Psychometric properties of the Dominic Interactive in a large French sample
10
Original Research Psychometric Properties of the Dominic Interactive in a Large French Sample Taraneh Shojaei, MD 1 ; Ashley Wazana, MD, FRCP 2 ; Isabelle Pitrou, MD, MSc 3 ; Fabien Gilbert, MSc 4 ; Lise Bergeron, PhD 5 ; Jean-Pierre Valla, MD 5 ; Viviane Kovess-Masfety, MD, PhD 6 Key Words: psychometrics, child psychiatry, school-aged children, questionnaire, mental health The Canadian Journal of Psychiatry, Vol 54, No 11, November 2009 W 767 Objectives: To examine the psychometric properties of the Dominic Interactive (DI) in school-aged children in a different cultural environment than Quebec. Methods: In a large French region, 100 schools and 25 children (aged 6 to 11 years) per school were randomly selected. Data were collected using self-administered questionnaires to children (DI), parents (sociodemographic characteristics, mental health services use), and teachers (child school achievement). DI psychometric properties were assessed by examining: the distribution of each DI diagnosis; comorbidity between diagnoses; alpha coefficients measuring internal consistency; and correlates of psychopathologies with sociodemographic status and health care services use. Estimates of DI properties were compared with those from a sample of community children in Quebec. Results: Complete data were available for 1274 children (54.4%). The internal consistency of each DI diagnosis of the French version was reasonable, with Cronbach’s alpha coefficients ranging from 0.62 to 0.89. The psychometric properties and comorbidity were consistent with the version from Quebec. Conclusions: The satisfactory psychometric properties of the DI along with other demonstrated advantages of this instrument (children enjoy the activity, parents approve of it, and it is cost-effective) and its cultural adaptability support the consideration of the DI for epidemiologic studies in diverse cultures. Can J Psychiatry. 2009;54(11):767–776. Clinical Implications · The psychometric performances of the DI were satisfactory and consistent in the French and Quebec samples. · Findings suggest the wider applicability of the DI to epidemiologic studies in diverse cultures. Limitations · The main limitation was the parents’ low response rate and Quebec study sample size. · DI does not make straightforward Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, (DSM-IV) diagnoses: it is only indicative of tendencies toward any DSM-IV disorder.
-
Upload
independent -
Category
Documents
-
view
7 -
download
0
Transcript of Psychometric properties of the Dominic Interactive in a large French sample

Original Research
Psychometric Properties of the Dominic Interactive ina Large French Sample
Taraneh Shojaei, MD1; Ashley Wazana, MD, FRCP
2; Isabelle Pitrou, MD, MSc
3;
Fabien Gilbert, MSc4; Lise Bergeron, PhD
5; Jean-Pierre Valla, MD
5;
Viviane Kovess-Masfety, MD, PhD6
Key Words: psychometrics, child psychiatry, school-aged children, questionnaire,mental health
The Canadian Journal of Psychiatry, Vol 54, No 11, November 2009 � 767
Objectives: To examine the psychometric properties of the Dominic Interactive (DI) in
school-aged children in a different cultural environment than Quebec.
Methods: In a large French region, 100 schools and 25 children (aged 6 to 11 years) per
school were randomly selected. Data were collected using self-administered questionnaires
to children (DI), parents (sociodemographic characteristics, mental health services use),
and teachers (child school achievement). DI psychometric properties were assessed by
examining: the distribution of each DI diagnosis; comorbidity between diagnoses; alpha
coefficients measuring internal consistency; and correlates of psychopathologies with
sociodemographic status and health care services use. Estimates of DI properties were
compared with those from a sample of community children in Quebec.
Results: Complete data were available for 1274 children (54.4%). The internal consistency
of each DI diagnosis of the French version was reasonable, with Cronbach’s alpha
coefficients ranging from 0.62 to 0.89. The psychometric properties and comorbidity were
consistent with the version from Quebec.
Conclusions: The satisfactory psychometric properties of the DI along with other
demonstrated advantages of this instrument (children enjoy the activity, parents approve of
it, and it is cost-effective) and its cultural adaptability support the consideration of the DI
for epidemiologic studies in diverse cultures.
Can J Psychiatry. 2009;54(11):767–776.
Clinical Implications
� The psychometric performances of the DI were satisfactory and consistent in the French andQuebec samples.
� Findings suggest the wider applicability of the DI to epidemiologic studies in diverse cultures.
Limitations
� The main limitation was the parents’ low response rate and Quebec study sample size.
� DI does not make straightforward Diagnostic and Statistical Manual of Mental Disorders,Fourth Edition, (DSM-IV) diagnoses: it is only indicative of tendencies toward any DSM-IVdisorder.

Child mental health assessment requires input from several
informants usually parents, teachers, and children them-
selves.1–3 Reliance on parent or teacher reports, excluding the
child, is problematic.4 Parents may be influenced by their own
psychopathology, or may have limited information about
norms for children or variation in intellectual abilities.5,6 Simi-
larly, teachers may not have adequate opportunities to observe
the child in other settings or might have limited access to child
internalizing psychopathology.
