INVITATION TO BID Implement Construction Works (ITB/GLED ...
Upload
khangminh22Category
view
5download
0
Breneol et al. Health Research Policy and Systems (2022) 20:64 https://doi.org/10.1186/s12961-022-00865-8
REVIEW
Strategies to adapt and implement health system guidelines and recommendations: a scoping reviewSydney Breneol1,2, Janet A. Curran1,2* , Robert Marten3, Kirti Minocha1, Catie Johnson1,2, Helen Wong1,4, Etienne V. Langlois5, Lori Wozney6, C. Marcela Vélez7, Christine Cassidy1,2, Sanjay Juvekar8, Melissa Rothfus9, Lydia Aziato10, Lisa Keeping‑Burke11, Samuel Adjorlolo12 and Daniel F. Patiño‑Lugo7
Abstract
Background: Evidence‑based health system guidelines are pivotal tools to help outline the important financial, policy and service components recommended to achieve a sustainable and resilient health system. However, not all guidelines are readily translatable into practice and/or policy without effective and tailored implementation and adaptation techniques. This scoping review mapped the evidence related to the adaptation and implementation of health system guidelines in low‑ and middle‑income countries.
Methods: We conducted a scoping review following the Joanna Briggs Institute methodology for scoping reviews. A search strategy was implemented in MEDLINE (Ovid), Embase, CINAHL, LILACS (VHL Regional Portal), and Web of Science databases in late August 2020. We also searched sources of grey literature and reference lists of potentially relevant reviews. All findings were reported following the Preferred Reporting Items for Systematic Reviews and Meta‑Analyses Extension for Scoping Reviews.
Results: A total of 41 studies were included in the final set of papers. Common strategies were identified for adapt‑ing and implementing health system guidelines, related barriers and enablers, and indicators of success. The most common types of implementation strategies included education, clinical supervision, training and the formation of advisory groups. A paucity of reported information was also identified related to adaptation initiatives. Barriers to and enablers of implementation and adaptation were reported across studies, including the need for financial sustain‑ability. Common approaches to evaluation were identified and included outcomes of interest at both the patient and health system level.
Conclusions: The findings from this review suggest several themes in the literature and identify a need for future research to strengthen the evidence base for improving the implementation and adaptation of health system guidelines in low‑ and middle‑income countries. The findings can serve as a future resource for researchers seeking to evaluate implementation and adaptation of health system guidelines. Our findings also suggest that more effort may be required across research, policy and practice sectors to support the adaptation and implementation of health system guidelines to local contexts and health system arrangements in low‑ and middle‑income countries.
Keywords: Health systems, Global health, Scoping review, Implementation science, Evidence‑informed guidelines
© The Author(s) 2022. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/. The Creative Commons Public Domain Dedication waiver (http:// creat iveco mmons. org/ publi cdoma in/ zero/1. 0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Open Access
*Correspondence: [email protected]
1 School of Nursing, Faculty of Health, Dalhousie University, Halifax, CanadaFull list of author information is available at the end of the article

Page 2 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
BackgroundEvidence-informed guidelines are pivotal to reform-ing healthcare and strengthening health systems for healthier communities worldwide [1, 2]. WHO concep-tualizes guidelines as a set of evidence-informed recom-mendations related to practice, public health or policy for informing and assisting decision-makers (e.g. policy-makers, healthcare providers or patients) [3]. In contrast to clinical practice guidelines focused on the appropriate-ness of clinical care activities, health system guidelines outline the required system, policy and/or finance com-ponents recommended to address health challenges [4, 5].
Despite the rigorous systematic synthesis of current research evidence focused on the development of high-quality guidelines, not all guidelines are readily and directly translatable into practice and/or policy [6, 7]. According to Balas and Boren, the small proportion of published evidence (approximately 14%) that does trans-late into practice can take upwards of 17 years from start to finish [8, 9]. Understanding implementation and adap-tation strategies that facilitate the uptake of evidence-informed guidelines and recommendations is an urgent research and policy priority [10–13]. Implementation strategies are often defined as “methods or techniques used to enhance the adaptation, implementation, and sustainability of a program or practice” [14]. Guideline adaptation strategies involve systematically modifying guidelines developed in a specific environment to be suitable for application in other contextual settings (e.g. organizational or cultural) [15].
A review of WHO guidelines by Wang et al. [16] revealed a lack of implementation strategies that were evidence-based and involved active techniques (e.g. workshops, evaluation surveys, training) within their relevant implementation sections. WHO is currently focused on enhancing the adaptability of guidelines [17] and integrating adaptation strategies into their imple-mentation plans [18]. For successful uptake, even high-quality international guidelines require adapting and tailoring to local contexts or circumstances [19]. To help achieve success, the Alliance for Health Policy and Sys-tems Research (a WHO-hosted partnership) created the Research to Enhance the Adaptation and Implementation of Health Systems Guidelines (RAISE) portfolio, which aims to support decision-making on policy and systems in six low- and middle-income countries (LMICs) [20]. However, much remains to be known about the factors and processes to enhance their adaptation and imple-mentation [16, 20]. Additional evidence is needed to inform good practices, effective methods and evidence-based implementation and adaptation recommendations for the utilization of health system guidelines.
Neglecting to consider the interaction between con-textual factors and guideline uptake is likely to lead to underperformance or failure [21–25]. It is important to recognize political, cultural and socioeconomic contexts and how these intersectional factors can influence health system guideline implementation and adaptation pro-cesses. Several methods have been derived for the selec-tion and tailoring of implementation strategies to address these contextual needs [26]. Various taxonomies have been established as a means to better describe and cate-gorize implementation strategies [27–33] and to concep-tualize context to allow for the analysis of determinants (e.g. barriers and enablers) of implementation outcomes [34]. Frameworks have also been identified for adapt-ing health-related guidelines, but often lack guidance on implementation [18, 35]. Therefore, the best methods for developing tailored implementation strategies and select-ing adaptation frameworks remain to be identified [12, 18].
We conducted a preliminary search of PROSPERO, MEDLINE, the Cochrane Database of Systematic Reviews, and the Joanna Briggs Institute (JBI) Database of Systematic Reviews and Implementation Reports. No reviews were identified that addressed adapting and implementing health system guidelines in LMICs. The search revealed a related overview of systematic reviews examining the effects of implementation techniques for health system initiatives that were deemed relevant to low-income countries (LICs) [36]. Despite this review and the acknowledged contextual differences between LICs and high-income countries (HICs), the findings were derived primarily from studies conducted in HICs, leaving a significant gap in the literature examining any contextual nuances of implementation and adaptation of health system guidelines specifically in LMICs.
The objective of this scoping review is unique, as it provides an overview of available evidence related to the implementation and adaptation of health system guidelines evaluated in LMICs. A focus on adaptation and implementation processes is a novel contribution in the literature by examining both of their strategies, interactions and influences. Recognizing the intricacy of contextual factors, we will only be examining implemen-tation and adaptation strategies that directly happened in LMICs. We adopted an integrated knowledge transla-tion approach by collaborating with a broad range of key informants, including the lead of each partner country in the WHO RAISE portfolio, throughout the review process to help ensure that the findings were relevant to knowledge users. Integrated knowledge translation is an approach to research where researchers and end-users work collaboratively to identify relevant knowledge gaps and ensure the production of actionable knowledge [37].

Page 3 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
The results of this scoping review provide critical insight into the development of evidence-based implementa-tion and adaptation recommendations for health system guidelines in LMICs.
Review aimsThis scoping review assessed and mapped the available evidence related to adapting and implementing health system guidelines and recommendations in LMICs. The following research questions guided the review:
1. What are the common strategies and approaches for implementing health system guidelines and recom-mendations in LMICs?
2. What are the common strategies and approaches for adapting health system guidelines and recommenda-tions in LMICs?
3. What are the commonly reported outcomes or indi-cators of success in adaptation and/or implementa-tion of health system guidelines and recommenda-tions in LMICs?
4. What are the commonly reported barriers and facili-tators with respect to adaptation and/or implemen-tation of health system guidelines and recommenda-tions in LMICs?
MethodsThis scoping review was guided by the methodologi-cal framework outlined by the JBI [38]. The framework includes six phases: (i) identifying the research ques-tion; (ii) searching for studies; (iii) selecting studies; (iv) extracting, charting and appraising data; (v) synthesizing and reporting findings; (vi) consulting with experts and key stakeholders [38].
Inclusion criteriaPopulationIn alignment with the Effective Practice and Organisation of Care (EPOC) taxonomy of health system interventions [39], this review considered articles including any health-care organizations, healthcare professionals or healthcare recipients targeted for change by health system guide-lines within LMICs.
ConceptThe concepts relevant for this review consist of the implementation and adaptation strategies, frameworks, and barriers and/or facilitators related to the adaptation and/or implementation of health system guidelines, poli-cies and/or recommendations. Articles were required to explicitly state their intent to implement and/or adapt any evidence-informed health system guideline to be
considered for inclusion. Health systems were concep-tualized to encompass any system responsible for the provision of health services, finances, and/or governance [40]. Our review considered any evidence-informed (as reported by author) health system guidelines, regardless of the developer. Articles that described their intent to implement and/or adapt clinical practice guidelines were excluded.
Implementation and adaptation, while often under-taken simultaneously, are two distinct concepts being examined by this review. Implementation strategies were defined as any “methods or techniques used to enhance the adaptation, implementation, and sustainability” [14]. Adaptation strategies were defined as a “process of thoughtful and deliberate alteration to the design or delivery of an intervention, with the goal of improving its fit or effectiveness in a given context” [41]. Articles were required to report on the implementation and/or adap-tation of health system guidelines to be considered for inclusion.
ContextContext in this review involved adaptation and/or imple-mentation strategies applied in LMICs at a health system level. LMICs were defined by the World Bank standards based on gross national income for the 2021 fiscal year [42]. Studies or data related to HICs were excluded from this review.
Types of sourcesThis scoping review considered any quantitative, quali-tative or mixed-methods studies that evaluated the implementation and/or adaptation of health system guidelines in any LMICs. Articles that were descriptive in nature (e.g. editorials, commentaries, opinion papers) or did not have evaluation processes for assessing the implementation/adaptation strategy were excluded. Lit-erature reviews that reported on relevant concepts were first reviewed for primary studies and then ultimately excluded. Studies published in English, not restricted by date of publication, were included.
Search strategyThe search strategy aimed to locate both published and unpublished studies. An initial search of MEDLINE (Ovid) was undertaken by a librarian scientist to iden-tify relevant studies of interest. The search strategy was developed using Medical Subject Headings (MeSH) terms and keywords contained in the titles and abstracts of relevant articles. A full search strategy for MEDLINE (Ovid) is included in our Additional file 1. This search strategy underwent peer review by another librarian using the Peer Review of Electronic Search Strategies

Page 4 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
(PRESS) [43] to ensure its accuracy. The search strategy was then adapted for each included information source. Lastly, primary studies from identified literature reviews were scanned for additional studies.
Information sourcesWe employed our search strategy in MEDLINE (Ovid), Embase, CINAHL (Cumulative Index to Nursing and Allied Health Literature), LILACS (Latin American and Caribbean Health Sciences Literature; VHL Regional Portal), and Web of Science databases. Sources of grey literature included a search of the CADTH (Canadian Agency for Drugs and Technologies in Health) Grey Mat-ters Tool, Google, Google Scholar, and ProQuest Disser-tations & Theses Global. These databases were chosen to capture potential articles across relevant countries.
Study selectionSearch results were uploaded into Covidence system-atic review software [45] for reference management. To ensure that eligibility criteria were uniformly applied by all reviewers, team members independently pilot-tested 20 citations and met to resolve any areas in need of clari-fication. Two reviewers then independently screened all titles and abstracts for assessment against the inclusion criteria. Full-text articles of potentially relevant stud-ies were retrieved, and two reviewers independently assessed the full-text studies for eligibility. Disagreements between reviewers were resolved through discussion at each stage of the study selection process. If consensus could not be achieved, a third reviewer made the final decision. Reasons for exclusion of full-text studies were documented and are reported in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Exten-sion for Scoping Reviews (PRISMA-ScR) flow diagram [46].
Data extractionData were extracted using a predetermined extrac-tion form to collect key findings relevant to the scoping review questions (Additional file 2). The main concepts in the data extraction form included year of publication, country, study aim(s), study population, setting, funding source, use of theoretical/conceptual frameworks, guide-line description, implementation strategies, adaptation strategies, outcomes of interest, study methods, barriers and enablers, key results and stakeholder engagement [38]. Details regarding implementation strategies were extracted based on Proctor and colleagues’ recommen-dations for operationalizing and reporting implemen-tation techniques [14]. This data extraction framework facilitated the collection of specific and pertinent data related to reported implementation strategies, such as
duration, dose and justification. Further, the Framework for Reporting Adaptations and Modifications–Enhanced (FRAME) was used to guide data extraction of adapta-tion strategies to capture the who, where, when, why and how aspects of modifications [41]. As this review seeks to examine implementation and adaptation as two dis-tinct concepts, data on implementation and adaptation strategies were extracted independently of each other. If articles reported on both implementation and adap-tation strategies, concepts related to processes such as barriers, enablers and outcomes were extracted indepen-dently. This could only be accomplished if authors explic-itly stated which indicators (e.g. barriers, enablers and outcomes) related to which concepts (implementation or adaptation). If this level of detail was not provided, the data were still extracted but we were unable to infer which indicators related to which concepts. Data were also extracted if authors reported using a theoretical/conceptual framework to guide/justify their implementa-tion and/or adaptation techniques. Two reviewers inde-pendently extracted details from the included articles, and disagreements were resolved with a third reviewer.
Quality assessmentThe quality of included studies was assessed using the JBI’s critical appraisal tools and the mixed-methods appraisal tool [47, 48]. Two reviewers independently completed the quality assessment. Any disagreements were resolved through discussion. The results of this quality assessment were not used to exclude studies from the review but rather to provide greater insight into the current body of literature on this topic.
Data analysisWe began by categorizing each health system guideline based on the six “building blocks” that WHO identifies as core components to strengthening health systems: (1) service delivery, (2) health workforce, (3) health informa-tion systems, (4) access to essential medicines, (5) financ-ing and (6) leadership or governance [49]. Health system guidelines were categorized into these building blocks based on their primary aim. Subsequently, directed con-tent analysis was used to map implementation strategies according to the list of 73 implementation strategies and definitions outlined in the Expert Recommendations for Implementing Change (ERIC) project [28]. The ERIC framework was developed through iterative consultations with experts and literature to derive a comprehensive list of known implementation strategies [28]. Analysis was completed by two reviewers independently, and disa-greements were resolved through consensus. Guided by the FRAME, thematic analysis was used to examine and group similarities in adaptation strategies and the who,
Page 5 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
what, where, why and when of any modification that took place. Lastly, the Capability, Opportunity and Motiva-tion Behaviour (COM-B) model guided the coding of the reported barriers to and enablers of implementation and adaptation [30, 50]. The COM-B model is a theoretically driven, evidence-based framework that outlines a sys-tematic process to identify and understand barriers and enablers with respect to implementation/adaptation of health initiatives [30, 50]. This model also links the iden-tified barriers and enablers to the required mechanisms needed to enact change [51]. Mapping the findings onto published taxonomies, such as the ERIC framework to classify implementation strategies, the FRAME to detail important considerations to adaptation techniques, and the COM-B model to map barriers and enablers, allows for the identification of possible gaps in current knowl-edge and opportunities for future research [52]. Further, results summaries were stratified per LMIC lending groups (low-, lower-middle and upper-middle-income)
and by using WHO’s six building blocks to assess for potential trends [49].
Descriptive summary tables of all included studies were created to outline extracted data specific to the health system guidelines, implementation strategies, adapta-tion strategies, outcomes/results, and article characteris-tics. Narrative summaries were included to address each research question.
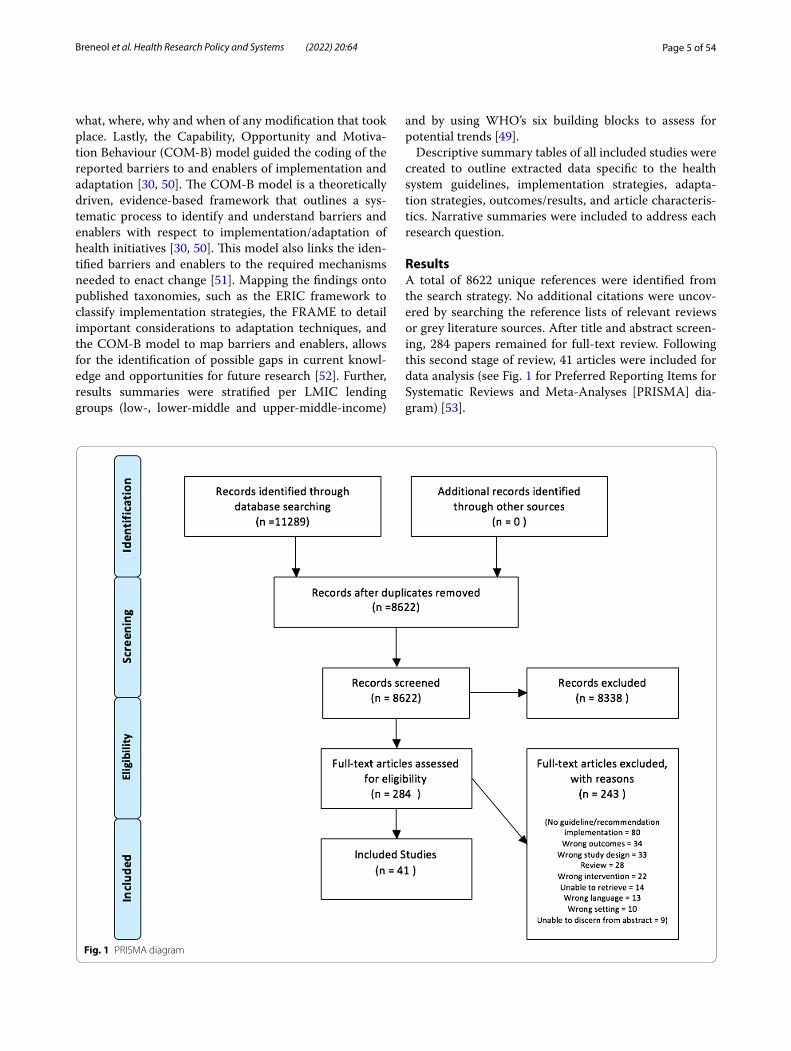
ResultsA total of 8622 unique references were identified from the search strategy. No additional citations were uncov-ered by searching the reference lists of relevant reviews or grey literature sources. After title and abstract screen-ing, 284 papers remained for full-text review. Following this second stage of review, 41 articles were included for data analysis (see Fig. 1 for Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA] dia-gram) [53].
Fig. 1 PRISMA diagram

Page 6 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Article summary characteristicsIdentified articles were published between 2005 and 2010 (n = 6), 2011–2015 (n = 10), and 2016 and beyond (n = 25) (see Fig. 2). Studies were most frequently con-ducted in upper-middle-income countries (n = 21), fol-lowed by lower-middle-income countries (n = 14) and LICs (n = 5) (see Fig. 3). One study reported on case study findings from low-, middle-, and upper-middle-income countries. Twenty-two studies used qualitative methods, 14 studies employed mixed methods, and five used cross-sectional methods to answer their research questions. Sources of funding varied among studies and often included multiple sources (see Fig. 4). Most studies reported funding from an HIC source (n = 21) (e.g. Irish Aid, and United Kingdom’s Wellcome Trust). Other studies reported funding from local country/context initiatives (n = 6) and high-income and local
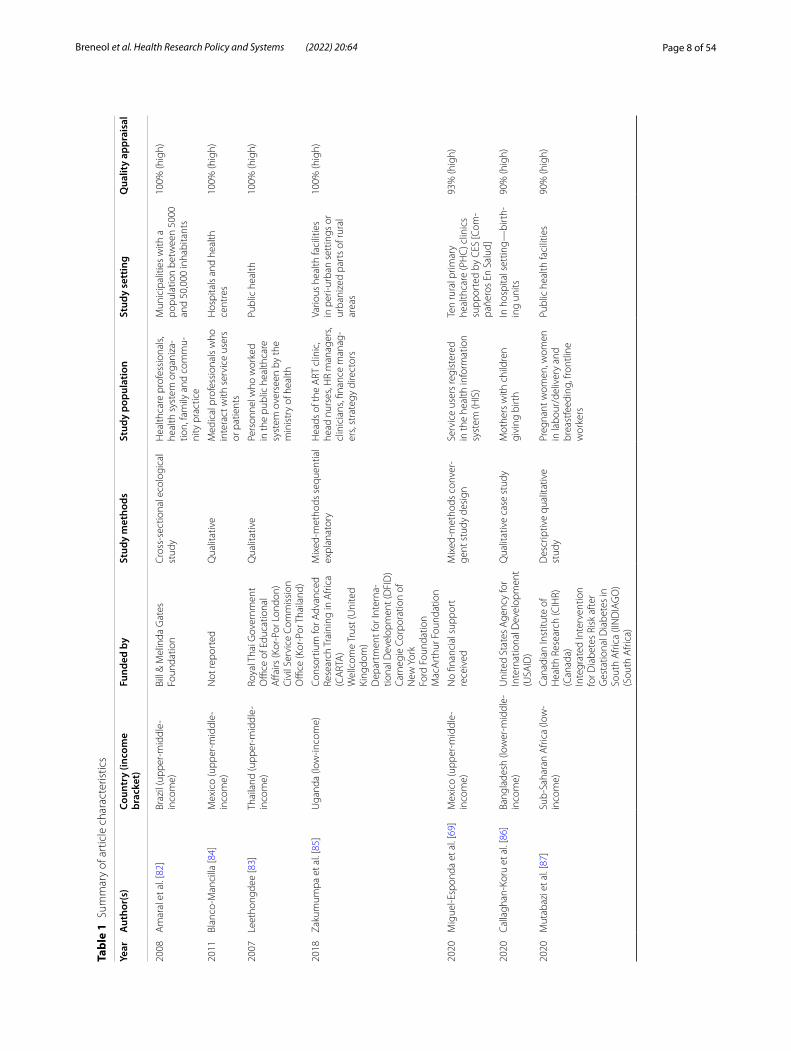
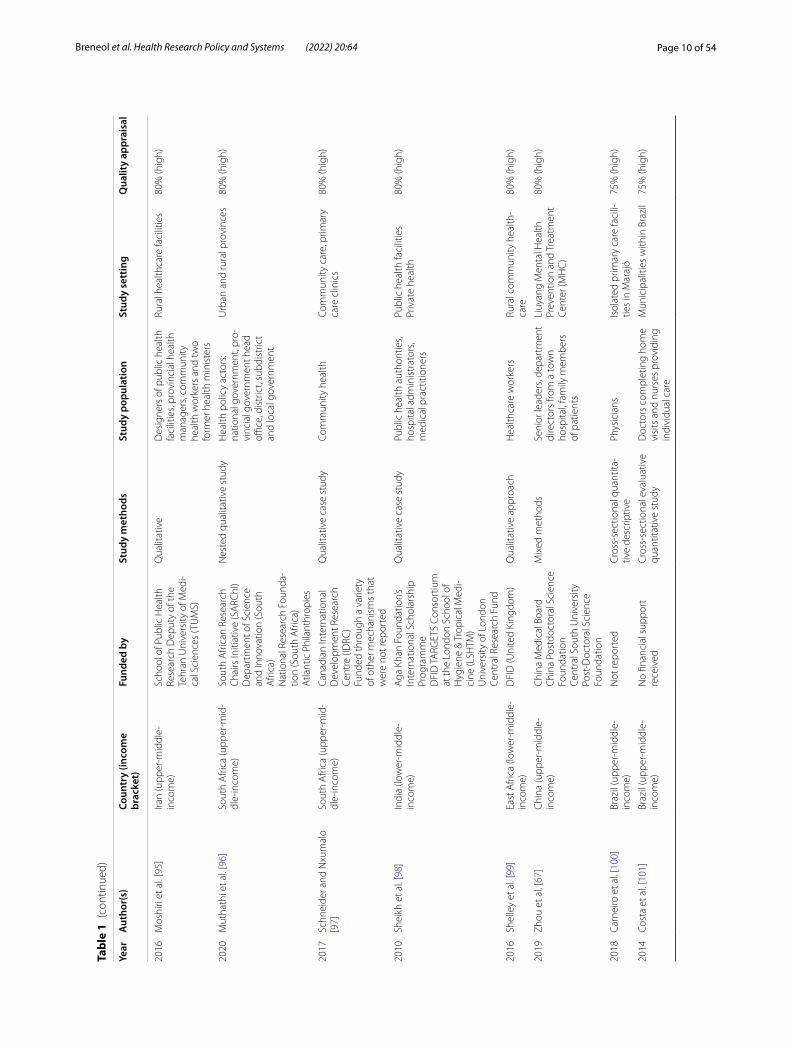
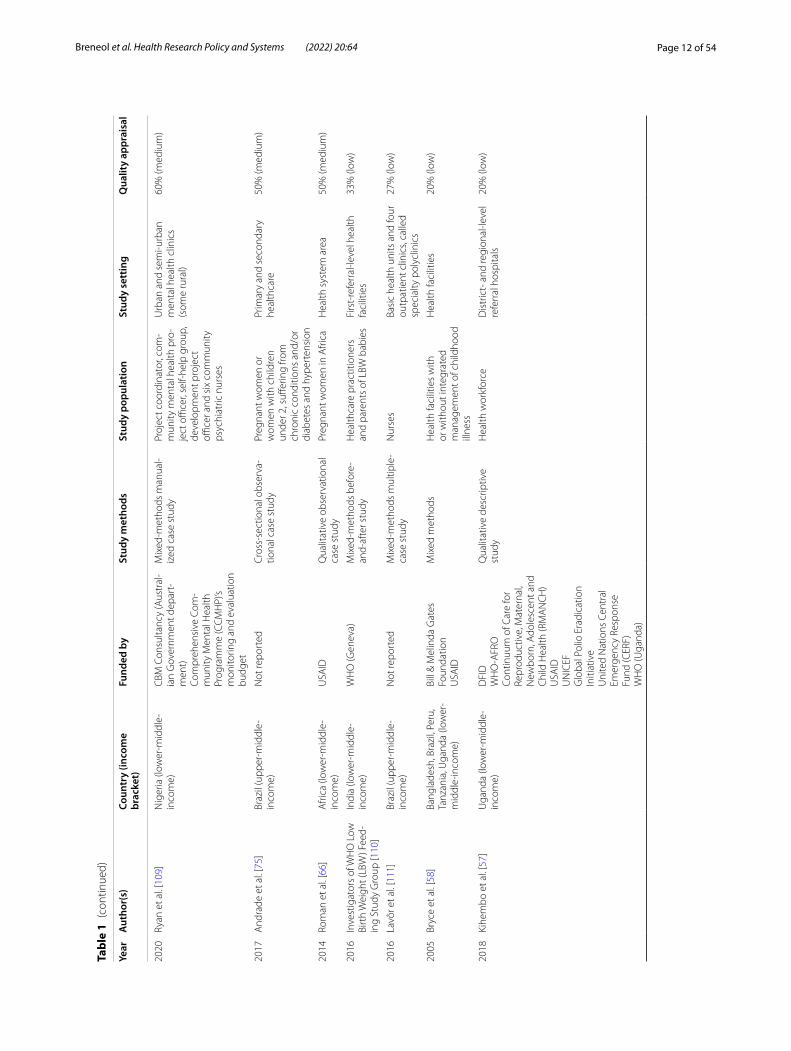
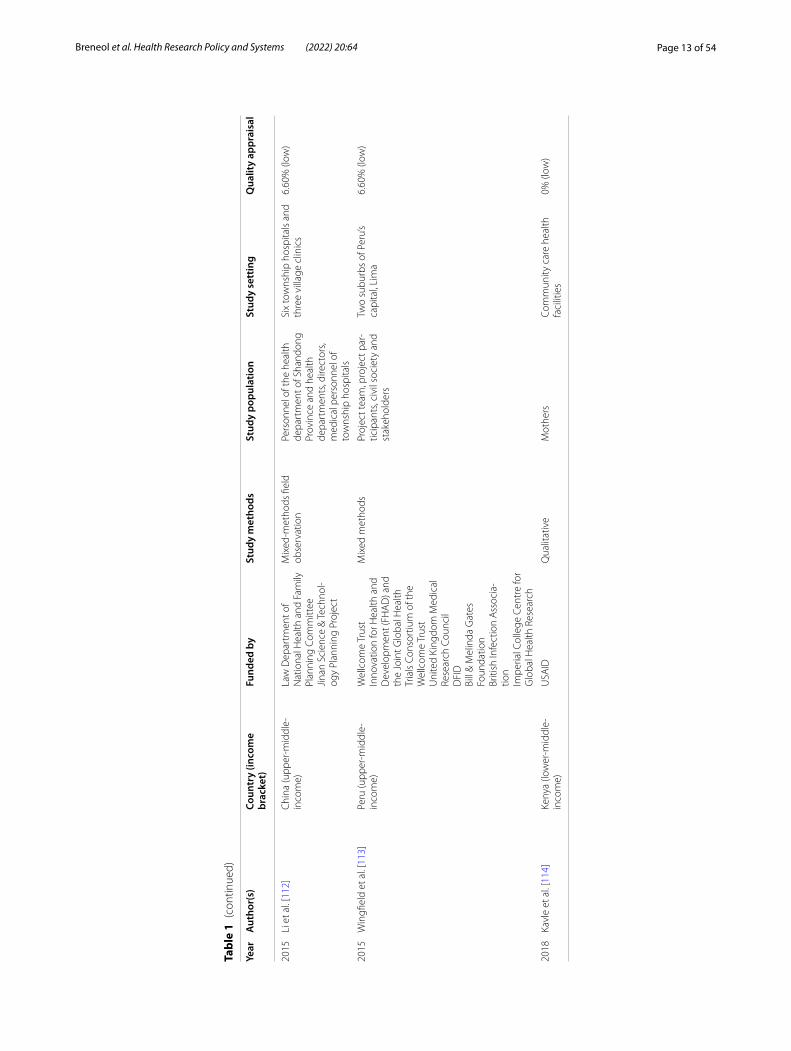
country partnerships (n = 5). The remaining reported that no funding was received (n = 2) or did not report information on funding (n = 7). Healthcare work-ers and end-users were the most commonly targeted study populations. Settings varied across urban and rural locations and community and hospital sites. Arti-cles reported implementing health system guidelines in urban hospitals (n = 7), both urban and rural com-munities (n = 7), only urban communities (n = 7), and both urban and rural hospitals (n = 5). Only one arti-cle reported on implementation of a guideline in both urban and rural clinics and hospitals. Please refer to Table 1 for a full summary of article characteristics. Any acronyms used in the tables can also be found in Additional file 3.
Fig. 2 Yearly publication trend
Fig. 3 Geographical clustering of health system initiatives

Page 7 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
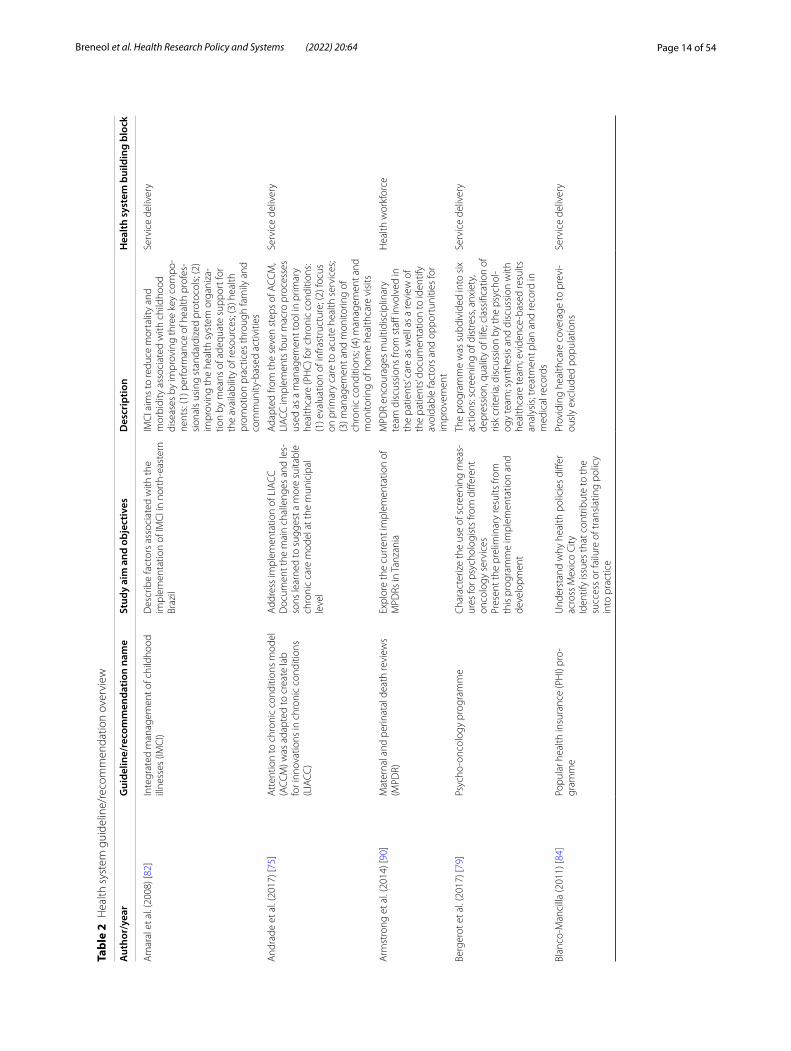
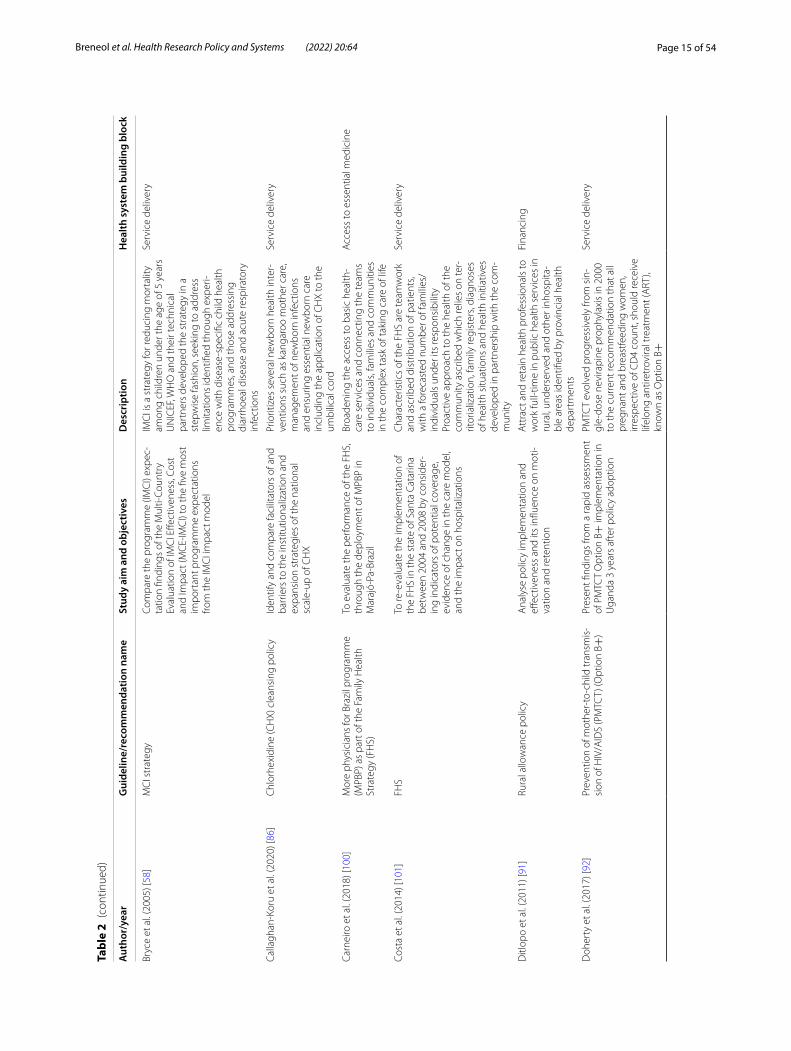
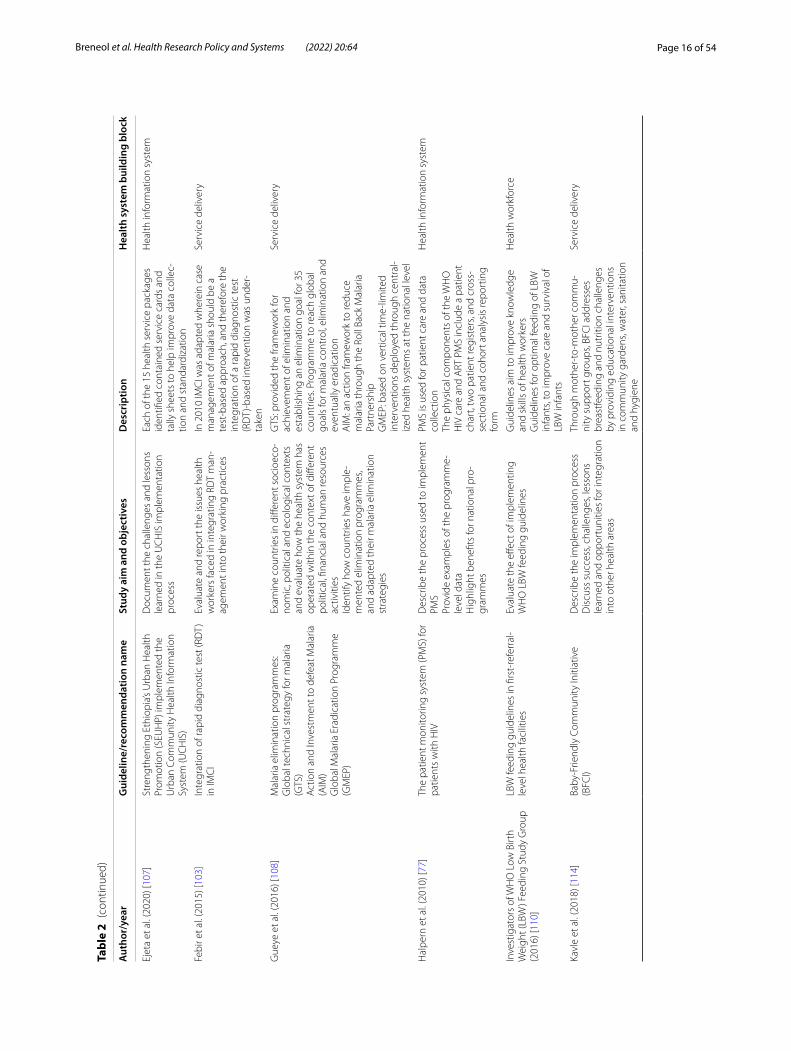
Health system guidelinesTable 2 summarizes the health system guidelines imple-mented in the included studies. While specific guidelines varied across studies, out of the total 41 studies, three reported on implementation of the Integrated Manage-ment of Childhood Illness (IMCI) guidelines and another three outlined the Prevention of Mother-to-Child Trans-mission of HIV/AIDS guidelines.
Service delivery was the health system building block most frequently targeted by the identified guidelines (n = 24). The remaining building blocks were targeted as follows, in descending order: health workforce (n = 5), financing (n = 4), access to essential medicine (n = 4), health information system (n = 2), and leadership and governance (n = 2).
Adaptation strategiesOnly 14 articles explicitly reported on the concept of adaptation. Rarely did articles specifically comment on the strategies used to determine what and why adapta-tions were necessary. Those that reported how adap-tations occurred often described any modifications as being suggested solutions to identified challenges dur-ing both pre- and post-implementation. Three articles also described a dedicated multidisciplinary working group aimed to gather feedback and identify required
modifications. Six articles reported adaptations to be reactive in nature and another six reported them to be proactively planned. Modifications made were frequently reported as adding, tailoring or tweaking content ele-ments, such as the addition of training sessions, expand-ing scope of practices and restructuring funding sources. None of the included articles reported using a guiding framework to help identify areas where adaptation could be beneficial and/or necessary. A full summary of the adaptation strategies and their related concepts accord-ing to the FRAME is given in Table 3.
Implementation strategiesEleven articles included in our review did not provide sufficient detail to adequately discern the strategies used to implement their health system guideline. 38 out of the 72 ERIC-defined implementation strategies were utilized across all 41 studies. A small number of reported imple-mentation strategies were determined by consensus to fall under two separate ERIC categories and were coded as such. Studies reported a range of one to eight strate-gies to implement their health system initiative, with an average of four distinct implementation strategies. Conducting ongoing training was identified as the most frequent implementation strategy (n = 11), followed by building a coalition (n = 8), use of advisory boards and workgroups (n = 6), conducting educational meetings
Fig. 4 Reported funding sources. *One article may have reported multiple funding sources
Page 8 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 1
Sum
mar
y of
art
icle
cha
ract
eris
tics
Year
Aut
hor(
s)Co
untr
y (in
com
e br
acke
t)Fu
nded
by
Stud
y m
etho
dsSt
udy
popu
latio
nSt
udy
sett
ing
Qua
lity
appr
aisa
l
2008
Am
aral
et a
l. [8
2]Br
azil
(upp
er‑m
iddl
e‑in
com
e)Bi
ll &
Mel
inda
Gat
es
Foun
datio
nC
ross
‑sec
tiona
l eco
logi
cal
stud
yH
ealth
care
pro
fess
iona
ls,
heal
th s
yste
m o
rgan
iza‑
tion,
fam
ily a
nd c
omm
u‑ni
ty p
ract
ice
Mun
icip
aliti
es w
ith a
po
pula
tion
betw
een
5000
an
d 50
,000
inha
bita
nts
100%
(hig
h)
2011
Blan
co‑M
anci
lla [8
4]M
exic
o (u
pper
‑mid
dle‑
inco
me)
Not
repo
rted
Qua
litat
ive
Med
ical
pro
fess
iona
ls w
ho
inte
ract
with
ser
vice
use
rs
or p
atie
nts
Hos
pita
ls a
nd h
ealth
ce
ntre
s10
0% (h
igh)
2007
Leet
hong
dee
[83]
Thai
land
(upp
er‑m
iddl
e‑in
com
e)Ro
yal T
hai G
over
nmen
tO
ffice
of E
duca
tiona
l A
ffairs
(Kor
‑Por
Lon
don)
Civ
il Se
rvic
e Co
mm
issi
on
Offi
ce (K
or‑P
or T
haila
nd)
Qua
litat
ive
Pers
onne
l who
wor
ked
in th
e pu
blic
hea
lthca
re
syst
em o
vers
een
by th
e m
inis
try
of h
ealth
Publ
ic h
ealth
100%
(hig
h)
2018
Zaku
mum
pa e
t al.
[85]
Uga
nda
(low
‑inco
me)
Cons
ortiu
m fo
r Adv
ance
d Re
sear
ch T
rain
ing
in A
frica
(C
ART
A)
Wel
lcom
e Tr
ust (
Uni
ted
King
dom
)D
epar
tmen
t for
Inte
rna‑
tiona
l Dev
elop
men
t (D
FID
)Ca
rneg
ie C
orpo
ratio
n of
N
ew Y
ork
Ford
Fou
ndat
ion
Mac
Art
hur F
ound
atio
n
Mix
ed‑m
etho
ds s
eque
ntia
l ex
plan
ator
yH
eads
of t
he A
RT c
linic
, he
ad n
urse
s, H
R m
anag
ers,
clin
icia
ns, fi
nanc
e m
anag
‑er
s, st
rate
gy d
irect
ors
Vario
us h
ealth
faci
litie
s in
per
i‑urb
an s
ettin
gs o
r ur
bani
zed
part
s of
rura
l ar
eas
100%
(hig
h)
2020
Mig
uel‑E
spon
da e
t al.
[69]
Mex
ico
(upp
er‑m
iddl
e‑in
com
e)N
o fin
anci
al s
uppo
rt
rece
ived
Mix
ed‑m
etho
ds c
onve
r‑ge
nt s
tudy
des
ign
Serv
ice
user
s re
gist
ered
in
the
heal
th in
form
atio
n sy
stem
(HIS
)
Ten
rura
l prim
ary
heal
thca
re (P
HC
) clin
ics
supp
orte
d by
CES
[Com
‑pa
ñero
s En
Sal
ud]
93%
(hig
h)
2020
Calla
ghan
‑Kor
u et
al.
[86]
Bang
lade
sh (l
ower
‑mid
dle‑
inco
me)
Uni
ted
Stat
es A
genc
y fo
r In
tern
atio
nal D
evel
opm
ent
(USA
ID)
Qua
litat
ive
case
stu
dyM
othe
rs w
ith c
hild
ren
givi
ng b
irth
In h
ospi
tal s
ettin
g—bi
rth‑
ing
units
90%
(hig
h)
2020
Mut
abaz
i et a
l. [8
7]Su
b‑Sa
hara
n A
frica
(low
‑in
com
e)Ca
nadi
an In
stitu
te o
f H
ealth
Res
earc
h (C
IHR)
(C
anad
a)In
tegr
ated
Inte
rven
tion
for D
iabe
tes
Risk
aft
er
Ges
tatio
nal D
iabe
tes
in
Sout
h A
frica
(IIN
DIA
GO
) (S
outh
Afri
ca)
Des
crip
tive
qual
itativ
e st
udy
Preg
nant
wom
en, w
omen
in
labo
ur/d
eliv
ery
and
brea
stfe
edin
g, fr
ontli
ne
wor
kers
Publ
ic h
ealth
faci
litie
s90
% (h
igh)

