Sarcomatoid renal cell carcinoma: Clinicopathologic. A study of 42 cases
11
Sarcomatoid Renal Cell Carcinoma: Clinicopathologic A Study of 42 Cases JAE Y. RO, MD,' ALBERT0 G. AYALA, MD,' AVISHAY SELLA, MD,t MELVIN L. SAMUELS, MD,t AND DAVID A. SWANSON, MD* Forty-two cases of sarcomatoid renal cell carcinoma were reviewed clinicopathologically. Twenty-four patients were men, and 18 women; average age was 56.2 years (range, 30-81 years). Eight, 9, 13, and 12 cases were Stages I, 11,111, and IV, respectively. Three morphologic patterns of sarcomatoid components were identified: malignant fibrous histiocytomatous (26 cases), fibrosarcomatous(6 cases), and unclassified sarcomatoid (10 cases). Mitotic count, degree of pleomorphism, cellularity, and amount of tumor matrix in the sarcomatoid areas, and similar morphologic parameters in the carcinomatous component all failed to correlate with prognosis, as did tumor size and renal vein involvement by tumor. Clinicopathologic stage was a most significant prognostic factor, with a survival of 49.7 months for Stage I and 6.8 months for combined Stages 11,111, and IV. Tumor necrosis in the sarcomatoid area and proportion of sarcomatoid components were also poor prognostic factors. When these factors were compared to the stage, necrosis was an independent variable, however, proportion of sarcomatoid components was a poor prognostic indicator only for Stages I and 11. Cancer 59516-526, 1987. ARCOMATOID RENAL CELL CARCINOMA is an un- S common, but not rare, neoplasm consisting of a typical renal cell carcinoma associated intimately with a sarcomatoid component.' It has been reported that sar- comatoid renal cell carcinoma constitutes approximately 1.0% to 1.5% of the total number of renal parenchymal tumors. ' 3 ' This tumor has received only scant and inci- dental attenti~n~-~; only two relatively large series',2have appeared in the literature. Although prognosis in sarcomatoid renal cell carcinoma is known to be extremely poor,'S2 little is known about what clinicopathologic information is prognostic. Fur- thermore, no studies have been done to correlate histologic features in this group of tumors with survival. Therefore, in an attempt to better understand this disease and to identify prognostic pathologic factors, we reviewed 42 cases of sarcomatoid renal cell carcinoma. Presented in part at the annual International Academy of Pathology (IAP) meeting, New Orleans, Louisiana, March 10-14, 1986. From the Departments of *Pathology, tMedical Oncology, and $Urology, The University of Texas M. D. Anderson Hospital and Tumor Institute at Houston, Houston, Texas. Address for reprints: Albert0 G. Ayala, MD, Department of Pathology, Box 85, U. T. M. D. Anderson Hospital, 6723 Bertner Avenue, Houston, TX 77030. The authors thank Ms. Barbara Newton for secretarial assistance, Ms. Terry L. Smith and Mr. Rick Shallenberger for statistical analysis of data, and Ms. Suzanne Simpson for editorial comments on the manu- script. Accepted for publication July 18, 1986. Materials and Methods All kidney tumors diagnosed as sarcomatoid renal cell carcinoma, carcinosarcoma, adult Wilms' tumor, and sarcoma of the kidney from 1973 to 1983 at The Uni- versity of Texas M. D. Anderson Hospital and Tumor Institute at Houston were analyzed. Cases were included in the study only if they contained recognizable renal cell carcinoma and a definite sarcomatoid component. All sarcomas not demonstrating epithelial elements were ex- cluded. Neoplasms with embryonal stroma that contained glomeruloid structures and lacked areas of typical adult renal cell carcinoma (adult Wilms' tumor) were also ex- cluded. Microscopic slides were reviewed without knowl- edge of the clinical information. The follow-up period was dated from the time of initial histologic diagnosis. The original slides were reviewed in all cases, and, when needed, the paraffin blocks were obtained and recut. The average number of slides per case was 10.5 (range, 5-25). The sarcomatoid components were analyzed according to patterns and proportion of the sarcomatoid compo- nents, mitotic count, degree of pleomorphism and necro- sis, cellularity, and the amount of tumor m a t r i ~ . ~ , ~ With respect to mitotic activity, the tumors were classified into three groups: a low mitotic group, when there were fewer than five mitoses per ten high-power fields (HPF); a me- dium mitotic activity group, when there were mitoses be- tween five and nine per ten HPF; and a high mitotic ac- tivity group, when there were ten or more mitoses per ten 5 16
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Sarcomatoid renal cell carcinoma: Clinicopathologic. A study of 42 cases

Sarcomatoid Renal Cell Carcinoma: Clinicopathologic
A Study of 42 Cases
JAE Y. RO, MD,' ALBERT0 G. AYALA, MD,' AVISHAY SELLA, MD,t MELVIN L. SAMUELS, MD,t AND DAVID A. SWANSON, MD*
Forty-two cases of sarcomatoid renal cell carcinoma were reviewed clinicopathologically. Twenty-four patients were men, and 18 women; average age was 56.2 years (range, 30-81 years). Eight, 9, 13, and 12 cases were Stages I, 11,111, and IV, respectively. Three morphologic patterns of sarcomatoid components were identified: malignant fibrous histiocytomatous (26 cases), fibrosarcomatous (6 cases), and unclassified sarcomatoid (10 cases). Mitotic count, degree of pleomorphism, cellularity, and amount of tumor matrix in the sarcomatoid areas, and similar morphologic parameters in the carcinomatous component all failed to correlate with prognosis, as did tumor size and renal vein involvement by tumor. Clinicopathologic stage was a most significant prognostic factor, with a survival of 49.7 months for Stage I and 6.8 months for combined Stages 11,111, and IV. Tumor necrosis in the sarcomatoid area and proportion of sarcomatoid components were also poor prognostic factors. When these factors were compared to the stage, necrosis was an independent variable, however, proportion of sarcomatoid components was a poor prognostic indicator only for Stages I and 11.
Cancer 59516-526, 1987.
ARCOMATOID RENAL CELL CARCINOMA is an un- S common, but not rare, neoplasm consisting of a typical renal cell carcinoma associated intimately with a sarcomatoid component.' It has been reported that sar- comatoid renal cell carcinoma constitutes approximately 1.0% to 1.5% of the total number of renal parenchymal tumors. '3' This tumor has received only scant and inci- dental a t t e n t i ~ n ~ - ~ ; only two relatively large series',2 have appeared in the literature.
Although prognosis in sarcomatoid renal cell carcinoma is known to be extremely poor,'S2 little is known about what clinicopathologic information is prognostic. Fur- thermore, no studies have been done to correlate histologic features in this group of tumors with survival. Therefore, in an attempt to better understand this disease and to identify prognostic pathologic factors, we reviewed 42 cases of sarcomatoid renal cell carcinoma.
