Racial differences in expectations of joint replacement surgery outcomes
15
Racial Differences in Expectations of Joint Replacement Surgery Outcomes Peter W. Groeneveld 1 , C. Kent Kwoh 2 , Maria K. Mor 2 , Cathleen J. Appelt 3 , Ming Geng 3 , Jennifer C. Gutierrez 4 , Damaris S. Wessel 4 , and Said A. Ibrahim 2 1 Philadelphia VAMC and University of Pennsylvania School of Medicine, Philadelphia 2 VA Pittsburgh Healthcare System and University of Pittsburgh, Pittsburgh, Pennsylvania 3 VA Pittsburgh Healthcare System, Pittsburgh, Pennsylvania 4 Philadelphia VAMC, Philadelphia, Pennsylvania Abstract Objective—Prior studies have indicated racial differences in patients’ expectations for joint replacement surgery outcomes. The goal of this study was to measure these differences using a well-validated survey instrument and to determine if the differences could be explained by racial variation in disease severity, socioeconomic factors, literacy, or trust. Methods—Detailed demographic, clinical, psychological, and social data were collected from 909 male patients (450 African American, 459 white) ages 50–79 years with moderate or severe osteoarthritis (OA) of the hip or knee receiving primary care at 2 veterans affairs medical centers. The previously validated Joint Replacement Expectations Survey was used to assess expectations for pain relief, functional improvement, and psychological well-being after joint replacement. Results—Among knee OA patients (n = 627), the unadjusted mean expectation score (scale 0– 76) for African American patients was 48.7 versus 53.6 for white patients (mean difference 4.9, P < 0.001). For hip OA patients (n = 282), the unadjusted mean expectation score (scale 0–72) for African Americans was 45.4 versus 51.5 for whites (mean difference 6.1, P < 0.001). Multivariable adjustment for disease severity, socioeconomic factors, education, social support, literacy, and trust reduced these racial differences to 3.8 points (95% confidence interval [95% CI] 1.2, 6.3) among knee OA patients and 4.2 points (95% CI 0.4, 8.0) among hip patients. Conclusion—Among potential candidates for joint replacement, African American patients have significantly lower expectations for surgical outcomes than white patients. This difference is not entirely explained by racial differences in demographics, disease severity, education, income, social support, or trust. © 2008, American College of Rheumatology Address correspondence to Peter W. Groeneveld, MD, MS, Philadelphia VAMC, 9 East, 3900 Woodland Avenue, Philadelphia, PA 19104-4155. [email protected]. AUTHOR CONTRIBUTIONS Dr. Groeneveld had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study design. Groeneveld, Kwoh, Ibrahim. Acquisition of data. Groeneveld, Kwoh, Appelt, Gutierrez, Wessel, Ibrahim. Analysis and interpretation of data. Groeneveld, Kwoh, Mor, Ibrahim. Manuscript preparation. Groeneveld, Kwoh, Mor, Appelt, Gutierrez, Wessel, Ibrahim. Statistical analysis. Groeneveld, Mor, Geng. NIH Public Access Author Manuscript Arthritis Rheum. Author manuscript; available in PMC 2011 July 11. Published in final edited form as: Arthritis Rheum. 2008 May 15; 59(5): 730–737. doi:10.1002/art.23565. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Transcript of Racial differences in expectations of joint replacement surgery outcomes
Racial Differences in Expectations of Joint Replacement SurgeryOutcomes
Peter W. Groeneveld1, C. Kent Kwoh2, Maria K. Mor2, Cathleen J. Appelt3, Ming Geng3,Jennifer C. Gutierrez4, Damaris S. Wessel4, and Said A. Ibrahim2
1Philadelphia VAMC and University of Pennsylvania School of Medicine, Philadelphia2VA Pittsburgh Healthcare System and University of Pittsburgh, Pittsburgh, Pennsylvania3VA Pittsburgh Healthcare System, Pittsburgh, Pennsylvania4Philadelphia VAMC, Philadelphia, Pennsylvania
AbstractObjective—Prior studies have indicated racial differences in patients’ expectations for jointreplacement surgery outcomes. The goal of this study was to measure these differences using awell-validated survey instrument and to determine if the differences could be explained by racialvariation in disease severity, socioeconomic factors, literacy, or trust.
Methods—Detailed demographic, clinical, psychological, and social data were collected from909 male patients (450 African American, 459 white) ages 50–79 years with moderate or severeosteoarthritis (OA) of the hip or knee receiving primary care at 2 veterans affairs medical centers.The previously validated Joint Replacement Expectations Survey was used to assess expectationsfor pain relief, functional improvement, and psychological well-being after joint replacement.
Results—Among knee OA patients (n = 627), the unadjusted mean expectation score (scale 0–76) for African American patients was 48.7 versus 53.6 for white patients (mean difference 4.9, P< 0.001). For hip OA patients (n = 282), the unadjusted mean expectation score (scale 0–72) forAfrican Americans was 45.4 versus 51.5 for whites (mean difference 6.1, P < 0.001).Multivariable adjustment for disease severity, socioeconomic factors, education, social support,literacy, and trust reduced these racial differences to 3.8 points (95% confidence interval [95% CI]1.2, 6.3) among knee OA patients and 4.2 points (95% CI 0.4, 8.0) among hip patients.
Conclusion—Among potential candidates for joint replacement, African American patients havesignificantly lower expectations for surgical outcomes than white patients. This difference is notentirely explained by racial differences in demographics, disease severity, education, income,social support, or trust.
© 2008, American College of RheumatologyAddress correspondence to Peter W. Groeneveld, MD, MS, Philadelphia VAMC, 9 East, 3900 Woodland Avenue, Philadelphia, PA19104-4155. [email protected] CONTRIBUTIONSDr. Groeneveld had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy ofthe data analysis.Study design. Groeneveld, Kwoh, Ibrahim.Acquisition of data. Groeneveld, Kwoh, Appelt, Gutierrez, Wessel, Ibrahim.Analysis and interpretation of data. Groeneveld, Kwoh, Mor, Ibrahim.Manuscript preparation. Groeneveld, Kwoh, Mor, Appelt, Gutierrez, Wessel, Ibrahim.Statistical analysis. Groeneveld, Mor, Geng.
NIH Public AccessAuthor ManuscriptArthritis Rheum. Author manuscript; available in PMC 2011 July 11.
Published in final edited form as:Arthritis Rheum. 2008 May 15; 59(5): 730–737. doi:10.1002/art.23565.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
INTRODUCTIONRacial variations in the utilization of major medical and surgical procedures and subsequenthealth care outcomes have been widely documented in the US health care system, includingthe Veterans Health Administration (VA) (1). Although the Department of Health andHuman Services, the Department of Veterans Affairs, and the National Institutes of Healthhave established the reduction of health care disparities among minorities as a majornational health policy goal (2), and many studies have documented the pervasiveness ofracial disparities in health care (3), relatively few studies have examined the root causes forracial variation in health care, such as racial differences in expectations of the outcomes ofmajor surgical procedures.
