Reflections on a virtual experiment addressing human behavior during epidemics
8
Keywords: participatory simulation, virtual experiments, behav- ioral economics, health psychology, epidemics Abstract We report on preliminary results from a pilot study using a vir- tual experiment to analyse human behavior during epidemics of an infectious disease. The experiment used a two-dimensional com- puter game representing an epidemic scenario, linked to an agent- based simulation of an epidemic spreading through a large popula- tion. 230 participants played the game and completed question- naires about their characteristics in relation to a psychological model of health behaviour, Protection Motivation Theory. The results show that participants responded to increasing infection load in their local neighbourhood by reducing their social contacts, as they would be expected to do in reality. However, there was no correlation between the strength of this response and a number of psychological factors that are known to be associated with health protective behavior in the real world. This suggests that partici- pants might not have responded to the game in the same way they would respond to a real epidemic. We discuss possible explana- tions for this mismatch, drawing on ideas from experimental be- havioral economics, psychology, computer game design, and the study of virtual worlds, and suggest ways in which our experimen- tal methodology could be improved to produce a more realistic response. 1. INTRODUCTION When faced with an epidemic of infectious disease people often respond by changing their behavior to protect them- selves, for example, by reducing their social contacts (social distancing). In previous work using agent-based simulation [21], we found that social distancing can be a highly effec- tive method for controlling and even stopping an epidemic if applied appropriately. However, if done incorrectly, social distancing can backfire, prolonging, rather than stopping the epidemic and causing worse economic impact than if people continued to behave as usual. A key parameter in this study was risk attitude, a measure of how strongly individuals respond to a given level of infection. This study prompted curiosity about how people respond during epidemics in the real world: do they display the ideal risk attitude as indi- cated by our simulations, or do they behave in a way that is less optimal? It is difficult to answer this question by looking at real world data: very little actual data exists because it is diffi- cult to collect, and what data there is, e.g., [3], [24], [25], does not provide sufficient detail about individuals’ daily social contacts to allow close comparison with our model. For obvious reasons, it is not possible to gather data by starting epidemics in the real world. We therefore turned to virtual experiments, using a simulated epidemic scenario in which the experimental subject interacts with other simu- lated members of a population through which an epidemic is spreading. The experiment is presented as a computer game (the Epidemic Game). An early version of this game was presented at SCSC 2011 [22]. There is obvious motivation for using virtual experiments for scenarios such as epidemics which cannot be reproduced in the real world. However, it is not at all clear whether such experiments are scientifically credible. Is it valid to use data about people’s responses to an artificial, simulated scenario to draw conclusions about responses in the real world? To address this question, in summer 2012 we carried out a pilot study using the Epidemic Game. The game was played by 230 participants at a public science centre and a university campus in central Scotland. Participants’ risk attitudes were calculated from their responses to the game and recorded automatically as they played. Participants also answered questions about their demographic characteristics, personal- ity, experiences, beliefs, and attitudes to disease and infec- tion. The questions were designed to gather data relating to factors used within a psychological theory of health protec- tive behavior, the Protection Motivation Theory [23]. The data from the pilot study has not yet been subjected to detailed statistical analysis. However, from preliminary analysis, two conclusions seem clear. First, the data shows that people playing the game did indeed respond to higher infection loads in the simulated epidemic by reducing their social contacts. This is a positive result, showing that people did not make random or perverse choices when playing the game, but responded as expected. However, the second ob- servation is quite surprising: there is no correlation between the risk attitudes people displayed when playing the game and their health-related beliefs according to Protection Mo- tivation Theory. Psychologists have found that these factors are predictors of how people respond to health threats in the Reflections on a Virtual Experiment Addressing Human Behavior During Epidemics Liam Delaney 1 , Adam Kleczkowski 2 , Savi Maharaj 2* , Susan Rasmussen 3 , Lynn Williams 4 1 Economics, University of Stirling, Stirling, Scotland 2 Computing Science and Mathematics, University of Stirling, Stirling, Scotland, *[email protected] 3 Psychology, University of Strathclyde, Glasgow, Scotland 4 School of Social Science, University of the West of Scotland, Paisley, Scotland
Transcript of Reflections on a virtual experiment addressing human behavior during epidemics

Keywords: participatory simulation, virtual experiments, behav-
ioral economics, health psychology, epidemics Abstract
We report on preliminary results from a pilot study using a vir-
tual experiment to analyse human behavior during epidemics of an
infectious disease. The experiment used a two-dimensional com-
puter game representing an epidemic scenario, linked to an agent-
based simulation of an epidemic spreading through a large popula-
tion. 230 participants played the game and completed question-
naires about their characteristics in relation to a psychological
model of health behaviour, Protection Motivation Theory. The
results show that participants responded to increasing infection
load in their local neighbourhood by reducing their social contacts,
as they would be expected to do in reality. However, there was no
correlation between the strength of this response and a number of
psychological factors that are known to be associated with health
protective behavior in the real world. This suggests that partici-
pants might not have responded to the game in the same way they
would respond to a real epidemic. We discuss possible explana-
tions for this mismatch, drawing on ideas from experimental be-
havioral economics, psychology, computer game design, and the
study of virtual worlds, and suggest ways in which our experimen-
tal methodology could be improved to produce a more realistic
response.
