
Statin therapy is associated with lower mortality among patients with severe heart failure
6
Statin Therapy Is Associated With Lower Mortality Among Patients With Severe Heart Failure Dariush Mozaffarian, MD, MPH, Regina Nye, MPH, and Wayne C. Levy, MD Experimental considerations suggest both potential harm and benefit from statin therapy in patients with severe heart failure. However, relations of statin therapy with clinical outcomes in severe heart failure are not well established. Using data from the Prospective Random- ized Amlodipine Survival Evaluation (PRAISE) trial, we evaluated associations of statin therapy with total mor- tality among 1,153 patients with severe heart failure (ejection fraction <30% and New York Heart Associa- tion class IIIB or IV symptoms) of ischemic and nonisch- emic etiologies. Statin therapy was administered to 134 patients (12%) during the study period. Over a 1.3-year mean follow-up, there were 413 deaths (29 deaths/100 person-years). Adjusting for age, gender, diabetes, smoking, heart failure etiology, ejection fraction, and New York Heart Association class, statin therapy was associated with a 62% lower risk of death (hazard ratio 0.38, 95% confidence interval 0.23 to 0.65), or 1 fewer death/5 patients taking statin therapy for 1 year. This association was not greatly altered by additional adjust- ment for a variety of other patient characteristics, includ- ing serum cholesterol levels. After propensity score anal- yses, statin therapy was still associated with a 48% lower risk of death (hazard ratio 0.52, 95% confidence interval 0.30 to 0.89). Although this observational study does not prove causality, further investigation of poten- tial benefits of statins in patients with severe heart fail- ure appears warranted. 2004 by Excerpta Medica, Inc. (Am J Cardiol 2004;93:1124 –1129) A lthough mortality from coronary artery disease is declining, the incidence and health burden of heart failure are rising. 1 In the United States, approx- imately 5 million persons have heart failure and 550,000 new cases are diagnosed annually; heart fail- ure is the most common cause of hospitalization among persons aged 65 years, and health care costs for heart failure exceed $20 billion annually. 1,2 Pa- tients with severely reduced left ventricular systolic function and severe symptoms are at particular risk, with mortality rates approaching 30%/year. The 3-hy- droxy-3-methylglutaryl coenzyme-A reductase inhib- itors (“statins”) are among the most frequently pre- scribed medications in clinical practice used for treating hypercholesterolemia and coronary artery dis- ease. However, clinical trials of statins for primary and secondary prevention of coronary artery disease excluded patients with chronic heart failure, 3–5 and despite the frequent intersection of coronary artery disease with heart failure, the relation of statin therapy to outcomes in heart failure is not well established. Additionally, many patients with heart failure do not have significant coronary artery disease, and the ap- propriateness of statin therapy in these patients is unclear. Experimental evidence suggests potential harm and potential benefit of statins in heart failure. Lower serum cholesterol predicts worse outcomes in heart failure, raising concern regarding use of lipid- lowering agents. 6 Statins also reduce ubiquinone (co- enzyme Q-10), which may adversely affect mitochon- drial and cardiac muscle function. 7,8 Conversely, statins modulate a variety of inflammatory and im- mune responses. 9 –12 Given the relation of systemic inflammation to morbidity and mortality in heart fail- ure, 13,14 statins may benefit patients with heart failure separately from or in addition to effects on cholesterol and coronary disease. Thus, experimental consider- ations are conflicting, and despite widespread clinical use of statins, data are sparse on the connection of statin therapy to clinical outcomes in heart failure. Before undertaking a large randomized trial, further assessment of the potential effects of statins in severe heart failure is needed. We therefore investigated whether statin therapy was associated with mortality among patients with severe heart failure enrolled in the Prospective Randomized Amlodipine Survival Evaluation (PRAISE). Our primary hypothesis was that statin therapy would be associated with lower all-cause mortality. From the Channing Laboratory, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, and the Depart- ments of Nutrition and Epidemiology, Harvard School of Public Health, Boston, Massachusetts; Pfizer PGRD, New London, Connect- icut; and Division of Cardiology, Department of Medicine, University of Washington, Seattle, Washington. Dr. Mozaffarian was supported in part by a Health Services Research & Development fellowship from the Veterans Affairs Puget Sound Health Care System, Seattle, Wash- ington; and an NRSA Training Grant in Academic Nutrition from the Harvard School of Public Health, Boston, Massachusetts.The PRAISE data were collected by the PRAISE Study Group and provided by Pfizer, New London, Connecticut. Manuscript received November 10, 2003; revised manuscript received and accepted January 2, 2004. Address for reprints: Dariush Mozaffarian, MD, MPH, 665 Hun- tington Avenue, Building 2, Room 315, Boston, Massachusetts 02115. E-mail: [email protected]. Pfizer did not provide funding for the present study design, analy- sis, or interpretation. 1124 ©2004 by Excerpta Medica, Inc. All rights reserved. 0002-9149/04/$–see front matter The American Journal of Cardiology Vol. 93 May 1, 2004 doi:10.1016/j.amjcard.2004.01.039
-
Upload
washington -
Category
Documents
-
view
4 -
download
0
Transcript of Statin therapy is associated with lower mortality among patients with severe heart failure

Ehsweiet(tepmps
Ahi5uaftfwdist
FWmHioitiHdP12
t0
s
1
Statin Therapy Is Associated With LowerMortality Among Patients With Severe
Heart Failure
Dariush Mozaffarian, MD, MPH, Regina Nye, MPH, and Wayne C. Levy, MDNa0damiylidtuI
xperimental considerations suggest both potentialarm and benefit from statin therapy in patients withevere heart failure. However, relations of statin therapyith clinical outcomes in severe heart failure are not wellstablished. Using data from the Prospective Random-zed Amlodipine Survival Evaluation (PRAISE) trial, wevaluated associations of statin therapy with total mor-ality among 1,153 patients with severe heart failureejection fraction <30% and New York Heart Associa-ion class IIIB or IV symptoms) of ischemic and nonisch-mic etiologies. Statin therapy was administered to 134atients (12%) during the study period. Over a 1.3-yearean follow-up, there were 413 deaths (29 deaths/100erson-years). Adjusting for age, gender, diabetes,moking, heart failure etiology, ejection fraction, and
iso
x-nd
t fatiosts
olicrishyibrefodi
eaeddtAhpuhLhledsmiusaausBahwatEtais, or interpretation.
