Reducing the barriers to accessing psychological therapies for Bengali, Urdu, Tamil and Somali...
26
This article was downloaded by: [University of Nottingham] On: 25 June 2014, At: 03:07 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK British Journal of Guidance & Counselling Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/cbjg20 Reducing the barriers to accessing psychological therapies for Bengali, Urdu, Tamil and Somali communities in the UK: some implications for training, policy and practice Del Loewenthal a , Ahmed Mohamed b , Samyukta Mukhopadhyay c , Kalai Ganesh d & Rhiannon Thomas e a Roehampton University , Whitelands College , London , UK b Department of Psychiatry , University of Cambridge , UK c Institute of Psychiatry , King's College London , UK d Independent Research Consultation e Psychotherapy in private practice Published online: 21 Oct 2011. To cite this article: Del Loewenthal , Ahmed Mohamed , Samyukta Mukhopadhyay , Kalai Ganesh & Rhiannon Thomas (2012) Reducing the barriers to accessing psychological therapies for Bengali, Urdu, Tamil and Somali communities in the UK: some implications for training, policy and practice, British Journal of Guidance & Counselling, 40:1, 43-66, DOI: 10.1080/03069885.2011.621519 To link to this article: http://dx.doi.org/10.1080/03069885.2011.621519 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Reducing the barriers to accessing psychological therapies for Bengali, Urdu, Tamil and Somali...
This article was downloaded by [University of Nottingham]On 25 June 2014 At 0307Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number 1072954 Registeredoffice Mortimer House 37-41 Mortimer Street London W1T 3JH UK
British Journal of Guidance ampCounsellingPublication details including instructions for authors andsubscription informationhttpwwwtandfonlinecomloicbjg20
Reducing the barriers to accessingpsychological therapies for BengaliUrdu Tamil and Somali communities inthe UK some implications for trainingpolicy and practiceDel Loewenthal a Ahmed Mohamed b Samyukta Mukhopadhyay c
Kalai Ganesh d amp Rhiannon Thomas ea Roehampton University Whitelands College London UKb Department of Psychiatry University of Cambridge UKc Institute of Psychiatry Kings College London UKd Independent Research Consultatione Psychotherapy in private practicePublished online 21 Oct 2011
To cite this article Del Loewenthal Ahmed Mohamed Samyukta Mukhopadhyay Kalai Ganeshamp Rhiannon Thomas (2012) Reducing the barriers to accessing psychological therapies for BengaliUrdu Tamil and Somali communities in the UK some implications for training policy and practiceBritish Journal of Guidance amp Counselling 401 43-66 DOI 101080030698852011621519
To link to this article httpdxdoiorg101080030698852011621519
PLEASE SCROLL DOWN FOR ARTICLE
Taylor amp Francis makes every effort to ensure the accuracy of all the information (theldquoContentrdquo) contained in the publications on our platform However Taylor amp Francisour agents and our licensors make no representations or warranties whatsoever as tothe accuracy completeness or suitability for any purpose of the Content Any opinionsand views expressed in this publication are the opinions and views of the authorsand are not the views of or endorsed by Taylor amp Francis The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information Taylor and Francis shall not be liable for any losses actions claimsproceedings demands costs expenses damages and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with in relation to orarising out of the use of the Content
This article may be used for research teaching and private study purposes Anysubstantial or systematic reproduction redistribution reselling loan sub-licensingsystematic supply or distribution in any form to anyone is expressly forbidden Terms ampConditions of access and use can be found at httpwwwtandfonlinecompageterms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Reducing the barriers to accessing psychological therapies for BengaliUrdu Tamil and Somali communities in the UK some implications fortraining policy and practice
Del Loewenthala Ahmed Mohamedb Samyukta Mukhopadhyayc Kalai Ganeshd
and Rhiannon Thomase
aRoehampton University Whitelands College London UK bDepartment of PsychiatryUniversity of Cambridge UK cInstitute of Psychiatry Kingrsquos College London UKdIndependent Research Consultation ePsychotherapy in private practice
(Received 20 October 2010 final version received 30 July 2011)
The aim of this research was to investigate the feasibility of achieving ImprovingAccess to Psychological Therapies (IAPT) for people from Black Asian andMinority Ethnic (BAME) communities living in the UK with specific referenceto Bengali Urdu Tamil and Somali speaking communities Focus groups werecarried out with each of the communities to investigate how they conceptualiseand experience lsquomental health issuesrsquo and what they do when faced with what theyregard as these issues A thematic analysis of the data suggested that participantsdid not fully understand common conceptualisations about mental health issuesnor did they know how to seek mental health support Implications of culturalbarriers and recommendations for IAPT outcomes for the four communities arediscussed
Keywords anxiety depression Improving Access to Psychological Therapies(IAPT) training Black Asian Minority Ethnic (BAME) thematic analysisBengali Urdu Tamil and Somali
Introduction
Disparities between Caucasian and Black Asian and Minority Ethnic (BAME)
communities in terms of access to experience with and outcomes in mental health
issues have been documented (Bhui Sashidharan Cannon McKenzie amp Sims 2003
Department of Health 2005 Health 2007a 2007b Fernando 2005 Health
Commission 2007) The Department of Health (2007a 2007b) stated that a key
mental health issue for BAME communities in the UK is low uptake of
psychologicaltalking therapies which it has been argued needs to change (Mulatu
amp Berry 2001) in order to achieve equality in mental health care across UK
communities It has been argued that a lsquocircle of fearrsquo (Sainsbury Centre for Mental
Health 2005) has developed preventing ethnic minorities from accessing mental
health services defined as services offering treatments support and advocacy to
persons experiencing disturbances to their mental health It was found that
individuals are frequently accessing services later and at a more critical stage than
Caucasian service users The Department of Health report conducted by Sashidhar-
Corresponding author Email dloewenthalroehamptonacuk
British Journal of Guidance amp Counselling
Vol 40 No 1 February 2012 4366
ISSN 0306-9885 printISSN 1469-3534 online
2012 Taylor amp Francis
httpdxdoiorg101080030698852011621519
httpwwwtandfonlinecom
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
an (2003) considered reasons that mental health services in the UK are failing to
meet the needs of BAME populations The report recommended the development of
the cultural capability of mental health services in the UK and the importance of
engaging the community in order to improve mental health services for thesepopulations
Providing better mental health care for BAME communities arguably requires
significantly more than the efforts currently made within our mental health care
system in the UK (Fowles 2007) The barriers for people from BAME communities
have been stated to include practicalities such as languages used for health
information through to attitudinal challenges faced by mainly Eurocentric-focused
health professionals in understanding the cultural diversity of both the expression
and treatment of mental health problems (Bhugra amp Ayonrinde 2004 Fernando2005) Related to this Sass Moffat Bhui and McKenzie (2009) have identified that
ethnic matching is a significant factor in enhancing care pathways for BAME
communities in the UK
A background to questions of cultural impact on access to psychological
therapies will now be presented followed by a discussion of language and the
categorisation of BAME communities and other cultural considerations such as
family ties and religion affecting access to psychological therapies for Bengali
Tamil Urdu and Somali speaking communities (the research group)
Cultural background
Research has indicated that mental health professionalsrsquo lack of understanding aboutthe cultural background of BAME communities negatively impacts on service usersrsquo
access to psychological therapies (Ager 1993 Beiser amp Hou 2002 Danso 2001
Silove Sinnerbrink Field Manicavasagar amp Steel 2000 Sinnerbrink Silove
Manicavasagar Steel amp Field 1996 Watters 2001 Watters amp Ingleby 2004) In
addition to this these professionalsrsquo attitudes during their interaction negative
positive or neutral left an impression on service users (Boi 2000)
McKenzie and Bhui (2007) explore the need for providing a coherent and
integrated service for minority ethnic communities They argue that emphasis isrequired on considering patientsrsquo needs improvising with existing techniques and
therapies highlighting resolutions integrated with respect for diversity at all times
evidence-based practice and success in long-term goals
There has also been criticism that in the UK diversity classification comes under
broad categories lacking specific and clear structures (McDowell Coleman amp
Ferner 2006) This is considered further below in relation to the use of terms such as
lsquoSouth Asianrsquo In addition to a loss of cultural specificity there is also the potential
difficulty inherent in defining and imposing mental health issues based onunderstandings applicable to a dominant culture This has previously been illustrated
from the perspective of transcultural psychiatry (Ellis Kia-Keating Yusuf Lincoln
amp Nur 2007 Ellis MacDonald Lincoln amp Cabral 2008 Fernando 2005)
The categorisation of communities and language issues
The use of the term lsquoSouth Asianrsquo community used to encompass individuals from
India Pakistan Bangladesh and Sri Lanka is in reality arguably too broad to enable
research on relevant factors that affect access to psychological therapies for these
44 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
linguistically religiously and culturally distinct communities Similarities in ethnicity
spoken languages or mother tongues may not imply similarities in culture These
have been shown to be distinctive in particular within the Tamil (Ravindran 2006)
and Bengali groups (Hossain amp Khan 2006) Only religion is considered as being acommon factor affecting access to mental health services for some individuals within
the South Asian community A lack of understanding of for example the geo-
political differences within the Bengali community is seen to create an instant barrier
between practitioner and service user (Gerrish 2000 2001)
Language emerges as a key barrier to peoplersquos use of health services (Murray amp
Buller 2007 Saha Fernandez amp Perez-Stable 2007) and requests for interpreters to
address mental health issues come particularly from four major linguistic minority
communities in the UK Bengali Somali Tamil and Urdu speakers Thesecommunities have been reported to ask for more translations when accessing mental
health services than other linguistic minority communities (Aspinall 2007) and these
communities were thus a particular focus for the National Health Service (NHS)
Trust which commissioned this work As such this research focused on these four
specific languages with regard to achieving Improving Access to Psychological
Therapies (IAPT) outcomes (IAPT 2008) The question of why these particular
communities request more interpreter services compared to other often larger
minority communities within the UK is an issue that is potentially of relevance butwhich fell outside of the scope of this research
Somalian service users may therefore be discouraged from accessing mental health
services due to language barriers (Bhui et al 2003 Fernando 2005 Health
Commission 2007 McCrone et al 2005 Pumroy 2008 Warfa et al 2006) An
example of this is the fact that the UK Department of Health has translated
psychological materials including computerised Cognitive Behaviour Therapy
(cCBT) into several languages but not as yet Somali (Department of Health 2007a)
In relation to primary care services in a more general sense rather thanspecifically psychological therapies Barron Holterman Shipster Batson and Alam
(2010) sought to investigate the awareness and views of ethnic minority community
members towards primary health care interpreting provision in Hertfordshire This
study identified the importance of the provision of high quality language
interpretation services for enabling access In particular this study highlighted the
importance of trust confidentiality accuracy and independence in an interpreter preferred to be from their own culture and gender (Barron et al 2010) This was an
issue that was also of concern for the participants in this research on access topsychological therapies
Other cultural considerations affecting access to psychological therapies for BengaliUrdu Tamil and Somali communities
Stigmas associated with mental health continue to exist within both majority and
minority communities living in the UK While the stigma associated with mental
health issues is thus not exclusively an issue for BAME communities there aredimensions of this which arise specifically for these minority groups For the
communities considered as the focus of this research negative connotations include
for example Somalis who have been shown to be not only shameful about mental
illnesses but also fearful of mental health professionals leading them to conceal
mental health issues (Whittaker Lewis amp Buchan 2005) Bradby et al (2007)
British Journal of Guidance and Counselling 45
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
pp 24162417) offer a similar view on the particular negative connotations attached
to mental illness among people of South Asian origin
Family ties are seen to be of particular importance within the research group
communities as they greatly impact on culture hence influencing both access to
psychological therapies as well as individualsrsquo openness to mental health profes-
sionals and researchers (Finnstrom amp Soderhamn 2006 Lavender Khondoker amp
Jones 2006) Thus family and community issues in relation to the accessing of
psychological therapies appear to be of more importance for the research group
communities than for the dominant culture
Religion is another aspect shown to significantly impact upon service usersrsquo
perspectives with regard to accessing psychological therapies (Guerin Guerin
Diiriye amp Yates 2004 Whittaker et al 2005 for Somali communities Ramakrish-
nan 1984 Ravindran 2006 for Tamil communities Gerrish 2001 King Weich
Nazroo amp Blizard 2006 Lavender et al 2006 for Bengali and Urdu communities)
Religious observance is often seen as an alternative means of alleviating symptoms of
psychological distress and as is discussed below in relation to Jinns mental health
concerns are frequently understood within a religious framework that is not the case
for the majority increasingly secular community within the UK The implications for
offering a clinically based secular psychological therapies service are that such a
service may not be seen by service users as relevant or able to respond to their needs
as they understand them As will be discussed below this study found that the
participants in the focus groups reinforced previous literature on the significance of
religion in relation to accessing psychological services The question as to the
accessing of psychological therapies for members of these communities who are not
religious was not raised within the focus groups conducted for this study This is an
area potentially of interest for further research but was outside the scope of this
particular studyThe intention of this research was twofold to understand how mental health
issues in particular anxiety and depression are conceptualised and experienced by
people from BAME communities with particular reference to Bengali Urdu Tamil
and Somali speaking communities in the UK (the research group) and to explore
any potential implications of this for the accessing of psychological therapies services
by the communities As part of the Department of Healthrsquos IAPT initiative (IAPT
2008) which highlighted the disparity in access to psychological therapy between the
BAME communities and the mainstream population in the UK this research
commissioned by a London NHS Mental Health Trust aimed to investigate how
specific BAME communities Bengali Urdu Tamil and Somali conceptualise and
experience anxiety and depression both directly and indirectly and how these differ
from majority conceptualisations Secondly it aimed to gain more knowledge about
the feasibility of increasing access to psychological therapies in order to address the
disparity highlighted in previous research within these communities (Department of
Health 2007a 2007b 2009 Health Commission 2007)
Method
Design
In terms of method quantitative or mixed methods approaches to data collection
and analysis were considered but rejected as the focus of the research lay in
46 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
explicating the lived experience of the participants as described A qualitative
approach to research was chosen which acts to gain insight into the individualrsquos
experiences (Corbin amp Strauss 1998) It was felt that in understanding the
significance of a given experience a method that allowed analysis of the participantrsquos
words and personal meanings that an experience might have for the individual would
be important (Harre amp Secord 1972) It is not suggested that a person may have
exact insight into their own motives but that one can gain an understanding of anexperience as lived through a description by the person who had the experience
Focus groups are group discussions organised to explore a specific set of issues
such as peoplersquos views and experience (Basch 1987 Kitzinger 1994) Although often
seen as a convenient way to simultaneously collect data from a number of
participants the method capitalises on communication between research participants
in the generation of data (Kitzinger 1995) This means that instead of the researcher
asking each person to respond to a question in turn participants are encouraged to
talk to one another interacting and commenting on each otherrsquos experiences and
points of view The method is particularly useful for exploring peoplersquos knowledge
and experiences
Previous research on mental illness within the research group communities
indicates that focus groups are frequently used as a research method (Barron et al
2010 Halcomb Gholizadeh Di Giacomo Phillips amp Davidson 2004) Focus groups
have been used in previous studies with the Somali community (Finnstrom amp
Soderhamn 2006 Gervais 2008 Green amp Thorogood 2004 Warfa et al 2006) the
Tamil community (Bradby et al 2007 Fernando 2005 Sadavoy Meier amp Yuk2004 Whitley amp Prince 2004) Urdu groups (Acharya amp Northcott 2007) and
Bengali groups (Hawthorne Rahman amp Pill 2003) suggesting their suitability for
researching issues within these communities
This study sought to consider community perspectives and the experiences and
understandings of members of these communities as part of these groups with
subsequent implications for them as individuals As such focus groups were chosen
as the most appropriate method for this type of research study to consider the
community perspective
Further vignettes followed by questionsprobes were chosen as the appropriate
method of enabling sharing of experiences within the focus groups Within the focus
group interview schedule vignettes of a person displaying anxiety and in turn
depression were presented to the focus group participants followed by questions
about the participantsrsquo experiences in relation to the vignette Vignettes have been
widely used as a data collection technique in qualitative research (Hazel 1995
Hughes 1998) Hughes (1998 p 381) describes vignettes as lsquostories about
individuals situations and structures which can make reference to important pointsin the study of perceptions beliefs and attitudesrsquo
Vignettes provide a valuable technique for exploring peoplersquos perceptions beliefs
and meanings about specific situations and are particularly useful in exploring
potentially sensitive topics that participants might otherwise find difficult to discuss
(Neale 1999) Use of vignettes within a lsquofocusrsquo group is becoming increasingly
popular with social researchers (Wilkinson 1998) Maclean (1999) writing on the
use of vignettes within focus groups commented that it encouraged even the quietest
group member to voice an opinion
According to principles that guide the use of vignettes in research the vignettes
were created in a way that made them appear plausible and real to participants and
British Journal of Guidance and Counselling 47
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that contained sufficient context for participants to understand the situation
depicted The researchers then endeavoured to follow the vignette with questions
directed towards the beliefs assumptions and experiences of the participants with
regard to personal experiences of anxiety depression how participants cope withmental health issues limitations of mental health services and possible solutions for
the community involved
As a result for the purposes of this study mental health services were defined as
services carried out by mental health professionals in which treatments support and
advocacy to persons are offered to people experiencing mental health issues
(disturbances to their mental health) As a result this incorporates a breadth of
mental health services and professionals such as General Practitioners (GPs)
community mental health teams mental health nurses counsellors psychotherapistsoccupational therapists and clinical and counselling psychologists
The research also made use of respondent validation conducted on an individual
basis to consider how if at all the perspectives of participants as individuals differed
from those of the particular community interviewed (Silverman 2000) In particular
the aim of the interviews was to clarify the themes emerging from the focus groups to
ensure that the themes derived from the focus groups interviews were captured
accurately As Herrel et al (2004) p 349) argue lsquo otherwise possible misinterpre-
tation due to translation can occur and responses can be influenced by other focusgroup membersrsquo
Participant recruitment
As previously mentioned Bengali Urdu Tamil and Somali speaking communities
were sampled specifically for this study They form a particular focus for the NHS
Trust in that they have been reported to ask for more translations when accessingmental health services than other linguistic minority communities (Aspinall 2007)
The four samples of participants were recruited through the various Bengali
Urdu Tamil and Somali community associations with which the NHS Trust was in
contact sometimes working directly on mental health issues and IAPT The process
of selection was opportunistic sampling based on those who volunteered to take part
after having been invited to do so verbally by senior members of these community
associations In particular the recruitment method was seen as one that was
culturally acceptable to the selected communities With permission posters were alsoplaced in community buildings to advertise the study Those who volunteered were
then supplied with additional information about the study and informed consent was
required from each participant
Participants
Bengali community participants
Two focus groups were conducted for Bengali speaking participants The first group
consisted of eight female participants and the second group consisted of four female
and two male participants As participants were recruited through opportunistic
sampling there was an inconsistency in the malefemale participation ratio
With regards to the six respondent validation interviews four female participants
were recruited and two male participants
48 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Demographically the age group of all participants was 50 and above All
participants reflected Bangladeshi heritage and identified with Islam as their religion
Urdu community participants
Two focus groups were conducted with 21 participants in total The first group
consisted of 15 female participants and the second group consisted of six maleparticipants marking a separation of the groups based on gender
A further six participants (three males and three females) were selected for the
respondent validation interviews
Demographically the age group of all participants was 40 and above A variety of
participants were recruited whose origins reflected a diversity of the Urdu speaking
population Even though most participants were of Pakistani origins some
participants stated their heritage to be East African and even Indian The majority
of the participants stated Islam to be their religion
Tamil community participants
The two focus groups were made up of 18 participants in total The first groupconsisted of 10 males and the second of eight female participants making a
separation of the groups based on gender
For the respondent validation interviews six interviews were carried out with
four males and two females
All participants fell within the age range of 40 and above
Somali community participants
Two focus groups were conducted with 24 participants in total The first group
consisted of 14 female participants and the second group consisted of 10 male
participants marking a separation of the groups based on gender
A further six participants three males and three females were selected for therespondent validation interviews
Demographically the age group of all participants was 40 and above
Data collection and analysis
Two open-ended focus groups were carried out with each of the separate Bengali
Urdu Tamil and Somali groups with the Community Development Workers
(CDWs) present The CDWs were involved due to their knowledge of the community
and ability to aid set up and implementation of the focus groups The respondent
validation interviews were then conducted with six individuals from each of the
community groupsDue to cultural considerations the four researchers all of whom were themselves
born outside of the UK and in terms of their languages and cultural backgrounds
members of the respective communities relevant to this study conducted the focus
groups and respondent validation interviews with the male and female participants
separately (with the exception of the Bengali participants who requested mixed
gender participant groups) The focus groups and respondent validations for each
British Journal of Guidance and Counselling 49
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