Presented in part at the annual International Academy of Pathology (IAP) meeting, New Orleans, Louisiana, March 10-14, 1986.
From the Departments of *Pathology, tMedical Oncology, and $Urology, The University of Texas M. D. Anderson Hospital and Tumor Institute at Houston, Houston, Texas.
Address for reprints: Albert0 G. Ayala, MD, Department of Pathology, Box 85, U. T. M. D. Anderson Hospital, 6723 Bertner Avenue, Houston, TX 77030.
The authors thank Ms. Barbara Newton for secretarial assistance, Ms. Terry L. Smith and Mr. Rick Shallenberger for statistical analysis of data, and Ms. Suzanne Simpson for editorial comments on the manu- script.
Accepted for publication July 18, 1986.
Materials and Methods
All kidney tumors diagnosed as sarcomatoid renal cell carcinoma, carcinosarcoma, adult Wilms' tumor, and sarcoma of the kidney from 1973 to 1983 at The Uni- versity of Texas M. D. Anderson Hospital and Tumor Institute at Houston were analyzed. Cases were included in the study only if they contained recognizable renal cell carcinoma and a definite sarcomatoid component. All sarcomas not demonstrating epithelial elements were ex- cluded. Neoplasms with embryonal stroma that contained glomeruloid structures and lacked areas of typical adult renal cell carcinoma (adult Wilms' tumor) were also ex- cluded. Microscopic slides were reviewed without knowl- edge of the clinical information. The follow-up period was dated from the time of initial histologic diagnosis. The original slides were reviewed in all cases, and, when needed, the paraffin blocks were obtained and recut. The average number of slides per case was 10.5 (range, 5-25).
The sarcomatoid components were analyzed according to patterns and proportion of the sarcomatoid compo- nents, mitotic count, degree of pleomorphism and necro- sis, cellularity, and the amount of tumor m a t r i ~ . ~ , ~ With respect to mitotic activity, the tumors were classified into three groups: a low mitotic group, when there were fewer than five mitoses per ten high-power fields (HPF); a me- dium mitotic activity group, when there were mitoses be- tween five and nine per ten HPF; and a high mitotic ac- tivity group, when there were ten or more mitoses per ten
5 16
No. 3 SARCOMATOID RENAL CELL CARCINOMA - Ro et al. 517
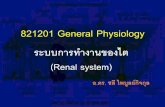
HPF. In terms of necrosis, the cases were categorized into four groups: no necrosis; minimal necrosis, when the ne- crotic areas did not exceed 15% of the tumor; moderate necrosis, when the necrotic areas were 15% to 50% of the tumor; and massive necrosis, when it was over 50% of the tumor. The necrosis was quantitated based on the gross and microscopic findings and only measured from the sarcomatoid areas, and compared with tumor size. Cel- lularity, amount of matrix, and degree of pleomorphism were estimated and categorized into high, intermediate, and low. The sarcomatoid patterns were evaluated and three major patterns were identified: (1) malignant fibrous histiocytomatous (MFH) pattern, (2) fibrosarcomatous pattern, and (3) unclassified sarcomatoid pattern. All tu- mors contained more than one pattern; however, each tumor was subclassified into one pattern based on pre- dominance. The tumors were divided into three categories based on the relative proportion of sarcomatoid and car- cinomatous elements in each tumor. Category I included cases in which carcinomatous elements predominated; Category 11, those in which the carcinomatous and sar- comatoid areas were roughly equal; and Category 111 comprised those composed predominantly of sarcomatoid elements.
The morphologic parameters of renal cell carcinoma were examined according to tumor patterns, cell types, nuclear grade, and mitotic count.8 The tumor patterns of carcinomatous areas were categorized into three basic patterns: solid, tubular or glandular, and papillary tumors. The composed tumor cells were divided into three types: tumors composed entirely of or more than 75% of clear cells, those composed entirely of or more than 75% of granular cells, and those composed of a mixture of both types (the minority populations were composed of at least >25%). Nuclear grade was determined utilizing the Fuhr- man et al. grading system': Grade I tumors were composed of cells with small, round, uniform nuclei (about 10 pm) with inconspicuous or absent nucleoli; Grade 2 had larger nuclei (about 15 pm) that exhibited irregularities in outline and nucleoli when examined under high power (400X); Grade 3 tumors had even larger nuclei (about 20 pm) with an obviously irregular outline and prominent large nucleoli even at lower power (1OOX); and Grade 4 exhib- ited features similar to the Grade 3 tumors, with the ad- dition of bizarre, often multilobated nuclei and heavy chromatin clumps. Mitoses were evaluated in the same way used for the sarcomatoid components. The tumor size, renal vein or vena caval involvement, capsular in- vasion, and presence of lymph node and distant metastases were also evaluated. Based on these parameters, pathologic stage was determined using the system of Robson et al.'
The Kaplan-Meier method" was used for all of the comparisons for survival curves, and the differences found were tested by the Gehan-Breslow modification of the Wilcoxon two-tailed test.' I
TABLE 1. Size of Sarcomatoid Renal Cell Carcinomas
Size (cm) No. of cases
<5 1 5-8 15 9-12 18
13-16 5 217 3
Results
Twenty-four of the patients were men and 18 were women. Patient ages ranged from 30 to 81 years (mean, 56.2 years). Twenty-two of the tumors occurred in the right kidney, and 20 in the left. There were no instances of bilateral tumors. The diameters of the lesions ranged from 4.2 to 18.5 cm, with a mean of 10.2 cm (Table 1).
Gross descriptions were available in 35 cases. No def- inite difference of gross findings from the typical renal cell carcinoma was noted; however, in six cases, the tu- mors revealed a dense, gray, fibrous appearance in large areas as well as the typical gross appearance of renal cell carcinoma.
Carcinomatous Components
In 25 of 42 cases, the tumor cells were arranged in a solid pattern; in 3 cases, the predominant pattern was papillary; in 6 cases, tubular or glandular; and in 8 cases, the pattern was mixed without a single predominant pat- tern. With respect to cell types, the predominant cell was clear cell in 18 cases (Fig. 1). In ten cases, the predominant cell type was granular, but one case showed oncocytes as the predominant cell type (Fig. 2). In 14 cases, the car- cinomatous areas were composed of mixed clear and granular cells without predominance. The distribution of patients according to nuclear grade was as follows: Grade 1,6 cases; Grade 2, 8 cases; Grade 3, 15 cases; and Grade 4, 13 cases.
