SLEEP QUALITY IN PROFESSIONAL BALLET DANCERS
15
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [Glos, Martin] On: 7 September 2009 Access details: Access Details: [subscription number 914458806] Publisher Informa Healthcare Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Chronobiology International Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713597233 Sleep Quality in Professional Ballet Dancers Ingo Fietze a ; Jutta Strauch a ; Martin Holzhausen b ; Martin Glos a ; Christiane Theobald c ; Hanna Lehnkering d ; Thomas Penzel a a Sleep Centre, CC13, Charité-Universitätsmedizin Berlin, Berlin, Germany b Institute for Biometrics and Medical Epidemiology, CC4, Charité-Universitätsmedizin Berlin, Berlin, Germany c National Ballet, Berlin, Germany d Research Group Chronobiology and Behavior, CC1, Charité-Universitätsmedizin Berlin, Berlin, Germany Online Publication Date: 01 August 2009 To cite this Article Fietze, Ingo, Strauch, Jutta, Holzhausen, Martin, Glos, Martin, Theobald, Christiane, Lehnkering, Hanna and Penzel, Thomas(2009)'Sleep Quality in Professional Ballet Dancers',Chronobiology International,26:6,1249 — 1262 To link to this Article: DOI: 10.1080/07420520903221319 URL: http://dx.doi.org/10.1080/07420520903221319 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of SLEEP QUALITY IN PROFESSIONAL BALLET DANCERS

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Glos, Martin]On: 7 September 2009Access details: Access Details: [subscription number 914458806]Publisher Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Chronobiology InternationalPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713597233
Sleep Quality in Professional Ballet DancersIngo Fietze a; Jutta Strauch a; Martin Holzhausen b; Martin Glos a; Christiane Theobald c; Hanna Lehnkering d;Thomas Penzel a
a Sleep Centre, CC13, Charité-Universitätsmedizin Berlin, Berlin, Germany b Institute for Biometrics andMedical Epidemiology, CC4, Charité-Universitätsmedizin Berlin, Berlin, Germany c National Ballet, Berlin,Germany d Research Group Chronobiology and Behavior, CC1, Charité-Universitätsmedizin Berlin, Berlin,Germany
Online Publication Date: 01 August 2009
To cite this Article Fietze, Ingo, Strauch, Jutta, Holzhausen, Martin, Glos, Martin, Theobald, Christiane, Lehnkering, Hanna and Penzel,Thomas(2009)'Sleep Quality in Professional Ballet Dancers',Chronobiology International,26:6,1249 — 1262
To link to this Article: DOI: 10.1080/07420520903221319
URL: http://dx.doi.org/10.1080/07420520903221319
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

SLEEP QUALITY IN PROFESSIONAL BALLET DANCERS
Ingo Fietze,1 Jutta Strauch,1MartinHolzhausen,2MartinGlos,1 Christiane
Theobald,3 Hanna Lehnkering,4 and Thomas Penzel1
1Sleep Centre, CC13, Charite-Universitatsmedizin Berlin, Berlin, Germany2Institute for Biometrics and Medical Epidemiology, CC4, Charite-UniversitatsmedizinBerlin, Berlin, Germany3National Ballet, Berlin, Germany4Research Group Chronobiology and Behavior, CC1, Charite-Universitatsmedizin Berlin,Berlin, Germany
Ballet dancers are competitive athletes who undergo extreme physical and mentalstress and work according to an irregular schedule, with long days of training, rehear-sal, and performance. Their most significant potential risks entail physical injury andaltered sleep. The elaborate training requirements for ballet dancers do not allowregular chronobiological patterns or a normal sleep-wake rhythm. Our aim was toinvestigate the sleep-wake rhythm and sleep quality during rehearsal phases prior toa ballet premiere. We used wrist actigraphy and sleep diaries for a period of 67 daysbefore the ballet premiere performance to study 24 classical ballet dancers. We likewiseapplied the Epworth Sleepiness Score (ESS), Pittsburgh Sleep Quality Index (PSQI),SF-12 Quality of life Assessment, and d2 Test of Attention to assess quality of sleep,aspects of cognitive performance, and health status. We found significant reductionin sleep duration, from 418+43 min to 391+42 min, and sleep efficiency, from81+4% to 79+5%, over the 67-day course of the rehearsal. We also found adecline in time in bed and an increase in wakefulness after sleep onset. Sleep onsetlatency did not change. However, the changes in sleep as documented by actigraphywere not reflected by the subjective data of the sleep diaries and sleep scores. As aresult of the facts that total sleep efficiency and sleep duration values were alreadylower than usual for the dancers’ age group at the beginning of the study and thatmental acuity, concentration, and speed were likewise impaired, we observed exacer-bated health deterioration in terms of sleep deprivation in ballet dancers during prep-aration for a premier. We conclude that individual activity-rest schedules, includingdaytime naps, may be helpful, especially during the stressful training and rehearsalexperienced prior to ballet premieres. (Author correspondence: [email protected])
Keywords Ballet dancers, Athletes, Actigraphy, Sleep efficiency, Sleep-wake rhythm
Submitted December 23, 2008, Returned for revision February 17, 2009, Accepted June 3, 2009Address correspondence toMartin Glos, Sleep Centre, CC13, Charice-Universitatsmedizin Berlin
Luisenstrasse 13, D-10117, Berlin, Germany. Tel.: 49-30 450 513 122; Fax: þ49-30 450 513 906;E-mail: [email protected]
Chronobiology International, 26(6): 1249–1262, (2009)Copyright # Informa Healthcare USA, Inc.ISSN 0742-0528 print/1525-6073 onlineDOI: 10.1080/07420520903221319
1249
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

