RSSSR 21 def PDF Unwin-Dickson pp161-174
14
GOAL FOCUSED HOPE, SPIRITUAL HOPE, AND WELL-BEING Jen Unwin and Joanne M. Dickson* Abstract e current study examined the relationship between goal focused hope and spiritual hope, and whether these constructs independently predicted subjective well-being (SWB). Two hundred and seven university staff and students completed measures of goal focused hope, spiritual hope, satisfaction with life, and positive affect. Goal focused and spiritual hope scores were not correlated. Via multiple regression analysis we found that goal focused hope, but not spiritual hope, was an independent pre- dictor of well-being. However the regression analysis also showed a significant goal- focused hope by spiritual hope interaction for subjective well-being, which suggests that spiritual hope may have a buffering effect when goal focused hope is low. Further studies of hope and SWB are suggested and implications for clinical interventions are discussed. ere is increasing evidence for the importance of subjective well- being in a number of domains (Sheldon & Lyubomirsky, 2004). In older adults, well-being protects against mortality and the onset of disability (Ostir, Markides, Black & Goodwin, 2000). Contrastingly, a lack of subjective well-being has been linked to depression and suicide (Keyes & Magyar-Moe, 2003). Ruini and Fava (2004) advocate well- being therapy as a means of counteracting and perhaps preventing psychological distress. Focusing on well-being in psychosocial inter- ventions aims for outcomes beyond the mere removal of suffering, to help people go “beyond zero” to achieve optimum functioning (Shel- don & Lyubomirsky, 2004). It is important that we further our understanding of the cognitive processes underpinning subjective well-being, as researchers and clini- cians are increasingly using this concept and designing interventions to enhance well-being. Well-being and hope are concepts much stud- ied in positive psychology and offer a new direction for researchers Research in the Social Scientific Study of Religion, Volume 21 © Koninklijke Brill NV, Leiden, 2010 * Author Note: Correspondence concerning this article should be addressed to Dr Jen Unwin (BSc, MSc, PsyD, CPsychol, AFBPSs),University of Liverpool, Division of Clinical Psychology, e Whelan Building, Brownlow Hill, Liverpool L69 3GB. Email: [email protected] Tel: +44-(0)151-7945657, Fax: +44-(0)151–7945537
Transcript of RSSSR 21 def PDF Unwin-Dickson pp161-174

GOAL FOCUSED HOPE, SPIRITUAL HOPE, AND WELL-BEING
Jen Unwin and Joanne M. Dickson*
Abstract
The current study examined the relationship between goal focused hope and spiritual hope, and whether these constructs independently predicted subjective well-being (SWB). Two hundred and seven university staff and students completed measures of goal focused hope, spiritual hope, satisfaction with life, and positive affect. Goal focused and spiritual hope scores were not correlated. Via multiple regression analysis we found that goal focused hope, but not spiritual hope, was an independent pre-dictor of well-being. However the regression analysis also showed a significant goal-focused hope by spiritual hope interaction for subjective well-being, which suggests that spiritual hope may have a buffering effect when goal focused hope is low. Further studies of hope and SWB are suggested and implications for clinical interventions are discussed.
There is increasing evidence for the importance of subjective well-being in a number of domains (Sheldon & Lyubomirsky, 2004). In older adults, well-being protects against mortality and the onset of disability (Ostir, Markides, Black & Goodwin, 2000). Contrastingly, a lack of subjective well-being has been linked to depression and suicide (Keyes & Magyar-Moe, 2003). Ruini and Fava (2004) advocate well-being therapy as a means of counteracting and perhaps preventing psychological distress. Focusing on well-being in psychosocial inter-ventions aims for outcomes beyond the mere removal of suffering, to help people go “beyond zero” to achieve optimum functioning (Shel-don & Lyubomirsky, 2004).
It is important that we further our understanding of the cognitive processes underpinning subjective well-being, as researchers and clini-cians are increasingly using this concept and designing interventions to enhance well-being. Well-being and hope are concepts much stud-ied in positive psychology and offer a new direction for researchers
Research in the Social Scientific Study of Religion, Volume 21© Koninklijke Brill NV, Leiden, 2010
* Author Note: Correspondence concerning this article should be addressed to Dr Jen Unwin (BSc, MSc, PsyD, CPsychol, AFBPSs),University of Liverpool, Division of Clinical Psychology, The Whelan Building, Brownlow Hill, Liverpool L69 3GB. Email: [email protected] Tel: +44-(0)151-7945657, Fax: +44-(0)151–7945537

162 jen unwin and joanne m. dickson
and clinicians seeking to identify and foster factors contributing to wellness (Naidoo, 2006). Folkman (2008), in reviewing studies relat-ing to the role of positive affect in the stress process, urges researchers to focus attention on the underlying cognitive processes that lead to adaptive coping, positive affect, and well-being.