This article may be used for research teaching and private study purposes Anysubstantial or systematic reproduction redistribution reselling loan sub-licensingsystematic supply or distribution in any form to anyone is expressly forbidden Terms ampConditions of access and use can be found at httpwwwtandfonlinecompageterms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Reducing the barriers to accessing psychological therapies for BengaliUrdu Tamil and Somali communities in the UK some implications fortraining policy and practice
Del Loewenthala Ahmed Mohamedb Samyukta Mukhopadhyayc Kalai Ganeshd
and Rhiannon Thomase
aRoehampton University Whitelands College London UK bDepartment of PsychiatryUniversity of Cambridge UK cInstitute of Psychiatry Kingrsquos College London UKdIndependent Research Consultation ePsychotherapy in private practice
(Received 20 October 2010 final version received 30 July 2011)
The aim of this research was to investigate the feasibility of achieving ImprovingAccess to Psychological Therapies (IAPT) for people from Black Asian andMinority Ethnic (BAME) communities living in the UK with specific referenceto Bengali Urdu Tamil and Somali speaking communities Focus groups werecarried out with each of the communities to investigate how they conceptualiseand experience lsquomental health issuesrsquo and what they do when faced with what theyregard as these issues A thematic analysis of the data suggested that participantsdid not fully understand common conceptualisations about mental health issuesnor did they know how to seek mental health support Implications of culturalbarriers and recommendations for IAPT outcomes for the four communities arediscussed
Keywords anxiety depression Improving Access to Psychological Therapies(IAPT) training Black Asian Minority Ethnic (BAME) thematic analysisBengali Urdu Tamil and Somali
Introduction
Disparities between Caucasian and Black Asian and Minority Ethnic (BAME)
communities in terms of access to experience with and outcomes in mental health
issues have been documented (Bhui Sashidharan Cannon McKenzie amp Sims 2003
Department of Health 2005 Health 2007a 2007b Fernando 2005 Health
Commission 2007) The Department of Health (2007a 2007b) stated that a key
mental health issue for BAME communities in the UK is low uptake of
psychologicaltalking therapies which it has been argued needs to change (Mulatu
amp Berry 2001) in order to achieve equality in mental health care across UK
communities It has been argued that a lsquocircle of fearrsquo (Sainsbury Centre for Mental
Health 2005) has developed preventing ethnic minorities from accessing mental
health services defined as services offering treatments support and advocacy to
persons experiencing disturbances to their mental health It was found that
individuals are frequently accessing services later and at a more critical stage than
Caucasian service users The Department of Health report conducted by Sashidhar-
Corresponding author Email dloewenthalroehamptonacuk
British Journal of Guidance amp Counselling
Vol 40 No 1 February 2012 4366
ISSN 0306-9885 printISSN 1469-3534 online
2012 Taylor amp Francis
httpdxdoiorg101080030698852011621519
httpwwwtandfonlinecom
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
an (2003) considered reasons that mental health services in the UK are failing to
meet the needs of BAME populations The report recommended the development of
the cultural capability of mental health services in the UK and the importance of
engaging the community in order to improve mental health services for thesepopulations
Providing better mental health care for BAME communities arguably requires
significantly more than the efforts currently made within our mental health care
system in the UK (Fowles 2007) The barriers for people from BAME communities
have been stated to include practicalities such as languages used for health
information through to attitudinal challenges faced by mainly Eurocentric-focused
health professionals in understanding the cultural diversity of both the expression
and treatment of mental health problems (Bhugra amp Ayonrinde 2004 Fernando2005) Related to this Sass Moffat Bhui and McKenzie (2009) have identified that
ethnic matching is a significant factor in enhancing care pathways for BAME
communities in the UK
A background to questions of cultural impact on access to psychological
therapies will now be presented followed by a discussion of language and the
categorisation of BAME communities and other cultural considerations such as
family ties and religion affecting access to psychological therapies for Bengali
Tamil Urdu and Somali speaking communities (the research group)
Cultural background
Research has indicated that mental health professionalsrsquo lack of understanding aboutthe cultural background of BAME communities negatively impacts on service usersrsquo
access to psychological therapies (Ager 1993 Beiser amp Hou 2002 Danso 2001
Silove Sinnerbrink Field Manicavasagar amp Steel 2000 Sinnerbrink Silove
Manicavasagar Steel amp Field 1996 Watters 2001 Watters amp Ingleby 2004) In
addition to this these professionalsrsquo attitudes during their interaction negative
positive or neutral left an impression on service users (Boi 2000)
McKenzie and Bhui (2007) explore the need for providing a coherent and
integrated service for minority ethnic communities They argue that emphasis isrequired on considering patientsrsquo needs improvising with existing techniques and
therapies highlighting resolutions integrated with respect for diversity at all times
evidence-based practice and success in long-term goals
There has also been criticism that in the UK diversity classification comes under
broad categories lacking specific and clear structures (McDowell Coleman amp
Ferner 2006) This is considered further below in relation to the use of terms such as
lsquoSouth Asianrsquo In addition to a loss of cultural specificity there is also the potential
difficulty inherent in defining and imposing mental health issues based onunderstandings applicable to a dominant culture This has previously been illustrated
from the perspective of transcultural psychiatry (Ellis Kia-Keating Yusuf Lincoln
amp Nur 2007 Ellis MacDonald Lincoln amp Cabral 2008 Fernando 2005)
The categorisation of communities and language issues
The use of the term lsquoSouth Asianrsquo community used to encompass individuals from
India Pakistan Bangladesh and Sri Lanka is in reality arguably too broad to enable
research on relevant factors that affect access to psychological therapies for these
44 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
linguistically religiously and culturally distinct communities Similarities in ethnicity
spoken languages or mother tongues may not imply similarities in culture These
have been shown to be distinctive in particular within the Tamil (Ravindran 2006)
and Bengali groups (Hossain amp Khan 2006) Only religion is considered as being acommon factor affecting access to mental health services for some individuals within
the South Asian community A lack of understanding of for example the geo-
political differences within the Bengali community is seen to create an instant barrier
between practitioner and service user (Gerrish 2000 2001)
Language emerges as a key barrier to peoplersquos use of health services (Murray amp
Buller 2007 Saha Fernandez amp Perez-Stable 2007) and requests for interpreters to
address mental health issues come particularly from four major linguistic minority
communities in the UK Bengali Somali Tamil and Urdu speakers Thesecommunities have been reported to ask for more translations when accessing mental
health services than other linguistic minority communities (Aspinall 2007) and these
communities were thus a particular focus for the National Health Service (NHS)
Trust which commissioned this work As such this research focused on these four
specific languages with regard to achieving Improving Access to Psychological
Therapies (IAPT) outcomes (IAPT 2008) The question of why these particular
communities request more interpreter services compared to other often larger
minority communities within the UK is an issue that is potentially of relevance butwhich fell outside of the scope of this research
Somalian service users may therefore be discouraged from accessing mental health
services due to language barriers (Bhui et al 2003 Fernando 2005 Health
Commission 2007 McCrone et al 2005 Pumroy 2008 Warfa et al 2006) An
example of this is the fact that the UK Department of Health has translated
psychological materials including computerised Cognitive Behaviour Therapy
(cCBT) into several languages but not as yet Somali (Department of Health 2007a)
In relation to primary care services in a more general sense rather thanspecifically psychological therapies Barron Holterman Shipster Batson and Alam
(2010) sought to investigate the awareness and views of ethnic minority community
members towards primary health care interpreting provision in Hertfordshire This
study identified the importance of the provision of high quality language
interpretation services for enabling access In particular this study highlighted the
importance of trust confidentiality accuracy and independence in an interpreter preferred to be from their own culture and gender (Barron et al 2010) This was an
issue that was also of concern for the participants in this research on access topsychological therapies
Other cultural considerations affecting access to psychological therapies for BengaliUrdu Tamil and Somali communities
Stigmas associated with mental health continue to exist within both majority and
minority communities living in the UK While the stigma associated with mental
health issues is thus not exclusively an issue for BAME communities there aredimensions of this which arise specifically for these minority groups For the
communities considered as the focus of this research negative connotations include
for example Somalis who have been shown to be not only shameful about mental
illnesses but also fearful of mental health professionals leading them to conceal
mental health issues (Whittaker Lewis amp Buchan 2005) Bradby et al (2007)
British Journal of Guidance and Counselling 45
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
pp 24162417) offer a similar view on the particular negative connotations attached
to mental illness among people of South Asian origin
Family ties are seen to be of particular importance within the research group
communities as they greatly impact on culture hence influencing both access to
psychological therapies as well as individualsrsquo openness to mental health profes-
sionals and researchers (Finnstrom amp Soderhamn 2006 Lavender Khondoker amp
Jones 2006) Thus family and community issues in relation to the accessing of
psychological therapies appear to be of more importance for the research group
communities than for the dominant culture
Religion is another aspect shown to significantly impact upon service usersrsquo
perspectives with regard to accessing psychological therapies (Guerin Guerin
Diiriye amp Yates 2004 Whittaker et al 2005 for Somali communities Ramakrish-
nan 1984 Ravindran 2006 for Tamil communities Gerrish 2001 King Weich
Nazroo amp Blizard 2006 Lavender et al 2006 for Bengali and Urdu communities)
Religious observance is often seen as an alternative means of alleviating symptoms of
psychological distress and as is discussed below in relation to Jinns mental health
concerns are frequently understood within a religious framework that is not the case
for the majority increasingly secular community within the UK The implications for
offering a clinically based secular psychological therapies service are that such a
service may not be seen by service users as relevant or able to respond to their needs
as they understand them As will be discussed below this study found that the
participants in the focus groups reinforced previous literature on the significance of
religion in relation to accessing psychological services The question as to the
accessing of psychological therapies for members of these communities who are not
religious was not raised within the focus groups conducted for this study This is an
area potentially of interest for further research but was outside the scope of this
particular studyThe intention of this research was twofold to understand how mental health
issues in particular anxiety and depression are conceptualised and experienced by
people from BAME communities with particular reference to Bengali Urdu Tamil
and Somali speaking communities in the UK (the research group) and to explore
any potential implications of this for the accessing of psychological therapies services
by the communities As part of the Department of Healthrsquos IAPT initiative (IAPT
2008) which highlighted the disparity in access to psychological therapy between the
BAME communities and the mainstream population in the UK this research
commissioned by a London NHS Mental Health Trust aimed to investigate how
specific BAME communities Bengali Urdu Tamil and Somali conceptualise and
experience anxiety and depression both directly and indirectly and how these differ
from majority conceptualisations Secondly it aimed to gain more knowledge about
the feasibility of increasing access to psychological therapies in order to address the
disparity highlighted in previous research within these communities (Department of
Health 2007a 2007b 2009 Health Commission 2007)
Method
Design
In terms of method quantitative or mixed methods approaches to data collection
and analysis were considered but rejected as the focus of the research lay in
46 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
explicating the lived experience of the participants as described A qualitative
approach to research was chosen which acts to gain insight into the individualrsquos
experiences (Corbin amp Strauss 1998) It was felt that in understanding the
significance of a given experience a method that allowed analysis of the participantrsquos
words and personal meanings that an experience might have for the individual would
be important (Harre amp Secord 1972) It is not suggested that a person may have
exact insight into their own motives but that one can gain an understanding of anexperience as lived through a description by the person who had the experience
Focus groups are group discussions organised to explore a specific set of issues
such as peoplersquos views and experience (Basch 1987 Kitzinger 1994) Although often
seen as a convenient way to simultaneously collect data from a number of
participants the method capitalises on communication between research participants
in the generation of data (Kitzinger 1995) This means that instead of the researcher
asking each person to respond to a question in turn participants are encouraged to
talk to one another interacting and commenting on each otherrsquos experiences and
points of view The method is particularly useful for exploring peoplersquos knowledge
and experiences
Previous research on mental illness within the research group communities
indicates that focus groups are frequently used as a research method (Barron et al
2010 Halcomb Gholizadeh Di Giacomo Phillips amp Davidson 2004) Focus groups
have been used in previous studies with the Somali community (Finnstrom amp
Soderhamn 2006 Gervais 2008 Green amp Thorogood 2004 Warfa et al 2006) the
Tamil community (Bradby et al 2007 Fernando 2005 Sadavoy Meier amp Yuk2004 Whitley amp Prince 2004) Urdu groups (Acharya amp Northcott 2007) and
Bengali groups (Hawthorne Rahman amp Pill 2003) suggesting their suitability for
researching issues within these communities
This study sought to consider community perspectives and the experiences and
understandings of members of these communities as part of these groups with
subsequent implications for them as individuals As such focus groups were chosen
as the most appropriate method for this type of research study to consider the
community perspective
Further vignettes followed by questionsprobes were chosen as the appropriate
method of enabling sharing of experiences within the focus groups Within the focus
group interview schedule vignettes of a person displaying anxiety and in turn
depression were presented to the focus group participants followed by questions
about the participantsrsquo experiences in relation to the vignette Vignettes have been
widely used as a data collection technique in qualitative research (Hazel 1995
Hughes 1998) Hughes (1998 p 381) describes vignettes as lsquostories about
individuals situations and structures which can make reference to important pointsin the study of perceptions beliefs and attitudesrsquo
Vignettes provide a valuable technique for exploring peoplersquos perceptions beliefs
and meanings about specific situations and are particularly useful in exploring
potentially sensitive topics that participants might otherwise find difficult to discuss
(Neale 1999) Use of vignettes within a lsquofocusrsquo group is becoming increasingly
popular with social researchers (Wilkinson 1998) Maclean (1999) writing on the
use of vignettes within focus groups commented that it encouraged even the quietest
group member to voice an opinion
According to principles that guide the use of vignettes in research the vignettes
were created in a way that made them appear plausible and real to participants and
British Journal of Guidance and Counselling 47
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that contained sufficient context for participants to understand the situation
depicted The researchers then endeavoured to follow the vignette with questions
directed towards the beliefs assumptions and experiences of the participants with
regard to personal experiences of anxiety depression how participants cope withmental health issues limitations of mental health services and possible solutions for
the community involved
As a result for the purposes of this study mental health services were defined as
services carried out by mental health professionals in which treatments support and
advocacy to persons are offered to people experiencing mental health issues
(disturbances to their mental health) As a result this incorporates a breadth of
mental health services and professionals such as General Practitioners (GPs)
community mental health teams mental health nurses counsellors psychotherapistsoccupational therapists and clinical and counselling psychologists
The research also made use of respondent validation conducted on an individual
basis to consider how if at all the perspectives of participants as individuals differed
from those of the particular community interviewed (Silverman 2000) In particular
the aim of the interviews was to clarify the themes emerging from the focus groups to
ensure that the themes derived from the focus groups interviews were captured
accurately As Herrel et al (2004) p 349) argue lsquo otherwise possible misinterpre-
tation due to translation can occur and responses can be influenced by other focusgroup membersrsquo
Participant recruitment
As previously mentioned Bengali Urdu Tamil and Somali speaking communities
were sampled specifically for this study They form a particular focus for the NHS
Trust in that they have been reported to ask for more translations when accessingmental health services than other linguistic minority communities (Aspinall 2007)
The four samples of participants were recruited through the various Bengali
Urdu Tamil and Somali community associations with which the NHS Trust was in
contact sometimes working directly on mental health issues and IAPT The process
of selection was opportunistic sampling based on those who volunteered to take part
after having been invited to do so verbally by senior members of these community
associations In particular the recruitment method was seen as one that was
culturally acceptable to the selected communities With permission posters were alsoplaced in community buildings to advertise the study Those who volunteered were
then supplied with additional information about the study and informed consent was
required from each participant
Participants
Bengali community participants
Two focus groups were conducted for Bengali speaking participants The first group
consisted of eight female participants and the second group consisted of four female
and two male participants As participants were recruited through opportunistic
sampling there was an inconsistency in the malefemale participation ratio
With regards to the six respondent validation interviews four female participants
were recruited and two male participants
48 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Demographically the age group of all participants was 50 and above All
participants reflected Bangladeshi heritage and identified with Islam as their religion
Urdu community participants
Two focus groups were conducted with 21 participants in total The first group
consisted of 15 female participants and the second group consisted of six maleparticipants marking a separation of the groups based on gender
A further six participants (three males and three females) were selected for the
respondent validation interviews
Demographically the age group of all participants was 40 and above A variety of
participants were recruited whose origins reflected a diversity of the Urdu speaking
population Even though most participants were of Pakistani origins some
participants stated their heritage to be East African and even Indian The majority
of the participants stated Islam to be their religion
Tamil community participants
The two focus groups were made up of 18 participants in total The first groupconsisted of 10 males and the second of eight female participants making a
separation of the groups based on gender
For the respondent validation interviews six interviews were carried out with
four males and two females
All participants fell within the age range of 40 and above
Somali community participants
Two focus groups were conducted with 24 participants in total The first group
consisted of 14 female participants and the second group consisted of 10 male
participants marking a separation of the groups based on gender
A further six participants three males and three females were selected for therespondent validation interviews
Demographically the age group of all participants was 40 and above
Data collection and analysis
Two open-ended focus groups were carried out with each of the separate Bengali
Urdu Tamil and Somali groups with the Community Development Workers
(CDWs) present The CDWs were involved due to their knowledge of the community
and ability to aid set up and implementation of the focus groups The respondent
validation interviews were then conducted with six individuals from each of the
community groupsDue to cultural considerations the four researchers all of whom were themselves
born outside of the UK and in terms of their languages and cultural backgrounds
members of the respective communities relevant to this study conducted the focus
groups and respondent validation interviews with the male and female participants
separately (with the exception of the Bengali participants who requested mixed
gender participant groups) The focus groups and respondent validations for each
British Journal of Guidance and Counselling 49
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

