Serum 25-hydroxyvitamin D level and the risk of mild cognitive impairment and dementia: the Korean...
15
Accepted Article This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. Please cite this article as doi: 10.1111/cen.12733 This article is protected by copyright. All rights reserved. Article Type: Original Article Serum 25-hydroxyvitamin D level and the risk of mild cognitive impairment and dementia: the Korean Longitudinal Study on Health and Aging (KLoSHA) Abbreviated Title: Serum 25-hydroxyitamin D and cognitive decline Jae Hoon Moon 1,* , Soo Lim 1,* , Ji Won Han 2 , Kyoung Min Kim 1 , Sung Hee Choi 1 , Ki Woong Kim 2,3 , Hak Chul Jang 1 1 Department of Internal Medicine, Seoul National University Bundang Hospital and Seoul National University College of Medicine, Seongnam-si, Gyeonggi-do, Korea 2 Department of Neuropsychiatry, Seoul National University Bundang Hospital and Seoul National University College of Medicine, Seongnam-si, Gyeonggi-do, Korea 3 Department of Brain and Cognitive Science, Seoul National University College of Natural Sciences, Seoul, Korea. *Authors equally contributed to this work. Corresponding author and reprint requests: Ki Woong Kim, M.D., Ph.D. Professor Department of Neuropsychiatry Seoul National University Bundang Hospital, Seoul National University College of Medicine 300 Gumi-dong, Bundang-gu, Seongnam-si, Gyeonggi-do 463-707, Korea Tel: +82-31-787-7432 E-mail: [email protected] Fax: +82-31-787-4052 Hak Chul Jang, M.D., Ph.D. Professor Department of Internal Medicine Seoul National University Bundang Hospital, Seoul National University College of Medicine 300 Gumi-dong, Bundang-gu, Seongnam-si, Gyeonggi-do 463-707, Korea Tel: +82-31-787-7005 E-mail: [email protected] Fax: +82-31-787-4052
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Serum 25-hydroxyvitamin D level and the risk of mild cognitive impairment and dementia: the Korean...

Acc
epte
d A
rtic
le
This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. Please cite this article as doi: 10.1111/cen.12733 This article is protected by copyright. All rights reserved.
Article Type: Original Article
Serum 25-hydroxyvitamin D level and the risk of mild cognitive impairment and dementia: the
Korean Longitudinal Study on Health and Aging (KLoSHA)
Abbreviated Title: Serum 25-hydroxyitamin D and cognitive decline
Jae Hoon Moon1,*, Soo Lim1,*, Ji Won Han2, Kyoung Min Kim1, Sung Hee Choi1, Ki Woong Kim2,3,
Hak Chul Jang1
1Department of Internal Medicine, Seoul National University Bundang Hospital and Seoul National
University College of Medicine, Seongnam-si, Gyeonggi-do, Korea 2Department of Neuropsychiatry, Seoul National University Bundang Hospital and Seoul National
University College of Medicine, Seongnam-si, Gyeonggi-do, Korea 3Department of Brain and Cognitive Science, Seoul National University College of Natural Sciences,
Seoul, Korea.
*Authors equally contributed to this work.
Corresponding author and reprint requests:
Ki Woong Kim, M.D., Ph.D.
Professor
Department of Neuropsychiatry
Seoul National University Bundang Hospital, Seoul National University College of Medicine
300 Gumi-dong, Bundang-gu, Seongnam-si, Gyeonggi-do 463-707, Korea
Tel: +82-31-787-7432 E-mail: [email protected] Fax: +82-31-787-4052
Hak Chul Jang, M.D., Ph.D.
Professor
Department of Internal Medicine
Seoul National University Bundang Hospital, Seoul National University College of Medicine
300 Gumi-dong, Bundang-gu, Seongnam-si, Gyeonggi-do 463-707, Korea
Tel: +82-31-787-7005 E-mail: [email protected] Fax: +82-31-787-4052
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Keywords: vitamin D, vitamin D deficiency, mild cognitive impairment (MCI), dementia
Acknowledgments
This study was supported by a National Research Foundation grant funded by the Korea Government
(Ministry of Education, Science, and Technology) (No. 2006-2005410) and by a grant from the Korean
Health Technology R&D Project, Ministry of Health, Welfare and Family Affairs, Republic of Korea (No.
A092077). The authors have nothing to disclose on conflicts of interest.
The authors thank the Medical Research Collaborating Center at Seoul National University Bundang
Hospital, as well as Prof. Soyeon Ahn for the reviewing statistical analyses.
Abstract
Objective: The association of low vitamin D status with mild cognitive impairment (MCI), a
preclinical condition that can lead to dementia, has not yet been fully explored. Our aim was to
investigate the association between vitamin D status and the future risk of MCI and dementia in older
adults.
Design, setting, and participants: We conducted a population-based prospective study as a part of
the Korean Longitudinal Study on Health and Aging. Four hundred and twelve elderly participants
who completed evaluations of cognitive function and metabolic parameters in 2005–2006 and 2010–
2011 were analyzed.
Major outcome measure: The rate of development of MCI or dementia during the study period was
compared according to baseline vitamin D status. Binary logistic regression analysis was performed to
investigate any independent association between vitamin D status and the risks of MCI or dementia.
Results: Among 405 subjects that remained after excluding seven demented subjects at baseline, 338
subjects remained unchanged or improved in their diagnosis for cognitive function during the study
period, whereas 67 subjects showed progression to MCI or dementia. When analyzing 236 subjects
whose baseline mini-mental state examination (MMSE) scores were <27, severe vitamin D deficiency
at baseline, defined as < 25 nmol/L, was independently associated with the progression of cognitive
impairment. Among 297 subjects who were normal at baseline, 50 acquired MCI and 247 remained
normal. Severe vitamin D deficiency was also independently associated with the development of MCI
when analyzing 145 subjects whose baseline MMSE scores were < 27.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Conclusion: Severe vitamin D deficiency was independently associated with the future risk of MCI
as well as dementia, especially in older adults whose baseline MMSE scores had decreased only
modestly.
Introduction
Vitamin D status is determined by the serum level of 25-hydroxyvitamin D, or 25(OH)D; and a low
vitamin D status is common and considered as a major health problem in elderly populations1-3. Several
studies have reported that low vitamin D status is associated with poor bone health and other conditions
including cardiovascular diseases, insulin resistance, autoimmune diseases, and certain malignancies4-6.
