Proceedings - Georgia Veterinary Medical Association
268
Proceedings October 15 - 17, 2021 The Hotel at Avalon, Alpharetta, GA
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Proceedings - Georgia Veterinary Medical Association

Proceedings October 15 - 17, 2021 The Hotel at Avalon, Alpharetta, GA

VetSouth 2021 Fall Veterinary Conference Proceedings Table of Contents
Page Number Friday, October 15 Dermatology —Michael Rossi, DVM, MNS, DACVD *No content provided by Author
LEAP CE/Wellness — Laura Smallwood, DVM, DACVIM – SA, RYT - 200 Changing How We Think About Stress: From Coping to Flourishing ............................................................................. 1 Changing How We Talk About Stress: From Venting to Processing .............................................................................. 5
Practice Management — Eric Garcia How to Stand Out in an Increasingly Competitive Marketplace ...................................................................................... 7 Avoiding Cat-astrophy: How to Engage Cat Owners in Life-Long Care ....................................................................... 10 Can You Help My Yelp?!: How to Handle Online Haters, Bullies, and More ............................................................... 12 Using Technology to Meet Client Expectations in Today’s World ................................................................................ 15
Shelter Medicine — Brenda Dines, DVM Ringworm 101: Diagnosis ............................................................................................................................................. 19 Ringworm 102: Treatment and Management ................................................................................................................ 21 Things You Wish You Knew: Most Common Diagnostic and Management Mistakes of Infectious Diseases in Shelters ....................................................................................................................................................................... 23 Behavior Management for the Shelter Population .......................................................................................................... 25
Wound Management — Mandy Wallace, DVM, MS, DACVS – SA Initial Wound Triage, Bandaging, and An Update on New Topical Wound Products ................................................... 26 Surgical Options for Wound Closure: Tension Relieving Techniques, Flaps and More ............................................... 32 Management of Burn Wounds, Non-Healing Wounds, and Other Challenging Wound Cases ...................................... 37 Choose Your Adventure: An Interactive Walk Through Challenging Would Management Cases ................................ 41
Saturday, October 16 Behavior — Lynne M Seibert, DVM, MS, PhD, DAC Separation-Related Anxiety in Dogs .............................................................................................................................. 43 Consequences of Aversive Training in Dogs .................................................................................................................. 47 Reducing Stress During Veterinary Visits ...................................................................................................................... 49 Keeping the Peace in Multi-Cat Households .................................................................................................................. 54
Dentistry — Barron Hall, DVM, FAVD, DAVDC Intraoral Imaging and Oral Surgery ................................................................................................................................ 57 Case Talk: What Would You Do? ................................................................................................................................. 59 Communicating with Clients Regarding Oral Health ..................................................................................................... 61
Internal Medicine — Jana Gordon, DVM, DACVIM Diagnostic and Management Strategies for Hypoadrenocorticism in Dogs ................................................................... 66 Updates Regarding Treatment and Management of Diabetes Mellitus in Cats and Dogs .............................................. 71 Diagnosis and Treatment of Immune-Mediated Hemolytic Anemia .............................................................................. 78 Review of Immunosuppressive Therapy......................................................................................................................... 86 A Review of Tests of Liver Disease in Companion Animals ......................................................................................... 91
Large Animal — Lee Jones, DVM, MS Bovine Anaplasmosis: A Blood Borne Disease in Cattle ............................................................................................... 96

Parasitology — Byron Blagburn, DVM, MS, PhD Four Heartworm Updates That Could Change Your Strategies .................................................................................... 100 The 10 Most Important Extra-Label Uses of Parasiticides for the Small Animal Practitioner ..................................... 103 Heartworm Testing: What to Do When Test Results and Experts Disagree ................................................................. 106 Broad-Spectrum Feline Parasite Control: The Time Has Come ................................................................................... 109 These Parasites Won’t Take No for an Answer ............................................................................................................ 115 Fleas, Ticks and Vector-Borne Diseases: Bad Things Come in Threes ........................................................................ 120 Techniques and Strategies in Fecal Diagnosis .............................................................................................................. 129
Veterinary Technicians — Kara Burns, MS, M.Ed, LVT, VTS, VTS-H FLUTD: What's All the Stress? .................................................................................................................................... 133 Feline Nutrition: Cats are Not Small Dogs ................................................................................................................... 137 4 Realities Exposed: A Visual Tour of Heartworm Disease ........................................................................................ 141 Fleas & Ticks: Talking it O.V.E.R. with Pet Owners .................................................................................................. 143 Nutritional Management of Pancreatitis ....................................................................................................................... 145 Keeping Pets Youthful with Senior Nutrition ............................................................................................................... 148 A Proactive Approach to Canine Osteoarthritis ............................................................................................................ 152
Sunday, October 17 Cardiology — Michael Aherne, MVB, MS, MANZCVS, DACVIM Tachyarrhythmias: Diagnosis & Treatment in General Practice .................................................................................. 154 Bradyarrhythmias & Conduction Disturbances: Diagnosis & Treatment in General Practice ..................................... 161 Identification & Management of Cardiac Disease in Cats ............................................................................................ 165 Feline Arterial Thromboembolism ............................................................................................................................... 170 Non-Inherited Dilated Cardiomyopathy Phenotypes in Dogs ....................................................................................... 173 Beyond Furosemide: A Guide to Cardiac Drugs for the General Practitioner .............................................................. 177 Tips from the Trenches: Avoiding Common Mistakes in the Management of Cardiac Disease .................................. 184
Nephrology/Urology — Andrew Specht, DVM, DACVIM-SAIM Myths & Misperceptions: Recognizing the Problems and Avoiding Common Mistakes ............................................. 185 Beyond Diet…What Else Should You Know about Chronic Kidney Disease ............................................................. 189 Beyond Azotemia…What You Need to Know about Oroteinuria in Dogs and Cats ................................................... 195 Bothersome Bugs: How to Deal with Persistent or Recurrent UTIs ............................................................................. 200 Trying Not to Let Cats Think Outside the Box – What We Know about Managing FIC ............................................. 205 Snippets on Stones: What to Do with the Really Challenging Urolith Cases ............................................................... 209 What’s New in Nephrology: Quick Hits and Hot Takes on a Variety of Topics .......................................................... 215
Pathology — Heather Wamsley, DVM, PhD, DACVP Urinalysis Tips and Tricks ............................................................................................................................................ 222 Urinalysis Sediment Microscopy Review ..................................................................................................................... 224 Cytology Submission and Review of Interpretation ..................................................................................................... 231 FNA Cytology Interactive Case Session ....................................................................................................................... 234 RBC, PLT and WBC Values ........................................................................................................................................ 236
Veterinary Technicians — Kara Burns, MS, M.Ed, LVT, VTS, VTS-H Pet Food Labels: Demystifying the Package ............................................................................................................... 241 Busting Nutritional Myths ............................................................................................................................................ 245 Discussing Diabetes Mellitus: Empowering Technicians ............................................................................................. 249 Calm the Angry GI Tract - Nutrition with GI ............................................................................................................... 255 You Are What You Eat: Helping Clients with Diet Choices ........................................................................................ 261 Let's Talk Lifestyle Vaccines: Having the Conversation with Pet Owners .................................................................. 264

Changing How We Think About Stress: From Coping to Flourishing Laura Jean Smallwood, DVM DACVIM (SAIM) RYT-200
What is Stress? Our traditional understanding of stress is rooted in scientific findings that date back to 1936, when Hungarian endocrinologist Hans Selye began to experiment with the effects of various hormones on rats. Seyle discovered that it didn’t matter which hormone he injected, the effects were the same—adrenal swelling, thymus atrophy, duodenal ulcers, and general illness. He eventually recognized that the effects that his experiments were having on the rats was not due to what he was injecting but, rather, due to what they were experiencing. He went on to demonstrate that he could also make his rats sick by exposing them to other things such as extreme temperature, loud noises, and near-drowning. Prior to his experimentation on rats, Seyle had been a physician. As a physician, he noticed that many of his patients with chronic conditions suffered symptoms that could not be attributed to their underlying diagnosis. At the time, he described this as “sick syndrome.” Drawing a correlation between what he observed in his patients what he later induced in his rats, Seyle gave “sick syndrome” a new name. Stress. Even before Seyle began to experiment on rats, physiologist Walter Cannon was experimenting on dogs and cats to see how pain, hunger, fear, and rage affected their physiology. In 1915 he coined the term fight-or-flight to describe the biological effects of adrenaline which included increased heart and respiratory rate, increased release of glucose from the liver into the bloodstream, increased blood flow to the muscles, and dampening down of non-urgent functions like digestion. For many decades, fight-or-flight and the ill-effects that stress can have on health have underpinned our collective narratives on stress and reasonably so. Fighting or fleeing is rarely an appropriate response to our circumstances in the context of modern life. Additionally, if stress is harmful to our health, it makes sense to avoid it. The mindset that stress is bad and to be managed or avoided is a well-entrenched belief and, for many generations, the stress research supported this narrative. More recent research on stress, however, is turning up some surprising findings. As it turns out, how our bodies respond to challenging circumstances is far more complex and nuanced than previously thought. There is also evidence that we have biological responses to stress that are protective against adverse outcomes rather than causative. Additionally, there is evidence that how we think about stress affects what happens in our bodies on a biological level and this can have an impact on long-term outcomes. In the context of this presentation stress will be defined as the mental, emotional, and physiological response to something that is challenging. Or as Kelly McGonigal describes it in her book The Upside of Stress: “Stress is what arises when something you care about is at stake.” I like this definition because this includes everything from the smallest inconvenience to the most major upheaval. It also points to three important realities:
• We don’t get stressed about things we don’t care about. • Our lives are meaningful because of the things we care about. • Stress is not our circumstances. Stress is an embodied response to a challenge that arises around something
we care about. The Stress Repertoire Stress has a bad reputation in part because we have long held a narrow view of how the stress response plays out and it looks something like this. Something “bad” happensmind interprets that something as an immediate threat to survival the sympathetic nervous system is activated adrenalin and cortisol is releasedthe body prepares to fight or fleeexcept that the something that started this whole thing was something a coworker said and now your
1
heart is racing, your blood pressure is through the roof, your blood sugar is elevated, your digestive system has shut down, your cognitive faculties are compromised and punching said coworker in the face and running away is not an option. The good news is that the stress response is far more complex and nuanced than advertised and baked into it are some biological chemicals that actually help us better respond to and recover from stress. These include:
• Adrenalin: activates the senses, increases awareness, and stops mind-wandering. • Dehydroepiandrosterone (DHEA): facilitates a quicker recovery from stress and improves post-stress
resilience. It has also been linked to reduced risk of diseases typically categorized as stress related including depression, anxiety, and heart disease.
• Oxytocin: restores autonomic balance and helps cardiac cells recover from micro-damage. • Testosterone, endorphins and dopamine: facilitate the “excite and delight” side of stress—think
skydivers and bungee jumpers. • Cortisol: decreases inflammation.
In her book the Upside of Stress, Kelly McGonigal describes something that reflects this complexity and she refers to as the “Stress Repertoire”. The stress repertoire includes these responses:
• Fight or Flight Response—fueled by adrenaline, testosterone, endorphins and dopamine, this response provides an energetic boost that can be motivating. If your survival is in immediate jeopardy (or you think it is), a full-blown fight-or-flight response will occur. It is also possible for this to be modulated by the perspective that you are being alerted to something important rather than something deadly.
• Challenge Response—the hallmark of this response is a higher DHEA:cortisol ratio, also known as the “growth index”, which results in greater self confidence and a greater capacity to learn from a stressful experience rather than be harmed by it. The Challenge Response represents a modulation of the fight-or-flight response.
• Tend-and-Befriend Response—the key hormone in this response is oxytocin. Oxytocin increases connectivity with others and also modulates the fight-or-flight response by dampening the inclination to fight or flea. Oxytocin release during this response increases courage, motivates caregiving, and strengthens social relationships.
So, perhaps, stress is not all bad. But how do we take advantage of the ways that stress might be beneficial without succumbing to the harm? One answer appears to be by changing our mindset. Mindsets and Stress Mindsets are sets of beliefs that we hold that substantively affect our view of the world. Typically, these are complex and acquired over time. Mindsets affect what we experience and, in turn, our experiences reinforces our mindsets. For instance, if your mindset about working a particular shift is that “this shift is always awful”, it is likely that your attentional bias will cause you to focus on what you expect (“awfulness”), you will find what you are looking for, you will experience the shift as awful, and your mindset will be reinforced. In short, the effect you expect is the effect you get and you will continue to expect that. Researcher Alia Crum has examined the impact of stress mindsets on health outcomes. Controlling for levels of stress, she has been able to demonstrate that individuals who believe that stress is inherently bad and to be avoided are likely to cope with stress by trying to avoid it while individuals who see stress in a more positive are more likely to have a proactive approach to stress. Rather than trying to avoid stress or numb themselves when they are feeling stress, these individuals are more likely to build internal and external resources that help them respond more skillfully to stressful situations. They are also less likely to be depressed and more likely to be satisfied with their lives that individuals with a stress-is-harmful mindset.
2

Mindfulness and Stress Mindfulness can be defined as the capacity to bring full attention to what is happening as it is happening with an awareness of when that experience is being clouded by pre-conceived ideas about what is happening that are not accurate. In the context of stress, a greater capacity for mindful awareness has a number of benefits:
• Increased body awareness and the capacity to recognize when the nervous system is being activated before a full-blown stress response is triggered.
• Increased capacity to observe thoughts, judgment and stories in order to perceive situations more accurately and less based on past experience.
• Decreased reactivity and increased capacity for emotional self-management. • Changes in perspective on self that can lead to seeing challenging situations as not personal.
Mindfulness practices are particularly helpful when it comes to recognizing mindsets. The increased capacity to observe thoughts separate from thinking that comes with regular meditation practice promotes a better ability to see mindsets for the collection of long-held beliefs that they are rather then accepting them as absolute truth. Mindfulness also practices also support a capacity to pay attention to how mindsets are working for us (or not) and offers us the possibility of intentionally modifying our mindsets in a skillful way. The Window of Tolerance When we consider the activation of the nervous system that occurs with the onset of a stress response, it can be helpful to think of this in terms of our window of tolerance for nervous system activation. Our autonomic nervous system is continually in flux—the sympathetic nervous system responding to things that are interesting or challenging to us and the parasympathetic nervous system modulating that effect—offering recovery from the effects of the sympathetic nervous system and the opportunity or “rest and digest”. Throughout the day we are in constant flux between arousal and recovery with the excursions varying between small (i.e., excited to see someone you know) to huge (i.e., almost crashing your car). Our window defines our tolerance for the intensity of these excursions. Within the window we are relatively comfortable as we cycle between nervous system activation and recovery. Outside the window we are in distress. At the edge, we bump up against challenge. And that edge is uncomfortable. Sometimes really uncomfortable. But it is not distress. And it is the sweet spot for learning and growth. Our mindset about stress affects the width of this window. If we believe that stress is bad and to be avoided, it is likely that we will find ourselves hurdling toward distress with the first signs of discomfort rather than viewing what we are experiencing as an opportunity to learn. Conversely, a positive mindset can make us more willing to be with the discomfort and learn from it. Over time, this positive mindset allows us build confidence and the window opens wider, bit by bit. In other words, the set point for the width of our window at any point in time depends on our past willingness to be with discomfort and learn from the challenges we face. The window of tolerance can also be affected by self-care. No matter how much resilience we have cultivated, the width of the window will narrow and our capacity to navigate challenge will be reduced if we are tired, poorly nourished, dehydrated, or overworked. Conversely, when we make time to sleep, rest, eat well, hydrate, exercise, and experience joy, the window of tolerance widens and our capacity to be with challenge expands. From Coping to Flourishing The invitation to change your stress mindset is an invitation to change your relationship with stress. Rather than thinking of stress as unnecessary, avoidable, and unfair, its possible to view stress as a normal part of having a meaningful life. A positive stress mindset allows us to take full advantage of the stress repertoire—the energy that comes with the release of adrenalin, the neuroplasticity that is enhanced by DHEA, and the possibility of greater connection to others that is mediated by oxytocin. A positive stress mindset decreases the likelihood that we will be
3
derailed by challenging experiences and increases the likelihood that we will learn from them. A positive stress mindset also appears to reduce the long-term adverse health impacts typically attributed to stress. This is not to say that there aren’t a lot of things in our lives, our communities, our workplaces, and our world that are badly in need of change. However, we are ill-prepared to address them if we find ourselves constantly derailed by the challenges that are inherent in the work we do, our relationships with others, and our occupancy of these human bodies. Perhaps if we adopt a positive stress mindset, we might find ourselves better able to effect the change we want to see in the world. Reference: McGonigal, Kelly, The Upside of Stress: Why stress is good for you and how to get good at it. 2015
4

Changing How Talk About Stress: From Venting to Processing Laura Jean Smallwood, DVM DACVIM (SAIM) RYT-200
Why What We Say Matters From a neurological perspective, what we say not only reflects what we think but reinforces those thought patterns. Perhaps you have encountered this is an acquaintance who is always complaining AND always dissatisfied with life. Language is inextricably tied to the meaning that we assign everything in our lives and how we talk about things has a lot to do with how we experience them. In the previous session on mindsets and stress, we discussed how mindsets affect outcomes. This effect is neither magical or mystical. Sometimes referred to as the placebo effect, what we expect is often what we get for a variety of reasons that include biological factors, what we pay attention to and don’t pay attention to, and the choices we make, large and small. Our cultural narrative around stress is that stress is bad for you and something to be avoided. Interestingly, there is research to suggest that this stress-is-bad mindset may have more to do with the adverse impact of stress on health than the stress itself. In one study people who reported that they were experiencing high levels of stress were more likely to die if they believed that stress was harming their health and less likely to die if they did not believe this. In the context of this study, perhaps it is worth considering that what we say about stress—to ourselves, our co-workers, our friends, and our loved ones—has the power to impact our own health and wellbeing and the health and well-being of others. Venting The belief that venting is a good way to “blow off steam” and manage stress is a myth that is deeply embedded in the veterinary culture. Venting certainly feels good in the moment as that feeling of righteous anger washes over us and we enjoy the camaraderie of coworkers gathering around to validate our experience of perceived injustice. However, venting is an ineffective way of managing stress and, for a number of reasons actually makes stress worse. Some things to consider include:
• Venting provides only short-term relief from strong emotions like anger. Sharing with coworkers makes us feel better for the moment but when we vent, we fail to engage with the full complexity of emotions that are being experienced. Underlying the anger may also be emotions like shame, guilt, sadness, or grief. Unrecognized, these emotions persist unaddressed.
• Having others agree with our outrage reinforces our behavior, keeps the anger alive longer, and reinforces the mindset that it is justified. When our coworkers validate our venting, they set us up not only to hang onto those feelings longer but to be negatively triggered again and again.
• Emotions are contagious. We have “mirror neurons” that wire us for empathy and, when activated we actually experience the emotions of another person. This is true for both positive and negative emotions but, unfortunately, negative emotions are far more contagious than positive ones. And just like an infectious disease, we don’t get rid of a negative emotion when we share it with another person. We get to hang on to our negativity while giving those around us their own copies. Negative emotions can quickly infect a workplace community and even spread to our families and communities as people take them home with them at the end of the day.
• Venting perpetuates a negative stress mindset. Venting is reaction to something we perceive as unfair, that shouldn’t be happening to us, that should be avoidable. When we vent, we perpetuate the idea that a stressful experience is unfair, shouldn’t be happening, and should be avoidable. The reality is that most things we vent about are neither avoidable or controllable. They are the challenges we run up against day in and day out in the work we do.
Processing Experience An alternative to venting is processing. Processing is an opportunity to fully acknowledge the experience—including the challenging and complicated emotions that arise and the discomfort of it all—in order to better
5

understand oneself, learn from the experience, and find meaning in the face of adversity. Unlike venting, this invites us to take a deep dive into what we are experiencing in order to cultivate greater resilience. Processing challenging experiences in this way, particular in the context of the workplace community, can be a powerful way of creating more supportive narratives and mindsets around the work that we do. This is particularly true when we share stories of challenging situations that we have successfully navigated or learned from in some way. Our capacity for resilience is not only expanded when we personally experience challenge and learn from it, it is also expanded when we hear the stories of others who have done the same. Vice versa, we have the opportunity to contribute to the resilience of others when we share our own stories of resilience. In the context of the veterinary workplace, this can be as simple as taking the time to process something challenging with a trusted colleague. It can also be more formal, setting aside time to talk in a group about challenges faced in the workplace—acknowledging the icky discomfort that comes with these situations and celebrating the ways that we can find meaning in them and learn from them. Talking About Stress How we talk about stress in the context of our work influences our personal stress mindset and well as the stress mindsets of our coworkers. When we complain about stress, we reinforce the mindset that stress is to be avoided and the fantasy that a life devoid of stress is either desirable or possible. When we vent about challenging experiences, we reinforce the mindset that stress is unfair and that it is personal. When we choose to suffer in silence, we deprive ourselves of the support of others and an opportunity for others in our workplace to learn from our experiences. Each day, when we talk about stress in the workplace, we have the opportunity to either model a stress mindset that contributes to well-being and resiliency or model a stress mindset that undermines well-being and resiliency. It’s up to us.
6
HOW TO STAND OUT IN AN INCREASINGLY COMPETITIVE MARKETPLACE
Eric D. Garcia, IT & Digital Marketing Consultant
Simply Done Tech Solutions Tampa, Florida, USA
The convenience of the internet is something we’ve all learned to enjoy in one way or another. Netflix, for example, makes for hours of satisfying home entertainment, especially when coupled with good popcorn. Google, as another example, allows us to index the entirety of the World Wide Web with just a keyword phrase and a vertical scroll. Facebook brings your childhood friends, college alumni and family under a single roof. This same convenience, however, can be dangerous at times and costly at others. Why? So much information is at our fingertips that the imagery and resources we access start to feel a lot like our own. After all, if I’m searching for new and savvy images on Google, I’m doing it on my Wi-Fi, in my home and on my laptop. This type of thinking, however natural, can spill over into nasty legal issues, especially in cases of copyright infringement. The situation is far more common and costly than most veterinarians and practice managers realize. A Costly Downside Veterinary practices using images found on the web that haven’t been properly licensed or authorized can lose the credibility of pet owners and wind up liable for thousands of dollars in damages. I have seen practices paying penalties of $500 to $20,000 for illegally using an image. While the repercussions might sound severe, courts are ruling in favor of image creators who made the effort to license their works and benefit from the protection of copyright law. This means that if you use a screengrab image on your website, social media or marketing brochure, you might face a steep fine faster than you can imagine. If you have illegally reused a web image, I wouldn’t hit the panic button. In my estimate, you’re like at least 99.9 percent of veterinary practices that have done it in some form or another. But know that if you keep the images live on your website or in marketing materials, you’re doing so at your own risk. What You Should Do Are you ready to fix the problem? Here are quick tips for avoiding copyright infringement and keeping your veterinary practice squeaky clean when copyright law is at issue:
1. Comb through your practice’s website, social networks and marketing materials from top to bottom. 2. If your practice doesn’t own the image or if you didn’t license it yourself, delete it. 3. On Facebook, make sure to delete (not just hide) images that you didn’t receive explicit permission to use.
Don’t worry, doing this won’t hurt the success or reach of your page. 4. Pay closer attention to your business page than your personal page. While both are liable for copyright
infringement, your business has more at stake and is more likely to be targeted for illegal use. 5. Memes count, too. While memes often provide a good laugh, these hilarious internet tidbits can be
infringed upon. Next Steps OK, so you’ve deleted the generic pet pics and just under 200 memes. Now what? It’s time to start thinking more holistically about your content and social media as a whole. Not only are illegally used stock images dangerous, they’re flat out boring. Simply put, these images no longer make the cut when it comes to the ability of modern veterinary practices to connect with pet owners. Social media and marketing today are not simply about cookie-cutter images but instead about the personal experience and connecting your practice in a deeper way. Your clients want to see you in your element, working with real pets and clients. That’s where the true story is, and that’s where the true value lies.
7

As you start to reclaim your veterinary practice’s message and imagery, it’s time to implement best practices. You can’t just start snapping shots with your new iPhone X. You must obtain explicit client permission if you want to show their pet in any photos or marketing materials. An easy way to do this is to collect a consent on your client registration forms. For existing clients, you can get a signature during drop-off or, if the owner is present, before you take a photo. Don’t forget that these photographs, even when authorized in a consent form, must be taken on a clinic-owned device. I recommend that you purchase a camera, perhaps an iPod Touch or a clinic cell phone, for your practice. Hospitals should go the extra mile by prohibiting the use of personal cameras for such purposes. This ensures that employees don’t take home images of clients, which can cause a wide range of fallout, and that selected images are approved by the appropriate decision makers before being posted. The Big Payoff Another benefit of these policies is that offering to take photos of a pet is an easy way to boost client engagement, as the owners are often proud to show off their adorable kitten turned Instagram superstar. For pets that can’t be photographed on the spot, invite the owner to email a photo after the visit. The key here is to boost client engagement by crafting a narrative around your veterinary practice and clients. Each pet and owner has a story to tell, and ultimately this becomes a part of your practice. When pet owners visit your website or social media page, they’re not looking for stock photos. They want the full picture. That is, they want the real story behind who you are and what your veterinary practice believes in most. It’s proven true time and time again that people gravitate toward a good story more so than just numbers or facts. We look for narrative when attributing meaning, simply because it resonates more deeply with us than an isolated statistic. Let’s look at some examples below:
Approach #1 – Not Recommended Simply Done Veterinary Clinic is a full service animal hospital. We offer state-of-the-art-care and advanced diagnostics. Approach #2 - Recommended Dr. Garcia founded our veterinary practice on the core belief that by enriching the lives of pets, we enrich the world around us. The staff and veterinarians at Simply Done Tech Clinic take immense pride in this philosophy, bringing this belief to action by implementing passionate, compassionate veterinary care. While Approach #1 is technically accurate, it won’t compel a pet owner to visit your hospital, and it won’t help to gain interest and trust like Approach #2 does. Let’s look at another example: Approach #1 – Not Recommended Dr. Garcia was born in Tampa, Florida. He graduated from the University of Florida in 2000. He has 2 dogs by the name of Elvis and Penny. Dr. Garcia is excited to meet both you and your pet! Approach #2 - Recommended Dr. Garcia knew from a young age that pets were his passion. The joy and wonder of a happy pet immediately inspired Eric to pursue a career in veterinary medicine after completing his undergraduate degree. Now, as the
8
founder of a successful veterinary practice, Dr. Garcia does what he loves each and everyday. Stop by soon, because Dr. Garcia can’t wait to meet you and your pet! As people, we crave a good story! Make sure that your veterinary practice is telling your tale, and you’ll be amazed at the results that can come from a more narrative-driven approach to marketing, social media and more.
9

AVOIDING CAT-ASTROHPY: HOW TO ENGAGE CAT OWNERS IN LIFE-LONG CARE
Eric D. Garcia, IT & Digital Marketing Consultant
Simply Done Tech Solutions Tampa, Florida, USA
How Case Studies Enhance Marketing Efforts The below resource was created by Eric Garcia, Cat Friendly Practice® (CFP) Advisory Council member and an IT and Digital Marketing consultant who works exclusively with veterinary practices. When it comes to helping veterinary practices streamline their technology and attract and retain clients, Eric Garcia has a proven track record of educating the industry and producing results. We are grateful to have Eric involved with our CFP program and share his knowledge with you.
TELL YOUR STORY People are often under the impression that Facebook is only for peer-to-peer interactions. This, however, couldn’t be further from the truth. Facebook is a platform that’s become as universal as the water cooler itself. Successful veterinary practices around the world leverage Facebook as a place to tell their unique story. Your veterinary practice has a story and details that make it entirely unique: the year it was founded; your founder (or two, or more); your Cat Friendly Practice® designation; and your practice style and perspective. Use Facebook to tell your story! It is a perfect platform where you can capture and captivate your audience. Tell your followers about success stories at your practice such as:
• How and why you chose to become a Cat Friendly Practice®? • How being a Cat Friendly Practice® has improved visits for cats and their caregivers? • What differences your practice has made today in the lives of cats and other animals?
Sharing this kind of information with your followers in a story format fosters community, trust, interactions, and keeps your trusted cat clients coming back to you. Stories like these are also known as: Case studies – a story particular to a specific cat client, place, and time. Case studies are crucially important for a variety of reasons, but primarily to help your audience know about the stellar care your Cat Friendly Practice® provides! When you are creating your case study, be sure to provide your audience with:
• The reason the cat came in to receive veterinary care. • Details regarding the type of care you provided for the cat. • How being a Cat Friendly Practice® improved the veterinary visit and overall care for the cat and the
caregiver. • An update on how the cat is doing today. • A photo, or quick video of the pet.
When you provide this level of in-depth information on a cat, you tell the story of your patient and demonstrate that you can deliver the same quality of care to any prospective client. You can to forge an immediate bond with cat caregivers who appreciate your attention to detail, and the accountability needed to provide optimal care for their cat. Your followers and their friends want to hear of your successes, which will brighten their day and instill them with confidence about your Cat Friendly Practice®. In exceptional circumstances, news coverage has even come about after particularly sincere and uplifting stories. This results in tremendous positive publicity, and simultaneously
10
helps you to market your services to a wider audience. This wider audience can soon grow and enhance your veterinary practice online, and in your local community. Case studies are also a great opportunity to educate your clients. By highlighting a particular health concern (like lily toxicity in cats), you can spread important information in your success story that will resonate with cat caregivers. These posts can be timed for specific times of year (the “chocolate holidays,” the start of flea season, holiday dangers) to help your clients stay aware of how to best care for their cat, and to keep your practice at the top of their minds. GET PERMISSION Yes, you should receive permission from the cat caregiver to share their story, pictures, or a video of their cat on social media or elsewhere. This is an important thing to note and emphasize, as some members of your staff may be appointed to collect signed photo/video release forms, to ensure that you’re permitted explicitly to share various types of media. Most cat caregivers don’t hesitate at the opportunity to share the joy of their cat with the world and online, but receiving permission firsthand is definitely a must. Sample topics for case studies can include:
• Dermatology: Before and after skin cases • Dental: Before and after dental care with photos • Surgical Case Examples • Laser Therapy Cases
By using Facebook with photos and videos to create and communicate compelling stories, you can enhance your marketing efforts, stay on the cutting edge, and attract more clients to your Cat Friendly Practice®.
11
CAN YOU HELP MY YELP?!: HOW TO HANDLE ONLINE HATERS, BULLIES AND MORE
Eric D. Garcia, IT & Digital Marketing Consultant
Simply Done Tech Solutions Tampa, Florida, USA
“Practices need to get involved if they want to thrive in the future.”
— Eric D. Garcia I’ve written at length about the importance of your online reputation and how you can protect and enhance it to ensure your veterinary practice thrives day in and day out. What’s less fun to discuss is how bad reviews can harm your business. It’s not a matter of if one happens but rather when. Ignoring negative reviews, however tempting it might be, is dangerous and can cause a situation involving a disgruntled client to snowball uncontrollably. I want to help you manage bad reviews by giving you proven techniques designed to mitigate any negative effects of a review before they become a thorn in your side. Here are six simple steps for resolving conflict and restoring online confidence in your practice. 1. Respond thoughtfully and apologize for the negative experience. Emphasize that a poor experience for your clients is not typical and that you as the owner or manager want to learn more about the incident. Provide your name and telephone number so that you can be reached easily. If you are comfortable doing so, provide the hours you work. The idea of extending yourself in this manner is to show your commitment to resolving the issue and to respond personally. To simply respond with, “We’re sorry to hear this, call us at …” feels disingenuous and can result in further backlash. 2. Next, do a bit of investigative research by pulling the client’s record. Contact the client with an understanding of where the experience or patient visit could have taken a turn for the worse. If the client does not contact you or you are unable to reach the pet owner, at least you responded personally and showcased your commitment to resolving the issue. After all, responding to reviews online should be considered an extension of your customer service efforts. 3. If the negative review involves specific details about the level of medicine or the treatment provided, do not respond publicly on the specifics. This is especially important because if you do respond in detail, you run the risk of breaching client confidentiality. It’s your responsibility to keep private any medical records and details about a patient’s condition. While veterinarians aren’t held to HIPAA-level standards — I’m referring to the Health Insurance Portability and Accountability Act — breaching confidentiality can get you reported to the state board. This is true even if a client initiated the conflict online. To respond online without divulging specifics, try something like this: “My name is Dr. Garcia and I’m the medical director of Simply Done Animal Hospital. We take your medically related concerns very seriously. As the medical director, I’d like to talk to you over the phone or in person. We want to do this to protect your privacy. Please contact me at XXX-XXX-XXXX. (Be sure to use your practice phone number and never a personal line.) I would like to discuss this case with you in further detail.” Again, if the client does not reply or contact you, you have a public response showing your willingness to alleviate the issue. 4. When you respond thoughtfully and personally, you dramatically increase the likelihood of resolving the matter. How do I know this? Practices around the world tell me about their bad reviews and how these techniques work 90 percent of the time at resolving the original complaint. Don’t assume that someone who leaves a bad review never wants to do business with you again. Clients usually want to get your attention by leaving the review. Your personalized response has the power to make the difference and bring them back for a second chance. You might be surprised by how much a client’s
12

tune changes after you’ve made the effort to reach out. It’s not uncommon to have clients update a review to show a better star ranking or to delete the review. 5. Now, you might find a review from the pet owner your staff calls “Mr. Crazy.” Yes, you know Mr. Crazy. He’s the one who yelled loudly in the waiting room, berated the receptionist and slammed the door on his way out while spooking other pets in the process. Mr. Crazy even WRITES HIS REVIEWS IN CAPITAL LETTERS BECAUSE HE’S THAT ANGRY. So, what do we do with the review from Mr. Crazy? We leave it alone! Why would we do that? Mr. Crazy is trying to set you up for a no-win scenario. He wants to know that his review affected you and even upset you. If you reply, do not be shocked if he deletes his review, deleting your response in the process, and writes again at twice the original length. He might even recruit his family and friends to attack you and will hunt down more websites where he can leave more reviews about you. The main takeaway here? Leave him alone. It’s not worth the battle. 6. Don’t assume that any and every negative review is crazy. Many client concerns are valid, and your response to them can turn a negative experience into a positive one. Think about it. If responding to a dissatisfied client helps to alleviate their concerns, and the pet owner is pleasantly surprised upon a return visit, you may have just saved a lifetime client. This person might then recommend you to family and friends. This is just one reason that responding to negative reviews patiently and thoughtfully is so important. Now that you know how to respond to a negative review, here are tips for disputing reviews posted on Google, Yelp and Facebook. 1. Yelp advocates for business owners by allowing them to remove erroneous reviews. You are probably laughing, but it’s true and is the one thing Yelp does do better than other review sites. If you have claimed your free Yelp listing — visit http://bit.ly/2Az5tY3 — you will be able to dispute reviews. For example, a practice I consulted with was accused of killing a client’s cat. The clinic, however, had no record of the client or such an incident. The “review” was likely intended as a personal attack against someone at the practice. We disputed the review with Yelp, saying we could furnish proof through the practice management software that the “client” was not associated with the practice. Soon after, we received this email from Yelp: “We’re writing to let you know that we’ve evaluated Larry C.’s review. … After assessing the review carefully against our content guidelines, we agree that this review should be removed. “We rely on community engagement to help keep Yelp useful. Thanks so much for taking the time to bring this matter to our attention!” Yelp swiftly removed the review. 2. When dealing with a negative review on Google, you are allowed to flag the review and submit a support request, so long as you have a Google business account and have claimed your business entry. (Learn more at www.google.com/business.) For instructions on flagging negative Google reviews, visit http://bit.ly/2DdpOVF. 3. Facebook is a bit different regarding reviews because the platform is significantly more conversational. If someone leaves a review and you reply, the person can simply reply back, generating a dialogue. I recommend posting only once and including your professional contact information — see tip No. 3 above — so that you can take the conversation offline. This will prevent the situation from escalating. Much like the advice regarding Mr. Crazy, if someone posts something about you or your practice in a local, private Facebook group, do not reply. It’s too easy for other people to jump in and for the conversation to veer closer to chaos. When dealing with local Facebook groups as a forum for discussion, oftentimes loyal clients will come to the rescue. This happens more often than you might think, especially if the claims are outrageous or offensive.
13

