 ± 0.27). Large LI differencesetween VOIs are not restricted to few patients. Betweenhe Broca’s and temporo-parietal VOI-LI differences >0.5 areound in 18 patients (27.7%). LI differences >1.0 are foundn six patients (9.2%). Between Broca’s and remaining pre-rontal LI differences >0.5 are seen in 20 patients (15.4%), >1n 2 patients (3.1%). Between temporo-parietal and remain-ng frontal, 18 patients (27.7%) had LI differences >0.5, 57.7%) over 1.
In the sub-group analysis, not only patients withtypical language dominance (N = 22) show strong dif-erences between VOIs (Broca’s vs. temporo-parietal:.02—1.55, mean 0.55 ± 0.41; Broca’s vs. remaining frontal:—1.08, 0.37 ± 0.32; remaining frontal vs. temporo-arietal: 0.02—1.11, 0.52 ± 0.33). Similar differences are
teralized activation in language fMRI of atypical dominant008), doi:10.1016/j.eplepsyres.2008.03.005
een in patients in whom the Wada-results are compati-le with the assumption of typical left dominance (N = 43)Broca’s vs. temporo-parietal: 0—1.61, mean 0.30 ± 0.38;roca’s vs. remaining frontal: 0—1.02, 0.19 ± 0.22; remain-
ng frontal vs. temporo-parietal: 0—1.21, 0.26 ± 0.33).

ARTICLE IN PRESS+ModelEPIRES-3950; No. of Pages 10
6 J. Wellmer et al.
Figure 4 Intra-individual differences of fMRI-LI between VOIs. On the individual patient level we find relevant LI differencesbetween any of the three functionally defined VOIs. This is irrespective from the underlying type of language dominance (atypicalo inted of at
Hetn>>4d7r7
ltpw(clii
(ae
R
Timtltowtf
r suspected typical). Panels A—C refer to the intra-individualominance; panels D—F refer to intra-individual LI differences
owever, the percentage of patients with large differ-nces is lower in the suspected typical dominant grouphan in the atypical dominant group: atypical domi-ant patients: Broca’s vs. temporo-parietal: >0.5 40.9%,1 13.6%; Broca’s vs. remaining frontal: >0.5 27.3%,1 4.5%; remaining frontal vs. temporo-parietal: >0.55.5%, >1 9.1%. Patients suspicious for typical languageominance—–Broca’s vs. temporo-parietal: >0.5 20.9%, >1.0%; Broca’s vs. remaining frontal: >0.5 9.3%, >1 2.3%;emaining frontal vs. temporo-parietal: >0.5 18.6%, >1.0%.
There is no uniform pattern regarding the most or leastateralized VOIs. Among patients with all VOIs lateralizingo the left hemisphere (N = 43—–not identical with the 43atients with IAP-suspected typical dominance) the VOIsith the strongest lateralization where temporo-parietal
Please cite this article in press as: Wellmer, J., et al., Strongly lapatients—–Implications for presurgical work-up, Epilepsy Res. (
24 cases), remaining frontal (21 cases) and Broca’s (20ases—–in some patients several VOIs were equally strongateralized). Negative fMRI-LIs were detected for Broca’sn 13, and for temporo-parietal and remaining frontaln 12 cases, each. When patients showed discordant LI
1aitf
r-VOI differences in patients with suspected typical languageypical dominant patients.
N = 17), negative LIs were found in Broca’s in eight cases,nd temporo-parietal and remaining frontal in seven casesach.
elationship between fMRI- and Wada-test results
he marked intra-individual differences between LI foundn the Broca’s, remaining frontal and temporo-parietal VOIake evident that the isolated inspection of neither of
he three functionally defined VOIs allow comprehensiveanguage assessment. This is supported by the observa-ion that especially in atypical dominant patients the rangef fMRI-LI within the three VOIs is wide. Among patientsith atypical language dominance according to the Wada-
est, fMRI-LI of the frontal and temporo-parietal VOI rangerom 1 to −1 each, in the remaining frontal VOI from
teralized activation in language fMRI of atypical dominant2008), doi:10.1016/j.eplepsyres.2008.03.005
to −0.93. In patients in whom the Wada-test resultsre compatible with the assumption of typical left dom-nance, the fMRI-LI ranges are 1 to −0.61 (frontal), 1o −0.26 (temporo-parietal) and 1 to −0.39 (remainingrontal).

