
Resurgent Malaria at the Millennium Control Strategies in Crisis
26
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Public Health Resources Public Health Resources 2000 Resurgent Malaria at the Millennium Control Strategies in Crisis J. Kevin Baird Parasitic Diseases Program, US Naval Medical Research Unit No. 2, Jakarta, Indonesia, [email protected] Follow this and additional works at: hp://digitalcommons.unl.edu/publichealthresources is Article is brought to you for free and open access by the Public Health Resources at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in Public Health Resources by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. Baird, J. Kevin, "Resurgent Malaria at the Millennium Control Strategies in Crisis" (2000). Public Health Resources. 331. hp://digitalcommons.unl.edu/publichealthresources/331
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Resurgent Malaria at the Millennium Control Strategies in Crisis
University of Nebraska - LincolnDigitalCommons@University of Nebraska - Lincoln
Public Health Resources Public Health Resources
2000
Resurgent Malaria at the Millennium ControlStrategies in CrisisJ. Kevin BairdParasitic Diseases Program, US Naval Medical Research Unit No. 2, Jakarta, Indonesia, [email protected]
Follow this and additional works at: http://digitalcommons.unl.edu/publichealthresources
This Article is brought to you for free and open access by the Public Health Resources at DigitalCommons@University of Nebraska - Lincoln. It hasbeen accepted for inclusion in Public Health Resources by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln.
Baird, J. Kevin, "Resurgent Malaria at the Millennium Control Strategies in Crisis" (2000). Public Health Resources. 331.http://digitalcommons.unl.edu/publichealthresources/331
Resurgent Malaria at the MillenniumControl Strategies in Crisis
J. Kevin Baird
Parasitic Diseases Program, US Naval Medical Research Unit No. 2, Jakarta, Indonesia
Abstract Completion of the Panama Canal in 1914 marked the beginning of an era ofvector control that achieved conspicuous success against malaria. In 1955 theWorld Health Organization (WHO) adopted the controversial Global EradicationCampaign emphasising DDT (dichlorodiphenyltrichloroethane) spraying inhomes. The incidence of malaria fell sharply where the programme was imple-mented, but the strategy was not applied in holoendemic Africa. This, along withthe failure to achieve eradication in larger tropical regions, contributed to disil-lusionment with the policy. The World Health Assembly abandoned the eradica-tion strategy in 1969. A resurgence of malaria began at about that time and todayreaches into areas where eradication or control had been achieved. A global ma-laria crisis looms. In 1993 the WHO adopted a Global Malaria Control Strategythat placed priority in control of disease rather than infection. This formalises apolicy that emphasises diagnosis and treatment in a primary healthcare setting,while de-emphasising spraying of residual insecticides. The new policy explicitlystresses malaria in Africa, but expresses the intent to bring control programmesaround the world into line with the strategy.This review raises the argument that a global control strategy conceived to
address the extraordinary malaria situation in Africa may not be suitable else-where. The basis of argument lies in the accomplishments of the Global Eradica-tion Campaign viewed in an historical and geographical context. Resurgent malariaaccompanying declining vector control activities in Asia and the Americas sug-gests that the abandonment of residual spraying may be premature given the toolsnow at hand. The inadequacy of vector control as the primary instrument ofmalaria control in holoendemic Africa does not preclude its utility in Asia andthe Americas.
CURRENT OPINION Drugs 2000 Apr; 59 (4): 719-7430012-6667/00/0004-0719/$25.00/0
© Adis International Limited. All rights reserved.
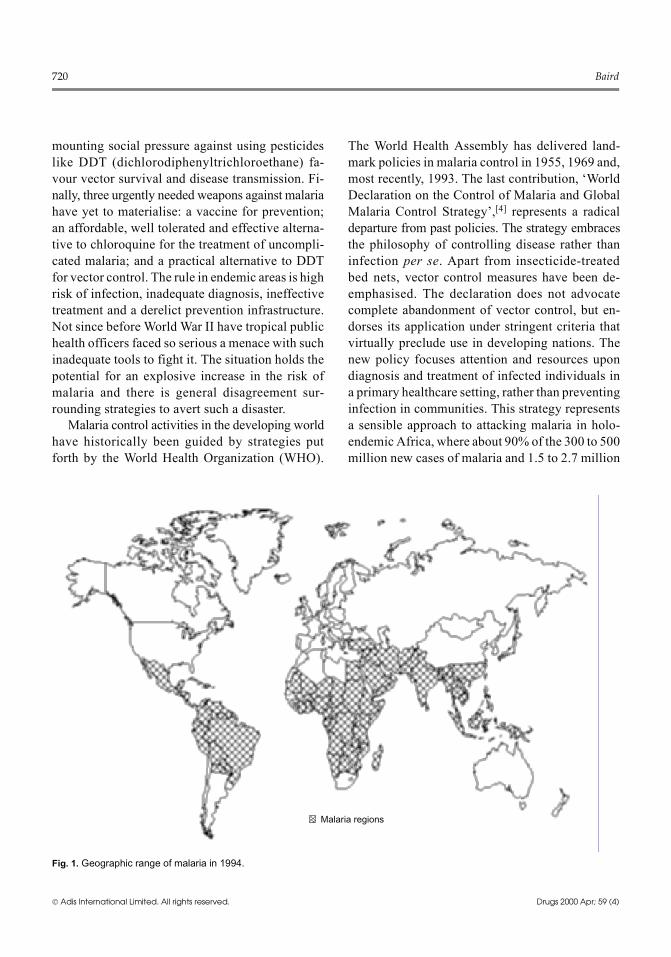
In 1955 the eradication of malaria seemed with-in reach.[1] Less than 50 years later malaria is re-surgent, causing an increasing number of infectionsacross an expanded geographic range (fig. 1).[2,3]Spreading resistance to available antimalarials hasrendered effective treatment increasingly difficultfor most people exposed to infection. In someareas, the possibility of untreatable multidrug-resistant malaria looms and economic realities in
many areas leave malaria essentially incurablewith the affordable antimalarials at hand. Parasitesurvival in the face of chemotherapeutic interven-tion is more likely than ever. In many areas, theability to perform a microscopic diagnosis of ma-laria has been lost with the retirement of a genera-tion of health workers trained during the heyday ofthe Global Eradication Campaign. Likewise, thedeterioration of vector control programmes and
proyster2
Text Box
This document is a U.S. government work and is not subject to copyright in the United States.
mounting social pressure against using pesticideslike DDT (dichlorodiphenyltrichloroethane) fa-vour vector survival and disease transmission. Fi-nally, three urgently needed weapons against malariahave yet to materialise: a vaccine for prevention;an affordable, well tolerated and effective alterna-tive to chloroquine for the treatment of uncompli-cated malaria; and a practical alternative to DDTfor vector control. The rule in endemic areas is highrisk of infection, inadequate diagnosis, ineffectivetreatment and a derelict prevention infrastructure.Not since before World War II have tropical publichealth officers faced so serious a menace with suchinadequate tools to fight it. The situation holds thepotential for an explosive increase in the risk ofmalaria and there is general disagreement sur-rounding strategies to avert such a disaster.Malaria control activities in the developing world
have historically been guided by strategies putforth by the World Health Organization (WHO).
The World Health Assembly has delivered land-mark policies in malaria control in 1955, 1969 and,most recently, 1993. The last contribution, ‘WorldDeclaration on the Control of Malaria and GlobalMalaria Control Strategy’,[4] represents a radicaldeparture from past policies. The strategy embracesthe philosophy of controlling disease rather thaninfection per se. Apart from insecticide-treatedbed nets, vector control measures have been de-emphasised. The declaration does not advocatecomplete abandonment of vector control, but en-dorses its application under stringent criteria thatvirtually preclude use in developing nations. Thenew policy focuses attention and resources upondiagnosis and treatment of infected individuals ina primary healthcare setting, rather than preventinginfection in communities. This strategy representsa sensible approach to attacking malaria in holo-endemic Africa, where about 90% of the 300 to 500million new cases of malaria and 1.5 to 2.7 million
Malaria regions
Fig. 1. Geographic range of malaria in 1994.
720 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

deaths occur each year.[5] However, the suitabilityof this explicitly African strategy for the rest of theworld has not been established. This is a critical issuebecause the resurgence of malaria most threatensendemic regions outside Africa.The debate over clinical- versus vector-based ap-
proaches to malaria control began soon after Ron-ald Ross identified anopheline mosquitoes as vec-tors in 1897. Ross’s vigorous advocacy of malariacontrol through attack on the mosquito sparkedcontroversy.[6] Completion of the Panama Canal in1914, made possible by controlling the vectors ofmalaria and yellow fever, vindicated Ross. Vectorcontrol came to dominate malaria control strategies,infrastructure and practice for the next 50 years.The most recent WHO policy represents a formaldeparture from that approach, essentially institut-ing the clinical approach to the control of malaria.However, no compelling body of work demonstratesthe utility of clinical management as the primaryinstrument of a broadly applied malaria control pro-gramme. The public health advantage gained througha focus on clinical management in lieu of vectorcontrol remains hypothetical. What explains thebroad advocacy of this approach? The history ofmalaria and its control in the 20th century offersinsights.This review examines the retreat and resurgence
of malaria in the 20th century. What has been doneto control malaria? What is being done? Whatshould be done? Discordant answers to the lastquestion in the community of malaria workers re-veal disagreement on strategies intended to bringmalaria under control. Clinical- versus vector-based control strategies form broad lines of divi-sion at the foundation of strategic thinking. Thisreview explores the basis of that division by exam-ining the global resurgence of malaria in an histor-ical and geographical context. The WHO’s 1993Global Malaria Control Strategy emerged from theperceived failure of its predecessor, the 1955 pol-icy that aimed for eradication. The earlier policywas neither applied to nor relevant to holoendemicmalaria in sub-Saharan Africa. The new policymaps out strategies that carry a distinctly African
point of view with respect to malaria as a publichealth issue. Therein lies the basis of discord: acontrol strategy conceived in an African contextmay not be globally applicable. Control of diseaserather than infection is sensible in holoendemicsub-Saharan Africa, where, by virtue of naturallyacquired immunity, each infection carries a rela-tively low risk of disease or death. Resources maybe focused on the minority at risk (infants, smallchildren and pregnant women). In Asia and theAmericas, however, each infection carries a rela-tively high risk of disease or death. Thus, late in-tervention in the clinical setting carries avoidablerisks, especially against a backdrop of the currentlypoor instruments of diagnosis and treatment. Con-trol of risk of infection by attacking the vector is asensible and, as the retreat of malaria earlier in thecentury demonstrated, practical approach.
1. Malaria in Retreat: 1904 to 1969
1.1 Malaria Revealed
An obscure French Army surgeon, AlphonseLaveran, ascertained the protozoan cause of ma-laria in 1880.[7] Leading malariologists of the dayinitially dismissed Laveran’s finding, instead cling-ing to the fashionable concept of a bacterial causeof malaria. Clinicians and scientists with access tomalaria patients and having ability with the micro-scope gradually affirmed Laveran. He received theNobel Prize in 1907. In 1897 Ronald Ross, then aBritish Indian Army medical officer, described theinfection of anopheline mosquitoes fed on para-sitaemic birds.[8] The prominent Italian malariolo-gists led by Grassi confirmed the findings of Rossin humans in 1899.[9] Ross received the NobelPrize in 1902. At the beginning of the 20th centurythe specific cause of malaria and its route of trans-mission was known with certainty.Ross advocated mosquito sanitation as the pri-
marymeans of controllingmalaria. During the 1900shis theories were tested in Senegal, Ghana andBurma,[6] with either limited success or none at all.Ross persisted in his advocacy of attacking the vec-tor and sparked acrimonious criticism from those
Resurgent Malaria at the Millennium 721
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

