Rapid immunomodulation by rosuvastatin in patients with ...
11
Clinical research Coronary heart disease Rapid immunomodulation by rosuvastatin in patients with acute coronary syndrome Andreas Link 1 * , Tarek Ayadhi 1 , Michael Bo ¨hm 1 , and Georg Nickenig 2 1 Klinik fu ¨r Innere Medizin III, Universita¨tsklinikum des Saarlandes, D-66421Homburg/Saar, Germany and 2 Medizinische Klinik und Poliklinik II, Universita¨tsklinikum Bonn, D-53105 Bonn, Germany Received 18 May 2006; revised 18 August 2006; accepted 11 September 2006; online publish-ahead-of-print 29 September 2006 See page 2916 for the editorial comment on this article (doi:10.1093/eurheartj/ehl376) Aims HMG-CoA reductase inhibitors (statins) reduce cardiovascular mortality and morbidity in patients with stable coronary artery disease as well as acute coronary syndrome (ACS). It is unclear how rapidly the beneficial effects of statins occur in patients with ACS and whether these drug properties are related to lipid lowering. Methods and results Patients with troponin-positive ACS (n ¼ 35) were randomized to 20 mg/day rosu- vastatin therapy or to placebo treatment. Anti-inflammatory effects of rosuvastatin measured by lym- phocyte intracellular cytokine production were taken before initiation of treatment and on days 1, 3, and 42. Compared with placebo, rosuvastatin treatment significantly reduced plasma concentrations of pro-inflammatory cytokines TNF-a and IFN-g at 72 h. Rosuvastatin also induced a rapid and significant reduction of TNF-a and IFN-g production in stimulated T-lymphocytes at 72 h. When compared with placebo, rosuvastatin inhibited the Th-1-immune response measured at 72 h. Conclusion Rosuvastatin exerts rapid immunomodulatory effects on the level of T-cell activation in patients with ACS. KEYWORDS Acute coronary syndromes; Inflammation; Th-1-immune response; Statins Introduction Acute coronary syndromes (ACSs) are associated with high morbidity and mortality. 1–3 The pathological features associ- ated with plaque instability and rupture are caused by inflammatory cell infiltration. Key players in this scenario are monocytes/macrophages and T-lymphocytes producing inflammatory cytokines that in turn stimulate macrophages and decrease the production of extracellular matrix by vas- cular smooth muscle cells. 4–6 In ACSs, Th-1 response that resembles the aggressive and deleterious action of T-lymphocytes producing inflammatory cytokines has been shown to be activated. 7 The first evidence of anti-inflammatory properties of HMG-CoA reductase inhibitors (statins) came from a retro- spective analysis of the CARE study, showing that statins reduced pro-inflammatory markers. 8 Two recent clinical trials (MIRACL 9 and PROVE IT-TIMI-22 10 ) have shown that high dose statin therapy reduced cardiovascular events in patients with ACS. Experiments in cultured cells and animals demonstrated that statins exert a wide array of immunomodulatory effects, such as reducing pro- inflammatory cytokines, activation and adhesion of mono- cytes, and activation and cytotoxicity of T-lymphocytes. 11–16 Thus, it would be desirable to treat ACSs not only with drugs interfering with platelets and the coagulation cascade but also those with anti-inflammatory effects. We evaluated possible immunomodulatory effects of rosu- vastatin in patients with ACSs in a double-blind, placebo- controlled, randomized prospective trial. To this end, cytokine plasma concentrations and specific intracellular cytokine expression in both monocytes and T-lymphocytes were assessed. Methods Patients Thirty-five patients with troponin-positive ACSs (NSTEMI or STEMI) not on cholesterol lowering drugs (including lipid-lowering drugs, dietary supplements, or food additives within the last 2 weeks) were randomized in a double-blind, placebo-controlled, mono- centric trial for 6 weeks testing rosuvastatin 20 mg or placebo once daily in oral tablet form. Randomization was done according to a defined unknown scheme. The randomization treatment codes were provided in sealed individual subject envelopes. The treatment code must not be broken except during medical emer- gencies. Primary endpoints were changes of the immune responses such as monocyte and lymphocyte intracellular cytokine expression. Four time points were investigated. After enrolment and randomiz- ation before initiating therapy, blood samples were taken for analy- sis of full clinical chemistry, haematology, and immunological markers (discussed subsequently). After 24 h, 72 h, and 6 weeks, further blood samples for the analysis of clinical chemistry, haema- tology, and immunological markers were taken. The exclusion cri- teria comprised any kind of inflammation. A patient flow chart was given (Figure 1). & The European Society of Cardiology 2006. All rights reserved. For Permissions, please e-mail: [email protected] * Corresponding author. Tel: þ49 6841 16 23372; fax: þ49 6841 16 23369. E-mail address: [email protected] European Heart Journal (2006) 27, 2945–2955 doi:10.1093/eurheartj/ehl277 Downloaded from https://academic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Rapid immunomodulation by rosuvastatin in patients with ...
Clinical researchCoronary heart disease
Rapid immunomodulation by rosuvastatin in patientswith acute coronary syndrome
Andreas Link1*, Tarek Ayadhi1, Michael Bohm1, and Georg Nickenig2
1Klinik fur Innere Medizin III, Universitatsklinikum des Saarlandes, D-66421Homburg/Saar, Germany and 2Medizinische Klinikund Poliklinik II, Universitatsklinikum Bonn, D-53105 Bonn, Germany
Received 18 May 2006; revised 18 August 2006; accepted 11 September 2006; online publish-ahead-of-print 29 September 2006
See page 2916 for the editorial comment on this article (doi:10.1093/eurheartj/ehl376)
Aims HMG-CoA reductase inhibitors (statins) reduce cardiovascular mortality and morbidity in patientswith stable coronary artery disease as well as acute coronary syndrome (ACS). It is unclear how rapidlythe beneficial effects of statins occur in patients with ACS and whether these drug properties are relatedto lipid lowering.Methods and results Patients with troponin-positive ACS (n ¼ 35) were randomized to 20 mg/day rosu-vastatin therapy or to placebo treatment. Anti-inflammatory effects of rosuvastatin measured by lym-phocyte intracellular cytokine production were taken before initiation of treatment and on days 1, 3,and 42. Compared with placebo, rosuvastatin treatment significantly reduced plasma concentrationsof pro-inflammatory cytokines TNF-a and IFN-g at 72 h. Rosuvastatin also induced a rapid and significantreduction of TNF-a and IFN-g production in stimulated T-lymphocytes at 72 h. When compared withplacebo, rosuvastatin inhibited the Th-1-immune response measured at 72 h.Conclusion Rosuvastatin exerts rapid immunomodulatory effects on the level of T-cell activation inpatients with ACS.