1. INTRODUCTION
When faced with an epidemic of infectious disease people often respond by changing their behavior to protect them-selves, for example, by reducing their social contacts (social distancing). In previous work using agent-based simulation [21], we found that social distancing can be a highly effec-tive method for controlling and even stopping an epidemic if applied appropriately. However, if done incorrectly, social distancing can backfire, prolonging, rather than stopping the epidemic and causing worse economic impact than if people continued to behave as usual. A key parameter in this study was risk attitude, a measure of how strongly individuals respond to a given level of infection. This study prompted curiosity about how people respond during epidemics in the real world: do they display the ideal risk attitude as indi-cated by our simulations, or do they behave in a way that is less optimal?
It is difficult to answer this question by looking at real world data: very little actual data exists because it is diffi-cult to collect, and what data there is, e.g., [3], [24], [25], does not provide sufficient detail about individuals’ daily social contacts to allow close comparison with our model. For obvious reasons, it is not possible to gather data by starting epidemics in the real world. We therefore turned to virtual experiments, using a simulated epidemic scenario in which the experimental subject interacts with other simu-lated members of a population through which an epidemic is spreading. The experiment is presented as a computer game (the Epidemic Game). An early version of this game was presented at SCSC 2011 [22].
There is obvious motivation for using virtual experiments for scenarios such as epidemics which cannot be reproduced in the real world. However, it is not at all clear whether such experiments are scientifically credible. Is it valid to use data about people’s responses to an artificial, simulated scenario to draw conclusions about responses in the real world? To address this question, in summer 2012 we carried out a pilot study using the Epidemic Game. The game was played by 230 participants at a public science centre and a university campus in central Scotland. Participants’ risk attitudes were calculated from their responses to the game and recorded automatically as they played. Participants also answered questions about their demographic characteristics, personal-ity, experiences, beliefs, and attitudes to disease and infec-tion. The questions were designed to gather data relating to factors used within a psychological theory of health protec-tive behavior, the Protection Motivation Theory [23].
The data from the pilot study has not yet been subjected to detailed statistical analysis. However, from preliminary analysis, two conclusions seem clear. First, the data shows that people playing the game did indeed respond to higher infection loads in the simulated epidemic by reducing their social contacts. This is a positive result, showing that people did not make random or perverse choices when playing the game, but responded as expected. However, the second ob-servation is quite surprising: there is no correlation between the risk attitudes people displayed when playing the game and their health-related beliefs according to Protection Mo-tivation Theory. Psychologists have found that these factors are predictors of how people respond to health threats in the
Reflections on a Virtual Experiment Addressing Human Behavior During Epidemics
Liam Delaney1, Adam Kleczkowski
2, Savi Maharaj
2*, Susan Rasmussen
3, Lynn Williams
4
1Economics, University of Stirling, Stirling, Scotland 2Computing Science and Mathematics, University of Stirling, Stirling, Scotland, *[email protected]
3Psychology, University of Strathclyde, Glasgow, Scotland 4School of Social Science, University of the West of Scotland, Paisley, Scotland

real world. The fact that these are uncorrelated to responses to the threats faced in the Epidemic game suggests that be-havior in this game might not match behavior in the real world.
Why is there this apparent mismatch, and what can be done to address it and make the Epidemic Game into a credible tool for studying health behavior? We look first for an answer in the field of behavioral economics, where it is common practice to use games (computerized or otherwise) as experimental tools. Results here suggest that the problem might be that the Epidemic Game was too formally struc-tured to elicit natural responses, or that the incentives and rewards built into the game somehow misled the partici-pants. Alternatively, perhaps the answer lies in the study of immersive, three-dimensional virtual worlds, some of which have been used in famous successful re-creations of classic experiments in psychology. Results here suggest that the Epidemic Game may need to be made more detailed and immersive to convince participants to respond in a realistic manner. Other possible explanations may lie in the timing of the experiments, or in the design of the game play and the information and cues given to players.
