
Computational Investigation of Gurney Flap Effects on Rotors in Forward Flight
Upload
universityofsydneyCategory
view
3download
0
ORIGINAL ARTICLE
SCAPULAR ANGLE OSTEOMYOGENOUS FLAPIN POSTMAXILLECTOMY RECONSTRUCTION: DEFECT,RECONSTRUCTION, SHOULDER FUNCTION,AND HARVEST TECHNIQUE
Jonathan R. Clark, BSc (Med), MBBS, FRACS,1,2,3 Martin Vesely, MD, FRCS,1,2
Ralph Gilbert, MD, FRCS(C)1,2
1 Department of Otolaryngology, Head and Neck Surgery, Princess Margaret Hospital,Toronto, Canada. E-mail: [email protected] Department of Plastic Surgery, Princess Margaret Hospital, Toronto, Canada3 Sydney Head and Neck Cancer Institute, Sydney, Australia
Accepted 19 February 2007Published online 16 July 2007 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/hed.20649
Abstract: Background. Maxillary reconstruction continues to
challenge in terms of optimal aesthetic and functional outcomes.
The aim of this study was to describe the utility of the scapular
angle osteomyogenous flap in a series of maxillectomy patients
and to examine the donor site morbidity.
Methods. This is a retrospective series of 14 patients under-
going maxillectomy and either primary or secondary reconstruc-
tion. The scapular angle can be oriented vertically and horizon-
tally. Aesthetic, functional, and operative morbidity is described.
The Disabilities of the Arm, Shoulder and Hand (DASH) question-
naire was used to examine shoulder and upper limb morbidity.
Results. Perioperative morbidity occurred in 4 patients. There
were no free flap failures. Functional and aesthetic outcomes were
acceptable with all patients having intelligible speech and none
requiring nutritional supplementation. The DASH was completed
by 12 of 14 patients. The mean and median DASH scores were
10.6 and 13, respectively. All patients gained full range of shoulder
movement by 6 months after surgery.
Conclusions. The scapular angle flap is well suited for maxillary
reconstruction and donor site morbidity is low. VVC 2007 Wiley
Periodicals, Inc.Head Neck 30: 10–20, 2008
Keywords: scapular angle; scapular tip; free flap; maxillec-
tomy; infrastructure; midface; reconstruction
Reconstruction of the midface following maxillec-tomy continues to be a major challenge for thehead and neck reconstructive surgeon. The max-illa is similar to the mandible in terms of its func-tional and aesthetic importance. However, thestructure of the midface is more complicated andcannot be completely replicated. When faced witha postmaxillectomy defect, the focus needs to beon determination of the essential components thatrequire restoration. Similar defects may be bettermanaged with either obturation or reconstruc-tion, depending on patient comorbidity, age, den-tal status, and underlying pathology. In contrastto the mandible, maxillary reconstruction is rela-tively uncommon, and previously it was avoidedto allow surveillance. As a result, even centerstreating large volumes of patients with head andneck cancer may not have extensive experience inreconstructing these patients.
Correspondence to: R. Gilbert
VVC 2007 Wiley Periodicals, Inc.
10 Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008

We have used the scapula osteocutaneous flap(based on the circumflex scapular vessels) exten-sively for mandibular reconstruction and havefound it useful in elderly head and neck patientswho frequently have peripheral vascular diseaseand find mobilizing following fibula harvest prob-lematic. Furthermore, the donor site has revealedremarkably little morbidity other than early re-stricted shoulder movement. Leading on fromthis, we have applied the scapular angle flap tomidface reconstruction. This is supplied by theangular branch of the thoracodorsal artery andcan be used as a composite flap with the teresmajor muscle. We report a series of patients inwhom this flap has been used for complex horizon-tal and vertical defects of the maxilla that usuallyperform poorly with standard prosthetic obtura-tion alone. This article focuses on the recipientand donor site with particular reference to har-vest technique and shoulder function followingsurgery.
MATERIALS AND METHODS
Clinical and Pathological Features. In total, 14patients underwent free flap reconstruction of apostablative maxillectomy defect using the scapu-lar angle osteomyogenous flap. This method ofreconstruction is a relatively recent techniqueand represents a small percentage of the total
number of patients undergoing maxillectomy atthe University Health Network, Toronto. The me-dian age was 61 years (range, 49–78 years); therewere 6 women and 8 men, and the median dura-tion of follow-up following reconstruction was 1year (range, 4 months to 3 years). Eleven patientsunderwent reconstruction primarily and 3 under-went delayed (secondary) reconstruction. Table 1details the individual clinicopathologic features,prior treatment, and defect classification for eachpatient.
Defect Classification and Reconstructive Philoso-
phy. Maxillectomy defects were classified pro-spectively according to Okay et al,1 as summar-ized in Table 2. This classification is based on thestability and retention of dentures dependent onthe residual palate and dentition, in particularthe terminal abutment teeth, to oppose the canti-lever forces encountered during mastication.There were 6 class II and 7 class III defects. Theremaining patient had maxillary resection includ-ing the orbital floor and zygoma (zf) without pala-toalveolar resection. Seven patients had orbitalfloor (f) involvement, and 8 patients had resectionof their zygoma (z).
