
Senate Community Affairs References Committee Inquiry into ...
16
Re: Senate Community Affairs References Committee Inquiry into Private Health Insurance Thank you for the opportunity to submit our views on suggested improvements to private health insurance in Australia. nib acknowledges Government, payers and providers all have a responsibility to improve market efficiency, as well as private health insurances access and affordability for consumers. nib supports the submission made by Private Health Australia, but we are keen to make some additional comments and suggestions of our own. I’d personally welcome the opportunity to further discuss and share our thoughts with the Committee on the items detailed in our submission. Yours sincerely Mark Fitzgibbon Chief Executive Officer nib health funds limited Senate Standing Committees on Community Affairs PO Box 6100 Parliament House Canberra ACT 2600 By email: [email protected] Value and affordability of private health insurance and out-of-pocket medical costs Submission 24
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Senate Community Affairs References Committee Inquiry into ...
Re: Senate Community Affairs References Committee Inquiry into Private Health Insurance
Thank you for the opportunity to submit our views on suggested improvements to private health insurance in Australia. nib acknowledges Government, payers and providers all have a responsibility to improve market efficiency, as well as private health insurances access and affordability for consumers.
nib supports the submission made by Private Health Australia, but we are keen to make some additional comments and suggestions of our own.
I’d personally welcome the opportunity to further discuss and share our thoughts with the Committee on the items detailed in our submission.
Yours sincerely
Mark Fitzgibbon Chief Executive Officer nib health funds limited
Senate Standing Committees on Community Affairs PO Box 6100 Parliament House Canberra ACT 2600 By email: [email protected]
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

nhfasx2007-2017
nib submission | July 2017
Senate Community Affairs References Committee Private Health Insurance Inquiry
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
i
Table of Contents
1 Executive summary
3 Introduction
4 Addressing regulatory failures
7 Expanding and improving PHI coverage and choice
9 Making PHI more attractive to younger people
11 Empowering PHI consumers with information
13 Conclusion
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
1
EXECUTIVE SUMMARYThe Senate Community Affairs References Committee Inquiry (Inquiry) into Private Health Insurance (PHI) is a timely examination of how our industry is regulated, and how it can maintain and enhance its future contribution to the Australian healthcare system.
nib welcomes the opportunity to submit our views on suggested improvements to PHI with the view to:
n Make our health care system more cost and service efficient;
n Deliver improved health outcomes;
n Provide better value and enhanced transparency for consumers; and
n Ensure taxpayers realise value from their investment through initiatives such as the PHI Rebate.
Our submission to the Inquiry has five themes:
1. The private healthcare sector, both service providers and PHI payers, must do more to help shoulder the overall cost and service delivery burden across primary, acute and preventive healthcare;
2. PHI should be able to take a greater role by expanding what it can cover;
3. Regulatory failures, not market failures, are constraining PHI’s ability to serve its policyholders better and more comprehensively than now;
4. To help rein in premium growth, and sustain community rating, PHI needs to be made more attractive and relevant to “young and healthy” people; and
5. Through reliable and easily accessible information, we can empower PHI policyholders to make better decisions and choices about their health, healthcare treatments and providers.
Within this framework, nib offers some policy and regulatory improvement proposals, and urges the Community Affairs References Committee to give them favourable consideration.
Key recommendations include:
Trialling Medicare SelectThe 2008 National Health and Hospitals Commission recommended a reorganisation of the relationship between purchaser, provider and consumer, called Medicare Select. This model removes federal-state and public-private healthcare funding splits, and makes Government and PHI work as partners to ensure patients get the best care and treatment for their needs.
As demand grows and service delivery gets more complex and costly, Medicare Select merits a trial and evaluation in real time and real localities.
Empowering patients with effective and reliable informationInformation asymmetry gives doctors and other health professionals too much power in the doctor-patient relationship. PHI regulation should enable insurers to share as much information as possible with their policyholders and, at a minimum, not preclude consumer and provider reviews of doctors, hospitals and other providers.
The very successful Whitecoat “TripAdvisor”-style reviewing service, founded by nib and now a joint venture with Bupa and HBF, is a practical example of what can be done to inform and empower consumers, without undermining the doctor-patient relationship.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
2
Excessive specialist chargingExcessive patient out-of-pockets are one of the biggest sources of complaint about PHI, even though these are the deliberate decisions of treating doctors, not insurers. These bad consumer experiences reflect unfairly not just on insurers, but the vast majority of specialists and surgeons who do the right thing by their patients.
The PHI industry is proposing regulatory intervention by Government to confront excessive specialist charging. nib endorses these industry proposals, and wants to work with provider groups sharing our concern about consumers’ medical bill shocks.