One such cognitive concept considered to underlie well-being is hope, commonly defined in dictionaries as to wish for something with expectation of its fulfilment. Scioli (2007) has suggested that hope is a primary indicator of subjective quality of life and reminds us that throughout history practitioners of every healing art have prescribed hope. And yet researchers and clinicians continue to struggle with defining and measuring hope and thus in reliably ameliorating it and understanding its relationship with well-being (Haase, Britt, Coward, Leidy & Penn, 1992). Clinicians in particular, long invested in the development of hope, have a paucity of information on which to base interventions to enhance this virtue (Lopez et al., 2004).
Hope has been thought of, on one hand, as akin to a sense of mas-tery over one’s goal related endeavours (Snyder, 2002); high hope indi-viduals believe the wished-for future will come about because they are confident that they can take the necessary steps to ensure it. Or con-trastingly, hope has been seen in terms of an integrating and creative energy based on a belief in, and a feeling of interconnectedness with, a power greater than self (Haase et al., 1992; Lynch, 1965; Marcel, 1962; Pruyser, 1986); high hope individuals believe in a positive future because there are greater external forces at work which we may not fully understand.
Snyder (2002) proposes that hope is a major contributor to well-being. Snyder et al. (2002) conceptualize hope as a person’s ability to perceive the pathways to desired goals and their sense of agency or effectiveness in being able to achieve those goals. Snyder and col-leagues have developed a measure of hope based on these ideas (Sny-der et al., 1991). In contrast there are large numbers of measures and studies which demonstrate that spirituality is of central importance to quality of life and well-being (Sawatzky, Ratner & Chiu, 2005; Gall et al., 2005; Goldstein, 2007). Gall et al. (2005) refer to an explosion of interest in this area. Indeed it seems impossible to overlook the importance of spiritual beliefs in a comprehensive understanding of well-being. In a large meta-analysis, Sawatzky, Ratner & Chiu (2005) confirmed that a random effects model of the bivariate correlation
goal focused hope, spiritual hope, and well-being 163
between spirituality and quality of life resulted in a moderate effect size (r = 0.34, 95% CI: 0.28–0.40). While numerous clinical protocols urge staff to care for a person’s spiritual needs, there is a lack of clar-ity about both how to achieve this and whether this links to any clear benefit in terms of outcomes (Stefanek, McDonald & Hess, 2005; Gall et al., 2005; Herbert, Weinstein, Martire & Schulz, 2006).
Scioli and his colleagues (Scioli, 2007; Scioli & Biller, 2009) have argued that Snyder’s goal focused approach to hope presents too nar-row a conceptualization of this complex virtue. He and his colleagues have proposed a broader model of hope drawn from psychology, theology, philosophy, and medicine which encompasses attachment, mastery, survival, and spirituality domains. Scioli et al. (in press) have developed a Comprehensive Hope Scale (CHS), encompassing these four domains of hope. Scores on this scale have been associated with self-reports of greater physical well-being among thyroid cancer sur-vivors. In addition, among HIV positive individuals, higher trait hope scores were predictive of higher CD4 (immune cell) levels, taken at 8 and 24 months later. In the development of the comprehensive mea-sure of hope, Scioli et al. (in press) found that those high in spiri-tual hope are more likely to feel empowered by a spiritual force or presence in order to achieve their life goals. Research of this kind may prove to be particularly useful to clinicians wishing to consider assessment protocols and interventions aimed at hope and well-being enhancement.
Well-being has been defined as a “person’s cognitive and affective evaluations of his or her life” (Diener et al., 2002; p. 63). Well-being can be evaluated by rating subjective life satisfaction, the presence of positive and the absence of negative emotions. The current study operationalizes subjective well-being in this way. Ryff (1989) however, has suggested that this approach may neglect other dimensions of well-being which are more enduring life challenges such as autonomy, purpose in life, and personal growth. Specifically, Ryff appeared to dis-tinguish happiness, or short-term affective well-being, from realizing one’s true potential over the longer term.
The aim of the present study was to examine simultaneously two different conceptualizations of hope and their relationships to well-being indicators. Using regression analysis, we also tested the relative contributions of goal focused hope and spiritual hope in predicting well-being.
164 jen unwin and joanne m. dickson
Method
The study consisted of an online self-report questionnaire investigation at a large university in the UK. Two hundred and forty eight individu-als endorsed the consent form after accessing the survey information. Two hundred and seven (80.2%) individuals went on to complete the survey. The total sample (N = 207) comprised 166 female participants (80.2%) and 41 male participants. One hundred and thirty six partici-pants were university staff members (65.7%) and 71 participants were university students. Mean age of participants was 36 years, with ages ranging from 22 to 64.
Measures
Hope Scale (Synder et al., 1991). This trait measure was designed to assess goal focused hope. The measure comprises 12–items, which includes four filler items. Items (e.g. “there are lots of ways around any problem”) are rated on 8–point scales ranging from 1 (definitely false) to 8 (definitely true). Possible scores range from 8 to 64. Snyder et al. (1991) have reported a mean normative sample score of 51.28 for a university college sample. The scale has shown high internal reliabil-ity and test-retest reliability (.84 and .85), and good convergent and discriminant validity with concepts such as optimism and hopeless-ness (Snyder et al., 1991). The Hope Scale has two sub-scales: “agency” (the sense of having the motivation to pursue goals) and “pathways” (seeing the steps that might lead to a goal). Good reliability was also shown in the present study (α = .87).