Like many things in life, the post shows that cooler heads will prevail. What is most important to keep in mind is that many minor issues can be smoothed over with dialogue. Intensive conflicts require more troubleshooting but can still be approached methodically based on the advice provided above. If you keep best practices in mind, a negative review here or there is certain to be the exception and not the rule. And if a negative review does spring up, you’ll be well-equipped to handle it.
14

USING TECHNOLOGY TO MEET CLIENT EXPECTATIONS IN TODAY’S WORLD
Eric Garcia
Simply Done Tech Solutions, LLC Tampa, Florida, USA
“Now more than ever your clients want to hear from you. We have a chance as a global veterinary community to make ourselves the resource for all things pets by helping our clients when they need us most.” - Eric D. Garcia We’re living in the midst of history, right now, in this very moment. It might seem like a far-off memory, but just a few months ago, most people were living lives normally: eating out at restaurants, spending time with friends and family, attending major sporting events and grocery shopping without fear of scarcity. In only a month or so, our entire world has been upended, as the global COVID-19 pandemic has spread fiercely throughout the world without consideration of country, race or ideology. If you’re reading this right now, I deeply hope that you and your family are healthy, and you’re staying safe through this truly trying time. I’m proud to have seen our veterinary community come together through this crisis, as they share ideas, techniques and methodology required to cope with this “new normal,” while continuing to give pets the care they need, even while the world around us shifts rapidly. Some of these areas of collaboration involve sharing ideas on how to adapt to curbside veterinary care, and adoption of modern technologies like telemedicine and online pharmacies. While these owner-centric benefits were once rare features of burgeoning veterinary clinics, they’re now vital necessities in a world of social distancing and economic uncertainty. I’ve seen veterinary practices across the country band together to share emerging best practices and I must say, I couldn’t be any prouder to be part of an amazing profession with incredibly talented and passionate people leading the way. In this vein, I want to take this opportunity to say, “Thank You” for your service as a veterinary healthcare provider in these trying times. Your sacrifice and dedication are nothing short of profound as you help hundreds of thousands of pets that continue to need veterinary care each day. As the situation around us evolves rapidly, social media has taken on a different feeling and as such, requires a new approach to implement evolving best practices. Many practices right now are asking the same questions: Is it appropriate to post on social media and market ourselves right now? What should we say and what if we come off as insensitive? What would help pet owners the most right now, and how do we convey it appropriately? These are perfectly normal questions to be asking at a time like this. Being concerned about the questions above shows an awareness of both our global environment, and the needs of pet owners enduring such changes. The pandemic has led some colleagues and clients to recommend that practices don’t saying anything to clients right now via email or social media; not wanting to add to their burden or worries. However, I would actually recommend the complete opposite. Pet owners need to hear from their vets, because they are dealing with uncertainty around their lives and the well-being of their family, loved ones and pets alike. They have pressing questions, too!
15

Are you open if my pet experiences a medical emergency? Can I still pick up medications for my pet? Is COVID-19 transmittable to pets, or can they give it to me? Now, more than ever before, pet owners want YOU to provide the insights and resources that they NEED. When pet owners are up at night wondering how this will all turn out, they find solace in both the people and institutions who provide leadership and a plan of action through the tumult. Google won’t always be able to answer these questions in real-time, but astute veterinary professionals will. Your clients need you to be the resource for information right now on all things related to pet care. So, I urge you, please, don’t abandon them by going silent now. Below, I will outline recommendations for what we should be sharing on social media. But before I do, I want to briefly shed more light on one more opportunity that has emerged from this situation. As many veterinary employees may not be able to work physically on location right now for a variety of reasons (including being immunocompromised, self-quarantine, other health considerations, etc.) now is actually a perfect time to work with employees remotely to develop and manage your social media strategy. You’ll need to provide them with images you take from within the practice, but they can focus on writing and posting the content and engaging with your audience in meaningful ways. While it’s totally acceptable to post on social media during COVID-19, it does require a different approach than our usual strategy. Let’s review the steps you can take to implement this successfully below:
1. First and foremost, write a letter to your clients so that they better understand the measures you’ll be taking to care for them and their pets during this pandemic.
2. I recommend sharing the FULL letter in a single social media post instead of posting a teaser and linking to
the full letter on your website. Since internet speeds around the world are slowing down due to overwhelming use and capacity issues, we want to be sensitive to the time pet owners have and create continuity with messaging. The best experience right now is the pet owner not needing to leave Facebook to continue reading.
3. This being said, ideally pet owners are able to read an entire letter in a single post, alongside an image that
shows your veterinary practice working or showing compassion with a pet. Label your image, IMPORTANT UPDATE RE: COVID-19 which you can create for free at canva.com. This will certainly capture their attention, like the image below for example:
4. As far as scheduling posts, 2-3 times per week is an acceptable amount of content. Focus on sharing value-
driven content, and don’t overwhelm pet owners with unnecessary insights or yourself with the task of creating too much content.
5. Emphasize important information that involves what you can do for pet owners. Are you open? Are you
closed? Are your hours adjusted? What about emergencies or vaccines? Similarly, what do we know about pet and animal health in relation to COVID-19? We know this information is in high-demand, as after a widely publicized incident of a tiger in a NY zoo contracted the virus, pet owners frantically Google-searched to see if their pets could contract or transmit the virus as well.
6. Share content that encourages the use of your telemedicine services and online pharmacy. If these features
of your practice aren’t up and running, or ready to scale, consider putting additional energy toward these areas immediately. If you do offer telemedicine, share an example of a veterinarian chatting with a client using this technology. If you offer an online pharmacy, find a photo of a pet at the door discovering their medicine delivered in a small package. This accessibility is huge right now and is something to focus on.
16
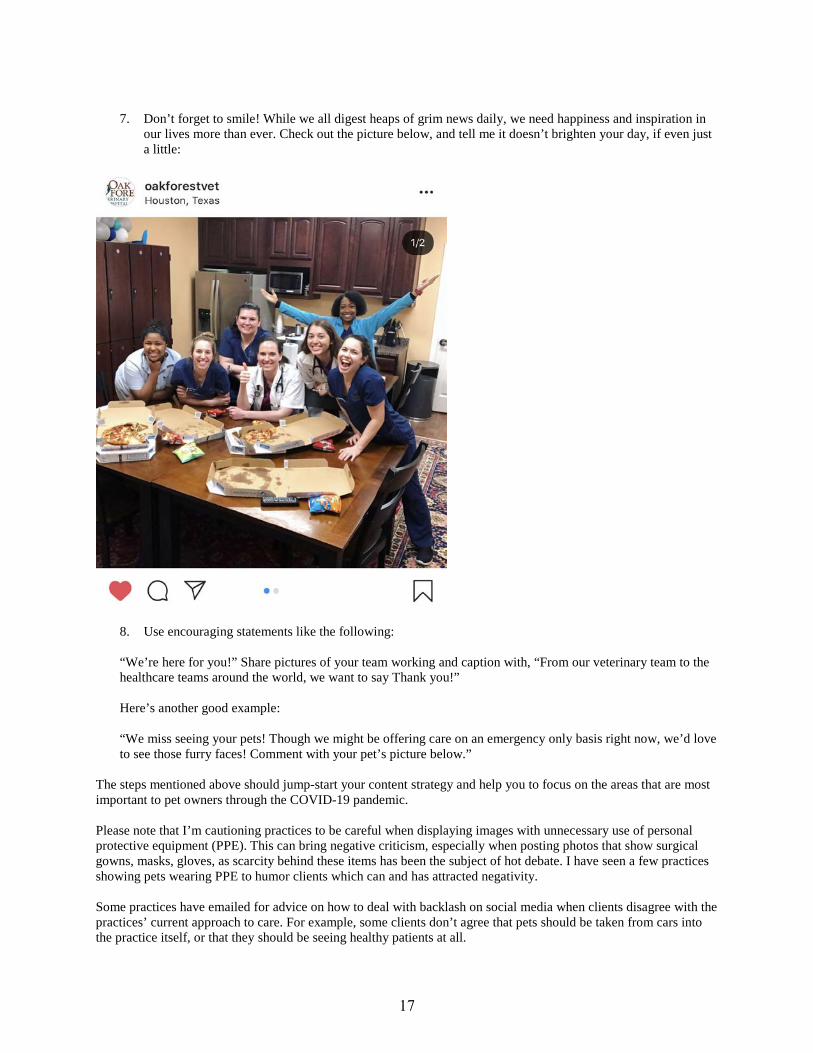
7. Don’t forget to smile! While we all digest heaps of grim news daily, we need happiness and inspiration in
our lives more than ever. Check out the picture below, and tell me it doesn’t brighten your day, if even just a little:
8. Use encouraging statements like the following:
“We’re here for you!” Share pictures of your team working and caption with, “From our veterinary team to the healthcare teams around the world, we want to say Thank you!”
Here’s another good example:
“We miss seeing your pets! Though we might be offering care on an emergency only basis right now, we’d love to see those furry faces! Comment with your pet’s picture below.”
The steps mentioned above should jump-start your content strategy and help you to focus on the areas that are most important to pet owners through the COVID-19 pandemic. Please note that I’m cautioning practices to be careful when displaying images with unnecessary use of personal protective equipment (PPE). This can bring negative criticism, especially when posting photos that show surgical gowns, masks, gloves, as scarcity behind these items has been the subject of hot debate. I have seen a few practices showing pets wearing PPE to humor clients which can and has attracted negativity. Some practices have emailed for advice on how to deal with backlash on social media when clients disagree with the practices’ current approach to care. For example, some clients don’t agree that pets should be taken from cars into the practice itself, or that they should be seeing healthy patients at all.
17
I recommend that if you’re subject to this type of negativity or criticism, you take these steps:
1. Don’t respond right away. Often times, we react negatively and too emotionally if we respond rapidly. Give yourself time to relax, cool down, and assess your response.
2. Review the comment at hand and construct a response. Share the response with multiple trusted people in
your practice to get their feedback before going live with your reply.
3. Consider contacting the person offline to have the discussion privately. This can often times be more productive than fueling a debate online via comments.
4. Remember compassion. Right now, both you and everyone around you, including our clients, have a
heightened sense of emotion and urgency (often rightfully so, but sometimes not). It’s easy to overreact in this environment, so try to keep calm and contextualize the interaction with the global situation at hand.
5. Emphasize the safety of your clients, their families, your team and their families. We are all doing our best
to honor and care for the ones we love, so keep this in mind and it might help you keep a more centered mindset.
6. Always keep responses simple, polite and with a focus on safety.
We are all in this together. While we continue to navigate this incredibly complex global situation, you are a valuable resource to communicate all things related to pet care, health and COVID-19. Now, more than ever before, clients want to hear from you. With this unprecedented scenario, comes an opportunity as a global veterinary community to make ourselves the resource that pet owners and pets need. Social media is ultimately an indispensable tool to bridge the gap that comes with social distancing and isolation. Use this tool for good to express how your veterinary practice is constructively handling the situation, and how you can help pets in need.
18

Ringworm 101: Diagnosis
Brenda Dines, DVM
Background
• Pathogenic Species o Microsporum canis
Wood’s positive Contagious Outbreaks Primary discussion point
o Trichophyton spp Very infrequent in cats Will not fluoresce under Wood’s lamp Can be contagious, but usually husbandry issues and rarely related to outbreaks
o Microsporum gypseum Not common or contagious Does not result in outbreaks or fluoresce under Wood’s lamp
• Risk Factors o Skin trauma o Group housing o Free-roaming o Exposure to dermatophytes o Warmer climates o Physiologic stress o Juvenile or geriatric
Physical Exam
• Perform in adequate white light • Make special note of areas of crusts or alopecia • Asymmetrical lesions common
Wood’s Lamp Exam
• Make sure the room is dark and allow your eyes time to adjust • Does NOT wipe off
o Lint, medication, fibers and crusts are common confounders • Much more animals fluoresce than what many of us were initially taught
o >72% spontaneous disease in one study o 100% experimental disease study
Direct Exam
• Some find challenging to see spores • Serves as a double check for hairs that fluoresce • Inexpensive
DTM + Cytology
• Color change does not automatically mean a diagnosis of ringworm
19
• M. canis color change can occur as early as 3-4 days • Colonies are usually white and fluffy with no pigment • 14 days is usually enough to assess for growth, but most will have recognizable growth
earlier • Tape touched to a colony + stain (lactophenol cotton blue or new methylene blue) + cover slip • M. canis is greater than 6 cells and canoe like
PCR
• Understand the pros/cons before use o Pros
Shorter turn around time than cultures Less labor intensive for shelter staff Staff training on obtaining samples, not analyzing samples
o Cons False positives are a concern
• Can detect dead spores • Can not discern from cats that have spores on their coat vs. those truly affected
Can not be used to monitor treatment efficacy (can be positive on dead spores) Cost
20
Ringworm 102: Treatment and Management
Brenda Dines, DVM
Treatment
Oral
• Itraconazole o (Itrafungol)
Only labeled drug for treatment of ringworm in cats Liquid, so tends to be easier to titrate and give
o COMPOUNDED IS NOT EFFECTIVE! o More expensive than terbinafine
• Terbinafine o Needs to be compounded if liquid desired
Comply with your local ordinances Ask for data on stability, not just USP guidelines
o Inexpensive
Topical
• Basics o Don’t clip hair
• Lime sulfur o 1st choice o Dilute 8oz/gallon
This is more concentrated than suggested on most labels Do NOT pre-wet, this makes it more dilute
o Let air dry, but keep your patients warm! • Azoles + Accelerated Hydrogen Peroxide
o Need at least 10 minute contact time with shampoo If using accelerated hydrogen peroxide rinse prior to shampoo, contact time with
shampoo can be 3 minutes o In vivo study, does not equal real word results
• Miconazole Cream o Helpful for hard-to-reach places o Not a primary therapy
DTM
• Used to monitor treatment progress • Requires some staff training and accountability • Should see decrease in colonies, if increase need to reassess
o Are treatments being performed? o Is housing being cleaned appropriately?
• One negative fungal culture in a healthy cat where treatment compliance is high is likely indicative of mycological cure
PCR
• Serious considerations before use for defining resolution in cats
21
o No cut-off data to discern resolved o May test positive due to dead spores on the coat
Management
Spread
• Staff are the largest concern for fomite transmission o Double-sided housing to limit concerns
Foster
• Can be treated in foster homes that can properly isolate, clean and administer medication
Environmental Decontamination
• Remove hair (organic debris) o This is the most important step (for any form of sanitation)
• Household cleaners labeled for Trichophyton spp work well when applied liberally • Accelerated hydrogen peroxide for shelter setting
o 1:16 dilution • Laundry can be washed in cold water without the addition of bleach for 2 cycles
Enrichment
• Time to cure can be long, make sure that animals receive extra enrichement • Remember kittens make up a majority of these patients and they critical windows for socialization
22
Things You Wish You Knew: Most Common Diagnostic & Management Mistakes of Infectious Disease in Shelters
Brenda Dines, DVM
Vaccination
• Use caution when considering intranasal FVRC vaccines o They do not have a modified live panleukopenia component and outbreaks have occurred due to
this vaccine use alone • Shelters that fail to immediately vaccinate on intake tend to have outbreaks
o If the animal is staying in the shelter, it requires vaccination This means injured or pregnant animals
• Vaccines can provide sterile immunity against diseases like parvovirus, panleukopenia, and distemper
Interpreting Tests After Vaccines
• PCR tests are very good at detecting DNA o Dogs and can remain parvovirus and panleukopenia positive on these tests for an extended time
after vaccination o Dogs can look like a distemper positive in the midst of an outbreak after vaccination
More testing will be needed to make the best choices • Know how the results are relayed
o Need quantitative results!
Not All Brands Are Created Equal
• Different sensitivity/specificity among brands of testing for in-house tests
Movement/Isolation of Animals
• Stress is one of the biggest risk factors for disease in cats o Moving cats through the shelter can be stressful o Consider options that do not result in movement
Altered cleaning order • Not isolating animals because there is “not a place to do so”
o Modifying areas and changing walking patterns can be very helpful if there are not physical barriers
• Do NOT mix species for contagious and stress concerns
Holding Animals
• Only for ill animals • Use titers with vaccine history to make guided decisions for animal movement and release
o Risk assessment! • Do NOT hold puppies/kittens to provide numerous series of vaccines
o Exposure in the shelter is the largest risk
Ringworm Specific
23

• ALWAYS screen each cat for ringworm, especially before group-housing • Do NOT give compounded itraconazole. It is not effective • NEVER make a diagnosis from a change of DTM media to red
o Use physical exam, Wood’s lamp exam, DTM colony morphology and DTM cytology to make a diagnosis
Sanitation
• Over-cleaning is a thing o Spot cleaning decreases stress and the likelihood for fomite transmission o Deep cleans should be performed prior to a new animal entering an enclosure
• Although quaternary ammonia products have labeling they do not reliably kill panleukopenia, parvovirus or calicivirus and have been shown to cause oral ulcerations if ingested by animals
When to Perform Additional Diagnostics
• Increased mortality • Increased morbidity • Increased severity of clinical signs
24
Behavior Management for the Shelter Population
Brenda Dines, DVM
Intake Questionnaires
• Schedule appropriate time to get the details o This is some of the most valuable information you will receive
• Obtain this information prior to relinquishment o Try to keep the pet with their people!
Moving Away from Single Point in Time Assessments
• Numerous studies advocate against formal behavior assessments • Resources should be invested in to normal daily interactions that are documented and can be disclosed to
potential adopters • Food bowl issues tended to not exist or were readily managed in homes • Dogs respond more aggressively to fake dogs than real ones
o Think of the body language a fake dog gives off o Can we have a playgroup instead (enrichment + info about interactions with other dogs)
Treat Behavioral Concerns like Medical Concerns (They really are!)
• Form a SOAP and modify your plan as needed (see the case study in presentation) • Become familiar with medications and start using them
o You wouldn’t deprive an animal with a bacterial infection antibiotics, so why would be deprive an animal with anxiety medications that could make their stay more comfortable?
Adoptability
• Focus on what makes a pet adoptable o Most of the time this is cage presence o Decreased length of stay = decreased likelihood of shelter acquired disorders o Ask the questions?
Was this an issue prior to entering the shelter? Is this a shelter acquired issue? Do we need to modify this behavior? Or do we need to make the pet more adoptable with working on cage presence? Can we show the pet in a different light? Where do they behave best?
Follow-Up
• Offering immediate follow-up and resources to keep adopted pets in the home opens the line of communication early on
• Trained volunteers if staff is limited o Resources available for common issues o Elevation of issues that involve aggression
25

Initial Wound Triage, Bandaging, and an Update on New Topical Wound Products
Mandy L. Wallace, DVM, MS, DACVS-SA Assistant Professor,
Small Animal Surgery University of Georgia College of Veterinary
Medicine [email protected]
Traumatic wounds are frequently encountered in both general practice and emergency medicine settings. The causes of these wounds vary greatly, and there are numerous factors that play into the decision making involved in how to manage the wound in the immediate post-trauma period. In this discussion, we will focus on how wounds heal, how to perform initial wound management, and how to navigate the ever-changing world of new wound healing products. Types of Traumatic Wounds Traumatic wounds occur in various different ways. In veterinary medicine, puncture wounds and lacerations caused by other animals are very common. These can be caused by other domestic animals or wild animals. Wild or unknown animals introduce another level of concern as exposure to Rabies must be considered. Every state has different laws and protocols regarding how these cases with potential exposure must be handled. In all cases, bite wounds will be contaminated even if they appear to be clean as they have been “injected” with bacteria from the other animal’s mouth. It is important to remember this fact as it will affect when you close the wound and how they are treated. Degloving wounds are another category of wounds that can be seen either with animal attacks or motor vehicle accidents. Degloving indicates that the skin has been pulled away from the underlying tissues. There are 2 types of degloving: mechanical and physiologic. Mechanical degloving occurs when the skin is ripped away completely from the underlying tissues and may be completely missing. These often occur on the limbs. Physiologic degloving occurs when the skin remains in place but has been pulled away from underlying tissues in such a way that the blood supply to the skin is removed. This leads to skin necrosis in the days following the initial injury and can cause any closure performed in the first 1-3 days to fail. It can also lead to a very large defect in the skin that was not expected. Laceration wounds are less common and are often caused by metal lawn edging or trauma from a sharp object that the dog or cat runs into accidentally. These can occur anywhere on the body and are often more clean than other types of wounds if treated quickly. Penetrating wounds refer to wounds that breach the thoracic or abdominal cavity or traverse deep within muscle tissue or bone. These can occur in various ways including animal attacks, gunshot wounds or stabbings, and running into a sharp object. These wounds can be dangerous as they can lead to pneumothorax, excessive internal bleeding, fractures, or septic peritonitis. It is very important to assess the animal for other injuries in addition to the external wounds that are present. Finally, burn wounds are a unique category of wounds in that they lead to severe physiological changes in various body systems in addition to the visible skin damage. These burns are typically of thermal origin; however, chemical burns can also occur from either accidental exposure or in animal abuse situations. Because of the variety of concurrent issues that can occur, the entire patient must be carefully evaluated daily to ensure that other organ systems are not failing or showing signs of damage. Wound Healing Steps In order to properly treat wounds, it is important to understand the steps that a wound goes through during healing. Immediately after a wound occurs, the vessels in the wound vasoconstrict to aid in hemostasis. Platelets are attracted to the exposed fibers and degranulate, which initiates hemostasis and causes release of inflammatory mediators. The platelets form a platelet plug, which is eventually remodeled into a fibrin seal.
26

The first stage of wound healing is the Inflammation phase. During this phase, which occurs over the first 1-3 days, vessels vasodilate allowing white blood cells, red blood cells, and platelets to enter the wound. The primary white blood cell present during the first 24 hours is the neutrophil. Neutrophils kill bacteria via phagocytosis and oxidative bursts. This begins the important task of cleaning up the wound bed; however, in wounds where there is a large bacterial burden, neutrophils on their own cannot neutralize all bacteria present. At 48 hours, macrophages become the primary white blood cell, which starts the process of debridement of the wound and leads to additional recruitment of inflammatory cells and growth factors as needed. The second phase of wound healing is the Debridement phase, which occurs during days 3-5 after wounding. During this phase, necrotic tissue and debris are removed from the wound by macrophages. At this point of wound healing, we can aid this process with proper wound management and manual debridement. The third phase of wound healing is the Proliferation phase, which typically occurs from 5-14 days after wound occurrence. During this phase, fibroblasts are present in the wound and are producing collagen. These fibroblasts and collagen, along with newly formed capillaries and hyaluronic acid, create a granulation bed. This granulation bed is extremely important to wound closure and epithelialization. Choice of appropriate materials for the wound at this point is paramount, as using materials that will damage the granulation tissue can delay healing. The final phase of wound healing, Maturation, can last for weeks to years depending on the location of the wound and what tissues are affected. During this phase, the collagen is reorganized along lines of tension to return the tissue to its original strength (if possible). Collagen is also converted from mostly Type 3 collagen to mostly Type 1 collagen. Initial Wound Triage When a dog with wounds arrives in your clinic, it is important that the patient is evaluated for systemic stability before the wounds are evaluated. During this time, if possible, the wounds should be covered with sterile materials that can easily be removed from the wound. Examples include sterile laparotomy pads, sterile gauze, and sterile operating room towels or drapes. This will prevent nosocomial infections from surfaces in the hospital and will keep cotton fibers from materials like cast padding out of the wound. If wounds are present over the thorax or abdomen, taking radiographs of those areas is advisable to determine if any penetration of those cavities has occurred. Indications of thoracic penetration may include a pneumothorax or pleural effusion. While rib fractures do not always indicate that the thoracic cavity has been penetrated, it does indicate that significant trauma has occurred. These cases should be carefully monitored for progression of respiratory signs, which may be caused by thoracic penetration. Abdominal cavity penetration may be indicated by herniation of abdominal contents, evidence of free gas in the peritoneal cavity, and free fluid in the peritoneal cavity, among others. If abdominal cavity penetration has occurred or is suspected to have occurred, surgical explore of the abdomen is advised to evaluate damage to any internal organs, which could lead to internal bleeding or septic peritonitis. Wounds over the neck should also be carefully evaluated as penetration of the trachea or esophagus or damage to a large artery or vein (carotid or jugular) could occur. Once the patient is determined to be stable and if no concern exists for penetration of a body cavity or vital structure, the patient should be sedated, and the wounds evaluated. Heavy sedation may be enough in the majority of patients; however, depending on the patient’s concurrent medical issues, general anesthesia may be the safest option for that patient. Once sedated or anesthetized, sterile lube should be placed in all punctures and lacerations, and the fur clipped from around any areas with wounds. It is a good idea to warn the owners ahead of time that their animal may have a lot of fur clipped in order to find all the wounds. The wounds should be explored with sterile instruments. Having a sterile wound pack available at all times containing hemostats, needle drivers, thumb forceps, a scalpel blade handle, and sterile gauze is useful in these situations and prevents you from having to open an entire surgical pack for just a few instruments. Wounds that are deeper than anticipated or have a large pocket may need to be opened further to ensure that no debris has been trapped in the pocketed area. If there are areas of necrotic tissue, those areas should be removed as they can help bacteria proliferate, increasing infection and decreasing healing. Once all wounds have been thoroughly evaluated, they should be flushed with sterile fluids (saline, LRS, etc.). There is not a set rule about how much to lavage, but this is your best chance to clean the wounds so a large amount of lavage fluid is advised. There are many acceptable ways to proceed with lavaging wounds. One option is to take a 1L bag of sterile fluids and attach an IV line to the bag. An 18 gauge over the needle IV catheter can be attached to
27

the end of that line. The bag can be placed in a pressure bag (as would be used to bolus IV fluids) to allow for the fluids to flow through the catheter in a pressurized fashion. If a pressure bag is not available, fluids can be drawn up into a 60 cc syringe with an 18 gauge needle or catheter on the end with the fluids manually pushed into the wound. As much as possible, all visible debris should be removed. One frequent question about lavage fluid is if tap water is an acceptable option for initial wound lavage. While it is not frequently used, it can be used for initial wound flushing situations, particularly if there is a lot of debris. It is very important to get that debris out of the wound. The concern with tap water in general is less about sterility and more about the pH of tap water and its effect on cell viability and wound healing. It should not be used after the initial wound lavage period if it is used at all. After wound lavage has occurred, this is the time for a culture to be taken. Cultures are encouraged if financially feasible for the owner as this can direct your antibiotic choices if the wound is not healing with appropriate wound management and empirical antibiotic choices. For the culture, a piece of tissue will give you the best results. It is important to ask the microbiology lab that your samples are sent to what their preferences are for how tissue samples are submitted for culture. Many labs do not want the tissue sample placed in a culturette tube. For example, the UGA diagnostic lab prefers that the sample be placed in a sterile gauze dampened with sterile saline and placed in a sterile cup. Typically, an aerobic culture and sensitivity will be enough for a traumatic wound. In select cases, anaerobic culture may be recommended, but this is rarely recommended for a traumatic wound. At this point, you must decide whether to close the wounds or to bandage them. In the majority of cases, bandaging the wounds rather than closing is advised. Closing the wounds too early can lead to development of deep wound infections, which can lead to skin necrosis and sepsis. Only very fresh (less than 6 hours old), minimally contaminated wounds should be closed at this point. It is advised that all animal bite wounds not be closed as these wounds are contaminated. If you are performing bandage changes for open wound management, this should be done with appropriate sterile technique each time. Sterile gloves should be used when replacing the primary layer and all things touching the wound should be sterile. This is to prevent nosocomial infection. Additionally, the bandage should always be changed if strikethrough has occurred, as strikethrough increases infection risk. Bandaging Tips Depending on the location of the wound or wounds, there may be limitations for the kind of bandage that can be used. For wounds over the limbs and ventral thorax, a soft padded bandage consisting of a primary layer (the sterile layer touching the wound), cast padding, Kling, and Vetrap can be useful and should provide the coverage needed to protect the wound or wounds. When these are placed on the limbs, tape “stirrups” can be placed on either side of the limb to help keep the bandage in place and also to allow for evaluation of the toes to ensure that they are not swelling or becoming cold, which may indicate that the bandage was placed too tightly or that the limb is swelling causing the bandage to become too tight. The toes should be checked under this bandage at least 3 times per day with the bandage removed and replaced if the toes are noted to be swelling. This is extremely important because the foot may not be getting appropriate blood supply, which can lead to tissue necrosis and in the worst case, lead to foot or limb amputation. When placing this bandage, cast padding should be placed from distal to proximal on the limb with several layers placed. It is hard to make this layer too tight as the material will tear before it gets to that point. Next, a single layer of Kling should be placed over the cast padding, again from distal to proximal. This layer is providing the stability of the bandage; therefore, it needs to be snug but not excessively tight. This layer can cause the most issues with bandages being too tight. After this layer is placed, the stirrups should be detached from each other and attached to the bandage. The final layer is the Vetrap. The Vetrap is a water-resistant layer and should be laid on top of the Kling layer. It should not be placed tightly as this can also easily cause the bandage to be too tight. The entire roll can be taken off the cardboard insert and re-rolled or it can be stretched and relaxed as it is being placed. Elasticon can be placed at the bottom of the bandage to allow the toes to be evaluated more easily and also to provide some traction on the bottom of the bandage. It can also be placed at the top of the bandage to help prevent bandage slippage; however, it can cause some irritation to dogs with thin or sensitive skin. The skin should be assessed during each bandage change before replacing any Elasticon to prevent ulcerations or other bandage complications from occurring. For areas where a soft padded bandage will not work, more unique options may need to be employed to keep the wounds covered. One of these unique options is a tie-over bandage. This bandage is very versatile and can be used
28

