
Ambient Air Pollution and Cardiovascular Malformations in Atlanta, Georgia, 1986-2003
Upload
khangminh22Category
view
1download
0
126
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
SumáRIo
A radiocirurgia se tornou uma alternativa popular à micro-cirurgia para pequenas malformações arteriovenosas (MAV). Diversos relatos documentaram uma alto índice de oblitera-ção (em torno de 80%) e um baixo índice de complicações induzidas pela radiação (em torno de 2%). A Gamma-Knife, aceleradores lineares e sistemas de partículas pesadas são opções de tecnologias viáveis para sua realização. A maior desvantagem da radiocirurgia é a de que o paciente perma-nece com risco de hemorragia até que a MAV esteja comple-tamente obliterada e este processo tipicamente leva em torno de 2 anos. As maiores vantagens são que o tratamento pode ser realizado de forma ambulatorial com anestesia local e que as potenciais sérias complicações da embolização e cirurgia aberta podem ser evitadas.
Palavras-chave: Malformações arteriovenosas, radiocirur-gia estereotáxica.
ABSTRACT
Radiosurgery has become a popular alternative to microsur-gery for small arteriovenous malformations (AVM). Numer-ous reports document high obliteration rates (around 80%) and low radiation induced complication rates (around 2%). Gamma knife, linear accelerator, and particle beam systems are all viable options. The major drawback of radiosurgery is that the patient remains at risk for hemorrhage until the AVM is completely obliterated and this process typically takes around 2 years. The major advantages are that the treatment can be performed on a outpatient basis with local anesthesia and that the potential serious complications of embolization and open surgery can be avoided.
Key-words: Arteriovenous malformations, stereotactic radio-surgery.
Radiosurgery for arteriovenous malformations Radiocirugia para malformações arteriovenosas cerebrais
William A. Friedman1 Frank J. Bova1
1 Department of Neurological Surgery, University of Florida, Gainesville, Florida.
Recebido em janeiro de 2009. Aceito em fevereiro de 2009.

127
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
introduCtion
Stereotactic radiosurgery is the term coined by Lars Leksell27 to describe the application of a single, high dose of radiation to a stereotactically defined target volume. In the 1970s reports be-gan to appear documenting the successful obliteration of arte-riovenous malformations (AVMs) with radiosurgery. When an AVM is treated with radiosurgery, a pathologic process appears to be induced that is similar to the response-to-injury model of atherosclerosis. Radiation injury to the vascular endothelium is believed to induce the proliferation of smooth-muscle cells and the elaboration of extracellular collagen, which leads to progressive stenosis and obliteration of the AVM nidus8,36,45,47 thereby eliminating the risk of hemorrhage.
The advantages of radiosurgery - compared to microsurgical and endovascular treatments - are that it is noninvasive, has minimal risk of acute complications, and is performed as an outpatient procedure requiring no recovery time for the pa-tient. The primary disadvantage of radiosurgery is that cure is not immediate. While thrombosis of the lesion is achieved in the majority of cases, it commonly does not occur until two or three years after treatment. During the interval between ra-diosurgical treatment and AVM thrombosis, the risk of hemor-rhage remains. Another potential disadvantage of radiosurgery is possible long term adverse effects of radiation. Finally, ra-diosurgery has been shown to be less effective for lesions over 10cc in volume. For these reasons, selection of the optimal tre-atment for an AVM is a complex decision requiring the input of experts in endovascular, open surgical, and radiosurgical treatment.
In the pages below, we will review the world’s literature on radiosurgery for AVMs. Topics reviewed will include the follo-wing: radiosurgical technique, radiosurgery results (gamma knife radiosurgery, particle beam radiosurgery, linear accele-rator radiosurgery), hemorrhage after radiosurgery, radiation induced complications, repeat radiosurgery, and radiosurgery for other types of vascular malformation.
RAdIoSuRgERy TEChNIquE
The radiosurgical paradigm been described at length in other publications17, but a brief description of radiosurgical techni-ques - with emphasis on points specifically applicable to AVM treatment - is in order. The fundamental elements of a suc-cessful radiosurgical treatment are the same regardless of the system (i.e. linear accelerator, gamma knife, or particle beam) being used to deliver the stereotactically focused radiation. They include:
1. appropriate patient selection,
2. application of a stereotactic head ring
3. acquisition of quality three-dimensional stereotactic images and transfer of this image database to a dose planning computer,
4. use of the computer to formulate an optimal plan (dose distribution) for radiation delivery,
5. selection of an appropriate treatment dose,
6. precision radiation delivery that faithfully executes the plan, and
7. careful clinical and radiographic follow-up.
All of these elements are critical, and poor performance of any step will result in suboptimal results.
pATIENT SELECTIoN
Open surgery is generally favored if an AVM is amenable to low-risk resection (e.g. low Spetzler-Martin grade, young he-althy patient) or is felt to be at high risk for hemorrhage during the latency period between radiosurgical treatment and AVM obliteration (e.g. associated aneurysm, venous outflow obs-truction).
Radiosurgery is favored when the AVM nidus is small (< 3cm) and compact, when surgery is judged to carry a high risk or is refused by the patient, and when the risk of hemorrhage is not felt to be extraordinarily high.
Endovascular treatment, although rarely curative alone, may be useful as a preoperative adjunct to either microsurgery or radiosurgery. If radiosurgery can be used alone, embolization should be avoided (see below) - embolic material typically makes radiosurgical targeting much more difficult and almost certainly reduces the success rate.