Sections 2-4 describe the theoretical concepts underlying the Epidemic game experiments, namely, Protection Moti-vation Theory, agent-based simulation of epidemics, and participatory simulation. Section 3 shows the design of the Epidemic game. Section 4 describes the experiments and summarizes the results. In Section 5 we consider ideas from behavioural economics, psychology, virtual worlds, and computer game design, and draw some lessons from these on how the Epidemic Game could be improved. Section 6 concludes with a discussion of the way forward.
2. PROTECTION MOTIVATION THEORY
Protection Motivation Theory (PMT) [23] is a psycho-
logical framework for understanding what motivates people
to change their behavior in order to protect their health. Ac-
cording to PMT, people’s motivation to protect themselves
from health threats is determined by four main factors: per-
ceived severity of the threat, perceived vulnerability to the
threat, perceived efficacy of the recommended protective
behavior (response-efficacy), and belief in one’s ability to
carry out this behavior (self-efficacy).
Support for various aspects of PMT as predictors of be-
havior during epidemics comes from studies assessing how
people responded to recent outbreaks of SARS, Avian Flu
and Swine Flu [4], [9], [10], [16], [17], [18], [19], [20], [24],
[25], [27]. For example, studies on responses to SARS and
to Avian Flu in Hong Kong indicate that higher perceived
vulnerability, and higher perceived severity of the disease
were associated with adopting recommended behaviors such
as washing hands, mask wearing, being vaccinated and so-
cial distancing. Studies also report associations between
perceived efficacy of protective behavior, and self-efficacy
in performing it, with the actual performance of the precau-
tionary behaviors.
Participants in our study were asked to state the extent to
which they agreed or disagreed with several statements de-
signed to measure their characteristics according to PMT.
Table 1 shows examples of these statements.
Perceived severity of illness:
• If I were to develop an infectious disease (e.g. flu) I
would suffer a lot of unpleasant symptoms.
• Developing an infectious disease would be unlikely to
cause me to die prematurely.
Perceived vulnerability:
• My chances of developing an infectious disease (e.g. flu)
in the future are likely.
• I am unlikely to develop an infectious disease (e.g. flu) in
the future.
Response efficacy:
• If I were to engage in social distancing (e.g. by avoiding
public transport and social events) I would lessen my
chance of developing an infectious disease.
Self efficacy:
• I am discouraged from engaging in social distancing dur-
ing times of infectious disease, because I feel it would be
difficult to do so.
• I feel confident in my ability to engage in social distanc-
ing during times of infectious disease.
Table 1: Example statements for measuring PMT beliefs.
3. SIMULATION MODEL
The Epidemic game uses an underlying agent-based
simulation of an epidemic spreading on a spatial network,
described more fully in [13] and [22]. The disease model is
based on the classic Susceptible-Infected-Recovered (SIR)
model [1] of the spread of infectious diseases. The spatial
network is a two-dimensional square lattice of 50x50 cells,
each of which is occupied by an individual. Initially, a few
individuals are infected and the remainder are susceptible,
meaning that they may become infected by contact with an
infected individual. Infected individuals eventually recover,
after which they are immune from further infection. These
transitions are governed by two parameters, p, the probabil-
ity that a single contact with an infected individual will
cause a susceptible to become infected, and q, the probabil-
ity at a given time-step that an infected individual will re-
cover.
Social distancing is modeled by making use of the spa-
tial structure of the network. Each individual has its own
contact radius, which is reduced or increased during the

course of the epidemic as the individual practices social
distancing. Contact takes place between individuals who are
within each other’s contact radius (as measured using
Euclidean distance).
An individual’s decision whether to practise social dis-
tancing is based upon the current infection load (ratio of
infected to non-infected individuals) within that individual’s
awareness radius. The awareness radius (also measured as
Euclidean distance) is the same for all individuals and re-
mains fixed through the duration of the simulation.
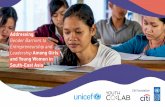
Figure 1 summarizes the processes that take place during
a single time-step of the simulation. Susceptible individuals
observe the infection load within their awareness radius and
modify their contact radius accordingly. They then make
contact with all their neighbours within their (new) contact
radius. This may result in the susceptible becoming infected
in the next time step. Currently infected individuals may
become recovered in the next time step.