advocating an approach focused on clinical treat-ment with quinine as a means of malaria control.Former colleagues in the Indian Medical Service,such as SP James, criticised mosquito control, citingresults obtained in Mian Mir (Pakistan). James[10](as cited by Nye and Gibson[6]) stated publicly inthe presence of Ross, ‘I will only say that anti-malarialmeasures and mosquito-destruction measures arenot, and have never been synonymous terms ... suc-cess in such operations has often been reported onevidence that will not bear criticism and is oftenridiculous’. This point of viewwas justifiable at thetime. There had been no compelling demonstrationof the utility of vector sanitation to control malaria.The Panama Canal changed all of that. It firmlyestablished vector control as a sound basis for dis-ease control.
1.2 The Panama Canal
The construction of the PanamaCanal by theUSrepresented more than a triumph of engineering ge-nius, tenacity and national will. The historian Mc-Cullough[11] wrote, ‘[i]n the history of finance cap-italism, in the history of medicine, it was an eventof signal consequence’. The importance of the ac-complishment to medicine may be best appreciatedby understanding the failure that preceded it. In1881 France began an effort to construct a canalacross the Isthmus of Panama. France invested $287million and the country’s national prestige. Theproject seized the attention of the world. Ferdinandde Lesseps, the national hero of France and builderof the Suez Canal, headed the effort.In 1881 Pasteur’s germ theory of disease had
gained broad acceptance among educated people.Laveran’s description of plasmodia as the cause ofmalaria, reported in 1880, was still 10 years fromsimilar acceptance. Proof of mosquitoes as vectorsof malaria and yellow fever would wait another 15years. Through the 8 years of intense French effortin Panama, McCullough[11] writes, ‘[c]ompany doc-tors advised staying out of the hot sun and to avoidgetting wet. ... New arrivals were warned againstthe night air and were told not to eat fruit’. Mostpeople earnestly believed that virtuous living pro-
tected against diseases like malaria and yellow fe-ver. Medical science had little to offer the buildersof the canal and catastrophe ensued.McCullough[11] wrote of the chief engineer in
Panama, ‘Bunau-Varilla estimated that of everyone hundred new arrivals at least twenty died, andof those who survived, only twentywere physicallystrong enough to do any real work; "and many ofthat number had lost the best of their intellectualvalue." Others calculated that of every four peoplewho came out of France at least two, often three,died of fever’. A cemetery at Gold Hill near theCulebra Cut holds the graves of nearly a thousandFrenchmen,womenandchildren from that era.Manymore thousands of lives were lost, mostly labourersimported from Jamaica and other French colonies.Among a peak workforce of just under 20 000, ap-proximately 200 died each month. Even those re-ceiving the best possible food, housing andmedicalcare were vulnerable. The senior French engineerin Panama, Dingler, in late 1883 brought his wife,son, daughter and the daughter’s fiancé to Panama,and all but Dingler were dead of yellow fever bythe end of 1884.In 1889 the effort in Panama collapsed under the
weight of sickness and death. Investor confidencecrumbled when reliable reports of the catastrophereached France. The failure precipitated a nationalscandal that ultimately toppled the government anddisgraced national figures of the time: de Lesseps,Alexandre Gustave Eiffel and Georges Clemenceau.Tropical vector-borne diseases defeated the mostdetermined effort of one of the most scientificallyand economically accomplished nations of the day.On 15August 1914 the ocean steamerAncon tran-
sited the Panama Canal, 10 years after the Americansbegan construction. Perhaps the single most impor-tant difference between the French and Americanefforts was the certain knowledge in 1904 that spe-cific mosquitoes transmitted malaria and yellowfever. Colonel William Crawford Gorgas had beenwithWalter Reed in Cuba and supervised the attackon mosquitoes in Havana that eradicated yellowfever and virtually eliminated malaria from whathad been a city of very high risk. Gorgas arrived in
722 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

Panama at the outset of the effort in 1904, person-ally tasked by President Theodore Roosevelt withrepeating the Havana accomplishment in PanamaCity, Colon and the Canal Zone.[11] The success ofvector control during construction at Panama, un-ambiguously measured in the health and accom-plishment of a peak workforce of 45 000, provedthat a rational and methodical approach to mos-quito sanitation prevented otherwise crippling tropi-cal fevers. An important point from this history isthe success enjoyed without benefit of modern in-secticides or antimalarials. Attacking the specificbreeding sites of known vectors using crude imple-ments and the disciplined application of a work-force of just 4000 men, as well as minimising hu-man contact with mosquitoes by use of nets andscreens, permitted construction of a canal across60 miles of deadly jungle. The success of Gorgasin Panama, made possible by the research accom-plishments of Ross[8] and Reed et al.,[12] markedthe beginning of the retreat of malaria in the 20thcentury and it showed the way. The stage had beenset for the struggle against the vectors of malaria.
1.3 The Global Eradication Campaign
The three decades following the opening ofthe Panama Canal brought powerful new weaponsagainst malaria. The aniline dye industry in Ger-many had produced families of compounds thatcured malaria and a wide variety of chemicals thatkilled or repelled mosquitoes. An important suc-cess using modern larvicides and household spray-ing before the advent of DDTwas the complete erad-ication of Anopheles gambiae from Brazil. Thatmosquito is the extraordinarily efficient vector ofmalaria in most of Africa. This work in Brazil wassponsored by the Rockefeller Foundation and di-rected by Fred Soper. According to Packard,[13]‘Soper’s apparent achievements revalidated an ap-proach to disease control that relied on narrowlydefined technical interventions directed solely atactivities of the mosquito’. The significance of thisachievement may be appreciated by imagining theintensemalaria transmission of sub-SaharanAfricaoccurring through tropical South America. Soper’s
vector eradication activities over 60 years agospared millions of lives and perhaps the economicvitality of the continent.The strategic urgencies of World War II spurred
a determined effort to refine and field the newchemical weapons against malaria. The unpublishedrecord of the Board for Coordination of MalariaStudies (5 bound volumes, Washington, DC, 1943-1946) begins with, ‘[w]hen the supply of quininewas suddenly cut off by the Japanese invasion ofPearl Harbor in December of 1941, our Army, Navy,and Marines faced a deadly serious problem. A longwar in the most malaria-infested areas of the worldlay before them and they were deprived of their onlyreliable therapeutic weapon, quinine’. The experi-ences of military forces in the European, Africanand Pacific theatres of action justified these con-cerns.[14] The strategic importance of malaria as aserious threat to military forces, reinforced by Amer-ican experiences in Korea and Vietnam,[14] contin-ues to influence malaria research across a broadfront.Chloroquine and DDTwere used by the USmil-
itary by 1944, and within just a few years were inuse around the globe. These chemicals were inex-pensive, effective and well tolerated with a goodsafety profile. Chloroquine cured with relativelyfew doses and without the sometimes severe ad-verse effects of drugs like quinine or atebrine. Per-haps more importantly, the history of the develop-ment of chloroquine in Nazi Germany and itswartime seizure by the US precluded commercial-isation.[15] The drug was broadly affordable at thepeak of its efficacy. For DDT, a single applicationto the interior of a home provided protection againstfeeding anophelines through a transmission season.The stability of DDT allowed maximum coverageof households at minimal cost. The agricultural ap-plication of DDT came later, and poisoned the landand public opinion against it.The new weapons against malaria spawned ex-
uberant optimism. The title of the book written byone of the pre-eminent malariologists of themiddleof the century, Paul Russel,[16] ‘Man’s Mastery ofMalaria’, epitomises this spirit. The eradication of
Resurgent Malaria at the Millennium 723
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

malaria seemed feasible and the leading scientistsof the day anticipated it. An uninterrupted string ofextraordinary successes justified the optimism ofthat time. Malaria had been fully eradicated fromplaces where it had always been endemic. For ex-ample, the eradication of malaria from the US hadbeen accomplished, where in 1914 an estimated600 000 cases of malaria had occurred.[17] Faustand Debakey[18] wrote in 1941, ‘[i]t is true that re-ported malaria deaths for 1940 were the lowest onrecord, totaling 1346 for the entire South, or a rateof 3.02 per 100,000 population’. Just 59 years latereven this ebbing incidence of death, appearing ‘low’at the time, seems almost inconceivable. Such arate in the US southern states today would yieldmore than 5000 deaths annually. The memory ofmalaria as a major cause ofmorbidity andmortalityin the US has vanished, but the eradication of ma-laria in the 1950s justified confidence in the weap-ons that accomplished the feat.In May 1955 theWorld Health Assembly adopted
the Global Malaria Eradication Campaign. Thestrategy rested on the concept of interruption of trans-mission by vector control followed by an emphasison case detection and treatment. MacDonald[19]had demonstrated mathematically the feasibility ofthis approach to eradication. The United StatesAgency for International Development (USAID)played a major supporting role around the globe interms of fiscal resources and technical guidance.[20]The accomplishment of reduced or eliminated riskof infection, virtually everywhere except holoen-demic Africa, was astonishing (fig. 2). Malaria dis-appeared from the US, Japan, Korea, Taiwan, Spain,Italy, the Balkans, Greece and northern Africa, re-gions that had been seasonally malarious throughhistory. Successes even occurred in the tropics.Malaria was eradicated across vast stretches of theSouth Pacific, including the tropical northern tierof Australia. Malaria disappeared from the Greaterand Lesser Antilles archipelagos, with the excep-tion of the island of Hispaniola (Haiti and Domi-nica). The significance of this accomplishmentmay be appreciated by British military statisticsfrom the Caribbean region for the period 1895 to
1904; 104.2 malaria admissions to hospital with1.42 deaths per 1000 European troops per year, and120 admissions and 2.5 deaths per 1000 West In-dian troops per year.[24]Success was not limited to eradication per se.
Malaria was brought under control across vast tropi-cal zones where meso-, hyper- and holoendemic ma-laria had always prevailed. On Java, an island over600 miles in length and home to almost 100 millionpeople, widespread hyper- and holoendemic ma-laria was rolled back to a few hypoendemic fociand occasional outbreaks at scattered locations.[23]The US International Cooperation Administration(the predecessor of USAID) in collaboration withWHO and the fledgling Republic of Indonesia be-gan DDT spraying campaigns in Java and else-where in 1951. In Central Java the slide positiverate fell from 24% to less than 1% between 1953and 1959.[23] Todaymalaria transmission rarely oc-curs in East and West Java, and fewer than a dozenhypoendemic foci persist in Central Java.[25] DDTspraying campaigns inMadagascar during the 1950s
1
10
100
1000
10 000
100 000
1 000 000
10 000 000
100 000 000
Rep
orte
d ca
ses
1940 1950 1960 1970
Year
TaiwanVenezuelaMauritiusBulgariaItalyRomaniaSpainTurkeyYugoslaviaSri LankaIndiaIndonesia
Fig. 2. The retreat of malaria between 1937 and 1969 (adaptedfrom data reported by Jukes,[21] Sharma[22] and Atmosoed-jono[23]).
724 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

pushed malaria transmission to vanishingly lowlevels on the vast central highland plateau.[3,26] InSri Lanka, the number of cases fell from over 2 mil-lion in 1946 to less than 100 in 1963.[21] In Guyana,George Giglioli supervised a DDT spraying cam-paign between 1947 and 1951 that eliminated ma-laria transmission from the heavily populated coastalarea.[27] Figure 2 illustrates data reported by Jukes[21]and other sources revealing the sharp decline inreported malaria between 1937 and 1969.Perhaps the most compelling successes of the
Global EradicationCampaign, by virtue of the daunt-ing scale of geography and human population,were Brazil and India. Brazil during the 1950s had5 million cases each year and by 1960 the numberof cases fell to just 50 000.[28] In India before 1945an estimated 75 million new cases occurred eachyear, with 800 000 deaths.[22] Out of a total popu-lation of 466 million people in 1965, 373 millionhad been freed of risk of malaria.[29] Eradicationhad been achieved in 56% of the population by 1968and only 10% remained in the DDT attack phase.In 1964 the annual parasite index (number of casesper 1000 population) was 0.00098, or roughly 1case of malaria among 1 million people.[22] Thebreathtaking success of the India story is recordedin the fact that no deaths caused by malaria wererecorded in 1968. The lives of nearly a million peo-ple each year had been spared and DDT sprayinglargely accounted for the accomplishment.In a retrospective view that includes the current
resurgence of malaria, the gain made against ma-laria during the period 1945 to 1965 stands out asan astonishing success by almost anymeasure. Thedegree of success appears all the more remarkablein view of the fact that few international agenciestook the campaign seriously enough to offer sub-stantial support. According to Packard,[30] ‘[m]anyhealth authorities, both within and outside the As-sembly, [WHO] viewed eradication as at best foolhardy, and at worst, potentially disastrous’. TheUSAID embraced the strategy and contributed$1.2 billion between 1950 and 1972.[20] In contrast,the WHO put up $20.3 million between 1956 and1963, and $17.5 million of that was contributed by
the US. Only $2.8 million was donated for the ef-fort by all other nations combined.[29] The GlobalEradication Campaign was, in a fiscal sense, a uni-lateral initiative of the US. Other leading developednations largely rejected the campaign. France andthe UK, with general accord among governmentsin Africa, stand out as examples.[29] The primary‘failure’ of the Global Eradication Campaign mayhave been political rather than operational or tech-nical. If one retrospectively supplants the unrealis-tic goal of eradication with one of control, the cam-paign appears brilliantly successful. Unfortunately,the value of the campaign has been measured inlarge part by its failure to actually eradicatemalariain much of the tropics, or to affect malaria inholoendemic Africa, where it was never applied.
1.4 Legacy of the Global Eradication Campaign
Unabated intense transmission in holoendemicAfrica contributed substantially to disillusionmentwith the Global Eradication Campaign. Ironically,the abatement of malaria almost everywhere elserendered the lack of progress in Africa especiallyconspicuous. Today, in the long shadow of the‘failure’ of eradication, global policy makers havefocuseduponholoendemicAfrica.Authoritativestra-tegic thinking in malaria control carries a distinctlyAfrican frame of reference. The emphasis on Af-rica in the World Declaration on the Control ofMalaria and Global Malaria Control Strategy is ex-plicit. According to Trigg and Kondrachine,[29] thedocument has been ‘confirmed by the World HealthAssembly in 1993, and by both the Forty-ninthSession of the United Nations General Assemblyand the Thirty-third Ordinary Session of the As-sembly of Heads of State and Government of theOrganisation of African Unity in 1994 and 1997,respectively’. Trigg and Kondrachine[29] summa-rise by writing, ‘[t]he strategy calls for disease-rather than parasite-oriented control programmes.... The strategy is firmly rooted in the primaryhealthcare approach ...’. This global strategy aimsto diminish disease caused by malaria through de-veloping effective diagnosis and treatment through
Resurgent Malaria at the Millennium 725
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