Our practice has been to offer all patients withclass III defects reconstruction unless prohibitedby patient morbidity. Although class I and IIdefects can be managed adequately with a dentalobturator, in young patients with minimal comor-
Table 1. Clinicopathological features, prior treatment and defect classification.
Age Sex FU yr Pathology Site
Prior
treatment Recon
Okay et al.
class of
defect Adj RT Status
1 66 M 1.7 SCC Alveolus palate
Upper lip
Surgery +
recon + RT
28 III – ANED
2 52 F 1.8 Recurrent SCC Maxillary sinus ChemoRT 18 III – AWD
3 69 M 0.8 SCC Lateral nasal wall – 18 IIfz Yes AWD
4 55 F 1.0 Recurrent ACC Maxillary sinus Surgery + RT 18 IIfz – ANED
5 55 M 3.0 Recurrent
ameloblastoma
Maxillary sinus Surgery 28 IIfz – ANED
6 49 F 2.4 SCC Maxillary sinus Surgery + RT 28 IIfz – ANED
7 71 F 2.2 SCC Alveolus – 18 IIIz Yes ANED
8 77 F 0.5 SCC Alveolus palate – 18 III – ANED
9 74 F 1.0 SCC Alveolus palate – 18 III – ANED
10 54 M 0.8 ACC Lateral nasal wall Surgery + RT 18 IIfz – AWD
11 61 M 0.8 SCC Nasal vestibule – 18 III – ANED
12 60 M 0.5 Recurrent SCC Maxillary sinus ChemoRT 18 IIfz – ANED
13 77 M 0.3 SCC Alveolus palate – 18 III ANED
14 78 M 0.5 Osteoradionecrosis Oropharynx
Maxilla
Surgery + RT 18 Izf – ANED
Abbreviations: FU yr, duration of follow-up in years; Adj RT, adjuvant (postoperative) radiotherapy; M, male; SCC, squamous cell carcinoma; RT, radio-therapy; 2 8, secondary; ANED, alive with no evidence of disease; F, female; 18, primary; f, resection of orbital floor; z, resection of zygoma; AWD, alivewith evidence of disease; ACC, adenoid cystic carcinoma; recon, reconstruction.
Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008 11
bidity, the option of a primary reconstruction isdiscussed. There are multiple reasons for provid-ing this option: class Ia defects can be closed with-out the need for any denture by either a local flapor thin fasciocutaneous free flap. Class Ib/IIdefects with extension to the maxillary antrumcan be closed with a thin fasciocutaneous flapmaintaining speech and swallowing with both anobturator in situ and when removed. Thin fascio-cutaneous flaps do not interfere with functionaldental restoration in patients with adequate re-sidual dentition. In class II defects with verticalextension to involve the orbital floor or zygoma,obturation perform poorly in terms of maintainingposition of the globe and projection of the midface.
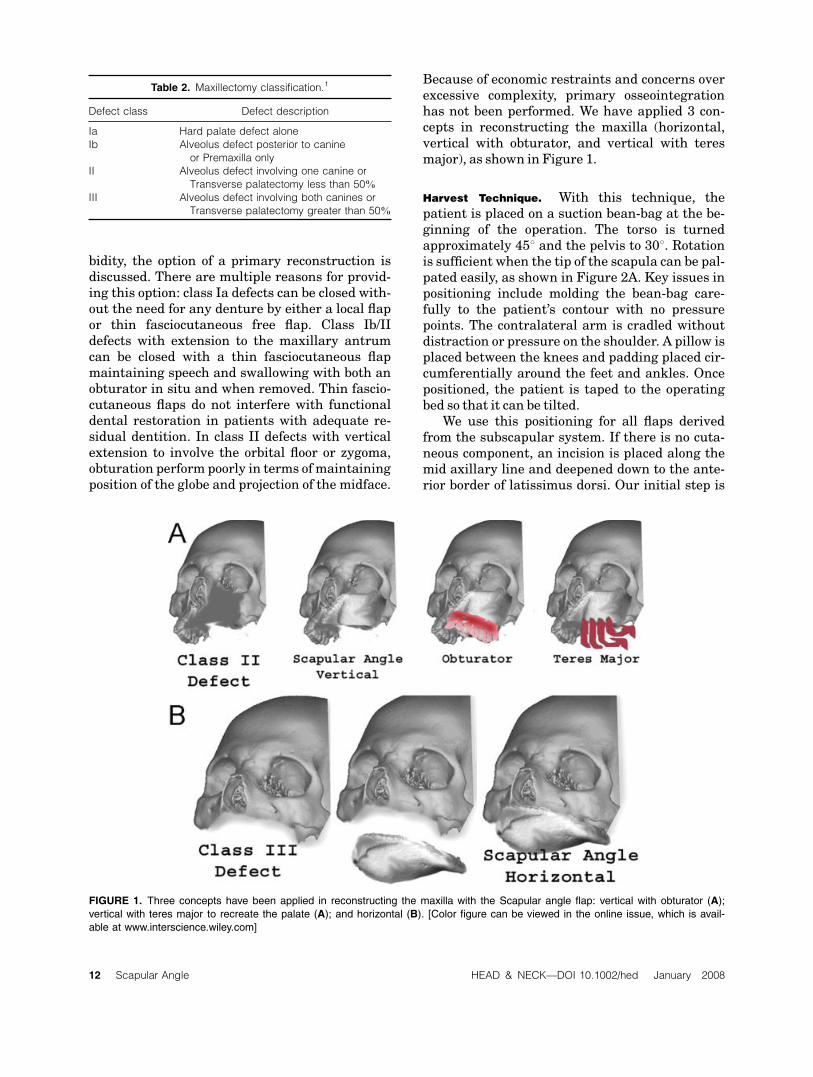
Because of economic restraints and concerns overexcessive complexity, primary osseointegrationhas not been performed. We have applied 3 con-cepts in reconstructing the maxilla (horizontal,vertical with obturator, and vertical with teresmajor), as shown in Figure 1.
