
return to - po - World Bank Documents & Reports
119
RETURN TO RESTRICTED PO|RS DESK FILE COPY Report No. WH-200a WITHIN 1N E WEEK This report was prepared for use within the Bank and its affiliated organizations. They do not accept responsibility for its accuracy or completeness. The report may not be published nor may it be quoted as representing their views. INTERNATIONAL BANK FOR RECONSTRUCTION AND DEVELOPMENT INTERNATIONAL DEVELOPMENT ASSOCIATION ECONOMIC GROWTH OF COLOMBIA: PROBLEMS AND PROSPECTS (in XII Volumes) VOLUME XI PUBLIC HEALTH November 1, 1970 South America Department Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of return to - po - World Bank Documents & Reports
RETURN TO RESTRICTED
PO|RS DESK FILE COPY Report No. WH-200a
WITHIN1N E WEEK
This report was prepared for use within the Bank and its affiliated organizations.They do not accept responsibility for its accuracy or completeness. The report maynot be published nor may it be quoted as representing their views.
INTERNATIONAL BANK FOR RECONSTRUCTION AND DEVELOPMENT
INTERNATIONAL DEVELOPMENT ASSOCIATION
ECONOMIC GROWTH OF COLOMBIA:
PROBLEMS AND PROSPECTS
(in XII Volumes)
VOLUME XI
PUBLIC HEALTH
November 1, 1970
South America Department
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
CURRENCY EQUIVALENTS
(Certificate Market Selling Rate of Exchange)
End 1968
1 US$ = 16.91 Pesos
1 Peso US$0.05913
End 1969
1 US$ = 17.90 Pesos
1 Peso US$o.o5586
End-March 1970
1 US$ = 18.20 Pesos
1 Peso = us$0.05494
End-June 1970
1 US$ = 18.h8 Pesos
1 Peso US$0.05411
End-September 1970
1 US$ = 18.80 Pesos
1 Peso = US$0.05319
TABLE OF COPJ TEi'CTS
Page No.
SUiM4ARY AND WNCLUSIONS
1. HEALTH AND M*EDICAL CAW4, AS Cktl'1ICAL ASPECTS OFECONOMIC AND SOCIAL DEVELOPAENT 1T4 CO4LOMBIA . . . . . 1 . .
A. Definitions and Orientations . . . . . . . . . . . . . 1
B. The Health Care System . . . . . . . . . . . . . . . . 4
1. Governmental Programs . . . . . . . . . . . . . . . 42. hne Private Sector . . . . . . . . . . . . . . . . 5
C. Sources of Funds arid Major Outlays for Healthand Medical Care . . . . . . . . . . . . . . . . . . . o
II. AS'SESSI1ENT OF THE PRESENT HEALLTH SITUATION . . . . . . . . 13
A. Significant Demographic Variables Associatedwith Health and Medical Care in Colombia . . . . . . . 13
1. Population Characteristics . . . . . . . . . . . . 132. Socio-Economic Characteristics . . . . . . . . . . 19
B. Morbidity Indices and 'Their Socio-EconomicRelationships . . . . . . . . . . . . . . . . . . 25
1. Illness and Restricted Activity . . . . . . . . . . 252. Utilization of Health Services . . . . . . . . . . 263. Socio-Economic Correlates of Morbidity and
the Utilization of Health Care Resources . . . . . 23
C. Major Categories of Health Problemus in Colombia . . . . 31
1. Di.arrheal Diseases and Blelated. Conditions . . . . . 312. 'The Common Acute In.f.ectious Diseases (of childhood) 313. Malnutrition . . . . . . . . . . . . . . . . . . . 324. Tuberculosis and Other Chronic Infectious iLiseases 325. High ithrtility aid Abortions . . . . . . . . . . . 356. Accidernts . . . . . . . . . . . . . . . . . . . . . 377. Dental D)isease . . . . . . . . . . . . . . . . . . l4od. Mental IlUless . . . . . . . . . . . . . . . . . . 40
D. lnstitutional Resources for Health . . . . . . . . . . 41
E. Health Personnel-Supply and Dis tribution . . . . . . . 45
1. Physicians . . . . . . . . . . . . . . . . . . . . 452. DenLLtists . . . . . . . . . . . . . . . . . . . . . 473. Professional Nurses . . . . . . . . . . . . . . . . 4714. Auxiliary Nurses . . . . . . . . . . . . . . . . . 45. Other Healti Manpower . . . . . . . . . . . . . . ..149
Page No.
F. Education and Training for the Health Occupations . . .49
1. Medical Biucation . . . . . . . . . . . . . . . . . 492. Nursing Education ................ . 513. Auxiliary Nurse Education . . . . . . . . . . . . . 514. Dental and Other Health Professions and
Occupations Education . . . . . . . . . . . . . . . 52
III. THE NATIONAL TEN YEAR HEALTH PLAN FOR COLOMBIA (1968-1977) 53
A. Origins and Evolution of the Plan . . . . . . . . . . . 53
B. Major Elements of the Plan . . . . . . . . . . . . . . 55
C. The Ten-Year Health Plan - Analysis and Comments . . . 56
1. National Support for the Plan . .. . . . . . . . .572. Support Within the Health Sector . . . . . . . . . 583. Financing of the Health Plan . . . . . . . . . . . 594. Manpower Requirements . . . . . . . . . . . . . . . 625. Suggested Areas for Further Development of the
Ten Year Health Plan ............... . 64
IV. RECOMMENDED PROJECT PROPOSALS . . . . . . . . . . . . . . . 71
A. Health Project Proposal Colombia - I . . . . . . . . . 72
B. Health Project Proposal Colombia - II . . . . . . . . . 73
C. Health Project Proposal Colombia - III . . . . . . . .7
D. Health Project Proposal Colombia - IV . . . . . . . . . 75
E. Health Project Proposal Colombia - V . . . . . . . . . 76
V. INVENTORY OF DEVELOPMENT STUDIES IN PROGRESS . . . . . . . 77,
A. Human Resources for Health - Phase II . . . . . . . . . 77
B. Experimental Study of Health Services in Colombia -Phase II . . . . . . . . . . . . . . . . . . . . . . . 78
C. Development of a Comprehensive Health PlanningSystem at the Local Level - Phase I . . . . . . . . . . 78
D. Integrated Nutrition Program of AppliedNutrition - Phase II . . . . . . . . . . . . . . . . . 79
E. Family Planning Programs in Colombia . . . . . . . . . 80
F. Nutrition and Development - Phase II . . . . . . . . . 81
Page No.
VI. RECOMMENDED PREINVESTMENT PROGRAM PROPOSALS . . . . . . . 83
VII. EXTERNAL ASSISTANCE IN THE COLOMBIAN HEALTH SECTOR . . . 84
VIII. BIBLIOGRAPHY AND REFERENCES . . . . . . . . . . . . . . . 85-
ANNEX 1 - -to Chapter VI.
APPENDIX A - to Chapter VII.

STJIfrD1A rr AND CONCLITJSIQNcl
1. This is the first time, in recent years, that the World Bankhas incluided a total survey of the health sector of a country as part ofa gene:ral appraisal of development problems, policies and prospects. Theinformation assembled in this general appraisal is to be utilized as thebasis for fur-ther discussion by the Bank, other international instituitions,goverrnmen-ets and inter-governmental agencies with the country concerned(Colombia) on its development policies and plans including those affectingthe health sector. Among the major objectives set for the survey andapplied in this report on the health sector are: (1) The assessment ofthe domestic and external financing requirements and of the possibilitiesthat those requirements can be met; (2) an analysis of the principal pre-invest;rnent surveys and studies required to carry out the development pro-gram; and (3) an analysis of the problems of investment and resourcemobilization within the health sector.
2. For this survey the hea-ilth sector has been Lroadly defined toincluide all planned and orginize7d publi a endeavor directed at the nationallevel toward the promotion of health, the prevention of illness and dis-abilli.ty, the care of the sick and the restoration to useful work or activit.-of all. those whose health statuis has been impaired. Part A of this renort,Chanters J-ITTT describes the (olombian health care system, assesses themna lor health problems of the country and provides a detailed analysis ofthe l'ational Ten Year Heal th Plan (.1.)A-19i77). Part FB, Chapters JV- _,cc.nsiders selected proposals and projects that could accelerate the pa-eof achievement or consolidate the sound obJectives of the Ten Year HealthPlzan. Separate reports consider the special health related problems o.fwater supply and sewage disposal ari( of housing and community development.
'S fiAs in many develc.ping oclin-tries thle health care system of Colon-i)J. is prelominantly a functioln of government. The Ministry of Health,th.( ugh at. the apex of this system, is only one of miultiple governmentalaghencies directly concerned wit.h the pro'vision of health and medicalservices. rn recent rears the 2cl.ombzia n or.i tute of 2oci.al Cccii vi ty:nri t-.h.he NLlJonal Caia',an (we:Lfare funr.l-s have ga31ined prcmi nence in the
hea-llth sector. I?ecrn t Jlegi s.].ali on has )dded tlo the oper:O iin;4l responnSi-TJi l ti ca of t.he Mr:ir s try o lIe Ith bJy an:ifJ grti.ng t.o .t .lle.rly ic f:i ned,in thri ti re for na; iJ ona,l healthh p1. nun ni a nd cl:o (li.na. t i 1n and for thec.ontinnirnv evaluation and supervision of all healt.h services at. regional--nd ic alcl levels. IJiLthin the last two ye:.rs, and For the first. t.ire,r(sl.mhi;in possesses an integrate(i network of heal Li programs and LJi. vi Li ef
wi lii hiifh potential for the e.rly dievel.orment of a comprehensive. and e.fi --i7ant heal lh ciJre systcem.
- ij -
heal t,h e, x end :i t.ires hi re r:isell t'] VEa-'P0l(d :iJ.- the rril ,period, i)1-1 , f'ro in T rvI Ii Jlion pesos a,nr .a; u J, to ? Y r"iiI I ipesos wittl a si.,eable furl'li(t,- increa.se budrge t.eX for CI ( h Il, pun i*,or goreTnrnnentally coat;ro' le ezipenldi Llres for he:eIlth fo ny r 'f i r'yconstantly at the level pI ercent are now t , ' r.ii ( in
GNP. Lip,nificant.Lly, e voen w:itr subsattarhLiai nro sin a,; ini3 i rto the TYirnistry of THeall,Ji its share oft thre ijncrea :fer- 1pu .Ihlr. exrlrendi!for health has faillen Iron 30 to 20 percent anc ie* c -i t_a e"ren ':i tu-E:sfor health services for t,ULe gener I.] poult Li o.;cr, are ric;i a t, the s:rie Level!they were 1(0 years ear:!ier, namineiy ;2 pesos per capitra. lin can O
expendliitures for hospi4t-S an( mcdi r'a care .for the f'.ive ,.-cfeo fpo'pula ti.i n covered by 11 se ri t, or the we:l.fare F'u :nds of i. ]
ini-L stries have risen hijr I ir, tle sarmF :i. tlrvnl tram i2r Lu 7"' -,; .
peI caT)ita and the a,ggr'i t, c rt .a Lhese ser-vice-s now reupreserni.over' h;lf (p53 percent ) oIL' a11 publAic expendi !,reg -f'or hP.i-L v , a.eexnen(iiLtures t'or he;a I h, thou''h s ubLiar Lia]l . 1 a nra. L re.L ii' y Uc 3d
Ca aJ ta-l invews, Lftfri ts made in t'he Tpas;l, 4'or he;al Lii th Li ,;equilpment have rint ber., si.ije.]t e:ither tLa aria.lyJs3s or p1la ever v t,h!an h-htfhere is abundant. evidenc- that .al:l evel.s of'' govermer,ent aind rnr-ny aIlbliuspiri ted in,dividuals ar-, groups !rave m.±de a? v.o Lahle si zerible fu idthese purposes. I?ecer,t.l,y , a. par 0of a new tIatria l. lHospi.1 a 1 Plan Ifn;:
with thfe recent incorra or *,f t.he NLion,i Al Tnst i tLte f'or 1'1 uni j v-,1
Development w:i thin the i.',11nistry o'' liea t,h.Lhat Minist r'v has LaVlishecran ordJerly system cf pl-mnng anzj budg,etiri for capitLal c i I'UC tior,,maderni zation and eui.,)rnerit, of health racilj Lies coverin g tiCe enti re
country. A rough arfiniryimltiun pl;rices the healtuh iinves tmente brudgelt. i n1970 at slightly un1der I() percernt, of to'al public expendi tures tr hor all, .
6. 'The health I)robleiis ari( needs of' Colombia are identil-iable witha rapidly growing population currenratly estimeated to number 21.6 mrdillj ian.The population is concentra3ted in the yonger age grours anr, increasinglyin urban centers al-t,hough almost half (ImP. percent) reside in small vi:],laggesand on farms. A high bLt nct precisely determined birth rate, coupledwith a declinring death rate - which may be associated niore wi.th a youth-ful vigorous poaulption anrd with imrroved levels of income and eduicationthan with widely availnble and successfully utilized publi.c health ser-vices -- has resul.ted in a high rate of n.atural increase in thle p07l.atlon.This high rate of population increase shows snme evidence of bavi.rlg ptoJssedlits peak yet it places heavy burdens on the current national effort toextend and irniprove heal.th ard medical. care services for all segment+s ofthe population. The impact; of this large and rapid.:Ly growing popnnlationis also bei.ng severe:ly felt in other areas of econcmic and social develo'-ment -- in the need for schoo-ls and teachers, in emplo,vrent opportulni.tiesin housing and coTmmuity development, in the per capita share of the grossdomestic product and in many others.
- iii -
7. The socio-econoric profile of the population is also charac-teristic of a developing society with a low median family income (1965)of 4348 pesos (U19$ 290) rising to 6645 pesos (US$ 443) in urban areasand falling to 2872 pesos (US$ 191) in rural households. The per capitashare of the gross domestic product is estimated (1967) at US!, 282 havingrisen from USI 246 ten years earlier. Occupational pursuits are heavilyweighted by unskilled employment. Educational levels are low with only13 percent of Colombians over the age of 15 having had some secondaryschooling and less than 2 percent with some university or professionaltraining. Thirty-five percent of rural dwellers have had no schoolingand only 3 percent have advanced to secondary school levels.
B. Rates for all illness, restricted activity and confinement tobed due to illness are high and are inversely correlated with low levelsof education, income and occupation. The same observations hold for theutilization of health care services, attendance by a physician or visitsto a hospital. Rural dwellers fare far less well than their urban counter-parts whether it be in relation to risk of illness or to the utilizationof health care services.
9. The major categorical disease problems of Colombia are, again,typical of a developing society. The foremost, diarrheal disease andrelated conditions, including intestinal parasitism, are clearly associatedwith low levels of environmental sanitation. Others include the acutecommunicable diseases (of childhood), malnutrition -- much of which isoccult rather than overt - tuberculosis, venereal disease, induced abor-tions, accidents, dental disease and mental illness. Many, if not allof these conditions are amenable to modern preventive measures and yetuntil very recently all but a fractional share of national health efforthas been consumed in attempting to cope with the huge burden of morbiditythese problems create. Other significant public health problems charac-teristic of Colombia's geographic and climatic circumstances -- malaria,yellow fever, yaws and leprosy -- are in sight of successful attack yetmajor efforts and continued vigilance are required to bring them undertotal control or possible eradication.
10. Sizeable investments have been made in the past in the build-ing equipment and operation of hospitals, health centers and health poststhroughout the country. These dispersed institutions have, until recently,been independently operated, usually inefficiently and without supervisionor regulation based on nationally agreed upon norms and standards. Anational hospital plan is now in operation with the objective of weavingtogether a nationally directed and supervised system of health institutionsand facilities. This plan, calling for modernization, regionalization andadequate staffing of the health care system gives promise of providingcomprehensive health services available to all segments of the Colombianpopulation.
- iv -
11. Shortages of all categories of essential health personnel andthe maldistribution of the limited health manpower supply comprise themost difficult and demanding problems currently being faced by the coun-try's health leaders. These shortages and maldistributions are severefor the higher professional categories -- physicians, dentists, profes-sional nurses, sanitary engineers, nutritionists, health educators,statisticians, hospital administrators and other supervisory levelpersonnel. A major problem also exists, due to the larger numbers re-quired, at middle levels -- auxiliary nurses, technicians of all types,medical and dental assistants, sanitarians, statistical assistants andhigher level clerical workers. Lower level supporting personnel arealso in short supply with insecurity of jobs and rapid turnover in em-ployment conspicuous problems.
12. These manpower problems require reorientation and augmentationof education and training at all levels and particularly for middle levelpersonnel. This will be feasible provided other educational institutions,in addition to the university medical schools, are fully mobilized for thispurpose. Special attention should be given to the need for close integra-tion of all training programs and the development of a national plan forthe training of all categories of required health manpower. Stabilizationof the available health manpower supply also requires a recasting of thesalary system, improved incentives and conditions of employment as well asthe acceleration and reinforcement of the adopted policy of delegation oftasks to trained middle and lower level personnel to be nerformed undercompetent supervision.
13. A sound Ten Year National Health Plan, 1968-1977, has beenadopted and is currently being implemented. This Plan has gained thesupport of the top levels of the national government and is backed byall significant elements within the health sector. Under the provisionsof the Plan, mechanisms have been created for the close integration ofall health activity in the country whether these be under governmentalor non-governmental auspices. Also, for the first time, national,regionaland local health programs are fully coordinated, under the direction ofthe Ministry of Health, and offer promise of the early institution of acomprehensive health and medical care system available to all segmentsof the population. For the present, the Ministry of Health retainsresponsibility for the administration of nation-wide campaigns that focuson major health problems requiring mass preventive measures, e.g., environ-mental sanitation inclucding water supplies and sewage disposal, malaria,leprosy, yaws and yellow fever eradication, nutrition and vaccinationagainst communicable disease but these programs too will ultimately bedecentralized.
1. Despite conspicuouis increases in public or governmentally con-trolled expenditures for health, current trends, sustained over the tenyear period 1961-1970, indicate that insufficient resources are beingdirected toward the improvement and extension of general health services,
-v-
the objectives of the National Health Plan. In response to a rapidlyrising demand for hospital and therapeutic care on the part of insuredworkers, a larger and larger share of expenditures is being consumedfor the benefit of this small but important element of the population.The balance of increased expenditures, at least on a per capita basis,is also being consumed by increases in the total population and thedepreciating purchasing power of the peso. To fully implement theNational Health Plan will require additional funds derived from publicsources and earmarked for general health services. A rise of 50 percentin such expenditures is desirable with emphasis on the utilization ofsuch increased expenditures for preventive measures.
15. An extension and consolidation of the social security system isunder consideration. Because such a system involves contributory mecha-nisms -- contributions by the workers, by the employer and by the govern-ment -- it has appeal to those who recognize the need for broadening thebase for the funding of essential health care services. Such an extension,however, warrants careful study of the current costs and the efficiencyof operation of the existing system and its more effective integrationwith the general health services directed by the Ministry of Health. Thereare already evidences that a two class system of health and medical careservices -- one for the employed, the other for the rest of the population --
is developing. Furthermore, preventive medicine and health promotive mea-sures should receive greater emphasis in the services available to socialsecurity and welfare fund beneficiaries.
16. A weakness in the existing mechanisms for the financing ofhealth services, now in the process of correction, has been insufficientattention to and the planning of long-term capital investments in requiredhealth care facilities and equipment. The establishment of the NationalHospital Fund and the National Institute for Municipal Development givepromise of correcting these deficiencies. External assistance in theform of long-term loans, on favorable terms, is needed to augment domesticresources.
17. Opportunities exist for further advances in the health statusof the Colombian population through the conjoint action of the Ministryof Health with other ministries of government: with the Ministry ofEducation for the education and training of health personnel and thehealth education of the public; with the Ministry of Agriculture innutrition and the adaptation of food resources to the feeding and nutri-tional needs of the population; and with the Ministries of Public Worksand Interior in housing and community development. Other examples couldbe cited including industry and agriculture in improving the health con-ditions of employment. The National Health Plan calls for more of suchendeavor and the Ministry of Health has already made significant stridesin this direction. National policy should encourage such efforts.
- vi-
18. The Government of Colombia has recognized the urgent and mountingproblems of a rapidly increasing population complicated by mass migrationsto urban centers and has launched a significant family planning program tocope with these problems. Family planning informational and medicalservices are being developed under both governmental and voluntary ausDicesto meet a genuine and increasing public demand. The limitations of theseprograms are related more to needs for trained manpower and the organiza-tions of health services than to the availability of funds for programfinancing. Social forces -- improved educational levels, increased familyincome, better housing and recreational opportunities and more ready accessto general health care -- have all been demonstrated to foster a decliningbirth rate. Improved knowledge of these forces and its translation intonational policy and social action is still required to bring the excessiverate of population increase under reasonable control.
19. At present, five significant health projects are sufficientlydeveloped in terms of plan, scope and cost to warrant careful considera-tion for external financial assistance. Each represents an area of highpriority determined by the National Health Plan. Domestic funds alreadycommitted to these projects in the annual budget of the Ministry are in-sufficient to realize their objectives as rapidly as the need dictates.These recommended projects are: (a) Development of Institutional Resourcesfor Health (Hospitals, Health Centers and Health Pcsts), (b) Control ofCommunicable Disease by Expansion and Acceleration of National Mass Vaccina-tion Programs, (c) Expansion and Completion of the National Taboratorv ofHealth, (d) Expansion and Development of the Colombian School of PublicHlealth, and (e) Fluoridation of Urban Wsater Supplies.
20. Developmental studies are currently in progress to refine andextend the National Health Plan. These studies are being funded fromboth domestic and external sources and several involve extensive collabora-tion with international assistance agencies and with scientific institu-tions in other countries. Six additional preinvestment program studiesare recommended for consideration at this time: (a) An Action Programfor Education and Training in the Health Sector, (b) Study of MedicalCare Institutions, (c) Nutrition Study - Phase III, (d) Health CareUnder the Social Security System, (e) Vital Statistics and MorbidityData - Registration and Analysis, and (f) Sample Studies of the HealthStatus and Health Resources of Colombia. More detailed outlines of theseproposed preinvestment program studies are provided.
I. HEALTH AND MEDICAL CARE AS CRITICAL ASPECTSOF ECONOMIC AND SOCIAL DEVELOPMENT IN COLOMBIA
A. Defiritions and Orientations
1. In the past, public health measures were commonly limited tothose governmental or philanthropic efforts initiated as a means ofmitigating the disruptiorn to commerce brouight about by the importationof epidemic infectious disease into a local population. The organizationof such services was invariably simple and discontinuous, and the healthpersonnel employed were usually housed in the basemenit of the local cityhall, not infrequently next to the city jail. Gradually, safeguardingthe community water supply, sanitary inspection of public places andother relatively simple activities were added functions of the publichealth officials. In enlightened communities episodic medical care wasalso extended through charity hospitals, dispensaries and custodialinstitutions to that segment of the population which, when incapacitatedby illness, was considered incapable of fending for itself through privatemeans. These institutions were autonomous, were answerable only to theirown independent boards of trustees, and dealt only with those problemswhich met their own admission policies. Services offered terminated withthe death or discharge of their patients.
2. Improved public understanding of the causes of illness and itseconomic and social consequences, technical advances in the medical andsocial sciences, and the assignment to government of greater responsibilitvand authority for promoting the total well-being of the population itserves, have made so limited a definition of public health obsolete and nolonger a tenable one. Today, the field of public health is almost univers-ally recogrnized as encompassing a planned and organized public endeavordirec-ted orn a national level toward the promotion of health, the preventionof illness and disability, the care of the sick, and the restoration touseful work or activity of all those whose health status has been impaired.As such, health care for many has lost the stigma of charity services, orthe beneficence of the rich for the poor, and has become an integral partof a rising tide of national aspirations for the interdependent goals ofbetter health, education, housing, and job opportunities.
3. So defined the scope of public health activity has been enlargedin many directions. It must involve a national network of programs andacti-vities reaching down through every jurisdiction of government to 1thelocal level where people live and work. It must engage the efforts ofevery ministry of the national government, and must incorporate the re-sources of professional groups and private enterprise outside the frame-work of government. Public health today includes the protection of thehuman population against all of the hazards of its environment, whetherthese hazards arise from naturally occurring noxious agents, or fromdangerous polutants of the environment created by man himself; it in-cl-21des l;hJe for-tification of man's ov resistance to disease by the applica-4-ion of the de-eloping sciences of nutrition, imntinization, and chemo-proply].axirs; the provis-ion of the ins4titu-tional reso-urces required to care
-2-
for the sick (hospitals, dispensaries, health centers, etc.); and thetraining and deployment of health personnel -- both professional andauxiliary -- required to staff the complex services demanded in a modernhealth and medical care system.
4. Two other essential ingredients of such a system should not beoverlooked. First, it is widely recognized -- and will be amply documentedin this report -- that an illiterate population is an unhealthy population,and a health-illiterate population cannot, or will not, take those measureswhich it alone must apply to safeguard or promote its own well-being, norwill it utilize effectively and efficiently the public health resourcesavailable to it to meet those needs which the individual alone cannot pro-vide. Thus, a national public education system, adapted to the specialneed for increasing enlightenment in matters of health, is an indispensablerequirement of a sound national public health program. Secondly, theremust be clearly defined leadership within -the national government --appropriately within the Ministry of Health -- to take stock of the ever-changing health situation, to plan and promote the needed programs, and tomobilize all resources -- governmental and private -- to the end that theservices required by the public are provided within the resources available.
5. In a developing country, such as Colombia, the burden of publichealth endeavor falls heavi:Ly on the national government, and particularly,on the national Ministry of Health. Despite its nominal designation andits legal authorities, the Ministry of Health does not always provide thesole, or even the major channel for the expenditure of funds for publichealth activity. Funds available for public health are at best limitedand other areas of national development are in severe competition for theresources of the national treasury. The tax base of local and state(Departmental) governments is severely limited and may be nonexistent;private enterprise in health and medical care is rudimentary, and public.philanthropy which has pioneered so extensively in expanding the scope ofpublic health endeavor in -the more advanced countries, is episodic andessentially unorganized.
6. Despite the above assessment, the public health system in Colombiais an extensive one, and many organizations within and outside of govern-ment, and at national, departmental and local levels are vigorously engagedin a modern public health program in Colombia that clearly meets the defini-tions and criteria set forth in this section. A unique attribute of thepublic health movement in Colombia is the availability of an extensivearray of basic data on the health situation and the available healthresources within the country. These were assembled in 1965-66 through acooperative enterprise of the Ministry of Health and the Association ofColombian Medical Schools with financial and other assistance provided bythe Milbank Memorial Fund of New York and the Pan American Health Organiza-tion (Regional Office for the Americas, World Health Organization). (3, 4)Many of these data were of fundamental value in the formulation by theMinistry of Health of a Ten-Year Health Program for Colombia (1968-77).(12)
7. A final point of orientation is in order. In reviewing thehealth problems of a developing country, such as Colombia, the observeris immediately made aware of the wide discrepancies that exist in themajor health indicators of that country when these are compared withsimilar indicators for the more advanced nations of the world, as for
example, those in Western Europe or in North America. A direct com-parison of such data is frequentlyodious and sometimes hazardous. Forexample, mnatching the infant mortality rate for all of Colombia and theU.S. national rate, fails to reflect the variable components withineach set of data or that approximately half of the Colombian populationresides in a rural setting where levels of literacy are low and familyincome meagre. The infant mortality rates of rural Negro communities inthe Mississippi Delta are of the same order of magnitude as those for alocal population in a rural Colombian village. Similar direct comparisonscould be made for a Bogotan barrio with an urban ghetto area in any oneof several mwajor U.S. cities.
8. Again, in Colombia the ratio of physicians to total populationis low, about 4X: 10,000, whereas, in the U.S. this ratio is 16.4:10,00C (1).The uneven distribution of physicians in the U.S. has evoked much concernbut nowhere does it approach the maldistribution recorded in Colombiawhere almost 3 out of 4 doctors reside in the principal cities, and serveless than 1/3 of the total population; only 10% of the medical manpower inColombia is available to the 2/3 of the populati-on residing in places of20,000 population or less. (4-o). Probably of even greater significance isthe observation that with the resources at present in sight, it would takeno less t;han 100 years for the medical training instituti-ons of Colombiato produce the number of physicians required to approach current U.S.physician/population ratios. Herein lies an importan-t -inference for Colom-bian health planners: It would be folly for them to set as their goalthe uncritical adoption of health care patterns and norms observed in theso-called advanced countries of the world. Rather, by applying innova-tive approaches they must devise new techniques and new concepts appropriateto their own health problems and their available or potential resources.For example, impressive evidence is rapidly accumulating in Colombia andelsewhere demonstrating that the skills and professional lkowledge of alimited number of physicians can be extended to serve a larger segment ofthe population. This can be accomplished by the greater utilization ofauxiliary worlcers trained to work as members of an integrated health careteam. The role of the physician rmairts a dominant one. However, hisfunctionas assume more of a directing and supervising nature and hebecomes more the manager of health services than the sole provider ofmedical care. Thus, in utilizing data presented in this report the purposeto be served is less to compare the Colombian situation unfavorably withthat of the more advan-taged areas of the world, but more to provide suit-able starting points or bench marks to Colombian health planiners, andthose who would assist them in their tasks, to develop unique and evenexperimental approaches to realistic goal objectives.
3. T'l :1 c tIJ t;, C;I'I ,
1. ri- t £ Ju;!ii i- . l Cr <U-;a 1':
9 CVF rumetalthJL hea lW I e; are c m;fivi t,td Oir ( ait 0 ' t'breeiidniistrative Ievels -- HatIl. l 11 I)F:rtml _tols -;j I1 I]nt;ealdar 10 1- or Corui-
sari as (29)), and at. the lo . vi e! iwhere servict.s l,o t1he pubi , ae
provided through-i 150() heal_t;h t:r, ir-id hiealth po:.uc ., disporruari .;, andsimilar f'ac-ili-ties for amju lat r y iredical care, andl through icuav r,('lflhospi-tals offering both i1-o wnbuAat:ry services. epuhlichospitaisi/ with about 412,.'.n41 b-_ ci i coYliIprjse W3f. ol' .al I slch facilitiesavailable in the country. ()pi. )
10. At the national lovel, t.he r i 11i-:;3.i lth is charged. by lawwith formulating na-tio o.ul h tbh I:,-1 i;V, "-th, poe_j),raUt oi of national
plans and programs, the supt erT.1 oslr>, r.-r inirJ tiud control of all activi-ties relative to health, t,he t.1 jr I Ie (; f c regirri Iationis arild. Upervisionf'or their fulfil.-Lment." ' There are oi.hei natioiial orgaiiizationis concernedwith the provision of' healt.1 services for specif.'ic popuLlatciori groups andthese include the Colombia' i:rbt.itrit. Lfor :-c;;:lo S-(ecurity, the MilitaryHealth Services, the Min.Jist-ries of F'rva1tlo.r0, labor, Public Works, Police,the National F ail-ways, thel Ports of ('Colo1nbia arnd other agencies with smallerprograms which ei.ther I-provide health ser-if.ces directly to their employeesor -through Welfare Funrds (_Jasas). These sn:ecial health programs, focusedon both publicly and prii/ately emrroloyed wro ke.rs, are limited to approxi-niately 1.3 million benefic lari.es- out -,! a la,or force estimatted in 1970 tobe about 6.5 million arnd a I-1otal populatio osf 91.6 million. (33). TheColombian National Red Cross Assc),. iatiorvn has also been recognized by theNational Government and assI:'ii -ied responsibilities for "attending to everyclass of accidents, calanri-ties, catastrophes, epidemics and other humani-tarian works." In addition , tlhr benefiericias and lotteries are legallyrecognized as autonomous reg. onial organizaitions which devote part of theirincome to the support of hospitals and. merdical care institutiorns.
11. As a consequence of recent legi-slation (Decrees 3224, (1963);1499, (1966); and 2470, (.1968) most, if not all, of these separatelyadministered programs are coo:rd-inated through a National Health Council,chaired by the Minister of Heal-th. This legislation also authorizedinternal reorganizations wi',hin the Ministry and provided for the coordina-tion of regional ard oc;al. health programT1s and -the unification of theirfinancial resources. For tire first -time a rnational network of healthactivity now exists with consolidated mechanisms established within theMin:istry for supervision, control, prograWdning and periodic evaluation
1/ Public hospitals, many of which are governed by independent or semi-
autonomous boards of directors, are defined as receiving all or partof their fumds from the public treasury; the medical care servicesthey provide are subject to the supervision of the Ministry of Health.
2/ In general, health benefits in these plans are restricted to the
employed workers; some provide limited, benefits to dependents ofinsured workers, e.g., maternity care and inLfarLt care during thefirst six months of life.
at all levels. In addition a series of semi-autonomous institutes wereeither assigned to or created under the aegis of the Ministry with theauthority and flexibility to undertake urgent and major health programsof national significance. As a consequence of these recent organizationaladaptations the Ministry of Health currently includes the following func-tional elements: (17).
a. Policy Determination and National Planning
i. Office of the Ministerii. Office of Planning
iii. Office of Human Resources for Healthiv. Office of the Legal Counsel
b. Assigned Agencies
i. Colombian Institute for Family Welfare (ICBF) (includesDivision of Nutrition -- formerly, National NutritionInstitute).
ii. National Institute for Municipal Development (INSFOPAL)(responsible for water supplies and sewerage systemsfor connunities over 2500 population).
iii. National Institute for Special Health Programs (INPES)(includes the formerly separately administered NationalInstitute of Health and is responsible for water suppliesand environmental sanitation in rural areas).
iv. National Hospital Fund (responsible for financing theconstruction of hospitals and health centers with fundsloaned by the Colombian Institute for Social Security).
v. National Cancer Institute.
vi. Supplies Corporation for Social Welfare Institutions(CORPAL).
c. Administrative Divisions
i. Medical Careii. Direct Campaigns
iii. Environmental Sanitationiv. General Administration
2. ThTe Private Secttor
12. In Colombia, as in many other developing countries, the privatelyoperated and financed health sector is of relatively small magnitude whencompared with governmentally directed or controlled operations. Throughvarious channiels, however, the private sector exerts considerable influenceon national policies and governmental programs. As was stated earlier,
approximately 20 percent of all hospitals, with about 12 percent of theavailable beds, are privately operated. Yet, the vast najority of thepublic hospitals throughout the counltry were established by local groupsand municipalities and continue to be directed by independenfli char-ity orother boards. These instit;utions are now dependent in prepond(erant degreefor support from the public treasury and the medical care provided issubject to the supervision of the Ministry of Health, yet they stillretain considerable autonoim and independence in their operations.
13. As for the medica:L profession, private practice appears to bethe ambition of most physiciains, though this may be as much due to lowerremuneration and less satisfac-tory working conditions in salaried posi-tions as to philosophical orientation. Only 14 percent of physicians inColombia are engaged exclusively in private practice and 24 percent ex-clusively in salaried positions; the majority, 62 percent, combine privateand non-private work in various proportions. However, after age 50, two-thirds or more physicians concentrate their efforts on the private sectorwhereas under age 35, over 75 percent of doctors are dependent on salariesas the major source of their income. (4o). Also in the privatesector the drug and pharmaceutical manufactu-riing arnd distribution indlustryappears to be a large and profitable one. In 1966, its gross productexceeded 1,200 million pesos, about 7 percent of total soft consumptiongoods manufacture in the country. (33). This sum is larger than thetotal public expenditures for health that year. (See paragraph 16 below).
14. No discussion of the role of the non-governmental sector inmeeting the health needs of the Colombian population would be completewithout reference to the Association of Colombian Medical Colleges. Thisassociation representing the seven (now nine) university medical schoolsin Colombia has provided outstanding leadership in the health sector overthe 10 years of its existence. It has contributed particularly to thedevelopment of public awareness of health as a necessary condition ofsocial and economic development of the country. In addition, it hascooperated with and supported the efforts of the Ministry of Health in aseries of unique studies encompassing a national health survey of Colombiaas well as an investigation of health manpower resources and professionaleducation. (3.4.5). These studies conducted in 1965-66 have placed inthe hands of Colombia policy makers and planners a wealth of vital datathat is the envy of their counterparts in many advanced countries of theworld. What is more, the Association has been instrumental in seeing thatmany of the findings, which are still in process of analysis and publica-tion, are utilized as the basis for new national programs now in process ofimplementation.
C. Sources of F'Lnds and Mlajor Outlaysfor Health and Mledical Care
15. In the 10 year irrLerval 1961-1970 there has been a dramatic risein recorded health expenditures in Colombia. In 1961, 543 million pesoswere devoted to these purposes at all levels of governmental expenditure
-7-
and by 1969 this figure had reached 2,763 million pesos, a five foldincrease. In the former year health expenditures represented 1.8 per-cent of the gross national product and in the latter, 2.5 percent. For1970 an additional rise is planned to 3,507 million pesos, 2.8 percentof the gross national product, a further reflection of the establishednational policy to give greater emphasis to health activity and an equi-valent reflection of the surging demand on the part of at least someelements of the Colombian population for health and medical care services.
16. Table I-1 shows the recorded expenditures for public health andmedical care for each of the years 1961-1969 and budget estimates for1970. The major sources of these funds are also displayed. It should benoted that expenditures for water and sewerage in urban communities(population 2,500 and over) have been omitted from the tabulation. Some,but probably a minor fraction, of the annual increases in total healthexpenditures is attributable to improved accounting and reporting procedures.The depreciation in the purchasing value of the pesos during this ten yearinterval also must be considered. However, the increase is so substantialand the accelerating rise in annual increments so notable in recent yearsthat there can be little question that with improving economic conditionsin the country the Government of Colombia has established as nationalpolicy the earmarking of larger and larger expenditures for public healthand medical care services.
17. In the same table it may be noted also that appropriations forthe Ministry of Health have risen from 162 million pesos in 1961 to 578million pesos in 1969. This represents a rise of approximately 140 percent,in terms of the 1961 purchasing power of the peso, in the eight year period.However, during this same interval appropriations for the Ministry of Healthhave become a significantly smaller fraction of the total expenditures forhealth and medical care, falling from 30 percent of the total in 1961 to 20percent in 1969. If expenditures through the National Institute for SocialSecurity, the Cajas and by other national agencies -- i.e., costs of providingmedical care for special employed groups -- are subtracted from the totalsit becomes apparent that general health care for the total Colombian popula-tion has not been as much the beneficiary of this rising tide of healthexpenditures as might be initially surmised. In 1961 general health carerepresented 72 percent of total costs and about 1 percent of the grossnational product; in 1969 general health care had fallen to 47 percent oftotal costs and remained at about 1 percent of gross national product.
18. Conversely, the beneficiaries of the social security system andof the Cajas and other special programs are now receiving a substantiallydifferent level of health care than that received by their own dependentsand by the balance of the population. It has been estimated that suchbeneficiaries now number about 1.3 million workers, or about 5 percent ofthe total population. In their behalf about 785 pesos were spent in 1969for medical care for each of them, an increase of 240 percent per individ-ual since 1961. For the general population about 52 pesos were expendedper individual in both 1961 and 1969 with the intervening yearsshowing lower average annual expenditures (see Table I-2). No
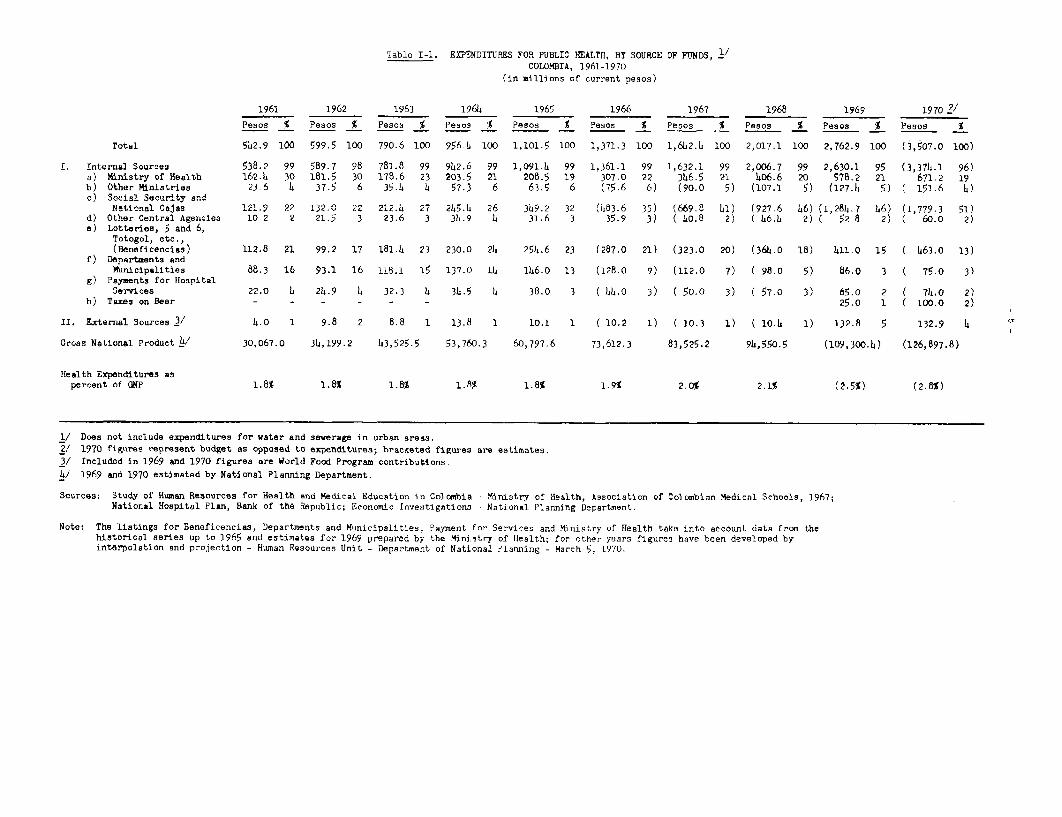
Table I-1. EXPENDITURES FOR PUBLIC HEALTH, BY SOURCE DF FUNDS, 2/COLOMBIA, 19l6-1970
(in millions of current pesos)
1961 1962 1963 1964 1965 1966 1967 1968 1969 1970 21
Pesos % Pesos % Pesos % Pesos % Pesos % Pesos % Pesos % Pesos % Pesos % Pesos %
Total 542.9 100 599.5 100 790.6 100 956.b 100 1,101.5 100 1,371.3 100 1,642.4 100 2,017.1 100 2,762.9 100 (3,5O7.0 100)
I. Internal Sources 538.2 99 589.7 98 781.8 99 942.6 99 1,091.4 99 1,361.1 99 1,632.1 99 2,006.7 99 2,630.1 95 (3,374.1 96)a) Ministry of Health 162.6 30 181.5 30 178.6 23 203.5 21 208.5 19 307.0 22 346.5 21 406.6 20 578.2 21 67i.2 19b) Other Ministries 23-6 4 37.5 6 35.4 Li 57.3 6 63.5 6 (75.6 6) (90.0 5) (107.1 5) (127.4 5) ( 151.6 4)c) Social Security and
National Cajas 121.9 22 132.0 22 212.L 27 245.2± 26 3r9.2 32 (483.6 35) (669.8 41) (927.6 46) (1,284.7 46) (1,779.3 51)d) Other Central Agencies 10 2 2 21.5 3 23.6 3 34.9 a 31.6 3 35.9 3) ( 40.8 2) ( 46.4 2) ( 52 8 2) ( 60.0 2)e) Lotteries, 5 and 6,
Totogol, etc.,(Beneficencias) 112.8 21 99.2 17 181.4 23 230.0 22 254.6 23 (287.0 21) (323.0 20) (364.o 18) 411 0 15 ( 463.0 13)
f) Departments andMunicipalities 88.3 16 93.1 16 118.1 15 137.0 14 146.0 13 (128.0 9) (112.0 7) ( 98-0 5) 86.0 3 ( 75.0 3)
g) Payments for HospitalServices 22.0 4 24.9 4 32.3 4 3h.5 4 38.0 3 ( 44.0 3) ( 50.0 3) C 57.0 3) 65.o 2 ( 74.0 2)
h) Taxes on Beer - - - - - - 25.0 1 ( 100.0 2)
II. External Sources 3/ 4.0 1 9.8 2 8.8 1 13.8 1 10.1 1 ( 10.2 1) ( 10.3 1) ( 10.4 1) 132-8 5 132.9 4 a
Gross National Product 4/ 30,067.0 34,199.2 h3,525.5 53,760.3 60,797.6 73,612.3 83,525.2 94,550.5 (109,300.4) (126,897.8)
Health Expenditures aspercent of GNP 1.8% 1.8% I-A% 1.8% 1.8S.9 2.0% 2.1% (2.5%) (2.8%)
1/ Does not include expenditures for water and sewerage in urban areas.2/ 1970 figures represent budget as opposed to expenditures; bracketed figures are estimates.3/ Included in 1969 and 1970 figures are World Food Program contributions-
4/ 1969 and 1970 estimated by National Planning Department.
Sources: Study of Human Resources for Health and Medical Education in Colombia - Ministry of Health, Association of Colombian Medical Schools, 1967;National Hospital Plan, Bank of the Republic; Economic rnvestigations National Planning Department.
Note: The listings for Beneficencias, Departments and MNnicipalities, Payment for Services and Ministry of Health take into account data from thehistorical series up to 1965 and estimates for 1969 prepared by the Ministry of Health: for other years figures have been developed byinterpolation and projection - Human Resources Unit - Department of National Planning - March 5, 1970.
data on medical care expenditures are available for the estimated 15 per-cent of the total Colombian population which is believed to receive suchservices through private channels. Roemer estimates that in other develop-ing countries of the world health services as a whole consumed between threeand four percent of the gross national product. (20). Assuming for Colombiaa median figure of 3.5 percent, this would imply -that the true health ex-penditures for Colombia are at the level of 3,526 million pesos (1969) ratherthan the 2,762 million pesos shown in Table I-1. It would follow that pri-vate medical care expenditures are at the level of 1,062 million pesosannually or about 328 pesos per person for the 15 percent of the total popu-lation that receives care through private channels. This figure is obviouslyquite low compared with expenditures under the ICSS - Caja systems suggestingthat Roemer's assumptions do not apply to Colombia, the 15 percent privatecare estimate is too high, or social security and other welfare fund bene-ficiaries are receiving an unusually costly form of medical care serviceswhen compared with recipients of private medical practice. It also followsthat public expenditures for medical care for the general population arevery low. These issues deserve further study and analysis.
