Standing orders for influenza and pneumococcal polysaccharide vaccination: Correlates identified in...
10
RESEARCH ARTICLE Open Access Standing orders for influenza and pneumococcal polysaccharide vaccination: Correlates identified in a national survey of U.S. Primary care physicians Steven M Albert 1* , Mary Patricia Nowalk 2 , Michael A Yonas 1,2 , Richard K Zimmerman 1,2 and Faruque Ahmed 3 Abstract Background: Standing orders programs (SOPs) allow non-physician medical staff to assess eligibility and administer vaccines without a specific physician’s order. SOPs increase vaccination rates but are underutilized. Method: In 2009, correlates of SOPs use for influenza vaccine and pneumococcal polysaccharide vaccination (PPV) were assessed in a nationally representative, stratified random sample of U.S. physicians (n = 880) in family and internal medicine who provided office immunization. The response rate was 67%. Physicians reporting no SOPs, only influenza SOPs, and joint influenza and PPV SOPs were compared using multinomial and logistic regression models to examine individual and practice-level correlates. Results: 23% reported using SOPs consistently for both influenza vaccine and PPV, and 20% for influenza vaccination only, with the remainder not using SOPs. Practice-level factors that distinguished practices with joint influenza-PPV SOPs included perceived practice openness to change, strong practice teamwork, access to an electronic medical record, presence of an immunization champion in the practice, and access to nurse/physician assistant staff as opposed to medical assistants alone. Discussion: Physicians in practices with SOPs for both vaccines reported greater awareness of ACIP recommendations and/or Medicare regulations and were more likely to agree that SOPs are an effective way to boost vaccination coverage. However, implementation of both influenza and PPV SOPs was also associated with a variety of practice-level factors, including teamwork, the presence of an immunization champion, and greater availability of clinical assistants with advanced training. Conclusions: Practice-level factors are critical for the adoption of more complex SOPs, such as joint SOPs for influenza and PPV. Keywords: Adult immunizations, Influenza vaccine, Pneumococcal pneumonia vaccine, Standing orders Background In the United States (U.S.) yearly adult influenza vacci- nation coverage remains less than optimal, with 65.6% of adults aged ≥ 65, 40.1% of adults aged 50-64, and 23% of adults aged 18-49 receiving influenza vaccine in 2009 [1]. Low vaccination coverage is evident for pneu- mococcal polysaccharide vaccination (PPV) as well. Among adults aged 65+, 60.6% report ever receiving PPV, and among those at high-risk aged 19-64, only 17.5% report ever receiving PPV [2]. Although self- reports of vaccination may be subject to inaccurate recall [3], it is clear that missed opportunities to vacci- nate adults in primary care are common and an importa77; manuscript, 77; manuscript, 77; manuscript, 77; manuscript, nt cause of low vaccination rates. Missed opportunities for vaccination often result from constraints on physician time and attendance to patients’ other priorities [4,5]. Cost or availability of * Correspondence: [email protected] 1 Department of Behavioral and Community Health Sciences, Graduate School of Public Health, University of Pittsburgh, Pittsburgh, PA, USA Full list of author information is available at the end of the article Albert et al. BMC Family Practice 2012, 13:22 http://www.biomedcentral.com/1471-2296/13/22 © 2012 Albert et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Standing orders for influenza and pneumococcal polysaccharide vaccination: Correlates identified in...
RESEARCH ARTICLE Open Access
Standing orders for influenza and pneumococcalpolysaccharide vaccination Correlates identifiedin a national survey of US Primary carephysiciansSteven M Albert1 Mary Patricia Nowalk2 Michael A Yonas12 Richard K Zimmerman12 and Faruque Ahmed3
Abstract
Background Standing orders programs (SOPs) allow non-physician medical staff to assess eligibility andadminister vaccines without a specific physicianrsquos order SOPs increase vaccination rates but are underutilized
Method In 2009 correlates of SOPs use for influenza vaccine and pneumococcal polysaccharide vaccination (PPV)were assessed in a nationally representative stratified random sample of US physicians (n = 880) in family andinternal medicine who provided office immunization The response rate was 67 Physicians reporting no SOPsonly influenza SOPs and joint influenza and PPV SOPs were compared using multinomial and logistic regressionmodels to examine individual and practice-level correlates
Results 23 reported using SOPs consistently for both influenza vaccine and PPV and 20 for influenzavaccination only with the remainder not using SOPs Practice-level factors that distinguished practices with jointinfluenza-PPV SOPs included perceived practice openness to change strong practice teamwork access to anelectronic medical record presence of an immunization champion in the practice and access to nursephysicianassistant staff as opposed to medical assistants alone
Discussion Physicians in practices with SOPs for both vaccines reported greater awareness of ACIPrecommendations andor Medicare regulations and were more likely to agree that SOPs are an effective way toboost vaccination coverage However implementation of both influenza and PPV SOPs was also associated with avariety of practice-level factors including teamwork the presence of an immunization champion and greateravailability of clinical assistants with advanced training
Conclusions Practice-level factors are critical for the adoption of more complex SOPs such as joint SOPs forinfluenza and PPV
Keywords Adult immunizations Influenza vaccine Pneumococcal pneumonia vaccine Standing orders
BackgroundIn the United States (US) yearly adult influenza vacci-nation coverage remains less than optimal with 656of adults aged ge 65 401 of adults aged 50-64 and23 of adults aged 18-49 receiving influenza vaccine in2009 [1] Low vaccination coverage is evident for pneu-mococcal polysaccharide vaccination (PPV) as well
Among adults aged 65+ 606 report ever receivingPPV and among those at high-risk aged 19-64 only175 report ever receiving PPV [2] Although self-reports of vaccination may be subject to inaccuraterecall [3] it is clear that missed opportunities to vacci-nate adults in primary care are common and animporta77 manuscript 77 manuscript 77 manuscript77 manuscript nt cause of low vaccination ratesMissed opportunities for vaccination often result fromconstraints on physician time and attendance topatientsrsquo other priorities [45] Cost or availability of
Correspondence smalbertpittedu1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USAFull list of author information is available at the end of the article
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
copy 2012 Albert et al licensee BioMed Central Ltd This is an Open Access article distributed under the terms of the Creative CommonsAttribution License (httpcreativecommonsorglicensesby20) which permits unrestricted use distribution and reproduction inany medium provided the original work is properly cited
vaccine is less important as a barrier to vaccination inthe US for two reasons 1) key national social insuranceprograms such as Medicare and Medicaid cover boththe costs of the vaccines and administration by recog-nized providers httpswwwcmsgovImmunizationsand 2) the Affordable Care Act mandates coverage ofvaccines by private insurersLess than optimal vaccination coverage is typical in
Europe as well A survey of the 27 member states of theEuropean Union plus Iceland and Norway during the2006-2007 influenza season found that influenza vacci-nation in people aged 65+ ranged from 321 in Austriato 821 in the Netherlands Western European coun-tries (except for Austria and Finland) achieved the 2006WHO goal of at least 50 coverage in the elderly butonly the Netherlands reached the 2010 WHO target of75 coverage [6] While most Western European coun-tries recommend PPV for the elderly countries vary inage guidelines and recommendations for repeat vaccina-tions A systematic review found large cross-nationaldifferences in vaccination coverage [7]Standing orders programs (SOPs) for immunization
are typically facility-based policies that enable non-phy-sician medical personnel to assess a patientrsquos immuniza-tion status and administer vaccines without directphysician involvement In 2002 US Medicare regula-tions prohibiting SOPs for medication administrationwere modified to exclude influenza and pneumococcalvaccinations [8]Introduction of SOPs has been shown to increase
influenza and pneumococcal vaccination rates in inpati-ent settings [910] In outpatient settings SOPsimproved influenza vaccination rates 27 in a generalelderly patient population [11] and among cardiovascu-lar patients attending a lipid clinic [12] In a study ofpatients in dialysis clinics SOPs did not increase influ-enza vaccination but significantly increased PPV andhepatitis B vaccination rates [13] In a systematic reviewcombination interventions which included SOPs werealso effective raising adult immunization rates by amedian of 16 [14] A meta-analysis of interventions toincrease adult immunizations found that organizationalchange had the highest impact though the effect ofSOPs was not explicitly assessed [15] The US AdvisoryCommittee on Immunization Practices (ACIP) [16] theTask Force for Community Preventive Services [14] andthe Southern California Evidence-Based Practice Center-RAND [17] have all endorsed SOPs to reduce missedopportunities and raise vaccination rates yet SOPs arenot commonly used in the outpatient setting Amongprimary care physicians outpatient use of SOPs was33 prior to the change in Medicare regulations [18]and since then has increased to just 42 for influenzavaccine [19]
Research on use of SOPs for influenza vaccine andPPV outside the United States is relatively scarce How-ever evidence suggests that implementation of SOPs iseffective in other countries In a Canadian antenatal set-ting for example a single nurse tasked with simplyapproaching patients to offer and administer vaccinewas able to boost influenza vaccination coverage tonearly half of clinic attendees [20] A similar approachto universal screening for vaccination in the case ofhepatitis B led to marked increases in uptake in Den-mark [21] Studies suggest that in the absence of SOPsor some other concerted effort opportunities to vacci-nate the elderly are routinely missed For example oneAustralian study found that hospitalized elderly whoexpressed interest in influenza vaccine and PPV wentunvaccinated in routine care [22] This situation may bechanging Recommendations from public health organi-zations in Europe now include use of SOPs ldquo Theclinician must be in the habit of using every visit oppor-tunity (for whatever reason) to check vaccination statusThis means empowering administrative reception andclerical staff to evaluate vaccination history eligibilityand contraindications through standing ordersrdquo [23]Suboptimal adult vaccination rates and low reported
use of SOPs suggest that there are barriers to SOPimplementation Primary care providers in outpatientsettings vary in their acceptance and use of SOPs forinfluenza vaccine and PPV [1324] The purpose of thisstudy was to identify factors that impede or promoteconsistent use of SOPs for adult vaccinations and toexamine factors that distinguish practices that consis-tently use SOPs for both influenza vaccine and PPVpractices that use SOPs for influenza vaccine alone andpractices that have no SOPs for either vaccine
MethodsSamplePhysicians selected to receive a mailed survey weresampled from the American Medical Associationrsquos(AMA) master list of outpatient-based family physicians(n = 45000) and general internists (n = 45000) toobtain a nationally representative sample The samplesize required to detect a 10 difference in proportionsof SOP implementation between the two specialtygroups with a power of 80 and alpha of P lt 005 was816 (408 per group) Assuming a 50 response rate andloss due to bad addresses we sampled 1640 physicians(820 internists and 820 family physicians) nationwide[19] A post hoc calculation of power based on thereported prevalence of SOPs in the sample suggests wehad 90 power to identify differences between SOPadopters and non-adopters as small as 10 in factorsassociated with adoption of SOPs No physician assis-tants or nurse practitioners were sampled
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 2 of 10
The survey was mailed with a cover letter signed byrepresentatives of the Centers for Disease Control andPrevention (CDC) the American Medical Association(AMA) and the principal investigator Attached to thesurvey was a $500 cash incentive to complete the ques-tionnaire Respondents were asked to return the com-pleted questionnaire in a self-addressed stampedenvelope Non-respondents received a second mailedsurvey approximately 8 weeks after the first Afteranother 8 weeks non-respondents were telephoned torequest participation or to complete the survey byphone Physicians were excluded if they were no longerin primary care practice did not immunize in theirpractice did not treat adult patients or did not answerquestions pertaining to influenza vaccination or PPV
Survey instrumentThe survey questionnaire (see Additional file 1) wasdeveloped using aspects of the Awareness-to-Adherencemodel [25] which predicts physician behavior regardingnew guidelines for care and diffusion of innovation the-ory which identifies predictable patterns of programadoption [2627] These topics were informed by find-ings from focus groups and interviews which were con-ducted beforehand The three focus groups involvedprimary care providers including physicians as well asnursing staff They were conducted in local sites selectedfor diversity in patient populations and variation in useof SOPs for adult immunizations Focus group discus-sions were facilitated by a qualitative researcher who fol-lowed a written protocol developed by the researchteamSurvey items were also informed by PRECEDE-PRO-
CEED a systematic process to evaluate health problemsand design intervention programs [28] PRECEDE is anacronym for Predisposing Reinforcing and EnablingConstructs in Educational Diagnosis and EvaluationThe questionnaire consisted of 22 closed-ended ques-tions and covered demographics practice characteristicsawareness agreement and use of SOPs for adult immu-nizations barriers to and facilitators of SOPs and physi-cian attitudes regarding SOPs It was designed to beconcise to encourage response by busy physicians Thequestionnaire was pilot tested with several local primarycare physicians and revised as appropriate
Data processing and analysesData from returned surveys were entered using a dou-ble-entry protocol and compared using an automatedprocedure to identify discordant values The files dif-fered in lt 5 of data points and differences were recon-ciled in each case The final survey data file was mergedwith the file provided by AMA to add physician demo-graphic training and practice indicators Missing values
overall accounted for lt 5 of the data For continuousvariables mean values for the appropriate measure werecalculated The survey and research protocol wereapproved by the University of Pittsburgh InstitutionalReview BoardFor the survey standing orders were defined as ldquoan
office policy that allows non-physician staff to screenadults for influenza and PPV and administer either vac-cine to eligible adults without getting a specific orderfrom the patientrsquos physicianrdquo The question used to elicitSOPs status asked physicians to choose among the fol-lowing categories of SOPs use in their practice (i) nostanding orders and no interest in implementing them(ii) no standing orders but interest in implementingthem (iii) standing orders but inconsistent use and (iv)consistent use of standing orders The question wasasked separately for influenza immunization and PPVCombining answers to the two questions allowed us toidentify physicians who reported no consistent use ofSOPs for either vaccine consistent use of SOPs forinfluenza vaccine only or consistent use of SOPs forboth vaccinations (Physicians rarely reported SOPs forPPV in the absence of SOPs for influenza vaccinationsee below) The three groups were compared in univari-ate analyses (c2 for proportions one-way analysis of var-iance for continuous measures) to identify significantcorrelates of SOPs statusMultinomial logistic regression models were developed
to examine differences between groups In multinomialmodels the two consistent SOP groups (influenza vac-cine only influenza vaccine and PPV) were each com-pared to physicians reporting no or inconsistent use ofSOPs A final logistic regression model was developedto examine how physicians reporting consistent SOPsfor both vaccines differed from those reporting consis-tent use of SOPs for influenza vaccine only For themultivariable analyses odds ratios and 95 confidenceintervals were estimated Interaction effects wereassessed but none was significant In developing theregression models we included variables significant inunivariate analyses (P lt 05) but also physician age andlength of time in practice because these may be corre-lated with knowledge of SOPs and attitudes toward theiruse An additional model was developed that excludedphysician age and length of time in practice as covari-ates Odds ratios from the alternative model did notappreciably differ and no changes in significant predic-tors were identifiedThe following predictors of SOPs status were
investigatedPhysician-Level Factors Indicators drawn from the
AMA file included age time since receiving medicaldegree medical specialty (family medicine or internalmedicine) and board certification The mailed survey
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 3 of 10
asked whether physicians had received their medicaldegrees outside the US and included the following indi-cators of physician knowledge of SOPs whether theywere aware of ACIP recommendations or Medicare reg-ulations and whether they agreed that SOPs are effectivein boosting vaccination coveragePractice-Level Factors Physicians reported on practice-
level factors likely to influence adoption or consistentuse of SOPs These included perceptions of how opentheir practice is to change or innovation whether theirstaff demonstrates strong teamwork and whether physi-cians are primary decision makers for the practiceAdditional factors included access to an electronic medi-cal record having an immunization champion (a clinicalstaff member who promotes and encourages immuniza-tion) on site size of practices (recorded as solo 2-4 or 5+ physicians) help available to physicians (how manyhelpers per provider recorded as 1 helper per 2+ provi-ders 1 helper per provider or two helpers per provider)type of help (advanced (PACRNP) nurse-level (RN orLPN) assistance or medical assistant) and organizationof the practice (comparing practices that are part oflarge health plans or corporations to other types) Thesurvey instrument can be found in the Additional file 1
ResultsOf the 1640 physicians contacted by mail 16 letterswere returned by the post office as undeliverable and107 physicians were no longer in practice no longer inprimary care (eg hospitalists) deceased or unknown atthe practice leaving 1517 eligible physicians Of these1015 physicians returned surveys for a response rate of67 Participation was higher among family physicians(689) than internists (648 P lt 01) and amongboard certified (689) than non-board certified (607P lt 01) physicians Participants and nonparticipants didnot vary by age (mean = 507 years) length of time inpractice (mean = 23 years) domestic vs internationaltraining or geographic region Among participating phy-sicians 819 received their medical degree in the USand 795 were board certified The modal practice pat-tern for physicians in the sample was an independentpractice (51) in a suburban setting (453) The nextmost common practice setting was to be based in alarge corporate health system (255) in an urban set-ting (312)Of the 1015 physicians who completed the survey 115
did not immunize adults in their practices leaving 900physicians in the sample Of these 900 20 did notrespond to questions specific to influenza vaccinationThus the analytic sample consisted of 880 physicianswho provided information on SOPs for influenza vacci-nation and PPV Consistent use of SOPs for pneumo-coccal vaccination in the absence of similar use of SOPs
for influenza vaccination was rare in fact only onerespondent in the sample fell into this category By con-trast SOPs for influenza vaccination without standingorders for PPV were common Given this distributionwe established three SOP groups no consistent use ofSOPs for either vaccination including the one physicianreporting SOP use for PPV only (n = 502 570) con-sistent use of SOPs for influenza vaccination only (n =175 199) and consistent use of SOPs for both vacci-nations (n = 203 231) Forty-three percent of thesample reported SOPs for influenza vaccination (with orwithout concomitant SOP for PPV) Physicians in thethree groups did not differ in age length of time inpractice US medical training board certification statusor specialtyDifferences among the three SOPs groups are shown
in Table 1 Across the three groups some correlatesincreased uniformly as use of SOPs increased for exam-ple awareness of ACIP recommendations andor Medi-care regulations belief that SOPs enhance adultvaccination rates having an immunization champion inthe practice agreement that SOPs are effective in boost-ing vaccination coverage access to an electronic medicalrecord (EMR) and having staff who are open to innova-tion and who work well together Training level andnumber of clinical assistants were significantly related touse of SOPs with practices reporting a greater staff toclinician ratio and those with more highly trained assis-tants (PACRNP or RNLPN) more often reporting con-sistent use of SOPs The proportion reporting 2 helpersper provider was 693 in the consistent influenzaPPVSOP group vs 563 in the consistent influenza onlygroup and 463 in the no consistent SOP group Pair-wise differences across these groupings were significantin post hoc comparisons Number of physicians in apractice was not a significant correlate of SOP groupTo investigate correlates of SOPs in more detail mul-
tinomial logistic regression models were developed toexamine the entire set of correlates These models allowa view of how physicians in each of the two SOP groupsdiffer from the group not using SOPs Table 2 showsodds ratios and 95 confidence intervals associated witheach correlate in a model that includes variables shownearlier in Table 1 adjusted for physician age and lengthof time in practiceIn the final adjusted model consistent use of SOPs
limited to influenza vaccine was independently and sig-nificantly associated with awareness of ACIP recommen-dations andor Medicare regulations (odds ratio [OR]235 95 confidence interval [CI] 160-346) agreementthat SOPs are an effective way to boost vaccination cov-erage (OR 297 95 CI 189-467) family medicine spe-cialty (OR 163 95 CI 110-242) greater amount ofhelp available to physicians (access to 2 assistants [OR
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 4 of 10
275 95 CI 131-579] access to 1 assistant [OR 230123-430] relative to the group with only 1 assistant for2+ providers)Consistent use of SOPs for both influenza vaccine and
PPV was associated with the same set of factors butadditional factors as well Shared correlates includedawareness of ACIP recommendations andor Medicareregulations (OR 446 95 CI 291-685) agreement thatSOPs are an effective way to boost vaccination coverage(OR 35 95 CI 214-571) family medicine specialty
(OR 127 95 CI 089-191 NS) and a greater staff toclinician ratio (OR 222 95 CI 109-454) Correlatesassociated only with combined influenza and PPV SOPsincluded a variety of practice-level factors practiceopenness to change and innovation (OR 215 95 CI133-347) strong practice teamwork (OR 278 95 CI149-521) access to an electronic medical record (OR190 95 CI 122-296) presence of an immunizationchampion in the practice (OR 194 95 127-298) andaccess to nursephysician assistant staff as opposed to
Table 1 Characteristics of PhysiciansPractices Reporting No Consistent Use of Standing Orders Programs (SOPs)Consistent Use of SOPs for Influenza Vaccine Only and Consistent Use of SOPs for Both Influenza Vaccine and PPV
No ConsistentUse of SOPs(n = 502)
Consistent Use of SOPs forInfluenza Vaccine Only
(n = 175)
Consistent Use of SOPs for BothInfluenza Vaccine and PPV
(n = 203)
P
Physician Indicators
Age 504 (101) 502 (94) 518 (99) 17
Years since medical degree 225 (104) 228 (100) 242 (98) 13
Family Medicine specialty 482 383 429 059
Board certified 797 811 783 53
Medical degree outside US 217 177 207 79
Physician is aware of ACIP recommendationsandor Medicare regulations
414 611 778 lt001
Physician believes SOPs are an effective way toboost adult vaccinations
602 794 823 lt001
Practice Indicators
Practice is open to change or innovation 516 611 783 lt001
Strong practice teamwork 657 737 906 lt001
Practice uses electronic medical record 456 566 591 001
Practice has immunization champion on site
233 274 389 lt001
Clinical support
2 helpers per provider 463 563 693 lt001
1 helper per provider 200 219 118
1 helper per 2+ providers 338 218 189
Number of physicians in practice
Solo 263 414 319 11
2-4 189 434 377
5+ 241 340 414
Type of clinical support
RNLPN 311 295 477 lt001
Medical Assistant 662 694 482
PACRNP 27 12 40
Practice is part of large health plan orcorporation
230 343 276 013
Physicians are primary decision makers forpractice
636 550 584 14
PPV = Pneumococcal polysaccharide vaccine
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 5 of 10
Table 2 Practice Characteristics Associated with Consistent Use of Standing Orders Programs (SOPs) for InfluenzaVaccination Only or Influenza and PPV Relative to No Consistent Use of SOPs in Multinomial Logistic Regression
Characteristic Consistent Use of SOPs for InfluenzaVaccine OnlyOR (95 CI)
Consistent Use of SOPs for Both InfluenzaVaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andorMedicare regulations
235 (160 346) Plt 001 446 (291 685) Plt 001
Physician believes that SOPs are an effective way toboost adult vaccinations
