Selected Manual Therapy Interventions and Functional ...
99
Student Session: Selected Manual Therapy Interventions and Functional Exercises for the Shoulder
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Selected Manual Therapy Interventions and Functional ...

Student Session: Selected Manual Therapy Interventions
and Functional Exercises for the Shoulder

• Dr Bob Boyles, PT, DSC, OCS, FAAOMPT– Associate Professor, University of Puget Sound,
Tacoma, WA
• Dr Danny McMillian, PT, DSc, OCS, CSCS– Assistant Professor, University of Puget Sound,
Tacoma, WA
Puget Sound. What is that?
• In 1792 George Vancouver gave the name "Puget's Sound" to the waters south of the Tacoma Narrows, in honor of Peter Puget, then a lieutenant accompanying him on the Vancouver expedition. The name later came to be used for the waters north of Tacoma Narrows as well


Agenda
• Brief evidence review• Selected thoracic interventions• Selected shoulder manual interventions• Selected functional rehab interventions

Structure and Function
“…a surprising lack of consensus as to even the most fundamental aspects of shoulder function” Bigliani et al. Clin Orthop 1996
Function
• The primary function of the shoulder girdle is placement of the hand to manipulate our environment
• The most mobile joint in the body: "sacrifices stability for mobility"
• Optimal function of the shoulder also depends on adequate motion or stabilization of the trunk

Think Regional

Green et al, Cochrane Database of Systematic Reviews, 2003
Physiotherapy Interventions for Shoulder Pain
• 26 RCTs included• Two broad categories of shoulder pain:
– Rotator cuff tendonitis disease– Adhesive capsulitis
• Results– Exercise is effective for short- and long-term
recovery in rotator cuff disease– Manual therapy provides added benefit to exercise– No evidence of US effectiveness in shoulder pain– No evidence that physiotherapy alone is of benefit
for adhesive capsulitis

• Design: Multi-site RCT• Population: N=150, painful shoulder
girdle • Outcomes:
– Baseline, during & end of treatment (6 &12 wks), follow-up (26 & 52 wks)
– Primary - patient perceived recovery– Secondary - severity of main complaint,
shoulder disability, additional care received
Bergman et al, Annals of Internal Medicine, 2004

Manipulative Therapy in Addition to Usual Medical Care for Patients with
Shoulder Dysfunction and Pain
• 150 patients w shoulder girdle dysfunction
• Usual medical care– Information, advise and therapy (2 weeks of NSAIDs)– Up to 3 corticosteroid injections if therapy ineffective– If no improvement after 6 weeks, physiotherapy began consisting
of exercise, massage and physical agents
• Usual medical care plus manipulative therapy ( 6 sessions over 12 weeks)
– Manipulative therapy consisting of manipulation (thrust) and mobilization techniques to shoulder girdle, cervical and thoracic spines and ribs. No other PT methods allowed.
Bergman, Ann Int Med, 2004

• Outcomes: patient-perceived recovery, severity of pain, shoulder pain, shoulder disability, and general health.
• 6 and 12 weeks (during and after treatment)26 and 52 weeks (follow-up)– No difference at 6wks– 12 weeks: 43% intervention & 21% control reported full
recovery– 52 weeks: same recovery rate as 12 weeks– All times consistent between-group difference in severity,
shoulder pain and disability and general health favored MT• Conclusion: Manipulative therapy for the shoulder
girdle in addition to usual medical care accelerates recovery.
Bergman, Ann Int Med, 2004
Manipulative Therapy in Addition to Usual Medical Care for Patients with
Shoulder Dysfunction and Pain
(Winters et al, BMJ, 1997)
• Subjects: (N= 198; 58 shoulder girdle group, 114 synovial group)• Treatment conditions:
– Group 1: Manipulation – Cx and Tx spine, ribs, AC and GH joints– Group 2: “Classic” Physiotherapy – therex, massage, modalities– Group 3: Corticosteroid Injection (1-3 injections)
• Results:– Manipulation was superior to Physiotherapy for the “shoulder
girdle group” – improved pain and lower drop-out rates– Injections were superior to Physiotherapy and Manipulation for
the “synovial group” – improved pain and lower drop-out rates• Conclusion: Manipulation seems to be preferred for shoulder
girdle disorders; Injections are preferred for synovial joint disorders
Comparison of Physiotherapy, Manipulation, And Corticosteroid Injection For Treating Shoulder Complaints In General Practice

Effectiveness of Rehabilitation for Patients with Impingement Syndrome:
A Systematic Review• Systematic review of 12 RCTs• Results:
– Therex more effective in reducing pain and increasing function than placebo. Mixed results when compared to surgery
– Adding MT to therex provides favorable outcomes compared to therex alone
– Does not support the use of US as a beneficial treatment
– Conflicting results in use of acupuncture
Michener LA et al, J Hand Ther, 2004
Comparison of Supervised Exercise With and Without Manual Physical Therapy for
Patients With Shoulder Impingement Syndrome
• Subjects (N= 52)• Treatment conditions
– Group 1: Manual therapy (upper quarter) and exercise– Group 2: Exercise alone; stretches and strengthening– 3-week intervention – biw for 6 Rx’s
• Results– Function: significantly more improvement in MT group
(35% vs 17%)– Pain: significantly less pain in MT group (70% vs 35%)– Strength: significant increase for MT group (16%)
• Conclusion: MT and exercise is superior to exercise alone for improving strength, function, and pain in patients with impingement syndrome
(Bang and Deyle, JOSPT, 2003)

Adhesive Capsulitis

Natural History
• Little agreement in the literature• “even the most severe cases recover with
or without treatment in about 2 years,”Codman – 1934
• “20-40 % of cases do not respond to conservative treatment”Castellarin – 2004
Duration of the Disease(with conservative treatment)
• Reeves – 1975• Prospective study, n = 41• Average duration; 30.1 months
• Shaffer et al. – 1992• Retrospective study, n = 62 • Average duration; 12 months
• Miller et al. – 1996• Retrospective study, n = 50• Average duration; 14 months
Long Term Effects• Reeves – 1975
– At 5 yr. f/u: 54% with limited ROM– 7% with functional limitation
• Shaffer et al. – 1992– At 7 year f/u: 43% with limited ROM– 11% had functional limitation
• Miller et al. – 1996– At 10 year f/u: 100% regained ‘functional ROM’
Treatment Options
• Wait and see• PT directed rehab• MD directed rehab• Oral corticosteroids• Steroid injections• Capsular distension• Long lever MUA• Arthroscopic release• Translational MUA
Traditional Manipulation (long-lever techniques)
• Common practice in some centers for patients who have failed conservative Rx.
» Sandor – 2000.
• M.U.A. is a useful way to treat frozen shoulder.
» Kivimaki et al. – 2001.
• Traditional manipulation risks fracture, especially in osteoporotic patients.
» Hannifan - 2000

• Markus et al. – 2005– 30 consecutive cases of recalcitrant AC received
MUA– “unequivocal acute intrarticular lesions were found
in 12 joints”• 4 Ant. labrum detachments- with 1 osteochondral
fragment• 3 SLAP tears• 2 Partial ruptures of GH ligaments• 2 Partial tears of subscapularis tendons
• “the joint should not be mobilized by force. In resistant shoulders, controlled endoscopic release is preferable.”
Traditional Manipulation (long-lever techniques)
GH Gliding Manipulation Following Scalene Block
• Subjects (N=8)– Average symptom duration = 7 mo (3-16 mo)
• Treatment– Slow progressive sustained hold– Translational small amplitude high velocity thrust– Post manipulation Rx: HVGS x 20’ with ice, US,
contralateral AAROM flexion 3-5 min/hr (daily PT for ~ 16 visits)
• Results – � PROM and Wolfgang’s functional score– � VAS pain– No complications
(Roubal et al, JOSPT, 1996)

Long Term Effectiveness of Translational Manipulation
• Subjects (N= 31)– Average symptom duration = 7.8 ± 2 mo
• Treatment– Slow progressive sustained hold– Translational small amplitude high velocity thrust– Post manipulation Rx: HVGS x 20’ with ice, US,
contralateral AAROM flexion 3-5 min/hr (daily PT for ~visits)
• Results– 5.3 ± 3.2 wks and at 14.4 ± 7.3 mo– � PROM and Wolfgang’s functional score– � VAS pain– No complications
(Placzek et al, Clin Orthop, 1998)

Manipulation Following Interscalene Block for Shoulder Adhesive Capsulitis: A
Case Series
• Subjects (N= 4)– Average Symptom Duration = 7.5 mo
• Treatment– Interscalene block followed by impairment-based
mobilizations/manipulations– Post manipulation Rx: mobilization, ROM,
strengthening exercises and ice (qd for one week then tiw for 2 weeks ~ 10 visits)
• Outcome Measures– PROM and SPADI– Video fluoroscopy recordings for 2 patients– Taken pre-rx, immediately post-rx, 6- and 12-week
(Boyles et al, Manual Therapy, 2005)

