
See-saw nystagmus and congenital nystagmus identified in the decussating retinal-fugal fiber...
22
Retinal-fugal fiber syndrome 143 Correspondence and reprint requests to: Patricia Apkarian Dept. Neurol. & Clin. Neurophysiol. Acad. Med. Ctr. Univ. Amsterdam Meibergdreef 9 1105 AZ Amsterdam The Netherlands Abstract purpose The purpose of the present study was to accurately docu- ment the oculomotor misalignments and instabilities associated with the non-decussating retinal-fugal fiber syndrome, a rare inborn, iso- lated, achiasmatic condition. 1–3 To date, the achiasmatic syndrome described has thus far been identified in three unrelated females. 1–4 A comparable achiasmatic condition has also been identified in a canine breed. 5,6 materials and methods The unique, inborn visual pathway mal- formation in the form of an isolated absence of the optic chiasm was confirmed by metabolic assay, the visual evoked potential (VEP) mis- routing paradigm and neuroradiological evaluation, including magnetic resonance imaging (MRI). 3,7–9 Horizontal and vertical, left and right eye, oculomotor scleral search coil recordings were measured, in one of the achiasmats, at 15 years of age. Comparable oculomotor record- ings were implemented in three controls, including a normal age- matched control, an adult control and an adult with idiopathic congenital nystagmus (CN). In addition to central and eccentric target fixation with binocular and monocular viewing, binocular and mono- cular pursuit and optokinetic nystagmus (OKN) also were recorded. results Following a binocular and monocular fixation paradigm, classic congenital nystagmus (CN) profiles were recorded in the achiasmat in the horizontal planes together with see-saw nystagmus (SSN) in the vertical planes; an alternating esotropia and vertical tropias also were documented. The CN showed interocular conjugacy and waveforms typically exhibited well-defined foveation periods. In general, both achiasmatic horizontal and vertical eye movements as well as corresponding interocular misalignments varied with stimu- lus and recording conditions. Moreover, horizontal eye movements Strabismus 0927-3972/01/$ 16.00 Strabismus – 2001, Vol. 9, No. 3, pp. 143–163 © Swets & Zeitlinger 2001 Accepted 9 May 2001 See-saw nystagmus and congenital nystagmus identified in the non- decussating retinal-fugal fiber syndrome Patricia Apkarian Lo J. Bour Department of Neurology & Clinical Neurophysiology, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands Original paper
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of See-saw nystagmus and congenital nystagmus identified in the decussating retinal-fugal fiber...

Retinal-fugal fiber syndrome 143
Correspondence and reprint requests to:Patricia ApkarianDept. Neurol. & Clin.Neurophysiol.Acad. Med. Ctr.Univ. AmsterdamMeibergdreef 91105 AZ AmsterdamThe Netherlands
Abstractpurpose The purpose of the present study was to accurately docu-ment the oculomotor misalignments and instabilities associated withthe non-decussating retinal-fugal fiber syndrome, a rare inborn, iso-lated, achiasmatic condition.1–3 To date, the achiasmatic syndromedescribed has thus far been identified in three unrelated females.1–4 Acomparable achiasmatic condition has also been identified in a caninebreed.5,6
materials and methods The unique, inborn visual pathway mal-formation in the form of an isolated absence of the optic chiasm wasconfirmed by metabolic assay, the visual evoked potential (VEP) mis-routing paradigm and neuroradiological evaluation, including magneticresonance imaging (MRI).3,7–9 Horizontal and vertical, left and righteye, oculomotor scleral search coil recordings were measured, in oneof the achiasmats, at 15 years of age. Comparable oculomotor record-ings were implemented in three controls, including a normal age-matched control, an adult control and an adult with idiopathiccongenital nystagmus (CN). In addition to central and eccentric targetfixation with binocular and monocular viewing, binocular and mono-cular pursuit and optokinetic nystagmus (OKN) also were recorded.
results Following a binocular and monocular fixation paradigm,classic congenital nystagmus (CN) profiles were recorded in the achiasmat in the horizontal planes together with see-saw nystagmus(SSN) in the vertical planes; an alternating esotropia and verticaltropias also were documented. The CN showed interocular conjugacyand waveforms typically exhibited well-defined foveation periods. Ingeneral, both achiasmatic horizontal and vertical eye movements aswell as corresponding interocular misalignments varied with stimu-lus and recording conditions. Moreover, horizontal eye movements
Strabismus 0927-3972/01/$ 16.00
Strabismus – 2001, Vol. 9, No. 3,pp. 143–163© Swets & Zeitlinger 2001
Accepted 9 May 2001
See-saw nystagmus and congenitalnystagmus identified in the non-
decussating retinal-fugal fiber syndrome
Patricia ApkarianLo J. Bour
Department of Neurology & Clinical Neurophysiology, Academic Medical Center, University of Amsterdam,
Amsterdam, The Netherlands
Original paper

showed sustained interocular conjugacy while vertical eye movementstypically showed disconjugacy. Previous oculomotor studies in theachiasmatic canine breed revealed comparable oculomotor instabili-ties, albeit the latter were reported to present primarily with unyokedeye movements and uniocular saccades.10,11 In the present study, inaddition to target fixation with binocular and monocular viewing,binocular and monocular pursuit and OKN responses also wererecorded. For the achiasmat, high-gain pursuit results, as with eccentricfixation, emphasized a preference for fixation with the adducting eye.Also at eccentric gaze with monocular viewing, the eye under covershowed, relative to the fixating eye, a hypodeviation concomitant withadduction and a hyperdeviation concomitant with abduction. OKNprofiles in the achiasmat with stimuli presented under both normalviewing and open-loop, retinal-field locked conditions proved rathercomplex; however, when an OKN response was identified, reversedOKN tracking was not apparent.
conclusions In general, the oculomotor results reported hereindemonstrate that the non-decussating retinal-fugal fiber syndrome isan afferent visual pathway disorder associated with vertical and hori-zontal misalignments concurrent with congenital nystagmus and alsowith the rarer see-saw nystagmus.
Key words Achiasmats; optic chiasm; congenital malformation;optic pathway misrouting; oculomotor instability; interocular misalign-ment; fixation; see-saw nystagmus; congenital nystagmus; optokineticnystagmus; scleral search coil; smooth pursuit; saccades; visual evokedpotentials; non-decussating retinal-fugal fiber syndrome
Introduction The non-decussating retinal-fugal fiber syndrome isan inborn malformation of the visual pathways in the form of an absentoptic chiasm.1–3 The uniqueness of this anomalous afferent condition isreflected in the fact that the ‘missing’ optic chiasm is an isolated onto-genetic anomaly without detectable, accompanying innate or acquiredcerebral midline defects, malformations, and/or endocrinologicalanomalies.12–19 In humans, the isolated achiasmatic anomaly has beenverified by metabolic and immunological assay, by neurological evalu-ation and neuroradiologic brain imaging and by non-invasive electrophysiology.1–3
To date, the non-decussating retinal-fugal fiber syndrome has beenidentified in three unrelated females1–4 as well as in a canine breed ofblack Belgium sheep dogs.5,6 The latter proved to be a colony of caninemutants who also presented with apparent inborn oculomotor insta-bilities. Anatomic investigations by Williams et al.6,20 revealed, in amajority of the canine mutants, that the chiasmal structure was com-pletely eliminated and that the optic nerves maintained a separation of5–8mm upon entering the thalamic structure. Moreover, as is charac-teristic of achiasmatic humans, no other midline abnormalities wereevident in the achiasmatic canines. After controlled inbreeding of the Belgium sheep dogs across three and as many as six generations,Williams et al. suggest that the isolated achiasmatic mutation presents
144 P. Apkarian & L.J. Bour

with an autosomal recessive genotype.5,6,20 Further genealogicalresearch on the achiasmatic canine breed is in progress.21
Of particular interest in the present report is that for both humansand the canine species, the achiasmatic condition is associated withstriking oculomotor instabilities1–6,10,11 and, at least for the human achiasmats, also reduced visual acuity, interocular misalignment andthe absence of binocular function.22,23 Auxiliary visual function such ascolor vision, contrast sensitivity (within spatial acuity range), and tem-poral responsivity as tested in the human achiasmats remains intact.24
In terms of visual pathway development, organization and function, amajor consequence of the achiasmatic visual system is that retinal-fugalafferents from the nasal retinal and corresponding temporal visual fieldinput are precluded from decussating at the optic chiasm. As shownfrom the canine achiasmatic models,6,11,20 the remarkable crossingblockage of nasal retinal input and disrupted retinal-fugal projectionscreates an unusual substrate of LGN misalignments and subsequentlyalso rather unusual higher order visual pathway organization and function.