Several studies reported that children aged as young as 5 or 6
years were capable of providing valid reports of depressed
mood and feelings.7–11 Few studies reported estimates of prev-
alence of child psychopathology using child self-report at a
young age (aged 6 years and older) as most instruments avail-
able are designed for children aged 9 years and older.12–15
Among the few self-report psychiatric instruments for
school-aged children, the Pictorial Instrument for Children
and Adolescents offered an attempt to assess DSM-III-R Axis
I psychiatric disorders in children aged 6 to 16 years using
drawings.16 Unfortunately, its development has been aban-
doned. Two recent studies have reported good evidence for
the reliability of young child (aged 5 years) self-report with
the structured Berkeley Puppet Interview5,17 but it is designed
for younger children and requires time and personnel
availability.
The DI is a self-report instrument for children aged as young
as 6 years, which is easy to administer in the general popula-
tion.18,19 Using 91 cartoon-based questions about symptoms
and strengths, probability diagnoses are generated for the
most prevalent DSM-IV psychopathologies.20 The original
version of the DI (Dominic-R) was a paper and pencil test
based on DSM-III-R criteria; the DI is a self-administered,
computerized version of the Dominic-R. DI was developed
and validated in Quebec originally in English and French, and
since has been translated into Spanish and German and has
been used in diverse settings and countries.19,21–24 The charac-
ter represented in the cartoon depicts the sex of the child
assessed, and can appear with a Caucasian (Dominic),
Hispanic (Gabi), African (Terry), or Asiatic (Ming) appear-
ance.19 In Europe, a French version has been adapted to the
French context through the modification of a few drawings
for a better acceptance.25 For example, the picture of Dominic
lying dead in a coffin was replaced by Dominic looking at a
grave in a cemetery to conform to norms in France, and the
French voice-over has been recorded with an accent from
France instead of from Quebec. More detailed information
on the instrument is available from the Dominic website.26
Several studies have reported on the performance of the orig-
inal Dominic-R. Reliability of the Dominic-R compared
favourably with that of other child assessment questionnaires
and was better than that of other structured interviews in
young children. Kappa values for the concordance between
Dominic-based diagnoses and clinical judgment-based
DSM-III-R diagnoses ranged from 0.64 to 0.88.18 The DI
computer version has been studied as well.23,25,27 In the
French version of the DI, internal consistency, as measured
by Cronbach’s alpha, ranged from 0.55 for SPh to 0.84 for
ADHD.25 Moderate to excellent internal consistency for each
DI diagnosis category has been reported for the Quebec
French version.28 Also it has been reported that the version
developed for African-American children (Terry) was a cul-
turally sensitive questionnaire with good reliability.22
Our study’s objective was to examine the psychometric prop-
erties of the DI computer version in a large regional French
sample and to compare the findings across 2 francophone
populations from different cultural backgrounds. To assess
the psychometric performances of the DI, we considered: the
distribution of each DI diagnosis; the comorbidity between
diagnoses; the internal consistency in our sample and that of a
convenience sample in Quebec; and the correlates of DI diag-
noses with known sociodemographic risk factors and health
care services use.
Methods
A cross-sectional survey was conducted from November
2004 to March 2005 in France’s south-eastern region of
Provence-Alpes-Côte d’Azur, with an estimated population
of 4 750 000 inhabitants.29 Key methodological aspects are
reported below; detailed methodology is reported exten-
sively in a previous paper.30
Participants
A stratified multistage probability sample was used to ensure
representativeness across schools of this area. The sampling
frame was the list of all primary schools: public and private,
urban and rural. Among the 100 primary schools randomly
selected, 99 accepted to participate. Twenty-five children
were randomly selected in each school, 5 from grades 1 to 5.
Contacts were attempted for 2341 children.
� La Revue canadienne de psychiatrie, vol 54, no 11, novembre 2009768
Original Research
Abbreviations used in this article
ADHD attention-deficit hyperactivity disorder
CD conduct disorder
DI Dominic Interactive
DSM Diagnostic and Statistical Manual of Mental Disorders
GAD generalized anxiety disorder
MDD major depressive disorder
ODD oppositional defiant disorder
SAD separation anxiety disorder
SPh specific phobia

The study design was approved by the French National Confi-
dentiality Committee. Participating parents received clear
information on the study, their written consent was manda-
tory, and anonymity was guaranteed.
Main Outcome Measures
Data were collected using questionnaires administered to 3
informants: parents (sociodemographic characteristics,
parental psychological distress, and health care services use);
children (DI)18; and teachers (child school achievement).
Measures of Child Psychopathology
The DI computer version allows screening for the following 7
disorders: SPh, MDD, SAD, GAD, ADHD, ODD, and CD. In
our study, children completed the DI at a computer station at
school, under the indirect supervision of a research assistant,
with 5 children in each session. During its administration, a
few introductory pictures familiarized the child with the soft-
ware. Colour cartoons and a voice-over depicted a child,
Dominic, in various daily life situations: at home, at school,
and with other children. The cartoons illustrated the abstract
emotional and behavioural content of DSM-IV
symptomatology. The voice-over describing the symptom
asked the child whether he or she feels or does what the child
in the picture is feeling or doing. Children responded by click-
ing on yes or no boxes, thus disclosing their own reactions
when they are faced with these situations. The children’s
answers were recorded on a floppy disk, leaving no informa-
tion on the computer’s hard drive.
Symptoms were scored as 0 for no and 1 for yes and were
summed for each of 7 diagnostic groups. An algorithm
assigned the child to 1 of the 3 diagnostic probability catego-
ries: likely absent, possible, and likely present using cut-off
points reported by Valla et al.19 For reporting purposes, and as
recommended by the author of the instrument, we considered
children in the category likely present as having one of the 7
screened disorders.
