Behavioral and Psychological Symptoms in Alzheimer’s Disease

lable at ScienceDirect
Behaviour Research and Therapy 55 (2014) 27e39
Contents lists avai
Behaviour Research and Therapy
journal homepage: www.elsevier .com/locate/brat
Provoking symptoms to relieve symptoms: A randomized controlleddismantling study of exposure therapy in irritable bowel syndrome
Brjánn Ljótsson a,*, Hugo Hesser b, Erik Andersson c, Jeffrey M. Lackner d, Samir El Alaoui c,Lisa Falk e, Kristina Aspvall a, Josefin Fransson a, Klara Hammarlund a, Anna Löfström a,Sanna Nowinski a, Perjohan Lindfors e,f, Erik Hedman a,g
aDepartment of Clinical Neuroscience, Division of Psychology, Karolinska Institutet, Nobels väg 9, 171 65 Stockholm, SwedenbDepartment of Behavioural Sciences and Learning, Linköping University, Linköpings universitet, 581 83 Linköping, SwedencDepartment of Clinical Neuroscience, Division of Psychiatry, Karolinska Institutet, Karolinska Universitetssjukhuset Huddinge, M46,141 86 Stockholm, SwedendDepartment of Medicine, University at Buffalo School of Medicine and Biomedical Science, ECMC, 462 Grider Street, Buffalo, NY 14215, USAeDepartment of Gastroenterology, Sabbatsbergs hospital, Olivecronas väg 1, 113 61 Stockholm, SwedenfDepartment of Medicine Huddinge, Karolinska Institutet, M54, Karolinska Universitetssjukhuset Huddinge, 141 86 Stockholm, SwedengDepartment of Clinical Neuroscience, Osher Center for Integrative Medicine, Karolinska Institutet, Retzius väg 8 171 77 Stockholm, Sweden
a r t i c l e i n f o
Article history:Received 26 April 2013Received in revised form10 January 2014Accepted 31 January 2014Available online 10 February 2014
Keywords:Irritable bowel syndromeDismantling studyExposureInternetRandomized controlled trial
Abbreviations: ACT, Acceptance and Commitmentfunctional bowel disorders; GSA, Gastrointestinal symDepression Scale; IBS, Irritable bowel syndrome; IBS-Internet-based cognitive behavior therapy without expWorking Alliance Inventory.* Corresponding author. Department of Clinical Neu
65 62.E-mail addresses: [email protected], brjann@g
(J.M. Lackner), [email protected] (S. El [email protected] (K. Hammarlund), [email protected] (E. Hedman).
http://dx.doi.org/10.1016/j.brat.2014.01.0070005-7967/� 2014 Elsevier Ltd. All rights reserved.
a b s t r a c t
An internet-delivered cognitive behavioral treatment (ICBT) based on systematic exposure exercises haspreviously shown beneficial effects for patients with irritable bowel syndrome (IBS). Exposure exercises maybeperceivedasdifficult forpatients toperformbecauseof theelicited short-termdistressandcliniciansmaybereluctant touse these interventions. Theaimof this studywas to compare ICBTwith the sameprotocolwithoutsystematic exposure (ICBT-WE) to assess if exposure had any incremental value. This randomized controlleddismantling study included 309 participants diagnosed with IBS. The treatment interventions lasted for 10weeks and included online therapist contact. ICBT-WE comprised mindfulness, work with life values, accep-tance, and encouraged reduced avoidance behaviors, while ICBT also included systematic exposure to IBSsymptomsand related situations. Severityof IBS symptomswasmeasuredwith theGastrointestinal SymptomRating Scalee IBS version (GSRS-IBS). The between-groupCohen’sd onGSRS-IBSwas 0.47 (95%CI: 0.23e0.70)at post-treatment and 0.48 (95% CI: 0.20e0.76) at 6-month follow-up, favoring ICBT. We conclude that thesystematic exposure included in the ICBT protocol has incremental effects over the other components in theprotocol. This study provides evidence for the utility of exposure exercises inpsychological treatments for IBS.
� 2014 Elsevier Ltd. All rights reserved.
Introduction
Irritable bowel syndrome (IBS) is a functional gastrointestinaldisorder with a prevalence of about 11% (Lovell & Ford, 2012) that isassociated with diminished work capacity, increased healthcare
Therapy; AUDIT, Alcohol Use Disorptom-specific anxiety; GSRS-IBS,QOL, Irritable Bowel Syndrome Quosure; MADRS-S, The Montgomer
roscience, Division of Psychology, K
mail.com (B. Ljótsson), hugo.hessoui), [email protected] (L. [email protected] (A. Löfström
used, reduced quality of life, and low responsiveness to pharmaco-logical treatments (Camilleri & Chang, 2008; Drossman et al., 1993;Halder et al., 2004; Talley, Gabriel, Harmsen, Zinsmeister, & Evans,1995). Several types of psychological treatments have been evalu-ated for IBS, including for example cognitive behavior therapy (CBT),
ders Identification Test; CBT, Cognitive behavior therapy; CSFBD, Cognitive scale forGastrointestinal Symptom Rating Scale e IBS version; HADS, Hospital Anxiety andality of Life Instrument; ICBT, Internet-based cognitive behavior therapy; ICBT-WE,yeÅsberg Depression Rating Scale e Self report; VSI, Visceral Sensitivity Index; WAI,
arolinska Institutet, Fogdevreten 2a, SE-171 65 Stockholm, Sweden. Tel.: þ46 70 717
[email protected] (H. Hesser), [email protected] (E. Andersson), [email protected]), [email protected] (K. Aspvall), [email protected] (J. Fransson),), [email protected] (S. Nowinski), [email protected] (P. Lindfors),

B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e3928
psychodynamic therapy, hypnotherapy, and mindfulness (Ford,Talley, Schoenfeld, Quigley, & Moayyedi, 2009; Gaylord et al., 2011;Lackner, Mesmer, Morley, Dowzer, & Hamilton, 2004). However,treatment effects are inconsistent across studies of the same treat-ment type andno single psychological treatment has emerged as themost effective treatment approach for IBS (Ljótsson et al., 2013).
One reason for the inconsistent effects between studies of psy-chological treatments for IBS may be that most treatments do nottarget gastrointestinal symptom-specific anxiety (GSA; Labus et al.,2004). GSA is an IBS-specific phenomenon that has been proposedto play a causal role in the maintenance of IBS symptoms and IBS-related disability and refers to heightened anxiety towards IBSsymptoms and IBS-associated situation (such as not being near atoilet) and behavioral attempts to avoid these stimuli (Labus et al.,2004). GSA has been shown to negatively impact symptom severityand quality of life in IBS (e.g., Craske et al., 2011; Labus, Mayer,Chang, Bolus, & Naliboff, 2007; Labus et al., 2004; Reme, Darnley,Kennedy, & Chalder, 2010). Recently, several studies have beenpublished where the treatments under investigation have includedinterventions that explicitly target GSA (Craske et al., 2011; Gaylordet al., 2011; Hunt, Moshier, & Milonova, 2009; Ljótsson, Andersson,et al., 2011; Ljótsson, Andréewitch, et al., 2010; Ljótsson, Falk, et al.,2010; Ljótsson, Hedman, Andersson, et al., 2011). These studieshave generally produced large treatment effects on IBS symptomsand quality of life and individual studies have demonstrated long-term societal cost-savings (Andersson et al., 2011; Ljótsson,Andersson, et al., 2011), maintenance of improvements over 12e18 months (Ljótsson, Andersson, et al., 2011; Ljótsson, Hedman,Lindfors, et al., 2011), and superiority over active treatment con-trols (Craske et al., 2011; Ljótsson, Hedman, Andersson, et al., 2011).Furthermore, process studies have indicated that symptom im-provements were mediated through decrease in GSA in several ofthese studies (Garland et al., 2011; Hunt et al., 2009; Ljótsson et al.,2013;Wolitzky-Taylor, Craske, Labus, Mayer, & Naliboff, 2012).Withthe exception of the study by Gaylord et al. (2011), which studiedmindfulness for IBS, these studies (Craske et al., 2011; Hunt et al.,2009; Ljótsson, Andersson, et al., 2011; Ljótsson, Andréewitch,et al., 2010; Ljótsson, Falk, et al., 2010; Ljótsson, Hedman,Andersson, et al., 2011) have investigated cognitive behavioraltreatments that have included exposure to target GSA. Exposuretherapy involves systematic and repeated contact with a stimulithat evokes conditioned aversive responses (e.g., fear) whileabstaining from behaviors that are consistent with the emotionalresponse (e.g., avoidance and safety behaviors) and/or engaging inbehaviors that are inconsistent with the emotional response (e.g.,approach; Barlow, Allen, & Choate, 2004; White & Barlow, 2002).Repeated exposure is proposed to lead to long-term extinction, orinhibition, of the emotional response to the aversive stimuli (Craskeet al., 2008). Exposure therapy is often used in CBT for anxietydisorders to decrease fear and avoidance of bodily (Forsyth & Fusé,2008) and situational (Hazlett-Stevens & Craske, 2008) stimuli.However, as noted above, most CBT protocols for IBS do not targetIBS-related fear or avoidance and, consequently, do not includeexposure as means of reducing GSA. An explanation for the lack oftreatments using exposure to target GSA may be that exposure toIBS symptoms and IBS-related aversive situations by definitionmeans short-term increase in symptom experience. This may makeboth patients and clinicians reluctant to try exposure-based in-terventions. Indeed, surveys have shown that some mental healthpractitioners and patients perceive exposure in psychologicaltreatments as an ineffective and unethical intervention (Olatunji,Deacon, & Abramowitz, 2009). Thus, showing that exposure has aunique value in treating IBS may have important clinical implica-tions for how IBS is conceptualized and managed, both withinmedical and psychological care.
