Report exploring the link between MSM, homophobia and HIV ...
104
Report exploring the link between MSM, homophobia and HIV/AIDS in countries: Bosnia and Herzegovina, Croatia, Montenegro and Serbia
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Report exploring the link between MSM, homophobia and HIV ...
Report exploring the link between MSM, homophobia and HIV/AIDS in countries: Bosnia and Herzegovina, Croatia, Montenegro and Serbia

Table of ContentsReport exploring the link between MSM, homophobia and HIV/AIDS in countries: Bosnia and Herzegovina, Croatia, Montenegro and SerbiaWithin the project:Developing UNDP Cross-Country Cooperation(Bosnia and Herzegovina, Croatia, Montenegro and Serbia)
Financially supported by UNDP Country Office Support Facility (COSF)
United Nations Development Programme (UNDP) is the UN’s global development network, advocating for changeand connecting countries to knowledge, experience and resources to help people build a better life. We are onthe ground in 166 countries, working with them on their own solutions to global and national developmentchallenges. As they develop local capacity, they draw on the people of UNDP and our wide range of partners.
Short extracts from this publication may be reproduced unaltered without authorisation, on condition that thesource is indicated.
The views expressed in this paper are those of the authors and do not necessarily represent the views of UNDP.
Copyright © 2010.
Editor in chief: Iva Jovović
Authors (in alphabetical order): Valerio Baćak, Zoran Dominković, Hrvoje Fuček, Kristijan Grđan, Branko Kolarić, Danijel Lončar and Dinko Štajduhar.
Published by: United Nations Development Programme (UNDP) in Croatia
Radnička cesta 41, 10 000 Zagreb, Hrvatska
Proofreading (English): Irena Bilić
Design and cover: Krešimir Kraljević
First edition: 2010
Acknowledgements:
Special thanks go to respondents who have taken the time to provide answers and inputs to the authors. We thank col-leagues from UNDP Regional HIV/AIDS Team under leadership of Mr. Shombi Sharp with support from colleagues Dudley Tarlton and John Macauley. We are grateful to our sub-regional UNDP Colleagues: Mrs. Miljana Grbić, Mrs. Itana Labović and Mr. Nešad Šeremet, who offered valuable advice, suggestions and contacts for their respective countries.
3
Executive Summary
1. Homophobia in South-eastern Europe - Prevalence, Consequences, and Prevention 91.1. Introduction 91.2. Meaning and Impact of Homophobia 91.3. A Snapshot of Homophobia in the Region 101.4. Local Responses to Homophobia 111.5. Recommendations for Homophobia Prevention 13
1.5.1.Young People and Schools 131.5.2. Law Enforcement and Homophobia 131.5.3. Social Marketing and the Media 141.5.4. Internalized Homophobia 14
1.6. Conclusion 15
2. MSM- men having sex with men 172.1. Introduction 172.2. The Term 182.3. “MSM” in the Region, Introduction 182.4. Silent men 192.5. What’s Sex Got to Do with It? 202.6. Continued: MSM in the Region 202.7. Instead of Conclusion 21
3. Legal Status of Sexual and Gender Minorities in South-eastern Europe 233.1. Introduction 233.2. Human Rights Standards 23
3.2.1. Human rights definition 233.2.2. Violations of human rights 233.2.3. The International Covenant on Civil and Political Rights (ICCPR) 243.2.4. First Optional Protocol to the ICCPR 263.2.5. Second Optional Protocol to the ICCPR 263.2.7. Protocol 12 to the ECHR 263.2.8. The European Charter on Human Rights and Fundamental Freedoms 273.2.9. The European documents relevant for sexual and gender minorities 273.2.10. The European Parliament Resolution A3-0028/94 273.2.11. The European Parliament Resolution A5-0050/00 273.2.12. The Council Directive 2000/78/EC 273.2.13. The European Parliament Resolution on Homophobia in Europe 283.2.14. The Council of Europe Recommendation CM/Rec (2010) 28
Table of Contents
4
3.3. Right to life, safety and protection from violence 283.3.1. Legal background in the region 283.3.2. Violence against sexual and gender minorities 293.3.3. Availability of effective remedies 303.3.4. Forced psychiatric treatment 313.3.5. Conclusions and recommendations 32
3.4. Right to expression and public assembly 333.4.1. Practice of the European Court on Human Rights 333.4.2. Zagreb Pride 343.4.3. Belgrade Pride 343.4.4. Queer festival Sarajevo 354.4.5. Conclusions and recommendations 35
3.5. Right to be protected from discrimination 363.5.2. Practice of the European Court on Human Rights 363.5.3. National anti-discrimination legislations 363.5.4. Conclusions and recommendations 39
3.6. Right to family life 403.6.1. European context 403.6.2. Situation in the region 413.6.3. Conclusions and recommendations 42
3.7. Summary of recommendations 42RIGHT TO LIFE, SAFETY AND PROTECTION FROM VIOLENCE 42RIGHT TO EXPRESSION AND PUBLIC ASSEMBLY 43RIGHT TO BE PROTECTED FROM DISCRIMINATION 43RIGHT TO FAMILY LIFE 44
4. Health of MSM 454.1. Introduction 454.2. Bosnia and Herzegovina 464.3. Croatia 494.4. Montenegro 524.5. Serbia 534.6. Instead of conclusion 564.7. References 57
5. Academic education on LGBT population in three helping professions in countries of South-eastern Europe 595.1. Summary 595.2. Introduction 595.3. On data collection 615.4. Overview of the data collected and discussion by country 62
5.4.1. Bosnia and Herzegovina 625.4.2. CROATIA 645.4.3. MONTENEGRO 695.4.4. SERBIA 70
5.5. Conclusion and recommendations 735.6. List of participants 745.7. References 75
5
6. Activism and non-governmental response 796.1. Introduction 796.2. Bosnia and Herzegovina 806.3. Croatia 816.4. Montenegro 836.5. Serbia 84
7. Prevention tips- manual on prevention activities 877.1. Prevention 87
7.1.1. Safer sex 877.1.2. Condoms and lubricants 88
7.2. Risk and vulnerability assessment 887.2.1. More than sex 887.2.2. Work with organizations in society (NGOs) 897.2.3. Work with “gatekeepers” 897.2.4. Work with health service providers 897.2.5. Principles obstructing HIV prevention 90
7.3. Strategies of HIV/STD prevention for MSM and with MSM 917.3.1. Health-promotion strategies focused on individuals 917.3.2. Under the open skies 917.3.3. On a secret mission 927.3.4. Materials 927.3.5. Groups 937.3.6. Workshops 937.3.7. Strategies for gradual increase, targeting and improvement of delivery of services and products 947.3.8. Condoms 947.3.9. Lubricants 957.3.10. Counselling 957.3.11. Ethical issues and confidentiality 967.3.12. Other services 96
7.4 Strategies for mobilizing the community 977.4.1. Celebration time 977.4.2. Safe house 977.4.3. On-line 987.4.4. In prison 987.5.1. Various settings 997.5.2. Visibility and representation 997.5.3. Link with the police 1007.5.4. Social advocacy 1007.5.5. Political advocacy 1017.6.6. Religion 101
Acronyms 103

6
7
Executive Summary
The term ‘Men who have sex with men’, frequently shortened to MSM - describes a behaviour rather than a specific group of people. It includes self-identified gay, bisexual, or heterosexual men, many of whom may not consider them-selves gay or bisexual including transgender populations.
MSM presents a topic that many governments and certain individuals would prefer not to talk about and choose to be silent on these issues, failing to acknowledge these behaviours and address them, which unfortunately helps the HIV and AIDS epidemic to grow. Therefore, the prevention programs addressing MSM are vitally important. However, this population is often seriously neglected because of official denial by governments, the relative invisibility of MSM, stig-matization of male-to-male sex, ignorance and/or lack of adequate information.
All four countries (Bosnia and Herzegovina, Croatia, Montenegro and Serbia) experience low level HIV/AIDS epidem-ics. The dominant way of HIV transmission in these countries is through sexual intercourses. Though a much lower proportion among all HIV cases are officially attributable to homosexual transmission, the problem of under-reporting of homosexual transmission among those diagnosed with HIV is often mentioned in the country reports. Many people feel uncomfortable to name MSM as a way of HIV transmission in their individual case when talking to doctors.
Since the year 2003 and the beginning of the Global Fund to fight AIDS, Tuberculosis and Malaria (GFTAM) donations to the countries in the sub-region, a significant amount of financial resources and technical assistance was poured into scaling up treatment and prevention activities. The prevention activities were also improved in both the coverage of us-ers as well as in the number and density of service delivery points.
There are still negative practices in place such as:
• National legislation and policies that hinder a creation enabling environment to prevent HIV among MSM;
• Lack of relevant data on stigma and discrimination (from quantitative surveys or qualitative research);
• Social, cultural and political circumstances that influence the level of stigma and discrimination towards MSM;
• Evidence of unlawful practices (e.g. in health services, workplace, etc).
Therefore, we prepared a report that would enable national authorities for better understanding of social and political context that would lead to comprehensive planning of prevention activities among MSM and other sexual minorities, even lead to a development of a larger scale sub-regional project.

9
Chapter 1Homophobia in South Eastern Europe- Prevalence, Consequences and Prevention
1. Homophobia in South-eastern Europe - Prevalence, Consequences, and PreventionPrepared by: Valerio Baćak
1.1. Introduction
Homophobia and its effects in the form of discrimination and violence remain widespread in South-eastern Europe. IIn this chapter we address the origin and meaning of the term followed by a discussion of the prevalence and manifesta-tions of homophobia in Croatia, Bosnia and Herzegovina, Montenegro, and Serbia. We also showcase a few notable campaigns to address homophobia in these countries designed by the local non-governmental organizations (NGOs). The final section outlines recommendations indicating the general direction for future efforts in preventing homopho-bia in the region. This is however not an exhaustive review of everything that has been done in response to homophobia in the four countries or globally in the past few decades.
1.2. Meaning and Impact of Homophobia
The term homophobia was coined by the clinical psychologist George Weinberg and popularized by the publication of his book Society and the Healthy Homosexual in 1972. He defined it as a “dread of being in close quarters with homo-sexuals – and in the case of homosexuals themselves, self-loathing”1. It is not the homosexuals who suffer from mental and emotional disorder, the argument goes, but the individuals with homophobic attitudes. He saw the phobia and prejudice directed at homosexual persons as a reflection of a larger fear that society has towards intimacy between men. In other words, homophobia can also be conceived as a social illness acting as a social norm. It can appear in various manifestations ranging from passive-aggressive hostility to overt violence2.
More recently it has been suggested that the concept should be expanded to include the other relevant constructs that define the way society and individuals deal with sexual difference such as sexual stigma, heterosexism, and sexual preju-dice3. Of these terms heterosexism may be the most appropriate as it captures well the essence of the sexual prejudice heterosexual persons have towards those with same-sex attractions4. In this chapter we use the word homophobia be-cause it is more widely used and better reflects the terminology of different organizations who are engaged in the human rights protection of sexual minorities5.
Homophobia is largely related to the wider processes of social exclusion of sexual minorities that are occurring through-out Eastern Europe6. Sex between men endures stigmatization globally, particularly in societies with widespread and
1 Weinberg, G. (1972). Society and the Healthy Homosexual. New York, NY: St. Martin’s Press; pg. 4.2 Kantor, M. (2009). Homophobia: The State of Sexual Bigotry Today. Westport, CT: Praeger Publishers.3 Herek, G. M. (2004). Beyond “Homophobia”: Thinking About Sexual Prejudice and Stigma in the Twenty-First Century. Sexuality Research and Social Policy, 1(2), 6-24. 4 Rothblum, E. D. & Bond, A. L. (eds.) (1996). Preventing Heterosexism and Homophobia. Thousand Oaks-London-New Delhi: SAGE Publications.5 It is important to note here the debates that are ongoing about the appropriate terms that should be used when addressing oppression based on sexual orientation, especially their political implications. For an incisive discussion of how language matters when talking about heterosexism see Kitzinger, C. (1996). “Speaking of Oppression: Psychology, Politics, and the Language of Power”, in Preventing Heterosexism and Homophobia, edited by Rothblum, E. D. & Bond, A. L. Thousand Oaks-London-New Delhi: SAGE Publications.6 Takacs. J. (2006). Social Exclusion of Young Lesbian, Gay, Bisexual and Transgender (LGBT) People in Europe. Brussels and Amster-dam: ILGA-Europe and IGLYO.
10
Chapter 1 Homophobia in South Eastern Europe- Prevalence, Consequences and Prevention
strong traditional views of gender roles. In addition to unfavourable social reactions to homosexuality, numerous coun-tries instituted laws that prohibit and sanction homosexual contact. As of 2009, 80 countries criminalize sexual in-tercourse between consenting adult men7. Hate crimes including those of the most violent kind are not a rarity. For instance, a recent report from the UNAIDS noted that every two or three days a person is killed in Brazil in violence connected with his or her sexuality, most of the victims being men who have sex with men8.
There have been laudable global improvements in the advancement of human rights of homosexual persons such as recent legalization of same-sex marriage in Argentina. Homophobia, though, is still omnipresent across the globe on both the structural and individual level. A 2005 nationally representative survey of gay, lesbian, and bisexual adults in the United States, for instance, found that around a half of the surveyed men experienced verbal harassment, and about 20% reported a person or property crime based on their sexual orientation9. Abundance of similar evidence from across the developed and less developed world strongly suggests that homophobia still remains a widespread and significant social problem.
Besides the informal and formal oppression experienced at the everyday level, men who have sex with men, along with women of alternative sexual orientation, suffer from multiple health problems related to their social exclusion. They are at a higher risk of suicidal behaviour, developing a mental disorder, and substance misuse and dependence compared to their heterosexual counterparts10. In many cases this is linked to either their direct experiences of homophobia or to the larger social environment unsupportive of homosexuality. Yet in many countries, such as England, with a long demo-cratic tradition, sexual identity has only recently been officially identified as a risk factor for suicide11.
1.3. A Snapshot of Homophobia in the Region
Research evidence about negative attitudes towards same-sex relationships in European post-communist countries clearly suggests its omnipresence. In particular, the revival of the influence of religious institutions has played a major role in this process. Countries such as Romania, Lithuania, Ukraine, and Belarus – with influential religious institu-tions – exhibited the strongest disapproval of homosexuality when compared to the countries from the so-called “old” Europe12. The four South-eastern European countries discussed in this report have an added burden of relatively recent wars which slowed down the development of the efforts to strengthen the protection of minority populations. The war and its aftermath were also responsible for the promotion of chauvinistic nationalism exclusive of ethnic, sexual, and other differences not in line with an idealized notion of a full-fledged citizen.
A compelling finding comes from a recent survey on a representative sample of 1049 adult participants in Montenegro13 - more than 60% reported believing that homosexuality is an illness and that it is immoral. In line with this is the finding that 62% think that homosexual persons do not have the right to freely and publicly express their sexuality by kissing, holding hands, or hugging. One of the rare encouraging results is that about only one in ten of the participants believed that physical violence against homosexuals is justified. In Croatia, a survey carried out in 2005 among 202 LGB persons
7 http://old.ilga.org/Statehomophobia/ILGA_State_Sponsored_Homophobia_2010.pdf8 http://www.unaids.org/en/KnowledgeCentre/Resources/FeatureStories/archive/2009/20090113_MSMLATAM.asp9 Herek, G. M. (2009). Hate Crimes and Stigma-Related Experiences among Sexual Minority Adults in the United States. Journal of Interpersonal Violence, 24(1), 54 -74.10 King, M., Semlyen, J., Tai, S. S., Killaspy, H., Osborn, D., Popelyuk, D., & Nazareth, I. (2008). A Systematic Review of Mental Disor-der, Suicide, and Deliberate Self Harm in Lesbian, Gay and Bisexual People. BMC Psychiatry, 8, 70-70; Meyer, I. H. (2003). Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychological Bulletin, 129(5), 674-697.11 King, M., Semlyen, J., Tai, S. S., Killaspy, H., Osborn, D., Popelyuk, D., & Nazareth, I. (2008). A Systematic Review of Mental Disor-der, Suicide, and Deliberate Self Harm in Lesbian, Gay and Bisexual People. BMC Psychiatry, 8, 70-70. 12 Štulhofer, A. & Rimac, I. (2009). Determinants of Homonegativity in Europe. Journal of Sex Research, 46(1), 24–32.13 Omladinski kulturni centar Juventas (2010). Rezultati istraživanja Homofobija u Crnoj Gori. Podgorica: Juventas.
11
Chapter 1Homophobia in South Eastern Europe- Prevalence, Consequences and Prevention
in three major cities revealed that every second participant experienced psychological or physical violence in the past four years due to their sexual orientation14.
A recent longitudinal survey of first-year students from the University of Zagreb reported that the disapproval of ho-mosexual intimacy increased among men15. In comparison to 1998, when 49% of the students expressed disapproval of sexual relationships between same-sex persons, the proportion increased to 63% in 2008. It is reasonable to expect that homonegativity among less educated young people with less access to information could be even higher. A Croatian National Institute of Public Health study found that 30% of the general practice physicians in Zagreb, the capital of Croatia, would prefer not to have men who have sex with men as their patients16 .
In a study among 214 members of the LGBTIQ population in Bosnia and Herzegovina17, social discrimination and exclu-sion were reported by the majority of the participants as the largest problem they face in the country. The sectors of society that have been identified as the most discriminatory have been the media, religion, and education. In the qualitative com-ponent of the study, where participants talked about their everyday experiences, school was commonly reported as a major place where they initially encountered homophobia and the homophobic discourse around the origins and depiction of homosexuality as a mental illness. One of the main messages that emerged from this survey is that LGBTIQ persons in Bosnia and Herzegovina fear violence and do not feel safe in their country.
There is also evidence of homophobia documented in numerous media reports across the region. The most appalling ex-ample is the eruption of anti-gay violence that ensued at the Gay Pride marches in Belgrade, the capital of Serbia, on June 30, 2001 and on October 10, 2010. In the latter thousands of right-wing extremists from across the country attempted to attack the march that was, with great difficulty, protected by more than 5500 strong police force. Another horrific example was the violent assaults by mainly religious extremists at the participants during the opening ceremony of the first Queer Sarajevo Festival in 2008. Police reaction was late and inadequate. Responding to the need for trained po-lice forces, governments in South-eastern European countries recently participated in the Law Enforcement Hate Crime Training program developed at the OSCE Office for Democratic Institutions and Human Rights (ODIHR)18.
1.4. Local Responses to Homophobia
Gay Pride march, as one of the most prominent means of sensitizing the public about the presence and rights of persons with same-sex attractions, has continuously taken place only in Zagreb, Croatia. With an ever increasing attendance but still violent opposition and under tight police supervision, the parade has been running annually since 2002. The efforts at similar marches in Serbia as briefly described in the previous section of the chapter faced better organized reactions from the extremist right-wing groups and relatively less institutional protection. The state of the human rights of sexual minorities and the pervasiveness of homophobia in Bosnia and Herzegovina and Montenegro is very well illustrated by the fact that there were no attempts at organizing similar events.
In spite of a vicious resistance to activities related to the human rights of homosexual persons in the region, successful activities were nonetheless implemented to tackle the problem of homophobia. Much of this effort was carried out un-
14 Pikić, A. & Jugović, I. (2006). Violence against Lesbians, Gays and Bisexuals in Croatia: Research Report. Zagreb: Lesbian group Kontra.15 Landripet, I., Šević, S., Car, D., Baćak, V., Mamula, M. & Štulhofer, A. (Forthcoming). Changing Sexuality? Results from Repeated Cross-sectional Studies of the University of Zagreb First-year Students, 1998-2008. Društvena istraživanja16 Cazin, I., Pristaš, I., & Kolarić, B. (2006). “Knowledge and Attitudes of Physicians about HIV/AIDS in Primary Health Care Prac-tice – A Pilot Study in the City of Zagreb and the Zagreb County,” in Second Generation of Surveillance in HIV Infection and AIDS in the Republic of Croatia, 2003–2006, edited by I. Gjenero-Margan & B. Kolarić. Zagreb: Croatian National Institute of Public Health.17 Đurković, S. (2007). Nevidljivo Q? Pitanje ljudskih prava i potreba LGBTIQ osoba u Bosni i Hercegovini. Sarajevo: Udruženje Q za promicanje i zaštitu kulture, identiteta i ljudskih prava queer osoba. 18 http://www.osce.org/publications/odihr/2006/09/20673_676_en.pdf

12
Chapter 1 Homophobia in South Eastern Europe- Prevalence, Consequences and Prevention
der the funding schemes of HIV prevention that focused on the men who have sex with men as a risk group in regard to HIV/AIDS. Stigma and discrimination related to homosexuality have been recognized by the UN and many other international organizations as one of the key social obstacles to preserving or improving the sexual health of sexual mi-norities. In addition to the campaigns on the local level, there were a number of important and positive legal advances nationally, one of which are the anti-discrimination laws implemented in all four countries19.
Non-governmental organizations, in particular, have been persistent in their laudable efforts to improve the quality of life for sexual minorities in Bosnia and Herzegovina, Croatia, Montenegro, and Serbia. Such activism appears to be the most developed in Croatia and Serbia where there are a number of organizations working on different issues related to LGBT persons, including homophobia. The photo below depicts the website set up in cooperation between NGOs “Kon-tra” and “Iskorak” in Croatia (see Figure 1). There they provide information about homophobia and the myths about homosexuality that support it. Most importantly, however, they provide information about the legal options for people who experienced violence or discrimination related to their sexual orientation.
Gay activism is especially difficult to carry out in Montenegro, and Bosnia and Herzegovina. In Montenegro NGO “Juventas” organized a public stand on May 17, 2009 (World Day against Homophobia) delivering information about homophobia. For a country where homosexuality is highly stigmatized setting up such a public presence was an impor-tant and brave20 step albeit a seemingly small one. Although men who have sex with men have been mentioned in docu-ments in Bosnia and Herzegovina that have outlined a set of proposed measures for tackling stigma and discrimination as part of the national response to the HIV/AIDS for the period 2010-2015, there are no specific measures targeting homophobia. In light of an increased public presence and influence of politically conservative movements associated with the Islam, along with a strong impact of both the Christian Orthodox and Catholic Church on the public opinion in the country, such measures are sorely needed.
An inspired and thoughtful educational project named “Vježbanka” was set up by the NGO “Q” from Bosnia and Herzegovina. Like the Croatian project described above, it is Internet-based (see Figure 2),21 although it is also printed as a hard copy. The publication provides comprehensive and visually appealing information on a range of topics from biological aspects of sexual development to queer theory. Gay activism in Serbia has been very successful in increasing its presence throughout the years especially online. The culmination of their efforts was the successful organization of the Gay Pride march in 2010 despite overwhelming opposition. Finally, people with same-sex attractions in all four countries have access to information and contacts trough a number of websites, most of which are maintained by the NGOs. These sites provide important and useful information on sexuality, including materials on safer sex, legal advice, and forums for anonymous discussion with peers22.
19 An encouraging move was made by the government of Montenegro on July 27, 2010 in which the parliament adopted an anti-dis-crimination law banning, among other, discrimination based on sexual orientation and gender identity. 20 For a brief report on the threats to the organizers during the event see: http://fellowship.birn.eu.com/en/main/news_and_upda-tes/19668/21 http://www.queer.ba/vjezbanka 22 These are the more popular regularly updated websites in the four countries: www.gay.hr (Croatia), www.queer.ba (Bosnia and Herzegovina), www.montenegro-gay.me (Montenegro), and www.gay-serbia.com (Serbia).
13
Chapter 1Homophobia in South Eastern Europe- Prevalence, Consequences and Prevention
1.5. Recommendations for Homophobia Prevention
1.5.1.Young People and Schools
School environment has to be the central location for preventing homophobia23. Targeting schools has proved effective in a number of Western European countries. In schools in the United Kingdom, for instance, officials work with both the victims of homophobic violence and its perpetrators. Another aspect of effective prevention efforts has been a series of surveys assessing the prevalence of homophobia in schools across the country. These efforts do not only enhance the knowledge about the presence of homophobia in schools, but they can also help with advocating for resources from lo-cal and national governments to address homophobic bullying. In the Netherlands, NGOs work in collaboration with state agencies and schools to design and implement locally tailored programs. The focus is on capacity building for the individual institutions so they do not have to depend on the outside expertise.
Effective prevention messages in schools can have a positive impact on young people who are otherwise exposed to homophobia as a socially desirable response to homosexuality. Curriculum change is particularly important24. Even though it seems unlikely that anything similar will soon happen in these four countries, the instructional materials in classrooms have to reflect the experiences of gay, lesbian, and transgender persons through subjects such as literature, history, and the social sciences. In addition to raising the awareness of and respect for sexual minorities among the students, prevention activities should also include the education of teachers. Finally, support for victims of homophobic violence as well as sanctions for those who engage in it have to be one of the principal components of any school-based prevention programs. The school has to have a clear and visible policy against any manifestations of homophobia that occurs either through verbal abuse or physical violence.
In order for schools to develop such activities, however, homophobic bullying in South-eastern Europe needs to be recognized as a pressing social problem by both school authorities and the relevant government agencies. In addition to attaining the support from the ministries of education, which is an advocacy challenge in itself, involving schools would also mean that teachers and school directors need to be educated and supportive of such efforts. It is, moreover, of fundamental importance to discuss sexual diversity in classroom settings in positive ways25. This can most effectively be achieved through comprehensive school-based sexual education programs. None of the countries in the region, however, have such programs in place and judging by the recent strong opposition to evidence-based sex-education26 from influential conservative groups it does not seem likely that such programs will be introduced in the near future.
1.5.2. Law Enforcement and Homophobia
Across the world only a small portion of homophobic incidents and crimes are reported in the news media and are doc-umented in the official hate crimes statistics27. Under-reporting of hate crimes can lead to false conclusions that abuse and violence against persons with same-sex attractions should not be a matter of public concern. A good example of the omnipresence of under-reporting, even in countries with well-developed criminal justice systems, is a recent estimate
23 Rothblum, E. D. & Bond, A. L. (eds.) (1996). Preventing Heterosexism and Homophobia. Thousand Oaks-London-New Delhi: SAGE Publications.24 Chan, C. (1996). “Combating Heterosexism in Educational Institutions: Strucutural Changes and Strategies,” in Preventing Hetero-sexism and Homophobia, edited by Rothblum, E. D. & Bond, A. L. Thousand Oaks-London-New Delhi: SAGE Publications.25 Sainsbury, J. (2009). Talking Straight: Finding New Ways to Challenge Homophobia in Australian schools. The Winston Churchill Memorial Trust of Australia.26 E.g. Bijelić, N. (2008). Sex Education in Croatia: Tensions between Secular and Religious Discourses. European Journal of Women’s Studies, 15(4), 329–343.27 Human Rights First (2007). Homophobia: 2007 Hate Crime Survey. New York, NY: Human Rights First.
14
Chapter 1 Homophobia in South Eastern Europe- Prevalence, Consequences and Prevention
from the police in the United Kingdom that 90% of hate crimes based on sexual orientation go unreported28. In addition to informing the responsible institutions about the gravity of these crimes, increasing the reporting and systematic doc-umentation of hate crimes can be used as a tool for advocating for more resources devoted to addressing and preventing homophobia-related crimes in the future. The same report points out that only Canada, Sweden, the United Kingdom, and the United States “have made a commitment to monitor such attacks in their official reporting on hate crimes”29.
Addressing homophobic violence also needs to involve expert psychological support for victims of such crimes. Preserv-ing psychological well-being has to be one of the priorities in dealing with homophobia. The focus should be on young people who are the most vulnerable, especially in school settings30. Cooperation between the NGOs and the public authorities is another important aspect of effective design and implementation of prevention policies. A good example of this practice comes from Bulgaria where the NGO “Gemini” has had a continually successful cooperation with the police by providing, for instance, training sessions for police officers on LGBT issues, with a particular emphasis on homophobia-based crimes31.
Victims of homophobic abuse and violence should be encouraged to report such incidents. This is especially important because many may believe that police will not adequately respond due to prejudice or the victims might be afraid that their sexual preferences will be exposed32. Part of the solution for the problem of under-reporting is to develop third-party reporting systems with someone else reporting the crime on behalf of the victim. Furthermore, appointing officers with special training in combating hate crimes can also prove beneficial. Sometimes NGOs keep track of hate crimes and in doing so either supplement the police records or provide the baseline information in the absence of systematic police statistics33. An additional significance of NGOs is that many victims may possibly feel more comfortable in expressing their problems to them then to the police.
1.5.3. Social Marketing and the Media
Social marketing campaigns can be a useful way of raising the public awareness about the detrimental effects of homo-phobic discrimination, abuse, and violence. One of the ways to promote prevention messages is to involve celebrities and prominent public figures to publicly support the campaign causes. One of the more prominent social marketing campaigns was developed by the Gay Lesbian and Straight Education Network (GLSEN) from the United States with the goal of eliminating the homophobic slang among young people (see Figure 3). Although less explored, using social media – including the social networking web sites – might also prove effective in addressing homophobia, particularly among young people. There are numerous ways in which these tools can be used to distribute information and messages that address respect for sexual diversity. However, in order to reach a wider population more conventional means of social marketing such as TV commercials and billboard ads may be more relevant.
1.5.4. Internalized Homophobia
Internalized homophobia is present worldwide, particularly in countries with higher rates of homonegativity and little institutional support for the protection of human rights of people with same-sex attractions. For two prominent scholars of the subject it represents ‘the gay person’s direction of negative social attitudes toward the self (…), and in its extreme
28 http://www.homeoffice.gov.uk/crime-victims/reducing-crime/hate-crime/29 Human Rights First (2007). Homophobia: 2007 Hate Crime Survey. New York, NY: Human Rights First; pg. 15.30 van Dijk, L & van Driel, B. (eds.) (2007). Challenging Homophobia: Teaching about Sexual Diversity. London, UK: Trentham.31 Polacek, R & Le Déroff, J. (2010). Joining Forces to Combat Homophobic and Transphobic Hate Crime: Cooperation between Police Forces and LGBT Organisations in Europe. Brussels: ILGA-Europe; pg. 57.32 Polacek, R & Le Déroff, J. (2010). Joining Forces to Combat Homophobic and Transphobic Hate Crime: Cooperation between Police Forces and LGBT Organisations in Europe. Brussels: ILGA-Europe. 33 van Dijk, L and van Driel, B. (Eds.) (2007). Challenging Homophobia: Teaching about Sexual Diversity. London, UK: Trentham; pg. 10-11.

15
Chapter 1Homophobia in South Eastern Europe- Prevalence, Consequences and Prevention
forms, it can lead to the rejection of one’s sexual orientation. Internalized homophobia is further characterized by an intrapsychic conflict between experiences of same sex affection or desire and feeling a need to be heterosexual.34” In-ternalized homophobia has been found correlated with a number of self-reported negative health outcomes such as depression, anxiety, and high-risk sexual behaviours35
One of the major obstacles to alleviating internalized homophobia are the often limited psychotherapeutic resources available for affected individuals who may not have recourse to trained and sensitive clinicians capable of providing adequate psychological support. This is often the case in countries that during medical education do not address the psychological distress that sexual minorities can experience as part of living in a social environment that condemns their sexual orientation and practices. The sexual prejudice of health professionals themselves, despite the availability of evidence-based information about homosexuality, can pose an additional barrier to delivering adequate psychological care to those affected by internalized homophobia.
1.6. Conclusion
In preventing homophobia and associated violence there is a need to mobilize and involve all the relevant social actors – educators, police, the legal and medical system, and the media. Only a holistic approach can create an atmosphere that will be respectful and protective of people with same-sex attractions. Human rights have to be a matter of concern for the entire society, not only of individual interest groups. Decentralized systems, such as those in the Netherlands, could also prove effective in South-eastern Europe. Idiosyncrasies present in particular organizational settings such as schools or companies might not always be best addressed with programs devised from top to bottom without the understanding of the local context. Furthermore, before any major campaign can be implemented on a national level, political support as well as sustained and appropriate public funding need to be secured.
The local NGOs in the four counties have done a remarkable job in placing the issue of homophobia into public view and advocating for changes in the legal system to address hate crimes and discrimination. A large number of their activities in homophobia prevention, however, have been predominantly Internet-based. And although Internet is undoubtedly an important venue for combating sexual prejudice, access to it may not be available to all who need such information and resources, especially not on a regular and uncontrolled basis. Thus more efforts seem to be needed that would bring the projects aimed at informing the public about homosexuality and promoting sexual diversity from the virtual to the real world36.
Considering the widespread negative public sentiments towards homosexuality, especially among men, in Croatia, Bosnia and Herzegovina, Montenegro, and Serbia, larger scale prevention efforts have to start immediately. The focus should be placed on schools where students have to have access to correct and positive information about human sexual diversity. Hopefully sex-education programs in the four countries will be set up and educate young people about sexual-ity in a non-judgmental fashion. The countries should also work on sharing best practices. Such exchange of knowledge and experiences has to involve the public institutions, and not only the NGO sector, since the former have the political and economic power. In the meantime, to avoid early disillusionment, it is important to bear in mind that any substan-tial social change requires time and patience.
34 Frost, D. M. & Meyer, I. H. (2009). Internalized Homophobia and Relationship Quality Among Lesbians, Gay Men, and Bisexuals. Journal of Counseling Psychology, 56(1), 97–109; pg. 97. 35 Williamson, I. (2000). Internalized Homophobia and Health Issues Affecting Lesbians and Gay Men. Health Education Research, 15(1), 97-107. 36 A great step in that direction was taken by the Croatian NGO “Iskorak” that was selected for the third place in the annual Croatian national competition for the best media campaign in the category of billboard ads for its campaign “U Krapini su svi homo sapiensi” (“Everybody in Krapina is homo sapiens”). Krapina is a Croatian town famous for its fossil remains of Homo sapiens neanderthalensis.
16
Chapter 1 Homophobia in South Eastern Europe- Prevalence, Consequences and Prevention
Figure 1
Figure 1
Figure 2
Screenshot of an anti-homophobia website designed and maintained by the Croatian NGO Iskorak.
From the “ThinkB4YouSpeak.com” campaign
Screenshot of a website designed and maintained by the NGO “Q” in Bosnia and Herzegovina with the information about sexual orientation and gender.
17
Chapter 2MSM- men having sex with men
2. MSM- men having sex with menPrepared by: Danijel Lončar
2.1. Introduction
In this chapter we will discuss men who have sex with men in general, taking into consideration regional particularities, as well as local masculinities and the way they interact with the image of manhood as perceived by men in the region. The region in question is that of Western Balkan, i.e. more specifically Bosnia and Herzegovina, Croatia, Montenegro and Serbia.
We will discuss the issues of sexuality, gender identity, taboos connected with sex and the relationship between sexuality and HIV epidemics. It will be of particular importance to avoid making any generalizations when describing the popula-tion in question as it will be shown that any such claims would diminish the complexity of the issue at hand. Questions discussed here have also been recognized as important in achieving the Millennium Development Goals:
“Promotion and protection of sexual rights are fundamental not only to achieving sexual health goals, but are also directly relevant to achieving the MDGs. The presence and accessibility of quality sexual and reproductive health ser-vices, information and education in relation to sexuality; protection of bodily integrity; and the guarantee of the right of people to freely choose sexual and marriage partners, to make decisions about child bearing, and to pursue satisfying, safe and pleasurable sexual lives are grounded in and contribute to gender equality and the empowerment of women (MDG 3); access to primary education, particularly for girls (MDG 2); reduction of infant and child mortality, especially of girl children (MDG 4); to improvements in maternal health and mortality (MDG 5); to decreasing vulnerability to HIV/AIDS, sexually transmitted infections and other health threats (MDG 6); and also to reduction of poverty (MDG 1). Thus, achieving sexual rights for all people will not only contribute to sexual and reproductive health, well-being and quality of life but will also advance the MDGs.”37
When trying to describe a population one finds oneself with a demanding task, especially if the population in question is not a population in the classic sense, as seen by the social sciences. “Men who have sex with men”38 is a term devised to describe a behaviour-based population that tends to avoid being perceived as one. In the discourse of social sciences, a population usually describes a group of people sharing some common trait often sharing same or similar identity. Yet, when the term MSM entered the public health discourse in 1990s it was used to avoid making assumptions about any-one’s identity or social group they identified with. Used to describe a certain type of sexual behaviour, men-to-men sex, it soon became a common denominator for alternative heterosexual and homosexual masculinities and behaviour. We will come back to the problem of heterosexual masculinity, as well as masculinity both in general and regional context later in the text. Before that, we feel, it would be important to better understand the term MSM and its use.
37 Ilkkaracan, P. and Jolly, S. (2007). Gender and Sexuality. Overview Report. BRIDGE38 In further text we will interchange the term “men who have sex with men” with acronym “MSM”.
18
Chapter 2 MSM- men having sex with men
2.2. The Term
Although conceived as a term that would allow discrimination-and-value-free reporting and monitoring of HIV epi-demic, expression “men who have sex with men“ is causing more misunderstanding and confusion. In its search for an adequate term, epidemiology has succeeded in “obscuring social dimensions of sexuality”39. From an epidemiological perspective, term MSM avoids “complex social and cultural connotations that, according to a strict biomedical view, have little to do with epidemiological investigation of diseases”40. However, we will show that social and cultural phe-nomena indeed influence the epidemiology of diseases – one example would be limited access we have to MSM popula-tion in the region due to discrimination and social stigma of homoeroticism. While we agree that behavioural aspect can be useful in certain situations, we believe, as do Young and Meyer, that indiscriminate use of the term is problem-atic on “theoretical, political, ethical and epidemiological grounds”. Our concern is “that the ubiquitous use of MSM undermines the self-determined sexual identity of members of sexual-minority groups; deflects attention from social dimensions of sexuality that are critical in understanding sexual health; and obscures elements of sexual behaviour that are important for public health research and intervention”41.
2.3. “MSM” in the Region, Introduction
In the beginning of the epidemic, AIDS was initially considered a “gay illness”, a health issue only for gay men and men who had sex with men42. However, it soon became evident that AIDS isn’t a disease of a certain group, race or nation. It doesn’t discriminate and it doesn’t have moral preferences. But, as statistics show, it is more common in some groups, like MSM. In fact, in the recent UNGASS Country Progress Report for Bosnia and Herzegovina, Croatia, Montenegro43 and Serbia it was stated that newly reported cases of HIV show a rising trend of HIV in the population of men who have sex with men. Also, in the same reports, male to male sex is still one of the dominant modes of transmission of HIV; 48.5% in Croatia44, 23% in Serbia45, 17.2% in Bosnia and Herzegovina4647.
For the countries in question, and probably for the entire region of South-eastern Europe, it is difficult to say if the term MSM is used correctly when gathering epidemiological data – it is often incorrectly used as a synonym for gay men. As Pitts et al have recognized “publications on MSM almost never offer a definition [of the term] or, if they do, proceed to bundle MSM with gay, bisexual and other homosexually active men into a single analysis.”48 In Croatia, for example, the official term for this mode of transmission is still “homo/bisexual”49. Apart from that, the reasons for this suspicion are numerous. As it will be mentioned in other chapters, homophobia is still quite common in the region, not only in gen-
39 Young, R. M. and Meyer, I. H. (2005) The Trouble With "MSM" and "WSW": Erasure of the Sexual-Minority Person in Public Health Discourse. American Journal of Public Health 95 (7).40 ibid.41 Ibid.42 Grmek, M. D. (1996). Povijest side. Zagreb: Nakladni zavod Globus.43 (2010). UNGASS Country Progress Report: Montenegro. UNAIDS.44 (2010). UNGASS Country Progress Report: Croatia. UNAIDS.45 (2010). UNGASS Country Progress Report: Serbia. UNAIDS.46 (2010). UNGASS Country Progress Report: Bosnia and Herzegovina. UNAIDS.47 At the time of the writing of this chapter we could not confirm the data for Montenegro as there are no clear information on popu-lation size estimates of most at risk groups.48 Pitts, M. K., Couch, M. A. and Smith, A. M. A. (2006). Men who have sex with men (MSM): how much to assume and what to ask? Medical Journal of Australia 185(8).49 Hrvatski zdravstveno-statistički ljetopis za 2008. Godinu. Zagreb: Hrvatski zavod za javno zdravstvo.

