Resident Surgical Practice Patterns for Vitreoretinal Surgery in Ophthalmic Training Programs in the...
7
Resident Surgical Practice Patterns for Vitreoretinal Surgery in Ophthalmic Training Programs in the United States Vinay A. Shah, MD, 1 Arun K. Reddy, BS, 1 Aaron J. Bonham, MS, 2 Nelson R. Sabates, MD, 1 Andrew G. Lee, MD 3 Purpose: To assess resident surgical experience in vitreoretinal surgery (VRS) in the United States. Design: Anonymous electronic survey over 2 consecutive years. Participants: A total of 287 third-year ophthalmology residents from US residency programs were included. Methods: To determine the type and amount of surgical experience in VRS. Residents were contacted via e-mail to complete the survey. A series of follow-up e-mails were sent to nonresponders. E-mail correspondence was sent to program directors of the US residency programs to encourage survey participation. An electronic survey instrument (Survey Monkey) was used to distribute the survey and collect the results. Participants were asked about vitrectomy and scleral buckle procedures as primary surgeon and about office procedures (e.g., intravitreal injections and retinal laser procedures). Questions regarding the self-described “comfort” level of the resident and the Accreditation Council for Graduate Medical Education (ACGME) vitreoretinal requirements for ophthalmology were also included. Main Outcome Measures: Vitreoretinal office and surgical procedures. Results: Of the 114 ophthalmology residency programs in the United States, 3 programs declined to participate and 103 of 228 programs (114 programs per year) did not respond to requests during a 2-year period. Of the 287 total respondents, approximately 59.1% had performed vitrectomy and 40.8% had performed a scleral buckle as the primary surgeon. In the survey of office procedures, 96.7% had performed intravitreal injections, 94.8% had performed macular laser therapy, and 99.6% had performed panretinal photocoagulation. In the self-reported resident “comfort” level section, 59% were “fairly comfortable” knowing the theoretic steps for VRS and 55.4% were “fairly satisfied” with VRS training. However, 72% of respondents were unaware of the correct ACGME minimum operative numbers for VRS. Conclusions: This self-reported electronic survey of third-year residents suggested that VRS experience at ACGME-accredited programs as primary surgeon was suboptimal for surgeries. A modest majority of residents reported comfort and satisfaction with VRS training for surgery, but a majority was satisfied and had adequate experience with office procedures such as intravitreal injection and laser treatment. Unfortunately, the majority of residents were unaware of the actual numeric ACGME VRS requirements for ophthalmology residency programs. Financial Disclosure(s): The author(s) have no proprietary or commercial interest in any materials discussed in this article. Ophthalmology 2009;116:783–789 © 2009 by the American Academy of Ophthalmology. Over the past several decades, vitreoretinal surgery (VRS) has advanced significantly with various new innovative techniques that have improved both anatomic and functional success for patients. VRS has always been considered one of the most complex and difficult surgical skills to master in ophthalmology. 1 It has been our experience that VRS is often performed by fellows in training in larger programs or by fellowship-trained specialists in smaller programs rather than eye residents as primary surgeons. The ophthalmology Residency Review Committee (RRC) and the Accreditation Council for Graduate Medical Education (ACGME) have established minimum requirements for operative experience for residents in VRS (http://www.acgme.org/acWebsite/ navPages/nav_240.asp, accessed October 6, 2008). In the United States, residency programs are accredited by the ACGME, and the documentation of compliance with national accreditation standards and requirements is verified by the specialty RRCs of the ACGME. Residency programs are required to meet “minimum operative numbers,” which are nationally benchmarked targets for ACGME accredita- tion purposes. Individuals (as opposed to accreditation for residency programs) are certified by the American Board of Ophthalmology. Board certification requires completion of an accredited residency program. Individual residents might graduate at, above, or below the target surgical numbers, and it is up to the program to attest to the American Board of Ophthalmology that the individual resident is surgically “competent” independently of the actual operative numbers. Evaluating surgical expertise of the residents is now con- sidered part of the core competencies by the RRC and ACGME for ophthalmology. 2–4 These numbers were re- cently modified (March 2007), and the minimum require- 783 © 2009 by the American Academy of Ophthalmology ISSN 0161-6420/09/$–see front matter Published by Elsevier Inc. doi:10.1016/j.ophtha.2008.11.010
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Resident Surgical Practice Patterns for Vitreoretinal Surgery in Ophthalmic Training Programs in the...
Resident Surgical Practice Patterns forVitreoretinal Surgery in OphthalmicTraining Programs in the United States
Vinay A. Shah, MD,1 Arun K. Reddy, BS,1 Aaron J. Bonham, MS,2 Nelson R. Sabates, MD,1
Andrew G. Lee, MD3
Purpose: To assess resident surgical experience in vitreoretinal surgery (VRS) in the United States.Design: Anonymous electronic survey over 2 consecutive years.Participants: A total of 287 third-year ophthalmology residents from US residency programs were included.Methods: To determine the type and amount of surgical experience in VRS. Residents were contacted via
e-mail to complete the survey. A series of follow-up e-mails were sent to nonresponders. E-mail correspondencewas sent to program directors of the US residency programs to encourage survey participation. An electronicsurvey instrument (Survey Monkey) was used to distribute the survey and collect the results. Participants wereasked about vitrectomy and scleral buckle procedures as primary surgeon and about office procedures (e.g.,intravitreal injections and retinal laser procedures). Questions regarding the self-described “comfort” level of theresident and the Accreditation Council for Graduate Medical Education (ACGME) vitreoretinal requirements forophthalmology were also included.
