
Serial assessment of biochemical changes in irradiated red blood cells
9
Serial assessment of biochemical changes in irradiated red blood cells Gopal Kumar Patidar a , Aparna Joshi a , Neelam Marwaha a,⇑ , Rajendra Prasad b , Pankaj Malhotra c , Ratti Ram Sharma a , Hari Krishan Dhawan a a Department of Transfusion Medicine, PGIMER, Chandigarh, India b Department of Biochemistry, PGIMER, Chandigarh, India c Department of Internal Medicine, PGIMER, Chandigarh, India article info Article history: Received 11 October 2013 Received in revised form 5 February 2014 Accepted 6 February 2014 Keywords: Irradiation Biochemical parameters Potassium abstract Background: Transfusion associated graft vs host disease (TA-GVHD) is delayed effect of blood component therapy with a very high mortality rate. The use of irradiated blood com- ponents is the only proven method to prevent TA-GVHD in susceptible patients. Aim: Our study was designed to analyze the quality of irradiated PRBCs in terms of their biochemical parameters during a storage period up to 28 days post irradiation. Methods: A total of 80 PRBC units were analyzed, 40 units each stored in CPDA-1 and addi- tive solution-SAGM. The units were evaluated serially for the following biochemical parameters, plasma/ supernatant potassium, sodium, pH, glucose, lactate, plasma/superna- tant hemoglobin and red cell ATP. We further evaluated the differences in these parameters between units irradiated on day 1 and day 7 of storage and stored these units up to 28 days and 35 days respectively. Ten units in each group were used as control. The assessment was done at weekly intervals from the day of irradiation. Results: Within each group of red cells, there was a rise in mean concentration of plasma potassium (K + ) from day 1 to last day of storage. There was a highly significant difference (P < 0.01) between irradiated and control units after first week of storage in both types of PRBCs. Irradiated CPDA-1 PRBC had significantly higher (K + ) than irradiated SAGM PRBC. Intergroup comparison revealed significantly higher (P < 0.05) mean hemoglobin in irradi- ated CPDA-1 PRBC as compared to SAGM PRBC. The mean pH was significantly higher (P < 0.05) in irradiated CPDA-1 PRBC as compared to irradiated SAGM PRBC only on day 7 of storage. ATP levels significantly decreased in irradiated units as compared to control units. SAGM PRBCs had significantly higher (P < 0.05) mean ATP concentration than CPDA-1PRBCs. Conclusion: Our study demonstrates that SAGM-PRBCs show better stability after irradia- tion compared to CPDA-1 PRBCs. The limits of safety for CPDA-1 PRBCs appear to be two weeks after irradiation. SAGM-PRBCs on the other hand show acceptable limits of safety up to three weeks of irradiation. The shelf life of irradiated PRBCs may vary depending upon the storage solution and day of irradiation. Ó 2014 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.transci.2014.02.002 1473-0502/Ó 2014 Elsevier Ltd. All rights reserved. ⇑ Corresponding author. Tel.: +91 9914209481. E-mail address: [email protected] (N. Marwaha). Transfusion and Apheresis Science 50 (2014) 479–487 Contents lists available at ScienceDirect Transfusion and Apheresis Science journal homepage: www.elsevier.com/locate/transci
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Serial assessment of biochemical changes in irradiated red blood cells

Transfusion and Apheresis Science 50 (2014) 479–487
Contents lists available at ScienceDirect
Transfusion and Apheresis Science
journal homepage: www.elsevier .com/ locate/ t ransc i
Serial assessment of biochemical changes in irradiated redblood cells
http://dx.doi.org/10.1016/j.transci.2014.02.0021473-0502/� 2014 Elsevier Ltd. All rights reserved.
⇑ Corresponding author. Tel.: +91 9914209481.E-mail address: [email protected] (N. Marwaha).
Gopal Kumar Patidar a, Aparna Joshi a, Neelam Marwaha a,⇑, Rajendra Prasad b,Pankaj Malhotra c, Ratti Ram Sharma a, Hari Krishan Dhawan a
a Department of Transfusion Medicine, PGIMER, Chandigarh, Indiab Department of Biochemistry, PGIMER, Chandigarh, Indiac Department of Internal Medicine, PGIMER, Chandigarh, India
a r t i c l e i n f o
Article history:Received 11 October 2013Received in revised form 5 February 2014Accepted 6 February 2014
Keywords:IrradiationBiochemical parametersPotassium
a b s t r a c t
Background: Transfusion associated graft vs host disease (TA-GVHD) is delayed effect ofblood component therapy with a very high mortality rate. The use of irradiated blood com-ponents is the only proven method to prevent TA-GVHD in susceptible patients.Aim: Our study was designed to analyze the quality of irradiated PRBCs in terms of theirbiochemical parameters during a storage period up to 28 days post irradiation.Methods: A total of 80 PRBC units were analyzed, 40 units each stored in CPDA-1 and addi-tive solution-SAGM. The units were evaluated serially for the following biochemicalparameters, plasma/ supernatant potassium, sodium, pH, glucose, lactate, plasma/superna-tant hemoglobin and red cell ATP. We further evaluated the differences in these parametersbetween units irradiated on day 1 and day 7 of storage and stored these units up to 28 daysand 35 days respectively. Ten units in each group were used as control. The assessmentwas done at weekly intervals from the day of irradiation.Results: Within each group of red cells, there was a rise in mean concentration of plasmapotassium (K+) from day 1 to last day of storage. There was a highly significant difference(P < 0.01) between irradiated and control units after first week of storage in both types ofPRBCs. Irradiated CPDA-1 PRBC had significantly higher (K+) than irradiated SAGM PRBC.Intergroup comparison revealed significantly higher (P < 0.05) mean hemoglobin in irradi-ated CPDA-1 PRBC as compared to SAGM PRBC. The mean pH was significantly higher(P < 0.05) in irradiated CPDA-1 PRBC as compared to irradiated SAGM PRBC only on day7 of storage. ATP levels significantly decreased in irradiated units as compared to controlunits. SAGM PRBCs had significantly higher (P < 0.05) mean ATP concentration thanCPDA-1PRBCs.Conclusion: Our study demonstrates that SAGM-PRBCs show better stability after irradia-tion compared to CPDA-1 PRBCs. The limits of safety for CPDA-1 PRBCs appear to be twoweeks after irradiation. SAGM-PRBCs on the other hand show acceptable limits of safetyup to three weeks of irradiation. The shelf life of irradiated PRBCs may vary dependingupon the storage solution and day of irradiation.
� 2014 Elsevier Ltd. All rights reserved.