Make PHI more relevant to younger peopleThe young and healthy need more convincing of the benefit from taking PHI cover. Current sticks and carrots, including the Medicare Levy Surcharge, Lifetime Health Cover and even the PHI Rebates, don’t do enough to make the product sufficiently attractive to healthy under 30s. It is this group that is essential to deepening the community-rated risk pool and therefore keeping premium growth down.
The next wave of PHI reform could look at measures including “Reverse” Lifetime Health Cover, whereby premiums are discounted for age steps under 30, as opposed to being loaded for age steps over 30. General reforms, especially extending the reach of the current Broader Health Cover for out-of-hospital wellness and condition management services, as well as administrative and purchaser-provider reforms that simply keep premiums lower, also enhance PHI’s appeal to the young and healthy.
Genuine PHI reform must tackle the rising costs of service provisionFinally, nib believes the reform of PHI regulation must be far wider than the Government so far is considering. The consumer offering concerns targeted by the Government, especially unpopular premium rises, restrictions and exclusions do need addressing. These, however, are driven by well above CPI growth in provider costs: doctors, hospitals, prostheses and other healthcare providers drive that growth, not insurers.
Reform that tackles PHI payers but not these powerful provider interests ultimately will be ineffective.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
3
INTRODUCTIONPrivate health insurance (PHI) is an integral and indispensable part of the Australian healthcare system.
Even in 2017, many people still believe PHI and the private health sector are indulgences of the wealthy, and that public investment in private health, especially PHI rebates, would be better spent on cash-hungry public hospitals and higher Medicare rebates for doctors.
Such ideologically-driven ideas must be continually challenged. The private health care sector can and must demonstrate that it is integral to the Australian healthcare system, and not an optional extra that can be discarded at will.
For that reason, nib welcomes the Senate Community Affairs References Committee’s inquiry into private health insurance. As the Turnbull Government is looking at ways to make PHI more consumer-friendly, the inquiry can drill down into challenges and opportunities facing the PHI industry, and test the water in exploring policy and regulatory innovation that goes further than what is currently proposed.
Recent history shows that even incremental healthcare reform is not easy. But that’s no reason not to try.
Support for key PHI policy settingsnib generally supports the submission made on behalf of the industry by Private Healthcare Australia (PHA). We endorse PHA’s defence of the “three pillars” of government support for PHI:
n Private health insurance rebates;
n The Medicare Levy Surcharge (MLS); and
n Lifetime Health Cover (LHC).
nib is also committed to:
n Community rating of PHI, so that everyone pays the same premium regardless of age or health status;
n The primacy of the relationship between patients and health professionals; and
n Ensuring a level playing field between PHI as payers for services and healthcare providers.
Proposals for policy and regulatory innovation in this submission are consistent with these principles.
Coverage of this submissionWhile PHA has made its submission on behalf our industry, nib’s submission makes complementary comments and proposals based on our own experience, and our reputation for being at the forefront of innovative policy thinking that is in the best interests of our customers.
The submission covers:
1. Addressing regulatory failures that put pressure on PHI costs and premiums;
2. Expanding PHI coverage and choice;
3. Making PHI more attractive and relevant to younger people; and
4. Empowering consumers to make better decisions about their healthcare.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
4
The private health sector will need to do moreAs a nation, we are spending $160 billion on healthcare, or about $6,600 for every man, woman and child. Government is the primary funder, currently funding approximately 70 per cent of our nation’s health expenditure.
According to Treasury’s 2015 Intergenerational Report, increasingly as a nation we (Government) are going to run out of sufficient working age people to fund the health care needs of our nation.
AN AGEING POPULATIONAustralians will live longer and continue to have the longest life expectancies in the world. The structure
of our population will also change which will have important implications for the demand for health care
services. The 2015 Intergenerational Report highlights that increasingly there will be fewer people of
traditional working age compared with the very young and elderly. The graph below shows the number of
working aged people (aged 15 – 64 years) to elderly (aged 65+ years) is declining. In 1974/75 there were
7.3 working aged people for every person aged 65 years and over, in 2014/15 it was 4.5 people and by
2054/55 it is expected to be 2.7.
1974–75 2014–15 2054–55
Source: 2015 Intergenerational report.
The challenges the Australian healthcare sector faces are very real. No stakeholder, whether they be a patient, provider or funder (both private and public) is immune from them.
ADDRESSING REGULATORY FAILURESThe current regulation of the PHI industry needs to be reviewed and reformed.
Making regulatory changes that help keep premium increases as low as possible and ending consumer out-of-pocket surprises requires more than simply making private health insurance more consumer-friendly. It means Government must:
n Trust insurers to act in the market responsibly, including when setting premiums and negotiating with hospitals, doctors and other providers; and
n Have the courage to take on vested provider interests.