Main Outcome Measures: Vitreoretinal office and surgical procedures.Results: Of the 114 ophthalmology residency programs in the United States, 3 programs declined to
participate and 103 of 228 programs (114 programs per year) did not respond to requests during a 2-year period.Of the 287 total respondents, approximately 59.1% had performed vitrectomy and 40.8% had performed ascleral buckle as the primary surgeon. In the survey of office procedures, 96.7% had performed intravitrealinjections, 94.8% had performed macular laser therapy, and 99.6% had performed panretinal photocoagulation.In the self-reported resident “comfort” level section, 59% were “fairly comfortable” knowing the theoretic stepsfor VRS and 55.4% were “fairly satisfied” with VRS training. However, 72% of respondents were unaware of thecorrect ACGME minimum operative numbers for VRS.
Conclusions: This self-reported electronic survey of third-year residents suggested that VRS experience atACGME-accredited programs as primary surgeon was suboptimal for surgeries. A modest majority of residentsreported comfort and satisfaction with VRS training for surgery, but a majority was satisfied and had adequateexperience with office procedures such as intravitreal injection and laser treatment. Unfortunately, the majorityof residents were unaware of the actual numeric ACGME VRS requirements for ophthalmology residencyprograms.
Financial Disclosure(s): The author(s) have no proprietary or commercial interest in any materials discussed
in this article. Ophthalmology 2009;116:783–789 © 2009 by the American Academy of Ophthalmology.Over the past several decades, vitreoretinal surgery (VRS)has advanced significantly with various new innovativetechniques that have improved both anatomic and functionalsuccess for patients. VRS has always been considered oneof the most complex and difficult surgical skills to master inophthalmology.1 It has been our experience that VRS isoften performed by fellows in training in larger programs orby fellowship-trained specialists in smaller programs ratherthan eye residents as primary surgeons. The ophthalmologyResidency Review Committee (RRC) and the AccreditationCouncil for Graduate Medical Education (ACGME) haveestablished minimum requirements for operative experiencefor residents in VRS (http://www.acgme.org/acWebsite/navPages/nav_240.asp, accessed October 6, 2008).
In the United States, residency programs are accredited
by the ACGME, and the documentation of compliance with© 2009 by the American Academy of OphthalmologyPublished by Elsevier Inc.
national accreditation standards and requirements is verifiedby the specialty RRCs of the ACGME. Residency programsare required to meet “minimum operative numbers,” whichare nationally benchmarked targets for ACGME accredita-tion purposes. Individuals (as opposed to accreditation forresidency programs) are certified by the American Board ofOphthalmology. Board certification requires completion ofan accredited residency program. Individual residents mightgraduate at, above, or below the target surgical numbers,and it is up to the program to attest to the American Boardof Ophthalmology that the individual resident is surgically“competent” independently of the actual operative numbers.Evaluating surgical expertise of the residents is now con-sidered part of the core competencies by the RRC andACGME for ophthalmology.2–4 These numbers were re-
cently modified (March 2007), and the minimum require-783ISSN 0161-6420/09/$–see front matterdoi:10.1016/j.ophtha.2008.11.010

Ophthalmology Volume 116, Number 4, April 2009
ment for VRS as primary surgeon was changed from 3 casesto 1 case as primary surgeon. The ACGME receives indi-vidual and program VRS data as part of the residencyaccreditation process in the United States, but the data areself-reported and may be prone to bias toward overreportingto meet the “minimum standards” requirement of the pro-cess. The ACGME accreditation and program review pro-cess includes anonymous individual survey data by theresidents of that program, which are then used to compareand contrast with the results reported by the program. Con-cordance (or disconcordance) between the 2 data sets can beused as an independent verification of compliance.
Although prior publications have described the surgicalexperience of residents in ophthalmology,5–8 to the best ofour knowledge this is the first direct survey of residents inVRS experience in the United States. We report the resultsof an electronic survey of third-year residents regardingexperience, type, and self-reported resident comfort leveland satisfaction with VRS in training programs over the last2 years.
Materials and Methods
A comprehensive 18-question survey was sent to every ACGME-accredited ophthalmology residency program in the United Statesfor 2 consecutive academic years. The anonymous survey wascompleted by the third-year ophthalmology (postgraduate year 4)residents in the program. First and second-year residents were notincluded in the survey. The surveys were collected electronicallyusing a commercially available Internet-based survey web service(www.surveymonkey.com, accessed December 1, 2006). Respon-dents provided the survey answers without any personal identify-ing information, and the data were collected anonymously and arereported in aggregate only. No specific identifiers were noted orcollected regarding individual survey participants or programname. The study was approved by the institutional review board ofthe University of Missouri, Kansas City, and was compliant withthe prevailing Health Insurance Portability and Accountability Actregulations.