0
100
200
300
400
500
600
Patient 1 Patient 2 Patient 3 Patient 4
De
gre
es
of
PR
OM
Pre-RxImmediateFinal
Total Passive ROM
0
10
20
30
40
50
60
70
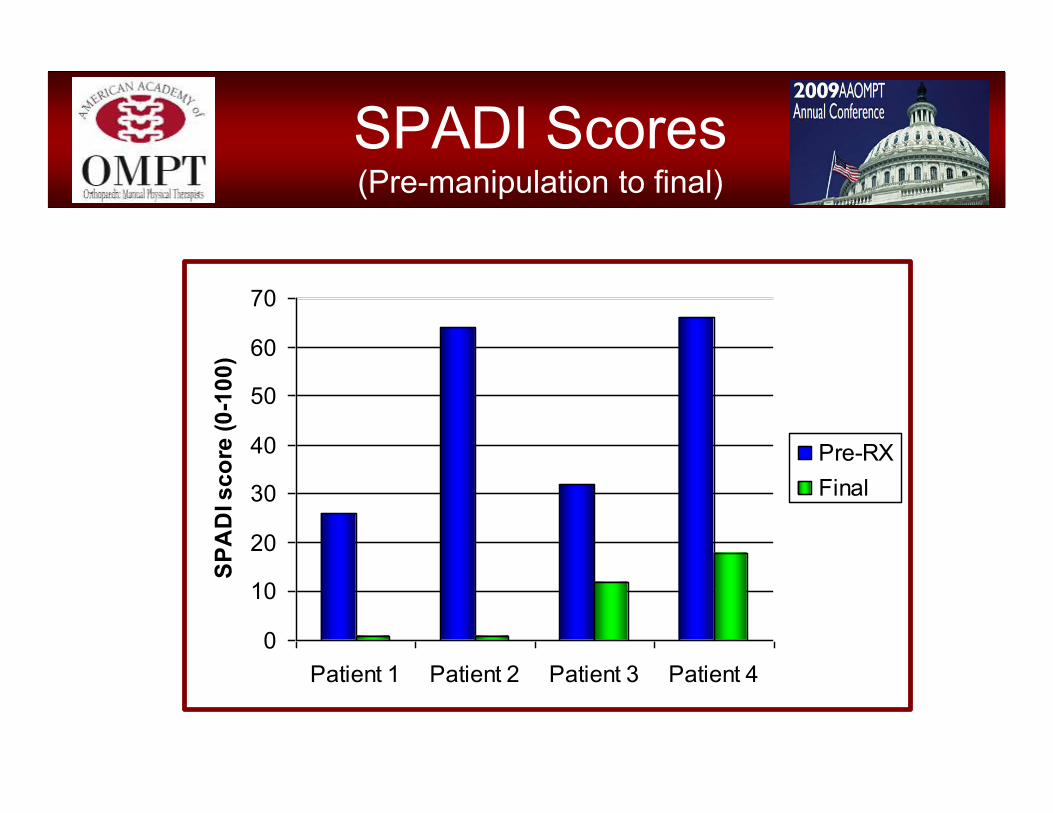
Patient 1 Patient 2 Patient 3 Patient 4
SPA
DI s
core
(0-1
00)
Pre-RXFinal
SPADI Scores (Pre-manipulation to final)
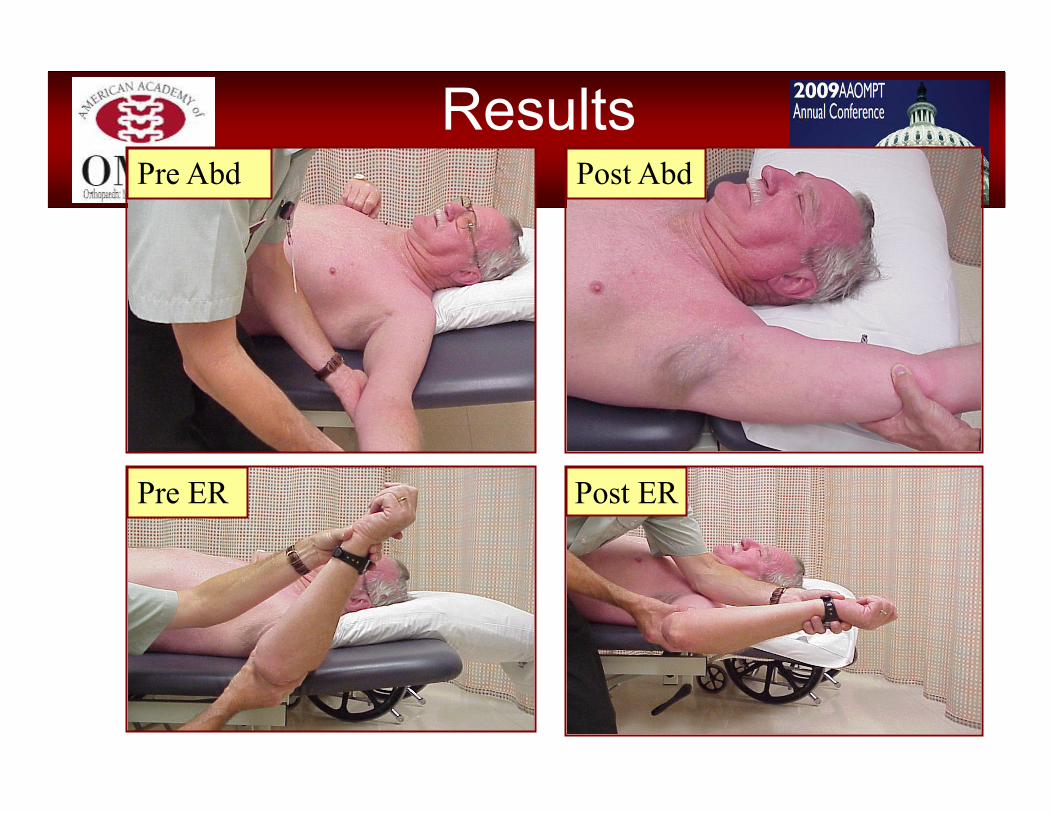
Results
Post ER
Post AbdPre Abd
Pre ER

Pre- Manipulation 6 wk Post- Manipulation
Video Fluoroscopy

Case Studies: Arthroscopic findings following
translational MUA.
• Arthroscopy performed immediately following translational manipulations
• Patient #1: 42 y.o. diabetic male. 14 month history of labral tear, impingement. AC x 7 months.
• Patient #2: 42 y.o.f., secondary AC s/p humeral neck fracture. AC x 14 months.

Patient #1 Diabetic male, AC x 7 months
Humeral head
Torn Scar tissue
Glenoid
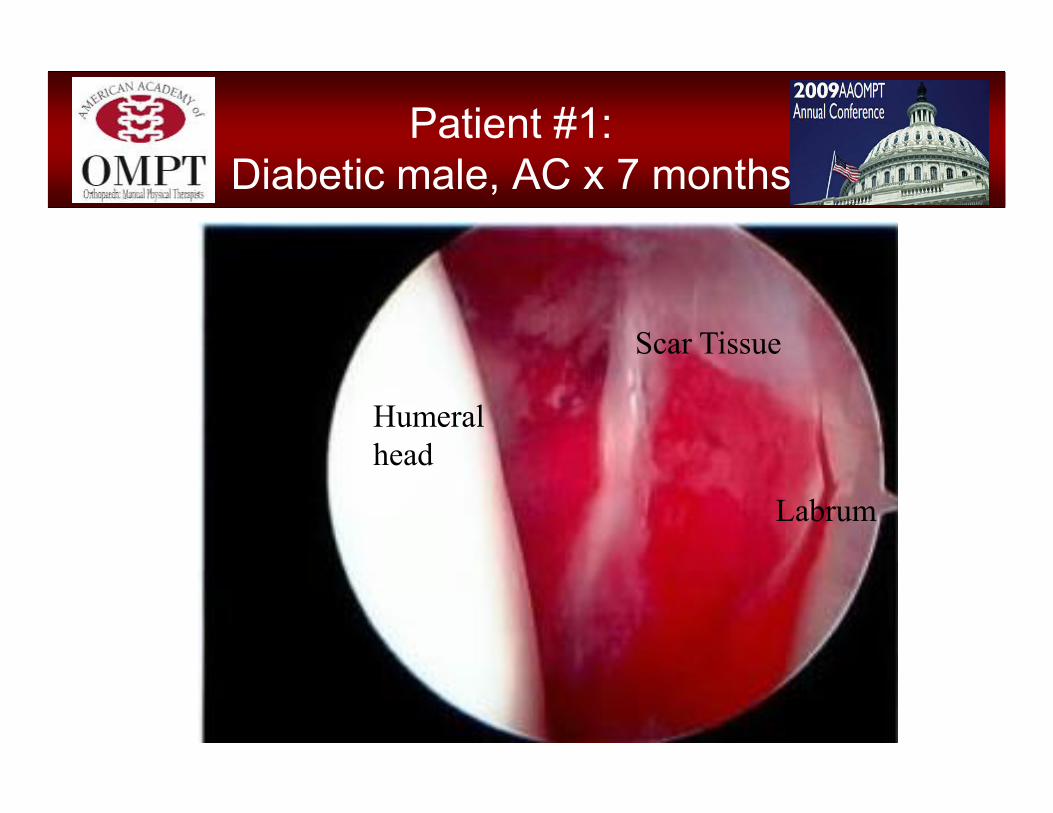
Patient #1: Diabetic male, AC x 7 months
Humeral head
Scar Tissue
Labrum

Patient #2:Secondary AC x 14 months.
Humeral head
‘Veil’ of scar tissue

Patient #2:Secondary AC x 14 months.
Humeral head
Scar tissue
Glenoid

Intra-articular Findings
• In both shoulders:– No acute intra-
articular lesions were found.Rotator cuff,
biceps tendon, subscapularis tendon, glenoid, labrum and humeral surfaces were found in perfect condition.

Translational Manipulation Theory
• “Translational manipulation attempts to restore the normal movements associated with angular GH motion.”
• “…the applied force moves the humeral head in a linear direction, parallel to the glenoid fossa.”
• Advantages over long-lever M.U.A include:– Minimizing GH joint compression– Improved operator control– Increased subacromial space– Isolates manipulative force to GH joint– Minimizes stress to brachial plexus
Placzek, et al, Amer J of Ortho– 2004
• Mounting and compelling evidence exists that translational manipulation following interscalene block is safe and effective treatment for the management of shoulder adhesive capsulitis.
• Patients should be offered this option early in the course of care rather than waiting out the pain and added expense of standard, less effective programs.
Adhesive Capsulitis Conclusions
RI: UE Associations
• Association between rib impairment and shoulder pain/impairment– Boyle, Man Ther, 1999
• Association between lateral elbow pain and shoulder impairment – Abbott, Man Ther, 2001
• Possible associations between upper quarter and CTS– Davis et al, JMPT, 1998
• Possible association between upper quarter and de Quervain’s Disease– Anderson & Tichenor, Phys Ther, 1994

Targeted Thoracic Spine for Shoulder Pain
The Short Term Effects of Thoracic Spine Thrust Manipulation on Patients with Shoulder Impingement Syndrome Manual Therapy Boyles et al, 2008, Manual Therapy
The Immediate Effects of Thoracic Spine Manipulation on Patients with Primary Complaints of Shoulder Pain.
Strunce et al, 2008, in review
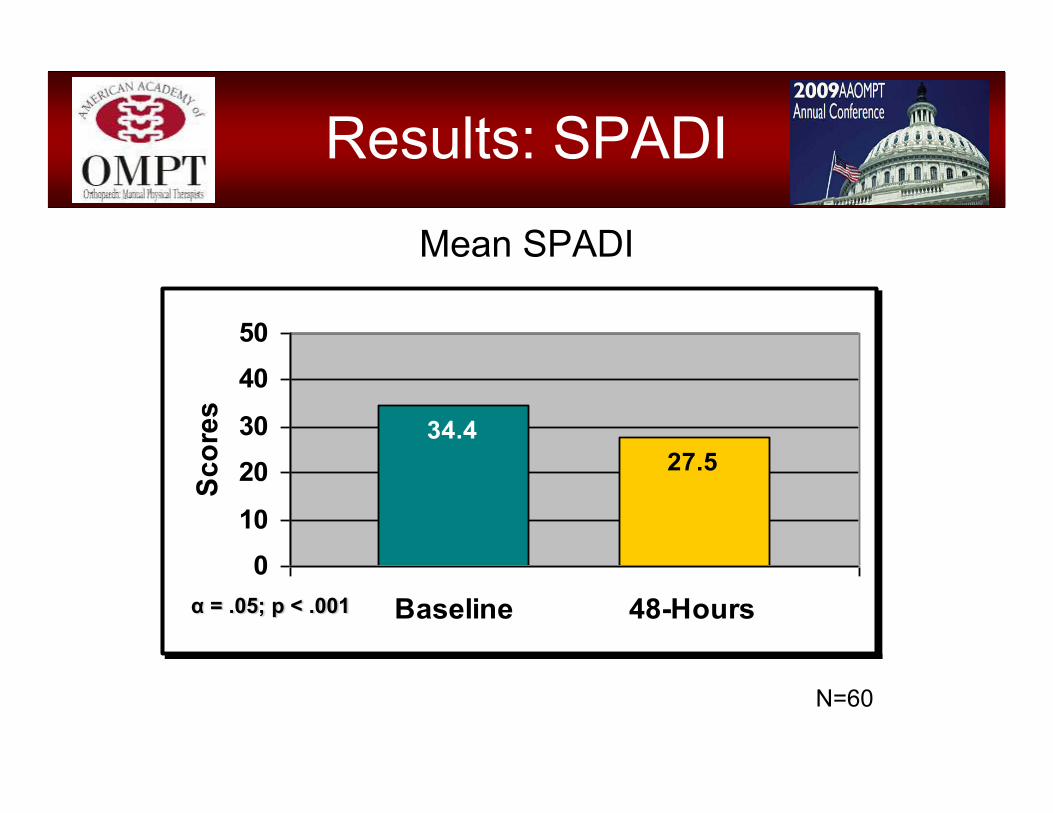
Results: SPADI
34.427.5
0
10
2030
4050
Baseline 48-Hours
Scor
esMean SPADI
α = .05; p < .001
N=60