1 9. Considerable difficulty is encountered in analyzi.ng availableColombian data to differentiate continuing operational expenses from thoseof an investment nature - expendituxres for the construction of new facilitiesand their initial equipment. This is in part die to recent changes -i-n theorganizational structure of agencies at the national level of governmentinvolved in the provision of health and medical care services and in part tochanging patterns of budget formulation, along with changing definitionsof "investments" as opposed to "operational expenditures".
20. For example, for 1965, 5 percent of the total expenditures forhealth of 1,101.5 million pesos, or 55.5 rrillion pesos, were allocated tocapital investment; 50.4 million pesos were devobed to construction ofhospitals and other facilities and 5.1 million pesos for constnrution ofrural water supplies. (3). Costs of construction of water supply andsewerage systems in cormunities larger than 2,500 popul1.-tion were omittedfrom this tabulation, presumably because national responsibility forfinancial assistance in this area to such communi.ties had been assigned tothe Ministry of Economic Development. This situati.on was changed in 1969with the transfer of the National Institute for Municipal Development (INSFOPAL)from the Ministry of Ecomomic Development to the Ministry of Health. Inthe 1970 national budget investment expenditures for water supply andsewerage systems are consolidated in the 507 million pesos Ministry of Healthcapital investment budget; 137 million pesos of these funds are earmarkedf'or INSFOPAL subsidies of water and sewerage systems in communities largerthan 2,500 population. An additional 61 million pesos are also earmarkedfor municipal water supplies and sewerage systems. (In Table I-1, these198 millio:n pesos are not included in the Total Tabullation for 1970 tomaintain the consistency of the historical seri.es of health expenditu-es).
21. On the other hand, more detailed scrutiny of the 1970 budge treveals that the 507 million pesos capital investrent budge-t of the Ministryof Health includes in addition to(a) the 198 million pesos, mentioned
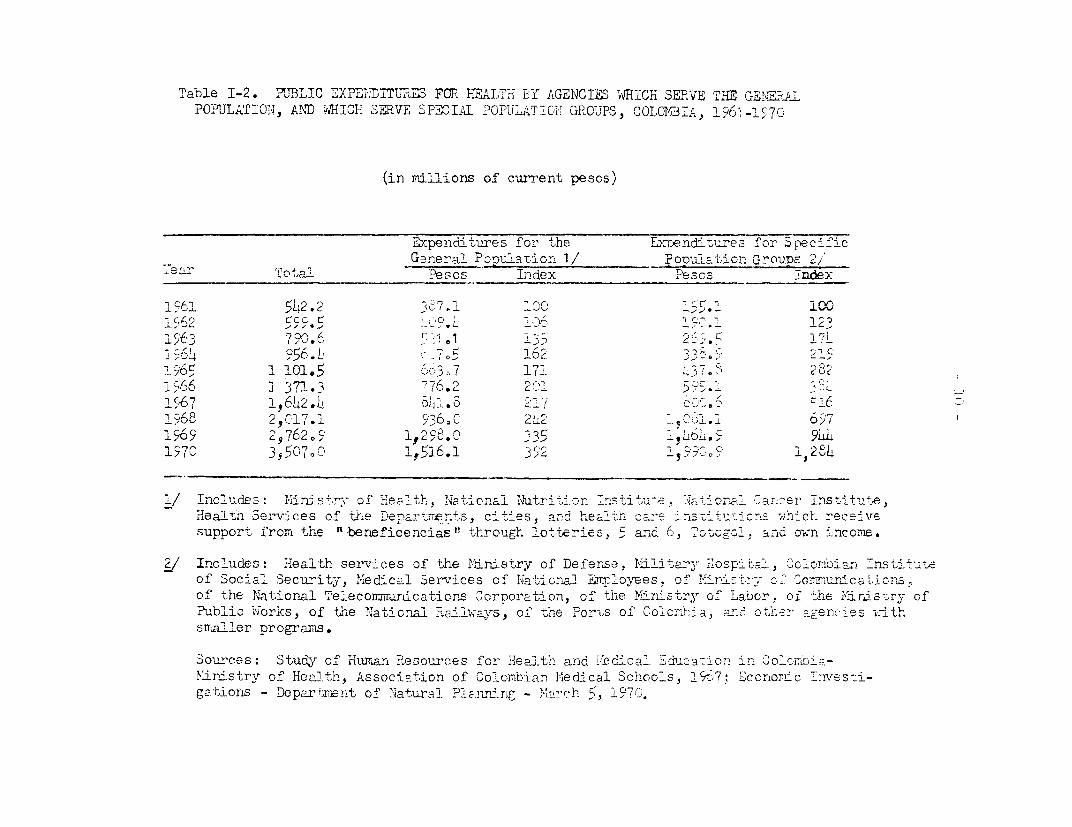
Table I-2. PUBLIC EXPE? .TT7L?3 FCOR HnAL7h T3Y AGENCIES ,W HICH SERVE THE GE!E,RAPOPULATION, AND WHICH SEPVE SPEACIA OPULATICL7 GORUPS, COLOICB 4", 196I -l "7
(in millions of current pescs)
Expenditltures for 'the ETenditiures for SpecificGereral PoDlaRtior 1/ _Poimiiation Gov-oups 2,
ear 'inota oPesos ILdex Pescs ndex
1'61 "L42.2 A c 100V~~~~~~
v / / * 5 ; C * / )rSO I C ~~~~~~~~~~~~~~~~~~~~~~ 1 )'j 196 3 7 . 0 I 2
; v v a v 5 ~64 A 1 196: 1 101.5 r-3z7 171, >'. 282'
1-66 71371. R 76,2 21 5 . 3,.
1567 196LL2.L _ LI.$ -
' 68 25,17.1 936.C 2 L -1965 29 762 O- 5c'1L. 9! CI
1 5 7 C 3 5 50 70 CO 15161 3 8 1, 28
1/ Includes in ns t of He -lt, Nat ionaI tatr4iti o,n m 7ti tu' - on.al Olarner Institute. JHeaItr. Ser-vices of the Depart`-'rnts, cities, anc healt. c-'e _es-ituticrLs which rece:vesupport from the "t beneficencias" through lotteries, W and 6, 5ot ool. and own -ncome.
2/ Includes : Health services of the l'Iinistry of Defense, Militr -osii.,-, Colcmvian ThsLst4 jt-of Social Security, Medical Services of INati-onal a mr -ees, of M'ni-, rty- oCf Cc=nufcin 7,
of the INIational Teleconmmun-iications CcrDoration, of the Yi>,nistryr of Labor. oL the MNris,-ry ofPublic ,;iorks, of th-,e Naticnal >a-ilways, of -.the For-,s of Ci olhcia, ad ot,.r agenoes withsmaller programs.
Soorces: Study of Human Resources for Health and M;ledical :dduc2- on ir inOC,ioRMinistry of Health, Association of Colombfian MFjedical Schools, 19,7; Econom,1 c Inesti-gations - Depariaen,t of Natura_ Planning -c L4ach ,, 1970.
- 11 -
above, for water and sewerage systems of communities writh populations of2,500 or more, (b) another 1 million pesos for Departmental water andwaste disposal plants, and (c) a fourth item for water and waste disposalresources, in this instance in rural areas, administered by INPES - theNational Institute for Special Health Program&s. Thus, in the aggregate, theIMEinistry of Health, in 1970, is making capital investments for water supplyand sewage disposal totaling 266 million pesos. The balance of the 507million pesos capital investment budget of the Ministry of Health includes:(d) about 47 million pesos for hospital and health center constructionand equipment, and (e) approximately 173 mi.llion pesos, for a variety ofactivities in which cons-tnlction or the purchase of fixed equipment - theusual basis for inclusion in a capital investment budget - are minor or absen-telements in the uses of these funds. Included in such "investnents' are thenmalJaria eradication campaign (61 million pesos). Mtass vaccination programs(24 million pesos), leprosy control (12 million pesos), tuberculosiscontrol (3 million pesos), maternal and child health services (49 millionpe.ios), and education and. training of personnr (17 million pesos).
22. Other factors to be considered in assembling a national invest-merit budget for health include the new roles recently assumed by theColombian Institute for Social Security and the National Hospital Fundin the direct construction or the funding of construction of medica.lcare facilities throughout Colombia. In 1969, for example, the formerbuilt,with its own funds, medical care facilities to meet the needs ofits beneficiaries and inffested for this purpose approximately 48 millionpesos; in 1970 its budget provides for about 56 million pesos for similarconstruction. In 1969 the National Hospital Fund borrowed from ICS about43 million pesos to assist the construction of hospitals and health centersmeeting the requirements of the now approved National Hospital Plan; in1970, the Fund anticipates similar borrowing in the range of 50 million pesos.
23. Based on the above, a reasonable approximation of a minimum investmentbudget for health facilities construction in Colombia assumes the followingproportions:
Total Health Budget - 1970
Prom Table I-1 3,507 million pesos+ Urban water & sewage 198 million pesos+ National. Hospital Fund 50 million pesos
Total ,755 million pesos
Investment Budget - 1Q70
Mii mstry of HealthHospital Construction 47 million pesosWater & Sewerage 286 million pesos
Institute for Social Security 56 million pesosNational Hospital Fund 50 million pesos
Total 39 mill.ic)n pesos
- 12 -
Accordingly, national capital investments in health facilities constructionin 1970 are estimated to be 11.7 percent of the total public expendituresfor health and medical care services this year. (439 million pesos/3,755 millionpesos). This ratio is not directly comparable with the figure of 5 percentfor 1965, quoted above, inasmuch as the estimation made for that earlieryear does not include capital expenditures made by the Ministry of EconomicDevelopment for water supply and sewerage systems in urban commu.nitiesor any investments for hospit.al construction that the Colombian Institutefor Social Security may have made that year. It also is not clear whetherDepartmental or municipal. expenditures for health facilities constructionare included in total health expenditures for either years (Table I-1).
24. For the period 1961-1968, financial assistance in the healthsector from external sources has been small ranging from 4.0 to 13.8 millionpesos per year with an average of 9.7 million pesos. Such assistance hasamounted to well under 2 percent of total public expenditures for healthand for the most part has been earmarked for special projects in the form ofstimrulatory or initiating grants. These figures undoubtedly under-reflectthe amount of external assistance received over the years by Colombia for manyof the assisting agencies have, in addition, provided substantial technicalconsultation and assistance, supplies and fellowships for the trainingof professional personnel abroad. The Pan American Health Organization andthe United Nations Children's Fund have been major donors as has been theU.S. Agency for Int&ernational Development and its predecessor agencies. Inthe non-governmental area the Rockefeller Foundation, the Milbank MemorialFund and the Hope prograum have been conspicuous for their assistance inrecent years. Since 1969, the World Food Program in cooperation withUNICEF ahd PAHO has been a substantial source of external financial assistanceto meet the requirements of the current country wide nutrition campaign.This aid, amounting to about 133 million pesos per year for five years, bringsthe percentage of foreign aid to the total health expenditures to just under5 percent in 1969.
II. ASSESSMENT OF THE PRESENT HEALTH SITUATION
A. Significant Demographic Variables Associatedwith Health and Medical Care in Colombia
1. Population Characteristics
25. The Colombian demographic picture is very similar to that of manycountries in the process of development: a fast growth in size of popula-tion, a high fecundity rate, a declining mortality rate, a concentrationof oopulation in childhood and young adult years, great movements in thespatial distribution of the population, a rapid growth of the urban nucleusand the incipient formation of a middle class (see Table I1-1).
26. In 1970, the population of Colombia is estimated to number 21.6million individuals. The next national census is planned for 1972; thelast, in 1964, which, because of technical problems may have resulted inan under-enumeration, placed the population at 17.5 million inhabitantsresiding in an area of 439,519 square miles. At that time about 98.7 per-cent lived in the Departments making up 53.6 percent of the nationalterritory. Population density of these Departments was about 73 inhabitantsper square mile. The remaining 1.3 percent of the population occupied the46.4 percent of the territory included in the Llanos Orientales. Thepopulation density of that area is about one inhabitant per square mile.
27. In 1905 the country had 4.4 million inhabitants; 33 years later, in1938 the population had doubled (8.7 million); 26 years later, (196h) thephenomenon was repeated (17.5 million) and it is possible that it willdouble aga:in in 22 years. This period of duplication is in contrast withthat of some other countries, such as Italy (117 years), Portugal (100years), Spain (88 years), Uruguay (58 years) and Argentina (47 years).
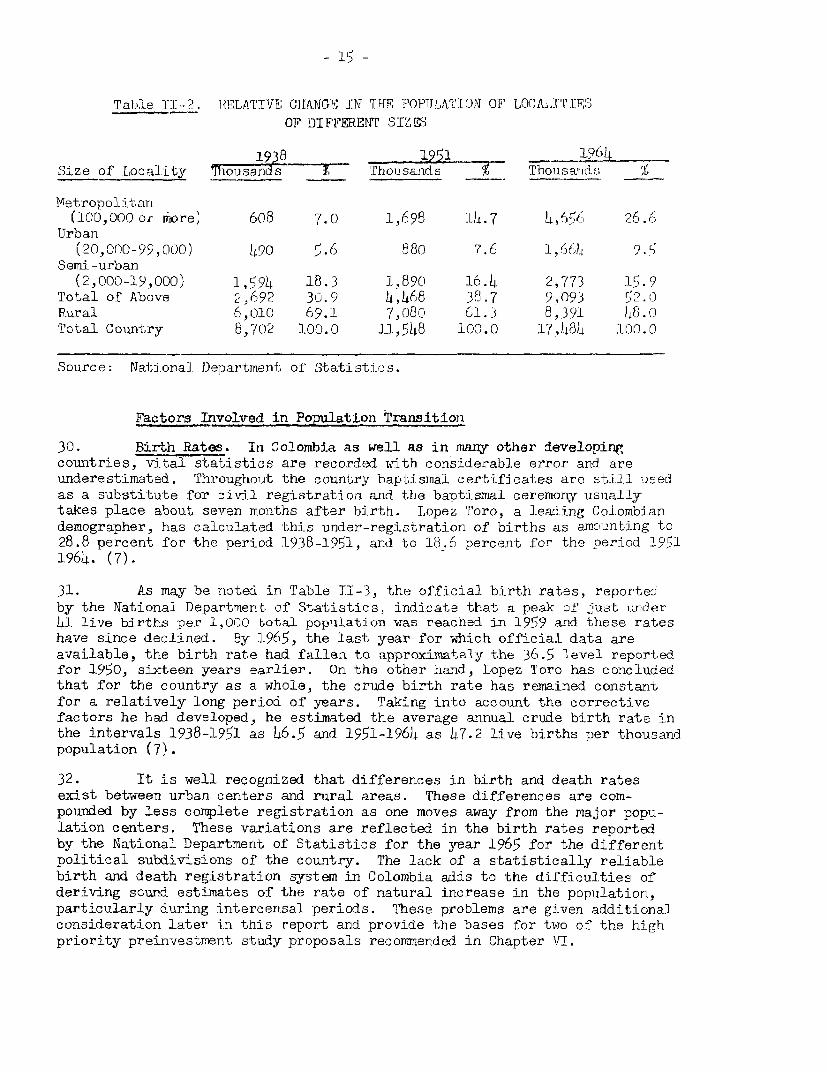
28. This rate of growth varies in different sections of the country.For example, Bogota, the capital city, is doubling its population every10-15 years, whereas some of the predominantly rural Departments require over55 years to double their population. Table II-2 illustrates the relativechange in the population of localities in the last three censuses. It maybe observed from this table that, over a brief span of years, the Colombianpopulation has shifted from predominantly rural (69 percent in 1938) to onealmost equally divided; the largest rate of growth may be seen in themetlropolitan centers. Estimates for 1970 place 41.5 percent of the country'sinhabitants in the 30 largest cities.
29. The economic resources of this population are limited. The averageper capita production in 1966 was 1,622 pesos, representing a 20 percentrise from the 1,300 pesos figure for 1950. (In dollar equivalents to 1958pesos these figures represent a rise in per capita production from $203 in1950 to $253 in 1966.) Associated with this low per capita production arethe umeven levels of family income: one-third of the population earns 3,600pesos or less per year and only 14 percent 12,000 pesos or more. In therural areas almost half (48 percent) have family incomes in the lowercategory and less than 5 percent in the higher.
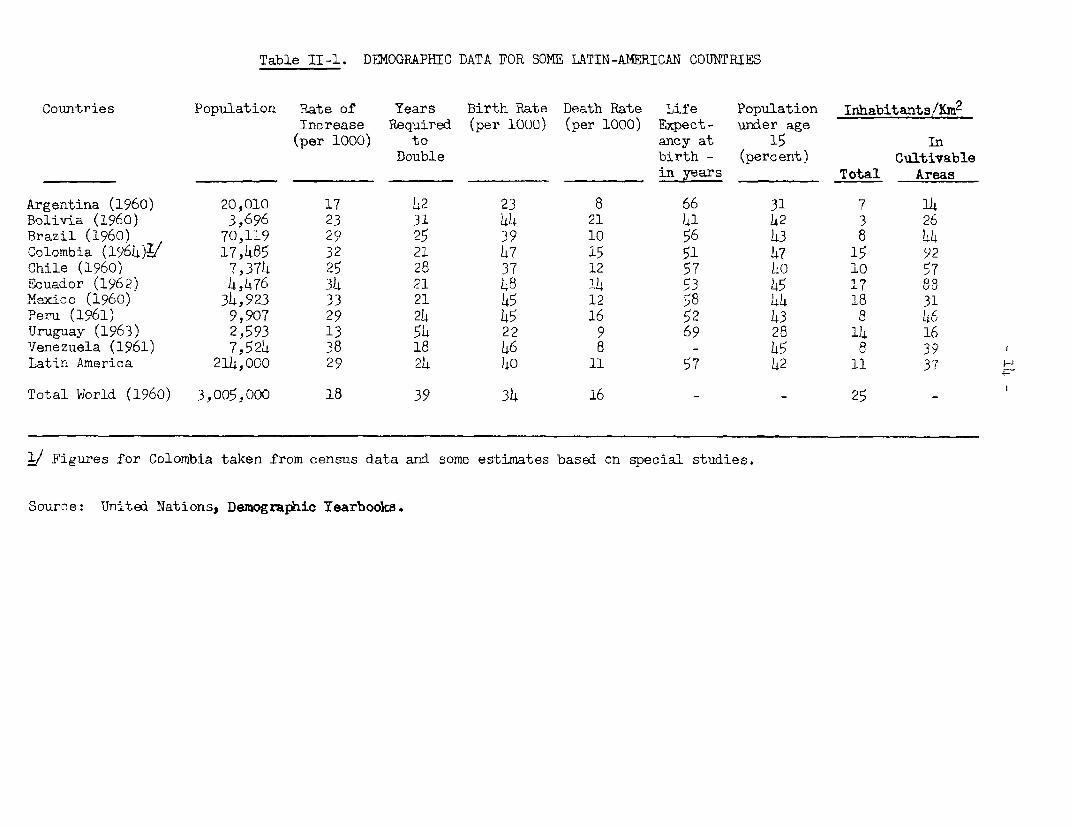
Table II-1. D4MOGRAPBIC DATA FOR SOME LATIN-AMERICAN COUNTRIES
Countries Population Rate of Years Birth Rate Death Rate Life Population Inhabitants/Km2
Increase Required (per booO) (per 1000) Expect- under age(per 1000) to ancy at 15 In
Double birth - (percent) Cultivablein yesars Total Areas
Argentina (1960) 20,010 17 42 23 8 66 31 7 14Bolivia (1960) 3,696 23 31 44 21 41 42 3 26Brazil (1960) 70,119 29 25 39 10 56 43 8 44Colombia (1964)1/ 17,485 32 21 47 15 51 47 15 92Chile (1960) 75374 25 28 37 12 57 0o 10 57Ecuador (1962) 4,476 34 21 48 1-4 53 45 17 88Mexico (1960) 34,923 33 21 45 12 58 44 18 31Peru (1961) 9,907 29 24 45 16 52 43 8 46Uruguay (1963) 2,593 13 54 22 9 69 28 14 16Venezuela (1961) 7,524 38 18 46 8 - 45 8 39Latin America 214,000 29 24 40 11 57 42 11 37 H
Total World (1960) 3,005,000 18 39 34 16 - - 25
j/ Figures for Colombia taken from census data and some estimates based on special studies.
Source: United Nations, Demographic Yearbooks.
- 15 -
Table 1I- 2. RELATIVE CHLANGE ITN THE POPUJLATION OF LOCAXITIFSOF DIFFERENT SITZSS
_ 1938 1951 l]6Size of Locality Tiosands- Tholsands r Thousan-idsf;
Metropolitan(100,000 or iiore, 608 7.0 1,6,9 14.7 l4,66 26 6 .6
Urban(20,no -99,000) 500 5.6 88o 7.6 1,646) 9.5
Semi-urban(2,000-19,000) 1,594 18.3 1,89c0 16.4 2,773 15.9
Total of Above '2, 692 30.9 ,468 38.7 9,093 52.0Rural 6,010 69.1 7,080 61.3 8,391 48.0Total Country 8,702 100.0 11,548 100.0 17,484 100.0
Source: National Department of Statistics.
Factors Involved in Po_lton transition
30. Birth Rates. In Colombia as well as in nirvn other developingcountries, vital statistics are recorded with considerable error and areunderestimated. Throughout the country baptismal certificates are still usedas a substitute for civil registration and the baptismal ceremony usuallytakes place about seven months after birth. Lopez Toro, a leading Colombiandemographer, has calculated this under-registration of births as amounting to28.8 percent for the period 1938-1951, and to 18.6 percent for the period 19511964. (7).
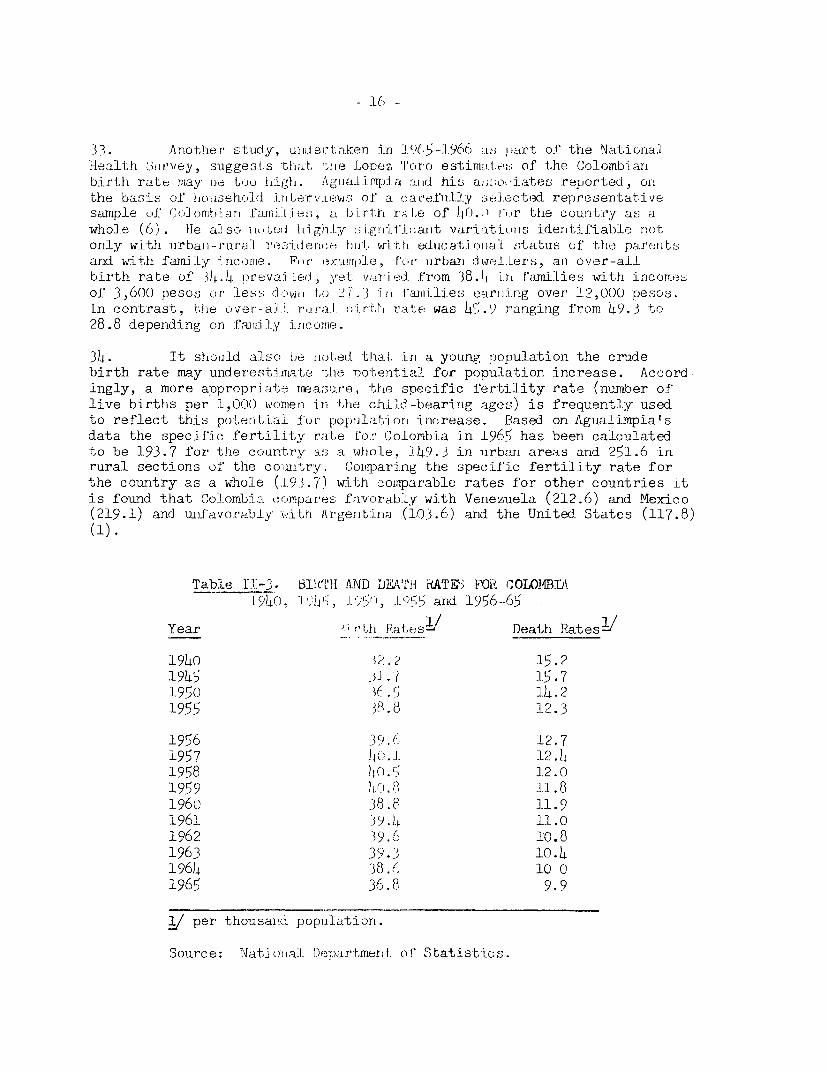
31. As may be noted in Table 1I-3, the official birth rates, reportedby the National Department of Statistics, indicate that a peak of Just under41 live births per 1,000 total population was reached in 1959 and these rateshave since declined. By 1965, the last year for which official. data areavailable, the birth rate had fallen to approximately the 36.5 level reportedfor 1950, sixteen years earlier. On the other hiand, Lopez Toro has concludedthat for the country as a whole, the crude birth rate has remained constantfor a relatively long period of years. Taking into account the correctivefactors he had developed, he estimated the average annual crude birth rate inthe intervals 1938-1951 as 46.5 and 1951-1964 as 47.2 live births per thousandpopulation (7).
32. It is well recognized that differences in birth and death ratesexist between urban centers and rural areas. These differences are com-pounded by less complete registration as one moves away from the major popu-lation centers. These variations are reflected in the birth rates reportedby the National Department of Statistics for the year 1965 for the differentpolitical subdivisions of the country. The lack of a statistically reliablebirth and death registration system in Colombia adds to the difficulties ofderiving sound estimates of the rate of natural increase in the populationparticularly during intercensal periods. These problems are given additionalconsideration later in this report and provide the bases for two of the highpriority preinvestment study proposals recommended in Chapter VI.
- 16 _
33. .Another' sLudy, Li-idartrtaken in ]9(>5-1966 a; ;.,rt o1' the NationalHealth Sil3nrvey, suggestLs that, 1-te Lopez Tlo-ro estimat.e:; of the Colomb-iarrbirth rate may he_ too higlh. 11giiaiirrq:i.a and his asso i.ates reported, onl
the basis otl household JuiLt errv-[euws of' a carefiilly sele(-ted representativesample oL f ombiari faini i -- at rhn :r.ll.e of b() . -.r tile country as awhole (6) . ie also ILO tel highll.y si.grl'i;aiit variatiotts identifiable notonly witlh irban-IraUral roniLderi(ce hot, wi-thlJ. ed-icatioiiaei -:tatus of the parentsand with fami:Ly irncorme. For 'exarVrrle, [or' urban diwel.lers, ani over-alLbirth rate of 34 4 prevai Led ,et vyre-t from 38.L i1.rt fawilies with incomesof 3,600 pesos or less dcm,i to :J7.,3 'i;r families earni.ng over, 12,000 pesos.In contrast, t;lhe over-al.l. r tral bi.rth ' rat.e was 45.. ranging from 4h9.3 to28.8 depending on TfTia-lny i-collie.
34. It should alsc. te tiot-.ed. that-l in a youngr population the crudebirth rate may underestimate the poltential for population increase. Accordingly, a more appropriate mea.3u.'e, the specific fertility rate (number oflive births per 1,000 -wonmen in the child-bearing ages) is frequently usedto reflect this potential fur p)opulation increase. Based on Agualimpia'sdata the specific fertility rate for' Colombia in 1965 has been calculatedto be 193.7 for the couintry as a whole, 1)49.3 in urban areas and 251.6 inrural sections of the cowitry. Comparing thie specific fertility rate forthe country as a whole (.1.93.7) with comparable rates for other countries itis found that Colombin. co(mpares favorab:Ly with Venezuela (212.6) and Mexico(219.1) and unifavorably -wit,h Irkgent1ina (103.6) and the United States (117.8)
(1).
Table 11-3. 1ItTrlf AND DEATH RATE3 FOR COLOJ'BDi194'].1;';:, I Y<t, 1,- and 1956-65
Year i- r'th Ratesl/ Death RateslJ
1940 W.? 15.21945 5i.7 15.71950 1. l4.21955 38.8 12.3
1956 39.E 12.71957 W.I. 12. I1958 l[C).L 12.01959 11. 81960 38.8 11.91961 39. 1 11.01962 19.6 10.81963 39-.3 l0.h1964 38.f, 10 01965 36.8 9.9
I/ per thousanid populatiorn.
Sou-rce: Natidloal D)epartmerLt of Statistics.
- 17 -
35. MortalitY Rates. As shown in Table II-4, under-registrationof deaths appears to be even greater than for births. Correction factors werecalculated by Lopez Toro for the period 1938-1951 as 37.7 percent and for1951-19614 as 32.8 percent indicating that about 1 out of 3 deaths are notofficially registered for the country as a whole.(7). To correct for thesedeficiencies, Lopez Toro estimated the average annual death rate for theperiod 1938-1951 as 22.4 and for 1951-1964 as 17.4 deaths per thousandpopulation. For 1965 a comparable estimate is 14.95 per thousand.
36. The infant mortality rate, deaths under one year per thousandlive births, is widely considered as one of the most sensitive indicators oflevels of public health accomplishment. In the IJ.S. this rate has remlainedalmost constant, around 25, for many years. In Colombia, the infant mortal-ity rate is reported to have declined from 114.4 to 88.5 between 1951 and196)4, a reduction of almost 23 percent. There is no basis for challengingthat a true decline has occurred. On the other hand the underreporting ofdeaths suggests that the "corrected" infant mortality rate is still over lb0indicating that one child in ten born alive fails to reach his first birthday.
37. Age specific death rates have been utilized to calculate lifeexpectancies at birth; these indicate that an infant born in 1965 has a 50-50 chance of surviving to age 57 whereas for children born earlier the com-parable figure for 1951 was 53 years and for 1938, 45 years.
38. Based on the calculated average annual birth and death rates (47.2and 14.95 respectively), and since immigration and emigration are negligiblefactors, Colombian authorities have assumed that the gross rate of populationincrease is in the range of 3 percent. For 1964 this figure has been set at3.3 percent. Obviously this estimate is an approximate one but until amarkedly improved system of vital registration is adopted, no better approxi-mations are available.
39. Compounding the problem of incomplete registration of deaths isthe fact that actual causes of death are not reliably identified. Fortypercent of registered deaths occur without medical certification; another17 percent, though medically certified, occur without a physician inattendance during the terminal illness. Thus, in only 43 percent of deaths,is there medical certitude of the cause of death.
40. Migration Patterns. Two classifications are used in Colombiafor the spat iaL disoributian of the population. The first, at the murnicipallevel, makes a distinction between the county seats and the rest of thecounty; the second, at locality levels, between the urban population (morethan 1,500 inhabitants) and the rural. At the national level the two class-ifications have a similar numerical value; however, at the regional levelthe differences become very large because many of the county seats are noturban (335 counties out of a total of 848). Boyaca, for example, with atotal of 127 counties in 1964, has 102 counties whose seats had less than1,500 population.
- 18 -
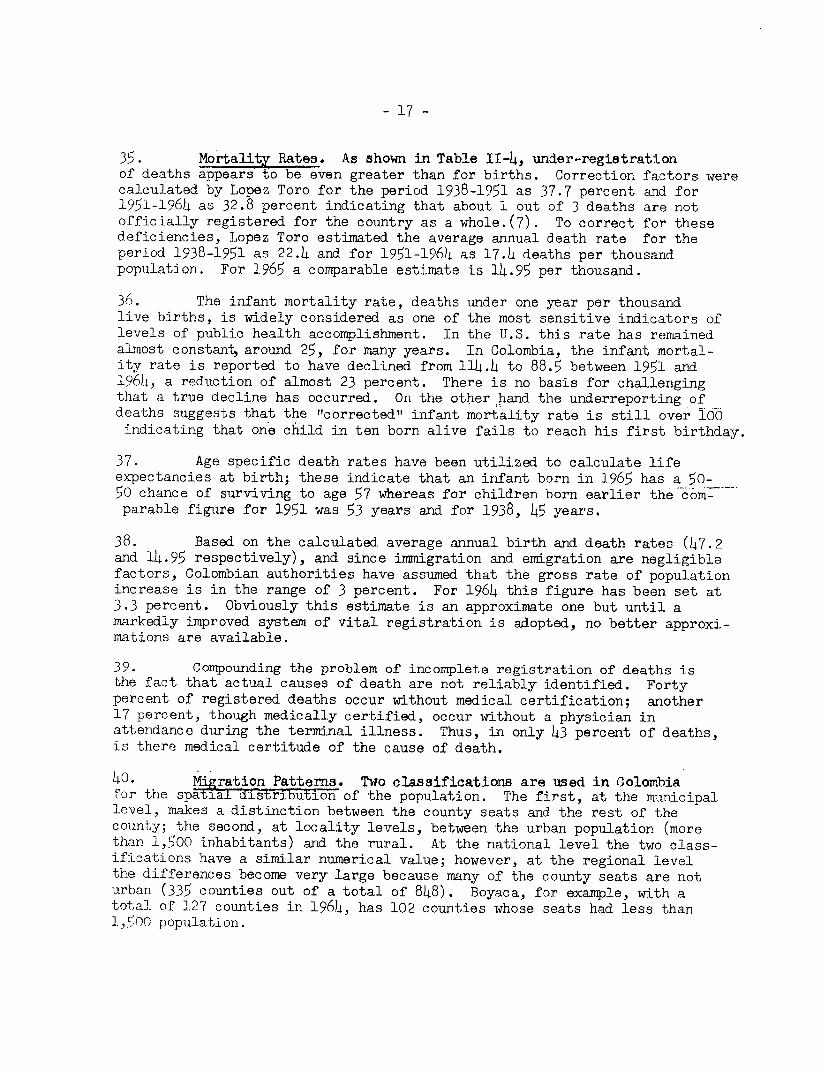
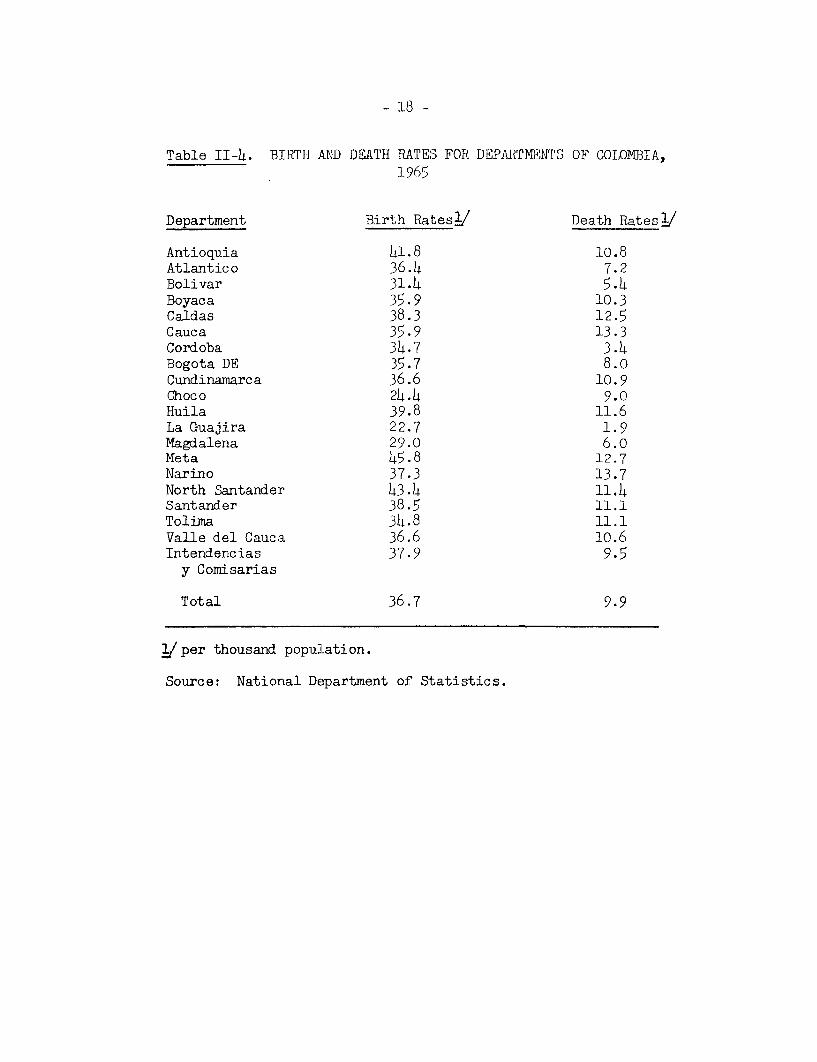
Table II-4. BIRTfI AND DEATH RATES FOR DEPARTMENTS OF COLOMETA,1965
Department Birth Rates / Death Rates /
Antioquia 41.8 10.8Atlantico 36.4 7.2Bolivar 31.4 5.4Boyaca 35.9 10.3Caldas 38.3 12.5Cauca 35.9 13.3Cordoba 34.7 3.4Bogota DE 35.7 8.oCundinamarca 36.6 10.9Choco 24.4 9.0Huila 39.8 11.6La Guajira 22.7 1.9Magdalena 29.0 6.oMeta 45.8 12.7Narino 37.3 13.7North Santander 43.4 11.4Santander 38.5 11.1Tolima 34.8 11.1Valle del Cauca 36.6 10.6Intendencias 37.9 9.5y Comisarias
Total 36.7 9.9
i/per thousand population.
Source: National Department of Statistics.
- 19 -
41. In Colombia, as in other Latin-American countries, urban popula-tion has grown much more rapidly than the rural population. For the period1951-1964 the population in county seats grew at the rate of 5.4 percentwhereas the population "'in the rest of the counties" increased at a rateof only 1.3 percent (see Table II-5). Also, while the urban populationhas grown faster than the rural, there is a strong tendency for these in-crements to concentrate in the major urban centers. In 1938, about 23percent of -the total population of county seats lived in cities with morethan 100,000 people; by 1964 this ratio was 51 percent. During the inter-censal periods (1938-1951 and l951-1964) the rmmicipalities that grew mostwere those with 200,000 and more inhabitants. Paralleling this, a slowerrate of growth may be observed in the smaller centers (2,000-4,999) and themedium ones (20,000-49,999). The growth of the big centers has caused thesmall neighboring muncipalities to become part of integrated social unitswhich can now be identified as urban complexes. This development is notablein the areas around the four major cities of the country - Bogota, Medellin,Cali and Barranquilla but similar patterns can be identified elsewhere.
42. uip to 1951 about 1.62 million people lived in another Departmentfrom where they were born; by 1964 this figure increased to 3.16 million.However, consolidating in 1964 the same politico-administrative jurisdic-tions prevailing in 1951, the inter-departmental migration fell to about2.76 million, the difference corresponding, in large measure, to the popula-tion flow between Cundinamarca and Bogota.
h3. For the period between the 1951 and 1964 censuses it may beobserved that the Departments registering positive migratory balances arethe most prosperous ones -- Cundinamarca together with Bogota, Valle,Atlantico, Antioquia, Meta and Magdalena, whereas those that have a lowdevelopment level, or were badly affected by guerrillas show negativebalances -- Choco, Boyaca, Narino, Toluna and Caldas (see Chart II-6).
44. The moverment registered in 1964 showed that outward flow fromcounty seats was exceeded by the inward flow to the same county seats. Inaddition, migration has been heavily concentrated among the economicallyactive segment of the population (ages 15-59), the majority being farmers,artisans,operators and domestic servants. However, when estimating theratio of immigrants to the resident population, the most mobile groups aremade up of professionals, technicians, officials, managers, salesmen anddomestic servants. These and related aspects of the migration of specialgroups within the countryhave been accelerating the regional imbalance ofvarious components of the Colombian population.
2. Socio-E2onomic CharacteristicsiJ
45. The Colombian National Health Survey, conducted during the years1965 and 1966 and previously referred to, provides a wealth of socio-economicdata which can be directly correlated with measurements of the amount of
/ The sources of data presented in this section, unless stated other-w-ise, are: Study on Health Manpower and Medical Education in Colombia,International Conference, Maracay, Venezuela, June 1967; Volume II - Pre-lirinary Fi:ndings (Reference 36) or Hechos Demograficos, 1968, Estudiosde Flecursos Hiumanos para la Saluid y FucacionMedica en Colombia, Investi-ga6ion lJac ional de Morbilidad, Ministerio de Salud Publica y Associacionde Pacultacles de Medicina (Reference 4-i).
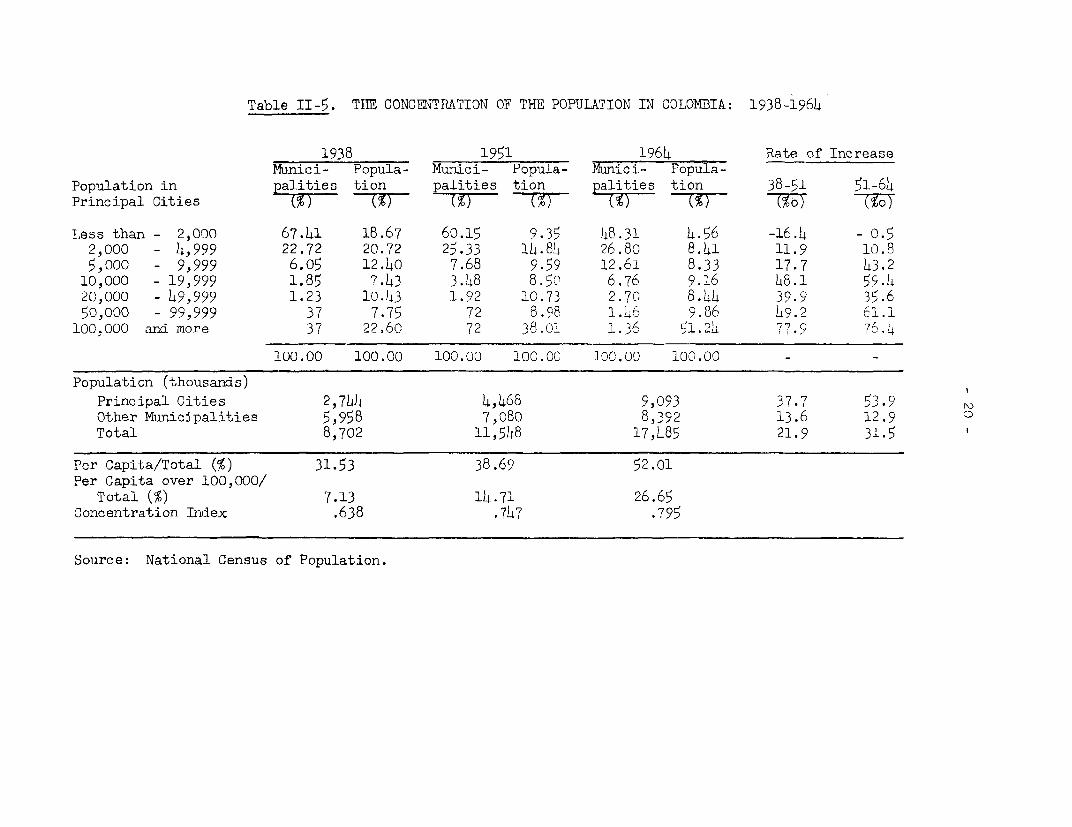
Table II-5. THE CONCENTRATION OF THE POPULATION IN COLOMBIA: 1938-1964
1938 1951 1964 Rate of IncreaseMunici- Popula- Munici- Popula- Munici- Popula-
Population in palities tion palities tion palities tion 38-51 51-64
Principal Cities (%) T%) (%) -Tl (M) 7M _JY 7%
Less than - 2,000 67.41 18.67 60.15 9.35 48.31 4.56 -16.4 - 0.52,000 - 4,999 22.72 20.72 25.33 14.84 26.80 8.41 11.9 10.8
5,000 - 9,999 6.05 12.40 7.68 9.59 12.61 8.33 17.7 43.2
10,000 - 19,999 1.85 7.43 3.48 8.5? 6.76 9.16 48.1 59.L20,000 - 49,999 1.23 1.43 1.92 10.73 2.70 8.44 39.9 35.650,000 - 99,999 37 7.75 72 8.98 1.4 9.86 L9.2 61.1
100,000 ard more 37 22.60 72 38.01 1.36 1.2L 77.9 76.4
100.00 100.00 100.00 100.00 100.00 100.00 - -
Population (thousands)
Principal Cities 2,744 4,468 9,093 37.7 53.9Other Municipalities 5,958 7,080 8,392 13.6 12.9 0
Total 8,702 11,548 17,485 21.9 31.5
Per Capita/Total (%) 31.53 38.69 52.01Per Capita over 100,000/
Total (%) 7.13 14.71 26.65Concentration Index .638 .747 .795
Source: National Census of Population.
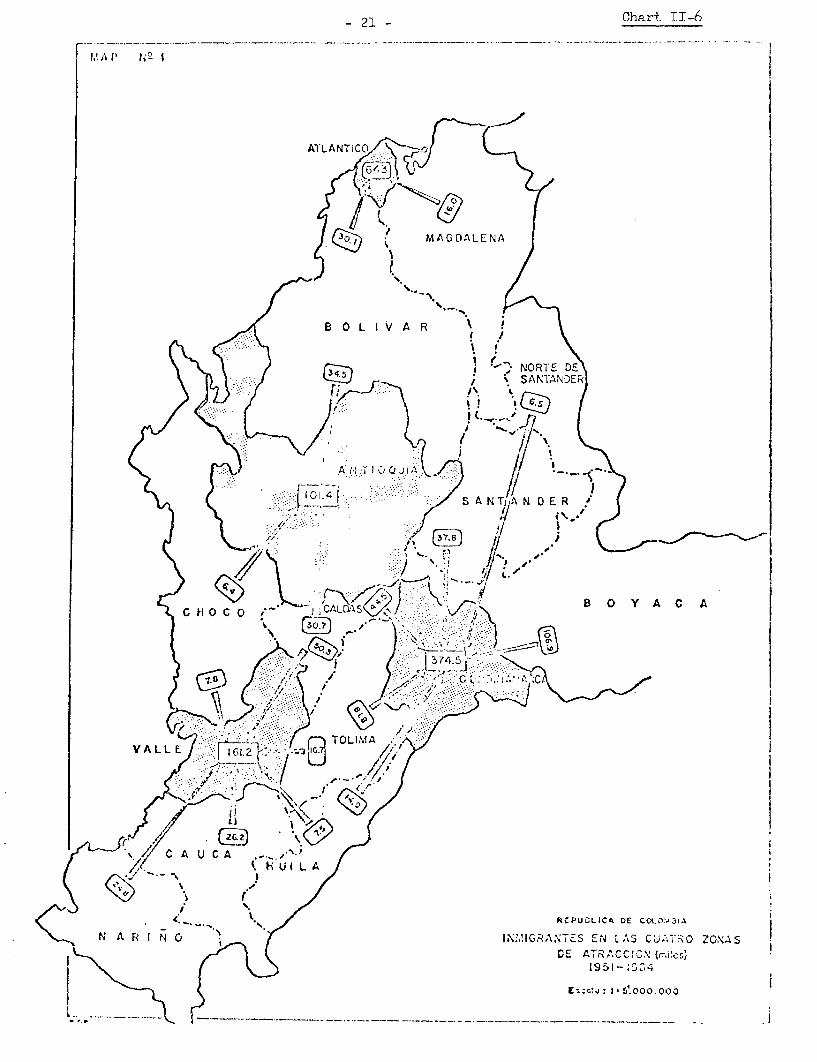
- 21 - Chart. II-6
1. A 1 I I
Al-LANTICO
l ( ( \ MAGDALENA
- ~ ~~ B L I V A R ! \
\> e ~~~~~~~~~~~A r o 1 Qul .... <_
) t i:: ilolt . g ~~~~~~~~~~S A NTy N D E R .