19
Chapter 2MSM- men having sex with men
eral population, but also in healthcare, among others. Furthermore, perception of heterosexuality is one-dimensional, and the entire system is still firmly hetero-normative, excluding other sexualities or the possibilities of a fluid sexuality. Of course, we must also take into consideration the possibility of false identification when taking HIV tests, but the reasons and motivations for such behaviour will be discussed later.
2.4. Silent men
Men who have sex with men are, for the most part, an invisible population in this region. We have no insight in the lives of men who have sex with other men that are outside common groups50 such as prisoners, soldiers, sailors, male sex workers etc. Part of the reason for this lack of information lays in the local perceptions of manhood and masculinity.Traditionally, a “real” man is exclusively heterosexual, religious and reproductively capable5152. Though those categories can be stretched, they are subjected to peer approval that can, at any point, strip man of his masculinity. As Michael Kimmel wrote, manhood is demonstrated for other men’s approval53, and as such is subjected to various social taboos. “… That men prove their manhood in the eyes of other men is both a consequence of sexism and one of its chief props… Masculinity is a homosocial enactment. We test ourselves, perform heroic feats, take enormous risks, all because we want other men to grant us our manhood…”54 A manly man’s worst fear would be to be denied the privilege of man-hood. Such fear of emasculation is described by Kimmel as homophobia. For our discussion in this chapter, this view on homophobia - as fear of emasculation - is important because it leads to shame that causes silence that contributes to the overall invisibility of MSM. As described by Kimmel, the shame of being afraid, of being labelled as a “lesser man” leads to silence that “keeps other people believing that we actually approve of the things that are done to women, to minorities, to gays and lesbians in our culture”55. Therefore, we could say that majority of men passively reinforce typical notion of masculinity. And this is certainly true when considering ideas of manhood in the Balkans. It can be implied that, for the reasons given, we can expect the majority of men who have sex with men to remain silent and invisible. In societies like the ones in the Balkans, where more and more women and men are rediscovering traditional values56, where religion can serve as a constant in one’s life, and where poverty, unemployment, corruption, authoritative governments, crime and violence are ever present, it is easy to give in to discrimination and intolerance, and human and minority rights are not high on the list of priorities. Having that in mind, one can understand why most MSM stay hidden, in fear of losing their social, political and other identities, as well as position and respect due to homophobia.
50 Men who identify themselves as gay, bisexual or transgender.51 Gutmann, M. (2007) Fixing Men: Sex, Birth Control, and AIDS in Mexico. Berkeley: University of California Press52In recent decades there have been numerous theories that tried to explain what it means to be a man, from biological and psycholo-gical to philosophical. Yet, all have failed in their attempt to discover “universal truths” about men. They certainly have been successful in creating new illusions about manhood and masculinity. One such theory tried to explain men through their “sexually rapacious appetites” and the “evolutionary” need to spread their semen (Gutmann, 2007). Such biological generalizations have failed to recognize, even within their own cultures, different expressions of masculinity removed from the need to procreate or indeed “spread their semen”.53 Kimmel, Michael S. (1994) “Masculinity as Homophobia: Fear, Shame, and Silence in the Construction of Gender Identity.” In The-orizing Masculinities, edited by Harry Brod and Michael Kaufman, 119–41. Thousand Oaks, CA: Sage.54 Ibid.55 Ibid.
56 Though this trend of returning to traditional values has been noted in many Western societies.

20
Chapter 2 MSM- men having sex with men
2.5. What’s Sex Got to Do with It?
The idea that there are only several limited and definite sexual categories has been refuted as early as 1948, when Kinsey and his associates published their report on “Sexual Behaviour in the Human Male” (followed in 1953 by a report on “Sexual Behaviour in the Human Female) where they described a plethora of various possibilities for sexual expression and therefore for numerous possible sexualities not limited by the conventional perceptions of sexuality. Despite that, it was not until feminist scholarship and queer theorists have started deconstructing the patriarchal ideas about sex and sexuality that the idea of a fluid sexuality has entered the discourse of the social sciences.
As it can be expected, theoretical assumptions about sexuality and its nature didn’t have an impact on society in general. In our region of interest, thinking about sex is still one-dimensional and role-governed. Sexual act is seen as the joining of two opposites, man and woman, masculinity and femininity. Through those terms people perceive roles during an intercourse. Man is always the penetrator, heterosexual, dominant and active, while the “submissive” partner (woman) is the one to be penetrated and is representing the passive feminine qualities. In many ways this perception of sex is similar to perception of intercourse in Latin America. The Balkan men can be seen as having the same qualities as the Latin American men have, and in that sense we can say that there is such a thing as Balkan “machismo” though with one exception, unlike in Latin America, sexual act between two men in the Balkan societies isn’t accepted on any level, no matter the role57. This is one more reason why MSM aren’t encouraged to become socially visible and as a result stay outside the reach of many organizations working with MSM.
2.6. Continued: MSM in the Region
By now it has become clear that, when we write about MSM in the countries of interest (Bosnia and Herzegovina, Croa-tia, Montenegro and Serbia), we write about those MSM that are in the reach of NGOs, meaning mostly gay and bisexual men. It can therefore be misleading to use this term when describing the epidemic in the region. Despite that, we feel it is important to present here the MSM population we have access to, gay and bisexual men.
Through the work of various NGOs in the region we have access, albeit limited, to gay and bisexual male population in Bosnia and Herzegovina, Croatia, Montenegro and Serbia.
It has been mentioned before that this region is still governed by traditional values imposed by religion and shared social and political history (hence the similarities between the countries). Homosexuality, although not on the list of medical disorders, is still seen by many people as a psychiatric condition58 that, if not dealt with, will cause the decay of traditional moral values and society in general. In most cases the reaction is ignorance, though it can, in its most serious form, escalate into full-blown violence, as demonstrated on 2010 Pride Parade in Belgrade, Serbia.
Homophobia is still present in all four countries, and it is expressed in various ways.
Gay people in the region are exposed to psychological and physical violence, though not every incident is reported (rea-sons for this are many, but it is usually the combination of fear, shame and lack of thrust in the State).
It is difficult to understand what kind of impact this situation has on MSM (especially gay men) in the region or how it affects intimate relationships between men. We can be certain that more men are “under the radar” and out of reach, in-visible and not covered by ongoing HIV prevention activities. Due to that, it is expected to see an even higher number of new HIV cases in this population. Unfortunately, we are not familiar with internal structures, behaviour and networks of this group as there are not enough studies directed to this population. That makes it difficult to better understand the social side of HIV epidemic in this population.
57 In many Latin American countries man who is the active partner is still seen as a “macho”, heterosexual with no social sanctions. The same can’t be said for the passive partner, who is often discriminated and ostracized.58 In Montenegro more than 60% of participants (representing general population) in a 2010 study by Juventas said that they believe homosexuality is an illness.

21
Chapter 2MSM- men having sex with men
2.7. Instead of Conclusion
In this chapter we have presented the issues of male sexuality, male gender identity, masculinity and the way they con-tribute to our understanding of men who have sex with men. Understanding that sexuality and identity are fluid terms that are constantly performed anew is important if we want to understand the population we are interested in - men who have sex with men - and if we want to create sustainable, population-friendly policies.
We have agreed with other authors that it is necessary to include understanding of social dimensions of sexuality if we want to better understand HIV epidemic. As Paula Treichler said “AIDS is simultaneously an epidemic of a transmis-sible lethal disease and an epidemic of meanings and significations”59. In the context of our region this is even more important, since people living with HIV/AIDS are exposed to discrimination, stigma and violence in public and private spheres and that contributes to lower rates of HIV testing done in these four countries. Furthermore, it is important to identify networks and understand the values and behaviour of men who have sex with men in this region, whereby MSM we mean all men who have sexual contact with other men.
Regrettably, we have to say that it was not possible to write a sociological or an anthropological overview of the MSM population in this region due to a lack of research and data. There is very little research on gay population also, apart from epidemiological and some behavioural studies.
59 Treichler, P. A. (1999) How to Have Theory in an Epidemic: Cultural Chronicles of AIDS. Durham: Duke University Press.

22
Chapter 2 MSM- men having sex with men
23
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
3. Legal Status of Sexual and Gender Minorities in South-eastern EuropePrepared by: Kristijan Grđan
3.1. Introduction
Protection of human rights is a core value of humanity. In the context of HIV and AIDS, the human rights protection has a significant value and is advocated by number of international documents. Effective addressing of HIV and AIDS issues across the countries in the world is undermined if human rights are not respected. Gay, lesbian, bisexual and transgender people (LGBT) usually face discrimination, hatred, violence and exclusion from the society.
In this analysis we report on developments in protection of human rights of LGBT people in Croatia, Bosnia and Her-zegovina, Serbia and Montenegro (hereinafter referred to as „region“). In the first part we describe the most important human rights standards applicable to the social and legal status of LGBT people, especially taking into account impor-tance of the European legislation and its possible influence on the countries in accession to the European Union. Then we analyze situation of LGBT people in four areas of social life: (1) right to life, safety and protection from violence, (2) right to expression and public assembly, (3) right to protection from discrimination and (4) right to family life, giving recommendations for improvement of legal and social status of LGBT people.
Due to methodological constraints we have not been able to do thorough analysis of national legislations, therefore we relied more on the resources provided by existing civil society organizations who are advocating for protection of rights of LGBT people at their respective national levels. Furthermore, we were faced with lack of relevant and accurate data, especially in Bosnia and Herzegovina and Montenegro. In countries such as Croatia and Serbia, where the LGBT activ-ism is more developed, it was easier to find accurate data and to compare this data with other resources. This research is therefore aimed at determining basic principles in protection of human rights of LGBT people across the region, while retaining possibilities of further and more comprehensive research in that field.
3.2. Human Rights Standards
3.2.1. Human rights definition
The wording of the Article 1 of the Universal Declaration on Human Rights entitles freedom and equality in dignity to all human beings. Human right is every right that is directly or indirectly attributed to human beings and their existence. For the purpose of this work, the discourse related to human rights of lesbian, gay, bisexual and transgender people will be used.
3.2.2. Violations of human rights
Some of the basic human rights are inviolable. Right to life is protected in every circumstance; almost all Member States of the Council of Europe signed and ratified Protocol no. 6 to abolish death penalty; only Russia signed but not ratified the Protocol. Right to life may be restricted by law in extreme situations, e.g. in enforcing authorities by state agents to immediately protect life and safety of others. According to Article 3 of the European Convention on Human Rights and

24
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
Fundamental Freedoms, every person is entitled to be protected from inhuman, degrading treatment or torture; this right is not allowed to be restricted not even in the state of emergency or war.
However, many human rights may be restricted in accordance with principles of proportionality. In legislation of coun-tries in the region, constitutional provisions containing principle of proportionality in restricting rights and freedom of other people are enforced. Modern legislation requires using proportionality test in determination why, when and how every specific human right may be restricted.60 The Universal Declaration on Human Rights does not define principle of proportionality, but in some specific situations the European Convention on Human Rights and Fundamental Free-doms does. The main principle is that the restriction of some human rights may be done only if necessary in democratic society and prescribed by law in the interest of national security or public safety, the prevention of disorder and crime, also the protection of health and morals and for the protection of rights and freedom of others. If being grounded in legal documents following international standards, the restriction of human rights would not be considered as violation.
The violation of rights exists when action that is undertaken, temporarily or permanently, deprives fully or partially a person of his/her rights, while having no basis under national or obligatory international legislation. There are different types of damage that may be suffered by the victim of such violation, and international legal sources provide obligation of the state to compensate pecuniary and non-pecuniary damage to victims of human rights violations.
Violations of human rights are always done by individuals or groups of people. Not only if state agents violated human rights, but also if anyone else under jurisprudence of the state violated the human rights of others, the state would be responsible for such violation. The state is due to protect rights of every citizen, and failure to do so would bring the state in breach of international legal standards.61
3.2.3. The International Covenant on Civil and Political Rights (ICCPR)
The United Nations General Assembly adopted the ICCPR and opened it for signature, ratification and accession by the Resolution 2200A (XXI) on December 16, 1996. The scope of human rights determined by this Covenant is:
• Right of self determination, to freely determine political status and to freely pursue economic, social and cultural development;
• Right to be equal in the rights prescribed by Covenant and by the law without distinction of any kind such as race, colour, sex, language, religion, political or other opinion, national or social origin, property, birth or other status;
• Right of persons whose rights are violated to receive an effective remedy;
• Equality of men and women in the enjoyment of all civil and political rights set forth in this Covenant;
• Inherent right that shall be protected by law. Therefore no one shall be arbitrary deprived of his life;
• If sentenced to death, that could be imposed only for most serious crimes, anyone shall have right to seek pardon or communication of the sentence. Sentence of death shall not be imposed for crimes committed by persons below 18 years of age and shall not be carried out on pregnant women;
• Protection from torture or cruel, inhuman or degrading treatment or punishment. It is prohibited to subject anyone to the medical or scientific experimentation without his free consent;
• Protection from slavery and slave-trade in all their forms. No one shall be held in servitude;
60 See case R v. Oakes, Supreme Court of Canada, 1982.61 The ECHR, case of Šečić v. Croatia, Application no. 40116/02; decision delivered on May 31, 2007.
25
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
• Right to liberty and security of a person. No one shall be subjected to arbitrary arrest or detention. No one shall be deprived of his liberty except on such grounds and in accordance with the procedure as established by law;
• Protection from imprisonment merely on the ground of inability to fulfil a contractual obligation;
• Within the territory of the State everyone legally has a right to liberty of movement and freedom to choose his residence;
• Rights of aliens lawfully in the territory of a State may be expelled only in pursuance of a decision reached in accor-dance with the law and to submit repeal against his/her expulsion;
• Equality before courts and tribunals;
• Right not to be retroactively prosecuted for criminal offence or for the activity that does not represent a criminal offence under national or international law;
• Right to recognition everywhere as a person before the law;
• Protection from the arbitrary or unlawful interference with private life, family, home or correspondence and from unlawful attacks on honour and reputation;
• Freedom of thought, conscience and religion. This right includes freedom to have or to adopt a religion or belief of his choice. Also the freedom, either individually or in community with others in public or in private, to manifest his religion or belief in worship, observance, practice and teaching;
• Right to hold opinions without interference;
• The right to peaceful assembly;
• Right to freedom of association with others, including the right to form and join trade unions for the protection of his interests;
• Right of men and women of marriageable age to marry and to found a family;
• Children have, without any discrimination as to race, colour, sex, language, religion, national or social origin, pro-perty or birth, the right to such measures of protection as are required by his status as a minor, on the part of his family, society and the State.
Furthermore, it shall be noted that advocacy of national, racial and religious hatred shall be prohibited by law, as Cov-enant prescribes. Religious hatred against homosexual and transgender people is common; the expression of hate speech against LGBT people, however, in many countries remains to be justified by freedom of expression rather than qualified as unlawful conduct.
In the case of public emergency which threatens the life of the nation and the existence of which is officially proclaimed (e.g. global terrorist attacks, natural disasters, epidemics, war and social disruption), the States parties may take mea-sures derogating from their obligations under the Covenant to the extent strictly required by the exigencies of the situation, provided that such measures are not inconsistent with their other obligations under international law and do not involve discrimination solely on the ground of race, colour, sex, language, religion or social origin. However, the derogation is not possible in some cases as when it is about (1) right to live, (2) prohibition of torture, cruel, inhuman or degrading treatment or punishment, (3) prohibition of slavery and servitude, (4) prohibition of imprisonment merely on the ground of inability to fulfil the contractual obligation, (5) prohibition of retroactive prosecution for criminal of-fences and those acts not representing criminal offences by national and international law, (6) right to be everywhere recognized as a person before the law and (7) freedom of thought, conscience and religion.
By the Covenant, the Human Rights Committee (HRC) is established to follow implementation of provisions set forth in the Covenant and to determine violations of rights in single cases.

26
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
3.2.4. First Optional Protocol to the ICCPR
The ICCPR-OP1 is an international document prescribing the competence of the HRC to receive and consider indi-vidual complaints brought before its jurisdiction. Individual complainants may be victims of violations of rights against legal provisions of the ICCPR. The same document defines procedural requirements for lodging complaints and per-forming process.
3.2.5. Second Optional Protocol to the ICCPR
This document was adopted and proclaimed by General Assembly Resolution 44/128 on December 15, 1989. It is aimed to the abolition of death penalty.
3.2.6. The Convention on the Protection of Human Rights and Fundamental Freedoms (ECHR)
This Convention, commonly known as the European Convention on Human Rights (ECHR), was adopted by the Council of Europe in Rome on November 4, 1950. By that time the Convention was amended and supplemented by additional protocols. Most importantly, the European Court on Human Rights and Fundamental Freedoms has been established to bring judgments on alleged violations of human rights among Member States of the Council of Europe.
3.2.7. Protocol 12 to the ECHR
The Protocol 12 to the ECHR was adopted by the Council of Europe in Rome on November 4, 2000. It was opened for signature, ratification or acceptance to any Member State of the Council of Europe which may determine which terri-tory this Protocol shall apply to. The Protocol 12 is very important for the reason that it extends the ECHR with all of the rights recognized at the national level. The general prohibition of discrimination is made to the enjoyment of any right set forth by law. It opens the competence of the ECHR to examine not only the cases where the rights and freedom prescribed by the ECHR and other adopted Protocols might be violated, but also where it is possible that some rights recognized only on the national level were violated against persons who alleged discriminatory treatment.
According to the explanatory Report of the Council of Europe62 the Protocol 12 concerns persons:
• in the enjoyment of any right specifically granted to an individual under national law;
• in the enjoyment of a right which may be inferred from a clear obligation of a public authority under national law, that is, where the public authority is under an obligation of national law to behave in a particular manner;
• by a public authority in the exercise of discretionary power (for example, granting certain subsidies);
• by any other act or omission by a public authority (for example, the behaviour of law enforcement officers when controlling a riot).
All the countries from the region signed the Protocol 12.
62 http://www.humanrights.coe.int
27
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
3.2.8. The European Charter on Human Rights and Fundamental Freedoms
The European Charter on Human Rights and Fundamental Freedoms is the first European document that includes prohibition of discrimination on the grounds of sexual orientation. However, it does not contain reference to gender identity. The non-discrimination provision is not „open-ended“which makes it difficult to apply to the transgender people.63 This document is obligatory to the Member States of the European Union and at this time not applicable to the countries in the region. However, when making judgments consider this document to be important for the interpreta-tion of the ECHR, therefore providing good advocacy arguments for the Member States of the Council of Europe which didn’t join the EU.64
3.2.9. The European documents relevant for sexual and gender minorities
In this subsection, other European documents protecting sexual and gender are closely described.
3.2.10. The European Parliament Resolution A3-0028/9465
The Resolution on Equal Rights for Homosexuals and Lesbians in the EC was adopted by the European parliament in 1994.66 The Resolution called the Member States to abolish all legal provisions which criminalize and discriminate against persons of the same sex, to recognize the same age of consent to apply to the homosexual and heterosexual ac-tivities and to stop with unequal treatment of persons with a homosexual orientation under administrative practices. It also urged to take measures and campaigns to fight against homophobia in society.
3.2.11. The European Parliament Resolution A5-0050/0067
By the European Parliament Resolution on Respect for Human Rights in the European Union adopted in the year of 2000, the Member States were urged to guarantee equality between the people irrespective of their sexual orientation, but more importantly, to guarantee same-sex couples’ equal rights that are entitled to the traditional families, particu-larly as regards to tax law, pecuniary rights and social rights. It is important to note that it was highlighted that the condition for membership in EU is a respect of human rights and that membership request to the state contrary to that would be denied.68
3.2.12. The Council Directive 2000/78/EC69
By this Council Directive Establishing a General Framework for Equal Treatment in Employment and Occupation, the direct and indirect discrimination on the basis of sexual orientation is prohibited.70
63 Article 21/1 of the European Charter on Human Rights and Fundamental Freedoms, OJ C 364/13, 18.12.2000.64 See below referrence to the case of Christine Goodwin v. the United Kingdom.65 Not binding document!66 OJ C 061 of February 28, 1994. The full text of the Resolution is not available in electronic form.67 Not binding document!68 Find full text of the Resolution on the webpage http://www.europarl.europa.eu69 Binding to all Member States of the Council of Europe!70 Official Journal of the European Communities L 303, pp. 16-22.
28
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
3.2.13. The European Parliament Resolution on Homophobia in Europe71
The Resolution on Homophobia in Europe was adopted in early 2006.72 It reaffirms earlier considerations, but strongly urges Member States to enact legislation to end discrimination faced by same-sex couples in the areas of inheritance, property arrangements, tenancies, pension, tax, social security and other rights. Furthermore, strongly condemning any kind of discrimination against people in relation to their sexual orientation, the Resolution urges the Member States to fight against hate speech and hate crimes committed against those people. The dignity of homosexual people was stressed so that Member States are even urged to accord full recognition of homosexuals as the victims of Nazi regime.
3.2.14. The Council of Europe Recommendation CM/Rec (2010)
On March 30, 2010 the Committee of Ministers of the Council of Europe enacted Recommendation on combating dis-crimination on the grounds of sexual orientation and/or gender identity. The Recommendation refers to (1) combating hate crimes and hate speech, (2) freedom of association, expression and peaceful assembly, (3) right to respect private and family life, (4) employment, (5) education, (7) housing, (8) sport and (9) right to asylum.
3.3. Right to life, safety and protection from violence
3.3.1. Legal background in the region
All the constitutions of the countries in the region are guaranteeing respect of human rights. In regards to sexual orien-tation and gender identity, this constitutional guarantee may be connected with the constitutional provisions guarantee-ing equal treatment before the law. Therefore, everyone, regardless of sexual orientation has a right to be protected from violence and from being exposed to life danger.
The restrictions are possible, but only in accordance to law when it’s necessary to protect freedom and rights of other people, legal system, public moral or health. However, in democratic society any interpretation that would bring to dis-crimination against persons on the ground of sexual orientation or gender identity is not considered to be necessary in protection of others, protection of legal system, public morale or health.
As the members of the Council of Europe, the countries in the region are due to guarantee protection of right to life to all citizens, and such obligation refers to implementation of special criminal policy against all perpetrators for criminal offences containing discriminatory motives, as such, for example, the violent physical attacks against the homosexual or transgender people.
The criminal legislation in all the countries in the region contain catalogue of criminal offences against life and personal safety. There are also specific criminal offences related to discrimination in place. However, only in Croatia partial hate crime legislation is in place. At the initiative of the coalition of civil society organizations protecting vulnerable social groups that are exposed to violence, in 2006 the Croatian Parliament passed amendment to the Croatian Criminal Code to implement term of “hate crime”.
“The hate crime is every criminal offence recognized by this Code that is committed against person on the ground of his/her … sexual orientation … or other characteristic.”
– Art. 89 Para 36 of the Croatian Criminal Code.
71 Not binding document!72 European Parliament, P6_TA-PROV(2006)0018

29
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
That definition itself did not give any clue about possible implementation in judiciary, except that the law enforcement bodies and consequently the judiciary qualified such criminal offences as hate crimes in individual proceedings. How-ever, by giving the qualification of the criminal offence to be a hate crime, the legislator did not raise an obligation of the criminal courts to recognize such qualification as an aggravating condition to the offenders. The second amendment implemented in the Criminal Code in 2006 refers to the most severe criminal offence against life – the aggravated mur-der, so that the murder motivated by the hate against the victim would be qualified form of criminal offence. The defini-tion of the hate crime, therefore, may only be used as a reference point in interpreting the meaning of “hate” considering criminal offence of aggravated murder. The perpetrator responsible for such a criminal offence may be sentenced up to forty years of imprisonment. Although judicial practice shows that there has been a small number of prosecutions con-nected to biased criminal offences, not even one case referred to the criminal offence of aggravated murder that would be motivated by hate on the grounds of sexual orientation or gender identity of the victim. Although the coalition of civil society organizations initially proposed that biased motives should be taken into account as aggravating condition of criminal offences, the Croatian Government did not accept such proposition. The reform of the criminal legislation is ongoing in Croatia and, since the “hate crime” provisions in the Croatian Criminal Code have been criticized by law enforcement, judiciary and legal experts, it is expected that reforms will affect hate crime policy. However, the proposi-tion of novel Criminal Code is still not finalized.
The provisions describing criminal offences in legislations across the region are rather “open-ended” than inclusive towards sexual orientation or gender identity. The criminal codes of countries in region are similar, but still containing some specific differences. While in Croatia, Serbia and Montenegro , the term of sexual orientation falls under “open-ended” provisions concerning criminal offence connected to discrimination, in Bosnia and Herzegovina the provision is closed but contains term of sexual orientation. In Croatia, Serbia and Montenegro criminal codes contain two criminal offences related to discrimination that are redundant, while most appropriate formulation is contained in the Criminal Code of the Federation of Bosnia and Herzegovina.
The criminal policy towards hate speech differs. The hate speech against LGBT people is banned in Croatia, while in Serbia and Montenegro hate speech is connected exclusively to racial context. In Bosnia and Herzegovina the criminal legislation refers to hate speech in ethnic, racial and religious context only.
No criminal legislation in countries in the region refers specifically to term of “gender identity”. Except for Bosnia and Herzegovina, all other countries in the region may apply criminal legislation to transgender victims of discrimination. In Bosnia and Herzegovina transgender victims of discrimination may only argue that they have been discriminated against on the ground of gender, since the term of gender is contained in the provision of the Criminal Code.
3.3.2. Violence against sexual and gender minorities
The violence against LGBT people is highly prevalent among countries in the region. The most documented examples of violence and hatred against LGBT people are given by civil society organizations acting in Croatia and Serbia. Except anecdotal examples in Bosnia and Herzegovina, Montenegro as well, there is no accurate data on incidence of violence against LGBT people. The modalities of violence are different, but commonly connected to physical attacks and verbal abuse. The exposition to violence is greater for people attending public events like Pride March or Queer Festival or visiting gay bars, venues and public places.
In Croatia and Serbia there are number of reports from recent years about inadequate police conduct in cases of violence against LGBT people. In Croatia, there is standardized practice of police officers to prosecute victims of violence for the misdemeanour against the public order if the violent attack happened on the street.73 . In 2009, the Gay-Straight Alliance
73 See the annual reports of the Team for Legal Changes of Iskorak and Kontra, available for download at: http://www.iskorak.org/promobox/publikacije
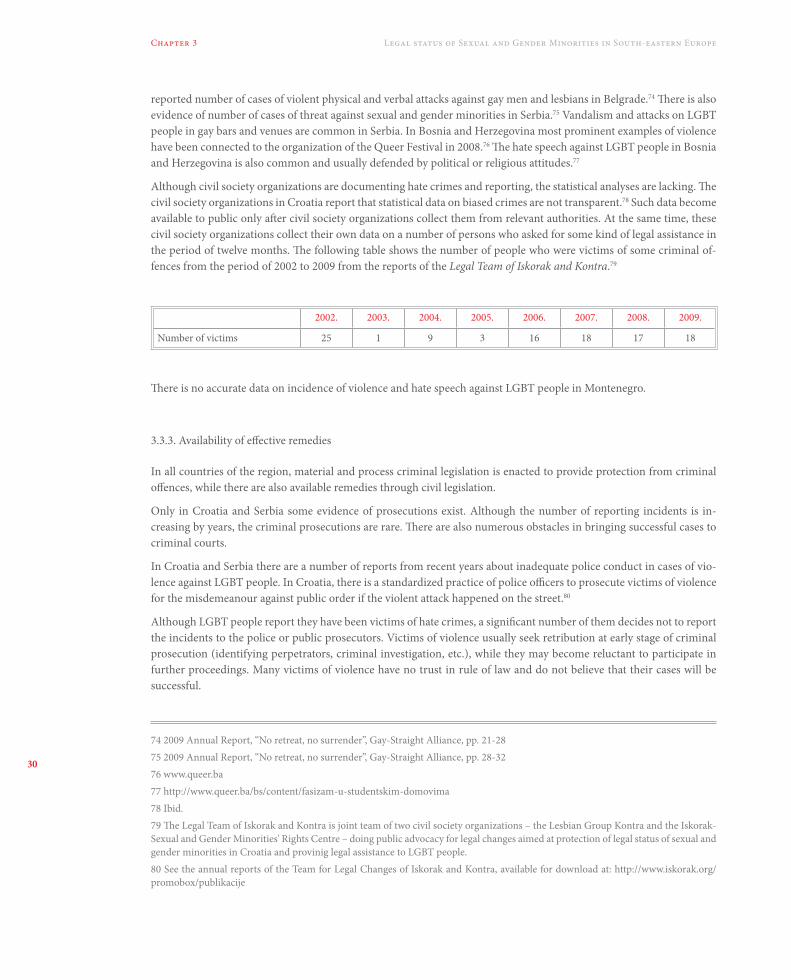
30
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
reported number of cases of violent physical and verbal attacks against gay men and lesbians in Belgrade.74 There is also evidence of number of cases of threat against sexual and gender minorities in Serbia.75 Vandalism and attacks on LGBT people in gay bars and venues are common in Serbia. In Bosnia and Herzegovina most prominent examples of violence have been connected to the organization of the Queer Festival in 2008.76 The hate speech against LGBT people in Bosnia and Herzegovina is also common and usually defended by political or religious attitudes.77
Although civil society organizations are documenting hate crimes and reporting, the statistical analyses are lacking. The civil society organizations in Croatia report that statistical data on biased crimes are not transparent.78 Such data become available to public only after civil society organizations collect them from relevant authorities. At the same time, these civil society organizations collect their own data on a number of persons who asked for some kind of legal assistance in the period of twelve months. The following table shows the number of people who were victims of some criminal of-fences from the period of 2002 to 2009 from the reports of the Legal Team of Iskorak and Kontra.79
2002. 2003. 2004. 2005. 2006. 2007. 2008. 2009.
Number of victims 25 1 9 3 16 18 17 18
There is no accurate data on incidence of violence and hate speech against LGBT people in Montenegro.
3.3.3. Availability of effective remedies
In all countries of the region, material and process criminal legislation is enacted to provide protection from criminal offences, while there are also available remedies through civil legislation.
Only in Croatia and Serbia some evidence of prosecutions exist. Although the number of reporting incidents is in-creasing by years, the criminal prosecutions are rare. There are also numerous obstacles in bringing successful cases to criminal courts.
In Croatia and Serbia there are a number of reports from recent years about inadequate police conduct in cases of vio-lence against LGBT people. In Croatia, there is a standardized practice of police officers to prosecute victims of violence for the misdemeanour against public order if the violent attack happened on the street.80
Although LGBT people report they have been victims of hate crimes, a significant number of them decides not to report the incidents to the police or public prosecutors. Victims of violence usually seek retribution at early stage of criminal prosecution (identifying perpetrators, criminal investigation, etc.), while they may become reluctant to participate in further proceedings. Many victims of violence have no trust in rule of law and do not believe that their cases will be successful.
74 2009 Annual Report, “No retreat, no surrender”, Gay-Straight Alliance, pp. 21-28 75 2009 Annual Report, “No retreat, no surrender”, Gay-Straight Alliance, pp. 28-3276 www.queer.ba 77 http://www.queer.ba/bs/content/fasizam-u-studentskim-domovima 78 Ibid.79 The Legal Team of Iskorak and Kontra is joint team of two civil society organizations – the Lesbian Group Kontra and the Iskorak-Sexual and Gender Minorities' Rights Centre – doing public advocacy for legal changes aimed at protection of legal status of sexual and gender minorities in Croatia and provinig legal assistance to LGBT people.80 See the annual reports of the Team for Legal Changes of Iskorak and Kontra, available for download at: http://www.iskorak.org/promobox/publikacije