Harvest Technique. With this technique, thepatient is placed on a suction bean-bag at the be-ginning of the operation. The torso is turnedapproximately 458 and the pelvis to 308. Rotationis sufficient when the tip of the scapula can be pal-pated easily, as shown in Figure 2A. Key issues inpositioning include molding the bean-bag care-fully to the patient’s contour with no pressurepoints. The contralateral arm is cradled withoutdistraction or pressure on the shoulder. A pillow isplaced between the knees and padding placed cir-cumferentially around the feet and ankles. Oncepositioned, the patient is taped to the operatingbed so that it can be tilted.
We use this positioning for all flaps derivedfrom the subscapular system. If there is no cuta-neous component, an incision is placed along themid axillary line and deepened down to the ante-rior border of latissimus dorsi. Our initial step is
Table 2. Maxillectomy classification.1
Defect class Defect description
Ia Hard palate defect alone
Ib Alveolus defect posterior to canine
or Premaxilla only
II Alveolus defect involving one canine or
Transverse palatectomy less than 50%
III Alveolus defect involving both canines or
Transverse palatectomy greater than 50%
FIGURE 1. Three concepts have been applied in reconstructing the maxilla with the Scapular angle flap: vertical with obturator (A);
vertical with teres major to recreate the palate (A); and horizontal (B). [Color figure can be viewed in the online issue, which is avail-
able at www.interscience.wiley.com]
12 Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008

to expose the dorsal aspect of the muscle (Figure2B) so that it can be mobilized completely. Dissec-tion of the pedicle will be anteromedial to latissi-mus (Figure 2D); however, the bone cuts will beperformed by retracting it forward (Figure 2C).
Next, the vascular anatomy is defined. Thepedicle is somewhat variable, and this may alterdissection considerably, especially if a compositeflap is planned. The angular branch usually arisesfrom the thoracodorsal artery2; however, it mayalso arise from the branch to serratus or form atrifurcation with these vessels. Usually there is aseparate branch supplying teres major which wepreserve. If a combination scapula or parascapu-lar cutaneous flap is planned, the proximal pedicleneeds to be defined, as the thoracodorsal arteryarises directly from the axillary artery in 5%. Inthis situation, a thoracodorsal-artery-based cuta-neous flap would be preferable.
There is some variability in the distal course ofthe angular branch, and there may be more than1 vessel. Sometimes the terminal vessels lie underthe fascia of the serrratus anterior and a cuff ofmuscle is included, taking care to preserve thelong thoracic nerve. The pedicle is fully mobilizedbefore the bone cuts are made to avoid injury tothe blood supply. Bone cuts depend on the desiredquantity and contour. Seneviratne et al2 havedemonstrated the length of bone supplied by theangular branch to be approximately 6 cm, usinginjection studies. This quantity is ideal for maxil-lary reconstruction; however, we have harvestedup to 14 cm of lateral scapula bone based on theangular branch alone. More bone is taken sepa-rately for a bone graft to reconstruct the orbitalfloor where required.
The final pedicle dissection is taken to the cir-cumflex scapular vessels, with assessment of flap
FIGURE 2. (A) A supine position is used for harvest. The latissimus dorsi (B) and teres major (C) muscles are identified. The angular
branch typically arises from the thoracodorsal artery (D) or branch to serratus anterior. [Color figure can be viewed in the online issue,
which is available at www.interscience.wiley.com]
Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008 13

viability before division. Seratus anterior, subsca-pularis, and teres major are reattached to thescapular bone using drill holes and heavy absorb-able suture. A large closed suction drain is usedbecause of the extensivemuscle dissection. Shouldermovement commences from day 1 postoperatively,and shoulder abduction exercises are given topractice daily on discharge. No formal physiother-apy is required, but patients are advised thatshoulder movement may take 6 months for fullrecovery.