;7. .... O LIVMAR.A-
41~ ~ ~ ~~*
Y~~~~~~ ~ ~~~~~~~~~~~~~~~~~~~~~ 0s Y A. A
x,,C H U C A __,-
y~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. _, .L
< _._ t., ;JCJUA DkC .. / 1
IC
N~~~~~~2 A R I N -b IRNEc NLSCA1R CA
C A U C A \ 80 YAC A
C K 1951 -D C :,1
7 -' I E:' I 5 0
I, ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ -5.0.0
- 22 -
illness and disability and the receipt of health services. Householdinterviews were conducted on a representative sample of 8,961 householdscomprised of 51,476 individuals. A clinical examination was made of asub-sample of 5,000 persons. The survey covered the civilian, ambulatory,non-institutional population of the 18 "Departments" existing in 1964.The universe from which the sample was drawn included 98.7 percent of thenational population living in 52.7 percent of the country's area.
46. In interpreting the following data it should be kept in mind thatthey are now five years old and that changes undoubtedly have taken place,patticularly in economic status, in several parts of the country. It isprobable that such changes are more pronounced in the urban centers of thecountry and that less or no changes have occurred in the rural areas. How-ever, these are surmises and though Colombia is fortunate among developingcountries to have such background information available on which to planits health programs the continuing need for current and precise data demandsspecial emphasis.
47. Urban-Rural Residence. The survey found 51.5 percent of the popula-tion living in towns with T70T or more inhabitants. The remainder, 48.5percent, lived in small villages or farms. For Colombia as a whole 49.1 per-cent of the males lived in towns and cities and 50.9 percent were countrydwellers. In contrast, 53.8 percent of females were town dwellers and 46.2percent were in rural areas.
48. Household Size. The average size of households for the nation is5.9 members. 24 percent of the population lived in households with five orsix members, 25 percent in households with seven to eight members, 18 per-cent in households with nine to ten members and 17 percent in householdswith eleven or more members. Thus only about 1 in 6 Colombians shareliving space with 3 or less other household members. In urban households,the average size is 5.8 members in comparison with 6.1 members among theirrural counterparts. Although large families are characteristic of bothurban and rural areas, small families are more prevalent in towns. Amongwomen who have reached the age of 30, the modal range of previous livebirths is 6-9, with significant nunbers having had 15 or more childrenborn alive.
49. Housing. Fifty-nine percent of households live in a house orapartment, 10 percent in a room, 26 percent in huts or shacks, 1 percent inother types of accommodations and information is lacking for the remaining4 percent of households. Among city dwellers 85 percent live in apartments,houses or rooms, with 10 percent in huts or shacks; in the country only 51percent reside in houses or rooms and 44 percent made their homes in hutsor shacks.
50. Over two-fifths (44 percent) of the households have water pipedinto their home, while an additional 25 percent had a source outside theirdwelling. Thus, almost one-third of the households (31 percent) had nowater supply. Twice as many of the homes in the towns and cities (89 per-cent) were supplied with water as rural homes (46 percent). (3b). Overhalf of the homes in the countryside (54 percent) do not have a nearsupply of water (Table II-7).
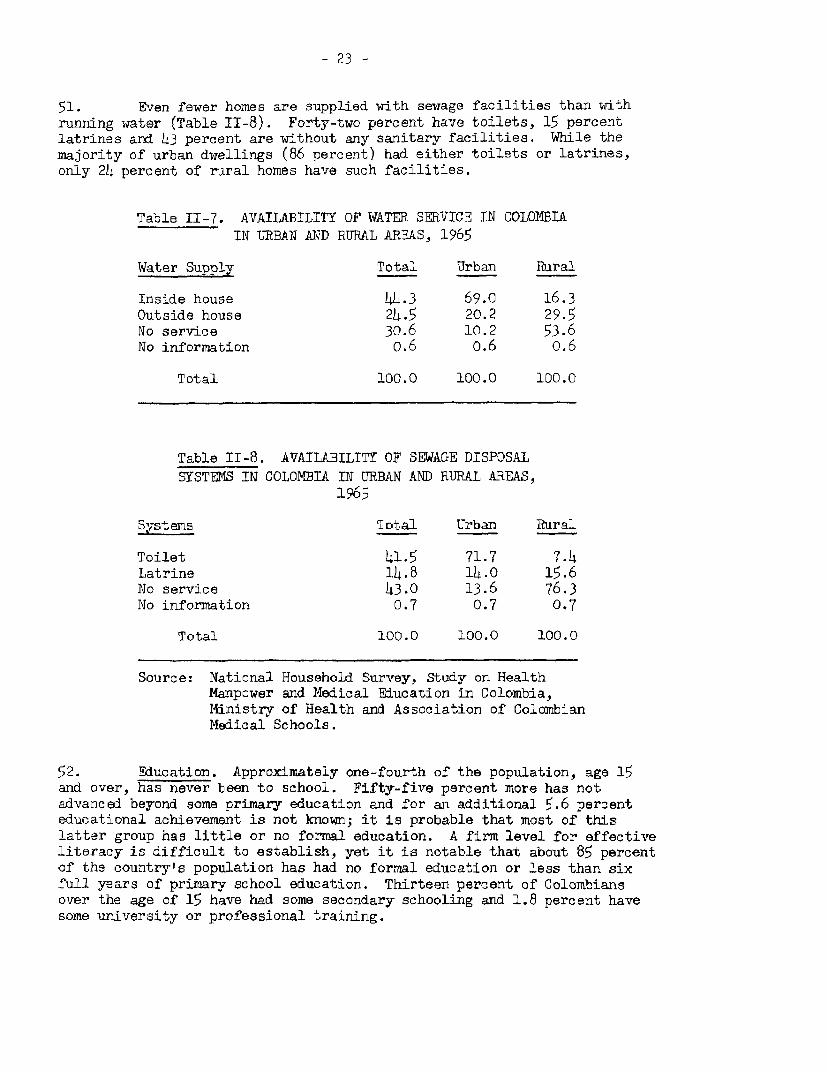
- 23 -
51. Even fewer homes are supplied with sewage facilities than withrunning water (Table II-8). Forty-two percent have toilets, 15 percentlatrines and 43 percent are without any sanitary facilities. While themajority of urban dwellings (86 percent) had either toilets or latrines,only 24 percent of rural homes have such facilities.
Table II-7. AVAILABILITY OF WATER SERVICE IN COLOMBIAIN URBAN AND RURAL AREAS, 1965
Water Supply Total Urban Rural
Inside house 44.3 69.0 16.3Outside house 24.5 20.2 29.5No service 30.6 10.2 53.6No information o.6 o.6 0.6
Total 100.0 100.0 100.0
Table II-8. AVAILABILITY OF SEWAGE DISPOSALSYSTEMS IN COLOMBIA TN URBAN AND RURAL AREAS,
1965
.t ems Iotal Urban Rura_
Toilet 41.5 71.7 7.4Latrine 14.8 14.0 15.6No service 43.0 13.6 76.3No information 0.7 0.7 0.7
Total 100.0 100.0 100.0
Source: National Household Survey, Study on HealthManpower and Medical Education in Colombia,Ministry of Health and Association of ColombianMedical Schools.
52. Education. Approximately one-fourth of the population, age 15and over, has never been to school. Fifty-five percent more has notadvanced beyond some primary education and for an additional 5.6 percenteducational achievement is not known; it is probable that most of thislatter group has little or no formal education. A firm level for effectiveliteracy is difficult to establish, yet it is notable that about 85 percentof the country's population has had no formal education or less than sixfull years of primary school education. Thirteen percent of Colombiansover the age of 15 have had some secondary schooling and 1.8 percent havesome university or professional training.
- 2)4 -
53. The educational experience of the population varies by residence.In general, people in cities have had more educational opportumity thanthose in rural areas. Over twice as many of those living in rural areas asin the cities (35 percent arnd 14 percent respectively) have had no -chooling.Twenty-six percent of the inhabitants of the cities have gone to secozidaryschools or to more advanced s-tuldies, but only 3 percent of' the r1uraJ.inhabitants (Table II-9).
54. Occupation. The most frequently reported occupations for theheads of households are farming and fishing (39 percent), followed in orderby- artisans and production workers (15 percent), salesmen (9 percent),housewives (8percent)and service workers '(8 percent). Relatively few areinvolved in professional (3 percent) managerial (2 percent) or clerical(3 percent) work. The occupations of the heads of the remaining 12 percentof households includes the armed forces, mining and transportation. Thesefindings do not yield an occupational profile for persons other than theheads of household, many of whom are gainfully employed. Nor do these dataindicate the degree of utilization of the manpower resources of the coimtryfor there are substantial evid'ences of unemployment, under-employment and,particularly in the agricultural sector, of seasonal employment.
55. Income. The median household annual income reported (1965) was4,348 pesos. (In their current equivalents - $290 U.S.). This varied byresidence, the median urban income being 6,645 pesos (U.S. $443) and themedian for rural households only 2,872:pesos (U.S. $191). (Table II-10).
56. The median income (1965) has been calculated for each occupationalgrouping. There is a close correlation between what a man does and howmuch income he reports. T'he highest median incomes are found for professionals(19,962 pesos), followed by business executives (13,309 pesos),office workers(11,183), transportation (7,540 pesos) and salesmen (7,134 pesos). Farmers,who constitute almost two-f'if hs of the heads of households, have a medianincome of 2,818 pesos and ranked next to the bottom.
57. The median amnual family income reported for each household variesnot only by occupation and residence but is also related to the level ofeducation of the head of the household and the size of his family. Forexample, 57.8 percent of those with a primary school education, 18.1 percentwho have attended secondary schools and only 2.5 percent with an educationbeyond the secondary school level report an income of 6,000 pesos or less.Over 81.8 percent of those with a superior education have an annual incomegreater than 6,000 pesos, 69.7 percent with a secondary education and only28.4 percent with a primary education earn a similar annual income.
58. Annual income also varies on a per capita basis by the size ofa household. The median per capita family income for families with onlytwo members was 1,715 pesos, for three to four member families 1,134 pesos,five to six mamber families 774 pesos, seven to eight member families 612pesos and nine to ten member families 528 pesos.
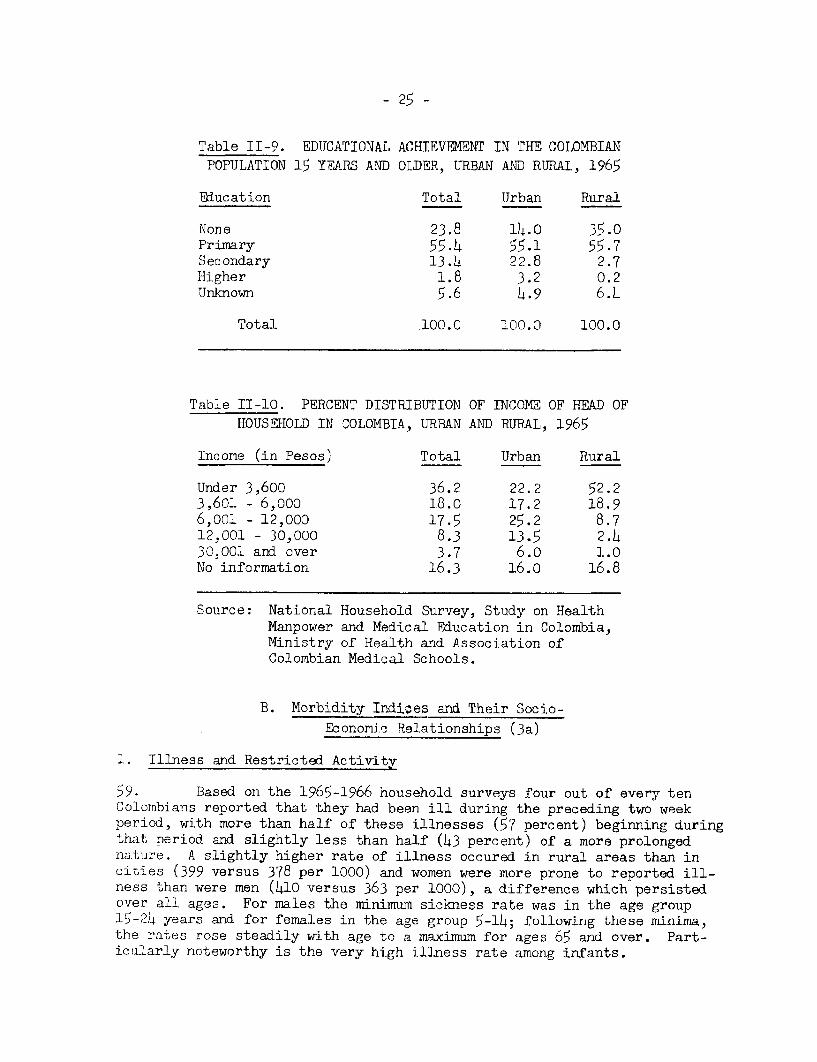
- 25 -
Table II-9. EDUJCATIONAL ACHIEVFMENT IN THE COLOMBIANPOPULATION 15 YEARS AND OLDER, URBAN AND RURAL, 1965
Education Total Urban Rural
None 23.8 14.0 35.0Primary 55.4 55.1 55.7Secondary 13.4 22.8 2.7Higher 1.8 3.2 0.2UJnknown 5.6 4.9 6.4
Total .100.0 100.0 100.0
Table II-10. PERCENT DISTRIBUTION OF INCOME OF HEAD OFHOUSEHOLD IN COLOMBIA, URBAN AND RURAL, 1965
Income (in Pesos) Total Urban Rural
Under 3,600 36.2 22.2 52.23,601 - 6,000 18.0 17.2 18.96,001 - 12,000 17.5 25.2 8.712,001 - 30,000 8.3 13.5 2.430,001 and over 3.7 6.o 1.0No information 16.3 16.0 16.8
Source: National Household Survey, Study on HealthManpower and Medical Education in Colombia,Ministry of Health and Association ofColombian Medical Schools.
B. Morbidity Indices and Their Socio-
Economic Relationships (3a)
1. Illness and Restricted Activity
59. Based on the 1965-1966 household surveys four out of every tenColombians reported that they had been ill during the preceding two weekperiod, with more than half of these illnesses (57 percent) beginning duringthat period and slightly less than half (43 percent) of a more prolongednature. A slightly higher rate of illness occured in rural areas than incities (399 versus 378 per 1000) and women were more prone to reported ill-ness than were men (4O0 versus 363 per 1000), a difference which persistedover all ages. For males the minimum sickness rate was in the age group15-2)4 years and for females in the age group 5-14; following these minima,the rates rose steadily with age to a maximum for ages 65 and over. Part-ictularly noteworthy is the very high illness rate among infants.
- 26 -
60. Many of the illnesses reported were mild and caused no restric-tion of activity or disability. However, the activity of approximatelyone person out of ten (108 per 1000) was restricted during this same twoweek period. Again, the rate for those in the country was higher than forcity dwellers (115 versus 164 per 1000). Females had a slightly higher rateof restricted activity than males (113 versus 103 per 1000) although overage 45 the rates for males were higher; for both males and females, re-stricted activity rates increased with age. From these data it has beencalculated that the average Colombian loses about 13.6 days per year fromhis usual activity because of illness. The rates for women are slightlyhigher than for men (14.5 days versus 12.7 days) and there is a sharpincrease with age. On the average, those between 25 and 44 years lose3 weeks per year (19.8 days) those between 45-64 years over four weeks(29.6 days) and those over age 65 years almost two months (53.6 days).
61. In the course of a year disability in bed due to illness averagedabout a week (7.3 days) for every Colombian. Variations by age and sexwere similar to those reported for the number of days of restricted activity.As might be expected, the annual average was higher for women than for men(8.6 days versus 5.8) and for both sexes there were sharp increases withage. Men over 65 years old had almost three weeks a year of illness whichconfined them to bed in contrast to four weeks for women. Although therural population reports more days of restricted activity they tend to beconfined to bed less frequently (6.9 days versus 7.7 days) than citydwellers. Tables II-ll, II-12 and TI-13 show some of the above illnessand restricted activity indices by age and sex.
2. Utilization of Health Services
62. How, when and to whom the Colombian population turns for medicalattention are questions of more than passing interest. These questions wereasked in the 1965 household sample survey for the two week period immediatelypreceding the interview. Almost 9 percent of the population (88.6 per 1000)sought consultation for reasons of health during that period. When personsare not ill they rarely seek consultation for health services (17.1 per 1000)but even when they are, only about one in five seek such aid (201.3 per 1000).The overall rate of consulting with a physician is 63.2 per thousand, con-stituting 72 percent of all contacts with health personnel. The rates forvisiting a doctor are three times greater for the urban population than therural.
63. When the sickness rates, reported above, are further comparedwith consultation rates it becomes even clearer that only a relatively smallproportion of individuals when they are ill are consulting any type of healthpersonnel for their complaints. In urban areas where the sickness rate was363 per 1000, the consultation rate was 118, only a third as much, and theconsultation rate for physicians was 93, about one-fourth of the sicknessrate. Among the rural population, these differentials are even more pro-nounced. With a sickness rate of 410, the total consultation rate was 57;consultation with a physician, 31 per thousand. Thus, when an individualliving in the country feels ill there is 1 chance in seven that he will seekany type of health assistance and 1 chance in 13 that he will be seen by aphysician.
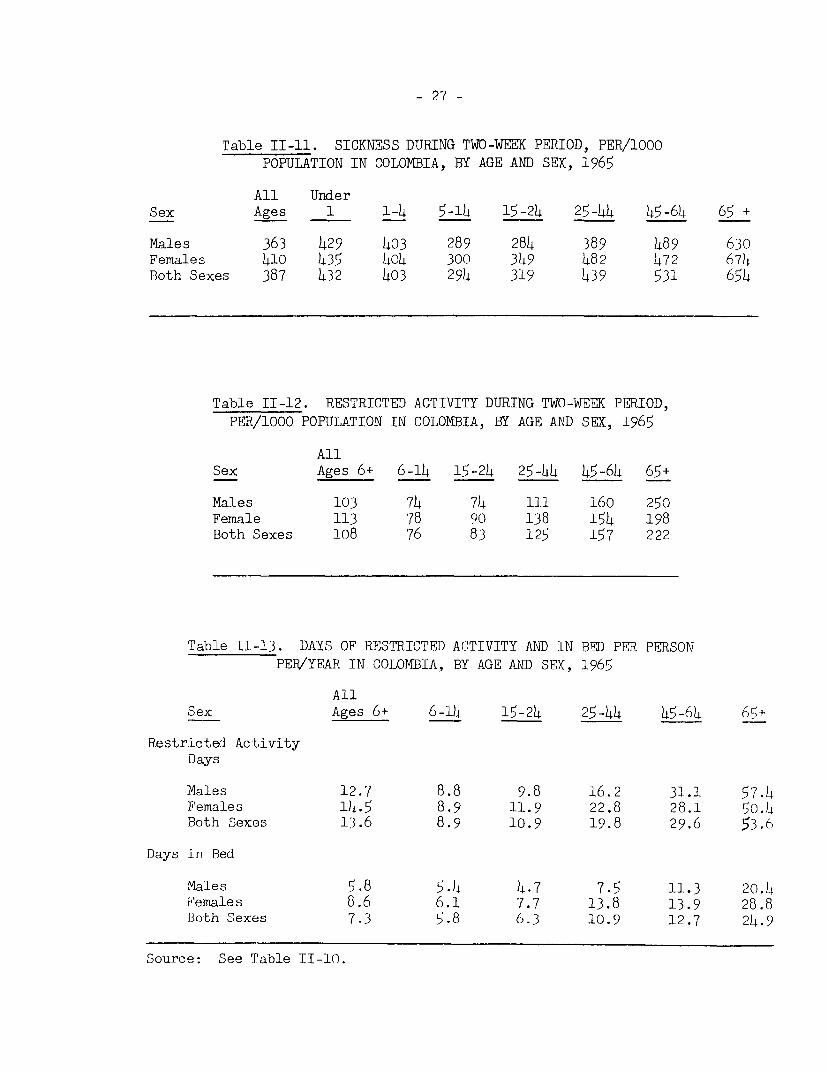
- 27 -
Table II-ll. SICKNESS DURING TWO-WEEK PERIOD, PER/1000
POPULATION IN COLOMBIA, BY AGE AND SEX, 1965
All UnderSex Ages 1 1-4 5-14 15-24 25-44 45-64 65 +
Males 363 429 403 289 284 389 489 630Females 410 435 404 300 349 482 472 674Both Sexes 387 432 403 294 319 439 531 654
Table II-12. RESTRICTED ACTIVITY DURING TWO-WEEK PERIOD,
PER/1000 POPULATION IN COLOMBIA, BY AGE AND SEX, 1965
AllSex Ages 6+ 6-14 15-24 25-44 45-64 65+
Males 103 74 74 111 160 250Female 113 78 90 138 154 198Both Sexes 108 76 83 125 157 222
Table II-13. DAYS OF RESTRICTED ACTIVITY AND IN BED PER PERSONPER/YEAR IN COLOMBIA, BY AGE AND SEX, 1965
AllSex Ages 6+ 6-14 15-24 25-44 45-64 65+
Restricted ActivityDays
Males 12.7 8.8 9.8 16.2 31.1 57.4Females 14.5 8.9 11.9 22.8 28.1 50.4Both Sexes 13.6 8.9 10.9 19.8 29.6 53.6
Days in Bed
Males 5.8 5.4 4.7 7.5 11.3 20.4Females 8.6 6.1 7.7 13.8 13.9 28.8Both Sexes 7.3 5.8 6.3 10.9 12.7 24.9
Source: See Table II-10.
- 2j8 -
64. Of aLl. consultatiors provided by a phys itiali abouit; one-thirdtook pl,ace i-ri IhJie physiciafns prjivate office, arn ecqual proportiorn in
institutitons fl0bt-pai.tienft departmen Lls, clinics, h^-alth cerlters, etc.),
11 percent in h-louse calls and the balan ce, about 17 percent. through otherarrar-gements. There is cor- i,derable variation between urbaii and ruiralareas. For the urban popiuLat;ioin, LW.*h per thousand saw physic(i.ans ininstitutions as compared to i11. 3 pet 1000 in ruralL areas, p.? per 1000urbarn residents,; had hoJuse 1alls but only 9.1 in rural areas.
65. After the physicianr, the mosit frequently consultedi hea.lth workerswere pharmacists (9.2 per l\00) arid nulrses (2.2 per 1000). The urhan-ruraldifference in the consultaltiorts -wil;h health personLnel persi3st:d but:. wereless pronounced. ,7Note: it is not pos;sible to difTerentiai:,e whet;her nurseconsultations were wit.h profeoisioncilly brainried nurses, pract ical nurses(auxiliary nurses) or aides_.7
66. Approximately 13 percent of the consultations about health arewith other types of health workers *-- the tegua, the midwif'e and others --unsanctioned and often unrecognized by the medical profession. Thesegroups provide a significant proportion of all medical care available tothe population. If patterns of heaL-th care consultation with unisanctioned,so-called indigenous, practitioners comnmon to ot.her parts of the world apply
in Colombia these figures may be gross understatements of the true pictureof the population's search f'or relief from their medical ills.
67. Hospital utilization - Almnost 23 percent of -the population hashad some past experience with hospitals and 5 percent has been hospitalizedwithin a year. Of the latter gIo'up 89 percent had been hospitalized once,8.6 percent twice and over 2 percen.t three or more times. More urban re-sidents seek hospitalization thatn rural dwellers. In a year, more womenare hospitalized than men, 64.2 and 35.9 per 1.000 respectively. Thi-sdifferential is everi more irw .ud in the age period l5-54 years when womenin the child bear ing period are hospitalized primarily because of complica-tions of pregnancy, delivery or in the post partem.
3. Socio-Economic Correlates of Morbidity and
the Utilization of Health Care Resources
68. The close associations of disease, malnutrition, lack of sanitation,poverty, crowding, illiteracy and. the other stigmata of underdevelopment areall well recognized aind well documented. In Colombia, data are availablefrom the National Health Survey to demonstrate sorme of these direct correla-tions and a few are selected in this section for illustrative purposes.(3b)
69. As shown in Table II-1)4 the rate of reported illness is twice ashigh for individuals wit;h no formal educational experience (oll per 1000) asfor those with education beyond the secondary level (199 per 1000). Similardifferences characterize the associationi of reported illness with income
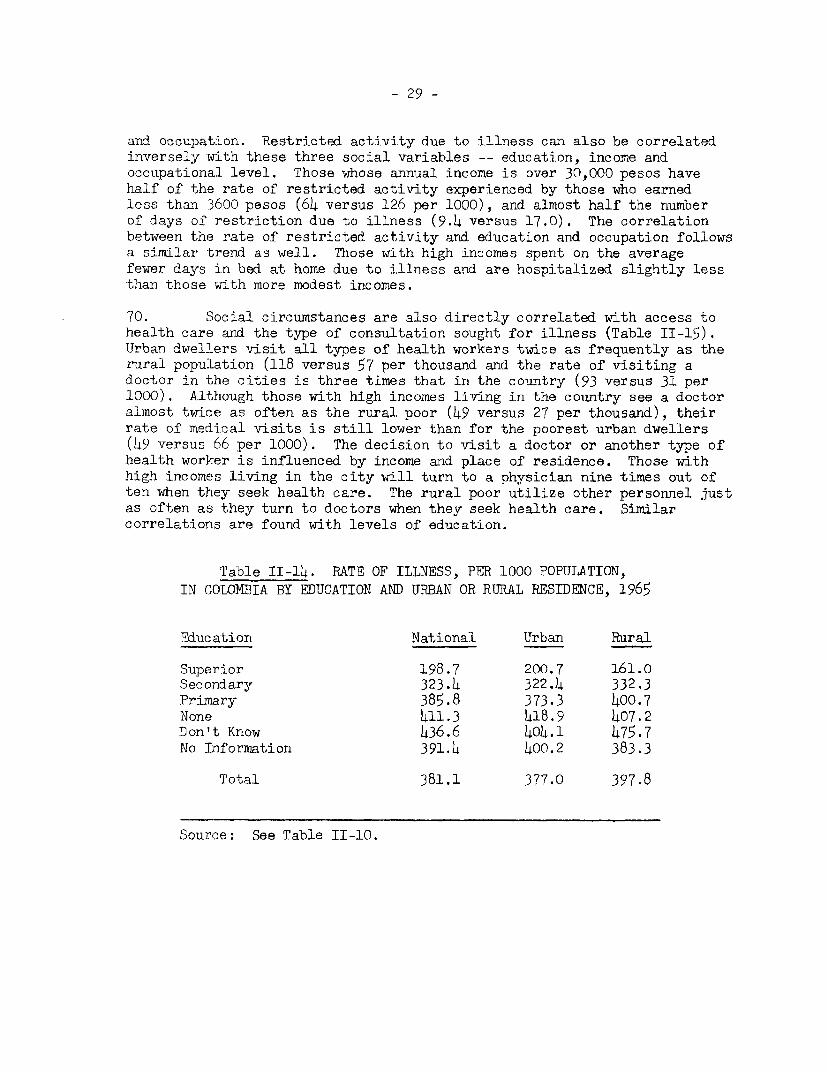
- 29 -
and occupation. Restricted activity due to illness can also be correlatedinversely with these three social variables -- education, income andoccupational level. Those whose annual income is over 30,000 pesos havehalf of the rate of restricted activity experienced by those who earnedless than 3600 pesos (64 versus 126 per 1000), and almost half the numberof days of restriction due to illness (9.4 versus 17.0). The correlationbetween the rate of restricted activity and education and occupation followsa similar trend as well. Those with high incomes spent on the averagefewer days in bed at home due to illness and are hospitalized slightly lessthan those with more modest incomes.
70. Social circumstances are also directly correlated with access tohealth care and the type of consultation sought for illness (Table II-15).Urban dwellers visit all types of health workers twice as frequently as therural population (118 versus 57 per thousand and the rate of visiting adoctor in the cities is three times that in the country (93 versus 31 per1000). Although those with high incomes living in the country see a doctoralmost twice as often as the rural poor (49 versus 27 per thousand), theirrate of medical visits is still lower than for the poorest urban dwellers(49 versus 66 per 1000). The decision to visit a doctor or another type ofhealth worker is influenced by income and place of residence. Those withhigh incomes living in the city will turn to a physician nine times out often when they seek health care. The rural poor utilize other personnel justas often as they turn to doctors when they seek health care. Similarcorrelations are found with levels of education.
Table II-14. RATE OF ILLNESS, PER 1000 POPULATION,IN COLOMBIA BY EDUCATION AND URBAN OR RURAL RESIDENCE, 1965
Fducation National Urban Rural
Superior 198.7 200.7 161.0Secondary 323.4 322.4 332.3Primary 385.8 373.3 400.7None 411.3 418.9 407.2Don't Know 436.6 404.1 475.7No Information 391.4 400.2 383.3
Total 381.1 377.0 397.8
Source: See Table II-10.
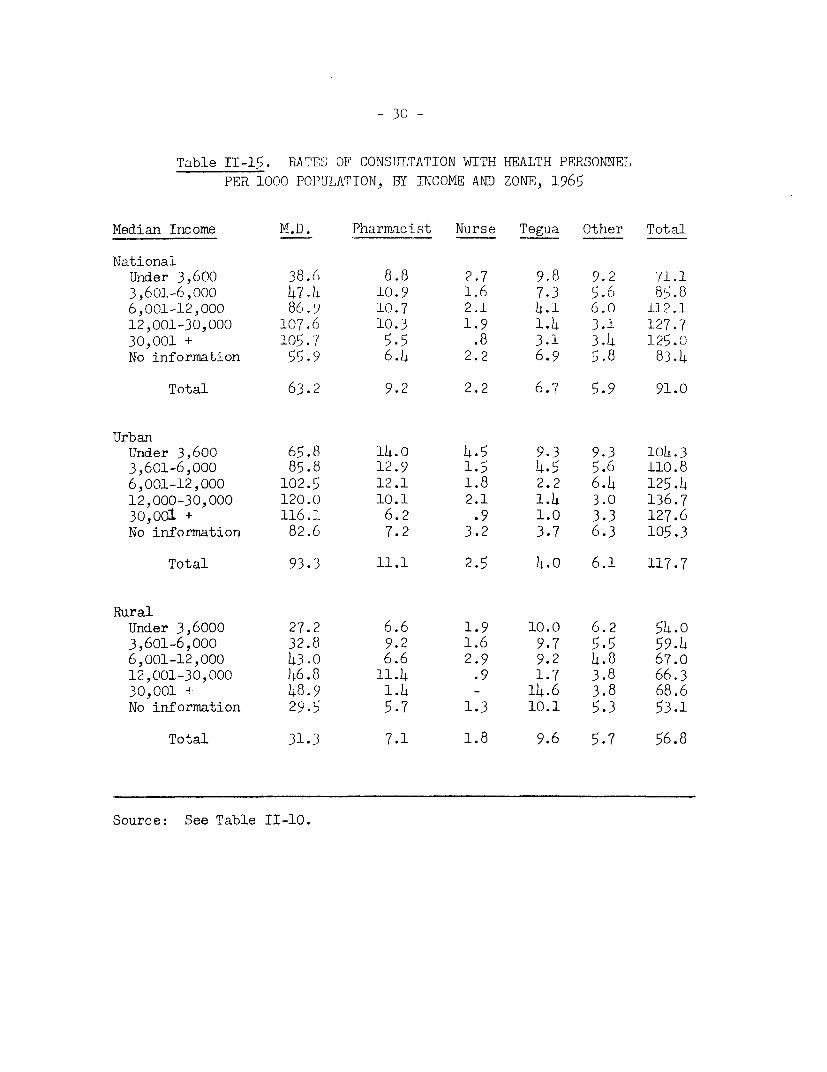
- 30 -
Table II-15. RATES' OF CONSUJLTATION WITH HEALTH PERSONNELPER 1000 POPULATION, BY INCOME AND ZONE, 1965
Median Income M.D. Pharmacist Nurse Tegua Other Total
NationalUnider 3,600 38.6 8.8 2.7 9.8 9.2 71.13,601-6,000 47.4 10.9 1.6 7.3 5.6 85.86,001-12,000 86.) 10.7 2.1 4.1 6.0 112.112,001-30,000 107.6 10.3 1.9 1.4 3.1 127.730,001 + 105o. 5.5 .8 3.1 3.4 125.0No information 55.9 6.4 2.2 6.9 5.8 83.4
Total 63.2 9.2 2.2 6.7 5.9 91.0
UrbanUnder 3,600 65.8 14.0 4.5 9.3 9.3 104.33,601-6,000 85.8 12.9 1.5 4.5 5.6 110.86,001-12,000 102.5 12.1 1.8 2.2 6.4 125.412,000-30,000 120.0 10.1 2.1 1.4 3.0 136.730,001 + 116.1 6.2 .9 1.0 3.3 127.6No information 82.6 7.2 3.2 3.7 6.3 105.3
Total 93.3 11.1 2.5 4.0 6.1 117.7
RuralUnder 3,6000 27.2 6.6 1.9 10.0 6.2 54.03,601-6,000 32.8 9.2 1.6 9.7 5.5 59.46,001-12,000 43.0 6.6 2.9 9.2 4.8 67.012,001-30,000 46.8 11.4 .9 1.7 3.8 66.330,001 d 48.9 1.4 - 14.6 3.8 68.6No information 29.5 5.7 1.3 10.1 5.3 53.1
Total 31.3 7.1 1.8 9.6 5.7 56.8
Source: See Table II-10.
- 21 -
C. Mfajor Categories of Health Problems in Colombia
71. Dependnble data on the frequency of specific disease enti ties orother major he1lnth problems - either as causes of death or of morbidity -are limited for a variety of reasons. First, there a:re severe shortnges ofrFlrysWIciars or cther hea7th -ersonnel qualified to reach even reasonablyaccurate diagnoses. Choose who are available Rre highly concentrated in theLew large cities of the country. Sncondly, the system for registration ofimnortant vital events is poorly mannred, inefficient., cumbersome and veryta.rdy in the t-abula-tion and of even annual sumnaries. Aspointed out; in a previous section (.Section B. 2), for large parts of thecountry, oniy I in 13 of those rep-ortng illness of any type were seen by aphysician during that illnRss . Also, it. has been esti-m,rated that up toone-third of the deaths occurrTIg in Colombia fail to reach the notice ofthe official registrars; of the notified deac,hs less than 60% are medicallycert.fied, even thougn such certificatin does not imply that the individualconcerned received m,edical attenti on durinL his- terminal- illness.
7.- The Natioln. HeltSh 5,JC\Oy of 1965 nndl ot,er speci.al studiesconducted more recently, indicate tha,t. this si tuatior! is improving, at least;in some areas of the country. Foweveer, considernble ca¢utjiorn must be appliedin interpreting currently a4va--iilable data for they undoubtedly underestimnatethe magnit)ude of each of the mna,jor deve-lopmenta9l henlt..h problems thatconf'ront the health auttonj ti es of the country. The following bri;efsunmaries of selected manjjor disease categori es and he_.lth problems are-ncluded for illus3trati-ve purposes.
1. Diarrheal Diseases and Related Conditions
'(3 T' Is grotin of conditJions Is clea3rly associ nted with the low levelsof envi ronrriental7 sanitation still prevalent in the country particul.,rlyauts`ide of the nmajor cities nd. n the rural areas (see Tables 11-7 and T1-B)It casn be estimated th.t no less thian orne in edgiht of a11 deaths are,ssoci ated with enterinc infections. They g,ive ri se t,o almost 8.5 percent
of all ronsiji tati oars w1 th heaI th personnel and compri se the second, orpo.sSiiJy t-he third, most frequent cause of' hosrpi fiKi ration. The toll of(i.rcheal iesses is grea-test in the early years of l.ife but no age group
s s -lored L] in kedi tc, tLiese condi t ors .-re the paras: i rc trfections of thegIsstrGin,testnal tract which i.n addition to causi tin' fhei r ownm morbidity anndmoI'tri.j Iy add a significant. burden to the nutritinnal requirements of thepopula-Jonr As n speci.al phlase of the National hlealth Su)rvey it was found-that over- 60 percent of the popula-tion harbors one or more variet.es ofp.athogenic: intestit al worms and other rarasites; infestation is h-alvest inchildhood and thne tyoung adultIt years and in the rural areas where lowet in-come and levels of educatiorn prevail and ;where there -s the least ac-ess t5o. tanmtation of rAamer supplies and sewq,age disoos.a] . (gp).
2. Th Corrmrorn Acute ITrfectious (iseases (of childhcod)
'I. fea; tsi ndi moBrbi di t;y ir i nr 'ncy a:n d early chiildhood rerri n hu:k i7in1 PcI omhi ilaivl e vonl thou gh. approlweci 7Abe reduc ti ens have heen nm....e it r ,n.n'yelrL . UulenlrlyJig mr lilut rI ;i on air-- gsn tIrolr oesti nal in fectionris are,in al
- '12 -
probability, the most si.gnJi'icant. factors for even in mild for- t.hey canaLso severely i.ncreasti t;he t.oil oJ lhe common infections of ch-i L.iood. Modernmedical technology has dievej nped simple a--nd re] ativeLy inexpensive immunizationprocedures to prevent many of' these common inf'ecti onF but on1 y 1imited successhns yet been attai ne( in protectirni the Colombi-a populi a Lion. For exim lp eonl y :13 percent of the susceptaible popul iti on (unde(r age .5) h:tve beernimmuinize(d a>gainst whooirigr cough , ' percent. (under ]5) ag-inst. diphtheri aand 5 percent against poi i eo (under age 5). VMeasles vracci nati on, one of thenewest yet most. usefull. pro)hyl .acti c procedures, ha.s not yet been sup)li edthrough publi c hea1 th channels aind tetanus toxoid has been gi ven to ibout1 percent ol' the general pop'ili.ati on. On the other hand smai] -oy vaccin;tionhas beern gyiven to 5z percentl. of a].l afge groups, a level of' protectionwhi.ch is considered low were this devas-t.ating infec tion to be rei.ntroducedinto the population. The neniiAh auijthorities have adopted the policy of'givingg BCG -vaiccinitdion as :i means of' protection against tuberculosis but;efforts to date have not e..oee.1e-l the immuni .- tien of B percent of thepodul -,ti on .
3. Malnutrition
75. Colombhi an authori-ities and external .ssi.st,Lnce agernci.es h-ve recog-ni.zed the needl for correcti.ng thle severe nutr;.tionnl deficiencies of' theColombian pooulatl 0!.on and curr0rent.I; i>'xtensi.ve progr.aims, costing in the rangeof U.S. $5 ail 1li orq arird a ar c nr s and lr1.1 be contin.ued for atleast. a f'ive ye. r per i o0 . o nt h r Pn,ior he.-lth problem in Colombia-i h.s beerso intensively studied, no naS 'h -a well. pla)nlirod o0 so imbitiou;s a program
been devisedi against otiher iriV jor health problems equivalent to tha-t current.lyunder way in this country-iride attack on mnalnutrit.ion. Yet the extent ofthe problem is so great, the liactors contri buting to it, so complex and theimplications for the tot.al economic and social (development, of' Colombia sopervasive that meazsures short of those plarned would be ill advised. TableII-16 shows the categories of nultritional deficiencies identified insampl]e studies conducted by the Insti Lute of Nutri Lion, according to urban-rural residence and fanilv i.nc-rte . For all classes of the population onlytwo nutri tional requi.rements are adequntely met - those for iron and vitamin C,whereas caloric, protein, minerail and other vitamin needs are significantlydeficient. Additiornal data- are avai.ilable demonstrating that malnutri ti onis heavily concent.rated ir! early childhood where growth requirements arehigh and where nutrit.ional deficits are directly reflected in increasedsusceptabili ty to intercurrent i nfections and retarded physica. and intel-lectual development. A second. highly vulnerable group i.s made up of pregnantrnd lactating mothers. Although direct measurements are lacking in Colombiasubstantial evidence derived f'ronm studies in other countries indicate thatthe efficiency and product:i.vity of t,he total working population is reducedwhen their nutritional requirements are unmet and that absente6ism andlearning curves of school children are comparably impaired under similarconditions.
. Tuberculosis and Other Chronic Infectious Diseases
76. In recent years both the mortalitty rate and the prevalence of
tuberculosis disease have been following a steadi:ly downward trend.
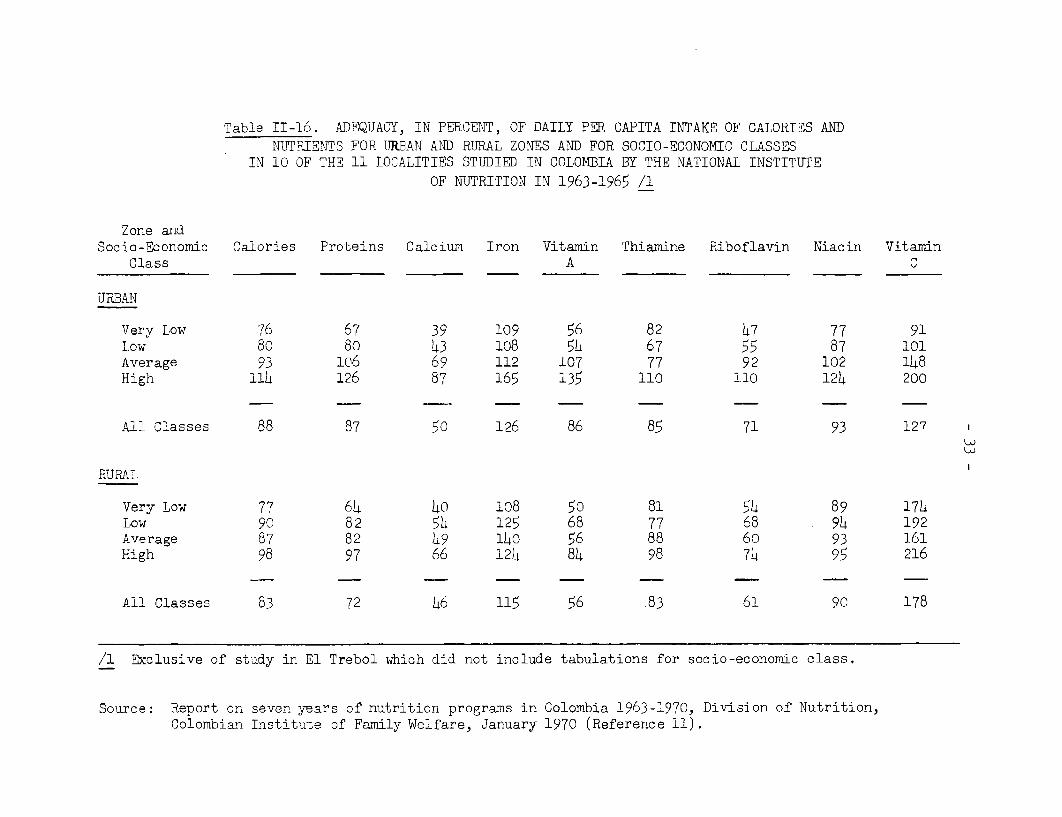
Table II-16. ADEQUACY, IN PERCENT, OF DAILY PaR CAPITA INTAKE OF CALORIES ANDNUTRIENTS FOR URBAN AND RURAL ZONES AND FOR SOCIO-ECONOMIC CLASSES
IN 10 OF THE 11 LOCALITIES STUDIED IN COLOMBIA BY THE NATIONAL INSTITUTEOF NUTRITION IN 1963-1965 /1
Zone andSocio-Economic Calories Proteins Calcium Iron Vitamin Thiamine Riboflavin Niacin Vitamin
Class A C
URBAN
Very Low 76 67 39 109 56 82 47 77 91Low 80 80 43 108 54 67 55 87 101Average 93 106 69 112 107 77 92 102 148High 1iL 126 87 165 135 110 110 124 200
All Classes 88 87 50 126 86 85 71 93 127
RURAT.
Very Low 77 64 4O 108 50 81 54 89 174Low 9C 82 54 125 68 77 68 94 192Average 87 82 49 140 56 88 60 93 161High 98 97 66 124 84 98 74 95 216
All Classes 83 72 46 115 56 83 61 90 178
/1 Exclusive of study in El Trebol which did not include tabulations for socio-economic class.
Source: Report on seven years of nutrition programs in Colombia 1963-1970, Division of Nutrition,Colombian Institute of Family Welfare, January 1970 (Reference 11).
- )4 -
These improventents are reflactions, in part, of better case finding pr,-cedures and tthe inst-itition of modern therapeutic inet1ioKt-;, including chemo-therapy, BCG imnlzization arLd chemoprophylaxis. C-u-rent death rates, in therange of 20 pe 10i0,000, can be comirpared favorably wJith those of other majorLatin American comintries b:ut, are B' or more t,imes higher than those currentlybeing observed in Korth America. Deaths and known cases are heavily concen-trated in the older age groups but the true extent of this, as yet lncontrolledproblem, is obscured by the seriouisly underreported number of cases. In orderto make international comparisons, -it is still necessary to adopt, ani arbitrar-ily selected "corrective factor" arid apply this -to the reported numrbher ofcases or deaths.
