Spectrum of Breast Cancer in Asian Women
10
Spectrum of Breast Cancer in Asian Women Gaurav Agarwal, MS, DNB, PDC (Endocr Surg), 1 P. V. Pradeep, MS, DNB, MRCS Ed, 1 Vivek Aggarwal, MS, 1 Cheng-Har Yip, MD FRCS (Glasg), FRCS Ed, 2 Polly S. Y. Cheung, FRCS, FRACS, FACS 3 1 Department of Endocrine and Breast Surgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Raebareli Road, Lucknow, 226014 Uttar Pradesh, India 2 Department of Surgery, University Malaya Medical Centre, Kuala Lumpur, Malaysia 3 Breast Care Center, Hong Kong Sanatorium and Hospital, Hong Kong, PeopleÕs Republic of China Abstract Introduction: Breast cancer is the leading cause of cancer-related deaths in Asia, and in recent years is emerging as the commonest female malignancy in the developing Asian countries, overtaking cancer of the uterine cervix. There have been no studies objectively comparing data and facts relating to breast cancer in the developed, newly developed, and developing Asian countries thus far. Material and Methods: This multi-national collaborative study retrospectively compared the demographic, clinical, pathological and outcomes data in breast cancer patients managed at participating breast cancer centers in India, Malaysia and Hong Kong. Data, including those on the availability of breast screening, treatment facilities and outcomes from other major cancer centers and cancer registries of these countries and from other Asian countries were also reviewed. Results: Despite an increasing trend, the incidence of breast cancer is lower, yet the cause- specific mortality is significantly higher in developing Asian countries compared with developed countries in Asia and the rest of the world. Patients are about one decade younger in developing countries than their counterparts in developed nations. The proportions of young patients (< 35 years) vary from about 10% in developed to up to 25% in developing Asian countries, which carry a poorer prognosis. In the developing countries, the majority of breast cancer patients continue to be diagnosed at a relatively late stage, and locally advanced cancers constitute over 50% of all patients managed. The stage-wise distribution of the disease is comparatively favorable in developed Asian countries. Pathology of breast cancers in young Asian women and the clinical picture are different from those of average patients managed elsewhere in the world. Owing to lack of awareness, lack of funding, lack of infrastructure, and low priority in public health schemes, breast cancer screening and early detection have not caught up in these under-privileged societies. Conclusions: The inadequacies of health care infrastructures and standards, sociocultural barri- ers, economic realities, illiteracy, and the differences in the clinical and pathological attributes of this disease in Asian women compared with the rest of the world together result in a different spectrum of the disease. Better socioeconomic conditions, health awareness, and availability of breast cancer screening in developed Asian countries seem to be the major causes of a favorable clinical picture and outcomes in these countries. Correspondence to: Gaurav Agarwal, MS, DNB, PDC (Endocr Surg), e-mail: [email protected] Ó 2007 by the Socie ´te ´ Internationale de Chirurgie World J Surg (2007) 31: 1031–1040 Published Online: 26 March 2007 DOI: 10.1007/s00268-005-0585-9
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Spectrum of Breast Cancer in Asian Women

Spectrum of Breast Cancer in Asian WomenGaurav Agarwal, MS, DNB, PDC (Endocr Surg),1 P. V. Pradeep, MS, DNB, MRCS Ed,1
Vivek Aggarwal, MS,1 Cheng-Har Yip, MD FRCS (Glasg), FRCS Ed,2
Polly S. Y. Cheung, FRCS, FRACS, FACS3
1Department of Endocrine and Breast Surgery, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Raebareli Road,
Lucknow, 226014 Uttar Pradesh, India2Department of Surgery, University Malaya Medical Centre, Kuala Lumpur, Malaysia3Breast Care Center, Hong Kong Sanatorium and Hospital, Hong Kong, People�s Republic of China
Abstract
Introduction: Breast cancer is the leading cause of cancer-related deaths in Asia, and in recent
years is emerging as the commonest female malignancy in the developing Asian countries,
overtaking cancer of the uterine cervix. There have been no studies objectively comparing data
and facts relating to breast cancer in the developed, newly developed, and developing Asian
countries thus far.
Material and Methods: This multi-national collaborative study retrospectively compared the
demographic, clinical, pathological and outcomes data in breast cancer patients managed at
participating breast cancer centers in India, Malaysia and Hong Kong. Data, including those on the
availability of breast screening, treatment facilities and outcomes from other major cancer centers
and cancer registries of these countries and from other Asian countries were also reviewed.
Results: Despite an increasing trend, the incidence of breast cancer is lower, yet the cause-
specific mortality is significantly higher in developing Asian countries compared with developed
countries in Asia and the rest of the world. Patients are about one decade younger in developing
countries than their counterparts in developed nations. The proportions of young patients
(< 35 years) vary from about 10% in developed to up to 25% in developing Asian countries, which
carry a poorer prognosis. In the developing countries, the majority of breast cancer patients
continue to be diagnosed at a relatively late stage, and locally advanced cancers constitute over
50% of all patients managed. The stage-wise distribution of the disease is comparatively favorable
in developed Asian countries. Pathology of breast cancers in young Asian women and the clinical
picture are different from those of average patients managed elsewhere in the world. Owing to
lack of awareness, lack of funding, lack of infrastructure, and low priority in public health schemes,
breast cancer screening and early detection have not caught up in these under-privileged
societies.
