Rapid weather changes are associated with increased ischemic stroke risk: a case-crossover study
10
CARDIOVASCULAR DISEASE Rapid weather changes are associated with increased ischemic stroke risk: a case-crossover study Florian Rakers 1,3 • Rene Schiffner 1 • Sven Rupprecht 1 • Antje Brandsta ¨dt 2 • Otto W. Witte 1 • Mario Walther 2 • Peter Schlattmann 2 • Matthias Schwab 1 Received: 26 March 2014 / Accepted: 12 June 2015 Ó Springer Science+Business Media Dordrecht 2015 Abstract Observational studies focusing on absolute meteorological values suggest an association between meteorological parameters and stroke risk but these results are inconsistent and conflicting. Since changes in weather can provoke atrial fibrillation, we examined the association between rapid weather changes and stroke risk in 1694 patients with determinable onset of stroke symptoms in a case-crossover study in central Germany. Days one to three before stroke onset were classified as hazard periods and day seven as the respective control period. Risk of ischemic stroke in relation to 24 h differences in mean ambient temperature, relative humidity and atmospheric pressure was determined. The association between tem- perature and stroke risk appears to be close to linear with an increase in stroke risk of 11 % (odds ratio 1.11, 95 % confidence interval 1.01–1.22) for each 2.9 °C temperature decrease over 24 h. In individuals with a higher cardio- vascular risk, stroke risk increased by 30 % (1.30, 1.06–1.61). Risk for cardioembolic strokes increased by 26 % (1.26, 1.06–1.50). Rapid positive or negative changes in relative humidity ( [ 5 %) and atmospheric pressure ( [ 10 hPa) increased stroke risk by a maximum of 30 % (1.30, 1.02–1.66) and 63 % (1.63, 1.10–2.42). In individuals with a higher cardiovascular risk, rapid changes in atmospheric pressure were associated with a four-times higher stroke risk (4.56, 1.26–16.43). Our results suggest that rapid decreases in ambient temperature and rapid changes in relative humidity and atmospheric pressure increase stroke risk under temperate climate conditions. Individuals with a high cardiovascular risk profile seem to be at greater risk. Keywords Cerebrovascular disease Á Stroke Á Infarction Á Stroke prevention Á Weather Introduction An increase in several significant risk factors for stroke can be attributed to long term or acute changes in weather. For example, onset of atrial fibrillation—the primary cause of cardioembolic strokes—can be provoked by cold weather [1, 2]. In addition, a low relative humidity is known to increase human blood viscosity [3] which is an established predictor for ischemic strokes [4]. Although a few obser- vational studies suggest that ambient temperature [5–8] and atmospheric pressure [9, 10] influence stroke risk, results are inconsistent and conflicting [11]. A humidity-related stroke risk could not be demonstrated so far [7, 9]. More- over, most of these studies focused on absolute meteoro- logical values and did not take rapid weather changes into account [5–7]. Lastly, study samples in the studies were often relatively small [8, 9, 12, 13]. Weather-related stroke risk is physiologically plausible and knowledge of an association between weather and stroke risk could help develop stroke prevention strategies and facilitate a shift in the awareness of health professionals regarding early signs of stroke in adverse weather conditions. & Florian Rakers fl[email protected] 1 Hans Berger Department of Neurology, Jena University Hospital, Bachstrasse 18, 07743 Jena, Thuringia, Germany 2 Institute of Medical Statistics, Computer Sciences and Documentation, Jena University Hospital, Bachstrasse 18, 07743 Jena, Thuringia, Germany 3 Department of Neurology, Helios Hospital Berlin-Buch, Schwanebecker Chaussee 50, 13125 Berlin, Germany 123 Eur J Epidemiol DOI 10.1007/s10654-015-0060-3
Transcript of Rapid weather changes are associated with increased ischemic stroke risk: a case-crossover study

CARDIOVASCULAR DISEASE
Rapid weather changes are associated with increased ischemic
stroke risk: a case-crossover study
Florian Rakers1,3 • Rene Schiffner1 • Sven Rupprecht1 • Antje Brandstadt2 •
Otto W. Witte1 • Mario Walther2 • Peter Schlattmann2 • Matthias Schwab1
Received: 26 March 2014 / Accepted: 12 June 2015
� Springer Science+Business Media Dordrecht 2015
Abstract Observational studies focusing on absolute
meteorological values suggest an association between
meteorological parameters and stroke risk but these results
are inconsistent and conflicting. Since changes in weather
can provoke atrial fibrillation, we examined the association
between rapid weather changes and stroke risk in 1694
patients with determinable onset of stroke symptoms in a
case-crossover study in central Germany. Days one to three
before stroke onset were classified as hazard periods and
day seven as the respective control period. Risk of
ischemic stroke in relation to 24 h differences in mean
ambient temperature, relative humidity and atmospheric
pressure was determined. The association between tem-
perature and stroke risk appears to be close to linear with
an increase in stroke risk of 11 % (odds ratio 1.11, 95 %
confidence interval 1.01–1.22) for each 2.9 �C temperature
decrease over 24 h. In individuals with a higher cardio-
vascular risk, stroke risk increased by 30 % (1.30,
1.06–1.61). Risk for cardioembolic strokes increased by
26 % (1.26, 1.06–1.50). Rapid positive or negative changes
in relative humidity ([5 %) and atmospheric pressure
([10 hPa) increased stroke risk by a maximum of 30 %
(1.30, 1.02–1.66) and 63 % (1.63, 1.10–2.42). In
individuals with a higher cardiovascular risk, rapid changes
in atmospheric pressure were associated with a four-times
higher stroke risk (4.56, 1.26–16.43). Our results suggest
that rapid decreases in ambient temperature and rapid
changes in relative humidity and atmospheric pressure
increase stroke risk under temperate climate conditions.