INTRODUCTION
Many factors influence the homeostatic and circadian regulation ofsleep and, in turn, its quality and quantity. Such factors include irregularsleep-wake schedules, irregular physical exercise, shiftwork, poor sleephygiene, physical disorders, medication, alcohol, nicotine, drugs, loudnoise, light at inappropriate times, as well as stress and sleep disorders(Akerstedt et al., 2007; Bliwise, 2008; Fischer et al., 2008; Muzet, 2007)Sleep disorders, such as sleep-related breathing disorders and periodiclimb movement, are common and must be excluded by the applicationof dedicated tests when investigating sleep quality, sleep duration, andother sleep characteristics of reference or special groups.
In concurrence with previous reference studies, we assumed that themajority of persons have a normal sleep efficiency (ratio of time spentasleep while in bed relative to the total time spent in bed for sleep) of.85% (Bliwise, 2005) and that the sleep duration is between 7 and 8 h(Ferrara & De Gennaro, 2001; Ohayon et al., 2004). Nonetheless, suffi-cient reference data on sleep are lacking, and subjects with healthy sleeppatterns are evidently rare (Fietze & Diefenbach, 2003). Curtailed sleepcan give rise to cognitive deficits and daytime sleepiness (Banks &Dinges, 2007). Moreover, insufficient sleep duration and quality impairwork ability, as is evident among day- and shiftworkers, such as nurses(Camerino et al., 2008).
There has been relatively little extensive investigation into the mannerin which sleep duration and sleep efficiency are altered among athleteswith lengthy exercise and training days, extended work periods, andwithout regular weekends (i.e., patterns not readily comparable to thoseof common shift systems) (Fischer et al., 2008; Knauth, 2007; Lehnkering& Siegmund, 2007). Ballet dancers are athletes who are routinely sub-jected to a high physical and mental work load, in addition to highstress, when training and rehearsing for performances (Koutedakis &Sharp, 2004). They are competitive performers in whom the sequenceof wakefulness and sleep, activity, and rest plays an important role, in amanner similar to that described for other athletes (Leger et al., 2005;Mellman & Podesta, 1997; Postolache et al., 2005). Training and publicperformances during the weekend preclude a conventional weekly workrhythm. Moreover, rehearsals for new performances, joint and musclepain, and the anxiety of suffering career-endangering injuries (Hincapieet al., 2008) constitute common stresses of ballet dancers (Milan, 1994).
We have investigated for the first time the sleep-wake pattern, sleepefficiency, and sleep duration of ballet dancers during three months oftraining prior to the premiere of a new ballet. We applied actigraphy, avalidated quantitative technique established to study sleep duration,sleep efficiency, and movement patterns during sleep (Acebo et al.,
I. Fietze et al.1250
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

1999; Morgenthaler et al., 2007), to assess the sleep-wake pattern. Wehypothesized that the increase in stress during the span before a premierealters sleep quality and duration, even among seasoned performers accus-tomed to performing in public and being involved in activity carried outunder a strictly disciplined work schedule.
METHODS
We performed a prospective field study of quantitative activity record-ing between 15 February and 3 May 2007. The premiere of the new per-formance took place on 28 April, shortly before the end of the recordingperiod.
Ballet dancers were invited to participate if they were not currentlyinvolved in another study, suffered from anymedical disorder, or reportedcurrent or past history of substance (alcohol, medication, drugs, or the like)abuse. A total of 28 members of the Berlin National Ballet volunteered. Ofthese 28 dancers, 24 completed the study (15 female/9 male). Fourdropped out early due to discomfort when wearing the actigraph or to per-ceived additional stress from completion of the daily sleep diary. The studysubjects were between 18 and 40 yrs of age (see Table 1). The femaledancers started their ballet careers at a younger age (6.57+2.47 yrs) thendid the male dancers (7.33+2.10 yrs). The male dancers smoked moreand consumed more alcohol than did the female dancers, and the femaledancers more frequently drank coffee than the male dancers (80.0% vs.44.4%). A total of 58.3% of the studied dancers took medication, primarilyvitamins, magnesium, and calcium as combined pills, and/or analgesicssuch as diclofenac (5 subjects). Their daily training consisted of an individ-ualwarming-upphase lastingup to60min, class trainingwith classical balletfor 90 min starting at 10 : 00 h., and 6.5 h of rehearsals. There was one30 min break. On each day of a public performance (110/yr), the casteddancers were allowed a 5 h time span to relax before preparing for thestage presentation.
TABLE 1 Summary of anthropometric data for the 24 ballet dancers
Subjects All Female Male
Number (N) 24 15 (62.5%) 9 (37.5%)Age (yrs) 27+5 28+4 27+7Height (cm) 172+6 169+3 179+4Weight (kg) 56.1+9.0 50.7+1.2 66.8+5.1BMI (kg/m2) 18.7+2.0 17.4+0.6 20.8+1.7
Ballet dancers were very lean young adults. The male dancers were somewhat taller and had higherBMI.
Sleep Quality in Professional Ballet Dancers 1251
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