297 (189 467) Plt 001 350 (214 571) Plt 001
Practice is open to change or innovation 136 (079 210) 215 (133 347) P= 002
Strong practice teamwork 118 (074 191) 278 (149 521) P= 001
Practice uses electronic medical record 135 (089 203) 190 (122 296) P= 005
Practice has immunization champion on site 112 (072 176) 194 (127 298) P= 002
Clinical support
2 helpers per provider 275 (131 579) P= 008 222 (109 454) P= 028
1 helper per provider 230 (123 430) P= 009 145 (078 267)
1 helper per 2+ providers 100 (ref) 100 (ref)
Number of physicians in practice
Solo 076 (041 138) 071 (039 130)
2-4 102 (065 160) 072 (045 117)
ge 5 100 (ref) 100 (ref)
Family Medicine specialty 163 (110 242) P= 015 127 (089 191)
Nurse-levelPA assistance rather than medical assistant 072 (048 109) 149 (099 224) P= 054
Practice is part of large health plan or corporation 134 (085 213) 104 (062 172)
Physicians are primary decision makers for practice 094 (061 145) 108 (068 170)
Model adjusted for physician age and time since medical degree Model x2 = 2397 p lt 0001 R2 = 026
Table 3 Practice Characteristics Associated with Consistent Use of SOPs for Both Influenza Vaccine and PPV Relativeto Influenza Vaccine Only in Logistic Regression
Characteristic Consistent Use of SOPsfor Both Influenza Vaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andor Medicare regulations 195 (118 324) P= 010
Physician believes that SOPs are an effective way to boost adult vaccinations 111 (060 206)
Practice is open to change or innovation 159 (092 275)
Strong practice teamwork 224 (110 454) P= 026
Practice uses electronic medical record 130 (077 221)
Practice has immunization champion on site 167 (101 454) P= 046
Clinical support
2 helpers per provider 086 (035 214)
1 helper per provider 066 (030 149)
1 helper per 2+ providers 100 (ref)
Number of physicians in practice
Solo 087 (042 180)
2-4 068 (039 119)
ge 5 100 (ref)
Family medicine specialty 078 (048 126)
Nurse-levelPA assistance rather than medical assistant 212 (131 345) P= 002
Practice is part of large health plan or corporation 083 (047 146)
Physicians are primary decision makers for practice 131 (078 221)
Model adjusted for physician age and time since MD Model Χ2 = 550 P lt 0001 R2 = 020
PPV = Pneumococcal Polysaccharide Vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 6 of 10
medical assistants alone (OR 149 95 CI 099-224 p= 054)The two SOP groups were directly compared in Table
3 Physicians reporting consistent use of SOPs for bothimmunizations were more likely to be aware of ACIPrecommendations andor Medicare regulations (OR195 95 CI 118-324) Practice-level factors distin-guishing consistent use of SOPs for both vaccinesincluded strong practice teamwork (OR 224 95 CI110-454) having an immunization champion on site(OR 167 95 CI 101-454) and access to nursephysi-cian assistant staff as opposed to medical assistants (OR221 95 CI 131-345)Finally we examined the number of physician and
practice characteristics associated with adoption ofSOPs and the prevalence of reported SOPs for eitherinfluenza vaccine or PPV We summed across the 12characteristics analyzed in the regression models andplotted adoption of SOPs against this index (Figure 1)In this sample of physicians few respondents reported 0or 1 characteristic (n = 3) and few reported all 12 (n =3) Physicians reported a median of six characteristicsassociated with adoption Figure 1 shows that adoption
of SOPs is as low as 105 when only 1 or 2 factors arepresent and as high as 769 in the presence of all 11 or12 factors
DiscussionIn this national survey of US primary care physicianstreating adults 231 reported using SOPs consistentlyfor both influenza vaccine and PPV and 199 usedSOPs only for influenza vaccination In total as we havereported elsewhere 43 of physicians reported consis-tent use of SOPs for influenza vaccine [19] Physiciansin practices with SOPs for both vaccines reportedgreater awareness of ACIP recommendations andorMedicare regulations and were more likely to agree thatSOPs are an effective way to boost vaccination coverageImplementation of both influenza and PPV SOPs wasassociated with a variety of practice-level factors as wellincluding more effective practice teamwork the pre-sence of an immunization champion and greater avail-ability of clinical assistants with more advanced trainingthan that of medical assistantsThe CDC has recommended SOPs for adult vaccina-
tion since 2000 [16] However the Center for Medicare
Prevalence of SOPs Relative to Number ofPhysician and Practice Characteristics Associated
with Adoption
Figure 1 Uploaded separately Prevalence of SOPs Relative to Number of Physician and Practice Characteristics Associated with Adoption
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 7 of 10
and Medicaid Services (CMS) prohibited SOPs for allmedications until 2002 when CMS modified its regula-tions to allow SOPs for influenza vaccine and PPV [8]It is understandable that physicians who were unawareof the change in CMS regulations might not haveadopted consistent use of SOPs as reflected in our dataGiven the myriad recommendations and policies
aimed at primary preventive care including immuniza-tions how can a practice keep current One solution isfor the practice to have an immunization championsomeone to interpret and communicate changes in vac-cine policies and recommendations as they occur Pre-vious research confirms the importance of animmunization champion to improve vaccination ratesOne study that included explicit training of immuniza-tion nurses to serve as clinical champions boosted influ-enza vaccination coverage rates in pregnant womenfrom 25 to 374 in 2008-2009 [29] However it isdifficult to determine the specific value of immunizationchampions relative to other practice-level factorsbecause most interventions designed to boost vaccina-tion coverage include a variety of elements Our findingssuggest the particular value of champions for practicesthat have SOPs for both influenza vaccine and PPV Itwould useful to determine which staff makes the mosteffective immunization champion and what sort of train-ing is most appropriate In most cases champions arenurses but recent efforts suggest that even non-clinicalstaff such as receptionists or medical records staff canbe trained as immunization champions httpwwwimmunizeusaorgiz-champions[30] It remains unclearhow such duties will be added to job descriptions orqualifications and whether additional compensation isappropriateAccess to physician assistants or licensed nursing per-
sonnel was a significant correlate of SOPs for PPV asopposed to SOPs for influenza Physicians in practiceswith access to these more highly trained personnel weretwice as likely to have SOPs for PPV and influenza(Table 3) This association may be related to the com-plexity of PPV dosing and recommendations for indivi-duals with high-risk medical conditions [31] Somephysicians may feel comfortable allowing clinical staffwith more extensive education and training to deter-mine eligibility for PPV and administer vaccine as iscommon practice for nurses Conversely US state lawsvary regarding licensing of medical assistants [32] thesedifferences may result in concerns about medical assis-tants administering PPV under SOPs Anecdotally weheard reports of hesitation by medical assistants to useSOPs for PPV despite physician guidance and trainingusing a toolkit In contrast influenza vaccine is adminis-tered in many locales where a physician is not evenpresent
The presence of an electronic medical record (EMR)was similarly associated with SOPs for PPV as opposedto SOPs for influenza Again this association may be afunction of the complexity of PPV dosing and recom-mendations for individuals with high-risk medical condi-tions The EMR makes it easier for practitioners to trackimmunization histories and to flag patients eligible forvaccinationTeamwork is the essence of SOPs and thus the asso-
ciation between self-reported teamwork in the practiceand use of SOPs for PPV is not surprising Teamwork isalso a key aspect of successful implementation of thepatient-centered medical home and accountable careorganization Both are quality improvement models inwhich providing timely and appropriate preventive ser-vices such as vaccination is a critical element Programsto educate staff in vaccination may help to improve per-ceived self-efficacy stimulate innovation and fosterteamwork These programs include ldquoWhat worksrdquo (avail-able at httpwww2acdcgovvaccinesedwhatworksceasp and toolkits that facilitate use of SOPs httpwwwimmunizeorgstanding-orders and httpwwwImmuni-zationEdorgstandingordersWe conclude that practice-level factors are critical for
the adoption of more complex SOPs such as joint SOPsfor influenza and PPV The greater clinical complexityof PPV administration may require access to electronicmedical records and more highly trained auxiliary stafffor example as well as better coordination betweenstaff reflected in greater perceived teamworkStrengths of this research include a survey that is
national in scope with a high response rate for physicianparticipants The questionnaire was based on theoreticalmodels designed around physician adoption of vaccinesHowever surveys are subject to the limitations of self-report While the survey covered many correlates ofSOP use it may not have captured all relevant correlatesof SOP use Also we relied on a single physician toreport on each practice and may therefore underesti-mate variance in delivery of vaccinationsSOPs are underused but can have a great public
health impact For example SOPs may help mitigatedisparities in vaccination coverage in underserved popu-lations though we have not been able to identifyresearch in this area Further national efforts at clinicianand medical assistant education should be considered toensure that physicians are aware of current vaccinerecommendations and policies and that all clinical staffcan competently administer recommended vaccinesPractical toolkits are available to facilitate adoption ofSOPs in primary care practices Teamwork and animmunization champion can help empower clinical sup-port staff to administer vaccines using SOPs thus help-ing to reduce missed opportunities for vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 8 of 10
Additional material
Additional file 1 National Survey of Physicians about StandingOrders Programs for Adult Immunizations
AcknowledgementsThis study was supported by the Centers for Disease Control and Preventionand the Association for Prevention Teaching and Research Grant No 5 U50CD300-860-21 Its contents are the responsibility of the authors and do notnecessarily reflect the official views of the CDC or the APTR
Author details1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USA2Department of Family Medicine and Clinical Epidemiology School ofMedicine University of Pittsburgh Pittsburgh PA USA 3Centers for DiseaseControl and Prevention Atlanta GA USA
Authorsrsquo contributionsSA performed the statistical analysis and drafted the manuscript SA RZ TNMAY and FA conceived of the study and participated in developing thedesign of the research SA and TN coordinated the survey component Allauthors revised the manuscript critically for important intellectual contentAll authors read and approved the final manuscript
Competing interestsAt the time of data analyses Drs Zimmerman and Nowalk had researchfunding and consultancy with Medimmune Inc and research funding fromMerck Inc about HPV vaccine Dr Zimmerman also had research fundingfrom Sanofi
Received 9 October 2011 Accepted 20 March 2012Published 20 March 2012
References1 CDCNCHS NHIS Influenza vaccination in the past 12 months among
adults 18 years of age and over by age United States 1999-2009 2010[httpwww cdc givnchshuscontents2010htmfig18] [cited 2011 May10]Available from URL [httpwwwcdcgivnchshuscontents2010htmfig18]
2 Centers for Disease Control and Prevention 2009 Adult VaccinationCoverage NHIS [httpwww cdc govvaccinesstats-survnhis2009-nhishtm2010 [cited 2011 Jan 27]
3 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Validity of self-reported influenza and pneumococcalvaccination status among a cohort of hospitalized elderly inpatientsVaccine 2007 25(25)4775-4783
4 Nowalk MP Zimmerman RK Feghali J Missed opportunities for adultimmunization in diverse primary care office settings Vaccine 2004223457-3463
5 Nowalk MP Zimmerman RK Cleary SM Bruehlman RD Missedopportunities to vaccinate older adults in primary care J Am Board FamPract 2005 1820-27
6 Sandrine IS Meacutegard Y Overview of vaccination policies for the elderly inWestern European countries Aging Clin Exp Res 2009 21(3)210-215
7 Kohlhammer Y Schnoor M Schwartz M Raspe H Schaumlfer T Determinantsof influenza and pneumococcal vaccination in elderly people asystematic review Public Health 2007 121(10)742-751
8 Centers for Medicare and Medicaid Series H Medicare and Medicaidprograms conditions of participation immunization standards forhospitals long-term care facilities and home health agencies final rulewith comment period Fed Regist 2002 6761808-61814
9 Middleton DB Lin CJ Smith KJ et al Economic Evaluation of StandingOrder Programs for Pneumococcal Vaccination of Hospitalized ElderlyPatients Infect Control Hosp Epidemiol 2008 29(5)385-394
10 Dexter PR Perkins SM Maharry KS Jones K McDonald CJ Inpatientcomputer-based standing orders vs physician reminders to increase
influenza and pneumococcal vaccination rates J Am Med Assoc 20042922366-2371
11 Goebel LJ Neitch SM Mufson MA Standing Orders in an AmbulatorySetting Increases Influenza Vaccine Usage in Older People J Am GeriatrSoc 2005 53(6)1008-1010
12 Loughlin SM Mortazavi A Garey KW Rice GK Birtcher KK Pharmacist-managed vaccination program increased influenza vaccination rates incardiovascular patients enrolled in a secondary prevention lipid clinicPharmacotherapy 2007 27(5)729-733
13 Bond TC Patel PR Krishner J et al Association of Standing-Order PoliciesWith Vaccination Rates in Dialysis Clinics A US-Based Cross-sectionalStudy Am J Kidney Dis 2009 54(1)6-9
14 Task Force on Community Preventive Services Recommendationsregarding interventions to improve vaccination coverage in childrenadolescents and adults Am J Prev Med 2000 1892-96
15 Stone EG Morton SC Hulscher ME et al Interventions that increase useof adult immunization and cancer screening services a meta-analysisAnn Intern Med 2002 136(9)641-651
16 Centers for Disease Control and Prevention Use of standing ordersprograms to increase adult vaccination rates MMWR Morb Mortal WklyRep 2000 49(RR01)15-26
17 Health Care Financing Administration Evidence Report and Evidence-BasedRecommendations Interventions that Increase the Utilization of Medicare-Funded Preventive Service for Persons Age 65 and Older Baltimore MA HealthCare Financing Administration 1999
18 Szilagyi PG Shone LP Barth R et al Physician practices and attitudesregarding adult immunizations Prev Med 2005 40(2)152-161
19 Zimmerman R Albert S Nowalk M Yonas M Ahmed F Use of standingorders for adult influenza vaccination A national survey of primary carephysicians Am J Prev Med 2010 40(2)144-148
20 Yudin MH Salaripour M Sgro MD Acceptability and feasibility of seasonalinfluenza vaccine administration in an antenatal clinic setting J ObstetGynaecol Can 2010 32(8)745-748
21 Harder KM Cowan S Eriksen MB Krarup HB Christensen PB Universalscreening for hepatitis B among pregnant women led to 96vaccination coverage among newborns of HBsAg positive mothers inDenmark Vaccine 2011 29(50)9303-9307
22 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Missed opportunities to vaccinate a cohort of hospitalisedelderly with pneumococcal and influenza vaccines Vaccine 2007285146-5154
23 Jean-Pierre B Pierre OL Jean-Pierre M Willingness to vaccinate and to bevaccinated in adults Aging Clin Exp Res 2009 21(3)244-249
24 Yonas MA Nowalk MP Zimmerman RK Ahmed F Albert S Examiningstructural and clinical factors associated with implementation ofstanding orders for adult immunization J Healthc Qual 2011
25 Pathman DE Konrad TR Freed GL Freeman VA Koch GG The awareness-to-adherence model of the steps to clinical guideline compliance MedCare 1996 34(9)873-889
26 Rogers EM Diffusion of Innovations 3 edition New York Free Press 198327 Green LW Gottlieb NH Parcel GS Diffusion Theory Extended and
Applied In Advances in Health Education and Promotion Greenwich Editedby Ward WB Conn JAI Press 1987
28 Gielen AC McDonald EM The PRECEDE-PROCEED Planning Model InHealth Behavior and Health Education Theory Research and Practice 3edition Edited by Glanz K Lewis FM Rimer BK San Francisco Jossey-BassPublishers 1997359-383
29 Mouzoon ME Flor MM Greisinger AJ et al Improving InfluenzaImmunization in Pregnant Women and Healthcare Workers Am J ManagCare 2010 16(3)209-216
30 The Immunization Partnership [httpwwwimmunizeusaorgiz-champions] Accessed Jan 20 2012
31 Centers for Disease Control and Prevention Updated recommendationsfor prevention of invasive pneumococcal disease among adults usingthe 23-valent pneumococcal polysaccharide vaccine (PSV23) MorbMortal Wkly Rep 2010 59(34)1102-1106
32 Stewart A Cox M Rosenbaum S The Epidemiology of US ImmunizationLaw Translating CDC immunization guidelines into practice State lawsrelated to the use of standing orders covering immunization practice2008 [httpwww gwumcedusphhshealthpolicychsrpdownloads
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 9 of 10
CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-

vaccine is less important as a barrier to vaccination inthe US for two reasons 1) key national social insuranceprograms such as Medicare and Medicaid cover boththe costs of the vaccines and administration by recog-nized providers httpswwwcmsgovImmunizationsand 2) the Affordable Care Act mandates coverage ofvaccines by private insurersLess than optimal vaccination coverage is typical in
Europe as well A survey of the 27 member states of theEuropean Union plus Iceland and Norway during the2006-2007 influenza season found that influenza vacci-nation in people aged 65+ ranged from 321 in Austriato 821 in the Netherlands Western European coun-tries (except for Austria and Finland) achieved the 2006WHO goal of at least 50 coverage in the elderly butonly the Netherlands reached the 2010 WHO target of75 coverage [6] While most Western European coun-tries recommend PPV for the elderly countries vary inage guidelines and recommendations for repeat vaccina-tions A systematic review found large cross-nationaldifferences in vaccination coverage [7]Standing orders programs (SOPs) for immunization
are typically facility-based policies that enable non-phy-sician medical personnel to assess a patientrsquos immuniza-tion status and administer vaccines without directphysician involvement In 2002 US Medicare regula-tions prohibiting SOPs for medication administrationwere modified to exclude influenza and pneumococcalvaccinations [8]Introduction of SOPs has been shown to increase
influenza and pneumococcal vaccination rates in inpati-ent settings [910] In outpatient settings SOPsimproved influenza vaccination rates 27 in a generalelderly patient population [11] and among cardiovascu-lar patients attending a lipid clinic [12] In a study ofpatients in dialysis clinics SOPs did not increase influ-enza vaccination but significantly increased PPV andhepatitis B vaccination rates [13] In a systematic reviewcombination interventions which included SOPs werealso effective raising adult immunization rates by amedian of 16 [14] A meta-analysis of interventions toincrease adult immunizations found that organizationalchange had the highest impact though the effect ofSOPs was not explicitly assessed [15] The US AdvisoryCommittee on Immunization Practices (ACIP) [16] theTask Force for Community Preventive Services [14] andthe Southern California Evidence-Based Practice Center-RAND [17] have all endorsed SOPs to reduce missedopportunities and raise vaccination rates yet SOPs arenot commonly used in the outpatient setting Amongprimary care physicians outpatient use of SOPs was33 prior to the change in Medicare regulations [18]and since then has increased to just 42 for influenzavaccine [19]
Research on use of SOPs for influenza vaccine andPPV outside the United States is relatively scarce How-ever evidence suggests that implementation of SOPs iseffective in other countries In a Canadian antenatal set-ting for example a single nurse tasked with simplyapproaching patients to offer and administer vaccinewas able to boost influenza vaccination coverage tonearly half of clinic attendees [20] A similar approachto universal screening for vaccination in the case ofhepatitis B led to marked increases in uptake in Den-mark [21] Studies suggest that in the absence of SOPsor some other concerted effort opportunities to vacci-nate the elderly are routinely missed For example oneAustralian study found that hospitalized elderly whoexpressed interest in influenza vaccine and PPV wentunvaccinated in routine care [22] This situation may bechanging Recommendations from public health organi-zations in Europe now include use of SOPs ldquo Theclinician must be in the habit of using every visit oppor-tunity (for whatever reason) to check vaccination statusThis means empowering administrative reception andclerical staff to evaluate vaccination history eligibilityand contraindications through standing ordersrdquo [23]Suboptimal adult vaccination rates and low reported
use of SOPs suggest that there are barriers to SOPimplementation Primary care providers in outpatientsettings vary in their acceptance and use of SOPs forinfluenza vaccine and PPV [1324] The purpose of thisstudy was to identify factors that impede or promoteconsistent use of SOPs for adult vaccinations and toexamine factors that distinguish practices that consis-tently use SOPs for both influenza vaccine and PPVpractices that use SOPs for influenza vaccine alone andpractices that have no SOPs for either vaccine
MethodsSamplePhysicians selected to receive a mailed survey weresampled from the American Medical Associationrsquos(AMA) master list of outpatient-based family physicians(n = 45000) and general internists (n = 45000) toobtain a nationally representative sample The samplesize required to detect a 10 difference in proportionsof SOP implementation between the two specialtygroups with a power of 80 and alpha of P lt 005 was816 (408 per group) Assuming a 50 response rate andloss due to bad addresses we sampled 1640 physicians(820 internists and 820 family physicians) nationwide[19] A post hoc calculation of power based on thereported prevalence of SOPs in the sample suggests wehad 90 power to identify differences between SOPadopters and non-adopters as small as 10 in factorsassociated with adoption of SOPs No physician assis-tants or nurse practitioners were sampled
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 2 of 10
The survey was mailed with a cover letter signed byrepresentatives of the Centers for Disease Control andPrevention (CDC) the American Medical Association(AMA) and the principal investigator Attached to thesurvey was a $500 cash incentive to complete the ques-tionnaire Respondents were asked to return the com-pleted questionnaire in a self-addressed stampedenvelope Non-respondents received a second mailedsurvey approximately 8 weeks after the first Afteranother 8 weeks non-respondents were telephoned torequest participation or to complete the survey byphone Physicians were excluded if they were no longerin primary care practice did not immunize in theirpractice did not treat adult patients or did not answerquestions pertaining to influenza vaccination or PPV
Survey instrumentThe survey questionnaire (see Additional file 1) wasdeveloped using aspects of the Awareness-to-Adherencemodel [25] which predicts physician behavior regardingnew guidelines for care and diffusion of innovation the-ory which identifies predictable patterns of programadoption [2627] These topics were informed by find-ings from focus groups and interviews which were con-ducted beforehand The three focus groups involvedprimary care providers including physicians as well asnursing staff They were conducted in local sites selectedfor diversity in patient populations and variation in useof SOPs for adult immunizations Focus group discus-sions were facilitated by a qualitative researcher who fol-lowed a written protocol developed by the researchteamSurvey items were also informed by PRECEDE-PRO-
CEED a systematic process to evaluate health problemsand design intervention programs [28] PRECEDE is anacronym for Predisposing Reinforcing and EnablingConstructs in Educational Diagnosis and EvaluationThe questionnaire consisted of 22 closed-ended ques-tions and covered demographics practice characteristicsawareness agreement and use of SOPs for adult immu-nizations barriers to and facilitators of SOPs and physi-cian attitudes regarding SOPs It was designed to beconcise to encourage response by busy physicians Thequestionnaire was pilot tested with several local primarycare physicians and revised as appropriate
Data processing and analysesData from returned surveys were entered using a dou-ble-entry protocol and compared using an automatedprocedure to identify discordant values The files dif-fered in lt 5 of data points and differences were recon-ciled in each case The final survey data file was mergedwith the file provided by AMA to add physician demo-graphic training and practice indicators Missing values
overall accounted for lt 5 of the data For continuousvariables mean values for the appropriate measure werecalculated The survey and research protocol wereapproved by the University of Pittsburgh InstitutionalReview BoardFor the survey standing orders were defined as ldquoan
office policy that allows non-physician staff to screenadults for influenza and PPV and administer either vac-cine to eligible adults without getting a specific orderfrom the patientrsquos physicianrdquo The question used to elicitSOPs status asked physicians to choose among the fol-lowing categories of SOPs use in their practice (i) nostanding orders and no interest in implementing them(ii) no standing orders but interest in implementingthem (iii) standing orders but inconsistent use and (iv)consistent use of standing orders The question wasasked separately for influenza immunization and PPVCombining answers to the two questions allowed us toidentify physicians who reported no consistent use ofSOPs for either vaccine consistent use of SOPs forinfluenza vaccine only or consistent use of SOPs forboth vaccinations (Physicians rarely reported SOPs forPPV in the absence of SOPs for influenza vaccinationsee below) The three groups were compared in univari-ate analyses (c2 for proportions one-way analysis of var-iance for continuous measures) to identify significantcorrelates of SOPs statusMultinomial logistic regression models were developed