Tumor necrosis and hemorrhage were frequently seen in the carcinomatous areas. Mitoses in carcinoma cells were infrequent, when compared to the sarcomatoid areas. In 33 cases, mitoses were less than five per ten HPF. Seven cases showed a mitotic count between five and nine per ten HPF, and only two cases showed mitoses of more than ten per ten HPF.
Sarcomatoid Components
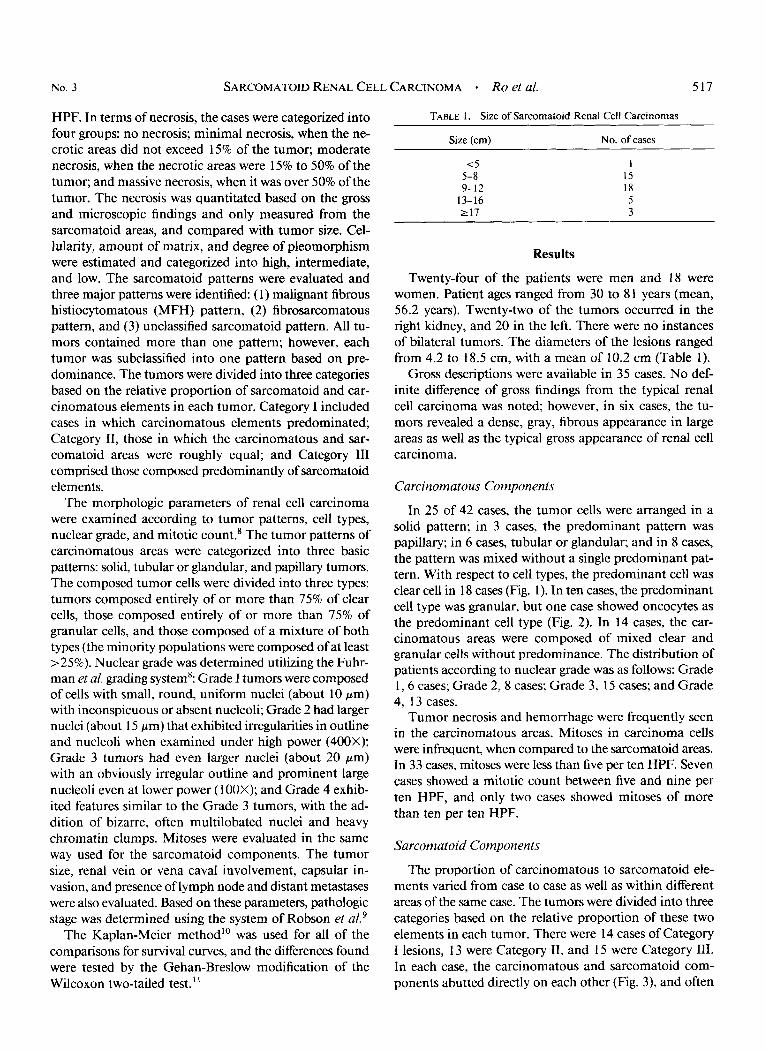
The proportion of carcinomatous to sarcomatoid ele- ments varied from case to case as well as within different areas of the same case. The tumors were divided into three categories based on the relative proportion of these two elements in each tumor. There were 14 cases of Category I lesions, 13 were Category 11, and 15 were Category 111. In each case, the carcinomatous and sarcomatoid com- ponents abutted directly on each other (Fig. 3), and often

518 CANCER February 1 1987 VOl. 59
FIG. 1 . Sarcomatoid renal cell carcinoma showing a clear cell type of renal cell carcinoma as well as a sarcomatoid component on the right (H & E, original magnification, X40).
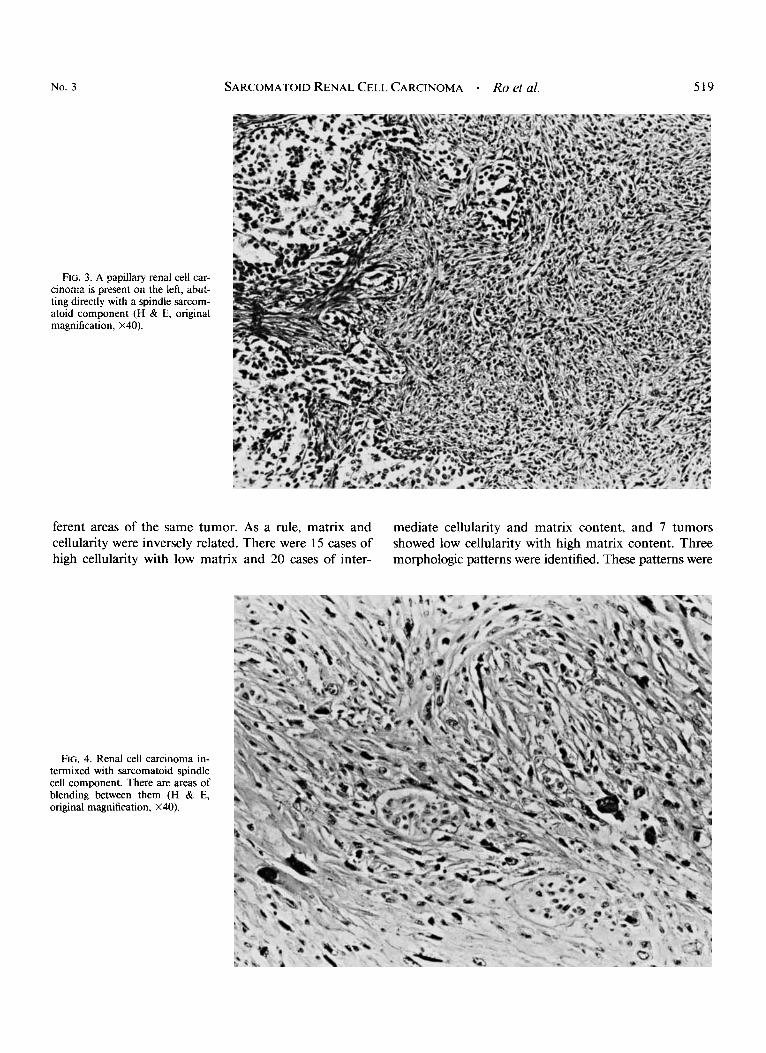
there were areas of blending between them (Fig. 4). The sarcomatoid portions of the tumors were composed pre- dominantly of spindle cells and, occasionally, round or
epithelioid cells. Pleomorphism was marked in 15 cases, moderate in 2 1 cases, and mild in 6 cases. The cellularity and matrix of tumor vaned from case to case and in dif-
FIG. 2. Oncocytes are the pre- dominant carcinoma component. The sarcomatoid component is present on the right (H & E, original magnification, X40).
