
Rationing in the Delivery of Healthcare
54
Rationing in the delivery of healthcare MSc in Pharmaceutical Medicine, Pharmacoeconomics Jonathan Guillemot, MA, MSc PhD candidate, Institute of Gerontology, King’s College London 1
Transcript of Rationing in the Delivery of Healthcare
Rationing in the delivery of healthcare
MSc in Pharmaceutical Medicine, Pharmacoeconomics
Jonathan Guillemot, MA, MScPhD candidate, Institute of Gerontology, King’s College London
1
Personal statement Jonathan Guillemot
MA Political ScienceMSc GerontologyPhD Candidate in Gerontology Consultant in Health Economics and Outcomes Research
2

Objectives Discuss the specificities of rationing
in the context of healthcare Support that rationing/priority-setting
does take place, whatsoever Not a question of if but how.
Discuss the importance of fairness as elementary value in Western and democratic countries
Introduce some national experiences of healthcare rationing around the world
3
Index1. Introduction to rationing2. Supply in healthcare3. Demand in healthcare4. Approaches to rationing5. International experiences of healthcare
rationing6. Specific issues associated with
healthcare rationing7. Conclusion 8. Literature
4

Introduction to rationing What does rationing mean?
Rationing is the controlled distribution of scarce resources, goods, or services.
Rationing is the artificial restriction of demand.
Examples: Civilian rationing during the WW2
Military rationingNavy (merchant or military)
Gas
5

Introduction to rationing In a free trade context: demand and supply meet at equilibriumIf supply decreases and demand increases: prices increase
For some goods, it is in the interest of the State to keep moderate pricesFuel, food
To keep prices moderate, rationing keeps demand artificially low
Rationing goods is a way to keep prices down, but encourages the development of a black market 6
Introduction to rationingObjective: sustainability
Reindeer population of Saint Matthews Island (USA, Alaska) went extinctReferred to as an example of overpopulationBut it is essentially an example of the importance of resources management (and consequences of mismanagement)
Officially, controlled rationingSupposes the existence of a rationing body with coercive power
Acceptability issues: communication strategies 7

Introduction to rationingIn what context does a society need healthcare rationing?Scarcity of supplyExcess of demand
Why is rationing healthcare complex?Difficulties of defining supplyDifficulties of defining demandDifficulties of implementing the policy
8
Supply in healthcareWhat does supply mean in the context of healthcare?Knowledge/researchWorkforce (doctors, nurses, etc.)Infrastructure (hospitals, ambulances, networks, etc.)
Consumables (pharmaceuticals, etc.)
9

Supply in healthcare“Health is priceless, but it comes at a
cost”What are the drivers to healthcare supply?The budget of the department of healthIndividual’s financial capacity (out-of-pocket)
Healthcare system management
10