ResultsMean NPRS
4.43
2.92 3.022.832.37
1.72 1.882.182.40
3.303.93
3.20
0
1
2
3
4
5
Neer Hawkins EmptyCan
IR ER ABD
Sco
re
Baseline 48-Hours
NeeNeereeeα = .05; p < .003
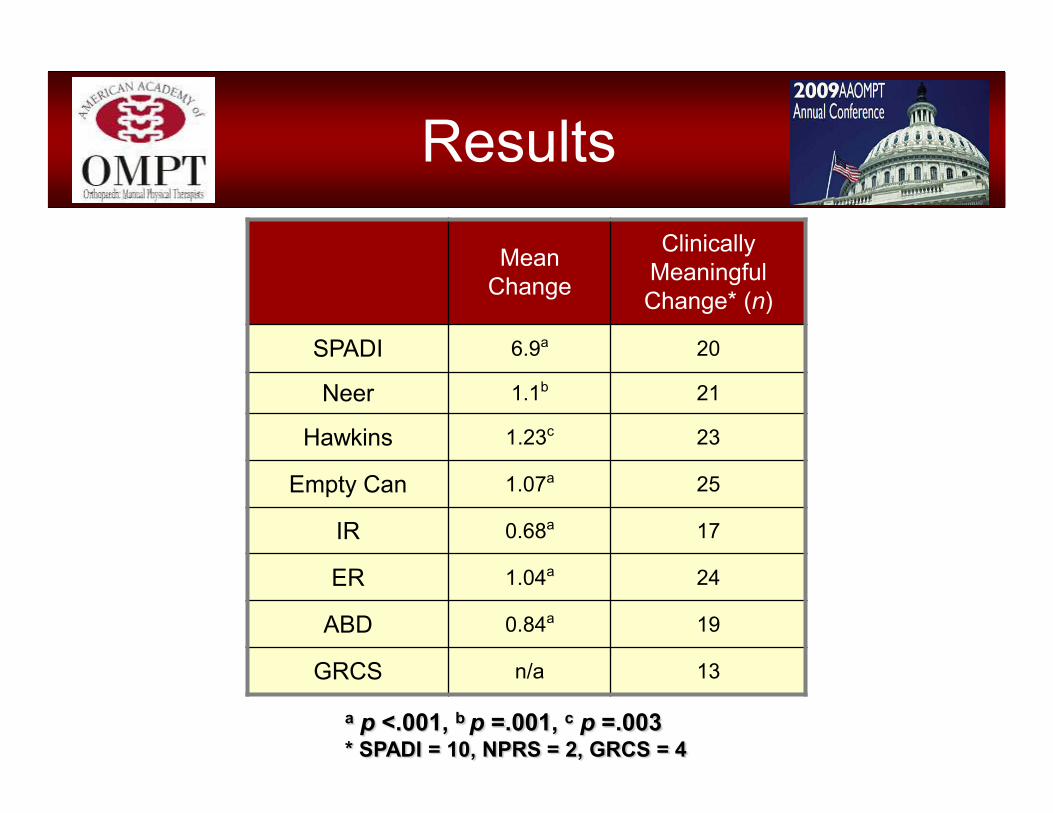
Results
a p <.001, b p =.001, c p =.003* SPADI = 10, NPRS = 2, GRCS = 4
Mean Change
Clinically Meaningful Change* (n)
SPADI 6.9a 20
Neer 1.1b 21
Hawkins 1.23c 23
Empty Can 1.07a 25
IR 0.68a 17
ER 1.04a 24
ABD 0.84a 19
GRCS n/a 13
Discussion
• Thoracic thrust manipulations were associated with statistically significant reduction of SPADI & NPRS
• Our findings may support recent studies that advocate the use of spinal thrust manipulation in the treatment of the upper extremity

Techniques
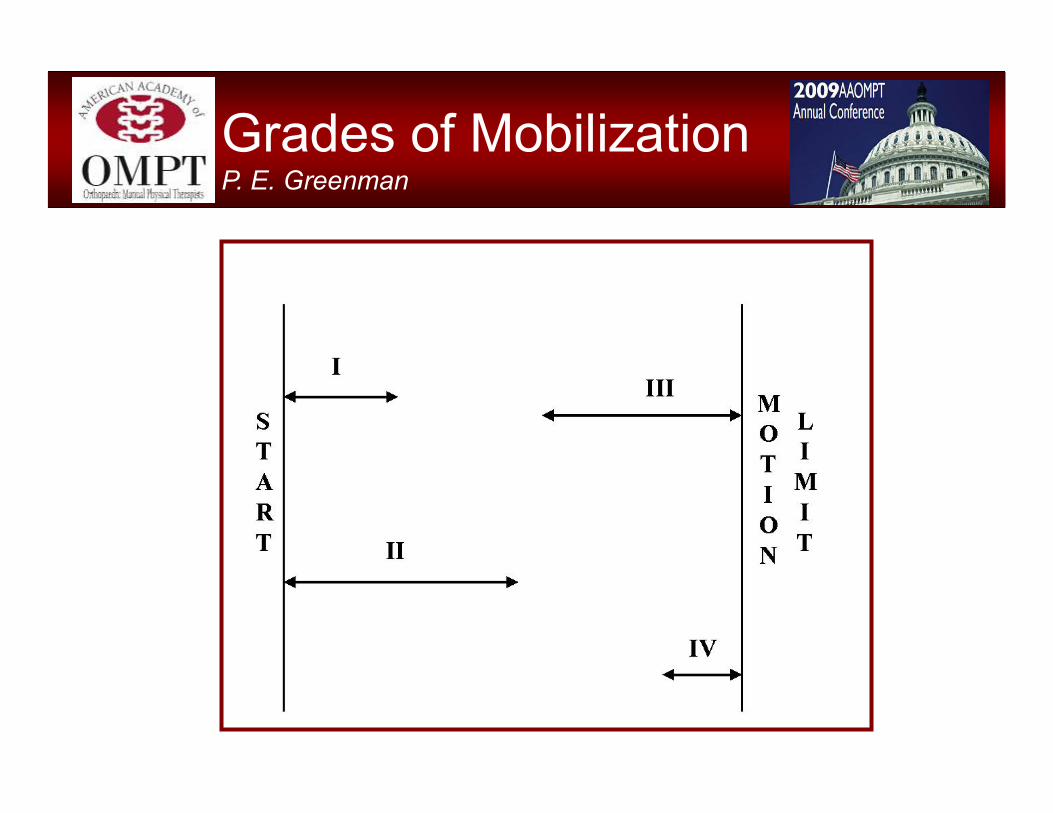
Grades of Mobilization P. E. Greenman

R2
L3/41/21/4R1
III++
III+
III
III-
IV+
IV++
IV
IV-
II+
II
I+
I
Grades of Mobilization G. D. Maitland

GRADE DESCRIPTIONI Small amplitude out of resistance (R1)II Large amplitude out of resistanceIII Large amplitude into resistanceIV Small amplitude into resistance
III- or IV- performed at 25% into restricted rangeIII or IV performed at 50% into restricted rangeIII+ or IV+ performed at 75% into restricted rangeIII++ or IV++ performed at restricted barrier (R2)
Grades I and II used to treat pain prior to reaching resistanceGrades III and IV used to treat resistance (joint restrictions) when pain is
not a limitation
Grades of Mobilization G. D. Maitland
• Patient must be completely relaxed• Operator must be relaxed• Patient must be comfortable and have complete
confidence in the operator’s grasp• Embrace the joint to be moved, hold around the joint to
feel movement• Move one joint, one motion at one time• Patient must be confident that the joint will not be hurt• Operator’s position must be comfortable and easy to
maintain• Operator’s position must afford him/her complete control
Mobilization PrinciplesG. D. Maitland; P. E. Greenman

Mid-Thoracic Manipulation
• Patient seated with back near edge of table
• Have patient grasp opposite shoulders, ensuring patient’s arm is over the other arm
• Fulcrum the patient’s thoracic spine into flexion by grasping the patient’s elbows and leaning into the patient with your upper body (J-stroke)
• Extend knees, lifting the patient vertically while emphasizing flexion and distraction of the thoracic spine
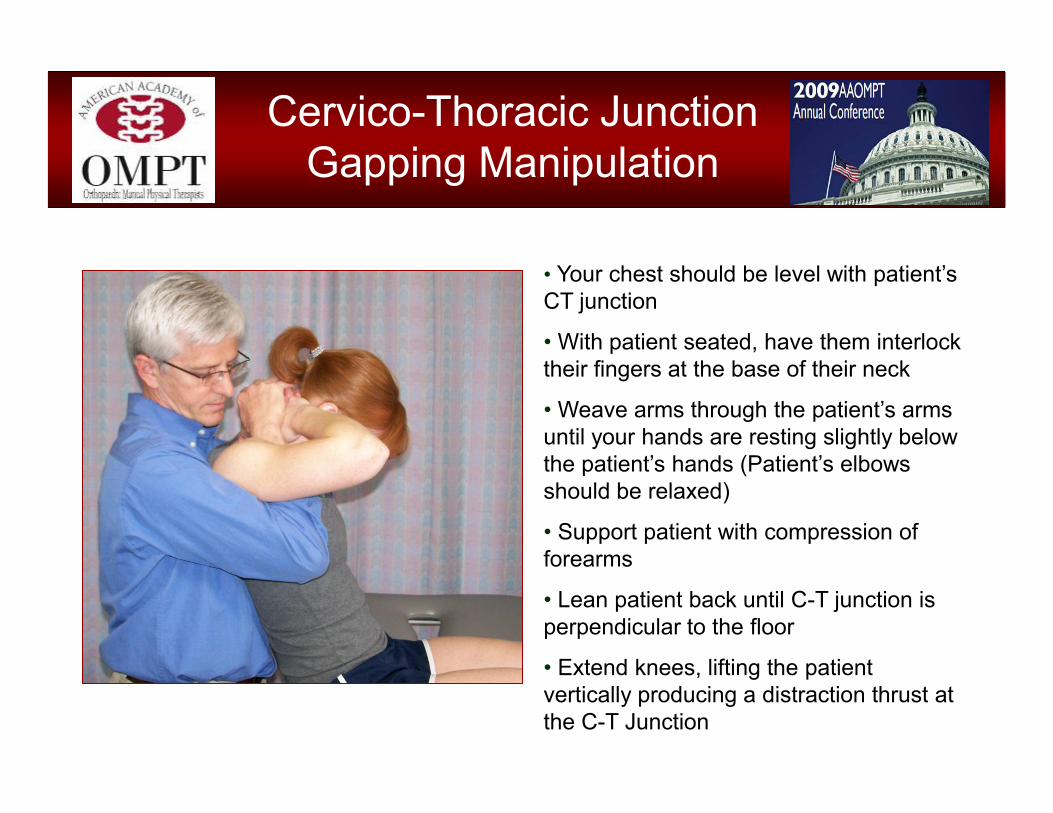
Cervico-Thoracic Junction Gapping Manipulation
• Your chest should be level with patient’s CT junction
• With patient seated, have them interlock their fingers at the base of their neck
• Weave arms through the patient’s arms until your hands are resting slightly below the patient’s hands (Patient’s elbows should be relaxed)
• Support patient with compression of forearms
• Lean patient back until C-T junction is perpendicular to the floor
• Extend knees, lifting the patient vertically producing a distraction thrust at the C-T Junction