77. Syphilis appeatrs t;o he on thle increase in oloJIi-a andl Wi. . <ehas been noted bhy somrte rIbL.ervers as reflecting greater fIrecluencY of' tsans,.ionto new cases -nd not. imereiy anf 1icrlC:rtease in recogrdbionr) and ILarger nuiibers.under treatmentO. Lprosy an l yaws are two other chronic infectious (diseasesnoted in Colombia and thought their frequency is nlot so great as -Io consti to.it.e
major health problems, they hlave absorbed significant pubblt: healt,h effortto maintain them ureder} reasonable control.
78. Malarl a. l3egiin-li;ori .-n 15i,8 an extensive program of mariaeradication was irnitiated iri l ooperat;on with PAHC' and UNICEF wit-h additionalbilateral,technical and financi.al assistance from the U.S. A survey coniductedat that timre iudicatec1 tba.t .Kar&lyn 8 percent of the population was infcictedand that it was the l4th i c;.use of illness in the country producingan annual economic 1 eso,.Oi:A-tedd in the range of 58 mil].ion pesos. Initialsuccess permlitted th(2 opeiJ4)- up of large areas of the country t,o ec-ploitat tonand colonil zation Lw hi, 0- '- moch of the campaign's momenltum was lostdue to tihe unavail. !:.y of .. icicent funds, Since 1966 theprcgraml has been reorg.an.i-'od 'e-2 rdow is art integral part of the 10 yearNational Health Prograv m u w',.Q-7'77) w.`th concenttroted attack operationsscheduled for -the first ft'vf- and the consolidati-on phase completingthe ten year schedu.le. Al, ;r,e cocl1usion of the rtuss campaigrn, continuedvigilence in the rphn ance nhise of eradication will rest with the local.decentralized heal. sL i vi ,Ies. -iTe highland areas of the country areessentially free of ri.k ot rriaIlatia transmission. (17 percent of the landarea and 44 percentof populationi have been desigrnated as free of malaria),An additional 22 percent of the land area and 42 percent of the populationare now designated a, in the consolidation phase; the balance, with 61percent of the lanid area but only 14 percent of the population,now fall intothe active attack area. (Most of the Llanos Area with less than 3 percent of thepopulation is excluded fromn: the ahove analysis.)
79. Based on the applic-ation of modern case finding methods, conductedin the field, less than 3 per 1,000 of the population is now believed toharbor malaria plasinodia, a significant reduction in the foci and sources ofinfection which were estimated to approach about 80 per thousand about tenyears earlier. The costs of this antimalarial program have been substantialwith no less than $36 million (U.S.) having been invested in the period 1958-1967. To bring it to its ultimate fruition in 1977, fund requirements willcontinue to be large with the National Health Plan calling for an additional$33 million (U.S.) needed for this purpose.
- 35 -
5. High Fertility and Abortions
80. Factors associated with high rates of population increase -- aphenomenon commonly identified with early stages of economic and socialdevelopment -- are not well known and even less well understood. The 1965-1966 National Health Survey has provided unique information for criticalappraisal of some of these factors. Many of these analyses should havesignificant implications for health planning not only in Colombia butelsewhere.
81. The Colombian population is young; 46.6 percent is less than 15years of age and only 6.8 percent is more than 5)4 years of age.I/ A lowerproportion of females less than 15 years old lives in the urban zone; ahigher proportion of women between 15 and 54 years of age lives in theurban zone. In the lower-income group 49.6 percent of the population isless than 15 years of age; in the higher-income group 38.5 percent is thatage. Inversely, the population between 15 and 54 year's old amounts to )42percent and 52.6 percent of the lower- and higher-income groups, respec-tively. The female population, age 15 to 54 years, is 24.2 percent of thetotal population of Colombia. Of that group, 22.7 percent has not attendedschool at all and on4y 16.1 percent has attended some years of intermediateor higher education.
82. The annual rate of pregnancies is 198.3 per 1,000 women of fertileage. The rate is higher in the rural zone (237.7) than in the urban zone(168.0), and diminishes as social and economic conditions improve.
83. Of each 100 pregnancies 11.7 terminate during the early fetalperiod, 2.0 in the intermediate fetal period and 86.3 in the late fetalperiod, 77 of which end at normal term. Fetal deaths account for 16.5 per-cent of the products of pregnancy.
84. The overall birth rate of the country is high. Even assuming thelower of the two rates discussed above (see para. 30) of 40.0 per 1,000inhabitants, this figure is 8.6 percent higher than that obtained throughthe record of baptisms. The urban and rural birth rates, adjusted to thepopulation of the country by age and sex, are 31.3 and 51.6 per 1,000 in-habitants, respectively.
85. The specific fertility rate is 165.0 per 1,000 women aged 15 to54 years; the urban rate is 129.4 and the rural rate is 211.3.1/ The
1/ These data are derived from the 1965-1966 National Health Survey (Ref-erence 3b). For age distribution of the population, 1970 populationestimates show no essential change; the percentage under age 15 isalso 46.6; and for 55 and over, 6.6 percent.
2/ These fertility rates are lower than those reported in para. 34 above.These differences arise from the fact that published rates for Colombiaare based on the use of ages 15-5)4 to define the child-bearing ageswhereas the usual practice is to include only women, ages 15-)4)4. Ratesreported in para. 34 were recalculated for the age period 15-44.
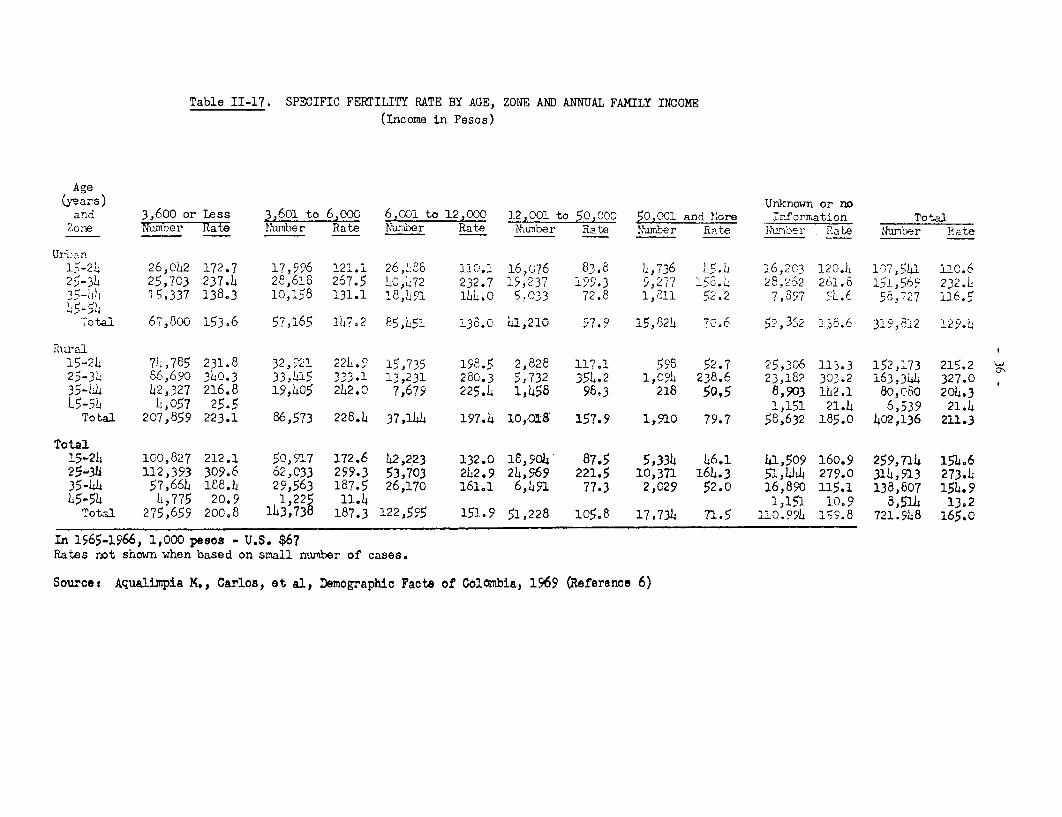
Table II-17. SPECIFIC FERTILITY RATE BY AGE, ZONE AND ANNUAL FAMILY INCOME
(Income in Pesos)
Age(years) Unknown or no
and 3,600 or less 3,601 to 6,ooo 6,001 to 12,000 12,001 to 50,000 50,001 and Nore T nfor maation TotalZori Numoer Rate Num.ber Rate Nurbaer Rate Nwnber Rate Nwmrer Rate Numr,ber Rate llzniber Rate
Urban26,042 172.7 17,99% 121.1 26,LP8 11C.1 16,076 8. 8 4,736 L5.L4 i6,203 120.4 107,S541 110.6
25-34 25,703 237.4 28,618 267.5 LO,L72 232.7 15,237 9.3 5,277 13 2-.262 261.8 15,.569 232.J35-I1)4 i5,337 138,3 10,158 131.1 18,41 1U4.0 5.033 72.8 1,S11 52.2 7,397 5L).6 58 727 16.5
Total 67,800 153,6 57,165 1,.2 85 451 138.0 4i,21 97.9 15,824 70.6 52,321 A ^ 82 129.'
PhLral15-24 714,785 231.8 32,921 224.9 15,735 198.5 2,828 117.1 598 52.7 25,306 113.3 152,173 215.225-3)4 86,690 340.3 33,L15 333.1 13,231 280.3 5,732 354.2 1,0,° 238.6 23,182 303.2 163,344 327.035-L4 L2,327 216.8 19,405 2 42.0 7,679 225.4 1,h58 98&3 218 50,5 8,903 162.1 80,080 204.3I5 45 4057 25.5 1,151 21.4 6,539 21.4
Total 207,859 223.1 86,573 228.4 37,11L) 197.4 10,018 157.9 1,910 79.7 58,632 185.0 402,136 211.3
Total15-21) 100,827 212.1 50,917 172.6 42,223 132.0 18,904 87.5 5,334 46.1 41,509 160.9 259,714 154.625-34 112,393 309.6 62,033 299.3 53,703 242.9 24,969 221,5 10,371 164.3 51,444 279.0 31)4,913 273.435-44 57,66h 168.) 29,563 187.5 26,170 161l1 6,)491 77.3 2,029 52.0 16,890 115.1 138,807 154.945-54 It, 775 20.9 1,225 11.4 1,151 10.9 8,514 13.2
Total 275,659 200.8 143,738 187.3 122,595 151.9 51,228 105.8 17,734 71.5 110. 99) 19.8 721.948 165.0
In 1565-1966, 1,000 pe3so - U.S. $67Rates not shonm when based on small number of cases.
Source, Aqualixnpia M., Carlos, et al, Demographic Facta of Colombia, 1969 (Reference 6)
- 37 -
highest fertility by age is among the women aged 25 to 34 years, with arate of 273.4 (see Table II-17). According to the specific fertility ratesof the country, a woman might have six children during the course of herreproductive life. That figure would vary from 4.7 children in the urbanzone to 7.7 in the rural zone. The different indicators of fertility con-sistently show that the fertility of rural women is 38 percent higher thanthat of urban women. In addition, fertility is 50 percent higher in someregions than in others. The differences are maintained in all age groupsby zone and family income, although the differences are more accentuatedin the extreme age groups.
86. The estimated 117,401 abortions among women aged 15 to 54 yearsamount to a rate of 136.1 abortions per 1,000 pregnancies, or one abortionfor every six live births (Table II-18). The risk of abortion increaseswith age, is higher in women without children and is reduced as the numberof children previously borne increases. The abortion rate is lower inwomen of rural areas with lower family income or little education. Therate is intermediate among women, urban or rural, who have more educationor higher income. The highest abortion rate is found in women of the urbanzone with a low level of education or low incomes.
87. The estimated number of induced abortions is 65,600 in one year.That figure corresponds to a rate of 76 per 1,000 pregnancies and is 65 per-cent of all abortions that occurred before 20 weeks gestation.
88. Rural women and women of low socio-economic level have a highfertility rate, probably attributable to their limited use of methods to con-trol fertility. Urban women and women of intermediate socio-economic levelhave a lower fertility rate achieved by increased rates of induced abortionsand prevented pregnancies. Women of high socio-economic level have the low-est fertility rate, a low rate of induced abortion and the highest rate ofprevented pregnancies. The comparisorn by regions reinforces the inverserelation between the fertility rates and abortion rates. (See Chart II-19).
89. A total of 23,241 still-births were reported; a rate of 26.9 per1,000 pregnancies or 32.9 per 1,000 live births. The risk of still-birthincreased with age, but no significant differences could be found relatedto socio-economic level of the mother.
6. Accidents (4 e.)
90. Accidents cause about 4.5 percent of all deaths in Colombia witha death rate of 4.4 per 10,000 population. Males experience three times therisk of females and risk increases with age. Transportation accounts formore than one-fourth of all fatal accidents, with falls and deaths from burnsfollowing in that order. No major trend has been noted. in recent years inthe rate of fatal accidents although accidental death due to vehicles appearsto be increasing slightly.
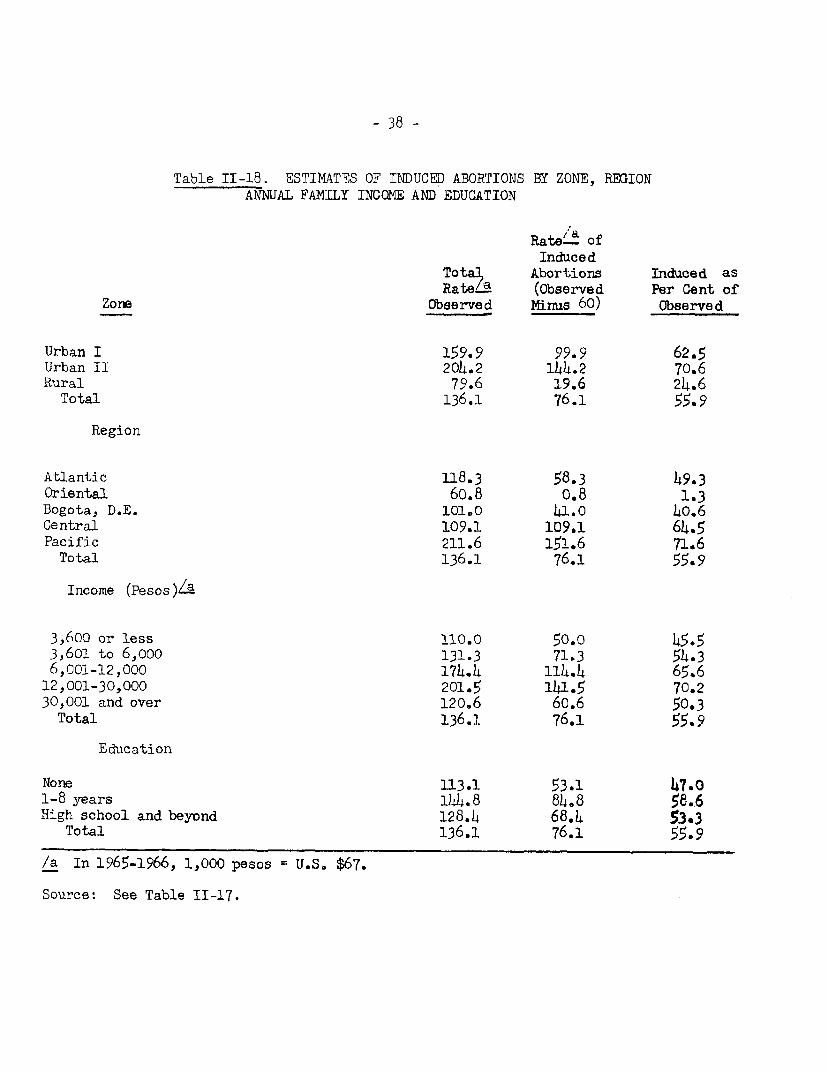
- 38 -
Table II-18. ESTIMATES OF INDUCED ABORTIONS BY ZONE, REGIONANNUAL FAMILY INCOQE AND EDUCATION
Rate'a ofInduced
TotaL Abortions Induced asR a tteLa (Observed Per Cent of
Zore Observed yinus 60) Observed
Urban I 159.9 99.9 62.5Urban II 204.2 i14.2 70.6Rural 79.6 19.6 24.6
Total 136.1 76.1 55.9
Region
Atlantic 118.3 58.3 49.3Oriental 60.8 0.8 1.3Bogota, D.E. 1010 441.0 40.6Central 109.1 109.1 64.5Pacific 211.6 151.6 71.6Total 136.1 76.1 55.9
Income (Pesos)/a
3,600 or less 110.0 50.0 45.53,602 to 6,ooo 131.3 71.3 54.36,001-12,000 174.4 114.4 65.612,001-30,000 201.5 141.5 70.230,001 and over 120.6 60.6 50.3Total 136.1 76.1 55.9
Education
None 113.1 53.1 47.O1-8 years 144.8 84.8 58.6High school and beyond 128.4 68.4 53*3
Total 136.1 76.1 55.9
/a In 1965-1966, 1,000 pesos U.S. $67.
Source: See Table II-17.
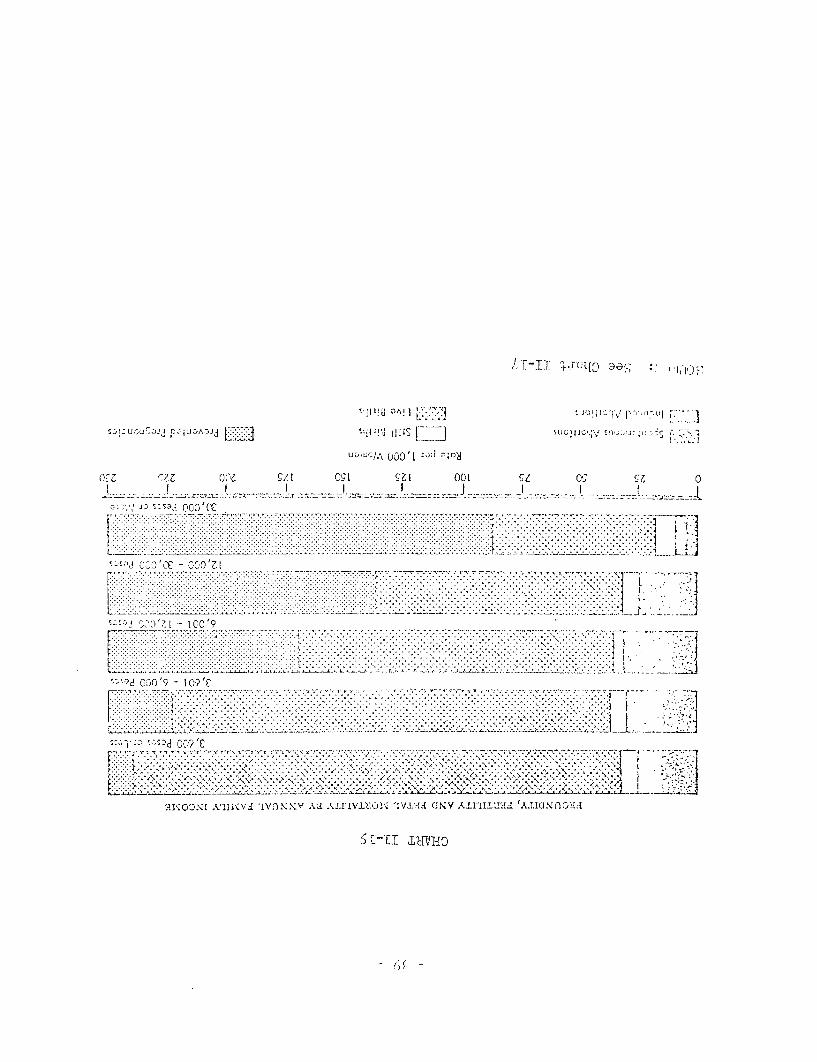
OAII!t !1 t -.. 3'J°!1'JQj,/ s.,,fl2<tUl i,7.
sv -):;Jj r !A,Jd , .St ll SloJ,. s;,.;,..r;-,,
56c §66 OC C/A CSI £61 COL (C OS 0_1__~~~~~~~~~~~~~~~~~~~~~~~~~~~ = _____1_> _z*:-~":. =:J*-=_ _, -;_, _ !_-
L I .'.'.. '. ... ......'5;'' CO19 CCfO'61
| -: - ~~~~~~~. T... . . . ....... . ..... ::.::. -:::: :- ;:::5_. ......
. . . .. . .. ... ; .
1 ..... ) . ................
.._ . .. _.. .. . .. _. . ._ . . .. . ... .,. ... . .. . . . . . . , . . _ . .
........ ..,,;;;.;;; ;,;, -, L;4 .. ,...........,. ,;,, .......... . ... ..., .. _ .. . ............. :,,,_,__,
'-'7d~ C-'[ ICC 9
.... ... . . . . . . . . . '. . .'. '.. * ... . . .. ... .. ..... , ..* ,,. ..., ,s ... . . ., - / o,h' ' ~~~~~~~~~~~~~~~. .; i.. ... ;.... ... .-*-*,* . A. ,................ ,..... s. rS.~.,, .,,,.... .... Ns.... ...... , . ..e....... . A>............. .... ......
5:351-8D %..§ 0!9 102..I - t C-0 q ~ ~ ~ ~ ~ ~ ~ ~ ~ I ... . . .... . K ... .. .. .
L .- ......... .2 A tX LX .i.2...2... .
5! :, 5 ;;; o, 9;,' - Is 0 c ;s 4t*
... \ .k . .\\ . .... '. k . . . .> IV.A , ..K 'U .' . .' , . .I
91. With respect. to morh)id:i Ly, inl any ornE yeal apfproxirlrtely .millicn accidents of' all ty,pes occur, a rate oj )426 per th-ousand po)Pula-LionI. Stated alte-naaive li , four ol every Letn (.olombians experience asignificant accidental inir; ry in any given year. More than one-fourth re-sult from falls, one-fifth from cnttirig and piercing inst-Irnments, 8 percentfrom falling or flying oh-Jects, 7 percent from vehicles an i c nercent fromfire and. biurning objects. ;cncluding vehicular accidenLs, the most hazardousplace from the point of view of aucideiital injury, :is the hlome, fol]owed bystreet accidents, farm accid(.den_-ts nUdJ a-LcciCide3lts Zait the place of work. Therisk of occupational accidents is highi, accounting for the 5;J2 acc;i.derntsper 1, 000 workers, a rate (.) perc.ent higher than- tihe rate experie-Lnced bynon-workers. Such occ upatiaOnal. aco:s!n ts are iqn,iivalent tI l()4 i.nca i.tat-ing acci(ientc; for each ni 1] wn hours of wrk.
92. All t-old, inL addition to. deaths, permanernt invalidity, dam.age toproperty and loss of incone, accidental injuries an aount in any one year for17 million days of invalid1ity, I 1 ILLi-ion medin:al -.are visit.i, 98 thousandhospitalizations (l perceent of all. hospitalizations, 12.7 percent of hospitaldays and 1.2 million days li- bed)
7. Dental Disease
93. In most co1uLtr:esq, dveJed or developing, the e.:-tent of dentalpathology is suiject only- to gros; :.s i!rates In o lombia, however, exten-siveinformation has been gathered i,icatinlriat ha.t , percent of the popula-tion over the age of three are in needi oi` d eiJal ( care with t:e highest pre-valance during the age span.--tb, reaching a nealz of 55.7 percent at ages15-24. No marked differentiaLs occuir with in ,mec levels or geographic loca-tion although women appear to have a higher need tJian mnen.
94. Not all those who need denital care receive such attention. Only24.3 percent of the population consilit dental attendants, slightly more thanhalf of those who express need for such c.are. Those who seek dental. assist-ance average 2.5 visits per year anrd this attention i.s concentrated in urbanareas, in the higher incomne croups anid. in the actije working age groups of thepopulation. Extractions account for o-ver two-thirds of services renderedwith fillings and dental prostheses making up most of the remainder ofcare given. Dental prophylaxis, so -imtportanit in early life, makes up onlya small fraction of dental care services.
8. Mental Illness
95. pubstantial evidence exists that mental illness and psychiatricdisorders are serious and Lmportant health problems in colombia. An estimatemade in 1967 indicates that; about 710,000 persons or almost 4 percent of thepopulation is disabled or chronically impaired by the psychoses, neluroses,mental deficiency, epilepsy and alcholismn. One in six of all hospital bedsare devoted to psychiatric care and almost 2 percent of all medical consulta-tions arise from mental health prolblems. About. 3 oercent of physiciansselect psychiatry as their area of specialty practice. ktegre-ttably neithertime nor opportunity perrnit-ted an appropriate survey of the mental healtharea or a proper evaluation of the proposed mental health program incorporatedin the Ten-Year National Health Plan.
- 41 -
D. Institutional Resources for Health
96. As of December 31, 1966, there were 658 hospitals in the countryproviding 46,735 beds (approximately 2.5 beds per 1000 population). 523of these hospitals, with 87.4 percent of the beds, receive all or partialsupport from the public treasury and their medical policies are guided bythe Ministry of Health. The remaining 135 hospitals, representing 12.6percent of total beds,make up the private sector. About one bed in fiveis devoted to special health problems: chronic diseases (tuberculosis)and mental illness. (Note: In the last four years the ratio of availablebeds has fallen slightly due in part to an increase in the population andto the closing of some hospitals and the deactivation of some beds.) Inaddition to these hospitals, there are operative about 1120 health centersand health posts rendering primarily preventive services and ambulatorycare.
97. Although the overall ratioiof available beds compares reasonablyfavorably with resources available in other countries, subdivision of thecountry reveals serious maldistribution of these essential health carefacilities. For example, dividing the country into three major categories:major towns of over 20,000 population (45.8 percent of total population),towns of 1,500 to 20,000 population (42.6 percent of the population).andsmaller communities with less than 1,500 inhabitants (11.6 percent of thetotal population) interesting disparities of availability of hospital carebecome apparent: (Table II-20). Whereas 23.2 percent of the population isjudged to lack access to hospital care this proportion rises from 1.1 per-cent in the more populous areas to 87.5 percent in small communities andrural areas. Concurrently the bed/population ratio falls from 3.5 per 1000in larger centers to 2.0 per 1000 in intermediate size communities and to0.8 per thousand for the rural balance of the country.
98. Other important comparisons indicate that hospital resources areutilized more efficiently in the more populous areas with shorter averagehospital stays (12.3, 10.9 and 15.1 days respectively per admission) andhigher occupancy rates (75.4, 51.5 and 53.3 percent respectively).
99. An interesting attribute of the health facilities situation isreflected in the number of partially constructed and unequipped and un-utilized hospital (or other health care) facilities scattered throughoutthe country. A recent inventory of these facilities places the number ofsuch structures in the vicinity of 856 buildings partially erected atvarious times during a 15 or more year interval. Political pressures,local charity boards and other sources contributed to this situation with-out reference to clearly assessed needs, national or regional plans and,alltoo often, with insufficient funds to either complete construction andequipment objectives or to initiate and maintain operation. One estimateplaces the already made investments in these structures in excess of 2,000million pesos. As will be noted in a later section, the new NationalHospital Plan has not only assessed these structures but proposes thecompletion, equipment, and placing in operation of such of these facilitiesas will contribute to a rational national plan for comprehensive healthcare coverage of the total population. Also as part of the NationalHospital Plan the estimated deficit of needed hospital beds by 1975 isin the range of 15,400 additional beds (see Table II-21).
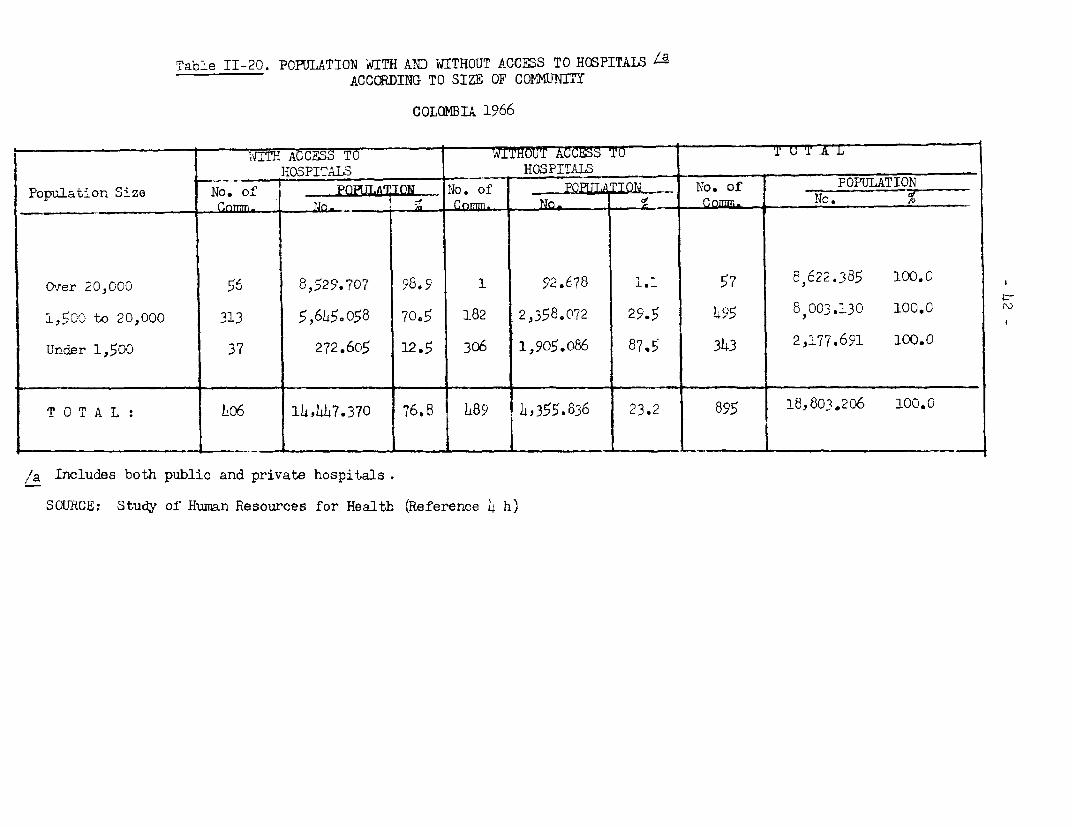
Table II-20. POPULATION -wITH AND WITHOUT ACCESS TO HOSPITALS /aACCCRDING TO SIZE OF COFMUNTY
COLOMBTA 1966
1.ITH ACCESS TO - T=hOUT ACCESS TO T u T A T LHOSPITALS HOSPITALS
Pooulation Size No. o No. of N TON m o. of POPULATIONCn _,__ Co . Io
Over 20,000 56 8,529.707 98.9 1 92.678 l. 57 8,622.385 100.C
1,50c to 20,000 313 5,645.058 70.5 182 2,358.072 29.5 145 8,003.130 100.0
Under 1,5GO 37 272.605 12.5 306 1,905.o86 87.5 343 2,177.691 100.0
T 0 T A L : |406 |14,447.370 76.8 1489 14,355.836 23.2 895 18,80.20$6 100.C
/a Includes both public and private hospitals.
SOURCE: Study of Human Resources for Health (Reference 14 h)
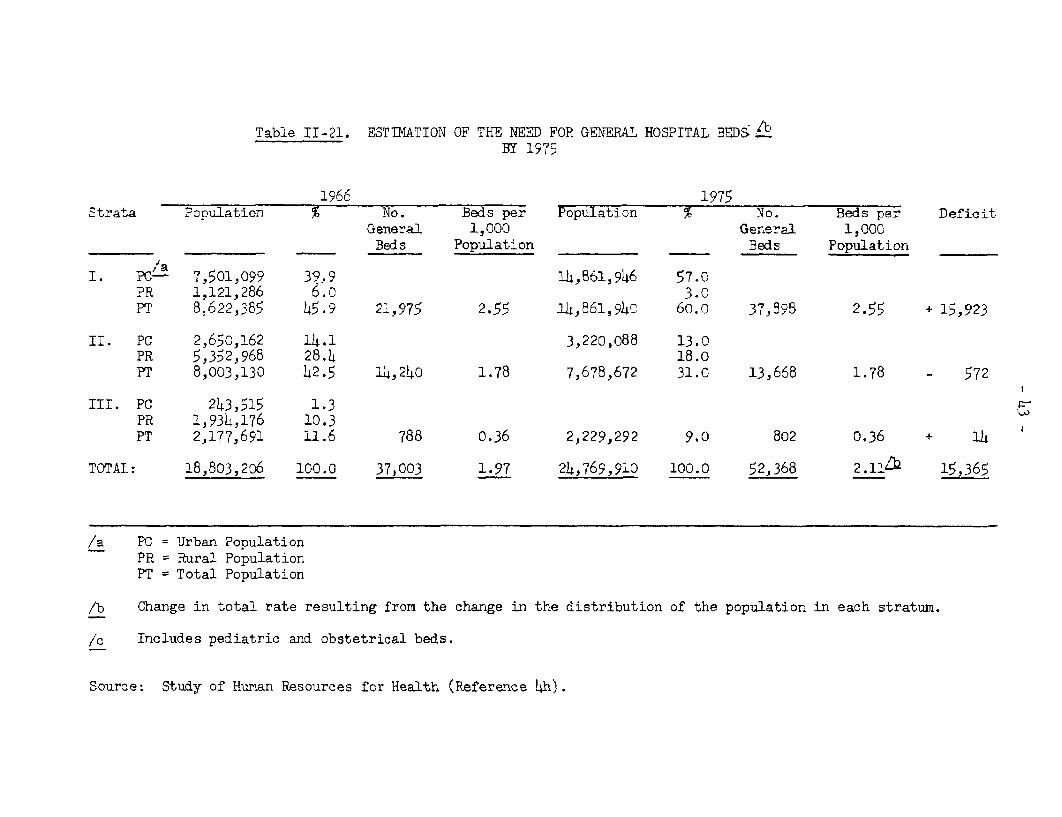
Table II-21. ESTIMATION OF THE NEED FOR GENERAL HOSPITAL BEDS it
BY 1975
1966 1975Strata PoDulation No. Beds per Population % No. Beds per Deficit
General 1,000 General 1,000________ __________ Beds Population Beds Population
I. PCL' 7,501,099 39.9 14h,61,946 57.0PR 1,121 286 6.0 3.0PT 8,622,385 45.9 42,975 2.55 14,961,94C 60.0 37,895 2.55 + 15,923
II. PC 2,650,162 14.1 3,220,088 13.0PR 5,352,968 28.4 18.0PT 8,003,130 42.5 14,240 1.78 7,678,672 31.0 13,668 1.78 - 572
III. PC 243,515 1.3PR 1,934,176 10.3PT 2,177,691 11.6 788 0.36 2,229,292 9.0 802 0.36 + 14
TOTAL: 18,803,206 100.0 37,003 1.97 24,769,910 100.0 52,368 2.11Zk 15,365
/a PC = Urban PopulationPR = Rural PopulationPT = Total Population
*b Change in total rate resulting from the change in the distribution of the population in each stratum.
/c Includes pediatric and obstetrical beds.
Source: Study of Hunan Resources for Health (Reference Lh).
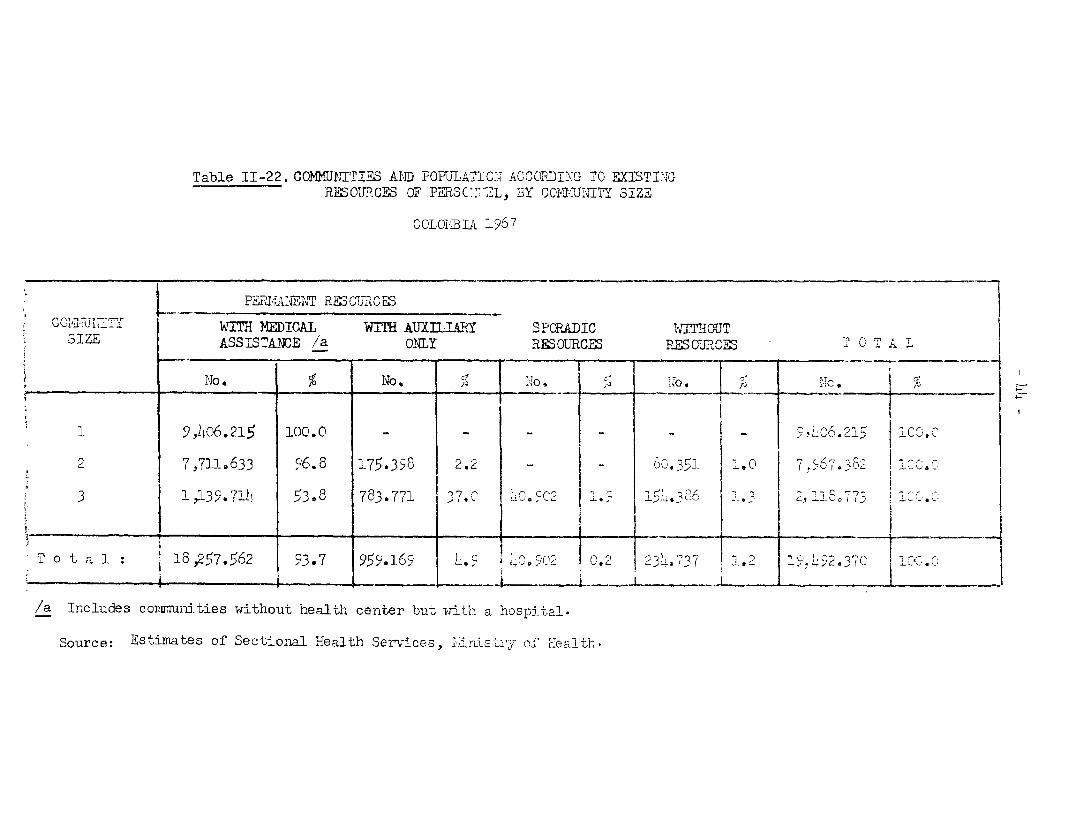
Table II-22. CON1LIUfITIES AiID POFuLAhTGIO AC1CORDIING TO EXISTINGRESOU.P.CES OF PL3C 2L, BY COI24ITY SIZE
COLOI31A 1967
2Q1 II 7 WITH ,E C M DIr WITH AUXILILRY SPORADIC WITMOUcIZE ASSISTANCE /a ONLY RES OTRCES PMSOU2C CI 0 T AL
_-- -. IG*1< l-T. to
1 9 ,146.215 100.0 _ _ - _ _ ,.G6.2l: Cv.C
2 7,7L11633 96.8 175.3<& 2.2 _ | _ ,-351 1.0 Q 796 7 .3& 2 1<t3 172.
3 ~ ~ 1139. 71L 53.8 783.771- _ _ _ _I_ __ _ __ _
tt, _ ~~~~~~I I I- -
i Total . 18: i la >257@62 | 93.7 |99.169 0.2 .7 71 32 |7C iC 5.C
/a Includes conrnmnities without health center butv ith a hospital-
Source: Estimates of Sectional 'Health Ser-vices, ; ristZ,r of HIealth.
100. Ambulatory care facilities -- of the total of 1120 health centersand health post facilities, 710 fall in the former category and 410 in thelatter. In addition, 657 hospitals provide out-patient or ambulatory careservices as do 205 offices of the Social Security System and the NationalWelfare Funds. About 5,500 private physicians offices and an indeterminatenumber of private care centers contribute to the ambulatory care servicesfor the population.
101. Based on the above compilation, it has been postulated that forthe country as a whole over 94 percent of the population has reasonableaccess to ambulatory care resources. This figure ranges from 95 percent inthe larger towns down to 90 percent in the less populated areas. However,the comprehensiveness of services available is disparate. For example, healthcenters and health posts which are called upon to render over 30 percent ofall consultations for the country as a whole (57 percent in small towns and83 percent in villages and rural areas) offer only limited facilities andequipment and limited personnel. Health centers are staffed primarily bynurse auxiliaries with occasional visits by physicians and health posts,many of which are open only on a sporadic basis, are staffed only by nurseauxiliaries. In consequence, as shown in Table II-22, whereas for the totalpopulation 94 percent is believed to have access to medical consultationwhen needed, an additional 5 percent to similar attention provided by a nurseauxiliary and less than 1.5 having access to none or only sporadic care, thissame situation does not prevail in the smallest communities and rural areas.There, only 54 percent has access to medical assistance and 37 percent mustdepend solely on the resources of a nurse auxiliary; the balance, 9 percent,is unprovided for or exposed only to sporadic and then severely limitedservices.
E. Health Personnel-Supply and Distribution
1. Physicians (4 -c)
102. Few countrieshave as much or as precise information on the number,qualifications, location and other characteristics of its medical profession.Using December 1966 as a reference point there were then 8100 physicianspractisirng in the country or a ratio of 4.5 physicians per 10,000 population(1 physician per 2,200 population). Much of the following analysis is basedon data received from each of the 6,323 physicians who responded to inquiriesincorporated in the 1965-1966 National Survey of Human Resources for Health.
103. Comparing physician resources in Colombia with those in othercountries, Colombia falls slightly below the mean of 6.0 physicians per10,000 population for South America and considerably below the national aver-ages of 15.1 for North American counltries; for Brazil the ratio is 4.0; Ecuador,3.3; Bolivia 2.9; Chile 5.8 and Argentina 14.9. The physician population inColombia is young with 56 percent under 40 years of age; 65 percent have com-pleted their medical training since 1950. The practice of medicine is essen-tially a male occupation with less than 2 percent women, a rate even lowerthan in the U.S. All but 3 percent are native born although 9 percent re-ceived their medical training abroad.
- 1ho -
illh. The distribLution of physicians is uneven wi-th 74 percent locatedin the principa:l cities of the country serving the needs of the 31 percentof the population that resides in such centers. Thus, in these citiesthere is one physician for 1000 of the population whereas elsewhere theratio drops to one for 6400 persons. Only 9 percent of physicians are inpractice in communi-ties of under 20,000 populat;ion, where almost 64 percentof the population reside. This disparity would. be even greater were it notfor the fact that since i95,7 every graduating physician is required to renderobligated service for at least two years, usually in a rural area designatedby the Ministry of Health.
105. Only 27 percent of physicians devote their energies to generalmedicine and an additional 53 percent are involv-ed in the specia]ized practiceof surgery, internal medicine, pediatrics and obste-trics. Orly a smal:L frac-tion of physicians specialize in public health, l.3 percent, and. an even smallerfraction, 2.5 percent, specialize in psychiatry.
106. Because the public treasury is responsible for funding so large afraction of health care services in Colombia it is not surprising that morethan half (53 percent) of the physicians indicate that all, or the majorshare, of their practice is devoted to non-private care. This figure varies,however, with non-private care rendered by 68.7 percent of physicians locatedin towns of under 20,000 population. In cities of intermediate size, thisproportion drops to 40 percent risiLg again to 54 percent in the capitalcities. It is also of interest that concentration of interest on privateversus non-private practice varies with the age of the physician. Early intheir careers up to 80 percent of physicians are totally or predominantlydependent on salaried income whereas beyond age 40 the emphasis in theirpractice turns more in the direction of private patient care. In maturelife only 25-40 percent of cloctors derive all or the majority of theirincome from salaries.
107. The mean income of physicians for the country as a whole is about92,000 pesos per year, this mean varying from 93,000 in the largest popula-tion centers down to 54,000 in communities under 20,000 population. In thelarger centers about one-third of physicians have incomes of over 100,000pesos and only 20 percent earn less than 50,000 pesos annually. In smallercommunities 40 percent fall into the lower category and only 4 percent inthe higher.
108. A significant finding of the 1965-1966 study focused on the utili-zation of the professional time and skills of the physicians; almost half(47.3 percent) is consumed in non-medical duties or tasks which in the viewof medically trained observers could be done as well, and in some instancesbetter, by other personnel without the long and expensive educational pre-paration requisite for the awarding of a medical degree. This observationand others to be considered later strengthen the argument for a greateruse of auxiliary personnel and thereby extending the availability of physi-cians for duties that cannot. be delegated to less well qualified workers.
- 47 -
109. As stated earlier, 3 percent of Colombian physicians were bornoutside of the country and a total of 9 percent are foreign trained. However,a recent development arousing the concern of Colombian authorities is theincreasing trend of Colombian physician,s to migrate to other countries,particularly to the U. S. In recent years this "professional drain" hasaveraged about 70 physicians a year equivalent to about 17 percent of theannual number of physicians graduating from Colombia medical schools.Regrettably,during the last several years this trend has been acceleratingand this migration rate may now be approaching 25 percent of production, aserious economic drain both on the limited educational facilities of thecountry and on its long-term social resources. Ostensibly the main motivationfor this emigration is to seek professional graduate training and experiencein U. S. hospitals and institutions and many such trained physicianscontemplate return to Colombia at the conclusion of this specializationexperience. However, data are incomplete or unavailable in this area and itis commonly believed that a large number remain as expatriates.
2. Dentists
110. Studies similar to those summarized above for physicians have re-cently been completed in Colombia for professional dentists. Unfortunately,delays in the publication of these more recent studies preclude the incorpora-tion of the major findings in this report. However, the 3,400 graduate dentistswho have been identified as in professional practice in the country establishesa dentist population ratio of 2.1 per 10,000, a figure slightly below the aver-age of 2.8 for all of South America and considerably below the average of 5.4for the North American countries. Comparable figures for several other LatinAmerican countries are: Argentina, 5.4; Bolivia, 1.6; Brazil, 2.7; Chile, 3.3;Ecuador, 1.2; Peru, 1.5; and Venezuela, 1.9.
3. Professional Nurses (4h)
111. Data similar to those covering the physician supply are also avail-able for a segment of the nursing resources; namely, the supply and distribu-tion of professional nurses, those who have had training beyond secondaryschool level, usually, if not exclusively provided in a university medicalcenter setting. The 1965 survey indicated that there were at that time justunder 2,000 nurses in Colombia of whom 82 percent (1618) responded to thestudy questionnaire. Of the respondents, 73 percent were engaged in nursingin Colombia, 21 percent were inactive and the balance, about 6 percent, wereoutside the country. Secular nurses made up 77 percent of those covered inthe survey but the balance, belonging to religious orders, constituted 25percent of the active professional nurse supply.
112. The ratio of nurses surveyed to the pcpulation as a whole was 8.2per 100,000; in the capital cities this ratio was 22.7, 15 times greater. thanin the rest of the country where it was 1.5 per 100,000. In contrast to someother countries where there are usually twice as many graduate nurses asphysicians, (e.g., U.S.), in Colombia, physicians outnumber nurses about 5.5
to 1. The internal distribution of nurses iri Colombia is further remaurkablein that about 67 percent of nurses are concentrated in the three principalcit;ies, Bogota, Medellin and Cali, whlich maike Up less than 19 percent of thetot,al population.