Conclusions: The inadequacies of health care infrastructures and standards, sociocultural barri-
ers, economic realities, illiteracy, and the differences in the clinical and pathological attributes of
this disease in Asian women compared with the rest of the world together result in a different
spectrum of the disease. Better socioeconomic conditions, health awareness, and availability of
breast cancer screening in developed Asian countries seem to be the major causes of a favorable
clinical picture and outcomes in these countries.
Correspondence to: Gaurav Agarwal, MS, DNB, PDC (Endocr Surg),e-mail: [email protected]
� 2007 by the Societe Internationale de Chirurgie World J Surg (2007) 31: 1031–1040
Published Online: 26 March 2007 DOI: 10.1007/s00268-005-0585-9

B reast cancer is the commonest cancer among wo-
men worldwide, with the lowest incidence being
reported from far eastern and south eastern Asian
countries.1,2 In recent years, breast cancer has emerged
as the commonest female malignancy in the majority of
Asian countries,3 but remains the second commonest
female malignancy in some regions of developing Asian
countries, next to the cancer of uterine cervix.4 Although
the incidence of breast cancer is lower in Asian countries,
the cause-specific mortality in most Asian countries is
much higher as compared to western countries.2 Higher
proportions of breast cancer patients in developing Asian
countries are younger than patients in developed Asian
and western countries.5,6 Given the huge population in
the developing Asian nations, and the fact that up to 25%
of all breast cancer patients here are young, there are a
large number of young breast cancer patients in Asia.
Young age by itself is a known indicator of poor prognosis
in breast cancer patients.
In most Asian societies, the majority of breast cancers
continue to be diagnosed at a relatively late stage. In
India, which represents a typical developing Asian
country with its multi-ethnic, multi-religious population
sharing similar peculiar economic, sociocultural chal-
lenges, health care facilities, and standards with the
majority of other developing Asian countries, locally ad-
vanced cancers constitute about 50% of the total.4 The
picture is, however, not so bleak in developed Asian
countries and regions such as Singapore, Hong Kong,
and Malaysia. Various factors such as lack of awareness,
unavailability of breast cancer screening and sociocul-
tural barriers of hesitation on the part of women to have
her breasts examined and seek treatment seem to result
in late stage at diagnosis in most Asian women. Besides
the poorer outcomes owing to late stage at diagnosis, and
relatively poorer breast cancer treatment opportunities
available to these patients, there seem to be other dif-
ferences in the clinical picture and pathology of breast
cancers in women in developing Asian countries, which
account for overall poorer outcomes. A lack of credible
and scientifically sound epidemiology data on breast
cancer from developing Asian countries makes it difficult
to understand the reasons for the different breast cancer
incidence, mortality, and outcomes in these countries
compared with developed countries in Asia and rest of
the world.
Asia, the largest and most populous continent in the
world, is a heterogeneous mix of nations that vary widely
in the cultural, social and economic structures, and in
geopolitical situations. All of these factors may have
some bearing on occurrence, progression, detection, and
management of breast cancer, and of most other malig-
nancies. The World Bank classifies India as a low in-
come, Malaysia as an upper-middle income, and Hong
Kong as a high income country7. These 3 countries are
very different in their socioeconomic as well as their
ethnic and cultural realities, and thus represent the
sociocultural and economic diversity of Asia. This survey
aimed at studying the overall picture of breast cancer
management in 3 Asian regions (Lucknow in India, Kuala
Lumpur in Malaysia, and Hong Kong, People�s Republic
of China) with an emphasis on the picture in young
women (< 35 years)
The objectives of this study were first, to study any
differences in incidence and mortality rates of breast
cancer, the spectrum of disease including age distribu-
tion, stages (TNM), tumor characteristics; and second, to
evaluate whether or not the comparative results from
participating centers and the available literature on these
issues point to any correlation of the differences with re-
gard to the social, cultural, and economic background,
and the availability of breast screening in various Asian
countries and regions.
MATERIALS AND METHODS
This collaborative and comparative multi-center retro-
spective study was carried out at 3 major Asian breast
cancer centers from India, Malaysia, and Hong Kong.
Demographic, clinical, pathological, and outcomes data
on breast cancer patients managed at the 3 participating
centers, namely, SGPGIMS, Lucknow, India; University
Malaya Medical Center, Kuala Lumpur, Malaysia; and
Hong Kong Sanatorium and Hospital, Hong Kong, were
collected and analyzed. Similar data, and data on the
availability of breast screening, treatment facilities, and
outcomes from other major cancer centers and cancer
registries of India, Hong Kong and Malaysia, as well as
from other Asian countries, were also reviewed. The
publications of the National Cancer Registry Program of
India, Indian Council of Medical Research—namely, the
2-year report on hospital-based cancer registries 1999–
2000, and the 2-year report of the population-based
cancer registries 1999–2000, assessing the burden and
care of cancer patients in India—were perused for this
purpose,8,9 with additional information on district-wise
distribution of breast cancers derived from the All India
Report 2001–2002 of the Development of an Atlas of
Cancer in India project of the National Cancer Registry
Program, ICMR and their website (http://www.cancerat-
lasindia.org/chapter6).3 The data for Malaysia and Hong
1032 Agarwal et al.: Breast Cancer in Asian Women

Kong were derived from the respective websites of
the National Cancer Registry of Malaysia (http://www.
crc.gov.my/ncr),10 and the Hong Kong Cancer Registry
(http://www.3.ha.org.hk/cancereg/stat.asp).11
A literature search was undertaken to unravel available
information on breast cancer demographics, detection,
treatment, and outcomes from various Asian countries in
the published scientific literature. Similar information was
also searched for on the internet, as well as other publi-
cations of cancer registries and organizations such as
the WHO, regional and national health agencies, institu-
tions and non-governmental organizations (NGOs), etc.
