
Retention of ventilation skills of emergency nurses after training with the SMART BAG ® compared to...
6
Resuscitation (2006) 68, 379—384 TRAINING AND EDUCATION Retention of ventilation skills of emergency nurses after training with the SMART BAG ® compared to a standard bag—valve—mask Melissa De Regge a , Catherine Vogels b , Koenraad G Monsieurs c,∗ , Paul A Calle c a Critical Care Department, Ghent University Hospital, De Pintelaan 185, 9000 Ghent, Belgium b Intensive Care Department, Cliniques Universitaires St. Luc, Avenue Hippocrate 10, 1200 Brussels, Belgium c Emergency Department, Ghent University Hospital, De Pintelaan 185, 9000 Ghent, Belgium Received 28 February 2005; received in revised form 8 July 2005; accepted 15 July 2005 KEYWORDS Bag—valve—mask; Gastric regurgitation; Training; Cardiopulmonary resuscitation (CPR); Airway management Summary Background and purpose: Studies show that nurses retain resuscitation skills poorly and that retention of ventilation skills is particularly difficult. We formed the hypoth- esis that the SMART BAG ® (SB, O-Two Medical Technologies Inc., Canada), i.e. a bag-valve-mask device with a pressure/flow responsive valve, would assist nurses in providing more efficient ventilation six months after training. Materials and methods: Prior to training, 39 emergency nurses performed CPR for 2 min, in pairs, using a standard bag-valve-mask device (STBVM, Laerdal, Norway) to assess their base line skills. A CPR training manikin (Simulaids, USA) equipped with a PEEP valve in the oesophagus set at 20 cm H 2 O was used to measure inspiratory time, tidal volume (Vt), peak pressure and gastric insufflation (GI). Immediately following training they were tested using an O-Two STBVM and a SB. Half of the nurses were retested after three months, the other half after six months. Efficient ventilation was defined as a mean Vt > 400 ml and GI < 50 ml in 1 min. Results: Before training, only 16% of nurses ventilated efficiently: 63% had GI and 28% had Vt < 400 ml. Three months after training the efficiency of the STBVM and the SB was high (81 and 75%, respectively). Six months after training, there was a trend towards higher efficiency for the SB (63%) compared to the STBVM (25%) (p = 0.07). For instances with the STBVM producing a Vt > 400 ml, those without GI had a lower peak pressure than those with GI (7.8 cm H 2 O versus 17.7 cm H 2 O, p = 0.0001) and showed a trend towards a longer inspiratory time (1.28 s versus 1.08 s, p = 0.08). Of all efficient ventilations with a STBVM, 26% had a Vt > 600 ml. A Spanish translated version of the summary of this article appears as Appendix in the online version at 10.1016/j.resuscitation.2005.07.013. ∗ Corresponding author. Tel.: +32 92402755; fax: +32 92404980. E-mail address: [email protected] (K.G. Monsieurs). 0300-9572/$ — see front matter © 2005 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.resuscitation.2005.07.013
Transcript of Retention of ventilation skills of emergency nurses after training with the SMART BAG ® compared to...