Individuals with a high cardiovascular risk profile seem to
be at greater risk.
Keywords Cerebrovascular disease � Stroke � Infarction �
Stroke prevention � Weather
Introduction
An increase in several significant risk factors for stroke can
be attributed to long term or acute changes in weather. For
example, onset of atrial fibrillation—the primary cause of
cardioembolic strokes—can be provoked by cold weather
[1, 2]. In addition, a low relative humidity is known to
increase human blood viscosity [3] which is an established
predictor for ischemic strokes [4]. Although a few obser-
vational studies suggest that ambient temperature [5–8] and
atmospheric pressure [9, 10] influence stroke risk, results
are inconsistent and conflicting [11]. A humidity-related
stroke risk could not be demonstrated so far [7, 9]. More-
over, most of these studies focused on absolute meteoro-
logical values and did not take rapid weather changes into
account [5–7]. Lastly, study samples in the studies were
often relatively small [8, 9, 12, 13]. Weather-related stroke
risk is physiologically plausible and knowledge of an
association between weather and stroke risk could help
develop stroke prevention strategies and facilitate a shift in
the awareness of health professionals regarding early signs
of stroke in adverse weather conditions.
& Florian Rakers
1 Hans Berger Department of Neurology, Jena University
Hospital, Bachstrasse 18, 07743 Jena, Thuringia, Germany
2 Institute of Medical Statistics, Computer Sciences and
Documentation, Jena University Hospital, Bachstrasse 18,
07743 Jena, Thuringia, Germany
3 Department of Neurology, Helios Hospital Berlin-Buch,
Schwanebecker Chaussee 50, 13125 Berlin, Germany
123
Eur J Epidemiol
DOI 10.1007/s10654-015-0060-3

In the current case-crossover study performed under
temperate climate conditions that prevail in large parts of
Europe and North America, we hypothesized firstly, that
rapid weather changes have an influence on ischemic
stroke risk; and secondly, that this risk applies specifically
to cardioembolic stroke because sympathetic autonomic
activity which promotes atrial fibrillation, increases with
lower temperature [1, 2].
Methods
Study design
Admission data were retrieved from the Jena University
Hospital’s patient data management system. Using the
International Classification of Diseases—10th Revision
(ICD-10) codes, we searched for transient cerebral
ischemic attack lasting between 1 and 24 h (G45.92) and
cerebral infarction (I63.X). Study period was the 1st of
January 2003 until 31st of December 2010 and the
catchment area involved a radius of\10 km around Jena
(filtered by postal codes). Accordingly, patient health
records and all medical reports (including self-reports or
accounts from accompanying caregivers) plus emergency
records together with CT/MRI results were individually
screened to verify the diagnosis and the date and time of
stroke onset. In wake-up strokes, stroke onset was defined
as the mean time between bedtime and wake-up time.
Additional data collected comprises age, sex and risk
factors to calculate the individual Framingham stroke risk
score [14]. Baseline systolic blood pressure needed for
this calculation was estimated from average systolic blood
pressure during the first 3 days of hospitalization. Stroke
subtypes were classified in accordance with the Trial of
ORG 10172 in Acute Stroke Treatment (TOAST) criteria
[15]. Severity of stroke symptoms was determined
according to the National Institutes of Health Stroke Scale
(NIHSS) [16]. Regular meetings were held during the
study period to ensure consistent stroke classification
procedures.
Exclusion criteria included: (1) inaccessible patient file,
(2) stroke occurring outside the 10 km zone around Jena
University Hospital, (3) diagnosis other than stroke due to
errors in hospital admission data, and, (4) inability to
determine the acute onset of stroke symptoms.
Temperature, relative humidity and atmospheric pres-
sure data were provided as hourly values for the entire
study period by the meteorological monitoring station of
the Jena University of Applied Sciences (longitude
11�340E/latitude 50�550N/altitude 215 m). The city of Jena
has a temperate climate with mild summers and moderately
cool winters [17].