a primary healthcare instrument. The details of ap-proach and the emphasis on Africa following thisstrategy may be found in the Multilateral InitiativeagainstMalaria in Africa and theRoll BackMalariacampaign. The WHO has emphasised the applica-tion of this strategy with priority given to the cre-ation of national malaria control programmes insub-Saharan Africa, and the ‘reorienting’ of exist-ing programmes in the rest of the world, ‘in linewith the principles of the global strategy’.[29]The rationale for the new WHO policy lies in
the epidemiology of disease and death caused bymalaria in holoendemic Africa. The risk of severeanaemia and cerebral malaria in infants, very youngchildren and pregnant women, especially primi-gravidae, is extraordinarily high in holoendemicAfrica. In contrast, older children and adults havelittle or no risk of disease despite virtually every-one being infected at least several times per year.Thus, abatement of severe anaemia and cerebral ma-laria among infants, young children and pregnantwomen lies at the core of strategic thinking in theGlobalMalaria Control Strategy. Improved clinicalmanagement of disease and protection measuresdirected at this narrow segment of the populationconstitute the basis of measures intended to reducethe burden of death and disease caused by malaria.The distinct epidemiology of disease and death
caused by malaria outside Africa bears consider-ation in formulating and accepting control strate-gies. In Asia and the Americas the risk of infectionis relatively low, but the risk of disease or deathwith infection is relatively high. This represents theconverse of the African scenario. Should interven-tion against low risk of infection and high risk ofdisease or death be deferred to the point of disease?Moreover, risk of disease and death is not focusedupon a narrow segment of the population. The bear-ing of resources intended to intervene against dis-ease and death may thus be expected to be corre-spondingly diffused and less efficacious. Finally,the focus onmalaria control in holoendemicAfrica,driven by the fact that most malaria now occursthere, defers engagement of the threat of resurgentmalaria. Malaria in other regions, largely the entire
length of southern Asia and Central and SouthAmerica, accounts almost entirely for the ‘global’resurgence of malaria. In contrast, malaria in mostof sub-SaharanAfrica is hyper- to holoendemic andhas been that way through history. Although in-creasing resistance to antimalarials threatens higherrisk of severe disease and death (in infants, youngchildren and pregnant women),[31] the absolutenumber of infections and the geographic range ofmalaria in holoendemic Africa remain stable. Ad-dressing the spreading geographic range and in-creasing incidence of malaria outside Africa mayrequire the development of intervention strategiesaimed at reducing risk of infection rather than dis-ease with infection.
2. Malaria in Resurgence: 1970 to Today
The resurgence of malaria that has occurredsince the late 1960s is generally acknowledged.According to Campbell,[32] ‘... there has been a dra-matic, worldwide increase in malaria-related ill-ness and death over the past two decades’. Accord-ing to Kondrachine and Trigg,[33] ‘[a]n increasingnumber of malaria epidemics has been documentedthroughout the world’. According to the Instituteof Medicine of the National Academy of Sci-ences,[34] ‘[m]alaria which had been eliminated oreffectively suppressed in many parts of the world,is undergoing a resurgence’. Incidence of clinicaldisease caused bymalaria has increased in endemicareas, and malaria has encroached into areas con-sidered free of risk for several decades.Even in the US, recent outbreaks of malaria have
occurred inCalifornia, Texas,NewJersey,NewYork,Michigan, Virginia and Florida[17] (unpublisheddata). Competent anopheline vectors are seasonallyabundant in North America, and repatriated travel-lers to or migrants from endemic areas carrying ga-metocytes may infect these mosquito populations.However, imported malaria accounts for the vastmajority of reported cases in the US. During the1960s and 1970s fewer than 50 cases of malariawere reported in US civilians. This number hasclimbed steadily to over 500 per year at present,
726 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)
and the number of actual cases is estimated to be 2to 3 times higher.[35]Increasingly frequent travel to and from the trop-
ics partly explains such statistics, but these trendsnonetheless reflect an overall greater risk of infec-tion. An enduring cycle of transmission in the USor Europe leading to endemic malaria is highly un-likely because the level of healthcare available toalmost all people virtually precludes the possibilityof permanent infectious pools of carriers. Never-theless, migration from endemic zones into sub-tropical and temperate areas lacking the higheststandards of medical care indeed threatens the rein-troduction of endemic malaria. Once re-established,the control or eradication of endemic malaria mayprove monumentally difficult in the absence of in-struments of control like chloroquine and DDT.Clear evidence of the global resurgence of ma-
laria emerges piecemeal from many sources, mostlyWHO surveillance statistics. Although some coun-tries still report relatively stable or declining ma-laria (e.g. Colombia, Ecuador, Mexico, Nepal,Bhutan, Thailand, Oman and Saudi Arabia[36,37]),encroachment and resurgence appears to be therule. Malaria had been eradicated from Armenia,Azerbaijan and Tadjikistan in the 1960s, and onlyabout 200 annual cases were recorded in the yearsbefore 1994, when suddenly over 3000 cases werereported.[37] Falciparum malaria has reappeared inTadjikistan for the first time in 35 years.[37] An es-timated 2 to 3 million annual cases of malaria nowoccur in Afghanistan.[36] There were 8700 cases ofvivax malaria in Turkey in 1990, and 84 345 casesin 1994.[37] In Iraq 3400 cases were reported in1989 compared with 98 222 cases in 1994.[36] Syriahas had increasing numbers of vivax malaria casessince the 1980s.[36]South Korea has seen a logarithmic increase in
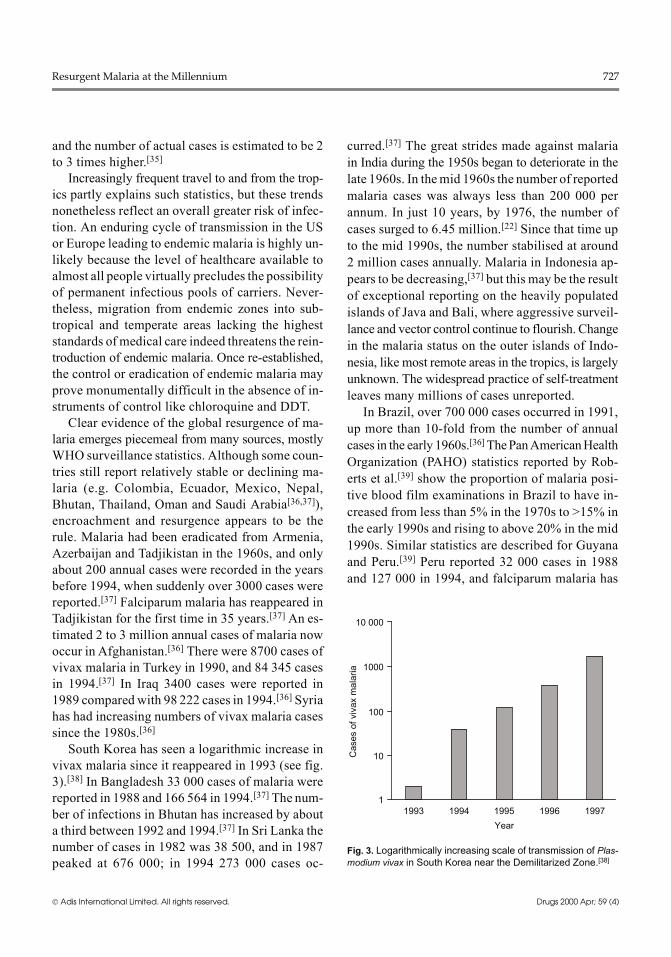
vivax malaria since it reappeared in 1993 (see fig.3).[38] In Bangladesh 33 000 cases of malaria werereported in 1988 and 166 564 in 1994.[37] The num-ber of infections in Bhutan has increased by abouta third between 1992 and 1994.[37] In Sri Lanka thenumber of cases in 1982 was 38 500, and in 1987peaked at 676 000; in 1994 273 000 cases oc-
curred.[37] The great strides made against malariain India during the 1950s began to deteriorate in thelate 1960s. In themid 1960s the number of reportedmalaria cases was always less than 200 000 perannum. In just 10 years, by 1976, the number ofcases surged to 6.45 million.[22] Since that time upto the mid 1990s, the number stabilised at around2 million cases annually. Malaria in Indonesia ap-pears to be decreasing,[37] but this may be the resultof exceptional reporting on the heavily populatedislands of Java and Bali, where aggressive surveil-lance and vector control continue to flourish. Changein the malaria status on the outer islands of Indo-nesia, like most remote areas in the tropics, is largelyunknown. The widespread practice of self-treatmentleaves many millions of cases unreported.In Brazil, over 700 000 cases occurred in 1991,
up more than 10-fold from the number of annualcases in the early 1960s.[36] ThePanAmericanHealthOrganization (PAHO) statistics reported by Rob-erts et al.[39] show the proportion of malaria posi-tive blood film examinations in Brazil to have in-creased from less than 5% in the 1970s to >15% inthe early 1990s and rising to above 20% in the mid1990s. Similar statistics are described for Guyanaand Peru.[39] Peru reported 32 000 cases in 1988and 127 000 in 1994, and falciparum malaria has
1
10
100
1000
10 000
Cas
es o
f viv
ax m
alar
ia
1993 1994 1995 1996 1997
Year
Fig. 3. Logarithmically increasing scale of transmission of Plas-modium vivax in South Korea near the Demilitarized Zone.[38]
Resurgent Malaria at the Millennium 727
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

