Mapping the Hallmarks of Lung Adenocarcinoma with Massively Parallel Sequencing
Upload
independentCategory
view
1download
0
1989;49:5748-5754. Published online October 1, 1989.Cancer Res Jens Benn Sørensen, Jens Henrik Badsberg and Jens Olsen A Multivariate Regression Analysis of 259 PatientsPrognostic Factors in Inoperable Adenocarcinoma of the Lung:
Updated Version http://cancerres.aacrjournals.org/content/49/20/5748
Access the most recent version of this article at:
Citing Articles http://cancerres.aacrjournals.org/content/49/20/5748#related-urls
This article has been cited by 4 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
[email protected] atTo order reprints of this article or to subscribe to the journal, contact the AACR Publications
To request permission to re-use all or part of this article, contact the AACR Publications
American Association for Cancer Research Copyright © 1989 on July 10, 2011cancerres.aacrjournals.orgDownloaded from

(CANCER RESEARCH 49, 5748-5754, October 15, 1989]
Prognostic Factors in Inoperable Adenocarcinoma of the Lung: A MultivariateRegression Analysis of 259 Patients1
Jens Benn S0rensen,2 Jens Henrik Badsberg, and Jens Olsen
Departments of Oncology ON K [J. B. S.J and Pathology fJ. O.], Finsen Institute/Rigshospitalet, and Statistical Research Unit [J. H. BJ, University of Copenhagen, 3Blegdamsvej, 2200 Copenhagen, Denmark
ABSTRACT
The prognostic factors for survival in advanced adenocarcinoma of thelung were investigated in a consecutive series of 259 patients treated withchemotherapy. Twenty-eight pretreatment variables were investigated byuse of Cox's multivariate regression model, including histológica!sub
types and degree of differentiation, the new international staging systemfor lung cancer, and seven laboratory parameters. Staging of the patientsincluded bone marrow examination but were otherwise nonextensivewithout routine bone, liver, and brain scans. Factors predicting poorsurvival were low performance status, stage IV disease, no prior nonrad-ical resection, liver métastases,high values of white blood cell count, andlactate dehydrogenase, and low values of aspartate aminotransaminase.The nonradical resection may not be a prognostic factor because of theresection itself but may rather serve as an indicator for patients havingminimal disease spread. Liver métastaseswere of limited clinical valueas a prognostic factor because they were detected in only seven cases inthis patient population. A new Cox analysis ignoring the influence of thisvariable revealed no other variables than those occurring in the formerCox model to be of importance (performance status, stage, surgicalresection, WBC, aspartate aminotransaminase, and lactate dehydrogenase). This simplified model appears to be a feasible clinical tool, allowingfor prognostic stratification of patients when first the inoperability of thepatient is known.
INTRODUCTION
Several examples exist of prognostic factors that have beenconclusively established and segregate the target patient population into subgroups with widely different outcomes. In thecase of advanced non-small cell lung cancer (squamous, ade-nò-,and large cell carcinoma) the treatment results are poor,and the magnitude of differences in outcome for categories ofthe strongest prognostic factors are larger than the types oftherapeutic differences (1-4).
Knowledge of prognostic factors is essential for predictingpatient outcome and for use in optimal trial design and analysis.However, prognostic factors are also used to understand theinterrelationship of such factors, not just their individual orunivariate effects. A way to obtain this knowledge is by multipleregression analysis (5). Among a number of theoretical models(6) Cox's multivariate regression model (7) is the most fre
quently applied when duration of survival is the measure ofinterest. Based on this model the dominating prognostic factorsmay be characterized, and results of this analysis permit theestimation of an expected survival probability.
The prognosis may vary with respect to the individual histo-logical types of non-small cell lung cancer (3, 8), although thisis not invariably observed and their contribution may be minorafter correction for the effects of other factors in a multivariate
Received 1/22/88; revised 10/28/88, 7/5/89; accepted 7/6/89.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1Supported by grants from the Danish Cancer Society.2To whom requests for reprints should be addressed, at the Department of
Oncology ONK, Finsen Institute, 49 Strandboulevarden, DK-2100 Copenhagen,Denmark.
regression analysis (9). ACL1 may be further subtyped according
to the classification by the WHO into acinar adenocarcinoma,papillary adenocarcinoma, bronchioloalveolar carcinoma, andsolid carcinoma with mucus formation (10). The subtypes havebeen reported previously to differ somewhat clinically; also thedegree of differentiation may have an impact (11,12), but thesevariables have never been evaluated for independent prognosticsignificance in a multivariate analysis. The new internationalstaging system for lung cancer (13) has not been evaluated in aCox analysis among non-small cell lung cancer patients, norhave several of the laboratory parameters, such as AST, pro-thrombin index, hemoglobin, platelet count, or WBC, some ofwhich been attributed to prognostic impact among patientswith small cell lung cancer (14, 15).
In order to clarify factors of dominating prognostic influenceand to establish a prognostic index for predicting the survivalexpectancy in advanced ACL, we performed an extensive multiple regression analysis of data collected from a series ofpatients consecutively entered into one prospective randomizedtrial of chemotherapy between 1981 and 1985. Data on thesubtyping of ACL, the degree of differentiation, the new international staging system, and seven laboratory parameters wereincluded among 18 other variables for evaluation of independent prognostic impact.