Reducing the barriers to accessing psychological therapies for BengaliUrdu Tamil and Somali communities in the UK some implications fortraining policy and practice
Del Loewenthala Ahmed Mohamedb Samyukta Mukhopadhyayc Kalai Ganeshd
and Rhiannon Thomase
aRoehampton University Whitelands College London UK bDepartment of PsychiatryUniversity of Cambridge UK cInstitute of Psychiatry Kingrsquos College London UKdIndependent Research Consultation ePsychotherapy in private practice
(Received 20 October 2010 final version received 30 July 2011)
The aim of this research was to investigate the feasibility of achieving ImprovingAccess to Psychological Therapies (IAPT) for people from Black Asian andMinority Ethnic (BAME) communities living in the UK with specific referenceto Bengali Urdu Tamil and Somali speaking communities Focus groups werecarried out with each of the communities to investigate how they conceptualiseand experience lsquomental health issuesrsquo and what they do when faced with what theyregard as these issues A thematic analysis of the data suggested that participantsdid not fully understand common conceptualisations about mental health issuesnor did they know how to seek mental health support Implications of culturalbarriers and recommendations for IAPT outcomes for the four communities arediscussed
Keywords anxiety depression Improving Access to Psychological Therapies(IAPT) training Black Asian Minority Ethnic (BAME) thematic analysisBengali Urdu Tamil and Somali
Introduction
Disparities between Caucasian and Black Asian and Minority Ethnic (BAME)
communities in terms of access to experience with and outcomes in mental health
issues have been documented (Bhui Sashidharan Cannon McKenzie amp Sims 2003
Department of Health 2005 Health 2007a 2007b Fernando 2005 Health
Commission 2007) The Department of Health (2007a 2007b) stated that a key
mental health issue for BAME communities in the UK is low uptake of
psychologicaltalking therapies which it has been argued needs to change (Mulatu
amp Berry 2001) in order to achieve equality in mental health care across UK
communities It has been argued that a lsquocircle of fearrsquo (Sainsbury Centre for Mental
Health 2005) has developed preventing ethnic minorities from accessing mental
health services defined as services offering treatments support and advocacy to
persons experiencing disturbances to their mental health It was found that
individuals are frequently accessing services later and at a more critical stage than
Caucasian service users The Department of Health report conducted by Sashidhar-
Corresponding author Email dloewenthalroehamptonacuk
British Journal of Guidance amp Counselling
Vol 40 No 1 February 2012 4366
ISSN 0306-9885 printISSN 1469-3534 online
2012 Taylor amp Francis
httpdxdoiorg101080030698852011621519
httpwwwtandfonlinecom
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
an (2003) considered reasons that mental health services in the UK are failing to
meet the needs of BAME populations The report recommended the development of
the cultural capability of mental health services in the UK and the importance of
engaging the community in order to improve mental health services for thesepopulations
Providing better mental health care for BAME communities arguably requires
significantly more than the efforts currently made within our mental health care
system in the UK (Fowles 2007) The barriers for people from BAME communities
have been stated to include practicalities such as languages used for health
information through to attitudinal challenges faced by mainly Eurocentric-focused
health professionals in understanding the cultural diversity of both the expression
and treatment of mental health problems (Bhugra amp Ayonrinde 2004 Fernando2005) Related to this Sass Moffat Bhui and McKenzie (2009) have identified that
ethnic matching is a significant factor in enhancing care pathways for BAME
communities in the UK
A background to questions of cultural impact on access to psychological
therapies will now be presented followed by a discussion of language and the
categorisation of BAME communities and other cultural considerations such as
family ties and religion affecting access to psychological therapies for Bengali
Tamil Urdu and Somali speaking communities (the research group)
Cultural background
Research has indicated that mental health professionalsrsquo lack of understanding aboutthe cultural background of BAME communities negatively impacts on service usersrsquo
access to psychological therapies (Ager 1993 Beiser amp Hou 2002 Danso 2001
Silove Sinnerbrink Field Manicavasagar amp Steel 2000 Sinnerbrink Silove
Manicavasagar Steel amp Field 1996 Watters 2001 Watters amp Ingleby 2004) In
addition to this these professionalsrsquo attitudes during their interaction negative
positive or neutral left an impression on service users (Boi 2000)
McKenzie and Bhui (2007) explore the need for providing a coherent and
integrated service for minority ethnic communities They argue that emphasis isrequired on considering patientsrsquo needs improvising with existing techniques and
therapies highlighting resolutions integrated with respect for diversity at all times
evidence-based practice and success in long-term goals
There has also been criticism that in the UK diversity classification comes under
broad categories lacking specific and clear structures (McDowell Coleman amp
Ferner 2006) This is considered further below in relation to the use of terms such as
lsquoSouth Asianrsquo In addition to a loss of cultural specificity there is also the potential
difficulty inherent in defining and imposing mental health issues based onunderstandings applicable to a dominant culture This has previously been illustrated
from the perspective of transcultural psychiatry (Ellis Kia-Keating Yusuf Lincoln
amp Nur 2007 Ellis MacDonald Lincoln amp Cabral 2008 Fernando 2005)
The categorisation of communities and language issues
The use of the term lsquoSouth Asianrsquo community used to encompass individuals from
India Pakistan Bangladesh and Sri Lanka is in reality arguably too broad to enable
research on relevant factors that affect access to psychological therapies for these
44 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
linguistically religiously and culturally distinct communities Similarities in ethnicity
spoken languages or mother tongues may not imply similarities in culture These
have been shown to be distinctive in particular within the Tamil (Ravindran 2006)
and Bengali groups (Hossain amp Khan 2006) Only religion is considered as being acommon factor affecting access to mental health services for some individuals within
the South Asian community A lack of understanding of for example the geo-
political differences within the Bengali community is seen to create an instant barrier
between practitioner and service user (Gerrish 2000 2001)
Language emerges as a key barrier to peoplersquos use of health services (Murray amp
Buller 2007 Saha Fernandez amp Perez-Stable 2007) and requests for interpreters to
address mental health issues come particularly from four major linguistic minority
communities in the UK Bengali Somali Tamil and Urdu speakers Thesecommunities have been reported to ask for more translations when accessing mental
health services than other linguistic minority communities (Aspinall 2007) and these
communities were thus a particular focus for the National Health Service (NHS)
Trust which commissioned this work As such this research focused on these four
specific languages with regard to achieving Improving Access to Psychological
Therapies (IAPT) outcomes (IAPT 2008) The question of why these particular
communities request more interpreter services compared to other often larger
minority communities within the UK is an issue that is potentially of relevance butwhich fell outside of the scope of this research
Somalian service users may therefore be discouraged from accessing mental health
services due to language barriers (Bhui et al 2003 Fernando 2005 Health
Commission 2007 McCrone et al 2005 Pumroy 2008 Warfa et al 2006) An
example of this is the fact that the UK Department of Health has translated
psychological materials including computerised Cognitive Behaviour Therapy
(cCBT) into several languages but not as yet Somali (Department of Health 2007a)
In relation to primary care services in a more general sense rather thanspecifically psychological therapies Barron Holterman Shipster Batson and Alam
(2010) sought to investigate the awareness and views of ethnic minority community
members towards primary health care interpreting provision in Hertfordshire This
study identified the importance of the provision of high quality language
interpretation services for enabling access In particular this study highlighted the
importance of trust confidentiality accuracy and independence in an interpreter preferred to be from their own culture and gender (Barron et al 2010) This was an
issue that was also of concern for the participants in this research on access topsychological therapies
Other cultural considerations affecting access to psychological therapies for BengaliUrdu Tamil and Somali communities
Stigmas associated with mental health continue to exist within both majority and
minority communities living in the UK While the stigma associated with mental
health issues is thus not exclusively an issue for BAME communities there aredimensions of this which arise specifically for these minority groups For the
communities considered as the focus of this research negative connotations include
for example Somalis who have been shown to be not only shameful about mental
illnesses but also fearful of mental health professionals leading them to conceal
mental health issues (Whittaker Lewis amp Buchan 2005) Bradby et al (2007)
British Journal of Guidance and Counselling 45
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
pp 24162417) offer a similar view on the particular negative connotations attached
to mental illness among people of South Asian origin
Family ties are seen to be of particular importance within the research group
communities as they greatly impact on culture hence influencing both access to
psychological therapies as well as individualsrsquo openness to mental health profes-
sionals and researchers (Finnstrom amp Soderhamn 2006 Lavender Khondoker amp
Jones 2006) Thus family and community issues in relation to the accessing of
psychological therapies appear to be of more importance for the research group
communities than for the dominant culture
Religion is another aspect shown to significantly impact upon service usersrsquo
perspectives with regard to accessing psychological therapies (Guerin Guerin
Diiriye amp Yates 2004 Whittaker et al 2005 for Somali communities Ramakrish-
nan 1984 Ravindran 2006 for Tamil communities Gerrish 2001 King Weich
Nazroo amp Blizard 2006 Lavender et al 2006 for Bengali and Urdu communities)
Religious observance is often seen as an alternative means of alleviating symptoms of
psychological distress and as is discussed below in relation to Jinns mental health
concerns are frequently understood within a religious framework that is not the case
for the majority increasingly secular community within the UK The implications for
offering a clinically based secular psychological therapies service are that such a
service may not be seen by service users as relevant or able to respond to their needs
as they understand them As will be discussed below this study found that the
participants in the focus groups reinforced previous literature on the significance of
religion in relation to accessing psychological services The question as to the
accessing of psychological therapies for members of these communities who are not
religious was not raised within the focus groups conducted for this study This is an
area potentially of interest for further research but was outside the scope of this
particular studyThe intention of this research was twofold to understand how mental health
issues in particular anxiety and depression are conceptualised and experienced by
people from BAME communities with particular reference to Bengali Urdu Tamil
and Somali speaking communities in the UK (the research group) and to explore
any potential implications of this for the accessing of psychological therapies services
by the communities As part of the Department of Healthrsquos IAPT initiative (IAPT
2008) which highlighted the disparity in access to psychological therapy between the
BAME communities and the mainstream population in the UK this research
commissioned by a London NHS Mental Health Trust aimed to investigate how
specific BAME communities Bengali Urdu Tamil and Somali conceptualise and
experience anxiety and depression both directly and indirectly and how these differ
from majority conceptualisations Secondly it aimed to gain more knowledge about
the feasibility of increasing access to psychological therapies in order to address the
disparity highlighted in previous research within these communities (Department of
Health 2007a 2007b 2009 Health Commission 2007)
Method
Design
In terms of method quantitative or mixed methods approaches to data collection
and analysis were considered but rejected as the focus of the research lay in
46 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
explicating the lived experience of the participants as described A qualitative
approach to research was chosen which acts to gain insight into the individualrsquos
experiences (Corbin amp Strauss 1998) It was felt that in understanding the
significance of a given experience a method that allowed analysis of the participantrsquos
words and personal meanings that an experience might have for the individual would
be important (Harre amp Secord 1972) It is not suggested that a person may have
exact insight into their own motives but that one can gain an understanding of anexperience as lived through a description by the person who had the experience
Focus groups are group discussions organised to explore a specific set of issues
such as peoplersquos views and experience (Basch 1987 Kitzinger 1994) Although often
seen as a convenient way to simultaneously collect data from a number of
participants the method capitalises on communication between research participants
in the generation of data (Kitzinger 1995) This means that instead of the researcher
asking each person to respond to a question in turn participants are encouraged to
talk to one another interacting and commenting on each otherrsquos experiences and
points of view The method is particularly useful for exploring peoplersquos knowledge
and experiences
Previous research on mental illness within the research group communities
indicates that focus groups are frequently used as a research method (Barron et al
2010 Halcomb Gholizadeh Di Giacomo Phillips amp Davidson 2004) Focus groups
have been used in previous studies with the Somali community (Finnstrom amp
Soderhamn 2006 Gervais 2008 Green amp Thorogood 2004 Warfa et al 2006) the
Tamil community (Bradby et al 2007 Fernando 2005 Sadavoy Meier amp Yuk2004 Whitley amp Prince 2004) Urdu groups (Acharya amp Northcott 2007) and
Bengali groups (Hawthorne Rahman amp Pill 2003) suggesting their suitability for
researching issues within these communities
This study sought to consider community perspectives and the experiences and
understandings of members of these communities as part of these groups with
subsequent implications for them as individuals As such focus groups were chosen
as the most appropriate method for this type of research study to consider the
community perspective
Further vignettes followed by questionsprobes were chosen as the appropriate
method of enabling sharing of experiences within the focus groups Within the focus
group interview schedule vignettes of a person displaying anxiety and in turn
depression were presented to the focus group participants followed by questions
about the participantsrsquo experiences in relation to the vignette Vignettes have been
widely used as a data collection technique in qualitative research (Hazel 1995
Hughes 1998) Hughes (1998 p 381) describes vignettes as lsquostories about
individuals situations and structures which can make reference to important pointsin the study of perceptions beliefs and attitudesrsquo
Vignettes provide a valuable technique for exploring peoplersquos perceptions beliefs
and meanings about specific situations and are particularly useful in exploring
potentially sensitive topics that participants might otherwise find difficult to discuss
(Neale 1999) Use of vignettes within a lsquofocusrsquo group is becoming increasingly
popular with social researchers (Wilkinson 1998) Maclean (1999) writing on the
use of vignettes within focus groups commented that it encouraged even the quietest
group member to voice an opinion
According to principles that guide the use of vignettes in research the vignettes
were created in a way that made them appear plausible and real to participants and
British Journal of Guidance and Counselling 47
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that contained sufficient context for participants to understand the situation
depicted The researchers then endeavoured to follow the vignette with questions
directed towards the beliefs assumptions and experiences of the participants with
regard to personal experiences of anxiety depression how participants cope withmental health issues limitations of mental health services and possible solutions for
the community involved
As a result for the purposes of this study mental health services were defined as
services carried out by mental health professionals in which treatments support and
advocacy to persons are offered to people experiencing mental health issues
(disturbances to their mental health) As a result this incorporates a breadth of
mental health services and professionals such as General Practitioners (GPs)
community mental health teams mental health nurses counsellors psychotherapistsoccupational therapists and clinical and counselling psychologists
The research also made use of respondent validation conducted on an individual
basis to consider how if at all the perspectives of participants as individuals differed
from those of the particular community interviewed (Silverman 2000) In particular
the aim of the interviews was to clarify the themes emerging from the focus groups to
ensure that the themes derived from the focus groups interviews were captured
accurately As Herrel et al (2004) p 349) argue lsquo otherwise possible misinterpre-
tation due to translation can occur and responses can be influenced by other focusgroup membersrsquo
Participant recruitment
As previously mentioned Bengali Urdu Tamil and Somali speaking communities
were sampled specifically for this study They form a particular focus for the NHS
Trust in that they have been reported to ask for more translations when accessingmental health services than other linguistic minority communities (Aspinall 2007)
The four samples of participants were recruited through the various Bengali
Urdu Tamil and Somali community associations with which the NHS Trust was in
contact sometimes working directly on mental health issues and IAPT The process
of selection was opportunistic sampling based on those who volunteered to take part
after having been invited to do so verbally by senior members of these community
associations In particular the recruitment method was seen as one that was
culturally acceptable to the selected communities With permission posters were alsoplaced in community buildings to advertise the study Those who volunteered were
then supplied with additional information about the study and informed consent was
required from each participant
Participants
Bengali community participants
Two focus groups were conducted for Bengali speaking participants The first group
consisted of eight female participants and the second group consisted of four female
and two male participants As participants were recruited through opportunistic
sampling there was an inconsistency in the malefemale participation ratio
With regards to the six respondent validation interviews four female participants
were recruited and two male participants
48 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Demographically the age group of all participants was 50 and above All
participants reflected Bangladeshi heritage and identified with Islam as their religion
Urdu community participants
Two focus groups were conducted with 21 participants in total The first group
consisted of 15 female participants and the second group consisted of six maleparticipants marking a separation of the groups based on gender
A further six participants (three males and three females) were selected for the
respondent validation interviews
Demographically the age group of all participants was 40 and above A variety of
participants were recruited whose origins reflected a diversity of the Urdu speaking
population Even though most participants were of Pakistani origins some
participants stated their heritage to be East African and even Indian The majority
of the participants stated Islam to be their religion
Tamil community participants
The two focus groups were made up of 18 participants in total The first groupconsisted of 10 males and the second of eight female participants making a
separation of the groups based on gender
For the respondent validation interviews six interviews were carried out with
four males and two females
All participants fell within the age range of 40 and above
Somali community participants
Two focus groups were conducted with 24 participants in total The first group
consisted of 14 female participants and the second group consisted of 10 male
participants marking a separation of the groups based on gender
A further six participants three males and three females were selected for therespondent validation interviews
Demographically the age group of all participants was 40 and above
Data collection and analysis
Two open-ended focus groups were carried out with each of the separate Bengali
Urdu Tamil and Somali groups with the Community Development Workers
(CDWs) present The CDWs were involved due to their knowledge of the community
and ability to aid set up and implementation of the focus groups The respondent
validation interviews were then conducted with six individuals from each of the
community groupsDue to cultural considerations the four researchers all of whom were themselves
born outside of the UK and in terms of their languages and cultural backgrounds
members of the respective communities relevant to this study conducted the focus
groups and respondent validation interviews with the male and female participants
separately (with the exception of the Bengali participants who requested mixed
gender participant groups) The focus groups and respondent validations for each
British Journal of Guidance and Counselling 49
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