re-emerged.[37] Reported malaria cases in Belizeincreased 3-fold between 1991 and 1994 (to 9957cases).[37]During the early 1970s the number of reported
malaria cases in South Africa totalled less than2000, whereas in 1993 and 1994 over 13 000 and10 000 cases, respectively, were reported.[40] InMadagascar, malaria suddenly reappeared in epi-demic fashion in 1987, quickly re-establishedhyperendemicity and remains so today.[41] High-land areas of Kenya have recently experienced anincreasing number of epidemics of malaria.[42]Djibouti and Somalia have also experienced sharpincreases in malaria rates in the wake of the disrup-tion of social services by war.[36]In the patchwork of data collected from many
sources and by as many means, an unmistakabletrend toward deterioration of the malaria situationemerges. Most of the available global data are atleast 5 years old and there is little reason to expectthat newer data will reveal anything but further de-terioration. Malaria is spreading at an alarmingrate, with more sharply rising numbers of cases inendemic areas, and encroachment into areas whereit had been nearly or completely eradicated. Theresurgence does not extend to the holoendemicareas of Africa for the simple reasons that its mea-sure in incidence normally resides at ceiling valuesand its geographic range has never retreated.
3. What Explains the Resurgence of Malaria?
Many factors account for the global resurgenceof malaria. The hierarchy of importance for thesefactors varies across a wide array of conditions.Political, social and economic forces may be espe-cially difficult to sort out and often profoundly in-fluence the risk of infection. The social upheavalof war in the tropics often provokes epidemic ma-laria. Likewise, region-specific physical and mete-orological factors create isolated outbreaks, e.g.unusually heavy monsoons causing epidemic ma-laria in Rajasthan during 1994,[43] and epidemicmalaria in the highlands of Irian Jaya, Indonesiaduring the El Nino weather anomalies (MJ Bangs
andMinistry of Health, Republic of Indonesia, per-sonal communications). Credible evidence sug-gests that global warming may be responsible foroutbreaks of malaria at higher elevations.[44] Theavailability of healthcare and its quality also influ-ence risk, as does the capacity to conduct sustain-able vector control activities.This review does not attempt a universal scope
of factors that may have contributed to the resur-gence of malaria. Instead, the analysis presentedhere accepts the premise that the increased risk ofmalaria relates to changes in key factors that broughtabout the global retreat of malaria. In that contextchloroquine treatment and DDT spraying standprominently as signposts to a broader explanation.These two substances played dominant roles againstmalaria between 1945 and 1965. The emergence ofresistance to chloroquine and the deterioration ofthe national programmes that applied DDT havebeen coincident with the resurgence of malaria. Abroad basis of evidence at least supports the viewthat these factors may be linked in a cause and ef-fect relationship. In any event, examination of thesefactors is useful because treatment and preventiondominate aspects of public health policies for thecontrol of malaria. Thus, examining the loss ofchloroquine to resistance and the sharp decline inDDT spraying may help the development of a ra-tionale for alternative strategies.
3.1 Resistance to Chloroquine
The emergence of resistance to chloroquine prob-ably represents the single most important factorcontributing to the global resurgence of malaria.Chloroquine now fails to cure most infections ac-quired in most endemic areas. The current impor-tance of chloroquine for the treatment of malariamay be difficult to grasp given its inferior thera-peutic properties compared with other standard an-timalarials. The generally sustained efficacy ofquinine and the availability of antimalarials suchas mefloquine and halofantrine seem to offer suit-able alternatives to chloroquine. The key to under-standing why that is not true for almost all of thepeople exposed to malaria may be found in the so-
728 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

cial and economic setting of the impoverished ruraltropics.Chloroquine remains widely used in the tropics
despite its inability to achieve cure (chloroquinesensitivity persists only in Central America, theCaribbean and parts of the Middle East). Peopleliving in rural areas with severely limited financialresources represent the vast majority of new ma-laria infections each year. In these areas chloroquineis sold over the counter at low cost. Most people inthe rural tropics do not have routine access to ahealthcare provider and treat themselves withoutbenefit of medical evaluation and counsel. In thiscontext the relatively infrequent use of quinine orother effective antimalarials may be understood.Most people taking quinine experience a range ofmildly to severely unpleasant adverse effects suchas tinnitus, vertigo and nausea lasting through the5 to 10 days of several daily doses. These adverseeffects often obscure the recovery from malaria.The punishing treatment costs about $5.00 (about1 day of wages) for the 20 to 30 tablets, and fewmanage the good compliance necessary for cure.In contrast, a regimen of chloroquine usually costsmuch less than $1.00 for the 5 to 10 tablets (oftenabout $US0.20), and the patient almost alwaysfeels better within 24 hours, with nearly completeclinical recovery after 72 hours. In Indonesia, vir-tually all patients experienced clinical recovery,even where the risk of RIII resistance was rela-tively high.[45] This was also true in Guyana, SouthAmerica (JK Baird & T Tiwari, unpublished data).The high risk of recurrent parasitaemia with chlor-oquine therapy must be weighed against that withinadequate compliance to quinine and the likeli-hood of reinfection within the month or two fol-lowing treatment. The self-treating poor of the ru-ral tropics will opt for more rapid recovery at lowercost, even if incomplete and with a high risk ofrecurrence. Most chloroquine users fail to appreci-ate that inadequate treatment contributes to the riskof infection among their family members andneighbours.In addition to poor therapeutic performance,
other characteristics of chloroquine account for the
heightened risk to the community in the face ofresistance. Chloroquine lingers in the bloodstreamlong after treatment. One month after a peak con-centration of about 1200 μg/L on day 2 of standardtherapy, concentrations averaging about 100 μg/Lwhole blood remain.[46] Chloroquine treatment hasno inhibitory effect on the infectivity of Plasmo-dium falciparum gametocytes to anopheline mos-quitoes. Chloroquine actually enhanced infectivityto anophelines relative to treatment with pyrimeth-amine/sulfadoxine in humans.[47] Aperson treatinga chloroquine-resistant infection with chloroquinewill (1) feel better quickly at relatively low cost,(2) maintain an asymptomatic parasitaemia forseveral weeks or more, (3) cull out chloroquine-sensitive parasites, leaving resistant trophozoitesto differentiate to gametocytes, and (4) remain in-fectious to anopheline mosquitoes. Chloroquinecreates the potential for large pools of asymptom-atic carriers of drug-resistant strains that readily in-fect mosquitoes.Chloroquine use in the face of resistance pro-
motes transmission. Effectively communicating thisproblem to lay chloroquine users may be very diffi-cult. Solving these problems may require supplant-ing chloroquine with a safely self-administereddrug that costs less and works better. The technicaland economic difficulty of doing so has proven oner-ous. There is no drug now available that approachesthe utility of chloroquine at the zenith of its effi-cacy, nor is one foreseen. The failure to develop analternative to chloroquine for people living in therural tropics virtually assures the longevity of theuse of this drug and the problems it engenders.Resistance to chloroquine byPlasmodium vivax
was first confirmed in 1989 from Papua NewGuinea.[48] It has since been documented in Indo-nesia, Myanmar, India and Guyana.[49-53] On thenorthern coast of Irian Jaya (Indonesian NewGuinea), half of the dozens of patients evaluatedwere again parasitaemic 14 days after receiving su-pervised chloroquine therapy.[50,54] Most patientsseeking treatment for confirmed vivax malaria atclinic in the same area already had ordinarily cura-tive concentrations of chloroquine in their blood.[55]
Resurgent Malaria at the Millennium 729
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)
In that region, one of the few adequately studied,resistance to chloroquine accounts for most clinicalvivax malaria. This problem poses a very seriousthreat to public health wherever vivax malaria oc-curs. The potential loss of chloroquine to resistanceby P. vivax in Asia and the Americas would almostcertainly exacerbate the resurgence of malaria al-ready occurring in those regions.
3.2 Repudiation of DDT and theDeterioration of Vector Control Programmes
In the public consciousness, DDT represents anicon of the capacity of technology to do harm. Thispesticide conjures the spectre of environmental de-struction and damaged health. This view fails tomakethe key conceptual separation of crop pest controlfrom the spraying of interior walls in homes to con-trol vectors of human disease.DDT applied to the interior of homes differs rad-
ically in terms of quantities and environmentalconsequence from DDT applied to large tracts ofarable, well drained land. In 1971, the year beforethe US banned the agricultural application of DDT,71million kilograms were sprayed in the US alone.This dusting of an appreciable portion of the USoccurred every year for more than 20 years. Therelative stability of DDT in the environment and itshigh affinity for fatty tissues established a markedbioaccumulation, notably in several raptor birdspecies, including the American bald eagle.[21] Themost serious adverse effect to human health wasreported in a study suggesting a link between DDTconcentrations in human adipose tissue and risk ofbreast cancer,[56] but definitive studies invalidatedthat association.[57-59] According to the 1991 Insti-tute of Medicine report on malaria,[60] DDT ‘re-mains one of the most effective insecticides for ma-laria control efforts in endemic countries. Comparedwith other available insecticides, it is inexpensiveand, importantly, is nontoxic to humans’. The re-port continues, ‘the use of DDT as a residual indoorspray does not introduceDDT into the environmentin amounts sufficient to enter the food chain, andthus this usage does not have adverse ecologicalconsequences’. It is difficult to reconcile the almost
complete retraction of DDT from strategic thinkingon malaria control with the sentiment expressed inthat report.Social pressure not to apply DDT, sometimes
extreme, comes from international aid agenciesand from non-governmental environmental groupsthat equate synthetic insecticide use with destruc-tion of the environment. According to Sharp and leSueur,[40] ‘[s]ocial attitudes against the use of DDThave increased to the degree that certain interna-tional research funding agencies will no longerfund research in any way associated with DDT’.Cursory inspection of funding opportunities froma wide variety of agencies engaged in malaria re-search bears out that sentiment. In the context ofmainstream scientific endeavour in the interest ofpublic health in the tropics, DDT appears to havebeen eliminated as a topic, except for explorationof harmful effects. Most informed people agreethat DDT creates risks to health and habitat, butdebate surrounds estimation of the risk-to-benefitratio that weighs the burden of vector-borne infec-tious diseases.The general repudiation of DDT spraying, to-
gether with the shift in policy away from sprayingstrategies, has contributed substantially to the de-terioration of vector control programmes in the de-veloping world. Trigg and Kondrachine[29] attrib-uted the resurgence in malaria during the 1980s and1990s in part to the reluctance of governments tomove away from ‘practices used during the eradi-cation era’, including the spraying of residual in-secticides such as DDT. The authors stressed inap-propriate application of DDT in this context, butthe assertion emphasises the extent to which au-thoritative agencies have turned away from vectorcontrol as a viable instrument of controlling infec-tion. The WHO has recently launched two impor-tant initiatives representing concrete steps towardimplementing the 1993 declaration of a new globalmalaria control strategy. The Roll Back Malariacampaign (WHO, UNICEF, UNDP and the WorldBank) lists objectives that do not include vectorcontrol activities beyond insecticide-treated bednets.[61] The Multilateral Initiative for Malaria also
730 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)
fails to address vector control issues outside Af-rica. Diminishing reliance on insecticide sprayingcampaigns as an instrument of control has beendescribed in the context of ‘progress’ in control bytheWHO.[62] TheWHOdoes not stand alone in thisposition. Many other leading agencies have ac-tively and passively discouraged national malariacontrol policies that focus on the spraying of insec-ticides, especially DDT. The decline to collapse ofvector control programmes, which has already oc-curred in many tropical nations, should be antici-pated in this social and political milieu.Apart from social pressures and the charac-
terisation of the spraying campaigns of the 1950sand 1960s as a failure, what accounts for the reluc-tance to sustain a commitment to residual sprayingprogrammes as an instrument of control? Some au-thorities obviously believe the clinical approachwill better control disease in the community, or thatresistance to DDT has rendered it ineffective as aninstrument of control. Many authorities argue thatvector control has not proven sustainable in devel-
oping nations. Compelling evidence to support theseviews is lacking. The best available evidence indi-cates that declining vector control, along with in-adequate treatment and diagnosis, may be drivingthe resurgence of malaria outside holoendemic Af-rica.
3.3 Vector Control Activity and MalariaAttack Rates
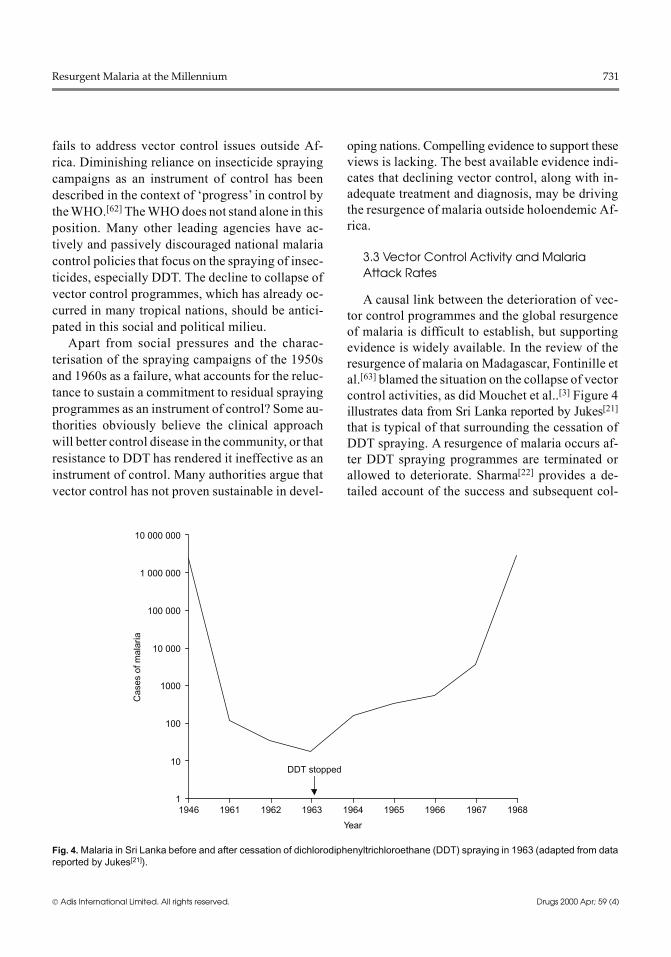
A causal link between the deterioration of vec-tor control programmes and the global resurgenceof malaria is difficult to establish, but supportingevidence is widely available. In the review of theresurgence of malaria on Madagascar, Fontinille etal.[63] blamed the situation on the collapse of vectorcontrol activities, as did Mouchet et al..[3] Figure 4illustrates data from Sri Lanka reported by Jukes[21]that is typical of that surrounding the cessation ofDDT spraying. A resurgence of malaria occurs af-ter DDT spraying programmes are terminated orallowed to deteriorate. Sharma[22] provides a de-tailed account of the success and subsequent col-
1
10
100
1000
10 000
100 000
1 000 000
10 000 000
1946 1961 1962 1963 1964 1965 1966 1967 1968
Cas
es o
f mal
aria
Year
DDT stopped
Fig. 4. Malaria in Sri Lanka before and after cessation of dichlorodiphenyltrichloroethane (DDT) spraying in 1963 (adapted from datareported by Jukes[21]).
Resurgent Malaria at the Millennium 731
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