113. About, )h2 percernt of active professiona]. nurses are work-ing in publ chospitals and an additional 1Lh percent, n private hospitals; together the:enurses provide a ratio of one graduate nurse to about )40 hospital beds.Another 1L3 percent of nnrses are emp]oyed, abou-t; equally divided amongpublic health servicen, Lh'oc i ;L Security and Nlaati oal. Welfare Fund cl-i:nicsandt in teaching. For tle! most- part. professionral rnurses provide little orno bedside care, inasmuch as 57 pecenLt serve as chiefs of nursing servicesanother 21 percent as direclto is, ass,srrant di.l.c tors or ,3upervis07or's ofhealth institutions, -t1 percent in t,eaching ro'les and Li pere¢nt in othersupervisory func-tions. url.y L percent are engagead in other duties includingprivate practice.
ll1. Nurses are lOt;il well reiaunerated with the average mont;hl..y v ncone ofreligious order nurses abaut 800 peso, per monti rind secular nursesaveraging about; 150)0 resos per nionth. In re(e,til ye:a-rs there h71s been aslightly upw-ard trend in F,he availthi-i1ty ot n.:roieiol nurse .; but thistrend is paralleled by a: increasing eigratLion of nurses from thie country,with about 11 percent of the graduate nurse supply in foreign residence,about haLf of these in the IJ.S.
4. Auxiliary Nurses
115. Auxiliary nurses or nurse aides provide the bulk of traditionalnursing services available in Colombia. However, no inventory comparableto those undertaken in medicine, dentistry and professional nursing has yetbeen initiated and thus only crude and somewhat contradictory estimates oftheir number in actual working si-tuations are available. One estimate(1965) places the number of nurse auxiliaries at about 11,000 or 8 for eachprofessional nurse. Another estimate (also in 1965) places the number ofemployed nurse auxiliaries at just under 4L,000 and a more recent assessment(1967) indicates that there were then 3,500 "certified" auxiliary nursesknown to health authorities and that an additional 12,000 "untrained"auxiliary nurses are employed by hospitals, health centers, and healthposts throughout the country. This estimate would place the total numberof "certified" and "unitrained'" auxiliary nurses in excess of 15,000.
116. These disparities arise, in part at least, as a consequence ofdifferences in definitlions and terminology. Until recently no formaleducational requirements were established for nurse auxiliaries and nurseaides,,both categories being trained on an in-service basis in hospitals orother health care institutions. In contrast, professional nurse traininghas been directed by acredited educationally oriented institutions. By-and-large, nurse auxiliaries have completed one or two years of secondary schooleducation and receive two years of supervised practical experience in a
- 49 -
hospital setting; nurse aides usually have less formal educational back-ground and receive less than a year of practical trainiing on the job.Accordingly, large numbers of young women employed in hospital or ambulatorycare services, many fulfilling complex and highly responsible tasks, cannotnow meet newly established standards for certification. Nor would many ofthe institutions in which they were prepared for work satisfy even modestcriteria for training accreditation of nurse auxiliaries or nurse aides.
5. Other Health Manpower
117. Modern medical. and health care services haVe become singlarlydlependenrt upon a large number of specialized aides, technicians, and othersupportling persormel. These skdlls vnor represent, in developed countriesat least, Ut.o 6a0 percent of the total supply of speciralized healthworkers. This ri.F'fere.iation of healthimanpower and the need fordelegation of responsbl-,e functions b,,r the phys;cia.n is clearly recogniz7edin Colombi-a particularlyf in the liJni Jesi Kr edical Centecs. However, thi.srecognition is orlfy now reach-ing We t.-ge at which national authorities arebegi ruing to bake invenl,ory of Lthis segmenlt, of the hewltl minpower pool andto establish standardcs an.] norrmts cY personmel reRuJrremenelts in order toassure the smiqo-oth and effecltive opoenlIicn of -ite health czaLre system. Amon-7gthie cat-egories of health workers Uiat aLrc jdue for sluch conTi&Lderation are:health adRministrators, phanri.pc:isCJa, op ti ciuL.s and optomettriL,ts, labora-tory.and other technircias, di.eti.c:ians and nu-1tr-itonis-ts, mnedical and dentaL aideslhealth educators arld hel. ibh promoters, ies t:i) and ci. i 't1l attendants,san:iJ. ti .i'S anId san:i ray r1nspec tors arnd engi n1001'.
F. EducatiorL anld Training for tue leaL-th Occupations
1 . Medical Education
118. In the 20 year periol si.nce 1'O the medical educmational system ofColombia has rnade a remarkable forward thru-st, Despite limited internalresources the ua-iversity medical schools making up the Association ofC,olomb'an Medical Faculties, have made ma0jor revi-sions in their organization,teaching programs and objec.tives and simultaneously have provided unprecedentedleaders,hip to the developmentl of'rogressive national health policies, resourcesand programs. (The reader is referred to the report: StLudy of Human Resourcesfor lHealth and Medical friucati on in Colombia, Methods and Results. JanuaryC1J9f>, Bogota, for an excel lent revi.ew of the soubject)
ILl). FPr-i.0or to l?'i, t-hree medi.cal schools gra-idu-ted .about 2i)iiph-sicianls annually. wasolltment ws open, I Ilul.te.; nre sm.xI- andalmost entirely part-time and the teachin.ng plan was based largely onthe older Continental [-uopean pattern. A relilit.;,ve? smLall fraction ofstudent,s beginning medical studies compIeted t;heJ r course and. raduateswere not. u-wi l'ormly iO f' high caliber. Four a-ddLtitional! -sehnoolls beganconI-Ibutirig graduates in -the earl'y IL'0s ndtrg`0,e i- .'he seven jrtvcalschool:-, hive -lineost dou)fleld 'thlle cpt . 1 piySJc:i- ans . Tr- sen(-:or schoc'satrc> nonJ accUenti_dg students a Ii i w Wl anincreweŽt s o t inioto -allsctools tlhe rnumber o]l' srrradua-e. s-oisl 4 approacli 600 a lLy by ±:rJ-
011 Ol;,viu of 'th;s ora ii t-r'i ly ned a al ii C. '. re s-,ori)eCisrJ r)-\
flwi-vate instti lti' n§ ; ,fir;i, t ) L :tei; L - -rrent,ly mat-
ri-j, 1 lated in the seven yc.n eiou';; a eyU et l ! , ii "'eon rlrrrir
aLre no-t complete:Ly -wri ror I l,iiOUfhtl ). .I'ii' I3iri'itS Is he le
:.qtreed to by al 'i 9 l 'I i . l t-i urnLi i r a i.!ll.,
with an overall aveol ci LII ) in Ii a'; li a' . tl. /-i ;i l. ion
lile to acadendic fail rn rH'r-it i ' k'h !,t. Lt.i, l i rndi to at ill. ()&rI,e
f'or the total seven ye ar ,)p- ;;rli tb l. ; nt-:tol wf. OC. .r l r th'rle
first two years. 'l'he en rnI fli"e r; , if wcrlniel ha,; iri.12l fran cider' ' ocr r r-
, ent to 12 percerit.
121 Th'e £ re''L :tp_; .1p:7.1:i i;ni0cr_. 1cii1e Canafl:ian Jnstitu liJons -j Jt nt r,. ul 51 ti.1 (Idli I . . ii e _ C i S -. 'a
trairring and carefull;r sur se,i n l i . ! ". pu - : . u ve n.e;3ie i ni
ind public health a.re "ei ri(i p. ' ! .. c'irrno in the
cir:riculium - irn view ,, Li r' 1jiLi. at .,; ii VUA . 1 . ; ! ec In 011
health problemis hoe-, ;.' -. i i u 'a o'v t ichiexcd. the saunedegree of acceut;oucc SI!O ia'; ; t ! ' ; I he muil> un ! ou;anid traditiornf,1 Iire ca. *. it I er' mrredi, a.! ci iL ies
are growiing wif.t ri or I a:i c-act L *.LUle Oil .. Ll Jt.
althoiugh half-!im aik p 1 1 -- In. J ,rntl I.' nt IIt. 'otinuc iO represent irtorethan 50 oerce I, o t ir mi i c:a:l ., r,il i-; tro. j i I In 2 i -in l*,onYundergraduate metir,cj edlm''' the I.,-alt.ies of rreica1 sntv'OS , w- a
in post-graduatoe edalO 'i thf 'n @1 va.tli; ti 1i the WI v ' tolosp:i tj.s , r'ese.arh'T't ani, i nc:''' '' V r' arm:i U "' hea] 'L '' S t -we Ii thfe Lra_iri j-i r, n' l l C ;;;JOtv t
122. The ruost of maintrairing tUe rriediLcal .,chools is iiij Ii aid the sixschools (of a total of 9) fo" which data are availabie required over 5C)million pesos a year for operatioi:.Ll costs, without reference to capitaloutlays or those for replacernerr -t or purrchase of new equipment. None ofthe schools has income of its own. The two private schools w,hi-ich receivethe smallest public contribuitions are aLmost entirely dependent on enroll-ment fees for their support. Only one school has received substantialfinancial aid from abroad and only three have private funds from Colombiansources. The seven public schoo:Ls charge an annual enrollment fee scaledto the income declared by the parerits of the stujdents; the two privateinstitutions charge a fixed enrollment fee considerably higher than is chargedat the public institutions. The degree -to which this system affects thechoice of medical careers is not clear; yet 'the sonls of merchants representmore than 25 percent of medical school Matriclan-ts.
123. Projections foIr the future supply of physicians have been developedby the Association of Colombian Medical Faculties based on current and anti-cipated resources of the training institutions. The population of Colombiais expected to rise from its present level (1969) of 20.5 million to 28.8million in 1980. With medical grad.uates rising -to about 600 annually andwith a loss by death of 70-90 physicians a year (emigration of physiciansis not considered) the physician popula-tion ratio will rise slightly from
- 51 -
its present level of 4.3 per 10,000 to about 4.9 in 1980. It is thus appar-ent that Colombian authorities are not counting on a major improvement inthe existing physician-population ratio as the means of overcoming the largebacklog of health problems now confronting the Colombian health system.
2. Nursing Education
12b. Nursing education in Colombia has remained relatively static overa period of years. Seven nursing schools were in opera-tion in 1956, thesame number as in 1965 when the survey of th-is field as well as of medicaleducation was made. One of the seven schools is not included in thatstudy; of the six schools providing data tlhree are located in Bogota andone each in Yedellin, Cali and Cartagena. Five of the six are integralparts of a university education system.
125. Between 1955 and 1963 the number of applications for acmission tothe six schools rose from 150 to 348 and the number of first year studentsfrom 1311 to 167. However, only one nursing school was able to selectone in four of its applicants; the other accepting all or a considerablemajority of theirs.
126. Two-thirds of all students come from major cities and less than1 percent from rural areas where half of the country's population resides.Three quarters of the matriculants completed their secondary education inprivate schools and though educational fees are low there is evidence tosuggest tha-t candidates for nursing education are drawn from reasonablywell-off economic strata of Colombia though perhaps somewhat less so thanare students choosing medicine as their career. On a national average 75percent of the students entering nmring school complete the program althoughthis figure ranges from 97 percent in one school down to 57 percent inanother.
127. The lack of appeal of nursing education appears to be linked withhigh academic requirements for admission to the schools and more recentlyto the lengthening of educational requirements. In the past the nursingtrairLing program varied from two to three years depending on theindividual school. More recently with the introduction of the generalstudies program in schools of nursing the duration of the required coursehas been lengthened to four years and on graduation the term "generalnurse" has progressively replaced "licenciate in nursing."
128. The cost of nursing education is also high and is largelyborne by the university budget. The range of cost per student per yearvaries from a low of 2,800 pesos in one school to 16,600 pesos wfithl anaverage of 6,740 pesos per student.
3. Auxiliary Nurse Education
129. It is stated that 30 schools of auxiliary nurse education are nowin operation in the country. Other information suggests that this figureis low and is limited to "accredited" training institutions. The M4inistryof Health estimates the number of "graduates" each year from these "accred-ited" schools in the range of 700. In all probability twice or three timesthat number of new recruits annually enter employment as auxiliary nurseswithout proper training or preparation. By crude calculation it is possibleto arrive at an estimate that no less than 100 "accredited" auxiliary nursetraining schools are needed with each turning out no less than 30 or 40graduates annually.
4. Dental and Other Health Professionsand Occupations Education
130. These systems have been or are in the process of being studiesbut published or other data are not presently available for inclusion inthis report.
- 53 -
III. TH, NATIONAL TEN YEAR HEALTH PL)N FOR COLOMBIA (:968-197?)
A. Origins and Evolution of the Plan
131. A number of strong, converging forces have been at work ininitiating and consolidating the Ten Year Health Plan now in effect inColombia. This document, Plan Nacional de Salud, 1968 -1°77, criti-cally assesses the significant health problems of the country,catalogues the resources available and needed to resolve these pro-blems and, eqlally inportantly, crysoalizes a series of long-termnational policies and -plans to guide tn'e governmental and privatesectors in achievirng attainabl-e national goals. In the brief periodof time in which it has been in effect miany of its innovations haveproven feasible. Moreover, though a period of ten years appears tobe a short span in whiTh to accomplish its mualtiple objectives itspractical directives have aroused the confidence of the healthadministrators of the country and have mustered widely based supportboth within the country and among international authorities and ob-servers.
132. Among the prominent forces that have givern rise to the planis the clear recognition, at the foreTwst levels of the Colombian Govern-ment, that economic and social development are inseparably interwovren,each with the other; advances in the former area cannot proceed at theexpense of parallel progress in the levels of health, the educationalstatus and the living conditions of the Colombian people. Stated alter-natively the development of modern social institutions are not dependentsolely on, and cannot be delayed until, the prior accumulation of indus-trial capital and economic vower. Rather, a healthy population, educatedto participate actively in a modern society and living in relative hoTneo-stasis with its domestic and working environment is, in fact, an essentialcondition of full economic development. Such a national determination hasalso been incorporated in the charter of the Alliance for Progress signedby Colombia and 18 other republics in 1961. That document calls for anational health plan as an integral element of a national plan for totaleconomic and social development.
133. But even in advance of the Pun Li. del Este, )eclaration, theGovernment of Colombia began in 1$(6 Io draft a lorng-Lterm publichealth plan. The technical .ssislance of [tie World H-ealth Organizationand the Pan Aierican hiealt.b Organization w;s en]iLred as was the helpof the United Nations Children's Fund. These efforts gave rise to aninitial ten-year hesll:h plan (-162-1971) Ibu-l, even more significantly.revealed many of the severe limilt-:ions and constraints under whichthe healt.L authorStiies in th' -t countciry were lorced to function. Dis-persed and fractionated responsibilities were the order of the day,ftinds fromi a mtlti[ ioiity u' source-s in Anadcluate amfJounts were expendedswithout, reference to prinr-l-v rjeeds or tt.itoLiorL1 planc, and unqualifiedpeis[noniel subrjecl l-: L ntron-age apc}oi.ntrnen i. and ramoUl.nl were) cosmpletely
5 4 -
devoid or pro 1' ,-;.si ori.L gl idti-cke andi Lu- i :)(-.V i.jiv.100 . Bt U, no, -t,he 1 eas1 ofthe (lil.ficul s idi llJ I-j i :d wa lh Ia oh ic-of reial)le data ch.-rackeri--ing eve tWe , mosL prev-i 'ti, nt o hefal j,lt pr'oldcoines and prov idi og areasonable ban.l.s forl evalm.;.itillor ttI.f' e lJTf'le;t-LiVeen.,,:; of, est LabLisho(]d aIc ,i-
vities or thie sliork1Jleon ieo,; of L.l Li urea I u Ile so.! ireil )-i&-tt.e ens someof which dated back I/(J lie wt e i ofa.
13L. I-t Wax i.in Q.t!iE; I &oeV(iw k e t1 t ai We Mi r-i:;l;ry ol I lealli wao;to respond creat.ively i )ri L.o Uhe ,V( P H d' thie C,o]lomb,i.a A s- a-tion of Medical. Facultie.s wh i oh was fi erei eci r g Ik, plan ai coo.rs : o,lact,ion f'or, itS own, th0erl tven,[�S! i t H I I (Hi I en m41 ers tor L duE dcveltcifereltof an adequate nat:icrnal UijI .ppy ofl ( ace! thier XLec I Lb manpowerand to adapt their eduect,eill t.is t.(-,oi Hr,reporary Cc ta,erVitionaLlryaccepted professional ,tarindards. TInhe an A`m.rici me [lea]Lb C) rga]Lza.Lio)and a private interjo ULOn,l ft1ulonda .i _on, thfe MiJlb:ji-jK Mem rwi Jal Fa0 ed uf NewYork, agreed to provide toedhnica.1 ars iistanLce an1d financial aid. 'lhus,the way was paved fCor the nati oriwiJd collaborative stud:j- of flealth Maan-power and Medical] EducationIre ir %)ombia (i'.nc-ut&e) incorpoirating ascientific apprai E.'_A of the health condition; an(d totl healthl rescurcesof the country - a trj.uly National Health Survey,
135. This National Hlealth Survey, a unicle undertaking in a develou-ing society, has placed, for t,he lirst timte, ire the hands of healthlauthorities and planners i.n Colombia a fund of scientdific knsowledge onwhich to base a sound nati-tunal health p_lan arid(1 pprogram. Its findingsform an integral part, of the Natiorial 'I'en) Year H1ealth Plaan, 1968-1977.But, its benefits have not stoPped there for, i.n addi-tion), the study'seconomic and soc.ial profile.s (-C the populat ien, its analyses of' ratesand patterns of population inerea-e an(d t' ot,her demographic characterist-ics have been of inval.uable , to other nati.onal ministries andagencies of government, as, For exaannple, th-e Ministries of Ed.ucaticn andLabor as well as the Nationa-l. Deto)arl-lmen-its of P1l,an,ning and Statistics. Itis also noteworthy that the *'-es.ign arid applications of' this nationalhealth planning procedure is beisrg inarearsaingl,y emulated in other LatinAmerican countries as well as elsewhere.
136. Important national legislative enactments have accompanied andparalleled the forrxRlatiore of' thle Nati(onral Healt,h Plan, incl.uding Decrees3224 of 1963, 1499 of 1_966 and 24Y( ol i.)6'8. These have authforized andlfoimalized institutional and( adninistrativee reorganizations required forsound development of national, reginal_ anld local, act-ivities in the healthfield. Specifically, the above legislation provides for the reorganizationof regional (Depart-amento) and local (Minnicipic) healt,h services as adescentralized functiorn of the Ministry of Hea'lth; fosters the coordinationthrough a National liealthli Counrcil-, chaired by the Minister of Health,ofthe efforts of previously dispersed entities of' government responsiblefor fractional health funct.ions and f'or- the unification of their financialresources; the organizatiori and consolidatdion wi.hin the Ministry ofHealth of the mechanisms for supervision, control, programming andperiodic evaluation of heal.th activity at all ILOvels of government; andfinally, defines the fields of' activity as well as creating the neworganizational structure required to carry out the new health programscalled for in the Nati.onal Plarn. A more deta.led appraisal of the new
organizational pattern in the health sector is presented elsewherein this report (See Chapter I, Section B, above).
B. Major Elements of the Plan
137. Following a general description of the geography and climateof Colombia, the major demographic attributes of' its population andthe significant economic and social circumstances influencing thestandards of life throughout the country, the National Health Plan,1966-1977, critically assesses current mortality and morbidity ratesfor Colombia and takes note of recent time trends. Each of the majorcauses of death and of illness are reviewed (see Chapter II, above)for various age groups of the population. An appraisal iE then made ofthe availability and utilization of health care resources in the variousgeographic zones and among the various social strata of the population.Thus, utilizing the extensive data assembled in the National HealthSurvey, the health authorities of Colombia, have been placed for thefirst time, in a position to formulate on defensible grounds a seriesof health priorities to guide both immediate and long-range programs.
136. For purposes of planning, diseases or other health problem,shave been arbitrarily categorizecd into those that are "reducible" or"non-reducible". Among the former a.re listed the major communicablediseases in the following order: the diarrheal diseases, intestinalparasitism, tuberculosis, measles, whooping cough, malaria, syphilisand gonorrhea, diphtheria, tet. nus, leprosy, polioomyelitis, smallpox,rabies and yellow fever. Two other conditions not of infectiousorigin, are includied in this list of "reducible" conditions - abortionsand endemic goitar -- and it i<. somewhat surprising that at least twoother condiLions known to be highly prevalent in the coujntry, contri-buting significantly to high morbidity and mortality and also clearlysusceptible to preventive measures, are conspiciously omitted fromthis list. Malnutrition and to a lesser extent, accidents are, infact, given high priorities in the subsequently developed health plan.Additional challenges can be raised to the justifications for placingother significant health problems in the category of "non-reducible"conditions, but, i.n the main, those too are covered in the subsequentdevelopmrent of programatic plans.
13Y. 'The major prograLms developedt in the Thn Year Plan are listedas follows:
(a) Reduction of morbidity and mortality from "reduciblecausqes":1. Program of basic sanitation (di.arrheal disease and
intestinal parasitism).
2. Tuberculosis program (prevenlive vaccination andtreatment of the sick).
3. Five-Year m; va( -,i.nition c.oi^ )aign (inca 1x;, wIo o pi nrF!di oh theri_La, T trn s F,()rjjio Inyyeliti ar)i (I `pox
ll. Teln-year iarii eradi.e a Lion MrI i af m.
5. venerea I iea n e r rg am.
t. Famdily planning, program (abortAonj.
7. Lepiosy con trol 2rogram.
O. Goiter control progrm.rM].
9S. R. hies control progra-m.
1). Aedes Aeg,ypti eraWI .ca,tion program (yelloow, ever
:11. Yaws eradication programn.
(b) Reduction of Mortality from "Inon-reducibleIi causes:
1. Nutrition and feedi ng vrogram.
'2, Occupa)8tiornal health program.
3. CoinnrehenFLve health and inedical care program (hospitals,health centers and healthn pol,ss).
L4. Mentail heall t.h program.
5. Dental he . tyh progr-m.
(c) Organi-zation of the health sector.
]. Develop-ment. of hea]lth paolicies and Programs.
2. Evnluattion and sip,errvision of decentralized healthactivities.
3. IThe training and organization of health personnel.
4. Health investigations and research.
5. Budgeting, for health operations and investments for health.
C. The Ten-Year Health Plan - Analysis and Comments
14 0. Neither space nor time permits a detailed analysis of eachof the programs and activities outlined in The Plan, and now in theprocess of implementation, beyond the observations and diEcuEsionsprovided in earlier sections of the report. In general however, each
of the projected programs and activities is based on a sound assess-ment of -the magnitude and vulnerability to attack of the problem, aclear appraisal of the resources needed and available and reasonableprojections of the time and funds required to achieve desirable ob-jectives. Whether the goals sought by the Plan will be achieve orwhether it will fail or fall short of its goal - as was the case inearlier Colombian efforts - depends Le;3s on its scientific and tech-nical elements - which appear sound - the n on tthe pol-itical climatein which this Plan has evolved. In this- connection a number of itemsbearing on the prospects for success of the Ten Ye;.ar Plan warran-tfurther consideration.
1. National Support for the Plan
LIll. In the past, and even in the present, health as one of thesocial sectors in development has not been assigned a high priorityby the governmental, industrial and economic leaders of the emergingnations. Erroneously, health and medical care expenditures have beenconsidlered consumer goods and prevailing oolicies have tended to favorinves,tment opportuntities in physical capital. Only with rising nationaloutput has there been a. willingnesis to devote part of -the increment to thefinancing of additional heal.th services. As mentioned above the charterof the Alliance for Progress did not precede the adoption of new policiesby the Colombian government for concerted social as well as economicdevelopment for the country. Since the mid-5Q'Js Colombia. has been seek-ing to formulate a national health plan. Furthermore, the supportgiven by the President of the country as well as by other high officialsof the government to the 1Wational Health Survey attest to a revisionof priorities that has been in process in Colombia for some time.
11h2. More recent legisl.ative enactments implementing the Ten YearPlan, and others now pending, indicate that thi. national level supporthas been maintained and perhaps even strenghtened (see next section).However, it should be recalled that these developments have all occorredduring a period of continuing risies in national productivity when therehas been a larger share of the gross national. product available for thesupport of the social in.stitutions of the country.
l4i3. The National Health Plan has been able to provide reasonableesti.xnates of the direct costs of he.l1th and medical care services nowavai, lab]Ie and ts:ome approximations of the indirect, costs accruing fromlo.;ses dule to premature death and preventable disabi]ity within itshuman capital resources. Unfortbnately, technical skills are not yet.sufficientl,y advanced to weigh in exact terms, the relative benefitsof equal investments in extending health care services or in, forexample, additional industrial plants. 'Thus, choices of alternativesor the determination of balance remains a. oolitical rather than a tech-ni.cal. judgeinent. At present in Colombia, there -i.; every indicationthat pulblic expenditures for, and thus national support of, the natiornk]Health Plan will continue to receive f..vorable corsi.clerition.
2. Support Within the Health Sector
Thb. As has been pointed out earlier, the Hinistry of Health,which has been responsible for the drafting of -the Ten Year Planand now has primary responsibility for its implementation,is onlyone of at least a score of national agencies - governmental, quasi-governmental and private - that share major responsibility for theprovision of henlth and medical care services. Moreover, atregional and local levels previou<sly independent acnd autonomoujsgovernmental agencies and their non-governmental cotunterpartsrender health care services to ..J greater or l.esser degree. (TOneNationa:l Health Plan identif.ied .2 Departanmernlrs, 3 Intendencias and5 Comisarias at th.e regional leve:l and t)90 municipios, ii(0 corregi-mentos and lLi)07 inspecc(ionei de polici.a at thFe local level).
145. The National Health Plan, as one of its major elements, hasprovided for a total organizationcal and functional reorientation ofthis multiplicity of agencies into a unified, yet regionalized, country-wide health program. At the national level a National Health Councilchaired by the Ministry of Healthl, provides representation for eachof the national bodies in policy and program formulation. In addition,the Ministry of Health has been transformed into a coordinating entity-with clearly defined responsibility for the supervision, evaluationand control of dece.6tratlized health activities.
l4o. Ii consept, such a plan fosters the establishment of clearlines ot authority andi accountability as well as the elimination ofcostly and w:asteful duplLication of scarce resources. However, theeffectiveness of tAins plan will depend on two major considerations:a) the administrative skill and leadership provided by the top echelonsof the Ministry of Health, backed up by a Lull complement of profes-sional staff within its own organization and b) the support providedby other health organizations and health personnel who have becomeaccustomed to functioning independently and who may have establishedloyalties to other power structures within the country.
147. The imolement.ation of the new organizational plan is stilltoo recent to aSsess its effectiveness. At the national level, how-ever, the observer can not fail to be impressed by the vigoroussupport being given the plan by leaders in the medical profession,particularly in academic circles, who through the Association ofColombian hledical Schools have worked so effectively with the HealthMinistry in conducting the National Health Survey and in developingthe total frarmtework of the N.tional. Health PXan. Professionalleadership within the Colombian Institute of Social Security andassociated with the Netional Welfare Funds, to some degree comrrpetingwith the Ministry in the provision of personal medical. care services,has strongly endorsed and praised the coordinating machinery providedthrough the National Health Council.
- 59 -
1-4d. The Ministry itself is unusually fortunate to have at theforemost: levels of administr ation a small group of dedicated healthauthorities who, having formulat,ed the 'Ten Year Plan, are now attempt-ing to make it work. Unfortunately this group iE severely limited i nnumber, is overworked and forced to depend on supporting staff farless experienced and subject to excessive turnover in professionalassignments. Several, high level posts are currently occupied by in-dividual.s relatively recently gradul,!ted from basic medical educationand whose graduate formal. training and experience provide them withmeager background for the responsibilities they now hold.
189. At the regional and local- levels, one also observes theunevenness of qualifications of responsible personnel. Even in majorpopulation centers, to find an outstanding heal.th professional in akey post is the except,ion rather than the rul.e. The principle ofintegrated and coordinated health services so strongl,y advocated andendorsed at the national planning level is only now beginning tofilter down to operational levels. These shortcomings are recognizedby the too levels of administration ;nd their correction depends onthe speed with which manpower training and organization plans, to bediscussed below, can be implemented.
3. Financing of the Health Plan
1o. As reported earlier (Chaspter I, Secti.on C) identifiab2eexpenditures for health and medical care serivice:s in Cclombia haverisen subUstantially since 1(-1. In that year 1.6( percent of thegross national product, or 543 mtillion pesos, was devoted to thesepurposes. Nine years later, in 1)69, these costs had risen to 2,763million peEos or 2.5 percent of the G.N.P. and budget estinates forthe current year, 1)'70, will bring these figures to 3,507 million pesos(2.8 percent of G.N.P.). It can be inferredc from these data thatgreater emphasis is being given to health care as a key elemnent ofnational economic and social policy.
151. There is al.o comple-mentary evidence that there is asurging dermiand for additional rrmediCal care services and this increaseddernand is particula:r ly conspicuous among social security and otherwelfare f>und beneficiaries. Expendi,tures for this small segment ofthe population, esti-mated to constitute no more thla.n 5 percent ofCol]ombia's total population, has risen Ž80,) percent per individuail.E-.penditures , for the-ir hos-pital anld medicl c.re now represent overhalf of' the total costs of health care in the country. The implicra-tions of this observation are worthy of special consideri tion withreference to the Ten Year 11,alth Plan, l906-lWyi. That Plan, havingtaken account of the major unmet health needs and the existing defi-ciencies and ineqpuiti-es in health resources aivailability, proposesnew= organizational arrangements and new,j heal3th programs for t;he bene-fit of the general po1nilamion. Yet expendituiires for suIch genere lservices have renmaired essentially constant on a per capita basis..(9165, 52.0 and 58.5 pesos per capita for I'?l, 1>c69 and 1)7`0 respectively).
- 60 -
i52. Grarited that, w1nitth the economies evii greater efficiency of operationcalled, for in tle Nati.onal Hea-l.:Lth P'lan adi i t` onal and irproved general healthservices will. e Jurthconing at lower per U-nit coSt; as the Plan becornes esta-blished. Yet it appears unrealistlic to zisslnie that evern the most urgent ofthe country's health prob)lems cani he overcome m(.reyIT throuagh the reallocationof available funId's and wit.h,out sJize;aibte incrente,;r L of new funds for generalhea:Lth services ,W-v the [t.o iO.: population fif (lombia
l-3. All. of hile 'Ilc'"-;it, . .ypitp 'J or hi I urnoc' slu-
t1le last ten ycars, ha ir\f(-ronu11 2 I I I ii' p1 :'ce i!i.".iJ).U O iin'0a5OC i i th(ct
popul ltion and tipre( v o- t; e .) i nUrtrn c. o.L Ulu peso. I gJ 'the varioll-o so c on ii! of tlleP i Lu :id t,n' l,,in e:lir or le,sser dUe, theamounts of fund;s cqu re lo h i ob icc 9;v s, -the d;t-a arc no ,rc-sented in a forwat pcit; i ci -) re;': nLiPo aplvOYimation o,f the totel:! b)udI,-getary nieeds fcri- a yii a (wil"i' i llis L),hI e .'..7 oi- 1975) for sOhealth programris conduc4i9d h,y or unde:r 1,il r cc Upeurt_iscllo of' i,he Lii ni si!f 0o
He a-lth. A crude calculation, which sho-l10. t.5 I .TrLed by i.:-tut,}hor Stulry ajidanalysis, would place t;hi.s aii:, to .t.boui; 7.-60 presos per capita cor.paro(owi th the present ,)l.5 [Xesos."3
L5h. tAn. ;,Jddiii.onYl ;-.ii fo lo so,;-;o.n tr i.hle fin.-aricial requircc--,ntsof the Tenl Yeav Plan and t.:lf . mp1et-cim.Jn ,!sli Jdon can be derived fron sspecial analys:is of 126$ t. I onI hTsalLlroxnendt_ lures Thereirl a dicho tomywas developed dJiv-idin.g coss lro i.tose J'or' ca.-i.re ol the sick -- hospitaliza-tioIn and cura.tive or poai;.i'L;vc cor.- ices; and, secondly, all other se.rvices,primatrily of a rirevontio ol he Lt. pro(iii;,live.! nature. Of' the ot',otI o. [,G9lmillion pesos exoended that ~y'r l neron'C.t (928 nrril]ion pesos) was devotedto the former category and only ' perceit iTu lillion pesos) to preventiveservices. There are, of course, serious It.imitat-i-ots to so sharp a d.Effereni-:iu-tion of one category from t,he ot.her since mrany dut;ies pe-rfformed by a physicianor other attendant in providing mTedical treatmienst have significant preventiveimplications. However, in a ucuntry sichI as Colombia where so many of itsserious health p.ob lensm. arc aLfienale l.o strictly preventive measuras suc.h adifferentiatior- ct serOe a usct:rul purpose. The Ten Year Plan maces a stronlgcase for the strengthening and reorientation of medical care services to pro-vide a more comprehensive and readily available program for the total popula-tion. But sound planning dictates that a larger segment of this program beoriented toward preventing illness and promoting health through such activi-ties as intensified maternal and child health activities, health eduicationincluding nutrition education, vaccination, and improved environmental healthservices. It would not be unreasonable to increase expenditures for preventiveservices to 20-25 percent of health care cost instead of maintaining it at itspresent level of 9 or less percent of -the total.
155. Another cribtco;l. insig,ht inwo the financial requiremnents of theTen Year Health Plan is provided by its initial recognition of the need forthe special funding of capital investments for health facilities. No conso-lidated estimate of construction and equi.pDent costs or the present valueof the existing health plant, of the country is available. In view of the658 operating hospitals (46,7-35 beds). the 1,120 health centers and healthposts and the large number oi'f;rater treatmen-t and sewerage systems existing
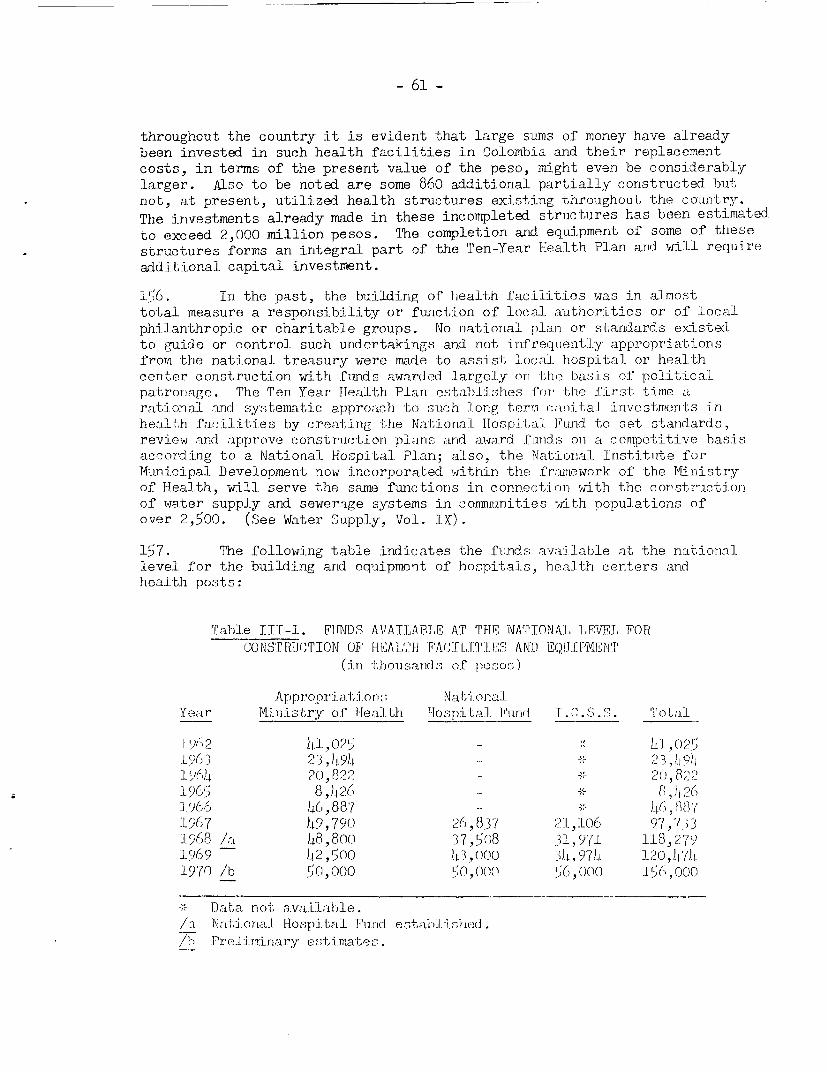
- 61 -
throughout the country it is evident that large sums of money have alreadybeen invested in such health facilities in Colombia and their replacementcosts, in terms of the present value of the peso, might even be considerablylarger. Also to be noted are some 860 additional partially constructed but;not, at present, utilized health structures existing throughout the country.The investments already made in these incompleted strluctures has been estimated.to exceed 2,000 million pesos. The completion and equipment of some of thesestructures forms an integral part of the Ten-Year Health Plan arni will requireadditional capital investment.
156. In the past, the building of hiealth facilities was in almosttotal measure a responsibility or function of loca.l authorities or of localphilanthropic or charitable groups. No nationial plan or standards existedto glide or control such undertakings and not infreq-uently appropriationsfrom the national treasury were made -to assist loc-al hospital or healthcenter construction with .funds awarded large:Ly on the basis of politicalpatronjage. The Ten Year Health Plan est'abliishef for the firs-t time arational and systematic approach to such long trermrnostal investmen-ts inhealt;h facilit.i-es by creating the National Hospi-tal i?and to set standards,review and approve construction plans and award fmids on a competitive basisaccording to a National Hospital Plan; also, the National Institulte forMunicipal Development now :incorporated within the fraunework of the M'inistryof Health, will serve the same functions in connection with the constructionof water supply and sewerage systems in communities with populations ofover 2,500. (See Water Supply, Vol. IX).
157. The following table indicates the funds available at the nationallevel for the building and eq.ipment of hospi-tals, health centers andhealth posts:
Tabl.e ITI-l. F[FNDS AVAIALNABLE AT THEll NATIONAI LEVE,L FORCONSTRUCTION OF HELALTH FACTI,.TT.E AND EQIJ I PMTBNT
(in -Lhou.sands of pesos.)
Appropr;iat-liJons Na-i;onalYear i nistry- of iHea:l.t Lb osp-ital_ Find T. (. .S. qTotal
'L t)2 O.,O25 1 1, 0 2519S6 3 23,)0.9)F 23,'L 9)1,9 64 20,, 82- 2 u, 8?25 '190'5 8,12(, _ ; 2(261'366 CS.46,87 - ,( ,I 96) 7 )49, 790 26,837 21,106 97,731968 /a 4.8,8oo 37,5()8 31,971 118,2791)969 - b.2,5no I.,()oO J, t, 974 12047.!71970 /b 50,000 51nC , 00( 5)i , COO 156,o0o
-Data not a.vailable./a Nati.onal. Hospital Funrid e.tabi iihod./l PreliMirlary estima-tes.
- 62 -
158. Iti may be seen that in recent1 years funds available from theN4ational level f'or hosp:i.tal, hea'Lth center and health post constructionand equipment are :i.ricreasi.ng subs1tantially. However, the NQationalHospital Plan, 1970-1972, assesses the immediate construction and equlp-ment needs in t.his area in excess of 800 million pesos. Future needs,part-,icularly t,hose f'or facilities recuired foIr the training of esser-tialpersonnel have not yet been firm.ly established (see Water Supply, Vol.TX, for estimates of capital requirements in that area).
159. As in the recent past both the Ministry of liealth and theC,olcmbian Institute for Social Socur:iurt,y will allocate f'rom their regularbudgets, funds earmarked for capital construction. To these will beadded the loan .unds availL able through the National Hospital Fund andborrowed from thie 1.C.S.S. trust funds. Repayment and the financing ofthese loans will ultimately be bornre by Ministry of' Health appropria-tions. Since the effect.ive life of constructed facilities and fixedequipment is a reasonabDly long one the new financing mechanism createdby the National Hospit.0l Fund offers a suitable dlevice for the satis-factory management of' external. investment funds that would acceleratethe constructioil and. equipment of' needed health facilities.
4. Manpower Requirements
1oO. Throughout tlhe various segments of the Ten Year National HealthPlan there are substlantial references to and documentation of seriousshortages of essent:ial health manpower. 'These sho-rt;ages apply notU onlyto physicians, dentists and nurses but also to auxiliary nurses, nursea:ides, nutrition workers, laboratory and other technicians, sanitaryengineers and inspectors, statisticians and medical record aides and toadministrative workers at all levels. These shortages are conmpoundedby such factors as the concentration of health personrnel in the largerurban areas at the expense of the smaller comumunities and rural areas,the emigration of trained personnel. abroad and. the lack of formal train-ing and rapid turnover of auxiliary supporting workers. The NationalHealth Survey further revealed thaL the full utilization of even thelimited supply of' trained professionals is crit,ically impaired byinad.equate facilities and equipment, the expenditure of too large a seg-ment of the physician's, dentist's and nurse's time in non-professionaltasks which. could be done as well by auxiliary workers and faults intraining which do not, prepare or encourage the professional workers touse their skills efficiently and effectively. 'rhus, the combined problemsof training, utilization and organization of health manpower give riseto probably the most difficult obstacle standing in the way of the fullimplementation of the National Health Plan within the ten year periodset for its accomplishment.
161. The traini'ng of higher level personnel is expensive both tothe individual and to the society which must underwrilte the ccsts ofneeded educational facilit:ies and subs,idize a Large fraction, if notall., of the operating expenses. Large investments of time are requiredbefore rormal- tra-ini.ng,, is completed; for the physiic:iar seven to ten yearsfor the dentist five or rnore and the nurse three t1o four years of univer-
- 63 -
sity level education are required. In Colombia, the Colombian Associationof Medical Schools has given much time and thought to developing ways ofimproving the educational patterns of all schools of the health professionsand to extend their influence to the training of auxiliary and supportingpersonnel. More recently, and as an outgrowth of the Ten Year Plan, theMinistry of Health has created a high-level adminis-trative unit Withinits organization to give direction and leadership in finding solutions tothe most pressing of the country's healt,h manpower problems.
162. At the present time, no consolidated and comprehensive planhas yet evolved for the whole heal t,h manpower area although there areindications that such an overall blueprint may be forthcoming within thenext 12 to 18 months. Nonetheless, a number of important guidelines havealready emerged indicating the direction this plan is expected to follow:
a. The nine medical schools, by increasing the combinednumber of their graduates from the present, level of under400 per year to 600, will be able to maintain the presentphysician-population ratio of il.32 per 10,000 and possi-bly raise it to close to 5.00 per 10,000 despite theanticipated increase in the total population of thecountry. Curriculum changes now in process will giveeven greater atterLion to preventive medicine and will.stress ttlie role of the physician as the health teamleader and the responsibility to delegal,e to and super-vise the work of o-ther members of -the team.
b. Education for professional nursing, which has not beenan attractive career with less lhan 150 graduates annually,must be greatly strengWhened to prcovide al, least 900 newtrainied professional mnrses each year. This would ultima-tely bring the nurse-population ratio from its presentlevel ol' 1 per 10,000 to i per 10),000, a figure comparableto the proposed physician-population ratio though stillgrossly below the avai:labilit,y of nurses in most developedcountries of the world. Concurrently the training ofauxiliary nurses will have to be increased. and improved toat least double the present numbers of 3500 certifiedworkers and at least s:imilar augmentation must be achievedin the training of nurse aides and rural health promoters.
c. Specialized training at all levels of public health activityat the Colombian School of Public Health, University ofAntioquia, is already underway and these programs are beingstrengthened.
ci. Intensive efforts must be made to improve the workingenvironmenl, of health workers in hospitals, health centersand heal]th posts l,hrough aupienlation of equipmentl andfacilities and, by better organization of health staff.Through such efforts and the delegaiirlon of tasks tosupervised auxiliary workurs the efficiency and productivityof the total staff' can be erdliarced.
i-, I1['rn C)wŽ(1 :7;::M. i fiiS * U:)p Fit'.tloi t,;,s Icrt' c'aP'ec P ;-liv;l 'j 'il''ri i,
0 TluL ) . - L .' ;i1 i ; ;iI }!l b) :np'. ULLS i i s h c ;ci, eu 1i Ld :/:IC' ( -4c2, iI .;t I L. I '. i . i r iA Iri :r I ,[, aI I. t J L I i 1.e l :.,, h ( ;
LiX l rV c_z.i rL p; :t rl t l uly rl;;u ,:CV nir te ria .
fll(l'e f'li 1..' .' i JI(! 4:(ui l. -/
L'. In ii j) : ii , I (J(t(:( j P7tZ.(,t-i- fl i -? c l r ' ioiri malt, c:^a c ' r-. f i i-e
iie fl¢i__ .-:,wrdi LI.i i.iiO 2'' tr1 1Li v i c .- ' s (I(Jw,I (:tAl ;'i
'I-[rea 1.'\ a-urt[''i.t' mr i4-if wili ELiiVe L;) 'I:.:7;liu r00'j ',l't,i r l :;ID<9!lSi~~~~ ~~~~ i1i ! f4>'< .}t),rt i ':i III tl } I.IJ i [i, f l ;l J '_tI :t'00 a S , 1 i.' ; 4]) t'. UKLO ']LulU i l,Y 4 0. I re:
r.D :V LIlF(l .t::; Wli -. I :1 f ! i k:)C p)fjti* 3 iIn i(uiii''A-lti ..
1o63. rh 3 1st, (t i.f i Ins 1 L'- ' i \ JiJljrI F li If l.i ri],;t j I j' r Mli
health manpower Irai n.n,g )I,L (J tar gel. ufldeLinLus cLxal. S a r,Uabl . we: 1beyond the presenLt o! inril cip;ated ! -)Si)UJ;; of LOu edauca l;)rla! in i.Iconcer-ned or of the M nistrv -)f (ea_ LG. Maz:reover, to da'.e, tihose gr i ):!i
with the problem have largel-, il nut ex(LUsi.vely been iji ' *i tL tnehealth professi-onals worki.nrg within t,he confines o-9f the hcaalth secI;orm 1t1e - '.Collaterally, t,here is lit.tLe evi-Ldeice thalt t,he Mini-1stry uf' .EiEduratlianr, aldmany educational insti. u Lions, o WLer thian til(i nine Utnivera.1 ties whilchopera-te a university medical school, h.vve yet considered Ihe roles theyultimately must, play in the pLeparatlio and training of auxiliary andsupporting health personnel.