Joint replacement surgery is a reliable and effective form of treatment for patients withmoderate to severe osteoarthritis (OA) of the hip or knee. Joint replacement providessubstantial pain relief and functional improvement in ~90% of patients undergoing surgery(4). Despite the effectiveness of joint replacement in reducing pain and improving functionalstatus and quality of life, racial and ethnic minority patients with advanced knee OA are halfas likely to receive knee replacement compared with white patients (5,6). Earlier studiesconducted in the VA reported that, compared with white patients, African American patientswith knee or hip OA perceived joint replacement as a less helpful treatment option (7,8).Moreover, a substantial number of minority patients with OA predicted that jointreplacement would have no significant effect on their health status (9).
Although these preliminary findings are suggestive of racial differences in attitudes towardjoint replacement, the magnitude of the racial differences remains unclear. It is alsouncertain if racial differences in expectations of surgical outcomes may be explained byracial variation in modulating factors such as disease severity, socioeconomic factors,education, literacy, social support, or trust in the health care system. Therefore, the goal ofthe present study was to measure these differences using a well-validated survey instrumentand to determine if the differences could be explained by confounders.
PATIENTS AND METHODSThe research protocol was approved by the institutional review boards for both thePhiladelphia and Pittsburgh VA Medical Centers. A comprehensive cross-sectional surveywas designed to measure clinical, psychological, and socioeconomic factors associated withexpectations for the outcomes of joint replacement. The survey was targeted specificallytoward patients with moderate to severe OA of the knee or hip between the ages of 50 and79 years, as these patients would generally be considered good candidates for jointreplacement surgery.
RecruitmentPatients were enrolled from October 2004 through September 2006 at the Pittsburgh and thePhiladelphia VA Medical Centers. Posters and pamphlets describing the study were placedin the waiting rooms of the primary care clinics and other areas of the hospitals, as well as in3 satellite outpatient clinics in the Pittsburgh VA Health Care System. In addition, letterswere sent to randomly selected patients who had upcoming primary care appointments ateach of these sites. These announcements invited patients ages 50–79 years who had chronicknee or hip pain on most days for at least 1 month during the past 6 months to enroll in thestudy. Patients were advised to contact research coordinators either in person (coordinatorswere situated in the clinic waiting areas) or by phone if they were interested in enrollment.None of the study publicity material specifically indicated that exploration of racial
Groeneveld et al. Page 2
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
disparities was a primary goal of the study, although this information was not withheld fromany participant who inquired.
Inclusion/exclusion criteriaAt the initial meeting with study personnel, potential enrollees were screened for inclusionand exclusion criteria by completing a brief, 3-stage face-to-face or telephone interview. Inscreening stage 1, patients were excluded from the study if they were not between ages 50and 79 years, or if they had a history of knee or hip replacement, lower extremityamputation, a medical illness with a life expectancy <12 months, inflammatory arthritis(e.g., rheumatoid arthritis, systemic lupus erythematosus, ankylosing spondylitis, psoriaticarthritis, gout), or dementia. In screening stage 2, the Arthritis Supplement of the FirstNational Health and Nutrition Examination Survey instrument was administered to identifyindividuals who were highly likely to have a diagnosis of knee or hip OA (10,11). Finally, inscreening stage 3, those patients who screened positive for OA in stage 2 were assessed forthe clinical severity of their OA using the Western Ontario and McMaster UniversitiesOsteoarthritis Index (WOMAC) (12), a reliable and valid scale designed to quantify painand functional status in patients with OA (13). Summary WOMAC scores range from 0 (nopain or disability) to 100 (severe pain with total disability), and patients with scores ≥39 arelikely to experience substantial symptom relief and functional improvement from jointreplacement surgery (14). Enrollment in this study was limited to patients with WOMACscores ≥39 on the screening assessment; these patients proceeded to the full interview.Patients who completed all study procedures were reimbursed $25 for their time and effort.
Data collectionThe full data collection interview consisted of an assessment of patients’ demographic andsocioeconomic characteristics, quality of life, pain level, functional status, literacy, trust inphysicians, social support, and expectations for joint replacement surgical outcomes. Qualityof life was measured using the Medical Outcomes Study (MOS) Short Form 12 (SF-12),version 2 (15). Pain level was measured using a 0–100 visual analog “thermometer.”Functional status was assessed using the WOMAC as described above. Medical literacy wasmeasured using the Rapid Estimate of Adult Literacy in Medicine-Revised (REALM-R)instrument (16). Patients’ trust in their physicians was measured using the Trust In PhysicianSurvey (17,18). The MOS Modified Social Support Survey was used to assess the quality ofpatients’ social support systems (19). Expectations of the effectiveness of joint replacementsurgery in improving quality of life were measured using the Hospital for Special SurgeryJoint Replacement Expectations Survey (JRES). This instrument, developed at an orthopedichospital in New York City, was separately developed by Mancuso et al for hip and kneesurgical candidates through an extensive process by which draft surveys containing 52potential categories of expectations were administered, and the survey elements with thehighest kappa statistics (intrarater reliability) were retained in the final instruments, whichwere subsequently rigorously tested in validation cohorts (20–22). The JRES contains 19(knee) or 18 (hip) items, with a 5-point Likert-scale response range for each item where astrong expectation of a particular (positive) outcome is scored as 4, while the absence of anexpectation for the outcome is scored as 0 (Appendices A and B, available at the ArthritisCare & Research Web site athttp://www.interscience.wiley.com/jpages/0004-3591:1/suppmat/index.html).
Patients self-identified their race and ethnicity, and only the responses of patients who self-identified as African American or white were included in this report. Additionally, becausefewer than 5% of our respondents were women, we excluded these responses from ouranalyses.
Groeneveld et al. Page 3
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Statistical analysesWe conducted comparative analyses comparing African American and white patients usingchi-square tests for categorical variables, t-tests for normally distributed continuousvariables, and Wilcoxon’s rank sum tests for non-normally distributed variables. Surveyresponses were subsequently analyzed using multivariable regression models. These modelswere fitted as an ordinary least squares regression with the JRES score as the dependentvariable. Independent variables in this model included race, age, sex, categorized income,categorized education, employment status, marital status, pain score, functional status(WOMAC score), location of interview (Pittsburgh or Philadelphia), literacy (REALM-R),social support, and trust in physicians. We then added interaction effects between race andother key predictors to our fully specified model to determine if the effect of these predictorswas modulated by race. Finally, we fit the fully specified model (excepting race) separatelyto white and African American patients to assess for any large differences in the effects ofpredictors.
All statistical analyses were performed using SAS 9.1 (SAS Institute, Cary, NC). Allsignificance tests were 2-sided, with a P value less than 0.05 assumed to be significant.