lapse of malaria control in India during the 1960sand 1970s. This extraordinary history provides aglimpse at the complexities and operational diffi-culties of a large nationalmalaria control programme.Sharma listed shortages of DDT and other opera-tional setbacks among the major factors behind theresurgence of malaria in India. He conceded thatvector resistance to DDT may have contributed, butpointed out that most important vectors in Indiafailed to develop resistance to DDT, and malariacarried by those species also resurged, ‘with equalvengeance’. Sharma noted sharp reductions in spray-ing activities as a permanent feature of control ac-tivities during 1992 to 1994, that ‘... produced arapid deterioration in the malaria situation’.An analysis by Roberts et al.[39] described an
inverse relationship between declining DDT housespray rates and rising standardised annual parasiteindex, using data from nations in the Americas be-tween 1959 and 1995 reported by PAHO. Increas-ing infection rates accompanied proportionately di-minishing house spray rates. Correlation does notprove causality, but the analysis begs an explana-tion. Likewise, the view that shifting malaria con-trol activities to diagnosis and treatment improvesthe malaria situation also demands proof. Unlikethe launch of vector control with the accomplish-ments of Gorgas in Panama and Soper in Brazil,there has been no compelling demonstration of theeffectiveness of the strategy for control in the pri-mary healthcare setting. Available data offer littleas a basis for confidence. For example, during a 5-year study at Antioquia, Colombia, the annual bloodexamination rate (ABER) increased from 17% to82% (reflecting a shift in emphasis), while the an-nual parasite index (API, cases per 1000 people atrisk) increased from 38 to 87.[64] This may be anartifact of more aggressive case detection, but theapproach demands vindication in data demonstrat-ing diminished risk of infection in communitieswhere it is applied. PAHO recently attributed a63% reduction in the P. falciparum crude mortalityrate (from 8.3 deaths/100 000 exposed in 1994 to3.0 in 1998) in the Americas to ‘Implementation ofthe GMCS [Global Malaria Control Strategy] in
the Region ...’, i.e. case detection and treatment.[65]However, the 307 deaths reported in 1998 werebased on preliminary data, and the accuracy of suchstatistics may vary to such an extent as to rendersuch comparisons unreliable. Advocates of controlbased on clinical interventions in lieu of vectorcontrol should execute and publish the results ofstudies designed to test the hypotheses relevant tothis issue. Such work may serve as a basis formeaningful deliberation of the issue in the scien-tific literature.
3.4 Vector Resistance to DDT and Resurgent Malaria
Resistance to DDT by anopheline vectors hasbeen widely cited as an important factor contribut-ing to the global resurgence of malaria. However,the available data fail to support that view. Nostudy has unequivocally linked DDT resistance toan increase in malaria attack rates. Brogdon andMcAllister[66] write, ‘careful scrutiny of current in-formation about vector resistance shows that the fulleffect of resistance on control efforts is not known’.The lack of evidence on this question raises thepossibility that DDT resistance has little effect oncontrol activities. Indeed, one hypothesis suggeststhat physiological resistance is of little or no con-sequence to control, and that so-called ‘behavioralresistance’ may actually enhance the performanceof DDT as an instrument of prevention.This concept was explained by Roberts and An-
dre.[67] Physiological or biochemical resistance isgauged by mortality, whereas behavioural resis-tance is a function of excito-repellency. Mosqui-toes may develop resistance to insecticides eitherby adapting behaviours that remove them fromcontact or by becoming repelled at the scent. Theprotective effects of DDT may rely upon repel-lency rather than mortality, i.e. simply reducing thelikelihood of contact between humans and mosqui-toes without necessarily killingmosquitoes.Wherethis is true, the importance of behavioural resis-tance supersedes that of resistance to killing (asmeasured in standardised tests for insecticide resis-tance), and may promote protection conferred by
732 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

DDT spraying in homes. This was the finding inthe exhaustive studies reported by Bangs.[68] It isremarkable that more than 50 years after the launchof DDT spraying on amassive scale, little is knownof how the insecticide actually works. This reflectsone of the true failures of the Global EradicationCampaign; its neglect of research as a necessarycomplement to operations left important questionsunanswered.
3.5 Social Momentum for the Elimination of DDT
A global ban on DDT production is being pur-sued by a number of organisations dedicated toprotecting the environment from human activities.TheWorldWildlife Fund has announced a strategicplan for accomplishing the global ban on DDT bythe year 2007.[69] TheUnitedNations Environmen-tal Programme (UNEP) appears to be the most likelyinstrument of such a ban. The argument presentedin this review is that DDT has been an extraordi-narily useful tool against malaria. The best availabledata suggest that DDT indoor spraying remains ef-fective and does not harm the environment or hu-man health, and authoritative sources have sup-ported this view.[60] On the other hand, leadinginternational agencies actively discourage DDTspraying campaigns. This contradiction largelycaptures the schism that exists in the communityof malaria workers. Residual DDT spraying as amethod of controlling malaria has been repudiatedby those believing a better approach is possible.Others perceive the failure to apply DDT in theface of a global malaria crisis as irresponsible inthe absence of proven or practical alternatives.Social pressure against DDT is immense. Many
communities in the tropics would almost certainlyreject its use in their homes. It seems likely, how-ever, that the decision would hinge upon the sever-ity of malaria in the community. The suddennessand cross-sectional attack of epidemic malaria ter-rifies. Stricken communities may embrace almostanymeasure of protection in the faceof such a seriousand immediate threat. The resurgence of malariaaround the globe allows a reasonable forecast of
more and more epidemics. Many millions of peo-ple with severely limited resources face a rapidlygrowing risk of epidemic malaria. What tools willbe brought to bear on the problem? If a global banon DDT production is realised, that tool vanishes.Tacit approval of the ban on DDT by the commu-nity of science, and the encouragement to disman-tle the infrastructure of residual insecticide spray-ing programmes, comes with a very heavy burdenof responsibility to the people facing resurgent ma-laria.
4. Regaining Control of Malaria
The global resurgence in malaria followed a gen-eral breakdown in malaria control programmes.The basis of failure has been attributed to the re-luctance to reorient away from vector control andtoward diagnosis and treatment,[29] whereas othersattribute it to deteriorating vector control activi-ties.[39] These opposing views may be reconciledthrough conceptual separation of malaria in Africafrom the rest of the world. Controlling malariamorbidity and mortality through emphasis on di-agnosis and treatment in a primary healthcare set-ting is a sensible approach in holoendemic Africabut not necessarily elsewhere. In Asia and the Amer-icas, where malaria is resurgent, the best availableevidence argues for control activities focused onthe vector, using residual repellent insecticides indwellings. There should be fundamentally distinctstrategies for Africa versus elsewhere, but in bothsettings poor people treating their infections needaffordable drugs that work well and safely withoutmedical supervision. Chloroquine needs to be abol-ished where it no longer cures, but nothing less thana drug that works better at lower cost could accom-plish that.
4.1 Conceptual Separation of Malaria inAfrica from Elsewhere
Malaria in holoendemic Africa is singular in itsintensity and intransigence. The global resurgenceofmalaria does not include holoendemicAfrica be-cause no substantial gains against risk of infectionhave been made (outside urban areas) on most of
Resurgent Malaria at the Millennium 733
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