Correlates of Child Psychopathology
A range of child, family, and socioeconomic factors known to
correlate with psychiatric disorders were collected in parents’
questionnaires.21,24 The correlates between DI scales and
those variables were examined as an external validation strat-
egy. Child and family characteristics included age, sex, birth-
place, chronic medical conditions, stressful life events, and
family structure (single- or 2-parent). Parents’ characteristics
included educational level (highest educational level), aver-
age family income (as compared with the national poverty
standard of €646 per month per capita, that is, US$824,
Can$974), occupational activity, unemployment (at least one
parent), and psychological distress (using Mental Health 5, a
5-item subscale measuring psychological distress, part of a
generic quality-of-life instrument: Short Form 3631–33). Other
factors collected were school area profile (disadvantaged or
not, urban, or rural) and school status (public or private).
School achievement was assessed by teachers by comparing
children’s school performance to that of other classmates,
using a 5-point Likert scale (very low to very good).
DI Comparisons
To compare French DI internal consistency with the original
Quebec French version, we considered results from a conve-
nience sample of 453 children aged 6 to 11 years who were
randomly selected in schools of a suburban area of
Montreal.28 To compare the comorbid diagnoses, we consid-
ered results from the Quebec Child Mental Health Survey.21
The details of the respective methodologies are previously
published but not for the internal consistency.
Statistical Analysis
Prior to statistical analyses, each subject was assigned a
weight computed as the product of the inverse probability of
being selected in the survey. To examine the performances of
the computer version of the DI, we first described the statisti-
cal distributions of each DI diagnosis. To assess internal con-
sistency, we calculated Cronbach’s alpha coefficient for each
diagnostic category and compared them to the Quebec data
available. Finally, we examined the comorbidity between the
different DI diagnosis and the correlates of psycho-
pathologies with sociodemographic status and health care
services use using logistic regression models.
The statistical analyses were performed with STATA SE,
Version 9 (Stata Corporation, College Station, TX).
ResultsAmong the 2341 eligible children, 462 parents (19.7%) did
not accept to participate and 531 (22.7%) did not return the
questionnaire. Response rates to the DI and parent question-
naires were 75.5% (n = 1767) and 57.6% (n = 1348), respec-
tively. Completed data were available for 1274 children
(54.4%).
Sociodemographic characteristics of children included are
reported in Table 1.
Distributions of DI Symptom Score
Score distribution and cut-off points of the 7 DI symptom
scales are reported by sex in Figure 1. Most internalizing dis-
orders (SAD, GAD, and MDD) seemed to have a Gaussian
density distribution for both sexes. SPh was normally distrib-
uted in girls, contrary to boys. The 3 externalizing disorders
(CD, ODD, and ADHD) were approximated by an asymp-
totic distribution. Distributions were compared for the 2 age
categories (ages 6 to 8 years and 9 to 11 years) and showed no
difference (data not shown).
Psychometric Properties of the Dominic Interactive in a Large French Sample
The Canadian Journal of Psychiatry, Vol 54, No 11, November 2009 � 769

Internal Consistency
The internal consistency (Table 2) measured by Cronbach’s
alpha coefficients was very good for internalizing and
externalizing disorders (� = 0.87 and � = 0.89, respec-
tively). SAD and SPh had the lowest internal consistency,
although fair (� = 0.62). In the Quebec sample, Cronbach’s
alpha coefficients were 0.90 and 0.89 for internalizing and
externalizing disorders, respectively, and 0.66 for SAD and
0.57 for SPh.
Comorbidity
According to the recommended cut-offs for the DI,19 25.4%
of children had at least one disorder, with no statistical signif-
icant difference between the sexes (26.9% for girls, com-
pared with 23.9% for boys, P = 0.30) and 10.6% had at least 2
diagnoses. The estimates ranged from 4.8% for MDD to
9.4% for SAD. The rate of SPh was higher in girls (10.8%,
compared with 5.5%, P < 0.001), while ADHD and CD were
significantly higher in boys (6.5%, compared with 3.6% for
ADHD; 8.6%, compared with 2.8% for CD, P � 0.001). The
likelihood of the association between internalizing disorders
(Table 3) ranged from OR 4.3 (95% CI 2.4 to 7.4, P � 0.001)
(MDD and SPh) to OR 23.5 (95% CI 14.1 to 39.3, P � 0.001)
(GAD and MDD). The strength of the association between
externalizing disorders ranged from OR 9.4 (95% CI 5.7 to
15.6, P � 0.001) (ODD and CD), OR 11.2 (95% CI 6.7 to
18.8, P � 0.001) (ADHD and CD), and OR 11.2 (95% CI 6.7
to 18.7, P � 0.001) (ADHD and ODD). There was a strong
overlap between externalizing disorders and MDD, with
odds ratios ranging from OR 8.5 (95% CI 4.9 to 14.6,
P � 0.001) (MDD and CD) to OR 19.7 (95% CI 11.5 to 33.6,
P < 0.001) (MDD and ADHD). The association was strong
between ADHD and GAD (OR 10.2, 95% CI 6.2 to 16.8,
P < 0.001), ODD and GAD (OR 13.7, 95% CI 8.5 to 22.1,
P � 0.001) and less important between externalizing disor-
ders and SAD (OR from 3.9 to 5.8, P < 0.001), externalizing
disorders and SPh (OR from 3.2 to 5.1, P � 0.001).