in nearly any location. With this bandage, loops of heavy gauge (0 to 2-0), non-absorbable suture are placed around the edges of the wound. Once the primary sterile layer is placed, sterile lap pads can be placed over the primary layer for additional fluid absorption. A layer of sterile drape material can be placed over the lap pads to create a water-resistant barrier, although this is not required. Umbilical tape or suture can be used to secure the bandage by placing the tape or suture through the pre-placed suture loops and tying the material on top of the bandage. Traditional Primary Layer Options There are many options available for primary bandage layers. This layer should be sterile and chosen based on the stage of wound healing which is occurring. In the initial period of the inflammation and debridement phases of wound healing, sterile gauze are often the material used to create the primary layer to create an adherent bandage. One common type of adherent bandage is a wet-to-dry bandage. With the wet-to-dry bandage, sterile gauze that are dampened with sterile fluid are placed within the wound. The fluid helps to dilute any purulent material and pulls it into the gauze. The gauze then dry over time (12-24 hours) and adhere to the underlying tissue, allowing for non-selective mechanical debridement at the time of bandage change. Various types of sterile fluid can be used for creation of the wet to dry bandage. Sterile saline, LRS, or other replacement fluids can all be used. Additionally, some fluids can be used to create a hyperosmotic dressing, which may have antimicrobial properties. Hypertonic saline is an example of a fluid that can be used in this manner. These wet-to-dry bandages should be changed at least every 24 hours, but in wounds that are highly exudative, they may need to be changed more often. If strikethrough is present on the outer layer of the bandage, the bandage should be changed as soon as possible in order to prevent contamination from entering through the bandage. In wounds that are highly exudative, another option is a dry-to-dry bandage. In this case, dry sterile gauze are placed onto the wound. This allows for more surface area to collect the fluid being produced by the wound and keeps the fluid from sitting within the wound too long. Ideally, the gauze within this bandage would also dry prior to bandage change at 12-24 hours, but in highly exudative wounds, this may not be the case. Once granulation tissue is present in the proliferation phase of wound healing, a non-adherent bandage should be placed over the wound bed to continue to promote granulation production and epithelialization, but without damaging the granulation tissue that is already present. Non-adherent primary layers typically consist of either a Telfa pad or a petroleum-impregnated dressing. The advantage of using a petroleum-impregnated dressing is that these dressings can stay moist for up to 3 days, providing moisture to the wound which further promotes healing and epithelialization. It also is easier to remove than Telfa pads, as those can become slightly adhered to the wound. One option if you do not have any petroleum-impregnated dressings available is to put triple-antibiotic ointment (from a new tube or a small sterile packet) onto the Telfa to recreate a similar effect to the petroleum-impregnated dressings. Depending on the state of the wound and its progress, these dressings can be left up to 72 hours without changing the bandage. New Options for Wound Management There are various new wound management options that are available in both the veterinary and human medicine markets. It is important when new options become available that you evaluate any research that has been performed with that new option to determine if it is actually superior to other options. Many of these products have not been evaluated and may not be better than what is currently being used. In the initial stages of wound management, antimicrobial agents have gained popularity and are easy to use. These agents, such as sugar and honey, are used to decrease the pre-existing bacterial load within the wound. Sugar is used for its hyperosmotic effects, which kills bacteria by changing the environment. This is effective even against some bacteria that are multi-drug resistant. There are no commercially available sugar dressings; however, no special type of sugar is needed. You can purchase regular white sugar and place that directly into the wound. Sterile gauze are placed on top of the sugar followed by the rest of the bandage. The sugar does tend to cause the wound to produce more exudate so using additional layers of gauze or lap pads to absorb the fluid is advised. These bandages should be changed every 24-48 hours depending on the state of the wound. Honey has become more popular over the past several years in veterinary medicine for wound management. Honey also has a hyperosmotic effect similar to sugar; however, it has additional properties that boost its antimicrobial
29

effects. One of these properties is that honey has a very small amount of hydrogen peroxide content within it. This amount is high enough to be antimicrobial but low enough that it does not damage the healthy cells. As with the sugar bandages, there can be quite a bit of fluid production in these bandages as the honey tends to pull edema out of the wound. These bandages should be changed every 24-48 hours, as based on the state of the wound. There are commercial honey preparations as well, such as Medihoney, or raw honey can be purchased. The advantage of medical honey preparations is that they are sterilized, minimizing risk of introducing contamination. Unpasteurized, raw honey provides the best antimicrobial activity of the over-the-counter options; however, there is a risk of introducing infection with purchased raw honey as it can contain spores from agents such as Clostridium. This risk is small, however. Silver is another option that is used for its antimicrobial properties. This can be used in any stage of wound repair; however, it can decrease inflammation, which can slow wound repair in the early phases. This can be in the form of silver sulfadiazine cream or in a commercial preparation (such as Acticoat). With some of the commercial preparations, there are specific ways that the dressing must be activated, and it is important that the instructions provided with the dressing are followed. For example, Acticoat must be activated with sterile water and will not work if not activated. SSD cream is often used in cases of thermal burns to prevent infection; however, more recent literature in human medicine has found that honey may provide better antimicrobial protection in those cases. No studies in veterinary medicine have compared the two agents. Specifically, for the debridement phase, there are two less commonly used options available. One of these options is use of an enzymatic dressing, such as collagenase-based dressings. These dressings dissolve collagenous tissue, which can lead to superficial sloughing of debris and other necrotic tissue. They are not good for heavily contaminated wounds or traumatic wounds, which excludes the majority of the wounds we treat. They are also fairly expensive to use. Another option is the use of medical maggots. Medical maggots are derived from larvae of the green blow fly and will not damage normal tissues, except for the epidermis; therefore, the epidermis must be protected from the maggots if they are to be used. Medical maggots can be obtained from various trusted sources over the internet and shipped to your hospital. Moisture-retentive dressings have become the standard of care in human medicine for all phases of open wound management. These include hydrogel, hydrocolloid, and alginate dressings. These dressings are hydrophilic, soaking up the wound exudate and turning it into a gel, which can improve debridement, granulation tissue development, and epithelialization. Human patients also report less discomfort when these dressings are used. The number of bandage changes can also be limited by using these types of dressings, which may also help with wound healing by maintaining a steady wound environment. Each type of dressing can take in various amounts of fluid, and it depends on the agent in the dressing and the size of the dressing. The best type of dressing depends on the wound that is being addressed. For example, alginate dressings work best for highly exudative wounds. These dressings have gained favor in veterinary medicine, but are not widely used mostly due to additional cost and need to have additional inventory in stock. Many of these products also have honey or silver within the dressing which can have additional positive properties when used for the appropriate wound. Platelet-rich plasma (PRP) has been a hot topic of wound healing research in veterinary medicine over the last 5 years. PRP can be created from blood taken from the patient and passed through a commercial system to create PRP. PRP contains growth factors and cytokines, which are thought to improve healing. While some of the research has been promising regarding improved and faster healing with PRP use, other studies have not shown a difference when PRP was used. Negative Pressure Wound Therapy, commonly referred to as VAC (vacuum assisted closure), is used frequently in human and veterinary medicine for traumatic wounds. This is an excellent option for very large wounds that need time to develop granulation tissue prior to closure. These systems increase development of new blood vessels, development of granulation tissue, aid in wound contraction, decrease dead space within the wound, and may decrease bacterial loads within the wound. With this option, a foam dressing is placed within the wound bed and an occlusive dressing is placed over the wound and foam. A small hole is cut in the dressing to attach a suction device with tubing. Once suction is initiated via the system (or wall suction), all of the air suctioned out of the foam and fluid from the wound is pulled into the system canister. The negative pressure exerted on the wound is typically -125 mmHg at a continuous setting, unless it is placed over a skin graft, open abdominal cavity, or other sensitive locations, where it may be decreased to -75mmHg. This should not be employed in wounds that are still requiring daily wound debridement. Once the VAC is applied, it can stay in place up to 3 days.
30

Antibiotic Use Another controversial topic with wound management is when to use antibiotics with wounds. As we are all aware of the concern for multi-drug resistant infections, it is important that we are judicious with our use of antibiotics. For clean lacerations that are closed soon after trauma occurs, antibiotics are likely not needed. However, for any animal attack wounds or other wounds that are infected, contaminated, or dirty, antibiotics should be employed to aid in decreasing the bacterial contamination within the wound. It is also recommended to obtain a culture from these wounds to aid in appropriate antibiotic selection. While waiting for the culture, a broad-spectrum antibiotic should be selected. A common choice is amoxicillin-clavulanic acid as it is broad spectrum and is generally well tolerated by dogs and cats. Once the culture results are available, the antibiotic selection can be adjusted as needed to select the best choice for that patient and that wound.
Suggested Reading
1. Hosgood G. Chapter 76: Open Wounds. In: Johnston SA, Tobias KM, eds. Veterinary Surgery: Small Animal. 2nd ed. St. Louis: Saunders Elsevier, 2018; 1410-1421.
2. Pavletic MM. Atlas of Small Animal Wound Management and Reconstructive Surgery. 4th ed. Hoboken: Wiley, 2018; 17-114.
31

Surgical Options for Wound Closure: Tension Relieving Techniques, Flaps, and More
Mandy L. Wallace, DVM, MS, DACVS-SA Assistant Professor, Small Animal Surgery
University of Georgia College of Veterinary Medicine [email protected]
Once wounds have been appropriately managed initially, the focus turns to when to close the wounds and how to close the wounds. Various factors must be considered when determining the best options for closure. This discussion will focus on the indications for wound closure, options for closing basic wounds, and options for closing more challenging wounds including flaps and grafts.
When to Close Wounds Determining when to close a traumatic wound is challenging and depends on various factors. The most important factors to determine when to close a wound are the state of the tissues within the wound and whether or not infection is present. The two most common types of closure in traumatic wounds are delayed primary closure and secondary closure. Delayed primary closure refers to closure within the first 3-5 days after the initial wound occurs and before granulation tissue develops. This is typically reserved for minimally contaminated wounds that do not require extensive debridement. Secondary closure occurs more than 3-5 days after the wound occurs and granulation tissue has developed. This is typically used in cases where there is contamination, infection, or tissue damage. Another important factor to consider when closing wounds is if a drain should be placed at the time of wound closure. Drains can be beneficial in wounds that have large subcutaneous pockets or if the wound still has a reasonable amount of effusion at the time of closure. There are two main types of drains that can be used: passive and active. The most common passive drain used is the Penrose drain. Penrose drains work by capillary action and gravity and therefore, should always be placed with the drain exiting the wound as ventrally as possible. There is not a need for the drain to exit from both the dorsal and ventral portion of the wound. This only increases the potential for contamination to enter the wound. The drain also should not exit through the wound opening. A new opening adjacent to the wound opening should be created to allow the drain to exit. The drain can be placed within the wound and secured dorsally adjacent to the wound opening with a suture placed through the skin, into the drain, and back through the skin. An opening can be made ventrally for the drain to exit through. The drain can also be secured to the skin at the opening with a suture to prevent the drain from being displaced inside the wound, where it will be difficult to retrieve for removal. After this, the wound opening can be closed primarily. The drain should be covered at all times to prevent contamination of the wound from the surrounding environment and to prevent drainage from the wound from exiting into the environment, whether that be the hospital or the patient’s home. Penrose drains should never be placed within the abdominal or thoracic cavity. Active drains are drains that create a vacuum within the wound to remove fluid from the wound bed. One example of this type of drain is a Jackson-Pratt drain. Jackson-Pratt drains consist of a fenestrated portion that is placed within the wound, tubing connected to the fenestrated portion, and a grenade connected to the tubing which collects the fluid from the wound. Another type of active drain can be made with items that can be found in many veterinary practices. It consists of a butterfly catheter and a red top tube. The end of the butterfly catheter (where the syringe is typically attached) is cut off, and fenestrations are created in the tubing. These fenestrations can be made with scissors or a #11 scalpel blade; however, they should not be greater than 50% of the circumference of the tubing, as larger fenestrations can weaken the tubing, causing a portion to break off inside the wound. The fenestrated tubing is placed within the wound bed with the butterfly portion exiting adjacent to the wound opening. The needle is placed into the red top tube, which creates the vacuum. The red top tube can be changed when it is full to a new red top tube. White tape can be used to create a holster for the red top tube, and this holster can be attached to the patient with suture. Because they create a vacuum, active drains can exit in any direction since gravity is not a factor in the
32

mechanism of drainage. These drains should also exit through a newly made opening adjacent to the wound opening. These drains decrease the risk of contamination seen with Penrose drains. Another advantage of active drains includes the ability to monitor fluid production volume, as well as cytology from the wound, which may indicate how the wound is healing and if an infection is present. Drains should be removed when the production decreases to a baseline level. Due to the irritation caused by the drain within the wound, there will almost always be some fluid production from the drain. Baseline fluid production is expected to be 1-2 mL per kg (body weight) per day; however, some wounds will not follow this rule. Typically, the fluid production is monitored, and the drain removed once the fluid production has plateaued. Wound Closure When the wound appears to be ready for closure, a plan should be developed for how to best close the wound. For many wounds, primary closure is possible and can be very straightforward; however, for more complex wounds, it is important to have a plan prior to going to surgery of what techniques may be necessary to close the wound completely. Even with the best plan in place, often the skin or wound do not behave as expected in surgery; therefore, it is important to have a back-up plan in place in case the original plan does not work. For straight-forward wound closures, the wound bed should be lavaged prior to closure with sterile saline. Depending on the results of the initial culture and how the wound is healing, taking a tissue sample for a new aerobic culture may be advisable to ensure that the appropriate antibiotics are being used. It may also be helpful to perform a culture at this point as unfortunately, nosocomial infections can occur during open wound management if there are breaks in sterile technique during bandage changes. Prior to closure, the edges of the wound should be debrided to create a fresh surface on each side of the wound to aid with healing. Wounds should be closed in three layers if possible. The deepest layer should be tacked down to the underlying muscle or granulation tissue if possible and include the fibrous hypodermal tissues for tension relief. This layer is often performed as buried simple interrupted or cruciate sutures rather than a simple continuous pattern since the tissues may be more friable. The next layer includes the more superficial subcutaneous tissues. This layer is often performed with a simple continuous pattern. Finally, in most cases, external skin sutures are recommended in an interrupted or cruciate pattern. Wounds Under Tension If the wounds are under tension at the time of closure, there are several tension relieving techniques that may be employed. The first option is undermining the skin to allow for additional movement of the skin without tension. It is extremely important that the undermining occurs below the cutaneous trunci muscle in areas that have this thin muscle layer under the skin. If this muscle is separated from the skin, the blood supply to the skin can be damaged. It is also important to preserve any penetrating blood vessels seen going to the skin. Depending on how much loose skin is present on the patient, this can provide a reasonable amount of skin movement. Stent sutures are another option to reduce tension on the wound. These sutures can be preplaced into the deeper tissues prior to primary wound closure as simple interrupted sutures. The wound can then be closed primarily. Once the wound is closed, the preplaced sutures are tied over a bolster of some sort, typically made of gauze, cast padding, or a lap pad rolled up. This will disperse the tension away from the suture line. These sutures can be removed 3-4 days after surgery as the skin will have had time to stretch, decreasing the overall tension. Walking sutures can be placed as another intra-operative option for tension relief. Simple interrupted sutures are placed from the dermis to the fascia, with the suture bite in the fascia taken further forward, thereby pulling the skin closer together. This will cause the skin to dimple if placed correctly; however, this is only a temporary cosmetic issue. There are other options for tension reduction that require additional incisions to be made, some of which are left to granulate for healing and require open wound management after closure of the initial wound. The two options that require open wound management are a simple relaxing incision and use of multiple smaller relaxing incisions. For a simple relaxing incision, an incision the length of the current wound is made parallel to the wound. This incision should be as far from the wound as the wound is wide. The length of this incision should also not be more than 4 times as long as the width of the skin bridge between the new incision and the wound. If the ratio between incision length and the width of the bridge is larger than this, it can lead to a compromised blood supply to the skin bridge, leading to necrosis. The alternative option to this, multiple smaller relaxing incisions, consists of rows of 1 cm stab
33

incisions that are 1 cm apart, parallel to the wound, starting 1 cm from the wound. If multiple rows are needed to relieve tension, the rows should be 1 cm apart with the stab incisions offset from each other. These incisions are also allowed to heal by second intention. Open wound management for both options should include a nonadherent primary layer, such as a Telfa pad or petroleum-impregnated gauze. One other option, called a V-Y plasty, requires additional incisions to be made, but these new incisions are closed at the time of the initial surgery. The V-Y plasty is typically used in areas where surrounding structures would be distorted, such as near the eye. With this option, a V-shaped incision is made in the skin adjacent to the wound with the point of the V away from the defect. The skin between the wound and the V is undermined allowing the wound to close. The created V wound is then able to be closed by converting it to a Y shape. Subdermal Plexus Flaps Subdermal plexus flaps can be used in areas where there is extra skin available adjacent to the wound that can be manipulated for use in closing the wound. These flaps are detached from the surrounding skin with the blood supply coming from whichever edge of the flap remains attached in its original location. Because of this, it is very important that the flap base is wide enough to support the length of the flap. In general, the length of the flap should be no longer than twice the width of the base. The base should be as wide or wider than the tip of the flap. It also important that when the flap is undermined that the subdermal plexus is not damaged as this is vital for the flap to have blood supply. The pros of the subdermal plexus flaps are that they are easy to develop, can be used in almost any location, and have a fairly good blood supply. The cons of these flaps are that they are limited in length by the width of base of the flap so they may not be useful to help close larger wounds. There are several variations of subdermal plexus flaps. The most common are advancement flaps, rotation flaps, and transposition flaps. Advancement flaps are typically developed by creating two incisions perpendicular to the wound at each end of the wound bed, allowing that skin to be pulled forward to close the wound. This creates a single pedicle flap (or a flap with only one source of collateral blood supply). This is the most straight-forward of the subdermal plexus flaps available. This flap should be developed in an area with ample loose skin. These flaps can be developed on each side of the wound, reducing the amount of stretching needed from each advancement flap and reduces flap length, which may aid in maintaining blood supply. This results in a wound closure that looks like an “H” and is called an H-plasty. Rotational flaps are another good option but do require a bit more planning to be successful. With this flap, the incision is started at one edge of the wound bed and is curved somewhat parallel to the wound. This incision is continued and the flap undermined until it is at a point where the wound can be covered and tension is minimal. Transposition flaps are similar in that the flap is rotated into the wound bed for closure; however, with this flap, an entire rectangular flap is created with one border being adjacent to the wound bed. This flap can be created at any angle up to 90 degrees from the wound bed. At angles closer to 90 degrees, there will be dog ears created, which decreases the cosmesis of the closure; however, the dog ears will decrease in size over time. One really unique type of subdermal plexus flap are skin fold flaps. This type of flap exploits the free skin present at the axillary and inguinal areas, at the junction of the limbs and the trunk. These can be used in a number of different directions depending on which attachments are incised. Each fold has 4 attachments: dorsal trunk, ventral trunk, lateral upper limb and medial upper limb. Three of these can be detached to allow maximum freedom of movement while still having adequate blood supply. Axial Pattern Flaps Axial pattern flaps are based upon a specific artery which, with its branches, supplies a distinct portion of the skin. Due to the robust blood supply within these flaps, they can be larger than subdermal plexus flaps. They also have a better survival rate than other flaps, even up to 100% survival in some studies. However, these flaps are very specific and can only be used in certain locations; therefore, their use can be limited. It is very important that if one of these flaps is to be used that the guidelines for that specific flap are followed strictly to prevent flap necrosis. The most useful and robust of these flaps is the caudal superficial epigastric flap. This flap is based off the caudal superficial epigastric artery and can be used to cover wounds over the caudal abdomen, contralateral or ipsilateral limb defects to the level of the stifle, and the ipsilateral flank. The medial incision of this flap is the ventral midline of the abdomen, and the lateral incision is made parallel to the medial incision. To determine where to make the
34

lateral incision, a measurement is taken from the teat to the medial incision. That same distance is marked from the teat moving laterally and that delineates the location of the lateral incision. The flap can include mammary glands 2- 5, if needed. Skin Grafts Skin grafts are the least robust of the more advanced closure options. These grafts are portions of skin removed from a part of the body with an abundance of loose skin and transplanted to the wound bed. These consist of either large pieces of skin used to cover the entire wound bed or island grafts, which are small pieces of skin that are embedded into a large granulation bed to promote epithelialization of the area. There are four main steps in the process of engraftment or “take” of the graft. The first step is adherence. During this stage, the graft becomes adhered to the underlying tissue via fibrin strands that keep the graft in close apposition to the wound bed. These fibrin attachments convert to fibrous attachments beginning on day 3 after surgery and continuing through day 10 after surgery. The next step is plasmatic imbibition. In this step, the blood components (red blood cells, white blood cells and serum) leak from the recipient site into the space between that site and the graft. These components are drawn into the graft by capillary action and nourish the graft until new blood vessels can form. The third step is inosculation, which typically begins in the first 2-3 days after graft placement. In this step, the remaining ends of the graft vessels anastomose with vessels in the recipient bed, which begins to allow new blood flow into the graft until new vessels form between the two. The final step is vascular ingrowth. This is the creation of new blood vessels between the recipient bed and graft tissue. In all cases, the grafted area must be bandaged appropriately to prevent the graft from being traumatized. A non- adherent layer should be placed directly over the graft to protect the graft during the bandage change. Typically, the first bandage change does not occur until 3 days after surgery. This allows the graft time to adhere and to start the engraftment process without disruption. At each bandage change, it is important to be extremely careful with removal of the primary layer. In some cases, sterile saline can be used to help with detaching the nonadherent layer from the graft if it has adhered in some way to the underlying tissue. Depending on the location of the graft, splints may be used as well to prevent motion in the graft area which can affect healing. A bandage should be in place for at least 10-14 days after graft placement. At each bandage change, the graft should be evaluated to determine how well the graft is taking. Dark purple or red is a good sign that vascularization is occurring. Any areas that are white or gray should be evaluated closely at the next bandage change as these areas may not survive. A common type of graft used in veterinary medicine is a full-thickness mesh graft. With this graft, no specialized equipment is needed to harvest or prepare the graft. A section of skin, approximately the size of the defect, is taken from the flank region. The donor site should be evaluated prior to taking the graft to ensure that it can be closed primarily. Once the skin has been removed, it is attached to a piece of sterilized cardboard with hypodermic needles to keep it stretched out. Any fat present on the underside of the graft skin must be removed to allow the best engraftment possible. Once the subcutaneous fat is removed, stab incisions are made in the graft. These stab incisions should be 1-2 cm long and around 1-2 cm apart. They should also be staggered apart in parallel rows. These meshes prevent seroma or hematoma formation between the recipient bed and the grafted skin. The wound bed should be prepared by freshening the edges prior to graft placement. Once the graft is in place, it is secured to the edges of the wound bed with sutures. Sutures can be placed in the middle of the graft at areas where the grafted tissue is lifting off of the recipient bed, if needed. These grafts have a lower survival rate than axial pattern flaps or subdermal plexus flaps as they do not have an inherent vascular supply; however, there can be 90-100% graft take if the graft is placed properly. Island grafts, as previously mentioned, are pieces of skin that are placed in a larger granulation bed to encourage epithelization. One example of this type of graft are punch grafts. The donor site is often the flank area as there is typically loose skin in this area. A 5 mm punch biopsy tool is used to create a perfectly circular graft of skin. The subcutaneous fat must be removed from this graft as well. The recipient bed is prepared by using a slightly smaller, 4 mm punch biopsy tool to create openings in the granulation tissue 1 to 2 cm apart. The skin graft is placed within the newly made openings in the granulation tissue. These grafts are bandaged as described for all grafts. These are easy to place and usually take quickly. The main disadvantage is that the cosmetic appearance afterward is generally poor and the new epithelium that is created by these grafts can be weaker than other skin and therefore more prone to trauma.
35

Suggested Reading 1. Stanley BJ. Chapter 77: Tension-Relieving Techniques. In: Johnston SA, Tobias KM, eds. Veterinary
Surgery: Small Animal. 2nd ed. St. Louis: Saunders Elsevier, 2018; 1422-1446. 2. Hunt GB. Chapter 78: Local or Subdermal Plexus Flaps. In: Johnston SA, Tobias KM, eds. Veterinary
Surgery: Small Animal. 2nd ed. St. Louis: Saunders Elsevier, 2018; 1446-1457. 3. Wardlaw JL, Lanz OI. Chapter 79: Axial Pattern and Myocutaneous Flaps. In: Johnston SA, Tobias KM,
eds. Veterinary Surgery: Small Animal. 2nd ed. St. Louis: Saunders Elsevier, 2018; 1457-1473. 4. Bohling MW, Swaim SF. Chapter 80: Skin Grafts. In: Johnston SA, Tobias KM, eds. Veterinary Surgery:
Small Animal. 2nd ed. St. Louis: Saunders Elsevier, 2018; 1473-1494. 5. Pavletic MM. Atlas of Small Animal Wound Management and Reconstructive Surgery. 4th ed. Hoboken:
Wiley, 2018; 265-492.
36

Management of Burn Wounds, Non-Healing Wounds, and Other Challenging Wound Cases
Mandy L. Wallace, DVM, MS, DACVS-SA Assistant Professor, Small Animal Surgery
University of Georgia College of Veterinary Medicine [email protected]
While many wounds are managed in similar ways, there are certain wounds that require special considerations either due to the inciting cause of the wound or due to inherent patient factors. These factors may affect the way the wound or the patient is managed and may affect wound healing. In this discussion, we will focus on these challenging cases and how we can best manage them to allow for healing. Wounds over Joints In general, there are several considerations when a wound occurs over a joint. First, the amount of motion over a joint can lead to significant issues with wound healing if not controlled. Second, there are often bony prominences near the wound that must be considered both during open wound management and during surgical closure. Another consideration is whether the joint has been compromised in the case of a traumatic wound in these areas. To address motion at the level of the elbow, stifle, tarsus or carpus, splints can be placed within soft padded bandages to limit motion at the joint. These splints can be made for each patient out of either casting material or Vet-lite depending on which is available. These splints will conform better to the patient’s limb than the premade splints and will decrease splint-related complications. Even with the splint in place, it is important that the owners keep the patient exercise restricted to further prevent excessive motion at the joint. Bony prominences can make wound management and closure more difficult by putting more pressure on the wound. One way to mitigate these prominences is to take the pressure off the prominence by creating “donuts” out of cast padding and kling materials. These can be placed so that the open part of the donut is over the bony prominence (such as the olecranon) and the remainder of the donut acts as a shock absorber. A common misconception is that the prominences should receive more padding than other portions to take pressure off them; however, this actually puts more pressure on the prominence which may lead to complications. When closing over these prominences, it is ideal to move the closure to the side of the prominence so that the incision is not directly over the pressure point Joint compromise is concerning as it can lead to infection within the joint, especially if not addressed. If present, the joint should be flushed and the joint closed as quickly as possible to prevent further contamination. The joint should be monitored closely to determine if a septic arthritis is developing. Signs of septic arthritis may include joint swelling, joint pain, and lameness of the affected limb. Arthrocentesis and cytology should be performed to confirm the diagnosis and to obtain a sample for culture. Joint fluid cultures are often more successful in growing the inciting bacteria when blood culture media is used. One particular type of wound that occurs over the elbow can develop from hygromas. Hygromas are pockets of serous fluid that occur over the olecranon process of the elbow. These tend to occur more frequently in large and giant breed dogs that tend to lay on hard surfaces rather than beds or cushions. While these are typically non-painful, they can grow and become ulcerated or infected. When this occurs, they must be managed as with any other open wound. As mentioned previously, “donuts” can be used during open wound management to take pressure away from the area. Once the wound is ready for closure, the wound should be closed away from the bony prominence, and all portions of the hygroma should be resected to prevent recurrence. In some cases, advancement or rotational flaps may be needed to help close the wound. After wound closure, the limb should be bandaged for 10-14 days to decrease pressure on the closure. The major concern with these wounds is the risk of recurrence. Environmental changes should be made including providing thick bedding and preventing the patient from laying on hard surfaces as much as possible. Another option is to purchase custom-made sleeves that protect the elbows from trauma when laying on hard surfaces. One option is available from DogLeggs. These can be used once the surgical closure wounds have healed.
37

Similarly, pressure sores over the joints can be seen in dogs hospitalized for long periods without appropriate bedding or those that are not moving much due to concurrent conditions. These dogs should have thick bedding available within their enclosure and should be flipped from side to side every 4-6 hours to prevent them from spending too much time on one side. If these sores occur, they should be treated similarly to hygromas, although once they are healed, if the patient has recovered from their concurrent conditions, they likely will not have long- term issues with recurrence. Distal Limb Wounds Distal limb wounds are common and often frustrating as there is limited extra skin in this area to aid in closure if skin is missing. It is also easy to close wounds in this area too tightly leading to a tourniquet effect and causing swelling distal to the closure. After initial open wound management, there are a few ways to manage closure. If the wound is less than 50% of the limb circumference, they can be allowed to heal by second intention. This option can take a long time to reach completion and requires bandage changes every few days. Once granulation tissue forms, non-adherent dressings can be used to encourage epithelialization and do not typically need to be changed daily. If the wound is greater than 50% of limb circumference, there is concern that if allowed to contract and close by this method, a tourniquet effect can be created. When considering surgical options, it depends on the patient and the location of the wound. Pouch or hinge flaps can be used for wounds below the elbow or stifle. With this closure, a single pedicle (hinge) or bipedicle (pouch) flap is developed on the flank. The limb is pulled forward or backward toward the flap, and the flap is secured to the open wound. The patient is bandaged with the limb secured next to the body for 2-3 weeks while the flap undergoes engraftment to the open wound area. After that time, another surgery is performed where the flap is detached from the flank, and the final portion of the flap is secured to the limb. The area where the flap was taken from undergoes primary closure. These work well as the flap maintains its inherent blood supply while engraftment takes place. The disadvantage is that the patient’s limb must be bandaged up and is unable to be used for ambulation during the 2-3-week engraftment process. This can be challenging for dogs with osteoarthritis as this period of immobilization can cause increased pain in their joints. It can also potentially hinder appropriate joint development in puppies as they are not weightbearing on that limb during a critical point of development. Other options are full-thickness mesh skin graft or punch grafts depending on the size of the wound and location. For more discussion of these grafts and how they are performed, please refer to the proceedings for “Surgical Management of Wounds”. Burn Wounds There are four main types of burns: thermal, chemical, electrical and radiation. Many of the burns that veterinarians deal with are thermal burns, typically caused by house fires or interaction with a very hot surface. These can range from superficial burns (first-degree) only affecting the epidermis to burns that extend to the bone (fifth degree). With any of these burns, there can be more damage than is evident on the surface. Thermal burns have three main zones based on the viability of the tissue within each. The area in the center of the burn is called the zone of coagulation, where no viable tissue remains. This entire area should be debrided. The next zone, just outside the first zone, is the zone of stasis. In this zone, there is reduced perfusion making the tissues vulnerable to further injury. Tissues in this zone are viable at first but can easily become non-viable depending on patient factors and how the wound is managed. The outermost zone, the zone of hyperemia, is where most of the inflammation is occurring. The tissues in this area are viable and should heal if treated appropriately. When burns occur, application of cool or cold running water for approximately 20 minutes can slow the tissue damage and has been shown to lead to improve healing. This should ideally be performed at the time that the burn occurs. After this, the burns should be covered with a non-adherent, sterile, occlusive dressing to prevent contamination and to decrease pain while the patient is being stabilized. Intravenous fluid therapy is important in burn patients as they lose significant amounts of fluid from the wound and can have a large shift of fluid out of the vascular system into the subcutaneous tissues, leading to hypovolemic shock. Additionally, it is important to keep the patient in a normovolemic state to allow perfusion to be restored to the zone of stasis. In addition to fluid therapy, in cases of structural fires, the patient may have smoke inhalation injury requiring oxygen therapy. The patient should be carefully monitored in the first few hours to determine if this has occurred and if oxygen is needed. After the initial triage, the wounds can be dealt with definitively. Large burns should have the necrotic or non-viable tissue debrided with sharp surgical debridement. This should be done carefully and in layers to prevent debridement of viable tissues. Tissues should be debrided to the level where bleeding occurs. Once bleeding is present,
38

debridement should stop in that area to keep the currently viable tissues. Development of infection is an important risk that must be mitigated in burn wound management. Often, silver sulfadiazine cream or honey are applied over all open areas prior to placement of sterile dressings to prevent infection in animals with large wounds. Open wound management continues until either the wounds close via second intention or with delayed primary surgical closure. Depending on the size of the wound with skin missing, advanced surgical techniques, such as flaps or grafts, may need to be employed to close all the wounds completely. Another recent development in the management of wounds in both people and animals is the use of sterilized fish skin as a barrier to protect the underlying burned tissue while epithelialization is occurring. These fish skins transfer collagen to the patient’s skin and can lead to fewer bandage changes. Tilapia is often used as it is inexpensive and readily available. There are also commercially available preparations; however, those that are commonly used in human medicine may be cost prohibitive in many veterinary patients. Nutrition is another factor that must be considered in burn victims with large burn wounds. They can lose a large amount of protein in the fluid lost from the wound. This is compounded by the fact that these patients are often being sedated or anesthetized daily for wound management and are held off food each night to prevent regurgitation and aspiration under anesthesia. Nutritional requirements should be calculated for the patient and adjusted based on measured protein levels to make up for losses. If the patient is unable or unwilling to eat the amount needed freely, feeding tubes such as nasogastric or esophageal tubes may be a good option to ensure that they obtain enough nutrition to maintain normal protein levels for adequate healing. Non-healing Wounds Non-healing wounds can occur for a variety of reasons. Examples of this type of wound include wounds that have not healed after an appropriate amount of time, wounds that heal partially or completely then re-open soon thereafter, and draining tracts that occur over different locations across the body either simultaneously or over a period of time. There are various reasons that a wound may not heal. The presence of a foreign body or foreign material within the wound or draining tract may lead to cycles of healing followed by eruption of draining tracts or infection. With foreign bodies, due to migration, the location of the wound or the draining tract location may change over time. Interestingly, the foreign material may enter the body through inhalation or ingestion and migrate out of the organs into the subcutaneous space. For those reasons, it can be challenging to know when or where the foreign body exposure occurred. Advanced imaging such as ultrasonography or computed tomography may be beneficial in locating foreign material if present; however, in many cases, the material may not be visible or it may have been broken down by the body already. Even if the foreign material is no longer present, these can introduce fastidious bacteria such as Nocardia or Actinomyces into spaces in the body which may be difficult to culture or treat. Appropriate treatment for these bacterial infections may require longer term antibiotic therapy (1-6 months). Additionally, exploration of the wound or draining tract may reveal the inciting foreign material, which should be removed if possible. Another cause of non-healing wounds are atypical bacteria, such as mycobacterium. Atypical mycobacterium are gram positive bacterial rods that are usually present in the environment or soil. This type of infection is more often seen in cats and often results from a penetrating injury. Clinical signs may include draining tracts, wounds that heal then reopen, “sterile” abscesses, and granulomas. The bacteria are often not seen on standard aerobic or anerobic culture or cytology. Diagnosis often requires obtaining tissue for histopathologic evaluation and for special mycobacterium culture at a human laboratory. The advantage of the culture over only performing histopathology is the opportunity to see what the bacteria are susceptible to in order to place the patient on appropriate antibiotic therapy. The disadvantage is that due to the slow growth of atypical mycobacterium it can take several weeks to get the culture and susceptibility results back. Once this has been diagnosed, treatment includes an aggressive surgical debridement of all affected areas as well as 6-12 months of antibiotics based on susceptibility results. An uncommon cause of non-healing wounds in Georgia that is seen more commonly in areas such as Florida or Louisiana is pythiosis. Pythiosis results from being infected with Pythium insidiosum, a fungal-like organism, and typically causes either skin lesions/granulomas or intestinal masses. Animals are usually infected by ingestion of or swimming in affected water sources (ponds, lakes, etc.). Skin lesions are similar to those seen with atypical mycobacterium. Similarly, diagnosis is typically via histopathological identification or a specific pythium culture. Treatment is challenging as even with complete removal of visible disease, the infectious agent may still be present within the body. For masses, aggressive surgical removal is indicated with follow-up specific anti-fungal therapy. Despite treatment, the prognosis for dogs with this disease is guarded to poor with recurrence likely.
39