Flap Fabrication, Fixation, and Vascular Anasto-
mosis. The boney component of the flap canbe placed either horizontally to replace the pal-atoalveolar complex (see Figure 3) or verticallyto restore the zygomaticomaxillary and naso-maxillary buttress (see Figure 4). The muscularcomponent can be used as a vascularized cover-
ing for the bone, or alternatively, when the boneis vertically positioned, the muscle acts as a fi-brous trampoline spanning from the bone (ante-riorly) to soft palate (posteriorly). The scapulaangle was placed horizontally in 7 patients andvertically in 7. The bone cannot be fully osteom-ized but can be ‘‘greenstick’’-fractured maintain-ing the periosteal blood supply, for contouring.This was performed in 4 patients with verticalplacement. Fixation was performed using rigidtitanium miniplates (1.3–2.0 mm), secured tothe residual maxilla and zygoma. Reconstruc-tion of the orbital floor was performed in 6patients using a graft of thin scapula bone(Figure 4c) or vascularized scapular bone fixedwith a cantilever miniplate.
Vascular anastomosis was performed using asingle recipient artery and vein in all patients.The facial artery and vein was used in 9 patients,
FIGURE 3. (A–C) Subtotal palate reconstruction for a class III defect. The angle of the scapular has a near-identical shape to the
native palate. The muscle atrophies and then mucosalises as shown immediately (D), 1 month (F), and 3 months (G) following sur-
gery. [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com]
14 Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008

with the pedicle tunneled through the buccalspace deep to the facial nerve over the mandible.In 2 patients, vascular anastomosis was to the su-perficial temporal vessels, and in the remainingpatient, anastomosis was to the facial artery andinternal jugular vein. Because of the long vascularpedicle, only 1 patient required a vein graft. Thispatient’s venous anastomosis was to the internaljugular vein due to absence of the anterior facialvein.
Assessment of Shoulder Function. Shoulder dis-ability was assessed using the Disabilities of theArm, Shoulder and Hand (DASH) questionnaire.This was completed by the patient in the surveil-lance clinic and applied using a cross-sectionaltechnique; hence, time from surgery to completionis different in each patient. The DASH is a region-specific upper limb disability outcome measure
that was developed by the American Academy ofOrthopedic Surgeons3 and has been shown to bereliable and valid in patient populations with avariety of upper-extremity disorders.4
RESULTS
A summary of reconstructive outcomes for eachpatient is shown in Table 3.
Perioperative Complications and Length of Hospital
Stay. There were no perioperative deaths. Do-nor site complications occurred in 2 patientsand consisted of seroma, which became infected in1 patient. There were no acute recipient site com-plications and no free flap failures or anastomoticrevisions. One patient developed deep venousthrombosis and pulmonary embolism on day 5after surgery. This patient had traveled on aninternational airflight 2 days prior to surgery. The
FIGURE 4. (A–D) Vertical bone orientation for a Class II defect. (C) A bone graft is used with a cantilever miniplate to support the or-
bital floor. Circumzygomatic wires are used to maintain the obturator until a scar band forms. [Color figure can be viewed in the online
issue, which is available at www.interscience.wiley.com]
Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008 15

Table
3.Reconstructivesummary.
Approach
Muscle/other
combinedwith
scapula
tip
Boneorientation/
other
Recipient
vessels
LOSday
Dentalrestoration
Morbidity
Revision
Diet
1Lip
resection
Latissim
usdorsi
RFFFforlip
reconstruction
Horizontal
Facial
10
Denture
Infectedseroma
back
–Norm
al
2WeberFergusson
Latissim
usdorsi
Horizontal
Facial
11
Secondary
OI
implant+denture
Lossofmidface
projection
Bonegraft
Vesitibulo-
plasty
Firm
3WeberFergusson
Teresmajor
Vertical+bonegraft
orbitalfloor
Facial
8Obturator
Pulm
onary
embolism
–Norm
al
4WeberFergusson
Teresmajor
Vertical+bonegraft
orbitalfloor
Facial
5Denture
+OI
Mild
ectropion
–Firm
5WeberFergusson
Teresmajor
Vertical+bonegraft
orbitalfloor
Superficialtemporal
6Obturator
Dystopia
+
ectropion
Lid
switch+
Cantho-plasty
Norm
al
6WeberFergusson
Teresmajor
Vertical(priororbital
floorbonegraft)
Facial
8Obturator
Seromascapula
+
ectropion
Cantho-plasty
planned
Firm
7Transoral
Latissim
usdorsi
+teresmajor
Horizontal
Facial
14
no
–Vestibulo-plasty
planned
Soft
8Transoral
Teresmajor
Horizontal
Facial
14
no
–Vestibulo-plasty
planned
Firm
9Lip
resection
Teresmajor+
subscapularis
Horizontal
Facial
12
no
––
Soft
10
WeberFergusson
Teresmajor
Vertical+bonegraft
orbitalfloor
Superficialtemporal
6Obturator
––
Norm
al
11
Rhinectomy/Lip
split
Teresmajor
Horizontal
Facial
8Nasalprosthesis
––
Soft
12
WeberFergusson
Latissim
usDorsi+
TeresMajor
Vertical+bonegraft
orbitalfloor
Facialartery
+IJV
14
Obturator
Inferiorrectus
dysfunction
–Firm
13
Lip
split
TeresMajor
Horizontal
Facial
29
no
Sialocoele
–Soft
14
Transfacial
(Mustarde)
Nil
Vertical+orbitalfloor
(vascularised)
Facial
4Denture
––
Norm
al
Abbreviations:LOS,length
ofhospitalstayin
days;RFFF,radialforearm
freeflap;OI,osseointegratedim
plants;IJV,internaljugularvein.