Distinctive in the present human achiasmatic cases is also the findingthat monocular visual fields are perfectly normal. Normal achiasmaticvisual field findings are in direct contradiction to previous publishedreports of either congenital or acquired pathological optic chiasm con-ditions; typically with anomalous involvement of the optic chiasm,there is an accompanying bitemporal hemianopsia.25–31
In an oculomotor study performed for clinical screening in one of theachiasmatic patients at the age of about 10 years,1,2 a three-channelrecording (left and right eye horizontal and right eye vertical) per-formed with a double magnetic induction method (DMI)32 revealedhorizontal, interocular conjugacy and congenital nystagmus waveformsin the horizontal planes and a pendular-like nystagmus in the singlevertical plane.With clinical verification of the isolated achiasmatic con-dition, and also the suggestion of accompanying horizontal and verti-cal oculomotor instabilities, the present study was undertaken with the scleral search coil technique33 to more accurately define, in both the horizontal and vertical planes, the achiasmatic oculomotor profile.Basically, the two-dimensional, four-channel recordings describedherein confirmed the presence of classic congenital nystagmus (CN) inthe horizontal planes together with pendular nystagmus and inter-ocular disconjugacy in the vertical planes. The latter appears to follow the profile of classic see-saw nystagmus (SSN) as originallydescribed by Maddox30 with elevation and intorsion of one eye andsimultaneous depression and extorsion of the fellow eye.A comparableoculomotor profile also has been confirmed in the two other humanachiasmats.1–4,34,35
Methods and materials
subjects Four subjects participated in the present study, including 1)a female achiasmat (AC1), tested at the age of 15 years, 2) the achias-mat’s unaffected fraternal twin sister (NR1), tested as an age-matchednormal control, 3) an adult male with hereditary congenital nystagmus
Retinal-fugal fiber syndrome 145
(CN1), and 4) an adult female with early-stage keratoconus (NR2); thelatter two subjects served as experimental controls. Subject participa-tion followed appropriate informed consent (including that of theguardians for AC1 and NR1). Test protocols and ethics committeeapproval were in accordance with the tenets of the Erasmus Univer-sity Medical Faculty, Amsterdam Medical Center and the Declarationof Helsinki.
The achiasmat (AC1) presented with corrected Snellen acuities at 6meters of 0.3 (20/60) OD, 0.2 (20/100) OS and 0.3 (20/60) ODS (bino-cular viewing). At 3 meters, binocular acuity slightly improved to 0.4 -(~20/50) and at a 20cm reading distance, binocular acuity reached 1(20/20). Refractive correction was S - 5.25 C - 1.5 axis 50° OD and S-6.75 OS. The fundus was lightly pigmented but was not evaluated as hypopigmented. Foveal and macular reflexes were present andnormal; papillae also were normal. Irides were blue but were notdiaphanous. Interocular alignment showed an alternating esotropia of20–25 prism diopters (10° to 12.5°) with a preference for right eye fix-ation. Torticollis and slight head shudder were present, intermittently;head tilt was towards the right shoulder. It is of particular interest tonote that static perimetry (Goldmann perimeter and Tübingen visualfield test) revealed normal visual fields;1–3,24 the blind spots for OD andOS were readily identified and plotted. Color vision (Ishihara plates)was also normal; stereopsis (Titmus, TNO and Julesz stereograms) wasabsent.
The fraternal twin control (NR1) presented with corrected Snellenacuities at 6 meters of 1 (20/20) OD, OS and ODS. Refractive correc-tion was S - 2.25 C - 0.5 axis 90° OD and S - 2.25, C - 0.5 axis 70° OS.The congenital nystagmus control (CN1) presented with correctedSnellen acuity at 3 meters of 0.5 (20/40) ODS. Refractive correctionwas S + 1.5 C - 2.5 axis 150° OD and S + 2 C - 2.75 axis 20° OS. Theadult control with early-stage keratoconus presented with correctedSnellen acuity at 3 meters of 1 (20/20) ODS. Refractive correction wasS + 1.50 C - 5 axis 60° OD and S - 0.5 C - 2.25 axis 90° OS. For allthree controls, visual fields, color vision and stereopsis were normal.Allfour subjects were tested with optimum optical correction.
stimulus For static target fixation, the stimulus consisted of redLED targets (radius = 0.09°, mean luminance ª 0.4cd/m2) fixed to a horizontal bar placed at distance of 130cm. The LED targets, posi-tioned at straight ahead (0°) and along the horizontal meridian to theleft and right of straight ahead (0°) at 10 eccentric loci from -25° to+25° in 5° intervals, subtended 0.18° in diameter and presented with amean luminance of about 0.4cd/m2. For smooth pursuit, a laser beamwas back projected via two servo-controlled mirrors onto a translucenttangent screen positioned at a test distance of 130cm and subtendinga visual angle of 85.4° in width and 69.4° in height. The laser stimulus(also a red spot subtending about 0.18° in diameter) was swept withconstant velocity (ramp profile) left and right from -25° to +25°through primary position at a rate of 8.3°/sec; duration of pursuit testepochs was 30 seconds. For the OKN paradigm, film templates placedaround a motor driven cylinder were projected by a central lamp onto
146 P. Apkarian & L.J. Bour

a translucent screen. The OKN stimulus field (85.4° ¥ 69.4°) consistedof high-contrast gratings subtending 2.2 cycles per degree and pre-sented with leftward or rightward drift at a rate of 10°/sec. Duration ofthe OKN test epochs also was 30 seconds.
eye movement recording method Horizontal and vertical rightand left eye movements were measured using scleral search coils in an AC magnetic field.33,36 The AC magnetic field with a frequency of 45kHz was generated by a coil system extending 2 ¥ 2 meters. An eyemovement monitor (Remmel Labs, Ashland, MA, USA) was used todrive the field coils and also to detect eye position. After the signaldetection stage, raw eye position data were low-pass filtered (-3dB at125Hz), and digitized with 12-bit precision at a sample rate of 250Hzvia an external data-acquisition system interfaced to a PC. The overallnoise level was less than 1min arc.
eye movement recording calibration Prior to in vivo recording,the scleral search coils, for in vitro calibration, were mounted onto aplexiglass gimbal system directed to a stimulus array of LEDs posi-tioned at zero degrees (i.e., straight ahead) and at various eccentrici-ties (±5, 10, 15, 20 and 25 degrees) across horizontal and verticalmeridians. In an off-line procedure, coil gains were obtained by sub-traction of raw signals of symmetrically positioned targets with respectto the reference target positioned at zero degrees. As coil offsets wereequal to the raw coil signals when directed to the reference target,measurements with the gimbal system obtained from the LED targetpositions across the horizontal and vertical meridians were used tocheck the accuracy of the calibrated signals. Erroneous magnetic pick-up from the search coil wires was minimized by directing the coils tothe reference position and also by on-line monitoring of all relatedoutput signals. Raw eye position signals were converted to Fick coor-dinates in degrees.36 Following Fick conversion, in vivo offsets due toslight inaccuracies from placement of the coil onto the sclera also weredetected and defined with an off-line interactive computer program(developed in-house) in which foveation periods and/or fixationperiods to the reference target (straight ahead) were successivelymarked and stored. For recorded oculomotor instabilities, foveationperiods were interactively computer marked with a first-stage criterionof a horizontal velocity of less than 4°/sec. In general, identification offoveation periods followed previously established definitions and pro-tocols.37–40 The average horizontal and corresponding vertical positionof all marked foveation periods were calculated. Subsequently, asecond-stage foveation filtering was implemented. For the latter, thefirst-stage cumulative foveation periods were filtered with additionalvertical position and velocity criteria. That is, the vertical position wasrequired to fall within ±30min/arc seconds of the fixation target; the4°/sec velocity criteria also was applied. Following the secondaryfoveation filtering procedure, the mean and standard deviation of thefinal selections of foveation periods were calculated; the final mean wasused as the horizontal and vertical in vivo offset and subsequently sub-tracted from the calibrated Fick angles.
Retinal-fugal fiber syndrome 147

eye movement recording protocol Subjects were positionedwithin the coil system such that the midsagittal plane of the body wasin the plane of the forward and vertical magnetic fields. To reduce headmovement artifacts and instabilities, patients/subjects were tested withforehead support, a bite bar with custom-molded dental impression andarm support. Both binocular and monocular testing were implementedfor the fixation, pursuit and OKN paradigms; monocular testing pro-ceeded with total occlusion of the fellow eye. During test trials, sub-jects were requested to minimize blinking. Testing took place primarilyin darkness with ambient room light (from computer monitors, variouslaboratory apparatus) minimized.