an (2003) considered reasons that mental health services in the UK are failing to
meet the needs of BAME populations The report recommended the development of
the cultural capability of mental health services in the UK and the importance of
engaging the community in order to improve mental health services for thesepopulations
Providing better mental health care for BAME communities arguably requires
significantly more than the efforts currently made within our mental health care
system in the UK (Fowles 2007) The barriers for people from BAME communities
have been stated to include practicalities such as languages used for health
information through to attitudinal challenges faced by mainly Eurocentric-focused
health professionals in understanding the cultural diversity of both the expression
and treatment of mental health problems (Bhugra amp Ayonrinde 2004 Fernando2005) Related to this Sass Moffat Bhui and McKenzie (2009) have identified that
ethnic matching is a significant factor in enhancing care pathways for BAME
communities in the UK
A background to questions of cultural impact on access to psychological
therapies will now be presented followed by a discussion of language and the
categorisation of BAME communities and other cultural considerations such as
family ties and religion affecting access to psychological therapies for Bengali
Tamil Urdu and Somali speaking communities (the research group)
Cultural background
Research has indicated that mental health professionalsrsquo lack of understanding aboutthe cultural background of BAME communities negatively impacts on service usersrsquo
access to psychological therapies (Ager 1993 Beiser amp Hou 2002 Danso 2001
Silove Sinnerbrink Field Manicavasagar amp Steel 2000 Sinnerbrink Silove
Manicavasagar Steel amp Field 1996 Watters 2001 Watters amp Ingleby 2004) In
addition to this these professionalsrsquo attitudes during their interaction negative
positive or neutral left an impression on service users (Boi 2000)
McKenzie and Bhui (2007) explore the need for providing a coherent and
integrated service for minority ethnic communities They argue that emphasis isrequired on considering patientsrsquo needs improvising with existing techniques and
therapies highlighting resolutions integrated with respect for diversity at all times
evidence-based practice and success in long-term goals
There has also been criticism that in the UK diversity classification comes under
broad categories lacking specific and clear structures (McDowell Coleman amp
Ferner 2006) This is considered further below in relation to the use of terms such as
lsquoSouth Asianrsquo In addition to a loss of cultural specificity there is also the potential
difficulty inherent in defining and imposing mental health issues based onunderstandings applicable to a dominant culture This has previously been illustrated
from the perspective of transcultural psychiatry (Ellis Kia-Keating Yusuf Lincoln
amp Nur 2007 Ellis MacDonald Lincoln amp Cabral 2008 Fernando 2005)
The categorisation of communities and language issues
The use of the term lsquoSouth Asianrsquo community used to encompass individuals from
India Pakistan Bangladesh and Sri Lanka is in reality arguably too broad to enable
research on relevant factors that affect access to psychological therapies for these
44 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
linguistically religiously and culturally distinct communities Similarities in ethnicity
spoken languages or mother tongues may not imply similarities in culture These
have been shown to be distinctive in particular within the Tamil (Ravindran 2006)
and Bengali groups (Hossain amp Khan 2006) Only religion is considered as being acommon factor affecting access to mental health services for some individuals within
the South Asian community A lack of understanding of for example the geo-
political differences within the Bengali community is seen to create an instant barrier
between practitioner and service user (Gerrish 2000 2001)
Language emerges as a key barrier to peoplersquos use of health services (Murray amp
Buller 2007 Saha Fernandez amp Perez-Stable 2007) and requests for interpreters to
address mental health issues come particularly from four major linguistic minority
communities in the UK Bengali Somali Tamil and Urdu speakers Thesecommunities have been reported to ask for more translations when accessing mental
health services than other linguistic minority communities (Aspinall 2007) and these
communities were thus a particular focus for the National Health Service (NHS)
Trust which commissioned this work As such this research focused on these four
specific languages with regard to achieving Improving Access to Psychological
Therapies (IAPT) outcomes (IAPT 2008) The question of why these particular
communities request more interpreter services compared to other often larger
minority communities within the UK is an issue that is potentially of relevance butwhich fell outside of the scope of this research
Somalian service users may therefore be discouraged from accessing mental health
services due to language barriers (Bhui et al 2003 Fernando 2005 Health
Commission 2007 McCrone et al 2005 Pumroy 2008 Warfa et al 2006) An
example of this is the fact that the UK Department of Health has translated
psychological materials including computerised Cognitive Behaviour Therapy
(cCBT) into several languages but not as yet Somali (Department of Health 2007a)
In relation to primary care services in a more general sense rather thanspecifically psychological therapies Barron Holterman Shipster Batson and Alam
(2010) sought to investigate the awareness and views of ethnic minority community
members towards primary health care interpreting provision in Hertfordshire This
study identified the importance of the provision of high quality language
interpretation services for enabling access In particular this study highlighted the
importance of trust confidentiality accuracy and independence in an interpreter preferred to be from their own culture and gender (Barron et al 2010) This was an
issue that was also of concern for the participants in this research on access topsychological therapies
Other cultural considerations affecting access to psychological therapies for BengaliUrdu Tamil and Somali communities
Stigmas associated with mental health continue to exist within both majority and
minority communities living in the UK While the stigma associated with mental
health issues is thus not exclusively an issue for BAME communities there aredimensions of this which arise specifically for these minority groups For the
communities considered as the focus of this research negative connotations include
for example Somalis who have been shown to be not only shameful about mental
illnesses but also fearful of mental health professionals leading them to conceal
mental health issues (Whittaker Lewis amp Buchan 2005) Bradby et al (2007)
British Journal of Guidance and Counselling 45
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
pp 24162417) offer a similar view on the particular negative connotations attached
to mental illness among people of South Asian origin
Family ties are seen to be of particular importance within the research group
communities as they greatly impact on culture hence influencing both access to
psychological therapies as well as individualsrsquo openness to mental health profes-
sionals and researchers (Finnstrom amp Soderhamn 2006 Lavender Khondoker amp
Jones 2006) Thus family and community issues in relation to the accessing of
psychological therapies appear to be of more importance for the research group
communities than for the dominant culture
Religion is another aspect shown to significantly impact upon service usersrsquo
perspectives with regard to accessing psychological therapies (Guerin Guerin
Diiriye amp Yates 2004 Whittaker et al 2005 for Somali communities Ramakrish-
nan 1984 Ravindran 2006 for Tamil communities Gerrish 2001 King Weich
Nazroo amp Blizard 2006 Lavender et al 2006 for Bengali and Urdu communities)
Religious observance is often seen as an alternative means of alleviating symptoms of
psychological distress and as is discussed below in relation to Jinns mental health
concerns are frequently understood within a religious framework that is not the case
for the majority increasingly secular community within the UK The implications for
offering a clinically based secular psychological therapies service are that such a
service may not be seen by service users as relevant or able to respond to their needs
as they understand them As will be discussed below this study found that the
participants in the focus groups reinforced previous literature on the significance of
religion in relation to accessing psychological services The question as to the
accessing of psychological therapies for members of these communities who are not
religious was not raised within the focus groups conducted for this study This is an
area potentially of interest for further research but was outside the scope of this
particular studyThe intention of this research was twofold to understand how mental health
issues in particular anxiety and depression are conceptualised and experienced by
people from BAME communities with particular reference to Bengali Urdu Tamil
and Somali speaking communities in the UK (the research group) and to explore
any potential implications of this for the accessing of psychological therapies services
by the communities As part of the Department of Healthrsquos IAPT initiative (IAPT
2008) which highlighted the disparity in access to psychological therapy between the
BAME communities and the mainstream population in the UK this research
commissioned by a London NHS Mental Health Trust aimed to investigate how
specific BAME communities Bengali Urdu Tamil and Somali conceptualise and
experience anxiety and depression both directly and indirectly and how these differ
from majority conceptualisations Secondly it aimed to gain more knowledge about
the feasibility of increasing access to psychological therapies in order to address the
disparity highlighted in previous research within these communities (Department of
Health 2007a 2007b 2009 Health Commission 2007)
Method
Design
In terms of method quantitative or mixed methods approaches to data collection
and analysis were considered but rejected as the focus of the research lay in
46 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
explicating the lived experience of the participants as described A qualitative
approach to research was chosen which acts to gain insight into the individualrsquos
experiences (Corbin amp Strauss 1998) It was felt that in understanding the
significance of a given experience a method that allowed analysis of the participantrsquos
words and personal meanings that an experience might have for the individual would
be important (Harre amp Secord 1972) It is not suggested that a person may have
exact insight into their own motives but that one can gain an understanding of anexperience as lived through a description by the person who had the experience
Focus groups are group discussions organised to explore a specific set of issues
such as peoplersquos views and experience (Basch 1987 Kitzinger 1994) Although often
seen as a convenient way to simultaneously collect data from a number of
participants the method capitalises on communication between research participants
in the generation of data (Kitzinger 1995) This means that instead of the researcher
asking each person to respond to a question in turn participants are encouraged to
talk to one another interacting and commenting on each otherrsquos experiences and
points of view The method is particularly useful for exploring peoplersquos knowledge
and experiences
Previous research on mental illness within the research group communities
indicates that focus groups are frequently used as a research method (Barron et al
2010 Halcomb Gholizadeh Di Giacomo Phillips amp Davidson 2004) Focus groups
have been used in previous studies with the Somali community (Finnstrom amp
Soderhamn 2006 Gervais 2008 Green amp Thorogood 2004 Warfa et al 2006) the
Tamil community (Bradby et al 2007 Fernando 2005 Sadavoy Meier amp Yuk2004 Whitley amp Prince 2004) Urdu groups (Acharya amp Northcott 2007) and
Bengali groups (Hawthorne Rahman amp Pill 2003) suggesting their suitability for
researching issues within these communities
This study sought to consider community perspectives and the experiences and
understandings of members of these communities as part of these groups with
subsequent implications for them as individuals As such focus groups were chosen
as the most appropriate method for this type of research study to consider the
community perspective
Further vignettes followed by questionsprobes were chosen as the appropriate
method of enabling sharing of experiences within the focus groups Within the focus
group interview schedule vignettes of a person displaying anxiety and in turn
depression were presented to the focus group participants followed by questions
about the participantsrsquo experiences in relation to the vignette Vignettes have been
widely used as a data collection technique in qualitative research (Hazel 1995
Hughes 1998) Hughes (1998 p 381) describes vignettes as lsquostories about
individuals situations and structures which can make reference to important pointsin the study of perceptions beliefs and attitudesrsquo
Vignettes provide a valuable technique for exploring peoplersquos perceptions beliefs
and meanings about specific situations and are particularly useful in exploring
potentially sensitive topics that participants might otherwise find difficult to discuss
(Neale 1999) Use of vignettes within a lsquofocusrsquo group is becoming increasingly
popular with social researchers (Wilkinson 1998) Maclean (1999) writing on the
use of vignettes within focus groups commented that it encouraged even the quietest
group member to voice an opinion
According to principles that guide the use of vignettes in research the vignettes
were created in a way that made them appear plausible and real to participants and
British Journal of Guidance and Counselling 47
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that contained sufficient context for participants to understand the situation
depicted The researchers then endeavoured to follow the vignette with questions
directed towards the beliefs assumptions and experiences of the participants with
regard to personal experiences of anxiety depression how participants cope withmental health issues limitations of mental health services and possible solutions for
the community involved
As a result for the purposes of this study mental health services were defined as
services carried out by mental health professionals in which treatments support and
advocacy to persons are offered to people experiencing mental health issues
(disturbances to their mental health) As a result this incorporates a breadth of
mental health services and professionals such as General Practitioners (GPs)
community mental health teams mental health nurses counsellors psychotherapistsoccupational therapists and clinical and counselling psychologists
The research also made use of respondent validation conducted on an individual
basis to consider how if at all the perspectives of participants as individuals differed
from those of the particular community interviewed (Silverman 2000) In particular
the aim of the interviews was to clarify the themes emerging from the focus groups to
ensure that the themes derived from the focus groups interviews were captured
accurately As Herrel et al (2004) p 349) argue lsquo otherwise possible misinterpre-
tation due to translation can occur and responses can be influenced by other focusgroup membersrsquo
Participant recruitment
As previously mentioned Bengali Urdu Tamil and Somali speaking communities
were sampled specifically for this study They form a particular focus for the NHS
Trust in that they have been reported to ask for more translations when accessingmental health services than other linguistic minority communities (Aspinall 2007)
The four samples of participants were recruited through the various Bengali
Urdu Tamil and Somali community associations with which the NHS Trust was in
contact sometimes working directly on mental health issues and IAPT The process
of selection was opportunistic sampling based on those who volunteered to take part
after having been invited to do so verbally by senior members of these community
associations In particular the recruitment method was seen as one that was
culturally acceptable to the selected communities With permission posters were alsoplaced in community buildings to advertise the study Those who volunteered were
then supplied with additional information about the study and informed consent was
required from each participant
Participants
Bengali community participants
Two focus groups were conducted for Bengali speaking participants The first group
consisted of eight female participants and the second group consisted of four female
and two male participants As participants were recruited through opportunistic
sampling there was an inconsistency in the malefemale participation ratio
With regards to the six respondent validation interviews four female participants
were recruited and two male participants
48 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Demographically the age group of all participants was 50 and above All
participants reflected Bangladeshi heritage and identified with Islam as their religion
Urdu community participants
Two focus groups were conducted with 21 participants in total The first group
consisted of 15 female participants and the second group consisted of six maleparticipants marking a separation of the groups based on gender
A further six participants (three males and three females) were selected for the
respondent validation interviews
Demographically the age group of all participants was 40 and above A variety of
participants were recruited whose origins reflected a diversity of the Urdu speaking
population Even though most participants were of Pakistani origins some
participants stated their heritage to be East African and even Indian The majority
of the participants stated Islam to be their religion
Tamil community participants
The two focus groups were made up of 18 participants in total The first groupconsisted of 10 males and the second of eight female participants making a
separation of the groups based on gender
For the respondent validation interviews six interviews were carried out with
four males and two females
All participants fell within the age range of 40 and above
Somali community participants
Two focus groups were conducted with 24 participants in total The first group
consisted of 14 female participants and the second group consisted of 10 male
participants marking a separation of the groups based on gender
A further six participants three males and three females were selected for therespondent validation interviews
Demographically the age group of all participants was 40 and above
Data collection and analysis
Two open-ended focus groups were carried out with each of the separate Bengali
Urdu Tamil and Somali groups with the Community Development Workers
(CDWs) present The CDWs were involved due to their knowledge of the community
and ability to aid set up and implementation of the focus groups The respondent
validation interviews were then conducted with six individuals from each of the
community groupsDue to cultural considerations the four researchers all of whom were themselves
born outside of the UK and in terms of their languages and cultural backgrounds
members of the respective communities relevant to this study conducted the focus
groups and respondent validation interviews with the male and female participants
separately (with the exception of the Bengali participants who requested mixed
gender participant groups) The focus groups and respondent validations for each
British Journal of Guidance and Counselling 49
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