Spiritual Hope questionnaire (Scioli et al. In press). This measure is a subscale of Scioli’s Comprehensive Hope Scale (trait) (CHS-T; Scioli et al., in press). The full version of the CHS-T comprises four hope subscales (Mastery, Attachment, Survival, Spirituality). Because of our study aim, we used the Spirituality subscale to assess spiritual hope, which Scioli et al. (in press) define as feeling empowered by a spiritual force or presence in order to achieve life goals. The Spirituality ques-tionnaire comprises 28-items (e.g., “my spiritual beliefs have empow-ered me to succeed in life,” “I believe in a benevolent (kind) higher power”). Items are rated on 4-point scales ranging from 0 (not me) to 3 (exactly like me). Some items are reversed scored. Possible scores range from 0 to 84. The Spirituality subscale has seven clusters made up of four items each: spiritual empowerment, spiritual openness, mystical
goal focused hope, spiritual hope, and well-being 165
experience, benign universe, spiritual terror management, symbolic immortality, and spiritual integrity. Scioli et al. (in press) report that each of the CHS-T subscales has been validated against established measures, and each subscale has shown good internal consistency, including Spirituality (α = .94). The present study also demonstrated good alpha reliability for this subscale (α = .96).
Satisfaction with Life Scale (SWLS; Pavot & Diener, 1993). This widely used measure was designed to assess individuals’ subjective satisfaction with life. The SWLS measure consists of five items (e.g., “If I could live my life over, I would change almost nothing”). Items are rated on scales ranging from 1 (strongly disagree) to 7 (strongly agree), with possible scores ranging from 5 to 35. Previous research has demonstrated good reliability (α = . 87) and test-retest correlation (r = .82) (e.g., Diener, Emmons, Larsen & Griffin, 1985). The SWL also showed good reliability in the present study (α = .86).
Positive and Negative Affect Scale (PANAS; Watson, Clark & Tel-legen, 1988). The PANAS was used to assess trait affect. The PANAS consists of two scales, comprising 10 positive affect (PA) items (e.g., “interested”) and 10 negative affect (NA) items (e.g., “upset”). Items are rated on 5-point scales ranging from 1 (very slightly or not at all) to 5 (extremely), with possible scores ranging from 10 to 50 for PA and NA, respectively. Crawford and Henry (2004) report a mean score of 31.31 for positive affect in a large normative general population sam-ple. The PANAS has shown good reliability (e.g., Crawford & Henry, 2004). Alpha reliabilities in the present study were .88 for PA and for NA.
We also calculated a composite score for well-being based on the SWL and affect measures. Consistent with past research, well-being scores were calculated by adding SWL and PA and subtracting NA (Deiner et al., 2002). This well-being measure also showed acceptable reliability (α = .75).
Procedure
After obtaining institutional approval, the study was made available via a web-link in an announcement to university staff and students. The link led potential participants to information about the study and a consent page. The questionnaires were preceded by brief demographic questions (gender, age, status). The questionnaires took approximately 10 minutes to complete.
166 jen unwin and joanne m. dickson
Information was given at the end of the survey regarding how par-ticipants could contact student and staff support services in the event of wanting to discuss any issues raised by participation in the study. Anonymous data from the questionnaires were downloaded from the website and entered into an SPSS 17 database for analysis.
Results
Preliminary analyses
Three participant scores were identified as univariate outliers (zs > 3.29) on each of the PA, SWL, and Hope variables, and one par-ticipant’s score was an extreme outlier on the composite well-being variable (z > 3.29). These scores were adjusted so that they were less extreme (cf. Tabachnik & Fidell, 2001).
Descriptive statistics
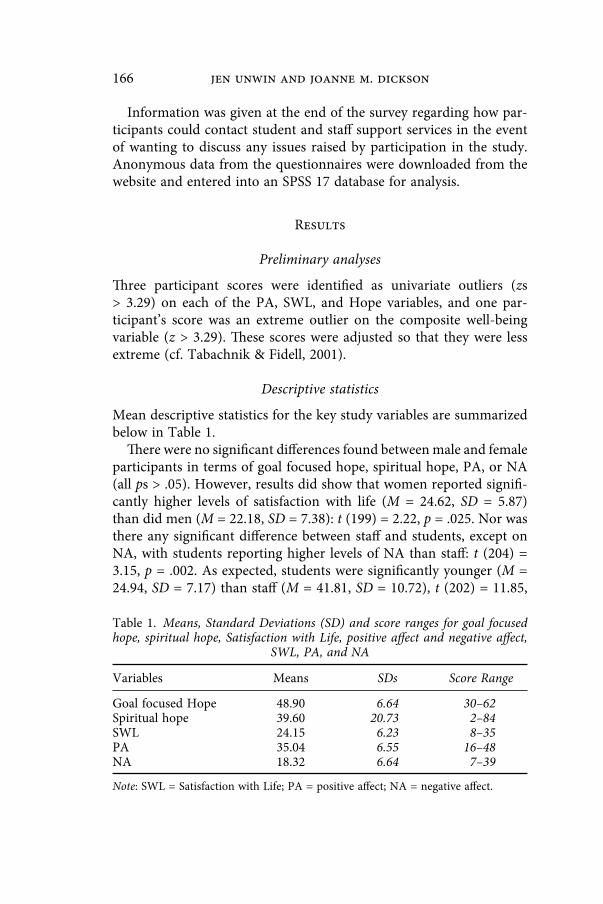
Mean descriptive statistics for the key study variables are summarized below in Table 1.