For the fixation paradigm, subjects were presented with a preview ofthe target position per trial. At the start of each trial, subjects wereinstructed to fixate the central target at primary position for one secondand then, upon auditory cueing (a tone), were requested to fixate aneccentric stimulus target for approximately 12 seconds. For subjectCN1, the fixation paradigm was somewhat modified such that targetfixation was of 3-second duration epochs with alternation betweenprimary position and eccentric target position within a given trial. Forall subjects, each fixation trial, which lasted a total of 15 sec, ended bya return to primary position. For the pursuit paradigm, tracking trialswere 60 sec each and subjects were requested to track the target to thebest of their ability. For the OKN paradigm subjects were requested togaze, with full attention, at the moving stripes but to avoid pursuing asingle stripe.
Eye movements also were measured during complete darknesswithout stimulus targets and during darkness while the subject imag-ined a stationary target. Lastly, a convergence paradigm was includedin which the subject fixated a pen-light tip as it was moved (by theexperimenter) from about a 100cm distance to within about 5cm of thebridge of the subject’s nose. Subjects AC1 and NR1 participated in twotest sessions over a three-day period; adult control CN1 participated inone session and adult control NR2 participated in multiple pilotstudies.
Results
binocular and monocular fixation In the horizontal planes, theeye movement recordings of the achiasmat demonstrated classic con-genital nystagmus.37–40 The presence of an alternating esotropia alsowas quantified. In the vertical planes, primarily a pendular nystagmuswas recorded. The latter, in contrast to the interocular conjugacyrecorded in the horizontal planes, showed striking interocular discon-jugacy. Although torsion was not measured in the present study, directobservation of the scleral vasculature indicated that the oculomotorprofile in the vertical and torsional planes followed that of classic see-saw nystagmus with intorsion and elevation of one eye and simultane-ous extorsion and depression of the fellow eye.3,30,39–47
An overview of the basic horizontal and vertical instabilities charac-teristic of the isolated achiasmatic condition during binocular viewingof a fixation target positioned at straight ahead (0°) is depicted in
148 P. Apkarian & L.J. Bour
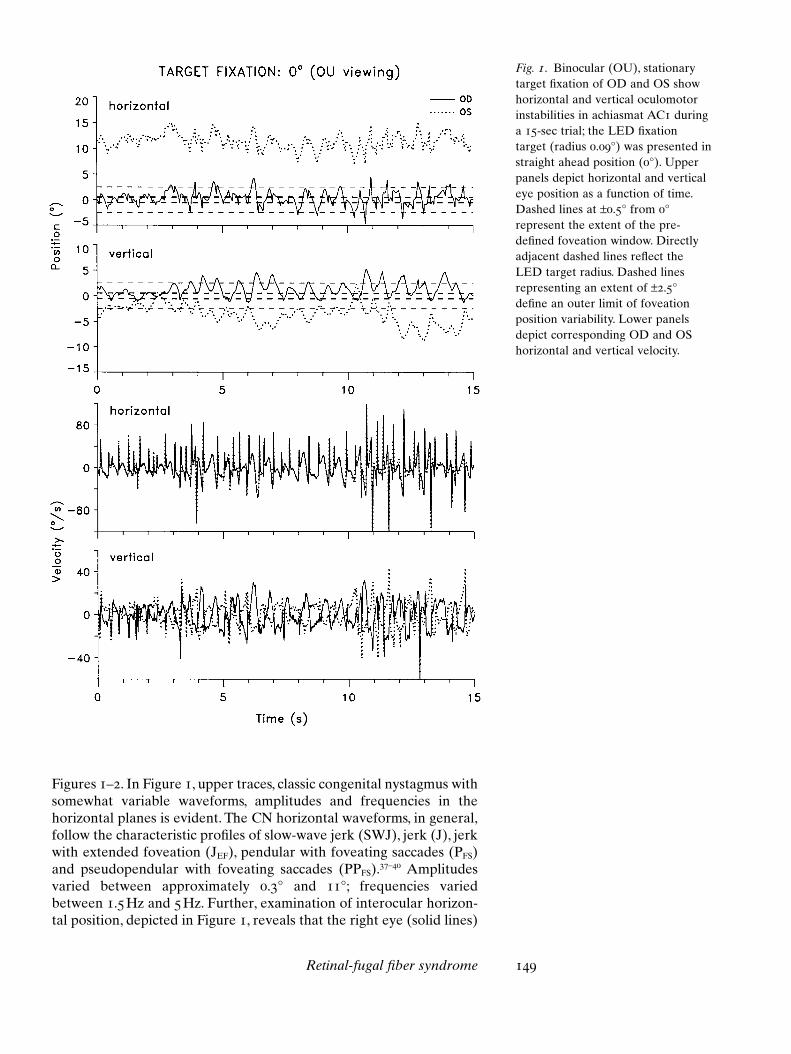
Fig. 1. Binocular (OU), stationarytarget fixation of OD and OS showhorizontal and vertical oculomotorinstabilities in achiasmat AC1 duringa 15-sec trial; the LED fixationtarget (radius 0.09°) was presented instraight ahead position (0°). Upperpanels depict horizontal and verticaleye position as a function of time.Dashed lines at ±0.5° from 0°represent the extent of the pre-defined foveation window. Directlyadjacent dashed lines reflect theLED target radius. Dashed linesrepresenting an extent of ±2.5°define an outer limit of foveationposition variability. Lower panelsdepict corresponding OD and OShorizontal and vertical velocity.
Figures 1–2. In Figure 1, upper traces, classic congenital nystagmus withsomewhat variable waveforms, amplitudes and frequencies in the horizontal planes is evident. The CN horizontal waveforms, in general,follow the characteristic profiles of slow-wave jerk (SWJ), jerk (J), jerkwith extended foveation (JEF), pendular with foveating saccades (PFS)and pseudopendular with foveating saccades (PPFS).37–40 Amplitudesvaried between approximately 0.3° and 11°; frequencies variedbetween 1.5Hz and 5Hz. Further, examination of interocular horizon-tal position, depicted in Figure 1, reveals that the right eye (solid lines)
Retinal-fugal fiber syndrome 149
typically fixates the target with foveation periods that lie primarilywithin a pre-defined fixation window extending ±0.5°; outer limits ofthe fixation window of ±2.5° also are denoted. During right-eye fixa-tion, the left-eye horizontal position shows a marked variable esotropiafrom about 10° to 15°. During right-eye fixation to the straight aheadLED target, vertical left-eye position shows a variable hypotropia ofmaximally 8°. The 10–12 second time interval of Figure 1 has beendefined and graphically shown in more detail in the left-hand columnof Figure 2. Corresponding phase-plane plots depicted in the rightcolumn of Figure 2 clearly illustrate that within the time epoch of about200ms in the horizontal plane, a leftward foveation saccade (see #1) isinitiated, returning the fovea of the fixating, right eye to the LEDtarget. Subsequently, a foveation period (see #2) with zero horizontaland approximately zero vertical eye velocity is evident when eye posi-tion is on (horizontal plane) or near (vertical plane) target. In general,horizontal position, velocity traces and the phase planes of Figures 1–2emphasize interocular horizontal conjugacy as well as less than 4°/secvelocity during foveations.
The interocular conjugacy in the horizontal planes depicted inFigures 1–2 gives way to a remarkable interocular disconjugacy in thevertical planes. The waveform of the vertical instabilities is primarilypendular; the slow-velocity components are clearly disjunctive, whereasfast-phase components of the vertical eye movements are generallyconjugate. In general, vertical instability amplitudes of the fixating eyereach a maximum of about 7° but, none the less, are smaller than thoseof the non-fixating eye. Vertical frequencies vary between 1Hz and 2Hz depending on viewing condition. Vertical velocity of the fixatingright eye, as with horizontal velocity, remains within ±4°/sec limit duringfoveation epochs; the corresponding vertical position also localizeswithin a narrow window. As vertical pendular velocities smaller than4°/sec were invariably associated with foveation periods, the verticalsee-saw nystagmus was phase-locked to the horizontal CN.