Shoulder Techniques
• GH Physiological Mvmts– Flexion (Grade 4)– Abduction (Grade 4)– External Rotation (Grade 4)– Internal Rotation (Grade 4)– Horiz. Flexion (Grade 4)
• GH Accessory Mvmts– AP Glides in Abduction– Caudal Glides in Abduction– Caudal Glides in Flexion
• AC Accessory Mvmts– AC Joint Caudal Glides– Clavicle Rotation (Wiggle)
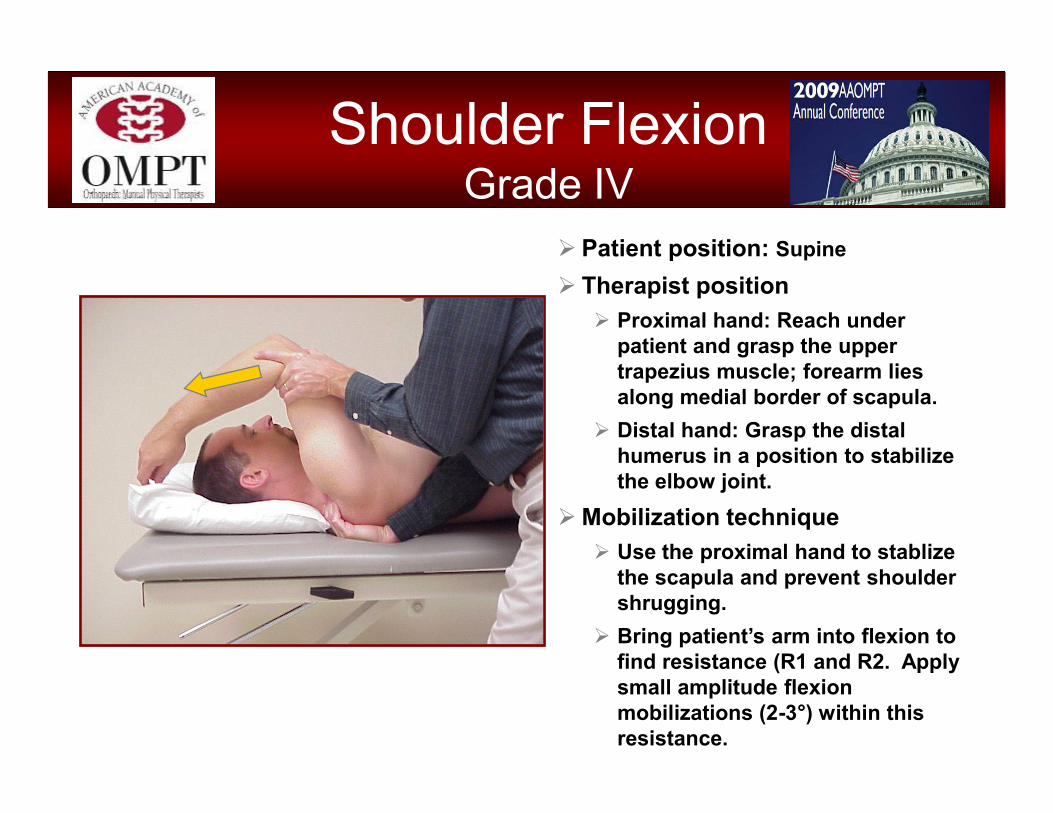
� Patient position: Supine
� Therapist position� Proximal hand: Reach under
patient and grasp the upper trapezius muscle; forearm lies along medial border of scapula.
� Distal hand: Grasp the distal humerus in a position to stabilize the elbow joint.
� Mobilization technique� Use the proximal hand to stablize
the scapula and prevent shoulder shrugging.
� Bring patient’s arm into flexion to find resistance (R1 and R2. Apply small amplitude flexion mobilizations (2-3°) within this resistance.
Shoulder Flexion Grade IV

Shoulder Abduction Grade IV
� Patient position: Supine
� Therapist position– Proximal hand: Reach under
patient and grasp the upper trapezius muscle; forearm lies along medial border of scapula.
– Distal hand: Grasp the distal humerus in a position to stabilize the elbow joint.
� Mobilization technique– Use the proximal hand to stabilize
the scapula and prevent shoulder shrugging.
– Bring patient’s arm into abduction to find resistance. Apply small amplitude abduction mobilizations (2-3°) within this resistance.

Shoulder External Rotation Grade IV
� Patient position– Supine, shoulder abducted and
elbow flexed to 90°, upper arm resting on plinth
� Therapist position– Proximal hand: Grasp the distal
humerus; lay forearm across anterior shoulder for stabilization
– Distal hand: Grasp wrist and hold in a neutral position
� Mobilization technique– Bring patient’s arm into external
rotation to find resistance. Apply graded mobilizations (~10°) within resistance.
– May be performed in various degrees of abduction based on patient symptoms and response
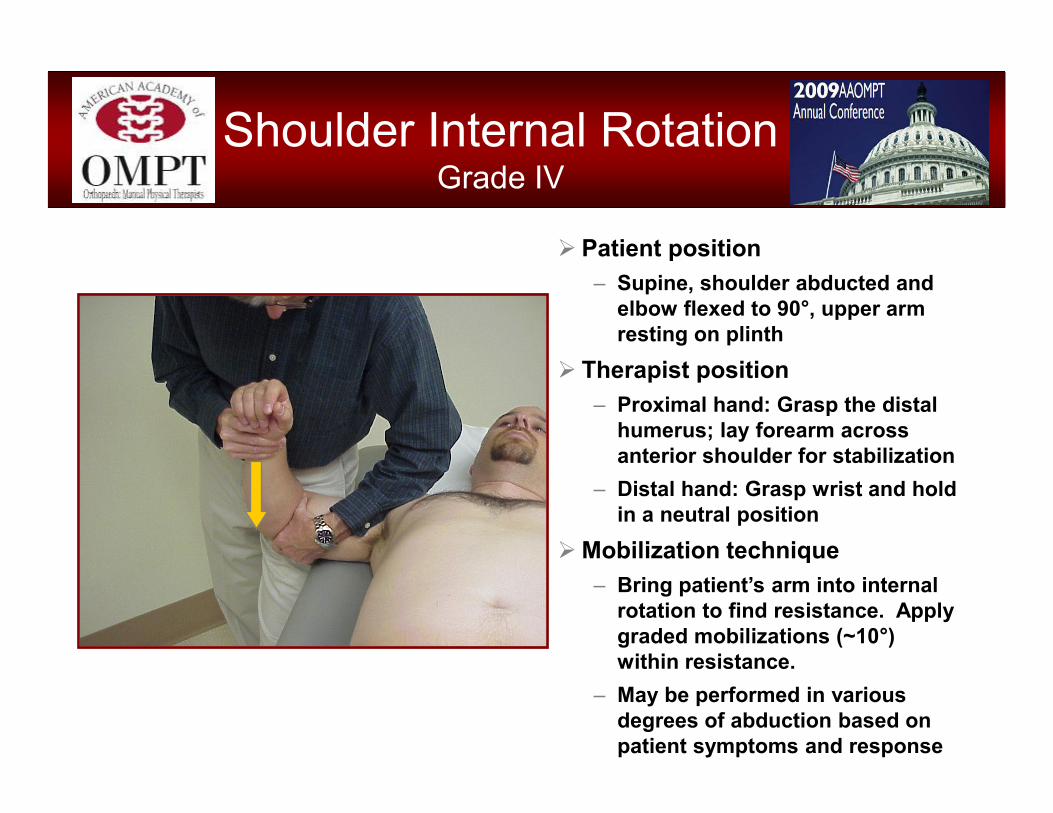
Shoulder Internal Rotation Grade IV
� Patient position– Supine, shoulder abducted and
elbow flexed to 90°, upper arm resting on plinth
� Therapist position– Proximal hand: Grasp the distal
humerus; lay forearm across anterior shoulder for stabilization
– Distal hand: Grasp wrist and hold in a neutral position
� Mobilization technique– Bring patient’s arm into internal
rotation to find resistance. Apply graded mobilizations (~10°) within resistance.
– May be performed in various degrees of abduction based on patient symptoms and response
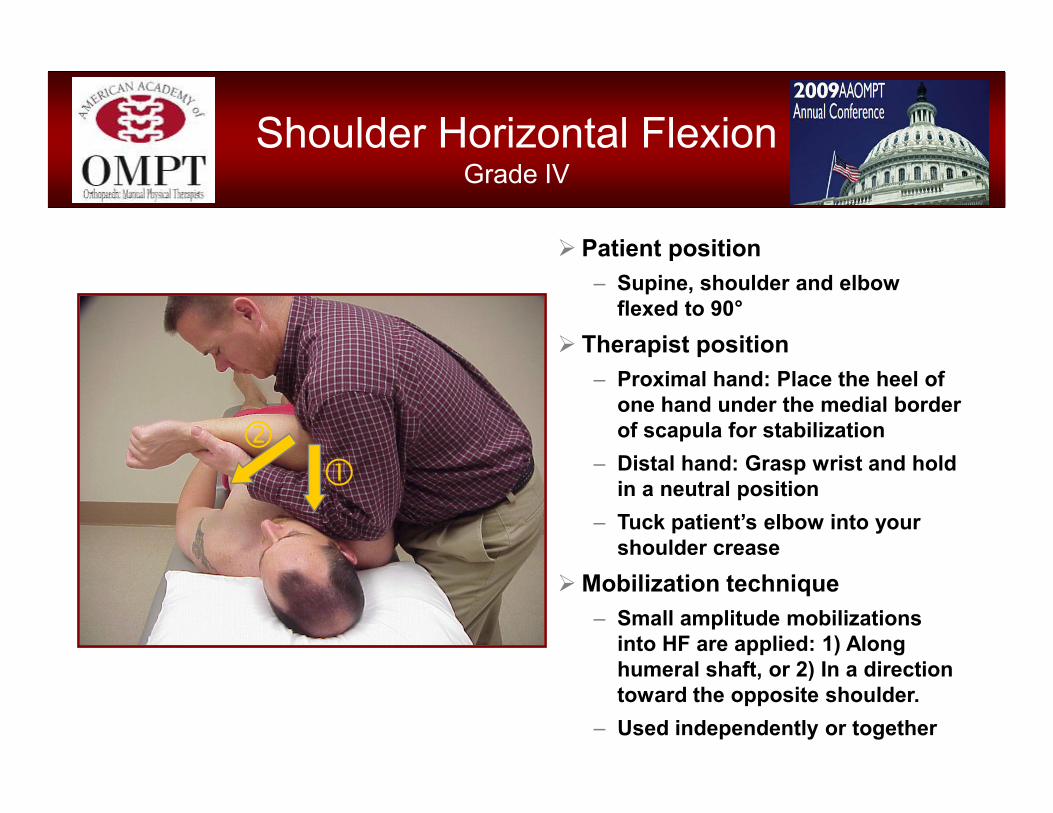
Shoulder Horizontal Flexion Grade IV
� Patient position– Supine, shoulder and elbow
flexed to 90°� Therapist position
– Proximal hand: Place the heel of one hand under the medial border of scapula for stabilization
– Distal hand: Grasp wrist and hold in a neutral position
– Tuck patient’s elbow into your shoulder crease
� Mobilization technique– Small amplitude mobilizations
into HF are applied: 1) Along humeral shaft, or 2) In a direction toward the opposite shoulder.
– Used independently or together
��
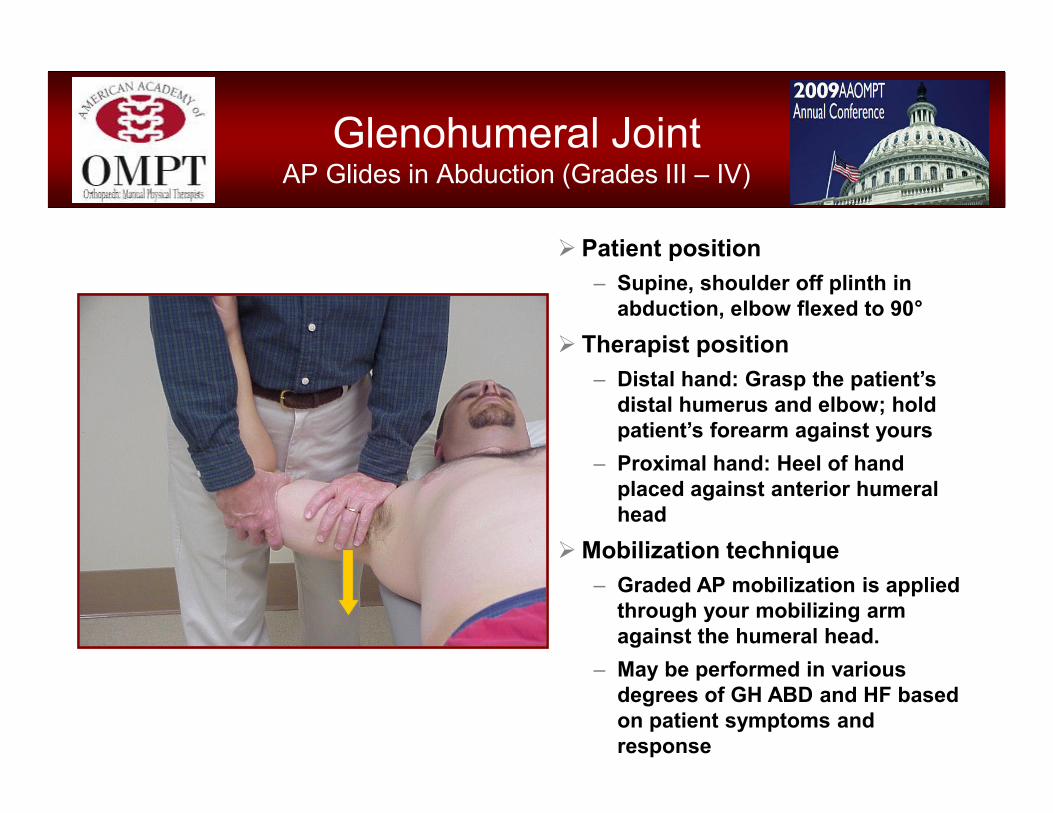
Glenohumeral Joint AP Glides in Abduction (Grades III – IV)
� Patient position– Supine, shoulder off plinth in
abduction, elbow flexed to 90°� Therapist position
– Distal hand: Grasp the patient’s distal humerus and elbow; hold patient’s forearm against yours
– Proximal hand: Heel of hand placed against anterior humeral head
� Mobilization technique– Graded AP mobilization is applied
through your mobilizing arm against the humeral head.
– May be performed in various degrees of GH ABD and HF based on patient symptoms and response