The pre-treatment evaluation of an AVM should ideally be a team effort: surgeons comfortable and experienced with open cerebrovascular surgery, endovascular surgery, and radiosur-gery should jointly pick the best method or combination of methods for each patient.
hEAd RINg AppLICATIoN
Radiosurgical treatment starts with head ring application. The rigidly attached ring enables the acquisition of spatially accu-rate information from angiography, CT, and MRI. The images obtained with the ring (and an attached stereotactic localizer) in place establish fixed relationships between the ring and the target lesion. These spatial relationships provide the substrate for computer-based treatment planning and are later translated from radiographic (virtual) space into real space so that the tre-

128
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
atment target can be accurately placed at the precise isocenter of the radiation delivery device. Of equal importance, because the stereotactic head ring is bolted to the treatment delivery device, it also immobilizes the patient during treatment. Most patients find it very difficult to remain motionless in frameless stereotactic systems, which limit their accuracy and utility.
At UF, patients are premedicated with 10mg of oral diazepam approximately one-half hour before ring application. No skin shaving or scalp preparation is required. The ring and posts are assembled and positioned to fit the patient, taking care to avoid accidental placement of pins into a burr hole, over a shunt path, or onto a bone flap from a prior craniotomy. The pin sites are anesthetized with a local injection of lidocaine plus bupivicai-ne, and the aluminum-tipped (CT-compatible) pins are hand-ti-ghtened with a wrench that is then attached to the ring to assure its ready availability for ring removal. At the conclusion of this procedure, the patient is transferred to a wheelchair and trans-ported to the radiology department for the next step (imaging) in the radiosurgery process.
STEREoTACTIC ImAgE ACquISITIoN
The most problematic aspect of AVM radiosurgery is target identification. In some series (see below), targeting error is listed as the most frequent cause of radiosurgical failure. The problem lies with imaging. While angiography very effectively defines blood flow (feeding arteries, nidus, and draining veins), it does so in only two dimensions. Using the two-dimensional data from stereotactic angiography to represent the three-di-mensional target results in significant errors of both overesti-mation and underestimation of AVM nidus dimensions7,11. Un-derestimation of the nidus size may result in treatment failure, while overestimation results in the inclusion of normal brain within the treatment volume. This can cause radiation damage to normal brain, which - when affecting an eloquent area - may result in a neurologic deficit. To avoid such targeting errors, a true three-dimensional image database is required. Both con-trast-enhanced CT and MRI are now commonly used for this purpose.
Diagnostic (non-stereotactic) angiography is used to charac-terize the AVM, but because of its inherent inadequacies as a treatment planning database, stereotactic angiography has been largely abandoned at our institution. We use contrast enhanced, stereotactic CT as a targeting image database for the vast majo-rity of AVMs. Our CT technique employs rapid infusion (1cc/sec) of contrast while scanning through the AVM nidus with 1-mm slices. This technique yields a very clear three dimen-sional picture of the nidus. Alternative approaches use MRI/MRA, as opposed to CT.
The images are transferred via Ethernet to the treatment plan-
ning computer. The fiducial markers on the stereotactic loca-lizer are automatically identified in each image and the dose planning software uses these reference points to define a three-dimensional Cartesian coordinate system relative to the head ring. Spatial coordinates are assigned to each point (pixel) in each CT slice. Because the ring remains fixed relative to the patient’s skull during treatment, any point in the virtual volume defined by the CT scan (including the entire head, and - most importantly - the AVM nidus) can be mapped precisely to a point in real space.
TREATmENT pLANNINg
Once the necessary stereotactic images have been acquired and transferred to the treatment-planning computer, treatment planning begins. This is accomplished through the use of a computer workstation and specialized treatment planning sof-tware “tools.” The methodology of treatment planning varies somewhat depending on the radiosurgery system and software employed, but the objectives and basic principles of radiosur-gery dose planning are universal.
The fundamental principle of radiosurgery is the delivery of focal, high dose radiation to a designated intracranial target - in this case the nidus of the AVM - while sparing the surrounding normal brain tissue - i.e. conformality. This is accomplished by focusing hundreds of non-parallel radiation beams on a ste-reotactically defined target. When the effect of these beams is averaged, a very high dose of radiation is delivered to the target volume (where all the beams intersect), while innocuously low doses are delivered to non-target tissues along the path of any given beam.
The primary goal of AVM radiosurgery treatment planning is to develop a plan with a target volume that conforms closely to the surface of the AVM nidus, while maintaining a steep dose gradient (the rate of change in dose relative to position) away from the nidal surface in order to minimize the radiation dose to surrounding brain. A number of treatment planning tools can be used to tailor the shape of the target volume to fit even hi-ghly irregular nidus shapes. Regardless of its shape, the entire nidus - not including the feeding arteries and draining veins - must lie within the target volume (the “prescription isodose shell”), with as little normal brain included as possible.
Dose planning is ideally a team effort, with the treating neuro-surgeon, radiation oncologist, and medical physicist contribu-ting to the development of an optimal plan.
doSE SELECTIoN
Once a satisfactory treatment plan has been developed, a dose must be selected. By convention, radiosurgical doses are pres-

129
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
cribed to the isodose shell (the set of all points in a dose plan that receive the same selected dose) that has been tailored to conform to the surface of the target. Isodose shells are com-monly designated as percentages of the maximum dose delive-red. For example, a typical AVM dose prescription might read “17.5 Gy to the 70% isodose line.” In this case, the 70% isodo-se shell has been tailored to conform closely to the surface of the AVM nidus and the minimum target dose of 17.5 Gy is de-livered to the periphery of the nidus. Higher doses are delivered within the nidus to a maximum of 25 Gy (17.5 = 70% of 25).