Various patient factors can also result in wounds that do not heal in an appropriate timeframe. Those may include patients that are immunocompromised either due to disease or current medications, patients with endocrine disease, or patients with Ehlers-Danlos syndrome. In these cases, often wound healing will progress appropriately once the underlying condition is stable or once we can safely decrease dosages of immunosuppressive medications. While the underlying conditions are being treated, the best option for non-healing wounds is to keep them clean and to prevent infection. This can be challenging and requires dedication from both the veterinarian and the owner to frequent wound management over weeks to months.
Suggested Reading
1. Hunt GB. Chapter 78: Local or Subdermal Plexus Flaps. In: Johnston SA, Tobias KM, eds. Veterinary Surgery: Small Animal. 2nd ed. St. Louis: Saunders Elsevier, 2018; 1446-1457.
2. Bohling MW, Swaim SF. Chapter 80: Skin Grafts. In: Johnston SA, Tobias KM, eds. Veterinary Surgery: Small Animal. 2nd ed. St. Louis: Saunders Elsevier, 2018; 1473-1494.
3. Bohling MW. Chapter 81: Burns. In: Johnston SA, Tobias KM, eds. Veterinary Surgery: Small Animal. 2nd
ed. St. Louis: Saunders Elsevier, 2018; 1495-1507. 4. Pavletic MM. Atlas of Small Animal Wound Management and Reconstructive Surgery. 4th ed. Hoboken:
Wiley, 2018; 173-252, 395-416.
40

Choose Your Adventure: An Interactive Walk Through Challenging Wound Management Cases
Mandy L. Wallace, DVM, MS, DACVS-SA Assistant Professor, Small Animal Surgery
University of Georgia College of Veterinary Medicine [email protected]
Wound management is a process that is unique to each individual case. Knowing what options are available and optimizing those options to create the best environment for wound healing will lead to better outcomes. During this session, various cases will be presented with the goal of discussing the topical wound product and surgical closure options available for that patient and how to decide which will result in the best outcome. Strategies for Wound Management When approaching a wound management case, there are various steps that can be worked through for each case to ensure that the appropriate management is occurring. #1: Patient Triage The first step in any wound management case is ensuring that the patient is stable. Wounds and orthopedic conditions should be the last things evaluated on a trauma patient. Evaluate the patient’s vital signs, cardiovascular and respiratory status and neurologic status prior to performing an orthopedic evaluation or in-depth wound evaluation. Patients should be stabilized prior to administration of any sedation (if possible). Additionally, any active bleeding should be addressed via compression, when possible, until appropriate evaluation can occur. #2 Wound Evaluation and Planning The second step after ensuring patient stability and treating any life-threatening issues such as shock or significant bleeding is to thoroughly evaluate the wounds under sedation and make a plan. While it may seem obvious, making a plan for how to manage the wounds will ensure that progress is being made daily toward the end goal of wound closure. For simple wounds, the plan may be as straightforward as placing a wet-to-dry bandage for 2-3 days with primary wound closure to occur once the wound bed appears healthy. However, for complex trauma cases with wounds across the entire body, developing a comprehensive plan will allow for the fewest possible anesthetic episodes and gives a global perspective of the best way to close each wound without interfering with closure of another wound. For example, if you have various wounds on the right side of a patient’s body, performing a caudal rotational flap to close a smaller wound over the scapula may limit the skin available or the options available to close a larger wound over the thorax. In that case, taking the rotational flap from a more cranial position may still allow the scapular wound to be closed without affecting the options for the thoracic wound. Using a body map can help with planning of complex wounds and allows for a record of wound size, wound health, topical wound products employed, and the plan for that wound. #3 Daily Wound Evaluation Failure to plan can lead to missed opportunities to close wounds at the optimal time. It can be easy to continue doing the same topical wound product and bandage every day without critically evaluating the wound. Each day, the following criteria should be evaluated:
• What stage of healing is this wound in currently? • Is the topical wound therapy and bandage being used appropriate for that stage of wound healing? • Is the wound bed progressing appropriately? Is there evidence of infection? • Is the wound ready to be closed? If yes, how and when can we close the wound? If no, what is preventing
the wound from being ready for closure and what steps can be taken to help the wound progress toward closure?
41

By working through this each day with each wound, progress is made in a more linear fashion, leading to improved wound outcomes. #4 Wound Closure When the wound is ready for closure, a plan for wound closure should be made prior to moving the patient into the procedure room or operating room. Often, the plan may change once the wound is evaluated when the patient is under general anesthesia. Knowing the plan prior to the patient entering the OR allows for optimal patient skin preparation and positioning. Without that, options may be limited if the original plan does not work as expected. For complex wounds, having 2-3 closure plans in mind can be helpful if it is determined that the original plan will not work. Also, be prepared that partial closure may be the only option and continued bandaging may be required for the remaining portion of the wound. #5 Post-operative Wound Bandaging and Evaluation Depending on the closure used, post-operative bandaging may also be necessary. For example, skin grafts must always be bandaged for 10-14 days after surgery. Additionally, some flaps may also benefit from bandaging. Bandages may also be useful depending on whether or not drains have been placed. Consider if bandaging is necessary prior to the patient waking up from wound closure as bandages and splints will be much easier to place at that time. If a bandage is placed, the bandage should be removed the following day to evaluate the closure and healing progression. The exception to this is if a skin graft has been performed, in which case the bandage should stay in place for 2-4 days after surgery. If wounds are not healing appropriately, there are several factors to consider. Is there too much tension on the wound? Is the wound showing signs of infection? If the patient is being managed as an outpatient, are the owners being compliant with E-collar placement and activity restriction? Are there other factors at work (atypical bacteria, fungal infection, immune compromise in the patient, patient nutritional status/albumin level) which can be investigated further? Determining the factors which may be contributing to poor wound healing earlier in the course of healing will allow for treatment changes which may save the wound closure performed. The longer the wound is allowed to progress in a negative fashion, the less likely it is to heal appropriately without further intervention.
In the end, after 10-14 days, hopefully the wounds have healed perfectly, and the patient can go back to their normal activity. With each patient, the opportunity exists to expand your knowledge of available options for management and closure. As one gets more experience with wound management, the subtle changes become more obvious, allowing for better decision making in these cases.
42
Separation-Related Anxiety in Dogs Lynne M. Seibert, DVM, MS, PhD, DACVB
Veterinary Behavior Consultants LLC Lawrenceville, GA USA
Anxiety is defined as the apprehensive anticipation of future danger accompanied by somatic symptoms of tension. Fear is a response that prompts an individual to remove or protect it from dangers or noxious stimuli. It has been suggested that fear and anxiety-related behaviors have evolved to promote survival in natural environments by enhancing the individual’s ability to avoid danger.
A phobia is a pathologic state of fear that is amplified beyond the adaptive response and is triggered by a normal environmental stimulus. Phobias are persistent over time, occur consistently with repeated exposure to a stimulus or situation, are irrational or unreasonable given the level of danger present, and usually lead to avoidance of the feared stimulus. Reactions may be intense (catatonia, hysteria, panic attacks).
Fears and phobias may develop because of genetic predispositions, lack of adequate exposure to various stimuli during development, traumatic experiences, or a combination of these factors. Fears and phobias can be debilitating and often require therapeutic intervention.
Fear-related behavior problems seen in dogs include thunderstorm and noise phobias, separation anxiety, social phobia, anthropophobia (fear of people), neophobia (fear of unfamiliar situations or novel items), and fear of other animals. Fear-related problems comprised approximately one-third of all cases in one behavior referral practice and were the most common reason for rejection of potential Guide Dogs in the United States.
Manifestations of anxiety in dogs include panting, salivation, pacing, whining, trembling, destructiveness, excessive vocalization, gastrointestinal upset, anorexia, withdrawal, inactivity, urination, defecation, and self-inflicted injuries.
In veterinary medicine, learning processes play important roles in the development, maintenance, and treatment of anxieties and phobias. Learning is defined as an enduring change in behavior that results from experience with environmental events, but not from fatigue, maturation, or alterations in physiological state.
Early experience and genetic predisposition may make some dogs more susceptible to developing anxiety-related disorders. Thus, there is a substantial range in the tolerance of individual dogs to experiencing potentially fear- inducing stimuli. Fear-related aggression problems account for most canine aggression cases in behavior practices.
Separation anxiety Separation anxiety is defined as a distress response to separation from an attachment figure. Its prevalence in the canine population is estimated to be about 15-17 percent. It is the second most common presenting complaint in behavior specialty practices.
Clinical signs of anxiety occur when the dog is completely separated from its human attachment figure(s). In a study conducted by Flannigan and Dodman (2001), the most common complaint made by owners was destructive behavior in the home during their absence.
The etiology of separation anxiety in dogs is unclear. An attachment disorder has been suspected, however, hyperattachment (excessive contact seeking with the owner) is not a consistent symptom for dogs with separation anxiety. In a study comparing clinically normal dogs with dogs that had separation anxiety, normal dogs were just as likely to follow their owners from room to room as were dogs with separation anxiety. Likewise, dogs with separation anxiety were no more likely to follow their owners around the house than were normal dogs.1 Contact seeking when the owner is at home or being a “Velcro dog” is not a reliable diagnostic criterion for separation anxiety. The gender of the dog, age when acquired, and presence or absence of other pets in the household does not appear to be significant risk factors for separation anxiety.
43
Dogs from shelters and dogs adopted as strays may be predisposed to develop separation anxiety, or prove more difficult to treat, but results of data have been equivocal. Dogs with separation anxiety do appear to have a higher reported incidence of noise phobia problems. The onset of separation anxiety often appears to be associated with minor disruptions to the normal schedule: changes to the owners’ work schedules, following boarding or a hospital stay, addition of new family members, and is often reported in geriatric patients with no historical evidence of schedule changes.
The diagnosis of separation anxiety is based on completing a physical evaluation and taking a behavioral history, establishing that the behavioral symptoms are occurring only in the owners’ absence, ruling out other potential causes of the behavioral symptoms (medical conditions, other anxiety conditions, lack of training, lack of environmental management, etc.). Videotaping the dog in the owner’s absence may provide the information necessary for making a diagnosis. Separation anxiety behaviors will typically occur within a short period after the owners’ departure.
Barrier Frustration and Confinement Distress Most dogs will quickly learn to accept confinement, especially if they are introduced to it in a process of positive reinforcement. However, some dogs will react anxiously to confinement regardless, because instincts drive them to roam and wander freely. Confinement anxiety may also be learned.
Symptoms Typical anxiety symptoms include restlessness, whining, barking, destructive behavior, escape attempts, and self- trauma. To distinguish the dog’s behavior from other types of anxiety, context is key: they exhibit signs of anxiety only when confined or when anticipating confinement.
Some key distinctions exist between separation anxiety and confinement distress. Confinement distress can occur with or without the presence of the owner, such as when the dog is crated for transport, denied access to an area, or simply placed in a room alone with the door closed. Separation anxiety, meanwhile, occurs with or without confinement, when the dog is physically separated from the owner or other family members.
Environmental management During the treatment process, it may be necessary for owners to arrange for daycare or pet sitters. Confinement can be dangerous, as many dogs with separation anxiety also suffer from barrier frustration/confinement distress and may injure themselves during escape attempts.
Behavior modification Many dogs with separation anxiety will display anxiety during the owner’s pre-departure routine (picking up keys, putting on shoes, setting the house alarm). Because the pre-departure cues are temporally associated with prolonged owner absences, these dogs develop classically conditioned fears of the elements of the pre-departure routine. Thus, anxiety begins before the owner ever gets out of the door. Classically conditioned fears can be extinguished by disrupting the pairing of the conditioned stimulus (keys, shoes, alarm) with the unconditioned stimulus (extended absences). This process of extinction can be accomplished if the owners will repeat elements of their pre-departure routine and stay home instead of leaving (pick up keys and put them down, put on shoes and hang out with dog instead of leaving).
Conditioned inhibition is a technique that can be used to teach anxious dogs to relax during their owner’s absence. These exercises involve using a safety signal (inhibitory conditioned stimulus) during ultrashort practice departures. The safety signal should be a signal that has never previously been associated with an extended owner absence and will be presented during brief departures. Over time, as the dog learns to associate this special signal with short, safe owner absences, the length of the practice departure can be gradually extended.
44
Pharmacotherapy Due to the intensity of anxiety, the severity of damage that can occur to property, the risk to the patient’s health and safety, and the frequency of exposure to anxiety–provoking owner absences, medication is often indicated to reduce suffering and hasten improvement. There are a variety of anxiolytic medication options available, including two products approved by the FDA for use in dogs with separation anxiety. Medication should always be used in combination with a behavior modification program. The duration of treatment will vary depending on severity and owner compliance with behavior modification. Separation anxiety is a treatable condition, especially with early intervention.
Maintenance medication therapies Selective serotonin reuptake inhibitors (SSRI’s) act through highly selective blockade of the reuptake of serotonin at the presynaptic neuron and may facilitate the downregulation of post-synaptic receptors.
• Fluoxetine (Prozac)
o DOG 1.0 – 2.0 mg/kg po q24h • Sertraline (Zoloft)
o DOG 1.0 – 3.0 mg/kg po q24h • Paroxetine (Paxil)
o DOG 1.0 mg/kg q12-24h Azapirones (Buspirone, Buspar) is a non-sedating anxiolytic drug that is a partial serotonin (5-HT1A) agonist (enhances neurotransmission of 5-HT) and a dopamine receptor agonist and D2 antagonist. Buspirone has a short half-life (2-11 hours). Side effects are uncommon, with mild gastrointestinal upset being most likely. Buspirone can be used in the treatment of separation anxiety in dogs, and for mild chronic fears and anxieties in non-aggressive dogs.
• 2.5 – 15.0 mg/dog po bid–tid
Tricyclic antidepressants As a group, tricyclic antidepressants affect serotonin, norepinephrine, acetylcholine, and histamine. They block the presynaptic reuptake of serotonin and norepinephrine to varying degrees. Tertiary amines (amitriptyline, doxepin, imipramine) are more potent inhibitors of serotonin reuptake, are more sedating, have more anticholinergic and cardiovascular side effects, and are metabolized to secondary amines (desipramine and nortriptyline). Metabolites are more potent inhibitors of norepinephrine reuptake. TCA’s have varying degrees of muscarinic, alpha-adrenergic, and H1 and H2 blocking activity.
The most common side effects seen in dogs are sedation and gastrointestinal upset. Peripheral and central anticholinergic effects can result in constipation, dry mouth, decreased tear production, urine retention, and mydriasis. TCA's can lower the seizure threshold and alter blood glucose levels. In humans, tricyclic antidepressants can cause cardiovascular, neurological, hematologic, gastrointestinal, and endocrine side effects. Testicular hypoplasia has also been reported.
Tricyclic antidepressants should never be used in combination with monoamine oxidase inhibitors, and should be used cautiously, if at all, with phenothiazines, anticholinergic agents, antidepressants, psychostimulants, anti-thyroid agents, cimetidine, thyroid supplements, and CNS depressants.
• Amitriptyline (Elavil)
o DOG 2.2 mg/kg po q12h • Clomipramine (Anafranil, Clomicalm)
o DOG 2.0 mg/kg po q12h
45

References 1. Parthasarathy, V, Crowell-Davis, SL. 2006. Relationship between attachment to owners and separation
anxiety in pet dogs. Journal of Veterinary Behavior 1:109-120.
46

Consequences of Aversive Training in Dogs Lynne M. Seibert, DVM, MS, PhD, DACVB
Veterinary Behavior Consultants LLC Lawrenceville, GA USA
Aversive training is training with consequences that dogs want to avoid, and often includes positive punishment and/or negative reinforcement. In our caseload, in metropolitan Atlanta, 37% of our clients admit to using shock collars to train their dogs (N = 165 canine patients seen in 2020). Shock collar training is equally as likely to be used in aggressive and non-aggressive patients. Negative outcomes of euthanasia, rehoming, or dental disarming occur in less than 2.5 percent of our caseload and are more likely in dogs that have been exposed to aversive training.
Veterinarians are legally and morally responsible for the behavioral health of their patients. In many states, only licensed veterinarians can legally diagnose, treat, correct, change, relieve, or prevent animal disease, deformity, defect, injury, or other physical or mental conditions, or render advice or recommendations regarding any of the above.
Veterinarians need to be directly involved in behavior case evaluations to make appropriate recommendations for training or behavior modification. Behavior case evaluations should include physical examination, thorough behavior history, diagnostic testing, diagnoses, behavior modification plan, behavior medications if indicated, and appropriate referrals. Obedience training is often not appropriate for pets with behavioral illness. Aggression and anxiety are not obedience training issues.
With aversive training, negative reinforcement (R-) and positive punishment (P+) may be employed, as well as flooding tactics and abusive treatment. Electronic (E, or E-stimulation) collars are collars that deliver a static electric stimulus, auditory signal, and often have a vibration setting. Devices may be remote, hand-operated, bark or noise- activated, or utilized in containment systems.
Is positive punishment (P+) effective? To use punishment tactics effectively, three conditions must be met: immediacy, consistency, and appropriate intensity. When attempts at punishment use high intensity punishers, like shock, fear or learned helplessness can result. Learned helplessness is a consequence when there is repeated exposure to uncontrollable stressors resulting in the individual failing to use any control options. Individuals learn that they lack behavioral control over environmental events, which undermines motivation. Conditioned emotional responses can also occur, causing the dog to become fearful of humans and less responsive to training.
Dogs with significant behavior problems were studied in a controlled study in which the dogs were assigned to three different training groups. In one group, twenty-one dogs were trained on basic obedience and recall over 5 training days, using only positive reinforcement techniques. In the second group, twenty-one dogs were trained on the same obedience tasks using active electronic collars pairing vibration cue with electric signal. The trainers could also use food rewards and lead pressure for training. In the third group, twenty-one additional dogs were trained by the same trainers from group two, using lead corrections, but no electronic corrections. All dogs wore identical E-collars, but only one group wore active collars. Blinded observers watched videotapes of the training sessions and scored latency to complete the response and the number of cues required.1
The group trained with positive reinforcement performed better than the other two groups. They exhibited a higher proportion of obeys after first command and had a shorter latency to comply with commands. The dogs trained with aversive tactics showed longer latencies as training progressed. Use of reward-based training was superior to negative reinforcement and positive punishment-based training (E-collar and lead corrections). Correction-based trainers were as effective at modifying undesirable behavior when they did not use e-collars but used leash corrections only.
In addition to the negative emotional and behavioral consequences of the use of aversive training in dogs, there are also potential physical consequences. Intraocular pressure was measured in healthy sled dogs who were trained to pull on a tether while wearing a nylon buckle collar and then while wearing a harness. A digital force gauge was used to measure the tension each dog generated against the leash for 10 seconds while wearing the collar and then
47
the harness. After 10 seconds of pulling on the leash at a consistent angle using previously determined tension, intraocular pressure was measured in both eyes. Under tension in a collar, IOP increased significantly more than when under tension with harness (P<0.05). IOP increased by a mean value of 7.4 mm Hg with collar and 2.3 mm Hg with the harness.2
Can aggression be corrected with positive punishment? Aggressive behaviors function to increase distance and can be highly effective. Growling and barking are warnings that a dog needs more space. Attempts to correct warnings will result in escalation of intensity of the aggressive display. Regardless of the handler’s response to aggression, aggressive behavior is often successful in terminating undesirable interactions. Furthermore, if the aggression is motivated by fear, fear cannot be successfully “punished.” Learning is difficult during times of heightened sympathetic arousal, so any attempt to “train” during an aggressive event is unlikely to be successful anyway.
Electronic containment systems (invisible fences) have been shown to be the least successful method of containment for dogs. In a study including over 1000 dogs, contained via either physical fencing (see-through or privacy), electronic fencing, or a tether system, the escape frequency was significantly highest for electronic fencing.3
In a review of the existing literature on the effects of using aversive training methods in dogs, the conclusion was that there is no evidence that aversive training methods are more effective than positive reinforcement-based training. Aversive training methods (positive punishment and negative reinforcement) can jeopardize physical and mental health of dogs.
References 1. China, L, Mills, DS, Cooper, JJ. 2020. Efficacy of dog training with and without remote electronic collars
versus a focus on positive reinforcement. Frontiers in Veterinary Science 7:508; 1-11. 2. Pauli, AM, Bentley, E, Diehl, KA, Miller, PE. 2006. The effects of application of neck pressure by collar or
harness on intraocular pressure in dogs; J Am Anim Hosp Assoc 42:207-211. 3. Starinsky, NS, Lord, LK, Herron, ME. 2017. Escape rates and biting histories of dogs confined to their owner’s
property though the use of various containment methods. JAVMA 250(3), 297-302. 4. Ziv, G. 2017. The effects of using aversive training methods in dogs – A Review. Journal of Veterinary
Behavior 19:50-60.
48

Reducing Stress During Veterinary Visits Lynne M. Seibert, DVM, MS, PhD, DACVB
Veterinary Behavior Consultants LLC Lawrenceville, GA USA
General safety principles In the veterinary hospital, animal bites and injuries associated with animal handling are the two leading sources of workers’ compensation losses. According to the AVMA PLIT, in a recent analysis of 605 veterinary workers’ compensation losses, 50 percent were due to animal bites. Cat bites are the most frequent and costly bite injuries. The average cat bite cost is $757, while the average dog bite cost is $495. Educating staff about animal behavior and how to approach, handle, and safely restrain patients will result in less expense, fewer injuries, safer procedures, and happier clients.
It is critical that each hospital have an established training protocol for new employees regarding animal handling protocols. Waiting areas should have signs posted requiring owners to keep pets on leashes or in carriers. Separate waiting areas may be designated for dogs and cats and smaller exotic species. Difficult patients should be taken to an examination room as quickly as possible since prolonged delays in the waiting area can exacerbate the patient’s anxiety. Scheduling difficult patients for the beginning or end of the day to reduce their waiting time may also be prudent. It is strongly recommended that employees hold or restrain all animals during examination or treatment procedures to prevent injury to owners.
Patients with a history of aggression during the veterinary visit should have notes in their files detailing the specific concerns. Patient file notes are most helpful when they detail specific interventions that were successful for that patient in the past. For hospitalized patients, cage cards should be labeled with client-friendly stickers that alert the staff to potential problem areas.
Most aggression in the veterinary hospital is due to fear or pain. Hospital staff may also see territorial, possessive, instrumental, drug-induced types of aggression. It is important to recognize when an animal is uncomfortable and likely to act defensively. Understanding the animals’ postural signals will help to determine the type of restraint that is indicated. Restraint must be safe for the humans as well as the patient. Avoid excessive neck pressure and do not position the animal in such a way that it could fall or be injured because of restraint.
Approaching animals The way staff members approach the patients can set the tone for the subsequent examination. Dogs are often overly sensitive to unfamiliar individuals reaching toward or over their heads, particularly if they are cornered or restricted by a leash. Hospital staff should avoid standing over, staring at, and reaching over canine patients. Any canine patient that shows excessively submissive postures (ears pinned back, caudal retraction of lip commissure, avoidance of eye contact, submissive urination) can potentially become frightened enough to bite. Dogs that are trembling, hiding, urinating, defecating, expressing anal sacs, yawning, or panting excessively, or any combination of these behaviors are frightened and could become aggressive.
Patients that are hiding under chairs or tables can be removed with their leashes before being restrained. It is never advisable to reach under a table or into a cage to remove a fractious patient. Cat carriers can be disassembled to safely remove the cat with a towel.
Handling cats Friendly cats greet with their tails straight up, ears forward, and back straight. Cats that are exhibiting an arched back, curved or tucked tail, or pin their ears back are frightened and may defensively bite or scratch.
No single approach will work for every patient, but most fractious cats can be wrapped in thick towels for a cursory examination. Gloves, collars, cat bags, squeeze boxes, muzzles, or chemical restraint are options if the cat is too
49
fractious to examine otherwise. All employees should be instructed on the proper handling of cats for transport (with forelimbs held to prevent scratching), restraint for venipuncture, and restraint for examinations.
Handling dogs For examination of difficult canine patients, towel holds, head collars, and/or muzzles can be used. If the patient is extremely fractious, the best approach might be to send the owner home with instructions for acclimating their dog to a basket style muzzle, and attempt the examination at another time, when the dog can comfortably return wearing the muzzle. Basket style muzzles do not restrict the dog’s ability to breathe but will prevent injury to handlers.
Larger examination rooms are preferred for difficult patients. Kennels and cages can aggravate defensive or territorial/protective responses, so patients may need to be removed from cages before handling is attempted.
Be cautious with chemical restraint. There is no perfect medication to address fear-induced aggression, unpredictable reactions can occur, and some medications can disinhibit aggressive tendencies.
Good restraint is informed, compassionate, attentive, and informed. Avoid scruffing, raising your voice, pinning, or rolling a patient. When physical force is used, you break your promise to “do no harm.” It can lead to aggression, injuries, and poor veterinary care.
Pets should be examined where they are most comfortable. It is rarely appropriate to “take a pet to the back.” Most pets will feel safer with their owners in the room. If an owner prefers not to be present for an examination and blood draw, simply ask them to step out of the examination room, rather than take a frightened pet to a noisy treatment area. Pet parents should be encouraged to visit with their pets in-between medical visits for benign visits to your hospital. High value treats should be offered during all visits.
Veterinary visits for cats Almost twice as many cats than dogs never visit the veterinarian: 41% of cat owners visit their veterinarians only for vaccinations, 39% of cat owners only take their cat to the veterinarian if their cat is sick, and 60% of cat owners report that their cat hates going to the veterinarian [2011 Bayer Healthcare, Brakke Consulting, Care Usage Study, American Pet Products Association, 2011-12 Pet Owners Survey]
Total team approach Receptionists can schedule appointments with behavior needs in mind, identify excessively anxious pets as they enter the hospital, and manage owner and pet traffic to minimize stress.
Kennel staff should be able to interpret species-specific postural signals, use humane handling techniques, and note problem behaviors that occur within the hospital.
Veterinary assistants can be trained to obtain behavioral histories, offer basic behavior advice, answer general behavior questions, and model good handling and pet interactions. Veterinary technicians or nurses can be trained to offer basic behavior counseling as instructed by the veterinarian, complete diagnostic tests requested by the doctor, and communicate the doctor’s discharge instructions to the client.
How to refer Provide timely referrals for behavior problems. Be clear to the client that referral is necessary and ensure that the behavior consultant is qualified to treat the pet. The client’s experience with any referral resource reflects on the referring veterinarian. Completion of an obedience class does not protect against behavior problems. The adverse effects of inappropriate training, especially if physical force is used, can result in significant morbidity and mortality.
50