ARTICLE IN PRESS+ModelEPIRES-3950; No. of Pages 10
Strongly lateralized activation in language fMRI of atypical dominant patients—–Implications for presurgical work-up 7
Figure 5 Distribution of the fMRI-LI found in the three functionally defined and the low-VOI, separately presented for atypicaland suspected typical dominant patients according to Wada-tests. In atypical dominant patients, all three functionally defined VOIsshow a very wide range of fMRI-LI making the prediction of language dominance from the evaluation of an individual VOI impossible.Among atypical dominant patients, the range of low-VOI fMRI-LI is also wide, but the highest detected LI is 0.84. In patients withsuspected typical dominance, there is a strong predominance of left lateralized fMRI-LI over all VOIs. However, in the functionally
ctivawith
ddVa
D
AWgiricramw
ripbudct
defined VOIs some patients show negative LI (right lateralized atypical dominance shows LI < 0. This implies that in no patientright.
Referring to the low-VOI, in the group of atypical dom-inant patients fMRI-LI range from 0.84 to −0.53, the rangeof fMRI-LI in the patients with suspected typical languagedominance is 1—0 (0 in the meaning of discordant lateral-ization). The distribution of fMRI-LI for both patient groupsand all four VOIs is shown in Fig. 5.
In order to exclude that the degree of language lateral-ization is a simple function of the cooperation of the patientsduring the task we performed a non-parametric correlationanalysis (Spearman’s rho) between the absolute value of thelaterality index and the number of correct presses for thelanguage and control condition. In this analysis, no signifi-cant correlation or trend could be observed (Broca’s r = 0.1;temporo-parietal r = −0.08; remaining frontal r = −0.01;low-VOI r = 0.5; all n.s.).
Consequences for previously proposed LIthresholds
Previous studies suggest the application of fMRI-LI thresholdsbetween ±0.1 and ±0.5 for the differentiation of atypicalfrom typical dominant patients. Our data regarding languagelateralization in atypical dominant patients show that theseLI thresholds may be too stringent for clinical application.This accounts in particular for the functionally defined VOIs,but also for the low-VOI. Analysis of low-VOI fMRI-LI found inatypical dominant patients shows that 17 of 22 patients have
Please cite this article in press as: Wellmer, J., et al., Strongly lapatients—–Implications for presurgical work-up, Epilepsy Res. (2
fMRI-LI between −0.53 and 0.1 or dissociated LI, respec-tively. However, five patients have fMRI-LI of 0.14, 0.25,0.38, 0.81 and 0.84. This means that depending on the cho-sen LI-threshold for unilateral language dominance between2 and 5 patients (9 and 23%) out of a sample of atypical
npLFf
tion) in single VOIs. In the low-VOI, no patient with suspectedsuspected typical dominance all three VOIs lateralized to the
ominant patients would have been misclassified as typicalominant. In our restricted sample only patients with low-OI fMRI-LI above ±0.84 could have been identified correctlys typical dominant.
iscussion
lthough fMRI offers some indisputable advantages over theada-test and it is therefore increasingly used in the presur-
ical work-up of patients with pharmacoresistant epilepsies,t suffers from some methodological limitations which refer-ing physicians should be aware of. One of these limitationss that bilateral activation patterns in fMRI cannot be con-lusively interpreted. This problem is relevant for clinicaloutine since some degrees of bilaterality are the rule in allpplied fMRI-protocols. Bilateral activation in fMRI is a basicethodological problem and not restricted to fMRI-protocolsith improper design (Desmond and Chen, 2002).