Statistical analysis
A case-crossover analysis was used to determine weather-
related stroke risk. This design was previously developed
to study the association between a transient exposure and a
risk factor for the development of an acute and rare event
[18]. The approach is a variation of the case–control
method, the difference being that every patient serves as
his or her own control. This allows controlling by design
for individual risks such as age, sex, socioeconomic status
or seasonal influences that do not change over a short
period of time. Interference is based on comparing the
potentially health-affecting conditions directly before the
event (hazard interval: 24 h weather changes between day-
2 and -1, -3 and -2 and between day-4 and -3 before onset
of stroke symptoms) with the same conditions in the
patient’s recent past (control interval: 24 h weather chan-
ges on respective days in previous week). The number of
days between weather change and stroke onset is referred
to as lag time. Three different lag times were used to
consider a potential delay before impact of the specific
meteorological variable. Conditional logistic regression
was used to take the self-matching structure of the case-
crossover design into account. The stratifying variable in
this case is the individual patient. The association between
mean daily changes in temperature, relative humidity and
atmospheric pressure and ischemic stroke risk is quantified
as the odds ratio that describes the change in odds for an
event according to alterations in the examined weather
characteristics. The hourly values of meteorological vari-
ables obtained from the meteorological station described
above were averaged over 24 h for day one, two and three
(hazard period) and day seven (control period) before
stroke occurrence. Averaged meteorological variables were
analyzed in two different models of conditional logistic
regression: (model one) as a continuous variable and
(model two) as a categorized variable with six categories.
For ambient temperature, cut off values were -5, -3, -1,
1, 3, 5 �C. Temperature changes between -1 and 1 �C
were taken as the reference category. For relative humidity,
cutoff values were the same as for temperature. For
atmospheric pressure, cutoff values were -10, -5, -2, 2,
5, 10 hPa with the changes in atmospheric pressure
between -2 and 2 hPa serving as the reference category.
These cutoff values were chosen according to values used
in previous studies to ensure comparability [12] or after
visual inspection of the appropriate distribution curve.
Confounding in a case-crossover study is only possible
among correlated transient exposures. In this study—given
the nature of weather—patients were exposed to all three
meteorological variables at the same time. To control for
this within-individual confounding, we used multivariable
conditional logistic regression. In addition, we regarded the
F. Rakers et al.
123

day of the week as a potential confounder as stroke risk
also depends on the day of the week [19]. By choosing a
7-day control period, both stroke occurrence and control
period shared the same day of the week and we adjusted for
this potential confounder. All analyses were performed for
the whole study population as well as for age (stratified by
older or younger than 60 years), sex and other risk factor
subgroups. The Framingham stroke risk score [14] was
grouped into three categories (mild risk: B12 points,
moderate risk: 13–17 points, high risk: C18) after visual
inspection of the distribution curve. The NIHSS was
grouped into two categories (less severe:\8 points, more
severe: C8 points) which is consistent with other stroke
studies [20]. Odds ratios in model one (weather as a con-
tinuous variable) refer to a 24 h change in the respective
meteorological variable that equals the 10th percentile of
all observed 24 h changes in this variable during the study
period (Table 2), i.e. we present odds ratios associated with
weather changes that are not uncommon and thus clinically
relevant.
Results
Study cohort
Of the 2066 patients admitted to Jena University Hospital
with a diagnosis of stroke, 177 (9 %) could not be pro-
cessed as patient files were not available during the
screening period. In 81 cases (4 %), we were unable to
retrospectively determine the date of acute onset of stroke
symptoms and a further 114 cases (5 %) did not meet the
ischemic stroke criteria. The remaining 1694 cases formed
the basis of this case-crossover study (Fig. 1). Character-
istics of the study population are described in Table 1. The
Framingham Stroke Risk could be calculated retrospec-
tively in 1645 cases and the NIHSS could be retrieved
electronically in 782 cases.
Meteorological variables
Table 2 summarizes the 24 h changes in mean daily values
of meteorological variables. During the study period, the
average daily temperature ranged from -14.0 to 28.6 �C.
Average daily atmospheric pressure and relative humidity
values ranged from 955.1 to 1017.1 hPa and 40.0–99.1 %,
respectively.
Stroke risk in relation to temperature
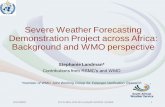
Figure 2 shows the association between stroke risk and the
change in ambient temperature analyzed as a continuous
variable. For each 2.9 �C decrease in mean daily ambient
temperature, the stroke risk in the overall population
increased by a maximum of 11 % [OR 1.10, 95 % confi-
dence interval (CI) 1.01–1.21, lag time: 1 day; 1.11,
1.01–1.22, lag time: 2 days]. Further, the risk for car-
dioembolic strokes increased by 26 % (1.26, 1.06–1.50, lag
1 day). The general risk of stroke in older patients
increased by a maximum of 13 % (1.13, 1.02–1.25, lag
1 day; 1.11, 1.01–1.23, lag 2 days). In women, the general
stroke risk increased by 14 % (1.14, 1.01–1.30, lag 2 days).
