
Self-efficacy, Psychosocial Factors, and Exercise Behavior in Traditional Versus Modified Cardiac...
11
Self-efficacy, Psychosocial Factors, and Exercise Behavior / 363 Self-efficacy, Psychosocial Factors, and Exercise Behavior in Traditional Versus Modified Cardiac Rehabilitation Joseph J. Carlson, RD, PhD; Gregory J. Norman, PhD; Deborah L. Feltz, PhD; Barry A. Franklin, PhD; Jeffrey A. Johnson, MS; Steven K. Locke, BS ■ BACKGROUND: Self-efficacy and social support are established determinants of exercise adherence and have potential usefulness for tailoring independent exercise regimens for cardiac patients. Highly supervised traditional cardiac rehabilitation programs may be a barrier for independent exercise self-efficacy in low - and moderate-risk patients. ■ PURPOSE: The authors evaluated changes in psychosocial measures including self-efficacy and social support in 80 cardiac patients with low to moderate risk randomized to a traditional cardiac rehabilitation protocol (TP) or modified protocol (MP). These measures also were assessed for their potential to predict subsequent exercise behavior. ■ METHODS: The TP (n = 38) emphasized a supervised exercise regimen and included continuous electrocardiogram (ECG) monitoring for 3 months. The lower cost MP (n = 42) emphasized independent exercise and included group education/support meetings, and gradually weaned patients from continuous ECG monitoring and direct medical supervision. ■ RESULTS: Repeated measures analyses of variance indicated that MP patients had higher levels of self-efficacy for independent exercise without continuous ECG monitoring (P .05). No other protocol differences were found. Multiple regression analyses using the pooled sample (excluding dropouts) indicated that self-efficacy for independent exercise was the only significant predictor of exercise over 6 months (R 2 =.28 [adjusted R 2 = .22] P .01). In contrast to previous reports, social support for exercise was not a significant predictor of exercise behavior. ■ CONCLUSIONS: These findings suggest cardiac rehabilitation programs for low- and moderate-risk patients should emphasize educational and patient monitoring methods that promote patient self-efficacy for independent exercise. Programs that emphasize highly supervised exercise including longer term use of continuous ECG monitoring may impair self-efficacy for independent exercise. Longer-term studies are needed to fully determine the value of using psychosocial measures for designing individualized exercise programs and predicting long-term exercise behavior in cardiac patients. K E Y W O R D S traditional and modified cardiac rehabilitation self-efficacy social support continuous ECG monitoring exercise behavior From Stanford Center for Research in Disease Prevention, Stanford University School of Medicine, Palo Alto, Calif (Dr Carlson, Dr Norman); the Department of Preventive Cardiology and Rehabilitation, Spectrum Health East (Formerly Blodgett Memorial Medical Center), Grand Rapids, Mich (Dr Carlson, Mr Johnson, and Mr Locke); the Department of Kinesiology, Michigan State University, East Lansing, Mich (Dr Feltz); the Division of Cardiology (Cardiac Rehabilitation), William Beaumont Hospital, Royal Oak, Mich (Dr Franklin). Supported by the Blodgett Memorial Medical Center Research Fund, and Kent County Health Department Cardiovascular Mini-Grant. Address correspondence to: Joseph J. Carlson, RD, PhD, Assistant Professor, The University of Utah, Division of Foods & Nutrition, College of Health, 250 South 1850 East, #239, Salt Lake City, UT 84112-0920.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Self-efficacy, Psychosocial Factors, and Exercise Behavior in Traditional Versus Modified Cardiac...

Self-efficacy, Psychosocial Factors, and Exercise Behavior / 363
Self-efficacy, Psychosocial Factors,and Exercise Behavior in TraditionalVersus Modified CardiacRehabilitation
Joseph J. Carlson, RD, PhD; Gregory J. Norman, PhD; Deborah L. Feltz, PhD; Barry A. Franklin, PhD; Jeffrey A. Johnson, MS; Steven K. Locke, BS
�� BACKGROUND: Self-efficacy and social support are establisheddeterminants of exercise adherence and have potential usefulness fortailoring independent exercise regimens for cardiac patients. Highlysupervised traditional cardiac rehabilitation programs may be a barrierfor independent exercise self-efficacy in low - and moderate-riskpatients.
�� PURPOSE: The authors evaluated changes in psychosocial measuresincluding self-efficacy and social support in 80 cardiac patients with lowto moderate risk randomized to a traditional cardiac rehabilitationprotocol (TP) or modified protocol (MP). These measures also wereassessed for their potential to predict subsequent exercise behavior.
�� METHODS: The TP (n = 38) emphasized a supervised exercise regimenand included continuous electrocardiogram (ECG) monitoring for 3months. The lower cost MP (n = 42) emphasized independent exerciseand included group education/support meetings, and gradually weanedpatients from continuous ECG monitoring and direct medicalsupervision.
�� RESULTS: Repeated measures analyses of variance indicated that MPpatients had higher levels of self-efficacy for independent exercisewithout continuous ECG monitoring (P � .05). No other protocoldifferences were found. Multiple regression analyses using the pooledsample (excluding dropouts) indicated that self-efficacy for independentexercise was the only significant predictor of exercise over 6 months(R2=.28 [adjusted R2= .22] P � .01). In contrast to previous reports,social support for exercise was not a significant predictor of exercisebehavior.
�� CONCLUSIONS: These findings suggest cardiac rehabilitation programsfor low- and moderate-risk patients should emphasize educational andpatient monitoring methods that promote patient self-efficacy forindependent exercise. Programs that emphasize highly supervisedexercise including longer term use of continuous ECG monitoring mayimpair self-efficacy for independent exercise. Longer-term studies areneeded to fully determine the value of using psychosocial measuresfor designing individualized exercise programs and predicting long-termexercise behavior in cardiac patients.
K E Y W O R D S
traditional and modified cardiacrehabilitation
self-efficacy
social support
continuous ECG monitoring
exercise behavior
From Stanford Center for Research inDisease Prevention, StanfordUniversity School of Medicine, PaloAlto, Calif (Dr Carlson, Dr Norman); theDepartment of Preventive Cardiologyand Rehabilitation, Spectrum HealthEast (Formerly Blodgett MemorialMedical Center), Grand Rapids, Mich(Dr Carlson, Mr Johnson, and MrLocke); the Department of Kinesiology,Michigan State University, EastLansing, Mich (Dr Feltz); the Divisionof Cardiology (Cardiac Rehabilitation),William Beaumont Hospital, RoyalOak, Mich (Dr Franklin).
Supported by the BlodgettMemorial Medical Center ResearchFund, and Kent County HealthDepartment Cardiovascular Mini-Grant.