Various analyses of AVM radiosurgery outcomes (described below) have elucidated an appropriate range of doses for the treatment of AVMs. Minimum nidal doses lower than 17.5 Gy have been associated with a significantly lower rate of AVM obliteration, while doses above 20 Gy have been associated with a higher rate of permanent neurological complications. We prescribe 20 Gy to the margin of the AVM nidus, whene-ver we feel it can be done safely, to optimize the chances of AVM obliteration. We choose the 80% isodose line for single isocenter plans and the 70% isodose line for multiple isocenter plans because these prescription isodoses are associated with the steepest dose gradients. As our experience has grown, the technology has evolved, and our ability to design very confor-mal plans has improved, we use this “optimal” dose on most AVMs less than 3cm in diameter, provided the nidus is well defined. Lower doses may be selected for larger AVMs, AVMs in very eloquent locations, or AVMs with more diffuse nidus morphology.
RAdIATIoN dELIvERy
The next step in the process is the execution of the treatment plan. The patient is placed supine on the couch of the treatment device and the head ring is secured to an immobilizing bracket. The patient’s head is positioned so that the focal point of the ra-diation delivery device coincides with the first isocenter in the treatment plan. An appropriately sized collimator is installed to determine the diameter of the beams; then many beams of radiation are directed at the isocenter from various directions. In the case of a LINAC-based system, this is accomplished by rotating the radiation source in several concentric arcs around the isocenter. The gamma knife achieves the same result by exposing the target simultaneously to 201 intersecting radia-tion beams from independent cobalt sources that are precisely aligned in a hemispherical array around the isocenter.
If the treatment plan includes multiple isocenters, the patient’s head is repositioned for each isocenter. Treatment of each iso-center typically takes about 5 minutes. Total treatment time is determined by the number of isocenters needed to achieve con-formality (more are needed for irregular shapes). An alternati-ve approach to treatment delivery with some LINAC systems
involves the use of a computer driven “micromultileaf colli-mator” and a radiation shaping method called intensity modu-lation. In general, intensity modulation is faster than multiple isocenter treatment, but not quite as conformal. Careful atten-tion to detail and the execution of various safety checks and redundancies (now usually entirely electronic) are necessary to ensure that the prescribed treatment plan is accurately and safely delivered. When radiation delivery has been completed, the head ring is removed, the patient is observed for approxi-mately thirty minutes, and is then discharged to resume her/his normal activities.
FoLLow-up
Standard follow-up after AVM radiosurgery typically consists of annual clinic visits with MRI/MRA to evaluate the effect of the procedure and monitor for neurologic complications. If the patient’s clinical status changes, she/he is followed more closely at clinically appropriate intervals.
Each patient is scheduled to undergo cerebral angiography at three years post-radiosurgery, and a definitive assessment of the success or failure of treatment is made based on the results of angiography (see below). If no flow is observed through the AVM nidus, the patient is pronounced cured and is discharged from follow-up. If the AVM nidus is incompletely obliterated, appropriate further therapy (most commonly repeat radiosur-gery on the day of angiography) is prescribed, and the treat-ment/follow-up cycle is repeated.
REpoRTEd EFFICACy oF Avm RAdIoSuRgERy (SEE TABLE 1)
Gamma Knife Radiosurgery
The gamma knife is a dedicated radiosurgery machine, inven-ted by Lars Leksell and his colleagues in 1968, in Sweden. Current gamma knife equipment contains 201 cobalt sources, held in a hemispherical array. These sources emit high energy photons (called gamma rays). Each source creates an indepen-dent beam path through normal brain to the radiosurgery tar-get. All of the beams coincide at the target, delivering a high dose of radiation, but each individual beam path has very little dose, creating a very steep dose gradient, with little risk to nor-mal tissue.
Steiner pioneered gamma knife radiosurgery for AVMs and has published multiple reports41,44. He has reported 1-year occlu-sion rates ranging from 33.7 to 39.5% and two-year occlusion rates ranging from 79 to 86.5%. However, these results were “optimized” by retrospectively selecting patients who received a high treatment dose. For example28, in one report he stated, “…a large majority of patients received at least 20-25 Gy of ra-

130
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
diation... Of the 248 patients treated before 1984, the treatment specification placed 188 in this group.” The reported thrombo-sis rates in this paper only applied to these 188 patients (76% of the total series).
Table 1. Major AVM radiosurgery series (over 100 patients) - when a group had multiple reports, the most recent results
are listed.