There were no significant differences found between male and female participants in terms of goal focused hope, spiritual hope, PA, or NA (all ps > .05). However, results did show that women reported signifi-cantly higher levels of satisfaction with life (M = 24.62, SD = 5.87) than did men (M = 22.18, SD = 7.38): t (199) = 2.22, p = .025. Nor was there any significant difference between staff and students, except on NA, with students reporting higher levels of NA than staff: t (204) = 3.15, p = .002. As expected, students were significantly younger (M = 24.94, SD = 7.17) than staff (M = 41.81, SD = 10.72), t (202) = 11.85,
Table 1. Means, Standard Deviations (SD) and score ranges for goal focused hope, spiritual hope, Satisfaction with Life, positive affect and negative affect,
SWL, PA, and NA
Variables Means SDs Score Range
Goal focused Hope 48.90 6.64 30–62Spiritual hope 39.60 20.73 2–84SWL 24.15 6.23 8–35PA 35.04 6.55 16–48NA 18.32 6.64 7–39
Note: SWL = Satisfaction with Life; PA = positive affect; NA = negative affect.
goal focused hope, spiritual hope, and well-being 167
p < .001. Finally, except for a negative correlation between age and NA (r (204) = –.28, p < .01), there were no other significant correlations between age and the variables for hope, PA, SWL.
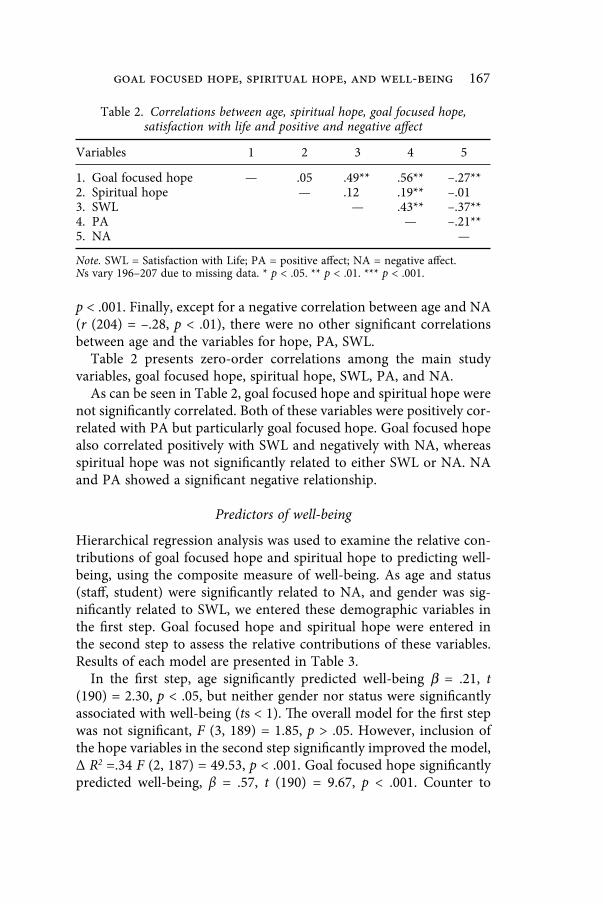
Table 2 presents zero-order correlations among the main study variables, goal focused hope, spiritual hope, SWL, PA, and NA.
As can be seen in Table 2, goal focused hope and spiritual hope were not significantly correlated. Both of these variables were positively cor-related with PA but particularly goal focused hope. Goal focused hope also correlated positively with SWL and negatively with NA, whereas spiritual hope was not significantly related to either SWL or NA. NA and PA showed a significant negative relationship.
Predictors of well-being
Hierarchical regression analysis was used to examine the relative con-tributions of goal focused hope and spiritual hope to predicting well-being, using the composite measure of well-being. As age and status (staff, student) were significantly related to NA, and gender was sig-nificantly related to SWL, we entered these demographic variables in the first step. Goal focused hope and spiritual hope were entered in the second step to assess the relative contributions of these variables. Results of each model are presented in Table 3.