Supply in healthcareWhy is the issue of resources allocation in healthcare (and rationing) is stronger in Western countries?Prominence of state-funded healthcare
The State is the PAYER: it is in its interest to provide the best healthcare at the lowest price
11
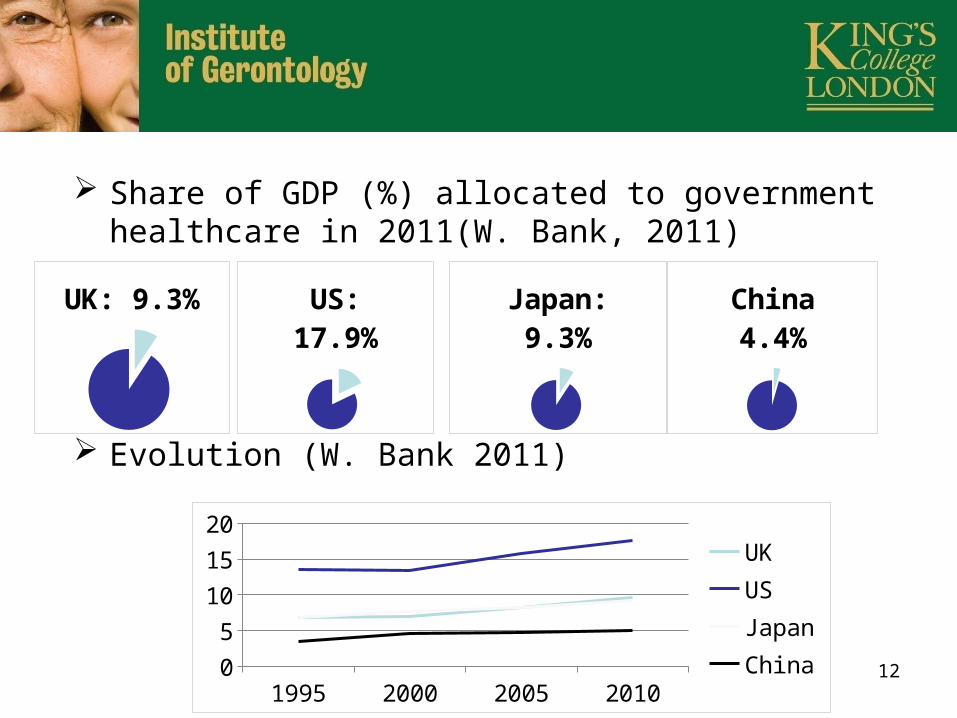
Share of GDP (%) allocated to government healthcare in 2011(W. Bank, 2011)
Evolution (W. Bank 2011)
UK: 9.3% US: 17.9%
Japan: 9.3%
1995 2000 2005 201005101520
UKUSJapanChina
China 4.4%
12
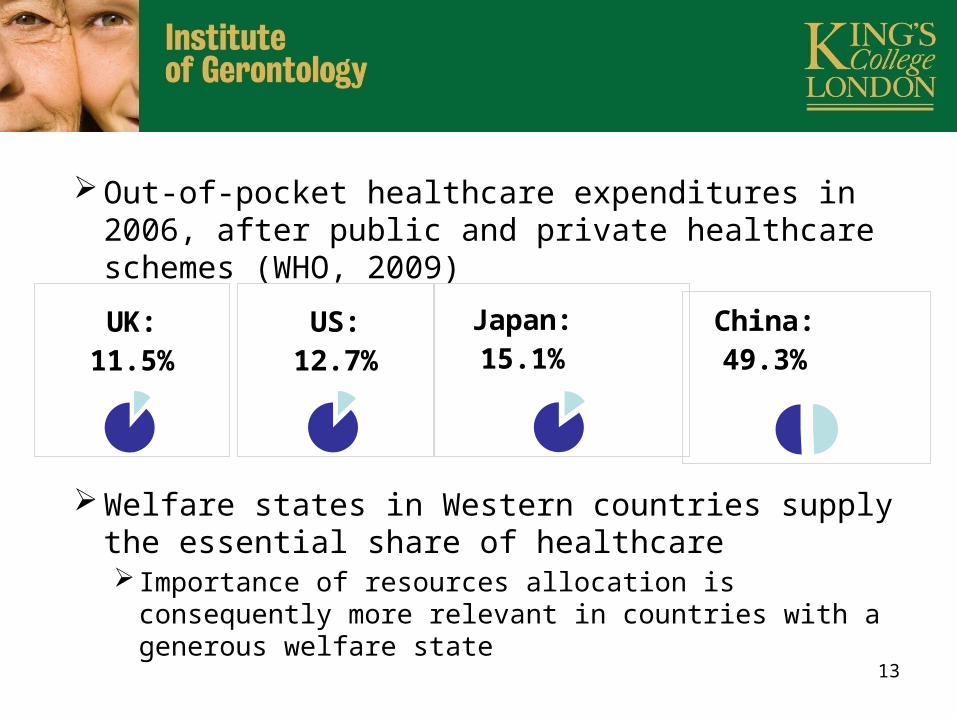
Out-of-pocket healthcare expenditures in 2006, after public and private healthcare schemes (WHO, 2009)
Welfare states in Western countries supply the essential share of healthcareImportance of resources allocation is consequently more relevant in countries with a generous welfare state
UK: 11.5%
US: 12.7%
Japan: 15.1%
China: 49.3%
13

Supply in healthcareWhy are health care resources
scarce?Government healthcare budgets are in competition with other budgetsDefense, education, development, etc.
Individuals’ budgets (spent on private healthcare or on healthcare directly) are also in competition with other budgetsHousing, alimentation, education, etc.14
Supply in healthcareDefinitions of rationing suggest that it is a temporary situation
Healthcare rationing or better presented: healthcare priority setting
Scarcity is a normal situation
15

Supply in healthcareRationalisation vs. rationing vs. prioritisationPrinciples can be linked but are different
Healthcare rationalisation (or more generally cost containment)Developing a strategy to have the most cost-effective systemHealthcare resources maximisationOr “doing better with the same resources (or with less)”
16
Supply in healthcareHealthcare rationalisation (or more generally cost containment) (continued)Includes cost-effective prevention policies, the selection of the most cost-effective drugs, encouraging generic drug use, etc.
May be seen by the public as hidden austerity measures
17