First Author Yamamoto74 Pollock52 Karlsson31,33 Steinberg61 Colombo8 Friedman21
Radio-surgical Device
Gamma Knife
Gamma Knife
Gamma Knife
Proton Beam
LINAC LINAC
Number of Pa-tients
40 313 945 86 180 388
Angio-graphic Cure Rate
65% 61% 56% 92% 80% 67%
Compli-cationsPerma-nent Ra-diation Induced
3 patients (7.5%)
30 patients
(9%)5% 11%
4 patients (2%)
7 patients (2%)
Hemor-rhage None 8 fatal 55 patients 10 patients
15 patients, 5 fatal
25 patients, 5 fatal
Yamamoto and colleagues reported on 25 Japanese patients treated on the gamma unit in Stockholm, but followed in Ja-pan49. The two-year thrombosis rate in those AVMs that were completely covered by the radiosurgical field was 64%. One additional patient had complete thrombosis at 3-year angio-graphy and one additional at 5-year angiography, for a total cure rate of 73%. In another paper48, these authors reported angiographic cures in 6/9 (67%) children treated in Stockholm or Buenos Aires and followed in Japan. Yamamoto et. al46., re-viewed the long-term follow-up results of a group of 40 Japa-nese patients undergoing gamma knife radiosurgery for AVMs in three different countries (Argentina, Sweden, and the Uni-ted States). In this group of patients, the mean lesion volume was only 3.7cc. Twenty-six patients (65%) were subsequently found to have angiographically confirmed nidus obliteration at 1-5 years after radiosurgery.
Kemeny reported on 52 AVM patients treated with gamma kni-fe radiosurgery20. They all received 25 Gy to the 50% isodose line. At one year, 16 patients (31%) had complete thrombosis and 10 patients (19%) had “almost complete” thrombosis. He found that the results were better in younger patients and in patients with relatively lateral location of their AVMs. There was no difference in outcome between small (<2cc), medium (2-3cc), and large (>3cc) AVMs.
Lunsford and colleagues reported on 227 AVM patients treated with gamma knife radiosurgery30. The mean dose delivered to
the AVM margin was 21.2 Gy. Multiple isocenters were used in 48% of the patients. Seventeen patients underwent 1-year an-giography, which confirmed complete thrombosis in 76.5%. As indicated in the paper, “this rate may be spurious since many of these patients were selected for angiography because their MR image had suggested obliteration.” Among 75 patients who were followed for at least two years, 2-year angiography was performed in only 46 (61%). Complete obliteration was confirmed in 37/46 (80%). This thrombosis rate strongly cor-related with AVM size, as follows: <1cc - 100%, 1-4cc - 85%, 4-10 cc - 58%. This group also reported on a group of 65 “ope-rable” AVMs, treated with radiosurgery34. Of 32 patients who subsequently underwent follow-up angiography, 84% showed complete thrombosis. In a later publication from this group, Pollock32 reported on 313 AVM patients - an angiographic cure rate of 61% was achieved.
Karlsson et al19 reported on 945 AVMs treated in Stockholm between 1970 and 1990, with the gamma knife. The overall occlusion rate was 56%. Shin and Maruyama reported on 400 cases treated with gamma knife radiosurgery37. They reported a 72% obliteration rate at 3 years post-treatment. Other groups have reported on gamma knife radiosurgery results for specific sites, like brainstem26,31, motor cortex18 or basal ganglia33, or groups, like children21.
Particle beam (proton or helium) Radiosurgery
Particle beam radiosurgery facilities use cyclotron like devices to accelerate subatomic particles to very high speeds before aiming them at patients. They have a unique physical property, called the Bragg - peak effect, which results in the vast majority of the beam’s energy being deposited at a predictable depth in tissue, with little exit dose. This property is theoretically ideal for radiosurgery but it’s utility has been limited by the need to spread out the Bragg peak to fit anatomic lesions, restrictions in beam number compared to gamma knife or LINAC systems, and the very high cost of the facilities needed for such systems.
Kjellberg and colleagues published multiple reports on the use of Bragg peak proton particle radiosurgery for AVMs22,24. Their NEJM article in 1983 provided details on long term follow-up of their first 75 patients23. It includes a well known diagram of doses versus complications. Unfortunately, only 20% of these patients had complete nidus obliteration on follow-up angio-graphy. Szeifert and colleagues45 reported on 63 patients refer-red to the United States for Bragg peak proton beam therapy and followed in Europe. Complete nidus obliteration was only seen in 10 patients (15.9%). A number of patients had radiation induced side effects.
In contrast, Steinberg and colleagues40, in an analysis of 86 AVMs treated with a helium particle-beam radiosurgical sys-

131
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
tem, reported a 29% one year thrombosis, 70% two year throm-bosis, and 92% three year thrombosis rate. The best results were obtained with smaller lesions and higher doses. Initially a treatment dose of 34.6 Gy was used but a higher than expected neurological complication rate (20% for the entire series) led to lower doses (7.7 - 19.2 Gy). No patients treated with the lower dose range had complications.
Linear Accelerator Radiosurgery
Linear accelerators are devices which use microwave energy to accelerate electrons to very high speeds. The energetic elec-trons collide with a heavy metal alloy in the head of the machi-ne. Most of the collision energy is lost as heat, but a small per-centage results in high energy photon radiation (called x-rays because they are electronically produced). These photons are virtually identical to those produced by the spontaneous decay of radioactive cobalt in the gamma knife. They are collimated and focused on the radiosurgical target. Linear accelerator sys-tems rotate the beam around the patient, from many different angles, to create the “hundreds of beams” approach used by the gamma knife to provide high doses at target but low doses to normal tissues.
Betti pioneered LINAC radiosurgery and reported on the re-sults of 66 AVMs treated with a linear accelerator radiosurgical system3,5. Doses of “no more than 40 Gy” were used in 80% of patients. He found a 66% two-year thrombosis rate. The percentage of cured patients was highest when the entire mal-formation was included in the 75% isodose line (96%) or the maximum diameter of the lesion was less than 12mm (81%).