to examine differences between groups In multinomialmodels the two consistent SOP groups (influenza vac-cine only influenza vaccine and PPV) were each com-pared to physicians reporting no or inconsistent use ofSOPs A final logistic regression model was developedto examine how physicians reporting consistent SOPsfor both vaccines differed from those reporting consis-tent use of SOPs for influenza vaccine only For themultivariable analyses odds ratios and 95 confidenceintervals were estimated Interaction effects wereassessed but none was significant In developing theregression models we included variables significant inunivariate analyses (P lt 05) but also physician age andlength of time in practice because these may be corre-lated with knowledge of SOPs and attitudes toward theiruse An additional model was developed that excludedphysician age and length of time in practice as covari-ates Odds ratios from the alternative model did notappreciably differ and no changes in significant predic-tors were identifiedThe following predictors of SOPs status were
investigatedPhysician-Level Factors Indicators drawn from the
AMA file included age time since receiving medicaldegree medical specialty (family medicine or internalmedicine) and board certification The mailed survey
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 3 of 10
asked whether physicians had received their medicaldegrees outside the US and included the following indi-cators of physician knowledge of SOPs whether theywere aware of ACIP recommendations or Medicare reg-ulations and whether they agreed that SOPs are effectivein boosting vaccination coveragePractice-Level Factors Physicians reported on practice-
level factors likely to influence adoption or consistentuse of SOPs These included perceptions of how opentheir practice is to change or innovation whether theirstaff demonstrates strong teamwork and whether physi-cians are primary decision makers for the practiceAdditional factors included access to an electronic medi-cal record having an immunization champion (a clinicalstaff member who promotes and encourages immuniza-tion) on site size of practices (recorded as solo 2-4 or 5+ physicians) help available to physicians (how manyhelpers per provider recorded as 1 helper per 2+ provi-ders 1 helper per provider or two helpers per provider)type of help (advanced (PACRNP) nurse-level (RN orLPN) assistance or medical assistant) and organizationof the practice (comparing practices that are part oflarge health plans or corporations to other types) Thesurvey instrument can be found in the Additional file 1
ResultsOf the 1640 physicians contacted by mail 16 letterswere returned by the post office as undeliverable and107 physicians were no longer in practice no longer inprimary care (eg hospitalists) deceased or unknown atthe practice leaving 1517 eligible physicians Of these1015 physicians returned surveys for a response rate of67 Participation was higher among family physicians(689) than internists (648 P lt 01) and amongboard certified (689) than non-board certified (607P lt 01) physicians Participants and nonparticipants didnot vary by age (mean = 507 years) length of time inpractice (mean = 23 years) domestic vs internationaltraining or geographic region Among participating phy-sicians 819 received their medical degree in the USand 795 were board certified The modal practice pat-tern for physicians in the sample was an independentpractice (51) in a suburban setting (453) The nextmost common practice setting was to be based in alarge corporate health system (255) in an urban set-ting (312)Of the 1015 physicians who completed the survey 115
did not immunize adults in their practices leaving 900physicians in the sample Of these 900 20 did notrespond to questions specific to influenza vaccinationThus the analytic sample consisted of 880 physicianswho provided information on SOPs for influenza vacci-nation and PPV Consistent use of SOPs for pneumo-coccal vaccination in the absence of similar use of SOPs
for influenza vaccination was rare in fact only onerespondent in the sample fell into this category By con-trast SOPs for influenza vaccination without standingorders for PPV were common Given this distributionwe established three SOP groups no consistent use ofSOPs for either vaccination including the one physicianreporting SOP use for PPV only (n = 502 570) con-sistent use of SOPs for influenza vaccination only (n =175 199) and consistent use of SOPs for both vacci-nations (n = 203 231) Forty-three percent of thesample reported SOPs for influenza vaccination (with orwithout concomitant SOP for PPV) Physicians in thethree groups did not differ in age length of time inpractice US medical training board certification statusor specialtyDifferences among the three SOPs groups are shown
in Table 1 Across the three groups some correlatesincreased uniformly as use of SOPs increased for exam-ple awareness of ACIP recommendations andor Medi-care regulations belief that SOPs enhance adultvaccination rates having an immunization champion inthe practice agreement that SOPs are effective in boost-ing vaccination coverage access to an electronic medicalrecord (EMR) and having staff who are open to innova-tion and who work well together Training level andnumber of clinical assistants were significantly related touse of SOPs with practices reporting a greater staff toclinician ratio and those with more highly trained assis-tants (PACRNP or RNLPN) more often reporting con-sistent use of SOPs The proportion reporting 2 helpersper provider was 693 in the consistent influenzaPPVSOP group vs 563 in the consistent influenza onlygroup and 463 in the no consistent SOP group Pair-wise differences across these groupings were significantin post hoc comparisons Number of physicians in apractice was not a significant correlate of SOP groupTo investigate correlates of SOPs in more detail mul-
tinomial logistic regression models were developed toexamine the entire set of correlates These models allowa view of how physicians in each of the two SOP groupsdiffer from the group not using SOPs Table 2 showsodds ratios and 95 confidence intervals associated witheach correlate in a model that includes variables shownearlier in Table 1 adjusted for physician age and lengthof time in practiceIn the final adjusted model consistent use of SOPs
limited to influenza vaccine was independently and sig-nificantly associated with awareness of ACIP recommen-dations andor Medicare regulations (odds ratio [OR]235 95 confidence interval [CI] 160-346) agreementthat SOPs are an effective way to boost vaccination cov-erage (OR 297 95 CI 189-467) family medicine spe-cialty (OR 163 95 CI 110-242) greater amount ofhelp available to physicians (access to 2 assistants [OR
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 4 of 10
275 95 CI 131-579] access to 1 assistant [OR 230123-430] relative to the group with only 1 assistant for2+ providers)Consistent use of SOPs for both influenza vaccine and
PPV was associated with the same set of factors butadditional factors as well Shared correlates includedawareness of ACIP recommendations andor Medicareregulations (OR 446 95 CI 291-685) agreement thatSOPs are an effective way to boost vaccination coverage(OR 35 95 CI 214-571) family medicine specialty
(OR 127 95 CI 089-191 NS) and a greater staff toclinician ratio (OR 222 95 CI 109-454) Correlatesassociated only with combined influenza and PPV SOPsincluded a variety of practice-level factors practiceopenness to change and innovation (OR 215 95 CI133-347) strong practice teamwork (OR 278 95 CI149-521) access to an electronic medical record (OR190 95 CI 122-296) presence of an immunizationchampion in the practice (OR 194 95 127-298) andaccess to nursephysician assistant staff as opposed to
Table 1 Characteristics of PhysiciansPractices Reporting No Consistent Use of Standing Orders Programs (SOPs)Consistent Use of SOPs for Influenza Vaccine Only and Consistent Use of SOPs for Both Influenza Vaccine and PPV
No ConsistentUse of SOPs(n = 502)
Consistent Use of SOPs forInfluenza Vaccine Only
(n = 175)
Consistent Use of SOPs for BothInfluenza Vaccine and PPV
(n = 203)
P
Physician Indicators
Age 504 (101) 502 (94) 518 (99) 17
Years since medical degree 225 (104) 228 (100) 242 (98) 13
Family Medicine specialty 482 383 429 059
Board certified 797 811 783 53
Medical degree outside US 217 177 207 79
Physician is aware of ACIP recommendationsandor Medicare regulations
414 611 778 lt001
Physician believes SOPs are an effective way toboost adult vaccinations
602 794 823 lt001
Practice Indicators
Practice is open to change or innovation 516 611 783 lt001
Strong practice teamwork 657 737 906 lt001
Practice uses electronic medical record 456 566 591 001
Practice has immunization champion on site
233 274 389 lt001
Clinical support
2 helpers per provider 463 563 693 lt001
1 helper per provider 200 219 118
1 helper per 2+ providers 338 218 189
Number of physicians in practice
Solo 263 414 319 11
2-4 189 434 377
5+ 241 340 414
Type of clinical support
RNLPN 311 295 477 lt001
Medical Assistant 662 694 482
PACRNP 27 12 40
Practice is part of large health plan orcorporation
230 343 276 013
Physicians are primary decision makers forpractice
636 550 584 14
PPV = Pneumococcal polysaccharide vaccine
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 5 of 10
Table 2 Practice Characteristics Associated with Consistent Use of Standing Orders Programs (SOPs) for InfluenzaVaccination Only or Influenza and PPV Relative to No Consistent Use of SOPs in Multinomial Logistic Regression
Characteristic Consistent Use of SOPs for InfluenzaVaccine OnlyOR (95 CI)
Consistent Use of SOPs for Both InfluenzaVaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andorMedicare regulations
235 (160 346) Plt 001 446 (291 685) Plt 001
Physician believes that SOPs are an effective way toboost adult vaccinations
297 (189 467) Plt 001 350 (214 571) Plt 001
Practice is open to change or innovation 136 (079 210) 215 (133 347) P= 002
Strong practice teamwork 118 (074 191) 278 (149 521) P= 001
Practice uses electronic medical record 135 (089 203) 190 (122 296) P= 005
Practice has immunization champion on site 112 (072 176) 194 (127 298) P= 002
Clinical support
2 helpers per provider 275 (131 579) P= 008 222 (109 454) P= 028
1 helper per provider 230 (123 430) P= 009 145 (078 267)
1 helper per 2+ providers 100 (ref) 100 (ref)
Number of physicians in practice
Solo 076 (041 138) 071 (039 130)
2-4 102 (065 160) 072 (045 117)
ge 5 100 (ref) 100 (ref)
Family Medicine specialty 163 (110 242) P= 015 127 (089 191)
Nurse-levelPA assistance rather than medical assistant 072 (048 109) 149 (099 224) P= 054
Practice is part of large health plan or corporation 134 (085 213) 104 (062 172)
Physicians are primary decision makers for practice 094 (061 145) 108 (068 170)
Model adjusted for physician age and time since medical degree Model x2 = 2397 p lt 0001 R2 = 026
Table 3 Practice Characteristics Associated with Consistent Use of SOPs for Both Influenza Vaccine and PPV Relativeto Influenza Vaccine Only in Logistic Regression
Characteristic Consistent Use of SOPsfor Both Influenza Vaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andor Medicare regulations 195 (118 324) P= 010
Physician believes that SOPs are an effective way to boost adult vaccinations 111 (060 206)
Practice is open to change or innovation 159 (092 275)
Strong practice teamwork 224 (110 454) P= 026
Practice uses electronic medical record 130 (077 221)
Practice has immunization champion on site 167 (101 454) P= 046
Clinical support
2 helpers per provider 086 (035 214)
1 helper per provider 066 (030 149)
1 helper per 2+ providers 100 (ref)
Number of physicians in practice
Solo 087 (042 180)
2-4 068 (039 119)
ge 5 100 (ref)
Family medicine specialty 078 (048 126)
Nurse-levelPA assistance rather than medical assistant 212 (131 345) P= 002
Practice is part of large health plan or corporation 083 (047 146)
Physicians are primary decision makers for practice 131 (078 221)
Model adjusted for physician age and time since MD Model Χ2 = 550 P lt 0001 R2 = 020
PPV = Pneumococcal Polysaccharide Vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 6 of 10
medical assistants alone (OR 149 95 CI 099-224 p= 054)The two SOP groups were directly compared in Table
3 Physicians reporting consistent use of SOPs for bothimmunizations were more likely to be aware of ACIPrecommendations andor Medicare regulations (OR195 95 CI 118-324) Practice-level factors distin-guishing consistent use of SOPs for both vaccinesincluded strong practice teamwork (OR 224 95 CI110-454) having an immunization champion on site(OR 167 95 CI 101-454) and access to nursephysi-cian assistant staff as opposed to medical assistants (OR221 95 CI 131-345)Finally we examined the number of physician and
practice characteristics associated with adoption ofSOPs and the prevalence of reported SOPs for eitherinfluenza vaccine or PPV We summed across the 12characteristics analyzed in the regression models andplotted adoption of SOPs against this index (Figure 1)In this sample of physicians few respondents reported 0or 1 characteristic (n = 3) and few reported all 12 (n =3) Physicians reported a median of six characteristicsassociated with adoption Figure 1 shows that adoption
of SOPs is as low as 105 when only 1 or 2 factors arepresent and as high as 769 in the presence of all 11 or12 factors
DiscussionIn this national survey of US primary care physicianstreating adults 231 reported using SOPs consistentlyfor both influenza vaccine and PPV and 199 usedSOPs only for influenza vaccination In total as we havereported elsewhere 43 of physicians reported consis-tent use of SOPs for influenza vaccine [19] Physiciansin practices with SOPs for both vaccines reportedgreater awareness of ACIP recommendations andorMedicare regulations and were more likely to agree thatSOPs are an effective way to boost vaccination coverageImplementation of both influenza and PPV SOPs wasassociated with a variety of practice-level factors as wellincluding more effective practice teamwork the pre-sence of an immunization champion and greater avail-ability of clinical assistants with more advanced trainingthan that of medical assistantsThe CDC has recommended SOPs for adult vaccina-
tion since 2000 [16] However the Center for Medicare
Prevalence of SOPs Relative to Number ofPhysician and Practice Characteristics Associated
with Adoption
Figure 1 Uploaded separately Prevalence of SOPs Relative to Number of Physician and Practice Characteristics Associated with Adoption
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 7 of 10
and Medicaid Services (CMS) prohibited SOPs for allmedications until 2002 when CMS modified its regula-tions to allow SOPs for influenza vaccine and PPV [8]It is understandable that physicians who were unawareof the change in CMS regulations might not haveadopted consistent use of SOPs as reflected in our dataGiven the myriad recommendations and policies
aimed at primary preventive care including immuniza-tions how can a practice keep current One solution isfor the practice to have an immunization championsomeone to interpret and communicate changes in vac-cine policies and recommendations as they occur Pre-vious research confirms the importance of animmunization champion to improve vaccination ratesOne study that included explicit training of immuniza-tion nurses to serve as clinical champions boosted influ-enza vaccination coverage rates in pregnant womenfrom 25 to 374 in 2008-2009 [29] However it isdifficult to determine the specific value of immunizationchampions relative to other practice-level factorsbecause most interventions designed to boost vaccina-tion coverage include a variety of elements Our findingssuggest the particular value of champions for practicesthat have SOPs for both influenza vaccine and PPV Itwould useful to determine which staff makes the mosteffective immunization champion and what sort of train-ing is most appropriate In most cases champions arenurses but recent efforts suggest that even non-clinicalstaff such as receptionists or medical records staff canbe trained as immunization champions httpwwwimmunizeusaorgiz-champions[30] It remains unclearhow such duties will be added to job descriptions orqualifications and whether additional compensation isappropriateAccess to physician assistants or licensed nursing per-
sonnel was a significant correlate of SOPs for PPV asopposed to SOPs for influenza Physicians in practiceswith access to these more highly trained personnel weretwice as likely to have SOPs for PPV and influenza(Table 3) This association may be related to the com-plexity of PPV dosing and recommendations for indivi-duals with high-risk medical conditions [31] Somephysicians may feel comfortable allowing clinical staffwith more extensive education and training to deter-mine eligibility for PPV and administer vaccine as iscommon practice for nurses Conversely US state lawsvary regarding licensing of medical assistants [32] thesedifferences may result in concerns about medical assis-tants administering PPV under SOPs Anecdotally weheard reports of hesitation by medical assistants to useSOPs for PPV despite physician guidance and trainingusing a toolkit In contrast influenza vaccine is adminis-tered in many locales where a physician is not evenpresent
The presence of an electronic medical record (EMR)was similarly associated with SOPs for PPV as opposedto SOPs for influenza Again this association may be afunction of the complexity of PPV dosing and recom-mendations for individuals with high-risk medical condi-tions The EMR makes it easier for practitioners to trackimmunization histories and to flag patients eligible forvaccinationTeamwork is the essence of SOPs and thus the asso-
ciation between self-reported teamwork in the practiceand use of SOPs for PPV is not surprising Teamwork isalso a key aspect of successful implementation of thepatient-centered medical home and accountable careorganization Both are quality improvement models inwhich providing timely and appropriate preventive ser-vices such as vaccination is a critical element Programsto educate staff in vaccination may help to improve per-ceived self-efficacy stimulate innovation and fosterteamwork These programs include ldquoWhat worksrdquo (avail-able at httpwww2acdcgovvaccinesedwhatworksceasp and toolkits that facilitate use of SOPs httpwwwimmunizeorgstanding-orders and httpwwwImmuni-zationEdorgstandingordersWe conclude that practice-level factors are critical for
the adoption of more complex SOPs such as joint SOPsfor influenza and PPV The greater clinical complexityof PPV administration may require access to electronicmedical records and more highly trained auxiliary stafffor example as well as better coordination betweenstaff reflected in greater perceived teamworkStrengths of this research include a survey that is
national in scope with a high response rate for physicianparticipants The questionnaire was based on theoreticalmodels designed around physician adoption of vaccinesHowever surveys are subject to the limitations of self-report While the survey covered many correlates ofSOP use it may not have captured all relevant correlatesof SOP use Also we relied on a single physician toreport on each practice and may therefore underesti-mate variance in delivery of vaccinationsSOPs are underused but can have a great public
health impact For example SOPs may help mitigatedisparities in vaccination coverage in underserved popu-lations though we have not been able to identifyresearch in this area Further national efforts at clinicianand medical assistant education should be considered toensure that physicians are aware of current vaccinerecommendations and policies and that all clinical staffcan competently administer recommended vaccinesPractical toolkits are available to facilitate adoption ofSOPs in primary care practices Teamwork and animmunization champion can help empower clinical sup-port staff to administer vaccines using SOPs thus help-ing to reduce missed opportunities for vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 8 of 10
Additional material
Additional file 1 National Survey of Physicians about StandingOrders Programs for Adult Immunizations
AcknowledgementsThis study was supported by the Centers for Disease Control and Preventionand the Association for Prevention Teaching and Research Grant No 5 U50CD300-860-21 Its contents are the responsibility of the authors and do notnecessarily reflect the official views of the CDC or the APTR
Author details1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USA2Department of Family Medicine and Clinical Epidemiology School ofMedicine University of Pittsburgh Pittsburgh PA USA 3Centers for DiseaseControl and Prevention Atlanta GA USA
Authorsrsquo contributionsSA performed the statistical analysis and drafted the manuscript SA RZ TNMAY and FA conceived of the study and participated in developing thedesign of the research SA and TN coordinated the survey component Allauthors revised the manuscript critically for important intellectual contentAll authors read and approved the final manuscript
Competing interestsAt the time of data analyses Drs Zimmerman and Nowalk had researchfunding and consultancy with Medimmune Inc and research funding fromMerck Inc about HPV vaccine Dr Zimmerman also had research fundingfrom Sanofi
Received 9 October 2011 Accepted 20 March 2012Published 20 March 2012
References1 CDCNCHS NHIS Influenza vaccination in the past 12 months among
adults 18 years of age and over by age United States 1999-2009 2010[httpwww cdc givnchshuscontents2010htmfig18] [cited 2011 May10]Available from URL [httpwwwcdcgivnchshuscontents2010htmfig18]
2 Centers for Disease Control and Prevention 2009 Adult VaccinationCoverage NHIS [httpwww cdc govvaccinesstats-survnhis2009-nhishtm2010 [cited 2011 Jan 27]
3 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Validity of self-reported influenza and pneumococcalvaccination status among a cohort of hospitalized elderly inpatientsVaccine 2007 25(25)4775-4783
4 Nowalk MP Zimmerman RK Feghali J Missed opportunities for adultimmunization in diverse primary care office settings Vaccine 2004223457-3463
5 Nowalk MP Zimmerman RK Cleary SM Bruehlman RD Missedopportunities to vaccinate older adults in primary care J Am Board FamPract 2005 1820-27
6 Sandrine IS Meacutegard Y Overview of vaccination policies for the elderly inWestern European countries Aging Clin Exp Res 2009 21(3)210-215
7 Kohlhammer Y Schnoor M Schwartz M Raspe H Schaumlfer T Determinantsof influenza and pneumococcal vaccination in elderly people asystematic review Public Health 2007 121(10)742-751
8 Centers for Medicare and Medicaid Series H Medicare and Medicaidprograms conditions of participation immunization standards forhospitals long-term care facilities and home health agencies final rulewith comment period Fed Regist 2002 6761808-61814
9 Middleton DB Lin CJ Smith KJ et al Economic Evaluation of StandingOrder Programs for Pneumococcal Vaccination of Hospitalized ElderlyPatients Infect Control Hosp Epidemiol 2008 29(5)385-394
10 Dexter PR Perkins SM Maharry KS Jones K McDonald CJ Inpatientcomputer-based standing orders vs physician reminders to increase
influenza and pneumococcal vaccination rates J Am Med Assoc 20042922366-2371
11 Goebel LJ Neitch SM Mufson MA Standing Orders in an AmbulatorySetting Increases Influenza Vaccine Usage in Older People J Am GeriatrSoc 2005 53(6)1008-1010
12 Loughlin SM Mortazavi A Garey KW Rice GK Birtcher KK Pharmacist-managed vaccination program increased influenza vaccination rates incardiovascular patients enrolled in a secondary prevention lipid clinicPharmacotherapy 2007 27(5)729-733
13 Bond TC Patel PR Krishner J et al Association of Standing-Order PoliciesWith Vaccination Rates in Dialysis Clinics A US-Based Cross-sectionalStudy Am J Kidney Dis 2009 54(1)6-9
14 Task Force on Community Preventive Services Recommendationsregarding interventions to improve vaccination coverage in childrenadolescents and adults Am J Prev Med 2000 1892-96
15 Stone EG Morton SC Hulscher ME et al Interventions that increase useof adult immunization and cancer screening services a meta-analysisAnn Intern Med 2002 136(9)641-651
16 Centers for Disease Control and Prevention Use of standing ordersprograms to increase adult vaccination rates MMWR Morb Mortal WklyRep 2000 49(RR01)15-26
17 Health Care Financing Administration Evidence Report and Evidence-BasedRecommendations Interventions that Increase the Utilization of Medicare-Funded Preventive Service for Persons Age 65 and Older Baltimore MA HealthCare Financing Administration 1999
18 Szilagyi PG Shone LP Barth R et al Physician practices and attitudesregarding adult immunizations Prev Med 2005 40(2)152-161
19 Zimmerman R Albert S Nowalk M Yonas M Ahmed F Use of standingorders for adult influenza vaccination A national survey of primary carephysicians Am J Prev Med 2010 40(2)144-148
20 Yudin MH Salaripour M Sgro MD Acceptability and feasibility of seasonalinfluenza vaccine administration in an antenatal clinic setting J ObstetGynaecol Can 2010 32(8)745-748
21 Harder KM Cowan S Eriksen MB Krarup HB Christensen PB Universalscreening for hepatitis B among pregnant women led to 96vaccination coverage among newborns of HBsAg positive mothers inDenmark Vaccine 2011 29(50)9303-9307
22 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Missed opportunities to vaccinate a cohort of hospitalisedelderly with pneumococcal and influenza vaccines Vaccine 2007285146-5154
23 Jean-Pierre B Pierre OL Jean-Pierre M Willingness to vaccinate and to bevaccinated in adults Aging Clin Exp Res 2009 21(3)244-249
24 Yonas MA Nowalk MP Zimmerman RK Ahmed F Albert S Examiningstructural and clinical factors associated with implementation ofstanding orders for adult immunization J Healthc Qual 2011
25 Pathman DE Konrad TR Freed GL Freeman VA Koch GG The awareness-to-adherence model of the steps to clinical guideline compliance MedCare 1996 34(9)873-889
26 Rogers EM Diffusion of Innovations 3 edition New York Free Press 198327 Green LW Gottlieb NH Parcel GS Diffusion Theory Extended and
Applied In Advances in Health Education and Promotion Greenwich Editedby Ward WB Conn JAI Press 1987