Address correspondence to:Joseph J. Carlson, RD, PhD, AssistantProfessor, The University of Utah,Division of Foods & Nutrition, Collegeof Health, 250 South 1850 East, #239,Salt Lake City, UT 84112-0920.

364 / Journal of Cardiopulmonary Rehabilitation 2001;21:363-373
The benefits of long-term participation in an exercise-based cardiac rehabilitation program include improve-ments in cardiovascular disease (CVD) risk factors,functional capacity, and reductions in CVD morbidityand all-cause mortality.1,2 Unfortunately, adherence tocardiac rehabilitation programs and subsequent long-term adherence to independent exercise regimens ispoor. By 6 months, approximately 50% of patients whoinitiate formal cardiac rehabilitation will drop out of theprogram. By 1 year, up to 80% of patients no longerparticipate.2-4 Among patients who discontinue super-vised cardiac rehabilitation, less than 25% continue toexercise at levels that will maintain or improve car-diorespiratory fitness.4,5
A number of elements characterize a traditional pro-tocol (TP) for cardiac rehabilitation.6 Typically, the TPemphasizes medically supervised exercise, with littleemphasis on independent off-site exercise. A significantamount of staff time is devoted to patient surveillancevia the use of continuous electrocardiogram (ECG)monitoring, which is required only for high-risk patientswho comprise less than 20% of patients in cardiac reha-bilitation.6-8 Nevertheless, continuous ECG monitoringremains a common practice that has been reinforced byinsurance reiumbursement.8
The format and number of supervised exercise reha-bilitation sessions patients receive has been debated formore than a decade.7-10 Presently, the number of ECG-monitored exercise sessions and the duration of super-vised rehabilitation programs are determined primarilyby a physiologically based risk stratification method thatincludes functional capacity, ejection fraction, fre-quency of threatening arrhythmias, and evidence ofmyocardial ischemia.6 A potential limitation to onlyusing physiological status to design cardiac patientsexercise regimen is that physiological status is not agood predictor of independent exercise in cardiacpatients.11-13 In contrast, psychosocial factors includingself-efficacy13-17 and social support18-20 have beenshown to be important predictors of exercise behaviorin cardiac patients, but are rarely considered formallywhen designing supervised and independent exerciseregimens.
According to Bandura,21,22 if people lack self-efficacythey will likely behave ineffectually, even if they knowwhat to do and how to do it. For example, a cardiacpatient who previously developed exercise skills andwas physiologically capable, may lack the self-efficacyto maintain an independent exercise program long-term.13 Low exercise self-efficacy may stem from con-cerns of a recurrent cardiac event, which could nega-tively effect exercise compliance, particularly in anon-monitored environment. In contrast, higher exer-cise self-efficacy in postcoronary bypass patients pre-dicted activities of daily living and physical, social, andleisure functional status at 1 month and 6 months after
surgery.15,23 Similarly, cardiac patients’ self-efficacy toperform specific physical activities (eg, walking or stairclimbing) predicted exercise behaviors, whereas per-ceived physical self-efficacy predicted home exerciseintensity and duration.11,12 It is possible that highlysupervised TPs that emphasize on-site exercise, partic-ularly those using continuous ECG monitoring, mayreduce self-efficacy for independent exercise.
To address concerns associated with poor rates ofsupervised program participation and independentexercise in the long term, we developed a reduced-costmodified protocol (MP) for low-to-moderate–risk car-diac patients designed to promote the adoption of inde-pendent exercise. The theoretical basis for the MP wasbased on Bandura’s theory of self-efficacy. The studyobjectives were to:
1. Determine if the MP patients, as compared with theTP patients, exhibited greater improvements in psy-chosocial predictors of exercise (self-efficacy,expectancy outcome, social support for exercise);
2. Determine if MP patients, as compared with TPpatients, perceived higher levels of self-efficacy forindependent exercise when not undergoing contin-uous ECG monitoring; and
3. To ascertain which psychosocial variables predictedindependent off-site exercise and total exercise (sumof on-site and off-site exercise).
METHODS
Study Design/Patients
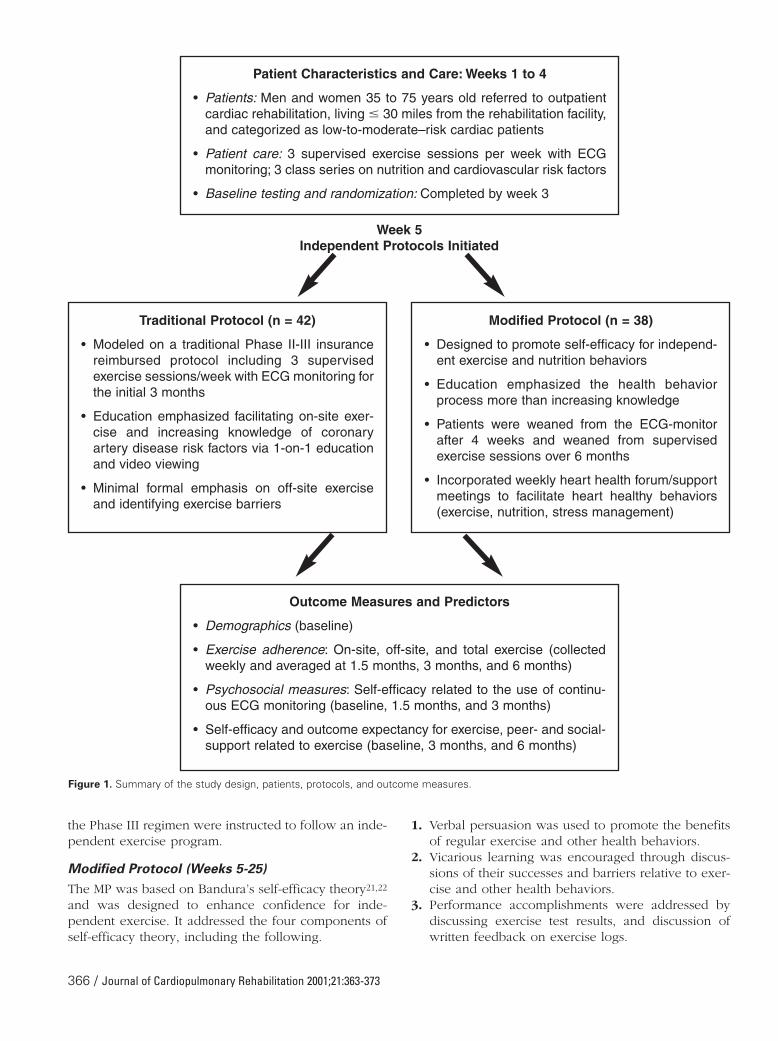
This 6-month randomized clinical trial was approved bythe institutional review board at a metropolitan hospitalin the mid-western United States. The study design,protocol, and outcome measures are summarized inFigure 1. Participants included patients who were first-time referrals to a cardiac rehabilitation program.Patients were recruited within 2 weeks of initiating car-diac rehabilitation and included men and womenbetween 35 and 75 years of age, who were classified aslow-to-moderate–risk,6 and who lived within 30 milesfrom the facility. Receptive patients were provided aninformed consent. Of the 106 patients approached, 13did not participate due to plans to leave the area formore than 1 month for business or vacation, and 3 addi-tional patients chose to enroll in a medically supervisedwork-site exercise program. During a 6.5-month recruit-ment period, 90 patients signed the informed consentand were randomized. Of these, 10 patients did notmeet the inclusion criteria: 4 were classified as highrisk6 within 1 week of baseline testing (2 had restingejection fractions �35%, 1 was referred for coronarybypass grafting, and 1 was hospitalized for congestive

heart failure); the remaining 6 patients had recurrentevents or conditions in the first 2 months that precludedexercise participation (2 required coronary bypass graft-ing, 2 developed unstable angina, and 2 experiencedmusculoskeletal injuries unrelated to exercise). Of 80eligible patients, 35 men and 7 women were assignedto the TP, and 31 men and 7 women were assigned tothe MP. Demographic and psychosocial measures weresimilar in the two groups. Table 1 summarizes the base-line characteristics of the 80 randomized patients.