With industry average Management Expense Ratios (MERs) at less than 10 per cent of revenue for a long time (nib’s FY16 MER was 8.9 per cent), consistently higher than CPI premium growth is not being driven by inefficient or greedy insurers.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
5
PHI INDUSTRY MARGINS (FY16)
Net Margin
Management Expense Ratio
Claims Ratio (including risk equalisation)
5.4%
86.1%
8.5%
Source: APRA (PHI Insurance Operations Report 2015/16)
They are being driven by strong, and sometimes excessive, growth in costs for medical, hospital and other healthcare services, including health professional fees and the use of expensive healthcare technologies. The PHA submission neatly summarises these supplier-drive cost pressures.1
Risk equalisationRisk equalisation – distributing a shared pool of funds between insurers reflecting differences in age and risk profiles of insured persons, with special provision for high-cost claims – is a fundamental underpinning of community rating.
Depending on their risk profiles, in any one year some insurers are net drawers from the pool and some are net payers.
The current system has been in place since the early 2000s. It is however, not geared to the increasing reality that insurers are dealing more and more with the consequences of chronic conditions rather than acute conditions. This pressure is going to intensify as the baby boom generation reaches 75 years and over in far greater numbers than previous elderly cohorts.
Even though ageing healthily is a public policy goal and the 2007 cover reforms introduced Broader Health Cover to allow PHI to cover condition management and wellness maintenance services, risk equalisation rules are stuck back in the days when PHI was all about covering acute, in-hospital treatment.
The current risk equalisation mechanism actively discourages insurers from working more extensively with their members to better manage their chronic conditions and health risks generally. This is because, under the current system, the benefits of any one insurer’s efforts to improve the health of its elderly customers are effectively shared with all other health insurers.
Conversely, the introduction of a prospective risk equalisation scheme would ensure insurers are encouraged to invest in proactively managing the health of their sickest members. It would also incentivise designing and offering PHI products taking full advantage of Broader Health Cover.
Furthermore, it would help make PHI more attractive and affordable to younger and healthier people not to mention deliver better health outcomes for the chronically ill.
In short, reforming and broadening risk equalisation is a win-win for everyone, including the Government as PHI regulator and subsidiser.
We therefore support the PHA’s2 recommendation to explore and improve regulatory reforms which could improve the relationship between PHI and public hospitals with the view to end the current State Government cost-shifting.
1. PHA submission, pages 5-10.2. PHA Submission, pages 31-35
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
6
Prostheses reformThe cost of prostheses – effectively, any medical or surgical device implanted or fitted into a patient’s body as part of a medical or surgical procedure – has long been a running sore for the PHI industry and successive governments.
Attempts to rein in prostheses costs were made by the Howard Government in 2000 and 2004, but research commissioned by the health insurance funds has clearly shown that Australian private health consumers could save $800 million annually in premiums if Australian prostheses prices were reset to levels paid in comparable markets overseas.
While we welcome and support the Government’s moves towards prostheses funding reform, we join PHA3 in urging the Committee to encourage the Government to go harder and further down the path of prostheses reform, to obtain lower prices for Australian health consumers, rather than allow windfall profits for manufacturers and suppliers.
As an insurer, nib has no problem with paying for prostheses and medical devices, if prices fairly reflect the true cost of developing, manufacturing and supplying a prosthesis, and it offers reasonable margins for manufacturers and suppliers. But we strongly object to being forced to pay through the nose for essential devices simply because outdated regulations let manufacturers and middlemen get away with it.
Reining in excessive specialist chargingTo help give our customers peace of mind at time of need, health insurers offer no-gap and known-gap fees to doctors that are well above MBS and generously reward their time and skill. nib will continue to make these fee incentives as generous as possible, in the best interests of our customers.
Nevertheless, some doctors insist on charging out-of-pockets, sometimes thousands of dollars more than what they would receive in Medicare and PHI benefits. This upsets consumers, many of whom are not well-off, and makes them doubt why they pay for private cover in the first place.
As an example, nib data shows there is a wide variation in specialist fees charged for removing a prostate gland in calendar year 2016. For this procedure, at the time:
n The Medicare schedule fee was $1,935.
n The nib Medigap (no gap) fee was $2,941.
n The Australian Medical Association recommended fee was $4,465.
3. PHA Submission, pages 28-29.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
7
As the graph below illustrates most specialists accepted nib’s Medigap fee. But the top fee recorded was a whopping and outrageous $13,300 – almost seven times the Medicare fee and more than four times the nib Medigap fee.