124 ©2004 by Excerpta Medica, Inc. All rights reserved.The American Journal of Cardiology Vol. 93 May 1, 2004
ew York Heart Association class, statin therapy wasssociated with a 62% lower risk of death (hazard ratio.38, 95% confidence interval 0.23 to 0.65), or 1 fewereath/5 patients taking statin therapy for 1 year. Thisssociation was not greatly altered by additional adjust-ent for a variety of other patient characteristics, includ-
ng serum cholesterol levels. After propensity score anal-ses, statin therapy was still associated with a 48%ower risk of death (hazard ratio 0.52, 95% confidencenterval 0.30 to 0.89). Although this observational studyoes not prove causality, further investigation of poten-
ial benefits of statins in patients with severe heart fail-re appears warranted. �2004 by Excerpta Medica,nc.
(Am J Cardiol 2004;93:1124–1129)
aryease
teryapyed.otap-
ts isntial
ure.s inid-
co-on-,im-icil-ureerolider-icaln ofre.hervere
atedalityd inivalas
wer
lthough mortality from coronary artery diseasedeclining, the incidence and health burden
eart failure are rising.1 In the United States, appromately 5 million persons have heart failure a50,000 new cases are diagnosed annually; hearre is the most common cause of hospitalizamong persons aged�65 years, and health care co
or heart failure exceed $20 billion annually.1,2 Pa-ients with severely reduced left ventricular systunction and severe symptoms are at particularith mortality rates approaching 30%/year. The 3-roxy-3-methylglutaryl coenzyme-A reductase inh
tors (“statins”) are among the most frequently pcribed medications in clinical practice usedreating hypercholesterolemia and coronary artery
rom the Channing Laboratory, Department of Medicine, Brigham andomen’s Hospital and Harvard Medical School, and the Depart-
ents of Nutrition and Epidemiology, Harvard School of Publicealth, Boston, Massachusetts; Pfizer PGRD, New London, Connect-
cut; and Division of Cardiology, Department of Medicine, Universityf Washington, Seattle, Washington. Dr. Mozaffarian was supported
n part by a Health Services Research & Development fellowship fromhe Veterans Affairs Puget Sound Health Care System, Seattle, Wash-ngton; and an NRSA Training Grant in Academic Nutrition from thearvard School of Public Health, Boston, Massachusetts.The PRAISEata were collected by the PRAISE Study Group and provided byfizer, New London, Connecticut. Manuscript received November0, 2003; revised manuscript received and accepted January 2,004.
Address for reprints: Dariush Mozaffarian, MD, MPH, 665 Hun-ington Avenue, Building 2, Room 315, Boston, Massachusetts2115. E-mail: [email protected].
Pfizer did not provide funding for the present study design, analy-
f
il-n
k,---rs-
ase. However, clinical trials of statins for primnd secondary prevention of coronary artery disxcluded patients with chronic heart failure,3–5 andespite the frequent intersection of coronary arisease with heart failure, the relation of statin ther
o outcomes in heart failure is not well establishdditionally, many patients with heart failure do nave significant coronary artery disease, and theropriateness of statin therapy in these patiennclear. Experimental evidence suggests potearm and potential benefit of statins in heart failower serum cholesterol predicts worse outcomeeart failure, raising concern regarding use of lip
owering agents.6 Statins also reduce ubiquinone (nzyme Q-10), which may adversely affect mitochrial and cardiac muscle function.7,8 Converselytatins modulate a variety of inflammatory andune responses.9–12 Given the relation of system
nflammation to morbidity and mortality in heart fare,13,14statins may benefit patients with heart faileparately from or in addition to effects on cholestnd coronary disease. Thus, experimental constions are conflicting, and despite widespread clinse of statins, data are sparse on the connectiotatin therapy to clinical outcomes in heart failuefore undertaking a large randomized trial, furtssessment of the potential effects of statins in seeart failure is needed. We therefore investighether statin therapy was associated with mortmong patients with severe heart failure enrolle
he Prospective Randomized Amlodipine Survvaluation (PRAISE). Our primary hypothesis w
hat statin therapy would be associated with lo
ll-cause mortality.0002-9149/04/$–see front matterdoi:10.1016/j.amjcard.2004.01.039

M
cpsbfHvwuirpt
sedcitcgttocvttwpptisg
agtccdwcfciaawof
tstahw
icwwcahtsadwcwcuujfiis2
R
oot7(pamwtlatofsmoaazs
uysdttdca[(o
ETHODSStudy design and population: PRAISE was a clini-
al trial of amlodipine versus placebo among 1,153atients with severe heart failure. The design, inclu-ion and exclusion criteria, and primary results haveeen described.15 Briefly, all patients had dyspnea oratigue at rest or on minimal exertion (New Yorkeart Association [NYHA] class IIIB or IV) and leftentricular ejection fraction �30% despite treatmentith angiotensin-converting enzyme inhibitors, di-retics, and digoxin. Patients with ischemic and non-schemic heart failure were enrolled. The institutionaleview boards of all 105 participating institutions ap-roved the study, and all subjects gave informed writ-en consent.