Previously, we reported that compared with the TP areduced-cost MP promoted greater program participa-tion (fewer dropouts), higher rates of independent exer-cise over 6 months, and higher rates overall of exerciseduring the final 3 months.24 Both study groups achievedcomparable improvements in physiological outcomesincluding functional capacity and blood lipids.24
Program Intervention Prior to IndependentInterventions (Entry to Week 4)
The initial 4 weeks of rehabilitation was identical for allpatients and included an orientation session and threeexercise sessions/week with continuous ECG monitor-
ing. During week 2, patients completed questionnaires toevaluate factors that may be predictive of exercise com-pliance, including employment status, smoking status,social support, income, and transportation barriers.18-20,25-
27 Additionally, baseline exercise testing was completedby week 3, which permitted patients to become accus-tomed to treadmill walking. Hospital-based exercise ses-sions included a warm-up, 30 to 40 minutes of aerobicexercise with continuous ECG monitoring, and a cool-down. Patients were instructed to regulate their exerciseintensity with a prescribed heart rate range correspon-ding to 60% to 85% of their aerobic capacity (maximumoxygen consumption), using perceived exertion as anadjunct intensity modulator. All patients were encour-aged to achieve five or more aerobic exercise sessionsper week (� 30 min/session) and were instructed to doc-ument their off-site exercise duration, intensity and fre-quency via exercise logs. Patients who failed to returntheir logs, or were absent from the facility for 2 consec-utive weeks, were contacted and interviewed about theiroff-site exercise program.
Patient education was provided in three forms: (a)individual, (b) three-group CVD risk factor/nutritionclasses, and (c) educational videos. Individual educa-tion was provided before and during exercise sessionsand included: (a) exercise training principles, (b) CVDrisk factors, (c) nutrition principles, (d) pharmacologicaltherapy, and (e) target outcome values (eg, lipids andblood pressure).
Independent Interventions (Weeks 5-25)
In week 5, the patients’ intervention diverged to theprotocol (TP or MP) according to randomization. Theprotocols are summarized in Figure 1 and are describedbelow.
Traditional Protocol (Weeks 5-12)
The TP patients were instructed to continue the sameregimen as the initial 4 weeks. This included three hos-pital-based ECG-monitored exercise sessions per week,CVD risk education, and reinforcement to exercise fiveor more sessions a week.
Traditional Protocol (Weeks 13-25)
During months 4 to 6, patients were encouraged toattend a Phase III maintenance regimen. This regimenwas similar to the Phase II program and included threeexercise sessions per week. Electrocardiogram monitor-ing was discontinued and staff supervision wasreduced; however, patients continued to receive educa-tional follow-up on CVD risk factors and medical issues.Phase III monitoring included a resting and postexer-cise blood pressure and instantaneous electrocardiogra-phy.28 Patients were asked to document their exerciseintensity and duration. Patients who chose not to attend
Self-efficacy, Psychosocial Factors, and Exercise Behavior / 365
Table 1 • BASELINE PATIENTCHARACTERISTICS*
Traditional ModifiedProtocol Protocol
Variables (n = 42) (n = 38)
Age (years) 59 ± 9 59 ± 10Gender (men/women) 80%/20% 84%/16%Marital status (married) 83% 90%Education
High school or less 47% 47%Some college or more 53% 53%
Annual Income�$25,000 13% 11%$25,000–$50,000 53% 54%�$50,000 34% 35%
Ethnicity (Caucasian) 92% 97%Cigarette Smoking Status
Current 7% 3%History of smoking 57% 66%Never smoked 36% 31%
Body mass index† 28.4 ± 3.0 28.1 ± 4.9Functional capacity (METs)‡ 6.4 ± 1.7 6.9 ± 1.6Reason for referral§
Coronary artery bypass 17 (40%) 12 (32%)Angioplasty 17 (40%) 21 (55%)Myocardial infaraction 11 (26%) 18 (47%)Positive angiography 2 (5%) 3 (8%)
*Mean ± SD or %.†Body weight in kilograms/height in meters squared.‡MET, metabolic equivalent. One MET = 3.5 mL O2/kg/min.§Selected patients had multiple reasons for referral and were included in
multiple columns.
the Phase III regimen were instructed to follow an inde-pendent exercise program.
Modified Protocol (Weeks 5-25)
The MP was based on Bandura’s self-efficacy theory21,22
and was designed to enhance confidence for inde-pendent exercise. It addressed the four components ofself-efficacy theory, including the following.
1. Verbal persuasion was used to promote the benefitsof regular exercise and other health behaviors.
2. Vicarious learning was encouraged through discus-sions of their successes and barriers relative to exer-cise and other health behaviors.
3. Performance accomplishments were addressed bydiscussing exercise test results, and discussion ofwritten feedback on exercise logs.