Several of the studies of the effect of exposure for IBS have beenconducted by our group, using the internet to deliver the treatment(Ljótsson, Andersson, et al., 2011; Ljótsson, Falk, et al., 2010;Ljótsson, Hedman, Andersson, et al., 2011). Internet-based CBT(ICBT) is a treatment format that been found produce treatmenteffects that are comparable to those of face-to-face CBT for bothsomatic and psychiatric diagnoses (Hedman, Ljótsson, & Lindefors,2012). We have previously shown that the ICBT protocol is superiorto a stress management treatment (Ljótsson, Hedman, Andersson,et al., 2011), which indicates that the treatment has specific ef-fects that cannot be attributed to expectation of improvement ortherapeutic attention. However, the ICBT protocol that we haveemployed has also included principles adapted from acceptanceand commitment therapy (ACT; Hayes, Strosahl, & Wilson, 1999),for example mindfulness training and emphasis on living a valuedlife together with IBS symptoms rather then letting the symptomscontrol your life (“values-based behavior change”) This means thata number of interventions besides the exposure exercises couldhave accounted for the superior improvement compared to stressmanagement. Work with life values and mindfulness has beenfound to reduce emotional reactivity and avoidance impulses(Levin, Hildebrandt, Lillis, & Hayes, 2012) andmindfulness has beensuccessfully evaluated as a stand-alone intervention for IBS(Gaylord et al., 2011). In a recently developed ACT protocol for IBS(Ferreira, Eugenicos, Morris, & Gillanders, 2011), the disabilityassociated with IBS is explained as a process of experientialavoidance (i.e., a model conceptually similar to GSA), but there ismuch less focus on systematic exposure with the purpose ofextinction and more focus on reducing avoidance in order to live afull live (i.e., values-based behavior change). A pilot study indicatedthat the ACT treatment led to improvement in IBS symptoms andquality of life for patients who completed the treatment (Ferreira,2011). Although the ACT-inspired components in the treatmentdeveloped by our group are not as comprehensive as in the full ACTtreatment developed by Ferreira et al. (2011), their work, studies onmindfulness for IBS, and the studies of values work in general,suggest that other treatment components than exposure couldhave accounted for the improvements we have observed in ourstudies. Furthermore, in CBT for depression, it has been observedthat patients’ acceptance of a treatment rationale for behaviorchange has an independent positive effect on outcome (Addis &Jacobson, 2000). Thus, if education about the maintaining andexacerbating effects of avoidance and control behaviors on IBSsymptoms is cogent and compelling, it may be enough to elicitbehavior change and consequently decrease symptoms.
In order to evaluate the incremental effect of exposure, weemployed a randomized controlled dismantling design inwhich thefull ICBT treatment package was compared to a treatment thatincluded all treatment interventions except for systematic exposureto IBS symptoms and IBS-related situations (“ICBT without expo-sure”; ICBT-WE). Thus,we controlled for both important non-specific(e.g., maturation, positive expectations, and therapist contact) andspecific technical components (e.g., psychoeducation, mindfulnesstraining, and values-based behavior change procedures) of thetreatment.Wepostulated that ICBTwould lead toamorepronouncedlong-term extinction effect through repeated exposure to condi-tioned stimuli in IBS, and hence larger improvements in symptoms,quality of life, and GSA than ICBT-WE.We also explored if therewereincremental effects of exposure on depression and anxiety and ifparticipation in the study was associated with any adverse events.
Methods
This study is reported in accordance with the CONSORT state-ment for non-pharmacological trials (Boutron, Moher, Altman,

B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e39 29
Schulz, & Ravaud, 2008). Clinicaltrials.gov registration ID:NCT01529567.
Recruitment and sample
Power considerationsIn our previous trial inwhich the exposure-based treatment was
compared to stress management, we obtained a post-treatmentbetween-group effect size of d ¼ 0.38 (Ljótsson, Hedman,Andersson, et al., 2011). Assuming a similar effect size in thisstudy, we aimed at recruiting 300 participants to obtain a 90%power with an a level of .05.
Inclusion criteriaParticipants were eligible for the study if they declared to have
had a previous diagnosis of IBS given by a physician, presently ful-filled the Rome III-criteria for IBS (Longstreth et al., 2006), and wereolder than 18 years of age. The following alarm symptoms that havebeen shown to predict presence ofmore serious organic diseases andmay warrant follow-up examination (Spiller et al., 2007) were causefor exclusion: (a) blood in stool without satisfactory medical expla-nation (such as known hemorrhoids), (b) diarrhea-predominant IBSwith no colonoscopy performed, (c) rapid weight loss that could notbe linked to change in diet, and (d) recent unexamined change instool frequencyor form if older than50years of age. In addition to thealarm symptoms, the following criteria were cause for exclusion: (e)any presence of current or previous inflammatory bowel disease, (f)lactose or gluten intolerance where proper dietary adjustments hadnot been made, (g) severe alcohol dependence, severe depressivesymptoms, or suicidal ideation, and (h) insufficient language orcomputer skills to perform an online text-based treatment.
ProcedureRecruitment for this study started on November 27, 2011 and
ended on December 31, 2011. Participants were recruited throughself-referral and information about the study was spread throughseveral channels, for example newspaper advertisments, an onlinediscussion forum about IBS, and a web portal for internet-basedtreatment studies. When applicants registered for the study, theywere given personal user accounts with unique usernames andpasswords. First they completed an online screening where theyconfirmed that they had been diagnosed with IBS by a physician,completed the Rome III Adult Questionnaire (Drossman et al.,2006), and answered questions about inclusion criteria aed (pres-ence of alarm symptoms) and inclusion criteria e, f and h. Thescreening also included the Alcohol Use Disorders IdentificationTest (Saunders, Aasland, Babor, la Fuente de, & Grant, 1993) and theMontgomeryeÅsberg Depression Rating Scale e Self report(MADRS-S; Svanborg & Åsberg, 1994).
After participants had completed the screening and submittedwritten consent, their answers were reviewed. Based on thefollowing assessment algorithm, participants were (I) excludeddirectly, (II) scheduled for a telephone interview, or (III) includeddirectly: I. Participants who lacked two or more criteria for fulfill-ment of an IBS diagnosis or did not fulfill criterion h were excludeddirectly. II. Participants who lacked one criterion for fulfillment ofIBS diagnosis, reported food intolerance but no adjustment in diet,confirmed any alarm symptom, or scored high on the AUDIT (�8) orthe MADRS-S (�30 total score or �4 on the suicide ideation item)were scheduled for an interview. The purpose of the interview wasto gather more information to enable a clinical assessment ofwhether the participants fulfilled all criteria for inclusion. Thestructured interviews were performed by advanced graduate psy-chology students. Throughout this process the graduate studentsreceived supervision by the principal investigator (BL), licensed
clinical psychologist, and a gastroenterologist (PL). BL and PL alsodecided on inclusion or exclusion based on the data collected.III. Participantswho fulfilled criteria for an IBS diagnosis at screeningand did not otherwise present any information that required furtherinvestigation were included directly after screening.
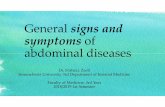
A total of 417 persons completed the screening and submittedwritten consent and 311 were included and randomized. Afterrandomization, two participants were excluded from the study. Oneparticipant had to undergo a medical procedure, not related to IBS,two weeks into treatment. Another participant informed theresearch team that he/she had been diagnosed with Crohn’s diseaseduring the follow-up period. Both these participants were excludedfrom all data analyses, and thus the study sample consisted of 309participants,156 in the ICBT-WEgroupand153 in the ICBTgroup. Theflow of participants through the trial is described in Fig. 1. Table 1contains participant demographics and medical history of the par-ticipants. Participants received no compensation for their participa-tion in the treatment. This studywasapprovedby the regional ethicalreview board in Stockholm, Sweden, on 23 November 2011.
RandomizationRandomization was performed by a researcher independent of
the research team. A list of anonymous participant identificationnumbers was sent to the researcher who used a true randomnumber service (www.random.org) to allocate the participants toeither the ICBT or ICBT-WE condition. Because some participantswere included directly based on their screening answers whileothers were interviewed before inclusion, the randomization wasstratified to control for the influence of the differential inclusionprocedure. After random allocation of the participants, the list wasreturned to the research team. The participants were then assignedto the treatment conditions by a member of the research team andthe assignments were double checked by the principal investigator.All participants were randomized simultaneously on 5 February2012 and the treatments started one day after randomization.
Interventions
Method of deliveryIn both conditions the respective treatment was delivered via
internet and lasted for 10 weeks. In this type of internet-based psy-chological treatment, participants read online self-help texts thatcontain both educationmaterial and instructions on how to performthe exercises that constitute the treatment. The general principle isthat the treatment should reflect face-to-face therapy in terms ofcontent, while using an online therapist to guide the participantsthrough the course of the treatment. Eleven therapists conducted thetreatments, five of whom were advanced graduate psychology stu-dents and six of whomwere clinical psychologists. Therapists wererandomly assigned to participants from both conditions in equalnumbers to control for any therapist-specific effects. During treat-ment, therapist contactwas usually initiated by the participantswhowere encouraged to send at least one message per week about theirwork with the treatment to their therapist. Participants were givenfeedback within 2e3 days after they had written a message. Threetypes of feedback were generally given by the online therapists: (1)Corrective psychoeducational information if the participant’s an-swers indicated thathe/shehadnot fullygrasped the rationale for thetreatment; (2) General support to maintain or increase the intensityof the participant’sworkwith the treatment; (3) Guidance on how toperform and evaluate the exercises prescribed by the treatment.
Difference between treatment conditionsThe two treatments were identical with the exception that ICBT,
but not ICBT-WE, included a component of systematic exposure to

Fig. 1. Participation flow through the study.
B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e3930
IBS-related situations and symptoms. Both treatments weredivided into successive steps that participants had to complete inorder to gain access to the next. The ICBT-WE treatment wasdivided into three successive steps and the ICBT condition also
included a fourth step comprising systematic exposure. The treat-ment steps are described in Table 2. Participants in the ICBT-WEcondition were encouraged to reach step 3 in three weeks andwork with the values-based behavior change until the last week of

Table 1Sample characteristics.
Total sample(n ¼ 309)
ICBT-WEGroup(n ¼ 156)
ICBT Group(n ¼ 153)
Female % 79.5% 75.2% 77.3%Age m (SD) 42.4 (14.5) 41.9 (14.9) 43.0 (14.1)Duration of IBS symptoms
m (SD) [median]15.9 (12.4)[12.0]
16.3 (12.9)[12.0]
15.5 (11.9)[12.0]
Years since diagnosis m(SD) [median]
8.4 (9.4) [5.0] 8.8 (9.7) [5.0] 7.9 (9.1) [5.0]
Years since last consultationwith physician because ofIBS m (SD) [median]
2.2 (2.5) [1.0] 2.2 (2.7) [1.0] 2.2 (2.2) [1.0]
Predominant bowel typeConstipation % 26.5% 29.5% 23.5%Diarrhea % 40.5% 37.8% 43.1%Mixed % 12.9% 12.2% 13.7%Unsubtyped % 20.1% 20.5% 20.5%
In relationship 72.8% 69.2% 76.5%EducationElementary school % 3.2% 3.9% 3.6%High school % 24.4% 19.6% 22.0%University <3 year % 17.3% 21.6% 19.4%University �3 years % 52.6% 52.3% 52.4%PhD degree % 2.6% 2.6% 2.6%
Employment statusEmployed % 68.3% 65.4% 71.2%Unemployed % 5.5% 5.8% 5.2%Student % 13.6% 16.0% 11.1%Retired % 12.6% 12.8% 12.4%
B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e39 31
the 10 week treatment, while participants in the ICBT conditionwere encouraged to reach step 4 in four weeks and work with thevalues-based behavior change and exposure exercises until the lastweek of treatment. After reaching the third or fourth step(depending on condition), participants were expected to returnweekly reports to their therapist, detailing their work with thebehavior changes prescribed in their respective condition. The re-ports in the ICBT-WE condition included questions about howparticipants had let their IBS interfere with their valued directionsin different life domains during the last week and how they had
Table 2Description of the treatment steps for both conditions.