Hospital design Consider accommodations to reduce stress: separate entrances for dogs and cats, sound-absorbing materials, towels draped over cages of frightened animals, surfaces that provide traction, large examination rooms, and taking reactive animals immediately to an examination room. Species segregation of hospitalized patients will reduce stress. Cat stress scores and urine cortisol-creatinine measurements were impacted by the extent of exposure to barking dogs. Cat enclosures should include soundproofing, natural light, elevated kennels, or perches, and hiding areas.
Psychoactive medications are in common use in many general veterinary practices, and pet parents often request these medications for their pets. Drugs with more immediate effects (event drugs) are useful for treating phobias and situational fears, such as veterinary visits and procedures.
Examples of event drugs include benzodiazepines (alprazolam, clonazepam, lorazepam), GABA analogues (gabapentin), direct-acting alpha-2 adrenergic agonists (clonidine, dexmedetomidine, Sileo), neuroleptic agents (acepromazine), and serotonin modulators (trazodone). Benzodiazepines should be used with caution, if at all, in cats, due to the rare occurrence of fatal hepatic necrosis, and the more common side effects of hyper-agitation and hyperphagia. Benzodiazepines and acepromazine can also cause idiosyncratic aggressive reactions.
Direct-acting alpha-2 adrenergic agonists Clonidine and dexmedetomidine are centrally acting sympatholytic agents with specificity toward presynaptic α2 receptors in the vasomotor center in the brainstem and locus ceruleus. They inhibit the release of norepinephrine and decrease sympathetic tone, resulting in reduction in fear and panic responses. Clonidine indications include treatment of fear or anxiety,1 adjunctive treatment of pain, and treatment of hypertension and glaucoma. Dexmedetomidine is approved for the treatment of noise aversion in dogs.
Clonidine is rapidly and almost completely absorbed after oral administration and reaches peak plasma level within one hour. The CNS effects of clonidine may be potentiated by benzodiazepines. At recommended doses, clonidine can be used for anxiolysis, but higher doses can increase anxiety via nonspecific activation of alpha-1-receptors. As an analgesic, clonidine may be synergistic with opioids.
Adverse events may include dry mouth, constipation, sedation, hypotension, and bradycardia. Clonidine should be used with caution with cardiovascular or renal disease and should not be used in combination with other antihypertensive drugs, beta-adrenergic blocking agents, or CNS depressants.
Clonidine Doses
• Dog: 0.01 – 0.05 mg/kg PO prn (or q12hrs) Dexmedetomidine oromucosal gel (Sileo)
• Dog: 125 mcg/m2 transmucosal
Gamma amino butyric acid analogues
Gabapentin is a structural analogue of GABA (gamma amino butyric acid), but does not alter GABA binding, reuptake, or degradation, and does not serve as a GABA-agonist in vivo. Instead, gabapentin binds to the alpha-2- delta-1 subunit of presynaptic voltage-gated calcium channels. It inhibits calcium influx by way of these channels and inhibits release of excitatory neurotransmitters (substance P, glutamate, norepinephrine) from primary afferent nerve fibers. Gabapentin has also been used as adjunctive therapy for pain, refractory seizures and for the treatment of anxiety.
Adverse events may include mild sedation or ataxia. Withdrawal-associated seizures are also possible. Avoid the use of gabapentin oral solution, which contains 300 mg/ml xylitol and may cause hypoglycemia and hepatotoxicity in veterinary patients. Potential drug interactions include antacids, hydrocodone, and morphine. In humans, gabapentin and pregabalin are not metabolized, but rather excreted unchanged in the urine.
Gabapentin can be used as event medication or as a maintenance medication. It is often a useful adjunctive maintenance medication for treatment of anxiety and arousal-related behaviors. It has also been used successfully
51
for sedation and control of intractable cats at a dose of 100-150 mg per cat. The event dose for dogs is 20-30 mg/kg, and the maintenance dose for dogs is 10 – 20 mg/kg bid. The maintenance dose for cats is 3 – 10 mg/kg bid.
Pregabalin, another GABA-analogue, has been used to treat partial-onset (focal) seizure disorders, neuropathic pain, diabetic neuropathy, and anxiety. In human patients, pregabalin has a higher oral bioavailability and longer half-life than gabapentin. Pregabalin is suspected to be a more potent anticonvulsant and anti-nociceptive agent based on experimental studies in rodents and clinical trials in humans. Pregabalin is a Schedule V controlled substance.
Benzodiazepines
Benzodiazepines potentiate binding of gamma amino butyric acid (GABA) at GABAA receptors and enhance GABAergic transmission. GABA is the major inhibitory neurotransmitter of the central nervous system, and regulates vigilance, anxiety, muscle tension, epileptogenic activity, and memory functions. Side effects of benzodiazepines may include sedation, muscle relaxation, hyperphagia, behavioral disinhibition, ataxia, tolerance, and acute hepatic necrosis (cats). Sudden termination of treatment with a benzodiazepine can result in rebound. Benzodiazepines are used routinely for acute management of situational anxiety, fear without aggression, and phobias, and as adjunctive treatment in combination with maintenance anxiety drugs.
Alprazolam
• Dog: 0.01 – 0.1 mg/kg PO prn • Cat: 0.125 - 0.25 mg/cat PO prn
Clonazepam • Dog: 0.05 – 0.2 mg/kg PO prn
Lorazepam • Dog: 0.02 – 0.2 mg/kg PO prn • Cat: 0.125 mg – 0.25 mg/cat prn
Serotonin Antagonist Reuptake Inhibitor, Phenylpiperazines
Trazodone is classified as a SARI, with actions that include serotonin 2 (5HT2A) antagonism, mild serotonin reuptake inhibition, alpha-1 adrenergic antagonism, and antihistaminic properties. Trazodone is most appropriately used to provide sedation and decrease anxiety during stressful events, such as thunderstorms or veterinary visits. Timing of onset is 30 – 60 minutes, with peak effects around 2 hours. The dose of trazodone for dogs ranges from 5.0 – 10.0 mg/kg PO prn up to q8 hours.
Pre-veterinary visit protocols o Trazodone (5 – 10 mg/kg, PO, 2 hours before travel/arrival) -- OR-- o Clonidine (0.02 mg/kg, PO, 1-2 hours before appointment) – OR -- o Dexmedetomidine (Sileo) (10 – 25 micrograms/kg, oral transmucosal, 20 min before visit), PLUS o Gabapentin (20-30 mg/kg, PO, 2 – 3 hours before travel/arrival)
o Trials at home are recommended to determine appropriate dose and which medications will produce adequate anxiety control and sedation.
o If these are insufficient, you can add transmucosal (OTM) acepromazine:
o Acepromazine (0.01 – 0.05 mg/kg), given via oral transmucosal route o Use your 10 mg/mL injectable formulation but give oral transmucosally o Give 20 minutes prior to procedure o Small volumes can be diluted with 0.9% saline for easier administration
A direct-acting alpha-2 adrenergic agonist (dexmedetomidine, Sileo, clonidine, guanfacine) is an option for pre- veterinary visit anxiety control. Some dogs will respond better to trazodone, while others will benefit more from the alpha-2 agonist. The disadvantage of using an alpha-2-agonist is that if the oral medications are not sufficient, you will not be able to use additional alpha-2-agonists (dexmedetomidine) for injectable sedation.
52

Higher doses of alpha-2-agonists can increase anxiety via nonspecific activation of alpha-1-receptors. Therefore, combining two different alpha-2 agonists is not desirable and may result in increased anxiety. If you do not anticipate needing to use injectable dexmedetomidine, then clonidine is fine, and can be combined with the other event medication if needed.
Additional options
o Phenobarbital (2-10 mg/kg dose PO, 2 hours prior to travel)
o A trial at home is recommended to determine appropriate dose and if this medication will produce adequate sedation
o Add gabapentin, 20 mg/kg, if needed OR
o Oral transmucosal dexmedetomidine or detomidine
o Doses range from 10-40 mcg/kg o 20 – 60 minutes to onset o Plus, opioid (hydromorphone, morphine) in buccal pouch o If the dog swallows some of the dose results are less predictable o Premedication with oral Cerenia at 8 mg/kg to avoid nausea
Additional Reading Bennett, K, Egger, C. Top five tips for sedation and anesthesia in fractious dogs. Clinician’s Brief, November 2018. Costa, RS, Karas, AZ, Borns-Weil, S. 2019. Chill protocol to manage aggressive and fearful dogs. Clinician’s Brief. Crowell-Davis, Seibert, Sung, et. al, 2003. Use of clomipramine, alprazolam, and behavior modification for treatment of storm phobia in dogs. JAVMA 222(6):744-751.
Ogata, Dodman, 2011. The use of clonidine in the treatment of fear-based behavior problems in dogs: An open trial. Journal of Veterinary Behavior 6,130-137.
53

Keeping the Peace in Multi-Cat Households Lynne M. Seibert, DVM, MS, PhD, DACVB
Veterinary Behavior Consultants LLC Lawrenceville, GA USA
The most common reasons for cat owners to seek assistance for a behavior problem are elimination outside the litter box, aggression between cats in the household, human-directed aggression, and destructive behavior. Intercat aggression is reported more frequently than human-directed aggression.
Feline social behavior and communication Cats are facultatively social, such that their degree of sociality in natural situations depends mainly on the distribution of resources. They can form stable bonds with other members of the colony. Free-living feral cats form matrilineal social groups and tend to be impermeable to new adult cats and solitary males. A housecat must tolerate close contact of other cats to live in a multi-cat household without displaying aggression. House cats are reported to engage in ‘time-sharing’, a phenomenon in which favorite areas are occupied in a temporal sequence, as well as physical sharing of an area.
Cats communicate with visual, auditory, and olfactory signals. Head rubbing results in deposition of scent from perioral glands, submandibular glands, and temporal glands. Scratching also results in release of olfactory cues from interdigital glands, as well as leaving a visual mark behind. Both male and female cats can mark with urine, although it is more common for males to spray urine than females. All forms of marking may become more frequent in situations where there are multiple cats housed in a limited area, or if there is social stress present.
Behavior problems can result from environments that are not compatible with cats’ needs. Environmental enrichment should provide sufficient outlets for species-typical behaviors, including playing, scratching, climbing, rest, and exploration.
Scratching Functions of scratching include nail grooming, muscle stretching, and marking territory. Use of designated scratching posts can be encouraged by providing posts with desirable surfaces, placed near resting areas, and using positive reinforcement for use of the posts.
Preferred textures include rope or woven sisal, loose pile carpet, cardboard, smooth wood, or non-toxic branches. Both vertical and horizontal scratching surfaces should be provided. Encouraging cats to scratch appropriate surfaces will help minimize undesirable damage to a home. Encouraging cats to mark surfaces with facial or interdigital scents may also minimize other forms of marking, such as scratching or urine marking.
Litter boxes Conflicts near litter boxes can result in avoidance of the litter box location or the litter box itself. Therefore, placement of litter boxes is especially important in multi-cat households. Boxes should be large, open, and positioned to avoid trapping a vulnerable cat. There is no established number of required litter boxes, but there should be enough locations to avoid competitive conflicts near the box.
Aggression between cats Frequent causes of inter-cat social stress or aggression are the introduction of a new cat to the household, fear or redirected aggression following a stressful incident, play aggression, status-related aggression, and medical conditions. For pairs of cats, the longer they have been together, the less overt aggression occurs. This is consistent with the formation of stable relationships which rely on agonistic signaling, rather than overt aggression. Introduction of a new cat should always be done gradually and combined with rewards for friendly behavior. The environment should meet the needs of the cats with provision of adequate resources that are accessible for all cats. Scent exchange between the cats can also help facilitate introductions.
54
In a retrospective study of 48 cases of intercat aggression, 30 cases were considered cured, and 18 were not cured. Male cats initiated aggression in more cases than did female cats; the aggression was equally likely to be directed toward a same sex or opposite sex victim. In most cases, there was clearly one aggressor and one victim.1
To identify the incidence of intercat aggression (scratching and/or biting) when a new cat is introduced into a household, a survey was mailed to individuals who adopted a cat from a local animal shelter.2
Among households with multiple cats, half (61/123) reported initial fighting between cats when the new cat was introduced. Number of cats in the household, age or gender of the adopted cat, age or gender of the original cats, or size of residence were not significantly associated with fighting at initial introduction.
Forty-four percent of people introduced the new cat into the home by simply putting the cats together immediately. Twenty-two percent of people kept the cats separated for a few days, and then put the cats together. Thirty-three percent of people kept the cats separated and gradually introduced the cats to each other, but the length of a gradual introduction varied among households from hours to weeks. Owners were asked how long it took for the new cat to be accepted by the original cat(s) in the household. Twenty-two percent of owners reported that the original cat(s) accepted the adopted cat immediately, 40% reported that acceptance occurred in less than one month, and 9% reported that the original cat(s) had not yet accepted the adopted cat.
Thirty-five percent of multi-cat households reported ongoing fighting 2–12 months after initial introductions. Neither age, sex, nor number of cats in the household was associated with ongoing fighting. Households in which any of the cats had outdoor access had significantly more fighting than households in which the cats remained strictly indoors (p = 0.03). Households where the initial meeting was perceived to be unfriendly/aggressive were more likely to have ongoing fighting (p = 0.003).
Status-related aggression
This problem can occur with cats that have previously established a relationship. The onset of aggression may have an identified event, such as illness of one of the cats, or addition of a new cat that disrupts the social order. The aggressor chases, growls, and attacks other cat or cats, while showing assertive postures, and may also control many of the resources, limiting the other cats’ access to the litter box or preferred resting spaces.
Treatment will require the owner to supervise interactions between the cats and intervene early in the event of escalating aggressive challenges, provide additional resources that subordinate cats can access, and possibly the use of medication. Selective serotonin reuptake inhibitors have been used in the management of assertive behavior in cats.
Fear and redirected aggression
A cat that hisses and growls at other cats when they come near while displaying signs of fear (ears back, tails tucked, crouching) is showing fear aggression. Fear aggression can occur between cats that have historically gotten along well together because of classical conditioning. Fear-related problems are best addressed using desensitization and counter-conditioning techniques, and possibly medication.
Play aggression
Play naturally involves elements of predation. Play aggression occurs when play becomes too rambunctious or causes injuries or distress. When cats have different play styles or energy levels, interventions may be needed. Pet parents can direct play time for younger, more energetic cats, or provide interactive toys.
General treatment recommendations Resources, particularly litter boxes, should be dispersed throughout the home, with particular attention to accommodating any submissive or fearful cats. Increasing vertical space will essentially increase the square footage for the cats’ use in crowded households. Resources should be distributed throughout the home to avoid competition.
55

Unfriendly cats should be physically separated when they cannot be supervised, and then gradually reintroduced. Gradual introductions Regardless of the cause of aggression, gradual introductions are always appropriate for cats that are unfriendly toward each other. Cats should never be left to ‘fight it out.’ Separate cats using a physical barrier, such as double- stacked pet gates, a screen, or a cracked door. Encourage the cats to play with each other under the door, or through the gates. Rotate the cats daily so that one cat is confined while the other has free access to the house. Provide each cat with food, water and a litter box, and individualized attention.
Place food dishes at a distance from the barrier that is acceptable for both cats (both cats will freely approach the food dish and eat without concern or stress). Each day, move both dishes several inches closer to the barrier. Once each cat can eat special treats on either side of the barrier without aggression or fear of the other cat, supervised interactions can proceed.
For supervised interactions, each cat should have a handler, and each cat should be engaged in a pleasant activity at a comfortable distance from each other. If both cats remain calm, the distance can be decreased gradually over several sessions. New cat introductions may require weeks to months.
References 1. Lindell EM, Erb HN, Houpt KA. 1997. Intercat aggression: a retrospective study examining types of
aggression, sexes of fighting pairs, and effectiveness of treatment. Appl Anim Behav Sci 55:153-162. 2. Levine E, Perry P, Scarlett J, Houpt KA. 2005. Intercat aggression in households following the introduction of a
new cat. Appl Anim Behav Sci 90:325–336.
56

Intraoral Imaging and Oral Surgery Barron P. Hall, DVM, Dipl. AVDC, FAVD, ZWD
Reasons for intraoral images: patient is having a dental procedure, missing teeth, fractured teeth, extra (supernumerary) teeth, discolored teeth, tooth resorption, pre-extraction, post-extraction, oral mass, epistaxis, halitosis, facial swelling, nasal discharge, gum recession, mobile teeth, oral inflammation, history of oral pain, jaws not aligned, medical records, evaluation of previous disease and treatment, client education, worn teeth, and displaced teeth to name a few. If you are providing any type of dental care, intraoral imaging is essential! You cannot treat what you cannot see and skull films do very little if anything to diagnose dental/oral problems. In order to obtain intraoral images the patient needs to be under general anesthesia, you need an x-ray source, and something to catch the x-rays. These images may be direct radiography (DR), Computed radiography (CR), or dental film. Many veterinarians use a DR system (Sopix 2 {Dental Focus}, Schick, Progeny {Midmark}). This type of system is fast and allows you to use less radiation than film (lower exposure times), however you are limited to a Size 2 or Size 1 sensor. If you are slightly computer literate, the programs are easy to use, images can be manipulated, easily shared, and storage takes up very little room physically, but lots of computer storage. CR uses phosphor plates in various sizes (0-4 and some special ones for exotics) to capture the images (CR 7 Vet {iM3}, Scan-X). It is not quite as fast as DR. The plates are inexpensive to replace and the images can be manipulated, shared, and stored on a computer. Dental film can be used. It comes in various sizes (0-4) and speeds (D, E, I). The amount of x-rays (mA) required and the exposure time (s) is based on the area being imaged and the speed of the film. Higher speed film requires less radiation. Film does need to be developed which can be done in a chairside darkroom or with an automatic processor that is made for dental film. This process requires more time than with DR or CR, the images cannot be manipulated, film must be developed and fixed properly, and the films need to be stored. One must take the time to learn normal oral/dental anatomy, how to take diagnostic images, and interpret them. This will only come from understanding of the basic techniques, taking dental radiology labs, and continued practice. An intraoral image is a two dimensional interpretation of a three dimensional structure. Without knowing what normal is, both radiographic artifacts and normal anatomy can be misinterpreted as pathology. Pathology stays with the tooth, artifacts go away, and normal anatomy moves independently from the tooth. These images combined with the oral exam findings will help lead you to a diagnosis. Once we have a diagnosis, then we can formulate a treatment plan. Dental terminology: Mesial – towards the midline (if the teeth were placed in a line instead of an arch) Distal – away from the midline (if the teeth were placed in a line instead of an arch) Labial – toward the lips (rostral teeth – incisors and canines) Buccal – toward the cheeks Facial – toward the cheeks or lips Palatal – toward the palate (maxilla) Lingual – toward the tongue (mandible) Coronal – toward the crown Apical – toward the root (apex) References: DuPont, GA, DeBowes, LJ. Atlas of Dental Radiography in Dogs and Cats. St. Louis (MO): Saunders; 2009 Coffman, CR, Brigdon, GM. Oral and Dental Imaging Equipment and Techniques for Small Animals. In: Holmstrom, SE, editor. Veterinary Clinics of North America: Small Animal Practice. May 2013 edition (43:3). Philadelphia (PA): Elsevier; 2013: 489-506.
57

Lemmons, M. Clinical Feline Dental Radiography. In: Holmstrom, SE, editor. Veterinary Clinics of North America: Small Animal Practice. May 2013 edition (43:3). Philadelphia (PA): Elsevier; 2013: 533-54. Bellows, J. Feline Dentistry Oral Assessment, Treatment, and Preventative Care. Ames (IA): Blackwell Publishing; 2010: 39-83.
58

Case Talk: What Would You Do? Barron P. Hall, DVM, Diplomate AVDC, FAVD, ZWD
Oncology Squamous cell carcinomas (SCC), while being the most common oral tumor in the feline, are the second most common oral tumor in the canine. SCC’s are usually found in medium to large breed dogs 7-9 years of age with no sexual predilection. There are two distinct forms that have been described: non-tonsillar and tonsillar. The prognosis and nature of these two forms is different. The non-tonsillar form is relatively slow growing and slow to metastasize, although it is locally invasive. This form tends to be found in the gingiva of the rostral oral cavity, but may also be found on the lips, hard or soft palate, buccal mucosa, or tongue. Its nature and rostral location provides for a better prognosis as they are commonly found sooner than those located in the caudal oral cavity. The tonsillar form is the most aggressive form. A large majority of this form (~98%) will metastasize early to regional lymph nodes, while almost 2/3 will have associated distant metastasis. The prognosis for this form is “grave”. The initial treatment of choice for SCC’s is primary surgical resection. CT scans are encouraged pre-operatively to better identify tumor margins and facilitate complete surgical excision. In my experience, incompletely excised SCC’s become very upset and return with a vengeance. Also in my experience, if the SCC is completely excised, no regional nor distant metastasis, and the histopathologic margins are “clean” the long term prognosis is “excellent”. I always encourage intraoral radiographs and incisional biopsies with a histopathologic diagnosis before deciding exactly what an oral mass is and how it should be treated. The four cases I will present involve four canine non-tonsillar oral SCC cases in four different breeds, three different locations, three different treatment options by the referring veterinarians, and two different out comes.
The mandible is made up of mirrored left and right halves that are firmly united rostrally at the intermandibular joint, known as the mandibular symphysis. This fibrous joint is a synchondrosis. The body of the mandible is the portion that contains eleven teeth. The mandibular canal lies within body of the mandible containing the neurovascular structures supplying the mandibular bone, teeth, and soft tissues. The ramus of the mandible is the distal portion that does not contain any teeth. The neurovascular complex enters through the mandibular foramen located on the lingual aspect of the caudoventral mandible. Its dorsal extent is the coronoid process and its most distal extent is the condyloid process. The condyloid process is part of the temporomandibular joint, a synovial joint. A thin articular disc within a loose joint capsule completely divides the joint cavity into dorsal and ventral compartments separating the articular cartilage covered surfaces of the condyloid process and the fossa of the temporal bone. ORTHOPEDICS In order to repair a fracture and stabilize the segments, forces placed on the bone need to be mitigated. The muscles of mastication place a variety of forces on the mandible. These forces may help or hinder fracture repair, so these muscles should be understood. There are five muscles of mastication. The four used to open the mouth are innervated by the trigeminal nerve, while the two bellied muscle used to open the mouth is innervated by both the trigeminal and facial nerves. The masseter muscle originates from the ventral border of the zygomatic arch extending caudolaterally to insert on the ventrolateral surface of the mandible (masseteric fossa) with some fibers extending around the ventral and caudal border to insert on its ventromedial surface. The temporalis muscle is the largest and strongest of these muscles. It originates primarily from the parietal bone and to a lesser extent from the temporal, frontal, and occipital bones. The muscle lies within the temporal fossa as fibers extend dorsally and ventrally beneath the zygomatic arch to insert on the coronoid process with some fibers reaching the ventral margin of the masseteric fossa were
59

they blend with the masseter muscle. On the medial aspect of the mandible they blend with the pterygoid muscles. The lateral pterygoid muscle is smaller and shorter than the medial pterygoid muscle. It originates from a small fossa on the sphenoid bone extending ventrolaterally and slightly caudal to insert on the medial aspect of the mandibular condyle just ventral to its articular surface. The medial pterygoid muscle originates from the lateral surface of the pterygoid, palatine, and sphenoid bones extend caudolaterally to insert on the medial and caudal surface of the angular process of the mandible. The digastricus muscle is the only muscle of mastication used to open the mouth. It originates from the paracondylar process of the occiput extending rostrally to attach on the ventral border of the mandible. The muscle appears to be a single bellied muscle, but a tendinous intersection divides the muscle into a rostral (trigeminal) and caudal belly (facial) with their own innervation. As with other orthopedic injuries, mandibular fracture repair can be very rewarding or very frustrating. There are usually more than one option for fracture stabilization based on your training and the equipment you have. The way you approach a fracture can vary on the way that you were trained. Those trained from the dental/oral surgery side usually opt for intraoral fixation using the teeth, wires, composite, and acrylic. Those surgically trained are more likely to use an extraoral approach with IM pins, External Skeletal Fixation (EXF), or plates and screws. There are multiple factors that need to be considered when planning on how to repair a fracture: patient, fracture, owner, and veterinarian. 1. The patient’s age, breed, neutered or not, size, skull type, dentition, oral health, overall health,
and other health issues all need to be considered. 2. How did the fracture occur? Is the dentition involved? What is the periodontal health? Was the
fracture pathologic? What is the bone health? Is there bone missing? Bilateral or unilateral? 3. What can the owner afford? What are the owner’s expectations? Do they comprehend their part
in this multiple week process? Where will the pet recuperate? Are there other pets in the home? Will the pet be left alone?
4. This may be the most difficult. You need to be honest with yourself and your client. Are you qualified? What advanced training have you had in the various methods of fracture repair? How mandibular many fracture repairs have you done? What equipment do you have? What is your comfort level with all of the above? ***Education:Equipment:Experience
A salvage procedure would be some type of mandibulectomy. This type of procedure is indicated when the fracture cannot be repaired or is a non-union. Based on answers to the above questions a salvage procedure may be the best option for all parties involved.
60

Communicating with Clients Regarding Oral Health Barron P. Hall, DVM, Diplomate, American Veterinary Dental College, FAVD, ZWD
Animal Dental Clinic Vienna, VA
Oral Exam A thorough oral examination is a vital part of every patient’s physical exam…every time. This includes puppies and kittens. The more you do, the better you will become. I was taught during veterinary school to be able to recognize “normal” on a physical exam. Once you have a grasp on normal, then you can better identify “abnormal”, even if you do not know what the pathologic process is. This methodology can be applied to the oral cavity, too; unfortunately none of us were taught normal in veterinary school. There are great changes in the size of animals during their first year of life. The oral cavity probably undergoes some of the greatest changes over this time period and should be monitored closely and regularly. From the beginning during the first puppy and kitten exam, the importance of good oral and dental health needs to be conveyed to the owners. This education and encouragement should be continued throughout the patient’s life. Oral healthcare is WIN - WIN – WIN! Embryology: Face, Head, Mouth, and Tooth DevelopmentThe face, head, and mouth develop from the first, second, and third branchial arches. The jaws (gnathostomata) are formed by modification of the first branchial arch. The primary palate, rostral maxilla, and the middle portion of the upper lip are formed by the fusion of the frontonasal process with both sides of the medial nasal processes. The merging of the two nasal processes forms the incisive bone, which contains the maxillary incisors. (NOTE: The anatomic term “premaxilla” is often misused in dogs and cats. This term should only be used with human and non-human primates.) The secondary palate is formed by the extension of each of the maxillary processes as palatine shelves towards the midline where they join with the downward growth of the nasal septum from the frontonasal process. This completes the separation of the oral and nasal cavities. The paired mandibles are formed from the ventral portion of the cartilage of the first arch extending to the midline where they are separated by a thin band of mesenchyme. The mandibles and maxilla grow independently of one another. Around the 25th day of embryonic development a thickening of the embryonic oral epithelium called the dental lamina forms two U-shaped structures that will give rise to the maxillary and mandibular dental arches. The ectoderm gives rise to the dental lamina, oral epithelium, and enamel organ. The dental papilla and dental sac are mesodermal in origin. Tooth development begins with the development of the enamel organ in 3 stages: bud, cap, and bell. The bud stage begins when the primary (baby) tooth bud comes off from the dental lamina. These primary buds give off lingual/palatal extensions referred to as successional lamina which will develop through their own bud, cap, and bell stage, giving rise to the secondary (adult) dentition. There are always more secondary teeth than primary teeth, so the nonsuccessional (adult teeth that did not come from a primary tooth) teeth will come directly from the dentinal lamina. The cap stage begins as a concavity and begins to form on the deepest aspect of the bud. As the concavity becomes much longer and thinner and the three parts of the enamel organ develop a fourth layer, the bell stage begins. This is the time amelogenesis (formation of enamel) and dentinogenesis (formation of dentin) begins. The mesenchymal cells surrounded by the extending enamel organ are the dental papilla. Those mesenchymal cells that surround the enamel organ are termed the dental follicle or dental sac. The mesodermal cells of the dental papilla form the dentin and pulp tissues, while the dental sac gives rise to cementum, periodontal ligament (PDL), and some alveolar bone. The formation of the root takes place after the form of the crown has developed. Sharpey’s fibers extend from the PDL attaching to the alveolar bone and the hard bone-like substance, cementum, that covers the root surface. Young secondary teeth are very thin walled and the apicies (root ends) are wide open, making these teeth impossible to perform a standard root canal on and more difficult to extract. The dentin layer that the tooth has prior to eruption is termed primary dentin and all of the dentin formed after eruption is termed secondary dentin. The secondary dentin is formed due to stresses placed on the teeth by masticating (chewing). As the tooth matures its dentinal
61

walls become thicker, the root will finish developing and the apex will close (~11-15 months of age), creating an apical foramen. Tooth Eruption The movement of the tooth into the oral cavity is termed tooth eruption. This occurs in three stages: preeruptive, eruptive/prefunctional, and posteruptive/functional. Preeruptive stage occurs as the crown is developing, which gives rise to the eruptive stage as the root begins to develop, and culminates with the functional stage when the teeth move into actual occlusion. It is quite common to see pericoronitis (normal gingival inflammation around the tooth during eruption). We do not fully understand why teeth erupt; however, there are four major theories for tooth eruption: root growth, pulpal tissue growth, bone deposition in alveolar crypt, and PDL force. Although the exact mechanism is not understood, the most plausible hypothesis is that the PDL’s driving force pushes the teeth into the oral cavity and maintains their occlusal contact. Eruption times can be quite varied due to the size of the breed and characteristics within that breed (ex. Tibetan terriers are slow to lose primary teeth). The exfoliation, or loss of the primary tooth, is believed to be caused by the developing secondary tooth bud causing resorption of the primary tooth root as it grows. Once enough root structure and support has been lost the crown and any remaining root will be shed. Dental Formulas: Canine, primary: 2 x (i 3/3 , c 1/1 , p 3/3) = 28 Canine, secondary: 2 x (I 3/3, C 1/1, P 4/4, M 2/3) = 42 Feline, primary: 2 x (i 3/3, c 1/1, p 3/2) = 26 Feline, secondary: 2 x (I 3/3, C 1/1, P 3/2, M 1/1) = 30 Eruption Times: Canine, primary (wks.): i 3-4, c 3, p 4-12 Canine, secondary (mos.): I 3-5, C 4-6, P 4-6, M 5-7 Feline, primary (wks.): i 2-3, c, 3-4, p 3-6 Feline, secondary (mos.): I 3-4, C 4-5, P 4-6, M 4-5 Pediatric Dental/Oral Problems Retained Primary Teeth RULE: You NEVER want two of the same type of tooth (primary and secondary) occupying the same spot at the same time. Retained primary teeth are most commonly found in toy breed dogs. These retained teeth predispose that area to premature periodontal disease and potential malocclusion due to abnormal eruption position of the secondary tooth before the primary tooth exfoliates.
NEEDED: Intraoral radiographs (before and after extraction), knowledge of pediatric oral anatomy, local anesthesia, small elevators, magnification and light, excellent extraction technique, adequate time, and patience Lingually Displaced Mandibular Canine Teeth Need treatment, usually seen with Class II Malocclusion (MAL 2) (short lower jaw), DO NOT just cut teeth! The sooner the primary teeth are extracted the better the chance of the mandible to grow to its genetic potential. Breeds: Standard poodle, Basset hound OPTIONS: Primary teeth – extraction, crown reduction (CAM) AND vital pulpotomy (VP) with direct pulp capping (PCD), orthodontics***inform owners that other dental procedures: endodontics +/- orthodontics +/- exodontics; will likely be needed as secondary mandibular canine teeth erupt
62
Secondary teeth – based on the occlusion: CAM AND VP with PCD +/- orthodontics +/- exodontics Fractured tooth with pulp exposure or discolored tooth (pink => black) “Do nothing” is NOT an option! Fractured teeth ARE painful. Oral bacteria will move through the pulp cavity of the fractured primary tooth and may adversely affect the developing secondary tooth bud. OPTIONS: Primary teeth – extraction Secondary teeth – VP/PCD within 48 hours of fracture, extraction, endodontics: apexification (APX) which will require multiple treatments for 3-6 months, then standard root canal therapy Jaw Fractures Puppy and kitten mandibles are primarily cartilage while they are developing. They will NOT hold screws and plates. When considering how to repair these fractures, the fact that we are dealing with young animals is positive in that they will heal in a relatively short period of time. The down side of these types of fractures is that these patients are growing, both the bone and the teeth. Many points must be considered when selecting methods of mandibular/maxillary fracture repair, however in many of these pediatric cases a tape muzzle may be the best and most practical choice. Any young animal that is bitten in the face/muzzle by a larger one requires time to thoroughly examine the wounds, including intraoral radiographic evaluation. There may be MUCH more going on than a small hole in the gingiva.
Electric Cord Trauma (electrocution) Puppies are known for chewing and they are no match for electricity. Emergency care for respiratory distress, especially pulmonary edema, is primary. Once the patient is stable, the oral cavity can be evaluated. Heat damage to the oral tissues can be seen in the tongue, palate, gingiva, and lips. Do not be in a hurry to rush in and debride charred tissues. It will take about 7-14 days for the soft tissues to show the full extent of the damage. Necrotic bone, if present, will need to be removed. Intraoral radiographs are needed to assess tooth damage. The electricity may cause bone or tooth death, so these patients need to be monitored closely while the secondary tooth erupt and jaw grows. If a tooth fails to erupt, intraoral radiographs are needed to evaluate the area to see if the secondary tooth is present and needs to be extracted or if the tooth has been resorbed.
Impacted Teeth Don’t confuse this with delayed eruption, commonly seen in Tibetan terriers and toy breed dogs. Impacted teeth may be fully or partially covered by soft tissue or bone. The thick soft tissue covering impacted teeth is termed an operculum. This tissue needs to be removed (operculectomy) using a scalpel, bur, radiosurgery unit, or laser. Be careful of damaging the tooth with the bur or excessive heat from the radiosurgery unit If teeth are not present, intraoral radiographs ARE NEEDED in order to determine if there is no tooth or if the tooth is impacted. Knowing if teeth are present or not is not only important for breeders, but impacted teeth can end up causing pathologic problems. The most common problem with an impacted tooth is a dentigerous cyst. This problem is more common in brachycephalic breeds. They are seen radiographically as a distinct radiolucent area surrounding the impacted crown. Caused by the dilation of the follicular space around the impacted crown, these cysts can be very invasive as they expand into surrounding tissues and destroy bone. They must be removed with thorough, aggressive surgery and curettage, including complete removal of the cyst lining. Histopathology will confirm the diagnosis. Boxers are known to have supernumerary (SN) (extra teeth) incisors and 1st premolars. This is of importance if a soft tissue swelling is noticed distal to the canine teeth, even if a 1st premolar is seen, as there could be a dentigerous cyst around an impacted SN 1st premolar.
63
Tooth Abnormalities Geminal tooth is a tooth where the tooth bud tried to divide and form a twin tooth, but never completely divided. The tooth appears to be slightly larger with a vertical cleft in the middle. There is still the normal number of teeth. Twinning happens when the original tooth bud completely divides allowing an identical tooth to form. There will be an increased number of teeth. Fusion tooth occurs when two tooth buds are joined at the crown. There is a decreased number of teeth. Concrescence occurs with the fusion of cementum between two teeth. Dilaceration of the root or crown is seen as bent or crooked structure from developmental causes. Dilacerated roots can be seen with intraoral radiographs of toy breed - especially brachycephalic - dog’s mandibular first molars where the roots are pointing towards each other. These teeth usually need to be extracted when discovered; hopefully this is before there is advanced periodontal disease, bone loss, fistulated tract, and/or pathologic fracture of the mandible. Palatal Clefts The palate, both hard and soft, separates the oral cavity from the nasal cavity. Non-traumatic clefts are failures in the development of the face and palate. Clefts can be unilateral or bilateral. Primary clefts are cleft lips and are formed along the incisivomaxillary suture lines. Secondary clefts are a failure of the medially extending palatine shelves to meet on the midline with the ventrally projecting nasal septum. Depending on the extent of the cleft, these may need to be surgically repaired. There are numerous techniques for repair based on the type and location of the cleft. A thorough knowledge of oral anatomy and oral surgery should be understood before attempting to repair these defects. This type of surgery is not for the casual surgeon. These surgeries can even be challenging for those veterinarians with some advanced oral surgical training. Tongue Disorders Microglossia (“bird tongue”) is an uncommon and lethal defect of the tongue. It is unlikely to be the primary complaint that a puppy is presented for. A newborn puppy shows an inability to nurse or no interest in nursing. These are sad cases that usually have other musculoskeletal, neurological, or ophthalmologic disorders termed “Fading Puppy Syndrome”. Typically these patients die or are euthanized. Inability or difficulty in nursing can also be caused by a short lingual frenulum. This can be surgically corrected to allow the puppy to have better use of its tongue. Lip Disorders Tight lip syndrome is a condition most commonly seen in Shar-peis where the lip can curl over the rostral mandible and lower incisors, interfering with occlusion, and inhibiting mandibular growth. Surgery is required to create a vestibule and release the tension on the rostral mandible. Equipment Intraoral radiographs are ESSENTIAL for the proper diagnosis and assessment of most oral pathology. Intraoral radiographs are legal documents and are excellent for marketing. As equipment goes, dental radiograph units are relatively inexpensive and the learning curve relatively small. The unit will pay for itself within a year if it is used. It will allow you to make better treatment decisions. Puppies and kittens are small; therefore you MUST have instruments and suture that are of appropriate size. Large elevators and extraction forceps are more likely to cause damage. You need to use finesse, not force, and have the appropriate amount of time to work on these patients. Although their neurological systems are developing they can still feel pain - remember to use appropriate multimodal pain management: pre-, intra-, and post-op.
Records Appropriate dental charts are essential for oral care, including use of appropriate abbreviations. Advise owners of your education, training, equipment, and abilities; either good or bad and do not be afraid to refer them if you feel it
64

is in the patient’s best interest. To the best of your abilities, make them aware of the good, the bad, and the ugly that may occur, while DOCUMENTING EVERYTHING!
65