366 / Journal of Cardiopulmonary Rehabilitation 2001;21:363-373
Patient Characteristics and Care: Weeks 1 to 4
• Patients: Men and women 35 to 75 years old referred to outpatientcardiac rehabilitation, living � 30 miles from the rehabilitation facility,and categorized as low-to-moderate–risk cardiac patients
• Patient care: 3 supervised exercise sessions per week with ECGmonitoring; 3 class series on nutrition and cardiovascular risk factors
• Baseline testing and randomization: Completed by week 3
Traditional Protocol (n = 42)
• Modeled on a traditional Phase II-III insurancereimbursed protocol including 3 supervisedexercise sessions/week with ECG monitoring forthe initial 3 months
• Education emphasized facilitating on-site exer-cise and increasing knowledge of coronaryartery disease risk factors via 1-on-1 educationand video viewing
• Minimal formal emphasis on off-site exerciseand identifying exercise barriers
Outcome Measures and Predictors
• Demographics (baseline)
• Exercise adherence: On-site, off-site, and total exercise (collectedweekly and averaged at 1.5 months, 3 months, and 6 months)
• Psychosocial measures: Self-efficacy related to the use of continu-ous ECG monitoring (baseline, 1.5 months, and 3 months)
• Self-efficacy and outcome expectancy for exercise, peer- and social-support related to exercise (baseline, 3 months, and 6 months)
Modified Protocol (n = 38)
• Designed to promote self-efficacy for independ-ent exercise and nutrition behaviors
• Education emphasized the health behaviorprocess more than increasing knowledge
• Patients were weaned from the ECG-monitorafter 4 weeks and weaned from supervisedexercise sessions over 6 months
• Incorporated weekly heart health forum/supportmeetings to facilitate heart healthy behaviors(exercise, nutrition, stress management)
Week 5Independent Protocols Initiated
Figure 1. Summary of the study design, patients, protocols, and outcome measures.

4. Physiological states were addressed by reviewingnormal and abnormal physiological responses toexercise.22 Moreover, the protocol integrated princi-ples from models that have cost effectively pro-moted adherence to health behaviors.29-31
Primary differences in the MP compared with the TPincluded: (a) a reduction in the total number of facility-based exercise sessions and sessions with continuousECG monitoring, (b) ongoing weekly education/sup-port group initiated in week 6, and (c) behaviorallybased education that emphasized overcoming barriersto independent exercise and nutrition behaviors overincreasing knowledge. The reduction of ECG-moni-tored exercise sessions was achieved by discontinuingmonitoring in week 5, at which time patients weregiven a personal heart rate monitor (Polar, PortWashington, NY) to use for 3 weeks for both on-siteand off-site exercise sessions.
In week 6, MP patients’ on-site exercise sessions werereduced to a maximum of two sessions per week, andweekly education and support meetings (called“hearthealth forums”) were initiated. The forums provided sup-plemental education and support for patients’ exercise andother coronary risk reducing behaviors. The forumsemphasized behavioral factors associated with exerciseand incorporated the four components of the self-efficacytheory. The first 15 minutes of each meeting included afacilitated interactive discussion regarding adherence toindependent exercise. Each participant had the opportu-nity to share their successes and barriers with the group.The group leader provided recommendations to over-come barriers and encouraged participant recommenda-tions. The final 45 minutes were devoted to interactive dis-cussion on topics involving exercise, nutrition, and stressreduction. To facilitate the adoption of independent exer-cise and avoid dependence on a facility-based exercise,during weeks 11 to 17 patients were encouraged to reducetheir on-site exercise visits to one session per week andduring weeks 18 to 25 were encouraged to reduce to oneexercise session every 2 weeks.
Measures
Exercise Adherence
Exercise frequency was documented weekly for super-vised on-site exercise, off-site independent exercise,and total exercise (on-site and off-site). Patients wereinstructed to include a variety of physical activities off-site, and were credited for non-traditional exercise ifthey met their exercise prescription guidelines. Off-siteexercise was self-reported on logs. For evaluation pur-poses, 30 minutes or more of aerobic activity a day wascounted as a session.
Psychosocial Measures for Exercise Behavior
These measures included several dimensions of exerciseself-efficacy, outcome expectancy, perceptions of physi-
cal condition, social support, and peer support for exer-cise. All questions were designed specifically for cardiacrehabilitation patients and were formulated based onprinciples and questions previously described,22,32,33 andwere piloted for readability. The questionnaires wereadministered at baseline, 3 months, and 6 months withthe exception of two questions that evaluated participantconfidence for exercise relative to using continuous ECGmonitoring, which were obtained at baseline, 1.5 months,and 3 months. To ensure uniform interpretation, the ques-tions were accompanied with written and standardizedverbal instructions provided by a trained professional.
SELF-EFFICACY FOR EXERCISE RELATED TO CONTINUOUS ECG MONITORING
Two questions addressed patients’ feelings of self-effi-cacy and safety relative to using continuous ECG moni-toring. The first question asked, “How comfortablewould you be (or are you) exercising in the cardiac reha-bilitation facility without an ECG heart monitor?” Thesecond question asked, “How comfortable are you exer-cising outside the cardiac rehabilitation facility withoutan ECG heart monitor?” “Comfortable” was defined andexplained to each patient as how confident and safe theyfelt exercising without the continuous ECG monitor withrespect to having an adverse cardiovascular event.Participants responded using a 5-point scale rangingfrom “very uncomfortable” to “very comfortable.” Thesetwo items were highly correlated at each assessmentpoint (r � .75) and were averaged to provide a compos-ite score. Internal consistency for the two-item scale washigh at each assessment point (Cronbach’s alpha � .85).
SELF-EFFICACY FOR EXERCISE FREQUENCY
Three questions measured self-efficacy for exercise fre-quency specific to on-site exercise, independent off-siteexercise, and total exercise (a combination of on-site andoff-site exercise sessions). Each question asked partici-pants to rate their self-efficacy regarding how many daysa week over the next 3 months they will exercise.Responses were made using an 11-increment probabilityscale (0%-100%) for each day (up to 3 days on-site, 7 daysoff-site, and 7 days combined). Self-efficacy levels for on-site exercise was highly skewed with most participantsindicating more than 90% confidence to complete super-vised exercise sessions at baseline. This negative skew ofthe distribution is understandable given the sample of low-to-moderate–risk participants. Off-site exercise and totalexercise frequency self-efficacy scores were highly corre-lated. Given our emphasis on promoting independentexercise, we chose to use only the off-site exercise fre-quency score for our self-efficacy measure for exercise fre-quency in the regression analysis.
SELF-EFFICACY FOR EXERCISE INTENSITY
One item measured exercise intensity based on theBorg rating of perceived exertion scale ranging from 6
Self-efficacy, Psychosocial Factors, and Exercise Behavior / 367

to 20.34 The question asked, “At what intensity/rate ofperceived exertion are you capable of being physicallyactive for 30 continuous minutes?”
SELF-EFFICACY FOR EXERCISE DURATION
Participants were asked, “How many minutes are youcapable of exercising at a rate of perceived exertionintensity of 12 to 13 (somewhat hard)?” Seven responseoptions were provided ranging from “15 minutes” to“105 minutes” in 15-minute increments.
OUTCOME EXPECTANCY FOR EXERCISE
One question evaluating outcome expectancy for exer-cise asked, “If you follow the exercise program sug-gested by the cardiac rehabilitation staff, what is yourlevel of confidence that it will play a role in improvingand maintaining your health?” Patients responded to an11-point scale that ranged from “no confidence” to“complete confidence.”