Step Contents
1 Both conditions. Explanation how symptom-related behaviors may maintamin exercise during which the patient observes and labels inner and outeimmediate awareness of current thoughts, GI symptoms, feelings, and b
2 Both conditions. Explanation of a psychological model of IBS. The learninganxiety on gastrointestinal functioning and how it increases awareness o
3 Both conditions. The role of negative thoughts in exacerbating IBS-relatedproposed as an alternative to attempts to control these experiences. Expawareness and fear of IBS symptoms and decrease quality of life. Participathen engage in values-based behavioral change where they focus on meexperiences. Instructions on how to use mindfulness as an aid to chooseobserving and labeling their environment during exposure, i.e., aversive, nfrom and suppression of thoughts and emotions. By attending to any impless inclined to act on these impulses. Comprehensive examples are givenexperienced symptom relief and increased quality of life by changing th
4 ICBT condition only. The ICBT participants continue their behavioral changgradual systematic exposure to IBS symptoms and related experiences bsymptoms by engaging in activities that provoke symptoms, such as eatincontrol behaviors, such as distraction, repeated toilet visits, eating certaiwhere symptoms are unwanted, such as attending a meeting when exper4) For constipation-predominant participants: scheduling of toilet visits.of urgency and toilet visits. Instructions on how to use mindfulness duriimportance of planning and repeating exposures is emphasized. Participatheir exposure exercises. The patient examples in step 3 are expanded w
Last step Both conditions. How to handle relapses into avoidance behaviors and howmain lessons learned, what has been gained through the treatment and
changed their behavior to be more in line with their valued direc-tion in these domains. The reports in the ICBT condition alsoincluded detailed descriptions of the exposure exercise(s) thatparticipants had engaged in during the last week. Therapists sentmobile text messages (SMS) with reminders to participants whodid not return a report for more than a week. Both treatmentconditions included identical information about relapse-prevention that was made available to all participants during thelast week of treatment.
In both conditions, participants examined their life values inimportant life domains such as close relationships, friendships,work and education, and leisure, analyzed how their IBS-relatedbehaviors interfered with these values, and set up behavioralgoals that were in line with those values. Thus, participants wereencouraged to spend less effort to avoid and control symptoms thatare essentially not under voluntary control. Mindfulness was taughtas a strategy to exercise observation of symptoms, thoughts, andfeelings without escaping them. Participants were informed thatfocusing on long-term valued goals instead of short-term distressavoidance would lead to several beneficial effects for them.Reduced behavioral avoidance would lead to extinction of fearassociated with symptoms, which in turn would relieve IBSsymptoms by affecting the positive feedback-loop between symp-toms, avoidance behaviors, and fear. The decoupling of behaviorfrom symptoms would also make the natural variations in IBSsymptoms less likely to induce disability and distress. Thereby, theparticipants would become less preoccupied with their symptomsand experience increased quality of life. The fourth step, presentonly in the ICBT condition, described how participants shouldsystematically and repeatedly challenge themselves by eliciting IBSsymptoms, engaging in aversive situations, and gradually weaningfrom safety and control behaviors. Participants in the ICBT condi-tion were informed that they would experience long-term reduc-tion of the distress associated with IBS-related stimuli by engagingin these systematic exposure exercises.
To ensure that the ICBT group received an additional interven-tion, which was not present in the ICBT-WE treatment, overarchingprinciples for all therapist communication in the two conditionswere established. In the ICBT-WE group, all therapist advice on
in focus on and vigilance towards symptoms. Two mindfulness exercises: 1. A 15-r experiences (practiced once daily). 2. A 20 s exercise that brings the patient intoehavioral impulses (practiced several times daily).of symptom-related fear through negative experiences of symptoms. The effect off threatening stimuli e specifically IBS-related stimuli.fear. A mindful and accepting stance towards negative thoughts and feelings is
lanation of how IBS-related avoidance and control behaviors maintain thents begin by recording how these behaviors prevent them from living a full life andaningful activities instead of trying to minimize symptoms and related negativemore functional ways of behaving in the presence of aversive experiences. Byeutral, and positive internal and external stimuli, patients will counter distractionulses to flee the situation or decrease the intensity of symptoms they will also beabout how IBS patients with different types of IBS symptoms and disability have
eir focus from avoidance of symptoms to living a valued life.e by recording all their avoidance, control and safety behaviors and then engage iny changing these behaviors. The exposure exercises include: 1) Exposure tog certain foods, physical activity, and stressful situations. 2) Reduction of safety andn foods, resting, and taking unprescribed medications. 3) Exposure to situationsiencing abdominal pain or riding the bus with fear of losing control of the bowels.5) For diarrhea-predominant participants: gradual increase in time between onsetng exposure to stay in contact with the aversive experience are also given. Thents are encouraged to formulate behavioral goals rather than emotional goals withith comprehensive descriptions on how to engage in exposure exercises.to maintain a widened behavioral repertoire. The participants also summarize thetheir future plans.

B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e3932
behavior change was based on whether the participants believedthat the behavior changewas in itself valuable andwould lead to anopportunity for them to live a richer life in important life domains.In contrast, participants in the ICBT group were also consistentlyencouraged to systematically challenge themselves through expo-sure exercises. The following example will illustrate this differencein therapeutic stance.
Many patients with IBS get up early in the morning to getenough time for a successful bowel movement in the morning. If,after carefully discussing the consequences of this habit with thetherapist, an ICBT-WE participant was satisfied with this routineand saw it as an opportunity to read the morning paper, she wouldnot have been encouraged to change the behavior. However, if theICBT-WE participant believed that this habit was a problem,because it took a lot of time or was a cause of frustration when thetoilet visits were unsuccessful, and these consequences negativelyaffected her family life or work, then the therapist would haveencouraged the participant to change the behavior and insteadfocus on performing morning behaviors that were in accordancewith her values. However, the therapist would not provide specificinstructions on how to engage in this behavior change. If theparticipant would ask for advice on how to conduct the behaviorchange, the therapist would encourage her to analyzewhat types ofalternative behaviors would bring her closer to living in accordancewith her values. This type of values-based analysis was also used inthe ICBT condition. However, the therapist would in addition alsohave recommended an ICBT participant to experiment with grad-ually changing the behavior regardless of whether it was regardedas problematic itself, to achieve extinction of morning-relateddistress. The participant would then formulate predictions aboutwhat could happen when leaving home without a successful toiletvisit, would planwhen to engage in the exposure exercises, analyzewhat possible safety behaviors she was at risk of using (e.g., eatingless breakfast, bringing medications when leaving home, still get-ting up an hour earlier to have the option to visit the toilet if any-thing unexpected happened), would formulate behavioral goals(e.g., not visit the toilet until one hour had passed after arriving towork), and would plan how to make the exercise increasingly morechallenging. After each exercise, the participant would evaluate theexercise in terms of behavioral goals met, the level of distressduring the exercise, and compare the experience with the pre-dictions that had been made. Participants were informed thatalthough the distress might not decrease during the exposure, theycould expect that over the course of several exposures, the distresswould gradually decrease.
Quality controlThe online therapists were supervised by the psychologist who
had developed the treatment manuals (BL). The therapist trainingincluded a half-day workshop and written material explaining theprincipal differences between the two treatment arms. During thestudy, all therapists had access to a closed online discussion forumwhere they could request advice on how to respond to participantenquiries. No assessments of the therapists’ treatment adherencewere made.
Assessments
Data collectionAll measures were administered online, a method which has
been shown to be reliable and produces results similar to tradi-tional paper-and-pencil administration (Hedman et al., 2010). Theoutcome measures were assessed at three time points; pre-treatment, post-treatment, and 6-month follow-up. Other
measures, which are not part of this report, were also administeredweekly during treatment.
Primary outcomeThe primary outcome measure of the study was the Gastroin-
testinal Symptom Rating Scale e IBS version (GSRS-IBS; Wiklundet al., 2003). The GSRS-IBS consists of 13 items covering severityof gastrointestinal symptoms. The items are scored between 1 (nodiscomfort at all) and 7 (very severe discomfort), rendering a totalscore between 13 and 91. The GSRS-IBS has demonstrated goodpsychometric properties for the different symptoms that areassessed, with an internal consistency (Cronbach’s a) ranging be-tween .74 and .85 and testeretest reliability between .55 and .70(Wiklund et al., 2003). Because IBS symptoms vary considerablyover time (Guilera, Balboa, & Mearin, 2005), the GSRS-IBS wasadministered weekly during four weeks at each of the threeassessment points. The mean GSRS-IBS score of these four weekswas used to get reliable estimates of the participants’ symptomlevels.
Secondary outcomesThe Irritable Bowel Syndrome Quality of Life Instrument (IBS-
QOL; Patrick, Drossman, Frederick, DiCesare, & Puder, 1998) is usedto assess the impact on quality of life for patients with IBS in severaldomains, including symptoms interference with activity, foodavoidance, dysphoric thoughts, and impact on relationships. TheIBS-QOL consists of 34 items scored between 1 and 6 and the totalscore is transformed to a 0e100 scale, where 0 represents mini-mum quality of life and 100 represents maximum quality of life.The IBS-QOL shows high internal consistency (Cronbach’s a ¼ .95)and testeretest reliability (r ¼ .86; Patrick et al., 1998).