Page 9 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 1
(con
tinue
d)
Year
Aut
hor(
s)Co
untr
y (in
com
e br
acke
t)Fu
nded
by
Stud
y m
etho
dsSt
udy
popu
latio
nSt
udy
sett
ing
Qua
lity
appr
aisa
l
2018
Sadd
i et a
l. [8
8]Br
azil
(upp
er‑m
iddl
e‑in
com
e)G
radu
ate
Stud
ies
Coor
di‑
natio
n Bo
ard
(Coo
rdin
atio
n fo
r the
Impr
ovem
ent o
f H
ighe
r Edu
catio
n Pe
rson
‑ne
l [C
APE
S])
Braz
ilian
Min
istr
y of
Edu
ca‑
tion
Fede
ral U
nive
rsity
of G
oiás
(U
FG) O
ffice
of t
he D
ean
of
Exte
nsio
n an
d Re
sear
ch
Cont
inge
nt m
ixed
‑met
h‑od
s ap
proa
chFr
ontli
ne h
ealth
wor
kers
; m
anag
ers,
nurs
esH
ealth
care
uni
ts in
G
oiân
ia; p
rimar
y ca
re
sett
ing
86%
(hig
h)
2015
Xia
et a
l. [8
9]C
hina
(upp
er‑m
iddl
e‑in
com
e)Ce
ntre
for E
nviro
nmen
t an
d Po
pula
tion
Hea
lth
(Griff
th U
nive
rsity
)
Mix
ed m
etho
dsPr
egna
nt w
omen
ser
vice
us
ers
Mat
erna
l and
chi
ld h
ealth
‑ca
re h
ospi
tals
86%
(hig
h)
2014
Arm
stro
ng e
t al.
[90]
Tanz
ania
(low
er‑m
iddl
e‑in
com
e)Ev
iden
ce fo
r Act
ion
Tanz
ania
Qua
litat
ive
Hea
lthca
re p
rofe
ssio
nals
, he
alth
sys
tem
coo
rdin
a‑to
rs, d
istr
ict,
regi
on a
nd
zona
l hea
lth a
dmin
istr
ator
s
One
regi
onal
refe
rral
ho
spita
l, on
e go
vern
men
t di
stric
t hos
pita
l and
one
fa
ith‑b
ased
dis
tric
t hos
pita
l
80%
(hig
h)
2011
Ditl
opo
et a
l. [9
1]So
uth
Afri
ca (u
pper
‑mid
‑dl
e‑in
com
e)Iri
sh A
idQ
ualit
ativ
e ca
se s
tudy
de
sign
Polic
y‑m
aker
s, ho
spita
l m
anag
ers,
nurs
es a
nd
doct
ors
Pred
omin
antly
dis
tric
t rur
al
hosp
itals
80%
(hig
h)
2017
Doh
erty
et a
l. [9
2]U
gand
a (lo
w‑in
com
e)Sw
edis
h an
d N
orw
egia
n go
vern
men
t age
ncie
sSo
uth
Afri
can
Med
ical
Re
sear
ch C
ounc
il
Des
crip
tive
qual
itativ
eIm
plem
enta
tion
part
ners
, M
inis
try
of H
ealth
, mul
tilat
‑er
al a
genc
ies
(UN
ICEF
and
W
HO
), di
stric
t man
age‑
men
t, co
mm
unity
‑ and
fa
cilit
y‑ba
sed
heal
th
wor
kers
All
four
regi
ons
of th
e co
untr
y80
% (h
igh)
2019
Love
ro e
t al.
[93]
Sout
h A
frica
(upp
er‑m
id‑
dle‑
inco
me)
Nat
iona
l Ins
titut
e of
Men
tal
Hea
lth (N
IMH
) Wai
nber
g/A
rbuc
kle
Trai
ning
Gra
ntU
nite
d St
ates
Pre
side
nt’s
Emer
genc
y Pl
an fo
r AID
S Re
lief (
PEPF
AR)
Mix
ed‑m
etho
ds e
xplo
ra‑
tory
des
ign
Dis
tric
t‑le
vel p
rogr
amm
e m
anag
ers
(DPM
s)U
rban
and
rura
l prim
ary
care
clin
ics
thro
ugho
ut
dist
rict
80%
(hig
h)
2014
Mko
ka e
t al.
[94]
Tanz
ania
(low
er‑m
iddl
e‑in
com
e)Sw
edis
h In
tern
atio
nal
Dev
elop
men
t Coo
pera
tion
Age
ncy
(Sid
a)
Qua
litat
ive
appr
oach
Dis
tric
t med
ical
offi
cer
(DM
O),
dist
rict n
ursi
ng
office
r (D
NO
), di
stric
t he
alth
offi
cer (
DH
O),
dis‑
tric
t hea
lth s
ecre
tary
(DH
S),
and
dist
rict p
harm
acis
t (D
P)
A ty
pica
l rur
al d
istr
ict
80%
(hig
h)
Page 10 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 1
(con
tinue
d)
Year
Aut
hor(
s)Co
untr
y (in
com
e br
acke
t)Fu
nded
by
Stud
y m
etho
dsSt
udy
popu
latio
nSt
udy
sett
ing
Qua
lity
appr
aisa
l
2016
Mos
hiri
et a
l. [9
5]Ira
n (u
pper
‑mid
dle‑
inco
me)
Scho
ol o
f Pub
lic H
ealth
Re
sear
ch D
eput
y of
the
Tehr
an U
nive
rsity
of M
edi‑
cal S
cien
ces
(TU
MS)
Qua
litat
ive
Des
igne
rs o
f pub
lic h
ealth
fa
cilit
ies,
prov
inci
al h
ealth
m
anag
ers,
com
mun
ity
heal
th w
orke
rs a
nd tw
o fo
rmer
hea
lth m
inis
ters
Rura
l hea
lthca
re fa
cilit
ies
80%
(hig
h)
2020
Mut
hath
i et a
l. [9
6]So
uth
Afri
ca (u
pper
‑mid
‑dl
e‑in
com
e)So
uth
Afri
can
Rese
arch
C
hairs
Initi
ativ
e (S
ARC
hI)
Dep
artm
ent o
f Sci
ence
an
d In
nova
tion
(Sou
th
Afri
ca)
Nat
iona
l Res
earc
h Fo
unda
‑tio
n (S
outh
Afri
ca)
Atla
ntic
Phi
lant
hrop
ies
Nes
ted
qual
itativ
e st
udy
Hea
lth p
olic
y ac
tors
: na
tiona
l gov
ernm
ent,
pro‑
vinc
ial g
over
nmen
t hea
d offi
ce, d
istr
ict,
subd
istr
ict
and
loca
l gov
ernm
ent
Urb
an a
nd ru
ral p
rovi
nces
80%
(hig
h)
2017
Schn
eide
r and
Nxu
mal
o [9
7]So
uth
Afri
ca (u
pper
‑mid
‑dl
e‑in
com
e)Ca
nadi
an In
tern
atio
nal
Dev
elop
men
t Res
earc
h Ce
ntre
(ID
RC)
Fund
ed th
roug
h a
varie
ty
of o
ther
mec
hani
sms
that
w
ere
not r
epor
ted
Qua
litat
ive
case
stu
dyCo
mm
unity
hea
lthCo
mm
unity
car
e, p
rimar
y ca
re c
linic
s80
% (h
igh)
2010
Shei
kh e
t al.
[98]
Indi
a (lo
wer
‑mid
dle‑
inco
me)
Aga
Kha
n Fo
unda
tion’
s In
tern
atio
nal S
chol
arsh
ip
Prog
ram
me
DFI
D TA
RGET
S Co
nsor
tium
at
the
Lond
on S
choo
l of
Hyg
iene
& T
ropi
cal M
edi‑
cine
(LSH
TM)
Uni
vers
ity o
f Lon
don
Cent
ral R
esea
rch
Fund
Qua
litat
ive
case
stu
dyPu
blic
hea
lth a
utho
ritie
s, ho
spita
l adm
inis
trat
ors,
med
ical
pra
ctiti
oner
s
Publ
ic h
ealth
faci
litie
sPr
ivat
e he
alth
80%
(hig
h)
2016
Shel
ley
et a
l. [9
9]Ea
st A
frica
(low
er‑m
iddl
e‑in
com
e)D
FID
(Uni
ted
King
dom
)Q
ualit
ativ
e ap
proa
chH
ealth
care
wor
kers
Rura
l com
mun
ity h
ealth
‑ca
re80
% (h
igh)
2019
Zhou
et a
l. [6
7]C
hina
(upp
er‑m
iddl
e‑in
com
e)C
hina
Med
ical
Boa
rdC
hina
Pos
tdoc
tora
l Sci
ence
Fo
unda
tion
Cent
ral S
outh
Uni
vers
ity
Post
‑Doc
tora
l Sci
ence
Fo
unda
tion
Mix
ed m
etho
dsSe
nior
lead
ers,
depa
rtm
ent
dire
ctor
s fro
m a
tow
n ho
spita
l, fa
mily
mem
bers
of
pat
ient
s
Liuy
ang
Men
tal H
ealth
Pr
even
tion
and
Trea
tmen
t Ce
nter
(MH
C)
80%
(hig
h)
2018
Carn
eiro
et a
l. [1
00]
Braz
il (u
pper
‑mid
dle‑
inco
me)
Not
repo
rted
Cro
ss‑s
ectio
nal q
uant
ita‑
tive
desc
riptiv
ePh
ysic
ians
Isol
ated
prim
ary
care
faci
li‑tie
s in
Mar
ajó
75%
(hig
h)
2014
Cost
a et
al.
[101
]Br
azil
(upp
er‑m
iddl
e‑in
com
e)N
o fin
anci
al s
uppo
rt
rece
ived
Cro
ss‑s
ectio
nal e
valu
ativ
e qu
antit
ativ
e st
udy
Doc
tors
com
plet
ing
hom
e vi
sits
and
nur
ses
prov
idin
g in
divi
dual
car
e
Mun
icip
aliti
es w
ithin
Bra
zil
75%
(hig
h)

Page 11 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 1
(con
tinue
d)
Year
Aut
hor(
s)Co
untr
y (in
com
e br
acke
t)Fu
nded
by
Stud
y m
etho
dsSt
udy
popu
latio
nSt
udy
sett
ing
Qua
lity
appr
aisa
l
2018
Sam
i et a
l. [1
02]
Sout
h Su
dan,
Afri
ca (l
ow‑
inco
me)
Save
the
Chi
ldre
n’s
Savi
ng
New
born
Liv
es p
ro‑
gram
me
ELM
A R
elie
f Fou
ndat
ion
Mix
ed‑m
etho
ds c
ase
stud
yN
ewbo
rns
and
mot
hers
Com
mun
ity/f
acili
ty‑b
ased
se
ttin
gs in
clud
ing
PHC
ce
ntre
, com
mun
ity h
ealth
pr
ogra
mm
e ce
ntre
s, ho
spi‑
tal a
nd c
amps
73%
(hig
h)
2015
Febi
r eta
al.
[103
]G
hana
(low
er‑m
iddl
e‑in
com
e)Bi
ll &
Mel
inda
Gat
es
Foun
datio
nA
CT
[art
emis
inin
‑bas
ed
com
bina
tion
trea
tmen
t]
Cons
ortiu
m
Qua
litat
ive
stud
yH
ealth
care
wor
kers
Dis
tric
t hos
pita
l, he
alth
ce
ntre
s an
d co
mm
unity
‑ba
sed
heal
th s
ervi
ces
70%
(hig
h)
2017
Pyon
e et
al.
[104
]Ke
nya
(low
er‑m
iddl
e‑in
com
e)D
FID
UKA
idQ
ualit
ativ
e m
etho
ds10
nat
iona
l‑lev
el p
olic
y‑m
aker
s, 10
cou
nty
heal
th
offici
als
and
19 h
ealth
care
pr
ovid
ers
10 d
istr
ict‑
and
cou
nty‑
leve
l hos
pita
ls a
nd o
ther
he
alth
faci
litie
s in
sel
ecte
d co
untie
s
70%
(hig
h)
2020
Rahm
an e
t al.
[105
]Ba
ngla
desh
(low
er‑m
iddl
e‑in
com
e)G
laxo
Smith
Klin
e (G
SK)
thro
ugh
PATH
(Sea
ttle
, U
SA)
Qua
litat
ive
desc
riptiv
eKe
y st
akeh
olde
rs, h
ealth
se
rvic
e pr
ovid
ers
and
care
give
rs
At b
oth
the
natio
nal a
nd
dist
rict l
evel
s of
Khu
lna
and
Laks
hmip
ur, s
pe‑
cific
ally
in tw
o su
bdis
tric
t pu
blic
hea
lthca
re fa
cilit
ies
70%
(hig
h)
2008
Stei
n et
al.
[106
]So
uth
Afri
ca (u
pper
‑mid
‑dl
e‑in
com
e)ID
RC (C
anad
a)Q
ualit
ativ
e m
etho
dsPH
C n
urse
sU
rban
and
rura
l PH
C
sett
ings
70%
(hig
h)
2017
Berg
erot
et a
l. [7
9]Br
azil
(upp
er‑m
iddl
e‑in
com
e)N
ot re
port
edM
ixed
met
hods
Psyc
holo
gist
s an
d on
col‑
ogy
staff
; pat
ient
s ag
ed
18 o
r old
er, w
ith c
ance
r tr
eatm
ent p
lan
Hos
pita
ls a
nd c
ance
r cen
‑tr
es fr
om d
iffer
ent B
razi
lian
citie
s
66.6
6% (m
ediu
m)
2010
Hal
pern
et a
l. [7
7]G
uyan
a (u
pper
‑mid
dle‑
inco
me)
Not
repo
rted
Cro
ss‑s
ectio
nal
Doc
tors
, nur
ses
and
data
en
try
cler
ks fr
om e
ach
care
an
d tr
eatm
ent s
ite
Clin
ics
acro
ss th
e na
tion
62.5
0% (m
ediu
m)
2020
Ejet
a et
al.
[107
]Et
hiop
ia (l
ow‑in
com
e)N
ot re
port
edQ
ualit
ativ
e de
scrip
tive
Thre
e ho
spita
ls in
Eth
iopi
aFa
mili
es w
ithin
The
heal
th fa
cilit
y si
tes
loca
ted
in A
ddis
Aba
ba,
Bish
oftu
and
Haw
assa
60%
(med
ium
)
2016
Smith
Gue
ye e
t al.
[108
]Bh
utan
, Mau
ritiu
s, N
amib
ia,
Phili
ppin
es, S
ri La
nka,
Tu
rkey
and
Tur
kmen
ista
n (lo
w‑,
mid
dle‑
and
upp
er‑
mid
dle‑
inco
me)
Bill
& M
elin
da G
ates
Fo
unda
tion
Mal
aria
Elim
inat
ion
Initi
a‑tiv
e of
the
Glo
bal H
ealth
G
roup
(USA
)
Qua
litat
ive
case
stu
dy
revi
ewH
ealth
care
and
pro
‑gr
amm
e st
affM
ostly
in d
ecen
tral
ized
he
alth
sys
tem
s60
% (m
ediu
m)
Page 12 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 1
(con
tinue
d)
Year
Aut
hor(
s)Co
untr
y (in
com
e br
acke
t)Fu
nded
by
Stud
y m
etho
dsSt
udy
popu
latio
nSt
udy
sett
ing
Qua
lity
appr
aisa
l
2020
Ryan
et a
l. [1
09]
Nig
eria
(low
er‑m
iddl
e‑in
com
e)C
BM C
onsu
ltanc
y (A
ustr
al‑
ian
Gov
ernm
ent d
epar
t‑m
ent)
Com
preh
ensi
ve C
om‑
mun
ity M
enta
l Hea
lth
Prog
ram
me
(CC
MH
P)’s
mon
itorin
g an
d ev
alua
tion
budg
et
Mix
ed‑m
etho
ds m
anua
l‑iz
ed c
ase
stud
yPr
ojec
t coo
rdin
ator
, com
‑m
unity
men
tal h
ealth
pro
‑je
ct o
ffice
r, se
lf‑he
lp g
roup
, de
velo
pmen
t pro
ject
offi
cer a
nd s
ix c
omm
unity
ps
ychi
atric
nur
ses
Urb
an a
nd s
emi‑u
rban
m
enta
l hea
lth c
linic
s (s
ome
rura
l)
60%
(med
ium
)
2017
And
rade
et a
l. [7
5]Br
azil
(upp
er‑m
iddl
e‑in
com
e)N
ot re
port
edC
ross
‑sec
tiona
l obs
erva
‑tio
nal c
ase
stud
yPr
egna
nt w
omen
or
wom
en w
ith c
hild
ren
unde
r 2, s
uffer
ing
from
ch
roni
c co
nditi
ons
and/
or
diab
etes
and
hyp
erte
nsio
n
Prim
ary
and
seco
ndar
y he
alth
care
50%
(med
ium
)
2014
Rom
an e
t al.
[66]
Afri
ca (l
ower
‑mid
dle‑
inco
me)
USA
IDQ
ualit
ativ
e ob
serv
atio
nal
case
stu
dyPr
egna
nt w
omen
in A
frica
Hea
lth s
yste
m a
rea
50%
(med
ium
)
2016
Inve
stig
ator
s of
WH
O L
ow
Birt
h W
eigh
t (LB
W) F
eed‑
ing
Stud
y G
roup
[110
]
Indi
a (lo
wer
‑mid
dle‑
inco
me)
WH
O (G
enev
a)M
ixed
‑met
hods
bef
ore‑
and‑
afte
r stu
dyH
ealth
care
pra
ctiti
oner
s an
d pa
rent
s of
LBW
bab
ies
Firs
t‑re
ferr
al‑le
vel h
ealth
fa
cilit
ies
33%
(low
)
2016
Lavô
r et a
l. [1
11]
Braz
il (u
pper
‑mid
dle‑
inco
me)
Not
repo
rted
Mix
ed‑m
etho
ds m
ultip
le‑
case
stu
dyN
urse
sBa
sic
heal
th u
nits
and
four
ou
tpat
ient
clin
ics,
calle
d sp
ecia
lty p
olyc
linic
s
27%
(low
)
2005
Bryc
e et
al.
[58]
Bang
lade
sh, B
razi
l, Pe
ru,
Tanz
ania
, Uga
nda
(low
er‑
mid
dle‑
inco
me)
Bill
& M
elin
da G
ates
Fo
unda
tion
USA
ID
Mix
ed m
etho
dsH
ealth
faci
litie
s w
ith
or w
ithou
t int
egra
ted
man
agem
ent o
f chi
ldho
od
illne
ss
Hea
lth fa
cilit
ies
20%
(low
)
2018
Kihe
mbo
et a
l. [5
7]U
gand
a (lo
wer
‑mid
dle‑
inco
me)
DFI
DW
HO
‑AFR
OCo
ntin
uum
of C
are
for
Repr
oduc
tive,
Mat
erna
l, N
ewbo
rn, A
dole
scen
t and
C
hild
Hea
lth (R
MA
NC
H)
USA
IDU
NIC
EFG
loba
l Pol
io E
radi
catio
n In
itiat
ive
Uni
ted
Nat
ions
Cen
tral
Em
erge
ncy
Resp
onse
Fu
nd (C
ERF)
WH
O (U
gand
a)
Qua
litat
ive
desc
riptiv
e st
udy
Hea
lth w
orkf
orce
Dis
tric
t‑ a
nd re
gion
al‑le
vel
refe
rral
hos
pita
ls20
% (l
ow)
Page 13 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 1
(con
tinue
d)
Year
Aut
hor(
s)Co
untr
y (in
com
e br
acke
t)Fu
nded
by
Stud
y m
etho
dsSt
udy
popu
latio
nSt
udy
sett
ing
Qua
lity
appr
aisa
l
2015
Li e
t al.
[112
]C
hina
(upp
er‑m
iddl
e‑in
com
e)La
w D
epar
tmen
t of
Nat
iona
l Hea
lth a
nd F
amily
Pl
anni
ng C
omm
ittee
Jinan
Sci
ence
& T
echn
ol‑
ogy
Plan
ning
Pro
ject
Mix
ed‑m
etho
ds fi
eld
obse
rvat
ion
Pers
onne
l of t
he h
ealth
de
part
men
t of S
hand
ong
Prov
ince
and
hea
lth
depa
rtm
ents
, dire
ctor
s, m
edic
al p
erso
nnel
of
tow
nshi
p ho
spita
ls
Six
tow
nshi
p ho
spita
ls a
nd
thre
e vi
llage
clin
ics
6.60
% (l
ow)
2015
Win
gfiel
d et
al.
[113
]Pe
ru (u
pper
‑mid
dle‑
inco
me)
Wel
lcom
e Tr
ust
Inno
vatio
n fo
r Hea
lth a
nd
Dev
elop
men
t (FH
AD
) and
th
e Jo
int G
loba
l Hea
lth
Tria
ls C
onso
rtiu
m o
f the
W
ellc
ome
Trus
tU
nite
d Ki
ngdo
m M
edic
al
Rese
arch
Cou
ncil
DFI
DBi
ll &
Mel
inda
Gat
es
Foun
datio
nBr
itish
Infe
ctio
n A
ssoc
ia‑
tion
Impe
rial C
olle
ge C
entr
e fo
r G
loba
l Hea
lth R
esea
rch
Mix
ed m
etho
dsPr
ojec
t tea
m, p
roje
ct p
ar‑
ticip
ants
, civ
il so
ciet
y an
d st
akeh
olde
rs
Two
subu
rbs
of P
eru’
s ca
pita
l, Li
ma
6.60
% (l
ow)
2018
Kavl
e et
al.
[114
]Ke
nya
(low
er‑m
iddl
e‑in
com
e)U
SAID
Qua
litat
ive
Mot
hers
Com
mun
ity c
are
heal
th
faci
litie
s0%
(low
)
Page 14 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 2
Hea
lth s
yste
m g
uide
line/
reco
mm
enda
tion
over
view
Aut
hor/
year
Gui
delin
e/re
com
men
datio
n na
me
Stud
y ai
m a
nd o
bjec
tives
Des
crip
tion
Hea
lth s
yste
m b
uild
ing
bloc
k
Am
aral
et a
l. (2
008)
[82]
Inte
grat
ed m
anag
emen
t of c
hild
hood
ill
ness
es (I
MC
I)D
escr
ibe
fact
ors
asso
ciat
ed w
ith th
e im
plem
enta
tion
of IM
CI i
n no
rth‑
east
ern
Braz
il
IMC
I aim
s to
redu
ce m
orta
lity
and
mor
bidi
ty a
ssoc
iate
d w
ith c
hild
hood
di
seas
es b
y im
prov
ing
thre
e ke
y co
mpo
‑ne
nts:
(1) p
erfo
rman
ce o
f hea
lth p
rofe
s‑si
onal
s us
ing
stan
dard
ized
pro
toco
ls; (
2)
impr
ovin
g th
e he
alth
sys
tem
org
aniz
a‑tio
n by
mea
ns o
f ade
quat
e su
ppor
t for
th
e av
aila
bilit
y of
reso
urce
s; (3
) hea
lth
prom
otio
n pr
actic
es th
roug
h fa
mily
and
co
mm
unity
‑bas
ed a
ctiv
ities
Serv
ice
deliv
ery
And
rade
et a
l. (2
017)
[75]
Att
entio
n to
chr
onic
con
ditio
ns m
odel
(A
CCM
) was
ada
pted
to c
reat
e la
b fo
r inn
ovat
ions
in c
hron
ic c
ondi
tions
(L
IACC
)
Add
ress
impl
emen
tatio
n of
LIA
CC
Doc
umen
t the
mai
n ch
alle
nges
and
les‑
sons
lear
ned
to s
ugge
st a
mor
e su
itabl
e ch
roni
c ca
re m
odel
at t
he m
unic
ipal
le
vel
Ada
pted
from
the
seve
n st
eps
of A
CCM
, LI
ACC
impl
emen
ts fo
ur m
acro
pro
cess
es
used
as
a m
anag
emen
t too
l in
prim
ary
heal
thca
re (P
HC
) for
chr
onic
con
ditio
ns:
(1) e
valu
atio
n of
infra
stru
ctur
e; (2
) foc
us
on p
rimar
y ca
re to
acu
te h
ealth
ser
vice
s; (3
) man
agem
ent a
nd m
onito
ring
of
chro
nic
cond
ition
s; (4
) man
agem
ent a
nd
mon
itorin
g of
hom
e he
alth
care
vis
its
Serv
ice
deliv
ery
Arm
stro
ng e
t al.
(201
4) [9
0]M
ater
nal a
nd p
erin
atal
dea
th re
view
s (M
PDR)
Expl
ore
the
curr
ent i
mpl
emen
tatio
n of
M
PDRs
in T
anza
nia
MPD
R en
cour
ages
mul
tidis
cipl
inar
y te
am d
iscu
ssio
ns fr
om s
taff
invo
lved
in
the
patie
nts’
care
as
wel
l as
a re
view
of
the
patie
nts’
docu
men
tatio
n to
iden
tify
avoi
dabl
e fa
ctor
s an
d op
port
uniti
es fo
r im
prov
emen
t
Hea
lth w
orkf
orce
Berg
erot
et a
l. (2
017)
[79]
Psyc
ho‑o
ncol
ogy
prog
ram
me
Cha
ract
eriz
e th
e us
e of
scr
eeni
ng m
eas‑
ures
for p
sych
olog
ists
from
diff
eren
t on
colo
gy s
ervi
ces
Pres
ent t
he p
relim
inar
y re
sults
from
th
is p
rogr
amm
e im
plem
enta
tion
and
deve
lopm
ent
The
prog
ram
me
was
sub
divi
ded
into
six
ac
tions
: scr
eeni
ng o
f dis
tres
s, an
xiet
y,
depr
essi
on, q
ualit
y of
life
; cla
ssifi
catio
n of
ris
k cr
iteria
; dis
cuss
ion
by th
e ps
ycho
l‑og
y te
am; s
ynth
esis
and
dis
cuss
ion
with
he
alth
care
team
; evi
denc
e‑ba
sed
resu
lts
anal
ysis
; tre
atm
ent p
lan
and
reco
rd in
m
edic
al re
cord
s
Serv
ice
deliv
ery
Blan
co‑M
anci
lla (2
011)
[84]
Popu
lar h
ealth
insu
ranc
e (P
HI)
pro‑
gram
me
Und
erst
and
why
hea
lth p
olic
ies
diffe
r ac
ross
Mex
ico
City
Iden
tify
issu
es th
at c
ontr
ibut
e to
the
succ
ess
or fa
ilure
of t
rans
latin
g po
licy
into
pra
ctic
e
Prov
idin
g he
alth
care
cov
erag
e to
pre
vi‑
ousl
y ex
clud
ed p
opul
atio
nsSe
rvic
e de
liver
y
Page 15 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 2
(con
tinue
d)
Aut
hor/
year
Gui
delin
e/re
com
men
datio
n na
me
Stud
y ai
m a
nd o
bjec
tives
Des
crip
tion
Hea
lth s
yste
m b
uild
ing
bloc
k
Bryc
e et
al.
(200
5) [5
8]M
CI s
trat
egy
Com
pare
the
prog
ram
me
(IMC
I) ex
pec‑
tatio
n fin
ding
s of
the
Mul
ti‑Co
untr
y Ev
alua
tion
of IM
CI E
ffect
iven
ess,
Cost
an
d Im
pact
(MC
E‑IM
CI)
to th
e fiv
e m
ost
impo
rtan
t pro
gram
me
expe
ctat
ions
fro
m th
e IM
CI i
mpa
ct m
odel
IMC
I is
a st
rate
gy fo
r red
ucin
g m
orta
lity
amon
g ch
ildre
n un
der t
he a
ge o
f 5 y
ears
UN
ICEF
, WH
O a
nd th
eir t
echn
ical
pa
rtne
rs d
evel
oped
the
stra
tegy
in a
st
epw
ise
fash
ion,
see
king
to a
ddre
ss
limita
tions
iden
tified
thro
ugh
expe
ri‑en
ce w
ith d
isea
se‑s
peci
fic c
hild
hea
lth
prog
ram
mes
, and
thos
e ad
dres
sing
di
arrh
oeal
dis
ease
and
acu
te re
spira
tory
in
fect
ions
Serv
ice
deliv
ery
Calla
ghan
‑Kor
u et
al.
(202
0) [8
6]C
hlor
hexi
dine
(CH
X) c
lean
sing
pol
icy
Iden
tify
and
com
pare
faci
litat
ors
of a
nd
barr
iers
to th
e in
stitu
tiona
lizat
ion
and
expa
nsio
n st
rate
gies
of t
he n
atio
nal
scal
e‑up
of C
HX
Prio
ritiz
es s
ever
al n
ewbo
rn h
ealth
inte
r‑ve
ntio
ns s
uch
as k
anga
roo
mot
her c
are,
m
anag
emen
t of n
ewbo
rn in
fect
ions
an
d en
surin
g es
sent
ial n
ewbo
rn c
are
incl
udin
g th
e ap
plic
atio
n of
CH
X to
the
umbi
lical
cor
d
Serv
ice
deliv
ery
Carn
eiro
et a
l. (2
018)
[100
]M
ore
phys
icia
ns fo
r Bra
zil p
rogr
amm
e (M
PBP)
as
part
of t
he F
amily
Hea
lth
Stra
tegy
(FH
S)
To e
valu
ate
the
perf
orm
ance
of t
he F
HS,
th
roug
h th
e de
ploy
men
t of M
PBP
in
Mar
ajó‑
Pa‑B
razi
l
Broa
deni
ng th
e ac
cess
to b
asic
hea
lth‑
care
ser
vice
s an
d co
nnec
ting
the
team
s to
indi
vidu
als,
fam
ilies
and
com
mun
ities
in
the
com
plex
task
of t
akin
g ca
re o
f life
Acc
ess
to e
ssen
tial m
edic
ine
Cost
a et
al.
(201
4) [1
01]
FHS
To re
‑eva
luat
e th
e im
plem
enta
tion
of
the
FHS
in th
e st
ate
of S
anta
Cat
arin
a be
twee
n 20
04 a
nd 2
008
by c
onsi
der‑
ing
indi
cato
rs o
f pot
entia
l cov
erag
e,
evid
ence
of c
hang
e in
the
care
mod
el,
and
the
impa
ct o
n ho
spita
lizat
ions
Cha
ract
eris
tics
of th
e FH
S ar
e te
amw
ork
and
ascr
ibed
dis
trib
utio
n of
pat
ient
s, w
ith a
fore
cast
ed n
umbe
r of f
amili
es/
indi
vidu
als
unde
r its
resp
onsi
bilit
yPr
oact
ive
appr
oach
to th
e he
alth
of t
he
com
mun
ity a
scrib
ed w
hich
relie
s on
ter‑
ritor
ializ
atio
n, fa
mily
regi
ster
s, di
agno
ses
of h
ealth
situ
atio
ns a
nd h
ealth
initi
ativ
es
deve
lope
d in
par
tner
ship
with
the
com
‑m
unity
Serv
ice
deliv
ery
Ditl
opo
et a
l. (2
011)
[91]
Rura
l allo
wan
ce p
olic
yA
naly
se p
olic
y im
plem
enta
tion
and
effec
tiven
ess
and
its in
fluen
ce o
n m
oti‑
vatio
n an
d re
tent
ion
Att
ract
and
reta
in h
ealth
pro
fess
iona
ls to
w
ork
full‑
time
in p
ublic
hea
lth s
ervi
ces
in
rura
l, un
ders
erve
d an
d ot
her i
nhos
pita
‑bl
e ar
eas
iden
tified
by
prov
inci
al h
ealth
de
part
men
ts
Fina
ncin
g
Doh
erty
et a
l. (2
017)
[92]
Prev
entio
n of
mot
her‑
to‑c
hild
tran
smis
‑si
on o
f HIV
/AID
S (P
MTC
T) (O
ptio
n B+
)Pr
esen
t find
ings
from
a ra
pid
asse
ssm
ent
of P
MTC
T O
ptio
n B+
impl
emen
tatio
n in
U
gand
a 3
year
s af
ter p
olic
y ad
optio
n
PMTC
T ev
olve
d pr
ogre
ssiv
ely
from
sin
‑gl
e‑do
se n
evira
pine
pro
phyl
axis
in 2
000
to th
e cu
rren
t rec
omm
enda
tion
that
all
preg
nant
and
bre
astfe
edin
g w
omen
, irr
espe
ctiv
e of
CD
4 co
unt,
shou
ld re
ceiv
e lif
elon
g an
tiret
rovi
ral t
reat
men
t (A
RT),
know
n as
Opt
ion
B+
Serv
ice
deliv
ery
Page 16 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 2
(con
tinue
d)
Aut
hor/
year
Gui
delin
e/re
com
men
datio
n na
me
Stud
y ai
m a
nd o
bjec
tives
Des
crip
tion
Hea
lth s
yste
m b
uild
ing
bloc
k
Ejet
a et
al.
(202
0) [1
07]
Stre
ngth
enin
g Et
hiop
ia’s
Urb
an H
ealth
Pr
omot
ion
(SEU
HP)
impl
emen
ted
the
Urb
an C
omm
unity
Hea
lth In
form
atio
n Sy
stem
(UC
HIS
)
Doc
umen
t the
cha
lleng
es a
nd le
sson
s le
arne
d in
the
UC
HIS
impl
emen
tatio
n pr
oces
s
Each
of t
he 1
5 he
alth
ser
vice
pac
kage
s id
entifi
ed c
onta
ined
ser
vice
car
ds a
nd
tally
she
ets
to h
elp
impr
ove
data
col
lec‑
tion
and
stan
dard
izat
ion
Hea
lth in
form
atio
n sy
stem
Febi
r et a
l. (2
015)
[103
]In
tegr
atio
n of
rapi
d di
agno
stic
test
(RD
T)
in IM
CI
Eval
uate
and
repo
rt th
e is
sues
hea
lth
wor
kers
face
d in
inte
grat
ing
RDT
man
‑ag
emen
t int
o th
eir w
orki
ng p
ract
ices
In 2
010
IMC
I was
ada
pted
whe
rein
cas
e m
anag
emen
t of m
alar
ia s
houl
d be
a
test
‑bas
ed a
ppro
ach,
and
ther
efor
e th
e in
tegr
atio
n of
a ra
pid
diag
nost
ic te
st
(RD
T)‑b
ased
inte
rven
tion
was
und
er‑
take
n
Serv
ice
deliv
ery
Gue
ye e
t al.
(201
6) [1
08]
Mal
aria
elim
inat
ion
prog
ram
mes
:G
loba
l tec
hnic
al s
trat
egy
for m
alar
ia
(GTS
)A
ctio
n an
d In
vest
men
t to
defe
at M
alar
ia
(AIM
)G
loba
l Mal
aria
Era
dica
tion
Prog
ram
me
(GM
EP)
Exam
ine
coun
trie
s in
diff
eren
t soc
ioec
o‑no
mic
, pol
itica
l and
eco
logi
cal c
onte
xts
and
eval
uate
how
the
heal
th s
yste
m h
as
oper
ated
with
in th
e co
ntex
t of d
iffer
ent
polit
ical
, fina
ncia
l and
hum
an re
sour
ces
activ
ities
Iden
tify
how
cou
ntrie
s ha
ve im
ple‑
men
ted
elim
inat
ion
prog
ram
mes
, an
d ad
apte
d th
eir m
alar
ia e
limin
atio
n st
rate
gies
GTS
: pro
vide
d th
e fra
mew
ork
for
achi
evem
ent o
f elim
inat
ion
and
esta
blis
hing
an
elim
inat
ion
goal
for 3
5 co
untr
ies.
Prog
ram
me
to re
ach
glob
al
goal
s fo
r mal
aria
con
trol
, elim
inat
ion
and
even
tual
ly e
radi
catio
nA
IM: a
n ac
tion
fram
ewor
k to
redu
ce
mal
aria
thro
ugh
the
Roll
Back
Mal
aria
Pa
rtne
rshi
pG
MEP
: bas
ed o
n ve
rtic
al ti
me‑
limite
d in
terv
entio
ns d
eplo
yed
thro
ugh
cent
ral‑
ized
hea
lth s
yste
ms
at th
e na
tiona
l lev
el
Serv
ice
deliv
ery
Hal
pern
et a
l. (2
010)
[77]
The
patie
nt m
onito
ring
syst
em (P
MS)
for
patie
nts
with
HIV
Des
crib
e th
e pr
oces
s us
ed to
impl
emen
t PM
SPr
ovid
e ex
ampl
es o
f the
pro
gram
me‑
leve
l dat
aH
ighl
ight
ben
efits
for n
atio
nal p
ro‑
gram
mes
PMS
is u
sed
for p
atie
nt c
are
and
data
co
llect
ion
The
phys
ical
com
pone
nts
of th
e W
HO
H
IV c
are
and
ART
PM
S in
clud
e a
patie
nt
char
t, tw
o pa
tient
regi
ster
s, an
d cr
oss‑
sect
iona
l and
coh
ort a
naly
sis
repo
rtin
g fo
rm
Hea
lth in
form
atio
n sy
stem
Inve
stig
ator
s of
WH
O L
ow B
irth
Wei
ght (
LBW
) Fee
ding
Stu
dy G
roup
(2
016)
[110
]
LBW
feed
ing
guid
elin
es in
firs
t‑re
ferr
al‑
leve
l hea
lth fa
cilit
ies
Eval
uate
the
effec
t of i
mpl
emen
ting
WH
O L
BW fe
edin
g gu
idel
ines
Gui
delin
es a
im to
impr
ove
know
ledg
e an
d sk
ills
of h
ealth
wor
kers
Gui
delin
es fo
r opt
imal
feed
ing
of L
BW
infa
nts,
to im
prov
e ca
re a
nd s
urvi
val o
f LB
W in
fant
s
Hea
lth w
orkf
orce
Kavl
e et
al.
(201
8) [1
14]
Baby
‑Frie
ndly
Com
mun
ity In
itiat
ive
(BFC
I)D
escr
ibe
the
impl
emen
tatio
n pr
oces
sD
iscu
ss s
ucce
ss, c
halle
nges
, les
sons
le
arne
d an
d op
port
uniti
es fo
r int
egra
tion
into
oth
er h
ealth
are
as
Thro
ugh
mot
her‑
to‑m
othe
r com
mu‑
nity
sup
port
gro
ups,
BFC
I add
ress
es
brea
stfe
edin
g an
d nu
triti
on c
halle
nges
by
pro
vidi
ng e
duca
tiona
l int
erve
ntio
ns
in c
omm
unity
gar
dens
, wat
er, s
anita
tion
and
hygi
ene
Serv
ice
deliv
ery
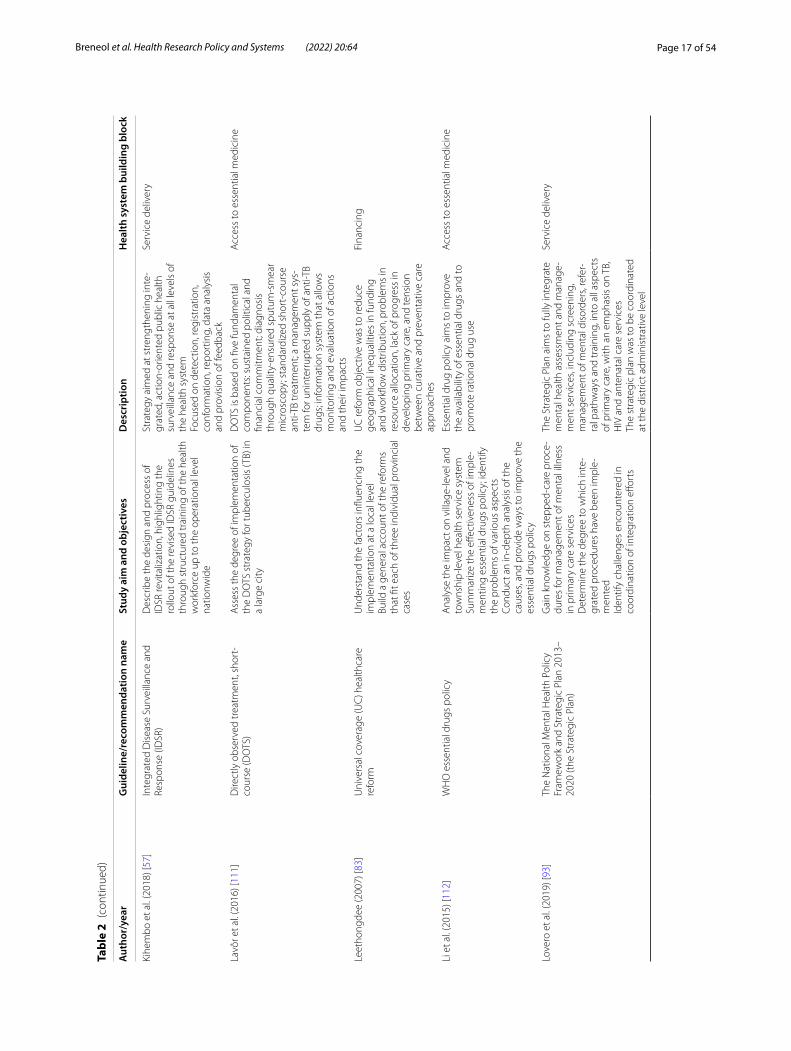
Page 17 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 2
(con
tinue
d)
Aut
hor/
year
Gui
delin
e/re
com
men
datio
n na
me
Stud
y ai
m a
nd o
bjec
tives
Des
crip
tion
Hea
lth s
yste
m b
uild
ing
bloc
k
Kihe
mbo
et a
l. (2
018)
[57]
Inte
grat
ed D
isea
se S
urve
illan
ce a
nd
Resp
onse
(ID
SR)
Des
crib
e th
e de
sign
and
pro
cess
of
IDSR
revi
taliz
atio
n, h
ighl
ight
ing
the
rollo
ut o
f the
revi
sed
IDSR
gui
delin
es
thro
ugh
stru
ctur
ed tr
aini
ng o
f the
hea
lth
wor
kfor
ce u
p to
the
oper
atio
nal l
evel
na
tionw
ide
Stra
tegy
aim
ed a
t str
engt
heni
ng in
te‑
grat
ed, a
ctio
n‑or
ient
ed p
ublic
hea
lth
surv
eilla
nce
and
resp
onse
at a
ll le
vels
of
the
heal
th s
yste
mFo
cuse
d on
det
ectio
n, re
gist
ratio
n,
conf
orm
atio
n, re
port
ing,
dat
a an
alys
is
and
prov
isio
n of
feed
back
Serv
ice
deliv
ery
Lavô
r et a
l. (2
016)
[111
]D
irect
ly o
bser
ved
trea
tmen
t, sh
ort‑
cour
se (D
OTS
)A
sses
s th
e de
gree
of i
mpl
emen
tatio
n of
th
e D
OTS
str
ateg
y fo
r tub
ercu
losi
s (T
B) in
a
larg
e ci
ty
DO
TS is
bas
ed o
n fiv
e fu
ndam
enta
l co
mpo
nent
s: su
stai
ned
polit
ical
and
fin
anci
al c
omm
itmen
t; di
agno
sis
thro
ugh
qual
ity‑e
nsur
ed s
putu
m‑s
mea
r m
icro
scop
y; s
tand
ardi
zed
shor
t‑co
urse
an
ti‑TB
trea
tmen
t; a
man
agem
ent s
ys‑
tem
for u
nint
erru
pted
sup
ply
of a
nti‑T
B dr
ugs;
info
rmat
ion
syst
em th
at a
llow
s m
onito
ring
and
eval
uatio
n of
act
ions
an
d th
eir i
mpa
cts
Acc
ess
to e
ssen
tial m
edic
ine
Leet
hong
dee
(200
7) [8
3]U
nive
rsal
cov
erag
e (U
C) h
ealth
care
re
form
Und
erst
and
the
fact
ors
influ
enci
ng th
e im
plem
enta
tion
at a
loca
l lev
elBu
ild a
gen
eral
acc
ount
of t
he re
form
s th
at fi
t eac
h of
thre
e in
divi
dual
pro
vinc
ial
case
s
UC
refo
rm o
bjec
tive
was
to re
duce
ge
ogra
phic
al in
equa
litie
s in
fund
ing
and
wor
kflow
dis
trib
utio
n, p
robl
ems
in
reso
urce
allo
catio
n, la
ck o
f pro
gres
s in
de
velo
ping
prim
ary
care
, and
tens
ion
betw
een
cura
tive
and
prev
enta
tive
care
ap
proa
ches
Fina
ncin
g
Li e
t al.
(201
5) [1
12]
WH
O e
ssen
tial d
rugs
pol
icy
Ana
lyse
the
impa
ct o
n vi
llage
‑leve
l and
to
wns
hip‑
leve
l hea
lth s
ervi
ce s
yste
mSu
mm
ariz
e th
e eff
ectiv
enes
s of
impl
e‑m
entin
g es
sent
ial d
rugs
pol
icy;
iden
tify
the
prob
lem
s of
var
ious
asp
ects
Cond
uct a
n in
‑dep
th a
naly
sis
of th
e ca
uses
, and
pro
vide
way
s to
impr
ove
the
esse
ntia
l dru
gs p
olic
y
Esse
ntia
l dru
g po
licy
aim
s to
impr
ove
the
avai
labi
lity
of e
ssen
tial d
rugs
and
to
prom
ote
ratio
nal d
rug
use
Acc
ess
to e
ssen
tial m
edic
ine
Love
ro e
t al.
(201
9) [9
3]Th
e N
atio
nal M
enta
l Hea
lth P
olic
y Fr
amew
ork
and
Stra
tegi
c Pl
an 2
013–
2020
(the
Str
ateg
ic P
lan)
Gai
n kn
owle
dge
on s
tepp
ed‑c
are
proc
e‑du
res
for m
anag
emen
t of m
enta
l illn
ess
in p
rimar
y ca
re s
ervi
ces
Det
erm
ine
the
degr
ee to
whi
ch in
te‑
grat
ed p
roce
dure
s ha
ve b
een
impl
e‑m
ente
dId
entif
y ch
alle
nges
enc
ount
ered
in
coor
dina
tion
of in
tegr
atio
n eff
orts
The
Stra
tegi
c Pl
an a
ims
to fu
lly in
tegr
ate
men
tal h
ealth
ass
essm
ent a
nd m
anag
e‑m
ent s
ervi
ces,
incl
udin
g sc
reen
ing,
m
anag
emen
t of m
enta
l dis
orde
rs, r
efer
‑ra
l pat
hway
s an
d tr
aini
ng, i
nto
all a
spec
ts
of p
rimar
y ca
re, w
ith a
n em
phas
is o
n TB
, H
IV a
nd a
nten
atal
car
e se
rvic
esTh
e st
rate
gic
plan
was
to b
e co
ordi
nate
d at
the
dist
rict a
dmin
istr
ativ
e le
vel
Serv
ice
deliv
ery
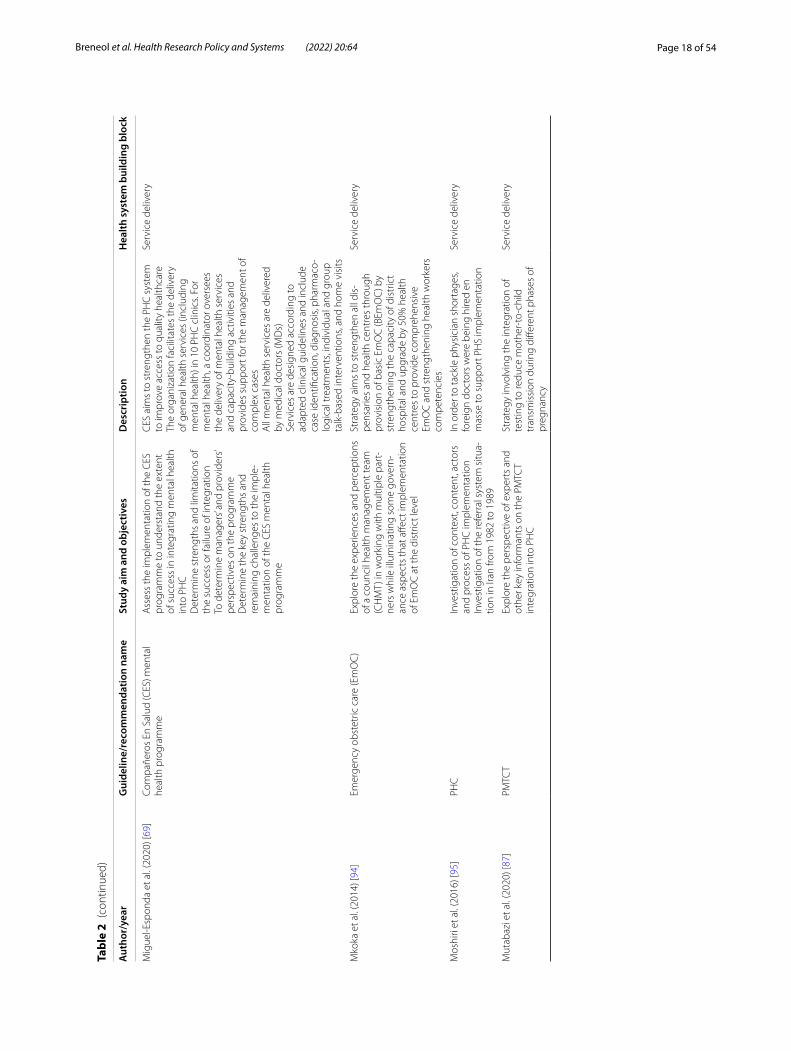
Page 18 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 2
(con
tinue
d)
Aut
hor/
year
Gui
delin
e/re
com
men
datio
n na
me
Stud
y ai
m a
nd o
bjec
tives
Des
crip
tion
Hea
lth s
yste
m b
uild
ing
bloc
k
Mig
uel‑E
spon
da e
t al.
(202
0) [6
9]Co
mpa
ñero
s En
Sal
ud (C
ES) m
enta
l he
alth
pro
gram
me
Ass
ess
the
impl
emen
tatio
n of
the
CES
pr
ogra
mm
e to
und
erst
and
the
exte
nt
of s
ucce
ss in
inte
grat
ing
men
tal h
ealth
in
to P
HC
Det
erm
ine
stre
ngth
s an
d lim
itatio
ns o
f th
e su
cces
s or
failu
re o
f int
egra
tion
To d
eter
min
e m
anag
ers’
and
prov
ider
s’ pe
rspe
ctiv
es o
n th
e pr
ogra
mm
eD
eter
min
e th
e ke
y st
reng
ths
and
rem
aini
ng c
halle
nges
to th
e im
ple‑
men
tatio
n of
the
CES
men
tal h
ealth
pr
ogra
mm
e
CES
aim
s to
str
engt
hen
the
PHC
sys
tem
to
impr
ove
acce
ss to
qua
lity
heal
thca
reTh
e or
gani
zatio
n fa
cilit
ates
the
deliv
ery
of g
ener
al h
ealth
ser
vice
s (in
clud
ing
men
tal h
ealth
) in
10 P
HC
clin
ics.
For
men
tal h
ealth
, a c
oord
inat
or o
vers
ees
the
deliv
ery
of m
enta
l hea
lth s
ervi
ces
and
capa
city
‑bui
ldin
g ac
tiviti
es a
nd
prov
ides
sup
port
for t
he m
anag
emen
t of
com
plex
cas
esA
ll m
enta
l hea
lth s
ervi
ces
are
deliv
ered
by
med
ical
doc
tors
(MD
s)Se
rvic
es a
re d
esig
ned
acco
rdin
g to
ad
apte
d cl
inic
al g
uide
lines
and
incl
ude
case
iden
tifica
tion,
dia
gnos
is, p
harm
aco‑
logi
cal t
reat
men
ts, i
ndiv
idua
l and
gro
up
talk
‑bas
ed in
terv
entio
ns, a
nd h
ome
visi
ts
Serv
ice
deliv
ery
Mko
ka e
t al.
(201
4) [9
4]Em
erge
ncy
obst
etric
car
e (E
mO
C)
Expl
ore
the
expe
rienc
es a
nd p
erce
ptio
ns
of a
cou
ncil
heal
th m
anag
emen
t tea
m
(CH
MT)
in w
orki
ng w
ith m
ultip
le p
art‑
ners
whi
le il
lum
inat
ing
som
e go
vern
‑an
ce a
spec
ts th
at a
ffect
impl
emen
tatio
n of
Em
OC
at t
he d
istr
ict l
evel
Stra
tegy
aim
s to
str
engt
hen
all d
is‑
pens
arie
s an
d he
alth
cen
tres
thro
ugh
prov
isio
n of
bas
ic E
mO
C (B
EmO
C) b
y st
reng
then
ing
the
capa
city
of d
istr
ict
hosp
ital a
nd u
pgra
de b
y 50
% h
ealth
ce
ntre
s to
pro
vide
com
preh
ensi
ve
EmO
C a
nd s
tren
gthe
ning
hea
lth w
orke
rs
com
pete
ncie
s
Serv
ice
deliv
ery
Mos
hiri
et a
l. (2
016)
[95]
PHC
Inve
stig
atio
n of
con
text
, con
tent
, act
ors
and
proc
ess
of P
HC
impl
emen
tatio
nIn
vest
igat
ion
of th
e re
ferr
al s
yste
m s
itua‑
tion
in Ir
an fr
om 1
982
to 1
989
In o
rder
to ta
ckle
phy
sici
an s
hort
ages
, fo
reig
n do
ctor
s w
ere
bein
g hi
red
en
mas
se to
sup
port
PH
S im
plem
enta
tion
Serv
ice
deliv
ery
Mut
abaz
i et a
l. (2
020)
[87]
PMTC
T Ex
plor
e th
e pe
rspe
ctiv
e of
exp
erts
and
ot
her k
ey in
form
ants
on
the
PMTC
T in
tegr
atio
n in
to P
HC
Stra
tegy
invo
lvin
g th
e in
tegr
atio
n of
te
stin
g to
redu
ce m
othe
r‑to
‑chi
ld
tran
smis
sion
dur
ing
diffe
rent
pha
ses
of
preg
nanc
y
Serv
ice
deliv
ery

