
Sports-related sudden cardiac death in a competitive and a noncompetitive athlete population aged 12...
23
Author's Accepted Manuscript Sports Related sudden Cardiac Death in a Compe- titive and Non-competitive Athlete Population aged 12 49 years: Data from an unselected Nationwide study in Denmark Bjarke Risgaard MD, Bo Gregers Winkel MD, PHD, Reza Jabbari MD, Charlotte Glinge BM, Ole Ingemann-Hansen MD, PHD, Jørgen Lange Thomsen MD, DMSc, Gyda Lolk Ottesen MD, DMSc, Stig Haunsø MD, DMSc, Anders Gaarsdal Holst MD, PHD, Jacob Tfelt-Hansen MD, DMSc PII: S1547-5271(14)00557-8 DOI: http://dx.doi.org/10.1016/j.hrthm.2014.05.026 Reference: HRTHM5789 To appear in: Heart Rhythm Cite this article as: Bjarke Risgaard MD, Bo Gregers Winkel MD, PHD, Reza Jabbari MD, Charlotte Glinge BM, Ole Ingemann-Hansen MD, PHD, Jørgen Lange Thomsen MD, DMSc, Gyda Lolk Ottesen MD, DMSc, Stig Haunsø MD, DMSc, Anders Gaarsdal Holst MD, PHD, Jacob Tfelt-Hansen MD, DMSc, Sports Related sudden Cardiac Death in a Competitive and Non-competitive Athlete Population aged 12 49 years: Data from an unselected Nationwide study in Denmark, Heart Rhythm, http://dx.doi.org/10.1016/j. hrthm.2014.05.026 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting galley proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. www.elsevier.com/locate/buildenv
Transcript of Sports-related sudden cardiac death in a competitive and a noncompetitive athlete population aged 12...

Author's Accepted Manuscript
Sports Related sudden Cardiac Death in a Compe-titive and Non-competitive Athlete Population aged12�49 years: Data from an unselected Nationwidestudy in Denmark
Bjarke Risgaard MD, Bo Gregers Winkel MD, PHD,Reza Jabbari MD, Charlotte Glinge BM, OleIngemann-Hansen MD, PHD, Jørgen LangeThomsen MD, DMSc, Gyda Lolk Ottesen MD,DMSc, Stig Haunsø MD, DMSc, Anders GaarsdalHolst MD, PHD, Jacob Tfelt-Hansen MD, DMSc
PII: S1547-5271(14)00557-8DOI: http://dx.doi.org/10.1016/j.hrthm.2014.05.026Reference: HRTHM5789
To appear in: Heart Rhythm
Cite this article as: Bjarke Risgaard MD, Bo Gregers Winkel MD, PHD, Reza JabbariMD, Charlotte Glinge BM, Ole Ingemann-Hansen MD, PHD, Jørgen Lange ThomsenMD, DMSc, Gyda Lolk Ottesen MD, DMSc, Stig Haunsø MD, DMSc, Anders GaarsdalHolst MD, PHD, Jacob Tfelt-Hansen MD, DMSc, Sports Related sudden Cardiac Deathin a Competitive and Non-competitive Athlete Population aged 12�49 years: Data froman unselected Nationwide study in Denmark, Heart Rhythm, http://dx.doi.org/10.1016/j.hrthm.2014.05.026
This is a PDF file of an unedited manuscript that has been accepted for publication. As aservice to our customers we are providing this early version of the manuscript. Themanuscript will undergo copyediting, typesetting, and review of the resulting galley proofbefore it is published in its final citable form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers that applyto the journal pertain.
www.elsevier.com/locate/buildenv

1
Sports related sudden cardiac death in a competitive and non-competitive athlete
population aged 12−49 years:
Data from an unselected nationwide study in Denmark
Bjarke Risgaard, MD1,2*
; Bo Gregers Winkel, MD, PHD1,2
; Reza Jabbari, MD1,2
; Charlotte Glinge, BM1,2
,
Ole Ingemann-Hansen, MD, PHD3; Jørgen Lange Thomsen, MD, DMSc
4; Gyda Lolk Ottesen, MD, DMSc
5;
Stig Haunsø, MD, DMSc1,2,6
; Anders Gaarsdal Holst, MD, PHD1,2
; Jacob Tfelt-Hansen, MD, DMSc1,2
Affiliations: 1The Danish National Research Foundation Centre for Cardiac Arrhythmia (DARC), Copenhagen,
Denmark; 2Laboratory of Molecular Cardiology, Department of Cardiology, The Heart Centre, Copenhagen University
Hospital Rigshospitalet, Copenhagen, Denmark; 3Department of Forensic Medicine, Aarhus University, Aarhus,
Denmark; 4Institute of Forensic Medicine, University of Southern Denmark, Odense, Denmark; 5Department of
Forensic Medicine, University of Copenhagen, Copenhagen, Denmark; and 6Department of Medicine and Surgery,
Faculty of Health Science, University of Copenhagen, Copenhagen, Denmark
Wordcount: 4744
Conflict of interest
AGH is an employee of Novo Nordisk A/S, Søborg, Denmark.
*Corresponding author: Bjarke Risgaard, MD. Address for correspondence: Laboratory of Molecular Cardiology, The
Heart Centre, Copenhagen University Hospital, Rigshospitalet, 9312, Juliane Maries Vej 20, 2100 Copenhagen Ø.
Tel: (+45) 35 45 65 01 Fax: (+45) 35 45 65 00 Email: [email protected]
2
Abstract
Background: Preparticipation screening programs have been suggested to reduce the numbers of sports
related sudden cardiac deaths (SrSCD).
Objective: To identify and characterize all SrSCD aged 12−49 years and to address the difference in
incidence rates between competitive and non-competitive athletes.
Methods: All deaths in persons aged 12−49 years in 2007−2009 were included. Death certificates were
reviewed. History of previous admissions to hospital was assessed, discharge summaries, and autopsy reports
were read. Sudden cardiac deaths (SCD) and SrSCD cases were identified.
Results: In the 3-year period there were 881 SCD of which we identified 44 SrSCD. In non-competitive
athletes aged 12−35 years the incidence rate of SrSCD was 0.43 (95% CI: 0.16 to 0.94) per 100,000 athlete
person-years whereas it was 2.95 (95% CI: 1.95 to 4.30) in non-competitive athletes aged 36−49 years. In
competitive athletes the incidence rate of SrSCD was 0.47 (95% CI: 0.10 to 1.14) and 6.64 (95% CI: 2.86 to
13.1) per 100,000 athlete person-years in those aged 12−35 years and 36−49 years, respectively. The
incidence rate of SCD in the general population was 10.7 (95% CI: 10.0 to 11.5) per 100.000 person-years.