480 G.K. Patidar et al. / Transfusion and Apheresis Science 50 (2014) 479–487
1. Introduction
The use of modified blood components has increased tosuit special requirements of immunosuppressed patients.These include leucoreduced and irradiated blood compo-nents. Established Indications of leukodepletions are to re-duce frequency of recurrent febrile nonhemolytictransfusion reactions to RBCs, reduce rate of alloimmuni-zation to leukocyte antigens for patients with malignantdisease, and reduce risk of transmission of cytomegalovi-rus among persons at risk of infection by transfusion.Transfusion associated graft vs host disease (TA-GVHD) isan adverse effect with a very high mortality rate and thisis not prevented by only leukodepletion. The use of irradi-ated blood components is the only proven method to pre-vent TA-GVHD in susceptible patients [1,2]. Irradiationeliminates the proliferative capacity of lymphocytes pres-ent in red cells, platelets and freshly collected plasma com-ponents, thereby inhibiting the production of cytokineswhich could act against patient’s tissues. Inhibiting lym-phocyte proliferation does not only inhibit production ofcytokines but also recognition of self and non-self (henceTA-GVHD). Groups at risk of GVHD include allogeneic/autologous bone marrow transplant recipients, congenitalimmune deficiency syndrome patients, recipients of intra-uterine transfusions and hematological malignancy pa-tients. However, irradiation leads to certain biochemicalchanges in blood, reducing its shelf life from 35 to 28 days.These include increase in hemolysis, changes in superna-tant potassium (K+), sodium (Na+), glucose, lactate, adeno-sine tri-phosphate (ATP) and decrease in pH.
We studied serial changes in the biochemical parame-ters of irradiated and stored PRBCs preserved in CPDA-1plasma and SAGM (sodium chloride, adenine, glucose andmannitol) to assess the feasibility of maintaining an inven-tory of these components. It is of great significance because
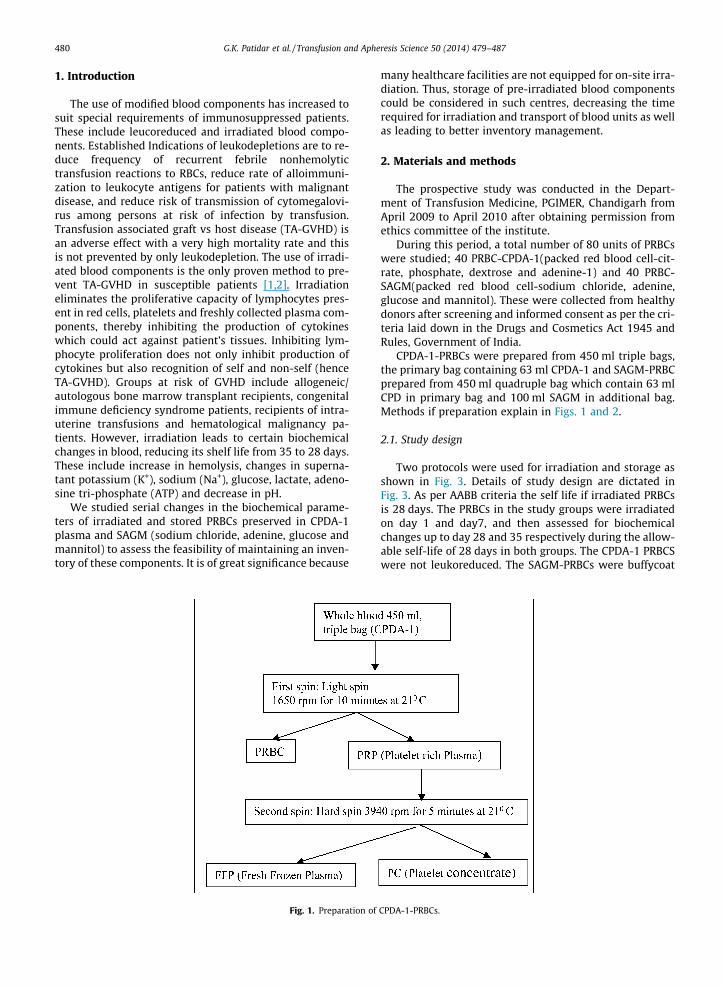
Fig. 1. Preparation of
many healthcare facilities are not equipped for on-site irra-diation. Thus, storage of pre-irradiated blood componentscould be considered in such centres, decreasing the timerequired for irradiation and transport of blood units as wellas leading to better inventory management.
2. Materials and methods
The prospective study was conducted in the Depart-ment of Transfusion Medicine, PGIMER, Chandigarh fromApril 2009 to April 2010 after obtaining permission fromethics committee of the institute.
During this period, a total number of 80 units of PRBCswere studied; 40 PRBC-CPDA-1(packed red blood cell-cit-rate, phosphate, dextrose and adenine-1) and 40 PRBC-SAGM(packed red blood cell-sodium chloride, adenine,glucose and mannitol). These were collected from healthydonors after screening and informed consent as per the cri-teria laid down in the Drugs and Cosmetics Act 1945 andRules, Government of India.
CPDA-1-PRBCs were prepared from 450 ml triple bags,the primary bag containing 63 ml CPDA-1 and SAGM-PRBCprepared from 450 ml quadruple bag which contain 63 mlCPD in primary bag and 100 ml SAGM in additional bag.Methods if preparation explain in Figs. 1 and 2.
2.1. Study design
Two protocols were used for irradiation and storage asshown in Fig. 3. Details of study design are dictated inFig. 3. As per AABB criteria the self life if irradiated PRBCsis 28 days. The PRBCs in the study groups were irradiatedon day 1 and day7, and then assessed for biochemicalchanges up to day 28 and 35 respectively during the allow-able self-life of 28 days in both groups. The CPDA-1 PRBCSwere not leukoreduced. The SAGM-PRBCs were buffycoat
CPDA-1-PRBCs.

Fig. 2. Preparation of SAGM-PRBC.
Fig. 3. Study design.
G.K. Patidar et al. / Transfusion and Apheresis Science 50 (2014) 479–487 481
depleted, hence only one log leukoreduced. The units werestored at 4 ± 2 �C in blood bank refrigerator from day 1 today 35. The parameters of visual examination, volumeand hematocrit were tested for quality control (as per na-tional standards criteria) [3].
2.2. Sampling procedure
Sampling was done at weekly intervals. After a hardspin at 3000 rpm for 10 min, the supernatant was takenand 0.5 ml was stored in a labeled cryovial at �70 �C forlactate estimation. Another 0.5 ml was tested for Na+, K+
and glucose in the Department of Biochemistry, PGIMER,Chandigarh while 1 ml was tested for supernatant Hband pH. The pH was measured at room temperature
(25–26 �C). The aliquots of packed cells were used to pre-pare hemolysate, which was also stored at �70 �C for test-ing ATP.