164. Based on the above considera-tions the time seems right for a con-certed extension of the analysis and planning activities of the Associationof Colombian Medical Colleges and the Ministry of Health to a new level ofnational planning for essential health manpower training and development.Essential data are now available, reasonable goals and objectives have beendetermined but the means for meeting these educational needs and require-ments have not been fully mobilized nor have the minimum costs and the appro-priate sources of funds for meeting these costs been clearly identified. Itis clear that the medical schools alone or even the nine universities whichsponsor them cannot by themselves find adequate solutions to all of the problemsand needs that must be met. Even the Ministry of Health working with theseinstitutions is not capable of mustering all of the required resources. Theoverall problem is a national one involving multiple ministries and agenciesof government and many other institutions as well. A tentative plan for animmediate and direct attack on these problems calls for a large scale develop-mental study over a period of 18 months to two years and is outlined in asuggested Preinvestment Studies Program (see Study 3-1 in appendix).
5. Suggested Areas for Further Developmentof the Ten Year Health Plan
165. During the period when the Plan was in process of preparation itwas clearly recognized that neither all of the major health problems norall of the possible approaches to their solution could be fully explored.Priorities, based on data then available or the liklehood of achieving rea-sonable goals in limited time spans, had to be established, leaving open forfuture consideration areas that might then warrant or be amenable to inten-sive study, analysis and planning efforts. Thus, the plan was offered not as a
static or fixed set of proposals but, preferable as a starting pointpossible of extension and revision as circumstances and opportunitiespermitted. Several areas touched on but not fully explored or developedin the original Plan, published in November 1967, now appear to meritspecial attention, 21½ years later.
Health Advances Dependent on or Arisingfrom Advances in Other Areas of Economicand Social Development
166. Throughout the various segments of the Plan extensive atten-tion is given to the positive correlations found in the National HealthSurvey of a wide range of social and economic variables with the fre-quency of illness and its severity and the equally significant negativecorrelations of these same variables with the availability or the utili-zation of health services. Such correlatiorns do not always establishcause and effect relationships hut they do, at least, confirm the inex-tricable bonds that make it impossible for the health planner to dependsolely upon his own limited resources. They also reinforce the need forthose responsible for planning at the overall level or in other sectorsto consider carefully the implications of their own planning efforts forthe health of the population.
167. Since 1968, and formalized by a legislative enactment, theMinistry of Health has been working cooperatively with the Ministry ofJustice in tackling the multiplicity of problems arising from the specialneed of protecting the welfare of mothers and children. Working throughthe Colombian Institute of Family Vklfare, a semi-autonomous agency attachedto the Ministry of Health, a concerted effort is now being made to bringtogether the previously uncoordinated and dispersed institutions of socialassistance under the policy guidance of the Colombian Council for SocialProtection of Minors and the Family. The former National Institute ofNutrition is now merged as an integral part of the new entity.
168. However, similar innovative approaches appear worthy of explora-tion in the fields of education, housing and commmnity development -- bothurban and ruiral -- and conjointly with agricultuire, industry, public worksand other sectors of economic and social development. In education twosignificant areas of activity deserve high priority. Even in developedcoulntries heal-th instruction in the school system has been sadly overlookedand downgraded. Content and teaching methods have completely escaped theattention or concern of qualified health experts. Health instructionmaterials devised 50 years ago, lacking relevance to modern day problemsand neglecting singular advances in techmical knowledge, are being used byunqualified teachers who do not filly understand the implica-tions of theirnstruction they are trying to transmit. This problem is serious enoughin an advanced society where deficiencies in the school may be made up byinstruction and example in the home. In a developinrg country such asColombia thfis augmentation of school instruction does not exist nor doesit capitalize on one of the few channels of bringing health instruction,via the children, into the home. Health care and the proper utilization
- 6E?) -
of commmunity health re.ource, have always depended oii an informed arid suL-ficiently motivated. pui) i: to (1o as mu(ch f1or thei r owrn health protectionas possible and to use rea-sonable discrimination in turning to availableresources for thlose melasitres which they camno-lt p)rovide for themselves.The transplantation o:t twode-n andi more c:omplex health systems to a develop-ing society will niot take)1 hold unless concerted efLfforts are nLade to infornand motivate, througlh pulblic. education, the people wlho are expec-ted tobenefit from improved heaLt,h knowledge and health resouirces. 'I'hese oppor-tujities offer a spe.-i.a:L clhalLenge to both educatlional aind health leaders.
160. A second opport-uttity- for conjo]intl health and educational effortlies in the training of sorely needej healt.h mannpower. rT'raditionally sucheducational needs have been left, to and anssinhed by the health profession andpar-ticularly by the sirJll fJration Of those professionals identified witha specialized ednacati-oiial program. (.olombi.an- leaders have now recogn.ized.that the healtlh probhiems of the courntry cannot, be resolved merely by inten-sified training of more physicians, deirtists, curses or other highest levelpersonnel. F.:ar more auxilixaries must b)e re(crutit-ed. and trained and. specifiedtasks within their connpetence to perform under supervision, rmust be assignedto them. It could. be argeed that, the ideal locus for such training of sulp-porting personnel is in tLhe same env:i.ronment in which higher level personnelare also being educaated. 4fO jEver, t1lie large :tnlbmbers of auxiliary workersnow needed in Colombia an^md 1,he tremend Jo;ns cost involved in adding requisitefacilities in .9. medJ_.(-.-...L :Sc:hbol. setti ug dictate that many other educationalinstitutions in the (nwt.irv reaching down to the secondary and vocationalsc.hool level, becomc' -ngaged in health !nanpowaer training commnensurate with theireducational capac:-it,as. Thea laiiversity medical centers should concentratetheir attention on -the I r ci nang of professional level personnel requiriniguniversity level instruc.ti._on. In addition, there are special responsibili-ties that they must share Jointly wit1h the entire educational system. Forexample, the establisfarieitt; of reasonable prerequisites, the development ofcurriculum content and.- tea(ching materials, the certification of accreditedinstitutions, the train.ing of teachers, the examination and licensure ofgraduates are all functions requi)ring the leadership and supervision of theh:ighest levels of com-petence drawn from the established health professionsand their institutions. To move in this directi.on appears to be *the mostpromising next step in resolving the health manpower problems of Colombia.An ou-tline of suggest,ed developmental plan is -included as an integral partof the Preinvestment Studi-es 'Program Study 3-1 (See Chapter VI).
170. The above are offered as examples of the types of multisectoralplanning and conjoint activity involving the health sector with otherprominent social and economic sectors. (A special report is devoted tothe area of housing and cumm-u-ity development). In agriculture, both theprotection of the health of the large number of workers engaged in thisessential occupation and the augmented and improved production, distributionand use of essential food resources offer special problems that cannot be
- 67 -
resolved by ef Sorts in either sector alone. In the area of nutrition(See Chapter II, Section C2) interesting innovative approaches arecurrently being explored and Preinvestment Studies Programn-tudy 3-3(,ee Chapter VI) suggests ways in which t,he amplification of theseefforts m.iglhlt be attempted. In the industrial area, the Ten Year Planrefers to the increasing problems of industr-lal and occupational illnes;and accidents. The plan suggests a minimumLL program wi-thin the MIinistryof Health's own operations designed to combat the inost serious of theseproblems. EBit the need will not be met until. industry itself recognizesthe magnitude of the burden of ill healt-h and loss of productivity iden-tified with industrial operations and joins with health authorities inseekcing jointly solutions to these problems. Closely associated withthis areaare the problems of air and w.j.ter pollution and of the dispo-sal of indusrial wastes. Colombia has not yet reached the stages nowfaced by the advanced countries of thle world where the costs of correct-ing mistakes in environmental sanitation in the past are reaching stag-gering pr.oport.ions. A preventive approach initiated early in Colombia'sindustrial development is certainly indicated.
Population Control
l71. In the Ten Year Plan itself no specific program was elabora-ted directed toward family -planning per se nor was reference made tothe already initiated national efforts to reduce or limit -tlle rate ofpopula-t:ion increase. However, shortly after the issuance of that Plan,the IMinis try of Health colla.boratedl in the preparation of a specialreport and statement of policy on population issued by- the NationalDepartment of Planning which reports directly t-o the Off'ice of thePresident. This more recent document (lh-b) is highly sensitive tothe cultural, religious and political framework in which the gove.rnmentof Colomlbia must function and also takes into critica'l account the vastarray of economic and social consequences of uncontrolled populationgrow-th in a developing society. These consequences are observable notonly in the he,-ialth sector but have direct, bearing on the educational,housing and community development needs, andl have serious impli-cationsfor employment, the per capita gross national product a.nd other componentsof -the general. s-tandard of living. It can be stated, without reservation,that no single developmentaL problem basically identified wi-th healthand medical -ervices has received so comprehensive a consideration froma multisectora.Tl vantage point. It is of interest,however, that themajor burden of effort to alLer the rate of populat-tion increase stil1rest-s on t,hc shoulders of the health sector whi.ch, as has been slhownithroughout this report, is seriously handicapped by severely limi-ted.financial, physical, manpower, organizational and even political resour-ces.
:1'72. Family planning activities in Colombia are not new. Dataassembled by the National IlHealth airvey in 1965-1966 clearly demonstratedthat women in the higher economic strata, with highest educational attain-ment and with greatestaccess to the healtlh care available in larger urban
- 6b -
centers have had notable success in lowering Vteir fertility ratethrough measures involving the prevention of pregnancies. Interestingly,induced abortions as a means of restraining fert-lility is most commonllyfound in women of the urban zone with a low leveL of education or lowincomers.
173. Since 1)6)1 t;he A ssocia3ti-on of (o:lomlnbiLlnl Medical Col.:legreshas made faiLily planni-rif servi-ces avai.lable through universitj hospiL Isand- affiliated health ccnters. In ;iddition it hia undertaken rat.herextensive educational programns at tec profess'ional level and has. been largely,responsible for suchl research, prim-a ril.y o: an operational. researchnaULure, as has been carried oni in tLhe country. A linost LsirmAitaneous aprivate group, the A ssoc;iat.iion for thle 'Je] f'.re of Lhe Colomli.lan Fami:iy,started to provide famil.y planninjg cornsu-l tations and service;* s on anextensive scale -throughi th oLfices of p riLvaLe inedical practi.tionersand through independenL cli.nics. 'These servi:Lc,es are a lso ailmost entirelyrestricted Lo urban centers.
174. More recently, the Mini;stry of leal-th, concentrating onthe less urbanized an(d rura.l population of the count',ry, has begun afamidly plannin1g program based lTargely on increasirig the availabilityr ofinformation and aporopria to medical consulLtations to those women whovo-Luntarily seek sLuach servi ces tLhrough its established maternal and childhealth programs. Elven more recently, L oie Colombian Insti tuL,e for SocialSecurity anid the t-atic; oa P1.fare FI'rids ihave similarly improved theircapability to respond to reqJuests I'or L'a.Mily planning assistance soughtby their beneiiuiarie.. h reasonable esLimite ofL funds currentLy be:ingspen i on these Camqily acALvitLies is in the ranifge of 2.5-3.O miilliondo-Llars annually wiL,h all but. minor amourtUs being derived from axternlsources, primarily fromi tLhe U1.5. It :is appare:tn that lack of funds,eanrarked specifical.ly for family planning purposes, i.s not inhibitingprog,ress in these -proram!ns.
175. Consolida.Led daita on -the exact nature and types of servicesrendered are ineagre as is information on the ninber of women reached andre-tention rates or on olilher indices essential. for scienLific appraisalsof the success oL these programs. This is riot surprising in theliglhtof the paucity, delayed nat,ure and unreliabilit\y of all vital statisticsdata f or Colombia ex(ceut those deri.vecd from special studies such as thoseconducrted in the National lMorbiditLy Survey of lq965-l966. (In a previoussection, Chapter 1I, Section A-!, the problems associated with analysisof birth rates were reviewed; see also PreinvestrlenLt Studies Prog-ra.m-S-tudyProposal 3-5). Barrin-g th?e availability of iar nmore accurate and currentbirth registration iniformation and associa-ted dato, a criti-cal reviewerof family planning activities in the present Colombian scene is unable tofo:recast, with any degree of confidence, future trends in the rate ofnatural increase of thWe poDulation. This rate appears to be high, in therange of 3 percentl per year. It, is either stable or gradually decliningbut whether present faimily planning efforts will or will. not have a de-monstrable impact in the rate is higlily conjectural.
176. The .above aissessmenti of present fami ly planning activity inColombia does not controvert; t-.he sounrd natoian-1l pol.-icies recently adopte?d.nor the sincere cletemTnninlt,ion and effort,s of najtional leaders both within-.and outside the governmenL tto apply ajvail.abl teLchni.ca.l knowledge and
- 69 -
capability to such ends within the social and political framework ofthe country. Other and perhaps even more important constraints on theseefforts are the limitations imposed by the sources of supporting fundswhich restrict expenditures to those which can be directly identifiedwith the immediate process of prevention of pregnancy. So narrowlydefined an approach to an objective could be self-defeating and underthe developmental circumstances, faced by Colombia, with particularreference to the current problems in the health sector, such limitationsmay be doubly so.
177. On superficial analysis the strategy of reachirg between 700and 750 thousand additional women with family planning services over thenext five years (increments of approximately 3 per cent of the women ofthe country, age 15-49, per year for each of the next five years) appearsto be a reasonable one. Calculations have been made indicating thatsuch efforts would cumulatively reduce the birth rate at least 4.4 perthousand and possibly as much as 12.5 per thousand. A substantial num-ber of physicians and nurses have been or are being brought up to dateon modern family planning techniques, health "promoters" are beingrecruited and given short training courses to prepare them to carrymaterial and child health instruction into the homes and ample fundsare available to support salaries and to purchase family planningcommodities for the program. Questions can be raised as to the relia-bility of the above predictions since these depend not only on thenumber of acceptors - those who initially volunteer to accept theseservices - but of equal and perhaps crucial importance the number ofwomen who are successful in adopting and continuing over long periodsof time effective contraceptive procedures. Such prevention of conceptionrequires medical instruction and supervision on a continuous basis andonly time and experience will demonstrate whether the programs now ini-tiated can meet these requirements.
178. The programs also appear vulnerable to serious shortfalls onother accounts. It remains to be seen whether the necessary responsescan be obtained from the child-bearing segment of the population in asocial and cultural milieu in which only 9 percent of the total populationseeks aid when it believes it needs health care for illness and in ruralareas only 3 percent turn to a physician for such assistance; less thanhalf of the pregnant women receive care during pregnancy; only 37 percenthave a physician in attendance at delivery, a figure dropping to 18 percentin rural areas. Even in the serious circumstances of a pregnancy terminat-ing in an abortion (about 1 in 7.5 pregnancies) only slightly more thanhalf (56 percent) are seen by a physician.
179. A strong case can be made for the view that an effective familyplanning program must be not only part of an inclusive maternal andchild health program but linked with a comprehensive and total healthand medical care program for the entire country. It is highly problematicalthat the infrastructure required for an effective family planning programcan be established for this purpose alone or can prepare the way for thebuilding of the same infrastructure required for more comprehensiveservices. Thus, it seems reasonable to question whether present family
- 70 -
plarmirig activi-ties in Colombia will really take hold until and unlessfar more adecluate provision is made l'or supplying the facilities :rndmanpower resources reqiuired for thie comprehensive h}ea:Lth and medicail careprogram call.ed for in the 'T'cn Year National lHealthi Plan ancl now in processof impl.ementation. IMloreover, as has been clearly dermonstrated by thedata available for Colombia, marked differentials in the acceptance andeffective utilization ot' f'amily planning practices can be identified withrising levels of education. and family incomc. It follows, then, that augmentedefforts to improve educational and job opportunities in Colombia alsooffer direct avenues to t,he effective slowing of the overall rate ofpopulation increase in the country.
- 71 -
IV. RECOM4ENDED PROJECT PROPOSALS
180. Many programs and activities, forming integral elements of theTen-Year National Health Plan, are now in variolls stages of implementa-tion. Some of high priority and following approved plans of developmentare moving forward at a slower pace than the need. for these programsdictate. This situation arises as a consequence of the severe competitionof the multiplicity of approved health programs for an appropriate shareof the Ministry of Health budget and the similar competition of the Ministryof Health with other ministries for an appropriate share of the nationalgovernment's available resources.
181. Some of these programs have been singled out for careful con-sideration for external financing as a means of accelerating and consoli-dating the full implementation of the Ten-Year National Health Plan. Thefive recommeended project proposals in this category are outlined on thefollowing pages. These outlines should serve as a hasis for furtherdiscussion with appropriate representa-tives of the Colombian government.
- 72 -
A. -- H[EALTH PPiOJWCT PROPOSAI,
COLOMBIA - I
1. Name of Project: Bevelopment of Instit-utional Resources for Health(Hospitals, I-lealth Centers anx] Health Posts)
2. Executing Agency: National Hiospital Fund (Ministry of Health)
3. Total Estimated Cost: 17S $50 million.
1X. Estimated External Finarncing Required: (IS $30 Million.
5. Description of the Project: A National fHospital Plan (1970-72) hasrecently been inauguirated calling for 1) the modernization andre-equipment of existing hospitals, health centers and health posts,and 2) the completion of construction and equipping of a substantialnumber of partially erected health facilities in key locations through-out the country that have been in various stages of construction forperiods up to 15 years. The National Health Survey (1965-1966) re-vealed large segmer]ts of the population failing to receive evenminimal standards of medical care services. For those attendingexisting facilities the quality of care rendered is inadequate. Thelimited availablity of professional health manpower heightens the needfor enhancing productivity and efficiency of the existing staff whichhas been severely impaired by the absence, oosolescence or malfunctionof basic and essential resources and equipment. In many instances theunsatisfactory w-orking environment in existing health facilitiesfrustrates efforts to recruit, train and -etain required personnel.The National Hospital Plan provides a practical and feasible programfor meeting the health care needs of all segments of the Colombianpopulation at reasonable cost. Operatioral and maintenance costs canbe covered through the regular operating budget of the Ministry ofHealth and other sources of operational income.
6. Present Status: The Ministry of Health has assigned this project highestpriority in the National Ten Year Health Plan. This project, brokendown into four component parts, appears on the list of 1970 projectsproposed by the Government of Colombia to the Joint Consultative Group.Since 1967, the National Hospital Fund a discrete national agencyadscribed to the Ministry of Health, has been charged with the legalresponsibility for reviewing and approving all proposals for theconstruction, renovation and major equipment of health facilitiesthroughout the country. It directs the investment of health facili-ties construction funds derived from long term loans made from thetrust fund reserves of the Colombia Institute of Social Security andearmarked for this purpose. Such funds are approaching 50 millionpesos annually. The FPnd is also responsible for evaluating andapprovring construction plans to be funded from the annual appropria-tions to the Ministry of Health also now fluctuating in the range of50 million pesos annually. The National Hospital Fund thus providesan instriiment of ,overnment to administer the management of externalfunds to be applie d to +he same plurposes.
- 73 -
B.- HEAlTH PROJECT PROPOSAI.
COLIOMBIA - II
1. Same of Project: Control of Communicable Disease by F7rpansion andAcceleration of National Mass Vaccination Programs
2. Executing Agency: Ministry of Health
3. Total Estimated Cost: US $5.6 million
L. Estimated External Financing Required: US 13.4 million
5. Description of the Project: An important group of communicable diseasesin Colombia are siusceptible to control, if not eradication, by sus-tained but relatively simple means of mass vaccination. These includesmallpox, diphtheria, whooping cough, tetanus, measles, poliomyelitiesand tuberculosis. Prevention of these illnesses would substantiallyreduce mortality and morbidity and would release scarce professionalmanpower and health facilities for other essential needs. Vaccina-tions can be given, under supervision, by trained sub-professionalpersonnel.
A nationally directed campaign is cuirrently under way toachieve satisfactory levels of protection in the most susceptiblesegments of the population. The aim of this project is to expand andaccelerate this campaign and attain sufficient momentum in the nextthree to five years to permit delegation of continuing responsibilityfor revaccination, when required, and vaccination of new susceptiblesto local health programs. The ultimate objective is to maintain thispreventive program as an irtegral part of the comprehensive healthservice coverage now in process of development for all segments of theColombian population.
6. Present Status: The Ministry of Health is now allocating approximately10 million pesos annually to this direct vaccination campaign and atthe present pace of accomplishments will require ten or more yearsof activity to realize desirable objectives. A doubling or triplingof the pace during the next three to four years, with externalassistance, would result in no additional direct operational costsyet could significantly reduce indirect costs in the long run.
- 74 -
C. - HEALTH PROJFECT ROPO'SAL
COLOMBIA - III
1. Name of Project: Expansion and Completion of the National Laboratoryof Health
2. Executing Agency: Ministry of Health
3. Total Estimated Cost: US $1. million
4. Estimated aXternal Financing Required: IJS $.5 million
5. Description of the Project: The National Laboratory of Health hasrecently been incorporated as art integral part of the new NationalInstitute for Special Health Programs, a semi-autonomous agency ofthe Ministry of Health. This laboratory is responsible for theproduction of biologicals and vaccines used in the prevention ofthe major communicable diseases in Colombia, the testing of drugproducts sold and distributed in the country and the scientificinvestigation of the significant health problems in the country bothin the laboratory and in the field. The laboratory has recently beeninstalled in a new and modernly equipped building in Bogota which,because of limitations of available funds, is only partially completedand does not meet the full requirements of its excellent scientificstaff. The attack on a number of important health problems will haveto be deferred pending acquisition of additional funds to complete andfully equiip desirable additional facilities particularly those thatwould be used for the specialized training of personnel required forthe operation of local health laboratories throughout the country andfor the quality control of such decentralized health laboratory services.The laboratory is also providing, at cost, its own manufactured vaccinesand other biological products to other Latin American countries and isserving as a regional reference laboratory in international public healthactivity.
6. Present Status: Construction and equipment costs of the recently inaugu-rated National Laboratory building have amounted to approximately US t 1million. The annually operating budget of the laboratory is approxi-mately US $ .5 million with increments contemplated up to a level ofapproximately US t .75 million by 1972. Doubling of existing facilitiesis a desirable objective in the next three years; additional operatingcosts could be absorbed in the annual Ministry of Health budget.
D. - HNALTH PROJtECT PROPOSAIL
COLOMBIA - IV
1. Name of Project: Expansion and Development of Training, Planning andResearch Programs - Colombia School of Public Health(1970-1971h)
2. Executing Agency: Ministry of Health
3. Total Estimated Cost: US $)J.2 million
4. Estimated External Financing Required: US l.6 million
5. Description of the Project: The Colombian School of Public Health(ITniversity of Antioquia, Medellin) constitut;es the sole specializedtraining facility for public health practice in the country. Itsmajor support (9n percent) is derived from annual subsidies fromthe Ministry of Health. During the five year period 1964-1968, 755individuals received graduate, post-graduate, intermediate or sub-professional training at the school. A plan has been developed toovercome the acute and severe shortages of public health personnelby training at this institution during the next five years a totalof 2700 physicians, dentists, nurses, engineers, statisticians,administrators, nutritionists, etc. The school is about to moveinto a new building constructed by the Ministry of Health whichwill facilitate the expanded training, research and consiultationprograms of this institution.
6. Present Status: A five year budget totaling approximately 75 millionpesos is required to finance this essential program. Reasonableforecasts indicate that the Ministry of Hea:Lth will he able toallocate about 2/3 of this amount (5( million pesos) from its annualappropriations during the next; five years. The balance, approxi-mately 25 million pesos is required from external sources to assurethe underwritirng of this hasic buidgetary financing.
' (!I ,( Will [Af - V!
1. Name of Pro-lect: ol'' h.Dko i. L.-tt; in o1 hart WaLer n>plins
2. lxe,,it,tiig Agency: Mirii.,tA!y 1 OlfEe:d] l
3 . Total Est;imated ci oct [: i;-L hrtiml1-i-on
1 h sLtmated External ai Lnao(:L lg he qic rod: [MI, I; nIih [01
D. Lescription of the P ro i(cc t: 'I-i p ecl;.aiit:; at thc redlp : jun by 1/-'to 2/7Yo.r7 deriL i:,.i. es in I It!, o :hJAi.lheoo,l onuliI on Li itreatlmeTnt, of 'r h i :ntrly l.Y at cp L l Up k c) o0.,o Or
the pu1pra!:t,i-r over lUie age. ofI lhI .- : piese. Y- ;.n rt(ned oi Petitacare W:it.l a pe-tck pr (-vaJ:-nl ot i.rl ,he aib' v.wrrmp 1E :II (5- 1) ( perce00t.LimitLedl resour es [utave re.st,v i.o U.ed cdrltaL care. I'he u1lk 0f ''ervi cc.sis corifiried Lo av I-Tac:j,f.ons [illjfi-Lig of cavitLies wwith reiativelylittle attel-tt ion givert to deitil-- _-)rophyiut s. T'wenLy-fi-ve years ofexperietnice in developed contvrties of the world has (demonstrated thatcontrolled addi.tion Or f UOFIia e ;oraiLs into commuity water suppliescarn significan-tly reduce cI .na.vities ;I] children (t minirnal costand withi no harmf'ul- effect,;. fAlIostc 90( percent of the uirban popula-tionl has. ac(cess tLo comnimn;.l l. rY sluppil,, provi(ling a sa.mple anddirect chattiel for l;n impi - t;.on of an est,.ah!iishel preventi.vemeasure benefitting a sultst i lracLtion olf the cotmntry's chliijIloodpopulatlorn.
f. Present Status: The denita I anh environmerita' health staffs of theMinistry of Healtht have developed detail.ec plans to reach P&C Dercenitof the urban popila.tion in1 the five year tp.eriod l'Y71-197".. Initia.alinvestments wi:l1l provide essen t.ial. eqniprmtent anoc t;he L.raining o1water supply p)ersonnriel. (OperatioraaI cos:ts and slppli.es for cottinmia-tion of the program are II:.LrrTPi.Itln.
- 77 -
V. INVENTORY OF DEVELOPMENT STUDIES IN PROGRESS
182. As stated in the main body of this report, the Ten-Year NationaLHealth Plan, 1968-1977, is not considered by the health authorities ofColornbia as a complete and all inclusive document. Rather it was designedto serve as a starting point of comprehensive activity based on dataavailable at the time of the Plan's preparation. Goals set were determinedby assessments of the urgency and priority of proposed programs and thereasonable likelihood of their attairvnent within the forseeable availabilityof resources. Thus, refinements and extensions of the Plan were viewed asessential and continuing responsibilities of the Ministry of Health andother concerned agencies and groups.
183. To this end a series of studies have been initiated and arecurrently in progress. During the course of this review of the Colombiarihealth sector a number of these developmental studies were exlored withthe principals engaged in their conduct. For purposes of illustration,six have been sirgled out here to indicate their nature and scope as wellas the prospects of the availability of new data and/or plans to guide thefurther implementation of the Ten-Year National Health Plan.
A. Human Resources for Health - Phase II
184. As one of the major objectives of their 1965-1966 cooperativeeffort the 1ifnistry of Health and the Association of Colombian MedicalColleges attempted -to take stock of the available supply of health manpowerin the country and the resources of the training institutions essential tomaintaining or increasing thLis supply. These efforts were limited almostentirely to physicians and nurses. More recently similar studies of dentalmanpower have been completed andi are shortly to be published. A continuingregistry of physicians was established and is being maintained providinguseful information on the location, na-ture of professional activity aniother significant characteristics of the available medical manpower supply.
185. C-urrentLy, the Ministry and the Association are jointly engaged(Phase II) in extendling this system of current registration to other healthoccupations and in adapting such a system to the need for a continuingevaluation of the critical manpower requirements of the new NationalHospital Plan now in process of imp,Lementation and designed to providecomprehensive health coverage for the entire population. Ou-t of these3tudies it is expected that within the next 12-18 months reasonably preciseinformation will be available on the number of health workers in eachcategory actually engaged in the general health care system, the numberof' currentl,y vacant positions, and appropriate norms required to make thesystem function at desirable levels of productivity and efficiency. Theseand re:Lated data to be obtained are essential to such important plannling.functiorns as: (1) the detailed organization of comprehentsive health ser-vices,(2) the basic training of all categories of health per;3onne'l; (3) the ectensioof graduat.e and continuing education oL' such persninncL; ().I) the fornu La tiori
_ 7 -
of appropriate salary scales and employment incen-tives; al-Et (5) the revisionof obligatory national. servi.ce requireinents now -limited to medical schoolgraduates. These studies are being L'inatced out of the regular appropriationsto the Ministry of Heal-th with some ass:i.s-tance from the Pan American HealthOrganization.
186. When these studies are completed it will still be necessary tomobilize an ambitious national program of health manpower training. Tothat end a preliminary proposal is suggested in Chapter VI, Section A below -An Action Program for Education and Training in the Health Sector. Referencesare also made in Chapter II. Sections C-4 and C5a to the need Cor such aprogram.
B. Experimerntal Study of Hea:Lth Servicesin Colombia. - Phase II
187. Since early 1969, the Ministry of Health and the Association ofColombian Medical Colleges have been conducting studies in the field designedto test the hypothesis that relatively- simple, yet, important, health taskscan be delegated by the physician and the professional nur3e and performeduinder supervision by au:xiliary nurses, nurse aides, and health promnoters -personnel who do not require as lengthy or as expensive a training periodas do the higher professional categries of+ heal-th workers. Success in thisprogram would reduce the cost. of ba;-3_: h.-aLtii services and extend the pro-ductivity and effectiveness of the oh.ysicialn. Studies are in progress inthree centers, under uniiversity medlcal center auspices, anxd are focusedprimarily on health services rendered in ambuLat.ory care facilities - healthcenters and health posts - find in home care services. The study designincludes the definition of tasiks appropriate for delegation. the developmentof health care manuals and instrictioncS, ithe recruitment, training andsupervision of necessary complements of' auxiliary personnel. and the carefulevaluation of performance and resuLts. P'hase I involved the technical andfield preparations for the study; Phase II - now in progress - is actuallytesting the plan under ..ie.l conditions. Completion of observations andanalysis of results is schedulled for early 1971. Tihe Pan American HealthOrganization ard the U.-. AgEoncy for International. Development are providingfinancial assistance to this tty.
C. Develoomte.it of a Compre'henisive Health PlanningSystem a,t; the L.ocal l.evel - Phase I
188. The Pan American Health Organization has long been in the forefrontin the development of systemnatic approaclies to the planrnirng of comprehensivehealth services in the developing countries. The success in applying thesetechniques in recent years in Co-Loabia can large'Ly be attributed to thepioneering program sponsored by P]AHO in association with the Institute ofEconomic and Social Planning in Santiago, Chile, in which more than 200health planners f'rom 20 countries have received intensive training since1962. Many of the leading hea'lth authorities in Colombia have benefitedby this program but the impact has Largely been felt on the national leveland is only now beginninrg to t'il-ter down to the Levels of Departmental andlocal health activity.
- 79 -
1 89. More recently, the Division of Research and Communications Science
(RECS) of WHO in Geneva has developed a plan of study and experimentationdesigned to foster comprehensive health planning approaches to local healthproblems based on the thesis that national programs should reflect soundplanning and development processes in the community rather than the otherway rolind.. Moreover, methodologies applicable to macro analysis and planningmnay not be applicable in small systems. Thus, new planning procedures mustbe de-vised and tested in the field specifically oriented to the types ofproblems encountered in the day to day operations of local health programsand within the framework i.n which the multiplicity of local health agenciesand personnel cope with speciLic health problems.
190. This study plan has gained the support; of the Ministry of Hea-Lthand other health organizations in Colombia. PAIiO and a number of Americanresearch and training institutions have manifested their interest and desireto cooperate. The site for the initial experiment has been chosen as theDepartment of del Val:Le in South Western Colombia incllding its regionalcenter and capital, the city of Cali. The University del Valle MedicalCenter has accepted responsibility for leading the study and WHO-RECS plansto install at least six of its staff members to work winth locally selectedcounterparts at least f'or the initial year or 18 months of exploratoryefforts. Financial support in the range of $150,000 a year has been pledgedby WHO. If exploratory efforts are successful and a decision is reached tocontinue these efforts for at least a five year period additional support,including external assistance, will be required.
D. Integrated Nutrition Program ofApplied Nutrition - Phase II
191. In the body of this report, Chapter II, Section C-3, the presentambitious program to combat malnutrition and to improve the feeding habitsas well as the food sources of the people of Colombia has been reviewed.Activities are centered in the Department of Nutrition of the ColombianInstitute for Family Welfare but affect the operations of all parts of theMinistry of Health, other ministries and agencies of the nationai government(Agriculture, Education, Interior and the Institute of Agricultural Marketing)and the decentralized health and other programs in the departments andcommunities. Such innovative programs are involved as the Integrated Programfor Appliecd Nutrition (PINA), the National Program for Nutrition Educationand Supplementary Feeding (PRONENCA) and the National Plan for the Developmentof Foods (PILANALDE). In brief, the total program consists of a wide varietyof activi-ties ranging from basic nutrition research, the trainirg of'nutritionists, technicians, teachers and "multipliers', the preparation ofmass education materials, applied research (preparation of new food supple-ments and genetic adaptations of foods to improve their nutritional qualitiesand at the sante time retairing their acceptability to Colomb:ian dietarypatterns), to iarge scale feeding programs and educational campaigns toimprove eal;ing and nutrition patterns.
- 8n -
192. Beginning in 1965, a pilot supplementary feeding program wasinitiated in Caldas Department (Nutrition Study - Phase I). The NationalFederation of Coffee Growers, assisted by the Inter-American Committee forDevelopment and using food supplements provided by WFP, demonstrated thebenefits accruing from special feedings for pre-school children and pregnantand nursing mothers. In 1969 this program was expanded (Nutrition Program -Phase II) to major scale and with its completion in 1975 will benefit noless than 900,000 pre-school and school children as well as pregnant andnursing mothers in all of *the 29 Departments of the country. The totalcost of the nutritional education and supplementary feeding of thesevulnerable groups is estimated to reach about 75 million pesos with theWFP providing 57 percent of the cost (42.3 million pesos) in the form offood commodities. UNICEF, PAHlO, AID and other irruernationa:L bodies arealso assisting.
193. As vital as this program is, it can only reach a fraction of thepopulation (5 percent and possibly 20 percent of the particularly vulnerablesegment). Moreover, althougrh this program does include the use of somelocal food supplies it is still largely dependent upon the importation ofsupplementary foods. The ultimate goal is, of course, the adequate nutritionof the total population, the full mobilization of indigenous food sources andthe education of the Colombian families to select and utilize in their dietnutritionally adequate foods that are available to them within their financialresources.
194. As stated above, the program is planned to continue for approxi-mately five more years, until 1975. However, there are indications thateven at its conclusion it will not have achieved an essential objective,namely that of assuring Colombia an adequate nutritional status based onan indigenous complete food supply available to the entire populationwithin the economic resources of each farnily and readily available tothese families at the local level. To further consolidate the gains ofthe present program an additional and relatively modest development studyis proposed as Phase III of the Integrated Program of Applied Nutritionand briefly outlined as Preinvestment Studies Program - Study 3-3 (seeChapter VI, Section C).
E. Family Planning Programs in Colombia
195. Although dating back to 1965, the family planning activities ofthe Association of Colombian Medical Schools, the Association for theWelfare of the Colombian Family and the Ministry of Health were intensifiedin 1969 through the combined technical and financial assistance of thePopulation Council, the Pan American Health Organization and the Inter-national Planned Parenthood Federation. Funds for all three of theseprograms originate in the U. S. Agency for In-ternational Development.Additional external assistance agencies are also involved, e.g., the FordFoundation and the Pathfinder Fund; the Governmen-t of Sweden has alsoindicated its intention to provide assistance in the very near future.It is estimated *that expenditure for these programs now approach $2 milliona year.
- 81 -
1L96. Responsibility for the coordination of the -otal program restswith the Ministry of Health which also has assumed responsibility for famiLlyplanning activities in the general hospitals of the country, the socialirnurance hospitals, largely in urban centers, and through local healthcen-ters and mobile units. The Association for the 'Welfare of the ColombianFamily is concentrating its efforts in providing family planning servicesin the larger towns, through private hospitals, in the preparation anddistribution of mass media pub.licity and working with other groups. TheAssociation of Colombian Medical colleges p:Lays a key role in conductingand directing both biomedical and sociological research through its ownDivision of Popu'Lation Research and through its member university medicalschools. It also plays a key ro:Le in conducting extensive sraining programs,evaluative Eollowup of the enLire program and by conducting post-par-.im
ami:ly planning services in the 20 or more university hospitals and healthcenters affiliated with its member me(dical schools. It is estimaGed thatfamily plauning services are niow available in a-t least 200 centers aniclinics and tha-t more than 300,000 women in the chi.-Ld-bearing ages havealready been reached with the goal of reaching over 700,000 more in thenext five years.
197. The objectives of' the Ministry of' Health programs have beenstated to be: (1) to increase coverage of prenatal care; (2) to preventprovoked abor-tions; (3) to gradually sa-tisfy demand for information andmedical services to space births or treat sterility- in the couples whojustifiably request them for medical and social reasons; and (4) tocontribute to the ear.ly detection of cancer of the female cervix throughvaginal cytology in women of reproductive age that request mother andchild protection.
198. In the text of this report (Chapter III, Section C5-6) some ofthe shortcomings and possible points of weakness of these programs havebeen touched upon. It is t,oo early to evaluate ful'Ly i-ts likelihood ofsuccess or failure but it is quite clear that its limitations are notidentit'iabl.e with lack of funds spec.i.Lically earmarked for family plarningacti-vities.
F. Nu-trition and Development - Phase II
199. Soujnd scientific data are lacking to firmly establish a causal.rela!,ionship of malnutrition irith physical and mental developmnen-t in ear'Lyc.h.ildhood and t;he e-tlenl; to wlhicihl supplementation of the diet wit,h essentialnutrienl,s can reverse developmental, deficJts once these stigmria, presumedto be due to malnutrition., appear. The Harvardt chool of Publi.c Healtthand Cornell University- are currently working wit,h the Colombian Instituteof Famil.y 'Jelfare (Department of Nutrition) in an ef'.t'ort to resolve thisint.terrnatLionally importarit scientific issue.
:N)0. The planrning phase of this study is now completed and a -two yearpilot study is currently in mid-passage. lf these preliminary investigations,beinLg condiucted in selected urban and suburban popul.ation groups in andarouiKl fogota, are successful thlie large research team plans to undertake

- 82 -
a 5-6 year definitive study involving no less than 600 study families. Amultidisciplinary team of nutritionists, psychologists, social anthro-pologists and ecologists are involved and have been drawn from universitycenters in the U.S. as well as from indigenous sources of trained researchworkers in Colombia. Approximately $250,000 have already been invested inthis scientific investigation; the cost of the total definitive study, ifundertaken, is not available at this time.
- 83 -
VI. RECOMMENDED PREINVESTME PROGRAM PROPOSALS
201. As a means of further refining and extending the Ten Year NationalHealth Plan, and to accelerate its full implementation, a number of key pro-gram areas have been identified for additional intensive study, includingthe development of detailed operational plans and reasonably precise esti-mates of program costs. Each of those areas selected for such a Preinvest-ment Studies Program merit high priority based both on the importance assignedto them by the Plan and on judgments made in the course of this survey's evalua-tion of the Colombian health sector, its development problems, policies andprospects.
202. The six proposals outlined in the following pages (ANNEX 1) focuson program areas vital to the present effective operation of the total healthand. medical care system and to its future development. These areas include:health manpower trairing and the education of the public in health, theefficiency of health care institutions, national nutrition, health careand the extension of social security, improved vital statistics and periodicstudies of improvement in the health status of the popullation. The pro-posals should serve as the basis for further discussions with appropriateColombian authorities.

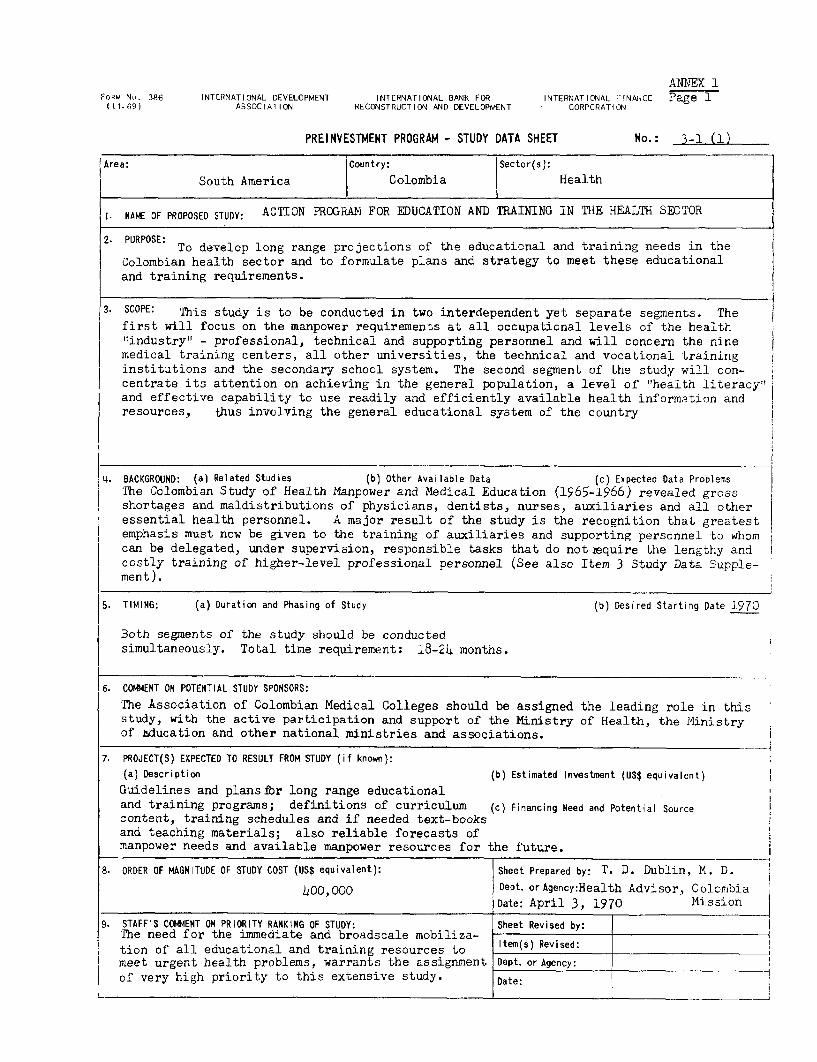
ANNTEX 1,ORM No. 386 INTERNATIONAL DEVELOPMENT INTERNATIONAL BANK FOR INTERNATIONAL FINAhCE Page I(11-69) ASSOCIATION RECONSTRUCTION AND DEVELOPMENT CORPORATiON
PREINVESTMENT PROGRAM - STUDY DATA SHEET No.: 3-1 (1)
IArea: Country: Sector(s):
South America I Colombia Health
1. NAME OF PROPOSED STUDY: ACTION PROGRAI FOR EDUCATION AND TRAINING IN THE HEALTH SECTOR
To develop long range projections of the educational and training needs in theColombian health sector and to formulate plans and strategy to meet these educationaland training requirements.
3. SCOPE: This study is to be conducted in two interdependent yet separate segments. Thefirst will focus on the manpower requirements at all occupational levels of the health"industry" - professional, technical and supporting personnel and will concern the ninemedical training centers, all other universities, the technical and vocational training iinstitutions and the secondary school system. The second segment of the study will con-centrate its attention on achieving in the general population, a level of "health literacy"'and effective capability to use readily and efficiently available health informetion andresources, thus involving the general educational system of the country
4%. BACKGROUND: (a) Related Studies (b) Other Available Data (c) Expected Data Problems
The Colombian Study of Health Manpower and Medical Education (1965-1966) revealed grossshortages and maldistributions of physicians, dentists, nurses, auxiliaries and all other
i essential health personnel. A major result of the study is the recognition that greatestemphasis must now be given to the training of auxiliaries and supporting personnel to whomcan be delegated, under supervision, responsible tasks that do not equire the lengthy andcostly training of higher-level professional personnel (See also Item 3 Study Data Supple-ment).
5. TIMING: (a) Duration and Phasing of Study (b) Desired Starting Date 1970
Both segments of the study should be conductedsimultaneously. Total time requirement: 18-24 months.
6. COMMENT ON POTENTIAL STUDY SPONSORS:
The Association of Colombian Medical Colleges should be assigned the leading role in thisstudy, with the active participation and support of the Ministry of Health, the Ministryof Education and other national ministries and associations.
7. PROJECT(S) EXPECTED TO RESULT FROM STUDY (if known):
(a) Description (b) Estimated Investment (US$ equivalent)
Guidelines and plansfor long range educationaland training programs; definitions of curriculum (c) Financing Need and Potential Sourcecontent, training schedules and if needed text-booksand teaching materials; also reliable forecasts ofmanpower needs and available manpower resources for the future.