The fMRI-protocol applied in this study fulfills the crite-ia for a robust and reliable language lateralization task. Its a tight comparison task (subtracting non-language com-onents such as visual exploration, decision making, andutton presses from the language > control contrast). Bysing an attention and decision demanding control con-ition, unspecific processing during the control conditionan be minimized. Additionally, the protocol offers con-inuous performance control which allows identification of
teralized activation in language fMRI of atypical dominant008), doi:10.1016/j.eplepsyres.2008.03.005
on-compliant patients. The applied functional VOIs arerotocol-specific, and the LI thresholds used to identifyI are activation-level adjusted (Fernandez et al., 2001).inally, the task shows good intra-subject re-test reliabilityor the evaluated VOIs (Fernandez et al., 2003). However,

INE
8
eo
s
•
•
•
•
dsgdmagaabrVdf1ttplr
iafatwlpeaentV
a
ifadvctgiracfoWllmcofipt
wbbpautiWahdfs
apdagtTfWdoind
L
ARTICLE+ModelPIRES-3950; No. of Pages 10
ven under these controlled conditions we find a wide rangef LI over patients and evaluated VOIs.
With regard to fMRI-based language lateralization on theingle patient level the core findings of this study are:
Even in carefully designed and closely monitored fMRI-protocols large intra-subject fMRI-LI differences existbetween VOIs. The prediction of the degree of languagelateralization in one VOI from another is not possible.Patients with Wada-test proven atypical language domi-nance can express a wide range of language lateralizationin any protocol-specific, functionally defined VOIs. Theprediction of typical or atypical language dominance fromone of these VOI is impossible on the single subject level.Referring the degree of individual language lateralizationto the least lateralized of several intra-individual VOIs(low-VOI) increases the sensitivity of fMRI for atypicallanguage dominance.Lateralization index thresholds between ±0.1 and ±0.5which have been suggested in earlier studies may be toostringent to discriminate atypical from typical dominantpatients with a safety that is needed in a presurgical set-ting.
The detection of large unsystematic intra-individual LIifferences between VOIs is the first relevant result of thetudy. This effect can be observed in the atypical dominantroup as well as in patients suspicious for being typicallyominant. The dimension of intra-individual LI differencesakes evident that the prediction of the LI of one VOI from
nother VOI is impossible. Therefore, comprehensive lan-uage dominance assessment based on a single VOI is notdmissible. The insufficiency of the isolated evaluation ofsingle VOI for language lateralization is further supportedy the second key result that the intra-subject comparisoneveals a wide range of LI in any of the functionally definedOIs. In patients with Wada-test proven atypical languageominance LI in the Broca’s and temporo-parietal VOI rangerom −1 to 1, in the remaining frontal VOI from −0.93 to, respectively. Hence, the detection of any LI in one ofhese VOIs does not allow attributing a given patient to anyype of underlying language dominance. This cannot be com-ensated by the fact that patients with suspected typicalanguage dominance according to the Wada-test are moreestricted with their LI range.
The observations of large LI differences between intra-ndividual VOIs and the wide range of LI in either VOI acrosstypical dominant patients have far-reaching consequencesor fMRI-application. They give a hint that fMRI-protocolsssessing predominantly frontally located language func-ions (such as object naming) or assessing only a singleherever located VOI might not be suited for presurgical
anguage lateralization. They are at the danger for missingatients with atypical language dominance. But also morelaborated fMRI-protocols known to activate both, frontalnd temporo-parietal neocortex and which are based on thevaluation of more than one VOI have to take precautions
Please cite this article in press as: Wellmer, J., et al., Strongly lapatients—–Implications for presurgical work-up, Epilepsy Res. (
ot to misclassify patients strongly language lateralized dueo over-interpretation of strong lateralization within singleOIs.