In general, the oculomotor profiles of Figures 1–2 reflect classic CNin the horizontal planes and see-saw nystagmus (SSN) in the verticalplanes. There are also, as briefly outlined, accompanying vertical andhorizontal interocular misalignments. Figure 3 emphasizes that the ocu-lomotor instabilities described as well as the interocular eye positionvary dramatically with gaze angle and viewing conditions. Typically, inthe achiasmatic patient, single binocular fixation is not observed;rather, fixation is effected via the preferred right eye. However, theupper left panels of Figure 3 show that after about 10 seconds of fixating a target in primary position with the right eye, suddenly, fol-lowing a saccade, fixation switches to the left eye. With initial right-eyefixation, the nystagmus recorded in Figure 4, in both horizontal and ver-tical planes, appears somewhat damped. Corresponding velocity tracesalso clearly show the presence of interocular conjugacy in the verticalplane. However, when fixation switches to the left eye, the pattern ofCN in the horizontal planes and SSN in the vertical planes reappears.The corresponding scan path depicted in the upper right panel ofFigure 3 emphasizes horizontal and vertical eye position across the 15-sec epoch; inspection of the switch from right- to left-eye fixation is
150 P. Apkarian & L.J. Bour

Retinal-fugal fiber syndrome 151
Fig. 2. Zoom-in of OD and OS horizontal and vertical position (left upper panels) and corresponding velocity (left lower panels)across the 10–12 second recording epoch derived from the corresponding time window of Figure 1. Foveation periods depicted(see, e.g., the foveation period numerically labeled with 1 and 2) follow the waveform of bidirectional jerk with extendedfoveation (Jef). Corresponding horizontal and vertical phase planes across the numerically labeled foveation period are plottedat the right upper and lower panels, respectively. In the horizontal phase plane, the esotropic left eye falls outside the horizon-tal position window of ±5°. Horizontal dashed lines depicted in the phase planes indicate a ±4°/sec, pre-defined velocity limitfor foveation; vertical dashed lines indicate a ±0.5°, pre-defined position limit for foveation with adjacent lines defining the LEDtarget radius. Note that the phase planes demonstrate zero velocity during foveation periods (label 2) in both horizontal andvertical planes.
further facilitated by the 5-sec epoch insert. Note for right-eye fixationthat the left eye is esotropic and variably hypotropic. The right lowerpanel of Figure 3 also clearly demonstrates horizontal conjugacy; notethe positive, one-to-one linear relationship between the positions of the
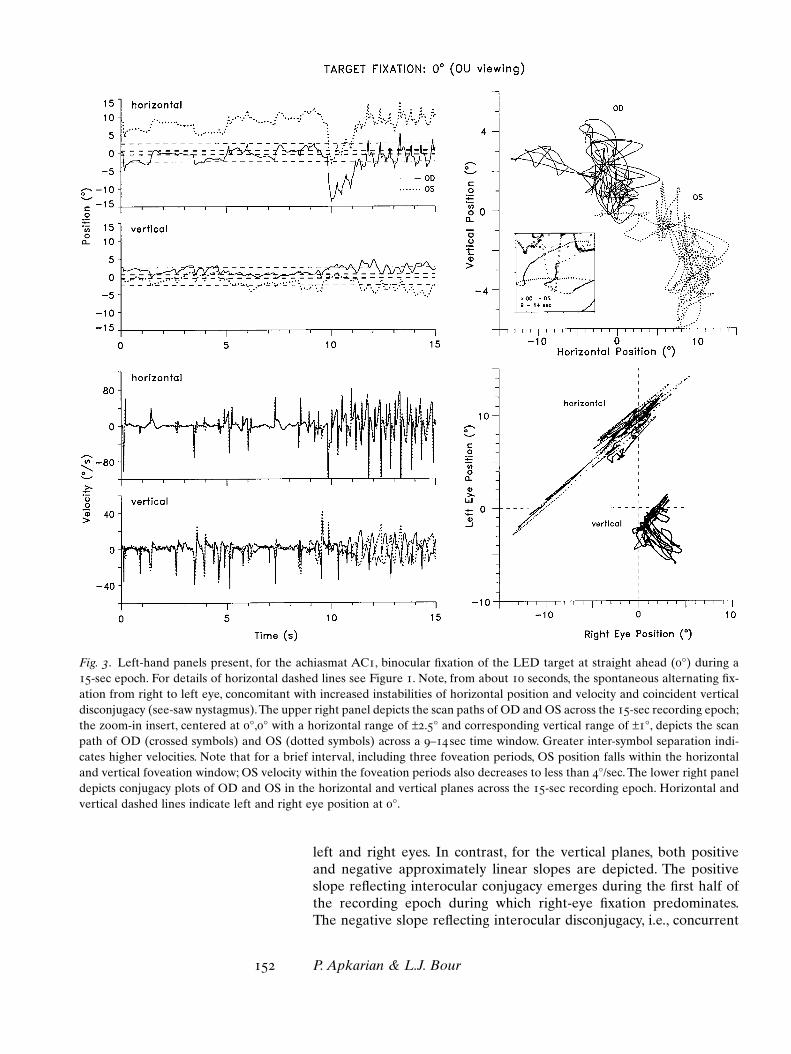
left and right eyes. In contrast, for the vertical planes, both positive and negative approximately linear slopes are depicted. The positiveslope reflecting interocular conjugacy emerges during the first half ofthe recording epoch during which right-eye fixation predominates.The negative slope reflecting interocular disconjugacy, i.e., concurrent
152 P. Apkarian & L.J. Bour
Fig. 3. Left-hand panels present, for the achiasmat AC1, binocular fixation of the LED target at straight ahead (0°) during a15-sec epoch. For details of horizontal dashed lines see Figure 1. Note, from about 10 seconds, the spontaneous alternating fix-ation from right to left eye, concomitant with increased instabilities of horizontal position and velocity and coincident verticaldisconjugacy (see-saw nystagmus).The upper right panel depicts the scan paths of OD and OS across the 15-sec recording epoch;the zoom-in insert, centered at 0°,0° with a horizontal range of ±2.5° and corresponding vertical range of ±1°, depicts the scanpath of OD (crossed symbols) and OS (dotted symbols) across a 9–14 sec time window. Greater inter-symbol separation indi-cates higher velocities. Note that for a brief interval, including three foveation periods, OS position falls within the horizontaland vertical foveation window; OS velocity within the foveation periods also decreases to less than 4°/sec. The lower right paneldepicts conjugacy plots of OD and OS in the horizontal and vertical planes across the 15-sec recording epoch. Horizontal andvertical dashed lines indicate left and right eye position at 0°.
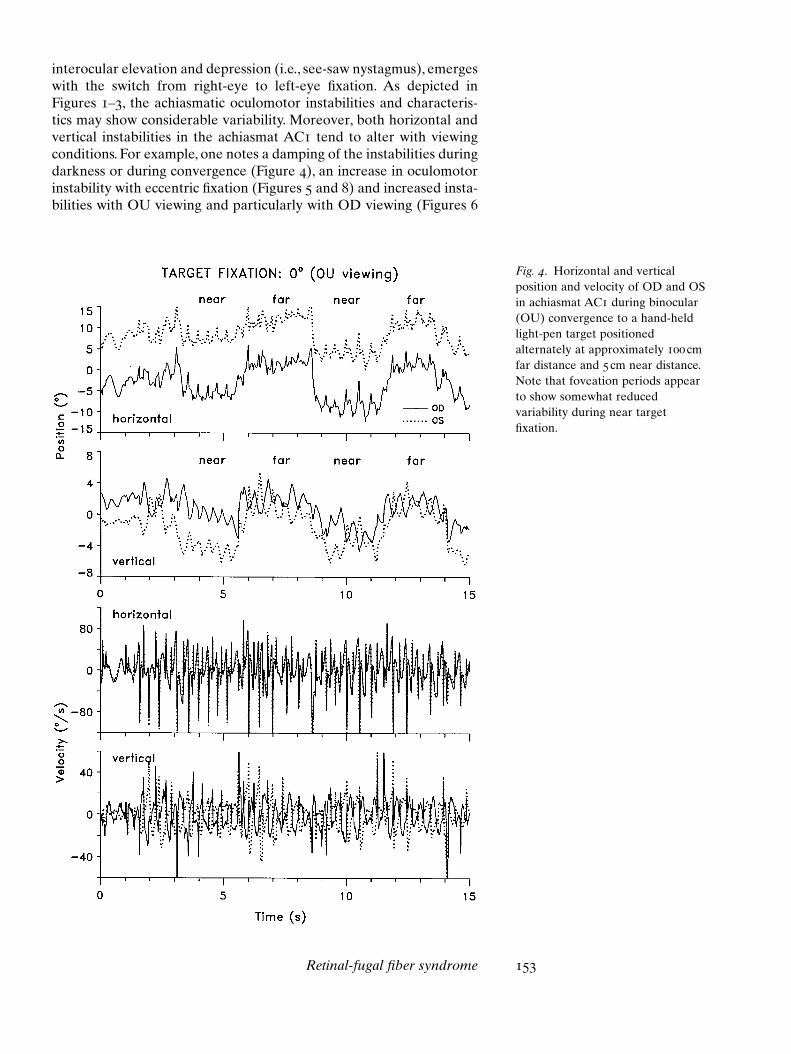
Fig. 4. Horizontal and verticalposition and velocity of OD and OSin achiasmat AC1 during binocular(OU) convergence to a hand-heldlight-pen target positionedalternately at approximately 100 cmfar distance and 5 cm near distance.Note that foveation periods appearto show somewhat reducedvariability during near targetfixation.