Supply in healthcareRationalisation vs. rationing vs. prioritisation
The R-word: rationingDecision not to deliver a healthcare service/not to meet a need
Prioritisation/priority-settingSystem used to prioritise healthcare access to certain disease areas or populations
It is often the case that these aspects are covered by one single institution and single policies may cover several aspects
18

Demand in healthcareHealthcare demand can be defined as healthcare needs
How do you know what you need? Healthcare knowledge and researchDiagnosis/tests (requiring techniques, knowledgeable professionals and facilities)
Management options for this needProduction capacities
19

Demand in healthcareHow are healthcare needs different from any other product demands?Individuals do not necessarily know what
they needBefore a diagnosis, a patient is not aware of his/her needs
An external actor – the doctor – informs people of their healthcare needs
20

Demand in healthcareWhat does it mean to die of natural
causes?Old? How old?Life expectancy vs. human life span
Life expectancy: statistical assessment from a population
Life span: “normal” duration of a lifetime at the end of which one dies of “natural causes”
Jeanne Calment dies in 1997 at age 122 (oldest human ever, with administrative proof)
Controversy on the existence of a maximum life span
21

Demand in healthcareAre all health problems [(leading to death or not) that a person encounters before their maximum life span] potentially unmet needs?Are there limits to healthcare needs?
No.
22

Demand in healthcare Needs are limitless, but some need more than
others Burden of diseases are unequal
At the international level (Tuberculosis, (WHO 2012))
At the national levels (HIV in the UK (Health Protection Agency 2010))
23

Demand in healthcare Across social groups (fractures according to age in Leicestershire (O’Neill 2005); diabetes according to ethnicities (AACC 2007))
Healthcare supply is scare (unequal, yet scarce)
Healthcare needs are limitless (unequal, yet limitless)
24
Approaches to rationing What are the possible ways to set priorities/ration healthcare?Priority to the wealthy? The powerful? The dominant?
Exclude others, like sexual minorities? Ethnicities? Sufferers from specific diseases?Wait, that’s unfair!
Implicitly or explicitly, such rules do exist everywhere Health care deserts (Healthcare geography), postcode lottery, waiting lines, etc.
Exclusion/restrictions of non-citizens from healthcare systems by creating administrative hurdles…
25
Approaches to rationingLet us rephrase: What are the possible ways to fairly set priorities/ration healthcare?Fairness/equity/social justice are essential ethical values and are inherently associated with the debate on healthcare rationing
But still, there are various solutions as these culturally embedded valuesThose with the greatest needs?Those with the greatest achievement capacities?
Those for whom healthcare resources can do best?
26
Approaches to rationingHaving to choose: the story from Grey’s Anatomy of the two patients impaled by one pole “How do you decide
who gets to live?” Age Gender Social importance Estimated quality-of-life after care
Survival prognosis People’s preferences
“It’s not fair either way”Grey’s anatomy, Season 2, Episode 6 27
Approaches to rationingHow does one know “for whom healthcare can do best”?By accumulating knowledge on the condition, its natural outcome, socio-economic impacts, the outcomes of possible various healthcare interventions, their socio-economic impacts, etc.
Aim: being able to choose according to a socially accepted (acceptable? To whom? The majority?) set of rules considered as fair and make the decision-making process a technical and objective issue rather than a subjective choice
28

Approaches to rationing The example of the QALYs as a way to objectively assess and compare the value of interventions QALY (Quality-Adjusted Life-Year) ICER threshold valid across disease areas, age groups, etc.
Values: Time gained from death, Quality of life and costs
UsageBuild a healthcare coverage threshold: the cost that society is ready to pay for an extra year of life (quality adjusted)
Develop a priority list (the most cost-effective to the least cost-effective)
Limits? Assumptions, knowledge evolution…
29

Approaches to rationing Explicit rationing: unpopular, politically challengingAt the individual level, it is tough to find negation of care acceptable
Other than simply refusing to explicitly setting priorities, there are other ways to “defuse the political bomb”Avoiding direct exclusion via healthcare recommendations
Delegating the responsibility to healthcare provider (gatekeepers)
Delegate the definition of the rules to an independent agency (which can be blamed for it)
30
Approaches to rationing The limits of the technical approach
The inclusion of social value judgments, usually using citizens groups
31

Approaches to rationing How do you compare disease areas to set priorities?Between life-threatening diseases (cancers, for example) and syndromes (irritable bowel syndrome(IBS)) associated, burdensome on society yet not having direct effects on life expectancy.
Budget impactTreatment A against cancer: cost-effective (health benefits outweigh the costs)
Treatment B against IBS: cost-saving (overall costs decrease due to the health technology)
32