16 Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008

median length of stay was 9 days (range, 4–29days).
Functional Outcomes Including Dental Restora-
tion. There were no primary osseointegratedimplants placed at the time of reconstruction. Onepatient underwent delayed osseointegration com-bined with vestibuloplasty to recreate the gingivo-labial sulcus. All patients with residual dentitionwere rehabilitated with a denture or obturator(n ¼ 8). No patient undergoing total palate recon-struction was able to retain a denture withoutosseointegrated implants. Despite this, dietaryintakes were indistinguishable from any edentu-lous patient. Five patients were able to maintaina normal diet (no restriction), and 9 were able totolerate a soft-to-firm diet.
Subtle changes in speech were noted by allpatients due to alterations in vocal resonance.Subjectively, 12 of 14 patients had excellent intel-ligibility with their denture or obturator in situ,and all patients had functional speech. Patientswithout dentures had (expected) difficulties withlabiodental or interdental articulation. One pa-tient with combined total upper lip reconstructionusing a radial forearm flap had noticeable changesin articulation, and 1 patient with combined softpalate/nasopharyngeal resection had velophar-yngeal insufficiency.
Aesthetic Outcomes. Despite all patients under-going maxillectomy and scapular angle free flapreconstruction, this represents a diverse range ofdefects and problems. Patients undergoing totalor near-total palatoalveolar reconstruction for
infrastructure maxillectomy defects had excellentearly and late aesthetic results, except for thepatient requiring revision total upper-lip recon-struction with a radial forearm flap. In contrast,patients undergoing supra-structure maxillecto-mies with resection of the zygoma and orbital floorhad less consistent results. Problems includedectropion, orbital dystopia, and loss of midfaceprojection. In this group, early aesthetic resultswere good; however, long-term effects of radio-therapy, including bone resorption and soft tissuefibrosis, were difficult to predict and counter.Finally, patients undergoing delayed (secondary)reconstruction were never able to achieve thesame level of soft tissue contouring that was possi-ble with primary reconstruction because of fibro-sis and scarring.
Shoulder Function. The DASH questionnairewas completed by 12 of 14 patients undergoingscapular osteomyogenous flap harvest. Onepatient, who had traveled overseas for surgery,was unavailable for follow-up assessment morethan 1month after surgery. Themedian time fromsurgery to completion of the DASH questionnairewas 9 months (range, 1–36 months). The medianand mean DASH scores were 13 and 10.6, respec-tively (range, 0–32). Individual patient dataincluding DASH score are summarized in Table 4.Range of shoulder movement was normal for allpatients followed more than 6 months after sur-gery. However, shoulder movement was typicallylimited to 90 to 120 degrees from vertical in thefirst month after surgery.
Table 4. Shoulder disability summary.
Age Sex
Time after
surgery
(mo) Pathology Site DASH Figure
1 66 M 18 SCC Alveolus palate Upper lip 13 Figures 3A and 3D
2 52 F 14 Recurrent SCC Maxillary sinus 2 Figure 3F
3 69 M – SCC Lateral nasal wall – Figure 7
4 55 F 12 Recurrent ACC Maxillary sinus 2 Figure 3E
5 55 M 36 Recurrent
ameloblastoma
Maxillary sinus 13 –
6 49 F 30 SCC Maxillary sinus 19 –
7 71 F 22 SCC Alveolus 0 –
8 77 F 2 SCC Alveolus palate 32 Figures 3B, 3C and 5
9 74 F 1 SCC Alveolus palate 19 Figure 4
10 54 M 6 ACC Lateral nasal wall 7 Figures 3G and 6
11 61 M 1 SCC Nasal vestibule 7 –
12 60 M 1 SCC Maxillary sinus 13 –
13 77 M – SCC Alveolus palate – Figure 2
14 78 M 4 Osteoradionecrosis Oropharynx Maxilla 0 –
Abbreviations: DASH, disabilities of the arm; shoulder and hand scale; M, male; SCC, squamous cell carcinoma; F, female.
Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008 17

DISCUSSION
We present a series of 14 patients with postmaxil-lectomy defects reconstructed using a scapula angleosteomyogenous flap. The length of follow-up wasshort and the group was heterogeneous in terms ofpathology and extent of resection, hence no conclu-sions can be made about the oncologic outcomes inthis series. Outcomes in terms of operative morbid-ity, function, aesthetics, and shoulder disabilitywere very acceptable considering the complex na-ture of this type of reconstruction. The angularbranch to the scapular bone was first described byDeraemaeker et al5 (1988) and then by Colemanand Sultan6 (1991); however, there are no large se-ries evaluating the angular bone flap in maxillaryreconstruction. Prior to these descriptions, thestandard scapular osseous flap based on the cir-cumflex scapular vessels has been used and contin-ues to be used for both mandibular and maxillaryreconstruction.7 The largest series in the literatureto date, by Uglesic et al,8 included 23 scapular boneflaps; however, this represents a very different pop-ulation with nearly all patients undergoing orbitalexenteration.
Reconstruction Versus Obturation. Continuingdiscussion persists over whether maxillectomydefects should be reconstructed or obturated.9
Prior arguments of surveillance have proven to beunfounded since reoperation is rarely an optionand modern imaging enables early detection. De-spite this, we use both obturation and reconstruc-tion based on individual patient parameters toachieve optimal functional and esthetic outcomes.Classification systems proposed by Okay et al1
and Brown et al10 have demonstrated the impor-tance of residual palate, alveolus, and dentition inpredicting patients who will perform poorly withobturation alone. These systems incorporate ahorizontal (functional) and a vertical (aesthetic)component and highlight the inadequacy of ana-tomic classifications,11–14 which do not incorpo-rate prosthodontic considerations.
Although quality of life data has not demon-strated a clear advantage of reconstruction overobturation for all maxillectomy patients,15,16 asthe defect increases, it is clear that functional out-comes and patient satisfaction diminish withobturation alone.15 This is because problems withstability, retention, leakage, and speech are com-mon in large palatomaxillary defects.13,15,17
Advantages of the Scapular Angle Osteomyogenous
Flap. Several authors have described other
excellent methods of reconstruction of the midfaceusing flaps based on the iliac crest,18,19 fibula,20
and radius.21,22 The scapular angle flap has anumber of advantages over these other recon-structions discussed below.
Pedicle Length. Pedicle length is particularly im-portant in maxillary reconstruction, and up to20 cm is achievable with the scapular angle.8 Bothfibula and iliac crest have relatively short pediclesand may require vein grafts to reach the neck.9,20
We have used the facial vessels for the majority ofanastomoses without vein graft. The superficialtemporal vessels may also be used; however, thevenous anatomy is less consistent.
Similar Structure to the Native Maxilla. The scapularbone is amixture of light-weight thin cortical bonemedially and more robust corticocancellous boneat the lateral border, averaging 28 6 7 mm inheight toward the scapular angle.23 The bonestock of the lateral border of the scapula isadequate to allow implantation,24,25 although in-ferior to iliac crest and fibula.26,27 The small num-ber of patients with implants in this series reflectsthe short follow-up, health care system, and eco-nomic restrictions of patients, rather than the ad-equacy of bone stock. As such, it parallels our ex-perience with mandibular reconstruction whereosseointegration is rarely performed.
Ease of Contouring and Harvest. Because of the uniquestructure of the scapula, ‘‘greenstick’’ fractures caneasily be achieved by cutting through 1 cortex andbending the bone by hand. This enables relativelyquick contouring and light-weight reconstructionof the maxilla when compared with other boneflaps with thick cortical bone. Although a 2-teamapproach is impractical and positioning is complex,the flap is harvested in a supine position28 and thepedicle is easier to dissect than a standard scapulabone flap, since it runs in a loose areolar planebetween latissimus and the chest wall.
Versatility. The scapular angle provides a large flatsection of bone that can be oriented both verticallyand horizontally. A single flap oriented verticallycan be used to reconstruct the entire hemimaxillaincluding orbital floor and palate. The teres majormuscle arises from the apex and is sutured to theresidual soft palate in the manner described byBrown et al18 and Genden et al,19 using the com-posite iliac crest and internal oblique flap. Futranet al20 described the limitations of the fibula in
18 Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008

restoring the entire maxillary form, and thisapplies equally to the radial forearm flap.21,22
Oriented horizontally, it can replace the entirepalato-aveolar complex without contouring or theneed for a skin paddle, which is unique.
Composite Options. The subscapular system of flapsis an extensive group of flaps derived from a singlepedicle. Possible combinations include muscle(teres major, latissimus dorsi, serratus anterior,and subscapularis myogenous flaps), skin (scap-ular, parascapular, latissimus dorsi musculocuta-neous, and thoracodorsal artery perforator flaps)and bone (lateral scapula, medial scapula, scapu-lar angle, and rib osseous flaps). Furthermore,these provide large amounts of soft tissue that canbe oriented free of the bone to allow reconstructionof very large and complex defects. The fibula, iliaccrest, and radial forearm flaps are limited to onlya few composite options and the skin paddle can-not be rotated independent of the bone.