the continent. North Africa, subtropical southernAfrica and the region of the Horn are exceptions.Malaria control activities based largely on DDTspraying brought about a retreat of malaria in thoseregions, and a resurgence has followed the deteri-oration of those programmes.[3] Although the geo-graphical range and number of infections in holo-endemic Africa cannot be considered resurgent, therising tide of resistance to available antimalarialsthreatens the effectiveness of treatment regimens.The threat of increasing risk of severe disease anddeath caused by drug resistance looms across holo-endemic Africa, but only for those at risk, i.e. in-fants, small children and pregnant women.The risk of severe disease among very young Af-
rican children and primigravid women is relativelyhigh even in the absence of drug resistance. Almosteveryone else in holoendemicAfrica has a very lowrisk of severe disease by virtue of naturally acquiredimmunity. The risk of severe disease among olderchildren and adults is vanishingly low despite veryhigh risk of infection (approximately >500% peryear). Thus, control of disease in young children andpregnant women, rather than limiting risk of infec-tion among everyone, constitutes the focus and hopeformalaria control inAfrica. However, the suitabil-ity of this approach for the rest of the world seemsdoubtful. The basis of doubt may be found in com-paring the dynamics of malaria transmission anddisease in Africa with that elsewhere (table I).The most important distinguishing feature of
Africanmalaria is the risk of infection. The incidence
of new infection in sub-Saharan Africa is muchhigher than any place else. Measured rates typicallyreach 8 infections per person-year.[70] The north coastof the island of New Guinea has the highest mea-sured attack rates outside the Sahel, ranging from1 to 5 infections per person-year.[71] In most otherplaces the risk of infection is relatively low. Theincidence of malaria in the rural Amazon of Brazil,for example, appears to be about 0.1 infections perperson-year.[72] Setting aside healthcare considera-tions, risk of infection by P. falciparum generallyequates with risk of death in most of the tropics.The risk of death without acquired immune or che-motherapeutic intervention is not known, but any-where between 5% and 50% seems probable. Incontrast, risk of death is a small fraction of the riskof infection in the Sahel. This distinction has far-reaching implications with regard to strategies in-tended to diminish morbidity and mortality causedby malaria.A hypothetical analysis illustrates this point. An
attack rate of 0.2 infections per person-year in aregion of 100 000 people would yield an annualaverage of 20 000 cases of malaria, or each personbeing infected about once every 5 years. Controlstrategies that reduce the risk of infection by 50%would prevent 10 000 cases, each case carrying amuch higher risk of death or debilitating diseaserelative to one in holoendemic Africa. In contrast,an attack rate of 5 infections per person-year in aregion of 100 000 people would yield 500 000 in-fections, or each person being infected 5 times an-
Table I. Distinctions between malaria in Asia and America, versus Africa
Endemic Asia and America Holoendemic Africa
Risk of infection Very low Very high
Risk of death with infection Very high Very low
Population at risk of death All ages Infants, small children andprimigravid women
Acquired immunity No Yes
Reduction in people infected with 50% effective control 50% 0%
Risk of control None Diminished naturally acquiredimmunity
History of vector control Effective Not applied
History of effective control Yes No
History of eradication Yes No
734 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)
nually. Reducing the risk of infection by 50% inthis instance would result in 2.5 infections per per-son per year. Thus, despite reducing the attack rate2-fold, the annual risk of infection would remainin excess of 100% for all residents. The efficacy ofcontrol measures with regard to preventing infec-tion among individuals depends upon the attackrate. Effective control measures in an area like Su-matra may have little utility in, for example, Bur-kina Faso. Likewise, control of malaria by focus-ing control resources on attacking clinical diseasein Sumatra may allow otherwise preventable expo-sure to risk of infection with attendant high risk ofsevere disease and death.An important variable in these considerations is
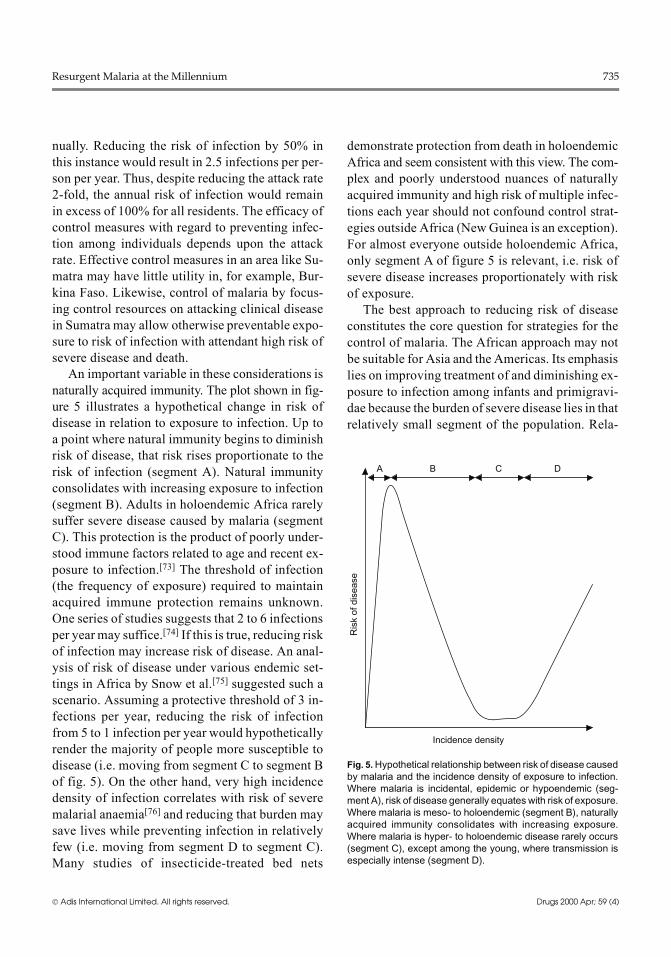
naturally acquired immunity. The plot shown in fig-ure 5 illustrates a hypothetical change in risk ofdisease in relation to exposure to infection. Up toa point where natural immunity begins to diminishrisk of disease, that risk rises proportionate to therisk of infection (segment A). Natural immunityconsolidates with increasing exposure to infection(segment B). Adults in holoendemic Africa rarelysuffer severe disease caused by malaria (segmentC). This protection is the product of poorly under-stood immune factors related to age and recent ex-posure to infection.[73] The threshold of infection(the frequency of exposure) required to maintainacquired immune protection remains unknown.One series of studies suggests that 2 to 6 infectionsper yearmay suffice.[74] If this is true, reducing riskof infection may increase risk of disease. An anal-ysis of risk of disease under various endemic set-tings in Africa by Snow et al.[75] suggested such ascenario. Assuming a protective threshold of 3 in-fections per year, reducing the risk of infectionfrom 5 to 1 infection per year would hypotheticallyrender the majority of people more susceptible todisease (i.e. moving from segment C to segment Bof fig. 5). On the other hand, very high incidencedensity of infection correlates with risk of severemalarial anaemia[76] and reducing that burden maysave lives while preventing infection in relativelyfew (i.e. moving from segment D to segment C).Many studies of insecticide-treated bed nets
demonstrate protection from death in holoendemicAfrica and seem consistent with this view. The com-plex and poorly understood nuances of naturallyacquired immunity and high risk of multiple infec-tions each year should not confound control strat-egies outside Africa (NewGuinea is an exception).For almost everyone outside holoendemic Africa,only segment A of figure 5 is relevant, i.e. risk ofsevere disease increases proportionately with riskof exposure.The best approach to reducing risk of disease
constitutes the core question for strategies for thecontrol of malaria. The African approach may notbe suitable for Asia and the Americas. Its emphasislies on improving treatment of and diminishing ex-posure to infection among infants and primigravi-dae because the burden of severe disease lies in thatrelatively small segment of the population. Rela-
A B C D
Ris
k of
dis
ease
Incidence density
Fig. 5. Hypothetical relationship between risk of disease causedby malaria and the incidence density of exposure to infection.Where malaria is incidental, epidemic or hypoendemic (seg-ment A), risk of disease generally equates with risk of exposure.Where malaria is meso- to holoendemic (segment B), naturallyacquired immunity consolidates with increasing exposure.Where malaria is hyper- to holoendemic disease rarely occurs(segment C), except among the young, where transmission isespecially intense (segment D).
Resurgent Malaria at the Millennium 735
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

tively expensive insecticide-treated bed net pro-grammes, as well as chemoprophylactic or chemo-therapeutic interventions, may be economically fo-cused upon those most at risk. Given the intensityof exposure in holoendemic Africa, the likelihoodof appreciably diminishing the number of peopleinfected may be considered remote by conven-tional vector control means. In contrast, in endemicareas outside holoendemic Africa, the entire popu-lation is at relatively low risk of infection but highrisk of severe disease with infection. In this settingreducing risk of severe disease through minimisingrisk of exposure to infection per se, i.e. vector con-trol, may be tenable. As sketched in this review,vector control has a proven record of effectivenessin a non-African setting. The economic and techni-cal difficulties of accomplishing effective diagno-sis and treatment in the rural tropics, given the toolsnow at hand, should further encourage activitiesdirected against the vectors of malaria.
4.2 Diagnosis and Treatment
The utility of reliable diagnosis and treatmentvaries with the risk of malaria among patients withfever. Where the risk is high, most people treat them-selves without the involvement of a medical pro-fessional. Under these circumstances improveddiagnostic capability may have little effect on thecontrol of malaria. Even where adequately staffedclinics are available, a presumptive clinical diag-nosis of malaria is often the rule. This practice posesno particular danger to patients actually infectedwith plasmodia, but it exposes people with other
illnesses to unnecessary treatment and may delayor preclude appropriate therapy.Reliable malaria diagnostic capability requires
an investment in a trained microscopist, micro-scope, staining supplies and reagents, and a commit-ment to exercise quality assurance. Given the pre-sumptive treatment of malaria in the absence ofdiagnostic services where the risk of malaria amongfebrile patients is high, it is difficult to see howdefinitive diagnosis would substantially improvethe control of malaria (table II). On the other hand,effective diagnosis where the risk of malaria amongfebrile patients is low may be an effective instru-ment of control. The minimal effort (assuming thenumber of febrile patients would be low comparedwith that in a highly endemic area) nets a relativelylarge benefit with respect to control. Assuming theavailability of effective treatment, the effort wouldsystematically diminish the small number of dis-ease carriers in the community and minimise trans-mission. Moreover, diagnostic capability enables ac-tive case detection and survey, i.e. identifying andtreating asymptomatic carriers. The clinical andpublic health importance of a definitive diagnosisof malaria is relatively high where the risk of ma-laria and presumptive therapy for it among febrilepatients is low.Whether used in a clinical or surveysetting, the public health utility of a definitive di-agnosis of malaria wilts without effective therapy.Effective treatment for malaria is the exception
in the rural tropics. The encroachment of resistanceto chloroquine or pyrimethamine/sulfadoxine largelyexplains this problem. The eroding efficacy of
Table II. Presumptive versus definitive diagnosis of malaria as an instrument of control
Malaria risk among febrile patients
low high
Febrile cases/unit time Few Many
Clinical diagnosis of malaria Infrequent Frequent
Usual misdiagnosis False negative False positive
Benefit of definitive diagnosis Appropriate treatment Avoid unnecessary treatment
Beneficiary Few with malaria Few without malaria
Cost/beneficiary High High
Effort/beneficiary Small Large
Control value of definitive diagnosis High Low
736 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

these drugs has contributed substantially to the re-surgence of malaria over the past 30 years. Althoughnew antimalarials have appeared in the marketplaceduring this time, none has yet supplanted chloro-quine. The characteristics of their cost, safety, tol-erability and efficacy have not matched those ofchloroquine. The prohibitive cost of most new an-timalarials precludes immediate clinical relevanceto the vast majority of people exposed to infection.Although the expiry of patent protection of thesedrugs may eventually see them more universallyavailable, drugs such asmefloquine or halofantrineare less well tolerated than chloroquine.[77] Thereare no drugs on the market at any cost or in ad-vanced development that appear to be as well tol-erated as chloroquine. Hope for such a product inthe foreseeable future appears dim.Combining blood schizonticidal antimalarials
represents an important or even imperative mea-sure to address the important problem of resistanceto available therapies. Combinations of existing an-timalarials, especially those now available in ruralclinics and marketplaces, hold great potential foreffective, self-administered therapies for uncompli-cated malaria. For example, combining chloroquineor pyrimethamine/sulfadoxine with an artemisininderivative may rescue an otherwise ineffectivetherapy while simultaneously guarding against theemergence of resistance to artemisinin. This ap-proach, as explained byWhite and others,[78,79] de-serves vigorous investigation. Applying combinedtherapies to the problem should demand a high stand-ard of proof of safety and efficacy in randomised,double-blind, placebo-controlled (i.e. monother-apy + placebo) trials. Among the many challengesto the use of combined therapies for malaria is de-velopment of the research capability needed togenerate proven formulations and administrationregimens. Current work on the artemisinin deriva-tives in combination with standard therapies suchas mefloquine[80-83] lays the foundation for clinicalresearch strategies for such endeavours in develop-ing nations.The availability of demonstrably well tolerated
and effective combined therapies constitutes the first
half of the journey to bringing the malaria problemunder control. Such products should move throughmeaningful licensing in order to realise the full mea-sure of impact against malaria. Licensing accom-plishes essential guarantees of safety, efficacy andgood manufacture, thereby protecting the productand the people receiving it. Licensing therapies re-quires special expertise and a commitment to meetchallenging regulatory requirements.Regulatory obstacles in the commercial devel-
opment of drugs in the developed nations add tre-mendously to the cost of drugs in the free market-place. Combined therapies using drugs that lackpatent protection, and the intrinsic difficulties inhaving industry competitors share InvestigationalNew Drug licences, largely cripple the commercialpharmaceutical industry in this arena. These indus-tries should not be looked to for progress in devel-oping and fielding combined antimalarial thera-pies. Noncommercial organisations must seize theinitiative of developing licensed combinations ofantimalarials. Seeing development of antimalarialsthrough to distribution at costs that undercut thedemand for inappropriately used drugs may radi-cally improve treatment of uncomplicated malariain remote areas of the tropics. The key is providingaccess to inexpensive and well tolerated therapythat can be administered with minimal medical su-pervision, if any at all.
4.3 Vector Control
The industry that creates insecticides uses a de-velopment paradigm that largely ignores applica-tions against insect vectors of human disease. It ishighly commercial and driven by agricultural mar-ket forces. Medically important insecticides such asmalathion and various pyrethroids have been inci-dental products developed for agricultural applica-tions. The licensing of insecticides for agriculturaluse demands minimal effect on the environment,i.e. rapid lethal activity and quick degradation.Low toxicity to plants and short residual actiondrive the design of agricultural pesticides, whilehuman toxicity and noxiousness apply largely todegradation products. The active product may be
Resurgent Malaria at the Millennium 737
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