Diagnostic and Management Strategies for Hypoadrenocorticism in Dogs Jana Gordon, DVM, DACVIM
Introduction
The adrenal glands are composed of an outer cortex and inner medulla. The outer cortex produces steroid hormones and the inner medulla produces catecholamines. The outer cortex is composed of three layers or zones: the outermost zona glomerulosa, the middle zona fasciculata and the inner zona reticularis. The zona glomerulosa produces the mineralocorticoid, aldosterone. The zona fasciculata produces the glucocorticoid, cortisol. The inner zona reticularis produces some cortisol and androgens such as testosterone, estradiol and progesterone.
Etiopathogenesis
Normally, neural stimulation of the hypothalamus produces corticotropin-releasing hormone (CRH). Corticotropin-releasing hormone stimulates the release of adrenocorticotropic hormone (ACTH) from the anterior pituitary. ACTH exerts its effects on the adrenal cortex and stimulates the zona fasciculata to release cortisol, the zona glomerulosa to release mineralocorticoids and the zona reticularis to release androgens. ACTH’s primarily effects are on cortisol release with minimal effects on mineralocorticoid and androgen production. Cortisol provides negative feedback to ACTH and CRH. Glucocorticoids are involved in many normal physiologic responses in the body.
Mineralocorticoid release form the zona glomerulosa is primarily mediated by the renin angiotensin aldosterone system and only minimally by ACTH. Renin is released from the juxtaglomerular apparatus of the kidney into circulation as a result of sympathetic stimulation, hypotension, hyponatremia, and hypochloremia. Renin then converts circulating angiotensinogen to angiotensin I. Angiotensin converting enzyme, in the pulmonary vascular endothelium, converts angiotensin I to angiotensin II. Angiotensin II, as well as being a potent vasoconstrictor, stimulates aldosterone secretion from the zona glomerulosa. High potassium can also directly stimulate aldosterone production at the adrenal. Aldosterone enhances sodium (water and chloride follow) retention in the proximal and distal tubules with hydrogen ion and potassium loss in the distal tubules and collecting ducts.
Hypoadrenocorticism occurs as a result of a deficiency in glucocorticoids and, in most cases, mineralocorticoids. Some dogs will have clinical evidence of only a glucocorticoid deficiency at the time of diagnosis, few of which develop clinical evidence of mineralocorticoid deficiency at a later date.1,2 Interestingly, aldosterone measures low in dogs with isolated clinical glucocorticoid deficiency and those with both glucocorticoid and mineralocorticoid deficiency, regardless if they develop clinical mineralocorticoid deficiency at a later date.1 Atypical hyperadrenocorticism is used to describe the isolated glucocorticoid deficiency. Initial mineralocorticoid deficiency with subsequent glucocorticoid deficiency is very rare.3 Primary hypoadrenocorticism (disease of the adrenal itself) is most common and the result of destruction of the adrenal cortices. Secondary hypoadrenocorticism occurs as a result of insufficient ACTH secretion from the pituitary leading to atrophy of certain zones of the adrenal cortices with primarily a glucocorticoid deficiency.
The majority of dogs with hypoadrenocorticism have idiopathic atrophy of the adrenal cortices likely secondary to immune-mediated destruction. In humans it is commonly seen as part of an immune-mediated polyglandular syndrome. In dogs polyglandular syndromes involving hypothyroidism, diabetes mellitus and/or hypoparathyroidism have rarely been documented. Hypoadrenocorticism may also occur secondary to cortical destruction as a result of adrenolytic therapy. In addition, chronic administration of glucocorticoids leads to cortical atrophy and rapid withdrawal can lead to a form of secondary hypoadrenocorticism. Infarcts, fungus and neoplasia can infiltrate the adrenals and trauma, infarcts and neoplastic infiltration of the pituitary can occur causing secondary hypoadrenocorticism.
Hypoadrenocorticism can occur in any breed but there may be an increased incidence in certain breeds with the mode of inheritance known in some. Females are affected more frequently than males in most dogs except the breeds with predispositions in which sexes are equally affected. Dogs up to 13 years of age can be affected but the disease is more common in young adult and middle-aged dogs.
66

Clinical Presentation The history can be variable and may consist of waxing and waning lethargy, inappetence, vomiting and diarrhea that often responds to symptomatic treatment. These signs may be present for weeks to months reflecting the progressive destruction of the adrenal glands and can mimic a chronic enteropathy.4 Dogs may also present for weakness, polyuria, polydipsia, muscle wasting, regurgitation, urinary incontinence and seizures. There may be a stressful event that precipitates these episodes. A more acute presentation with anorexia, vomiting, diarrhea, melena, collapse and shock can occur. These dogs may or may not have a history of more chronic signs. Dogs may be weak (cortisol, sodium, potassium), lethargic (cortisol, sodium), exhibit muscle wasting (cortisol), and have abdominal pain (cortisol). In a more acute presentation the dog may be laterally recumbent with pale tacky mucous membranes, increased capillary refill, poor pulse quality, bradycardia (potassium), and hypothermia. Components of cardiovascular collapse are primarily due to mineralocorticoid deficiency (hypovolemia) with some contribution from glucocorticoid deficiency (vascular tone). Diagnosis Routine Laboratory Evaluation The most common finding on the CBC is a mild non-regenerative anemia (cortisol on enterocyte health & bone marrow). Studies are conflicting regarding the absence of a stress leukogram to differentiate hypoadrenocorticism from non-adrenal illness with one study saying the absence of a stress leukogram is more common with cortisol deficiency but another stating this is also found in dogs with non-adrenal illness.5,6 The classic electrolyte abnormalities are increased potassium, decreased sodium and decreased chloride. These occur due to mineralocorticoid deficiency because of a lack of aldosterone and its effects on the renal tubules. Increased BUN and creatinine are primarily prerenal secondary to dehydration but intestinal hemorrhage can cause increases in BUN. It is possible that these dogs can develop acute renal failure if their prerenal factors (hypovolemia, hypotension) are not addressed in a timely fashion or if they have underlying renal disease but this is uncommon. Liver enzymes may be normal or mildly increased likely due to poor perfusion of the liver. Hypoglycemia may also be seen with cortisol deficiency. A mild to moderate hypercalcemia (total +/- ionized) is fairly common and the exact cause unknown but does not appear to be related to parathyroid hormone or parathyroid related protein. Alterations due to increased bone resorption, an increase in intestinal absorption, decreased glomerular filtration rate and increased renal tubular reabsorption may play a role. Mild hypoalbuminemia is also seen frequently and likely due to increased losses through the intestinal tract. Hypocholesterolemia can also occur and may be due to decreased intestinal absorption of fats or decreased mobilization from tissues, both cortisol-dependent functions. A metabolic acidosis occurs secondary to decreased hydrogen ion excretion (aldosterone deficiency), poor tissue perfusion (generates lactic acid) and decreased renal excretion of acids (↓ GFR). Sodium Potassium Ratio Sodium potassium ratios have been relied upon historically to suggest mineralocorticoid deficiency. Dogs with mineralocorticoid deficiency should have low sodium and increased potassium. Many dogs do not have decreased sodium but all should have increased potassium.7 The lower the sodium potassium ratio the more likely the dog has hypoadrenocorticism. In one study of 34 dogs considered to have low sodium potassium ratios (< 24), 8 had hypoadrenocorticism.7 Of these 8, 2 had a ratio from 20 – 24, 2 had a ratio from 15 – 20 and 4 were less than 15. Interestingly, all dogs with a ratio < 15 had hypoadrenocorticism. The problem is the specificity of these ratios. Other diseases associated with low sodium potassium ratios are acute kidney injury, pancreatitis, intestinal parasitism, intestinal salmonellosis, neoplasia, pregnancy, mushroom toxicity, pyometra, pyoderma, pneumonia and diabetes mellitus.7,8,9,10 A later study looked at ratios in 37 dogs with hypoadrenocorticism and electrolyte disorders.11 As ratios decreased from 32 to 15, the sensitivity decreased (less able to identify dogs with hypoadrenocorticism) and specificity increased (easier to identify dogs without hypoadrenocorticism). ACTH Stimulation Test The ACTH stimulation test is the test recommended to diagnose this disease. A baseline cortisol is taken followed by administration of synthetic cosynotropin (250 mcg/dog or 5 mcg/kg) with a second sample obtained an hour later. Alternatively, synthetic ACTH gel is given IM followed by a blood draw at 1 and 2 hours. There should be no to
67

minimal stimulation and cortisol levels are almost always less than 2.0 µg/dl. This is usually the only test run for this disease. It appears 1 mcg/kg is equally as effective as 5 mcg/kg in screening for this disease and may help decrease costs of testing.12 Critical illness relative cortisol insufficiency (CIRCI) occurs in severely ill animals with non-adrenal illness and they typically have baseline cortisols above 2 mcg/dl, even in the normal range, but with no to minimal stimulation. Basal Cortisol Synthetic cosynotropin is typically used to perform the ACTH stimulation test in the dog. Synthetic ACTH gel can also be used. Due to the cost of cosynotropin. the ACTH stimulation test is cost prohibitive for some. Availability has also been limited at times. This is the driving force behind investigating less expensive alternatives to the traditional tests. Basal cortisol is one of these tests. It is important to note that a single baseline cortisol is inadequate for diagnosis and may be low or undetectable in normal dogs and dogs with non-adrenal illness. Studies evaluating basal cortisol in dogs with hypoadrenocorticism reported that all dogs with hypoadrenocorticism have a baseline cortisol < /= 2 but up to 37% of dogs with non-adrenal illness may have baseline cortisol < 2 mcg/dl.13,14 If using < 1 mcg/dl as a cut-off up to 15% of dogs may be missed (have baseline cortisol > 1 mcg/dl) but only up to 9% of dogs with non-adrenal illness have a cortisol < 1 mcg/dl.13,14 Cortisol to Endogenous ACTH Ratio Because the majority of dogs have disease secondary to adrenal dysfunction the cortisol is decreased, the negative feedback to ACTH production is lost, and ACTH increased. The result is a decrease in the ratio of cortisol to ACTH. This test was has been evaluated as an alternative to the ACTH stimulation test and is able to differentiate dogs with hypoadrenocorticism from healthy dogs and dogs with non-adrenal illness.15 This test is also able to differentiate primary from secondary hypoadrenocorticism. In primary hypoadrenocorticism ACTH is increased, as mentioned above, and with secondary hypoadrenocorticism ACTH is low to low normal due to failed secretion from the pituitary. In reality, synthetic cosynotropin is typically available, there is low cost synthetic ACTH gel available and endogenous ACTH is an expensive test so it is unlikely this ratio will replace the ACTH stimulation test at this time. It is also important to remember that an ACTH stim is typically only required once for diagnosis of hypoadrenocorticism whereas when diagnosing and treating hyperadrenocorticism the test is often repeated several times. Aldosterone In dogs with mineralocorticoid deficiency, aldosterone levels would be expected to be decreased to absent and if an attempt was made to stimulate production with an ACTH stimulation test, aldosterone would not increase. In normal dogs and dogs with atypical hypoadrenocorticism the expectation would be aldosterone levels would be ‘normal’ and stimulation would occur. Unfortunately, there is significant overlap between normal dogs, dogs with non-adrenal illness and dogs with hypoadrenocorticism regarding baseline and post stimulation aldosterone levels.1 As mentioned earlier, there is overlap in aldosterone measurements between dogs that have clinical evidence of mineralocorticoid and those that don’t meaning both are low.1 This is surprising because it suggests that even in the absence of electrolyte abnormalities, aldosterone is decreased. Aldosterone is not routinely measured in cases of hypoadrenocorticism. Diagnostic Imaging Thoracic radiographs might reveal microcardia (hypovolemia), decreased diameter of the caudal vena cava (hypovolemia) and megaesophagus (cortisol on muscle). On abdominal ultrasound, adrenal glands might be normal, or occasionally small, in size. Normal adrenal size ion ultrasound was noted in approximately 30% of dogs in one study.11 Treatment and Monitoring Mineralocorticoid Deficiency
68

Mineralocorticoids should be given as soon as mineralocorticoid deficiency is diagnosed. Options for initial mineralocorticoid replacement are injectable desoxycorticosterone pivalate (DOCP) or oral fludrocortisone acetate. DOCP has historically been given at 2.2 mg/kg SC or IM but it appears a starting dose of 1.1 mg/kg is as effective.16 Initially, IM administration of DOCP might be preferred over oral fludrocortisone due to possibilities of poor GI absorption of oral medications. There are two approaches to maintenance protocols. The more common method focuses on stretching out the dosing interval as long as possible by monitoring electrolytes every week starting at week three. Most dogs require injections every 22 to 30 days with some requiring injections as infrequently as every 90 days.17 Another protocol keeps the dosing interval at 28 days but determines the lowest dose needed by monitoring electrolytes at 14 and 28 days to make adjustments.18 DOCP is started at 1.5 mg/kg and weaned by 10% every 28 days, if indicated, until the appropriate dose is obtained to avoid hyperkalemia. The dose can be reduced if on day 14 the potassium is normal and on day 28 the potassium is normal or increased. DOCP has very little glucocorticoid activity so supplementation with glucocorticoids is necessary. Fludrocortisone is an alternative in a dog that can take oral medications. Fludrocortisone is given at 0.02 mg/kg once to twice daily. Some dogs are not stabilized on once daily (absence of clinical signs, sodium:potassium of > 27:1) but then will improve with twice daily administration.19 Long term fludrocortisone may be administered without glucocorticoids, but glucocorticoids should be given initially and then tapered to the lowest dose necessary to maintain appetite and normal activity levels while minimizing signs of glucocorticoid excess. In some dogs mineralocorticoid requirements may increase over the first several months so monitoring is recommended. Sodium and chloride often remain low despite normal potassium. Salt can be supplemented to help normalize sodium and chloride but is usually not necessary long term as mild hyponatremia is well tolerated. The goals of therapy are to normalize potassium and control clinical signs. Glucocorticoid Deficiency Parenteral glucocorticoids should be given as soon as possible. The glucocorticoids used most commonly in emergent cases are dexamethasone, dexamethasone sodium phosphate, prednisolone sodium succinate and hydrocortisone hemisuccinate. If considering glucocorticoids prior to, or during, the ACTH stimulation test, dexamethasone-containing formulations are recommended because dexamethasone will not directly interfere with measuring cortisol during the ACTH stimulation test. Initially, higher doses of glucocorticoids are used more frequently. Dexamethasone sodium phosphate is given at 0.1 to 0.2 mg/kg IV twice a day. This can be followed up by dexamethasone or dexamethasone sodium phosphate at 0.1 mg/kg once daily, hydrocortisone sodium succinate at 0.5 mg/kg/hr CRI or prednisolone sodium succinate at 0.25 to 1.0 mg/kg IV BID. Parenteral glucocorticoids are given until the dog is no longer vomiting and eating and drinking regularly. At this time, dogs can be switched to oral prednisone at 0.5 mg/kg BID while hospitalized, then tapered to lowest dose necessary once at home and feeling well. Maintenance doses of glucocorticoids can be as low as 0.1 mg/kg every other day but it might take several weeks until the dog can be safely weaned to this dose with most dogs requiring daily administration. If utilizing fludrocortisone as a mineralocorticoid, it may be possible to discontinue glucocorticoids because fludrocortisone contains some glucocorticoid. Some dogs are very sensitive to the side effects of glucocorticoids and a dose of prednisone or prednisolone cannot be used without causing significant side effects. In these dogs, alternative glucocorticoids are hydrocortisone and methylprednisolone. Hydrocortisone is started at 0.5 – 1.0 mg/kg BID then increase dose as needed. Doses may be up to 5 mg/kg BID. Methyl prednisolone is initiated at approximately 50% the most recent dose of prednisone or prednisolone then the dose is increased gradually if signs of hypocortisolism develop. Follow Up and Prognosis These dogs do very well. Because dogs can develop progressive aldosterone deficiency, it is recommended to monitor electrolytes for 6 months in patients with glucocorticoid and mineralocorticoid deficiency. References
1. Baumstark ME, et al. Evaluation of aldosterone concentrations in dogs with hypoadrenocorticism. J Vet Int Med 2014;28:154-9.
69
2. Thompson AL, et al. Comparison of classic hypoadrenocorticism with glucocorticoid-deficient hypoadrenocorticism in dogs: 46 cases (1985-2005). J Am Vet Med Assoc 2007; 230:1190-1194.
3. McGonigle KM, et al. Mineralocorticoid before glucocorticoid deficiency in a dog with primary
hypoadrenocorticism and hypothyroidism. J Am Anim Hosp Assoc 2013;Jan-Feb 49:54-57.
4. Hauck C, et al. Prevalence and characterization of hypoadrenocorticism in dogs with signs of chronic intestinal disease: A multicenter study. J Vet Int Med 2019;34:1399-1405.
5. Gold AJ, et al. Evaluation of basal serum or plasma cortisol concentrations for the diagnosis of
hypoadrenocorticism in dogs. J Vet Int Med 2016;30:1798-1805.
6. Seth M, et al. White blood cell counts and the sodium to potassium ratio to screen for hypoadrenocorticism in dogs. J Vet Int Med 2011:25:1351-1356.
7. Roth L. Evaluation of low sodium:potassium ratios in dogs. J Ve Diag Invest 1999 Jan;11(1):60-4.
8. Schaer M, et al. Combined hyponatremia and hyperkalemai mimicking acute hypoadrenocorticism in three
pregnant dogs. J Am Vet Med Assoc 2001 Mar 15;218(6):897-9.
9. DiBartola SP, et al. Clinicopathologic findings resembling hypoadrenocorticism in dogs with primary gastrointestinal disease. J Am Vet Med Assoc 1985 Jul1;187(1):60-3.
10. Pak SI. The clinical implication of sodium-potassium ratios in dogs. J Vet Sci 2000 Jun;1(1):61-5.
11. Adler JA, et al. Abnormalities of serum electrolyte concentrations in dogs with hypoadrenocorticism. J Vet
Int Med 2007 Nov-Dec;21(6)1168-73.
12. Botsford A, et al. Low-dose ACTH stimulation testing in dogs suspected of hypoadrenocorticism. J Vet Int Med 2018;32:1886-1890.
13. Bovens C, et al. Basal serum cortisol concentration as a screening test for hypoadrenocorticism in dogs. J
vet Inte Med 2014;28:1541-1545.
14. Gold AJ, et al. Evaluation of basal serum or plasma cortisol concentrations for the diagnosis of hypoadrenocorticism in dogs. J Vet Int Med 2016 Nov;30(6):1798-1805.
15. Lathan P, et al. Use of the cortisol-to-ACTH ratio for the diagnosis of primary hypoadrenocorticism in
dogs. J vet Int Med 2014;28:1546-1550.
16. Vincent AM, et al. Low-dose desoxycorticosterone pivalate treatment of hypoadrenocorticism in dogs: A randomized clinical trial. J Vet Int Med 2020;35:1720-1728.
17. Jaffey JA, et al. Desoxycorticosterone pivalate duration of action and individualized dosing intervals in
dogs with primary hypoadrenocorticism. J Vet Int Med 2017;31:1649-1657.
18. Sieber-Ruckstuhl NS, et al. Evaluation of low-dose desoxycorticosterone pivalate treatment protocol for long-term management of dogs with primary hypoadrenocorticism. J Vet Int Med 2018;33:1266-1271.
19. Roberts E, et l. Factors that affect stabilization times of canine spontaneous hypoadrenocorticism, Vet Rec
2016 Jul 23;179(4):98
70

Updates Regarding Treatment and Management of Diabetes Mellitus in Cats and Dogs
Jana Gordon, DVM, DACVIM Background Diabetes mellitus is a common endocrine disorder of dogs and cats. In dogs it is almost always classified as type 1 because there is a permanent deficiency in insulin and, if provoked with glucose, no increase in insulin secretion from the pancreas would be observed. In cats, type 2 diabetes mellitus occurs almost exclusively. These cats retain some ability to produce insulin, and insulin secretion can be stimulated from pancreatic cells, but insulin resistance and/or damaged beta cells have resulted in inadequate amounts of insulin to maintain euglycemia. Our goals of treatment of the diabetic dog and cat are to optimize glucose control. In cats, diabetic remission is also a goal. Diabetic remission occurs when the clinical signs of diabetes mellitus resolve, blood glucose levels normalize and the pet no longer requires insulin. Diabetic remission is uncommon in dogs. In dogs, remission may occur with ‘other’ types of diabetes mellitus that may occur with certain diseases. Acute pancreatitis, hyperadrenocorticism, exogenous glucocorticoid or progestin administration and insulin resistance secondary to reproductive hormones (e.g. diestrus, pregnancy) can result in forms of reversible diabetes mellitus in dogs. Unfortunately, even with management of these conditions a permanent diabetic state often occurs . In cats, insulin resistance is a much more common cause of diabetes mellitus. As a result, if the cause of resistance is eliminated and the remaining functional beta cells protected it is possible that insulin will not be required long term. While well-designed studies with large numbers of cats are lacking, some factors that might contribute to achieving remission are early treatment, use of longer acting insulins, insulin administration twice daily, use of low carbohydrate diets and weight loss. Treatment Diet In diabetic dogs, it initially appeared that diets high in insoluble and soluble fiber improved glycemic control.1,2,3 A more recent study suggests that higher fiber diets are no better than moderate fiber diets regarding glycemic control but that limiting dietary fat may help control serum lipids in diabetic dogs who are already predisposed to hyperlipidemia.4 For this reason the current recommendation is to feed a moderate to high fiber, low fat diet based on the body condition of the pet. In dogs the goal of dietary therapy is to promote ideal body weight and minimize glucose fluctuations. This means for overweight and obese dogs a diet high in fiber to promote weight loss may be appropriate but this diet would be inappropriate in underweight patients. Concurrent disorders requiring specific dietary management (e.g. inflammatory bowel disease, food allergy, chronic kidney disease) should be considered and may take priority in diet selection. In cats, diets high in fiber were initially used to manage diabetes for reasons described above for dogs. With a better understanding of type 2 diabetes mellitus and feline metabolism, low carbohydrate diets were developed because of the concern that carbohydrates increased postprandial hyperglycemia, endogenous insulin production and insulin requirements in diabetic cats. Obesity, rather than dietary carbohydrates are believed to lead to diabetes mellitus in cats but higher dietary carbohydrates can contribute to obesity. For many years, low carbohydrate diets have been considered critical in obtaining diabetic remission. There have been several studies using low carbohydrate diets in diabetic cats that have resulted in diabetic remission and the current recommendation is to use them to optimize remission.5,6,7,8 Despite the apparent benefits of the low carbohydrate diets, other studies have documented diabetic remission with other diet types.9,10 As a result, while low carbohydrate diets appear to be superior to moderate carbohydrate diets, remission can occur with variable carbohydrate content. This is probably because all diets must meet AAFCO requirements which are for higher protein content in the feline at the expense of carbohydrates. It is recommended to feed twice daily with concurrent insulin administration. For dogs and cats that refuse to meal feed frequent smaller meals are recommended to avoid large glucose fluctuations. Oral Hypoglycemics
71
Oral hypoglycemics are commonly used alone, or with insulin, in human diabetic patients because of the high incidence of type 2 diabetes. Their mechanisms include; decreased intestinal absorption of glucose, increased insulin release from the pancreas, decreased glucose production by the liver and increased tissue sensitivity to insulin. In our companion animal species they are generally ineffective, not readily available and/or cost prohibitive limiting their use. Below is a general review. Alpha glucosidase inhibitors (acarbose) – The mechanism of action is inhibition of pancreatic amylase and intestinal brush border enzymes that digest complex carbohydrates. The end result is a delay in the digestion and thus absorption of glucose which lowers blood glucose levels. A single study in a small number of dogs has been published and has shown that acarbose did not lower insulin requirements but did decrease glucose and glycosylated hemoglobin levels in treated dogs.11 Three of 5 dogs did develop loose feces with administration. In cats acarbose is given less often because they are typically given a low carbohydrate diet. In an early study using acarbose, low carbohydrate diet and insulin or glipizide in 18 diabetic cats, 11 went into remission. These were also the cats that were classified as obese so it is possible that correction of obesity is what led to the remission rather than any benefit from acarbose.12 In fact a study in healthy cats showed little benefit to giving cats acarbose with a low carbohydrate diet.13 Another study looked at acarbose, sitagliptin (DDP-4 inhibitor) or combination therapy on postprandial glucose, insulin levels and incretin hormone (glucagon-like peptide 1, glucose dependent insulinotropic hormone) production in a small number of healthy cats.14 In this study acarbose did decrease postprandial glucose and insulin. In summary, acarbose and other alpha glucosidase inhibitors, have more value in decreasing glucose in diabetics that are not on carbohydrate restricted diets but may not decrease insulin requirements. Sulfonylureas - The sulfonylureas stimulate pancreatic beta cells directly to secrete insulin. For this reason they only work on individuals still able to produce insulin which are type 2 and ‘other’ diabetics. Glipizide is the sulfonylurea that has been used most in cats. This drug class is not used in dogs because they do not typically have enough functional insulin producing cells to have effect. In cats response rates up to 65% are reported with remission in up to 27% of cats though diabetes recurred in some.15,16 Despite a response in cats, the use of sulfonylureas is discouraged because any of the drugs that increase insulin secretion from the pancreas are thought to place increased demand on damaged or small numbers of functional beta cells which could lead to cell exhaustion and loss. Sulfonylureas are not used in dogs because they have type 1 diabetes mellitus in most instances. Side effects are hypoglycemia, vomiting, increased liver enzymes and icterus. Meglitinides – The meglitinides also stimulate insulin production from beta cells but for a shorter period of time. There is a single report of the use of nateglinide and a longer acting sulfonylurea, glimepiride, in healthy cats.17
Nateglinide was short in duration but potent compared to the longer-acting less potent sulfonylurea. No studies have been done in diabetic cats.
Glucagon-like Peptide 1 (GLP-1) agonists – (Exenatide, Exenatide ER) GLP-1 is normally produced by cells in the intestinal tract. This is an incretin hormone stimulated by the presence of ingesta that increases insulin production as well as decreases glucagon, decreases gastric emptying and increases satiety. There have been several studies of the pharmacokinetics and pharmacodynamics of injectable formulations of exenatide, exenatide extended release and liraglutide in healthy cats.18,19,20 There is a study of exenatide ER in 30 newly diagnosed diabetic cats.21 These cats were given exenatide ER or placebo subcutaneously once weekly as well as glargine insulin and a low carbohydrate diet for 16 weeks or until diabetic remission. Remission rates were 40% on exenatide ER vs. 20% in control cats. No weight gain was seen. It appears there may be a role for exenatide ER in the treatment of diabetes mellitus in cats. Mild intestinal side effects may be seen. Somatostatin Receptor Ligands - (octreotide, pasireotide) These drugs are used commonly in humans with acromegaly to decrease insulin like growth factor-1 (IGF-1). Pasireotide has been investigated in cats with acromegaly and diabetes mellitus and resulted in decreased IGF-1, decreased insulin requirements and improved insulin sensitivity when administered over 5 days with the short-acting formulation.22 Another study in diabetic acromegalic cats given pasireotide ER (6 – 8 mg/kg SC) monthly for 6 months, saw 3 of 8 cats that completed the study (n = 14 cats) go into remission.23 The drug is expensive limiting its use. Dipeptidyl Peptidase-4 (DDP-4) inhibitors – DDP-4 is an enzyme that degrades GLP-1. Because of the positive effects of GLP-1 on insulin production and body weight it is logical a drug that inhibits its breakdown would be beneficial in type 2 diabetes mellitus. All studies done to date have been with oral sitagliptin in healthy cats. There
72
is evidence that sitagliptin increases insulin levels in healthy cats.14,24,25 No studies have been done in diabetic cats. Mild intestinal side effects may be seen. Biguanide/Metformin – Therapeutic benefits from metformin are primarily a result of decreased glucose production by the liver and increased glucose uptake by muscle. Metformin requires the presence of insulin to work. Unfortunately, the biguanides have not been very effective in dogs or cats. Thiazolidinediones – Also known as glitazones these drugs primarily act by increasing insulin sensitivity in the fat and less in the liver and muscle. They require the presence of insulin to be effective. They are used most often in people in combination with other oral hypoglycemics and insulin. Limited studies have been done in cats with troglitazone, pioglitazone and darglitazone evaluating pharmacokinetics, glucose-lowering effects and lipid profiles.26,27,28 The thiazolidinediones have insulin sensitizing and lipid lowering effects in normal cats.26,28,29 No studies have been done in diabetic cats. Insulin Insulin preparations have changed over time to better suit the needs of human diabetics and, more recently, our veterinary patients. Most maintenance preparations for dogs and cats are meant for once to twice daily administration but there is research into newer hybrid preparations that could be used for weekly administration in cats.30 Neutral protamine Hagedorn (NPH) is a human recombinant formulation that is potent with a variable but relatively short duration, even more so in cats than dogs. For this reason I do not consider this insulin a good choice for cats in general. NPH is the least expensive insulin in the United States because it can be purchased through a discount program which makes it popular in our veterinary patients. Dogs should be started on twice daily administration and this may be too infrequent for some dogs. This insulin does come in mixes that contain either 25% (25/75), 30% (70/30) or 50% (50/50) regular along with the NPH. The idea is that the regular portion addresses post-prandial increases in glucose and the NPH addresses glucose production between meals as a result of glycogenolysis and gluconeogenesis. While we don’t use these insulin mixes commonly in dogs they have been used successfully by some practitioners. The starting dose of NPH is 0.25 U/kg in the dog BID (large dog’s lower dose). Because this is a human insulin the concentration is U-100. Pork lente insulin has been used in dogs and cats for many years. Cats have been able to achieve diabetic remission with low carbohydrate diets and pork lente insulin.8,10,31 There is a single study that shows superior remission rates of twice daily lente to ONCE daily glargine in 13 cats with 3 of 7 lente and 1 of 6 glargine cats obtaining remission.32 Lente is a preferred insulin in dogs because of its more predictable behavior in this species. Most dogs require twice daily administration so it is started twice daily but some dogs may be well regulated on once daily insulin.33 A double nadir is often seen with this insulin in dogs at 4 and 11 hours.33 Cats require twice daily administration. Because this is a veterinary insulin it is a U-40 formulation. The dose is 0.25 U/kg in the dog BID or 1 to 2 units BID in cats. Protamine zinc insulin (PZI) is considered long acting and historically was administered twice daily in dogs and cats. This insulin was originally used in cats because it was largely composed of beef insulin which was thought to be more compatible with cats, less insulin antibody formation. The current formulation used in the US is a veterinary U-40 product that is composed of human recombinant regular insulin, protamine and zinc. PZIr is emerging as a good initial insulin choice in dogs, particularly if once daily administration is desired. In a study of 276 dogs comparing once and twice daily PZIr in naïve and previously treated diabetic dogs, there was improvement in both clinical and laboratory parameters in 71% and 74% of dogs, respectively.34 PZIr is less predictable in dogs regarding time to onset, nadir and duration than in cats.35 In addition, its prolonged duration in some dogs resulted in hypoglycemia when given twice daily in one study.36 The dose is 0.25 U/kg in the dog BID or 1 to 2 units BID in cats. Glargine insulin is the most common initial insulin recommendation in cats because of high remission rates in studies. This is an ultra-long-acting insulin that is not as potent as the insulins previously described but has a duration greater than 24 hours in many cats. The prolonged duration is due to the acidic pH of the formulation that forms a precipitate when injected subcutaneously. While diabetic remission occurs in cats on PZI, lente and glargine insulins; glargine and detemir given twice daily are more likely to result in remission.8,37,38 Once daily
73