Therefore, vitamin D is now considered to play an important role in muscle function, immunity,
metabolic signaling, and protection against cardiovascular diseases and malignancies7.
The global population is aging and the prevalence and economic burdens of dementia are rapidly
increasing worldwide as well as in Korea8, 9. Low vitamin D status has also received attention as a
potential metabolic risk factor for dementia. A number of studies have shown that a low serum 25(OH)D
concentration was associated with an increased risk of dementia and Alzheimer’s disease in older adults10,
11. However, the association of low vitamin D status with mild cognitive impairment (MCI), a preclinical
condition that can lead to dementia12, 13, has not yet been fully explored. Considering the possibility of
“critical periods” at older ages during which an adequate vitamin D level might prevent neurocognitive
loss, it is important to evaluate any association of low vitamin D status with MCI so that we can screen
and manage low vitamin D status in the elderly as early as possible to reduce the future risk of dementia.
Here we investigated the association between vitamin D status and the future risk of MCI and dementia in
a population-based prospective cohort of Korean elders. Comprehensive cognitive domains with other
potential confounding factors that could affect cognitive function were examined.
Materials and Methods
Subjects
This study was conducted as a part of the Korean Longitudinal Study on Health and Aging (KLoSHA),
which was designed as a population-based prospective cohort study on health, aging, and common
geriatric diseases in elderly Korean subjects aged 65 years or older14. Four hundred and twelve elderly
participants (mean age, 72.5 ± 7.0 years; 203 men and 209 women) who completed evaluations for
cognitive function and metabolic parameters during 2005–2006 and 2010–2011 were analyzed. Vitamin
D adequacy was defined according to the serum 25(OH)D concentration; levels of <25(OH)D and 25.0–

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
49.9 nmol/L indicate severe vitamin D deficiency and vitamin D deficiency, respectively. Adequate
serum vitamin D status was defined as 50.0 nmol/L or more of serum 25(OH)D. The subjects were
grouped according to this definition. This study was approved by the Institutional Review Board of the
Seoul National University Bundang Hospital. The subjects were fully informed regarding study
participation and written informed consent was obtained from each individual or their legal guardians.
Baseline lifestyle characteristics
Smoking status was divided into three categories: “current smoker” if the individual had smoked currently
for at least 1 year; “nonsmoker” if the individual had never smoked; and “ex-smoker” if the individual
had smoked but quit. For alcohol consumption, subjects were divided into the categories: “current
drinker” or “nondrinker”. A current drinker was defined as a person who consumed more than four
standard drinks per week (50 g/week of ethanol).
Anthropometric and biochemical parameters
We measured the height and weight of subjects in light clothing and without shoes to the nearest 0.1 cm
and 0.1 kg, respectively. The body mass index (BMI) was calculated by determining the ratio between
weight and the square of the height (expressed in kg/m2). A standard mercury sphygmomanometer was
used to measure blood pressure. The mean of two measurements was used to determine systolic and
diastolic blood pressures (SBP and DBP, respectively). Serum 25(OH)D concentrations were measured
using Diels–Alder derivatization and ultrahigh performance liquid chromatography–tandem mass
spectrometry (Waters, Milford, MA, USA), which is a “gold standard” for evaluating 25(OH)D
concentration15. Calibration was performed with standard reference material 972 from the National
Institute of Standards and Technology, and the intra- and interassay coefficients of variation were 4.0%
and 7.7% at 29.0 ng/ml, respectively. Fasting plasma glucose concentration was measured using the
glucose-oxidase method (YSI 2300 STAT glucose analyzer, Yellow Springs Instrument Co., Yellow
Springs, OH, USA).
Diagnoses of hypertension and diabetes mellitus
SBP/DBP below 120/80 mmHg was defined as normal on two consecutive measurements;
prehypertension was defined as 120/80 to 139/89 mmHg; and hypertension was defined as at least 140/90
mmHg or if the subjects were on antihypertensive medication. Normal glucose regulation was defined as
a fasting glucose concentration below 100 mg/dl, and a 2-h postprandial glucose concentration below 140
mg/dl; prediabetes was defined as 100–125 mg/dl (fasting) or 140–199 mg/dl (2-h postprandial); and
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
diabetes mellitus was defined as at least 126 mg/dl (fasting) or at least 200 mg/dl (2-h postprandial), or if
the subjects were on antidiabetic medication.
Diagnosis of cognitive impairment, and assessment of mood, general health status, and exercise
For the diagnosis of MCI, dementia, and other psychiatric disorders, the Korean version of the
Consortium to Establish a Registry for Alzheimer’s Disease Clinical Assessment Battery16 and the Korean
version of the Mini International Neuropsychiatric Interview17 were used by geriatric psychiatrists. In
addition, the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease Clinical
Assessment Battery Neuropsychological Assessment Battery18, a lexical fluency test19, and a digit span
test20 were performed on the subjects as described21. These assessment tools for cognitive function have
been validated in previous studies16-20. MCI was diagnosed according to the revised diagnostic criteria for
MCI proposed by the International Working Group on MCI using established neuropsychological tests21.
Dementia was defined by the diagnostic features of dementia described in the Diagnostic and Statistical
Manual of Mental Disorders, fourth edition22. All types of MCI and dementia were included in the
diagnosis. Mood was assessed using the Korean version of the Geriatric Depression Scale (GDS-K)23, and
the Cumulative Illness Rating Scale (CIRS) was used to assess the general health status of older adults24.
All final diagnoses of psychiatric disorders were determined by a panel of four research psychiatrists as
described21. Exercise was measured using a questionnaire asking for the number of hours of moderate to
hard exercise taken per day.
Data analysis
Values with normal distributions are expressed as mean ± SD. One-way ANOVA and the linear-by-linear
association tests for linear association analysis were used for the comparison of baseline characteristics
according to vitamin D status and for estimating the relationships between vitamin D status and cognitive
decline. Binary logistic regression analysis was used to test for any multiple correlations between
cognitive impairment and other risk factors and potential confounders. All statistical analyses were
performed with SPSS software (version 18.0; SPSS, Chicago, IL, USA), and p < 0.05 was considered
significant.