linguistically religiously and culturally distinct communities Similarities in ethnicity
spoken languages or mother tongues may not imply similarities in culture These
have been shown to be distinctive in particular within the Tamil (Ravindran 2006)
and Bengali groups (Hossain amp Khan 2006) Only religion is considered as being acommon factor affecting access to mental health services for some individuals within
the South Asian community A lack of understanding of for example the geo-
political differences within the Bengali community is seen to create an instant barrier
between practitioner and service user (Gerrish 2000 2001)
Language emerges as a key barrier to peoplersquos use of health services (Murray amp
Buller 2007 Saha Fernandez amp Perez-Stable 2007) and requests for interpreters to
address mental health issues come particularly from four major linguistic minority
communities in the UK Bengali Somali Tamil and Urdu speakers Thesecommunities have been reported to ask for more translations when accessing mental
health services than other linguistic minority communities (Aspinall 2007) and these
communities were thus a particular focus for the National Health Service (NHS)
Trust which commissioned this work As such this research focused on these four
specific languages with regard to achieving Improving Access to Psychological
Therapies (IAPT) outcomes (IAPT 2008) The question of why these particular
communities request more interpreter services compared to other often larger
minority communities within the UK is an issue that is potentially of relevance butwhich fell outside of the scope of this research
Somalian service users may therefore be discouraged from accessing mental health
services due to language barriers (Bhui et al 2003 Fernando 2005 Health
Commission 2007 McCrone et al 2005 Pumroy 2008 Warfa et al 2006) An
example of this is the fact that the UK Department of Health has translated
psychological materials including computerised Cognitive Behaviour Therapy
(cCBT) into several languages but not as yet Somali (Department of Health 2007a)
In relation to primary care services in a more general sense rather thanspecifically psychological therapies Barron Holterman Shipster Batson and Alam
(2010) sought to investigate the awareness and views of ethnic minority community
members towards primary health care interpreting provision in Hertfordshire This
study identified the importance of the provision of high quality language
interpretation services for enabling access In particular this study highlighted the
importance of trust confidentiality accuracy and independence in an interpreter preferred to be from their own culture and gender (Barron et al 2010) This was an
issue that was also of concern for the participants in this research on access topsychological therapies
Other cultural considerations affecting access to psychological therapies for BengaliUrdu Tamil and Somali communities
Stigmas associated with mental health continue to exist within both majority and
minority communities living in the UK While the stigma associated with mental
health issues is thus not exclusively an issue for BAME communities there aredimensions of this which arise specifically for these minority groups For the
communities considered as the focus of this research negative connotations include
for example Somalis who have been shown to be not only shameful about mental
illnesses but also fearful of mental health professionals leading them to conceal
mental health issues (Whittaker Lewis amp Buchan 2005) Bradby et al (2007)
British Journal of Guidance and Counselling 45
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
pp 24162417) offer a similar view on the particular negative connotations attached
to mental illness among people of South Asian origin
Family ties are seen to be of particular importance within the research group
communities as they greatly impact on culture hence influencing both access to
psychological therapies as well as individualsrsquo openness to mental health profes-
sionals and researchers (Finnstrom amp Soderhamn 2006 Lavender Khondoker amp
Jones 2006) Thus family and community issues in relation to the accessing of
psychological therapies appear to be of more importance for the research group
communities than for the dominant culture
Religion is another aspect shown to significantly impact upon service usersrsquo
perspectives with regard to accessing psychological therapies (Guerin Guerin
Diiriye amp Yates 2004 Whittaker et al 2005 for Somali communities Ramakrish-
nan 1984 Ravindran 2006 for Tamil communities Gerrish 2001 King Weich
Nazroo amp Blizard 2006 Lavender et al 2006 for Bengali and Urdu communities)
Religious observance is often seen as an alternative means of alleviating symptoms of
psychological distress and as is discussed below in relation to Jinns mental health
concerns are frequently understood within a religious framework that is not the case
for the majority increasingly secular community within the UK The implications for
offering a clinically based secular psychological therapies service are that such a
service may not be seen by service users as relevant or able to respond to their needs
as they understand them As will be discussed below this study found that the
participants in the focus groups reinforced previous literature on the significance of
religion in relation to accessing psychological services The question as to the
accessing of psychological therapies for members of these communities who are not
religious was not raised within the focus groups conducted for this study This is an
area potentially of interest for further research but was outside the scope of this
particular studyThe intention of this research was twofold to understand how mental health
issues in particular anxiety and depression are conceptualised and experienced by
people from BAME communities with particular reference to Bengali Urdu Tamil
and Somali speaking communities in the UK (the research group) and to explore
any potential implications of this for the accessing of psychological therapies services
by the communities As part of the Department of Healthrsquos IAPT initiative (IAPT
2008) which highlighted the disparity in access to psychological therapy between the
BAME communities and the mainstream population in the UK this research
commissioned by a London NHS Mental Health Trust aimed to investigate how
specific BAME communities Bengali Urdu Tamil and Somali conceptualise and
experience anxiety and depression both directly and indirectly and how these differ
from majority conceptualisations Secondly it aimed to gain more knowledge about
the feasibility of increasing access to psychological therapies in order to address the
disparity highlighted in previous research within these communities (Department of
Health 2007a 2007b 2009 Health Commission 2007)
Method
Design
In terms of method quantitative or mixed methods approaches to data collection
and analysis were considered but rejected as the focus of the research lay in
46 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
explicating the lived experience of the participants as described A qualitative
approach to research was chosen which acts to gain insight into the individualrsquos
experiences (Corbin amp Strauss 1998) It was felt that in understanding the
significance of a given experience a method that allowed analysis of the participantrsquos
words and personal meanings that an experience might have for the individual would
be important (Harre amp Secord 1972) It is not suggested that a person may have
exact insight into their own motives but that one can gain an understanding of anexperience as lived through a description by the person who had the experience
Focus groups are group discussions organised to explore a specific set of issues
such as peoplersquos views and experience (Basch 1987 Kitzinger 1994) Although often
seen as a convenient way to simultaneously collect data from a number of
participants the method capitalises on communication between research participants
in the generation of data (Kitzinger 1995) This means that instead of the researcher
asking each person to respond to a question in turn participants are encouraged to
talk to one another interacting and commenting on each otherrsquos experiences and
points of view The method is particularly useful for exploring peoplersquos knowledge
and experiences
Previous research on mental illness within the research group communities
indicates that focus groups are frequently used as a research method (Barron et al
2010 Halcomb Gholizadeh Di Giacomo Phillips amp Davidson 2004) Focus groups
have been used in previous studies with the Somali community (Finnstrom amp
Soderhamn 2006 Gervais 2008 Green amp Thorogood 2004 Warfa et al 2006) the
Tamil community (Bradby et al 2007 Fernando 2005 Sadavoy Meier amp Yuk2004 Whitley amp Prince 2004) Urdu groups (Acharya amp Northcott 2007) and
Bengali groups (Hawthorne Rahman amp Pill 2003) suggesting their suitability for
researching issues within these communities
This study sought to consider community perspectives and the experiences and
understandings of members of these communities as part of these groups with
subsequent implications for them as individuals As such focus groups were chosen
as the most appropriate method for this type of research study to consider the
community perspective
Further vignettes followed by questionsprobes were chosen as the appropriate
method of enabling sharing of experiences within the focus groups Within the focus
group interview schedule vignettes of a person displaying anxiety and in turn
depression were presented to the focus group participants followed by questions
about the participantsrsquo experiences in relation to the vignette Vignettes have been
widely used as a data collection technique in qualitative research (Hazel 1995
Hughes 1998) Hughes (1998 p 381) describes vignettes as lsquostories about
individuals situations and structures which can make reference to important pointsin the study of perceptions beliefs and attitudesrsquo
Vignettes provide a valuable technique for exploring peoplersquos perceptions beliefs
and meanings about specific situations and are particularly useful in exploring
potentially sensitive topics that participants might otherwise find difficult to discuss
(Neale 1999) Use of vignettes within a lsquofocusrsquo group is becoming increasingly
popular with social researchers (Wilkinson 1998) Maclean (1999) writing on the
use of vignettes within focus groups commented that it encouraged even the quietest
group member to voice an opinion
According to principles that guide the use of vignettes in research the vignettes
were created in a way that made them appear plausible and real to participants and
British Journal of Guidance and Counselling 47
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that contained sufficient context for participants to understand the situation
depicted The researchers then endeavoured to follow the vignette with questions
directed towards the beliefs assumptions and experiences of the participants with
regard to personal experiences of anxiety depression how participants cope withmental health issues limitations of mental health services and possible solutions for
the community involved
As a result for the purposes of this study mental health services were defined as
services carried out by mental health professionals in which treatments support and
advocacy to persons are offered to people experiencing mental health issues
(disturbances to their mental health) As a result this incorporates a breadth of
mental health services and professionals such as General Practitioners (GPs)
community mental health teams mental health nurses counsellors psychotherapistsoccupational therapists and clinical and counselling psychologists
The research also made use of respondent validation conducted on an individual
basis to consider how if at all the perspectives of participants as individuals differed
from those of the particular community interviewed (Silverman 2000) In particular
the aim of the interviews was to clarify the themes emerging from the focus groups to
ensure that the themes derived from the focus groups interviews were captured
accurately As Herrel et al (2004) p 349) argue lsquo otherwise possible misinterpre-
tation due to translation can occur and responses can be influenced by other focusgroup membersrsquo
Participant recruitment
As previously mentioned Bengali Urdu Tamil and Somali speaking communities
were sampled specifically for this study They form a particular focus for the NHS
Trust in that they have been reported to ask for more translations when accessingmental health services than other linguistic minority communities (Aspinall 2007)
The four samples of participants were recruited through the various Bengali
Urdu Tamil and Somali community associations with which the NHS Trust was in
contact sometimes working directly on mental health issues and IAPT The process
of selection was opportunistic sampling based on those who volunteered to take part
after having been invited to do so verbally by senior members of these community
associations In particular the recruitment method was seen as one that was
culturally acceptable to the selected communities With permission posters were alsoplaced in community buildings to advertise the study Those who volunteered were
then supplied with additional information about the study and informed consent was
required from each participant
Participants
Bengali community participants
Two focus groups were conducted for Bengali speaking participants The first group
consisted of eight female participants and the second group consisted of four female
and two male participants As participants were recruited through opportunistic
sampling there was an inconsistency in the malefemale participation ratio
With regards to the six respondent validation interviews four female participants
were recruited and two male participants
48 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Demographically the age group of all participants was 50 and above All
participants reflected Bangladeshi heritage and identified with Islam as their religion
Urdu community participants
Two focus groups were conducted with 21 participants in total The first group
consisted of 15 female participants and the second group consisted of six maleparticipants marking a separation of the groups based on gender
A further six participants (three males and three females) were selected for the
respondent validation interviews
Demographically the age group of all participants was 40 and above A variety of
participants were recruited whose origins reflected a diversity of the Urdu speaking
population Even though most participants were of Pakistani origins some
participants stated their heritage to be East African and even Indian The majority
of the participants stated Islam to be their religion
Tamil community participants
The two focus groups were made up of 18 participants in total The first groupconsisted of 10 males and the second of eight female participants making a
separation of the groups based on gender
For the respondent validation interviews six interviews were carried out with
four males and two females
All participants fell within the age range of 40 and above
Somali community participants
Two focus groups were conducted with 24 participants in total The first group
consisted of 14 female participants and the second group consisted of 10 male
participants marking a separation of the groups based on gender
A further six participants three males and three females were selected for therespondent validation interviews
Demographically the age group of all participants was 40 and above
Data collection and analysis
Two open-ended focus groups were carried out with each of the separate Bengali
Urdu Tamil and Somali groups with the Community Development Workers
(CDWs) present The CDWs were involved due to their knowledge of the community
and ability to aid set up and implementation of the focus groups The respondent
validation interviews were then conducted with six individuals from each of the
community groupsDue to cultural considerations the four researchers all of whom were themselves
born outside of the UK and in terms of their languages and cultural backgrounds
members of the respective communities relevant to this study conducted the focus
groups and respondent validation interviews with the male and female participants
separately (with the exception of the Bengali participants who requested mixed
gender participant groups) The focus groups and respondent validations for each
British Journal of Guidance and Counselling 49
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
pp 24162417) offer a similar view on the particular negative connotations attached
to mental illness among people of South Asian origin
Family ties are seen to be of particular importance within the research group
communities as they greatly impact on culture hence influencing both access to
psychological therapies as well as individualsrsquo openness to mental health profes-
sionals and researchers (Finnstrom amp Soderhamn 2006 Lavender Khondoker amp
Jones 2006) Thus family and community issues in relation to the accessing of
psychological therapies appear to be of more importance for the research group
communities than for the dominant culture
Religion is another aspect shown to significantly impact upon service usersrsquo
perspectives with regard to accessing psychological therapies (Guerin Guerin
Diiriye amp Yates 2004 Whittaker et al 2005 for Somali communities Ramakrish-
nan 1984 Ravindran 2006 for Tamil communities Gerrish 2001 King Weich
Nazroo amp Blizard 2006 Lavender et al 2006 for Bengali and Urdu communities)
Religious observance is often seen as an alternative means of alleviating symptoms of
psychological distress and as is discussed below in relation to Jinns mental health
concerns are frequently understood within a religious framework that is not the case
for the majority increasingly secular community within the UK The implications for
offering a clinically based secular psychological therapies service are that such a
service may not be seen by service users as relevant or able to respond to their needs
as they understand them As will be discussed below this study found that the
participants in the focus groups reinforced previous literature on the significance of
religion in relation to accessing psychological services The question as to the
accessing of psychological therapies for members of these communities who are not
religious was not raised within the focus groups conducted for this study This is an
area potentially of interest for further research but was outside the scope of this
particular studyThe intention of this research was twofold to understand how mental health
issues in particular anxiety and depression are conceptualised and experienced by
people from BAME communities with particular reference to Bengali Urdu Tamil
and Somali speaking communities in the UK (the research group) and to explore
any potential implications of this for the accessing of psychological therapies services
by the communities As part of the Department of Healthrsquos IAPT initiative (IAPT
2008) which highlighted the disparity in access to psychological therapy between the
BAME communities and the mainstream population in the UK this research
commissioned by a London NHS Mental Health Trust aimed to investigate how
specific BAME communities Bengali Urdu Tamil and Somali conceptualise and
experience anxiety and depression both directly and indirectly and how these differ
from majority conceptualisations Secondly it aimed to gain more knowledge about
the feasibility of increasing access to psychological therapies in order to address the
disparity highlighted in previous research within these communities (Department of
Health 2007a 2007b 2009 Health Commission 2007)
Method
Design
In terms of method quantitative or mixed methods approaches to data collection
and analysis were considered but rejected as the focus of the research lay in
46 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
explicating the lived experience of the participants as described A qualitative
approach to research was chosen which acts to gain insight into the individualrsquos
experiences (Corbin amp Strauss 1998) It was felt that in understanding the
significance of a given experience a method that allowed analysis of the participantrsquos
words and personal meanings that an experience might have for the individual would
be important (Harre amp Secord 1972) It is not suggested that a person may have
exact insight into their own motives but that one can gain an understanding of anexperience as lived through a description by the person who had the experience
Focus groups are group discussions organised to explore a specific set of issues
such as peoplersquos views and experience (Basch 1987 Kitzinger 1994) Although often
seen as a convenient way to simultaneously collect data from a number of
participants the method capitalises on communication between research participants
in the generation of data (Kitzinger 1995) This means that instead of the researcher
asking each person to respond to a question in turn participants are encouraged to
talk to one another interacting and commenting on each otherrsquos experiences and
points of view The method is particularly useful for exploring peoplersquos knowledge
and experiences
Previous research on mental illness within the research group communities
indicates that focus groups are frequently used as a research method (Barron et al
2010 Halcomb Gholizadeh Di Giacomo Phillips amp Davidson 2004) Focus groups
have been used in previous studies with the Somali community (Finnstrom amp
Soderhamn 2006 Gervais 2008 Green amp Thorogood 2004 Warfa et al 2006) the
Tamil community (Bradby et al 2007 Fernando 2005 Sadavoy Meier amp Yuk2004 Whitley amp Prince 2004) Urdu groups (Acharya amp Northcott 2007) and
Bengali groups (Hawthorne Rahman amp Pill 2003) suggesting their suitability for
researching issues within these communities
This study sought to consider community perspectives and the experiences and
understandings of members of these communities as part of these groups with
subsequent implications for them as individuals As such focus groups were chosen
as the most appropriate method for this type of research study to consider the
community perspective
Further vignettes followed by questionsprobes were chosen as the appropriate
method of enabling sharing of experiences within the focus groups Within the focus
group interview schedule vignettes of a person displaying anxiety and in turn
depression were presented to the focus group participants followed by questions
about the participantsrsquo experiences in relation to the vignette Vignettes have been
widely used as a data collection technique in qualitative research (Hazel 1995
Hughes 1998) Hughes (1998 p 381) describes vignettes as lsquostories about
individuals situations and structures which can make reference to important pointsin the study of perceptions beliefs and attitudesrsquo
Vignettes provide a valuable technique for exploring peoplersquos perceptions beliefs
and meanings about specific situations and are particularly useful in exploring
potentially sensitive topics that participants might otherwise find difficult to discuss
(Neale 1999) Use of vignettes within a lsquofocusrsquo group is becoming increasingly
popular with social researchers (Wilkinson 1998) Maclean (1999) writing on the
use of vignettes within focus groups commented that it encouraged even the quietest
group member to voice an opinion
According to principles that guide the use of vignettes in research the vignettes
were created in a way that made them appear plausible and real to participants and
British Journal of Guidance and Counselling 47
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that contained sufficient context for participants to understand the situation
depicted The researchers then endeavoured to follow the vignette with questions
directed towards the beliefs assumptions and experiences of the participants with
regard to personal experiences of anxiety depression how participants cope withmental health issues limitations of mental health services and possible solutions for
the community involved
As a result for the purposes of this study mental health services were defined as
services carried out by mental health professionals in which treatments support and
advocacy to persons are offered to people experiencing mental health issues
(disturbances to their mental health) As a result this incorporates a breadth of
mental health services and professionals such as General Practitioners (GPs)
community mental health teams mental health nurses counsellors psychotherapistsoccupational therapists and clinical and counselling psychologists
The research also made use of respondent validation conducted on an individual
basis to consider how if at all the perspectives of participants as individuals differed
from those of the particular community interviewed (Silverman 2000) In particular
the aim of the interviews was to clarify the themes emerging from the focus groups to
ensure that the themes derived from the focus groups interviews were captured
accurately As Herrel et al (2004) p 349) argue lsquo otherwise possible misinterpre-
tation due to translation can occur and responses can be influenced by other focusgroup membersrsquo
Participant recruitment
As previously mentioned Bengali Urdu Tamil and Somali speaking communities
were sampled specifically for this study They form a particular focus for the NHS
Trust in that they have been reported to ask for more translations when accessingmental health services than other linguistic minority communities (Aspinall 2007)
The four samples of participants were recruited through the various Bengali
Urdu Tamil and Somali community associations with which the NHS Trust was in
contact sometimes working directly on mental health issues and IAPT The process
of selection was opportunistic sampling based on those who volunteered to take part
after having been invited to do so verbally by senior members of these community
associations In particular the recruitment method was seen as one that was
culturally acceptable to the selected communities With permission posters were alsoplaced in community buildings to advertise the study Those who volunteered were
then supplied with additional information about the study and informed consent was
required from each participant
Participants
Bengali community participants
Two focus groups were conducted for Bengali speaking participants The first group
consisted of eight female participants and the second group consisted of four female
and two male participants As participants were recruited through opportunistic
sampling there was an inconsistency in the malefemale participation ratio
With regards to the six respondent validation interviews four female participants
were recruited and two male participants
48 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Demographically the age group of all participants was 50 and above All
participants reflected Bangladeshi heritage and identified with Islam as their religion
Urdu community participants
Two focus groups were conducted with 21 participants in total The first group
consisted of 15 female participants and the second group consisted of six maleparticipants marking a separation of the groups based on gender
A further six participants (three males and three females) were selected for the
respondent validation interviews
Demographically the age group of all participants was 40 and above A variety of
participants were recruited whose origins reflected a diversity of the Urdu speaking
population Even though most participants were of Pakistani origins some
participants stated their heritage to be East African and even Indian The majority
of the participants stated Islam to be their religion
Tamil community participants
The two focus groups were made up of 18 participants in total The first groupconsisted of 10 males and the second of eight female participants making a
separation of the groups based on gender
For the respondent validation interviews six interviews were carried out with
four males and two females
All participants fell within the age range of 40 and above
Somali community participants
Two focus groups were conducted with 24 participants in total The first group
consisted of 14 female participants and the second group consisted of 10 male
participants marking a separation of the groups based on gender
A further six participants three males and three females were selected for therespondent validation interviews
Demographically the age group of all participants was 40 and above
Data collection and analysis
Two open-ended focus groups were carried out with each of the separate Bengali
Urdu Tamil and Somali groups with the Community Development Workers
(CDWs) present The CDWs were involved due to their knowledge of the community
and ability to aid set up and implementation of the focus groups The respondent
validation interviews were then conducted with six individuals from each of the
community groupsDue to cultural considerations the four researchers all of whom were themselves
born outside of the UK and in terms of their languages and cultural backgrounds
members of the respective communities relevant to this study conducted the focus
groups and respondent validation interviews with the male and female participants
separately (with the exception of the Bengali participants who requested mixed
gender participant groups) The focus groups and respondent validations for each
British Journal of Guidance and Counselling 49
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
explicating the lived experience of the participants as described A qualitative
approach to research was chosen which acts to gain insight into the individualrsquos
experiences (Corbin amp Strauss 1998) It was felt that in understanding the
significance of a given experience a method that allowed analysis of the participantrsquos
words and personal meanings that an experience might have for the individual would
be important (Harre amp Secord 1972) It is not suggested that a person may have
exact insight into their own motives but that one can gain an understanding of anexperience as lived through a description by the person who had the experience
Focus groups are group discussions organised to explore a specific set of issues
such as peoplersquos views and experience (Basch 1987 Kitzinger 1994) Although often
seen as a convenient way to simultaneously collect data from a number of
participants the method capitalises on communication between research participants
in the generation of data (Kitzinger 1995) This means that instead of the researcher
asking each person to respond to a question in turn participants are encouraged to
talk to one another interacting and commenting on each otherrsquos experiences and
points of view The method is particularly useful for exploring peoplersquos knowledge
and experiences
Previous research on mental illness within the research group communities
indicates that focus groups are frequently used as a research method (Barron et al
2010 Halcomb Gholizadeh Di Giacomo Phillips amp Davidson 2004) Focus groups
have been used in previous studies with the Somali community (Finnstrom amp
Soderhamn 2006 Gervais 2008 Green amp Thorogood 2004 Warfa et al 2006) the
Tamil community (Bradby et al 2007 Fernando 2005 Sadavoy Meier amp Yuk2004 Whitley amp Prince 2004) Urdu groups (Acharya amp Northcott 2007) and
Bengali groups (Hawthorne Rahman amp Pill 2003) suggesting their suitability for
researching issues within these communities
This study sought to consider community perspectives and the experiences and
understandings of members of these communities as part of these groups with
subsequent implications for them as individuals As such focus groups were chosen
as the most appropriate method for this type of research study to consider the
community perspective
Further vignettes followed by questionsprobes were chosen as the appropriate
method of enabling sharing of experiences within the focus groups Within the focus
group interview schedule vignettes of a person displaying anxiety and in turn
depression were presented to the focus group participants followed by questions
about the participantsrsquo experiences in relation to the vignette Vignettes have been
widely used as a data collection technique in qualitative research (Hazel 1995
Hughes 1998) Hughes (1998 p 381) describes vignettes as lsquostories about
individuals situations and structures which can make reference to important pointsin the study of perceptions beliefs and attitudesrsquo
Vignettes provide a valuable technique for exploring peoplersquos perceptions beliefs
and meanings about specific situations and are particularly useful in exploring
potentially sensitive topics that participants might otherwise find difficult to discuss
(Neale 1999) Use of vignettes within a lsquofocusrsquo group is becoming increasingly
popular with social researchers (Wilkinson 1998) Maclean (1999) writing on the
use of vignettes within focus groups commented that it encouraged even the quietest
group member to voice an opinion
According to principles that guide the use of vignettes in research the vignettes
were created in a way that made them appear plausible and real to participants and
British Journal of Guidance and Counselling 47
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that contained sufficient context for participants to understand the situation
depicted The researchers then endeavoured to follow the vignette with questions
directed towards the beliefs assumptions and experiences of the participants with
regard to personal experiences of anxiety depression how participants cope withmental health issues limitations of mental health services and possible solutions for
the community involved
As a result for the purposes of this study mental health services were defined as
services carried out by mental health professionals in which treatments support and
advocacy to persons are offered to people experiencing mental health issues
(disturbances to their mental health) As a result this incorporates a breadth of
mental health services and professionals such as General Practitioners (GPs)
community mental health teams mental health nurses counsellors psychotherapistsoccupational therapists and clinical and counselling psychologists
The research also made use of respondent validation conducted on an individual
basis to consider how if at all the perspectives of participants as individuals differed
from those of the particular community interviewed (Silverman 2000) In particular
the aim of the interviews was to clarify the themes emerging from the focus groups to
ensure that the themes derived from the focus groups interviews were captured
accurately As Herrel et al (2004) p 349) argue lsquo otherwise possible misinterpre-
tation due to translation can occur and responses can be influenced by other focusgroup membersrsquo
Participant recruitment
As previously mentioned Bengali Urdu Tamil and Somali speaking communities
were sampled specifically for this study They form a particular focus for the NHS
Trust in that they have been reported to ask for more translations when accessingmental health services than other linguistic minority communities (Aspinall 2007)
The four samples of participants were recruited through the various Bengali
Urdu Tamil and Somali community associations with which the NHS Trust was in
contact sometimes working directly on mental health issues and IAPT The process
of selection was opportunistic sampling based on those who volunteered to take part
after having been invited to do so verbally by senior members of these community
associations In particular the recruitment method was seen as one that was
culturally acceptable to the selected communities With permission posters were alsoplaced in community buildings to advertise the study Those who volunteered were
then supplied with additional information about the study and informed consent was
required from each participant
Participants
Bengali community participants
Two focus groups were conducted for Bengali speaking participants The first group
consisted of eight female participants and the second group consisted of four female
and two male participants As participants were recruited through opportunistic
sampling there was an inconsistency in the malefemale participation ratio
With regards to the six respondent validation interviews four female participants
were recruited and two male participants
48 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Demographically the age group of all participants was 50 and above All
participants reflected Bangladeshi heritage and identified with Islam as their religion
Urdu community participants
Two focus groups were conducted with 21 participants in total The first group
consisted of 15 female participants and the second group consisted of six maleparticipants marking a separation of the groups based on gender
A further six participants (three males and three females) were selected for the
respondent validation interviews
Demographically the age group of all participants was 40 and above A variety of
participants were recruited whose origins reflected a diversity of the Urdu speaking
population Even though most participants were of Pakistani origins some
participants stated their heritage to be East African and even Indian The majority
of the participants stated Islam to be their religion
Tamil community participants
The two focus groups were made up of 18 participants in total The first groupconsisted of 10 males and the second of eight female participants making a
separation of the groups based on gender
For the respondent validation interviews six interviews were carried out with
four males and two females
All participants fell within the age range of 40 and above
Somali community participants
Two focus groups were conducted with 24 participants in total The first group
consisted of 14 female participants and the second group consisted of 10 male
participants marking a separation of the groups based on gender
A further six participants three males and three females were selected for therespondent validation interviews
Demographically the age group of all participants was 40 and above
Data collection and analysis
Two open-ended focus groups were carried out with each of the separate Bengali
Urdu Tamil and Somali groups with the Community Development Workers
(CDWs) present The CDWs were involved due to their knowledge of the community
and ability to aid set up and implementation of the focus groups The respondent
validation interviews were then conducted with six individuals from each of the
community groupsDue to cultural considerations the four researchers all of whom were themselves
born outside of the UK and in terms of their languages and cultural backgrounds
members of the respective communities relevant to this study conducted the focus
groups and respondent validation interviews with the male and female participants
separately (with the exception of the Bengali participants who requested mixed
gender participant groups) The focus groups and respondent validations for each
British Journal of Guidance and Counselling 49
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