administration may control clinical signs but twice daily is better for obtaining remission.32,37 In dogs insulin glargine was reported to be less predictable in one small study but in a more recent study 10 dogs were given BID glargine and all were regulated.40,41 The dose is 0.25 U/kg twice daily in both species not to exceed 2 units in a large cat. This is a human insulin analogue so is U-100. There is now a glargine U-300 (Tujeo®) that has been shown to be less potent in humans so less risk of hypoglycemia. This insulin is 14 – 30% less potent in people and in a study comparing IV and SC glargine U-100 and U-300 glargine U-300 in normal beagle dogs, a slower and less pronounced decrease in glucose was seen with U-300 vs U-100.42 The assumption is that this is due to slower absorption of the U-300 glargine. Detemir insulin is similar to glargine in that it is ultra-long acting and less potent than NPH, lente or PZI. The long duration of detemir is due to alterations in its structure that result in binding to albumin which slows absorption and decreases the amount available free to bind receptors. It is longer in duration and more often associated with hypoglycemia so starting doses are lower at 0.10 mg/kg/dose BID in dogs and cats.38,43,44 This insulin is also a good choice to put cats in remission.38,43,44.45 Detemir is marketed for people so is a U-100 formulation. Insulin Degludec (Tresiba® Novo-Nordisk®) is an ultra-long-acting synthetic insulin that acts like glargine in that when injected under the skin it forms soluble multi-hexamers with a duration of action of over 42 hours in humans. A study of Degludec was done in 8 cats, 5 novel and 3 previously diagnosed, treated over a 12 month period.46 They were dosed 0.5 to 2 units/cat once to twice daily to start. Adjustments were made based on clinical signs and fructosamine. Most were on a low carbohydrate diet. Glucose curves were done every 3 months in 4 cats and fructosamine followed in all 8 cats. There was one clinical hypoglycemic event but no other adverse effects. No cats went into remission but fructosamine decreased in all cats and weight gain was observed. In summary, pork lente is a good initial insulin for dogs because of its well-known predictable behavior. NPH is an acceptable inexpensive alternative but may be too short in duration for some dogs to administer twice daily. Response to PZI, glargine and detemir is variable in dogs but are good longer acting alternatives to NPH and lente. Glargine twice daily is a good initial choice for cats if your goals include diabetic remission. Detemir is a good alternative but may be more difficult to dose in cats. Pork lente and PZI are also options and may control clinical signs but are less likely to result in remission. Patient Monitoring Clinical signs and body weight - Recall the goals of treatment are to eliminate clinical signs of hyperglycemia and hypoglycemia as well as diabetic remission in cats. The presence of diabetic neuropathy or cataracts suggests poor regulation. Cataracts are irreversible but the polyneuropathy improves in most cats with regulation. Because clinical signs and body weight are so important they should be discussed with every visit. Signs of hyperglycemia are easy to identify because they are related to why the animal presented. Signs of hypoglycemia can be missed, particularly in cats that are less interactive than dogs. It is important to use clinical signs with other methods to optimize treatment decisions. Glucose curves – Glucose curves are the most frequently used method of monitoring diabetics. I can’t emphasize enough the importance of using clinical signs along with blood glucose measurements. The goal of a curve is to determine if the insulin dose and duration are appropriate. Remember that initial insulin doses are supposed to be low in order to be safe so it should be expected to have to make adjustments. It can take 2 to 3 months to regulate a dog or cat on insulin. It is also important to remember that cats can go into remission within a few months. When evaluating a glucose curve we are most interested in how high the glucose is at the time of insulin administration, if the glucose decreases after insulin administration (responds to insulin), how low the glucose becomes (nadir) and the duration of insulin (time from administration to when is above renal threshold). The traditional insulins we have used that are more potent (NPH, pork lente, PZI) create an inverse bell shape glucose curve with a pronounced glucose differential (difference between pre insulin glucose and nadir) and nadir that is placed in a more classic position midway between administrations of insulin. The less potent, ultra-long insulins will often curve with a smaller differential and nadirs that often occur late or just before the next dose. This has changed how we perform glucose curves. For the more potent insulins or in patients whose curves are more classic more frequent glucose measurements may be necessary than in patients on ultra-long acting insulins with relatively flat curves to identify the nadir. In addition, for twice daily insulin administration, a 12 hour curve is the minimum. For once daily insulin a curve closer to 24 hours is recommended. I recommend to all clients that these curves are performed at home
74
because of the effects of stress (travel, hospitalization) on glucose levels and food intake. In addition, the limited activity of the hospital environment may not mimic activity at home. Despite this there are situations in which in hospital curves have to be done. Glucose curves are performed weekly until the appropriate insulin dose is identified. There are also intense glucose monitoring programs described for cats using glargine and detemir insulin with the overall goal of putting cats in to diabetic remission more quickly.34,35 The premise is that early use of insulin at appropriate doses to maintain euglycemia will preserve the functional insulin-producing cells of the pancreas so a cat may not always be insulin dependent. Diabetic remission is more common in recently diagnosed cats but can occur less often in previously diagnosed diabetic cats. Basically, cats are given twice daily ultra-long-acting insulin and placed on a low carbohydrate diet. Owners perform at least 3 glucose measurements per day with a glucose goal of 50 – 100 mg/dl on an Alpha TRAK glucometer (80 – 130 mg/dl on human glucometers). The first phase is 3 days of monitoring that requires only adjustments for certain cats that stay above 300 mg/dl or those that drop below 50 mg/dl. Phase 2 begins on day 4 and you increase the dose every 3 days by a certain amount depending on what your glucose is. If glucose is low you will be dose reducing. If within a certain range no change in dose is made. For phase 3 the glucose is kept between 50 – 200 mg/dl all day long. The end of this phase is when all glucose measurements are less than 100 mg/dl and the nadir is in the normal range for a week. Phase 4 is a dose reduction period where the cat is slowly weaned off insulin to determine if the cat is in remission. Remission is defined as euglycemia for at least 14 days with no insulin. It is recommended these cats continue on the low carbohydrate diet to prevent relapse. Glucose curves can be done periodically on stable diabetics to support adequate control. Continuous glucose monitors allow for the collection of more data points without having to obtain blood samples. Sensors read up to 14 days. In dogs they are more easily displaced so adding some tissue glue to the sensor pad may help. Cat skin is more fragile and adheres to the sensor better so glue is not typically needed or recommended. There is some concern that readings from the sensor, which is in the subcutaneous space, may be erroneous with dehydration so may be more reliable in a well hydrated patient. This is relevant with diabetic ketoacidosis because using a sensor is valuable in this setting. A disadvantage of the CGM’s is that they give so much data that can take time to evaluate. You can use these systems to make a more traditional curve and just have spot reads taken rather than look at extensive tracings. Fructosamine – Fructosamine is the measurement of glycosylated proteins in the blood. Since albumin is the most abundant protein in the blood, fructosamine correlates with the serum half-life of albumin which is 1 to 2 weeks in the dog and cat. Frucotsamine is sometimes used to diagnose diabetes in cats whose clinical signs are not highly suggestive of or specific for diabetes mellitus and for monitoring patients but is not reliable on cats with mild hyperglycemia. Fructosamine is also used to help further define control when glucose curves are difficult to interpret as well as in stable diabetics as an alternative to glucose curves. Fructosamine can be artifactually affected by hypoproteinemia, hyperproteinemia, hypothyroidism, hyperthyroidism, hyperlipidemia, azotemia and hemolysis. Glycosylated hemoglobin – Glycoslylated hemoglobin is the measurement of glucose bound to red blood cells which means it describes glycemic control over 2 to 3 months. This test has not historically been used in dogs and cats as often but there is renewed interest in its use for stable diabetics. Glycosylated hemoglobin, with reference ranges, is also not as readily available as fructosamine. Urine glucose and ketones – The renal threshold for glucose is approximately 180 mg/dl in the dog and 280 mg/dl in the cat. Urine glucose is not a reliable indicator of glycemic control but repeated high urine glucose and urine ketones may suggest too little insulin. Frequent negative urine glucose tests could suggest remission in cats or an insulin overdose. It is important to remember the urine collected reflects blood glucose over several hours. Conclusion Advancements in treatment of human diabetics gives veterinarians more options for companion animals. While we cannot incorporate many of the traditional non-insulin options used in people some, like exenatide, are showing utility in a subpopulation of our veterinary patients. In addition, human and veterinary insulin development continues to allow us access to insulins that work better in our patients. As we have better tools and a better understanding of how to monitor our patients, we may be able to involve our clients in more day-to-day control of their pets diabetes as they would their own. References
75
1. Nelson RW, et al. Effect of dietary insoluble fiber on control of glycemia in dogs with naturally occurring diabetes mellitus. J Am Vet Med Assoc 1998 Feb 1;212(3):380-6.
2. Kimmel SE, et al. Effects of insoluble and soluble dietary fiber on glycemic control in dogs with naturally occurring insulin-dependent diabetes mellitus. J Am Vet Med Assoc 2000 Apr 1;216(7):1076-81
3. Graham PA, et al. Influence of a high fibre diet on glycaemic control and quality of life in dogs with diabetes mellitus. J Sm Anim Pract 2002 Feb;43(2):67-73.
4. Fleeman LM, et al. Lack of advantage of high fibre, moderate carbohydrate diets in dogs with stabilized diabetes mellitus. J Sm Animal Pract 2009 Nov;50(11):604-14.
5. Frank G, et al. Use of a high-protein diet in the management of feline diabetes mellitus. Vet Ther 2001 Summer;(2):238-46.
6. Weaver KE, et al. Use of glargine and lente insulins in cats with diabetes mellitus. J Vet Int Med 2006 Mar-Apr;20(2):234-8.
7. Bennett N, et al. Comparison of a low carbohydrate-low fiber diet and a moderate carbohydrate-high fiber diet in the management of feline diabetes mellitus. J Fel Med Surg 2006 Apr;8(2):73-84.
8. Marshall RD, et al. Treatment of newly diagnosed diabetic cats with glargine insulin improves glycaemic control and results in higher probability of remission than protamine zinc and lente insulins. J Fel Med Surg 2009 Aug;11(8):683-91.
9. Hall TD, et al. Effects of diet on glucose control in cats with diabetes mellitus treated with twice daily glargine insulin. J Fel Med Surg 2009 Feb;11(2):125-30.
10. Michiels L, et al. Treatment of 46 cats with porcine lente insulin-a prospective , multicenter study. J Fel Med Surg 2008 Oct;10(5):439-51.
11. Nelson RD, et al. Effect of the alpha-glucosidase inhibitor acarbose on control of glycemia in dogs with naturally acquired diabetes mellitus. J Am Vet Med Assoc 2000 Apr 15;216(8):1265-9.
12. Mazzaferro EM, et al. Treatment of feline diabetes mellitus using an alpha-glucosidase inhibitor and a low-carbohydrate diet. J Fel Med Surg 2003 Jun;5(3):183-9.
13. Singh R, et al. Effect of acarbose on postprandial blood glucose concentrations in healthy cats fed low and high carbohydrate diets. J Fel Med Surg 2015 Oct:17(10):848-57.
14. Mori A, et al. Effect of acarbose, sitagliptin and combination therapy on blood glucose, insulin, and incretin hormone concentrations in experimentally induced postprandial hyperglycemia of healthy cats. Res Vet Sci 2016 Jun;106:131-4.
15. Nelson RW, et al. Effect of an orally administered sulfonylurea, glipizide, for treatment of diabetes mellitus in cats. J Am Vet Med Assoc 1993 Sep 15;203(6):821-7.
16. Feldman EC, et al. Intensive 50-week evaluation of glipizide administration in 50 cats with previously untreated diabetes mellitus. J AM Vet Med Assoc 1997 Mar 15;210(6):772-7.
17. Mori A, et al. Effect of glimepiride and nateglidine on serum insulin and glucose concentration in healthy cats. Vet Res Comm 2009 Dec:33(8):957-70.
18. Gilor C, et al. The GLP-1 mimetic exenatide potentiates insulin secretion in healthy cats. Domest Anim End 2011 Jul;41(1):42-9.
19. Rudinsky AJ, et al. Pharmacology of the glucagon-like peptide-1 analogue exenatide extended-release in healthy cats. Domest Animal End 2015 Apr;51:78-85
20. Hall MJ. et al. Pharmacokinetics and pharmacodynamics of the glucagon-like peptide-1 analogue liraglutide in healthy cats. Domest Animal End 2015 Apr;41:114-21.
21. Riederer A, et al. Effect of the glucagon-like peptide-1 analogue exenatide extended release in cats with newly diagnosed diabetes mellitus. J Vet Int Med 2016 Jan-Feb;30(1):92-100.
22. Scudder CJ, et al. Pasireotide for the medical management of feline hypersomatotropism. J Vet Int Med 2015; 29: 1074 – 1080.
23. Gostelow et al. Pasireotide long-acting release treatment for diabetic cats with underlying hypesomatotropism. J Vet Int med 2017 Mar;31(2):355-64.
24. Nishii N, et al. Effects of sitagliptin on plasma incretin concentrations after glucose administration through an esophagostomy tube or feeding in healthy cats. Domest Anim End 2014 Oct;49:14-9.
76

25. Padrutt I, et al. Effects of the glucagon-like peptide-1 (GLP-1) analogues exenatide, exenatide extended release, and of the dipeptidylpeptidase-4 (DDP-4) inhibitor sitagliptin on glucose metabolism in healthy cats. Res Ve Sci 2015 Apr:99:23-9.
26. Michels GM, et al. Pharmacokinetics of the insulin-sensitizing agent troglitazone in cats. Am J Vet Res 2000 Jul;61(7):775-8.
27. Hoenig M, Ferguson DC. Effect of darglitazone on glucose clearance and lipid metabolism in obese cats. Am J Vet Res 2003 Nov 64;(11):1409-13.
28. Clark MH, et al. Pharmacokinetics of pioglitazone in lean and obese cats. J Vet Pharm Ther 2012 Oct;35(5):428-36.
29. Clark M, et al. Effects of pioglitazone on insulin sensitivity and serum lipids in obese cats. J Vet Int Med 2014 Jan-Feb;28(1):166-74.
30. Gilor C, et al. An ultra-long-acting recombinant insulin for the treatment of diabetes mellitus in cats. J Vet Int Med 2021 Jun;1 – 8.
31. Martin GJ, Rand JS. Control of diabetes mellitus in cats with porcine insulin zinc suspension. Vet Rec 2007 Jul 21;161(3):88-94.
32. Weaver KE, et al. Use of glargine and lente insulins in cats with diabetes mellitus. J Vet Int Med 2006 Mar-Apr;20(2):234-8.
33. Graham PA, et al. Pharmacokinetics of a porcine insulin zinc suspension in diabetic dogs. J Small Anim Pract 1997 oct;38(10):434-8.
34. Ward CR, et al. Field efficacy and safety of protamine zinc recombinant human insulin in 276 dogs with diabetes mellitus. Dom Anim End 2021 Apr; 75:1 – 13.
35. Clark M, et al. Pharmacokinetics and pharmacodynamics of protamine zinc recombinant human insulin in healthy dogs. J Vet Pharm Ther 2012 Aug;35(4):342-50.
36. Maggiore AD, et al. Efficacy of protamine zinc recombinant human insulin for controlling hyperglycemia in dogs with diabetes mellitus. J Vet Int Med 2012 Jan-Feb;26(1):109-15.
37. Roomp K, Rand J. Intensive blood glucose control is safe and effective in diabetic cats using home monitoring and treatment with glargine. J Fel Med Surg 2009 Aug;11(8):668-82
38. Roomp K, Rand J. Evaluation of detemir in diabetic cats managed with a protocol for intensive blood glucose control. J Fel Med Surg 2012 Aug;14(8):566-72.
39. Baori A, et al. Glargine insulin and high-protein-low-carbohydrate diet in cats with diabetes mellitus. Vet Res Comm 2008 Sep:32 Suppl 1:S243-5.
40. Francassi F, et al. Use of insulin glargine in dogs with diabetes mellitus. Vet Rec 2012 Jan;170(2):52. 41. Hess RS, Drobatz KJ. Glargine insulin for treatment of naturally occurring diabetes mellitus in dogs. J AM
Vet Med Assoc 2013 Oct 15;243(8):1154-61. 42. Werner U, et al. Equipotency of insulin glargine 300 and 100 U/ml with intravenous dosing but differential
bioavailability with subcutaneous dosing in dogs. Diabetes Obes Metab 2021 Jan;23(1):166-174. 43. Sako T, et al. Time-action profiles of insulin detemir in normal and diabetic dogs. Res Vet Sci 2011
Jun;90(3):396-403. 44. Fracassi F, et al. Detemir insulin for the treatment of diabetes mellitus in dogs. J AM Vet Med Assoc 2015
Jul 1;247(1):73-8. 45. Hoelmkjaer KM, et al. Insulin detemir treatment in diabetic cats in a practice setting. J Fel Med Surg 2015
Feb:17(2):144-51. 46. Hitomi O, et al. The effect of insulin Degludec on glycemic control in diabetic cats over a 12-month period.
J Vet Med Sci Jun;82(6):695-698.
77

Diagnosis and Treatment of Immune-Mediated Hemolytic Anemia Jana Gordon, DVM
Introduction Immune-mediated diseases are common in our companion animals. They affect all organ systems and oftentimes more than one at a time. These diseases require intense management and are associated with life-threatening comorbidities as well as treatment complications and failure. Immune-mediated hemolytic anemia (IMHA), and a variant, precursor immune-mediated anemia (PIMA), are common of diseases we see as internists. It is important to have a good understanding of this disease to optimize care and outcomes. This session will be a review of what we know about IMHA and PIMA with information regarding IMHA in dogs and cats drawn from the literature as well as The ACVIM Consensus Statement on The Diagnosis of Immune-Mediated Hemolytic Anemia in Dogs and The ACVIM Consensus Statement on The Treatment of Immune-Mediated Hemolytic Anemia in dogs. References to these statements will be referred to as CS. Etiopathogenesis A portion of the CS discusses the terminology we have historically used to describe IMHA and a move to the use of associative and non-associative IMHA. Idiopathic forms of the disease were those in which we did not identify a cause and secondary are those we assumed were secondary to another disease. The CS asks for different terminology based on the fact that idiopathic assumes no underlying cause but an alternative term non-associative allows for our poor understanding of causation and inability to identify a cause. Along this same line of thinking secondary implies a causal relationship that, in most cases, is tenuous at best but associative avoids commitment to a direct link. From this point forward the terms non-associative and associative will be used. IMHA is a complex manifestation of immune dysregulation that results in direct and indirect targeting of red blood cell antigens. IgG and IgM antibodies produced by B lymphocytes may activate complement leading to intravascular hemolysis or, more commonly, these antibodies coat red blood cells and are removed by the reticuloendothelial system within the liver and spleen. PIMA is a related disease targeting the immature red cells in the bone marrow. PIMA lacks the hemolytic component because the destruction is at the level of the bone marrow. Pro-inflammatory cytokines, platelet activation and damage to vascular endothelium play a role in disease and development of complications with immune-mediated anemia. The result is tissue hypoxia, a pro-inflammatory state and disorders of coagulation, primarily hypercoagulability.1-5 The signalment has been well established in previous studies but I feel it is important to realize that any breed, sex, neuter status or age can be affected. The tendency is for adult, female, small breed dogs with more miniature schnauzers and Cocker spaniels to be affected in spring and summer months.6-12 There have been a lot of retrospective studies and case reports of diseases associated with IMHA but the numbers are often small and evidence of causality weak. We have been told over the years to evaluate our patients for any drug or biologic exposure, infectious disease, cancer or toxicity because these may have set off the immune dysregulation. various infectious organisms, drugs, biologics and neoplasms have been implicated. Unfortunately, we haven’t made a lot of progress in identifying associated conditions so it is still important to evaluate the patient history, perform a thorough physical exam and utilize basic laboratory tests to determine if further testing is warranted. Diseases and conditions may not be truly associated but may complicate treatment. Below is a discussion that is based on highlights from the literature reviewed to formulate the CS. Infection Many infectious agents have been implicated in the pathophysiology of IMHA but in the dog, Babesia gibsonii, Bartonella vinsonii, Leishmania infantum and Dirofilaria immitis infections have a documented association with immune-mediated hemolytic anemia.13-18 This is the reason for the recommendation to test for these organisms as well as Ehrlichia spp. in the dog. The current recommendation is for antibody and PCR techniques be utilized when available, excepting D. immitis in which an antigen test is highly sensitive and specific for infection in the dog. In cats, there is evidence of immune-mediated hemolytic anemia occurring with Babesia felis and Mycoplasma haemofelis. There are a lot of studies in FeLV positive cats with immune-mediated hemolytic anemia but they have
78

comorbidities that confound the diagnosis. The recommendation in cats is to PCR all cats for M. haemofelis, PCR and antibody cats in endemic areas for B. felis and test for FeLV status. Other infections may be associated with IMHA and should be considered based on geographical region and individual patient assessment. Drugs and vaccines There have been many studies looking at the relationship between drugs and biologics and the development of IMHA. Regarding drugs, there are no drugs we use commonly here in the United States that have been associated with IMHA. Regarding vaccines there are some good studies looking at an association but they both support and refute a relationship.10,22 For this reason there is not a clear understanding of the relationship between vaccines and development of IMHA. Other There are case reports of immune-mediated hemolytic anemia associated with pregnancy and a bee sting in dogs.23,24 There is not strong evidence of immune-mediated hemolytic anemia as a paraneoplastic syndrome in dogs and cats. Diagnosis Diagnostic tests are dictated by a detailed history, a complete physical examination and general laboratory assessment. For the diagnosis of IMHA we look for specific indicators of immune-mediated destruction of red cells and hemolysis. Indicators of immune-mediated destruction Autoagglutination/SAT – Autoagglutination occurs as a result of red blood cells clumping. In IMHA it is due to red blood cells being coated with antibodies. Rouleaux is an artifactual stacking of red cells that often occurs with high protein levels in plasma. To eliminate this artifact a saline agglutination test is performed in which 1 drop of blood is placed on a slide and 4 drops saline added (saline agglutination test = SAT). To further decrease false positives, red cells can be washed 3 times with saline at a 1:4 ratio. Autoagglutination can also cause artifacts on CBC’s including; increased red blood cell numbers, mean corpuscular cell volume (MCV) and mean corpuscular hemoglobin concentration (MCHC).25 Coombs/DAT – A direct Coombs test or direct antibody test (DAT) detects antibodies against red blood cells. There are different techniques used that may affect sensitivity.26,27 They may use a single anti-antibody (monovalent) reagent or a polyvalent antibodies to look for multiple antigens (IgM, IgG, other) and be performed at 4 and/or 37 ֯ ֯ ֯°C. P
26 PCoombs is positive in 60% to 100% of dogs with IMHA. P
11,28,29P Coombs can also be positive with PIMA. P
30P In a
study of 19 cats with associative hemolytic anemia, 15 had positive Coombs. P
31 PA single study demonstrated that
glucocorticoids or previous transfusions did not affect Coombs, but the current recommendation is to test before drugs or transfusion because of variability in testing methods. P
28P
Flow cytometry – Flow cytometry defines cells by looking at cell number, size and composition using a flow cytometer. This technique is much less commonly used for looking for RBC antibodies than SAT or DAT so is not a preferred method at this time. Indicators of hemolysis Spherocytes – These should be identified by a pathologist because of concerns over misinterpreting other cell types. Spherocytes are reported in 67 to 80% of dogs with IMHA.7,11 Spherocytes can be found in stored blood products and hemolytic reactions so should be counted pretransfusion. There are non-immune causes of spherocytes or pyknocytes (distorted, irregular small red cells) such as oxidative damage, envenomation, hypersplenism, PK deficiency and diseases that cause erythrocyte fragmentation. For IMHA you want to detect ≥ 5 spherocytes /hpf, which is equivalent to 1+ on slide evaluation. Seeing 3-4 spherocytes/hpf is acceptable if other causes of spherocytosis mentioned above are ruled out. Spherocytes suggest extravascular hemolysis. Hyperbilirubinemia/hyperbilirubinuria – Increased serum bilirubin without evidence of a hepatic or post hepatic cause suggests hemolysis. A dipstick bilirubin reading of > 2 is considered abnormal in dog urine. Any positive bilirubin in cat urine is abnormal.
79

Hemoglobinemia/hemoglobinuria – Serum can be visualized for gross hemolysis or measurement of cell free hemoglobin (hemolytic index). Artifact can be created with difficult blood draw (prolonged, small needle, through a catheter) and poor sample handling (force into tube, temperature extremes). A positive hemoglobin on a urine test strip without gross red cells on urine sediment suggest hemoglobinuria. A low urine specific gravity or highly alkaline urine may cause to red cell lysis and artifactual hemolysis. RBC ghosts – These are pale red cells with no internal content and suggest intravascular hemolysis. To avoid artifact, it is recommended a blood smear be made right after collection. Diagnostic algorithm for IMHA The diagnostic algorithm used in the CS is based on the premise that you first look for evidence of immune destruction and then evidence of hemolysis. Evidence of immune destruction was either a positive saline agglutination after RBC washing or 2 of the following:
- Spherocytes - Positive autoagglutination w/o washing - Positive Coombs/DAT or flow cytometry
If evidence of immune destruction criteria are satisfied, then more than one of the following indicators of hemolysis must be noted for the dog to have IMHA:
- Increased bilirubin - Hemoglobinemia - Hemoglobinuria - Ghost cells
If more than one indicator of hemolysis is not found, then rule out other causes of destruction to diagnose IMHA If only 1 sign of destruction was found then > 1 sign of hemolysis must be present
- If more than 1 sign of hemolysis is present, rule out other causes of destruction then diagnose IMHA - If only 1 sign of hemolysis present then there is a suspicion of IMHA
The algorithm gives allowances for the variable clinical presentations and sensitivity of tests utilized. For instance, intravascular hemolysis is less common than extravascular with reports of around 10%.11 This means that hemoglobinemia and hemoglobinuria are unlikely to be seen and these are two criteria for hemolysis. Other common findings seen in dogs with IMHA are concurrent thrombocytopenia in up to 68% of dogs.7,9,11,29 Interestingly, even though you would expect an anemia secondary to destruction to be regenerative, a non-regenerative anemia can be seen in 25 – 33% of dogs and 57% of cats with IMHA based on reticulocyte count.7,11,31 Bone marrow evaluation is often performed in dogs and cats suspected of PIMA. Erythroid hyperplasia, red cell aplasia, myelofibrosis, phagocytosis, lymphocyte hyperplasia and plasma cell hyperplasia may be found.32,33 Treatment Hematologic interventions Blood transfusion – Blood transfusions are indicated when there are sigs suggesting tissue hypoxia such as lethargy, collapse, tachycardia and tachypnea. Blood typing and cross matching may be difficult to interpret because animals with autoagglutination also ‘autoagglutinate’ on type cards and cross match. This means a truly compatible cross match may look incompatible. Packed cells are preferred over whole blood to avoid volume overload. Ideally blood should be fresh or < 7 days old because older cells are more likely to cause a transfusion reaction. Plasma – Dogs with IMHA are often thrombocytopenic and hypercoagulable.1,2,3,7,9,11,29 Because these dogs are in hypercoagulable DIC, and not hypocoagulable, plasma is not indicated. Human IVIg – Human immunoglobulin has been used in refractory IMHA with variable results. A study of 10 dogs given 1g/kg noted no obvious adverse but 6 developed thrombocytopenia and 7 died, 5 with thromboembolic
80
disease.34 In this study there was no improved survival. Another randomized blind prospective study of 28 dogs given IVIg on initial presentation saw no improved short term response, hospitalization time or survival to discharge.35 A larger study of 22 dogs that received IVIg based on disease severity, saw similar hospitalization times and mortality between groups given IVIg and those who were not, but it was proposed the IVIg may have been beneficial because it was likely given to more severely affected with similar results.36 There are several reports of human IVIg use in dogs with PIMA that did not respond to initial immunosupressants.37,38 In these dogs there are very few side effects. Human IVIg has been given more than once to the same patient successfully. Plasmapheresis – There is a case report of plasmapheresis being used in a Maltese dog that was treated unsuccessfully with prednisone, cyclosporine and multiple transfusions.39 The dog experienced hypocalcemia during the process but no other complications occurred and the anemia resolved. Plasmapheresis has been used safely and effectively for several other acute and fulminating immune disorders in dogs. The two most common methods are plasma exchange and membrane filtration. In plasma exchange, blood is removed, plasma pulled off and red cells given back with a substitute for the plasma. One or two filters can also be used in membrane filtration techniques to remove microparticles but preserve plasma. Obviously, these are more time intensive and technically difficult procedures. Immunosuppressive Drugs Glucocorticoids – Glucocorticoids are a staple of treatment because they act most quickly and consistently. Even though glucocorticoids are unlikely to affect the Coombs test, it is recommended all diagnostics are complete prior to initiating therapy. Start prednisone or prednisolone at 2.3 mg/kg/day or 50-60 mg/m2 if > 25 kg. The dose can be given once daily or split into two doses. Dexamethasone injection is an option at 0.2-0.4 mg/kg/day for those animals unable to tolerate oral glucocorticoids. If giving prednisone/prednisolone at > 2 mg/kg/day (or large breeds on high doses of glucocorticoids), begin taper as soon as PCV is >30%, PCV is stable for 14 days and other markers of destruction and hemolysis decrease or are absent. Tapering every 3 weeks is recommended based on PCV. Adjunct immunosuppressants – Adjuncts are commonly used with this disease for two reasons. One is the concern with disease severity, a poor response or relapse can occur. The second is how poorly large and giant breeds tolerate glucocorticoids as an earlier back up. The author uses adjuncts to more rapidly taper glucocorticoids in most of our canine patients, regardless of size. The criteria the authors of the CS use for adding adjuncts include a PCV drop of > 5% within 7 days, requirement for transfusion for > 7 days post diagnosis, a dog larger than 25 kg and an animal expected to have bad side effects. Care should also be taken in how additional immunosuppressants are added. As you consider adding another drug ask if there are reasons why current drugs might not be working such as administration techniques affecting bioavailability (e.g. fed vs non fed, drug-drug interactions)? If therapeutic drug monitoring is available (e.g cyclosporine Il-2 levels)? Do you anticipate additional immunosuppression without therapeutic benefit (no more than 3 immunosuppressants)? Are the signs you are seeing due to failed therapy or another disorder? Some drug specifics follow:
- Azathioprine is given at 2 mg/kg/day or 50 mg/m2/day for 2-3 weeks then EOD. Monitor CBC and ALT every 2 weeks for 2 months then every 1-2 months. Hepatotoxicity is most common in the first month, but an idiosyncratic non-dose dependent marked myelosuppression and hepatotoxicity can be seen.
- Cyclosporine is initiated at 5 mg/kg twice daily. Monitoring is liver tests every 2 to 3 months. An advantage of this drug is that an assay is available that determines physiologic effects (pharmacodynamic assay). Drug adjustments can be made based on physiologic response.
- Mycophenolate is initiated at 8 - 12 mg/kg twice daily. No marrow side effects have been observed
but based on the mechanism of action a CBC is recommended at 2 weeks and then every 2 - 3 months. Diarrhea is the most common side effect and can be hemorrhagic and seen 1 to 2 weeks after initiation. This often responds to a lower dose.
- Leflunomide is given at 2 mg/kg/day. A CBC is done every 2 weeks for 2 months then every 2 months
throughout treatment. Leflunomide is usually a tertiary immunosuppressant because of a less consistent response.
81