PROSTATECTOMY COST VARIATION (CY16)
0
10
20
30
40
50
Ser
vice
s p
aid
($)
Charge range
Up
to
1,50
0
1,50
1 to
2,0
00
2,00
1 to
2,5
00
2,50
1 to
3,0
00
3,00
1 to
3,5
00
3,50
1 to
4,0
00
4,00
1 to
4,5
00
4,50
1 to
5,0
00
5,00
1 to
5,5
00
5,50
1 to
6,0
00
6,00
1 to
6,5
00
6,50
1 to
7,0
00
7,00
1 to
7,5
00
7,50
1 to
8,0
00
8,00
1 to
8,5
00
8,50
1 to
9,0
00
9,00
1 to
9,5
00
9,50
1 to
10,
000
10,0
01 +
Item code 37211
MBS Fee $1,935
MediGap Fee $2,941
AMA Fee $4,465
Source: nib
The problem of excessive specialist charging needs consideration in any regulatory reform of PHI. PHA makes some proposals on patient out-of-pockets in its submission4, which nib endorses. We are also very willing to work with provider organisations, such as the Royal Australasian College of Surgeons, which share our concern about isolated high-charging outlier specialists.
EXPANDING AND IMPROVING PHI COVERAGE AND CHOICEKeeping PHI attractive and affordable is more than improving the regulatory framework and how the PHI market operates. It is also expanding and improving the breadth of the PHI choice.
nib has some comments and proposals on this over and above the PHA industry submission.
Trial a “Medicare Select” approachNo single reform is a panacea for the various challenges facing the Australian healthcare system. Nevertheless, a good starting point would be a “single payer” model which would allow a payer to cover the full spectrum of healthcare including primary care (e.g. GP and specialist out-patient visits, diagnostic and radiology, pharmaceuticals), outpatient specialist visits, as well as in-hospital treatment.
4. PHA submission, pages 39-40.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
8
Under current arrangements, multiple payers are involved in funding any one person’s health care with State Governments, the Federal Government, private health insurers and individuals providing different combinations depending on the type of care being provided.
These arrangements are cumbersome compromises, born out of a long battle between those who would mandate a British-style public healthcare monopoly versus free market forces for choice and accessibility.
It is dysfunctional. No one payer has a “full view” of the consumer and incentives to better manage and coordinate care are significantly blunted. The economic benefit of any effort invested by any one payer towards managing health risks is effectively free-ridden by the other payers. It creates massive duplication of systems and infrastructure. And it creates enormous confusion for consumers who so often don’t understand why for example, nib will pay for their specialist within the hospital but not outside.
The idea of a single payer system is not new. A proposal, Medicare Select, was outlined in the Rudd Government’s National Health and Hospital Reform Commission’s Report of 2010. In essence:
n Private health insurers (the carriers) design a Medicare Select model that covers the full healthcare – both acute and primary – requirements of individuals aged over 65 who currently have private health insurance (the insured).
n The insured are given the choice to opt into Medicare Select or stay with existing dual funding arrangements (i.e. Medicare and PHI).
n Commonwealth and state governments (Government) jointly set health performance targets and subject to targets being met, pay the carrier an annual amount equivalent to their otherwise expected expense for the insured (i.e. a risk- adjusted capitation).
n A portion of financial savings achieved by the carrier in managing the healthcare of the insureds’ care are shared with Government.
This is not US-style managed care, and is consistent with the key PHI principles we support.
Indeed, Government funding following the insured under Medicare Select make the model, and the healthcare market, contestable. In nib’s view, Medicare Select would promote cost efficiency, better use of scarce healthcare resources and give the insured more control over their own healthcare choices, in partnership with their Medicare Select provider.
After almost ten years, and with current and future cost pressure on Government and private healthcare payers continuing to mount, it is timely to at least revisit the Medicare Select concept, and to consider trialling it.
Should Government pursue that possibility, nib would be enthusiastic in helping to design and implement a Medicare Select trial to operate in a region or regions of Australia. That includes our taking a financial stake in such a trial.
Broadening Broader Health Cover (BHC)Approximately one per cent of nib’s hospital customers account for more than half our hospital benefits paid before risk equalisation is applied. No doubt other insurers would report similar profiles.
Intervening, monitoring and better managing customers who are at risk of poor health outcomes is aimed at providing them with the right care, in the right place at the right time. By better managing the health and well-being of our “frequent fliers”, we are also reducing pressure on claims inflation and premium increases.
Under BHC introduced in 2007, PHI insurers can pay hospital table benefits in limited out-of-hospital care environments, including patients’ homes, primary and community care. Currently, BHC has two main areas of focus; Hospital Substitute Care and Chronic Disease Management programs.