Assessment of statin therapy: Medications were as-essed at baseline and every 3 months during clinicxaminations or phone interviews. Medications, exactates of initiation and cessation, and doses were re-orded. Statin use (any brand) was the exposure ofnterest and was evaluated as time spent on statinherapy during follow-up. Thus, persons not on statinsontributed time-at-risk (person-time) to the no-statinroup until death, study end, or initiation of statinherapy, whereas persons taking statins contributedime-at-risk to the statin group until death, study end,r cessation of statin therapy. When statin usehanged, patients were compared only with those sur-iving to that point, avoiding survivor bias. Becauseherapy with statins may be discontinued when pa-ients become acutely ill, all person-time and deathsithin 2 weeks of statin cessation were counted aserson-time and events in the statin group; we alsoerformed sensitivity analyses (i.e., considering pa-ients as statin-treated even after cessation of use),ncluding the entirety of person-time and deaths aftertatin cessation as person-time and events in the statinroup.
Ascertainment of mortality: Events were centrallydjudicated using medical records, electrocardio-rams, chest x-ray reports, autopsy reports, death cer-ificates, and witness statements.15,16 Our primary out-ome was all-cause mortality; we also evaluatedause-specific cardiac mortality. Sudden death wasefined as death from cardiac or unknown causes thatas unexpected and occurred after an abrupt loss of
onsciousness in a previously stable patient. Pumpailure death was defined as progressive heart failureulminating in death, not due to acute myocardialnfarction or observed or suspected life-threateningrrhythmia; these included cardiac transplants (n � 8)t time of transplantation. Fatal myocardial infarctionas defined as death �60 minutes from symptomnset during hospitalization for acute myocardial in-arction. No patient was lost to follow-up.
Statistical analysis: Differences in baseline charac-eristics were evaluated using t tests and chi-squaretatistics. Kaplan-Meier survival methods were usedo compare unadjusted survival rates with statin ther-py. Univariate and multivariate Cox proportional-azards models were used to evaluate risks associated
ith statin therapy. To minimize potential confound- cHEA
ng, age, gender, heart failure etiology, and NYHAlass were prespecified covariates; other covariatesere evaluated based on previously published data asell as associations with exposures or outcomes in the
urrent data set. Two final models are presented: (1)djusted for age, gender, diabetes, smoking status,eart failure etiology, NYHA class, and ejection frac-ion; and (2) further adjusted for systolic blood pres-ure, treatment assignment (amlodipine or placebo),llopurinol use, serum cholesterol, triglycerides, so-ium, blood urea nitrogen, creatinine, hematocrit,hite blood cell count, and lymphocyte count. Other
ovariates that did not materially alter the results andere therefore excluded from the final models in-
luded heart rate, diastolic blood pressure, furosemidese and dose, metolazone use, potassium-sparing di-retic use, and serum uric acid. Propensity score ad-ustment and stratification were also used to accountor potential bias in use of statin therapy.17 Potentialnteractions were assessed using likelihood ratio test-ng. Analyses were performed using the Stata 7.0ystem (College Station, Texas). All p values are-tailed (� � 0.05).
ESULTSPatient characteristics: In all, 134 participants were
n statin therapy during the study period, including 93n statin therapy at baseline and 41 who began statinherapy during follow-up (average time of initiation,8 days; range 0 to 736). These included lovastatin69% of subjects; mean � SD dose 24 � 12 mg),ravastatin (16% of subjects; mean dose 19 � 8 mg),nd simvastatin (15% of subjects; mean dose 12 � 4g). Patients on statin therapy were more likely to beomen, to have an ischemic etiology of heart failure,
o be taking less furosemide, and to have a higherymphocyte count (Table 1). Patients on statins werelso more likely to have higher serum cholesterol andriglycerides, consistent with indications for cholester-l-lowering medication. There were no significant dif-erences in age, prevalence of diabetes or currentmoking, ejection fraction, NYHA class, use of otheredications, or other laboratory parameters indicative
f heart failure severity, such as serum sodium, cre-tinine, hematocrit, or white blood cell count. Nearlyll patients (99%) were on angiotensin-converting en-yme inhibitors, diuretics, and digoxin (data nothown).