Conclusion: The incidence rates of SrSCD in non-competitive and competitive athletes are not different. The
study showed an increase in the incidence rate of SrSCD in persons aged 36−49 years in both non-
competitive and competitive athletes compared to those aged 12−35 years. Importantly, SCD in the general
population is much more prevalent than SrSCD in all age groups.
Key words: Sudden cardiac death; Athletes; epidemiology, preparticipation screening
Abbreviations
ARVC – Arrhythmogenic right ventricular cardiomyopathy
CAD – coronary artery disease
HCM – Hypertrophic cardiomyopathy
3
SCD – Sudden cardiac death
SrSCD – Sports related sudden cardiac death
SUD – Sudden unexplained death
Introduction
Sports-related sudden cardiac deaths (SrSCD) are tragic occurrences that receive significant media attention
and have become highly debated public health issues.(1) Several epidemiological studies on SrSCD in young
competitive athletes have estimated the incidence rate, the causes, and the proportion of these deaths that are
potentially preventable.(2–6) In this regard, it is heavily debated if preparticipation screening programs
prevent some of these deaths.(1,7) Data that favours such a strategy mainly comes from a prospective,
initially retrospective, Italian study in which it has been shown that preparticipation screening lowers the
incidence rate of SrSCD in young competitive athletes.(3) However, several other studies have suggested
that screening will be of limited value.(1,2,6,8,9) Today, preparticipation screening programs are
recommended by the European Society of Cardiology (10) and have been implemented on different levels in
many countries with the most extensive ones in Italy and Israel.(2,3)
According to the most frequently used definition, initially proposed by Maron and colleagues,(11) a
competitive athlete is a person who participates in individual sports or in an organized team that requires
systematic training and regular competition against others. On the other hand, non-competitive athletes
participates in a variety of recreational sports activities within a wide range of exercise levels ranging from
moderate to vigorous activity.(7) Until now, studies on SrSCD have mainly been conducted on competitive
athletic populations aged less than 35 years(3–6,8,12). While studies on SrSCD during non-competitive
athletic activities remain sparse(13,14), it has been shown that the risk of cardiac arrest is transiently
increased during vigorous exercise, but that habitual exercise is associated with an overall decreased
mortality.(15)
To our knowledge, only one study has prospectively evaluated the incidence rate of all sports related sudden
deaths (SD).(12) To fully understand the epidemiology of sports related SrSCD, several issues still need to
be addressed. First, the incidence rate of SrSCD in the non-competitive athletic population is unknown.

4
Second, it is not known whether non-competitive athletes are in a higher risk of SrSCD than competitive
athletes. Third, studies on SrSCD in competitive athletes have mainly been conducted on young individuals,
and incidence rates for the population aged >35 years is largely unknown.
We have previously identified all sudden cardiac deaths (SCD) including all SrSCD in competitive athletes
aged 12-35 years in Denmark 2000-2006.(6,16) The aim of this first nationwide study on persons aged
12−49 years was to identify and characterize all SrSCD and to address the difference in incidence rates
between competitive and non-competitive athletes.
Methods
Study design
The methods used for this study have previously been described in detail.(17) In short, this is a nationwide
retrospective study using the availability of all death certificates, the registration of all in- and outpatient
activity in Danish hospitals and emergency rooms together with access to all medical records and autopsy
reports. We included all deaths in a 3-year period (2007−2009) in persons aged 12−49 years. The study was
approved by the local ethics committee (H−KF−272484), The Danish Data Protection Agency
(2011−41−5767), and the Danish National Board of Health (7−505−29−58/6).
Danish registries:
All Danish citizens have a unique and personal civil registration number which can be linked to national
registries on an individual level. The Danish National Patient Registry contains information on all in- and
outpatient activities in Denmark since 1978. Diagnoses are coded according to the corresponding
International Classification of Diseases, the 8th revision (ICD-8) until 1993 and since 1994 the 10
th revision
(ICD-10) has been used.
Review of death certificates:

5
Death certificates were read independently by two physicians in order to identify deaths that were sudden
and unexpected. In case of disagreement a consensus were reached after re-evaluating the circumstances
surrounding the death, including a review of previous medical history which was taken into account in every
single case. Danish death certificates are informative and suitable to identify sudden unexpected deaths as
they have a supplemental information field (see supp. Data, Winkel et. al (16)). This field contains
information describing circumstances surrounding the death including interviews with eyewitnesses and
relatives, previous medical conditions, an external examination of the body, and the preliminary conclusion
before autopsy. This field is mandatory in all medico-legal external examinations (external examinations),
including cases in which it is decided not to conduct an autopsy. The Danish Death certificates can only be
issued by a medical doctor. In cases where citizens or patients are found dead and/or the death is sudden and
unexpected, external examinations are mandatory by law. Information from these examinations can be found
in the supplemental information field on the Danish death certificate. Due to this great level of detail, the
Danish death certificates are highly suitable to identify cases of sudden unexpected death during sports.
Discharge summaries:
Discharge summaries were available through an electronic hospital records system. We had access to
information describing the time surrounding the death, including a description of the treatment and
management in the emergency room or hospital department. Discharge summaries were also available from
the prehospital trauma and emergency doctors.
Conduct of autopsies:
In Denmark there are three forensic departments conducting around 1500 autopsies per year. All forensic
autopsies are supervised by another forensic pathologist and follow a protocol in which all organs are
thoroughly examined. Toxicology screens are performed in unexplained adolescent and adult cases of
sudden unexpected death. Cardiac pathologists are available if deemed necessary.
Definitions

6
We defined the sudden unexpected death as the sudden, natural unexpected death; in witnessed cases as an
acute change in cardiovascular status with time to death being <1 h and in unwitnessed cases as a person last
seen alive and functioning normally <24 h before being found dead.
Sudden cardiac death (SCD) in autopsied cases was defined as the natural unexpected death of unknown or
cardiac cause; in witnessed cases as an acute change in cardiovascular status with time to death being <1 and
in unwitnessed cases as a person last seen alive and functioning normally <24 h before being found
dead.(16–19)
Autopsied SCD was subdivided in two groups: 1) Explained SCD, in which a cardiac cause of death was
established and 2) Sudden unexplained death (SUD), where causes of death after autopsy remained
unknown.
In non-autopsied deaths the same criteria were used in cases presumed to be of cardiac origin based on the
circumstances relating to the death including all information from death certificates and discharge
summaries. Non-autopsied cases with no competing causes of death were considered to be of cardiac origin.