Our approach is to work together with our customers, and a collective network of health professionals including General Practitioners, Primary Care providers, by partnering with other private insurers, Local Health Districts and other health services.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24
X
nib
sub
missio
n | J
ULY
20
17
9
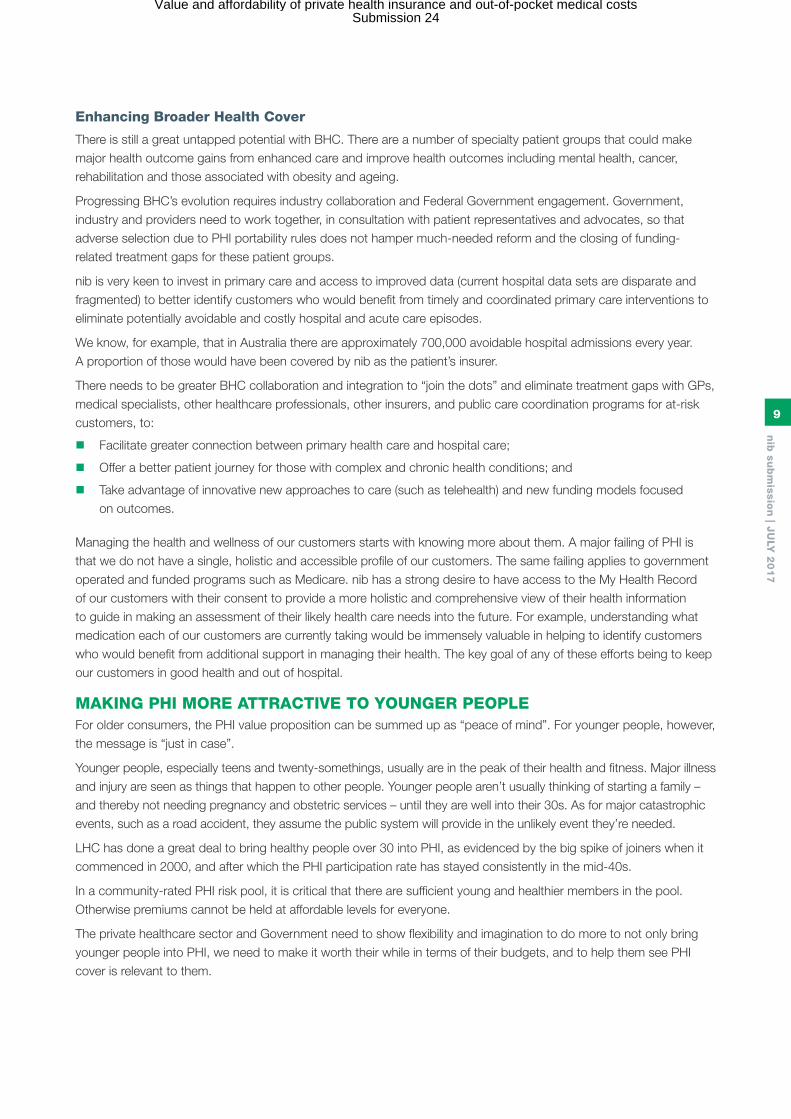
Enhancing Broader Health Cover
There is still a great untapped potential with BHC. There are a number of specialty patient groups that could make major health outcome gains from enhanced care and improve health outcomes including mental health, cancer, rehabilitation and those associated with obesity and ageing.
Progressing BHC’s evolution requires industry collaboration and Federal Government engagement. Government, industry and providers need to work together, in consultation with patient representatives and advocates, so that adverse selection due to PHI portability rules does not hamper much-needed reform and the closing of funding-related treatment gaps for these patient groups.
nib is very keen to invest in primary care and access to improved data (current hospital data sets are disparate and fragmented) to better identify customers who would benefit from timely and coordinated primary care interventions to eliminate potentially avoidable and costly hospital and acute care episodes.
We know, for example, that in Australia there are approximately 700,000 avoidable hospital admissions every year. A proportion of those would have been covered by nib as the patient’s insurer.
There needs to be greater BHC collaboration and integration to “join the dots” and eliminate treatment gaps with GPs, medical specialists, other healthcare professionals, other insurers, and public care coordination programs for at-risk customers, to:
n Facilitate greater connection between primary health care and hospital care;
n Offer a better patient journey for those with complex and chronic health conditions; and
n Take advantage of innovative new approaches to care (such as telehealth) and new funding models focused on outcomes.