Those with increased risk for vascular disease showed a
30 % (1.30, 1.06–1.61, lag 1 day) higher general stroke
risk for a medium Framingham score and a 16 % (1.16,
1.01–1.32, lag 2 days) higher risk for a high Framingham
score. The magnitude of all associations decreased over
time and associations were non-significant following a lag
time of[2 days.
In the categorized model, positive odds ratios indicate
an increased stroke risk in the overall population following
a decrease in mean daily ambient temperature between 3
and 5 �C (1.15, 0.87–1.51, lag 2 days) and more so for a
decrease of greater than 5 �C (1.47, 0.85–2.52, lag 2 days;
Fig. 5). However, the CI included 1.00. Increases in tem-
perature of more than 5 �C were associated with an up to
47 % (0.53, 0.28–1.00, lag 1 day; 0.57, 0.29–1.05, lag
2 days) decrease in stroke risk (Fig. 5). In subgroups,
stroke risk in women increased by 30 % (1.30, 1.01–1.68,
lag 2 days) after a temperature decrease of 1–3 �C. Stroke
risk more than tripled (3.25, 1.03–10.25, lag 2 days) in
those with a medium Framingham risk score following a
decrease in temperature of more than 5 �C. Risk for less
severe strokes increased by 74 % (1.74, 1.06–2.87, lag
2 days) after a temperature decrease of 3–5 �C. The risk for
cardioembolic strokes tended to be more than two times
higher (2.77, 0.97–7.89, lag 1 day) after a temperature
decrease of more than 5 �C. For cardioembolic strokes,
stroke risk decreased by 22 % (0.78, 0.47–1.29, lag 3 days)
following a temperature increase of 1–3 �C. In males,
stroke risk decreased by 67 % (0.33, 0.12–0.93, lag 1 day)
after a temperature increase of more than 5 �C.
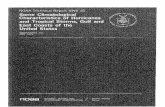
Stroke risk in relation to relative humidity
Figure 3 depicts the association between stroke risk and the
mean daily relative humidity analyzed as a continuous
variable. For each mean daily decrease in relative humidity
of 4.1 %, the general stroke risk in the overall population
increased by 4 % (1.04, 1.01–1.07, lag 1 day) and the risk
for cardioembolic strokes by 6 % (1.06, 1.00–1.12, lag
1 day). The general stroke risk in women increased by 6 %
(1.06, 1.01–1.11, lag 1 day), and in younger individuals by
9 % (1.09, 1.00–1.18, lag 1 day). In patients with a low
Framingham score, the general risk of stroke was raised by
7 % (1.07, 1.01–1.14, lag 1 day).
Rapid weather changes are associated with increased ischemic stroke risk: a case-crossover…
123

Analysis of the mean daily relative humidity as a cate-
gorized variable demonstrated a increase in stroke risk of
maximal 30 % (1.26, 1.01–1.59, lag 1 day; 1.30,
1.02–1.66, lag 2 days, Fig. 5) in the overall population
following a more than 5 % decrease in relative humidity. A
comparable increase in stroke risk was observed after an
increase in relative humidity of 3–5 % (1.34, 0.98–1.84,
lag 1 day; 1.39, 1.01–1.90, lag 2 days; Fig. 5). In sub-
groups, the stroke risk generally increased in males by a
maximum of 48 % (1.48, 1.07–2.05, lag 1 day; 1.38,
0.98–1.93, lag 2 days; 1.45, 1.03–2.05, lag 3 days) after
exposure to a decrease in relative humidity of more than
5 % and by a maximum of 72 % (1.45, 0.90–2.32, lag
1 day; 1.48, 0.93–2.35, lag 2 days; 1.72, 1.07–2.75, lag
3 days) after exposure to an increase in relative humidity
between 3 and 5 %. In patients with a low Framingham
score, stroke risk increased by 71 % (1.71, 1.02–2.88, lag
1 day) after a decrease in relative humidity of more than
5 %. Risk for strokes due to large artery atherosclerosis
was about three times higher (2.72, 1.11–6.7, lag 1 day;
3.11, 1.28–7.53, lag 2 days) after an increase in relative
humidity between 3 and 5 %.