Figure 1: Transitions of an individual in the model
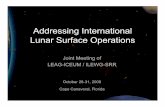
The extent to which a susceptible individual reduces its
contact radius in response to a given infection load is gov-
erned by another key parameter, the risk attitude, α. Figure
2 shows how α relates to the social distancing response for
different values of α. Lower values of α represent a more
cautious, or risk-averse response, i.e., there is a greater re-
duction in the contact radius in response to a given infection
load.
In earlier work [21] using this model to study social dis-
tancing we determined that for social distancing to be effec-
tive, α should either be very low (so that the epidemic is
quickly suppressed) or, if such a strong social distancing
response is not feasible, then α should be relatively high (so
that the epidemic runs its course, perhaps affecting most of
the population, but social contacts are maintained so there is
no economic cost from the loss of social contact). The worst
outcome occurs if α is between these extremes, resulting in
a lukewarm response which does not stop the epidemic but
prolongs its spread while causing significant economic cost
from the loss of social contacts. One of the purposes of the
Epidemic Game is to allow us to compare these results with
the values of α adopted when real people participate in the
simulation.
4. THE EPIDEMIC GAME
The design of the Epidemic Game is based on the idea of
participatory simulation [29], where users interact with an
agent-based simulation by controlling the behavior of one or
more agents. Underlying the game is a simulation of an epi-
demic spreading through a large population. The player con-
trols the actions of a single susceptible individual in this
population. A round in the game represents a single day in
the epidemic (or a time step in the underlying simulation).
On each day, the player is informed about the infection load
within his/her local neighbourhood (corresponding to the
awareness radius of the individual controlled by the player).
The player must then choose how many contacts to make
that day. The player’s choice is used to calculate his/her
effective risk attitude α for that day. The player’s chosen α
is then adopted as the global risk attitude to be used by all
the simulated susceptible individuals in modifying their
contact radius during the current time step. In other words,
if the player has been very cautious, then the simulated sus-
ceptibles will mirror this caution in their own response;
similarly, if the player behaves recklessly, the simulated
susceptibles will follow suit. The reason for introducing this
mirroring is to magnify the effect of the player’s choices so
that they can have a real influence on the course of the epi-
demic, making the game more engaging for the player.
Figure 2: Social distancing response to infection load for
different risk attitudes (α). Susceptible
Infected
Recovered
recover, probability q become infected after con-
tact with an infected person,
probability p
modify contact radius in
response to local infec-
tion load

The game is played via an interactive user interface writ-
ten in Java which communicates with a back-end agent-
based model created with NetLogo [30]. The player is
greeted with a welcome screen and then shown instructions
(Figure 3). The instructions state that the player must try to
achieve two goals: to earn money by making as many social
contacts as possible, and to remain uninfected. Because
making more social contacts raises the risk of infection,
these two goals create a tension which the player must re-
solve.
On each “day” in the game, the player is shown a repre-
sentation of the current infection load in his/her local
neighbourhood (Figure 4). Red figures represent infected
neighbours and green figures represent uninfected
neighbours (which may be either susceptible or recovered in
the underlying simulation model). The player uses the
mouse to modify his/her contact radius, represented as a
light blue circle on the screen, and then clicks a button to
proceed. The figures are animated and move too quickly for
the player to control which figures are within the circle
when the button is pressed. This means that the player can
control how many neighbours to contact, but cannot dis-
criminate between infected and uninfected neighbours.
There are a number of possible outcomes after the
choice is submitted (Figure 5). If the player remains unin-
fected and the epidemic is ongoing, then he/she is credited
with earnings corresponding to the number of contacts made
and play continues to the next day. If the player is infected,
the game ends, and the player is told how long he/she sur-
vived and how much was earned during the epidemic.
If the player is well and the epidemic is over (i.e., there are
If the player is well and the epidemic is over (i.e., there are
no infected individuals remaining in the total population)
the game ends, the player is congratulated on helping to stop
the epidemic, and the earnings during the epidemic are re-
ported. In addition, the player is credited with additional
earnings for contacts made “after” the epidemic; the purpose
of this is to prevent the player being unfairly penalized for
ending the epidemic early and thereby having fewer oppor-
tunities to make contacts during the epidemic.
Figure 3: Epidemic game instruction screen
Figure 4: A day in the game
Figure 5: Three responses to clicking the submit button:
game continues another day; game ends when player is in-
fected; game ends because epidemic is over.