8. ORDER OF MAGNITUDE OF STUDY COST (US$ equivalent): Sheet Prepared by: T. D. Dublin, M. D.
400O,000 Dept. orAgency:Health Advisor, ColombiaDate: April 3, 1970 Mission A
9. STAFF'S COMMENT ON PRIORITY RANKING OF STUDY: Sheet Revised by:The need for the immediate and broadscale mobiliza- Ition of all educational and training resources to em(s) Revised:meet urgent health problems, warrants the assignment Dept. or Agency:
of very high priority to this extensive study. Date:
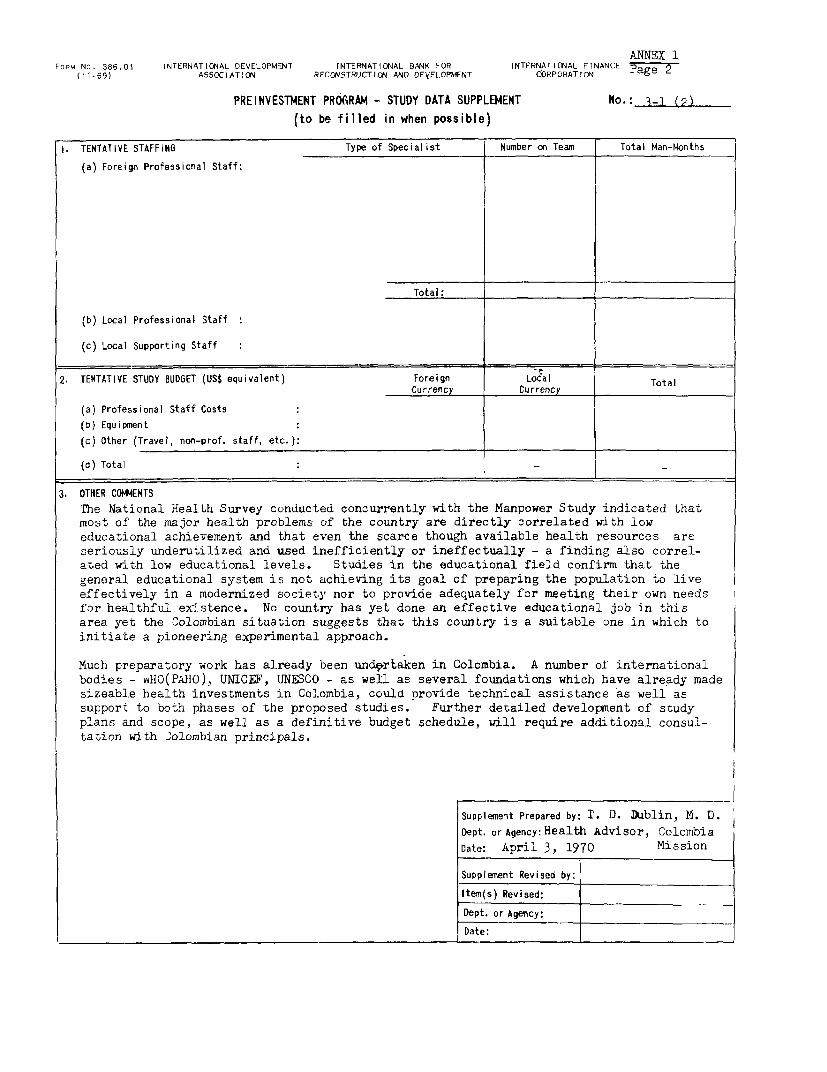
ANNEX 1FORM NO. 386.01 INTERNATIO!AL OEVELOPMENT INTERNATIONAL BANK FOR INTERNATIONAL FINANCE Page 2
(I1-69) ASS0CIATION RECONSTRUCTION AND DEVELOPMENT CORPORATION
PREINVESTMENT PRO(RAM - STUDY DATA SUPPLEMENT No.:R- .(to be filled in when possible)
i. TENTATIYE STAFFING Type of Specialist Number on Team Total Man-Months
(a) Foreign Professional Staff:
Total:
(b) Local Professional Staff
(c) Local Supporting Staff
2. TENTATIVE STUDY BUDGET (US$ equivalent) Foreign Local TotalCurrency Currency
(a) Professional Staff Costs(8) Equipment
(c) Other (Travel, non-prof. staff, etc.):
(d) Total
3. OTHER CO4ENTSThe National Health Survey conducted concurrently with the Manpower Study indicated thatmost of the major health problems of the country are directly correlated with loweducational achievement and that even the scarce though available health resources areseriously underutilized and used inefficiently or ineffectually - a finding also correl-ated with low educational levels. Studies in the educational field confirm that thegeneral educational system is not achieving its goal of preparing the population to liveeffectively in a modernized society nor to provide adequately for meeting their own needsfor healthful existence. No country has yet done an effective educational job in thisarea yet the Colombian situation suggests that this country is a suitable one in which toinitiate a pioneering experimental approach.
Much preparatory work has already been und9ortaken in Colombia. A number ol internationalbodies - wHO(PAHO), UNICEF, UNESCO - as well as several foundations which have already madesizeable health investments in Colombia, could provide technical assistance as well assupport to both phases of the proposed studies. Further detailed development of studyplans and scope, as well as a definitive budget schedule, will require additional consul-tation with ,olombian principals.
Supplement Prepared by: T. D. Dublin, M. D.Dept. or Agency: Health Advisor, Colcmbia
Date: April 3, 1970 Mission
Supplement Revised by:
Item(s) Revised:
Dept. or Agency:
Date:
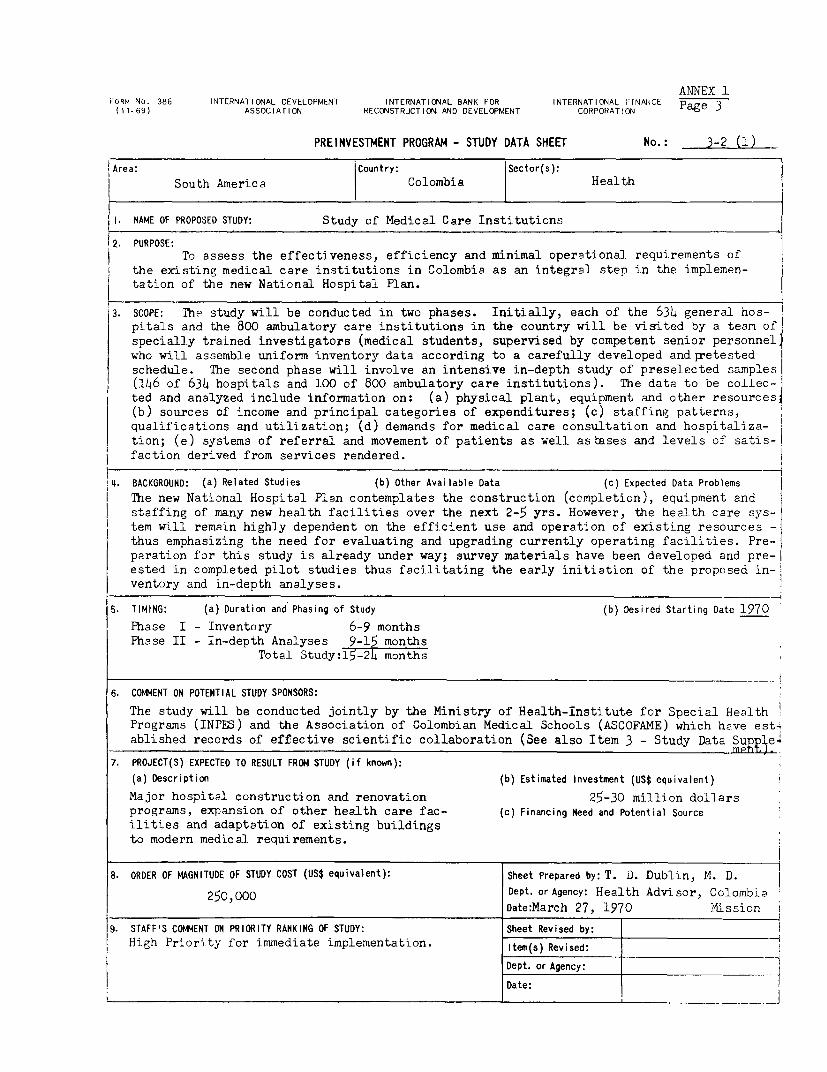
ANNEX 1FORM No. 386 INTERNATIONAL DEVELOPMENT INTERNATIONAL BANK FOR INTERNATIONAL HINANCE Pae 3(11-69) ASSOCIATION RECONSTRUCTION AND DEVELOPMENT CORPORATION ag
PREINVESTMENT PROGRAM - STUDY DATA SHEET No.: 3-2 (1)
I Area: Country: Sector(s):
South America Colombia Health
I. NAME OF PROPOSED STUDY: Study of Medical Care Institutions
2. PURPOSE:To assess the effectiveness, efficiency and minimal operational requirements of
the existing medical care institutions in Colombia as an integral step in the implemen-
tation of the new National Hospital Plan.
3. SCOPE: The study will be conducted in two phases. Initially, each of the 634 general hos-pitals and the 800 ambulatory care institutions in the country will be visited by a team of
specially trained investigators (medical students, supervised by competent senior personnel"
who will assemble uniform inventory data according to a carefully developed and getested
schedule. The second phase will involve an intensive in-depth study of preselected samples
(146 of 634 hospitals and 100 of 800 ambulatory care institutions). The data to be collec-
ted and analyzed include information on: (a) physical plant, equipment and other resources1
(b) sources of income and principal categories of expenditures; (c) staffing patterns,
qualifications and utilization; (d) demands for medical care consultation and hospitaliza-
tion; (e) systems of referral and movement of patients as well asbases and levels of satis-
faction derived from services rendered. |
4. BACKGROUND: (a) Related Studies (b) Other Available Data (c) Expected Data Problems
The new National Hospital Plan contemplates the construction (completion), equipment andstaffing of many new health facilities over the next 2-5 yrs. However, the health care sys-tem will remain highly dependent on the efficient use and operation of existing resources -
thus emphasizing the need for evaluating and upgrading currently operating facilities. Pre-
paration for this study is already under way; survey materials have been developed and pre-I
ested in completed pilot studies thus facilitating the early initiation of the proposed in-
ventory and in-depth analyses.
5. TIMING: (a) Duration and Phasing of Study (b) Desired Starting Date 1970
Phase I - Inventory 6-9 monthsPhase II - In-depth Analyses 9-15 months
Total Study:15-24 months
6. COMMENT ON POTENTIAL STUDY SPONSORS:
The study will be conducted jointly by the Ministry of Health-Institute for Special HealthPrograms (INPES) and the Association of Colombian Medical Schools (ASCOFAME) which have est4
ablished records of effective scientific collaboration (See also Item 3 - Study Data SupJ3e
7. PROJECT(S) EXPECTED TO RESULT FROM STUDY (if known):
(a) Description (b) Estimated Investment (US$ equivalent)
Major hospital construction and renovation 25-30 million dollars
programs, expansion of other health care fac- (c) Financing Need and Potential Source
ilities and adaptation of existing buildingsto modern medical requirements.
8. ORDER OF MAGNITUDE OF STUDY COST (US$ equivalent): Sheet Prepared by: T. J. Dublin, M. D.
250,000 Dept. or Agency: Health Advisor, ColombiaDate:March 27, 1970 AMission
9. STAFF'S COMMENT ON PRIORITY RANKING OF STUDY: Sheet Revised by:
High Priority for immediate implementation. Item(s) Revised:
Dept. or Agency: -
Date:
,~~~~~~~~~~~~~~~~~~~~~~~~~~~______________ . _________________
ANNEX 1FoaM No. 386.01 INTERNATIONAL DEVELOPMENT MNTERNAT ONAL PA1K FOR INTERNATIOVAL FINANCE
t I 1.692 ASSOCIATION RECCwSTRJCTI1ON AND DEVELOPMENT CORPORATION Pag 4PREINVESTMENT PROGRAM - STUDY DATA SUPPLEMIENT No.: 3-2 (2)
(to be filled in when possible)
I. TENTATiVE STAFFING Type of Specialist Number cn Team Total Man-Months(a) Foreign Professional Staff:
See detailed budget incorporated in proposal: Studyof Medical Care Institutions, Ministry of Health(INPES) and Association of Colombian Medical Colleges,Bogota, 14ovember 1969.
Total:
(b) Local Professional Staff
(c) Local Supporting Staff
2. TENTATIVE STUDY BUDGET (US$ equivalent) Foreign Local TotalCurrency Currency
(a) Professional Staff Costs
(b) Equipment
(c) Other (Travel, non-prof. staff, etc.):
(d) Total 250,000
3. OTHER COMENTSDNo high level consultative and technical committees will assist the study, the former toinclude the Minister of Health, the President of ASCOFAME, the Director of the ColombianInstitute for Social Security, the Director of the National Hospital Fund and the Execu-tive Secretary of the Colombian hospital Association. International advisors will becalled on as needed. The technical committee will be comprised of the co-directors ofthe study. Three representatives of the Itinistry of Health (Medical Care, Office ofPlanning and Cfiice oi Administralion of Human Resources for Health) and two representa-tives of the Colombian School of Public Health. Such sponsorship and srticipation pro-vide assurances that tne study will be well executed and its findings utilized. Thisstudy has been under consideration by FONADE but was rejected for local funding as notthe type of study funded by tnat agency. In discussions iath FONADE the question was raisedas to whether the in-depth phase should not include all institutions rather than only sell-ected sampiles. Based on other findings of the health phase of the current Economic andSocial Development Survey of Colombia the medical care problems of the Country are toocentral to the critical issues now being faced by the Government in implementing its newten year National Health Plan- to warrant either the abandonment or delay of this study.Investments in medical care Jacilities and equipment either already made or contemplatedduring the next few years are sizeable and operating costs oI the health and medical caresystem are mounting rapidly from 1.1 billion pesos in 1965 to 3.4 billion pesos budgetedfor 1970. The p-opoGed study will assist the country in deternining how to obtain themaximum return on expenditures.
Supplement Prepared by: T. D. Dublin, .A. D.Dept. or Agency: HIealth Advisor, ColombiaDate: March 27, 1970 M4ission
Supplement Revised by:
Item(s) Revised:
Dept. or Agency:
Date:
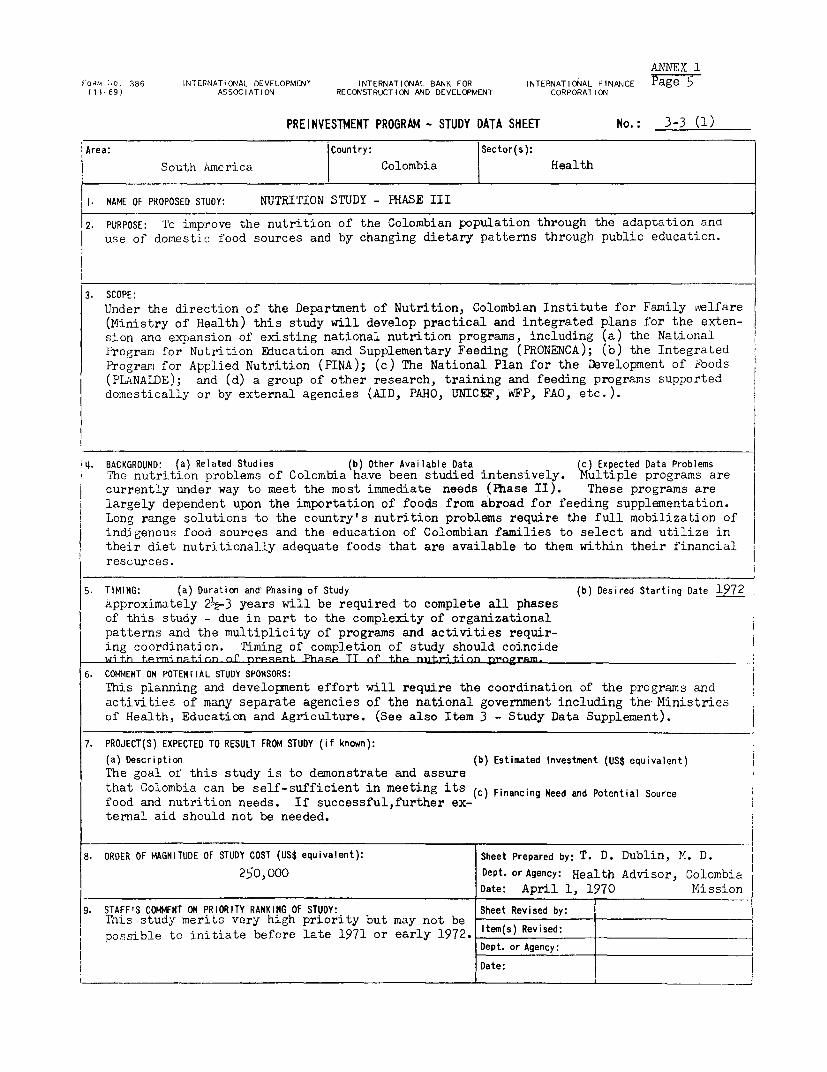
ANNEX 1
! ORM 10. 386 INTERNATIONAL DEVELOPMENT INTERNATIONAL BANK FOR INTERNATIONAL FINANCE Page 5(11-69) ASSOCIATION RECONSTRUCTION AND DEVELOPMENT CORPORATION
PREINVESTMENT PROGRAM - STUDY DATA SHEET No.: 3-3 (1)
Area: |Country: |Sector(s):
Area: South America | Colombia Health
1. NAME OF PROPOSED STUDY: NUTRITION STUDY - PHASE III
2. PURPOSE: Tc improve the nutrition of the Colombian population through the adaptation antuse of domestic food sources and by changing dietary patterns through public education.
3. SCOPE:Under the direction of the Department of Nutrition, Colombian Institute for Family ivelfare(Ministry of Health) this study will develop practical and integrated plans for the exten-sion and expansion of existing national nutrition programs, including (a) the NationalProgram for Nutrition Education and Supplementary Feeding (PRONENCA); (b) the IntegratedPro-ram for Applied Nutrition (PINA); (c) The National Plan for the Development of Noods(PLANALDE); and (d) a group of other research, training and feeding programs supporteddomestically or by external agencies (AID, PAHO, UNICEF, WFP, FAO, etc.).
I4. BACKGROUND: (a) Related Studies (b) Other Available Data (c) Expected Data Problems
I The nutrition problems of Colombia have been studied intensively. Multiple programs arecurrently under way to meet the most immediate needs (Phase II). These programs are
a largely dependent upon the importation of foods from abroad for feeding supplementation.Long range solutions to the country's nutrition problems require the full mobilization ofindigenous food sources and the education of Colombian families to select and utilize in
their diet nutritionally adequate foods that are available to them within their financial
rescurces.
5. TIMING: (a) Duration and Phasing of Study (b) Desired Starting Date 1972Approximately 21½-3 years will be required to complete all phasesof this study - due in part to the complexity of organizationalpatterns and the multiplicity of programs and activities requir-ing coordination. Timing of completion of study should coincidewi t.h trrnyi nqtJi nn nf present. Ph;.p TT of thp niit ri tion progrAm._
6. COMMENT ON POTENTIAL STUDY SPONSORS:This planning and development effort will require the coordination of the programs and
activities of many separate agencies of the national government including the Ministriesof Health, Education and Agriculture. (See also Item 3 - Study Data Supplement).
7. PROJECT(S) EXPECTED TO RESULT FROM STUDY (if known):
(a) Description (b) Estimated Investment (US$ equivalent)
The goal of this study is to demonstrate and assurethat Colombia can be self-sufficient in meeting its (c) Financing Need and Potential Source
food and nutrition needs. If successful,further ex-ternal aid should not be needed.
8. ORDER OF MAGNITUDE OF STUDY COST (US$ equivalent): Sheet Prepared by: T. D. Dublin, M. D.
250,000 Dept. or Agency: Health Advisor, ColombiaDate: April 1, 1970 Mission
9. STAFF'S COMMENT ON PRIORITY RANKING OF STUDY: Sheet Revised by:This study merits very high priority but may not be
possible to initiate before late 1971 or early 1972. Item(s) Revised: -Dept. or Agency: l
Date: X
I _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ . _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ -
ANNEX 1FopM NC. 386.01 INTERNAT1CmAL DEVELOPM1ENT INTERNATIONAL BANK FOR NTERNATINAL FINANCE Page 6
(11-69) ASSOCI ATION R:CONSTRJCTIOtN AND DEVELOPMENT CORPORATION
PREINVESTMENT PROGRAM - STUDY DATA SUPPLEMENT No.: 3I-3 2
(to be filled in when possible)
1. TENTATIVE STAFFING Type of Specialist Number on Team Total Man-Months
(a) Foreign Professional Staff:
Total:
(b) Local Professional Staff
(c) Local Supporting Staff
2. TENTATIVE STUDY BUDGET (US$ equivalent) Foreign Local TotalCurrency Currency
(a) Professional Staff Costs
(b) Equipment
(c) Other (Travel, non-prof. staff, etc.):
(d) Total 250,000
3. OTHER COMMENTS
Additional con.sultations with Colombian principals are required tc develop the detailedplan ana scope of the proposed studies and an appropriate budget. As a bare mriimml 4$-millicn (US) per year are now being invested in applied nutrition programs and these ex-cenditures will be continued over the next five years. If the costs of other nutriticnand food activities, the economic lcsses due to malnutrition and the costs attributableto the medicaa care of nutritional disease are added, the costs to the Colombian eccnomyare far greater. Thus a relatively smaller expenditure for planning and developrment ofa self sufficient and continoin-, nutrition pro, ram for the total populations should be asound investment.
Supplement Prepared by:T. D. Dublin, M. D.
Dept. or Agency: Health Advisor, ColombiaDate: April 1, 1970 FIVssion
Supplement Revised by:
Item(s) Revised:
Dept. or Agency:
Date:
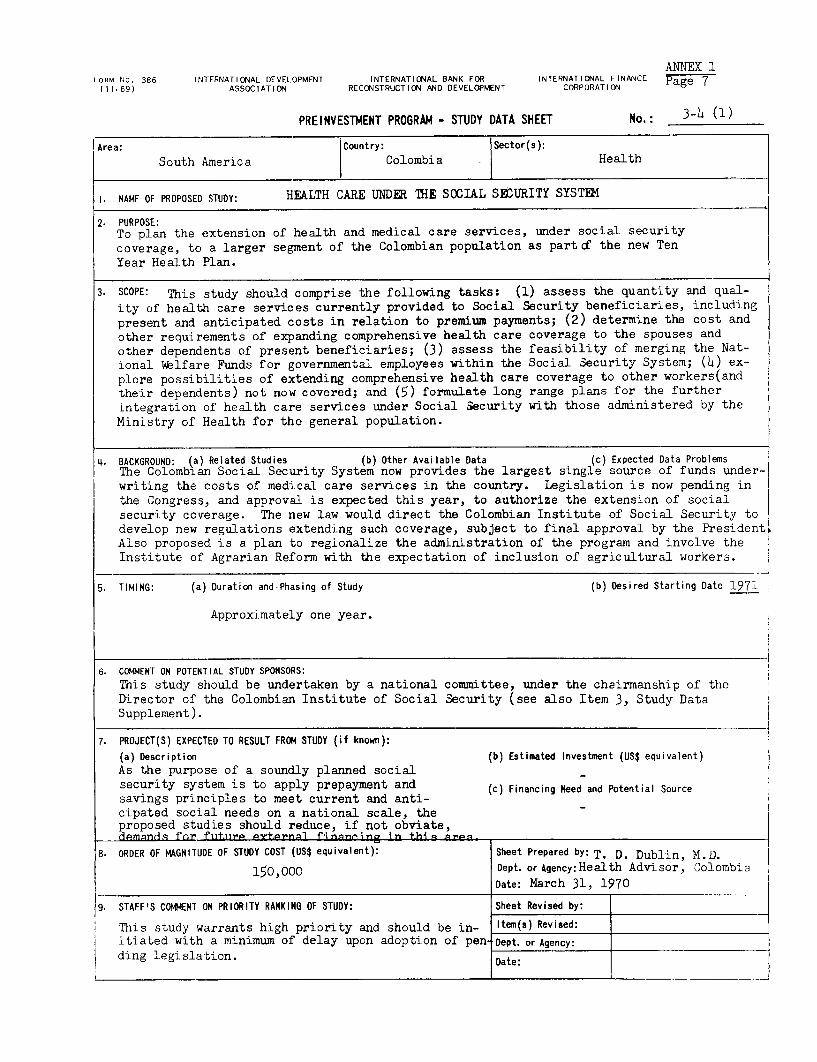
ANNEX 1I ORM No. 386 ItJTERNATIONAL DEVELOPMENT INTERNATIONAL BANK FOR INTERNATIONAL FINANCE Page 7
(11.69) ASSOCIATION RECONSTRUCTION AND DEVELOPMENT CORPORATION
PREINVESTMENT PROGRAM - STUDY DATA SHEET No.: 3-h (1)
IArea: Country: Sector(s):
South America Colombia Health
I NAME OF PROPOSED STUDY: HEALTH CARE UNDER THiE SOCIAL SEURITY SYSTEBM
2. PURPOSE:To plan the extension of health and medical care services, under social securitycoverage, to a larger segment of the Colombian population as part d the new TenYear Health Plan.
3. SCOPE: This study should comprise the following tasks: (1) assess the quantity and qual-ity of health care services currently provided to Social Security beneficiaries, includingpresent and anticipated costs in relation to premium payments; (2) determine the cost andother requirements of expanding comprehensive health care coverage to the spouses andother dependents of present beneficiaries; (3) assess the feasibility of merging the Nat-ional Wblfare Funds for governmental employees within the Social Security System; (4) ex-plore possibilities of extending comprehensive health care coverage to other workers(andtheir dependents) not now covered; and (5) formulate long range plans for the furtherintegration of health care services under Social Security with those administered by theMinistry of Health for the general population.
4. BACKGROUND: (a) Related Studies (b) Other Available Data (c) Expected Data ProblemsThe Colombian Social Security System now provides the largest single source of funds under-writing the costs of medical care services in the country. Legislation is now pending inthe Congress, and approval is expected this year, to authorize the extension of socialsecurity coverage. The new law would direct the Colombian Institute of Social Security todevelop new regulations extending such coverage, subject to final approval by the PresidentAlso proposed is a plan to regionalize the administration of the program and involve theInstitute of Agrarian Reform with the expectation of inclusion of agricultural workers.
5. TIMING: (a) Duration and-Phasing of Study (b) Desired Starting Date 1971
Approximately one year.
6. COMMENT ON POTENTIAL STUDY SPONSORS:
This study should be undertaken by a national committee, under the chairmanship of the
Director of the Colombian Institute of Social Security (see also Item 3, Study DataSupplement).
7. PROJECT(S) EXPECTED TO RESULT FROM STUDY (if known):
(a) Description (b) Estimated Investment (US$ equivalent)
As the purpose of a soundly planned socialsecurity system is to apply prepayment and (c) Financing Need and Potential Source
savings principles to meet current and anti-cipated social needs on a national scale, theproposed studies should reduce, if not obviate,ds]mqnd&q for fitiir P trrngl finnn^ring in his nr.en
8. ORDER OF MAGNITUDE OF STUDY COST (US$ equivalent): Sheet Prepared by: T. D. Dublin, M.D.
150,000 Dept. or Agency:Health Advisor, ColombiaDate: March 31, 1970
9. STAFF'S COMMENI ON PRIORITY RANKING OF STUDY: Sheet Revised by:
This study warrants high priority and should be in- Item(s) Revised:itiated with a minimum of delay upon adoption of pen- Dept. or Agency: L
ding legislation. Date:____ ____ ____ ____ ____ ____ ____ ____ L __ ____ ____ ____ ____ ____ ____ ___ _ _ __
ANNEX 1FORM No. 386.01 INTERNATIONAL DEVELOPMENT INTERNATIONAL BANK FOR INTERNATIONAL FINANCE Page o(11-69) ASSOCIATION RECONSTRUCTION AND DEVELOPMENT CORPORATION g
PREINVESTMENT PROGRAM - STUDY DATA SUPPLEMENT No.: 3-4 (2)(to be filled in when possible)
1. TENTATIVE STAFFING Type of Specialist Number on Team Total Man-Months
(a) Foreign Professional Staff:
Total:
(b) Local Professional Staff
(c) Local Supporting Staff
2. TENTATIVE STUDY BUDGET (US$ equivalent) Foreign Local rotalCurrency Currency
(a) Professional Staff Costs
(b) Equipment
(c) Other (Travel, non-prof. staff, etc.):
(d) Total
3. OTHER CtMENTS
The ColDmbuan Institute for Social Security, the Ministry of Health, the r.inistry of Labor,the National C2jas, the Nationnl Hospital Fund, the Institute for Agrarian Reform, theNational Decartment of Planning and the AssociatLon of Colombian Medical Co'leges are someo the naticnal bodies that should be represented in the national study committee. Inter-nat-onal bodies (WHO, ILO) and external consultants could make significant contributions tothe findings and reccmmendaticns of that cbmmittee.
Further details on scope, study plani Pnd budget require supplementary discussion withColombian princiaals. Travel to and study in other countries on the part of committeemembers and the extensive use of external consultants is essential to the study in thelight of exoerience gained and mistakes made in recent years in other national socialsecurity systems. A significant fraction of the domestic costs can and should be borneby internal sources such as the Social Security System itself.
Supplement Prepared by: T. D. Dublin, M. U.
Dept. or Agency: Health Advisor, ColombiaDate: March 31, 1970 Mission
Supplement Revised by:
Item(s) Revised:
Dept. or Agency:
Date:
ANNEX 1rORM No. 386 INTERNATIONAL DEVELOPMENT INTERNATIONAL BANK FOR INTERNATIONAL FINANCE Page 9
(11.69) ASSOCIATION RECONSTRUCTION AND DEVELOPMENT CORPORATION
PREINVESTMENT PROGRAM - STUDY DATA SHEET No.: 3-5 (1)
Area: Country: Sector(s):South America I Colombia Health
1. NAME OF PROPOSED STUDY: VITAL STATISTICS AND MORBIDITY DATA - RE1lISTRATION AND ANALYSIS
2. PURPOSE:To modernize and improve the Colombian national system of registration, tabula-tion and analysis of essential vital statistics and current morbidity data.
3. SCOPE: This study should comprise the following tasks: (1) prepare recommendations for therevision of existing national legislation pertaining to the registration, collection, com-pilation, analysis and dissemination of essential vital statistics data on the populationof Colombia; (2) develop detailed plans for a revitalized and efficient national vital sta-tistics system; (3) define the requirements of physical resources, equipment and personnelneeded to establish and maintain this new system at the national level and for decentral-ized activities, including capital investments and operating budget; and (4) prescribe theprofessional and technical job descriptions to be incorporated within national civil ser-vice personnel requirements for employment in the new vital statistics system and proposelong range educational programs for the appropriate training of both professional andtechnical personnel.
4. BACKGROUND: (a) Related Studies (b) Other Available Data (c) Expected Data ProblemsAccurate, complete and current vital statistics data are required for the effective and ef-ficient administration of the new 10 Year National Health Plan - particularly in connectionwith its recently decentralized health care services. The marked underregistration ofbirths and deaths and the cumbersome, delayed and unreliable mechanisms for handling theseand other essential vital statistics data, seriously impede appropriate program evaluationand planning not only in the health sector but in other critical areas of national economicand social development. Some preparatory work for the proposed studies has already beenuinrJrt.,qk-n hy P-geh nf thbe natie Zn7l hnr;ieg that. will 'he JuvolvAd
5. TIMING: (a) Duration and Phasing of Study (b) Desired Starting Date 1971
Approximately one year.
6. COMENT ON POTENTIAL STUDY SPONSORS: A national Committee, under the chairmanship of the Minister ofHealth, and utilizing the advice of appropriate international agencies (e.g. PAHO and WHO)and consultants, should undertake this study. The Ministry of Health, the National Depart-}ment of Statistics and the National Department of Planning are directly concerned and shoulhp invnlud in +he stuldy IINlP, IINTCTF ns TSATn y y mipprt t.his stlndy.-
7. PROJECT(S) EXPECTED TO RESULT FROM STUDY (if known):
(a) Description (b) Estimated Investment (US$ equivalent)
A new system for the registration and analysisof vital statistics and morbidity data. (c) Financing Need and Potential Source
8. ORDER OF MAGNITUDE OF STUDY COST (US$ equivalent): Sheet Prepared by: T. D. Dublin, M.D.75,000 Dept. or Agency: Health Advisor, Colombia
Date: March 30, 1970 Mission.
9. STAFF'S COW4ENT ON PRIORITY RANKING OF STUDY: Sheet Revised by: P. EngelmannAs the absence of a proper system of vital statis- Item(s) Revised: 5(b) & 6tics affects investment decisions in many areas,this study warrants high priority and early initia- Dept. or Agency: IBRD/O.D.P.tion. Date: October 18, 1970
i _~~_ I
ANNEX 1FORM No. 386.01 INTERNATICNAL DEVELOPMENT INTERNATIONAL BANK FOR INTERNATICNAL FINANCE Page 10
(11-69) ASSOCIATICN RECONSTRUCTION AND DEVELOPMENT CORPORATION
PREINVESTMENT PROGRM - STUDY DATA SUPPLEMENT No.: 3-5 (2)(to be filled in when possible)
I. TENTATIVE STAFFING Type of Specialist Number on Team Total Man-Months
(a) Foreign Professional Staff:
Total:
(b) Local Professional Staff
(c) Local Supporting Staff
2. TENTATIVE STUDY BUDGET (US$ equivalent) Foreign Local TotalCurrency Currency T
(a) Professional Staff Costs
(b) Equipment
(c) Other (Travel, non-prof. staff, etc.):
(d) Total
3. OTHER COfMENTSOnly the general outline of this proposed preinvestment study has been developed at thzstime. For additional and more specific details, further discussions with the Ministry ofHealth nnd the National Department of Statistics would be required. The suggested budgetis offered as an initial approximation. Registration of births is still dependent on bap-tisms, a ceremony usually delayed for a period of approximately 7 months; underregistra-tion of births has been calculated to range between 29 and 19 percent with even greater var-iations noted in different parts of the country. Underregistration in mortality rates appearsto be even larger than in birth rates (between 38 and 33 percent) with most marked deficitsIn the early yesrs of life. Procedures currently being followed involve an overcentraliza-t>on of the registration system in Bogota with insufficient attention being given to the ac-curacy, completeness and quality of data being registered at the local level. Essential dataremain unt-bulated and unpublished for long periods of time (up to 5 years). The registrat-iorof not-ifiable diseases and morbidtty indices (admissions, discharges and duration of medicalcare) are equally cumbersome, delayed and unreliable.
For a period of more than 17 years, the Ministry of Health, the agency most dependent on theavailability and reliability of vital statistics, has lacked direct responsibility and in-volvement in the major phases of vital record collection and tabulation. The National Dep-artment of Statistics, which enjoys a fine reputation for the quality of data it produces inother sectors of the national economy, is well equipped in Bogota with computer and othernecessary central facilities. However, it lacks qualified and experienced staff in theheelth ares and is dependent on an outmoded system oflocal registration employing untrained and technically Supplement Prepared by: T. D. Dublin, M.D.unqualified personr.el. Dept. or Agency: Health Advisor, Colombia
Date: March 30, 1970 Mission
Supplement Revised by:
Item(s) Revised:
Dept. or Agency:
Date:
ANNEX 1FORM No. 386 IN1ERNATIONAL DEVELOPMENT INTERNATIONAL BANK FOR INTERNATIONAL FINAJ'4CE P(11-69) ASSOCIATION RECONSTRUCTIClt' AND DEVELOPMENT CORPORATION Page 1
PREINVESTMENT PROGRAM - STUDY DATA SHEET No.: 3-6 (1)
Area: Country: Sector(s):South America Colombia Health
SAMPLE STUDIES OF THE HEALTH STATUS AND HFALTH RESOURCES OF COLOMBIA1. NAME OF PROPOSED STUDY:
2. PUROSE
To reappraise the major health problems, health facilities and health manpowerof the country in order to determine progress achieved since 1965 in meeting nationalgoals and to establish objective bases for revision of national health programs and acti-vities.
3. SCOPE: Under the aegis of the Ministry of Health and the Association of Colombia MedicalColleges a second series of investigations will be undertaken, utilizing modern samplingtechniques and linked with the periodic national population census (1972), to determinethe needs and demands of the country for health and medical services. These studies willtake into account the socio-economic status of the population. They will be modeled onthe pioneering and highly successful national studies of 1965-66, to facilitate comparisonsand reliable measurement of progress and change, but will also incorporate newly developedsurvey methods and examination procedures.
4. BACKGROUND: (a) Related Studies (b) Other Available Data (c) Expected Data ProblemsSince the initial surveys in 1965-66 major reorganizations and reorientations of healthprograms and activities have occurred in Colombia. Concurrently significant advances havetaken place in other sectors of the country's total economic and social development whichhave either direct or indirect bearing on the country's complex health picture. The scien-ltific measurement of these interrelated changes, through national sample surveys, will pro-lvide essential data useful for program evaluation and planning in the health and otherrelated sectors of national development.
5. TIMING: (a) Duration and Phasing of Study (b) Desired Starting Date 1971Three and one-half years will be required to complete the study
Planning and Preparatory Phase (1971) - 12 monthsField Studies and Surveys (1972) - 12 monthsAnalysis and Publication of Data (1973-7 4)- 18 months
6. COMMENT ON POTENTIAL STUDY SPONSORS:The Ministry of Health and the Association of Colombian Medical Colleges have demonstratedtheir capacities to undertake this type of national health survey and their pioneering iefforts are now being emulated in many of other developing countries.
-I7. PROJECT(S) EXPECTED TO RESULT FROM STUDY (if known):
(a) Description (b) Estimated Investment (US$ equivalent)A more efficient and effective health and medicalcare system appropriately responsive to the health (c) Financing Need and Potential Sourcecare needs and demands of the Colombian population.
8. ORDER OF MAGNITUDE OF STUDY COST (US$ equivalent): Sheet Prepared by: T. D. Dublin, M. D.400,000 Dept. or Agency: Health Advisor, Colombia
Date: April 2, 1970 Mission9. STAFF'S COMMENT ON PRIORITY RANKING OF STUDY: Sheet Revised by:
High priority - initiation in 1971 Item(s) Revised:
Dept. or Agency:
Date:
ANNEX 1FORM NO. 386.Of INTERNATICNAL DEVELOPMENT INTERNATIONAL SANX FOR INTERNATICNeAL FINANCE P
(11-69) ASSOCIATION RECONSTRUCTIcON AND DEVELOPMENT CORPORATION Page 12
PREINVESTMENT PROGRAM - STUDY DATA SUPPLEMENT No.(to be filled in when possible)
1- TENTATIVE STAFFING Type of Specialist Number on Team Total Man-Months
(a) Foreign Professional Staff:
Total:
(b) Local Professiona) Staff
(c) Local Supporting Staff
2. TENTATIVE STUDY BUDGET (US$ equivalent) Foreign Local TotalCurrency Currency
(a) Professiona1 Staff Costs
(b) Equipnment
(c) Other iTravel. nor-prof. staff. etc.):
(d) Total
3. OTHER CODMENTS
Additional consultations with Colombian principals will be required to develop thedetailed plan and scope of the proposed studies. Preliminary cost estimate is basedon expenditures of 165-66 studies (covering the period July 1, 1968-June 30, 1967)which amounted to $382,000. Forty percent of the cost of that study was defrayed byColombi.an sources.
'This proposed study complements rather than competes with preinvestment study proposal3-5; Vital Statistics and Current Morbidity Data - Registration and Analysis; and willalso complement the next Colombian National Census of 1972.
Supplement Prepared by: T. D. Dublin, M. D.Dept. or Agency: Health Advisor, Colcmbia
Date: April 2, 1970. Mission
Supplement Revised by:
Item(s) Revised:
Dept. or Agency:
Date:
- 8L4 -
VTT. EXTERNAL ASSISTANCE IN TH}E COt O1MBIAN HEALTH SECTOR
203. Over a period of manyr years,irite.rnatioonal. agencies, the govern-ments of other countries andl philanthropic foundations have extendedtechnical assistance, commodities and equipment as Iel as financial aidto the health sector of Colomrbia. No list, of the donors or a tabulationof the amounts of their contributions has been compiled. Conspicuousamong the assisting international organizations are the World HealthOrganization and its Regional. Office for the Amnericas, the Pan AmericanHealth Organization, the United Nations Chi.ldrens Fundl andc the World FoodProgram (FAO), The U.S. Agency for International Developrent and itsprediecessor agencies has supported many important hea.lth activities inthe country for maany years. The Rockefeller Foundation, the KelloggFounidation and the Milbank emorial FlFnd have also been involved in sup-porting specific health projects, particl.arly those related to mecdicaleduication and research.
204. To illustrate the extent and natiure of this assistance a recentcompilation of PATIO aidl to Colombia can ble found in Appendix A.


APPENDTX APage 1
PAN MIRCNHEALTH ORGTANIZATION PROJECTS5 IN COLOMIBIA_(1960)
COLOMBiA-.0200, Malaria Eradicaition Financing th~e program hlas inot presented problems., inas-much as the Government has assigned it ani annual butdgetJPurpttsc: Eradication of malaria, of 52 million pesos; moreover, the administr-ative organiza-l
IProballc flth-ation: ] 957- lionl is effective./lssisi(fqIC providcd: 2 uticdical ollicers, ( I (ifi he posts Mieclt gs" Were hield wi tli mnalariologists from Veneztuela,
witS vacant (11hiring JiarTt of the ye:ar), I Sanitary cnginecer, anti at oilier meetinigs ilie campaign staff discuissed prob-.I vi'ipttniologist, awil 4 Sanitary itrsptc:itrs: antiulalaria drugs li-inis aniti e-siatllisijed chitirirels of collaboration andi coirdlini-
arnd vitt-noligiaal sutptlolis: 'tidt 2 short-termu fel lowslhips. tutul.WForIc dieno: IKi~rly ill I961 ini tIrle b,asis of hel cv.alua- liesearch wats stat-ted itt diei fl(ieds (if tlitrativ itic! ettlo-
hiim cctndlt:iocl in Ntos'tmlme- '1907, the( intti;triotis are.a of mo.ligy.
C'0I0fTbiZL Wa dtVidV LIS 1.'j .:PAHO/RB, PAHO/SMF UNICEF'I act 1 ~~~~~~~~1 222.(J00 100 970,1149 1 IX)
C onsolidmationt phlse 7.ttl:t.lOO 69.5 1 54.458 16.0 COLOMBIA-0201, Study of the ChemotherapyAttack phtiise 3,202,000 28.5 769,391 79. 2 o aaiPrep)aratory pthasc 2171,000 2.0 47,000 4.8 o aai
Dunring ili he 1ittI spt-ay rtg cycle,, icCtrriedi tint rit lit, first I'uirlosc : Asse~ssmlent of tire usefulness of a 3-day, 3-druglrat uterit fo r tine ruiaila I atre of Plcasntodi ori vivpax in fee-htalif of lth Yc eair. 449,4331 Itlse Iti S' vci'! tsprat et ( 92.8%, -ili
itT the~ Target), withi 2,120.499( iiuletl,iiiaol, sprotected., 'Tic hurts. : 96.98218)Ii ('yflo wa ltt bg titi ini . ijly; itcl!riCtInitg lit esti naf es. A.~N so /t *ir oltOid.-d AdisSir;- y n-rvictis iby stall i-f litad -47-4.556 tiiistcs wi-me to) lit spirayied. At Olt end- otf No- 11re,alIo 14jul01.tbaP10,aI bvmnber-, 394.,281 liouses (83.1%," of tlie target h bailiteeri t2 thrira trdim ifiitiitttiic (it)ltinivriip-4211(I aizrttt~ 41a cotsSprayeid, with] 1.934,145 iiniialitattts JIriltcit(A. li ado-ljjkin .irdiitiSt~et pr i i i-ltiss4- Ituarerly- spmrayings wi7re ;trmrnt iist':it riie ithite: A fiti:i trial wtas iitade of Ctiii Cxi'riiitt11-1iitt
eleCts, treat rut-itt ~~~~~~~~~~~~~ ~~~~~~~~withll] tiitit' ptriniaqii. aid, 111 i yrritliviariunmlcgkii't otit 31 (v ars ;t raicjial -tire (if P. tCivfi irifi'ci-il
6t,f33 iiitsms i ti: hst t ttttilr trll .5 t) iittsis i ii,' ot-il tts1c Isictl1--is lyct' titeittiii'rtd witl mltlitnit (t1iiie citl il h6J I' ttjPv int fl uit Ii l m 0t o.miiprith (tJ7am l 6, i1 hitciis.s il tlf -3i 1i
AS f,f No~vembriic- 7i91.2:2i) liltiil sititttar ai I, tad cx it-ll x IIri' is wit- sit- t11. rrt;tcht-io' III vxS', agc grittt p, attd tll cIrtnlittii-d, is-ili 25,527 3.2'-; b,ido tti loll tisitlivt. 'PrItacpr- ft-.il'ti 2 mue tjte -- e'.iCti.r-si-tmtl-
i-t-tttacm-- if ltii-.i ivity [ti-- tttsi,hilci tot- Cttti attai-k-jhtttse a ill thehi:xtme-iutt'rrtalariilathe ilsaui-al hea hint ; (limits ace(.6';-' amit 5.2<.rtFt'ttiiy tltiril, zi ltritnita Nitltitirt niatiria. was tni'ati'd with1 pritirri;tiintm'[lit-anti --ti I-rriett ittms ill rttst tltit rrsmt 1mtolt- iltti-iig H-I olamvs tti itsti- I'r tltctt fitt latent1 infect ion was pmmt'sei't.
(t)ot tCIitmtpii ii ork. it IeMtn-i 'itliitii iie li"tr itl Was Iteitin iti April 1946 ainti (iintintri~dm'(lttilSI> itXi i iirti t it l i ucttlielfs ill t i- c Y11 w . fil riijc- 19641. hitc tsc if thei hii g rate Ill p piittlation inobti ity
Thi-'itfat irii200 ni t-y.av. rua
(-lio i-al tO1 (f .111 Ci -)0( l) , ,1 ,' l it tpt-tIut'rIctI i tt I ICICtSIiICCII 1 lt t09 1 rIt i-hurst,- ideti ! IIf l It I s t ItI.
SW-IMi kmi - '.igm im i,it •t-tmi-itli- I. t1, -r-: 2 71w . 20tuit-0V i r s ; itliCii IItlt f IK was IlaI-t I o -i I- Ii flIt- tII u IIs I t I l fit- II tti-lirltirtCt- I ftistilI mhtI. - (Ii I-t It t
Jirnign.~~~~~~~~~~~~~~~~~~~~~~~~~i 1-nmlijroflloi. raniTtw~liiltl at-
APPENDIX A
Page 2
117irk r/l,Ii: lirhteatli c-vili:ro I,:l. pl;irirll jol COLOMBIA-3103, Special Public HealthtIrecilyif C.:nt coriiiicll Il.Ie ar.1li,o '.it, Will, g-ir Administration Programs
rcsullts. ThuI p1itt-: lrinpr-trvc-rrernt iii adinhiiistrlative iiitirrods andlDur ing tilie year a rt.ineSrr)r:sthit n % rt i f s PI IN Ijs tr\ -d in I " c . 1Io'lI p caI111lr Ie t1 iim l ~ lim p o
Surveillance rif airports; and plorts riurig Ilie Atl:uiltic Pro/ftildlrl' uti oni: I (07-19t70,coast WasitS coritjllLIC(l -1ssistaric-i- ploviillii/: I Shlor-teylli co01511 Itarit andii hil-
Eleven ellow feVelr cajst'S were pu -'Irtei 11zi ,I' e 11rti vikr-v svv,c l)y file PAI I0 /WllO Country lcpr:Jtt:s-i;I-dUr-ing thle veal.