Correlates of Child Mental Health Problems
Internalizing and externalizing disorders were less frequent
in older children (aged 9 to 11 years) (OR 0.6, 95% CI 0.4 to
0.8, P � 0.001) (Table 4). Girls were more likely to have inter-
nalizing disorders (OR 1.4, 95% CI 1.1 to 2.0, P � 0.02), but
less likely to have externalizing disorders (OR 0.7, 95% CI
0.4 to 1.0, P � 0.03). Children born outside of France had a
2-fold higher rate of internalizing disorders (OR 2.1, 95% CI
1.1 to 4.0, P � 0.02). Teacher-reported low performance at
school was associated with an increase of OR 1.9 (95% CI 1.3
to 2.9, P � 0.01) and OR 2.8 (95% CI 1.7 to 4.4, P � 0.001) of
internalizing and for externalizing disorders, respectively.
� La Revue canadienne de psychiatrie, vol 54, no 11, novembre 2009770
Original Research
Table 1 Sociodemographic characteristics of aFrench regional sample of children aged 6 to 11years (n = 1274)
Variable n (%)
Child characteristics
Sex
Boys 636 (50.2)
Girls 638 (49.8)
Age, years
6–8 735 (59.2)
9–11 526 (40.8)
Family structure
2-parent 1109 (86.7)
Single-parent 165 (13.3)
Birthplace
France 1217 (95.5)
Outside of France 57 (4.5)
Socioeconomic characteristics
Demographic area
Rural 198 (7.6)
Urban 1076 (92.4)
Disadvantaged school area
No 1142 (89.5)
Yes 132 (10.5)
School status
Public 1110 (89.0)
Private 164 (11.0)
Parent characteristics
Responding parent
Mother 1049 (82.3)
Father 225 (17.7)
Parental education
<High school 462 (37.7)
�High school 801 (62.3)
Unemployment (at least 1
parent)
No 1106 (87.4)
Yes 152 (12.6)
Incomea
High 951 (81.7)
Low 200 (18.3)
aCompared with the national poverty standard of €646 per month percapita

High parental education was protective both for internalizing
and for externalizing disorders. Parental unemployment was
associated with an increased risk of 1.6-fold (95% CI 1.0 to
2.3, P � 0.03) of any psychopathology, whereas a parent being
an executive was a protective factor for internalizing and
externalizing disorders, compared with employees category.
No association was found for chronic conditions, stressful life
events, family structure, and parental psychological distress.
Both internalizing and externalizing disorders were associ-
ated with low performance at school as reported by the
teacher.
Correlates of Child Mental Services Contact
In the past 12 months, 150 children (11.8%) had contact with a
mental health service. Children with externalizing disorders
were more likely to have contact with a mental health profes-
sional (OR 3.2, 95% CI 2.0 to 5.0, P � 0.001) and the
association was statistically significant for boys (OR 3.5,
95% CI 2.0 to 6.2, P � 0.001) and girls (OR 2.4, 95% CI 1.1 to
5.4, P � 0.03). There was no overall association with internal-
izing disorders (OR 1.4, 95% CI 0.9 to 2.2, P � 0.13). Glob-
ally, boys were more likely to have contact with mental health
professionals than girls: OR 2.6, 95% CI 1.5 to 4.3, P � 0.01
and OR 1.1, 95% CI 0.6 to 2.0, P � 0.5, respectively. Boys
with internalizing disorders had increased services use
(OR 2.2, 95% CI 1.3 to 3.9, P � 0.01) and use was signifi-
cantly higher for GAD (OR 4.2, 95% CI 1.8 to 9.5, P � 0.001)
and MDD (OR 3.9, 95% CI 1.7 to 9.0, P � 0.001). For
externalizing disorders, the association was statistically sig-
nificant for ADHD (OR 2.6, 95% CI 1.2 to 5.8, P � 0.02), CD
(OR 3.9, 95% CI 2.0 to 7.7, P � 0.001), and ODD (OR 3.5,
95% CI 1.6 to 7.8, P � 0.01). In girls, mental health services
Psychometric Properties of the Dominic Interactive in a Large French Sample
The Canadian Journal of Psychiatry, Vol 54, No 11, November 2009 � 771
Table 2 Internal consistency (Cronbach alpha coefficient) of DI diagnosis according to age and sex in a Frenchregional sample of children aged 6 to 11 years (n = 1274) and Quebec sample (n = 453)
Total Aged 6–8 years Aged 9–11 years Boys Girls
Mental disorder
(number of items per
scale)
France
n = 1767
Canada
n = 453
France
n = 1009
Canada
n = 231
France
n = 742
Canada
n = 222
France
n = 903
Canada
n = 225
France
n = 864
Canada
n = 228
SPh (n = 9) 0.62 0.57 0.62 0.59 0.57 0.55 0.65 0.56 0.55 0.53