MATERIALS AND METHODS
Patients. The present series includes 259 consecutive patients withinoperable ACL who participated in a prospective randomized trial ofcytostatic treatment from February 1981 to August 1985 at the FinsenInstitute, Bispebjerg Hospital, and Herlev Hospital, Copenhagen, Denmark, and Renstr0mska Hospital, Gothenburg, Sweden. The treatmentwas either vindesine alone; a combination of lomustine, cyclophospha-mide, and methotrexate; or a combination of all 4 drugs. The overallresponse rate was 24% and the median survival was 29 weeks, with nodifferences between the treatment arms (4). All patients had a Karnofskyperformance status of 50% or better and a maximum age of 70 years.No patient had previously received chemotherapy or radiotherapy, but35 patients had undergone a surgical resection of the lung tumorbecause they were believed to be resectable. However, all tumor tissuecould not be removed and the operations were thus nonradical, rendering these patients candidates for the chemotherapy trial. The mediantime from diagnosis to start of chemotherapy was 23 days.
Histológica!or cytological materials from all patients were evaluatedin accordance with the WHO classification (10) by the pathologists atthe respective hospitals and only patients satisfying the criteria for ACLwere included. Subtyping of ACL was done retrospectively and blindedfor the clinical results by one pathologist (J. O.) based on histológica!material from 220 patients while 39 patients only had cytologicalmaterial (11). The poorly differentiated acinar and papillary adenocarcinoma and the solid carcinoma with mucus formation were classifiedas poorly differentiated tumors while all others were classified as welldifferentiated tumors for the purpose of this analysis.
Routine pretreatment evaluation consisted of a complete history withregistration of pulmonary and extrapulmonary symptoms as well asweight loss during the previous 6 months, general physical examination
3The abbreviations used are: ACL, adenocarcinoma of the lung; AST, aspartate
aminotransaminase; LDH, lactate dehydrogenase.
5748
American Association for Cancer Research Copyright © 1989 on July 10, 2011cancerres.aacrjournals.orgDownloaded from

PROGNOSTIC FACTORS IN LUNG ADENOCARCINOMA
with biopsy or needle aspiration from suspected superficial foci, bonemarrow biopsy from posterior iliac crest, and chest X-ray. Additionally,bilateral mammography and pelvic examination were performed infemales if the diagnosis of ACL was not based upon cytological orhistológica! bronchial material. Extensive staging was not done. Boneor liver scans were not routinely undertaken and brain scans werecarried out only in symptomatic patients. Various biochemical testswere obtained prior to therapy including complete blood counts andplasma values of prothrombin index, AST, LDH, and alkaline phos-phatase.
Patients were characterized as having either limited or extensivedisease, the latter referring to spread outside one lung with the regionallymph nodes, including the ipsi- and contralateral supraclavicularnodes. Also informations about stages Ilia, Illb, and IV according tothe new international staging system for lung cancer (13) were included.
Survival was recorded from the day of randomization to the day ofdeath or the most recent update (February 1987).
Statistical Analyses. Twenty-eight pretreatment variable (Tables 1-3) were chosen for analysis either because previous studies had indicateda possible effect on prognosis or because such an effect seemed likely.The univariate effect of individual variables on prognosis was examinedby grouping the patients on the basis of each variable in turn andcomputing the log rank test for the survival times of the respectivegroups (16).
Continuous variables were evaluated without transformation, withlogarithmic transformation, dichotomized, and as quartiles. The division points were chosen according to the reference intervals for alllaboratory variables, according to description in other studies (weightloss), or according to median values (age). Each variable was tested forproportional intensity of death.
All variables were to be evaluated for prognostic significance in anextensive regression analysis using Cox's proportional hazards model
(7). A stepwise procedure based on partial likelihood ratios was usedin the analysis.
All patients from whom the regression model was derived were finallyassigned a value of prognostic index. The values of the individualsignificant prognostic factors were multiplied with the regression coefficients and added together to form the prognostic index for theparticular patient. Grouping was carried out based on this prognosticindex and survival curves and rates for 1- and 2-year survival werecalculated for patients in the separate groups.
RESULTS
Survival Related to Individual Variables. Results of the univariate analyses are summarized in Tables 1, 2, and 3 and thisgrouping was the basis for the subsequent multiple regressionanalyses. Nonparametric univariate testing using the log ranktest was done to characterize the material. In these nonpara-metric univariate analyses a statistically significant (P < 0.05)prognostic influence was observed for performance status; surgery; brain, liver, and bone métastases;stage; weight loss; WBC;hemoglobin; prothrombin index; LDH; extrapulmonary symptoms; and number of metastatic sites below the diaphragm(Tables 1-3).
From Table 1 the variables describing histopathological subtypes, histopathological differentiation, extent of disease, sex,age, chest X-ray complications, and disease parameter werewithout significant influence. No prognostic importance wasfound for treatment regimen, platelet count, alkaline phospha-tase, or AST in Table 2 or for pulmonary symptoms, lymphnode métastases, bone marrow examination, or number ofmetastatic sites above the diaphragm in Table 3.
