Radiation Biology Workbook.pdf - gnssn
41
Distance Assisted Training Programme for Nuclear Medicine Technologists Edited by: Heather E. Patterson, Brian F. Hutton Radiation Biology Authors: Ansto (Australian Nuclear Science & Technical Organisation) Heather Patterson John Cormack Module 2 Unit 2c The material within this document should be regarded as the property of the International Atomic Energy Agency and should be reproduced or used only in accordance with the attached statement of ownership. (version 4.1) REGIONAL COOPERATIVE AGREEMENT INTERNATIONAL ATOMIC ENERGY AGENCY
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Radiation Biology Workbook.pdf - gnssn

Distance Assisted Training Programme for
Nuclear Medicine Technologists
Edited by: Heather E. Patterson, Brian F. Hutton
Radiation Biology
Authors: Ansto (Australian Nuclear Science
& Technical Organisation) Heather Patterson
John Cormack
Module 2 Unit 2c
The material within this document should be regarded as the property of the International
Atomic Energy Agency and should be reproduced or used only in accordance with the attached
statement of ownership. (version 4.1)
REGIONAL COOPERATIVE AGREEMENT
INTERNATIONAL ATOMIC ENERGY AGENCY

b
Statement of ownership
All materials which form part of the project ‘Distance Assisted Training for Nuclear
Medicine Professionals’, including any translation of these materials, remain the
property of the IAEA, Vienna. In addition, the names of the original authors and
editors of the material shall be acknowledged at all times. If the materials are to be
reproduced or printed in any manner, the statement of ownership, as well as names
of original authors and editors shall be included.
The project materials are freely available to lecturers and students for use in
Nuclear Medicine training, provided they are not used for commercial purposes.
The IAEA, authors and editors make no guarantee regarding the accuracy of
material presented and accept no responsibility for any action arising from use of
the materials.
The materials will normally be made available only as part of national formal
training programmes approved by the IAEA. This is encouraged to ensure that
students undertaking the training have adequate supervision and guidance. Also
formal recognition of students training will only be provided subject to formal
student assessment via national training programmes.
Your respect for the use of these materials will be very much appreciated.
Please direct any queries regarding these materials or their use to:
Nuclear Medicine Section
International Atomic Energy Agency
P.O. Box 100
A‐1400 Vienna
Austria

c
Radiation Biology
Biological effects of exposure to ionizing radiation
CONTENTS page
Flowchart d
Outline 1
1. The Human Body – an introduction 3
1.1 Respiratory System 4 1.2 Digestive System 5 1.3 Circulatory System 6 1.4 Lymphatic System 7 1.5 Urinary System 7
Summary of Body Systems
2. Cells and the Biological Damage from Radiation 9 2.1 Cell Structure 9 2.2 Cell Division 10 2.3 Radiation Damage 11
2.3.1 Cell damage 2.3.2 Cell repair 13
2.4 Cell Survival 14
3. Effects of Radiation on Humans 15 3.1 Doses from natural background radiation 3.2 Deterministic Effects 19
3.2.1 Response of skin to radiation 20 3.2.2 Response of gastrointestinal tract to radiation 21
Cataract induction 22 Fertility effects
3.3 Stochastic Effects 24 3.2.1 Hereditary effects 25 3.2.2 Radiation carcinogenesis
3.4 Tissue weighting factors 27 3.5 Exposure of the Foetus 28 3.6 Wholebody radiation effects 30 Summary of Radiation Effects
4. Radiobiology in Nuclear Medicine 33
Glossary 35

d
Radiation Biology
Biological Effects of Exposure to Ionizing Radiation
Flowchart
Outline
Introduction to Human Body
Respiratory Digestive Circulatory Lymphatic Urinary System System System System System
Cells and the Biological Damage from Radiation
Cell Structure Radiation damage Cell Repair Cell Survival Cell damage Effects of Cell damage
Natural radioactivity
Effects of radiation on humans
Deterministic Stochastic Assessing the risks Exposure to foetus Early and late effects Radiation protection & the pregnant worker Response of skin Hereditory effect Response of GI tract Carcinogenises Cataracts
Whole-body radiation effects
Radiobiology in Nuclear Medicine
On-line exercise
OL R1
R1
OL
Revision exercise

1
Radiation Biology Adapted from ‘Biological Effects of Exposure to Ionizing Radiation’
As produced by Australian Nuclear Science and Technical Organization (Ansto) For IAEA project RAS/06/027 – Radiation Protection by Distance Learning
Reviewer: John Cormack Production Editor: Heather Patterson
Outline: As a nuclear medicine technologist, you should understand what the possible consequences of exposure to ionizing radiation are and why safety precautions should be practiced. In this unit you will learn how ionizing radiation can affect the human body. In Module 1, Radiation Safety unit 2a you learned about the ALARA principle where the exposure to radiation workers should be ‘As Low as Reasonably Achievable’. It is important to follow the ‘Golden Rule’ and reduce external radiation through Time, Distance and Shielding and prevent internal exposure through contamination control – Minimize, Contain and Protect. This unit will help you to understand the biological effects of radiation exposure to the human body and reinforce the necessity for care and attention to safety. In nuclear medicine diagnostic studies the risk of damaging radiation exposure to staff and patients is minimal providing safety and care are practiced at all times. However you should be aware of what can happen if the human body is exposed to high doses of radiation such as in radionuclide therapy, radiation oncology (radiotherapy) or large scale radiation accidents involving whole body exposure, for example; the nuclear reactor accident at Chernobyl in 1986.
As an introduction to this subject, you will be given a basic understanding of how the human body works. In Radiation Safety Part 2, Unit 2b, ‘Assessing radiation risks to the patient’ and ‘the biological effects of radiation’ were briefly described however in this unit there will be discussion on the effects of ionizing radiation at a cellular level and the resulting effects to the total body. You will then learn about the terms used to describe these effects.
Pre-requisite:
To understand the terms and units of radiation doses you are expected to have already studied Radiation Safety – Part 2, Unit 2a, Module 2,
Time Check:
Allow 6 hrs to study this subject and complete the exercises in your Workbook.

2
Objectives: This unit aims to inform the nuclear medicine technologist of the biological effects on the human body following exposure to ionizing radiation.
On completion of this unit you will: Understand the general functions of body organs and how inhaled and
ingested materials may eventually be deposited in them. Understand the basic structure of body cells and how direct and indirect
radiation can alter and damage them. Be able to identify and give examples of deterministic and stochastic
effects Be able to describe the possible effects of ionizing radiation on a
developing foetus, members of the public, radiation workers and in accident situations.

3
Introduction: The anatomy, physiology and pathophysiology of the major body organs will be described in detail in the clinical subjects of this course, however for the purpose of understanding the general effects of ionizing radiation on the human body this subject will only provide an overview of various bodily functions.
Objectives: On completion of this section you will be able to:
Describe the functions of the respiratory, digestive, circulatory, lymphatic and urinary systems of the body.
Explain how inhaled and ingested materials may eventually be deposited in body organs
General functions of the body:
The human body is affected by ionizing radiation from sources outside the body (an external source) and from radioactive materials which have entered the body (internal contamination). This is illustrated by Figure 1.
Internal Contamination
From radioactivematerial which has entered the
body.
External Radiation
From a source outside the body
Figure 1
External and Internal Radiation Hazards
For external sources to cause harm they must be able to penetrate the body and affect our cells. As alpha particles and low energy beta particles cannot penetrate the skin (unless through an open wound or through chemical absorption), only high energy beta particles, gamma rays, x-rays and neutrons present an external radiation hazard. This is further explained in Module 2, Unit 2b, Radiation Safety Part 2.
1. The Human Body

4
If radioactive materials are taken into the body either by inhalation, ingestion, through an open wound or through chemical absorption, they are in direct contact with cells and can therefore irradiate all of the cells surrounding them. In this case, alpha and beta particles are of most concern as they both have short ranges in biological tissue and will dissipate their energy in a small volume. This is further explained in Unit2a, Radiation Safety. However, when considering sources inside the body, it is important to have some knowledge of how the human body works and how radionuclides can become deposited in the various parts of the body. The human body is based around a bony structure called a skeleton, and consists of a number of functional units known as organs. The skin covers and protects the body and also helps to control body temperature and fluid balance. Within the body there are systems for the intake of air, food and water, the transport of material and removal of wastes. Knowledge of these systems is important as they are the means by which radionuclides may enter, be transported around and finally leave the body. These body systems are known as the respiratory, digestive, circulatory, lymphatic and urinary systems.
1.1 Respiratory system
The function of the respiratory system is to bring air close enough to the circulatory system so that oxygen can enter the blood and carbon dioxide can leave. The respiratory system consists of the nose, trachea, breathing bronchi and the lungs. The lung is full of small air sacs called alveoli which are surrounded by a network of blood capillaries (see Figure 2). This is where the exchange of gases occurs.
Nose
Bronchi
Trachea
Lung
Alveoli
Figure 2
The Respiratory System
In situations from industrial mining of uranium ore to lung ventilation studies in nuclear medicine, airborne radioactive materials (especially particulates) enter the body through inhalation and affect the lungs and other organs. The overall effect of the radioactive material is dependent