interocular elevation and depression (i.e., see-saw nystagmus), emergeswith the switch from right-eye to left-eye fixation. As depicted inFigures 1–3, the achiasmatic oculomotor instabilities and characteris-tics may show considerable variability. Moreover, both horizontal andvertical instabilities in the achiasmat AC1 tend to alter with viewingconditions. For example, one notes a damping of the instabilities duringdarkness or during convergence (Figure 4), an increase in oculomotorinstability with eccentric fixation (Figures 5 and 8) and increased insta-bilities with OU viewing and particularly with OD viewing (Figures 6
Retinal-fugal fiber syndrome 153
and 8). Regarding convergence, Figure 4 depicts a 15-second recordingepoch in which fixation alternates between near and far viewing con-ditions. Note, in the horizontal planes, the improvement in foveationperiods and reduced average velocity, particularly in the vertical planes,during convergence. Damping of the SSN also is evident during convergence.
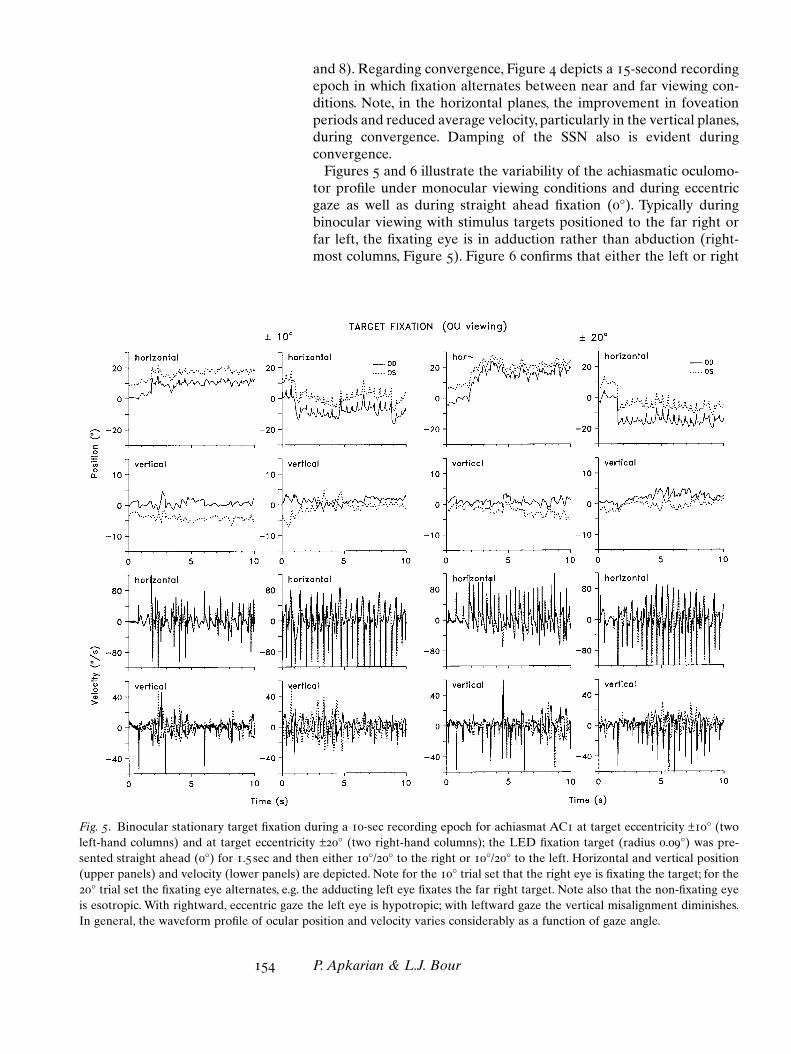
Figures 5 and 6 illustrate the variability of the achiasmatic oculomo-tor profile under monocular viewing conditions and during eccentricgaze as well as during straight ahead fixation (0°). Typically duringbinocular viewing with stimulus targets positioned to the far right orfar left, the fixating eye is in adduction rather than abduction (right-most columns, Figure 5). Figure 6 confirms that either the left or right
154 P. Apkarian & L.J. Bour
Fig. 5. Binocular stationary target fixation during a 10-sec recording epoch for achiasmat AC1 at target eccentricity ±10° (twoleft-hand columns) and at target eccentricity ±20° (two right-hand columns); the LED fixation target (radius 0.09°) was pre-sented straight ahead (0°) for 1.5 sec and then either 10°/20° to the right or 10°/20° to the left. Horizontal and vertical position(upper panels) and velocity (lower panels) are depicted. Note for the 10° trial set that the right eye is fixating the target; for the20° trial set the fixating eye alternates, e.g. the adducting left eye fixates the far right target. Note also that the non-fixating eyeis esotropic. With rightward, eccentric gaze the left eye is hypotropic; with leftward gaze the vertical misalignment diminishes.In general, the waveform profile of ocular position and velocity varies considerably as a function of gaze angle.
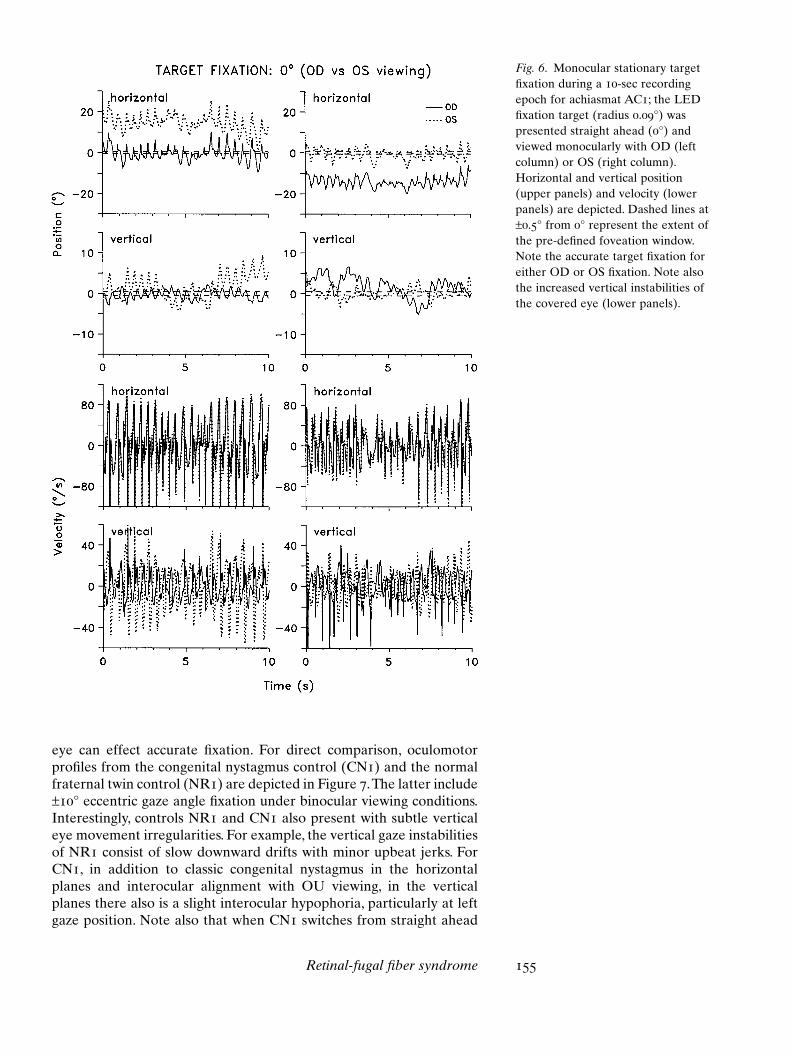
Fig. 6. Monocular stationary targetfixation during a 10-sec recordingepoch for achiasmat AC1; the LEDfixation target (radius 0.09°) waspresented straight ahead (0°) andviewed monocularly with OD (leftcolumn) or OS (right column).Horizontal and vertical position(upper panels) and velocity (lowerpanels) are depicted. Dashed lines at±0.5° from 0° represent the extent ofthe pre-defined foveation window.Note the accurate target fixation foreither OD or OS fixation. Note alsothe increased vertical instabilities ofthe covered eye (lower panels).