Resuscitation (2006) 68, 379—384
TRAINING AND EDUCATION
Retention of ventilation skills of emergencynurses after training with the SMART BAG®
compared to a standard bag—valve—mask�
Melissa De Reggea, Catherine Vogelsb, Koenraad G Monsieursc,∗,Paul A Callec
a Critical Care Department, Ghent University Hospital, De Pintelaan 185, 9000 Ghent, Belgiumb Intensive Care Department, Cliniques Universitaires St. Luc, Avenue Hippocrate 10,
1200 Brussels, Belgiumc Emergency Department, Ghent University Hospital, De Pintelaan 185, 9000 Ghent, BelgiumReceived 28 February 2005; received in revised form 8 July 2005; accepted 15 July 2005
KEYWORDSBag—valve—mask;Gastric regurgitation;Training;Cardiopulmonaryresuscitation (CPR);Airway management
SummaryBackground and purpose: Studies show that nurses retain resuscitation skills poorlyand that retention of ventilation skills is particularly difficult. We formed the hypoth-esis that the SMART BAG® (SB, O-Two Medical Technologies Inc., Canada), i.e. abag-valve-mask device with a pressure/flow responsive valve, would assist nurses inproviding more efficient ventilation six months after training.Materials and methods: Prior to training, 39 emergency nurses performed CPR for2 min, in pairs, using a standard bag-valve-mask device (STBVM, Laerdal, Norway) toassess their base line skills. A CPR training manikin (Simulaids, USA) equipped with aPEEP valve in the oesophagus set at 20 cm H2O was used to measure inspiratory time,tidal volume (Vt), peak pressure and gastric insufflation (GI). Immediately followingtraining they were tested using an O-Two STBVM and a SB. Half of the nurses wereretested after three months, the other half after six months. Efficient ventilationwas defined as a mean Vt > 400 ml and GI < 50 ml in 1 min.Results: Before training, only 16% of nurses ventilated efficiently: 63% had GI and28% had Vt < 400 ml. Three months after training the efficiency of the STBVM and theSB was high (81 and 75%, respectively). Six months after training, there was a trendtowards higher efficiency for the SB (63%) compared to the STBVM (25%) (p = 0.07).For instances with the STBVM producing a Vt > 400 ml, those without GI had a lowerpeak pressure than those with GI (7.8 cm H2O versus 17.7 cm H2O, p = 0.0001) andshowed a trend towards a longer inspiratory time (1.28 s versus 1.08 s, p = 0.08). Ofall efficient ventilations with a STBVM, 26% had a Vt > 600 ml.
� A Spanish translated version of the summary of this article appears as Appendix in the online version at10.1016/j.resuscitation.2005.07.013.
∗ Corresponding author. Tel.: +32 92402755; fax: +32 92404980.E-mail address: [email protected] (K.G. Monsieurs).
0300-9572/$ — see front matter © 2005 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.resuscitation.2005.07.013

380 M. De Regge et al.
Conclusions: Six months after training, nurses ventilated at least as efficiently withthe SB, compared with the STBVM. This illustrates the ability of the SB to compensatefor the deterioration over time in skill. On the other hand, training with a STBVMshould focus primarily on prolonging the inspiratory time, and therefore the peakpressure, whilst maintaining an adequate Vt.© 2005 Elsevier Ireland Ltd. All rights reserved.
Introduction
The European Resuscitation Council (ERC) 2000Guidelines recommend tidal volumes (Vt) of400—600 ml and inspiratory times between 1 and2 s to reduce gastric insufflation (GI)1 when ven-tilation is provided with a bag—valve—mask (BVM)and supplemental oxygen. The SMART BAG® (SB, O-Two Medical Technologies Inc., Canada) is a BVMwith a pressure/flow responsive valve limiting theflow rate to a maximum of 40 l/min.2—4 The valveprevents rescuers who squeeze the bag too force-fully from generating excessively high upper airwaypressures which contribute to GI.
It is not known how the SB influences the ventila-tion skills of rescuers six months after training when
Materials
tilation skills of 39 emergency nurses of GhentUniversity Hospital, a tertiary teaching hospitalinvolved in prehospital emergency care. To assessbase line basic life support (BLS) skills all nurseswere tested prior to training. A manikin was placedsupine on the floor. The nurses were asked to per-form BLS in pairs for 2 min, alternating two ventila-tions using a Laerdal STBVM with 15 chest compres-sions, without interruption and without any helpfrom the testing team. The nurses were retrainedsubsequently in two-rescuer CPR, combining chestcompression and BVM ventilation using an O-TwoSTBVM and a SB, focussing on avoiding excessiveVt and GI. The total duration of practical BLS train-ing was 60 min, with one instructor per six nurses.Immediately after training, the nurses completed
months, the other half (19) after six months. Inthese retesting sessions, the STBVM was alwaysused before the SB to prevent bias by a potential
We used a CPR training manikin (Simulaids, USA)specifically equipped with an oesophagus and aPEEP valve set at 20 cm H2O to simulate thelower oesophageal sphincter pressure. Ventila-tion variables (Vt, inspiratory time, and peakpressure) were measured with CPRview® soft-ware (Michigan Instruments, USA). GI was mea-sured with a volume meter (Medishield, UK).The total volume of GI collected over 2 min wasrecorded.