SrSCD was defined as a SCD occurring during or within 1 hour after moderate- to high-intensity exercise.
Using all the information available, we subdivided SrSCD into whether the deceased was considered a
competitive or non-competitive athlete. The deceased was considered a competitive athlete if he or she did
moderate to high intensity sports on a regular level and took part in competitions. For the purpose of this
study, a non-competitive athlete was defined as a person not participating in competitions, but who did
moderate to high intensity sports on a regular level in the months prior to death.
Media search
To apply a method used by others when identifying SrSCD, an additional extensive retrospective media
search was performed as a supplement to the main approach. The Danish media surveillance database
Infomedia (www.infomedia.dk), a database of approximately 400 printed, 2,200 web-based, and the major
radio and television Danish media, was used.
Sport activities in the general population
7
To estimate the size of the background population performing competitive and non-competitive sports
activities, on a regular level (the denominator), we used data from the Danish National Institute of Public
Health.(20) They conducted, in collaboration with the five regions of Denmark, the Ministry of Interior and
Public Health, a major study “How are you?” from 2010 in which they, among other things, investigated the
occurrence of physical activity in Denmark. Through questionnaires they collected information on physical
activity throughout the country from persons aged 16 years and above.
The respondents were asked to choose one of the following categories fitting their daily activity level the
best; 1) Doing hard exercise at a competition level regularly several times a week, 2) Doing recreational
sports or hard physical demanding work at least 4 hours a week, 3) Walking, biking, or doing other less
demanding recreation sports at least 4 hours a week, or 4) Reading, watching television or doing other
sedentary activities. All data were stratified on age, gender, geographic area, education, civil status as well as
ethnicity and weighted for non-response by statistic Denmark.(21)
For the purpose of this study, respondents choosing category one was considered competitive athletes, and
respondents choosing category two was considered non-competitive athletes. As the age range in the “How
are you?” study not matched ours, the assumption was made, that we could extrapolate information from the
population aged 16−49 years to the population aged 12−49 years.
Cardiac symptoms prior to death
We defined prodromal symptoms as symptoms in the hours to minutes leading up to the death and
antecedent symptoms as symptoms in the years to days leading up to the death. Previous contacts to general
practitioners with cardiac symptoms were investigated by collecting all records as previously described in
detail.(22)
Statistical analysis
All calculations and data analysis were performed with the use of Stata software package (StataCorp,
Collage Station, Texas, version 11.0). Incidence rates were calculated using the mean age group population
as a denominator. Confidence intervals for incidence rates were calculated using the Poisson distribution.

8
Sensitivity analysis was carried out using autopsied cases only. Categorized nominal data were compared
using the chi-square test. If any cell values were <5, the Fisher exact test was used. Medians were compared
using the Wilcoxon rank-sum test. We considered a two sided p-value <0.05 to be statistically significant.
Results
Review of death certificates
In the study period, Denmark had a mean population of 5.48 million inhabitants, of whom, 2.73 million were
aged 12−49 years equalling 8.20 million person-years for the three year study period. From 2007−2009 there
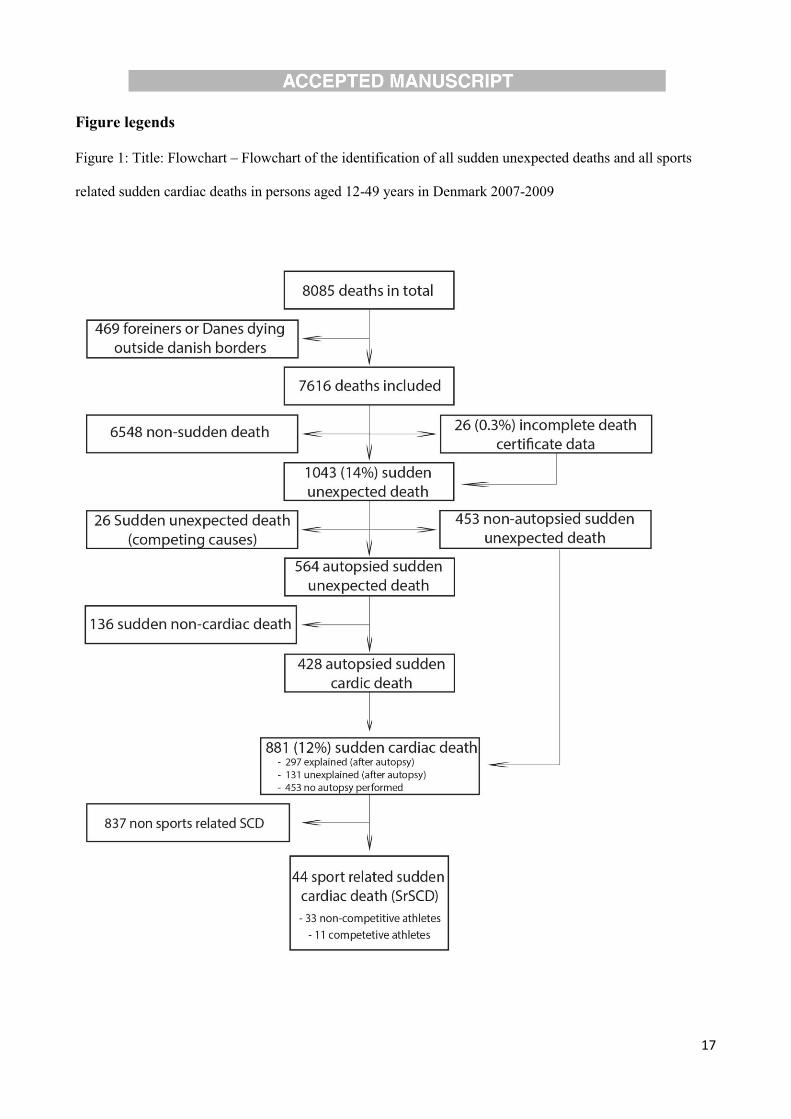
were 8085 deaths among persons aged 12−49 years. There were 7616 death certificates issued during this
period. The 469 death certificates missing represented foreigners or Danes dying outside Danish borders.
Twenty-six (<1%) cases were initially excluded due to incomplete data on the death certificate (figure 1).
Media search
By searching the national media database through 2007−2009, we identified and read 580 relevant articles.
The following search query was used (in Danish); Cardiac arrest (258 hits), Cardiac death (86 hits), Sports
death (11 hits), Sudden death (115 hits), and drop dead (110 hits). We identified 11 SrSCD occurring outside
Danish borders, and 7 cases inside Danish borders. Five of these 7 cases were not included in this study due
to successful resuscitation (n = 2), and age >49 years (n = 3).