PERCEPTION OF PHYSICAL CONDITION
Two items assessed participants’ perceptions of theirphysical condition. The first item read, “In my presentphysical condition, I can do the daily and leisure phys-ical activities I desire.” The second statement was, “Ibelieve I am in good physical condition.” Participantsresponded to each statement using a 5-point scale rang-ing from “strongly disagree” to “strongly agree.” Thesetwo items were summed to form a composite score.Internal consistency for the two-item scale was high ateach assessment point (Cronbach’s alpha �.75).
SIGNIFICANT OTHER SUPPORT FOR EXERCISE
Three questions addressed the role of significant othersocial support as it related to exercise behavior:
1. Do you have someone who is close to you who pro-vides positive feedback when you follow the exer-cise recommendations provided to you by cardiacrehabilitation?
2. Do you have someone who is close to you to exer-cise with during non-rehabilitation exercise sessions?
3. Do you have a person close to you who providessupport if you are having a difficult time followingyour suggested exercise regimen?
Each question ranged from “never” to “very often” ona 5-point scale. Responses were summed to form a com-posite score. Internal consistency for the 3-item scale washigh at each assessment point (Cronbach’s alpha �.75).
PEER SUPPORT FOR EXERCISE
One question evaluated the role of other cardiac reha-bilitation participants in relation to supporting theirexercise behavior. This question asked, “How importantdo you feel fellow rehabilitation participants are in
helping you follow the exercise regimen suggested byyour cardiac rehabilitation staff?” Participants respondedusing a 5-point scale ranging from “no importance” to“extremely important.”
Statistics
Statistical significance was set at P � .05. Analysesincluded 2 � 3 repeated measures analysis of variance(protocol � time) to evaluate protocol differences inexercise frequency and psychosocial measures. Threemultiple regression analyses were conducted to deter-mine the role of eight psychosocial factors in predictingindependent off-site exercise and total exercise (on-siteand off-site). For regression analyses, first, baseline lev-els of both demographic characteristics and independ-ent measures were evaluated to determine how theypredicted exercise frequency over 6 months. Second,the same predictors were evaluated to determine howthey predicted the first 3 months of exercise. Finally, thepredictors measured at 3 months were evaluated todetermine how they predicted exercise during months4 to 6. For each regression analyses, demographic vari-ables were entered first, then stepwise entry was usedto include the statistically significant psychosocial pre-dictors. We used stepwise entry to create regressionmodels due to multiple predictors with limited degreesof freedom given the relatively small sample size.
During the 6-month study, exercise frequency datawere obtained on 78 patients, which included 13dropouts. Complete demographic and psychosocial datawere obtained on 64 patients, while follow-up psychoso-cial and exercise data were obtained on 52 patients at 3months and 57 patients at 6 months. Reasons for missingdata included patients who failed to return for their 3- and6-month evaluations (dropouts) or patients who failed tocomplete the psychosocial questions.
RESULTS
Group Education Attendance
The nutrition/risk factor classes offered to both proto-cols during the first month were well attended. Seventypercent of the TP and 79% of the MP attended all threeclasses, whereas 86% of the TP and 92% of the MPattended two of three classes. The MP support meetings(called Heart Health Forums) were well attended with87% of participants attending more than three sessions,58% more than five sessions, 44% more than eight ses-sions, and 31% 10 or more sessions.
Exercise Adherence by Protocol
Patients in the MP demonstrated higher rates of off-siteindependent exercise over 6 months and total exercise
368 / Journal of Cardiopulmonary Rehabilitation 2001;21:363-373

(on-site and off-site) during the final 3 months as com-pared with TP patients. These results were previouslyreported with physiological outcomes22 and are sum-marized in Table 2.
Self-efficacy for Exercise Related toContinuous ECG Monitoring
The 2 � 3 repeated measures analysis of variance (pro-tocol � time) indicated the MP had significantly higherlevels of self-efficacy while exercising without continu-ous ECG monitoring (F[1,55] = 4.2, P = .045) as com-pared with the TP over 3 months. Also, based on timeeffects (F[1,55] = 18.9, P � .001) the patients’ self-effi-cacy levels improved significantly in both protocols. Asshown in Table 3, the mean scores increased in the MPfrom baseline at each time point (1.5 months and 3months), while confidence levels in the TP improvedonly from baseline to 1.5 months, but remainedunchanged thereafter.
Although these findings were statistically significant,we questioned whether a score of 5 corresponding to“very comfortable” and 4 corresponding to“comfortable”were clinically relevant. A post hoc analysis of the fre-quency distribution of scores using the two questionscomprising the composite score was conducted. Whileexercising off-site without ECG monitoring, 63% (20 of32) of the MP answered “very comfortable” but only 33%(11 of 33) of the TP answered “very comfortable.”Similarly, while exercising on-site without ECG monitor-ing, 56% of the MP participants (18 of 32) answered “verycomfortable” and only 30% (10 of 33) of the TP patientsanswered “very comfortable.” These data support thefinding that MP patients had greater self-efficacy whileexercising without the continuous ECG monitoring.
Psychosocial Factors Related to the Exercise Prescription
No statistically significant protocol main effects or proto-col by time interactions were found for the eight meas-
ures. However, significant main time effects indicated thatfour of the measures were dynamic (Table 4). Two meas-ures increased (self-efficacy for exercise duration andphysical condition) and two measures decreased (self-efficacy for total exercise frequency and social support).Self-efficacy for exercise duration increased from between30 to 45 minutes to 45 minutes from baseline to 3 months,and these levels were maintained from 3 to 6 months. Theself-efficacy scores for physical condition improved froma baseline level of “slightly agree” to a level of “agree.”The self-efficacy for total exercise frequency (on-site andoff-site) decreased significantly in both protocols frombaseline to 6 months. The social support measures forexercise indicated that patients in both protocols had ahigh level of social support at baseline. These scoresremained relatively high, but decreased significantly(P = .038) during the 6-month study.
Psychosocial Factors as Predictors ofExercise Behavior
Because both protocols were effective in promoting phys-iological improvements22 and the only statistically signifi-cant protocol differences in the psychosocial variableswere those specific to the use of ECG monitoring, we usedthe pooled sample to examine psychosocial predictors ofexercise behavior. Correlations among the eight psy-chosocial variables and the total exercise frequency at 3and 6 months were assessed. The strongest associationbetween the predictors and exercise behavior at 3 and 6months was found for self-efficacy for independent exer-cise frequency (r = .46 and .43, respectively; P � .001).Examination of the correlation among the eight variablesat 3 months and exercise frequency for months 4 to 6revealed a similar pattern. Correlations among the predic-tors were low to moderate in magnitude, with thestrongest association found between self-efficacy for phys-ical condition and self-efficacy for exercise without ECGmonitoring (r = .50, P � .001). These correlations indi-cated that multicollinearity among the predictors wouldnot be a concern for the multiple regression models.