31
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
Police misconduct is common in cases of violence against LGBT people. Victims of violence and discrimination are usu-ally faced with rude and offensive behaviour of police officers when investigating their case. Police officers at basic posts, due to low education and lack of knowledge about LGBT issues, may be offensive and insult victims on the grounds of sexual orientation and/or gender identity. In Croatia, for example, if incident was to be reported to the police, in major-ity of cases the proper criminal investigation would not be done and police would not even send a report to the prosecu-tor’s office. On the other hand, the proper criminal investigation would be done exclusively if a victim brought criminal complaint directly to the prosecutor’s office. Furthermore, police officers rather recognize violence against LGBT people as misdemeanors against public peace and order than as relevant criminal offences, resulting in under-reporting of in-cidents to prosecutor’s office. In early 2006, the group of violent perpetrators attacked participants of public gay party in Zagreb. Since the victims defended from the attackers, the police concluded that there is no evidence that perpetrators committed criminal offence of “Violent Behaviour” because victims “participated in a fight”.81
Investigations of cases of violence against LGBT people when the offender is not known are long lasting and of uncertain outcome. In majority of cases police is unable to identify perpetrators and no criminal prosecution is initiated. The Team for Legal Changes of Iskorak and Kontra in Croatia reported that successful investigations are usually done when public pressure is made towards the police.
In Croatia, the Ministry of Justice established a mechanism aimed at provision of support to victims and witnesses in criminal proceedings before national courts, there are no specific measures provided for sexual and gender minorities.82 It is not known whether the victims and witnesses of biased crimes received any kind of support within that mechanism. Although in 2008 the Croatian Parliament passed the legislation to improve accessibility of legal services for citizens with low social standard, no civil society organizations protecting sexual and gender minorities registered in the Ministry of Justice as an organization able to provide such support and therefore is eligible to be funded by the state. However, some civil society organizations such as the Lesbian Group Kontra, are providing direct legal support to victims of hate crimes that are funded by other sources.
The LGBT organizations in Serbia have established systems in providing direct legal assistance to victims of hate crimes. Some of them have a profound documenting methods and are able to report on hate crime incidents. The existing state based victims and witnesses support mechanism refers to war crimes only, while there has been initiative to develop such mechanism for victims of other crimes following good practice from other countries.83 The Ministry of Justice recently announced the Free Legal Aid Act will be enacted to provide free legal aid to people with low social standard.84
3.3.4. Forced psychiatric treatment
In Croatia, in the middle of 2008, the mass media reported about abuse of minors, forced treatment, placing in seclusion and under restraints in the Psychiatric hospital „Lopača“ near town of Rijeka. The civil society organization protecting rights of people with mental disabilities immediately urged the People’s Ombudsman to undertake all necessary mea-sures within his competence and to induce investigation of alleged violations of human rights in that hospital.85 As the result from the oversight by the national authorities, director of the hospital has been replaced, and the hospital released some patients. One of them was Ms. Ana Dragičević who alleged she was detained in that hospital in the period of more than two years only on the ground of being a lesbian. About conditions and treatment she was subjected, even the inter-national organization Human Rights Watch reported recently.86
81 2006 Annual Report on Status of Rights of Sexual and Gender Minorities in the Republic of Croatia, Team for Legal Changes of Iskorak and Kontra, 2007., pp. 22-2382 The Guidelines for providing informations to victims of criminal offences in criminal pre-trials and trials, The Ministry of Justice, 2007.83 From the speech of Ms. Snežana Malović, the minister of justice, the Ministry of Justice, 25.11.2008.84 Public announcment given by Ms. Snežana Malović, the minister of justice, 09.10.2010.85 2008 Annual Report of the People's Ombudsman. http://www.ombudsman.hr 86 McRae A., 2010. „Once You Enter, You Never Leave“, Human Rights Watch

32
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
In 2002, well known psychiatrist Mr. Vladimir Gruden publicly said that he has the ability to cure homosexual people.87 In 2003 the Croatian Medical Chamber concluded that attitudes of Mr. Vladimir Gruden are not in line with medical standards; however, although warned, he was not reprimanded for public statements that homosexuality was a mental disorder. The Croatian Psychiatric Association also expressed a public statement that homosexuality is not a mental disorder.88 In 2006, the child psychiatrist and judicial expert Mrs. Dubravka Kocijan-Hercigonja publicly said that homosexuality is a form of a gender identity disorder; although civil society brought complaint to the Croatian Medical Chamber, there have been no disciplinary consequences.89 In September 2010, an alternative therapist in Serbia alleged homosexuality is a mental disorder and it can be effectively cured. Although he was not a medical doctor, the Serbian Ministry of Health and Social Welfare reaffirmed attitude of the World Health Organization that homosexuality is not a mental disorder.90
Forced psychiatric treatment is a form of violence against sexual minorities and represents severe violation of human rights. Forced psychiatric treatment may raise interference into right to freedom, self-determination and physical integ-rity; furthermore, such treatment may also be inhuman and degrading for subjected persons.
3.3.5. Conclusions and recommendations
High prevalence of violence against sexual and gender minorities in countries in the region and lack of effective rem-edies show that protection of life and personal safety of persons concerned is not in line with the international human rights standards. Although there have been some improvements in legislation, especially in Croatia, the implementation of existing legislation is insufficient. There is no accurate statistical data on incidence of hate crimes committed against members of sexual and gender minorities, the state based support to victims and witnesses of hate crimes is absent, and the investigations undertaken by the police are usually ineffective. There is a low number of judicial cases, and only a few, usually publicly covered cases are successful. The forms of violence are various, and sometimes members of sexual mi-norities are subjected to involuntary psychiatric treatment. There is a lack of involvement of civil society organizations in developing mechanisms that are necessary for the implementation of enacted legislation. The situation in the whole region raises possibility of violations of articles 2, 3, 5, 8 in conjunction with article 14 of the European Convention on Human Rights; however, there is no judgement of the European Court on Human Rights that would refer to situation of sexual and gender minorities in countries in the region.
The improvements in legislation and development of mechanisms of implementation are necessary. In doing so, follow-ing steps should be undertaken:
1. Criminal legislation in all countries in the region should be amended in order to recognize hatred against sexual and gender minorities as an aggravating condition to criminal offences against life, physical integrity, personal safety, personal rights and freedom of victims;
2. Hate speech should be effectively addressed in order to prevent spreading of hatred against sexual and gender mi-norities;
3. Biased criminal offences should have a priority at all stages of criminal proceedings, starting even in pre-criminal phases;
4. Police, law enforcement bodies and the judiciary should be educated and trained to appropriately respond to biased criminal offences;
87 The statement was done at the round table of the Croatian Episcopal Conference in 2002.88 From the archives of the Iskorak – Sexual and Gender Minorities' Rights Center. 89 See “Depresija, osamljenost i nevjerovanje u vlastitu vrijednost – najčešći su problemi”, Glas Koncila, 2006.90 Press release of the Serbian Ministry of Health, 20.09.2010.
33
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
5. Countries should develop state-based mechanisms aimed at provision of support and accessible legal services to victims of biased criminal offences;
6. Police, law enforcement bodies and the judiciary should collect and analyze statistical data showing incidence of biased crimes against sexual and gender minorities;
7. Medical doctors, especially psychiatrists, should be educated on standards in providing psychiatric care and support to avoid medicalization of homosexuality;
8. Capacities of civil society organizations should be developed in order to raise their abilities to design and advocate appropriate mechanisms of implementation of enacted legislation;
9. Comprehensive outreach activities should be conducted to inform members of sexual and gender minorities on their rights and to encourage them in reporting violence they suffered.
3.4. Right to expression and public assembly
3.4.1. Practice of the European Court on Human Rights
The right to expression and public assembly is a fundamental human right protected by the Article 11 of the European Convention on Human Rights and Fundamental Freedoms. The most visible event of the LGBT community is Gay Pride manifestation. In its recent case of Alekseyev v. Russia,91 the European Court on Human Rights found violation of the Article 11 taken into conjunction with the Articles 13 and 14 of the Convention. The decision referred to three applica-tions by the same applicant who alleged that Russia violated his right to public assembly by banning Gay Pride marches in that country from the period from 2006 to 2008. The Russian Government defended their reasons for banning gay pride marches in two fundamental reasons: (1) that decisions on banning were result of public pressure towards the Government and fear from escalation of violence and (2) that the event in question had had to be banned for the protec-tion of morals, since under the view of the Government, homosexuality was incompatible with the „religious doctrines for the majority of population” (§§ 57, 59). The Court, however, was not persuaded by the arguments of the Russian Government, and the judgment delivered some principles that are of fundamental importance for further consider-ations of such public events in members of the Council of Europe.
The first principle is that Pride March itself cannot be automatically considered to have a potential to cause public disor-der regardless the possibility of counter demonstration. According to the Court, „the participants must be able to hold the demonstration without having to fear that they will be subjected to physical violence by their opponents.“ Therefore, the duty of Contracting States to take reasonable and appropriate measures to enable lawful demonstrations to proceed peacefully is imposed (§§ 73-74).
The second important principle set forth by the Court is that „it would be incompatible with the underlying values of the Convention if the exercise of Convention rights by a minority group were made conditional on its being accepted by the majority“ (§ 81).
The third principle is that there is no wide margin of appreciation in case of banning Pride marches. The stance of the Court is that „any decision restricting the exercise of freedom of assembly must be based on an acceptable assessment of the relevant facts“(§ 85).
And finally, the forth principle, Pride marches cannot be banned by the reasoning officials while „spontaneously ex-pressing uniformed views which they considered popular“ (§ 86).
91 The ECHR, Applications nos. 4916/07, 25924/08 and 14599/09, judgment delivered on October 21, 2010.

34
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
3.4.2. Zagreb Pride
Zagreb Pride manifestations have been regularly organized once a year since 2002. The occasion of the first Zagreb Pride, organized by the civil society organizations Iskorak and Kontra, was accompanied by extreme violence and hatred against gay and lesbian community. In following years, the extent of violence against participants of pride marches was different. In 2007 one person tried to throw a Molotov cocktail at the march while the participants were passing the central square. Although the participants of the march receive immediate protection from the police, after leaving the event, many of them are subjected to verbal and physical violence if recognized as being participants to such events.
In 2009 and 2010 the counter demonstrations organized by extremist fascistic groups were allowed by the Ministry of Interior Affairs. Even the LGBT civil society organizations urged the authorities such counter demonstrations to be banned, there was no appropriate reaction. In 2009, as reported by the Lesbian Group Kontra, the counter demonstra-tion against Zagreb Pride was publicly announced as „Antigay demonstration“ while attitudes of the organizers were grounded in Nazi ideas on the superiority of the white race. The website of the organizers even contained fascistic sym-bols and a guide on how to prepare the Molotov cocktails. 92 The Ministry of Interior Affairs never replied to the requests of the Lesbian Group Kontra to ban such a fascistic counter-demonstration. The same situation repeated in 2010, while the Lesbian Group Kontra even urged the competent court about the failure of the Ministry of Interior Affairs to ban such counter demonstration – there was no response.93
The growing incidence of violence and hatred connected to the event of Pride March manifestation in Croatia, in recent years, is highly concerning. The lack of police protection provided to the participants of the Pride marches, insufficient criminal investigations in finding perpetrators and bringing them before justice system, allowing fascistic counter dem-onstrations to be held expressing hatred against sexual and gender minorities, undermine Croatian efforts to fulfil the standards in protection of human rights. The right of LGBT community to peaceful assembly cannot be placed in the same line with the „right“ of extremist social groups to organize hate-based public assemblies! Principle of such equal-ization that is clearly imposed by the Croatian Government is contrary to the principles derived by the interpretation of the Article 11 of the European Convention on Human Rights and Fundamental Freedoms. The European Court on Human Rights expressed a view that right to public assembly set forth by the Convention applies to all assemblies „except those where the organizers and participants have violent intentions or otherwise deny the foundations of a democratic society“.94 Failure of the state to ban fascistic counter demonstrations at the occasion of Pride March events may constitute failure of the state to protect participants of such events from violence, bringing Croatia in breach of the international human rights standards.
3.4.3. Belgrade Pride
The first Belgrade Pride was organized in 2001. The manifestation was followed by the extreme violence against par-ticipants of the Pride March with hundreds of people injured. In 2009, a number of civil society organizations from Serbia joined into coalition to organize Pride March. As reported by Labris – Lesbian Human Rights Organization, the organizers faced number of difficulties in ensuring the safety for Pride March participants.95 The police did not develop operational plans to protect participants of the Pride March from violence. Due to inability to adequately protect the participants of the Pride March, the Serbian authorities changed the location of the event, therefore banning event to be
92 2009 Annual Report on Status of Rights of Sexual and Gender Minorities in the Republic of Croatia, 2010. Lesbian Group Kontra, p. 593 Press release issued by the Lesbian Group Kontra, 2010. Exact date not available.94 The ECHR, case of Alekseyev v. Russia, Applications nos. 4916/07, 25924/08 and 14599/09, judgment delivered on October 21, 2010. § 8095 The full chronology of the events surrounding Pride March 2009 could be found in the 2009 Annual Report on Rights of LGBTIQ People in Serbia, 2010, Labris, pp. 5-9

35
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
organized at the place selected by the organizers. Therefore, the Belgrade Pride 2009 has been cancelled. In December 2009, the five members of the organization committee lodged the complaint to the European Court on Human Rights. On October 10, 2010 the first Belgrade Pride manifestation was organized in Serbia, after 2001. Unfortunately, this event was also followed by the extreme violence targeted against sexual and gender minorities. However, the police was successful in protecting the participants of the Pride March, while they had to encounter with more than 6.000 anti-gay demonstrators. Police arrested 249 people in total, almost a half of them for disorderly conduct and damaging the property, while 158 were injured – in majority of them policemen, according to the media reports. On the same day, the President of the Republic of Serbia, Mr. Boris Tadić, strongly condemned violence and vandalism surrounding the event of Belgrade Pride 2010, ensuring that all vandals and hooligans who endangered the safety of Serbian citizens will be brought to justice.96 Many international media and organizations have monitored the event of Belgrade Pride 2010.97
3.4.4. Queer festival Sarajevo
Association Q in Sarajevo has organized the Sarajevo Queer Festival 2008 on September 24-28, 2008. The event was sur-rounded by violence committed by the extremist religious groups. The Amnesty International reported that „attacks at the end of the first day left eight people injured“ after which organizer had been forced to close the rest of the festival and cancel the whole event. The Amnesty International urged the national authorities to promptly and thoroughly investigate the at-tacks, bring those responsible to justice and to provide adequate security for the organizers and participants of the festival even after the festival has finished.98 As reported by the organizers the whole „organizational team became a target of hate speech and threats received constantly month before and after the opening of the Festival.“ Six injured persons reported attacks to the police, and the Prosecutor’s office of the Cantonal Ministry of Interior Affairs raised indictments against two persons.99 There is no accurate data of what have been legal consequences of prosecution in these cases.
On September 30, 2008, by the Resolution 1626(2008) the Parliamentary Assembly of the Council of Europe strongly condemned the discrimination and violence against LGBT people and attacks against organizers and participants of the Sarajevo Queer Festival, calling the national authorities to condemn such violence and discrimination and to thoroughly investigate any attacks against them with consequent bringing of those responsible to the justice system.
4.4.5. Conclusions and recommendations
The circumstance of high prevalence of violence against LGBT people is directly reflecting their right of expression and assembly in all countries in the region. While there is no accurate data on the situation in the Montenegro, there are well documented reports by civil society organizations in Croatia, Serbia, and Bosnia and Herzegovina. All the major and most visible public events are surrounded by extremist expression of hatred and violence, requiring the authorities to ensure protection to participants as organizers while considering such events to be of a high risk of causing public disorder. The negative practice in Serbia, perhaps based on the example in Russia, to ban Pride marches, seems to be changed by allowing the recent Belgrade Pride March 2010 and providing protection by the police to the participants and organizers. However, the existence of such high quantity of hatred against sexual and gender minorities in the re-gion is highly concerning. An example of „equalizing positions“ of sexual and gender minorities with extremist fascistic groups, as reported in Croatia, brings concerns about how serious national authorities take the right of people on ex-pression and public assembly. Therefore, these steps should be done by the national authorities in the region to ensure right of everyone to expression and public assembly is respected:
96 „President reacts to Belgrade violence“, B92, October 10, 2010.97 For full coverage please visit: www.parada.rs 98 Public statement by the Amnesty International, September 30, 2008.99 Narrative report of the Sarajevo Queer Festival 2008, The Association Q, Sarajevo, Bosnia and Herzegovina.

36
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
1. National authorities shall ensure adequate level of protection from violence to the participants and organizers of public events, prior, immediately and after the event.
2. National authorities shall ban all the extremist public assemblies aimed at disturbing public, expressing hatred and violent attacking against participants and the organizers of LGBT public events;
3. National authorities shall thoroughly investigate all violent attacks against participants and the organizers of LGBT public events and bring the perpetuators to the justice system ensuring effective legal remedies to victims;
4. National authorities should do public campaigning to address hatred against LGBT people in the region with pur-pose of raising level of respect, tolerance and humanity to LGBT people.
3.5. Right to be protected from discrimination
3.5.1. Protocol 12 of the European Convention on Human Rights
All the countries in the region have ratified the Protocol 12 to the European Convention on Human Rights. Although some countries in the EU have not ratified Protocol 12 yet, the fact that countries in the region respond so quickly in its ratification may rely on the fact that all the countries have signed documents to start process of stabilization and joining to the EU.
3.5.2. Practice of the European Court on Human Rights
Fundamentally, all the cases that have been lodged before the European Court on Human Rights argue about dis-crimination. Virtually violation of any right enacted by the European Convention on Human Rights and Fundamental Freedoms, and in the countries of the region, violation of any right enacted by the national legislation (effect of Proto-col 12), if committed against sexual and gender minorities may be connected with discrimination. There have been a number of judgments of the European Court on Human Rights concerning following areas that have been connected with discrimination: (1) banning criminalization of the same-sex activities between consenting adults, (2) equalizing age of consent for same- or opposite-sexual activities, (3) equal opportunities in employment, (4) custody over biologi-cal child, (5) adoption procedures, (6) right to expression and peaceful assembly, and (7) rights of same-sex couples.100 The well established practice of the European Court on Human Rights, while allowing certain margin of appreciation to member states, shows that, except in regards to right to marry, the discrimination on the grounds of sexual orientation is prohibited in all areas of social life.
3.5.3. National anti-discrimination legislations
In this part we refer to most important and current legislation, which is, at this moment, comprised of the comprehen-sive anti-discrimination laws. Although having in mind that during the recent years different other legal documents containing anti-discrimination provisions (e.g. labour or media legislation) have been enacted by countries in the re-gion, since they are redundant and unnecessary when special anti-discrimination acts are enacted, we leave them out of this analysis.
100 Wintemute R., 2006. “Sexual Orientation and Gender Identity Discrimination: The Case Law of the European Court on Human Rights and the European Court of Justice”, ILGA Europe
37
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
Croatia was the first country in the region to enact the Anti-Discrimination Act in 2008. The Act came in force on January 1, 2009.101 The discrimination on the ground of sexual orientation and/or gender identity is prohibited.102 The exclusions of discrimination are set in accordance with the international human rights principles. However, after the pressure of the Catholic Church, the Croatian Parliament enacted amendments excluding discrimination in family law when privileges have been given to married heterosexual couples.103 Furthermore, activities of religious organizations also cannot be considered as discriminatory. Although the Anti-Discrimination Act brought new mechanisms aimed at protection of sexual and gender minorities, especially in building effective remedies to victims of discrimination, the protection from discrimination on the ground of sexual orientation has been granted in Croatia from 2003 by the Gender Equality Act.104 The Same-Sex Union’s Act also contained provision banning the discrimination on the grounds of sexual orientation and living in the same-sex union.105 Although the Croatian legislator practised to implement anti-discrimination provisions into other laws (e.g. Media Act, Electronic Media Act, Labour Act, Voluntarism Act), the Gender Equality Act and the Same-Sex Unions’ Act were most important since they covered all the aspects of social life, while anti-discrimination provisions in other laws were redundant. The Office of the Ombudswoman for Gender Equal-ity is established as the central anti-discrimination body. Since 2003 that office became the first state-based mechanism that could be effectively used in responding to discrimination based on sexual orientation and the Ombudswoman for Gender Equality was usually publicly condemning violence and discrimination against sexual minorities, urged police and law enforcement bodies to conduct proper investigations, supported advocacy activities of civil society organiza-tions and supported these organizations in organizing public events.
The countries in the region soon followed Croatian example by adopting the comprehensive anti-discrimination legisla-tion. Serbia adopted the Anti-Discrimination Act on February 29, 2009; Bosnia and Herzegovina adopted the Act on July 23, 2009; and Montenegro adopted the Act on July 27, 2010.
While in Croatia there is closed provision concerning grounds of discrimination, provisions banning discrimination in laws of other countries in the region are „open-ended“. Surprisingly, although after some debate and pressure of various religious communities, all countries implemented „gender expression“ as a ground of discrimination in their laws.106 The exclusion of discrimination in all countries is recognized for (1) activities of religious communities and (2) when giving privileges to married heterosexual couples. The anti-discrimination legislation in all countries in the region is comprehensive, setting up central bodies in combating discrimination, determining judicial mechanisms, and allowing civil society organizations to bring complaints or to intervene in existing judicial proceeding.
There are, however, some fundamental concerns surrounding the existing anti-discrimination legislation, as follows:
1. In Croatia the legislator missed to enact „open-ended“ provision when defining grounds of discrimination, which would, in case of any further social development and appearance of some other grounds, require amending the existing Act;
2. Under the pressure of religious communities all the countries in the region passed an excuse for discrimination if committed while doing religious-based activities. Therefore, the legal way to religious-based hate speech against sexual and gender minorities is opened;
101 Official Gazette no. 85/08102 There has been huge public discussion surrounding proposition of the Anti-Discrimination Bill to the Croatian Parliament regar-ding term of „gender identity“, because Catholic church made a pressure towards the Government not to implement such term into the Bill.103 Article 9/2/10 of the Anti-Discrimination Act.104 Article 6/2 of the Gender Equality Act, Official Gazette no. 116/03.105 Article 21 of the Same-Sex Union's Act – the part of the provision concerning same-sex unions have never been applied in order to recognize broader scope of rights of same-sex partners, although the Act was lex specialis to the Family Act.106 See Article 2/1 of the Anti-Discrimination Act of Bosnia and Herzegovina; Article 2/2 of the Montenegro Anti-Discrimination Act; Article 2/1 of the Serbian Anti-Discrimination Act.

38
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
3. Under the above mentioned circumstances, all the countries in the region passed an excuse for giving privileges to married heterosexual couples. Although possible formal recognition of the same-sex partnerships in a form of marriage falls within the margin of appreciation of the Council of Europe member states, such excluding provisions in anti-discrimination legislation are not well balanced considering recent practice of the European Court on Hu-man Rights and recognition of same-sex union within the notion of „family life“ under the European Convention on Human Rights and Fundamental Freedoms;
4. The provisions concerning interveners in Serbia, Montenegro, and Bosnia and Herzegovina are not in line with general rules of civil procedure. Namely, such provisions allow legal or a natural person to intervene in civil procee-dings regarding discrimination, however, regardless the outcome of the proceeding, the intervener is due to cover expenses of its participation to the proceeding. In Croatia, originally, the Government also proposed such legal solution – however, after civil society organizations107 warned the Croatian Parliament about inequality between interveners in civil proceedings, the Bill has been amended by the Government. Provisions requiring interveners to cover the expenses of their participation to the civil proceedings regardless the outcome may be challenged under the constitutional guarantees of equality before the law;
5. The consideration of discrimination to constitute different forms of misdemeanours, while having in place criminal legislation proscribing discrimination to be the criminal offence, and possible prosecution of offenders for both criminal offence and misdemeanours, are contrary to the legal principle ne bis in idem and to the existing practice of the European Court on Human Rights.108 Furthermore, while considering discrimination to be a misdemeanour, the legislators overruled their earlier policy that offenders who committed criminal offence of discrimination actually committed serious offence, sending wrong message to the society that discrimination is a less serious offence.109
Regarding implementation of the above described anti-discrimination legislation, there have been a few examples in Croatia. The Croatian Ombudswoman for Gender Equality immediately started to implement the Anti-Discrimination Act after entered in force. According to the Ombudswoman’s 2009 Annual Report there have been a few individual complaints concerning discrimination on the ground of sexual orientation.110 The civil society organizations reported on several cases of discrimination, usually connected with violence, of which one case of discrimination at workplace was successfully solved; however, there have not been any civil judicial proceedings in cases of discrimination initiated in 2009.111 According to the media reports and public statements by the Lesbian Group Kontra, in 2010 first collective complaint against discrimination has been brought before the County Court in Zagreb.112 The collective complaint has been brought against the episcopal teacher in elementary public school who allegedly taught pupils that homosexuality is a mental disorder. During the civil proceeding, a number of civil society organizations joined complaint as the inter-veners. The case is still pending before the Court.
107 The Team for Legal Changes of Iskorak and Kontra.108 The ECHR, case of Maresti v. Croatia, Application no. 55759/07, judgement delivered on June 25, 2009.109 In Croatia, the Government argued that by enacting misdemeanour offences for discrimination, the procedures before the courts will be faster, comparing that situation with domestic violence. That was true, because magistrates' courts are faster that regular crimi-nal courts, however, the domestic violence represents different situation than discrimination does. Cases of domestic violence require urgency because immediate protection of victims of violence is necessary and has to be enforced by competent judicial decision, while in discrimination cases such an urgency is not necessarily required.110 2009 Annual Report of the Ombudswoman for Gender Equality, pp. 145-149.111 2009 Annual Report on the Status of Rights of Sexual and Gender Minorities in the Republic of Croatia, 2010, Lesbian Group Kontra pp. 34-42112 Public statement by the Lesbian Group Kontra, Croatia, May 25, 2010.
39
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
The People’s Defender (ombudsman) in Serbia paid a special attention to the position of sexual minorities in its 2009 Annual Report. As the main problems, the People’s Defender pointed out (1) endangering right to public assembly, (2) hate speech in public sphere and (3) a lack of safety for LGBT human rights defenders.113 The People’s Defender ex-pressed clear supportive policy towards rights of LGBT persons, although there is a lack of description of concrete cases of discrimination reported to his Office and there is no information about possible outcomes. The civil society organiza-tion Gay-Straight Alliance reported in 2010 about initiating civil complaint to the First Municipal Court in Belgrade in case of hate speech in the newspaper; until the writing of their report, the hearing at the Court was not even scheduled, contrary to the legal provisions about urgency in discrimination matters.114
Although having received a number of complaints against discrimination, majority on the ground of national origin, the Human Rights Institution of Ombudsman in Bosnia and Herzegovina did not refer to any case of discrimination on the grounds of sexual orientation or gender identity.115 There is no relevant data about cases of discrimination or possible judicial proceedings in Bosnia and Herzegovina. The same situation is with the Office of the Human Rights Defender of Montenegro, also there is no accurate data on implementation of Anti-Discrimination Act concerning sexual or gender minorities.
3.5.4. Conclusions and recommendations
The most significant evolvement regarding human rights of sexual and gender minorities in the region is, naturally, development of comprehensive anti-discrimination legislation. This is, at the same time, an important positive example in protection of rights of sexual and gender minorities, with possibility of promising outcomes. However, there are a few gaps in existing legislations that may be filled by:
1. enacting clear prohibition of hate speech against sexual and gender minorities even if being religious-based;
2. considering recent developments in the judicial practice of the European Court on Human Rights regarding reco-gnition of same-sex unions under the notion of „family life“;
3. developing clear criminal policy against offenders who committed discrimination;
4. equalizing status of interveners according to fundamental principles of civil proceedings;
5. enacting „open-ended“ provision regarding grounds of discrimination (Croatia only).
Although existing, the anti-discrimination legislation is rarely implemented. Having in place advocacy projects and doing strategic litigation before national authorities, civil society organizations in Croatia and Serbia more often use criminal than civil legislation to address discrimination. In Montenegro, and Bosnia and Herzegovina, there isn’t even any evidence on use of existing legislation in protecting members of sexual and gender minorities from discrimination. Although comprehensive anti-discrimination legislation covering grounds of sexual orientation and gender identity have developed in all countries from the region, it remains unclear which specific measures have been undertaken to en-sure their effective implementation, while civil society organizations pay more attention to political activities instead of participating in building and developing mechanisms of implementation (e.g. education of law enforcement, judiciary, social workers, creating networks of support, etc.). Therefore:
113 2009 Regular Annual Report of the People's Defender, March 2010, p. 17.114 „No Surrender, No Retreat“, 2010. Gay-Straight Alliance, p. 37.115 Annual Report of the Human Rights Institution of Ombudsman in Bosnia and Herzegovina, 2010.
40
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
1. The capacities of civil society organizations to participate in building mechanisms of implementation of anti-discri-mination legislation should be developed in terms of funding and providing professional support;
2. More attention should be paid to the situation in Montenegro, and Bosnia and Herzegovina; development of legal services provided by civil society organizations should be supported by national and international donors.
3.6. Right to family life
3.6.1. European context
Across the European Union there is no political consensus on recognizing right to marry for the same-sex unions. Al-though same-sex unions should be considered and treated as families, the member states of the Council of Europe are not obliged to legally recognize same-sex marriages.116 While some countries in the EU allow same-sex partners to marry (e.g. Spain, Netherlands and Belgium), some of them enacted registered partnerships legislation (e.g. UK, France and Ger-many), while in other countries, even if legally recognized, the same-sex union is considered to be informal cohabitation. At the international level, the attitude determining scope of rights entitled to same-sex partners falls under margin of ap-preciation of every state. While member states of the Council of Europe have to ensure that there will be no discrimination on the ground of sexual orientation in adoption procedures,117 the issue of adoption remains to be opened.
In the period from 1983 to 1996 the European Commission on Human Rights (now the European Court on Human Rights) did not pass any decision that would be favourable to same-sex couples; instead, all the applications have been declared as inadmissible.118 However, in 2003 the case of Karner v. Austria overruled earlier admissibility decisions of the Commission and the Court, by the judgment that same-sex partners should be equally treated when considering tenancy.119 In recent decision in the case of Schalk and Kopf v. Austria,120 the Court considered that situation of same-sex partners’ falls within the notion of “family life” under the Convention since “a rapid evolution of social attitudes towards same-sex couples has taken place in many member States” (§ 93). Following that conclusion, the Court found that “the relationship of the applicants, cohabiting same-sex couples living in a de facto stable partnership, falls within the notion of ‘family life’, just as the relationship of a different-sex couple in the same situation would” (§ 94). However, the Court did not find that state violated human rights of applicants by denying them right to marry, which right is avail-able to different-sex couples, since “the question whether or not to allow same-sex marriage is left to regulation by the national law of the Contracting State” (§ 61).This decision, however, is not final and is pending the referral to the Grand Chamber. One month later, in the case of P.B. and J.S. v. Austria, the Court found violation of right to equal treatment against same-sex couple regarding insurance, since the exclusion of persons living in a homosexual relationship from the insurance policies has not been necessary in democratic society (§ 42).121 Furthermore, in case of J.M. v. the United Kingdom the Court found that making difference between heterosexual and homosexual couples in determining child maintenance represents discrimination.122
The recent decisions of the European Court on Human Rights showed significant developments in recognizing equality
116 The ECHR, case of Schalk and Kopf v. Austria, Application no. 30141/04; decision delivered on June 24, 2010.117 See case of E.B. v. France (2007), the European Court on Human Rights, Application no. 43546/02118 Wintemute R., 2006. “Sexual Orientation and Gender Identity Discrimination: The Case Law of the European Court on Human Rights and the European Court of Justice”, ILGA Europe119 The ECHR, Application no. 120 The ECHR, Application no. 30141/04, delivered on June 24, 2010.121 The ECHR, Application no. 18984/02, delivered on July 20, 2010.122 The ECHR, Application no. 37060/06, delivered on September 28, 2010.