Appropriate similar publications and reports from other
geographic regions outside Asia, including those from the
International Agency for Research on Cancer (IARC),12
and its GLOBOCAN database,6 were used for the pur-
pose of comparing the incidence, clinical picture, pathol-
ogy, and outcomes of breast cancer between the Asian
and non-Asian regions and countries studied.
RESULTS
The databases of participating centers provided valid
and complete information on 544 patients managed dur-
ing 1998–2004 at SGPGIMS, Lucknow, India; 2,009 pa-
tients managed at the UMMC Kuala Lumpur, Malaysia
during 1995–2004, and 901 patients managed at HKSH,
Hong Kong during 2003–2005. Published data from TMH,
Mumbai—another dedicated breast center in India—are
incorporated into the study for comparison of results.
Incidence, Demography and Mortality of BreastCancer in Asia
Breast cancer incidence in various Asian countries and
a comparison with other WHO regions, including USA
and France, are provided in Table 1. The numbers of new
breast cancers diagnosed in all 4 WHO regions is much
smaller than the numbers diagnosed in USA and France.2
Data from all urban and rural population-based cancer
registries (PBCR) in India suggest a rising incidence of
this disease in India. Yet, the age-adjusted rates reported
from various urban registries range from 24.8 to 33.4 per
100,000 of the population,3 which amount to about one-
third of the incidence reported from western countries
such as the USA (San Francisco, CA: non-Hispanic white
109.6 per 100,000) and Uruguay (Montevideo 114.9 per
100,000).12 The minimum age-adjusted rate reported
from the only rural population-based cancer registry in
India is even less at a mere 7.2 per 100,000,3 and is
somewhat similar to the incidence reported from other
developing countries such as the Gambia and Jiashan,
China.12 Breast cancer accounts for about one-quarter of
all cancers in Indian women, about half of all cancer-
related deaths. With the exception of Chennai, all urban
PBCRs in India report breast cancer to be the commonest
female malignancy over the years 2000–2001.3 This is a
different pattern from the earlier reports where cancer of
the uterine cervix was the commonest type of cancer,
even in urban centers. In the Chennai urban PBCR and
the Barshi rural PBCR, breast cancer remains the second
commonest female malignancy reported, with cancer of
the uterine cervix still remaining the number one cancer
problem.3,8,9
As per the National Cancer Registry of Malaysia, the
age-adjusted rate (incidence) of breast cancer in the year
2003 was 42.9 per 100,000 of the population.10 One in 20
Malaysian women is estimated to be affected by breast
cancer in her life time. However, the incidence of breast
cancer is reported to vary considerably among the 3
ethnic groups that constitute Malaysian society. The age-
adjusted rates in ethnic Chinese (59.7 per 100,000) and
Indians (55.8 per 100,000) are considerably higher than
Table 1.Number of new breast cancer patients diagnosed and deaths in various WHO regions2
WHO regions Number of new cases (thousands) Number of cancer deaths (thousands)
India, Nepal, Pakistan (SEARO D) 109 67Indonesia, Thailand, Singapore (SEARO B) 53.9 29China, Korea, Mongolia (WPRO B1) 102.1 57.5Cambodia, Myanmar (WPRO B2) 10.2 6.3Iran, Kuwait, Saudi Arabia, UAE (EMRO B) 10.2 5.1Egypt, Iraq, Yemen (EMRO D) 13.6 7USA (AMRO A) 226.5 53.3France, Germany (EURO A) 221.8 91.8
SEARO: South East Asian Regional Office; WPRO: Western Pacific Regional Office; EMRO: Eastern Mediterranean RegionalOffice; AMRO: Americas Regional Office; EURO: European Regional Office.
Agarwal et al.: Breast Cancer in Asian Women 1033

that in ethnic Malays (33.9 per 100,000).10 In Hong Kong,
2,059 new cases of breast cancer were registered in
2002. The crude rate was 59.0 and the age-adjusted rate
42.0 per 100,000 of the population. The relative fre-
quency of breast cancer amongst all malignancies in fe-
males was 20.8%, and its incidence doubled in the 1990s,
overtaking lung cancer as the number one cancer
affecting Hong Kong women. One in 23 women is ex-
pected to be affected in her life time. The mortality to
incidence ratio is 0.21.11
The breast cancer incidences in young women vary
widely amongst various Asian countries, with countries
like Pakistan having a high incidence and Japan a very
low incidence (Table 2).5,6 In the current study, 26% of
patients managed at SGPGIMS, Lucknow were younger
than 35 years of age, with the peak incidence in the age
group of 35–40 years. Data from TMH, Mumbai in India,
shows this proportion to be 11%.3 Of the 2,009 patients
managed between 1995 and 2004 at the UMMC, Kuala
Lumpur, Malaysia, 7.6% were younger than 35 years
age. The National Cancer Registry of Malaysia reports
13.4% of patients being younger than 40 years of age,
and a peak incidence in the age group of 50–59 years.10
Data from the Hong Kong Cancer Registry reports 11.6%
of patients to be younger than 40 years of age, and the
peak incidence of breast cancer in the age group of 50–
54 years.11 Data on the proportions of young patients in
various other countries and societies show that 7.4% of
American patients,13 29.3% of Taiwanese patients,
12.6% of patients in Singapore, and 8% of Australian
patients are under 40 years of age.14 These data indicate
that a higher proportion of breast cancer patients in
developing Asian countries are young, compared with
developed Asian countries and western countries.