Glenohumeral Joint Caudal Glides in Abduction (Grades III – IV)
� Patient position– Supine, shoulder off plinth in
abduction, elbow flexed to 90°� Therapist position
– Distal hand: Grasp the patient’s distal humerus and elbow; hold patient’s forearm against yours
– Proximal hand: 1st web space or heel of hand placed against head of humerus (adjacent to acromion)
� Mobilization technique– Graded mobilization is applied
through your mobilizing hand to glide the humeral head caudally.
– Elbow may be held stationary, or carried on line with humerus or further distally– depending on irritability
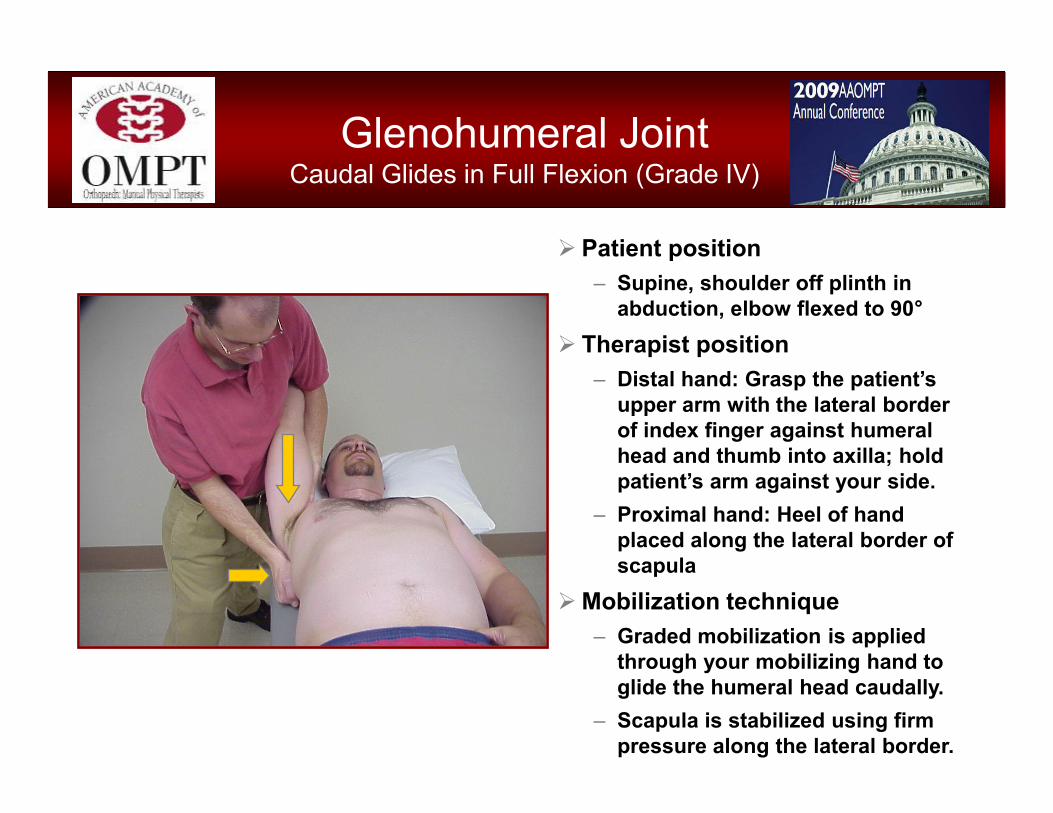
Glenohumeral Joint Caudal Glides in Full Flexion (Grade IV)
� Patient position– Supine, shoulder off plinth in
abduction, elbow flexed to 90°� Therapist position
– Distal hand: Grasp the patient’s upper arm with the lateral border of index finger against humeral head and thumb into axilla; hold patient’s arm against your side.
– Proximal hand: Heel of hand placed along the lateral border of scapula
� Mobilization technique– Graded mobilization is applied
through your mobilizing hand to glide the humeral head caudally.
– Scapula is stabilized using firm pressure along the lateral border.
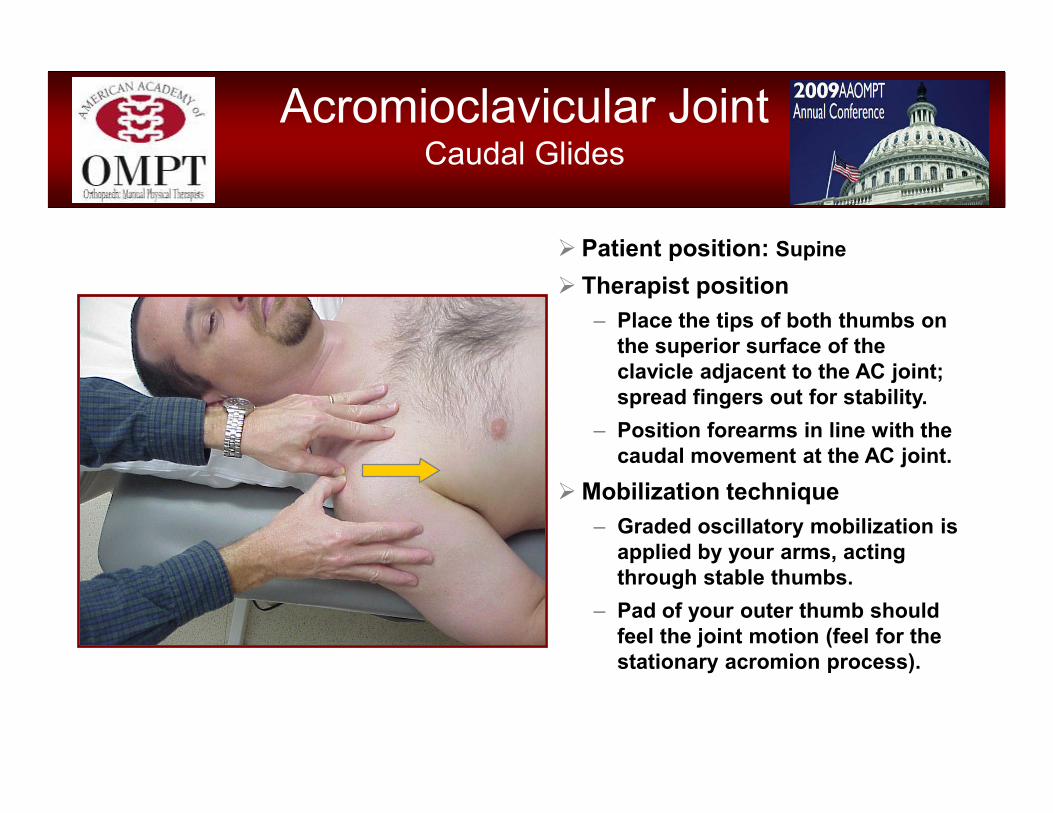
Acromioclavicular Joint Caudal Glides
� Patient position: Supine
� Therapist position– Place the tips of both thumbs on
the superior surface of the clavicle adjacent to the AC joint; spread fingers out for stability.
– Position forearms in line with the caudal movement at the AC joint.
� Mobilization technique– Graded oscillatory mobilization is
applied by your arms, acting through stable thumbs.
– Pad of your outer thumb should feel the joint motion (feel for the stationary acromion process).