Page 19 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 2
(con
tinue
d)
Aut
hor/
year
Gui
delin
e/re
com
men
datio
n na
me
Stud
y ai
m a
nd o
bjec
tives
Des
crip
tion
Hea
lth s
yste
m b
uild
ing
bloc
k
Mut
hath
i et a
l. (2
020)
[96]
Idea
l clin
ic re
aliz
atio
n an
d m
aint
enan
ce
(ICRM
) pro
gram
me
Gen
erat
e kn
owle
dge
on th
e po
licy
impl
emen
tatio
nEx
amin
e th
e in
fluen
ce o
f mot
ivat
ion,
co
gniti
on a
nd p
erce
ived
pow
er o
f the
po
licy
acto
rs a
nd h
ow it
influ
ence
d IC
RM
impl
emen
tatio
nEx
plor
e po
licy
cohe
renc
e in
the
ICRM
pr
ogra
mm
eEx
plor
e th
e pe
rcep
tions
of s
take
hold
‑er
s at
the
natio
nal,
prov
inci
al a
nd lo
cal
gove
rnm
ent l
evel
s
The
goal
of t
he IC
RM p
rogr
amm
e is
to
prep
are
all P
HC
faci
litie
s to
mee
t the
qu
ality
sta
ndar
ds s
et b
y th
e O
ffice
of
Hea
lth S
tand
ards
Com
plia
nce
(OH
SC)
An
idea
l clin
ic is
defi
ned
as a
clin
ic
with
goo
d in
frast
ruct
ure,
ade
quat
e st
aff, a
dequ
ate
med
icin
es a
nd s
uppl
ies,
and
good
adm
inis
trat
ive
proc
esse
s, w
ith s
uffici
ent b
ulk
supp
lies;
it us
es
appl
icab
le c
linic
al p
olic
ies,
prot
ocol
s an
d gu
idel
ines
, and
it h
arne
sses
par
tner
and
st
akeh
olde
r sup
port
Hea
lth w
orkf
orce
Pyon
e et
al.
(201
7) [1
04]
Free
mat
erni
ty s
ervi
ces
(FM
S) p
olic
yU
nder
stan
d ho
w th
e po
licy
chan
ged
heal
th s
yste
m g
over
nanc
e in
Ken
ya a
nd
use
the
insi
ghts
to in
form
pol
icy
impl
e‑m
enta
tion
in K
enya
and
in o
ther
LM
ICs
FMS
was
par
t of a
nat
iona
l str
ateg
y to
re
duce
mat
erna
l and
neo
nata
l mor
tal‑
ity, a
llevi
ate
pove
rty
and
achi
eve
the
Mill
enni
um D
evel
opm
ent G
oal t
arge
ts;
abol
ish
user
fees
for a
ll he
alth
ser
vice
s an
d di
spen
sarie
s, an
d pr
ovid
e FM
S in
all
leve
ls o
f car
e of
the
gove
rnm
ent h
ealth
se
ctor
Fina
ncin
g
Rahm
an e
t al.
(202
0) [1
05]
Mat
erna
l, ne
onat
al, c
hild
and
ado
lesc
ent
heal
th (M
NC
&AH
) and
com
mun
ity‑b
ased
he
alth
care
(CBH
C),
repr
oduc
tive
and
adol
esce
nt h
ealth
(MC
R&A
H)
Und
erst
and
key
driv
ers
for i
mpl
emen
ta‑
tion
of W
HO
reco
mm
enda
tions
for t
he
case
man
agem
ent o
f chi
ldho
od p
neu‑
mon
ia a
nd p
ossi
ble
serio
us b
acte
rial
infe
ctio
n (P
SBI)
with
am
oxic
illin
dis
pers
‑ib
le ta
blet
s (D
T)G
ener
ate
evid
ence
to s
tren
gthe
n ne
wbo
rn a
nd c
hild
hea
lth p
rogr
amm
es
in B
angl
ades
h
The
Min
istr
y of
Hea
lth a
nd F
amily
W
elfa
re (M
OH
FW) i
n Ba
ngla
desh
pro
‑vi
des
heal
thca
re s
ervi
ces
for c
hild
hood
pn
eum
onia
and
PSB
I in
the
PHC
set
ting
thro
ugh
both
the
dire
ctor
ate
of h
ealth
se
rvic
es a
nd d
irect
orat
e of
fam
ily p
lan‑
ning
, und
er th
ree
oper
atio
nal p
lans
Inco
rpor
ate
child
‑frie
ndly
am
oxic
illin
DT
for t
he c
ase
man
agem
ent o
f chi
ldho
od
pneu
mon
ia a
nd P
SBI w
hen
refe
rral
for
oral
am
oxic
illin
is n
ot fe
asib
le
Serv
ice
deliv
ery
Rom
an e
t al.
(201
4) [6
6]M
alar
ia in
pre
gnan
cy (M
IP)
Ass
ess
how
thre
e co
untr
ies
in A
frica
w
ere
able
to a
chie
ve g
reat
er p
rogr
ess
in
MIP
con
trol
Iden
tify
the
prac
tices
and
str
ateg
ies
that
sup
port
ed th
e su
cces
s of
the
MIP
pr
ogra
mm
eId
entif
y bo
ttle
neck
s in
MIP
pro
gram
me
impl
emen
tatio
n pr
oces
ses
Shar
e le
sson
s le
arne
d
The
MIP
fram
ewor
k ai
ms
to p
reve
nt
and
cont
rol m
alar
ia d
urin
g pr
egna
ncy
by fo
cusi
ng o
n th
ree
met
hods
that
st
abili
ze tr
ansm
issi
on: (
1) in
term
itten
t pr
even
tativ
e tr
eatm
ent w
ith s
ulfa
doxi
ne/
pyrim
etha
min
e (S
P) a
ntim
alar
ial d
rug;
(2)
use
of p
hysi
cal i
nsec
ticid
e ne
ts; (
3) e
ffec‑
tive
case
man
agem
ent b
ased
on
sign
s an
d sy
mpt
oms
Serv
ice
deliv
ery
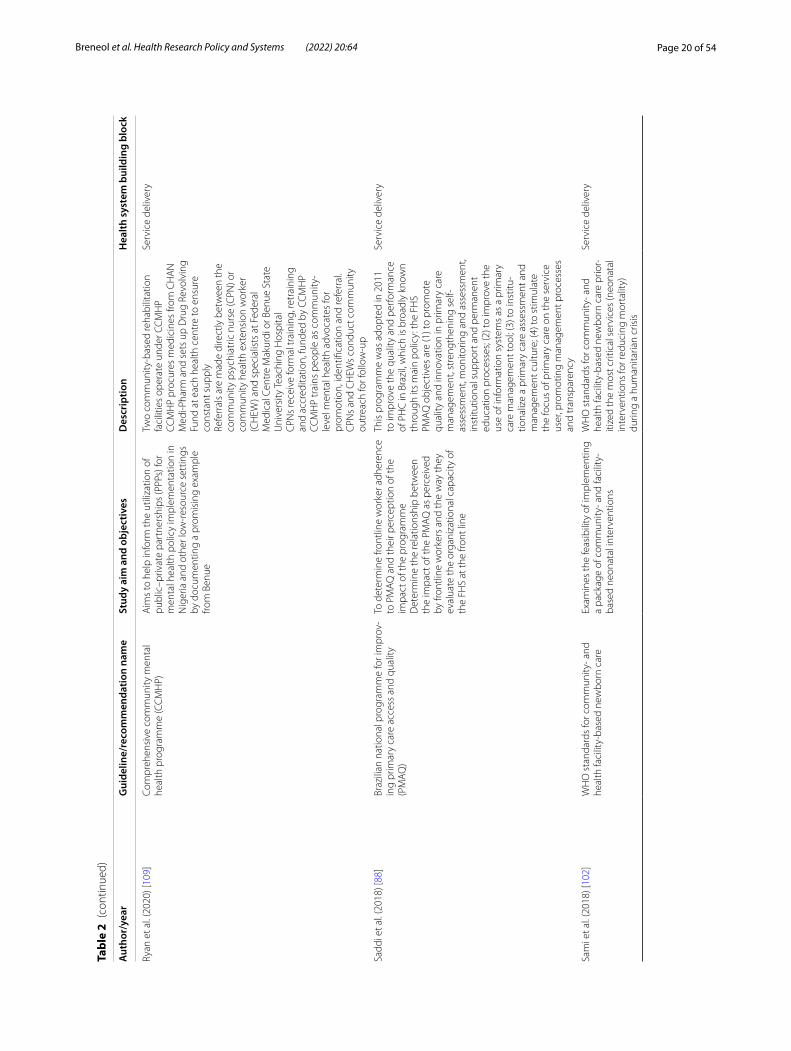
Page 20 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 2
(con
tinue
d)
Aut
hor/
year
Gui
delin
e/re
com
men
datio
n na
me
Stud
y ai
m a
nd o
bjec
tives
Des
crip
tion
Hea
lth s
yste
m b
uild
ing
bloc
k
Ryan
et a
l. (2
020)
[109
]Co
mpr
ehen
sive
com
mun
ity m
enta
l he
alth
pro
gram
me
(CC
MH
P)A
ims
to h
elp
info
rm th
e ut
iliza
tion
of
publ
ic–p
rivat
e pa
rtne
rshi
ps (P
PPs)
for
men
tal h
ealth
pol
icy
impl
emen
tatio
n in
N
iger
ia a
nd o
ther
low
‑res
ourc
e se
ttin
gs
by d
ocum
entin
g a
prom
isin
g ex
ampl
e fro
m B
enue
Two
com
mun
ity‑b
ased
reha
bilit
atio
n fa
cilit
ies
oper
ate
unde
r CC
MH
PCC
MH
P pr
ocur
es m
edic
ines
from
CH
AN
M
edi‑P
harm
and
set
s up
Dru
g Re
volv
ing
Fund
at e
ach
heal
th c
entr
e to
ens
ure
cons
tant
sup
ply
Refe
rral
s ar
e m
ade
dire
ctly
bet
wee
n th
e co
mm
unity
psy
chia
tric
nur
se (C
PN) o
r co
mm
unity
hea
lth e
xten
sion
wor
ker
(CH
EW) a
nd s
peci
alis
ts a
t Fed
eral
M
edic
al C
entr
e M
akur
di o
r Ben
ue S
tate
U
nive
rsity
Tea
chin
g H
ospi
tal
CPN
s re
ceiv
e fo
rmal
trai
ning
, ret
rain
ing
and
accr
edita
tion,
fund
ed b
y CC
MH
PCC
MH
P tr
ains
peo
ple
as c
omm
unity
‑le
vel m
enta
l hea
lth a
dvoc
ates
for
prom
otio
n, id
entifi
catio
n an
d re
ferr
al.
CPN
s an
d C
HEW
s co
nduc
t com
mun
ity
outr
each
for f
ollo
w‑u
p
Serv
ice
deliv
ery
Sadd
i et a
l. (2
018)
[88]
Braz
ilian
nat
iona
l pro
gram
me
for i
mpr
ov‑
ing
prim
ary
care
acc
ess
and
qual
ity
(PM
AQ
)
To d
eter
min
e fro
ntlin
e w
orke
r adh
eren
ce
to P
MA
Q a
nd th
eir p
erce
ptio
n of
the
impa
ct o
f the
pro
gram
me
Det
erm
ine
the
rela
tions
hip
betw
een
the
impa
ct o
f the
PM
AQ
as
perc
eive
d by
fron
tline
wor
kers
and
the
way
they
ev
alua
te th
e or
gani
zatio
nal c
apac
ity o
f th
e FH
S at
the
front
line
This
pro
gram
me
was
ado
pted
in 2
011
to im
prov
e th
e qu
ality
and
per
form
ance
of
PH
C in
Bra
zil,
whi
ch is
bro
adly
kno
wn
thro
ugh
its m
ain
polic
y: th
e FH
SPM
AQ
obj
ectiv
es a
re (1
) to
prom
ote
qual
ity a
nd in
nova
tion
in p
rimar
y ca
re
man
agem
ent,
stre
ngth
enin
g se
lf‑as
sess
men
t, m
onito
ring
and
asse
ssm
ent,
inst
itutio
nal s
uppo
rt a
nd p
erm
anen
t ed
ucat
ion
proc
esse
s; (2
) to
impr
ove
the
use
of in
form
atio
n sy
stem
s as
a p
rimar
y ca
re m
anag
emen
t too
l; (3
) to
inst
itu‑
tiona
lize
a pr
imar
y ca
re a
sses
smen
t and
m
anag
emen
t cul
ture
; (4)
to s
timul
ate
the
focu
s of
prim
ary
care
on
the
serv
ice
user
, pro
mot
ing
man
agem
ent p
roce
sses
an
d tr
ansp
aren
cy
Serv
ice
deliv
ery
Sam
i et a
l. (2
018)
[102
]W
HO
sta
ndar
ds fo
r com
mun
ity‑ a
nd
heal
th fa
cilit
y‑ba
sed
new
born
car
eEx
amin
es th
e fe
asib
ility
of i
mpl
emen
ting
a pa
ckag
e of
com
mun
ity‑ a
nd fa
cilit
y‑ba
sed
neon
atal
inte
rven
tions
WH
O s
tand
ards
for c
omm
unity
‑ and
he
alth
faci
lity‑
base
d ne
wbo
rn c
are
prio
r‑iti
zed
the
mos
t crit
ical
ser
vice
s (n
eona
tal
inte
rven
tions
for r
educ
ing
mor
talit
y)
durin
g a
hum
anita
rian
cris
is
Serv
ice
deliv
ery
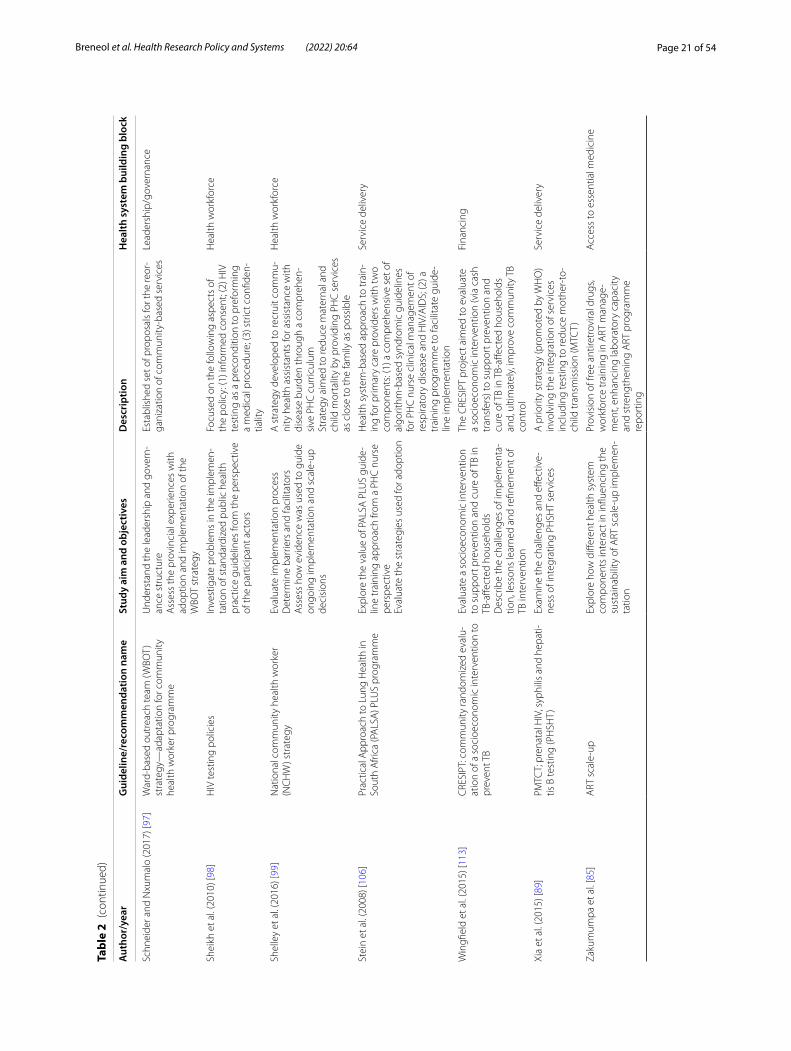
Page 21 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 2
(con
tinue
d)
Aut
hor/
year
Gui
delin
e/re
com
men
datio
n na
me
Stud
y ai
m a
nd o
bjec
tives
Des
crip
tion
Hea
lth s
yste
m b
uild
ing
bloc
k
Schn
eide
r and
Nxu
mal
o (2
017)
[97]
War
d‑ba
sed
outr
each
team
(WBO
T)
stra
tegy
—ad
apta
tion
for c
omm
unity
he
alth
wor
ker p
rogr
amm
e
Und
erst
and
the
lead
ersh
ip a
nd g
over
n‑an
ce s
truc
ture
Ass
ess
the
prov
inci
al e
xper
ienc
es w
ith
adop
tion
and
impl
emen
tatio
n of
the
WBO
T st
rate
gy
Esta
blis
hed
set o
f pro
posa
ls fo
r the
reor
‑ga
niza
tion
of c
omm
unity
‑bas
ed s
ervi
ces
Lead
ersh
ip/g
over
nanc
e
Shei
kh e
t al.
(201
0) [9
8]H
IV te
stin
g po
licie
sIn
vest
igat
e pr
oble
ms
in th
e im
plem
en‑
tatio
n of
sta
ndar
dize
d pu
blic
hea
lth
prac
tice
guid
elin
es fr
om th
e pe
rspe
ctiv
e of
the
part
icip
ant a
ctor
s
Focu
sed
on th
e fo
llow
ing
aspe
cts
of
the
polic
y: (1
) inf
orm
ed c
onse
nt; (
2) H
IV
test
ing
as a
pre
cond
ition
to p
refo
rmin
g a
med
ical
pro
cedu
re; (
3) s
tric
t con
fiden
‑tia
lity
Hea
lth w
orkf
orce
Shel
ley
et a
l. (2
016)
[99]
Nat
iona
l com
mun
ity h
ealth
wor
ker
(NC
HW
) str
ateg
yEv
alua
te im
plem
enta
tion
proc
ess
Det
erm
ine
barr
iers
and
faci
litat
ors
Ass
ess
how
evi
denc
e w
as u
sed
to g
uide
on
goin
g im
plem
enta
tion
and
scal
e‑up
de
cisi
ons
A s
trat
egy
deve
lope
d to
recr
uit c
omm
u‑ni
ty h
ealth
ass
ista
nts
for a
ssis
tanc
e w
ith
dise
ase
burd
en th
roug
h a
com
preh
en‑
sive
PH
C c
urric
ulum
Stra
tegy
aim
ed to
redu
ce m
ater
nal a
nd
child
mor
talit
y by
pro
vidi
ng P
HC
ser
vice
s as
clo
se to
the
fam
ily a
s po
ssib
le
Hea
lth w
orkf
orce
Stei
n et
al.
(200
8) [1
06]
Prac
tical
App
roac
h to
Lun
g H
ealth
in
Sout
h A
frica
(PA
LSA
) PLU
S pr
ogra
mm
eEx
plor
e th
e va
lue
of P
ALS
A P
LUS
guid
e‑lin
e tr
aini
ng a
ppro
ach
from
a P
HC
nur
se
pers
pect
ive
Eval
uate
the
stra
tegi
es u
sed
for a
dopt
ion
Hea
lth s
yste
m‑b
ased
app
roac
h to
trai
n‑in
g fo
r prim
ary
care
pro
vide
rs w
ith tw
o co
mpo
nent
s: (1
) a c
ompr
ehen
sive
set
of
algo
rithm
‑bas
ed s
yndr
omic
gui
delin
es
for P
HC
nur
se c
linic
al m
anag
emen
t of
resp
irato
ry d
isea
se a
nd H
IV/A
IDS;
(2) a
tr
aini
ng p
rogr
amm
e to
faci
litat
e gu
ide‑
line
impl
emen
tatio
n
Serv
ice
deliv
ery
Win
gfiel
d et
al.
(201
5) [1
13]
CRE
SIPT
: com
mun
ity ra
ndom
ized
eva
lu‑
atio
n of
a s
ocio
econ
omic
inte
rven
tion
to
prev
ent T
B
Eval
uate
a s
ocio
econ
omic
inte
rven
tion
to s
uppo
rt p
reve
ntio
n an
d cu
re o
f TB
in
TB‑a
ffect
ed h
ouse
hold
sD
escr
ibe
the
chal
leng
es o
f im
plem
enta
‑tio
n, le
sson
s le
arne
d an
d re
finem
ent o
f TB
inte
rven
tion
The
CRE
SIPT
pro
ject
aim
ed to
eva
luat
e a
soci
oeco
nom
ic in
terv
entio
n (v
ia c
ash
tran
sfer
s) to
sup
port
pre
vent
ion
and
cure
of T
B in
TB‑
affec
ted
hous
ehol
ds
and,
ulti
mat
ely,
impr
ove
com
mun
ity T
B co
ntro
l
Fina
ncin
g
Xia
et a
l. (2
015)
[89]
PMTC
T; p
rena
tal H
IV, s
yphi
lis a
nd h
epat
i‑tis
B te
stin
g (P
HSH
T)Ex
amin
e th
e ch
alle
nges
and
effe
ctiv
e‑ne
ss o
f int
egra
ting
PHSH
T se
rvic
esA
prio
rity
stra
tegy
(pro
mot
ed b
y W
HO
) in
volv
ing
the
inte
grat
ion
of s
ervi
ces
incl
udin
g te
stin
g to
redu
ce m
othe
r‑to
‑ch
ild tr
ansm
issi
on (M
TCT)
Serv
ice
deliv
ery
Zaku
mum
pa e
t al.
[85]
ART
sca
le‑u
pEx
plor
e ho
w d
iffer
ent h
ealth
sys
tem
co
mpo
nent
s in
tera
ct in
influ
enci
ng th
e su
stai
nabi
lity
of A
RT s
cale
‑up
impl
emen
‑ta
tion
Prov
isio
n of
free
ant
iretr
ovira
l dru
gs,
wor
kfor
ce tr
aini
ng in
ART
man
age‑
men
t, en
hanc
ing
labo
rato
ry c
apac
ity
and
stre
ngth
enin
g A
RT p
rogr
amm
e re
port
ing
Acc
ess
to e
ssen
tial m
edic
ine
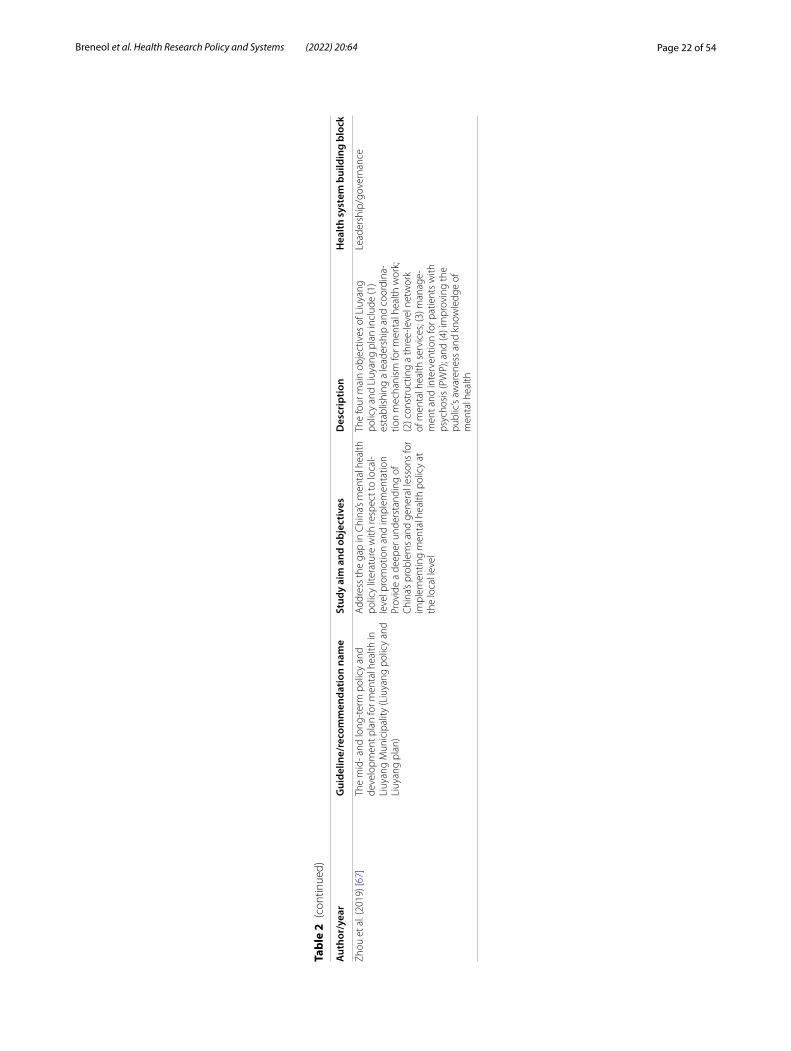
Page 22 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 2
(con
tinue
d)
Aut
hor/
year
Gui
delin
e/re
com
men
datio
n na
me
Stud
y ai
m a
nd o
bjec
tives
Des
crip
tion
Hea
lth s
yste
m b
uild
ing
bloc
k
Zhou
et a
l. (2
019)
[67]
The
mid
‑ and
long
‑ter
m p
olic
y an
d de
velo
pmen
t pla
n fo
r men
tal h
ealth
in
Liuy
ang
Mun
icip
ality
(Liu
yang
pol
icy
and
Liuy
ang
plan
)
Add
ress
the
gap
in C
hina
’s m
enta
l hea
lth
polic
y lit
erat
ure
with
resp
ect t
o lo
cal‑
leve
l pro
mot
ion
and
impl
emen
tatio
nPr
ovid
e a
deep
er u
nder
stan
ding
of
Chi
na’s
prob
lem
s an
d ge
nera
l les
sons
for
impl
emen
ting
men
tal h
ealth
pol
icy
at
the
loca
l lev
el
The
four
mai
n ob
ject
ives
of L
iuya
ng
polic
y an
d Li
uyan
g pl
an in
clud
e (1
) es
tabl
ishi
ng a
lead
ersh
ip a
nd c
oord
ina‑
tion
mec
hani
sm fo
r men
tal h
ealth
wor
k;
(2) c
onst
ruct
ing
a th
ree‑
leve
l net
wor
k of
men
tal h
ealth
ser
vice
s; (3
) man
age‑
men
t and
inte
rven
tion
for p
atie
nts
with
ps
ycho
sis
(PW
P); a
nd (4
) im
prov
ing
the
publ
ic’s
awar
enes
s an
d kn
owle
dge
of
men
tal h
ealth
Lead
ersh
ip/g
over
nanc
e
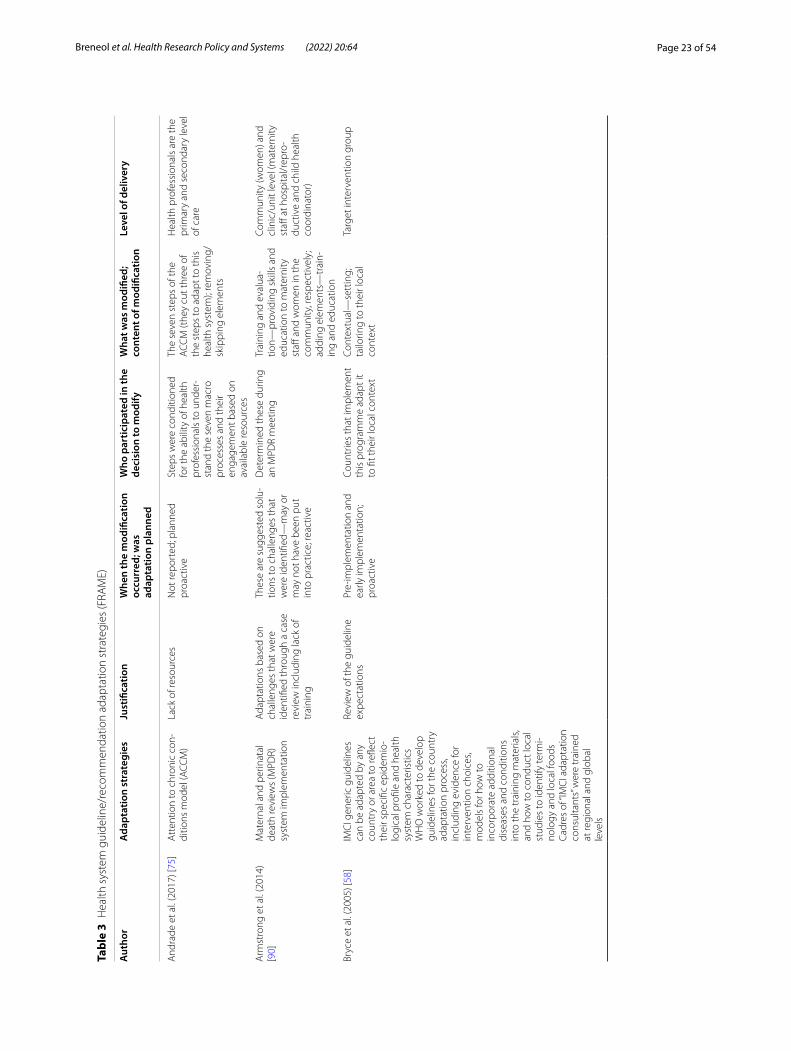
Page 23 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 3
Hea
lth s
yste
m g
uide
line/
reco
mm
enda
tion
adap
tatio
n st
rate
gies
(FRA
ME)
Aut
hor
Ada
ptat
ion
stra
tegi
esJu
stifi
catio
nW
hen
the
mod
ifica
tion
occu
rred
; was
ad
apta
tion
plan
ned
Who
par
ticip
ated
in th
e de
cisi
on to
mod
ifyW
hat w
as m
odifi
ed;
cont
ent o
f mod
ifica
tion
Leve
l of d
eliv
ery
And
rade
et a
l. (2
017)
[75]
Att
entio
n to
chr
onic
con
‑di
tions
mod
el (A
CCM
)La
ck o
f res
ourc
esN
ot re
port
ed; p
lann
ed
proa
ctiv
eSt
eps
wer
e co
nditi
oned
fo
r the
abi
lity
of h
ealth
pr
ofes
sion
als
to u
nder
‑st
and
the
seve
n m
acro
pr
oces
ses
and
thei
r en
gage
men
t bas
ed o
n av
aila
ble
reso
urce
s
The
seve
n st
eps
of th
e A
CCM
(the
y cu
t thr
ee o
f th
e st
eps
to a
dapt
to th
is
heal
th s
yste
m);
rem
ovin
g/sk
ippi
ng e
lem
ents
Hea
lth p
rofe
ssio
nals
are
the
prim
ary
and
seco
ndar
y le
vel
of c
are
Arm
stro
ng e
t al.
(201
4)
[90]
Mat
erna
l and
per
inat
al
deat
h re
view
s (M
PDR)
sy
stem
impl
emen
tatio
n
Ada
ptat
ions
bas
ed o
n ch
alle
nges
that
wer
e id
entifi
ed th
roug
h a
case
re
view
incl
udin
g la
ck o
f tr
aini
ng
Thes
e ar
e su
gges
ted
solu
‑tio
ns to
cha
lleng
es th
at
wer
e id
entifi
ed—
may
or
may
not
hav
e be
en p
ut
into
pra
ctic
e; re
activ
e
Det
erm
ined
thes
e du
ring
an M
PDR
mee
ting
Trai
ning
and
eva
lua‑
tion—
prov
idin
g sk
ills
and
educ
atio
n to
mat
erni
ty
staff
and
wom
en in
the
com
mun
ity, r
espe
ctiv
ely;
ad
ding
ele
men
ts—
trai
n‑in
g an
d ed
ucat
ion
Com
mun
ity (w
omen
) and
cl
inic
/uni
t lev
el (m
ater
nity
st
aff a
t hos
pita
l/rep
ro‑
duct
ive
and
child
hea
lth
coor
dina
tor)
Bryc
e et
al.
(200
5) [5
8]IM
CI g
ener
ic g
uide
lines
ca
n be
ada
pted
by
any
coun
try
or a
rea
to re
flect
th
eir s
peci
fic e
pide
mio
‑lo
gica
l pro
file
and
heal
th
syst
em c
hara
cter
istic
sW
HO
wor
ked
to d
evel
op
guid
elin
es fo
r the
cou
ntry
ad
apta
tion
proc
ess,
incl
udin
g ev
iden
ce fo
r in
terv
entio
n ch
oice
s, m
odel
s fo
r how
to
inco
rpor
ate
addi
tiona
l di
seas
es a
nd c
ondi
tions
in
to th
e tr
aini
ng m
ater
ials
, an
d ho
w to
con
duct
loca
l st
udie
s to
iden
tify
term
i‑no
logy
and
loca
l foo
dsCa
dres
of “
IMC
I ada
ptat
ion
cons
ulta
nts”
wer
e tr
aine
d at
regi
onal
and
glo
bal
leve
ls
Revi
ew o
f the
gui
delin
e ex
pect
atio
nsPr
e‑im
plem
enta
tion
and
early
impl
emen
tatio
n;
proa
ctiv
e
Coun
trie
s th
at im
plem
ent
this
pro
gram
me
adap
t it
to fi
t the
ir lo
cal c
onte
xt
Cont
extu
al—
sett
ing;
ta
ilorin
g to
thei
r loc
al
cont
ext
Targ
et in
terv
entio
n gr
oup
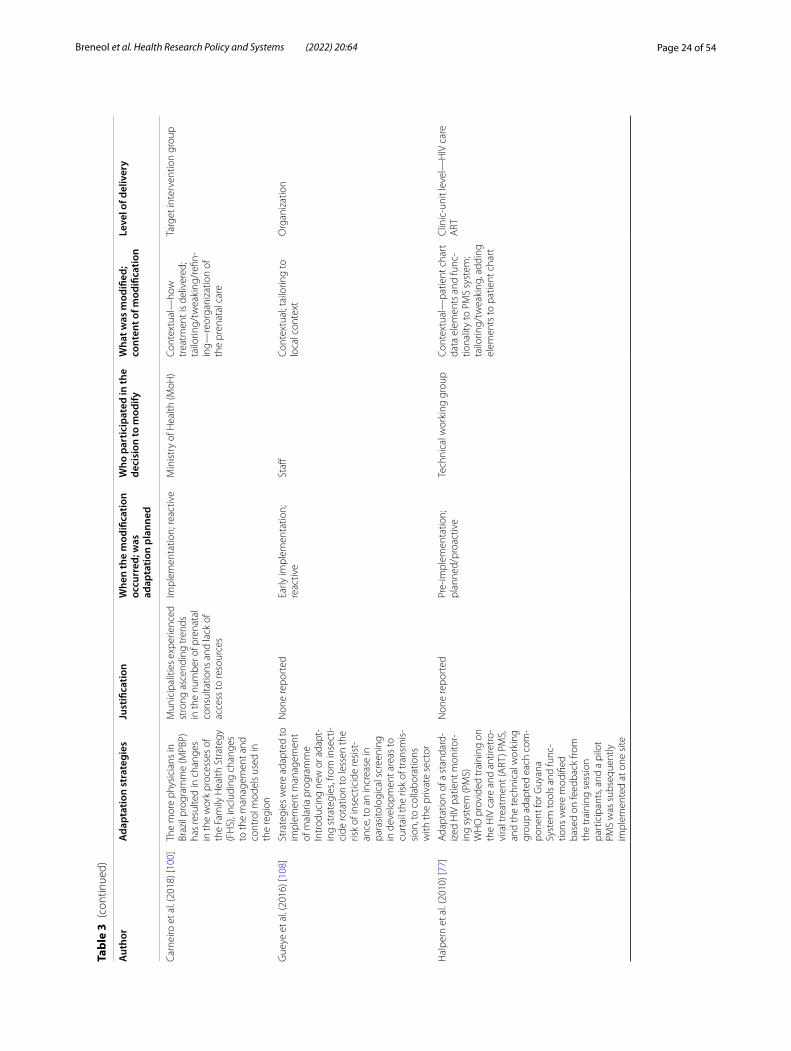
Page 24 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 3
(con
tinue
d)
Aut
hor
Ada
ptat
ion
stra
tegi
esJu
stifi
catio
nW
hen
the
mod
ifica
tion
occu
rred
; was
ad
apta
tion
plan
ned
Who
par
ticip
ated
in th
e de
cisi
on to
mod
ifyW
hat w
as m
odifi
ed;
cont
ent o
f mod
ifica
tion
Leve
l of d
eliv
ery
Carn
eiro
et a
l. (2
018)
[100
]Th
e m
ore
phys
icia
ns in
Br
azil
prog
ram
me
(MPB
P)
has
resu
lted
in c
hang
es
in th
e w
ork
proc
esse
s of
th
e Fa
mily
Hea
lth S
trat
egy
(FH
S), i
nclu
ding
cha
nges
to
the
man
agem
ent a
nd
cont
rol m
odel
s us
ed in
th
e re
gion
Mun
icip
aliti
es e
xper
ienc
ed
stro
ng a
scen
ding
tren
ds
in th
e nu
mbe
r of p
rena
tal
cons
ulta
tions
and
lack
of
acce
ss to
reso
urce
s
Impl
emen
tatio
n; re
activ
eM
inis
try
of H
ealth
(MoH
)Co
ntex
tual
—ho
w
trea
tmen
t is
deliv
ered
; ta
ilorin
g/tw
eaki
ng/r
efin‑
ing—
reor
gani
zatio
n of
th
e pr
enat
al c
are
Targ
et in
terv
entio
n gr
oup
Gue
ye e
t al.
(201
6) [1
08]
Stra
tegi
es w
ere
adap
ted
to
impl
emen
t man
agem
ent
of m
alar
ia p
rogr
amm
eIn
trod
ucin
g ne
w o
r ada
pt‑
ing
stra
tegi
es, f
rom
inse
cti‑
cide
rota
tion
to le
ssen
the
risk
of in
sect
icid
e re
sist
‑an
ce, t
o an
incr
ease
in
para
sito
logi
cal s
cree
ning
in
dev
elop
men
t are
as to
cu
rtai
l the
risk
of t
rans
mis
‑si
on, t
o co
llabo
ratio
ns
with
the
priv
ate
sect
or
Non
e re
port
edEa
rly im
plem
enta
tion;
re
activ
eSt
affCo
ntex
tual
; tai
lorin
g to
lo
cal c
onte
xtO
rgan
izat
ion
Hal
pern
et a
l. (2
010)
[77]
Ada
ptat
ion
of a
sta
ndar
d‑iz
ed H
IV p
atie
nt m
onito
r‑in
g sy
stem
(PM
S)W
HO
pro
vide
d tr
aini
ng o
n th
e H
IV c
are
and
antir
etro
‑vi
ral t
reat
men
t (A
RT) P
MS,
an
d th
e te
chni
cal w
orki
ng
grou
p ad
apte
d ea
ch c
om‑
pone
nt fo
r Guy
ana
Syst
em to
ols
and
func
‑tio
ns w
ere
mod
ified
ba
sed
on fe
edba
ck fr
om
the
trai
ning
ses
sion
pa
rtic
ipan
ts, a
nd a
pilo
t PM
S w
as s
ubse
quen
tly
impl
emen
ted
at o
ne s
ite
Non
e re
port
edPr
e‑im
plem
enta
tion;
pl
anne
d/pr
oact
ive
Tech
nica
l wor
king
gro
upCo
ntex
tual
—pa
tient
cha
rt
data
ele
men
ts a
nd fu
nc‑
tiona
lity
to P
MS
syst
em;
tailo
ring/
twea
king
, add
ing
elem
ents
to p
atie
nt c
hart
Clin
ic‑u
nit l
evel
—H
IV c
are
ART