RESULTSBaseline cohort characteristics
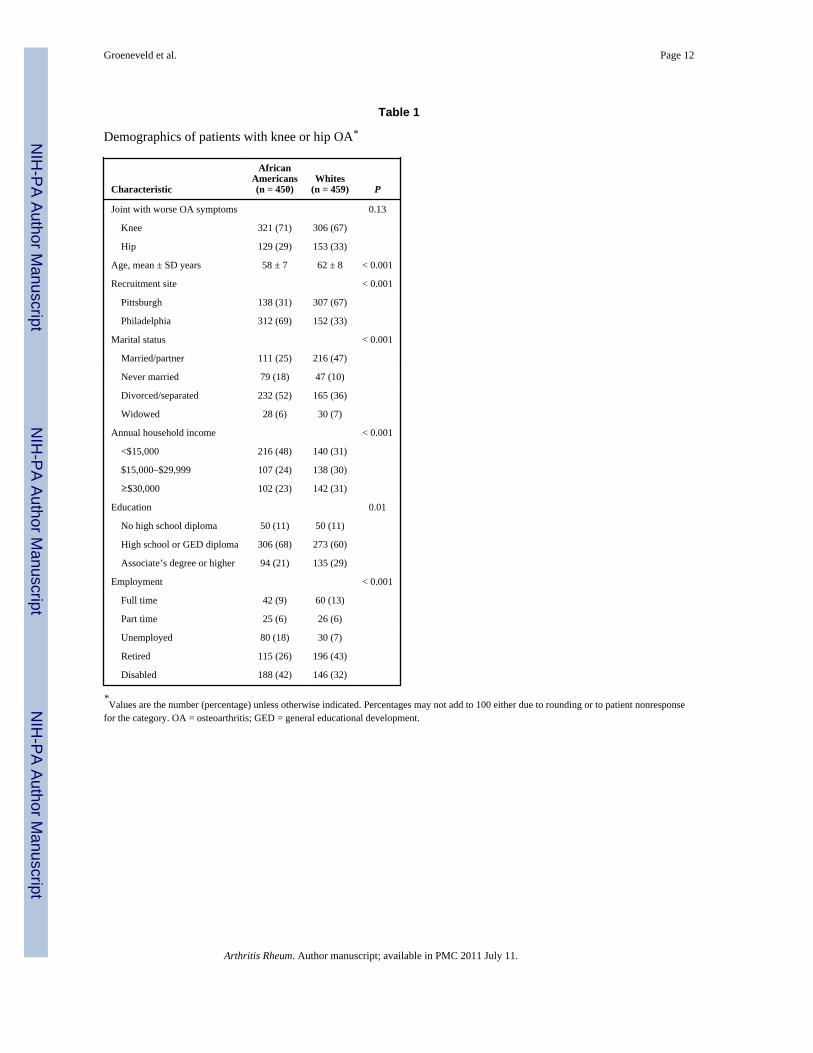
The final survey cohort comprised 909 primary care patients with chronic knee or hip OAwho identified themselves as either white or African American. Characteristics of white (n =459) and African American (n = 450) enrollees are summarized in Table 1. AfricanAmerican patients were younger, predominantly from Philadelphia, less likely to be married,more likely to have household incomes below the poverty level, and less likely to havereceived an associate’s degree or other higher education degree than white enrollees. MoreAfrican American respondents (42%) than white respondents (32%) reported receivingdisability payments due to their knee/hip OA (P < 0.001).
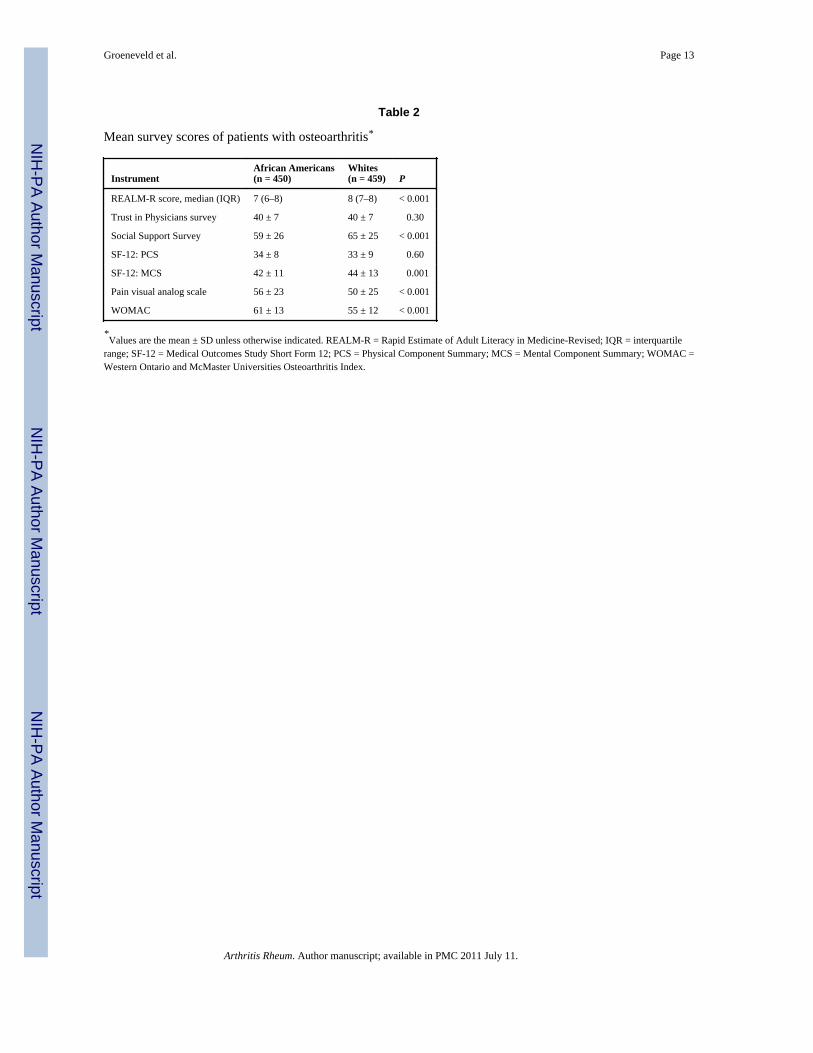
Mean survey instrument scores are summarized by race in Table 2. African Americanpatients had lower health literacy and lower social support than whites, although there wasno racial difference in trust in physicians. African American and white patients had similarPhysical Component Summary scores on the SF-12, although African American patients hadsignificantly lower Mental Component Summary scores (P = 0.01). African Americanpatients had significantly higher mean pain scores as reported on a visual analog scale (P <0.001), and African American patients had significantly more functional impairment fromtheir OA as measured by the WOMAC index (P < 0.001).
To assess reliability of the JRES instrument in our patient population, we calculatedCronbach’s alpha for the entire cohort of knee OA respondents (α = 0.96) and hip OArespondents (α = 0.95). Because the JRES was primarily developed and validated amongwhite patients (20,21), we then calculated Cronbach’s alpha separately for African Americanknee OA patients (α = 0.95) and white knee OA patients (α = 0.96), as well as AfricanAmerican hip OA patients (α = 0.93) and white hip OA patients (α = 0.96). All alpha valuesexceeded 0.9, indicating extremely high reliability of the scale among both AfricanAmericans and whites.