both, provided its degradation yields safe and welltolerated derivatives. Malathion typifies such prod-ucts: it is mildly toxic and appreciably noxious tohuman beings but it rapidly degrades to innocuousproducts. These characteristics make it an ideal ag-ricultural pesticide. The criteria that bring success-ful agricultural pesticides to the marketplace arenot necessarily favourable for the control of medi-cally important arthropods. The fact that DDT wasdeveloped as amedical insecticide and then appliedagriculturally suggests that the converse may alsobe true. Medical insecticides should be developedindependently of agricultural pesticides.The properties of DDT, with the effective per-
formance evident in its extraordinary accomplish-ments, should serve as the ‘gold standard’ for de-velopment criteria. The ideal pesticide for the controlof vector-borne diseases would be stable in the in-terior environment, unstable outdoors, have a lowcapacity for bioaccumulation (e.g. partition poorlyinto vertebrate tissue) and be powerfully repellentto human blood meal-seeking insects. The safetyof such a pesticide to plants would be almost irrel-evant, while mammalian toxicity and tolerancewould be critically important. Likewise, the dispo-sition of the compound on surfaces in the home,rather than on crops, would appropriately narrowthe search. This development equation differs rad-ically from that for products for agricultural use.Important insecticides for the control of malariashould not be expected from the agricultural sector.Thus, it may be essential to commit to the de novodesign and development of pesticides intendedspecifically for the control of vector-borne dis-eases.The resurgence of malaria that now threatens pub-
lic health through the tropics into subtropical zonesdemands immediate measures. New insecticides, ifthe challenge to develop them were taken up, wouldenter into long range plans for turning back malaria.The development, licensing, manufacture and dis-tribution of a new pesticide would take at least 5years under the best of circumstances. In the mean-time, consideration should be given to the use ofDDT itself. Although authoritative sources cite vec-
tor resistance to DDT as an important contributingfactor in the global resurgence ofmalaria,[29,33,34,65]evidence supporting that contention is broadlylacking. Likewise, the propensity for DDT to accu-mulate in human and animal tissues is beyonddoubt, but there has been no unequivocal demon-stration of serious adverse effects on human health.Finally, the medical application of DDT has notbeen shown to cause significant harm to the envi-ronment. If DDT remains a well tolerated and ef-fective means of preventing human morbidity andmortality caused by malaria, policy makers shouldoffer compelling arguments for its exclusion fromthe practice of control.Proponents of the ban on DDT point to its pirat-
ing from intended medical uses into the agricul-tural sector. This practice undoubtedly occurs, butits effect must be minimal given the relatively smallquantities of DDT needed for medical versus agri-cultural applications. Some farmersmay cheat withpirated DDT, but short of the near total capture ofmedical DDT for illicit agricultural use, the con-tamination of the environment may be reasonablyforecast as minimal. Formulating ‘medical DDT’with a herbicide or any other substance that farmersfind intolerable on crops would largely solve thisproblem. The difficulty lies in securing the exper-tise and political will to formulate, license andmanufacture medical DDT.The rising tide of malaria may ultimately force
the application of residual pesticides. Meaningfuldeliberation of the risks and benefits of DDT as atool to be applied againstmalaria should take place.Also, a commitment to development of medical in-secticides would represent an important step for-ward in the long term. The social pressure for out-lawing DDT may be irresponsible with regard toprotecting human health against diseases that killmillions, but no less so than the failure of the com-munity of science to develop socially and environ-mentally acceptable pesticides specifically suitedfor use against medically important arthropods. Itis a stunning realisation that we almost completelylack such capability in the face of the vector-bornediseases that threaten public health everywhere.
738 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

5. Conclusions
The retreat of vector control as the primary in-strument of limiting morbidity and mortality causedby malaria outside holoendemic Africa is beingdriven by loosely conceived concepts of its failure.These are listed below.• Vector control is unsustainable in developingnations. This view largely ignores the extraor-dinary achievements realised relatively quicklyand with little or no political and fiscal supportfrom anywhere in the developed world outsidethe US. The sustainability of vector control witha broader commitment to support it seemslikely. The maintenance of extremely low levelsof malaria on the islands of Java and Bali inIndonesia for a period of over 30 years dem-onstrates that committed developing nationssustain such programmes and reap their bene-fits.
• DDT harms human health and the environment.There is no direct evidence to support this con-cept, and much of the indirect evidence derivesfrom the impact of the agricultural applicationof DDT. Despite the many millions of tons ofDDT applied liberally to crops for more than 20years (a practice that ceased in the US almost 30years ago), exposure to DDT in the environmentdoes not increase the risk of any human disease.Thus, it seems likely that the medical applica-tion of DDT in homes rather than dusted ontocrops represents a lesser risk to both human andwildlife health. Claims of subtle health effectsof DDT pale in comparison to the unambiguousand lethal threat of malaria.
• Vector resistance to DDT has rendered it inef-fective. This concept appears repeatedly in themedical literature without substantiation. Re-ports of diminished susceptibility to the lethaleffects of DDT by anopheline mosquitoes maynot be relevant in the practice of malaria con-trol. Excito-repellency apparently representsthe basis of preventing malaria, i.e. diminishingvector contact with humans without killingmosquitoes. Credible reviews of the available
evidence do not show resistance to influenceDDT effectiveness in controlling malaria.
• DDT is socially unacceptable. This concept islargely true, but the tendency to leverage thisliability against vector control in general shouldbe resisted. The medical application of DDT issocially unacceptable in the same manner thatmost Americans find the metric system intoler-able; the prevailing view is not necessarily cor-rect, nor does it disqualify efforts to address it.More importantly, misconceptions about DDTdo not relieve the community of science fromthe duty to field a better product. Reliance uponagricultural industry to develop and supply in-secticides of medical importance is unaccept-able.
• DDT spraying programmes do not work. Thisconcept captures elements of all of the above,but also includes the failure to eradicate malariaduring the Global Eradication Campaign, or tohave an impact on malaria in holoendemic Af-rica. Even strident advocates of DDT do not ar-gue for a return to the eradication strategy, norwould most recommend such an objective forholoendemicAfrica. Nonetheless, the campaignshowed that control through spraying a stableresidual insecticide that repels mosquitoesachieves control. In the face of an increasinglyvolatile malaria situation in Asia and the Amer-icas, this history bears recall.The momentum to control malaria through clin-
ical management outside holoendemic Africa car-ries important risks. Gauging these is difficult be-cause the strategy represents venturing into largelyuncharted territory. Diagnosis and treatment hasnot been the primary instrument of control acrossvast endemic regions, except in Africa. The impor-tant risks are summarised below.• Malaria is poised to spiral out of control. Aglobal malaria crisis may not be the time to ex-plore untried strategies of dealing with the prob-lem.Theconsequencesof failuremaybe toogreat.
• Diagnostic performance is poor in most en-demic areas. Although new dipstick technolo-gies promise some day to improve the reliability
Resurgent Malaria at the Millennium 739
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

of the diagnosis of malaria, today these tests arerelatively insensitive (sensitivity is uniformlysuperior only above 100 parasites/μl). In endemicareas where the author has worked, more thanthree-quarters of parasitaemias fall below thisthreshold. Expense of the dipstick assays is alsoa problem. Even at the cut-rate cost of $US1.00per test, this is too expensive for most peopleexposed to malaria. Today, in the face of crisis,diagnostic capabilities in many endemic areasare either poor or nonexistent. Reliance upondiagnosis as a foundation of control is risky un-der these circumstances.
• Treatment is inadequate in most endemic areas.The benefit of prompt and reliable diagnosis van-ishes with inadequate treatment. Chloroquineand pyrimethamine/sulfadoxine overwhelm-ingly dominate the antimalarial pharmacies ofhealthcare providers and merchants in the im-poverished rural tropics. These drugs fail toachieve cure more often than not. Promisingnew therapies and therapeutic strategies are onthe horizon, but none is broadly fielded wherethe malaria crisis looms. Reliance upon treat-ment as a foundation of control is risky underthese circumstances.
• Asians and Americans exposed to malaria arenot immune. Compared with the risk to Africansliving in holoendemic areas (except possibly in-fants, small children and pregnant women) therisk of severe disease and death with infectionin any Asian or American is very much higher.Thus, an infection in Sumatra carries a muchhigher probability of morbidity or mortalitythan one in Burkina Faso. Acontrol strategy thatdoes not intervene until clinical illness mani-fests in the patient from Sumatra seems unnec-essarily risky. Moreover, the reluctance to abaterisk of exposure for fear of diminishing naturallyacquired immunity is irrelevant in Sumatra.Turning back resurgent malaria requires ac-
knowledgement that the problem lies predomi-nantly outside holoendemic Africa. The severe andworsening malaria situation in most of that regionrevolves around evidence of deteriorating efficacy
of chemotherapeutic agents. Malaria in holoende-micAfrica remains stable but appears to be increas-ingly difficult to manage in the clinic or throughappropriate treatment at home. The best route toaddressing this problem has been set forth by theWHO 1993 policy on control strategies. In contrast,the worsening malaria situation in Asia and theAmericas revolves around an alarming increase inthe number and geographic range of reported infec-tions. The two most important factors contributingto this resurgence may be clinical resistance to avail-able chemotherapeutic agents, and a general degra-dation in the will and ability to conduct sustainablevector control activities. The latter problem mayworsen with applying an African solution to anAmerican and Asian problem. Separating policiesfor holoendemic Africa from those suitable in theAmericas and Asia may help solve both problems.A focused policy with greatly intensified effort toreduce childhoodmorbidity andmortality in Africahas been accomplished under the leadership of theWHO. However, the resurgence in numbers of ma-laria cases and the encroachment of the disease intoareas where it had been virtually eradicated outsideholoendemic Africa may continue unabated with-out a parallel policy focused on that unique prob-lem.The best available evidence suggests that vector
control programmes applying DDT or other resid-ual insecticides offer the best hope for turning backresurgent malaria in Asia and the Americas. If theuse of DDT is socially impractical, an effort shouldbe made to develop more suitable medical pesti-cides through a rational process driven by medicalrather than agricultural entomology needs. The cri-teria that drive the development of agricultural pes-ticides conflict with those needed for the creationofmedically important products. The historical andcontinuing reliance upon the agricultural pesticideindustry for medical applications offers no brightprospects. The lack of will to attack this problemby seizing themedical insecticide development ini-tiative from agricultural interests may be the great-est impediment to achieving great strides against
740 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