A Laerdal STBVM (Laerdal, Norway) was used tomeasure base line ventilation skills of the nursesbecause this BVM is used routinely in our hospi-tal. During and after training, an O-Two STBVMand a SB were used because both have identicalmechanical properties except for the valve in theSB.
Methods
On the occasion of a new in-house advanced lifesupport training programme, we studied the ven-
learning effect from the SB on the STBVM (theopposite being unlikely). After initial training, thenurses were asked to rate subjective efficiencyand ease of use of the SB and STBVM on a 0—10scale. Before the three and six months retentiontest, they were asked about their exposure to CPRsince their initial training. Efficient ventilationwas defined as a mean Vt > 400 ml and GI < 50 mlcollected over 1 min. All tests were taken over2 min, for GI the mean volume collected over 1 minis reported. The paired t-test, Mann—WhitneyU-test and Fisher’s exact test were applied whereappropriate using InStat3 (Graphpad Software Inc.,USA). A p ≤ 0.05 was considered significant. Thepower of the study to detect a difference of 3 cmH2O in peak pressure after six months was 95%.
Results
For the evaluation of the retention of ventilationskills we included only the complete series of venti-
compared with a STBVM. We formed the hypothesisthat after six months the SB would assist nurses inventilating efficiently. This hypothesis was tested ina group of emergency nurses.
a questionnaire collecting demographic data andinformation on previous CPR training and exposure,after which they were tested using an O-Two STBVMand a SB (the order of testing was randomised usingsealed envelopes).
Half of the nurses (20) were retested after three
Retention of ventilation skills of emergency nurses 381
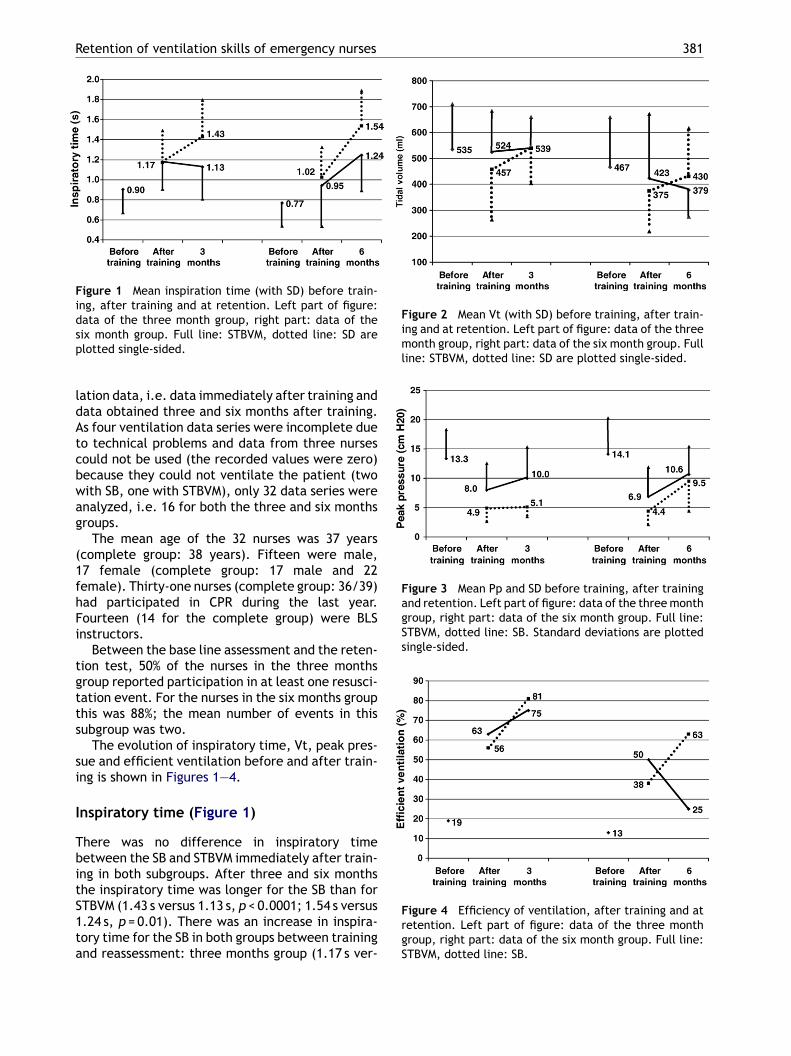
Figure 1 Mean inspiration time (with SD) before train-ing, after training and at retention. Left part of figure:data of the three month group, right part: data of thesix month group. Full line: STBVM, dotted line: SD areplotted single-sided.
lation data, i.e. data immediately after training anddata obtained three and six months after training.As four ventilation data series were incomplete dueto technical problems and data from three nursescould not be used (the recorded values were zero)because they could not ventilate the patient (twowith SB, one with STBVM), only 32 data series wereanalyzed, i.e. 16 for both the three and six monthsgroups.