In the first step, age significantly predicted well-being β = .21, t (190) = 2.30, p < .05, but neither gender nor status were significantly associated with well-being (ts < 1). The overall model for the first step was not significant, F (3, 189) = 1.85, p > .05. However, inclusion of the hope variables in the second step significantly improved the model, Δ R2 =.34 F (2, 187) = 49.53, p < .001. Goal focused hope significantly predicted well-being, β = .57, t (190) = 9.67, p < .001. Counter to
Table 2. Correlations between age, spiritual hope, goal focused hope, satisfaction with life and positive and negative affect
Variables 1 2 3 4 5
1. Goal focused hope — .05 .49** .56** –.27**2. Spiritual hope — .12 .19** –.013. SWL — .43** –.37**4. PA — –.21**5. NA —
Note. SWL = Satisfaction with Life; PA = positive affect; NA = negative affect.Ns vary 196–207 due to missing data. * p < .05. ** p < .01. *** p < .001.
168 jen unwin and joanne m. dickson
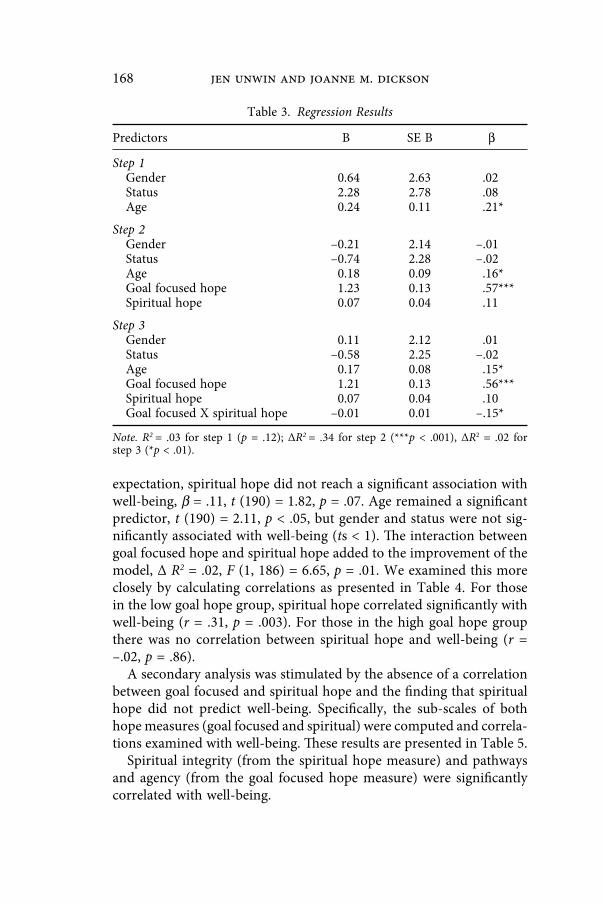
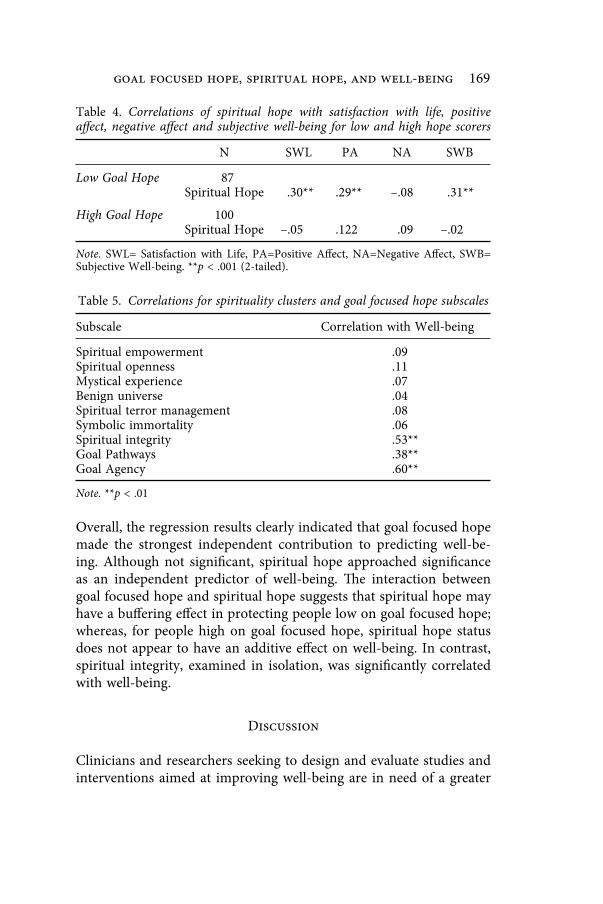
expectation, spiritual hope did not reach a significant association with well-being, β = .11, t (190) = 1.82, p = .07. Age remained a significant predictor, t (190) = 2.11, p < .05, but gender and status were not sig-nificantly associated with well-being (ts < 1). The interaction between goal focused hope and spiritual hope added to the improvement of the model, Δ R2 = .02, F (1, 186) = 6.65, p = .01. We examined this more closely by calculating correlations as presented in Table 4. For those in the low goal hope group, spiritual hope correlated significantly with well-being (r = .31, p = .003). For those in the high goal hope group there was no correlation between spiritual hope and well-being (r = –.02, p = .86).