Self-efficacy, Psychosocial Factors, and Exercise Behavior / 369
Table 2 • EXERCISE FREQUENCY (MEAN ± SD) OVER 6 MONTHS BY PROTOCOL
Exercise Type Group/n Weeks 1–6 Weeks 7–12 Weeks 13–25 6 Month Sum
On-site exercise TP/40 13.3 ± 3.7 11.1 ± 6.5 4.3 ± 6.7 28.8 ± 13.0MP/38 13.5 ± 2.7 8.5 ± 4.3 6.9 ± 7.6 29.2 ± 10.7
Off-site exercise TP/39 15.3 ± 7.1 16 ± 7.8 40 ± 21 69.5 ± 33.6MP/37 16.5 ± 7.5 21 ± 6.9* 49 ± 15 83.5 ± 25.6*
Total exercise TP/39 27.6 ± 7.7 26 ± 8.2 44 ± 21 98.1 ± 33.4(on site + off site)
MP/37 29.4 ± 7.7 29 ± 8.6 54 ± 26† 111.8 ± 29.1Total Exercise TP/39 4.6 ± 1.3 4.4 ± 1.4 3.4 ± 1.6 3.8 ± 1.3Weekly average MP/37 4.9 ± 1.3 4.8 ± 1.4 4.2 ± 1.5† 4.3 ± 1.2
TP, traditional protocol; MP, modified protocol.Analysis of variance main effects indicating protocol differences; P � .05*P � .005.†P � .03.

Three multiple regression models were tested. Fortwo of the models, we regressed baseline to 3 monthsand baseline to 6 months for exercise behavior on psy-chosocial predictors assessed at baseline. In a thirdmodel, 4- to 6-month exercise behavior was regressedon psychosocial predictors assessed at 3 months.Demographic variables including gender, income, edu-cation, and marital status were entered in the first blockand remained in each of the models. In the secondblock, the eight psychosocial predictors were enteredstepwise resulting in only statistically significant predic-tors remaining in the final regression models. Table 5shows the standardized � weights and their associatedt value statistics for the three regression models. Eachoverall model was statistically significant with adjustedR2s ranging from .15 to .22. In all three models, onlyself-efficacy for independent exercise frequency wasstatistically significant after controlling for demographicvariables.
DISCUSSION
Over 6 months, we prospectively evaluated exercise fre-quency rates and changes in self-efficacy and psychoso-cial measures related to exercise behavior in low- andmoderate-risk patients randomized to either a TP or MPfor cardiac rehabilitation. The present study was uniquein that it measured factors associated with independentoff-site exercise. Several studies on cardiac patients’ self-efficacy have shown that self-efficacy predicts exercisebehavior; however, these studies have primarily focusedon exercise in a supervised setting.13,15,16 To our knowl-edge, this is the first study to report on the effect of arehabilitation protocol designed specifically to promoteself-efficacy for off-site exercise.
We anticipated the MP patients would exhibit higherself-efficacy levels for independent exercise as comparedwith the TP patients, due to the MP’s emphasis on pro-moting self-efficacy for independent exercise, and theirhigher rates of exercise frequency. The only protocol dif-ferences in the psychosocial measures were the higherlevels of self-efficacy for exercise without continuousECG monitoring in the MP compared with the TP.
Although there were no other significant protocol differ-ences, both protocols had significant increases in self-efficacy for exercise intensity and self-efficacy in physicalcondition, and significant decreases in self-efficacy forexercise frequency and social support for exercise.
Based on the pooled sample, we hypothesized thatself-efficacy and social support would predict exercisebehavior; however, the only significant predictor wasself-efficacy for exercise frequency. The lack of predic-tion by social support was likely precluded by the clus-tering of scores at the upper end of the scale at base-line, and that the social support level decreased overtime. Another potential predictor, outcome efficacy(also known as outcome expectancy),35 did not predictexercise behavior. Generally, outcome efficacy is likelynot as strong a predictor as self-efficacy because the for-mer assesses the consequence of a behavior (ie, if Iexercise, I will be healthier) whereas the latter measuresone’s perceived ability to perform behaviors.22,33,35
The higher self-efficacy levels in the MP patients whileexercising without continuous ECG monitoring may par-tially be attributed to methodological differences. The MPfacilitated independent exercise by weaning patientsfrom ECG monitoring and supervised exercise sessions,and provided ongoing weekly support meetings for off-site exercise. In contrast, the TP patients followed a facil-ity-based program three times/week for 6 months withcontinuous ECG monitoring during the initial 3 months.The lower levels of self-efficacy in the TP patients sug-gests that emphasis on supervised exercise and extendedECG monitoring for some patients may be a barrier toindependent exercise. However, because the MP alsoincluded a specialized educational program we cannotconclude that the attenuated ECG monitoring per se inthe MP was the only factor responsible for the observedself-efficacy difference between groups. There are sev-eral plausible reasons why there were no significant dif-ferences in most of the psychosocial measures. Averagebaseline levels for exercise frequency self-efficacy, socialsupport, and outcome expectancy approached the upperrange of the scales for all patients and may have pre-cluded improvements in these measures. Also, the TPwas not a sedentary or “usual care” control, but was anestablished intervention that supported regular exercise
370 / Journal of Cardiopulmonary Rehabilitation 2001;21:363-373
Table 3 • MEAN (± SD) PATIENT COMFORT AND SELF-EFFICACY LEVEL WHILE EXERCISINGWITHOUT CONTINUOUS ELECTROCARDIOGRAM MONITORING*
Protocol Baseline Score 1.5-month Score 3-month Score
Traditional protocol (n = 30) 3.30 ± 1.1 4.05 ± .76 4.03 ± .97Modified protocol (n = 27) 3.69 ± 1.0 4.37 ± .78 4.43 ± .85†
*Scores reflect a composite mean of 2 questions assessing patient comfort and self-efficacy levels while exercising without continuous ECG monitoring bothin the rehabilitation facility and off-site. Scoring was based on a 5-point scale ranging from 1 = very uncomfortable to 5 very comfortable. Comfortable wasdefined and explained to each patient as how confident and safe they felt exercising without continuous ECG monitoring relative to having a cardiovascularevent.
†Analysis of variance indicated significant protocol differences, P � .05, and time effects P � .001.