2.3. Preparation of hemolysate [4]
Two ml of packed red cells were washed three timeswith normal saline. Equal quantity of distilled water wasadded and mixed thoroughly with the cells using vortexmixer for 5 min. Then equal volume of carbon-tetra chlo-ride (Qualigens Fine Chemicals) was added and againmixed thoroughly using vortex mixer for 1 min. Tube wasgiven hard spin at 2000 rpm for 20 min. The clear superna-tant was collected in a cryovial and hemoglobin wasmeasured using automated cell counter (SYSMEX KX-21,

482 G.K. Patidar et al. / Transfusion and Apheresis Science 50 (2014) 479–487
Kobe, Japan). The cryovial with the hemolysate was thenstored at �70 �C till ATP estimation.
The units were irradiated by gamma irradiation, using aCesium137, self contained, turn-table, gamma cell irradiator(BIOBEAM 8000, STS, Braunschweig, Germany). The dosedelivered to each bag was 25 Gray (Gy) requiring 9 min55 s of exposure. Quality control of irradiated productswas done using radiation exposure indicator strips (RAD-SURE, ISP Technologies Inc. – Wayne, NJ).
Supernatant potassium, sodium and glucose levels wereestimated by automated analyzer (Hitachi 902, RocheDiagnostics, Germany). Supernatant plasma lactate wasestimated by commercial kits (CENTRONIC GmbH, Ger-many). Plasma supernatant hemoglobin was determinedby HemoCue AB (Angelholm, Sweden). An estimation ofsupernatant pH of each PRBC unit was done by using thepH indicator solution (UNIVERSAL INDICATOR, Glaxo-SmithKline Pharmaceuticals Limited, India). Red cell ATPconcentration was determined using a commercial kitATP Colorimetric Assay Kit (Bio Vision Inc, USA) as permanufacturer’s instructions [18].
All the parameters were estimated weekly from day 1till day 28 in Group 1 bags and from day 7 till day 35(28 days after irradiation) in Group 2 bags.
3. Statistical analysis
In this study we compared the biochemical parametersbetween Non-IR and IR red cells of SAGM PRBC and CPDA-1PRBC. This was normally distributed data. The observationsrecorded for all the RBC parameters were expressed interms of the following descriptive statistical measures asmean, range and standard deviation. Independent ‘t’ testwas applied where we found significant difference in ourresult.
To assess the correlation between several biochemicalparameters during red cells’ storage, Pearson’s correlationcoefficient (r) was applied. A p value <0.05 was consideredto indicate statistically significant difference. All analyseswere performed with the software package SPSS Version13.0 for windows (USA).
4. Results
In this study various red cell preparations were as-sessed for serial changes in biochemical parameters on dif-ferent days of storage.
All total 80 units of red cells selected satisfied the initialquality control criteria as per national standards criteria[3]. The mean volume and mean hematocrit of two differ-ent types of red cells is shown in Table 1.
Table 1Volume and hematocrit of PRBCs.
Parameters CPDA-1 PRBC (n = 40) SAGM-PRBC (n = 40)
Volume (ml) 291.70 ± 21.20 355.07 ± 9.41Mean ± SD (range) (248–319) (333–367)Hematocrit (%) 68.47 ± 1.97 60.77 ± 2.46Mean ± SD (range) (65.6–73.2) (56–64.9)
4.1. Group-1
There was a progressive rise in plasma/supernatantpotassium, lactate, and hemoglobin concentration withstorage, in both CPDA-1 and SAGM PRBCs. This increasewas significantly greater in irradiated as compared tonon-irradiated PRBCs. For potassium levels significant in-crease was observed from day 7 to day 28 (p < 0.001) inboth CPDA-1 and SAGM PRBCs. Significant changes in lac-tate levels were observed in CPDA-1 PRBCs from day 14onwards and in SAGM-PRBCs from day-1 itself. Superna-tant Hb concentration increased significantly from day 7to day 28 in IR-SAGM PRBCs while in IR- CPDA-1 PRBCsit was increased significantly on day-14.
A Progressive decline was observed in levels of plasma/supernatant sodium, glucose, pH and ATP. The decline wassignificantly more in IR-PRBCs (as shown in Table 2).
4.2. Group-2
There was a progressive rise in plasma/supernatantpotassium, lactate, and hemoglobin concentration withstorage, in both CPDA-1 and SAGM PRBCs from day 7 today 35 (as shown in Table 3). This increase was signifi-cantly greater in irradiated as compared to non-irradiatedPRBCs. For potassium levels significant increase was ob-served from day 21 to day 35 (p < 0.001) in both CPDA-1and SAGM PRBCs. Significant changes in lactate levels wereobserved from day 14 onwards in both CPDA-1 and SAGMPRBCs.
Supernatant Hb concentration increased significantlyfrom day 7 to day 35 in SAGM PRBCs while in CPDA-1PRBCs it was increased significantly on day-14.
A progressive decline was observed in levels of plasma/supernatant sodium, glucose, pH, and ATP. The decline wassignificantly more in irradiated PRBCs as compared to non-irradiated PRBCs. For sodium levels significant decline wasobserved on day-7 and day 35 in both CPDA-1 PRBCs andSAGM PRBCs. For glucose levels significant decline was ob-served from day 28 to day 35 in CPDA-1 PRBCs while inSAGM PRBCs it was significantly decline from day 14 today 35. For pH levels significant decline was observed fromday 7 to day 14 in SAGM PRBCs while in CPDA-1 PRBCs itwas on day 14 and on day 35. Decline in ATP levels wasnot significant in CPDA-1 PRBCs while in SAGM PRBCs itwas statistically significantly from day 14 to day 35 (asshown in Table 3).
4.3. Correlation between various parameters
A negative correlation was observed between pH andlactate (r = �0.097, �0.238 (p < 0.05), �0.077, �0.106,�0.2 and �0.292), plasma Hemoglobin and ATP(r = 0.417, 0.596, 0.741, 0.868, 0.898 and 0.838), PlasmaPotassium (K+) and ATP (r = �0.397, �0.581, �0.576,�0.605, �0.47 and �0.497), glucose and lactate lev-els(r = �0.522, �0.258, �0.376, �0.484, �0.518 and�0.308) and Lactate and ATP (r = 0.009, �0.599, �0.62,�0.487, �0.245 (p < 0.05) and �0.245) in both studygroups and in both IR and Non-IR PRBCs. There was a posi-tive correlation between plasma/supernatant potassium

Tabl
e2
Seri
alch
ange
sin
bioc
hem
ical
para
met
ers
inno
n-IR
and
IRPR
BCs
onda
ys1–
28.
Day
1D
ay7
Day
14D
ay21
Day
28
Non
-IR
IRN
on-I
RIR
Non
-IR
IRN
on-I
RIR
Non
-IR
IR
Pota
ssiu
mm
ean
±SD
(ran
ge)
(mm
ol/L
)C
PDA
-16.
01±
0.5
6.29
±0.
7116
.17
±2.
1⁄42
.80
±9.
1⁄⁄
24.6
0±
3.8⁄
73.3
2±
8.3⁄⁄
30.4
7±
4.4⁄
90.2
±11
.9⁄⁄
38.8
6±
3.7⁄
103
±11
.2⁄⁄
SAG
M3.