28 Gielen AC McDonald EM The PRECEDE-PROCEED Planning Model InHealth Behavior and Health Education Theory Research and Practice 3edition Edited by Glanz K Lewis FM Rimer BK San Francisco Jossey-BassPublishers 1997359-383
29 Mouzoon ME Flor MM Greisinger AJ et al Improving InfluenzaImmunization in Pregnant Women and Healthcare Workers Am J ManagCare 2010 16(3)209-216
30 The Immunization Partnership [httpwwwimmunizeusaorgiz-champions] Accessed Jan 20 2012
31 Centers for Disease Control and Prevention Updated recommendationsfor prevention of invasive pneumococcal disease among adults usingthe 23-valent pneumococcal polysaccharide vaccine (PSV23) MorbMortal Wkly Rep 2010 59(34)1102-1106
32 Stewart A Cox M Rosenbaum S The Epidemiology of US ImmunizationLaw Translating CDC immunization guidelines into practice State lawsrelated to the use of standing orders covering immunization practice2008 [httpwww gwumcedusphhshealthpolicychsrpdownloads
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 9 of 10
CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-

The survey was mailed with a cover letter signed byrepresentatives of the Centers for Disease Control andPrevention (CDC) the American Medical Association(AMA) and the principal investigator Attached to thesurvey was a $500 cash incentive to complete the ques-tionnaire Respondents were asked to return the com-pleted questionnaire in a self-addressed stampedenvelope Non-respondents received a second mailedsurvey approximately 8 weeks after the first Afteranother 8 weeks non-respondents were telephoned torequest participation or to complete the survey byphone Physicians were excluded if they were no longerin primary care practice did not immunize in theirpractice did not treat adult patients or did not answerquestions pertaining to influenza vaccination or PPV
Survey instrumentThe survey questionnaire (see Additional file 1) wasdeveloped using aspects of the Awareness-to-Adherencemodel [25] which predicts physician behavior regardingnew guidelines for care and diffusion of innovation the-ory which identifies predictable patterns of programadoption [2627] These topics were informed by find-ings from focus groups and interviews which were con-ducted beforehand The three focus groups involvedprimary care providers including physicians as well asnursing staff They were conducted in local sites selectedfor diversity in patient populations and variation in useof SOPs for adult immunizations Focus group discus-sions were facilitated by a qualitative researcher who fol-lowed a written protocol developed by the researchteamSurvey items were also informed by PRECEDE-PRO-
CEED a systematic process to evaluate health problemsand design intervention programs [28] PRECEDE is anacronym for Predisposing Reinforcing and EnablingConstructs in Educational Diagnosis and EvaluationThe questionnaire consisted of 22 closed-ended ques-tions and covered demographics practice characteristicsawareness agreement and use of SOPs for adult immu-nizations barriers to and facilitators of SOPs and physi-cian attitudes regarding SOPs It was designed to beconcise to encourage response by busy physicians Thequestionnaire was pilot tested with several local primarycare physicians and revised as appropriate
Data processing and analysesData from returned surveys were entered using a dou-ble-entry protocol and compared using an automatedprocedure to identify discordant values The files dif-fered in lt 5 of data points and differences were recon-ciled in each case The final survey data file was mergedwith the file provided by AMA to add physician demo-graphic training and practice indicators Missing values
overall accounted for lt 5 of the data For continuousvariables mean values for the appropriate measure werecalculated The survey and research protocol wereapproved by the University of Pittsburgh InstitutionalReview BoardFor the survey standing orders were defined as ldquoan
office policy that allows non-physician staff to screenadults for influenza and PPV and administer either vac-cine to eligible adults without getting a specific orderfrom the patientrsquos physicianrdquo The question used to elicitSOPs status asked physicians to choose among the fol-lowing categories of SOPs use in their practice (i) nostanding orders and no interest in implementing them(ii) no standing orders but interest in implementingthem (iii) standing orders but inconsistent use and (iv)consistent use of standing orders The question wasasked separately for influenza immunization and PPVCombining answers to the two questions allowed us toidentify physicians who reported no consistent use ofSOPs for either vaccine consistent use of SOPs forinfluenza vaccine only or consistent use of SOPs forboth vaccinations (Physicians rarely reported SOPs forPPV in the absence of SOPs for influenza vaccinationsee below) The three groups were compared in univari-ate analyses (c2 for proportions one-way analysis of var-iance for continuous measures) to identify significantcorrelates of SOPs statusMultinomial logistic regression models were developed
to examine differences between groups In multinomialmodels the two consistent SOP groups (influenza vac-cine only influenza vaccine and PPV) were each com-pared to physicians reporting no or inconsistent use ofSOPs A final logistic regression model was developedto examine how physicians reporting consistent SOPsfor both vaccines differed from those reporting consis-tent use of SOPs for influenza vaccine only For themultivariable analyses odds ratios and 95 confidenceintervals were estimated Interaction effects wereassessed but none was significant In developing theregression models we included variables significant inunivariate analyses (P lt 05) but also physician age andlength of time in practice because these may be corre-lated with knowledge of SOPs and attitudes toward theiruse An additional model was developed that excludedphysician age and length of time in practice as covari-ates Odds ratios from the alternative model did notappreciably differ and no changes in significant predic-tors were identifiedThe following predictors of SOPs status were
investigatedPhysician-Level Factors Indicators drawn from the
AMA file included age time since receiving medicaldegree medical specialty (family medicine or internalmedicine) and board certification The mailed survey
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 3 of 10
asked whether physicians had received their medicaldegrees outside the US and included the following indi-cators of physician knowledge of SOPs whether theywere aware of ACIP recommendations or Medicare reg-ulations and whether they agreed that SOPs are effectivein boosting vaccination coveragePractice-Level Factors Physicians reported on practice-
level factors likely to influence adoption or consistentuse of SOPs These included perceptions of how opentheir practice is to change or innovation whether theirstaff demonstrates strong teamwork and whether physi-cians are primary decision makers for the practiceAdditional factors included access to an electronic medi-cal record having an immunization champion (a clinicalstaff member who promotes and encourages immuniza-tion) on site size of practices (recorded as solo 2-4 or 5+ physicians) help available to physicians (how manyhelpers per provider recorded as 1 helper per 2+ provi-ders 1 helper per provider or two helpers per provider)type of help (advanced (PACRNP) nurse-level (RN orLPN) assistance or medical assistant) and organizationof the practice (comparing practices that are part oflarge health plans or corporations to other types) Thesurvey instrument can be found in the Additional file 1
ResultsOf the 1640 physicians contacted by mail 16 letterswere returned by the post office as undeliverable and107 physicians were no longer in practice no longer inprimary care (eg hospitalists) deceased or unknown atthe practice leaving 1517 eligible physicians Of these1015 physicians returned surveys for a response rate of67 Participation was higher among family physicians(689) than internists (648 P lt 01) and amongboard certified (689) than non-board certified (607P lt 01) physicians Participants and nonparticipants didnot vary by age (mean = 507 years) length of time inpractice (mean = 23 years) domestic vs internationaltraining or geographic region Among participating phy-sicians 819 received their medical degree in the USand 795 were board certified The modal practice pat-tern for physicians in the sample was an independentpractice (51) in a suburban setting (453) The nextmost common practice setting was to be based in alarge corporate health system (255) in an urban set-ting (312)Of the 1015 physicians who completed the survey 115
did not immunize adults in their practices leaving 900physicians in the sample Of these 900 20 did notrespond to questions specific to influenza vaccinationThus the analytic sample consisted of 880 physicianswho provided information on SOPs for influenza vacci-nation and PPV Consistent use of SOPs for pneumo-coccal vaccination in the absence of similar use of SOPs
for influenza vaccination was rare in fact only onerespondent in the sample fell into this category By con-trast SOPs for influenza vaccination without standingorders for PPV were common Given this distributionwe established three SOP groups no consistent use ofSOPs for either vaccination including the one physicianreporting SOP use for PPV only (n = 502 570) con-sistent use of SOPs for influenza vaccination only (n =175 199) and consistent use of SOPs for both vacci-nations (n = 203 231) Forty-three percent of thesample reported SOPs for influenza vaccination (with orwithout concomitant SOP for PPV) Physicians in thethree groups did not differ in age length of time inpractice US medical training board certification statusor specialtyDifferences among the three SOPs groups are shown
in Table 1 Across the three groups some correlatesincreased uniformly as use of SOPs increased for exam-ple awareness of ACIP recommendations andor Medi-care regulations belief that SOPs enhance adultvaccination rates having an immunization champion inthe practice agreement that SOPs are effective in boost-ing vaccination coverage access to an electronic medicalrecord (EMR) and having staff who are open to innova-tion and who work well together Training level andnumber of clinical assistants were significantly related touse of SOPs with practices reporting a greater staff toclinician ratio and those with more highly trained assis-tants (PACRNP or RNLPN) more often reporting con-sistent use of SOPs The proportion reporting 2 helpersper provider was 693 in the consistent influenzaPPVSOP group vs 563 in the consistent influenza onlygroup and 463 in the no consistent SOP group Pair-wise differences across these groupings were significantin post hoc comparisons Number of physicians in apractice was not a significant correlate of SOP groupTo investigate correlates of SOPs in more detail mul-
tinomial logistic regression models were developed toexamine the entire set of correlates These models allowa view of how physicians in each of the two SOP groupsdiffer from the group not using SOPs Table 2 showsodds ratios and 95 confidence intervals associated witheach correlate in a model that includes variables shownearlier in Table 1 adjusted for physician age and lengthof time in practiceIn the final adjusted model consistent use of SOPs
limited to influenza vaccine was independently and sig-nificantly associated with awareness of ACIP recommen-dations andor Medicare regulations (odds ratio [OR]235 95 confidence interval [CI] 160-346) agreementthat SOPs are an effective way to boost vaccination cov-erage (OR 297 95 CI 189-467) family medicine spe-cialty (OR 163 95 CI 110-242) greater amount ofhelp available to physicians (access to 2 assistants [OR
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 4 of 10
275 95 CI 131-579] access to 1 assistant [OR 230123-430] relative to the group with only 1 assistant for2+ providers)Consistent use of SOPs for both influenza vaccine and
PPV was associated with the same set of factors butadditional factors as well Shared correlates includedawareness of ACIP recommendations andor Medicareregulations (OR 446 95 CI 291-685) agreement thatSOPs are an effective way to boost vaccination coverage(OR 35 95 CI 214-571) family medicine specialty
(OR 127 95 CI 089-191 NS) and a greater staff toclinician ratio (OR 222 95 CI 109-454) Correlatesassociated only with combined influenza and PPV SOPsincluded a variety of practice-level factors practiceopenness to change and innovation (OR 215 95 CI133-347) strong practice teamwork (OR 278 95 CI149-521) access to an electronic medical record (OR190 95 CI 122-296) presence of an immunizationchampion in the practice (OR 194 95 127-298) andaccess to nursephysician assistant staff as opposed to
Table 1 Characteristics of PhysiciansPractices Reporting No Consistent Use of Standing Orders Programs (SOPs)Consistent Use of SOPs for Influenza Vaccine Only and Consistent Use of SOPs for Both Influenza Vaccine and PPV
No ConsistentUse of SOPs(n = 502)
Consistent Use of SOPs forInfluenza Vaccine Only
(n = 175)
Consistent Use of SOPs for BothInfluenza Vaccine and PPV
(n = 203)
P
Physician Indicators
Age 504 (101) 502 (94) 518 (99) 17
Years since medical degree 225 (104) 228 (100) 242 (98) 13
Family Medicine specialty 482 383 429 059
Board certified 797 811 783 53
Medical degree outside US 217 177 207 79
Physician is aware of ACIP recommendationsandor Medicare regulations
414 611 778 lt001
Physician believes SOPs are an effective way toboost adult vaccinations
602 794 823 lt001
Practice Indicators
Practice is open to change or innovation 516 611 783 lt001
Strong practice teamwork 657 737 906 lt001
Practice uses electronic medical record 456 566 591 001
Practice has immunization champion on site
233 274 389 lt001
Clinical support
2 helpers per provider 463 563 693 lt001
1 helper per provider 200 219 118
1 helper per 2+ providers 338 218 189
Number of physicians in practice
Solo 263 414 319 11
2-4 189 434 377
5+ 241 340 414
Type of clinical support
RNLPN 311 295 477 lt001
Medical Assistant 662 694 482
PACRNP 27 12 40
Practice is part of large health plan orcorporation
230 343 276 013
Physicians are primary decision makers forpractice
636 550 584 14
PPV = Pneumococcal polysaccharide vaccine
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 5 of 10
Table 2 Practice Characteristics Associated with Consistent Use of Standing Orders Programs (SOPs) for InfluenzaVaccination Only or Influenza and PPV Relative to No Consistent Use of SOPs in Multinomial Logistic Regression
Characteristic Consistent Use of SOPs for InfluenzaVaccine OnlyOR (95 CI)
Consistent Use of SOPs for Both InfluenzaVaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andorMedicare regulations
235 (160 346) Plt 001 446 (291 685) Plt 001
Physician believes that SOPs are an effective way toboost adult vaccinations
297 (189 467) Plt 001 350 (214 571) Plt 001
Practice is open to change or innovation 136 (079 210) 215 (133 347) P= 002
Strong practice teamwork 118 (074 191) 278 (149 521) P= 001
Practice uses electronic medical record 135 (089 203) 190 (122 296) P= 005
Practice has immunization champion on site 112 (072 176) 194 (127 298) P= 002
Clinical support
2 helpers per provider 275 (131 579) P= 008 222 (109 454) P= 028
1 helper per provider 230 (123 430) P= 009 145 (078 267)
1 helper per 2+ providers 100 (ref) 100 (ref)
Number of physicians in practice
Solo 076 (041 138) 071 (039 130)
2-4 102 (065 160) 072 (045 117)
ge 5 100 (ref) 100 (ref)
Family Medicine specialty 163 (110 242) P= 015 127 (089 191)
Nurse-levelPA assistance rather than medical assistant 072 (048 109) 149 (099 224) P= 054
Practice is part of large health plan or corporation 134 (085 213) 104 (062 172)
Physicians are primary decision makers for practice 094 (061 145) 108 (068 170)
Model adjusted for physician age and time since medical degree Model x2 = 2397 p lt 0001 R2 = 026
Table 3 Practice Characteristics Associated with Consistent Use of SOPs for Both Influenza Vaccine and PPV Relativeto Influenza Vaccine Only in Logistic Regression
Characteristic Consistent Use of SOPsfor Both Influenza Vaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andor Medicare regulations 195 (118 324) P= 010
Physician believes that SOPs are an effective way to boost adult vaccinations 111 (060 206)
Practice is open to change or innovation 159 (092 275)
Strong practice teamwork 224 (110 454) P= 026
Practice uses electronic medical record 130 (077 221)
Practice has immunization champion on site 167 (101 454) P= 046
Clinical support
2 helpers per provider 086 (035 214)
1 helper per provider 066 (030 149)
1 helper per 2+ providers 100 (ref)
Number of physicians in practice
Solo 087 (042 180)
2-4 068 (039 119)
ge 5 100 (ref)
Family medicine specialty 078 (048 126)
Nurse-levelPA assistance rather than medical assistant 212 (131 345) P= 002
Practice is part of large health plan or corporation 083 (047 146)
Physicians are primary decision makers for practice 131 (078 221)
Model adjusted for physician age and time since MD Model Χ2 = 550 P lt 0001 R2 = 020
PPV = Pneumococcal Polysaccharide Vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 6 of 10
medical assistants alone (OR 149 95 CI 099-224 p= 054)The two SOP groups were directly compared in Table
3 Physicians reporting consistent use of SOPs for bothimmunizations were more likely to be aware of ACIPrecommendations andor Medicare regulations (OR195 95 CI 118-324) Practice-level factors distin-guishing consistent use of SOPs for both vaccinesincluded strong practice teamwork (OR 224 95 CI110-454) having an immunization champion on site(OR 167 95 CI 101-454) and access to nursephysi-cian assistant staff as opposed to medical assistants (OR221 95 CI 131-345)Finally we examined the number of physician and
practice characteristics associated with adoption ofSOPs and the prevalence of reported SOPs for eitherinfluenza vaccine or PPV We summed across the 12characteristics analyzed in the regression models andplotted adoption of SOPs against this index (Figure 1)In this sample of physicians few respondents reported 0or 1 characteristic (n = 3) and few reported all 12 (n =3) Physicians reported a median of six characteristicsassociated with adoption Figure 1 shows that adoption
of SOPs is as low as 105 when only 1 or 2 factors arepresent and as high as 769 in the presence of all 11 or12 factors
DiscussionIn this national survey of US primary care physicianstreating adults 231 reported using SOPs consistentlyfor both influenza vaccine and PPV and 199 usedSOPs only for influenza vaccination In total as we havereported elsewhere 43 of physicians reported consis-tent use of SOPs for influenza vaccine [19] Physiciansin practices with SOPs for both vaccines reportedgreater awareness of ACIP recommendations andorMedicare regulations and were more likely to agree thatSOPs are an effective way to boost vaccination coverageImplementation of both influenza and PPV SOPs wasassociated with a variety of practice-level factors as wellincluding more effective practice teamwork the pre-sence of an immunization champion and greater avail-ability of clinical assistants with more advanced trainingthan that of medical assistantsThe CDC has recommended SOPs for adult vaccina-
tion since 2000 [16] However the Center for Medicare
Prevalence of SOPs Relative to Number ofPhysician and Practice Characteristics Associated
with Adoption
Figure 1 Uploaded separately Prevalence of SOPs Relative to Number of Physician and Practice Characteristics Associated with Adoption
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 7 of 10
and Medicaid Services (CMS) prohibited SOPs for allmedications until 2002 when CMS modified its regula-tions to allow SOPs for influenza vaccine and PPV [8]It is understandable that physicians who were unawareof the change in CMS regulations might not haveadopted consistent use of SOPs as reflected in our dataGiven the myriad recommendations and policies
aimed at primary preventive care including immuniza-tions how can a practice keep current One solution isfor the practice to have an immunization championsomeone to interpret and communicate changes in vac-cine policies and recommendations as they occur Pre-vious research confirms the importance of animmunization champion to improve vaccination ratesOne study that included explicit training of immuniza-tion nurses to serve as clinical champions boosted influ-enza vaccination coverage rates in pregnant womenfrom 25 to 374 in 2008-2009 [29] However it isdifficult to determine the specific value of immunizationchampions relative to other practice-level factorsbecause most interventions designed to boost vaccina-tion coverage include a variety of elements Our findingssuggest the particular value of champions for practicesthat have SOPs for both influenza vaccine and PPV Itwould useful to determine which staff makes the mosteffective immunization champion and what sort of train-ing is most appropriate In most cases champions arenurses but recent efforts suggest that even non-clinicalstaff such as receptionists or medical records staff canbe trained as immunization champions httpwwwimmunizeusaorgiz-champions[30] It remains unclearhow such duties will be added to job descriptions orqualifications and whether additional compensation isappropriateAccess to physician assistants or licensed nursing per-
sonnel was a significant correlate of SOPs for PPV asopposed to SOPs for influenza Physicians in practiceswith access to these more highly trained personnel weretwice as likely to have SOPs for PPV and influenza(Table 3) This association may be related to the com-plexity of PPV dosing and recommendations for indivi-duals with high-risk medical conditions [31] Somephysicians may feel comfortable allowing clinical staffwith more extensive education and training to deter-mine eligibility for PPV and administer vaccine as iscommon practice for nurses Conversely US state lawsvary regarding licensing of medical assistants [32] thesedifferences may result in concerns about medical assis-tants administering PPV under SOPs Anecdotally weheard reports of hesitation by medical assistants to useSOPs for PPV despite physician guidance and trainingusing a toolkit In contrast influenza vaccine is adminis-tered in many locales where a physician is not evenpresent
The presence of an electronic medical record (EMR)was similarly associated with SOPs for PPV as opposedto SOPs for influenza Again this association may be afunction of the complexity of PPV dosing and recom-mendations for individuals with high-risk medical condi-tions The EMR makes it easier for practitioners to trackimmunization histories and to flag patients eligible forvaccinationTeamwork is the essence of SOPs and thus the asso-
ciation between self-reported teamwork in the practiceand use of SOPs for PPV is not surprising Teamwork isalso a key aspect of successful implementation of thepatient-centered medical home and accountable careorganization Both are quality improvement models inwhich providing timely and appropriate preventive ser-vices such as vaccination is a critical element Programsto educate staff in vaccination may help to improve per-ceived self-efficacy stimulate innovation and fosterteamwork These programs include ldquoWhat worksrdquo (avail-able at httpwww2acdcgovvaccinesedwhatworksceasp and toolkits that facilitate use of SOPs httpwwwimmunizeorgstanding-orders and httpwwwImmuni-zationEdorgstandingordersWe conclude that practice-level factors are critical for
the adoption of more complex SOPs such as joint SOPsfor influenza and PPV The greater clinical complexityof PPV administration may require access to electronicmedical records and more highly trained auxiliary stafffor example as well as better coordination betweenstaff reflected in greater perceived teamworkStrengths of this research include a survey that is
national in scope with a high response rate for physicianparticipants The questionnaire was based on theoreticalmodels designed around physician adoption of vaccinesHowever surveys are subject to the limitations of self-report While the survey covered many correlates ofSOP use it may not have captured all relevant correlatesof SOP use Also we relied on a single physician toreport on each practice and may therefore underesti-mate variance in delivery of vaccinationsSOPs are underused but can have a great public
health impact For example SOPs may help mitigatedisparities in vaccination coverage in underserved popu-lations though we have not been able to identifyresearch in this area Further national efforts at clinicianand medical assistant education should be considered toensure that physicians are aware of current vaccinerecommendations and policies and that all clinical staffcan competently administer recommended vaccinesPractical toolkits are available to facilitate adoption ofSOPs in primary care practices Teamwork and animmunization champion can help empower clinical sup-port staff to administer vaccines using SOPs thus help-ing to reduce missed opportunities for vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 8 of 10
Additional material
Additional file 1 National Survey of Physicians about StandingOrders Programs for Adult Immunizations
AcknowledgementsThis study was supported by the Centers for Disease Control and Preventionand the Association for Prevention Teaching and Research Grant No 5 U50CD300-860-21 Its contents are the responsibility of the authors and do notnecessarily reflect the official views of the CDC or the APTR
Author details1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USA2Department of Family Medicine and Clinical Epidemiology School ofMedicine University of Pittsburgh Pittsburgh PA USA 3Centers for DiseaseControl and Prevention Atlanta GA USA
Authorsrsquo contributionsSA performed the statistical analysis and drafted the manuscript SA RZ TNMAY and FA conceived of the study and participated in developing thedesign of the research SA and TN coordinated the survey component Allauthors revised the manuscript critically for important intellectual contentAll authors read and approved the final manuscript
Competing interestsAt the time of data analyses Drs Zimmerman and Nowalk had researchfunding and consultancy with Medimmune Inc and research funding fromMerck Inc about HPV vaccine Dr Zimmerman also had research fundingfrom Sanofi
Received 9 October 2011 Accepted 20 March 2012Published 20 March 2012
References1 CDCNCHS NHIS Influenza vaccination in the past 12 months among