eye can effect accurate fixation. For direct comparison, oculomotorprofiles from the congenital nystagmus control (CN1) and the normalfraternal twin control (NR1) are depicted in Figure 7.The latter include±10° eccentric gaze angle fixation under binocular viewing conditions.Interestingly, controls NR1 and CN1 also present with subtle verticaleye movement irregularities. For example, the vertical gaze instabilitiesof NR1 consist of slow downward drifts with minor upbeat jerks. ForCN1, in addition to classic congenital nystagmus in the horizontalplanes and interocular alignment with OU viewing, in the verticalplanes there also is a slight interocular hypophoria, particularly at leftgaze position. Note also that when CN1 switches from straight ahead
Retinal-fugal fiber syndrome 155

Fig. 7. Binocular, eccentric (±10°),stationary target fixation during a 10-sec recording epoch for nystagmuscontrol CN1 (left two columns) andnormal control NR1 (right twocolumns); the LED fixation target(radius 0.09°) was presented straightahead (0°), 10° to the right (1st and3rd columns) or 10° to the left (2nd
and 4th columns). Horizontal andvertical position (upper panels) andvelocity (lower panels) also aredepicted. Note that the CN controlpresents with a slight vertical phoria(OD over OS) which is more evidentduring fixation from straight aheadto left eccentric gaze position. Notealso that the normal control, NR1,presents with a micro-upbeatnystagmus as evinced in the verticalvelocity functions.
target fixation to eccentric fixation, concurrent saccades show a slightvertical component.
Figure 8 illustrates cumulative scan paths of horizontal tracking totargets of varying eccentricities for the achiasmat, ACI; the scan pathsreveal extreme oculomotor instabilities in both horizontal and verticalplanes. Note also that during OU viewing (Figure 8, upper row) as wellas during OD viewing (Figure 8, center row), vertical instabilities aremore intense for OS than for OD. Note that the latter, OD, is the preferred eye for fixation. From the tilt of the cumulative scan path forOS with either OU or OD viewing (Figure 8, left columns), it can beobserved that with rightward gaze, the non-fixating left eye showshypodeviation during right-eye adduction and hyperdeviation duringright-eye abduction. With OS viewing, note the tilt of the right eye(Figure 8, lower panel, center column). Herein, the non-fixating righteye shows a hyperdeviation during left-eye adduction and a hypo-deviation during left-eye abduction Esotropia also is readily apparentfrom both the binocular and monocular cumulative scan paths (Figure8). Monocular viewing, particularly for the eye under cover, showsincreased vertical instability compared to binocular viewing (centerrow, Figure 8). Comparison of OU, OD and OS viewing as depicted in
156 P. Apkarian & L.J. Bour

Fig. 8. Cumulative OS and OD scanpaths for achiasmat AC1, derivedfrom fixation trials during binocularand monocular viewing. Scan pathswere derived across fixation trials atvarious gaze angles along thehorizontal meridian. Rightmostpanels represent the mean andstandard deviation of horizontal andvertical peak-to-peak nystagmusamplitude measured for each fixationtrial. Note, during OU viewing, apreference to fixate eccentric targetswith the adducting eye. Note, underOD or OS, increased vertical andhorizontal instabilities as well asincreased horizontal and verticalmisalignments, particularly for thecovered eye. Note also, particularlyduring OD viewing (center row),that the amplitude of OS verticalinstabilities increases significantlycompared to OD.
Figure 8 further demonstrates that vertical instabilities are greatest forOS during OD viewing.
smooth pursuit and okn As depicted in Figure 9 and in accor-dance with previous studies,48–52 under either binocular or monocularviewing, the smooth pursuit responses of achiasmat AC1 clearly showsuperimposition of the ongoing CN upon the smooth tracking com-ponent. Eye position during foveation periods is approximately ontarget and the corresponding average horizontal eye position followsthe continuous displacement of the target, which moved in a horizon-tal trajectory (±25°) at a rate of 8.3°/sec. In general, for either binocu-lar or monocular viewing, gain of the smooth pursuit performance,evaluated when CN and SSN velocities approximated zero, was high(approximating 1); reversed smooth pursuit was not observed. Undervariable viewing conditions and during tracking, a directional asym-metry was noted; that is, when the target was tracked from right to left,concomitant oculomotor instabilities appeared to damp. Also as illus-trated in Figure 9, under binocular viewing conditions, achiasmat AC1switched the fixating eye when the direction of target movement wasreversed. Preferentially, the eye in adduction pursued the target. Thus,target direction rightward was tracked with OD while target direction
Retinal-fugal fiber syndrome 157
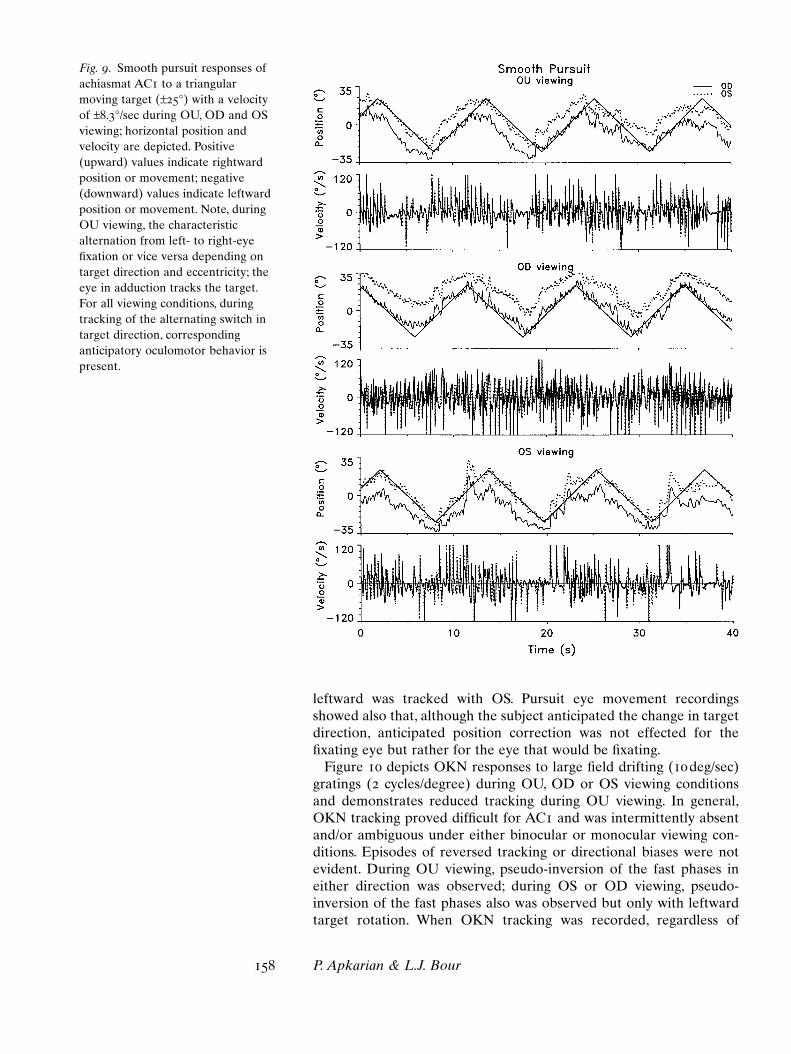
Fig. 9. Smooth pursuit responses ofachiasmat AC1 to a triangularmoving target (±25°) with a velocityof ±8.3°/sec during OU, OD and OSviewing; horizontal position andvelocity are depicted. Positive(upward) values indicate rightwardposition or movement; negative(downward) values indicate leftwardposition or movement. Note, duringOU viewing, the characteristicalternation from left- to right-eyefixation or vice versa depending ontarget direction and eccentricity; theeye in adduction tracks the target.For all viewing conditions, duringtracking of the alternating switch intarget direction, correspondinganticipatory oculomotor behavior ispresent.
leftward was tracked with OS. Pursuit eye movement recordingsshowed also that, although the subject anticipated the change in targetdirection, anticipated position correction was not effected for the fixating eye but rather for the eye that would be fixating.