The mean age of the 32 nurses was 37 years(complete group: 38 years). Fifteen were male,17 female (complete group: 17 male and 22female). Thirty-one nurses (complete group: 36/39)had participated in CPR during the last year.Fourteen (14 for the complete group) were BLSinstructors.
Between the base line assessment and the reten-tion test, 50% of the nurses in the three monthsgroup reported participation in at least one resusci-tation event. For the nurses in the six months groupthis was 88%; the mean number of events in thissubgroup was two.
The evolution of inspiratory time, Vt, peak pres-sue and efficient ventilation before and after train-ing is shown in Figures 1—4.
I
TbitS1ta
Figure 2 Mean Vt (with SD) before training, after train-ing and at retention. Left part of figure: data of the threemonth group, right part: data of the six month group. Fullline: STBVM, dotted line: SD are plotted single-sided.
Figure 3 Mean Pp and SD before training, after trainingand retention. Left part of figure: data of the three monthgroup, right part: data of the six month group. Full line:STBVM, dotted line: SB. Standard deviations are plottedsingle-sided.
Figure 4 Efficiency of ventilation, after training and atretention. Left part of figure: data of the three monthgroup, right part: data of the six month group. Full line:STBVM, dotted line: SB.
nspiratory time (Figure 1)
here was no difference in inspiratory timeetween the SB and STBVM immediately after train-ng in both subgroups. After three and six monthshe inspiratory time was longer for the SB than forTBVM (1.43 s versus 1.13 s, p < 0.0001; 1.54 s versus.24 s, p = 0.01). There was an increase in inspira-ory time for the SB in both groups between trainingnd reassessment: three months group (1.17 s ver-

382 M. De Regge et al.
Table 1 Efficiency of ventilation before training and at three and six months
Before training After training Retention
Laerdal BVM STBVM SB STBVM SB
Three months (n = 16)GI 11 3 0 3 0Volumes GI/min 2295 ml 1350 ml 0 ml 783 ml 0 mlVt > 400 ml 14 13 9 15 13Vt > 400 ml + GI < 50 ml 3 10 9 12 13Efficient 19% 63% 56% 75% 81%
Six months (n = 16)GI 9 1 0 5 0Volumes GI/min 4178 ml 5800 ml 0 ml 3488 ml 0 mlVt > 400 ml 9 9 6 5 10Vt > 400 ml + GI < 50 ml 2 8 6 4 10Efficient 13% 50% 38% 25% 63%
GI, gastric insufflation in 1 min and Vt, tidal volume.
sus 1.43 s, p = 0.0075) and six months group (1.02 sversus 1.54 s, p = 0.0002).