KEYWORDSAcute coronary syndromes;
Inflammation;
Th-1-immune response;
Statins
Introduction
Acute coronary syndromes (ACSs) are associated with highmorbidity and mortality.1–3 The pathological features associ-ated with plaque instability and rupture are caused byinflammatory cell infiltration. Key players in this scenarioare monocytes/macrophages and T-lymphocytes producinginflammatory cytokines that in turn stimulate macrophagesand decrease the production of extracellular matrix by vas-cular smooth muscle cells.4–6 In ACSs, Th-1 response thatresembles the aggressive and deleterious action ofT-lymphocytes producing inflammatory cytokines has beenshown to be activated.7
The first evidence of anti-inflammatory properties ofHMG-CoA reductase inhibitors (statins) came from a retro-spective analysis of the CARE study, showing that statinsreduced pro-inflammatory markers.8 Two recent clinicaltrials (MIRACL9 and PROVE IT-TIMI-2210) have shown thathigh dose statin therapy reduced cardiovascular events inpatients with ACS. Experiments in cultured cells andanimals demonstrated that statins exert a wide array ofimmunomodulatory effects, such as reducing pro-inflammatory cytokines, activation and adhesion of mono-cytes, and activation and cytotoxicity of T-lymphocytes.11–16
Thus, it would be desirable to treat ACSs not only withdrugs interfering with platelets and the coagulation
cascade but also those with anti-inflammatory effects.We evaluated possible immunomodulatory effects of rosu-vastatin in patients with ACSs in a double-blind, placebo-controlled, randomized prospective trial. To this end,cytokine plasma concentrations and specific intracellularcytokine expression in both monocytes and T-lymphocyteswere assessed.
Methods
Patients
Thirty-five patients with troponin-positive ACSs (NSTEMI or STEMI)not on cholesterol lowering drugs (including lipid-lowering drugs,dietary supplements, or food additives within the last 2 weeks)were randomized in a double-blind, placebo-controlled, mono-centric trial for 6 weeks testing rosuvastatin 20 mg or placeboonce daily in oral tablet form. Randomization was done accordingto a defined unknown scheme. The randomization treatmentcodes were provided in sealed individual subject envelopes. Thetreatment code must not be broken except during medical emer-gencies. Primary endpoints were changes of the immune responsessuch as monocyte and lymphocyte intracellular cytokine expression.Four time points were investigated. After enrolment and randomiz-ation before initiating therapy, blood samples were taken for analy-sis of full clinical chemistry, haematology, and immunologicalmarkers (discussed subsequently). After 24 h, 72 h, and 6 weeks,further blood samples for the analysis of clinical chemistry, haema-tology, and immunological markers were taken. The exclusion cri-teria comprised any kind of inflammation. A patient flow chartwas given (Figure 1).
& The European Society of Cardiology 2006. All rights reserved. For Permissions, please e-mail: [email protected]
* Corresponding author. Tel: þ49 6841 16 23372; fax: þ49 6841 16 23369.E-mail address: [email protected]
European Heart Journal (2006) 27, 2945–2955doi:10.1093/eurheartj/ehl277
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022
The study was performed in accordance with the ethical prin-ciples in the Declaration of Helsinki and Good Clinical Practice.Informed consent was obtained from all patients and the study pro-tocol was approved by the Ethics Committee of the University ofSaarland, Germany.
Blood sampling
At each visit, 20 mL of heparinized and 10 mL of EDTA-bufferedblood were drawn from a venous canula.
Intracellular cytokine measurement by flowcytometry
Heparinized whole blood samples were stimulated with lipopolysac-charide (LPS) (100 ng/mL LPS, Sigma, Germany) for monocytecytokine expression, with Staphylococcus aureus enterotoxin B(2.5 mg/mL SEB) in the presence of CD28 (clone Leu-28, BDPharmingen, Germany) and CD49d (clone 9F10, BD Pharmingen)for CD3-T-lymphocyte cytokine expression, or with phorbol-2-myristate-13-acetate (PMA, Sigma) and ionomycin (Sigma) forCD4-T-cell cytokine expression. Cells were incubated in polypropy-lene tubes at 378C for a total of 6 h. During the last 4 h, 10 mg/mLBrefeldin A (Sigma) was added to block extracellular secretion ofcytokines. Cell fixation was done with 2 mM EDTA for 15 min forplanned measurement of monocyte or lymphocyte cytokineexpression or with paraformaldehyde 4% for 5 min for plannedmeasurement of CD4-T-cell cytokine expression. Erythrocytes werelysed for 10 min by using lysing solution (BD Pharmingen), accordingto the manufacturer’s instructions. Cell membranes were reversiblypermeabilized with saponine 0.1% (Sigma) in PBS containing 5% milkpowder and 0.1% bovine serum albumin (Sigma). Cell surfacemarkers and intracellular cytokines were labelled with mouse anti-human antibodies conjugated to fluorescent dyes at saturating con-centrations in permeabilization buffer. For staining the cell surface
markers, we used PE-Cy5-labelled anti-CD14 (clone RMO52,Beckmann/Coulter, Germany) for monocytes; PerCP-labelledanti-CD3 (clone SK7, BD Pharmingen) for lymphocytes; andPerCP-labelled anti-CD4 (clone SK3, BD Pharmingen) for theT-helper-cells (Th-cells). For staining the intracellular cytokines,we used for monocyte intracellular cytokines FITC-labelledanti-TNF-a (clone MAb11, BD Pharmingen) and PE-labelledanti-IL-6 (clone MQ2-13A5, BD Pharmingen); for lymphocyte intra-cellular cytokines FITC-labelled anti-TNF-a (clone MAb11, BDPharmingen) and PE-labelled anti- IFN-g (clone 4s.B3, BDPharmingen); and for Th-cells FITC-labelled anti-IFN-g (clone4S.B3, BD Pharmingen) and PE-labelled anti-IL4 (clone 8D4-8, BDPharmingen). After 45 min of incubation at 48C, cells were washedthree times in permeabilization buffer and twice in FACS buffer.Subsequently, stained antigens were fixed with 1% paraformalde-hyde. Measurements were performed on a Becton DickinsonFACScan flow cytometer and the Cellquest software system.Normal ranges of the per cent of cytokine positive producingT-cells and monocytes are given in Table 1.