No. 3 SARCOMATOID RENAL CELL CARCINOMA - Ro et al. 519
FIG. 3. A papillary renal cell car- cinoma is present on the left, abut- ting directly with a spindle sarcom- atoid component (H & E, original magnification, X40).
ferent areas of the same tumor. As a rule, matrix and cellularity were inversely related. There were 15 cases of high cellularity with low matrix and 20 cases of inter-
mediate cellularity and matrix content, and 7 tumors showed low cellularity with high matrix content. Three morphologic patterns were identified. These patterns were
FIG. 4. Renal cell carcinoma in- termixed with sarcomatoid spindle cell component. There are areas of blending between them (H & E, original magnification, X40).
520 CANCER February 1 1987 Vol. 59
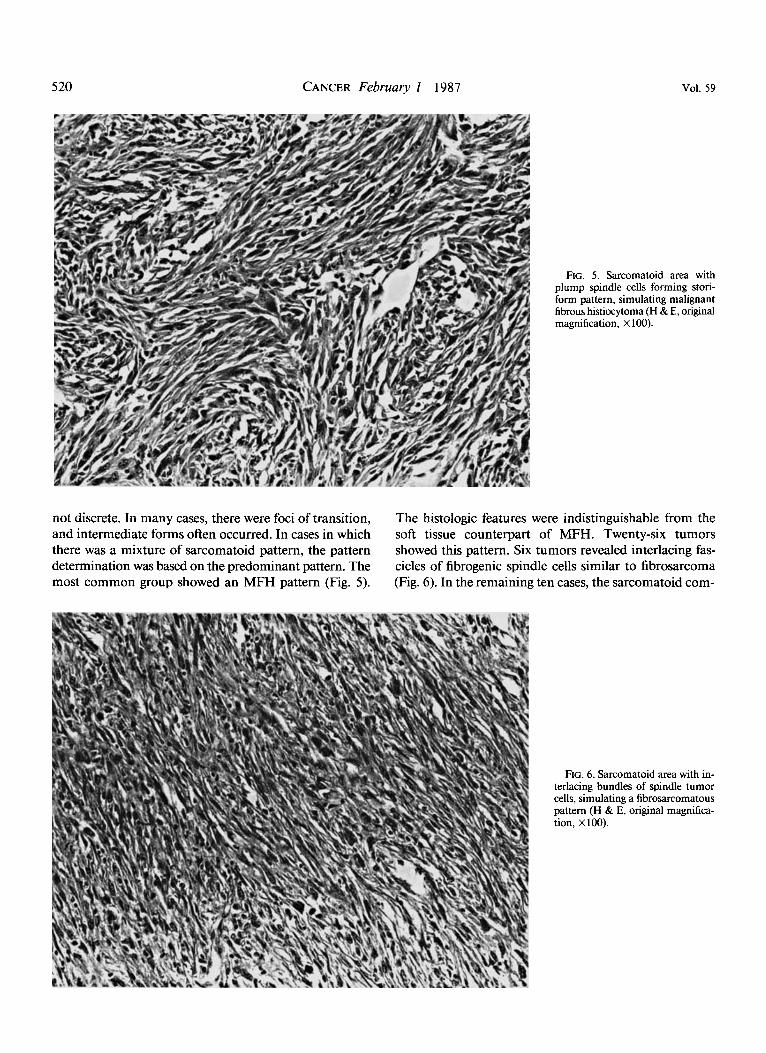
FIG. 5. Sarcomatoid area with plump spindle cells forming stori- form pattern, simulating malignant fibrous histiocytoma (H & E, original magnification, X 100).
not discrete. In many cases, there were foci of transition, and intermediate forms often occurred. In cases in which there was a mixture of sarcomatoid pattern, the pattern determination was based on the predominant pattern. The most common group showed an MFH pattern (Fig. 5).
The histologic features were indistinguishable from the soft tissue counterpart of MFH. Twenty-six tumors showed this pattern. Six tumors revealed interlacing fas- cicles of fibrogenic spindle cells similar to fibrosarcoma (Fig. 6). In the remaining ten cases, the sarcomatoid com-
FIG. 6. Sarcomatoid ai terlacing bundles of spir cells, simulating a fibrosa pattern (H & E, original tion, XIOO).
-ea with in- idle tumor ucomatous magnifica-
SARCOMATOID RENAL CELL CARCINOMA 0 Ro el al. 52 1
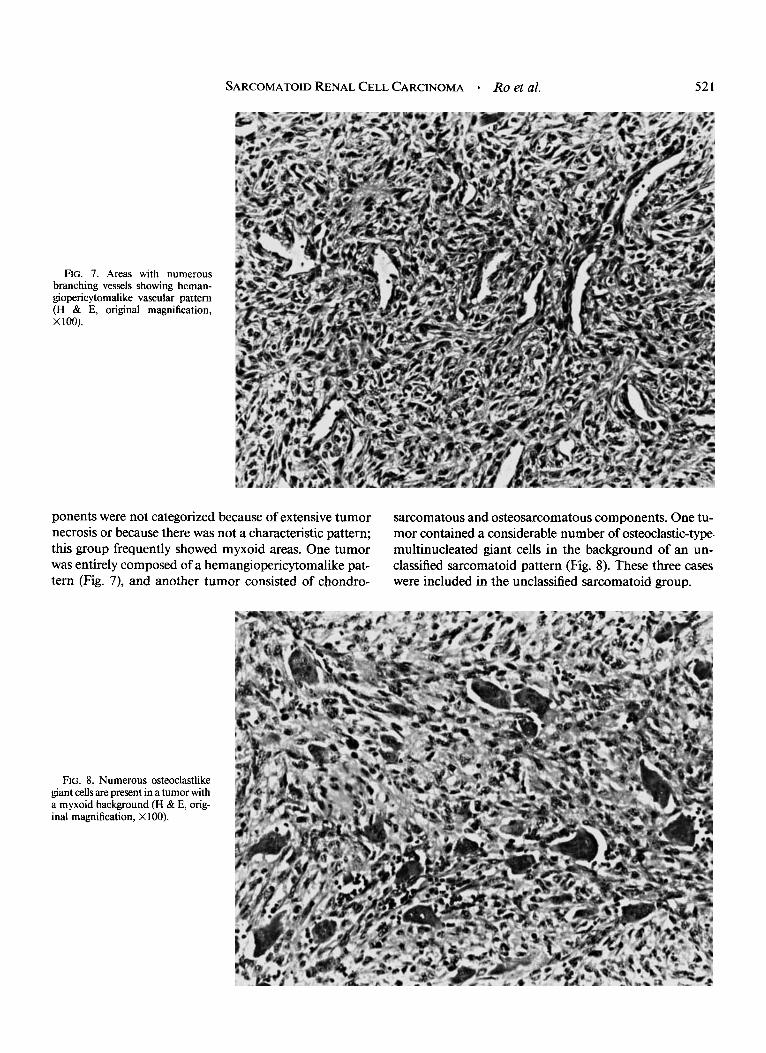
FIG. 7. branching giopericytl (H 8~ E, x 100).