Managing the health and wellness of our customers starts with knowing more about them. A major failing of PHI is that we do not have a single, holistic and accessible profile of our customers. The same failing applies to government operated and funded programs such as Medicare. nib has a strong desire to have access to the My Health Record of our customers with their consent to provide a more holistic and comprehensive view of their health information to guide in making an assessment of their likely health care needs into the future. For example, understanding what medication each of our customers are currently taking would be immensely valuable in helping to identify customers who would benefit from additional support in managing their health. The key goal of any of these efforts being to keep our customers in good health and out of hospital.
MAKING PHI MORE ATTRACTIVE TO YOUNGER PEOPLEFor older consumers, the PHI value proposition can be summed up as “peace of mind”. For younger people, however, the message is “just in case”.
Younger people, especially teens and twenty-somethings, usually are in the peak of their health and fitness. Major illness and injury are seen as things that happen to other people. Younger people aren’t usually thinking of starting a family – and thereby not needing pregnancy and obstetric services – until they are well into their 30s. As for major catastrophic events, such as a road accident, they assume the public system will provide in the unlikely event they’re needed.
LHC has done a great deal to bring healthy people over 30 into PHI, as evidenced by the big spike of joiners when it commenced in 2000, and after which the PHI participation rate has stayed consistently in the mid-40s.
In a community-rated PHI risk pool, it is critical that there are sufficient young and healthier members in the pool. Otherwise premiums cannot be held at affordable levels for everyone.
The private healthcare sector and Government need to show flexibility and imagination to do more to not only bring younger people into PHI, we need to make it worth their while in terms of their budgets, and to help them see PHI cover is relevant to them.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24
X
nib
sub
missio
n | J
ULY
20
17
10
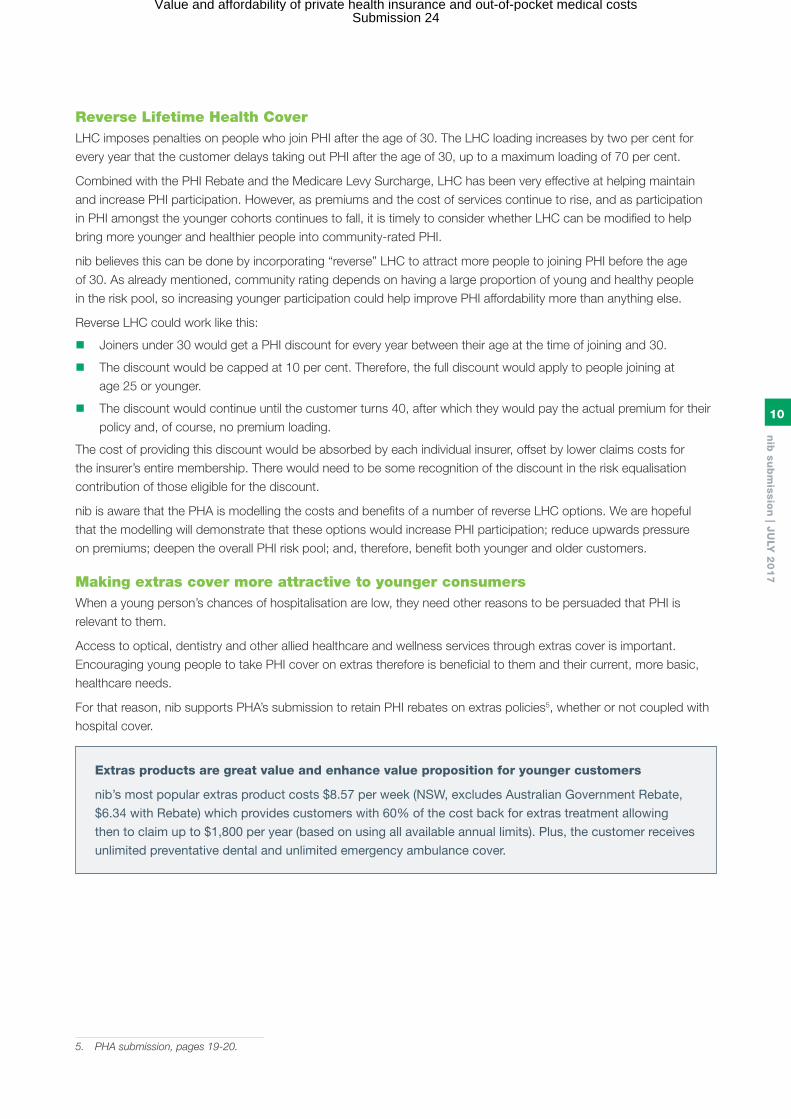
Reverse Lifetime Health Cover LHC imposes penalties on people who join PHI after the age of 30. The LHC loading increases by two per cent for every year that the customer delays taking out PHI after the age of 30, up to a maximum loading of 70 per cent.