Results
Baseline characteristics according to serum 25(OH)D concentration
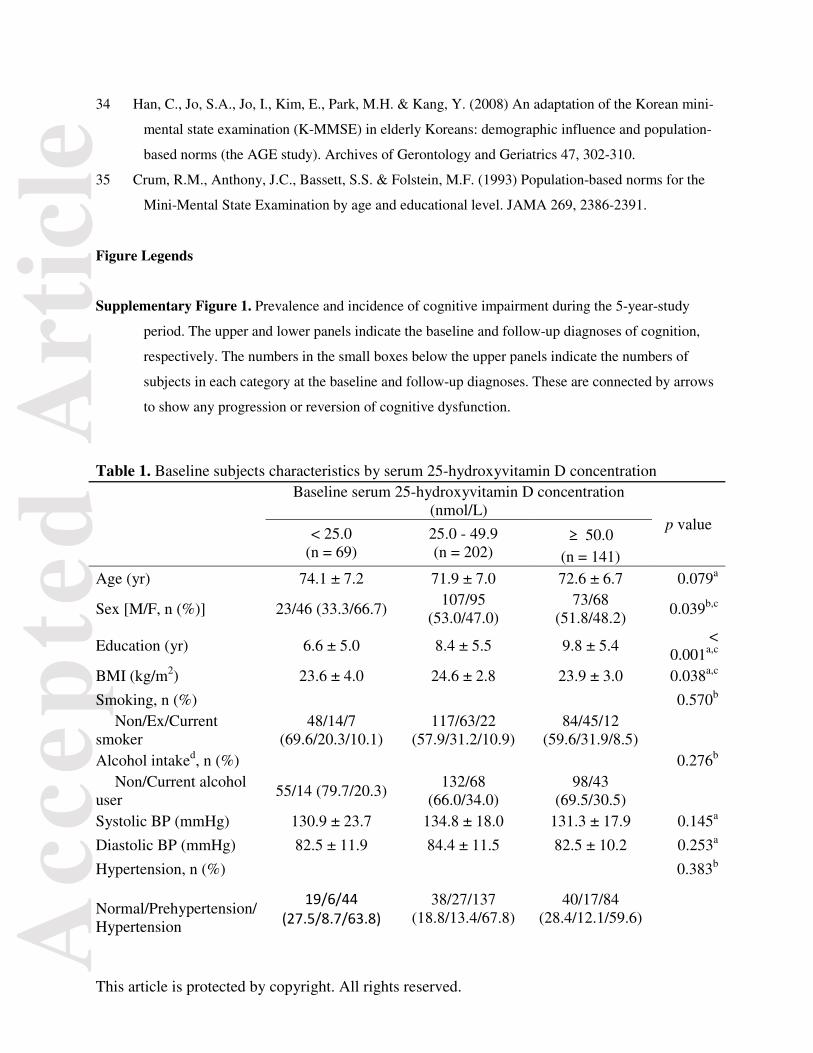
Baseline demographic, metabolic, and neuropsychiatric characteristics are shown in Table 1. At the
baseline evaluation, 141 subjects showed adequate serum 25(OH)D levels (≥ 50.0 nmol/L), 202 had
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
25(OH)D deficiency (25.0–49.9 nmol/L), and 69 had severe deficiency (< 25.0 nmol/L). Subjects with
severe vitamin D deficiency were less educated and tended to be older than those with higher serum
25(OH)D levels. The group with severe vitamin D deficiency also showed a higher ratio of female
subjects and more depressive mood (higher GDS-K score) than did the others. Although the fasting
plasma glucose concentration was lower in the subjects with adequate vitamin D status than in the
deficient and severely deficient subjects, the prevalence of diabetes mellitus was not different among
these groups. There was no difference in smoking habit, alcohol intake, hypertension, stroke history, or
general health status (CIRS score) according to vitamin D status.
Prevalence and incidence of cognitive impairment during the 5-year-study period
At the baseline evaluation, 304 subjects were cognitively normal, 101 had MCI, and seven had dementia.
By the time of the follow-up evaluation, 295 subjects were normal, 94 had MCI, and 23 had dementia.
The specific changes in each category of cognitive status are summarized in Supplementary Figure 1.
Prospective association between baseline serum 25(OH)D levels and the progression of cognitive
impairment
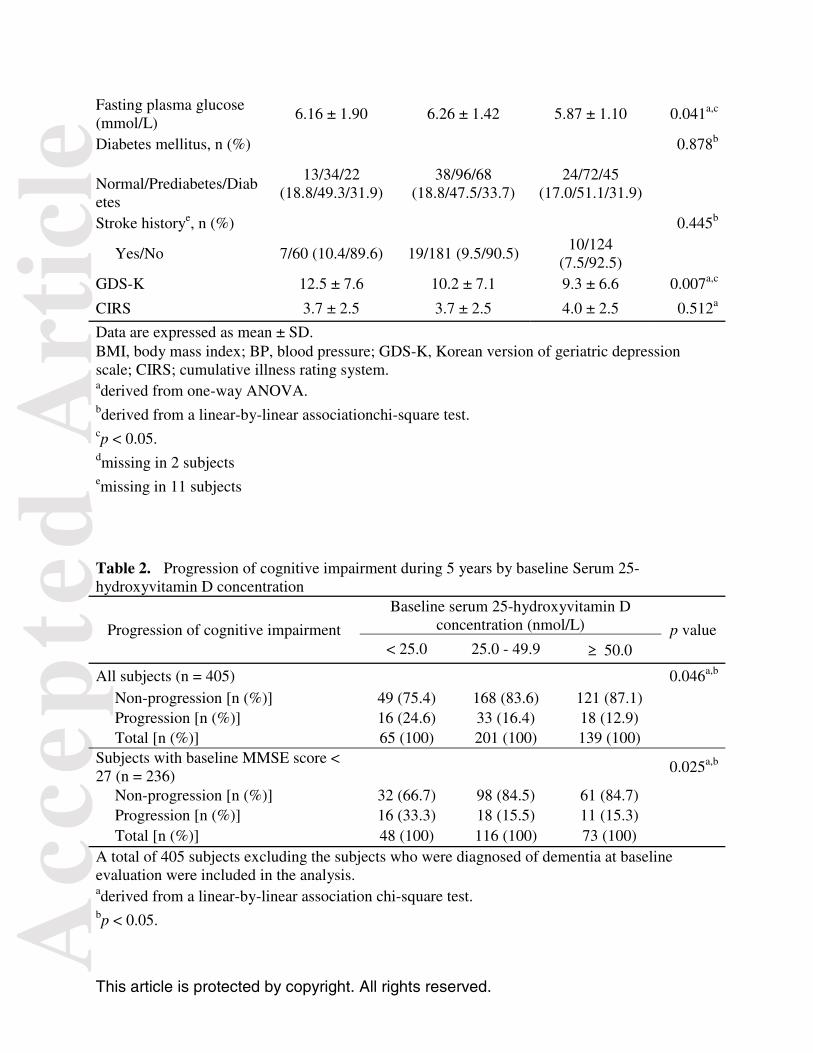
Among 405 subjects who were cognitively normal or had MCI at baseline, 338 remained unchanged or
improved in their diagnosis for cognitive function during the study period, whereas 67 subjects showed a
progression to MCI or dementia. In unadjusted analyses, a lower serum 25(OH)D concentration was