Areas with numerous vessels showing heman-
malike vascular pattern original magnification,
ponents were not categorized because of extensive tumor necrosis or because there was not a characteristic pattern; this group frequently showed myxoid areas. One tumor was entirely composed of a hemangiopericytomalike pat- tern (Fig. 7), and another tumor consisted of cbondro-
sarcomatous and osteosarcomatous components. One tu- mor contained a considerable number of osteoclastic-type. multinucleated giant cells in the background of an un- classified sarcomatoid pattern (Fig. 8). These three cases were included in the unclassified sarcomatoid group.
FIG. 8. Numerous osteoclastlike giant cells are present in a tumor with a myxoid background (H & E, orig- inal magnification, X 100).
522 CANCER February 1 1987 Vol. 59
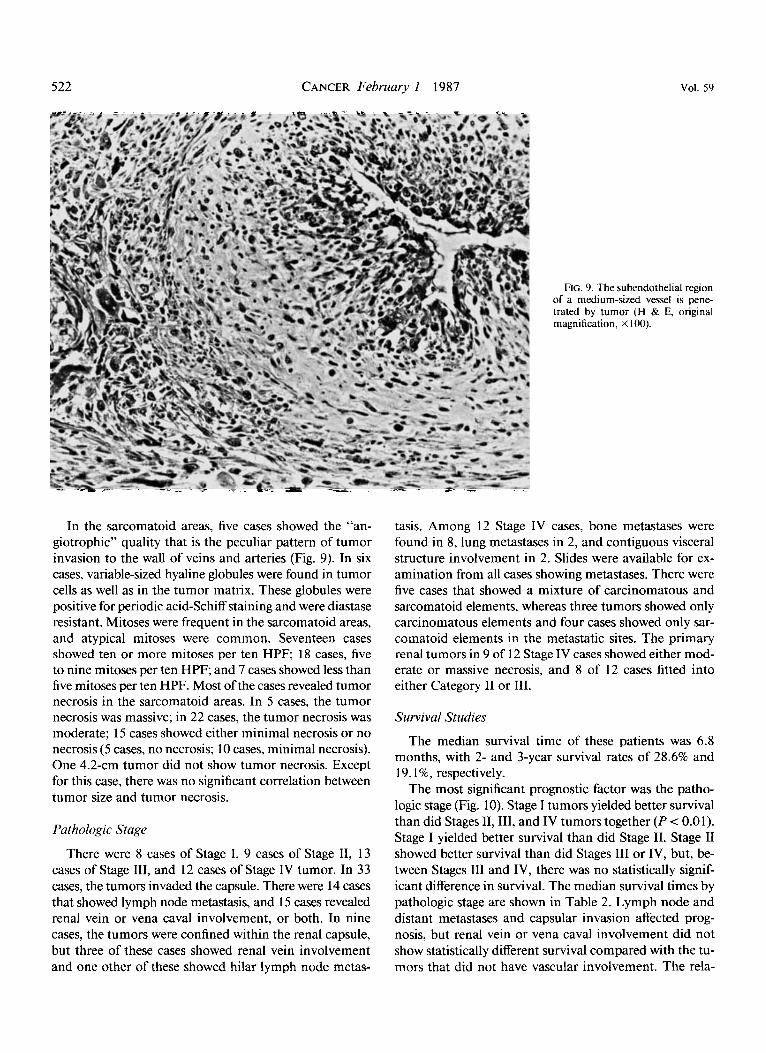
FIG. 9. The subendothelial region of a medium-sized vessel is pene- trated by tumor (H & E, original magnification, X 100).
In the sarcomatoid areas, five cases showed the “an- giotrophic” quality that is the peculiar pattern of tumor invasion to the wall of veins and arteries (Fig. 9). In six cases, variable-sized hyaline globules were found in tumor cells as well as in the tumor matrix. These globules were positive for periodic acid-Schiff staining and were diastase resistant. Mitoses were frequent in the sarcomatoid areas, and atypical mitoses were common. Seventeen cases showed ten or more mitoses per ten HPF; 18 cases, five to nine mitoses per ten HPF; and 7 cases showed less than five mitoses per ten HPF. Most of the cases revealed tumor necrosis in the sarcomatoid areas. In 5 cases, the tumor necrosis was massive; in 22 cases, the tumor necrosis was moderate; 15 cases showed either minimal necrosis or no necrosis ( 5 cases, no necrosis; 10 cases, minimal necrosis). One 4.2-cm tumor did not show tumor necrosis. Except for this case, there was no significant correlation between tumor size and tumor necrosis.
Pathologic Stage
There were 8 cases of Stage I, 9 cases of Stage 11, 13 cases of Stage 111, and 12 cases of Stage IV tumor. In 33 cases, the tumors invaded the capsule. There were 14 cases that showed lymph node metastasis, and 15 cases revealed renal vein or vena caval involvement, or both. In nine cases, the tumors were confined within the renal capsule, but three of these cases showed renal vein involvement and one other of these showed hilar lymph node metas-
tasis. Among 12 Stage IV cases, bone metastases were found in 8, lung metastases in 2, and contiguous visceral structure involvement in 2. Slides were available for ex- amination from all cases showing metastases. There were five cases that showed a mixture of carcinomatous and sarcomatoid elements, whereas three tumors showed only carcinomatous elements and four cases showed only sar- comatoid elements in the metastatic sites. The primary renal tumors in 9 of 12 Stage IV cases showed either mod- erate or massive necrosis, and 8 of 12 cases fitted into either Category I1 or 111.
Survival Studies
The median survival time of these patients was 6.8 months, with 2- and 3-year survival rates of 28.6% and 19. I %, respectively.