The Visceral Sensitivity Index (VSI; Labus et al., 2004) is ameasure of GSA (i.e., distress, avoidance, and safety behaviors inresponse to IBS-related stimuli). The VSI contains 15 items, whichare scored between 1 and 6, rendering a total score between0 (minimum GSA) and 75 (maximum GSA). The VSI has demon-strated high internal consistency (Cronbach’s a ¼ .90e.92) and hasbeen shown to be associated with symptom severity (Craske et al.,2011) and diagnostic status of IBS (Labus, 2007) and also to be amediator of the effect of exposure-based CBT on IBS symptoms(Ljótsson et al., 2013; Wolitzky-Taylor et al., 2012).
The Cognitive Scale for Functional Bowel Disorders (Toner et al.,1998) measures negative thoughts about bowel function and per-sonality characteristics thought to be linked to IBS, for exampleperfection and need for social approval. The CSFBD includes 25items scored from 1 (strongly disagree) to 7 (strongly agree) with atotal score between 25 and 175. The CSFBD has demonstrated highinternal consistency (Cronbach’s a¼ .93) and is associated with lifeinterference due to bowel symptoms (Toner et al., 1998).
The Hospital Anxiety and Depression Scale (HADS; Zigmond &Snaith, 1983) measures the levels of anxiety and depression ontwo subscales, with 7 items each. Each item reflects a symptom ofdepression or anxiety and is scored between 0 and 3, with higherscores indicating more severe symptoms (total score range persubscale, 0e21). The instrument has shown good psychometricproperties within somatic healthcare with a testeretest reliabilityof r ¼ .72 and Cronbach’s a ¼ .89e.93 (Zigmond & Snaith, 1983).
Measures of non-specific factorsThe treatment credibility scale (Borkovec & Nau, 1972) consists
of five 10 point items and is used to measure how credible atreatment seems and how successful participants predict thetreatment will be in alleviating the target problems. The internalconsistency (Cronbach’s a) of the questions ranges between .69 and.83 and the testeretest reliability ranges between .75 and .82

B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e39 33
(Devilly & Borkovec, 2000). In this study, the treatment credibilityscale was administered after 2 weeks of treatment.
TheWorking Alliance Inventory (WAI; Tracey & Kokotovic, 1989)measures the alliance between patient and therapist in a psycho-logical treatment. The WAI measures the alliance in terms ofagreement on goal, agreement on treatment tasks, and personalbond between patient and therapist. Therapeutic alliance in face-to-face psychological treatments has been shown to be associatedwith the outcome of treatment (Martin, Garske, & Davis, 2000). Inthe present study, the 10-item version of the WAI was used, witheach item being scored between 1 and 7, giving a total score be-tween 10 and 70. The 10-itemWAI has demonstrated high internalconsistency (Cronbach’s a ¼ .97) (Busseri & Tyler, 2003). In thisstudy, the WAI was administered after 4 weeks of treatment.
Adverse eventsAt both post-treatment and 6-month follow-up, participants
were asked if they had experienced any adverse events that theyassociated with their participation in the study. For all adverseevents that were reported, participants rated the discomfort causedby the effect both when it occurred and the residual discomfort atthe time of assessment (i.e., the level of discomfort at the post-treatment or follow-up assessment). The ratings were made be-tween 0 (‘did not affect me at all’) and 3 (‘affected me verynegatively’).
Additional measuresParticipants who during treatment notified the research team
that they wished to discontinue treatment were asked to completean exist questionnaire detailing their reasons for discontinuation.Even though they had discontinued, these participants were askedto complete the post-treatment and follow-up up assessments. Atpost-treatment, participants were asked if they had started anyother pharmacological or non-pharmacological treatment duringthe treatment period. At follow-up, participants were asked abouthealthcare visits specifically related to IBS in the period betweentreatment completion and the 6-month follow-up.
Analysis
Continuous and repeatedly measured outcomes were analyzedusing mixed-effects regression for repeated-measures data(Muthén & Curran, 1997). This data analytic approach takes de-pendency in data into account by incorporating random effects (i.e.,individual differences in level and slope) in themodel in addition tofixed (i.e., average level and slope) and provides unbiased param-eters estimates in the presence of missing data under fairly unre-strictive assumptions (Gueorguieva & Krystal, 2004; Lane, 2008;Muthén & Curran, 1997). Given that the approach made use of allavailable data and all participants had at least one valid observation(i.e., the pre-treatment assessment), this made it a full intention-to-treat analysis. The inclusion of random effects and associatedcovariance structure were determined analytically using likelihoodratio tests. To adequately model the functional form of populationchange across all measurement points (pre, post, 6-month follow-up), change was modeled using linear and quadratic polynomialterms and error variance was held equal across time. Differences inlinear rates of change (i.e., slopes) were compared for the twoconditions. Estimated means (and variances) were obtained fromthe model and unstandardized and standardized between-groupeffect sizes (i.e., mean difference divided by the baseline standarddeviation) were calculated at post and 6-month follow-up using themodel-implied mean difference at these time points.
For non-repeated assessments, independent groups t-tests andchi-2 tests were used to assess differences between the treatment
conditions, depending on the scale of the measure. We alsoexplored the association between behavior change and symptom-atic improvement by correlating the post-treatment GSRS-IBS scorewith the number of reports about behavior change that participantsreturned, controlling for the pre-treatment GSRS-IBS score.
Results
Missing data
The number of participants completing the continuous outcomemeasures at each assessment point is detailed in Table 3. If par-ticipants did not complete the post-treatment and follow-upquestionnaires after several reminders, they were given the op-portunity to complete a reduced assessment battery including onlythe questionnaires of primary interest. Thus, the attrition differssomewhat between measures, with the main outcome GSRS-IBShaving the highest completion rate. One hundred and forty-sixICBT-WE participants (93.6%) and 146 ICBT participants (95.4%)completed the GSRS-IBS at post-treatment, while the correspond-ing numbers at follow-up were 135 ICBT-WE participants (86.5%)and 134 ICBT participants (87.6%). Given the small amount ofmissing data overall, we relied on full information maximumlikelihood estimation using all available data to return unbiasedestimates and standard errors under the assumption of ignorableconditional missing (Lane, 2008).
Discontinuation of treatment
In the ICBT-WE condition, 17 participants (10.9%) reported thatthey wished to discontinue treatment in comparison with 15participants (9.8%) in the ICBT condition. The most common rea-sons for discontinuation were insufficient time for participation(n ¼ 16), improvement since treatment start (n ¼ 7), low faith inthe treatment (n ¼ 7), not satisfied with the treatment format(n ¼ 7), and wanted to or had started another treatment (n ¼ 6).As presented below, 60.3% ICBT-WE and 54.9% ICBT participantsactually engaged in the behavior changes prescribed in theirtreatment arm. Thus, about 30% of the sample did neithercommence behavior change nor formally discontinue theirparticipation. These participants were not asked for their reasonfor not completing the treatment.
Continuous outcomes
Descriptive statistics for the continuous outcome measures andresults of the repeated-measures mixed effect regression analysisof the outcomes are presented in Table 3. For all outcome measuresthere were significant improvements over time across treatments(all p’s < .001). The coefficient in the model that tests for differentaverage linear rates of change across all time points (pre, post andfollow-up) as a function of treatment was significant for GSRS-IBS,IBS-QOL, VSI, and the HADS anxiety and depression subscales, fa-voring ICBT over ICBT-WE in all cases. Between-group effect sizes,derived from the mixed effect regression analyses, were small tomoderate at post-treatment and at 6-month follow-up. The largesteffect sizes at post and follow-up, d ¼ 0.47 and 0.48 respectively,were observed on the primary outcome GSRS-IBS. On the CSFBD, nosignificant difference in average rates of change between thegroups was observed (p > .05).
Treatment activity
During the treatment, participants in the ICBT-WE group sent amean of 9.5, SD ¼ 6.3, messages to their therapist and received 9.1,

Table 3Continuous treatment outcome measures.
ICBT-WE ICBT Between-group contrasts(Estimates from the mixed-effects regression analysis)
(95% CI)
n M SD n M SD Mean difference Effect size D in linear slope
GSRS-IBSPre 156 47.5 11.0 153 46.1 10.2Post 146 38.2 14.5 146 31.8 11.4 5.3 (2.6e7.9) 0.47 (0.23e0.70)Follow-up 135 37.3 13.4 134 32.2 12.3 5.4 (2.3e8.6) 0.48 (0.20e0.76) 2.0*** (0.8e3.2)VSIPre 156 38.8 16.7 153 37.2 17.1Post 144 26.5 17.4 142 21.5 16.4 4.9 (1.1e8.7) 0.30 (0.07e0.53)Follow-up 131 24.3 17.5 133 19.3 17.3 4.8 (0.5e9.0) 0.29 (0.03e0.55) 1.7*** (0.3e3.1)IBS-QOLPre 156 57.5 20.7 153 59.6 20.3Post 146 73.6 20.4 146 79.2 16.7 5.2 (0.8e9.5) 0.26 (0.04e0.49)Follow-up 134 76.5 19.8 133 81.4 18.2 5.1 (0.5e5.1) 0.26 (0.02e0.49) 1.6* (0.0e3.2)CSFBDPre 156 133.8 36.9 153 130.9 38.9Post 145 105.2 41.3 142 97.9 39.1 7.2 (1.5e15.9) 0.19 (0.04e0.42)Follow-up 118 99.0 40.1 129 88.8 40.6 10.2 (0.0e20.4) 0.27 (0.00e0.54) 2.1ns (�1.1 to 5.3)HADS anxietyPre 156 8.3 3.9 153 8.0 4.0Post 145 7.1 4.2 142 5.7 3.6 1.4 (0.5e2.3) 0.36 (0.13e0.59)Follow-up 118 6.7 4.0 129 5.7 4.2 1.1 (0.1e2.1) 0.29 (0.03e0.54) 0.6*** (0.2e0.9)HADS depressionPre 156 5.1 3.9 153 5.2 4.0Post 145 4.3 3.9 142 3.6 3.5 0.7 (0.2e1.5) 0.18 (0.05e0.40)Follow-up 118 3.9 4.0 129 3.3 3.4 0.7 (0.2e1.5) 0.17 (0.06e0.41) 0.4* (0.1e0.8)
CSFBD: Cognitive scale for functional bowel disorders; GSRS-IBS: Gastrointestinal Symptom Rating Scalee IBS version; HADS: Hospital Anxiety and Depression Scale; IBS-QOL:Irritable Bowel Syndrome Quality of Life Instrument; ICBT: Internet-based cognitive behavior therapy; ICBT-WE: Internet-based cognitive therapy without exposure; VSI:Visceral Sensitivity Index.Note. Observed means and standard deviations are presented. Mean differences and effect sizes are based on estimated means (and variances) from repeated-measuresmixed-effects regression analysis. Effect sizes are calculated as standardized mean difference using the baseline standard deviation (positive effect sizes always indicatefavorable treatment effects of ICBT as compared with ICBT-WE). D in linear slope denotes the average linear difference in change score between conditions across allmeasurement points (as a function of one unit change in time). ***p < .001, *p < .05.