5
on the chemical and physical characteristics of the inhaled material, particularly the size of the particles and how easily they can be dissolved. If we now consider the whole process of inhalation and exchange of gases, we can see how the radioactive materials can become deposited in the body. Firstly, particles of dust can enter the body with the air we breathe. If the dust particles are large (>10m in diameter) most of them will be trapped in the upper parts of the respiratory system (e.g. the hairs in the nose) and do not enter the lungs. However, smaller dust particles are more likely to travel further into the respiratory system (see Figure 3).
Figure 3
The Process of Inhalation of Particulates
The dust particles will remain in the respiratory system until removed either physically by the sweeping action of fine hairs (cilia) lining the bronchi (aided by coughing) or chemically (e.g. by being dissolved). The removal of dust particles from the lungs by movement of the cilia and coughing is usually followed by swallowing. This means that inhaled material may end up in the digestive system. If the dust particles are soluble they will dissolve in the alveoli. The dissolved material enters the bloodstream and is transported to other areas of the body. Insoluble material will remain in the lungs or adjacent lymph nodes.
1.2 Digestive System
The digestive system is the means by which food and water are taken into the body and broken down so that they can be absorbed into the bloodstream. The digestive system is a continuous tube consisting of the mouth, oesophagus, stomach, small intestine and large intestine (see Figure 4).
Dust particles inhaled with air
Particles >10m removed by nose hairs
Particles 10m enter lungs
Particles removed from lungs by coughing
Particles go to digestive system
Soluble particles dissolve into blood stream
Particles transported to other areas of the body
Insoluble material remains in lungs or
nearby lymph nodes

6
Mouth
Oesophagus
Stomach
Small intestineLarge intestine
Liver
Figure 4 The Digestive System
During digestion, food is broken down into simple chemical compounds which are absorbed from the small intestine into the bloodstream and transferred via the liver to body tissues. The unabsorbed food has most of the water removed as it passes through the large intestine and is passed out of the body as solid waste (faeces). The digestive system is also a major route by which radionuclides may enter the body. Soluble radionuclides in food, water and other material entering the mouth (e.g. by chewing fingernails) will be absorbed into the bloodstream and transported to body tissue. Insoluble radioactive material will pass through the digestive system and be excreted in the faeces. The amount of radioactive material which enters the circulatory system depends on many factors including the chemical and physical characteristics of the ingested material.
1.3 Circulatory System
The circulatory system is the means by which material is transported throughout the body. The circulatory system consists of the heart and a network of arteries, capillaries and veins which carry blood throughout the human body. Red and white blood cells and a liquid called plasma are the main components of blood. The circulatory system carries oxygen and essential nutrients to all places in the body and takes waste products away for removal from the body. The circulatory system also is important for the body’s protection from infection as it carries the defensive and repair units to the source of the infection.
The circulatory system is the major mechanism by which radionuclides may be transported within the body. Radionuclides may enter the circulatory system directly (i.e. if the skin is broken due either to wounds or injection) or indirectly (via the respiratory or digestive systems). The part of the body to which radionuclides are transported depends on the chemical properties of the radionuclide. For example, calcium is extracted from our food and deposited in bone tissue. Elements which have similar chemical properties to calcium (e.g. strontium, barium and radium) will

7
also go to the bones whether the atoms are radioactive or not. Iodine is required by the thyroid gland in the neck so any intake of iodine will go to the thyroid. In fact, this aspect of radionuclide deposition is very useful for medical imaging and therapy purposes as particular radionuclides may be attached to a special chemicals so that they are transported to the region of interest in the body. Such substances are known as radiopharmaceuticals.
1.4 Lymphatic System
The lymphatic system is really a part of the circulatory system. It consists of a fluid, called the lymph, which fills all the spaces in body tissue, lymph vessels and numerous lymph glands or nodes (such as in the groin and under the arm). The lymphatic system has no central pump but relies on body movement to move fluid around. It is responsible for the transfer of material between the circulatory system and all cells of the body. It also plays an important part in protecting the body. Lymph nodes filter out substances like bacteria, small particles and even cancerous cells, preventing them from entering the blood system and spreading to other areas of the body. If the skin is broken, the lymphatic system is one of the means by which the radionuclide may be taken up by the body. The lymphatic system will transport the radionuclide within the local area of the wound prior to being taken into the blood and transported within the circulatory system.
1.5 Urinary System The urinary system is the primary means by which soluble radionuclides are removed from the body. The urinary system consists of the kidneys, the ureters, the bladder and the urethra (see Figure 5).
Kidney
Pelvis
Renal Vein
Urethra
Ureter
Renal artery
Bladder
ofkidney
Figure 5. The Urinary System
8
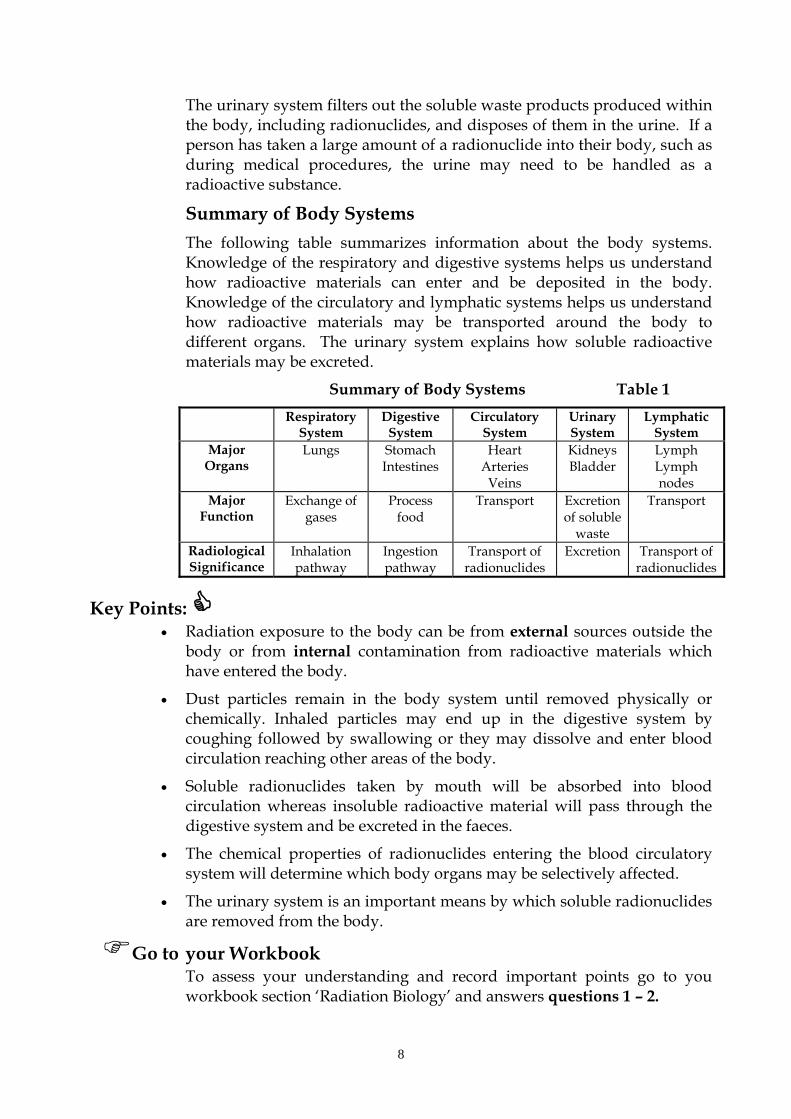
The urinary system filters out the soluble waste products produced within the body, including radionuclides, and disposes of them in the urine. If a person has taken a large amount of a radionuclide into their body, such as during medical procedures, the urine may need to be handled as a radioactive substance.
Summary of Body Systems
The following table summarizes information about the body systems. Knowledge of the respiratory and digestive systems helps us understand how radioactive materials can enter and be deposited in the body. Knowledge of the circulatory and lymphatic systems helps us understand how radioactive materials may be transported around the body to different organs. The urinary system explains how soluble radioactive materials may be excreted.
Summary of Body Systems Table 1
Respiratory System
Digestive System
Circulatory System
Urinary System
Lymphatic System
Major Organs
Lungs Stomach Intestines
Heart Arteries
Veins
Kidneys Bladder
Lymph Lymph nodes
Major Function
Exchange of gases
Process food
Transport Excretion of soluble
waste
Transport
Radiological Significance
Inhalation pathway
Ingestion pathway
Transport of radionuclides
Excretion
Transport of radionuclides
Key Points: Radiation exposure to the body can be from external sources outside the
body or from internal contamination from radioactive materials which have entered the body.
Dust particles remain in the body system until removed physically or chemically. Inhaled particles may end up in the digestive system by coughing followed by swallowing or they may dissolve and enter blood circulation reaching other areas of the body.
Soluble radionuclides taken by mouth will be absorbed into blood circulation whereas insoluble radioactive material will pass through the digestive system and be excreted in the faeces.
The chemical properties of radionuclides entering the blood circulatory system will determine which body organs may be selectively affected.
The urinary system is an important means by which soluble radionuclides are removed from the body.
Go to your Workbook To assess your understanding and record important points go to you workbook section ‘Radiation Biology’ and answers questions 1 – 2.