Clavicle Rotation (Wiggle)
� Patient position: Supine
� Therapist position– Stand near the patient’s shoulder,
facing towards the clavicle.– Gently grip the mid clavicle using
your thumbs on the inferior edge and finger tips superiorly.
� Mobilization technique– Apply a gentle mobilization force
using a rocking or “wiggling” motion through repetitive wrist flexion and extension.
– Works as a nice easing technique following direct AC and/or SC joint mobilizations.

Therapeutic Exercise: The Shoulder
Danny McMillian, PT, DSc, OCS, CSCS AAOMPT OCT 09
Shoulder Function
• Integrated not isolated– Define integrated
• GHJ, ACJ, SCJ, Scapula-Thoracic Articulation?
• Why are there no chairs on a pitcher’s mound?
– Re-define integrated• Regional interdependence
considerations• C-spine to the foot (and
everything in between)Functional Movement Screen
(FMS) – Deep Squat

• Janda has written extensively on neuromuscular imbalances as they affect function of the upper quarter. – Prone to tightness
• upper trapezius• pectoralis major/minor• upper cervical extensors
– Prone to weakness • middle/lower trapezius• rhomboids• serratus anterior• deep neck flexors
Shoulder Impairment
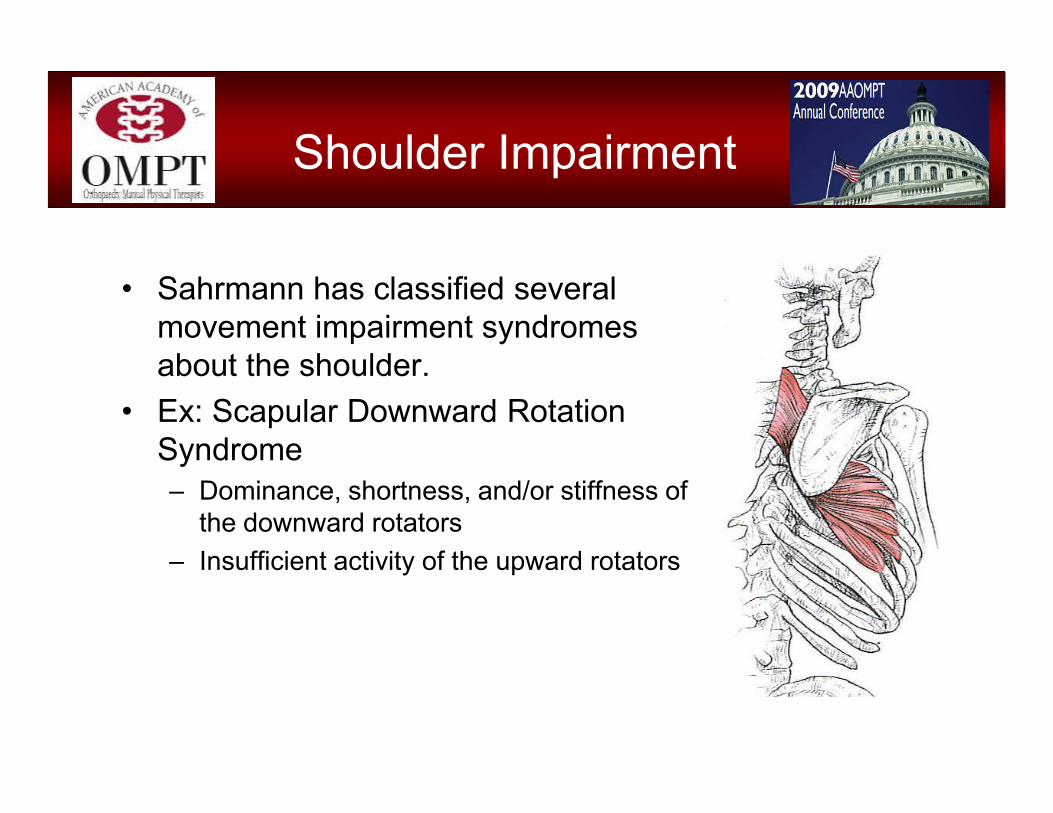
• Sahrmann has classified several movement impairment syndromes about the shoulder.
• Ex: Scapular Downward Rotation Syndrome– Dominance, shortness, and/or stiffness of
the downward rotators– Insufficient activity of the upward rotators
Shoulder Impairment

Examination
• Ensure full, 3D view of all segments contributing to motion
• Death by special tests– 35+ Magee/Cleland– Let a viewing of integrated
motion be your guide to a more focused examination
• Hx:– Consider previous spine or
LE problems– Loss of power from LE

• The SICK scapula– Scapular malposition– Inferior medial border
prominence– Coracoid pain and
malposition– dysKinesis of scapular
movement
• Adjunct tests– Scapular assistance
• Assess ROM– Scapular retraction
• Assess– Strength– Relocation test
Examination

Regional Interdependence with the SICK scapula
• Burkhart & Kibler 2003– 48% poor lumbar
flexibility– 44% exhibited
Trendelenburg sign with SLS sequence
– 39% exhibited decreased hip IR on contralateral side
• By altering proximal mobility/stability distal mobility and force production suffer– “Breaks the kinetic chain”– What effect does
decrease T-Spine extension/rotation have on this player’s force production?
Regional Interdependence with the SICK scapula

Regional Interdependence
• Kinetic link model– Proximal to distal stability– 50-60% of the force
transmitted through the shoulder is generated from the lower extremity and trunk (tennis & baseball)
• Kinetic Chain Roles– Legs/trunk - force
generation– Shoulder – force regulation– Arm- force delivery

ShoulderPrimary Synergists
• Lower Extremities:– Generating drive for
overhead lifts– Decelerating throws
The Core: An unstable core = unstable, length:tension
relationships about the shoulder girdle
ShoulderPrimary Synergists
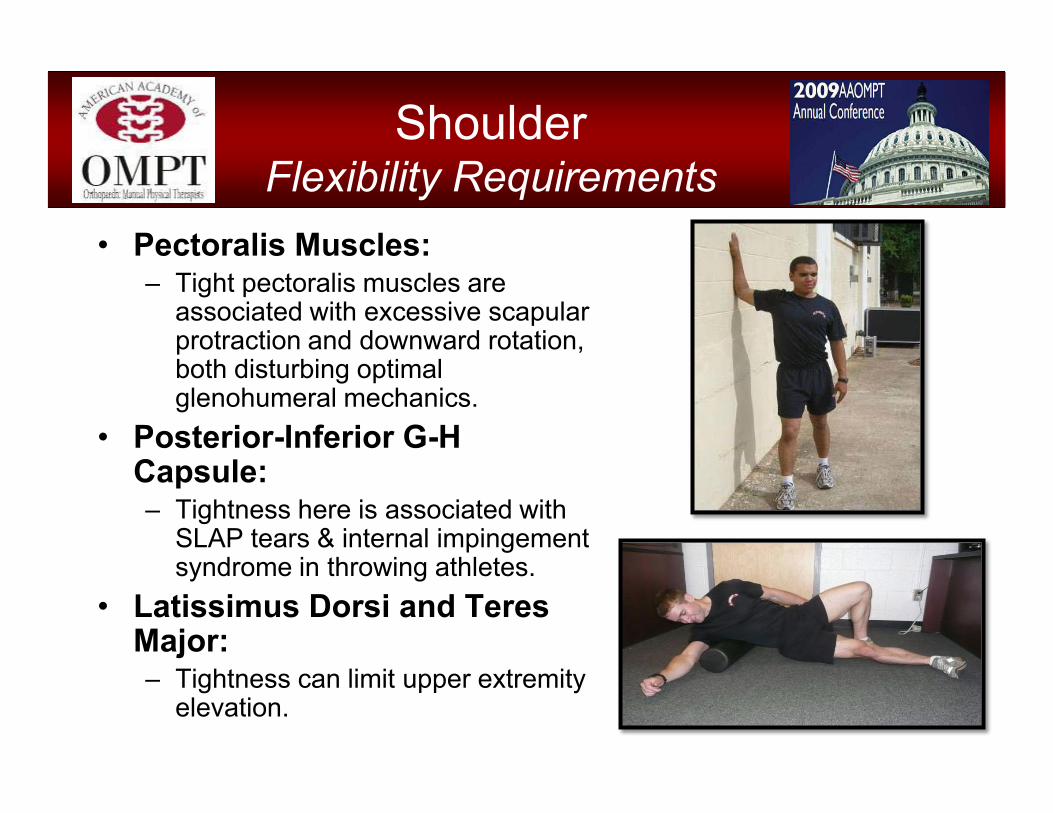
• Pectoralis Muscles: – Tight pectoralis muscles are
associated with excessive scapular protraction and downward rotation, both disturbing optimal glenohumeral mechanics.
• Posterior-Inferior G-H Capsule: – Tightness here is associated with
SLAP tears & internal impingement syndrome in throwing athletes.
• Latissimus Dorsi and Teres Major:– Tightness can limit upper extremity
elevation.
ShoulderFlexibility Requirements

� Thoracic Rotation & Extension: For throwing/punching motions, inability to optimally move the thoracic spine in the transverse plane may create pathological compensations at the shoulder.
• Hip & Trunk Extension: Lack of extension will result in compensations up the chain to enable continuation of functional performance.
ShoulderFlexibility Requirements
Functional Shoulder Exercise
• Foundational principles guide exercise selection and progression
– Train movements, not mm*– Train in 3D– Don’t fear speed– Challenge proprioception
*Discrete mm performance impairments may need isolation first, then integration with more functional movement patterns.
• Training Considerations– Isolated shoulder movement
versus integrated activity with the trunk and LEs
– Both or single arm demand – Symmetry of weight distribution– Stability of surface and base of
support– Dynamic versus static demand
• Repetitive motion or sustained postures
Functional Shoulder Exercise