Data Collection
A comprehensive 18-question questionnaire was designed on thesurveymonkey.com website. An e-mail web address link wascreated (http://www.surveymonkey.com/s.asp?u�82042846428,accessed November 11, 2008) for the survey. E-mail addresses ofthe programs were acquired from the San Francisco Matchingprogram website (www.sfmatch.org, accessed November 6, 2008).An initial request was sent to program directors or chairs as listedin the San Francisco matching program for the e-mail addresses ofthird-year residents. Alternatively, programs were offered the op-tion of forwarding the link directly to their residents withoutproviding the individual e-mail addresses. The initial survey re-quest was sent in December 2006. Serial requests were repeatedapproximately every 4 weeks until the middle of March, and all theresponses collected were included before March 13, 2007, onlycollected via the Internet through the website. There was noincentive offered to the participants for participation, and there wasno implied or offered penalty for nonparticipation. Surveys wereautomatically entered into a database, and the responses to eachquestion were tabulated. The second-year survey was sent out
similarly from December 2007 to March 2008.784
The survey was designed to determine the following: (1) thenumber of VRS procedures performed by a resident both asprimary surgeon (formerly Class 1) versus assistant surgeon (for-merly Class III) and the various steps of the procedures performed;(2) the number of office procedures (e.g., retina lasers and intra-vitreal injections) performed by residents; (3) the degree of self-reported resident satisfaction with VRS training at their program;(4) the degree of self-reported “comfort” level (e.g., theoretic stepsof VRS); (5) the number of residents who were aware of theminimum operative numbers required by the ACGME for VRS;and (6) the number of residents proceeding to fellowship, includ-ing VRS and the impact of VRS fellowship plans on residentexperience in VRS.
Statistical Analysis
Frequency data were tabulated, and frequencies were used fordescriptive statistics. Chi-square analyses were used to performgroup comparisons of categoric outcomes.
Results
A total of 114 e-mails were sent to the program directors of all theACGME-accredited ophthalmology programs around the UnitedStates for 2 consecutive years. Of the 228 e-mails to ophthalmol-ogy residency programs in the United States over 2 years, 3programs (3 in 2006 and 0 in 2007) declined to participate forvarious reasons and 103 programs (46/114 in 2006 and 57/114 in2007) did not respond to the initial or follow-up e-mail request. Ofthe 868 third-year ophthalmology residents (434 per year over 2years) in the country, 287 (33%) completed the survey. The surveydata were collected from December 2006 to March 2007 (145/434), and a second set of data were collected from December 2007to March 2008 (142/434). Of the 287 respondents, 192 (66.9%)responded that they had definite plans to do a fellowship afterresidency (Table 1). Sixty-two respondents (21.6%) indicatedplans to proceed to a surgical retina fellowship after residency, 5respondents (1.7%) had plans to proceed to a medical retinafellowship after residency, and 125 respondents (43.6%) had plansto proceed to another type of fellowship after residency.
Location (i.e., state) data were provided by 284 of the 287respondents. The state data were used to categorize each respon-dent into 1 of 4 major US census regions (Northeast, Midwest,South, and West). Sixty-five respondents (22.9%) were from theNortheast, 103 respondents (36.3%) were from the Midwest, 84respondents (29.6%) were from the South, and 32 respondents(11.3%) were from the West. We were unable to determine how
Table 1. Fellowship Plans after Residency (N � 287)
Fellowship Plan Frequency %
None 95 33.1Retina (Medical) 5 1.7Retina (Surgical) 62 21.6Cornea 51 17.8Glaucoma 37 12.9Oculoplastics 18 6.3Pediatrics 11 3.8Uveitis 2 0.7Neuro-ophthalmology 1 0.3International 1 0.3Do not know 4 1.4
Total 287 100
Shah et al � Resident Surgical Practice Patterns for VRS in the United States
representative this distribution of residents was because data wasnot available regarding the national distribution of residents.