A solution to this problem can be the low-VOI approachs suggested in this study. By focusing to the least lateral-
MobnW
PRESSJ. Wellmer et al.
zed of three evaluated VOIs we increase the sensitivity ofMRI for atypical language dominance. The idea behind thispproach is putting the decision about underlying languageominance on the evaluation of more than one VOI and toerify if any of the tested VOI gives rise for a doubt con-erning underlying unilateral language dominance. Notably,he detection of weakly or even dissociated lateralized lan-uage functions within one VOI does not mean that a patients necessarily atypical language dominant. There are severaleasons why LI might be artificially low. Weakly or dissoci-ted lateralized low-VOI fMRI-activation merely allows theonclusion ‘‘typical language dominance not detected byMRI’’. Hence, if clinically relevant, a more definite methodf language lateralization should be applied, namely theada-test. If, however, the low-VOI shows strongly left
ateralized language functions, then all VOIs are stronglyateralized and the diagnosis of typical language dominanceight be justified. In this case, performance of a Wada-test
ould be redundant. In this point we follow the suggestionsf Abou-Khalil (2007) who also regards the fMRI only as arst step in an algorithm with Wada-test performance inatients, in whom language lateralization is clinically essen-ial but fMRI not appropriate.
However, what remains unsolved is the question belowhat degree of fMRI-lateralization atypical dominance muste suspected. Earlier studies suggested that LI thresholdsetween ±0.1 and ±0.5 might be discriminative. Althoughrotocols vary and require individual thresholds (Jansen etl., 2006), these values are obviously relatively low. Evennder application of the low-VOI approach, in this studyhese thresholds would have led to a misdiagnosis of typ-cal language dominance in up to 5 of 22 patients withada-test proven atypical language dominance. Withoutpplication of low-VOIs, discordance would have been evenigher. Although this study is no formal LI threshold vali-ation study, our data indicate that the low-VOI thresholdor the protocol applied here must be at least 0.84 to gainufficient diagnostic safety on the single patient level.
In summary our data indicate that fMRI should not bepplied uncritically in the presurgical work-up of epilepsyatients. Patients with Wada-test proven atypical languageominance can show strongly lateralized fMRI-activation inny VOI, pretending unilateral language dominance. Strate-ies have to be found to allow discriminating atypical fromypical dominant patients with sufficient diagnostic safety.he low-VOI approach may be a step in this direction. IfMRI does not allow conclusive language lateralization aada-test should be performed. The Wada-test is not thatangerous, that its replacement must be forced for the costf inaccurate preoperative language lateralization which,n the worst case, may finally result in avoidable perma-ent morbidity (for example aphasia or relevant memoryecline).
imitations of the study
teralized activation in language fMRI of atypical dominant2008), doi:10.1016/j.eplepsyres.2008.03.005
ost patients in this study had only unilateral Wada-tests (56ut of 65, for reasons see Wellmer et al., 2005). This mighte seen as a limitation of the study. However, this study doesot claim to be a full fMRI vs. Wada-test validation study.ith regard to the primary target of this study, the detection

INomi
otnto
tceefjsrti
C
W
A
PFmJoaDBDa
R
A
A
B
B
B
D
D
D
ARTICLE+ModelEPIRES-3950; No. of Pages 10
Strongly lateralized activation in language fMRI of atypical d
of the range of fMRI-LI found in atypical dominant patients,unilateral Wada-tests are no relevant restriction. Unilat-eral Wada-tests allow the diagnosis of atypical languagedominance with certainty (see ‘‘Materials and methods’’section). Yet, the identification of patients with typical lan-guage dominance is not possible with certainty. Instead weclassify patients in whom unilateral Wada-test does not con-tradict unilateral left dominance as ‘‘suspicious for’’ or‘‘compatible with’’ typical language dominance. However,some of the 43 patients classified this way may be positiveor negative bilateral dominant and thereby atypical domi-nant. These patients might be missed in the spectrum of LIfound in atypical dominant patients. An estimation of thenumber of negative or positive bilateral dominant patientsamong the 43 patients is difficult. On the one hand ourpatient sample has a bias towards atypical language domi-nance (focal epilepsy, early onset, clinical hints for atypicallanguage dominance). On the other hand there are no datareporting the incidence of positive or negative bilaterality incomparable samples. Since the range of fMRI-LI found in theatypical dominant patients is already very large, an addi-tional identification and evaluation of these patients wouldprobably not modify the result relevantly.