5. PRELIMINARY EXPERIMENTAL RESULTS
In summer 2012 the Epidemic Game was played by 230
participants, who were recruited from two locations. The
majority of participants were recruited during their visit to
the Glasgow Science Centre, a large science museum open
to the general public and popular with families. In addition,
participants were recruited from the population of the cam-
pus of the University of the West of Scotland. Subjects
ranged in age from 18 to 89, with a mean age of 32.4 years.
There were 109 males, and 121 females. All participants
played the game at least three times (with the first game
designated as a “practice run”) and completed a question-
naire which assessed the PMT variables, personality and
social support.
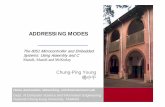
The full analysis of the data from these experiments is
still in progress. However, from a preliminary analysis,
there are two striking results. The first is that the majority of
participants do indeed respond to increased infection load
by reducing their contact radius. Figure 6 shows one partici-
pant’s responses during four games. The black solid circles
represent the practice run, when the participant was playing
the game for the first time and, presumably, experimenting
with different responses to discover how the game worked.
The single cross is from a very short game, where the player
unfortunately became infected on the first day. The open
triangles and circles, however, are from longer games where
the player was exposed to a variety of infection loads and
responded accordingly. The player’s behavior in these
games closely matches a theoretical response with α = 0.42,
shown by the red line on the graph.
Not all participants’ responses matched the theory so
neatly, and there were a few participants whose responses
were bizarre, suggested that they did not understand the
game or chose not to engage with it in the intended way. But
most participants did appear to respond in accordance with
some theoretical α, though the actual value of α varied
greatly among participants. This first result is reassuring, as
it indicates that most people were able to understand what
the game was about and responded to it in a logical fashion.
The second preliminary result, although unexpected, is
even more interesting. Data from the questionnaires was
used to measure for each participant the four factors of Pro-
tection Motivation Theory, namely, perceived severity of
illness, perceived vulnerability, response-efficacy, and self-
efficacy. Figure 7 shows scatter-plots of the participants’
mean risk attitude during all games, plotted against these
four measures. There is a striking lack of correlation: the
factors of PMT, which are known to be predictors of how
people respond to health threats in the real world, appear to
bear no relation to their response to threats in the Epidemic
Game. This is an unexpected result which raises questions
about the usefulness of the virtual experiment methodology.
Given the practical importance of learning ways to control
epidemics and the unfeasibility of doing experiments with
epidemics in the real world, it is worth investigating further
to understand why this has happened and explore possibili-
ties for improving the methodology. We discuss this in more
detail in the next section.
Figure 6: A participant’s actual responses to different in-
fection loads during four games, represented by four differ-
ent symbols. Black solid circles represent the days of the
first, “practice”, game. The line shows the theoretical re-
sponse with α = 0.42.
Figure 7: A preliminary analysis of participants’ risk atti-
tude (vertical axis) plotted against PMT factors.

6. DISCUSSION
In this section we consider what can be learned from
other areas of study in which games and simulations have
been used with apparent success to carry out experiments on
human behavior. Our hope is to find ways to improve the
Epidemic Game and make it into a more useful tool.
Insights from behavioral economics
Behavioral economics is a modern departure from tradi-
tional neoclassical economics in which ideas from psychol-
ogy and cognitive science are incorporated into the study of
human economic decision-making. The use of experimental
methods is fundamental and many experiments are pre-
sented as games, which may be played face-to-face in a
laboratory setting, or on a computer.
A key part of behavioral economics is prospect theory
[12] [2], a model of risk attitudes and risk evaluation in ex-
perimental settings. Prospect theory includes the idea of loss
aversion: people are much more strongly affected by losses,
even small losses, than to gains of the same magnitude. In
the Epidemic Game players did not experience any losses:
the consequence of becoming infected was that the game
ended and the player missed out on the potential bonus for
earnings “after” the epidemic. Loss aversion could be incor-
porated into the game by giving players an initial number of
points, some of which would be lost if the player became ill.
This could be explained as the cost of medical treatment.
There is strong evidence that loss aversion is an important
component in economic decision making in the real world,
so adding it into the Epidemic Game might help to evoke a
more realistic response.