Colombo reported on 97 AVM patients treated with a linear accelerator system9. Doses from 18.7-40 Gy were delivered in one or two sessions. Of 56 patients who were followed longer than 1 year, 50 underwent 12-month follow-up angiography. In 26 patients (52%), complete thrombosis was demonstrated. Fifteen of 20 patients (75%) undergoing two-year angiography had complete thrombosis. He reported a definite relationship between AVM size and thrombosis rate, as follows: Lesions <15mm in diameter had a one year obliteration rate of 76% and a two year rate of 90%. Lesions 15-25mm in diameter had a one-year thrombosis rate of 37.5% and a two-year rate of 80%. Lesions greater than 25mm in diameter had a one-year thrombosis rate of 11% and a two-year rate of 40%. In a later report10, Colombo and colleagues reported follow-up on 180 radiosurgically treated AVMs. The one-year thrombosis rate was 46%, and the two-year rate was 80%.
Souhami reported on 33 AVMs treated with a linear accelerator system38. The prescribed dose at isocenter varied from 50-55 Gy. A complete obliteration rate of 38% was seen on one-year angiography. For patients whose arteriovenous malformation
nidus was covered by a minimum dose of 25 Gy, the total obli-teration rate was 61.5 % whereas none of the patients who had received less than 25 Gy at the edge of the nidus obtained a total obliteration.
Loeffler reported on 16 AVMs treated with a linear accelerator system29. The peripheral prescribed dose was 15-25 Gy, typi-cally to the 80-90% line. The total obliteration rate was 5/11 (45%) at one year and 8/11 (73%) at two years after treatment.
Engenhart and colleagues12 reported on the treatment of 212 patients in Heidelberg. “Above a threshold dose of 18Gy, the obliteration rate was 72%. Radiation induced late complica-tions were seen in 4.3%.
Schlienger and colleagues35 reported on 169 patients treated in Paris. The overall obliteration rate was 64%. Success ra-tes were higher in smaller lesions, in lesions not embolized, in lesions treated with higher doses, and lesions treated with one isocenter. Two patients experienced radiation induced side effects.
Andrade and colleagues1 reported on 38 rolandic area AVMs treated in Toronto. Complete nidus obliteration was seen in 60.5%. Two patients experienced radiation induced side effects.
Friedman and colleagues have published multiple reports on the University of Florida experience with radiosurgery for AVMs13,17. They have documented occlusion rates of 80% for lesions less than 10cc in volume, with radiation induced complications in the 2% range. Factors favoring occlusion in-clude; smaller AVM size, lower Spetzler-Martin score, higher peripheral radiation dose, and compact nidus morphology. De-tailed dosimetric analysis suggested that 12 Gy volume and eloquent location correlated with transient radiation induced complications. Detailed, updated UF results follow below:
RESuLTS oF Avm RAdIoSuRgERy AT uF
Between 5/18/88 and 5/1/08, 617 AVMs were treated on the University of Florida radiosurgery system (see Figure 1). There were 307 men and 310 women in the series. The mean age was 39 (range: 4 - 78). Patients presented with hemorrhage (203), seizure (250), headache/incidental finding (218), and progres-sive neurological deficit27. Thirty-eight patients had undergone prior subtotal microsurgical AVM excision. Fifty-five patients had undergone at least one embolization procedure. Patients were screened with a vascular neurosurgeon prior to conside-ration of radiosurgery.
The median lesion volume was 6.9cc (0.1 - 52.3 cc). The treat-ment volume was determined in all cases by performing a com-puterized dose volume histogram of the treatment isodose shell (which was constructed to conform closely to the AVM nidus). Lesion volumes were stratified as follow: A - <1cc, B - 1-4cc,

132
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
C - 4-10cc, D - >10cc. Spetzler-Martin grades were distributed as follows: grade I - 37 patients, grade II - 208 patients, grade III - 254 patients, and grade IV - 107 patients. The median ra-diation dose to the periphery of the lesion was 17.5 Gy (range: 7.5 - 25 Gy). This treatment dose was delivered to the 80% isodose line when single isocenter plans were used, and to the 70% line when multiple isocenters were employed. Two hun-dred eighty nine patients were treated with a single isocenter, 84 patients with two isocenters, 42 patients with three isocen-ters, 21 patients with four isocenters, and 124 patients with five isocenters or more.
Mean follow-up duration for the entire AVM group was 33 months (2 - 166 mos.). Follow-up generally consists of clini-cal examination and MRI scanning at one-year intervals after treatment, unless clinical symptoms indicate more frequent follow-up. When possible, follow-up is performed in Gaines-ville, otherwise scan and exam results are forwarded by the patient’s local physician.
Initially, all patients were asked to undergo angiography at ye-arly intervals, regardless of the MRI findings. After the first 50 patients were treated, it was decided to defer angiography until MRI/MRA strongly suggested complete thrombosis. Further-more, if complete thrombosis was not identified three years after radiosurgery, repeat radiosurgery was undertaken in an effort to obliterate any remaining nidus (see below).
An angiographic cure required that no nidus or shunting re-main on the study, as interpreted by a neuroradiologist and the treating neurosurgeon. Of the 192 follow-up angiograms per-formed to date, 147 (77%) have demonstrated complete AVM obliteration. Using this traditional method of reporting, the following angiographic cure rates were seen in the various size categories: A - 93%, B - 86%, C - 83%, D - 53%. But angiogra-phic success rates can be misleadingly high, since angiography may not be done if MRI shows residual nidus. If angiography or MRI followup results at 3 years are accepted, the following results are seen in 367 patients: A - 93%, B - 83%, C - 63%, D - 35%. Finally, if one includes radiosurgical retreatments (which will salvage a number of initial failures, see below), the patient success rates are as follows: A - 100%, B - 93%, C - 84%, D - 75%.