adults 18 years of age and over by age United States 1999-2009 2010[httpwww cdc givnchshuscontents2010htmfig18] [cited 2011 May10]Available from URL [httpwwwcdcgivnchshuscontents2010htmfig18]
2 Centers for Disease Control and Prevention 2009 Adult VaccinationCoverage NHIS [httpwww cdc govvaccinesstats-survnhis2009-nhishtm2010 [cited 2011 Jan 27]
3 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Validity of self-reported influenza and pneumococcalvaccination status among a cohort of hospitalized elderly inpatientsVaccine 2007 25(25)4775-4783
4 Nowalk MP Zimmerman RK Feghali J Missed opportunities for adultimmunization in diverse primary care office settings Vaccine 2004223457-3463
5 Nowalk MP Zimmerman RK Cleary SM Bruehlman RD Missedopportunities to vaccinate older adults in primary care J Am Board FamPract 2005 1820-27
6 Sandrine IS Meacutegard Y Overview of vaccination policies for the elderly inWestern European countries Aging Clin Exp Res 2009 21(3)210-215
7 Kohlhammer Y Schnoor M Schwartz M Raspe H Schaumlfer T Determinantsof influenza and pneumococcal vaccination in elderly people asystematic review Public Health 2007 121(10)742-751
8 Centers for Medicare and Medicaid Series H Medicare and Medicaidprograms conditions of participation immunization standards forhospitals long-term care facilities and home health agencies final rulewith comment period Fed Regist 2002 6761808-61814
9 Middleton DB Lin CJ Smith KJ et al Economic Evaluation of StandingOrder Programs for Pneumococcal Vaccination of Hospitalized ElderlyPatients Infect Control Hosp Epidemiol 2008 29(5)385-394
10 Dexter PR Perkins SM Maharry KS Jones K McDonald CJ Inpatientcomputer-based standing orders vs physician reminders to increase
influenza and pneumococcal vaccination rates J Am Med Assoc 20042922366-2371
11 Goebel LJ Neitch SM Mufson MA Standing Orders in an AmbulatorySetting Increases Influenza Vaccine Usage in Older People J Am GeriatrSoc 2005 53(6)1008-1010
12 Loughlin SM Mortazavi A Garey KW Rice GK Birtcher KK Pharmacist-managed vaccination program increased influenza vaccination rates incardiovascular patients enrolled in a secondary prevention lipid clinicPharmacotherapy 2007 27(5)729-733
13 Bond TC Patel PR Krishner J et al Association of Standing-Order PoliciesWith Vaccination Rates in Dialysis Clinics A US-Based Cross-sectionalStudy Am J Kidney Dis 2009 54(1)6-9
14 Task Force on Community Preventive Services Recommendationsregarding interventions to improve vaccination coverage in childrenadolescents and adults Am J Prev Med 2000 1892-96
15 Stone EG Morton SC Hulscher ME et al Interventions that increase useof adult immunization and cancer screening services a meta-analysisAnn Intern Med 2002 136(9)641-651
16 Centers for Disease Control and Prevention Use of standing ordersprograms to increase adult vaccination rates MMWR Morb Mortal WklyRep 2000 49(RR01)15-26
17 Health Care Financing Administration Evidence Report and Evidence-BasedRecommendations Interventions that Increase the Utilization of Medicare-Funded Preventive Service for Persons Age 65 and Older Baltimore MA HealthCare Financing Administration 1999
18 Szilagyi PG Shone LP Barth R et al Physician practices and attitudesregarding adult immunizations Prev Med 2005 40(2)152-161
19 Zimmerman R Albert S Nowalk M Yonas M Ahmed F Use of standingorders for adult influenza vaccination A national survey of primary carephysicians Am J Prev Med 2010 40(2)144-148
20 Yudin MH Salaripour M Sgro MD Acceptability and feasibility of seasonalinfluenza vaccine administration in an antenatal clinic setting J ObstetGynaecol Can 2010 32(8)745-748
21 Harder KM Cowan S Eriksen MB Krarup HB Christensen PB Universalscreening for hepatitis B among pregnant women led to 96vaccination coverage among newborns of HBsAg positive mothers inDenmark Vaccine 2011 29(50)9303-9307
22 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Missed opportunities to vaccinate a cohort of hospitalisedelderly with pneumococcal and influenza vaccines Vaccine 2007285146-5154
23 Jean-Pierre B Pierre OL Jean-Pierre M Willingness to vaccinate and to bevaccinated in adults Aging Clin Exp Res 2009 21(3)244-249
24 Yonas MA Nowalk MP Zimmerman RK Ahmed F Albert S Examiningstructural and clinical factors associated with implementation ofstanding orders for adult immunization J Healthc Qual 2011
25 Pathman DE Konrad TR Freed GL Freeman VA Koch GG The awareness-to-adherence model of the steps to clinical guideline compliance MedCare 1996 34(9)873-889
26 Rogers EM Diffusion of Innovations 3 edition New York Free Press 198327 Green LW Gottlieb NH Parcel GS Diffusion Theory Extended and
Applied In Advances in Health Education and Promotion Greenwich Editedby Ward WB Conn JAI Press 1987
28 Gielen AC McDonald EM The PRECEDE-PROCEED Planning Model InHealth Behavior and Health Education Theory Research and Practice 3edition Edited by Glanz K Lewis FM Rimer BK San Francisco Jossey-BassPublishers 1997359-383
29 Mouzoon ME Flor MM Greisinger AJ et al Improving InfluenzaImmunization in Pregnant Women and Healthcare Workers Am J ManagCare 2010 16(3)209-216
30 The Immunization Partnership [httpwwwimmunizeusaorgiz-champions] Accessed Jan 20 2012
31 Centers for Disease Control and Prevention Updated recommendationsfor prevention of invasive pneumococcal disease among adults usingthe 23-valent pneumococcal polysaccharide vaccine (PSV23) MorbMortal Wkly Rep 2010 59(34)1102-1106
32 Stewart A Cox M Rosenbaum S The Epidemiology of US ImmunizationLaw Translating CDC immunization guidelines into practice State lawsrelated to the use of standing orders covering immunization practice2008 [httpwww gwumcedusphhshealthpolicychsrpdownloads
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 9 of 10
CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-

asked whether physicians had received their medicaldegrees outside the US and included the following indi-cators of physician knowledge of SOPs whether theywere aware of ACIP recommendations or Medicare reg-ulations and whether they agreed that SOPs are effectivein boosting vaccination coveragePractice-Level Factors Physicians reported on practice-
level factors likely to influence adoption or consistentuse of SOPs These included perceptions of how opentheir practice is to change or innovation whether theirstaff demonstrates strong teamwork and whether physi-cians are primary decision makers for the practiceAdditional factors included access to an electronic medi-cal record having an immunization champion (a clinicalstaff member who promotes and encourages immuniza-tion) on site size of practices (recorded as solo 2-4 or 5+ physicians) help available to physicians (how manyhelpers per provider recorded as 1 helper per 2+ provi-ders 1 helper per provider or two helpers per provider)type of help (advanced (PACRNP) nurse-level (RN orLPN) assistance or medical assistant) and organizationof the practice (comparing practices that are part oflarge health plans or corporations to other types) Thesurvey instrument can be found in the Additional file 1
ResultsOf the 1640 physicians contacted by mail 16 letterswere returned by the post office as undeliverable and107 physicians were no longer in practice no longer inprimary care (eg hospitalists) deceased or unknown atthe practice leaving 1517 eligible physicians Of these1015 physicians returned surveys for a response rate of67 Participation was higher among family physicians(689) than internists (648 P lt 01) and amongboard certified (689) than non-board certified (607P lt 01) physicians Participants and nonparticipants didnot vary by age (mean = 507 years) length of time inpractice (mean = 23 years) domestic vs internationaltraining or geographic region Among participating phy-sicians 819 received their medical degree in the USand 795 were board certified The modal practice pat-tern for physicians in the sample was an independentpractice (51) in a suburban setting (453) The nextmost common practice setting was to be based in alarge corporate health system (255) in an urban set-ting (312)Of the 1015 physicians who completed the survey 115
did not immunize adults in their practices leaving 900physicians in the sample Of these 900 20 did notrespond to questions specific to influenza vaccinationThus the analytic sample consisted of 880 physicianswho provided information on SOPs for influenza vacci-nation and PPV Consistent use of SOPs for pneumo-coccal vaccination in the absence of similar use of SOPs
for influenza vaccination was rare in fact only onerespondent in the sample fell into this category By con-trast SOPs for influenza vaccination without standingorders for PPV were common Given this distributionwe established three SOP groups no consistent use ofSOPs for either vaccination including the one physicianreporting SOP use for PPV only (n = 502 570) con-sistent use of SOPs for influenza vaccination only (n =175 199) and consistent use of SOPs for both vacci-nations (n = 203 231) Forty-three percent of thesample reported SOPs for influenza vaccination (with orwithout concomitant SOP for PPV) Physicians in thethree groups did not differ in age length of time inpractice US medical training board certification statusor specialtyDifferences among the three SOPs groups are shown
in Table 1 Across the three groups some correlatesincreased uniformly as use of SOPs increased for exam-ple awareness of ACIP recommendations andor Medi-care regulations belief that SOPs enhance adultvaccination rates having an immunization champion inthe practice agreement that SOPs are effective in boost-ing vaccination coverage access to an electronic medicalrecord (EMR) and having staff who are open to innova-tion and who work well together Training level andnumber of clinical assistants were significantly related touse of SOPs with practices reporting a greater staff toclinician ratio and those with more highly trained assis-tants (PACRNP or RNLPN) more often reporting con-sistent use of SOPs The proportion reporting 2 helpersper provider was 693 in the consistent influenzaPPVSOP group vs 563 in the consistent influenza onlygroup and 463 in the no consistent SOP group Pair-wise differences across these groupings were significantin post hoc comparisons Number of physicians in apractice was not a significant correlate of SOP groupTo investigate correlates of SOPs in more detail mul-
tinomial logistic regression models were developed toexamine the entire set of correlates These models allowa view of how physicians in each of the two SOP groupsdiffer from the group not using SOPs Table 2 showsodds ratios and 95 confidence intervals associated witheach correlate in a model that includes variables shownearlier in Table 1 adjusted for physician age and lengthof time in practiceIn the final adjusted model consistent use of SOPs
limited to influenza vaccine was independently and sig-nificantly associated with awareness of ACIP recommen-dations andor Medicare regulations (odds ratio [OR]235 95 confidence interval [CI] 160-346) agreementthat SOPs are an effective way to boost vaccination cov-erage (OR 297 95 CI 189-467) family medicine spe-cialty (OR 163 95 CI 110-242) greater amount ofhelp available to physicians (access to 2 assistants [OR
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 4 of 10
275 95 CI 131-579] access to 1 assistant [OR 230123-430] relative to the group with only 1 assistant for2+ providers)Consistent use of SOPs for both influenza vaccine and
PPV was associated with the same set of factors butadditional factors as well Shared correlates includedawareness of ACIP recommendations andor Medicareregulations (OR 446 95 CI 291-685) agreement thatSOPs are an effective way to boost vaccination coverage(OR 35 95 CI 214-571) family medicine specialty
(OR 127 95 CI 089-191 NS) and a greater staff toclinician ratio (OR 222 95 CI 109-454) Correlatesassociated only with combined influenza and PPV SOPsincluded a variety of practice-level factors practiceopenness to change and innovation (OR 215 95 CI133-347) strong practice teamwork (OR 278 95 CI149-521) access to an electronic medical record (OR190 95 CI 122-296) presence of an immunizationchampion in the practice (OR 194 95 127-298) andaccess to nursephysician assistant staff as opposed to
Table 1 Characteristics of PhysiciansPractices Reporting No Consistent Use of Standing Orders Programs (SOPs)Consistent Use of SOPs for Influenza Vaccine Only and Consistent Use of SOPs for Both Influenza Vaccine and PPV
No ConsistentUse of SOPs(n = 502)
Consistent Use of SOPs forInfluenza Vaccine Only
(n = 175)
Consistent Use of SOPs for BothInfluenza Vaccine and PPV
(n = 203)
P
Physician Indicators
Age 504 (101) 502 (94) 518 (99) 17
Years since medical degree 225 (104) 228 (100) 242 (98) 13
Family Medicine specialty 482 383 429 059
Board certified 797 811 783 53
Medical degree outside US 217 177 207 79
Physician is aware of ACIP recommendationsandor Medicare regulations
414 611 778 lt001
Physician believes SOPs are an effective way toboost adult vaccinations
602 794 823 lt001
Practice Indicators
Practice is open to change or innovation 516 611 783 lt001
Strong practice teamwork 657 737 906 lt001
Practice uses electronic medical record 456 566 591 001
Practice has immunization champion on site
233 274 389 lt001
Clinical support
2 helpers per provider 463 563 693 lt001
1 helper per provider 200 219 118
1 helper per 2+ providers 338 218 189
Number of physicians in practice
Solo 263 414 319 11
2-4 189 434 377
5+ 241 340 414
Type of clinical support
RNLPN 311 295 477 lt001
Medical Assistant 662 694 482
PACRNP 27 12 40
Practice is part of large health plan orcorporation
230 343 276 013
Physicians are primary decision makers forpractice
636 550 584 14
PPV = Pneumococcal polysaccharide vaccine
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 5 of 10
Table 2 Practice Characteristics Associated with Consistent Use of Standing Orders Programs (SOPs) for InfluenzaVaccination Only or Influenza and PPV Relative to No Consistent Use of SOPs in Multinomial Logistic Regression
Characteristic Consistent Use of SOPs for InfluenzaVaccine OnlyOR (95 CI)
Consistent Use of SOPs for Both InfluenzaVaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andorMedicare regulations
235 (160 346) Plt 001 446 (291 685) Plt 001
Physician believes that SOPs are an effective way toboost adult vaccinations
297 (189 467) Plt 001 350 (214 571) Plt 001
Practice is open to change or innovation 136 (079 210) 215 (133 347) P= 002
Strong practice teamwork 118 (074 191) 278 (149 521) P= 001
Practice uses electronic medical record 135 (089 203) 190 (122 296) P= 005
Practice has immunization champion on site 112 (072 176) 194 (127 298) P= 002
Clinical support
2 helpers per provider 275 (131 579) P= 008 222 (109 454) P= 028
1 helper per provider 230 (123 430) P= 009 145 (078 267)
1 helper per 2+ providers 100 (ref) 100 (ref)
Number of physicians in practice
Solo 076 (041 138) 071 (039 130)
2-4 102 (065 160) 072 (045 117)
ge 5 100 (ref) 100 (ref)
Family Medicine specialty 163 (110 242) P= 015 127 (089 191)
Nurse-levelPA assistance rather than medical assistant 072 (048 109) 149 (099 224) P= 054
Practice is part of large health plan or corporation 134 (085 213) 104 (062 172)
Physicians are primary decision makers for practice 094 (061 145) 108 (068 170)
Model adjusted for physician age and time since medical degree Model x2 = 2397 p lt 0001 R2 = 026
Table 3 Practice Characteristics Associated with Consistent Use of SOPs for Both Influenza Vaccine and PPV Relativeto Influenza Vaccine Only in Logistic Regression
Characteristic Consistent Use of SOPsfor Both Influenza Vaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andor Medicare regulations 195 (118 324) P= 010
Physician believes that SOPs are an effective way to boost adult vaccinations 111 (060 206)
Practice is open to change or innovation 159 (092 275)
Strong practice teamwork 224 (110 454) P= 026
Practice uses electronic medical record 130 (077 221)
Practice has immunization champion on site 167 (101 454) P= 046
Clinical support
2 helpers per provider 086 (035 214)
1 helper per provider 066 (030 149)
1 helper per 2+ providers 100 (ref)
Number of physicians in practice
Solo 087 (042 180)
2-4 068 (039 119)
ge 5 100 (ref)
Family medicine specialty 078 (048 126)
Nurse-levelPA assistance rather than medical assistant 212 (131 345) P= 002
Practice is part of large health plan or corporation 083 (047 146)
Physicians are primary decision makers for practice 131 (078 221)
Model adjusted for physician age and time since MD Model Χ2 = 550 P lt 0001 R2 = 020
PPV = Pneumococcal Polysaccharide Vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 6 of 10
medical assistants alone (OR 149 95 CI 099-224 p= 054)The two SOP groups were directly compared in Table
3 Physicians reporting consistent use of SOPs for bothimmunizations were more likely to be aware of ACIPrecommendations andor Medicare regulations (OR195 95 CI 118-324) Practice-level factors distin-guishing consistent use of SOPs for both vaccinesincluded strong practice teamwork (OR 224 95 CI110-454) having an immunization champion on site(OR 167 95 CI 101-454) and access to nursephysi-cian assistant staff as opposed to medical assistants (OR221 95 CI 131-345)Finally we examined the number of physician and
practice characteristics associated with adoption ofSOPs and the prevalence of reported SOPs for eitherinfluenza vaccine or PPV We summed across the 12characteristics analyzed in the regression models andplotted adoption of SOPs against this index (Figure 1)In this sample of physicians few respondents reported 0or 1 characteristic (n = 3) and few reported all 12 (n =3) Physicians reported a median of six characteristicsassociated with adoption Figure 1 shows that adoption
of SOPs is as low as 105 when only 1 or 2 factors arepresent and as high as 769 in the presence of all 11 or12 factors
DiscussionIn this national survey of US primary care physicianstreating adults 231 reported using SOPs consistentlyfor both influenza vaccine and PPV and 199 usedSOPs only for influenza vaccination In total as we havereported elsewhere 43 of physicians reported consis-tent use of SOPs for influenza vaccine [19] Physiciansin practices with SOPs for both vaccines reportedgreater awareness of ACIP recommendations andorMedicare regulations and were more likely to agree thatSOPs are an effective way to boost vaccination coverageImplementation of both influenza and PPV SOPs wasassociated with a variety of practice-level factors as wellincluding more effective practice teamwork the pre-sence of an immunization champion and greater avail-ability of clinical assistants with more advanced trainingthan that of medical assistantsThe CDC has recommended SOPs for adult vaccina-
tion since 2000 [16] However the Center for Medicare
Prevalence of SOPs Relative to Number ofPhysician and Practice Characteristics Associated
with Adoption
Figure 1 Uploaded separately Prevalence of SOPs Relative to Number of Physician and Practice Characteristics Associated with Adoption
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 7 of 10
and Medicaid Services (CMS) prohibited SOPs for allmedications until 2002 when CMS modified its regula-tions to allow SOPs for influenza vaccine and PPV [8]It is understandable that physicians who were unawareof the change in CMS regulations might not haveadopted consistent use of SOPs as reflected in our dataGiven the myriad recommendations and policies
aimed at primary preventive care including immuniza-tions how can a practice keep current One solution isfor the practice to have an immunization championsomeone to interpret and communicate changes in vac-cine policies and recommendations as they occur Pre-vious research confirms the importance of animmunization champion to improve vaccination ratesOne study that included explicit training of immuniza-tion nurses to serve as clinical champions boosted influ-enza vaccination coverage rates in pregnant womenfrom 25 to 374 in 2008-2009 [29] However it isdifficult to determine the specific value of immunizationchampions relative to other practice-level factorsbecause most interventions designed to boost vaccina-tion coverage include a variety of elements Our findingssuggest the particular value of champions for practicesthat have SOPs for both influenza vaccine and PPV Itwould useful to determine which staff makes the mosteffective immunization champion and what sort of train-ing is most appropriate In most cases champions arenurses but recent efforts suggest that even non-clinicalstaff such as receptionists or medical records staff canbe trained as immunization champions httpwwwimmunizeusaorgiz-champions[30] It remains unclearhow such duties will be added to job descriptions orqualifications and whether additional compensation isappropriateAccess to physician assistants or licensed nursing per-
sonnel was a significant correlate of SOPs for PPV asopposed to SOPs for influenza Physicians in practiceswith access to these more highly trained personnel weretwice as likely to have SOPs for PPV and influenza(Table 3) This association may be related to the com-plexity of PPV dosing and recommendations for indivi-duals with high-risk medical conditions [31] Somephysicians may feel comfortable allowing clinical staffwith more extensive education and training to deter-mine eligibility for PPV and administer vaccine as iscommon practice for nurses Conversely US state lawsvary regarding licensing of medical assistants [32] thesedifferences may result in concerns about medical assis-tants administering PPV under SOPs Anecdotally weheard reports of hesitation by medical assistants to useSOPs for PPV despite physician guidance and trainingusing a toolkit In contrast influenza vaccine is adminis-tered in many locales where a physician is not evenpresent
The presence of an electronic medical record (EMR)was similarly associated with SOPs for PPV as opposedto SOPs for influenza Again this association may be afunction of the complexity of PPV dosing and recom-mendations for individuals with high-risk medical condi-tions The EMR makes it easier for practitioners to trackimmunization histories and to flag patients eligible forvaccinationTeamwork is the essence of SOPs and thus the asso-
ciation between self-reported teamwork in the practiceand use of SOPs for PPV is not surprising Teamwork isalso a key aspect of successful implementation of thepatient-centered medical home and accountable careorganization Both are quality improvement models inwhich providing timely and appropriate preventive ser-vices such as vaccination is a critical element Programsto educate staff in vaccination may help to improve per-ceived self-efficacy stimulate innovation and fosterteamwork These programs include ldquoWhat worksrdquo (avail-able at httpwww2acdcgovvaccinesedwhatworksceasp and toolkits that facilitate use of SOPs httpwwwimmunizeorgstanding-orders and httpwwwImmuni-zationEdorgstandingordersWe conclude that practice-level factors are critical for
the adoption of more complex SOPs such as joint SOPsfor influenza and PPV The greater clinical complexityof PPV administration may require access to electronicmedical records and more highly trained auxiliary stafffor example as well as better coordination betweenstaff reflected in greater perceived teamworkStrengths of this research include a survey that is
national in scope with a high response rate for physicianparticipants The questionnaire was based on theoreticalmodels designed around physician adoption of vaccinesHowever surveys are subject to the limitations of self-report While the survey covered many correlates ofSOP use it may not have captured all relevant correlatesof SOP use Also we relied on a single physician toreport on each practice and may therefore underesti-mate variance in delivery of vaccinationsSOPs are underused but can have a great public
health impact For example SOPs may help mitigatedisparities in vaccination coverage in underserved popu-lations though we have not been able to identifyresearch in this area Further national efforts at clinicianand medical assistant education should be considered toensure that physicians are aware of current vaccinerecommendations and policies and that all clinical staffcan competently administer recommended vaccinesPractical toolkits are available to facilitate adoption ofSOPs in primary care practices Teamwork and animmunization champion can help empower clinical sup-port staff to administer vaccines using SOPs thus help-ing to reduce missed opportunities for vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 8 of 10
Additional material
Additional file 1 National Survey of Physicians about StandingOrders Programs for Adult Immunizations
AcknowledgementsThis study was supported by the Centers for Disease Control and Preventionand the Association for Prevention Teaching and Research Grant No 5 U50CD300-860-21 Its contents are the responsibility of the authors and do notnecessarily reflect the official views of the CDC or the APTR
Author details1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USA2Department of Family Medicine and Clinical Epidemiology School ofMedicine University of Pittsburgh Pittsburgh PA USA 3Centers for DiseaseControl and Prevention Atlanta GA USA
Authorsrsquo contributionsSA performed the statistical analysis and drafted the manuscript SA RZ TNMAY and FA conceived of the study and participated in developing thedesign of the research SA and TN coordinated the survey component Allauthors revised the manuscript critically for important intellectual contentAll authors read and approved the final manuscript
Competing interestsAt the time of data analyses Drs Zimmerman and Nowalk had researchfunding and consultancy with Medimmune Inc and research funding fromMerck Inc about HPV vaccine Dr Zimmerman also had research fundingfrom Sanofi
Received 9 October 2011 Accepted 20 March 2012Published 20 March 2012
References1 CDCNCHS NHIS Influenza vaccination in the past 12 months among
adults 18 years of age and over by age United States 1999-2009 2010[httpwww cdc givnchshuscontents2010htmfig18] [cited 2011 May10]Available from URL [httpwwwcdcgivnchshuscontents2010htmfig18]
2 Centers for Disease Control and Prevention 2009 Adult VaccinationCoverage NHIS [httpwww cdc govvaccinesstats-survnhis2009-nhishtm2010 [cited 2011 Jan 27]
3 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Validity of self-reported influenza and pneumococcalvaccination status among a cohort of hospitalized elderly inpatientsVaccine 2007 25(25)4775-4783