50±
1.15
4.14
±1.
3311
.12
±2.
3⁄23
.00
±4.
3⁄⁄
20.1
0±
4.4⁄
35.0
4±
4.3⁄⁄
28.8
0±
5.1⁄
45.3
0±
6.1⁄⁄
36.4
0±
3.2⁄
56.9
0±
6.2⁄⁄
Sodi
um
mea
n±
SD(r
ange
)(m
mol
/L)
CPD
A-1
156.
34±
3.09
156.
28±
3.20
152.
74±
2.3⁄
145.
18±
3.7⁄⁄
150.
40±
3.11
140.
25±
3.18
146.
16±
2.86
136.
60±
2.43
143.
05±
2.1⁄
132.
80±
1.5⁄⁄
SAG
M14
8.0
±2.
6914
6.8
±3.
2014
5.6
±2.
1714
4.1
±2.
4114
2.9
±20
a13
8.6
±2.
5#14
0.6
±2.
32a
134.
8±
2.1#
138.
2±
1.68
a12
9.9
±1.
3#
Glu
cose
mea
n±
SD(r
ange
)(m
mol
/L)
CPD
A-1
20.5
0±
1.87
21.7
7±
1.52
16.6
2±
2.94
16.5
9±
1.53
12.8
0±
1.50
13.5
6±
1.11
11.0
5±
1.53
10.4
1±
1.37
9.43
±1.
01a
8.16
±0.
52#
SAG
M36
.74
±1.
4037
.14
±1.
6430
.09
±3.
1130
.51
±59
.34
26.8
5±
3.23
25.3
6±
1.40
22.3
8±
2.79
21.7
1±
1.34
19.5
3±
1.47
19.5
7±
1.40
Lact
ate
mea
n±
SD(r
ange
)(m
mol
/L)
CPD
A-1
6.95
±1.
376.
61±
0.70
13.2
4±
0.97
12.8
4±
1.27
15.1
9±
1.03
a17
.63
±2.
22#
15.9
0±
1.16⁄
19.4
8±
1.74⁄⁄
17.4
9±
1.13⁄
22.6
2±
2.93⁄⁄
SAG
M5.
58±
0.59
a6.
29±
0.73
#8.
92±
0.79
a10
.80
±1.
94#
11.2
7±
0.76⁄
15.2
4±
1.46⁄⁄
13.7
5±
0.99⁄
19.5
2±
1.43⁄⁄
15.4
7±
0.79⁄
24.3
0±
2.34⁄⁄
pHm
ean
±SD
(ran
ge)
CPD
A-1
7.25
±0.
267.
15±
0.24
7.05
±0.
156.
95±
0.15
6.75
±0.
266.
60±
0.21
6.55
±0.
156.
50±
0.00
6.50
±0.
006.
45±
0.15
SAG
M7.
20±
0.25
7.10
±0.
217.
00±
0.00
a6.
70±
0.25
#6.
65±
0.24
6.50
±0.
006.
50±
0.00
6.50
±0.
006.
50±
0.00
6.35
±0.
24Su
pern
atan
tH
bm
ean
±SD
(ran
ge)
(g/L
)C
PDA
-10.
65±
0.2
0.61
±0.
151.
47±
0.3
1.44
±0.
231.
97±
0.4a
2.05
±0.
36#
2.5
±0.
223.
03±
0.54
3.61
±0.
23.
85±
0.25
SAG
M0.
36±
0.06
0.37
±0.
130.
59±
0.07⁄
1.30
±0.
33⁄⁄
0.73
±0.
08⁄
2.10
±0.
37⁄⁄
0.91
±0.
14⁄
2.72
±0.
26⁄⁄
1.43
±0.
22⁄
3.40
±0.
25⁄⁄
ATP
mea
n±
SD(r
ange
)(l
mol
/gm
Hb)
CPD
A-1
3.42
±0.
063.
38±
0.10
3.23
±0.
08a
3.00
±0.
20#
2.87
±0.
10⁄
2.57
±0.
08⁄⁄
2.49
±0.
15⁄
2.24
±0.
07⁄⁄
2.05
±0.
082.
05±
0.08
SAG
M3.
54±
0.1
3.47
±0.
083.
48±
0.1
3.31
±0.
083.
3±
0.09
a3.
20±
0.04
#3.
3±
0.04⁄
3.00
±0.
07⁄⁄
3.2
±0.
06⁄
2.84
±0.
08⁄⁄
Non
-IR
–N
on-i
rrad
iate
d,IR
–Ir
radi
ated
.a
vs#
(p<
0.05
),⁄
vs⁄⁄
(p<
0.00
1).
G.K. Patidar et al. / Transfusion and Apheresis Science 50 (2014) 479–487 483
and hemoglobin (r = 0.522, 0.258, 0.376, 0.484, 0.518 and0.308), glucose and ATP levels (r = 0.417, 0.596, 0.741,0.868, 0.898 and 0.838) in all groups of PRBCs and duringall days of storage (Fig. 4).
4.3.1. Intergroup comparisons of various biochemicalparameters in irradiated PRBCs
Intergroup comparison of potassium, pH and ATP showsno statistically significant difference between Group 1 andGroup 2 in both kinds of PRBCs after irradiation.
In CPDA-1 PRBCs (Group 1) K+ levels increased frommean baseline value of 6.29 meq/L to 7 times (42.8 meq/L)the initial value in one week and 17 times (103 meq/L)after four weeks after irradiation. In Group 2 the equivalentincrease was fourfold in one week (to 69.89 meq/L) and 7times (113.6 meq/L) in four weeks starting from baselinevalue of 15.66 meq/L after irradiation. In SAGM-PRBCs K+
levels in Group 1 units increased from baseline value of4.14 meq/L to 5 times (23 meq/L) in one week and 14 times(56.9 meq/L) in four weeks after irradiation. In Group 2the equivalent increase was two times in one week(to 32.5 meq/L) and 4 times (62.15 meq/L) in four weeksstarting from baseline value of 14.84 meq/L after irradia-tion (Fig. 5).
In CPDA-1 PRBCs (Group 1) Hb levels increased frommean baseline value of 0.61 g/L to 2 times (1.44 g/L) theinitial value in one week and 6 times (3.85 g/L) after fourweeks after irradiation. In Group 2 the equivalent increasewas 1.5 times in one week (2.07 g/L) and 3.5 times(4.87 meq/L) in four weeks starting from baseline valueof 1.44 g/L after irradiation. In SAGM-PRBCs Hb levels inGroup 1 units increased from baseline value of 0.37 to 3times (1.3 g/L) in one week and 9 times (3.4 g/L) in fourweeks after irradiation. In Group 2 the equivalent increasewas 1.5 times in one week (1.93 g/L) and 4 times (4.8 g/L)in four weeks starting from baseline value of 1.22 g/L afterirradiation (Fig. 6).