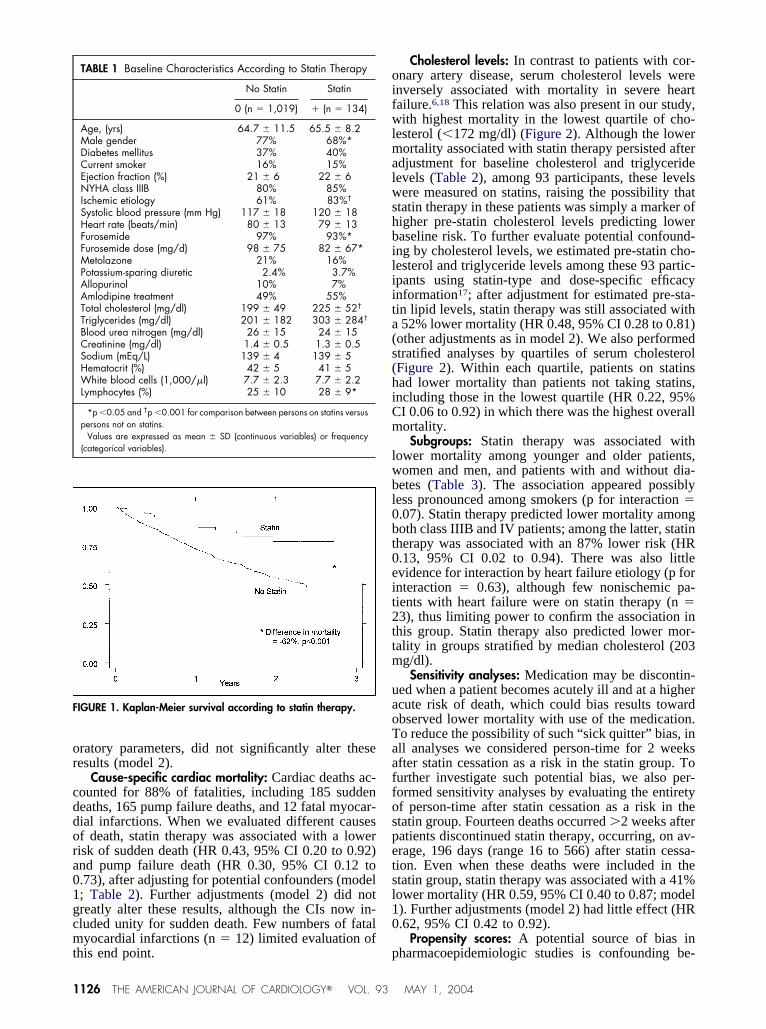
Total mortality: During 15 months of mean follow-p, there were 413 deaths (29 deaths/100 person-ears). In unadjusted analyses, statin therapy was as-ociated with 62% lower risk of death (31 vs 12eaths/100 person-years, p �0.001) (Figure 1), equalo approximately 1 fewer death/5 patients on statinherapy for 1 year. After adjustment for age, gender,iabetes, smoking, heart failure etiology, NYHAlass, and ejection fraction, statin therapy was stillssociated with 62% lower risk of death (hazard ratioHR] 0.38, 95% confidence interval [CI] 0.23 to 0.65)model 1; Table 2). Further adjustment for a variety ofther potential confounding or mediating factors, in-
luding serum cholesterol, triglycerides, and other lab-RT FAILURE/STATINS AND MORTALITY IN HEART FAILURE 1125
or
cddora01gcmt
oifwlmalwshbiliita(s(hiCm
lwbl0bt0eit2ttm
uaoTaaffospetsl10
F
1
ratory parameters, did not significantly alter theseesults (model 2).
Cause-specific cardiac mortality: Cardiac deaths ac-ounted for 88% of fatalities, including 185 suddeneaths, 165 pump failure deaths, and 12 fatal myocar-ial infarctions. When we evaluated different causesf death, statin therapy was associated with a lowerisk of sudden death (HR 0.43, 95% CI 0.20 to 0.92)nd pump failure death (HR 0.30, 95% CI 0.12 to.73), after adjusting for potential confounders (model; Table 2). Further adjustments (model 2) did notreatly alter these results, although the CIs now in-luded unity for sudden death. Few numbers of fatalyocardial infarctions (n � 12) limited evaluation of
TABLE 1 Baseline Characteristics According to Statin Therapy
No Statin Statin
0 (n � 1,019) � (n � 134)
Age, (yrs) 64.7 � 11.5 65.5 � 8.2Male gender 77% 68%*Diabetes mellitus 37% 40%Current smoker 16% 15%Ejection fraction (%) 21 � 6 22 � 6NYHA class IIIB 80% 85%Ischemic etiology 61% 83%†
Systolic blood pressure (mm Hg) 117 � 18 120 � 18Heart rate (beats/min) 80 � 13 79 � 13Furosemide 97% 93%*Furosemide dose (mg/d) 98 � 75 82 � 67*Metolazone 21% 16%Potassium-sparing diuretic 2.4% 3.7%Allopurinol 10% 7%Amlodipine treatment 49% 55%Total cholesterol (mg/dl) 199 � 49 225 � 52†
Triglycerides (mg/dl) 201 � 182 303 � 284†
Blood urea nitrogen (mg/dl) 26 � 15 24 � 15Creatinine (mg/dl) 1.4 � 0.5 1.3 � 0.5Sodium (mEq/L) 139 � 4 139 � 5Hematocrit (%) 42 � 5 41 � 5White blood cells (1,000/�l) 7.7 � 2.3 7.7 � 2.2Lymphocytes (%) 25 � 10 28 � 9*
*p �0.05 and †p �0.001 for comparison between persons on statins versuspersons not on statins.
Values are expressed as mean � SD (continuous variables) or frequency(categorical variables).
IGURE 1. Kaplan-Meier survival according to statin therapy.