41
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
for same-sex unions. Although the Court holds attitude that right to marry for same-sex couples falls under margin of appreciation of the Council of Europe member states, the practice of the Court undoubtedly requires from the member states to apply scope of rights falling within the notion of family life to same-sex unions in the same way such as scope of rights would be applied to different-sex couples.
3.6.2. Situation in the region
In all the countries in the region the family laws do not allow same-sex couples to marry. The marriage is defined as living union of a man and a woman; the opposite-gender combination is necessary for marriage being legally allowable and crucial to its existence.
Croatia is the only country in the region that legally recognizes same-sex union. In 2003, the Croatian Parliament en-acted the Same-Sex Union’s Act with limited scope of rights.123 There are only three rights directly deriving from the Same-Sex Union’s Act: (1) right to mutual maintenance, (2) right to acquire mutual property and (3) right to mutual assistance.124 The later developments in legislation slightly broaden the scope of rights; the violence between same-sex partners is recognized as domestic violence.125 Furthermore, the legislator recently announced that the novel Social Welfare Act is going to be enacted by the end of 2010 and will recognize same-sex unions as families.126 Until the time of finalization of this report, the Croatian Government still did not publicly present the Social Welfare Bill. The same-sex unions in Croatia are considered as informal cohabitation of two persons of same-sex, which means that to be eligible to exercise some of the rights enacted by the Same-Sex Union’s Act partners need to prove the existence of the same-sex union at the court. Such rule is excluded in cases of domestic violence where courts have discretion in determining existence of same-sex unions in every concrete situation. How the existence of same-sex union would be determined in social welfare system remains to be questioned, while at the same time the discretion of social workers in such determi-nation is also possible. In 2010, the civil society organizations reported about positive practice in prison system to allow visits to same-sex couples under the same circumstances as allowed for heterosexual married or non-married couples. 127
The analysis of the civil society organizations the Iskorak and the Kontra in 2006 showed that same-sex couples are able to use only 2% of rights under the scope of rights given to the married heterosexual couples. At the same time, these or-ganizations warned that extramarital heterosexual couples had possibility to use only 46% of rights available to married heterosexual couples.128 Therefore, at the initiative of these organizations, two members of the Croatian Parliament pro-posed in 2006, the Registered Partnership Bill to be enacted. Such legal solution would almost fully equalize same-sex unions and extramarital heterosexual unions with married couples.129 The reactions from other members of the Croa-tian Parliament have been extremely homophobic and the proposition didn’t pass the Parliament. After that, no propo-sition to broaden the scope of rights to same-sex couples has been done due to unfavourable political circumstances.
The possibility of registration is a crucial issue when considering rights of same-sex couples. While heterosexual couples living in extramarital unions have the possibility to marry and therefore to register their living union, such possibility is not available for same-sex partners. If not being able to register, same-sex couples would never have access to the same scope of rights that are available to married heterosexual couples.
123 Official Gazette no. 116/03124 Article 4 of the Same-Sex Union's Act.125 Article 7 of the Act on Protection from Domestic Violence, Official Gazette 137/09.126 http://www.gay.hr/magazin/4010 127 2009 Annual Report on Status of Rights of Sexual and Gender Minorities in the Republic of Croatia, Lesbian Group Kontra, pp. 36-37.128 The Registered Partnership Bill, 2006.129 The adoption was excluded!
42
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
There is no accurate data about use of scope of rights enacted by the Same-Sex Union’s Act in Croatia. There are no examples from the judicial practice. The civil society organizations reported that only possible use of that Act was in contracting property issues between same-sex partners.
In 2008, the Anti-Discrimination Act was enacted by the Croatian Parliament. The provisions of the Act exclude dis-crimination in cases when married heterosexual couples are placed in favourable position.130
3.6.3. Conclusions and recommendations
Although the states are not obliged to allow same-sex couples to marry, the European Court on Human Rights set the standard that scope of rights exercised by families should be available to same-sex partners. The form of the legal recog-nition falls under the margin of appreciation of every country; however, the more important is that the Court urges for certain quality of legislation in order to equalize rights of same-sex couples compared with different-sex couples. These developments open possibility for civil society organizations and political stakeholders in further advocacy for social and legal changes. In the context of above mentioned, the least that should be done in order to improve social and legal position of same-sex couples in the region are these steps:
1. the same-sex partners should enjoy at least the same scope of rights that are available to heterosexual couples living in extramarital cohabitation;
2. the Croatian Same-Sex Unions’ Act should be amended to broaden the scope of rights available to same-sex unions in at least the areas of housing, inheritance, insurance and tax system;
3. Serbia, Montenegro, Bosnia and Herzegovina should legally recognize same-sex unions and entitle them with appropriate scope of rights following the standards set by the European Court on Human Rights;
4. the campaigning targeting negative social attitudes towards same-sex unions should be implemented;
5. the efforts of the civil society organizations advocating legal recognition of same-sex couples should be supported in terms of funding and developing professional capacities.
3.7. Summary of recommendations
RIGHT TO LIFE, SAFETY AND PROTECTION FROM VIOLENCE
1. Criminal legislation in all countries in the region should be amended in order to recognize hatred against sexual and gender minorities as aggravating condition to criminal offences against life, physical integrity, personal safety, personal rights and freedom of victims;
2. Hate speech should be effectively addressed in order to prevent spreading of hatred against sexual and gender mi-norities;
3. Biased criminal offences should have priority at all stages of criminal proceedings, starting even in pre-criminal phases;
130 Article 9/2/10 of the Anti-Discrimination Act, OG 85/08
43
Chapter 3Legal status of Sexual and Gender Minorities in South-eastern Europe
4. Police, law enforcement bodies and the judiciary should be educated and trained to appropriately respond to biased criminal offences;
5. Countries should develop state-based mechanisms aimed at provision of support and accessible legal services to victims of biased criminal offences;
6. Police, law enforcement bodies and the judiciary should collect and analyze statistical data showing incidence of biased crimes against sexual and gender minorities;
7. Medical doctors, especially psychiatrists, should be educated on standards in providing psychiatric care and support to avoid medicalization of homosexuality;
8. Capacities of civil society organizations should be developed in order to raise their abilities to design and advocate appropriate mechanisms of implementation of enacted legislation;
9. Comprehensive outreach activities should be conducted to inform members of sexual and gender minorities on their rights and to encourage them in reporting violence they suffered.
RIGHT TO EXPRESSION AND PUBLIC ASSEMBLY
1. National authorities shall ensure adequate level of protection from violence to the participants and organizers of public events, prior to, immediately and after the event.
2. National authorities shall ban all the extremist public assemblies aimed at disturbing public, expressing hatred and violent attacks against participants and the organizers of LGBT public events;
3. National authorities shall thoroughly investigate all violent attacks against participants and the organizers of LGBT public events and bring the perpetuators to the justice system ensuring effective legal remedies to victims;
4. National authorities should do public campaigning to address hatred against LGBT people in the region with the purpose of raising level of respect, tolerance and humanity to LGBT people.
RIGHT TO BE PROTECTED FROM DISCRIMINATION
1. Enacting clear prohibition of hate speech against sexual and gender minorities even if being religious-based;
2. Considering recent developments in the judicial practice of the European Court on Human Rights regarding reco-gnition of same-sex unions under the notion of „family life“;
3. Developing clear criminal policy against offenders who committed discrimination;
4. Equalizing status of interveners according to fundamental principles of civil proceedings;
5. Enacting „open-ended“provision regarding grounds of discrimination (Croatia only).
6. The capacities of civil society organizations to participate in building mechanisms of implementation of anti-discri-mination legislation should be developed in terms of funding and providing professional support;
7. More attention should be paid to the situation in Montenegro, and Bosnia and Herzegovina; development of legal services provided by civil society organizations should be supported by national and international donors.
44
Chapter 3 Legal status of Sexual and Gender Minorities in South-eastern Europe
RIGHT TO FAMILY LIFE
1. The same-sex partners should enjoy at least the same scope of rights that is available to heterosexual couples living in extramarital cohabitation;
2. The Croatian Same-Sex Unions’ Act should be amended to broaden the scope of rights available to same-sex unions in at least the areas of housing, inheritance, insurance and tax system;
3. Serbia, Montenegro, Bosnia and Herzegovina should legally recognize same-sex unions and entitle them with appropriate scope of rights following the standards set by the European Court on Human Rights;
4. The campaigning targeting negative social attitudes towards same-sex unions should be implemented;
5. The efforts of the civil society organizations advocating legal recognition of same-sex couples should be supported in terms of funding and developing professional capacities.
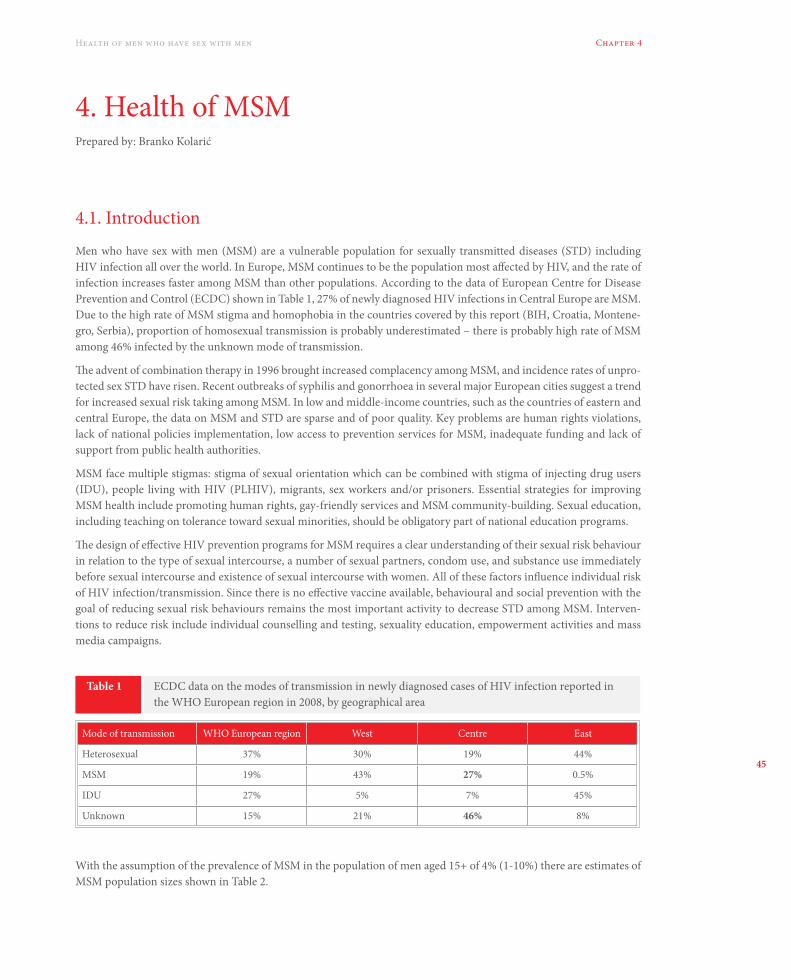
45
Chapter 4Health of men who have sex with men
4. Health of MSMPrepared by: Branko Kolarić
4.1. Introduction
Men who have sex with men (MSM) are a vulnerable population for sexually transmitted diseases (STD) including HIV infection all over the world. In Europe, MSM continues to be the population most affected by HIV, and the rate of infection increases faster among MSM than other populations. According to the data of European Centre for Disease Prevention and Control (ECDC) shown in Table 1, 27% of newly diagnosed HIV infections in Central Europe are MSM. Due to the high rate of MSM stigma and homophobia in the countries covered by this report (BIH, Croatia, Montene-gro, Serbia), proportion of homosexual transmission is probably underestimated – there is probably high rate of MSM among 46% infected by the unknown mode of transmission.
The advent of combination therapy in 1996 brought increased complacency among MSM, and incidence rates of unpro-tected sex STD have risen. Recent outbreaks of syphilis and gonorrhoea in several major European cities suggest a trend for increased sexual risk taking among MSM. In low and middle-income countries, such as the countries of eastern and central Europe, the data on MSM and STD are sparse and of poor quality. Key problems are human rights violations, lack of national policies implementation, low access to prevention services for MSM, inadequate funding and lack of support from public health authorities.
MSM face multiple stigmas: stigma of sexual orientation which can be combined with stigma of injecting drug users (IDU), people living with HIV (PLHIV), migrants, sex workers and/or prisoners. Essential strategies for improving MSM health include promoting human rights, gay-friendly services and MSM community-building. Sexual education, including teaching on tolerance toward sexual minorities, should be obligatory part of national education programs.
The design of effective HIV prevention programs for MSM requires a clear understanding of their sexual risk behaviour in relation to the type of sexual intercourse, a number of sexual partners, condom use, and substance use immediately before sexual intercourse and existence of sexual intercourse with women. All of these factors influence individual risk of HIV infection/transmission. Since there is no effective vaccine available, behavioural and social prevention with the goal of reducing sexual risk behaviours remains the most important activity to decrease STD among MSM. Interven-tions to reduce risk include individual counselling and testing, sexuality education, empowerment activities and mass media campaigns.
Table 1 ECDC data on the modes of transmission in newly diagnosed cases of HIV infection reported in the WHO European region in 2008, by geographical area
Mode of transmission WHO European region West Centre East
Heterosexual 37% 30% 19% 44%
MSM 19% 43% 27% 0.5%
IDU 27% 5% 7% 45%
Unknown 15% 21% 46% 8%
With the assumption of the prevalence of MSM in the population of men aged 15+ of 4% (1-10%) there are estimates of MSM population sizes shown in Table 2.
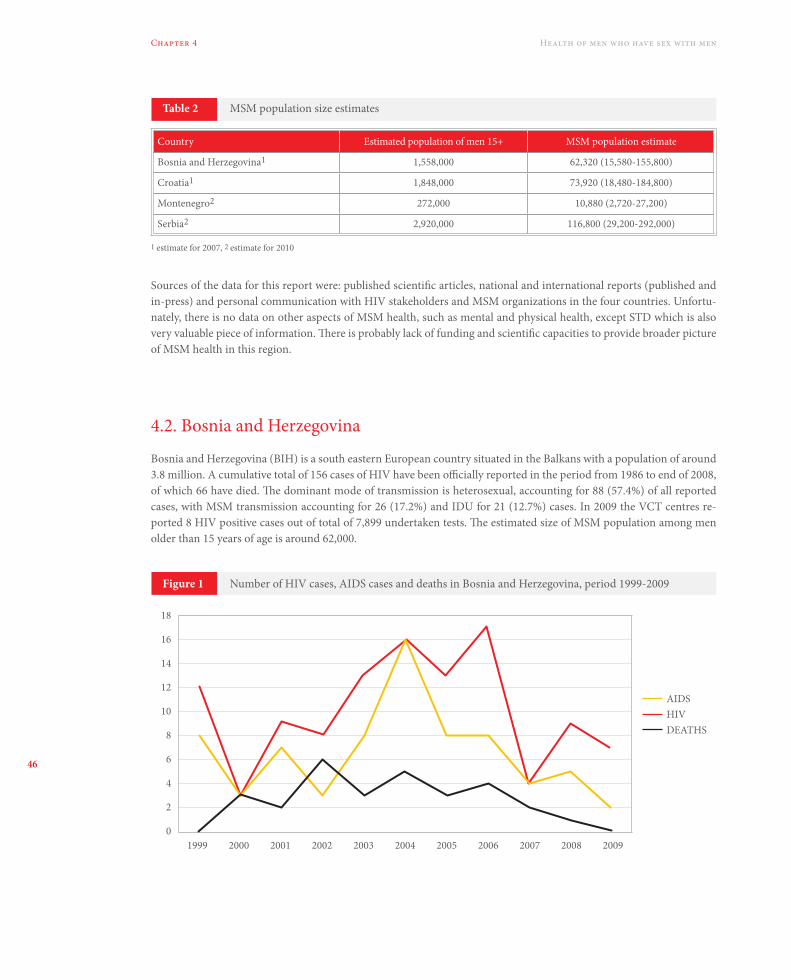
46
Chapter 4 Health of men who have sex with men
Sources of the data for this report were: published scientific articles, national and international reports (published and in-press) and personal communication with HIV stakeholders and MSM organizations in the four countries. Unfortu-nately, there is no data on other aspects of MSM health, such as mental and physical health, except STD which is also very valuable piece of information. There is probably lack of funding and scientific capacities to provide broader picture of MSM health in this region.
4.2. Bosnia and Herzegovina
Bosnia and Herzegovina (BIH) is a south eastern European country situated in the Balkans with a population of around 3.8 million. A cumulative total of 156 cases of HIV have been officially reported in the period from 1986 to end of 2008, of which 66 have died. The dominant mode of transmission is heterosexual, accounting for 88 (57.4%) of all reported cases, with MSM transmission accounting for 26 (17.2%) and IDU for 21 (12.7%) cases. In 2009 the VCT centres re-ported 8 HIV positive cases out of total of 7,899 undertaken tests. The estimated size of MSM population among men older than 15 years of age is around 62,000.
1 estimate for 2007, 2 estimate for 2010
Table 2
Figure 1
MSM population size estimates
Number of HIV cases, AIDS cases and deaths in Bosnia and Herzegovina, period 1999-2009
Country Estimated population of men 15+ MSM population estimate
Bosnia and Herzegovina1 1,558,000 62,320 (15,580-155,800)
Croatia1 1,848,000 73,920 (18,480-184,800)
Montenegro2 272,000 10,880 (2,720-27,200)
Serbia2 2,920,000 116,800 (29,200-292,000)
19990
2
4
6
8
10
12
14
16
18
2000
AIDSHIVDEATHS
2001 2002 2003 2004 2005 2006 2007 2008 2009
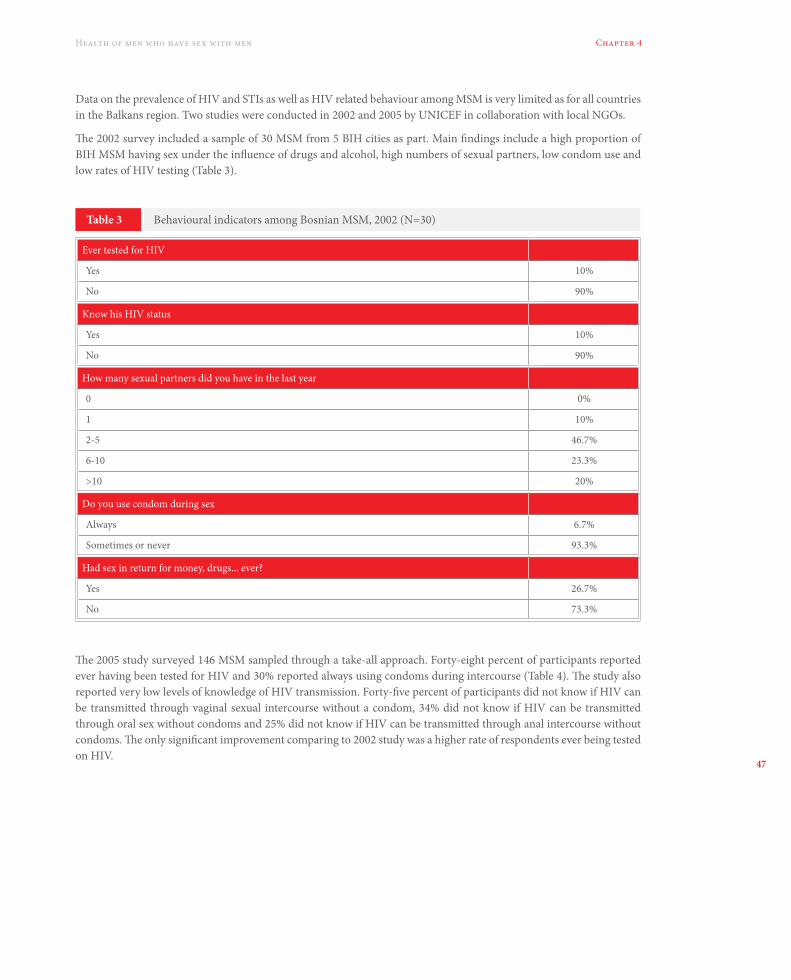
47
Chapter 4Health of men who have sex with men
Data on the prevalence of HIV and STIs as well as HIV related behaviour among MSM is very limited as for all countries in the Balkans region. Two studies were conducted in 2002 and 2005 by UNICEF in collaboration with local NGOs.
The 2002 survey included a sample of 30 MSM from 5 BIH cities as part. Main findings include a high proportion of BIH MSM having sex under the influence of drugs and alcohol, high numbers of sexual partners, low condom use and low rates of HIV testing (Table 3).
Table 3 Behavioural indicators among Bosnian MSM, 2002 (N=30)
Ever tested for HIV
Yes 10%
No 90%
Know his HIV status
Yes 10%
No 90%
How many sexual partners did you have in the last year
0 0%
1 10%
2-5 46.7%
6-10 23.3%
>10 20%
Do you use condom during sex
Always 6.7%
Sometimes or never 93.3%
Had sex in return for money, drugs... ever?
Yes 26.7%
No 73.3%
The 2005 study surveyed 146 MSM sampled through a take-all approach. Forty-eight percent of participants reported ever having been tested for HIV and 30% reported always using condoms during intercourse (Table 4). The study also reported very low levels of knowledge of HIV transmission. Forty-five percent of participants did not know if HIV can be transmitted through vaginal sexual intercourse without a condom, 34% did not know if HIV can be transmitted through oral sex without condoms and 25% did not know if HIV can be transmitted through anal intercourse without condoms. The only significant improvement comparing to 2002 study was a higher rate of respondents ever being tested on HIV.
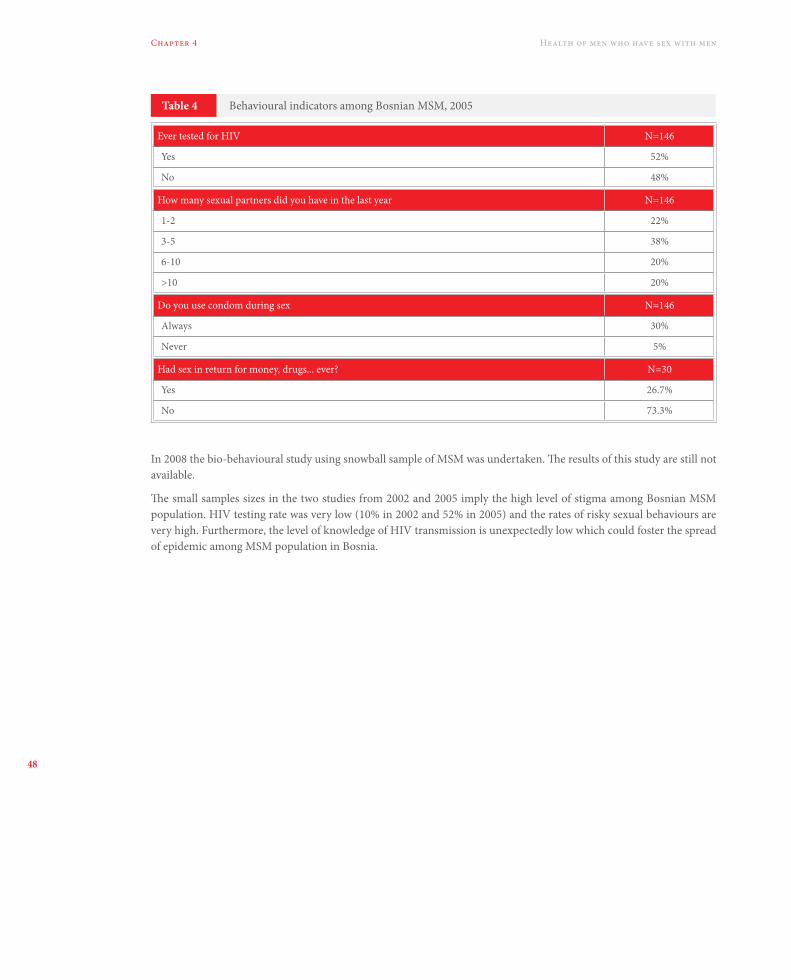
48
Chapter 4 Health of men who have sex with men
Table 4 Behavioural indicators among Bosnian MSM, 2005
Ever tested for HIV N=146
Yes 52%
No 48%
How many sexual partners did you have in the last year N=146
1-2 22%
3-5 38%
6-10 20%
>10 20%
Do you use condom during sex N=146
Always 30%
Never 5%
Had sex in return for money, drugs... ever? N=30
Yes 26.7%
No 73.3%
In 2008 the bio-behavioural study using snowball sample of MSM was undertaken. The results of this study are still not available.
The small samples sizes in the two studies from 2002 and 2005 imply the high level of stigma among Bosnian MSM population. HIV testing rate was very low (10% in 2002 and 52% in 2005) and the rates of risky sexual behaviours are very high. Furthermore, the level of knowledge of HIV transmission is unexpectedly low which could foster the spread of epidemic among MSM population in Bosnia.

49
Chapter 4Health of men who have sex with men
4.3. Croatia
Croatia is a south eastern European country with a population of 4,437,460 citizens. According to the National HIV Registry, a total of 792 cases of HIV have been officially registered in the period from 1985 to 2009 (Figure 2). Estimated size of MSM population among men older than 15 years of age is approximately 74,000.
Figure 2
Figure 3
Number of registered HIV cases, AIDS cases and deaths (“SMRTI”) in Croatia, period 1985-2009
Percentage of homosexual transmission in HIV registered cases in Croatia, period 1985-2008
1999
1998
1997
1996
1995
1994
1993
1992
1991
1990
1989
1988
1987
1986
1985
0
10
20
30
40
50
60
70
80
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
AIDSHIVSMRTI
1999
1998
1997
1996
1995
1994
1993
1992
1991
1990
1989
1988
1987
1986
1985
0
10
20
30
40
50
60
70
80
2000
2001
2002
2003
2004
2005
2006
2007
2008
The dominant mode of transmission is through a homosexual intercourse; 48.5% of all registered cases are MSM. The proportion of MSM among HIV cases rises in the last few years (Figure 3.) and in period 2006 – 2008 more than 60% of newly diagnosed cases are MSM.
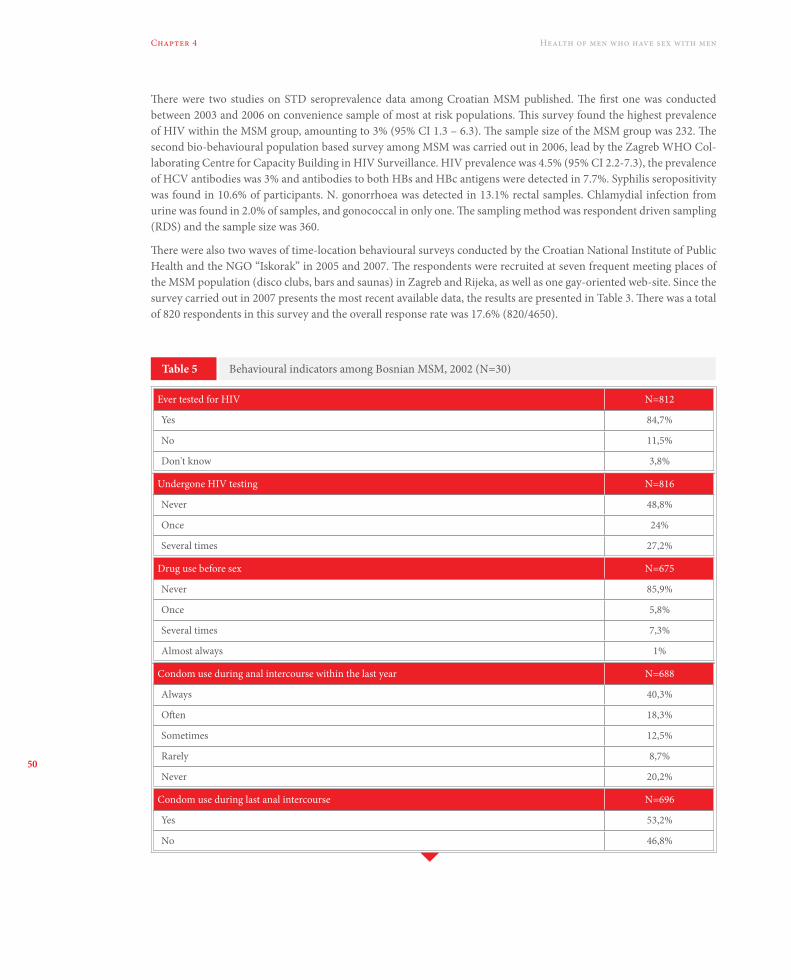
50
Chapter 4 Health of men who have sex with men
There were two studies on STD seroprevalence data among Croatian MSM published. The first one was conducted between 2003 and 2006 on convenience sample of most at risk populations. This survey found the highest prevalence of HIV within the MSM group, amounting to 3% (95% CI 1.3 – 6.3). The sample size of the MSM group was 232. The second bio-behavioural population based survey among MSM was carried out in 2006, lead by the Zagreb WHO Col-laborating Centre for Capacity Building in HIV Surveillance. HIV prevalence was 4.5% (95% CI 2.2-7.3), the prevalence of HCV antibodies was 3% and antibodies to both HBs and HBc antigens were detected in 7.7%. Syphilis seropositivity was found in 10.6% of participants. N. gonorrhoea was detected in 13.1% rectal samples. Chlamydial infection from urine was found in 2.0% of samples, and gonococcal in only one. The sampling method was respondent driven sampling (RDS) and the sample size was 360.
There were also two waves of time-location behavioural surveys conducted by the Croatian National Institute of Public Health and the NGO “Iskorak” in 2005 and 2007. The respondents were recruited at seven frequent meeting places of the MSM population (disco clubs, bars and saunas) in Zagreb and Rijeka, as well as one gay-oriented web-site. Since the survey carried out in 2007 presents the most recent available data, the results are presented in Table 3. There was a total of 820 respondents in this survey and the overall response rate was 17.6% (820/4650).
Table 5 Behavioural indicators among Bosnian MSM, 2002 (N=30)
Ever tested for HIV N=812
Yes 84,7%
No 11,5%
Don't know 3,8%
Undergone HIV testing N=816
Never 48,8%
Once 24%
Several times 27,2%
Drug use before sex N=675
Never 85,9%
Once 5,8%
Several times 7,3%
Almost always 1%
Condom use during anal intercourse within the last year N=688
Always 40,3%
Often 18,3%
Sometimes 12,5%
Rarely 8,7%
Never 20,2%
Condom use during last anal intercourse N=696
Yes 53,2%
No 46,8%
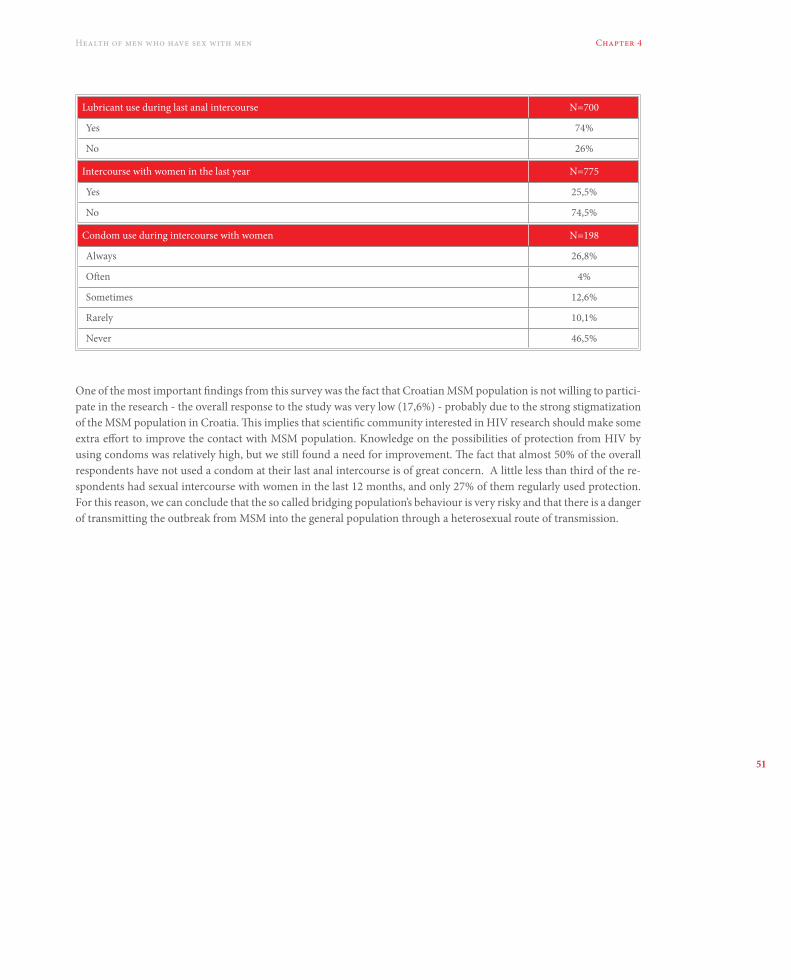
51
Chapter 4Health of men who have sex with men
One of the most important findings from this survey was the fact that Croatian MSM population is not willing to partici-pate in the research - the overall response to the study was very low (17,6%) - probably due to the strong stigmatization of the MSM population in Croatia. This implies that scientific community interested in HIV research should make some extra effort to improve the contact with MSM population. Knowledge on the possibilities of protection from HIV by using condoms was relatively high, but we still found a need for improvement. The fact that almost 50% of the overall respondents have not used a condom at their last anal intercourse is of great concern. A little less than third of the re-spondents had sexual intercourse with women in the last 12 months, and only 27% of them regularly used protection. For this reason, we can conclude that the so called bridging population’s behaviour is very risky and that there is a danger of transmitting the outbreak from MSM into the general population through a heterosexual route of transmission.
Lubricant use during last anal intercourse N=700
Yes 74%
No 26%
Intercourse with women in the last year N=775
Yes 25,5%
No 74,5%
Condom use during intercourse with women N=198
Always 26,8%
Often 4%
Sometimes 12,6%
Rarely 10,1%
Never 46,5%