A further possible restriction of the current study is thatit only addresses the discrimination of typical (unilateralleft) from atypical language dominance (all others). We donot address the identification of unilateral right dominantpatients who must be regarded as a separate subgroup inthe presurgical work-up. Yet, as in most studies assessing thedistribution of language dominance across epilepsy patients,among our patients there is a strong skewness towards leftlateralized language functions (see Fig. 2). In consequencewe have too few patients with right hemispheric languageorganization to allow a respective evaluation. However, itis common practice to apply symmetrical LI thresholds forleft and right unilateral dominance in virtually all fMRI-and Wada-studies. We therefore assume that the princi-ples outlined for the identification of typical (unilateral left)dominant patients can be symmetrically applied for unilat-eral right dominant patients.
It might be seen as another restriction of our studythat we only evaluate a single fMRI-activation task ratherthan relying language lateralization to a test battery. Infact, some groups propose to use multiple fMRI-tasks todetermine individual language lateralization patterns (e.g.combined task analysis (CTA); Ramsey et al., 2001; Jansenet al., 2006). Certainly, the more language sub-functions aretested, the more reliable the result of language lateraliza-tion should become. However, a central shortcoming of CTAas applied thus far is that it usually merges activation pat-terns of different language tasks to a single fMRI-LI. Althoughthis LI may be statistically robust, it is an arithmetical con-struct which delivers a different quality of information thanthat which is desirable in individual presurgical languagelateralization. Relying to the principles of electrocorticos-timulation where usually the detection of only one out ofseveral tested language sub-functions already means pres-
Please cite this article in press as: Wellmer, J., et al., Strongly lapatients—–Implications for presurgical work-up, Epilepsy Res. (2
ence of relevant eloquent cortex in the tested hemisphere,one might rather consider the following procedure: applica-tion of a battery of several complementary fMRI-tasks. Eachtask is then analyzed separately the way suggested in thisstudy (with specific VOIs and a task-specific low-VOI thresh-
D
PRESSnant patients—–Implications for presurgical work-up 9
ld). If then the fMRI-activation pattern of any of the appliedasks raises doubt about global unilateral language domi-ance, performance of a Wada-test should be considered. Ifhis procedure is finally more reliable than the applicationf single semantic decision task remains to be evaluated.
Further criticism of the current study may arise fromhe fact that we neither address patients’ compliance norerebral lesions in detail. Both are factors potentially influ-ncing the degree of language lateralization and mightventually belong to an algorithm which helps identifyingMRI-language lateralization-suited patients. Yet, these sub-ects are very complex and need to be examined in separatetudies. We feel that even without this information theesults of our study are sufficiently interpretable and con-ribute to the understanding of the role that fMRI can playn the presurgical language lateralization of individuals.
onflict of interest
e have no conflict of interest.
cknowledgements
K was funded via an institutional grant of the Deutscheorschungsgemeinschaft (DFG SFB/TR3) given to the Depart-ent of Epileptology, University of Bonn. All authors, except
R, were funded by the University of Bonn, Departmentf Medicine without extramural sources. JR worked as
self-employed neuroradiologist at the Department ofiagnostic and Therapeutic Neuroradiology, Medical Centeronn, Bonn, Germany. The authors would also like to thankeidre Mahkorn-Cooper, M.D., for her help in proof-readingn earlier version of this article.