Intraplasmatic cytokine measurement bycytometric bead array
To measure intraplasmatic cytokines, serum samples were separ-ated from EDTA whole blood. According to the manufacturer’sinstructions, we used the Cytometric Bead Array System (CBA,Becton Dickinson, Heidelberg, Germany) for quantitative measure-ment of the following cytokines by flow cytometry: IL-6; TNF-a;IFN-g; IL-4; and IL-10. Measurements were performed on a BectonDickinson FACScan flow cytometer and the BD-CBA softwaresystem. The detection limits of the cytokine assays were measuredby 0.5 pg/mL. Normal ranges of the levels of intraplasmatic cyto-kines are given in Table 1.
Statistical methods
The size of the trial population has been calculated to the nullhypothesis that rosuvastatin and placebo therapy were not differentfor the primary endpoints (immunological markers). A sample size of17 patients in each group had a power of 80% to detect an effect sizeof 1.00 SD using a two-group t-test with a 0.05 two-sided significantlevel.
For all immunological markers and lipid data, the following stat-istical parameters were calculated: median, the value of the 25thand 75th percentile, and the percentage of change from baselineto 24 h, 72 h, or 42 days. All immunological parameters and lipiddata were normally distributed, tested by the analysis of variance.The type I error rate was fixed as a ¼ 0.05 (two-sided; 95% confi-dence limit). Differences were considered significant if P , 0.05.
Results
Patient baseline characteristics
Thirty-five patients with troponin-positive ACS (NSTEMI orSTEMI) and angiographically documented coronary arterydisease were randomized to receive rosuvastatin 20 mg/day(n ¼ 18) or placebo (n ¼ 17). The groups were well matchedwith respect to age [rosuvastatin group 55.5 (48.0–69.0) vs.placebo group 60.0 (51.0–69.5) years], gender, infarctionsize measured by the maximum of creatine kinase 872(180.8–2837.5) vs. 787 (320.8–1478.0) U/L, and the use ofadditional standard infarction therapy (Table 2).
Lipid profile
Thebaseline lipid levels in both groupswere equivalent for totalcholesterol 201 (178.0–235.0) vs. 208 (190.0–219.0) mg/L, LDLcholesterol 134 (103.9–143.8) vs. 134 (115.3–144.4) mg/L, HDL
Figure 1 Study flow chart for registered and randomized patients with ACS.
2946 A. Link et al.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022

Table 1 Measured parameters were presented as absolute amounts (described as median and value of the 25th and 75th percentiles) and per cent changes from baseline
Normal range Placebo group Rosuvastatin group
Baseline Day 1 Day 3 Day 42 Baseline Day 1 Day 3 Day 42
CholesterinAbsolute counts(mg/dL)
,200 208 (190, 219) 219 (190, 245) 221 (205, 257) 225 (210, 255) 201 (178, 235) 194 (179, 216) 176 (159, 200) 154 (132, 179)
Relative changes (%) þ5 þ8 þ15 22; P ¼ 0.01 216; P ¼ 0.008 226; P ¼ 0.001LDL cholesterin
Absolute counts(mg/dL)
,135 134 (115, 144) 147 (122, 165) 162 (127, 187) 158 (129, 174) 134 (104, 144) 135 (111, 158) 117 (101, 137) 76 (56, 94)
Relative changes (%) þ9 þ15 þ19 þ1; P ¼ 0.296 216; P ¼ 0.002 249; P ¼ 0.001HDL cholesterin
Absolute counts(mg/dL)
45+ 10 39 (34, 47) 49 (42–59) 42 (31, 50) 42 (35, 52) 43 (39, 47) 45 (41, 51) 44 (40, 52) 49 (45, 56)
Relative changes (%) þ23 þ10 þ7 þ7; P ¼ 0.032 0; P ¼ 0.318 þ13; P ¼ 0.597Triglycerides
Absolute counts(mg/dL)
,200 143 (121, 212) 152 (142, 223) 156 (141, 191) 224 (144, 250) 119 (90, 177) 137 (106, 164) 132 (112, 173) 116 (89, 190)