52
Chapter 4 Health of men who have sex with men
4.4. Montenegro
Montenegro is a south eastern European country situated in the Balkans with a population of around 680,000. A cu-mulative total of 101 cases of HIV have been officially reported in the period from 1989 to end of 2009, out of which 50 had developed AIDS and 29 died (Figure 4). In 2009 the VCT centres reported 6 HIV positive results out of total of 738 undertaken tests. The estimated size of MSM population among men older than 15 years of age is approximately 11,000.
Figure 4 Number of registered HIV cases in Montenegro, period 1989-2009
1999
1998
1997
1996
1995
1994
1993
1992
1991
1990
1989
0
5
10
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
HIV/AIDS
The dominant mode of transmission is through heterosexual intercourse (46% of all infected), followed by homosexual/bisexual intercourses (37%).
Montenegro seems to be facing the highest degree of stigma and homophobia among four countries covered by this report. Namely, due to the mentioned reasons, RDS survey among MSM conducted from March to September 2007 failed to be carried out. Consequently, Public health institute of Montenegro started formative research among MSM population and the report from this research is yet to be published. According to personal communication, there were 123 MSM included in formative research. Hopefully, formative research would provide some information on Montene-gro MSM population in order to improve contact with this particular population and enable further research in the area of MSM health and HIV risk behaviours.
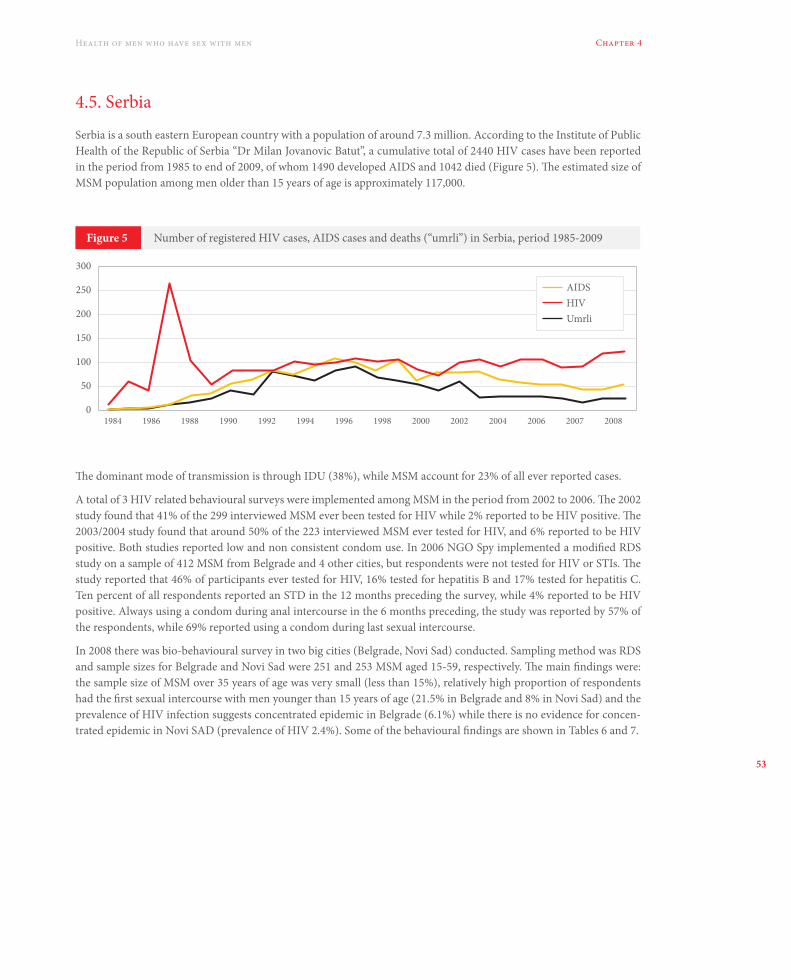
53
Chapter 4Health of men who have sex with men
4.5. Serbia
Serbia is a south eastern European country with a population of around 7.3 million. According to the Institute of Public Health of the Republic of Serbia “Dr Milan Jovanovic Batut”, a cumulative total of 2440 HIV cases have been reported in the period from 1985 to end of 2009, of whom 1490 developed AIDS and 1042 died (Figure 5). The estimated size of MSM population among men older than 15 years of age is approximately 117,000.
Figure 5 Number of registered HIV cases, AIDS cases and deaths (“umrli”) in Serbia, period 1985-2009
199819961994199219901988198619840
50
100
150
200
250
300
2000 2002 2004 2006 2007 2008
AIDSHIVUmrli
The dominant mode of transmission is through IDU (38%), while MSM account for 23% of all ever reported cases.
A total of 3 HIV related behavioural surveys were implemented among MSM in the period from 2002 to 2006. The 2002 study found that 41% of the 299 interviewed MSM ever been tested for HIV while 2% reported to be HIV positive. The 2003/2004 study found that around 50% of the 223 interviewed MSM ever tested for HIV, and 6% reported to be HIV positive. Both studies reported low and non consistent condom use. In 2006 NGO Spy implemented a modified RDS study on a sample of 412 MSM from Belgrade and 4 other cities, but respondents were not tested for HIV or STIs. The study reported that 46% of participants ever tested for HIV, 16% tested for hepatitis B and 17% tested for hepatitis C. Ten percent of all respondents reported an STD in the 12 months preceding the survey, while 4% reported to be HIV positive. Always using a condom during anal intercourse in the 6 months preceding, the study was reported by 57% of the respondents, while 69% reported using a condom during last sexual intercourse.
In 2008 there was bio-behavioural survey in two big cities (Belgrade, Novi Sad) conducted. Sampling method was RDS and sample sizes for Belgrade and Novi Sad were 251 and 253 MSM aged 15-59, respectively. The main findings were: the sample size of MSM over 35 years of age was very small (less than 15%), relatively high proportion of respondents had the first sexual intercourse with men younger than 15 years of age (21.5% in Belgrade and 8% in Novi Sad) and the prevalence of HIV infection suggests concentrated epidemic in Belgrade (6.1%) while there is no evidence for concen-trated epidemic in Novi SAD (prevalence of HIV 2.4%). Some of the behavioural findings are shown in Tables 6 and 7.
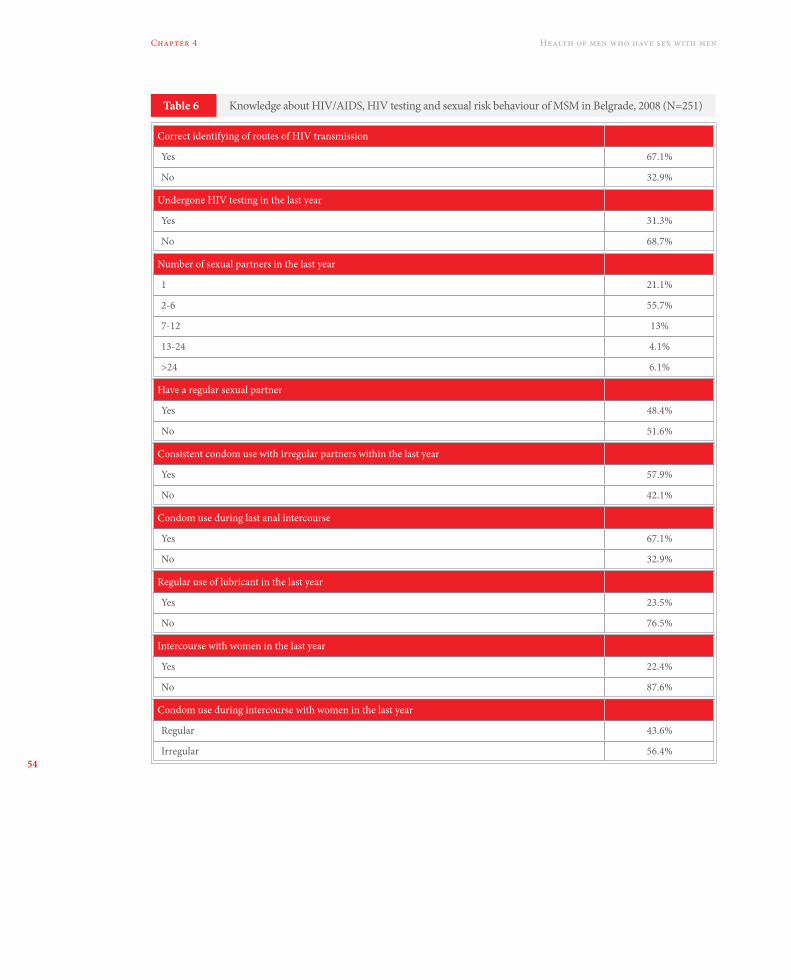
54
Chapter 4 Health of men who have sex with men
Table 6 Knowledge about HIV/AIDS, HIV testing and sexual risk behaviour of MSM in Belgrade, 2008 (N=251)
Correct identifying of routes of HIV transmission
Yes 67.1%
No 32.9%
Undergone HIV testing in the last year
Yes 31.3%
No 68.7%
Number of sexual partners in the last year
1 21.1%
2-6 55.7%
7-12 13%
13-24 4.1%
>24 6.1%
Have a regular sexual partner
Yes 48.4%
No 51.6%
Consistent condom use with irregular partners within the last year
Yes 57.9%
No 42.1%
Condom use during last anal intercourse
Yes 67.1%
No 32.9%
Regular use of lubricant in the last year
Yes 23.5%
No 76.5%
Intercourse with women in the last year
Yes 22.4%
No 87.6%
Condom use during intercourse with women in the last year
Regular 43.6%
Irregular 56.4%

55
Chapter 4Health of men who have sex with men
Table 7 Knowledge about HIV/AIDS, HIV testing and sexual risk behaviour of MSM in Novi Sad, 2008 (N=253)
Correct identifying of routes of HIV transmission
Yes 59%
No 41%
Undergone HIV testing in the last year
Yes 16%
No 84%
Number of sexual partners in the last year
1 32.8%
2-6 57.6%
7-12 6.8%
13-24 2.8%
>24 0%
Have a regular sexual partner
Yes 51.2%
No 48.8%
Consistent condom use with irregular partners within the last year
Yes 45.1%
No 54.9%
Condom use during last anal intercourse
Yes 58.4%
No 41.6%
Regular use of lubricant in the last year
Yes 16.3%
No 83.7%
Intercourse with women in the last year
Yes 31.6%
No 69.4%
Condom use during intercourse with women in the last year
Regular 31.6%
Irregular 69.4%
56
Chapter 4 Health of men who have sex with men
The main findings of surveys among MSM in Serbia are similar to the rest of the region: the rate of risk behaviours for STD is very high, HIV testing rate to low and the bridging population does not use condom with women regularly. The rate of MSM who are involved in sexual activities very young (under 15 years of age) in Belgrade suggests the need of special intervention for youth. The response rate of MSM above 35 years of age reaffirms the fact that older population is specially hidden and hard to reach. The great benefit from the 2008 RDS survey is the fact that there is significant dif-ference in MSM behaviour patterns between regions/cities in the same countries which implies the need of sub-national research and intervention approach.
4.6. Instead of conclusion
At the end, we can summarize that there is no data on MSM health in the region beside the data connected to STD/HIV. For Montenegro there is no data on MSM health at all. In other three countries included in this report we can observe the following similarities: the rate of HIV testing among MSM is very low and the prevalence of risk behaviours is rather high. Background for some amount of the presented results is the presence of high level of stigma and homophobia in the region (the most recent example is gay pride in Belgrade, October 2010). In the future, we should strengthen public health, social and political activities to provide higher level of social security which will enable environment for health research among MSM population in the region.
57
Chapter 4Health of men who have sex with men
4.7. References
1. WHO Regional Office for Europe. HIV and other STIs among MSM in the European Region – Report on a con-sultation. WHO Europe, 2008.
2. European Centre for Disease Prevention and Control. Technical report – Effectiveness of behavioural and psycho-social HIV/STI prevention interventions for MSM in Europe. ECDC, 2009.
3. European Centre for Disease Prevention and Control/WHO Regional Office for Europe. HIV/AIDS surveillance in Europe 2008. Stockholm: European Centre for Disease Prevention and Control; 2009.
4. Joint United Nations Programme on HIV/AIDS (UNAIDS). 2008 AIDS Epidemic Update [retrieved 02.10.2010].
5. Republic of Serbia, National AIDS Commision, Ministry of Health, Institute of Public Health of Serbia “Dr Milan Jovanovic Batut”. UNGASS country progress report. March 2010.
6. The Republic of Croatia, The Ministry of Health and Social Welfare. UNGASS country progress report. March 2010.
7. UNGASS country progress report Bosnia and Herzegovina. March 2010.
8. UNGASS country progress report Montenegro. March 2010.
9. Sapienca R. Young people selling sex in Bosnia and Herzegovina: research on sexual behaviour amongst men ha-ving sex with men. UNICEF; 2005.
10. Wong E: Rapid assessment and response on HIV/AIDS among especially vulnerable young people in South Ea-stern Europe. CIDA/UNICEF; 2002.
11. Republic of Serbia, Ministry of Health. Surveys among HIV most –at-risk populations and persons living with HIV. (In Serbian); 2008.
12. http://www.hzjz.hr/epidemiologija/hiv.htm.
13. Kolaric B, Pavlić J. HIV/AIDS Surveillance in Croatia. Croatian National Institute of Public Health. Zagreb 2007.
14. Kolaric B, Bielen L, Gjenero-Margan I. Risk behaviours for getting HIV among the Croatian men who have sex with men. Coll Antropol. 32(3):687-91, 2008.
15. Kolaric B, Stajduhar D. Risk Behaviors for Getting HIV Infection among the Croatian Men Who Have Sex With Men in 2007. Coll Antropol. In press.
16. Bozicevic I, Djakovic Rode O, Lepej Zidovec S, Johnston LG, Stulhofer A, Dominkovic Z, Bacak V, Lukas D, Bego-vac J. Prevalence of sexually transmitted infections among men who have sex with men in Zagreb, Croatia. AIDS Behav. 3:303-9; 2009.
17. Stulhofer A, Bacak V, Bozicevic I, Begovac J. HIV-related Sexual Risk Taking Among HIV-negative Men Who Have Sex with Men in Zagreb, Croatia. AIDS Behav. 12:505-12; 2008.

58
Chapter 4 Health of men who have sex with men
59
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
5. Academic education on LGBT population in three helping professions in countries of South-eastern EuropePrepared by: Dinko Štajduhar
5.1. Summary
This text will give a brief overview on the representation of contents relating to LGBT persons in programs of academic education in three helping professions: medicine, social work and psychology, for the countries of Bosnia and Herze-govina, Croatia, Montenegro and Serbia. The problem of representation of programmatic contents on LGBT popula-tion in academic education of helping professions might be reduced to a mere question of attitudes and preferences of department heads and lecturers at particular Universities, if we were not aware of the fact that LGBT persons in communities of considerably more liberal countries than those of South-eastern Europe are subject to significant stig-matization and discrimination131, as to a range of various other permanent social pressures which for this population amounts to not only inequality in realization of basic human rights, but also to a notably lower quality of life, as well as considerable and very tangible health risks. One relatively simple and cheap – but perhaps not the most efficient – way in which the development of tolerance for differences in sexual orientations and practices could be influenced – and thus reduce the social pressures mentioned – is the inclusion of contents on same-sex orientation in academic programs, and encouraging research among this population in the region, with the assumption that helping professionals with developed affirmative viewpoint towards this population will have certain influence on attitudes of the population as a whole. This article shows the collected data on inclusion of contents on LGBT populations into programs of institutions of higher education in the fields of medicine, psychology and social work in countries of South-eastern Europe. Even though incomplete and selective, the results point to the need of active work on encouraging inclusion of these issues into academic programs.
5.2. Introduction
It has been 36 years since the members of the American psychiatric association, after a longer period of data collection and debate, voted to exclude homosexuality from the Diagnostic statistical manual of mental disorders132. The World Health Organization removed homosexuality from the classification of mental disorders in 1994. Some of the important evidence for depathologizing homosexuality was the research results of inability of blind psychodiagnostic differentia-tion of groups of non clinical homosexual and heterosexual men133. Even though it was for quite a while considered that various mental disorders were no more common in LGBT population in relation to overall population, a range of cross-sectional studies conducted in the last twenty years shows the opposite: the incidence of depressive disorders, addiction
131 Within the frame of this monograph V. Bačak wrote on the incidence, consequences and prevention of homophobia in countries of South-eastern Europe. 132 Stoller R, Marmor J, Bieber I, Gold R et al. (1973) A Symposium: Should Homosexuality be in the APA nomenclature. Am J Psychiatry 130:1207-1216.133 Hooker E. (1957) The Adjustment of the Male Overt Homosexual. Journal of projective techniques. XXI: 18-31.

60
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
and anxiety disorders is higher in this group, and so is the suicide rate134,135,136. The traditional (and a very wrong) medi-cal explanation would be: homosexual orientation is a factor that leads to a higher incidence of mental disorders and suicides in this group, in the way that hypercholesterolemia “leads” to heart attacks. Thus, as a risk factor, homosexuality in itself would present a disorder. However, it would be very naive to reduce this very complex phenomenon such as sexual orientation to a risk factor and assume simple causal relationships.
For this purpose it will be sufficient to say that in order to label homosexuality as a disorder, it would be necessary that it always and without exception, in each homosexually oriented individual, be linked with another psychiatric disorder, that is, that the causal relationship between homosexuality and another disorder be nomic. This however is not the case, and thus, even without being familiar with the fact that problems of LGBT persons are caused by constant social pres-sures, data on higher risk for a range of mental disorders is not and cannot be a criteria basing on which homosexuality could be defined as a mental disorder.
On the other hand, the evidence grew stronger on the increased risks for mental disorders and suicide in LGBT popu-lation are a result of a life surrounded by stigma, discrimination137,138,139 and other forms of social oppression140. For instance, a group of researchers from the University of Yale showed that in those states of the USA that banned gay marriage as a legal option, there is a significantly higher psychiatric morbidity in LGBT persons141. The same group of researchers pointed to the relationship of a significantly higher psychiatric morbidity in LGBT persons with residence in those federal states of USA that do not have specific regulations that protect this population from hate crimes and employment discrimination142, with a direct recommendation of the author that a change of the legal framework is a direct question of prevention of psychiatric morbidity. One might thus say that problems of this population should become a subject of interest of preventive medicine and public health143,144, with cooperation of a range of professions that deal with problems of marginalized groups, all with the assumption that various activities in development of social tolerance could lead to a reduction in social oppression towards LGBT persons, and finally, to a reduction of the men-tioned health risks.
134 King M, Semlyen J, See Tai S, Killaspy H, Osborn D, Popelyuk D, Nazareth I. (2008) A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry 2008, 8:70.135 Remafedi G. (1999) Sexual Orientation and Youth Suicide. JAMA 282:1291.136 King M, Mc Keown E, Warner J, Ramsay A, Johnson K, Cort C, Wright L, Blizard R, Davidson O. (2003) Mental Health and Quality of Life of Gay Men and Lesbians in England and Wales. British Journal of P sychiatry 183:552-558137 Mays V.M, Cochran S.D. (2001) Mental Health Correlates of Perceived Discrimination Among Lesbian, Gay, and Bisexual Adults in the United States American. Am J Public Health. 2001;91:1869–1876138 Meyer I.H. (2003) Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychol Bull. 129(5): 674–697139 Warner J, Mc Keown E, Griffin M, Johnson K, Ramsay A, Cort C, King M. (2004) Rates and Predictors of Mental Illness in Gay Men, Lesbians and Bisexual Men and Women. British Journal of Psychiatry 185:479-485.140 Newcomb M.E, Brian Mustanski B. (2010) Internalized Homophobia and Internalizing Mental Health Problems: A Meta-analytic Review. Clinical Psychology Review 30:1019-1029.141Hatzenbuehler M.L, McLaughlin K.A, Keyes K.M, Hasin D.S. (2010) The Impact of Institutional Discrimination on Psychiatric Disorders in Lesbian, Gay, and Bisexual Populations: a Prospective Study. Am J Public Health. 100(3):452-459. 142 Hatzenbuehler M.L, Keyes K.M, Hasin D.S. (2009) State-level Policies and Psychiatric Morbidity in Lesbian, Gay, and Bisexual Populations. Am J Public Health. 99(12):2275-81.143 King M, Nazareth I. (2006) The Health of People Classified as Lesbian, Gay and Bisexual Attending Family Practitioners in London: a Controlled Study. BMC Public Health 6:127144 Corliss H.L, Shankle M.D, and Moyer M.B. (2007) Research, Curricula, and Resources Related to Lesbian, Gay, Bisexual, and Transgender Health in US Schools of Public Health. Am J Public Health. 97:1023–1027.

61
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
In spite of all just stated, a lack interest for research of problems of this population in various fields of medical and social sciences is more than obvious145,146,147,148. Also, the lack of presence of contents related to this population in academic programs149 and public health preventive programs is evident. What should be a rule, is in fact an exception150.
The motivation for this overview lies in the assumption that those professionals of helping professions (social workers, psychologists, physicians) who develop affirmative attitudes towards the LGBT population during their education will become an important factor in forming such attitudes in the society in general. Additionally, development of affirmative attitudes of the mentioned professionals towards their patients would be made easier. Also, research among this popula-tion would also be encouraged, and finally also the development of public health programs with the goal of correcting prejudice towards LGBT population.
This questionnaire was conducted primarily with the goal of gathering information on various programmatic views and approaches to questions of LGBT population in those academic institutions of South-eastern Europe that educate physicians, social workers and psychologists. Another goal was to gather data on possible public actions of members of the mentioned professions in their home countries focused on developing tolerance towards different lifestyles and sexual orientations. Even though the primary subject of this text is academic education, research work was also added into consideration due to the fact that it represents an essential part of quality high education and is necessary for bring-ing about the generation of local knowledge on LGBT population in societies of this region. On the other hand, public action of professional societies and institutions is, in my opinion, important not only as a factor of influence on society attitudes and tolerance, but also as a model of professional standards and ethics of generations to come.
5.3. On data collection
Data on which this overview was based, I gathered from a number of different sources. The primary source were the answers to written queries I sent using the electronic mail to the addresses of lecturers of departments of a larger number of the universities in the region that educate social workers, psychologists and physicians. The addresses were collected partly from web sites of the high education institutions in question and from University administration offices, as well as from survey respondents who often themselves recommended persons who have additional information. I have sent queries to a total of 55 addresses, out of which 7 cases the mail came returned to sender for reasons of inactive e-mail accounts; of the remaining e-mail sent 23 I received answers from all 23 persons. For one institution of higher education I contacted, I obtained the data from a graduate student. who graduated from that institution. I sent queries also to 5 professional medical associations, and received an answer from one address.
The letter contained the following questions: (1) does the curriculum of pre-graduate studies for students at a particular department of a university include contents related to homosexuality and normalization of homosexuality; (2) is the educational material (i.e. educational text published in a university textbook) on sexual orientation mandatory litera-ture for students and within which course; (3) has any research in a particular country been conducted on attitudes of students or graduate social workers, psychologists of physicians towards homosexually oriented persons; (4) has a
145 Rothblum E.D. (1994) "I only read about myself on bathroom walls": the Need for Research on the Mental Health of Lesbians and Gay Men. J Consult Clin Psychol. 62(2):213-20. 146 Coyle A, Kitzinger C. (2002) Lesbian & Gay Psychology: New Perspectives. Oxford: Blackwell. 147 Clarke V. et al (2010) Lesbian, Gay, Bisexual, Trans, Queer Psychology: An Introduction. Cambridge: Cambridge University Press. 148 Clark W.M, Serovich J.M. (1997) Twenty Years and Still in the Dark? Content Analysis of Articles Pertaining to Gay, Lesbian and Bisexual Issues in Marriage and Family Therapy Journals. Journal of Marital and Family Therapy, 23:239-253.149 Harrison A.E, Silenzio V.M.B. (1996) Comprehensive Care of Lesbian and Gay Patients and Families. Primary Care 23:31-46. 150 Warwick I, Aggleton P. (2002) Gay Men's Physical and Emotional Well-Being: Re-orienting Research and Health Promotion. In: Coyle A, Kitzinger C. (2002) Lesbian & Gay Psychology: New Perspectives. Oxford: Blackwell. Pp. 135-153)

62
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
professional association of a certain profession issued a public statement with an affirmative standpoint related to LGBT population and (5) has it issued a public statement as a reaction on possible inadequate publicly stated information and attitudes in the media towards persons of same-sex orientation. To a larger number of respondents I sent additional questions relating to whether the contents presented in the curricula, i.e. textbook materials contain: (1) a definition of homosexuality, homophobia and heterosexism, (2) prevalence of homosexuality, (3) specificities in psychosocial de-velopment of LGBT persons, (4) psychiatric morbidity and suicide mortality in homosexual persons, (5) problem of discrimination and stigma of LGBT persons, (6) problem of gay parenthood.
I also gathered information from descriptions of programmatic contents of courses in psychology studies, social work studies and medical studies available on web sites of a large number of universities. A part of additional information I obtained by analyzing textual contents related to homosexuality and questions of sexual orientation in university text-books used in particular countries, and from various other publicly available publications.
5.4. Overview of the data collected and discussion by country
5.4.1. Bosnia and Herzegovina
Medicine
The following overview is based on data obtained from two out of five academic institutions to which a request was sent for information on educational curricula.
According to information obtained from lecturers at the Medical school of the University of Sarajevo, medical students study psychiatry from a textbook of psychiatry in which homosexuality is presented within the chapter on sexual per-versities and deviations but unfortunately, as I do not have the title at my disposal, I cannot present it in this overview151. The material of the prescribed mandatory literature does not include any determinant on LGBT questions; there is no data on definition, normalization nor prevalence of homosexuality as well as data on specificity of psychosocial devel-opment of LGBT persons, psychiatric morbidity or of problems of stigmatization and discrimination of LGBT persons and gay parenthood. The curriculum for medical students includes however the subject of stigmatization and prejudice against mental patients, other nationalities and races which also includes homosexual persons. According to available data obtained from a lecturer at Medical school of the University of Sarajevo, some psychiatrists consider that same-sex orientation is a disorder and engage in treating such persons, often at the request of their parents.
An example of a publication pointing to a significant prejudice towards homosexuality of some physicians in Bosnia and Herzegovina can be found in the translation of a book “The AIDS crisis: An Islamic Socio-Cultural Perspective”152 by Malik Badri, an Indonesian university professor of psychology. Preparing the translation of this book, filled with ex-plicit phrases showing extreme prejudice against LGBT persons153, two lectures from Medical school in Tuzla took part, from which no other conclusion can be made except they agree with attitudes stated in the book. It is worth mention-ing offhandedly, that the mentioned book represents officially recommended additional literature for students of social pedagogy at the Islam pedagogy faculty of the University of Zenica154.
151 Loga S. (Ed) (1999) Klinička psihijatrija. Sarajevo i Tuzla: Medical school in Sarajevo and Tuzla.152 Badri M. (2002) The AIDS crisis: An Islamic Socio-Cultural Perspective. Sarajevo: El-Kalem. Duh i vrijeme.153 Excerpts from the mentioned book speak for themselves: „… groups under heightened risk for AIDS such as: homosexuals, pro-miscuous and bisexual men and prostitutes are walking time bombs …“ (p.p. 42); „… AIDS is a subject of slander and disgrace due to its unambiguous link to morals, homosexuality, bisexualism and promiscuity …“ (p.p. 42); „… These abnormalities, that would disgust even the citizens of Sodom, are practiced without any restrictions in bars for homosexuals (…). If modern westerners think they can continue with such perversities with no punishment, then they are truly not aware of the moral reality and history of earlier civilizations …“ (p.p.str. 125). 154 http://www.ipf.unze.ba/fileadmin/user_upload/TEKSTOVI/NPP_SP_-_bosanski_01.pdf

63
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
At the Medical school in Mostar, according to available information obtained from students who graduated, the ques-tions of homosexuality, i.e. LGBT population are not included into the educational curriculum. Similarly to examples from practically all medical schools in the region, this program does not include questions on prevalence of homo-sexuality; there is no data on specificity of psychosocial development of LGBT persons, on psychiatric morbidity, nor problems of stigmatization and discrimination of LGBT persons or gay parenthood. In existing educational literature there are no materials on LGBT population.
According to available data, until today no research has been conducted on attitudes of medical students or physicians towards LGBT persons.
Professional associations of psychiatrists in Bosnia and Herzegovina have not until today publicly reacted to possible publicly stated inadequate information or attitudes towards LGBT persons.
Psychology
The overview is based on information obtained from lecturers of one institution.
According to information obtained by courtesy of lecturers of the Department of Psychology of the Faculty of Philoso-phy of the University of Banja Luka, the program of studies of psychology at this faculty does not have a separate course or a specific part of a program in one of existing courses that would refer to questions of LGBT population. Within the framework of the course “Developmental psychology”, students are familiarized with the standpoint that the process of affectionate bonding progresses in the same way with both persons of homosexual and heterosexual orientation. Ho-mosexuality is within the course “Psychopathology” being covered as a drive disorder. There is no separate educational material that would refer to questions of LGBT population. In several researches conducted within the framework of diploma paper preparations which were primarily focused on researching ethnic distances, students investigated into social distance towards marginalized social groups, also towards homosexual persons. One student wrote her diploma paper using the observational experience of child development in a homosexual (lesbian) partnership she acquired in the USA155. The Association of Psychologists of the Republic of Srpska has not until today commented on possible nega-tive public statements against same-sex oriented persons.
On the web site of the Department of Psychology of the Faculty of Philosophy of the University of Sarajevo, a detailed presentation of the curriculum for school year 2008/2009 can be found along with a textual commentary and introduc-tion. In the description of each course there is a description of the contents of the respective course, including a list of educational units. I found no mandatory or optional course with specific part that would address LGBT population. In the framework of the optional course of “Psychology of parenthood” for instance, there is specific mention of “Parent-hood in specific circumstances” following which there is a list numbering six specific family situations to which this content refers, gay parenthood not being one of them.
In the program of psychology studies at the Department of Psychology of the University of Mostar, available on the web site of the University156, there is no course that would specifically address LGBT population as such. However, an optional course in psychology of human sexuality is offered to students of the first and second semester of graduate studies, a detailed view into which I was not able to obtain. Within the course on psychopathology questions of LGBT population are not addressed.
155 I do not have a specific reference at my disposal for the time being. All diploma papers are available at the library of the Faculty of philosophy at the University in Banja Luka. 156 http://www.ffmo.ba/index.php?option=com_content&view=section&layout=blog&id=10&Itemid=12

64
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
Social work
According to data obtained by courtesy of lecturers at the Faculty of Political Sciences of the University of Sarajevo, in both pre-graduate and graduate studies, there are no contents included into the curriculum that would be related to homosexual orientation, i.e. LGBT population. According to the available data, no research on attitudes of students of social work or of graduate social workers towards LGBT persons in Bosnia and Herzegovina has been conducted. Also, there were no public reactions to possible inadequate articles or statements in the media in relation to same-sex oriented persons.
5.4.2. CROATIA
The study of medicine and psychiatry
Having in mind that I myself, as the author of this text, am a psychiatrist that has been educated and lives in Croatia, I have the best knowledge of the situation regarding the education of medical students and psychiatrists, and their work in this country. It is precisely due to this fact that this part of the report will be un-proportionally detailed.
Reviewing The Catalogue of knowledge and competences157 with respect to the study of medicine at the medical school of the universities of Zagreb, Rijeka, Osijek and Split, I have come to realize that there is no course within the study of medicine which follows a programmatic determinant that would relate to same-sex orientation. Besides psychiatry, there is one separate course in psychology, that is, psychological medicine. The program of the study of medicine at the University of Zagreb does not cover homosexual orientation in the curriculum of neither psychiatry nor psychologi-cal medicine as a separate educational unit, but within the description of the psychiatric classification briefly defines homosexuality as excluded from the list of disorders. In order to illustrate this lack of organized education, I would like to mention that two weeks prior to compiling this report I have heard, in a conversation with two students who recently graduated from Medical School of the University of Zagreb who came to the ward I work at to do their internship, that they are not familiar with the fact whether homosexuality is a disease or not. In the textbook of psychiatry or psycholog-ical medicine158 for medical students at the University of Zagreb there is no separate chapter on sexual orientation and students cannot gain adequate information from the sources mentioned. There are no extracurricular courses within the study of medicine at four Croatian medical schools dedicated to this subject. Within the residency program in psychia-try such contents are not to be found nor is a candidate required to answer questions on this topic within the framework of his regular examinations, even though they are represented in literature recommended for preparation of the exam159.
I have obtained similar information investigating the curricula of two other Medical schools. Medical school of the University of Rijeka has no separate educational unit dedicated to same-sex orientation, but according to the obtained information, students are made familiar with the fact that this is not a disorder, and with other information on specific-ity of psychosocial development of homosexual persons. Medical school of the University of Split does not cover these subjects in the curriculum. I obtained no direct information from Medical school of the University of Osijek, but as this particular Medical school uses the same material that is used at the Medical school of the University of Zagreb, a conclu-sion follows that they do not cover the programmatic content in question in the curriculum.
When it comes to psychiatry, in university textbooks for medical students, when compared to the 1990-ies, there has been a significant progress in attitudes towards homosexuality. Namely, in the textbook for medical students of the
157 Medicinski fakultet (MF) u Zagrebu, MF u Rijeci, MF u Splitu, MF u Osijeku (2008) Katalog znanja i vještina za studij medici-ne. Zagreb, Rijeka, Split i Osijek: MF Zagreb, MF Rijeka, MF Split, MF Osijek. Available at: http://cms.mef.hr/meddb/slike/pisac1/file1210p1.pdf 158 Klain E. (Ed) (1999) Psihološka medicina. Zagreb: Golden Marketing. 159 Eg. Sadock B.J., Sadock V.A. (2007) Kaplan and Sadock's Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. Phila-delphia: Lippincott Williams & Wilkins.

65
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
Medical school of the University of Zagreb published in 1995160, the author of a short paragraph on homosexuality161 of-fers an arbitrary elaboration on why homosexuality is a disease, going against the standpoint of the WHO, which at that time had already published the ICD-10162 in which such a category was explicitly excluded. In psychiatric periodicals published following the publication of this textbook, it is not possible to find any correction or reaction of other psy-chiatrists on these statements. Still, it is worth mentioning that the same year a widely used textbook of psychiatry for nursing college has also been published, giving no review of homosexuality but also not showing it as a disorder, in con-cordance with the standpoint of psychiatry experts of the day163. In 2006, a new psychiatry textbook for medical students in Zagreb was published164, one that clearly defines homosexual orientation as excluded from psychiatric classification. Still, in the mentioned textbook, homosexuality is mentioned within the chapter on modern psychiatric classifications in a way that it is being stated that “homosexuality, in itself, is not included as a diagnostic category” 165, without any further comments. Thus, this information is not presented in a way that students could understand its wider meaning, and certainly is not sufficient so that they could accept an affirmative attitude towards alternative sexual orientations.
Almost no recent publication intended to educate psychiatrists deals with the problem of sexuality. The following ex-ample shows however, that pathologizing attitudes towards homosexual orientation in Croatian psychiatry are still pres-ent to a significant degree. In the book “Psychiatric evaluations – a collection of expertise”166 from the author Miroslav Goreta it is possible to find a separate chapter dedicated to forensic meaning of homosexuality with examples of psychi-atric evaluations, while at the same time, there is no chapter entitled heterosexuality is missing, which probably unin-tentionally speaks of the stigma of homosexual orientation. The authors pathologizing attitude towards homosexuality is apparent in the fact that in the mentioned monograph, the chapter entitled “Homosexuality” is preceded by chapters entitled “Pedophilia and incest”, and is followed by the chapter entitled “Paraphiliae – other”, which unambiguously clas-sifies homosexuality into paraphiliae. In the text itself, the author states that: “Even though homosexuality is no longer a psychiatric diagnosis (…) it still holds a considerable meaning in forensic psychiatric evaluations, which many psychia-trists now defensively negate ‘because this is a diagnosis that no longer exists’, while others still cannot make peace with the exclusion of this ‘pathology’ from the chapter on paraphiliae and consider it should be returned to its ‘right place’”. The author, being a person of a long experience and considerable knowledge, evidently basing on his personal knowl-edge, describes two groups of (Croatian) psychiatrists who are burdened with considerable prejudice against homosexu-ally oriented persons: one that defensively negates this problem because this diagnosis no longer exists (but still is a diagnosis), and the other that considers that this “pathology” needs to be reintroduced to psychiatric classification. Un-fortunately, aside from an overview of the problem, the author offers no third standpoint, nor has he himself definitely given an opinion on the problem. The author of this text is not aware that Croatian medical periodicals have, until today, published a review that would critically point to the problem of description of homosexuality in the mentioned book.
Professional associations of physicians in Croatia in the last twenty years have not used any opportunity to publicly correct possible inadequate information and prejudice against LGBT persons stated in the public, of which there were of course, plenty. However, at the request of Mr. Dorino Manzin, an activist of the organization of persons of same-sex orientation “Iskorak”, then-president of the Croatian psychiatric association, Professor Ljubomir Hotujac, wrote a letter167 with a detailed explanation of historic development of current standpoint of psychiatry towards homosexual
160 Muačević V. (ur) (1995) Psihijatrija. Zagreb: Medicinska naklada.161 The author of the mentioned paragraph is prof. Vladimir Gruden, MD, PhD.162 Acronym meanings: WHO – World Health Organization, ICD – International Statistical Classification of Diseases and Related Health Problems.163 Jakovljević M. (Ed) (1995) Psihijatrija za studente više medicinske škole. Samobor: AG Matoš.164 Hotujac Lj. (ur) (2006) Psihijatrija. Zagreb: Medicinska naklada.165 Hotujac Lj. (2006), str. 84. 166 Goreta M, Peko-Čović I, Buzina N. (2004) Psihijatrijska vještačenja – zbirka ekspertiza (knjiga prva – kazneno pravo). Zagreb: Naklada Zadro. Pp. 326.167 Letter of prof. dr. Ljubomir Hotujac to Dorino Manzin, 9.4.2002., available at: http://www.gay-u-obitelji.com/site/index.php?option=com_content&task=view&id=13&Itemid=30