Combined with the PHI Rebate and the Medicare Levy Surcharge, LHC has been very effective at helping maintain and increase PHI participation. However, as premiums and the cost of services continue to rise, and as participation in PHI amongst the younger cohorts continues to fall, it is timely to consider whether LHC can be modified to help bring more younger and healthier people into community-rated PHI.
nib believes this can be done by incorporating “reverse” LHC to attract more people to joining PHI before the age of 30. As already mentioned, community rating depends on having a large proportion of young and healthy people in the risk pool, so increasing younger participation could help improve PHI affordability more than anything else.
Reverse LHC could work like this:
n Joiners under 30 would get a PHI discount for every year between their age at the time of joining and 30.
n The discount would be capped at 10 per cent. Therefore, the full discount would apply to people joining at age 25 or younger.
n The discount would continue until the customer turns 40, after which they would pay the actual premium for their policy and, of course, no premium loading.
The cost of providing this discount would be absorbed by each individual insurer, offset by lower claims costs for the insurer’s entire membership. There would need to be some recognition of the discount in the risk equalisation contribution of those eligible for the discount.
nib is aware that the PHA is modelling the costs and benefits of a number of reverse LHC options. We are hopeful that the modelling will demonstrate that these options would increase PHI participation; reduce upwards pressure on premiums; deepen the overall PHI risk pool; and, therefore, benefit both younger and older customers.
Making extras cover more attractive to younger consumersWhen a young person’s chances of hospitalisation are low, they need other reasons to be persuaded that PHI is relevant to them.
Access to optical, dentistry and other allied healthcare and wellness services through extras cover is important. Encouraging young people to take PHI cover on extras therefore is beneficial to them and their current, more basic, healthcare needs.
For that reason, nib supports PHA’s submission to retain PHI rebates on extras policies5, whether or not coupled with hospital cover.
Extras products are great value and enhance value proposition for younger customers
nib’s most popular extras product costs $8.57 per week (NSW, excludes Australian Government Rebate,
$6.34 with Rebate) which provides customers with 60% of the cost back for extras treatment allowing
then to claim up to $1,800 per year (based on using all available annual limits). Plus, the customer receives
unlimited preventative dental and unlimited emergency ambulance cover.
5. PHA submission, pages 19-20.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
11
EMPOWERING PHI CONSUMERS WITH INFORMATIONThe most fundamental market failure in healthcare is the information asymmetry that currently exists between the buyers of health care (consumers) and the sellers of health care (doctors). Most patients, at time of urgent need, don’t argue with their doctors, nor feel empowered to seek a second opinion. They do what they’re told, and go where they’re told. If they’re told they need a given procedure, they take that advice at face value.
There are wide variations in the medical sector when it comes to the volume and cost of medical and surgical procedures, to the point that questions must be asked about why it is, and whether the patient’s best interests were serviced, or whether it was the doctor’s financial interests that were the real focus of the doctor-patient transaction.
The Atlas of Healthcare Variation, recently updated by the Australian Commission on Safety and Quality
in Healthcare, shows just how much our chances of having surgery, and particular types of surgery, can
depend upon where we live. The Commission argues that redressing unwarranted regional variation can
only be achieved by a range of actions that mitigate hospitalisation in the first place, promote the latest
clinical science/evidence about treatment or surgery and most importantly, empower patients to make
more informed choices.
Variation examples cited by the Commission include:
n The likelihood of having a knee replacement in Hawkesbury, NSW (443 per 100,000 per person)
was 3.5 times higher than in Darwin, NT (128);
n The likelihood of having a hysterectomy in Ballarat, VIC (744 per 100,000 women) was more than
5.5 times higher than in Manly, NSW (134); and
n The likelihood of having a caesarean section in Cockburn, WA (356 per 1,000 women) was almost
double that of Norwood, SA (192).
As the Commission notes, some variation by geography is reasonable if it reflects “a response to
differences in patient needs or choice of treatment”. This, however, cannot account for the massive
variation reported.
The bottom line is this. If procedures are being performed simply because they’re readily available, not because of clinical necessity, then they are an avoidable cost putting upward pressure on PHI premiums. If no-gap fees aren’t accepted by doctors, individuals can be stuck with significant out-of-pocket costs, and taxpayers with the subsidy costs of Medicare are the PHI rebates.
Far worse, is the inevitable conclusion that some patients are receiving costly, risky and often invasive health care treatment that they don’t need.
The solution: more information and transparencyPatients not only deserve reliable and independent information about their treatment and provider options, they are entitled to it.
We must get reliable data and information into the palms of patients, and their doctors, so they are able to make more informed choices about treatment and doctor options. That includes not only treatments themselves, but the quality of their experience as a consumer.