SAD (n = 8) 0.62 0.66 0.61 0.64 0.62 0.66 0.59 0.65 0.64 0.67
GAD (n = 15) 0.75 0.74 0.76 0.75 0.73 0.73 0.73 0.72 0.76 0.75
MDD (n = 20) 0.80 0.80 0.80 0.81 0.79 0.80 0.80 0.80 0.79 0.81
Internalizing disorders 0.87 0.90 0.88 0.90 0.85 0.89 0.87 0.89 0.87 0.89
ADHD (n = 19) 0.83 0.86 0.83 0.86 0.83 0.85 0.84 0.87 0.82 0.84
ODD (n = 9) 0.72 0.76 0.70 0.75 0.75 0.76 0.71 0.77 0.73 0.74
CD (n = 14) 0.80 0.74 0.82 0.78 0.77 0.67 0.83 0.79 0.71 0.63
Externalizing disorders 0.89 0.90 0.89 0.91 0.89 0.89 0.90 0.91 0.87 0.88
Table 3 Comorbidity between DI diagnoses in a French regional sample of children aged 6 to 11 years (n = 1274)using OR (95% CIs)
Mental health
disorder
SPh
n = 140
SAD
n = 165
GAD
n = 120
MDD
n = 84
ADHD
n = 91
ODD
n = 107
CD
n = 105
SPh — 4.4 (2.8–6.8) 6.5 (4.1–10.3) 4.3 (2.4–7.4) 3.2 (1.8–5.6) 3.9 (2.3–6.6) 5.1 (3.1–8.4)
SAD — 9.2 (6.0–14.2) 10.7 (6.6–17.5) 5.8 (3.5–9.4) 5.3 (3.3–8.4) 3.9 (2.4–6.3)
GAD — 23.5
(14.1–39.3)
10.2 (6.2–16.8) 13.7 (8.5–22.1) 3.8 (2.2–6.6)
MDD — 19.7
(11.5–33.6)
11.7 (6.9–19.9) 8.5 (4.9–14.6)
ADHD — 11.2 (6.7–18.7) 11.2 (6.7–18.8)
ODD — 9.4 (5.7–15.6)
CD —
— = OR 1
� La Revue canadienne de psychiatrie, vol 54, no 11, novembre 2009772
Original Research
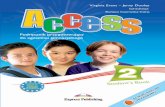
Table 4 Child and family correlates of DI psychopathology scales in a French regional sample of children aged 6to 11 years (n = 1274) using OR (95% CIs)
Variable Internalizing disorders Externalizing disorders Any disorders
Child characteristics
Aged 9 to 11 years 0.5 (0.4–0.7) 0.8 (0.5–1.2) 0.6 (0.4–0.8)a
Sex
Boys 1 1 1
Girls 1.4 (1.1–2.0)b
0.7 (0.4–1.0)b
1.2 (0.9–1.5)
Birthplace
France 1 1 1
Outside of France 2.1 (1.1–4.0)b
1.8 (0.8–4.0) 2.0 (1.1–3.7)b
Stressful life events
0 or 1 1 1 1
�2 1.1 (0.8–1.6) 1.3 (0.8–2.1) 1.3 (0.9–1.8)
School achievement
High 1 1 1
Low 1.9 (1.3–2.9)c
2.8 (1.7–4.4)a
2.3 (1.6–3.3)a
Chronic physical illness
No 1 1 1
Yes 0.9 (0.6–1.4) 1.0 (0.6–1.6) 0.9 (0.6–1.3)
Parent and family characteristics
Family structure
2-parent 1 1 1
Single-parent 1.3 (0.8–2.0) 0.9 (0.5–1.6) 1.2 (0.8–1.7)
Parental education
Low 1 1 1
High 0.6 (0.4–0.8)a
0.6 (0.4–0.9)c
0.6 (0.4–0.7)a
Unemployment
No 1 1 1
Yes (at least 1 parent) 1.5 (0.9–2.3) 1.4 (0.8–2.4) 1.6 (1.0–2.3)b
Occupational activity
Employees 1 1 1
Agricultural, craft, and trade 0.8 (0.5–1.3) 0.6 (0.3–1.0) 0.8 (0.5–1.2)
Executives 0.4 (0.3–0.7) 0.5 (0.3–1.0)b
0.4 (0.3–0.7)a
Intermediate 0.8 (0.5–1.3) 0.5 (0.3–1.0)b
0.7 (0.4–1.0)
Manual workers 1.0 (0.6–1.8) 0.9 (0.4–1.8) 0.9 (0.5–1.6)
No activity 1.3 (0.8–2.3) 1.3 (0.7–2.4) 1.4 (0.9–2.3)
Parents’ psychological distress
No 1 1 1
Yes 1.1 (0.8–1.7) 1.5 (1.0–2.3) 1.4 (0.9–1.9)
All analyses are univariate.
aP < 0.001;
bP < 0.05;
cP < 0.01

Psychometric Properties of the Dominic Interactive in a Large French Sample
The Canadian Journal of Psychiatry, Vol 54, No 11, November 2009 � 773
Figure 1 Score distribution and cut-off points of the 7 DI symptom scales according to sex (n = 1274)
Legend
Dash lines indicate cut-off points and separate
probability diagnostic zones into 3:
– 1: likely absent
– 2: possible
– 3: likely present

use was significantly higher for MDD and ODD: OR 3.1, 95%
CI 1.1 to 8.8, P � 0.03 and OR 4.1, 95% CI 1.7 to 10.1, P �
0.01, respectively.
Discussion
Limitations
One limit comes from parents low response rate. To assess a
possible response bias, responding and nonresponding par-
ents were compared according to school area and status, and
child characteristics (age and sex), and did not reveal statisti-
cal differences. Despite this low response rate, it is important
to note that our study’s objective was to report data related to
the psychometric properties of the DI and not to provide prev-
alence rates of mental health disorders in the general popula-
tion. A second limit is related to the Quebec convenience
sample, whose size was limited to 453 children and used a
sampling strategy different from ours. In the Quebec survey,
children were randomly selected from the general population
and outpatients clinics; in the French sample, only children
from the general population were selected.