66
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
orientation, clearly stating that psychiatry does not consider homosexuality a disorder. At the request of the same or-ganization, the Croatian medical chamber gave a brief written information on the fact that medicine does not consider homosexuality a disease. Towards the end of 2002, university professor of psychiatry, Vladimir Gruden publicly stated that homosexuality is a disease168, and in 2007, university professor Dubravka Kocijan-Hercigonja stated in an interview she gave to the catholic paper “Glas Koncila” (Voice of the Council), that according to contemporary psychiatric clas-sifications homosexuality represented a disorder of sexual identity and could be treated successfully. Both of these cases were reported to responsible authorities of the Croatian medical chamber who in turn assessed that the statements men-tioned did not represent a disciplinary violation169. In spite of this, it seems that such statements are indeed exceptions: from my personal contact with numerous colleagues, I have come to know that Croatian psychiatrists’ predominant viewpoint is that same-sex orientation is not a disorder. However, it is precisely on this level that the interest of Croatian medicine for same-sex oriented persons ceases: the majority of my colleagues are of the opinion that if homosexuality is not a disorder, medicine has nothing to do with persons of same-sex orientation.
Until today, no research has been conducted in Croatia that would be primarily focused on attitudes of medical stu-dents or physicians towards LGBT persons. In 2006, a group of authors170 published the results of research on attitudes of medical students toward HIV positive persons, and into this research an evaluation of attitudes towards same-sex oriented persons was included. Even though the research showed a significant presence of negative attitudes towards homosexually oriented persons among medical students, this information published in an indexed publication has not resulted in programmatic changes of education for medical students.
To conclude, it can be said that in the Republic of Croatia not a single one of four Medical schools has organized pro-grammatic contents dedicated to familiarizing medical students with questions of same-sex orientation or building ad-equate affirmative attitudes, in spite of the fact that a research conducted on medical students showed a significant pres-ence of negative attitudes towards same-sex oriented persons. Curricular materials contain no adequate texts that would with sufficient in-depth present this issue. The program of residency in psychiatry does not contain these subjects nor are they required as knowledge at the occasion of regular examinations of knowledge in particular fields of psychiatry.
Psychology
The data collected refer to three of a total of five higher educational institutions that are responsible for education of future psychologists in Croatia.
According to data obtained by courtesy of lecturers at the Department of Psychology of the Faculty of Philosophy of the University of Zagreb, not a single one of the courses in psychology studies covers subjects related to the LGBT popula-tion, even though students come across the questions of homosexuality within a range of courses, such as “Criteria of normality”, “Social perception and attitudes” and several courses from the domain of clinical psychology. Many students take the optional course “Sociology of sexuality” at the Department of Sociology, which covers this field in detail171. In the academic year 2010/2011 this Department will start teaching two new optional courses “Psychology of gender and sex” and “Psychology of partner relationships”, which plan to cover subjects relating to sexual orientation. This depart-ment has no educational material as of yet on sexual orientation that would be referred to as mandatory literature for students.
168 Hrvatska biskupska konferencija, dana 20. Studenog 2002. godine.169 For more detail see: Stewart C. (2010) The Greenwood Encyclopedia of LGBT Issues Worldwide, Vol. 2. Pp. 89-90. Santa Barbara: Greenwood Press.170 Tešić V, Kolarić B, Begovac J. (2006) Attitudes towards HIV/AIDS among Four Year Medical Students at the University of Zagreb Medical School – Better in 2002 than in 1993 but Still Unfavorable. Coll. Antropol. 30(2006) Suppl. 2:89-97171 The head of this course is Aleksandar Štulhofer, a person of rich public activity and equally rich research practice. The program of the course is truly all-encompassing at first glance already and can be found at: http://www.ffzg.hr/socio/astulhof/sexispit.htm.
67
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
According to data obtained from lecturers at the Department of Psychology of the Faculty of Philosophy of the Uni-versity of Rijeka, contents related to the LGBT population are covered during pre-graduate studies within the course “Introduction to psychology of abnormal experience and behavior” and in graduate studies within the courses “Basics of counseling and psychotherapy” and “Groups and social processes”. In conducting the curriculum of the course “Groups and social processes” regular guests are also the members of a non government organization dedicated to lesbian popu-lation “Lori”, with which some of the staff of the Department collaborate. The education includes contents related to definition of homosexuality and LGBT population, prevalence of homosexuality, the problem of psychiatric morbidity of LGBT persons, the problem of discrimination and stigmatization and questions of gay parenthood. In the program of graduate studies of psychology an optional course entitled “Psychology of sexuality” is planned but not held at the mo-ment. Within the framework of the course on “Basics of counseling and psychotherapy” a textbook is used that offers no separate chapter referring to sexual orientation, but in exercises within the course work with LGBT persons is covered and non mandatory literature on this field is offered to the students.
According to data obtained from lecturers of the Department of Psychology of the Faculty of Philosophy of the Uni-versity of Zadar, pre-graduate studies offer no specific and organized program that would refer to LGBT questions, but these subjects are covered, similarly to other Psychology departments in Croatia, included into a range of other courses. As optional courses, graduate students are offered “Psychology of human sexuality I and II”, and within the framework of that course subjects related to sexual orientation are covered. Literature in this course includes a title specifically focused on homosexuality172.
University textbooks for psychology studies in Croatia are for the major part translations of textbooks from Anglo-Saxon countries, which certainly accurately present particular areas of psychology. But, as an example of – even though isolated – implicitly uncovered subjects related to LGBT population, that might be (although even unintended) a consequence of prejudice, a textbook should be mentioned that is used at the Zagreb university “Psychology of marriage and family” from the authors Mira Čudina Obradović and Josip Obradović173. The field of psychology which represents, as can be seen from examples abroad, an ideal framework for the normalization and destigmatization of LGBT population, and the building up of positive attitudes of future helping professionals, is in this textbook brought down to portraying traditional family forms in an account that is normatively saturated. In a textbook that is by its format and contents fairly comprehensive, there is not even a mention of same-sex partnership (or marriage), nor of parenthood of same-sex oriented persons, even though the authors must have come in contact with at least some of the abroad publications that as a rule, dedicate whole chapters to these questions174,175,176 . Even if certain authorial licenses or preferences are taken into consideration, since this is a textbook aspiring to present university students with one field of science, the least it can and should be expected from it is to state the viewpoints of other authors in the family psychology field – otherwise the scientific character of the textbook is compromised, and gives away an image of a local publication, in essence of one conveying oppressive values, of a publica-tion that passes up the opportunity to be a bearer of improvement of attitudes in a society.
On the web site of Faculty of Philosophy of the University of Zagreb created and maintained by the students themselves, educational material from Introduction to psychopathology177 from school year 2007/2008 can be found (dates of held lectures are indicated as well). The author has not been named and the material was obviously compiled by the students, based on the lectures delivered to them, and questions on exclusions of homosexuality from psychiatric classification have been elaborated on. The material contains the information on higher suicide mortality of homosexual adolescents. Partly incorrect data is given as well, stating that in homosexual persons relative risk for development of depression
172 Green, B., Herek, G.M. (1999). Psihologija ženske i muške homoseksualnosti: teorija, znanstvena istraživanja i kliničke primjene, Zagreb: Impressum.173 Čudina-Obradović M, Obradović J. (2006) Psihologija braka i obitelji. Zagreb: Golden Marketing – Tehnička knjiga. 174 Bray J.H., Stanton M. (Ed.) (2009) The Wiley-Blackwell Handbook of Family Psychology. Chichester: Wiley-Blackwell.175 Walsh F. (Ed.) (2003) Normal Falimy Processes. New York: Guilford.176 Ponzetti J.J. (Ed.) (2003) International Encyclopedia of Marriage and Family, 2nd Ed. New York: Macmillan Reference.177 http://www.ffzg.hr/psiho/stup/SKRIPTE/III%20godina/V%20semestar/Psihopatologija/UVOD%20U%20bip%20bip.doc.

68
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
and other mental disorders is not higher than in heterosexual persons (data on equal prevalence of schizophrenia and bipolar disorders is correct). It is however confusing, that in the same material homosexuality is unambiguously defined as a sexual orientation disorder.
Lecturers of the Department of Psychology of the Faculty of Philosophy of the University of Zagreb have thus far conducted one research of attitudes of general population towards homosexual persons178. One graduate student while writing her diploma paper conducted a research of attitudes of students of various studies from Zagreb, Rijeka and Split towards persons of homosexual orientation179. At the Department of Psychology of the Faculty of Philosophy of the University of Zadar, some years ago, a diploma paper was written referring to questions on attitudes towards persons of homosexual orientation180.
When it comes to actions of the Croatian Psychology Association, it has until today, in only one case reacted to inad-equate attitudes towards homosexuality in the Croatian public. To the statement of an eminent Croatian psychiatrist towards the end of 2002 (see text above) that homosexuality is a disorder, the Croatian psychology association reacted by issuing a statement that psychologists do not consider homosexuality in itself to be a disorder.
Social work
The data collected refer to one higher educational institution responsible for education of graduate social workers – Study center for social work at the Faculty of Law of the University of Zagreb. Even though the study of social work does not have a program that would in an organized manner specifically refer to homosexuality, nor a specific course on LGBT population, questions of homosexual orientation are covered in a range of courses within the framework of certain subjects. For example, the course on “Social psychology” in the part of its program devoted to prejudice and discrimination covers examples of persons of Roma nationality and persons of homosexual orientation. Also, lecturers of the Center have made contact and collaboration with one non government organization that promotes the rights of LGBT population (“Iskorak”), so that in the near future inclusion of members of this organization is expected in the education of students of social work within the course “Social work and youth” in the total of 2 school hours, with the possibility for students to attend workshops of the mentioned organization on questions related to LGBT population.
The study of social work in Zagreb does not list any publication that would be specifically focused on questions of LGBT population, but these subjects are included in educational material used as mandatory literature in various courses181.
While compiling her diploma paper, one graduate student has conducted a research on attitudes of female students of social work towards persons of same-sex orientation182.
The professional association of social workers in Croatia has not until today publicly reacted on possible inadequate, publicly stated information and attitudes towards LGBT persons.
178 Kamenov Ž., Jokić-Begić N. i Lauri Korajlija A. (2003) Stigmatizacija tjelesnih invalida, psihičkih bolesnika, narkomana, alkoholi-čara i homoseksualaca. XVI Dani Ramira Bujasa, Zagreb. 179 Parmač M. (2005) Stavovi studenata prema osobama homoseksualne orijentacije. (Diploma paper). Zagreb: Filozofski fakultet, Odsjek za psihologiju. Available at: http://darhiv.ffzg.hr/132/1/MajaParmač.pdf 180 Reference not available.181 Vasta R., Haith M.M. i Miller S.A. (1998) Dječja psihologija. Jastrebarsko: Naklada Slap. Mandatory literature for students among other represents also the chapter on „Development of sexual roles and difference among the genders” (p.p. 561-599), and within the framework of this chapter two pages of text devoted to comparison of development of sexual roles in same-sex and traditional families. As optional literature chapters from this textbook are used: Smith E.E., Nolen-Hoeksema S., Frederickson B.L., Loftus G.R., Bem D.J. i Maren S. (2007) Atkinson/Hilgard Uvod u psihologiju. Jastrebarsko: Naklada Slap, referring more directly to sexual orientation. 182 I do not have a full reference. The author of the diploma paper is Mara Kraljević. It is available at the library of the Study center of social work.

69
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
5.4.3. MONTENEGRO
Medicine
According to information obtained by courtesy of lecturers of the Medical school of the University of Montenegro, and according to information obtained from the University web site183, the curriculum does not include contents relating to LGBT questions as a part of one course nor as a separate course either mandatory or optional one. According to available data, until today no research has been conducted on attitudes of medical students or physicians towards LGBT persons. At the suggestion of the non-government association “Juventas”, The Medical Chamber of Montenegro and The Asso-ciation of psychiatrists of Montenegro have issued a public statement as a reaction to inadequate information on LGBT persons released in the media.
Psychology
In Montenegro, the study of psychology is organized at the Faculty of Philosophy of the University of Montenegro in the city of Nikšić.
The program of psychology studies available from the University web site184 does not mention no specific determinant that would refer to LGBT population. The program for the course on “Family psychology” mentions a unit entitled “Un-usual family constellations”, which is followed by three examples, none addressing directly neither homosexual families nor parenthood.
The program of psychology studies at the Faculty of Philosophy of the University of Montenegro also shows that the courses entitled “Basics of clinical psychology”, “General psychopathology” and “Psychology of mental health” are in part held by Jelena Vlajković, a professor at Department for psychology of the University of Belgrade, from which it can be concluded that programs at these two universities are similar for this field. As the Department of Psychology of the University of Belgrade gave us the information that there is no organized part of the curriculum dedicated to homosexu-ality, with some degree of certainty, it can be concluded that a similar situation is to be found also at the Department for Psychology of the University of Montenegro. With the respect to this, more precise information should be gathered.
Social work
According to data obtained by courtesy of lecturers at the study of social work at the University of Political Sciences in Podgorica, there is no course that would in its program address the LGBT population specifically, but these contents are covered within the framework of other programmatic areas as part of courses in psychology, family law, sociology and sociology of family. Until today, according to the data obtained, no research has been conducted on attitudes of stu-dents of social work or graduate social workers towards LGBT population. According to the standpoint of the lecturer interviewed for this report, very little has been done when it comes to questions of attitudes towards LGBT population to educate on matters same-sex orientation in all levels of education. In this sense, non-government organizations rep-resent the main source of activities in this field.
183 http://www.medf.ac.me/ 184 http://www.ff.ac.me/15Psihologija/01os.htm
70
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
5.4.4. SERBIA
Medicine
According to data obtained by courtesy of the faculty staff of the Medical School of the University of Belgrade, which hence refer to that institution exclusively, the curriculum for medical students includes the question of definition of ho-mosexuality (of course, including more specifically that this is not a disorder), while no other specific contents are pres-ent (prevalence of sexual orientations, specificity of psychosocial development of LGBT persons, psychiatric morbidity and suicidal mortality, the problem of discrimination and stigma of LGBT persons and the problem of gay parenthood). No separate course on psychology is offered to medical students. Residency programs in psychiatry do not include contents relating to LGBT population185.
According to the data obtained by courtesy of lecturers at the Medical School of the University of Niš, the curriculum for medical students does not contain structured contents relating to LGBT persons, with the exception of data on the definition of homosexuality and the problem of stigmatization and discrimination of homosexual persons. In clinical work with LGBT population at the Psychiatry clinic which is also the academic base of the mentioned University the clear viewpoint that this is a variation of health is promoted, however this is not explicitly articulated in the curriculum or educational material for medical students.
According to the information obtained from the web site of the Medical School of the University of Belgrade, official textbooks of psychiatry for medical students are those authored by Jovan Marić, i.e. Slavka Morić-Petrović. The two mentioned textbooks, which are at the same time primary literature for medical students, were not available at the time of writing this report. As recommended literature the psychiatry textbook by Petar Kaličanin186 published in 2003 in re-printed edition is also mentioned, which was available to me for the purposes of this report. In this book the chapter on “Psychological functions and their disorders” describes homosexuality within the framework of a drive disorder187, even though along with the information that the majority of psychiatrists today do not consider this a disorder. The chapter on “Disorders of sexual life” 188 contains a subtitle “Disorders of gender identity”. Under the subtitle “Disorders of gender identity”, to which an ICD-10 code is added in the title, in the introductory part, a classification of disorders of sexual life is shown according to ICD-9, which includes a definition of homosexuality as a mental disorder. This is followed by a separate paragraph giving a relatively detailed account of homosexuality as a form of psychopathology. In comparison to any other disorders form the class of disorders of gender identity and disorders of sexual preference, homosexual-ity is described in most detail. Even though with some other diagnostic categories, a standpoint of earlier psychiatric classification is presented (for example in the chapter on dissociative disorders), following such presentations for other diagnostic categories, this is followed by a presentation of the latest psychiatric classification (ICD-10). However, in the chapter on disorders of gender identity, the status of homosexuality within the ICD-10 is not presented, in spite of the fact that some other disorders from the same category are presented according to this most recent classification. From the description of homosexuality in this psychiatry textbook, that is most probably used in specialist education, there is almost no doubt that the viewpoint of the author is that homosexuality is a disorder. By leaving out a review of a recent knowledge and the attitudes on homosexuality, at the same time giving a detailed pathologizing account of same-sex orientation, the reader is implicitly suggested that homosexuality is a disease.
It is worth stressing that the above mentioned textbook by Petar Kaličanin, as an example of inadequate presentation of the problem of homosexuality, finds itself in an apparent minority in relation to other publications that present the questions of sexual orientation according to the views of psychiatry today. Among recent monographs in the field of
185 (Republika Srbija). Ordinance on specializations and sub-specializations of health workers and helping health professionals. Offi-cial courier RS No. 111/93, 46/97, 33/2000, 44/2000, 27/2004 i 36/2004. Source: http://www.med.bg.ac.rs/?sid=1362 186 Kaličanin P. (2003) Klinička psihijatrija. Beograd: Institut za mentalno zdravlje. 187 Kaličanin (2003), p.p. 37: „Homosexuality is one of the most common disorders of sexual drive “, continuing with „The majority of psychiatrists today does not consider homosexuality a sexual deviation, but an alternative form of sexual behavior “ 188 Kaličanin (2003),p.p. 398-400.
71
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
psychiatry in that sense, a textbook of a Belgrade professor Ljubomir Erić entitled “Psychodynamic psychiatry – volume III” is worth mentioning, which refers to questions of sexuality, sexual and gender disorders and homosexuality. As I do not have this book at my disposal, I am unable to present it here to greater detail. According to the information I obtained by courtesy of colleagues psychiatrists whom I contacted, it is an informed work that covers the questions of sexual orientation in accordance with recent knowledge and attitudes in psychiatry.
The subject of sexual orientation is also taken up in the publication “Normal and disordered sexual behavior” 189which came to be published as an almanac of lectures from an interdisciplinary seminar held in 2003 at the Clinic for psychiatry of the Clinical center of Serbia. Among others, this monograph includes a chapter on the rights of transsexual persons on respect of private lives as in the practice of the European court for human rights. The information on the monograph and its contents were obtained by the courtesy of my Belgrade colleagues, but is not available to be presented in this report.
It is an important piece of information to mention that at the Clinical center of Serbia in the last twenty years, there is a multidisciplinary team for assessing gender dysphoric persons, a team in which psychiatrists from the Clinic for psychiatry are also included. One psychiatrist received her master and doctor titles from the field of transgender conditions190,191.
According to the data available, there has been no research conducted in Serbia on attitudes of physicians or psychia-trists towards LGBT population. However, a research into the attitudes of medical students is planned192.
The Serbian psychiatric association has until today issued no public statement related to persons of homosexual orien-tation or in relation to the “Pride parade”, nor has in any of its statements so far reacted to possible inadequate infor-mation stated in public. Non-government organization of LGBT persons “Labris” has insisted, several years ago, on psychiatrists in Serbia to state their viewpoint towards homosexuality and so contribute to the destigmatization of this population, upon which Mrs. Miroslava Jašović Gašić, professor of psychiatry at the Medical school of the University of Belgrade, then-president of the Psychiatry section of the Medical association of Serbia, wrote a letter shortly explain-ing that the official viewpoint of psychiatry as medical profession is that homosexuality is considered a variation of the normal state. At the time the “Pride Parade” was held at the beginning of October 2010, one psychiatrist active in politics, but not active in the psychiatric profession, stated in the media that the “brain of a homosexual has some kind of anomaly”, and has not undergone any kind of disciplinary procedure, even though according to available data, a large number of psychiatrists in Serbia consider his statement a breach of ethics.
According to the obtained data, some psychiatrists in Serbia, similarly to Croatia, and probably in other countries of the region as well, perceive the evident dissonance of the variety of attitudes (from pathologizing to affirmative) that can be heard in professional public in relation to LGBT population.
Psychology
Information gathered here relates to the Department of Psychology of the Faculty of Philosophy at the University of Belgrade. In the curriculum of psychology studies in this institution there are, for the time being, no contents devoted to questions of LGBT population. There are no textbook articles that would systematically and in an organized man-ner cover this field. Until now, no research has been conducted into the attitudes of students of psychology or graduate psychologists towards LGBT population.
189 Duišin D, Nikolić-Balkoski G, Barišić-Rojnič J. (2003) Heteroseksualnost, homoseksualnost, transseksualnost. In: Marić J, editor. Normalno i poremećeno polno ponašanje. Beograd: Megraf. p.49-59.190 Duišin D. (2004) Analiza tipologije ličnosti u odnosu na rodni identitet. [doctoral dissertation]. Beograd: Medicinski fakultet Univerziteta u Beogradu.191 Duišin D, Nikolić-Balkoski G, Batinić B. (2009) Sociodemographic Profile of Transsexual Patients. Psychiatria Danubina 2009, 21:220-223.192 Data obtained by courtesy of dr. D. Duišin.

72
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
At the time of publishing this publication at an expert meeting in Belgrade, two psychologists will present the overview of research on gay parenthood, but unfortunately up to the moment of publishing this report, I am unable to obtain more detailed information on the authors, the title of their work or the title of the meeting
According to the available information, the professional association of psychologists of Serbia has not publicly reacted to possible inadequate publicly stated information and attitudes towards LGBT persons.
Social work
The data obtained refer to one institution of high education that educated graduate social workers – the Department of social policy and social work of the Faculty of Political Sciences at the University of Belgrade.
During the last ten years or so, the contents related to homosexuality have been included into the curriculum as part of the optional courses related to gender studies. Before the curricular changes in accordance to the Bologna declaration, implemented four years ago, students of social work were able to choose an optional course “Female studies”, followed by “Gender studies”, with a large number of both male and female students choosing the aforementioned courses. Upon implementing the “Bologna” curricular changes, the students were offered an optional course “Policies of gender equali-ties”, where in the framework of Queer theories contents related to homosexual orientation are taught. The mentioned course also offers the students with printed educational material. In the framework of several other courses such as “Mental health”, “Social work with individuals”, “Social psychology” and “Community social work”, contents related to homosexuality are covered alongside questions on, for instance, tolerance and social marginalization. However, accord-ing to the lecturer from the mentioned Department who was contacted for the purposes of this report, these contents, for the time being are not covered systematically enough nor given sufficient curricular space.
Even though no research was conducted on attitudes of students of social work or graduate social workers towards LGBT populations, the faculty of this institution published preliminary results193 of research on attitudes of students and lecturers from various departments of University of Belgrade (social, science, technical and medical studies) towards gender equality in the system of high education. The research also included students of social work, and among other subjects it also addressed the questions of homosexuality.
According to available information, the professional association of social workers in Serbia has until today, issued no public statement as a reaction to possible inadequate articles or statements in the media related to same-sex oriented persons.
193 Džamonja Ignjatović, T, Žegarac, N. Popović, D. i Duhaček, D. (2009). "Istraživanje stavova prema rodnoj ravnopravnosti u sistemu visokoškolskog obrazovanja", u: Vujačić, I. (ur.) Godišnjak 2009, Beograd: Univerzitet u Beogradu - Fakultet političkih nauka, Godina III, Broj 3, 697-712.
73
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
5.5. Conclusion and recommendations
The data collected is by all means very noninclusive, scarce and selective that they could be taken as a comprehensive overview of the contents of academic programs of education relating to LGBT persons for students of psychology, social work or medicine in this region. What I have gained by this survey and from other sources, and what was certainly worthwhile, is an incomplete overview of the situation and trends in university programs, which still allows drawing some preliminary conclusions.
Overviews relating to particular countries are unequally detailed due to different – but mostly low – response rates to the survey, and other used sources are very selective and undoubtedly incomplete. Both facts represent a source of possible significant interpretation errors and thus the data available obviously do not present a relevant comparison basis for uni-versity programs in different countries of the region. In spite of this, from the data obtained it can be broadly indicated that (1) the inclusion of the contents related to questions and problems of LGBT population in all university mandatory courses for students of the three helping professions is still insufficient; (2) that university departments of social work and psychology in the region currently significantly stand out from medical schools in the degree of innovation and integration of educational contents related to questions of LGBT persons in educational programs and research work of students and professors; (3) that there is minimal research activity in this field, which is primarily present in Croatia and Serbia; (4) that professional associations of physicians, psychologists and social workers in the region in planned public activities do not include public actions that might help build social tolerance and affirmative attitudes towards LGBT population. The information we did obtain on relation of particular countries of the region could scenically be described as a metaphor of various tones of the same colour, in line with different stages in the process of recognizing the importance of including contents on LGBT population into the curriculum.
It is also important to mention that university textbooks and other publications that represent negative examples are shown in more detail, in most part because they vividly portray a significant dissonance in the attitudes of the profes-sional elite of a particular country, but these examples certainly cannot be interpreted as a predominant viewpoint of professional community of a certain country in the region.
As I already stated in the introduction, our current knowledge on problems of LGBT population should change the status of these programmatic contents in academic education of helping professions: the inclusiveness of contents on LGBT population into academic programs can now not be viewed as a matter of preference, but this question needs to be understood as a question of ethic obligation. Adequate informedness and development of affirmative attitudes to-wards the LGBT population, according to current knowledge, are a matter of prevention of mental disorders and suicide mortality in this population.
What can be done to speed up the process of including contents on LGBT population into academic programs and the subsequent development of these programs and their maximal social utilization? As I am not an expert whose primary field is development of academic programs, I will recommend only a few ideas that to me, basing on contact with the respondents of this questionnaire, seem to be meaningful:
• Organize interdisciplinary scientific-professional meetings on regional level with specific subjects related to LGBT persons, in which also the members of non-government organizations of LGBT persons would be included, and also ensure financial support for such meetings;
• Encourage inclusion of members of non-government organizations of LGBT persons into conducting programs in academic institutions that refer to LGBT population (among other, in order to enable students a direct and personal experience of dialogue with LGBT persons);
• Encourage research with LGBT population, but also research of attitudes of general and professional population towards LGBT persons;
• Encourage the development of public health programs in development and implementation of which various hel-ping professions should take part, also the faculty from higher education institutions that deal with questions of LGBT populations, with the goal of improving attitudes of the general population towards LGBT population;
74
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
• Organize interdisciplinary scientific-professional bodies in countries of the region, the obligation of which would be adequate informing (in line with recent standpoint of international science) of the legislating authorities and the public in procedures of finding legal solutions that refer to LGBT population; the same bodies would have the task of developing guidelines on a minimum of programmatic content on LGBT population that should be included into curricula of higher education programs for each helping profession.
Even though the primary subject of this text is academic education, research work was also added into consideration due to the fact that it represents an essential part of quality high education. It is necessary for bringing about the generation of local knowledge on LGBT population in societies of this region. On the other hand, public action of professional societies and institutions is, in my opinion, important not only as a factor of influence on society attitudes and tolerance, but also as a model of professional standards and ethics of generations to come.
At last, a few words about the respondents to the survey. The response rate to the request for information on program-matic content was surprisingly modest, even though this is a survey in which the goals of conducting this questionnaire were explained, and I also have introduced myself to all the respondents. Some I contacted by phone – and still received no answer. I have already said that such a low response rate significantly limits the interpretation of the collected data. However, those respondents that did reply to my query, have invested a considerable amount of time to provide me with detailed answers and literature references and the research, even when the data given spoke only of partial or complete omission of the LGBT subject from the programs they were reporting on. For this reason, it is my impression that the respondents have in fact shown motivation, openness and interest for innovation and change, and it is exactly such people that could be the pioneers of program change at high education institutions they work at. I would like to use this opportunity to heartily thank all those who took part by providing data and interpretations and were open for dialogue.
5.6. List of participants
Prof. Marina Ajduković, PhD, Social Work Study Centre, Faculty of Law, University of Zagreb, Croatia
Prof. Lidija Arambašić, PhD, Department for Psychology, Faculty of Humanities and Social Sciences, University of Zagreb, Croatia
Prof. Suada Buljubašić, PhD, Social Work Study, Faculty of Political Sciences, University of Sarajevo, Bosnia and Her-zegovina
Anđela Delale, PhD, Social Work Study Centre, Faculty of Law, University of Zagreb, Croatia
Prof. Aleksandar Dimitrijević, PhD, Department for Psychology, Faculty of Humanities and Social Sciences, University of Belgrade, Serbia Dragana Duišin, MD, PhD, Institute for Psychiatry, Clinical Centre of Serbia, Belgrade, and Faculty of Medicine, Uni-versity of Belgrade, Serbia
Alma Džubur Kulenović, MD, PhD, Department for Psychiatry, Clinical Centre Sarajevo, and Faculty of Medicine, University of Sarajevo, Bosnia and Herzegovina
Prof. Tanja Frančišković, MD, PhD, Department for Psychiatry, Clinical Hospital Center Rijeka, Faculty of Medicine, University of Rijeka, Croatia
Nino Grbavac, MD, Neuropsychiatric Hospital „Dr Ivan Barbot“ Popovača, Croatia
Prof. Grozdanko Grbeša, MD, PhD, Department for Psychiatry, Clinical Centre Niš, and Faculty of Medicine, Univer-sity of Niš, Serbia

75
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
Lidija Injac, MD, MSc, Department for Psychiatry, Clinical Centre Podgorica and Faculty of Medicine, University of Montenegro, Montenegro
Uglješa Janković, MSc, Department for Social Work and Social Policy, Faculty of Political Sciences, University of Mon-tenegro, Montenegro
Prof. Miroslava Jašović-Gašić, MD, PhD, Institute for Psychiatry, Clinical Centre of Serbia, Belgrade, and Faculty of Medicine, University of Belgrade, Serbia
Prof. Željka Kamenov, PhD, Department for Psychology, Faculty of Humanities and Social Sciences, University of Za-greb, Croatia
Assist. Prof. Srđan Milovanović, MD, PhD, Institute for Psychiatry, Clinical Centre of Serbia, Belgrade, and Faculty of Medicine, University of Belgrade, Serbia
Prof. Marija Mitić, PhD, Department for Psychology, Faculty of Humanities and Social Sciences, University of Belgrade, Serbia
Marina Nekić, PhD, Department for Psychology, Faculty of Humanities and Social Sciences, University of Zadar, Croatia
Assist. Prof. Milena Pašić, PhD, Department for Psychology, Faculty of Humanities and Social Sciences, University of Banja Luka, Bosnia and Herzegovina
Prof. Nina Pećnik, PhD, Social Work Study Centre, Faculty of Law, University of Zagreb, Croatia
Prof. Zoran Sušanj, PhD, Department for Psychology, Faculty of Humanities and Social Sciences, University of Rijeka, Croatia
Prof. Kristina Urbanc, PhD, Social Work Study Centre, Faculty of Law, University of Zagreb, Croatia
Prof. Ivan Urlić, MD, PhD, The Chair of psychological medicine, Faculty of Medicine, University of Split, Croatia, and Department for psychology, Faculty of Humanities and Social Sciences, University of Mostar, Bosnia and Herzegovina
Prof. Nevenka Žegarac, PhD, Department for Social Policy and Social Work, Faculty of Political Sciences, University of Belgrade, Serbia
Prof. Ivanka Živčić-Bećirević, PhD, Department for Psychology, Faculty of Humanities and Social Sciences, University of Rijeka, Croatia
5.7. References
Badri M. (2002) AIDS/SIDA i kriza modernog svijeta u svjetlu islama. Sarajevo: El-Kalem. Duh i vrijeme.
Bray J.H., Stanton M. (Ed.) (2009) The Wiley-Blackwell Handbook of Family Psychology. Chichester: Wiley-Blackwell.
Clark W.M, Serovich J.M. (1997) Twenty Years and Still in the Dark? Content Analysis of Articles Pertaining to Gay, Les-bian and Bisexual Issues in Marriage and Family Therapy Journals. Journal of Marital and Family Therapy, 23:239-253.
Clarke V. et al (2010) Lesbian, Gay, Bisexual, Trans, Queer Psychology: An Introduction. Cambridge: Cambridge Uni-versity Press.
Corliss H.L, Shankle M.D, and Moyer M.B. (2007) Research, Curricula, and Resources Related to Lesbian, Gay, Bisexual, and Transgender Health in US Schools of Public Health. Am J Public Health. 97:1023–1027.
Coyle A, Kitzinger C. (2002) Lesbian & Gay Psychology: New Perspectives. Oxford: Blackwell.
Čudina-Obradović M, Obradović J. (2006) Psihologija braka i obitelji. Zagreb: Golden Marketing – Tehnička knjiga.