associated with a higher risk of such progression. This applied when all subjects were considered, as well
as when only the subjects whose baseline MMSE scores were <27 were considered (Table 2). In the
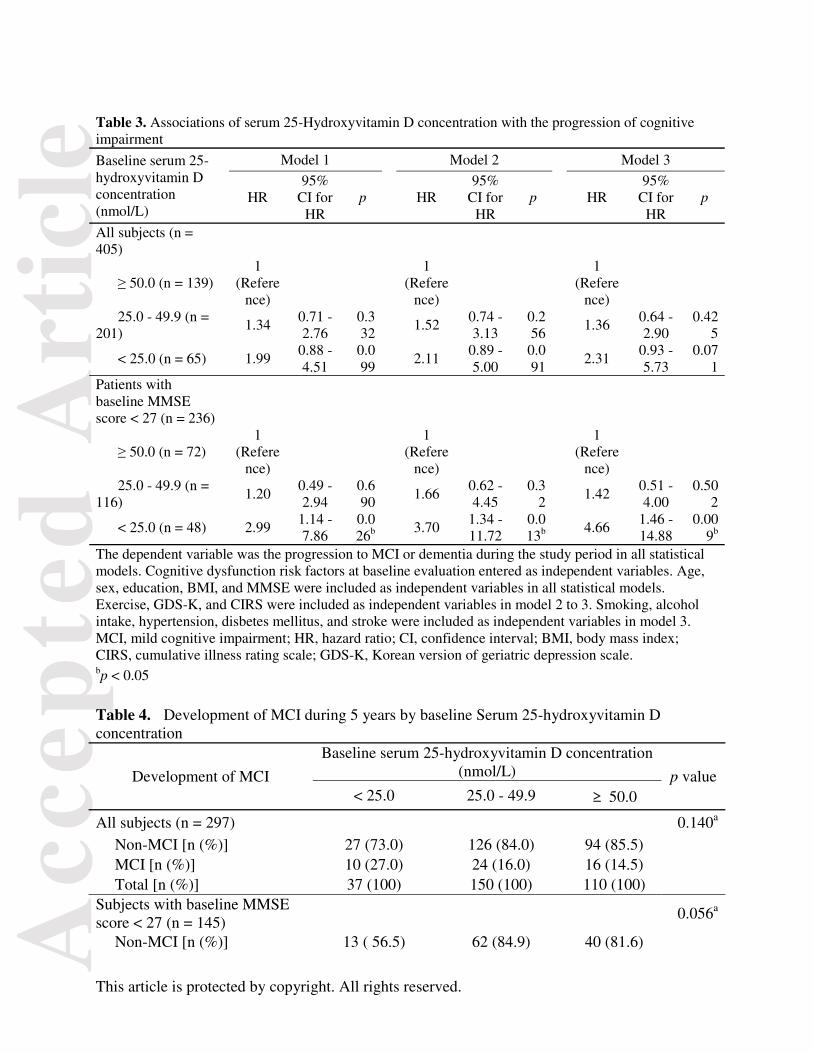
analysis with all subjects, the adjusted risk of progression to MCI or dementia tended to be higher in the
subjects with severe vitamin D deficiency than in those with adequate vitamin D status (Table 3). When
we analyzed only the subjects whose baseline MMSE scores were <27, subjects with severe vitamin D
deficiency showed a higher risk of progression of cognitive impairment than did the subjects with
adequate vitamin D status. This was after adjusting for other confounding factors including age, sex,
education duration, BMI, baseline MMSE, exercise level, GDS-K and CIRS scores, smoking habit,
alcohol intake, and the presence of hypertension, diabetes mellitus, and stroke history (Table 3).
Prospective association between baseline serum 25(OH)D levels and the development of MCI
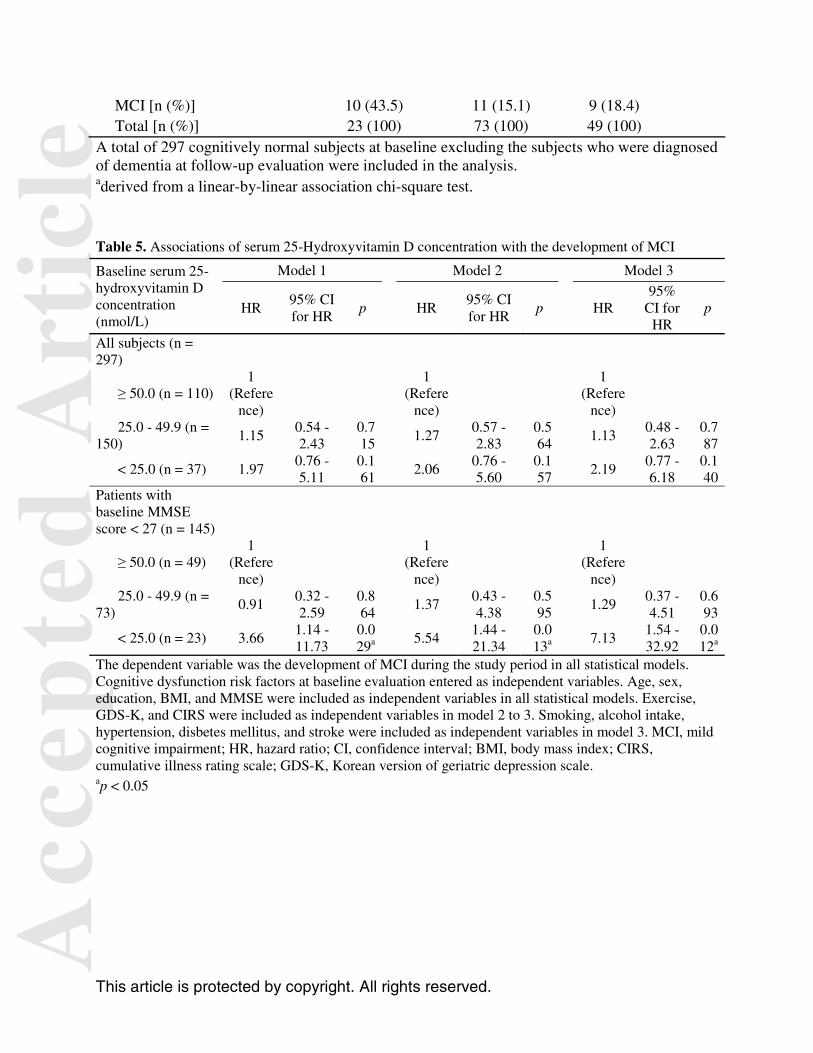
Among 297 subjects who were cognitively normal at the baseline evaluation, MCI developed in 50 of
them during the 5-year study period and 247 remained normal. In all these subjects, the development of
MCI was not associated with lower serum 25(OH)D concentration in both unadjusted and adjusted
analyses (Table 4 and 5). However, unadjusted analyses on 145 subjects with a baseline MMSE score <27
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
demonstrated that a lower serum 25(OH)D concentration tended to be associated with a higher risk of
developing MCI (Table 4). This association also showed statistical significance in adjusted analyses. The
group of severe vitamin D deficiency showed a higher risk of developing MCI compared with the vitamin
D adequate group, after adjusting for other confounding factors in the subjects whose baseline MMSE
scores were <27 (Table 5).