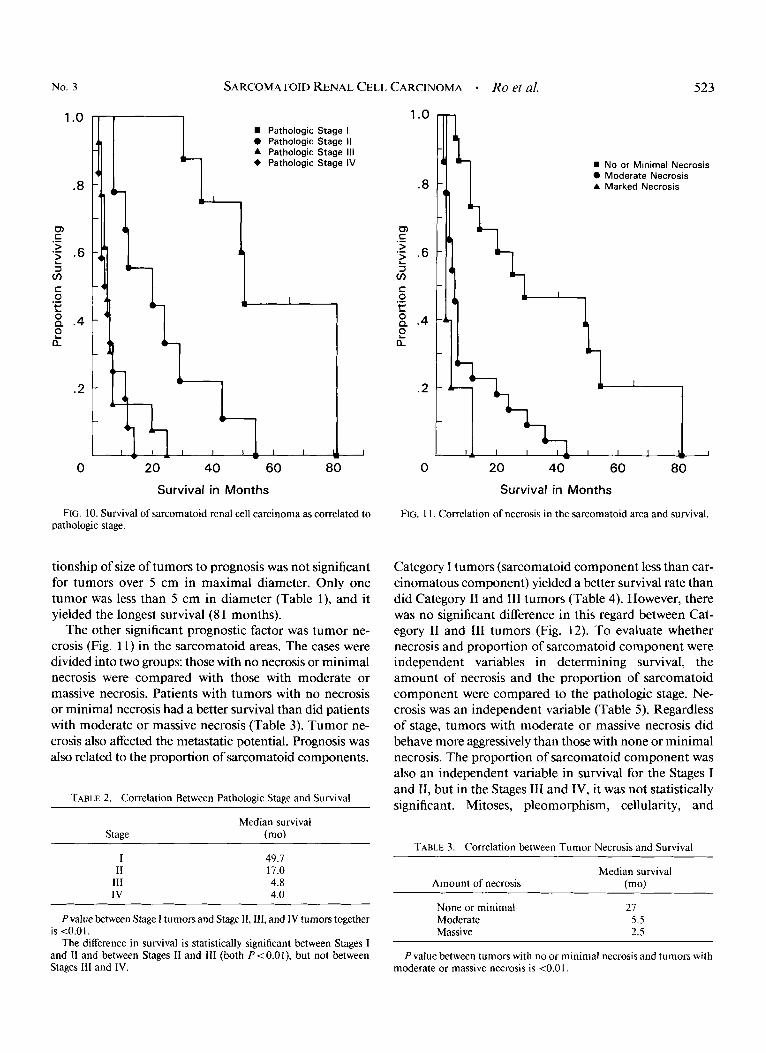
The most significant prognostic factor was the patho- logic stage (Fig. 10). Stage I tumors yielded better survival than did Stages 11,111, and IV tumors together ( P < 0.01). Stage I yielded better survival than did Stage 11. Stage I1 showed better survival than did Stages 111 or IV, but, be- tween Stages 111 and IV, there was no statistically signif- icant difference in survival. The median survival times by pathologic stage are shown in Table 2. Lymph node and distant metastases and capsular invasion affected prog- nosis, but renal vein or vena caval involvement did not show statistically different survival compared with the tu- mors that did not have vascular involvement. The rela-
No. 3
1 .o
.8
m c >
3 cn c 0
.-
.- .6 L
.- t: g .4 2 a
.2
0
SARCOMATOID RENAL CELL CARCINOMA - Ro et al.
0 A +
Pathologic Pathologic Pathologic Pathologic
Stage I Stage II Stage 111 Stage IV
20 40 60 80
Survival in Months
FIG. 10. Survival of sarcomatoid renal cell carcinoma as correlated to pathologic stage.
tionship of size of tumors to prognosis was not significant for tumors over 5 cm in maximal diameter. Only one tumor was less than 5 cm in diameter (Table l), and it yielded the longest survival (8 1 months).
The other significant prognostic factor was tumor ne- crosis (Fig. 11) in the sarcomatoid areas. The cases were divided into two groups: those with no necrosis or minimal necrosis were compared with those with moderate or massive necrosis. Patients with tumors with no necrosis or minimal necrosis had a better survival than did patients with moderate or massive necrosis (Table 3). Tumor ne- crosis also affected the metastatic potential. Prognosis was also related to the proportion of sarcomatoid components.
TABLE 2. Correlation Between Pathologic Stage and Survival
Median survival Stage (mo)
I 11
111 IV
49.7 17.0 4.8 4.0
Pvalue between Stage I tumors and Stage 11,111, and IV tumors together is <O.O I .
The difference in survival is statistically significant between Stages I and I1 and between Stages I1 and 111 (both P<O.Ol), but not between Stages I11 and IV.
1 .o
.8
m c >
3 v)
c 0
.-
.- .6 L
.- c.’ z P .4 ? a
.2
0
523
No or Minimal Necrosis 0 Moderate Necrosis A Marked Necrosis
20 40 60 80 Survival in Months
FIG. 1 I . Correlation of necrosis in the sarcomatoid area and survival.
Category I tumors (sarcomatoid component less than car- cinomatous component) yielded a better survival rate than did Category I1 and 111 tumors (Table 4). However, there was no significant difference in this regard between Cat- egory I1 and I11 tumors (Fig. 12). To evaluate whether necrosis and proportion of sarcomatoid component were independent variables in determining survival, the amount of necrosis and the proportion of sarcomatoid component were compared to the pathologic stage. Ne- crosis was an independent variable (Table 5). Regardless of stage, tumors with moderate or massive necrosis did behave more aggressively than those with none or minimal necrosis. The proportion of sarcomatoid component was also an independent variable in survival for the Stages I and 11, but in the Stages 111 and IV, it was not statistically significant. Mitoses, pleomorphism, cellularity, and
TABLE 3. Correlation between Tumor Necrosis and Survival
Median survival Amount of necrosis (mo)
None or minimal Moderate Massive
21 5.5 2.5
P value between tumors with no or minimal necrosis and tumors with moderate or massive necrosis is <O.O I .

524 CANCER February I 1987 VOl. 59
TABLE 4. Correlation between Category and Survival
Category* Median survival
(mo)
I I1 111
29.0 5.5 5.8
* Categories indicate proportion of histologic components: I, predom- inantly carcinomatous; 11, carcinomatous and sarcomatoid roughly equal; 111, predominantly sarcomatoid. P value between Category I and Categories I1 and 111 is <0.01.
amount of tumor matrix in the sarcomatoid areas did not show significant differences in survival and were poor prognosticators of outcome. The patterns of sarcomatoid components had no prognostic significance.
Attempts to correlate cell types, patterns, nuclear grade, and mitoses of carcinomatous components to the prog- nosis failed to reveal any significant results.
Discussion
Sarcomatoid renal cell carcinoma has been recognized as a distinct renal tumor since it was first named by Farrow er al.' in 1968. The renal cell carcinomatous components and the sarcomatoid components abut directly on each
Category I 0 Category II A Category 111
1 I I I I1 I I I I1 I
0 20 40 60 80 Survival in Months
FIG. 12. Correlation of the proportion ofsarcomatoid component and survival.