Vt (Figure 2)
There were no differences in Vt between the SBand STBVM at any time. The increase in Vt for theSB between training and at retention was not sig-nificant: three months group 457 ml versus 539 ml,p = 0.10; six months group 375 ml versus 430 ml,p = 0.36.
Peak pressure (Figure 3)
After training, the SB had lower peak pressures thanthe STBVM in both subgroups (4.9 cm versus 8.0 cmH2O; p = 0.0001 in the three months group; 4.4 cmversus 6.9 cm H2O, p = 0.06 in the six months group).At three months, the difference remained (5.1 cmversus 10.0 cm H2O, p < 0.0001) but at six monthspeak pressure increased for the SB to the same levelas the STBVM.
Efficiency (Figure 4)
At three months, both the SB and STBVM showeda trend towards higher efficiency when comparedwith their efficiency immediately after training.At six months, the SB showed a tendancy towardshigher efficiency and the STBVM towards lower effi-ciency but both results were statistically not signif-icant. When the SB was compared with the STBVMat six months, there was a trend towards higherefficiency for the SB (63%) over the STBVM (25%)(p = 0.07). Table 1 shows data of Vt and GI relatedto efficiency. None of the SB users had GI.
At total of 128 data series (SB and STBVM) aftertraining and at retention were available (64 imme-diately after training, 32 after three months, 32after six months). Immediately after training, only58% (37/64) of all recordings had a Vt > 400 ml, afterthree months this reached 88% (28/32), and aftersix months 47% (15/32). Table 2 illustrates all casesimmediately after training and at retention with
l
GI
547.1.0
I, ga
Table 2 Ventilation variables for cases with Vt > 400 m
STBVM Vt > 400 ml (n = 42)
GI+ (n = 8)
Vt (ml) 651 (147; 424—849)Pp (cm H2O) 17.7 (5.5; 8.8—22.8)Ti (s) 1.08 (0.32; 0.59—1.64)GI (ml) 2423 (2658; 100—7180)
Vt, tidal volume; Pp, peak pressure; Ti, inspiratory time; Grange).
SB Vt > 400 ml (n = 38)
− (n = 34) GI− (n = 38)
4 (106; 401—785) 568 (107; 429—884)8 (2.1; 4.5—12.8) 7.6 (3.7; 2.9—18.0)28 (0.24; 0.82—1.81) 1.47 (0.30; 1.02—2.20)
0
stric insufflation in 1 min. Mean values (standard deviation;

Retention of ventilation skills of emergency nurses 383
Table 3 High tidal volumes with and without gastric insufflation
STBVM Vt > 600 ml (n = 15) SB Vt > 600 ml (n = 13)
GI+ (n = 6) GI− (n = 9) GI− (n = 13)
Vt (ml) 715 (98; 593—849) 688 (65; 603—785) 683 (91; 619—884)Pp (cm H2O) 18.3 (4.6; 9.8—22.5) 9.1 (2.1; 6.3—12.8) 8.2 (3.9; 4.8—18.0)Ti (s) 1.17 (0.30; 0.83—1.64) 1.43 (0.22; 1.07—1.81) 1.71 (0.27; 1.34—2.20)GI (ml) 2897 (2930; 100—7180) 0 0
Vt, tidal volume; Pp, peak pressure; Ti, Inspiratory time; GI, gastric insufflation in 1 min. Mean values (standard deviation;range).