Page 25 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 3
(con
tinue
d)
Aut
hor
Ada
ptat
ion
stra
tegi
esJu
stifi
catio
nW
hen
the
mod
ifica
tion
occu
rred
; was
ad
apta
tion
plan
ned
Who
par
ticip
ated
in th
e de
cisi
on to
mod
ifyW
hat w
as m
odifi
ed;
cont
ent o
f mod
ifica
tion
Leve
l of d
eliv
ery
Kihe
mbo
et a
l. (2
018)
[57]
Impl
emen
t nat
ionw
ide
ISD
R tr
aini
ng to
hea
lth
faci
litie
s ba
sed
on th
e re
vise
d gu
idel
ines
dev
el‑
oped
Post
‑tra
inin
g su
ppor
t th
roug
h in
tegr
ated
su
perv
isio
n
Two
chal
leng
es fr
om th
e fir
st im
plem
enta
tion:
Lack
of f
undi
ng re
sulte
d in
a la
ck o
f res
ourc
es a
nd
capa
citie
s at
the
oper
a‑tio
nal l
evel
A n
eed
for a
har
mon
ized
ou
tbre
ak re
spon
se a
nd
info
rmat
ion
flow
at t
he
dist
rict l
evel
Pre‑
impl
emen
tatio
n;
plan
ned
Min
istr
y of
hea
lth a
long
w
ith k
ey p
artn
ers
Aim
ed to
enh
ance
the
capa
city
of d
istr
icts
to
prom
ptly
det
ect,
acce
ss
and
effec
tivel
y re
spon
d to
pu
blic
hea
lth e
mer
gen‑
cies
; add
ing
elem
ents
—tr
aini
ng
Hea
lth w
orkf
orce
all
the
way
up
to th
e op
erat
iona
l na
tiona
l lev
el
Leet
hong
dee
(200
7) [8
3]G
over
nmen
t dec
ided
to
fund
the
sche
me
by p
ool‑
ing
the
Min
istr
y of
Pub
lic
Hea
lth (M
oPH
) bud
gets
fo
r pub
lic h
ospi
tals
, oth
er
heal
th fa
cilit
ies,
and
Med
i‑ca
l Wel
fare
Sch
eme
(MW
S)
and
volu
ntar
y he
alth
car
d sc
hem
e an
d pr
ovid
ing
addi
tiona
l mon
ey
The
initi
al p
lan
met
resi
st‑
ance
from
qua
rter
s su
ch
as th
e ci
vil s
ervi
ce a
nd th
e la
bour
uni
ons
Pre‑
impl
emen
tatio
n;
reac
tive
Civ
il se
rvic
e an
d la
bour
un
ions
reje
cted
the
initi
al
plan
, gov
ernm
ent t
hen
had
to re
asse
ss
Impl
emen
tatio
n an
d sc
ale‑
up a
ctiv
ities
; su
bstit
utin
g th
e fu
ndin
g st
ruct
ures
Targ
et in
terv
entio
n gr
oup
Mut
abaz
i et a
l. (2
020)
[87]
Ove
r the
yea
rs, t
he p
re‑
vent
ion
of m
othe
r‑to
‑chi
ld
tran
smis
sion
of H
IV/A
IDS
(PM
TCT)
gui
delin
es h
ave
been
ada
pted
, but
no
stra
tegi
es re
port
ed
Non
e re
port
edN
one
repo
rted
Non
e re
port
edN
one
repo
rted
Non
e re
port
ed
Ryan
et a
l. (2
020)
[109
]Co
mpr
ehen
sive
com
‑m
unity
men
tal h
ealth
pr
ogra
mm
e (C
CM
HP)
A s
cale
‑up
initi
ativ
e fo
r th
e ge
nera
l men
tal h
ealth
po
licy
impl
emen
tatio
n in
N
iger
ia th
roug
h pu
blic
–pr
ivat
e pa
rtne
rshi
p in
he
alth
care
del
iver
y
Abs
ence
of m
ore
clin
ical
re
sour
ces
Scal
e‑up
; rea
ctiv
eN
one
repo
rted
Phon
e ps
ychi
atris
ts a
s ne
eded
; add
ing
elem
ent
Com
mun
ity p
sych
iatr
ic
nurs
es (C
PNs)
and
com
‑m
unity
hea
lth e
xten
sion
w
orke
r (C
HEW
s)
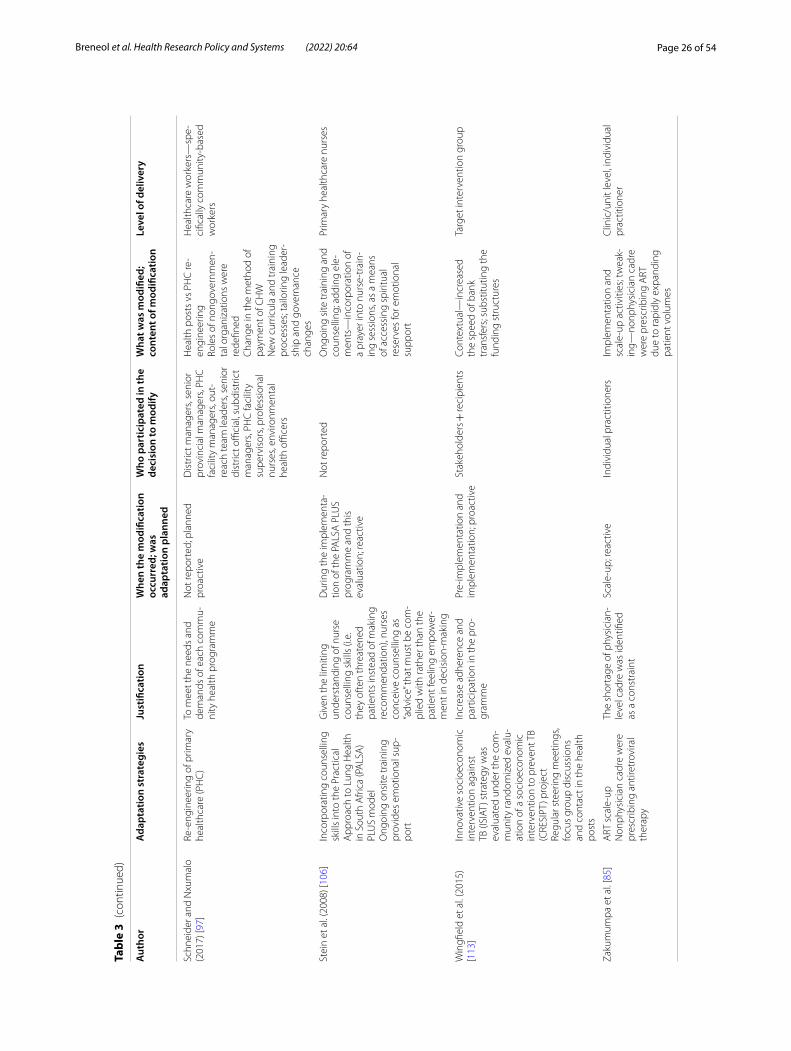
Page 26 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 3
(con
tinue
d)
Aut
hor
Ada
ptat
ion
stra
tegi
esJu
stifi
catio
nW
hen
the
mod
ifica
tion
occu
rred
; was
ad
apta
tion
plan
ned
Who
par
ticip
ated
in th
e de
cisi
on to
mod
ifyW
hat w
as m
odifi
ed;
cont
ent o
f mod
ifica
tion
Leve
l of d
eliv
ery
Schn
eide
r and
Nxu
mal
o (2
017)
[97]
Re‑e
ngin
eerin
g of
prim
ary
heal
thca
re (P
HC
)To
mee
t the
nee
ds a
nd
dem
ands
of e
ach
com
mu‑
nity
hea
lth p
rogr
amm
e
Not
repo
rted
; pla
nned
pr
oact
ive
Dis
tric
t man
ager
s, se
nior
pr
ovin
cial
man
ager
s, PH
C
faci
lity
man
ager
s, ou
t‑re
ach
team
lead
ers,
seni
or
dist
rict o
ffici
al, s
ubdi
stric
t m
anag
ers,
PHC
faci
lity
supe
rvis
ors,
prof
essi
onal
nu
rses
, env
ironm
enta
l he
alth
offi
cers
Hea
lth p
osts
vs
PHC
re‑
engi
neer
ing
Role
s of
non
gove
rnm
en‑
tal o
rgan
izat
ions
wer
e re
defin
edC
hang
e in
the
met
hod
of
paym
ent o
f CH
WN
ew c
urric
ula
and
trai
ning
pr
oces
ses;
tailo
ring
lead
er‑
ship
and
gov
erna
nce
chan
ges
Hea
lthca
re w
orke
rs—
spe‑
cific
ally
com
mun
ity‑b
ased
w
orke
rs
Stei
n et
al.
(200
8) [1
06]
Inco
rpor
atin
g co
unse
lling
sk
ills
into
the
Prac
tical
A
ppro
ach
to L
ung
Hea
lth
in S
outh
Afri
ca (P
ALS
A)
PLU
S m
odel
Ong
oing
ons
ite tr
aini
ng
prov
ides
em
otio
nal s
up‑
port
Giv
en th
e lim
iting
un
ders
tand
ing
of n
urse
co
unse
lling
ski
lls (i
.e.
they
oft
en th
reat
ened
pa
tient
s in
stea
d of
mak
ing
reco
mm
enda
tion)
, nur
ses
conc
eive
cou
nsel
ling
as
“adv
ice”
that
mus
t be
com
‑pl
ied
with
rath
er th
an th
e pa
tient
feel
ing
empo
wer
‑m
ent i
n de
cisi
on‑m
akin
g
Dur
ing
the
impl
emen
ta‑
tion
of th
e PA
LSA
PLU
S pr
ogra
mm
e an
d th
is
eval
uatio
n; re
activ
e
Not
repo
rted
Ong
oing
site
trai
ning
and
co
unse
lling
; add
ing
ele‑
men
ts—
inco
rpor
atio
n of
a
pray
er in
to n
urse
‑tra
in‑
ing
sess
ions
, as
a m
eans
of
acc
essi
ng s
pirit
ual
rese
rves
for e
mot
iona
l su
ppor
t
Prim
ary
heal
thca
re n
urse
s
Win
gfiel
d et
al.
(201
5)
[113
]In
nova
tive
soci
oeco
nom
ic
inte
rven
tion
agai
nst
TB (I
SIAT
) str
ateg
y w
as
eval
uate
d un
der t
he c
om‑
mun
ity ra
ndom
ized
eva
lu‑
atio
n of
a s
ocio
econ
omic
in
terv
entio
n to
pre
vent
TB
(CRE
SIPT
) pro
ject
Regu
lar s
teer
ing
mee
tings
, fo
cus
grou
p di
scus
sion
s an
d co
ntac
t in
the
heal
th
post
s
Incr
ease
adh
eren
ce a
nd
part
icip
atio
n in
the
pro‑
gram
me
Pre‑
impl
emen
tatio
n an
d im
plem
enta
tion;
pro
activ
eSt
akeh
olde
rs +
reci
pien
tsCo
ntex
tual
—in
crea
sed
the
spee
d of
ban
k tr
ansf
ers;
subs
titut
ing
the
fund
ing
stru
ctur
es
Targ
et in
terv
entio
n gr
oup
Zaku
mum
pa e
t al.
[85]
ART
sca
le‑u
pN
onph
ysic
ian
cadr
e w
ere
pres
crib
ing
antir
etro
vira
l th
erap
y
The
shor
tage
of p
hysi
cian
‑le
vel c
adre
was
iden
tified
as
a c
onst
rain
t
Scal
e‑up
; rea
ctiv
eIn
divi
dual
pra
ctiti
oner
sIm
plem
enta
tion
and
scal
e‑up
act
iviti
es; t
wea
k‑in
g—no
nphy
sici
an c
adre
w
ere
pres
crib
ing
ART
du
e to
rapi
dly
expa
ndin
g pa
tient
vol
umes
Clin
ic/u
nit l
evel
, ind
ivid
ual
prac
titio
ner

Page 27 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
(n = 6) and developing educational materials (n = 5). The least prevalent ERIC-defined implementation strategies included, but were not limited to, revision of professional roles (n = 2), alterations of incentives/allowance structure (n = 2), assessments for readiness and identification of barriers and facilitators (n = 1), and tailoring of strategies (n = 1). A full breakdown of all 38 implementation strate-gies and their frequencies can be found in Table 4. None of our included studies explicitly reported the use of a theoretical/conceptual framework to guide their selec-tion of implementation strategies.
Outcomes of interestTable 5 summarizes the outcomes of interest and key results of included studies. Nineteen articles reported the involvement of key stakeholders in various aspects of their design and implementation processes. Stakehold-ers varied from frontline healthcare workers to policy-makers, government organizations and nongovernmental organizations (NGOs). Outcomes of interest were related primarily to documenting and evaluating the implemen-tation process, as well as the impact of the guideline on the health system (n = 39). These included assessing the barriers to and enablers of implementation, eliciting end-users’ experiences and perspectives, monitoring system and service changes, evaluating resource use, identify-ing future steps and comparing guideline expectations to real-world impacts. Additionally, one article explic-itly specified the documentation of an implementation framework as an outcome of interest. Patient-level out-comes were noted as an indicator of success and included measuring health outcomes and quality of care delivery (n = 3). While many outcomes of interest were indicators of the overall success of the health system guideline inte-gration, there were no outcomes of interest specifically reported as related to adaptations.
Outcome measuresOutcome measures included interviews/focus groups (n = 29), document/policy analysis (n = 10), surveys/questionnaires (n = 9), health administrative data and medical records (n = 8), field visits/observations (n = 4), secondary data from literature/guideline reviews (n = 2), individual case studies (n = 2), clinical assessment tools (n = 1), performance assessment tools (n = 1) and patient observations (n = 1). A full breakdown of outcomes is presented in Table 5.
Barriers and enablers related to implementationReported barriers to and enablers of implementation of health system guidelines were coded using the COM-B framework [54]. Barriers and enablers that were most frequently reported by identified studies were associated
with physical (n = 36) or social (n = 22) opportunity. Physical opportunities are defined as the environmental context and resources, whereas social opportunities refer to the social influences, such as norms and cultural fac-tors [54]. Financial constraints, access to resources, and training (or lack thereof ) were persistent physical oppor-tunity factors described. Language and communication, political instability and power imbalances are all exam-ples of reported barriers or enablers related to social opportunities.
Implementation barriers and enablers related to psy-chological (n = 15) and physical capabilities (n = 19) were the second most frequently coded category in the COM-B framework. Physical capabilities describe the skills and abilities required, while psychological capa-bilities refer to the concepts of knowledge, memory, decision-making and behavioural regulation [54]. Identi-fied articles reported barriers and enablers related to the knowledge about implemented guidelines, the emotional toll on frontline workers and the resistance to change. Physical capabilities included adapting training materials specific to the needs of end-users and ongoing training/mentorship with supervision.
Reflective (n = 4) and automatic (n = 10) motivations were the least often coded barrier and enabler in our review. Reflective motivation refers to the roles, iden-tities and beliefs about consequences [54]. Resistance to or acceptance of change, trust in the guidelines, and defining role and responsibility attributes are all exam-ples noted among the reflective motivation category. Automatic motivation refers to the emotion and rein-forcement influencing target behaviour [54]. Dedicated commitment, enthusiasm and motivation to implement health system guidelines were reported as a barrier and/or enabler. A summary of the COM-B analysis can be found in Tables 6 and 7. A full breakdown of extracted and analysed data can be found in Additional file 4.
Barriers and enablers related to adaptationEight articles reported barriers and enablers related to adaptation of the health system guidelines. Of these, physical opportunities were the most commonly reported barriers and enablers, with articles describing the use of technical working groups to adjust and manage unexpected changes, ensure flexibility in initiatives, and create new structures/systems to facilitate local adapta-tion (n = 6). Strong multisectoral collaboration, proac-tive leadership and culturally appropriate support are all examples of barriers and enablers related to social oppor-tunities that were reported (n = 3). Reflective motivation (n = 2) was the only other COM-B category captured in reported barriers and enablers with respect to adaptation by this review. This related to a lack of available evidence
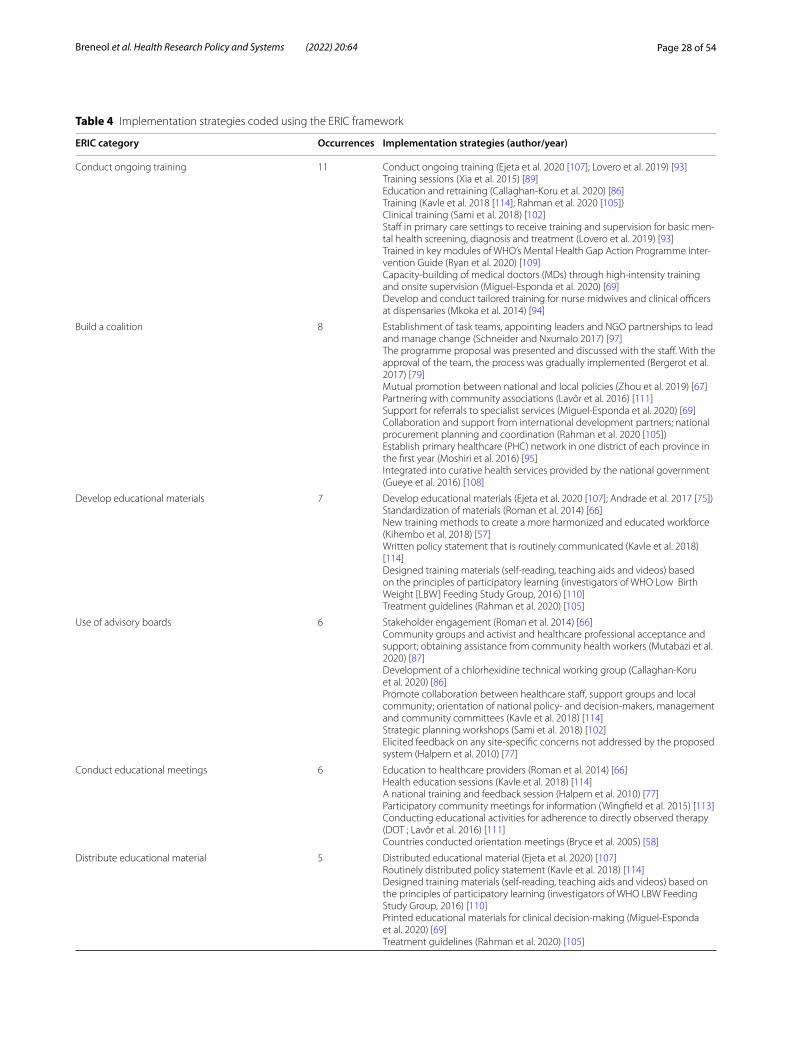
Page 28 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Table 4 Implementation strategies coded using the ERIC framework
ERIC category Occurrences Implementation strategies (author/year)
Conduct ongoing training 11 Conduct ongoing training (Ejeta et al. 2020 [107]; Lovero et al. 2019) [93]Training sessions (Xia et al. 2015) [89]Education and retraining (Callaghan‑Koru et al. 2020) [86]Training (Kavle et al. 2018 [114]; Rahman et al. 2020 [105])Clinical training (Sami et al. 2018) [102]Staff in primary care settings to receive training and supervision for basic men‑tal health screening, diagnosis and treatment (Lovero et al. 2019) [93]Trained in key modules of WHO’s Mental Health Gap Action Programme Inter‑vention Guide (Ryan et al. 2020) [109]Capacity‑building of medical doctors (MDs) through high‑intensity training and onsite supervision (Miguel‑Esponda et al. 2020) [69]Develop and conduct tailored training for nurse midwives and clinical officers at dispensaries (Mkoka et al. 2014) [94]
Build a coalition 8 Establishment of task teams, appointing leaders and NGO partnerships to lead and manage change (Schneider and Nxumalo 2017) [97]The programme proposal was presented and discussed with the staff. With the approval of the team, the process was gradually implemented (Bergerot et al. 2017) [79]Mutual promotion between national and local policies (Zhou et al. 2019) [67]Partnering with community associations (Lavôr et al. 2016) [111]Support for referrals to specialist services (Miguel‑Esponda et al. 2020) [69]Collaboration and support from international development partners; national procurement planning and coordination (Rahman et al. 2020 [105])Establish primary healthcare (PHC) network in one district of each province in the first year (Moshiri et al. 2016) [95]Integrated into curative health services provided by the national government (Gueye et al. 2016) [108]
Develop educational materials 7 Develop educational materials (Ejeta et al. 2020 [107]; Andrade et al. 2017 [75])Standardization of materials (Roman et al. 2014) [66]New training methods to create a more harmonized and educated workforce (Kihembo et al. 2018) [57]Written policy statement that is routinely communicated (Kavle et al. 2018) [114]Designed training materials (self‑reading, teaching aids and videos) based on the principles of participatory learning (investigators of WHO Low Birth Weight [LBW] Feeding Study Group, 2016) [110]Treatment guidelines (Rahman et al. 2020) [105]
Use of advisory boards 6 Stakeholder engagement (Roman et al. 2014) [66]Community groups and activist and healthcare professional acceptance and support; obtaining assistance from community health workers (Mutabazi et al. 2020) [87]Development of a chlorhexidine technical working group (Callaghan‑Koru et al. 2020) [86]Promote collaboration between healthcare staff, support groups and local community; orientation of national policy‑ and decision‑makers, management and community committees (Kavle et al. 2018) [114]Strategic planning workshops (Sami et al. 2018) [102]Elicited feedback on any site‑specific concerns not addressed by the proposed system (Halpern et al. 2010) [77]
Conduct educational meetings 6 Education to healthcare providers (Roman et al. 2014) [66]Health education sessions (Kavle et al. 2018) [114]A national training and feedback session (Halpern et al. 2010) [77]Participatory community meetings for information (Wingfield et al. 2015) [113]Conducting educational activities for adherence to directly observed therapy (DOT ; Lavôr et al. 2016) [111]Countries conducted orientation meetings (Bryce et al. 2005) [58]
Distribute educational material 5 Distributed educational material (Ejeta et al. 2020) [107]Routinely distributed policy statement (Kavle et al. 2018) [114]Designed training materials (self‑reading, teaching aids and videos) based on the principles of participatory learning (investigators of WHO LBW Feeding Study Group, 2016) [110]Printed educational materials for clinical decision‑making (Miguel‑Esponda et al. 2020) [69]Treatment guidelines (Rahman et al. 2020) [105]