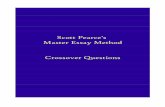
Stroke risk in relation to atmospheric pressure
Figure 4 shows the association between stroke risk and
mean daily atmospheric pressure analyzed as a continuous
variable. We found no association between a change in
atmospheric pressure over 24 h and the general stroke risk
in the overall population at all lag times. However, for each
Fig. 1 Flowchart of the patient
data selection process for the
case-crossover study
Table 1 Characteristics of patients admitted to the Jena University
Hospital with a verified diagnosis of ischemic stroke or transient
ischemic attack (TIA) between 1st January 2003 and 31st December
2010
No. %
Overall population 1694 100
Median age (years) 75
Young (\60) 246 15
Old (C60) 1448 85
Men 824 49
Previous stroke/TIA 526 31
Pathogenesis
Small artery occlusion 696 41
Cardioembolism 541 32
Large artery atherosclerosis 272 16
Undetermined 185 11
Median Framingham stroke risk score 18
Low (B12) 381 23
Middle (13–17) 401 24
High (C17) 863 53
Median NIHSS score 4
Less severe (\8) 504 64
More severe (C8) 278 36
F. Rakers et al.
123

Table 2 Percentiles of 24 h
changes of mean daily
meteorological parameters over
the study period 1st January
2003–31st December 2010
Percentiles
5th 10th 25th 50th 75th 90th 95th
Temperature (�C) -3.8 -2.9 -1.4 0.1 1.5 2.8 3.6
Atmospheric pressure (hPa) -4.1 -3.2 -1.9 -0.2 1.6 3.7 5.1
Relative humidity (%) -5.9 -4.1 -1.8 0.2 2.1 3.8 4.9
Fig. 2 Odds ratios for the
association of stroke risk with a
decrease of 2.9 �C in mean
daily ambient temperature over
24 h for lag times of 1, 2 and
3 days before onset of stroke
symptoms in the overall
population and subgroups.
Square size is proportional to
the number of cases, bars
indicate 95 % CI, adjusted for
relative humidity and
atmospheric pressure, filled
squares mark odds ratios with
confidence intervals not
including 1.00
Fig. 3 Odds ratios for the
association of stroke risk with a
decrease of 4.1 % in mean daily
relative humidity over 24 h for
lag times of 1–3 days before
onset of stroke symptoms in the
overall population and
subgroups. Square size is
proportional to the number of
cases, bars indicate 95 % CI,
adjusted for temperature and
atmospheric pressure, filled
squares mark odds ratios with
confidence intervals not
including 1.00
Rapid weather changes are associated with increased ischemic stroke risk: a case-crossover…
123

3.2 hPa increase in atmospheric pressure over 24 h, the risk
for clinically severe strokes decreased by 11 % (0.89,
0.80–0.99, lag 1 day). In younger individuals, the general
stroke risk also decreased by 14 % (0.86, 0.76–0.96, lag
2 days).
Analyzed as a categorized variable, a decrease of mean
daily atmospheric pressure of more than 10 hPa over 24 h
was associated with an increase in stroke risk by up to
46 % (1.32, 0.86–2.04, lag 1 day; 1.46, 0.96–2.11, lag
3 days; Fig. 5) in the overall population. Comparably, after
an increase in atmospheric pressure of more than 10 hPa,
stroke risk increased in the overall population by a maxi-
mum of 63 % (1.56, 1.06–2.29, lag 1 day; 1.63, 1.10–2.42,
lag 3 days; Fig. 5). Increases in stroke risk were observed
after a decrease in atmospheric pressure between 2 and
5 hPa (1.38, 1.14–1.69, lag 3 days; Fig. 5) and after an
increase in atmospheric pressure between 2 and 5 hPa
(1.29, 1.03–1.63, lag 3 days; Fig. 5). Within subgroups,
stroke risk increased in older patients by 79 % (1.79,
1.10–2.91, lag 1 day) after a decrease in atmospheric
pressure of more than 10 hPa, by 37 % (1.37, 1.11–1.69,
lag 3 days) after a decrease in atmospheric pressure
between 2 and 5 hPa and by a maximum of 58 % (1.55,
1.03–2.36, lag 1 day; 1.58, 1.06–2.43, lag 2 days) after an
increase in atmospheric pressure of more than 10 hPa. In
males, stroke risk increased by a maximum of 67 % (1.35,
1.01–1.81, lag 1 day; 1.67, 1.26–2.21, lag 3 days) follow-
ing a decrease in atmospheric pressure between 2 and 5 and
by 84 % (1.84, 1.03–3.27, lag 1 day) after an increase in
atmospheric pressure of more than 10 hPa. Those with a
medium Framingham score showed a more than four-times
higher stroke risk after a decrease in atmospheric pressure
of more than 10 hPa (4.56, 1.26–16.43, lag 1 day). In
patients with a high Framingham score, stroke risk
increased by 46 % (1.46, 1.11–1.92, lag 3 days) after a
decrease in atmospheric pressure between 2 and 5 hPa and
by 71 % (1.71, 1.02–2.94, lag 3 days) after an increase in
atmospheric pressure of more than 10 hPa. Risk for strokes
due to large artery atherosclerosis approximately doubled
following a decrease in atmospheric pressure between 5
and 10 hPa (2.30, 1.29–4.10, lag 3 days) and after an
increase in atmospheric pressure between 5 and 10 hPa
(1.88, 1.01–3.50, lag 3 days). Risk for strokes due to small
artery occlusion was more than doubled (2.22, 1.16–4.22,
lag 3 days) after an increase in atmospheric pressure of
more than 10 hPa.