The study protocol was submitted to and approved by the InstitutionalEthics Review Committee of the Charite University Medical Centre inBerlin, which administers general guidelines for clinical studies, andadhered to the ethical standards of the journal (Portaluppi et al., 2008).The study was initiated in 2007 as the initial activity of a new health part-nership between the Berlin National Ballet and the Charite UniversityMedical Centre.
All subjects underwent a medical interview and physical examinationby a physician. The baseline exam included assessment of body massindex (BMI), blood pressure, heart rate, ambulatory polygraphy (with avalidated system [Embletta PDS, Embla systems, Broomfield, Colorado,USA] for exclusion of sleep-related breathing disorders and periodic legmovements), and application of specific sleep questionnaires. We appliedthe Epworth Sleepiness Score (ESS) for assessment of sleepiness (Johns,2001), Pittsburgh Sleep Quality Index (PSQI) for sleep habits (Buysseet al., 1989), Quality of Life Questionnaire for general wellbeing in itsSF-12 short form for health status (Gandek et al., 1998), and d2 Test ofAttention for cognitive performance (Brickenkamp, 1994). In addition,we identified the individual chronotype using the Horne and Ostbergquestionnaire for English-speaking dancers (Horne & Ostberg, 1976)and the validated German version of the same questionnaire for theother dancers (Griefahn et al., 2001). All questionnaires were appliedone time at the beginning of the investigations.
Continuous recording of activity over the 67-spanwas performed usingMinimitterMonitors (Actiwatch AW-64, IM Systems, Baltimore, Maryland,USA). Actigraphs were worn continuously, except for short intervals whenthey could otherwise have been exposed towater and/or during special ath-letic activities or performances on stage. The actigraphs were worn on thenon-dominant wrist according to standard criteria (Morgenthaler et al.,2007). Acceleration of the wrist to which the actigraph is affixed is sensedby miniature piezo-electric sensors with bi-axial detection, with the outputdigitized at a sampling rate of 40 Hz and with storage at 1 min intervals inthe actigraph memory. Calculation of the sleep-time and activity-restindex were scored by the software Activity & Sleep Analysis 5 (Version5.48, CamNtech Ltd., Cambridge, UK) provided with the Actiwatch.
Eloquent sleep-wake scoring can be reliably obtained only withadditional information provided inmanually completed sleep logs. All par-ticipants were therefore requested to complete daily sleep diaries. Thesleep log items were selected according to common recommendations(Koutedakis & Sharp, 2004; Middelkoop et al., 1997). The subjects wereasked to record the times of going to bed, falling asleep, waking up, andleaving the bed. On this basis, as well as the completion of the various ques-tionnaires/forms, we evaluated subjective sleep quality, work schedule,health problems, and activity periods during the day.
I. Fietze et al.1252
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

Data Analysis
Activity recordings were rated usable if �80% of the recorded nightswere complete. The automatic sleep-scoring algorithm employedadditional information from the actigraphic recordings. Total sleep time(TST), sleep efficiency (SE), and number of movements/min (NMM)were calculated daily over the entire recording period. Additional par-ameters were sleep onset latency (SL, lapse in time between retiring tobed and attaining sleep), wake after sleep onset (WASO, total amount oftime spent awake after first sleep occurred), and time in bed (TIB).
Statistical Analysis
Nonparametric tests for statistical analysis (SPSS version 15.0, SASversion 9.1) were applied because the data were not normally distributed.The level of significance was set to p , 0.05. TST, SE, SL,WASO, TIB, andNMM were investigated. We evaluated recordings between 20 Februaryand 27 April 2007 (i.e., the night before the premiere performance) fora sum total of 67 days completed for all subjects. We used a statistical analy-sis to check for trends and a multi-level regression model with randomintercept to determine the effect of the recorded number of minutes onsubjects’ sleep efficiency (level 1 being the time course, level 2 the individ-ual participant). Model 1 shows the individual stability of sleep time by suc-cessively adding the factors of time (Model 2) and number of minutesmoving (Model 3) as predictors. We used non-parametric Brunnermodels for small sample sizes that allow for multiple missing data(,20% allowed/subject) to determine changes in SL, WASO, and TIB.The Student’s t-test was applied to compare the SF-12 and d2 Test ofAttention with respective questionnaire reference norms (Brickenkamp,1994; Gandek et al., 1998), and the Mann-Whitney U-rank test was usedto compare the groups for PSQI, ESS, SF-12, and d2 Test of Attention.Pearson’s correlation coefficients were derived to investigate relationshipsamong the scores of the PSQI and ESS, age, BMI, and mean SE at thebeginning of the study, as well as changes in mean SE and/or NMMbetween the beginning and end of the 67-day recording period. Sex differ-ences in values of these parameters were assessed by the Mann-WhitneyU-rank test.
RESULTS
All 24 subjects completed the medical interview, physical examination,SF-12, PSQI, ESS, d2 Test, and ambulatory polygraphy study. The SF-12values of the ballet dancers were similar to normal (reference) subjects;however, the mental sum score was significantly lower (p , 0.02) than
Sleep Quality in Professional Ballet Dancers 1253
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