Page 29 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Table 4 (continued)
ERIC category Occurrences Implementation strategies (author/year)
Promote network‑weaving 5 Leading and managing change—establishment of task teams, appointing leaders and NGO partnerships (Schneider and Nxumalo 2017) [97]Collaboration between national reproductive health programmes and national malaria control programmes (Roman et al. 2014) [66]Coordination of Community Cadres within the health system (Shelley et al. 2016) [99]Multi‑department participation and collaboration to better implement the national essential drugs policy (Li et al. 2015) [112]Targeted interactions of PHC designers with local actors shaped a wide net‑work of friends before the implementation phase (Moshiri et al. 2016) [95]
Conduct educational outreach visits 4 Education to healthcare providers (Roman et al. 2014) [66]Ongoing onsite training provides emotional support (Stein et al. 2008) [106]Monthly visits from a member of the working group to validate reports and address any implementation issues (Halpern et al. 2010) [77]Developed management and training capacity in a limited number of districts (Bryce et al. 2005) [58]
Access new funding 4 Ensuring financial stability (Roman et al. 2014) [66]Financial guarantee from the central government (Zhou et al. 2019) [67]Distribution of amoxicillin by UNICEF (Rahman et al. 2020) [105]Programme financing (Miguel‑Esponda et al. 2020) [69]
Stage implementation scale‑up 4 Implementation scale‑up (Callaghan‑Koru et al. 2020) [86]Pilot project was evaluated first; when it was deemed successful, the guideline was implemented at all existing care sites, one site at a time (Halpern et al. 2010) [77]End of one phase was marked with a review meeting with the objective of synthesizing early implementation experience and planning for expansion (Bryce et al. 2005) [58]Policies were implemented in a series of stages (Leethongdee, 2007) [83]
Develop and organize monitoring systems 4 Surveillance system and performance and monitoring framework (Kihembo et al. 2018) [57]Programme monitoring (Kavle et al. 2018 [114]; Bryce et al. 2005) [58]Following each assessment, quality improvement plans are generated and provided to facility managers to guide their improvement actions (Muthathi et al. 2020) [96]
Develop resource‑sharing agreements 4 Management of resource availability; commodities/resources availability (Roman et al. 2014) [66]Distribution of medical commodities (Sami et al. 2018) [102]Ensuring medication supply (Miguel‑Esponda et al. 2020) [69]Supply and distribution of amoxicillin dispersible tablets (Rahman et al. 2020) [105]
Provide clinical supervision 4 Provide clinical supervision (Sami et al. 2018 [102]; Lovero et al. 2019 [93])Staff in primary care settings to receive training and supervision (Lovero et al. 2019) [93]Capacity‑building of MDs through high‑intensity training and onsite supervi‑sion (Miguel‑Esponda et al. 2020) [69]
Develop a formal implementation blueprint 3 Five‑year strategic plan with workplans (Kihembo et al. 2018) [57]Planning and early implementation, developed national strategy and plan (Bryce et al. 2005) [58]Network expansion plan; required budget was estimated and suggested to government; establish PHC network in one district of each province in the first year (Moshiri et al. 2016) [95]
Develop and implement tools for quality monitoring 3 Develop and implement tools for quality monitoring (Ejeta et al. 2020) [107]Standardization of materials; performance assessments (indicators); monitor‑ing and evaluating (Roman et al. 2014) [66]Monitoring through a health information system (Miguel‑Esponda et al. 2020) [69]
Change physical structure and equipment 3 Provide essential equipment and supplies; build/improve infrastructure for service delivery (Mkoka et al. 2014) [94]Availability of basic equipment (Rahman et al. 2020) [105]Providing containers to collect sputum and other inputs in the laboratory (Lavôr et al. 2016) [111]
Use train‑the‑trainer strategies 2 Train‑the‑trainer strategies (Ejeta et al. 2020 [107]; Kihembo et al. 2018) [57]
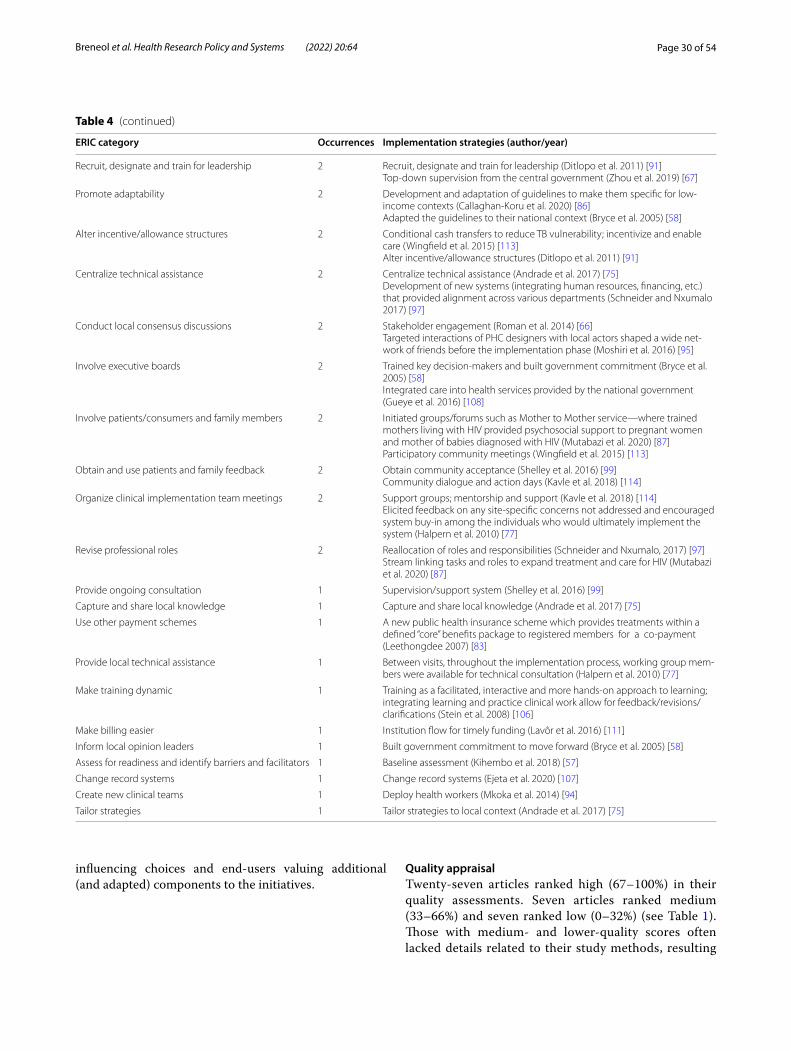
Page 30 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
influencing choices and end-users valuing additional (and adapted) components to the initiatives.
Quality appraisalTwenty-seven articles ranked high (67–100%) in their quality assessments. Seven articles ranked medium (33–66%) and seven ranked low (0–32%) (see Table 1). Those with medium- and lower-quality scores often lacked details related to their study methods, resulting
Table 4 (continued)
ERIC category Occurrences Implementation strategies (author/year)
Recruit, designate and train for leadership 2 Recruit, designate and train for leadership (Ditlopo et al. 2011) [91]Top‑down supervision from the central government (Zhou et al. 2019) [67]
Promote adaptability 2 Development and adaptation of guidelines to make them specific for low‑income contexts (Callaghan‑Koru et al. 2020) [86]Adapted the guidelines to their national context (Bryce et al. 2005) [58]
Alter incentive/allowance structures 2 Conditional cash transfers to reduce TB vulnerability; incentivize and enable care (Wingfield et al. 2015) [113]Alter incentive/allowance structures (Ditlopo et al. 2011) [91]
Centralize technical assistance 2 Centralize technical assistance (Andrade et al. 2017) [75]Development of new systems (integrating human resources, financing, etc.) that provided alignment across various departments (Schneider and Nxumalo 2017) [97]
Conduct local consensus discussions 2 Stakeholder engagement (Roman et al. 2014) [66]Targeted interactions of PHC designers with local actors shaped a wide net‑work of friends before the implementation phase (Moshiri et al. 2016) [95]
Involve executive boards 2 Trained key decision‑makers and built government commitment (Bryce et al. 2005) [58]Integrated care into health services provided by the national government (Gueye et al. 2016) [108]
Involve patients/consumers and family members 2 Initiated groups/forums such as Mother to Mother service—where trained mothers living with HIV provided psychosocial support to pregnant women and mother of babies diagnosed with HIV (Mutabazi et al. 2020) [87]Participatory community meetings (Wingfield et al. 2015) [113]
Obtain and use patients and family feedback 2 Obtain community acceptance (Shelley et al. 2016) [99]Community dialogue and action days (Kavle et al. 2018) [114]
Organize clinical implementation team meetings 2 Support groups; mentorship and support (Kavle et al. 2018) [114]Elicited feedback on any site‑specific concerns not addressed and encouraged system buy‑in among the individuals who would ultimately implement the system (Halpern et al. 2010) [77]
Revise professional roles 2 Reallocation of roles and responsibilities (Schneider and Nxumalo, 2017) [97]Stream linking tasks and roles to expand treatment and care for HIV (Mutabazi et al. 2020) [87]
Provide ongoing consultation 1 Supervision/support system (Shelley et al. 2016) [99]
Capture and share local knowledge 1 Capture and share local knowledge (Andrade et al. 2017) [75]
Use other payment schemes 1 A new public health insurance scheme which provides treatments within a defined “core” benefits package to registered members for a co‑payment (Leethongdee 2007) [83]
Provide local technical assistance 1 Between visits, throughout the implementation process, working group mem‑bers were available for technical consultation (Halpern et al. 2010) [77]
Make training dynamic 1 Training as a facilitated, interactive and more hands‑on approach to learning; integrating learning and practice clinical work allow for feedback/revisions/clarifications (Stein et al. 2008) [106]
Make billing easier 1 Institution flow for timely funding (Lavôr et al. 2016) [111]
Inform local opinion leaders 1 Built government commitment to move forward (Bryce et al. 2005) [58]
Assess for readiness and identify barriers and facilitators 1 Baseline assessment (Kihembo et al. 2018) [57]
Change record systems 1 Change record systems (Ejeta et al. 2020) [107]
Create new clinical teams 1 Deploy health workers (Mkoka et al. 2014) [94]
Tailor strategies 1 Tailor strategies to local context (Andrade et al. 2017) [75]
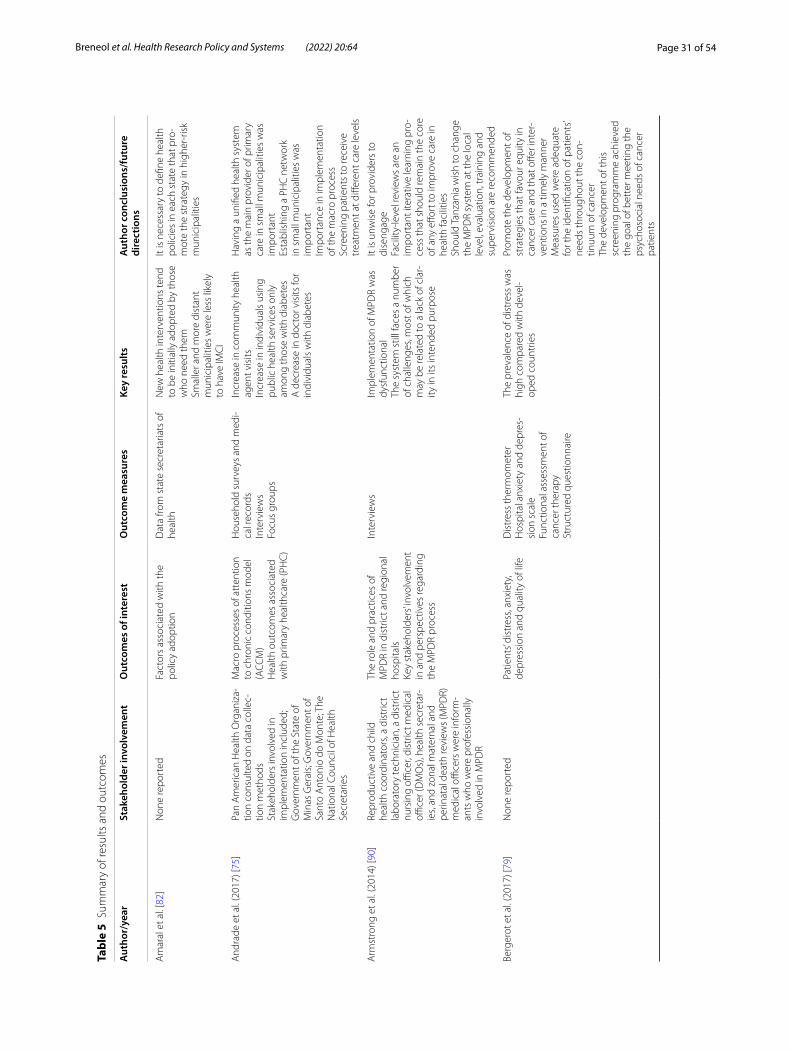
Page 31 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
Sum
mar
y of
resu
lts a
nd o
utco
mes
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Am
aral
et a
l. [8
2]N
one
repo
rted
Fact
ors
asso
ciat
ed w
ith th
e po
licy
adop
tion
Dat
a fro
m s
tate
sec
reta
riats
of
heal
thN
ew h
ealth
inte
rven
tions
tend
to
be
initi
ally
ado
pted
by
thos
e w
ho n
eed
them
Smal
ler a
nd m
ore
dist
ant
mun
icip
aliti
es w
ere
less
like
ly
to h
ave
IMC
I
It is
nec
essa
ry to
defi
ne h
ealth
po
licie
s in
eac
h st
ate
that
pro
‑m
ote
the
stra
tegy
in h
ighe
r‑ris
k m
unic
ipal
ities
And
rade
et a
l. (2
017)
[75]
Pan
Am
eric
an H
ealth
Org
aniz
a‑tio
n co
nsul
ted
on d
ata
colle
c‑tio
n m
etho
dsSt
akeh
olde
rs in
volv
ed in
im
plem
enta
tion
incl
uded
; G
over
nmen
t of t
he S
tate
of
Min
as G
erai
s; G
over
nmen
t of
Sant
o A
nton
io d
o M
onte
; The
N
atio
nal C
ounc
il of
Hea
lth
Secr
etar
ies
Mac
ro p
roce
sses
of a
tten
tion
to c
hron
ic c
ondi
tions
mod
el
(ACC
M)
Hea
lth o
utco
mes
ass
ocia
ted
with
prim
ary
heal
thca
re (P
HC
)
Hou
seho
ld s
urve
ys a
nd m
edi‑
cal r
ecor
dsIn
terv
iew
sFo
cus
grou
ps
Incr
ease
in c
omm
unity
hea
lth
agen
t vis
itsIn
crea
se in
indi
vidu
als
usin
g pu
blic
hea
lth s
ervi
ces
only
am
ong
thos
e w
ith d
iabe
tes
A d
ecre
ase
in d
octo
r vis
its fo
r in
divi
dual
s w
ith d
iabe
tes
Hav
ing
a un
ified
hea
lth s
yste
m
as th
e m
ain
prov
ider
of p
rimar
y ca
re in
sm
all m
unic
ipal
ities
was
im
port
ant
Esta
blis
hing
a P
HC
net
wor
k in
sm
all m
unic
ipal
ities
was
im
port
ant
Impo
rtan
ce in
impl
emen
tatio
n of
the
mac
ro p
roce
ssSc
reen
ing
patie
nts
to re
ceiv
e tr
eatm
ent a
t diff
eren
t car
e le
vels
Arm
stro
ng e
t al.
(201
4) [9
0]Re
prod
uctiv
e an
d ch
ild
heal
th c
oord
inat
ors,
a di
stric
t la
bora
tory
tech
nici
an, a
dis
tric
t nu
rsin
g offi
cer,
dist
rict m
edic
al
office
r (D
MO
s), h
ealth
sec
reta
r‑ie
s, an
d zo
nal m
ater
nal a
nd
perin
atal
dea
th re
view
s (M
PDR)
m
edic
al o
ffice
rs w
ere
info
rm‑
ants
who
wer
e pr
ofes
sion
ally
in
volv
ed in
MPD
R
The
role
and
pra
ctic
es o
f M
PDR
in d
istr
ict a
nd re
gion
al
hosp
itals
Key
stak
ehol
ders
’ invo
lvem
ent
in a
nd p
ersp
ectiv
es re
gard
ing
the
MPD
R pr
oces
s
Inte
rvie
ws
Impl
emen
tatio
n of
MPD
R w
as
dysf
unct
iona
lTh
e sy
stem
stil
l fac
es a
num
ber
of c
halle
nges
, mos
t of w
hich
m
ay b
e re
late
d to
a la
ck o
f cla
r‑ity
in it
s in
tend
ed p
urpo
se
It is
unw
ise
for p
rovi
ders
to
dise
ngag
eFa
cilit
y‑le
vel r
evie
ws
are
an
impo
rtan
t ite
rativ
e le
arni
ng p
ro‑
cess
that
sho
uld
rem
ain
the
core
of
any
effo
rt to
impr
ove
care
in
heal
th fa
cilit
ies
Shou
ld T
anza
nia
wis
h to
cha
nge
the
MPD
R sy
stem
at t
he lo
cal
leve
l, ev
alua
tion,
trai
ning
and
su
perv
isio
n ar
e re
com
men
ded
Berg
erot
et a
l. (2
017)
[79]
Non
e re
port
edPa
tient
s’ di
stre
ss, a
nxie
ty,
depr
essi
on a
nd q
ualit
y of
life
Dis
tres
s th
erm
omet
erH
ospi
tal a
nxie
ty a
nd d
epre
s‑si
on s
cale
Func
tiona
l ass
essm
ent o
f ca
ncer
ther
apy
Stru
ctur
ed q
uest
ionn
aire
The
prev
alen
ce o
f dis
tres
s w
as
high
com
pare
d w
ith d
evel
‑op
ed c
ount
ries
Prom
ote
the
deve
lopm
ent o
f st
rate
gies
that
favo
ur e
quity
in
canc
er c
are
and
that
offe
r int
er‑
vent
ions
in a
tim
ely
man
ner
Mea
sure
s us
ed w
ere
adeq
uate
fo
r the
iden
tifica
tion
of p
atie
nts’
need
s th
roug
hout
the
con‑
tinuu
m o
f can
cer
The
deve
lopm
ent o
f thi
s sc
reen
ing
prog
ram
me
achi
eved
th
e go
al o
f bet
ter m
eetin
g th
e ps
ycho
soci
al n
eeds
of c
ance
r pa
tient
s
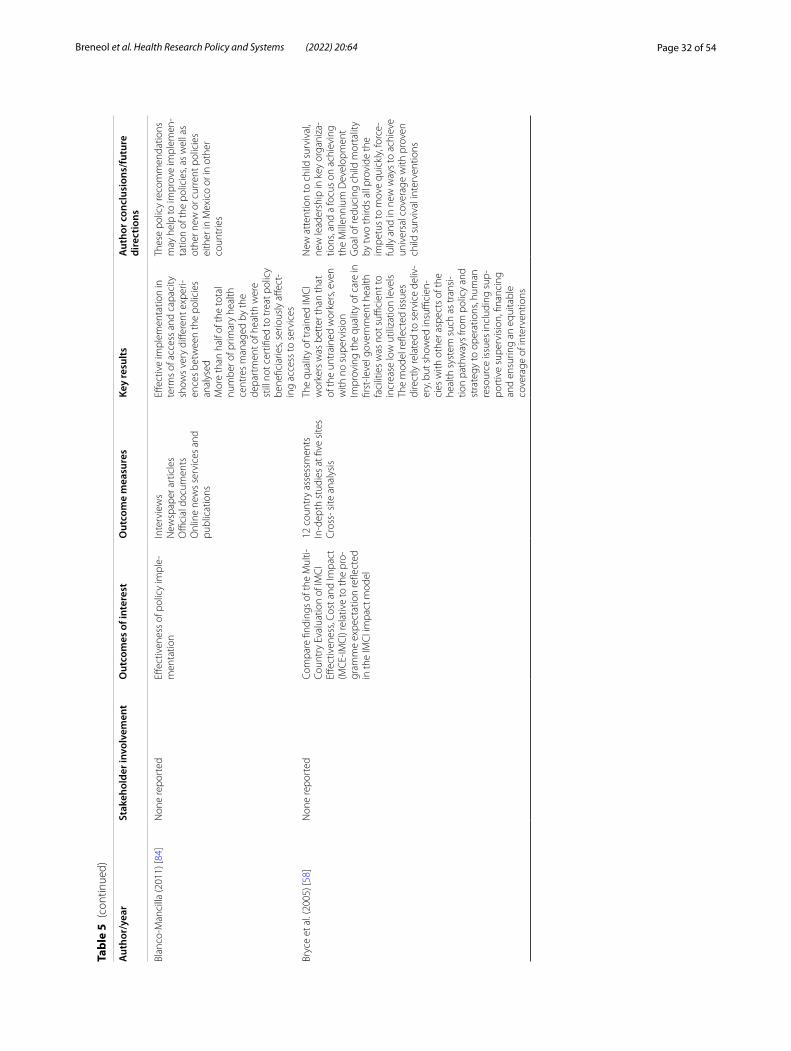
Page 32 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Blan
co‑M
anci
lla (2
011)
[84]
Non
e re
port
edEff
ectiv
enes
s of
pol
icy
impl
e‑m
enta
tion
Inte
rvie
ws
New
spap
er a
rtic
les
Offi
cial
doc
umen
tsO
nlin
e ne
ws
serv
ices
and
pu
blic
atio
ns
Effec
tive
impl
emen
tatio
n in
te
rms
of a
cces
s an
d ca
paci
ty
show
s ve
ry d
iffer
ent e
xper
i‑en
ces
betw
een
the
polic
ies
anal
ysed
Mor
e th
an h
alf o
f the
tota
l nu
mbe
r of p
rimar
y he
alth
ce
ntre
s m
anag
ed b
y th
e de
part
men
t of h
ealth
wer
e st
ill n
ot c
ertifi
ed to
trea
t pol
icy
bene
ficia
ries,
serio
usly
affe
ct‑
ing
acce
ss to
ser
vice
s
Thes
e po
licy
reco
mm
enda
tions
m
ay h
elp
to im
prov
e im
plem
en‑
tatio
n of
the
polic
ies,
as w
ell a
s ot
her n
ew o
r cur
rent
pol
icie
s ei
ther
in M
exic
o or
in o
ther
co
untr
ies
Bryc
e et
al.
(200
5) [5
8]N
one
repo
rted
Com
pare
find
ings
of t
he M
ulti‑
Coun
try
Eval
uatio
n of
IMC
I Eff
ectiv
enes
s, Co
st a
nd Im
pact
(M
CE‑
IMC
I) re
lativ
e to
the
pro‑
gram
me
expe
ctat
ion
refle
cted
in
the
IMC
I im
pact
mod
el
12 c
ount
ry a
sses
smen
tsIn
‑dep
th s
tudi
es a
t five
site
sC
ross
‑ site
ana
lysi
s
The
qual
ity o
f tra
ined
IMC
I w
orke
rs w
as b
ette
r tha
n th
at
of th
e un
trai
ned
wor
kers
, eve
n w
ith n
o su
perv
isio
nIm
prov
ing
the
qual
ity o
f car
e in
fir
st‑le
vel g
over
nmen
t hea
lth
faci
litie
s w
as n
ot s
uffici
ent t
o in
crea
se lo
w u
tiliz
atio
n le
vels
The
mod
el re
flect
ed is
sues
di
rect
ly re
late
d to
ser
vice
del
iv‑
ery,
but
sho
wed
insu
ffici
en‑
cies
with
oth
er a
spec
ts o
f the
he
alth
sys
tem
suc
h as
tran
si‑
tion
path
way
s fro
m p
olic
y an
d st
rate
gy to
ope
ratio
ns, h
uman
re
sour
ce is
sues
incl
udin
g su
p‑po
rtiv
e su
perv
isio
n, fi
nanc
ing
and
ensu
ring
an e
quita
ble
cove
rage
of i
nter
vent
ions
New
att
entio
n to
chi
ld s
urvi
val,
new
lead
ersh
ip in
key
org
aniz
a‑tio
ns, a
nd a
focu
s on
ach
ievi
ng
the
Mill
enni
um D
evel
opm
ent
Goa
l of r
educ
ing
child
mor
talit
y by
two
third
s al
l pro
vide
the
impe
tus
to m
ove
quic
kly,
forc
e‑fu
lly a
nd in
new
way
s to
ach
ieve
un
iver
sal c
over
age
with
pro
ven
child
sur
viva
l int
erve
ntio
ns
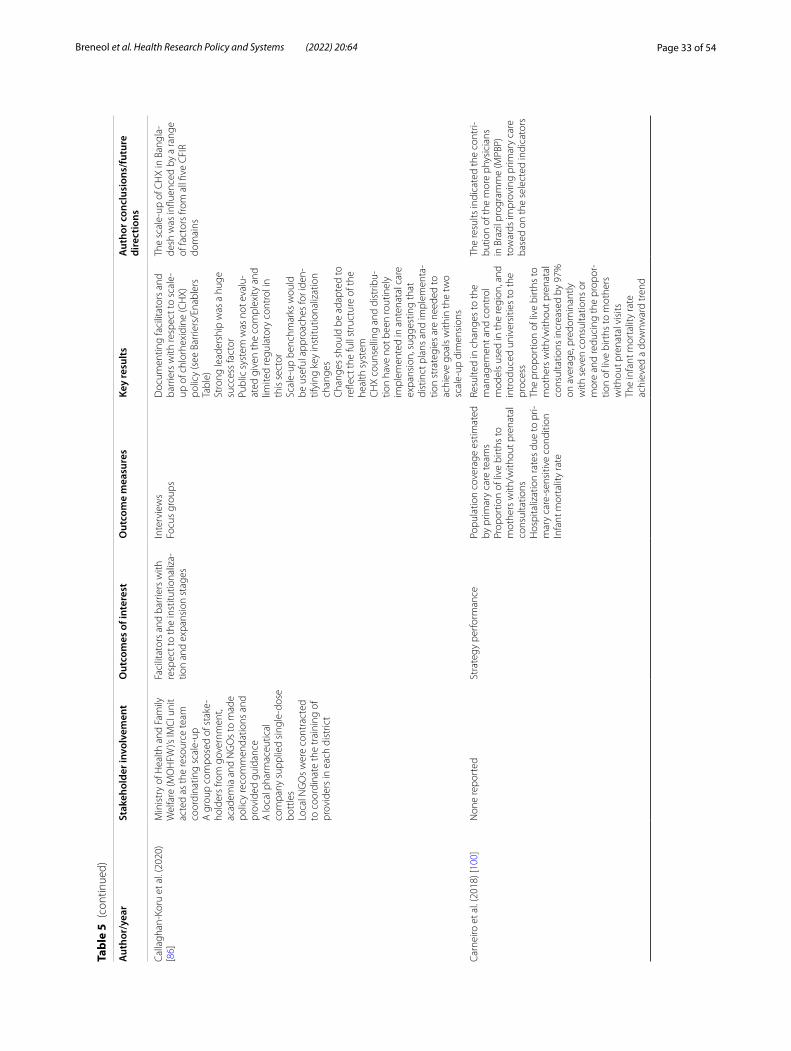
Page 33 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Calla
ghan
‑Kor
u et
al.
(202
0)
[86]
Min
istr
y of
Hea
lth a
nd F
amily
W
elfa
re (M
OH
FW)’s
IMC
I uni
t ac
ted
as th
e re
sour
ce te
am
coor
dina
ting
scal
e‑up
A g
roup
com
pose
d of
sta
ke‑
hold
ers
from
gov
ernm
ent,
acad
emia
and
NG
Os
to m
ade
polic
y re
com
men
datio
ns a
nd
prov
ided
gui
danc
eA
loca
l pha
rmac
eutic
al
com
pany
sup
plie
d si
ngle
‑dos
e bo
ttle
sLo
cal N
GO
s w
ere
cont
ract
ed
to c
oord
inat
e th
e tr
aini
ng o
f pr
ovid
ers
in e
ach
dist
rict
Faci
litat
ors
and
barr
iers
with
re
spec
t to
the
inst
itutio
naliz
a‑tio
n an
d ex
pans
ion
stag
es
Inte
rvie
ws
Focu
s gr
oups
Doc
umen
ting
faci
litat
ors
and
barr
iers
with
resp
ect t
o sc
ale‑
up o
f chl
orhe
xidi
ne (C
HX)
po
licy
(see
Bar
riers
/Ena
bler
s Ta
ble)
Stro
ng le
ader
ship
was
a h
uge
succ
ess
fact
orPu
blic
sys
tem
was
not
eva
lu‑
ated
giv
en th
e co
mpl
exity
and
lim
ited
regu
lato
ry c
ontr
ol in
th
is s
ecto
rSc
ale‑
up b
ench
mar
ks w
ould
be
use
ful a
ppro
ache
s fo
r ide
n‑tif
ying
key
inst
itutio
naliz
atio
n ch
ange
sC
hang
es s
houl
d be
ada
pted
to
refle
ct th
e fu
ll st
ruct
ure
of th
e he
alth
sys
tem
CH
X co
unse
lling
and
dis
trib
u‑tio
n ha
ve n
ot b
een
rout
inel
y im
plem
ente
d in
ant
enat
al c
are
expa
nsio
n, s
ugge
stin
g th
at
dist
inct
pla
ns a
nd im
plem
enta
‑tio
n st
rate
gies
are
nee
ded
to
achi
eve
goal
s w
ithin
the
two
scal
e‑up
dim
ensi
ons
The
scal
e‑up
of C
HX
in B
angl
a‑de
sh w
as in
fluen
ced
by a
rang
e of
fact
ors
from
all
five
CFI
R do
mai
ns
Carn
eiro
et a
l. (2
018)
[100
]N
one
repo
rted
Stra
tegy
per
form
ance
Popu
latio
n co
vera
ge e
stim
ated
by
prim
ary
care
team
sPr
opor
tion
of li
ve b
irths
to
mot
hers
with
/with
out p
rena
tal
cons
ulta
tions
Hos
pita
lizat
ion
rate
s du
e to
pri‑
mar
y ca
re‑s
ensi
tive
cond
ition
Infa
nt m
orta
lity
rate
Resu
lted
in c
hang
es to
the
man
agem
ent a
nd c
ontr
ol
mod
els
used
in th
e re
gion
, and
in
trod
uced
uni
vers
ities
to th
e pr
oces
sTh
e pr
opor
tion
of li
ve b
irths
to
mot
hers
with
/with
out p
rena
tal
cons
ulta
tions
incr
ease
d by
97%
on
ave
rage
, pre
dom
inan
tly
with
sev
en c
onsu
ltatio
ns o
r m
ore
and
redu
cing
the
prop
or‑
tion
of li
ve b
irths
to m
othe
rs
with
out p
rena
tal v
isits
The
infa
nt m
orta
lity
rate
ac
hiev
ed a
dow
nwar
d tr
end
The
resu
lts in
dica
ted
the
cont
ri‑bu
tion
of th
e m
ore
phys
icia
ns
in B
razi
l pro
gram
me
(MPB
P)
tow
ards
impr
ovin
g pr
imar
y ca
re
base
d on
the
sele
cted
indi
cato
rs
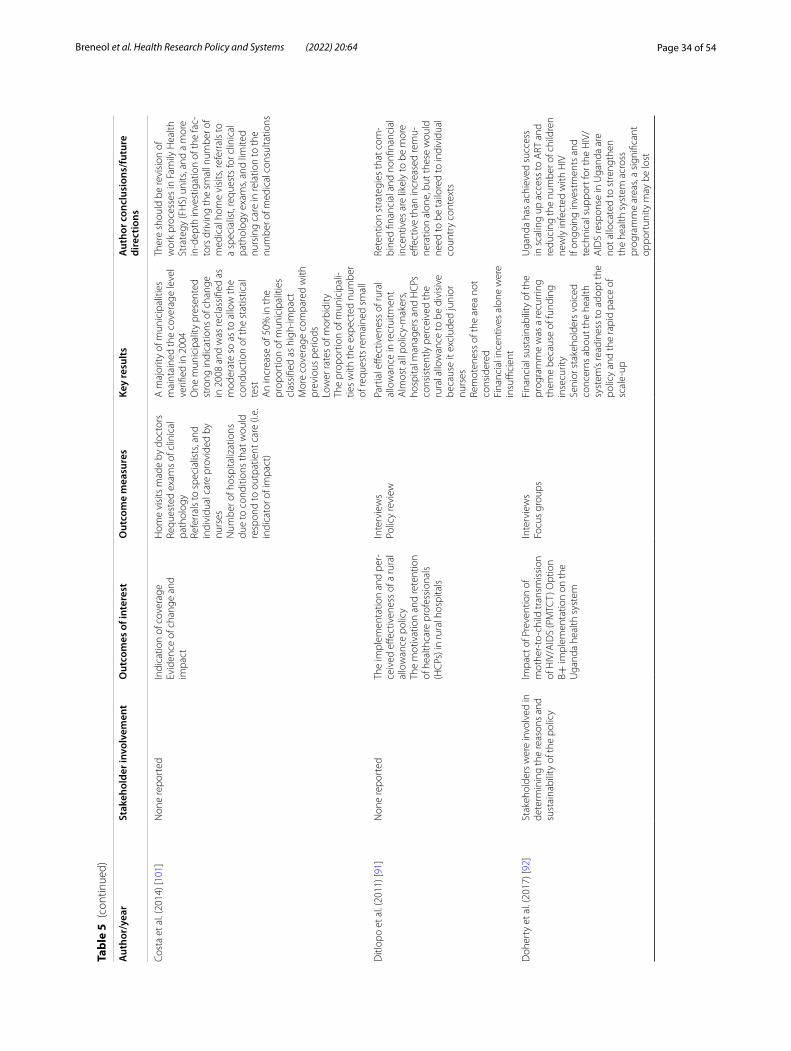
Page 34 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Cost
a et
al.
(201
4) [1
01]
Non
e re
port
edIn
dica
tion
of c
over
age
Evid
ence
of c
hang
e an
d im
pact
Hom
e vi
sits
mad
e by
doc
tors
Requ
este
d ex
ams
of c
linic
al
path
olog
yRe
ferr
als
to s
peci
alis
ts, a
nd
indi
vidu
al c
are
prov
ided
by
nurs
esN
umbe
r of h
ospi
taliz
atio
ns
due
to c
ondi
tions
that
wou
ld
resp
ond
to o
utpa
tient
car
e (i.
e.
indi
cato
r of i
mpa
ct)
A m
ajor
ity o
f mun
icip
aliti
es
mai
ntai
ned
the
cove
rage
leve
l ve
rified
in 2
004
One
mun
icip
ality
pre
sent
ed
stro
ng in
dica
tions
of c
hang
e in
200
8 an
d w
as re
clas
sifie
d as
m
oder
ate
so a
s to
allo
w th
e co
nduc
tion
of th
e st
atis
tical
te
stA
n in
crea
se o
f 50%
in th
e pr
opor
tion
of m
unic
ipal
ities
cl
assi
fied
as h
igh‑
impa
ctM
ore
cove
rage
com
pare
d w
ith
prev
ious
per
iods
Low
er ra
tes
of m
orbi
dity
The
prop
ortio
n of
mun
icip
ali‑
ties
with
the
expe
cted
num
ber
of re
ques
ts re
mai
ned
smal
l
Ther
e sh
ould
be
revi
sion
of
wor
k pr
oces
ses
in F
amily
Hea
lth
Stra
tegy
(FH
S) u
nits
, and
a m
ore
in‑d
epth
inve
stig
atio
n of
the
fac‑
tors
driv
ing
the
smal
l num
ber o
f m
edic
al h
ome
visi
ts, r
efer
rals
to
a sp
ecia
list,
requ
ests
for c
linic
al
path
olog
y ex
ams,
and
limite
d nu
rsin
g ca
re in
rela
tion
to th
e nu
mbe
r of m
edic
al c
onsu
ltatio
ns
Ditl
opo
et a
l. (2
011)
[91]
Non
e re
port
edTh
e im
plem
enta
tion
and
per‑
ceiv
ed e
ffect
iven
ess
of a
rura
l al
low
ance
pol
icy
The
mot
ivat
ion
and
rete
ntio
n of
hea
lthca
re p
rofe
ssio
nals
(H
CPs
) in
rura
l hos
pita
ls
Inte
rvie
ws
Polic
y re
view
Part
ial e
ffect
iven
ess
of ru
ral
allo
wan
ce in
recr
uitm
ent
Alm
ost a
ll po
licy‑
mak
ers,
hosp
ital m
anag
ers
and
HC
Ps
cons
iste
ntly
per
ceiv
ed th
e ru
ral a
llow
ance
to b
e di
visi
ve
beca
use
it ex
clud
ed ju
nior
nu
rses
Rem
oten
ess
of th
e ar
ea n
ot
cons
ider
edFi
nanc
ial i
ncen
tives
alo
ne w
ere
insu
ffici
ent
Rete
ntio
n st
rate
gies
that
com
‑bi
ned
finan
cial
and
non
finan
cial
in
cent
ives
are
like
ly to
be
mor
e eff
ectiv
e th
an in
crea
sed
rem
u‑ne
ratio
n al
one,
but
thes
e w
ould
ne
ed to
be
tailo
red
to in
divi
dual
co
untr
y co
ntex
ts
Doh
erty
et a
l. (2
017)
[92]
Stak
ehol
ders
wer
e in
volv
ed in
de
term
inin
g th
e re
ason
s an
d su
stai
nabi
lity
of th
e po
licy
Impa
ct o
f Pre
vent
ion
of
mot
her‑
to‑c
hild
tran
smis
sion
of
HIV
/AID
S (P
MTC
T) O
ptio
n B+
impl
emen
tatio
n on
the
Uga
nda
heal
th s
yste
m
Inte
rvie
ws
Focu
s gr
oups
Fina
ncia
l sus
tain
abili
ty o
f the
pr
ogra
mm
e w
as a
recu
rrin
g th
eme
beca
use
of fu
ndin
g in
secu
rity
Seni
or s
take
hold
ers
voic
ed
conc
erns
abo
ut th
e he
alth
sy
stem
’s re
adin
ess
to a
dopt
the
polic
y an
d th
e ra
pid
pace
of
scal
e‑up
Uga
nda
has
achi
eved
suc
cess
in
sca
ling
up a
cces
s to
ART
and
re
duci
ng th
e nu
mbe
r of c
hild
ren
new
ly in
fect
ed w
ith H
IVIf
ongo
ing
inve
stm
ents
and
te
chni
cal s
uppo
rt fo
r the
HIV
/A
IDS
resp
onse
in U
gand
a ar
e no
t allo
cate
d to
str
engt
hen
the
heal
th s
yste
m a
cros
s pr
ogra
mm
e ar
eas,
a si
gnifi
cant
op
port
unity
may
be
lost