his end point. p
126 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 93
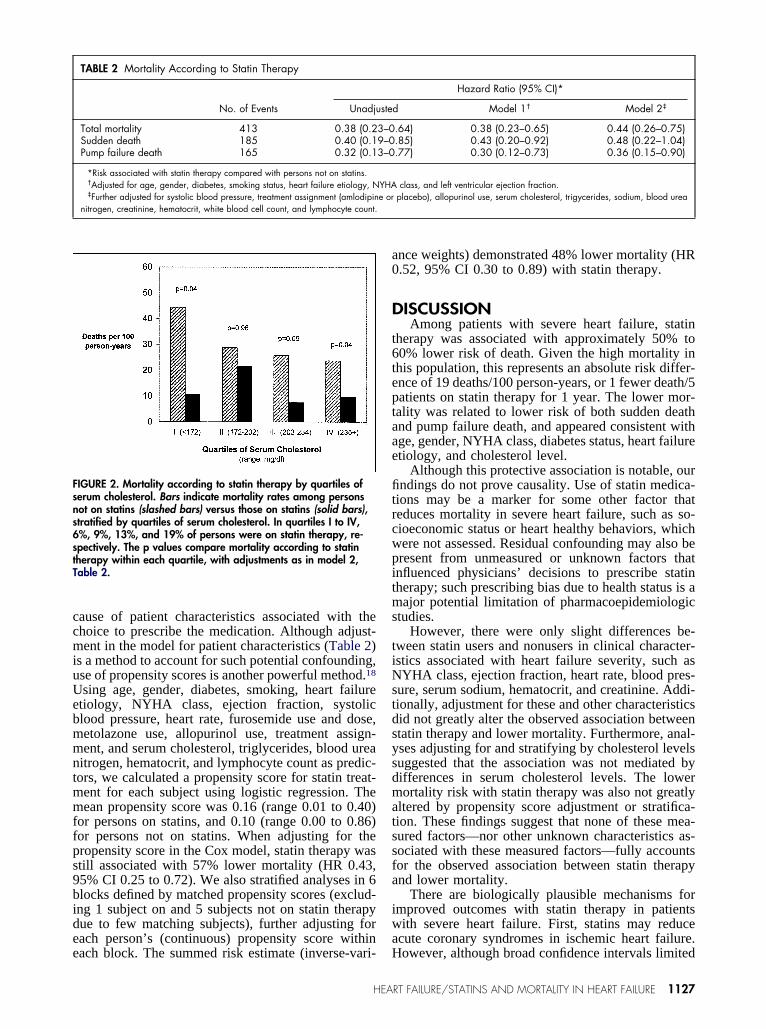
Cholesterol levels: In contrast to patients with cor-nary artery disease, serum cholesterol levels werenversely associated with mortality in severe heartailure.6,18 This relation was also present in our study,ith highest mortality in the lowest quartile of cho-
esterol (�172 mg/dl) (Figure 2). Although the lowerortality associated with statin therapy persisted after
djustment for baseline cholesterol and triglycerideevels (Table 2), among 93 participants, these levelsere measured on statins, raising the possibility that
tatin therapy in these patients was simply a marker ofigher pre-statin cholesterol levels predicting loweraseline risk. To further evaluate potential confound-ng by cholesterol levels, we estimated pre-statin cho-esterol and triglyceride levels among these 93 partic-pants using statin-type and dose-specific efficacynformation17; after adjustment for estimated pre-sta-in lipid levels, statin therapy was still associated with52% lower mortality (HR 0.48, 95% CI 0.28 to 0.81)
other adjustments as in model 2). We also performedtratified analyses by quartiles of serum cholesterolFigure 2). Within each quartile, patients on statinsad lower mortality than patients not taking statins,ncluding those in the lowest quartile (HR 0.22, 95%I 0.06 to 0.92) in which there was the highest overallortality.Subgroups: Statin therapy was associated with
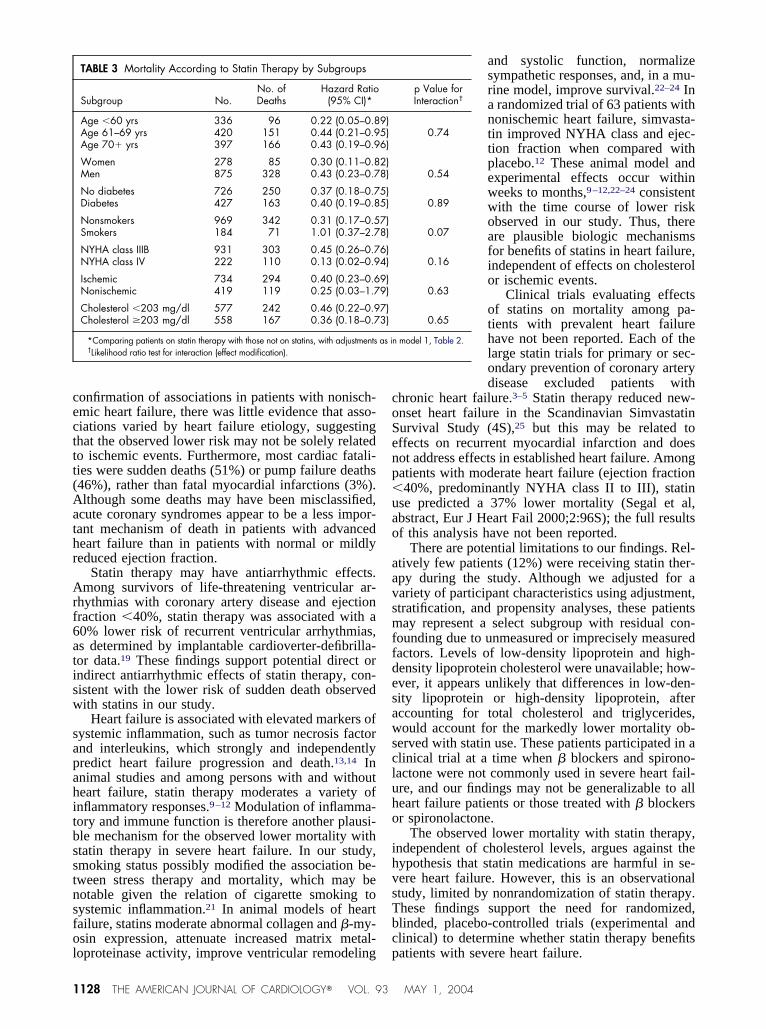
ower mortality among younger and older patients,omen and men, and patients with and without dia-etes (Table 3). The association appeared possiblyess pronounced among smokers (p for interaction �.07). Statin therapy predicted lower mortality amongoth class IIIB and IV patients; among the latter, statinherapy was associated with an 87% lower risk (HR.13, 95% CI 0.02 to 0.94). There was also littlevidence for interaction by heart failure etiology (p fornteraction � 0.63), although few nonischemic pa-ients with heart failure were on statin therapy (n �3), thus limiting power to confirm the association inhis group. Statin therapy also predicted lower mor-ality in groups stratified by median cholesterol (203
g/dl).Sensitivity analyses: Medication may be discontin-
ed when a patient becomes acutely ill and at a highercute risk of death, which could bias results towardbserved lower mortality with use of the medication.o reduce the possibility of such “sick quitter” bias, inll analyses we considered person-time for 2 weeksfter statin cessation as a risk in the statin group. Tourther investigate such potential bias, we also per-ormed sensitivity analyses by evaluating the entiretyf person-time after statin cessation as a risk in thetatin group. Fourteen deaths occurred �2 weeks afteratients discontinued statin therapy, occurring, on av-rage, 196 days (range 16 to 566) after statin cessa-ion. Even when these deaths were included in thetatin group, statin therapy was associated with a 41%ower mortality (HR 0.59, 95% CI 0.40 to 0.87; model). Further adjustments (model 2) had little effect (HR.62, 95% CI 0.42 to 0.92).