ATP value in CPDA1-PRBCs (Group 1) declined by 60%(2.05 lmol/gm Hb) of initial value of 3.38 lmol/gm Hbby day 28; and in Group 2 it was 55% (1.86 lmol/gm Hb)of day 1 values of 3.24 lmol/gm Hb after 28 days of storageafter irradiation. In SAGM-PRBCs the ATP value was declineby 81% (2.84 lmol/gm Hb) of initial value of 3.47 lmol/gmHb after irradiation; in Group 2 it was 72% of baseline va-lue of 3.38 lmol/gm Hb (Fig. 7).
4.4. Comparison with AABB standards for biochemicalparameters
The biochemical alterations observed in our study werewithin accepted safe values as per AABB standards, exceptfor concern regarding ATP, pH and K+. CPDA-1 PRBCs(Groups 1 and 2) exceeded safe K+ and pH levels afterday 14 of irradiation. In Group-1 SAGM-PRBCs plasma K+
exceeded safe levels after day 28 of storage while inGroup-2 it exceeded after day 21. SAGM-PRBCs (irradiatedday 7) exceeded safe K+ levels after day 21 of storage andsafe pH levels after day 28 of storage (Table 4).
We also compared our study with different publishedstudies it will discuss in discussion part (Table 5).

Tabl
e3
Seri
alch
ange
sin
bioc
hem
ical
para
met
ers
inno
n-IR
and
IRPR
BCs
onda
ys7–
35.
Day
7(D
-1of
IR)
Day
14(D
-7af
ter
IR)
Day
21(D
-14
afte
rIR
)D
ay28
(D-2
1af
ter
IR)
Day
35(D
-28
afte
rIR
)
Non
-IR
IRN
on-I
RIR
Non
-IR
IRN
on-I
RIR
Non
-IR
IR
Pota
ssiu
mm
ean
±SD
(ran
ge)
(mm
ol/L
)C
PDA
-115
.62
±2.
2615
.66
±2.
1326
.80
±2.
1269
.89
±11
.135
.52
±2.
8⁄88
.3±
12.9⁄⁄
45.0
8±
4.1⁄
103
±12
.4⁄⁄
52.8
5±
4.6⁄
113.
6±
10.6⁄⁄
SAG
M14
.77
±3.
0214
.84
±1.
8125
.60
±3.
3032
.50
±6.
4031
.60
±2.
4⁄43
.60
±4.
9⁄⁄
38.0
7±
2.7⁄
55.4
5±
3.8⁄⁄
46.1
4±
2.9⁄
62.1
5±
6.4⁄⁄
Sodi
um
mea
n±
SD(r
ange
)(m
mol
/L)
CPD
A-1
153.
46±
2.36
a15
0.64
±2.
96#
149.
67±
1.22
a14
3.99
±2.
74#
147.
11±
2.4a
138.
07±
2.2#
144.
34±
2.1
133.
55±
2.7
141.
27±
1.7a
128.
87±
2.5#
SAG
M14
4.2
±1.
6a14
2.3
±2.
0#14
1.9
±1.
6⁄13
7.0
±1.
9⁄⁄
139.
8±
1.1⁄
133.
1±
1.9⁄⁄
138.
6±
1.1⁄
130.
9±
1.1⁄⁄
137.
1±
1.5⁄
128.
6±
1.0⁄⁄
Glu
cose
mea
n±
SD(r
ange
)(m
mol
/L)
CPD
A-1
17.1
8±
2.02
17.0
3±
1.94
13.1
0±
1.56
13.2
4±
1.09
11.2
2±
1.14
10.5
0±
1.62
9.28
±0.
64⁄
7.84
±0.
70⁄⁄
8.05
±0.
47⁄
6.73
±0.
44⁄⁄
SAG
M27
.98
±1.
9430
.53
±3.
1923
.37
±1.
83a
27.2
6±
2.93
#20
.17
±0.
99a
23.9
3±
2.40
#18
.78
±0.
67a
20.8
4±
1.84
#17
.06
±0.
39a
18.1
2±
1.28
#
Lact
ate
mea
n±
SD(r
ange
)(m
mol
/L)
CPD
A-1
12.2
7±
0.77
11.9
1±
1.16
14.6
7±
0.67
a17
.68
±2.
18#
15.9
±0.
62⁄
2.15
±1.
75⁄⁄
17.2
7±
0.63⁄
22.5
2±
2.97⁄⁄
19.1
2±
0.71⁄
25.2
4±
2.66⁄⁄
SAG
M6.
85±
0.69
7.08
±2.
2611
.14
±1.
35a
12.8
0±
1.49
14.0
±1.
18a
15.8
9±
2.20
#15
.62
±0.
84⁄
21.5
±1.
44⁄⁄
17.2
7±
0.86⁄
27.5
3±
1.97⁄⁄
pHm
ean
±SD
(ran
ge)
CPD
A-1
7.11
±0.
217.
05±
0.15
6.95
±0.
15a
6.60
±0.
21#
6.65
±0.
246.
50±
0.00
6.50
±0.
006.
50±
0.00
6.50
±0.
00a
6.25
±0.
26#
SAG
M7.
00±
0.23
a6.
70±
0.25
#6.
80±
0.25
a6.
50±
0.00
#6.
50±
0.00
6.50
±0.
006.
50±
0.00
6.50
±0.
006.
35±
0.24
6.20
±0.
25Su
pern
atan
tH
bm
ean
±SD
(ran
ge)
(g/L
)C
PDA
-11.
64±
0.26
1.44
±0.
352.
49±
0.19
a2.
07±
0.45
#3.
54±
0.35
3.13
±0.
544.
32±
0.20
4.05
±0.
385.
72±
0.35
4.87
±0.
49SA
GM
0.72
±0.
07⁄
1.22
±0.
33⁄⁄
1.05
±0.
19⁄
1.93
±0.
38⁄⁄
1.40
±0.
13⁄
2.79
±0.
33⁄⁄
1.88
±0.
14⁄
3.64
±0.
40⁄⁄
2.59
±0.
16⁄
4.80
±0.
28⁄⁄
ATP
mea
n±
SD(r
ange
)(l
mol
/gm
Hb)
CPD
A-1
3.19
±0.
073.
24±
0.09
2.89
±0.
152.
94±
0.27
2.57
±0.
142.
45±
0.17
2.01
±0.
202.
14±
0.18
1.76
±0.
201.
86±
0.12
SAG
M3.
41±
0.05
3.38
±0.
043.
32±
0.06⁄
3.22
±0.
04⁄⁄
3.24
±0.
07⁄
3.04
±0.
07⁄⁄
3.14
±0.
08⁄
2.88
±0.
04⁄⁄
2.95
±0.
12⁄
2.44
±0.
08⁄⁄
Non
-IR
–N
on-i
rrad
iate
d,IR
–Ir
radi
ated
.a
vs#
(p<
0.05
),⁄
vs⁄⁄
(p<
0.00
1).