Figure 1A: This patient presented with a grand mal seizure disorder and was ini-tially treated with embolization. This AP angiogram shows the targeted AvM nidus at the time of his first radiosurgical treatment in 1991. He received 1500 cGy to the periphery of the nidus.
Figure 1B: Lateral angiography at the time of the first radiosurgical treatment.
133
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
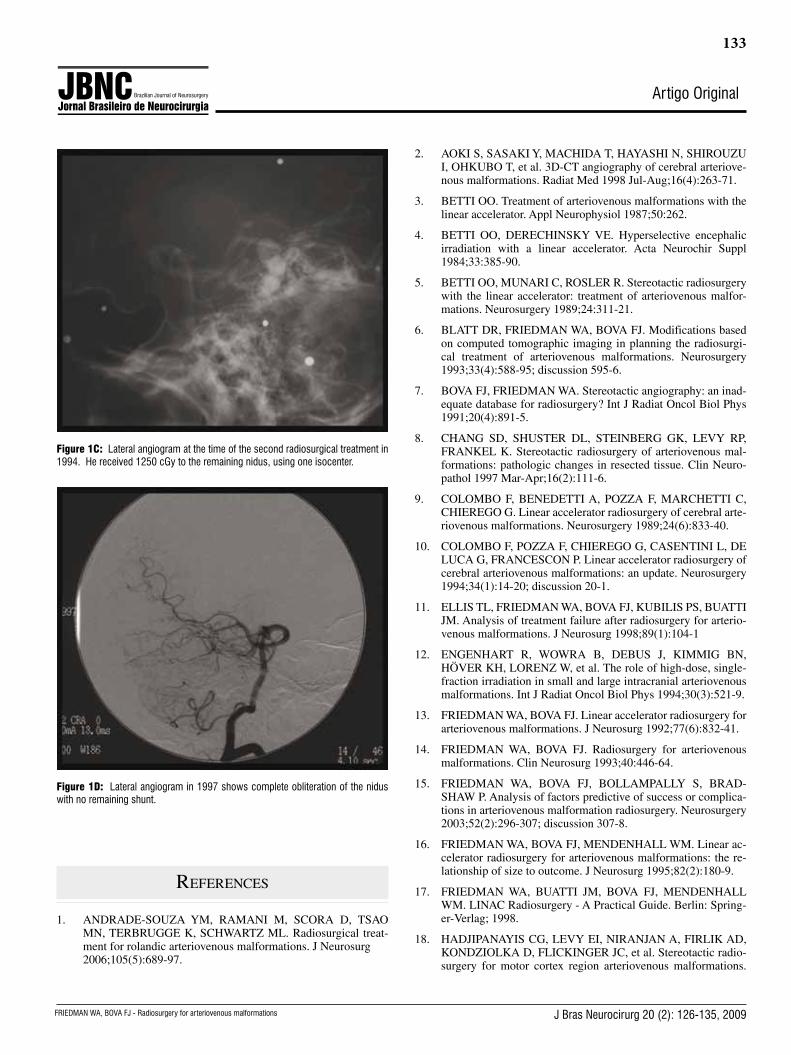
Figure 1C: Lateral angiogram at the time of the second radiosurgical treatment in 1994. He received 1250 cGy to the remaining nidus, using one isocenter.
Figure 1D: Lateral angiogram in 1997 shows complete obliteration of the nidus with no remaining shunt.
referenCes
1. ANDRADE-SOUZA YM, RAMANI M, SCORA D, TSAO MN, TERBRUGGE K, SCHWARTZ ML. Radiosurgical treat-ment for rolandic arteriovenous malformations. J Neurosurg 2006;105(5):689-97.
2. AOKI S, SASAKI Y, MACHIDA T, HAYASHI N, SHIROUZU I, OHKUBO T, et al. 3D-CT angiography of cerebral arteriove-nous malformations. Radiat Med 1998 Jul-Aug;16(4):263-71.
3. BETTI OO. Treatment of arteriovenous malformations with the linear accelerator. Appl Neurophysiol 1987;50:262.
4. BETTI OO, DERECHINSKY VE. Hyperselective encephalic irradiation with a linear accelerator. Acta Neurochir Suppl 1984;33:385-90.
5. BETTI OO, MUNARI C, ROSLER R. Stereotactic radiosurgery with the linear accelerator: treatment of arteriovenous malfor-mations. Neurosurgery 1989;24:311-21.
6. BLATT DR, FRIEDMAN WA, BOVA FJ. Modifications based on computed tomographic imaging in planning the radiosurgi-cal treatment of arteriovenous malformations. Neurosurgery 1993;33(4):588-95; discussion 595-6.
7. BOVA FJ, FRIEDMAN WA. Stereotactic angiography: an inad-equate database for radiosurgery? Int J Radiat Oncol Biol Phys 1991;20(4):891-5.
8. CHANG SD, SHUSTER DL, STEINBERG GK, LEVY RP, FRANKEL K. Stereotactic radiosurgery of arteriovenous mal-formations: pathologic changes in resected tissue. Clin Neuro-pathol 1997 Mar-Apr;16(2):111-6.