Approaches to rationingSo economically, it is more meaningful to fund treatment B in priority
So if comfort has more value than survival, should it be given priority?Should life threatening healthcare solutions have priority on others?
33

International experiences of healthcare rationing: England and the NICE National Institute for Health and Care Excellence (NICE)Created in 1999British rationing body
One of the most advanced rationing regulation system
Essential principleICER: Incremental Cost-Effectiveness Ratio
The cost that the British society is ready to pay for an extra year of life (quality adjusted) has a limit£20,000 ( later tolerated up to £30,000) per QALY
34
International experiences: England and the NICE Pharmacological treatments recommended by the NICE are funded by the NHS
Recommendations are developed on the basis of a health technology assessment (HTA)Outcome: cost per QALY
The first rationing case of Lenalidomide Lenalidomide (Revlimid): treatment for multiple myeloma (cancer of plasma cells)
ICER = £43,800, therefore not initially recommended
TA171later recommended lenalidomideSee documentary BBC (Wishart 2009)
35

International experiences: England and the NICE Where cost-containment and rationing policies overlap/collide The Quality and Outcomes Framework (QOF)
financial incentive program to encourage GP adherence to official recommendations via a set of indicators
Prioritisation of disease areas and interventions
Organised by the NICE and the Department of Health 36

International experiences: England and the NICE
Leads to extra expendituresNot rationing policy, right?
What does it encourage exactly? The nature of the policy depends on the recommendations themselves
It can be a healthcare expansion policy, as well as a cost-containment or a rationing policy.
37
International experiences: England and the NICEThe limits of pragmatic rationing: Social value judgements via the Citizens Council when facing difficult moral and ethical issues 15 reports since 2002
Report 2: Are there circumstances in which the age of a person should be taken into account when NICE is making a decision about how treatments should be used in the NHS?
Report 6: Is there a preference to save the life of people in imminent danger of dying?
http://www.nice.org.uk/aboutnice/howwework/citizenscouncil/reports.jsp
38
International experiences: GermanyRationalisation processes being implemented
In Germany viaThe HTA agency IQWIG (Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen) develops cost-effectiveness assessments (2004)
The Federal Joint Committe (Gemeinsamer Bundesausschuss (G-BA)) regulates the benefit package (Leistungskatalog) and commissions the IQWIG
39
International experiences: France Rationalisation processes being implemented
In France via The HTA agency HAS (Haute Autorité de Santé)
The Sécurité SocialeThe ANSM (Agence Nationale de Sécurité du Médicament)
40

International experiences: France & Germany Not yet explicit rationing policies, but on their waysIn Germany, citizens disagreed with the principles of imposing limits to the benefit package or to politician-based rationing (preferring tax increases)
Implicit rationing/prioritisationIncrease of out-of-pocket expenditure via drug de-reimbursement in France, therefore leaving the choice to patients
Cost control (consultation fees re-evaluation) have led to decreasing interest in some professions or increases in fees outside the reimbursed framework
41
International experiences: USA & Oregon Mixed healthcare system, between private insurance
and public coverage Public coverage faces similar issues as in other
welfare states Medicare (65+)/Medicaid (poorer people)
Oregon and priority setting experience (1990s) Developed a list of morbidities to tackle in priority and a treatment cut-off list
Very negatively perceived although the goal was to simplify eligibility criteria for Medicaid, but was instead seen as “rationing for the poor”
Organ donation: priority lists Gray areas: quality reductions, time limits for care (veiled/implicit rationing?)…
Private insurance-based healthcare
42

International experiences: Australia HTA agency (Pharmaceutical Benefits Advisory Committee (PBAC))Conducts HTARecommends which HC technology can be reimbursed
The Ministry of Health and AgeingCan decide not to reimburse a cost-effective technology
Cannot decide to reimburse a cost-ineffective technology
The Ministry is, in this case the rationing body while the PBAC is a rationalising/cost-containment body
43

International experiences: Japan One of the oldest populations Which is not associated with the most costly healthcare system
Efficient cost-containment policiesHigh levels of out-patient careEfficient payment system (despite generalised private insurance)
Strict price control (od healthcare services and technologies)
No explicit rationing policiesDecrease in service quality 44