Discussion
Here we found that a low 25(OH)D concentration (< 25.0 nmol/L) at baseline was associated with
cognitive decline in elderly subjects. The association between vitamin D status and cognitive performance
in elderly population has been reported over the past decade10, 11, 25-28. In addition, several potential
mechanisms explaining this association have been suggested. Thus, hypovitaminosis D and inefficient
utilization of vitamin D have been reported to induce oxidative stress, altered immune responses,
disruption of calcium homeostasis, dysregulation of neurotrophic factors and neurotransmitters, and
disruption of amyloid β clearance in the central nervous system29.
However, most previous studies evaluated the prevalence and incidence of dementia or used specific
cognitive function tests to estimate cognitive decline. To the best of our knowledge, only one cross-
sectional study has evaluated the association between poor vitamin D status and the clinical entity of MCI
diagnosed according to the consensus criteria of the International Working Group on MCI30. MCI is
characterized by noticeable cognitive decline with preserved basic activities of daily living; clinically, it is
a risk state of progression to dementia but is not sufficient in itself to be diagnosed as dementia31. This
prodromal stage of dementia can be further classified according to the number of impaired cognitive
domains: single-and multiple-domain type MCI. Approximately 15– 42% of people aged 65 or older are
estimated to have MCI, and 5–15% of them progress to dementia annually regardless of their subtype21, 32.
Furthermore, MCI increases both health-related resource use and costs, not only as a risk state of
dementia, but also as an independent disease entity33. Therefore, discovering modifiable risk factors for
developing MCI will be helpful for its early detection and the prevention of progressed, severe cognitive
dysfunction such as dementia. Here for the first time we have demonstrated that a low vitamin D status
increased the risk of MCI as well as dementia in this prospective study with a community-based cohort of
the elderly. Moreover, our results suggest that vitamin D status can be a useful clinical marker for
selecting groups at risk of developing MCI as well as dementia. Although we demonstrated that subjects
with multiple-domain type MCI had a lower chance of reversion to normal cognition compared with the
single-domain type MCI in our previous study21, there was no difference in vitamin D status between
single- and multiple-domain type MCI at the baseline in the present study (data not shown).

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
In this study, it is notable that the adjusted hazard ratios of cognitive decline were higher and had
statistical significance when the subjects whose baseline MMSE score was ≥27 were excluded. The
MMSE is a brief screening test for cognitive impairment and estimates global cognitive function with a
30-point questionnaire. The population-based norms for the MMSE score are influenced by age and
education34, 35, and the mean baseline MMSE score was 25 in our study population consisting of subjects
with old age and a medium level of education (mean age at baseline, 72.5 ± 7.0 years; education duration,
8.6 ± 5.5 years). Considering that the mean MMSE score is 27 in young adults aged 18–29 years with an
education duration of 5–8 years35, our results suggest that severe vitamin D deficiency is a more important
predictor for the development of MCI and dementia in older adults who cannot maintain their cognitive
function to the level of young adults.
This study had strengths as a prospective cohort study. Our results are less likely to be due to the reverse
causality which could be resulted from less outdoor physical activity in demented patients. Moreover, we
adjusted for physical activity and other confounding factors including age, sex, education period, BMI,
baseline MMSE, depressive mood, cumulative illness, smoking, alcohol use, hypertension, diabetes
mellitus, and stroke. This intensive adjustment for possible confounding factors made such reverse
causality less likely.
Our study also had some limitations. In the baseline characteristics, subjects with severe vitamin D
deficiency tended to be older; they were more likely to be women, were less educated, and were more
depressed. Although we adjusted for age, sex, education, and depressive mood, vitamin D deficiency
could simply be a marker of diseases and aging processes that also contribute to risks for cognitive
impairment, rather than being a pathologic cause of dementia per se. The relatively low follow-up rate of
our cohort allowed only a limited number of subjects to be included in the analysis. Among the initial
1000 subjects of the KLoSHA study, about 50% did not participate in the 5-year follow-up evaluation.
This low follow-up rate could lead to some selection bias in the analyses. In addition, health behavior
patterns including sun exposure time, exercise habits, and dietary patterns might also have changed after
the baseline evaluation because we provided the participants with standard education outlining factors in a
healthy lifestyle. In addition, we could not exclude incident dementia occurring within 1 year because we
did not follow up on a yearly basis. We also included subjects with stroke or other comorbidities
including hypertension and diabetes mellitus in the analyses. However, we excluded prevalent dementia
at baseline and adjusted for these comorbidities and CIRS, as mentioned above.
In conclusion, we demonstrated here that a lower serum 25(OH)D concentration was associated with the
progression of cognitive decline and the development of MCI after a 5-year follow-up in elderly subjects.
This association was maintained after extensive adjusting for conventional risk factors. These results

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
suggest that elderly subjects with lower serum 25(OH)D concentrations might require a more intensive
follow-up program for the earlier detection of cognitive dysfunction.