Although the incidence rates in Asian countries are less
than in western developed countries, the mortality rates
are disproportionately higher (Table 1).2 Breast cancer
thus remains the single largest cause of cancer deaths in
Asians, similar to the rest of the world. Globally, it ac-
counts for about 15% of all cancer deaths in women,
killing some 471.2 women per 100,000 of the population
annually.2
Breast Cancer Screening and Detectionin Asian Countries
An organized large-scale breast cancer screening
program is almost non-existent in India. The few breast
cancer screening programs available are largely targeted
at small communities, covering a minuscule proportion of
the Indian population, and rely on funds derived from
research grants or the screened individuals� own re-
sources. There is no government-funded or -aided mass
breast screening program available, and the experts also
advocate screening based on periodic breast examina-
tion by a physician and breast self examination.15 The
approach to breast cancer screening in Malaysia is more
or less identical to that in India, and population-based
breast cancer screening is not recommended due to
limited resources, and a lack of local statistics on mam-
mography and breast cancers.16
In Hong Kong, the first breast screening program was
set up in 1990 at Kwong Wah Hospital, with private
funding from a voluntary organization, the Tung Wah
Group. From its first pilot study of 3,829 asymptomatic
women, 2 cancers were detected per 1,000 women.
Since then, more well-women clinics have been set up
by voluntary organizations such as Tung Wah Eastern
Table 2.Number of new breast cancer patients diagnosed per 100,000 of the young populations in Asian countries5,6
10–14 years 15–19 years 20–24 years 25–29 years 30–34 years
Pakistan (1995–1997) – 1.2 6.3 14.0 48.4Israel (Jews) 0.1 0.2 2.1 9.7 33.3Singapore – – – 6.3 29.9Egypt – 0 1.4 8.5 29.9Bahrain – 0 0 0 27.7China (Beijing; 1993–1997) – 0.7 3 11 26.9Kuwait – 0 0 2.9 22.7Philippines (Manila) 0.1 0.5 1.9 8.2 22.1Jordan – 0 0.8 6.5 21.7Mali 0.5 1.9 2.9 8.5 21.7Oman – 1.9 2.9 8.5 21.7Korea (Seoul) – 0.3 1.5 6.1 17.3Japan (Nagasaki) – 0.4 1.8 3.1 16Thailand – 0.4 1.2 4.8 15.2Vietnam – 0.9 7.6 11.5 13.8
1034 Agarwal et al.: Breast Cancer in Asian Women

Hospital, the Family Planning Association and private
hospitals. The Hong Kong Government also set up 3
women�s health centers providing mammogram facilities
and breast screening advice with a fee charged for the
service. To date, the longest serving breast screening
program has served 46,637 women, with a cancer
detection rate of 5 per 1,000 women. However, the Hong
Kong government in its ‘‘Report on Cancer Prevention
and Screening’’ in December 2004, does not recommend
‘‘screening mammogram and breast self examination,’’
based on available local data, despite the admission that
Hong Kong has the highest incidence of breast cancer
among Asian countries (http://www.info.gov.hk/dh/dis-
eases/index.htm).
Clinical Picture of Breast Cancer in AsianWomen
Table 3 summarizes the stage-wise distribution of
breast cancer patients managed at the participating In-
dian, Malaysian, and Hong Kong centers of this study.
These data, together with those from other Asian coun-
tries, suggest that nearly all the patients are clinically
detected, and that almost none are screen-detected in
developing Asian countries. Local invasion occurs in up to
two-thirds and metastases in 6% to 25% of Indian and
Saudi patients.5,18 Significant proportions of patients
present with T2/T3 tumors, and even more strikingly, up
to one-third of all patients present with skin and/or chest
wall involvement (T4a–c). Inflammatory breast cancers
are seen more often in younger patients, putting them at
considerable risk.
Half of the young patients managed at SGPGIMS,
Lucknow, India, had Stage III disease. Similarly, in earlier
reports, 50%–60% of Malaysian women had stage III or
IV disease,19 compared with only 14% of young American
women presenting at Stage III.20 The stage-wise distri-
bution of patients is worse in the case of younger pa-
tients, as revealed in Table 4, which provides a stage-
wise comparison of young breast cancer patients man-
aged at some centers in India, USA, and Singa-
pore.18,20,21 The proportion of Stage III patients in
Singapore is reported to be 22%,21 which is closer to the
American rather than the Asian figures. At the University
of Malaya Medical Centre, Kuala Lumpur, Malaysia, of
the 2,009 breast cancer patients managed, 152 were
under the age of 35 years. In this group of young women,
69% were at Stages 1 and 2, while 31% were at Stages 3
and 4, which is marginally higher than the 27% of patients
Table 4.Stage-wise comparison of young breast cancer patients managed at centers in Asia and the USA
SGPGIMS, Lucknow,India (%)
RCC, Trivandrum,India17 (%)
Changi,Singapore20 (%)
New York,USA19 (%)
Tx 3 6 – –T1 9 12 30 54T2 24 47 59 36T3 32 27 11 10T4 32 9 – –LN + 67 60 53 51
SGPGIMS: Sanjay Gandhi Postgraduate Institute of Medical Sciences; RCC: Regional Cancer Center; Tx to T4: tumor stages(TNM-AJCC classification); LN+: metastatic lymph nodes.