International experiences: less developed countriesPriority-setting is more difficult in developing countriesBurden of underdevelopment (supply difficulties)
Lack of information (knowledge management for evidence-based decision-making)
Multiple players, various agendas (corruption?)
Lack of systematic decision-making processes
Implementation obstacles (political instability, weak institutions, social inequalities)
45
International experiences: less developed countries Less comprehensive welfare state than developed economies More burden on citizens the essential share of the costs is supported via out-of-pocket expenditures
Extra-national health care resources: a significant and increasing role (17% in 2006 (WHO 2009))
Government healthcare spending <$20 per capita per year (WHO 2008) making priority setting even more important!
Progressively structures are being developedWHO/World Bank: Essential health care package: a solution to overcome the challenges of setting the basis of an efficient and sustainable priority-setting system
46
International experiences: less developed countriesDo older people cost too much?
The red herring argument: cost of proximity to death rather than ageing (McGrail 2000)
Explanatory argument: the rectangularisation of survival curve (Wilmoth 1999)
Life expectancy in good health: the vain pursuit of immortality
Chronological age as a poor proxy as age expectancy grows
47
International experiences: age and ageingPriority to the young to reach a fair lifespan?Priority based expected lifespan (priority to the younger)? The fair innings argument (Williams 1997)
Going towards more equality? Is the role of healthcare to provide citizens with an equal life experience
Going towards more efficiency? Is the role of healthcare to support those who can benefit the most?
48
International experiences: other issues Life-threatening situations: should we be ready to allocate more resources in cases of emergency life-threatening situations (mountain rescues…)
Socially important people: breadwinners, parents, political figures, historical figures…
New technologies: should we accept excess expenditures regarding healthcare improvements to encourage innovations and progress?
Children: should we allocate more resources to children because society values children more?
Orphan diseases: should a society be ready to spend more for rare diseases sufferers when funding would create unbalance in the budget?
49

Conclusion The question is not to approve or oppose rationing policies But rather, how one does best allocate resources
How does one tackle the most difficult ethical issues? (in a democratic context)
How does one develop a socially acceptable AND transparent/explicit priority-setting system?
Is it adaptable to changing economic situation (resource-shrinking economies)
Is the resource allocation/priority setting system cost-effective? 50

Conclusion The debate on rationing questions the very basis of societyWhat is the goal of the healthcare system?To support the weak or the most capable?
Can societies build a fairer system than natural selection? (play God?)
On what basis do government allocate resources?Evidence-based decision-making in healthcare (in other areas?)
The capacity to ration resources is the result of our capacity to plan and anticipate (with more or less success)
51
Literature Wishart, A. The Price of Life, BBC documentary,
broadcasted on BBC2 July 5th 2009, freely accessible on http://vimeo.com/4796083
PRI’s The World, Rationaing Health. Who lives? Who Decides? www.rationinghealth.org/ (see also audio post and forum discussion)
Ham, C. and Robert, G. (Eds). Reasonable Rationing: International experience of priority setting in health care.
Ham, C. & Coulter A. Explicit and implicit rationing: taking responsibility and avoiding blame for health care choices. J Health Serv Res Policy July 1, 2001 vol. 6 issue 3, 163-169
Robinson, S. Williams, L. et al. Priority-setting and rationing in healthcare: Evidence from the English experience. Social Science & Medicine, December 2012, vol. 75, issue 12, 2386–2393
Wilmoth, J.R. & Horiuchi, S. Rectangularization revisited: Variability of age at death within human populations. Demography, November 1999, vol. 36, Issue 4, 475-495
52

Literature McGrail, K., Green, B. et al. Age, costs of acute and
long-term care and proximity to death: evidence for 1987-88 and 1994-95 in British Columbia. Vol. 29, issue 3, 249-253.
Williams, A. The rationing debate: Rationing health care by age: The case for. BMJ, March 1997, vol. 314, 820.
Oduncu, F.S. Priority-setting, rationing and cost-effectiveness in the German Health Care System, Med Health Care and Philos, June 2012, 1-13
Youngkong, S. et al. Setting priorities for health interventions in developing countries: a review of empirical studies. Tropical Medicine and International Health, August 2009, vol. 14, issue 8, 930-939
Kapiriri L. & Martin D.K. (2007) A strategy to improve priority setting in developing countries. Health Care Analysis, 2007, vol. 15, 159–167.
Kapiriri L. How effective has the essential health package been in improving priority setting in low income countries? Social Science & Medicine, vol. 85, May 2013, 38–42
53
Literature Gallego, G., Taylor S.J. and Brian, J.E. Setting
priorities for high-cost medications in public hospitals in Australia: should the public be involved? Australian Health Review, 2011, 35, 191–196
www.nice.org.uk : Citizens Council, Quality and Outcomes Framework and NICE guideline development methods
Hashimoto, H. et al. Cost containment and quality of care in Japan: is there a trade-off? Lancet, 2011, vol. 378, 1174–82
54




