resurgent malaria and, incidentally or intention-ally, other vector-borne disease as well.A well tolerated and affordable treatment for
malaria with a high likelihood of compliance isequally important to bringing resurgent malariaunder control. The heart of the problem has impor-tant parallels with the insecticides. Reliance on thepharmaceutical industry to provide such antimalar-ials is unrealistic. Even the US Department of De-fense, which produced chloroquine and prima-quine, rationally turns over hugely expensivedevelopment costs to pharmaceutical partners thatsubsequently market relatively expensive prod-ucts, e.g. mefloquine or halofantrine. The initiativeto develop well tolerated and affordable antimalar-ials should be seized by the governments of nationsstruggling with malaria and the international agen-cies that support their efforts in public health.Combining available antimalarials and evaluatingthese in rigorous clinical trials may be the best ap-proach to accomplishing a useful product in theshortest time.Malaria affects the poor. Solutions that poor peo-
ple can afford and independently manage at the vil-lage level offer the brightest hope. This may be oneof the few characteristics that solutions for Africa,the Americas and Asia share. Otherwise, these re-gions face fundamentally distinct problems. Thepoor rely upon the community of science for guid-ance on relieving themselves from the onerous bur-den of malaria. The challenge for national govern-ments and international agencies is to offer guidancethat proves practical across a spectrum of environ-mental, social and economic conditions.Current con-ditions in the rural tropics such as poor diagnosis,inadequate treatment, and an enfeebled vector con-trol infrastructure underpin the forecast of an in-creasingly serious problem. Averting the onslaughtof malaria thus expected in the first decade of thenew millennium defines a monumental challenge.
Acknowledgements
The author is grateful to Stephen L. Hoffman, Donald J.Roberts, James R. Campbell and Michael J. Bangs for theirthoughtful reviews of this manuscript. The views of the
author are his own and are not to be construed as representingthose of the US Department of Defence or of the US Navy.
References1. Harrison G. Mosquitoes, malaria and man: a history of the hos-
tilities since 1880. London: John Murray, 1978: 3142. Krogstad DJ. Malaria as a reemerging disease. Epidemiol Rev
1996; 18: 77-893. Mouchet J, Manguin S, Sircoulon J, et al. Evolution of malaria
in Africa for the past 40 years: impact of climatic and humanfactors. J Am Mosquito Control Assoc 1998; 14: 121-30
4. World Health Organization. Implementation of the global ma-laria control strategy. WHO Technical Report Series no. 839.Geneva: WHO, 1993
5. World Health Organization. Malaria fact sheet no.94. Geneva:WHO, 1998
6. Nye ER, Gibson ME. Ronald Ross: malariologist and poly-math. London: Macmillan Press, 1996: 316
7. Boyd MF. Historical review, In: Boyd MF, editor. Malariology.Philadelphia: WB Saunders, 1949: 3-25
8. Ross R. On some peculiar pigmented cells found in two mos-quitoes fed on malarial blood. BMJ 1897; ii: 1786-8
9. Grassi B, Bignami A, Bastianelli G. Ulteriori ricerche sul ciclodei parassitimalarici umani nel corpo del zanarone. Atti RealeAccademia dei Lincei 1899 S.5; 8: 21
10. James SP. Malaria in Mian Mir. In: Jennings WE, editor. Trans-actions of the Bombay Medical Conference, 1909. Bombay:Bennett, Coleman, 1909: 84-9
11. McCullough D. The path between the seas: the creation of thePanama Canal, 1870-1914. New York: Simon & Schuster,1978: 698
12. Reed W, Carroll J, Agramonte A. Experimental yellow fever.Trans Assoc Am Physicians 1901; 16: 45-70
13. Packard RM. Malaria dreams: postwar visions of health anddevelopment in the third world. Med Anthropol 1997; 17:279-96
14. Beadle C, Hoffman SL. History of malaria in the United Statesnaval forces at war:WorldWar I through theVietnam conflict.Clin Infect Dis 1993; 16: 320-9
15. Coatney GR. Pitfalls in a discovery: the chronicle of chloro-quine. Am J Trop Med Hyg 1963; 12: 121-8
16. Russel PF. Man’s mastery of malaria. London: Oxford Univer-sity Press, 1955
17. Zucker JR. Changing patterns of autochthonous malaria trans-mission in the United States: a review of recent outbreaks.Emerg Infect Dis 1996; 2; 37-43
18. Faust EC, Debakey L. Malaria mortality in the Southern UnitedStates for the year 1940, with supplementary data on malariain other states. J Natl Malaria Soc 1942; 1: 125-31
19. MacDonald G. The epidemiology and control of malaria. Lon-don: Oxford University Press, 1957
20. United States Agency for International Development. Malaria:meeting the global challenge. AID science & technology indevelopment series. Boston: Oelgeschlager, Gunn, & HainPublishers, 1985
21. Jukes TH. Insecticides in health, agriculture and the environ-ment. Naturwissenschaften 1974; 61: 6-16
22. Sharma VP. Re-emergence of malaria in India. Indian J MedRes 1996; 103; 26-45
23. Atmosoedjono S. Malaria control in Indonesia sinceWorldWarII. Wageningen Agricultural University Papers 1990; 90-7:141-54
Resurgent Malaria at the Millennium 741
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)
24. Curtin PD. Malarial immunities in Nineteenth Century WestAfrica and the Caribbean. Parassitologia 1994; 36: 69-82
25. Baird JK, Sismadi P,Masbar S, et al. Afocus of endemicmalariain Central Java. Am J Trop Med Hyg 1996; 54: 98-104
26. Lepers JP, Fontinille D, Rason MD, et al. Transmission andepidemiology of newly transmitted falciparum malaria in thecentral highland plateau of Madagascar. Ann Trop MedParasitol 1991; 85: 297-304
27. Reynolds DJ. The Demerara doctor. Perspectives in Health1996; 1 (2) [online]. Available from: URL: http://www.paho.org/english/DPImag/Number2/dpi2pdemerara.html [Accessed2000 Feb 29]
28. CruzMA. Humanmigration and the spread of malaria in Brazil.Parasitol Today 1987; 3: 166-70
29. Trigg PI, Kondrachine AV. Commentary: malaria control in the1990s. Bull WHO 1998; 76: 11-6
30. Packard RM. ‘No other logical choice’: global malaria eradica-tion and the politics of international health in the post-war era.Parassitologia 1998; 40: 217-29
31. Butler D, Maurice J, O’Brien C. Time to put malaria control onthe global agenda. Nature 1997; 386: 535-6
32. Campbell CC. Malaria: an emerging and re-emerging globalplague. FEMS Immunol Med Microbiol 1997; 18: 325-31
33. Kondrachine AV, Trigg PI. Global overview of malaria. IndianJ Med Res 1997; 106: 39-52
34. National Academy of Sciences (US). Vaccines Against malaria:hope in a gathering storm. Washington: National AcademyPress, 1996
35. Greenberg AE, Lobel HO. Mortality from plasmodiumfalciparum malaria in travelers from the United States, 1959to 1987. Ann Intern Med 1990; 113: 326-7
36. World Health Organization. World malaria situation in 1994:Part II, the Americas. Wkly Epidemiol Rec 1997; 72: 277-84
37. World Health Organization. World malaria situation in 1994:Part III. Wkly Epidemiol Rec WHO 1997; 72: 285-90
38. Feighner BH, Pak SI, Novakoski WL, et al. Reemergence ofPlasmodium vivax malaria in the Republic of Korea. EmergInfect Dis 1998; 4: 295-7
39. Roberts DR, Laughlin LL,Hsheih P. DDT, global strategies, anda malaria control crisis. Emerg Infect Dis 1997; 3: 295-302
40. Sharp BL, le Sueur D. Malaria in South Africa: the past, thepresent and selected implications for the future. S Afr Med J1996; 86: 83-9
41. Lepers JP, Deloron P, Andriamagatiana-RasonMD, et al. Newlytransmitted plasmodium falciparum malaria in the centralhighland plateaux of Madagascar: assessment of clinical im-pact in a rural community. Bull WHO 1990; 68: 217-22
42. Malakooti MA, Biomndo K, Shanks GD. Reemergence of epi-demic malaria in the highlands of western Kenya. Emerg In-fect Dis 1998; 4: 671-6
43. Shukla RP, Pandey AC, Mathur A. Investigation of malaria out-break in Rajasthan. Indian J Malariol 1995; 32: 119-28
44. MartensWJ, Niessen LW, Rotmans J. Potential impact of globalclimate change on malaria risk. Environ Health Perspect1995; 103: 458-64
45. Baird JK, Basri H, Jones TR, et al. Resistance to antimalarialsin northeastern Irian Jaya, Indonesia. Am J Trop Med Hyg1991; 44: 640-4
46. Baird JK, Leksana B, Masbar S, et al. Diagnosis of resistanceto chloroquine by Plasmodium vivax: timing of recurrenceand whole blood chloroquine levels. Am J Trop Med Hyg1997; 56: 621-6
47. Hogh B, Gamage-Mendis A, Butcher GA, et al. The differingimpact of chloroquine and pyrimethamine/sulfadoxine upon
the infectivity of malaria species to the mosquito vector. AmJ Trop Med Hyg 1998; 58: 176-82
48. Rieckmann KH, Davis DR, Halton DC. Plasmodium vivax re-sistance to chloroquine? Lancet 1989; II: 1183-4
49. Schwartz IK, Lackritz EM, Patchen LC. Chloroquine-resistantPlasmodium vivax from Indonesia. N Engl J Med 1991;324: 927
50. Baird JK, Basri H, Subianto B, et al. Treatment of chloroquineresistant Plasmodium vivax with chloroquine and primaquineor halofantrine. J Infect Dis 1995; 171: 1678-82
51. Than M, Kyaw MP, Soe AY, et al. Development of resistance tochloroquine by Plasmodium vivax in Myanmar. Trans R SocTrop Med Hyg 1995; 89: 307-8
52. Garg M, Gopinathan N, Bodhe P, et al. Vivax malaria resistantto chloroquine: case reports from Bombay. Trans R Soc TropMed Hyg 1995; 89: 656-7
53. Phillips EJ, Keystone JS, Kain KC. Failure of combined chloro-quine and high-dose primaquine therapy for Plasmodiumvivax acquired in Guyana, South America. Clin Infect Dis1996; 23: 1171-3
54. Baird JK,Wiady I, Fryauff DJ, et al. In vivo resistance to chloro-quine by Plasmodium vivax and Plasmodium falciparum atNabire, Irian Jaya, Indonesia. Am J Trop Med Hyg 1997; 56:627-31
55. Baird JK, Leksana B, Masbar S, et al. Whole blood chloroquineconcentrations with Plasmodium vivax in Irian Jaya, Indone-sia. Am J Trop Med Hyg 1997; 56: 618-20
56. Wolff MS, Toniolo PG, Lee EW, et al. Blood levels of organo-chlorine residues and risk of breast cancer. J Natl Cancer Inst1993; 85: 648-52
57. Krieger N, Wolff MS, Hiatt RA, et al. Breast cancer and serumorganochlorines: a prospective study among white, black, andAsian women. J Natl Cancer Inst 1994; 86: 589-99
58. Hunter DJ, Hankinson SE, Laden F, et al. Plasma organochlo-rine levels and risk of breast cancer. N Engl J Med 1997; 337:1253-8
59. Longnecker MP, Rogan WJ, Lucier G. The health effects ofDDT and PCBS and an overview of organochlorines in publichealth. Ann Rev Public Health 1997; 18: 211-44
60. Institute of Medicine. Malaria: obstacles & opportunities. In:Oaks Jr SC, Mitchell VS, Pearson GW, et al, editors. Wash-ington DC: National Academy Press, 1991
61. World Health Organization. Four international organizationsunite to roll back malaria, World Health Organization PressRelease WHO/77 of 30 October 1998. Accessed at http://www.who.ch/
62. World Health Organization. Multilateral perspective on malariabegins to take shape: tropical diseases newsletter no. 55, Feb-ruary 1998. Geneva: WHO, 1998
63. Fontinille D, Lepers JP, Campbell GH, et al. Malaria transmis-sion and vector biology in Manarintsoa, high plateau of Mad-agascar. Am J Trop Med Hyg 1990; 43: 107-15
64. Pan American Health Organization. Status of malaria programsin the Americas. XLII Report. Washington, DC: Pan Ameri-can Health Organization, 1994
65. Pan American Health Organization. Report on the status of ma-laria programs in theAmericas.HCP/HCT/149/99,August1999
66. Brogdon WG, McAllister JC. Insecticide resistance and vectorcontrol. Emerg Infect Dis 1998; 4: 605-14
67. Roberts DR, Andre RG. Insecticide resistance issues in vector-borne disease control. Am J Trop Med Hyg 1994; 50 Suppl.:21-34
68. Bangs MJ. Doctoral dissertation. Bethesda (MD): UniformedServices University of the Health Sciences, 1998
742 Baird
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)

69. World Wildlife Fund News. WWF urges World Health Assem-bly delegates to phase out deadly DDT pesticide (May 21 1999)[online]. Available from: URL: http://www.worldwildlife.org/toxics/whatsnew [Accessed 2000 Mar 3]
70. Beadle C, McElroy PD, Oster CN, et al. Impact of transmissionintensity and age on Plasmodium falciparum density and as-sociated fever: implications for malaria vaccine trial design.J Infect Dis 1995; 172: 1047-54
71. Jones TR, Baird JK, Bangs MJ, et al. Malaria vaccine study sitein Irian Jaya, Indonesia: plasmodium falciparum incidencemeasurements, epidemiologic considerations in sample sizeestimation. Am J Trop Med Hyg 1994; 50: 210-8
72. Pan American Health Organization. Status of malaria programsin theAmericas. XLVReport.WashingtonDC: PanAmericanHealth Organization, 1997
73. Baird JK. Age-dependent characteristics of protection vs. sus-ceptibility to Plasmodium falciparum. Ann Trop Med Para-sitol 1998; 92: 367-90
74. Baird JK. Host age as a determinant of naturally acquired im-munity to Plasmodium falciparum. Parasitol Today 1995; 11:105-11
75. SnowRW,Omumbo JA, LoweB, et al. Relation between severemalaria morbidity in children and level of Plasmodiumfalciparum transmission in Africa. Lancet 1997; 349: 1650-4
76. McElroy PD, Beier JC, Oster CN, et al. Dose- and time-depend-ent relations between infective Anopheles inoculation and
outcomes of Plasmodium falciparum parasitemia among chil-dren in Western Kenya. Am J Epidemiol 1997; 145: 945-56
77. Baird JK, Hoffman SL. Prevention of malaria in travelers. MedClin North Am 1999; 83: 923-44
78. White NJ, Nosten F, Looareesuwan S, et al. Averting a malariadisaster. Lancet 1999; 353: 1965-7
79. White N. Antimalarial drug resistance and combination chemo-therapy. Phil Trans R Soc Lond B Biol Sci 1999; 354: 739-49
80. Price R, van Vugt M, Phaipun L, et al. Adverse effects in pa-tients with acute falciparum malaria treated with artemisininderivatives. Am J Trop Med Hyg 1999; 60: 547-55
81. Nosten F, Hien TT,White NJ. Use of artemisinin derivatives forthe control of malaria. Med Trop (Mars) 1998; 58 Suppl. 3:45-9
82. Price RN, Nosten F, Luxemberger C, et al. Artesunate/mefloqu-ine treatment of multi-drug resistant falciparum malaria.Trans R Soc Trop Med Hyg 1997; 91: 574-7
83. Van VugtM, BrockmanA,Gemperli B, et al. Randomized com-parison of artemether-benflumetol and artesunate-mefloquinein treatment of multi-drug resistant falciparum malaria. Anti-microb Agents Chemother 1998; 42: 135-9
Correspondence and offprints: Dr J. Kevin Baird, ParasiticDiseases Program, US Naval Medical Research Unit No.2,American Embassy, Jakarta, FPO AP 96520-8132, USA.
Resurgent Malaria at the Millennium 743
© Adis International Limited. All rights reserved. Drugs 2000 Apr; 59 (4)




