TABLE 5. Correlation Between Pathologic Stage and Amount of Tumor Necrosis in Survival
Necrosis
None or Moderate No. of Stage minimal or massive cases
Stage I 6 (67.7)* 2 (30.0): 8 Stage 11, 111 and IV 9 (12.5): 25 (5.0)* 34 No. of Cases 15 27 42
* Number in parenthesis indicates median survival time in months. In Chi-square, I degree of freedom = 6.64; P value is t O . O 1 .
other, and often areas of transition are found between This tumor is a highly aggressive malignancy
with a dismal prognosis. This kind of renal tumor has also been referred to in
the literature as carcinosar~oma, '~-~~ renal carcinoma of sarcomatoid type,'-4 and mixed tumor of the kidney." The derivation of the sarcomatoid component in renal cell carcinoma is still being debated. Bennington and Beckwithk2 considered the sarcomatoid portion to be de- rived from the stroma, whereas Farrow er al.' suggested that it is derived from metaplastic transformation of the cells of the adenocarcinoma. Cecil et a l l5 reported that most of the tumors reported in the literature as carcino- sarcomas or mixed tumors of the kidney are probably a sarcomatoid variant of renal cell carcinoma. However, these last authors believed that there remains a small group of renal neoplasms with definite epithelial and mesen- chymal differentiation. Recently, we had a chance to study sarcomatoid renal cell carcinomas using immunohisto- chemical and electron microscopic studies. In most cases, the spindle cells of sarcomatoid components reacted with antikeratin antibody and showed ultrastructural features of epithelial origin. However, some cases neither reacted with epithelial markers nor showed ultrastructural features of epithelial origin. Three of them demonstrated smooth muscle components either by immunostaining or electron microscopic study (or both). These findings suggest that some mixed epithelial and sarcomatoid tumors of the kidney could be true carcinosarcomas. Details of this study are reported separately." Nonetheless, Farrow et al.' have suggested that, given the incomplete state of knowledge about these unusual malignancies, "sarcomatoid" is at present an appropriate term.
In the current study, the histologic features of sarcoma- toid renal cell carcinomas varied from case to case, and in different areas in the same tumor. The carcinomatous components were composed of either clear cells, granular cells, or mixed cells with varying nuclear grades. Solid pattern was the most frequent tumor pattern. Occasion- ally, tubular or glandular pattern and papillary pattern were found in the carcinomatous areas. The incidence

No. 3 SARCOMATOID RENAL CELL CARCINOMA * Ro et al. 525
and proportion of cell types and tumor patterns were not that different from those in usual renal cell carcinoma; however, high nuclear grades (Grades 3 and 4) were more frequently seen in sarcomatoid renal cell carcinoma than overall in renal cell carcinoma.8 In one tumor in our cur- rent series, the carcinomatous components were entirely composed of oncocytes.
In accordance with the findings of Tomera et a/.,2 the sarcomatoid components of our cases generally demon- strated features that could be compatible with either ma- lignant fibrous histiocytoma (MFH) or fibrosarcoma. Twenty-six tumors mimicked MFH and six cases resem- bled fibrosarcoma, whereas ten cases could not be accu- rately categorized. This result is comparable to the Tomera et a/. description of 11 tumors of MFH and 2 tumors of fibrosarcomatous features in their series of sarcomatoid renal cell carcinomas. The MFH pattern has also been described as the predominant sarcomatoid pattern in spindle squamous carcinoma of the head and neck'' and in sarcomatoid breast carcinomas,' thus providing further testimony to the nonspecificity of the histologic pattern of MFH. Among ten unclassified sarcomas in our current series, one tumor showed large areas of osteosarcomatous and chondrosarcomatous components and another tumor contained numerous osteoclastlike giant cells scattered in the spindle sarcomatoid tumor. The osteoclastlike giant cell component has been reported in sarcomatoid carci- noma of other organs, such as thyroid, renal pelvis, breast, lung, pancreas, ovary, and salivary Farrow et ul.,' Hou and Willis,16 Macke et a/.,22 and Elliott et a/.23 reported cases of renal cell carcinoma with sarcomatoid areas resembling osteosarcoma.
In 15 of 42 cases from this study, the sarcomatoid com- ponents were the predominant elements (Category III), with 5 of these cases composed almost entirely of sarco- matoid components at the first examination. Nevertheless, further sampling of these tumors disclosed foci of renal cell carcinoma allowing for a diagnosis of sarcomatoid renal cell carcinoma. Therefore, since primary sarcomas of the kidney are extremely rare, renal neoplasms that appear to be sarcomas should always be extensively sam- pled to exclude a carcinomatous component. If only a small biopsy sample is available, electron microscopic ex- amination or immunohistochemical study is required to unveil the epithelial component of the potential sarcoma- toid tumor.3
Many previous studies have attempted to identify mor- phologic parameters that correlate with biologic behavior in general of renal cell ~ a r c i n o m a . ~ . ~ . ~ ~ - ~ ' Th e results, however, have often been contradictory, and only a few concepts have achieved clinical importance and are widely used by practicing pathologists. The pathologic stage has been known to be the best single prognostic factor in renal cell carcinoma. Other factors, including cell type, tumor
grade, and tumor cell arrangement, have been found to be associated with clinical outcome. Recently, Fuhrman et aL8 introduced nuclear grade into the analysis and found it to be the most significant prognostic criterion for the outcome of Stage I renal cell carcinoma.
Our median survival time of 6.8 months is comparable to the median survival of 6.2 months of Tomera et aL2 Sarcomatoid renal cell carcinomas in our series were ad- vanced at the time of diagnosis. Thirty-four of 42 of our cases (8 1%) and 1 1 of 13 of the Tomera et aL2 cases (85%) had Stages I1 through IV tumors at the time of diagnosis. Like other reports8,9*24*26 of renal cell carcinomas, the cur- rent study indicates that the pathologic stage is the single best parameter for predicting overall survival in sarcoma- toid renal cell carcinoma.
Recently, Costa et aL6 reported results of a clinicohis- topathologic correlation in soft tissue sarcomas, finding necrosis to be the most important prognostic factor. Kaufman et aL7 studied sarcomatoid breast carcinomas and noted that patients with tumor composed predomi- nantly of sarcomatoid elements had a worse prognosis than those with predominantly epithelial components.
We applied these morphologic parameters to sarcoma- toid renal cell carcinomas. We found that those tumors with no or minimal necrosis yielded a favorable prognosis, both in terms of survival and metastases, whereas those with moderate or massive necrosis yielded a significantly poorer survival time. The amount of necrosis, regardless of pathologic stage, was an independent variable indicating a separate prognosticator. The proportion of sarcomatoid components also appeared to be an important factor. The more the sarcomatoid components present, the worse the prognosis was. When the proportion of sarcomatoid com- ponent was compared to the stage, however, this factor was a poor prognosticator only for Stages I and 11, but not for Stages I11 and IV.