that contained sufficient context for participants to understand the situation
depicted The researchers then endeavoured to follow the vignette with questions
directed towards the beliefs assumptions and experiences of the participants with
regard to personal experiences of anxiety depression how participants cope withmental health issues limitations of mental health services and possible solutions for
the community involved
As a result for the purposes of this study mental health services were defined as
services carried out by mental health professionals in which treatments support and
advocacy to persons are offered to people experiencing mental health issues
(disturbances to their mental health) As a result this incorporates a breadth of
mental health services and professionals such as General Practitioners (GPs)
community mental health teams mental health nurses counsellors psychotherapistsoccupational therapists and clinical and counselling psychologists
The research also made use of respondent validation conducted on an individual
basis to consider how if at all the perspectives of participants as individuals differed
from those of the particular community interviewed (Silverman 2000) In particular
the aim of the interviews was to clarify the themes emerging from the focus groups to
ensure that the themes derived from the focus groups interviews were captured
accurately As Herrel et al (2004) p 349) argue lsquo otherwise possible misinterpre-
tation due to translation can occur and responses can be influenced by other focusgroup membersrsquo
Participant recruitment
As previously mentioned Bengali Urdu Tamil and Somali speaking communities
were sampled specifically for this study They form a particular focus for the NHS
Trust in that they have been reported to ask for more translations when accessingmental health services than other linguistic minority communities (Aspinall 2007)
The four samples of participants were recruited through the various Bengali
Urdu Tamil and Somali community associations with which the NHS Trust was in
contact sometimes working directly on mental health issues and IAPT The process
of selection was opportunistic sampling based on those who volunteered to take part
after having been invited to do so verbally by senior members of these community
associations In particular the recruitment method was seen as one that was
culturally acceptable to the selected communities With permission posters were alsoplaced in community buildings to advertise the study Those who volunteered were
then supplied with additional information about the study and informed consent was
required from each participant
Participants
Bengali community participants
Two focus groups were conducted for Bengali speaking participants The first group
consisted of eight female participants and the second group consisted of four female
and two male participants As participants were recruited through opportunistic
sampling there was an inconsistency in the malefemale participation ratio
With regards to the six respondent validation interviews four female participants
were recruited and two male participants
48 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Demographically the age group of all participants was 50 and above All
participants reflected Bangladeshi heritage and identified with Islam as their religion
Urdu community participants
Two focus groups were conducted with 21 participants in total The first group
consisted of 15 female participants and the second group consisted of six maleparticipants marking a separation of the groups based on gender
A further six participants (three males and three females) were selected for the
respondent validation interviews
Demographically the age group of all participants was 40 and above A variety of
participants were recruited whose origins reflected a diversity of the Urdu speaking
population Even though most participants were of Pakistani origins some
participants stated their heritage to be East African and even Indian The majority
of the participants stated Islam to be their religion
Tamil community participants
The two focus groups were made up of 18 participants in total The first groupconsisted of 10 males and the second of eight female participants making a
separation of the groups based on gender
For the respondent validation interviews six interviews were carried out with
four males and two females
All participants fell within the age range of 40 and above
Somali community participants
Two focus groups were conducted with 24 participants in total The first group
consisted of 14 female participants and the second group consisted of 10 male
participants marking a separation of the groups based on gender
A further six participants three males and three females were selected for therespondent validation interviews
Demographically the age group of all participants was 40 and above
Data collection and analysis
Two open-ended focus groups were carried out with each of the separate Bengali
Urdu Tamil and Somali groups with the Community Development Workers
(CDWs) present The CDWs were involved due to their knowledge of the community
and ability to aid set up and implementation of the focus groups The respondent
validation interviews were then conducted with six individuals from each of the
community groupsDue to cultural considerations the four researchers all of whom were themselves
born outside of the UK and in terms of their languages and cultural backgrounds
members of the respective communities relevant to this study conducted the focus
groups and respondent validation interviews with the male and female participants
separately (with the exception of the Bengali participants who requested mixed
gender participant groups) The focus groups and respondent validations for each
British Journal of Guidance and Counselling 49
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Demographically the age group of all participants was 50 and above All
participants reflected Bangladeshi heritage and identified with Islam as their religion
Urdu community participants
Two focus groups were conducted with 21 participants in total The first group
consisted of 15 female participants and the second group consisted of six maleparticipants marking a separation of the groups based on gender
A further six participants (three males and three females) were selected for the
respondent validation interviews
Demographically the age group of all participants was 40 and above A variety of
participants were recruited whose origins reflected a diversity of the Urdu speaking
population Even though most participants were of Pakistani origins some
participants stated their heritage to be East African and even Indian The majority
of the participants stated Islam to be their religion
Tamil community participants
The two focus groups were made up of 18 participants in total The first groupconsisted of 10 males and the second of eight female participants making a
separation of the groups based on gender
For the respondent validation interviews six interviews were carried out with
four males and two females
All participants fell within the age range of 40 and above
Somali community participants
Two focus groups were conducted with 24 participants in total The first group
consisted of 14 female participants and the second group consisted of 10 male
participants marking a separation of the groups based on gender
A further six participants three males and three females were selected for therespondent validation interviews
Demographically the age group of all participants was 40 and above
Data collection and analysis
Two open-ended focus groups were carried out with each of the separate Bengali
Urdu Tamil and Somali groups with the Community Development Workers
(CDWs) present The CDWs were involved due to their knowledge of the community
and ability to aid set up and implementation of the focus groups The respondent
validation interviews were then conducted with six individuals from each of the
community groupsDue to cultural considerations the four researchers all of whom were themselves
born outside of the UK and in terms of their languages and cultural backgrounds
members of the respective communities relevant to this study conducted the focus
groups and respondent validation interviews with the male and female participants
separately (with the exception of the Bengali participants who requested mixed
gender participant groups) The focus groups and respondent validations for each
British Journal of Guidance and Counselling 49
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
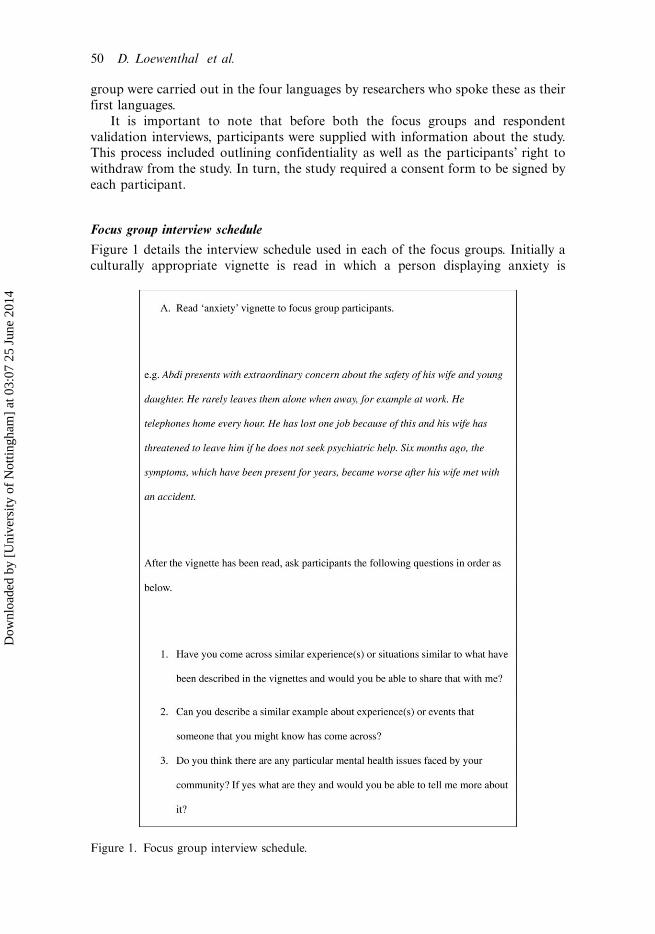
group were carried out in the four languages by researchers who spoke these as their
first languages
It is important to note that before both the focus groups and respondent
validation interviews participants were supplied with information about the studyThis process included outlining confidentiality as well as the participantsrsquo right to
withdraw from the study In turn the study required a consent form to be signed by
each participant
Focus group interview schedule
Figure 1 details the interview schedule used in each of the focus groups Initially a
culturally appropriate vignette is read in which a person displaying anxiety is
Figure 1 Focus group interview schedule
50 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

Figure 1 Continued
British Journal of Guidance and Counselling 51
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
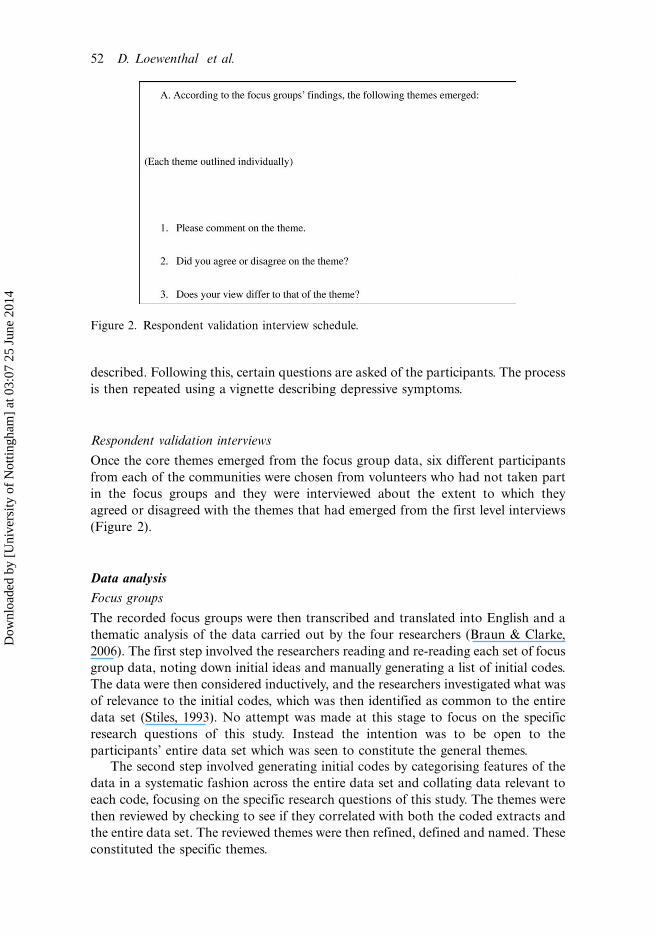
described Following this certain questions are asked of the participants The process
is then repeated using a vignette describing depressive symptoms
Respondent validation interviews
Once the core themes emerged from the focus group data six different participants
from each of the communities were chosen from volunteers who had not taken part
in the focus groups and they were interviewed about the extent to which they
agreed or disagreed with the themes that had emerged from the first level interviews
(Figure 2)
Data analysis
Focus groups
The recorded focus groups were then transcribed and translated into English and a
thematic analysis of the data carried out by the four researchers (Braun amp Clarke
2006) The first step involved the researchers reading and re-reading each set of focus
group data noting down initial ideas and manually generating a list of initial codes
The data were then considered inductively and the researchers investigated what was
of relevance to the initial codes which was then identified as common to the entire
data set (Stiles 1993) No attempt was made at this stage to focus on the specific
research questions of this study Instead the intention was to be open to the
participantsrsquo entire data set which was seen to constitute the general themes
The second step involved generating initial codes by categorising features of the
data in a systematic fashion across the entire data set and collating data relevant to
each code focusing on the specific research questions of this study The themes were
then reviewed by checking to see if they correlated with both the coded extracts and
the entire data set The reviewed themes were then refined defined and named These
constituted the specific themes
Figure 2 Respondent validation interview schedule
52 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

Respondent validation interviews
If the respondent validation interviews presented different perspectives on the
question to that of the focus groups the comments and criticisms from the
respondent validation interviews would be incorporated within the thematic data
analysis Alongside this incorporation the analysis would specify that the particular
information was provided as part of the respondent validation
However the data collected from the respondent validation interviews concurredwholly with the data collected from the focus groups and therefore the thematic
analysis did not require any modification to the data gathered as part of the focus
group stage indicating that the individual community members agreed with the
researcherrsquos findings from the focus group
Researcher reflexivity
Within this study the researchers acknowledged the requirement for reflexivity in
qualitative research in the self-exploration of the presuppositions held and decisions
made by the researchers This was particularly important as within the datacollection stages the four researchers collected data from their respective commu-
nities Therefore it was important that the researchers were transparent and reflexive
about their research process theoretical perspectives and researcher values in
maintaining the quality of the research (Seale Gobo Gubrium amp Silverman 2004)
As Nightingale and Cromby (1999 p 228) suggest personal reflexivity urges us lsquoto
explore the ways in which a researcherrsquos involvement with a particular study
influences acts upon and informs such researchrsquo
Further epistemological reflexivity requires us to engage with questions such ashow the research has been defined and how the methods have lsquoconstructedrsquo the
findings Thus epistemological reflexivity encourages us to reflect upon the
assumptions about knowledge that we have made in the course of the research
enabling us to consider the implications of the assumptions for the research (Willig
2001)
The researchers attempted to achieve researcher reflexivity through frequent
group supervision both prior to and throughout the research process where the
researchers would discuss their assumptions and processes with regard to theresearch as a group Researchers were also encouraged to keep research diaries
within which they reflected on different aspects of the research process and their role
within the construction of research knowledge (Blaxter Hughes amp Tight 2001) The
sharing of this information in group supervision sessions was paramount in enabling
researchers to consider the place they took in the research thereby ensuring the
quality of the research
Results
Following the thematic analysis (Braun amp Clarke 2006) the participantsrsquo experiences
were characterised by four common themes in relation to accessing psychological
therapies which emerged across all groups
(1) Understanding of lsquomental health issuesrsquo and available mental health services
(2) Cultural barriers to approaching service providers
British Journal of Guidance and Counselling 53
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