With the use of log rank analysis, the 26 patients treated atRenstromska Hospital had a significantly longer survival thanthe other 233 patients (P = 0.012). This difference might becaused by uneven distribution of prognostic factors, althoughthere were no significant differences in univariate comparison
Table 1 Median duration of survival: influence of histopathology and clinicalfeatures
VariableHistopathological
subtypingAeinarPapillaryBronchioloalveolarSolid
carcinomaDegree
ofdifferentiationWellPoorlyPerformance
status90-100%70-80%50-60%Age==57
yr>57yrSexMaleFemaleWeight
loss0-5%>5%Chest
X-rayNocomplications*ComplicationsSurgeryNonradical
resectionNosurgeryDisease
parameterMeasurableEvaluableNo
parameterBrain
métastasesNoYesLiver
métastasesNoYesBone
métastasesNoYesDisease
extentLimitedExtensiveStageIliaIllbIVNo.
ofpatients130231332521468811556123136139120150971371193522411010841234252527222371071526571123Median
survival(days)2042192751502251903402039420321120620925016224017744219221519222521814621562222155241182312236160pa0.730.19<0.00010.580.500.0140.140.040.290.02<0.00010.0020.170.005
" Result of log rank test.* Chest X-ray complications: atelectasis; pleural effusion; elevated hemidia-
phragm.
between the institutions with respect to the variables from thefinal Cox model. To evaluate this point further, the institutionswere included among the other variables in the Cox regressionmodel, and this variable showed an independent impact onprognosis. However, as one of the purposes of this study wasto derive a prognostic index which might be useful to otherinvestigative groups as well, the institutions were not includedamong the variables in the final Cox analysis or the prognosticindex in Table 4.
Multivariate Regression Analyses. Multivariate regressionanalyses were used to examine the joint effects of the variables.These analyses were based on the groupings in Tables 1 to 3.
5749
American Association for Cancer Research Copyright © 1989 on July 10, 2011cancerres.aacrjournals.orgDownloaded from
PROGNOSTIC FACTORS IN l.l'NCi ADKNOCARCINOMA
Table 2 Median duration of survival: influence of treatment and pretreatmentlaboratory values
VariableTreatment
regimenOnedrugThree
drugsFourdrugsWBCs9
xlO'/liter>9xlO'/literPlatelets<400x
lOVliter>400xlO'/literHemoglobin>7.5
ITIM<7.5mMProthrombin
index20.70<0.70ASTs40
units/liter>40units/literAlkaline
phosphatase<275units/liter>275
units/literLDHS450
units/liter>450units/literNo.
ofpatients84888711913813512219S5913524241151569914382Median
survival(days)200204225264161225187221129218100210162241165259129P"0.740.0070.100.00170.00140.850.14<0.0001"
Result of logrank test.
Table 3 Median duration of survival: influence of symptoms anil number ofmetastatic sites
VariablePulmonary'symptomsNoYesExtrapulmonary
symptomsNoYesLymph
nodemétastasesNoYesBone
marrowexaminationNegativePositiveMetastatic
sites abovediaphragm0-1>1Metastatic
sites belowdiaphragm0>0No.
ofpatients4121713012799158176171728722039Median
survival(days)225201263166212203198165216193229135P"0.210.0040.860.950.730.006
" Result of logrank test.
The candidate variables selected first were those in Table 1which themselves had a significant univariate correlation withsurvival. Variables without significant additional informationin this model were excluded one by one. Then variables fromTable 1 without prognostic impact in the univariate analyseswere included if they supplied additional information to themultivariate model.
Variables which lost their impact on the model during thisprocedure were excluded. When this process was completed forthe variables in Table 1, the procedure was repeated withinclusion of the variables from Table 2 and, finally, with the
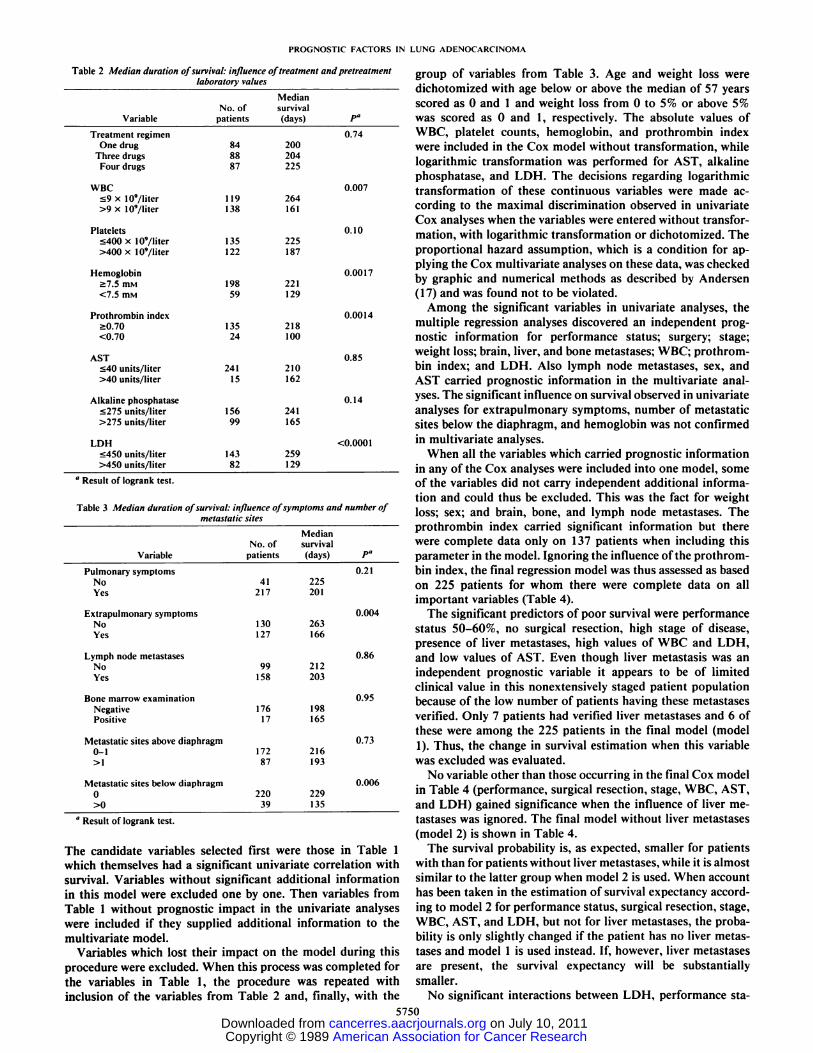
group of variables from Table 3. Age and weight loss weredichotomized with age below or above the median of 57 yearsscored as 0 and 1 and weight loss from 0 to 5% or above 5%was scored as 0 and 1, respectively. The absolute values ofWBC, platelet counts, hemoglobin, and prothrombin indexwere included in the Cox model without transformation, whilelogarithmic transformation was performed for AST, alkalinephosphatase, and LDH. The decisions regarding logarithmictransformation of these continuous variables were made according to the maximal discrimination observed in univariateCox analyses when the variables were entered without transformation, with logarithmic transformation or dichotomized. Theproportional hazard assumption, which is a condition for applying the Cox multivariate analyses on these data, was checkedby graphic and numerical methods as described by Andersen(17) and was found not to be violated.