Relative changes (%) þ5 þ5 þ39 þ1; P ¼ 0.428 23; P ¼ 0.490 þ8; P ¼ 0.105IFN-g
Absolute amount(pg/mL)
,50 67 (29.9, 128.8) 105 (31.8, 118.7) 75 (49.6, 141.9) 39 (22.3, 91.8) 124 (90.2, 155.7) 74 (30.9, 126.6) 41 (24.2, 106.1) 30 (8.6, 50.8)
Relative changes (%) þ18 þ21 220 221; P ¼ 0.002 247; P ¼ 0.001 267; P ¼ 0.001IL-6
Absolute amount(pg/mL)
,10 19 (13.8, 30.5) 22 (17.4, 35.3) 12 (8.9, 18.4) 4 (2.9, 6.4) 36 (28.4, 45.2) 20 (15.5, 43.6) 13 (7.8, 18.6) 4 (3.1, 8.4)
Relative changes (%) 23 248 282 221; P ¼ 0.053 260; P ¼ 0.035 288; P ¼ 0.029TNF-a
Absolute amount(pg/mL)
,10 2 (1.6, 4.2) 3 (2.2, 4.2) 3 (2.4, 4.1) 2 (1.5, 3.5) 4 (3.9, 4.7) 3 (2.2, 4.1) 2 (1.8, 3.7) 2 (1.7, 2.6)
Relative changes (%) þ14 þ13 0 237; P ¼ 0.001 236; P ¼ 0.001 249; P ¼ 0.021IL-4
Absolute amount(pg/mL)
,10 6 (3.3, 11.7) 6 (4.0, 10.6) 11 (9.1, 16.4) 7 (3.7, 12.7) 6 (3.2, 11.9) 13 (7.8, 16.99 8 (5.9, 10.2) 4 (2.8, 9.1)
Relative changes (%) þ45 þ95 235 þ86; P ¼ 0.259 þ12; P ¼ 0.102 22; P ¼ 0.465IL-10
Absolute amount(pg/mL)
,10 4 (2.8, 6.4) 5 (3.4, 7.7) 4 (3.4, 7.3) 3 (2.2, 4.5) 3 (2.1, 5.0) 5 (3.2, 5.7) 2 (1.7, 6.2) 3 (1.9, 5.6)
Relative changes (%) þ20 211 230 þ20; P ¼ 0.917 25; P ¼ 0.826 25; P ¼ 0.126C-reactive protein
Absolute amount(mg/L)
,5 11 (5.1, 45.8) 18 (12.0, 58.9) 33 (11.7, 46.4) 3 (3.0, 20.3) 11 (6.4, 38.9) 20 (16.6, 82.7) 18 (11.3, 92.5) 3 (3.0, 3.9)
Relative changes (%) þ47 þ43 0 þ56; P ¼ 0.757 þ44; P ¼ 0.355 269; P ¼ 0.133
Continued
Rap
idim
munom
odulation
byrosuvastatin
2947
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022

Table 1 Continued
Normal range Placebo group Rosuvastatin group
Baseline Day 1 Day 3 Day 42 Baseline Day 1 Day 3 Day 42
IL-6 in monocytes(%) 30.0+ 10% 31 (21.2, 43.7) 25 (18.8, 39.9) 28 (19.5, 37.5) 27 (18.9, 59.3) 18 (8.5, 35.6) 22 (14.6, 38.4) 23 (11.7, 34.7) 48 (27.8, 63.1)Relative changes (%) þ16 216 þ36 þ11; P ¼ 0.480 þ12; P ¼ 0.524 þ31; P ¼ 0.07
TNFa in monocytes(%) 45.0+ 10% 53 (43.6, 63.9) 48 (39.1, 55.0) 50 (38.3, 60.4) 72 (59.2, 75.9) 47 (22.6, 63.6) 38 (34.5, 63.7) 57 (28.3, 67.2) 71 (62.4, 77.4)Relative changes (%) 26 26 þ30 22; P ¼ 0.692 24; P ¼ 0.387 þ35; P ¼ 0.813
IFNg in lymphocytes(%) 5.0+ 2.5% 3 (2.5, 5.4) 4 (2.7, 5.4) 4 (2.6, 5.3) 3 (2.7, 4.9) 5 (2.6, 11.7) 3 (1.9, 5.1) 3 (2.2, 3.6) 3 (1.9, 4.3)Relative changes (%) þ4 21 þ2 217; P ¼ 0.026 233; P ¼ 0.008 218; P ¼ 0.018
TNFa in lymphocytes(%) 5.0+ 2.5% 7 (4.4, 8.5) 7 (4.6, 9.7) 6 (5.1, 12.4) 5 (4.1, 7.4) 10 (6.6, 18.3) 6 (4.4, 9.6) 6 (5.2, 6.4) 5 (3.9, 7.4)Relative changes (%) þ4 þ7 213 237; P ¼ 0.007 238; P ¼ 0.001 237; P ¼ 0.018
IFNg in Th-cells(%) 9.0+ 4.0% 24 (20.9, 37.3) 26 (21.8, 36.4) 24 (12.9, 36.8) 29 (22.9, 39.1) 34 (23.9, 48.6) 26 (18.1, 38.3) 22 (13.6, 27.1) 13 (5.3, 17.4)Relative changes (%) þ2 22 þ4 217; P ¼ 0.035 244; P ¼ 0.032 269; P ¼ 0.001
IL4 in Th-cells(%) 2.0+ 1.5% 3 (1.4, 3.4) 2 (0.3, 2.8) 3 (0.8, 3.4) 2 (0.5, 2.6) 4 (1.2, 4.9) 2 (0.8, 4.1) 1 (0.1, 3.5) 1 (0.2, 2.3)Relative changes (%) þ1 þ6 24 252; P ¼ 0.457 277; P ¼ 0.039 271; P ¼ 0.056
All parameters include cholesterin, LDL cholesterin, HDL cholesterin, triglycerides, interferon-gamma (IFN-g), interleukin-6 (IL-6), tumour-necrosis factor-alpha (TNF-a), interleukin-4 (IL-4), interleukin-10 (IL-10),C-reactive protein, inducible cytokine expressin in monocytes and lymphocytes, and the T-helper-(Th)-cell-subpopulation. P-values are obtained from the analyses of the per cent changes.