(3) Interpreter and General Practitioner (GP) services
(4) Religion
Each theme will now be discussed in turn using verbatim examples from theindividual participants to illuminate the theme
(1) Understanding of lsquomental health issuesrsquo and available mental health services
The findings across all focus groups indicate a lack of understanding of the Western
conceptions of depression and anxiety to differing degrees All 10 members of the
Urdu female focus group struggled with the concept of anxiety partially as stated
because there is no directly equivalent concept available in Urdu The Somali male
and female groups spoke of anxiety as a lsquonon-clinical disorderrsquo conceptualised by a
male Somali participant as lsquoa fleeting situational discomfort that passes awayrsquo even ifit lasts for a significant period of time Further the Somali participants indicated an
understanding of anxiety as a physical as well as emotional experience For Tamil
participants there was also a lack of knowledge of what are termed psychological
diagnoses such as anxiety As a female Tamil participant with a medical background
stated
Lots of people who come to us [GP surgery] do not have a clue of what they are goingthrough and that they suffer and live with it I am so surprised that therersquos still lack ofknowledge and awareness among this community
Similarly within the Somali community depression is conceptualised in a way that is
indistinguishable from everyday life struggles and survival Somali female partici-
pants had more understanding of lsquodisappointmentsrsquo lsquodepressive statesrsquo as well as
lsquobroken spiritsrsquo Female participants commented that families were lsquodrowning withthis plaguersquo and lsquothis darknessrsquo because they are lsquoalways downrsquo lsquothinking too deeprsquo
lsquobeing full with thoughtsrsquo and lsquofed up with life in generalrsquo They also described
hopelessness and commented that in some families lsquothe lights have been turned off rsquo
which could indicate something of how the family was functioning
However with regard to the concepts of lsquomental healthrsquo and lsquomental issuesrsquo the
participants related more easily to this concept It appeared that when discussing
lsquomental healthrsquo through the way in which the conversation flowed participants
across all four community groups and genders demonstrated more familiarity withthis as a conceptual framework Within the male and female groups a discussion of
lsquoPagolrsquo took place (the Bengali variation of the Hindi word lsquoPagalrsquo which directly
translates to denote stereotypes of intense madness and conjures images of
institutionalisation) which have a highly positive correlation to thoughts of shame
guilt and the urge to conceal any pertinent mental health problems Male and female
Somali participants used metaphors such as lsquoHe has jumped over the fencersquo or
lsquocrossed to the other sidersquo to describe the lsquomentally ill personrsquo
At the same time both the female and mixed gender Bengali focus groups spokeof a desire for more community-based interventions such as group sessions and
other talking therapies to increase awareness of this concept within the community
and as a means of enabling members of the community to access available services
The Urdu female group stated they were interested in lsquoinformal talksrsquo and awareness-
raising forums but to fulfil the same purpose All 10 of the Urdu female group felt
54 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

that group sessions would be a good way to start a dialogue for one to then move on
to one-on-one sessionsIn contrast to the Somali men the women generally were not aware of alternative
ways to receive mental health support Men on the other hand were more
knowledgeable about available psychotherapy and counselling services They
commented that they would refer people to use counselling services or a
psychotherapist if that professional was knowledgeable about the Somali culture
Only one of the youngest female participants commented that talking to the patient
can alleviate common mental disorders if such talking was specifically related to
asking the patient about how he was feeling not just lsquohow are you questionsrsquo
Somali participants asked for education about lsquocommon mental disordersrsquo as
they are understood within mental health in order to better understand the provision
of available services However the participants particularly mothers in the Somali
female group and fathers in the Somali male group raised fears about the role of
social services in terms of a fear that their children will be lsquosnatchedrsquo by social
services if they asked for support They distinctly requested more information on the
role of social services
(2) Cultural barriers to approaching service providers
While both the female and male Bengali participant groups identified isolation as a
major factor affecting depression and anxiety within the Tamil community there was
a strong feeling that speaking about psychological problems to others is wrong This
feeling was thought to be rooted in the culture Tamil participants admitted that they
keep their worries to themselves although this seemed to be more dominant among
the female group A discussion in the female Tamil group suggested participants were
more interested in seeing professionals lsquooutside the communityrsquo Further another
Tamil female spoke of how
My friendrsquos husband knows she has a problem and he blames her and because that canlead to divorce or separation she does not talk about it she just keeps it to herself andsuffering inside
Particularly the Bengali and Tamil focus groupsrsquo discussions focused on the negative
associations with lsquomadnessrsquo leading to thoughts of shame guilt and the urge to
conceal any pertinent mental health problems due to fears of being ostracised by the
community
Within the Urdu community the issue of lsquocoping alonersquo and not having an outlet
also arose Their need to cope alone was often spoken of in regard to being seen to be
lsquoPagolrsquo as a female Urdu participant suggested
Yoursquore still aware of words like pagal which can make you very aware of what you needto do to not be pagal and therefore it stops you from exploring what is really affectingyou because yoursquore too busy trying to not act lsquopagalrsquo what is pagal anyway
However the Urdu female participants also felt that they would rather cope on their
own because sometimes it is hard to articulate and particularly shameful to speak of
the experience of mental illness as a female Urdu participant described
British Journal of Guidance and Counselling 55
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

It can be seen to be shameful to admit to having any problems the best reaction is tocope alone and express your pain through physical reactions like crying
Similarly five Urdu male participants specified that it can be a cultural factor to
want to cope alone due to the patriarchal nature of the community They felt that
culturally some men are still bound to not display their emotions because of a need
to appear to remain strong for others
For the Somali groups an important theme that emerged was related to a
perceived need to escape from the community if a sufferer was diagnosed with mental
illness Participants commented that they know of people especially mothers with
children who have mental health problems but these mothers move out of the area as
they feel ashamed and stigmatised by the community It was expressed by the Somali
male focus group participants that issues surrounding mental health were not
tolerated well within the community
Seven of the Somali women in particular expressed a sense of helplessness in the
face of mental illness either their own or those of others because of their place
within the Somali community As stated within the male and female Somali focus
groups one perceived solution was to provide distraction For example they said
that they would consider getting the person married so that as a female participant
stated lsquothe wedding can take such things off their mindrsquo This also seemed apparent
within the Tamil participants One male participant spoke of how
In our community when we are depressed we make our hearts strong ourselves engaging in something perhaps to get that diversion
(3) Interpreter and General Practitioner (GP) services
Two female Tamil participants referred to the potential use of lsquotalking to
professionalsrsquo as useful when experiencing psychological problems because as a
female Tamil participant suggested lsquogetting five minutes to talk to someone itself is a
big thingrsquo or as a second female suggested lsquofor example middle of the night you
might feel suicidal you canrsquot sleep at 2am and feel like talking to someonersquo
However within the Tamil male focus group the issue of language was spoken of as
a barrier to Tamils seeking GP support for a psychological problem A male Tamil
participant suggested
Typically Tamil people hesitate to talk in English so language becomes a barrier when itcomes to explaining their psychological problems to the GP When we approach a GPwe never specify we have a problem
One elderly Tamil female participant from India highlighted that she had been so
accustomed to her own way of culture back home and added that because she was
not able to converse well in English she felt that the GP did not understand her
problems properly resulting in an interpretation that was not correctHowever across the focus groups participants spoke of finding interpreter
services unreliable and non-confidential The Bengali participants in particular
expressed that they were generally wary of interpreters even if as one female
participant felt they lsquoare perhaps now being trained betterrsquo They expressed that they
56 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

wanted the independence and freedom to talk about their issues directly with the
health professional rather than relying on someone to speak for them Within the
Urdu male and female groups although there seemed to be a general view that an
interpreter would be helpful when they visit the GP there was general disagreement
among the more elderly participants from both male and female Urdu focus groups
as a consequence of experiences where interpreters have not translated correctly to
the GP
Within the Tamil female focus group as discussion took place around
misinterpretation by interpreters one female participant said
I took my mom to see the GP because she cannot speak well in English she had a lot ofpain in her leg that day I couldnrsquot go and she needed an interpreter by luck I couldgo that day and mom said since interpreter was there let her explain the interpreterwas not explaining things properly what my mom was going through you know likethat so GP started asking me questions
There was a similar concern within the Somali groups in relation to interpreters
specifically in relation to concerns about not being able to find a professional
interpreter who would keep their problems in confidence A significant proportion of
the Somali focus group participants were worried and anxious about disclosing a
mental health problem both to the general practitioner and most importantly to
the interpreter There was a general consensus amongst the Somali male and female
participants that interpreters can gossip among themselves and within the commu-
nity and this can cause huge distress to the Somali mental health sufferer who is then
labelled for lifeIt was also expressed that once someone is known to have sought treatment for a
mental health issue they will be immediately stigmatised within the community and
this causes an indirect experience of anxiety in men and depression in women Using
interpreters thus caused most of the Somali participants considerable worry As
mentioned previously being ostracised was also a related and major concern for
them and indirectly influenced their willingness to access psychological therapy A
common solution to increase access to psychological therapies that Somali
participants asked for included the provision of lsquoprofessionally trained interpretersrsquoThe majority of the participants from the research group felt that their needs were
not addressed by their GP Most of the participants felt anxious and even depressed
when their GP did not understand and address their mental health problems because
of language and cultural barriers As such participants felt that GPs were not able to
clearly understand the concerns and distress from the participantsrsquo perspective
Perhaps unsurprisingly this view was different from for example those Urdu
and Tamil participants who were able to converse well in English often those from
younger generations though they also said that they would not normally go and see
the GP unless their problems were severe
Both Bengali focus groups however stated that their GP was the first port of call
for physical and psychological ailments However these Bengali participants stated
that they were adverse to the notion of medication as a solution to psychological
issues and preferred the option of talking therapies if supported within a cohesive
structural framework and particularly if based within the community
British Journal of Guidance and Counselling 57
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

(4) Religion
Religion seemed to play a dominant role for the Tamil community regardless of
whether they are Hindu Muslim or Christian in determining whether they want to
access mental health services For example when describing how he coped with
lsquosadness and depressionrsquo an elderly male Tamil participant also spoke of lsquokeeping it
within mersquo by lsquopraying to Godrsquo
Within the Bengali community religion seemed to still be a factor albeit less so
Three participants mentioned that when trying to cope with symptoms they would
on a few occasions turn to religion as a meditative and therapeutic outlet especially
if they felt that they did not want to burden another person with their problems or if
they wanted to remain strong for their other family members This was especially the
case if there had been a major traumatic event experienced by everyone such as the
death of a family member
For the Urdu community there was a significant emphasis on how religion and
culture impact on an individual Religion was discussed with particular reference to
Jinns supernatural creatures in Arab folklore and Islamic teachings which occupy a
parallel world to that of mankind as a concept Participants felt that within Islam a
belief in Jinns influences the conception of mental health within the relevant
communities and how mental health can be treated but is little understood by most
Western health professionals One participant stated that lsquowhether professionals
believe it or not they need to at least respect the privacy of onersquos thoughtsrsquo The
Urdu male group discussed the potential helpfulness of community-based interven-
tions that took into account the religious needs of Urdu speakers who are
predominantly Muslim and wanted interventions that could where appropriate
be used alongside religious teaching
Of the Somali participants a majority commented that they use the Qurrsquoan to
deal with mental illness This for example means that they would shower holy water
all over the patient in an attempt to lsquorescuersquo them and lsquowash away the bad spiritsrsquo
The groups expressed that increased understanding by the service providers of the
significance of religious beliefs would allow an appreciation by mental health
professionals of how people view mental well-being and the potential to tailor
services accordingly
Discussion
Given the Department of Healthrsquos (2007a 2007b) focus on increasing the low uptake
of psychologicaltalking therapies from BAME communities the findings in this
study seem to hold an important significance in uncovering and exploring some of
the cultural religious and language barriers to access to these services
In particular the findings support previous studies that suggest that deliberate
measures may need to be put in place in enabling BAME communities to seek
psychological support In general the study supported previous findings that suggest
that barriers to improving access for BAME communities may include cultural and
community-specific language disadvantages differences in cultural interpretations of
mental health and illness and mental health services through to problems accessing
available psychotherapeutic services (Bhugra amp Ayonrinde 2004 Fernando 2005)The findings of this study may particularly be seen to highlight the potential
problems that arise by imposing what may be considered medical conceptions of
58 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo onto minority
communities It is not to say that Bengali Urdu Somali and Tamil speaking
communities do not experience what from a Western perspective would be
understood as anxiety and depression but that the conceptualisation and under-
standing of this was shown to be significantly different from the focus group data
This highlights previous findings that suggest the potential danger in imposing
mental health issues based on understandings applicable to a dominant culture
without taking the patientrsquos culture into consideration (Ellis et al 2007 2008
Fernando 2005)In contrast it appeared that while lsquoanxietyrsquo and lsquodepressionrsquo were concepts that
were less culturally transferable between the majority and minority community group
samples lsquomental healthrsquo or lsquomental illnessrsquo seemed more universally understood by
these communities
Importantly the participant focus groups addressed the potential barriers to
accessing mental health advice and support such as language (both in practice and
in concept) and attitudinal challenges of the patient themselves (both cultural and
religious) as located in previous work (Bhugra amp Ayonrinde 2004 Fernando 2005)
A particular highlighted concern in the focus groups across the communities was a
distrust in interpreter services emerging as a potential key barrier to peoplersquos use of
health services (Murray amp Buller 2007 Saha et al 2007) as previously noted by
Bengali Somali Tamil and Urdu speakers
However in considering how one may increase knowledge and understanding of
available services to the Bengali Urdu Tamil and Somali populations the lsquogrouprsquo or
lsquocommunityrsquo was considered a potentially valuable asset in increasing access to
available psychological therapy services This may highlight the sense of the
importance for the research group of community-focused programmes often
managed within and by the community itself
The implications of this study in particular for improving access to psychological
therapies are important As Sashidharan (2003) recommended there must be a
development of the cultural capability of mental health services in the UK to form a
coherent and integrated service for minority ethnic communities which meets the
needs of patients (McKenzie amp Bhui 2007)
While three female participants mentioned the usefulness of seeking psycholo-
gical support from lsquoa professionalrsquo either the perception of participants in the focus
groups of services available and at times past impressions of service use acted as a
barrier to future use (Boi 2000) The findings suggest a need to develop specialist
primary mental health care and culturally sensitive GP services that can be easily and
flexibly accessed by BAME communities such as Bengalis Urdus Tamils and
Somalis and particularly for people whose first language is not English Such
specialist services should focus on understanding socio-cultural issues within the
specific communities as well as recognising shared common features Of significance
here would be to improve the understanding of GPs and other primary care
professionals as to cultural and religious influences potentially affecting access and
referral to mental health services such as the psychological therapies Similarly there
is a need to develop the training of interpreters to have more relevant knowledge of
dialects and develop greater awareness of the importance of confidentiality in this
culturally sensitive area (Saha et al 2007) These findings support the Barron et al
(2010) study which highlighted the importance of the provision of high quality
British Journal of Guidance and Counselling 59
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

language interpretation services for enabling access and the importance of trust
confidentiality accuracy and independence in an interpreter
With reference to IAPT a focus on what are understood within the majority
community to be specific conditions and the design of psychological treatment based
on this model can be seen to create a situation where many people within minority
communities such as those who were the focus of this study do not recognise the
relevance of the service for them In particular as within the male Somali community
focus group depression was conceptualised in a way that is indistinguishable from
everyday life struggles and survival for lsquodepressionrsquo to be treated as a separate
clinical condition both by GPs and within the psychological therapies would appear
an unfamiliar concept As explored by the participantsrsquo increased understanding of
the term lsquomental illnessrsquo framing the issues in these terms may be of benefit
At the same time if the service provision is to be focused on lsquocommon mental
disordersrsquo an alternative or parallel approach is to familiarise minority commu-
nities with these terms through for example the use of local education providers
(such as English for Speakers of Other Languages [ESOL] classes) and through
community workshops Such an approach arguably does not seek to impose Western
conceptions of mental health on minority communities but instead enhances
awareness of the context in which psychological therapy services are provided and
enables potential service users to understand the potential relevance of such
provisions for them
Further it has implications for the use of psychological therapies in that
approaches which seek to treat symptoms rather than to consider the individual in
the context of the community may be particularly inappropriate for the research
group communities
A further importance of lsquocommunityrsquo emerged from the research in that it was
felt that if understanding of the conditions that might cause a person to seek
psychological therapy particularly within the framework of UK NHS provision
were increased within the community the stigma could potentially be lessened The
distinction drawn here by the participants was thus one of the significance of an
initial change in attitude at community rather than individual level with consequent
implications for individuals
Of further significance for providers of psychological therapy services is the
acknowledgement of the wariness that many members of the research groupsrsquo
communities may have in approaching health professionals This seems particularly
important given that it has been noted that Asian Bangladeshi Asian Pakistani and
Black African individuals have more difficulties in engaging with and benefiting from
talking therapy services than the average non-BAME client (Gilleard Dennis amp
Ziyal 2005) Currently therefore despite the perception that GPs could not
understand the participants or their issues while this was mainly related to language
and cultural barriers arguably such concerns could be seen as projections of shame
about mental health issues onto the GPs and the NHS
Improving access to psychological therapies is perhaps in this context about
improving the accessibility of psychological therapies through improving relations
with communities in order to increase trust in the service providers This could allow
for improved accessibility to information and education for specific services such as
social services as it could be argued that the Somalisrsquo fear of social services had a
significant impact on the way they access therapeutic services and it could also
60 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