Another possible explanation for the Epidemic Game re-
sults is that people may be modeling their initial decisions
as an information-seeking tradeoff [11]. When first faced
with the game, people may be uncertain of the rules and the
best strategies to use, and therefore try out various options
in order to learn how the game works. The design of the
Epidemic Game permits the subject to play the game as
many times as desired to perform this exploration. Aware
that he/she has been asked to play a structured game with
defined rules and rewards, and lacking a full understanding
of these, the player experiments by trying out different op-
tions in order to get information about the rules and work
out the best strategy. This kind of behavior is very far re-
moved from a person’s real world experience of dealing
with epidemics (where there are no second chances) and
much closer to how someone might behave when solving a
crossword puzzle or learning to play chess.
If the problem is indeed that the highly structured design
of the Epidemic Game leads subjects to treat it as a puzzle
to be solved rather than an experience to be lived, it might
be possible to fix this by redesigning the game to make it
much less structured with open-ended options for players to
explore.
The behavioral economics literature also contains many
interesting results and guidelines about the measurement of
risk attitudes and risk aversion, much of which is relevant to
the Epidemic Game. For example, it has been found that
risk attitudes may be domain-specific [28], meaning that the
same individual may display different risk attitudes in dif-
ferent contexts. It is important to take this into account, as it
could mean that risk taking behavior when playing a com-
puter game is not representative of behavior when faced
with health threats in the real world. Other relevant results
include gender differences in risk attitudes [7] and the phe-
nomenon of ambiguity aversion, where people prefer to take
options with known probabilities [5] rather than options
whose probabilities are uncertain.
Insights from virtual environments research
Figure 8: Screenshots from a prototype of a more realis-
tic Epidemic Game.
The Epidemic Game presented players with a simple,
two-dimensional, cartoon-like representation of an epi-
demic, lacking in realistic detail and immersive content.
Virtual worlds, of which the best known is Second Life, are
highly immersive three-dimensional simulated scenarios
containing high levels of realistic detail. It has been claimed
that virtual worlds evoke in the user a sense of “presence”
within the simulated world [6], [15], leading to realistic so-
cial behaviour that mimics that in the real world. Virtual
worlds have also been used successfully to re-create classic
experiments in psychology, such as the famous Milgram
Obedience experiments [26]. This suggests that it might be
possible to improve the Epidemic Game by making it more
detailed, realistic and immersive, perhaps by re-
implementing it within a three-dimensional virtual environ-

ment. Figure 8 shows screenshots from a prototype version
of this [14] which is currently under development.
There is a fair amount of evidence that virtual worlds
prompt users to behave according to social norms similar to
those that govern real world behaviour. Examples include
proxemics (social norms about personal space) in Second
Life [8], and eye gaze and eye contact in massively-
multiplayer online role-playing games (MMORPGs) [31].
However, it is undeniable that not all behaviors in virtual
worlds translate to the real world: the inhabitants of Second
Life can fly and teleport, and in MMORPGs players fight
and kill, and death is not permanent. In moving the Epi-
demic Game into a virtual environment, where the player is
expected to become immersed and to suspend disbelief in
the scenario presented, great care will need to be taken to
ensure that this illusion cannot be accidentally dispelled by
some mishap or unanticipated action by the player.
Another important aspect to consider when considering
the use of virtual worlds for scientific experimentation is the
experimental control / mundane realism trade-off [3]. The
more detailed the virtual world, the more difficult it be-
comes to design controlled experiments, as the number of
experimental factors grows with every new detail that is
added. However, it may be that realistic detail is necessary
in order to make participants forget that they are in an ex-
periment and behave in a natural way. A balance will need
to be struck between the need for realistic, immersive envi-
ronments and the requirement to keep experiments as simple
as possible and reduce the number of confounding factors.
Game design issues
An alternative to re-implementing the Epidemic Game in
a virtual world is to improve the interface and playability of
the existing game. The current interface was designed to
faithfully represent the underlying agent-based simulation:
neighbours are shown as anonymous stick figures, and
awareness and contact radii are depicted literally as circles.
The resulting interface is rather abstract and perhaps un-
engaging for the player. There are several ways in which the
interface could be made more engaging, for example by
presenting information differently, or by giving more varied
and entertaining feedback. Increasing players’ engagement
with the game may encourage them to treat it less as an ab-
stract exercise and more as a real, role-playing scenario.
Timing issues
A final observation about the experiments is that they
were carried out during the summer months, when seasonal
influenza is at its lowest ebb in Scotland. Participants were
therefore less likely to have had recent experience of an
influenza outbreak, and this may have reduced their ability
to identify with the scenario presented in the game and in-
fluenced their responses to the questionnaire. This suggests
that the experiment should be repeated during the winter,
when seasonal influenza is at its peak, so that the results can
be compared.