484 G.K. Patidar et al. / Transfusion and Apheresis Science 50 (2014) 479–487
5. Discussion
Prevention of TA-GVHD is of paramount importance asit cannot be treated successfully. Patients at risk must beidentified and transfused with irradiated cellular bloodproducts, as it is the only proven way of preventing TA-GVHD. However irradiation itself increases storage lesionsin red cells affecting the shelf-life. As per AABB guidelines[15] shelf life is reduced to 28 days after irradiation, as perBCHS guidelines [16] 14 days after irradiation, while as perJapanese guidelines [17] it can be stored up to 3 weeksafter irradiation (or the original date of expiry, whicheveris earlier). Increase in these adverse lesions is evident fromthe day of irradiation itself. This study was planned to as-sess the biochemical changes in red cells stored after irra-diation and their implication for the shelf-life of PRBCs.
In this study, two types of red cells were includedCPDA-1 and SAGM. In each group, 40 units of red bloodcells were taken, thus a total of 80 units of red cells wereassessed. Red cells were taken after they satisfied the qual-ity control criteria [3]. Quality control parameters checkedwere visual examination, volume (ml) and hematocrit (%)as required as per national standard.
Biochemical parameters which assume importance fortransfusion were tested in each of two types of red cells.These parameters were supernatant plasma potassium,sodium, glucose, lactate levels, supernatant plasmahemoglobin, pH and red cell ATP. These were tested atweekly intervals. The red cells units were stored in bloodbank refrigerator at 20–60 �C equipped with audiovisualalarms.
Irradiation affects the red cell membrane with an in-creased loss of potassium from the cell as well as increasein supernatant plasma hemoglobin. In CPDA-1 PRBCs K+
levels (Group 1) increased to 7 times the initial value inone week and 17 times in four weeks after irradiation. K+
levels (Group 2) increased less exponentially; to 4 timesthe initial value in one week and 7 times in four weeksafter irradiation however baseline values and storage ac-tual value were higher. In our study K+ level rise up to103 mmol/L after 28 days of irradiation which is almostequal to Janatpour et al. [5] study in which it was rise upto 111 mmol/L. In SAGM-PRBCs K+ levels in units (Group 1)increased to 5 times the initial value in one week and 14times in four weeks after irradiation. K+ levels (Group 2)increased less exponentially; to 2 times the initial valuein one week and 4 times in four weeks after irradiation.In our study for SAGM-PRBCs K+ levels till 35 days of stor-age was 62.1 mmol/L which is comparable to other studieslike Moroff et al. [6] (72.3 mmol/L on day 28) , Brugnaraand Churchill [7] (60–70 mmol/L on day 41), and Daveyand colleagues [8] (78.1 mmol/L on day 42). Lower valuein our study may be because of lesser days of storage ascompared to studied by Moroff et al. [6], and Brugnaraand Churchill [7]. The transfusion dose in a neonate is15 ml/kg and in a one kg neonate only 0.3–0.4 meq K willbe infused. This dose is even smaller than the usual dailyrequirement of 2–3 meq/kg. However, this rationale willnot apply to large volume transfusions (>25 ml/kg) suchas for exchange transfusions [19,20].

Fig. 4. Correlations between various parameters.
Fig. 5. Increase in plasma potassium from day 1 to day 28 of storage inboth groups of PRBCs.
Fig. 6. Decrease in pH from day 1 to day 28 of storage in both groups ofPRBCs.
Fig. 7. Decrease in ATP from day 1 to day 28 of storage in both groups ofPRBCs.
G.K. Patidar et al. / Transfusion and Apheresis Science 50 (2014) 479–487 485
Further, for equal days of storage after irradiation, in-crease in K+ levels was more significant in CPDA-1 PRBCscompared to SAGM-PRBCs (p < 0.001). This could be dueto greater dilution of K+ in SAGM additive solution.
Apart from visual assessment, plasma hemoglobin mea-surement in the supernatant from red cell units providesan objective measure of the extent of hemolysis duringstorage. The extent of hemolysis in blood components isan important indicator of cellular integrity and qualityparameters. In CPDA-1 PRBCs Hb levels (Group 1) in-creased to more than double the initial value in one weekand 6 times in four weeks after irradiation. Hb levels(Group 1) increased less exponentially to 1.5 times the ini-tial value in one week and 3.5 times in four weeks afterirradiation. Janatpour et al. [5] have reported the rise inHb concentration in irradiated stored blood by day 28 ofstorage; a 5-fold increase in four weeks, Davey and col-leagues [8] have reported in SAGM-PRBCs; 16-fold riseover 6 weeks similarly observed in Leitner et al. [10] studysupernatant hemoglobin was rise up to 2.06 g/L after35 days of storage. In our study, Hb levels in SAGM-PRBCsincreased from mean of 0.37 g/L on day 1 to 3.4 g/L on day28 and to 4.8 g/L on day 35 of storage. Hb levels (Group 1)increased to 3 times the initial value in one week to 9 timesin four weeks. Hb levels (Group 2) increased to 1.5 timesthe initial value in one week to 4 times in four weeks.
In our study, glucose levels in CPDA-1 PRBCs decreasedfrom mean of 21.77 mmol/L on day 1 to 8.16 mmol/L onday 28 and to 6.73 mmol/L on day 35 of storage. By the lastday of storage, glucose levels in both groups of irradiatedunits decreased to 1/3rd of initial values. In SAGM-PRBCglucose level decrease up to 18.12 mmol/L till 35 daysof storage and it is comparable to study by Moroff et al.[6] (30.58 mmol/L on day 28), and Zimmermann andcolleagues [11] (19.97 mmol/L on day 42).
Further, for equal days of storage after irradiation, theglucose levels were almost double in SAGM-PRBCs com-pared to CPDA-1 PRBCs. This may be attributed to differ-ence in composition of CPDA-1 anticoagulant (2 gdextrose in 63 ml, a part of which is removed while makingplasma and platelet components from whole blood) andSAGM additive solution (2.2 g dextrose in 100 ml additivesolution is added to the PRBCs).