eferences
bou-Khalil, B., 2007. An update on determination of language dom-inance in screening for epilepsy surgery: the Wada test andnewer noninvasive alternatives. Epilepsia 48, 442—455.
dcock, J.E., Wise, R.G., Oxbury, J.M., et al., 2003. QuantitativefMRI assessment of the differences in lateralization of language-related brain activation in patients with temporal lobe epilepsy.Neuroimage 18, 423—438.
enson, R.R., FitzGerald, D.B., LeSueur, L.L., et al., 1999. Languagedominance determined by whole brain functional MRI in patientswith brain lesions. Neurology 52, 798—809.
inder, J.R., Swanson, S.J., Hammeke, T.A., et al., 1996. Deter-mination of language dominance using functional MRI: acomparison with the Wada test. Neurology 46, 978—984.
inder, J.R., Frost, J.A., Hammeke, T.A., et al., 1999. Conceptualprocessing during the conscious resting state. A functional MRIstudy. J. Cogn. Neurosci. 11, 80—95.
esmond, J.E., Sum, J.M., Wagner, A.D., et al., 1995. FunctionalMRI measurement of language lateralization in Wada-testedpatients. Brain 118, 1411—1419.
esmond, J.E., Chen, S.H., 2002. Ethical issues in the clinical appli-cation of fMRI: factors affecting the validity and interpretationof activations. Brain Cogn. 50, 482—497.
etre, J.A., 2004. fMRI: applications in epilepsy. Epilepsia 45 (Suppl.
teralized activation in language fMRI of atypical dominant008), doi:10.1016/j.eplepsyres.2008.03.005
4), 26—31.onaldson, D.I., Buckner, R.L., 2001. Effective paradigm design. In:
Mathews, P.M., Jezzard, P., Evans, A.C. (Eds.), Functional Mag-netic Resonance Imaging of the Brain: Methods for Neuroscience.Oxford University Press, pp. 177—195.

INE
1
F
F
H
H
H
H
J
K
L
L
L
L
M
R
R
S
S
S
S
S
S
W
W
W
W
ARTICLE+ModelPIRES-3950; No. of Pages 10
0
ernandez, G., de Greiff, A., von Oertzen, J., et al., 2001. Languagemapping in less than 15 min: real-time functional MRI duringroutine clinical investigation. Neuroimage 14, 585—594.
ernandez, G., Specht, K., Weis, S., et al., 2003. Intrasubject repro-ducibility of presurgical language lateralization and mappingusing fMRI. Neurology 60, 969—975.
elmstaedter, C., Kurthen, M., Linke, D.B., Elger, C.E., 1997. Pat-terns of language dominance in focal left and right hemisphereepilepsies: relation to MRI findings, EEG, sex and age at onset ofepilepsy. Brain Cogn. 33, 135—150.
elmstaedter, C., 2004. Neuropsychological aspects of epilepsysurgery. Epilepsy Behav. 5, S45—S55.
ertz-Pannier, L., Gaillard, W.D., Mott, S.H., et al., 1997. Non-invasive assessment of language dominance in children andadolescents with functional MRI: a preliminary study. Neurology48, 1003—1012.
und-Georgiadis, M., Lex, U., von Cramon, D.Y., 2001. Languagedominance assessment by means of fMRI: contributions from taskdesign, performance, and stimulus modality. J. Magn. Reson.Imaging 13, 668—675.
ansen, A., Menke, R., Sommer, J., et al., 2006. The assessmentof hemispheric lateralization in functional MRI—–robustness andreproducibility. Neuroimage 33, 204—217.
urthen, M., Helmstaedter, C., Linke, D.B., et al., 1994. Quantita-tive and qualitative evaluation of patterns of cerebral languagedominance. An amobarbital study. Brain Lang. 46, 536—564.