Sports related sudden cardiac death population
From the review of the death certificates, registry information on previous medical history, discharge
summaries, and the media search we identified 881 SCD of which 44 cases were SrSCD. Thirty-three of the
44 SrSCD occurred in a non-competitive athlete whereas 11 cases occurred in a competitive athlete (figure
2). Of the 2 cases identified through media search, one was identified from the review of the death
certificates. The remaining case was identified and included after review of discharge summaries among the
26 cases with incomplete death certificate data (page 2 of death certificate missing, figure 1.
Sport activities in Denmark
9
The Danish National Institute of Public Health received 172,639 questionnaires (60% of those invited).
Based on 96,075 questionnaires, received from persons aged 16−49 years, we estimated the size of the non-
competitive and competitive athlete population in the background population. Overall, 8.9% and 28.1% were
classified as competitive and non-competitive athletes, respectively. This equals to 730,166 competitive
athletic person-years and 2,305,355 non-competitive athletic person-years for the 3-year study period (table
1).
Incidence rates
In persons aged 12−49 years we report an incidence rate of SrSCD in the general population of 0.54 (95%
confidence interval [CI]: 0.39 to 0.72) per 100,000 person-years. The incidence rate of SCD in the general
population was 10.7 (95% CI: 10.0 to 11.5) using the same methodology.
In non-competitive athletes aged 12−35 years the incidence rate of SrSCD was 0.43 (95% CI: 0.16 to 0.94)
per 100,000 athlete person-years whereas it was 2.95 (95% CI: 1.95 to 4.30) in those aged 36-49 years. In
competitive athletes the incidence rate of SrSCD was 0.47 (95% CI: 0.10 to 1.14) and 6.64 (95% CI: 2.86 to
13.1) per 100,000 athlete person-years in those aged 12−35 years and 36-49 years, respectively.
The incidence rate of SCD in the general population was 3.15 (95% CI: 2.67 to 3.69) per 100.000 person-
years in those aged 12−35 years and it was 21.7 (95% CI: 20.1-23.4) per 100.000 person-years in those 36 to
49 years (table 1).
Characterisation of SrSCD in competitive and non-competitive athletes
Forty-four cases of SrSCD were identified in the 3-year study period with a median of 16 cases per year
(range 12−16). The median age was 41.5 years (range 12−49 years, mean 38 years) and there were a marked
male predominance (n=41, 93%) (See clinical characteristics in table 2 and table 3).
The predominant sport was running (n=17) followed by cycling (n=13). In 33 out of 44 (75%) cases, death
occurred during non-competitive athlete activities. In 30 out of 44 (68%) cases death occurred in a public
area; in 33 of 44 (75%) cases death was witnessed. Prodromal symptoms were observed in 16 out of 33
(48%) witnessed cases, and antecedent symptoms were reported in 21 out of 44 (47%) cases.

10
An autopsy was conducted in 35 of 44 cases (autopsy ratio 80%). After review of the autopsy reports, 15
deaths were found to be caused by coronary artery disease (CAD), 5 were caused by arrhythmogenic right
ventricular cardiomyopathy (ARVC), 4 were caused by hypertrophic heart (HH), 4 were sudden and
unexplained (SUD), 2 were caused by myocarditis, and 1 was caused by each of the following: valve disease,
malformation of coronary artery, hypertrophic cardiomyopathy (HCM), congenital heart disease, and non-
concentric hypertrophy of left ventricle. In the 4 cases of HH, left ventricular hypertrophy was found, but no
definite diagnoses of HCM could be made as the histopathology showed no signs of disarray of the
myofibrils. In supplemental material, see comparisons of SrSCD in competitive and non-competitive athletes
as well as macroscopic and histological definitions.
Discussion
Using death certificates, registry entries, discharge summaries, and a media search along with autopsy
reports we have conducted a study on SrSCD in Denmark 2007−2009 in the age group 12-49 years. The aim
was to identify and characterize all SrSCD and to address the difference in incidence rates between
competitive and non-competitive athletes. We found 44 SrSCD of which 33 deaths occurred in a non-
competitive athlete. This equals an overall incidence rate of SrSCD in the general population of 0.54 per
100,000 person-years. In the non-competitive and competitive athlete populations the incidence rate of
SrSCD was 1.43 and 1.51 per 100,000 athlete person-years, respectively. In contrast, the incidence rate of
SCD in the general population was 10.7 per 100,000 person-years.
Risk of SrSCD during sports
There is an on-going debate whether competitive athletes are at increased risk of SrSCD, but also whether
recreational sport activities confer an increased risk.(12,14,15,23,24) Physical activity may be regarded as a
“two-edged sword” as vigorous exercise acutely increases the risk of SCD,(25) while physical activity in the
long-term may offer protection against several cardiovascular diseases.(23,26)
11
In France, it has recently prospectively been shown that SD during sports more often occur in young
competitive athletes compared to young non-competitive participants (0.98 vs. 0.22 per 100,000 person-
years).(12) However, although prospective in design, Marijon and colleagues calculated the incidence rates
for non-competitive athletes using the general population as the denominator. As mentioned by the authors
themselves, they had variability in the reported incidence rates throughout the country, and this might be
explained by some degree of underreporting.
We find that SrSCD in Denmark is uncommon. In young competitive athletes aged 12−35 years, we report a
very low incidence rate of 0.47 per 100,000 athlete person-years. This is lower than we have previously
reported in Denmark (1.21 per 100,000), but also lower than Minnesota (0.93 per 100,000), the Veneto
region (0.87 per 100,000), France (0.98 per 100,000) and in the entire United States (0.61 per 100,000).(3–
6,8,12) In competitive athletes aged 36-49 years there is a significantly higher incidence rate of SrSCD
reaching 6.64 per 100.000 person-years (table 1). To our knowledge, incidence rates of SrSCD in competitive
athletes have not previously been reported in this age group. In young non-competitive athletes, we also
report a significantly higher incidence rate of SrSCD in those aged 36−49 years compared to those aged 12-
35 years; 2.95 vs. 0.43 per 100.000 athlete person-years. It is noteworthy, that the incidence rate of SCD in
the general population was much higher reaching 3.15 per 100.000 person-years in those aged 12−35 years
and 21.7 per 100.000 person-years in those aged 36−49 years. Like previous studies, we find a male
predominance.(6,27)
Preparticipation screening programs
In order to reduce the burden of SrSCD in competitive athletes, there has been an increasing focus on the
most realistic and optimal strategy for mass preparticipation screening programs. On one side the Italian
investigators have implemented and promoted nationally mandated screening programs of all athletes with
routine electrocardiograms (ECGs) and a medical examination. In the Veneto region they have shown that
after the implementation of the mandatory preparticipation screening program, launched in the 1980s, the
incidence rate of SrSCD in the competitive athletes have declined remarkably.(3) On the other hand the

12
American Heart Association have underscored the many obstacles in administering a massive and expensive
program with little or doubtful effect.(28,29)
Even though preparticipation screening programs has been debated for several years, knowledge on
outcomes, risks and benefits of screening, and cost efficiency remain incomplete.(1) In Denmark, it has
recently been proposed that screening of competitive athletes probably will be of limited value, and
screening is not recommended by the Danish Society of Cardiology.(6,30) That is, no systematic screening
of athletes has been in place during or before the study period. However, due to requirements from, for
example, the Union of European Football Associations preparticipation screening of a small group of athletes
has been carried out in the study period.