Among the significant variables in univariate analyses, themultiple regression analyses discovered an independent prognostic information for performance status; surgery; stage;weight loss; brain, liver, and bone métastases;WBC; prothrombin index; and LDH. Also lymph node métastases,sex, andAST carried prognostic information in the multivariate analyses. The significant influence on survival observed in univariateanalyses for extrapulmonary symptoms, number of metastaticsites below the diaphragm, and hemoglobin was not confirmedin multivariate analyses.
When all the variables which carried prognostic informationin any of the Cox analyses were included into one model, someof the variables did not carry independent additional information and could thus be excluded. This was the fact for weightloss; sex; and brain, bone, and lymph node métastases.Theprothrombin index carried significant information but therewere complete data only on 137 patients when including thisparameter in the model. Ignoring the influence of the prothrombin index, the final regression model was thus assessed as basedon 225 patients for whom there were complete data on allimportant variables (Table 4).
The significant predictors of poor survival were performancestatus 50-60%, no surgical resection, high stage of disease,presence of liver métastases,high values of WBC and LDH,and low values of AST. Even though liver metastasis was anindependent prognostic variable it appears to be of limitedclinical value in this nonextensively staged patient populationbecause of the low number of patients having these métastasesverified. Only 7 patients had verified liver métastasesand 6 ofthese were among the 225 patients in the final model (model1). Thus, the change in survival estimation when this variablewas excluded was evaluated.
No variable other than those occurring in the final Cox modelin Table 4 (performance, surgical resection, stage, WBC, AST,and LDH) gained significance when the influence of liver métastases was ignored. The final model without liver métastases(model 2) is shown in Table 4.
The survival probability is, as expected, smaller for patientswith than for patients without liver métastases,while it is almostsimilar to the latter group when model 2 is used. When accounthas been taken in the estimation of survival expectancy according to model 2 for performance status, surgical resection, stage,WBC, AST, and LDH, but not for liver métastases,the probability is only slightly changed if the patient has no liver métastases and model 1 is used instead. If, however, liver métastasesare present, the survival expectancy will be substantiallysmaller.
No significant interactions between LDH, performance sta-
5750
American Association for Cancer Research Copyright © 1989 on July 10, 2011cancerres.aacrjournals.orgDownloaded from

PROGNOSTIC FACTORS [N LUNG ADENOCARCINOMA
Table 4 Prognostic factors in ACL: results of Cox regression analysis in 225 patients, with (model I) or without (model 2) the variable describing liver métastases
Variable-Performance
status = 50-60% (0/1)"Surgery(0/1)"Stage
WBCLn (AST)Ln (LDH)Liver métastases(0/1)°CoefficientW1.0232
-0.78080.21690.0470
-0.34290.71341.0511Model
1SE0.1978
0.21450.08920.01840.15250.16030.4705P<0.0001
0.00030.0150.010.025
<0.00010.025Coefficient(fi)0.9548
-0.76360.23710.0519
-0.29070.7751
IgnoredModel
2SE0.1958
0.21460.08840.01810.15010.1528
IgnoredP<0.0001
0.00040.0070.0040.05
<O.OOOIIgnored
' 0 = no; 1 = yes.
tus, liver métastases,or stage could be detected. For the interaction between LDH and performance status the significancelevel was P = 0.13, while P > 0.5 was noted for the otherinteractions evaluated.
The finding of a poor prognosis for patients having low ASTvalues was unexpected and thus analyzed further. The distribution of patients in different groups of AST values is shownat Table 5 together with the median survivals. The normalrange in our laboratory is 10-40 units/liter. The mean valuewas 22.2 units/liter (range, 5-176). AST was not correlated toweight loss (r = —¿�0.048).Mean AST values for patients withliver métastaseswas 35.1 units/liter compared to 21.9 units/liter for patients without (P = 0.02).