Third, the DI does not make straightforward DSM-IV diagno-
ses but rather DSM-IV–based diagnostic approximates. Con-
sequently the DI is only indicative of tendencies toward any
DSM-IV disorder. The DI does not collect information about
frequency, duration of symptoms, or age of onset because the
cognitive maturity of children aged 6 to 11 years limits their
comprehension of abstract concepts.18,34 To compensate for
the lack of severity assessment at the symptom level and the
lack of assessment of significant distress or impairment
accompanying the disorder, frequency and duration criteria
have been replaced with a cut-off point of increasing severity
at the disorder level. These differences between DI diagnostic
approximations and straightforward DSM-IV diagnoses limit
the instrument’s ability to diagnose children.
Main Findings
Our study reports on the psychometric properties of a child
instrument, the DI, in a large epidemiologic sample of French
children aged 6 to 11 years, by analyzing statistical distribu-
tions, internal consistency, and correlates of DI diagnosis.
Externalizing disorders were approximated by an asymptotic
distribution, whereas internalizing disorders seemed to have a
normal density distribution. These findings open up an inter-
esting research perspective to explain how children
self-report a normal level of internalizing symptoms, whereas
external disorders are reported in a different manner where no
or few symptoms is the norm. Interestingly, the distribution of
SPh in girls is a Gaussian curve, whereas it is an asymptotic
curve in boys, underlying the scarcity for boys. These results
can contribute substantively to establishing the norms of psy-
chiatric assessments of children.
Second, our paper establishes the consistency of the DI
across the francophone culture by comparing French and
Quebec DI psychometric properties. The internal consis-
tency coefficients were very similar to the Quebec sample,
with a Cronbach’s alpha of 0.90 both for externalized and for
internalized disorders. The lowest alpha coefficients were for
SAD (0.62) and SPh (0.62) as in the Quebec sample (0.66 and
0.57). The internal consistency estimates remained consis-
tent across age groups and sex as in the Quebec sample. The
main difference between French and Quebecois results was
for CD coefficients, which were higher in the French sample.
The comorbidity between externalizing and internalizing
disorders was similar to that from the Quebec Child Mental
Heal th Survey. Correlates of mental heal th
psychopathologies reported here (aged 6 to 8 years, low
school achievement, low parental education, parental unem-
ployment) are consistent with results of previous epidemio-
logic studies.35–37 The association between DI and such
theoretically related constructs as known sociodemographic
risk factors and services use further contribute to the validity
(face and external validity, and coherence) of this
self-reported instrument.38
Clinical Implications
The psychometric properties of the DI were satisfactory and
results were consistent with those of the Quebec sample. The
DI could then contribute more widely to the field of clinical
and epidemiologic assessment. In a clinical setting, it offers a
simple assessment specially designed for children aged 6 to
11 years that is both appealing to children and easy to use by
professional. At initial interview, the DI provides a system-
atic overview of the child’s symptoms as the child perceives
them. This offers an alternative to the often lengthy process
needed to build up a trustworthy relationship with the child.
The DI can be particularly helpful with questions that might
trigger uneasiness, provoke denial, or jeopardize the relation-
ship with the child, or for children who might find it difficult
to talk about sensitive topics, for example, suicidal thoughts.
Although the DI instrument does not replace clinical assess-
ment, it can provide a helpful and rapid screening of child
psychopathologies.
Moreover, the adaptation of the DI to different cultures is
very easy to implement. Contrary to most psychiatric instru-
ments, it only requires the translation of 91 short phrases ask-
ing if the child has experienced what the drawing is showing.
For this reason, the DI has been selected, together with parent
and teacher the Strengths and Difficulties Questionnaire, in a
current European project, whose main objective is to produce
a kit for measuring child mental health in Europe. The DI has
been translated for 5 of the 7 participating countries (Italy,
� La Revue canadienne de psychiatrie, vol 54, no 11, novembre 2009774
Original Research

Romania, Lithuania, Bulgaria, and Turkey); German and
Dutch versions were already available.
Psychometric performances have been assessed in other
versions of the DI as, for example, Terry, developed for
African-American children; test–retest reliability and internal
consistency were satisfactory, with intraclass correlations
coefficients ranging from 0.75 to 0.80, and Cronbach’s alpha
from 0.78 to 0.90.22 The instrument’s reliability and its easy
adaptability added to other advantages of the DI (children
enjoy the activity, parents approve of it, and it is cost-
effective) suggest its wider applicability in epidemiologic
studies in other cultures, especially for immigration studies
where children from diverse cultures could be compared with
the children living in the country of origin.
Conclusion
Performances estimated for each DI diagnosis were satisfac-
tory and psychometric properties were consistent in the
French and Quebec samples. In epidemiologic studies, DI
permits young children to achieve informant status and the
pictorial design allows transposition in diverse cultures and
languages. The satisfactory psychometric performances and
the adaptability of the DI to other cultures suggest its wider
applicability to epidemiologic studies in diverse cultures.
Funding and Support
Our research was funded by la Mutuelle d’Assurances des Eleves,Mutuelle d’Assurances des Instituteurs de France Foundation,Mutuelle Générale de l’Education Nationale Foundation for PublicHealth, Federation Nationale de la Mutualité Francaise and theRegional Directorate for Health and Social Affairs (DirectionRégionale des Affaires Sanitaires et Sociales) of theProvence-Alpes-Côte d’Azur region, France.