the published reference values (45.9 vs. 51.9 points) (Gandek et al., 1998).The PSQI was normal in most subjects (Buysse et al., 1989), and in 12ballet dancers the PSQI was .5. The mean ESS was 7.6, but a high ESSvalue .9 was found in four (16.7%) of the dancers. The ballet dancersdemonstrated a significantly (p , 0.049) lower speed in processingletters (434.8+74.2 number of letters processed) and lower concentrationperformance (166.6+36.6 number of correct checked letters minuswrong checked letters) relative to the age-adjusted normal values for thed2 Test of Attention (Brickenkamp, 1994). Dancers who exhibited lowersleep quality according to the PSQI also scored lower on the SF-12mental health component (p ¼ 0.034; Z ¼ 22,117). Dancers with a clini-cally elevated PSQI also demonstrated higher effort rates in the d2 Testof Attention (p ¼ 0.022), and dancers with a higher ESS also scoredworse on the SF-12 physical health component (p ¼ 0.008). Of the 22ballet dancers who completed the Horne and Ostberg or German chron-otype questionnaire, one male was definitely a morning type, one femalewas a moderate morning type, 15 (5 males/10 females) were intermediatetype, and 5 (2 males/3 females) were moderate evening types. Polygraphicsleep recordings revealed that 21 of the 24 dancers were normal sleepers.Their mean apnea/hypopnea index (AHI) was 3.95+6.2/h, mean oxygensaturation 96.6+1.4%, mean nocturnal pulse rate 55.2+6 beats/min, andmean periodic limb movement index (PLMI) 4.9+5.4/h. One dancer evi-denced sleep apnea, with an AHI of 29.8/h, and two others showed peri-odic leg movement syndrome, with PLMI .10/h.
Over the 67-day span of study, the mean time of falling asleep was00 : 52 h, and mean the time of rising was 08:40 h according to the sleepdiaries.
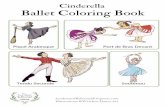
ThemeanTST, as determined by actigraphy, for the subjects in the firstweek of the study was 418.31+42.86min. It decreased significantly duringthe study (B ¼ 3.26, df ¼ 12.10, p , 0.001; see Figure 1). During the lastweek before the performance, TST declined to 391.75+41.80 min.
The mean SE in the first week of the study was 81.12+4.36%, and itdecreased significantly over time (B ¼ 2.58, df ¼ 13.10, p , 0.001), inde-pendent of sex (see Figure 1). During the last week of recordings, prior tothe premiere, mean SE was 78.61+4.68%. Statistical analyses disclosedsignificant effects on SE over time (i.e., decrease by 0.057 SE units/day)as well as on nocturnal activity (0.108 SE units/NMM units). There wasno relation among the alterations in SE and the PSQI and ESS scores,age, or BMI.
Themean SL value the first week of the study was 18.05+9.48 min. SLdid not vary significantly over the course of the study (B ¼ 1.97, df ¼ 5.68,p ¼ 0.069), even though the mean SL the week prior to performancedecreased to 15.38+6.93 min. There was no sex difference (p ¼ 0.364),
I. Fietze et al.1254
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

nor was there an interaction between the time course of training andrehearsal and sex (p ¼ 0.329).
The mean WASO was 72.13+27.68 min the first week. It varied signifi-cantly over the course of the study (B ¼ 1.95, df ¼ 9.92, p ¼ 0.035). ThemeanWASO increased the week prior to the premiere to 74.22+27.01 min.
FIGURE 1 Actigraphy over 68 days for all 24 ballet dancers aligned, with day zero marking the day ofthe premiere (a few more days were recorded after the premiere and are shown here) and data aver-aged per study day. The upper panel shows sleep efficiency calculated as percent total sleep time overtime spent in bed. The regression line indicates the clear decline during the period before the premiereperformance. The lower panel shows the total sleep time, which also demonstrates a decline, though toa lesser extent.
Sleep Quality in Professional Ballet Dancers 1255
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