References
1 Pearce, S.H. & Cheetham, T.D. (2010) Diagnosis and management of vitamin D deficiency. BMJ
(Clinical Research ed.) 340, b5664.
2 Formiga, F., Ferrer, A., Almeda, J., San Jose, A., Gil, A. & Pujol, R. (2011) Utility of geriatric
assessment tools to identify 85-years old subjects with vitamin D deficiency. The Journal of
Nutrition, Health & Aging 15, 110-114.
3 Holick, M.F. (2007) Vitamin D deficiency. New England Journal of Medicine 357, 266-281.
4 Perez-Lopez, F.R., Chedraui, P. & Fernandez-Alonso, A.M. (2011) Vitamin D and aging: beyond
calcium and bone metabolism. Maturitas 69, 27-36.
5 Holick, M.F. (2012) Vitamin D: A D-Lightful Vitamin for Health. Endocrinology and Metabolism
27, 255-267.
6 Lim, S., Shin, H., Kim, M.J., Ahn, H.Y., Kang, S.M., Yoon, J.W., Choi, S.H., Kim, K.W., Song,
J.H., Choi, S.I., Chun, E.J., Shin, C.S., Park, K.S. & Jang, H.C. (2012) Vitamin D inadequacy is
associated with significant coronary artery stenosis in a community-based elderly cohort: the
Korean Longitudinal Study on Health and Aging. The Journal of Clinical Endocrinology and
Metabolism 97, 169-178.
7 Cherniack, E.P., Florez, H., Roos, B.A., Troen, B.R. & Levis, S. (2008) Hypovitaminosis D in the
elderly: from bone to brain. The Journal of Nutrition, Health & Aging 12, 366-373.
8 Wimo, A., Jonsson, L., Bond, J., Prince, M., Winblad, B. & Alzheimer Disease, I. (2013) The
worldwide economic impact of dementia 2010. Alzheimer's & Dementia 9, 1-11 e13.
9 Kim, K.W., Park, J.H., Kim, M.H., Kim, M.D., Kim, B.J., Kim, S.K., Kim, J.L., Moon, S.W., Bae,
J.N., Woo, J.I., Ryu, S.H., Yoon, J.C., Lee, N.J., Lee, D.Y., Lee, D.W., Lee, S.B., Lee, J.J., Lee,
J.Y., Lee, C.U., Chang, S.M., Jhoo, J.H. & Cho, M.J. (2011) A nationwide survey on the
prevalence of dementia and mild cognitive impairment in South Korea. Journal of Alzheimer's
Disease : JAD 23, 281-291.
10 Balion, C., Griffith, L.E., Strifler, L., Henderson, M., Patterson, C., Heckman, G., Llewellyn, D.J.
& Raina, P. (2012) Vitamin D, cognition, and dementia: a systematic review and meta-analysis.
Neurology 79, 1397-1405.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
11 Littlejohns, T.J., Henley, W.E., Lang, I.A., Annweiler, C., Beauchet, O., Chaves, P.H., Fried, L.,
Kestenbaum, B.R., Kuller, L.H., Langa, K.M., Lopez, O.L., Kos, K., Soni, M. & Llewellyn, D.J.
(2014) Vitamin D and the risk of dementia and Alzheimer disease. Neurology 83, 920-928.
12 Ritchie, K. (2004) Mild cognitive impairment: an epidemiological perspective. Dialogues in
Clinical Neuroscience 6, 401-408.
13 Ward, A., Arrighi, H.M., Michels, S. & Cedarbaum, J.M. (2012) Mild cognitive impairment:
disparity of incidence and prevalence estimates. Alzheimer's & Dementia 8, 14-21.
14 Park, J.H., Lim, S., Lim, J.Y., Kim, K.I., Yoon, I.Y., Kim, J.M., Chang, Y.S., Chang, C.B., Chin,
H.J., Choi, E.A., Lee, S.B., Park, Y.J., Paik, N.J., Kim, T.K., Jang, H.C. & Kim, K.W. (2007) An
overview of the Korean Longitudinal Study on Health and Aging. Psychiatry Investigation 4, 84-
95.
15 Holick, M.F. (2009) Vitamin D status: measurement, interpretation, and clinical application.
Annals of Epidemiology 19, 73-78.
16 Lee, J.H., Lee, K.U., Lee, D.Y., Kim, K.W., Jhoo, J.H., Kim, J.H., Lee, K.H., Kim, S.Y., Han, S.H.
& Woo, J.I. (2002) Development of the Korean version of the Consortium to Establish a Registry
for Alzheimer's Disease Assessment Packet (CERAD-K): clinical and neuropsychological
assessment batteries. The Journals of Gerontology. Series B, Psychological Sciences and Social
Sciences 57, P47-53.
17 Yoo, S., Kim, Y., Noh, J., Oh, K., Kim, C., Namkoong, K., Chae, J., Lee, G., Jeon, S. & Min, K.
(2006) Validity of Korean version of the mini-international neuropsychiatric interview. Anxiety
Mood 2, 50-55.
18 Lee, D.Y., Lee, K.U., Lee, J.H., Kim, K., Jhoo, J., Kim, S.Y., Yoon, J.C., Woo, S.I., Ha, J. & Woo,
J.I. (2004) A normative study of the CERAD neuropsychological assessment battery in the
Korean elderly. Journal of the International Neuropsychological Society 10, 72-81.
19 Ruff, R.M., Light, R.H., Parker, S.B. & Levin, H.S. (1996) Benton Controlled Oral Word
Association Test: reliability and updated norms. Archives of Clinical Neuropsychology 11, 329-
338.
20 Wechsler, D. (1987) WMS-R: Wechsler Memory Scale--Revised: manual. Psychological
Corporation San Antonio.
21 Han, J.W., Kim, T.H., Lee, S.B., Park, J.H., Lee, J.J., Huh, Y., Park, J.E., Jhoo, J.H., Lee, D.Y. &
Kim, K.W. (2012) Predictive validity and diagnostic stability of mild cognitive impairment
subtypes. Alzheimer's & Dementia 8, 553-559.
22 Association Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-
IV-TR. Arlington, VA: American Psychiatric Publishing, Inc.; 2000.

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
23 Bae, J.N. & Cho, M.J. (2004) Development of the Korean version of the Geriatric Depression Scale
and its short form among elderly psychiatric patients. Journal of Psychosomatic Research 57,
297-305.