Acknowledgements
We are indebted to Dr Christine Chan-Chee, Dr Robert Goodman,French Ministry of Health and Social Affairs, French Ministry ofEducation, Provence-Alpes-Côte d’Azur Regional Directorate forHealth and Social Affairs, Aix-Marseille and Nice EducationalAuthority, as well as children, parents, teachers, and principals ofparticipating schools.
References
1. Achenbach TM, McConaughy SH, Howell CT. Child/adolescent behavioral and
emotional problems: implications of cross-informant correlations for situational
specificity. Psychol Bull. 1987;101:213–232.
2. Bird HR, Gould MS, Staghezza B. Aggregating data from multiple informants in
child psychiatry epidemiological research. J Am Acad Child Adolesc Psychiatry.
1992;31:78–85.
3. Jensen PS, Rubio-Stipec M, Canino G, et al. Parent and child contributions to
diagnosis of mental disorder: are both informants always necessary? J Am Acad
Child Adolesc Psychiatry. 1999;38:1569–1579.
4. Deater-Deckard K, O’Connor TG. Parent-child mutuality in early childhood: two
behavioral genetic studies. Dev Psychol. 2000;36(5):561–570.
5. Arseneault L, Moffitt TE, Caspi A, et al. Strong genetic effects on
cross-situational antisocial behaviour among 5-year-old children according to
mothers, teachers, examiner-observers, and twins’ self-reports. J Child Psychol
Psychiatry. 2003;44:832–848.
6. Kagan J, Snidman N, Arcus D. Childhood derivatives of high and low reactivity
in infancy. Child Dev. 1998;69:1483–1493.
7. Ialongo NS, Edelsohn G, Kellam SG. A further look at the prognostic power of
young children’s reports of depressed mood and feelings. Child Dev.
2001;72:736 –747.
8. McClellan JM, Werry JS. Introduction—research psychiatric diagnostic
interviews for children and adolescents. J Am Acad Child Adolesc Psychiatry.
2000;39:19–27.
9. Rebok G, Riley A, Forrest C, et al. Elementary school-aged children’s reports of
their health: a cognitive interviewing study. Qual Life Res. 2001;10:59–70.
10. Christman A, Egger H, Compton SN, et al. Assessment of childhood
depression. Child Adolesc Psychiatry Ment Health. 2006;11(2):111–116.
11. Warren SL, Dadson N. Assessment of anxiety in young children. Curr Opin
Pediatr. 2001;13:580–585.
12. Goodman R. The extended version of the Strengths and Difficulties
Questionnaire as a guide to child psychiatric caseness and consequent burden.
J Child Psychol Psychiatry. 1999;40:791–799.
13. Goodman R, Ford T, Simmons H, et al. Using the Strengths and Difficulties
Questionnaire (SDQ) to screen for child psychiatric disorders in a community
sample. Br J Psychiatry. 2000;177:534–549.
14. Angold A, Costello EJ. The Child and Adolescent Psychiatric Assessment
(CAPA). J Am Acad Child Adolesc Psychiatry. 2000;39:39–48.
15. Angold A, Prendergast M, Cox A, et al. The Child and Adolescent Psychiatric
Assessment (CAPA). Psychol Med. 1995;25:739–753.
16. Ernst M, Cookus BA, Moravec BC. Pictorial Instrument for Children and
Adolescents (PICA-III-R). J Am Acad Child Adolesc Psychiatry.
2000;39:94–99.
17. Arseneault L, Kim-Cohen J, Taylor A, et al. Psychometric evaluation of 5- and
7-year-old children’s self-reports of conduct problems. J Abnorm Child
Psychol. 2005;33:537–550.
18. Valla JP, Bergeron L, Berube H, et al. A structured pictorial questionnaire to
assess DSM-III-R-based diagnoses in children (6–11 years): development,
validity, and reliability. J Abnorm Child Psychol. 1994;22:403–423.
19. Valla JP, Bergeron L, Smolla N. The Dominic-R: a pictorial interview for 6- to
11-year-old children. J Am Acad Child Adolesc Psychiatry. 2000;39:85–93.
20. American Psychiatric Association. Diagnostic and statistical manual of mental
disorders. 4th ed. Washington (DC): APA; 1994.
21. Bergeron L, Valla JP, Breton JJ, et al. Correlates of mental disorders in the
Quebec general population of 6 to 14-year olds. J Abnorm Child Psychol.
2000;28:47–62.
22. Bidaut-Russell M, Valla JP, Thomas JM, et al. Reliability of the Terry: a mental
health cartoon-like screener for African-American children. Child Psychiatry
Hum Dev. 1998;28:249–263.
23. Scott TJ, Short EJ, Singer LT, et al. Psychometric properties of the Dominic
interactive assessment: a computerized self-report for children. Assessment.
2006;13:16–26.
24. Bergeron L, Valla JP, Smolla N, et al. Correlates of depressive disorders in the
Quebec general population 6 to 14 years of age. J Abnorm Child Psychol.
2007;35:459–474.
25. Chan Chee C, Kovess V, Valla JP, et al. Validation d’un questionnaire interactif
sur la santé mentale des enfants de 6 à 11 ans. Annal Medic Psy. 2003:439–445.
26. Digital Interactive Multimedia Assessment Tools Inc. The Dominic Interactive
[Internet]. Westmount (QC):Digital Interactive Multimedia Assessment Tools
Inc; 2004 [cited 2009 Oct 1]. Available from:
http://www.dominicinteractive.com.