Warming up the shoulder“Priming the Cannon”
• Light loads through full range– Roll-outs on physioball– Medicine ball chop/lift– Overhead squat– Lunge and reach– Standing row and rotate– Windshield wiper
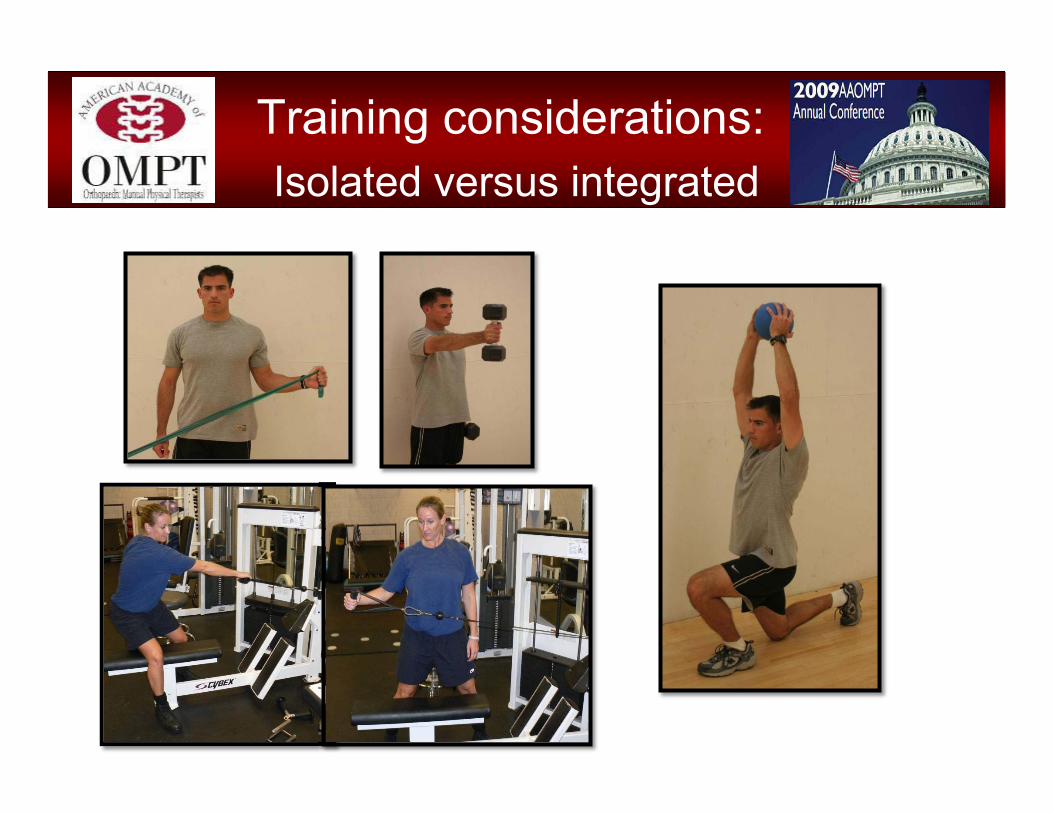
Training considerations:Isolated versus integrated

Training considerations:Both or single arm demand

Training considerations:Symmetry of weight distribution
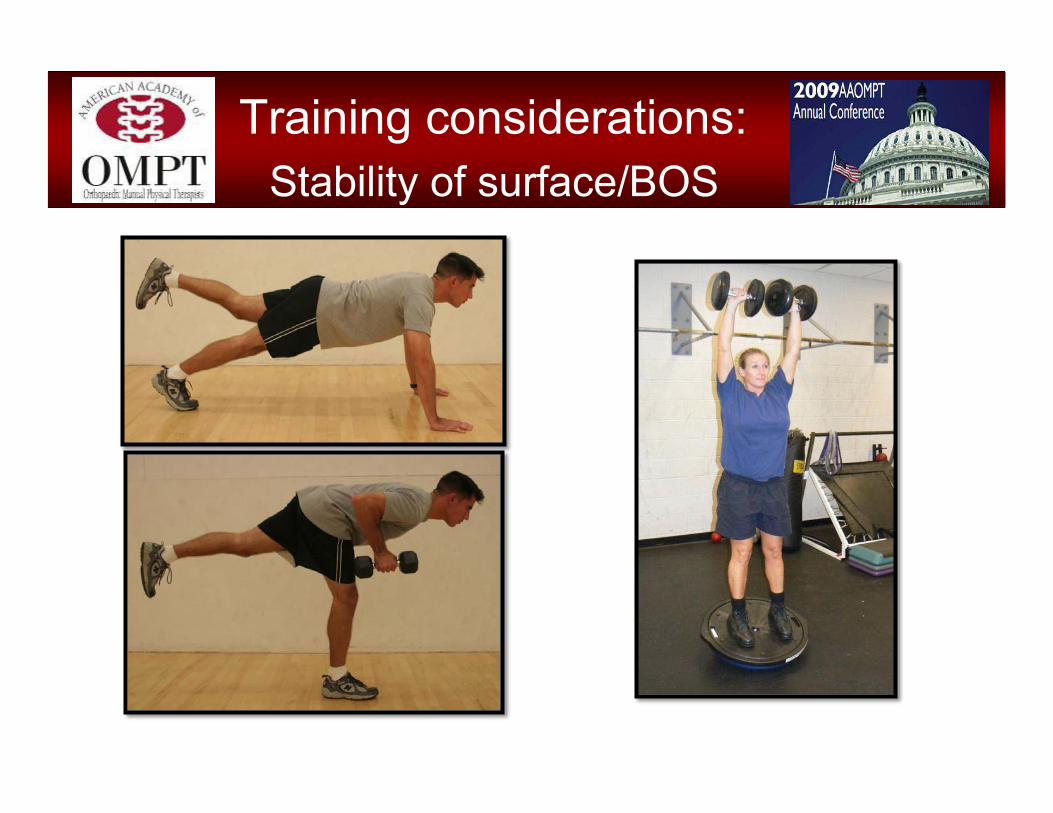
Training considerations:Stability of surface/BOS
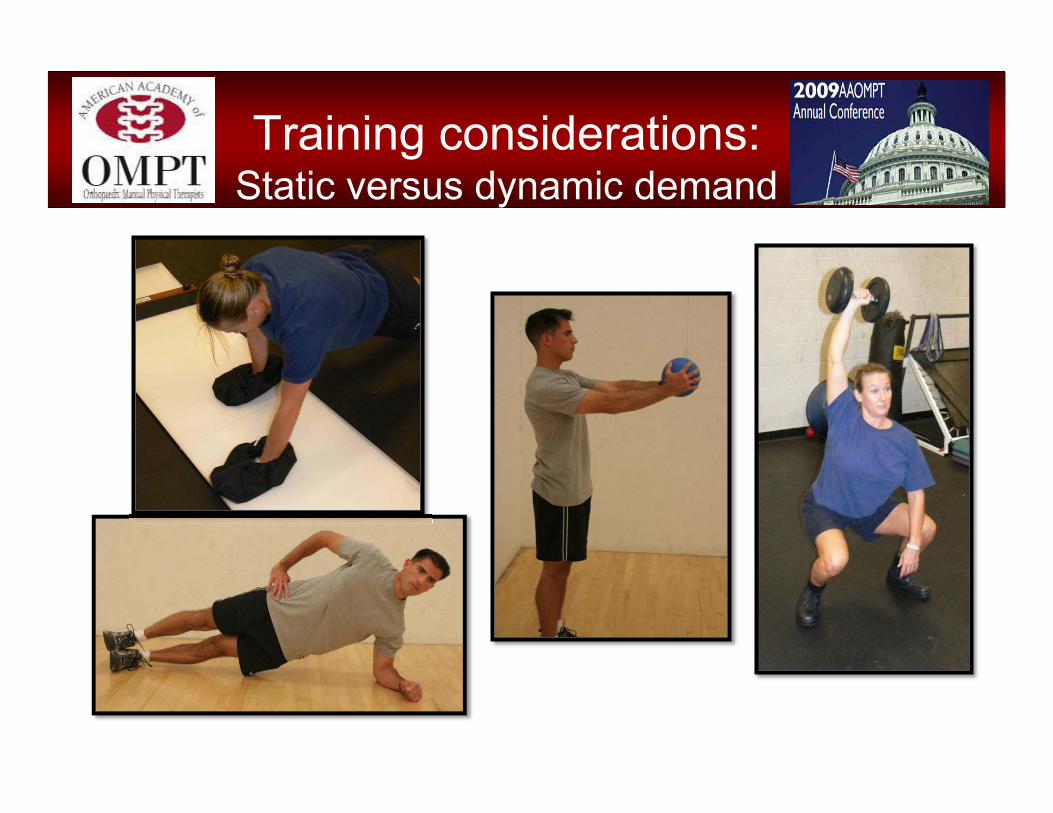
Training considerations:Static versus dynamic demand
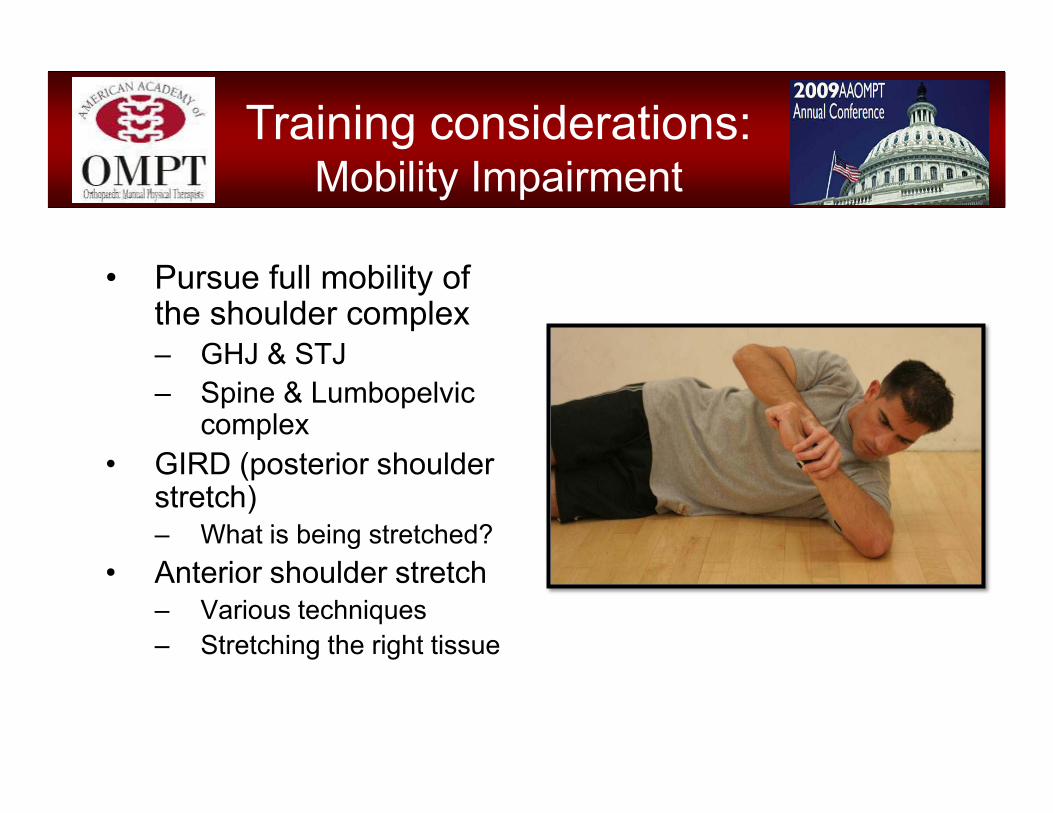
• Pursue full mobility of the shoulder complex– GHJ & STJ– Spine & Lumbopelvic
complex• GIRD (posterior shoulder
stretch)– What is being stretched?
• Anterior shoulder stretch– Various techniques– Stretching the right tissue
Training considerations:Mobility Impairment