Page 35 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Ejet
a et
al.
(202
0) [1
07]
City
/tow
n he
alth
offi
ces
Sub‑
city
and
dis
tric
t offi
ces
Com
mun
ity le
ader
sRe
gion
al h
ealth
bur
eaus
Ethi
opia
n Fe
dera
l Min
istr
y of
H
ealth
Mem
bers
of t
he S
EUH
P pr
o‑gr
amm
eH
ealth
cen
tres
Less
ons
lear
ned
Cha
lleng
es to
impl
emen
tatio
nIn
terv
iew
sD
ocum
ent r
evie
wTh
e pi
lot t
est e
nabl
ed th
e ur
ban
heal
th e
xten
sion
pro
fes‑
sion
als
(UH
E‑Ps
) to
com
pre‑
hens
ivel
y fo
cus
on th
e 15
he
alth
ser
vice
pac
kage
sU
se o
f tal
ly s
heet
hel
ped
colle
ct h
igh‑
qual
ity d
ata
and
repo
rt it
to c
ity/t
own
heal
th
office
sSy
stem
atic
cat
egor
izat
ion
of
hous
ehol
ds, b
ased
on
thei
r ec
onom
ic s
tatu
s an
d he
alth
se
rvic
e ne
eds
allo
wed
for
effec
tive
time
man
agem
ent
and
deliv
ery
of s
ervi
ces
to
vuln
erab
le p
opul
atio
ns
Plan
s ar
e m
ade
to s
cale
up
the
prog
ram
me
to m
ajor
citi
es
Febi
r et a
l. (2
015)
[103
]N
one
repo
rted
Perc
eptio
ns o
f hea
lthca
re
wor
kers
(HC
Ws)
rega
rdin
g th
e is
sues
face
d
Inte
rvie
ws
Impl
emen
tatio
n fa
ced
chal
‑le
nges
giv
en th
e w
eak
heal
th
syst
ems
in m
ost d
evel
opin
g co
untie
sTh
e pe
rcep
tions
of f
ront
‑lin
e H
CW
s on
the
accu
racy
an
d ne
ed fo
r the
gui
delin
e to
geth
er w
ith th
e ca
paci
ty
of h
ealth
sys
tem
s to
sup
port
im
plem
enta
tion
play
ed a
cr
ucia
l rol
eG
uide
lines
on
finan
cing
of
diag
nost
ics
and
trea
tmen
ts a
re
influ
enci
ng c
linic
al d
ecis
ion‑
mak
ing
in th
is s
ettin
g
Furt
her r
esea
rch
is n
eede
d to
un
ders
tand
the
impa
ct o
f the
N
atio
nal H
ealth
Inte
rvie
w S
urve
y (N
HIS
) on
the
feas
ibili
ty o
f int
e‑gr
atin
g te
st‑b
ased
man
agem
ent
for m
alar
ia o
f the
IMC
I gui
delin
esFi
ndin
gs s
ugge
st th
at th
e pr
oble
m is
hei
ghte
ned
by
belie
fs a
nd h
abits
of f
ront
line
heal
th s
taff
in h
ealth
faci
litie
s in
de
velo
ping
cou
ntrie
s th
at a
re
used
to p
resu
mpt
ive
trea
tmen
t an
d pe
rcei
ve e
very
feve
r to
be
mal
aria
Gue
ye e
t al.
(201
6) [1
08]
Non
e re
port
edW
ays
in w
hich
cou
ntrie
s ha
ve
impl
emen
ted
elim
inat
ion
prog
ram
mes
The
deve
lopm
ent a
nd a
dop‑
tion
of p
rogr
amm
esH
ow p
rogr
amm
es o
pera
ted
with
in th
eir c
onte
xt
Revi
ew o
f cas
e st
udy
repo
rts
Mal
aria
pro
gram
mes
did
not
sh
ow a
hig
h le
vel o
f cap
acity
fo
r ant
icip
atio
n of
thre
ats
to
elim
inat
ion
Ther
e w
ere
man
y ex
ampl
es o
f m
ajor
dev
elop
men
t pro
jec‑
tions
that
com
bine
d a
pote
n‑tia
l for
incr
ease
d re
cept
ivity
an
d vu
lner
abili
tyM
onito
ring
and
eval
ua‑
tion
incl
uded
mon
itorin
g pr
ogra
mm
e ou
tput
s an
d ev
alu‑
atio
n of
impa
ct
Glo
bal m
alar
ia e
radi
catio
n w
ill re
quire
wel
l‑man
aged
m
alar
ia p
rogr
amm
es p
rovi
ding
hi
gh‑q
ualit
y im
plem
enta
tion
of e
vide
nce‑
base
d st
rate
gies
, fo
unde
d up
on s
tron
g su
rvei
l‑la
nce
and
resp
onse
str
ateg
ies
tailo
red
to th
e su
bnat
iona
l lev
el
tran
smis
sion
con
text
Ade
quat
e fu
ndin
g an
d hu
man
re
sour
ces
to s
usta
in m
alar
ia
elim
inat
ion
and
prev
entio
n of
re
intr
oduc
tion
is a
lso
requ
ired
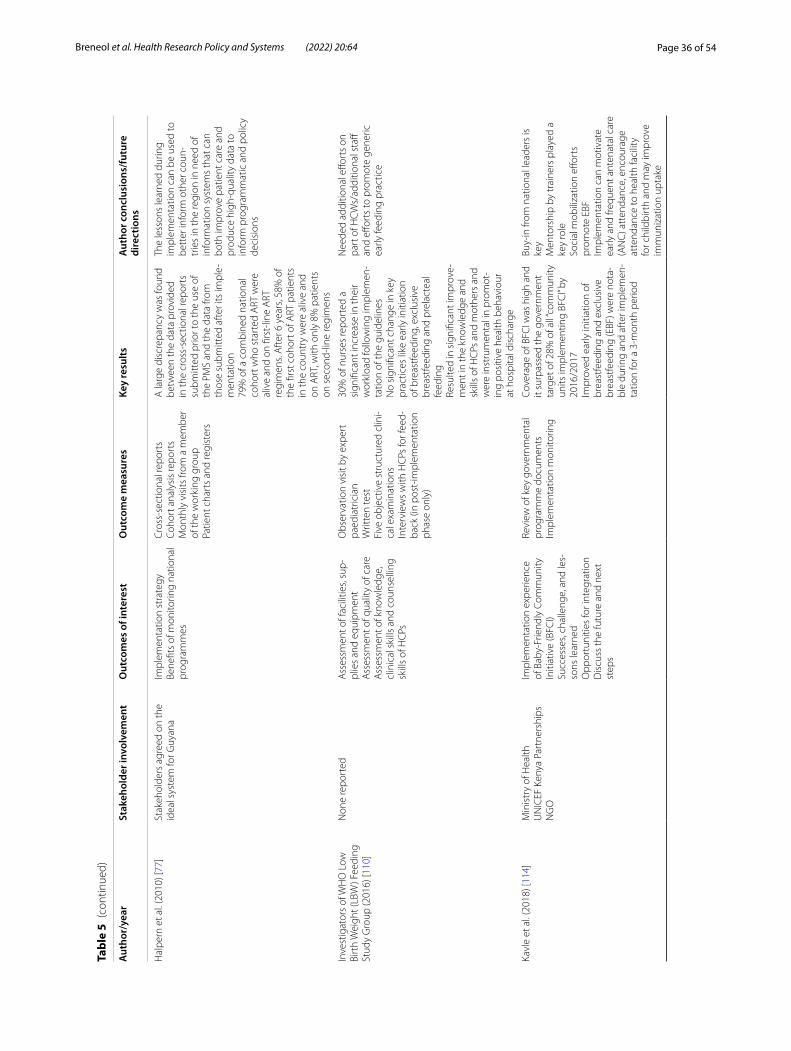
Page 36 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Hal
pern
et a
l. (2
010)
[77]
Stak
ehol
ders
agr
eed
on th
e id
eal s
yste
m fo
r Guy
ana
Impl
emen
tatio
n st
rate
gyBe
nefit
s of
mon
itorin
g na
tiona
l pr
ogra
mm
es
Cro
ss‑s
ectio
nal r
epor
tsCo
hort
ana
lysi
s re
port
sM
onth
ly v
isits
from
a m
embe
r of
the
wor
king
gro
upPa
tient
cha
rts
and
regi
ster
s
A la
rge
disc
repa
ncy
was
foun
d be
twee
n th
e da
ta p
rovi
ded
in th
e cr
oss‑
sect
iona
l rep
orts
su
bmitt
ed p
rior t
o th
e us
e of
th
e PM
S an
d th
e da
ta fr
om
thos
e su
bmitt
ed a
fter
its
impl
e‑m
enta
tion
79%
of a
com
bine
d na
tiona
l co
hort
who
sta
rted
ART
wer
e al
ive
and
on fi
rst‑
line
ART
re
gim
ens.
Aft
er 6
yea
rs, 5
8% o
f th
e fir
st c
ohor
t of A
RT p
atie
nts
in th
e co
untr
y w
ere
aliv
e an
d on
ART
, with
onl
y 8%
pat
ient
s on
sec
ond‑
line
regi
men
s
The
less
ons
lear
ned
durin
g im
plem
enta
tion
can
be u
sed
to
bett
er in
form
oth
er c
oun‑
trie
s in
the
regi
on in
nee
d of
in
form
atio
n sy
stem
s th
at c
an
both
impr
ove
patie
nt c
are
and
prod
uce
high
‑qua
lity
data
to
info
rm p
rogr
amm
atic
and
pol
icy
deci
sion
s
Inve
stig
ator
s of
WH
O L
ow
Birt
h W
eigh
t (LB
W) F
eedi
ng
Stud
y G
roup
(201
6) [1
10]
Non
e re
port
edA
sses
smen
t of f
acili
ties,
sup‑
plie
s an
d eq
uipm
ent
Ass
essm
ent o
f qua
lity
of c
are
Ass
essm
ent o
f kno
wle
dge,
cl
inic
al s
kills
and
cou
nsel
ling
skill
s of
HC
Ps
Obs
erva
tion
visi
t by
expe
rt
paed
iatr
icia
nW
ritte
n te
stFi
ve o
bjec
tive
stru
ctur
ed c
lini‑
cal e
xam
inat
ions
Inte
rvie
ws
with
HC
Ps fo
r fee
d‑ba
ck (i
n po
st‑im
plem
enta
tion
phas
e on
ly)
30%
of n
urse
s re
port
ed a
si
gnifi
cant
incr
ease
in th
eir
wor
kloa
d fo
llow
ing
impl
emen
‑ta
tion
of th
e gu
idel
ines
No
sign
ifica
nt c
hang
e in
key
pr
actic
es li
ke e
arly
initi
atio
n of
bre
astfe
edin
g, e
xclu
sive
br
east
feed
ing
and
prel
acte
al
feed
ing
Resu
lted
in s
igni
fican
t im
prov
e‑m
ent i
n th
e kn
owle
dge
and
skill
s of
HC
Ps a
nd m
othe
rs a
nd
wer
e in
stru
men
tal i
n pr
omot
‑in
g po
sitiv
e he
alth
beh
avio
ur
at h
ospi
tal d
isch
arge
Nee
ded
addi
tiona
l effo
rts
on
part
of H
CW
s/ad
ditio
nal s
taff
and
effor
ts to
pro
mot
e ge
neric
ea
rly fe
edin
g pr
actic
e
Kavl
e et
al.
(201
8) [1
14]
Min
istr
y of
Hea
lthU
NIC
EF K
enya
Par
tner
ship
sN
GO
Impl
emen
tatio
n ex
perie
nce
of B
aby‑
Frie
ndly
Com
mun
ity
Initi
ativ
e (B
FCI)
Succ
esse
s, ch
alle
nge,
and
les‑
sons
lear
ned
Opp
ortu
nitie
s fo
r int
egra
tion
Dis
cuss
the
futu
re a
nd n
ext
step
s
Revi
ew o
f key
gov
ernm
enta
l pr
ogra
mm
e do
cum
ents
Impl
emen
tatio
n m
onito
ring
Cove
rage
of B
FCI w
as h
igh
and
it su
rpas
sed
the
gove
rnm
ent
targ
et o
f 28%
of a
ll “co
mm
unity
un
its im
plem
entin
g BF
CI”
by
2016
/201
7Im
prov
ed e
arly
initi
atio
n of
br
east
feed
ing
and
excl
usiv
e br
east
feed
ing
(EBF
) wer
e no
ta‑
ble
durin
g an
d af
ter i
mpl
emen
‑ta
tion
for a
3‑m
onth
per
iod
Buy‑
in fr
om n
atio
nal l
eade
rs is
ke
yM
ento
rshi
p by
trai
ners
pla
yed
a ke
y ro
leSo
cial
mob
iliza
tion
effor
ts
prom
ote
EBF
Impl
emen
tatio
n ca
n m
otiv
ate
early
and
freq
uent
ant
enat
al c
are
(AN
C) a
tten
danc
e, e
ncou
rage
at
tend
ance
to h
ealth
faci
lity
for c
hild
birt
h an
d m
ay im
prov
e im
mun
izat
ion
upta
ke
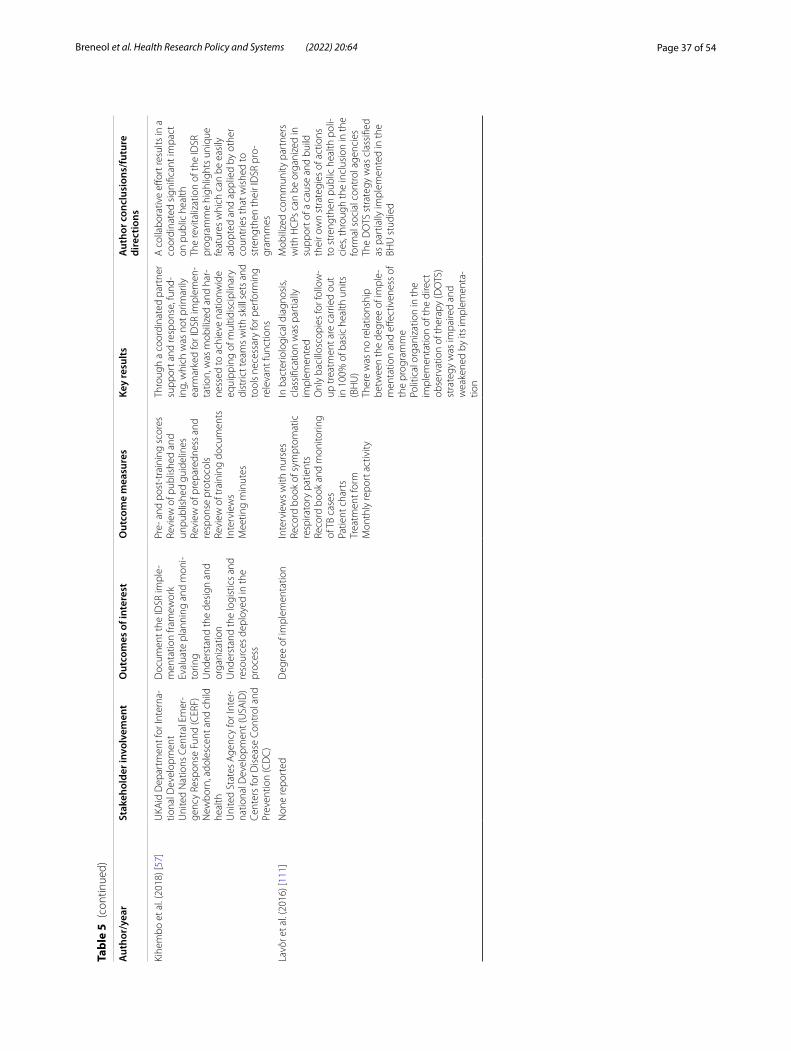
Page 37 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Kihe
mbo
et a
l. (2
018)
[57]
UKA
id D
epar
tmen
t for
Inte
rna‑
tiona
l Dev
elop
men
tU
nite
d N
atio
ns C
entr
al E
mer
‑ge
ncy
Resp
onse
Fun
d (C
ERF)
New
born
, ado
lesc
ent a
nd c
hild
he
alth
Uni
ted
Stat
es A
genc
y fo
r Int
er‑
natio
nal D
evel
opm
ent (
USA
ID)
Cent
ers
for D
isea
se C
ontr
ol a
nd
Prev
entio
n (C
DC
)
Doc
umen
t the
IDSR
impl
e‑m
enta
tion
fram
ewor
kEv
alua
te p
lann
ing
and
mon
i‑to
ring
Und
erst
and
the
desi
gn a
nd
orga
niza
tion
Und
erst
and
the
logi
stic
s an
d re
sour
ces
depl
oyed
in th
e pr
oces
s
Pre‑
and
pos
t‑tr
aini
ng s
core
sRe
view
of p
ublis
hed
and
unpu
blis
hed
guid
elin
esRe
view
of p
repa
redn
ess
and
resp
onse
pro
toco
lsRe
view
of t
rain
ing
docu
men
tsIn
terv
iew
sM
eetin
g m
inut
es
Thro
ugh
a co
ordi
nate
d pa
rtne
r su
ppor
t and
resp
onse
, fun
d‑in
g, w
hich
was
not
prim
arily
ea
rmar
ked
for I
DSR
impl
emen
‑ta
tion,
was
mob
ilize
d an
d ha
r‑ne
ssed
to a
chie
ve n
atio
nwid
e eq
uipp
ing
of m
ultid
isci
plin
ary
dist
rict t
eam
s w
ith s
kill
sets
and
to
ols
nece
ssar
y fo
r per
form
ing
rele
vant
func
tions
A c
olla
bora
tive
effor
t res
ults
in a
co
ordi
nate
d si
gnifi
cant
impa
ct
on p
ublic
hea
lthTh
e re
vita
lizat
ion
of th
e ID
SR
prog
ram
me
high
light
s un
ique
fe
atur
es w
hich
can
be
easi
ly
adop
ted
and
appl
ied
by o
ther
co
untr
ies
that
wis
hed
to
stre
ngth
en th
eir I
DSR
pro
‑gr
amm
es
Lavô
r et a
l. (2
016)
[111
]N
one
repo
rted
Deg
ree
of im
plem
enta
tion
Inte
rvie
ws
with
nur
ses
Reco
rd b
ook
of s
ympt
omat
ic
resp
irato
ry p
atie
nts
Reco
rd b
ook
and
mon
itorin
g of
TB
case
sPa
tient
cha
rts
Trea
tmen
t for
mM
onth
ly re
port
act
ivity
In b
acte
riolo
gica
l dia
gnos
is,
clas
sific
atio
n w
as p
artia
lly
impl
emen
ted
Onl
y ba
cillo
scop
ies
for f
ollo
w‑
up tr
eatm
ent a
re c
arrie
d ou
t in
100
% o
f bas
ic h
ealth
uni
ts
(BH
U)
Ther
e w
as n
o re
latio
nshi
p be
twee
n th
e de
gree
of i
mpl
e‑m
enta
tion
and
effec
tiven
ess
of
the
prog
ram
me
Polit
ical
org
aniz
atio
n in
the
impl
emen
tatio
n of
the
dire
ct
obse
rvat
ion
of th
erap
y (D
OTS
) st
rate
gy w
as im
paire
d an
d w
eake
ned
by it
s im
plem
enta
‑tio
n
Mob
ilize
d co
mm
unity
par
tner
s w
ith H
CPs
can
be
orga
nize
d in
su
ppor
t of a
cau
se a
nd b
uild
th
eir o
wn
stra
tegi
es o
f act
ions
to
str
engt
hen
publ
ic h
ealth
pol
i‑ci
es, t
hrou
gh th
e in
clus
ion
in th
e fo
rmal
soc
ial c
ontr
ol a
genc
ies
The
DO
TS s
trat
egy
was
cla
ssifi
ed
as p
artia
lly im
plem
ente
d in
the
BHU
stu
died