Table 3.Stage-wise distribution of patients at 3 Asian centers
Stage(TNM-AJCC classification)
SGPGIMS, Lucknow,India
(n = 544, 1998–2004; %)
UMMC, KualaLumpur, Malaysia (n = 2,009,
1995–2004; %)
HKSH, Hong Kong(n = 901,
2003–2005; %)
0 1 3 13I 4 23 34II 34 47 43III 51 16 9IV 9 11 1
SGPGIMS: Sanjay Gandhi Postgraduate Institute of Medical Sciences; UMMC: University Malaya Medical Center; HKSH: HongKong Sanatorium and Hospital.
Agarwal et al.: Breast Cancer in Asian Women 1035

of all age groups with Stages 3 and 4 disease. Similarly,
of the young patients managed at the Breast Cancer
Center of HKSH, Hong Kong, the majority were managed
at Stages 0 to 2, with Stages 3–4 disease comprising less
than 10% of all patients. Both the Malaysian and Hong
Kong centers recorded a trend toward larger tumor size,
more lymph nodal metastases, and poorer histological
grade and hormone receptor status.
Pathology
Data on the pathology of breast cancer in Asian women
revealed a pattern of a higher proportion of patients with
high tumor grade (grade 3 of the Bloom and Richardson
grading system), and hormone receptor-negative tumors.
About 60% of SGPGIMS breast cancer patients had
grade 3 tumors, 66% had axillary lymph nodal metasta-
ses, and 58% are estrogen (ER) and progesterone (PR)
receptor-negative. Data from Mumbai, India, showed a
slightly better ER- and PR-negative rates of 47%.4 Data
from the University of Malaya Medical Center Registry
showed that in all patients, 11.4% patients had Grade 1,
52.5% had Grade 2 while 36.1% had Grade 3 cancers.
56.4% were ER-positive. In Hong Kong, of all the invasive
cancers, 83.6% were ductal and 3.8% lobular. Grade 3
tumors were present in 48.3%. Lymph vascular invasion
was present in 30.7%. Estrogen receptor was positive in
76.6%. The data on HER-2neu immunoreactivity in Asian
patients are scarce, but the available information hints at
low rates of positive HER-2neu status. Seventeen of 100
recent breast cancer patients managed at SGPGIMS
Lucknow were found to over-express HER-2neu (immu-
nohistochemical evaluation). HER-2 over expression was
present in 22.6% of patients managed at the Breast Care
Center, HKSH, Hong Kong. In the young Malaysian pa-
tients (less than 35 years old) from the UMMC data, the
median tumor size was 4.0 cm with a mean of 5.1 cm.
About 52% were ER-positive. Only 5.6% had Grade 1
(Bloom and Richardson) tumors, while 55.1% of patients
had Grade 2 and 39.3% Grade 3 tumors. On the whole,
women < 35 years age presented with larger tumors and
at a later stage. They were also more likely to be ER-
negative and with a higher grade of cancer compared
with the overall average.
DISCUSSION
Comparisons among various regions of the world show
a 3-tier distribution of the magnitude of the breast cancer
problem. The number of new cases and age-standard-
ized incidence rates of breast cancer are low in Asia,
intermediate in South America and eastern Europe, and
high in North America and western Europe.2 China,
Korea, Thailand and Japan—all Asian countries—are
amongst the countries with the lowest incidence of breast
carcinoma. Besides the geographic differences, breast
cancer incidence seems directly proportionate to the level
of industrial development of a country, although there are
numerous exceptions to this rule. The age-adjusted rate
is 37.4 per 100,000 for the global female population, but
the rate in developed countries (67.8 per 100,000) is
nearly 3 times that in the developing countries (23.8 per
100,000).6 Japan with its high level of industrial devel-
opment yet moderate breast cancer incidence and Uru-
guay with only a moderate level of development yet high
breast cancer incidence provide contradictions to this
rule.