7. SUMMARY AND FUTURE WORK
This Epidemic Game experiment was a pilot study in the
use of virtual experiments and participatory simulation to
study human behaviour during epidemics. The results
showed that although participants responded to the threats
faced in the game, the risk attitudes they displayed were
uncorrelated with their psychological characteristics accord-
ing to Protection Motivation Theory, and therefore might
not have been representative of their responses to health
threats in the real world.
Insights from behavioral economics suggest a number of
factors influencing decision-making under risk that should
be considered in order to improve the Epidemic Game.
These include incorporating loss aversion, making the game
less structured so as to prompt a natural response rather than
strategic information-seeking behavior, and considering
whether domain-specific risk attitudes and ambiguity aver-
sion have a role to play.
Insights from the study of virtual worlds suggest that re-
implementing the Epidemic Game within a realistically de-
tailed three-dimensional virtual environment might prompt a
greater sense of immersion and presence in the players, and
cause them to respond more naturally. However there are
tradeoffs to consider between the desire for more realism
and the need to be able to carry out controlled experiments.
Other possibilities to consider are whether the current
two-dimensional game interface could be improved so as to
make it more engaging for the players, and whether differ-
ent results might be obtained if the experiments were to be
repeated in the winter, when seasonal influenza is at its
peak.
Our immediate next step is to complete the comprehen-
sive statistical analysis of the data from the already com-
pleted experiments. In future work we will explore a num-
ber of lines of investigation, including redoing the experi-
ments at a different time of year, improving the game play
in the current two-dimensional Epidemic Game, and devel-
oping a more realistic three-dimensional version. Our long
term goal is to create a framework that can be used for ex-
perimental study of human behaviour within simulations of
scenarios, of which epidemics are just one example, which
cannot practicably be studied experimentally in the real
world.

References
[1] Anderson, RM; May, RM. 1991. Infectious Diseases of
Humans: Dynamics and Control. OUP.
[2] Barberis, N. 2012. “Thirty Years of Prospect Theory in
Economics: A Review and Assessment”. Available at
SSRN: http://ssrn.com/abstract=2177288.
[3] Blascovich, J; Loomis, J; Beall, AC; Swinth, KR; Hoyt,
CL; Bailenson, JN. 2002. “Immersive Virtual Environ-
ment Technology as a Methodological Tool for Social
Psychology”. Psychological Inquiry 13(2).
[4] Beutels, P; Jia, N; Zhou, Q; Smith, R; Cao, W; Sake
JD. 2009. “The Economic Impact of SARS in Beijing,
China”, Tropical Medicine and International Health, 14.
[5] Borghans, L; Golsteyn, BHH; Heckman, JJ, Meijers, H.
2009. “Gender Differences in Risk Aversion and Ambi-
guity Aversion”. Journal of the European Economic As-
sociation, MIT Press, 7(2-3).
[6] Cummings, JJ; Bailenson, JN; Fidler, MJ. 2012. “How
Immersive is Enough?”. Proceedings of the International
Society for Presence Research Conference, 2012.
[7] Dohnen, T; Falk, A; Huffman, D; Sunde, U; Schupp, J;
Wagner, GG. 2011. “Individual Risk Attitudes: Meas-
urement, Determinants and Behavioral Consequences”.
Journal of the European Economic Association, 9 (3), 5.
[8] Friedman, D; Steed, A; Slater, M. 2007. “Spatial Social
Behavior in Second Life”. Intelligent Virtual Agents
2007, LNAI 4722.
[9] Jones, JH; Salathé, M. 2009. “Early Assessment of
Anxiety and Behavioral Response to Novel Swine-
Origin Influenza A (H1N1)”, PLoS ONE, 4(12): e8032.
[10] Goodwin, R; Haque, S; Neto, F; Myers, LB. 2009. “Ini-
tial psychological responses to Influenza A, H1N1”,
BMC Infectious Diseases, 9:166.
[11] Hertwig, R; Erev, I. 2009. “The description-experience
gap in risky choice”. Trends in Cognitive Sciences, 13.
[12] Kahneman, D; Tversky, A. 1979. “Prospect Theory: An
Analysis of Decision Under Risk”. Econometrica 47(2).
[13] Kleczkowski, A; Maharaj, S. 2010. “Stay at Home:
Wash Your Hands: Epidemic Dynamics with Awareness
of Infections”. Summer Computer Simulation Confer-
ence, 2010. ACM Digital Library.