27. Valla JP, Kovess V, Chan Chee C, et al. A French study of the Dominic
Interactive. Soc Psychiatry Psychiatr Epidemiol. 2002;37:441–448.
28. Bergeron L, Smolla N, Valla JP, et al. Psychometric properties of the Dominic
Interactive in children aged 6–11. Annual meeting of the American Academy of
Child and Adolescent Psychiatry (AACAP); 2007 Oct; Boston (MA).
29. Oger P. Provence-Alpes-Cotes d’Azur : la région compte 4 743 000 habitants
[Internet]. Provence-Alpes-Cotes d’Azur (FR) : Institut national des statistiques
économiques (INSEE); 2006. Available from: http://www.insee.fr/fr/
insee_regions/provence/themes/sud_essentiel/sie88/sie88.pdf.
30. Shojaei T, Wazana A, Pitrou I, et al. The strengths and difficulties
questionnaire: validation study in French school-aged children and
cross-cultural comparisons. Soc Psychiatry Psychiatr Epidemiol.
2009;44(9):740–747. Epub 2008 Dec 19.
31. Aaronson NK, Acquadro C, Alonso J, et al. International Quality of Life
Assessment (IQOLA) Project. Qual Life Res. 1992;1:349–351.
32. Korkeila J, Lehtinen V, Bijl R, et al. Establishing a set of mental health
indicators for Europe. Scand J Public Health. 2003;31:451–459.
33. McCabe CJ, Thomas KJ, Brazier JE, et al. Measuring the mental health status
of a population: a comparison of the GHQ-12 and the SF-36 (MHI-5). Br J
Psychiatry. 1996;169:516–521.
34. Yates T. Theories of cognitive development. In: Lewis M, editor. Child and
adolescent psychiatry. Baltimore (MD): Williams & Wilkins; 1990.
35. Costello EJ, Angold A, Burns BJ, et al. The Great Smoky Mountains Study of
Youth. Goals, design, methods, and the prevalence of DSM-III-R disorders.
Arch Gen Psychiatry. 1996;53:1129–1136.
36. Bird HR, Gould MS, Yager T, et al. Risk factors for maladjustment in Puerto
Rican children. J Am Acad Child Adolesc Psychiatry. 1989;28:847–850.
Psychometric Properties of the Dominic Interactive in a Large French Sample
The Canadian Journal of Psychiatry, Vol 54, No 11, November 2009 � 775
37. Velez CN, Johnson J, Cohen P. A longitudinal analysis of selected risk factors
for childhood psychopathology. J Am Acad Child Adolesc Psychiatry.
1989;28:861–864.
38. Westen D. Quantifying construct validity: two simple measures. J Pers Soc
Psychol. 2003;84(3):608–618.
Manuscript received November 2008, revised, and accepted February2009.1Public Health Practitioner, EA 4069 Paris Descartes University,Fondation MGEN pour la Santé Publique, Paris, France.2Assistant Professor, McGill University, Institute of Community andFamily Psychiatry; Montreal, Quebec; Child Psychiatrist, Jewish GeneralHospital, Montreal, Quebec.
3Public Health Practitionner, EA 4069 Paris Descartes University,Fondation MGEN pour la Santé Publique, Paris, France.4Statistician, EA 4069 Paris Descartes University, Fondation MGEN pourla Santé Publique, Paris, France.5Researcher, Department of Psychiatry, Rivière-des-Prairies Hospital,Fernand-Seguin Research Center, Université de Montréal, Montreal,Quebec.6Psychiatrist Head, EA 4069 Paris Descartes University Paris, France.Address for correspondence: Pr V Kovess, EA 4069 Paris DescartesUniversity, 15 rue de l’école de médecine 75270 Paris Cedex 06, France;[email protected]
� La Revue canadienne de psychiatrie, vol 54, no 11, novembre 2009776
Original Research
Résumé : Propriétés psychométriques du Dominique interactif dans un vaste
échantillon français
Objectifs : Examiner les propriétés psychométriques du Dominique interactif (DI) chez des enfants
d’âge scolaire dans un environnement culturel différent de celui du Québec.
Méthodes : Dans une grande région française, 100 écoles et 25 enfants (de 6 à 11 ans) par école ont
été choisis au hasard. Les données ont été recueillies par des questionnaires auto-administrés aux
enfants (DI), aux parents (caractéristiques sociodémographiques, utilisation des services de santé
mentale), et aux enseignants (rendement scolaire). Les propriétés psychométriques du DI ont été
évaluées en examinant : la distribution de chaque diagnostic du DI; la comorbidité entre les
diagnostics; les coefficients alpha mesurant la cohésion interne; et les corrélations des
psychopathologies avec le statut sociodémographique et l’utilisation des services de santé. Les
estimations des propriétés du DI ont été comparées avec celles d’un échantillon de la population
d’enfants du Québec.
Résultats : Des données complètes étaient disponibles pour 1274 enfants (54,4 %). La cohésion
interne de chaque diagnostic du DI de la version française était raisonnable, les coefficients alpha de
Cronbach allant de 0,62 à 0,89. Les propriétés psychométriques et de comorbidité concordaient
avec celles de la version québécoise.
Conclusions : Les propriétés psychométriques satisfaisantes du DI ainsi que d’autres avantages
démontrés de cet instrument (les enfants aiment l’activité, les parents l’approuvent, il est rentable) et
son adaptabilité culturelle soutiennent que le DI soit considéré pour des études épidémiologiques
dans diverses cultures.