When dichotomized according to elevated levels or not according to the limits shown in Table 2, neither AST nor WBCcarried significant information in the final Cox model. However, LDH was still significant (P = 0.006). The grouping ofAST values according to the group limits in Table 5 were alsoentered into the final Cox model. In this model the five intervalsof AST values could be simplified to three intervals: 0-19 units/liter, 20-40 units/liter, and >40 units/liter (P = 0.38). Theintervals 0-19 and 20-40 could not be grouped together (P =0.025) but the intervals 20-40 and >40 could be reduced to oneinterval, i.e., >20 (P = 0.95). Thus, a significantly highermortality rate for patients having AST values above 40 units/liter was not demonstrated in the multivariate model.
The 35 nonradically resected patients were compared to theother 224 patients with respect to all important variables, i.e.,the significant variables in the final Cox model. No significantdifferences were noted with respect to stage, liver métastases,AST, WBC, or LDH. However, the resected patients hadsignificantly better performance status than other patients.There were 19 (54%) resected patients in performance status90-100% compared to 69 (31%) nonresected patients (P <0.01). Testing the final Cox model without the 35 resectedpatients, the important variables changed only slightly. All theprevious variables except WBC remained significant, while nonew variables achieved significance. WBC approached significance (P = 0.07).
Risk Groups Based on Prognostic Index. The 225 patients onwhom the final models were based, either with (model 1) orwithout (model 2) the variable describing liver métastases,weregrouped in Table 6 according to the prognostic index. The
Table 5 Survival of patients grouped according to pretreatment values of AST
AST(units/liter)0-910-1920-2930-40>40No.nlpatients"12135633115Median
survival(days)159210201239162
corresponding survival curves for model 1 are given in Fig. 1.The level of statistical significance between the survival curveswas P < 0.0001. The estimation of the prognostic index isbased on regression coefficients in Table 4.
DISCUSSION
Although chemotherapy has been widely used in the treatment of patients with advanced ACL the results remain unsatisfactory, with respect to both single agent treatment (18) andcombination chemotherapy regimens (19). Differences in efficacy among different regimens tend to be smaller than theprognostic influence from other factors which must be considered in the interpretation of treatment results. No previousattempts have been made to disclose the independent prognosticvariables of relevance for survival in a patient population solelywith ACL but this type of lung cancer has been included inmultiple regression analyses of prognostic factors in sevenstudies of non-small cell lung cancer (2, 3, 20-24) and in twostudies including all major types of lung cancer (9, 25).
The positive prognostic factors for survival from these studiesare listed in Table 7. It must be emphasized that none of the
Table 6 Number of I- and 2-year survivors and median survivals according toprognostic indices for the final Cox models with (model I) and without (model 2)
liver métastases
No. ofpatientsSurvival"PrognosticindexModel
1*<3.753.75-4.25>4.25Model
2d<4.54.5-5.0>5.0Total/dead63/5784/8178/7784/7575/7566/65lyr34
(54)'18(21)6(8)43(51)9(12)6(9)2yr15(24)3(4)KD19(23)0(0)1(2)Median(days)3822209737918594
" Kaplan-Meier estimates.* Performance status, surgery, stage. WBC. AST. LDH. and liver métastases.' Numbers in parentheses, percentage.J Same as above, but liver métastasesignored.
200 400 600 800 1000 1200Days
" Total number, 256 patients: 3 had missing information.
Fig. 1. Survival in 3 prognostic categories in the Cox model (model 1). Theprognostic categories were based on values of prognostic indices being <3.75 (63patients). 3.75-4.25 (84 patients, and >4.25 (78 patients).
5751
American Association for Cancer Research Copyright © 1989 on July 10, 2011cancerres.aacrjournals.orgDownloaded from

PROGNOSTIC FACTORS IN LUNG ADENOCARCINOMA
Table 7 Studies of independent prognostic factors including patients with non-small cell lung cancer: factors with positive influence on survival
ReferenceTotal no. of patientsACL patientsWHO histológica!types1'Good
PS'LowwtlossLimited
diseaseNewinternationalstagingFemale
sexAgeChemotherapyNo
livermétastasesExtrathoracicmétastases,0/1
nonbonysitesNobonemétastasesNobrainmétastasesNos.c.métastasesNosupraclavicularlymphnode
métastasesNocontralaterallungmétastasesNonradical
resectionHistologyAlbuminLDHWBCAST9"
5138761
I. II, III,IV+*++00-0—0——_--0-000025
316102
I, II, III,IV+++0—+0+0++—++Ü-00002"452dIII,IV+0+0+-0—0——000000000y893383
I, III,IV++00+-0+0+0+0-—+*000020
12458
I, III,IV+——000000000000-000021
90dI,
III,IV-+00000+00000000+00022
378257
I, III,IV+—00+-0—++—000—-0+0023
13761
1. Ill,IV++—0—-+00000000+'0—0024
190134
I, III,IV•f000+-0—0——0000-0000Current
studv259259III+——+—-0+0——000+00+++No.
ofpositivestudies/total no.
evaluated9/105/83/61/14/71/81/14/81/13/71/61/31/21/31/32/71/12/31/11/1
" Solely male patients; Cox analysis not applied.* Histology not included in Cox analysis.' Prognostic factors for 1-year survival.J —¿�,not reported.* I, squamous cell carcinoma, II, small cell carcinoma; III, adenocarcinoma; IV, large cell carcinoma.^PS, performance status.* +. significant prognostic factor; —¿�,evaluated, but not a significant prognostic factor; 0, not evaluated.* Non-large cell histology is positive prognostic factor.' Non-squamous cell histology is positive prognostic factor.