4 Nowalk MP Zimmerman RK Feghali J Missed opportunities for adultimmunization in diverse primary care office settings Vaccine 2004223457-3463
5 Nowalk MP Zimmerman RK Cleary SM Bruehlman RD Missedopportunities to vaccinate older adults in primary care J Am Board FamPract 2005 1820-27
6 Sandrine IS Meacutegard Y Overview of vaccination policies for the elderly inWestern European countries Aging Clin Exp Res 2009 21(3)210-215
7 Kohlhammer Y Schnoor M Schwartz M Raspe H Schaumlfer T Determinantsof influenza and pneumococcal vaccination in elderly people asystematic review Public Health 2007 121(10)742-751
8 Centers for Medicare and Medicaid Series H Medicare and Medicaidprograms conditions of participation immunization standards forhospitals long-term care facilities and home health agencies final rulewith comment period Fed Regist 2002 6761808-61814
9 Middleton DB Lin CJ Smith KJ et al Economic Evaluation of StandingOrder Programs for Pneumococcal Vaccination of Hospitalized ElderlyPatients Infect Control Hosp Epidemiol 2008 29(5)385-394
10 Dexter PR Perkins SM Maharry KS Jones K McDonald CJ Inpatientcomputer-based standing orders vs physician reminders to increase
influenza and pneumococcal vaccination rates J Am Med Assoc 20042922366-2371
11 Goebel LJ Neitch SM Mufson MA Standing Orders in an AmbulatorySetting Increases Influenza Vaccine Usage in Older People J Am GeriatrSoc 2005 53(6)1008-1010
12 Loughlin SM Mortazavi A Garey KW Rice GK Birtcher KK Pharmacist-managed vaccination program increased influenza vaccination rates incardiovascular patients enrolled in a secondary prevention lipid clinicPharmacotherapy 2007 27(5)729-733
13 Bond TC Patel PR Krishner J et al Association of Standing-Order PoliciesWith Vaccination Rates in Dialysis Clinics A US-Based Cross-sectionalStudy Am J Kidney Dis 2009 54(1)6-9
14 Task Force on Community Preventive Services Recommendationsregarding interventions to improve vaccination coverage in childrenadolescents and adults Am J Prev Med 2000 1892-96
15 Stone EG Morton SC Hulscher ME et al Interventions that increase useof adult immunization and cancer screening services a meta-analysisAnn Intern Med 2002 136(9)641-651
16 Centers for Disease Control and Prevention Use of standing ordersprograms to increase adult vaccination rates MMWR Morb Mortal WklyRep 2000 49(RR01)15-26
17 Health Care Financing Administration Evidence Report and Evidence-BasedRecommendations Interventions that Increase the Utilization of Medicare-Funded Preventive Service for Persons Age 65 and Older Baltimore MA HealthCare Financing Administration 1999
18 Szilagyi PG Shone LP Barth R et al Physician practices and attitudesregarding adult immunizations Prev Med 2005 40(2)152-161
19 Zimmerman R Albert S Nowalk M Yonas M Ahmed F Use of standingorders for adult influenza vaccination A national survey of primary carephysicians Am J Prev Med 2010 40(2)144-148
20 Yudin MH Salaripour M Sgro MD Acceptability and feasibility of seasonalinfluenza vaccine administration in an antenatal clinic setting J ObstetGynaecol Can 2010 32(8)745-748
21 Harder KM Cowan S Eriksen MB Krarup HB Christensen PB Universalscreening for hepatitis B among pregnant women led to 96vaccination coverage among newborns of HBsAg positive mothers inDenmark Vaccine 2011 29(50)9303-9307
22 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Missed opportunities to vaccinate a cohort of hospitalisedelderly with pneumococcal and influenza vaccines Vaccine 2007285146-5154
23 Jean-Pierre B Pierre OL Jean-Pierre M Willingness to vaccinate and to bevaccinated in adults Aging Clin Exp Res 2009 21(3)244-249
24 Yonas MA Nowalk MP Zimmerman RK Ahmed F Albert S Examiningstructural and clinical factors associated with implementation ofstanding orders for adult immunization J Healthc Qual 2011
25 Pathman DE Konrad TR Freed GL Freeman VA Koch GG The awareness-to-adherence model of the steps to clinical guideline compliance MedCare 1996 34(9)873-889
26 Rogers EM Diffusion of Innovations 3 edition New York Free Press 198327 Green LW Gottlieb NH Parcel GS Diffusion Theory Extended and
Applied In Advances in Health Education and Promotion Greenwich Editedby Ward WB Conn JAI Press 1987
28 Gielen AC McDonald EM The PRECEDE-PROCEED Planning Model InHealth Behavior and Health Education Theory Research and Practice 3edition Edited by Glanz K Lewis FM Rimer BK San Francisco Jossey-BassPublishers 1997359-383
29 Mouzoon ME Flor MM Greisinger AJ et al Improving InfluenzaImmunization in Pregnant Women and Healthcare Workers Am J ManagCare 2010 16(3)209-216
30 The Immunization Partnership [httpwwwimmunizeusaorgiz-champions] Accessed Jan 20 2012
31 Centers for Disease Control and Prevention Updated recommendationsfor prevention of invasive pneumococcal disease among adults usingthe 23-valent pneumococcal polysaccharide vaccine (PSV23) MorbMortal Wkly Rep 2010 59(34)1102-1106
32 Stewart A Cox M Rosenbaum S The Epidemiology of US ImmunizationLaw Translating CDC immunization guidelines into practice State lawsrelated to the use of standing orders covering immunization practice2008 [httpwww gwumcedusphhshealthpolicychsrpdownloads
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 9 of 10
CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-

275 95 CI 131-579] access to 1 assistant [OR 230123-430] relative to the group with only 1 assistant for2+ providers)Consistent use of SOPs for both influenza vaccine and
PPV was associated with the same set of factors butadditional factors as well Shared correlates includedawareness of ACIP recommendations andor Medicareregulations (OR 446 95 CI 291-685) agreement thatSOPs are an effective way to boost vaccination coverage(OR 35 95 CI 214-571) family medicine specialty
(OR 127 95 CI 089-191 NS) and a greater staff toclinician ratio (OR 222 95 CI 109-454) Correlatesassociated only with combined influenza and PPV SOPsincluded a variety of practice-level factors practiceopenness to change and innovation (OR 215 95 CI133-347) strong practice teamwork (OR 278 95 CI149-521) access to an electronic medical record (OR190 95 CI 122-296) presence of an immunizationchampion in the practice (OR 194 95 127-298) andaccess to nursephysician assistant staff as opposed to
Table 1 Characteristics of PhysiciansPractices Reporting No Consistent Use of Standing Orders Programs (SOPs)Consistent Use of SOPs for Influenza Vaccine Only and Consistent Use of SOPs for Both Influenza Vaccine and PPV
No ConsistentUse of SOPs(n = 502)
Consistent Use of SOPs forInfluenza Vaccine Only
(n = 175)
Consistent Use of SOPs for BothInfluenza Vaccine and PPV
(n = 203)
P
Physician Indicators
Age 504 (101) 502 (94) 518 (99) 17
Years since medical degree 225 (104) 228 (100) 242 (98) 13
Family Medicine specialty 482 383 429 059
Board certified 797 811 783 53
Medical degree outside US 217 177 207 79
Physician is aware of ACIP recommendationsandor Medicare regulations
414 611 778 lt001
Physician believes SOPs are an effective way toboost adult vaccinations
602 794 823 lt001
Practice Indicators
Practice is open to change or innovation 516 611 783 lt001
Strong practice teamwork 657 737 906 lt001
Practice uses electronic medical record 456 566 591 001
Practice has immunization champion on site
233 274 389 lt001
Clinical support
2 helpers per provider 463 563 693 lt001
1 helper per provider 200 219 118
1 helper per 2+ providers 338 218 189
Number of physicians in practice
Solo 263 414 319 11
2-4 189 434 377
5+ 241 340 414
Type of clinical support
RNLPN 311 295 477 lt001
Medical Assistant 662 694 482
PACRNP 27 12 40
Practice is part of large health plan orcorporation
230 343 276 013
Physicians are primary decision makers forpractice
636 550 584 14
PPV = Pneumococcal polysaccharide vaccine
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 5 of 10
Table 2 Practice Characteristics Associated with Consistent Use of Standing Orders Programs (SOPs) for InfluenzaVaccination Only or Influenza and PPV Relative to No Consistent Use of SOPs in Multinomial Logistic Regression
Characteristic Consistent Use of SOPs for InfluenzaVaccine OnlyOR (95 CI)
Consistent Use of SOPs for Both InfluenzaVaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andorMedicare regulations
235 (160 346) Plt 001 446 (291 685) Plt 001
Physician believes that SOPs are an effective way toboost adult vaccinations
297 (189 467) Plt 001 350 (214 571) Plt 001
Practice is open to change or innovation 136 (079 210) 215 (133 347) P= 002
Strong practice teamwork 118 (074 191) 278 (149 521) P= 001
Practice uses electronic medical record 135 (089 203) 190 (122 296) P= 005
Practice has immunization champion on site 112 (072 176) 194 (127 298) P= 002
Clinical support
2 helpers per provider 275 (131 579) P= 008 222 (109 454) P= 028
1 helper per provider 230 (123 430) P= 009 145 (078 267)
1 helper per 2+ providers 100 (ref) 100 (ref)
Number of physicians in practice
Solo 076 (041 138) 071 (039 130)
2-4 102 (065 160) 072 (045 117)
ge 5 100 (ref) 100 (ref)
Family Medicine specialty 163 (110 242) P= 015 127 (089 191)
Nurse-levelPA assistance rather than medical assistant 072 (048 109) 149 (099 224) P= 054
Practice is part of large health plan or corporation 134 (085 213) 104 (062 172)
Physicians are primary decision makers for practice 094 (061 145) 108 (068 170)
Model adjusted for physician age and time since medical degree Model x2 = 2397 p lt 0001 R2 = 026
Table 3 Practice Characteristics Associated with Consistent Use of SOPs for Both Influenza Vaccine and PPV Relativeto Influenza Vaccine Only in Logistic Regression
Characteristic Consistent Use of SOPsfor Both Influenza Vaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andor Medicare regulations 195 (118 324) P= 010
Physician believes that SOPs are an effective way to boost adult vaccinations 111 (060 206)
Practice is open to change or innovation 159 (092 275)
Strong practice teamwork 224 (110 454) P= 026
Practice uses electronic medical record 130 (077 221)
Practice has immunization champion on site 167 (101 454) P= 046
Clinical support
2 helpers per provider 086 (035 214)
1 helper per provider 066 (030 149)
1 helper per 2+ providers 100 (ref)
Number of physicians in practice
Solo 087 (042 180)
2-4 068 (039 119)
ge 5 100 (ref)
Family medicine specialty 078 (048 126)
Nurse-levelPA assistance rather than medical assistant 212 (131 345) P= 002
Practice is part of large health plan or corporation 083 (047 146)
Physicians are primary decision makers for practice 131 (078 221)
Model adjusted for physician age and time since MD Model Χ2 = 550 P lt 0001 R2 = 020
PPV = Pneumococcal Polysaccharide Vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 6 of 10
medical assistants alone (OR 149 95 CI 099-224 p= 054)The two SOP groups were directly compared in Table
3 Physicians reporting consistent use of SOPs for bothimmunizations were more likely to be aware of ACIPrecommendations andor Medicare regulations (OR195 95 CI 118-324) Practice-level factors distin-guishing consistent use of SOPs for both vaccinesincluded strong practice teamwork (OR 224 95 CI110-454) having an immunization champion on site(OR 167 95 CI 101-454) and access to nursephysi-cian assistant staff as opposed to medical assistants (OR221 95 CI 131-345)Finally we examined the number of physician and
practice characteristics associated with adoption ofSOPs and the prevalence of reported SOPs for eitherinfluenza vaccine or PPV We summed across the 12characteristics analyzed in the regression models andplotted adoption of SOPs against this index (Figure 1)In this sample of physicians few respondents reported 0or 1 characteristic (n = 3) and few reported all 12 (n =3) Physicians reported a median of six characteristicsassociated with adoption Figure 1 shows that adoption
of SOPs is as low as 105 when only 1 or 2 factors arepresent and as high as 769 in the presence of all 11 or12 factors
DiscussionIn this national survey of US primary care physicianstreating adults 231 reported using SOPs consistentlyfor both influenza vaccine and PPV and 199 usedSOPs only for influenza vaccination In total as we havereported elsewhere 43 of physicians reported consis-tent use of SOPs for influenza vaccine [19] Physiciansin practices with SOPs for both vaccines reportedgreater awareness of ACIP recommendations andorMedicare regulations and were more likely to agree thatSOPs are an effective way to boost vaccination coverageImplementation of both influenza and PPV SOPs wasassociated with a variety of practice-level factors as wellincluding more effective practice teamwork the pre-sence of an immunization champion and greater avail-ability of clinical assistants with more advanced trainingthan that of medical assistantsThe CDC has recommended SOPs for adult vaccina-
tion since 2000 [16] However the Center for Medicare
Prevalence of SOPs Relative to Number ofPhysician and Practice Characteristics Associated
with Adoption
Figure 1 Uploaded separately Prevalence of SOPs Relative to Number of Physician and Practice Characteristics Associated with Adoption
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 7 of 10
and Medicaid Services (CMS) prohibited SOPs for allmedications until 2002 when CMS modified its regula-tions to allow SOPs for influenza vaccine and PPV [8]It is understandable that physicians who were unawareof the change in CMS regulations might not haveadopted consistent use of SOPs as reflected in our dataGiven the myriad recommendations and policies
aimed at primary preventive care including immuniza-tions how can a practice keep current One solution isfor the practice to have an immunization championsomeone to interpret and communicate changes in vac-cine policies and recommendations as they occur Pre-vious research confirms the importance of animmunization champion to improve vaccination ratesOne study that included explicit training of immuniza-tion nurses to serve as clinical champions boosted influ-enza vaccination coverage rates in pregnant womenfrom 25 to 374 in 2008-2009 [29] However it isdifficult to determine the specific value of immunizationchampions relative to other practice-level factorsbecause most interventions designed to boost vaccina-tion coverage include a variety of elements Our findingssuggest the particular value of champions for practicesthat have SOPs for both influenza vaccine and PPV Itwould useful to determine which staff makes the mosteffective immunization champion and what sort of train-ing is most appropriate In most cases champions arenurses but recent efforts suggest that even non-clinicalstaff such as receptionists or medical records staff canbe trained as immunization champions httpwwwimmunizeusaorgiz-champions[30] It remains unclearhow such duties will be added to job descriptions orqualifications and whether additional compensation isappropriateAccess to physician assistants or licensed nursing per-
sonnel was a significant correlate of SOPs for PPV asopposed to SOPs for influenza Physicians in practiceswith access to these more highly trained personnel weretwice as likely to have SOPs for PPV and influenza(Table 3) This association may be related to the com-plexity of PPV dosing and recommendations for indivi-duals with high-risk medical conditions [31] Somephysicians may feel comfortable allowing clinical staffwith more extensive education and training to deter-mine eligibility for PPV and administer vaccine as iscommon practice for nurses Conversely US state lawsvary regarding licensing of medical assistants [32] thesedifferences may result in concerns about medical assis-tants administering PPV under SOPs Anecdotally weheard reports of hesitation by medical assistants to useSOPs for PPV despite physician guidance and trainingusing a toolkit In contrast influenza vaccine is adminis-tered in many locales where a physician is not evenpresent
The presence of an electronic medical record (EMR)was similarly associated with SOPs for PPV as opposedto SOPs for influenza Again this association may be afunction of the complexity of PPV dosing and recom-mendations for individuals with high-risk medical condi-tions The EMR makes it easier for practitioners to trackimmunization histories and to flag patients eligible forvaccinationTeamwork is the essence of SOPs and thus the asso-
ciation between self-reported teamwork in the practiceand use of SOPs for PPV is not surprising Teamwork isalso a key aspect of successful implementation of thepatient-centered medical home and accountable careorganization Both are quality improvement models inwhich providing timely and appropriate preventive ser-vices such as vaccination is a critical element Programsto educate staff in vaccination may help to improve per-ceived self-efficacy stimulate innovation and fosterteamwork These programs include ldquoWhat worksrdquo (avail-able at httpwww2acdcgovvaccinesedwhatworksceasp and toolkits that facilitate use of SOPs httpwwwimmunizeorgstanding-orders and httpwwwImmuni-zationEdorgstandingordersWe conclude that practice-level factors are critical for
the adoption of more complex SOPs such as joint SOPsfor influenza and PPV The greater clinical complexityof PPV administration may require access to electronicmedical records and more highly trained auxiliary stafffor example as well as better coordination betweenstaff reflected in greater perceived teamworkStrengths of this research include a survey that is
national in scope with a high response rate for physicianparticipants The questionnaire was based on theoreticalmodels designed around physician adoption of vaccinesHowever surveys are subject to the limitations of self-report While the survey covered many correlates ofSOP use it may not have captured all relevant correlatesof SOP use Also we relied on a single physician toreport on each practice and may therefore underesti-mate variance in delivery of vaccinationsSOPs are underused but can have a great public
health impact For example SOPs may help mitigatedisparities in vaccination coverage in underserved popu-lations though we have not been able to identifyresearch in this area Further national efforts at clinicianand medical assistant education should be considered toensure that physicians are aware of current vaccinerecommendations and policies and that all clinical staffcan competently administer recommended vaccinesPractical toolkits are available to facilitate adoption ofSOPs in primary care practices Teamwork and animmunization champion can help empower clinical sup-port staff to administer vaccines using SOPs thus help-ing to reduce missed opportunities for vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 8 of 10
Additional material
Additional file 1 National Survey of Physicians about StandingOrders Programs for Adult Immunizations
AcknowledgementsThis study was supported by the Centers for Disease Control and Preventionand the Association for Prevention Teaching and Research Grant No 5 U50CD300-860-21 Its contents are the responsibility of the authors and do notnecessarily reflect the official views of the CDC or the APTR
Author details1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USA2Department of Family Medicine and Clinical Epidemiology School ofMedicine University of Pittsburgh Pittsburgh PA USA 3Centers for DiseaseControl and Prevention Atlanta GA USA
Authorsrsquo contributionsSA performed the statistical analysis and drafted the manuscript SA RZ TNMAY and FA conceived of the study and participated in developing thedesign of the research SA and TN coordinated the survey component Allauthors revised the manuscript critically for important intellectual contentAll authors read and approved the final manuscript
Competing interestsAt the time of data analyses Drs Zimmerman and Nowalk had researchfunding and consultancy with Medimmune Inc and research funding fromMerck Inc about HPV vaccine Dr Zimmerman also had research fundingfrom Sanofi
Received 9 October 2011 Accepted 20 March 2012Published 20 March 2012
References1 CDCNCHS NHIS Influenza vaccination in the past 12 months among
adults 18 years of age and over by age United States 1999-2009 2010[httpwww cdc givnchshuscontents2010htmfig18] [cited 2011 May10]Available from URL [httpwwwcdcgivnchshuscontents2010htmfig18]
2 Centers for Disease Control and Prevention 2009 Adult VaccinationCoverage NHIS [httpwww cdc govvaccinesstats-survnhis2009-nhishtm2010 [cited 2011 Jan 27]
3 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Validity of self-reported influenza and pneumococcalvaccination status among a cohort of hospitalized elderly inpatientsVaccine 2007 25(25)4775-4783
4 Nowalk MP Zimmerman RK Feghali J Missed opportunities for adultimmunization in diverse primary care office settings Vaccine 2004223457-3463
5 Nowalk MP Zimmerman RK Cleary SM Bruehlman RD Missedopportunities to vaccinate older adults in primary care J Am Board FamPract 2005 1820-27
6 Sandrine IS Meacutegard Y Overview of vaccination policies for the elderly inWestern European countries Aging Clin Exp Res 2009 21(3)210-215
7 Kohlhammer Y Schnoor M Schwartz M Raspe H Schaumlfer T Determinantsof influenza and pneumococcal vaccination in elderly people asystematic review Public Health 2007 121(10)742-751
8 Centers for Medicare and Medicaid Series H Medicare and Medicaidprograms conditions of participation immunization standards forhospitals long-term care facilities and home health agencies final rulewith comment period Fed Regist 2002 6761808-61814
9 Middleton DB Lin CJ Smith KJ et al Economic Evaluation of StandingOrder Programs for Pneumococcal Vaccination of Hospitalized ElderlyPatients Infect Control Hosp Epidemiol 2008 29(5)385-394
10 Dexter PR Perkins SM Maharry KS Jones K McDonald CJ Inpatientcomputer-based standing orders vs physician reminders to increase
influenza and pneumococcal vaccination rates J Am Med Assoc 20042922366-2371
11 Goebel LJ Neitch SM Mufson MA Standing Orders in an AmbulatorySetting Increases Influenza Vaccine Usage in Older People J Am GeriatrSoc 2005 53(6)1008-1010
12 Loughlin SM Mortazavi A Garey KW Rice GK Birtcher KK Pharmacist-managed vaccination program increased influenza vaccination rates incardiovascular patients enrolled in a secondary prevention lipid clinicPharmacotherapy 2007 27(5)729-733
13 Bond TC Patel PR Krishner J et al Association of Standing-Order PoliciesWith Vaccination Rates in Dialysis Clinics A US-Based Cross-sectionalStudy Am J Kidney Dis 2009 54(1)6-9
14 Task Force on Community Preventive Services Recommendationsregarding interventions to improve vaccination coverage in childrenadolescents and adults Am J Prev Med 2000 1892-96
15 Stone EG Morton SC Hulscher ME et al Interventions that increase useof adult immunization and cancer screening services a meta-analysisAnn Intern Med 2002 136(9)641-651
16 Centers for Disease Control and Prevention Use of standing ordersprograms to increase adult vaccination rates MMWR Morb Mortal WklyRep 2000 49(RR01)15-26
17 Health Care Financing Administration Evidence Report and Evidence-BasedRecommendations Interventions that Increase the Utilization of Medicare-Funded Preventive Service for Persons Age 65 and Older Baltimore MA HealthCare Financing Administration 1999
18 Szilagyi PG Shone LP Barth R et al Physician practices and attitudesregarding adult immunizations Prev Med 2005 40(2)152-161
19 Zimmerman R Albert S Nowalk M Yonas M Ahmed F Use of standingorders for adult influenza vaccination A national survey of primary carephysicians Am J Prev Med 2010 40(2)144-148
20 Yudin MH Salaripour M Sgro MD Acceptability and feasibility of seasonalinfluenza vaccine administration in an antenatal clinic setting J ObstetGynaecol Can 2010 32(8)745-748
21 Harder KM Cowan S Eriksen MB Krarup HB Christensen PB Universalscreening for hepatitis B among pregnant women led to 96vaccination coverage among newborns of HBsAg positive mothers inDenmark Vaccine 2011 29(50)9303-9307
22 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Missed opportunities to vaccinate a cohort of hospitalisedelderly with pneumococcal and influenza vaccines Vaccine 2007285146-5154
23 Jean-Pierre B Pierre OL Jean-Pierre M Willingness to vaccinate and to bevaccinated in adults Aging Clin Exp Res 2009 21(3)244-249
24 Yonas MA Nowalk MP Zimmerman RK Ahmed F Albert S Examiningstructural and clinical factors associated with implementation ofstanding orders for adult immunization J Healthc Qual 2011
25 Pathman DE Konrad TR Freed GL Freeman VA Koch GG The awareness-to-adherence model of the steps to clinical guideline compliance MedCare 1996 34(9)873-889
26 Rogers EM Diffusion of Innovations 3 edition New York Free Press 198327 Green LW Gottlieb NH Parcel GS Diffusion Theory Extended and
Applied In Advances in Health Education and Promotion Greenwich Editedby Ward WB Conn JAI Press 1987
28 Gielen AC McDonald EM The PRECEDE-PROCEED Planning Model InHealth Behavior and Health Education Theory Research and Practice 3edition Edited by Glanz K Lewis FM Rimer BK San Francisco Jossey-BassPublishers 1997359-383
29 Mouzoon ME Flor MM Greisinger AJ et al Improving InfluenzaImmunization in Pregnant Women and Healthcare Workers Am J ManagCare 2010 16(3)209-216
30 The Immunization Partnership [httpwwwimmunizeusaorgiz-champions] Accessed Jan 20 2012
31 Centers for Disease Control and Prevention Updated recommendationsfor prevention of invasive pneumococcal disease among adults usingthe 23-valent pneumococcal polysaccharide vaccine (PSV23) MorbMortal Wkly Rep 2010 59(34)1102-1106
32 Stewart A Cox M Rosenbaum S The Epidemiology of US ImmunizationLaw Translating CDC immunization guidelines into practice State lawsrelated to the use of standing orders covering immunization practice2008 [httpwww gwumcedusphhshealthpolicychsrpdownloads
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 9 of 10
CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-

Table 2 Practice Characteristics Associated with Consistent Use of Standing Orders Programs (SOPs) for InfluenzaVaccination Only or Influenza and PPV Relative to No Consistent Use of SOPs in Multinomial Logistic Regression
Characteristic Consistent Use of SOPs for InfluenzaVaccine OnlyOR (95 CI)
Consistent Use of SOPs for Both InfluenzaVaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andorMedicare regulations
235 (160 346) Plt 001 446 (291 685) Plt 001
Physician believes that SOPs are an effective way toboost adult vaccinations
297 (189 467) Plt 001 350 (214 571) Plt 001
Practice is open to change or innovation 136 (079 210) 215 (133 347) P= 002
Strong practice teamwork 118 (074 191) 278 (149 521) P= 001
Practice uses electronic medical record 135 (089 203) 190 (122 296) P= 005
Practice has immunization champion on site 112 (072 176) 194 (127 298) P= 002
Clinical support