Progression
• Options galore– Amplitude
• partial to full
– Speed of movement • slow to fast
– Volume• Repetitions or Time
– Amount of resistance
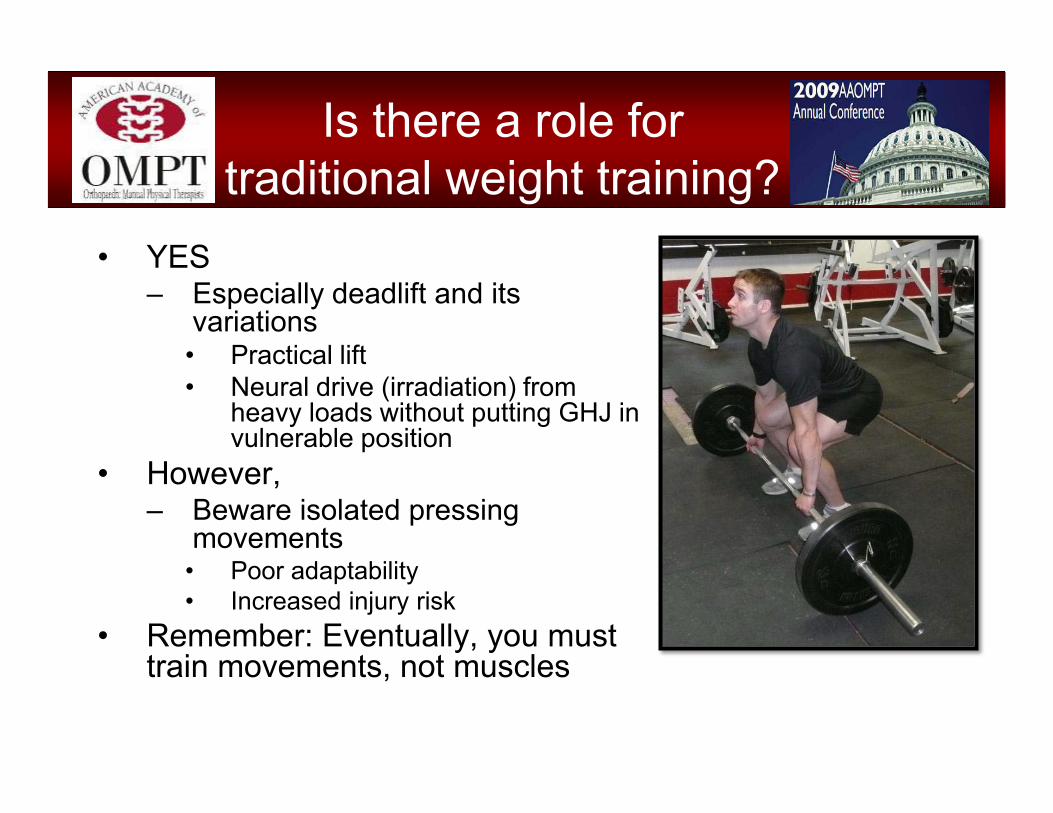
• YES – Especially deadlift and its
variations• Practical lift• Neural drive (irradiation) from
heavy loads without putting GHJ in vulnerable position
• However,– Beware isolated pressing
movements• Poor adaptability• Increased injury risk
• Remember: Eventually, you must train movements, not muscles
Is there a role for traditional weight training?
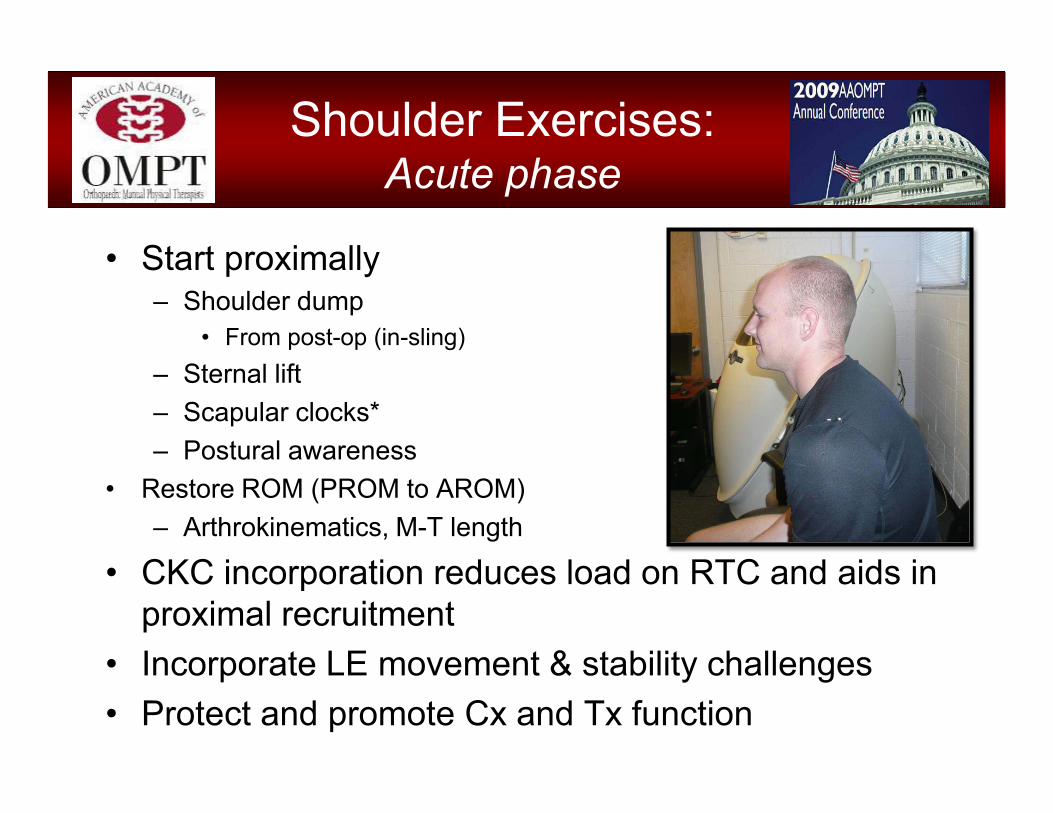
• Start proximally– Shoulder dump
• From post-op (in-sling) – Sternal lift– Scapular clocks*– Postural awareness
• Restore ROM (PROM to AROM)– Arthrokinematics, M-T length
• CKC incorporation reduces load on RTC and aids in proximal recruitment
• Incorporate LE movement & stability challenges• Protect and promote Cx and Tx function
Shoulder Exercises:Acute phase

• Upper Body Ergometer– Consider impairment when choosing forward/rearward
cycle• Unloaded movements
– Large-amplitude, integrated ROM• Pain-free• Integrated PNF patterns• Throwing patterns
• Light resistance– Isolate PRN
Shoulder Exercises:Sub-acute phase

Shoulder Exercises:Sub-acute phase
– Incorporate movement & stability challenges
• Pushup+• Physioball roll/reach• Progressive push-ups • PU+ w/Rotation• Telescoping/Punching • Bow Hunter

• Integrate LE/trunk– Step up/down w/single-arm
shoulder press– Squat w/arms overhead – Lunge and Reach Variations
• MedBall, etc
Shoulder ExerciseFunctional Progression

• Increase load, speed, and/or complexity of kinetic chain movement– Lunge & Reach– Overhead squat with
unequal load– Turkish Get Up– “Battling Ropes”– Deadlift
Shoulder ExerciseFunctional Progression

Shoulder ExerciseFunctional Progression

Shoulder Exercises:Reconditioning End Stage
“Finish-Line” Functional TrainingConsiderations in this stage must focus on individual-
specific occupational or sports goals

• Malliou PC, et al. Effective ways of restoring muscular imbalances of the rotator cuff muscle group: a comparative study of various training methods. BJSM 38:766-772, 2004.
• Wise MB, et al. The effect of limb support on muscle activation during shoulder exercises. JSES 13:614-620, 2004
• Krabak BJ, et al. Practical nonoperative management of rotator cuff injuries. CJSM 13:102-105, 2003.
• Burkhart SS, et al. The disabled throwing shoulder: spectrum of pathology part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 19:641-661, 2003.
• McMullen J, Uhl TL. A kinetic chain approach for shoulder rehabilitation. JAT 35:329-337, 2000.
• Jonsson P, et al. Eccentric training in chronic painful impingement syndrome of the shoulder: results of a pilot study. KSSTA 2006;14:76-81.
• Smith J, et al. Electromyographic activity in the immobilized shoulder girdle musculature during scapulothoracic exercises. APMR 2006;87:923-927.
References

• Bak K, Fauno P. Clinical findings in competitive swimmerss with shoulder pain. AJSM 1997;25(2):254-260.
• Gross ML, et al. Anterior shoulder instability in weight lifters. AJSM 1993;21(4):599-603.
• Scavenius M, Iversen BF. Nontraumatic clavicular osteolysis in weight lifters. AJSM 1992;20(4):463-467.
• Ronai P. Exercise modifications and strategies to enhance shoulder function. Strength and Conditioning Journal 2005;27(4):36-45.
• Sauers EL. Effectiveness of rehabilitation for patients with subacromial impingement syndrome. JAT 2005;40(3):221-223.
• Buss DD, et al. Nonoperative management for in-season athletes with anterior shoulder instability. AJSM 2004;32(6):1430-33.
• Kibler WB. The role of the scapula in athletic shoulder function. AJSM 1998;26(2):325-336.
References
• Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part II: evaluation and treatment of SLAP lesions in throwers. Arthroscopy. 2003;19(5):531-539.
• Fees M, et al. Upper extremity weight-training modifications for the injured athlete. A clinical perspective. AJSM 1998;26(5):732-742.
• Placzek JD, et al. Shoulder outcome measures. A comparison of 6 functional tests. AJSM 2004;32(5):1270-1277.
• Reinold MM, et al. Electromyographic analysis of the rotator cuff and deltoid musculature during common shoulder external rotation exercises. JOSPT 2004;34:385-94.
• Cools AM, et al. Rehabilitation of scapular muscle balance. Which exercises to prescribe. AJSM 2007;35(10):1744-51.
• Kibler WB, et al. Evaluation of apparent and absolute supraspinatus strength in patients with shoulder injury using the scapular retraction test. ASJM 2006;34:1643-1647.
References






![“Ekomo’s Interventions” [María Nsue Angüe]](https://static.fdokumen.com/doc/165x107/632104d980403fa2920c8b06/ekomos-interventions-maria-nsue-anguee.jpg)