[14] Kleczkowski, A; Maharaj, S; Rasmussen, S; Williams,
L. 2011. “Studying Human Behaviour with Virtual Ex-
periments and Participatory Simulation”. Poster pre-
sented at SISCA DemoFest, Edinburgh, 2011.
[15] La, C-A; Michiardi, P. 2008. “Characterizing User Mo-
bility in Second Life”. Proceedings of the first Work-
shop on Online Social Networks, ACM Digital Library.
[16] Lau, JTF; Yang, X; Tsui, H; Kim, JH. 2003. “Monitor-
ing community responses to the SARS epidemic in
Hong Kong: from day 10 to day 62”. J. Epidemiol.
Community Health 2003;57.
[17] Lau, JTF; Tsui, H; Lau, M; Yang, X. 2004. “SARS
Transmission, Risk Factors, and Prevention in Hong
Kong”. Emerg. Infect. Dis. 2004 April; 10(4).
[18] Lau, JT; Kim, JH; Tsui, H; Griffiths S. 2007. “Percep-
tions related to human avian influenza and their associa-
tions with anticipated psychological and behavioral re-
sponses at the onset of outbreak in the Hong Kong Chi-
nese general population”. Am. J. Infect. Control 35(1).
[19] Lau, JTF; Kim, JH; Tsui, HY; Griffiths, S. 2008. “Per-
ceptions related to bird-to-human avian influenza, influ-
enza vaccination and use of face mask”. Infection 36(5)
[20] Leung, GM; Quah, S; Ho, LM; Ho, SY; Hedley, AJ;
Lee, HP; Lam, TH. 2004. “A tale of two cities: commu-
nity psychobehavioral surveillance and related impact on
outbreak control in Hong Kong and Singapore during
the severe acute respiratory syndrome epidemic”. Infect
Control Hosp. Epidemiol. 25(12).
[21] Maharaj, S; Kleczkowski, A. 2012. “Controlling Epi-
demic Spread by Social Distancing: Do it well or not at
all”. BMC Public Health, 12(1):679.
[22] Maharaj, S; McCaldin, T; Kleczkowski. 2011. “A Par-
ticipatory Simulation Model for Studying Attitudes to
Infection Risk”, Summer Computer Simulation Confer-
ence 2011, ACM Digital Library.
[23] Rogers, RW (1975) “A Protection Motivation Theory
of Fear Appeals and Attitude Change”, Journal of Psy-
chology, 91.
[24] Rubin, GK; Amlôt, R; Page, L; Wessely, S. 2009.
“Public perceptions, anxiety, and behavior change in re-
lation to the swine flu outbreak”, BMJ 2009; 339:b2651,
doi: 10.1136/bmj.b2651
[25] Sadique, MZ; Edmunds, WJ; Smith, RD; Meerding,
WJ; de Zwart, O; Brug, J; Beutels, P. 2007. “Precaution-
ary Behavior in Response to Perceived Threat of Pan-
demic Influenza”, Emerging Infectious Diseases 13(9).
[26] Slater, M; Antley, A; Davison, A; Swapp, D; Guger, C;
Barker, C; Pistrang, N; Sanchez-Vives, MV. 2006. “A
Virtual Reprise of the Stanley Milgram Obedience Ex-
periments”. PLoS ONE 1(1): e39
[27] Tang, CSK; Wong, C. 2003. “An Outbreak of the Se-
vere Acute Respiratory Syndrome: Predictors of Health
Behaviors and Effect of Community Prevention
Measures in Hong Kong, China”, Am. J. Public Health.
93(11).
[28] Weber, EU; Blais, A; Betz, NE. 2002. “A Domain-
specific Risk-attitude Scale”. Journal of Behavioral De-
cision Making, 15.
[29] Wilensky, U; Stroup, W. 1999. “Learning through Par-
ticipatory Simulations”, Computer Supported Collabo-
rative Learning (CSCL ’99). 1999.
[30] W Wilensky, U., 1999. NetLogo.
http://ccl.northwestern.edu/netlogo/ Center for Con-
nected Learning and Computer-Based Modeling,
Northwestern University, Evanston, IL.
[31] Yee, N; Bailenson, JN; Urbanek, M; Chang, F; Merget,
D. 2007. “The Unbearable Likeness of Being Digital:
The Persistence of Nonverbal Social Norms in Online
Virtual Environments”. Cyber Psych. and Behav. 10 (1).