Propensity scores: A potential source of bias in
harmacoepidemiologic studies is confounding be-MAY 1, 2004
ccmiuUebmmntmmffps9bidee
a0
D
t6teptaae
fitrcwpitms
tiNstdsysdmatssfa
iwa
Fsns6stT
ause of patient characteristics associated with thehoice to prescribe the medication. Although adjust-ent in the model for patient characteristics (Table 2)
s a method to account for such potential confounding,se of propensity scores is another powerful method.18
sing age, gender, diabetes, smoking, heart failuretiology, NYHA class, ejection fraction, systoliclood pressure, heart rate, furosemide use and dose,etolazone use, allopurinol use, treatment assign-ent, and serum cholesterol, triglycerides, blood urea
itrogen, hematocrit, and lymphocyte count as predic-ors, we calculated a propensity score for statin treat-ent for each subject using logistic regression. Theean propensity score was 0.16 (range 0.01 to 0.40)
or persons on statins, and 0.10 (range 0.00 to 0.86)or persons not on statins. When adjusting for theropensity score in the Cox model, statin therapy wastill associated with 57% lower mortality (HR 0.43,5% CI 0.25 to 0.72). We also stratified analyses in 6locks defined by matched propensity scores (exclud-ng 1 subject on and 5 subjects not on statin therapyue to few matching subjects), further adjusting forach person’s (continuous) propensity score within
TABLE 2 Mortality According to Statin Therapy
No. of Events Unadju
Total mortality 413 0.38 (0.2Sudden death 185 0.40 (0.1Pump failure death 165 0.32 (0.1
*Risk associated with statin therapy compared with persons not on statins.†Adjusted for age, gender, diabetes, smoking status, heart failure etiology, N‡Further adjusted for systolic blood pressure, treatment assignment (amlodipin
nitrogen, creatinine, hematocrit, white blood cell count, and lymphocyte count.
IGURE 2. Mortality according to statin therapy by quartiles oferum cholesterol. Bars indicate mortality rates among personsot on statins (slashed bars) versus those on statins (solid bars),tratified by quartiles of serum cholesterol. In quartiles I to IV,%, 9%, 13%, and 19% of persons were on statin therapy, re-pectively. The p values compare mortality according to statinherapy within each quartile, with adjustments as in model 2,able 2.
ach block. The summed risk estimate (inverse-vari- H
HEA
nce weights) demonstrated 48% lower mortality (HR.52, 95% CI 0.30 to 0.89) with statin therapy.
ISCUSSIONAmong patients with severe heart failure, statin
herapy was associated with approximately 50% to0% lower risk of death. Given the high mortality inhis population, this represents an absolute risk differ-nce of 19 deaths/100 person-years, or 1 fewer death/5atients on statin therapy for 1 year. The lower mor-ality was related to lower risk of both sudden deathnd pump failure death, and appeared consistent withge, gender, NYHA class, diabetes status, heart failuretiology, and cholesterol level.
Although this protective association is notable, ourndings do not prove causality. Use of statin medica-
ions may be a marker for some other factor thateduces mortality in severe heart failure, such as so-ioeconomic status or heart healthy behaviors, whichere not assessed. Residual confounding may also beresent from unmeasured or unknown factors thatnfluenced physicians’ decisions to prescribe statinherapy; such prescribing bias due to health status is aajor potential limitation of pharmacoepidemiologic
tudies.However, there were only slight differences be-
ween statin users and nonusers in clinical character-stics associated with heart failure severity, such asYHA class, ejection fraction, heart rate, blood pres-
ure, serum sodium, hematocrit, and creatinine. Addi-ionally, adjustment for these and other characteristicsid not greatly alter the observed association betweentatin therapy and lower mortality. Furthermore, anal-ses adjusting for and stratifying by cholesterol levelsuggested that the association was not mediated byifferences in serum cholesterol levels. The lowerortality risk with statin therapy was also not greatly
ltered by propensity score adjustment or stratifica-ion. These findings suggest that none of these mea-ured factors—nor other unknown characteristics as-ociated with these measured factors—fully accountsor the observed association between statin therapynd lower mortality.
There are biologically plausible mechanisms formproved outcomes with statin therapy in patientsith severe heart failure. First, statins may reduce
cute coronary syndromes in ischemic heart failure.
Hazard Ratio (95% CI)*
d Model 1† Model 2‡
.64) 0.38 (0.23–0.65) 0.44 (0.26–0.75)
.85) 0.43 (0.20–0.92) 0.48 (0.22–1.04)
.77) 0.30 (0.12–0.73) 0.36 (0.15–0.90)
class, and left ventricular ejection fraction.placebo), allopurinol use, serum cholesterol, trigycerides, sodium, blood urea
ste
3–09–03–0
YHAe or
owever, although broad confidence intervals limited
RT FAILURE/STATINS AND MORTALITY IN HEART FAILURE 1127
cecttt(Aathr
Arf6atisw
sapahitbsstnsfol
coSenp�uao
aavsmffdesawscluho
ihvsTbc
1
onfirmation of associations in patients with nonisch-mic heart failure, there was little evidence that asso-iations varied by heart failure etiology, suggestinghat the observed lower risk may not be solely relatedo ischemic events. Furthermore, most cardiac fatali-ies were sudden deaths (51%) or pump failure deaths46%), rather than fatal myocardial infarctions (3%).lthough some deaths may have been misclassified,
cute coronary syndromes appear to be a less impor-ant mechanism of death in patients with advancedeart failure than in patients with normal or mildlyeduced ejection fraction.