Therewas,however,no sexdifference (p ¼ 0.849)or interactionbetween timecourse of the study span and sex (p ¼ 0.721).
In the first week, the mean TIB was 516.89+59.88 min. However, theTIB was not stable over the course of the study (B ¼ 2.94, df ¼ 10.55,p ¼ 0.001). The mean TIB in the week prior to the premiere decreasedto 498.71+49.93 min. There was no sex difference (p ¼ 0.345) or inter-action between the time course of the study and sex (p¼0.463).
The mean NMM during the nights of the first week of the study was66.97+21.84 min. Activity during sleep increased slightly during thestudy (B ¼ 1.58, df ¼ 11.12, p ¼ 0.097). The mean NMM during thenight during the week prior to the premiere was 69.07+21.46 min.There was no significant sex difference in the NMM (p ¼ 0.967), andthere was no significant relation between the time course of training andsex (p ¼ 0.493). Moreover, there was no relation between the increase inNMM and PSQI and ESS scores, age, and BMI.
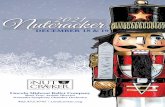
Subjective sleep durationwas derived from the sleepdiaries as values foreach single day (see Figure 2). No significant changes in subjective sleepduration were found. The mean sleep duration was 467.78+20.99 minduring the first week of the study and 455.23+43.65 min the week priorto the premiere. Subjective sleep quality was derived from the subjectivesleep scores provided in the diaries of the dancers. The scores rangedbetween 1 (good sleep quality) to 3 (bad sleep quality). The overall meanscore was 1.33+0.17, although there was great variability in subjective
FIGURE 2 Subjectively reported sleep time derived from the daily sleep diaries over 68 days for the 24ballet dancers presented in the same manner as Figure 1. The regression line indicates no significantchange in subjective sleep time during the period before the premiere performance.
I. Fietze et al.1256
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

ratings of sleep quality betweendancers and betweendays.We foundno sig-nificant changes in the subjective ratings of sleep quality during the studyand no significant changes when comparing the scores of first and lastweek of the study.
DISCUSSION
Our 67-day study of the sleep-wake schedule in professional balletdancers during a period of high physical andmental stress due to prepara-tory training for a ballet premiere revealed that SE and sleep durationwere impaired. In addition, TIB decreased and WASO increased. Thesechanges occurred even though SE and sleep duration were already rela-tively low at the beginning of the study. SL did not change over thecourse of study. Changes in sleep parameters, as derived by actigraphy,indicate that the specific extended work schedule of ballet dancers influ-ences their sleep-wake schedule, especially in the months preparatory toa ballet premiere. This effect exacerbates the low SE that was found tobe present in the group of dancers at the onset of the study and producesresults comparable to those of patients suffering from mild insomnia oreffects of shiftwork (Knauth, 2007; Pilcher, 2000). Stress is one of thefactors that may significantly influence the sleep of the ballet dancers.Other factors that are capable of influencing sleep duration and time inbed are daily working time, smoking, drinking habits, irregular physicalexercise, and the sleep-wake cycle variables of napping and socialization,as shown in adolescents (Fischer et al., 2008).
We determined that the time needed to fall asleep (SL) and amount ofactivity during sleep (NMM) did not change over the two months of studybefore the ballet premiere, but that sleep quality, sleep duration, TIB, andWASO did. This finding is noteworthy, as experienced and very well-trained dancers perform in approximately five ballet premieres perseason, which leads one to assume that they should be well adapted tothis situation. Based on the reported disciplined sleep-wake schedule, wedid not expect lower sleep quality or reduced sleep duration during thisperiod. Our ballet dancers intended to obtain sufficient sleep. As an indi-cation of this, the reported TIB at the beginning of the study was 517 min,decreasing to 499 min in the final week, but which is still a long duration.In healthy subjects, the SE is .85% (Bliwise, 2005); however, in our balletdancers, the SE was below average, being only 78.8%. Such a reduced SE istypically found in young and less well-trained adults (Lee & Lin, 2007). Wedid not detect significant sex differences, perhaps owing to the smallsample size of the study. We found no change in sleep quality based onthe subjective sleep-quality scores or reported duration of sleep in thediaries (see Figure 2). We thus assume that the dancers do not recognize
Sleep Quality in Professional Ballet Dancers 1257
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