There seem to be many plausible reasons for differ-
ences in breast cancer incidence. The low average life
expectancy of women in developing Asian countries has
a bearing on the incidence of breast cancer, which has a
known correlation with increasing age. However, even the
age-adjusted incidence rates of this disease are lower in
Asia. Probable explanations for this are: shorter life span
of estrogen exposure in Asian women, late menarche
related to under-nutrition, and early menopause. In the
majority of Asian societies, bearing many children, having
the first child at an early age, and feeding children for long
periods are the norm. All of these are factors known to
protect against breast cancer.22 In a study on breast
cancer risk factors among Asian–American ethnic
groups, 68.5% of Chinese, 75.5% of Japanese, and
72.1% of Asian women as a whole were below the age of
30 at the time of their first delivery.23 Asian diets in gen-
eral have less fat and higher fiber content, and many of its
ingredients contain soy proteins, which have been sug-
gested, albeit with questionable validity, to have some
protective effect against breast cancer.24,25 Furthermore,
the usage of oral contraceptive pills and hormone
replacement therapies, known risk-enhancing factors, is
rather low in Asians. The putative protection afforded by
these factors in Asians is strengthened by increased
incidence rates of breast cancer in urban Asian societies
that are fast adopting the western life-style and food
habits, and that second generation immigrant Asians in
the USA are found to have a similar breast cancer risk to
other American women.26
Lack of breast cancer awareness, inaccessible health
care and screening, unaffordable treatment, competing
health care needs such as communicable diseases,
1036 Agarwal et al.: Breast Cancer in Asian Women

some of which get higher priority than neoplastic dis-
eases, sociocultural barriers (Purdah, unwillingness to
expose oneself due to sociocultural compulsions) and
reliance on low-cost traditional/alternative medicines are
a few of the risk factors unique to Asian and Indian wo-
men that culminate in poorer outcomes for breast cancer
in these societies. Women in developing Asian countries
are ill-aware of breast cancer. As a result, many of them
ignore an evident breast problem or lump, resulting in a
delay in diagnosis, which is reflected in the outcome. It is
not uncommon for women to be aware of a breast lump
for many years before seeking medical attention. Many
such patients seem to have an attitude of denial of this
fact, postponing seeking medical attention until an overt
secondary change of the disease such as skin edema or
ulceration (Fig. 1), or symptomatic metastatic disease. At
SGPGIMS, Lucknow, India, about 55% of patients pre-
senting with locally advanced breast cancer were well
aware of the presence of a possibly life-threatening
cancerous breast lump, yet sought treatment only when
the disease had progressed to that stage.
Most Asian countries, barring a few relatively developed
ones, do not have an organized breast cancer screening
program serving the entire or a substantial part of the
population, owing to the high costs involved and the low
yield of such programs. The social and cultural beliefs also
make women hesitate to subject themselves to screening
breast examinations and imaging. Breast self-examination
is an alternative in countries with limited resources, though
with its known limitations.27 Teaching breast self-exami-
nation does help in improving awareness about breast
health issues as a whole, and about breast cancer in
particular. Many studies have shown that periodic physical
examination by a physician as a screening modality is at
least as effective in reducing breast cancer mortality.
The clinical picture of breast cancer is more favorable in
Malaysia and Hong Kong. Population-based mammo-
graphic screening is not recommended in Malaysia due to
limited resources and lack of infrastructure, expertise,
and local standards for mammography.16 Because of
this, ductal carcinoma in situ is rare, comprising only 2.7%
of the total number of cancers seen. Screening by clinical
breast examination is opportunistic, i.e., when a woman
sees a doctor, a clinical breast examination is encour-
aged. Women are also taught breast self-examination by
nurses when they attend the community maternal and
child health clinics. The emphasis currently is on creating
‘‘breast-awareness’’ among the public, utilizing the media
as the main source of information. With this approach, it
is hoped that women will present earlier to their doctor
with breast lumps.
Among 901 consecutive cancer patients at the HKSH
breast care centre, Hong Kong from September 2003 to
November 2005, the mode of presentation of breast
cancer was mostly by incidental discovery by the patient
(81.4%), the remaining were discovered by regular breast
screening, which included monthly breast self-examina-
tion, annual clinical examination by a doctor, screening
mammogram, and additional screening ultrasound when
the breast density was high. The introduction of breast
cancer screening programs in Hong Kong has resulted in
a major change in the disease pattern of breast cancer. In
the pre-screening era in the 1980s in Hong Kong, stage 0
cancer was limited to the diagnosis of Paget�s disease
only in < 2% of cases, around 40% to 50% were at stages
3 and 4 at first diagnosis, which was quite different from
the data just quoted from a local breast centre in the
years 2003–2005.28 Yet, owing to the lack of appropriate
resources, and unsure of the overall cost-effectiveness of
the mammographic screening, the Hong Kong govern-
ment still does not recommend this as a routine screening
procedure for the masses.17
The impact of breast cancer awareness and cost-effec-
tive screening on the outcome of this disease is well
understood by health policy planners in the majority of
Asian countries. In countries like India, such efforts are
coming mostly from non-governmental and volun-
tary organizations. The community initiatives of the
SGPGI Breast Health Program (http://www.sgpgibreast-
health.org) in creating awareness, teaching breast self-
examination to women, providing periodic screening
physical examination, and investigative work-up including
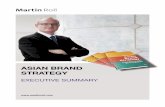
Figure 1. Clinical picture of breast cancer inAsian women: the good, a T2N0 tumor managedwith breast conservation surgery and sentinellymph node biopsy; the bad, an inflammatorybreast carcinoma (T4dN1M0); the ugly, fungatingbreast cancer with chest wall fixity (T4cN2M0).
Agarwal et al.: Breast Cancer in Asian Women 1037

breast screening only for the high-risk individuals over the
past decade or so in and around Lucknow, India, have re-
sulted in somewhat better acceptance of breast cancer
screening by educated urban women in the region. A minor
shift to earlier stages at diagnosis has also resulted
simultaneously, as has better acceptance of contemporary
breast cancer treatment strategies such as breast con-
servation, sentinel lymph node studies, breast recon-
struction, and comprehensive multi-modal treatment
protocols, which are all provided by SGPGIMS, Lucknow,
at a subsidized cost and on a ‘‘no professional fee’’ basis.
Similar benefits, albeit reaching a minuscule proportion of
the huge Indian population, have resulted from the efforts
and initiatives of other institutions, agencies, and non-
governmental organizations such as the Cancer Patients
Aid Society, Mumbai (http://www.cpaaindia.org).