To determine whether mass preparticipation screening should be recommended, we decided to measure, on a
nationwide basis, the incidence rate of SrSCD in non-competitive and competitive athletes aged 12-49. This
has not been done before. Typically, pre-participation screening programs are only available to those young
people who choose to be involved in competitive sports. However, the current results suggest that being a
non-competitive athlete confers the same risk of SrSCD. Hence, it is questionable whether these programs, if
recommended, only should be available to those who choose to do sports on a competitive level.
Furthermore, the current findings suggest that SCD in the general population is much more common than
SrSCD and it might be argued that it would be ethically unacceptable to screen only those participating in
sports and not the general population.(31)
We believe that the present study indicate that screening probably will be of limited value. Most
preparticipation programs are only available to those who are young, and those who choose to do
competitive sports, which cannot, in our point of view, be ethically acceptable. Furthermore and importantly,
the present study indicates that the majority of these deaths could not have been prevented by screening with
an ECG and a physical examination. That is, we believe that only 12 of these cardiac diseases would be
potentially detectable (ARVC [5], HH [4], valve disease [1], HCM [1], congenital heart disease [1]).
13
We found that prodromal symptoms were observed in 16 out of 33 (48%) witnessed cases, and antecedent
symptoms were reported in 21 out of 44 (46%) cases, suggesting that raising awareness on symptoms during
sport among athletes may present an alternative strategy for preventions of SrSCD.
Limitation
It is a limitation that the study was retrospective. We used data from questionnaires from the Danish
National Institute of Public Health, to estimate the non-competitive and competitive athlete background
population in Denmark. As the age range not matched ours, the assumption was made, that we could
extrapolate information from the population aged 16−49 years to the population aged 12−49 years.
Furthermore, the assumption was made that the information from this survey from 2010 could be
extrapolated to the years 2007−2009. The present study does not provide any insight into arrhythmia
mechanisms of a SrSCD. It is a limitation that 26 (0.3%) death certificates were incomplete. As shown in the
sensitivity analysis, lack of autopsies brings some uncertainty into estimates of the SrSCD incidence rates.
Not all SrSCD cases were evaluated by a pathologist with expertise in sports-cardiology.
To conclude, the present study suggests that preparticipation screening will be of limited value, and probably
ethically unacceptable, if only provided to those (young people) who choose to be involved in competitive
sports. Cardiac symptoms prior to death are often found, suggesting that raising awareness on symptoms
during sport among athletes may present an alternative strategy for preventions of SrSCD.
Funding Sources
This work was supported by the Danish National Research Foundation Centre for Cardiac Arrhythmia
(DARC), University of Copenhagen, Copenhagen, Denmark; Laboratory of Molecular Cardiology, The
Heart Centre, Department of Cardiology, University Hospital Rigshospitalet, Copenhagen, Denmark; The
John and Birthe Meyer Foundation; The Danish Heart Foundation (12-04-R91-A3790-22689); The Research
Fund of Rigshospitalet, Copenhagen University Hospital.

14
Acknowledgement
The Danish Health Profile 2010 was funded by The Capital Region, Region Zealand, The South Denmark
Region, The Central Denmark Region, The North Denmark Region, The Danish Ministry of Interior and
Health, and the National Institute of Public Health, University of Southern Denmark.
References
1. Link MS, Estes NAM 3rd. Sudden cardiac death in the athlete: bridging the gaps between evidence, policy, and practice. Circulation. 2012;125:2511–2516.
2. Steinvil A, Chundadze T, Zeltser D, Rogowski O, Halkin A, Galily Y, Perluk H, Viskin S. Mandatory electrocardiographic screening of athletes to reduce their risk for sudden death proven fact or wishful thinking? J Am Coll Cardiol. 2011;57:1291–1296.
3. Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G. Trends in Sudden Cardiovascular Death in Young Competitive Athletes After Implementation of a Preparticipation Screening Program. JAMA: The Journal of the American Medical Association. 2006;296:1593 –1601.
4. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden Deaths in Young Competitive Athletes. Circulation. 2009;119:1085 –1092.
5. Corrado D, Basso C, Rizzoli G, Schiavon M, Thiene G. Does sports activity enhance the risk of sudden death in adolescents and young adults? J Am Coll Cardiol. 2003;42:1959–1963.
6. Holst AG, Winkel BG, Theilade J, Kristensen IB, Thomsen JL, Ottesen GL, Svendsen JH, Haunsø S, Prescott E, Tfelt-Hansen J. Incidence and etiology of sports-related sudden cardiac death in Denmark--implications for preparticipation screening. Heart Rhythm. 2010;7:1365–1371.
7. Corrado D, Schmied C, Basso C, Borjesson M, Schiavon M, Pelliccia A, Vanhees L, Thiene G. Risk of sports: do we need a pre-participation screening for competitive and leisure athletes? Eur Heart J. 2011;32:934–944.
8. Maron BJ, Haas TS, Doerer JJ, Thompson PD, Hodges JS. Comparison of U.S. and Italian experiences with sudden cardiac deaths in young competitive athletes and implications for preparticipation screening strategies. Am J Cardiol. 2009;104:276–280.
9. Roberts WO, Stovitz SD. Incidence of sudden cardiac death in Minnesota high school athletes 1993-2012 screened with a standardized pre-participation evaluation. J Am Coll Cardiol. 2013;62:1298–1301.