their shortened sleep duration and lower objective sleep quality, and thatthey do not complain about these changes.
The extent of daily ballet training did not increase over the studyperiod. It is accordingly more likely that mental factors are responsiblefor the stress encountered (e.g., learning new roles, anxiety of takingpart in the premiere performance, and ongoing fear of physical injury).This stress was reflected in the mental health score (SF-12) of thedancers, which was lower than normal (Gandek et al., 1998). Extremephysical demands and mental stress may also be responsible for the lowperformance, with regard to speed and concentration, recorded on thed2 Test of Attention (Spreen & Strauss, 1998).
One factor that may explain the objective changes in sleep quality andduration is the very late time that the dancers went to bed (i.e., 00 : 52 h onaverage). In this context, we determined a delayed sleep-wake rhythm aswell as loss of the seven-day rhythm because rehearsals were scheduledeach day of the week, including the weekend days. We observed that theTIB was rather long, as an indication to get sleep, but the TST and SEwere low, as an indication of sleep deprivation. The late mental and phys-ical stress occasioned by evening performances, the missing recoverybetween an “end of work” session and usual bedtime under possibleunder normal daytime work conditions, and the absence of free days asregular weekends markedly influenced sleep. Physical pain, most oftenof the joints at night, might have also played a role in fragmenting sleep(Hincapie et al., 2008). Therefore, dancers occasionally resort to the usepain relievers in the evening; however, during our study, we did notobserve increased use of these medications.
Our dancers experienced a short basal TST of 6.43 h on average. Thisis below the suggested requirements of 7–8 h (Carskadon & Dement,2005; Ferrara & De Gennaro, 2001; Ohayon, 2004), and it is less thanthe subjective sleep duration in Germany overall (Meier, 2004; Ohayon& Zulley, 2001) and below the sleep duration among German medical stu-dents of nearly the same age range (Lehnkering & Siegmund, 2007).Indeed, this sleep duration is rather comparable to that of shiftworkers(Knauth et al., 1980; Pilcher, 2000).
Although the short sleep duration itself may lead to additional stressand health consequences (McEwen, 2006; Van Cauter et al., 2007) and alowering work ability and performance in shiftworkers (Camerino et al.,2008; Knauth, 2007), the influence of disturbed or shortened sleep on ath-letic performance is still unclear (Leger et al., 2005). Even a slight degreeof less than optimal sleep may be accompanied, for example, by the wor-sening of reaction time. This is particularly relevant here, as reactiontime is an ubiquitous element of athletic performance. Because sleep isimportant for memory consolidation, including retention of psychomotorskills, sleep loss may be associated with decreased cognitive performance
I. Fietze et al.1258
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

(Fulda & Schulz, 2001). This may explain the low speed and low concen-tration on the d2 Test of Attention among our ballet dancers.
Sleepiness may likewise be one complaint often observed in dancers.Although the ESS showed a normal mean value of ,10 (Johns, 1991),an observed increase in sleepiness (ESS) correlates well with a decreasein physical health, as concluded from the findings of the SF-12. Otherwise,a pathological PSQI is correlated with impairment of concentrationderived from the d2 Test of Attention. We were therefore able toconfirm in our young healthy subjects the well-known relationshipbetween decline in self-perceived physical and mental performance,well-being, and sleepiness (Samuels, 2008). It is worthy of mention herethat the questionnaires were filled out only once, at the beginning of thestudy, without another evaluation upon study completion. Accordingly,we were unable to explore correlations over the course of the study spanbetween objective sleep changes that were evaluated by actigraphy andsubjective changes that were evaluated by specific questionnaires forsleep, cognition, and quality of life (QoL).
Resting periods and sleep-wake schedules are normally planned forthe entire ballet team, regardless of individual distinctions. On the basisof the findings of the present study, it would be more effective to plan indi-vidualized schedules. Another possibility for compensation of shortenedsleep duration is strategic napping, a simple technique for functionalimprovement also recommended for shiftworkers before a night shift(Morgenthaler et al., 2007). Napping reduces sleep pressure (Werthet al., 1996) and can be more effective than merely a short break(Horner & Foster, 1995) or a break with light exercise (Sallinen et al.,2008). For ballet dancers, athletes, or persons with common extendedwork schedules, we especially recommend a short nap. It has beenshown that a nap as short as 10–20 min may reduce sleepiness under con-ditions of prior sleep deficit (Hayashi et al, 1999; Takahashi & Arito, 2000;Tietzel & Lack, 2002). Ballet dancers begin their training at 10 : 00 h andare required to perform at their peak at 20 : 00 h for public performances.Their schedule includes two to three public performances per week, total-ling 110/yr during 43 working weeks. The greatest effort is requiredduring the evening, when psychomotor vigilance and subjective alertnessnormally decrease after a typical day of activity (Wyatt et al., 1999). Onecompensation for this situation may be the so-called wake-maintenancezone that occurs roughly 3 h prior to falling asleep (Lack et al., 2008).During this time, psychomotor, cognitive, and physical abilities, as wellas their coordination, are almost at peak.
In summary, the objective decrease in sleep duration and sleep effi-ciency during the period prior to a premiere performance was not subjec-tively reflected, and performance was evidently unimpaired, based uponthe subjective reporting by the ballet master. Moreover, the number of
Sleep Quality in Professional Ballet Dancers 1259
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