24 Miller, M.D., Paradis, C.F., Houck, P.R., Mazumdar, S., Stack, J.A., Rifai, A.H., Mulsant, B. &
Reynolds, C.F., 3rd (1992) Rating chronic medical illness burden in geropsychiatric practice and
research: application of the Cumulative Illness Rating Scale. Psychiatry Research 41, 237-248.
25 Soni, M., Kos, K., Lang, I.A., Jones, K., Melzer, D. & Llewellyn, D.J. (2012) Vitamin D and
cognitive function. Scandinavian Journal of Clinical and Laboratory Investigation.
Supplementum 243, 79-82.
26 Annweiler, C., Montero-Odasso, M., Llewellyn, D.J., Richard-Devantoy, S., Duque, G. & Beauchet,
O. (2013) Meta-analysis of memory and executive dysfunctions in relation to vitamin D. Journal
of Alzheimer's Disease : JAD 37, 147-171.
27 van der Schaft, J., Koek, H.L., Dijkstra, E., Verhaar, H.J., van der Schouw, Y.T. & Emmelot-Vonk,
M.H. (2013) The association between vitamin D and cognition: A systematic review. Ageing
Research Reviews 12, 1013-1023.
28 Annweiler, C., Dursun, E., Feron, F., Gezen-Ak, D., Kalueff, A.V., Littlejohns, T., Llewellyn, D.J.,
Millet, P., Scott, T., Tucker, K.L., Yilmazer, S. & Beauchet, O. (2014) 'Vitamin D and cognition
in older adults': updated international recommendations. Journal of Internal Medicine.
29 Gezen-Ak, D., Yilmazer, S. & Dursun, E. (2014) Why vitamin D in Alzheimer's disease? The
hypothesis. Journal of Alzheimer's Disease : JAD 40, 257-269.
30 Annweiler, C., Fantino, B., Schott, A.M., Krolak-Salmon, P., Allali, G. & Beauchet, O. (2012)
Vitamin D insufficiency and mild cognitive impairment: cross-sectional association. European
Journal of Neurology 19, 1023-1029.
31 Winblad, B., Palmer, K., Kivipelto, M., Jelic, V., Fratiglioni, L., Wahlund, L.O., Nordberg, A.,
Backman, L., Albert, M., Almkvist, O., Arai, H., Basun, H., Blennow, K., de Leon, M., DeCarli,
C., Erkinjuntti, T., Giacobini, E., Graff, C., Hardy, J., Jack, C., Jorm, A., Ritchie, K., van Duijn,
C., Visser, P. & Petersen, R.C. (2004) Mild cognitive impairment--beyond controversies, towards
a consensus: report of the International Working Group on Mild Cognitive Impairment. Journal of
Internal Medicine 256, 240-246.
32 Petersen, R.C., Caracciolo, B., Brayne, C., Gauthier, S., Jelic, V. & Fratiglioni, L. (2014) Mild
cognitive impairment: a concept in evolution. Journal of Internal Medicine 275, 214-228.
33 Zhu, C.W., Sano, M., Ferris, S.H., Whitehouse, P.J., Patterson, M.B. & Aisen, P.S. (2013) Health-
related resource use and costs in elderly adults with and without mild cognitive impairment.
Journal of the American Geriatrics Society 61, 396-402.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
34 Han, C., Jo, S.A., Jo, I., Kim, E., Park, M.H. & Kang, Y. (2008) An adaptation of the Korean mini-
mental state examination (K-MMSE) in elderly Koreans: demographic influence and population-
based norms (the AGE study). Archives of Gerontology and Geriatrics 47, 302-310.
35 Crum, R.M., Anthony, J.C., Bassett, S.S. & Folstein, M.F. (1993) Population-based norms for the
Mini-Mental State Examination by age and educational level. JAMA 269, 2386-2391.
Figure Legends
Supplementary Figure 1. Prevalence and incidence of cognitive impairment during the 5-year-study
period. The upper and lower panels indicate the baseline and follow-up diagnoses of cognition,
respectively. The numbers in the small boxes below the upper panels indicate the numbers of
subjects in each category at the baseline and follow-up diagnoses. These are connected by arrows
to show any progression or reversion of cognitive dysfunction.
Table 1. Baseline subjects characteristics by serum 25-hydroxyvitamin D concentration
Baseline serum 25-hydroxyvitamin D concentration (nmol/L)
p value < 25.0
(n = 69) 25.0 - 49.9 (n = 202)
≥ 50.0 (n = 141)
Age (yr) 74.1 ± 7.2 71.9 ± 7.0 72.6 ± 6.7 0.079a
Sex [M/F, n (%)] 23/46 (33.3/66.7) 107/95
(53.0/47.0) 73/68
(51.8/48.2) 0.039b,c
Education (yr) 6.6 ± 5.0 8.4 ± 5.5 9.8 ± 5.4 <
0.001a,c
BMI (kg/m2) 23.6 ± 4.0 24.6 ± 2.8 23.9 ± 3.0 0.038a,c
Smoking, n (%) 0.570b
Non/Ex/Current smoker
48/14/7 (69.6/20.3/10.1)
117/63/22 (57.9/31.2/10.9)
84/45/12 (59.6/31.9/8.5)
Alcohol intaked, n (%) 0.276b
Non/Current alcohol user
55/14 (79.7/20.3) 132/68
(66.0/34.0) 98/43
(69.5/30.5) Systolic BP (mmHg) 130.9 ± 23.7 134.8 ± 18.0 131.3 ± 17.9 0.145a
Diastolic BP (mmHg) 82.5 ± 11.9 84.4 ± 11.5 82.5 ± 10.2 0.253a
Hypertension, n (%) 0.383b
Normal/Prehypertension/Hypertension
19/6/44 (27.5/8.7/63.8)
38/27/137 (18.8/13.4/67.8)
40/17/84 (28.4/12.1/59.6)
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Fasting plasma glucose (mmol/L)
6.16 ± 1.90 6.26 ± 1.42 5.87 ± 1.10 0.041a,c
Diabetes mellitus, n (%) 0.878b
Normal/Prediabetes/Diabetes
13/34/22 (18.8/49.3/31.9)
38/96/68 (18.8/47.5/33.7)
24/72/45 (17.0/51.1/31.9)
Stroke historye, n (%) 0.445b
Yes/No 7/60 (10.4/89.6) 19/181 (9.5/90.5) 10/124
(7.5/92.5) GDS-K 12.5 ± 7.6 10.2 ± 7.1 9.3 ± 6.6 0.007a,c
CIRS 3.7 ± 2.5 3.7 ± 2.5 4.0 ± 2.5 0.512a