Statin therapy may have antiarrhythmic effects.mong survivors of life-threatening ventricular ar-
hythmias with coronary artery disease and ejectionraction �40%, statin therapy was associated with a0% lower risk of recurrent ventricular arrhythmias,s determined by implantable cardioverter-defibrilla-or data.19 These findings support potential direct orndirect antiarrhythmic effects of statin therapy, con-istent with the lower risk of sudden death observedith statins in our study.
Heart failure is associated with elevated markers ofystemic inflammation, such as tumor necrosis factornd interleukins, which strongly and independentlyredict heart failure progression and death.13,14 Innimal studies and among persons with and withouteart failure, statin therapy moderates a variety ofnflammatory responses.9–12 Modulation of inflamma-ory and immune function is therefore another plausi-le mechanism for the observed lower mortality withtatin therapy in severe heart failure. In our study,moking status possibly modified the association be-ween stress therapy and mortality, which may beotable given the relation of cigarette smoking toystemic inflammation.21 In animal models of heartailure, statins moderate abnormal collagen and �-my-sin expression, attenuate increased matrix metal-
TABLE 3 Mortality According to Statin Therapy by Subgroups
Subgroup No.No. ofDeaths
Hazard Ratio(95% CI)*
Age �60 yrs 336 96 0.22 (0.05–0.8Age 61–69 yrs 420 151 0.44 (0.21–0.9Age 70� yrs 397 166 0.43 (0.19–0.9
Women 278 85 0.30 (0.11–0.8Men 875 328 0.43 (0.23–0.7
No diabetes 726 250 0.37 (0.18–0.7Diabetes 427 163 0.40 (0.19–0.8
Nonsmokers 969 342 0.31 (0.17–0.5Smokers 184 71 1.01 (0.37–2.7
NYHA class IIIB 931 303 0.45 (0.26–0.7NYHA class IV 222 110 0.13 (0.02–0.9
Ischemic 734 294 0.40 (0.23–0.6Nonischemic 419 119 0.25 (0.03–1.7
Cholesterol �203 mg/dl 577 242 0.46 (0.22–0.9Cholesterol �203 mg/dl 558 167 0.36 (0.18–0.7
*Comparing patients on statin therapy with those not on statins, with adjustments†Likelihood ratio test for interaction (effect modification).
oproteinase activity, improve ventricular remodeling p
128 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 93
and systolic function, normalizesympathetic responses, and, in a mu-rine model, improve survival.22–24 Ina randomized trial of 63 patients withnonischemic heart failure, simvasta-tin improved NYHA class and ejec-tion fraction when compared withplacebo.12 These animal model andexperimental effects occur withinweeks to months,9–12,22–24 consistentwith the time course of lower riskobserved in our study. Thus, thereare plausible biologic mechanismsfor benefits of statins in heart failure,independent of effects on cholesterolor ischemic events.
Clinical trials evaluating effectsof statins on mortality among pa-tients with prevalent heart failurehave not been reported. Each of thelarge statin trials for primary or sec-ondary prevention of coronary arterydisease excluded patients with
hronic heart failure.3–5 Statin therapy reduced new-nset heart failure in the Scandinavian Simvastatinurvival Study (4S),25 but this may be related toffects on recurrent myocardial infarction and doesot address effects in established heart failure. Amongatients with moderate heart failure (ejection fraction40%, predominantly NYHA class II to III), statin
se predicted a 37% lower mortality (Segal et al,bstract, Eur J Heart Fail 2000;2:96S); the full resultsf this analysis have not been reported.
There are potential limitations to our findings. Rel-tively few patients (12%) were receiving statin ther-py during the study. Although we adjusted for aariety of participant characteristics using adjustment,tratification, and propensity analyses, these patientsay represent a select subgroup with residual con-
ounding due to unmeasured or imprecisely measuredactors. Levels of low-density lipoprotein and high-ensity lipoprotein cholesterol were unavailable; how-ver, it appears unlikely that differences in low-den-ity lipoprotein or high-density lipoprotein, afterccounting for total cholesterol and triglycerides,ould account for the markedly lower mortality ob-
erved with statin use. These patients participated in alinical trial at a time when � blockers and spirono-actone were not commonly used in severe heart fail-re, and our findings may not be generalizable to alleart failure patients or those treated with � blockersr spironolactone.
The observed lower mortality with statin therapy,ndependent of cholesterol levels, argues against theypothesis that statin medications are harmful in se-ere heart failure. However, this is an observationaltudy, limited by nonrandomization of statin therapy.hese findings support the need for randomized,linded, placebo-controlled trials (experimental andlinical) to determine whether statin therapy benefits
p Value forInteraction†
0.74
0.54
0.89
0.07
0.16
0.63
0.65
model 1, Table 2.
9)5)6)
2)8)
5)5)
7)8)
6)4)
9)9)
7)3)
as in
atients with severe heart failure.
MAY 1, 2004
b
1T2v13tS4Boa15pc6L7Jop8om9c21Sii1a1ic1
Oh1f1MoS1GaP1sp51o1cf2ItC2Lcs2lri2Jim2a22o
Acknowledgment: The PRAISE data were collectedy the PRAISE study group and provided by Pfizer.