9
2. Cells and the Biological Damage from Radiation Introduction:
The different parts of the human body are made up of microscopic building blocks called cells. Cells which have the same function are grouped together to form tissue e.g. muscle tissue. Different tissues can group together to form an organ e.g. the heart. Organs group together to form body systems such as the systems considered in the previous section.
For the purpose of this unit ‘Radiation Biology’ we will briefly describe cell structure, division, repair and survival to help you understand how ionizing radiation can alter and damage cell function. However, in the course in Module 9; Unit 16a, ‘Introductory Human Biology’ you will learn in more detail the cellular level of organisation in bodily functions.
Objectives: On completion of the following section you will
understand the basic structure of body cells. be able to identify ionizing radiation exposures as either acute or chronic be able to describe the difference between direct and indirect radiation
damage to cells in terms of ionization, free radicals and damage to DNA.
Time Check: Allow 1.5 hrs to study this section and complete the exercises in your Workbook.
2.1 Cell Structure
Most body cells have three main parts: the cell membrane which forms the boundary of the cell. Materials move
in and out of the cell through the cell membrane. the nucleus which controls the functions of the cell, particularly growth
and division. the cytoplasm which is a fluid-like substance within the cell and contains
many of its functional parts. Most of the chemical changes taking place in a cell occur in the cytoplasm. The basic structure of a body cell is shown in Figure 6.
Cell membraneCytoplasm
Nuclear membrane
Nucleus

10
Figure 6 Basic Structure of a Body Cell
The nucleus in the human body contains 46 chromosomes which each consist of fine fibrous strands made up of genes. These genes are composed of proteins and small segment of deoxyribonucleic acid (DNA). This DNA carries all the genetic information about the physical and mental characteristics of a person. It also enables this information to be passed from one generation of cells to the next. [The picture on the left shows the structure of DNA strands]
The different parts of human body cells are summarised Table 2a.
Summary of Cell Structure Table 2a Cell Part Description
Cell membrane Allows the movement of material in and out of the cell.
Cytoplasm Where most chemical processes occur.
Nucleus Controls the cell.
Chromosomes Consist of fibrous strands of genes.
Genes Consist of proteins and DNA.
DNA Carries genetic information.
2.2 Cell Division A feature of most body cells is that they pass through a stage of reproduction during which they divide and form exact copies of themselves. Each cell divides to form two new ones and it is the chromosomes in the nucleus that are the main participants. Red blood cells do not have a nucleus and so are unable to divide. This means that new red blood cells must continuously be manufactured, a process that occurs in the bone marrow.
Remember
Cell division is a continuous process in some parts of the body such as the lining of the digestive tract. For adults cell division may take hours or even days. For a child or unborn baby it is more rapid and can be as short as about 20 minutes. If radiation damage to cells occurs at the phase of mitosis, which is the most sensitive cell cycle phase, the damage is likely to be more extensive. Hence young children and the unborn, because of more rapid cell division, are considered to be more at risk from the effects of radiation. For the same reason, cancerous tumours (rapidly dividing cells) are also more likely to be damaged by radiation than normal tissue.
Both male and females carry reproductive cells. In males these are known as sperm and in females they are known as the ova. They are manufactured in the reproductive organs or gonads (the testes in a male and the ovaries in a female). These cells only contain half the number of chromosomes (23 instead of 46) and during sexual reproduction, a sperm and ovum are joined to create a cell with 46 chromosomes. The

11
reproductive cells are important as they pass inherited characteristics onto the next generation.
2.3 Radiation Damage
To help you understand reactions to cells interfered with by ionizing radiation let us revise the structure of atoms. The human body is composed of many different types of cells. Cells are composed of many different types of molecules. Molecules consist of one or more atoms of one or more elements joined by chemical bonds. Atoms consist of a nucleus, neutrons, protons and electrons. In general the number of electrons is equal to the number of protons for any one atom. For example: the atom of oxygen has eight electrons circling around a center with eight protons. Since protons have a positive electrical charge, and electrons have a negative charge, this atom would be balanced, and have no charge. If one electron is taken away, there would then be seven electrons and eight protons -- providing a net positive charge. If you could add one extra electron to an oxygen atom, there would then be nine (negative) electrons and eight (positive) protons -- for a net negatively charged atom.
2.3.1 Cell damage
Radiation damage occurs when ionizing radiation interferes with the normal operation of a cell causing direct and indirect damage to the cell.
Direct damage occurs when radiation strikes a critical area of the cell (such as the DNA) and causes direct ionization in the molecule itself.
Indirect damage occurs as the result of the formation of very chemically reactive atom groups, called free radicals, within the cell.
What are ‘free radicals’?
Free radicals are atoms or groups of atoms that have at least one unpaired electron in the orbital position. Since electrons like to be paired with other electrons, this makes free radicals very reactive. To find a mate for its unpaired electron, a free radical (symbolized by a dot e.g. OH• or H•) will "steal" an electron from a nearby molecule, thus leaving the nearby molecule with a single electron. To fix this, the nearby molecule will steal an electron from yet another molecule. This turns into a chain of chemical reactions, that damages each new molecule that has an electron stolen from it. This can be especially bad if one of those molecules is a molecule of DNA.
About 80% of the cell is water. When radiation ionizes water molecules the ions formed interact with other water molecules.

12
Initial Phase:
H2O radiation H2O+ + e’
Second Phase:
H2O+ H+ + OH• or: H2O + e’ H2O’
H2O’ H• + OH’
Two of the products formed, H• (hydrogen free radical) and OH• (hydroxyl free radical) are very reactive because they have unpaired electrons. Another reaction product in the cell is hydrogen peroxide (H2O2) which is also very reactive. OH• + OH• H2O2
These reactive atom groups can interfere with normal cellular processes by breaking chemical bonds such as the bonds between carbon atoms in the DNA molecule. In living systems, the hydroxyl free radical does not normally occur, because of the strength of the bonds holding the water molecules together. But if anyone is exposed to radiation, these bonds can be broken by the radiation so that hydroxyl radicals result. This is the basis of the dreadful, often fatal, damage that occurs in people with radiation sickness. If hydroxyl radicals attack DNA, chain reactions run along the DNA molecule causing damage to, and mutations in, the genetic material or even actual breakage of the DNA strands. The body does its best to repair this damage by the natural processes of DNA replication, but imperfect repair leaves altered DNA and can give rise to cancer. When strong X- and gamma radiation is deliberately used to kill cancers, it does by producing large numbers of hydroxyl free radicals.
Note !
Free radicals promote beneficial oxidation that produces energy and kills bacterial invaders. In excessive amounts, however, they produce harmful oxidation that can damage cell membranes and cell contents.
Radiation is not the only way free radicals are produced, and free radicals are not only produced from water. But radiation is the only common way that hydroxyl free radicals are formed in the body from water. Unfortunately, there are other ways in which hydroxyl radicals can be formed and there are several other kinds of free radicals, especially the super-oxide radical, that can be produced in other ways. They are produced by many disease processes, by poisons, drugs, metals, cigarette smoke, car exhausts, heat, lack of oxygen, even by sunlight. Free radicals may also cause damage to enzymes (chemicals which are important for the functioning of the cell) or to membranes (affecting transport of materials). This sequence of events is summarized in the diagram below.
13
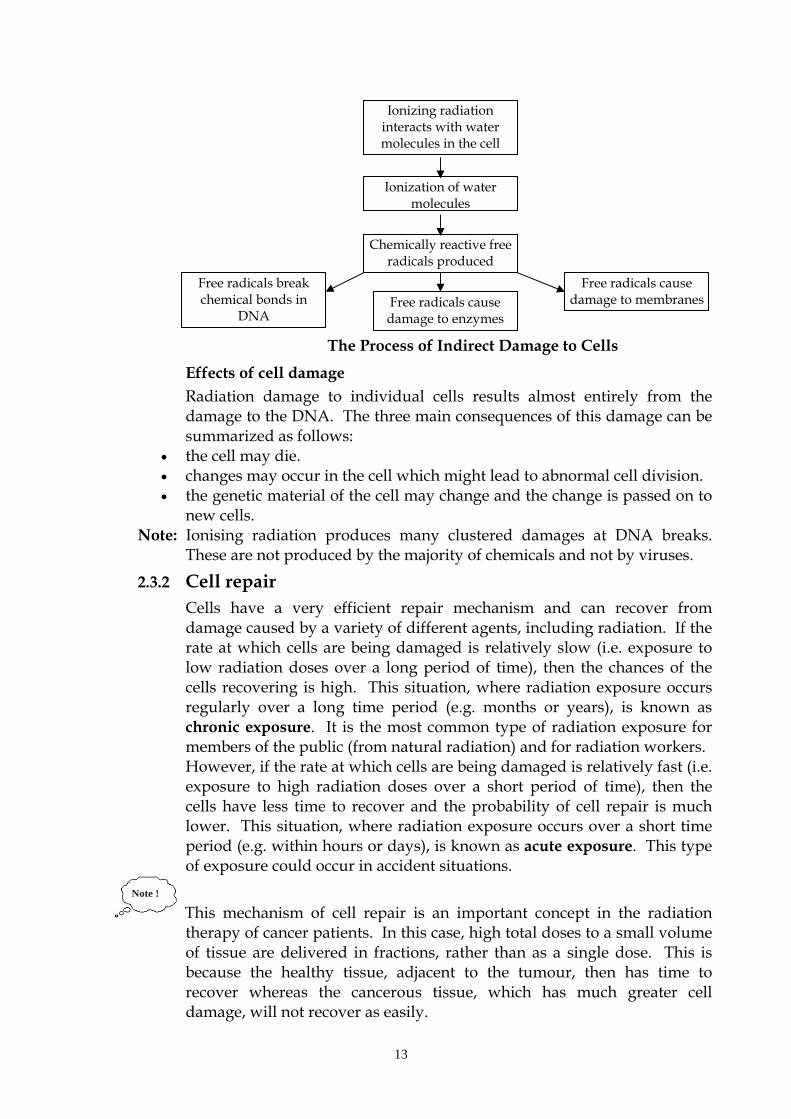
The Process of Indirect Damage to Cells
Effects of cell damage Radiation damage to individual cells results almost entirely from the damage to the DNA. The three main consequences of this damage can be summarized as follows:
the cell may die. changes may occur in the cell which might lead to abnormal cell division. the genetic material of the cell may change and the change is passed on to
new cells. Note: Ionising radiation produces many clustered damages at DNA breaks.
These are not produced by the majority of chemicals and not by viruses.
2.3.2 Cell repair
Cells have a very efficient repair mechanism and can recover from damage caused by a variety of different agents, including radiation. If the rate at which cells are being damaged is relatively slow (i.e. exposure to low radiation doses over a long period of time), then the chances of the cells recovering is high. This situation, where radiation exposure occurs regularly over a long time period (e.g. months or years), is known as chronic exposure. It is the most common type of radiation exposure for members of the public (from natural radiation) and for radiation workers. However, if the rate at which cells are being damaged is relatively fast (i.e. exposure to high radiation doses over a short period of time), then the cells have less time to recover and the probability of cell repair is much lower. This situation, where radiation exposure occurs over a short time period (e.g. within hours or days), is known as acute exposure. This type of exposure could occur in accident situations.
Note !
This mechanism of cell repair is an important concept in the radiation therapy of cancer patients. In this case, high total doses to a small volume of tissue are delivered in fractions, rather than as a single dose. This is because the healthy tissue, adjacent to the tumour, then has time to recover whereas the cancerous tissue, which has much greater cell damage, will not recover as easily.
Ionizing radiation interacts with water molecules in the cell
Ionization of water molecules
Chemically reactive free radicals produced
Free radicals break chemical bonds in
DNA Free radicals cause damage to enzymes
Free radicals cause damage to membranes
14
2.4 Cell Survival:
A cell is said to have retained its reproductive integrity if it is capable of sustained proliferation, that is, if it can grow into a macroscopic colony of 60 cells or more. A survivor that has retained its reproductive integrity is said to be clonogenic. Some cells also die by apoptosis without attempted division. For differentiated cells that do not proliferate, such as nerve muscle or secretory cells, huge doses of radiation are needed to cause them to be unable to function.
Go to your Workbook and answer questions 3 – 7 to record your understanding of this section
Key Points: Most body cells reproduce through division and form 2 cells.
Red blood cells do not have a nucleus and can not divide but are manufactured in the bone marrow.
Cells ‘die’ only when they attempt to divide.
Radiation damage to cells is more extensive if it occurs during cell division.
As cell division is more rapid in young children and unborn than in adults so they are considered more at risk from effects of radiation.
Cancerous tumours have rapidly dividing cells and are more likely to be damaged by radiation than normal tissue.
Direct damage causes direct ionization in the molecule Indirect damage occurs as a result of formation of ‘free radicals’ within
the cell.
Some free radicals are formed when water within a cell is ionized.
Free radicals can attack and alter DNA which can lead to cancer.
Chronic exposure: exposure due to low radiation doses over a long period of time - high chance of cell recovery or repair
Acute exposure: exposure to high a radiation dose over a short period of time - cells have less time to recover and lower probability of cell repair
Mechanism of cell repair is an important concept for radiation therapy.