Myogenous Flap. Bulky skin flaps are undesirablein palatoalveolar reconstruction for several rea-sons: first, they may make dental restorationimpossible without implants; second, for class IIIdefects, the flap ptosis into the oral cavity andadversely affects articulation, resonance, andswallowing; and last, aesthetic outcomes are infe-rior. Muscle is a near-ideal lining for the palateand nasal cavity. Although muscle contracts andatrophies, when splinted by bone it provides athin and rigid lining that mucosalises rapidly andfunctions similarly to native gingiva (see Figure3). Kakibuchi et al29 have demonstrated that thenasal lining that forms over the vascularizedmus-cle is nearly identical histologically to nativemucosa.
Reliability. Anastomotic revision and failure ratesdescribed for maxillary reconstruction using fib-ula20 and iliac crest9 are high compared withthose of flaps derived from the subscapular sys-tem. Furthermore, the cutaneous components areless reliable.
Minimal Donor Site Morbidity. We believe that the fib-ula is best avoided in elderly patients and thosewith peripheral vascular disease. The iliac cresthas its own associated morbidity with abdominalwall weakness, hip pain, and contour defect,although this can be minimized by using a split-thickness bone flap and polypropylene mesh. Thepotential for fracture limits the use of the radial
forearm bone flap in the elderly and osteoporoticpatients.
Disability of Arm Shoulder and Hand Outcome
Measure. There is minimal literature describingdonor site morbidity after scapular flap harvest.Coleman et al30 used subjective and objectivemeasures to assess shoulder function and morbid-ity in 4 patients undergoing a standard scapularosteocutaneous flap harvest (lateral border ofscapular based on circumflex scapular vessels).They found that morbidity in this small subset ofpatients was quite acceptable and should not dis-courage reconstructive surgeons from using thisversatile flap.
The DASH is an objective and validated out-come measure for assessing shoulder disability. Ithas been compared with several scales and foundto be the best clinimetric scale for assessing upperlimb morbidity.31 Normative values for the gen-eral population have been calculated with a meanscore of 10.1 (SD 14.68).32 The original DASH wasadministered to 368 patients with upper-extrem-ity conditions, with a mean score of 38 (SD 22) andmedian of 35.3 It is somewhat remarkable that themedian13 and mean (10.6) scores following scapu-lar angle harvest were the same as that of thenormal population. The only score to lie outside 1standard deviation was in a patient within 2months of surgery.
CONCLUSIONS
The scapular angle osteomyogenous free flap iswell suited to midface reconstruction, in particu-lar total and near-total palatoalveolar defects.The long vascular pedicle, boney structure, adja-cent soft tissue supplied by the same vascular sys-tem and minimal donor site morbidity make thisflap a versatile reconstructive option for selectpost-maxillectomy defects.
REFERENCES
1. Okay DJ, Genden E, Buchbinder D, et al. Prosthodonticguidelines for surgical reconstruction of the maxilla: aclassification system of defects. J Prosthetic Dent 2001;86:352–363.
2. Seneviratne S, Duong C, Taylor GI. The angular branchof the thoracodorsal artery and its blood supply to theinferior angle of the scapula: an anatomical study. PlastReconstr Surg 1999;104:85–88.
3. Hudak PL, Amadio PC, Bombardier C. Development ofan upper extremity outcome measure: the DASH (dis-abilities of the arm, shoulder and hand). The Upper Ex-tremity Collaborative Group (UECG). Am J Ind Med 1996;29:602–608.
Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008 19

4. McConnel S, Beaton DE, Bombardier C. Disabilities ofthe arm, shoulder and hand: the DASH outcome mea-sure user’s manual, 1st ed. Toronto, ON: Institute forWork and Health; 1999.
5. Deraemaeker R, Tienen CV, Lejour M, et al. The serra-tus anterior-scapula free flap. A new osteomuscular unitfor reconstruction after radical head and neck surgery(abstract). Proceedings of the Second International Con-ference on Head and Neck Cancer, Boston, MA, 1988.
6. Coleman JJ, Sultan MR. The bipedicled osteocutaneousscapula flap: a new subscapular system free flap. PlastReconstr Surg 1991;87:682–692.
7. Schwartz WM, Banis JC, Newton ED, et al. The osteocu-taneous scapular flap for mandibular and maxillaryreconstruction. Plast Reconstr Surg 1986;77:530–545.
8. Uglesic V, Virag M, Varga S, et al. Reconstruction follow-ing radical maxillectomy with flaps supplied by the sub-scapular artery. J Cranio-Maxillo-Facial Surg 2000;28:153–160.