2 helpers per provider 275 (131 579) P= 008 222 (109 454) P= 028
1 helper per provider 230 (123 430) P= 009 145 (078 267)
1 helper per 2+ providers 100 (ref) 100 (ref)
Number of physicians in practice
Solo 076 (041 138) 071 (039 130)
2-4 102 (065 160) 072 (045 117)
ge 5 100 (ref) 100 (ref)
Family Medicine specialty 163 (110 242) P= 015 127 (089 191)
Nurse-levelPA assistance rather than medical assistant 072 (048 109) 149 (099 224) P= 054
Practice is part of large health plan or corporation 134 (085 213) 104 (062 172)
Physicians are primary decision makers for practice 094 (061 145) 108 (068 170)
Model adjusted for physician age and time since medical degree Model x2 = 2397 p lt 0001 R2 = 026
Table 3 Practice Characteristics Associated with Consistent Use of SOPs for Both Influenza Vaccine and PPV Relativeto Influenza Vaccine Only in Logistic Regression
Characteristic Consistent Use of SOPsfor Both Influenza Vaccine and PPV
OR (95 CI)
Physician is aware of ACIP recommendations andor Medicare regulations 195 (118 324) P= 010
Physician believes that SOPs are an effective way to boost adult vaccinations 111 (060 206)
Practice is open to change or innovation 159 (092 275)
Strong practice teamwork 224 (110 454) P= 026
Practice uses electronic medical record 130 (077 221)
Practice has immunization champion on site 167 (101 454) P= 046
Clinical support
2 helpers per provider 086 (035 214)
1 helper per provider 066 (030 149)
1 helper per 2+ providers 100 (ref)
Number of physicians in practice
Solo 087 (042 180)
2-4 068 (039 119)
ge 5 100 (ref)
Family medicine specialty 078 (048 126)
Nurse-levelPA assistance rather than medical assistant 212 (131 345) P= 002
Practice is part of large health plan or corporation 083 (047 146)
Physicians are primary decision makers for practice 131 (078 221)
Model adjusted for physician age and time since MD Model Χ2 = 550 P lt 0001 R2 = 020
PPV = Pneumococcal Polysaccharide Vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 6 of 10
medical assistants alone (OR 149 95 CI 099-224 p= 054)The two SOP groups were directly compared in Table
3 Physicians reporting consistent use of SOPs for bothimmunizations were more likely to be aware of ACIPrecommendations andor Medicare regulations (OR195 95 CI 118-324) Practice-level factors distin-guishing consistent use of SOPs for both vaccinesincluded strong practice teamwork (OR 224 95 CI110-454) having an immunization champion on site(OR 167 95 CI 101-454) and access to nursephysi-cian assistant staff as opposed to medical assistants (OR221 95 CI 131-345)Finally we examined the number of physician and
practice characteristics associated with adoption ofSOPs and the prevalence of reported SOPs for eitherinfluenza vaccine or PPV We summed across the 12characteristics analyzed in the regression models andplotted adoption of SOPs against this index (Figure 1)In this sample of physicians few respondents reported 0or 1 characteristic (n = 3) and few reported all 12 (n =3) Physicians reported a median of six characteristicsassociated with adoption Figure 1 shows that adoption
of SOPs is as low as 105 when only 1 or 2 factors arepresent and as high as 769 in the presence of all 11 or12 factors
DiscussionIn this national survey of US primary care physicianstreating adults 231 reported using SOPs consistentlyfor both influenza vaccine and PPV and 199 usedSOPs only for influenza vaccination In total as we havereported elsewhere 43 of physicians reported consis-tent use of SOPs for influenza vaccine [19] Physiciansin practices with SOPs for both vaccines reportedgreater awareness of ACIP recommendations andorMedicare regulations and were more likely to agree thatSOPs are an effective way to boost vaccination coverageImplementation of both influenza and PPV SOPs wasassociated with a variety of practice-level factors as wellincluding more effective practice teamwork the pre-sence of an immunization champion and greater avail-ability of clinical assistants with more advanced trainingthan that of medical assistantsThe CDC has recommended SOPs for adult vaccina-
tion since 2000 [16] However the Center for Medicare
Prevalence of SOPs Relative to Number ofPhysician and Practice Characteristics Associated
with Adoption
Figure 1 Uploaded separately Prevalence of SOPs Relative to Number of Physician and Practice Characteristics Associated with Adoption
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 7 of 10
and Medicaid Services (CMS) prohibited SOPs for allmedications until 2002 when CMS modified its regula-tions to allow SOPs for influenza vaccine and PPV [8]It is understandable that physicians who were unawareof the change in CMS regulations might not haveadopted consistent use of SOPs as reflected in our dataGiven the myriad recommendations and policies
aimed at primary preventive care including immuniza-tions how can a practice keep current One solution isfor the practice to have an immunization championsomeone to interpret and communicate changes in vac-cine policies and recommendations as they occur Pre-vious research confirms the importance of animmunization champion to improve vaccination ratesOne study that included explicit training of immuniza-tion nurses to serve as clinical champions boosted influ-enza vaccination coverage rates in pregnant womenfrom 25 to 374 in 2008-2009 [29] However it isdifficult to determine the specific value of immunizationchampions relative to other practice-level factorsbecause most interventions designed to boost vaccina-tion coverage include a variety of elements Our findingssuggest the particular value of champions for practicesthat have SOPs for both influenza vaccine and PPV Itwould useful to determine which staff makes the mosteffective immunization champion and what sort of train-ing is most appropriate In most cases champions arenurses but recent efforts suggest that even non-clinicalstaff such as receptionists or medical records staff canbe trained as immunization champions httpwwwimmunizeusaorgiz-champions[30] It remains unclearhow such duties will be added to job descriptions orqualifications and whether additional compensation isappropriateAccess to physician assistants or licensed nursing per-
sonnel was a significant correlate of SOPs for PPV asopposed to SOPs for influenza Physicians in practiceswith access to these more highly trained personnel weretwice as likely to have SOPs for PPV and influenza(Table 3) This association may be related to the com-plexity of PPV dosing and recommendations for indivi-duals with high-risk medical conditions [31] Somephysicians may feel comfortable allowing clinical staffwith more extensive education and training to deter-mine eligibility for PPV and administer vaccine as iscommon practice for nurses Conversely US state lawsvary regarding licensing of medical assistants [32] thesedifferences may result in concerns about medical assis-tants administering PPV under SOPs Anecdotally weheard reports of hesitation by medical assistants to useSOPs for PPV despite physician guidance and trainingusing a toolkit In contrast influenza vaccine is adminis-tered in many locales where a physician is not evenpresent
The presence of an electronic medical record (EMR)was similarly associated with SOPs for PPV as opposedto SOPs for influenza Again this association may be afunction of the complexity of PPV dosing and recom-mendations for individuals with high-risk medical condi-tions The EMR makes it easier for practitioners to trackimmunization histories and to flag patients eligible forvaccinationTeamwork is the essence of SOPs and thus the asso-
ciation between self-reported teamwork in the practiceand use of SOPs for PPV is not surprising Teamwork isalso a key aspect of successful implementation of thepatient-centered medical home and accountable careorganization Both are quality improvement models inwhich providing timely and appropriate preventive ser-vices such as vaccination is a critical element Programsto educate staff in vaccination may help to improve per-ceived self-efficacy stimulate innovation and fosterteamwork These programs include ldquoWhat worksrdquo (avail-able at httpwww2acdcgovvaccinesedwhatworksceasp and toolkits that facilitate use of SOPs httpwwwimmunizeorgstanding-orders and httpwwwImmuni-zationEdorgstandingordersWe conclude that practice-level factors are critical for
the adoption of more complex SOPs such as joint SOPsfor influenza and PPV The greater clinical complexityof PPV administration may require access to electronicmedical records and more highly trained auxiliary stafffor example as well as better coordination betweenstaff reflected in greater perceived teamworkStrengths of this research include a survey that is
national in scope with a high response rate for physicianparticipants The questionnaire was based on theoreticalmodels designed around physician adoption of vaccinesHowever surveys are subject to the limitations of self-report While the survey covered many correlates ofSOP use it may not have captured all relevant correlatesof SOP use Also we relied on a single physician toreport on each practice and may therefore underesti-mate variance in delivery of vaccinationsSOPs are underused but can have a great public
health impact For example SOPs may help mitigatedisparities in vaccination coverage in underserved popu-lations though we have not been able to identifyresearch in this area Further national efforts at clinicianand medical assistant education should be considered toensure that physicians are aware of current vaccinerecommendations and policies and that all clinical staffcan competently administer recommended vaccinesPractical toolkits are available to facilitate adoption ofSOPs in primary care practices Teamwork and animmunization champion can help empower clinical sup-port staff to administer vaccines using SOPs thus help-ing to reduce missed opportunities for vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 8 of 10
Additional material
Additional file 1 National Survey of Physicians about StandingOrders Programs for Adult Immunizations
AcknowledgementsThis study was supported by the Centers for Disease Control and Preventionand the Association for Prevention Teaching and Research Grant No 5 U50CD300-860-21 Its contents are the responsibility of the authors and do notnecessarily reflect the official views of the CDC or the APTR
Author details1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USA2Department of Family Medicine and Clinical Epidemiology School ofMedicine University of Pittsburgh Pittsburgh PA USA 3Centers for DiseaseControl and Prevention Atlanta GA USA
Authorsrsquo contributionsSA performed the statistical analysis and drafted the manuscript SA RZ TNMAY and FA conceived of the study and participated in developing thedesign of the research SA and TN coordinated the survey component Allauthors revised the manuscript critically for important intellectual contentAll authors read and approved the final manuscript
Competing interestsAt the time of data analyses Drs Zimmerman and Nowalk had researchfunding and consultancy with Medimmune Inc and research funding fromMerck Inc about HPV vaccine Dr Zimmerman also had research fundingfrom Sanofi
Received 9 October 2011 Accepted 20 March 2012Published 20 March 2012
References1 CDCNCHS NHIS Influenza vaccination in the past 12 months among
adults 18 years of age and over by age United States 1999-2009 2010[httpwww cdc givnchshuscontents2010htmfig18] [cited 2011 May10]Available from URL [httpwwwcdcgivnchshuscontents2010htmfig18]
2 Centers for Disease Control and Prevention 2009 Adult VaccinationCoverage NHIS [httpwww cdc govvaccinesstats-survnhis2009-nhishtm2010 [cited 2011 Jan 27]
3 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Validity of self-reported influenza and pneumococcalvaccination status among a cohort of hospitalized elderly inpatientsVaccine 2007 25(25)4775-4783
4 Nowalk MP Zimmerman RK Feghali J Missed opportunities for adultimmunization in diverse primary care office settings Vaccine 2004223457-3463
5 Nowalk MP Zimmerman RK Cleary SM Bruehlman RD Missedopportunities to vaccinate older adults in primary care J Am Board FamPract 2005 1820-27
6 Sandrine IS Meacutegard Y Overview of vaccination policies for the elderly inWestern European countries Aging Clin Exp Res 2009 21(3)210-215
7 Kohlhammer Y Schnoor M Schwartz M Raspe H Schaumlfer T Determinantsof influenza and pneumococcal vaccination in elderly people asystematic review Public Health 2007 121(10)742-751
8 Centers for Medicare and Medicaid Series H Medicare and Medicaidprograms conditions of participation immunization standards forhospitals long-term care facilities and home health agencies final rulewith comment period Fed Regist 2002 6761808-61814
9 Middleton DB Lin CJ Smith KJ et al Economic Evaluation of StandingOrder Programs for Pneumococcal Vaccination of Hospitalized ElderlyPatients Infect Control Hosp Epidemiol 2008 29(5)385-394
10 Dexter PR Perkins SM Maharry KS Jones K McDonald CJ Inpatientcomputer-based standing orders vs physician reminders to increase
influenza and pneumococcal vaccination rates J Am Med Assoc 20042922366-2371
11 Goebel LJ Neitch SM Mufson MA Standing Orders in an AmbulatorySetting Increases Influenza Vaccine Usage in Older People J Am GeriatrSoc 2005 53(6)1008-1010
12 Loughlin SM Mortazavi A Garey KW Rice GK Birtcher KK Pharmacist-managed vaccination program increased influenza vaccination rates incardiovascular patients enrolled in a secondary prevention lipid clinicPharmacotherapy 2007 27(5)729-733
13 Bond TC Patel PR Krishner J et al Association of Standing-Order PoliciesWith Vaccination Rates in Dialysis Clinics A US-Based Cross-sectionalStudy Am J Kidney Dis 2009 54(1)6-9
14 Task Force on Community Preventive Services Recommendationsregarding interventions to improve vaccination coverage in childrenadolescents and adults Am J Prev Med 2000 1892-96
15 Stone EG Morton SC Hulscher ME et al Interventions that increase useof adult immunization and cancer screening services a meta-analysisAnn Intern Med 2002 136(9)641-651
16 Centers for Disease Control and Prevention Use of standing ordersprograms to increase adult vaccination rates MMWR Morb Mortal WklyRep 2000 49(RR01)15-26
17 Health Care Financing Administration Evidence Report and Evidence-BasedRecommendations Interventions that Increase the Utilization of Medicare-Funded Preventive Service for Persons Age 65 and Older Baltimore MA HealthCare Financing Administration 1999
18 Szilagyi PG Shone LP Barth R et al Physician practices and attitudesregarding adult immunizations Prev Med 2005 40(2)152-161
19 Zimmerman R Albert S Nowalk M Yonas M Ahmed F Use of standingorders for adult influenza vaccination A national survey of primary carephysicians Am J Prev Med 2010 40(2)144-148
20 Yudin MH Salaripour M Sgro MD Acceptability and feasibility of seasonalinfluenza vaccine administration in an antenatal clinic setting J ObstetGynaecol Can 2010 32(8)745-748
21 Harder KM Cowan S Eriksen MB Krarup HB Christensen PB Universalscreening for hepatitis B among pregnant women led to 96vaccination coverage among newborns of HBsAg positive mothers inDenmark Vaccine 2011 29(50)9303-9307
22 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Missed opportunities to vaccinate a cohort of hospitalisedelderly with pneumococcal and influenza vaccines Vaccine 2007285146-5154
23 Jean-Pierre B Pierre OL Jean-Pierre M Willingness to vaccinate and to bevaccinated in adults Aging Clin Exp Res 2009 21(3)244-249
24 Yonas MA Nowalk MP Zimmerman RK Ahmed F Albert S Examiningstructural and clinical factors associated with implementation ofstanding orders for adult immunization J Healthc Qual 2011
25 Pathman DE Konrad TR Freed GL Freeman VA Koch GG The awareness-to-adherence model of the steps to clinical guideline compliance MedCare 1996 34(9)873-889
26 Rogers EM Diffusion of Innovations 3 edition New York Free Press 198327 Green LW Gottlieb NH Parcel GS Diffusion Theory Extended and
Applied In Advances in Health Education and Promotion Greenwich Editedby Ward WB Conn JAI Press 1987
28 Gielen AC McDonald EM The PRECEDE-PROCEED Planning Model InHealth Behavior and Health Education Theory Research and Practice 3edition Edited by Glanz K Lewis FM Rimer BK San Francisco Jossey-BassPublishers 1997359-383
29 Mouzoon ME Flor MM Greisinger AJ et al Improving InfluenzaImmunization in Pregnant Women and Healthcare Workers Am J ManagCare 2010 16(3)209-216
30 The Immunization Partnership [httpwwwimmunizeusaorgiz-champions] Accessed Jan 20 2012
31 Centers for Disease Control and Prevention Updated recommendationsfor prevention of invasive pneumococcal disease among adults usingthe 23-valent pneumococcal polysaccharide vaccine (PSV23) MorbMortal Wkly Rep 2010 59(34)1102-1106
32 Stewart A Cox M Rosenbaum S The Epidemiology of US ImmunizationLaw Translating CDC immunization guidelines into practice State lawsrelated to the use of standing orders covering immunization practice2008 [httpwww gwumcedusphhshealthpolicychsrpdownloads
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 9 of 10
CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-
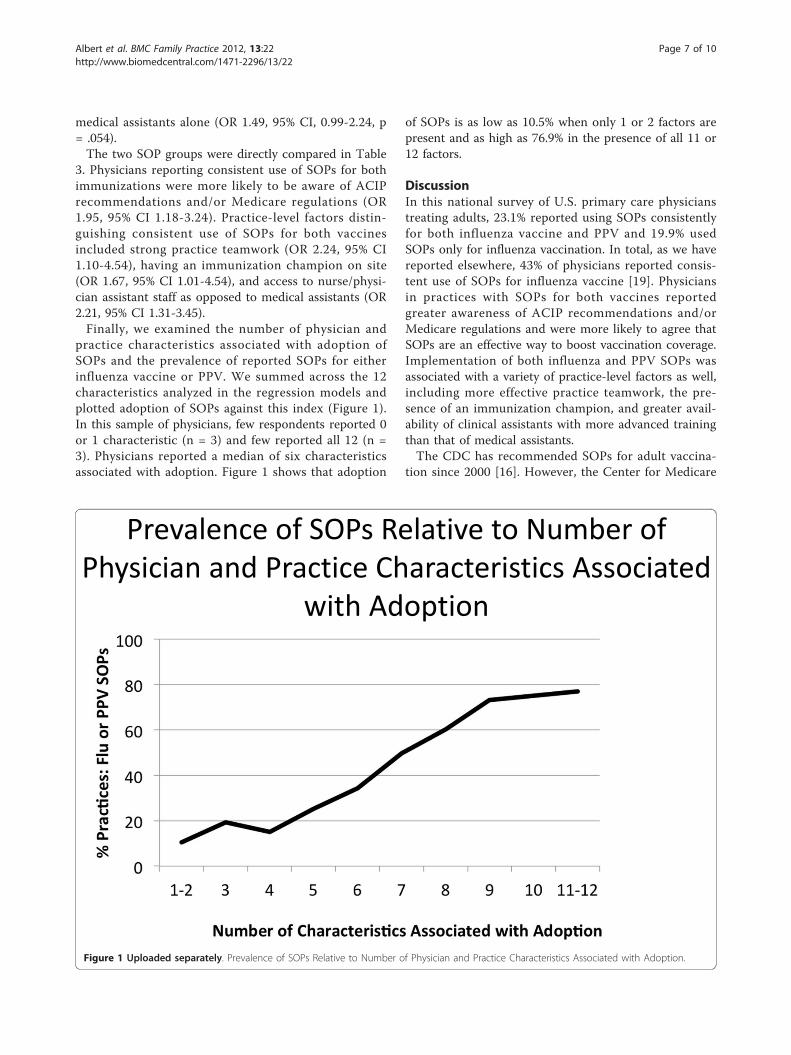
medical assistants alone (OR 149 95 CI 099-224 p= 054)The two SOP groups were directly compared in Table
3 Physicians reporting consistent use of SOPs for bothimmunizations were more likely to be aware of ACIPrecommendations andor Medicare regulations (OR195 95 CI 118-324) Practice-level factors distin-guishing consistent use of SOPs for both vaccinesincluded strong practice teamwork (OR 224 95 CI110-454) having an immunization champion on site(OR 167 95 CI 101-454) and access to nursephysi-cian assistant staff as opposed to medical assistants (OR221 95 CI 131-345)Finally we examined the number of physician and
practice characteristics associated with adoption ofSOPs and the prevalence of reported SOPs for eitherinfluenza vaccine or PPV We summed across the 12characteristics analyzed in the regression models andplotted adoption of SOPs against this index (Figure 1)In this sample of physicians few respondents reported 0or 1 characteristic (n = 3) and few reported all 12 (n =3) Physicians reported a median of six characteristicsassociated with adoption Figure 1 shows that adoption
of SOPs is as low as 105 when only 1 or 2 factors arepresent and as high as 769 in the presence of all 11 or12 factors
DiscussionIn this national survey of US primary care physicianstreating adults 231 reported using SOPs consistentlyfor both influenza vaccine and PPV and 199 usedSOPs only for influenza vaccination In total as we havereported elsewhere 43 of physicians reported consis-tent use of SOPs for influenza vaccine [19] Physiciansin practices with SOPs for both vaccines reportedgreater awareness of ACIP recommendations andorMedicare regulations and were more likely to agree thatSOPs are an effective way to boost vaccination coverageImplementation of both influenza and PPV SOPs wasassociated with a variety of practice-level factors as wellincluding more effective practice teamwork the pre-sence of an immunization champion and greater avail-ability of clinical assistants with more advanced trainingthan that of medical assistantsThe CDC has recommended SOPs for adult vaccina-
tion since 2000 [16] However the Center for Medicare
Prevalence of SOPs Relative to Number ofPhysician and Practice Characteristics Associated
with Adoption
Figure 1 Uploaded separately Prevalence of SOPs Relative to Number of Physician and Practice Characteristics Associated with Adoption
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 7 of 10
and Medicaid Services (CMS) prohibited SOPs for allmedications until 2002 when CMS modified its regula-tions to allow SOPs for influenza vaccine and PPV [8]It is understandable that physicians who were unawareof the change in CMS regulations might not haveadopted consistent use of SOPs as reflected in our dataGiven the myriad recommendations and policies
aimed at primary preventive care including immuniza-tions how can a practice keep current One solution isfor the practice to have an immunization championsomeone to interpret and communicate changes in vac-cine policies and recommendations as they occur Pre-vious research confirms the importance of animmunization champion to improve vaccination ratesOne study that included explicit training of immuniza-tion nurses to serve as clinical champions boosted influ-enza vaccination coverage rates in pregnant womenfrom 25 to 374 in 2008-2009 [29] However it isdifficult to determine the specific value of immunizationchampions relative to other practice-level factorsbecause most interventions designed to boost vaccina-tion coverage include a variety of elements Our findingssuggest the particular value of champions for practicesthat have SOPs for both influenza vaccine and PPV Itwould useful to determine which staff makes the mosteffective immunization champion and what sort of train-ing is most appropriate In most cases champions arenurses but recent efforts suggest that even non-clinicalstaff such as receptionists or medical records staff canbe trained as immunization champions httpwwwimmunizeusaorgiz-champions[30] It remains unclearhow such duties will be added to job descriptions orqualifications and whether additional compensation isappropriateAccess to physician assistants or licensed nursing per-
sonnel was a significant correlate of SOPs for PPV asopposed to SOPs for influenza Physicians in practiceswith access to these more highly trained personnel weretwice as likely to have SOPs for PPV and influenza(Table 3) This association may be related to the com-plexity of PPV dosing and recommendations for indivi-duals with high-risk medical conditions [31] Somephysicians may feel comfortable allowing clinical staffwith more extensive education and training to deter-mine eligibility for PPV and administer vaccine as iscommon practice for nurses Conversely US state lawsvary regarding licensing of medical assistants [32] thesedifferences may result in concerns about medical assis-tants administering PPV under SOPs Anecdotally weheard reports of hesitation by medical assistants to useSOPs for PPV despite physician guidance and trainingusing a toolkit In contrast influenza vaccine is adminis-tered in many locales where a physician is not evenpresent
The presence of an electronic medical record (EMR)was similarly associated with SOPs for PPV as opposedto SOPs for influenza Again this association may be afunction of the complexity of PPV dosing and recom-mendations for individuals with high-risk medical condi-tions The EMR makes it easier for practitioners to trackimmunization histories and to flag patients eligible forvaccinationTeamwork is the essence of SOPs and thus the asso-
ciation between self-reported teamwork in the practiceand use of SOPs for PPV is not surprising Teamwork isalso a key aspect of successful implementation of thepatient-centered medical home and accountable careorganization Both are quality improvement models inwhich providing timely and appropriate preventive ser-vices such as vaccination is a critical element Programsto educate staff in vaccination may help to improve per-ceived self-efficacy stimulate innovation and fosterteamwork These programs include ldquoWhat worksrdquo (avail-able at httpwww2acdcgovvaccinesedwhatworksceasp and toolkits that facilitate use of SOPs httpwwwimmunizeorgstanding-orders and httpwwwImmuni-zationEdorgstandingordersWe conclude that practice-level factors are critical for
the adoption of more complex SOPs such as joint SOPsfor influenza and PPV The greater clinical complexityof PPV administration may require access to electronicmedical records and more highly trained auxiliary stafffor example as well as better coordination betweenstaff reflected in greater perceived teamworkStrengths of this research include a survey that is
national in scope with a high response rate for physicianparticipants The questionnaire was based on theoreticalmodels designed around physician adoption of vaccinesHowever surveys are subject to the limitations of self-report While the survey covered many correlates ofSOP use it may not have captured all relevant correlatesof SOP use Also we relied on a single physician toreport on each practice and may therefore underesti-mate variance in delivery of vaccinationsSOPs are underused but can have a great public
health impact For example SOPs may help mitigatedisparities in vaccination coverage in underserved popu-lations though we have not been able to identifyresearch in this area Further national efforts at clinicianand medical assistant education should be considered toensure that physicians are aware of current vaccinerecommendations and policies and that all clinical staffcan competently administer recommended vaccinesPractical toolkits are available to facilitate adoption ofSOPs in primary care practices Teamwork and animmunization champion can help empower clinical sup-port staff to administer vaccines using SOPs thus help-ing to reduce missed opportunities for vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 8 of 10
Additional material
Additional file 1 National Survey of Physicians about StandingOrders Programs for Adult Immunizations
AcknowledgementsThis study was supported by the Centers for Disease Control and Preventionand the Association for Prevention Teaching and Research Grant No 5 U50CD300-860-21 Its contents are the responsibility of the authors and do notnecessarily reflect the official views of the CDC or the APTR
Author details1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USA2Department of Family Medicine and Clinical Epidemiology School ofMedicine University of Pittsburgh Pittsburgh PA USA 3Centers for DiseaseControl and Prevention Atlanta GA USA
Authorsrsquo contributionsSA performed the statistical analysis and drafted the manuscript SA RZ TNMAY and FA conceived of the study and participated in developing thedesign of the research SA and TN coordinated the survey component Allauthors revised the manuscript critically for important intellectual contentAll authors read and approved the final manuscript
Competing interestsAt the time of data analyses Drs Zimmerman and Nowalk had researchfunding and consultancy with Medimmune Inc and research funding fromMerck Inc about HPV vaccine Dr Zimmerman also had research fundingfrom Sanofi
Received 9 October 2011 Accepted 20 March 2012Published 20 March 2012
References1 CDCNCHS NHIS Influenza vaccination in the past 12 months among
adults 18 years of age and over by age United States 1999-2009 2010[httpwww cdc givnchshuscontents2010htmfig18] [cited 2011 May10]Available from URL [httpwwwcdcgivnchshuscontents2010htmfig18]