ehericy, S., Cohen, L., Bazin, B., et al., 2000. Functional MR eval-uation of temporal and frontal language dominance comparedwith the Wada test. Neurology 54, 1625—1633.
iegeois, F., Connelly, A., Cross, J.H., et al., 2004. Languagereorganization in children with early-onset lesions of the lefthemisphere: an fMRI study. Brain 127, 1229—1236.
oring, D.W., Meador, K.J., Lee, G.P., et al., 1990. Cerebral lan-guage lateralization: evidence from intracarotid amobarbitaltesting. Neuropsychologia 28, 831—838.
oring, D.W., Meador, K.J., Allison, J.D., et al., 2002. Now you see
Please cite this article in press as: Wellmer, J., et al., Strongly lapatients—–Implications for presurgical work-up, Epilepsy Res. (
it, now you don’t: statistical and methodological considerationsin fMRI. Epilepsy Behav. 3, 539—547.
edina, L.S., Aguirre, E., Bernal, B., Altman, N.R., 2004. Func-tional MR imaging versus Wada test for evaluation of languagelateralization: cost analysis. Radiology 230, 49—54.
W
PRESSJ. Wellmer et al.
amsey, N.F., Sommer, I.E.C., Rutten, G.J., Kahn, R.S., 2001. Com-bined analysis of language tasks in fMRI improves assessmentof hemispheric dominance for language functions in individualsubjects. Neuroimage 13, 719—733.
utten, G.J., Ramsey, N.F., van Rijen, P.C., van Veelen, C.W., 2002.Reproducibility of fMRI-determined language lateralization inindividual subjects. Brain Lang. 80, 421—437.
abbah, P., Chassoux, F., Leveque, C., et al., 2003. FunctionalMR imaging in assessment of language dominance in epilepticpatients. Neuroimage 18, 460—467.
absevitz, D.S., Swanson, S.J., Hammeke, T.A., et al., 2003. Useof preoperative functional neuroimaging to predict languagedeficits from epilepsy surgery. Neurology 60, 1788—1792.
altzman-Benaiah, J., Scott, K., Smith, M.L., 2003. Factors asso-ciated with atypical speech representation in children withintractable epilepsy. Neuropsychologia 41, 1967—1974.
preer, J., Arnold, S., Quiske, A., et al., 2002. Determination ofhemisphere dominance for language: comparison of frontal andtemporal fMRI activation with intracarotid amytal testing. Neu-roradiology 44, 467—474.
pringer, J.A., Binder, J.R., Hammeke, T.A., et al., 1999. Languagedominance in neurologically normal and epilepsy subjects: afunctional MRI study. Brain 122, 2033—2046.
zaflarski, J.P., Binder, J.R., Possing, E.T., et al., 2002. Languagelateralization in left-handed and ambidextrous people: fMRIdata. Neurology 59, 238—244.
ada, J., Rasmussen, T., 1960. Intracarotid injection of sodiumamytal for the lateralization of cerebral speech dominance. J.Neurosurg. 17, 266—282.
eber, B., Wellmer, J., Schur, S., et al., 2006a. Presurgical lan-guage fMRI in patients with drug-resistant epilepsy: effects oftask performance. Epilepsia 47, 880—886.
eber, B., Wellmer, J., Reuber, M., et al., 2006b. Left hippocampalpathology is associated with atypical language lateralization inpatients with focal epilepsy. Brain 129, 346—351.
ellmer, J., Fernandez, G., Linke, D.B., et al., 2005. Unilateral
teralized activation in language fMRI of atypical dominant2008), doi:10.1016/j.eplepsyres.2008.03.005
intracarotid amobarbital procedure for language lateralization.Epilepsia 46, 1764—1772.
oermann, F.G., Jokeit, H., Luerding, R., et al., 2003. Language lat-eralization by Wada test and fMRI in 100 patients with epilepsy.Neurology 61, 699—701.
Copyright © 2022 FDOKUMEN




