15
3. Radiation Exposure to the Human Population
Introduction:
The potential hazards associated with ionizing radiation were recognised soon after the discovery of X-rays by Roentgen in 1895 and of radioactive materials by Bequerel in 1896. One of the earliest published records of radiation injury was by Thomas Edison, who reported that he and an assistant suffered severe smarting of the eyes after working with an X-ray tube.
Since then radiological and epidemiological research has led to the development of radiation protection standards, which take age, gender and type of exposed tissue into consideration. The effect of ionizing radiation on the biologic system is often not predictable and this is related to several factors among which are total radiation dose, dose rate, radiation quality and several other environmental factors. Research has also been concerned with genetic (heritable) as well as somatic effects.
The following section will compare various sources of radiation, discuss the effects on humans and the response of body tissues and organs to ionizing radiation.
Objectives: On completion of this section you will be able to:
Identify various sources of radiation to which the general population is exposed.
Describe the somatic effects of radiation exposure to specific body organs. Describe differences between deterministic and stochastic effects List body organs in increasing radiosensitivity by analysis of a list of
tissue weighting factors Explain the effects of ionizing radiation on a developing foetus. Describe signs and symptoms of the prodromal radiation syndrome.
Time Check:
Allow 3 hrs to study the following section and answer questions in your Workbook.
3.1 Doses from natural background radiation
Natural sources of radiation include cosmic rays from outer space, terrestrial radiation from natural radioactive materials in the ground, and radiation from radionuclides naturally present in the body, inhaled, or ingested. The sources of natural background radiation are illustrated in Figure 7.
Enhanced natural sources are sources that are natural in origin but to which exposure is increased as a result of human activity. An example of an enhanced natural source is air travel at high altitude.

16
Our BodiesPlants
Radioactive Soil and Rocks Indoor Radon
Figure 7: Radiation is everywhere!
There are three principle components of natural background radiation: 1. cosmic rays from solar flares in the sun or from outer space; 2. ingested radioactivity, principally potassium-40 in food, and inhaled
radioactivity, principally radon. 3. radiation from the Earth's crust, which in practice means from building
materials because most persons spend much of their lives indoors.
Cosmic radiation
Cosmic rays are made up of radiation originating from outside the solar system and from charged particles (largely protons) emanating from the surface of the sun. The intensity of cosmic rays arriving at the earth’s surface varies with both latitude and altitude above sea level. The variation with latitude is a consequence of the magnetic properties of the earth. Consequently, cosmic-ray intensity is least in equatorial regions and rises towards the poles (it is this radiation arriving at the poles which gives rise to the spectacular flickering lights of the Aurora Borealis and Aurora Australis see Figure 8). There is an even larger variation in cosmic-ray intensity with altitude, because at high elevations there is less atmosphere to absorb the cosmic rays, and so intensity is greater.
Natural radioactivity in the earth’s crust
Naturally occurring radioactive materials are widely distributed throughout the earth’s crust, and as a consequence, humans are exposed to the rays from them. There is a big variation between rocky land masses, where the stones and soil contain radioactive thorium and uranium, and areas under the ocean, where radioactivity is low

17
Figure 8: Aurora Borealis as seen from Aberdeen, Scotland
(The “Northern Lights”).
Man-made radiation sources
There are various sources of radiation to which the human population is exposed which result from human activity. In developed countries the effective dose is dominated by medical radiation. Radiation dose from medical procedures has for the first time in history overtaken all other sources, both natural and man-made, as the most important contributor to exposure of humans. Diagnostic imaging is by far the largest contributing factor, with CT and molecular imaging alone contributing 75 percent of total medical radiation exposure. As an indication of the magnitude of this dose, the population radiation risk from diagnostic imaging in the USA is equivalent to two Chernobyl, or twenty Fukushima, nuclear reactor accidents every year! For individual patients undergoing diagnostic imaging procedures, the benefits will generally far outweigh the risks; the above facts, however, do stress the extreme importance of radiation monitoring, regulation and control.
Internal Exposure
Small traces of radioactive materials are normally present in the human body, ingested from the tiny quantities present in food supplies or inhaled as airborne particles. The biggest source of natural background radiation is radon gas, which seeps into the basement of houses from rocks underground. It is a decay product in the uranium series. Radon itself is a noble gas that does little harm, but in the confined space of an underground mine or basement of a house, it decays with a 3-day half-life to form solid progeny that stick to dust particles and if inhaled become lodged on the surface of the bronchus or lung.
Radon progeny emit particles that, it is believed, can cause lung cancer.

18
Comparison of radiation doses from natural sources and human activities The exposure of the human population to a variety of sources of radiation resulting from human activity is given in the table below. The average annual effective dose from all sources amounts to 2.8 mSv.
Table 2b Average per capita annual effective doses from various natural and
man‐made radaition sources. Adapted from data by UNSCEAR and Clarke
AVERAGE PER CAPITA ANNUAL DOSE
EFFECTIVE DOSE (mSv per Year)
SOURCE MEAN RANGE
Natural background
Cosmic radiation 0.36 0.2 ‐ 0.5 (a)
Terrestrial radioactivity 0.42 0.2 ‐ 20 (b)
Internal radioactivity 0.36 (c)
Radon in dwellings 1.26 0.5 ‐ 100
Total from natural background 2.4
Man Made Sources
Diagnostic X‐rays 0.28
Nuclear medicine 0.11
Consumer products 0.1 (e)
Weapons fall‐out <0.01 0.08 in 1960ʹs (d)
Occupational <0.01
Nuclear fuel cycle <0.01
Total from man made sources 0.4
Notes:
(a) Cosmic radiation dose varies with latitude and altitude. The maximum of
the range corresponds to an altitude of about 1500 metres at middle latitudes.
(b) Very high values up to about 20 mSv per year are measured on thorium
beach sands in Kerala, India. 70,000 people live in this area, 25% receiving
more than 5 mSv per year, 9% more than 10 mSv per year, and 1% more than 20
mSv per year.
(c) This is largely due to potassium‐40, a naturally occuring radionuclide (half‐
life 1.3 x 109 years) found in all potassium. An average man contains about 140g
of potassium located mostly in muscle tissue.
(d) Fall‐out from nuclear weapons tests varies with latitude and differs between
hemispheres; it has been decreasing since the cessation of atmospheric testing in
the 1960ʹs.
(e) Miscellaneous consumer sources include:‐
‐ luminous dials (mostly watches) 0.01 ‐ 0.05 mSv per year;
‐ TV watching (children) 0.004 mSv per year;
‐ jet travel 0.007 mSv per hour.