B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e3934
SD ¼ 5.1, messages from their therapist, while the correspondingnumbers were 10.7, SD ¼ 6.8, and 10.0, SD ¼ 5.2, in the ICBT group.There were no significant differences in the number of messagessent, t(307) ¼ 1.69, p ¼ .093, or received, t(307) ¼ 1.38, p ¼ .170, bythe participants. The therapists spent a mean of 8.3 min, SD ¼ 6.7,per participant and week writing messages to the participants inthe ICBT-WE group and they spent 9.9 min (SD¼ 8.2) per week andparticipant the ICBT group, t(307) ¼ 1.88, p ¼ .061.
In the ICBT-WE condition, 93 participants (59.6%) completedtheir third step and began the values-based behavior change. In theICBT condition, 84 (54.9%) participants completed the fourth stepand began the exposure exercises (in addition to the values-basedbehavior change), a non-significant difference, c2(1) ¼ 0.70,p¼ .402. After completing the third and fourth steps (depending ontreatment condition), participants submitted weekly reports abouttheir behavior change (i.e., values-based behavior change in theICBT-WE condition and both values-based behavior change andexposure exercises in the ICBT condition). Participants returned 26.,SD ¼ 2.9, and 2.3, SD ¼ 2.7, behavior change reports on average inthe ICBT-WE and ICBT conditions, respectively, and the two treat-ment groups did not differ significantly in this regard t(309)¼ 0.94,p ¼ .35. The average number of behavior change reports alsoinclude the participants who did not complete the third and fourthsteps in the ICBT-WE and ICBT condition, respectively, and there-fore returned no behavior change reports. Removing these partic-ipants increased the average number of reports to 4.3 and 4.2 forthe two groups, respectively.
To investigate whether treatment activity (as prescribed by therespective treatments) was related to outcome, the number ofsubmitted behavior change reports was correlated with the post-
treatment GSRS-IBS score, while controlling for the pre-treatmentGSRS-IBS score. The correlation coefficients were r(143) ¼ �.16,p ¼ .052, and r(143) ¼ �.177, p ¼ .033 for the ICBT-WE and IBCTgroups, respectively. These correlations suggest that for the ICBTgroup, there was a significant relationship between the number ofreports returned and the improvement at post-treatment.
Treatment credibility and alliance
After 2 weeks of treatment, there was not a significant differ-ence in treatment credibility scores between the ICBT-WE,M ¼ 31.5, SD ¼ 10.1, and ICBT, M ¼ 33.0, SD ¼ 9.6, conditions,t(281) ¼ 1.26, p ¼ 0.209. On the WAI, there was no difference in therated alliance with the online therapist between the ICBT-WE,M ¼ 57.4, SD ¼ 16.5, and ICBT, M ¼ 60.1, SD ¼ 16.7, conditions af-ter 4 weeks of treatment, t(248) ¼ 1.33, p ¼ 0.183.
Other treatment seeking
At post-treatment, 20 of 144 (13.9%) ICBT-WE participants and17 of 142 (12.0%) ICBT participants reported that they had startedanother pharmacological or non-pharmacological treatment orconsulted a health-care professional during the study treatmentperiod, a non-significant difference, c2(1) ¼ 0.233, p ¼ .725. Themost common types of treatment seeking during treatment werecontact with a psychologist/psychotherapist (nICBT-WE ¼ 5,nICBT ¼ 5), consulting a dietitian and/or changing diet (nICBT-WE ¼ 6,nICBT ¼ 4), consulting a physician (nICBT-WE ¼ 4, nICBT ¼ 5), andchanging medication (nICBT-WE ¼ 4, nICBT ¼ 2). At the follow-upassessment, 27 of 126 (21.4%) ICBT-WE participants and 30 of 131

B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e39 35
(22.9%) ICBT participants reported further treatment seeking in theperiod between treatment completion and 6-month follow-up, alsoa non-significant difference, c2(1) ¼ 0.081, p ¼ .881. The mostcommon types of treatment seeking after treatment completionwere consulting a general practitioner (nICBT-WE ¼ 21, nICBT ¼ 15),specialist (nICBT-WE ¼ 13, nICBT ¼ 15), dietitian (nICBT-WE ¼ 9,nICBT ¼ 8), psychologist/psychotherapist (nICBT-WE ¼ 7, nICBT ¼ 8),and physical therapist (nICBT-WE ¼ 7, nICBT ¼ 2).
Adverse events
There were no significant differences in the proportion of par-ticipants reporting adverse events at post-treatment or follow-up.At post-treatment, 19 of 145 (13.1%) ICBT-WE participants and 29of 142 ICBT participants (20.4%), c2(1) ¼ 2.76, p ¼ .097, reported atotal of 55 adverse events from their participation in treatment.Twenty-two adverse events were given the highest severity rating(‘affected me very negatively’) when the effect occurred and 5adverse events were given the highest rating of residual discomfortat the time of the post-treatment assessment. On the 0e3 scale, themean severity when the effect occurred was 2.0 and the meanrating of residual discomfort was 0.8. The most common adverseevents were worsening of symptoms (n ¼ 31), stress because of thestudy (n ¼ 12) and depressed or anxious mood (n ¼ 6). At follow-up, 9 of 127 (7.1%) ICBT-WE participants and 3 of 131 (2.3%) ICBTparticipants, c2(1) ¼ 3.35, p ¼ .067, reported a total of 14 adverseevents after the treatment had been completed. Seven of the eventswere rated with the highest severity at the time of occurrence(mean rating ¼ 2.3) and 3 had the highest rate of residualdiscomfort at the 6-month follow-up (mean rating¼ 1.5). Increasedsymptoms (n ¼ 8) and depressed or anxious mood (n ¼ 4) were themost common adverse events after treatment completion.
Discussion
This studywas designed to investigate the incremental effects ofsystematic exposure in an empirically validated treatment of IBS.Compared to a package including psychoeducation, mindfulness,acceptance, and values work, all targeting a proposed behavioralpattern of maladaptive avoidance and control behaviors in IBS, theinclusion of systematic exposure in addition to these componentslead to larger improvements in IBS symptoms, quality of life, IBS-related fear and avoidance (i.e., GSA), and depression and anxiety.We observed no difference in treatment credibility, alliance withthe online therapist, the amount of therapist contact, or reportedtreatment activity between the groups. The effect of exposure isfurther underlined by the correlation between the somewhat crudemeasure of number of exposure exercises reports and symptomaticimprovement in the ICBT group. Although significant time effectswere observed on all measures, we did not observe a differencebetween treatment conditions in effect on the CSFBD. The CSFBDnot only measures negative thoughts about IBS symptoms, but alsocovers other themes such as perfectionism and social desirability(Toner et al., 1998). Thus, the CSFBD may be too general for it tocapture the specific benefits of the exposure interventions, sincethey did not target perfectionism or social desirability.
When interpreting the results from the study, it is important toremember that the ICBT-WE condition was designed to control forall interventions that could not be conceptualized as systematicexposure, i.e., the systematic and repeated contact with a stimulithat evokes conditioned aversive responses while abstaining frombehaviors that are consistent with the emotional response and/orengaging in behaviors that are inconsistent with the emotionalresponse (Barlow et al., 2004; White & Barlow, 2002). Informing apatient that exposure will lead to extinction of a fear response does
not in itself constitute, or necessarily lead to, systematic exposure.We therefore chose to add this information to the ICBT-WE group.Had the information about extinction processes not been present inthe ICBT-WE conditions, it would not have been possible to sepa-rate the effects of learning about exposure and extinction from theeffects of actual systematic and repeated exposure. Consequently,we observed that many participants in the ICBT-WE conditionspontaneously engaged in exposure-like behaviors, that were notonly based on living valued life but also had clear elements ofputting oneself in difficult and aversive situations primarily to getused to them. Despite this contamination between the conditions,the ICBT condition still showed a clear advantage on almost alloutcomemeasures and the between-group effect sizes were largeston the measure of IBS symptoms (i.e., GSRS-IBS), d ¼ 0.47 andd ¼ 0.48 at post and follow-up, respectively. As any contaminationbetween the groups would obscure the actual additive effects ofexposure, we interpret these results as strong support for thebeneficial long-term effects of the procedures involved in system-atic exposure for IBS. Thus, themechanisms of both treatmentsmayhave been quite similar and the results could be interpreted as adoseeresponse effect. The ICBT-WE agenda of a behavioral changethat steers away from the avoidance and control behaviors thatmaintain disability and symptoms and proposes an acceptingstance towards aversive experiences while focusing on living avalued life, encourages exposure. Adding the challenging and oftenpainful systematic exposure exercises may therefore haveenhanced processes that were already present in the ICBT-WEcondition, leading to even larger improvements in symptoms andquality of life.
The full treatment protocol constitutes a somewhat unusual mixof both acceptance- and mindfulness-based interventions andsystematic exposure and is presented to lead to both long-termhabituation as well increased quality of life through increased fre-quency of valued behaviors. In contrast, it has been explicitly statedthat in ACT, exposure is not used to achieve habituation but topractice behavioral flexibility in the presence of avoided stimuli(Hayes, Villatte, Levin, & Hildebrandt, 2011). We believe that theparticipants in our studies of ICBT for IBS have been presented witha coherent treatment rationale that emphasizes practicing amindful and accepting stance towards daily variations in symptomlevel that are essentially not under willful control (or the behaviorsthat are available to exert symptom control often lead to an un-wanted increase in symptoms and disability). Adding systematicexposure with the aim of decreasing symptoms through mecha-nisms of extinction does not necessarily introduce a “controlagenda” that contradicts acceptance of symptoms in the present.Because exposure seldom leads to immediate symptom relief(Craske et al., 2008) it has instead been presented as way to practicehaving symptoms in difficult situations, which will lead to symp-tom improvement through the natural process of extinction, andmindfulness and acceptance have been used as strategies to stay intouch with the aversive experience during the exposure. At thesame time, reduced avoidance will increase quality of life whichwill make the symptoms less interfering and reduce stress,decreasing both awareness of symptoms and symptom levels.