Page 38 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Leet
hong
dee
(200
7) [8
3]N
one
repo
rted
Influ
ence
s of
impl
emen
tatio
nIn
terv
iew
sFo
cus
grou
psD
ocum
enta
ry a
naly
sis
Mai
n ch
ange
s fo
cuse
d on
the
role
of p
ublic
org
aniz
atio
ns,
and
tens
ions
bet
wee
n th
e ol
d an
d ne
w a
dmin
istr
ativ
e st
ruct
ures
The
choi
ce o
f fun
ding
mec
ha‑
nism
was
an
impo
rtan
t are
a of
lo
cal d
iscr
etio
nM
any
resp
onde
nts,
espe
‑ci
ally
at l
ower
leve
ls, h
ad a
po
or u
nder
stan
ding
of t
he
purc
hase
r/pr
ovid
er s
plit
abou
t to
be
impl
emen
ted
in th
e Th
ai
syst
em, w
hich
hig
hlig
hted
th
e hu
ge s
hift
in c
ultu
re th
at
wou
ld b
e re
quire
d in
the
new
sy
stem
Ther
e w
as a
mac
ro‑le
vel
prob
lem
con
cern
ing
the
dist
ribut
ion
of fi
nanc
e an
d th
e w
orkf
orce
acr
oss
the
natio
nTh
ere
was
a m
icro
‑leve
l pr
oble
m c
once
rnin
g th
e di
strib
utio
n of
reso
urce
s by
co
ntra
ctin
g un
its fo
r prim
ary
care
(CU
Ps) t
o ho
spita
ls a
nd
heal
th c
entr
es
Ther
e w
as a
cyc
le o
f pol
icy
pres
crip
tions
, loc
al a
dapt
atio
ns
and
high
er‑le
vel p
olic
y re
visi
ons
that
affe
cted
sev
eral
asp
ects
of
the
refo
rms
and
part
icul
arly
the
finan
cing
mec
hani
sm, w
hich
re
sulte
d in
the
low
er‑le
vel a
ctor
s ha
ving
the
mos
t im
pact
Li e
t al.
(201
5) [1
12]
Non
e re
port
edIm
pact
of e
ssen
tial d
rug
polic
y on
prim
ary
care
ser
vice
sEff
ectiv
enes
s of
impl
emen
ting
esse
ntia
l dru
g po
licy
Fiel
d ob
serv
atio
nM
ain
oper
atio
n in
dica
tors
Impl
emen
tatio
n w
as v
ery
stab
leTh
e he
alth
adm
inis
tra‑
tive
depa
rtm
ents
sho
uld
stre
ngth
en th
e ch
oice
, co
nfirm
atio
n, a
sses
smen
t and
co
ntro
l of d
istr
ibut
ion
com
‑pa
nies
, est
ablis
h th
e in
dust
ry
stan
dard
s of
dru
g di
strib
utio
n in
dust
ry a
s so
on a
s po
ssib
le,
and
impr
ove
the
acce
ss
thre
shol
d
Thro
ugh
the
inve
stig
atio
n of
gr
assr
oots
med
ical
inst
itutio
ns,
we
can
dete
rmin
e th
e pr
inci
ples
, va
rietie
s an
d pr
ices
of s
peci
fical
ly
supp
lied
drug
s, an
d th
e st
ate
can
desi
gnat
e sp
ecia
lized
man
u‑fa
ctur
ers
for d
rug
man
ufac
turin
g an
d go
vern
men
t can
pro
vide
fin
anci
al s
ubsi
dies
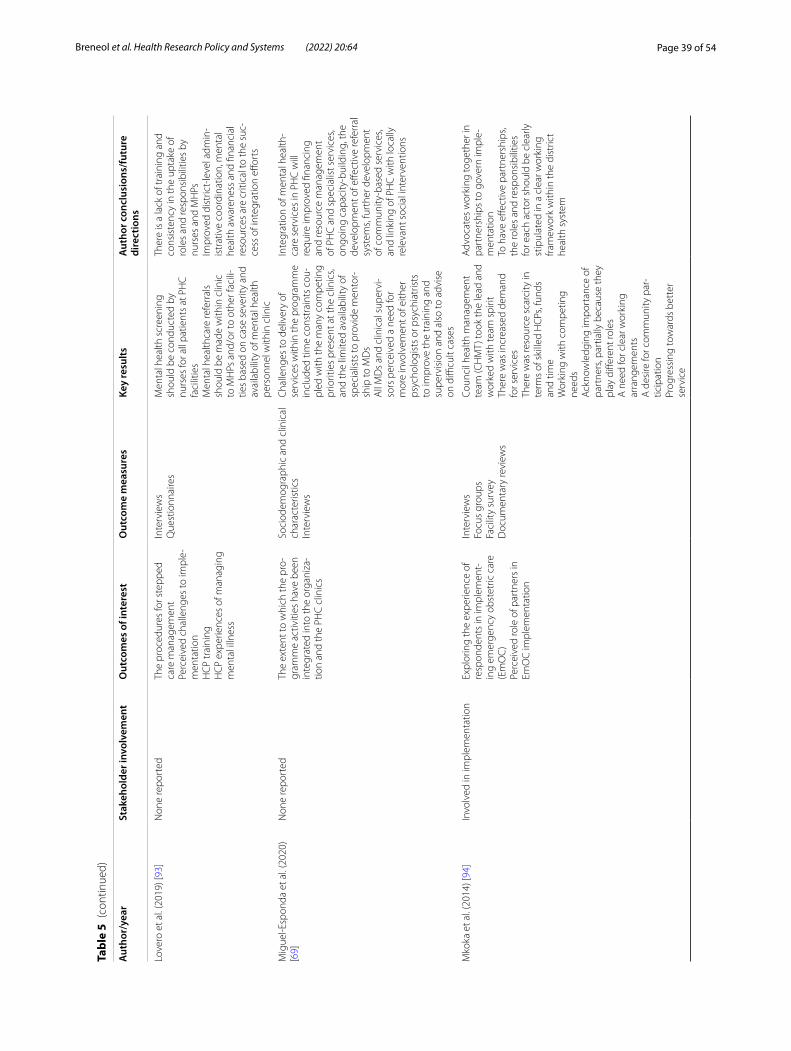
Page 39 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Love
ro e
t al.
(201
9) [9
3]N
one
repo
rted
The
proc
edur
es fo
r ste
pped
ca
re m
anag
emen
tPe
rcei
ved
chal
leng
es to
impl
e‑m
enta
tion
HC
P tr
aini
ngH
CP
expe
rienc
es o
f man
agin
g m
enta
l illn
ess
Inte
rvie
ws
Que
stio
nnai
res
Men
tal h
ealth
scr
eeni
ng
shou
ld b
e co
nduc
ted
by
nurs
es fo
r all
patie
nts
at P
HC
fa
cilit
ies
Men
tal h
ealth
care
refe
rral
s sh
ould
be
mad
e w
ithin
clin
ic
to M
HPs
and
/or t
o ot
her f
acili
‑tie
s ba
sed
on c
ase
seve
rity
and
avai
labi
lity
of m
enta
l hea
lth
pers
onne
l with
in c
linic
Ther
e is
a la
ck o
f tra
inin
g an
d co
nsis
tenc
y in
the
upta
ke o
f ro
les
and
resp
onsi
bilit
ies
by
nurs
es a
nd M
HPs
Impr
oved
dis
tric
t‑le
vel a
dmin
‑is
trat
ive
coor
dina
tion,
men
tal
heal
th a
war
enes
s an
d fin
anci
al
reso
urce
s ar
e cr
itica
l to
the
suc‑
cess
of i
nteg
ratio
n eff
orts
Mig
uel‑E
spon
da e
t al.
(202
0)
[69]
Non
e re
port
edTh
e ex
tent
to w
hich
the
pro‑
gram
me
activ
ities
hav
e be
en
inte
grat
ed in
to th
e or
gani
za‑
tion
and
the
PHC
clin
ics
Soci
odem
ogra
phic
and
clin
ical
ch
arac
teris
tics
Inte
rvie
ws
Cha
lleng
es to
del
iver
y of
se
rvic
es w
ithin
the
prog
ram
me
incl
uded
tim
e co
nstr
aint
s co
u‑pl
ed w
ith th
e m
any
com
petin
g pr
iorit
ies
pres
ent a
t the
clin
ics,
and
the
limite
d av
aila
bilit
y of
sp
ecia
lists
to p
rovi
de m
ento
r‑sh
ip to
MD
sA
ll M
Ds
and
clin
ical
sup
ervi
‑so
rs p
erce
ived
a n
eed
for
mor
e in
volv
emen
t of e
ither
ps
ycho
logi
sts
or p
sych
iatr
ists
to
impr
ove
the
trai
ning
and
su
perv
isio
n an
d al
so to
adv
ise
on d
ifficu
lt ca
ses
Inte
grat
ion
of m
enta
l hea
lth‑
care
ser
vice
s in
PH
C w
ill
requ
ire im
prov
ed fi
nanc
ing
and
reso
urce
man
agem
ent
of P
HC
and
spe
cial
ist s
ervi
ces,
ongo
ing
capa
city
‑bui
ldin
g, th
e de
velo
pmen
t of e
ffect
ive
refe
rral
sy
stem
s, fu
rthe
r dev
elop
men
t of
com
mun
ity‑b
ased
ser
vice
s, an
d lin
king
of P
HC
with
loca
lly
rele
vant
soc
ial i
nter
vent
ions
Mko
ka e
t al.
(201
4) [9
4]In
volv
ed in
impl
emen
tatio
nEx
plor
ing
the
expe
rienc
e of
re
spon
dent
s in
impl
emen
t‑in
g em
erge
ncy
obst
etric
car
e (E
mO
C)
Perc
eive
d ro
le o
f par
tner
s in
Em
OC
impl
emen
tatio
n
Inte
rvie
ws
Focu
s gr
oups
Faci
lity
surv
eyD
ocum
enta
ry re
view
s
Coun
cil h
ealth
man
agem
ent
team
(CH
MT)
took
the
lead
and
w
orke
d w
ith te
am s
pirit
Ther
e w
as in
crea
sed
dem
and
for s
ervi
ces
Ther
e w
as re
sour
ce s
carc
ity in
te
rms
of s
kille
d H
CPs
, fun
ds
and
time
Wor
king
with
com
petin
g ne
eds
Ack
now
ledg
ing
impo
rtan
ce o
f pa
rtne
rs, p
artia
lly b
ecau
se th
ey
play
diff
eren
t rol
esA
nee
d fo
r cle
ar w
orki
ng
arra
ngem
ents
A d
esire
for c
omm
unity
par
‑tic
ipat
ion
Prog
ress
ing
tow
ards
bet
ter
serv
ice
Adv
ocat
es w
orki
ng to
geth
er in
pa
rtne
rshi
ps to
gov
ern
impl
e‑m
enta
tion
To h
ave
effec
tive
part
ners
hips
, th
e ro
les
and
resp
onsi
bilit
ies
for e
ach
acto
r sho
uld
be c
lear
ly
stip
ulat
ed in
a c
lear
wor
king
fra
mew
ork
with
in th
e di
stric
t he
alth
sys
tem
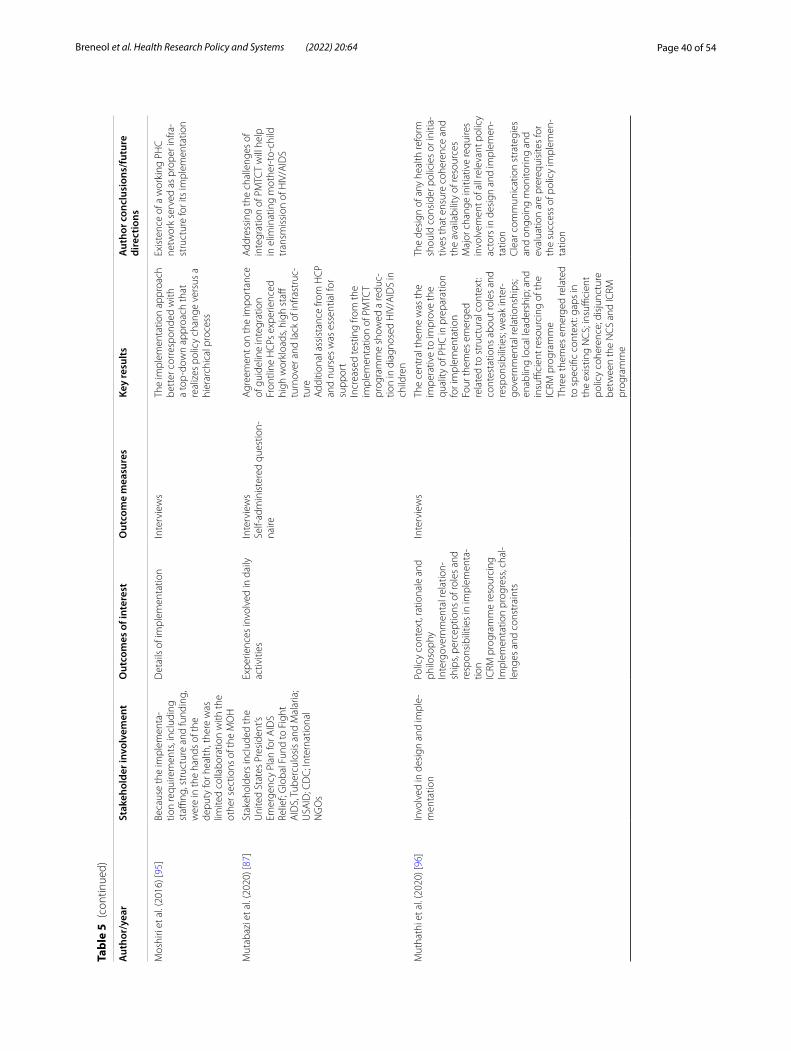
Page 40 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Mos
hiri
et a
l. (2
016)
[95]
Beca
use
the
impl
emen
ta‑
tion
requ
irem
ents
, inc
ludi
ng
staffi
ng, s
truc
ture
and
fund
ing,
w
ere
in th
e ha
nds
of th
e de
puty
for h
ealth
, the
re w
as
limite
d co
llabo
ratio
n w
ith th
e ot
her s
ectio
ns o
f the
MO
H
Det
ails
of i
mpl
emen
tatio
nIn
terv
iew
sTh
e im
plem
enta
tion
appr
oach
be
tter
cor
resp
onde
d w
ith
a to
p‑do
wn
appr
oach
that
re
aliz
es p
olic
y ch
ange
ver
sus
a hi
erar
chic
al p
roce
ss
Exis
tenc
e of
a w
orki
ng P
HC
ne
twor
k se
rved
as
prop
er in
fra‑
stru
ctur
e fo
r its
impl
emen
tatio
n
Mut
abaz
i et a
l. (2
020)
[87]
Stak
ehol
ders
incl
uded
the
Uni
ted
Stat
es P
resi
dent
’s Em
erge
ncy
Plan
for A
IDS
Relie
f; G
loba
l Fun
d to
Fig
ht
AID
S, T
uber
culo
sis
and
Mal
aria
; U
SAID
; CD
C; I
nter
natio
nal
NG
Os
Expe
rienc
es in
volv
ed in
dai
ly
activ
ities
Inte
rvie
ws
Self‑
adm
inis
tere
d qu
estio
n‑na
ire
Agr
eem
ent o
n th
e im
port
ance
of
gui
delin
e in
tegr
atio
nFr
ontli
ne H
CPs
exp
erie
nced
hi
gh w
orkl
oads
, hig
h st
aff
turn
over
and
lack
of i
nfra
stru
c‑tu
reA
dditi
onal
ass
ista
nce
from
HC
P an
d nu
rses
was
ess
entia
l for
su
ppor
tIn
crea
sed
test
ing
from
the
impl
emen
tatio
n of
PM
TCT
prog
ram
me
show
ed a
redu
c‑tio
n in
dia
gnos
ed H
IV/A
IDS
in
child
ren
Add
ress
ing
the
chal
leng
es o
f in
tegr
atio
n of
PM
TCT
will
hel
p in
elim
inat
ing
mot
her‑
to‑c
hild
tr
ansm
issi
on o
f HIV
/AID
S
Mut
hath
i et a
l. (2
020)
[96]
Invo
lved
in d
esig
n an
d im
ple‑
men
tatio
nPo
licy
cont
ext,
ratio
nale
and
ph
iloso
phy
Inte
rgov
ernm
enta
l rel
atio
n‑sh
ips,
perc
eptio
ns o
f rol
es a
nd
resp
onsi
bilit
ies
in im
plem
enta
‑tio
nIC
RM p
rogr
amm
e re
sour
cing
Impl
emen
tatio
n pr
ogre
ss, c
hal‑
leng
es a
nd c
onst
rain
ts
Inte
rvie
ws
The
cent
ral t
hem
e w
as th
e im
pera
tive
to im
prov
e th
e qu
ality
of P
HC
in p
repa
ratio
n fo
r im
plem
enta
tion
Four
them
es e
mer
ged
rela
ted
to s
truc
tura
l con
text
: co
ntes
tatio
ns a
bout
role
s an
d re
spon
sibi
litie
s; w
eak
inte
r‑go
vern
men
tal r
elat
ions
hips
; en
ablin
g lo
cal l
eade
rshi
p; a
nd
insu
ffici
ent r
esou
rcin
g of
the
ICRM
pro
gram
me
Thre
e th
emes
em
erge
d re
late
d to
spe
cific
con
text
: gap
s in
th
e ex
istin
g N
CS;
insu
ffici
ent
polic
y co
here
nce;
dis
junc
ture
be
twee
n th
e N
CS
and
ICRM
pr
ogra
mm
e
The
desi
gn o
f any
hea
lth re
form
sh
ould
con
side
r pol
icie
s or
initi
a‑tiv
es th
at e
nsur
e co
here
nce
and
the
avai
labi
lity
of re
sour
ces
Maj
or c
hang
e in
itiat
ive
requ
ires
invo
lvem
ent o
f all
rele
vant
pol
icy
acto
rs in
des
ign
and
impl
emen
‑ta
tion
Cle
ar c
omm
unic
atio
n st
rate
gies
an
d on
goin
g m
onito
ring
and
eval
uatio
n ar
e pr
ereq
uisi
tes
for
the
succ
ess
of p
olic
y im
plem
en‑
tatio
n
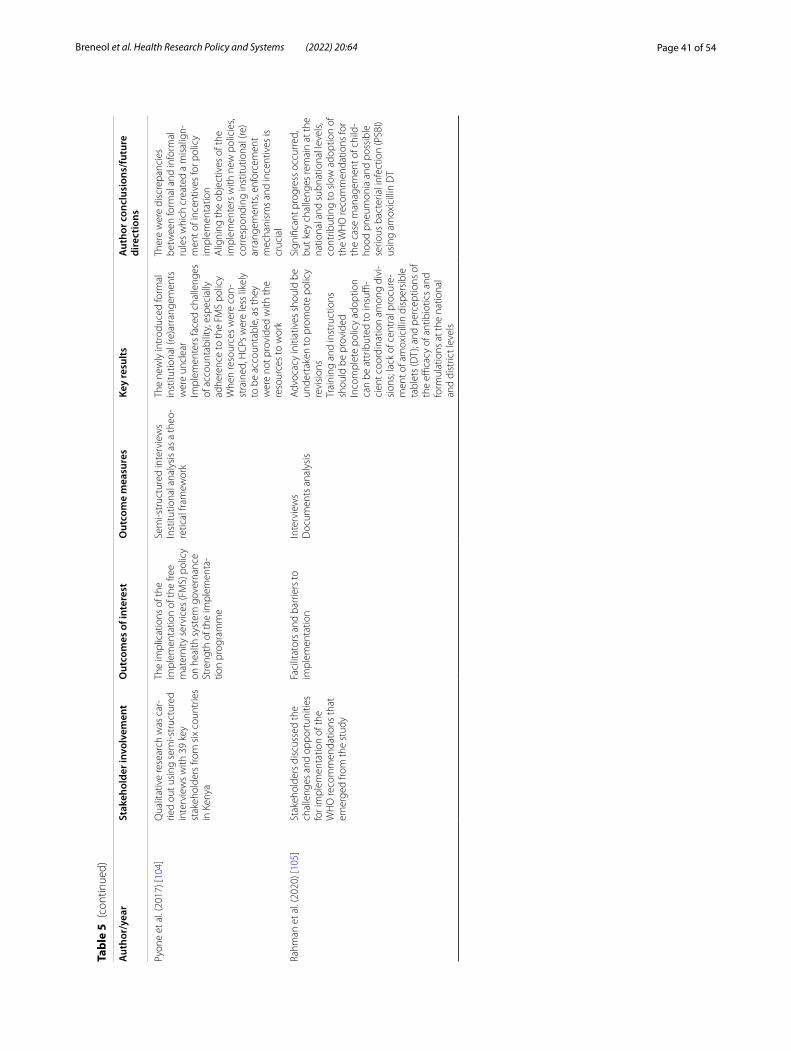
Page 41 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Pyon
e et
al.
(201
7) [1
04]
Qua
litat
ive
rese
arch
was
car
‑rie
d ou
t usi
ng s
emi‑s
truc
ture
d in
terv
iew
s w
ith 3
9 ke
y st
akeh
olde
rs fr
om s
ix c
ount
ries
in K
enya
The
impl
icat
ions
of t
he
impl
emen
tatio
n of
the
free
mat
erni
ty s
ervi
ces
(FM
S) p
olic
y on
hea
lth s
yste
m g
over
nanc
eSt
reng
th o
f the
impl
emen
ta‑
tion
prog
ram
me
Sem
i‑str
uctu
red
inte
rvie
ws
Inst
itutio
nal a
naly
sis
as a
theo
‑re
tical
fram
ewor
k
The
new
ly in
trod
uced
form
al
inst
itutio
nal (
re)a
rran
gem
ents
w
ere
uncl
ear
Impl
emen
ters
face
d ch
alle
nges
of
acc
ount
abili
ty, e
spec
ially
ad
here
nce
to th
e FM
S po
licy
Whe
n re
sour
ces
wer
e co
n‑st
rain
ed, H
CPs
wer
e le
ss li
kely
to
be
acco
unta
ble,
as
they
w
ere
not p
rovi
ded
with
the
reso
urce
s to
wor
k
Ther
e w
ere
disc
repa
ncie
s be
twee
n fo
rmal
and
info
rmal
ru
les
whi
ch c
reat
ed a
mis
alig
n‑m
ent o
f inc
entiv
es fo
r pol
icy
impl
emen
tatio
nA
ligni
ng th
e ob
ject
ives
of t
he
impl
emen
ters
with
new
pol
icie
s, co
rres
pond
ing
inst
itutio
nal (
re)
arra
ngem
ents
, enf
orce
men
t m
echa
nism
s an
d in
cent
ives
is
cruc
ial
Rahm
an e
t al.
(202
0) [1
05]
Stak
ehol
ders
dis
cuss
ed th
e ch
alle
nges
and
opp
ortu
nitie
s fo
r im
plem
enta
tion
of th
e W
HO
reco
mm
enda
tions
that
em
erge
d fro
m th
e st
udy
Faci
litat
ors
and
barr
iers
to
impl
emen
tatio
nIn
terv
iew
sD
ocum
ents
ana
lysi
sA
dvoc
acy
initi
ativ
es s
houl
d be
un
dert
aken
to p
rom
ote
polic
y re
visi
ons
Trai
ning
and
inst
ruct
ions
sh
ould
be
prov
ided
Inco
mpl
ete
polic
y ad
optio
n ca
n be
att
ribut
ed to
insu
ffi‑
cien
t coo
rdin
atio
n am
ong
divi
‑si
ons;
lack
of c
entr
al p
rocu
re‑
men
t of a
mox
icill
in d
ispe
rsib
le
tabl
ets
(DT)
; and
per
cept
ions
of
the
effica
cy o
f ant
ibio
tics
and
form
ulat
ions
at t
he n
atio
nal
and
dist
rict l
evel
s
Sign
ifica
nt p
rogr
ess
occu
rred
, bu
t key
cha
lleng
es re
mai
n at
the
natio
nal a
nd s
ubna
tiona
l lev
els,
cont
ribut
ing
to s
low
ado
ptio
n of
th
e W
HO
reco
mm
enda
tions
for
the
case
man
agem
ent o
f chi
ld‑
hood
pne
umon
ia a
nd p
ossi
ble
serio
us b
acte
rial i
nfec
tion
(PSB
I) us
ing
amox
icill
in D
T
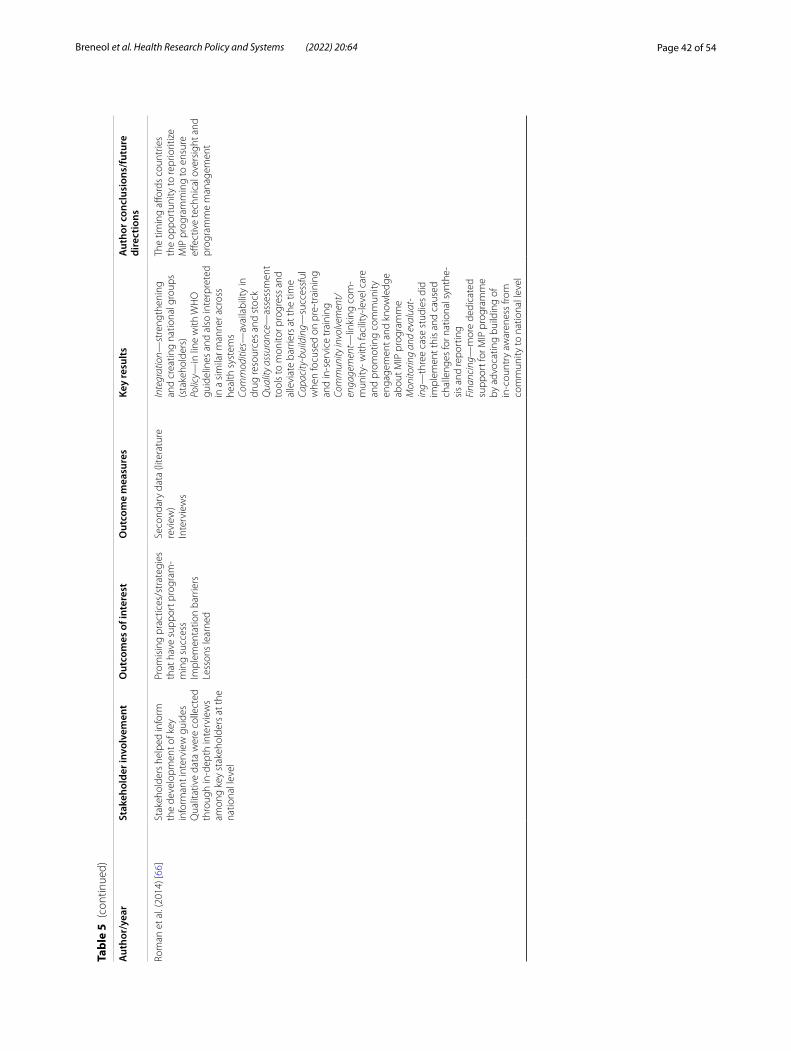
Page 42 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Rom
an e
t al.
(201
4) [6
6]St
akeh
olde
rs h
elpe
d in
form
th
e de
velo
pmen
t of k
ey
info
rman
t int
ervi
ew g
uide
sQ
ualit
ativ
e da
ta w
ere
colle
cted
th
roug
h in
‑dep
th in
terv
iew
s am
ong
key
stak
ehol
ders
at t
he
natio
nal l
evel
Prom
isin
g pr
actic
es/s
trat
egie
s th
at h
ave
supp
ort p
rogr
am‑
min
g su
cces
sIm
plem
enta
tion
barr
iers
Less
ons
lear
ned
Seco
ndar
y da
ta (l
itera
ture
re
view
)In
terv
iew
s
Inte
grat
ion—
stre
ngth
enin
g an
d cr
eatin
g na
tiona
l gro
ups
(sta
keho
lder
s)Po
licy—
in li
ne w
ith W
HO
gu
idel
ines
and
als
o in
terp
rete
d in
a s
imila
r man
ner a
cros
s he
alth
sys
tem
sCo
mm
oditi
es—
avai
labi
lity
in
drug
reso
urce
s an
d st
ock
Qua
lity
assu
ranc
e—as
sess
men
t to
ols
to m
onito
r pro
gres
s an
d al
levi
ate
barr
iers
at t
he ti
me
Capa
city
-bui
ldin
g—su
cces
sful
w
hen
focu
sed
on p
re‑t
rain
ing
and
in‑s
ervi
ce tr
aini
ngCo
mm
unity
invo
lvem
ent/
enga
gem
ent—
linki
ng c
om‑
mun
ity‑ w
ith fa
cilit
y‑le
vel c
are
and
prom
otin
g co
mm
unity
en
gage
men
t and
kno
wle
dge
abou
t MIP
pro
gram
me
Mon
itorin
g an
d ev
alua
t-in
g—th
ree
case
stu
dies
did
im
plem
ent t
his
and
caus
ed
chal
leng
es fo
r nat
iona
l syn
the‑
sis
and
repo
rtin
gFi
nanc
ing—
mor
e de
dica
ted
supp
ort f
or M
IP p
rogr
amm
e by
adv
ocat
ing
build
ing
of
in‑c
ount
ry a
war
enes
s fro
m
com
mun
ity to
nat
iona
l lev
el
The
timin
g aff
ords
cou
ntrie
s th
e op
port
unity
to re
prio
ritiz
e M
IP p
rogr
amm
ing
to e
nsur
e eff
ectiv
e te
chni
cal o
vers
ight
and
pr
ogra
mm
e m
anag
emen
t
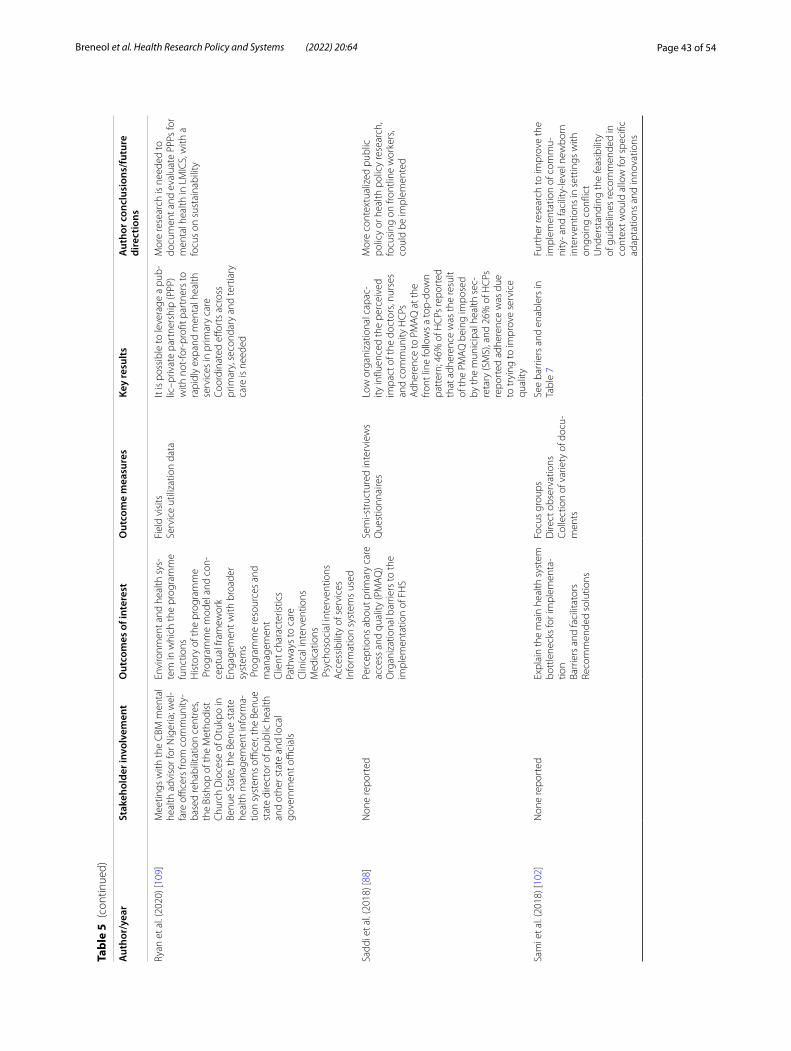
Page 43 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Ryan
et a
l. (2
020)
[109
]M
eetin
gs w
ith th
e C
BM m
enta
l he
alth
adv
isor
for N
iger
ia; w
el‑
fare
offi
cers
from
com
mun
ity‑
base
d re
habi
litat
ion
cent
res,
the
Bish
op o
f the
Met
hodi
st
Chu
rch
Dio
cese
of O
tukp
o in
Be
nue
Stat
e, th
e Be
nue
stat
e he
alth
man
agem
ent i
nfor
ma‑
tion
syst
ems
office
r, th
e Be
nue
stat
e di
rect
or o
f pub
lic h
ealth
an
d ot
her s
tate
and
loca
l go
vern
men
t offi
cial
s
Envi
ronm
ent a
nd h
ealth
sys
‑te
m in
whi
ch th
e pr
ogra
mm
e fu
nctio
nsH
isto
ry o
f the
pro
gram
me
Pro
gram
me
mod
el a
nd c
on‑
cept
ual f
ram
ewor
kEn
gage
men
t with
bro
ader
sy
stem
s P
rogr
amm
e re
sour
ces
and
man
agem
ent
Clie
nt c
hara
cter
istic
sPa
thw
ays
to c
are
Clin
ical
inte
rven
tions
Med
icat
ions
Psy
chos
ocia
l int
erve
ntio
nsA
cces
sibi
lity
of s
ervi
ces
Info
rmat
ion
syst
ems
used
Fiel
d vi
sits
Serv
ice
utili
zatio
n da
taIt
is p
ossi
ble
to le
vera
ge a
pub
‑lic
–priv
ate
part
ners
hip
(PPP
) w
ith n
ot‑fo
r‑pr
ofit p
artn
ers
to
rapi
dly
expa
nd m
enta
l hea
lth
serv
ices
in p
rimar
y ca
reCo
ordi
nate
d eff
orts
acr
oss
prim
ary,
sec
onda
ry a
nd te
rtia
ry
care
is n
eede
d
Mor
e re
sear
ch is
nee
ded
to
docu
men
t and
eva
luat
e PP
Ps fo
r m
enta
l hea
lth in
LM
ICS,
with
a
focu
s on
sus
tain
abili
ty
Sadd
i et a
l. (2
018)
[88]
Non
e re
port
edPe
rcep
tions
abo
ut p
rimar
y ca
re
acce
ss a
nd q
ualit
y (P
MA
Q)
Org
aniz
atio
nal b
arrie
rs to
the
impl
emen
tatio
n of
FH
S
Sem
i‑str
uctu
red
inte
rvie
ws
Que
stio
nnai
res
Low
org
aniz
atio
nal c
apac
‑ity
influ
ence
d th
e pe
rcei
ved
impa
ct o
f the
doc
tors
, nur
ses
and
com
mun
ity H
CPs
Adh
eren
ce to
PM
AQ
at t
he
front
line
follo
ws
a to
p‑do
wn
patt
ern;
46%
of H
CPs
repo
rted
th
at a
dher
ence
was
the
resu
lt of
the
PMA
Q b
eing
impo
sed
by th
e m
unic
ipal
hea
lth s
ec‑
reta
ry (S
MS)
, and
26%
of H
CPs
re
port
ed a
dher
ence
was
due
to
tryi
ng to
impr
ove
serv
ice
qual
ity
Mor
e co
ntex
tual
ized
pub
lic
polic
y or
hea
lth p
olic
y re
sear
ch,
focu
sing
on
front
line
wor
kers
, co
uld
be im
plem
ente
d
Sam
i et a
l. (2
018)
[102
]N
one
repo
rted
Expl
ain
the
mai
n he
alth
sys
tem
bo
ttle
neck
s fo
r im
plem
enta
‑tio
nBa
rrie
rs a
nd fa
cilit
ator
sRe
com
men
ded
solu
tions
Focu
s gr
oups
Dire
ct o
bser
vatio
nsCo
llect
ion
of v
arie
ty o
f doc
u‑m
ents
See
barr
iers
and
ena
bler
s in
Ta
ble
7Fu
rthe
r res
earc
h to
impr
ove
the
impl
emen
tatio
n of
com
mu‑
nity
‑ and
faci
lity‑
leve
l new
born
in
terv
entio
ns in
set
tings
with
on
goin
g co
nflic
tU
nder
stan
ding
the
feas
ibili
ty
of g
uide
lines
reco
mm
ende
d in
co
ntex
t wou
ld a
llow
for s
peci
fic
adap
tatio
ns a
nd in
nova
tions
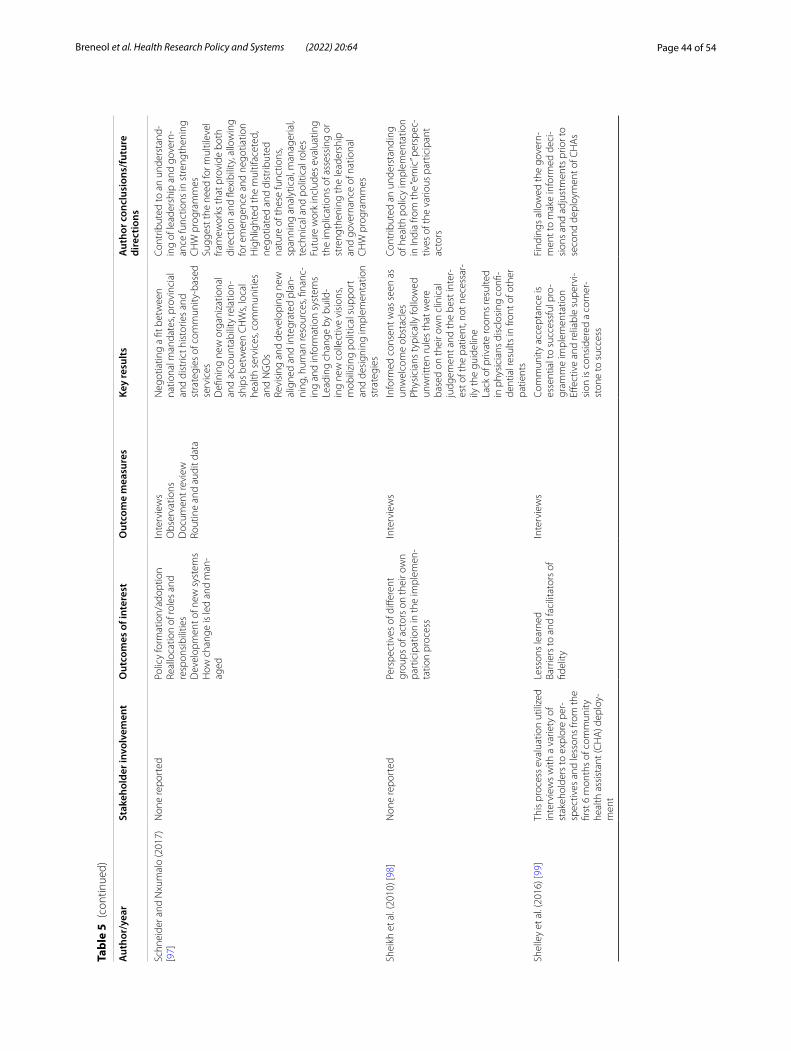
Page 44 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Schn
eide
r and
Nxu
mal
o (2
017)
[9
7]N
one
repo
rted
Polic
y fo
rmat
ion/
adop
tion
Real
loca
tion
of ro
les
and
resp
onsi
bilit
ies
Dev
elop
men
t of n
ew s
yste
ms
How
cha
nge
is le
d an
d m
an‑
aged
Inte
rvie
ws
Obs
erva
tions
Doc
umen
t rev
iew
Rout
ine
and
audi
t dat
a
Neg
otia
ting
a fit
bet
wee
n na
tiona
l man
date
s, pr
ovin
cial
an
d di
stric
t his
torie
s an
d st
rate
gies
of c
omm
unity
‑bas
ed
serv
ices
Defi
ning
new
org
aniz
atio
nal
and
acco
unta
bilit
y re
latio
n‑sh
ips
betw
een
CH
Ws,
loca
l he
alth
ser
vice
s, co
mm
uniti
es
and
NG
Os
Revi
sing
and
dev
elop
ing
new
al
igne
d an
d in
tegr
ated
pla
n‑ni
ng, h
uman
reso
urce
s, fin
anc‑
ing
and
info
rmat
ion
syst
ems
Lead
ing
chan
ge b
y bu
ild‑
ing
new
col
lect
ive
visi
ons,
mob
ilizi
ng p
oliti
cal s
uppo
rt
and
desi
gnin
g im
plem
enta
tion
stra
tegi
es
Cont
ribut
ed to
an
unde
rsta
nd‑
ing
of le
ader
ship
and
gov
ern‑
ance
func
tions
in s
tren
gthe
ning
C
HW
pro
gram
mes
Sugg
est t
he n
eed
for m
ultil
evel
fra
mew
orks
that
pro
vide
bot
h di
rect
ion
and
flexi
bilit
y, a
llow
ing
for e
mer
genc
e an
d ne
gotia
tion
Hig
hlig
hted
the
mul
tifac
eted
, ne
gotia
ted
and
dist
ribut
ed
natu
re o
f the
se fu
nctio
ns,
span
ning
ana
lytic
al, m
anag
eria
l, te
chni
cal a
nd p
oliti
cal r
oles
Futu
re w
ork
incl
udes
eva
luat
ing
the
impl
icat
ions
of a
sses
sing
or
stre
ngth
enin
g th
e le
ader
ship
an
d go
vern
ance
of n
atio
nal
CH
W p
rogr
amm
es
Shei
kh e
t al.
(201
0) [9
8]N
one
repo
rted
Pers
pect
ives
of d
iffer
ent
grou
ps o
f act
ors
on th
eir o
wn
part
icip
atio
n in
the
impl
emen
‑ta
tion
proc
ess
Inte
rvie
ws
Info
rmed
con
sent
was
see
n as
un
wel
com
e ob
stac
les
Phys
icia
ns ty
pica
lly fo
llow
ed
unw
ritte
n ru
les
that
wer
e ba
sed
on th
eir o
wn
clin
ical
ju
dgem
ent a
nd th
e be
st in
ter‑
est o
f the
pat
ient
, not
nec
essa
r‑ily
the
guid
elin
eLa
ck o
f priv
ate
room
s re
sulte
d in
phy
sici
ans
disc
losi
ng c
onfi‑
dent
ial r
esul
ts in
fron
t of o
ther
pa
tient
s
Cont
ribut
ed a
n un
ders
tand
ing
of h
ealth
pol
icy
impl
emen
tatio
n in
Indi
a fro
m th
e “e
mic
” per
spec
‑tiv
es o
f the
var
ious
par
ticip
ant
acto
rs
Shel
ley
et a
l. (2
016)
[99]
This
pro
cess
eva
luat
ion
utili
zed
inte
rvie
ws
with
a v
arie
ty o
f st
akeh
olde
rs to
exp
lore
per
‑sp
ectiv
es a
nd le
sson
s fro
m th
e fir
st 6
mon
ths
of c
omm
unity
he
alth
ass
ista
nt (C
HA
) dep
loy‑
men
t
Less
ons
lear
ned
Barr
iers
to a
nd fa
cilit
ator
s of
fid
elity
Inte
rvie
ws
Com
mun
ity a
ccep
tanc
e is
es
sent
ial t
o su
cces
sful
pro
‑gr
amm
e im
plem
enta
tion
Effec
tive
and
relia
ble
supe
rvi‑
sion
is c
onsi
dere
d a
corn
er‑
ston
e to
suc
cess
Find
ings
allo
wed
the
gove
rn‑
men
t to
mak
e in
form
ed d
eci‑
sion
s an
d ad
just
men
ts p
rior t
o se
cond
dep
loym
ent o
f CH
As
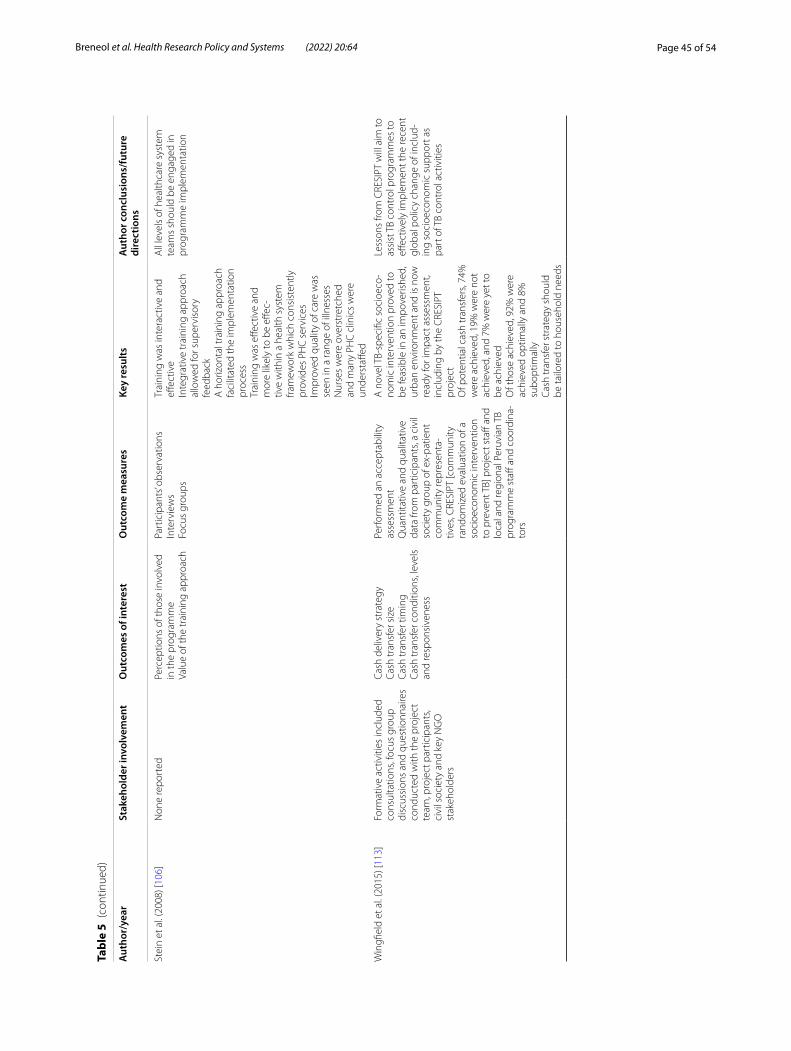
Page 45 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Stei
n et
al.
(200
8) [1
06]
Non
e re
port
edPe
rcep
tions
of t
hose
invo
lved
in
the
prog
ram
me
Valu
e of
the
trai
ning
app
roac
h
Part
icip
ants
’ obs
erva
tions
Inte
rvie
ws
Focu
s gr
oups
Trai
ning
was
inte
ract
ive
and
effec
tive
Inte
grat
ive
trai
ning
app
roac
h al
low
ed fo
r sup
ervi
sory
fe
edba
ckA
hor
izon
tal t
rain
ing
appr
oach
fa
cilit
ated
the
impl
emen
tatio
n pr
oces
sTr
aini
ng w
as e
ffect
ive
and
mor
e lik
ely
to b
e eff
ec‑
tive
with
in a
hea
lth s
yste
m
fram
ewor
k w
hich
con
sist
ently
pr
ovid
es P
HC
ser
vice
sIm
prov
ed q
ualit
y of
car
e w
as
seen
in a
rang
e of
illn
esse
sN
urse
s w
ere
over
stre
tche
d an
d m
any
PHC
clin
ics
wer
e un
ders
taffe
d
All
leve
ls o
f hea
lthca
re s
yste
m
team
s sh
ould
be
enga
ged
in
prog
ram
me
impl
emen
tatio
n
Win
gfiel
d et
al.
(201
5) [1
13]
Form
ativ
e ac
tiviti
es in
clud
ed
cons
ulta
tions
, foc
us g
roup
di
scus
sion
s an
d qu
estio
nnai
res
cond
ucte
d w
ith th
e pr
ojec
t te
am, p
roje
ct p
artic
ipan
ts,
civi
l soc
iety
and
key
NG
O
stak
ehol
ders
Cash
del
iver
y st
rate
gyCa
sh tr
ansf
er s
ize
Cash
tran
sfer
tim
ing
Cash
tran
sfer
con
ditio
ns, l
evel
s an
d re
spon
sive
ness
Perf
orm
ed a
n ac
cept
abili
ty
asse
ssm
ent
Qua
ntita
tive
and
qual
itativ
e da
ta fr
om p
artic
ipan
ts, a
civ
il so
ciet
y gr
oup
of e
x‑pa
tient
co
mm
unity
repr
esen
ta‑
tives
, CRE
SIPT
[com
mun
ity
rand
omiz
ed e
valu
atio
n of
a
soci
oeco
nom
ic in
terv
entio
n to
pre
vent
TB]
pro
ject
sta
ff an
d lo
cal a
nd re
gion
al P
eruv
ian
TB
prog
ram
me
staff
and
coo
rdin
a‑to
rs
A n
ovel
TB‑
spec
ific
soci
oeco
‑no
mic
inte
rven
tion
prov
ed to
be
feas
ible
in a
n im
pove
rishe
d,
urba
n en
viro
nmen
t and
is n
ow
read
y fo
r im
pact
ass
essm
ent,
incl
udin
g by
the
CRE
SIPT
pr
ojec
tO
f pot
entia
l cas
h tr
ansf
ers,
74%
w
ere
achi
eved
, 19%
wer
e no
t ac
hiev
ed, a
nd 7
% w
ere
yet t
o be
ach
ieve
dO
f tho
se a
chie
ved,
92%
wer
e ac
hiev
ed o
ptim
ally
and
8%
su
bopt
imal
lyCa
sh tr
ansf
er s
trat
egy
shou
ld
be ta
ilore
d to
hou
seho
ld n
eeds
Less
ons
from
CRE
SIPT
will
aim
to
assi
st T
B co
ntro
l pro
gram
mes
to
effec
tivel
y im
plem
ent t
he re
cent
gl
obal
pol
icy
chan
ge o
f inc
lud‑
ing
soci
oeco
nom
ic s
uppo
rt a
s pa
rt o
f TB
cont
rol a
ctiv
ities
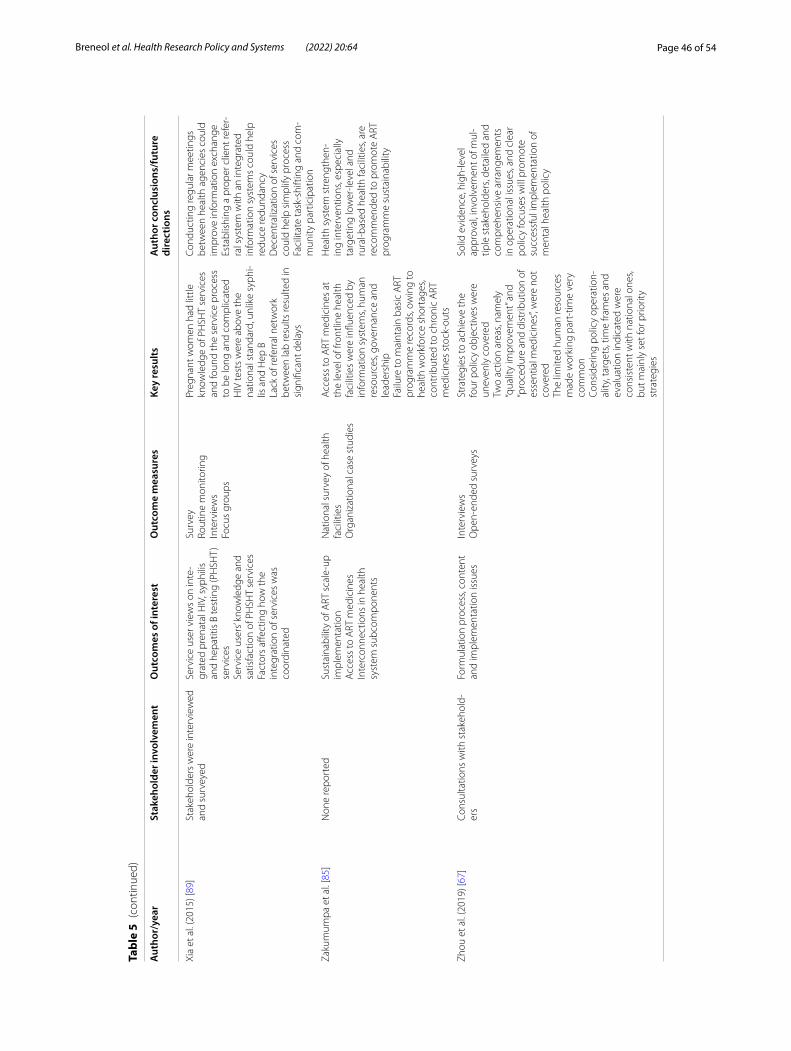
Page 46 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
Tabl
e 5
(con
tinue
d)
Aut
hor/
year
Stak
ehol
der i
nvol
vem
ent
Out
com
es o
f int
eres
tO
utco
me
mea
sure
sKe
y re
sults
Aut
hor c
oncl
usio
ns/f
utur
e di
rect
ions
Xia
et a
l. (2
015)
[89]
Stak
ehol
ders
wer
e in
terv
iew
ed
and
surv
eyed
Serv
ice
user
vie
ws
on in
te‑
grat
ed p
rena
tal H
IV, s
yphi
lis
and
hepa
titis
B te
stin
g (P
HSH
T)
serv
ices
Serv
ice
user
s’ kn
owle
dge
and
satis
fact
ion
of P
HSH
T se
rvic
esFa
ctor
s aff
ectin
g ho
w th
e in
tegr
atio
n of
ser
vice
s w
as
coor
dina
ted
Surv
eyRo
utin
e m
onito
ring
Inte
rvie
ws
Focu
s gr
oups
Preg
nant
wom
en h
ad li
ttle
kn
owle
dge
of P
HSH
T se
rvic
es
and
foun
d th
e se
rvic
e pr
oces
s to
be
long
and
com
plic
ated
HIV
test
s w
ere
abov
e th
e na
tiona
l sta
ndar
d, u
nlik
e sy
phi‑
lis a
nd H
ep B
Lack
of r
efer
ral n
etw
ork
betw
een
lab
resu
lts re
sulte
d in
si
gnifi
cant
del
ays
Cond
uctin
g re
gula
r mee
tings
be
twee
n he
alth
age
ncie
s co
uld
impr
ove
info
rmat
ion
exch
ange
Esta
blis
hing
a p
rope
r clie
nt re
fer‑
ral s
yste
m w
ith a
n in
tegr
ated
in
form
atio
n sy
stem
s co
uld
help
re
duce
redu
ndan
cyD
ecen
tral
izat
ion
of s
ervi
ces
coul
d he
lp s
impl
ify p
roce
ssFa
cilit
ate
task
‑shi
ftin
g an
d co
m‑
mun
ity p
artic
ipat
ion
Zaku
mum
pa e
t al.
[85]
Non
e re
port
edSu
stai
nabi
lity
of A
RT s
cale
‑up
impl
emen
tatio
nA
cces
s to
ART
med
icin
esIn
terc
onne
ctio
ns in
hea
lth
syst
em s
ubco
mpo
nent
s
Nat
iona
l sur
vey
of h
ealth
fa
cilit
ies
Org
aniz
atio
nal c
ase
stud
ies
Acc
ess
to A
RT m
edic
ines
at
the
leve
l of f
ront
line
heal
th
faci
litie
s w
ere
influ
ence
d by
in
form
atio
n sy
stem
s, hu
man
re
sour
ces,
gove
rnan
ce a
nd
lead
ersh
ipFa
ilure
to m
aint
ain
basi
c A
RT
prog
ram
me
reco
rds,
owin
g to
he
alth
wor
kfor
ce s
hort
ages
, co
ntrib
uted
to c
hron
ic A
RT
med
icin
es s
tock
‑out
s
Hea
lth s
yste
m s
tren
gthe
n‑in
g in
terv
entio
ns, e
spec
ially
ta
rget
ing
low
er‑le
vel a
nd
rura
l‑bas
ed h
ealth
faci
litie
s, ar
e re
com
men
ded
to p
rom
ote
ART
pr
ogra
mm
e su
stai
nabi
lity
Zhou
et a
l. (2
019)
[67]
Cons
ulta
tions
with
sta
keho
ld‑
ers
Form
ulat
ion
proc
ess,
cont
ent
and
impl
emen
tatio
n is
sues
Inte
rvie
ws
Ope
n‑en
ded
surv
eys
Stra
tegi
es to
ach
ieve
the
four
pol
icy
obje
ctiv
es w
ere
unev
enly
cov
ered
Two
actio
n ar
eas,
nam
ely
“qua
lity
impr
ovem
ent”
and
“pro
cedu
re a
nd d
istr
ibut
ion
of
esse
ntia
l med
icin
es”, w
ere
not
cove
red
The
limite
d hu
man
reso
urce
s m
ade
wor
king
par
t‑tim
e ve
ry
com
mon
Cons
ider
ing
polic
y op
erat
ion‑
ality
, tar
gets
, tim
e fra
mes
and
ev
alua
tion
indi
cate
d w
ere
cons
iste
nt w
ith n
atio
nal o
nes,
but m
ainl
y se
t for
prio
rity
stra
tegi
es
Solid
evi
denc
e, h
igh‑
leve
l ap
prov
al, i
nvol
vem
ent o
f mul
‑tip
le s
take
hold
ers,
deta
iled
and
com
preh
ensi
ve a
rran
gem
ents
in
ope
ratio
nal i
ssue
s, an
d cl
ear
polic
y fo
cuse
s w
ill p
rom
ote
succ
essf
ul im
plem
enta
tion
of
men
tal h
ealth
pol
icy

Page 47 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
in an unclear understanding of the implementation and initiative fidelity. Results from these studies should be considered with this in mind.
DiscussionThis scoping review located, mapped and codified pub-lished literature exploring the adaptation and implemen-tation of health system guidelines in LMICs to assess trends and identify potential gaps. Through the synthesis of available evidence, we were able to identify common strategies for adapting and implementing health system guidelines, related barriers and enablers, and indicators of success.
Overall, the most common type of implementation strategies used to facilitate the integration of health system guidelines involved education, training, clinical supervision and the formulation of working groups and advisory boards. Examples of education and training include the development of standardized educational materials, as well as national training and feedback sessions (see Table 4 for a breakdown of all exam-ples). While this review can comment on the types of implementation strategies utilized, specific details such as the duration and dose of these techniques were largely underreported by the authors of the included studies (e.g. 1-day vs month-long workshops). The reported educational and collaborative implementation
Table 6 Implementation barriers and enablers coded using the COM‑B framework (summary table)
COM-B category COM-B subcategory COM-B definition Frequency of occurrence
Examples of barriers and enablers
Opportunity Physical Environmental context and resources 36 ○ Financial constraints and budgets○ Physical resources to support guideline implementation (water lines, lack of transpor‑tation, etc.)○ Need for extensive human resources○ Stakeholder support and buy‑in○ Site check‑ins○ Training for end‑users and stakeholders○ Supportive policies and laws○ Ensuring basic needs are met for workers to support motivation and reduce attrition○ Local leadership○ Incentives○ Strategic implementation and operation plans
Social Social influences, norms, cultural, social pressures, conformity
22 ○ Cultural context○ Political instability/stability○ Political commitment○ Stigma (e.g. HIV+ mothers counselling other HIV+ mothers)○ Power imbalances
Capabilities Psychological Knowledge, memory, decision‑making, behavioural regulation
15 ○ Knowledge of the guideline and its practices○ Emotional toll on frontline clinicians work‑ing with vulnerable populations○ Resistance to change
Physical Skills and abilities 19 ○ Adapting training materials for all (e.g. adapting materials for those who are illiterate)○ Hosting training meetings○ Continued implementation through train‑ing, mentorship, supportive supervision and follow‑up documentation
Motivation Reflective Roles and identity, beliefs about conse‑quences and optimism
4 ○ Resistance to/acceptance of change○ Trust in guidelines○ More clear definition of roles and respon‑sibilities
Automatic Emotions and reinforcement 10 ○ Enthusiasm and commitment to imple‑mentation○ Motivation to implement and perform duties