9. Brown JS, Re: Brown JS, Jones DC, Summerwill A,et al. Vascularised iliac crest with internal oblique mus-cle for immediate reconstruction after maxillectomy. Br JOral Maxillofac Surg 2002;40:183–190, 2003;41:364.
10. Brown JS, Rogers SN, McNally DM, et al. A modifiedclassification for the maxillectomy defect. Head Neck2000;22:17–26.
11. Spiro RH, Strong EW, Shah JP. Maxillectomy and itsclassification. Head Neck 1997;19:309–314.
12. Yamamoto Y, Kawashima K, Sugihara T, et al. Surgicalmanagement of maxillectomy defects based on the con-cept of buttress reconstruction. Head Neck 2004;26:247–256.
13. Davison SP, Sherris DA, Meland NB. An algorithm formaxillectomy defect reconstruction. Laryngoscope 1998;108:215–219.
14. Cordeiro PG, Santamaria E. A classification system andalgorithm for reconstruction of maxillectomy and mid-face defects. Plast Reconstr Surg 2000;105:2331–2346.
15. Rogers SN, Lowe D, Brown JS, et al. Health-relatedquality of life after maxillectomy: a comparison betweenprosthetic obturation and free flap. Br J Oral MaxillofacSurg 2003;61:174–181.
16. Genden EM, Okay D, Stepp MT, et al. Comparison offunctional and quality-of-life outcomes in patients withand without palatomaxillary reconstruction: a prelimi-nary report. Arch Otolaryngol Head Neck Surg 2003;129:775–780.
17. Funk GF, Arcuri MR, Frodel JL Jr. Functional dentalrehabilitation of massive palatomaxillary defects: casesrequiring free tissue transfer and osseointegratedimplants. Head Neck 1998;20:38–51.
18. Brown J. Deep circumflex iliac artery free flap with in-ternal oblique muscle as a new method of immediate
reconstruction of maxillectomy defect. Head Neck 1996;18:412–421.
19. Genden EM, Wallace D, Buchbinder D, et al. Iliac crestinternal oblique osteomusculocutaneous free flap recon-struction of the postablative palatomaxillary defect. ArchOtolaryngol Head Neck Surg 2001;127:854–861.
20. Futran ND, Wadsworth JT, Villaret D, et al. Midfacereconstruction with the fibula free flap. Arch OtolaryngolHead Neck Surg 2002;128:161–166.
21. Chepeha DB, Moyer JS, Bradford CR, et al. Osseocuta-neous radial forearm free tissue transfer for repair ofcomplex midfacial defects. Arch Otolaryngol Head NeckSurg 2005;131:513–517.
22. Villaret DB, Futran NA. The indications and outcomesin the use of osteocutaneous radial forearm free flap.Head Neck 2003;25:475–481.
23. Shimizu T, Ohno K, Michi K, et al. Morphometric exami-nation of the free scapular flap. Plast Reconstr Surg1997;99:1947–1953.
24. Schmelzeisen R, Neukam FW, Shirota T, et al. Postoper-ative function after implant insertion in vascularizedbone grafts in maxilla and mandible. Plast ReconstrSurg 1996;97:719–725.
25. Urken ML, Buchbinder D, Costantino PD, et al. Oro-mandibular reconstruction using microvascular compos-ite flaps: report of 210 cases. Arch Otolaryngol HeadNeck Surg 1998;124:46–55.
26. Frodel JL, Funk GF, Capper DT, et al. Osseointegratedimplants: a comparative study of bone thickness in fourvascularized bone flaps. Plast Reconstr Surg 1993;92:449–458.
27. Moscoso JF, Keller J, Gender MS, et al. Vascularisedbone flaps in oro-mandibular reconstruction: a compara-tive study of suitability for endosseous implants. ArchOtolaryngol Head Neck Surg 1994;120:36–42.
28. Nishimura T, Furukawa M, Koshima I. Scapular boneflap harvests of patients in a supine position. Laryngo-scope 2004;114:1130–1102.
29. Kakibuchi M, Fujikawa M, Hosokawa K, et al. Func-tional reconstruction of maxilla with free latissimusdorsi-scapular osteomusculocutaneous flap. Plast ReconstrSurg 2002;109:1238–1244.
30. Coleman SC, Burkey BB, Day TA, et al. Increasing useof the scapula osteocutaneous free flap. Laryngoscope2000;110:1419–424.
31. Bot SD, Terwee CB, van der Windt DA, et al. Clinimetricevaluation of shoulder disability questionnaires: a sys-tematic review of the literature. Ann Rheumatic Dis 2004;63:335–341.
32. Hunsaker FG, Cioffi DA, Amadio PC, et al. The Ameri-can Academy of Orthopaedic Surgeons outcomes instru-ments—normative values from the general population.J Bone Joint Surg A 2002;84:208–215.
20 Scapular Angle HEAD & NECK—DOI 10.1002/hed January 2008
Copyright © 2022 FDOKUMEN




