PAHO/RB Il ia/~~~~~~~~~~~~~~~~~It'lliu: 'I'lir letgal s Incic- rea id fr n'it ions o, f tlit- NaPAHO/RB ~~~~~~~~~~~~~~~ii.oial Institirir for Spec(iail I Iraltlh lPrrtgiariis I NIEIS.
ItI'Irlo]ir I hatI ItI,. wr It vstI a I rishiud Ity cxrrcli i vi dIrrr ItI
slifatit es zi-airI 1909 ltimdllg: wc:r appit~rovedl. iri acc:tIdarl r-I %il iCOLOMBIA-31 00, -Health Services tlet ii,.iv lr-;;il plorviSirtis. It, orrghrrri,atirrri, ifilttii:il ir-glili-
I'n;jtit l'i IldIlirtli f a ifi lInat1 IrritirII tzi Lt; It rr:iigtli. i4 Ils, ann41S sa If wt:e rrrrlt:rc r st IrIdv. I [I(],l t Ilhe 1rr-g~ P aii1izti.l r)
Ciling oif tlr rinstyit Mlii- IIrIltlr:dIc Irillih a-l ld i rljuw tir:i olrf tile NillinSt, tltr: Iristitriti:' s -lSt worikirig rr-lituiri.lirtili-md ti--ilsn:vir: rxltisitil n) irt-giitrr lialti srvil: wifiti li O Nliiii-[r-y war- rIri;lyv tlrfincdt.
Midttr localt ex iitrlti nsio nl t1 rillii rif.Siirra in 1INPES is rrspollnsibilr frtr it4 forllowinig piogranis: trainl-
all X ha lY Ilerstrri Ire1
rig~~ ~~ I f ptrti-srrir:l. jlo~irsial ardif-clurctnr, ircseai-i;l prottcctt.,l',-tibu/r/c dr,rolio,i.: 195I-1 99~I~) i,i-isrt rral Saritait iorr, riie:i inlpetiiion, chldii we1 far,. rirllo-
lngn, arid I irn administrative iitirl.I nurilse, I sanit iiv PAHO/RBcrigilneer. 5 short-termi oiriusrlailts tiii (Pf luicn mnade
Nsits), anrd I ternp)lrirary ailvis,e :r,flipii ur-n t al( sitt Sipttiest-mminiri services;~, airri 2(0 shor -tcrn auIit 7 iiii-19-tiril ti-I- COLOMBIA-3301 , National Institute of Healthin ws lips. (Carlos Finlay)
Ifnrk: i/tine: DuorinIg tie yr-ar tire otigri.tnr f lit'! I'nrplos: St iingtiliciirg nif tire serivir:is rendlricd biy [lir-lkinlistry otf Pubilic Health Avis -aierIr(il tnt git rig II gredite eriirw Ft:vt:r Srctriii rrf tirt! National Instiliftt (of IlIraitl t4.adilirnjvtrat ivc tIexihilitv ki-rd Irlorir altlittoilly Cver thle dc- oiii i r o unt irS ini vnrniertiio withi the lienisplierrr-widlicent rjlalized iisjitlites engagitd in, rcali ir A,i k. r-auripaigil agailist yt:ltrw ICever. illitith ar-eas 4rf Ir svir-ch.1
hias breconi il the keystonic 4ifithi- lr-alt I, itcli-int rs. IMajot /urrol,uI/i/ (11,1i : 195(1.Inleflinigs were eldt- to u;otrsidiialac tlir ptotc.~s~ i:ihlal-ii it. 'Issishinri- ptrtird>/ih: I iabirratlirx riolistiltairt andl adlvinijrarid pit it uIl ritit itnrtion iii 196i9. civics Io ieit I'AII0,/WIIO Cirroitr Irtrsriat,Efotitits it ttlrtiilliate~ t i-l- t iis tii rIi vii i- ial its.
tinlt id, wit I a view to est altishuiti a fatikirral healthi sysicini JF"olk P/inlc: Urtiiler tl liecrernre rerirganlizilig tw l iitMrst rx(::ir:iitiill f a atirnil helth (.iuiiiii -nt in oirrstuill I f l'iililicI; I:altlh, tire National tirstittirti of lraltlh beceane
level Signirfiidi nrajri)r ptroignr .Ss il II IrIIis PIi1iritllll. i-ln agi'lrlv ltr.f-Iivnsible 1nt tile Nat irnal nstlit ni: filn StuCCialA tillicy anrn spnecific ~ir-grailirlr-lri.wt ua s-ti II-ll Pnrogi i-urS ii IE1S).
SUtiplieS Wcie siildierd and tdrawri rip. tliritirglr tiei-ir aciil of A i-onimrilicit. tliesidi:i irver by tire D)irlicttr oft INI1 lS,
Tle ili-isil- saitrationiul 11gr.win-i hits air irrrprcssivn s,tiittiiic of tiht Inistiliti:. Woik trii ilt icinw iistallai-ionirriVCirird of ;tt--ltmplilhniclit, wvis ci:i -ioiit Ia hwart
1It I nurr:l was15 iitii iririeil.
aspiect lviii liecilllic tilte ir:sptrnSibllty ,I' hr Nat iriial inst i- Rf!scvrarlh un1 arltrrviiiis infectionis, letrir-Sy. tfrvpaintsolitmhr
riefrl Spiecial Ilea-klthr Irrgrarnls, sit ;is t) vinsure gri:i-itrr sris, anti entomolorlrgy was carried fonrwardl.rilnuinist rt iv.: fii:xlii ity. nT:c lnrduclli:tin oif 1niologic:als dutrinug tire, pnerod was as
lireoluject tniniaternial and1 chlrir lair: arid famiily ptirt I ow~ yellow fryer vai:lint:: 1,625,000 dtises (30.1,50(1teci inn was in itsOnna I stages. .ltses; diis rliritind inl the Crouintry arid 908.00)) airotad)
teclie wnrgasln for Iiiolstagesin:i itgfit-lln tl ya rneozc-flricrl srinl;nhpnx vacinrie: 7.992.200) dlii.ss (III whniichof l t pio raimnfo l tipprintw inth helth- iacvi tafs ri y alilrj 3)1(,0001 welt: Shiipiped to Ecuadori)r ; awiirahie.S vai:cirre fti
\tChaiigc o cr.ulbtcntl elhsrifso Iltj iriirriarr us.:: 4(1.629 ]14-uolnnvctu-aimenits (8,)10)t fri:aatru:itsaind tire .javeriana University ( Bogtti i-) Ithas cninh t ited aird
wt:re shipped t(i Veneznnlai *t antirablies vaccine ftir Cnn
I'lielieafli prmoter por was reourgan izedl, aie 25, 6 us( 21,(0viiiutheiiEu d 'theano phealtcipromoter nurse lowl l iram c arnn lie vaccine: 6)10,000) ilidivid rial diises; diphitheria to)x,irin 32,(000
teogamof thyscin deandnrsmesta wevo willli tiaii hred ifte doses : Sehiick toxini 60,000) (i)Ses ; antit yploid vai;cine,:(irogam atthe dpartmntal evel as trined.180,00(1 (loses; BCG initradlermic vaccinle: 3.1 43,000) dilris;
A major, large-scale stupervisioni programn was counductedl- arld BCG oral vacicine: 125,10(0 doses.
at the iiatit-otial level. As~~~~\t of Octobier, 6 cases of ye1Iow fever were- diagvni -ed.
PAHO/RB, WHO/RB, WHO/UINDP PAHO/RB
APPENDIX A
Page 3
"Shooild ilii- 4-Ixt-inriirian l recatinentl hi; SliiiWri to lbe Usable, Itogoiit. National aitjlhoiit ii; andIi th, P-AHOI( Zone ;dvisi;rlarge siitis couild lie saved in trfea1nicnt i;oss anin maniy inirde inispec;tion t ripos toi all tIhe tuberi-iulosis programls.er-adicat ion pirograms WoUld lie aile to give radical-ciire mnkiiig it pissilIi to ~vstvimatizc t1le work in aicordanei
treatmnctt ini iirciiirnstances in which it is niot feasibile to do withi istabilishied guide-lincs. At ithe Girard(iit Pilot Ceiiter.
so) witlh the classical 14-day scheiiiiie. Ohi thic other hand. whiich faiced a crisis earlyI inii th Year, thie apptiintirient ofsliotld]( thn t reatmerit he provenl t(o he low in per;ccidtage of a flill-tiniw dlirectoir iointrililteild to a notahle imnprivicint
radic;al cueiis cffccIti;d t hi; Organiization will have evidlience in li1i Aiork hiriing tlic siecoind half iof lie year. li noidil ofwitlh whiiihi io cionvinice nialioinal servic;es that its use wouild iperations jirvtarcdl iy (irardoip was aidiiptcd in ithier partslie ciirniter-pirdicln;ive arid( watsteful of recsoiiries. iif ti1 le iiiinty. tart iclarly in Cali.
As a h)y-firoiuiie-t oif the priiject, a mnarkeid effict hais beiie A conisililtii stiiiialiteil in BIC( tiroduct n ihser%eid tilenoted on the powduatiiin iof the sttijily area. '[his toiiiirltionl, tnitpara limi iif vacc;iiiti tl 1 ;w National Institutie of Heialthilivinig in an areat which latiks general or i)rivate hecalth scr- and sihilnitted a scrii~ (if recoitinrneidatiiiis. Nsvlitii we-re,vices, was at first r'ather ci- ispiiioiis of the mriazlii c;radliia- lh-ing tilt iliiti ilfit-4.
tioiri opecrations bln LlItiMately caime to retly upon the naz- At hiw Sclo1l if I'ihliic 11ialtih of Antioiijiia 1[iivi'isity.tionatl irojct persiirncel andi to caill uipon them iifi- assistance in Mi;illl in. t lii si;iiud couirsc (3 inonths) intiiirilii
withi their nialaria attacks and( also withi othier hiealthi prob- cpididcmioliigy and cont 'il wNas held, with 1S national stil-lenms. Ilii,s thcir attitude tiiwaril tIe G(;vcrnnwnen's healthl dents; ili attvildani..acitivities was comipletely altere-d.
PAHO/5MF COLOMBIA-2200, Water Supplies
hirlfji)im: I nrlli'ii(l~Ii'i0cit On f thC nnatioinal W1'11t- SHlitilyCOLOMBIA-0300, Smallpox Eradication priigrainu inc-liuding ilit pilannrinig, design. finanicing. i*iiii-
Puarposc: 1'radiicatiiin of the idisiase froinr tlin- coijiiitry by strucltioli. alld iterlir l oi if nnuniniiipah walten- suppitly sci;viiecs.
niwalis iof vaciia;intiig 9()t% (iit lie popital iiii in a 4-year, P J1 oliI/i i/Iiir(1tiiii i :1960 1970.pl iodil. AIssislllif iii piivu/i'i/ I sari itaIry cligiticir., 3 shli ertt nn
Prcoboiebc (dnratitiori 190(7-1972 init.nt in admiliii'irat ivc not liilos. nilt( advisory si'r-viceAssi.sloici; providi'el: Adlvisiory swirvi;i;s liy tIlii' inn-fiial liy Zione I V OJtlici -. alf.
thificir assigtic;d tii truicji; AMIHO-0304, etuiptirilin and1( sotp- IP'pirk do,ii: Recoiimmii-ndirit us in teichnic;al aiidi all-
plies; aii(i I short-te~rn felloiwshipi. Inilinist at ye aspi-its (of hi program icontinued to lie inl-II' ork dlories Duiring [tii! year, 4,597At092 pci;rso were jlncniid anid an iiitiriven 't1-1, Wals note(ill Iin Ip inIVestnieiit
vaci;inatedl. Sinice thet start iof tii;( i;anliaigii in uldy 1967, a aild otpeiationral i:upilidilyit of tile National NIuinicipal De-
35S.2%,,, coverage nf itIn population has l)cii;i achuievi;d. A v-lpiunienit I nstitutti- I IN,S'FOP'AL,I. A good( deal if emi-total of 203,0l34 persons were vai;iinatedl furf the( fir-st tiine phuasis was jila-ud on adiminuist ratlive, operational. andlandh 16.3.283 wer.je ru;vaci;uinatedl the propourtions iif takis m1aintienanlce aspecu-s if1 tlii; water snupply systemls.
were 89.9'j~, aridi 77.7%.( respiectively. I NSFOP'A I ucontinum-d tii initpleninet IDII Plan Nii. I,
'[hei mor,Hiidity rate has renuainedl at zero sinuce 1967. Whuich as oif 30 sutitenihiir iripri-sented an inuvcSi;tniu- (of'Iule hotrizontal naltiire (if the tirugrain was setting a niew Coil$317,356.467.7o t 1807'~;; iif tIe total fijnuds) . liii; invest-
pace cif uipiratiuunu fir lthe locual hlealthi eirviuics if tIe 22 mliuIr malic idirini- Ihc veor wvas CiiI$49.]tt6.040.83.dep)artmentls ini whiich it is Ibeinug caririedi htl, aniti oliii Althlii sanie tunei. withi national fundi(s, INSFOPAL con-
irrunuirnuizatioon activities. sticil is 11CG, DF)I', alld Yc yilowi ii nuiii;il t :iruay utl p iii4l u ndur the 1967.1970 Fol ii-Yv:u1fi-vir vail inatioini.. %Arre luicing incoipojuiuatud iiitii li- trip- P~lan. ( ;il13.13 3,0 53,3t having, lucen inuvu;siti-d ufliluinu itw
gri n. l'i-st lItl f oftlu' year. lyv cseiiutive, hdecree tIhe fihlds (if
WHO/1R1 act ion were dii iii'id and liw in list it its thatt will assrimle respilni-
uinnldc; the1 dliriut-cii,ui of ilii- Ministry o~f l'iih1ii ilcalili. It isCOLOMBIA-0400, Tuberculosis Control bIi ul-v' il 1t at t his luc;isunu'4 a ill leadtii ti rajuun- ilentuiilts iti
troil puuuguannl, beuginnuing withi a1 %vi:ricluaioru area ill I '['lie Autiorionimiiis N111iuuiuiial \Vatclr Supply anal Se-winagitari uialtlh disitrict, wbich incidiu;iis 12 ljnlunic;itialitii;s of Ainlioiilitcs u;arrivil wl a laurgu-su;alc iniprovrivimilt anid
ilii; Dpitaitnclnlts ofi C1i)(imillunrat j o ujill I ntl! ionl prougirai iiiiiigil t1w ycar.
P'robaleoi durettion: I 966-19i70) WHO/ RBAIs.sisitini c purov;ided: Ad vi siory se rv icc b~ y te P AHIO /
WIHO (:iiirt riy Rcimtieseiitativi; arid biy .lie niu;iical ofiicierass~igincdi Ii proiject AMIHO-040t4. COLOMBIA-2300, Aedes aegypti Eradication
Wlor-k (lone: Wiitluiii tle struititmir of the MIinist ry oifl'tiill, I healthi, tuilii;iiulosis conitroul ceased tii bei a vertical P'arpise: 1trai dllatlil iif A. unigypti.Iriigririn and was illi;irpoiralted iriti tire Divisiinli of Mediical Prohah/lc d/nu rr,/i(oi : I1951I-
Caiii;. 'Illii riti;gra-itiiiri of tun1,luuuiuluusis prigr;iliis iritii this /Issisu'nii' piroiideiuI I saniiiary iinstiel;tor and adivisoiryreguldar ac ivitii;s of lthe huu;;il1t I services piroceueded niurnil;lly. sur-vilus liv t Ib P AlHO/W\ 10 l() inilry Hkpcii.sciitative; equtip.
Ill tIlis cionniictiioni a roIpichiu1 l- o granill was dlrawnl Ut1 ill Uliil t and 'Ii ppl ii'.
AP:PENBTX A.
COLOMvBIA-61 00, School of Public l-Health 41144 on1 cinb1ical 4144m 11414'4114y wa's ollied'1 al Iilit /Nationa44l
(of i lic IInI4cr'4,i[Ly (o1 Aniifiqi411i4I ill 1(4rdcr Io adc1
4111iatI'y p414- 'I' i:I44lall4 uIlrdi,4al I14111c1in (.arlet, tnf;difw'4 rmIt in11d1444144 j('14('5i14II1 I44111 ~ii NI 144'V II 4445444 ill 4 41441 I IV 'lm ld iIwdN14 disfi (41441Ii1r MI'- 111481- I.111'4'llI'oi '4444' roii>-
I wn (ledls of tile Ilolirit r'4.
/'4144411/4 I/11'44'.464 - 96. )(4I.ssist41(inc p1'1iorided: 2 s1111 -14c4(144il4I8IS I 141.11144. PAHO/RB
iriry aIdvistr4. and11 ad(visoty "I4vivicrs .y li 'A lW/Wli(ColI(iltfry Rl4lrescl4Ia1ive' 44ililiil4lvlt :1114l1I sholr-II'rill 141I COLOMvBIA~-6203, Center for the Teaching of14W51hi1(. Pathology
Wir' on'1/4u41: 114hiricenI4gi~ 4441554 '4 11''4It~: 44.,44~ I'41la15flf1114('It ill ol4l1j4inn'-I 1441.1 ll 1141
lotal4 of 2(1) '.11d44'411 I,rl of 141 1144111 ojlj441 4'1111'I..11'15If liallIioloy Iof lh14: rN4t 4io1a UJ4ii.'14sily, flt- Ul IIi'4'I'4.sit '
441l14S A''(4'4'4IItII1441o4 11114 'c4 1441tl' 14,1 1111 II'ltrinling oIf t148clli41g. II(1514it4al. a41d II.-
DIfril'iuig IfiI yoi4ll' tIll' Sc'41441d l'4IS 4'~lI'IId III Il li- 4144' s4 (*4j* 4 h 1I(rsonn44iIlII in 14 lio 1 fiId f j1Ia1holo4gy in Lailini Anwica:144
inAl4' ct4'lt4'." int1IlIdling a1 4'4'14I4dgist. al(4 4''4I44lonl", '' 4'i444(llelidicIng Iof Ila14i1(ig 1111.gian111 for techn14ical1 4144d a14xilia11'v
1141ntr11111nist. pcismi~~1llI ill Illis fi4l1hl 441111 viw44444'ag144n1Cnt (If i'I'51car44h a'1
WHO/RB [lift poA.I I'dnlc levell.
Ass141istfnl prm/14d1'i/Id. I shil irml con sult4111ant. a11d ad6. isory4)
COLOMBIA-6200, Health Manpower anid Medical ,:rvicc ('' Ifi' Ined1(icl('1 (Iiler a(ssignedl to 4')ro.I('fIt AM IBO-Education Studies 4513 4141 1I)'r lie 1"AAH0/WII0( Cmintry ReCprCesentative:.
Ifo(Ik (/44,41: Atu assssier5(it wa(s made (If illtC I)roIlrI's (If
1'u4rpo44: Stijily oIf 111:4114 4144444JIp1'4cr 4'411114i;cl4i'lt'.1; 41441l Ill4' p4441ining i4tciviIii4S IwIinlg carr'4i(4d 14141 tIlli' tIl 18tinitIe 44(e441IS for inicoeting t1wlinl 4(41iltil clletion41 of~ dz114 foi ;i A\41Ir'ica4 Pro'1gram44 for lII'iIIiIiig ill PathoIIlogy f11 l'l. i.wo4IriIIntatiIn oIf medical44( ed(lcaii4111 ar44( 11w411114 J4al414i41g :4144 II'i lIroI5pIc41't oS f fil inrIgram1 was dra'4fted this 1tarnplle1t
f(4r developing a1 wo'rkintg Iinethdll4lIIgv tlaf 4(114) s41r44 :t5 ~t is ii(44i4(y concl14rn'd1wilh411 dIescrIibing thi cuie 14(''I(I .14t14 (If
mnodel for o(tlier c114 1tr'iIs. paihollllgy a4nd( witl promot'iniIg thiis Sj(1411tC ly. 'I'li 114'4Ift wa1,Nitration:I 1 964-1908. -evewcdI hI) Illc444e( Inc eidws fit Ilic :41(1441 Colia in Go(inin(It
AssistlSf1c1' prIllidiI'd: A'1
iol'Iy ~ltlviles l~iv I44lcal 4ltiar'ls, :414d for'warde(d to) PAHOI I Headquar41 t11ers f(14' f1441l r4Viuw,
Re 14If 5I-S 'lta Itive 1 II (S111 1.4 1(v14r tIll'jIItI iII, I,1": :11111 jI iIIlI iI I di SI i'iI((i Ii(oIf( (81)' Iy e XI ye444r.
a4141o11 t. (If su4IjP1jvs. Al iei( incelinIg o(f th~e P'LAP' Coord4(inlating (>mnllttle held
11 fork 1/4o11: '1 mb' 1411 :4144 .'ifilII4 111 Health1/ /l/114;1,mlool'r 14(114 inl Jl. 11 4(' (h)rganfizaItionr (44 r(tpri's.entC4d by) Il inedllli-(11d41 A dl/il/ Edi/alion1 01 i14 (CIII4loi /1i4, V' / I. It/, 4 44111 M1('4(1i(I ca officcr' zis1ign Id to pi 'i I'l AMHI -35 13.I/4'ports ofJ f/h iI'Il//'cI/V C(nfrlf'ri'ce 1bIll' 19671) Nv45 iS- D)oring the1 flust 4( lilf of Ihc yc4444, 11h14 delCtartnicnis of Ila-
S14(41d iII 14141 S14441isli 4111(1 Eaiglis'1i. 1t wa widrk1'14 disiH'l11t1ici, IhlllIgy tIf An4ini(414l]4iVI44'11,f-y, fli(4 Na4tional4 UivcrIiV4'ity, 4(4dparl4'i1444lrly to the Ii(44a1111 aniorlt ics'tj' If 1141c 1. ''4 iiiinci'IIts On,1 Unl(Irsily 1 f Vail44 r(c'Iivttd tl1(4 laborator11(4y equj(4ij44(1tII ll 441 '444 .AnwC4iiran4 l'(cdera411in oIf As4'o,i4i:ltionI' IIl NII',4I;iIl ac(Clii4ii-ed by PAul) will funll(s alloca44te4d iri 19)67.
~'4'lIII1. II ie444111(141 4541'lIt1145.4(11 utIl SlllIk If A c1(145ultani( visiled 3 Centrl( AmIeri'ca1n coun04tries4 411n1p14'1i'1b1. 441c1 l44'4(ll4l,lllil-, IIi id4g 41(1 I'llit 5IWy m 1111 I k' exi4-o iln ordo11r toI pr1(rn41it tIle i4'(Igra44n, int14rviI'w poilliaelt41
PAHO/OF Milbank Memorial Fund ii144rns4 11t1 silIjbicts rla'41td1 tIl w(itlhol((gy. lie also( 44tter(ded111(4 PathololIgy ( Ai,rlg(s, Iof Central Arneri'ca4 anld Nlexi'o tlhatw.as held in M4I'jt(l:l, Y~444tict4i.n Vlexic'o, iln Deemer4lfl(1.
COLOMBIA-6201 , Continuing Medical Education IFhe s(411c1 i(1n (If felIlIws V.w4s I(4gl41 tIle first fedl Iwxshili.(waidedI will goinlo(1 I-GT4 i4t) J44an4fnar(y 1969.
liar1ticu14arI'y fIoll' tinofcss5i4n141 vNi44kinIg iII sinall clon14m4fli4-
1i4!s: and4( jIniblicaLiiifn (of a 1wr(iiival4I1141 in :iI 14111 ltl Im
lIiz ngii loillitogra44)hici; Ilcial'4 444(d Ilipicld in4fIrinaifuI 4 COLOMBIA-6204, Experimental Sfudies on Health1'rohld/u1I1/4: l//1/iIrII I 65- 197.74 Services,'.'siSbohlee prelllid/1d: Advisliy) byriIC lI4 (4"Itu1't4'
4/rposI': D)('5i4.n of an414 (j(ral 1411al sIllIly 1(4451d 4(f4 the4
a444d /'onc~ [V( ()f1i1 e s14(fT and4( bv' ( I'i AI IO/)WfIO C(ISIIiIIr\ find1 ings of tIlc I lealthi Wr4i((ow(4r a1n(1 MedIical4 Edncilit 1n
hiellres(4t:nitlke: gra11ts: 4441d 2 shol-41tter(4( 44f4(1 I lon4g-tI'lln StUid% a144(1 aimf(4d at tcstinIg in1 sp(ecially s1l4t(4ct( health 441'(aa
fIl lwsliips. ~~~~~~~~~~the oIptinlot'm systfems flIr thef trainin ', and i. til izationl of
II 444/4 '/444'. NVith the I'IvlIIie-i':4i14n ('if tlie Naii4444 44444di4'al au4\1i3iary Ier-onnel.
Schols(41. illIrI' tl444ii 50) p1445t r:(dllltC courscs44 w44rtrI offered, Prob/i (le/ dIlrtition: 1967-1969.37 living held at IilC Unkers'1'it"4, (if 'VJite. ApproxIiminaetev .ssistanI' proiidd4d: 1141 PItin 1)',ar a(dvi-er alIl( adviso5rv
611 1)hvs4Yic'ians1 114(V ioipaled in fthese! cmilrsI's. ser'vices by) tie 1'AHO/WI't( C.onnI ry RelIir('5nt4itt lve
It coiii''4irs4'es we-re held in tIlic depa4rtmnental ' apitals : gr4(nts : (4quiIrrment and il(j)ldi(4s.
APIiENDLX A
COLOMBIA-41 01, Clinical and Social Pediatrics \1 ilk ,ctittples w~i cii vri-il iruary for analyses.A Colonihia irigiitiir i%;s sentiii 1'io erti Rico for- sptc-
I'llrpiosc: U-gairi iiatiott if yicail) soia It I ti I ili trics cotl sis- ialIiyc41Il I t:in in g.
for jI)to fessours otf ji)ediat trics c IttirSes o(I vI dijat ItItIf IIs ill III(( Ii -
seri ees to- pjitilrtt ic hospit als. COLOMBIA-4601 , Air PollutionI'ro)aible tbiraiio,t 1904 (tinder AM BO-4-1IOtj-196'.
As.sistanitce proirt)ded: Ishoi,rt-lecrtn contsutiIant anti adl- Pu rpoisv Planitntitg andl est aidinsitent of a iiit itjoralI oc-.
vistirv scrviccs b) thle PA11O/WHl( Countttry Btepresenittlive; cnplat,ional health nuti.; and insiallationt of air- samupling
eqtItIi patfieit t a 1id suLi 1Ii es. stat ions, ill the nutijot itlics of Ilse c,-otuntry.Wlor-k donv 'rite I\V Lat itt Anttriciican Coi i sc in Clinical Pr'oliithlc dn ration: I907- (1070
anti S)ocial Pcediatrics was held on scheilujle anti withi suec- Assisiurti -irotold: Ailvisorysrie tytl A 0
vesin thei DJepartnitit of Social Pedliatrics of theq Sitool of WI ()(i0 i Coli1v B1 nstttv
Metdicinte of Aritioquiaii Untiversity (Medlellin ) ?-if was lVoiuk i/one: Wit t tiut O rganization's assistancie, a 70-
:ittended by 16 students, 5 'if theita l'AIIO fellows fronit hoitti riitrTMc ott inditsni al Itygitne was olletrtd to 5t. poio-
Birazil, I-aiti, Paraguay, 1'erti, andl Vnezncttla. 'I'ite colirse fes'-ioitals. A 1 .00Ot-pap! ntitiiiial oni the cotirse was prie-
lasted fromn 5 Auigust to 31 October. and for Ilie fir-st timeif tiartcil.4 itiirses took part, f(ir piurtposes o,f a tclani-trainitig trial. Duriing I I!( year several stuieiiis related to) ventilation piriil-
As- part of the- iwitrse, anil witlstIte assistancee i-f za social- If-ills were calrriedl ou[t.
og,ist anti at planner, a fieII ldsiolv qf a titiial conintitnity It Blt.oi`t Ii te pieriniaiuctt stat ions for the dletermIination of
was carruetl outi. air tlolhiitont andl rt(ialaioni levels continuted their operationis,
The1 StUdJeats were gjveit a fieldi assignment on h'iert-o antol plaits wire startedl for thc insisallation oif anothler station
B3errioi, where thecy cundlucetl a ritittilitin suirvev anrul a semni- it Nlicdcllin.
nar in maternal antI eltild serviCes. One of t lie- ittises in- Basic satu;plittg, for airi piolIltitou wais carriedl fttiward inl
~trciwtors spent a nmonth atl. dlie Clinicial aitd Social l'ediat ries several privitt.iail tttitills.
Coilse littid ill Chile, ini order. to guii lt fdit ioieil ixpieriencte Afu octitipliotntitl Inalih i tiit Iflueant alterations in thse S;pe-
in coiit ses (of this kindl. cial I)sritof Ittigit:,
WHO/RBCOLOMBIA-4900, Health and Population
COLOMBIA-4202, Nutrition Training Center DnmcPtI 1) J.%/i'S I:xtciisitii of inaletital autd chil licai:lth i and
I'irp)osc linroviricienett (if tlti nittritiiinal stattis,i iii the famnily phibining s,ivtit-s ti rittal arias.count ry, i)v ptrovi(ling traininug int appl1 ied nut ntrio ittitnil fooid Prilmid,c u/uruntion. : P)OB1-19'70).
e'Conomnies tii 1ersons lioldinig key goverrimetit , managemenet, lIssistircec ptovit,did I niit-ilival ofi iier.
antd tei-ching posts relatcd itii agrictultitt-c andf fid poi ify. 117ikr, dorte: Wor-k was startedl on thle dlevelopmentt of ithe
A1ssisl(lftce p)iiiidcdl: Aulvisiry services- hy tlt, VAMIO/ iti:tiialda fiihutret
WHO0 Counttry Repre.sentative. PAHO/OF AIDlVork eloIte: Atpprival waIs givent lwe tpin if opetratioins
6or puffting minii etfeu:t this jointi prjiti iif the Nationial Utti-versity. thle NationaLl Nitrit ion Intstlititfc, IiJNI CEF, FAO, COLOMBIA-6000, Medical Textbooks andaf( ii (Itli Or ga nizat ioni. Teaching Materials
Airttntgerntents for stpite luh( '4itipiticnitt fi,t- the Cctlter
were Ieing ma-d. IPurpose: Estabilisinitin iif af systeml fit- the distriliutiiin.
[Ilie bst curitse ott 1tttt it iiin wvas held, withk cotshidiraltle sale, aniti riestld if ticxtIti)ks
sincuess ;18 stitiflerits from several etmitt-it is p1:1- tititteId. 1'rol(ti)lel duruliuii: 190i7-Plans Ncl.(- flade fo loddig a "imlar coli-sc in1909, issis.ince p'firid ihud: At v isior y services I iy tlite PA11O/I iuit ueit tuate fr I iil ig s tii I icii rs ii 169 WHlO. Coii,, ry Retr citistt live.
Work doune: All Ilie aitedlical sechoiols of the 9 itiiversittics
COLOMBIA-4500 (-4507), Radiation Protection ilii the coinititry lhaul ~igiicul tlti- ictter-agcellent etof lil-hittettce to tliti Ilasic agut itiiwiit witl Ilhe Cove'tinniint.
Ii iroui,: Estalilishitnent of a ritutlitont prtuttitont service 'Ilt, 0 rganiizt ion itutdl av;tilaloli 1i Ilie schiuiols thc Ilirst 2
oll It naitolnal scale! iii itlo coitpi witl Ittlie oivir-allI tirili- t xtil ,,ks issitil( tiolcii Off ittigrihi i I'atuuii i ehc 1 Ji/)i)g
le,nt of rail at iiit cxptosit ir, 1),li it t ctutpat itna Initel if t lii: arid I?/oqu/lliiku.I lir (list ri hutiiiri i i I lii l:tsis itf ret-itcsts.
girl-ttlil 1dict At ilii yi-i" cids Ittl8 schoiis htiol rciliiisteil a otai-tl f 1.078
b'hai ( c/b du/ratint: 1 907-197tt. tuitics tif tlof furnwtr itol 1.1072 tif tlie, litlir.
Alssisfaui,iu jiroviri(b: AdIvisorv' sur-vites lIy t li PA IIO/ lIn aItfilititi. t liv latuitl ii Aulutiiristrativt anuuiluu. td
WIlO Coiii l i t- t u ii,s itutlfitrins for tIli proitiutu (sO Ics an( r 1 tital liccip t-
ll'ol/ ii: lIt Iiglitisuttvill:iucu satitiu uuoiiiituil tiril turds. tnotrthi1lvupiurust w;re tprtvidcul.
its tf-guillar t tu i- tiling stiitlltIs ful.rio-a.litiii aiial- Ettii siliotul atptuuittl ;t staff inmnetr Iio liutinIc thec

APPENIDIX APacge 6
RUork done: Ini accordanice' w Ivi ll) ii;:- plan I opejlatioireS Ii nildc, ;i (lcpaIi lirtll 1, riI\ flic ,;cthoois of AMledicine andpreparation of the theoretical iridetl of at ivilivs wvas 90',i , o I Irr )IIisI t i .cachII of IIrose arIivI isit ic : anII d SI taIIl IsIelli tcomipleted arid: preparation t0f the Inarorals f.ir 1that InOdlil ,F a ;,airer fur rescarir.1 in ;,,wl g i- l and pnlbie li,;iltli (ien.-
wals 8)1,1, completed. According to pi-c(le:ti:rici,:dl ,,rinti;,, Iist rV.all III eXI erirneTCal) stlody areas were sel:t(cl ziid i liarilinilig piohleiI/c dlrIa// io. 19(0 1-1)97 1.of tlie model for the initial appraisal of tlhes lsts wa- s wt AIsislm/un p)rovioed: :3 ho -e(.rrl colistiltaillts :1 erinpo-COnCluded. Application of tile model in a test rtimricipllity rary adlvisers. andl advisory servirs by the( dentlal Ceul.slIttitnt
vtas earneid iriit, as were the seletion <ii 1a illirig of Il. as,igrt(d lo prf jcct A ll()-4ll09 I g-rant; (lu1ilinrlient and
iw cesY alr) personnel andfl tre eritlection of dalta f(or i it initial Sliptplit s; atll(l 1. sliol-term PFl lwvshiip.
appraisal ill 2 if thle 3 exper iienrIital Ir Iras. ' .ls 011;1a I,1- 1lV k: (fim : In tIeI I )D.I al I ll i of l'reritiv arid Socialainr:d were analyzed. i-ttlistry of tlii- Ulniversity of Antioqinia. changes were
lrriruleralerrtatioriru of tic tlheOretiCal taModel proigrare-4 trill ra;dIld in t1 l clrrictlliim in orficl to ioitroduci:e tlhe tetrclirgtleir i;vallriatiorn wiet siliedi(tlel 1or 19(9'). F1 til(irt vi:k ;aspects Of orl hIdnloic s aidi ipedodorltics. Irvairn-
ring i rograrris ini ear-iolgy and rricrbiologv were i on-PAHO/OF AID -tidin:cl for dcntists working in local instititiurs, arid a
ill sr ci ltific irivesligit ion wvas given for the facilty.
COLOMBIA-6300, Nursing Education A s(raininar waVs cInd tO disetiss the( ritilizalioin of aiixiliaryd1-nii:al ltcrtsoiciil in healtlh programs in Colomnlia.
PIrpose: Ilprovenirtnt ill tlie niisilng care iiIroiVid( in In Novvermnhr tle D)epartnr:nt condicted art internationalhealtai services. throLlgll the estahlishmriient of contiriuring eilII- c:omrise in (rial niciolriology For 12 prlofessors of this nlisci-Cdtirii programs in administratioir anidl supelvisiin. Jrn e1IVoI plilnrr f-tnm otlier d(neitl schools irn tfi Hermispihere. Stildlics
traininlg, and training in specialized fieils. wi-re :oirilltir l tip evaluatce l htle I. ii.. r' iof flrtiriiditedProlbiadle (d,irdtiio: 1968-1971). iabl salt fir the Ii( ve nrtio n i f nltaal aries.
Assistance prrov;id/edl: Advisory services bjy tlie nurse as- At tliv Natiirnal University, aftemipls were being mnadesignreld to project AMI)O-3204. to 'Ittsigrl aur irll:graltd diarltarrnwi;ill st rrrct ire which wu(illil
U or/k donrir 'Ihe Standing C(rrrmiiltcr in Njrsikng F of ili' st r-rgtn ! til teaichring of trrv;ritnion in dcntal In alth asCohionibiarr Associatiorn of tiriversities coniliriled s-ILking tI%ll as in tin: otlier medical scirni:es. '[he program oftoward coordinationi of the tirririg r tlri-tl arlit pigr varls. stindmes wvias kling revised ti give emphasis to p,reventive
During the year tile niuirbilw .,i stilrills, irrot'lltid inl d iivst Stitnidis u tnie tiaininig a,d uitilizatiin (of auixiliarynursirig aLuxiliary cotirseS inervasel. t tlir a bigi,4, mad stir i l talld 1an 11 letniiilires fur tle frirniishin,,. of dte,ntal care
in tire basic programi of tite Unliviirsity of Valil C (ali 1 ,11 wVt'l in'e way ill at field renter.a trial lbasis, stutdlenits rrniy b1 grolrwird azir lild, to thleir
abilitics after 2l1% ye;ins; byv otinritming thi U shidices for PAHO/RBart ariditiotial 11/, years they can it-u (-ivc a b;aic;ilatireate
degre(e in nUilsing or. if tIIey i(: lit tic t li d stictin:s fijr (i
ririrtlr i thl T cal biecnrel gene ;ral rru1is;
COLOMBIA-6400, Sanitary Engineering Education
Puorpose: lIpr-iivernent in tire tnaliniial i :inining rof tiroi-
fessionial personnel engaged ill saniit;rrx r1iIWVroe( : prr-
mpotin of researcih and( txpiarr.iuil anti oIb ur'ili'-atiui if
salnital)' erigirieeririg dnicatioirn in thi ricgidart t nil crgirncer-
ing courses at t1w Naliorral lUnivetsily.
Probalule (Ittrrrtion: 1964-1971.Assistance prorvided: Advisory stivir:es by tie sariitatv
etngineer assigned to project AMNRTO-(fl1)(t; grants: eqtuip-
merit arid supplies; and 1 long-tcrmt felNloship.WVork d/one: A sihort coourse oin svytemn, analysis in
waler resources was helni at the U[nivri-Sitv Of thr Andes. aridanothier on indiustrial hygiene was ofiereil dtfit, Natiotinal
Urriversity. A total of 96 persorius atteinddil hit t i-scs.'Ilree research proje-cts weri siart-d 41nitirig tii: vyar.
PAHO/RB, PAHO/OF IDB
COLOMBIA-6600, Teaching of PreventiveMedicine and Dentistry
Purtrpose: lrtfegratioit of thi tu tach;rg (if prrc-cltivi mnedi-
rine antl preventive derutistry at ilt liniversity of AntitttilLiain Medellirn. and at the National (Iiiiversity in looigrtA,
- 85 -
VIII. BIBLIOGRAPHY AND REFERENCES
A. Health Conditions and Health Resources in Colombia
1. Health Conditions in the Americas, 1961-1964, Pan American Health Organi-zatJion, Pan American Sanitary Bureau - Regional office of the WorldHealth Organization, Scientific Publication #138, Second Printing,October 1967.
2. Facts on Health Progress, goals in the charter of Punta del Este, Scien-tific Publication #166, Pan American Health Organization, Second Print-ing, July 1969.
3. Study on Health Manpower and Medical Education in Colombia - InternationalConference on Health Manpower and Medical Education, MKracay, Venezuela,June 1967 - Ministry of Public Health of Colombia and the ColombianAssociation of Medical Schools - a) Vol. I - Methodology; b) Vol. II -Preliminary Findings; c) Vol. III - Karacay Conference, Working Docu-ments and Reports.
4. Estudlo de Recursos Humanos Para la Salud y Educacion Medica en Colombia,Investigacion Nacional de Morbilidad, Ministerio de Salud Publica,Associacion de Facultades de Medicina,
a. Educacion Medica en Colombia 1965b. Las Escuelas de Enfermeria en Colombia frente a las necesidades
y utilizacion de recursos disponibles, 1966c. Recurso de Enfermeria, 1967d. Resultados Preliminares de Entrevistas Domnicliaria, 1967e. Analisis del Gasto Publico en Salud (1961-1965), 1966f. Estudio de Poblacion, 1967g. Estudio de la Mortalidad, 1967h. Analisis de la informacion basica sobre la utilizacion y
disponibilidad de los recursos para la Atencion Medica enColombia, 1967
i. Hechos Demograficos, 1968J. Diagnosticos de Consulta Externa, 1968k. Dlirectorio Medico Colombiano, 19681. Accidentes, 1968m. Atencion Modica 1968n. La Muestra, 1966o. La Profesion Medica, 1968p. Parasitismo Intestinal, 1969q. Metodos y Resultados, 1969
5. Recursos Humanos Para la Salud y la Educacion Medica en Colombia, ConferenciaNational de Rssultados, Bogota, Agosto 1967, Asociacion Colombiana deFacultades de Medicina.
6. Agualimpia M., Carlos et al, Demographic Facts of Colombia, The NationalInvestigation of Morhidity, Milbank Memorial Fund Quarterly, XLVII,Number 3: 255-296, July, 1969.
7. Lopez Toro, Alvaro, Ana]isis Demographico de los Censos Colombianos: 1951y 1964, Centro do Estudios Sobre Desarrollo Economico (CEDE) Universidadde los Andes, Bogota, 1968.
8. Anuario General de Estadistica - 1965, Poblacion, Asistencia Social eHigiene, Tomo 1, Departamento Administrativo Nacional de Estadistica,Republica de Colombia.
9. Departamento administrativo nacional de estadistica (DANE), informe alcongreso nacional, Republica de Colombia, 1968.
10. Instituto Colombiano de Seguros Sociales, Cartilla Informativa del SeguroSocial Colombiano, 1969.
11. Informe Sobre Siete Anos de Programas de Nutricion en Colombia - Enero de1963 a Enero de 1970, Instituto Qolombiano de Bienstar Familiar,Direccion de Nutricion Ministerio de Salud Publica, 1970.
B. Health Plans and Health Programs in Colombia
12. Plan National de Salud, 1968-1977, Resumen de la primera aproximacion(Documento de trabajo - Version preliminar); Republic of Colombia,Ministerio de Salud hPblica, Bogota, Noviembre 16 a 17 de 1967.
13. Plan Nacional de Salud, 1968-1977, Tablas, Cuadros y Resumenes, Ministeriode Salud ibJlica, Republica de Colombia, Noviembre, 1967.
1h. Planes y Programas de Desarrollo, 1969-1972, Departamento Nacional dePlaneacion, Republico de ;olombia, Documento DNP-417J, Diciembre, 1969,
a) Salud, (Capitulo v, Analisis y Politicas Sectoriales)b) Politica de Poblacion, (Capitulo * , Analisis y Politicas
Generales).
15. Planes y ProFramas de Desarrollo, 1969/72. Plan de Inversiones Publicas,Sectores Salud, Vivenda y Seguridad, Tomo 4 , Departamento National dePlaneacion, Republica de Colombia.
16. Planes y Progrsmas de Desarrollo, Sector Salud, Departamento Nacional dePlanencion, Unidad de Recursos Humanos, Republica de Colombia, Noviembrede 1969.
17. Ordonez Plaja, Antonio, Ministro de Salud Publica, Informe al HonorableCongreso de la RepubJica de Colombia,
agosto de 1967 - julio de 1966agosto de 1968 - julio de 1969
18. Ministerio de Salud Publica Apropriaciones 1970.
19. Current Economic Position and Prospects of Colombia - International BankfSor RcconstruotiO r an6 Dpvelopment. - International Development Associa-tion, ae-ori. #WH-188a (Restricted), Dec. 30, 1968, Volume III, Annex V,Human Resources.
- 87 -
20. Social. Science andI Health Planning - Culture, Disease and Healt.h Servieesin Colombia, The Milbank Memorial Fund Quarterly, XLVT, Number 2, April196'8, Part 2.
21. P]an Hospita]ario Nacional-,Plan de Construccion, Dotacton y Operacion de!Hospitales, Colombia 1970-1972, Ministerio de Salud ubliica, Oct.ubre de1969.
22. Estudio de InstitAuciones de Atencion Medica, Prospect.o Ministerio de Salud,INPES Asociaciozi Colombiana de Facu].tades de Medic-ina, Noviembre, 1969.
23. Experiment.al St,udy of Hea:lth Services in Colombia, Plan oi' Operatiorns, Pha....eII, Revised June 1969.
21h. A Program for Research to Develop a Comprehensive Healtlh Plarnrning System,Health Plnnninrg Research Team, Division of Research in Epidemology andC,ommunications Science, WHO, Geneva, 1969.
?5. Ordonez Plaja, Antonio, Bienestar Social en Colombia, Bogota, 1968.
26. Plan Nacional de Alimentos para el desarrollo (PLANALDE) Programa Nacionalde Educacion Nutricional y Complementacion Alimentaria (PRONENCA)(RequLest to World Food Programme) 1969.
27. Extension de Servicios de Atencion Materna e Infantil, Estudio Preparatoria,Ministerio de Salud Publica, INPES; Asociacion Col. de Facultades deMedicina, 1969.
28. Programa de Extension de Servicios de Proteccion Materna e Infanti] y deBienestar Familiar. Plan de Operaciones Republica de Colombia, Ministeriode Salud Publica, Division de Atencion Medica, Grupo Materno Infantil,March 1969.
29. Manual Para el Adiestramiento de Promotoras Rurales de Salud, ConocimientosBasicos Minisalud, Division de Atencion Medica, Enero de 1969.
30. Propuesta Estadistica para el Sector Salud, DANE, 1969.
31. Plan Quinquenal de Desarrollo, 1969-1973, Escuela de Salud Publica.
32. Asociacion Coloombiana de Facultades de Medicina, Informe de Actividades1959-1968.
33. National. Planning DApartirant - Economic Stud(lies.

![Panasonic SIVI-IS! ~~~ [}(]oo[po](https://static.fdokumen.com/doc/165x107/631d3a1b76d2a4450503e6ab/panasonic-sivi-is-oopo.jpg)


