Discussion
The present study identifies a rapid decrease of ambient
temperature as well as rapid changes in relative humidity
and atmospheric pressure as risk factors for ischemic stroke
in a large study population from a primary care hospital in
central Germany using two different models of conditional
logistic regression analysis.
In the firstmodel, meteorological variables were analyzed
as continuous variables and thus a linear association between
weather and stroke risk was assumed (Figs. 2, 3, 4). This
assumption was then further explored by analyzing the
Fig. 4 Odds ratios for the
association of stroke risk with a
decrease of 3.2 hPa in mean
daily atmospheric pressure over
24 h for lag times of 1, 2 and
3 days before onset of stroke
symptoms in the overall
population and subgroups.
Square size is proportional to
the number of cases, bars
indicate 95 % CI, adjusted for
temperature and relative
humidity, filled squares mark
odds ratios with confidence
intervals not including 1.00
F. Rakers et al.
123

appropriate variable in a categorized model. Here, a rapid
drop in temperature was generally associated with an
increased stroke risk, whereas large increases in temperature
were associatedwith a decreased stroke risk both in the entire
study population (Fig. 5) and in the subgroups. Even though
the protective effects of a temperature increase are more
distinct than the increased risk of a temperature drop, the
association between ambient temperature and stroke risk
appears to be close to linear. For changes in relative humidity
and atmospheric pressure, the assumption of linearity could
generally not be met. Larger increases as well as larger
decreases of these variableswithin 24 hwere associatedwith
an increased stroke risk resulting in an almost U-shaped
association curve (Fig. 5).
Fig. 5 Odds ratios for the association of stroke risk with categorized
24 h changes of ambient temperature, relative humidity and atmo-
spheric pressure for different cut off points and lag times in the
overall study population. Overlaid with 2nd order polynomial
trendline to illustrate the observed associations. Bars indicate 95 %
confidence inverval. Asterisks marks odds ratios with confidence
intervals not including 1.00. Each odds ratio is adjusted for the two
respective other meteorological variables. Non-filled boxes represent
the reference category
Rapid weather changes are associated with increased ischemic stroke risk: a case-crossover…
123

A rapid decrease in temperature over 24 h was associ-
ated with an increased risk for cardioembolic strokes in
both logistic regression analysis models. This is compatible
with the mechanistic explanation of a temperature-related
onset of atrial fibrillation—the primary cause of car-
dioembolic strokes—which is also provoked by cold
weather [1, 2]. Other possible mechanisms for the raised
incidence of cardioembolic strokes include increased sys-
tolic blood pressure at low temperatures and a consecu-
tively increased left atrial dilatation promoting atrial
fibrillation [1, 2]. In line with this, the odds ratios from
both models indicate that in those with an increased vas-
cular risk profile for vascular disease—in whom the inci-
dence of atrial fibrillation is greatest [21]—the association
between acute temperature changes and stroke risk is most
pronounced. In women and elderly patients, stroke risk
seems to increase following decreasing temperatures.
However, these associations were significant only when
temperature was analyzed as a continuous variable and the
odds ratios were close to those in the overall population.
Thus, our results do not allow a final conclusion about
whether stroke risk associated with temperature is gender
or age dependent. While gender effects have previously
been reported in Asia [5, 8], two previous European reports
failed to show a significant gender effect for temperature-
related ischemic stroke risk [12, 13].
In contrast to our results, two recent studies undertaken
in Italy [10] and Scotland [22] reported a positive corre-
lation between an increase in temperature and ischemic
stroke risk. A further study from Israel has shown an
increased stroke risk in the Negev Desert on hot days [23].
However, the Mediterranean climate found in Italy, the
maritime climate of western Scotland and the desert cli-
mate in Israel are not comparable to central Europe’s cli-
mate [17], and accordingly these findings do not
necessarily contradict our results. Moreover, the Italian and
Scottish studies differed significantly in design, as both
analyses specified the first day of hospitalization as the
onset of stroke and not the time of actual onset of stroke
symptoms. This approach might have introduced a bias in
the two European studies, since it is estimated that
10–30 % of all stroke patients present to the emergency
department with a delay of more than 24 h [24]. In
agreement with our findings, a small case-crossover study
from South Korea [8] also showed an association between
a drop in temperature and increased risk for stroke.
To date, the impact of humidity on ischemic stroke risk
has received little attention. In a Spanish study and in one
large intercontinental analysis [7, 9], relative humidity
and/or rainfall were not associated with stroke risk,
although a Japanese study reported a positive association
between rainfall and stroke risk in women [5]. However,
this association was not sustained after adjusting for other
meteorological factors. While these studies focused on
mid- and long-term changes of meteorological variables,
our results suggest that especially rapid changes in relative
humidity increase stroke risk, regardless of whether these
changes are positive or negative. In the categorized model,
a consistently higher odds ratio was observed in males after
large changes in relative humidity at all lag times. Our
findings might be partly explained by a physiological
response to a drop in relative humidity leading to increased
blood viscosity [3] that may promote ischemic strokes via
increased thrombogenesis [4].