a Vt > 400 ml in order to evaluate the differencesbetween cases with GI and without GI. For STBVMcases with a Vt > 400 ml (42/64), cases without GIhad lower peak pressures (7.8 cm versus 17.7 cmH2O, p = 0.0001) and showed a trend towards longerinspiratory time (1.28 s versus 1.08 s, p = 0.08) thancases with GI (Table 2). SB cases with a Vt > 400 ml(38/64 all without GI) compared with STBVM caseswithout GI had significantly longer inspiratory times(1.47 s versus 1.28 s, p = 0.02) but peak pressureswere similar (7.6 cm versus 7.8 cm H2O, p = 0.17).Of all 34 efficient ventilations with a STBVM aftertraining and at retention sessions, 9 (26%) hadVt > 600 ml. Table 3 analyses these cases becausethey are prone to GI. The only significant differ-ence between STBVM with and without GI was peakpressure (18.3 cm versus 9.1 cm H2O, p = 0.003).Between STBVM without GI versus SB, inspiratorytimes were different (1.43 s versus 1.71 s, p = 0.02).Between STBVM with GI and SB, both inspiratorytimes and peak pressures were different (1.17 s ver-sus 1.71 s, p = 0.002 and 18.3 cm versus 8.2 cm H2O,p = 0.001).
The nurses rated the efficiency of the SB 8.4 and8.0 for the STBVM (p = 0.03). Ease of use was rated8
D
Nisucesisaaucu
thetists but none of 29 EMTs were unable to produceeven one effective Vt (defined as >434 ml) during a3 min assessment.9 However, 16/29 EMTs comparedto 1/26 anaesthetists caused at least one episode ofGI. Following studies showing that lowering Vt canreduce GI, the ERC 2000 guidelines recommendedto limit Vt and prolong inspiratory time.1,10,11
The SB is designed to provide controlled ventila-tion and to limit GI. Wagner-Berger et al. studied20 nurses using a bench model of an unprotectedairway with a PEEP valve at 20 cm H2O.2 Peak pres-sure was lower with the SB (12 cm H2O) than withSTBVM (17 cm H2O), there was less GI with the SBand inspiratory time was longer (1.9 s for SB versus1.5 s for STBVM). The same researchers studied theSB in 60 adult patients undergoing routine inductionof anaesthesia.3 Peak pressure was 13 cm H2O for SBand 17 cm H2O for STBVM. Von Goedecke et al. com-pared the skills of 191 emergency physicians usinga STBVM and a SB on a bench model of an unpro-tected airway with a PEEP valve set at 19 cm H2O.4
The incidence of GI was 4% for SB versus 39% forSTBVM (Vt was comparable between groups, peakpressure was not reported).
The long-term efficiency of ventilation aftertwsomiwltaimfttsinf
.1 versus 7.7 (p = 0.10).
iscussion and conclusion
urses from our emergency department reportednfrequent exposure to resuscitation. This is noturprising as in Belgium emergency ventilation issually performed by emergency medical techni-ians or by physicians.5 Lack of regular training andxposure therefore explains their poor base linekill level. The infrequent exposure to resuscitations not different from observations of other hospitaltaff.6 Inadequate CPR skills is a known problemmongst various groups of health care workers.7 GInd subsequent pulmonary aspiration is of partic-lar clinical concern. A registry of 996 in-hospitalardiac arrest patients found that GI caused by BVMse was 12%.8 Walsh et al. found that 6/27 anaes-
raining with SB and STBVM is not known. Therefore,e assessed differences in retention of ventilation
kills between the SB and a STBVM. We believe thatvercautious ventilation was the main reason whyany nurses had a low Vt immediately after train-
ng. At up to three months the ventilatory efficiencyith both devices was maintained, but in the group
eft for six months before retesting, there was arend towards a decline with STBVM while it wast least maintained with the SB. The increase innspiratory time with the SB after three and sixonths is remarkable, most likely caused by the
act that the SB provides more controlled ventila-ion compared with a STBVM. At six months bothhe SB and the STBVM group had higher peak pres-ues and longer inspiratory times (compared withmmediately after training). This is explained by aumber of nurses squeezing the bag longer and tooorcefully. In the STBVM group this resulted in GI,

384 M. De Regge et al.
but not in the SB group. These data illustrate theability of the SB to compensate for the skill deterio-ration over time. Table 2 highlights the importanceof inspiratory time and peak pressure in limitingGI. The message of Table 3 is that a Vt exceeding600 ml does not cause GI in our model as long asinspiratory time and peak pressure are controlled.Training should therefore focus on prolonging inspi-ratory time whilst maintaining adequate Vt.