2948A.Link
etal.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022

Table 2 Baseline characteristics of both treatment groups: age, gender, lipid profile, infarction size,and concomitant therapy
Placebo group Rosuvastatin group
n 17 18Age (years) 60 (51.0, 69.5) 55.5 (48.0, 69.0)Men/women (n/n) 11/6 12/6Cholesterin (mg/L) 208 (190.0, 219.0) 201 (178.0, 235.0)LDL cholesterin (mg/L) 134 (115.3, 144.4) 134 (103.9, 143.8)HDL cholesterin (mg/L) 39 (33.7, 47.3) 43 (38.9, 46.9)Triglyceride (mg/L) 143 (121.2, 211.8) 118 (90.0, 177.0)Non-ST-elevation infarction (NSTEMI) 10 12ST-elevation infarction (NSTEMI) 7 6Infarction size (CKmax U/L) 787 (320.8, 1478.0) 872 (180.8, 2837.5)Ejection fraction (%) 58 (38.2, 72.0) 59 (36.2, 68.5)GPIIb/IIIa-antagonism (n) 8 11ASS (n) 17 18Clopidogrel (n) 17 17b-blockers (n) 17 18ACE-inhibitors (n) 17 17
Parameters are described as median and value of the 25th and 75th percentiles or as nominal data.
Figure 2 Relative changes to baseline of the pro-inflammatory cytokine interferon-g (IFN-g) during a therapy with rosuvastatin or placebo over 42 days. In orderto examine the values of significance, individual patient data separated in a placebo or rosuvastatin group are shown before therapy and at days 1, 3, and 42.
Rapid immunomodulation by rosuvastatin 2949
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022

cholesterol 43 (38.9–46.9) vs. 39 (33.7–47.3) mg/L, andtriglycerides 118 (90.0–177.0) vs. 143 (121.2–211.8) mg/L.Rosuvastatin decreased total cholesterol significantly morethan placebo at 72 h (rosuvastatin: 216% vs. placebo: þ8%,P¼ 0.0008) and after 6 weeks (rosuvastatin: 226% vs.placebo: þ15%, P¼ 0.0001). LDL cholesterol was reduced by16% at 72 h and by 49% after 6 weeks of statin treatment(both P, 0.0002 vs. placebo). There was no significant treat-ment effect at 24 h for any of the lipids (Table 1).
Cytokine plasma concentrations and C-reactiveprotein
In all patients, the baseline levels of the pro-inflammatorycytokines IFN-g, TNF-a, and IL-6 were above the normalranges. Although there were no differences in baselinecharacteristics and severity of the ACSs between the treat-ment groups, by chance the median baseline levels of
the pro-inflammatory cytokines IFN-g, TNF-a, and IL-6 weregreater in the rosuvastatin group than in the placebogroup at baseline: IFN-g (rosuvastatin: 124 pg/L vs. placebo:67 pg/L), TNF-a (rosuvastatin: 4 pg/L vs. placebo: 2 pg/L),and IL-6 (rosuvastatin: 36 pg/L vs. placebo: 19 pg/L).Rosuvastatin reduced IFN-g (Figure 1; Table 1), TNF-a(Figure 2; Table 1), and IL-6 (Table 1) significantly more thanplacebo at 72 h. These reductions were sustained for up to 6weeks. We found no rapid effect of rosuvastatin on C-reactiveprotein. Plasma concentrations of the anti-inflammatory cyto-kines IL-4 and IL-10 remained unaltered (Table 1).
Changes in the inducible intracellular monocytecytokine expression
Monocyte activity was measured after LPS stimulationin vitro. The inducible intracellular cytokine expressionof IL-6 and TNF-a in monocytes was measured by
Figure 3 Relative changes to baseline of the pro-inflammatory cytokine tumour necrosis factor-a (TNF-a) during therapy with rosuvastatin or placebo over42 days. In order to examine the values of significance, individual patient data separated in a placebo or rosuvastatin group are shown before therapy and atdays 1, 3, and 42.
2950 A. Link et al.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022
immunofluorescent staining and flow cytometry. Baselinedata showed no differences in median values of the induci-ble production of IL-6 or TNF-a in monocytes in the rosu-vastatin group or in the placebo group. Furthermore, nosignificant modulation during the experimental time courseby placebo or rosuvastatin was observed (Table 1).
Changes in the inducible intracellularT-lymphocyte cytokine expression
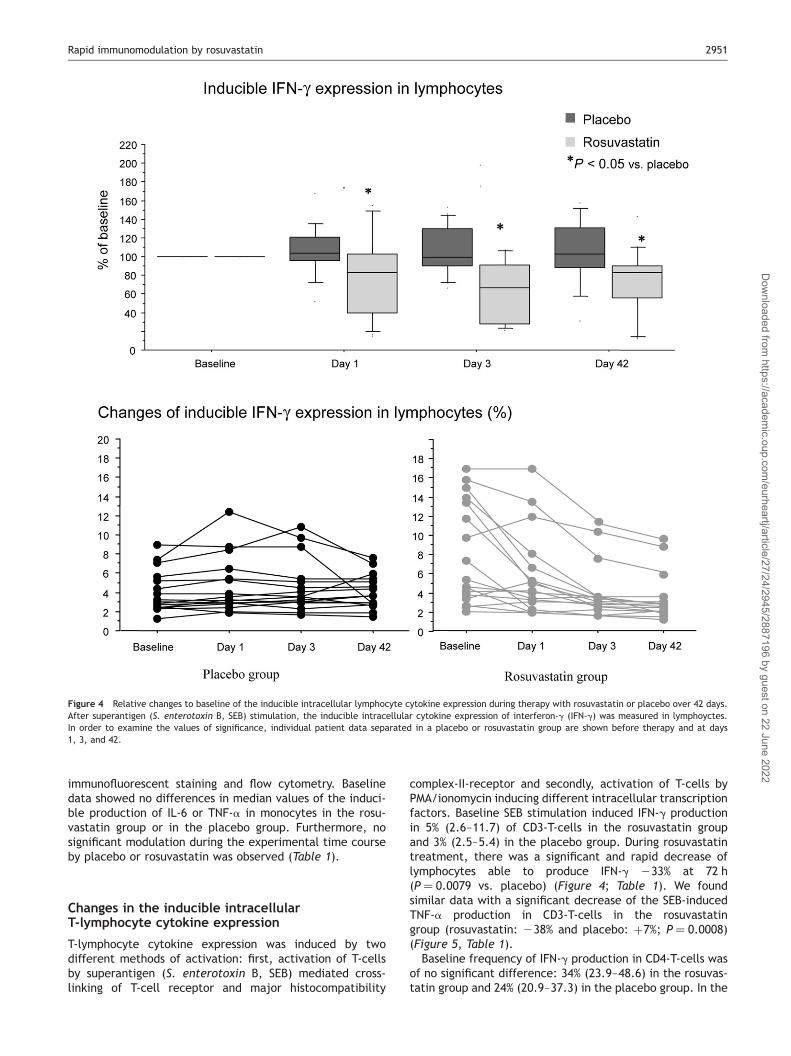
T-lymphocyte cytokine expression was induced by twodifferent methods of activation: first, activation of T-cellsby superantigen (S. enterotoxin B, SEB) mediated cross-linking of T-cell receptor and major histocompatibility