It has been reported that, in renal cell carcinoma, the larger the tumor, the greater the likelihood of local exten- sion, vascular invasion, and metastasis. However, in 1968, Kay25 reported that the relationship of size of tumor to prognosis was significant only for tumors under 5 cm in maximal dimension, and Fuhrman et a/.8 in 1982 indi- cated that, with the exception of patients with tumors at the extremes of size ( 1 3 cm or >8 cm), knowledge of size offered no clue for the outcome.
As in the series of Tomera et aL2 our examples of sar- comatoid renal cell carcinomas were large in size (mean diameter, 10.2 cm). Except for the one tumor of less than 5 cm, which did not show tumor necrosis and which yielded the longest survival time, there was no correlation in our series between tumor size and degree of tumor necrosis and between tumor size and prognosis.
There is some controversy regarding the relationship of prognosis and renal vein involvement by renal cell car-

526 CANCER February 1 1987 VOl. 59
cinoma. Several reports indicated that renal vein involve- ment is associated with significantly worse prognosi~'*~~*~'; however, other reports claimed that renal vein or vena caval involvement by itself does not adversely affect the clinical outcome.8,26*28 Our results with sarcomatoid renal cell carcinoma concurred with the latter in finding that prognosis did not correlate with vascular involvement by tumor. In our study, the pathologic parameters of carci- nomatous components and certain morphologic features of sarcomatoid components, including patterns, mitotic count, degree of pleomorphism, cellularity, and the amount of matrix, were not found to be of significant prognostic importance. But the pathologic stage, degree of tumor necrosis, and proportion of sarcomatoid com- ponents are important prognosticators of outcome.
REFERENCES
I . Farrow GM, Hamson EG, Utz DC. Sarcomas and sarcomatoid and mixed malignant tumors of the kidney in adults: Part 111. Cancer
2. Tomera KV, Farrow GM, Lieber MM. Sarcomatoid renal carci- noma. J Urol 1983; 130:657-659.
3. Deitchman B, Sidhu GS. Ultrastructural study of a sarcomatoid variant of renal cell carcinoma, Cancer 1980; 46: I 152- 1 157.
4. Krutchik AN, Sullivan C, Sinkovics JG, Ayala A. Chemo-immu- notherapy of sarcomatoid renal cell carcinoma, Med Pediatr Oncol 1978;
5. Tannenbaum M. Ultrastructural pathology of human renal cell tumors. Pathol Annu 197 I ; 6:249-277.
6. Costa J, Wesley RA, Glatstein E, Rosenberg SA. The grading of soft tissue sarcomas: Results of a clinicohistopathologic correlation in a series of 163 cases. Cancer 1984; 53530-541.
7. Kaufman MW, Marti JR, Gallager HS, Hoehn JL. Carcinoma of the breast with pseudosarcomatous metaplasia. Cancer 1984; 53: 1908- 1917.
8. Fuhrman SA, Lasky LC, Limas C. Prognostic significance of mor- phologic parameters in renal cell carcinoma. Am JSurg Pathol 1982; 6:
9. Robson C, Churchill B, Anderson W. The results of radical ne-
10. Kaplan EL, Meier P. Nonparametric estimation from incomplete
1968; 221556-563.
5:9-13.
655-663.
phrectomy for renal cell carcinoma. J Urol 1969; 101:297-301.
observations. J Am Stat Assoc 1958; 53:457-48 I .
I I . Gehan E. A generalized Wilcoxon test for comparing arbitrarily singly-censored samples. Brometrika 1965; 52:203-223.
12. Bennington JL, Beckwith JB. Tumors of the Kidney, Renal Pelvis, and Ureter. In: Atlas of Tumor Pathology, series 2, fascicle 12. Wash- ington, DC: Armed Forces Institute of Pathology, 1975; 229-23 1.
13. Fisher ER, Davis ER. Carcinosarcoma of kidney. J Urol 1962;
14. Rao MS, Lotuaco LG, McGregor DH. Carcinosarcoma of the adult kidney. Postgrad Med J 1977; 53:408-411.
15. Cecil B, Woodard B, Mickey DD, Pizzo S. Renal carcinosarcoma: Ultrastructure and transplantation into athymic mice. Arch Pathol Lab Med 1980; 104:276-279.
16. Hou LT, Willis RA. Renal carcinosarcoma, true and false. J Pathol Bacteriol 1963; 85:139-144.
17. JuhPsz J, Sebok J, Galambos J, Kiss P. Renal carcinosarcoma (mixed tumours) of the kidney. Int Urd Nephrol 1980 12:103-108.
18. Khorsand J, Ro JY, Mackay B, Ayala AG, Ordonez NG. Sar- comatoid renal cell carcinoma. An immunocytochemical and ultra- structural study of 26 cases (Abstr 182). Lab Invest 1986; 54:31A.
19. Leventon GS, Evans HL. Sarcomatoid squamous cell carcinoma of the mucous membranes of the head and neck: A clinicopathologic study of 20 cases. Cancer 1981; 48:994-1003.
20. Kenney RM, Prat J, Tabernero M. Giant-cell tumor-like prolif- eration associated with a papillary transitional cell carcinoma of the renal pelvis. Am J Surg Pathol 1984; 8:139-144.
2 I . Carcangiu ML, Steeper T, Zampi G, Rosai J. Anaplastic thyroid carcinoma: A study of 70 cases. Am J Clin Pathol 1985; 83: 135-158.
22. Macke RA, Hussain MB, Imray TJ, Wilson RB, Cohen SM. Os- teogenic and sarcomatoid differentiation of a renal cell carcinoma. Cancer 1985; 56:2452-2457.
23. Elliott JT, Pontius EE, McCallum DC. Carcinosarcoma of the kidney. Urology 1973; 1:151-153.
24. Selli C, Hinshaw WM, Woodard BT, Paulson DF. Stratification of risk factors in renal cell carcinoma, Cancer 1983; 52:899-903.
25. Kay S. Renal carcinoma: A 10-year study. Am J Clin Pathol 1968; 50:428-432.
26. Skinner DG, Colvin RB, Vermillion CD, Pfister RC, Leadbetter WF. Diagnosis and management of renal cell carcinoma: A clinical and pathologic study of 309 cases. Cancer 1971; 28:1165-1177.
27. Rafla SR. Renal cell carcinoma: Natural history and results of treatment. Cancer 1970; 25:26-40.
28. Waters WB, Richie JP. Aggressive surgical approach to renal cell carcinoma: Review of 130 cases. J Urol 1979; 122:306-309.
29. Holland JM. Cancer of the kidney: Natural history and staging. Cancer 1973; 32:1030-1042.
30. Meyers G Jr, Fehrenbaker L, Kelalis P. Prognostic significance of renal vein invasion by hypernephroma. J Urol 1968; 100:420-423.
3 I . Petel N, Lavengood R. Renal cell carcinoma: Natural history and results of treatment. J Urol 1978; 119:722-726.
87:109-118.