Among patients with knee OA, white patients had a mean ± SD unadjusted JRES(expectation) score of 53.6 ± 14.5, whereas African American patients had a mean ± SDscore of 48.7 ± 14.6 (P < 0.001 for the difference). More African American patients (24%)than white patients (15%; P = 0.004) had JRES scores below the midpoint of the scale,
Groeneveld et al. Page 4
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
indicating predominantly low expectations for the outcomes of surgery. JRES scores forwhite and African American patients with knee OA are shown in Figure 1.
Among hip OA patients, white patients had a mean ± SD unadjusted JRES score of 51.5 ±14.3, whereas African American patients had a mean ± SD score of 45.4 ± 14.2 (P < 0.001for the difference). Approximately 25% of African American patients, compared with 16%of white patients (P = 0.06), had JRES scores below the scale midpoint. JRES scores forwhite and African American patients with hip OA are shown in Figure 2.
Race and expectations: results of multivariable regression modelsIn fitting the ordinary least squares multivariable regression models, we performedKolmogorov-Smirnov tests for normality of the regression residuals for the fully specifiedmodels. These tests failed to reject the null (P > 0.05 in all cases), indicating that the modelsmet the normality assumption for ordinary least squares regression.
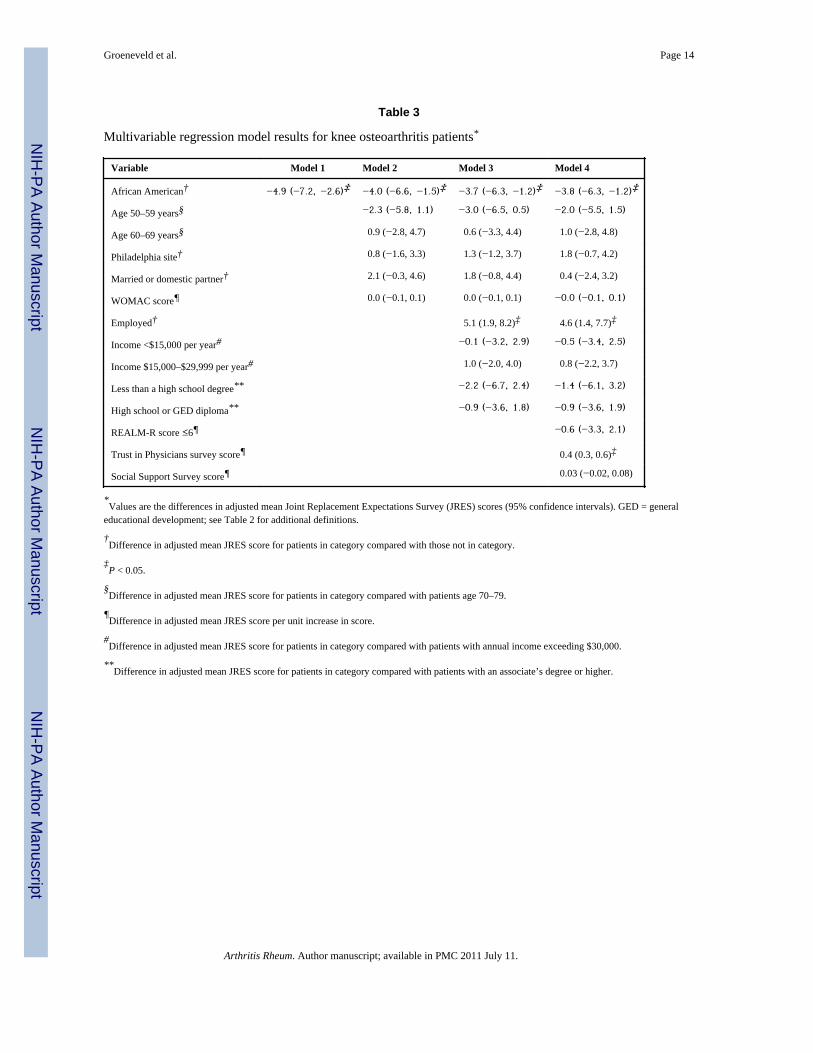
Results from multivariable ordinary least squares regression models are summarized inTable 3. For knee OA patients, adjustment for WOMAC score, age, sex, marital status, andclinical site (Philadelphia or Pittsburgh) reduced the mean racial difference in knee JRESscores from an unadjusted difference of 4.9 points (95% confidence interval [95% CI] 2.6,7.2) to a difference of 4.0 points (95% CI 1.5, 6.6). Addition of employment status, income,and education to the model further reduced the race difference to 3.7 points (95% CI 1.2,6.3). Addition of the REALM-R literacy score, Trust in Physician score, and MOS SocialSupport score did not materially influence the racial difference in mean scores, which was3.8 points (95% CI 1.2, 6.3).
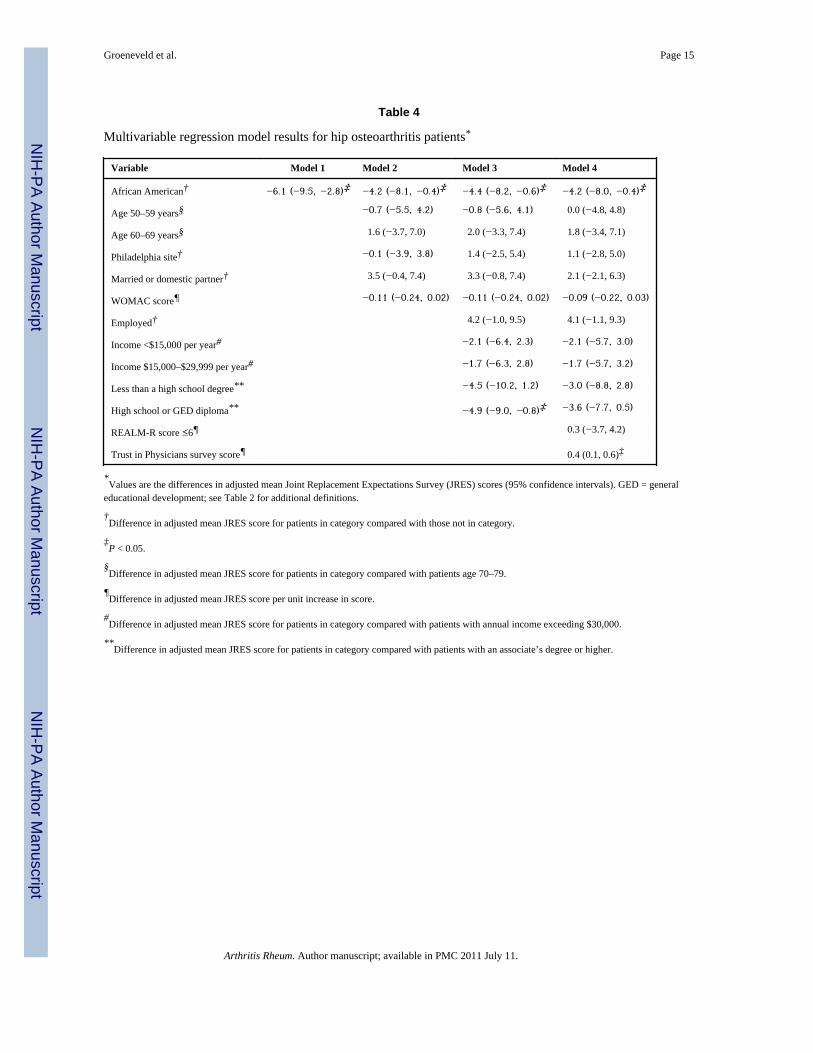
For hip OA patients (Table 4), adjustment for the WOMAC score, age, sex, marital status,and clinical site (Philadelphia or Pittsburgh) reduced the mean racial difference in hip JRESscores from an unadjusted mean difference of 6.1 points (95% CI 2.8, 9.5) to 4.2 points(95% CI 0.4, 8.1). Addition of employment status, income, and education to the model didnot materially change the racial difference in means scores, which was 4.4 points (95% CI0.6, 8.2). Addition of the REALM-R literacy score, trust score, and social support score alsohad a minimal effect on the race difference in mean scores, which was 4.2 points (95% CI0.4, 8.0).