76
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
Duišin D, Nikolić-Balkoski G, Barišić-Rojnič J. (2003) Heteroseksualnost, homoseksualnost, transseksualnost. In: Marić J, editor. Normalno i poremećeno polno ponašanje. Beograd: Megraf. p.49-59.
Duišin D, Nikolić-Balkoski G, Batinić B. (2009) Sociodemographic Profile of Transsexual Patients. Psychiatria Danu-bina 2009, 21:220-223.
Duišin D. (2004) Analiza tipologije ličnosti u odnosu na rodni identitet. [doktorska disertacija]. Beograd: Medicinski fakultet Univerziteta u Beogradu.
Džamonja Ignjatović, T, Žegarac, N. Popović, D. i Duhaček, D. (2009). “Istraživanje stavova prema rodnoj ravno-pravnosti u sistemu visokoškolskog obrazovanja”, u: Vujačić, I. (ur.) Godišnjak 2009, Beograd: Univerzitet u Beogradu - Fakultet političkih nauka, Godina III, Broj 3, 697-712.
Filozofski fakultet u u Nikšiću, Univerzitet Crne Gore. Nastavni plan i program studija psihologije na službenim inter-netskim stranicama Fakulteta: http://www.ff.ac.me/15Psihologija/01os.htm
Goreta M, Peko-Čović I, Buzina N. (2004) Psihijatrijska vještačenja – zbirka ekspertiza (knjiga prva – kazneno pravo). Zagreb: Naklada Zadro. Pp. 326.
Green, B., Herek, G.M. (1999). Psihologija ženske i muške homoseksualnosti: teorija, znanstvena istraživanja i kliničke primjene, Zagreb: Impressum.
Harrison A.E, Silenzio V.M.B. (1996) Comprehensive Care of Lesbian and Gay Patients and Families. Primary Care 23:31-46.
Hatzenbuehler M.L, Keyes K.M, Hasin D.S. (2009) State-level Policies and Psychiatric Morbidity in Lesbian, Gay, and Bisexual Populations. Am J Public Health. 99(12):2275-81.
Hatzenbuehler M.L, McLaughlin K.A, Keyes K.M, Hasin D.S. (2010) The Impact of Institutional Discrimination on Psy-chiatric Disorders in Lesbian, Gay, and Bisexual Populations: a Prospective Study. Am J Public Health. 100(3):452-459.
Hooker E. (1957) The Adjustment of the Male Overt Homosexual. Journal of projective techniques. XXI: 18-31.
Hotujac Lj. (2002) Letter to Dorino Manzin, 9.4.2002., available at: http://www.gay-u-obitelji.com/site/index.php?option=com_content&task=view&id=13&Itemid=30 (in croatian language)
Hotujac Lj. (ur) (2006) Psihijatrija. Zagreb: Medicinska naklada.
Jakovljević M. (Ed) (1995) Psihijatrija za studente više medicinske škole. Samobor: AG Matoš.
Kaličanin P. (2003) Klinička psihijatrija. Beograd: Institut za mentalno zdravlje.
Kamenov Ž., Jokić-Begić N. i Lauri Korajlija A. (2003) Stigmatizacija tjelesnih invalida, psihičkih bolesnika, narkomana, alkoholičara i homoseksualaca. XVI Dani Ramira Bujasa, Zagreb.
King M, Mc Keown E, Warner J, Ramsay A, Johnson K, Cort C, Wright L, Blizard R, Davidson O. (2003) Mental Health and Quality of Life of Gay Men and Lesbians in England and Wales. British Journal of P sychiatry 183:552-558
King M, Nazareth I. (2006) The Health of People Classified as Lesbian, Gay and Bisexual Attending Family Practitioners in London: a Controlled Study. BMC Public Health 6:127
King M, Semlyen J, See Tai S, Killaspy H, Osborn D, Popelyuk D, Nazareth I. (2008) A systematic review of mental dis-order, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry 2008, 8:70.
Klain E. (Ed) (1999) Psihološka medicina. Zagreb: Golden Marketing.
Mays V.M, Cochran S.D. (2001) Mental Health Correlates of Perceived Discrimination Among Lesbian, Gay, and Bi-sexual Adults in the United States American. Am J Public Health. 2001;91:1869–1876.
Medicinski fakultet (MF) u Zagrebu, MF u Rijeci, MF u Splitu, MF u Osijeku (2008) Katalog znanja i vještina za studij medicine. Zagreb, Rijeka, Split i Osijek: MF Zagreb, MF Rijeka, MF Split, MF Osijek. Available at: http://cms.mef.hr/meddb/slike/pisac1/file1210p1.pdf
77
Chapter 5Academic education of LGBT population in three helping professions in countries of South-eastern Europe
Medicinski fakultet Univerziteta Crne Gore. (2010) Program nastave psihijatrije za studente medicine na službenim internetskim stranicama: http://www.medf.ac.me/
Meyer I.H. (2003) Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychol Bull. 129(5): 674–697
Muačević V. (ur) (1995) Psihijatrija. Zagreb: Medicinska naklada.
(Nepoznati autor) (2007) Uvod u psihopatologiju – slajdovi i bilješke s predavanja 26.10.2007-25.1.2008. Available at: http://www.ffzg.hr/psiho/stup/SKRIPTE/III%20godina/V%20semestar/Psihopatologija/UVOD%20U%20bip%20bip.doc.
Newcomb M.E, Brian Mustanski B. (2010) Internalized Homophobia and Internalizing Mental Health Problems: A Meta-analytic Review. Clinical Psychology Review 30:1019-1029.
Odsjek za psihologiju, Filozofski fakultet Sveučilišta u Mostaru. (2010) Program preddiplomskog i diplomskog studija psihologije. Dostupno na: http://www.ffmo.ba/index.php?option=com_content&view=section&layout=blog&id=10&Itemid=12
Odsjek za socijalnu pedagogiju Islamskog pedagoškog fakulteta Univerziteta u Zenici. (2010) Nastavni plan i program dodiplomskog studija socijalne pedagogije, na službenim internetskim stranicama Fakulteta. Available at: http://www.ipf.unze.ba/fileadmin/user_upload/TEKSTOVI/NPP_SP_-_bosanski_01.pdf
Parmač M. (2005) Stavovi studenata prema osobama homoseksualne orijentacije. (Diplomski rad). Zagreb: Filozofski fakultet, Odsjek za psihologiju. Available at: http://darhiv.ffzg.hr/132/1/MajaParmač.pdf
Ponzetti J.J. (Ed.) (2003) International Encyclopedia of Marriage and Family, 2nd Ed. New York: Macmillan Reference.
Remafedi G. (1999) Sexual Orientation and Youth Suicide. JAMA 282:1291.
(Republika Srbija). Pravilnik o specijalizacijama i užim specijalizacijama za zdravstvenih radnika i zdravstvenih sarad-nika. Službeni glasnik RS br. 111/93, 46/97, 33/2000, 44/2000, 27/2004 i 36/2004. Source: http://www.med.bg.ac.rs/?sid=1362
Rothblum E.D. (1994) “I only read about myself on bathroom walls”: the Need for Research on the Mental Health of Lesbians and Gay Men. J Consult Clin Psychol. 62(2):213-20.
Sadock B.J., Sadock V.A. (2007) Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. Philadelphia: Lippincott Williams & Wilkins.
Stewart C. (2010) The Greenwood Encyclopedia of LGBT Issues Worldwide, Vol. 2. Pp. 89-90. Santa Barbara: Green-wood Press.
Stoller R, Marmor J, Bieber I, Gold R et al. (1973) A Symposium: Should Homosexuality be in the APA nomenclature. Am J Psychiatry 130:1207-1216.
Štulhofer A. (2010) Sociologija spolnosti za preddiplomske studente sociologije na Filozofskom fakultetu Sveučilišta u Zagrebu: silabus i literatura. Available at: http://www.ffzg.hr/socio/astulhof/sexispit.htm.
Tešić V, Kolarić B, Begovac J. (2006) Attitudes towards HIV/AIDS among Four Year Medical Students at the University of Zagreb Medical School – Better in 2002 than in 1993 but Still Unfavorable. Coll. Antropol. 30(2006) Suppl. 2:89-97
Vasta R., Haith M.M. i Miller S.A. (1998) Dječja psihologija. Jastrebarsko: Naklada Slap.
Walsh F. (Ed.) (2003) Normal Falimy Processes. New York: Guilford.
Warner J, Mc Keown E, Griffin M, Johnson K, Ramsay A, Cort C, King M. (2004) Rates and Predictors of Mental Illness in Gay Men, Lesbians and Bisexual Men and Women. British Journal of Psychiatry 185:479-485.
Warwick I, Aggleton P. (2002) Gay Men’s Physical and Emotional Well-Being: Re-orienting Research and Health Pro-motion. In: Coyle A, Kitzinger C. (2002) Lesbian & Gay Psychology: New Perspectives. Oxford: Blackwell. Pp. 135-153)

78
Chapter 5 Academic education of LGBT population in three helping professions in countries of South-eastern Europe
79
Chapter 6Activism and non- governmental response
6. Activism and non-governmental responsePrepared by: Hrvoje Fuček
6.1. Introduction
In the dawn of a new century, things seemed almost radically changed for the LGBT populations in the Balkans. Several gay or gay friendly clubs were opened in Croatia, as well as in Serbia and Bosnia-Herzegovina. The Croatian lesbian organizations Lori and Kontra, the Croatian LGBT association Iskorak, as well as several similar groups and organiza-tions in Serbia (Arkadija, Labris, Queeria, Deve, later on GAYTEN), have started with their work, organizing various campaigns, public discussions and lectures, launching websites and internet forums. They were soon followed by two LGBT associations in Macedonia and Bosnia-Herzegovina (Centre for Civic and Human Rights in Skopje and in Sara-jevo, Bosnia, later known as organization Q BIH). Such turnover created a positive ground for different cultural under-takings, but strange enough, the culture stayed behind the activism for a few more years. Maybe the severe incidents that occurred during the Belgrade Pride (2001) discouraged the queer artists to go public at that time.
In the recent years, however, the LGBT culture in the Balkans apparently became more visible than ever. Various ar-ticles, essays, stories and poems appeared in renowned cultural magazines in Croatia, Serbia and Bosnia-Herzegovina, such as Zarez, Libra Libera, Album, Lica, Kolaps, Iza, Teorija Koja Hoda, etc. The Serbian cultural and LGBT activists have launched two gay magazines - Decko and GAY(TO). A few exhibitions of queer visual artists were held in Belgrade, organized by the Center for Contemporary Arts and RotoR. Likewise, some alternative Serbian theatres have organized several domestic queer performances. As well, one of the clearest signs that something is changing in the Balkans was the victory of the Slovenian transvestite trio Sestre at the national contest for Eurosong contest in 2002, and their almost immediate visits and shows all over the countries of ex-Yugoslavia. In Bosnia-Herzegovina, the theatre shows of Slove-nian gay director Damir Zlatar Fray were very positively received, while Bosnian queer visual artists Boris Majstorovic and Danis Fejzic have held various exhibitions and performances. The first LGBT radio program - called the Gay Ming – was also broadcasted in Serbia.
In 2004 Croatia got its first Festival Queer Zagreb. Challenging the existence of post-socialist queer identity, it presented selected works of queer artists from the Balkans for the first time ever. When we talk about culture, the Queer Zagreb festival has become one of the most important queer festivals in the Balkans.
After years of invisible presence and hidden cultural activities, it seems that the time has come for this region’s queer population to stand up together and offer its local and global public a specific and authentic culture.
As well, the LGBT activists from the Balkans have gathered together in order to create a new regional network - SEE Queer Network. One of the main objectives of this regional network is to work together on deeper queer cultural inte-grations.
The legal position of homosexuals in the former Yugoslavia significantly changed during the seventies of the twentieth century. Slovenia was the first country to lead a debate on decriminalization of homosexuality. Along with Croatia and Montenegro, Slovenia decriminalized homosexuality in 1977 whereas Serbia did so in 1994.
According to the latest report of the European Commission, Serbia has been assessed as a country with a large number of incidents of hate speech, threats and physical attacks on the LGBT population, while in Montenegro the anti-gay at-titudes are deeply rooted. In the countries of the former Yugoslavia it is not forbidden to be gay, that is, it is not forbidden to be gay only at home. It is obvious that homophobia will be a great obstacle for the Western Balkans in terms of the EU.
There is no doubt that homophobia exists in the Balkans, especially when it comes to Serbia and Montenegro. It is obvious that these countries are lagging a lot behind other Balkan countries, such as Slovenia and Croatia, but since the European path has undoubtedly been chosen, the attitude towards the LGBT populations will have to be changed very quickly.

80
Chapter 6 Activism and non- governmental response
6.2. Bosnia and Herzegovina
Bosnia and Herzegovina has ratified Protocol No. 12 to the Convention for the Protection of Human Rights and Fun-damental Freedoms and was a signatory to the 2007 UN Declaration on Sexual Orientation and Gender Identity. The age of consent is equal for all sexual acts including consenting same-sex sexual act. Bosnia and Herzegovina does not provide any legal recognition of same-sex partnerships. Neither joint nor second parent adoption is available to same-sex couples. Discrimination on the basis of sexual orientation is prohibited in the areas of employment, membership in professional organizations, education, training, housing, health, social protection, goods and services. Laws on hate and violence do not refer to sexual orientation or gender identity and do not recognize sexual orientation or gender identity as being an aggravating factor.
Although activism in Bosnia and Herzegovina is at very limited and small scale, several noteworthy projects were es-tablished over the years.
Organization Logos has issued the Baseline Study on Faith-based Development in Bosnia and Herzegovina: Challenges of Non-patriarchal Approaches and Communities, which deals with the complex and vehement issue of place and treat-ment of LGBTIQ persons in the religious communities present in Bosnia and Herzegovina (Islam, Roman Catholic and Eastern Orthodox Christianity, Judaism, Buddhism, Hinduism, etc.). It is a cross-sectoral research that evaluates religious, cultural and institutional responsiveness to LGBTIQ faith-oriented individuals, including various background analyses on legal, social and theological framework for protection from discrimination on the basis of one’s sexual ori-entation, gender identity and gender expression. It is the only study of this format and volume in the region.
The First Queer Sarajevo Festival (QSF) was organized by Organization Q on September 24, 2008 with the aim to pres-ent the ‘life stories’ of LGBTIQ persons through art and to mainstream queer theory, art and culture into the Sarajevo cultural scene. The festival’s organizational team prepared a five day program, including exhibitions, films (documentary and featured), round tables, and performances with the opening of three art exhibitions on September 24, at the Gallery of the Academy of Fine Arts in Sarajevo, Bosnia and Herzegovina. Although protests against QSF were evident before its scheduled date, physical violence against the QSF, guests and organizers ensued at the opening ceremony. Due to the violence that occurred on the night of September 24 and the serious threats during the following days, the activities of the QSF were cancelled in the evening of September 26. Although the police was informed and was present during the opening of the Festival, adequate protection was not provided for the participants. There is no information on whether any of the perpetrators of violence have actually been prosecuted.
Organization Q started the project ‘’Campaign to promote the human rights of sexual and gender minorities in BIH’’ in May 2005. The project had the following objectives: to educate the public about human LGBT rights, primarily on the existence of Article 2 Law on Gender Equality, which bans discrimination based on gender and sexual orientation, as well as to inform the LGBT population throughout the country about their human rights.
Organization Q works on scale up IEC/BCC in population with increased risk for HIV/AIDS with its partners UG PROI, Sarajevo, and Association XY, Sarajevo, along with the NGO ‘Action Against AIDS’, Banja Luka, and UG Vikto-rija, Banja Luka, specifically implementing full harm reduction and outreach services in the Federation of Bosnia and Herzegovina, Brčko District of BIH, and the Republika Srpska. UNDP is the Principal Recipient of the implementation of the HIV/AIDS Programme, funded by the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM). The whole project responds effectively to the “Priority Activities for Poverty Reduction” of the national Poverty Reduction Strategy Paper (PRSP). It contributes to the adequacy of social protection, provides to the poor, aims to reduce corrup-tion, contributes to public awareness of human rights, contributes to public health and prevention education, and it will improve the quality of life for the minority groups. The expected outcome of the implementation of the GFATM grant to BIH is the following: the prevention of the spread of HIV in BIH will be improved, the survival rates of PLWHA will be increased and the national capacity to manage GFATM grants in BIH will be built.

81
Chapter 6Activism and non- governmental response
6.3. Croatia
Croatia, as a whole, is still considered to be rather conservative, especially in public reactions regarding LGBT rights and visibility of LGBT people. In the last few years there has been no mass organized or group violence towards LGBT activism and manifestations, however, hate speech and severe incidents against LGBT community and individuals occasionally hap-pen, including an attempt to throw five or six Molotov cocktails on Zagreb Pride in 2007.
Croatia has ratified Protocol No. 12 to the Convention for the Protection of Human Rights and Fundamental Freedoms and was a signatory to the 2007 UN Declaration on Sexual Orientation and Gender Identity. The age of consent is equal for all sexual acts including consenting same-sex sexual act. Cohabiting same-sex couples enjoy a set of limited rights, while joint or second parent adoption is not available to same-sex couples. Sexual orientation is included in the law on hate and violence, and is recognized as an aggravating factor.
Over the last decades, Croatia has undergone unprecedented progress. Since the fall of Communism in the late 1980s and the struggle for independence and democracy in the early 1990s life has taken on a new dimension. The gay scene has begun to develop in Zagreb and the society is moving towards liberation of its view o homosexuality.
The last six years have marked a great milestone for the LGBT community in Croatia on the legal level. However, although some of the rights of the LGBT population are now protected by the Croatian law, implementation of these newly-passed laws is made difficult by discriminatory actions of state institutions in specific cases. Most of the time, victims do not even report discrimination or violence, since they have no confidence in the Croatian legal system, es-pecially the police. The community is especially discouraged by homophobia within the institutions, even within the Croatian Parliament which passed the above laws but whose members publicly use hate speech aimed at sexual and gender minorities, breaking these same laws and showing the public how little they value the very laws they raised their hands in favour of in the hope of endearing themselves to the international community.
In recent years homosexuals have become more visible in the media. Debates with the participation of LGBT organiza-tions have been held on national television. Both newspapers and television programs have focused on gay issues by interviewing gays and lesbians and highlighting annual events such as the Queer Zagreb festival and Zagreb Pride.
Many important politicians and political parties have officially supported the struggle for an equal society. Although the LGBT organizations are trying to promote gay and lesbian rights by informing and educating a large number of the public, many still consider homosexuality to be an illness. In general, homosexuality is tolerated as long as it is not obvi-ous. People in larger cities [Zagreb, Rijeka and Osijek] have a more open-minded attitude towards homosexuality while people in rural areas often view it negatively.
Croatia’s homosexual community, and especially the younger generation, is aiming to show with an active fight for its rights and against strong odds, that one should not be ashamed or discriminated against for being gay. The annual Pride Parade and Festival in downtown Zagreb reflect this new age of courage. Despite threats from skinheads and rightist protesters who rail against any form of homosexual expression and oppose all pro-gay legislation, the brave marchers have stepped out of the shadows.
The first Pride event in 2002 saw a mere couple hundred celebrants surrounded by hundreds of policemen who were there to keep the peace. The marchers, numbering about 200, were subjected to jeering and heckling from some by-standers and , in spite of the presence of police, a tear gas canister was thrown at them.
Currently there are several NGOs working with sexual and gender minorities in Croatia. They are Iskorak - Sexual and gender minorities rights centre, Lesbian group Kontra, Lesbian group Lori, Domino - Queer Zagreb and Zagreb Pride.
Iskorak - Sexual and gender minorities’ rights centre was established in 2002. and is one of the oldest NGOs in Croa-tia. They primarily focus on the prevention of HIV/AIDS in the MSM population as well as on providing counselling services to the sexual and gender minorities. Together with Kontra they are also focused on advocating changes in the legislature and on empowering the community.

82
Chapter 6 Activism and non- governmental response
Lesbian Group Kontra is a non-governmental organization that promotes lesbian human rights. It was registered in 2002 in Zagreb. They are actively involved in providing support, education, counselling and empowerment of lesbians and bisexual women in seeking acceptance of their identity, accomplishing social visibility, or coming out of anonymity and isolation. Together with Iskorak they advocate changes in the legislature.
Both Iskorak and Kontra and their activities are primarily responsible for several major accomplishments in Croatia: organization of the first, and several sequential Pride marches in Croatia, participation in the creation and advocated of the Act on Same Sex Civil Unions; as a result of their advocating, anti-discriminatory provisions were implemented into Law on Sex Equality, Law on Media, Law on Electronic Media, Law on Croatian Radio Television, Law on Changes to Law on Labour, Law on Science Activity and High Education, Law on Changes to Penal Code (Hate Crime was accepted in Penal Code), and the Textbooks Standards. They publish annual reports on the rights of sexual and gender minorities in the Republic of Croatia.
Lesbian group Lori was formed in 2000 and is the only NGO that works in the field of protection of LGBT rights outside of Croatia’s capital of Zagreb, in the town of Rijeka. The aim of this association is general protection and promotion of LGBT human rights, with the primary focus on lesbian human rights. Their activities are mainly focused on education and counselling, media watch and local community empowerment.
Domino - Queer Zagreb is an international cultural festival which has been taking place in Croatia since 2003. It has become the biggest event of this kind in Central and Eastern Europe. The Queer Zagreb festival contributes each year to the cultural and social diversity of Croatia, as the program attracts a wide audience and allows it to see things in a different manner. The festival has been making its mark by presenting artists who challenge the norms of aesthetics and contents within which the vast majority of the local culture in Croatia remains.
Zagreb Pride Association is the youngest LGBT organization in Croatia registered in late 2008 as an organization with primary focus on organizing Pride marches in Croatia. Zagreb Pride is a queer-feminist, anti-fascist, non-hierarchical group that advocates for the LGBT community’s solidarity, and opposes violence and discrimination against the LGBT population. Zagreb Pride mostly consists of an open volunteer group of people which is gathered in the Zagreb Pride Organizing Committee (OOZP). In addition to the Pride march they organize several community events (mostly par-ties) for the LGBT population throughout the year.
LGBT activism in Croatia is quite pronounced with a number of different activities directed towards the community and society in general. One of the most visible LGBT events in Croatia was the first Pride which took place in Zagreb in 2002, with extremely strong police security. Many believe that without the aid of the police, Pride would be turned into a massacre, as was the case in Belgrade in 2001. In subsequent years, the resistance of society to the Pride Parade was smaller, however in 2007 there was an attempted attack with Molotov cocktail on Pride, but because of the rapid reaction of the police, and the attempted attack was prevented. In 2009, for the first time the police allowed the organization of anti-pride protest on the same day of the Pride Parade. However the number of participants in the Pride Parade widely exceeds the number of anti-pride protesters. In addition to the parade, the organizers organized a series of additional events such as banner workshops, parties, public coming outs etc.
In addition to Pride Parades, theQueer Zagreb Festival has been organized in Zagreb on a regular basis since 2003 and since 2009, the festival Perforacije has joined the tradition. Both festivals have a regional and world-wide cultural range of theatrical productions and film screenings and parties. The content of festivals often transcends other topics related to sexual and gender identity, and includes promoting all socio-unknown groups that resist traditional social values.
Since 2002, a number of public campaigns aimed at awareness of society about sexual and gender minorities have been launched. The first campaign “Love is love” was launched by Lori, whose spot was never broadcasted on national televi-sion due to high levels of homophobia has. The second campaign called “And homophobes are people” was started by the organization Domino - Queer Zagreb and its billboards were displayed throughout Croatia. In addition to these campaigns Iskorak launched a campaign “in Krapina all Homosapiens” which premiered in seven major Croatian cities, and the cam-paign “Stepping Up Against Homophobia”, during which a video featuring famous Croatian cultural, political and public figures who speak out for first time against homophobia by was premiered. A step forward was taken together an anti-discrimination campaign was run: “Different love, same rights” and “Right to work without discrimination.”
83
Chapter 6Activism and non- governmental response
There is only one gay club in Zagreb, three gay saunas (one in Rijeka) and two gay cruising bars and regular gay parties in Rijeka in Zagreb, and several gay-friendly/gay-safe places in the rest of the country. The situation develops every year. Most of the saunas, cruising bars and beaches in the coastal areas are often visited by older men, while younger genera-tions are more visible at the parties and in the club(s).
The development of the LGBT rights and culture in Croatia is contributed by LGBT sites such as Gay.hr and crolportal.com which are important online points for organizing gay activism and for meeting other gay and gay-tolerant people.
6.4. Montenegro
On the basis of a referendum held on 21 May 2006, Montenegro declared independence on 3 June 2006. On 28 June 2006, it became the 192nd member state of the United Nations, and on 11 May 2007 the 47th member state of the Council of Europe. On 15 December 2008, Montenegro presented its official application to the European Union, with the hopes of gaining EU candidate status by 2009. Montenegro decriminalized homosexual sex in 1977. The age of consent legislation was equalized in 1977. Homosexuals are not banned from military service. Gays and lesbians continue to face discrimination and harass-ment in Montenegro. The gay scene is very small. Anti-gay attitudes are deeply ingrained. The invisibility of homosexuals and lesbians in public and social spheres is further slowing efforts to overcome homophobia in this conservative society.
Persons’ alternative sexual orientations remain closely-guarded secrets.
The first conference for gay rights was held without an incident, and the first Montenegrin gay portal was launched. However, last year was also marked by a series of homophobic statements by politicians, but above all by a statement by Montenegrin Minister of Human and Minority Rights Ferhat Dinosa. After that statement, some NGOs and activists for human rights demanded his resignation several times, but he has not yet filed it. As they say, the Minister violated, un-der Article 44 of the protector of human rights and freedoms, the Articles of the Constitution relating to human rights. Dinosa has denied stating earlier that he does not know if there is a man in Montenegro who would say that he is gay or a woman who would say that she is a lesbian, and that according to the findings of the ministry, there is not a registered association that deals with the protection of the LGBT groups. Although Montenegro was one of the first republics of the former Yugoslavia to decriminalize homosexuality, the majority of its citizens still believe that homosexuality is a disease, and so far there are no indicators that show that these views could change soon. Although Article 19 of the Law on Prohibition of Discrimination states that everyone has the right to publicly express their sexual identity and sexual orientation, the members of a different sexual orientation in Montenegro are forced to pretend not to exist, as was con-firmed by several failed attempts to organize the Pride Parade. The only person who has publicly called for the organiza-tion of the Pride Parade in Montenegro was the Serbian activist Atila Kovac, who was stoned in front of the state televi-sion by Montenegrin supporters after that statement. The police detained three people, but to date there is no answer.
The current state of the LGBT population in this country can be described as a “black spot of Europe” and the protection of all citizens should be a prerequisite for Montenegro’s membership in the EU.
According to research by the European Agency for Fundamental Rights, Serbia and Montenegro are currently in a poor position when it comes to respecting human rights, and the EU will continue to monitor whether there will be prog-ress in implementing the provisions of the European Convention on Human Rights, which is one of the conditions for convergence of the EU countries.
Montenegro is the last of the Western Balkan countries to adopt the anti-discrimination law. The Employment Agency of Montenegro and the NGO Juventas signed a Memorandum of Understanding to promote and support human rights of the LGBT population in Montenegro. In the recommendations of the Committee of Ministers of the Council of Eu-rope (March 2010) it is stated that the LGBT population is discriminated against in many areas of which one of the most important is the right to employment and decent work. The recommendations on measures to combat discrimination based on sexual orientation and gender identity are addressed to the Member States of the Committee of Ministers of the Council of Europe, including Montenegro.

84
Chapter 6 Activism and non- governmental response
One of the main objectives of the adopted recommendation relates to the activities and actions that member states should undertake to ensure respect for human rights of those with a “different” sexual orientation, and to promote toler-ance towards them.
The small number of registered incidents of homophobia in Montenegro should not be interpreted as a sign of tolerance. Even if they report attacks, victims of homophobic violence tend to avoid any mention of sexual orientation. Conse-quently, statistical data does not reflect the actual level of homophobia in the country.
Juventas is the NGO that works with the LGBT community in Montenegro. Since 2008 they have launched several projects and programs in order to improve the overall LGBT rights in that country. They put emphasis on two projects: “Health and Rights” which deals with HIV/AIDS prevention among the MSM population and the Promotion of LGBT human rights in Montenegro and the West Balkans.
In December 2009, The NGO Juventas, in partnership with the Centre for Monitoring of Podgorica, started the project “Montenegro - a bright spot on the gay map,” whose main goal is to promote and support human rights of the LGBT population in Montenegro. The project’s goal is also to promote and support the activities against the discrimination aimed at people with a different sexual orientation and gender identity in Montenegro, as well as provide compensation for the violations of human rights. Beneficiaries are LGBT people, while the target groups include LGBT activists, the general population, government institutions (including professionals and service providers) as well as nongovernmental organizations, political parties and the media.
In addition to the above mentioned organizations, the Institute of Public Health, Podgorica, NGO Forum MNE, CA-ZAS, SOS Podgorica, as well as UNAIDS collaborate on the project. For the first time in Montenegro, there is a formed coalition at the national level, “Together for LGBT Rights” to promote the realization of the rights of sexual minorities.
The development of the LGBT rights and culture in Montenegro is contributed by the LGBT site montenegro-gay.me which is an important online point for organizing gay activism and for meeting other gay and gay-tolerant people.
6.5. Serbia
Gays and lesbians continue to face discrimination and harassment in Serbia. The majority of the Serbian people display great anti-gay attitudes. There have been numerous instances of violent gay-bashing, the most extreme during the first Belgrade Gay Pride. Three other Pride Day celebrations were planned in Serbia: one in Belgrade in 2004 initiated by activists from GSA and another in Novi Sad initiated by LGBT Vojvodina in 2007. However, due to low cooperation between the activist groups and the inability to provide adequate safety against violence generated by limited funding, these two were never realized. The third one, Belgrade Pride 2009, was cancelled for similar reasons – the police could not guarantee security to the participants.
Official medical textbooks that classify homosexuality under “Sexual Deviations and Disorders” are widely used throughout the country. Upon several requests, the Serbian Medical Society finally stated in an official letter to Labris in 2008 that same-sex orientation is not a disease.
The gay scene in Serbia is rather small and clubs that proclaim themselves as LGBT (friendly) open and close frequently. As of 2008, Loud & Queer which operates in Belgrade is the only official LGBT club. In addition, there are few gay and gay-friendly cafes are located in the downtown areas of Belgrade and Novi Sad, but their existence is a public secret.
The protection of LGBT people in Serbia is further complicated by the existence of various nationalist and pro-fascist associations such as ‘Obraz’, ‘1389’ and ‘Stormfront’, which are well-funded and supported by some right-wing political parties. These groups have, on several occasions, made their threats to the LGBT population publicly known, with little or no reaction from the media and the police. The previous year was challenging for the LGBT population in Serbia, and the state has not done anything to protect them. Although the results of the Gay-Straight Alliance show a shift when it
85
Chapter 6Activism and non- governmental response
comes to human rights of the LGBT population, and although the European anti-discrimination law has been passed, it is obvious that Serbia is still not a country of tolerance in which everyone has equal rights and freedoms.
Lazar Pavlović (LGBT activist) was a victim of discrimination and threats several times. He was threatened by unknown young men with beatings and even death, and just a year later he was the victim of attempted attacks by violent youth in the park Kalemegdan in Belgrade. Both cases have been reported to the police, and the attacker was arrested, which led to this being the first case in Serbia that was fined by a court on grounds of sexuality.
The police has raised the level of professionalism in their work with the LGBT population, but the courts and the pros-ecution are a bottleneck in the protection of human rights in Serbia, since they are unacceptably slow and inefficient and as often self-declared incompetent when it comes to cases of violence against the LGBT population. Despite great op-position by the Serbian Orthodox Church, the anti-discrimination law was adopted in March last year, and many were convinced that they the conditions to hold the parade were finally created. Just days after the organizers announced that they will organize the LGBT Parade, they received threats in the open media. Igor Marinkovic, member of the Govern-ing Board of the Serbian People’s Movement 1389 said that this organization has never called for attacks on the LGBT population, but they only warned of what could happen if the parade took place. The majority of the citizens did not want the parade to take place.
The day before the parade, the event was cancelled due to the fact that the police could not guarantee the safety of the participants, which clearly showed that the state is not really ready to equally protect the rights of all of its citizens. The failure to hold the Pride Parade was a serious political blow to Serbia. The European institutions monitor very carefully what happens to the LGBT population in Serbia, because they test the potential future members in terms of respect for fundamental human rights.
This year the Parade was held successfully for the first time and 9 years after the first parade that was held in Belgrade and that ended in bloodshed. The event was seen as a new test of tolerance in Serbia which seeks to join the European Union. The parade was a success with 2000 participants in the Belgrade city centre and no incidents, as the authorities kept the violence confined to another neighbourhood of the capital city. In these neighbourhoods, more than 100 Ser-bian policemen and civilians were injured and dozens more were arrested in skirmishes that broke out less than a mile away from the Pride Parade. The police tossed tear-gas canisters in order to disperse anti-gay protesters and three fire trucks were dispatched to the headquarters of the Democratic Party of Serbian President Boris Tadić, where a Molotov cocktail set a part of the building on fire. Overall, 85 police and more than a dozen civilians were hurt, while 60 protest-ers were arrested. This clearly shows the high level of homophobia in that country.
The following organizations are currently active in the field of protection of LGBTIQ human rights in the Republic of Serbia: Association Rainbow (Asocijacija Duga, Šabac), Gayten LGBT (Beograd), Gay Lesbian Info Center (Beograd), GayStraight Alliance (GejStrejt Alijansa, Beograd), Queeria (Kvirija, Beograd), Gay Men Support Group (Novi Sad), LABRIS - organization for lesbian human rights (Beograd), Lesbian Organization Novi Sad (Novi Sad), SPY - Safe Puls of Youth (Siguran puls mladih, Beograd), Queer Beograd (Beograd).
The development of the LGBT rights and culture in Serbia is aided by LGBT sites, such as the oldest Adriatic LGBT Ac-tivism mailing list in the region, Gay-Serbia and Queeria which are important online points for organizing gay activism and for meeting other gay and gay-tolerant people.
The LGBT activism in Serbia is now focused on the development and lobbying for the registered partnership law as well on the implementation of the anti-discrimination law. Cases of discrimination and violence against the LGBT population are being processed and monitored by the leading NGOs. Many of the LGBT organizations in Serbia continue to work on outreach programs and community empowerment.