10. Corrado D, Pelliccia A, Bjørnstad HH, Vanhees L, Biffi A, Borjesson M, Panhuyzen-Goedkoop N, Deligiannis A, Solberg E, Dugmore D, Mellwig KP, Assanelli D, Delise P, van-Buuren F, Anastasakis A, Heidbuchel H, Hoffmann E, Fagard R, Priori SG, Basso C, Arbustini E,

15
Blomstrom-Lundqvist C, McKenna WJ, Thiene G. Cardiovascular pre-participation screening of young competitive athletes for prevention of sudden death: proposal for a common European protocol. Consensus Statement of the Study Group of Sport Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J. 2005;26:516–524.
11. Maron BJ, Chaitman BR, Ackerman MJ, Bayés de Luna A, Corrado D, Crosson JE, Deal BJ, Driscoll DJ, Estes NAM 3rd, Araújo CGS, Liang DH, Mitten MJ, Myerburg RJ, Pelliccia A, Thompson PD, Towbin JA, Camp SP Van. Recommendations for physical activity and recreational sports participation for young patients with genetic cardiovascular diseases. Circulation. 2004;109:2807–2816.
12. Marijon E, Tafflet M, Celermajer DS, Dumas F, Perier M-C, Mustafic H, Toussaint J-F, Desnos M, Rieu M, Benameur N, Heuzey J-Y Le, Empana J-P, Jouven X. Sports-related sudden death in the general population. Circulation. 2011;124:672–681.
13. Whittington RM, Banerjee A. Sport-related sudden natural death in the City of Birmingham. J R Soc Med. 1994;87:18–21.
14. Thompson PD, Funk EJ, Carleton RA, Sturner WQ. Incidence of death during jogging in Rhode Island from 1975 through 1980. JAMA. 1982;247:2535–2538.
15. Siscovick DS, Weiss NS, Fletcher RH, Lasky T. The incidence of primary cardiac arrest during vigorous exercise. N Engl J Med. 1984;311:874–877.
16. Winkel BG, Holst AG, Theilade J, Kristensen IB, Thomsen JL, Ottesen GL, Bundgaard H, Svendsen JH, Haunsø S, Tfelt-Hansen J. Nationwide study of sudden cardiac death in persons aged 1-35 years. Eur Heart J. 2011;32:983–990.
17. Risgaard B, Winkel B, Jabbari R, Behr ER, Ingemann-Hansen O, Thomsen JL, Ottesen GL, Gislason GH, Bundgaard H, Haunsø S, Holst AG, Tfelt-Hansen J. The burden of sudden cardiac death in persons aged 1-49 years - a nationwide study in Denmark. Circ Arrhythm Electrophysiol. 2014;Accepted for publication.
18. Kong MH, Fonarow GC, Peterson ED, Curtis AB, Hernandez AF, Sanders GD, Thomas KL, Hayes DL, Al-Khatib SM. Systematic review of the incidence of sudden cardiac death in the United States. J Am Coll Cardiol. 2011;57:794–801.
19. Margey R, Roy A, Tobin S, O’Keane CJ, McGorrian C, Morris V, Jennings S, Galvin J. Sudden cardiac death in 14- to 35-year olds in Ireland from 2005 to 2007: a retrospective registry. Europace. 2011;13:1411–1418.
20. Statistik [Internet]. [cited 2013 Apr 17]. Available from: http://www.si-folkesundhed.dk/Statistik.aspx

16
21. Danmarks Statistik [Internet]. 2013 [cited 2013 Mar 4]. Available from: http://www.dst.dk/da/
22. Jabbari R, Risgaard B, Holst AG, Nielsen JB, Glinge C, Engstrøm T, Bundgaard H, Svendsen JH, Haunsø S, Winkel BG, Tfelt-Hansen J. Cardiac symptoms before sudden cardiac death caused by coronary artery disease: a nationwide study among young Danish people. Heart. 2013;99:938–943.
23. Albert CM, Mittleman MA, Chae CU, Lee IM, Hennekens CH, Manson JE. Triggering of sudden death from cardiac causes by vigorous exertion. N Engl J Med. 2000;343:1355–1361.
24. Tunstall Pedoe DS. Marathon cardiac deaths : the london experience. Sports Med. 2007;37:448–450.
25. Maron BJ. The paradox of exercise. N Engl J Med. 2000;343:1409–1411.
26. Lemaitre RN, Siscovick DS, Raghunathan TE, Weinmann S, Arbogast P, Lin DY. Leisure-time physical activity and the risk of primary cardiac arrest. Arch Intern Med. 1999;159:686–690.
27. Marijon E, Bougouin W, Périer M-C, Celermajer DS, Jouven X. Incidence of sports-related sudden death in France by specific sports and sex. JAMA. 2013;310:642–643.
28. Maron BJ, Thompson PD, Ackerman MJ, Balady G, Berger S, Cohen D, Dimeff R, Douglas PS, Glover DW, Hutter AM Jr, Krauss MD, Maron MS, Mitten MJ, Roberts WO, Puffer JC, American Heart Association Council on Nutrition, Physical Activity, and Metabolism. Recommendations and considerations related to preparticipation screening for cardiovascular abnormalities in competitive athletes: 2007 update: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: endorsed by the American College of Cardiology Foundation. Circulation. 2007;115:1643–1455.
29. Maron BJ, Thompson PD, Puffer JC, McGrew CA, Strong WB, Douglas PS, Clark LT, Mitten MJ, Crawford MH, Atkins DL, Driscoll DJ, Epstein AE. Cardiovascular preparticipation screening of competitive athletes. A statement for health professionals from the Sudden Death Committee (clinical cardiology) and Congenital Cardiac Defects Committee (cardiovascular disease in the young), American Heart Association. Circulation. 1996;94:850–856.
30. Dansk Cardiologisk Selskab - Holdningspapirer [Internet]. [cited 2013 Jun 12]. Available from: http://www.cardio.dk/rapporter/holdningspapir-menu
31. Maron BJ. Diversity of views from Europe on national preparticipation screening for competitive athletes. Heart Rhythm. 2010;7:1372–1373.