complex-II-receptor and secondly, activation of T-cells byPMA/ionomycin inducing different intracellular transcriptionfactors. Baseline SEB stimulation induced IFN-g productionin 5% (2.6–11.7) of CD3-T-cells in the rosuvastatin groupand 3% (2.5–5.4) in the placebo group. During rosuvastatintreatment, there was a significant and rapid decrease oflymphocytes able to produce IFN-g 233% at 72 h(P ¼ 0.0079 vs. placebo) (Figure 4; Table 1). We foundsimilar data with a significant decrease of the SEB-inducedTNF-a production in CD3-T-cells in the rosuvastatingroup (rosuvastatin: 238% and placebo: þ7%; P ¼ 0.0008)(Figure 5, Table 1).Baseline frequency of IFN-g production in CD4-T-cells was
of no significant difference: 34% (23.9–48.6) in the rosuvas-tatin group and 24% (20.9–37.3) in the placebo group. In the
Figure 4 Relative changes to baseline of the inducible intracellular lymphocyte cytokine expression during therapy with rosuvastatin or placebo over 42 days.After superantigen (S. enterotoxin B, SEB) stimulation, the inducible intracellular cytokine expression of interferon-g (IFN-g) was measured in lymphoyctes.In order to examine the values of significance, individual patient data separated in a placebo or rosuvastatin group are shown before therapy and at days1, 3, and 42.
Rapid immunomodulation by rosuvastatin 2951
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022

statin group, there was also a significant decrease of lym-phocytes able to produce IFN-g at 72 h (rosuvastatin:244% vs. placebo: 22%; P ¼ 0.0318) (Th-1 immuneresponse) (Figure 6; Table 1). This effect was sustained forup to 42 days. PMA/ionomycin induced IL-4 production in3–4% of CD4-positive T-cells (Th-2 immune response)before treatment (Figure 7). Within the statin group, theTh2-immune response declined significant at 72 h (rosuvas-tatin: 277% vs. placebo: þ6%; P ¼ 0.0397) (Th-2 immuneresponse) (Figure 7; Table 1).
Discussion
The lipid-lowering properties of statins have been suggestedas the main reason for the reduction of morbidity and mor-tality rates.17–20 However, in addition, multiple investi-gations have indicated the possibility that statins may
evoke beneficial effects via LDL cholesterol-independentmechanisms. By blocking the HMG-CoA reductase, not onlycholesterol biosynthesis but also numerous additional inter-mediates are diminished. These factors, such as geranylgera-nylpyrophosphate, are involved in a wide array of cellularevents which makes it conceivable that statins exertadditional effects beyond cholesterol reduction.21 Many ofthese investigations concentrated on the effect of statinson vascular cells, as atherosclerosis predominately takesplace in the vessel wall.22–24 In addition, it is well establishedthat atherosclerosis resembles a systemic inflammatorydisease.1 Therefore, findings of diverse immunomodulatoryeffects of statins on circulating monocytes and lymphocyteshave been of special interest.12,13 These drugs exert versatilechanges in inflammatory cells such as reduction of cytokinesand adhesion molecules.25 Most of these results werederived from studies on isolated cells and animal models.
Figure 5 Relative changes to baseline of the inducible intracellular lymphocyte cytokine expression during therapy with rosuvastatin or placebo over 42 days.After superantigen (S. enterotoxin B, SEB) stimulation, the inducible intracellular cytokine expression of tumour necrosis factor-a (TNF-a) was measured in lym-phoyctes. In order to examine the values of significance, individual patient data separated in a placebo or rosuvastatin group are shown before therapy and atdays 1, 3, and 42.
2952 A. Link et al.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022

In agreement with this, statins were found to suppressglobal inflammatory markers such as high sensitiveC-reactive protein and cytokines in various types ofpatients.26,27 In contrast to these larger studies, ourpatients have no significant difference in C-reactiveprotein values between placebo and rosuvastatin groups.This might be due to the observation that in our patients,only mild elevations in C-reactive protein could bedetected. Nevertheless, these studies were not able to dis-tinguish anti-inflammatory effects on the basis of the vascu-lar healing from direct impact of statins on circulating whiteblood cells. More mechanistic insight came from studiesdemonstrating that statins alter the immunity by reducingthe Th-1 response in animals with experimental autoimmunemyocarditis,28 in patients with chronic graft vs. hostdisease,29 and in patients with ACSs.30 However, thesesmall-scale studies were not able to differentiate putativeacute effects and were, therefore, not designed to pointat potentially lipid independent effects.