Surgical Procedures
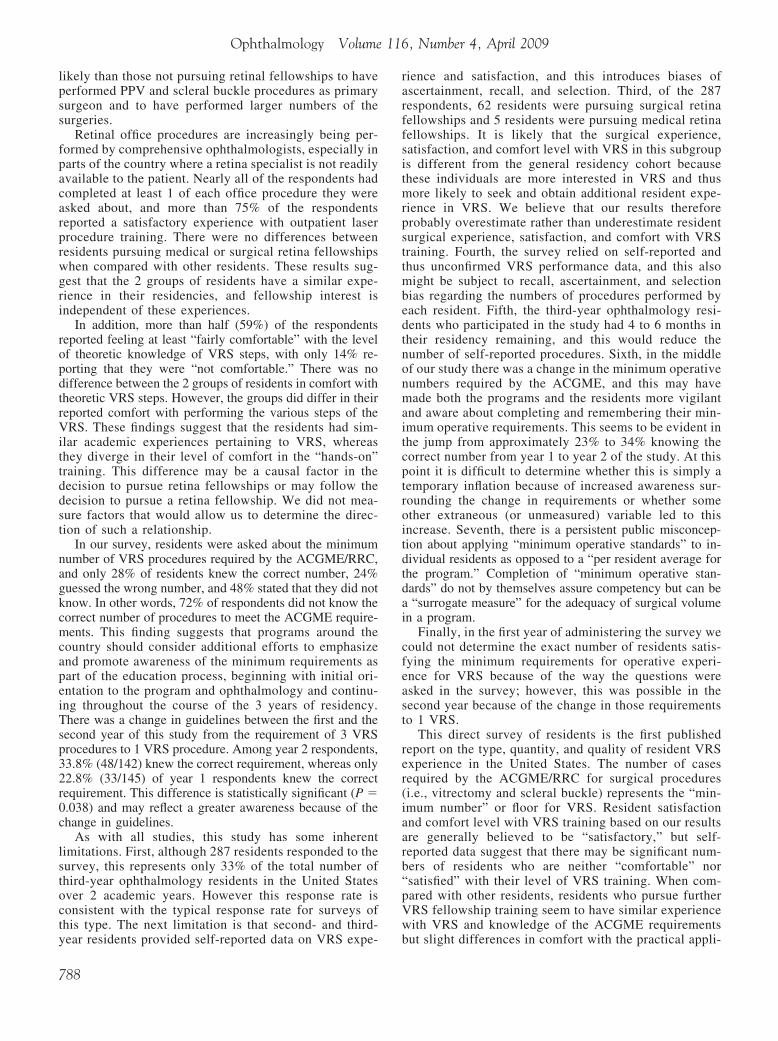
Scleral Buckle. Frequency and percentage data for the number ofscleral buckles performed as assistant (Table 2) and primary(Table 3) surgeon were calculated for each survey year and acrosssurvey years. Chi-square analysis revealed that there were nostatistically significant differences between the year 1 and year 2respondents in the number of scleral buckles performed as assis-tant surgeon (P � 0.088) or as primary surgeon (P � 0.633). Morethan half (59.2%) of respondents reported never having completeda scleral buckle procedure as primary surgeon.
Among residents pursuing a retina fellowship plan, 65.7%(44/67) reported performing at least 1 scleral buckle as primarysurgeon, compared with only 33.2% (73/220) of residents notpursuing a retina fellowship. A chi-square analysis found thisdifference to be statistically significant (P�.001). Also, 17.9% ofresidents (12/67) pursuing a retina fellowship had completed morethan 5 scleral buckles as primary surgeon, which was a signifi-cantly larger percentage than the 3.2% of those (7/220) not pur-suing a retina fellowship (P�.001). There was no differencebetween those with and without retina fellowship plans in thenumber of scleral buckles performed as assistant surgeon (P �0.080).
Pars Plana Vitrectomy. Frequency and percentage data for thenumber of pars plana vitrectomies (PPVs) performed as assistant(Table 2) and primary (Table 3) surgeon were calculated for eachsurvey year and across survey years. Chi-square analysis revealedthat there were no statistically significant differences between theyear 1 and year 2 respondents in the number of PPVs performed asassistant surgeon (P � 0.652) or as primary surgeon (P � 0.709).There was a significant number of respondents (40.9%) reportingthat they had not performed a single PPV as primary surgeon.
Among residents pursuing a retina fellowship, 67.2% (45/67)reported performing at least 1 PPV as primary surgeon, comparedwith 56.4% (124/220) of residents not pursuing a retina fellowship.A chi-square analysis found that this difference was not statisti-cally significant (P � 0.125). Among those with retina fellowshipplans, 28.4% (19/67) had performed more than 5 PPVs as primarysurgeon compared with only 8.7% (19/219) of those without retinafellowship plans. This difference was statistically significant(P�0.001). There was no difference between those with andwithout retina fellowship plans in the number of PPVs performedas assistant surgeon (P � 0.544). Table 4 displays the distributionof various PPV steps performed by residents as primary surgeon.
Overall, residents with plans to pursue a retina fellowshipreported having more experience with scleral buckle and PPV
Table 2. Number of Scleral Buckle and PPV ProceduresPerformed as Assistant Surgeon by Study Year
Study Year None 1–5 6–10 >11
Scleral BuckleYear 1 (2007) 12 (8.3%) 64 (44.1%) 29 (20.0%) 40 (27.6%)Year 2 (2008) 7 (4.9%) 80 (56.3%) 30 (21.1%) 25 (17.6%)Total 19 (6.6%) 144 (50.2%) 59 (20.6%) 65 (22.6%)
PPVYear 1 (2007) 2 (1.4%) 20 (13.8%) 23 (15.9%) 100 (69.0%)Year 2 (2008) 5 (3.5%) 21 (14.8%) 24 (16.9%) 92 (64.8%)Total 7 (2.4%) 41 (14.3%) 47 (16.4%) 192 (66.9%)
PPV � pars plana vitrectomy.
procedures. Residents pursuing retina fellowships were also morelikely to have performed a vitrectomy before the beginning of theirpostgraduate year 4 than other residents (65.2% vs. 48.2%, P �0.045). Only 2 of 287 respondents (0.7%) reported performingneither a scleral buckle nor a PPV as either primary or assistantsurgeon, both from the second year of the survey.