Data are expressed as mean ± SD. BMI, body mass index; BP, blood pressure; GDS-K, Korean version of geriatric depression scale; CIRS; cumulative illness rating system. aderived from one-way ANOVA. bderived from a linear-by-linear associationchi-square test. cp < 0.05. dmissing in 2 subjects emissing in 11 subjects
Table 2. Progression of cognitive impairment during 5 years by baseline Serum 25-hydroxyvitamin D concentration
Progression of cognitive impairment
Baseline serum 25-hydroxyvitamin D concentration (nmol/L) p value
< 25.0 25.0 - 49.9 ≥ 50.0
All subjects (n = 405) 0.046a,b
Non-progression [n (%)] 49 (75.4) 168 (83.6) 121 (87.1) Progression [n (%)] 16 (24.6) 33 (16.4) 18 (12.9) Total [n (%)] 65 (100) 201 (100) 139 (100) Subjects with baseline MMSE score < 27 (n = 236)
0.025a,b
Non-progression [n (%)] 32 (66.7) 98 (84.5) 61 (84.7) Progression [n (%)] 16 (33.3) 18 (15.5) 11 (15.3) Total [n (%)] 48 (100) 116 (100) 73 (100) A total of 405 subjects excluding the subjects who were diagnosed of dementia at baseline evaluation were included in the analysis. aderived from a linear-by-linear association chi-square test. bp < 0.05.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Table 3. Associations of serum 25-Hydroxyvitamin D concentration with the progression of cognitive impairment
Baseline serum 25-hydroxyvitamin D concentration (nmol/L)
Model 1 Model 2 Model 3
HR 95%
CI for HR
p HR 95%
CI for HR
p HR 95%
CI for HR
p
All subjects (n = 405)
≥ 50.0 (n = 139) 1
(Reference)
1 (Refere
nce)
1 (Refere
nce)
25.0 - 49.9 (n = 201)
1.34 0.71 - 2.76
0.332
1.52 0.74 - 3.13
0.256
1.36 0.64 - 2.90
0.425
< 25.0 (n = 65) 1.99 0.88 - 4.51
0.099
2.11 0.89 - 5.00
0.091
2.31 0.93 - 5.73
0.071
Patients with baseline MMSE score < 27 (n = 236)
≥ 50.0 (n = 72) 1
(Reference)
1 (Refere
nce)
1 (Refere
nce)
25.0 - 49.9 (n = 116)
1.20 0.49 - 2.94
0.690
1.66 0.62 - 4.45
0.32
1.42 0.51 - 4.00
0.502
< 25.0 (n = 48) 2.99 1.14 - 7.86
0.026b 3.70
1.34 - 11.72
0.013b
4.66 1.46 - 14.88
0.009b
The dependent variable was the progression to MCI or dementia during the study period in all statistical models. Cognitive dysfunction risk factors at baseline evaluation entered as independent variables. Age, sex, education, BMI, and MMSE were included as independent variables in all statistical models. Exercise, GDS-K, and CIRS were included as independent variables in model 2 to 3. Smoking, alcohol intake, hypertension, disbetes mellitus, and stroke were included as independent variables in model 3. MCI, mild cognitive impairment; HR, hazard ratio; CI, confidence interval; BMI, body mass index; CIRS, cumulative illness rating scale; GDS-K, Korean version of geriatric depression scale. bp < 0.05
Table 4. Development of MCI during 5 years by baseline Serum 25-hydroxyvitamin D concentration
Development of MCI
Baseline serum 25-hydroxyvitamin D concentration (nmol/L) p value
< 25.0 25.0 - 49.9 ≥ 50.0
All subjects (n = 297) 0.140a
Non-MCI [n (%)] 27 (73.0) 126 (84.0) 94 (85.5) MCI [n (%)] 10 (27.0) 24 (16.0) 16 (14.5) Total [n (%)] 37 (100) 150 (100) 110 (100) Subjects with baseline MMSE score < 27 (n = 145)
0.056a
Non-MCI [n (%)] 13 ( 56.5) 62 (84.9) 40 (81.6)
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
MCI [n (%)] 10 (43.5) 11 (15.1) 9 (18.4) Total [n (%)] 23 (100) 73 (100) 49 (100) A total of 297 cognitively normal subjects at baseline excluding the subjects who were diagnosed of dementia at follow-up evaluation were included in the analysis. aderived from a linear-by-linear association chi-square test. Table 5. Associations of serum 25-Hydroxyvitamin D concentration with the development of MCI
Baseline serum 25-hydroxyvitamin D concentration (nmol/L)
Model 1 Model 2 Model 3
HR 95% CI for HR
p HR 95% CI for HR
p HR 95%
CI for HR
p
All subjects (n = 297)
≥ 50.0 (n = 110) 1
(Reference)
1 (Refere
nce)
1 (Refere
nce)
25.0 - 49.9 (n = 150)
1.15 0.54 - 2.43
0.715
1.27 0.57 - 2.83
0.564
1.13 0.48 - 2.63
0.787
< 25.0 (n = 37) 1.97 0.76 - 5.11
0.161
2.06 0.76 - 5.60
0.157
2.19 0.77 - 6.18
0.140
Patients with baseline MMSE score < 27 (n = 145)
≥ 50.0 (n = 49) 1
(Reference)
1 (Refere
nce)
1 (Refere
nce)
25.0 - 49.9 (n = 73)
0.91 0.32 - 2.59
0.864
1.37 0.43 - 4.38
0.595
1.29 0.37 - 4.51
0.693
< 25.0 (n = 23) 3.66 1.14 - 11.73
0.029a
5.54 1.44 - 21.34
0.013a
7.13 1.54 - 32.92
0.012a
The dependent variable was the development of MCI during the study period in all statistical models. Cognitive dysfunction risk factors at baseline evaluation entered as independent variables. Age, sex, education, BMI, and MMSE were included as independent variables in all statistical models. Exercise, GDS-K, and CIRS were included as independent variables in model 2 to 3. Smoking, alcohol intake, hypertension, disbetes mellitus, and stroke were included as independent variables in model 3. MCI, mild cognitive impairment; HR, hazard ratio; CI, confidence interval; BMI, body mass index; CIRS, cumulative illness rating scale; GDS-K, Korean version of geriatric depression scale. ap < 0.05