19
There are several conclusions. 1) radon represents the largest source of radiation to the general population. 2) medical diagnostic x rays represent by far the largest source of radiation
resulting from human activities. 3) the overall effective dose from medical radiation is about equal to that
from natural background, excluding radon, and only about a quarter of the total effective dose to which the population is exposed if radon is included.
Somatic effects of radiation on humans
As you have already learnt, ionizing radiation acts on the cells of the human body. If the cells do not repair themselves, permanent effects of radiation damage can be seen as biological changes in tissues and organs. These changes may be manifested as medical symptoms which are classified into two mechanisms of action, somatic stochastic (nondeterminant) effects and somatic deterministic (certainty). These effects are of particular concern in the case of the developing foetus.
3.2 Deterministic Effects
The most common result of radiation damage is for the cell to die. If only a few cells are affected, it is not usually a problem as there are many cells in the body and new cells will replace the dead cells. However, as the amount of radiation absorbed (i.e the dose increases), a point will be reached where sufficient cells are killed to affect the overall operation of the organ. The result of this is a loss of organ function which will become more serious as the number of affected cells is increased. The different types of radiation damage resulting from tissue injury such as erythema are known as deterministic effects. These effects are characterised by having a threshold dose, below which there is no observable effect, followed by a response where the severity of the effect increases with increasing radiation dose (see Figure 8).
Threshold dose
Dose
Severity of Effect
Figure 9: Deterministic Dose Response Curve
An example of a deterministic effect is erythema or skin reddening. Exposure to a low dose of ionizing radiation, below the threshold dose,
20
will not cause the skin to redden. If the dose is increased to a value just above the threshold dose the skin will redden, in the same way that fair skinned people experience mild sunburn. If the dose is increased further, blistering will occur (like severe sunburn) and higher doses will result in death of the skin tissue and ulceration.
3.2.1 Response of skin to radiation.
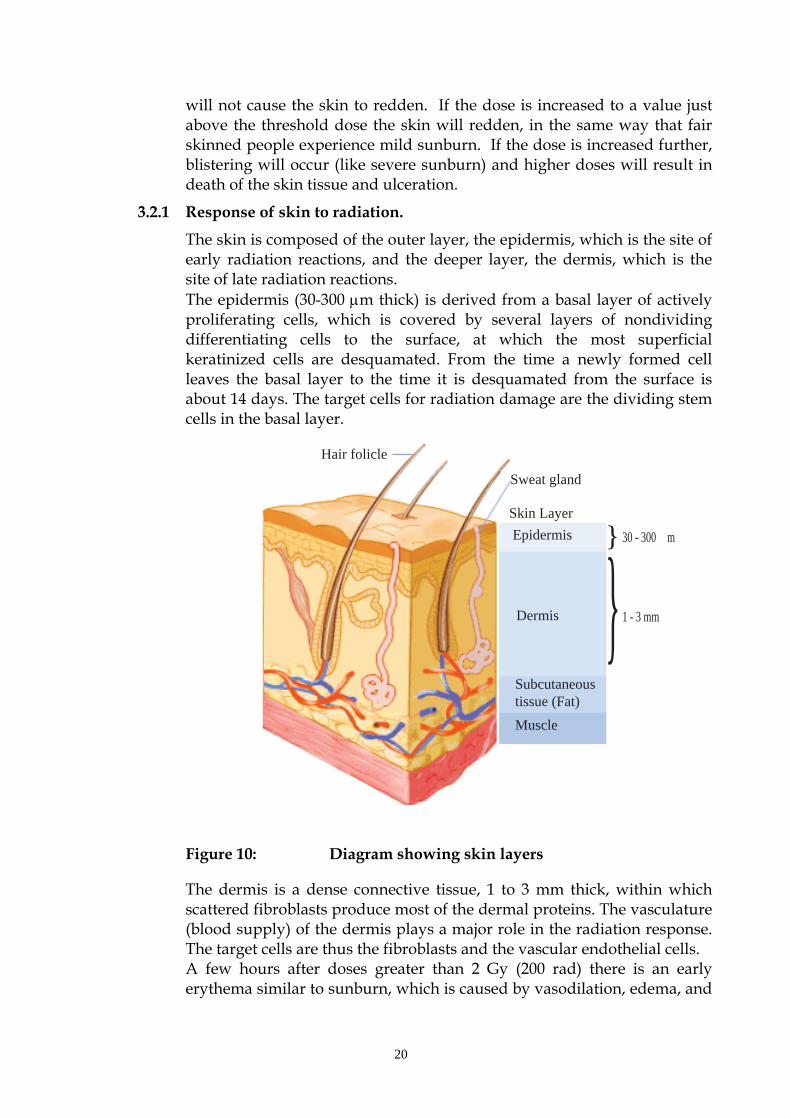
The skin is composed of the outer layer, the epidermis, which is the site of early radiation reactions, and the deeper layer, the dermis, which is the site of late radiation reactions. The epidermis (30-300 m thick) is derived from a basal layer of actively proliferating cells, which is covered by several layers of nondividing differentiating cells to the surface, at which the most superficial keratinized cells are desquamated. From the time a newly formed cell leaves the basal layer to the time it is desquamated from the surface is about 14 days. The target cells for radiation damage are the dividing stem cells in the basal layer.
Hair folicle
Sweat gland
Skin Layer
Epidermis
Dermis
Subcutaneoustissue (Fat)
Muscle
}
}30 - 300 m
1 - 3 mm
Figure 10: Diagram showing skin layers
The dermis is a dense connective tissue, 1 to 3 mm thick, within which scattered fibroblasts produce most of the dermal proteins. The vasculature (blood supply) of the dermis plays a major role in the radiation response. The target cells are thus the fibroblasts and the vascular endothelial cells. A few hours after doses greater than 2 Gy (200 rad) there is an early erythema similar to sunburn, which is caused by vasodilation, edema, and

21
loss of plasma constituents from capillaries. Reactions resulting from stem cell death take longer to develop.
Examples of skin responses following a course of radiation therapy include:
Initial erythema develops in the second to third week of a fractionated regimen of radiation therapy,
followed by dry or moist desquamation resulting from depletion of the basal cell population. At lower doses, islets of skin may regrow from surviving stem cells.
At higher doses, at which there are no surviving stem cells within the area treated, moist desquamation is complete, and healing must occur by migration of cells from outside the treated area.
The clinical appearance of radiation fibrosis results from atrophy leading to contraction of the irradiated area.
Skin appendages are a special case. Within a few days after irradiation, the death of germinal cells results in hair dysplasia (i.e., short, thin hair). The proportion of dysplastic hair is dose-dependent. Epilation (hair loss) occurs during the third week, and regrowth may occur after 1 to 3 months. Sebaceous glands are as sensitive as hair, but sweat glands are less radiosensitive. Regenerated skin may be dry and hairless.
While these effects are common-place in radiation oncology, where large doses are used in the treatment of malignant disease, observable skin reactions are only seen in a diagnostic setting following prolonged (or repeated) fluoroscopy during interventional radiology. One of the most common factors in injuries reported so far occur in the more obese or muscular the patient, who experience more chance of injury as exposure factors are automatically increased by the X-Ray machine. Erythema is not uncommon, while even a few cases of necrosis have been reported.
3.2.2 Response of the Gastro – Intestinal tract to radiation
The lining of the gastro-intestinal (G.I.) tract is a classic example of a self-renewal system. The cells in the crypts divide rapidly and provide a continuous supply of cells that move up the villi, differentiate, and become the functioning cells. The cells at the top of the folds of the villi are slowly but continuously sloughed off in the normal course of events and are replaced continuously by cells that originate from mitoses in the crypts.

22
A
Longitudinal
Circular
Submucosa Crypts
Villi
muscle
muscle
B
crypt
villi
Figure 11: A. Cross section of large intestine B. magnified section
A large dose of radiation will sterilize a significant proportion of the dividing cells in the crypts but has essentially no effect on the differentiated cells in the villi. Consequently, crypt degeneration appears early after irradiation, and the villi remain long and their epithelial covering of differentiated cells shows little change. With the further passage of time, the tips of the villi continue to be sloughed away by normal use but no replacement cells are available from the depopulated crypts, and so the villi begin to shorten and shrink. At sufficiently high doses the surface lining of the jejunum is completely denuded of villi. This can be fatal, death occurs 9-10 days later. There were examples of death by this mechanism in the workers at Chernobyl. While all of the GI tract is sensitive to radiation, the small intestine is the most sensitive.
Cataract Induction.
The lens of the eye differs from other organs in that dead and injured cells are not removed. Recent analyses of Chernobyl data have indicated that, for protracted exposures, the threshold for opacity and cataract induction may be as low as 1 Sv (100 rem). Although this is unlikely to be a problem for nuclear medicine workers, it may well have an impact on radiologists and other workers performing interventional fluoroscopic procedures.
Fertility effects.
The cells of the reproductive system are highly sensitive to radiation effects.
In the human male, stem cells and proliferating spermatogonia (male germ cells) are highly sensitive. However, spermatids (developing sperm cells) and mature sperm show considerable resistance. With a turnover time for the spermatognesis (stem cell to mature sperm) of 64 – 72 days, sterility is never seen immediately after the radiation dose, because mature sperm are resistant to the killing effects of radiation. However, they can sustain heritable genetic damage. Doses of a few Sv to the human testes can lead to permanent sterility; smaller doses cause only temporary reduction in the number of sperm cells.