To assess whether key predictor variables interacted with race, we then fit our full regressionmodel including interaction terms between race and marital status, employment, education,income, trust in physicians, and social support. None of the race-interaction coefficientswere significant (P > 0.1 for all) for either knee or hip OA patients. To further test fordifferences in the effects of predictors by race, we next fit the full regression models(excepting the race variable) separately for white patients and African American patients.For knee OA patients, a single-point increase in the Trust in Physicians scale was associatedwith a 0.46 higher JRES score (P = 0.04) for whites, and a 0.41 higher JRES score (P =0.001) for African Americans. Higher WOMAC scores were associated with a lower JRESscore for white knee OA patients (−0.16 per unit increase in WOMAC; P = 0.04) but not forAfrican American knee OA patients (0.04 per unit increase in WOMAC; P = 0.51). Forwhite hip OA patients, increased trust in physicians was associated with a 0.31 higher JRESscore (P = 0.08), and this effect was slightly more pronounced for African Americans (0.66higher score; P = 0.002). White hip OA patients who were employed had higher adjustedJRES scores (4.6 higher; P = 0.05), as did employed African American hip OA patients (5.2higher; P = 0.03). No other covariates were significant predictors of JRES score for eitherracial group among hip OA patients.
Groeneveld et al. Page 5
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
DISCUSSIONIn this sample of primary care patients with chronic knee/hip pain who were potentialcandidates for joint replacement, we found significant racial differences in expectations forjoint replacement surgery outcomes using a comprehensive, well-validated surveyinstrument. These differences were not explained by racial variation in the age or sexdistribution of the patient populations, nor were they explained by differences in geographiclocation, socioeconomic status, educational level, health literacy, trust in physicians, orsocial support between African American and white patients.
The clinical or policy significance of a modest, 4–6-point difference in JRES scores,equivalent to a standardized difference (i.e., fraction of a standard deviation) of 0.3–0.4, isuncertain. Because our study was a cross-sectional design, it was not possible to ascertain ifpatients with lower JRES scores were actually less likely to undergo surgery in subsequentmonths and years. However, a growing body of evidence suggests a strong correlationbetween patients’ expectations of joint replacement surgery and their stated willingness toundergo surgery (9,23,24). Future longitudinal studies are necessary to clearly quantify therelationship between patients’ expectations and joint replacement surgery rates.
Our findings add to substantial research that has explored the root causes for racialdifferences in the utilization of joint replacement surgery for knee and hip OA. Ibrahim et alpreviously reported that, compared with white patients, African American patients with kneeor hip OA are less likely to perceive joint replacement as an effective treatment option (8).Another study by Ibrahim et al assessing patient familiarity with joint replacement andexpectations of surgical outcomes found that African American patients were less familiarwith the details of joint replacement surgery and the duration of the expected recoveryperiod (23). The current study expands on these previous findings by using a morecomprehensive (i.e., 17- or 18-item), integrated (i.e., single composite score), well-validatedmeasure of joint replacement surgery expectations. We also enrolled sufficient numbers ofpatients to verify these findings separately among patients with knee OA and those with hipOA. Additionally, in multivariable analyses, we adjusted for several factors likely toconfound the relationship between race and joint replacement expectations, including otherdemographic factors, socioeconomic variables, literacy, social support, and trust. Indeed,African American and white patients in our sample differed markedly in age, geographiclocation, socioeconomic status, educational attainment, health literacy, and social support.These factors are all likely to influence patient expectations of surgery independent of race,yet when we adjusted for the independent effect of these variables, racial differences inpatient expectations persisted. Additionally, we found little evidence of interaction betweenrace and other predictors of expectations. Generally, significant predictors of higherexpectations, such as employment and greater trust in physicians, were similarly influentialin both racial groups.
If racial differences in joint replacement expectations are not mediated by the many factorsthat we explored, what are the central causes for these racial differences? Among theremaining possibilities are racial differences in the composition of patients’ social networks,through which trusted information regarding the benefit of knee and hip replacement may beobtained, as well as differences in access to other sources of information about jointreplacement such as the Internet. Our own prior research suggests that information receivedthrough informal channels (rather than, for example, a physician visit) is often critical ininfluencing patients’ attitudes toward medical technology (25).
With any elective surgery, it is vital that patient-physician decision making truly be shared,and that patient autonomy be respected (26). As such, a decision to decline elective joint
Groeneveld et al. Page 6
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
replacement surgery by a patient with moderate or severe arthritis is not necessarilyirrational, and may reflect an accurate self-assessment of individual circumstances and/orrisk preferences (27). However, a decision to decline beneficial therapy based on erroneous,incomplete, or outdated information is not an issue of autonomy or preference, but ofdisparity in knowledge (9). More African American patients may lack access to accurateinformation (e.g., interpersonal networks where receipt of joint replacement is common,etc.) about the experiences after surgery than do white patients. In a context in which trust inthe health system is low, African American patients may therefore discount the benefits ofsurgery as described by health care providers (28).
Interventions designed to improve the accuracy of, and reduce racial differences in, patients’understanding of the outcomes of joint replacement surgery may be a particularly effectiveway of reducing racial disparities in utilization of this effective treatment option. To beeffective, such interventions should not only increase the quality and quantity of informationavailable to patients, but also increase the number and variety of sources of trustedinformation. Weng et al have pilot tested an educational intervention (a video and tailoreddecision aid) designed to reduce disparities in expectations of knee replacement, measuredby the anticipated WOMAC score after surgery (29). This intervention lowered the expectedWOMAC score for both pain and physical function among African American participants.Although these findings are preliminary, they suggest that racial differences in expectationsare modifiable. Peer counselors, testimonials, compelling presentations of race- andethnicity-specific outcome data, culturally competent media presentations, and theestablishment of patient networks all may be effective in reducing racial differences inexpectations and consequently improve equity in joint replacement surgery rates.