studies has included all the variables cited.The studies were each based on different clinical groups of
patients and resulted in somewhat different multivariate modelsof prognostic factors. However, all studies except one discovered initial performance status as a very important prognosticindicator while other factors of importance varied, includingthe relative importance of histological type. No information isavailable regarding the role of either subtyping or the degree ofdifferentiation in a previous regression model for survival butunivariate analyses have suggested clinical differences amongsubtypes of ACL (11, 12). The current study thus contributesnew information to the literature, inasmuch as it is the firstmultivariate evaluation of prognostic impact of subtypes anddegree of differentiation in ACL, the new international stagingsystem, and paraclinical parameters such as hemoglobin, platelet count, WBC, AST, and prothrombin index. The prognosticimpact of the new international staging system was confirmedin this multivariate analyses, as was previously documented inunivariate analyses by Mountain (13). The prognostic impactof LDH, which was shown by O'Connell et al. (22), was also
confirmed. The finding of a prognostic impact for WBC andAST has never been reported before.
In the present study no independent significant influences onsurvival were noted for the individual subtypes of ACL or forthe different degrees of differentiation. The data should not bemisinterpreted to imply that absence of substantial survivalcorrelation with subtype or differentiation precludes importantdifferences relating to other aspects of the biological behaviorof the tumors, e.g., with respect to etiology or metastatic spread.A possible observer variability in this histological evaluationmay partially account for the lack of survival correlation, butthere are at present no data on the extent of such a variability.However, with the present data at hand it does not seem
necessary to take these histological variables into considerationin the planning of treatment for patients with inoperable ACL.
The prognostic index for survival in the present patientpopulation was composed of performance status, prior nonrad-ical surgical resection, stage, presence of liver metastasis, WBC,AST, and LDH (Table 4). The importance of performancestatus was not unexpected because it was almost uniformlyreported to be important variables in other regression models(2, 3, 9, 20, 22-25). Although it is a somewhat subjectivemeasure of current symptom status (26) the performance statusscore remains still a very important prognostic stigma.
The occurrence of metastasis in specific organs may indicatea poor prognosis but in a regression model of prognostic factorsthe influence may be diminished with the inclusion of othersummarizing variables, e.g., as extent of disease. This is thecase in studies by Miller et al. (2) and Stanley (9). In the presentstudy no significant prognostic information was observed forextent of disease either in univariate or in multivariate analyses,but the stage of disease was a significant variable in bothanalyses.
Also the nonradical resection, which was attributed independent prognostic information in the present study, may notbe a prognostic factor because of the resection itself. It mayrather serve as a summarizing variable, depicting patients ingood performance status with only minimal and local diseasespread at the time of resection. However, because resectedpatients differed from nonresected ones only with respect toperformance status and because the Cox model remained almost unchanged when the 35 resected patients was omitted, itappears to be reasonable to include these patients in the analysis.
Information regarding métastasesto brain, liver, bone, orlymph nodes carried significant information in multivariate
5752
American Association for Cancer Research Copyright © 1989 on July 10, 2011cancerres.aacrjournals.orgDownloaded from

PROGNOSTIC FACTORS IN LUNG ADENOCARCINOMA
analyses, which is in accordance with observations by Finkel-stein et al. (3), Evans et al. (21), and Lanzotti et al. (25), but inthéfinal model only liver métastasessupplied independentprognostic information (Table 4). However, liver metastasis isof limited clinical value as a prognostic variable in a nonexten-sively staged patient group like the present one. The 7 patientshaving liver metastasis may be regarded as a minimum figurebecause the patients were not routinely liver scanned. Thehigher frequencies of elevated values of LDH (36% of patients)and alkaline phosphatase (39%) and of low prothrombin index(15%) may partially reflect the presence of occult liver métastases in a substantially higher number of patients.
When ignoring the influence of liver métastases,the resultingsimplified model (model 2) consisted of the remaining 6 variables from the original Cox analysis (model 1). The simplifiedmodel may serve as a feasible clinical tool, allowing for prognostic stratification of patients when first the inoperability ofthe patients is known.
The interaction effects of the potentially prognostic variableson the survival was explored. An interaction between LDH andvariables such as performance status, liver métastasesor stagewould be interesting for the interpretation of this biochemicalvariable. However, such interactions could not be discovered inthe present study.
Biochemical variables have not been extensively studied inother regression analyses of prognostic factors in non-small celllung cancer. Overall, the laboratory variables previously evaluated was lymphocyte count (9), serum albumin concentration(21), alkaline phosphatase (23), and LDH (22,23). Lymphocytecount was an important variable in univariate analysis in thestudy by Stanley (9) although not among the variables in thefinal multivariate model. Serum albumin concentrations contributed significant information on survival in a study by Evanset al. (21), while alkaline phosphatase was not significant at P= 0.05 in a study by Rapp et al. (23). Conflicting data havebeen reported for LDH, which was among the significant prognostic factors in a multivariate analysis by O'Connell et al. (22),
but not in the study by Rapp et al. (23). Several studies in small-cell lung cancer have disclosed laboratory parameters as important prognostic variables in that disease entity (14, 15, 27) andthe present material enabled evaluation in patients with ACL.WBC, AST, and LDH were all included in the final regressionmodel, each providing separate and additional power in predicting prognosis. These laboratory assessments are inexpensive and readily available and may thus represent advantagescompared to more complex and invasive investigations.