Because of the categoric response options for year 1, it isdifficult to discern who actually completed the ACGME VRSrequirement, yet we can do so for year 2 respondents. Among the142 respondents from year 2 of the survey, 31.7% (N � 45) did notmeet the ACGME requirement of at least 1 scleral buckle or PPVprocedure as primary surgeon when the survey was administered.A chi-square test showed that the percentage of residents attainingthe ACGME requirement was greater for residents pursuing aretina fellowship (82.9%, 29/35) than for those with other fellow-ship plans (63.6%, 68/107); this difference was statistically signif-icant (P � 0.033).
Office Procedures
We also inquired from the respondents to answer questions regard-ing their experience with 3 office procedures: panretinal photoco-agulation (PRP), focal macular laser, and intravitreal injections.
Panretinal Photocoagulation
Of the 287 total respondents, 285 responded to an item askingabout their experience conducting PRP and 99.6% (284/285) ofthese respondents had performed at least 1 PRP, with a singlerespondent (0.4%) having performed none. Among these 285respondents, the majority (61.8%) had performed more than 20PRPs, 13.7% (39/285) had performed between 11 and 20 PRPs,and 12.3% (35/285) had performed 10 or fewer PRPs.
Focal Macular Laser
Of the 287 total respondents, 286 responded to an item askingabout their experience conducting focal macular procedures;94.8% (271/286) of these respondents had performed at least 1focal macular procedure, and 5.2% (15/286) had performed none.Among these respondents, 44.1% (126/186) had performed morethan 20 of the procedures, 22.7% (65/286) had performed between11 and 20 procedures, and 28% (80/286) had performed 10 orfewer procedures.
Intravitreal Injections
Of the 287 respondents, 96.7% (278/286) had performed at least 1
Table 3. Number of Scleral Buckle and PPV ProceduresPerformed as Primary Surgeon
Study Year None 1–2 >3
Scleral BuckleYear 1 (2007) 82 (56.6%) 35 (24.1%) 28 (19.3%)Year 2 (2008) 88 (62.0%) 31 (21.8%) 23 (16.2%)Total 170 (59.2%) 66 (23.0%) 51 (17.8%)
PPVYear 1 (2007) 57 (39.6%) 41 (28.5%) 46 (31.9%)Year 2 (2008) 60 (42.3%) 43 (30.3%) 39 (27.5%)Total 117 (40.9%) 84 (29.4%) 85 (29.7%)
PPV � pars plana vitrectomy.
intravitreal injection and only 3.1% (9/287) had performed none.
785

0
Ophthalmology Volume 116, Number 4, April 2009
There were 33.4% (96/287) who had performed more than 20 ofthe injections, 20.2% (58/287) who had performed between 11 and20 injections, and 43.2% (124/287) who had performed 10 orfewer.
Table 5 displays the frequency distribution of each procedurefor residents planning on pursuing either medical or surgical retinafellowships (n � 67) compared with those not entering generalophthalmology or other fellowships (n � 220). Although thegeneral trend shows increased numbers of procedures for residentspursuing retina fellowships, there was no difference between the 2groups of residents in any of the 3 office procedures (PRP: P �0.182; focal macular laser: P � 0.343; intravitreal injection: P �0.176).
Comfort Level with VRS
When asked about comfort with their knowledge of the theoreticsteps of a vitreoretinal procedure, 285 residents provided a re-sponse. Table 6 displays the distribution of responses for residentspursuing a retina fellowship and those pursuing other types offellowship or no fellowship. Chi-square analysis found no signif-icant difference between the 2 groups of residents in their comfortwith the theoretic steps of VRS (P � 0.296).
There were 284 responses to an item asking about comfort withperforming vitrectomy. The distributions of responses for residentspursuing retina fellowships and those pursuing other fellowshipsor no fellowship are displayed in Table 6. Chi-square analysisshowed that the groups differed from one another in their comfortlevel with performing the VRS (P � 0.004). This difference is areflection of the larger portion of residents without retina fellow-ship plans (56%) reporting that they are “not comfortable” per-
Table 4. Number of Pars Plana Vitrecto
Procedure None 1–5 (%)
Open/close sclerotomy 61 (21.3) 108 (37.6)Core vitrectomy 102 (35.5) 133 (46.3)Membrane peel 266 (92.7) 20 (7.0)
Table 5. Frequency Retina Fellowship Plan vers
Retina Fellowship Other/
Frequency % Frequency
PRP0–5 2 3.0 166–10 2 3.0 1611–20 7 10.4 3221–50 22 32.8 79�50 34 50.7 75
FML0–5 2 3.0 136–10 0 0.0 011–20 0 0.0 021–50 65 97.0 206�50 0 0.0 0
IVI0–5 19 28.4 546–10 11 16.4 4911–20 9 13.4 49�20 28 41.8 68
FML � focal macular laser; IVI � intravitreal injection; PRP � panretinal ph
786
forming VRS compared with those with retina fellowship plans(33.3%), which was statistically significant (P � 0.001).