We observed a considerably higher stroke risk after
sudden positive or negative changes in atmospheric pres-
sure in the categorized model. Our results may appear to be
in conflict with other studies in which no significant
association between atmospheric pressure and ischemic
stroke risk was ascertained [13, 22, 25]. However, these
studies assumed a linear association between atmospheric
pressure and stroke risk and as such are comparable to our
first model that did not show a relationship between
atmospheric pressure and stroke risk. Further, it has been
suggested that changes in atmospheric pressure may lead to
a plaque rupture in the carotid arteries [29]. Even though
this speculation would support our finding of an association
between changes in atmospheric pressure and stroke risk
related to large artery pathogenesis, to date, there are no
data in the literature that provide a validated mechanism
for this association [11].
Our study includes several important features. This is
the first analysis to show a weather-related stroke risk in
the prevailing temperate climate of large parts of Europe
and North America. Secondly, the large study population
allows the determination of a weather-related cardioem-
bolic stroke risk and identification of an increased stroke
risk in the subgroup of individuals with an increased risk
profile for vascular disease. Thirdly, by using the onset of
stroke symptoms instead of the date of hospital admission
or mortality data for our analysis, we avoided a potential
bias that might have affected the outcome in previous
studies [5–8].
It is important to note a few limitations of our hospital-
based study. Firstly, since we had no way of determining
the number of stroke patients not admitted to the hospital, a
selection bias might have altered the results. However,
since the Jena University Hospital is the only hospital with
a stroke unit within the defined study radius and all
emergencies are referred to the emergency department, this
minimizes a potential selection bias. Secondly, we were
unable to control for air-pollution. Air-pollution can result
in respiratory infections which are not only potential
stroke-risk factors but also linked to changes in meteoro-
logical parameters [26, 27]. However, average air-pollution
in the rural Jena region is low [28] compared to
F. Rakers et al.
123

metropolitan areas like Seoul [26]. In addition, our data did
not include microclimate information, such as room tem-
perature and room humidity. However, extensive heating
and air conditioning is relatively uncommon in the climate
examined. Moreover, we did not consider weather-related
physical activity that may have an impact on individual
exposure to outdoor temperatures and humidity.
Conclusions
Our findings show a marked association between stroke
risk and rapid weather changes. Sudden decreases in
ambient temperature as well as rapid changes in relative
humidity and atmospheric pressure over 24 h increase
stroke risk under temperate climate conditions. Analyzing a
large cohort, we identified that individuals with a higher
risk profile for vascular disease are at particular risk. In the
general population, this risk applies mainly but not exclu-
sively to cardioembolic strokes. The knowledge of the
association between weather and stroke risk may encour-
age healthcare authorities to implement stroke prevention
strategies by means of shifting the attention of health
professionals to early signs of stroke under adverse weather
conditions, by raising public awareness and educating
subgroups at risk.
Acknowledgments We thank Nasim Kroegel (Jena University
Hospital) for critical reading of the manuscript and her helpful
suggestions.
Conflict of interest None.
References
1. Kiu A, Horowitz JD, Stewart S. Seasonal variation in AF-related
admissions to a coronary care unit in a ‘‘hot’’ climate: fact or
fiction? J Cardiovasc Nurs. 2004;19(2):138–41.
2. Frost L, Johnsen SP, Pedersen L, Husted S, Engholm G, Sorensen
HT, et al. Seasonal variation in hospital discharge diagnosis of
atrial fibrillation: a population-based study. Epidemiology.
2002;13(2):211–5.
3. Doi T, Sakurai M, Hamada K, Matsumoto K, Yanagisawa K,
Kikuchi N, et al. Plasma volume and blood viscosity during h
sitting in a dry environment: effect of prehydration. Aviat Space
Environ Med. 2004;75(6):500–4.
4. Lowe GD, Lee AJ, Rumley A, Price JF, Fowkes FG. Blood
viscosity and risk of cardiovascular events: the Edinburgh Artery
Study. Br J Haematol. 1997;96(1):168–73.
5. Matsumoto M, Ishikawa S, Kajii E. Cumulative effects of
weather on stroke incidence: a multi-community cohort study in
Japan. J Epidemiol. 2010;20(2):136–42.
6. Feigin VL, Nikitin YP, Bots ML, Vinogradova TE, Grobbee DE.
A population-based study of the associations of stroke occurrence
with weather parameters in Siberia, Russia (1982–92). Eur J
Neurol. 2000;7(2):171–8.
7. Chang CL, Shipley M, Marmot M, Poulter N. Lower ambient
temperature was associated with an increased risk of
hospitalization for stroke and acute myocardial infarction in
young women. J Clin Epidemiol. 2004;57(7):749–57.