. American Heart Association. 2002 Heart and Stroke Statistical Update. Dallas,exas: American Heart Association; 2001.. Health Care Financing Administration. Heart Failure National Project Over-iew. Available at: http://www.hcfa.gov/quality/download/3s.pdf. Accessed May2, 2001.. Scandinavian Simvastatin Survival Study Group. Randomized trial of choles-
erol lowering in 4444 patients with coronary heart disease: the Scandinavianimvastatin Survival Study (4S). Lancet 1994;344:1383–1389.. Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG,rown L, Warnica JW, Arnold JM, Wun CC, Davis BR, Braunwald E. The effectf pravastatin on coronary events after myocardial infarction in patients withverage cholesterol levels. CARE Trial investigators. N Engl J Med 1996;335:001–1009.. LIPID Study Group. Prevention of cardiovascular events and death withravastatin in patients with coronary heart disease and a broad range of initialholesterol levels. N Engl J Med 1998;339:1349–1357.. Rauchhaus M, Coats AJ, Anker SD. The endotoxin-lipoprotein hypothesis.ancet 2000;356:930–933.. De Pinieux G, Chariot P, Ammi-Said M, Louarn F, Lejonc JL, Astier A,acotot B, Gherardi R. Lipid-lowering drugs and mitochondrial function: effectsf HMG-CoA reductase inhibitors on serum ubiquinone and blood lactate/yruvate ratio. Br J Clin Pharmacol 1996;42:333–337.. Marz W, Siekmeier R, Muller HM, Wieland H, Gross W, Olbrich HG. Effectsf lovastatin and pravastatin on the survival of hamsters with inherited cardio-yopathy. J Cardiovasc Pharmacol Ther 2000;5:275–279.. Ridker PM, Rifai N, Lowenthal SP. Rapid reduction in C-reactive protein witherivastatin among 785 patients with primary hypercholesterolemia. Circulation001;103:1191–1193.0. Holm T, Andreassen AK, Ueland T, Kjekshus J, Froland SS, Kjekshus E,imonsen S, Aukrust P, Gullestad L. Effect of pravastatin on plasma markers of
nflammation and peripheral endothelial function in male heart transplant recip-ents. Am J Cardiol 2001;87:815–818.1. Palinski W, Tsimikas S. Immunomodulatory effects of statins: mechanismsnd potential impact on arteriosclerosis. J Am Soc Nephrol 2002;13:1673–1681.2. Node K, Fujita M, Kitakaze M, Hori M, Liao JK. Short-term statin therapy
mproves cardiac function and symptoms in patients with idiopathic dilatedardiomyopathy. Circulation 2003;108:839–843.
3. Kapadia S, Dibbs Z, Kurrelmeyer K, Kalra D, Seta Y, Wang F, Bozkurt B, dHEA
ral H, Sivasubramanian N, Mann DL. The role of cytokines in the failing humaneart. Cardiol Clin 1998;16:645–656.4. Blum A, Miller H. Pathophysiological role of cytokines in congestive heartailure. Annu Rev Med 2001;52:15–27.5. Packer M, O’Connor CM, Ghali JK, Pressler ML, Carson PE, Belkin RN,iller AB, Neuberg GW, Frid D, Wertheimer JH, Cropp AB, DeMets DL. Effect
f amlodipine on morbidity and mortality in severe chronic heart failure. PRAISEtudy Group. N Engl J Med 1996;335:1107–1114.6. O’Connor CM, Carson PE, Miller AB, Pressler ML, Belkin RN, NeubergW, Frid DJ, Cropp AB, Anderson S, Wertheimer JH, DeMets DL. Effect of
mlodipine on mode of death among patients with advanced heart failure in theRAISE trial. Am J Cardiol 1998;82:881–887.7. Jones P, Kafonek S, Laurora I, Hunninghake D. Comparative dose efficacytudy of atorvastatin versus simvastatin, pravastatin, lovastatin, and fluvastatin inatients with hypercholesterolemia (the CURVES study). Am J Cardiol 1998;81:82–587.8. Rosenbaum PR, Rubin DB. The central role of the propensity score inbservational studies for causal effects. Biometrika 1983;70:41–55.9. Horwich TB, Hamilton MA, Maclellan WR, Fonarow GC. Low serum totalholesterol is associated with marked increase in mortality in advanced heartailure. J Card Fail 2002;8:216–224.0. Mitchell LB, Powell JL, Gillis AM, Kehl V, Hallstrom AP, and the AVIDnvestigators. Are lipid-lowering drugs also antiarrhythmic drugs? An analysis ofhe Antiarrhythmics versus Implantable Defibrillators (AVID) trial. J Am Collardiol 2003;42:81–87.1. Tracy RP, Psaty BM, Macy E, Bovill EG, Cushman M, Cornell ES, KullerH. Lifetime smoking exposure affects the association of C-reactive protein withardiovascular disease risk factors and subclinical disease in healthy elderlyubjects. Arterioscler Thromb Vasc Biol 1997;17:2167–2176.2. Bauersachs J, Galuppo P, Fraccarollo D, Christ M, Ertl G. Improvement of
eft ventricular remodeling and function by hydroxymethylglutaryl coenzyme aeductase inhibition with cerivastatin in rats with heart failure after myocardialnfarction. Circulation 2001;104:982–985.3. Hayashidani S, Tsutsui H, Shiomi T, Suematsu N, Kinugawa S, Ide T, Wen, Takeshita A. Fluvastatin, a 3-hydroxy-3-methylglutaryl coenzyme a reductasenhibitor, attenuates left ventricular remodeling and failure after experimentalyocardial infarction. Circulation 2002;105:868–873.4. Pliquett RU, Cornish KG, Peuler JD, Zucker IH. Simvastatin normalizesutonomic neural control in experimental heart failure. Circulation 2003;107:493–2498.5. Kjekshus J, Pedersen TR, Olsson AG, Faergeman O, Pyorala K. The effectsf simvastatin on the incidence of heart failure in patients with coronary heart
isease. J Card Fail 1997;3:249–254.RT FAILURE/STATINS AND MORTALITY IN HEART FAILURE 1129




