injuries did not increase over the course of training and rehearsal for theperformance. However, our sleep data reflect ongoing stress in balletdancers that increases before a premiere performance. This phenomenon,in conjunction with the fact that baseline sleep duration and sleep effi-ciency were already lower in this group than in the normal population,leads us to recommend that ballet dancers should focus attention notonly on their physical condition and nutrition, but also on their relaxation,including their sleep-wake behavior. These results furthermore supportthe emphasis of European policies on increasing the resources availableto persons with extended work periods (e.g., sufficient time for adequateregeneration in order to protect their health and well-being). This situ-ation might be improved by intentional short naps during the daytimeto compensate for sleep deficit. Awareness of these factors could assistdancers or persons with typically extended work schedules, such asother athletes or shiftworkers, toward improving their training orworking intensity, enhancing physical and psychological fitness, and avoid-ing injuries or fatal errors. An immediate consequence of the findings ofthis study has been the installation of a dedicated napping room inBerlin for professional ballet dancers as part the new health partnershipbetween the Berlin National Ballet and the Charite University MedicalCentre. A follow-up study is planned to investigate the effect of this inter-vention (i.e., napping) on sleep duration and sleep quality.
ACKNOWLEDGMENTS
This study was solely funded by Charite University funds. Weespecially thank the Berlin National Ballet dancers for their support andunderstanding of issues related to clinical research. The authors wish toexpress special thanks to Wladimir Malakhov, the intendant of the balletcompany and to Dr. Dirk Kowalski, the chair of the association offriends and supporters for the Staatsballet Berlin.
DECLARATION OF INTEREST
The authors report no conflicts of interest. The authors alone areresponsible for the content and writing of the paper.
REFERENCES
Acebo C, Sadeh A, Seifer R, Tzischinsky O, Wolfson AR, Hafer A, Carskadon MA. (1999). Estimatingsleep patterns with activity monitoring in children and adolescents: How many nights are necess-ary for reliable measures? Sleep 22:95–103.
Akerstedt T, Kecklund G, Gillberg M. (2007). Sleep and sleepiness in relation to stress and displacedwork hours. Physiol. Behav. 92:250–255.
I. Fietze et al.1260
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

Banks S, Dinges DF. (2007). Behavioral and physiological consequences of sleep restriction. J. Clin.Sleep Med. 15:519–528.
Bliwise DL. (2005). Normal aging. In Kryger M, Roth T, Dement WC (eds). Principles and practice ofsleep medicine. Philadelphia, Pa.: Elsevier Saunders, pp. 24–38.
Bliwise DL. (2008). Invited commentary: Cross-cultural influences on sleep—broadening the environ-mental landscape. Am. J. Epidemiol. 168:1365–1366.
Brickenkamp R. (1994). Test d2. Aufmerksamkeits-Belastungs-Test. Goettingen: Hogrefe.Buysse DJ, Reynolds CF, III, Monk TH, Berman SR, Kupfer DJ. (1989). The Pittsburgh Sleep Quality
Index: A new instrument for psychiatric practice and research. Psychiatry Res. 28:193–213.Camerino D, Conway PM, Sartori S, Campanini P, Estryn-Behar M, van der Heijden BI, Costa G.
(2008). Factors affecting work ability in day and shift-working nurses. Chronobiol. Int. 25:425–442.Carskadon MA, Dement WC. (2005). Normal human sleep: An overview. In Kryger M, Roth T,
Dement WC (eds). Principles and practice of sleep medicine. Philadelphia, Pa.: Elsevier Saunders,pp. 13–23.
Ferrara M, De Gennaro L. (2001). How much sleep do we need? Sleep Med. Rev. 5:155–179.Fietze I, Diefenbach K. (2003). Healthy sleepers are rare: Problems and success rates in establishing a
control group for sleep studies. Neuropsychopharmacology 28:558–561.Fischer FM, Nagai R, Teixeira LR. (2008). Explaining sleep duration in adolescents: The impact of
socio-demographic and lifestyle factors and working status. Chronobiol. Int. 25:359–372.Fulda S, Schulz H. (2001). Cognitive dysfunction in sleep disorders. Sleep Med. Rev. 5:423–445.Gandek B, Ware JE, Aaronson NK, Apolone G, Bjorner JB, Brazier JE, Bullinger M, Kaasa S, Leplege
A, Prieto L, SullivanM. (1998). Cross-validation of item selection and scoring for the SF-12HealthSurvey in nine countries: Results from the IQOLA Project. International Quality of Life Assess-ment. J. Clin. Epidemiol. 51:1171–1178.
Griefahn B, Kunemund C, Brode P, Mehnert P. (2001). The validity of a German version of the morn-ingness-eveningness-questionnaire developed by Horne and Ostberg. Somnology 5:71–80.
Hayashi M, Watanabe M, Hori T. (1999). The effects of a 20 min nap in the mid-afternoon on mood,performance and EEG activity. Clin. Neurophysiol. 110:272–279.
Hincapie CA, Morton EJ, Cassidy JD. (2008). Musculoskeletal injuries and pain in dancers: A systema-tic review. Arch. Phys. Med. Rehabil. 89:1819–1829.
Horne JA, Ostberg O. (1976). A self-assessment questionnaire to determine morningness-eveningnessin human rhythms. Int. J. Chronobiol. 4:97–110.
Horner JA, Foster SC. (1995). Can exercise overcome sleepiness? Sleep Res. 24A:437.Johns MW. (1991). A new method for measuring daytime sleepiness: The Epworth sleepiness scale.
Sleep 14:540–545.Knauth P. (2007). Extended work periods. Ind. Health 45:125–136.Knauth P, Landau K, Droge C, Schwitteck M, Widynski M, Rutenfranz J. (1980). Duration of sleep
depending on the type of shift work. Int. Arch. Occup. Environ. Health 46:167–177.Koutedakis Y, Sharp NC. (2004). Tight-muscles strength training, dance exercise, dynamometry, and
anthropometry in professional ballerinas. J. Strength Cond. Res. 18:714–719.Lack LC, Gradisar M, van Someren EJ, Wright HR, Lushington K. (2008). The relationship between
insomnia and body temperature. Sleep Med. Rev. 12:307–317.Lee AJ, Lin WH. (2007). Association between sleep quality and physical fitness in female young adults.
J. Sports Med. Phys. Fitness 47:462–467.Leger D, Metlaine A, Choudat D. (2005). Insomnia and sleep disruption: Relevance for athletic per-
formance. Clin. Sports Med. 24:269–285.Lehnkering H, Siegmund R. (2007). Influence of chronotype, season, and sex of subject on sleep
behaviour of young adults. Chronobiol. Int. 24:875–888.McEwen BS. (2006). Sleep deprivation as a neurobiologic and physiologic stressor, allostasis and allo-
static load. Metabolism 55:S20–S23.Meier U. (2004). Das Schlafverhalten der deutschen Bevolkerung- eine reprasentative Umfrage.
Somnologie 8:87–94.Mellman MF, Podesta L. (1997). Common medical problems in sports. Clin. Sports Med. 16:635–662.Middelkoop HA, van Dam EM, Smilde-van den Doel DA, van Dijk G. (1997). 45-hour continuous
quintuple-site actimetry: Relations between trunk and limb movements and effects of circadiansleep-wake rhythmicity. Psychophysiology 34:199–203.
Sleep Quality in Professional Ballet Dancers 1261
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009

