Screening for distant metastases in patients with head and neck cancer: what is the current clinical...
152
Diagnostic imaging in detecting recurrent and metastatic head and neck cancer
Transcript of Screening for distant metastases in patients with head and neck cancer: what is the current clinical...
Diagnostic imaging in detecting recurrent
and metastatic head and neck cancer
The studies described in this thesis were performed at the Department of
Otolaryngology / Head and Neck Surgery of the Vrije Universiteit Medical
Center, Amsterdam, Th Netherlands.
The research was supported by CVZ/VAZ (projectnumber 00154)
Cover design and lay-out: Jolanda Looijen - Schaake
Printed by Ponsen & Looijen BV, Wageningen, the Netherlands
Publication of this thesis was financially supported by:
GlaxoSmithKline, Sanofi-Aventis Netherlands B.V., Schering-Plough,
Merck Serono, Artu Biologicals, Stallergenes B.V., Atos Medical B.V.
VRIJE UNIVERSITEIT
Diagnostic imaging in detecting recurrent and metastatic head and neck cancer
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad Doctor aan
de Vrije Universiteit Amsterdam,
op gezag van de rector magnificus
prof.dr. L.M. Bouter,
in het openbaar te verdedigen
ten overstaan van de promotiecommissie
van de faculteit der Geneeskunde
op dinsdag 30 september 2008 om 10.45 uur
in de aula van de universiteit,
De Boelelaan 1105
door
Jolijn Brouwer
geboren te Veenendaal

promotoren: prof.dr. C.R. Leemans
prof.dr. R. de Bree
prof.dr. J.A. Castelijns
copromotor: prof.dr. E.F.I. Comans

to my parents to Vincent and Tijs

Contents Chapter 1 Introduction 9 Chapter 2 Detecting recurrent laryngeal carcinoma 31
after radiotherapy: room for improvement
Chapter 3 Systematic review: Accuracy of imaging tests in 47
the diagnosis of recurrent laryngeal carcinoma after
radiotherapy
Chapter 4 Improved detection of recurrent laryngeal tumor after 65
radiotherapy using 18FDG-PET as initial method
Chapter 5 The cost-effectiveness of 18FDG-PET in selecting patients 75
with suspicion of recurrent laryngeal carcinoma after
radiotherapy for direct laryngoscopy
Chapter 6 Screening for distant metastases in patients with head and 89
neck cancer: what is the current clinical practice?
Chapter 7 Screening for distant metastases in patients with head and 101
neck cancer: is chest computed tomography sufficient?
Chapter 8 Screening for distant metastases in patients with head and 115
neck cancer: Is there a role for 18FDG-PET?
Chapter 9 Summary and future prospects 127
Chapter 10 Samenvatting en vooruitzichten 135 List of publications, Dankwoord en CV 145

1 Introduction
Introduction
10
1. Head and neck cancer 1.1 Head and neck carcinomas
1.1.1 Etiology and risk factors Head and neck squamous cell carcinomas originate from the mucosal linings of the
upper aerodigestive tract. Squamous cell carcinomas represent roughly 90% of all
cancers in the head and neck region. In The Netherlands more than 2500 new
patients are diagnosed with head and neck squamous cell carcinomas (HNSCC)
each year. Globally, the incidence is 500.000 per year with a mortality of 270.000.
The incidence and mortality of HNSCC vary geographically by race and gender. The
highest incidence is observed in Melanesia (Papua, New Guinea and adjacent
islands), South-Western Europe and South-Central Asia [1-4].
Cigarette smoking is the single most important risk factor for head and neck cancer.
Other ways of consuming tobacco, cigar and pipe smoking or chewing tobacco, also
increase this risk. Another major contributor to developing head and neck cancer is
alcohol abuse. An especially strong association is seen between alcohol and
pharyngeal carcinomas, cancer of the supraglottis and oral cavity. A combination of
heavy tobacco and excessive alcohol use is often seen in patients with HNSCC.
Other associations with HNSCC are the carcinogens betel quid and maté, infections
with Human Papilloma Virus (i.e. tonsil), Human Immunodeficiency Virus and
Ebstein-Barr Virus (nasopharynx), genetic predisposition, occupational exposure
(organic chemicals) and poor oral hygiene. High intake of fruits and vegetables
decrease the risk of HNSCC in some studies [5-22].
1.1.2 Staging and treatment
Staging of HNSCC is performed according to the TNM system of the International
Union Against Cancer / American Joint Committee on Cancer [23]. This classification
describes the anatomical extent of the primary tumour as well as the involvement of
regional lymph nodes and distant metastases [24]. Based on this classification,
clinical stages I-IV can be assessed. About one-third of the patients present with
early stage (I-II) disease and two-thirds with advanced stage (III-IV) [25]. Patients
with early stage HNSCC can usually be treated with either surgery or radiotherapy,
while patients with advanced stage disease mostly need a combination of treatment
modalities.
Introduction
11
1.1.3 Primary tumour
The vast majority (90%) of the HNSCC originate from any part of the lining mucosa in
the head and neck region. A discrimination of areas has led to different sites: lip and
oral cavity, oro-, hypo- and nasopharynx, larynx, maxillary sinus and nasal cavity and
ethmoid sinus. For each of these sites, a classification for the T-stage has been
made.
Size and extension are important to classify the primary tumour. Staging the primary
tumour will dictate the choices of treatment.
1.1.4 Lymph node metastases
Primary HNSCC tumours can spread and cause metastases. The most important
route of spreading is through the lymphatic system towards regional lymph nodes,
rather than haematogenous causing distant metastases. Distant metastases occur in
almost 50% of patients with extensive lymph node metastases and in 7% of patients
without nodal neck metastases [26]. Prognosis for survival is importantly diminished
by the presence, localisation and number of lymph node metastases and extranodal
spread [27-31]. It is clear that if metastases in the neck are diagnosed, the neck
should be treated [32]. Management of the clinically negative (N0) neck is
controversial: there is general agreement that so called elective treatment of the neck
is indicated when there is a certain (10-20%) likelihood of occult (clinically
undetectable) lymph node metastases or when the neck needs to be entered for
surgical treatment of the primary tumour, or when the patient will be unavailable for
regular follow-up. Arguments that defend elective neck dissection are that occult
metastases will always become manifest, they may develop in extensive or
inoperable disease despite regular follow-up and it may spread to distant metastases
when still occult. Arguments against elective neck dissection are that it means
overtreatment in the majority of patients, it may inflict futile morbidity and the
treatment may destroy a barrier to cancer spread in case of recurrence or second
primary disease.
The assessment of the status of the neck nodes is often based on palpation,
although this is generally accepted to be inaccurate. The overall error in the
assessment of the presence or absence of cervical lymph node metastasis is 20 to
30%. Histopathological evaluations have demonstrated that both the false-positive
and the false-negative rate are unsatisfactorily high, causing over- and
undertreatment in many patients. Modern imaging techniques, such as computed
tomography (CT), magnetic resonance imaging (MRI), ultrasound (US) and

Introduction
12
especially US-guided fine-needle aspiration cytology, are more reliable than
palpation.18FDG-PETshowed no additional value [33,34].
A positive lymph node can be the only symptom of a malignant tumour. This has
been shown to be the case in 1%–2% of head and neck malignancies. In case of
lymph node metastases in the neck of unknown origin, thorough investigations are
performed in order to discover an occult primary tumour in the head and neck region.
The following diagnostic modalities are performed after medical history and specialist
head and neck examination: fine-needle aspiration cytology, imaging by means of CT
or MRI, 18FDG-PET and panendoscopy under general anaesthesia with tonsillectomy
and directed biopsies of the base of tongue and nasopharynx. If the primary tumour
is not detected by these methods, there is a diagnosis of cervical metastasis of an
unknown primary tumour. Treatment often consists of a (modified) radical neck
dissection and irradiation of the neck and areas of the head and neck where the
primary tumour is likely to be located [35].
1.1.5 Distant metastases
Head and neck tumours tend to spread to regional lymph nodes before spreading
haematogenous. When distant metastases occur, prognosis changes dramatically.
This clinical problem is discussed in chapter 1.3.
1.1.6 Recurrent disease
Survival rates of HNSCC have only moderately improved over the last decades, in
part due to the relatively high local recurrence rate. Even when surgical margins are
histopathologically tumour-free local recurrence rate is 10 to 30% [36]. A local
recurrence is clinically defined as the occurrence of another squamous cell
carcinoma within 3 years after and less than 2 centimetres away from the index
tumour. This definition has recently been adapted based on molecular analysis of the
index and second tumour [37].
There are 2 theoretical explanations for local recurrences. First, cancer cells have
remained in the patient. This is likely to concern a small number of cancer cells and
is called (local) minimal residual disease. Second, tumour related mucosal precursor
lesions, genetically altered ‘fields’ surrounding the tumour, may be left behind and
these may give rise to new invasive carcinomas. This phenomenon is known as
second field tumours [36].

Introduction
13
1.1.7 Second primary tumour
One of the strongest predictors of head and neck cancer is a history of previous
HNSCC. The risk of second primary tumour (SPT) is related to long-term tobacco
and excessive alcohol exposure and genetic predisposition. Smokers have a 5 times
increased risk, whereas with alcohol abuse the risk is doubled [38].
Definition of SPT is still debated since Warren and Gates first described it in 1932
[39]. Clinically tumours are considered SPT when occurring more than 2 centimetres
away from the primary tumour and arising after 3 years or more. The second field
tumour however may meet these criteria, but should be distinguished from SPT as it
is in fact a tumour arising from the same genetically altered field as the index tumour
has developed from [40].
SPT can occur synchronous or metachronous. Synchronous if they appear at the
same time or within 6 months of the index tumour and metachronous if developed
after 6 months [40]. Development of a SPT usually results in a poor prognosis,
especially when unfavourably situated in lungs or oesophagus [42]. Another reason
for the poor prognosis is that a SPT often arises in previously irradiated or operated
areas. The choices of treatment are then limited by the treatment of the index tumour
i.e., radiation or prior surgery. Detection of simultaneous SPT is of great importance.
The primary tumour and an SPT can then be treated at the same time.
1.2 Larynx carcinomas In The Netherlands laryngeal cancers account for 1.5-2 percent of all cancers, with a
slightly decreasing incidence in the last few years. Ninety percent or more are of
squamous cell origin. The main risk factor for laryngeal carcinoma is tobacco usage.
Laryngeal carcinomas situated in the glottic region usually present at an early stage
with the typical complaint of hoarseness. In North-Western Europe two-thirds of the
laryngeal carcinomas originate in the glottic region, of which 60% are diagnosed in
stage I. Carcinomas originating from the supraglottic region mostly present at a later
stage with swallowing complaints, dyspnoea, odynophagia and otalgia. Cancers of
the subglottic region are rare [43,44].
When treating patients for laryngeal cancer, the goal is not only curation but also
preservation of its unique functions; phonation, breathing and swallowing. Early stage
laryngeal cancer can usually be managed successfully with either radiotherapy or
surgery. Advanced stage disease is often treated with a combination of modalities:
surgery with or without postoperative radiotherapy or (chemo)radiation with salvage
surgery. With the aim of preservation of organ and function without jeopardising

Introduction
14
survival, chemoradiation with surgical salvage kept in reserve has become a frequent
treatment policy. Selected advanced lesions may be successfully treated by altered
fractionation irradiation schedules alone [45].
The local control rate of T1 laryngeal cancer after radiotherapy is high [46]. However,
in more advanced laryngeal cancer the recurrence rate after radiotherapy is between
25-50% [45,47-49]. In most of these cases, surgical salvage of recurrent or residual
carcinoma is successful [50,51]. Early detection of recurrent laryngeal carcinoma is
an important prognostic factor [52]. In very selected cases of limited recurrence,
partial laryngectomy is an option [53-57].
Distinguishing between recurrent carcinoma and radiotherapeutic sequels can be a
difficult clinical problem [58]. Postradiotherapy changes include fibrosis, oedema and
soft tissue and cartilage necrosis. Approximately 50% of patients with severe
oedema or necrosis following radiotherapy will have a recurrence [59]. The need for
biopsy itself can present a dilemma as this may exacerbate postradiotherapy
changes. This is the perplexing decision of whether to see the patient regularly in
clinical follow-up, treating the patient with antibiotics, steroids or even hyperbaric
oxygen, or to perform biopsies of the larynx. The first alternatives run the risk of
missing the recurrent tumour, while the trauma of multiple biopsies in heavily radiated
tissue may initiate superimposed infection, chondritis, failure to heal, and further
oedema [58].
1.3 Distant metastases
The detection of distant metastases changes the prognosis and influences the
selection of treatment modality in patients with HNSCC. Distant metastases usually
occur late in the course of the disease. The lungs (45-83%), bone (10-41%) and liver
(6-24%) are the most frequent sites of distant metastases. Incidence of distant
metastases at presentation varies from 2 to 17%. The incidence of clinically detected
distant metastases in HNSCC is 4 to 26%, while at autopsy higher incidences have
been reported (37-57%) [60-63]. Approximately 50% of the terminal HNSCC patients
have distant metastases.
Patients with distant metastases are generally not considered curable and almost
always receive only palliative treatment [64].
Development of distant metastases is related to the site and stage of the primary
tumour. Several clinical risk factors for development of distant metastases were
identified: three or more neck metastases, bilateral or low-jugular metastases,
metastases larger than 6 centimetres, primary site or neck recurrences or second
Introduction
15
primary tumours. Screening for distant metastases has been performed by multiple
modalities; Laboratory biochemical tests were used as screening method for bone
and liver metastases. X-ray of the chest was performed to detect lung metastases.
Bone scintigraphy was the most widely accepted method of determining spread to
the skeletal system and US of the liver was often the first choice for liver metastases
because of the widespread availability, lack of ionizing radiation and low costs.
However, the yield of these techniques in screening procedures is very low. Only
chest CT appeared to be of value in screening for distant metastases [65].
Despite negative screening and locoregional tumour control some patients develop
distant metastases. These distant metastases must have been present at diagnostic
work-up, but were apparently below the detection limit of screening tests. If distant
spread occurs early after major surgery with curative intent these patients probably
underwent futile extensive treatment [66]. Roughly 90% percent of the patients with
distant metastases will die within 12 months.
2. Positron Emission Tomography 2.1 General principles
There is a fundamental difference between positron emission tomography (PET) and
the other major techniques, X-ray computed tomography (CT) and magnetic
resonance imaging (MRI). The latter methods utilise physical properties of the
organism such as tissue dependent absorption of X-rays (CT) and proton densities or
relaxation times in an externally induces nuclear magnetisation (MRI). As such they
are primarily anatomical techniques in which changes in size and structure are used
to differentiate abnormal tissue from normal tissue. PET detects the distribution, and
dynamic redistribution, of specific tracers, whose properties are tailored to be
sensitive to monitor specific biochemical and physiological processes.
The PET scan is therefore a functional imaging technique based on a combination of
advanced detection equipment and the use of radioactive tracers. The radioactive
isotopes send out positrons. Positrons are the antimatter counterpart of electrons and
therefore have the same mass but a positive charge. As positrons travel through
matter, they loose energy through ionisation and excitation of nearby atoms and
molecules. After losing enough energy and travelling a distance of about 2 to 3 mm,
the positron annihilates with an electron. This causes two photons or gamma rays
with an energy of 511 keV, emitted at an angle of 180°. This emission in opposite
Introduction
16
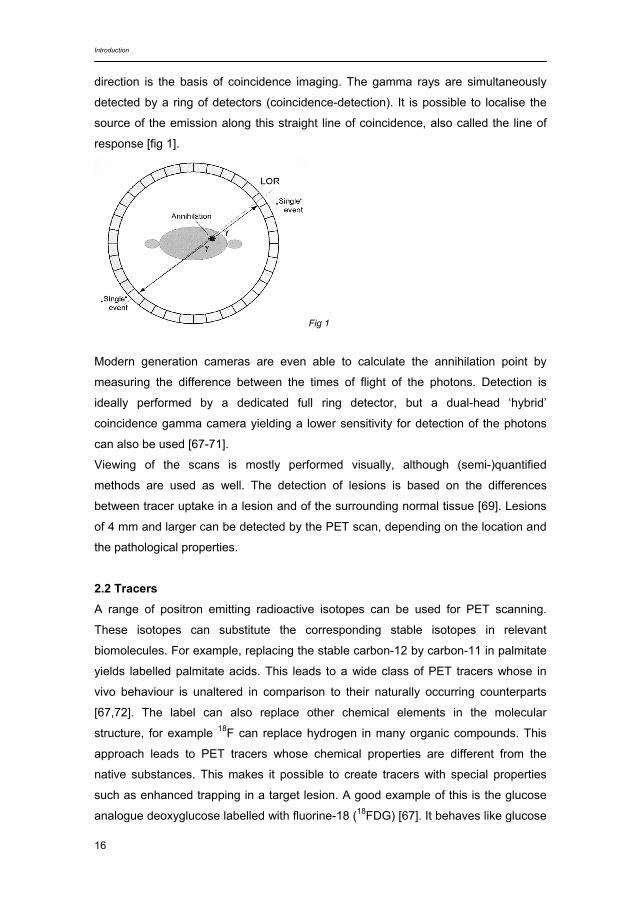
direction is the basis of coincidence imaging. The gamma rays are simultaneously
detected by a ring of detectors (coincidence-detection). It is possible to localise the
source of the emission along this straight line of coincidence, also called the line of
response [fig 1].
Fig 1
Modern generation cameras are even able to calculate the annihilation point by
measuring the difference between the times of flight of the photons. Detection is
ideally performed by a dedicated full ring detector, but a dual-head ‘hybrid’
coincidence gamma camera yielding a lower sensitivity for detection of the photons
can also be used [67-71].
Viewing of the scans is mostly performed visually, although (semi-)quantified
methods are used as well. The detection of lesions is based on the differences
between tracer uptake in a lesion and of the surrounding normal tissue [69]. Lesions
of 4 mm and larger can be detected by the PET scan, depending on the location and
the pathological properties.
2.2 Tracers A range of positron emitting radioactive isotopes can be used for PET scanning.
These isotopes can substitute the corresponding stable isotopes in relevant
biomolecules. For example, replacing the stable carbon-12 by carbon-11 in palmitate
yields labelled palmitate acids. This leads to a wide class of PET tracers whose in
vivo behaviour is unaltered in comparison to their naturally occurring counterparts
[67,72]. The label can also replace other chemical elements in the molecular
structure, for example 18F can replace hydrogen in many organic compounds. This
approach leads to PET tracers whose chemical properties are different from the
native substances. This makes it possible to create tracers with special properties
such as enhanced trapping in a target lesion. A good example of this is the glucose
analogue deoxyglucose labelled with fluorine-18 (18FDG) [67]. It behaves like glucose
Introduction
17
with respect to uptake in a (cancer) cell, however after the 18FDG is phosphorylated 18FDG-6 phosphate is not recognized as a substrate for further metabolic
degradation (glycolysis) or storage in glycogen. Therefore, in the absence of
sufficient activity of the enzyme its exit from the cells is prevented. Glucose uptake is
high in brain cells, muscle cells, inflammatory tissues (macrophages, plasma cells,
lymphocytes and granulocytes) and most types of tumour cells. However some
tumours are not 18FDG avid, e.g. neuro-endocrine tumours. 18FDG is administered intravenously approximately 1 hour before scanning, after a
fasting period of at least 6 hours. Physiological uptake is seen in the brain, some
muscles (myocardium) and the colon (especially the proximal part). All other areas of
diffuse or focal uptake are either malignant tumours or inflammatory lesions [68].
2.3 Applications 18FDG-PET is used in cardiology and neurology, but mostly in the oncologic field,
where it is commonly used for primary staging and restaging after therapy. The
technique has a high sensitivity in FDG avid tumour types, allowing the detection of
tumours with a diameter of 4 mm (depending on the location and the FDG avidity). In
addition 18FDG-PET can often differentiate between vital tumour tissue and fibrosis or
necrosis following therapy, yielding a higher specificity compared to conventional
imaging techniques (CT and MRI).
In oncology, 18FDG-PET is routinely used among others in the diagnostic work-up of
patients with non-small cell lung cancer, malignant lymphomas, melanomas, gastro-
intestinal carcinomas and squamous cell carcinomas of the head and neck.
2.3.1 18FDG-PET in head and neck
Research is being conducted to determine the optimal use of 18FDG-PET in head
and neck tumours.
Occult primary tumours: Lymph node metastasis in the neck is the first symptom. In
most patients a primary tumour is identified through extensive diagnostics. In 1.5-3%
of HNSCC patients, however, the primary tumour remains occult. 18FDG-PET studies
show additional value for detecting a primary tumour in 21-47% of these patients
[73,74].
Lymph node metastases: Detection of lymph node metastases in the neck in patients
with a biopsy proven primary head and neck tumour is an important step in deciding
the best possible treatment for a patient. Using 18FDG-PET in this setting yields a
sensitivity of 74-93% with a specificity of 93-94%. In comparison to CT, MRI and
Introduction
18
ultrasound, 18FDG-PET appeared to be more reliable [75,76]. However, in detecting
occult metastases in a clinically negative neck, 18FDG-PET is not helpful [34,77]. This
can be explained by the small size of occult (micro)metastases.
Tumour response to non-surgical treatment: Organ preservation treatment
(radiotherapy with or without chemotherapy) is an increasingly important modality in
head and neck oncology. Since 18FDG-PET detects biological parameters in tissue, it
may be able to give prognostic information of tumour response, both in the pre-
treatment phase and in an early phase of treatment. An early identification of
nonresponders to (chemo)radiation would refrain a substantial number of patients
from the morbidity and costs of a futile extensive treatment and the complications of
salvage surgery and may improve survival due the remaining option of postoperative
irradiation. So far however, studies have not been unambiguous about the use of 18FDG-PET for this purpose, although some show promising results. [78-80].
Residual tumour after non-surgical treatment: Radiotherapy with or without
chemotherapy invariably changes the anatomy of tissues resulting in a difficulty
differentiating residual tumour from fibrosis, oedema or necrosis on CT or MRI. In
residual mass of the neck, negative aspiration cytology does not rule out vital tissue.
Neck dissection shows in roughly 40% no vital tumour, and has a high risk of post-
operative complications after (chemo)radiation. Studies using 18FDG-PET to
discriminate between residue tumour and post- (chemo)radiation changes show
promising results, but need to be extended [81].
Tumour recurrence after non-surgical treatment: Many laryngeal carcinomas are
treated with radiation therapy with or without chemotherapy. It is of the utmost
importance that organ preservation can be carried out without compromising
locoregional disease control. Approximately 50% of patients with severe oedema or
necrosis following radiotherapy will have a recurrence. The need for biopsy itself can
present a dilemma as this may exacerbate postradiotherapy changes. There may be
a role for 18FDG-PET in detecting recurrent carcinoma in this setting.
Distant metastases and second primary tumours: Detecting distant metastases or
second primary tumours may alter the choice of treatment in patients with head and
neck carcinomas. Since PET is a whole body technique, 18FDG-PET may be helpful
in screening for distant metastases.
Planning of radiotherapy: In radiotherapy, setting exact limits for the target-volume,
has become even more important with the introduction of ‘three-dimensional
conformal radiation therapy’ and ‘intensity-modulated radiation therapy’, to reduce
the impact on healthy surrounding tissue. Comparing tumour-volumes estimated by

Introduction
19
CT, MRI and 18FDG-PET showed promising results for the latter technique, and most
likely especially for PET-CT [82].
Hybrid PET-CT scanners: Fusion of 18FDG-PET and CT provides information on both
anatomy and function. Mainly because of the complex anatomy and normal
biodistribution of 18FDG in the head and neck region (especially following treatment),
fusion of CT and 18FDG-PET images will simplify the interpretation of PET images
compared to visual correlation of the two modalities [83]. More studies on this subject
are needed to define the surplus value of integrating these techniques.
3. Screening, efficiency and statistics 3.1 Screening
Screening may have different objectives. It can be defined as routine testing of
people that do not show any signs of the disease that is being tested. Wilson and
Jungner made directives about screening in 1968 for the World Health Organisation
[84]. These state that screening a healthy population is useful when the disease is an
important health risk, the mechanism of the disease is well understood and there
should be a detectable early stage that can be treated better than more advanced
stages. The early stage must be detected by effective and acceptable tests in which
the interval between different tests must be stated. Adequate measures should be
taken so the health care system is able to cope with the extra work. The physical and
psychological risks should be minor compared to the benefits and the cost should be
balanced to the benefits [85].
The effect of screening is often difficult to decide. The only true outcome in cancer
research is death, but since this may take long follow-up, it is easier to take an
intermediate end-point. This, however, is prone to introduce inaccuracies, such as
lead time bias (diseases discovered through screening at an earlier stage), length
time bias (only the slowly progressive form of the disease is found during screening)
and overdiagnosis bias (during screening disease is found that would otherwise not
have become clinically significant) [85-88].
In the adult population in The Netherlands, nationwide screening programmes are
active for breast and cervical cancer, as in many countries in Western Europe and
the USA [87,89,90]. There is still an ongoing discussion about the effect, risks and
harms of these screening programmes. The discussion based on the aforementioned
known biases focuses on the health and survival benefits of screening for both the

Introduction
20
individual and society as a whole compared to the risks. The main problem seems to
be that screening is usually performed in a healthy, low risk population. It might be
more useful to screen a population that is at risk, for example Human Papilloma Virus
positive patients for cervical cancer [85,87,89-91]. We applied this form of screening
in a population at risk, to detect distant metastases in patients with advanced stage
head and neck cancers. Our aim of screening was different: rather than to find
disease at an early stage and be able to curably treat the patient, disseminated
disease without curative options is detected to prevent the patient from undergoing
futile extensive treatment and provide the patients with the best quality of life
possible. In the literature screening and staging are often used to indicate similar
meaning, although, in fact they are not interchangeable. Looking for distant
metastases of a given primary tumour should be considered staging of the disease.
Looking for second primary tumours is a screening process. Herein, screening is
sometimes used when staging would have been more appropriate.
3.2 Cost effectiveness and efficiency
In the last few decades there has been an increasing focus on costs in health care.
The government, health insurances, and medical professionals emphasise the
importance of developing guidelines that promote cost-effectiveness [92]. Guidelines
are viewed as useful tools for making care more consistent and efficient and for
closing the gap between what clinicians do and what scientific evidence supports.
Interest in clinical guidelines is widespread and has its origin in issues faced by most
healthcare systems: rising costs; variation in service delivery with the presumption
that at least some of this variation originates from inappropriate care; the intrinsic
desire of healthcare professionals to offer and patients to receive the best care
possible [93]. When looking at cost-effectiveness there is a difference in interest
between society and the individual. The value of one’s life is nearly infinite for the
individual, while society places a far more conservative value on our lives; disease
causes economic loss due to missed days of work or early death [94]. In continuation
to this, there are 5 types of costs: direct costs within healthcare, direct costs outside
healthcare, indirect costs within healthcare, indirect costs outside healthcare and
intangible costs. The direct costs within healthcare include the actual amount of the
health services resources directly involved in illness diagnosis and treatment. Direct
costs outside healthcare include patient costs like travelling costs. Indirect costs
within healthcare are medical costs of diseases not related to the therapy under
study which arise as a consequence of life years gained. Indirect costs outside
Introduction
21
healthcare involve the economic loss of a worker’s production secondary to the
illness. The intangible costs of disease are described as the changes in the quality of
life for the patient and family [95-98].
There is no widely accepted successful way of incorporating economic
considerations into guidelines. However it is clear that healthcare is expensive while
resources are limited and therefore diagnostics and effects of treatment should be in
balance with total costs. Economic evaluation can be looked at in 3 ways; first, a
cost-identification analysis in which the financial consequences for providing care
according to the guidelines is outlined. In this, all outcomes should be equivalent in
terms of quality of life, survival and functional indices. The costs are the only metric
examined. Second, a cost-effectiveness (or cost-utility) balance can be performed in
which the costs of an intervention are measured against a particular intervention or
effect. A separate balance can be made for each effect. The effects measured can
be diagnosing a patient with a disease, longer survival or better quality of life. To
calculate a cost-effectiveness balance is not easy. The effect is calculated against a
reference script. This reference script should consist of the diagnostics or treatments
used in best practice. Third, a cost-benefit analysis produces a ratio of the costs to
an estimation of the monetised benefit of an intervention [92,93,99].
Cost analyses are complex and difficult to perform. It is unlikely that the majority of
cost analyses measure up to the ideal standards of society perspective, outcome
measurement, comprehensive accounting of costs, appropriate comparison
interventions, discounting cost over time and sensitivity analysis for uncertainty.
However, a deliberate cost analysis with acknowledged imperfections is preferable to
none [100].
3.3 Statistics
We analysed the accuracy of the screening or diagnostic modalities comparing the
results of the test under evaluation with the results of a reference standard. The
reference standard is regarded as the best available modality to establish the
presence or absence of disease. This is (mostly) a combination of histopathology and
follow-up. The results were then analysed in a 2 x 2 table, in which the results of the
new diagnostic test are compared to the results of the reference standard. An ideal
test would show a true positive rate and true negative rate of 1.0 with a false positive
rate and false negative rate both equal to 0 [101]. From this table outcome measures
as sensitivity, specificity, positive predictive value and negative predictive value can
be extracted. Sensitivity is the chance of a positive result in a patient with malignant

Introduction
22
tumour, while specificity is the chance of a negative result in a tumour negative
patient. Positive predictive value shows the probability of actually having e.g. distant
metastases or recurrent laryngeal carcinoma when having a positive test result.
Negative predictive value shows the probability of not having tumour when having a
negative test result.
Where interobserver variability was determined a weighted kappa was used. This
shows the level of agreement between the observers, beyond the level expected by
chance. The higher the weighted kappa, the higher the level of agreement, with a
maximum of 1.0.
In a systematic review the main findings of several original studies were summarised
in order to assess the overall diagnostic estimates of sensitivity and specificity
according to the (former) guidelines for meta-analyses evaluating diagnostic tests
[102]. For each original study, the sensitivity, specificity, positive predictive value,
negative predictive value and their 95% confidence intervals (CI) in the detection of
recurrent larynx carcinoma were calculated from the original data. Summary pooled
estimates of sensitivity and specificity can only be established if heterogeneity (the
inconsistency of findings) between studies was rejected through constructing forest
plots and by performing the Q test, which is used to verify the assumption that the
treatment effect should be homogenous between trials and the estimated treatment
effect of each trial should have a normal distribution [103-105]. Because the Q test
has limited power and may fail to detect heterogeneity, it was rejected if the p-value
was above 0.10. In the presence of mild heterogeneity across studies, a random-
effects model is considered preferable in meta-analysis, because this approach
produces wider 95% CIs [106]. We used weighted models in which the weight of
each study is its sample size.
Furthermore, we plotted the pairs of sensitivity and specificity of each study in
receiver operating characteristic (ROC) space and used the approach of Moses and
Littenberg to summarise the data by fitting the summary ROC curve [101,107].
Sensitivity (percentage of true positives) is plotted against the percentage of false
positive (1-specificity, defined as the percentage of true negatives). The Q-point is
the maximum joint sensitivity and specificity, closest to the optimal upper left corner
of the summary ROC curve. The overall quality of the test performance is reflected by
its ability to raise the sensitivity without compromising the specificity [88].
All these tests show the relationship between test findings and a reference standard.
Therefore, it should be noted that the results are dependent on the population
studied, in which the prevalence and the population size can be of influence on the
Introduction
23
results of the tests. The lower the prevalence and number of patients included, the
less precise the test results are.
4. Aim of the study and outline of this thesis
In order to detect recurrent disease after prior treatment and metastases in patients
with extended primary disease, new imaging techniques have been developed in the
last decades.
In case of a recurrent laryngeal carcinoma, it is important to detect it as early as
possible in order to be able to cure the patient. So far, a direct laryngoscopy under
general anaesthesia is mostly considered the only reliable tool in detecting these
recurrences. A reliable imaging technique would ease the burden on these patients.
In patients having extensive primary disease, many techniques are used to find
possible distant metastatic disease. When this is found, curation is mostly an illusion.
Therefore, in many cases only palliative care is given to improve the quality of the
remaining life, instead of undergoing major treatment which would turn out to be
futile.
The aims of the research described in this thesis were to evaluate the daily practice
and the possibilities of imaging techniques in order to detect recurrent laryngeal
carcinoma after prior radiotherapy (Chapters 2-5) and distant metastases in patients
with extensive primary head and neck carcinomas (Chapters 6-8).
Chapter 2 describes a comprehensive analysis of the extent and yield of diagnostic
work-up in a cohort of patients clinically suspected of a recurrence, which had
undergone direct laryngoscopy between 1986 and 1998 in our institution. Also an
evaluation of the current care and its usefulness was surveyed by means of a
questionnaire send to different physicians in the major institutions treating head and
neck cancer in The Netherlands.
In Chapter 3 a systematic review of the available literature was performed to
summarise the available evidence and determining the diagnostic accuracy of CT,
MRI and 18FDG-PET in selecting patients for the invasive procedure of direct
laryngoscopy under general anaesthesia.
Chapter 4 describes patients undergoing 18FDG-PET before direct laryngoscopy in
order to examine the possibility be able to stratify patients for this procedure.
Interobserver variability for 18FDG-PET was determined in a group of 9 observers.