It is, however, disturbing to see many women ignoring
their disease until they have large fungating tumors with
sepsis (Fig. 1). High proportions of women have axillary
node-positive disease. Striking features reflecting tumors
that have been ignored for a long time are large tumor
size, skin ulceration or fungation in up to 10%, and
more than 3 metastatic lymph nodes in the majority
(4, SGPGIMS Lucknow data).
Even basic clinical data on breast cancer from Asian
countries are scarce, which is a reflection of either a total
lack of or ineffective cancer registries in this region. If
available, the quality of data is often questioned, with the
majority of data coming from hospital-based registries in
large cities, rather than from community studies and reg-
istries. The multi-modal comprehensive breast cancer
treatment is out of reach of the average woman in a
developing Asian country. The cost of chemotherapy or
surgery at government-run hospitals is at times more than
the average monthly income of Asian households. Treat-
ment at more convenient private and corporate hospitals,
which are many times more costly, though do not always
offer better quality treatment and services, is reserved for
the few in the upper echelon of society who can afford it.4
The high quality contemporary surgical and adjuvant
treatments are available and affordable for only a minority
of the population. Besides, most Asian societies are male-
dominated, where women occupy a relatively inferior so-
cial position. The health care and nutritional needs of
women are thus often ignored, and the scarce finances
reserved for the men-folk of the family.
Governments of developing Asian countries spend a
minuscule proportion of their GDP on health care, and
only a fraction of this small budget is allocated to neo-
plastic diseases. There are important medical problems
that need more urgent attention and financial support, like
epidemics of communicable diseases, malnutrition, infant
mortality, vaccination programs, and natural calamities.
The infrastructure for managing neoplastic diseases is
even less developed. For example, in India, there are
fewer than 100 surgical oncology centers to cater for the
population of more than one billion. The numbers of
radiotherapy units are far less than the WHO recom-
mendations of a minimum of 0.4 units per million of the
population. There is little emphasis on neoplastic dis-
eases in the undergraduate medical education curricu-
lum, and no country-specific guidelines or protocols that
take into account the local health care infrastructure and
health economics are available. As a result, even those
patients who do seek medical attention for a breast lump
often do not get sufficient and timely advice and appro-
priate multi-modal treatment, other than that at special-
ized centers of excellence.
Only a minority of patients benefit from less invasive
surgical techniques and other contemporary management
strategies. Even at the few centers offering breast
conservational surgery, breast conservation rates are low
due to the late presentation and low acceptance of breast
conservation surgery.29 Reports from other developing
Asian countries indicate similarly poor breast conservation
rates and the unavailability of comprehensive treatment
opportunities to breast cancer patients. In comparison,
comprehensive multi-modal therapy is available to the
majority of patients in Hong Kong. Of the Malaysian
patients managed at the University Malaya Medical Cen-
ter, some 27% underwent breast conservational surgery.
An even smaller proportion of patients can be offered
the benefits of sentinel lymph node studies as the
majority present with clinically palpable axillary lymph
nodes. In India, only 3 centers offer sentinel lymph node
studies, using a combination of radio-pharmaceutical and
blue dye, on a consistent basis. In a validation study, 70
consecutive sentinel lymph node procedures at SGPG-
IMS, Lucknow, using in-house prepared low-cost Tc-
antimony colloid and blue dye, have resulted in achieving
a negative predictive value of sentinel lymph node pro-
cedures in ruling out axillary metastases of 95.65%; the
positive predictive value was 100% and overall accuracy
97%, while the cost incurred was only 2% of that of the
commercially available dyes.30 Such innovations may
perhaps be useful for other developing countries where
costs are a major deterrent.
In conclusion, the overall picture of breast cancer is
strikingly variable among Asian countries, and among
regions and ethnic groups within individual countries.
Although the incidence is comparatively lower in east and
southeastern Asia, breast cancer has emerged as the
1038 Agarwal et al.: Breast Cancer in Asian Women

largest cancer problem in Asian women, and the largest
cause of cancer-related deaths. It remains the second
commonest malignancy in women in the rural areas of
developing Asian countries. A high proportion of Asian
breast cancer patients are young. Poor awareness, a lack
of breast cancer screening programs, limited health care
facilities, sociocultural barriers, and faith in low-cost tra-
ditional alternative medicine systems are responsible for
the delayed presentation and advanced stage at diag-
nosis in the majority of patients in developing Asian
countries. The availability of screening programs has
instigated a change toward earlier staging of breast
cancer in most urban Asian societies, but the benefits do
not yet seem to have reached the rural areas and under-
developed regions.
Owing to the limitations of the quality of data and
information available on these issues, the authors do not
make any claims that this study is an epidemiologically
and scientifically perfect account of breast cancer in
various regions and countries in Asia. However, the
information provided should be seen as an attempt to
bridge the divide.
ACKNOWLEDGEMENTS
Gaurav Agarwal wishes to thank Dr A. Nandakumar,
DyDG-ICMR and Officer In-Charge NCRP, for providing
the detailed reports of the National Cancer Registry
Program; the Faculty and Residents of the Departments
of Endocrine and Breast Surgery, and Radiotherapy for
the upkeep of data; and the organizers of the Breast
Surgery International Symposium on ‘‘Breast Cancer in
Developing Countries’’ at the International Surgical
Week, 2006, Durban, South Africa.