Lactate levels (Group 1) almost doubled the initial valuein one week and increased to 3 times in four weeks afterirradiation. Lactate levels (Group 2) increased less expo-nentially to 1.5 times the initial value in one week and 2times in four weeks after irradiation. Lactate levels in both
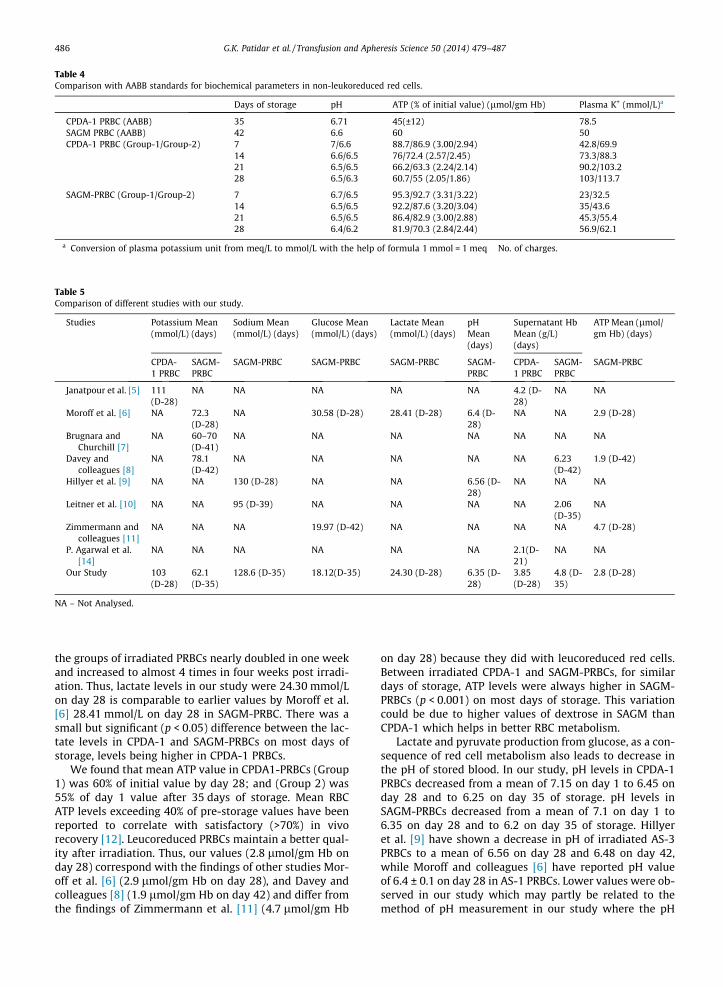
Table 4Comparison with AABB standards for biochemical parameters in non-leukoreduced red cells.
Days of storage pH ATP (% of initial value) (lmol/gm Hb) Plasma K+ (mmol/L)a
CPDA-1 PRBC (AABB) 35 6.71 45(±12) 78.5SAGM PRBC (AABB) 42 6.6 60 50CPDA-1 PRBC (Group-1/Group-2) 7 7/6.6 88.7/86.9 (3.00/2.94) 42.8/69.9
14 6.6/6.5 76/72.4 (2.57/2.45) 73.3/88.321 6.5/6.5 66.2/63.3 (2.24/2.14) 90.2/103.228 6.5/6.3 60.7/55 (2.05/1.86) 103/113.7
SAGM-PRBC (Group-1/Group-2) 7 6.7/6.5 95.3/92.7 (3.31/3.22) 23/32.514 6.5/6.5 92.2/87.6 (3.20/3.04) 35/43.621 6.5/6.5 86.4/82.9 (3.00/2.88) 45.3/55.428 6.4/6.2 81.9/70.3 (2.84/2.44) 56.9/62.1
a Conversion of plasma potassium unit from meq/L to mmol/L with the help of formula 1 mmol = 1 meq � No. of charges.
Table 5Comparison of different studies with our study.
Studies Potassium Mean(mmol/L) (days)
Sodium Mean(mmol/L) (days)
Glucose Mean(mmol/L) (days)
Lactate Mean(mmol/L) (days)
pHMean(days)
Supernatant HbMean (g/L)(days)
ATP Mean (lmol/gm Hb) (days)
CPDA-1 PRBC
SAGM-PRBC
SAGM-PRBC SAGM-PRBC SAGM-PRBC SAGM-PRBC
CPDA-1 PRBC
SAGM-PRBC
SAGM-PRBC
Janatpour et al. [5] 111(D-28)
NA NA NA NA NA 4.2 (D-28)
NA NA
Moroff et al. [6] NA 72.3(D-28)
NA 30.58 (D-28) 28.41 (D-28) 6.4 (D-28)
NA NA 2.9 (D-28)
Brugnara andChurchill [7]
NA 60–70(D-41)
NA NA NA NA NA NA NA
Davey andcolleagues [8]
NA 78.1(D-42)
NA NA NA NA NA 6.23(D-42)
1.9 (D-42)
Hillyer et al. [9] NA NA 130 (D-28) NA NA 6.56 (D-28)
NA NA NA
Leitner et al. [10] NA NA 95 (D-39) NA NA NA NA 2.06(D-35)
NA
Zimmermann andcolleagues [11]
NA NA NA 19.97 (D-42) NA NA NA NA 4.7 (D-28)
P. Agarwal et al.[14]
NA NA NA NA NA NA 2.1(D-21)
NA NA
Our Study 103(D-28)
62.1(D-35)
128.6 (D-35) 18.12(D-35) 24.30 (D-28) 6.35 (D-28)
3.85(D-28)
4.8 (D-35)
2.8 (D-28)
NA – Not Analysed.
486 G.K. Patidar et al. / Transfusion and Apheresis Science 50 (2014) 479–487
the groups of irradiated PRBCs nearly doubled in one weekand increased to almost 4 times in four weeks post irradi-ation. Thus, lactate levels in our study were 24.30 mmol/Lon day 28 is comparable to earlier values by Moroff et al.[6] 28.41 mmol/L on day 28 in SAGM-PRBC. There was asmall but significant (p < 0.05) difference between the lac-tate levels in CPDA-1 and SAGM-PRBCs on most days ofstorage, levels being higher in CPDA-1 PRBCs.
We found that mean ATP value in CPDA1-PRBCs (Group1) was 60% of initial value by day 28; and (Group 2) was55% of day 1 value after 35 days of storage. Mean RBCATP levels exceeding 40% of pre-storage values have beenreported to correlate with satisfactory (>70%) in vivorecovery [12]. Leucoreduced PRBCs maintain a better qual-ity after irradiation. Thus, our values (2.8 lmol/gm Hb onday 28) correspond with the findings of other studies Mor-off et al. [6] (2.9 lmol/gm Hb on day 28), and Davey andcolleagues [8] (1.9 lmol/gm Hb on day 42) and differ fromthe findings of Zimmermann et al. [11] (4.7 lmol/gm Hb
on day 28) because they did with leucoreduced red cells.Between irradiated CPDA-1 and SAGM-PRBCs, for similardays of storage, ATP levels were always higher in SAGM-PRBCs (p < 0.001) on most days of storage. This variationcould be due to higher values of dextrose in SAGM thanCPDA-1 which helps in better RBC metabolism.