Introduction
24
An estimation of the cost-effectiveness of 18FDG-PET in the selection for direct
laryngoscopy in patients with suspicion of recurrent laryngeal carcinoma after
radiotherapy was performed in Chapter 5.
Chapter 6 describes a questionnaire on current practice concerning the diagnostic
work-up in HNSCC patients in screening for distant metastases in the departments
treating head and neck cancer in The Netherlands.
In Chapter 7 the accuracy of screening for distant metastases with chest CT in 109
consecutive patients with head and neck squamous cell carcinoma with previously
established risk factors between 1997 and 2000 was retrospectively analysed.
In Chapter 8 a prospective comparison in 34 consecutive HNSCC patients of the
yield of whole body 18FDG-PET and chest CT to detect distant metastases and
synchronous primary tumours was performed.
Chapter 9 contains a summary and future prospects, followed by a Dutch summary
(Chapter 10).
Introduction
25
Literature
1. Muir C, Weiland L (1995) Upper aerodigestive tract cancers. Cancer 75:147-153 2. Parkin DM, Pisani P, Ferlay J (1999) Global cancer statistics. CA Cancer J Clin 49:33-64 3. Parker SL, Davis KJ, Wingo PA, Ries LA, Heath CW Jr. (1998) Cancer statistics by race and
ethnicity. CA Cancer J Clin 48:31-48 4. Raitiola HS, Pukander JS (1997) Etiological factors of laryngeal cancer. Acta Otolaryngol
Suppl 529:215-217 5. Blot WJ, McLaughlin JK, Winn DM, Austin DF, Greenberg RS, Preston-Martin S, Bernstein L,
Schoenberg JB, Stemhagen A, Fraumeni JF jr (1988) Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res 48:3282-3287
6. Mashberg A, Boffetta P, Winkelman R, Garfinkel L (1993) Tobacco smoking, alcohol drinking, and cancer of the oral cavity and oropharynx among U.S. veterans. Cancer 72:1369-1375
7. Muscat JE, Richie JP Jr, Thompson, Wynder EL (1996) Gender differences in smoking and risk for oral cancer. Cancer Res 56:5192-5197
8. Morse DE, Katz RV, Pendrys DG, Holford TR, Krutchkoff DJ, Eisenberg E, Kosis D, Mayne ST (1996) Smoking and drinking in relation to oral epithelial dysplasia. Cancer Epidemiol Biomarkers Prev 5:769-777
9. Maier H, Sennewald E, Heller GF, Weidauer H (1994) Chronic alcohol consumption – the key risk factor for pharyngeal cancer. Otolaryngol Head Neck Surg 110:168-173
10. Brugere J, Guenel P, Leclerc A, Rodriguez J (1986) Differential effects of tobacco and alcohol in cancer of the larynx, pharynx, and mouth. Cancer 57:391-395
11. Lu CT, Yen YY, Ho CS, Ko YC, Tsai CC, Hsieh CC, Lan SJ (1996) A case-control study of oral cancer in Changhua County, Taiwan. J Oral Pathol Med 25:245-248
12. Pintos J, Franco EL, Oliviera BV, Kowalski LP, Curado MP, Dewar R (1994) Maté, coffee, and tea consumption and risk of cancers of the upper aerodigestive tract in southern Brazil. Epidemiology 5:583-590
13. McKaig RG, Baric RS, Olshan AF (1998) Human papillomavirus and head and neck cancer: epidemiology and molecular biology. Head Neck 20:250-265
14. Braakhuis BJ, Snijders PJ, Keune WJ, Meijer CJ, Ruijter-Schippers HJ, Leemans CR, Brakenhoff RH (2004) Genetic patterns in head and neck cancers that contain or lack transcriptionally active human papillomavirus. J Natl Cancer Inst 96:998-1006
15. Singh B, Balwally AN, Shaha AR, Rosenfeld RM, Har-El G, Lucente FE (1996) Upper aerodigestive tract squamous cell carcinoma. The human immunodeficiency virus connection. Arch Otolaryngol Head Neck Surg 122:639-643
16. Kassim KH, Daley TD (1988) Herpes simplex virus type 1 proteins in human oral squamous cell carcinoma. Oral Surg Oral Med Oral Pathol 65:445-448
17. Hørding U, Nielsen HW, Albeck H, Daugaard S (1993) Nasopharyngeal carcinoma: histopathological types and association with Epstein-Barr Virus. Eur J Cancer B Oral Oncol 29B:137-139
18. Cruz IB, Snijders PJ, Meijer CJ, Braakhuis BJ, Snow GB, Walboomers JM, van der Waal I (1998) p53 expression above the basal cell layer in oral mucosa is an early event of malignant transformation and has predictive value for developing oral squamous cell carcinoma. J Pathol 184:360-368
Introduction
26
19. Schildt EB, Eriksson M, Hardell L, Magnuson A (1999) Occupational exposure as risk factors for oral cancer evaluated in a Swedish case-control study. Oncol Rep 6:317-320
20. Marshall JR, Graham S, Haughey BP, Shedd D, O’Shea R, Brasure J, Wilkinson GS, West D (1992) Smoking, alcohol, dentition and diet in the epidemiology of oral cancer. Eur J Cancer B Oral Oncol 28B:9-15
21. De Stefani E, Deneo-Pellegrini H, Mendilaharsu M, Ronco A (1999) Diet and risk of cancer of the upper aerodigestive tract – I. Foods. Oral Oncol 35:17-21
22. De Stefani E, Ronco A, Mendilaharsu M, Deneo-Pellegrini H (1999) Diet and risk of cancer of the upper aerodigestive tract – II. Nutrients. Oral Oncol 35:22-26
23. Sobin LH, Wittekind Ch, Eds (2002) TNM classification of malignant tumours 6th edition. UICC, International Union Against Cancer
24. Patel SG, Shah JP (2005) TNM Staging of cancers of the head and neck: striving for uniformity among diversity. CA Cancer J Clin 55:242-258
25. Tabor MP, Brakenhoff RH, Houten van VMM, Kummer JA, Snel MHJ, Snijders PJF, Snow GB, Leemans CR, Braakhuis BJM (2001) Persistence of genetically altered fields in head and neck cancer patients: Biological and clinical implications. Clin Cancer Res 7:1523-1532
26. Leemans CR, Tiwari R, Nauta JJP, Waal van der I, Snow GB (1993) Regional lymph node involvement and its significance in the development of distant metastases in head and neck cancer patients. Cancer 71:452-456
27. Snow GB, Annyas AA, Slooten van EA Bartelink H, Hart AA (1982) Clin Otolaryngol 7:185-192 28. Shah JP (1990) Cervical lymph node metastases—diagnostic, therapeutic and prognostic
implications. Oncology 4:61-69 29. Leemans CR, Tiwari R, Waal van der I, Karim AB, Nauta JJ, Snow GB (1990) The efficacy of
comprehensive neck dissection with or without postoperative radiotherapy in nodal metastases of squamous cell carcinoma of the upper respiratory and digestive tracts. Laryngoscope 100:1194-1198
30. Stell PM, Morton RP, Singh SD (1983) Cervical lymph node metastases: the significance of the level of the lymph node. Clin Oncol 9:101-107
31. Jones AS, Roland NJ, Field JK, Phillips DE (1994) The level of cervical lymph node metastases: their prognostic relevance and relationship with head and neck squamous carcinoma primary sites. Clin Otolaryng 19:63-69
32. Nieuwenhuis EJC, Waal van der I, Leemans CR, Kummer A, Pijpers R, Castelijns JA, Brakenhoff RH, Snow GB (2005) Histopathologic validation of the sentinel node concept in oral and oropharyngeal squamous cell carcinoma. Head Neck 27:150-158
33. Bondt RBJ de, Nelemans PJ, Hofman PAM, Casselman JW, Kremer B, Engelshoven JMA van, Beets-Tan RGH (2007) Detection of lymph node metastases in head and neck cancer: A meta-analysis comparing US, USgFNAC, CT and MR imaging. Eur J Radiol 64:266-272
34. Brouwer J, Bree R de, Comans EFI, Castelijns JA, Hoekstra OS, Leemans CR (2004) Positron emission tomography using (18F) fluorodeoxyglucose (FDG-PET) in the clinically negative neck: is it likely to be superior? Eur Arch Otolaryngol 261:479-483
35. Regelink G, Brouwer J, Bree R de, Pruim J, Laan BF van der, Vaalburg W, Hoekstra OS, Comans EFI, Vissink A, Leemans CR, Roodenburg JL (2002) Detection of unknown primary tumours and distant metastases in patients with cervical metastases: value of FDG-PET versus conventional modalities. Eur J Nucl Med Mol Imaging 29:1024-1030
36. Tabor MP, Brakenhoff RH, Ruijter-Schippers HJ, Kummer JA, Leemans CR, Braakhuis BJM (2004) Genetically altered fields as origin of locally recurrent head and neck cancer: a retrospective study. Clin Cancer Res 10:3607-3613
Introduction
27
37. Braakhuis BJ, Tabor MP, Leemans CR, van der Waal I, Snow GB, Brakenhoff RH (2002) Second primary tumors and field cancerization in oral and oropharyngeal cancer: molecular techniques provide new insights and definitions. Head Neck 24:198-206
38. Lin K, Patel SG, Matsuo JM, Singh B, Wong RJ, Kraus DH, Shaha AR, Shah JP, Boyle JO (2005) Second primary malignancy of the aerodigestive tract in patients treated for cancer of the oral cavity and larynx. Head Neck 27:1042-1048
39. Warren S, Gates O (1932) Multiple primary malignant tumors. A survey of the literature and a statistical study. Am J Cancer 16:1358-1414
40. Tabor MP, Brakenhoff RH, Ruijter-Schippers HJ, Wal JE van der, Snow GB, Leemans CR, Braakhuis BJM (2002) Multiple head and neck tumors frequently originate from a single preneoplastic lesion. Am J Pathol 161:1051-1060
41. Léon X, Ferlito A, Myer III CH, Saffiotti U, Shaha AR, Bradley PJ, Brandwein MS, Anniko M, Elluru RG, Rinaldo A (2002) Second primary tumors in head and neck cancer patients. Acta Otolaryngol 122:765-778
42. Schwartz LH, Ozsahin M, Zhang GN, Touboul E, Vataire F de, Andolenko P, Lacau-Saint-Guily J, Laugier A, Schlienger M (1994) Synchronous and metachronous head and neck carcinomas. Cancer 74:1933-1938
43. Dutch Cancer registration http://www.ikcnet.nl 44. Shah JP, Karnell LH, Hoffman HT, Ariyan S, Brown GS, Fee WE, Glass AG, Goepfert H,
Ossoff RH, Fremgen A (1997) Patterns of care for cancer of the larynx in the United States. Arch Otolaryngol Head Neck Surg 123:475-483
45. Parsons JT, Mendenhall WM, Stringer SP, Cassisi NJ (1998) T4 laryngeal carcinoma: radiotherapy alone with surgery reserved for salvage. Int J Radiat Oncol Biol Phys 40:549-552
46. Spector JG, Sessions DG, Chao KS, Haughey BH, Hanson JM, Simpson JR, Perez CA (1999) Stage I (T1N0M0) squamous cell carcinoma of the laryngeal glottis: therapeutic results and voice preservation. Head Neck 21:707-717
47. Terhaard CH, Hordijk GJ, Broek van den P, Jong de PC, Snow GB, Hilgers FJ, Annyas BA, Tjho-Heslinga RE, Jong de JM (1992) T3 laryngeal cancer: a retrospective study of the Dutch Head and Neck Oncology Cooperative Group: study design and general results. Clin Otolaryngol 17:393-402
48. Moose BD, Greven KM (1997) Definitive radiation management for carcinoma of the glottic larynx. Otolaryngol Clinic North Am 30:131-143
49. Medini E, Medini I, Lee CK, Gapany M, Levitt SH (1998) Curative radiotherapy for stage II-III squamous cell carcinoma of the glottic larynx. Am J Clin Oncol 21:302-305
50. Shamboul K, Doyle-Kelly W, Bailey D (1984) Results of salvage surgery following radical radiotherapy for laryngeal carcinoma. J Laryngol Otol 98:905-907
51. Fisher AJ, Calderelli DD, Chacko DC, Holinger LD (1986) Glottic cancer. Surgical salvage for radiation failure. Arch Otolaryngol Head Neck Surg 112:519-521
52. Brenner B, Marshak G, Sulkes A, Rakowsky E (2001) Prognosis of patients with recurrent laryngeal carcinoma. Head Neck 23:531-535
53. DelGaudio JM, Fleming DJ, Esclamado RM, Carroll WR, Bradford CR (1994) Hemilaryngectomy for glottic carcinoma after radiation therapy failure. Arch Otolaryngol Head Neck Surg 120:959-963
54. Lydiatt WM, Shah JP, Lydiatt KM (1996) Conservation surgery for recurrent carcinoma of the glottic larynx. Am J Surg 172:662-664
55. Nibu K, Kamata S, Kawabata K, Nakamizo M, Nigauri T, Hoki K (1997) Partial laryngectomy in the treatment of radiation-failure of early glottic carcinoma. Head Neck 19:116-120
Introduction
28
56. Watters GW, Patel SG, Rhys-Evans PH (2000) Partial laryngectomy for recurrent laryngeal carcinoma. Clin Otolaryngol 25:146-152
57. Kooper DP, Broek P van den, Manni JJ, Tiwari RM, Snow GB (1995) Partial laryngectomy for recurrent glottic carcinoma. Clin Otolaryngol 20:167-170
58. Bahadur S, Amatya RC, Kacker SK (1985) The enigma of post-radiation oedema and residual or recurrent carcinoma of the larynx and pyriform sinus. J Laryngol Otol 99:763-765
59. O’Brien PC (1996) Tumour recurrence or treatment sequelae following radiotherapy for larynx cancer. J Surg Oncol 63:130-135
60. Leon X, Quer M, Orus C, del Prado Venegas M, Lopez M (2000) Distant metastases in head and neck cancer patients who achieved locoregional control. Head Neck 22:680-686
61. Ferlito A, Shaha AR, Silver CE, Rinaldo A, Mordin V (2001) Incidence and sites of distant metastases from head and neck cancer. ORL J Otorhinolaryngology Relat Spec 63:202-207
62. Alvi A, Johnson JT (1997) Development of distant metastasis after treatment of advanced-stage head and neck cancer. Head Neck 9:500-505
63. Leemans CR, Tiwari R, Nauta JJ, van der Waal I, Snow GB (1993) Regional lymph node involvement and its significance in the development of distant metastases in head and neck carcinoma. Cancer 71:452-456
64. Buckley JG, Ferlito A, Shaha AR, Rinaldo A (2001) The treatment of distant metastases in head and neck cancer - present and future. ORL J Otorhinolaryngology Relat Spec 63:259-264
65. Bree R de, Deurloo EE, Snow GB, Leemans CR (2000) Screening for distant metastases in patients with head and neck cancer. Laryngoscope 110:397-401
66. McGuirt WF, Greven K, Williams D, Keyes JW, Watson N, Cappellari JO, Geisinger KR (1998) PET scanning in head and neck oncology: a review. Head Neck 20:208-215
67. Hoff J van den (2005) Principles of quantitative positron emission tomography. Amino Acids 29:341-353
68. Kole AC, Nieweg OE (1996) Applications of positron-emission tomography in oncology [Toe-passingen van positron-emissie tomografie in de oncologie]. Ned Tijdschr Geneeskd 140:244-248
69. Comans EFI, Hoekstra OS, Hoekman K, Hoeven JJM van der, Golding RP, Teule GJJ (2000) Added value of positron emission tomography with fluoro-18-deoxyglucose as the tracer (FDG-PET) in clinical problem cases in oncology [Meerwaarde van positronemissietomografie met als tracer fluor-18-deoxyglucose (FDG-PET) bij klinische probleemgevallen in de oncologie]. Ned Tijdschr Geneeskd 144:1520-1528
70. Bree R de, Brouwer J, Senft A, Putten L van der, Comans EFI, Hoekstra OS, Leemans CR (2006) Clinical applications of FDG-PET in patients with squamous cell carcinoma of the head and neck [Klinische toepassingen van FDG-PET bij patiënten met een plaveiselcelcarcinoom in het hoofd-halsgebied]. Ned Tijdschr Oncol 3:95-101
71. Turkington TG (2001) Introduction to PET instrumentation. J Nucl Med Technol 29:1-8 72. Fischman AJ, Alpert NM, Babich JW, Rubin RH (1997) The role of positron emission
tomography in pharmacokinetic analysis. Drug Metab Rev 29:923-956 73. Regelink G, Brouwer J, Bree R de, Pruim J, Laan BF van der, Vaalburg W, Hoekstra OS,
Comans EFI, Vissink A, Leemans CR, Roodenburg JL (2002) Detection of unknown primary tumours and distant metastases in patients with cervical metastases: value of FDG-PET versus conventional modalities. Eur J Nucl Med Mol Imaging 29:1024-1030
Introduction
29
74. Regelink G, Pruim J, Bree R de, Laan BF van der, Hoekstra OS, Roodenburg JL (2004) The role of FDG-PET in the diagnostics of patients with a neck metastasis of an unknown primary tumour [De rol van FDG-PET voor de diagnostiek van patiënten met een halskliermetastase van een onbekende primaire tumor]. Ned Tijdschr Oncol 1:49-53
75. Adams S, Baum RP, Stuckensen T, Bitter K, Hör G (1998) Prospective comparison of 18F-FDG PET with conventional imaging modalities (CT,MRI,US) in lymph node staging of head and neck cancer. Eur J Nucl Med 25:1255-1260
76. Ng AH, Yen TC, Liao CT, Chang JTC, Chan SC, Ko SF, Wang HM, Wong HF (2005) 18F-FDG PET and CT/MRI in oral cavity squamous cell carcinoma: a prospective study in 124 patients with histological correlation. J Nucl Med 46:1136-1143
77. Wensing BM, Vogel WV, Marres HA, Merkx MA, Postema EJ, Oven WJ, Hoogen FJ van den (2006) FDG-PET in the clinically negative neck in oral squamous cell carcinoma. Laryngoscope 116:809-813
78. Rege S, Safa AA, Chaiken L, Hoh C, Juillard G, Withers HR (2000) Positron emission tomography: an independent indicator of radiocurability in head and neck carcinomas. Am J Clin Oncol 23:164-169
79. Halfpenny W, Hain SF, Biassoni L, Maisey MN, Sherman JA, McGurk M (2002) FDG-PET. A possible prognostic factor in head and neck cancer. Br J Cancer 86:512-516
80. Brun E, Kjellén E, Tennvall J, Ohlsson T, Sandell A, Perfekt R, Wennerberg J, Strand SE (2002) FDG PET studies during treatment: prediction of therapy outcome in head and neck squamous cell carcinoma. Head Neck 24:127-135
81. Wong RJ, Lin DT, Schőder H, Patel SG, Gonen M, Wolden S, Pfister DG, Shah JP, Larson SM, Kraus DH (2002) Diagnostic and prognostic value of [18F] Fluorodeoxyglucose positron emission tomography for recurrent head and neck squamous cell carcinoma. J Clin Oncol 20:4199-4208
82. Daisne JF, Duprez T, Weynand B, Lonneux M, Hamoir M, Reychler H, Gregoire V (2004) Tumour volume in pharyngolaryngeal squamous cell carcinoma: comparison at CT, MR imaging, and FDG PET and validation with surgical specimen. Radiology 233:93-100
83. Goerres GW, Schulthess GK von, Steinert HC (2004) Why most PET of lung and head-and-neck cancer will be PET/CT. J Nucl Med 45 Suppl 1:66S-71S
84. Wilson JM, Jungner YG (1968) Principles and practice of mass screening for disease. Bol Oficina Sanit Panam 65:281-393
85. Veerman E (2004) Sense and nonsense of screening. [Zin en onzin van screening]. Med Contact 59:10-13
86. Black WC (2000) Overdiagnosis: an underrecognizes cause of confusion and harm in cancer screening. J Natl Cancer Inst 92:1280-1282
87. Giard RWM, Bonneux LGA (2001) Breast cancer screening lacking effectiveness. [Borstkanker-screening onvoldoende effectief]. Ned Tijdschr Geneeskd 145:2205-2208
88. Craanen ME, Kuipers EJ (2001) Advantages and disadvantages of population screening for cancer and surveillance of at-risk groups. Best Pract Res Clin Gastroenterol 15:211-26
89. Bonneux L (2004) Harms and benefits of screening to prevent cervical cancer. Lancet 364:1483
90. Bonneux L (2003) Mortality reduction by breast-cancer screening. Lancet 362:245 91. Tabár L, Gad A, Holmberg LH, Ljungquist U, Kopparberg County Project Group, Fagerberg
CJG, Baldetorp L, Gröntoft O, Lundström B, Månson JC, Östergötland County Project Croup, Eklund G, Day NE, Pettersson F (1985) Reduction in mortality from breast cancer after mass screening with mammography. Lancet 1:829-32
Introduction
30
92. Casparie AF, Hout van BA, Simoons ML (1998) Guidelines and costs [Richtlijnen en kosten]. Ned Tijdschr Geneeskd 142:2075-2077
93. Eccles M, Mason J (2001) How to develop cost-conscious guidelines. Health Technol Assess 5:1-69
94. Schweitzer SO (1974) Cost effectiveness of early detection of disease. Health Serv Res 9:22-32
95. Tsue TT, Desyatnikova SS, Deleyiannis FWB, Futran ND, Stack BC, Weymuller EA, Glenn MG (1997) Comparison of cost and function in reconstruction of the posterior oral cavity and oropharynx. Arch Otolaryngol Head Neck Surg 123:731-737
96. Agthoven M van, Ineveld BM van, Boer MF de, Leemans CR, Knegt PP, Snow GB, Uyl-de Groot CA (2001) The costs of head and neck oncology: primary tumours, recurrent tumours and long-term follow-up. Eur J Cancer 37:2204-2211
97. Drummond MF, Sculpher MJ, Torrance GW, O’Brien BJ, Stoddart GL (2005) Methods for the economic evaluation of health care programmes 3rd ed. Oxford; New York: Oxford University Press.
98. Gold MR, Siegel JE, Russell LB, Weinstein MC (1996) Cost-effectiveness in health and medicine. New York: Oxford university press.
99. Petruzzelli GJ, Brockenbrough JM, Vandevender D, Creech SD (2002) The influence of recon-structive modality on cost of care in head and neck oncologic surgery. Arch Otolaryngol Head Neck Surg 128:1377-1380
100. Funk GF, Karnell LH, Whitehead S, Paulino A, Ricks J, Smith RB (2002) Free tissue transfer versus pedicled flap cost in head and neck cancer. Otolaryngol Head Neck Surg 127:205-12
101. Moses LE, Shapiro D, Littenberg B (1993) Combining independent studies of a diagnostic test into a summary ROC curve: data-analytic approaches and some additional considerations. Stat Med 12:1293-1316
102. Deville W, Buntinx F, Bouter LM, Montori VM, de Vet HC, van der Windt DA, Bezemer PD (2002) Conducting systematic reviews of diagnostic studies: didactic guidelines. BMC Med Res Methodol 2:9
103. Irwig L, Tosteson AN, Gatsonis C, Lau J, Colditz G, Chalmers TC, Mosteller F (1994) Guidelines for meta-analyses evaluating diagnostic tests. Ann Intern Med 120:667-676
104. Deeks JJ (2001) Systematic reviews of evaluations of diagnostic and screening tests. In: Egger M, Smith GD, Altman DG, eds. Systematic Reviews in Health Care: Meta-Analysis in Context. London, England: BMJ Publishing Group: 248-282
105. Baujat B, Mahé C, Pignon J-P, Hill C (2002) A graphical method for exploring heterogeneity in meta-analyses: application to a meta-analysis of 65 trials. Statist Med 21:2641-2652
106. Deville W, Buntinx F (2002) Guidelines for conducting systematic reviews of studies evaluating the accuracy of diagnostic studies. In: Knottnerus JA, ed. The Evidence Base of Clinical Diagnosis. London, England: BMJ Publishing Group:145-165
107. Littenberg B, Moses LE (1993) Estimating diagnostic accuracy from multiple conflicting reports: a new meta-analytic method. Med Decis Making 13:313-321
2
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
Jolijn Brouwer, Evelien J. Bodar, Remco de Bree, Johannes A. Langendijk, Jonas A. Castelijns,
Otto S. Hoekstra , C. René Leemans
Eur Arch Otorhinolaryngol (2004) 261:417-422

Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
32
Abstract
Detecting recurrent laryngeal carcinoma after radiotherapy for a primary tumour can
be difficult. Early detection however, is an important prognostic factor. Although a
biopsy should be performed in case of clinical suspicion, repeated negative biopsies
do not exclude the presence of viable tumour. The trauma caused by biopsies in
irradiated tissue may initiate infection, further oedema and failure to heal. We
investigated these problems and evaluated the current care and its usefulness. A
survey of the current practice concerning diagnostic procedures for detecting
recurrent laryngeal carcinoma after radiotherapy in the major institutions treating
head and neck cancer in The Netherlands was performed by means of a
questionnaire. Furthermore, we performed a comprehensive analysis of the extent
and yield of diagnostic work-up in a cohort of patients clinically suspected of a
recurrence, who had undergone direct laryngoscopy between 1986 and 1998 in our
institution, with a follow-up of at least 6 months. In case of suspected recurrence,
94% of the departments use direct laryngoscopy under general anaesthesia with the
taking of biopsies as a diagnostic technique. Imaging does not play an important role.
In our department 207 laryngoscopies were evaluated in 131 patients. In 70 patients
the first laryngoscopy was negative. Of these initial negative laryngoscopies, 22
(31%) turned out to be false negative within 6 months. Thirty-seven patients
remained disease free. They underwent 65 unnecessary laryngoscopies to come to
this conclusion. In the decision to perform direct laryngoscopy, the conventional work
up leaves room for improvement. Too many unnecessary laryngoscopies are
performed. New imaging techniques such as FDG-PET or new applications of CT or
MRI may improve the yield of direct laryngoscopy.
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
33
Introduction
Laryngeal carcinoma is the most common head and neck cancer. When treating
patients for laryngeal cancer, the goal is not only to cure, but also to preserve
function. Early laryngeal cancer can usually be managed successfully with either
radiotherapy or surgery. Advanced stage disease is often treated with a combination
of surgery and radiotherapy. Selected advanced lesions may be successfully treated
by irradiation, with surgery in reserve for salvage treatment [1]. With the emphasis on
preservation of organ and function, investigative treatment regimes using modified
fractionation schedules of radiation, and the combination of chemotherapy and
radiation have recently emerged.
The local control rate of T1 laryngeal cancer after radiotherapy is high [2]. However,
in T2 to T4 laryngeal cancer the recurrence rate after radiotherapy is between 25–
50% [1,3,4,5]. In most of these cases, surgical salvage of recurrent or residual
carcinoma after radical radiotherapy is successful [6,7]. In selected cases, of limited
recurrence, partial laryngectomy is an option [9-13]. Early detection of recurrent
laryngeal carcinoma is therefore an important prognostic factor [8].
Distinguishing between recurrent carcinoma and radiotherapeutic sequels can be a
difficult clinical problem [14]. Postradiotherapy changes include fibrosis, oedema and
soft tissue and cartilage necrosis. Approximately 50% of patients with severe
oedema or necrosis following radiotherapy will have a recurrence [15]. The need for
biopsy itself can present a dilemma as this may exacerbate postradiotherapy
changes. This requires the perplexing decision of whether to see the patients
regularly in clinical follow-up, treating them with antibiotics, steroids or even
hyperbaric oxygen, or to perform biopsies of the larynx. The first alternatives run the
risk of missing the recurrent tumour, while the trauma of multiple biopsies in heavily
radiated tissue may initiate superimposed infection, chondritis, failure to heal and
further oedema [14].
It has been claimed that imaging techniques such as computer tomography (CT),
magnetic resonance imaging (MRI) and positron emission tomography using (18F)
fluorodeoxyglucose (FDG-PET) may be useful in this setting [5]. However, at present,
there are no clear guidelines for the diagnostic policy in case of clinical suspicion on
recurrent laryngeal carcinoma after radiotherapy. Prior to the potential introduction of
new CT and MRI techniques and new technologies such as FDG-PET, the nature
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
34
and yield of current clinical practice need to be assessed. Such data may be helpful
to define and prospectively evaluate new diagnostic algorithms.
To evaluate the current standard of care and its usefulness, we made a survey of the
practice concerning these diagnostics in the major institutions treating head and neck
cancer in The Netherlands. Furthermore, we analysed symptoms, smoking
behaviour, diagnostic techniques and results of direct laryngoscopy under general
anaesthesia in patients with suspicion of recurrent laryngeal carcinoma after
radiotherapy in our institution. Our policy during the study period was to perform
direct laryngoscopy with taking of biopsies in case of clinical suspicion on recurrent
laryngeal carcinoma.
Subjects and methods
Questionnaire on current clinical practice
The questionnaire on the practice concerning diagnostic policy in case of clinical
suspicion of recurrent laryngeal carcinoma after radiotherapy was sent to
investigators in 20 institutions: 12 institutions with an otolaryngology/head and neck
surgery department and a radiation oncology department and 8 radiation oncology
institutions treating head and neck cancer in The Netherlands. The questionnaire
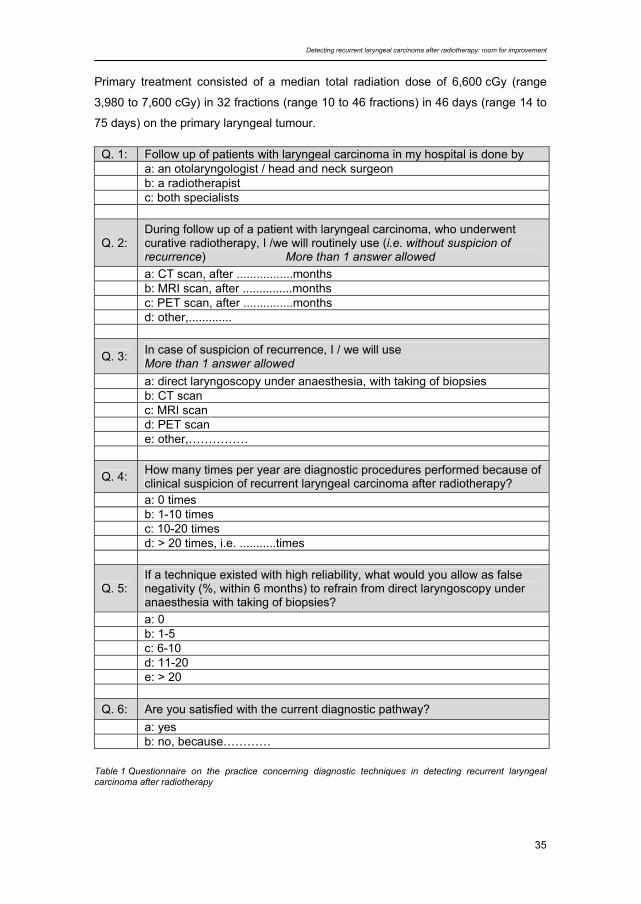
consisted of six questions (Table 1) and was accompanied by an explaining letter.
Retrospective study Between 1986 and 1998, 246 direct laryngoscopies under general anaesthesia in
158 patients were performed because of suspected recurrent laryngeal squamous
cell carcinoma (SCC) after radiotherapy in our institution. Data on ten laryngoscopies
in ten of these patients were incomplete. In another 17 patients (29 laryngoscopies),
the first laryngoscopy was performed more than 3 years after the end of
radiotherapy, and a tumour in these patients should be considered a second primary
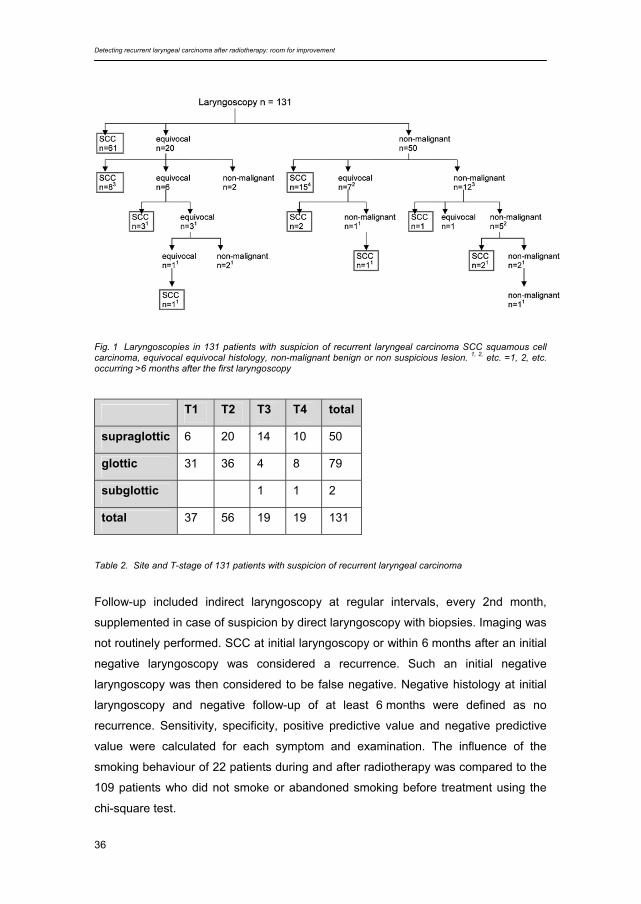
tumour instead of a recurrence [16]. Therefore, 207 direct laryngoscopies in 131
patients were considered eligible for analysis (Fig. 1).
The group consisted of 112 men and 19 women. The median age of these patients
was 63 years, with a range of 40 to 88 years. Seventy-nine patients (60%) suffered
from glottic carcinoma, 50 from supraglottic carcinoma (38%) and 2 from subglottic
carcinoma (2%). The majority of the primary tumours (71%) had been staged T1 or
T2 (Table 2).
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
35
Primary treatment consisted of a median total radiation dose of 6,600 cGy (range
3,980 to 7,600 cGy) in 32 fractions (range 10 to 46 fractions) in 46 days (range 14 to
75 days) on the primary laryngeal tumour.
Table 1 Questionnaire on the practice concerning diagnostic techniques in detecting recurrent laryngeal carcinoma after radiotherapy
Q. 1: Follow up of patients with laryngeal carcinoma in my hospital is done by a: an otolaryngologist / head and neck surgeon b: a radiotherapist c: both specialists
Q. 2: During follow up of a patient with laryngeal carcinoma, who underwent curative radiotherapy, I /we will routinely use (i.e. without suspicion of recurrence) More than 1 answer allowed
a: CT scan, after .................months b: MRI scan, after ...............months c: PET scan, after ...............months d: other,.............
Q. 3: In case of suspicion of recurrence, I / we will use More than 1 answer allowed
a: direct laryngoscopy under anaesthesia, with taking of biopsies b: CT scan c: MRI scan d: PET scan e: other,……………
Q. 4: How many times per year are diagnostic procedures performed because of clinical suspicion of recurrent laryngeal carcinoma after radiotherapy?
a: 0 times b: 1-10 times c: 10-20 times d: > 20 times, i.e. ...........times
Q. 5: If a technique existed with high reliability, what would you allow as false negativity (%, within 6 months) to refrain from direct laryngoscopy under anaesthesia with taking of biopsies?
a: 0 b: 1-5 c: 6-10 d: 11-20 e: > 20 Q. 6: Are you satisfied with the current diagnostic pathway? a: yes b: no, because…………
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
36
Fig. 1 Laryngoscopies in 131 patients with suspicion of recurrent laryngeal carcinoma SCC squamous cell carcinoma, equivocal equivocal histology, non-malignant benign or non suspicious lesion. 1, 2, etc. =1, 2, etc. occurring >6 months after the first laryngoscopy
T1 T2 T3 T4 total
supraglottic 6 20 14 10 50
glottic 31 36 4 8 79
subglottic 1 1 2
total 37 56 19 19 131
Table 2. Site and T-stage of 131 patients with suspicion of recurrent laryngeal carcinoma
Follow-up included indirect laryngoscopy at regular intervals, every 2nd month,
supplemented in case of suspicion by direct laryngoscopy with biopsies. Imaging was
not routinely performed. SCC at initial laryngoscopy or within 6 months after an initial
negative laryngoscopy was considered a recurrence. Such an initial negative
laryngoscopy was then considered to be false negative. Negative histology at initial
laryngoscopy and negative follow-up of at least 6 months were defined as no
recurrence. Sensitivity, specificity, positive predictive value and negative predictive
value were calculated for each symptom and examination. The influence of the
smoking behaviour of 22 patients during and after radiotherapy was compared to the
109 patients who did not smoke or abandoned smoking before treatment using the
chi-square test.
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
37
Results Questionnaire on current clinical practice All institutions returned the questionnaire. In 18 institutions (90%), both the
otolaryngologist and the radiation-oncologist performed the clinical follow-up after
radiotherapy. Two radiation-oncologists stated that an otolaryngologist in another
hospital also performed clinical follow-up of the patients.
During follow-up of patients with laryngeal carcinoma, 19 investigators (95%) used
physical examination with indirect and/or fiberoptic laryngoscopy. MRI was performed
in one hospital (5%), after 4 months, CT and FDG-PET were never routinely
performed.
Diagnostic procedures because of suspicion of recurrent laryngeal carcinoma were
performed more than 20 times a year by five investigators (25%), 11–20 times a year
by three (15%), 1–10 times a year by nine (45%) and never by one investigator. Two
investigators were not able to give an estimation.
In case of clinical suspicion, 11 investigators (55%) performed CT, 9 MRI (45%) and
8 FDG-PET (40%). Four investigators used additional examinations to screen for
regional recurrence and distant metastasis (ultrasound of the neck, CT scan of the
thorax).
In case of suspected recurrent laryngeal carcinoma during follow-up, all investigators
use direct laryngoscopy under anaesthesia, with the taking of biopsies.
Sixteen investigators (80%) would accept 1–5% false negativity of a diagnostic
technique with a high reliability in order to refrain from direct laryngoscopy under
general anaesthesia with taking of biopsies. Four (20%) would accept 6–10%. None
of the investigators would accept a false negativity over 10%.
To the question whether the current diagnostic path was satisfactory, 13 investigators
(65%) responded affirmatively. The remaining seven (35%) were dissatisfied. The
most important reason given for this dissatisfaction was that it may be difficult to
prove a recurrent laryngeal carcinoma after radiotherapy with either biopsy or
imaging by CT or MRI scan despite high suspicion, which can result in a
considerable delay of correct diagnosis. Biopsy taken during direct laryngoscopy
results in a relatively high percentage of false negativity. Imaging techniques also
pose problems in distinguishing recurrent tumour from infection. It may therefore be
difficult for the surgeon to decide whether to take biopsies or not, since it is known
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
38
that taking them in irradiated tissue can be damaging. Furthermore, multiple
investigators commented that they would like to have easier access to PET scan,
because of its expected high predictive value and they expect that this technique
may contribute to the diagnostic pathway. At the time of the questionnaire three PET
scans were available in The Netherlands, two whole rings and one dual head.
Analysis of direct laryngoscopies for possible recurrent laryngeal carcinoma
Patient characteristics
The site and T-stage distribution of the original laryngeal tumours are shown in
Table 2. Suspicion of recurrence arose with a median of 5.7 months (interquartile
range [IQR; 25%–75%]: 3.4–10.7) after the end of radiotherapy. Overall, 94 patients
(72%) had a proven recurrence and 37 patients (28%) had no recurrence. In 78% the
first direct laryngoscopy was performed more than 4 months after radiotherapy.
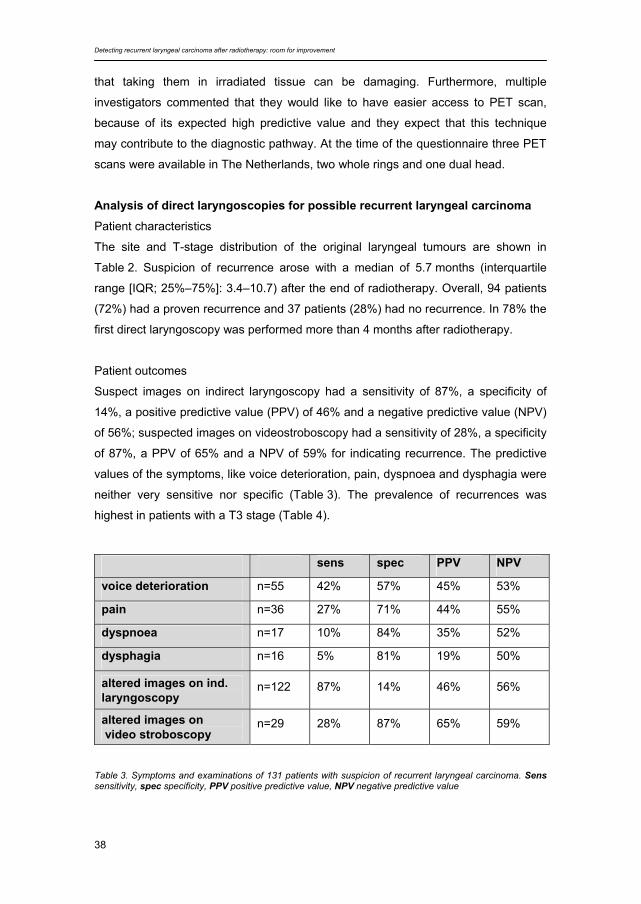
Patient outcomes
Suspect images on indirect laryngoscopy had a sensitivity of 87%, a specificity of
14%, a positive predictive value (PPV) of 46% and a negative predictive value (NPV)
of 56%; suspected images on videostroboscopy had a sensitivity of 28%, a specificity
of 87%, a PPV of 65% and a NPV of 59% for indicating recurrence. The predictive
values of the symptoms, like voice deterioration, pain, dyspnoea and dysphagia were
neither very sensitive nor specific (Table 3). The prevalence of recurrences was
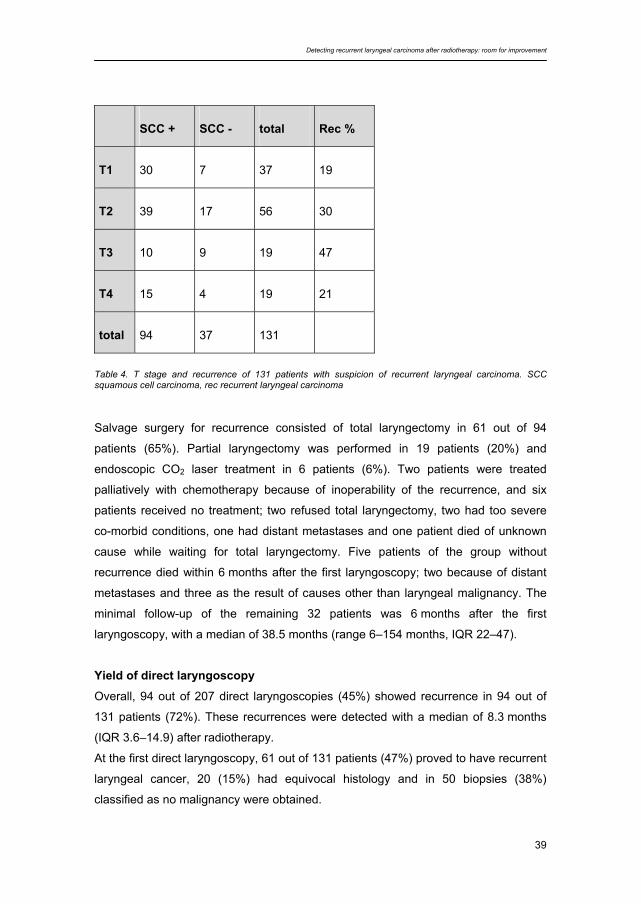
highest in patients with a T3 stage (Table 4).
sens spec PPV NPV
voice deterioration n=55 42% 57% 45% 53%
pain n=36 27% 71% 44% 55%
dyspnoea n=17 10% 84% 35% 52%
dysphagia n=16 5% 81% 19% 50%
altered images on ind. laryngoscopy
n=122 87% 14% 46% 56%
altered images on video stroboscopy
n=29 28% 87% 65% 59%
Table 3. Symptoms and examinations of 131 patients with suspicion of recurrent laryngeal carcinoma. Sens sensitivity, spec specificity, PPV positive predictive value, NPV negative predictive value
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
39
SCC + SCC - total Rec %
T1 30 7 37 19
T2 39 17 56 30
T3 10 9 19 47
T4 15 4 19 21
total 94 37 131
Table 4. T stage and recurrence of 131 patients with suspicion of recurrent laryngeal carcinoma. SCC squamous cell carcinoma, rec recurrent laryngeal carcinoma Salvage surgery for recurrence consisted of total laryngectomy in 61 out of 94
patients (65%). Partial laryngectomy was performed in 19 patients (20%) and
endoscopic CO2 laser treatment in 6 patients (6%). Two patients were treated
palliatively with chemotherapy because of inoperability of the recurrence, and six
patients received no treatment; two refused total laryngectomy, two had too severe
co-morbid conditions, one had distant metastases and one patient died of unknown
cause while waiting for total laryngectomy. Five patients of the group without
recurrence died within 6 months after the first laryngoscopy; two because of distant
metastases and three as the result of causes other than laryngeal malignancy. The
minimal follow-up of the remaining 32 patients was 6 months after the first
laryngoscopy, with a median of 38.5 months (range 6–154 months, IQR 22–47).
Yield of direct laryngoscopy
Overall, 94 out of 207 direct laryngoscopies (45%) showed recurrence in 94 out of
131 patients (72%). These recurrences were detected with a median of 8.3 months
(IQR 3.6–14.9) after radiotherapy.
At the first direct laryngoscopy, 61 out of 131 patients (47%) proved to have recurrent
laryngeal cancer, 20 (15%) had equivocal histology and in 50 biopsies (38%)
classified as no malignancy were obtained.

Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
40
In the 70 patients with a first negative laryngoscopy, 76 follow-up laryngoscopies
were performed; 50 were within 6 months after the first laryngoscopy. Follow-up
laryngoscopies detected 33 recurrences (12 of which were in the initial equivocal
group and 21 in the initial non-malignant group), 22 of which occurred within
6 months after the first negative direct laryngoscopy (7 in the equivocal group and 15
in the benign group). Therefore, the risk of developing a recurrence within 6 months
after negative direct laryngoscopy was still 31% (22/70).
A total number of 81 laryngoscopies was needed to detect the remaining number of
33 recurrences in the group that had an initial negative laryngoscopy. In the group of
37 patients finally classified as disease free, a total of 65 laryngoscopies were
performed. Patients with a T3 stage laryngeal carcinoma needed the highest amount
of direct laryngoscopies to diagnose recurrence; the mean number performed was
4.9 within 6 months. For T1 tumours this was 1.7, for T2 2.1 and for T4 1.7 times,
respectively.
In the 22 patients who continued smoking during and after radiotherapy the mean
number of direct laryngoscopies was 2.4, and it took an average of four
laryngoscopies to detect a recurrence, while these numbers were 1.4 and 1.9 for the
109 patients who did not smoke. The difference between the mean numbers of
laryngoscopies performed in both groups was significant (P=0.001). The number of
recurrences found in just one laryngoscopy instead of a number of laryngoscopies
was significantly higher in the non-smoking group (P=0.002)
Discussion
Persistence of significant laryngeal oedema following radiotherapy confronts the
surgeon with a diagnostic dilemma. Though oedema may represent a response to
irradiation, the possibility of residual carcinoma must be considered. Biopsy itself can
cause problems as this may exacerbate postradiotherapy changes, although if
reasonable clinical suspicion of recurrence exists a biopsy should be performed. The
negative predictive value of multiple deep biopsies is limited. If there is residual
tumour, it is often present as submucosal tiny nests throughout the previous tumour
site, which may be missed by the biopsies. On the other hand, if one chooses to
observe the delayed oedematous larynx until tumour is clinically apparent, the
chances for surgical cure may be markedly diminished or even lost [14].

Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
41
In our series, 70 (53%) of the first direct laryngoscopies performed because of
suspicion of recurrent laryngeal carcinoma after radiotherapy were negative.
However, 22 (31%) of these biopsies were proven false negative, confirming the
difficulty of obtaining positive biopsies. In another 11 (16%) patients, recurrence was
proven more than 6 months after a first negative laryngoscopy, the majority of these
within 12 months.
It is often supposed that a recurrent laryngeal tumour after radiotherapy is harder to
reveal when the primary tumour was of a larger volume. In this study this hypothesis
was confirmed. Original T3 tumours, sometimes of a larger volume than T4 tumours,
needed the highest number of direct laryngoscopies to detect a recurrence, while
there was no difference in the number of laryngoscopies needed between original T1
and T4 tumours.
If unnecessary laryngoscopies could be prevented it would save costs and the risk of
damage to the larynx through the taking of biopsies. In this study, the group of
patients in whom unnecessary laryngoscopies theoretically could have been
prevented includes the 48 patients who underwent 95 laryngoscopies and did not
have a recurrent laryngeal carcinoma within 6 months. Therefore, reliable diagnostic
tests are needed to avoid a number of these unnecessary laryngoscopies. These
diagnostic tests should be sensitive enough to detect recurrence in a stage at which
surgical salvage (total laryngectomy, in some circumstances partial laryngectomy)
remains possible.
On the other hand, these tests should be specific enough to minimize the number of
unnecessary laryngoscopies. One of the questions in the questionnaire was intended
to reveal what is considered to be a worthwhile novel diagnostic technique. It showed
that all of the institutions questioned would accept some false negativity of this
diagnostic test, 80% a maximum of 5% and 20% a maximum of 10% false negativity.
The false negativity of the method now accepted as the gold standard (direct
laryngoscopy) is however higher than 5%, in this study almost 17%.
We also analysed the diagnostic values of voice complaints, pain, dyspnoea,
dysphagia, altered images on indirect laryngoscopy and videolaryngostroboscopy.
The sensitivity, specificity, positive predicting value and negative predicting value of
all these diagnostic tests were limited.
Radiological investigations, without a post-treatment baseline scan for comparison,
seem to be less effective in patients suspected of having a recurrent or residual
tumour after previous irradiation treatment due to diffuse tissue changes including
varying amounts of fibrosis and oedema [17]. This especially seems to be true for

Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
42
laryngeal recurrences. [18]. At this moment neither on CT nor on MRI can reliable
distinction be made between cancer, oedema and irradiation fibrosis or necrosis [17].
Baseline and follow-up post treatment CT or MRI may well improve detection of
recurrent laryngeal carcinoma after radiotherapy. Follow-up CT, after an initial post-
treatment CT, was shown in a study by Hermans et al. to detect about 40% of local
failures earlier than with clinical examination. Furthermore, the use of follow-up CT
scans could substantially reduce the number of patients needing biopsy [19,29].
FDG-PET can distinguish tumour recurrence from radiation sequelae in patients
treated for laryngeal carcinoma [20]. Positive and negative predictive values of 67–
89% and 80–100%, respectively, have been reported [21-24]. FDG-PET was more
sensitive than conventional methods such as CT or MRI in detecting recurrent
carcinoma. However, these studies did not use a baseline CT or MRI for follow-up. In
contrast to anatomic imaging methods, FDG-PET produces images that reflect the
physiologic and biochemical process of tissues. Because FDG-PET relies on
neoplastic cell metabolic function, its greatest potential will be in detecting small,
submucosal recurrences.
Immediately after radiotherapy FDG-PET may show increased uptake in the
irradiated area. Therefore, Greven et al. found that 1 month after radiotherapy FDG-
PET was inaccurate for predicting the presence of carcinoma. Four months after
radiotherapy FDG-PET was a better predictor for the presence of residual or
recurrent carcinoma [23]. In our patient group the vast majority (78%) of the direct
laryngoscopies were performed more than 4 months after radiotherapy. Therefore, it
can be anticipated that many of these patients would have benefited from selection
based on FDG-PET through the avoidance of unnecessary direct laryngoscopies.
The yield of direct laryngoscopy in the detection of recurrent laryngeal carcinoma
after radiotherapy can be improved by patient selection based on imaging
techniques. If the sensitivity of a diagnostic technique is high, delayed diagnosis of
recurrent laryngeal carcinoma is minimised. In selected cases a partial laryngectomy
is then still possible. A high negative predicting value of a diagnostic technique is
warranted to avoid unnecessary direct laryngoscopies as much as possible.
Currently, the highest diagnostic values seem to be found with FDG-PET.
The vast majority of the recurrences were diagnosed within the first 2 years (79%),
while the most (61%) were within 1 year after radiotherapy. These figures are in
concordance with the literature [25,26]. Patients who continued smoking during and
after radiotherapy underwent more direct laryngoscopies, probably as the result of
oedema caused by the effect of tobacco on the irradiated mucosa.

Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
43
In the present series using the conventional work-up 20% of the patients with
recurrent laryngeal carcinoma after radiotherapy underwent partial laryngectomy,
while 65% of these patients underwent total laryngectomy. In most series more than
half of the patients who experienced recurrence after irradiation originally had
tumours of such extent that they would have required total laryngectomy anyway if
surgery had been recommended instead of radiotherapy for initial treatment
[7,25,27]. Postoperative complications, such as necrosis or fistulae, are significantly
higher after salvage laryngectomies after radiation therapy than after primary
surgery. However, partial laryngectomies for salvage after radiotherapy with a high
success rate of 82 to 97% have been reported [9-13,27,28].
In conclusion, in the decision making to perform a direct laryngoscopy under general
anaesthesia for suspicion of recurrent laryngeal carcinoma after radiotherapy, the
conventional work up leaves room for improvement. If criteria are based on
conventional techniques, too many direct laryngoscopies are performed. The yield of
direct laryngoscopy in the detection of recurrent laryngeal carcinoma after
radiotherapy can probably be improved by patient selection based on new imaging
techniques such as FDG-PET or performing post-treatment baseline CT or MRI
scans for comparison. FDG-PET during follow-up should preferably be performed
4 months and baseline post-treatment CT or MRI scans should be done 3 months
after completion of radiotherapy. There is a need for comparative studies between
such techniques and the effect of their implementation.
Acknowledgements
The authors would like to thank Drs. Baatenburg de Jong, Botke, Burlage, Copper,
Croll, Franssen, Helle, Hilgers, van den Hoogen, de Jong, Kaanders, Keus, Kremer,
de Kuyper, B.F.A.M. van der Laan, K.T. van der Laan, Levendag, Lubsen, Meeuwis,
Noach, Oei, Oldenburger, Rasch, van der Sangen, Schimmel, Tabak, Terhaard,
Teunissen, Timmer, Uppelschoten, Vonk and Wiggenraad for filling out the
questionnaire on the practice concerning diagnostic techniques in detecting recurrent
laryngeal carcinoma after radiotherapy.
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
44
Literature 1. Parsons JT, Mendenhall WM, Stringer SP, Cassisi NJ (1998) T4 laryngeal carcinoma:
radiotherapy alone with surgery reserved for salvage. Int J Radiat Oncol Biol Phys 40:549–
552
2. Spector JG, Sessions DG, Chao KS, Haughey BH, Hanson JM, Simpson JR, Perez CA
(1999) Stage I (T1N0M0) squamous cell carcinoma of the laryngeal glottis: therapeutic
results and voice preservation. Head Neck 21:707–717
3. Terhaard CH, Hordijk GJ, Broek van den P, Jong de PC, Snow GB, Hilgers FJ, Annyas
BA, Tjho-Heslinga RE, Jong de JM (1992) T3 laryngeal cancer: a retrospective study of the
Dutch Head and Neck Oncology Cooperative Group: study design and general results. Clin
Otolaryngol 17:393–402
4. Moose BD, Greven KM (1997) Definitive radiation management for carcinoma of the glottic
larynx. Otolaryngol Clinic North Am 30:131–143
5. Medini E, Medini I, Lee CK, Gapany M, Levitt SH (1998) Curative radiotherapy for stage II-
III squamous cell carcinoma of the glottic larynx. Am J Clin Oncol 21:302–305
6. Shamboul K, Doyle-Kelly W, Bailey D (1984) Results of salvage surgery following radical
radiotherapy for laryngeal carcinoma. J Laryngol Otol 98:905–907
7. Fisher AJ, Calderelli DD, Chacko DC, Holinger LD (1986) Glottic cancer. Surgical salvage
for radiation failure. Arch Otolaryngol Head Neck Surg 112:519-521
8. Brenner B, Marshak G, Sulkes A, Rakowsky E (2001) Prognosis of patients with recurrent
laryngeal carcinoma. Head Neck 23:531–535
9. DelGaudio JM, Fleming DJ, Esclamado RM, Carroll WR, Bradford CR (1994)
Hemilaryngectomy for glottic carcinoma after radiation therapy failure. Arch Otolaryngol
Head Neck Surg 120:959–963
10. Lydiatt WM, Shah JP, Lydiatt KM (1996) Conservation surgery for recurrent carcinoma of
the glottic larynx. Am J Surg 172:662–664
11. Nibu K, Kamata S, Kawabata K, Nakamizo M, Nigauri T, Hoki K (1997) Partial
laryngectomy in the treatment of radiation-failure of early glottic carcinoma. Head Neck
19:116–120
12. Watters GW, Patel SG, Rhys-Evans PH (2000) Partial laryngectomy for recurrent laryngeal
carcinoma. Clin Otolaryngol 25:146–152
13. Kooper DP, Broek P van den, Manni JJ, Tiwari RM, Snow GB (1995) Partial laryngectomy
for recurrent glottic carcinoma. Clin Otolaryngol 20:167–170
14. Bahadur S, Amatya RC, Kacker SK (1985) The enigma of post-radiation oedema and
residual or recurrent carcinoma of the larynx and pyriform sinus. J Laryngol Otol 99:763–
765
15. O Brien PC (1996) Tumour recurrence or treatment sequelae following radiotherapy for
larynx cancer. J Surg Oncol 63:130–135
Detecting recurrent laryngeal carcinoma after radiotherapy: room for improvement
45
16. Braakhuis BJM, Tabor MP, Leemans CR, Waal I van der, Snow GB, Brakenhoff RH (2002)
Second primary tumors and field cancerization in oral and oropharyngeal cancer:
Molecular techniques provide new insights and definitions. Head Neck 24:198–206
17. Castelijns JA, Hermans R, Brekel MW van den, Mukherji SK (1998) Imaging of laryngeal
cancer. Semin Ultrasound CT MRI 19:492–504
18. Gussack GS, Hudgins PA (1991) Imaging modalities in recurrent head and neck tumors.
Laryngoscope 101:119–124
19. Mukherji SK, Mancuso AA, Kotzur IM, Mendenhall WM, Kubilis PS, Tart RP, Freeman D,
Lee WR (1994) Radiological appearance of the irradiated larynx. Part II. Primary site
response. Radiology 193:149–154
20. Greven KM, Williams III DW, Keyes Jr JW, McGuirt WF, Harkness BA, Watson Jr NE,
Raben M, Frazier LC, Geisinger KR, Cappellari JO (1994) Distinguishing tumor recurrence
from irradiation sequelae with positron emission tomography in patients treated for larynx
cancer. Int J Radiat Oncol Biol Phys 29:841–845
21. Greven KM, Williams III DW, Keyes Jr JW, McGuirt WF, Watson Jr NE, Randall ME,
Raben M, Geisinger KR, Cappellari JO (1994) Positron emission tomography of patients
with head and neck carcinoma before and after high dose irradiation. Cancer 74:1355–
1359
22. Austin JR, Wong FC, Kim EE (1995) Positron emission tomography in the detection of
residual laryngeal carcinoma. Otolaryngol Head Neck Surg 113:404–407
23. Greven KM, Williams III DW, McGuirt Sr WF, Harkness BA, D Agostino Jr RB, Keyes Jr
JW, Watson Jr NE (2001) Serial positron emission tomography scans following radiation
therapy of patients with head and neck cancer. Head Neck 23:942–946
24. Terhaard CH, Bongers V, Rijk van PP, Hordijk GJ (2001) F-18-fluoro-deoxy-glucose
positron-emission tomography scanning in detection of local recurrence after radiotherapy
for laryngeal/pharyngeal cancer. Head Neck 23:933–941
25. McLaughlin MP, Parsons JT, Fein DA, Stringer SP, Cassisi NJ, Mendenhall WM, Million
RR (1996) Salvage surgery after radiotherapy failure in T1-T2 squamous cell carcinoma of
the glottic larynx. Head Neck 18:229–235
26. Jones AS, Husband D, Rowley H (1998) Radical radiotherapy for squamous cell
carcinoma of the larynx, oropharynx and hypopharynx: patterns of recurrence, treatment
and survival. Clin Otolaryngol 23:496–511
27. Shaw HJ (1991) Role of partial laryngectomy after irradiation in the treatment of laryngeal
cancer: a view from the United Kingdom. Ann Otol Rhinol Laryngol 100:268–273
28. Lavey RS, Calcaterra TC (1991) Partial laryngectomy for glottic cancer after high-dose
radiotherapy. Am J Surg 162:341–344
29. Hermans R, Pameijer FA, Mancuso AA, Parsons JT, Mendenhall WM (2000) Laryngeal or
hypopharyngeal squamous cell carcinoma: can follow-up CT after definitive radiation
therapy be used to detect local failure earlier than clinical examination alone? Radiology
214:683–687

3
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
Jolijn Brouwer, Lotty Hooft, Otto S. Hoekstra, Ingrid I. Riphagen, Jonas A. Castelijns, Remco de Bree, C. René Leemans
Head Neck (2008) 30:889-897

Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
48
Abstract
Diagnosing recurrent laryngeal tumour after radiotherapy is challenging. The most
reliable method is direct laryngoscopy under general anaesthesia. However, many
futile laryngoscopies are performed in disease-free patients. Imaging tests selecting
patients for this invasive procedure would be useful. The aim of this systematic
review was summarizing the available evidence and determining the diagnostic
accuracy of CT, MRI, thallium-201 (201Tl) scintigraphy, and F-18-fluorodeoxyglucose
positron emission tomography (18FDG-PET). A systematic review was performed
according to the guidelines of the Cochrane Collaboration. Two reviewers scored the
articles according to A-, B-, and C-items. Statistical meta-analysis was performed
producing summary pooled estimates of sensitivity and specificity. There were 8
eligible studies on 18FDG-PET. The validity of the 18FDG-PET studies was
reasonable; the pooled estimates (95% CI) for sensitivity and specificity were 89%
and 74%. The diagnostic accuracy of 18FDG-PET is promising and warrants a
randomized trial comparing a strategy based on conventional diagnostic work-up to
one based on 18FDG-PET.
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
49
Introduction
Radiotherapy is a commonly used, curative treatment for laryngeal carcinomas. The
local control rate of T1 laryngeal cancer after radiotherapy is high [1]. However, in T2
to T4 laryngeal cancer, the recurrence rate after radiotherapy is 25% to 50% [2-5].
Diagnosis of recurrent tumour at an early stage will increase the chance of curative
surgery, in some cases with laryngeal preservation. Radiation treatment may induce
oedema, fibrosis, and necrosis. Differentiation between these postradiation changes
and recurrence can be challenging. Hoarseness, pain, stridor, and swallowing
complaints may be caused by recurrent tumour but may also result from radiation
itself. In a previous study, we found that indirect laryngoscopy had a sensitivity of
87% and a specificity of 14% [6]. Signs and symptoms, like voice deterioration, pain,
dyspnoea, and dysphagia were neither very sensitive nor specific. Direct
laryngoscopy under general anaesthesia with taking of biopsies is the most reliable
diagnostic approach, but biopsies in irradiated tissue may lead to infection,
chondritis, failure to heal, and further oedema [7]. In the aforementioned study, we
evaluated 207 laryngoscopies performed in 131 consecutive patients: in 70 patients
the first laryngoscopy was negative, but 22 (31%) still had a proven recurrence within
6 months. Thirty-seven patients remained disease free, but to come to this
conclusion they underwent 65-futile laryngoscopies [6].
Therefore, a reliable imaging test would be useful to select patients for direct
laryngoscopy. At present, CT or MRI scans, thallium-201 (201Tl) scintigraphy, and F-
18-fluorodeoxyglucose positron emission tomography (18FDG-PET) are used to
evaluate clinically suspected lesions. The aim of this systematic review was to
summarize the available evidence in a systematic manner and to determine the
diagnostic accuracy of these 4 tests in patients with suspicion of recurrent laryngeal
carcinoma after radiotherapy.
The literature search was performed according to the guidelines of the Cochrane
Collaboration for systematic reviews in Medline and Embase using a time frame from
January 1990 until April 2006 without language restrictions. The search strategy was
a modified version of a previously developed search strategy for PET and 18FDG,
combined with keywords and MESH terms for ‘computed tomography’, ‘magnetic
resonance imaging’, ‘thallium’, ‘carcinoma’, ‘recurrence’, ‘head and neck’ and ‘larynx’

Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
50
[8,9]. The terms were modified for each database, and the search was for title words,
text words, and keywords. Two independent reviewers selected eligible studies. A
manual cross-reference search of eligible studies was done to find other relevant
studies. Differences were resolved by consensus.
Inclusion criteria were radiotherapy with curative intent for a primary laryngeal
carcinoma; imaging during follow-up with CT/MRI/201Tl scintigraphy/18FDG-PET;
languages English, German, French, Dutch; and at least 7 patients. For PET we
included dual head gamma cameras with coincidence detection as well as full ring
scanners. The exclusion criteria were case reports, editorials, letters, commentaries,
reviews, duplicate publications on the same patient population, treatment with
chemoradiation, CT or MRI articles published before 1990 (since we considered
older scanning techniques inferior in quality). For 18FDG-PET, 1990 is about the time
of launch of clinical PET applications.
The methodological quality of the included articles was independently judged by the
same 2 reviewers, using the criteria list for diagnostic tests, recommended by the
Cochrane Methods Group on Screening and Diagnostic Tests. The list consists of
criteria to judge the internal validity of the studies (A-items) and of criteria that pertain
to the external validity; generalisability (B-items), and detailed information on the
index-test (C-items).
We assessed 8 internal validity criteria. First, application of a valid reference (‘gold’)
standard. We considered biopsy taken during direct laryngoscopy and clinical follow-
up of 12 months as valid reference tests: tumour recurrence was considered proven
in case of positive histopathology, and absence of recurrence was considered proven
in case of negative biopsies, but only in combination with a negative clinical follow-up
of 12 months. Second, use of the same reference tests for every patient. Third,
performance of those reference tests in a standardized manner. When
histopathology was used as reference test, we assumed that the biopsies had been
taken in a standardized manner, unless specified otherwise. For clinical follow-up, we
required that at least its duration was specified. Fourth, independence of the tests
(i.e., blinding of the interpretation of ‘index’- [CT, MRI, 201Tl scintigraphy, 18FDG-PET]
and reference tests) to avoid bias caused by knowledge of the reference test results
or vice versa (review bias). Fifth, uniform applicability of the reference test. The
purpose of this was to prevent work-up bias: when the results of a diagnostic test
have an influence on whether or not the patient will undergo confirmation by a
reference test, the characteristics of the diagnostic test are altered. Sixth, valid
comparison of different index tests. When more than 1 index test was compared in a

Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
51
study, this was considered valid if all index tests were performed and interpreted
independently of each other in every patient. Interpretation of an index test can be
influenced by knowledge of the results of another index test. Seventh, the study was
characterized as prospective or retrospective. Eighth, the occurrence and method for
reporting missing data. Description of missing data is essential since patients those
who are not available for evaluation might have different results than evaluable
patients, and this is a threat for the validity of the study. A mismatch between data in
a table and data in the text was considered as missing data.
To assign positive scores with respect to external validity, we required a clear
description of the selection, demographics, and the inclusion and exclusion criteria of
the population, as well as a good description of the index test. A small patient
spectrum was a population of only laryngeal carcinomas. We classified studies as
having a broad spectrum if they contained a variety of malignancies of which we
could extract the larynx patients' results.
Data were independently extracted by 2 reviewers using a standardized form, which
included patient characteristics, index test characteristics, and outcome measures.
Differences in judgment of the methodological quality were solved through
consensus. When the original article did not supply enough data to score the A-, B-,
and C-items, additional information was requested from the corresponding author.
Statistical analysis
For all included studies, an attempt was made to extract the 2 × 2 table by each
reviewer independently. From these tables, sensitivity, specificity, and their 95%
confidence intervals (CIs) were calculated. We added 0.5 to a cell frequency of 0 in
order to calculate the estimates. Meta-analysis to produce summary pooled
estimates of sensitivity and specificity were performed if heterogeneity (the
inconsistency of findings) was rejected [10,11]. Potential heterogeneity of results
among different studies was assessed graphically by constructing forest plots (Figure
1) and statistically by the Q test. Because the Q test has limited power and may fail
to detect heterogeneity, it was rejected if the p value was above .10 instead of p >
.05. In the presence of mild heterogeneity across studies, a random-effects model is
considered preferable in meta-analysis, because this approach produces wider 95%
Cis [12]. This allowed for a more conservative interpretation of the results. Analyses
were performed using MetaDisc software (version Beta 1.1.0), specially designed for
meta-analysis of diagnostic and screening tests. We used weighted models in which
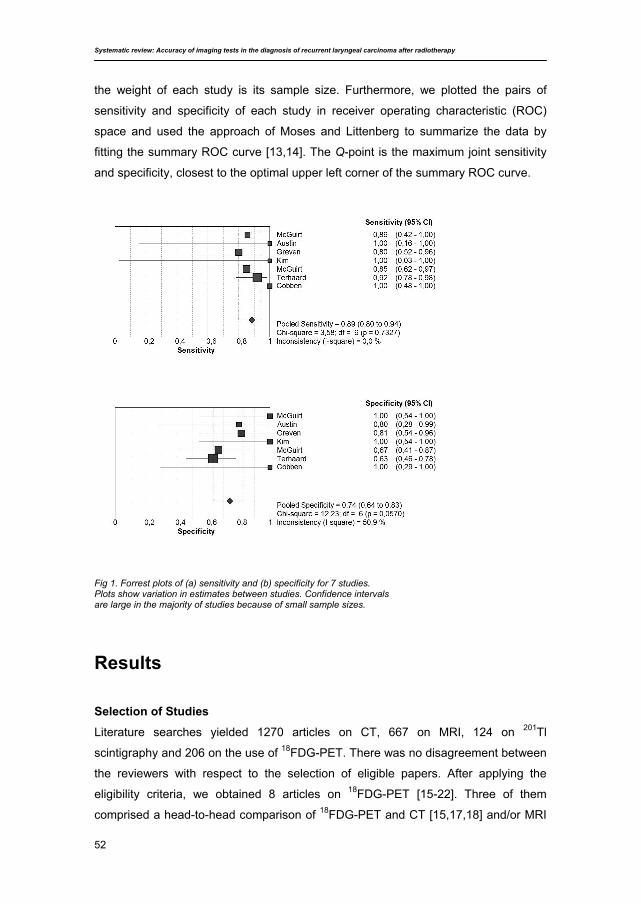
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
52
the weight of each study is its sample size. Furthermore, we plotted the pairs of
sensitivity and specificity of each study in receiver operating characteristic (ROC)
space and used the approach of Moses and Littenberg to summarize the data by
fitting the summary ROC curve [13,14]. The Q-point is the maximum joint sensitivity
and specificity, closest to the optimal upper left corner of the summary ROC curve.
Fig 1. Forrest plots of (a) sensitivity and (b) specificity for 7 studies. Plots show variation in estimates between studies. Confidence intervals are large in the majority of studies because of small sample sizes.
Results Selection of Studies
Literature searches yielded 1270 articles on CT, 667 on MRI, 124 on 201Tl
scintigraphy and 206 on the use of 18FDG-PET. There was no disagreement between
the reviewers with respect to the selection of eligible papers. After applying the
eligibility criteria, we obtained 8 articles on 18FDG-PET [15-22]. Three of them
comprised a head-to-head comparison of 18FDG-PET and CT [15,17,18] and/or MRI
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
53
[17,18] and 1 study reported on the comparison of F-18-fluorothymidine positron
emission tomography (18FLT-PET) with 18FDG-PET [22]. One study [20] was included
despite the fact that it did not completely meet with the criteria. The population
consisted of 75 patients, 67 larynx and 8 hypo/oropharynx. We decided to include the
study reasoning that 90% of the data indeed concerned laryngeal cancer.
Unexpectedly, we found no articles on CT, MRI, or 201Tl scintigraphy that met the
inclusion criteria. Apart from exclusion of studies on tumours other than laryngeal, the
most frequent reasons for ineligibility were as follows: primary treatment not
radiotherapy, but surgery or chemo(radio)therapy; scans performed before
radiotherapy, not after; the results of patients with laryngeal carcinoma could not be
distinguished from those of patients with other head and neck malignancies; the
results of patients who underwent radiotherapy could not be distinguished from those
of patients who underwent other forms of treatment; the results of CT and MRI could
not be extracted separately.
The included 18FDG-PET studies were published between 1995 and 2004. The total
number of patients was 181, and per study, the number of patients included varied
from 7 to 75. The prevalence of recurrent tumour varied from 29% to 63%. Two
studies used a dual head camera [20,21] and all others a full ring PET camera.
Methodological Quality Assessment Internal Validity Criteria (A-Items)
There was disagreement between the 2 reviewers in 26 of 176 scores (15%). All
disagreements were resolved by consensus. In 2 (of the 8 included) studies [15,20]
all patients underwent a valid reference test: histopathology from biopsies taken
during direct laryngoscopy and appropriate follow-up. In the remaining 5, not all
patients had a valid reference test; Kim et al. [16] took biopsies in 4 of the 8 patients.
In 3, these were negative after which the follow-up was not clearly described. The
other 4 patients underwent a follow-up of 10 to 24 months. In McGuirt et al. [17], 32
patients underwent biopsies. The other 6 were followed-up for 8 to 40 months. In
Greven et al. [18], 3 of the 31 patients did not have biopsies taken and had a follow-
up of 9 to 38 months. Austin et al. [19] performed biopsies in 3 of the 7, 1 patient with
a negative biopsy had a follow-up of 7 months. Of the other 4, 1 had a follow-up of
less than 12 months. Stokkel et al. [21] took biopsies in 6 patients, the other 5 had a
follow-up of less than 12 months. Cobben et al. [22] took biopsies in all 8 patients
without further follow-up, and the reference test was therefore incomplete in the 3
patients without tumorpositive biopsies. In all studies the histopathological
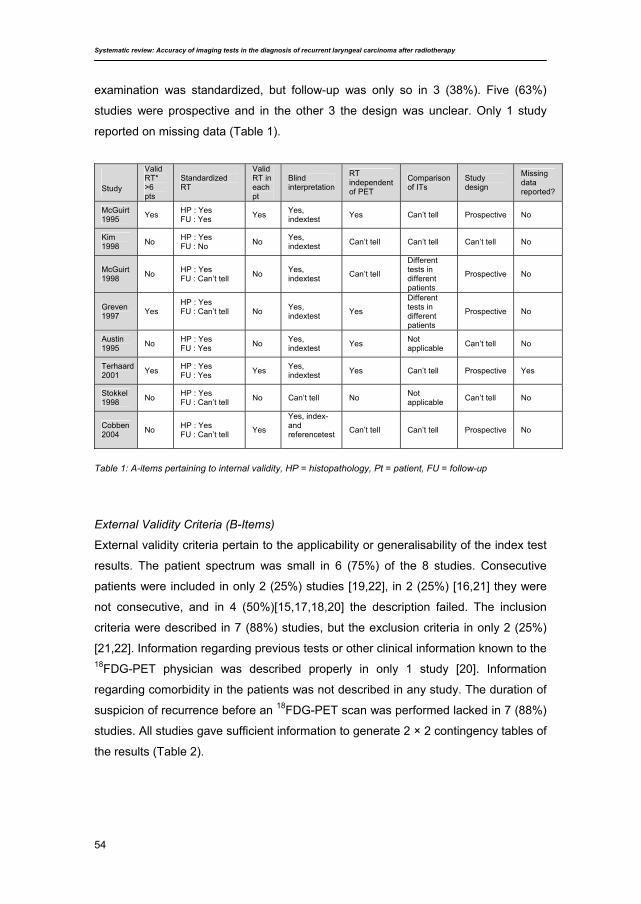
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
54
examination was standardized, but follow-up was only so in 3 (38%). Five (63%)
studies were prospective and in the other 3 the design was unclear. Only 1 study
reported on missing data (Table 1).
Study
Valid RT* >6 pts
Standardized RT
Valid RT in each pt
Blind interpretation
RT independent of PET
Comparison of ITs
Study design
Missing data reported?
McGuirt 1995 Yes HP : Yes
FU : Yes Yes Yes, indextest Yes Can’t tell Prospective No
Kim 1998 No HP : Yes
FU : No No Yes, indextest Can’t tell Can’t tell Can’t tell No
McGuirt 1998 No HP : Yes
FU : Can’t tell No Yes, indextest Can’t tell
Different tests in different patients
Prospective No
Greven 1997 Yes
HP : Yes FU : Can’t tell
No Yes, indextest Yes
Different tests in different patients
Prospective No
Austin 1995 No HP : Yes
FU : Yes No Yes, indextest Yes Not
applicable Can’t tell No
Terhaard 2001 Yes HP : Yes
FU : Yes Yes Yes, indextest Yes Can’t tell Prospective Yes
Stokkel 1998 No HP : Yes
FU : Can’t tell No Can’t tell No Not applicable Can’t tell No
Cobben 2004 No HP : Yes
FU : Can’t tell Yes
Yes, index- and referencetest
Can’t tell Can’t tell Prospective No
Table 1: A-items pertaining to internal validity, HP = histopathology, Pt = patient, FU = follow-up
External Validity Criteria (B-Items)
External validity criteria pertain to the applicability or generalisability of the index test
results. The patient spectrum was small in 6 (75%) of the 8 studies. Consecutive
patients were included in only 2 (25%) studies [19,22], in 2 (25%) [16,21] they were
not consecutive, and in 4 (50%)[15,17,18,20] the description failed. The inclusion
criteria were described in 7 (88%) studies, but the exclusion criteria in only 2 (25%)
[21,22]. Information regarding previous tests or other clinical information known to the 18FDG-PET physician was described properly in only 1 study [20]. Information
regarding comorbidity in the patients was not described in any study. The duration of
suspicion of recurrence before an 18FDG-PET scan was performed lacked in 7 (88%)
studies. All studies gave sufficient information to generate 2 × 2 contingency tables of
the results (Table 2).
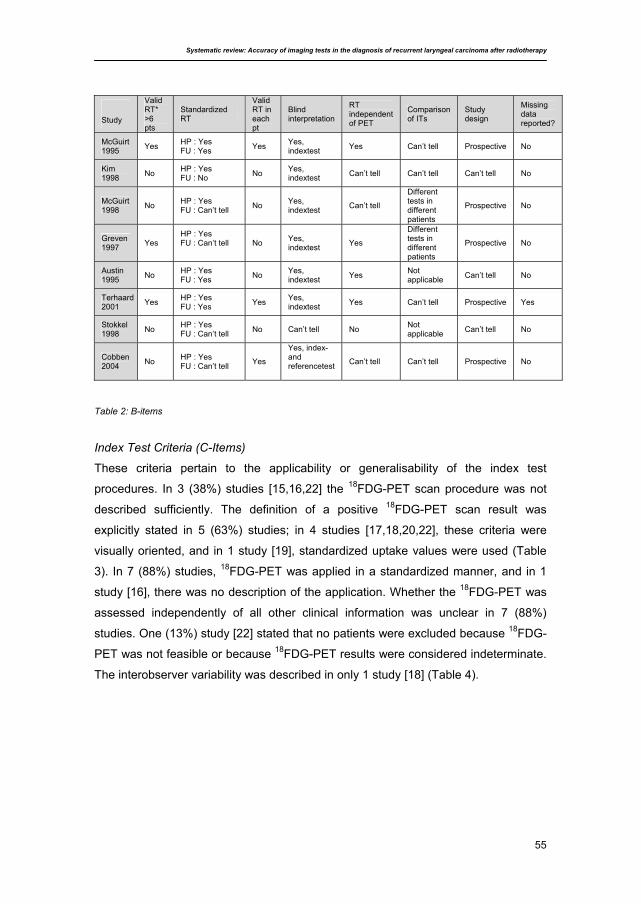
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
55
Table 2: B-items
Index Test Criteria (C-Items)
These criteria pertain to the applicability or generalisability of the index test
procedures. In 3 (38%) studies [15,16,22] the 18FDG-PET scan procedure was not
described sufficiently. The definition of a positive 18FDG-PET scan result was
explicitly stated in 5 (63%) studies; in 4 studies [17,18,20,22], these criteria were
visually oriented, and in 1 study [19], standardized uptake values were used (Table
3). In 7 (88%) studies, 18FDG-PET was applied in a standardized manner, and in 1
study [16], there was no description of the application. Whether the 18FDG-PET was
assessed independently of all other clinical information was unclear in 7 (88%)
studies. One (13%) study [22] stated that no patients were excluded because 18FDG-
PET was not feasible or because 18FDG-PET results were considered indeterminate.
The interobserver variability was described in only 1 study [18] (Table 4).
Study
Valid RT* >6 pts
Standardized RT
Valid RT in each pt
Blind interpretation
RT independent of PET
Comparison of ITs
Study design
Missing data reported?
McGuirt 1995 Yes HP : Yes
FU : Yes Yes Yes, indextest Yes Can’t tell Prospective No
Kim 1998 No HP : Yes
FU : No No Yes, indextest Can’t tell Can’t tell Can’t tell No
McGuirt 1998 No HP : Yes
FU : Can’t tell No Yes, indextest Can’t tell
Different tests in different patients
Prospective No
Greven 1997 Yes
HP : Yes FU : Can’t tell
No Yes, indextest Yes
Different tests in different patients
Prospective No
Austin 1995 No HP : Yes
FU : Yes No Yes, indextest Yes Not
applicable Can’t tell No
Terhaard 2001 Yes HP : Yes
FU : Yes Yes Yes, indextest Yes Can’t tell Prospective Yes
Stokkel 1998 No HP : Yes
FU : Can’t tell No Can’t tell No Not applicable Can’t tell No
Cobben 2004 No HP : Yes
FU : Can’t tell Yes
Yes, index- and referencetest
Can’t tell Can’t tell Prospective No
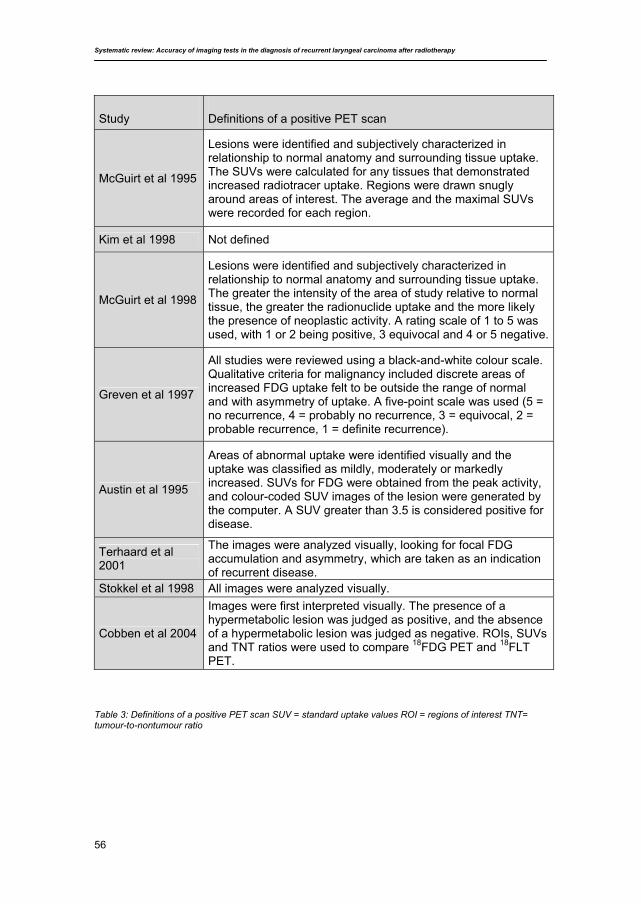
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
56
Table 3: Definitions of a positive PET scan SUV = standard uptake values ROI = regions of interest TNT= tumour-to-nontumour ratio
Study Definitions of a positive PET scan
McGuirt et al 1995
Lesions were identified and subjectively characterized in relationship to normal anatomy and surrounding tissue uptake. The SUVs were calculated for any tissues that demonstrated increased radiotracer uptake. Regions were drawn snugly around areas of interest. The average and the maximal SUVs were recorded for each region.
Kim et al 1998 Not defined
McGuirt et al 1998
Lesions were identified and subjectively characterized in relationship to normal anatomy and surrounding tissue uptake. The greater the intensity of the area of study relative to normal tissue, the greater the radionuclide uptake and the more likely the presence of neoplastic activity. A rating scale of 1 to 5 was used, with 1 or 2 being positive, 3 equivocal and 4 or 5 negative.
Greven et al 1997
All studies were reviewed using a black-and-white colour scale. Qualitative criteria for malignancy included discrete areas of increased FDG uptake felt to be outside the range of normal and with asymmetry of uptake. A five-point scale was used (5 = no recurrence, 4 = probably no recurrence, 3 = equivocal, 2 = probable recurrence, 1 = definite recurrence).
Austin et al 1995
Areas of abnormal uptake were identified visually and the uptake was classified as mildly, moderately or markedly increased. SUVs for FDG were obtained from the peak activity, and colour-coded SUV images of the lesion were generated by the computer. A SUV greater than 3.5 is considered positive for disease.
Terhaard et al 2001
The images were analyzed visually, looking for focal FDG accumulation and asymmetry, which are taken as an indication of recurrent disease.
Stokkel et al 1998 All images were analyzed visually.
Cobben et al 2004
Images were first interpreted visually. The presence of a hypermetabolic lesion was judged as positive, and the absence of a hypermetabolic lesion was judged as negative. ROIs, SUVs and TNT ratios were used to compare 18FDG PET and 18FLT PET.
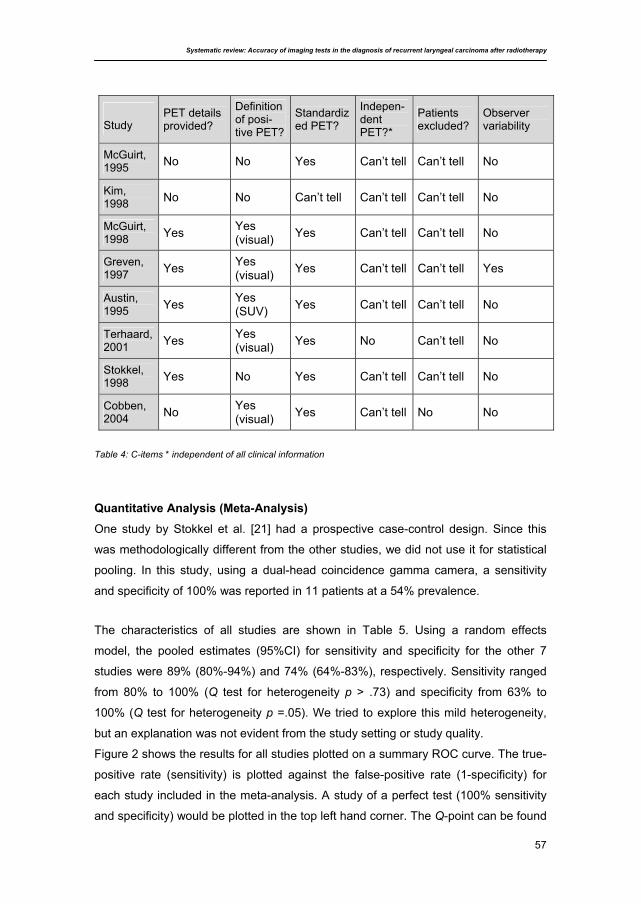
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
57
Table 4: C-items * independent of all clinical information
Quantitative Analysis (Meta-Analysis)
One study by Stokkel et al. [21] had a prospective case-control design. Since this
was methodologically different from the other studies, we did not use it for statistical
pooling. In this study, using a dual-head coincidence gamma camera, a sensitivity
and specificity of 100% was reported in 11 patients at a 54% prevalence.
The characteristics of all studies are shown in Table 5. Using a random effects
model, the pooled estimates (95%CI) for sensitivity and specificity for the other 7
studies were 89% (80%-94%) and 74% (64%-83%), respectively. Sensitivity ranged
from 80% to 100% (Q test for heterogeneity p > .73) and specificity from 63% to
100% (Q test for heterogeneity p =.05). We tried to explore this mild heterogeneity,
but an explanation was not evident from the study setting or study quality.
Figure 2 shows the results for all studies plotted on a summary ROC curve. The true-
positive rate (sensitivity) is plotted against the false-positive rate (1-specificity) for
each study included in the meta-analysis. A study of a perfect test (100% sensitivity
and specificity) would be plotted in the top left hand corner. The Q-point can be found
Study PET details provided?
Definition of posi-tive PET?
Standardized PET?
Indepen-dent PET?*
Patients excluded?
Observer variability
McGuirt, 1995 No No Yes Can’t tell Can’t tell No
Kim, 1998 No No Can’t tell Can’t tell Can’t tell No
McGuirt, 1998 Yes Yes
(visual) Yes Can’t tell Can’t tell No
Greven, 1997 Yes Yes
(visual) Yes Can’t tell Can’t tell Yes
Austin, 1995 Yes Yes
(SUV) Yes Can’t tell Can’t tell No
Terhaard, 2001 Yes Yes
(visual) Yes No Can’t tell No
Stokkel, 1998 Yes No Yes Can’t tell Can’t tell No
Cobben, 2004 No Yes
(visual) Yes Can’t tell No No
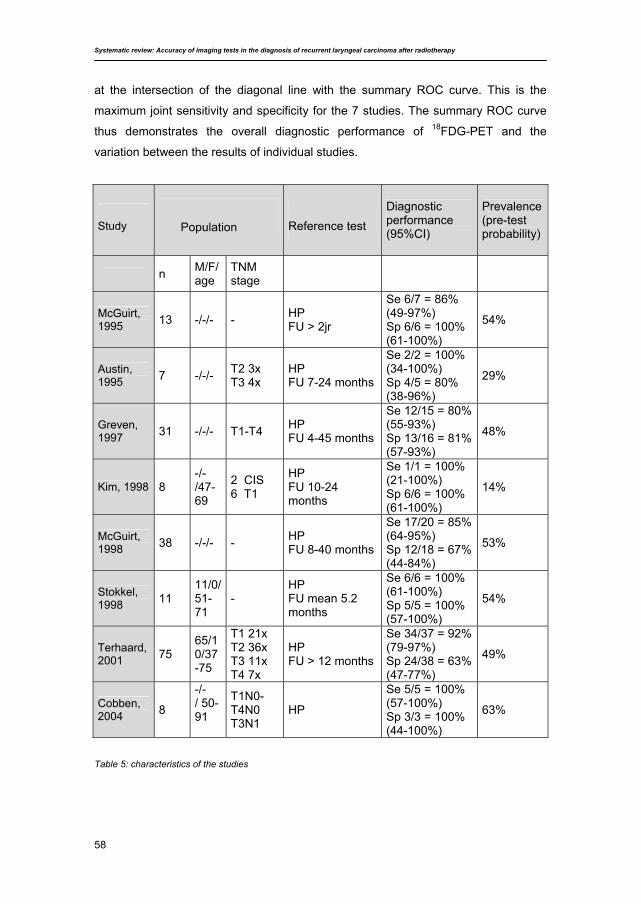
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
58
at the intersection of the diagonal line with the summary ROC curve. This is the
maximum joint sensitivity and specificity for the 7 studies. The summary ROC curve
thus demonstrates the overall diagnostic performance of 18FDG-PET and the
variation between the results of individual studies.
Study
Reference test Diagnostic performance (95%CI)
Prevalence (pre-test probability)
n M/F/age
TNM stage
McGuirt, 1995 13 -/-/- - HP
FU > 2jr
Se 6/7 = 86% (49-97%) Sp 6/6 = 100% (61-100%)
54%
Austin, 1995 7 -/-/- T2 3x
T3 4x HP FU 7-24 months
Se 2/2 = 100% (34-100%) Sp 4/5 = 80% (38-96%)
29%
Greven, 1997 31 -/-/- T1-T4 HP
FU 4-45 months
Se 12/15 = 80% (55-93%) Sp 13/16 = 81% (57-93%)
48%
Kim, 1998 8 -/-/47-69
2 CIS 6 T1
HP FU 10-24 months
Se 1/1 = 100% (21-100%) Sp 6/6 = 100% (61-100%)
14%
McGuirt, 1998 38 -/-/- - HP
FU 8-40 months
Se 17/20 = 85% (64-95%) Sp 12/18 = 67% (44-84%)
53%
Stokkel, 1998 11
11/0/51-71
- HP FU mean 5.2 months
Se 6/6 = 100% (61-100%) Sp 5/5 = 100% (57-100%)
54%
Terhaard, 2001 75
65/10/37-75
T1 21x T2 36x T3 11x T4 7x
HP FU > 12 months
Se 34/37 = 92% (79-97%) Sp 24/38 = 63% (47-77%)
49%
Cobben, 2004 8
-/-/ 50-91
T1N0-T4N0 T3N1
HP
Se 5/5 = 100% (57-100%) Sp 3/3 = 100% (44-100%)
63%
Table 5: characteristics of the studies
Population
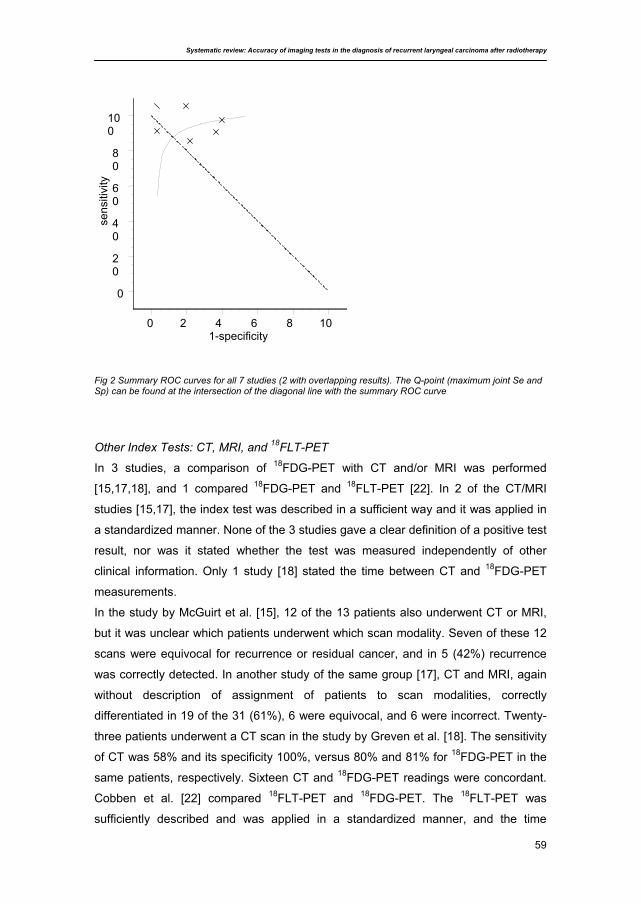
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
59
Fig 2 Summary ROC curves for all 7 studies (2 with overlapping results). The Q-point (maximum joint Se and Sp) can be found at the intersection of the diagonal line with the summary ROC curve
Other Index Tests: CT, MRI, and 18FLT-PET
In 3 studies, a comparison of 18FDG-PET with CT and/or MRI was performed
[15,17,18], and 1 compared 18FDG-PET and 18FLT-PET [22]. In 2 of the CT/MRI
studies [15,17], the index test was described in a sufficient way and it was applied in
a standardized manner. None of the 3 studies gave a clear definition of a positive test
result, nor was it stated whether the test was measured independently of other
clinical information. Only 1 study [18] stated the time between CT and 18FDG-PET
measurements.
In the study by McGuirt et al. [15], 12 of the 13 patients also underwent CT or MRI,
but it was unclear which patients underwent which scan modality. Seven of these 12
scans were equivocal for recurrence or residual cancer, and in 5 (42%) recurrence
was correctly detected. In another study of the same group [17], CT and MRI, again
without description of assignment of patients to scan modalities, correctly
differentiated in 19 of the 31 (61%), 6 were equivocal, and 6 were incorrect. Twenty-
three patients underwent a CT scan in the study by Greven et al. [18]. The sensitivity
of CT was 58% and its specificity 100%, versus 80% and 81% for 18FDG-PET in the
same patients, respectively. Sixteen CT and 18FDG-PET readings were concordant.
Cobben et al. [22] compared 18FLT-PET and 18FDG-PET. The 18FLT-PET was
sufficiently described and was applied in a standardized manner, and the time
sens
itivi
ty
0
20
40
60
80
100
1-specificity0 2 4 6 8 10

Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
60
between 18FDG-PET and 18FLT-PET was stated. It was unclear whether the 2
measurements were independent of each other. Both PET scans revealed all 5
recurrences, but 18FLT-PET had 1 false-positive result versus none with 18FDG-PET.
Discussion
The first striking point in the search for literature was our observation that there was
so little literature on the specific question: we found no eligible studies on CT, MRI,
and 201Tl scintigraphy and only 8 18FDG-PET articles. One study [18] compared both
CT and 18FDG-PET and 2 studies [15,17] compared CT and MRI with 18FDG-PET.
The most frequent reason of ineligibility was that studies comprised an array of head
and neck tumours rather than only laryngeal cancers. The reason we focused our
analysis merely on a specific site, the larynx, is the very specific diagnostic clinical
dilemma of delayed diagnosis in laryngeal carcinomas or increasing complaints
because of postradiation changes, which may not be similar or comparable with other
head and neck sites. Moreover, especially the larynx is prone to develop
postradiation alternations (it is a critical organ in radiotherapy) which may affect the
diagnostic performance of imaging tests. This may be less so with tumours at other
sites. Another reason to exclude studies was treatment with chemoradiation instead
of radiotherapy alone. It could be discussed whether adding chemotherapy will give
very different problems in detecting recurrent laryngeal carcinoma; however, we
decided to keep the search as clear as possible.
The quality of the 18FDG-PET studies was variable. Therefore, many explanations for
(mild) heterogeneity are possible, but since the total number of studies is low,
subgroup analysis is not possible. We can only describe the variability. First of all, the
range of sample sizes was large: there were 3 larger studies [17,18,20]. In the
studies with a smaller population, the sensitivity and specificity were higher than in
the larger studies. The prevalence was about equal in 6 studies; in 2 it was much
lower [16,19]. The definition of a positive scan varied. Five studies gave a clear
definition of a positive 18FDG-PET scan. In 4, this was visual (higher uptake of tracer
vs. background), which is subjective. Data on observer variation were scarce. Our
requirement of 12 months of clinical follow-up to obtain a valid reference test posed
another problem, since many studies included patients with a shorter follow-up;
however, in the 3 larger studies, this potential bias appeared limited since a shorter
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
61
follow-up could maximally pertain to an overall 6% of the patients (0% [20] to 10%
[18] and 16% [15,17]).
In 3 studies [15,17,18], 18FDG-PET results were not strictly dichotomized but an
’equivocal’ category was added. This may be more resembling clinical practice, and it
allows scenario analyses: in a ‘sensitive reading strategy’, equivocal findings would
be considered positive, whereas in a conservative approach, only ‘very positive’
findings would be classified as positive. Consequently, in a sensitive approach, the
sensitivity is higher and the specificity is lower when compared with a conservative
approach. From 7 of the reviewed articles, it is not clear which approach has been
used. Greven et al. [18] used a conservative approach. Since the chance of missing
a recurrence outweighs the risk of a futile direct laryngoscopy, a sensitive strategy
will mostly be used in daily clinical practice.
In a questionnaire on the practice concerning the diagnostic policy in case of clinical
suspicion of recurrent laryngeal carcinoma after radiotherapy, we found that all
clinicians use direct laryngoscopy under general anaesthesia with taking of biopsies
in all patients. However, the conventional work-up is insufficient and leaves room for
improvement [6].
Stratification for direct laryngoscopy using conventional techniques is inefficient to
the extent that too many invasive procedures are performed. The yield of direct
laryngoscopy in the detection of recurrent laryngeal carcinoma after radiotherapy can
probably be improved by patient selection based on imaging techniques. The
perspective is that if the results of a reliable imaging technique are negative (i.e., the
chance of recurrent tumour is very low) direct laryngoscopy is not needed. A
prerequisite for such a strategy is a high sensitivity of the diagnostic test to diagnose
recurrent tumour accurately.
To select the diagnostic modality of choice in these patients, studies using head-to-
head comparisons of different modalities in the same population can be very efficient.
The alternative design to determine the clinical utility and cost-effectiveness of 18FDG-PET in a randomized trial in which a strategy based on conventional
diagnostic work up is compared with one based on 18FDG-PET [23]. The aim of such
trial is then to investigate whether application of 18FDG-PET can reduce the number
of futile direct laryngoscopies under general anaesthesia without increase of
incurable recurrences and its cost-effectiveness compared with conventional
diagnostic work-up. In our opinion, the diagnostic accuracy of 18FDG-PET, with a
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
62
sensitivity of 89% and a specificity of 74%, suggested by this systematic review
justifies such trial.
Acknowledgements
The authors thank Hans Reitsma for his help in the statistical analysis.
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
63
Literature
1. Spector JG, Sessions DG, Chao KS, Haughey BH, Hanson JM, Simpson JR, Perez CA
(1999) Stage I (T1N0M0) squamous cell carcinoma of the laryngeal glottis: therapeutic
results and voice preservation. Head Neck 21:707-717
2. Parsons JT, Mendenhall WM, Stringer SP, Cassisi NJ (1998) T4 laryngeal carcinoma:
radiotherapy alone with surgery reserved for salvage. Int J Radiat Oncol Biol Phys
40:549-552
3. Terhaard CH, Hordijk GJ, Broek van den P, Jong de PC, Snow GB, Hilgers FJ, Annyas
BA, Tjho-Heslinga RE, Jong de JM (1992) T3 laryngeal cancer: a retrospective study of
the Dutch Head and Neck Oncology Cooperative Group: study design and general
results. Clin Otolaryngol 17:393-402
4. Moose BD, Greven KM (1997) Definitive radiation management for carcinoma of the
glottic larynx. Otolaryngol Clinic North Am 30:131-143
5. Medini E, Medini I, Lee CK, Gapany M, Levitt SH (1998) Curative radiotherapy for stage
II-III squamous cell carcinoma of the glottic larynx. Am J Clin Oncol 21:302-305
6. Brouwer J, Bodar EJ, Bree de R , Langendijk JA, Castelijns JA, Hoekstra OS, Leemans
CR (2004) Detecting recurrent laryngeal carcinoma after radiotherapy: Room for
improvement? Eur Arch Otorhinolaryngol 261:417-422
7. Bahadur S, Amatya RC, Kacker SK (1985) The enigma of post-radiation oedema and
residual or recurrent carcinoma of the larynx and pyriform sinus. J Laryngol Otol 99:763-
765
8. Mijnhout GS, Hooft L, Tulder MW van, Devillé WLJM, Teule GJJ, Hoekstra OS (2000)
How to perform a comprehensive search for FDG-PET literature? Eur J Nucl Med
27:91-97
9. Mijnhout GS, Hoekstra OS, Tulder MW van, Teule GJJ, Devillé WLJM (2001)
Systematic review of the diagnostic accuracy of 18F-FDG PET in melanoma patients.
Cancer 91:1530-1542
10. Irwig L, Tosteson AN, Gatsonis C, Lau J, Colditz G, Chalmers TC, Mosteller F(1994)
Guidelines for meta-analyses evaluating diagnostic tests. Ann Intern Med 120:667-676
11. Deeks JJ (2001) Systematic reviews of evaluations of diagnostic and screening tests.
In: Egger M, Smith GD, Altman DG, eds. Systematic Reviews in Health Care: Meta-
Analysis in Context. London, England: BMJ Publishing Group; p 248-282
12. Devillé W, Buntinx F (2002) Guidelines for conducting systematic reviews of studies
evaluating the accuracy of diagnostic studies. In: Knottnerus JA, ed. The Evidence Base
of Clinical Diagnosis. London, England: BMJ Publishing Group; p 145-165
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal carcinoma after radiotherapy
64
13. Moses LE, Shapiro D, Littenberg B (1993) Combining independent studies of a
diagnostic test into a summary ROC curve: data-analytic approaches and some
additional considerations. Stat Med 12:1293-1316
14. Littenberg B, Moses LE (1993) Estimating diagnostic accuracy from multiple conflicting
reports: a new meta-analytic method. Med Decis Making 13:313-321
15. McGuirt WF, Greven KM, Keyes Jr JW, Williams DW 3rd, Watson NE Jr, Geisinger KR,
Cappellari JO (1995) Positron emission tomography in the evaluation of laryngeal
carcinoma. Ann Otol Rhinol Laryngol 104:274-278
16. Kim HD, Boyd J, Dunphy F, Lowe V (1998) F-18 FDG PET scan after radiotherapy for
early stage larynx cancer. Clinical Nuclear Medicine 23:750-752
17. McGuirt WF, Greven KM, Williams III DW, Keyes Jr JW, Watson Jr NE (1998)
Laryngeal radionecrosis versus recurrent cancer: a clinical approach. Ann Otol Rhinol
Laryngol 107:293-296
18. Greven KM, Williams III DW, Keyes Jr JW, McGuirt WF, Watson Jr NE, Case LD (1997)
Can positron emission tomography distinguish tumour recurrence from radiation
sequellae in patients treated for larynx cancer? Cancer J Sci Am 3:353-357
19. Austin JR, Wong FC, Kim EE (1995) Positron emission tomography in the detection of
residual laryngeal carcinoma. Otol Head Neck Surg 113:404-407
20. Terhaard CH, Bongers V, Rijk PP van, Hordijk GJ (2001) F-18-fluoro-deoxy-glucose
positron-emission-tomography scanning in detection of local laryngeal/pharyngeal
cancer. Head Neck 23:933-941
21. Stokkel MP, Terhaard CH, Mertens IJ, Hordijk GJ, Rijk PP van (1998) Fluorine-18-FDG
detection of laryngeal cancer postradiotherapy using dual-head coincidence imaging. J
Nucl Med 39:1385-1387
22. Cobben DCP, Laan BFAM van der, Maas B, Vaalburg W, Suurmeijer AJ, Hoekstra HJ,
Jager PL, Elsinga PH (2004) 18F-FLT PET for visualization of laryngeal cancer:
comparison with 18F-FDG PET. J Nucl Med 45:226-231
23. Bree R de, Putten L van der, Hoekstra OS, Kuik DJ, Uyl-de Groot CA, Tinteren H van,
Leemans CR, Boers M: RELAPS Study Group (2007) A randomized trial of PET
scanning to improve diagnostic yield of direct laryngoscopy in patients with suspicion of
recurrent laryngeal carcinoma after radiotherapy. Contemp Clin Trials 28:705-712
4
Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
Jolijn Brouwer, Remco de Bree, Emile F.I. Comans, Mohammed Akarriou, Johannes A. Langendijk, Jonas A. Castelijns, Otto S. Hoekstra,
C. René Leemans
Radiother Oncol (2008) 87:217-220
Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
66
Abstract
Timely detection of recurrent laryngeal tumour after radiation is an important
predictive factor for curation as well as preservation of laryngeal function. Direct
laryngoscopy under general anaesthesia with taking of biopsies is the standard
diagnostic procedure to detect recurrence when suspicion is raised. This, however, is
an invasive and potentially damaging technique. Hence, a non-invasive diagnostic
procedure, such as 18FDG-PET to stratify patients for direct laryngoscopy could be
useful. 18FDG-PET is interpreted visually so that observer variation may affect clinical
practice. In the present study, we therefore investigated this aspect of reproducibility.
Thirty consecutive patients suspected of recurrent laryngeal carcinoma after
radiotherapy underwent 18FDG-PET and direct laryngoscopy under general
anaesthesia with taking of biopsies. 18FDG-PET scans were reported by nine nuclear
medicine physicians and residents, using a three-point scaling system. The reference
was the absence or appearance of a local recurrence in the 12 months following 18FDG-PET. Eight patients had biopsy proven recurrent laryngeal carcinoma.
Sensitivity of 18FDG-PET was 88% (95% CI 53–98%) and specificity was 82% (95%
CI 62–93%). The observers had a moderate to reasonable agreement (weighted
kappa 0.45 (95% CI 0.20–0.69)) vs. the clinical gold standard and interobserver
kappa was 0.54 (95% CI 0.40–0.69). 18FDG-PET seems to be a promising technique
to detect recurrent laryngeal carcinoma after radiotherapy, and selecting patients for
direct laryngoscopy. This will avoid futile invasive procedures. Interobserver
agreement and variability is reasonable using this technique, but training is
necessary. Studies comparing different strategies to select patients for direct
laryngoscopy in case of suspected recurrence are warranted.

Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
67
Introduction
The objectives of treatment of patients with laryngeal cancer are cure and
preservation of laryngeal function. Patients with early staged laryngeal tumours are
treated with radiotherapy or conservation-surgery, but advanced staged disease is
currently often managed by combined radiotherapy and chemotherapy, if
laryngectomy is to be avoided. Laryngectomy is thus reserved for the very advanced
cases and for recurrences [1]. Local failure rates of early staged laryngeal cancer
after radiotherapy are 10–25%, while recurrence rates of advanced staged tumours
after (chemo)radiation are 25–50% [1-5].
Timely diagnosis in case of residual or recurrent laryngeal tumour is of great
importance to increase the possibility of cure and in some cases even with
preservation of laryngeal function. Diagnosing residual or recurrent tumour is,
however, challenging due to post-radiation changes, i.e., oedema, inflammation,
fibrosis and necrosis.
In a previous study we evaluated the yield of 207 direct laryngoscopies under general
anaesthesia with biopsies in 131 patients, who were suspected of having recurrent
laryngeal carcinoma after radiotherapy [6]. We found that the first laryngoscopy was
negative in 53% of patients and that 37 patients (28%) remained disease-free after
65 futile laryngoscopies. Moreover, taking biopsies in irradiated tissue has the
potential to cause infection, chondritis, failure to heal and further oedema [7].
The yield of direct laryngoscopy in the detection of recurrent laryngeal carcinoma
after radiotherapy could possibly be improved by patient selection based on imaging
techniques. Only a limited number of studies have been performed in this setting,
using computed tomography (CT), magnetic resonance imaging (MRI), thallium-201
(201Tl) scintigraphy and F-18-fluorodeoxyglucose positron emission tomography
(18FDG-PET). 18FDG-PET has been studied most extensively. Most authors report
promising accuracy data [8,15]. However, observer variation is scarcely reported.
The aim of the present study was to evaluate the value of 18FDG-PET in detecting
recurrent laryngeal carcinoma after radiotherapy, and to measure its observer
variation to determine its usefulness in routine clinical practice.
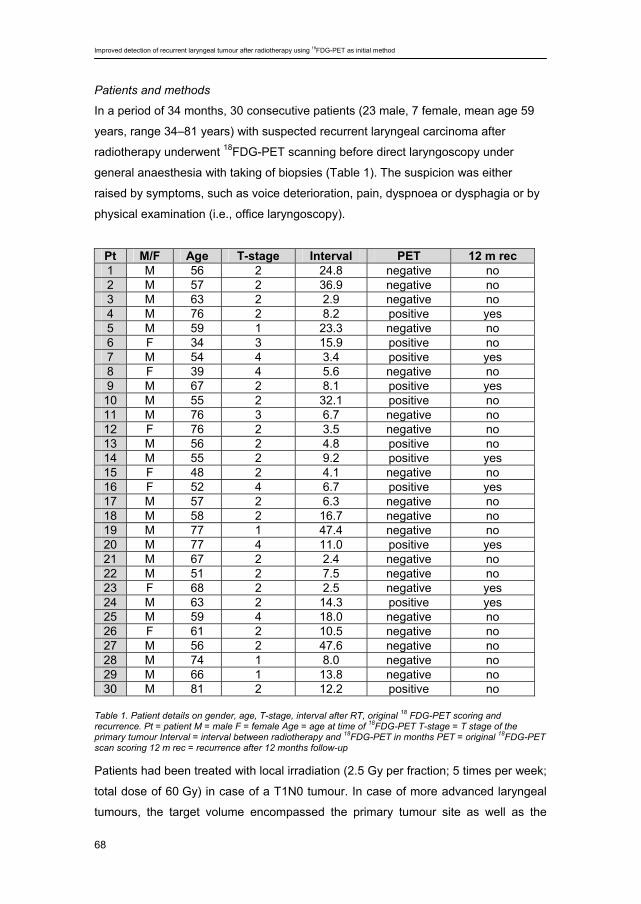
Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
68
Patients and methods
In a period of 34 months, 30 consecutive patients (23 male, 7 female, mean age 59
years, range 34–81 years) with suspected recurrent laryngeal carcinoma after
radiotherapy underwent 18FDG-PET scanning before direct laryngoscopy under
general anaesthesia with taking of biopsies (Table 1). The suspicion was either
raised by symptoms, such as voice deterioration, pain, dyspnoea or dysphagia or by
physical examination (i.e., office laryngoscopy).
Table 1. Patient details on gender, age, T-stage, interval after RT, original 18 FDG-PET scoring and recurrence. Pt = patient M = male F = female Age = age at time of 18FDG-PET T-stage = T stage of the primary tumour Interval = interval between radiotherapy and 18FDG-PET in months PET = original 18FDG-PET scan scoring 12 m rec = recurrence after 12 months follow-up Patients had been treated with local irradiation (2.5 Gy per fraction; 5 times per week;
total dose of 60 Gy) in case of a T1N0 tumour. In case of more advanced laryngeal
tumours, the target volume encompassed the primary tumour site as well as the
Pt M/F Age T-stage Interval PET 12 m rec 1 M 56 2 24.8 negative no 2 M 57 2 36.9 negative no 3 M 63 2 2.9 negative no 4 M 76 2 8.2 positive yes 5 M 59 1 23.3 negative no 6 F 34 3 15.9 positive no 7 M 54 4 3.4 positive yes 8 F 39 4 5.6 negative no 9 M 67 2 8.1 positive yes
10 M 55 2 32.1 positive no 11 M 76 3 6.7 negative no 12 F 76 2 3.5 negative no 13 M 56 2 4.8 positive no 14 M 55 2 9.2 positive yes 15 F 48 2 4.1 negative no 16 F 52 4 6.7 positive yes 17 M 57 2 6.3 negative no 18 M 58 2 16.7 negative no 19 M 77 1 47.4 negative no 20 M 77 4 11.0 positive yes 21 M 67 2 2.4 negative no 22 M 51 2 7.5 negative no 23 F 68 2 2.5 negative yes 24 M 63 2 14.3 positive yes 25 M 59 4 18.0 negative no 26 F 61 2 10.5 negative no 27 M 56 2 47.6 negative no 28 M 74 1 8.0 negative no 29 M 66 1 13.8 negative no 30 M 81 2 12.2 positive no
Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
69
nodal areas, with an elective dose of 2.0 Gy per fraction, 6 times a week, to a total
dose of 46 Gy and a total dose of 70 Gy at the primary tumour site.
All patients underwent 18FDG-PET after at least a 6 h fasting period. Sixty minutes
after intravenous administration of 370 MBq of 18FDG, patients with more weight than
85 kg received 555 MBq, imaging of the base of skull to the clavicles was started.
Two bedpositions were scanned, 5 min per position, using a full ring BGO PET
scanner (ECAT EXACT HR + CRI/ Siemens) without a rigid customized mask.
Iterative reconstruction (OSEM) with 2 iterations and 16 subsets was performed. A
transmission scan of each bed position (68-Ge source, 3 min) was used for
attenuation correction. 18FDG-PET was considered positive in case of focally enhanced tracer uptake,
incompatible with physiological tracer distribution. For the accuracy measurement the
scans were assessed by 2 experienced nuclear medicine physicians, with knowledge
of all clinically relevant information. Scoring was performed on a 2-point scale, either
positive or negative, no equivocals.
In the data-analysis, we classified patients as positive or negative with respect to the
presence of recurrent laryngeal carcinoma using a follow-up of at least 12 months: 18FDG-PET was considered true positive in case of a positive scan confirmed by a
tumour positive biopsy within 12 months. False positive if the scan was positive but
biopsies or follow-up were negative for 12 months after 18FDG-PET. 18FDG-PET was
classified as true negative in case of a negative scan in combination with negative
biopsies and a negative follow-up of 12 months. A false negative scan was a
negative scan but a positive biopsy within 12 months. Sensitivity, specificity, positive
predictive value, negative predictive value, accuracy and 95% confidence interval
(95% CI) were determined.
Subsequently, 18FDG-PET scans were revised and assessed by nine nuclear
medicine physicians and residents in training. Contrary to the initial scoring, the
observers were now blinded to clinical information. The observers were requested to
classify the scans using a 3-point ordinal scale (negative, equivocal, positive). The
interobserver variability was determined and expressed in a linear weighted kappa
which corrects for agreement by chance. Kappa statistics are used as a measure for
(fraction of) agreement. The higher the weighted kappa, the higher the agreement,
with a maximum of 1.0: <0.2 = little agreement, 0.21–0.4 = moderate agreement,
0.41–0.6 = reasonable agreement, 0.61–0.8 = substantial agreement, 0.81–
0.99 = almost perfect agreement [16].
Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
70
Results
Clinical suspicion of recurrence was raised at a median of 8.7 months (range 2.4–
47.6) after radiotherapy. Initial tumour T-stages included 23 early T-stage tumours (4
T1 and 19 T2), and 7 advanced T-stage tumours (2 T3 and 5 T4). All patients had
been treated by radiotherapy with curative intent. After one year of clinical follow-up 8
patients had a biopsy proven recurrent laryngeal carcinoma.
In the clinical setting, 7 recurrences were detected by 18FDG-PET; one patient had a
negative 18FDG-PET, but proven recurrence within 12 months. 18FDG-PET was
considered false positive in 4 patients, since increased uptake on the scan could not
be confirmed. 18FDG-PET was true negative in 18 patients. Sensitivity of 18FDG-PET
was 88% (95% CI 53–98%) at a specificity of 82% (95% CI 62–93%) with
corresponding positive and negative predictive values of 64% and 95%, respectively,
and an accuracy of 83%.
At revision of the 18FDG-PET scans, the observers had a kappa of 0.45 (95% CI
0.20–0.69; i.e., reasonable agreement vs. the clinical gold standard). Sensitive
reading (equivocal scores considered to be positive) showed a kappa of 0.40 (95%
CI 0.16–0.64), and conservative reading (equivocal scores negative) a kappa of 0.50
(95% CI 0.27–0.74). The sensitivity of individual observers with sensitive and
conservative reading ranged from 88% to 63–88%, respectively, and their specificity
from 41–68% to 55–95%.
The interobserver variability showed a kappa of 0.54 (95% CI 0.40–0.69; i.e.,
reasonable agreement), with no variation on sensitive and conservative reading
strategies. To explore potential differences between the 6 board-certified physicians
and the 3 residents, we calculated kappa’s for either group (Table 2), and found that
the differences were not statistically significant. Diagnostic certainty was slightly
higher in the experienced group, due to less equivocal scores (total proportion of
13% equivocal scores vs. 19%).
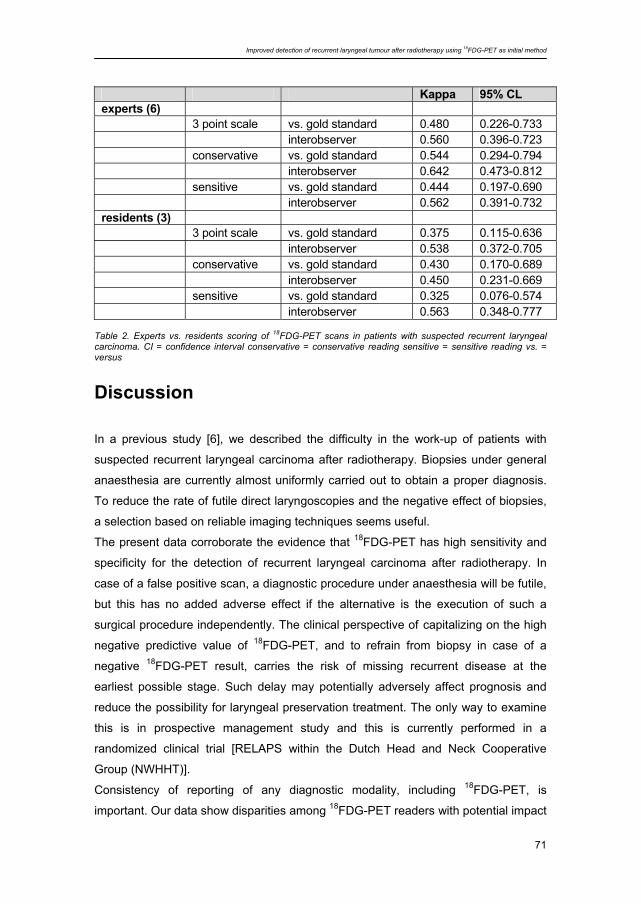
Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
71
Table 2. Experts vs. residents scoring of 18FDG-PET scans in patients with suspected recurrent laryngeal carcinoma. CI = confidence interval conservative = conservative reading sensitive = sensitive reading vs. = versus
Discussion
In a previous study [6], we described the difficulty in the work-up of patients with
suspected recurrent laryngeal carcinoma after radiotherapy. Biopsies under general
anaesthesia are currently almost uniformly carried out to obtain a proper diagnosis.
To reduce the rate of futile direct laryngoscopies and the negative effect of biopsies,
a selection based on reliable imaging techniques seems useful.
The present data corroborate the evidence that 18FDG-PET has high sensitivity and
specificity for the detection of recurrent laryngeal carcinoma after radiotherapy. In
case of a false positive scan, a diagnostic procedure under anaesthesia will be futile,
but this has no added adverse effect if the alternative is the execution of such a
surgical procedure independently. The clinical perspective of capitalizing on the high
negative predictive value of 18FDG-PET, and to refrain from biopsy in case of a
negative 18FDG-PET result, carries the risk of missing recurrent disease at the
earliest possible stage. Such delay may potentially adversely affect prognosis and
reduce the possibility for laryngeal preservation treatment. The only way to examine
this is in prospective management study and this is currently performed in a
randomized clinical trial [RELAPS within the Dutch Head and Neck Cooperative
Group (NWHHT)].
Consistency of reporting of any diagnostic modality, including 18FDG-PET, is
important. Our data show disparities among 18FDG-PET readers with potential impact
Kappa 95% CL experts (6) 3 point scale vs. gold standard 0.480 0.226-0.733 interobserver 0.560 0.396-0.723 conservative vs. gold standard 0.544 0.294-0.794 interobserver 0.642 0.473-0.812 sensitive vs. gold standard 0.444 0.197-0.690 interobserver 0.562 0.391-0.732 residents (3) 3 point scale vs. gold standard 0.375 0.115-0.636 interobserver 0.538 0.372-0.705 conservative vs. gold standard 0.430 0.170-0.689 interobserver 0.450 0.231-0.669 sensitive vs. gold standard 0.325 0.076-0.574 interobserver 0.563 0.348-0.777
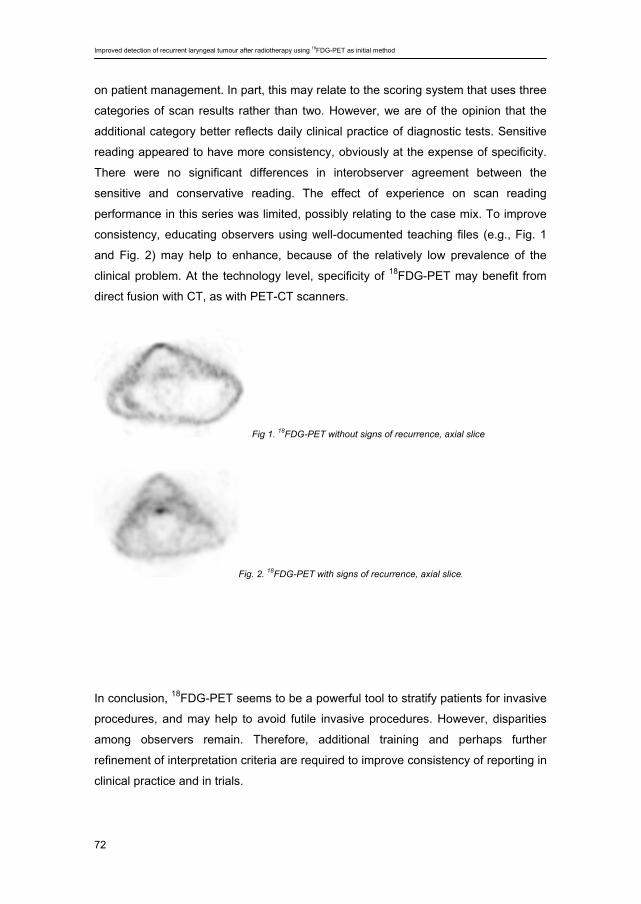
Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
72
on patient management. In part, this may relate to the scoring system that uses three
categories of scan results rather than two. However, we are of the opinion that the
additional category better reflects daily clinical practice of diagnostic tests. Sensitive
reading appeared to have more consistency, obviously at the expense of specificity.
There were no significant differences in interobserver agreement between the
sensitive and conservative reading. The effect of experience on scan reading
performance in this series was limited, possibly relating to the case mix. To improve
consistency, educating observers using well-documented teaching files (e.g., Fig. 1
and Fig. 2) may help to enhance, because of the relatively low prevalence of the
clinical problem. At the technology level, specificity of 18FDG-PET may benefit from
direct fusion with CT, as with PET-CT scanners.
Fig 1. 18FDG-PET without signs of recurrence, axial slice
Fig. 2. 18FDG-PET with signs of recurrence, axial slice.
In conclusion, 18FDG-PET seems to be a powerful tool to stratify patients for invasive
procedures, and may help to avoid futile invasive procedures. However, disparities
among observers remain. Therefore, additional training and perhaps further
refinement of interpretation criteria are required to improve consistency of reporting in
clinical practice and in trials.
Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
73
Literature
1. Parsons JT, Mendenhall WM, Stringer SP, Cassisi NJ (1998) T4 laryngeal carcinoma:
radiotherapy alone with surgery reserved for salvage. Int J Radiat Oncol Biol Phys
40:549-552
2. Spector JG, Sessions DG, Chao KS, Haughey BH, Hanson JM, Simpson JR, Perez CA
(1999) Stage I (T1N0M0) squamous cell carcinoma of the laryngeal glottis: therapeutic
results and voice preservation. Head Neck 21:707-717
3. Terhaard CH, Hordijk GJ, Broek van den P, Jong de PC, Snow GB, Hilgers FJ, Annyas
BA, Tjho-Heslinga RE, Jong de JM (1992) T3 laryngeal cancer: a retrospective study of
the Dutch Head and Neck Oncology Cooperative Group: study design and general
results. Clin Otolaryngol 17:393-402
4. Moose BD, Greven KM. (1997) Definitive radiation management for carcinoma of the
glottic larynx. Otolaryngol Clinic North Am 30:131-143
5. Medini E, Medini I, Lee CK, Gapany M, Levitt SH (1998) Curative radiotherapy for stage
II-III squamous cell carcinoma of the glottic larynx. Am J Clin Oncol 21:302-305
6. Brouwer J, Bodar EJ, Bree R de, Langendijk JA, Castelijns JA, Hoekstra OS, Leemans
CR (2004) Detecting recurrent laryngeal carcinoma after radiotherapy: Room for
improvement? Eur Arch Otorhinolaryngol 261:417-422
7. Bahadur S, Amatya RC, Kacker SK (1985) The enigma of post-radiation oedema and
residual or recurrent carcinoma of the larynx and pyriform sinus. J Laryngol Otol 99:763-
765
8. McGuirt WF, Greven KM, Keyes Jr JW, Williams III DW, Watson Jr NE, Geisinger KR,
Cappellari JO (1995) Positron emission tomography in the evaluation of laryngeal
carcinoma. Ann Otol Rhinol Laryngol 104:274-278
9. Kim HD, Boyd J, Dunphy F, Lowe V (1998) F-18 FDG PET scan after radiotherapy for
early stage larynx cancer. Clin Nucl Med 23:750-752
10. McGuirt WF, Greven KM, Williams III DW, Keyes Jr JW, Watson Jr NE (1998)
Laryngeal radionecrosis versus recurrent cancer: a clinical approach. Ann Otol Rhinol
Laryngol 107:293-296
11. Greven KM, Williams III DW, Keyes Jr JW, McGuirt WF, Watson Jr NE, Case LD (1997)
Can positron emission tomography distinguish tumour recurrence from radiation
sequellae in patients treated for larynx cancer? Cancer J Sci Am 3:353-357
12. Austin JR, Wong FC, Kim EE (1995) Positron emission tomography in the detection of
residual laryngeal carcinoma. Otol Head Neck Surg 113:404-407
13. Terhaard CH, Bongers V, Rijk PP van, Hordijk GJ (2001) F-18-fluoro-deoxy-glucose
positron-emission-tomography scanning in detection of local laryngeal/pharyngeal
cancer. Head Neck 23:933-941
Improved detection of recurrent laryngeal tumour after radiotherapy using 18FDG-PET as initial method
74
14. Stokkel MP, Terhaard CH, Mertens IJ, Hordijk GJ, Rijk PP van (1998) Fluorine-18-FDG
detection of laryngeal cancer postradiotherapy using dual-head coincidence imaging. J
Nucl Med 39:1385-1387
15. Cobben DCP, Laan BFAM van der, Maas B, Vaalburg W, Suurmeijer AJH, Hoekstra HJ,
Jager PL, Elsinga PH (2004) 18F-FLT PET for visualization of laryngeal cancer:
comparison with 18F-FDG PET. J Nucl Med 45:226-231
16. Landis JR, Koch GG (1977) The measurement of observer agreement for categorical
data. Biometrics 33:159-174
5
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
Addy C.G. van Hooren, Jolijn Brouwer, Remco de Bree, Otto S. Hoekstra, C. René Leemans, Carin A. Uyl-de Groot
Submitted
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
76
Abstract
The aim of this study was to estimate the cost-effectiveness of 18FDG-PET in the
selection for direct laryngoscopy in patients with suspicion of recurrent laryngeal
carcinoma after radiotherapy. In a retrospective study the direct medical costs of 30
patients with suspicion of recurrent laryngeal carcinoma after radiotherapy were
calculated from the first visit with suspicion of recurrent laryngeal cancer until one
year after. A conventional strategy, in which all these patients underwent direct
laryngoscopy under general anaesthesia with taking of biopsies, was compared to an 18FDG-PET strategy in which only patients with a positive or equivocal 18FDG-PET underwent direct laryngoscopy. A sensitivity analysis was performed to examine the
influence of the type of camera (PET, PET-CT, mobile PET) and ‘setting’ (academic,
non-academic hospital). The sensitivity, specificity, positive (PPV) and negative
predictive value (NPV) for the direct laryngoscopy were 1.0. These figures were for 18FDG-PET 1.0, 0.83, 0.64 and 1.0, respectively. The mean costs for the detection of
recurrent laryngeal cancer with direct laryngoscopy in the conventional strategy were
€ 13.230. The mean costs of an 18FDG-PET strategy were € 399 less than
performing a direct laryngoscopy in all patients. The costs of the 18FDG-PET strategy, expressed as costs saved per avoided direct laryngoscopy, were € 630.
The type of camera and setting had no influence on the cost-effectiveness of 18FDG-
PET. In patients with suspicion for recurrent laryngeal carcinoma after radiotherapy 18FDG-PET seems to be effective and not more costly in selecting patients for direct
laryngoscopy under general anaesthesia.
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
77
Introduction
The most common cancer of the head and neck is laryngeal cancer. Each year
around 700 new cases of laryngeal carcinoma are diagnosed in The Netherlands [1].
Early laryngeal cancer can usually be managed successfully with either radiotherapy
or surgery. Advanced stage disease is often treated with a combination of treatment
modalities. Many laryngeal carcinomas are treated with radiotherapy with or without
chemotherapy with surgery for salvage in case of recurrence. Depending on tumour
stage, the local recurrence rate varies from 10 to 50% [2]. Distinguishing between
recurrent carcinoma and radiotherapeutic sequels frequently poses a difficult clinical
problem. Computed tomography (CT) and magnetic resonance imaging (MRI) are
the most commonly used diagnostic methods in primary laryngeal carcinoma. When
recurrent laryngeal cancer is suspected they seem to be less effective, unless a
base-line posttreatment scan is performed [3-7]. Therefore, patients with clinical
suspicion of recurrent laryngeal cancer almost invariably undergo a direct
laryngoscopy under general anaesthesia with taking of biopsies. It has been shown
that less than 50% of these procedures show recurrence. Therefore, more than 50%
of these direct laryngoscopies are futile with unnecessary general anaesthesia and
risk of exacerbation of postradiotherapy changes [6]. F18-deoxyglucose (18FDG)
Positron Emission Tomography (PET) could be able to distinguish between recurrent
tumour and radiation sequelae and the first results of 18FDG-PET in the diagnosis of
recurrent laryngeal cancer are promising. In previous studies a specificity of 80-
100%, a positive predictive value of 67-89% and negative predictive value of 80-
100% has been reported [8-12].
Current health policy makers rightfully dictate the need for economic evaluations of
new expensive diagnostic techniques, such as 18FDG-PET [13]. Next to accuracy
data, the cost effectiveness of 18FDG-PET in the diagnosis of recurrent laryngeal
cancer thus needs to be investigated. In fact two diagnostic strategies have to be
compared: In the conventional strategy all patients undergo direct laryngoscopy
under general anaesthesia with taking of biopsies if necessary. In the 18FDG-PET
strategy only patients with a positive or equivocal 18FDG-PET undergo direct
laryngoscopy. In the latter strategy 18FDG-PET was used as selection method for
performing direct laryngoscopy. The aim of the present study was to compare the
costs of both strategies.
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
78
Patients and Methods Patients and clinical procedures
In this retrospective study, data of 30 patients who were seen between 1998-2001
with suspicion of recurrent laryngeal cancer after radiotherapy was analysed. All
patients had radiotherapy for a primary laryngeal carcinoma. The distribution of
tumour subsites was 63% glottis, 33% supraglottis and 3% subglottis. Ten percent of
the patients were staged T1, 43% T2, 20% T3 and 27% T4 (Table 1).
N0 N1 N2
T1 3 0 0
T2 10 2 1
T3 5 1 0
T4 6 1 1
Table 1. Number of patients in the several tumour and lymph node (N) stages of the primary laryngeal
carcinoma
All patients underwent a direct laryngoscopy with biopsies under general
anaesthesia as well as a single 18FDG-PET scan. They were all studied after fasting
overnight. Preceding the 18FDG-PET studies, the patients’ plasma glucose level was
measured. Sixty minutes after intravenous administration of 370MBq, 18FDG imaging
of the head and neck region was performed by scanning two bed positions. The 18FDG-PET scans were done by two technologists and a nuclear physician and
performed before the laryngoscopy to avoid false-positive 18FDG-PET findings as a
result of trauma due to the biopsies taken.
In both (modelled) strategies patients had regular follow-up visits after 18FDG-PET
and direct laryngoscopy. Histopathological examination of the biopsy taken or
primary tumour status after 12 months follow-up were used as the reference
standard. With the results of both diagnostic tests a decision tree with five paths was
constructed (Figure 1). Salvage laryngectomy was advised in case of recurrence.
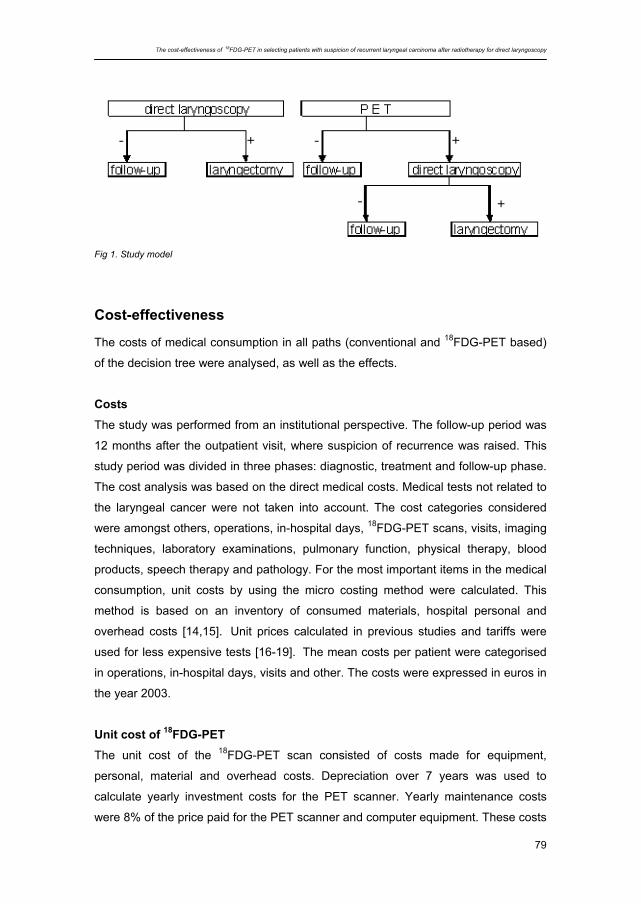
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
79
Fig 1. Study model
Cost-effectiveness
The costs of medical consumption in all paths (conventional and 18FDG-PET based)
of the decision tree were analysed, as well as the effects.
Costs
The study was performed from an institutional perspective. The follow-up period was
12 months after the outpatient visit, where suspicion of recurrence was raised. This
study period was divided in three phases: diagnostic, treatment and follow-up phase.
The cost analysis was based on the direct medical costs. Medical tests not related to
the laryngeal cancer were not taken into account. The cost categories considered
were amongst others, operations, in-hospital days, 18FDG-PET scans, visits, imaging
techniques, laboratory examinations, pulmonary function, physical therapy, blood
products, speech therapy and pathology. For the most important items in the medical
consumption, unit costs by using the micro costing method were calculated. This
method is based on an inventory of consumed materials, hospital personal and
overhead costs [14,15]. Unit prices calculated in previous studies and tariffs were
used for less expensive tests [16-19]. The mean costs per patient were categorised
in operations, in-hospital days, visits and other. The costs were expressed in euros in
the year 2003.
Unit cost of 18FDG-PET The unit cost of the 18FDG-PET scan consisted of costs made for equipment,
personal, material and overhead costs. Depreciation over 7 years was used to
calculate yearly investment costs for the PET scanner. Yearly maintenance costs
were 8% of the price paid for the PET scanner and computer equipment. These costs
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
80
were accounted according to the 18FDG-PET utilisation time for a head and neck 18FDG-PET scan and the time the PET scanner was used per year. The costs of 18FDG were based on the price paid per month for a fixed number of patient
injections. The cost of staff was valued by internal unit costs of the hospital
accounting system. To account for the overhead costs for infrastructure service, a
standard mark up percentage of 35% on all operating costs was used.
For the calculation of a unit cost of 18FDG-PET it is important to distinguish between
a covered and a non-covered setting, i.e. in a situation of using 18FDG-PET for
research purposes. When not all 18FDG-PET scans are covered, than these scans
should be ascribed to the unit costs of the 18FDG-PET scan which are covered. In
this study this is called the non-covered academic setting. The unit cost price of the 18FDG-PET and the 18FDG-PET-CT in an academic setting and in a non-covered
academic setting were calculated for the standard procedure of 15 minutes. The cost
of the mobile PET scanner was based on the rent paid for the mobile PET scanner
and the hospital personal needed. The cost of 18FDG was based on the mean price
of 370 MBq charged by Tyco Healthcare (Zaltbommel, The Netherlands). The total
costs of both strategies were calculated for the various 18FDG-PET and 18FDG-PET-
CT settings.
Effectiveness
The effects were expressed as the number of direct laryngoscopies avoided, mean
cost per strategy within 12 months and costs saved per avoided direct laryngoscopy
Sensitivity analysis
The cost of 18FDG-PET could be influenced by the type of camera (PET, PET-CT,
mobile PET) and ‘setting’ (academic, non-covered academic hospital). Because there
were no studies, which compare 18FDG-PET and 18FDG-PET-CT for this specific
indication, it is assumed in this analysis that both imaging techniques detect residual
laryngeal carcinoma after radiotherapy equally well. The efficiency of 18FDG-PET in
the diagnosis of recurrent laryngeal cancer could also depend on the sensitivity and
specificity of 18FDG-PET, examination time of 18FDG-PET as well as the prevalence
of recurrences in the studied population. The influence of these parameters on the
efficiency of 18FDG-PET was therefore analysed in the sensitivity analysis.
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
81
Statistical analysis
In this study the mean costs per patient per cost category are reported. The 95%
variance was calculated for each category in each phase. Statistical significance
between the various strategies was not calculated due to the small number of
patients.
Results
Clinical results
The direct costs of 30 patients, 22 men and 8 women (mean age 64.0; range 52-82)
were examined. The prevalence of recurrent laryngeal cancer in this study was
0.233.
For direct laryngoscopy the sensitivity, specificity, positive as well as the negative
predictive value in this study were 1.0 since no additional recurrences were detected
during 12 months follow-up. The positive test probability was 0.233. The negative test
probability was 0.767. For 18FDG-PET the sensitivity was 1.0, the specificity was
0.86. The positive and negative predictive value was respectively 0.64 and 1.0. The
positive test probability was 0.367. The sensitivity of 1.0 in this study implied that no
patient was withheld a direct laryngoscopy if selection was based on 18FDG-PET. In
total 19 direct laryngoscopies would have been avoided if 18FDG-PET was used for
selection.
There were four false-positive 18FDG-PET scans in the 18FDG-PET strategy for which
no obvious explanation other than post-radiotherapy inflammatory changes was
found. Four patients with recurrent laryngeal cancer had a total laryngectomy. One
patient refused, another patient died within one month and in one patient the tumour
was inoperable. Two patients underwent microlaryngoscopy and CO2-laser treatment
of oedema because of dyspnoea complaints. The costs of these operations were
also taken into account.
Cost analysis
The unit cost price of 18FDG-PET amounted to € 521 (Personal (P) €29; Material (M)
€356; Overhead (O) €135). The cost price of 18FDG-PET in a non-covered academic
setting, amounted to € 1156 (P €333; M € 523; O €300). The cost price of a mobile 18FDG-PET was € 611 (P € 29; M € 423; O € 158).
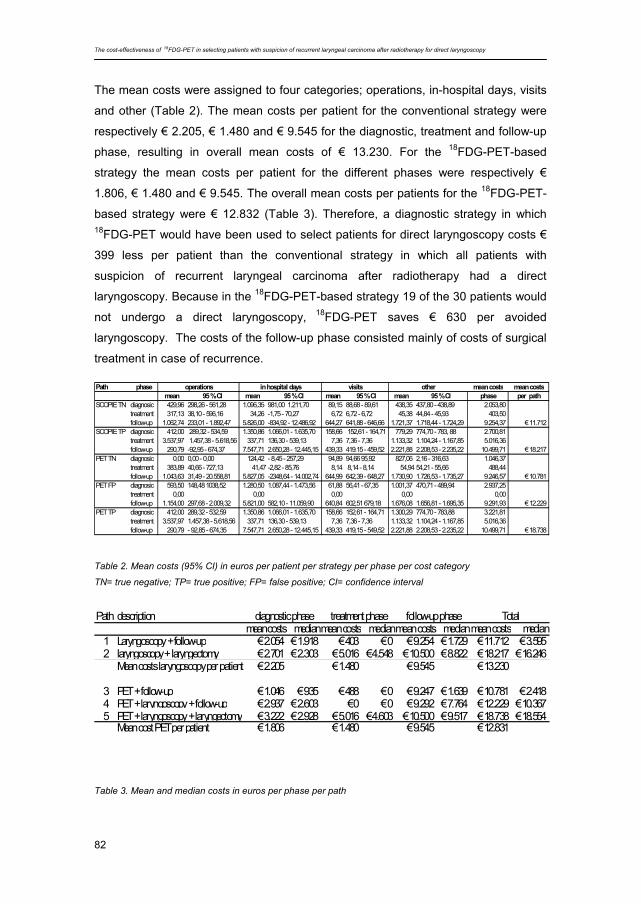
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
82
The mean costs were assigned to four categories; operations, in-hospital days, visits
and other (Table 2). The mean costs per patient for the conventional strategy were
respectively € 2.205, € 1.480 and € 9.545 for the diagnostic, treatment and follow-up
phase, resulting in overall mean costs of € 13.230. For the 18FDG-PET-based
strategy the mean costs per patient for the different phases were respectively €
1.806, € 1.480 and € 9.545. The overall mean costs per patients for the 18FDG-PET-
based strategy were € 12.832 (Table 3). Therefore, a diagnostic strategy in which 18FDG-PET would have been used to select patients for direct laryngoscopy costs €
399 less per patient than the conventional strategy in which all patients with
suspicion of recurrent laryngeal carcinoma after radiotherapy had a direct
laryngoscopy. Because in the 18FDG-PET-based strategy 19 of the 30 patients would
not undergo a direct laryngoscopy, 18FDG-PET saves € 630 per avoided
laryngoscopy. The costs of the follow-up phase consisted mainly of costs of surgical
treatment in case of recurrence.
Table 2. Mean costs (95% CI) in euros per patient per strategy per phase per cost category TN= true negative; TP= true positive; FP= false positive; CI= confidence interval
Table 3. Mean and median costs in euros per phase per path
Path description mean costs medianmean costs medianmean costs medianmean costs median
1 Laryngoscopy + follow-up € 2.054 € 1.918 € 403 € 0 € 9.254 € 1.729 € 11.712 € 3.5952 laryngoscopy + laryngectomy € 2.701 € 2.303 € 5.016 € 4.548 € 10.500 € 8.822 € 18.217 € 16.246
Mean costs laryngoscopy per patient € 2.205 € 1.480 € 9.545 € 13.230
3 PET + follow-up € 1.046 € 935 € 488 € 0 € 9.247 € 1.639 € 10.781 € 2.4184 PET + laryngoscopy + follow-up € 2.937 € 2.603 € 0 € 0 € 9.292 € 7.764 € 12.229 € 10.3675 PET + laryngoscopy + laryngectomy € 3.222 € 2.928 € 5.016 € 4.603 € 10.500 € 9.517 € 18.738 € 18.554
Mean cost PET per patient € 1.806 € 1.480 € 9.545 € 12.831
diagnostic phase treatment phase follow-up phase Total
Path phase mean costs mean costsmean 95 % CI mean 95 % CI mean 95 % CI mean 95 % CI phase per path
SCOPIE TN diagnosic 429,96 298,26 - 561,28 1.096,35 981,00 1.211,70 89,15 88,68 - 89,61 438,35 437,80 - 438,89 2.053,80treatment 317,13 38,10 - 596,16 34,26 -1,75 - 70,27 6,72 6,72 - 6,72 45,38 44,84 - 45,93 403,50follow-up 1.062,74 233,01 - 1.892,47 5.826,00 -834,92 - 12.486,92 644,27 641,88 - 646,66 1.721,37 1.718,44 - 1.724,29 9.254,37 € 11.712
SCOPIE TP diagnosic 412,00 289,32 - 534,59 1.350,86 1.066,01 - 1.635,70 158,66 152,61 - 164,71 779,29 774,70 - 783, 88 2.700,81treatment 3.537,97 1.457,38 - 5.618,56 337,71 136,30 - 539,13 7,36 7,36 - 7,36 1.133,32 1.104,24 - 1.167,85 5.016,36follow-up 290,79 -92,95 - 674,37 7.547,71 2.650,28 - 12.445,15 439,33 419.15 - 459,52 2.221,88 2.208,53 - 2.235,22 10.499,71 € 18.217
PET TN diagnosic 0,00 0,00 - 0,00 124,42 - 8,45 - 257,29 94,89 94,66 95,92 827,06 2,16 - 316,63 1.046,37treatment 383,89 40,66 - 727,13 41,47 -2,82 - 85,76 8,14 8,14 - 8,14 54,94 54,21 - 55,66 488,44follow-up 1.043,63 31,49 - 20.558,81 5.827,05 -2348,64 - 14.002,74 644,99 642,39 - 648,27 1.730,90 1.726,53 - 1.735,27 9.246,57 € 10.781
PET FP diagnosic 593,50 148,48 1038,52 1.280,50 1.087,44 - 1.473,56 61,88 56,41 - 67,35 1.001,37 470,71 - 489,94 2.937,25treatment 0,00 0,00 0,00 0,00 0,00follow-up 1.154,00 297,68 - 2.009,32 5.821,00 582,10 - 11.059,90 640,84 602,51 679,18 1.676,08 1.656,81 - 1.695,35 9.291,93 € 12.229
PET TP diagnosic 412,00 289,32 - 532,59 1.350,86 1.066,01 - 1.635,70 158,66 152,61 - 164,71 1.300,29 774,70 - 783,88 3.221,81treatment 3.537,97 1.457,38 - 5.618,56 337,71 136,30 - 539,13 7,36 7,36 - 7,36 1.133,32 1.104,24 - 1.167,85 5.016,36follow-up 290,79 - 92,85 - 674,35 7.547,71 2.650,28 - 12.445,15 439,33 419,15 - 549,52 2.221,88 2.208,53 - 2.235,22 10.499,71 € 18.738
in hospital daysoperations visits other
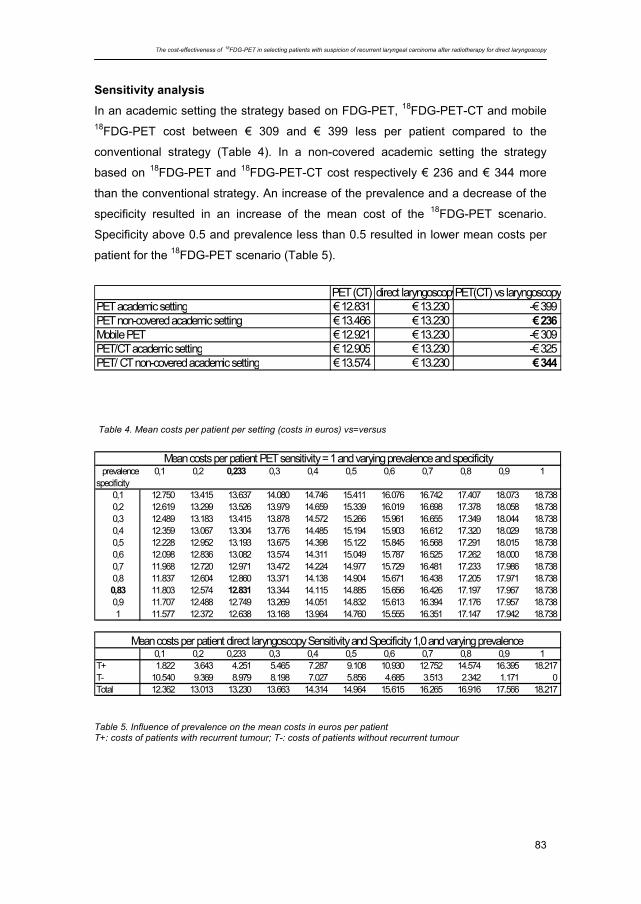
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
83
Sensitivity analysis
In an academic setting the strategy based on FDG-PET, 18FDG-PET-CT and mobile 18FDG-PET cost between € 309 and € 399 less per patient compared to the
conventional strategy (Table 4). In a non-covered academic setting the strategy
based on 18FDG-PET and 18FDG-PET-CT cost respectively € 236 and € 344 more
than the conventional strategy. An increase of the prevalence and a decrease of the
specificity resulted in an increase of the mean cost of the 18FDG-PET scenario.
Specificity above 0.5 and prevalence less than 0.5 resulted in lower mean costs per
patient for the 18FDG-PET scenario (Table 5).
Table 4. Mean costs per patient per setting (costs in euros) vs=versus
Table 5. Influence of prevalence on the mean costs in euros per patient T+: costs of patients with recurrent tumour; T-: costs of patients without recurrent tumour
PET (CT) direct laryngoscopyPET(CT) vs laryngoscopyPET academic setting € 12.831 € 13.230 -€ 399PET non-covered academic setting € 13.466 € 13.230 € 236Mobile PET € 12.921 € 13.230 -€ 309PET/CT academic setting € 12.905 € 13.230 -€ 325PET/ CT non-covered academic setting € 13.574 € 13.230 € 344
prevalence 0,1 0,2 0,233 0,3 0,4 0,5 0,6 0,7 0,8 0,9 1specificity
0,1 12.750 13.415 13.637 14.080 14.746 15.411 16.076 16.742 17.407 18.073 18.7380,2 12.619 13.299 13.526 13.979 14.659 15.339 16.019 16.698 17.378 18.058 18.7380,3 12.489 13.183 13.415 13.878 14.572 15.266 15.961 16.655 17.349 18.044 18.7380,4 12.359 13.067 13.304 13.776 14.485 15.194 15.903 16.612 17.320 18.029 18.7380,5 12.228 12.952 13.193 13.675 14.398 15.122 15.845 16.568 17.291 18.015 18.7380,6 12.098 12.836 13.082 13.574 14.311 15.049 15.787 16.525 17.262 18.000 18.7380,7 11.968 12.720 12.971 13.472 14.224 14.977 15.729 16.481 17.233 17.986 18.7380,8 11.837 12.604 12.860 13.371 14.138 14.904 15.671 16.438 17.205 17.971 18.7380,83 11.803 12.574 12.831 13.344 14.115 14.885 15.656 16.426 17.197 17.967 18.7380,9 11.707 12.488 12.749 13.269 14.051 14.832 15.613 16.394 17.176 17.957 18.7381 11.577 12.372 12.638 13.168 13.964 14.760 15.555 16.351 17.147 17.942 18.738
0,1 0,2 0,233 0,3 0,4 0,5 0,6 0,7 0,8 0,9 1T+ 1.822 3.643 4.251 5.465 7.287 9.108 10.930 12.752 14.574 16.395 18.217T- 10.540 9.369 8.979 8.198 7.027 5.856 4.685 3.513 2.342 1.171 0Total 12.362 13.013 13.230 13.663 14.314 14.964 15.615 16.265 16.916 17.566 18.217
Mean costs per patient PET sensitivity = 1 and varying prevalence and specificity
Mean costs per patient direct laryngoscopy Sensitivity and Specificity 1,0 and varying prevalence
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
84
Discussion
In this retrospective study the cost-effectiveness of an 18FDG-PET-based strategy in
comparison with a conventional strategy in patients with suspicion of recurrent
laryngeal carcinoma after radiotherapy was determined. 18FDG-PET had a sensitivity
and specificity of 1.0 and 0.86, respectively. The costs of the 18FDG-PET-strategy
were € 399 lower per patient than the conventional method using a direct
laryngoscopy for all patients. Therefore, it can be concluded that 18FDG-PET is
effective and not more costly in selecting patients with suspicion of recurrent
laryngeal carcinoma after radiotherapy for direct laryngoscopy under general
anaesthesia. This was the case for all settings of 18FDG-PET and 18FDG-PET-CT,
except from cases when the costs of research are not fully covered.
The need for economic evaluations of new technologies like PET has been
recognised. Nevertheless economic evaluations have remained under-utilised in
nuclear medicine. Furthermore economic evaluation studies in nuclear medicine
differed widely in terms of form of evaluation, outcome measures and costing [20].
Only one study calculated the costs of 18FDG-PET in the diagnosis of recurrent
laryngeal cancer. In a limited cost-effectiveness study Bongers et al. found that
implementation of 18FDG-PET using a dual-head camera in the detection of recurrent
laryngeal cancer has additional costs of 64 Euro per patient [21]. In the present study
a more extensive cost-analysis is performed using a dedicated full-ring PET-scanner.
The quality of life of patients was not taken into account, although there were
probably more negative side effects in the conventional strategy. As in all diagnostic
imaging techniques, there is an interobserver variability in reporting the scans. This
may influence the overall cost-effectiveness of 18FDG-PET. A calculation of this was
not performed in this study.
The 18FDG-PET-based strategy in this study showed no false-negative test results.
Therefore, no patients would have been wrongly withheld further diagnostics and
eventual therapy. Although the patientgroup was originally included consecutively,
some patients were lost in retrospect because not enough data were available to
calculate the costs. This led to a group with a coincidental high sensitivity of 18FDG-
PET of 100%. In a systematic review by Brouwer et al.[22] the pooled sensitivity was
89% and this is a more valid number than 100%. False negative results in a 18FDG-
PET strategy will carry the risk of missing recurrent disease at the earliest possible
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
85
stage. Such delay may potentially adversely affect prognosis and reduce the
possibility for laryngeal preservation treatment. It may also induce extra costs.
The results of this study though, are in agreement with the results of a study by
Terhaard et al. [12]. They concluded that a18FDG-PET scan should be the first
diagnostic step when a local recurrence is suspected after radiotherapy and in case
of a negative 18FDG-PET scan no direct laryngoscopy with taking of biopsies is
needed.
In this study the prevalence was only 23%. However, in a study by Brouwer et al. the
prevalence was 45% [3]. Differences in prevalence between studies are commonly
found. In the present study half of the patients had advanced primary tumours. The
probability of recurrence in advanced primary tumours is considered higher. There is
a tendency to treat advanced laryngeal cancer with concomitant radiotherapy and
chemotherapy. If the percentage of patients treated for advanced primary tumours
would have been higher, the prevalence of recurrent disease would be higher and
consequently the 18FDG-PET-based strategy would have been less cost effective. On
the other hand, in a previous study, it was shown that patients with advanced stage
laryngeal carcinoma needed most direct laryngoscopies [3]. From that point of view it
can be anticipated that patients with advanced primary tumours may particularly
benefit from an 18FDG-PET based strategy.
Since both the conventional and the 18FDG-PET-based strategy showed no false-
negative test results in this study, these pathways are absent in the decision model
used. An estimation of the costs and the effects of false-negative findings can not be
made. Secondly, because of the absence of false-negative 18FDG-PET scans, the
influence of sensitivity of 18FDG-PET can therefore not be tested in a sensitivity
analysis.
As previously stated, cost-effectiveness studies differ in terms of evaluation and
costing. The costs of an 18FDG-PET scan depends e.g. on the number of 18FDG-PET
studies per PET camera, type of PET camera, number of bed positions, time per bed
position, costs of 18FDG, number of technologists and nuclear physicians. For an 18FDG-PET scan of the head and neck two bed positions were scanned with a total
time of 15 minutes per patient. 18FDG-PET as whole-body technique may be
performed when screening for distant metastases is indicated in patient with risk
factors [23]. Because of the different indications a whole-body 18FDG-PET was not
used in this study. If a whole-body scan is used there is a possible risk that false
positive lesions are found elsewhere in the body. This would induce extra costs for
further investigation. Since a whole-body scan was not used in this study, these costs
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
86
were not calculated. The extra costs of false positive results within the larynx were
included.
For the delivery of 18FDG there is only one distributor in The Netherlands. Probably
the price of 18FDG can be reduced when more distributors enter the market, resulting
in a lower price per 18FDG-PET scan.
Although there are differences between health systems between countries, we think
that our findings could largely be generalised to other countries. The results largely
depend on the price of 18FDG-PET scan or18FDG-PET-CT scan and the costs of
follow-up treatment. In this respect, we calculated with real cost prices instead of
using tariffs. The used prices are therefore not depended of a health care financing
system.
Since non-surgical treatments with salvage surgery in reserve are being popularised,
the clinical problem of detecting recurrent laryngeal carcinoma after radiotherapy is
increasingly important. Therefore, cost-effectiveness is also one of the endpoints in
an ongoing randomised multi-center trial [24].
In conclusion, 18FDG-PET seems to be effective and not more costly in selecting
patients for direct laryngoscopy under general anaesthesia to detect recurrent
laryngeal carcinoma after radiotherapy. These findings have to be confirmed in a
prospective randomised clinical trial.
Acknowledgement The authors like to thank A.J.G.A. van Heiningen for critical review of the manuscript.
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
87
Literature 1. Siesling S, van Dijck JA, Visser O, Coebergh JW (2003) Trends in incidence of and
mortality from cancer in The Netherlands in the period 1989-1998. Eur J Cancer 39:2521-
2530
2. O’Brien PC (1996) Tumor recurrence of treatment sequela following radiotherapy for larynx
cancer. J Surg Oncol 63:130-135
3. Brouwer J, Bodar EJ, de Bree R, Langendijk JA, Castelijns JA, Hoekstra OS, Leemans CR
(2004) Detecting recurrent laryngeal carcinoma after radiotherapy: Room for improvement.
Eur Arch Otorinolaryngol 261:417-422
4. Lell, M, Baum U, Greess H, Noymar A, Nkenke E, Koester M, Lenz M, Bautz W (2000)
Head and neck tumours: imaging recurrent tumor and post-therapeutic changes with CT
and MRI. Eur J Radiol 33:239-247
5. Lowe VJ, Kim H, Boyd JH, Eisenbeis JF, Dunphy FR, Fletcher JW (1999) Primary and
recurrent early stage laryngeal cancer: Preliminary results of 2-[Fluorine 18] Fluoro-2-
deoxy-D-glucose PET imaging. Radiology 212:799-802
6. Zinreich SJ (2002) Imaging in laryngeal cancer: computed tomography, magnetic
resonance imaging, positron emission tomography. Otolaryngol Clin North America
35:971-991
7. Hermans R, Pameijer FA, Mancuso AA, Parsons JT, Mendenhall WM (2000) Laryngeal or
hypopharyngeal squamous cell carcinoma: can follow-up CT after definitive radiation
therapy be used to detect local failure earlier than clinical examination alone? Radiology
214:683–687
8. Farber LA, Benard F, Machtay M, Smith RJ, Weber RS, Weinstein GS, Chalian AA, Alavi
A, Rosenthal DI (1999) Detection of recurrent head and neck squamous cell carcinomas
after radiation therapy with 2-18F-fluoro-2-deoxy-D-glucose positron emission tomography.
Laryngoscope 109:970-975
9. Greven KM, Williams III DW, Keyes Jr JW, McGuirt FW, Watson NE Jr, Case LD (1997)
Can Positron Emission Tomography distinguish tumor recurrence from irradiation sequelae
in patients treated for larynx cancer? Cancer 3:353-357
10. Greven, KM., Williams III DW, McGuirt DW Sr, Harkness BA, D’Agostino RB Jr, Keyers JW
Jr (2001) Serial Positron Emission Tomography scans following radiation therapy of
patients with head and neck cancer. Head Neck 23:942-946
11. Lapela, M, Grenman R, Kurki T, Joensuu H, Leskinen S, Lindholm P, Haaparanta M,
Ruotsalainen U, Minn H (1995) Head and neck cancer: detection of recurrence with PET
and 2-[F18]fluoro-2-deoxy-D-glucose. Radiology 197:205-211
The cost-effectiveness of 18FDG-PET in selecting patients with suspicion of recurrent laryngeal carcinoma after radiotherapy for direct laryngoscopy
88
12. Terhaard C.H., Bongers V, van Rijk P, Hordijk GJ (2001) F-18-Fluoro-Deoxyglucose
positron emission tomography scanning in detection of local recurrence after radiotherapy
for laryngeal / pharyngeal cancer. Head Neck 23:933-941
13. Valk PE, Pounds TR, Tesar RD, Hopkins DM, Haseman MK (1996) Cost-effectiveness of
PET imaging in clinical oncology. Nucl Med Biol 23:737-743
14. Drummond, MF, O’Brien B, Stoddart GL, Torrance GW (1997) Methods for the economic
evaluation of health care programmes. Toronto: Oxford University Press
15. Oostenbrink JB, Koopmanschap MA, Rutten FFH (2000) Manual for costing research
[Handleiding voor kostenonderzoek]. Amstelveen: Health Care Board
16. http://www.ctgzorg.nl
17. van Agthoven M, Heule-Dieleman HA, Knegt PP, Kaanders JH, Baatenburg de Jong RJ,
Kremer B, Leemans CR, Marres HA, Manni JJ, Langendijk JA, Levendag PC, Tjho-
Heslinga RE, Jong de JM, Boer de MF, Uyl-de Groot CA (2006) Compliance and efficiency
before and after implementation of a clinical practice guideline for laryngeal carcinomas.
Eur Arch Otorhinolaryngol 263:729-732
18. Agthoven M van, van Ineveld BM, de Boer MF, Leemans CR, Knegt PP, Snow GB, Uyl-de
Groot CA (2001) The costs of head and neck oncology: primary tumours, recurrent
tumours and long-term follow-up. Eur J Cancer 27:2204-2211
19. Goor KM, Mahieu HF, Leemans CR, Peeters AJ, Langendijk JA, van Aghthoven M (2003)
CO2-laser decortication: an efficient alternative to radiotherapy in the treatment of T1a
carcinomas of the glottis [Decorticatie met CO2 laser; een doelmatig alternatief voor
radiotherapie in de behandeling van T1a-carcinomen van de glottis] Ned Tijdschr Geneesk
147:1177-1181
20. Dietlein W, Knapp H, Lauterbach KW, Schicha H (1999) Economic evaluation studies in
nuclear medicine. Eur J Nucl Med 26:663-680
21. Bongers V, Hobbelink MG, van Rijk PP, Hordijk GJ (2002) Cost-effectiveness of dual-head
18F-fluorodeoxyglucose PET for the detection of recurrent laryngeal cancer. Cancer
Biother Radiopharm 17:303-306
22. Brouwer J, Hooft L, Hoekstra OS, Riphagen II, Castelijns JA, Bree R de, Leemans CR
(2008) Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal
carcinoma after radiotherapy. Head Neck 30:889-897
23. Brouwer J, Senft A, Bree R de, Comans EFI, Golding RP, Castelijns JA, Hoekstra OS,
Leemans CR (2006) Screening for distant metastases in patients with head and neck
cancer: is there a role for 18 FDG-PET? Oral Oncol 42:275-280
24. Bree R de, Putten L van der, Hoekstra OS, Kuik DJ, Uyl-de Groot CA, Tinteren H van,
Leemans CR, Boers M: RELAPS Study Group (2007) A randomized trial of PET scanning
to improve diagnostic yield of direct laryngoscopy in patients with suspicion of recurrent
laryngeal carcinoma after radiotherapy. Contemp Clin Trials 28:705-7
6
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
Jolijn Brouwer, Remco de Bree, Otto S. Hoekstra,
Johannes A. Langendijk, Jonas A. Castelijns, C. René Leemans
Clin Otolaryngol (2005) 30:438-443

Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
90
Abstract
The detection of distant metastases during screening influences the choice of
treatment in patients with head and neck squamous cell carcinoma (HNSCC). There
is no consensus on the diagnostic technique that has to be used nor on the subgroup
of HNSCC patients that may benefit from screening. Questionnaire on current
practice concerning the diagnostic work-up in HNSCC patients for screening for
distant metastases. Investigators in the 12 otolaryngology / head and neck and seven
oromaxillofacial departments treating head and neck cancer in the Netherlands. The
response rate was 100%. Indications for screening were cervical lymph node
metastases (63%), mutilating surgery (58%), locoregional recurrence (47%),
advanced T-stage (32%), second primary tumour (21%). Diagnostic techniques
routinely used for screening besides chest X-ray were chest CT (84%), liver
ultrasound (53%), liver CT (16%) and bone scintigraphy (42%). Forty-two per cent of
the clinicians were not satisfied with the current methods of screening. This survey
shows a substantial variation in indications and diagnostic techniques used for
screening for distant metastases between the major institutions treating head and
neck cancer in the Netherlands. There is a need for guidelines for screening for
distant metastases in patients with head and neck cancer.
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
91
Introduction
Head and neck squamous cell carcinomas (HNSCC) grow locally invasive and have
a proclivity to metastasize to regional lymph nodes rather than to spread
haematogenous. Distant metastases usually occur late during the course of the
disease. If distant metastases are present, the general opinion dictates that no
curative options are available. Thus, the presence of distant metastases changes the
prognosis and influences the choice of treatment in patients with HNSCC [1].
The incidence of distant metastases in HNSCC patients is relatively low in
comparison with other malignancies. The reported incidence of clinically detected
distant metastases in HNSCC patients ranges from 4% to 24% [2-7], while mainly
historical autopsy studies demonstrated an incidence of distant metastases of 11–
47% [8]. The incidence of distant metastases at presentation varies from 2% to 17%
of HNSCC patients [5,6].
The incidence of distant metastases of HNSCC is directly related to the stage of the
tumour, particularly the presence and extension of lymph node metastases, and
regional control above the clavicles [2-5]. The presence of lymph node metastases
increases the risk of developing distant metastases [8-10]. Particularly patients with
multiple lymph node metastases, especially three or more, have a greater risk of
developing distant metastases [9,11]. Almost 50% of all HNSCC patients with more
than three lymph node metastases will develop distant metastases [9]. Moreover,
low-jugular lymph node metastases are also associated with a higher risk for distant
metastases [10]. Locoregional control also significantly influences development of
distant metastases [2,5,8,12].
Once distant metastases occur, the prognosis is dismal. The median time to death
from the diagnosis of distant metastases ranges from 1 to 12 months [3,4]. About
88% of the patients with distant metastases will be dead within 12 months [3].
Although locoregional control in HNSCC has improved significantly with the use of
multimodality treatment, the overall survival rate has not improved during the last
decades. This was mainly caused by the increased incidence of distant metastases
[7]. If this trend continues, detection and treatment of distant metastases become
increasingly important.
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
92
The lungs (45–83%), bone (10–41%) and liver (6–24%) are the most common sites
of haematogenous metastases from HNSCC [3-5]. Distant spread to other sites is
less frequent.
Screening can be defined as the examination of asymptomatic patients to classify
them as likely or unlikely to have the disease in question. It has become increasingly
common to offer varied screening recommendations based on perceived risk for
disease. However, there are no clear guidelines for screening for distant metastases
in patients with HNSCC [13]. There is neither consensus on the diagnostic technique
that has to be used nor on the subgroup of HNSCC patients that may benefit from
screening.
To evaluate current practice concerning the diagnostic work-up in HNSCC patients,
we performed a questionnaire among surgeons in the major institutions treating head
and neck cancer in the Netherlands.
Materials and Method
The questionnaire on current clinical practice concerning screening for distant
metastases in patients with locoregional advanced HNSCC was sent to clinicians in
12 otolaryngology/head and neck surgery and seven oromaxillofacial surgery
departments treating head and neck cancer in the Netherlands. The questionnaire
[Fig. 1] was accompanied by an explanatory letter.
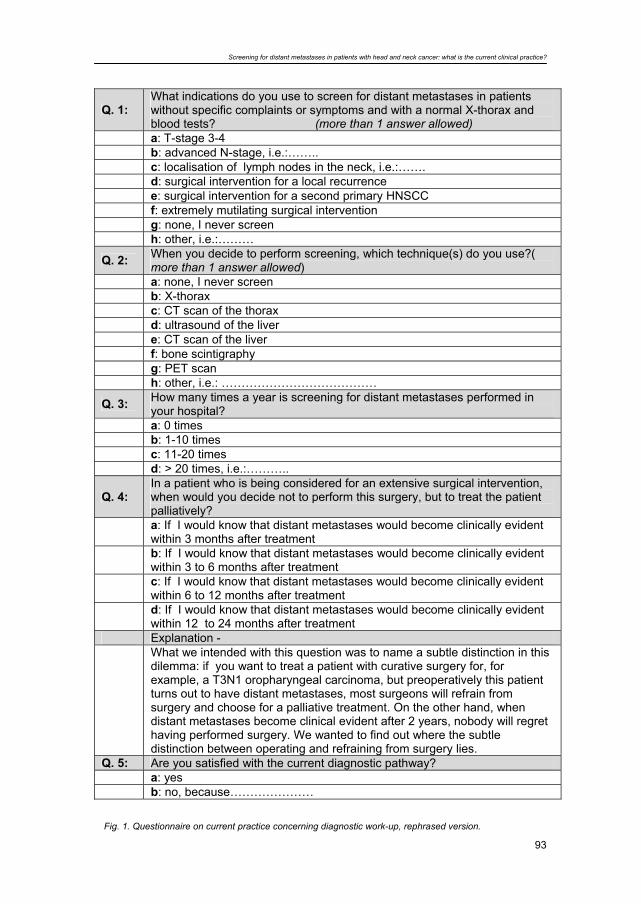
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
93
Q. 1: What indications do you use to screen for distant metastases in patients without specific complaints or symptoms and with a normal X-thorax and blood tests? (more than 1 answer allowed)
a: T-stage 3-4 b: advanced N-stage, i.e.:…….. c: localisation of lymph nodes in the neck, i.e.:……. d: surgical intervention for a local recurrence e: surgical intervention for a second primary HNSCC f: extremely mutilating surgical intervention g: none, I never screen h: other, i.e.:………
Q. 2: When you decide to perform screening, which technique(s) do you use?( more than 1 answer allowed)
a: none, I never screen b: X-thorax c: CT scan of the thorax d: ultrasound of the liver e: CT scan of the liver f: bone scintigraphy g: PET scan h: other, i.e.: …………………………………
Q. 3: How many times a year is screening for distant metastases performed in your hospital?
a: 0 times b: 1-10 times c: 11-20 times d: > 20 times, i.e.:………..
Q. 4: In a patient who is being considered for an extensive surgical intervention, when would you decide not to perform this surgery, but to treat the patient palliatively?
a: If I would know that distant metastases would become clinically evident within 3 months after treatment
b: If I would know that distant metastases would become clinically evident within 3 to 6 months after treatment
c: If I would know that distant metastases would become clinically evident within 6 to 12 months after treatment
d: If I would know that distant metastases would become clinically evident within 12 to 24 months after treatment
Explanation -
What we intended with this question was to name a subtle distinction in this dilemma: if you want to treat a patient with curative surgery for, for example, a T3N1 oropharyngeal carcinoma, but preoperatively this patient turns out to have distant metastases, most surgeons will refrain from surgery and choose for a palliative treatment. On the other hand, when distant metastases become clinical evident after 2 years, nobody will regret having performed surgery. We wanted to find out where the subtle distinction between operating and refraining from surgery lies.
Q. 5: Are you satisfied with the current diagnostic pathway? a: yes b: no, because…………………
Fig. 1. Questionnaire on current practice concerning diagnostic work-up, rephrased version.
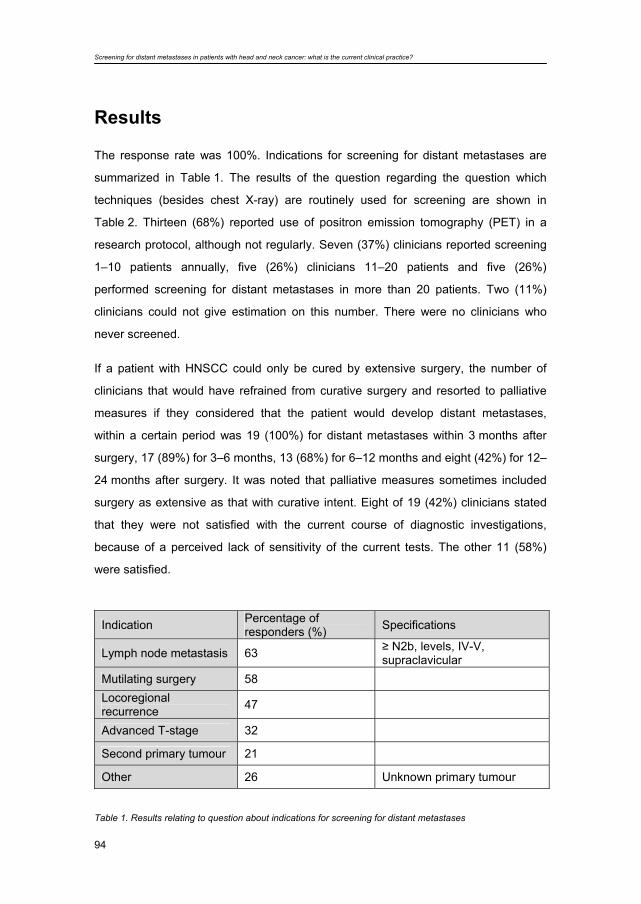
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
94
Results
The response rate was 100%. Indications for screening for distant metastases are
summarized in Table 1. The results of the question regarding the question which
techniques (besides chest X-ray) are routinely used for screening are shown in
Table 2. Thirteen (68%) reported use of positron emission tomography (PET) in a
research protocol, although not regularly. Seven (37%) clinicians reported screening
1–10 patients annually, five (26%) clinicians 11–20 patients and five (26%)
performed screening for distant metastases in more than 20 patients. Two (11%)
clinicians could not give estimation on this number. There were no clinicians who
never screened.
If a patient with HNSCC could only be cured by extensive surgery, the number of
clinicians that would have refrained from curative surgery and resorted to palliative
measures if they considered that the patient would develop distant metastases,
within a certain period was 19 (100%) for distant metastases within 3 months after
surgery, 17 (89%) for 3–6 months, 13 (68%) for 6–12 months and eight (42%) for 12–
24 months after surgery. It was noted that palliative measures sometimes included
surgery as extensive as that with curative intent. Eight of 19 (42%) clinicians stated
that they were not satisfied with the current course of diagnostic investigations,
because of a perceived lack of sensitivity of the current tests. The other 11 (58%)
were satisfied.
Indication Percentage of
responders (%) Specifications
Lymph node metastasis 63 ≥ N2b, levels, IV-V, supraclavicular
Mutilating surgery 58
Locoregional recurrence 47
Advanced T-stage 32
Second primary tumour 21
Other 26 Unknown primary tumour
Table 1. Results relating to question about indications for screening for distant metastases
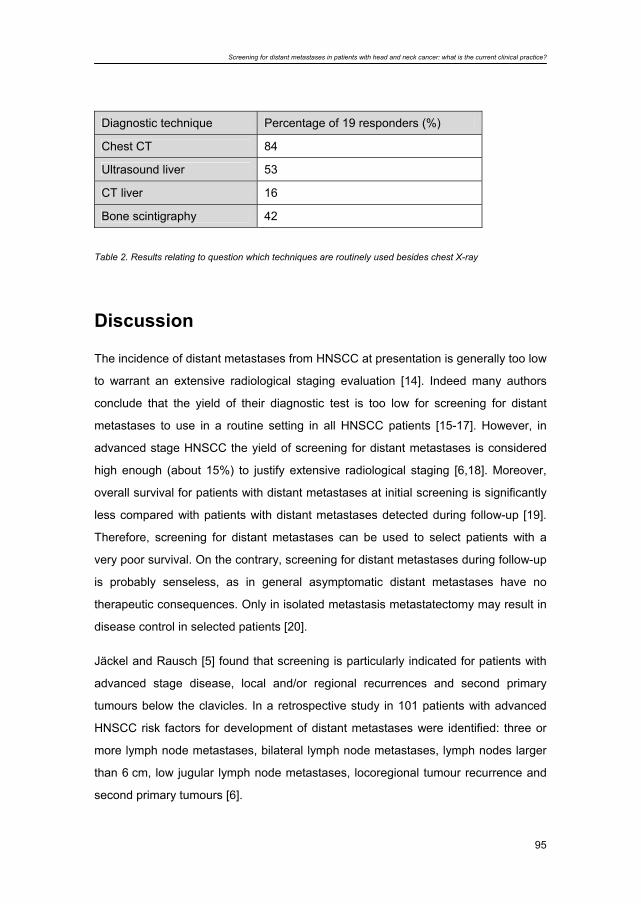
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
95
Diagnostic technique Percentage of 19 responders (%)
Chest CT 84
Ultrasound liver 53
CT liver 16
Bone scintigraphy 42
Table 2. Results relating to question which techniques are routinely used besides chest X-ray
Discussion
The incidence of distant metastases from HNSCC at presentation is generally too low
to warrant an extensive radiological staging evaluation [14]. Indeed many authors
conclude that the yield of their diagnostic test is too low for screening for distant
metastases to use in a routine setting in all HNSCC patients [15-17]. However, in
advanced stage HNSCC the yield of screening for distant metastases is considered
high enough (about 15%) to justify extensive radiological staging [6,18]. Moreover,
overall survival for patients with distant metastases at initial screening is significantly
less compared with patients with distant metastases detected during follow-up [19].
Therefore, screening for distant metastases can be used to select patients with a
very poor survival. On the contrary, screening for distant metastases during follow-up
is probably senseless, as in general asymptomatic distant metastases have no
therapeutic consequences. Only in isolated metastasis metastatectomy may result in
disease control in selected patients [20].
Jäckel and Rausch [5] found that screening is particularly indicated for patients with
advanced stage disease, local and/or regional recurrences and second primary
tumours below the clavicles. In a retrospective study in 101 patients with advanced
HNSCC risk factors for development of distant metastases were identified: three or
more lymph node metastases, bilateral lymph node metastases, lymph nodes larger
than 6 cm, low jugular lymph node metastases, locoregional tumour recurrence and
second primary tumours [6].
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
96
In the questionnaire, 63% of the investigators mentioned lymph node status as an
indication for screening for distant metastases. Most of these indications fit in the
identified risk profile described above. Recurrent HNSCC was previously identified as
risk factor and mentioned to be an indication to screen for 75% of the investigators in
the questionnaire. An advanced T-stage was mentioned as an indication for
screening in 13%, but is not clearly identified as independent risk factor. Mutilating
surgery was mentioned in 23%, but did not appear to be an independent risk factor
for distant metastases [6].
When it is decided to screen for distant metastases, the question arises which
diagnostic technique has to be used. In the questionnaire the investigators
mentioned chest CT, ultrasound or CT of the liver, bone scintigraphy and PET as the
techniques used for screening.
Laboratory biochemical tests are used as screening method for bone and liver
metastases, but are not sensitive and extremely non-specific, especially because of
malnourishment and alcohol abuse, not uncommon in head and neck cancer patients
[4,6].
The lungs are the most frequent initial sites of distant metastases. Moreover, lung
metastases occur in 61–91% in combination with distant metastases at other sites.
Distant metastases at other sites without simultaneous lung metastases are found in
only 6–25% [5,6,8,10,12]. Because of the high incidence of lung metastases and the
frequent combination of distant metastases at other sites with lung metastases,
examination of the thorax is most important in screening for distant metastases.
The diligence with which technique the lungs should be screened remains
controversial. The most commonly performed test for the detection of pulmonary
metastases is an X-ray of the chest. If there is a high likelihood of pulmonary
metastases, a CT scan of the chest may be more informative than a chest X-ray
alone. CT is more sensitive in the detection of pulmonary nodules than plain chest
radiography, because of the superiority of CT in detecting small nodules. Also axial
scans give better visualization of those areas of the lungs that may be hidden using
plain chest X-ray [21]. Chest X-ray detects only 28–60% of all malignant pulmonary
lesions detected by CT [4,18].
For the detection of liver metastases several diagnostic imaging techniques are
available, e.g. ultrasound (US), CT, MRI and PET. US is often the first choice
because of the widespread availability, lack of ionizing radiation and low costs [22]. If
the initial US examination is not adequate, CT should be used [23].
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
97
Bone scintigraphy is the most widely accepted method of determining spread to the
skeletal system. However, bone scintigraphy is non-specific because any bone
disease, regardless of aetiology and histology, will cause increased uptake of the
radioisotope, e.g. fractures, arthritis, degenerative disease of the spine and
osteoporosis [15].
Because of the low incidence and high percentage of equivocal findings,
necessitating additional examinations and, consequently, delay, cost and confusion
for patients and physicians, routine bone scintigraphy and abdominal ultrasound are
not recommended for screening in HNSCC patients [6,15]. Therefore, CT scan of the
thorax (eventually extended to the liver) is the single most important conventional
diagnostic technique for screening for distant metastases at initial evaluation [6].
Although chest CT frequently detects distant metastases, not all distant metastases
were detected as appeared during follow-up. This is partly because of limited
sensitivity and partly due to localization of the malignant lesions. Therefore, a more
sensitive whole body technique is needed. 18-F-fluorodeoxyglucose (FDG) PET
might be able to offer more sensitive screening of the whole body [19].
Positron emission tomography using FDG is able to detect distant metastases in
HNSCC patients. However, a straightforward meta-analysis of the literature on FDG-
PET for screening for distant metastases is not possible because of the large
variation in methods used by different authors to assess the presence or absence of
disease [24].
Decisions regarding radical resection of the HNSCC and appropriate reconstruction
rest heavily on the presence or absence of distant metastases. In selected
circumstances, such as an advanced fungating tumour or airway occlusive tumour,
appropriate surgical treatment may be considered for best palliation. In other
circumstances palliative treatment is usually given, because of the dismal prognosis
when distant metastases are present. In evaluating diagnostic techniques it is
important to realize how important missing of occult distant metastases is considered
to be in clinical practice. In screening for distant metastases a more sensitive
technique is needed [19]. For the evaluation of new diagnostic techniques, like FDG-
PET, demands have to be defined. Therefore, we tried to determine the length of
interval between screening and detection of clinically evident distant metastases
within which extensive treatment is considered futile. The majority of the investigators
in this questionnaire would refrain from extensive treatment if an HNSCC patient
would develop clinically manifest distant metastases within 12 months.

Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
98
Although screening for distant metastases is performed frequently and almost half of
the clinicians are not satisfied with the current diagnostic screening pathway, there is
no consensus or direct guideline on the indications and diagnostic techniques for
screening for distant metastases in HNSCC patients. In the Dutch guidelines for
diagnostics, treatment, supportive care and rehabilitation of laryngeal carcinoma the
recommendation was rightfully not strongly formulated because of a low level of
evidence at that time [25]. At the moment we propose to screen only patients with
risk factors for distant metastases using chest CT (eventually extended to the liver)
only [6,19]. Further studies evaluating new diagnostic techniques for screening for
distant metastases have to include a follow-up of 12 months in the gold standard, as
this period is considered important in the decision to treat with curative intent or
palliatively.
Conclusion
This questionnaire shows a substantial variation in indications and diagnostic
techniques used for screening for distant metastases between the major institutions
treating head and neck cancer in The Netherlands. There is a need for clear
guidelines for screening for distant metastases in patients with head and neck
cancer.
Acknowledgements
The authors would like to thank Drs R.J. Baatenburg de Jong, R.J. Bun, M.P.
Copper, G.A. Croll, E.J.M. Hannen, F.J.M. Hilgers, F.J.A. van den Hoogen, B.
Kremer, G.T.M. de Kuyper, R. Koole, B.F.A.M. van der Laan, K.T. van der Laan, H.
Lubsen, C.A. Meeuwis, M.A.W. Merkx, J.L.N. Roodenburg, L.E. Smeele, E.J.C.
Teunissen and J.G.A.M. Visscher for filling out the questionnaire.
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
99
Literature 1. Ferlito A, Buckley JG, Rinaldo A, Mondin V (2001) Screening tests to evaluate distant
metastases in head and neck cancer. ORL J Otorhinolaryngol Relat Spec 63:208-211
2. Merino OR, Linberg RD, Fletcher GH (1977) An analysis of distant metastases from
squamous cell carcinoma of the upper respiratory and digestive tracts. Cancer 40:145-151
3. Calhoun KH, Fulmer P, Weiss R, Hokanson JA (1994) Distant metastases from head and
neck squamous cell carcinomas. Laryngoscope 104:1199-1205
4. Troell RJ, Terris DJ (1995) Detection of metastases from head and neck cancers.
Laryngoscope 105:247-250
5. Jäckel MC, Rausch H (1999) Distant metastasis of squamous epithelial carcinomas of the
upper aerodigestive tract. The effect of clinical tumor parameters and course of illness
[Fernmetastasierung von Plattenepithelkarzinomen des oberen Aerodigestivtrakts. Der
Einfluss klinischer Tumorparameter und des Krankheitsverlauf]. HNO 47:38-44
6. Bree R de, Deurloo EE, Snow GB, Leemans CR (2000) Screening for distant metastases
in patients with head and neck cancer. Laryngoscope 110:397-400
7. Taneja C, Allen H, Koness J, Radie-Keane K, Wanebo HJ (2002) Changing patterns of
failure of head and neck cancer. Arch Otolaryngol Head Neck Surg 128:324-327
8. Nishijima W, Takooda S, Tokita N, Takayama S, Sakura M (1993) Analyses of distant
metastases in squamous cell carcinoma of the head and neck and lesions above the
clavicle at autopsy. Arch Otolaryngol Head Neck Surg 119:65-68
9. Matsuo JM, Patel SG, Singh B, Wong RJ, Boyle JO, Kraus DH, Shaha AR, Zelefsky MJ,
Pfister DG, Shah JP (2003) Clinical nodal stage is an independently significant predictor of
distant failure in patients with squamous cell carcinoma of the larynx. Ann Surg 238:412-
421
10. Leemans CR, Tiwari R, Nauta JJP, Waal van der I, Snow GB. (1993) Regional lymph node
involvement and its significance in the development of distant metastases in head and
neck carcinoma. Cancer 71:452-456
11. Shingaki S, Takada M, Sasai K, Bibi R, Kobayashi T, Nomura T, Saito C (2003) Impact of
lymph node metastasis on the pattern of failure and survival in oral carcinomas. Am J Surg
185:278-284
12. Leibel SA, Scott CB, Mohiuddin M, Marcial VA, Coia LR, Davis LW, Fuks Z (1991) The
effect of local-regional control on distant metastatic dissemination in carcinoma of the head
and neck. Results from an analysis of the RTOG head and neck database. In J Radia
Oncol Biol Phys 21:549-556
13. Johnson JT (2001) Proposal of standardization on screening tests for detection of distant
metastases from head and neck cancer. ORL J Otorhinolaryngol Relat Spec 63:256-258
Screening for distant metastases in patients with head and neck cancer: what is the current clinical practice?
100
14. Shah JP, Lydiatt W (1995) Treatment of cancer of the head and neck. CA Cancer J Clin
45:352-368
15. Brown DH, Leakos M (1998) The value of a routine bone scan in a metastatic survey. J
Otlaryngol 27:187-189
16. Nilssen ELK, Murthy P, McClymont L, Denholm S (1999) Radiological staging of chest and
abdomen in head and neck squamous cell carcinoma: are computed tomography and
ultrasound necessary? J Laryngol Otol 113:152-154
17. Tan LKS., Greener CC, Seikaly H, Rassekh CH, Calhoun KH (1999) Role of screening
chest computed tomography in patients with advanced head and neck cancer. Otolaryngol
Head Neck Surg 120:689-692
18. Warner GC, Cox GJ (2001) Evaluation of chest radiography versus chest computed
tomography in screening for pulmonary malignancy in advanced head and neck cancer. J
Otolaryngol 32:107-109
19. Brouwer J, Bree R de, Hoekstra OS, Golding RP, Langendijk JA, Castelijns JA, Leemans
CR (2005) Screening for distant metastases in patients with head and neck cancer: is
chest CT sufficient? Laryngoscope 115:1813-1817
20. Wedman J, Balm AJ, Hart AA, Loftus BM, Hilgers FJ, Gregor RT, van Zandwijk N,
Zoetmulder FA (1996) Value of resection of pulmonary metastases in head and neck
cancer patients. Head Neck 18:311-316
21. Chalmers N, Best JJ (1991) The significance of pulmonary nodules detected by CT but not
by chest radiography in tumour staging. Clin Radiol 44:410-412
22. Nelson RC (1994) Radiological evaluation of metastases to the liver. Cancer Treat Res
69:129-146
23. Kruskal JB, Kane RA (1996) Imaging of primary and metastatic liver tumors. Surg Oncol
Clin 5:231-260
24. Vermeersch H, Loose D, Ham H, Otte A, Wiele van de C (2003) Nuclear medicine imaging
for the assessment of primary and recurrent head and neck carcinoma using routinely
available tracers. Eur J Nucl Med Mol Imaging 30:1689-1700
25. Kaanders JH, Hordijk GJ (2002) Dutch Cooperative Head and Neck Oncology Group.
Carcinoma of the larynx: the Dutch national guideline for diagnostics, treatment, supportive
care and rehabilitation. Radiother Oncol 63:299-307
7
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
Jolijn Brouwer, Remco de Bree, Otto S. Hoekstra, Richard P. Golding, Johannes A. Langendijk, Jonas A. Castelijns, C. René Leemans
Laryngoscope (2005) 115:1813-1817

Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
102
Abstract
The detection of distant metastases during screening influences the choice of
treatment in patients with head and neck squamous cell carcinoma. A previous study
in the authors' institution showed that chest computed tomography (CT) scan was the
most important screening technique. Different clinical risk factors in patients with
head and neck squamous cell carcinoma for the development of distant metastases
were identified. To evaluate the authors' diagnostic strategy, the accuracy of
screening for distant metastases with chest CT in 109 consecutive patients with head
and neck squamous cell carcinoma with risk factors between 1997 and 2000 was
retrospectively analysed. Preoperative screening with CT revealed 20 patients (18%)
with lung metastases and 1 liver metastasis. Despite negative screening with chest
CT, 9 (11%) patients developed distant metastases within 12 months during follow-
up. Sensitivity of the chest CT was 73%; the specificity was 80%. Although chest CT
frequently detects distant metastases, there seems to be a need for a more sensitive
and whole-body screening technique.

Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
103
Introduction
The presence of distant metastases influences prognosis and choice of treatment in
patients with head and neck squamous cell carcinoma (HNSCC). Patients with
HNSCC and distant metastases are generally not considered curable, and treatment
is mostly palliative. In both clinical and autopsy studies, the lungs are the most
frequent site of distant metastases in patients with head and neck cancer [1,2].
Although there has been an improvement in locoregional control of disease in
patients with head and neck cancer over the last decades, improvement in survival is
hampered by the development of distant metastases in these patients. For patients
who have reached locoregional control and develop distant metastases, it is thought
that these distant metastases were already subclinically present at the time of
treatment for the primary tumour [3]. Therefore, screening for distant metastases at
that time point may be important.
In a previous study, we evaluated preoperative screening with chest CT scan,
ultrasound or CT scan of the liver, and bone scintigraphy [1]. We identified several
clinical risk factors in patients with HNSCC for the development of distant
metastases: three or more cervical lymph node metastases, bilateral lymph node
metastases, lymph nodes larger than 6 cm, low-level jugular lymph node metastases,
locoregional tumour recurrence, and second primary tumours. It was concluded that
chest CT was the single most important diagnostic technique for screening for distant
metastases. Since then, in patients with at least one of the above mentioned risk
factors a chest CT was performed to screen for distant metastases [1]
There are no guidelines for screening for distant metastases in patients with
locoregional advanced HNSCC [4]. There is no consensus on the diagnostic
technique that must be used or on the subgroup of patients with HNSCC that may
benefit from screening.
In the present study, we validated the proposed diagnostic screening algorithm using
chest CT in a cohort of consecutive patients with risk factors for distant metastases.
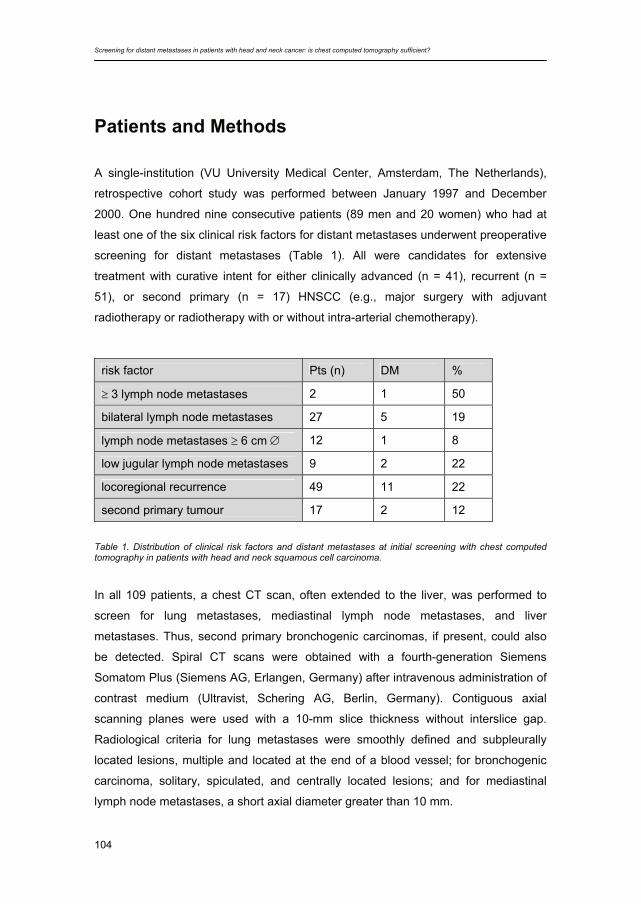
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
104
Patients and Methods
A single-institution (VU University Medical Center, Amsterdam, The Netherlands),
retrospective cohort study was performed between January 1997 and December
2000. One hundred nine consecutive patients (89 men and 20 women) who had at
least one of the six clinical risk factors for distant metastases underwent preoperative
screening for distant metastases (Table 1). All were candidates for extensive
treatment with curative intent for either clinically advanced (n = 41), recurrent (n =
51), or second primary (n = 17) HNSCC (e.g., major surgery with adjuvant
radiotherapy or radiotherapy with or without intra-arterial chemotherapy).
Table 1. Distribution of clinical risk factors and distant metastases at initial screening with chest computed tomography in patients with head and neck squamous cell carcinoma.
In all 109 patients, a chest CT scan, often extended to the liver, was performed to
screen for lung metastases, mediastinal lymph node metastases, and liver
metastases. Thus, second primary bronchogenic carcinomas, if present, could also
be detected. Spiral CT scans were obtained with a fourth-generation Siemens
Somatom Plus (Siemens AG, Erlangen, Germany) after intravenous administration of
contrast medium (Ultravist, Schering AG, Berlin, Germany). Contiguous axial
scanning planes were used with a 10-mm slice thickness without interslice gap.
Radiological criteria for lung metastases were smoothly defined and subpleurally
located lesions, multiple and located at the end of a blood vessel; for bronchogenic
carcinoma, solitary, spiculated, and centrally located lesions; and for mediastinal
lymph node metastases, a short axial diameter greater than 10 mm.
risk factor Pts (n) DM %
≥ 3 lymph node metastases 2 1 50
bilateral lymph node metastases 27 5 19
lymph node metastases ≥ 6 cm ∅ 12 1 8
low jugular lymph node metastases 9 2 22
locoregional recurrence 49 11 22
second primary tumour 17 2 12

Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
105
Screening result was considered to be true-positive when there were evident
metastases on chest CT, when lesions on chest CT were progressive on two
successive CT scans with an interval of 3 months, or when histopathological
examination of tissue obtained by bronchoscopy, thoracoscopy, or thoracotomy
revealed malignancy. Follow-up was performed by regular visits to the outpatient
clinic. In case of suspicion of distant metastases (e.g., on routine chest radiographs),
additional diagnostic examinations were performed, such as a follow-up chest CT
scan and bronchoscopy. Similar additional workup was performed if there was a
lesion suspect for a second primary tumour. Patients were classified as clinically
positive or negative with respect to the presence of distant metastasis using a follow-
up period of 12 months because the majority of the distant metastases become
evident in that period [5].
If a patient had a negative finding on chest CT scan but developed distant
metastases during follow-up of 12 months, the screening result was considered false-
negative. If chest CT scan during screening was abnormal but further preoperative
workup remained inconclusive, patients were treated as scheduled. If follow-up of 12
months did not reveal metastases, the CT results were classified as false-positive.
Patients were divided into those with and without locoregional control in whom distant
metastases became manifest during 12 months of follow-up despite negative
screening result, since no distinction can be made between growth of metastases
already present at time of screening or reseeding by the locoregional recurrent
tumour.
During follow-up, the dates of the detection of distant metastases and death were
recorded. For the groups of patients who had negative results for distant metastases
during screening, locoregional recurrence, and/or development of distant metastases
during follow-up, Kaplan-Meier survival curves of estimated distant metastases–free
survival and estimated overall survival were calculated.
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
106
Results
The 109 patients had a total of 112 tumours at the time of preoperative
investigations: 3 patients had synchronous multiple primary HNSCC tumours. The
tumours were located in the oral cavity (n = 24), oropharynx (n = 34), hypopharynx (n
= 10), larynx (n = 20), cervical oesophagus (n = 2), nose and paranasal sinus (n = 3),
and lymph node metastases of unknown primary origin (n = 2). Recurrent tumours
were located in lymph nodes (n = 10), skin/tracheostoma (n = 4), and neopharynx (n
= 3). Initial TNM classification varied from T2 to T4 and N1 to N3. Most represented
were T2N3 (n = 6), T3N2c (n = 10), and T4N2c (n = 12). Preoperative screening with
CT revealed 20 patients (18%) with lung metastases and 1 liver metastasis. The
incidence of distant metastases for the different risk factors varied from 8% to 50%
(Table 1). Also, three synchronous second primary bronchogenic tumours were
detected. In 15 patients, chest CT findings were evident, whereas in the other 8
patients the diagnosis of malignancy was made based on rapid progression on
follow-up CT scan or by bronchoscopy. Abnormalities in 10 other CT scans could not
be confirmed clinically by progression on chest CT (n = 7), by mediastinoscopy (n =
1), or by bronchoscopy (n = 2). These patients were treated as negative for distant
metastases, and follow-up revealed no chest metastases in these patients.
Therefore, these initial CT findings were classified as false-positive (Fig. 1). In 58
patients, the chest CT scan was extended to the liver. In 13 of these patients (22%)
an ultrasound of the liver was advised and performed. In 12 patients no metastases
were found, but in 1 patient suspicion remained. In this patient ultrasound-guided
needle aspiration cytological examination was negative, but laparoscopy showed a
histologically proven liver metastasis.
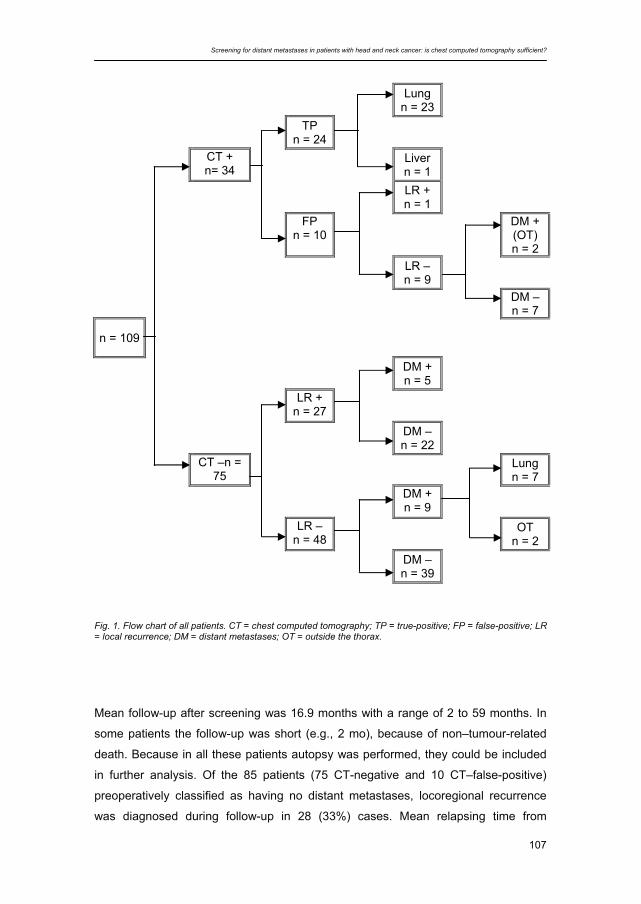
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
107
Lung n = 23
TP n = 24
CT + n= 34 Liver
n = 1
LR + n = 1
FP
n = 10 DM +
(OT) n = 2
LR – n = 9
DM – n = 7
n = 109
DM + n = 5
LR + n = 27
DM – n = 22
CT –n = 75 Lung
n = 7
DM + n = 9
LR – n = 48 OT
n = 2
DM – n = 39
Fig. 1. Flow chart of all patients. CT = chest computed tomography; TP = true-positive; FP = false-positive; LR = local recurrence; DM = distant metastases; OT = outside the thorax.
Mean follow-up after screening was 16.9 months with a range of 2 to 59 months. In
some patients the follow-up was short (e.g., 2 mo), because of non–tumour-related
death. Because in all these patients autopsy was performed, they could be included
in further analysis. Of the 85 patients (75 CT-negative and 10 CT–false-positive)
preoperatively classified as having no distant metastases, locoregional recurrence
was diagnosed during follow-up in 28 (33%) cases. Mean relapsing time from
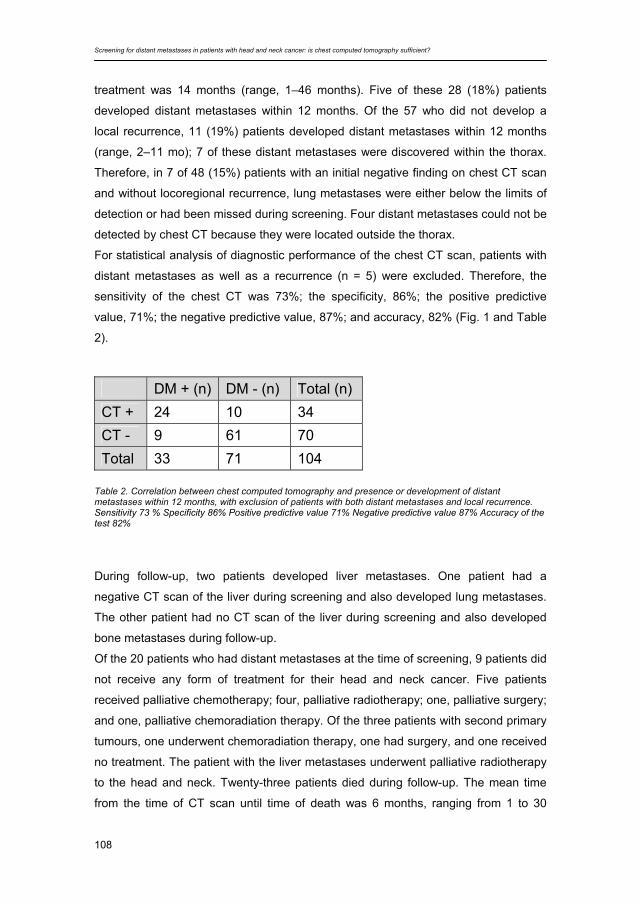
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
108
treatment was 14 months (range, 1–46 months). Five of these 28 (18%) patients
developed distant metastases within 12 months. Of the 57 who did not develop a
local recurrence, 11 (19%) patients developed distant metastases within 12 months
(range, 2–11 mo); 7 of these distant metastases were discovered within the thorax.
Therefore, in 7 of 48 (15%) patients with an initial negative finding on chest CT scan
and without locoregional recurrence, lung metastases were either below the limits of
detection or had been missed during screening. Four distant metastases could not be
detected by chest CT because they were located outside the thorax.
For statistical analysis of diagnostic performance of the chest CT scan, patients with
distant metastases as well as a recurrence (n = 5) were excluded. Therefore, the
sensitivity of the chest CT was 73%; the specificity, 86%; the positive predictive
value, 71%; the negative predictive value, 87%; and accuracy, 82% (Fig. 1 and Table
2).
DM + (n) DM - (n) Total (n) CT + 24 10 34 CT - 9 61 70 Total 33 71 104
Table 2. Correlation between chest computed tomography and presence or development of distant metastases within 12 months, with exclusion of patients with both distant metastases and local recurrence. Sensitivity 73 % Specificity 86% Positive predictive value 71% Negative predictive value 87% Accuracy of the test 82% During follow-up, two patients developed liver metastases. One patient had a
negative CT scan of the liver during screening and also developed lung metastases.
The other patient had no CT scan of the liver during screening and also developed
bone metastases during follow-up.
Of the 20 patients who had distant metastases at the time of screening, 9 patients did
not receive any form of treatment for their head and neck cancer. Five patients
received palliative chemotherapy; four, palliative radiotherapy; one, palliative surgery;
and one, palliative chemoradiation therapy. Of the three patients with second primary
tumours, one underwent chemoradiation therapy, one had surgery, and one received
no treatment. The patient with the liver metastases underwent palliative radiotherapy
to the head and neck. Twenty-three patients died during follow-up. The mean time
from the time of CT scan until time of death was 6 months, ranging from 1 to 30
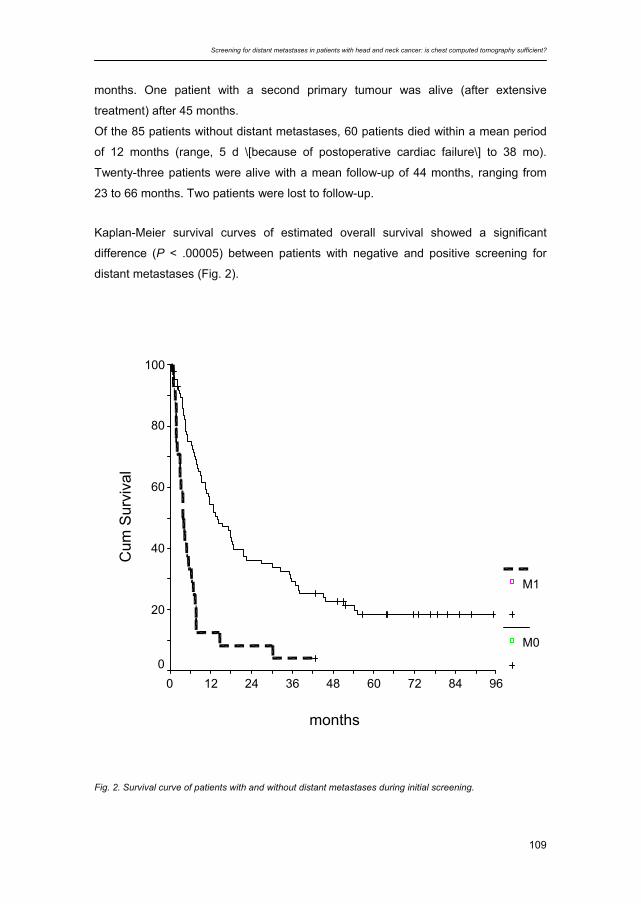
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
109
months. One patient with a second primary tumour was alive (after extensive
treatment) after 45 months.
Of the 85 patients without distant metastases, 60 patients died within a mean period
of 12 months (range, 5 d \[because of postoperative cardiac failure\] to 38 mo).
Twenty-three patients were alive with a mean follow-up of 44 months, ranging from
23 to 66 months. Two patients were lost to follow-up.
Kaplan-Meier survival curves of estimated overall survival showed a significant
difference (P < .00005) between patients with negative and positive screening for
distant metastases (Fig. 2).
months
96847260483624120
Cum
Sur
viva
l
100
80
60
40
20
0
M1
M0
Fig. 2. Survival curve of patients with and without distant metastases during initial screening.
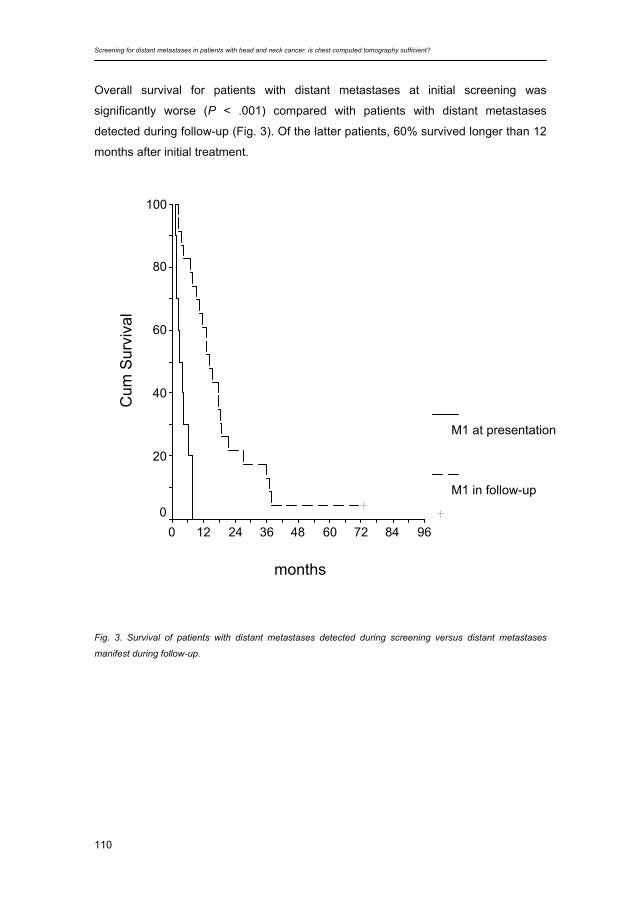
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
110
Overall survival for patients with distant metastases at initial screening was
significantly worse (P < .001) compared with patients with distant metastases
detected during follow-up (Fig. 3). Of the latter patients, 60% survived longer than 12
months after initial treatment.
months
96847260483624120
Cum
Sur
viva
l
100
80
60
40
20
0
M1 at presentation
M1 in follow-up
Fig. 3. Survival of patients with distant metastases detected during screening versus distant metastases
manifest during follow-up.
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
111
Discussion
In the present study, most distant metastases at screening were found in the thorax,
whereas in one patient a liver metastasis was detected. In 21 of the 32 (66%)
patients with distant metastases, these distant metastases were detected during
screening. In the previous study, this rate was 17 of 32 (53%) [1]. The incidence
(18%) is similar to that found in the previous study (17%) [1] which seems to be high
enough to justify a screening procedure. The 3% incidence of synchronous second
primary bronchogenic tumours is as would be expected from the literature [6]. The
percentages of distant metastases at screening in the present study and in the
previous study 1 are higher than in other reports [7,8], presumably because only
patients with clinical risk factors for development of distant metastases were included
in our study.
Of the 58 patients who underwent CT scan of the liver, 1 patient (2%) had a liver
metastasis. During follow-up, another two patients developed liver metastases. One
of these had a false-negative CT scan of the liver at screening and developed both
liver and lung metastases. The other patient had no CT scan of the liver at screening
and developed liver metastases and bone metastases during follow-up. Moreover,
based on CT findings, ultrasound of the liver was performed in 13 patients, which
resulted in the confirmation of only one liver metastasis. Therefore, chest CT scan
with extension to the liver may not be the proper technique to detect liver
metastases.
During follow-up, 16 of the 85 patients (21%) developed distant metastases within 12
months, despite negative screening. Eleven of these patients had no signs of
locoregional recurrence at the time of detection of distant metastases. Seven of
these were located in the thorax. From this, two conclusions can be extrapolated.
First, previous studies concluded that chest CT was the single most effective tool to
screen for distant metastases in patients with head and neck malignancies. However,
with this technique, 11 of 32 (34%) of the distant malignancies were still missed at
screening. Chest CT failed to detect malignant abnormalities in the thorax in at least
7 of 32 (22%) patients. Second, 2 (2%) patients developed distant metastases
outside the thorax, suggesting that a whole-body screening technique would be more
suitable for screening. Therefore, a more sensitive technique that would cover the
whole body would seem to be required in diagnostic screening tests for distant
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
112
metastases and second primary tumours. 18F fluorodeoxyglucose (FDG) positron
emission tomography (PET) scan is currently under investigation for this indication in
various centers.
Prognosis of patients with distant metastases found during screening was worse
compared with patients with distant metastases detected during follow-up. Thus, the
sooner a distant metastasis is found, the worse the prognosis for the patients.
Therefore, screening for distant metastases using chest CT can be used to select
patients with a poor survival. This screening procedure may be useful to exclude
patients for extensive treatment.
There is no difference in distant metastasis–free survival found in patients with and
without locoregional recurrence. Probably in patients with locoregional recurrence at
least part of the distant metastases develops from the initial tumour instead of the
recurrence. If this hypothesis is true, the incidence of missed distant metastases on
chest CT is even higher, although it is highly unlikely that diagnostic imaging
techniques will ever be able to detect micrometastases.
Concerning the need for whole-body screening, conflicting results have been
reported for the use of FDG PET scanning. Hanasono et al. [9] reported that FDG
PET scan detected two of four distant metastases in a group of eight patients,
whereas CT scan found all metastases. Keyes et al. [10] studied a group of 56
patients with various head and neck tumours before therapy. FDG PET detected
three lung tumours, and CT scan detected two. However, FDG PET had six false-
positive results. In a study by Manolidis et al. [11], in a group of 29 patients with
various tumour types and stages, FDG PET detected 9 of 10 histopathologically
confirmed distant metastases. In a review by McGuirt et al. [12], PET scanning of the
chest was performed combined with CT scanning of the head and neck in 97
patients. Seventeen pulmonary lesions were found, of which six proved to be
malignant. Wax et al. [13] performed a follow-up of the clinical course of 15 head and
neck cancer patients with intrathoracic lesions detected by FDG-PET, and in 9
patients the diagnosis was confirmed. Schmidt et al. [14] found an incidence of 13%
for distant metastases with a sensitivity of 100% and specificity of 98%. The balance
of these studies would appear to favour FDG-PET as the most suitable option for
more reliable screening for distant metastases in head and neck cancer patients at
present. However, it should be pointed out that imaging techniques are still
advancing. In this regard, the efficacy of multidetector CT scanners is still being
assessed.

Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
113
Conclusion
Although chest CT frequently detects distant metastases and synchronous second
primary tumours during screening, not all intrathoracic malignancies were detected
that appeared during follow-up. This is partly due to limited sensitivity and partly to
localization of the malignant lesions. Therefore, a more sensitive whole-body
technique is needed. FDG PET might be able to offer more sensitive screening of the
whole body. A pilot study is currently being analysed in which the value of whole-
body FDG-PET and chest CT for screening for distant metastases and second
primary tumours in HNSCC patients at risk are compared.
Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
114
Literature
1. Bree R de, Deurloo EE, Snow GB, Leemans CR (2000). Screening for distant metastases
in patients with head and neck cancer. Laryngoscope 110:397-401
2. Ferlito A, Rinaldo A, Buckley JG, Mondin V (2001) General considerations on distant
metastases from head and neck cancer. ORL J Otorhinolaryngol Relat Spec 63:189-191
3. León X, Quer M, Orus C, Del Prado Venegas M, Lopez M (2000) Distant metastases in
head and neck cancer patients who achieved loco-regional control. Head Neck 22:680-686
4. Johnson JT (2001) Proposal of standardization on screening tests for detection of distant
metastases from head and neck cancer. ORL J Otorhinolaryngol Relat Spec 63:256-258
5. Leemans CR, Tiwari R, Nauta JJ, Waal I van der, Snow GB (1993) Regional lymph node
involvement and its significance in the development of distant metastases in head and
neck carcinoma. Cancer 71:452-456
6. Haughey BH, Gates GA, Arfken CL, Harvey J (1992) Meta-analysis of second malignant
tumors in patients with head and neck cancer: the case for an endoscopic screening
protocol. Ann Otol Rhinol Laryngol 101:105-112
7. Dennington ML, Carter DR, Meyers AD (1980) Distant metastases in head and neck
epidermoid carcinoma. Laryngoscope 90:196-201
8. Black RJ, Gluckman JL, Shumrick DA (1984) Screening for distant metastases in head and
neck cancer patients. Aust N Z J Surg 54:527-530
9. Hanasono MM, Kunda LD, Segall GM, Ku GH, Terris DJ (1999) Uses and limitation of
FDG Positron Emission Tomography in patients with head and neck cancer. Laryngoscope
109:880-885
10. Keyes Jr JW, Chen MYM, Watson NE Jr, Greven KM, McGuirt WF, Williams DW 3rd (2000)
FDG PET evaluation of head and neck cancer: value of imaging the thorax. Head Neck
22:105-110
11. Manolidis S, Donald PJ, Volk P, Pounds TR (1998) The use of PET scanning in occult and
recurrent head and neck cancer. Acta Otolaryngol suppl 534:5-11
12. McGuirt WF, Greven K, Williams D 3rd, Keyes JW Jr, Watson N, Cappellari JO, Geisinger
KR (1998) PET scanning in head and neck oncology: a review. Head Neck 20:208-215
13. Wax MK, Myers LL, Gabalski EC, Husain S, Gona JM, Nabi H (2002) Positron emission
tomography in the evaluation of synchronous lung lesions in patients with untreated head
and neck cancer. Arch Otolaryngol Head Neck Surg 128:703-707
14. Schmidt M, Schmalenbach M, Jüngehülsing M, Theissen P, Dietlein M, Schröder U,
Eschner W, Stennert E, Schicha H (2004) 18F-FDG PET for detecting recurrent head and
neck cancer, local lymph node involvement and distant metastases. Nuklearmedizin 43:91-
101
8
Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
Jolijn Brouwer, Asaf Senft, Remco de Bree, Emile F.I. Comans, Richard
P. Golding, Jonas A. Castelijns, Otto S. Hoekstra and C. René Leemans
Oral Oncology (2006) 42:275–280

Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
116
Abstract
The detection of distant metastases and second primary tumours at the time of initial
evaluation changes the prognosis and influences the selection of treatment modality
in patients with HNSCC. Until recently chest CT was the single most effective test to
screen for distant metastases in HNSCC patients. In this observational cohort study
we prospectively compared the yield of whole body 18FDG-PET and chest CT to
detect distant metastases and synchronous primary tumours. The results of whole
body 18FDG-PET and chest CT were analysed in 34 consecutive HNSCC patients
with previously established risk factors for the presence of distant metastases. Four
patients were diagnosed with distant metastases or second primary tumours: CT as
well as 18FDG-PET identified one patient with lung metastases and another with
primary lung cancer. In addition, 18FDG-PET detected second primary tumours in two
patients (hepatocellular carcinoma and abdominal adenocarcinoma). However
increased uptake sites at 18FDG-PET in lung, liver and pelvis in five patients were not
confirmed by other imaging modalities. The added value of whole body 18FDG-PET
versus chest CT was to identify unknown malignancy in 6% of the patients.
Confirmation of positive 18FDG-PET findings is feasible and necessary.

Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
117
Introduction
The detection of distant metastases at the time of initial evaluation changes the
prognosis and influences the selection of treatment modality in patients with head
and neck squamous cell carcinoma (HNSCC). Distant metastases usually occur late
in the course of the disease. The lungs, bone and liver are the most frequent sites of
distant metastases. The prevalence of distant metastases in HNSCC at autopsy (37–
57%) is much higher than in clinical studies (4–26%) [1-4]. Distant metastases that
appear during follow-up in patients who achieved locoregional control must have
arisen from subclinical distant spread already present at the time of treatment.
Patients with distant metastases are generally not considered curable and almost
always receive only palliative treatment [5].
Because of the relatively low incidence of distant metastases at presentation, only
patients with risk factors should undergo evaluation for distant metastases. In a
previous study [6] in the 1990s, we evaluated the value of screening for distant
metastases retrospectively in 101 patients with advanced stage HNSCC, scheduled
for major surgery, who underwent chest radiographs, chest computer tomography
(CT), ultrasound or CT scan of the liver and bone scintigraphy. We identified several
risk factors for development of distant metastases and found that chest CT was the
single most important technique that was available for screening for distant
metastases in HNSCC patients at that time. Besides lung metastases, chest CT can
also detect primary lung cancer, mediastinal lymph node metastases, bone
metastases in spine and ribs, and can be extended to the liver. Therefore, we
continued performing chest CT only in screening for distant metastases in HNSCC
patients with risk factors: three or more cervical metastases, bilateral or low-jugular
(level IV) cervical metastases, cervical metastases larger than 6 cm, recurrence or
second primary tumours.
Despite negative screening and locoregional tumour control some patients develop
distant metastases. These distant metastases must have been present at diagnostic
work-up, but were apparently below the detection limit of screening tests. If distant
spread occurs early after major surgery with curative intent these patients probably
underwent inappropriate extensive treatment.
Thus a more sensitive diagnostic technique which preferably examines the whole
body is needed. Positron emission tomography (PET) using the radiolabeled glucose

Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
118
analogue 18-fluoro-2-deoxy-glucose (18FDG) offers a functional imaging approach for
the entire body. 18FDG-PET is shown to be able to detect various types of tumours,
among which HNSCC [7]. However, false positive results can occur and confirmation
of PET findings can be problematic. The current study evaluates the value of 18FDG-
PET in screening for distant metastases in HNSCC patients. The 18FDG-PET results
are compared with the results of chest CT in HNSCC patients with risk factors for
distant metastases.
Materials and methods
Between May 1998 and August 1999, 34 consecutive HNSCC patients (12 females
and 22 males, mean age 59 years, range 25–85), who had risk factors for developing
distant metastases underwent screening for distant metastases and synchronous
second primary tumours. Primary tumour sites included oral cavity, oropharynx,
hypopharynx, larynx, nasopharynx and lymph node metastases of unknown primary
tumour. Some patients were already known with secondary primary HNSCC at the
time of screening. These patients had the following risk factors for development of
distant metastases: three or more lymph node metastases (n = 1), bilateral lymph
node metastases (n = 11), lymph node metastases of 6 cm or larger (n = 10), low-
jugular (level IV) lymph node metastases (n = 1), locoregional recurrence (n = 6) and
second primary tumour (n = 5). In all 34 patients a spiral chest CT was performed
using a fourth-generation Siemens Somatom Plus (Siemens AG, Erlangen,
Germany) after intravenous administration of contrast medium (Ultravist, Schering
AG, Berlin, Germany). Contiguous axial scanning planes were used at 10 mm slice
thickness without interslice gap. Radiological criteria for lung metastases were:
smoothly defined and subpleurally located lesions, multiple and located at the end of
a blood vessel; for bronchogenic carcinoma, solitary, spiculated, and centrally
located lesions; and for mediastinal lymph node metastases, a minimal axial
diameter of more than 10 mm.
All patients underwent 18FDG-PET after at least a 6 h fast. Sixty minutes after
intravenous administration of 370 MBq of 18FDG, imaging of the midfemur–cranial
vault trajectory was started using a full ring BGO PET scanner (ECAT EXACT
HR + CRI/Siemens). A PET scan was considered positive if there was an abnormal
focally enhanced tracer uptake, which could not be attributed to normal physiological
uptake.
Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
119
Patients were classified as positive or negative with respect to the presence of
distant metastases using a follow-up of 12 months. Initial screening for distant
metastases was classified as true positive if the findings on chest CT were
pathognomonic for metastases, if suspected lesions on chest CT or 18FDG-PET were
progressive or if biopsy revealed malignancy. Patients were followed regularly
according to our standard clinical practice. In case of suspicion of distant metastases
or second primary tumours during follow-up, additional diagnostic examinations were
performed.
If a patient had a negative chest CT or 18FDG-PET, but developed distant
metastases within the follow-up of 12 months, screening was considered false
negative. If chest CT or 18FDG-PET during initial screening was abnormal but further
pre-operative work-up remained inconclusive, patients were regarded as negative for
distant metastases and treated as scheduled. If in case of preoperatively
unconfirmed positive 18FDG-PET or CT the 12 months follow-up did not reveal
metastases, the CT or 18FDG-PET results were classified as false positive. We
separately evaluated negative screening test results for patients with and without
locoregional control in whom distant metastases became manifest during 12 months
of follow-up, since no distinction can be made between metastases attributable to the
primary tumour or due to reseeding of the recurrent tumour. Since only lesions inside
the thorax can be detected by CT scan of the thorax as well as whole body 18FDG-
PET these were analysed separately.
Finally, the 18FDG-PET scans were retrospectively scored by two independent
experienced nuclear medicine physicians (OSH, EFC). Different than at initial
scoring, the observers were now blinded to the results of the other examinations and
the final clinical diagnoses. The observers used a five point scale to score the scans;
negative, probably negative, equivocal, probably positive, positive. Disagreement
was solved through consensus. The interobserver variability was determined and
expressed in a weighted kappa. The higher the weighted kappa, the higher the
agreement, with a maximum of 1.0.
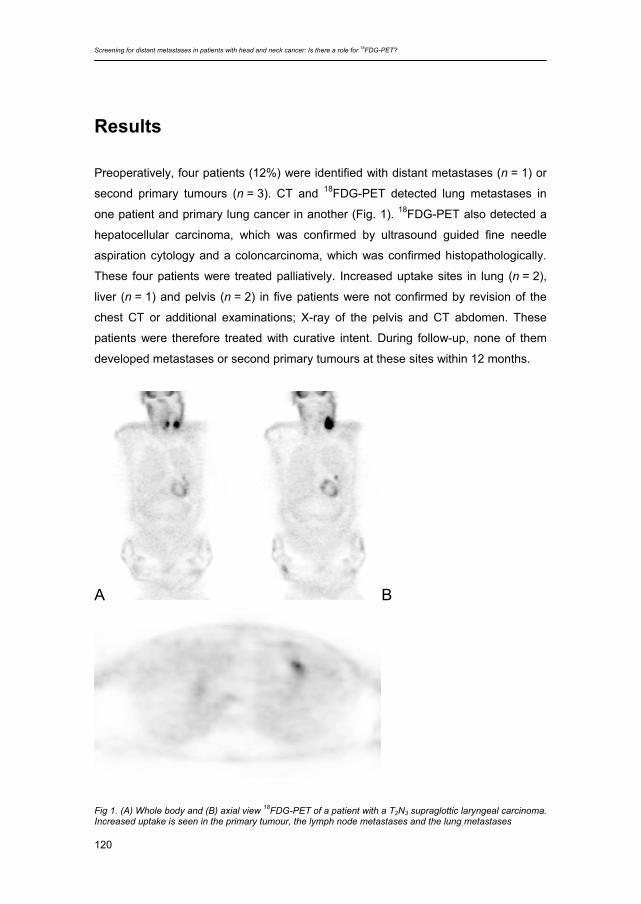
Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
120
Results
Preoperatively, four patients (12%) were identified with distant metastases (n = 1) or
second primary tumours (n = 3). CT and 18FDG-PET detected lung metastases in
one patient and primary lung cancer in another (Fig. 1). 18FDG-PET also detected a
hepatocellular carcinoma, which was confirmed by ultrasound guided fine needle
aspiration cytology and a coloncarcinoma, which was confirmed histopathologically.
These four patients were treated palliatively. Increased uptake sites in lung (n = 2),
liver (n = 1) and pelvis (n = 2) in five patients were not confirmed by revision of the
chest CT or additional examinations; X-ray of the pelvis and CT abdomen. These
patients were therefore treated with curative intent. During follow-up, none of them
developed metastases or second primary tumours at these sites within 12 months.
A
↑
B
Fig 1. (A) Whole body and (B) axial view 18FDG-PET of a patient with a T2N3 supraglottic laryngeal carcinoma. Increased uptake is seen in the primary tumour, the lymph node metastases and the lung metastases
Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
121
Outcome of the 30 patients without distant metastases or second primary tumours
below the clavicles was analysed. Eight patients developed distant metastases within
12 months after surgery; three of these eight patients also had locoregional
recurrence. The median time to detection of distant metastases (lung, n = 3; bone,
n = 2) in the five relapsing patients without evidence of locoregional recurrence was
five months (range 3–7). All these eight patients died of disease within 12 months
after initial treatment. During the period of extended follow-up after 12 months,
another five patients developed distant metastases. Two of these patients developed
also a locoregional recurrence, while the other three had locoregional control.
Six of the other 17 patients with negative initial screening by 18FDG-PET and CT died
within 12 months (median 2, range 1–4) without signs of distant metastases Three
died of disease and three due to other causes.
If corrected for localisation inside the thorax, chest CT and 18FDG-PET both detected
two lung lesions during screening, both missing three lesions that appeared during
follow-up.
During revision of the 18FDG-PET scans, the observers found nine (26%) out of 34
scans to be suspicious for distant metastases or second primary tumours. Of these
scans three (9%) were true positive (1× distant metastases and 2× second primary
tumours). 18FDG-PET was equivocal in four (12%) patients of which one was positive
for second primary tumour. During follow-up, the other six (18%) positive and three
(9%) patients with equivocal scans were free of distant metastases. Initial
disagreement between the examiners occurred in eight (24%) 18FDG-PET
examinations. The examiners could reach consensus in all cases. The interobserver
variability was expressed in a weighted kappa; 0.77 (95% CI 0.59–0.96).
Discussion
In patients at risk for disseminated head and neck cancer, the added value of PET to
chest CT in detecting distant metastases and second primary tumours was 6%
(95%CI 2–19%). In this relatively small study, this added value consisted of the
identification of second primary tumours outside of the thorax. The observer
agreement of PET readings was substantial.
Our data stipulate that abnormal 18FDG-PET findings should be confirmed otherwise,
and that patients with unconfirmed foci should be given the benefit of the doubt. In
our study, such unconfirmed 18FDG-PET foci were found in lungs, liver and pelvis.
Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
122
The first step in validation of the former two categories consists of revision of the CT
scan. It is unlikely that pulmonary 18FDG-PET abnormalities have no anatomical
substrate at CT, but they may have been missed at CT reading. Alternatively, the
aspect of lesions at CT may help to determine their nature. In HNSCC patients with
locally advanced disease, pulmonary infiltrates may be more prevalent than in other
malignancies. All distant metastases and second primary tumours found during
screening had implications for the choice of treatment. In all these cases the planned
treatment with curative intent changed to palliative treatment. This emphasizes the
importance of screening for distant metastases.
Screening for disseminated cancer to avoid patients being subjected to aggressive
therapy from which they will not derive benefit is likely to be most effective in subsets
of patients at substantial risk of such findings. Otherwise, the cost and delay caused
by adding tests and the likelihood of obtaining many false positive test results may be
counterproductive. In current literature, specific studies to support this supposition
are lacking. Only a few studies have reported on the detection of distant metastases
or synchronous second primary tumours in head and neck cancer patients by 18FDG-
PET [7-25]. In most studies 18FDG-PET findings were confirmed by conventional
radiological techniques and also some false positive findings were reported. The
studies on distant metastases included only a limited number of patients or reported
on a low incidence of distant metastases in the studied groups. The latter is mainly
due to the fact that only four studies investigated head and neck cancer patients with
advanced stage disease only [9,12,18,20]. Some studies investigated heterogeneous
groups with regard to tumour types (not only squamous cell carcinoma)
[7,8,13,14,16,21]. Four studies report on follow-up, although not in detail [8,9,13,21].
Only three studies compared 18FDG-PET with conventional radiological diagnostic
techniques (e.g., chest X-ray or CT) to screen for distant metastases [11,12,18].
It is difficult to compare the results of the aforementioned studies with the presented
results of this study due to different tumour types and stages, lack of comparison with
conventional diagnostic techniques and a low number of patients included. To the
best of our knowledge, no study has reported a direct comparison of 18FDG-PET and
CT while applying an adequate follow-up. The report of Teknos et al. [12] is the only
limited study in which 18FDG-PET was compared with CT. Unfortunately, they did not
report on the follow-up of their patients who were negative during screening.
To confirm the value of 18FDG-PET in detecting lung lesions, Nabi et al. [22]
reviewed the clinical course of 15 head and neck cancer patients with intrathoracic
lesions detected by 18FDG-PET. In nine of these patients malignant lesions were

Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
123
confirmed histopathologically or on repeated CT scans during follow-up. They
recommend that the chest be routinely surveyed during 18FDG-PET evaluation of
head and neck cancer patients. Wax et al. [23] reported that 18FDG-PET detected in
15 (25%) of the 59 patients with several types of untreated head and neck cancer at
different stages synchronous lung lesions (distant metastases or second primary
tumours). There were no data on follow-up or comparison with CT mentioned.
Stokkel et al. [24] found in 12 of 68 head and neck cancer patients a synchronous
primary tumour located in the head and neck or thorax. Nishiyama et al. [25] found
synchronous primary tumours in five of 53 (9%) of previously untreated head and
neck cancer patients using 18FDG-PET.
It is obvious that identification of distant metastases and second primary tumours, for
which no curative treatment is available is important because of the impact on quality
of remaining life. From our previous study and other studies it was clear that
screening with chest CT was the most efficient diagnostic strategy for detection of
distant metastases and that chest CT should therefore be the preferred investigation
for screening for distant metastases in high-risk HNSCC patients [5,6]. In conclusion,
our findings suggest that whole body 18FDG-PET may have additional value in
screening for distant metastases and second primary tumours, if applied to the
subset of patients who is at substantial risk. Whether this application of 18FDG-PET
will indeed be (cost-)effective, is now studied in a larger cohort of patients in a
multicenter study. Finally, these initial data suggest that in this patient population, the
use of PET-CT scanners might be productive since apparent discrepancies can be
solved readily while preserving the yield of whole body 18FDG-PET.
Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
124
Literature
1. Leon X, Quer M, Orus C, Del Prado Venegas M, Lopez M (2000) Distant metastases in
head and neck cancer patients who achieved locoregional control. Head Neck 22:680-686
2. Ferlito A, Shaha AR, Silver CE, Rinaldo A, Mordin V (2001) Incidence and sites of distant
metastases from head and neck cancer. ORL J Otorhinolaryngology Relat Spec 63:202-
207
3. Alvi A, Johnson JT (1997) Development of distant metastasis after treatment of advanced-
stage head and neck cancer. Head Neck 9:500-505
4. Leemans CR, Tiwari R, Nauta JJ, van der Waal I, Snow GB (1993) Regional lymph node
involvement and its significance in the development of distant metastases in head and
neck carcinoma. Cancer 71:452-456
5. Buckley JG, Ferlito A, Shaha AR, Rinaldo A (2001) The treatment of distant metastases in
head and neck cancer - present and future. ORL J Otorhinolaryngology Relat Spec
63:259-264
6. Bree R de, Deurloo EE, Snow GB, Leemans CR (2000) Screening for distant metastases
in patients with head and neck cancer. Laryngoscope 110:397-401
7. McGuirt WF, Greven K, Williams D, Keyes JW, Watson N, Cappellari JO, Geisinger KR
(1998) PET scanning in head and neck oncology: a review. Head Neck 20:208-215
8. Manolidis S, Donald PJ, Volk P, Pounds TR (1998) The use of positron emission
tomography scanning in occult and recurrent head and neck cancer. Acta Otolaryngol
suppl 534:5-11
9. Kunkel M, Wahlman U, Grotz KA, Benz P, Kuffner HD, Spitz J, Wagner W (1998) Value of
(F18)-2-fluorodeoxyglucose PET scanning in staging mouth cavity carcinoma.
Comparative evaluation of PET findings before and after preoperative radiochemotherapy
with histological and computerized tomography findings [Stellenwert der [F18]-2-Fluor-
desoxyglukose-PET im Staging des Mundhölenkarzinoms]. Mund Kiefer Gesichts Chir
2:181-187
10. Hanasono MM, Kunda LD, Segall GM, Ku GH, Terris DJ (1999) Uses and limitations of
FDG positron emission tomography in patients with head and neck cancer. Laryngoscope
109:880-885
11. Keyes JW, Chen MYM, Watson NE, Greven KM, McGuirt WF, Williams DW (2000) FDG
PET evaluation of head and neck cancer: value of imaging the thorax. Head Neck 22:105-
110
Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
125
12. Teknos TN, Rosenthal EL, Lee D, Taylor R, Marn CS (2001) Positron emission
tomography in the evaluation of stage III and IV head and neck cancer. Head Neck
23:1056-1060
13. Kresnik E, Mikosch P, Gallowitsch HJ, Kogler D, Wieser S, Heinisch M, Unterweger O,
Raunik W, Kumnig G, Gomez I, Grunbacher G, Lind P (2001) Evaluation of head and neck
cancer with 18FDG-PET: a comparison with conventional methods Eur J Nucl Med 28:816-
821
14. Stuckensen T, Kovacs AF, Adams S, Baum RP (2000) Staging of the neck in patients with
oral cavity SCC: a prospective comparison of PET, ultrasound, CT and MRI. J Cran
Maxillofac Surg 28:319-324
15. Nakasono Y, Inoue T, Oriuchi N, Takeuchi K, Negishi A, Endo K, Mogi K (2001) The role of
whole-body FDG-PET in preoperative assessment of tumor staging in oral cancers. Ann
Nucl Med 15:505-512
16. Kitagawa Y, Nishizawa S, Sano K, Sadato N, Maruta Y, Ogasawara T, Nakamura M,
Yonekura Y (2002) Whole-body 18-FDG-PET in patients with head and neck cancer. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 93:202-207
17. Regelink G, Brouwer J, Bree R de, Pruim J, Laan BFAM van der, Vaalburg W, Hoekstra
OS, Comans EFI, Vissink A, Leemans CR, Roodenburg JLN (2002) Detection of unknown
primary tumours and distant metastases in patients with cervical metastases: value of
FDG-PET versus conventional modalities. Eur J Nucl Med 29:1024-1030
18. Schmid DT, Stoeckli SJ, Bandhauer F, Huguenin P, Schmid S, Schulthess GK von,
Goerres GW (2003) Impact of PET on initial staging and therapy in locoregional advanced
scc of the head and neck. Laryngoscope 113:888-891
19. Goerres GW, Schmid DT, Gratz KW, von Schulthess GK, Eyrich GK (2003) Impact of
whole body positron emission tomography on initial staging and therapy in patients with
squamous cell carcinoma of the oral cavity. Oral Oncol 39:547-551
20. Schwartz DL, Rajendran J, Yueh B, Coltrera M, Anzai Y, Krohn K, Eary J (2003) Staging of
head and neck squamous cell cancer with extended-field FDG-PET.
Arch Otolaryngol Head Neck Surg 129:1173-1178
21. Schmidt M, Schmalenbach M, Jungehulsing M, Theissen P, Dietlein M, Schroder U,
Eschner W, Stennert E, Schicha H (2004) 18F-FDG PET for detecting recurrent head and
neck cancer, local lymph node involvement and distant metastases. Comparison of
qualitative visual and semiquantitative analysis. Nuklearmedizin 43:91-101
22. Nabi HA, Spaulding M, Farrell E, Lamonica D (1998) Detection of synchronous lung
lesions by FDG-PET imaging: influence on management of patients with head and neck
cancer. J Nucl Med 39:248P
23. Wax MK, Myers LL, Gabalski EC, Syed Husain, Gona JM, Nabi H (2002) Positron
emission tomography in the evaluation of synchronous lung lesions in patients with
untreated head and neck cancer. Arch Otolaryngol Head Neck Surg 128:703-707

Screening for distant metastases in patients with head and neck cancer: Is there a role for 18FDG-PET?
126
24. Stokkel MPM, Moons KGM, Broek FW ten, Rijk PP van, Hordijk GJ (1999) 18F-
Fluorodeoxyglucose dual-head positron emission tomography as a procedure for detecting
simultaneous primary tumors in case of head and neck cancer. Cancer 86:2370-2377
25. Nishiyama Y, Yamamoto Y, Yokoe K, Miyabe K, Ogawa T, Toyama Y, Satoh K, Ohkawa M
(2005) FDG PET as a procedure for detecting simultaneous tumours in head and neck
cancer patients. Nuc lMed Comm 26:239-244
9
Summary and future prospects