Satisfaction with VRS TrainingWhen asked to rate “satisfaction” with their VRS experience, 285residents responded. The distribution of responses is displayed inTable 6. Chi-square analysis found no statistically significant dif-ference between the 2 groups of residents (P � 0.541).
Knowledge of ACGME Requirements of VRSThe final question of the survey inquired about what was theminimum number of VRS procedures required by the ACGME fora resident to graduate in ophthalmology. There was a change inguidelines between the first and the second year of this study.During year 1 the minimum required was 3, and during year 2 theminimum was reduced to 1. Table 6 displays the percentage ofresponses that were over, under, and correct for each group in eachyear of the study. Among year 2 respondents, 33.8% (48/142)knew the correct requirement, whereas only 22.8% (33/145) ofyear 1 respondents knew the correct requirement. This differenceis statistically significant (P � 0.038). There was no difference inknowledge of the requirement between residents with plans for aretina fellowship compared with residents with other fellowshipplans (P � 0.077).
Discussion
The ACGME and RRC for ophthalmology are responsiblefor residency program accreditation. These organizations
teps Performed by Residents (N � 287)
10 (%) 11–20 (%) 21–50 (%) >50 (%)
(15.7) 37 (12.9) 26 (9.1) 10 (3.5)(10.5) 14 (4.9) 3 (1.0) 5 (1.7)(0.0) 0 (0.0) 1 (0.3) 0 (0.0)
ther/No Fellowship Plan for Categoric Variables
ellowship Total
% Frequency % P
0.1827.3 18 6.37.3 18 6.3
14.7 39 13.736.2 101 35.434.4 34 38.2
0.3435.9 15 5.20.0 0 0.00.0 0 0.0
94.1 271 94.80.0 0 0.0
0.17624.5 73 25.422.3 60 20.922.3 58 20.230.9 96 33.4
my S
6–
4530
us O
No F
otocoagulation.

A
A*
Shah et al � Resident Surgical Practice Patterns for VRS in the United States
set the minimum average number and variety of proceduresresidents should complete during training, including VRS.The Association of University Professors in Ophthalmologyacts in a complementary and advisory role to the ACGMEand RRC.9 At the time that this survey was designed andadministered in 2006–2007, the ACGME/RRC require-ments as a primary surgeon were as follows: 45 cataractsurgeries, 5 glaucoma filtering surgeries, 3 VRS procedures,and 10 “other” retinal cases. These numbers have undergoneand continue to undergo review and revision by theACGME and RRC in ophthalmology. The present mini-mum operative numbers as primary surgeon are 86 cataractsurgeries, 5 glaucoma filtering surgeries, 1 VRS, and 25“other” retinal cases (http://acgme.org/acWebsite/RRC_240/240_MinimumsOperativeTable.pdf, accessed November 6,2008). It remains to be seen whether performing 1 VRS caseis even necessary for “surgical competency” in VRS. Al-though the concept of minimum numbers is the basis ofquantitative benchmark comparison of programs for accred-itation by the ACGME and RRC, we believe that thisprocess has significant limitations and implications not justfor VRS but for all ophthalmic surgical procedures per-formed by residents. For example, if an individual resident(resident A) were to have performed 286 cataract surgeries,this far exceeds the “minimum” number, but what if everyone of these cases had vitreous loss or some other compli-cation? However, if a different resident (resident B) hadcompleted just 76 cataract surgeries (i.e., below the mini-mum), but every case was perfect with an ideal outcomethen, “Who would be the better the surgeon?” In addition,what if resident A had 286 perfect surgical outcomes butwas an uncaring, selfish person who operated on patients
Table 6. Frequency Retina Fellowship Plan versus OtherACGME
Retina Fellowship
Frequency %
VRS comfort (Theoretic steps)Not comfortable 9 13.8Somewhat 18 27.7Fairly 18 27.7Very 20 30.8
VRS comfort (Performing)Not comfortable 22 33.3Somewhat 29 28.8Fairly/very 25 37.9
VRS satisfactionNot satisfied 13 19.7Somewhat 13 19.7Fairly 19 28.8Very 21 31.8CGME VRS requirementsUnderestimate 5 7.5Correct 13 19.4Overestimate 31 26.9Do not know 67 46.3
CGME � Accreditation Council for Graduate Medical Education; VRStatistically significant at � � 0.05.
who did not need or ask for surgery? These issues remain to
be clarified in future assessments of all of the ACGMEcompetencies, including “surgical competency.”