9. COLOMBO F, BENEDETTI A, POZZA F, MARCHETTI C, CHIEREGO G. Linear accelerator radiosurgery of cerebral arte-riovenous malformations. Neurosurgery 1989;24(6):833-40.
10. COLOMBO F, POZZA F, CHIEREGO G, CASENTINI L, DE LUCA G, FRANCESCON P. Linear accelerator radiosurgery of cerebral arteriovenous malformations: an update. Neurosurgery 1994;34(1):14-20; discussion 20-1.
11. ELLIS TL, FRIEDMAN WA, BOVA FJ, KUBILIS PS, BUATTI JM. Analysis of treatment failure after radiosurgery for arterio-venous malformations. J Neurosurg 1998;89(1):104-1
12. ENGENHART R, WOWRA B, DEBUS J, KIMMIG BN, HÖVER KH, LORENZ W, et al. The role of high-dose, single-fraction irradiation in small and large intracranial arteriovenous malformations. Int J Radiat Oncol Biol Phys 1994;30(3):521-9.
13. FRIEDMAN WA, BOVA FJ. Linear accelerator radiosurgery for arteriovenous malformations. J Neurosurg 1992;77(6):832-41.
14. FRIEDMAN WA, BOVA FJ. Radiosurgery for arteriovenous malformations. Clin Neurosurg 1993;40:446-64.
15. FRIEDMAN WA, BOVA FJ, BOLLAMPALLY S, BRAD-SHAW P. Analysis of factors predictive of success or complica-tions in arteriovenous malformation radiosurgery. Neurosurgery 2003;52(2):296-307; discussion 307-8.
16. FRIEDMAN WA, BOVA FJ, MENDENHALL WM. Linear ac-celerator radiosurgery for arteriovenous malformations: the re-lationship of size to outcome. J Neurosurg 1995;82(2):180-9.
17. FRIEDMAN WA, BUATTI JM, BOVA FJ, MENDENHALL WM. LINAC Radiosurgery - A Practical Guide. Berlin: Spring-er-Verlag; 1998.
18. HADJIPANAYIS CG, LEVY EI, NIRANJAN A, FIRLIK AD, KONDZIOLKA D, FLICKINGER JC, et al. Stereotactic radio-surgery for motor cortex region arteriovenous malformations.

134
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
Neurosurgery 2001;48(1):70-6; discussion 76-7.
19. KARLSSON B, LINDQUIST C, STEINER L. Prediction of obliteration after gamma knife surgery for cerebral arteriove-nous malformations. Neurosurgery 1997; 40(3):425-30; discus-sion 30-1.
20. KEMENY AA, DIAS PS, FORSTER DM. Results of stereotac-tic radiosurgery of arteriovenous malformations: an analysis of 52 cases. J Neurol Neurosurg Psychiatry 1989;52(5):554-8.
21. KIRAN NA, KALE SS, VAISHYA S, KASLIWAL MK, GUP-TA A, SHARMA MS, et al. Gamma Knife surgery for intra-cranial arteriovenous malformations in children: a retrospective study in 103 patients. J Neurosurg 2007;107(6 Suppl):479-84.
22. KJELLBERG RN. Stereotactic Bragg peak proton beam radio-surgery for cerebral arteriovenous malformations. Ann Clin Res 1986;18 Suppl 47:17-9.
23. KJELLBERG RN, HANAMURA T, DAVIS KR, LYONS SL, ADAMS RD. Bragg-peak proton-beam therapy for arteriovenous malformations of the brain. N Engl J Med 1983;309(5):269-74.
24. KJELLBERG RN, POLETTI CE, ROBERSON GH, ADAMS RD. Bragg-peak proton beam treatment of arteriovenous mal-formation of the brain. ExcMed 1977;433:181-6.
25. KONDZIOLKA D, LUNSFORD LD, KANAL E, TALAGALA L. Stereotactic magnetic resonance angiography for target-ing in arteriovenous malformation radiosurgery. Neurosurgery 1994;35(4):585-90; discussion 90-1.
26. KURITA H, KAWAMOTO S, SASAKI T, SHIN M, TAGO M, TERAHARA A et al. Results of radiosurgery for brain stem arteriovenous malformations. J Neurol Neurosurg Psychiatry 2000;68(5):563-70.
27. LEKSELL L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand 1951;102:316-9.
28. LINDQUIST C, STEINER L. Stereotactic radiosurgical treat-ment of malformations of the brain. In: Lunsford LD, ed. Mod-ern Stereotactic Neurosurgery. 1 ed. Boston: Martinus Nijhoff; 1988:491-506.
29. LOEFFLER JS, ALEXANDER E, 3RD, SIDDON RL, SAUN-DERS WM, COLEMAN CN, WINSTON KR. Stereotactic radiosurgery for intracranial arteriovenous malformations us-ing a standard linear accelerator. Int J Radiat Oncol Biol Phys 1989;17(3):673-7.
30. LUNSFORD LD, KONDZIOLKA D, FLICKINGER JC, BIS-SONETTE DJ, JUNGREIS CA, MAITZ AH et al. Stereotac-tic radiosurgery for arteriovenous malformations of the brain. J Neurosurg 1991;75(4):512-24.
31. MARUYAMA K, KONDZIOLKA D, NIRANJAN A, FLICK-INGER JC, LUNSFORD LD. Stereotactic radiosurgery for brainstem arteriovenous malformations: factors affecting out-come. J Neurosurg 2004;100(3):407-13.