Difference between treatment conditions
Our previous mediational study of the ICBT protocol showedthat the superior effects of ICBT on IBS symptoms when comparedto an internet-delivered stress management protocol was largelyexplained by change in GSA (Ljótsson et al., 2013). The results in thepresent trial further underline the central role of GSA in IBS. Severalcognitive behavioral treatments that have not focused on GSA asthe primary maintaining mechanism in IBS have failed to show

B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e3936
superiority over attention control conditions (Blanchard et al.,2007; Boyce, Talley, Balaam, Koloski, & Truman, 2003; Drossmanet al., 2003). However, including this study, there are now threestudies that show that exposure-based and GSA-focused treat-ments lead to larger symptomatic improvement than attentioncontrol conditions (Craske et al., 2011; Ljótsson, Hedman,Andersson, et al., 2011). The congruency between the assumedrole of GSA in IBS and the seemingly specific effects of an inter-vention (i.e., exposure) that is supposed to target the processes ofGSA (i.e., fear and avoidance) strongly suggest that GSA plays asimilar role in IBS as fear and avoidance do in anxiety disorders andchronic pain (Clark, 1999; Vlaeyen & Linton, 2000). GSA may notthen simply constitute a process that exacerbates the symptoms ofa medical disorder, but could be a core process involved in thedevelopment, maintenance, and course of IBS. Future researchshould further investigate the properties of GSA in terms of thebehavioral, cognitive, and affective processes that are involved,how they maintain IBS, and how these processes can be targeted todecrease disability.
Although exposure may have specific effects it is possible thatother interventions could also be used to target GSA and achievesimilar effects. Mindfulness as a stand-alone intervention, forexample mindfulness-based cognitive therapy, includes at least 4e5 times more training in mindfulness (Hofmann, Sawyer, Witt, &Oh, 2010) and may therefore be more potent than the ICBT-WEcondition in this study. The value of mindfulness is highlightedby our recentmediational study of the ICBT protocol, that suggestedthat the mindfulness and exposure exercises were both indepen-dently associated with improvement in GSA (Ljótsson et al., 2013)as well as the mediational study by Garland et al. (2011) thatshowed that the effects of mindfulness on IBS symptoms weremediated through reduced GSA. However, the studies that havebeen conducted on mindfulness as a stand-alone intervention forIBS (Gaylord et al., 2011; Kearney, 2012; Zernicke et al., 2013) showlarge variations in results and only the study by Gaylord et al. (2011)demonstrated effects similar to those we have obtained in this andprevious studies. Cognitive interventions may also have additionalvalue or could even replace exposure as means of reducing fear andworry about IBS-related stimuli. The issue of the effects of specificcomponents could be addressed by using a “full” dismantling oradditive component design, which investigates the value of eachtreatment component in isolation and in combination with othercomponents (Borkovec, 1990).
This is the first study of psychological treatment for IBS thatreports adverse treatment events. Generally, negative effects ofpsychological treatments have received little attention in theresearch, even though they are known to exist (Barlow, 2010). Intotal, about 17% of participants reported to have experienced atleast one adverse effect during treatment and 40% of these eventswere given the highest severity rating at the time of occurrence.There were no significant differences between the two groups onthe number of reported adverse events. The most common events(78%) were related to increased IBS symptoms and stress, which isnot surprising given the nature of the treatments (to changesymptom-controlling behaviors in both conditions and to provokesymptoms in the ICBT condition) and the time and effort requiredby the treatment. However, the effects seemed to be transient asonly 10% of all events had the highest severity rating of residualeffects at the post-treatment assessment and the mean residualrating of severity was about 60% lower than the mean severityrating at the time of occurrence. In addition, about 5% of the par-ticipants reported at least one adverse event in the period betweentreatment completion and follow-up, and again increased symp-toms were the most common effects. Further studies shouldexplore the impact of these events on treatment outcome and how
participants perceive them, for example, are they considered un-comfortable but necessary consequences of a demanding behav-ioral change treatment or as unwanted effects of a painful andineffective intervention? An important finding was also that therewas no significant difference in treatment discontinuation betweenthe two treatments and the proportions of participants whoengaged in behavior change were similar in both treatment arms.That is, including systematic exposure did not seem to lead toincreased dropout or decreased adherence compared to the ICBT-WE. We find these observations encouraging in the light of howexposure is often negatively perceived by mental health pro-fessionals and patients (Olatunji et al., 2009) and the low number ofcognitive behavioral treatments for IBS that include exposureinterventions.
However, only 55% of the participants in ICBT conditioncompleted all the treatment steps and began exposure exercises. Inour first study of ICBT for IBS (Ljótsson, Falk, et al., 2010), 74% of theparticipants initiated the exposure exercises. Given that there doesnot seem to be a remarkable difference in treatment efficacy of theICBT condition in this study and the first study (the mean decreaseon the GSRS-IBS from pre- to post-treatment was 14.3 in this studyand 16.1 in the original study; Ljótsson, Falk, et al., 2010), this is aninteresting finding. If fewer participants engaged in behaviorchange in this study it would be natural to assume that lessimprovement would have been observed. We believe that in theoriginal study, which only included 42 participants in the ICBTcondition, therapists spent more time in trying to engage inactiveparticipants to work with the treatment than was possible in thisstudy with more than 300 participants in treatment. However, aparticipant whose inactivity is due to a lack of interest or belief inthe treatment may not improve further even if he or she isencouraged to progress with the treatment. Therefore, we believethat the 55% completion rate observed in the ICBT condition in thisstudy is a more accurate estimate of the treatment engagement inthis population. This leads to important conclusions. First, almosthalf of a self-referred sample will not engage in the treatment ex-ercises prescribed in the ICBT protocol (although it does not seem tobe the systematic exposure per se that discourages treatment ac-tivity). Second, despite this engagement rate, the ICBT producestreatment effects that are well at par with treatment effects thathave been observed in studies of individual face-to-face CBT for IBS.It is also important to underline that the IBS population is notdefined based on the presence of GSA but on their symptomaticprofile. Thus, it is possible that many patients with IBS do not fit thetheoretical model underlying this treatment. The treatmentcompletion rate of 55% in this study could be taken as an indicationthat all participants may not recognize themselves in this model.Future research should investigate if the ICBT protocol can beadapted to fit more patients and/or if there are patient character-istics that predict low adherence and gain from the ICBT protocol.
There are some important limitations that have to be consideredwhen interpreting the results in this study. First, as in two of ourprevious ICBT studies (Ljótsson, Falk, et al., 2010; Ljótsson, Hedman,Andersson, et al., 2011), participants were self-recruited andalthough diagnostic criteria were confirmed, we relied on theirprevious diagnosis of IBS for inclusion. In this study, we also pro-vided a “fast-track” into the study for applicants who fulfilled allRome III-criteria and did not report any alarm symptoms. However,after treatment completion, one participant reported to have beendiagnosed with Crohn’s disease. This participant was interviewedbecause of reported alarm symptoms at screening (i.e., was notincluded through the fast-track), and was judged to have under-gone proper medical examination. Upon review of the case, we didnot judge that the correct diagnosis had been delayed by the in-clusion of this participant in the study. Second, as observed in a

B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e39 37
previous study, in which participants were recruited consecutivelyat a gastroenterological clinic (Ljótsson, Andersson, et al., 2011),clinical patients seem to be less impaired and suffer from lesssymptoms than participants recruited by self-referral (Ljótsson,Falk, et al., 2010; Ljótsson, Hedman, Andersson, et al., 2011).However, it is difficult to judge how this impacts the generaliz-ability of these results regarding the specific effects of systematicexposure. Third, although we made an effort to collect reportsabout adverse events related to the participation in the trial, theseevents were not collected with the same scrutiny as employed inpharmacological trials. We did not collect reports continuouslythroughout the trial but rather at the post-treatment assessment.Nor did we collect reports about all adverse event during treatmentbut asked the participants about events that they specificallyassociated with their participation in the treatment. Thus, alladverse events associated with the treatment may not have beencollected. However, we believe that this rudimentary collection ofadverse events provides valuable information about the possiblenegative effects of participating in a study such as this, especiallyconsidering that reporting negative effects in psychological treat-ment studies is rarely done (Barlow, 2010). Fourth, the addition ofblinded clinician-rated outcome measure could have providedvaluable additional information about the efficacy of our condi-tions. We emphasized subjective data because there is growingunderstanding that an accurate understanding of the therapeuticvalue of a treatment comes from the patient’s perspective unfil-tered by others (e.g., a clinician; Lackner et al., 2011). Fifth, inaccordance with convention we measured treatment credibilityalliance when it was reasonable that participants had formed anopinion of the treatment and alliance with their therapist, butbefore the improvements caused by behavior change could beassumed to confound these measures. However, since the two armsdid not diverge in terms of content until after the third step, i.e.,after 3 or 4 weeks for most participants, the treatment credibilitymeasurement after 2 weeks would not have captured any differ-ence in treatment credibility due to the divergence after the thirdstep and similarly, any difference in alliance due to the divergencemay not have been captured at 4 weeks. Therefore, it would havebeen preferable to administer the measures of treatment credibilityand alliance somewhat later in the study than at the second andfourth week. Finally, no assessments were made of the therapistadherence in the two treatment arms. It is reasonable to assumethat ICBT, due to its structure, gives larger control over how par-ticipants are exposed to the treatment interventions compared toconventional CBT, and therefore therapist adherence may be of lessimportance in ICBT than in conventional CBT. However, a recentstudy of ICBT for generalized anxiety disorder demonstrated thatonline therapists’ written reinforcements of participants’ taskcompletion were associated with treatment outcome and patients’adherence to the treatment (Paxling et al., 2013). Thus, it wouldhave been preferable if therapists’ adherence had beenmeasured inthe two arms to investigate any differences in therapists’ writtenmessages to the participants.
To our knowledge, this is the first IBS study that has used acontrolled component randomized design to examine if systematicexposure has specific beneficial effects in a psychological treatmentfor IBS. Furthermore, this is the largest study of any psychologicaltreatment that has been published for IBS and the fourth in a seriesof studies that have demonstrated consistent and beneficial effectson IBS symptoms of an internet-delivered treatment based pri-marily on exposure. We believe that this and our previous studiesprovide strong evidence for the beneficial effects of exposure in-terventions in IBS. This has important implications, since mostpsychological treatments for IBS do not include exposure. Althoughthe clinician working with IBS may view it as counterintuitive,
provoking symptoms seems to be an effective way to actuallyreduce symptom complaints and disability. Given the generally loweffect of pharmacological treatments for IBS and the many psy-chological treatments that purport to reduce symptoms but withinconsistent results, it may be time to change how IBS is managed.If initial pharmacological interventions and life style adjustmentsdo not give satisfactory results, there is a risk that further treatmentinterventions following the same agenda of symptom reductionmay actually maintain and exacerbate both symptoms anddisability. Instead, systematic exposure as part of a comprehensivepsychological treatment may be one of the most effective in-terventions for a patient with IBS who does not benefit from usualcare.