Figure 10 depicts OKN responses to large field drifting (10deg/sec)gratings (2 cycles/degree) during OU, OD or OS viewing conditionsand demonstrates reduced tracking during OU viewing. In general,OKN tracking proved difficult for AC1 and was intermittently absentand/or ambiguous under either binocular or monocular viewing con-ditions. Episodes of reversed tracking or directional biases were notevident. During OU viewing, pseudo-inversion of the fast phases ineither direction was observed; during OS or OD viewing, pseudo-inversion of the fast phases also was observed but only with leftwardtarget rotation. When OKN tracking was recorded, regardless of
158 P. Apkarian & L.J. Bour
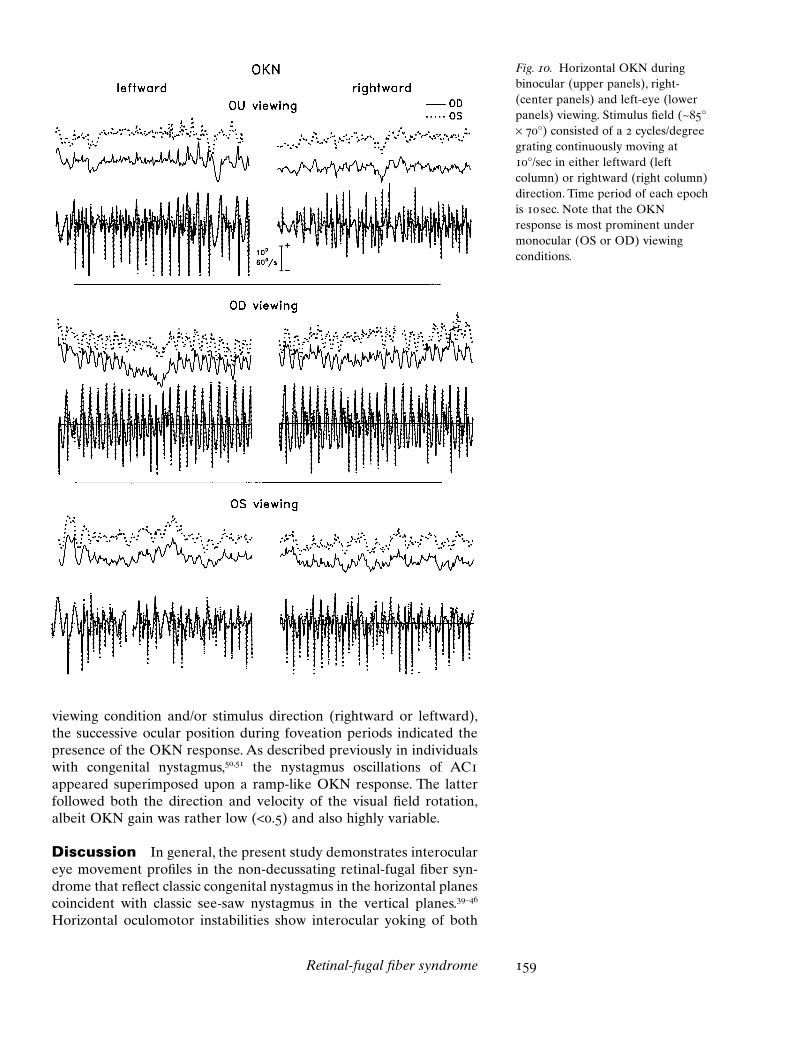
Fig. 10. Horizontal OKN duringbinocular (upper panels), right-(center panels) and left-eye (lowerpanels) viewing. Stimulus field (~85°¥ 70°) consisted of a 2 cycles/degreegrating continuously moving at10°/sec in either leftward (leftcolumn) or rightward (right column)direction. Time period of each epochis 10 sec. Note that the OKNresponse is most prominent undermonocular (OS or OD) viewingconditions.
viewing condition and/or stimulus direction (rightward or leftward),the successive ocular position during foveation periods indicated thepresence of the OKN response. As described previously in individualswith congenital nystagmus,50,51 the nystagmus oscillations of AC1appeared superimposed upon a ramp-like OKN response. The latterfollowed both the direction and velocity of the visual field rotation,albeit OKN gain was rather low (<0.5) and also highly variable.
Discussion In general, the present study demonstrates interoculareye movement profiles in the non-decussating retinal-fugal fiber syn-drome that reflect classic congenital nystagmus in the horizontal planescoincident with classic see-saw nystagmus in the vertical planes.39–46
Horizontal oculomotor instabilities show interocular yoking of both
Retinal-fugal fiber syndrome 159

References1 Apkarian P, Barth PG, Wenniger-
Prick L, Bour L. Non-decussatingretinal fugal fibre syndrome: VEPdetection of a visual system anomalyassociated with visual loss,
nystagmus and aberrant opticchiasm. Invest Ophthalmol Vis Sci.(suppl) 1993;34:711.
2 Apkarian P, Bour L, Barth PG. Aunique achiasmatic anomalydetected in non-albinos with
160 P. Apkarian & L.J. Bour
fast and slow phases while vertical instabilities show yoking of pri-marily only the fast phases. In addition to multiplanar oculomotorinstabilities, the isolated achiasmatic condition also demonstrates con-comitant vertical and horizontal interocular misalignments.1–4,10,11,34,35
The achiasmatic eye movement profiles of oculomotor instabilitiesshow that during fixation attempts, periods of zero or near zero veloc-ity in the horizontal planes coincide with zero (near zero) velocityperiods in the vertical planes. Consequently, horizontal and verticalinstabilities appear, at least to some degree, to perform in a function-ally coupled manner, albeit with considerable variability. The achias-matic oculomotor (mis)alignments as well as amplitude and frequencyinstabilities also are dependent upon viewing parameters, includinggaze position, convergence and binocular versus monocular fixation.
While see-saw nystagmus is an uncommon and/or rarely documentedcondition, the simultaneous occurrence of both congenital nystagmusand congenital see-saw nystagmus is most unusual,41,52–54 although casesof albinos with congenital nystagmus and concomitant ‘micro’ see-sawnystagmus have been reported.34 While oculomotor instabilities andparticularly see-saw nystagmus have been observed in various midlinedisorders,42 the association between conjugate horizontal eye move-ment instabilities and disconjugate vertical (and torsional) instabilitiesremains poorly understood. Further, whereas horizontal oculomotorinstabilities and misalignments occur with high incidence in conditionsof optic pathway misrouting associated with albinism, a visual pathwaymisrouting condition nearly opposite to that of the achiasmats, therobust CN and SSN reported herein as well as in two additional unre-lated achiasmatic patients,1–4 appears unique to the isolated achiasmaticcondition. Indeed, a most perplexing finding in the isolated achiasmatic,i.e., in the non-decussating retinal-fugal fiber syndrome, is that despitethe absence of single binocular vision, conjugacy of horizontal (but notvertical) oculomotor instabilities is generally preserved. As alsoemphasized in the present achiasmatic oculomotor study, the relation-ship between afferent anomalies of the visual pathways, oculomotorinstabilities and concomitant oculomotor binocular coordination is acomplex issue requiring further investigation. Eye movement studiesthat characterize the achiasmatic see-saw nystagmus with greater pre-cision by torsional measurements as well as direct comparison withocular instabilities associated with chiasmal crossing defects in albinismare now in progress.35,47 Finally, although the etiology of various hori-zontal, vertical and torsional instabilities and corresponding inter-ocular interactions remains enigmatic, emerging studies concerningcongenital visual system miswiring and concomitant aberrant oculo-motor function promise to contribute toward a better understandingof optic pathway misrouting-related oculomotor irregularities.53–55

Retinal-fugal fiber syndrome 161
misrouted retinal-fugal projections.Eur J Neurosci. 1994;6:501–507.
3 Apkarian P, Bour LJ, Barth PG,Wenniger-Prick L, Verbeeten B Jr.Non-decussating retinal-fugal fibresyndrome. An inborn achiasmaticmalformation associated withvisuotopic misrouting, visual evokedpotential ipsilateral asymmetry andnystagmus. Brain. 1995;118:1195–1216.
4 Apkarian P, Bour LJ. ConcurrentDMI ocular motor and patternonset VEP measures in patients withmetabolic and/or chiasmal midlinedisorders. Invest Ophthalmol Vis Sci.(suppl) 2001;42:844.
5 Williams RW, Garraghty PE,Goldowitz D. A new visual systemmutation: achiasmatic dogs withcongenital nystagmus. Soc NeurosciAbstr. [suppl] 1991;17:187.
6 Williams RW, Hogan D, GarraghtyPE. Target recognition and visualmaps in the thalamus of achiasmaticdogs. Nature. 1994;367:637–639.
7 Apkarian P, Reits D, Spekreijse H,Van Dorp D. A decisiveelectrophysiological test for humanalbinism. Electroencephalogr ClinNeurophysiol. 1983;55:513–531.
8 Apkarian P, Reits D, Spekreijse H.Component specificity in albinoVEP asymmetry: maturation of thevisual pathway anomaly. Exp BrainRes. 1984;53:285–294.
9 Apkarian P, Tijssen R. Detectionand maturation of VEP albinoasymmetry: an overview and alongitudinal study from birth to 54weeks. Behav Brain Res. 1992;49:57–67.