23
In the female, radiation destroys both ovum and maturing follicles. This reduces hormone production. Therefore radiogenic sterility in females can be accompanied by artificial menopause with significant effects on sexual characteristics. A single dose of 4 Sv (400rem) to the ovaries is required to produce permanent sterility; at 0.5 Sv (50 rem) temporary amenorrhea can occur. Younger women seem better able to recover fertility than do older women.
Note !
The effect of radiation dose on a particular person depends on genetic and biological factors (e.g. age and general health) as well as on chemical factors (e.g. the amount of oxygen present in tissue). Therefore in any population there will be a range of sensitivity to radiation. Hence, the threshold dose in a given tissue will be reached at lower doses in more sensitive individuals. As the dose increases more individuals will show the effect, up to a dose above which all exposed people will show the effect. Deterministic effects are most often seen in cases of high doses of radiation delivered in a short period of time (i.e. in the case of acute exposure). Other than for controlled medical exposure, high doses are not usual in the workplace. Hence deterministic effects are only seen in accident situations and do not occur routinely in the workplace.
Remember
Deterministic effects do not occur routinely in the workplace. They are the result of accident situations. Table 3 shows the deterministic effects to specific organs which occur following an acute exposure. Note that the doses in the table are given in units of millisieverts (mSv). The definition of these dose units are explained in Radiation Safety Part 2, Unit 2b, Module 2. Effects of Acute Exposures to Specific Organs Table 3
Most of the effects shown in Table 3 are classed as early effects as they are normally observed within a few days or weeks of exposure. The exception to this is the formation of cataracts following irradiation of the eye. This effect takes several years to develop and is therefore classified as
Dose (mSv)
Organ Effect
3 500 Testes Permanent sterility 1000 Eye Cataracts and lens opacities 3 000 Ovaries Sterility
2 500+ Skin Skin reddening (erythema) and possible permanent hair loss
500 Bone marrow Reduced blood cell formation 150+ Testes Temporary sterility
60 Foetus Probable minimum dose causing effect (possible malformation)

24
a late effect. It is still a deterministic effect because there is a threshold dose below which cataracts will not occur.
The severity of the deterministic effects mentioned in Table 3 depends on the size of the dose and the period over which the dose was received. In fact, if the dose is received over several weeks rather than all at once, the threshold dose at which the effect occurs increases considerably, usually by about 100%. Very high doses of radiation to the whole body can cause sufficient damage to the organs to stop their function and this may ultimately cause death. Radiation sickness (nausea, vomiting diarrhoea) is an early deterministic effect resulting from an acute high dose to the whole body. Other effects resulting from acute exposure to the whole body are shown in Table 4.

25
Effects of Acute Whole Body Exposure to Radiation Table 4
Dose (mSv)
Effect
50 000+ Severe damage to central nervous system rapidly lethal. 8 000 - 50 000 Destruction of lining of intestine and white blood cells
death within two weeks. 4 000 Fatal for half those irradiated within 30 days without
medical treatment. 2 000 - 8 000 Damage to white blood cells and gut lining. Death may
result from secondary infection but can be avoided in many cases with special medical treatment.
1 000 - 2 000 Possible radiation sickness nausea, vomiting, diarrhoea not lethal.
3.3 Stochastic Effects
Sometimes, the effect of radiation is not to kill the cell but to alter it in some way. In most cases this alteration will not affect the cell significantly so there will be no observable effect. However there is a possibility that the injury might affect the control system of the cell, subsequently causing it to divide more rapidly than normal. If the affected cell does begin to divide in this way, an increasing number of abnormal daughter cells will be produced. If these abnormal cells invade normal tissue they are called malignant cells and this results in cancer. The type of cancer formed is dependent on the type of the original cell which was altered. Cancers do not appear immediately after radiation exposure but appear after a latency period in which no effects are observable. The latency period is dependent on the type of cancer but can vary from two years for leukemia to thirty years or possibly longer for some solid cancers. For this reason the concept of latency has been replaced by a combination of “age at exposure” and “time since exposure”. Hence, cancer is classified as a late effect.
Unlike deterministic effects, the amount of radiation exposure does not change the severity of the cancer but it does alter the chance of getting cancer. In other words, exposure to a high dose can increase the risk of getting a cancer but if cancer occurs (whether it be at low or high dose) the severity of the cancer is the same. This is rather like a lottery prize in that even a single ticket could win the first prize but the more tickets you buy the more chance you have of winning. However, the value of the prize does not change. Effects of ionizing radiation which rely on chance are referred to as stochastic effects.
For the purposes of radiation protection, it is assumed that the probability of a stochastic effect increases linearly as the dose increases and that there is no threshold dose; however, there is still much scientific debate regarding the exact shape of the dose-response curve at the relatively low doses experienced in medical imaging (see Figure 12). If there is no

26
threshold dose then it is considered that even small doses of radiation might cause cancer.
Figure 12 Stochastic Dose Response Curve
Remember
Stochastic effects are the only effects possible at low doses and hence, radiation protection is aimed at preventing deterministic effects and reducing the chances of stochastic effects occurring. The risk of stochastic effects is the primary reason for limiting doses to both the public and radiation workers.
3.3.1 Hereditary Effects Some facts about the hereditary effects of radiation:
Exposure of a population can cause adverse health effects in the descendants as a consequence of mutations induced in germ cells.
Hereditary diseases are classified into three principal categories: Mendelian, chromosomal, and multifactorial.
Radiation does not produce new, unique mutations but increases the incidence of the same mutations that occur spontaneously.
Information on the hereditary effects of radiation comes almost entirely from animal experiments.
If one of the reproductive cells (either the sperm or the ovum) is damaged by ionizing radiation, there is a chance that this damage may affect either the immediate child or subsequent generations. This type of effect is therefore known as a hereditary effect. Hereditary effects are based on chance and hence are stochastic. However, the risk of hereditary effects is much lower than the risk of cancer.

27
Experimental studies on plants and animals have shown that hereditary effects can occur after exposure to large doses of radiation. However, there have been no cases identified in humans where radiation has resulted in hereditary effects.
Note !
Hereditary effects from exposure to ionizing radiation have not been identified in humans.
3.3.2 Radiation Carcinogenesis Radiation carcinogensis is a stochastic effect. Cancer induction is the most important somatic effect of low-dose ionizing radiation. In sharp contrast to the case for the hereditary effects of radiation, risk estimates for leukemogenesis and carcinogenesis do not rely on animal data but can be based on experience in humans. The human experience of radiation-induced carcinogenesis includes the survivors of the atomic-bomb attacks on Hiroshima and Nagasaki in Japan, patients exposed to medical irradiation, and early workers exposed occupationally. Some examples include:
Leukemia and solid tumors in Japanese survivors of the atomic bomb Leukemia in patients irradiated for ankylosing spondylitis Thyroid cancer in children irradiated for benign conditions of the head
and neck, such as enlarged thymus or tonsils, and children who suffered hair loss following treatment for ringworm of the scalp.
Breast cancer in patients treated with x-rays for postpartum mastitis and patients who had repeated fluoroscopy during the management of tuberculosis
Lung cancer in uranium miners Bone cancer in painters of luminous watch-dial dials who licked their
paintbrushes and thus ingested radium and patients who had injections of radium for tuberculosis or ankylosing spondylitis
Figure: 13 Marie Curie (seated) at work with Irene Curie, her daughter.
Both Marie Curie (left) and her
daughter Irene Curie (right) died
from leukaemia almost certainly
induced by radiation from handling
radioactive materials.