Acknowledgments
The authors would like to express their gratitude to Viktor Kaldofor assisting in the randomization procedure and Per Carlbring forallowing us to use his website www.studie.nu to recruitparticipants.
References
Addis, M., & Jacobson, N. (2000). A closer look at the treatment rationale andhomework compliance in cognitive-behavioral therapy for depression. Cogni-tive Therapy and Research, 24(3), 313e326. http://dx.doi.org/10.1023/A:1005563304265.
Andersson, E., Ljótsson, B., Smit, F., Paxling, B., Hedman, E., Lindefors, N., et al.(2011). Cost-effectiveness of internet-based cognitive behavior therapy for ir-ritable bowel syndrome: results from a randomized controlled trial. BMC PublicHealth, 11, 215. http://dx.doi.org/10.1186/1471-2458-11-215.
Barlow, D. H. (2010). Negative effects from psychological treatments: a perspective.The American Psychologist, 65(1), 13e20. http://dx.doi.org/10.1037/a0015643.
Barlow, D. H., Allen, L., & Choate, M. (2004). Toward a unified treatment foremotional disorders. Behavior Therapy, 35(2), 205e230. http://dx.doi.org/10.1016/S0005-7894(04)80036-4.
Blanchard, E. B., Lackner, J. M., Sanders, K., Krasner, S., Keefer, L., Payne, A., et al.(2007). A controlled evaluation of group cognitive therapy in the treatment ofirritable bowel syndrome. Behaviour Research and Therapy, 45(4), 633e648.http://dx.doi.org/10.1016/j.brat.2006.07.003.
Borkovec, T. D. (1990). Control groups and comparison groups in psychotherapyoutcome research. NIDA Research Monograph, 104, 50e65.
Borkovec, T., & Nau, S. (1972). Credibility of analogue therapy rationales. Journal ofBehavior Therapy and Experimental Psychiatry, 3, 257e260. http://dx.doi.org/10.1016/0005-7916(72)90045-6.
Boutron, I., Moher, D., Altman, D., Schulz, K., & Ravaud, P. (2008). Extending theCONSORT statement to randomized trials of nonpharmacologic treatment:explanation and elaboration. Annals of Internal Medicine, 148(4), 295e309.
Boyce, P., Talley, N. J., Balaam, B., Koloski, N., & Truman, G. (2003). A randomizedcontrolled trial of cognitive behavior therapy, relaxation training, and routineclinical care for the irritable bowel syndrome. American Journal of Gastroen-terology, 98(10), 2209e2218. http://dx.doi.org/10.1111/j.1572-0241.2003.07716.x.
Busseri, M., & Tyler, J. (2003). Interchangeability of the Working Alliance Inventoryand Working Alliance Inventory, Short Form. Psychological Assessment, 15(2),193e197.
Camilleri, M., & Chang, L. (2008). Challenges to the therapeutic pipeline for irritablebowel syndrome: end points and regulatory hurdles. Gastroenterology, 135(6),1877e1891. http://dx.doi.org/10.1053/j.gastro.2008.09.005.
Clark, D. M. (1999). Anxiety disorders: why they persist and how to treat them.Behaviour Research and Therapy, 37(Suppl. 1), S5eS27. http://dx.doi.org/10.1016/S0005-7967(99)00048-0.
Craske, M. G., Kircanski, K., Zelikowsky, M., Mystkowski, J., Chowdhury, N., &Baker, A. (2008). Optimizing inhibitory learning during exposure therapy.Behaviour Research and Therapy, 46(1), 5e27. http://dx.doi.org/10.1016/j.brat.2007.10.003.
Craske, M. G., Wolitzky-Taylor, K. B., Labus, J., Wu, S., Frese, M., Mayer, E. A., et al.(2011). A cognitive-behavioral treatment for irritable bowel syndrome usinginteroceptive exposure to visceral sensations. Behaviour Research and Therapy,49(6), 413e421. http://dx.doi.org/10.1016/j.brat.2011.04.001.
Devilly, G., & Borkovec, T. (2000). Psychometric properties of the credibility/ex-pectancy questionnaire. Journal of Behavior Therapy and Experimental Psychiatry,31(2), 73e86. pii: S0005791600000124.
Drossman, D. A., Corazziari, E., Delvaux, M., Spiller, R. C., Talley, J., Thompson, W. G.,et al. (2006). Rome III: The functional gastrointestinal disorders. McLean, VA:Degnon Associates.
Drossman, D. A., Li, Z., Andruzzi, E., Temple, R., Talley, N. J., Thompson, W., et al.(1993). U.S. householder survey of functional gastrointestinal disorders.

B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e3938
Prevalence, sociodemography, and health impact. Digestive Diseases and Sci-ences, 38(9), 1569e1580. http://dx.doi.org/10.1007/BF01303162.
Drossman, D. A., Toner, B., Whitehead, W., Diamant, N., Dalton, C., Duncan, S., et al.(2003). Cognitive-behavioral therapy versus education and desipramine versusplacebo for moderate to severe functional bowel disorders. Gastroenterology,125(1), 19e31. http://dx.doi.org/10.1016/S0016-5085(03)00669-3.
Ferreira, N. B. (2011). Investigating the role of psychological flexibility and the use of anacceptance and commitment therapy based intervention in irritable bowel syn-drome (Doctoral dissertation). The University of Edinburgh. Retrieved fromhttp://hdl.handle.net/1842/6312.
Ferreira, N. B., Eugenicos, M., Morris, P. G., & Gillanders, D. (2011). Using acceptanceand commitment therapy in irritable bowel syndrome. Gastrointestinal Nursing,9(9), 28e35.
Ford, A., Talley, N. J., Schoenfeld, P., Quigley, E., & Moayyedi, P. (2009). Efficacy ofantidepressants and psychological therapies in irritable bowel syndrome: sys-tematic review and meta-analysis. Gut, 58(3), 367e378. http://dx.doi.org/10.1136/gut.2008.163162.
Forsyth, J. P., & Fusé, T. (2008). Interoceptive exposure for panic disorder. InW. T. O’Donohue, & J. E. FIsher (Eds.), Cognitive behavior therapy (2nd ed.).Hoboken, NJ: John Wiley & Sons, Inc.
Garland, E. L., Gaylord, S. A., Palsson, O., Faurot, K., Mann, J. D., & Whitehead, W. E.(2011). Therapeutic mechanisms of a mindfulness-based treatment for IBS:effects on visceral sensitivity, catastrophizing, and affective processing of painsensations. Journal of Behavioral Medicine. http://dx.doi.org/10.1007/s10865-011-9391-z.
Gaylord, S. A., Palsson, O. S., Garland, E. L., Faurot, K. R., Coble, R. S., Mann, J. D., et al.(2011). Mindfulness training reduces the severity of irritable bowel syndromein women: results of a randomized controlled trial. American Journal ofGastroenterology, 106(9), 1678e1688. http://dx.doi.org/10.1038/ajg.2011.184.
Gueorguieva, R., & Krystal, J. (2004). Move over ANOVA: progress in analyzingrepeated-measures data and its reflection in papers published in the Archives ofGeneral Psychiatry. Archives of General Psychiatry, 61(3), 310e317. http://dx.doi.org/10.1001/archpsyc.61.3.310.
Guilera, M., Balboa, A., & Mearin, F. (2005). Bowel habit subtypes and temporalpatterns in irritable bowel syndrome: systematic review. American Journal ofGastroenterology, 100(5), 1174e1184. http://dx.doi.org/10.1111/j.1572-0241.2005.40674.x.
Halder, S., Locke, G., Talley, N. J., Fett, S., Zinsmeister, A., & Melton, L. (2004). Impactof functional gastrointestinal disorders on health-related quality of life: apopulation-based case-control study. Alimentary Pharmacology and Therapeu-tics, 19(2), 233e242. http://dx.doi.org/10.1111/j.0269-2813.2004.01807.x.
Hayes, S. C., Strosahl, K., & Wilson, K. (1999). Acceptance and commitment therapy:An experiential approach to behavior change. New York, NY: Guilford Press.
Hayes, S. C., Villatte, M., Levin, M., & Hildebrandt, M. (2011). Open, aware, andactive: contextual approaches as an emerging trend in the behavioral andcognitive therapies. Annual Review of Clinical Psychology, 7, 141e168. http://dx.doi.org/10.1146/annurev-clinpsy-032210-104449.
Hazlett-Stevens, H., & Craske, M. G. (2008). Live (in vivo) exposure. InW. T. O’Donohue, & J. E. Fisher (Eds.), Cognitive behavior therapy (2nd ed.).Hoboken, NJ: John Wiley & Sons, Inc.
Hedman, E., Ljótsson, B., & Lindefors, N. (2012). Cognitive behavior therapy via theInternet: a systematic review of applications, clinical efficacy and cost-effec-tiveness. Expert Review of Pharmacoeconomics & Outcomes Research, 12(6), 745e764. http://dx.doi.org/10.1586/erp.12.67.
Hedman, E., Ljótsson, B., Rück, C., Furmark, T., Carlbring, P., Lindefors, N., et al.(2010). Internet administration of self-report measures commonly used inresearch on social anxiety disorder: a psychometric evaluation. Computers inHuman Behavior, 26(4), 736e740. http://dx.doi.org/10.1016/j.chb.2010.01.010.
Hofmann, S., Sawyer, A., Witt, A., & Oh, D. (2010). The effect of mindfulness-basedtherapy on anxiety and depression: a meta-analytic review. Journal of Consul-ting and Clinical Psychology, 78(2), 169e183. http://dx.doi.org/10.1037/a0018555.
Hunt, M., Moshier, S., & Milonova, M. (2009). Brief cognitive-behavioral internettherapy for irritable bowel syndrome. Behaviour Research and Therapy, 47, 797e802. http://dx.doi.org/10.1016/j.brat.2009.05.002.
Kearney, D. J. (2012). Mindfulness meditation for women with irritable bowelsyndromeeevidence of benefit from a randomised controlled trial. EvidenceBased Nursing, 15(3), 80e81. http://dx.doi.org/10.1136/ebnurs-2012-100488.