10 Williams RW, Dell’Osso LF. Ocularmotor abnormalities in achiasmaticmutant Belgian sheepdogs. InvestOphthalmol Vis Sci. (suppl) 1993;34:1125.
11 Dell’Osso LF, Williams RW. Ocularmotor abnormalities in achiasmaticmutant Belgian sheepdogs: unyokedeye movements in a mammal. VisRes. 1995;35:109–116.
12 Bataini JP, Delanian S, Ponvert D.Chiasmal gliomas: results ofirradiation management in 57
patients and review of literature. IntJ Radiat Oncol Biol Phys. 1991;21:615–623.
13 Barkovich AJ, Fram EK, Norman D.Septo-optic dysplasia: MR imaging.Radiology. 1989;171:189–192.
14 Benner JD, Preslan MW, Gratz E,Joslyn J, Schwartz M, Kelman S.Septo-optic dysplasia in two siblings.Am J Ophthalmol. 1990;109:632–637.
15 Dutton JJ. Gliomas of the anteriorvisual pathway. Surv Ophthalmol.1994;38:427–452.
16 Iraci G, Gerosa M, Tomazzoli L,Pardatscher K, Fiore DL, Javicoli R,Secchi AG. Gliomas of the opticnerve and chiasm. A clinical review.Child’s Brain. 1981;8:326–349.
17 Kaufman LM, Miller MT, MafeeMF. Magnetic resonance imaging ofpituitary stalk hypoplasia. A discretemidline anomaly associated withendocrine abnormalities in septo-optic dysplasia. Arch Ophthalmol.1989;107:1485–1489.
18 MacCarty CS, Boyd AS, Childs DS.Tumors of the optic nerve and opticchiasm. J Neurosurg. 1970;33:439–444.
19 Roessmann U. Septo-optic dysplasia(SOD) or DeMorsier syndrome. JClin Neuro-Ophthalmol. 1989;9:156–159.
20 Hogan D, Garraghty PE, WilliamsRW. Abnormal retinofugalprojections and visual cortical mapsin a mutant with unilateralmisrouting at the optic chiasm. SocNeurosci Abstr. [suppl] 1996;22:1611.
21 Tang O, Williams RW, Goldowitz D.Mapping the achiasmatic mutationin the dog: A Progress Report. SocNeurosci Abstr. [suppl] 1994;20:1504.
22 Apkarian P. Chiasmal crossingdefects in disorders of binocularvision. Eye. 1996;10:222–232.
23 Apkarian P, De Faber JTHN,Wenniger-Prick L. Alternatingesotropia, torticollis and headtremor in non-decussating retinalfugal fibre syndrome. ESA Trans.22nd meeting. Proceedings (editor, M.Spiritus). Buren, Netherlands:Aeolus Press, 1996;130–133.
24 Victor JD, Apkarian P, Hirsch J,Conte MM, Packard M, Relkin NR,Kim KHS, Shapley RM. Visualfunction and brain organization innon-decussating retinal-fugal fibresyndrome. Cerebral Cortex. 2000;10:2–22.
25 Traquair HM, Dott NM, RussellWR. Traumatic lesions of the opticchiasma. Brain. 1935;58:398–411.
26 Østerberg G. Traumatic bitemporalhemianopia (sagittal tearing of theoptic chiasma). Acta Ophthalmol.1938;16:466–474.
27 Fisher NF, Jampolsky A, Scott AB.Traumatic bitemporal hemianopsia.Part I. Diagnosis of macularsplitting. Am J Ophthalmol. 1968;65:237–242.
28 Fisher NF, Jampolsky A, Flom MC.Traumatic bitemporal hemianopsia.Part II. Binocular cooperation.Am J Ophthalmol. 1968;65:574–577.
29 Fisher NF, Jampolsky A, Scott AB,Morris A, Lehmann D, Alden J.Traumatic bitemporal hemianopsia.Part III. Nasal versus temporalretinal function. Am J Ophthalmol.1968;65:578–581.
30 Maddox EE. See-saw nystagmuswith bitemporal hemianopia. Proc RSoc Med. 1914;7:12–13.
31 Little WS. Absence of the opticchiasm and other cerebralcommissures; temporal hemianopia.Trans Am Ophthalmol Soc. 1886;22:367–369.
32 Bour LJ, Van Gisbergen JAM,Bruijns J, Ottes FP. The doublemagnetic induction method formeasuring eye movement–results inmonkey and man. IEEE TransBiomed Engin. 1984;31:419–427.
33 Collewijn H, Van der Mark F, JansenTC. Precise recording of human eyemovements. Vis Res. 1975;15:447–450.
34 Apkarian P, Bour LJ, Wenniger-Prick L, De Faber JTHN. How doesalbino or achiasmatic misrouting ofthe visual pathways affect visualfunction and concomitant ocularmotor control? Tschr Nederl VerOrthopt. 1997;2:39–49.
35 Apkarian P, Bour LJ, Van der SteenJ, Collewijn H. Ocular motordisorders associated with inbornchiasmal crossing defects; multi-planar eye movement recordings insee-saw and congenital nystagmus.In: Becker W, Deubel H, Mergner T,editors. Current OculomotorResearch; Physiological andPsychological Aspects. PlenumPublishing Co., 1999;403–413.
36 Robinson DA. A method ofmeasuring eye movement using ascleral coil in a magnetic field. IEEETrans Biomed Electron. 1963;BME-10:137–145.
37 Abadi RV, Dickinson CM.Waveform characteristics incongenital nystagmus. DocOphthalmol. 1986;64:153–167.
38 Dell’Osso LF, Daroff RB.Congenital nystagmus waveformsand foveation strategy. DocOphthalmol. 1975;39:155–182.
39 Glaser JS. Neuro-ophthalmology.Lippincott, 1990.
40 Leigh RJ, Zee DS. The Neurology ofEye Movements. 3rd Edition. OxfordUniversity Press, 1999;442–444.
41 Schmidt D, Kommerell G.Congenitaler Schaukelnystagmus(Seesaw Nystagmus). Ein Fall miterhaltenen Gesichtsfeldern,vertikaler Blickparese undKopftremor. Albrecht v GraefesArch Klin Exp Ophthalmol. 1974;191:265–272.
42 Arnott EJ, Miller SJH. See sawnystagmus. Trans Ophthalmol SocUK. 1970;90:491–496.
43 Drachman DA. See-saw nystagmus.J Neurol Neurosurg Psychiatr. 1966;29:356–361.
44 Jensen OA. Seesaw nystagmus. BrJ Ophthalmol. 1959;43:225–229.
45 Lourie H. Seesaw nystagmus. Casereport elucidating the mechanism.Arch Neurol. 1963;9:531–533.
46 Williams IM, Dickinson P, RamsayRJ, Thomas L. See-saw nystagmus.Austr J Ophthalmol. 1982;10:19–25.
47 Apkarian P, Bour L, Bruno P, Vanden Berg AV. Three dimensional eyemovement recordings in non-decussating retinal fugal fibre
162 P. Apkarian & L.J. Bour

Retinal-fugal fiber syndrome 163
syndrome: An inborn achiasmaticmalformation identified withcongenital and see saw nystagmus.Invest Ophthalmol Vis Sci. 1995:36[suppl]:175.
48 Kurzan R, Büttner U. Smoothpursuit mechanisms in congenitalnystagmus. Neuro-Ophthalmology.1989;9:313–325.
49 Gresty MA, Barratt HJ, Page NG,Ell JJ. Assessment of vestibulo-ocular reflexes in congenitalnystagmus. Ann Neurol. 1985;17:129–136.
50 Yee RD, Baloh RW, Honrubia V.Study of congenital nystagmus:optokinetic nystagmus. Br JOphthalmol. 1980;64:926–932.
51 Yee RD, Baloh RW, Honrubia V,Kim YS. A study of congenital
nystagmus: vestibular nystagmus.J Otolaryngol. 1981;10:89–98.
52 Kommerell G. Congenitalnystagmus: Control of slow trackingmovements by target offset from thefovea. Graefe’s Arch Clin ExpOphthalmol. 1986;224:295–298.
53 Zauberman H, Magora A.Congenital ‘see-saw’ movement. Arare anomaly of ocular motility. Br JOphthalmol. 1969;53:173–175.
54 Zelt RP, Biglan AW. Congenitalseesaw nystagmus. J PediatrOphthalmol Strabismus. 1985;22:13–16.
55 Freedman HL, Kushner BJ.Congenital ocular aberrantinnervation-new concepts. J PediatrOphthalmol Strabismus 1997;34:10–16.





