A secondary analysis was stimulated by the absence of a correlation between goal focused and spiritual hope and the finding that spiritual hope did not predict well-being. Specifically, the sub-scales of both hope measures (goal focused and spiritual) were computed and correla-tions examined with well-being. These results are presented in Table 5.
Spiritual integrity (from the spiritual hope measure) and pathways and agency (from the goal focused hope measure) were significantly correlated with well-being.
Table 3. Regression Results
Predictors B SE B β
Step 1Gender 0.64 2.63 .02Status 2.28 2.78 .08Age 0.24 0.11 .21*
Step 2Gender –0.21 2.14 –.01Status –0.74 2.28 –.02Age 0.18 0.09 .16*Goal focused hope 1.23 0.13 .57***Spiritual hope 0.07 0.04 .11
Step 3Gender 0.11 2.12 .01Status –0.58 2.25 –.02Age 0.17 0.08 .15*Goal focused hope 1.21 0.13 .56***Spiritual hope 0.07 0.04 .10Goal focused X spiritual hope –0.01 0.01 –.15*
Note. R2 = .03 for step 1 (p = .12); ΔR2 = .34 for step 2 (***p < .001), ΔR2 = .02 for step 3 (*p < .01).
goal focused hope, spiritual hope, and well-being 169
Overall, the regression results clearly indicated that goal focused hope made the strongest independent contribution to predicting well-be-ing. Although not significant, spiritual hope approached significance as an independent predictor of well-being. The interaction between goal focused hope and spiritual hope suggests that spiritual hope may have a buffering effect in protecting people low on goal focused hope; whereas, for people high on goal focused hope, spiritual hope status does not appear to have an additive effect on well-being. In contrast, spiritual integrity, examined in isolation, was significantly correlated with well-being.
Discussion
Clinicians and researchers seeking to design and evaluate studies and interventions aimed at improving well-being are in need of a greater
Table 4. Correlations of spiritual hope with satisfaction with life, positive affect, negative affect and subjective well-being for low and high hope scorers
N SWL PA NA SWB
Low Goal Hope 87Spiritual Hope .30** .29** –.08 .31**
High Goal Hope 100Spiritual Hope –.05 .122 .09 –.02
Note. SWL= Satisfaction with Life, PA=Positive Affect, NA=Negative Affect, SWB= Subjective Well-being. **p < .001 (2-tailed).
Table 5. Correlations for spirituality clusters and goal focused hope subscales
Subscale Correlation with Well-being
Spiritual empowerment .09Spiritual openness .11Mystical experience .07Benign universe .04Spiritual terror management .08Symbolic immortality .06Spiritual integrity .53**Goal Pathways .38**Goal Agency .60**
Note. **p < .01

170 jen unwin and joanne m. dickson
understanding of the factors underpinning this important variable. These factors need to be measurable and have clinical utility. The cur-rent study sought to examine two contrasting methods of conceptual-izing and measuring hope in terms of their relationship to each other and their relative contributions to well-being indicators.
Correlations
These two forms of hope were found not to be correlated with each other indicating that two distinct and independent constructs exist. Goal focused hope was found to be significantly correlated with sat-isfaction with life and positive affect, confirming findings from previ-ous research. Spiritual hope was found to be significantly correlated with positive affect, as would be predicted from previous research, but not satisfaction with life. The lack of a relationship between spiritual hope and satisfaction with life is somewhat puzzling but does reflect previous research that has found negative results in this area (Herbert et al., 2006).
Regression
When both forms of hope were entered into a multiple regression analysis alongside age, gender, and status, some interesting differences emerged. Goal focused hope explained significant variance in subjec-tive well-being whereas spiritual hope did not. In addition however, the interaction effect of the two forms of hope made a significant con-tribution to the model and seems to suggest that when goal focused hope scores are low, then spiritual hope scores may have a buffering or protective effect on well-being. This finding makes intuitive sense. Age remains a significant factor in the model of well-being, and this is in line with previous findings in this area (Janson & Mueller, 1983).
When the subscales of the spiritual hope measure were examined individually, it was the spiritual integrity cluster that was significantly correlated with well-being. The items in this cluster are “I have a pur-pose in life,” “My life has meaning,” “I have made (or will make) a difference in this world,” and “I have a reason to live,” lending support to Ryff ’s (1989) claims that purpose in life is essential to well-being.