8. Hong YC, Rha JH, Lee JT, Ha EH, Kwon HJ, Kim H. Ischemic
stroke associated with decrease in temperature. Epidemiology.
2003;14(4):473–8.
9. Jimenez-Conde J, Ois A, Gomis M, Rodriguez-Campello A,
Cuadrado-Godia E, Subirana I, et al. Weather as a trigger of
stroke. Daily meteorological factors and incidence of stroke
subtypes. Cerebrovasc Dis. 2008;26(4):348–54.
10. Morabito M, Crisci A, Vallorani R, Modesti PA, Gensini GF,
Orlandini S. Innovative approaches helpful to enhance knowl-
edge on weather-related stroke events over a wide geographical
area and a large population. Stroke. 2011;42(3):593–600.
11. McArthur K, Dawson J, Walters M. What is it with the weather
and stroke? Expert Rev Neurother. 2010;10(2):243–9.
12. Kyobutungi C, Grau A, Stieglbauer G, Becher H. Absolute
temperature, temperature changes and stroke risk: a case-cross-
over study. Eur J Epidemiol. 2005;20(8):693–8.
13. Magalhaes R, Silva MC, Correia M, Bailey T. Are stroke
occurrence and outcome related to weather parameters? Results
from a population-based study in northern portugal. Cerebrovasc
Dis. 2011;32(6):542–51.
14. Wolf PA, D’Agostino RB, Belanger AJ, Kannel WB. Probability
of stroke: a risk profile from the Framingham Study. Stroke.
1991;22(3):312–8.
15. Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB,
Gordon DL, et al. Classification of subtype of acute ischemic
stroke. Definitions for use in a multicenter clinical trial. TOAST.
Trial of Org 10172 in Acute Stroke Treatment. Stroke.
1993;24(1):35–41.
16. Brott T, Adams HP Jr, Olinger CP, Marler JR, Barsan WG, Biller
J, et al. Measurements of acute cerebral infarction: a clinical
examination scale. Stroke. 1989;20(7):864–70.
17. Peel MC, Finlayson BL, McMahon TA. Updated world map of
the Koppen–Geiger climate classification. Hydrol Earth Syst Sci.
2007;11(5):1633–44.
18. Maclure M. The case-crossover design: a method for studying
transient effects on the risk of acute events. Am J Epidemiol.
1991;133(2):144–53.
19. Turin TC, Kita Y, Murakami Y, Rumana N, Sugihara H, Morita
Y, et al. Increase of stroke incidence after weekend regardless of
traditional risk factors: Takashima Stroke Registry, Japan;
1988–2003. Cerebrovasc Dis. 2007;24(4):328–37. doi:10.1159/
000106978.
20. Briggs DE, Felberg RA, Malkoff MD, Bratina P, Grotta JC.
Should mild or moderate stroke patients be admitted to an
intensive care unit? Stroke. 2001;32(4):871–6.
21. Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, inci-
dence, prognosis, and predisposing conditions for atrial fibrilla-
tion: population-based estimates. Am J Cardiol. 1998;82(8A):
2N–9N.
22. Dawson J, Weir C, Wright F, Bryden C, Aslanyan S, Lees K,
et al. Associations between meteorological variables and acute
stroke hospital admissions in the west of Scotland. Acta Neurol
Scand. 2008;117(2):85–9.
23. Berginer VM, Goldsmith J, Batz U, Vardi H, Shapiro Y. Clus-
tering of strokes in association with meteorologic factors in the
Negev Desert of Israel: 1981–1983. Stroke. 1989;20(1):65–9.
24. The International Stroke Trial (IST). A randomised trial of
aspirin, subcutaneous heparin, both, or neither among 19435
patients with acute ischaemic stroke. Int Stroke Trial Collab
Group. Lancet. 1997;349(9065):1569–81.
25. Field TS, Hill MD. Weather, Chinook, and stroke occurrence.
Stroke. 2002;33(7):1751–7.
26. Hong YC, Lee JT, Kim H, Kwon HJ. Air pollution: a new risk
factor in ischemic stroke mortality. Stroke. 2002;33(9):2165–9.
Rapid weather changes are associated with increased ischemic stroke risk: a case-crossover…
123

27. Smeeth L, Thomas SL, Hall AJ, Hubbard R, Farrington P, Val-
lance P. Risk of myocardial infarction and stroke after acute
infection or vaccination. N Engl J Med. 2004;351(25):2611–8.
28. Geologie TLfUu. Umweltberichterstattung. http://www.tlug-jena.
de/de/tlug/uw_bericht/2013/luft/luftqualitaet/. 2013. http://www.
tlug-jena.de/de/tlug/uw_bericht/2013/luft/luftqualitaet/. Accessed
15 May 2013.
29. Houck PD, Lethen JE, Riggs MW, Gantt DS, Dehmer GJ.
Relation of atmospheric pressure changes and the occurrences of
acute myocardial infarction and stroke. Am J Cardiol. 2005;96
(1):45–51.
F. Rakers et al.
123