The observation of lower AST values predicting poor prognosis was unexpected. Because of the occurrence of elevatedAST in patients with liver métastasesit was anticipated thatthe inverse correlation would appear if AST was of significantinfluence on survival. The mean AST value was higher forpatients with liver métastasesthan for patients without, but asignificantly higher mortality rate for patients having elevatedAST levels, i.e., >40 units/liter, compared to other patientswere not observed either in univariate or in multivariate analyses. It is difficult to establish the theoretical background forthis finding. One simple explanation is that it might be a typeI error; the risk for this is, however, only 2.5%.
Another reason may be the correlation between total musclemass and AST. According to this, a low AST value would depictpatients with low muscle mass because of poor nutritional statuswho would have a poor prognosis. However, this theory is notsupported by the lack of correlation between AST and weightloss, although this is only an indirect evaluation of the problem.
The prognostic impact of AST needs further confirmation.The staging program applied is therefore of potential impor
tance for the prognostic index. The nonextensive staging program used in the present study might be the reason why extentof disease and métastasesto specific organs other than liverwas found to be of minor importance for prognosis in contrastto some other studies. A more extensive staging would tend toclassify more patients as having metastasis to specific organs,thus having extensive disease. Likewise, some patients wouldmove into the stage IV category. The conclusions on the relativeimportance of métastasesto various sites and the effect ofactual organ involvement on potentially important variablessuch as AST are hampered by the shortcomings of the limitedstaging procedure. It is, however, interesting that a prognosticdiscrimination is achievable based on simple and cheap investigations when first the inoperability of the patient is known.
This study presents an analysis of a large number of variablesfor potential prognostic information. The problem of false-positive errors when the ratio of the number of patients suffering endpoints to the number of potential predictors is small(say <10) has previously been addressed (28). The ratio in thepresent study is close to that border (28 potential predictors,259 patients) which, however, is arbitrary. The present verythorough evaluation was made to achieve the maximal information from this clinical study, but the problem lies in theinterpretation of the analysis (5). There may be false-positiveerrors due to simple stochastic variation. The prognostic importance of laboratory tests in ACL has not been reportedpreviously and obviously needs further confirmation in subsequent studies for evidence as truly prognostic factors or refutation as false-positive results (5, 29). A collective considerationof such studies together with the present one diminishes therisk of incorrect assessment of the prognostic effect for thesevariables.
The current prospect for cytostatic treatment of advancedACL is not satisfactory (18, 19). Increased knowledge of prog-nostically different groups of patients gives options for a rational selection of treatment. Additionally, the proper use ofprognostic information is important for the reliability, efficiency, and interpretability of clinical trials and may lead tomore rapid progress and with less costs than seen until now.
REFERENCES
1. Ruckdeschel. J. C, Finkelslein. D. M., Ettinger. D. S.. Creech, R. H.. Mason.B. A., Joss, R. A., and Vogel, S. A randomized trial of the four most activeregimens for metastatic non-small cell lung cancer. J. Clin. Oncol., 4: 14-22, 1986.
2. Miller, T. P., Chen, T. T., Coliman, C. A., O'Bryan, J. M., Vance, R. B.,
Weiss, G. B., Fletcher, W. S., Stephens, R. L., and Livingston, R. B. Effectof alternating combination chemotherapy on survival of ambulatory patientswith metastatic large-cell and adenocarcinoma of the lung. A SouthwestOncology Group study. J. Clin. Oncol.. 4: 502-508, 1986.
3. Finkelstein, D. M., Ettinger, D. S., and Ruckdeschel, J. C. Long-termsurvivors in metastatic non-small cell lung cancer: an Eastern CooperativeOncology Group study. J. Clin. Oncol., 4: 702-709, Õ986.
4. S0rensen, J. B., Hansen, H. H., Dombernowsky, P., Bork, E., Malmberg, R.,Aabo, K., Bgdker, B., and Hansen. M. Chemotherapy for adenocarcinomaof the lung (WHO III): A randomized study of vindesine versus lomustine,cyclophosphamide and methotrexate versus all four drugs. J. Clin. Oncol., 5:1169-1177, 1987.
5. Sather, H. N. The use of prognostic factors in clinical trials. Cancer (Phila.).58: 461 -467, 1986.
6. Kalbfleisch, J. D., and Prentice, R. L. The Statistical Analysis of FailureTime Data. New York: John Wiley & Sons. Inc., 1980.
7. Cox, D. R. Regression models and life-tables. J. R. Statistics Soc., 34: 187-220, 1972.
8. Mountain. C. F., Carr, D. T., and Anderson. W. A. D. A system for theclinical staging of lung cancer. Am. J. Roentgenol. Radiât.Ther. NucÃ.Med.,120: 130-138, 1974.
9. Stanley. K. E. Prognostic factors for survival in patients with inoperable lung
5753
American Association for Cancer Research Copyright © 1989 on July 10, 2011cancerres.aacrjournals.orgDownloaded from

PROGNOSTIC FACTORS IN LUNG ADENOCARCTNOMA
cancer. J. Nail. Cancer Inst.. 65: 25-32, 1980. 2110. World Health Organization. Histological Typing of Lung Tumours, Ed. 2.
Geneva: World Health Organization, 1981.11. S0rensen, J. B., Hirsch. F. R., and Olsen, J. The prognostic implication of
histopathologic subtyping of pulmonary adenocarcinoma according to theclassification of the World Health Organization. An analysis of 259 consecutive patients with advanced disease. Cancer (Phila.), 62: 361-367, 1988. 22
12. Saijo. N.. Niitani. H., Tominaga. K., Eguchi, K., Koketsu. H., Fujino, T.,and Ishikawa. S. Comparison of survival in nonresected well differentiatedand poorly differentiated adenocarcinoma of the lung. J. Cancer Res. Clin.Oncol.. »7:71-79. 1980.