86
Chapter 6 Activism and non- governmental response
87
Chapter 7Prevention tips- manual on prevention activities
7. Prevention tips- manual on prevention activitiesPrepared by: Hrvoje Fuček and Zoran Dominković
7.1. Prevention
The best cure for any sexually transmitted disease is prevention – the most important issue is not to become infected. This paragraph covers the activities that individuals can undertake in order to protect themselves and their partners. However, it is also important to take into consideration the social and psychological influences that can prevent a num-ber of people from behaving in a desirable way.
7.1.1. Safer sex
Prevention can be ensured in four ways: abstinence, mutual fidelity, use of condoms, and non-penetrative sex. Penetra-tive sex without a condom is very risky. Consistent use of condoms and non-penetrative sex are known as safer sex, because they decrease the risk of HIV infection to a considerable degree, as well as the risk of contracting other sexually transmitted diseases (STDs).
Even though abstinence guarantees full protection from STDs, it is a viable option for a very small number of people. Sex fulfils a number of needs. It is a unique and usually free source of pleasure, which tends to strengthen the emotional connection between partners, and for many men it is a confirmation of their personality.
Mutual fidelity – where both partners are HIV-tested and they know that they are not infected, while no partner engages in sex outside of the relationship – constitutes an option that is possible for few men who have sex with men. Many of them do not have a permanent partner, or they live in a society which renders the finding and retention of a permanent partner rather difficult. Many are married and have sexual relations with their wives because of a feeling of duty, and with one or more men for pleasure. Those who are not married and have a permanent male partner may not be in a position to see their partner as much as they might want to, which may result in frustration, and in one partner or both partners entering sexual relations with other persons.
Non-penetrative sex is the stimulation of a penis by hand, or between the legs, or in some other manner that does not include insertion into the mouth, vagina, or anus. That ensures safety, because the contact of infected sperm with undamaged skin cannot result in the infection entering the blood stream. Mutual masturbation and other forms of non-penetrative sex are usually practiced by men who have sex with men, but as an occasional alternative to sexual intercourse, rather than as its replacement.
Given the fact that few people wish or are able to limit themselves to abstinence, mutual fidelity and non-penetrative sex, all the men who have sex with men should be aware of the importance of consistent and successful use of condoms when these options are not available. When a condom is not used, or is unavailable, the extraction of the penis out of the anus or mouth prior to ejaculation can decrease the risk, but it does not eliminate it.
88
Chapter 7 Prevention tips- manual on prevention activities
7.1.2. Condoms and lubricants
If both partners cannot prove that they are HIV-negative, which includes blood testing and abstinence from sexual ac-tivities or drug injecting in a manner that may lead to infection for a period of at least three months, a condom should be used in every anal or vaginal intercourse. When used in an appropriate manner, the male condom prevents the transfer of STDs in 99 percent of cases. Thicker condoms are recommended for use in anal intercourse; however, recent studies indicate that condom thickness does not play a part, provided that a lubricant is used.
The use of condoms may seem simple, but it requires practice. When not used properly – for example, if air remains trapped in the tip of the condom, or if the condom is not fully unwrapped throughout the length of the penis – the con-dom may slip or break. When they are with their partners, men tend to act in a hurry and do not put on the condom in a right manner. Men ought to practice placing the condom on their own penis first, and also practice taking it off upon ejaculation: that will simplify the use of the condom with their partner.
Given the fact that the anus is not able to produce moisture, friction can cause rupture of the condom. In order to avoid that, many men use saliva; however, it dries quickly and such an approach is not recommended. Water-based lubricants are more desirable, but they can be inaccessible or too expensive for many men. Oil-based lubricants, such as vaseline or cooking oil, must not be used, given the fact that they destroy latex. A key activity in working with men who have sex with men is to ensure easy access to adequate lubricants.
Although the transmission risk for HIV and a number of other STDs is significantly smaller in oral sex, some experts recommend condoms to be used in oral sex as well. However, the taste and the feeling are so unpleasant for many men that they prefer not to do that. According to studies, ejaculation into the mouth elevates the risk of infection. Extraction of the penis out of the mouth prior to ejaculation decreases the risk.
There are significant differences in penis size. Male condoms are used in various sizes; using the wrong size may lead to discomfort, or the condom may slip off during sex. Organizations in charge of condom distribution should therefore make condoms accessible in various sizes for their clients. It should also be recognized that male condoms can decrease the level of sensation for a certain number of men. That can be prevented by lubricating the internal side of the condom with saliva, in the area where the condom gets in contact with the glans of the penis.
Condoms can be available free of charge, at subsidized prices, or at commercial prices from a number of sources, in-cluding health clinics, retail stores and NGOs. The method of ensuring the availability of condoms for men who have sex with men, demonstration of condom use, and methods used to persuade clients to use condoms, constitute vital implementation areas for programs focused on men who have sex with men (MSM).
7.2. Risk and vulnerability assessment
7.2.1. More than sex
Human sexual behaviour and attitudes on sex are motivated by much more than just knowledge. Behaviour change is a complex process, motivated by several factors, including awareness of the need for change, and of the benefits stem-ming from change; practicing new skills, such as persuading the partner to use condoms; and trust in one’s own ability to adopt new behaviour, changing the circumstances regardless of obstacles and mistakes.
HIV/AIDS prevention must therefore include not only the physical aspects of prevention, but also the social and psycho-logical context in which sex is taking place. For MSM, such context may include the issues of sexuality, culture, gender, health, social status, religion, politics, legislation, self-respect and power. For many men, the key issues are poverty and fun-damental needs, such as food and clothing, as well as the obligation to marry and take care of their own wife and children. Wider social attitudes, such as stigmatisation of sex between men, and abuse of men who practice it, are also a fundamental issue. Interventions that do not focus on these issues as the very core of prevention strategy will therefore fail.
89
Chapter 7Prevention tips- manual on prevention activities
7.2.2. Work with organizations in society (NGOs)
Prevention strategies are more effective when implemented by people whom they are intended to benefit. Same as in the process of evaluation, men who have sex with men (MSM) must be included in all the intervention planning and implementation stages. That frequently takes place through an existing group or an NGO led by MSM and working with MSM. An NGO can then take the responsibility for some interventions. Such an organization may already exist; if not, its establishment should be supported. Establishing an NGO with men who have sex with men requires time and care-ful support. Attention should be focused on accepting the autonomy of such an organization, as well as accepting the need for those involved in the organization to reach their own decisions on whether they wish to continue operating. The establishment process typically begins in an informal fashion, with reliable individuals who gradually take over the leading role.
The concept of leaders is closely connected with such NGOs. Leaders are those individuals in a community who are rec-ognized as representatives of the community and/or whose sexual or social practice the community is admiring. Leaders have a decisive influence: in one US study, risky sexual behaviour among MSM decreased by 30 percent in small towns where the most accepted clients in bars were trained in HIV prevention and encouraged to promote safer sex with their acquaintances. Training for leaders is increasingly recognized as a tool for maximizing the potential of a leader to build the concord necessary among MSM for various HIV/STD prevention strategies.
Other forms of capacity building aimed at supporting the establishment of NGOs may include administrative and strate-gic skills; partnership building and the development of services that persons may be directed to; high-quality insurance, in particular for health services; assistance in the development and implementation of advocacy strategies. Equally im-portant is the development of the financial system; strengthening governance and system of responsibility; development of documenting activities, monitoring, evaluation and communication functions; resource mobilization.
Given the fact that NGOs are usually small and have relatively few resources, and having in mind that cooperation can provide additional strength and resources, mechanisms aimed at networking with other NGOs should also be developed.
7.2.3. Work with “gatekeepers”
Gatekeepers are men or women who control access to the desired public, either indirectly or directly. They include the owners of commercial meeting venues where MSM meet; the police, which controls access to public places where men are “cruising” (looking for sexual partners); and prison guards, who can allow or disable HIV and other interventions in prisons.
Work with the gatekeepers is a crucial aspect of every prevention strategy. Interventions that have the approval and assistance of gatekeepers will reach many more men than those interventions that the gatekeepers are opposing. In negotiations with the gatekeepers, however, it is important to ensure that the control over interventions is retained by the NGO, and it is also important to make it clear that inappropriate messages that might come from the gatekeepers are unacceptable.
7.2.4. Work with health service providers
MSM have specific health needs, which may be satisfied only by the medical staff that is fully aware of such problems and has the sensibility for them. That includes the possibility of working with MSM in a non-judgmental manner (use of neutral or supportive language and behaviour) upon the disclosure of their sexual history. That also includes the famil-iarity with and possibility of treatment of infection in anus, and also in the genital area and mouth.
When working with MSM, confidentiality must be ensured. That is also true for behaviour and gender/sexual identity (respecting the right of an individual not to discover his sexual behaviour and identity to others), as well as health, in particular when an individual is infected by HIV or a sexually transmitted disease.
90
Chapter 7 Prevention tips- manual on prevention activities
Ideally, all health workers should be aware of the fact that some men have sex with other men; however, voluntary and confi-dential HIV and STD counselling and testing rarely target this group. Capable and compassionate counsellors and staff should be trained for the provision of such services. Although a number of issues surrounding HIV are similar both for MSM and other populations, there are many other issues to consider, such as safer sex, HIV-positive status upon rape, informing the partner and care in family, and these issues require a different approach both for the counsellor and for the client.
7.2.5. Principles obstructing HIV prevention
Debates are sometimes taking place on whether HIV transmission among men might be stopped if men would be pre-vented to have sex with men. Instead of ensuring the provision of services, such as STD clinics, condoms and lubricants, there is an idea that the prevention programs should be focused on decreasing the frequency of sex among men. That can theoretically be achieved by:
• Religious bans;
• Social stigmatization;
• Placing sex among men outside of the boundaries of the law, and introducing penalties such as imprisonment, fines, and – in several countries – execution;
• Police actions aimed at the closure of commercial establishments and prevention of sex among men in public venues;
• Decreasing the number of locations where MSM can meet;
• Discrimination against MSM, or support for social, economic or legal sanctions targeting sex among men;
• Decrease of supply of or demand for sexual services provided by men;
• “Cures” against homosexuality.
These strategies have been widely implemented in a number of societies, both prior to and after the appearance of HIV/AIDS. However, they consistently fail to prevent sex among men, thus also failing to prevent HIV transmission among men.
Furthermore, by denying men access to adequate prevention programs, such strategies have actually contributed to the spread of the virus among men and onto their female partners in a number of communities. In addition to that, stigma-tising sex among men does not only deny a number of men the possibility of leading happy and fulfilled lives, but it can also cause significant psychological and social problems for men, their wives and children.
Given the fact that such an approach to HIV prevention is counterproductive, and leading to the denial of human rights, it is neither recommendable nor supported by the International HIV/AIDS Alliance. However, high profile of such strategies in a number of societies cannot be ignored, and it is therefore important for NGOs to discuss them, with the aim of reacting appropriately to the institutions and individuals that propose them. Given the importance of developing appropriate response, it is frequently important to work with stakeholders who share the same views, such as human rights organizations, sex worker organizations, politicians and all those who understand the need for rejecting inap-propriate strategies.
91
Chapter 7Prevention tips- manual on prevention activities
7.3. Strategies of HIV/STD prevention for MSM and with MSM
The strategy includes the following categories:
• Promoting health with a focus on an individual;
• Gradual increase, targeting and improvement of the delivery of services and products;
• Mobilizing the community;
• Advocacy, political changes and informing the community.
Effective programs aimed at decreasing HIV transmission among MSM will include strategies from all these categories, having in mind local conditions and needs, and deciding on the relative importance attached to each strategy.
The studies confirm that strategies emphasized in this section have raised awareness of HIV/AIDS and STDs in various communities, and they have also resulted in a certain increase of condom use. However, there is unfortunately very little evidence from the developing world on such strategies leading to a significant decrease of HIV transmission, or to a continuously small HIV level among MSM. That does not mean that such strategies do not function, but merely that there is not much research conducted in this area.
7.3.1. Health-promotion strategies focused on individuals
This sub-section is dedicated to strategies aimed at shaping individual attitudes and views of men on sexuality and sexu-al behaviour, with the purpose of raising the frequency of safer sex practice, and the demand for counselling and testing.
Individual interventions include outreach (visits to parks, bars and other meeting points, and talking to men individu-ally); distribution of leaflets; video presentations; counselling; workshops and group discussions; official presentations. The content of the interventions includes skill building in the use of condoms and lubricants; provision of STD testing; therapy opportunities; and the promotion and provision of voluntary HIV counselling and testing.
Peer education is important; whenever possible, individual interventions should be implemented by men who have sex with men, with adequate training, compensation and support.
Obstacles facing the promotion of health focused on individuals include: low level of information on HIV/STD; resistance towards being identified as a man who has sex with men; negative attitudes on condoms; low self-confidence. The hostil-ity of gatekeepers and other HIV/STD service providers can also constitute a barrier that needs to be tackled in practice.
7.3.2. Under the open skies
Throughout the world, men cruise in public spaces, most frequently in parks, on the streets and beaches known among the local population to serve for such activities. Major share of men that one can come across in such public spaces are poor, with low education or illiterate, socially excluded and/or unsure about their sexual identity. In a number of societ-ies, men cruise in such venues because they cannot meet other men anywhere else; however, even in areas where there are alternatives, such as bars and saunas, meeting points under open skies are popular nevertheless. Sex can take place in these public spaces, especially if there are areas providing a certain degree of privacy, or it can take place somewhere else. A number of sexual encounters are anonymous, with few exchanged words, if any.
Interventions in public spaces usually include trained workers who regularly visit the locations and speak to men whom they meet there. They provide leaflets if possible, explain safer sex techniques, propagate STD testing and treatment,
92
Chapter 7 Prevention tips- manual on prevention activities
as well as voluntary counselling and testing, and they distribute condoms and lubricants. Outreach requires skills such as how to access the strangers and avoid attacks of those who target meeting points of men. The police can also have a hostile attitude, which is why the safety of outreach workers must be carefully taken into consideration. Given the fact that men who have sex with men are frequently facing problems much more difficult than HIV, such as hunger, family problems and violence, the information provided orally or in the leaflets frequently needs to extend beyond HIV/STD. For example, the Blue Diamond Society in Kathmandu, Nepal, supports togetherness among men who use public parks, in order to protect each other from blackmailers, theft, and the police.
The best outreach workers are usually men who cruise public spaces themselves, and who fully understand the concerns of the men they meet. In order to avoid confusion between their private lives and their work, ethical standards need to be developed as part of their training program. That may include working in pairs, partly because of safety, and partly to decrease the possibility of workers becoming confused by sexual offers.
Once their trust is won, men in public spaces, generally speaking, react well to the care shown for their benefit. Some men may show interest for other activities, such as the development of information and communication materials, and some may offer their services for training purposes, where propensity for such kind of activity is important.
7.3.3. On a secret mission
Outreach activities can also be implemented in commercial meeting points, such as bars, night clubs, saunas and cin-emas. Possible activities include conversations with customers, placing posters, distributing leaflets and condoms, and cultural or cabaret-style performances.
One-on-one conversations on HIV and other topics can be held without the permission of the owner or manager; how-ever, activities are much more efficient with the support of that person. In the beginning, achieving the goal may prove to be difficult, even when the owner himself is a man who has sex with men. The owners may not necessarily display readiness to confirm that their venue is a meeting place for men who have sex with men, or they may believe that HIV- and STD-related promotional activities are bad for business.
One argument for persuading the owners to change their minds can be the fact that HIV itself is bad for business, be-cause it decreases the number of potential customers. Also, the material and presentations that are nicely designed, or even erotically if appropriate, are more likely to attract customers. When one owner allows outreach to take place in his venue, it is usually easier to persuade others to follow suit. Their interest may be purely commercial – permanent clien-tele is good for business – or it may be personal, given the fact that an owner himself may be a man who has sex with men. Whatever their motivation, these individuals are crucial as gatekeepers, in the process of assisting the development of successful prevention programs. Interventions must be continuous in order to be effective: condoms and leaflets should always be accessible; cabaret performances may be held once per month, and on the occasion of the World AIDS Day each year.
7.3.4. Materials
Men who have sex with men should be included in the designing of posters, leaflets, video materials, theatre shows, and all the other types of material. This process includes all the phases: development, pre-testing and distribution.
The development stage may be the continuation of participatory evaluation. In this process, the target group is con-firmed; the most adequate means of presenting information (written or figurative) is determined; the most adequate language and information is also selected. Pre-testing is the presentation of finished material to a representative group of men who are not included into the development process. Their reaction is important, given the fact that they may identify the strengths and the weaknesses that were not apparent to the development team. Only when the material is successfully pre-tested can it be distributed to the target audience.

93
Chapter 7Prevention tips- manual on prevention activities
7.3.5. Groups
One-on-one interventions provide basic information and enable men to focus on issues that are particularly problem-atic for them; group discussions and workshops promote wider discussion, and help create the sense of unity. The more people there are, providing as many opinions as possible, the more potential answers there are, and these answers can then be recommended for problems which impact upon either the individuals, or the group. Groups can also provide psychological support that many individuals need in order to practice safer sex and develop self-esteem.
Meetings should be held in places where the participants feel at ease, but also in locations where they cannot easily be disturbed. Anonymity is important in this process, and notifications on the meeting should not refer to sex among men. Various formats should be used, ranging from regular weekly meetings without the obligation to participate, to day-long or weekend workshops where the participants have the obligation to be present the entire time. Group discussions typically do not last longer than one or two hours. They can be relatively informal and non-structured, although they are more efficient with a facilitator who can guide the discussion without forcing it, ensuring that all participants have the possibility to express their opinion, and to have a feeling of participating in the process and the freedom to express their ideas.
Discussions should cover not only sexual behaviour and safer sex, but also other issues that are troubling men who have sex with men. It is important to allow the participants to voice negative experiences, including the issue of unprotected sex, without the disapproval of others; such experiences are customary, and discussion about them is part of the process of adopting safer sex.
7.3.6. Workshops
Workshops tend to be longer than group discussions; they require extensive preparation, and – preferably – two trained facilitators. Basic issues that can be covered by the workshops include:
• HIV/AIDS;
• STD diagnostics and treatment, including oral and anal STDs;
• Use of condoms and lubricants;
• Changing risky behaviour;
• Sexual identity and gender;
• Social / cultural / religious issues;
• Marriage and family;
• Wives and other female partners;
• Legal issues and issues pertaining to human rights;
• Discrimination and stigmatisation;
• Sex work;
• Development of the community and mobilization;
• Economic topics and poverty.

94
Chapter 7 Prevention tips- manual on prevention activities
As the organization is growing, and members develop their skills, other topics that may be covered include the following:
• Needs of the community;
• Participation in the health promotion program;
• Sexual health products and services;
• Educational and information strategies;
• Support for people living with HIV/AIDS;
• Advocacy.
Techniques used in workshops include: games, role play, case studies, working in small groups, and discussions. Lectures are not recommendable, unless they are brief and used as an introduction to discussion, rather than at the very end.
7.3.7. Strategies for gradual increase, targeting and improvement of delivery of services and products
Advising men to use condoms is one step towards HIV prevention; to make these condoms available is the second step. Other steps include organizing STD treatment and enabling voluntary HIV counselling and testing. In other words, wherever possible, individual interventions must be supported by the provision of clinical services and products – con-doms and lubricants.
7.3.8. Condoms
Consistent and appropriate use of condoms is the only tool for decreasing the risk of HIV transmission in anal and vaginal intercourse, but the availability of condoms is limited. A number of factors can prevent men from buying condoms, includ-ing the price, the fact that the number of locations where they are sold is limited, and shame associated with the purchase.
Therefore, the key element in the work of NGOs is to make condoms available. Male condoms are usually obtained at donor organizations, at low prices or free of charge. They can be distributed by outreach workers, or they can be provided at commercial meeting points for customers to take them – although, if latter is the case, a mechanism must be established to prevent individuals from taking large quantities and then selling them to others. Although condoms may seem simple, condom use is a skill that needs to be developed, partly through workshops, and partly through use. Furthermore, several factors must be taken into consideration in order to make condoms acceptable for men who have sex with men. These factors include:
Wrapping/motives: wherever possible, wrapping should be culturally acceptable, and the assumption that a condom can only be used for sex with a woman should be avoided.
Instructions for use: printed instructions should be written in adequate, simple language, combined with culturally ac-ceptable explicit images for illiterate persons.
Size: condom size is a problem for some men; condoms are produced in three sizes, but NGOs usually have only one size available.
Female condoms: as the alternative to male condoms, female condoms can be used for anal intercourse; the internal ring is usually extracted, and the condom placed on the penis prior to penetration. Advantages include the fact that it is more comfortable for men with a big penis, and that full erection is not needed prior to use; downsides include the appearance and the high price of female condoms.
One-on-one outreach, group discussions and workshops may assist men become better acquainted with condoms.
95
Chapter 7Prevention tips- manual on prevention activities
7.3.9. Lubricants
Given the fact the anus is not producing moisture, an alternative solution is needed in order for intercourse to be pleas-ant. Men usually use saliva, even though such an approach tends to be insufficient, and the saliva dries quickly; alterna-tively, seminal fluid (“pre-cum”) is used, which is dangerous, as it may contain HIV. Cooking oil or body cream are also used, but they should not be used with condoms because of the fact that they destroy latex. Only water-based lubricants may be used with condoms.
Few men have access to water-based lubricants. They are usually sold only in pharmacies, at a price that is above reach for most men who need them. While NGOs distribute free-of charge lubricants for one-time use that they receive from the donors, many others do not have such sources. Finding a regular supply of free or cheap lubricants is a problem that many NGOs in developing countries have not managed to resolve.
Providing conditions for the diagnostics and treatment of STDs, and for HIV testing and counselling, constitutes a fundamental element of all HIV prevention efforts. However, even where such possibilities are available, many men, regardless of whether they have sex with men or women, do not use them. That can happen because of several reasons, including the lack of awareness of individuals that they might become infected; the inability to pay for counselling or treatment; believing that “real men” cannot get sick; and in some cases, because of fear of being identified as a man who has sex with men.
Encouraging men to look for treatment for STDs and to undergo HIV testing has an important impact on the epidemics. The wish to be tested reflects the recognition of risk, and men who display that wish also adopt and practice safer sex techniques, independently of the results of the testing process, practicing them much more consistently that men who do not subject themselves to testing. Opportunities of this kind must always be available on a voluntary basis, and an NGO should at no point in time allow for any form of mandatory or obligatory testing and counselling.
Diagnostics and treatment of STDs requires medical staff educated to recognize the symptoms, and access to a well-equipped laboratory is sometimes needed as well. When men who have sex with men are clients, even when they do not self-identify as such, the doctors and other medical staff must be educated to be able to recognize and treat infections in the mouth and anus. It is also helpful when MSM learn to recognize and properly describe their symptoms.
HIV testing requires access to laboratory, and auxiliary medical staff trained in the taking of blood samples. Pre-testing and post-testing counselling should be included in the testing process, which also requires trained staff. There are HIV tests for saliva that can be self-administered, but they are not widely available and are not recommended, given the fact that they do not provide for the possibility of counselling.
7.3.10. Counselling
Pre-test and post-test counselling with a compassionate counsellor familiar with MSM not only assists in the transfer of information on HIV/STD and safer sex, but it also creates an opportunity for clients to learn about NGOs and other organizations working with MSM. When a client’s test is HIV-positive, that person can also be provided with details on organizations for persons living with HIV. Various forms of counselling may be needed, depending on cultural issues and the needs of clients.
Problems that typically occur in counselling include internalised homophobia (men may lack readiness to admit that they are attracted by men, and may therefore lack the readiness to undertake preventive measures); poverty (including the inability to practice safer sex, because the paying partner refuses to do so); and manhood (attitude that “real men do not get sick” discourages the use of condoms). One counselling session rarely results in a consistent change of behaviour, although two sessions – prior to and after the testing – have shown to decrease the rate of new STD infections in the USA. Regular counselling is ideal; where impossible, clients should be directed towards NGOs which provide group discussions and workshops.

96
Chapter 7 Prevention tips- manual on prevention activities
Many NGOs do not have the medical resources that would allow for STD diagnostics and treatment, although they may have the space available for HIV counselling and for the taking of blood samples. These organizations frequently collaborate with other service providers, in order to ensure adequate HIV and STD services for men who have sex with men. That includes the organization of counselling at the available time and place, for a low amount of money or free of charge, and such approaches are usually not publicly identified as being dedicated for men who have sex with men, or even as STD clinics.
7.3.11. Ethical issues and confidentiality
Medical staff and counsellors must be trained for work with men who have sex with men in a non-judgmental manner. Ideally, many doctors and counsellors will be MSM themselves, although the confidentiality for staff, as well as clients, must be respected. Initial training for counsellors that does not require prior experience may be short in terms of dura-tion, especially in communities where working with MSM is a novelty, but it should be continuous, in order to ensure that lessons learned in working with clients are shared with other counsellors, and that counselling skills are continu-ously developed.
Confidentiality should always be preserved in HIV/STD services. That includes the issue of health, in particular when an individual has become HIV- or STD-infected, as well as behaviour and sexual/gender identity – taking into account the right of the individual not to reveal his sexual behaviour and identity to others. Confidentiality in regard to HIV should be respected regardless of the result, in particular when the readiness of one client to announce his status is directly con-nected with the assumption that the status of the other person is HIV-positive.
Every person with a diagnosed HIV faces a number of concerns, which may include the current health condition, the issue of how to inform the partners, and stigmatisation connected to HIV/AIDS and its consequences, such as the loss of one’s job or home. A man who has sex with men, and finds out that he is HIV-positive, frequently faces additional difficulties, including the possibility of his sexual activity being discovered, and the problem with preserving the rela-tionship. Counselling may help men to identify some of these problems, but long-term assistance is more desirable, in particular by groups of MSM who also live with HIV.
7.3.12. Other services
NGOs can enable a number of services for MSM, in addition to condoms and HIV/STD services. That includes work-shops and group discussions, as mentioned above, and educational possibilities as well, such as literacy programs and legal advice. That is usually provided within the framework of a safe house, as we shall describe in the following chapter.

97
Chapter 7Prevention tips- manual on prevention activities
7.4 Strategies for mobilizing the community
While some MSM have strong social networks, many are either physically or socially isolated from their peers. The existence of a NGO, even if involving only a couple of members, helps build and mobilize the community as a whole. That community in formation can help strengthen the sense of identity and unity among individual men, strengthening their decision to practice safer sex.
The community can only grow out of the needs and desires of men themselves, and cannot be imposed from the out-side. It may be impossible to achieve one single community in one geographical area: experience from several countries shows that middle-class men are more likely to feel as being part of the community with a Western gay identity, while men with lower salaries, those who are less educated, are more likely to promote local identities. Some groups, in par-ticular those focused on human rights, can include women who have sex with women, while other groups prefer work-ing only with men.
As we have already mentioned, NGOs usually have a large number of volunteers, and it is likely that, at least in the be-ginning, they require assistance in capacity building. Organizations that function well are able to identify key problems, such as the procurement of condoms, hostile police actions, or repressive policy, and they develop strategies in order to respond to these challenges. They also develop their assets in order to preserve the projects, and in order to decrease the need for external support.
7.4.1. Celebration time
In addition to the basic year-long work through outreach and counselling, the wider community (or communities) of men who have sex with men can be mobilized around specific national and international events or celebrations, such as the World AIDS Day (December 1) and Gay Pride. That can play a dual role: introducing Pride into the community on the one hand, together with awareness raising among the general population on the existence and needs of MSM on the other. A number of various events may take place, including public marches and demonstrations; art and photo exhibi-tions; cinema, theatre and dance shows. Some of the key events, in particular the World AIDS Day, can include other communities hurt by the infection, such as sexual workers and persons infected with HIV.
While the World AIDS Day is focused specifically on HIV, Gay Pride is a much more fluid concept. It can be connected with an international event (such as the commemoration connected with riots in the gay Stonewall Bar in New York in June 1969), or with a national celebration. In the Netherlands, for example, the Queen’s birthday towards the end of April is also the national Gay Pride day. The word “gay” itself can be perceived as inappropriate, or it can be included into a wider concept: LGBTQ – lesbian, gay, bisexual, transgender and questioning – which is used by some groups.
Stronger visibility both for individuals and the community as a whole can have negative consequences, such as increased police repression, violence and homophobia by political and religious leaders. The general impact of public celebrations, however, is almost always positive. Men who participate in the planning and implementation achieve a strong sense of togetherness and self-respect, while those following the events feel a decreased sense of isolation. The society at large also begins to think over its perceptions and opinions on the group that they previously knew little about.
7.4.2. Safe house
In a number of societies, men who have sex with men, in particular those with low salaries and those living with their families, have few opportunities to relax and get to know their peers in an environment in which they are not forced to hide their sexuality. A number of NGOs therefore perceive safe houses as a priority, especially where commercial meet-ing points do not exist, or where men cannot afford visiting such meeting points.
98
Chapter 7 Prevention tips- manual on prevention activities
A safe house can range from one room rented on a weekly basis by an NGO, to a building owned by an NGO. The more available it is for the community, the bigger role it will play in its development. Depending on the size and availability, it can act as an office, an informal meeting place, or a place for holding a number of various activities. These activities can range from discussion groups, workshops and the planning process for WAD, to acting rehearsals, literacy classes and movie nights. If the venue permits, a safe house can also accommodate the counselling and testing service, as well as a library.
Safe house poses a continuous obligation, because it creates important order and bureaucracy. The structures must be designed in such a way to enable the volunteers to participate in the management of the house, and to become educated in computer skills, defence and accounting.
The location of the safe house must be carefully selected. Even when the exact location is anonymous, the neighbours might probably become curious as to who is coming there. Instead of an area with housing units, perhaps it might be better to place the safe house in a commercial zone and near a park, or some other cruising zone.
7.4.3. On-line
Although it still has its limitations as far as the rural areas are concerned, the Internet has become a virtual community for many men using the web for social and sexual contact with other men. The available content includes international websites, such as www.gayromeo.com, and in the area of Croatia there is a website with a national focus which can be accessed at www.gay.hr.
While the Internet provides an increase of possibilities for men to explore their sexual identity, some activists argue that it allows men to have more sex with other men, but without building a sense of community needed to break down the homophobia. However, websites and chat-rooms provide important opportunities for HIV prevention. In Singapore, par-ticipants who are recognized as resource persons for HIV frequently respond to private inquiries about safer sex and AIDS.
7.4.4. In prison
Sex among men is a particular aspect of life in prisons around the world. When it happens, it can take place because of sexual relaxation, as an expression of loyalty, or as an act of violence, when one or more men impose their will to another man. Many, if not most men who have sex with men in prison would not engage in such practices in other cir-cumstances. Condoms are regularly accessible, and drug injecting may be customary. HIV infection rates are regularly higher in prison than in the general population.
HIV prevention projects for prisons focused on sex and drug injecting are necessary, but face a number of shortcom-ings. It is possible that the authorities do not wish to acknowledge the extent of the problem, nor allow an external person to become part of the prison management. Prisoners are usually suspicious towards educational efforts. Despite that, projects for prisoners have been initiated in a number of countries, ranging from Costa Rica to Zambia, usually by ex-prisoners. While some of these projects are focused on HIV prevention, others respond to a wide range of prisoner needs, such as literacy classes, self-respect workshops and the issue of drug taking.
Determined by quite diverse environment and circumstances, the community in prisons is quite different from the com-munity of men who have sex with men elsewhere. Despite that, the sense of community does exist, and constitutes the foundation upon which the community can be built.
Strategies for advocacy, political changes and informing the community
Attitudes and activities of men who have sex with men are strongly influenced by the wider community in which these men live. Social environment which stigmatises sex among men regularly leads to poor self-esteem and/or fear of rec-ognition, both of which prevent safer sex. Advocacy interventions ensure that organizations of men who have sex with men are perceived as part of the solution for HIV/AIDS epidemics. Men whose social environment is supportive of the right to engage in safer sex with other men are more likely to protect themselves and their partners.
99
Chapter 7Prevention tips- manual on prevention activities
7.5.1. Various settings
People live in a range of overlapping social settings, including friends, family, colleagues at work, neighbourhood in which they live, legislation, culture and religious rules. Wider settings, including the legislation and religion, impact upon the narrower settings, such as the attitudes of family and neighbourhood. There are very few countries where most of these settings are supportive of the right of men to have sex with men. Much more frequently, there is a conflict between the desires of men, their activities and settings in which they live.
While community mobilization is mostly focused on men who have sex with men, the development of interventions in the surrounding environment is focused on the wider community. Direct goal of these interventions is recognizing the right of men who have sex with men to access adequate information, skills, services and products that can enable them to protect themselves and their partners. Long-term goal may be focused on full legal and social equality.
Advocacy activities depend on the social and political situation at the local level, and on the local needs of men who have sex with men. At the national level, activities may include research on political trends, lobbying and discussions leading towards legislative reforms. At the local level, possible interventions in the environment may include:
• Lobbying in order to enable information and services, combating violence against men who have sex with men;
• Basic information and education for the general population, aimed at combating stigmatisation;
• Promoting the participation of men who have sex with men in policy-making bodies, such as advisory groups on health care and HIV/AIDS committees;
• Educational initiatives with the police, religious leaders and others who shape the rules of the community;
• Providing information to the general population, which allows men and their female partners confronted with the risk to find the relevant information and services.
Advocacy interventions may face considerable difficulties in overcoming intense stigmatisation which is frequently linked with men who have sex with men. The initial goals may therefore be limited, but medium- and long-term goals ought to decrease the stigmatisation and discrimination against men who have sex with men, while increasing the en-gagement of the wider community in the fight against the epidemics within this group of men.
7.5.2. Visibility and representation
The first fundamental goal in advocacy is to raise awareness of the problem. Ideally, that would require one or more men willing to publicly acknowledge that they have sex with men, with the ability to discuss the appropriate interven-tions. Although the number of men who come out is rising in more and more countries, some societies still harbour an extremely hostile attitude; in such societies, it may be safer and much more appropriate to discuss these matters in the name of the community, rather than as a member of the community. Also, wherever possible, men should not speak on their own behalf, but rather as NGO representatives.
Representing the institutions with a direct or indirect impact upon the lives of men who have sex with men is crucial. There are many such organizations, ranging from the HIV/AIDS national committees, to management boards of health clinics; from human rights organizations to city authorities. Some organizations consist of elected representatives, some have appointed members, and some are self-declared. The NGOs should determine which organizations are most in-fluential, and also which ones are most likely to accept the representatives of men who have sex with men; that is an important issue even prior to the planning process dedicated to achieving successes in advocacy as quickly as possible.
When it comes to serving as a member of such a body, advocacy is likely to be more effective when a representative has an active role in the decision making process regarding the decisions that also have an impact on other groups. For
100
Chapter 7 Prevention tips- manual on prevention activities
example, one can try to achieve a situation where a local clinic ensures adequate protection for men who have sex with men, but also ensures adequate counselling for women victims of rape, emphasizing the fact that men who have sex with men are part of the wider community, deserving the same respect that the community provides to others.
Furthermore, it is important that a representative indeed comes from the group he is representing, or that he has re-ceived support from that group. In cases when education and professional skills are at a low level, a representative of men who have sex with men may need a certain level of support and training.
7.5.3. Link with the police
Wherever possible, the NGOs should work with the police in order to create an environment where it is possible to implement HIV education with minimal risk and maximum effect. That may be difficult to achieve, especially if invita-tions for meetings with the police are ignored. The success frequently depends on the goodwill of one or two key police officers to hear out NGO representatives. Alternative approach may be possible through local or national politicians, through other NGOs, or through NGOs that already have well-established liaisons.
The content of the discussions and activities depends on the local situation. The emphasis may be on health, rather than on human rights, and it can include unofficial discussions, official discussions regarding the membership in the liaison committee of the police, and sessions aimed at awareness raising, held with the high-ranking police officials. Compro-mises may be important, given the fact that the police will most frequently not be willing to give up on its authority, or to forgive a criminal offence.
7.5.4. Social advocacy
The stronger they become, NGOs usually want to work, either alone or with others, on national advocacy. In that re-spect, it is possible to have two mutually linked goals: raising public awareness and accepting men who have sex with men (social advocacy) on the one hand; legal protection of the rights of men who have sex with men (political advocacy) on the other. In some countries, these may be long-term goals. Potential partners include NGOs representing men who have sex with men from other regions of a country; human rights groups; health organizations; ethnic minorities; drug users; sexual workers; other marginalized groups.
Public opinion is most frequently influenced by the media, while changes in the legislation depend on intensive lobbying of politicians and other decision makers. Changes in religious views may also be the result of lobbying of religious leaders.
Messages should always be adjusted to the capacity of understanding among the audience. It is certainly a reality that stigmatisation and repression of men who have sex with men places both them and their female partners under the same risk; however, local circumstances will dictate whether it is best to address the audience through the issue of health, and the importance of protecting those who are facing the risk; through the issue of human rights; or through the combination of these two. Invoking the history of a country, if there was a period when sex among men used to be accepted, is also an option that can be utilized. Finally, however, the public must become aware that the repression and stigmatisation of men who have sex with men is preventing educational activities, subjecting both men and their female partners to risk.
Access to the media can be used in several ways, including press releases, articles ready for publication, contacts with journalists creating sympathetic programs or articles, interviews and appearances in talk shows and in broadcasts in-volving the input from the audience. A number of topics can be subject to a press release or a statement, such as NGO initiatives, or reactions to events or statements of others: for example, condemning someone’s statement which stigma-tised sex among men. Another topic may be the appearance of a policy promoting HIV-related information for men who are facing the risk. Other approaches focused on the public may include the use of posters, leaflets and brochures, as well as the participation in public discussions and events; for example, during the elections, theatre performances, etc.

101
Chapter 7Prevention tips- manual on prevention activities
NGOs should be aware of the fact that there is frequently a strong reaction to awareness raising on sex among men, including negative media coverage and violence against men noticed to have sex with other men; however, long-term success is more important that short-term difficulties.
7.5.5. Political advocacy
Efforts aimed at changing the public opinion constitute an important groundwork for political advocacy, the goal of which is legislative change. Long-term goals of political advocacy may include the revision of existing laws and drafting of legislative proposals. That may include legalization of sex among men on the same foundation as sex among men and women, or anti-discrimination laws. Goals of a more short-term nature, which are also easier to implement, may include statements of the minister of health, the national AIDS committee, or leading donor agencies that recognize the right of men who have sex with men to receive adequate information and services.
Political advocacy, to be exact, requires specific skills, but these skills can be adopted either through internal training, or through training outside of the organization.
7.6.6. Religion
Religious leaders are frequently the most vocal critics of sex among men, and negative attitudes of the community and political leaders are frequently based on religion. The dialogue with religious leaders is therefore important. Further-more, some religious leaders have sex with men, and their fear of being discovered makes them hostile towards any discussion on sex among men. On the other hand, many religious leaders admit that sex among men is a reality and that men need to be supported and enabled to protect themselves and their partners. Such leaders can provide assistance, although that may take place in private rather than in public.

102
Chapter 7 Prevention tips- manual on prevention activities

Acronyms
AIDS- Acquired immunodeficiency syndrome
BCC- Behaviour Change Communication
BIH- Bosnia and Herzegovina
COSF- Country Office Support Facility
EC- European Commission
ECHR- European Convention on the Protection of Human Rights and Fundamental Freedoms
GFATM- Global Fund to fight AIDS, tuberculosis and malaria
GLSEN- Gay Lesbian and Straight Education Network
HIV- Human immunodeficiency virus
HRC- Human Rights Committee
ICCPR- International Covenant on Civil and Political Rights
ICCPR- OP1- First Optional Protocol to International Covenant on Civil and Political Rights
ICD- International Statistical Classification of Diseases and Related Health Problems
IDU- injecting drug users
IEC- Information, Education and Communication
ILGA- International Lesbian and Gay Association
LGBT- lesbian/gay/bisexual/transgender
LGBTIQ- lesbian/gay/bisexual/transgender/intersexed/queer
MDG- Millennium Development Goal
MSM- men having sex with men
NGO- nongovernmental organisation
ODIHR- Office for Democratic Institutions and Human Rights, OSCE
OSCE- Organization for Security and Co-operation in Europe
PLHIV- people living with HIV
PRSP- Poverty Reduction Strategy Paper
STD- Sexually transmitted disease
UN- United Nations
UNAIDS- United Nations Joint Programme on HIV/AIDS
UNDP- United Nations Development Programme
UNGASS- United Nations General Assembly Special Session
UNICEF- United Nations Children’s Fund
USA- United States of America
VCT- Voluntary counselling and testing
WHO- World Health Organisation
Acronyms