In interpreting our results, it is appropriate to acknowledge several limitations. First, thisresearch is a cross-sectional study, which limits causal inference. In particular, we did notassess whether patients were anticipating surgery in the near future, nor did we laterdetermine who had undergone surgery subsequent to the survey. Respondents who werefacing the tangible prospect of joint replacement surgery may have responded differentlythan those patients for whom surgery was a more hypothetical option. Second, although ourrecruitment of nearly 1,000 patients over 2 years’ time improved our likelihood of attractingsomewhat more reluctant participants to enter the research cohort, it is possible that ourmethod of enrollment selected patients who were generally more trusting of the healthsystem or of the VA in particular. Patients with frequent visits to the medical centers alsohad more opportunities to be enrolled, so we may have inadvertently enrolled a cohort ofpatients who were more connected to the health system than typical veterans. Third, thisstudy excluded patients who previously had undergone joint replacement surgery. If oneracial group had greater access to surgery than the other regardless of expectations, it ispossible that the racial differences we observed were an artifact created by the pool ofpresurgical knee/hip OA patients in one racial group being depleted faster than the otherracial group. However, we believe this phenomenon likely would have diminished theapparent racial difference in expectations, because it is probable that white patients wouldhave had more facilitated access to surgery. As such, it would have been less likely for us tohave enrolled white patients who were both highly favorable of joint replacement surgerybut who had not yet undergone surgery, thus potentially reducing the mean expectationsscore among white participants compared with African American participants. Finally, theracial difference we observed could have been an artifact produced by the JRES instrumentitself, if the instrument performed differently across racial groups. However, the highlysimilar distributional form of the responses, the nearly identical Cronbach’s alpha values,and the similar results of the regression analyses stratified by race suggest this is unlikely.
Groeneveld et al. Page 7
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
In this study of primary care patients with chronic knee/hip pain who were potentialcandidates for joint replacement, we found significant racial differences in patientexpectations regarding joint replacement surgery. These findings were independentlyobserved for both hip OA and knee OA patients. The racial differences in expectationspersisted despite adjustment for multiple potential confounders. Future studies shouldexplore interventions designed to reduce racial disparities in expectations of the benefits andrisks of joint replacement. Such interventions are likely to improve the quality of patientdecision making, while potentially reducing racial differences in utilization of jointreplacement and subsequent quality of life for patients with OA.
AcknowledgmentsThe authors gratefully acknowledge the assistance in manuscript preparation provided by Alexis Greenhut, MPH,statistical advice provided by Samuel Field, PhD, and graphical expertise provided by Janell Olah, MFA.
Supported by a Merit Review grant (HSR&D IIR 03-201-1) from the VA Health Services Research andDevelopment Service (Washington, DC). Drs. Groeneveld and Ibrahim’s work was supported by CareerDevelopment awards from the VA Health Services Research and Development Service (Washington, DC). Dr.Ibrahim’s work was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (grantK24-AR0-55259).
REFERENCES1. Fiscella K, Franks P, Gold MR, Clancy CM. Inequality in quality: addressing socioeconomic, racial,
and ethnic disparities in health care. JAMA. 2000; 283:2579–2584. [PubMed: 10815125]2. Department of Health and Human Services. Healthy people 2010: midcourse review. Goal 2:
eliminate health disparities. 2005. URL:http://www.healthypeople.gov/data/midcourse/html/execsummary/Goal2.htm
3. Smedley, BD.; Stith, AY.; Nelson, AR., editors. the Committee on Understanding and EliminatingRacial and Ethnic Disparities in Health Care, Board on Health Sciences Policy, and the Institute ofMedicine. Unequal treatment: confronting racial and ethnic disparities in health care. Washington(DC): National Academies Press; 2003.
4. Callahan CM, Drake BG, Heck DA, Dittus RS. Patient outcomes following tricompartmental totalknee replacement: a meta-analysis. JAMA. 1994; 271:1349–1357. [PubMed: 8158821]
5. Wilson MG, May DS, Kelly JJ. Racial differences in the use of total knee arthroplasty forosteoarthritis among older Americans. Ethn Dis. 1994; 4:57–67. [PubMed: 7742733]
6. Skinner J, Weinstein JN, Sporer SM, Wennberg JE. Racial, ethnic, and geographic disparities inrates of knee arthroplasty among Medicare patients. N Engl J Med. 2003; 349:1350–1359.[PubMed: 14523144]
7. Ibrahim SA, Siminoff LA, Burant CJ, Kwoh CK. Variation in perceptions of treatment and self-carepractices in elderly with osteoarthritis: a comparison between African American and white patients.Arthritis Rheum. 2001; 45:340–345. [PubMed: 11501721]
8. Ibrahim SA, Siminoff LA, Burant CJ, Kwoh CK. Understanding ethnic differences in the utilizationof joint replacement for osteoarthritis: the role of patient-level factors. Med Care. 2002; 40(1Suppl):I44–I51. [PubMed: 11789631]