In a previous survey, program directors reported a widerange of total number of cases as a primary surgeon from 70to 400.9 In previous studies, the trends in resident surgicalexperience have been studied in both cataract and glaucomasurgery.5,6 Both studies surveyed the program directorsinquiring about the average number of surgeries performedby their residents before graduation.
The trends in resident surgical experience for VRS havenot been previously reported. In March 2007, the ophthal-mology ACGME/RRC requirements changed (website up-dated March 14, 2007), and the minimum operative numberrequirements for a graduating ophthalmology resident as aprimary surgeon went from 3 cases to 1 case effective for thegraduating class of residents in June 2008 (www.acgme.org,accessed November 6, 2008). The RRC reported that thismodification was made “in response to the growing data-base from the operative logs and the Committee’s carefulreview” (www.acgme.org, accessed November 6, 2008).Our second set of responses (December 2007 to March2008) was collected from the residents who required 1 VRSto graduate.
The majority (59%) of respondents had no primaryscleral buckle experience, and a significant minority(41%) had no primary PPV experience. Approximatelyone third of residents who completed the survey (30%[85/287]) did not perform a single scleral buckle or PPVas primary surgeon. On the contrary, a large percentagehad VRS experience as assistant surgeon (93.4% forscleral buckle and 97.6% for PPV), and only 2 (0.7%) ofthe respondents had performed no VRS at all. In addition,
Fellowship Plan for Comfort and Satisfaction Items andirements
ther/No Fellowship Total
quency % Frequency % P
0.29632 14.5 41 14.458 26.4 76 26.784 38.2 102 35.846 20.9 66 23.2
0.004*122 56.0 144 50.748 22.0 67 23.648 22.0 25 25.7
0.54144 20.1 57 20.057 26.0 70 24.666 30.1 85 29.852 31.8 73 25.6
0.0778 3.6 13 4.5
68 30.9 81 28.237 16.8 55 19.2
107 48.6 138 48.1
itreoretinal surgery.
/NoRequ
O
Fre
S � v
residents entering surgical retina fellowship were more
787
Ophthalmology Volume 116, Number 4, April 2009
likely than those not pursuing retinal fellowships to haveperformed PPV and scleral buckle procedures as primarysurgeon and to have performed larger numbers of thesurgeries.
Retinal office procedures are increasingly being per-formed by comprehensive ophthalmologists, especially inparts of the country where a retina specialist is not readilyavailable to the patient. Nearly all of the respondents hadcompleted at least 1 of each office procedure they wereasked about, and more than 75% of the respondentsreported a satisfactory experience with outpatient laserprocedure training. There were no differences betweenresidents pursuing medical or surgical retina fellowshipswhen compared with other residents. These results sug-gest that the 2 groups of residents have a similar expe-rience in their residencies, and fellowship interest isindependent of these experiences.
In addition, more than half (59%) of the respondentsreported feeling at least “fairly comfortable” with the levelof theoretic knowledge of VRS steps, with only 14% re-porting that they were “not comfortable.” There was nodifference between the 2 groups of residents in comfort withtheoretic VRS steps. However, the groups did differ in theirreported comfort with performing the various steps of theVRS. These findings suggest that the residents had sim-ilar academic experiences pertaining to VRS, whereasthey diverge in their level of comfort in the “hands-on”training. This difference may be a causal factor in thedecision to pursue retina fellowships or may follow thedecision to pursue a retina fellowship. We did not mea-sure factors that would allow us to determine the direc-tion of such a relationship.
In our survey, residents were asked about the minimumnumber of VRS procedures required by the ACGME/RRC,and only 28% of residents knew the correct number, 24%guessed the wrong number, and 48% stated that they did notknow. In other words, 72% of respondents did not know thecorrect number of procedures to meet the ACGME require-ments. This finding suggests that programs around thecountry should consider additional efforts to emphasizeand promote awareness of the minimum requirements aspart of the education process, beginning with initial ori-entation to the program and ophthalmology and continu-ing throughout the course of the 3 years of residency.There was a change in guidelines between the first and thesecond year of this study from the requirement of 3 VRSprocedures to 1 VRS procedure. Among year 2 respondents,33.8% (48/142) knew the correct requirement, whereas only22.8% (33/145) of year 1 respondents knew the correctrequirement. This difference is statistically significant (P �0.038) and may reflect a greater awareness because of thechange in guidelines.