17
Figure legends
Figure 1: Title: Flowchart – Flowchart of the identification of all sudden unexpected deaths and all sports
related sudden cardiac deaths in persons aged 12-49 years in Denmark 2007-2009
18
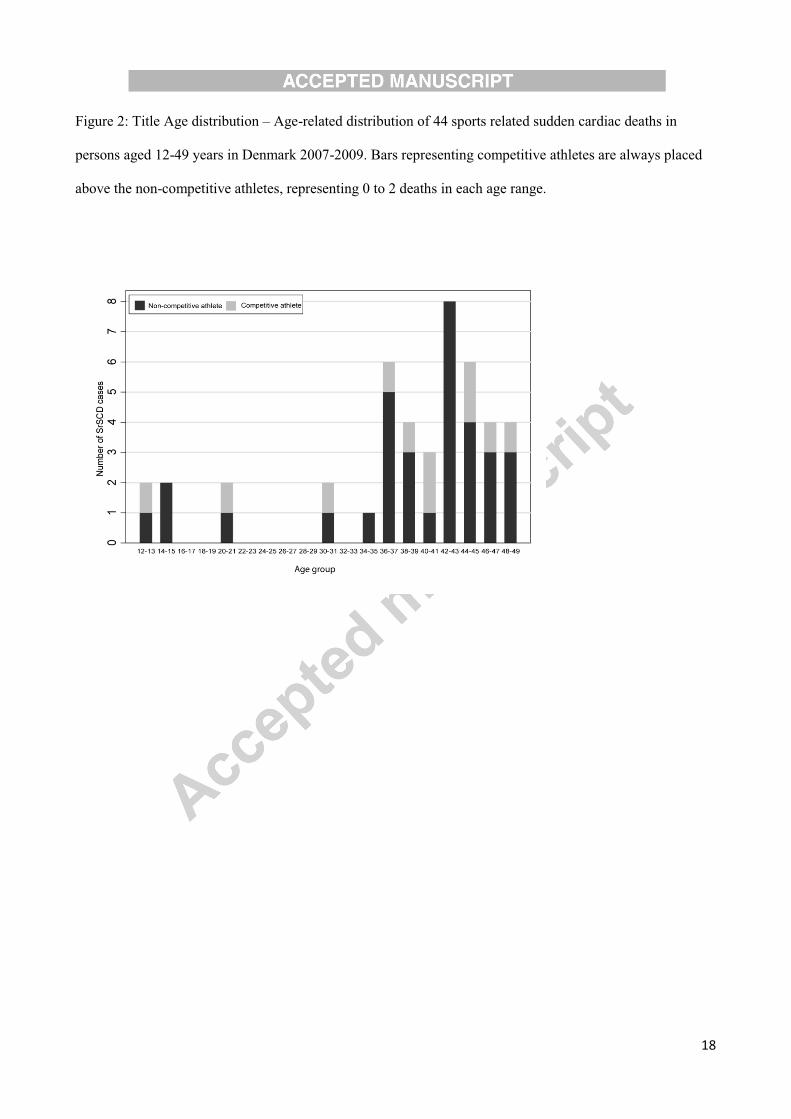
Figure 2: Title Age distribution – Age-related distribution of 44 sports related sudden cardiac deaths in
persons aged 12-49 years in Denmark 2007-2009. Bars representing competitive athletes are always placed
above the non-competitive athletes, representing 0 to 2 deaths in each age range.

19
Tables
Table 1: Sports-related sudden cardiac death by different age groups in Denmark 2007-2009
*SCD, sudden cardiac death; †SrSCD, sports related sudden cardiac death;
Age group (years) 12-49 12-35 36-49
SrSCD† cases (n) 44 9 35
Of whom were competitive athletes (n) 11 3 8
Age group population, in thousands 2,735 1,618 1,116
Active competitive athletes* 8.9% 13.2% 3.6%
Active non-competitive athletes* 28.1% 28.7% 27.3%
Incidence rates per 100.000 person-years
(denominator) (95% CI) (95% CI) (95% CI)
SCD* (general population) 10.7 (10.0-11.5)
3.15 (2.67-
3.69) 21.7 (20.1-23.4)
SrSCD† (general population) 0.54 (0.39-0.72)
0.19 (0.08-
0.35) 1.05 (0.73-1.45)
Non-competitive athletes (non-competitive athletes) 1.43 (0.99-2.01) 0.43 (0.16-
0.94) 2.95 (1.95-4.30)
Competitive athletes (competitive athletes) 1.51 (0.75-2.71) 0.47 (0.10-
1.14) 6.64 (2.86-13.1)
Sensitivity analyses: Incidence rates per 100,000
person-years (denominator)
Autopsied cases only:
Non-competitive athletes (non-competitive
athletes) 1.08 (0.6-2.5)
0.43 (0.16-
0.94) 2.08 (2.3-12.0)
Competitive athletes (competitive athletes) 1.37 (0.7-1.6) 0.47 (0.10-
1.14) 5.81 (1.3-3.3)

20
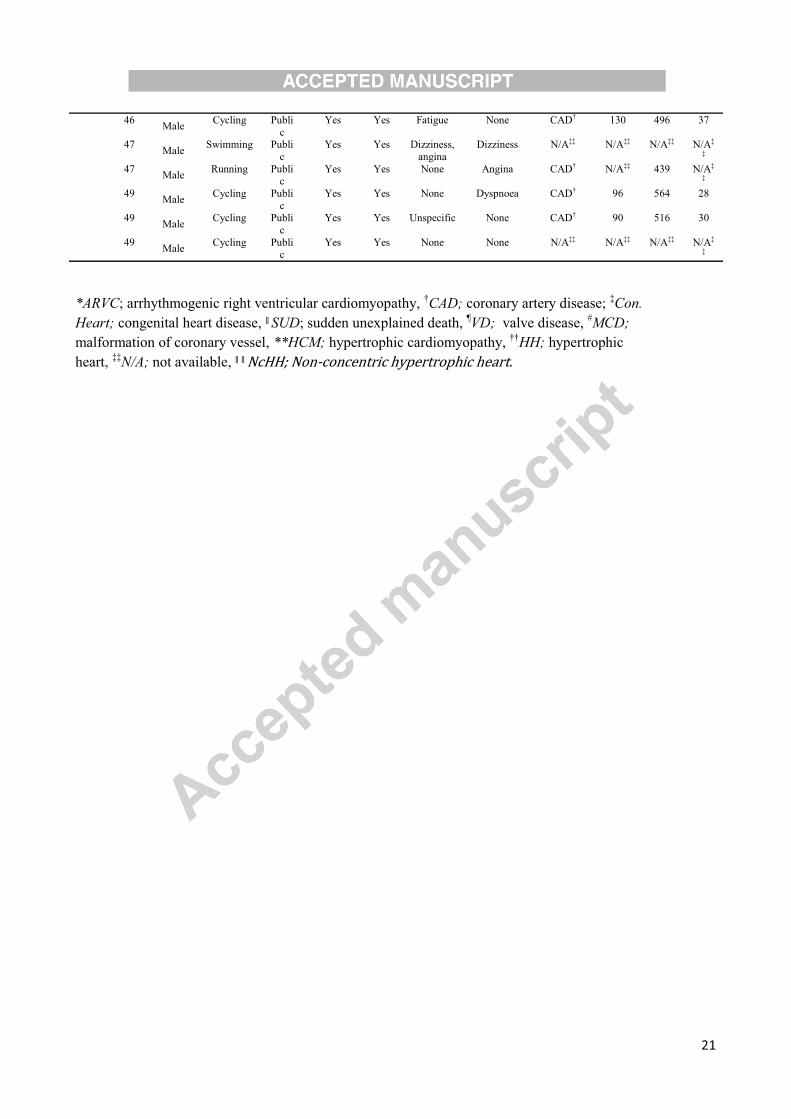
Table 2: Characterisation of sports-related sudden deaths in non-competitive athletes by age in Denmark,
2007 to 2009
SrSCD in non-competitive athletes Age
grou
p
Age
at
deat
h
Gende
r
Sport Place Witnesse
d
HL
R
Prodromal
symptoms
Antecedent
symptoms
Autopsy Body
weigh
t
Heart
weigh
t
Body
mass
inde
x
≤35
years
12 Male
Running Public
Yes Yes None Angina ARVC* 110 422 36
14 Male
Football Publi
c
Yes Yes None None Con. Heart† 70 572 23
15 Male
Running Publi
c
Yes Yes Dizziness,
dyspnoea
Syncope,
presyncope SUDǁ 66 378 21
20 Female
Dancing Public
Yes Yes None Syncope VD¶ 50 360 19
30 Male
Running Publi
c
Yes Yes None None CAD† 158 730 40
34 Male
Running Publi
c
Yes Yes None Syncope ARVC N/A‡‡ 520 N/A‡
‡
>35
years
36 Male
Running Publi
c
Yes Yes Unspecific Angina,
dyspnoea
ARVC* 75 410 23
36 Male Cycling Home No No None None CAD† 110 522 31 36
Male Running Publi
c
No Yes None None Myocarditi
s
114 412 32
36 Male
Running Public
No Yes None Angina, dyspnoea
ARVC 89 526 24
37 Male Running Home Yes Yes Unspecific None CAD† 80 450 25
38 Male
Running Public
Yes Yes None None NcHH 82 364 25
39 Male
Running Publi
c
No No None None N/A‡‡ N/A‡‡ N/A‡‡ N/A‡
‡ 39
Male Running Publi