9. Suarez-Almazor ME, Souchek J, Kelly PA, O’Malley K, Byrne M, Richardson M, et al. Ethnicvariation in knee replacement: patient preferences or uninformed disparity? Arch Intern Med. 2005;165:1117–1124. [PubMed: 15911724]
10. Davis MA, Ettinger WH, Neuhaus JM. Obesity and osteoarthritis of the knee: evidence from theNational Health and Nutrition Examination Survey (NHANES I). Semin Arthritis Rheum. 1990;20 Suppl 1(3):34–41. [PubMed: 2287947]
11. Tepper S, Hochberg MC. Factors associated with hip osteoarthritis: data from the First NationalHealth and Nutrition Examination Survey (NHANES-I). Am J Epidemiol. 1993; 137:1081–1088.[PubMed: 8317437]
Groeneveld et al. Page 8
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
12. Roos EM, Klassbo M, Lohmander LS. and Western Ontario and McMaster Universities. WOMACosteoarthritis index: reliability, validity, and responsiveness in patients with arthroscopicallyassessed osteoarthritis. Scand J Rheumatol. 1999; 28:210–215. [PubMed: 10503556]
13. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: ahealth status instrument for measuring clinically important patient relevant outcomes toantirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840. [PubMed: 3068365]
14. Hawker GA, Wright JG, Coyte PC, Williams JI, Harvey B, Glazier R, et al. Differences betweenmen and women in the rate of use of hip and knee arthroplasty. N Engl J Med. 2000; 342:1016–1022. [PubMed: 10749964]
15. Gandhi SK, Salmon JW, Zhao SZ, Lambert BL, Gore PR, Conrad K. Psychometric evaluation ofthe 12-item Short-Form Health Survey (SF-12) in osteoarthritis and rheumatoid arthritis clinicaltrials. Clin Ther. 2001; 23:1080–1098. [PubMed: 11519772]
16. Bass PF III, Wilson JF, Griffith CH. A shortened instrument for literacy screening. J Gen InternMed. 2003; 18:1036–1038. [PubMed: 14687263]
17. Freburger JK, Callahan LF, Currey SS, Anderson LA. Use of the Trust in Physician Scale inpatients with rheumatic disease: psychometric properties and correlates of trust in therheumatologist. Arthritis Rheum. 2003; 49:51–58. [PubMed: 12579593]
18. Anderson LA, Dedrick RF. Development of the Trust in Physician scale: a measure to assessinterpersonal trust in patientphysician relationships. Psychol Rep. 1990; 67:1091–1100. [PubMed:2084735]
19. Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 1991; 32:705–714.[PubMed: 2035047]
20. Mancuso CA, Sculco TP, Wickiewicz TL, Jones EC, Robbins L, Warren RF, et al. Patients’expectations of knee surgery. J Bone Joint Surg Am. 2001; 83-A:1005–1012. [PubMed:11451969]
21. Mancuso CA, Salvati EA, Johanson NA, Peterson MG, Charlson ME. Patients’ expectations andsatisfaction with total hip arthroplasty. J Arthroplasty. 1997; 12:387–396. [PubMed: 9195314]
22. Mancuso CA, Sculco TP, Salvati EA. Patients with poor preoperative functional status have highexpectations of total hip arthroplasty. J Arthroplasty. 2003; 18:872–878. [PubMed: 14566742]
23. Ibrahim SA, Siminoff LA, Burant CJ, Kwoh CK. Differences in expectations of outcome mediateAfrican American/white patient differences in “willingness” to consider joint replacement.Arthritis Rheum. 2002; 46:2429–2435. [PubMed: 12355491]
24. Toye FM, Barlow J, Wright C, Lamb SE. Personal meanings in the construction of need for totalknee replacement surgery. Soc Sci Med. 2006; 63:43–53. [PubMed: 16473445]
25. Groeneveld PW, Sonnad SS, Lee AK, Asch DA, Shea JE. Racial differences in attitudes towardinnovative medical technology. J Gen Intern Med. 2006; 21:559–563. [PubMed: 16808736]
26. Thompson AG. The meaning of patient involvement and participation in health care consultations:a taxonomy. Soc Sci Med. 2007; 64:1297–1310. [PubMed: 17174016]
27. Hudak PL, Clark JP, Hawker GA, Coyte PC, Mahomed NN, Krder HJ, et al. “You’re perfect forthe procedure! Why don’t you want it? ” Elderly arthritis patients’ unwillingness to consider totaljoint arthroplasty surgery: a qualitative study. Med Decis Making. 2002; 22:272–278. [PubMed:12058784]
28. Margolis ML, Christie JD, Silvestri GA, Kaiser L, Santiago S, Hansen-Flaschen J. Racialdifferences pertaining to a belief about lung cancer surgery: results of a multicenter survey. AnnIntern Med. 2003; 139:558–563. [PubMed: 14530226]
29. Weng HH, Kaplan RM, Boscardin WJ, MacLean CH, Lee IY, Chen W, et al. Development of adecision aid to address racial disparities in utilization of knee replacement surgery. ArthritisRheum. 2007; 57:568–575. [PubMed: 17471558]
Groeneveld et al. Page 9
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Distribution of Joint Replacement Expectations Survey (JRES) scores for white patients andAfrican American patients with knee osteoarthritis. Dot plots indicate individual responses,with the horizontal black lines indicating the mean. The corresponding box-and-whiskersplot indicates the median (horizontal line), interquartile range (box), and 2.5th to 97.5thpercentiles (whiskers). The y-axis indicates the total JRES score.
Groeneveld et al. Page 10
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
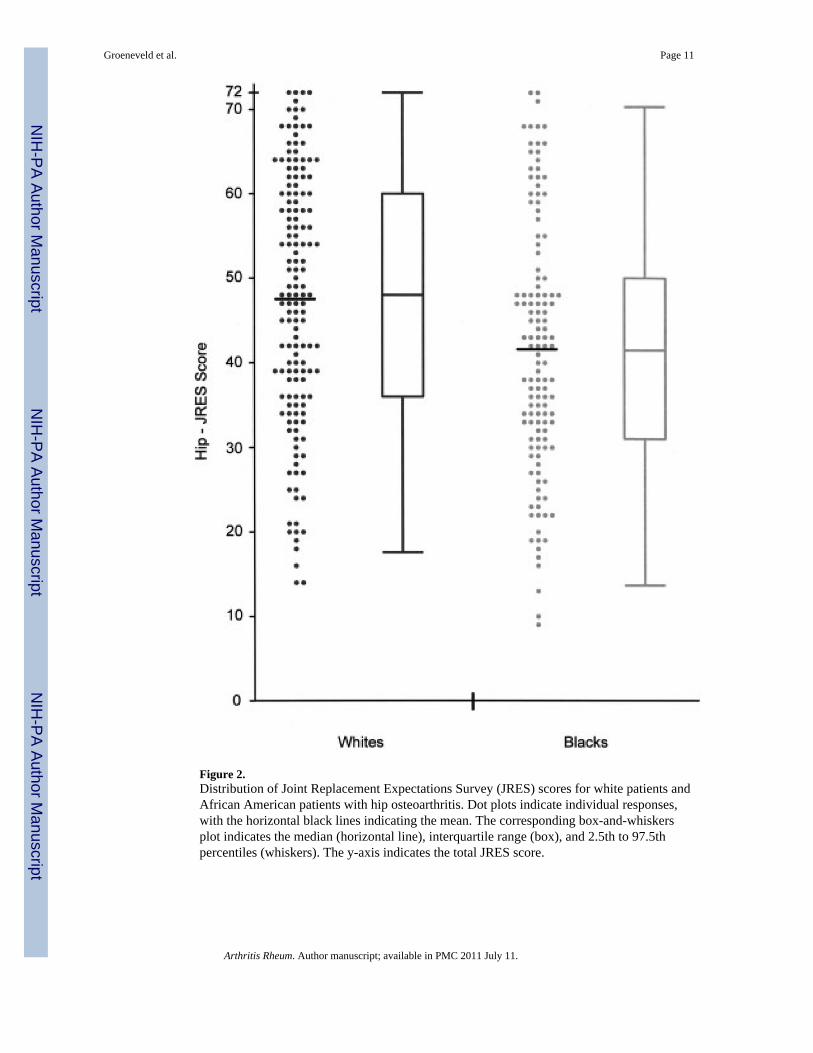
Figure 2.Distribution of Joint Replacement Expectations Survey (JRES) scores for white patients andAfrican American patients with hip osteoarthritis. Dot plots indicate individual responses,with the horizontal black lines indicating the mean. The corresponding box-and-whiskersplot indicates the median (horizontal line), interquartile range (box), and 2.5th to 97.5thpercentiles (whiskers). The y-axis indicates the total JRES score.