As with all studies, this study has some inherentlimitations. First, although 287 residents responded to thesurvey, this represents only 33% of the total number ofthird-year ophthalmology residents in the United Statesover 2 academic years. However this response rate isconsistent with the typical response rate for surveys ofthis type. The next limitation is that second- and third-
year residents provided self-reported data on VRS expe-788
rience and satisfaction, and this introduces biases ofascertainment, recall, and selection. Third, of the 287respondents, 62 residents were pursuing surgical retinafellowships and 5 residents were pursuing medical retinafellowships. It is likely that the surgical experience,satisfaction, and comfort level with VRS in this subgroupis different from the general residency cohort becausethese individuals are more interested in VRS and thusmore likely to seek and obtain additional resident expe-rience in VRS. We believe that our results thereforeprobably overestimate rather than underestimate residentsurgical experience, satisfaction, and comfort with VRStraining. Fourth, the survey relied on self-reported andthus unconfirmed VRS performance data, and this alsomight be subject to recall, ascertainment, and selectionbias regarding the numbers of procedures performed byeach resident. Fifth, the third-year ophthalmology resi-dents who participated in the study had 4 to 6 months intheir residency remaining, and this would reduce thenumber of self-reported procedures. Sixth, in the middleof our study there was a change in the minimum operativenumbers required by the ACGME, and this may havemade both the programs and the residents more vigilantand aware about completing and remembering their min-imum operative requirements. This seems to be evident inthe jump from approximately 23% to 34% knowing thecorrect number from year 1 to year 2 of the study. At thispoint it is difficult to determine whether this is simply atemporary inflation because of increased awareness sur-rounding the change in requirements or whether someother extraneous (or unmeasured) variable led to thisincrease. Seventh, there is a persistent public misconcep-tion about applying “minimum operative standards” to in-dividual residents as opposed to a “per resident average forthe program.” Completion of “minimum operative stan-dards” do not by themselves assure competency but can bea “surrogate measure” for the adequacy of surgical volumein a program.
Finally, in the first year of administering the survey wecould not determine the exact number of residents satis-fying the minimum requirements for operative experi-ence for VRS because of the way the questions wereasked in the survey; however, this was possible in thesecond year because of the change in those requirementsto 1 VRS.
This direct survey of residents is the first publishedreport on the type, quantity, and quality of resident VRSexperience in the United States. The number of casesrequired by the ACGME/RRC for surgical procedures(i.e., vitrectomy and scleral buckle) represents the “min-imum number” or floor for VRS. Resident satisfactionand comfort level with VRS training based on our resultsare generally believed to be “satisfactory,” but self-reported data suggest that there may be significant num-bers of residents who are neither “comfortable” nor“satisfied” with their level of VRS training. When com-pared with other residents, residents who pursue furtherVRS fellowship training seem to have similar experiencewith VRS and knowledge of the ACGME requirements
but slight differences in comfort with the practical appli-
Shah et al � Resident Surgical Practice Patterns for VRS in the United States
cation of their learning. Future work is needed to estab-lish the need for, the type of, and the amount of VRSexperience that provide the optimal level of training for ageneral ophthalmologist to acquire during residencytraining. We hope that our work will stimulate furtherinvestigation into the quality and quantity of residentVRS training in the United States.
References
1. Jonas JB, Rabethge S, Bender HJ. Computer-assisted trainingsystem for pars plana vitrectomy. Acta Ophthalmol Scand2003;81:600–4.
2. Lee AG. The new competencies and their impact on residenttraining in ophthalmology. Surv Ophthalmol 2003;48:651–62.
3. Lee AG, Volpe N. The impact of the new competencies on
pitals and Clinics, Iowa City, Iowa.
resident education in ophthalmology. Ophthalmology2004;111:1269–70.
4. Oetting TA, Lee AG, Beaver HA, et al. Teaching and assess-ing surgical competency in ophthalmology training programs.Ophthalmic Surg Lasers Imaging 2006;37:384–93.
5. Golden RP, Krishna R, DeBry PW. Resident glaucoma sur-gical training in United States residency programs. J Glau-coma 2005;14:219–23.
6. Rowden A, Krishna R. Resident cataract surgical training inUnited States residency programs. J Cataract Refract Surg2002;28:2202–5.
7. Aaron MM, Aaberg TM. Ophthalmology resident training inrefractive surgery. Am J Ophthalmol 2001;131:241–3.
8. LeBoyer RM, Deutsch TA, Rubenstein JB. Results ofresident-performed laser in situ keratomileusis. J CataractRefract Surg 2005;31:771–5.
9. Binenbaum G, Volpe NJ. Ophthalmology resident surgicalcompetency: a national survey. Ophthalmology 2006;113:
1237–44.Footnotes and Financial Disclosures
Originally received: August 24, 2008.Final revision: November 7, 2008.Accepted: November 11, 2008. Manuscript no. 2008-1015.
1 Department of Ophthalmology, University of Missouri-Kansas City,Kansas City, Missouri.
2 Department of Basic Medical Science, University of Missouri-KansasCity, School of Medicine, Kansas City, Missouri.
3 Departments of Ophthalmology, Neurology, and Neurosurgery and the H.Stanley Thompson Neuro-ophthalmology Clinic, University of Iowa Hos-
Financial Disclosure(s):The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article.
Supported in part by an unrestricted grant from Research to PreventBlindness, Inc., New York, New York.
The views and opinions expressed herein are the personal views of theauthors and are not intended to reflect the views or opinions of theResidency Review Committee for ophthalmology.
Presented at The annual meeting of the American Academy of Ophthal-mology Atlanta, Georgia, November 2008.
Correspondence:Vinay A. Shah, MD, Department of Ophthalmology, 2300 Holmes Street,
Kansas City, MO 64108.789