REFERENCES
1. Lacey JV Jr, Devesa SS, Brinton LA. Recent trends in
breast cancer incidence and mortality. Environ Mol Mutagen
2002;39:(2–3) 82–88.
2. Shibuya K, Mathers CD, Boschi-Pinto C, et al. Global and
regional estimates of cancer mortality and incidence by site.
II. Results for the global burden of disease 2000. BMC
Cancer 2002;2:37.
3. Summary of Specific Sites: Breast (ICD-10:C50)—Fe-
males. In: Nandakumar A, Gupta PC, Gangadharan P,
Visweswara RN (editors). Development of an atlas of can-
cer in India: first all India report: 2001–2002, vol 1. National
Cancer Registry Program, Indian Council for Medical Re-
search, Bangalore, India, April 2004.
4. Chopra R. The Indian scene. J Clin Oncol 2001;19:(18)
106–111.
5. Amr SS, Sa�di ARM, Ilahi F, et al. The spectrum of breast
diseases in Saudi Arab females: a 26 year pathological
survey at Dhahran health center. Ann Saudi Med
1995;15:(2) 125–132.
6. Breast Cancer Incidence in different regions GLOBOCAN
2002, IARC. http://www.-dep.iarc.fr/GLOBOCAN 2002.
7. http://web.worldbank.org/WBSITE/EXTERNAL/DATASTA-
TISTICS/0,,contentMDK:20421402~pagePK:64133150~
piPK:64133175~theSitePK:239419,00.html.
8. Indian Council of Medical Research. Two year report of the
hospital based cancer registries 1999–2000. An assess-
ment of the burden and care of cancer patients. National
Cancer Registry Program (Indian Council of Medical
Research), Bangalore, August 2005.
9. Indian Council of Medical Research. Two year report of the
population based cancer registries 1999–2000. Incidence
and distribution of cancer. National Cancer Registry Pro-
gram (Indian Council of Medical Research), Bangalore,
April 2005.
10. National Cancer Registry Malaysia. http://www.crc.gov.my/
ncr, 2003.
11. Hong Kong Cancer Registry. http://www.ha.org.hk/cance-
reg.
12. Parkin DM, Wheelan SL, Ferlay J, et al. (editors). Cancer
incidence in five continents, vol VIII, IARC, no. 155, 2002,
Lyon.
13. Shavers VL, Harlan LC, Stevens JL. Racial/ethnic variation
in clinical presentation, treatment, and survival among
breast cancer patients under age 35. Cancer 2003;97:(1)
134–147.
14. Foo CS, Su D, Chong CK, et al. Breast cancer in young
Asian women: study on survival. ANZ J Surg 2005;75:566–
572.
15. Mittra I. Breast screening: the case for physical examination
without mammography. Lancet 1994;343:342–344.
16. Clinical Practice Guideline for the management of breast
cancer in Malaysia. http://www.moh.gov.my/medical/cpg.
htm, 2002.
17. http://www.info.gov.hk/dh/diseases/index.htm.
18. Mathew A, Rajan B, Pandey M. Do younger women with
non-metastatic and non-inflammatory breast carcinoma
have poor prognosis? World J Surg Oncol 2004;2:2.
19. Hisham AN, Yip CH. Spectrum of breast cancer in
Malaysian women: overview. World J Surg 2003;27:921–
923.
20. Gajdos C, Tartter PI, Bleiweiss IJ, et al. Stage 0 to stage III
breast cancer in young women. J Am Coll Surg 2000;
190:(5) 523–529.
21. Menon M, The CH, Chua CL. Clinical and social problems in
young patients with breast carcinoma. ANZ J Surg
1992;62:364–367.
22. Collaborative Group on Hormonal Factors in Breast Can-
cerBreast cancer and breastfeeding: collaborative reanaly-
Agarwal et al.: Breast Cancer in Asian Women 1039

sis of individual data from 47 epidemiological studies in 30
countries, including 50302 women with breast cancer and
96973 women without the disease. Lancet 2002;360:(9328)
187–195.
23. Chan N. Breast cancer risk factors among Asian American
ethnic groups. http://www.students.washington.edu/nlchan/
thesis/thesisnov2000.ppt#13.
24. Breast Cancer and Nutrition. http://www.fauxpress.com/
kimball/med/candiet/breastnutr.html.
25. Hirose K, Imaeda N, Tokudome Y, et al. Soybean products
and reduction of breast cancer risk: a case-control study in
Japan. Br J Cancer 2005;93:(1) 15–22.
26. Ziegler RG, Hoover RN, Pike MC, et al. Migration patterns
and breast cancer risk in Asian-American women. J Natl
Cancer Inst 1993;85:(22) 1819–1827.
27. Harris R, Kinsinger LS. Routinely teaching breast self-
examination is dead. What does this mean?. J Natl Cancer
Inst 2002;94:(19) 1420–1142.
28. Cheung PSY. Breast cancer in Hong Kong—the need for
early detection. J Hong Kong Med Assoc 1992;44:(4) 248–
252.
29. Raina V, Bhutani M, Bedi R, et al. Clinical features and
prognostic factors of early breast cancer at a major cancer
center in North India. Indian J Cancer 2005;42:(1) 40–45.
30. Agarwal G, Gambhir S, Kheruka S, et al. Low-cost sentinel
node studies in breast cancer with indigenous blue dye
and 99mTc-antimony colloid [abstract]. J Japan Surg Soc
2005;106:221.
1040 Agarwal et al.: Breast Cancer in Asian Women