and elicited significant improvements in physiologicaloutcomes.24 Furthermore, the TP had significantly moredropouts (n = 10) compared with the MP (n = 3), there-fore, the former likely reflects a subset of more compli-ant patients and did not reflect the TP patients whodropped out. Finally, these low-to-moderate–risk patientswere discharged from the hospital with a walking pro-gram and did not initiate outpatient rehabilitation for 2.5
to 3 weeks after the event. Consequently, it is possiblethese patients realized physiological and psychosocialimprovements from exercise prior to their baseline test-ing, and thus were less likely to improve further.
Perceptions of physical condition and self-efficacy forexercise duration improved in both protocols (Table 4).These improvements suggest the patients became morecomfortable with their physical capabilities and their abil-
Self-efficacy, Psychosocial Factors, and Exercise Behavior / 371
Table 4 • TRADITIONAL AND MODIFIED PROTOCOL MEAN (± SD) SCORES OF SELF-EFFICACYRELATED TO THE EXERCISE PRESCRIPTION AND SOCIAL AND PEER SUPPORT FOR EXERCISE
Question Type Protocol/Sample Size Baseline 3-month 6-month
Total exercise frequency SE*TP/24 5.6 ± 1.4 5.1 ± 1.7 5.1 ± 1.3MP/28 5.3 ± 1.0 4.9 ± 1.4 4.8 ± 1.2
Off-site exercise frequency SETP/24 5.1 ± 1.4 5.0 ± 1.7 5.0 ± 1.3MP/28 4.9 ± 1.3 4.8 ± 1.3 4.6 ± 1.3
Exercise intensity SETP/23 12.7 ± 1.1 12.7 ± 1.0 13.1 ± 1.6MP/30 12.6 ± 1.0 13.1 ± 1.2 14.8 ± 1.8
Exercise duration SE*TP/24 2.7 ± 1.0 2.9 ± 1.1 3.1 ± 1.0MP/30 2.8 ± 0.9 3.2 ± 1.0 3.2 ± 0.8
Perception of physical condition*TP/24 3.3 ± .91 3.9 ± .68 3.9 ± .85MP/31 3.6 ± .81 4.0 ± .71 4.1 ± .70
Outcome expectancyTP/24 8.6 ± 1.1 8.5 ± 1.3 8.6 ± 1.0MP/31 8.7 ± 1.0 8.7 ± 1.3 8.6 ± 1.2
Social support for exercise*TP/24 11.5 ± 2.8 10.5 ± 3.3 11.0 ± 3.6MP/31 11.9 ± 1.7 11.0 ± 2.1 11.1 ± 2.2
Peer support for exerciseTP/23 2.2 ± 1.0 2.1 ± 1.1 2.2 ± 1.1MP/31 2.3 ± 1.3 2.2 ± 1.2 2.1 ± 1.3
SE, self-efficacy; TP, traditional protocol; MP, modified protocol.*Refers to significant time effects: total exercise frequency SE, P = .004; exercise duration SE, P = .02; perception of physical condition, P � .001; social
support, P = .001.
Table 5 • PSYCHOSOCIAL PREDICTORS OF TOTAL EXERCISE (ON-SITE + OFF-SITE) INCARDIAC REHABILITATION PATIENTS
Exercise Sessions Completed
Weeks 1–12* Weeks 13–25† Total Weeks 1–25*(Adjusted R2 = .18)‡ (Adjusted R2 = .15)§ (Adjusted R2 = .22)‡
Predictor Variable � t � t � t
Gender (female) �.200 �1.49 .033 0.25 �.133 �1.03Income (�$50,000 annually) �.057 �0.45 .025 0.18 �.086 �0.69Education (some college or more) .078 0.63 .019 0.15 .219 1.77Marital status (not married) �.037 �0.28 �.023 �0.17 .010 0.08Self-efficacy for independent exercise frequency .485 4.19* .450 3.45* .527 4.61*
*Exercise for Weeks 1–12 and Total Weeks 1–25 were regressed onto psychosocial variables assessed at baseline.†Exercise for Weeks 13–25 were regressed onto psychosocial variables assessed at 3 months.‡P � .01.§P � .05.

ity to sustain aerobic exercise. Analysis of the associatedphysiological data showed improvements in functionalcapacity and physical performance, lending support tothese findings. Both protocols elicited significantincreases in maximum oxygen consumption anddecreases in submaximal rate pressure product (heart rate� systolic blood pressure) from baseline to 6 months.24
Levels of exercise frequency self-efficacy and socialsupport for exercise significantly decreased in both pro-tocols, suggesting that at the program onset patientsmay have been overly optimistic about the number ofexercise sessions they would perform (Table 4). Thedecrease in self-efficacy paralleled modest declines inexercise frequency over 6 months. The reductions inthe perceived level of social support for exercise maybe attributed to reducing staff supervision over time orless support from significant others, as patients werefurther from their cardiac event.
Overall, these findings suggest that cardiac rehabili-tation programs for low- and moderate-risk patientsshould emphasize educational and monitoring methodsthat promote self-efficacy for independent exercise.Moreover, selected self-efficacy measures may be help-ful in determining when patients can be weaned froma supervised exercise program and be successful inde-pendently. Larger studies with longer follow-up periodsare needed to fully determine the usefulness of psy-chosocial measures in designing individualized exerciseregimens and predicting off-site exercise adherence incardiac patients.
Applications
The MP or a similar protocol that incorporates supportmeetings appears to be a feasible method for address-ing the four components of self-efficacy (verbal persua-sion, vicarious learning, performance accomplishments,and physiological states) and facilitating the adoption ofindependent exercise in low-to-moderate–risk patients.The finding that self-efficacy for independent exercisepredicted subsequent exercise behavior highlights theimportance of using methods that promote self-efficacyfor independent exercise, particularly because most car-diac patients do not follow a supervised program forlonger than 6 months.3,4 The availability of psychosocialmeasures to be used in conjunction with physiologicalstratification criteria to determine when patients can beweaned from a supervised program with a high proba-bility of long-term success would have significantpatient and program outcome implications.
Although self-efficacy for exercise frequency was theonly statistically significant predictor of exercise, thereare associated clinical applications for the battery ofself-efficacy questions to help patients tailor their exer-cise regimen. For example, if a clinician was preparinga patient’s exercise prescription based on his or her
treadmill test, simultaneously addressing psychosocialmeasures could be helpful in promoting exercise com-pliance. For instance, assessing exercise self-efficacycould identify a patient with a low self-efficacy forindependent exercise, despite having a high functionalcapacity. In this case, the clinician could use the infor-mation to help the patient identify the primary barrier(s)for off-site exercise, such as determining the patient isuncomfortable exercising in a non-monitored environ-ment due to concerns of experiencing a recurrent car-diac event. This information would prompt the need toaddress the patient’s concerns and help determinewhen to wean the patient to an off-site regimen. In con-trast, if a patient reported 100% confidence in exercis-ing independently for more than 30 minutes 5 days aweek, the clinician could likely reduce the requirednumber of supervised sessions after the patient demon-strates the proper self-monitoring skills.