Groeneveld et al. Page 11
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Groeneveld et al. Page 12
Table 1
Demographics of patients with knee or hip OA*
Characteristic
AfricanAmericans(n = 450)
Whites(n = 459) P
Joint with worse OA symptoms 0.13
Knee 321 (71) 306 (67)
Hip 129 (29) 153 (33)
Age, mean ± SD years 58 ± 7 62 ± 8 < 0.001
Recruitment site < 0.001
Pittsburgh 138 (31) 307 (67)
Philadelphia 312 (69) 152 (33)
Marital status < 0.001
Married/partner 111 (25) 216 (47)
Never married 79 (18) 47 (10)
Divorced/separated 232 (52) 165 (36)
Widowed 28 (6) 30 (7)
Annual household income < 0.001
<$15,000 216 (48) 140 (31)
$15,000–$29,999 107 (24) 138 (30)
≥$30,000 102 (23) 142 (31)
Education 0.01
No high school diploma 50 (11) 50 (11)
High school or GED diploma 306 (68) 273 (60)
Associate’s degree or higher 94 (21) 135 (29)
Employment < 0.001
Full time 42 (9) 60 (13)
Part time 25 (6) 26 (6)
Unemployed 80 (18) 30 (7)
Retired 115 (26) 196 (43)
Disabled 188 (42) 146 (32)
*Values are the number (percentage) unless otherwise indicated. Percentages may not add to 100 either due to rounding or to patient nonresponse
for the category. OA = osteoarthritis; GED = general educational development.
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Groeneveld et al. Page 13
Table 2
Mean survey scores of patients with osteoarthritis*
InstrumentAfrican Americans(n = 450)
Whites(n = 459) P
REALM-R score, median (IQR) 7 (6–8) 8 (7–8) < 0.001
Trust in Physicians survey 40 ± 7 40 ± 7 0.30
Social Support Survey 59 ± 26 65 ± 25 < 0.001
SF-12: PCS 34 ± 8 33 ± 9 0.60
SF-12: MCS 42 ± 11 44 ± 13 0.001
Pain visual analog scale 56 ± 23 50 ± 25 < 0.001
WOMAC 61 ± 13 55 ± 12 < 0.001
*Values are the mean ± SD unless otherwise indicated. REALM-R = Rapid Estimate of Adult Literacy in Medicine-Revised; IQR = interquartile
range; SF-12 = Medical Outcomes Study Short Form 12; PCS = Physical Component Summary; MCS = Mental Component Summary; WOMAC =Western Ontario and McMaster Universities Osteoarthritis Index.
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Groeneveld et al. Page 14
Table 3
Multivariable regression model results for knee osteoarthritis patients*
Variable Model 1 Model 2 Model 3 Model 4
African American† −4.9 (−7.2, −2.6)‡ −4.0 (−6.6, −1.5)‡ −3.7 (−6.3, −1.2)‡ −3.8 (−6.3, −1.2)‡
Age 50–59 years§ −2.3 (−5.8, 1.1) −3.0 (−6.5, 0.5) −2.0 (−5.5, 1.5)
Age 60–69 years§ 0.9 (−2.8, 4.7) 0.6 (−3.3, 4.4) 1.0 (−2.8, 4.8)
Philadelphia site† 0.8 (−1.6, 3.3) 1.3 (−1.2, 3.7) 1.8 (−0.7, 4.2)
Married or domestic partner† 2.1 (−0.3, 4.6) 1.8 (−0.8, 4.4) 0.4 (−2.4, 3.2)
WOMAC score¶ 0.0 (−0.1, 0.1) 0.0 (−0.1, 0.1) −0.0 (−0.1, 0.1)
Employed† 5.1 (1.9, 8.2)‡ 4.6 (1.4, 7.7)‡
Income <$15,000 per year# −0.1 (−3.2, 2.9) −0.5 (−3.4, 2.5)
Income $15,000–$29,999 per year# 1.0 (−2.0, 4.0) 0.8 (−2.2, 3.7)
Less than a high school degree** −2.2 (−6.7, 2.4) −1.4 (−6.1, 3.2)
High school or GED diploma** −0.9 (−3.6, 1.8) −0.9 (−3.6, 1.9)
REALM-R score ≤6¶ −0.6 (−3.3, 2.1)
Trust in Physicians survey score¶ 0.4 (0.3, 0.6)‡
Social Support Survey score¶ 0.03 (−0.02, 0.08)
*Values are the differences in adjusted mean Joint Replacement Expectations Survey (JRES) scores (95% confidence intervals). GED = general
educational development; see Table 2 for additional definitions.
†Difference in adjusted mean JRES score for patients in category compared with those not in category.
‡P < 0.05.
§Difference in adjusted mean JRES score for patients in category compared with patients age 70–79.
¶Difference in adjusted mean JRES score per unit increase in score.
#Difference in adjusted mean JRES score for patients in category compared with patients with annual income exceeding $30,000.
**Difference in adjusted mean JRES score for patients in category compared with patients with an associate’s degree or higher.
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Groeneveld et al. Page 15
Table 4
Multivariable regression model results for hip osteoarthritis patients*
Variable Model 1 Model 2 Model 3 Model 4
African American† −6.1 (−9.5, −2.8)‡ −4.2 (−8.1, −0.4)‡ −4.4 (−8.2, −0.6)‡ −4.2 (−8.0, −0.4)‡
Age 50–59 years§ −0.7 (−5.5, 4.2) −0.8 (−5.6, 4.1) 0.0 (−4.8, 4.8)
Age 60–69 years§ 1.6 (−3.7, 7.0) 2.0 (−3.3, 7.4) 1.8 (−3.4, 7.1)
Philadelphia site† −0.1 (−3.9, 3.8) 1.4 (−2.5, 5.4) 1.1 (−2.8, 5.0)
Married or domestic partner† 3.5 (−0.4, 7.4) 3.3 (−0.8, 7.4) 2.1 (−2.1, 6.3)
WOMAC score¶ −0.11 (−0.24, 0.02) −0.11 (−0.24, 0.02) −0.09 (−0.22, 0.03)
Employed† 4.2 (−1.0, 9.5) 4.1 (−1.1, 9.3)
Income <$15,000 per year# −2.1 (−6.4, 2.3) −2.1 (−5.7, 3.0)
Income $15,000–$29,999 per year# −1.7 (−6.3, 2.8) −1.7 (−5.7, 3.2)
Less than a high school degree** −4.5 (−10.2, 1.2) −3.0 (−8.8, 2.8)
High school or GED diploma** −4.9 (−9.0, −0.8)‡ −3.6 (−7.7, 0.5)
REALM-R score ≤6¶ 0.3 (−3.7, 4.2)
Trust in Physicians survey score¶ 0.4 (0.1, 0.6)‡
*Values are the differences in adjusted mean Joint Replacement Expectations Survey (JRES) scores (95% confidence intervals). GED = general
educational development; see Table 2 for additional definitions.
†Difference in adjusted mean JRES score for patients in category compared with those not in category.
‡P < 0.05.
§Difference in adjusted mean JRES score for patients in category compared with patients age 70–79.
¶Difference in adjusted mean JRES score per unit increase in score.
#Difference in adjusted mean JRES score for patients in category compared with patients with annual income exceeding $30,000.
**Difference in adjusted mean JRES score for patients in category compared with patients with an associate’s degree or higher.
Arthritis Rheum. Author manuscript; available in PMC 2011 July 11.