Lactate and pyruvate production from glucose, as a con-sequence of red cell metabolism also leads to decrease inthe pH of stored blood. In our study, pH levels in CPDA-1PRBCs decreased from a mean of 7.15 on day 1 to 6.45 onday 28 and to 6.25 on day 35 of storage. pH levels inSAGM-PRBCs decreased from a mean of 7.1 on day 1 to6.35 on day 28 and to 6.2 on day 35 of storage. Hillyeret al. [9] have shown a decrease in pH of irradiated AS-3PRBCs to a mean of 6.56 on day 28 and 6.48 on day 42,while Moroff and colleagues [6] have reported pH valueof 6.4 ± 0.1 on day 28 in AS-1 PRBCs. Lower values were ob-served in our study which may partly be related to themethod of pH measurement in our study where the pH

G.K. Patidar et al. / Transfusion and Apheresis Science 50 (2014) 479–487 487
indicator solution was used and the reading was on a dif-ference in scale of 0.5 units. A mathematical deduction ofthe pH curve of many samples of stored blood in variousstorage solutions revealed a lower limit of pH 6.2 belowwhich RBCs had decreased ATP generation [21].
The biochemical alterations observed in our study onirradiated PRBCs were within recommended values as perinternational (AABB) [13] standards, except for concernregarding pH and K+. In Group-1 SAGM-PRBCs plasma K+
exceeded recommended levels after day 28 of storagewhile in Group-2 it exceeded after day 21. SAGM-PRBCs(irradiated day 7) exceeded recommended K+ levels afterday 21 of storage and safe pH levels after day 28 of storage.The quality of stored irradiated PRBCs was better and long-er preserved in SAGM additive solution than CPDA-1PRBCs. Zimmermann and colleagues [11] have furthershowed that quality of irradiated PRBCs is even better inleucoreduced SAGM-PRBCs. Their study on units irradiatedwith 30 Gy on day 14 and stored till day 42 showed thatPRBCs maintained their in vitro quality till 28 days postirradiation.
6. Conclusion
Hence, we conclude that SAGM-PRBCs show better sta-bility after irradiation compared to CPDA-1 PRBCs. The lim-its of recommended levels for CPDA-1 PRBCs appear to betwo weeks after irradiation and thus the shelf life shouldbe limited to this period. SAGM-PRBCs on the other handshow acceptable limits of safety up to three weeks of irra-diation. The shelf life of irradiated red cell is different invarious countries. The shelf life of irradiated PRBCs shouldbe determined by taken into consideration the storagesolution, day of irradiation after blood collection andleukoreduction.
References
[1] Anderson KC, Weinstein HJ. Transfusion-associated graft versus-hostdisease. N Engl J Med 1990;323:315–21.
[2] Leitman SF. Use of blood cell irradiation in the prevention ofposttransfusion graft-versus-host disease. Transfus Sci 1989;10:2219–32.
[3] Saran RK. Transfusion medicine – technical manual, vol. 32, 2nded. New Delhi, India: Directorate General of Health Services (DGHS),Ministry of Health and Family Welfare, Government of India; 2003.p. 352–3.
[4] Lewis SM, Bain BJ, Bates I. Dacie and Lewis practical hematology.10th ed. Elsevier; 2008. p. 281–2.
[5] Janatpour K, Denning L, Nelson K, Betlach B, Mackenzie M, Holland P.Comparison of X-ray vs. gamma irradiation of CPDA-1 red cells. VoxSang 2005;89:215–9.
[6] Moroff G, Holme S, AuBuchon JP, Heaton WA, Sweeney JD, FriedmanLI. Viability and in-vitro properties of AS-1 red cells after gammairradiation. Transfusion 1999;39:128–34.
[7] Brugnara C, Churchill WH. Effect of irradiation on red cell cationcontent and transport. Transfusion 1992;32:246–52.
[8] Davey RJ, McCoy NC, Yu M, Sullivan JA, Spiegel DM, Leitman SF. Theeffect of pre-storage irradiation on post-transfusion red cell survival.Transfusion 1992;32:525–8.
[9] Hillyer CD, Tiergerman KO, Berkman EM. Evaluation of the red cellstorage lesion after irradiation in filtered packed red cell units.Transfusion 1991;31:497–9.
[10] Leitner GC, Neuhauser M, Weigel G, Kurze S, Fischer MB, Höcker P.Altered intracellular purine nucleotides in gamma-irradiated redblood cell concentrates. Vox Sang 2001;81:113–8.
[11] Zimmermann R, Wintzheimer S, Weisbach V, Strobel J, Zingsem J,Eckstein R. Influence of prestorage leucoreduction and subsequentirradiation on in vitro red blood cell (RBC) storage variables of RBCsin additive solution saline–adenine–glucose–mannitol. Transfusion2009;49:75–80.
[12] Peck CC, Moore GL, Bolin RB. Adenine in blood preservation. Crit RevClin Lab Sci 1981;13:173–212.
[13] Brecher ME. Components from whole blood donations. AmericanAssociation of Blood Banks. Technical Manual 16th ed.; 2008. p.288–89.
[14] Agarwal P, Ray VL, Choudhary N, Chaudhary RK. Effect of prestoragegamma irradiation on red blood cells. Indian J Med Res 2005;122:385–7.
[15] Menitove JE. Standards for blood banks and transfusion services,19th ed. Bethesda, MD: American Association of Blood Banks; 1999.
[16] Chapman J, Fineey RD, Farman K, Kesley P, et al. Guidelines ongamma irradiation of blood components for the prevention oftransfusion-associated-graft-versus-host disease. Transfus Med1996;6:261–71.
[17] Asai T, Inaba S, Ohto H, Osada K, Suzuki G, Takahashi K, et al.Guidelines for irradiation of blood and blood components to preventpost-transfusion graft vs host disease in Japan. Transfus Med 2000;10:312–20.
[18] Ambruso DR, Hawkins B, Johnson DL, Fritzberg AR, KlingensmithWC, McCabe ER. Measurement of adenosine triphosphate and 2,3-diphosphoglycerate in stored blood with 31P nuclear magneticresonance spectroscopy. Biochem Med Metab Biol 1986;35(3):376–83.
[19] Seghatchian MJ, Vickers M, Ip AH, Stivala JF, de Silva PM. Thepotassium haemoglobin and acid content of CPDA-1 whole blood,plasma reduced red cells and red cells suspended in SAG-M over 35days. Transfus Med 1993;3(Suppl. 2):58–9.
[20] Hall TL, Barnes A, Miller JR, Bethencourt DM, Nestor L. Neonatalmortality following transfusion of red cells with high plasmapotassium levels. Transfusion 1993;33:606–9.
[21] Valeri CR, Hirsch NM. Restoration in vivo of erythrocyte adenosinetriphosphate, 2,3-diphosphoglycerate, potassium ion, and sodiumion concentrations following the transfusion of acidcitrate-dextrose-stored human red blood cells. J Lab Clin Med 1969;73:722–33.
![North Carolina register [serial] - NC OAH](https://static.fdokumen.com/doc/165x107/633bb631a24651471c0221d8/north-carolina-register-serial-nc-oah.jpg)

![Yackety yack [serial] - Internet Archive](https://static.fdokumen.com/doc/165x107/63276564e491bcb36c0b431c/yackety-yack-serial-internet-archive.jpg)

