Implications
Further studies are need with both the general population and clinical samples to more fully understand the relationships between various

goal focused hope, spiritual hope, and well-being 171
aspects of hope and a person’s subjective well-being. As this was a university sample, it may be that the buffering effects of spiritual hope seen here may be amplified in patient groups, particularly those facing adverse circumstances such as illness and disability. In addition, long term studies of hope and well-being will help us to understand the buffering effects of goal focused and spiritual hope against adversity over time. In this regard, there is growing interest in the area of mean-ing making and meaning focused coping (Folkman, 2008). It is likely that both goal focused hope and spiritual hope are related to meaning making and meaning focused coping in adverse circumstances and that these efforts are linked to well-being. In illness and disability, which are potentially challenging for those who are very highly goal focused or by nature very low on this variable, it may be that spiritual hope plays a protective role in terms of well-being. Moreover, it may be that the effects of spirituality on affect are mediated by a sense of life having meaning. Similarly those with a sense of meaning in life are likely to have congruent goals which they aspire to achieve, which may or may not be spiritually derived. Highly goal focused individuals who lack a coherent sense of meaning in life may, regardless of their spiritual orientation, have less satisfaction in life and find experiences such as illness more challenging. Similarly, individuals may be highly spiritual yet still lack a coherent sense of meaning for their own lives. Such links between meaning, goal directed activity, and well-being have already been posited (Lightsey, 2006). Such links may help us to understand the positive effects of seemingly different therapeutic and religious experiences. Those with secular belief systems should not be regarded as inherently disadvantaged from a well-being point of view. Spiritual hope did contribute significantly to the prediction of positive affect in this study. The role of positive emotions in coping is an area of increasing interest (Folkman, 2008), and further exploration of the contribution of spiritual hope is clearly warranted. These relationships warrant further exploration perhaps with large samples which would allow for structural equation modelling and path analyses.
Goal focused hope is easy to understand and measure. The Hope Scale can easily be introduced into busy clinical settings as a screening tool (Unwin, Kacperek, & Clarke, 2009). The same can also be said of Scioli’s measure of spiritual hope. The CHS is fairly long, but further study of the utility of the separate sub-scales and clusters in clinical situations would be useful. It has also been possible to demonstrate that interven-tions are successful in increasing goal focused hope (Linley & Joseph, 2004). Encouraging individuals to identify and move towards personally

172 jen unwin and joanne m. dickson
valued goals is the ultimate client centered therapy and is at the heart of approaches such as solution focused therapy and acceptance and commitment therapy for which there is growing evidence of effective-ness (Kim, 2008; Hayes et al., 2006).
There have been some early attempts to increase spirituality (Gold-stein, 2007), but the mechanisms of action and effectiveness require further study. It may be that the increased mindfulness related to paying attention to sacred moments and reduced engagement with negative thinking allows individuals relatively more mental energy to reflect on the meaning of their lives, to plan and engage in valued goals (Brown and Ryan, 2004).
Methodological issues
The current study, although adequately powered, certainly has a range of limitations. The study participants were self selected volunteers in an online study in a university setting and as such cannot be regarded as representative of the general population and no doubt differ sig-nificantly on the study variables as compared to a clinical population. More females than males took part in the study and this will also bias the results. Further studies simultaneously studying goal focused and spiritual hope will serve to build on this research.
Conclusion
This study sought to understand the relationship of goal focused and spiritual hope to each other and to subjective well-being. The results show that goal focused and spiritual hope are independent concepts and that goal focused hope is of importance in the prediction of well-being. Results also indicate that spiritual hope has a buffering effect on well-being when goal focused hope is low and that experiencing one’s life as meaningful is important.
References
Brown, K. & Ryan, R. (2004). Fostering health self-regulation from within and with-out: A self-determination theory perspective. In Linley, P. & Joseph, S. (Eds.) Posi-tive psychology in practice (pp. 105–124). Hoboken, NJ: Wiley.
Crawford, J. & Henry, D. (2004). The positive and negative affect schedule (PANAS): Construct validity, measurement properties and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 43, 245–265.
goal focused hope, spiritual hope, and well-being 173
Diener, E., Emmons, R. A., Larsen, R., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49, 71–75.
Diener, E., Lucas, R., & Oishi, S. (2002). Subjective well-being: The science of happi-ness and life satisfaction. In Snyder, C. & Lopez, S. (Eds.) The handbook of positive psychology (pp. 63–73). Oxford: Oxford University Press.
Folkman, S. (2008). The case for positive emotions in the stress process. Anxiety, Stress and Coping, 21(1), 3–14.
Gall, T., Charbonneau, C., Clarke, N., Grant, K., Joseph, A. & Shouldice, L. (2005). Understanding the nature and role of spirituality in relation to coping and health: A conceptual framework. Canadian Psychology, 46(2), 88–104.
Goldstein, E. (2007). Sacred moments: Implications on well-being and stress. Journal of Clinical Psychology, 63, 1001–1019.
Hayes, S., Luoma, J., Bond, F., Masuda, A., & Lillis, J. (2006). Acceptance and commit-ment therapy: Model, processes, and outcomes. Behaviour Research and Therapy, 44(1), 1–25.
Haase, J., Britt, T., Coward, D. D., Leidy, N. & Penn, P. (1992). Simultaneous concept analysis of spiritual perspective, hope, acceptance and self-transcendence. Journal of Nursing Scholarship, 24(2), 141–147.