13. Mountain. C. F. A new-international staging system for lung cancer. Chest 23(Suppl.). 89: 225s-233s. 1986.
14. Souhami, R. L., Bradbury. I.. Geddes. D. M., Spiro, S. G., Harper, P. G.,and Tobias, J. S. Prognostic significance of laboratory parameters measuredat diagnosis in small cell carcinoma of the lung. Cancer Res.. 45: 2878-2882,1985.
15. 0sterlind. K., and Andersen, P. K. Prognostic factors in small cell lung 24cancer: multivariatc model based on 778 patients treated with chemotherapywith or without irradiation. Cancer Res., 46: 4149-4194. 1986.
16. Peto. R., Pike, M. C.. Armitage. P., Breslow. N. E., Cox, D. R., Howard, S.V., Mantel, N.. McPherson, K., Peto, J., and Smith. P. G. Design andanalysis of randomized clinical trials requiring prolonged observation of each 25.patient. II. Analysis and examples. Br. J. Cancer, 35: 1-39, 1977.
17. Andersen, P. K. Testing goodness of fit of Cox's regression and life model.Biometrics. 38: 67-77. 1982.
18. S0rensen, J. B., Clerici, M., and Hansen, H. H. Single agent chemotherapy 26.for advanced adenocarcinoma of the lung. A review. Cancer Chcmother.Pharmacol.,2/: 89-102. 1988. 27.
19. S0rensen. J. B., and Hansen. H. H. Combination chemotherapy for advancedadenocarcinoma of the lung. A review. Cancer Chemother. Pharmacol., 21:103-116, 1988.
20. Einhorn, L. E., Loehrer, P. J., Williams, S. D., Meyers, S., Gabrys, T.. 28.Nattan, S. R., Woodburn, R., Drasga. R.. Songer, J., Fisher, W., Stephens.D., and Hui, S. Random prospective study of vindesine versus vindesine plushigh-dose cisplatin versus vindesine plus cisplatin plus mitomycin C in 29.advanced non-small-cell lung cancer. J. Clin. Oncol.. 4: 1037-1043. 1986.
Evans. W. K.. Nixon, D. W.. Daly. J. M.. Ellenberg. S. S.. Gardner, L.,Wolfe. E.. Shepherd. F. A.. Feld. R.. Gralla. R.. Fine. S., Kemeny, N..Jeejeebhoy. K. N.. Heymsfield. S.. and Hoffman. F. A. A randomized studyof oral nutritional support versus ad Uh nutritional intake during chemotherapy for advanced colorectal and non-small-cell lung cancer. J. Clin. Oncol..5: 113-124. 1987.O'Connell. J. P.. Kris. M. G., Gralla. R. J.. Groshen, S., Trust, A.. Fiore, J.
J., Kclsen. D. P.. Heelan. R. T.. and Golbey, R. B. Frequency and prognosticimportance of pretreatment clinical characteristics in patients with advancednon-small-cell lung cancer treated with combination chemotherapy. J. Clin.Oncol.. 4: 1604-1614, 1986.Rapp. E., Pater. J. L., Willan. A., Cormier, Y., Murray. N.. Ewans. W. K..Hodson, D. I., Clark, D. A., Feld, R.. Arnold. A. M., Ayoub, J. I.. Wilson,K. S., Latreille, J.. Wierzbicki. R. F., and Hill, D. P. Chemotherapy canprolong survival in patients with advanced non-small-cell lung cancer: reportof a Canadian multicenter randomized trial. J. Clin. Oncol.. 6: 633-641.1988.Sukurai. M., Shinkai. T.. Eguchi, K.. Sasaki. V., Tamura. T.. Miura. K..Fujiwara, Y., Otsu. A.. Horiuchi, N.. Nakano. H.. Nakagawa, K.. Hong. W..and Saijo. N. Prognostic factors in non-small cell lung cancer: mulliregrcssionanalysis in the National Cancer Center Hospital (Japan). J. Cancer Res. Clin.Oncôl..7/5:563-566, 1987.Lanzotti. V. J.. Thomas, D. R.. Boyle, L. E., Smith. T. L.. Gehan. E. A., andSamuels, M. L. Survival with inoperable lung cancer. An integration ofprognostic variables based on simple clinical criteria. Cancer (Phila.). 39:303-313. 1977.Orr, S. T., and Aisner. J. Performance status assessment among oncologypatients: a review. Cancer Treat. Rep., 70: 1423-1429. 1986.Cohen. M. H., Makuch, R.. Johnston-Early. A., Ihde. D. C., Bunn, P. A.,Fossieck. B. E., and Minna, J. D. Laboratory parameters as an alternative toperformance status in prognostic stratification of patients with small celllung cancer. Cancer Treat. Rep.. 65: 187-195, 1981.Harrell, F. E., Lee, K. L., Matchar. D. B.. and Reichert, T. A. Regressionmodels for prognostic prediction: advantages, problems, and suggested solutions. Cancer Treat. Rep., 69: 1071-1077, 1985.Simon, R. Importance of prognostic factors in cancer clinical trials. CancerTreat. Rep.. 66: 185-192, 1984.
5754
American Association for Cancer Research Copyright © 1989 on July 10, 2011cancerres.aacrjournals.orgDownloaded from
Copyright © 2022 FDOKUMEN