Milan KR. (1994). Injury in ballet: A review of relevant topics for the physical therapist. J. Ortho. SportsPhys. Ther. 19:121–129.
Morgenthaler T, Alessi C, Friedman L, Owens J, Kapur V, Boehlecke B, Brown T, Chesson A Jr,Coleman J, Lee-Chiong T, Pancer J, Swick TJ. (2007). Practice parameters for the use ofactigraphy in the assessment of sleep and sleep disorders: An update for 2007. Sleep 30:519–529.
Muzet A. (2007). Environmental noise, sleep and health. Sleep Med. Rev. 1:135–142.OhayonMM, Zulley J. (2001). Correlates of global sleep dissatisfaction in the German population. Sleep
24:780–787.Ohayon MM, Carskadon MA, Guilleminault C, Vitiello MV. (2004). Meta-analysis of quantitative sleep
parameters from childhood to old age in healthy individuals: Developing normative sleep valuesacross the human lifespan. Sleep 27:1255–1273.
Pilcher JJ, Lambert BJ, Huffcutt AI. (2000). Differential effects of permanent and rotating shifts on self-report sleep length: A meta-analytic review. Sleep 23:155–163.
Portaluppi F, Touitou Y, Smolensky MH. (2008). Ethical and methodological standards for laboratoryand medical biological rhythm research. Chronobiol. Int. 25:999–1016.
Postolache TT, Hung TM, Rosenthal RN, Soriano JJ, Montes F, Stiller JW. (2005). Sports chronobiol-ogy consultation: From the lab to the arena. Clin. Sports Med. 24:415–456.
SallinenM,Holm J, Hirvonen K, HarmaM, Koskelo J, Letonsaari M, Luukkonen R, Virkkala J, MullerK. (2008). Recovery of cognitive performance from sleep debt: Do a short rest pause and a singlerecovery night help? Chronobiol. Int. 25:279–296.
Samuels C. (2008). Sleep, recovery, and performance: The new frontier in high-performance athletics.Neurol. Clin. 26:169–180.
Spiegel K, Leproult R, Van Cauter E. (1999). Impact of sleep debt on metabolic and endocrine func-tion. Lancet 354:1435–1439.
SpreenO, Strauss E. (1998).A compendium of neuropsychological tests. OxfordUniversity Press, NewYork.Takahashi M, Arito H. (2000). Maintenance of alertness and performance by a brief nap after lunch
under prior sleep deficit. Sleep 23:813–819.Tietzel AJ, Lack LC. (2002). The recuperative value of brief and ultra-brief naps on alertness and cog-
nitive performance. J. Sleep Res. 11:213–218.Van Cauter E, Holmback U, Knutson K, Leproult R, Miller A, Nedeltcheva A, Pannain S, Penev P,
Tasali E, Spiegel K. (2007). Impact of sleep and sleep loss on neuroendocrine and metabolic func-tion. Horm. Res. 67(Suppl. 1):2–9.
Werth E, Dijk DJ, Achermann P, Borbely AA. (1996). Dynamics of the sleep EEG after an early eveningnap: Experimental data and simulations. Am J Physiol. 271:R501–R510.
Wyatt JC, Ritz-De Cecco A, Czeisler CA, Dijk DJ. (1999). Circadian temperature and melatoninrhythms, sleep, and neurobehavioral function in humans living on a 20 h-day. Am. J. Physiol.277:R1152–R1163.
I. Fietze et al.1262
Downloaded By: [Glos, Martin] At: 11:32 7 September 2009