Labus, J. (2007). In search of mechanisms of change in treatment outcome research:mediators and moderators of psychological and pharmacological treatments forirritable bowel syndrome. Gastroenterology, 133(2), 702e705. http://dx.doi.org/10.1053/j.gastro.2007.06.052.
Labus, J., Bolus, R., Chang, L., Wiklund, I., Naesdal, J., Mayer, E. A., et al. (2004). TheVisceral Sensitivity Index: development and validation of a gastrointestinalsymptom-specific anxiety scale. Alimentary Pharmacology and Therapeutics,20(1), 89e97. http://dx.doi.org/10.1111/j.1365-2036.2004.02007.x.
Labus, J., Mayer, E. A., Chang, L., Bolus, R., & Naliboff, B. (2007). The central role ofgastrointestinal-specific anxiety in irritable bowel syndrome: further validationof the visceral sensitivity index. Psychosomatic Medicine, 69(1), 89e98. http://dx.doi.org/10.1097/PSY.0b013e31802e2f24.
Lackner, J. M., Jaccard, J., Baum, C., Smith, A., Krasner, S., Katz, L., et al. (2011). Pa-tient-reported outcomes for irritable bowel syndrome are associated with pa-tients’ severity ratings of gastrointestinal symptoms and psychological factors.Clinical Gastroenterology and Hepatology, 9(11), 957e964.e1. http://dx.doi.org/10.1016/j.cgh.2011.06.014.
Lackner, J. M., Mesmer, C., Morley, S., Dowzer, C., & Hamilton, S. (2004). Psycho-logical treatments for irritable bowel syndrome: a systematic review and meta-analysis. Journal of Consulting and Clinical Psychology, 72(6), 1100e1113. http://dx.doi.org/10.1037/0022-006X.72.6.1100.
Lane, P. (2008). Handling drop-out in longitudinal clinical trials: a comparison ofthe LOCF and MMRM approaches. Pharmaceutical Statistics, 7(2), 93e106. http://dx.doi.org/10.1002/pst.267.
Levin, M. E., Hildebrandt, M. J., Lillis, J., & Hayes, S. C. (2012). The impact of treat-ment components suggested by the psychological flexibility model: a meta-analysis of Laboratory-based component studies. Behavior Therapy, 43(4),741e756. http://dx.doi.org/10.1016/j.beth.2012.05.003.
Ljótsson, B., Andersson, G., Andersson, E., Hedman, E., Lindfors, P., Andréewitch, S.,et al. (2011). Acceptability, effectiveness, and cost-effectiveness of internet-based exposure treatment for irritable bowel syndrome in a clinical sample: arandomized controlled trial. BMC Gastroenterology, 11, 110. http://dx.doi.org/10.1186/1471-230X-11-110.
Ljótsson, B., Andréewitch, S., Hedman, E., Rück, C., Andersson, G., & Lindefors, N.(2010). Exposure and mindfulness based therapy for irritable bowel syndromee an open pilot study. Journal of Behavior Therapy and Experimental Psychiatry,41(3), 185e190. http://dx.doi.org/10.1016/j.jbtep.2010.01.001.
Ljótsson, B., Falk, L., Vesterlund, A. W., Hedman, E., Lindfors, P., Rück, C., et al. (2010).Internet-delivered exposure and mindfulness based therapy for irritable bowelsyndromeea randomized controlled trial. Behaviour Research and Therapy,48(6), 531e539. http://dx.doi.org/10.1016/j.brat.2010.03.003.
Ljótsson, B., Hedman, E., Andersson, E., Hesser, H., Lindfors, P., Hursti, T., et al. (2011).Internet-delivered exposure-based treatment vs. stress management for irri-table bowel syndrome: a randomized trial. American Journal of Gastroenterology,106(8), 1481e1491. http://dx.doi.org/10.1038/ajg.2011.139.
Ljótsson, B., Hedman, E., Lindfors, P., Hursti, T., Lindefors, N., Andersson, G., et al.(2011). Long-term follow-up of internet-delivered exposure and mindfulnessbased treatment for irritable bowel syndrome. Behaviour Research and Therapy,49(1), 58e61. http://dx.doi.org/10.1016/j.brat.2010.10.006.
Ljótsson, B., Hesser, H., Andersson, E., Lindfors, P., Hursti, T., Rück, C., et al. (2013).Mechanisms of change in an exposure-based treatment for irritable bowelsyndrome. Journal of Consulting and Clinical Psychology, 81(6), 1113e1126. http://dx.doi.org/10.1037/a0033439.
Longstreth, G., Thompson, W., Chey, W., Houghton, L., Mearin, F., & Spiller, R. C.(2006). Functional bowel disorders. Gastroenterology, 130(5), 1480e1491. http://dx.doi.org/10.1053/j.gastro.2005.11.061.
Lovell, R. M., & Ford, A. C. (2012). Global prevalence of and risk factors for irritablebowel syndrome: a meta-analysis. Clinical Gastroenterology and Hepatology,10(7), 712e721.e4. http://dx.doi.org/10.1016/j.cgh.2012.02.029.
Martin, D. J., Garske, J. P., & Davis, M. K. (2000). Relation of the therapeutic alliancewith outcome and other variables: a meta-analytic review. Journal of Consultingand Clinical Psychology, 68(3), 438e450. http://dx.doi.org/10.1037/0022-006X.68.3.438.
Muthén, B. O., & Curran, P. J. (1997). General longitudinal modeling of individualdifferences in experimental designs: a latent variable framework for analysisand power estimation. Psychological Methods, 2(4), 371e402. http://dx.doi.org/10.1037/1082-989X.2.4.371.
Olatunji, B. O., Deacon, B. J., & Abramowitz, J. S. (2009). The cruelest cure? Ethicalissues in the implementation of exposure-based treatments. Cognitive andBehavioral Practice, 16(2), 172e180. http://dx.doi.org/10.1016/j.cbpra.2008.07.003.
Patrick, D., Drossman, D. A., Frederick, I., DiCesare, J., & Puder, K. (1998). Quality oflife in persons with irritable bowel syndrome: development and validation of anew measure. Digestive Diseases and Sciences, 43(2), 400e411. http://dx.doi.org/10.1023/A:1018831127942.
Paxling, B., Lundgren, S., Norman, A., Almlöv, J., Carlbring, P., Cuijpers, P., et al.(2013). Therapist behaviours in internet-delivered cognitive behaviour therapy:analyses of e-Mail correspondence in the treatment of generalized anxietydisorder. Behavioural and Cognitive Psychotherapy, 41(3), 280e289. http://dx.doi.org/10.1017/S1352465812000240.
Reme, S. E., Darnley, S., Kennedy, T., & Chalder, T. (2010). The development of theirritable bowel syndrome-behavioral responses questionnaire. Journal of Psy-chosomatic Research, 69(3), 319e325. http://dx.doi.org/10.1016/j.jpsychores.2010.01.025.
Saunders, J., Aasland, O., Babor, T., la Fuente de, J., & Grant, M. (1993). Developmentof the alcohol use disorders identification test (AUDIT): WHO CollaborativeProject on early Detection of persons with Harmful alcohol ConsumptioneII.Addiction, 88(6), 791e804. http://dx.doi.org/10.1111/j.1360-0443.1993.tb02093.x.
Spiller, R. C., Aziz, Q., Creed, F., Emmanuel, A., Houghton, L., Hungin, P., et al. (2007).Guidelines on the irritable bowel syndrome: mechanisms and practical man-agement. Gut, 56(12), 1770e1798. http://dx.doi.org/10.1136/gut.2007.119446.
Svanborg, P., & Åsberg, M. (1994). A new self-rating scale for depression and anxietystates based on the Comprehensive Psychopathological Rating Scale. Acta Psy-chiatrica Scandinavica, 89(1), 21e28. http://dx.doi.org/10.1111/j.1600-0447.1994.tb01480.x.
Talley, N. J., Gabriel, S., Harmsen, W., Zinsmeister, A., & Evans, R. (1995). Medicalcosts in community subjects with irritable bowel syndrome. Gastroenterology,109(6), 1736e1741. pii: S0016508595003891.
Toner, B., Stuckless, N., Ali, A., Downie, F., Emmott, S., & Akman, D. (1998). Thedevelopment of a cognitive scale for functional bowel disorders. PsychosomaticMedicine, 60(4), 492e497.

B. Ljótsson et al. / Behaviour Research and Therapy 55 (2014) 27e39 39
Tracey, T., & Kokotovic, A. (1989). Factor structure of the Working Alliance In-ventory. Psychological Assessment, 1(3), 207e210. http://dx.doi.org/10.1037/1040-3590.1.3.207.
Vlaeyen, J. W., & Linton, S. J. (2000). Fear-avoidance and its consequences in chronicmusculoskeletal pain: a state of the art. Pain, 85(3), 317e332. http://dx.doi.org/10.1016/S0304-3959(99)00242-0.
White, K. S., & Barlow, D. H. (2002). Panic disorder and agoraphobia. In D. H. Barlow(Ed.), Anxiety and its disorders (2nd ed.). New York, NY: Guilford Publication.
Wiklund, I., Fullerton, S., Hawkey, C., Jones, R., Longstreth, G., Mayer, E. A., et al.(2003). An irritable bowel syndrome-specific symptom questionnaire: devel-opment and validation. Scandinavian Journal of Gastroenterology, 38(9), 947e954. http://dx.doi.org/10.1080/00365520310004209.
Wolitzky-Taylor, K., Craske, M. G., Labus, J. S., Mayer, E. A., & Naliboff, B. D. (2012).Visceral sensitivity as a mediator of outcome in the treatment of irritable bowelsyndrome. Behaviour Research and Therapy, 50(10), 647e650. http://dx.doi.org/10.1016/j.brat.2012.05.010.
Zernicke, K. A., Campbell, T. S., Blustein, P. K., Fung, T. S., Johnson, J. A., Bacon, S. L., &Carlson, L. E. (2013). Mindfulness-based stress reduction for the treatment ofirritable bowel syndrome symptoms: a randomized wait-list controlled trial.International Journal of Behavioral Medicine, 20(3), 385e396. http://dx.doi.org/10.1007/s12529-012-9241-6.
Zigmond, A., & Snaith, R. (1983). The hospital anxiety and depression scale. ActaPsychiatrica Scandinavica, 67(6), 361e370. http://dx.doi.org/10.1111/j.1600-0447.1983.tb09716.x.
Copyright © 2022 FDOKUMEN