28
Both Marie and Irene Curie are thought to have died of leukemia as a result of the radiation exposure they received during their experiments with radioactivity.
The belief that stochastic effects have no dose threshold is based on the molecular mechanisms involved. There is no reason to believe that even a single x-ray photon could not result in a base change leading to a mutation that could cause cancer or a hereditary defect. For this reason it is considered prudent to assume that no dose is too small to be effective. For this reason the concept of latency has been replaced by a combination of “age at exposure” and “time since exposure”. Hence, cancer is classified as a late effect.
Assessing the Risk
To determine risk estimates for radiation-induced cancer from observed data (the Japanese atomic-bomb survivors), a model must be assumed because: Data must be projected out to a full lifespan, because no exposed
population has yet lived out its lifespan; Data must be extrapolated from high to low doses; Risks must be “transferred” from (for example) a Japanese to Western
population with different natural cancer rates.
There are two principal risk models.
1. The absolute risk model assumes that radiation produced a discrete “crop” of cancers, over and above the spontaneous level and unrelated to the spontaneous level.
2. The relative risk model assumes that radiation increases the spontaneous incidence by a factor. Because the natural cancer incidence increases with age, this model predicts a large number of excess cancers appearing late in life after irradiation.
The International Commission on Radiological Protection (ICRP) estimates that, on average, 13 to 15 years of life are lost for each radiation-induced cancer and that death occurs at age 68 to 70 years.
Importantto
Remember
The risk of radiation-induced cancer varies considerably with age at the time of exposure. The overall risk drops dramatically with age; children and young adults are much more susceptible to radiation-induced cancer than the middle-aged and old.
3.4 Tissue weighting factors
Some organs or tissue are more sensitive to radiation than others and will have an increased probability of developing stochastic effects. Also some cancers are more likely to result in death or serious problems than others. Hence, when determining the overall effect of ionizing radiation on

29
humans, a factor known as the tissue weighting factor (wT) is applied. Basically, this factor takes into account the varying radiosensitivity of organs and tissues and the severity of the resulting cancer. The values for radiation weighting factors given in Table 5 have been recommended internationally in ICRP Report Number 103. The higher the value of the weighting factor, the greater is the probability of serious stochastic effects occurring following a specific exposure. Although different people respond to radiation doses differently the radiation weighting factors are approximated so that they can be applied to everybody.
Note: The total of all radiation weighting factors for all tissues and organs adds up to give a whole body exposure factor of 1.
Weighting Factors for Human Tissues and Organs Table 5
Organ/Tissue Number of wT Total Tissues Contribution Lung, stomach, colon 6 0.12 0.72 bone marrow, breast remainder Gonads 1 0.08 0.08 Thyroid, oesophagus, 4 0.04 0.16 bladder, liver Bone surface, skin, brain 4 0.01 0.04 salivary glands 1. The wT for gonads is applied to the mean of the doses to testes and
ovaries 2. The dose to the colon is taken to be the mass-weighted mean of ULI and
LLI doses, as in the Publication 60 formulation. The specified remainder tissues (14 in total, 13 in each sex) are: Adrenals, extrathoracic tissue (ET), gall bladder, heart, kidneys, lymphatic nodes, muscle, oral mucosa, pancreas, prostate (♂), small intestine (SI), spleen, thymus, uterus/cervix (♀).
The above values imply that the probability of serious stochastic effects from lung exposure is three times higher than that from the thyroid (0.12 divided by 0.04 equals 3).
3.5 Exposure of the Foetus In a foetus, or unborn child, the number of cells is less than in the adult and the cells are rapidly dividing. As radiation damage is more extensive on dividing cells, the foetus is particularly sensitive to radiation damage and exposure to high doses could result in possible malformation or even death. For this reason and because it is possible that exposure to radiation at any
30
time in pregnancy may increase the probability of cancer in the child, special radiation protection measures are necessary to protect the foetus Research on the biological effects of ionizing radiation on developing foetus has mainly concentrated on the Hiroshima and Nagasaki bomb victims as well as the Chernobyl accident in 1986. These studies have indicated that exposure to radiation during the first two weeks of pregnancy has not resulted in deterministic or stochastic effects to the child.
Moderate doses of radiation can produce catastrophic effects on the developing embryo and foetus. In determining the effects of radiation on a developing embryo or foetus, the principal factors of importance are the dose and the stage of gestation at which the dose is delivered. Dose rate is also a factor, since many pathologic effects on the embryo are reduced significantly by reducing the dose rate.
Gestation in humans is divided into
Preimplantation - 0 through 9 days Organogenesis - 10 days through 6 weeks foetal period - 6 weeks through term The principal effects of radiation on the developing embryo and foetus are: growth retardation; embryonic, neonatal, or foetal death; congenital malformations; functional impairment, such as mental retardation.
The foetal thyroid, which starts to concentrate iodine at about the 12th week of pregnancy, can be damaged if it is exposed to iodine-131. Radioactive iodine-131 is widely used for treatment of hyperthyroidism and thyroid cancer. Typically, a therapeutic treatment results in a total-body dose of 50 to 150 mGy (5-15 rad) from the isotope circulating in the blood. Pregnancy is, of course, a contraindication to the treatment with iodine-131. Treatment should be delayed, if possible, to eliminate the potential effects during pregnancy. Additionally, one must consider that the foetal thyroid begins to function after ten to twelve weeks of pregnancy and that by the third trimester the foetal thyroid avidly takes up iodine.
Importantto
Remember
For these reasons, radionuclide therapy or scans using 131I must not be given to pregnant women.
Radiation protection and the pregnant worker
When a pregnancy is declared, the maximum permissible dose to the abdomen of the mother is 2 mSv (200 mrem) over the remainder of the pregnancy. Until a pregnancy is declared, no special limits apply to the mother other than those applicable to any radiation worker.

31
When a pregnancy is declared, the duties of a radiation worker should be reviewed to ensure that this limit is not exceeded.
A dose of 0.1 Gy (10 rad) to the embryo during the sensitive period of gestation (10 days to 26 weeks) often is regarded as the cut-off point above which a therapeutic abortion should be considered to avoid the possibility of an anomalous child. The recommendation to terminate a pregnancy should be flexible and must depend on many factors in addition to dose.
Patient / Personnel Exposure; Risk-Benefit
Irradiation in the foetal period leads to the greatest degree of permanent growth retardation The radiation doses involved in diagnostic radiology, other than interventional procedures, are seldom sufficiently large to result in immediate deterministic effects. The one exception is irradiation of the developing embryo or foetus, of which a possible consequence is reduced head diameter (microcephaly) and mental retardation. This is usually considered to be a "deterministic effect"; that is, it requires damage to a large number of cells, there is a practical dose threshold, and the severity of the response increases with dose. The threshold for radiation-induced mental retardation, thought to be 0.1 to 0.2 Gy (10-20 rad), is such that few procedures are likely to cause this effect.
Note !
Some of the largest doses in diagnostic radiology are associated with fluoroscopy and often the dose rate is greatest at the skin, where the x-ray beam first enters the patient. It is not difficult to understand why CT scans involve relatively larger effective doses because larger volumes of tissue are exposed to higher doses than with common X-rays. Surveys have emphasized wide variations in dose with different model scanners and different techniques. However, in general, effective doses from typical procedures are in the range of 2 to 4 mGy (200- 400 mrad) for head scans and 10 to20 mGy (1-2 rad) for body scans.
3.6 Whole-Body Radiation Effects Soon after irradiation, early symptoms appear, which last for a limited period of time; this is referred to as the prodromal radiation syndrome. The eventual survival time and mode of death depend on the magnitude of the dose. In most mammals three distinct modes of death can be identified, although in actual accidental exposures some overlap is frequently seen.
Cerebrovascular syndrome: At very high doses, in excess of about 100 Gy (10,000 rad), death occurs 24 to 48 hours after exposure and appears to result from neurologic and cardiovascular breakdown;
Gastrointestinal syndrome: At intermediate dose levels, in the order of 5 to 12 Gy (500 – 1,200 rad), death occurs in a matter of days and is associated with extensive bloody diarrhea and destruction of the gastrointestinal mucosa.
32
Hematopoietic syndrome or bone-marrow death: At low dose levels, in the order of 2.5 to 5 Gy (250-500 rad), death occurs several weeks after exposure and is caused by effects on the blood-forming organs.
The signs and symptoms of the human post-irradiation syndrome can be divided into two main groups: gastrointestinal and neuromuscular.
1. Gastrointestinal symptoms are anorexia, nausea, vomiting, diarrhea, intestinal cramps, salivation, fluid loss, dehydration, and weight loss.
2. Neuromuscular symptoms include easily fatigued, apathy or listlessness, sweating, fever, headache, and hypotension.
Summary of Radiation Effects
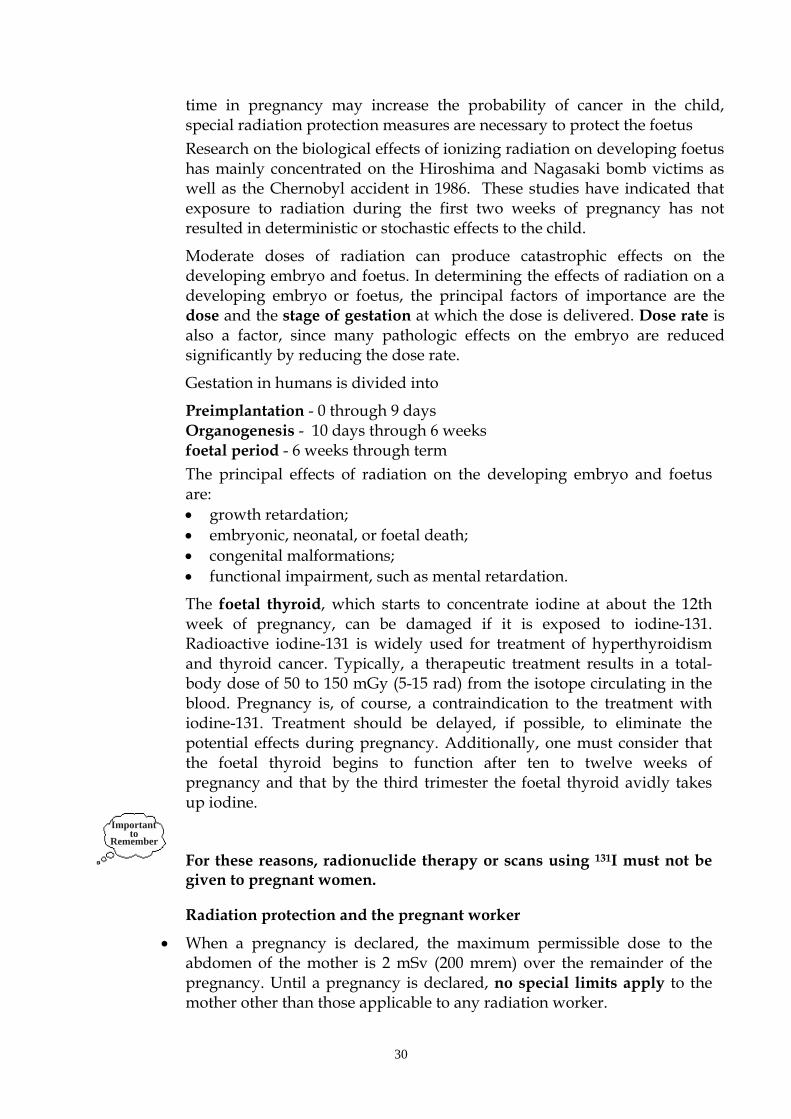
Several new terms have been introduced in this section and Figure 13 shows how all these terms are related.
Remember
Acute exposures may lead to early or late effects which may be either
stochastic or deterministic.
High level chronic exposures could lead to late effects which may be either deterministic or stochastic.
In Figure 13, deterministic effects are shown in bold type and stochastic effects are shown in normal type.
*Never observed in humans
Figure 13: Summary of Radiation Effects
Acute Exposure
Chronic Exposure
Early Effects Late Effects
Cancer Sterility
Cataracts Hereditary Effects*
RADIATION EXPOSURE
ErythemaRadiation Sickness
33
Key Points: The major systems in the body are the respiratory, digestive, circulatory,
lymphatic and urinary systems. Through various processes, inhaled and ingested materials may
eventually be deposited in body organs. From this position they can irradiate nearby organs and tissues.
The human body is made up of small building blocks called cells which are grouped to form tissues and organs.
Each cell has a cell membrane, nucleus and cytoplasm. The nucleus consists of 46 chromosomes. Chromosomes consist of genes made up of proteins and molecules of
DNA. DNA carries genetic material concerning the physical and mental
characteristics of a person. Cells divide to produce more cells and during division the cell is more
sensitive to radiation. Ionizing radiation can damage a cell directly or indirectly by creating free
radicals. Free radicals can break the chemical bonds in the DNA molecule, damage
the enzymes or damage the membranes of a cell. Radiation damage may result in cell death, abnormal cell division or cell
modification. Radiation exposure may be acute (over a short period of time) or chronic
(over a long period of time). Radiation effects may be early effects or late effects. Deterministic effects have a threshold below which there is no effect and
above which the severity of the effect increases with dose. Deterministic effects are associated with high doses and dose rates.
Stochastic effects depend on chance and have a latency period before the effect occurs. There is thought to be no threshold for stochastic effects, and the chance of an effect increases as the dose increases. The severity of the effect is not dependent on the size of the dose.
Hereditary affects may occur if a reproductive cell is changed by radiation and this may be passed to future generations. Hereditary effects have not been observed in humans.
Stochastic effects are the only possible effects at low doses. Radiation protection is aimed at preventing deterministic effects and
reducing the chances of stochastic effects occurring. Different organs within the body have different responses to radiation.
Weighting factors are used to allow for the different radiosensitivities of the various organs.
The unborn child is very sensitive to radiation and special protective measures are required to protect the foetus.
Go to your Workbook and answer questions 5 –10 to record your understanding of this section