32. POLLOCK BE, FLICKINGER JC, LUNSFORD LD, MAITZ A, KONDZIOLKA D. Factors associated with successful ar-teriovenous malformation radiosurgery. Neurosurgery 1998 Jun;42(6):1239-44; discussion 44-7.
33. POLLOCK BE, GORMAN DA, BROWN PD. Radiosurgery for arteriovenous malformations of the basal ganglia, thalamus, and
brainstem. J Neurosurg 2004;100(2):210-4.
34. POLLOCK BE, LUNSFORD LD, KONDZIOLKA D, MAITZ A, FLICKINGER JC. Patient outcomes after stereotactic radio-surgery for ‘operable’ arteriovenous malformations. Neurosur-gery 1994;35:1-8.
35. SCHLIENGER M, ATLAN D, LEFKOPOULOS D, MERI-ENNE L, TOUBOUL E, MISSIR O, et al. Linac radiosurgery for cerebral arteriovenous malformations: results in 169 pa-tients. Int J Radiat Oncol Biol Phys 2000;46(5):1135-42.
36. SCHNEIDER BF, EBERHARD DA, STEINER LE. Histopa-thology of arteriovenous malformations after gamma knife ra-diosurgery [see comments]. J Neurosurg 1997 Sep;87(3):352-7.
37. SHIN M, MARUYAMA K, KURITA H, KAWAMOTO S, TAGO M, TERAHARA A, et al. Analysis of nidus obliteration rates after gamma knife surgery for arteriovenous malformations based on long-term follow-up data: the University of Tokyo ex-perience. J Neurosurg 2004;101(1):18-24.
38. SOUHAMI L, OLIVIER A, PODGORSAK EB, PLA M, PIKE GB. Radiosurgery of cerebral arteriovenous malformations with the dynamic stereotactic irradiation. IntJRadiation Oncology BiolPhys 1990;19:775-82.
39. SPIEGELMANN R, FRIEDMAN WA, BOVA FJ. Limitations of angiographic target localization in planning radiosurgical treatment. Neurosurgery 1992;30(4):619-23; discussion 23-4.
40. STEINBERG GK, FABRIKANT JI, MARKS MP, LEVY RP, FRANKEL KA, PHILLIPS MH et al. Stereotactic heavy-charged-particle Bragg-peak radiation for intracranial arteriove-nous malformations. N Engl J Med 1990;323(2):96-101.
41. STEINER L. Radiosurgery in cerebral arteriovenous malforma-tions. In: Fein JM, Flamm ES, eds. Cerebrovascular Surgery, Vol 4. Wien/New York: Springer Verlag, 1985, vol 4, p.1161-215.
42. STEINER L. Treatment of arteriovenous malformations by radiosurgery. In: Wilson CB, Stein BM, eds. Intracranial Ar-teriovenous Malformations. Baltimore/London: Williams and Wilkins; 1984:295-313.
43. STEINER L, LEKSELL L, FORSTER DM, GREITZ T, BACK-LUND EO. Stereotactic radiosurgery in intracranial arterio-venous malformations. Acta Neurochir (Wien) 1974; Suppl 21:195-209.
44. STEINER L, LEKSELL L, GREITZ T, FORSTER DM, BACKLUND EO. Stereotaxic radiosurgery for cerebral arte-riovenous malformations. Report of a case. Acta Chir Scand 1972;138(5):459-64.
45. SZEIFERT GT, KEMENY AA, TIMPERLEY WR, FORSTER DM. The potential role of myofibroblasts in the obliteration of arteriovenous malformations after radiosurgery. Neurosurgery 1997 Jan;40(1):61-5; discussion 65-6.
46. YAMAMOTO M, JIMBO M, HARA M, SAITO I, MORI K. Gamma knife radiosurgery for arteriovenous malformations: long-term follow-up results focusing on complications occurring more than 5 years after irradiation. Neurosurgery 1996;38:906-14.
47. YAMAMOTO M, JIMBO M, IDE M, JIMBO M, HIRAI T, NAKAMURA Y. Gamma knife radiosurgery for cerebral arte-riovenous malformations: an autopsy report focusing on irradia-

135
FRIEDMAN WA, BOvA FJ - Radiosurgery for arteriovenous malformations J Bras Neurocirurg 20 (2): 126-135, 2009
Artigo Original
tion-induced changes observed in nidus-unrelated arteries. Surg Neurol 1995 Nov;44(5):421-7.
48. YAMAMOTO M, JIMBO M, IDE M, TANAKA N, LINDQUIST C, STEINER L. Long-term follow-up of radiosurgically treated arteriovenous malformations in children: report of nine cases. SurgNeurol 1992;38:95-100.
49. YAMAMOTO M, JIMBO M, KOBAYASHI M, et al. Long-term results of radiosurgery for arteriovenous malformation: Neurodi-agnostic imaging and histological studies of angiographically confirmed nidus obliteration. Surg Neurol 1992;37:219-30.
Corresponding author
William A. Friedman, M.D.Professor and ChairmanDepartment of Neurological SurgeryP.O. Box 100265, MBIUniversity of FloridaGainesville, Florida 32610Phone: 352 273-9000Fax: 352 392-8413E-mail: [email protected]
Parque Barigüi - Curitiba, PR
Copyright © 2022 FDOKUMEN



