Summary and future prospects
128
Summary
When treating patients with laryngeal carcinoma, preservation of the functions of the
larynx, phonation, breathing and swallowing, is a vital goal. Therefore, non-surgical
treatment options have gained popularity. Surgical salvage is kept in reserve for
recurrence. In a previously radiated larynx, however, recurrent carcinoma is not
easily distinguished from radiotherapeutic sequels. Since early detection is essential
for successful salvage surgery, this creates a clinical problem. Chapters 2-5 of this
thesis address this problem.
When distant metastases are detected in head and neck squamous cell carcinoma
(HNSCC) patients with primary disease, treatment is altered and prognosis is
unfavourable. These patients are usually not considered curable and will receive
palliative treatment. Screening for distant metastases is performed to spare these
patients from undergoing futile extensive treatment. The optimal screening method
for these patients is still debated. Chapters 6-8 of this thesis address this clinical
problem.
The aims of this thesis were the evaluation of the daily clinical practice and the
possibilities of imaging techniques in order to detect recurrent laryngeal carcinoma
after prior radiotherapy (Chapters 2-5) and distant metastases in patients with
extensive primary head and neck carcinomas (Chapters 6-8).
In Chapter 2 the current daily practice is described through a questionnaire among
clinicians and retrospective analysis of a cohort of patients clinically suspected of a
recurrent laryngeal carcinoma after radiotherapy. The questionnaire showed that
94% of the physicians in departments in the major institutions treating head and neck
cancer in The Netherlands used direct laryngoscopy as a diagnostic technique.
Imaging (MRI, CT, 18FDG-PET) did not play an important role.
All 131 patients in the cohort suspected of recurrence had undergone 207 direct
laryngoscopies under general anaesthesia with biopsies. In 70 (53%) patients the
first laryngoscopy was negative. Twenty-two (31%) of them turned out to be false
negative within 6 months. Sixty-five (31%) futile laryngoscopies were performed in 37
patients that remained disease free.
A systematic review is described in Chapter 3. This was performed to summarise the
available evidence in patients with suspicion of recurrent laryngeal carcinoma after
radiotherapy. An attempt was made to determine the diagnostic accuracy of CT and
MRI scans, 201Tl scintigraphy and 18FDG-PET in these patients.
Summary and future prospects
129
Surprisingly, no articles on CT, MRI or 201Tl scintigraphy were found which met the
inclusion criteria. Eight articles on 18FDG-PET were available. In 3 articles 18FDG-
PET was compared to CT or MRI.
The internal and external validity of the articles was described to compare their
quality. Because of the small number of studies, it was not possible to create
subgroups. A quantitative analysis using a random effects model was performed. The
pooled estimates (95% confidence interval) for sensitivity and specificity of 18FDG-
PET were 89% (80%-94%) and 74% (64%-83%).
Chapter 4 is a pilot study on 18FDG-PET in detecting recurrent laryngeal carcinoma
after radiotherapy, in which interobserver variation was measured to determine its
usefulness in routine clinical practice.
Thirty consecutive patients underwent 18FDG-PET and direct laryngoscopy under
general anaesthesia with taking of biopsies. The reference was the absence or
appearance of a local recurrence within the 12 months following 18FDG-PET. Eight
patients had biopsy proven recurrent laryngeal carcinoma. First the scans were
evaluated by 2 observers. This showed a sensitivity of 88% and a specificity of 82%
Then the scans were reviewed by 9 observers to determine interobserver variability.
The observers had a moderate to reasonable agreement with a weighted kappa of
0.45 vs. the clinical gold standard. The weighted kappa for interobserver variability
was 0.54.
An estimation of the cost-effectiveness of 18FDG-PET in the selection for direct
laryngoscopy in patients with suspicion of recurrent laryngeal carcinoma after
radiotherapy is performed in Chapter 5. The direct medical costs of 30 patients were
calculated from the first visit where suspicion was raised till 12 months later. A
strategy in which all patients undergo direct laryngoscopy was compared to an 18FDG-PET strategy in which only patients with a positive or equivocal 18FDG-PET
undergo direct laryngoscopy.
The mean costs for the detection of recurrent laryngeal cancer with direct
laryngoscopy in the conventional strategy were € 13.230. The mean costs of an 18FDG-PET strategy were € 12.831. Therefore an 18FDG-PET strategy is not more
costly than the conventional strategy.
To evaluate the daily practice concerning screening for distant metastases
preoperatively, a questionnaire was performed among investigators in the 12
departments treating head and neck cancer in The Netherlands in Chapter 6.
All investigators returned the questionnaire. There was no uniformity and indeed a
substantial variation in the indications for screening and methods of screening. There
Summary and future prospects
130
is a need for clear guidelines for screening for distant metastases in patients with
head and neck cancer.
Chapter 7 describes the evaluation of a diagnostic strategy. In a previous study, risk
factors for developing distant metastases in patients with head and neck cancer were
established. Chest CT scan turned out to the best diagnostic tool for pretreatment
screening in these patients. In this study 109 consecutive patients with HNSCC
scheduled for extensive treatment and at least one risk factor underwent chest CT.
A total of 20 lung metastases and 1 liver metastasis were found. The chest CT had a
sensitivity of 73% and a specificity of 80%. To better detect distant metastases
before treatment and thus to avoid futile extensive treatment, a more sensitive,
preferably whole-body, technique is desirable.
In order to improve the sensitivity of screening described in Chapter 6, Chapter 8
prospectively compared the yield of whole-body 18FDG-PET and chest CT to detect
distant metastases and synchronous primary tumours in a pilot study. Thirty-four
consecutive patients, with extended HNSCC, underwent both techniques. Both chest
CT and 18FDG-PET detected 2 lung lesions, but 18FDG-PET detected 2 additional
second primary tumours in the abdomen. There was an added value in 6% of the
patients of whole-body 18FDG-PET versus chest CT.
Future prospects
The results described in this thesis warrant further investigation of the possibilities of 18FDG-PET. In the population of patients who are suspected of a recurrent laryngeal
carcinoma after radiotherapy for a T2-T4 tumour, a prospective randomised clinical
trial, the RELAPS study, is currently performed within the Dutch Head and Neck
Cooperative Group [1]. To avoid futile direct laryngoscopies under general
anaesthesia, selection based on 18FDG-PET is investigated. A conventional strategy
is compared to a strategy based on 18FDG-PET. In the conventional arm, patients
undergo direct laryngoscopy with biopsies. When recurrence is found, treatment
obviously follows. When histopathology is equivocal or negative, direct laryngoscopy
is performed again after 6 weeks, unless the symptoms subside. In the 18FDG-PET
arm, patients first undergo 18FDG-PET. When the result is positive or equivocal,
direct laryngoscopy is performed. When negative, a follow-up period of 3 months is
started, unless symptoms progress. Reference standard is a follow-up of 6 months
and results of direct laryngoscopy with biopsies.
Summary and future prospects
131
To further investigate the value of whole-body 18FDG-PET in detecting distant
metastases and synchronous primary tumours in patients with extensive primary
HNSCC, a prospective observational study was started, the SCHOOL study, in 3
Head and Neck Centres in The Netherlands. In this study patients underwent both 18FDG-PET and conventional chest CT. The yield of the 2 techniques separately and
in combination was determined as well as interobserver agreement of CT and 18FDG-
PET, the costs of diagnostic work-up and extensive treatment for advanced HNSCC
with palliative or curative intent, and the cost-effectiveness of screening based on
conventional diagnostic work-up and 18FDG-PET [2]. In addition, a validation of the
reviewing criteria found in the SCHOOL study will be performed as well as a study to
determine the value (accuracy, reduction of futile extensive treatments and
associated costs) of integrated PET-CT in screening for distant metastases and
second primary tumours in head and neck cancer patients, as compared to CT, PET
and visual correlation of PET and CT.
So far, 18FDG is the most commonly used tracer in PET imaging in head and neck.
Ongoing studies are examining the possibilities of new tracers. As described in
chapter 3, Cobben et al. [3] compared fluorine-18 labelled thymidine with 18FDG in
laryngeal cancer. Carbon-11 labelled methionine showed promising results in
differentiating between inflammation and malignant tumour in rats in a study by Zhao
et al. [4]. Pre-treatment C11 labelled tyrosine PET was compared to post-treatment
tyrosine PET for therapy evaluation in laryngeal cancer patients by De Boer et al. [5].
Both sensitivity and specificity were 100%. Börjesson et al. [6] combined PET and
the monoclonal antibody U36 (immuno-PET) labelled with Zirconium-89 to detect
HNSCC lymph node metastases. However, till now none of these tracers has found
its way into daily practice.
To improve imaging in HNSCC, cross-sectional imaging techniques (CT and MRI)
are combined with functional imaging (PET). The disease can then be characterised
both anatomically and functionally. The fusion of PET and CT has already proven to
be more accurate for the detection of malignancy in the head and neck region than
either modality alone. Agarwal et al. [7] describe in a recent review the surplus value
of PET/CT in staging advanced HNSCC, finding unknown primary tumours, radiation
treatment planning, monitoring treatment response, restaging and identifying
recurrent HNSCC.
PET/MRI is a new and promising multi-modality imaging device successfully studied
in a preclinical setting [8]. Advantages of MRI over CT: MRI uses no ionising
radiation and produces high soft-tissue contrast and provides spectroscopic
Summary and future prospects
132
information and functional MRI. Furthermore PET/MRI allows for simultaneous data
acquisition. Pichler et al. [9] describe an overview of current working prototypes.
Both CT and MRI by themselves, not just in fusion techniques, show new possibilities
in oncology. Recent technical developments may improve the results of CT and MRI
found in this thesis. At present, a chest CT is performed using a multidetector CT
scanner during breath-holding. The slices currently used are much thinner than
before and this is likely to improve the sensitivity. MRI has improved both due to the
introduction of faster MR imaging techniques (whole-body MR imaging) and newer
pulse sequences (short term inversion recovery (STIR) and diffusion MRI). Due to the
introduction of multi-receiver channel MR, whole-body MRI has become clinically
feasible, with substantially reduced examination times [10]. Whole-body MRI shows
potential in detecting metastasis of primary head and neck tumours [11]. STIR
imaging uses an alternative MR imaging sequence that provides suppression of
signal from fat and additive effects of T1 and T2 mechanisms on tissue brightening.
Because most tumour-related abnormalities have both long T1 and long T2
relaxation times, such an additive effect on tissue brightening may improve lesion
conspicuity and sensitivity of lesion detection [12]. Whole-body STIR can be used for
the primary tumour, but showed especially good results in metastastic spread to
bone, liver and central nervous system and bone marrow disease [10,13,14].
Diffusion weighted MRI attempts to assess the diffusion capacity of tissue. Due to
tumour proliferation, the tumour regions have increased cellular density and this
results in a reduction of diffusion of water molecules through these regions. It
provides information on extracellular space tortuosity, tissue cellularity and the
integrity of cellular membranes [15-18]. This technique has a very short scanning
time and adds no extra cost to patients who are already undergoing MRI. The
molecular motion can be determined by calculating the apparent diffusion coefficient
(ADC) with diffusion-weighted MRI. Hypercellular tissue, such as in malignant
tumours will show low ADC values. Diffusion weighted whole-body MR imaging may
be used for characterisation of neck lymph nodes, to diferentiate between persistent
or recurrent cancer and treatment-induced tissue changes and to confirm or exclude
metastatic disease or a second primary tumour [19-21]. Both techniques can be used
in whole-body MRI scanning. However, the role of these new (whole-body) MR
techniques in clinical management is yet to be established by additional studies.
In the next few years, it might be expected that the indications for 18FDG-PET will
become clearer and promising new tracers and scanners will find their way into the
daily clinical setting, after first establishing their applicability.
Summary and future prospects
133
Literature 1. Bree R, Putten L van der, Hoekstra OS, Kuik DJ, Uyl-de Groot CA, Tinteren H van,
Leemans CR, Boers M: RELAPS Study Group (2007) A randomized trial of PET scanning
to improve diagnostic yield of direct laryngoscopy in patients with suspicion of recurrent
laryngeal carcinoma after radiotherapy. Contemp Clin Trials 28:705-712
2. Senft A, Bree R de, Hoekstra OS, Kuik DJ, Golding RP, Oyen WJG, Pruim J, Hoogen FJ
van den, Roodenburg JLN, Leemans CR (2008) Screening for distant metastases in head
and neck cancer patients by chest CT or whole body FDG-PET: A prospective multitrial
study. Radiother Oncol 87:221-229
3. Cobben DCP, Laan BFAM van der, Maas B, Vaalburg W, Suurmeijer AJ, Hoekstra HJ,
Jager PL, Elsinga PH (2004) 18F-FLT PET for visualization of laryngeal cancer:
comparison with 18F-FDG PET. J Nucl Med 45:226-231
4. Zhao S, Kuge Y, Kohanawa M, Takahashi T, Zhao Y, Yi M, Kanegae K, Seki K, Tamaki N
(2008) Usefulness of 11C-methionine for differentiating tumors from granulomas in
experimental rat models: a comparison with 18F-FDG and 18F-FLT. J Nucl Med 49:135-
141
5. De Boer JR, Pruim J, Burlage F, Krikke A, Tiebosch AT, Albers FW, Vaalburg W, Van Der
Laan BF (2003) Therapy evaluation of laryngeal carcinomas by tyrosine-pet. Head Neck
25:634-644
6. Börjesson PK, Jauw YW, Boellaard R, Bree R, Comans EFI, Roos JC, Castelijns JA,
Vosjan MJ, Kummer JA, Leemans CR, Lammertsma AA, Dongen GA (2006) Performance
of immuno-positron emission tomography with zirconium-89-labeled chimeric monoclonal
antibody U36 in the detection of lymph node metastases in head and neck cancer patients.
Clin Cancer Res 12:2133-2140
7. Agarwal V, Branstetter IV BF, Johnson JT (2008) Indications for PET/CT in the Head and
Neck. Otolaryngol Clin N Am 41:23-49
8. Judenhofer MS, Wehrl HF, Newport DF, Catana C, Siegel SB, Becker M, Thielscher A,
Kneilling M, Lichy MP, Eichner M, Klingel K, Reischl G, Widmaier S, Röcken M, Nutt RE,
Machulla H-J, Uludag K, Cherry SR, Claussen CD, Pichler BJ (2008) Simultaneous PET-
MRI: a new approach for functional and morphological imaging. Nat Med 14:459-465
9. Pichler BJ, Wehrl HF, Kolb A, Judenhofer MS (2008) Positron Emission
Tomography/Magnetic Resonance Imaging: The next generation of multimodality imaging?
Semin Nucl Med 38:199-208
10. Schmidt GP, Kramer H, Reiser MF, Glaser C (2007) Whole-body Magnetic Resonance
Imaging and Positron Emission Tomography-Computed Tomography in oncology. Top
Magn Reson Imaging 18:193-202
Summary and future prospects
134
11. Herborn CU, Unkel C, Vogt FM, Massing S, Lauenstein TC, Neumann A (2005) Whole-
body MRI for staging patients with head and neck squamous cell carcinoma. Acta
Otolaryngol 125:1224-1229
12. Shuman WP, Patten RM, Baron RL, Liddell RM, Conrad EU, Richardson ML (1991)
Comparison of STIR and spin-echo MR imaging at 1.5 T in 45 suspected extremity tumors:
lesion conspicuity and extent. Radiology 179:247-252
13. Antoch G, Vogt FM, Freudenberg LS, Nazaradeh F, Goehde SC, Barkhausen J, Dahmen
G, Bockisch A, Debatin JF, Rühm SG (2003) Whole-body dual-modality PT/CT and whole-
body MRI for tumor staging in oncology. JAMA 290:3199-3206
14. Schmidt GP, Schönberg SO, Schmid R, Stahl R, Tiling R, Becker CR, Reiser MF, Baur-
Melnyk A (2007) Screening for bone metastases: whole-body MRI using a 32-channel
system versus dual-modality PET-CT. Eur Radiol 17:939-949
15. Khoo VS, Joon DL (2006) New developments in MRI for target volume delineation in
radiotherapy. Br J Radiol 79 Spec No 1:S2-15
16. Patterson DM, Padhani AR, Collins DJ (2008) Technology insight: water diffusion MRI—a
potential new biomarker of response to cancer therapy. Nat Clin Pract Oncol 5:220-233
17. Koh DM, Collins DJ (2007) Diffusion-weighted MRI in the body: applications and
challenges in oncology. AJR Am J Roentgenol 188:1622-1635
18. Zbären P, Weidner S, Thoeny HC (2008) Laryngeal and hypopharyngeal carcinomas after
(chemo)radiotherapy: a diagnostic dilemma. Curr Opin Otolaryngol Head Neck Surg
16:147-153
19. Abdel Razek AAK, Kandeel AY, Soliman N, El-shenshawy HM, Kamel Y, Nada N,
Denewar A (2007) Role of diffusion-weighted echo-planar MR imaging in differentiation of
residual or recurrent head and neck tumors and posttreatment changes. AJNR Am J
Neuradiol 28:1146-1152
20. Hermans R, Vandecaveye V (2007) Diffusion-weighted MRI in head and neck cancer.
Cancer Imaging 7:126-127
21. Vandecaveye V, Keyzer F de, Nuyts S, Deraedt K, Dirix P, Hamaekers P, Poorten V
vander, Delaere P, Hermans R (2007) Detection of head and neck squamous cell
carcinoma with diffusion weighted MRI after (chemo)radiotherapy: correlation between
radiologic and histopathologic findings. Int J Radiat Oncol Biol Phys 67:960-971
10
Samenvatting en vooruitzichten
Samenvatting en vooruitzichten
136
Samenvatting Bij het behandelen van patiënten met een larynxcarcinoom is het behoud van de
functies van de larynx, fonatie, ademhaling en slikken, een belangrijk doel. Om die
reden hebben niet-chirurgische behandelingen aan populariteit gewonnen.
Chirurgische interventie, de zogenaamde ‘salvage’ chirurgie, wordt achter de hand
gehouden in geval van recidief. In een voorheen bestraalde larynx is het echter niet
gemakkelijk om recidief carcinoom te onderscheiden van radiotherapeutische
veranderingen. Dit creëert een klinisch probleem omdat vroege detectie essentieel is
voor succesvolle ’salvage’ chirurgie. De hoofdstukken 2-5 van deze dissertatie
besteden aandacht aan dit probleem. Als er afstandsmetastasen worden gevonden bij patiënten met een primair hoofd-
halscarcinoom, wijzigt de behandeling en wordt de prognose ongunstiger. Deze
patiënten worden meestal niet meer als curabel beschouwd en ondergaan palliatieve
behandeling. Het opsporen van afstandmetastasen wordt verricht om deze patiënten
een onnodige uitgebreide behandeling te besparen. De meest optimale manier voor
het screenen op afstandsmetastasen is nog niet gevonden. De hoofdstukken 6-8
richten zich op dit klinische probleem.
Het doel van deze dissertatie was een evaluatie te verrichten van de dagelijkse
klinische praktijk en van de mogelijkheden van beeldvormende technieken om
recidief larynxcarcinomen na eerdere radiotherapie (hoofdstukken 2-5) en
afstandsmetastasen bij patiënten met uitgebreide primaire hoofd-halscarcinomen
(hoofdstukken 6-8) te detecteren.
In Hoofdstuk 2 wordt de huidige klinische praktijk beschreven door middel van een
enquête onder klinische artsen en wordt een retrospectieve analyse verricht op een
cohort patiënten die klinische verdenking hadden op een recidief larynxcarcinoom na
radiotherapie. Uit de enquête kwam naar voren dat 94% van de artsen, werkzaam op
afdelingen van Nederlandse centra waar hoofd-halskanker wordt behandeld, directe
laryngoscopie onder narcose gebruiken als diagnostische techniek. Beeldvorming
(MRI, CT, 18FDG-PET) speelde geen grote rol.
Alle 131 patiënten in het cohort verdacht voor een recidief larynxcarcinoom,
ondergingen in totaal 207 laryngoscopieën onder narcose met het nemen van
biopten. Bij 70 (53%) patiënten was de eerste laryngoscopie negatief. Hiervan bleken
er 22 (31%) foutnegatief binnen 6 maanden. Er werden 65 (31%) onnodige
laryngoscopieën verricht bij 37 patiënten die ziektevrij bleven.
Samenvatting en vooruitzichten
137
Een systematische review wordt beschreven in Hoofdstuk 3. Deze werd verricht om
alle beschikbare informatie samen te vatten over patiënten met verdenking op
recidief larynxcarcinoom na radiotherapie. Er werd een poging gedaan om in deze
populatie de diagnostische accuraatheid te bepalen van CT en MRI scans, 201Tl
scintigrafie en 18FDG-PET.
Verrassend genoeg werden er geen artikelen gevonden over CT, MRI of 201Tl
scintigrafie, die voldeden aan de inclusiecriteria. Er waren 8 artikelen beschikbaar
over 18FDG-PET. In 3 van deze artikelen werd 18FDG-PET vergeleken met CT of
MRI. Om de kwaliteit van de artikelen te vergelijken, werd hun interne en externe
kwaliteit beschreven. Gezien het kleine aantal artikelen, was het onmogelijk om
subgroepen te maken. De samengevoegde schattingen (95% betrouwbaarheids-
interval) voor sensitiviteit en specificiteit van 18FDG-PET waren respectievelijk 89%
(80%-94%) en 74% (64%-83%).
Hoofdstuk 4 beschrijft een pilot studie over het gebruik van 18FDG-PET bij de
detectie van recidief larynxcarcinoom na radiotherapie, waarin de interobserver
variatie werd gemeten om de bruikbaarheid in de klinische praktijk te bepalen.
Dertig opeenvolgende patiënten ondergingen 18FDG-PET en directe laryngoscopie
onder algehele narcose met het nemen van biopten. De referentiestandaard was de
aan- of afwezigheid van een lokaal recidief binnen 12 maanden na 18FDG-PET. Acht
patiënten hadden een door biopten bevestigd recidief larynxcarcinoom. Eerst werden
de scans bekeken door 2 beoordelaars. Een sensitiviteit van 88% en een specificiteit
van 82% werden gevonden. Daarna werden de scans gereviseerd door 9
beoordelaars om de interobserver variatie te bepalen. De beoordelaars hadden een
matige tot redelijke overeenstemming met een gewogen kappa van 0.45 ten opzichte
van de referentiestandaard. De gewogen kappa voor de interobserver variatie was
0.54.
Een schatting van de kosteneffectiviteit van 18FDG-PET voor de selectie voor directe
laryngoscopie bij patiënten met verdenking op recidief larynxcarcinoom na
radiotherapie wordt beschreven in Hoofdstuk 5. De directe medische kosten van 30
patiënten werden berekend over een periode vanaf het eerste polikliniek bezoek
waarbij verdenking op recidief was tot 12 maanden later. Een strategie waarin alle
patiënten een directe laryngoscopie ondergingen werd vergeleken met een 18FDG-
PET strategie waarin alleen patiënten met een positieve of twijfelachtige 18FDG-PET
uitslag een directe laryngoscopie kregen.
Samenvatting en vooruitzichten
138
De gemiddelde kosten voor de detectie van recidief larynxcarcinoom door middel van
directe laryngoscopie in de conventionele strategie waren € 13.230. De gemiddelde
kosten van een 18FDG-PET strategie waren € 12.831. Een 18FDG-PET strategie is
daarom niet duurder dan de conventionele strategie.
Om de dagelijkse praktijk met betrekking tot het preoperatief screenen naar
afstandsmetastasen te evalueren, werd in Hoofdstuk 6 een enquête verricht onder
artsen in de 12 afdelingen die hoofd-halskanker behandelen in Nederland.
Allen retourneerden de enquête. Er was geen consensus en zelfs een behoorlijke
variatie tussen de indicaties en de methoden van screenen. Er is behoefte aan
duidelijke richtlijnen voor screenen op afstandsmetastasen in patiënten met hoofd-
halskanker.
Hoofdstuk 7 beschrijft de evaluatie van een diagnostische strategie. In een eerdere
studie werden risicofactoren vastgesteld voor het ontwikkelen van afstands-
metastasen bij hoofd-halskanker patiënten. CT scan van de thorax bleek het beste
diagnosticum voor het screenen van deze patiënten voor aanvang van de
behandeling. In deze studie ondergingen 109 hoofd-halskankerpatiënten met
tenminste 1 risicofactor, die gepland waren voor uitgebreide behandeling, een CT
scan van de thorax.
In totaal werden er bij 20 patiënten longmetastasen en bij 1 patiënt levermetastasen
gevonden . De CT scan van de thorax had een sensitiviteit van 73% en een
specificiteit van 80%. Om afstandsmetastasen nog beter te kunnen detecteren
voorafgaand aan een behandeling, en om zo onnodige uitgebreide behandeling te
voorkomen, is een sensitievere en bij voorkeur ‘whole-body’ techniek wenselijk.
Om de sensitiviteit van screenen zoals beschreven in hoofdstuk 6, te verbeteren,
wordt in Hoofdstuk 8 in een prospectieve pilot studie een vergelijking gemaakt
tussen de opbrengst van whole-body 18FDG-PET en CT scan van de thorax bij het
opsporen van afstandsmetastasen en synchrone primaire tumoren. Vierendertig
opeenvolgende patiënten, met uitgebreide hoofd-halskanker, ondergingen beide
technieken. Zowel CT scan van de thorax als 18FDG-PET detecteerden 2
longmetastasen, echter 18FDG-PET ontdekte daarbij nog 2 tweede primaire tumoren
in het abdomen. Er was een toegevoegde waarde in 6% van de patiënten in 18FDG-
PET ten opzichte van CT thorax.
Samenvatting en vooruitzichten
139
Vooruitzichten
De resultaten die beschreven zijn in deze dissertatie rechtvaardigen nadere
onderzoeken naar de mogelijkheden van 18FDG-PET. In de populatie van patiënten
met verdenking op een recidief larynxcarcinoom na radiotherapie voor een T2-T4
tumor, wordt op dit moment een prospectieve gerandomiseerde klinische studie
verricht binnen de Nederlandse Werkroep Hoofd Hals Tumoren, de RELAPS studie
[1]. Om onnodige directe laryngoscopieën onder narcose te kunnen voorkomen,
wordt een selectie op basis van 18FDG-PET onderzocht. Een conventionele strategie
wordt vergeleken met een strategie gebaseerd op 18FDG-PET. In de conventionele
arm ondergaan patiënten directe laryngoscopie met biopten. Als er een recidief wordt
gevonden, volgt uiteraard behandeling. Als de histopathologie negatief of twijfelachtig
is, wordt de directe laryngoscopie herhaald na 6 weken, tenzij de symptomen
verminderen. In de 18FDG-PET arm ondergaan patiënten eerst 18FDG-PET. Als de
uitslag positief of twijfelachtig is, wordt directe laryngoscopie verricht. Als de uitslag
negatief is volgt een follow-up periode van 3 maanden, tenzij de symptomen
toenemen. De referentie standaard is een negatieve follow-up van 6 maanden of
directe laryngoscopie met biopten.
Om de waarde van whole-body 18FDG-PET, bij de detectie van afstandsmetastasen
en synchrone tweede primaire tumoren van patiënten met uigebreide hoofd-
halskanker, nader te onderzoeken, werd een prospectieve observationele studie
gestart in 3 Hoofd Hals centra in Nederland, de SCHOOL studie. In deze studie
ondergingen patiënten zowel 18FDG-PET als CT scan van de thorax. De opbrengst
van de 2 technieken apart en in combinatie werd bepaald evenals de ‘interobserver’
overeenstemming van CT en 18FDG-PET, de kosten van het diagnostische traject en
uitgebreide behandeling voor gevorderde hoofd-halskanker met palliatieve of
curatieve opzet, en de kosteneffectiviteit van screenen gebaseerd op het
conventionele traject en op 18FDG-PET [2]. Daarnaast zal er een validatie van de
beoordelingscriteria zoals gevonden in de SCHOOL studie plaatsvinden, alsmede
een studie om de waarde (accuraatheid, vermindering van overbodige uitgebreide
ingrepen en geassocieerde kosten) van een geïntegreerde PET-CT te bepalen voor
het screenen op afstandsmetastasen en 2e primaire tumoren bij hoofd-halskanker
patiënten, vergeleken met CT, PET en visuele correlatie van CT en PET.
Tot nu toe is 18FDG de meest gebruikte tracer voor PET in het hoofd-halsgebied.
Lopende onderzoeken bestuderen de mogelijkheden van nieuwe tracers. Zoals
Samenvatting en vooruitzichten
140
beschreven in hoofdstuk 3, vergeleken Cobben et al. [3] flourine-18 gelabeld
thymidine met 18FDG bij larynxcarcinomen. Koolstof-11 gelabeld methionine liet, in
een studie door Zhao et al. [4], veelbelovende resultaten zien bij het differentiëren
tussen ontsteking en maligne tumor bij ratten. Een koolstof-11 gelabelde thyrosine
PET werd vergeleken voor en na behandeling bij patiënten met een larynxcarcinoom
door De Boer et al. [5]. Zowel de sensitiviteit als de specificiteit was 100%. Börjesson
et al. [6] combineerden PET en het monoklonaal antilichaam U36 (immuno-PET)
gelabeld met Ziconium-89, om lymfekliermetastasen te detecteren van hoofd-
halscarcinomen. Tot op heden heeft geen van deze tracers echter zijn weg gevonden
in de dagelijkse praktijk.
Om beeldvorming in hoofd-halskanker te verbeteren worden anatomische
beeldvormende technieken (CT en MRI) gecombineerd met functionele beeldvorming
(PET). Op deze manier kan de ziekte zowel anatomisch als functioneel
gekarakteriseerd worden. De fusie van PET en CT heeft al bewezen meer accuraat
te zijn voor de detectie van maligne tumoren in het hoofd-halsgebied dan één van
beide technieken apart. Agarwal et al. [7] beschrijven in een recente review de
meerwaarde van PET/CT bij stadiëring van voortgeschreden hoofd-halskanker,
detectie van onbekende primaire tumoren, radiotherapie planning, respons
monitoren, her-stadiëring en de identificatie van recidieven.
PET/MRI is een nieuwe veelbelovende beeldvormende multi-modaliteit scanner,
welke succesvol werd getest in de preklinische setting [8]. Voordelen van MRI boven
CT: MRI gebruikt geen ioniserende straling en produceert een hoog weke delen
contrast en verschaft spectroscopische en functionele data. Daarnaast maakt
PET/MRI simultane data acquisitie mogelijk. Pichler et al. [9] geven een overzicht
van werkende prototypes.
Zowel CT als MRI op zich, niet slechts in fusie technieken, hebben nieuwe
mogelijkheden in de oncologie. Recente technische ontwikkelingen kunnen de
resultaten van de CT en MRI, zoals beschreven in deze dissertatie, verbeteren.
Tegenwoordig wordt een CT scan van de thorax verricht met een multi-detector CT
scanner tijdens inademing. De coupes, die nu gebruikelijk zijn, zijn veel dunner dan
voorheen en hierdoor is het heel aannemelijk dat de sensitiviteit verbeterd is. MRI is
verbeterd door zowel door de introductie van snellere MRI technieken (whole-body
MRI) en door nieuwere puls-sequenties (short term inversion recovery (STIR) en
diffusie MRI). Door de introductie van de multi-channel MRI, is whole-body MRI
klinisch mogelijk geworden, met substantieel gereduceerde onderzoekstijden [10].
Whole-body MRI heeft mogelijkheden bij de detectie van metastasen van primaire
Samenvatting en vooruitzichten
141
hoofd-halstumoren [11]. STIR beeldvorming is gebaseerd op een alternatieve MR
beeldvormende sequentie, welke een verminderd vet signaal geeft en extra effecten
aangaande T1 en T2 mechanismen bij beeldvorming van weefsels. Omdat de
meeste tumor gerelateerde afwijkingen zowel lange T1 als T2 relaxatie tijden
kennen, kan een dergelijk effect op weefsel een verbetering geven van zichtbaarheid
en sensitiviteit van detectie van de laesie [12]. Whole-body STIR kan worden
gebruikt voor de primaire tumor maar laat met name goede resultaten zien bij
metastasering naar bot, lever, het centrale zenuwstelsel en bij beenmerg ziekten
[10,13,14].
Diffusie gewogen MRI toont de diffusie capaciteit van het weefsel. Door tumor
proliferatie, heeft de tumor regio een verhoogde cellulaire dichtheid en dat resulteert
in een vermindering van de diffusie van watermoleculen in deze regio. Op deze
manier wordt er informatie verschaft over de richting van de extracellulaire ruimte, de
weefsel cellulariteit en de integriteit van de celmembraan [15-18]. Deze techniek
heeft een heel korte scan tijd en voegt geen extra kosten toe voor de patiënten die
toch al een MRI ondergaan. The moleculaire beweging kan bepaald worden door het
berekenen van de apparant diffusion coefficient (ADC) op basis van diffusie MRI:
hypercellulair weefsel, zoals in maligne tumoren, laat lage ADC waarden zien.
Diffusie gewogen whole-body MRI zou gebruikt kunnen worden ter karakterisering
van halskliermetastasen, ter differentiatie tussen residu of recidief tumor en weefsel
veranderingen als gevolg van een behandeling en om gemetastaseerde ziekte en 2e
primaire tumoren aan te tonen of uit te sluiten [19-21]. Beide technieken kunnen
worden gebruikt bij whole-body MRI. De rol van deze nieuwe (whole-body) MRI
technieken in de klinische setting moet verder worden aangetoond in vervolg studies.
In de komende jaren is de verwachting dat de indicaties voor 18FDG-PET duidelijker
worden en dat veelbelovende nieuwe tracers and scanners hun weg zullen vinden
naar de dagelijkse klinische praktijk, nadat eerst hun toepasbaarheid is aangetoond.
Samenvatting en vooruitzichten
142
Literatuur 1. Bree R, Putten L van der, Hoekstra OS, Kuik DJ, Uyl-de Groot CA, Tinteren H van,
Leemans CR, Boers M: RELAPS Study Group (2007) A randomized trial of PET scanning
to improve diagnostic yield of direct laryngoscopy in patients with suspicion of recurrent
laryngeal carcinoma after radiotherapy. Contemp Clin Trials 28:705-712
2. Senft A, Bree R de, Hoekstra OS, Kuik DJ, Golding RP, Oyen WJG, Pruim J, Hoogen FJ
van den, Roodenburg JLN, Leemans CR (2008) Screening for distant metastases in head
and neck cancer patients by chest CT or whole body FDG-PET: A prospective multitrial
study. Radiother Oncol 87:221-229
3. Cobben DCP, Laan BFAM van der, Maas B, Vaalburg W, Suurmeijer AJ, Hoekstra HJ,
Jager PL, Elsinga PH (2004) 18F-FLT PET for visualization of laryngeal cancer:
comparison with 18F-FDG PET. J Nucl Med 45:226-231
4. Zhao S, Kuge Y, Kohanawa M, Takahashi T, Zhao Y, Yi M, Kanegae K, Seki K, Tamaki N
(2008) Usefulness of 11C-methionine for differentiating tumors from granulomas in
experimental rat models: a comparison with 18F-FDG and 18F-FLT. J Nucl Med 49:135-
141
5. De Boer JR, Pruim J, Burlage F, Krikke A, Tiebosch AT, Albers FW, Vaalburg W, Van Der
Laan BF (2003) Therapy evaluation of laryngeal carcinomas by tyrosine-pet. Head Neck
25:634-644
6. Börjesson PK, Jauw YW, Boellaard R, Bree R, Comans EFI, Roos JC, Castelijns JA,
Vosjan MJ, Kummer JA, Leemans CR, Lammertsma AA, Dongen GA (2006) Performance
of immuno-positron emission tomography with zirconium-89-labeled chimeric monoclonal
antibody U36 in the detection of lymph node metastases in head and neck cancer patients.
Clin Cancer Res 12:2133-2140
7. Agarwal V, Branstetter IV BF, Johnson JT (2008) Indications for PET/CT in the Head and
Neck. Otolaryngol Clin N Am 41:23-49
8. Judenhofer MS, Wehrl HF, Newport DF, Catana C, Siegel SB, Becker M, Thielscher A,
Kneilling M, Lichy MP, Eichner M, Klingel K, Reischl G, Widmaier S, Röcken M, Nutt RE,
Machulla H-J, Uludag K, Cherry SR, Claussen CD, Pichler BJ (2008) Simultaneous PET-
MRI: a new approach for functional and morphological imaging. Nat Med 14:459-465
9. Pichler BJ, Wehrl HF, Kolb A, Judenhofer MS (2008) Positron Emission
Tomography/Magnetic Resonance Imaging: The next generation of multimodality imaging?
Semin Nucl Med 38:199-208
10. Schmidt GP, Kramer H, Reiser MF, Glaser C (2007) Whole-body Magnetic Resonance
Imaging and Positron Emission Tomography-Computed Tomography in oncology. Top
Magn Reson Imaging 18:193-202
Samenvatting en vooruitzichten
143
11. Herborn CU, Unkel C, Vogt FM, Massing S, Lauenstein TC, Neumann A (2005) Whole-
body MRI for staging patients with head and neck squamous cell carcinoma. Acta
Otolaryngol 125:1224-1229
12. Shuman WP, Patten RM, Baron RL, Liddell RM, Conrad EU, Richardson ML (1991)
Comparison of STIR and spin-echo MR imaging at 1.5 T in 45 suspected extremity tumors:
lesion conspicuity and extent. Radiology 179:247-252
13. Antoch G, Vogt FM, Freudenberg LS, Nazaradeh F, Goehde SC, Barkhausen J, Dahmen
G, Bockisch A, Debatin JF, Rühm SG (2003) Whole-body dual-modality PT/CT and whole-
body MRI for tumor staging in oncology. JAMA 290:3199-3206
14. Schmidt GP, Schönberg SO, Schmid R, Stahl R, Tiling R, Becker CR, Reiser MF, Baur-
Melnyk A (2007) Screening for bone metastases: whole-body MRI using a 32-channel
system versus dual-modality PET-CT. Eur Radiol 17:939-949
15. Khoo VS, Joon DL (2006) New developments in MRI for target volume delineation in
radiotherapy. Br J Radiol 79 Spec No 1:S2-15
16. Patterson DM, Padhani AR, Collins DJ (2008) Technology insight: water diffusion MRI—a
potential new biomarker of response to cancer therapy. Nat Clin Pract Oncol 5:220-233
17. Koh DM, Collins DJ (2007) Diffusion-weighted MRI in the body: applications and
challenges in oncology. AJR Am J Roentgenol 188:1622-1635
18. Zbären P, Weidner S, Thoeny HC (2008) Laryngeal and hypopharyngeal carcinomas after
(chemo)radiotherapy: a diagnostic dilemma. Curr Opin Otolaryngol Head Neck Surg
16:147-153
19. Abdel Razek AAK, Kandeel AY, Soliman N, El-shenshawy HM, Kamel Y, Nada N,
Denewar A (2007) Role of diffusion-weighted echo-planar MR imaging in differentiation of
residual or recurrent head and neck tumors and posttreatment changes. AJNR Am J
Neuradiol 28:1146-1152
20. Hermans R, Vandecaveye V (2007) Diffusion-weighted MRI in head and neck cancer.
Cancer Imaging 7:126-127
21. Vandecaveye V, Keyzer F de, Nuyts S, Deraedt K, Dirix P, Hamaekers P, Poorten V
vander, Delaere P, Hermans R (2007) Detection of head and neck squamous cell
carcinoma with diffusion weighted MRI after (chemo)radiotherapy: correlation between
radiologic and histopathologic findings. Int J Radiat Oncol Biol Phys 67:960-971

List of publications Dankwoord Curriculum Vitae auctoris
146
List of publications
Bree R de, Brouwer J, Comans EFI, Hoekstra OS, Snow GB, Leemans CR (2001)
The preliminary results of FDG-PET in screening for distant metastases and
synchronous primary tumors below the clavicles in patients with head and neck
cancer at initial evaluation. In: Metastases in head and neck cancer. Proceedings of
the 2nd International Symposium. Tectum Verlag, Marburg Germany 155-159
Regelink G, Brouwer J, Bree R de, Pruim J, Laan BF van der, Vaalburg W, Hoekstra
OS, Comans EF, Vissink A, Leemans CR, Roodenburg JL (2002) Detection of
unknown primary tumours and distant metastases in patients with cervical
metastases: value of FDG-PET versus conventional modalities. Eur J Nucl Med Mol
Imaging 29:1024-1030
Brouwer J, Bodar EJ, Bree R de, Langendijk JA, Castelijns JA, Hoekstra OS,
Leemans CR (2004) Detecting recurrent laryngeal carcinoma after radiotherapy:
room for improvement. Eur Arch Otorhinolaryngol 261:417-422
Brouwer J, Bree R de, Comans EF, Castlijns JA, Hoekstra OS, Leemans CR (2004)
Positron emission tomography using [18F] fluorodeoxyglucose (FDG-PET) in the
clinically negative neck: is it likely to be superior? Eur Arch Otorhinolaryngol 261:479-
483
Brouwer J, Bree R de, Hoekstra OS, Langendijk JA, Castelijns JA, Leemans CR
(2005) Screening for distant metastases in patients with head and neck cancer: what
is the current clinical practice? Clin Otolaryngol 30:438-443
Brouwer J, Bree R de, Hoekstra OS, Golding RP, Langendijk JA, Castelijns JA,
Leemans CR (2005) Screening for distant metastases in patients with head and neck
cancer: is chest computed tomography sufficient? Laryngoscope 115:1813-1817
Brouwer J, Senft A, Bree R de, Comans EF, Golding RP, Castelijns JA, Hoekstra
OS, Leemans CR (2006) Screening for distant metastases in patients with head and
neck cancer: is there a role for (18)FDG-PET? Oral Oncol 42:275-280
147
Putten L van der, Akarriou M, Brouwer J, Bree R de, Kuik DJ, Comans EF, Leemans
CR, Hoekstra OS (2006) 18 FDG-PET in suspicion on recurrent larynxcarcinoma:
interobserver variation and RELAPS study [18 FDG-PET bij verdenking op recidief
larynxcarcinoom: interobserver variatie en RELAPS studie]. Tijdschr Nucl Geneesk
28:49-51
Bree R de, Brouwer J, Senft A, Putten L van der, Comans EF, Hoekstra OS,
Leemans CR (2006) Clinical applications of FDG-PET in patients with squamous cell
carcinoma of the head and neck [Klinische toepassingen van FDG-PET bij patiënten
met een plaveiselcelcarcinoom in het hoofd-halsgebied]. Ned Tijdschr Oncol 3:95-
101
Brouwer J, Bree R de, Comans EF, Akarriou M, Langendijk JA, Castelijns JA,
Hoekstra OS, Leemans CR (2008) Improved detection of recurrent laryngeal tumour
after radiotherapy using 18FDG-PET as initial method. Radiother Oncol 87:217-220
Brouwer J, Hooft L, Hoekstra OS, Castelijns JA, Bree R de, Leemans CR (2008)
Systematic review: Accuracy of imaging tests in the diagnosis of recurrent laryngeal
carcinoma after radiotherapy. Head Neck 30:889-897
148
Dankwoord
Mijn dank gaat uit naar allen die hebben bijgedragen aan het tot stand komen van dit
proefschrift. Een aantal van hen wil ik in het bijzonder bedanken voor hun motivatie,
inspiratie, tijd en energie;
Mijn promotoren: Prof.dr. C.R. Leemans, beste René. Promotor en opleider, hartelijk dank voor je
interesse, waardevolle inbreng en kritische blik op al het werk in dit proefschrift.
Daarnaast dank ik je voor de gelegenheid die je mij hebt geboden om dit
promotieonderzoek uit te voeren naast mijn opleiding. Met veel plezier maak ik nu
deel uit van je staf.
Prof.dr. R. de Bree, beste Remco. Ik ken niemand binnen of buiten de KNO die zo
hard werkt als jij. Dat is een ongelooflijke inspiratie voor iedereen om je heen, maar
ook een erg hoge lat. Zonder jou was dit boekje er nooit gekomen, waarvoor ik je
zeer dankbaar ben. Excuus voor de grijze haren.
Prof.dr. J.A. Castelijns, beste Jonas. Vanuit een andere hoek, de radiologie, had jij
een frisse kijk op alle stukken en in het bijzonder dank ik je voor je hulp in het laatste
hoofdstuk.
Mijn copromotor: Prof.dr. E.F.I. Comans, beste Emile. Naast de onmisbare aanvullingen op alle
artikelen, heb jij veel tijd besteed aan het reviseren van alle scans. Veel dank
daarvoor.
De leden van de leescommissie en de promotiecommissie, prof.dr. R. Hermans,
prof.dr. O.S. Hoekstra, prof.dr. B.F.A.M. van der Laan, prof.dr. J.A. Langendijk,
prof.dr. H.A.M. Marres, prof.dr. W.J.G. Oyen, en prof.dr. I. van der Waal ben ik zeer
erkentelijk voor het nauwgezet doornemen van het manuscript en voor het zitting
nemen in de promotiecommissie.
149
De mede-auteurs van de artikelen, dank voor jullie inbreng en beoordeling van de
artikelen. In het bijzonder wil ik Otto Hoekstra danken voor zijn grote aandeel in
verschillende artikelen en Hans Langendijk voor de radiotherapeutische blik. Lotty
‘GG’ Hooft dank ik voor haar werk bij de systematische review.
Alle collega stafleden, arts-assistenten, onderzoekers en medewerkers van de
afdeling KNO, huidige en voormalige, dank ik voor hun interesse, adviezen en
nuchterheid.
Medewerkers van de afdelingen Nucleaire Geneeskunde en Radiologie bedank ik
voor de logistieke facilitatie bij het reviseren van de scans.
Mijn paranimfen, Eline Vriens-Nieuwenhuis en Asaf Senft, omdat zij mij bij willen
staan.
Mijn familie en vrienden dank ik voor hun geduld, steun en interesse tijdens het
schrijven van dit proefschrift maar vooral ook daarbuiten, want uiteindelijk zijn zij het
die het leven kleur geven.
151
Curriculum Vitae auctoris
Jolijn Brouwer is geboren op 19 oktober 1973 te Veenendaal. In 1992 behaalde zij
haar V.W.O. diploma aan het Christelijk Lyceum in haar geboorteplaats. Datzelfde
jaar startte zij met de studie Geneeskunde aan de Vrije Universiteit te Amsterdam.
Tijdens haar co-schappen deed zij een wetenschappelijk onderzoek binnen de
afdeling KNO naar gehoorgangcarcinomen en volgde een keuze co-schap KNO in
het National University Hospital te Singapore. Aansluitend op het afronden van de
studie in februari 2000, begon zij als AGNIO te werken op de afdeling KNO van het
VU medisch centrum. December 2000 begon zij aan een onderzoek dat heeft geleid
tot deze dissertatie.
Van oktober 2002 tot februari 2008 werd zij opgeleid tot Keel-, Neus-, en Oorarts aan
het VU medisch centrum te Amsterdam (prof.dr. C.R. Leemans), het Spaarne
Ziekenhuis te Haarlem (dr. E.B.J. van Nieuwkerk) en het Westfriesgasthuis te Hoorn
(dr. H.F. Nijdam).
Sinds het afronden van de opleiding is zij werkzaam als staflid KNO in het VUmc.
Jolijn is getrouwd met Vincent Krocké en zij hebben een zoon, Tijs (2007).