2 Centers for Disease Control and Prevention 2009 Adult VaccinationCoverage NHIS [httpwww cdc govvaccinesstats-survnhis2009-nhishtm2010 [cited 2011 Jan 27]
3 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Validity of self-reported influenza and pneumococcalvaccination status among a cohort of hospitalized elderly inpatientsVaccine 2007 25(25)4775-4783
4 Nowalk MP Zimmerman RK Feghali J Missed opportunities for adultimmunization in diverse primary care office settings Vaccine 2004223457-3463
5 Nowalk MP Zimmerman RK Cleary SM Bruehlman RD Missedopportunities to vaccinate older adults in primary care J Am Board FamPract 2005 1820-27
6 Sandrine IS Meacutegard Y Overview of vaccination policies for the elderly inWestern European countries Aging Clin Exp Res 2009 21(3)210-215
7 Kohlhammer Y Schnoor M Schwartz M Raspe H Schaumlfer T Determinantsof influenza and pneumococcal vaccination in elderly people asystematic review Public Health 2007 121(10)742-751
8 Centers for Medicare and Medicaid Series H Medicare and Medicaidprograms conditions of participation immunization standards forhospitals long-term care facilities and home health agencies final rulewith comment period Fed Regist 2002 6761808-61814
9 Middleton DB Lin CJ Smith KJ et al Economic Evaluation of StandingOrder Programs for Pneumococcal Vaccination of Hospitalized ElderlyPatients Infect Control Hosp Epidemiol 2008 29(5)385-394
10 Dexter PR Perkins SM Maharry KS Jones K McDonald CJ Inpatientcomputer-based standing orders vs physician reminders to increase
influenza and pneumococcal vaccination rates J Am Med Assoc 20042922366-2371
11 Goebel LJ Neitch SM Mufson MA Standing Orders in an AmbulatorySetting Increases Influenza Vaccine Usage in Older People J Am GeriatrSoc 2005 53(6)1008-1010
12 Loughlin SM Mortazavi A Garey KW Rice GK Birtcher KK Pharmacist-managed vaccination program increased influenza vaccination rates incardiovascular patients enrolled in a secondary prevention lipid clinicPharmacotherapy 2007 27(5)729-733
13 Bond TC Patel PR Krishner J et al Association of Standing-Order PoliciesWith Vaccination Rates in Dialysis Clinics A US-Based Cross-sectionalStudy Am J Kidney Dis 2009 54(1)6-9
14 Task Force on Community Preventive Services Recommendationsregarding interventions to improve vaccination coverage in childrenadolescents and adults Am J Prev Med 2000 1892-96
15 Stone EG Morton SC Hulscher ME et al Interventions that increase useof adult immunization and cancer screening services a meta-analysisAnn Intern Med 2002 136(9)641-651
16 Centers for Disease Control and Prevention Use of standing ordersprograms to increase adult vaccination rates MMWR Morb Mortal WklyRep 2000 49(RR01)15-26
17 Health Care Financing Administration Evidence Report and Evidence-BasedRecommendations Interventions that Increase the Utilization of Medicare-Funded Preventive Service for Persons Age 65 and Older Baltimore MA HealthCare Financing Administration 1999
18 Szilagyi PG Shone LP Barth R et al Physician practices and attitudesregarding adult immunizations Prev Med 2005 40(2)152-161
19 Zimmerman R Albert S Nowalk M Yonas M Ahmed F Use of standingorders for adult influenza vaccination A national survey of primary carephysicians Am J Prev Med 2010 40(2)144-148
20 Yudin MH Salaripour M Sgro MD Acceptability and feasibility of seasonalinfluenza vaccine administration in an antenatal clinic setting J ObstetGynaecol Can 2010 32(8)745-748
21 Harder KM Cowan S Eriksen MB Krarup HB Christensen PB Universalscreening for hepatitis B among pregnant women led to 96vaccination coverage among newborns of HBsAg positive mothers inDenmark Vaccine 2011 29(50)9303-9307
22 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Missed opportunities to vaccinate a cohort of hospitalisedelderly with pneumococcal and influenza vaccines Vaccine 2007285146-5154
23 Jean-Pierre B Pierre OL Jean-Pierre M Willingness to vaccinate and to bevaccinated in adults Aging Clin Exp Res 2009 21(3)244-249
24 Yonas MA Nowalk MP Zimmerman RK Ahmed F Albert S Examiningstructural and clinical factors associated with implementation ofstanding orders for adult immunization J Healthc Qual 2011
25 Pathman DE Konrad TR Freed GL Freeman VA Koch GG The awareness-to-adherence model of the steps to clinical guideline compliance MedCare 1996 34(9)873-889
26 Rogers EM Diffusion of Innovations 3 edition New York Free Press 198327 Green LW Gottlieb NH Parcel GS Diffusion Theory Extended and
Applied In Advances in Health Education and Promotion Greenwich Editedby Ward WB Conn JAI Press 1987
28 Gielen AC McDonald EM The PRECEDE-PROCEED Planning Model InHealth Behavior and Health Education Theory Research and Practice 3edition Edited by Glanz K Lewis FM Rimer BK San Francisco Jossey-BassPublishers 1997359-383
29 Mouzoon ME Flor MM Greisinger AJ et al Improving InfluenzaImmunization in Pregnant Women and Healthcare Workers Am J ManagCare 2010 16(3)209-216
30 The Immunization Partnership [httpwwwimmunizeusaorgiz-champions] Accessed Jan 20 2012
31 Centers for Disease Control and Prevention Updated recommendationsfor prevention of invasive pneumococcal disease among adults usingthe 23-valent pneumococcal polysaccharide vaccine (PSV23) MorbMortal Wkly Rep 2010 59(34)1102-1106
32 Stewart A Cox M Rosenbaum S The Epidemiology of US ImmunizationLaw Translating CDC immunization guidelines into practice State lawsrelated to the use of standing orders covering immunization practice2008 [httpwww gwumcedusphhshealthpolicychsrpdownloads
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 9 of 10
CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-

and Medicaid Services (CMS) prohibited SOPs for allmedications until 2002 when CMS modified its regula-tions to allow SOPs for influenza vaccine and PPV [8]It is understandable that physicians who were unawareof the change in CMS regulations might not haveadopted consistent use of SOPs as reflected in our dataGiven the myriad recommendations and policies
aimed at primary preventive care including immuniza-tions how can a practice keep current One solution isfor the practice to have an immunization championsomeone to interpret and communicate changes in vac-cine policies and recommendations as they occur Pre-vious research confirms the importance of animmunization champion to improve vaccination ratesOne study that included explicit training of immuniza-tion nurses to serve as clinical champions boosted influ-enza vaccination coverage rates in pregnant womenfrom 25 to 374 in 2008-2009 [29] However it isdifficult to determine the specific value of immunizationchampions relative to other practice-level factorsbecause most interventions designed to boost vaccina-tion coverage include a variety of elements Our findingssuggest the particular value of champions for practicesthat have SOPs for both influenza vaccine and PPV Itwould useful to determine which staff makes the mosteffective immunization champion and what sort of train-ing is most appropriate In most cases champions arenurses but recent efforts suggest that even non-clinicalstaff such as receptionists or medical records staff canbe trained as immunization champions httpwwwimmunizeusaorgiz-champions[30] It remains unclearhow such duties will be added to job descriptions orqualifications and whether additional compensation isappropriateAccess to physician assistants or licensed nursing per-
sonnel was a significant correlate of SOPs for PPV asopposed to SOPs for influenza Physicians in practiceswith access to these more highly trained personnel weretwice as likely to have SOPs for PPV and influenza(Table 3) This association may be related to the com-plexity of PPV dosing and recommendations for indivi-duals with high-risk medical conditions [31] Somephysicians may feel comfortable allowing clinical staffwith more extensive education and training to deter-mine eligibility for PPV and administer vaccine as iscommon practice for nurses Conversely US state lawsvary regarding licensing of medical assistants [32] thesedifferences may result in concerns about medical assis-tants administering PPV under SOPs Anecdotally weheard reports of hesitation by medical assistants to useSOPs for PPV despite physician guidance and trainingusing a toolkit In contrast influenza vaccine is adminis-tered in many locales where a physician is not evenpresent
The presence of an electronic medical record (EMR)was similarly associated with SOPs for PPV as opposedto SOPs for influenza Again this association may be afunction of the complexity of PPV dosing and recom-mendations for individuals with high-risk medical condi-tions The EMR makes it easier for practitioners to trackimmunization histories and to flag patients eligible forvaccinationTeamwork is the essence of SOPs and thus the asso-
ciation between self-reported teamwork in the practiceand use of SOPs for PPV is not surprising Teamwork isalso a key aspect of successful implementation of thepatient-centered medical home and accountable careorganization Both are quality improvement models inwhich providing timely and appropriate preventive ser-vices such as vaccination is a critical element Programsto educate staff in vaccination may help to improve per-ceived self-efficacy stimulate innovation and fosterteamwork These programs include ldquoWhat worksrdquo (avail-able at httpwww2acdcgovvaccinesedwhatworksceasp and toolkits that facilitate use of SOPs httpwwwimmunizeorgstanding-orders and httpwwwImmuni-zationEdorgstandingordersWe conclude that practice-level factors are critical for
the adoption of more complex SOPs such as joint SOPsfor influenza and PPV The greater clinical complexityof PPV administration may require access to electronicmedical records and more highly trained auxiliary stafffor example as well as better coordination betweenstaff reflected in greater perceived teamworkStrengths of this research include a survey that is
national in scope with a high response rate for physicianparticipants The questionnaire was based on theoreticalmodels designed around physician adoption of vaccinesHowever surveys are subject to the limitations of self-report While the survey covered many correlates ofSOP use it may not have captured all relevant correlatesof SOP use Also we relied on a single physician toreport on each practice and may therefore underesti-mate variance in delivery of vaccinationsSOPs are underused but can have a great public
health impact For example SOPs may help mitigatedisparities in vaccination coverage in underserved popu-lations though we have not been able to identifyresearch in this area Further national efforts at clinicianand medical assistant education should be considered toensure that physicians are aware of current vaccinerecommendations and policies and that all clinical staffcan competently administer recommended vaccinesPractical toolkits are available to facilitate adoption ofSOPs in primary care practices Teamwork and animmunization champion can help empower clinical sup-port staff to administer vaccines using SOPs thus help-ing to reduce missed opportunities for vaccination
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 8 of 10
Additional material
Additional file 1 National Survey of Physicians about StandingOrders Programs for Adult Immunizations
AcknowledgementsThis study was supported by the Centers for Disease Control and Preventionand the Association for Prevention Teaching and Research Grant No 5 U50CD300-860-21 Its contents are the responsibility of the authors and do notnecessarily reflect the official views of the CDC or the APTR
Author details1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USA2Department of Family Medicine and Clinical Epidemiology School ofMedicine University of Pittsburgh Pittsburgh PA USA 3Centers for DiseaseControl and Prevention Atlanta GA USA
Authorsrsquo contributionsSA performed the statistical analysis and drafted the manuscript SA RZ TNMAY and FA conceived of the study and participated in developing thedesign of the research SA and TN coordinated the survey component Allauthors revised the manuscript critically for important intellectual contentAll authors read and approved the final manuscript
Competing interestsAt the time of data analyses Drs Zimmerman and Nowalk had researchfunding and consultancy with Medimmune Inc and research funding fromMerck Inc about HPV vaccine Dr Zimmerman also had research fundingfrom Sanofi
Received 9 October 2011 Accepted 20 March 2012Published 20 March 2012
References1 CDCNCHS NHIS Influenza vaccination in the past 12 months among
adults 18 years of age and over by age United States 1999-2009 2010[httpwww cdc givnchshuscontents2010htmfig18] [cited 2011 May10]Available from URL [httpwwwcdcgivnchshuscontents2010htmfig18]
2 Centers for Disease Control and Prevention 2009 Adult VaccinationCoverage NHIS [httpwww cdc govvaccinesstats-survnhis2009-nhishtm2010 [cited 2011 Jan 27]
3 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Validity of self-reported influenza and pneumococcalvaccination status among a cohort of hospitalized elderly inpatientsVaccine 2007 25(25)4775-4783
4 Nowalk MP Zimmerman RK Feghali J Missed opportunities for adultimmunization in diverse primary care office settings Vaccine 2004223457-3463
5 Nowalk MP Zimmerman RK Cleary SM Bruehlman RD Missedopportunities to vaccinate older adults in primary care J Am Board FamPract 2005 1820-27
6 Sandrine IS Meacutegard Y Overview of vaccination policies for the elderly inWestern European countries Aging Clin Exp Res 2009 21(3)210-215
7 Kohlhammer Y Schnoor M Schwartz M Raspe H Schaumlfer T Determinantsof influenza and pneumococcal vaccination in elderly people asystematic review Public Health 2007 121(10)742-751
8 Centers for Medicare and Medicaid Series H Medicare and Medicaidprograms conditions of participation immunization standards forhospitals long-term care facilities and home health agencies final rulewith comment period Fed Regist 2002 6761808-61814
9 Middleton DB Lin CJ Smith KJ et al Economic Evaluation of StandingOrder Programs for Pneumococcal Vaccination of Hospitalized ElderlyPatients Infect Control Hosp Epidemiol 2008 29(5)385-394
10 Dexter PR Perkins SM Maharry KS Jones K McDonald CJ Inpatientcomputer-based standing orders vs physician reminders to increase
influenza and pneumococcal vaccination rates J Am Med Assoc 20042922366-2371
11 Goebel LJ Neitch SM Mufson MA Standing Orders in an AmbulatorySetting Increases Influenza Vaccine Usage in Older People J Am GeriatrSoc 2005 53(6)1008-1010
12 Loughlin SM Mortazavi A Garey KW Rice GK Birtcher KK Pharmacist-managed vaccination program increased influenza vaccination rates incardiovascular patients enrolled in a secondary prevention lipid clinicPharmacotherapy 2007 27(5)729-733
13 Bond TC Patel PR Krishner J et al Association of Standing-Order PoliciesWith Vaccination Rates in Dialysis Clinics A US-Based Cross-sectionalStudy Am J Kidney Dis 2009 54(1)6-9
14 Task Force on Community Preventive Services Recommendationsregarding interventions to improve vaccination coverage in childrenadolescents and adults Am J Prev Med 2000 1892-96
15 Stone EG Morton SC Hulscher ME et al Interventions that increase useof adult immunization and cancer screening services a meta-analysisAnn Intern Med 2002 136(9)641-651
16 Centers for Disease Control and Prevention Use of standing ordersprograms to increase adult vaccination rates MMWR Morb Mortal WklyRep 2000 49(RR01)15-26
17 Health Care Financing Administration Evidence Report and Evidence-BasedRecommendations Interventions that Increase the Utilization of Medicare-Funded Preventive Service for Persons Age 65 and Older Baltimore MA HealthCare Financing Administration 1999
18 Szilagyi PG Shone LP Barth R et al Physician practices and attitudesregarding adult immunizations Prev Med 2005 40(2)152-161
19 Zimmerman R Albert S Nowalk M Yonas M Ahmed F Use of standingorders for adult influenza vaccination A national survey of primary carephysicians Am J Prev Med 2010 40(2)144-148
20 Yudin MH Salaripour M Sgro MD Acceptability and feasibility of seasonalinfluenza vaccine administration in an antenatal clinic setting J ObstetGynaecol Can 2010 32(8)745-748
21 Harder KM Cowan S Eriksen MB Krarup HB Christensen PB Universalscreening for hepatitis B among pregnant women led to 96vaccination coverage among newborns of HBsAg positive mothers inDenmark Vaccine 2011 29(50)9303-9307
22 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Missed opportunities to vaccinate a cohort of hospitalisedelderly with pneumococcal and influenza vaccines Vaccine 2007285146-5154
23 Jean-Pierre B Pierre OL Jean-Pierre M Willingness to vaccinate and to bevaccinated in adults Aging Clin Exp Res 2009 21(3)244-249
24 Yonas MA Nowalk MP Zimmerman RK Ahmed F Albert S Examiningstructural and clinical factors associated with implementation ofstanding orders for adult immunization J Healthc Qual 2011
25 Pathman DE Konrad TR Freed GL Freeman VA Koch GG The awareness-to-adherence model of the steps to clinical guideline compliance MedCare 1996 34(9)873-889
26 Rogers EM Diffusion of Innovations 3 edition New York Free Press 198327 Green LW Gottlieb NH Parcel GS Diffusion Theory Extended and
Applied In Advances in Health Education and Promotion Greenwich Editedby Ward WB Conn JAI Press 1987
28 Gielen AC McDonald EM The PRECEDE-PROCEED Planning Model InHealth Behavior and Health Education Theory Research and Practice 3edition Edited by Glanz K Lewis FM Rimer BK San Francisco Jossey-BassPublishers 1997359-383
29 Mouzoon ME Flor MM Greisinger AJ et al Improving InfluenzaImmunization in Pregnant Women and Healthcare Workers Am J ManagCare 2010 16(3)209-216
30 The Immunization Partnership [httpwwwimmunizeusaorgiz-champions] Accessed Jan 20 2012
31 Centers for Disease Control and Prevention Updated recommendationsfor prevention of invasive pneumococcal disease among adults usingthe 23-valent pneumococcal polysaccharide vaccine (PSV23) MorbMortal Wkly Rep 2010 59(34)1102-1106
32 Stewart A Cox M Rosenbaum S The Epidemiology of US ImmunizationLaw Translating CDC immunization guidelines into practice State lawsrelated to the use of standing orders covering immunization practice2008 [httpwww gwumcedusphhshealthpolicychsrpdownloads
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 9 of 10
CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-
Additional material
Additional file 1 National Survey of Physicians about StandingOrders Programs for Adult Immunizations
AcknowledgementsThis study was supported by the Centers for Disease Control and Preventionand the Association for Prevention Teaching and Research Grant No 5 U50CD300-860-21 Its contents are the responsibility of the authors and do notnecessarily reflect the official views of the CDC or the APTR
Author details1Department of Behavioral and Community Health Sciences GraduateSchool of Public Health University of Pittsburgh Pittsburgh PA USA2Department of Family Medicine and Clinical Epidemiology School ofMedicine University of Pittsburgh Pittsburgh PA USA 3Centers for DiseaseControl and Prevention Atlanta GA USA
Authorsrsquo contributionsSA performed the statistical analysis and drafted the manuscript SA RZ TNMAY and FA conceived of the study and participated in developing thedesign of the research SA and TN coordinated the survey component Allauthors revised the manuscript critically for important intellectual contentAll authors read and approved the final manuscript
Competing interestsAt the time of data analyses Drs Zimmerman and Nowalk had researchfunding and consultancy with Medimmune Inc and research funding fromMerck Inc about HPV vaccine Dr Zimmerman also had research fundingfrom Sanofi
Received 9 October 2011 Accepted 20 March 2012Published 20 March 2012
References1 CDCNCHS NHIS Influenza vaccination in the past 12 months among
adults 18 years of age and over by age United States 1999-2009 2010[httpwww cdc givnchshuscontents2010htmfig18] [cited 2011 May10]Available from URL [httpwwwcdcgivnchshuscontents2010htmfig18]
2 Centers for Disease Control and Prevention 2009 Adult VaccinationCoverage NHIS [httpwww cdc govvaccinesstats-survnhis2009-nhishtm2010 [cited 2011 Jan 27]
3 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Validity of self-reported influenza and pneumococcalvaccination status among a cohort of hospitalized elderly inpatientsVaccine 2007 25(25)4775-4783
4 Nowalk MP Zimmerman RK Feghali J Missed opportunities for adultimmunization in diverse primary care office settings Vaccine 2004223457-3463
5 Nowalk MP Zimmerman RK Cleary SM Bruehlman RD Missedopportunities to vaccinate older adults in primary care J Am Board FamPract 2005 1820-27
6 Sandrine IS Meacutegard Y Overview of vaccination policies for the elderly inWestern European countries Aging Clin Exp Res 2009 21(3)210-215
7 Kohlhammer Y Schnoor M Schwartz M Raspe H Schaumlfer T Determinantsof influenza and pneumococcal vaccination in elderly people asystematic review Public Health 2007 121(10)742-751
8 Centers for Medicare and Medicaid Series H Medicare and Medicaidprograms conditions of participation immunization standards forhospitals long-term care facilities and home health agencies final rulewith comment period Fed Regist 2002 6761808-61814
9 Middleton DB Lin CJ Smith KJ et al Economic Evaluation of StandingOrder Programs for Pneumococcal Vaccination of Hospitalized ElderlyPatients Infect Control Hosp Epidemiol 2008 29(5)385-394
10 Dexter PR Perkins SM Maharry KS Jones K McDonald CJ Inpatientcomputer-based standing orders vs physician reminders to increase
influenza and pneumococcal vaccination rates J Am Med Assoc 20042922366-2371
11 Goebel LJ Neitch SM Mufson MA Standing Orders in an AmbulatorySetting Increases Influenza Vaccine Usage in Older People J Am GeriatrSoc 2005 53(6)1008-1010
12 Loughlin SM Mortazavi A Garey KW Rice GK Birtcher KK Pharmacist-managed vaccination program increased influenza vaccination rates incardiovascular patients enrolled in a secondary prevention lipid clinicPharmacotherapy 2007 27(5)729-733
13 Bond TC Patel PR Krishner J et al Association of Standing-Order PoliciesWith Vaccination Rates in Dialysis Clinics A US-Based Cross-sectionalStudy Am J Kidney Dis 2009 54(1)6-9
14 Task Force on Community Preventive Services Recommendationsregarding interventions to improve vaccination coverage in childrenadolescents and adults Am J Prev Med 2000 1892-96
15 Stone EG Morton SC Hulscher ME et al Interventions that increase useof adult immunization and cancer screening services a meta-analysisAnn Intern Med 2002 136(9)641-651
16 Centers for Disease Control and Prevention Use of standing ordersprograms to increase adult vaccination rates MMWR Morb Mortal WklyRep 2000 49(RR01)15-26
17 Health Care Financing Administration Evidence Report and Evidence-BasedRecommendations Interventions that Increase the Utilization of Medicare-Funded Preventive Service for Persons Age 65 and Older Baltimore MA HealthCare Financing Administration 1999
18 Szilagyi PG Shone LP Barth R et al Physician practices and attitudesregarding adult immunizations Prev Med 2005 40(2)152-161
19 Zimmerman R Albert S Nowalk M Yonas M Ahmed F Use of standingorders for adult influenza vaccination A national survey of primary carephysicians Am J Prev Med 2010 40(2)144-148
20 Yudin MH Salaripour M Sgro MD Acceptability and feasibility of seasonalinfluenza vaccine administration in an antenatal clinic setting J ObstetGynaecol Can 2010 32(8)745-748
21 Harder KM Cowan S Eriksen MB Krarup HB Christensen PB Universalscreening for hepatitis B among pregnant women led to 96vaccination coverage among newborns of HBsAg positive mothers inDenmark Vaccine 2011 29(50)9303-9307
22 Skull SA Andrews RM Byrnes GB Kelly HA Nolan TM Brown GVCampbell DA Missed opportunities to vaccinate a cohort of hospitalisedelderly with pneumococcal and influenza vaccines Vaccine 2007285146-5154
23 Jean-Pierre B Pierre OL Jean-Pierre M Willingness to vaccinate and to bevaccinated in adults Aging Clin Exp Res 2009 21(3)244-249
24 Yonas MA Nowalk MP Zimmerman RK Ahmed F Albert S Examiningstructural and clinical factors associated with implementation ofstanding orders for adult immunization J Healthc Qual 2011
25 Pathman DE Konrad TR Freed GL Freeman VA Koch GG The awareness-to-adherence model of the steps to clinical guideline compliance MedCare 1996 34(9)873-889
26 Rogers EM Diffusion of Innovations 3 edition New York Free Press 198327 Green LW Gottlieb NH Parcel GS Diffusion Theory Extended and
Applied In Advances in Health Education and Promotion Greenwich Editedby Ward WB Conn JAI Press 1987
28 Gielen AC McDonald EM The PRECEDE-PROCEED Planning Model InHealth Behavior and Health Education Theory Research and Practice 3edition Edited by Glanz K Lewis FM Rimer BK San Francisco Jossey-BassPublishers 1997359-383
29 Mouzoon ME Flor MM Greisinger AJ et al Improving InfluenzaImmunization in Pregnant Women and Healthcare Workers Am J ManagCare 2010 16(3)209-216
30 The Immunization Partnership [httpwwwimmunizeusaorgiz-champions] Accessed Jan 20 2012
31 Centers for Disease Control and Prevention Updated recommendationsfor prevention of invasive pneumococcal disease among adults usingthe 23-valent pneumococcal polysaccharide vaccine (PSV23) MorbMortal Wkly Rep 2010 59(34)1102-1106
32 Stewart A Cox M Rosenbaum S The Epidemiology of US ImmunizationLaw Translating CDC immunization guidelines into practice State lawsrelated to the use of standing orders covering immunization practice2008 [httpwww gwumcedusphhshealthpolicychsrpdownloads
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 9 of 10
CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-

CDC_guidelines_translationpdf] Available from URL wwwgwumcedusphhshealthpolicyimmunizationreportscfm
Pre-publication historyThe pre-publication history for this paper can be accessed herehttpwwwbiomedcentralcom1471-22961322prepub
doi1011861471-2296-13-22Cite this article as Albert et al Standing orders for influenza andpneumococcal polysaccharide vaccination Correlates identified in anational survey of US Primary care physicians BMC Family Practice 20121322
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Albert et al BMC Family Practice 2012 1322httpwwwbiomedcentralcom1471-22961322
Page 10 of 10
- Abstract
-
- Background
- Method
- Results
- Discussion
- Conclusions
-
- Background
- Methods
-
- Sample
- Survey instrument
- Data processing and analyses
-
- Results
- Discussion
- Acknowledgements
- Author details
- Authors contributions
- Competing interests
- References
- Pre-publication history
-