34
4. Radiobiology in Nuclear Medicine
A small percentage of the population is exposed to Nuclear Medicine procedures and these procedures result in low radiation doses. However there are still potential biologic risks to the patient, personnel, foetuses and future generations.
Radiopharmaceuticals are chosen for their property of localizing in different organs of the body, for which diagnostic information is required. The organ of interest is called the ‘target’ organ. Some radiopharmaceuticals have an affinity for organs that are not the organ of interest; these are termed ‘critical organs’. Because the critical organ is the organ that concentrates most of the radiopharmaceutical, it is this organ that will determine the activity of radiopharmaceutical that can be administered. Because radiopharmaceuticals are transported throughout the body by the bloodstream, the whole body dose is also important. Information regarding critical organ and whole body doses are found in the package inserts for most radiopharmaceuticals.
Refer to Radiation Safety-Part 2 for using this data to calculate radiation dose from injected activity.
The dose absorbed by an organ is calculated from the dose rate i.e. the fraction of the administered dose reaching the organ, and the duration of exposure. The duration of exposure depends on biologic processes and physical properties of the radionuclide. Physical and biological variables are the two general factors that need to be considered when estimating patient exposure in nuclear medicine.
Physical factors:
The type of radiation emitted
The energy of the emissions
The physical half-life
Biological factors:
Unlike physical factors these are less well defined and contribute to uncertainties regarding estimation of exposure.
Most patients undergo nuclear medicine procedures because they are ill but critical organ values represent exposure to healthy individuals
Disease may affect the size and function of the organ thus influencing the uptake by that organ.
Age of patient. Physiological processes, metabolic rates alter with age and organ sizes in children differ from those of adults.
The biological effect of a radionuclide is dependent on both the physical and biological half-life. When considered together the resultant process is

35
referred to in terms of ‘effective half-life’. Physical decay and biological processes are both exponential decreases; therefore the resultant ‘effective’ half-life is also exponential.
Although dose estimates in nuclear medicine are difficult, nuclear medicine procedures do not deliver excessive doses and are usually lower than those from diagnostic x-rays. The risk of inducing late effects (particularly leukaemia) is very small. Because children are more sensitive to radiation, doses from diagnostic procedures are more of a hazard to children than adults.
Dose Reduction
The nuclear medicine technologist can greatly contribute to dose reduction. Methods available for reducing exposure are:
Using small amounts of radionuclides that are pure gamma emitters, have low energies and short half-lives
Use of agents that selectively block and decrease uptake in critical organs (e.g. Lugol’s solution to reduce thyroid uptake of radioactive iodine)
Using radiopharmaceuticals with short effective half-lives
Ensuring that the correct amount of radiopharmaceutical is administered for each procedure, taking into account the weight and age of patients
Ensuring that instrumentation used to measure doses is properly calibrated and that all quality control procedures necessary are carried out as specified
Refer to Radiation Safety-Part 2; Section 3-radiation Safety and the Patient
***Important Reference:***
The following IAEA website is an excellent resource for supplementary
and additional information:
http://rpop.iaea.org/RPOP/RPoP/Content/AdditionalResources/Training/1
_TrainingMaterial/NuclearMedicine.htm
Go to DAT website for on‐line exercise OL1 LINK where you are required
to follow a powerpoint presentation on:
Biological Effects, Hazards and Risks
On completion then complete the Revision Exercise R1 answering
questions relating to information in the presented powerpoint.
***Remember completing Revision Exercises is part of Completion
towards Final Results for this course.

36
Glossary of terms and words
Acute exposure Exposure to radiation over a short time period (a few hours or less).
Ankylosing Spondylitis
Inflammation of the vertebrae caused by rheumatoid arthritis.
Apoptosis Programmed cell death, the body's normal method of disposing of damaged, unwanted, or unneeded cells
Chronic exposure Exposure to radiation over a long time period (months or years).
Cell membrane The boundary of the cell.
Chromosomes Fine fibrous strands of genes.
Cytoplasm The fluid-like substance within a cell which contains many functional part of the cell.
Desquamate of skin) come off in scales like thin flakes.
Deterministic effect An effect of radiation (e.g. skin reddening) which is characterised by having a threshold dose.
Deoxyribonucleic acid (DNA)
A molecule which carries all the genetic material concerning the physical and mental characteristics of a human being.
Dose Energy absorbed per unit mass
Early effect A radiation effect which occurs within a few days or weeks of exposure.
Epilation Removal of hair by the roots
Foetus An unborn child.
Free radical A chemically reactive atom group which may be formed by the ionization of water in the cell.
Gene The part of a chromosome consisting of proteins and a segment of DNA with specific base sequence.
Gestation Carrying developing young in uterus during pregnancy.
Germ cell Formative stage of a spermatozoon or an ovum
Hereditary effect An effect of radiation which could be passed on to future generations.
Late effect A radiation effect which occurs years after exposure.
Necrosis The pathologic death of a cell or group of cells in contact with living cells
Nucleus The part of a cell which controls the functions of a cell.

37
Ovum Female germ cell (plural Ova).
Postpartum mastitis Inflammation of the breast following childbirth
Progeny Offspring. Product of radioactive decay
Radiogenic Pertaining to a substance or state resulting from a radioactive transformation.
Somatic effect Effects of radiation on the exposed individual, as distinguished from genetic effects, which may also affect subsequent unexposed generations.
Spermatid
Spermatogenesis
Spermatogonia
Spermatozoon
Male germ cell immediately before assuming its final typical form.
The production of sperm
Primative male germ cell
Mature male germ cell (plural: spermatozoa)
Stochastic effect An effect of radiation (e.g. cancer) where the probability of the effect is proportional to the dose received. The severity of the effect is, however, independent of the dose.
Stem cell A formative cell.
Threshold dose The dose of radiation below which there is no observable radiation injury.
Tissue weighting factor
A factor which considers the differences in probability of fatal cancer for different organs and tissues.