Patients want to have to hand (preferably via their mobile) the very latest clinical evidence about their condition and treatment options. They want to be able to:
n Compare feedback from previous patients about their treatment outcomes and doctor experience.
n Do cost comparisons, understand any out-of-pocket expenses and make a doctor appointment online and in the case of a specialist, an electronic referral.
n Share their own experience and maybe engage a virtual community with similar medical conditions.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
12
Variation in health outcomes is a world-wide problem
Outcome customer measurement and transparency is key to driving down variation.
Prostate cancer survival rates are the same across Germany, but by using outcomes data to drive
improvements, Hamburg’s Martini-Klinik ensures better quality of life post-surgery.
As the chart below shows the five-year survival rate – of around 95 per cent – for cancer patients having
their prostate gland removed at Martini-Klinik, is in line with the rest of Germany.
But although that obviously is an important measure of the clinic’s performance, it says nothing about the
quality of life of men who have had a radical prostatectomy.
Removing the prostate can lead to urinary incontinence and erectile dysfunction. It turns out that around
43 per cent of men undergoing radical prostatectomy in Germany as a whole suffer incontinence one year
after surgery. At the Martini-Klinik the figure is 6.5 per cent.
Similarly, three quarters of German patients report severe erectile dysfunction after one year, compared to
just over one third for Martini-Klinik patients.
At the core of this approach is understanding the outcomes that matter to patients.
Source: Science Business Publishing
Measuring outcomes of prostate cancer care
Focusing on mortality alone…. …may obscure large differences in outcomes that matter most to patients
Germany
Sweden
Best in class: Martini Klinik
Germany
Sweden
Best in class: Martini Klinik
94.0%
94.0%
95.0%
43.3%
50.0%
6.5%
Germany
Sweden
Best in class: Martini Klinik
75.5%
80.0%
34.7%
5 year survival 1 year incontinence 1 year severe erectile dysfunction
Swedish data rough estimates from graphs; Source: National quality report for the year of diagnosis 2012 from the National Prostate Cancer Register (NPCR) Sweden, Martini Klinik, BARMER GEK Report Krankenhaus 2012, Patient-reported outcomes (EORTC-PSM), 1 year after treatment, 2010.
nib, Bupa and HBF are working quickly to meet these customer needs through the Whitecoat website. One of the primary goals of Whitecoat is to ensure that consumers have access to information that allows them to make an informed decision about their treatment options, which doctor is best for them and transparency as to any out-of-pocket costs they will bear.
Some specialists, and the Australian Medical Association, fear Whitecoat: they are not used to being questioned or reviewed. Many providers however have embraced the concept, and see that positive Whitecoat reviews and feedback benefit them not only with potential patients, but with referring GPs and other specialists as well.
We are grateful that the Government has been very positive about services like Whitecoat. When nib and our joint venture partners launched Whitecoat’s expansion into specialist services in 2016, the then Minister for Health, Ms Ley, publicly welcomed it as a great advance for consumers.
It is clear that consumers are hungry for this information. The Government is on strong ground with consumers and PHI members in ensuring that services like Whitecoat not only continue as they are doing, but expand and grow. It is meeting a real need.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24

X
nib
sub
missio
n | J
ULY
20
17
13
CONCLUSIONThe suggestions and proposals in this submission are not magic healthcare reform bullets.
They are, however, constructive ideas about practical and implementable policy and regulatory reform that can make the private health choice more attractive, affordable and sustainable into the future. These ideas will benefit the whole Australian healthcare system – both public and private.
Our message is the Government’s exploration of PHI regulatory reform is welcomed, but concentrating simply on policies and how they are marketed to consumers is addressing an effect of deep-set problems in the system, not their root causes.
Government needs political courage to confront the real source of those problems: the spiraling cost of the services that PHI buys for its customers through their premiums.
As an industry leader, nib wants to work with Government, industry, providers and consumers to keep PHI, and the private health choice, relevant and affordable. All of us who believe in the private health choice – including both payers and private providers – must work together for the common cause of keeping that choice as Australians’ preferred point of access to their healthcare needs.
Public policy and government regulation should be flexible and innovative enough to promote the private healthcare value proposition in a time when the political pendulum is swinging back to the notion that “government must always provide”, with all the implications for higher taxes and public debt that entails.
If we do no not innovate while there is some political will to do so, the private health sector will continue to face uphill challenges in terms of consumer affordability, inefficiency and undesirable health outcomes, while the public sector – especially public hospitals – will, in coming decades, be in grave danger of collapsing under the strain of patient demand.
Value and affordability of private health insurance and out-of-pocket medical costsSubmission 24




