Page 48 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
strategies are in direct alignment with current literature and support similar emerging themes in other health-care and income settings [55, 56]. A recent review of techniques used to implement nursing practice guide-lines across different health settings reveals that educa-tion-based strategies were almost always incorporated in the implementation plan [55]. Our findings are consistent with other works in LMICs cited in Imam-arua et al.’s (2017) literature synthesis of implementa-tion strategies to deliver maternal practice guidelines [56]. While these reviews identified the involvement of local opinion leaders in their implementation tactics, the formal creation of advisory groups (such as devel-oping technical working groups) appears to be more common in health system-based implementation ini-tiatives than in clinical practice guidelines. This could be reflective of the complex nature of health systems, social norms and values in local communities regard-ing decision-making, and the various actors that need to be thoughtfully and proactively engaged to facili-tate implementation. Furthermore, included studies used an average of four implementation strategies, and less than half of potential strategies available to them (38/73 techniques defined by ERIC). Thus, our review highlights the potential need to leverage and combine a
wider variety of implementation techniques to address known barriers to changes and to achieve policy/pro-gramme goals.
Though most of the included articles detailed ration-ales for implementing their targeted health system guidelines, the selection of implementation strategies did not appear to be guided by foundational knowledge, theory or conceptual frameworks. Further, only three studies applied a formal implementation plan [57–59]. Implementation science literature highlights the criti-cal importance of identifying and tailoring implementa-tion techniques to successfully transition evidence into real-world practice [60, 61]. Conducting behavioural analyses to identify barriers and facilitators can then be used to guide the selection of evidence-based strategies and to mitigate potential challenges while simultaneously amplifying promising facilitators [54, 60, 61]. Differing levels of available human and physical resources, politi-cal structures, professional roles and responsibilities, and cultural and religious practices are all salient and intersectional factors that need to be considered within an implementation plan for health system initiatives [62, 63]. These contextual factors are of particular importance to consider in potentially resource-limited settings to optimize strengths and attend to weaknesses [63]. One
Table 7 Barriers and enablers related to adaption (COM‑B analysis—opportunities, motivation)
Author (year) Opportunities
Physical Social
Andrade et al. (2017) [75]
○ Unable to implement an electronic system (enabler) ○ None reported
Bryce et al. (2005) [58] ○ Adapting guidelines to context (enabler) ○ None reported
Gueye et al. (2016) [108]
○ Programme showed flexibility over time, as it was able to mobilize a large number of staff
○ None reported
Halpern et al. (2010) [77]
○ A technical working group is crucial to help develop the country‑specific systems, oversee implementation, and adjust or deal with unexpected changes (enabler)
○ None reported
Leethongdee (2007) [83]
○ Created a new catchment area which increased the budget (enabler)
○ None reported
Rahman et al. (2020) [105]
○ Readiness of the health system to execute the policy (ena‑bler/barrier)
○ Proactive leadership from national programmes, advocacy, technical and resource support from international develop‑ment partners (enabler)
Stein et al. (2008) [106] ○ None reported ○ The spiritual adaptation/incorporation provided culturally appropriate support (enabler)
Wingfield et al. (2015) [113]
○ None reported ○ Strong multisectoral collaboration (enabler)
Motivation
Automatic Reflective
Stein et al. (2008) [106]
○ None reported ○ Nurses valued counselling skills that were built as an adapta‑tion to the guideline (enabler)
Wingfield et al. (2015) [113]
○ None reported ○ Lack of available evidence, and thus deciding on the transfer amounts and timing was difficult (barrier)

Page 49 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
component necessary for building a resilient health sys-tem is an awareness of the current strengths and weak-nesses within existing structures to inform practice and policy planning [64]. There are various evidence-based frameworks and taxonomies that provide structured and systematic processes to identify existing barriers and enablers in specific contexts [26, 28, 54, 65]. Exist-ing tools such as the COM-B model can be used to help identify and map known implementation barriers and enablers and assist in selecting targeted techniques to influence change at the health system level [54]. The use of evidenced-based conceptual and theoretical frame-works could help to improve the selection of individual-ized implementation techniques and ultimately improve the successful integration of health system guidelines in LMICs.
Lack of consistent funding was a noted barrier to the implementation of health system guidelines. Despite this, only a handful of articles reported accessing new fund-ing sources as part of their implementation plan [66–69]. While seven studies were conducted in an LIC setting, reports of financial constraints were not limited to those within LICs. Our findings suggest that securing imple-mentation research funding is arduous, irrespective of a country’s income level. Recent work from Ritchie et al. [62] explored the challenges experienced among LMICs when translating maternal health evidence into practice and revealed that lack of health system funding was one of the most common barriers to evidence implementa-tion in LMICs. This barrier, however, may not be unique to LMICs, with sustained funding being challenging even among high-income contexts [70]. As highlighted in the implementation science literature, this is of particular importance when considering the ability to sustain the delivery of health system guidelines beyond their ini-tial implementation [71]. Partnering with NGOs was one strategy utilized by some of our included articles to help fund initiatives. However, while initial finan-cial support may provide the necessary seed money and resources to help launch initiatives, projects with-out sustained sources of funding risk being shut down [70]. It is also noteworthy that over half of the included studies reported funding sources stemming solely from high-income funding initiatives (e.g. Irish Aid, Austral-ian government funding, Canada’s International Devel-opment Research Centre), with only 11 studies utilizing funds from their local country (i.e. Brazilian Ministry of Education, China’s Medical Board). Financial commit-ments and sustained funding from health ministries is essential to supporting implementation efforts and facili-tating the longevity and sustainability of moving evidence into practice and strengthening implementation of health system guidelines into the real-world context.
When stratifying our findings by WHO’s health sys-tem building blocks, it became clear that change at the health system level is often dependent on addressing all intersecting concepts. For example, a majority of our identified health system guidelines targeted the service delivery building block, and yet their related barriers included lack of financing, resources and/or leadership and government commitment. Guidelines that targeted the health workforce building block reported barriers specific to the lack of knowledge about the guidelines, human resources and funding. These findings highlight the intersectional nature of all health system building blocks and the critical need to look across components to facilitate successful system-level change. When exploring Rwanda’s great success in improving health outcomes, Sayinzoga and Bijlmakers [72] discovered that one of the key factors influencing their successes was the recogni-tion of the need for multiple and interconnected health system initiatives to achieve set goals. Without account-ing for this intersectional nature, initiatives are unlikely to be successful, resulting in wasted time and efforts [63]. Strengthening health systems requires purposeful plan-ning and action across building blocks to enact reform across all health, social and political structures [73, 74]. Researchers and decision-makers are encouraged to incorporate WHO’s health system building blocks as a framework to identify essential elements that may require additional support during the implementation and adap-tation of health system guidelines.
Our review revealed a dearth of reported information related to the adaptation of health system guidelines in comparison to implementation strategies. We could find only one study that reported having tailored its guidelines to the needs of the local context as an implementation strategy [75], and only 14 studies reported adaptation techniques. Adapting both health system and clinical practice guidelines is critical to enhancing applicability to the specific setting and to account for differing cultural, organizational and environmental factors [76]. Adapta-tion of these initiatives can lead to increased local uptake by engaging stakeholders and end-users throughout the process [76]. However, this customization must be car-ried out carefully to ensure the correct application of evi-dence and recommendations. Utilizing evidence-based adaptation frameworks provides systematic guidance to ensure that the required modifications are made while still honouring the authenticity of the guideline [76]. Unfortunately, the use of adaptation frameworks was not reported in any of our included articles. While some articles reported on their adaptation techniques, such as Halpern et al.’s [77] detailed description of the crea-tion of a technical working group to adapt each guide-line component, most articles did not provide sufficient

Page 50 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
detail of their processes or reasoning. Rigorous research is needed to explore and identify the most effective adap-tation strategies to enhance a guideline’s applicability and uptake at the health system level and support the use of these strategies in practice.
The most frequent indicators of success when imple-menting and adapting health system guidelines were related to assessing contextualized barriers and facili-tators, end-user experiences, and monitoring system changes. Choosing outcomes and indicators is still a debated topic within implementation science literature [8]. As this review identified, many distinguish imple-mentation success by evaluating the process itself (i.e. challenges and successes). Limited studies reported on cost as a critical implementation outcome. Without evaluating implementation cost, sustainability of the health system change is difficult to discern. Conduct-ing cost–benefit analyses and verifying areas of poten-tial cost savings could provide decision-makers with further evidence to support the granting of sustainable funding for implementation of health system guide-lines—a major barrier identified in this review.
An alternative ideology asserts success as being related to a health system guideline’s ability to achieve its recommended target and improve care [78]. Only a small proportion of studies included in our review compared guideline targets with real-world changes or leveraged patient-level outcomes to identify improve-ments in quality of life and health outcomes [75, 79]. The integration of patient- and population-level out-comes may be an important component in the evalu-ation of health system guidelines in LMICs, as an ultimate goal of a resilient and sustainable health sys-tem is to better serve patients and families. There are also a variety of evaluation frameworks that can help guide researchers in the selection of outcomes and indicators of success at the health system level [49]. While flexibility is necessary in evaluation plans, uti-lizing these frameworks can provide structure and evi-dence-based processes to ensure comparable outcomes are being selected and reported. This would allow for the streamlined comparison and shared learning across LMICs and could facilitate a more transpar-ent understanding of key factors that drive successful implementation of health system guidelines.
The findings from our quality appraisal and the lack of detail that we were able to extract related to certain concepts (i.e. adaptation strategies) highlight the need to improve adherence to reporting guidelines within this body of literature. By following reporting guide-lines in the dissemination of study findings, we can help increase the transparency and completeness of research initiatives [80], ensuring that articles contain
the important components and active ingredients for their implementation and adaptation strategies, evalu-ation methods and health system initiatives. Without this information, it is difficult for readers to discern how implementation and adaptation plans were devel-oped, the techniques employed, and the trustworthi-ness of findings [81].
LimitationsIt is important to consider our findings considering potential limitations. First, our search strategy was lim-ited to reports published in English. We consulted with our knowledge users, who advised that they did not believe this would influence our review findings; how-ever, we acknowledge that not all initiatives conducted in LMICs are reported in this language. This may also partly explain our finding that most initiatives were funded by HICs. Second, given the variation in how authors describe health system guidelines (e.g. recommendations, policies), we may not have captured all potentially rele-vant studies. Further, it is worth noting that authors may not uniformly use the term “adaptation” when referring to the concept definition adopted in this work. Variations in terminology could have impacted our identification and/or extraction of data. However, our search strategy was carefully developed by an experienced library scien-tist to mitigate such challenges and comprehensively cap-ture pertinent studies.
ConclusionsIdentifying evidenced-based strategies to successfully move evidence into practice continues to be a growing and critical area of research. Health system guidelines are pivotal tools to optimize, strengthen and develop resilient healthcare infrastructures and provisions. This scoping review provides a comprehensive overview of published literature examining the adaptation and implementa-tion of health system guidelines in LMICs. Our findings revealed the most common strategies for implementing health system guidelines in LMICs, including education, training, clinical supervision and formation of advisory groups. There is a need to explore the impact of lever-aging and combining a wider variety of implementa-tion techniques to achieve policy/programme goals. The reporting of adaptation strategies was an evident gap in this body of literature, highlighting the need for more primary research aimed at identifying effective adapta-tion techniques to enhance a guideline’s applicability and uptake at the health system level. Given the lack of theoretical frameworks identified in included studies, research teams can turn to established implementation and adaptation frameworks as a starting point to help

Page 51 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
guide their work. Furthermore, while the absence of sus-tained funding and financial commitments was identified as a salient barrier to the implementation of health sys-tem guidelines, there was a lack of studies reporting cost as an evaluation outcome. Future researchers are encour-aged to consider conducting cost analyses to create a case for decision-makers to support the granting of sustain-able funding for health system guidelines. Our findings suggest that more effort may be required across research, policy and practice sectors to support the adaptation and implementation of health system guidelines to local con-texts and health system arrangements in LMICs.
AbbreviationsLMICs: Low‑ and middle‑income countries; LIC: Low‑income country; HIC: High‑income country; EPOC: Effective Practice and Organisation of Care; COM‑B: Capability, Opportunity and Motivation Behaviour model; RAISE: Research to Enhance the Adaptation and Implementation of Health Systems Guidelines.
Supplementary InformationThe online version contains supplementary material available at https:// doi. org/ 10. 1186/ s12961‑ 022‑ 00865‑8.
Additional file 1. Search strategy.
Additional file 2. Data extraction form.
Additional file 3. Acronyms.
Additional file 4. Barriers to and enablers of implementation categorized by the COM‑B framework (opportunities category).
AcknowledgementsWe would like to acknowledge and thank those who helped us during the citation screening and/or data extraction phases: Benjamin Rose‑Davis, Kiyana Kamali, Zohra Khatoon, and Daniel Crowther.
Author contributionsSB performed citation screening, data extraction and data analysis, and wrote the initial draft of this manuscript. JAC directly supervised all phases of the work, provided substantial content expertise, contributed to data interpreta‑tion, and provided substantial revisions on the initial and final manuscript. RM supervised all phases of the work, provided substantial content expertise, con‑tributed to data interpretation, and provided substantial revisions on the initial and final manuscript. KM and CJ performed citation screening, data extraction, data analysis and provided significant revisions to the manuscript. HW helped draft the initial protocol for this work, performed citation screening, and provided significant revisions to the manuscript. LW, CC, MR and LK‑B pro‑vided methodological expertise during all phases of the work and provided significant revisions to the manuscript. EV, MV, SJ, LA, SA and DP provided methodological expertise, provided key stakeholder and content expertise to ensure the relevancy of this work, and provided significant revisions to the final manuscript. All authors read and approved the final manuscript.
FundingThis work was jointly funded by the SPOR Evidence Alliance (Award Number: 201705GSR‑386588‑GSR‑CEAJ‑157857) and WHO Alliance for Health Policy and Systems Research.
Availability of data and materialsAll data generated or analysed during this study are included in this published article and its additional files.
Declarations
Ethics approval and consent to participateNo ethical approval was required, as this work is a secondary analysis of published literature.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Author details1 School of Nursing, Faculty of Health, Dalhousie University, Halifax, Canada. 2 Strengthening Transitions in Care Lab, IWK Health Centre, 8th Floor Chil‑dren’s Site, 5850/5980 University Ave, Halifax, NS B3K 6R8, Canada. 3 Alliance for Health Policy and Systems Research, World Health Organization, Geneva, Switzerland. 4 Faculty of Health, Dalhousie University, Halifax, Canada. 5 Partner‑ship for Maternal, Newborn & Child Health (PMNCH), World Health Organiza‑tion, Geneva, Switzerland. 6 Nova Scotia Health Authority Policy and Planning, Dartmouth, Canada. 7 Facultad de Medicina, Universidad de Antioquia, Medellín, Antioquia, Colombia. 8 Vadu Rural Health Program, KEM Hospital Research Centre, Pune, India. 9 W.K. Kellogg Health Science Library, Dalhousie University, Halifax, Canada. 10 School of Nursing and Midwifery, University of Ghana, Legon, Accra, Ghana. 11 Department of Nursing & Health Sciences, University of New Brunswick, St. John, Canada. 12 Department of Mental Health Nursing, University of Ghana, Legon, Accra, Ghana.
Received: 21 December 2021 Accepted: 9 May 2022
References 1. Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder‑DeWan S,
et al. High‑quality health systems in the sustainable development goals era: time for a revolution. Lancet Glob Health. 2018;6(11):e1196–252.
2. Moberg J, Oxman AD, Rosenbaum S, Schünemann HJ, Guyatt G, Flottorp S, et al. The GRADE evidence to decision (EtD) framework for health system and public health decisions. Health Res Policy Syst. 2018;16(1):45.
3. World Health Organization. WHO handbook for guideline development. 2nd ed. Geneva: WHO Press; 2014.
4. Brouwers MC, Lavis JN, Spithoff K, Vukmirovic M, Florez ID, Velez M, et al. Assessment of health systems guidance using the appraisal of guidelines for research and evaluation‑health systems (AGREE‑HS) instrument. Health Policy. 2019;123(7):646–51.
5. National Center for Complementary and Integrative Health. Clinical practice guidelines clinical practice guidelines. 2021. https:// www. nccih. nih. gov/ health/ provi ders/ clini calpr actice. Accessed 23 Nov 2021.
6. McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635–45.
7. Sheldon TA, Cullum N, Dawson D, Lankshear A, Lowson K, Watt I, et al. What’s the evidence that NICE guidance has been implemented? Results from a national evaluation using time series analysis, audit of patients’ notes, and interviews. BMJ. 2004;329(7473):999.
8. Westfall JM, Mold J, Fagnan L. Practice‑based research—“Blue High‑ways” on the NIH roadmap. JAMA. 2007;297(4):403–6.
9. Balas AE, Boren SA. Managing clinical knowledge for health care improvement. In: Bemmel J, McCray A, editors. Yearbook of medical informatics 2000: patient‑centered systems. Stuttgart: Schattauer Verlagsgesellschaft mbH; 2000. p. 65–70. http:// hdl. handle. net/ 10675.2/ 617990.
10. Institute of Medicine. Initial national priorities for comparative effectiveness research: health and medicine division. Washington, DC: The National Academies Press; 2009. http:// natio nalac ademi es. org/ hmd/ repor ts/ 2009/ compa rativ eeffe ctive nessr esear chpri oriti es. aspx. Accessed 14 Dec 2019.
Page 52 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
11. Agency for Healthcare Research and Quality (AHRQ). PA‑18‑793: AHRQ health services research demonstration and dissemination grants (R18). https:// grants. nih. gov/ grants/ guide/ pa‑ files/ pa‑ 18‑ 793. html. Accessed 14 Dec 2019.
12. Powell BJ, Fernandez ME, Williams NJ, Aarons GA, Beidas RS, Lewis CC, et al. Enhancing the impact of implementation strategies in healthcare: a research agenda. Front Public Health. 2019. https:// doi. org/ 10. 3389/ fpubh. 2019. 00003.
13. Glandon D, Meghani A, Jessani N, Qiu M, Bennett S. Identifying health policy and systems research priorities on multisectoral collaboration for health in low‑income and middle‑income countries. BMJ Glob Health. 2018;3(Suppl 4): e000970.
14. Proctor EK, Powell BJ, McMillen JC. Implementation strategies: recom‑mendations for specifying and reporting. Implement Sci. 2013;8:139.
15. Guidelines International Network. Working groups/adaptation. 2019. https://g‑ i‑n. net/ worki ng‑ groups/ adapt ation. Accessed 14 Dec 2019.
16. Wang Z, Norris SL, Bero L. Implementation plans included in World Health Organisation guidelines. Implement Sci. 2016;11(1):76.
17. Dedios MC, Esperato A, De‑Regil LM, Peña‑Rosas JP, Norris SL. Improv‑ing the adaptability of WHO evidence‑informed guidelines for nutri‑tion actions: results of a mixed methods evaluation. Implement Sci. 2017;12(1):39.
18. Wang Z, Norris SL, Bero L. The advantages and limitations of guideline adaptation frameworks. Implement Sci. 2018;13(1):72.
19. Schünemann HJ, Fretheim A, Oxman AD. Improving the use of research evidence in guideline development: 13. Applicability, transferability and adaptation. Health Res Policy Syst. 2006;4(1):25.
20. World Health Organization. Request for proposals: technical support centre—research to enhance the adaptation and implementation of health systems guidelines (RAISE). 2019. https:// www. who. int/ allia nce‑ hpsr/ calls forpr oposa ls/ allia nce‑ rfp‑ tsc‑ RAISE. pdf? ua=1.
21. McCormack B, Kitson A, Harvey G, Rycroft‑Malone J, Titchen A, Seers K. Getting evidence into practice: the meaning of “context.” J Adv Nurs. 2002;38(1):94–104.
22. Kaplan HC, Brady PW, Dritz MC, Hooper DK, Linam WM, Froehle CM, et al. The influence of context on quality improvement suc‑cess in health care: a systematic review of the literature. Milbank Q. 2010;88(4):500–59.
23. Taylor SL, Dy S, Foy R, Hempel S, McDonald KM, Ovretveit J, et al. What context features might be important determinants of the effectiveness of patient safety practice interventions? BMJ Qual Saf. 2011;20(7):611–7.
24. Tomoaia‑Cotisel A, Scammon DL, Waitzman NJ, Cronholm PF, Halladay JR, Driscoll DL, et al. Context matters: the experience of 14 research teams in systematically reporting contextual factors important for practice change. Ann Fam Med. 2013;11(Suppl 1):S115–23.
25. Edwards N, Barker PM. The importance of context in implementation research. J Acquir Immune Defic Syndr. 2014;67(Suppl 2):S157–62.
26. Powell BJ, Beidas RS, Lewis CC, Aarons GA, McMillen JC, Proctor EK, et al. Methods to improve the selection and tailoring of implementation strategies. J Behav Health Serv Res. 2017;44(2):177–94.
27. Powell BJ, McMillen JC, Proctor EK, Carpenter CR, Griffey RT, Bunger AC, et al. A compilation of strategies for implementing clinical innovations in health and mental health. Med Care Res Rev. 2012;69(2):123–57.
28. Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, et al. A refined compilation of implementation strategies: results from the expert recommendations for implementing change (ERIC) project. Implement Sci. 2015;10:21.
29. Mazza D, Bairstow P, Buchan H, Chakraborty SP, Van Hecke O, Grech C, et al. Refining a taxonomy for guideline implementation: results of an exercise in abstract classification. Implement Sci. 2013;8:32.
30. Michie S, Richardson M, Johnston M, Abraham C, Francis J, Harde‑man W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95.
31. Kok G, Gottlieb NH, Peters GJY, Mullen PD, Parcel GS, Ruiter RAC, et al. A taxonomy of behaviour change methods: an intervention mapping approach. Health Psychol Rev. 2016;10(3):297–312.
32. Alvarez E, Lavis JN, Brouwers M, Carmona Clavijo G, Sewankambo N, Solari L, et al. Developing evidence briefs for policy: a qualitative case
study comparing the process of using a guidance‑contextualization workbook in Peru and Uganda. Health Res Policy Syst. 2019;17(1):89.
33. Cochrane Effective Practice and Organisation of Care Review Group. Data collection checklist. 2002. https:// www. ncbi. nlm. nih. gov/ pub‑med/ 18624 603.
34. Nilsen P, Bernhardsson S. Context matters in implementation science: a scoping review of determinant frameworks that describe contextual determinants for implementation outcomes. BMC Health Serv Res. 2019;19(1):189.
35. Darzi A, Abou‑Jaoude EA, Agarwal A, Lakis C, Wiercioch W, Santesso N, et al. A methodological survey identified eight proposed frame‑works for the adaptation of health related guidelines. J Clin Epidemiol. 2017;86:3–10.
36. Pantoja T, Opiyo N, Lewin S, Paulsen E, Ciapponi A, Wiysonge CS, et al. Implementation strategies for health systems in low‑income countries: an overview of systematic reviews. Cochrane Database Syst Rev. 2017;12(9):CD011086.
37. Kothari A, McCutcheon C, Graham ID. Defining integrated knowledge translation and moving forward: a response to recent commentaries. Int J Health Policy Manag. 2017;6(5):299–300.
38. Peters M, Godfrey C, McInerney P, Soares C, Khalil H, Park P. Methodol‑ogy for JBI scoping reviews. In: The Joanna Briggs institute reviewers’ manual. Adelaide: The Joanna Briggs Institute; 2015. p. 1–24.
39. Effective Practice and Organisation of Care (EPOC). The EPOC taxonomy of health systems interventions. EPOC resources for review authors. Oslo: Norwegian Knowledge Centre for the Health Services. 2016. https:// epoc. cochr ane. org/ epoc‑ taxon omy. Accessed 14 Dec 2019.
40. World Health Organization. WHO | health systems strengthening glos‑sary. WHO. World Health Organization; 2011. https:// www. who. int/ healt hsyst ems/ hss_ gloss ary/ en/ index5. html. Accessed 12 Aug 2020.
41. Wiltsey Stirman S, Baumann AA, Miller CJ. The FRAME: an expanded framework for reporting adaptations and modifications to evidence‑based interventions. Implement Sci. 2019;14(1):58.
42. The World Bank. World Bank country and lending groups. https:// datah elpde sk. world bank. org/ knowl edgeb ase/ artic les/ 906519‑ world‑ bank‑ count ry‑ and‑ lendi ng‑ groups. Accessed 14 Feb 2020.
43. Sampson M, McGowan J, Cogo E, Grimshaw J, Moher D, Lefebvre C. An evidence‑based practice guideline for the peer review of electronic search strategies. J Clin Epidemiol. 2009;62(9):944–52.
44. EndNote. EndNote | clarivate analytics . EndNote. n.d. https:// endno te. com/. Accessed 12 Aug 2020.
45. Covidence Systematic Review Software. Covidence systematic review software. Covidence. 2018. https:// www. covid ence. org/.
46. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA‑ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
47. Critical Appraisal Tools—JBI. http:// joann abrig gs. org/ resea rch/ criti cal‑ appra isal‑ tools. html. Accessed 22 Dec 2017.
48. Hong QN, Pluye P, Fabregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed methods appraisal tool (MMAT) version 2018: user guide . 2018. https:// files. zotero. net/ eyJle HBpcm VzIjo xNTkw MTk1O TEzLC JoYXN oIjoi Y2NlN DAxYj E4ZDR jYmQy ZGJmZ mVhZD A2Nzk zN2I1 NmYiL CJjb2 50ZW5 0VHlw ZSI6I mFwcG xpY2F 0aW9u XC9wZ GYiLC JjaGF yc2V0 IjoiI iwiZm lsZW5 hbWUi OiJNT UFUXz IwMTh fY3Jp dGVya WEtbW FudWF sXzIw MTgtM DgtMD FfRU5 HLnBk ZiJ9/ f9320 95093 a0e05 566f0 96b08 349ae d6adf 9e176 2c9a3 2b5d3 f87b4 882ae f83c/ MMAT_ 2018_ crite ria‑ manual_ 2018‑ 08‑ 01_ ENG. pdf.
49. World Health Organization. Monitoring the building blocks of health systems: a handbook of indicators and their measurement strategies. 2010. https:// www. who. int/ healt hinfo/ syste ms/ WHO_ MBHSS_ 2010_ full_ web. pdf.
50. What is NVivo? | QSR international. http:// www. qsrin terna tional. com/ what‑ is‑ nvivo. Accessed 11 Sep 2017.
51. Michie S, Ashford S, Sniehotta FF, Dombrowski SU, Bishop A, French DP. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO‑RE taxonomy. Psychol Health. 2011;26(11):1479–98.
52. Gagliardi AR, Alhabib S, the members of the Guidelines International Network Implementation Working Group. Trends in guideline imple‑mentation: a scoping systematic review. Implement Sci. 2015;10(1):54.
Page 53 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
53. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA‑ScR): checklist and explanation. Ann Internal Med. 2018. https:// doi. org/ 10. 7326/ M18‑ 0850.
54. Michie S, Atkins L, West R. The behaviour change wheel: a guide to designing interventions. 1st ed. Great Britain: Silverback Publishing; 2014.
55. Spoon D, Rietbergen T, Huis A, Heinen M, van Dijk M, van Bodegom‑Vos L, et al. Implementation strategies used to implement nursing guide‑lines in daily practice: a systematic review. Int J Nurs Stud. 2020;111: 103748.
56. Imamura M, Kanguru L, Penfold S, Stokes T, Camosso‑Stefinovic J, Shaw B, et al. A systematic review of implementation strategies to deliver guidelines on obstetric care practice in low‑ and middle‑income coun‑tries. Int J Gynaecol Obstet. 2017;136(1):19–28.
57. Kihembo C, Masiira B, Nakiire L, Katushabe E, Natseri N, Nabukenya I, et al. The design and implementation of the re‑vitalised integrated disease surveillance and response (IDSR) in Uganda, 2013–2016. BMC Public Health. 2018;18(1):879.
58. Bryce J, Victora CG, Habicht J‑P, Black RE, Scherpbier RW. Program‑matic pathways to child survival: results of a multi‑country evaluation of integrated management of childhood illness. Health Policy Plan. 2005;20(suppl_1):i5‑17.
59. Moshiri E, Arab M, Khosravi A. Using an analytical framework to explain the formation of primary health care in rural Iran in the 1980s. Arch Iran Med. 2016;19(1):16–22.
60. Straus S, Tetroe J, Graham I. Knowledge translation in health care: mov‑ing from evidence to practice. 2nd ed. Oxford: Wiley; 2013.
61. Waltz TJ, Powell BJ, Fernandez ME, Abadie B, Damschroder L. Choosing implementation strategies to address contextual barriers: diversity in recommendations and future directions. Implement Sci. 2019;14(42):1–15.
62. Ritchie LM, Khan S, Moore JE, Timmings C, van Lettow M, Vogel JP, et al. Low‑ and middle‑income countries face many common barriers to implementation of maternal health evidence products. J Clin Epide‑miol. 2016;1(76):229–37.
63. van Olmen J, Marchal B, Van Damme W, Kegels G, Hill PS. Health sys‑tems frameworks in their political context: framing divergent agendas. BMC Public Health. 2012;12(1):774.
64. Kruk ME, Myers M, Varpilah ST, Dahn BT. What is a resilient health sys‑tem? Lessons from Ebola. Lancet. 2015;385(9980):1910–2.
65. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation sci‑ence. Implement Sci. 2009;4:50.
66. Roman E, Wallon M, Brieger W, Dickerson A, Rawlins B, Agarwal K. Moving malaria in pregnancy programs from neglect to priority: experience from Malawi, Senegal, and Zambia. Glob Health Sci Pract. 2014;2(1):55–71.
67. Zhou W, Yu Y, Zhao X, Xiao S, Chen L. Evaluating China’s mental health policy on local‑level promotion and implementation: a case study of Liuyang Municipality. BMC Public Health. 2019;19(1):24.
68. Rahman M, Delarosa J, Luies SK, Alom KR, Quintanar‑Solares M, Jabeen I, et al. Understanding key drivers and barriers to implementation of the WHO recommendations for the case management of childhood pneumonia and possible serious bacterial infection with amoxicillin dispersible tablets (DT) in Bangladesh: a qualitative study. BMC Health Serv Res. 2020;20(1):142.
69. Miguel‑Esponda G, Bohm‑Levine N, Rodríguez‑Cuevas FG, Cohen A, Kakuma R. Implementation process and outcomes of a mental health programme integrated in primary care clinics in rural Mexico: a mixed‑methods study. Int J Ment Health Syst. 2020;14(1):21.
70. Bégin HM, Eggertson L, Macdonald N. A country of perpetual pilot projects. CMAJ. 2009;180(12):1185–1185.
71. Proctor E, Luke D, Calhoun A, McMillen C, Brownson R, McCrary S, et al. Sustainability of evidence‑based healthcare: research agenda, methodological advances, and infrastructure support. Implement Sci. 2015;10(1):88.
72. Sayinzoga F, Bijlmakers L. Drivers of improved health sector perfor‑mance in Rwanda: a qualitative view from within. BMC Health Serv Res. 2016;16(123):1–10.
73. Kutzin J, Sparkes SP. Health systems strengthening, universal health coverage, health security and resilience. Bull World Health Organ. 2016;94(1):2.
74. Taghreed A. Advancing the application of systems thinking in health. Health Res Policy Syst. 2014;12(50):1–5.
75. Andrade MV, Noronha K, Cardoso CS, Oliveira CDL, Calazans JA, Souza MN. Challenges and lessons from a primary care intervention in a Brazil‑ian municipality. Rev Saúde Pública. 2019;53:45.
76. Harrison MB, Legare F, Graham ID, Fervers B. Adapting clinical practice guidelines to local context and assessing barriers to their use. Can Med Assoc J. 2010;182(2):E78–84.
77. Halpern M, Lachmansingh B, Minior T, Hasbrouck LM, Persaud N, Foo A. Implementation of a standardized HIV patient monitoring system in Guyana. Rev Panam Salud Pública. 2010;28(2):107–13.
78. Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, et al. Outcomes for implementation research: conceptual distinctions, meas‑urement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65–76.
79. Bergerot CD, Zayat CG, de Azevedo IM, Okuma GY, Pedras RN, Manhães MFM, et al. Implementation of a psycho‑oncology program according to international recommendations applied in a Brazilian Public Service. Estud Psicol. 2017;22(4):350–7.
80. Marušić A, Campbell H. Reporting guidelines in global health research. J Glob Health. 2016;6(2): 020101.
81. Simera I, Moher D, Hirst A, Hoey J, Schulz KF, Altman DG. Transparent and accurate reporting increases reliability, utility, and impact of your research: reporting guidelines and the EQUATOR Network. BMC Med. 2010;8:24.
82. Amaral J, Victora C, Leite AJ, Da Cunha A. Implementation of the inte‑grated management of childhood illnesses strategy in Northeastern Brazil. Rev Saúde Pública. 2008;42:598–606.
83. Leethongdee S. Health sector reform in Thailand: Policy implementa‑tion in three provinces. Swansea University; 2007.
84. Blanco‑Mancilla G. Implementation of health policies in Mexico City: What factors contribute to more effective service delivery? London, UK: Department of Social Policy of London School of Economics; 2011.
85. Zakumumpa H, Dube N, Damian RS, Rutebemberwa E. Understand‑ing the dynamic interactions driving the sustainability of ART scale‑up implementation in Uganda. Glob Health Res Policy. 2018;3:23.
86. Callaghan‑Koru JA, Islam M, Khan M, Sowe A, Islam J, Mannan II, et al. Factors that influence the scale up of new interventions in low‑income settings: a qualitative case study of the introduction of chlorhexidine cleansing of the umbilical cord in Bangladesh. Health Policy Plan. 2020;35(4):440–51.
87. Mutabazi JC, Gray C, Muhwava L, Trottier H, Ware LJ, Norris S, et al. Integrating the prevention of mother‑to‑child transmission of HIV into primary healthcare services after AIDS denialism in South Africa: perspectives of experts and health care workers ‑ a qualitative study. BMC Health Serv Res. 2020;20:582.
88. Saddi F da C, Harris MJ, Coelho GA, Pêgo RA, Parreira F, Pereira W, et al. Perceptions and evaluations of front‑line health workers regarding the Brazilian National Program for Improving Access and Quality to Primary Care (PMAQ): a mixed‑method approach. Cad Saúde Pública. 2018;34. Available from: http:// www. scielo. br/j/ csp/a/ YpYHf ZJzFG jcs8Y qH6pt 8NB/? lang= en.
89. Xia J, Rutherford S, Ma Y, Wu L, Gao S, Chen T, et al. Obstacles to the coordination of delivering integrated prenatal HIV, syphilis and hepatitis B testing services in Guangdong: using a needs assessment approach. BMC Health Serv Res. 2015;15(1):1–9.
90. Armstrong CE, Lange IL, Magoma M, Ferla C, Filippi V, Ronsmans C. Strengths and weaknesses in the implementation of maternal and peri‑natal death reviews in Tanzania: perceptions, processes and practice. Trop Med Int Health. 2014;19(9):1087–95.
91. Ditlopo P, Blaauw D, Bidwell P, Thomas S. Analyzing the implementation of the rural allowance in hospitals in North West Province, South Africa. J Public Health Policy. 2011;32(1):S80‑93.
92. Doherty T, Besada D, Goga A, Daviaud E, Rohde S, Raphaely N. “If donors woke up tomorrow and said we can’t fund you, what would we do?” A health system dynamics analysis of implementation of PMTCT option B+ in Uganda. Glob Health. 2017;13(1):51.
Page 54 of 54Breneol et al. Health Research Policy and Systems (2022) 20:64
• fast, convenient online submission
•
thorough peer review by experienced researchers in your field
• rapid publication on acceptance
• support for research data, including large and complex data types
•
gold Open Access which fosters wider collaboration and increased citations
maximum visibility for your research: over 100M website views per year •
At BMC, research is always in progress.
Learn more biomedcentral.com/submissions
Ready to submit your researchReady to submit your research ? Choose BMC and benefit from: ? Choose BMC and benefit from:
93. Lovero KL, Lammie SL, van Zyl A, Paul SN, Ngwepe P, Mootz JJ, et al. Mixed‑methods evaluation of mental healthcare integration into tuber‑culosis and maternal‑child healthcare services of four South African districts. BMC Health Serv Res. 2019;19(1):1–12.
94. Mkoka DA, Kiwara A, Goicolea I, Hurtig AK. Governing the implementa‑tion of Emergency Obstetric Care: experiences of Rural District Health Managers, Tanzania. BMC Health Serv Res. 2014;14:333.
95. Moshiri E, Rashidian A, Arab M, Khosravi A. Analyzing the implementa‑tion of the rural allowance in hospitals in North West Province, South Africa. 2016;19(1):2–8.
96. Muthathi IS, Rispel LC. Policy context, coherence and disjuncture in the implementation of the Ideal Clinic Realisation and Maintenance pro‑gramme in the Gauteng and Mpumalanga provinces of South Africa. Health Res Policy Syst. 2020;18(1):55.
97. Schneider H, Nxumalo N. Leadership and governance of community health worker programmes at scale: a cross case analysis of provincial implementation in South Africa. Int J Equity Health. 2017;16(1):72.
98. Sheikh K, Porter J. Discursive gaps in the implementation of public health policy guidelines in India: the case of HIV testing. Soc Sci Med. 2010;71(11):2005–13.
99. Shelley KD, Belete YW, Phiri SC, Musonda M, Kawesha EC, Muleya EM, et al. Implementation of the community health assistant (CHA) cadre in Zambia: a process evaluation to guide future scale‑up decisions. J Community Health. 2016;41(2):398–408.
100. Carneiro VB, Maia CRM, Ramos EMLS, Castelo‑Branco S. Tecobé in Marajó: trend of indicators for the monitoring of primary care before and during the More Physicians for Brazil Program. Ciênc Saúde Cole‑tiva. 2018;23:2413–22.
101. Costa FF, Calvo MCM. Evaluation of the family health strategy imple‑mentation in Santa Catarina in 2004 and 2008. Rev Bras Epidemiol. 2014;17:557–70.
102. Sami S, Amsalu R, Dimiti A, Jackson D, Kenyi S, Meyers J, et al. Under‑standing health systems to improve community and facility level newborn care among displaced populations in South Sudan: a mixed methods case study. BMC Pregnancy Childbirth. 2018;18(1):325.
103. Febir LG, Baiden FE, Agula J, Delimini RK, Akpalu B, Tivura M, et al. Implementation of the integrated management of childhood illness with parasitological diagnosis of malaria in rural Ghana: health worker perceptions. Malar J. 2015;14(1):174.
104. Pyone T, Smith H, van den Broek N. Implementation of the free mater‑nity services policy and its implications for health system governance in Kenya. BMJ Glob Health. 2017;2(4):e000249.
105. Rahman M, Delarosa J, Luies SK, Alom KR, Quintanar‑Solares M, Jabeen I, et al. Understanding key drivers and barriers to implementation of the WHO recommendations for the case management of childhood pneumonia and possible serious bacterial infection with amoxicillin dispersible tablets (DT) in Bangladesh: a qualitative study. BMC Health Serv Res. 2020;20(1):1–12.
106. Stein J, Lewin S, Fairall L, Mayers P, English R, Bheekie A, et al. Building capacity for antiretroviral delivery in South Africa: A qualitative evalu‑ation of the PALSA PLUS nurse training programme. BMC Health Serv Res. 2008.
107. Ejeta LT, Leta Y, Abuye M, Yasin C, Tebekaw Y, Giday T, et al. Implement‑ing the Urban Community Health Information System in Ethiopia: Les‑sons from the pilot‑tests in Addis Ababa, Bishoftu and Hawassa. Ethiop J Health Dev. 2020. Available from: https:// www. ajol. info/ index. php/ ejhd/ artic le/ view/ 198793.
108. Smith Gueye C, Newby G, Tulloch J, Slutsker L, Tanner M, Gosling RD. The central role of national programme management for the achieve‑ment of malaria elimination: a cross case‑study analysis of nine malaria programmes. Malar J. 2016;15(1):488.
109. Ryan GK, Nwefoh E, Aguocha C, Ode PO, Okpoju SO, Ocheche P, et al. Partnership for the implementation of mental health policy in Nigeria: a case study of the Comprehensive Community Mental Health Pro‑gramme in Benue State. Int J Ment Health Syst. 2020;14(1):10.
110. Investigators of WHO LBW Feeding Study Group D India. World Health Organization Guidelines for feeding low birth weight infants: effects of implementation in first referral level health facilities in India. Indian J Pediatr. 2016;83(6):522–8.
111. Lavôr DC, Pinheiro JD, Gonçalves MJ. Evaluation of the implementation of the directly observed treatment strategy for tuberculosis in a large city. Rev Esc Enferm USP. 2016;50:247–54.
112. Li Z, Shu D, Xia M, Gao D, Lu D, Huang N, et al. The assessment on impact of essential drugs policy on primary health care system in rural areas of Shandong Province policy and regulation division of the Health Department of Shandong Province. Technol Health Care. 2015;23(s1):S169‑76.
113. Wingfield T, Boccia D, Tovar MA, Huff D, Montoya R, Lewis JJ, et al. Designing and implementing a socioeconomic intervention to enhance TB control: operational evidence from the CRESIPT project in Peru. BMC Public Health. 2015;15(1):810.
114. Kavle JA, Ahoya B, Kiige L, Mwando R, Olwenyi F. From national guide‑lines to implementation: opportunities and challenges for scale‑up of baby‑friendly community initiative (BFCI) in Kenya. In Breastfeeding Medicine; 2018. p. A‑26.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in pub‑lished maps and institutional affiliations.
Copyright © 2022 FDOKUMEN