perhaps explain why members of the Somali community are reluctant to seek mental
health advice (McCrone et al 2005 Pumroy 2008)
While this study reinforces many of the arguments put forward by for example
Wharfa et al (forthcoming) McKenzie and Bhui (2007) the findings here are
perhaps limited by a number of factors Firstly by carrying out consultation through
community associations the emphasis on the importance of the community and
community interventions may have been over-emphasised in that the volunteers who
came forward were those already involved with those community associations
Similarly the particular emphasis on religion as an influence on the conception of
mental health as of relevance for members of for example Somali and Urdu
communities may again have been drawn into particular focus due to contacting the
participants through their respective community associations which were often
religiously based
Additionally while the researchers were all themselves immigrants to the UK who
spoke either Bengali Urdu Tamil or Somali as their first languages it is perhaps of
significance that female researchers interviewed the Bengali Urdu and Tamil male
and female groups while a male researcher interviewed the Somali groups In relation
to the importance of cultural sensitivity acknowledged through the separation of the
focus groups into male and female the gender of the researchers and indeed the age
of the researchers two of whom were in their early twenties may have influenced
the findings in terms of their own place within the community they were researching
for example when speaking to older members or those of the opposite sex Parallel
to this is the issue that while the dangers of projection were discussed with the
researchers before the empirical phase was carried out the question arises as to
whether in the interpretation of the data as a thematic analysis it is possible to
bracket out fully the researcherrsquos own perspectives on the research question
In terms of the question of language which was a central issue for this study
while the interviews were conducted in the relevant community languages by a
researcher for whom that language was the first language it is acknowledged here
that in terms of validation the translation of the focus group findings into English
and then back into the original languages prior to the respondent validation phase
could have enhanced the reliability of these findings The limitation here was one of
time constraints but it is acknowledged that this could potentially have enhanced
understanding of the conceptualisations and provided a more developed idea of the
level of accuracy they achieved
There are implications of this study for individual and community-based
interventions and in particular for the training and professional development of
GPs interpreters and psychological therapists working with such BAME commu-
nities Further research into the design of training programmes for these groups is
now required
In turn this study has highlighted ethical implications for cross-cultural research
It has been suggested that researchers who are sensitive to and knowledgeable of
cross-cultural issues increase their chances of working in an ethical manner
particularly with participants from ethnic minority backgrounds (Ponterotto amp
Casas 1993) This study has suggested that research procedures can become more
ethically appropriate through an acknowledgement and incorporating of practices
relevant to the culture through activities such as cultural matching of researcher and
participant and awareness of specific issues such as gender during interview
British Journal of Guidance and Counselling 61
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

processes particularly when interviewing groups of participants or communities (Sue
amp Sue 1990)
This study has also highlighted the fact that researchers particularly when
researching different cultures need to be aware of the potential incongruence
between the researcherrsquos views and theoretical frameworks and those views of the
group or culture being researched Furthermore where differences occur they must
be respected and the researcher must take care not to project their own views ontothe research process or to judge the participantsrsquo views (Lee 1995) Thomason
(1999) suggests this is particularly important for cross-cultural research which
focuses on mental health issues in that researchers have tended to adopt Western
definitions of what constitutes healthy and normal functioning
Further research is needed to consider the impact of accessing talking therapies
primarily through doctors and the NHS One of the main endeavours of the Layard
Report (2006) was to move to a talking therapies intervention rather than a medical
one for mental health issues However the medicalisation of terms such as
lsquodepressionrsquo and the regarding of such conditions as lsquodisordersrsquo is different to what
is ordinarily meant by depression or anxiety
At the same time while this paper raises issues as to the different understandings
of these terms between what is assumed to be the dominant culture and those of the
research group communities a question arises as to what extent understanding of
lsquoanxietyrsquo and lsquodepressionrsquo as clinical disorders is different between health service
professionals and lay persons within the majority culture The findings here are that
the research groups have different understandings of what is meant by these terms
which may impact upon the extent to which they access psychological therapies
However it is possible that for example reluctance to accept pharmacological
intervention and to approach health service professionals and GPs is not somethingthat can be understood exclusively in terms of minority cultural factors
Conclusion
In conclusion this study aimed to explore how the Bengali Urdu Tamil and Somali
communities conceptualise and experience what health professionals term lsquoanxietyrsquo
and lsquodepressionrsquo and what they do when faced with what they regard as mental
health issues with implications of this for the training of staff involved Overall it is
suggested that common mental disorders such as lsquoanxietyrsquo and lsquodepressionrsquo were not
clearly understood within the focus group discussions across the four community
groups The findings highlight that cultural language and religious barriers were
thought to exist for the participants in seeking mental health support This may hold
important implications in particular for IAPT in creating culturally sensitive
psychological programmes programmes which through increased knowledge within
the minority communities could be more relevant for the clients Further education
at a community level could be useful in promoting services alongside promoting
mental health issues and in turn decreasing the associated stigma
Notes on contributors
Professor Del Loewenthal is Director of the Research Centre for Therapeutic EducationDepartment of Psychology Roehampton University He is also in private practice inWimbledon and Brighton He trained as an existential analytic psychotherapist at the
62 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

Philadelphia Association and is a chartered psychologist His publications include Post-existentialism and the Psychological Therapies Towards a Therapy without Foundations(-Karnac) and Critically Engaging CBT (co-edited with Richard House 2010 PCCS Books)He is currently writing Phototherapy and Therapeutic Photography in a Digital Age(Routledge)
Ahmed Mohamed worked as a Research Assistant for the Research Centre for TherapeuticEducation He is currently doing a PhD at the Department of Psychiatry University ofCambridge focusing on neuroethics of cognitive enhancement Ahmed is interested inclinically and ethically investigating the best way of using cognitive enhancement drugs andneuroimaging techniques on healthy volunteers and patients with neuropsychiatric disorders
Samyukta Mukhopadhyay completed her undergraduate degree BSc(Hons) in Psychology atGoldsmiths University of London in 2008 and then worked as a Research Assistant at theResearch Centre for Therapeutic Education She is currently pursuing an MSc in ForensicMental Health Sciences at the Institute of Psychiatry Kingrsquos College London with an interestin re-victimization of individuals with mental health needs and their experiences of theCriminal Justice System In future she hopes to work within the mental health and disabilitysector
Kalai Ganesh-Hari was a research assistant at the Research Centre for Therapeutic Educationfollowing her PhD with the School of Education Communication and Language SciencesUniversity of Newcastle upon Tyne UK which explored the area of organizational andcognitive psychology with particular emphasis on emotional intelligence predictors andoutcomes leadership and emotions in the workplace
Dr Rhiannon Thomas is a psychotherapeutic counsellor in private practice She has previouslyworked as a counsellor in a school for children diagnosed with learning and behaviouraldifficulties and has just completed her PhD carried out at the Research Centre forTherapeutic Education Roehampton University on language and experience with particularreference to the experience of psychotherapy of mothers with children diagnosed as having asignificant language delay
References
Acharya MP amp Northcott HC (2007) Mental distress and the coping strategies of elderlyIndian immigrant women Transcultural Psychiatry 44 614636
Ager A (1993) Mental health issues in refugee populations A review Working Paper of theHarvard Centre for the Study of Culture and Medicine Department of Management andSocial Sciences Queen Margaret College Edinburgh UK
Aspinall P (2007) Language ability A neglected dimension in the profiling of populationsand health service users Health amp Education Journal 66(1) 90106
Barron D Holterman C Shipster P Batson S amp Alam M (2010) Seen but not heard Ethnic minoritiesrsquo views of primary health care interpreting provision A focus group studyPrimary Health Care Research and Development 11 132141
Basch C (1987) Focus group interview An under-utilised research technique for improvingtheory and practice in health education Health Education Quarterly 41 18
Beiser M amp Hou F (2002) Language acquisition unemployment and depressive disorderamong Southeast Asian refugees A 10-year study Social Science amp Medicine 53(10) 13211334
Bhugra D amp Ayonrinde O (2004) Depression in migrants and ethnic minorities Advancesin Psychiatric Treatment 10 1317
Bhui K Sashidharan SP Cannon M McKenzie K amp Sims A (2003) Should there beseparate services for ethnic minority groups British Journal of Psychiatry 182 1012
Blaxter L Hughes C amp Tight M (2001) How to research (2nd edn) Buckingham OpenUniversity Press
British Journal of Guidance and Counselling 63
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Boi S (2000) Nursesrsquo experiences in caring for patients from different cultural backgroundsNT Research 5(5) 382389
Bradby H Varyani M Oglethorge R Raine W White I amp Helen M (2007) BritishAsian families and the use of child and adolescent mental health services A qualitativestudy of a hard to reach group Social Science amp Medicine 65 24132424
Braun V amp Clarke V (2006) Using thematic analysis in psychology Qualitative Research inPsychology 3 77101
Corbin J amp Strauss A (1998) Basics of Qualitative Research London SageDanso R (2001) From there to here An investigation of the initial settlement experiences of
Ethiopian and Somali refugees in Toronto Geo Journal 55 314Department of Health (2005) Delivering race equality in mental health care An action plan for
reform and outside services Retrieved from http213121207229uploadDRE20ACtion20Planpdf
Department of Health (2007a) Improving access to psychological therapies Computerisedcognitive behaviour therapy (cCBT) implementation guidance 126
Department of Health (2007b) Improving access to psychological therapies Specification forthe commissioner-led Pathfinder programme Retrieved from httpwwwmhchoicecsiporgukpsychological-therapies-iapt-commissionerled-pathfinder-sitesresourceshtml
Department of Health (2009) Improving access to psychological therapies Black and MinorityEthnic (BME) Positive practice guide Retrieved from httpwwwdhgovukprod_consum_dhgroupsdh_digitalassetsdocumentsdigitalassetdh_094201pdf
Ellis BH Kia-Keating M Yusuf S Lincoln A amp Nur A (2007) Ethical research inrefugee communities and the use of community participatory methods TransculturalPsychiatry 44(3) 459481
Ellis BH MacDonald HZ Lincoln AK amp Cabral HJ (2008) Mental health of Somaliadolescent refugees The role of trauma and perceived discrimination Journal of Consultingand Clinical Psychology 76(2) 184193
Fernando S (2005) Multicultural mental health services Projects for minority ethniccommunities in England Transcultural Psychiatry 42 420436
Finnstrom B amp Soderhamn O (2006) Concepts of pain among Somali women Issues andInnovations in Nursing Practice 54(4) 418425
Fowles J (2007) Positive steps supporting race equality in mental health care Department ofHealth Retrieved from httpwwwdhgovukenPublicationsandstatisticsPublicationsPublicationsPolicyAndGuidanceDH_066059
Gerrish K (2000) Individualized care Its conceptualisation and practice within a multiethnicsociety Journal of Advanced Nursing 32(1) 9199
Gerrish K (2001) The nature and effect of communication difficulties arising frominteractions between district nurses and South Asian patients and their careers Journal ofAdvanced Nursing 33(5) 566574
Gervais MC (2008) The drivers of Black and Asian peoplersquos perceptions of racialdiscrimination by public services A qualitative study Paper for Communities and LocalGovernments
Gilleard C Dennis M amp Ziyal L (2005) Ethnicity and access to talking therapies inWandsworth Report to Wandsworth PCT
Green J amp Thorogood N (2004) Qualitative methods for health research London SageGuerin B Guerin P Diiriye RO amp Yates S (2004) Somali conceptions and expectations
concerning mental health Some guidelines for mental health professionals New ZealandJournal of Psychology 33 5967
Halcomb E Gholizadeh L Di Giacomo M Phillips J amp Davidson P (2007) Literaturereview Considerations in undertaking focus group research with culturally and linguisti-cally diverse groups Journal of Clinical Nursing 16(6) 10001011
Harre R amp Secord P (1972) The explanation of social behaviour Oxford BlackwellHawthorne K Rahman J amp Pill R (2003) Working with Bangladeshi patients in Britain
Perspectives from primary health care Family Practice 20(2) 185191Hazel N (1995) Elicitation techniques with young people Social Research Update 12
Department of Sociology University of Surrey Retrieved from httpwwwsocsurreyacuksruSRU12html
64 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

Health Commission (2007) Count me in Census report 2007 Retrieved fromhttpwwwblackmentalhealthorgukindexphpoptioncom_contentamptaskviewampid150ampItemid63]
Herrel N Olevitch L DuBois DK Terry P Thorp D Kind E amp Said A (2004)Somali refugee women speak out about their needs for care during pregnancy and deliveryThe Journal of Midwifery amp Womenrsquos Health 49(40) 345349
Hossain I amp Khan MH (2006) The rift within an imagined community Understandingnationalism(s) in Bangladesh Asian Journal of Social Science 34(2) 324339
Hughes R (1998) Considering the vignette technique and its application to a study of druginjecting and HIV risk and safer behaviour Sociology of Health and Illness 20(3) 381400
IAPT (2008) Improving access to psychological therapies Key performance indicators andtechnical guidance Retrieved from httpwwwiaptnhsuk
King M Weich S Nazroo J amp Blizard B (2006) Religion mental health and ethnicityEMPIRIC A national survey of England Journal of Mental Health 15(2) 153162
Kitzinger J (1994) Focus groups Method or madness In M Boulton (Ed) Challenge andinnovation Methodological advances in social research on HIVAIDS (pp 159175)London Taylor and Francis
Kitzinger J (1995) Introducing focus groups British Medical Journal 311 299302Lavender H Khondoker AH amp Jones R (2006) Understanding of depression An
interview study of Yoruba Bangladeshi and White British people Family Practice 23(6)651658
Lee CC (Ed) (1995) Counselling for diversity Needham Heights MA Allyn and BaconMaclean C (1999) Children family community and work An ethnography of the oil and gas
industry in Scotland Retrieved from httpwwwabdnacukirrarkletonpublicationschildrenshtml
McCrone P Bhui K Craig T Mohamed S Warfa N Stansfeld AS Thornicroft G ampCurtis S (2005) Mental health needs service use and cost among Somali refugees in theUK Acta Psychiatrica Scandinavica 111(5) 351357
McDowell SE Coleman JJ amp Ferner RE (2006) Systematic review and meta-analysis ofethnic differences in risks of adverse reactions to drugs used in cardiovascular medicineBritish Medical Journal 332 11771181
McKenzie K amp Bhui K (2007) Better mental healthcare for ethnic minority groups moving away from the blame game and putting patients first Commentary on Institu-Institutional racism in psychiatry Psychiatric Bulletin 31 368369
Mulatu MS amp Berry JW (2001) Health care practice in a multicultural context Westernand non-Western assumptions In SS Kazarian amp DR Evans (Eds) Handbook of culturalhealth psychology (pp 4663) San Diego CA Academic Press
Murray S amp Buller AM (2007) Exclusion on grounds of language ability a reporting gapin health services research Journal of Health Services Research amp Policy 12(4) 205208
Neale B (1999) Post divorce childhoods Retrieved from httpwwwleedsacukfamilyNightingale DJ amp Cromby J (Eds) (1999) Social constructionist psychology A critical
analysis of theory and practice Buckingham Open University PressPonterotto JG amp Casas JM (1993) Handbook of ethnicracial minority counseling research
Springfield IL Charles C ThomasPumroy S (2008) Treating mental illness in a country with no psychiatrists Retrieved from
httpwwwutnecom2008-04-03GreatWritingTreating-Mental-Illness-in-a-Country-with-No-Psychiatristsaspxblogid38
Ramakrishnan S (1984) The living culture of the Tamils Tamil Nadu Retrieved from httpwwwtamilnationorgcultureramakrishnanhtml
Ravindran G (2006) Negotiating identities in the diasporic space Transnational Tamil cinemaand Malaysian Indians Retrieved from httpwwwtamilnationorgculturedramaravindranpdf
Sadavoy J Meier R amp Yuk MO (2004) Barriers to access to mental health services forethnic seniors The Toronto study The Canadian Journal of Psychiatry 49(3) 192199
Saha S Fernandez A amp Perez-Stable E (2007) Reducing language barrier and racialethnic disparities in health care An investment in our future Journal of General InternalMedicine 22(2) 371372
British Journal of Guidance and Counselling 65
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014
Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014

Sainsbury Centre for Mental Health (2005) Breaking the circles of fear A review of therelationship between mental health services and African and Caribbean communitiesRetrieved from httpwwwscmhorguk
Sashidharan S (2003) Inside outside Improving mental health services for Black and MinorityEthnic communities in England London Department of Health
Sass B Moffat J Bhui K amp Mckenzie K (2009) Enhancing pathways to care for blackand minority ethnic populations A systematic review International Review of Psychiatry21(5) 430438
Seale C Gobo G Gubrium JF amp Silverman D (Eds) (2004) Qualitative researchpractice London Sage
Silove S Sinnerbrink I Field A Manicavasagar V amp Steel Z (1997) Anxiety depressionand PTSD in asylum seekers Association with pre-migration trauma and post-migrationstressors British Journal of Psychiatry 170 351357
Silverman D (2000) Doing qualitative research London SageSinnerbrink I Silove S Manicavasagar V Steel S amp Field A (1996) Asylum seekers
General health status and problems with access to health care Medical Journal of Australia165 634637
Stiles WB (1993) Quality control in qualitative research Clinical Psychology Review 13593618
Sue DW amp Sue D (1990) Counselling the culturally different New York John Wiley ampSons
Thomason TC (1999) Psychological and vocational assessment of Native Americans ERICDocument ED432428 Greensboro NC ERIC Clearinghouse on Counseling and StudentServices
Warfa N Bhui K Craig T Curtis S Mohamud S Stansfled S McCrone P ampThornicroft G (2006) Post-migration geographical mobility mental health and healthservice utilisation among Somali refugees in the UK A qualitative study Health and Place12 503515
Warfa N Bhui K Watters C Craig T Mohamud S amp Curtis S (forthcoming)Prevalence and predictors of psychological distress among Somali immigrants A cross-national comparative study (Forthcoming)
Watters C (2001) Emerging paradigms in the mental health care of refugees Social Science ampMedicine 52 17091718
Watters C amp Ingleby D (2004) Locations of care Meeting the mental health and social careneeds of refugees in Europe International Journal of Law and Psychiatry 27 549570
Whitley R amp Prince M (2004) Is there a link between rates of common mental disorder anddeficits in social capital in Gospel Oak London Results from a qualitative study Health ampPlace 11 237248
Whittaker S Lewis K amp Buchan L (2005) An exploration of psychological well-beingwith young Somali refugees and asylum-seeker women Clinical Child Psychology andPsychiatry 10(2) 177196
Wilkinson S (1998) Focus group methodology A review International Journal of SocialResearch Methodology Theory and Practice 1(3) 181203
Willig C (2001) Introducing qualitative research in psychology Adventures in theory andmethod Buckingham Open University Press
66 D Loewenthal et al
Dow
nloa
ded
by [
Uni
vers
ity o
f N
ottin
gham
] at
03
07 2
5 Ju
ne 2
014