c
Yes Yes Dyspnoea Palpitations N/A‡‡ N/A‡‡ N/A‡‡ N/A‡
‡
40 Male
Running Public
Yes Yes None Presyncope, angina,
dyspnoea
MCD# 103 510 29
42 Male
Running Public
Yes Yes Angina None HCM** 110 712 33
42 Male
Cycling Publi
c
Yes Yes Angina None Myocarditi
s
89 486 29
42 Female
N/A Publi
c
Yes Yes None None SUDǁ 81 340 26
42 Male Cycling Home No Yes Angina
Angina, palpitations
, and
presyncope (in pain)
CAD† 102 561 31
42
Male
Gymnastic
s
Home N/A Yes Dyspnoea,
Palpitations
None HH†† 71 468 23
43 Male
Running Public
Yes Yes Unspecific Dyspnoea HH†† 118 588 32
43 Male Cycling Publi
c No Yes None
Syncope,
angina, dyspnoea
treated as
asthma
CAD† 86 581 28
43 Male
Cycling Publi
c
Yes Yes Unspecific Angina N/A‡‡ N/A‡‡ N/A‡‡ N/A‡
‡
44 Female
Cycling Public
No No None Dyspnoea, unspecific
N/A‡‡ N/A‡‡ N/A‡‡ N/A‡
‡
44 Male Stepping Home No No None None CAD† 76 430 24
44 Male
Cycling Home Yes Yes Presyncope Angina N/A‡‡ N/A‡‡ N/A‡‡ N/A‡
‡
45 Male
Ice skating Publi
c
Yes Yes None Angina N/A‡‡ N/A‡‡ N/A‡‡ N/A‡
‡
21
46 Male
Cycling Publi
c
Yes Yes Fatigue None CAD† 130 496 37
47 Male
Swimming Publi
c
Yes Yes Dizziness,
angina
Dizziness N/A‡‡ N/A‡‡ N/A‡‡ N/A‡
‡
47 Male
Running Public
Yes Yes None Angina CAD† N/A‡‡ 439 N/A‡
‡
49 Male
Cycling Publi
c
Yes Yes None Dyspnoea CAD† 96 564 28
49 Male
Cycling Publi
c
Yes Yes Unspecific None CAD† 90 516 30
49 Male
Cycling Public
Yes Yes None None N/A‡‡ N/A‡‡ N/A‡‡ N/A‡
‡
*ARVC; arrhythmogenic right ventricular cardiomyopathy, †CAD; coronary artery disease;
‡Con. Heart; congenital heart disease, ǁSUD; sudden unexplained death,
¶VD; valve disease, #MCD;
malformation of coronary vessel, **HCM; hypertrophic cardiomyopathy, ††HH; hypertrophic
heart, ‡‡N/A; not available, ǁ ǁNcHH; Non-concentric hypertrophic heart.

22
Table 3: Characterisation of sports-related sudden deaths in competitive athletes by age in Denmark, 2007 to
2009
SrSCD in competitive athletes Age
group Age
at
death
Gender Sport Place Witnessed HLR Prodromal
symptoms
Antecedent
symptoms
Autopsy Body
weight
Heart
Weight
Body
mass
index
≤35
years
13 Male Running Public Yes Yes None None ARVC* 54 248 19
20 Male Football Arena Yes Yes None None SUD‡ 74 384 21
31 Male Squash Home No Yes Presyncope, palpitations
Syncope SUD‡ N/A¶ 522 N/A¶
>35
years
37 Male Handball Arena Yes Yes Unspecific None CAD† 92 474 29 38 Male Cycling Public Yes Yes None None CAD† 85 568 24
40 Male Football Home Yes Yes Angina Unspecific CAD† 73 367 24
41 Male Handball Arena Yes Yes Angina None CAD† N/A¶ 428 N/A¶ 44 Male Cycling Public Yes Yes None None HHǁ 91 587 25
45 Male Football Arena Yes Yes Unspecific None N/A¶ N/A¶ N/A¶ N/A¶
47 Male Running Public No Yes None None CAD† 82 450 25
48 Male Football Arena Yes Yes None Angina HHǁ N/A¶ 560 N/A¶
*ARVC; arrhythmogenic right ventricular cardiomyopathy, †CAD; coronary artery
disease; ‡SUD; sudden unexplained death, ǁHH; Hypertrophic heart,
¶N/A; not
available




