Limitations of the study
This is an in vitro study and our observations mightdiffer from the performance of nurses in real situa-tions. The sequence of testing at retention (STBVMbefore SB) may have been advantageous for the SB.However, no feedback was offered to the candi-dates after STBVM ventilation, and we thereforebelieve influence has been minimal. The airwaypressures generated by the Simulaids manikin arelower than in most other models reported in theliterature, but even at these lower pressures, sig-nificant GI occurred.
study was presented as an abstract at the seventhCongress of the European Resuscitation Council inBudapest, Hungary, September 8—11 2004.
References
1. de Latorre F, Nolan J, Robertson C, et al. European Resus-citation Council Guidelines 2000 for Adult Advanced LifeSupport. Resuscitation 2001;48:211—21.
2. Wagner-Berger HG, Wenzel V, Stallinger A, et al. Decreas-ing peak flow rate with a new bag—valve—mask device:effects on respiratory mechanics, and gas distribution ina bench model of an unprotected airway. Resuscitation2003;57(2):193—9.
3. Wagner-Berger HG, Wenzel V, Voelckel WG, et al. Apilot study to evaluate the SMART BAG: a new pressure-responsive, gas-flow limiting bag—valve—mask device.Anesth Analg 2003;97(6):1686—9.
4. Van Goedecke A, Wagner-Berger H, Stadlbauer K, etal. Effects of decreasing peak flow rate on stomachinflation during bag—valve—mask ventilation. Resuscitation2004;63:131—6.
5. Bossaert L, Van Hoeyweghen R. Evaluation of cardiopul-monary resuscitation (CPR) techniques Cerebral Resuscita-tion Study Group. Resuscitation 1989;17 Suppl.: S99—109;discussion S199—206.
6. Buck-Barret I, Squire I. The use of basic life support skillsby hospital staff: what skills should be taught? Resuscitation
1
1
Conflict of interest
None of the authors have a conflict of interestrelated to this study.
Acknowledgements
We thank the nursing management of Ghent Uni-versity Hospital, the advanced life support train-ers and the emergency nurses who participatedin the study. O-Two Medical Technologies providedthe SB and STBVM for the duration of the study.We are indebted to Mitchell Baldwin from Michi-gan Instruments (Ontario, Canada) for providingthe CPR manikin and the CPRview software. This
2004;60:39—44.7. Kaye W, Mancini ME. Retention of cardiopulmonary resusci-
tation skills by physicians, registered nurses, and the generalpublic. Crit Care Med 1986;14(7):620—2.
8. Stone B, Chantler P, Baskett P. The incidence of regurgi-tation during cardiopulmonary resuscitation: a comparisonbetween the bag—valve—mask and the laryngeal mask air-way. Resuscitation 1998;38:3—6.
9. Walsh K, Loveday K, O’Rathaille M. A comparison of theeffectiveness of pre-hospital bag—valve—mask ventilationperformed by Irish emergency medical technicians andanaesthetists working in a tertiary referral teaching hospi-tal. IMJ 2003;96(3):77—9.
0. Wenzel V, Keller C, Idris A, et al. Effects of smaller tidalvolumes during basic life support ventilation in patients withrespiratory arrest: good ventilation, less risk? Rescusitation1999;43:25—9.
1. Wenzel V, Volker MD, Idris A, et al. Influence of tidal volumeon the distribution of gas between the lungs and stomach inthe nonintubated patient receiving positive-pressure venti-lation. Crit Care Med 1998;26(2):364—8.



