Herbert, R., Weinstein, E., Martire, L. & Schulz, R. (2006). Religion, spirituality and the well-being of informal caregivers: A review, critique, and research prospectus. Aging and Mental Health, 10(5), 497–520.
Janson, P. & Mueller, K. (1983). Age, ethnicity & well-being. Research on Aging, 53, 353–367.
Kim, J. (2008). Examining the effectiveness of solution-focused brief therapy: A meta-analysis. Research on Social Work Practice, 18(2), 107–116.
Keyes, C. & Magyar-Moe, J. (2003). The measurement and utility of adult subjective well-being. In Lopez, S. & Snyder, C. (2003). Positive psychological assessment (pp. 411–425). Washington, DC: American Psychological Association.
Lightsey, O. (2006). Resilience, meaning and well-being. The Counseling Psychologist, 34(1), 96–107.
Linley, P. & Joseph, S. (2004). Applied positive psychology: A new perspective for clinical practice. In Linley, P & Joseph, S. (Eds.) Positive psychology in practice (pp. 3–12). Hoboken, NJ: Wiley.
Lopez, S., Snyder, C., Magyar-Moe, J., Edwards, L., Pedrotti, J., Janowski, K., et al. (2004). Strategies for accentuating hope. In Linley, P & Joseph, S. (Eds.) Positive psychology in practice (pp. 388–404). Hoboken, NJ: Wiley.
Lynch, W. F. (1965). Images of hope: Imagination as healer of the hopeless. Baltimore: Helicon Press.
Marcel, G. (1962). Homo viator: Introduction to a metaphysic of hope. New York: Harper and Row.
Naidoo, P. (2006). Potential contributions to disability theorizing and research from positive psychology. Disability and Rehabilitation, 28(9), 595–602.
Ostir, G., Markides, K., Black, S. & Goodwin, J. (2000). Emotional well-being predicts subsequent functional independence and survival. Journal of the American Geriat-rics Society, 48, 473–478.
Pavot, W. & Diener, E. (1993). Review of the satisfaction with life scale. Psychological Assessment, 5, 164–172.
Pruyser, P. W. (1986). Maintaining hope in adversity. Pastoral Psychology, 35, 120–131.Ruini, C. & Fava, G. (2004). Clinical applications of well-being therapy. In Linley, P.
& Joseph, S. (Eds.) Positive psychology in practice (pp. 371–387). Hoboken, NJ: Wiley.
Ryff, C. (1989). Happiness is everything, or is it? Explorations on the meaning of psy-chological well-being. Journal of Personality and Social Psychology, 57, 1069–1081.

174 jen unwin and joanne m. dickson
Sawatzky, R., Ratner, P. & Chiu, L. (2005). A meta-analysis of the relationship between spirituality and quality of life. Social Indicators Research, 72, 153–188.
Scioli, A. (2007). Hope and spirituality in the age of anxiety. In R.J. Estes (Ed.), Advancing quality of life in a turbulent world (pp. 135–150). New York: Springer.
Scioli, A., Ricci, M., Nyugen, T. Biller, H. B. & Scioli, E. R. (in press). Hope: Its nature and measurement. Psychology of Religion and Spirituality.
Scioli, A. & Biller, H. B. (2009). Hope in the age of anxiety. New York: Oxford Uni-versity Press.
Sheldon, K. & Lyubomirsky, S. (2004). Achieving sustainable new happiness: pros-pects, practices and prescriptions. In Linley, P. & Joseph, S. (Eds.) Positive Psychol-ogy in Practice (pp. 127–145). Hoboken, NJ: Wiley.
Snyder, C. R., Harris, C., Anderson, J. R., Holleran, S. A., Irving, L. M., Sigman, S. T. et al. (1991). The will and the ways: Development and validation of an individual-differences measure of hope. Journal of Personality and Social Psychology, 60, 4, 570–585.
Snyder, C. R. (2002). Hope theory: Rainbows in the mind. Psychological Inquiry, 13(4), 249–275.
Snyder, C., Rand, K. & Sigmon, D. (2002). Hope theory: A member of the positive psychology family. In Snyder, C. & Lopez, S. (Eds.) Handbook of positive psychology (pp. 257–276). Oxford: Oxford University Press.
Stefanek, M., McDonald, P. & Hess, S. (2005). Religion, spirituality and cancer: Cur-rent status and methodological challenges. Psycho-oncology, 14, 450– 463.
Stotland, E. (1969). The psychology of hope. San Francisco: Jossey-Bass.Tabachnick, B. G., & Fidell, L. S. (2001). Using multivariate statistics. Pearson US:
Pearson Education, Inc.Unwin, J., Kacperek, L. & Clarke, C. (2009). Adjustment to lower limb amputation.
Clinical Rehabilitation, 23, 1044–1050.Watson, D., Clark, L. & Tellegen, A. (1988). Development and validation of brief
measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070.