References
1. Hedback B, Perk J, Wodlin P. Long-term reduction of cardiacmortality after myocardial infarction: 10-year results of a compre-hensive rehabilitation programme. Eur Heart J. 1993;14:831-835.
2. Balady GJ, Fletcher BJ, Froelicher ES, et al. American HeartAssociation Medical/Scientific Statement. Position statement: car-diac rehabilitation programs: a statement for health care profes-sionals from the American Heart Association. Circulation.1994;90:1602-1610.
3. Oldridge NB. Cardiac rehabilitation exercise programme: compli-ance and compliance-enhancing strategies. Sports Med. 1988;6:42-55.
4. Radtke KL. Exercise compliance in cardiac rehabilitation.Rehabilitation Nursing. 1989;14(4):182-186.
5. Daltroy LH. Improving cardiac patient adherence to exercise reg-imens: a clinical trial of health education. J Cardiopulm Rehabil.1985;5:40-49.
6. American Association of Cardiovascular and PulmonaryRehabilitation. Guidelines for Cardiac Rehabilitation Programs.2nd ed. Champaign, Ill: Human Kinetics Publishers; 1995.
7. Labrador PM, Vongvanich P, Merz BC. Risk stratification for exer-cise training in cardiac patients: do the proposed guidelineswork? J Cardiopulm Rehabil. 1999;19:118-125.
8. Keteyian SJ, Mellett, PA, Fedel FJ, McGowan CM, Stein PD.Electrocardiographic monitoring during cardiac rehabilitation.Chest. 1995;107(5):1242-1246.
9. Mitchell M, Franklin BA, Johnson S, Rubenfire M. Cardiac exer-cise programs: role of continuous electrocardiographic monitor-ing. Arch Phys Med Rehabil. 1984;65:463-466.
10. Greenland P, Pomilla PV. ECG monitoring in cardiac rehabilita-tion: is it needed? The Physician and Sports Medicine. 1989;17:75-82.
11. Ewart CK. Psychological effects of resistive weight training: impli-cations for cardiac patients. Med Sci Sports Exer. 1989;21(6):683-688.
12. Ewart CK, Stewart KJ, Gillilan RE, Kelemen MH. Self-efficacymediates strength gains during circuit weight training in men withcoronary artery disease. Med Sci Sports Exer. 1986;185:531-540.
13. Lemanski K. The use of self-efficacy in cardiac rehabilitation.Prog Cardiovasc Nurs. 1990;5(4):114-117.
14. McAuley E, Courneya KS. Adherence to exercise and physicalactivity as health promoting behaviors: attitudinal and self-efficacyinfluences. Applied and Preventative Psychology. 1993;2:65-77.
372 / Journal of Cardiopulmonary Rehabilitation 2001;21:363-373

15. Sullivan MD, LaCroix AZ, Russo J, Katon WJ. Self-efficacy andself-reported functional status in coronary heart disease: a six-month prospective study. Psychosom Med. 1998;60(4):473-478.
16. Perkins S, Jenkins LS. Self-efficacy expectation, behavior per-formance, and mood status in early recovery from percutaneoustransluminal coronary angioplasty. Heart Lung. 1998;27(1):37-46.
17. Oxman TE, Hull JG. Social support, depression, and activities ofdaily living in older heart surgery patients. J Gerontol B PsycholSci Soc Sci. 1997;52(1):1-14.
18. Friis R, Armstrong G. Social support and social networks, andcoronary heart disease and rehabilitation. J Cardiopulm Rehabil.1986;6:132-147.
19. Erling J, Oldridge NB. Effect of a spousal support program oncompliance with cardiac rehabilitation. Med Sci Sports Exer.1985;17:284-289.
20. Kulik JA, Mahler HIM. Emotional support as a moderator ofadjustment and compliance after coronary artery bypass surgery:A longitudinal study. J Behav Med. 1992;16(1):45-63.
21. Bandura A. Self-efficacy mechanism in human agency. AmPsychol. 1982;37:122-147.
22. Bandura A. Self-efficacy: toward a unifying theory of behavioralchange. Psychol Rev. 1977;84(2):191-215.
23. Allen JK, Becker DM, Swank RT. Factors related to functional sta-tus after coronary artery bypass surgery. Heart Lung. 1990;19:337-343.
24. Carlson JJ, Johnson JA, Franklin BA, VanderLaan RL. Program par-ticipation, exercise adherence, cardiovascular outcomes, and pro-gram cost of traditional versus modified cardiac rehabilitation.Am J Cardiol. 2000;86:17-23.
25. Harlan WR, Sandler SA, Lee KL, Lam LC, Mark DB. Importance ofbaseline functional and socioeconomic factors for participation in
cardiac rehabilitation. Am J Cardiol. 1995;76:36-39.26. Mirotznik J, Feldman L, Stein R. The health belief model and adher-
ence with a community center-based, supervised coronary heartdisease exercise program. Journal of Community Health.1995;20(3):233-247.
27. Oldridge NB, Spencer J. Exercise habits and perceptions beforeand after graduating or dropout from supervised cardiac exerciserehabilitation. J Cardiopulm Rehabil. 1985;5:313-319.
28. Franklin BA, Reed PS, Gordon S, Timmis GC. Instantaneous elec-trocardiography: a simple screening technique for cardiac exer-cise programs. Chest. 1989;96:174-177.
29. DeBusk RF, Miller NH, Superko HR, et al. A case-managementsystem for coronary risk factor modification after acute myocar-dial infarction. Ann Intern Med. 1994;120:721-729.
30. Robison JI, Rogers MA, Carlson JJ, et al. Effects of a 6-monthincentive-based exercise program on adherence and work capac-ity. Med Sci Sports Exerc. 1992;24:85-93.
31. Stofflemeyer BE, Mavis BE, Stachnik TL, et al. A program modelto enhance adherence in worksite-based fitness programs. JOccup Med. 1993;Feb:156-161.
32. Courneya K, McAuley E. Are there different determinants of thefrequency, intensity, and duration of physical activity? BehavMed. 1994;20:84-90.
33. Feltz DL. Self-confidence and sports performance. Exerc SportsSci Rev. 1988;16:423-458.
34. Borg G. Ratings of perceived exertion and heart rates duringshort-term cycle exercise and their use in a new cycling strengthtest. Int J Sports Med. 1982;3:153-158.
35. Desharnais R, Bouillon J, Godin G. Self-efficacy and outcomeexpectations as determinants of exercise adherence. Psychol Rep.1986;59:1155-1159.
Self-efficacy, Psychosocial Factors, and Exercise Behavior / 373




