Patients with ACS are at very high risk of immediate car-diovascular complications. Pathophysiologically, this isbased on an inflammatory distress which causes plaquerupture and ultimately vessel occlusion, indicating thatthese individuals are candidates for an instant immunomo-dulatory treatment.The data presented herein suggest that rosuvastatin
treatment is accompanied by a rapid anti-inflammatoryeffect at 72 h in patients with ACS. This is evidenced bythe reduction of the circulating pro-inflammatory cytokinesIL-6, TNF-a, and IFN-g. Most inflammatory cytokines arederived from either vascular cells, monocytes, or lympho-cytes. In order to provide more mechanistic insight, induci-ble cytokine expression was assessed in monocytes andlymphocytes. Whereas rosuvastatin showed no significanteffect on monocytes, TNF-a and IFN-g expression was pro-foundly reduced in lymphocytes, indicating that statins pre-dominately target the adaptive immune response in patientswith ACS. In agreement with these data, Th-1 response
Figure 6 Relative changes to baseline of the inducible intracellular cytokine expression in T-helper-cells (Th-cells) during therapy with rosuvastatin orplacebo over 42 days. After PMA/ionomycin stimulation, the inducible intracellular cytokine expression of interferon-g (IFN-g) and Th-1 immune responsewas measured. In order to examine the values of significance, individual patient data separated in a placebo or rosuvastatin group are shown before therapyand at days 1, 3, and 42.
Rapid immunomodulation by rosuvastatin 2953
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022

evidenced as IFN-g expression in T-helper cells was reduced,whereas there was no effect on anti-inflammatory cytokinessuch as IL-4 or IL-10, shifting the immune system to a lessaggressive state.In most patients, the inflammatory markers (TNF-a and
IFN-g as well as inducible TNF-a and IFN-g expression in lym-phocytes) showed a rapid suppression 24 h after initiation ofrosuvastatin therapy. However, different kinetics of inflam-matory suppression could be observed in individual patientsat that point of time, making it difficult to interpret the 24 hdata. However at 72 h, all patients showed a similardepression of inflammatory parameters in contrast to theplacebo-treated patients. Therefore, the interval of 72 hwas considered to be the time when inflammatorydepression was clearly evident.It is reasonable to suggest that these anti-inflammatory
properties confer clinical benefit. Interventional trials suchas MIRACL and PROVE-IT-TIMI-22 demonstrated that patients
with ACS benefit from statin treatment.9,10 However, itis not known whether this is due to lipid lowering orthe so-called pleiotropic, lipid-independent effects ofHMG-CoA reductase inhibitors. Of note, the anti-inflammatory effects of rosuvastatin appeared at 72 h andthe magnitude of anti-inflammation was not appreciablyincreased over the 6 weeks observation period.
The present study shows for the first time in patients withACS that statins inhibit T-cell immune response by down-regulation of pro-inflammatory intracellular cytokines andsuppressing Th-1-immune response, thereby targeting adap-tive immunity of T-lymphocytes rather than monocytes.These effects appear rapidly at 72 h. Function and cytokineexpression of circulatory monocytes were not depressed byrosuvastatin. This part of the innate immunity was notmodulated by our rosuvastatin patients. This defence mech-anism is always present, ready to recognize, and eliminatesmicrobes. In contrast, activated marcophages are able to be
Figure 7 Relative changes to baseline of the inducible intracellular cytokine expression in T-helper-cells (Th-cells) during therapy with rosuvastatin or placeboover 42 days. After PMA/ionomycin stimulation, the inducible intracellular cytokine expression of interleukin-4 (IL-4) and Th-2 immune response was measured.In order to examine the values of significance, individual patient data separated in a placebo or rosuvastatin group are shown before therapy and at days 1, 3,and 42.
2954 A. Link et al.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022

modulated by statins. Statins diminish the pro-inflammatoryactivity of activated macrophage, their endothelialadhesion, and ability to bind to the vessel wall but not ofmonocytes.These data suggest that in patients with ACSs, statins
rapidly inhibit the activity of Th-1 response independentlyof the present plasma lipid levels. Thus, clinical studiesare necessary to evaluate the cardiovascular outcome byrapidly suppressing the Th-1-immune response in patientswith ACS by statins.
Acknowledgement
The study was supported by the Deutsche Forschungsgemeinschaftand an unrestricted grant of AstraZeneca.
Conflict of interest: none declared.
References
1. Lusis AJ. Atherosclerosis. Nature 2000;407:233–241.2. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis.
Circulation 2002;105:1135–1143.3. Ross R. Atherosclerosis: an inflammatory disease. N Engl J Med
1999;340:115–126.4. Liuzzo G, Goronzy JJ, Yang H, Kopecky SL, Holmes DR, Frye RL, Weyand
CM. Monoclonal T-cell proliferation and plaque instability in acute coron-ary syndromes. Circulation 2000;101:2883–2888.
5. Liuzzo G, Angiolillo DJ, Buffon A, Rizello V, Colizzi C, Ginnetti F,Biasucci LM, Maseri A. Enhanced response of blood monocytes to invitro lipopolysaccharide-challenge in patients with recurrent unstableangina. Circulation 2001;103:2236–2241.
6. Weyand CM, Goronzy JJ, Liuzzo G, Kopecky Sl, Holmes DR Jr, Frye RL.T-cell immunity in acute coronary syndromes. Mayo Clin Proc2001;76:1011–1020.
7. Soejima H, Irie A, Miyamoto S, Kajiwara I, Kojima S, Hokamaki J,Sakamoto T, Tanaka T, Yoshimura M, Nishimura Y, Ogawa H. Preferencetoward a T-helper type 1 response in patients with coronary spasticangina. Circulation 2003;107:2196–2200.
8. Ridker PM, Rifai N, Pfeffer MA, Sacks F, Braunwald E. Long-term effects ofpravastatin on plasma concentration of C-reactive protein. TheCholesterol and Recurrent Events (CARE) Investigators. Circulation1999;100:230–235.
9. Schwartz GG, Olsson AG, Ezekowitz MD, Ganz O, Oliver MF, Waters D,Zeiher A, Chaitman BR, Leslie S, Stern T. Effects of atorvastatin onearly recurrent ischaemic events in acute coronary syndromes: theMIRACL study: a randomized controlled trial. JAMA 2001;285:1711–1718.
10. Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R,Joyal SV, Hill KA, Pfeffer MA, Skene AM. Intensive versus moderate lipidlowering with statins after acute coronary syndromes. N Engl J Med2004;350:1495–1504.
11. Aikawa M, Rabkin E, Sugiyama S, Voglic SJ, Fukumoto Y, Furukawa Y,Shiomi M, Schoen FJ, Libby P. An HMG-CoA reductase inhibitor, cerivasta-tin, suppresses growth of macrophages expressing matrix metalloprotei-nases and tissue factor in vivo and in vitro. Circulation2001;103:276–283.
12. Kwak B, Mulhaupt F, Myit S, Mach F. Statins as a newly recognized type ofimmunomodulator. Nat Med 2000;6:1399–1402.
13. Mach F. Statins as immunomodulatory agents. Circulation 2004;109(Suppl. 1):II15–II17.
14. Blanco-Colio LM, Munoz-Garcia B, Martin-Ventura JL, Lorz C, Diaz C,Hernandez G, Egido J. 3-Hydroxy-3-methylglutaryl coenzyme A reductase
inhibitors decrease Fas ligand expression and cytotoxicity in activatedhuman T lymphocytes. Circulation 2003;108:1506–1513.
15. Hakamada-Taguchi R, Uehara Y, Kuribayashi K, Numabe A, Saito K,Negoro H, Fujita T, Toyo-oka T, Kato T. Inhibition ofhydroxymethylglutaryl-coenzyme a reductase reduces Th1 developmentand promotes Th2 development. Circ Res 2003;93:948–956.
16. Ghittoni R, Patrussi L, Pirozzi K, Pellegrini M, Lazzerini PE, Capecchi PL,Pasini FL, Baldari CT. Simvastatin inhibits T-cell activation by selectivelyimpairing the function of Ras superfamily GTPases. FASEB J2005;19:605–607.
17. Scandinavian Simvastatin Study Group. Randomised trial of cholesterollowering in 4444 patients with coronary heart disease: theScandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383–1389.
18. Sacks FM, Pfeffer MA, Move LA, Rouleau JL, Rutherford JD, Cole TG,Brown L, Warnica JW, Arnold JM, Wun CC, Davis BR, Braunwald E. Theeffect of pravastatin on coronary events after myocardial infarction inpatients with average cholesterol levels. Cholesterol and RecurrentEvents Trial investigators. N Engl J Med 1996;335:1001–1009.
19. The Long-Term Investigation with Pravastatin in Ischaemic Disease (LIPID)Study Group. Prevention of cardiovascular events and death with pravas-tatin in patients with coronary heart disease and a broad range of initialcholesterol levels. N Engl J Med 1998;339:1349–1357.
20. Heart Protection Study Collaborative Group. MRC/BHF Heart ProtectionStudy of cholesterol lowering with simvastatin in 20.536 high-risk individ-uals: a randomised placebo-controlled trial. Lancet 2002;360:7–22.
21. Goldstein JL, Brown MS. Regulation of the mevalonate pathway. Nature1990;343:425–430.
22. Dimmeler S, Fleming I, Fisslthaler B, Hermann C, Busse R, Zeiher AM.Activation of nitric oxide synthase in endothelial cells by Akt-dependentphosphorylation. Nature 1999;399:601–605.
23. Kureishi Y, Luo Z, Shiojima I, Bialik A, Fulton D, Lefer DJ, Sessa WC,Walsh K. The HMG-CoA reductase inhibitor simvastatin activates theprotein kinase Akt and promotes angiogenesis in normocholesterolemicanimals. Nat Med 2000;6:1004–1010.
24. Dimmeler S, Aicher A, Vasa M, Mildner-Rihm C, Adler K, Tiemann M,Rutten H, Fichtlscherer S, Martin H, Zeiher AM. HMG-CoA reductaseinhibitors (statins) increase endothelial progenitor cells via the PI3-kinase/Akt pathaway. J Clin Invest 2001;108:391–397.
25. Weitz-Schmidt G, Welzenbach K, Brinkmann V, Kamata T, Kallen J,Bruns C, Cottens S, Takada Y, Hommel U. Statins selectively inhibit leuko-cyte function antigen-1 by binding to a novel regulatory integrin site. NatMed 2001;7:687–692.
26. Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein andother markers of inflammation in the prediction of cardiovasculardisease in women. N Engl J Med 2000;342:836–843.
27. Ridker PM, Rifai N, Clearfield M, Downs JR, Weis SE, Miles JS, Gotto Am Jr.Air Force/Texas Coronary Atherosclerosis Prevention Study Investigators.Measurement of C-reactive protein for the targeting of statin therapy inthe primary prevention of acute coronary events. N Engl J Med2001;344:1959–1965.
28. Azuma RW, Suzuki J, Ogawa M, Futamatsu H, Koga N, Onai Y, Kosgue H,Isobe M. HMG-CoA reductase inhibitor attenuates experimental auto-immune myovcarditis through inhibition of T cell activation. CardiovascRes 2004;64:412–420.
29. Hori A, Kanda Y, Goyama S, Onishi Y, Komeno Y, Mitani K, Kishi Y, Ogawa S,Imataki O, Chiba S, Kojima R, Hamaki T, Sakiyama M, Kami M,Makimoto A, Tanosaki R, Takaue Y, Hirai H; Japan Hematology OncologyClinical Study Group. A prospective trial to evaluate the safety and effi-cacy of pravastatin for the treatment of refractory chronicgraft-versus-host disease. Transplantation 2005;79:372–374.
30. Shimada K, Miyauchi K, Daida H. Early intervention with atorvastatinmodulates TH1/TH2 imbalance in patients with acute coronary syn-drome: from bedside to bench. Circulation 2004;109:e213–e214.
Rapid immunomodulation by rosuvastatin 2955
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/27/24/2945/2887196 by guest on 22 June 2022