Novel therapeutics C1-INCH – Intravascular hemolysis is mediated through complement. Complement is activated by interaction of complement (C1) with antibody-coated cells and consists of a sequentially activated proteins that eventually form an attack complex which binds to a cell leading to its destruction. A C1-inhibitor is an acute phase protein that binds to C1r and C1s proteases in the C1 complex preventing complement activation. In addition, C1-inhibitors prevent activation of C2 and C4 as well as inhibiting fibrinolytic (hemostasis), clotting and kinin-kallikrein pathways (blood pressure, inflammation). Recombinant human C1 esterase inhibitor has been used in people to treat conditions such as hereditary angioedema, myocardial infarction/reperfusion injury, sepsis and prevention of organ transplant rejection.40-43 In humans there is a complement-mediated syndrome paroxysmal nocturnal hemoglobinuria that is treated with C1 inhibitors successfully.44 It would make sense to employ this therapeutic strategy in IMHA with intravascular hemolysis which is known to be complement-mediated.45,46 Limited administration is recommended because of concerns of antibody formation to this foreign protein. A single dose of 50 IU/kg has been administered to dogs with no adverse side effects with a recommended dosing of 50 IU/kg slow IV q 8 ours for 3 doses.47 There is currently a study being done using C1-INCH in dogs with IMHA. Relapse If relapse occurs it is important to make sure it is due to the IMHA or PIMA and not secondary to treatment or the result of another disease? Relapse can occur at any time. Cats have a reported relapse rate of 27 – 30%.29,31 Dogs a relapse rate of 15% in one study.8 If the drug taper hasn’t been initiated, another drug should be added. If giving more than one drug, and one is cyclosporine, consider therapeutic drug monitoring. If a dramatic decrease in PCV has occurred, increase drugs to the original dose. If a small decrease has occurred, increase the dose appropriately. After a relapse, consider tapering over a period twice as long. If there have been multiple relapses, consider lifelong treatment or splenectomy. Intact females should be ovariectomized. Thromboprophylaxis Unfortunately, thromboembolic disease is the most common complication of IMHA and the leading cause of death.7,8,29,34 Hypercoagulability has been documented repeatedly with IMHA.2,3,7 While glucocorticoids are known to also cause hypercoagulability, with IMHA the primary concern is the effects of the IMHA on coagulation.48,49 The recommendation is to use thromboprophylaxis in acute IMHA except in hemorrhagic DIC or with platelets < 30k/ul. Venous thrombi are most common and form in a low sheer environment that is rich in fibrin and platelet poor. For this reason, anticoagulants are recommended over platelet inhibitors. Platelet inhibitors are not discouraged in combination with anticoagulants and only recommended for sole thromboprophylaxis if anticoagulants cannot be administered or are not affordable. The anticoagulants recommended are unfractionated heparin, low molecular weight heparin and the factor Xa inhibitors. Dosing recommendations are as follows:
- Unfractionated heparin optional load at 100 U/kg IV then 900 U/kg/d as an IV CRI or 150-300 U/kg SC q 6 hours
- Low molecular weight heparin dalteparin 150-175 U/kg q 8 hours; enoxaparin 0.8-1 mg/kg q 6-8 hours - Factor X a inhibitor rivaroxaban 1 – 2 mg/kg PO daily - Clopidogrel 1 – 4 mg/kg daily
It is the authors opinion that prophylactic anticoagulants are most crucial during active disease when there is evidence of inflammation, red cell destruction and hypercoagulability due to immune dysregulation. Administration during prolonged glucocorticoid administration is not continued unless other risk factors for clot formation are present. Gastroprotectants Gastrointestinal bleeding can occur for various reasons with IMHA and PIMA. Dogs with IMHA often present with melena likely due to poor perfusion of the intestinal tract secondary to anemia and thromboembolism. Glucocorticoids are known to cause gastric ulceration in dogs and used chronically with this disease.50,51 It seems intuitive to use gastroprotectants and antacids in these patients. Unfortunately, these agents are only active in the proximal intestinal tract (stomach, proximal duodenum) and with IMHA the lesions are not necessarily in these regions. In addition, the ulceration seen with glucocorticoid administration is not associated with clinical signs so treatment may not be necessary.50,51 The recommendation is to utilize these drugs with active gastroduodenal ulceration or esophagitis.
82
Prognosis Mortality rates up to 70% have been reported with IMHA.7,8,9,11,30,52 Fortunately, the higher mortality rates were in earlier studies with therapeutics no longer utilized today. There are also advances in knowledge of immunomodulatory therapeutics and use of thromboprophylaxis that have improved survival rates. Seventy-five percent of deaths were within 3 weeks in dogs in one study.22 Mortality risks for IMHA include marked reticulocytosis, lower PCV at diagnosis, intravascular hemolysis, a bilirubin > 10 mg/dl and persistent autoagglutination during therapy.11,22,53 PIMA mortality rates are reported lower and this is the authors experience as well.30 The appearance of reticulocytes is a good prognostic indicator in dogs with PIMA.30 References
1. Mischke R. Hemostatic disorders as a complication of autoimmune hemolytic anemia in dogs. Dtsch Tierarztl Wochenschr 1998 Jan;105(1):13-6.
2. Goggs R, et al. Serial assessment of coagulation status of dogs with immune-mediated haemolytic anaemia using thromboelastography. Vet J 2012 Mar;191(3):347-53.
3. Sinnott VB, et al. Use of thromboelastography in dogs with immune-mediated hemolytic anemia: 39 cases (2000-2008). J Vet Emerg Crit Care 2009 Oct;19(5):484-8.
4. Griebsch C, et al. C-reactive protein concentration in dogs with primary immune-mediated hemolytic anemia. Vet Clin Path 2009 Dec;38(4):421-5.
5. Johnson V, et al. Comparison of cytokine responses between dogs with sepsis and dogs with immune-mediated hemolytic anemia. Vet Immunol Immunopath 2016 Nov 1;180:15-20.
6. Jacobs RM, et al. Use of a microtiter Coombs: test for study of age, gender, and breed distributions in immunohemolytic anemia of the dog. J Am Vet Med Assoc 1984 Jul 1;185(1):66-9.
7. Scott-Moncrieff JC, et al. Hemostatic abnormalities in dogs with primary immune-mediated hemolytic anemia. J Am Anim Hosp Assoc 2001 May-Jun;3793)”220-7.
8. Weinkle TK, et al. Evaluation of prognostic factors, survival rates, and treatment protocols for immune-mediated hemolytic anemia in dogs: 151 cases (1993-2002). J Am Vet Med Assoc 2005 Jun1;226(11):1869-80.
9. Burgess K, et al. Treatment of immune-mediated hemolytic anemia in dogs with cyclophosphamide 2000 Jul-Aug;14(4):456-62.
10. Carr AP, et al. Prognostic factors for mortality and thromboembolism in canine immune-mediated hemolytic anemia: a retrospective study of 72 dogs. J Vet Int Med Sep-Oct;16(5):504-9.
11. Klag AR, et al. Idiopathic immune-mediated hemolytic anemia in dogs: 42 cases (1986-1990). J Am Vet Med Assoc 1993 Mar 1;202(5):783-8.
12. Woolhead VL, et al. Breed predispositions, clinical findings, and prognostic factors for death in dogs with non e immune-mediated anemia. J Vet Int Med 2021 Jan;35(1):252-60.
13. Birkenheuer AJ, et al. Geographic distribution of babesiosis among dogs in the United States and association with dog bites: 150 cases (2000-2003). J Am Vet Med Assoc Sep 15;227(6):942-7.
14. Birkenheuer AJ, et al. Babesia gibsonii infections in dogs from North Carolina. J Am Anim Hosp Assoc 1999 Mar-Apr;35(2):125-8
15. Antognoni MT, et al. Natural infection of Anaplasma platys in dogs from Umbria region (Central Italy). Vet Ital 2014 Jan-Mar;50(1):49-56.
16. Breitschwerdt EB, et al. Clinicopathological abnormalities ant treatment response in 24 dogs seroreactive to Bartonella vinsonii (berkhoffii) antigens. J Am Anim Hosp 2004 Mar-Apr:40(2):92-101.
17. Ciaramella P, et al. A retrospective clinical study of canine leishmaniasis in 150 dogs naturally infected by Leishmania infantum. Vet Rec 1997 Nov 22;141(21):539-43.
18. Werner LL, et al. An investigation of the role of immunologic factors in anemia associated with canine heartworm disease. Vet Immunol Immunopath. 1984 Oct;7(3-4):285-92.
19. Schoeman T, et al. Feline babesiosis: signalment, clinical pathology and concurrent infections. J S Afr Vet Assoc 2001 Mar;72(1):4-11.
20. Zulty JC, et al. Cold agglutinins in cats with haemobartonellosis. J Am Vet Med Assoc 1990 Mar 15;196(6):907-10.
21. Tasker S, et al. Description of outcomes of experimental infection with feline heamoplasmas: copy numbers, haematology, Coombs’ testing and blood glucose concentrations. Vet Microb 2009 Nov 18;139(3-4):323-32.
83
22. Duval D, et al. Vaccine=associated immune-mediated hemolytic anemia in the dog. J Vet Int Med 1996 Sep-Oct;10(5):290-5
23. Fernandez Y, et al. Pregnancy-associated immune-mediated hemolytic anemia in a dog. J Vet Emerg Crit Care 2020 May;30(3):308-11.
24. Noble SJ, et al. Bee sting envenomation resulting in secondary immune-mediated hemolytic anemia in two dogs. J Am Vet Med Assoc 1999 Apr 1;214(7):1026-7.
25. Porter RE, et al. Effect of immune-mediated erythrocyte agglutination on analysis of canine blood using a multichannel blood cell counting system. Vet Clin Path 1990;19(2):45-50.
26. Warman SM, et al. Pattern of Coombs’ test reactivity has diagnostic significance in dogs with immune-mediated haemolytic anaemia. J Small Anim Pract 2008 Oct;49(10):525-30.
27. Chaudhary R, et al. Application of flow cytometry in detection of red-cell-bound IgG in Coombs-negative AIHA. Hematology 2006 Aug;11(4):295-300.
28. Caviezel LL, et al. Comparison of 4 direct Coombs; teat methods with polyclonal antiglobulins in anemic and nonanemic dogs for in-clinic or laboratory use. J Vet Int Med 2014 Mar-Apr;28(2):583-91.
29. Day MJ. Serial monitoring of clinical, haemotological and immunological parameters in canine autoimmune haemolytic anaemia, J Small Animal Pract 1996 Nov;37(11):523-34.
30. Stokol T, et al. Idiopathic pure red cell aplasia and nonregenerative immune-mediated anemia in dogs: 43 cases (1988-1999). J Am Vet Med Assoc 2000 May 1;216(9):1429-36.
31. Kohn B, et al. Primary immune-mediated hemolytic anemia in 19 cats: diagnosis, therapy, and outcome (1998 – 2004). J Vet Int Med 2006 Jan-Feb;20(1):159-66.
32. Lucidi CA, et al. Histologic and cytologic bone marrow findings in dogs with suspected precursor-targeted immune-mediated anemia and associated phagocytosis of erythroid precursors. Vet Clin Pathol 2017 Sep;46(3):401-15.
33. Weiss DJ. Bone marrow pathology in dogs and cats with non-regenerative immune-mediated haemolytic anaemia and pre red cell aplasia. J Comp Pathol 2008 Jan;138(1):46-53.
34. Scott-Moncrieff JC, et al. Intravenous administration of human immune globulin in dogs with immune-mediated hemolytic anemia. J Am Vet Med Assoc 1997 Jun 1;210(11):1623-7.
35. Whelan MF, et al. Use of human immunoglobulin in addition to glucocorticoids for the initial treatment of dogs with immune-mediated hemolytic anemia. J Vet Emerg Crit Care 2009 Apr;19(2):158-64.
36. Gerber B, et al. Use of human immunoglobulin in dogs with primary immune mediated hemolytic anemia. Schweiz Arch Tierheilkd 2002 Apr;144(4):180-5.
37. Yuki M. A case of non-regenerative immune-mediated anemia treated by combination therapy of human immune globulin and mycophenolate mofetil in a dog. Open Vet J 2011;1(1):46-9.
38. Scott-Moncrieff JC, et al. Treatment of nonregenerative anemia with human gamma-globulin in dogs. J Am Vet Med Assoc 1995 Jun 15;206(12):1895-1900.
39. Crump KL, et al. Use of therapeutic plasmapheresis in a case if canine immune-mediated hemolytic anemia. J Vet Emerg Crit Care 2009 Aug;19(4):375-80
40. Busse PJ, et al. Hereditary angioedema. N Eng J Med 2020 Mar;19;382(12):1136-48. 41. Panagiotou A, et al. The lectin pathway of complement in myocardial ischemia/reperfusion injury – review
of its significance and the potential impact of therapeutic interference by C1 esterase inhibitor. Front Immunol 2018 May 25;9:1151.
42. Singer M, et al. Bench-to-bedside review: the role of C1-esterase inhibitor in sepsis and other critical illnesses. Crit Care 2011 Jan 26;15(1):203.
43. Berger M, et al. Update on C1 esterase inhibitor in human solid organ transplantation. Transplantation 2019 Sep;103(9):1763-775.
44. Brodsky RA. Paroxysmal nocturnal hemoglobinuria. Blood 2014 Oct 30;124(18):2804-11. 45. Goggs R, et al. C1 inhibitor in canine intravascular hemolysis (C1INCH): study protocol for a randomized
controlled trial. BMC Vet Res 2019 Dec 30;15(1):475 46. Hernandez DM, et al. In vitro inhibition of canine complement-mediated hemolysis. J Vet Int Med 2018
Jan;32:(1):142-6. 47. Wong C, et al. Pharmacokinetics of human recombinant C1-esterase inhibitor and development of anti-drug
antibodies in healthy dogs. Vet Immunol Immunopath 2018 Sep;203:66-72. 48. Flint SK, et al. Independent and combined effects of prednisone and acetylsalicylic acid on
thromboelastography variables in healthy dogs. Am J Vet Res 2011 Oct;72(10):1325-32. 49. Rose LJ, et al. Effect of prednisone administration on coagulation variables in healthyBeagle dogs. Vet
Clin Pathol 2011 Dec;40(4):426-34.
84
50. Whittemore JC, et al. Clinical, clinicopathologic, and gastrointestinal changes from administrations of clopidogrel, prednisone, or combination in healthy dogs: A double-blind reandomized trial. J Vet Int Med 2019 Nov-Dec;33(6):2618-27.
51. Whittemore JC, et al. Clinical, clincopathologic, and gastrointestinal changes from aspirin, prednisone, or combination treatment in healthy research dogs: A double-blind randomized trial. J Vet Int Med 2019 Sep-Oct;33(5):1977-87.
52. Reimer ME, et al. Immune-mediated hemolytic anemia: 70 cases )1988-1996). J Am Anim Hos Assoc 1999 Sep-Oct;35(5):384-91.
53. Mills JN, et al. Autoimmune haemolytic anaemia in dogs. Aust Vet J 1985 Apr;62(4):121-3. 54. Garden OA, et al. ACVIM consensus statement on the diagnosis of immune-mediated hemolytic anemia in
dogs and cats. J Vet Int Med 2019 Mar;33(2):313-34. 55. Garden OA, et al. ACVIM consensus statement on the treatment of immune-mediated hemolytic anemia in
dogs. J Vet Int Med 2019 Mar;33(2):313-34.
85

Review of Immunosuppressive Therapy Jana Gordon, DVM, DACVIM
Introduction Immune-mediated diseases are commonly diagnosed in dogs and, occasionally, in cats. In some cases we are able to identify a drug, infectious agent or neoplasm that is responsible for the condition but in many of our patients no cause is found. Regardless, the immune response must be controlled and for that we rely primarily on pharmaceutical intervention. For many years we have had a relatively small number of therapeutic options, which has made the decision-making process easy but has also subjected many of our patients to serious side effects and treatment failure. This is a review and update on the use of immunosuppressants in companion animals.
Glucocorticoids Glucocorticoids have been used for decades in veterinary medicine. They have been used at their lowest dose to treat various forms of hypocortisolism, at a higher dose to treat inflammatory conditions and at even higher doses to treat immune-mediated conditions. Of all the immunosuppressives currently and previously available, glucocorticoids, in their most common formulations, are singularly the most effective in controlling many immune-mediated diseases. Unfortunately, practitioners are often treating conditions for extended periods of time and our patients, particularly canine patients, suffer because of it. While some side effects of glucocorticoids are merely inconvenient (e.g. polyuria, polydipsia, polyphagia, panting) others are more difficult to tolerate or even life-threatening (e.g. aggression, insulin resistance, recurrent infection, thromboembolic disease). Some of the difficulty we have in controlling disease and side effects of this type of drug could be related to our dosing. What actually constitutes an immunosuppressive dose is not completely clear. We know that cats may have a problem with the bioavailability or metabolism of the pro drug, prednisone, to prednisolone so prednisolone is recommended in this species.1 In addition, cats that are obese appear to have higher plasma concentrations of prednisone than cats with a normal body condition which might explain why obese cats are more susceptible to detrimental effects of glucocorticoids.1 For this reason cats should be dosed on lean body mass.
Historically dosing of prednisone and prednisolone has been done on a mg/kg basis and immunosuppressive doses reported as 2 mg/kg/day in dogs and up to twice that in cats, who reportedly are more resistant to the effects (good and bad) of glucocorticoids. This has led to overdosing of large breed dogs that appear more susceptible to side effects of glucocorticoids.2 Alternatively, dosing of 40 to 50 mg/m2/day based on body surface area has been recommended and not to exceed a total of 60 mg/day in large and giant breeds.2 Doses higher than this are not believed to provide additional therapeutic benefits but lead to more severe muscle wasting and weakness.
The glucocorticoids we use most often to treat chronic immune conditions (prednisone, prednisolone) are oral and intermediate in duration. Intermediate acting injectable glucocorticoids are occasionally used when oral medications are not tolerated for short periods of time. Long-acting depot glucocorticoids do not provide consistent immune suppression and are more often associated with the development of complications such as diabetes mellitus so are not recommended. A long-acting glucocorticoid that is used in our veterinary patients is budesonide. Budesonide is a long acting potent glucocorticoid (15 x more potent than prednisone) that is metabolized extensively by the liver on first pass.3 Commercially available capsules are formulated to resist degradation in the stomach (requires pH > 5.5).3 Budesonide is used most often for ‘topical’ effects and as a topical in patients in which persistent serum glucocorticoid levels are not desirable. In veterinary patients we use it most often for IBD but there are additional applications such as an inhalant for asthma, topical for atopic dermatitis and potentially for chronic hepatitis.4 Budesonide, short or long release, does suppress the hypothalamic-pituitary-adrenal axis despite relatively few clinical side effects.5,6 The extended release formulation is used most often at 3 mg/m2 daily in the dog and 1 mg/day in the cat.7 Alternatively dogs are dosed by range of weight at: 1mg (3-7 kg), 2 mg (7.1-15 kg), 3 mg (15.1-30 kg) and 5 mg (> 30 kg).8 In one study similar side effects and clinical effects were seen in dogs treated with prednisone at 1 mg/kg PO BID for 3 weeks then 0.5 mg/kg PO BID for 3 weeks or budesonide dosed by range of weight.8
Azathioprine Azathioprine has been used to treat immune-mediated diseases in dogs for many years. Cats and some people lack, or have a marked decrease in, thiopurine methyltransferase, an enzyme involved in the azathioprine metabolism. This makes them more susceptible to bone marrow suppression which is why azathioprine is not used in cats.
86

Azathioprine is metabolized by the liver into an active metabolite whose exact mechanism is unknown but results in interference with T cell function. An idiosyncratic bone marrow suppression and hepatotoxicity are reported so monitoring is required. Initial dose in dogs is 2 mg/kg/day for 1 to 2 weeks followed by 2 mg/kg EOD or 1 mg/kg/day. There is concern that azathioprine takes time to achieve effect but there is no evidence to support this drug takes any longer than other adjunct immunosuppressants. Azathioprine is a relatively inexpensive drug. Chlorambucil Chlorambucil is a cell cycle non-specific alkylating agent used historically in dogs and cats for both neoplasia and immune-mediated diseases. Compared to other alkylating agents it has fewer side effects including gastrointestinal upset and bone marrow suppression. Chlorambucil has historically been used as the feline adjunct immunosuppressant because cats did not tolerate the other immunosuppressants, like azathioprine and cyclophosphamide, available at the time. To this day it is used in cats with various immune-mediated conditions that are refractory to glucocorticoids. Chlorambucil was used in dogs primarily as an anti-neoplastic but looks promising as an immunosuppressant in this species. In a retrospective study in 27 dogs, prednisolone and chlorambucil were compared to prednisolone and azathioprine for protein-losing enteropathy.9 The dogs in the chlorambucil/prednisolone group had significantly greater weight gain, albumin and survival times than the azathioprine/prednisolone group. There are a lot of dosing recommendations in dogs and cats for various diseases. In the study mentioned above, 4 to 6 mg/m2 was the initial dose in dogs. For cats the dose is 2 mg every 24 to 48 hours to start or compound at same dose recommendations as dogs (0.1 to 0.2 mg/kg day or 4 to 6 mg/m2/day). The drug is tapered to the lowest effective dose. Although chlorambucil is less marrow suppressive than other alkylating agents, dose-dependent myelosuppression can occur so periodic monitoring of CBC’s is required. In addition, breeds that continuously grow hair will experience alopecia. Vomiting, diarrhea and neurologic signs (cats) can also be seen. Chlorambucil is manufactured in 2 mg tablets that should not be divided. Chlorambucil tablets are expensive and doses difficult to determine with the limited tablet size which has led to the use of compounded formulations. There are inconsistent reports concerning the efficacy of compounded products, liquid more of a concern than capsules, but they are commonly used in practice. Cyclosporine Cyclosporine is a potent immunosuppressant that primarily works through inhibition of T cell function. This drug is derived from various fungal organisms. Initial use in dogs and cats was in renal transplant patients but over the years cyclosporine has been used in dogs and cats for numerous inflammatory and immune-mediated processes. It is now approved for use in dogs for atopy and cats for allergic skin disease. Keep in mind that there are differences in the bioavailability between preparations. Preparations that are microemulsified should be used because they have better bioavailability so more dependable absorption and blood levels. This means that in solution it forms a microemulsion to aid absorption. For many life-threatening conditions it is desirable to attain immunosuppression as soon as possible. For this reason, higher doses of 5 mg/kg BID and drug monitoring are recommended. For more stable conditions (atopy, anal forunculosis, IBD, hepatitis, etc) therapy is often initiated at 5 mg/kg once daily and therapeutic drug monitoring may or may not be needed based on response. Historically we would measure cyclosporine levels with peak values being used to look for risk of toxicity and trough for treatment failure. Unfortunately, there is a poor correlation between cyclosporine levels and clinical response. This has led to the development of pharmacodynamic assays to determine the action of the drug in the individual patient. There is a ‘pharmacodynamic’ T cell assay that has been developed at the University of Mississippi that utilizes quantitative real time PCR to evaluate expression of IL-2 and IFN-γ as measures of T cell suppression.10 The idea is that measuring cyclosporine levels (the previous methodology) tells you about pharmacokinetics but measuring T cell function tells you about actual pharmacologic effects (pharmacodynamics). Cyclosporine has been used for almost every immune condition described in dogs with variable success and for many conditions in cats. In a study looking at prednisone alone and cyclosporine alone for treating primary immune-mediated polyarthritis (IMPA) in a small number of dogs equal numbers of dogs in each group (7/10) responded to each therapy suggesting cyclosporine alone may be a viable option for treating IMPA and likely other immune-mediated conditions.11 Side effects of cyclosporine are primarily intestinal but idiosyncratic hepatotoxicity has been reported. Gingival hyperplasia, increased hair growth and secondary infections may also be seen with chronic administration. While this drug can be compounded, compounded formulations are not recommended for more life-threatening conditions over the FDA approved product that has more proven bioavailability. Atopica® is available in capsules as well as a 100 mg/ml oral solution.
87

Mycophenolate Mycophenolate is a derivative of a fungus and a prodrug of the active metabolite, mycophenolic acid. Mycophenolic acid is an irreversible inhibitor of an enzyme involved in the synthesis of purines and thus inhibits B and T cell proliferation. This drug was originally used in humans (and in canine research) to prevent organ rejection but has since been used for multiple immune-mediated conditions. The original product was prohibitively expensive but now that generics are available, mycophenolate has been used much more commonly in veterinary medicine. While use of this drug has been published for numerous immune-mediated conditions in dogs (IMHA, myasthenia gravis, ITP, meningoencephalomyelitis, glomerulonephritis, sterile panniculitis, etc), there are case reports of the successful use of mycophenolate in two cats with primary IMHA and one with IMPA.12,13 The dose for dogs and cats is 10 to 15 mg/kg twice daily. In a dog study looking at lymphocyte function with oral mycophenolate, 10 mg/kg BID did not suppress lymphocyte function so higher doses might be needed in some patients. Tablets, capsules, oral suspensions and injectable formulations are available. For the injectable formulation in cats, plasma levels consistent with immunosuppression in humans were not attained until 20 mg/kg BID was given in one study. Bioavailability is variable in dogs. There is evidence that it may take about 2 weeks to see therapeutic benefits from this drug in dogs. Blood levels can be measured at Auburn University. Intestinal side effects, particularly diarrhea, are most common in dogs but marked myelosuppression has been noted in people. For this reason, and our limited experience with this drug, it is recommended to periodically monitor CBC’s. This drug has a similar mechanism of action as azathioprine so there are concerns about additive toxicity when used together. Leflunomide Leflunomide is also a prodrug whose active metabolite is teriflunomide. Teriflunomide reversibly blocks an enzyme in pyrimidine synthesis so it affects T and B cell synthesis. Interestingly the half-life of this metabolite is 2 weeks in humans but only 24 hours in dogs. This drug has been used in people for rheumatoid arthritis and to prevent organ rejection. Once again, its cost made its use in veterinary species prohibitive but it has become more affordable. There are a few individual case reports of its use in dogs in the literature and less in cats. Availability as a generic and a study from 2010 regarding use in immune-mediated polyarthropathy in dogs brought awareness to its potential use in our patients.14 In this study 8 dogs had a complete response, 5 had a partial response and 1 dog had no response based on clinical impression (a single dog had follow-up arthrocentesis) with no side effects. This drug is now used as an adjunct immunosuppressant in many immune diseases. The dose recommended is 2 mg/kg once daily in dogs.15 Drug levels can be measured at Auburn University. Side effects are very uncommon but lethargy, anorexia, diarrhea, anemia, bleeding, thrombocytopenia, and elevated liver enzymes can be seen. Leflunomide may decrease platelet function in dogs. Because of severe myelosuppression and hepatotoxicity in people occasional monitoring is recommended until we know more about the safety of this drug. Cytarabine This is an injectable medication frequently used as an antineoplastic for CNS neoplasms because it penetrates the BBB. Cytarabine is cytotoxic to many proliferating cells through a cell phase specific inhibition of DNA synthesis so is beneficial in other diseases. It has become the first line adjunct int eh treatment of granulomatous meningoencephalomyelitis (GME) and meningoencephalitis of unknown etiology/origin (MUE).16 It is given preferentially as a CRI over several hours to achieve longer steady state concentrations.17,18 Monitoring is necessary because cytarabine can cause bone marrow suppression and neurologic side effects. Human Intravenous Immunoglobulin Human intravenous immunoglobulin is a pooled sample of normal human immunoglobulin collected from several thousand donors. The product is almost exclusively IgG monomers with a small percentage of IgG dimers, IgM and IgA. Human immunoglobulin infusions work by modulating complement activation, blocking activation of Fcy receptors on monocytes and macrophages (reduces activation of these cells), upregulates inhibitory FcyRIIB (inhibits pathogenic autoantibody consumption of cells), binding FcRn receptors on macrophages in place of endogenous IgG (endogenous pathogenic autoantibody free to be more readily destroyed), interaction with idiotypic (bad) antibodies (blocks interaction of autoantibodies with target autoantigens), increases anti-inflammatory cytokines and suppressing inflammatory mediators. IVIG is most commonly used in poorly responsive cases of autoimmune hemolytic anemia with varying success but has also been used in other poorly responsive or acute severe immune-mediated diseases successfully such as SLE, IMTP, fulminant myasthenia gravis and cutaneous
88
erythema multiforme.19,20,21 The recommended dose is 0.5 to 1 g per kg IV. This is infusion of a foreign protein so allergic reactions are possible and believe to be more common with repeated administration.
Plasmapharesis Plasmapheresis refers to removal of components from blood using a system located outside of the body resulting in a filtered plasma. This can be done with centrifugation techniques or using semipermeable membranes to remove cells. Double filtration plasmapheresis refers to the use of two semipermeable membranes in the process. With this technique larger, more pathogenic components can be removed and smaller, more valuable substances can be returned to the patient. Plasmapheresis has been used in dogs with intoxications, hyperviscosity syndrome, IMHA, ITP, SLE.22,23,24,25,26 Complications include hypotension, hypocalcemia and hypothermia.
References: 1. Center SA, Randolph JF, et al. Influence of body condition on plasma prednisolone and prednisone in
clinically healthy cats after single oral dose administration. Res Vet Sci 2013 Aug;95(1):225-30.2. Wang HB, Kim SM, et al. Pharmacokinetic comparison of body surface area and body weight based
prednisolone dose on small and large breed dogs. Abstract ACVIM 2015.3. Plumb DC. Plumbs Veterinary Drug Book. 5th ed. 2005 Blackwell Publishing .4. Malamies M, Vainio O, et al. Endocrine effects of inhaled budesonide compared with inhaled fluticasone
proprionate and oral prednisolone in healthy beagle dogs. Vet J 2012 Dec;194(3):1209-15.5. Tumulty JW, Broussard JD, et al. Clinical effects of short term oral budesonide on the hypothalamic-
pituitary-adrenal axis in dogs with inflammatory bowel disease. J Am Anim Hosp 2004 Mar-Apr;40(2):120-3.
6. Stroup ST, Behrend ET, et al. Effects of oral administration of controlled-ileal-release budesonide andassessment of pituitary-adrenocortical axis suppression in clinically normal dogs. Am J Vet Res 2006Jul;67(7):1173-8.
7. Pietra M, Fracassi F, et al. Plasma concentrations and therapeutic effects of budesonide in dogs withinflammatory bowel disease. Am J vet Res 2013 Jan;74(1):78-83.
8. Dye TL, Diehle KJ, et al. Randomized, controlled trial of budesonide and prednisone for the treatment ofidiopathic inflammatory bowel disease in dogs. J Vet Int Med 2013 Nov-Dec; 27(6):1385-91.
9. Dandreaux JR, Noble PM, et al. Comparison of a chlorambucil-prednisolone combination with anazathioprine-prednisolone combination for treatment of chronic enteropathy with concurrent protein-losingenteropathy in dogs: 27 cases (2007 – 2010) J Am Vet Med Assoc 2013 Sep 15;243(6):1705-14.
10. Fellman CL, Archer TM, et al. Effects of oral cyclosporine on canine T-cell expression of IL-2 and IFN-gamma across a 12-h dosing interval. J Vet Pharmacol Therap 2016 Jun;39(3):237-44.
11. Rhoades AC, Vernau W, et al. Comparison of the efficacy of prednisone and cyclosporine for treatment ofdogs with primary immune-mediated polyarthritis. J Am Vet Med Assoc Feb 15;248(4):395-404.
12. Bacek LM, MacIntire DK. Treatment of primary immune-mediated hemolytic anemia with mycophenolatemofetil in two cats, J Vet Emerg Crit Care 2010 Feb;212(1): 45-9.
13. Tamura Y, et al. Successful treatment and long-term follow up of idiopathic immune-mediated polyarthritiswith mycophenolate mofetil in a cat. J Fel Med Surg 2020 Nov;6(2):1-5.
14. Colopy SA, Baker TA, et al. Efficacy of leflunomide for treatment of immune-mediated polyarthritis indogs: 14 cases (2006-2008). J Am Vet Med Assoc 2010 Feb 1;236(3):312-8.
15. Sato M, et al. A retrospective study on the safety and efficacy of leflunomide in dogs. J Vet Int Med 2017Sep-Oct;32(5):52-57.
16. Zarfos M, et al. Combined cytosine arabinoside and prednisone therapy for meningoencephalitis ofunknown etiology in 10 dogs. J Small Anima Pract 2006 Oct;47(10):588-95.
17. Crook KI, et al. The pharmacokinetics of cytarabine in dogs when administered via subcutaneous andcontinuous infusion routes, j Vet Pharma col Ther 2013 Aug;36(4):408-11.
18. Lowrie M, et al. Effect of a constant rate infusionof cytosine arabinosideonmortalityin dogs withmeningoencephalitisof unknown origin, The Vet J 2016:213:1-5.
19. Balog K, et al. A prospective randomized clinical trial of vincristine versus human intravenousimmunoglobulin for acute adjunctive management of presumptive primary immune-mediatedthrombocytopenia in dogs. J Vet Int Med 2013 May/Jun;27(536-41.
89
20. Ramos SJ, et al. Erythema multiforme major in a dog treated with intravenous human immunoglobulin andimmunosuppressive therapy. J Am Anim Hosp Assoc 2020 Mar/Apr;56(2):133-8.
21. Whelan MF, et al. Use of human immunoglobulin in addition to glucocorticoids for the initial treatment ofdogs with immune-mediated hemolytic anemia. J Vet Emerg Crit Care 2009 Apr;19(2):158-64.
22. Crump KL, et al. Use of therapeutic plasmapheresis in a case of canine immune-mediated hemolyticanemia. J Vet Emerg Crit Care 2009 Aug;19(4):375-80.
23. Heather GG, et al.. Successful management of acute bilirubin encephalopathy in a dog with immune-mediated hemolytic anemia using therapeutic plasma exchange. J Vet Emerg Crit Care 2019Sep;29(5):549-57.
24. Scagnelli AM, et al. Effects of therapeutic plasma exchange on serum immunoglobulin concentrations in adog with refractory immune-mediated hemolytic anemia. J Am Vet Med Assoc 2018 May 1;252(9):1108-12
25. Kopecny L, et al. Application of therapeutic plasma exchange in dogs with immune-mediatedthrombocytopenia, J Vet Int Med 2020 Jul-Aug:34(4):1576-81.
26. Matus RE, et al. Plasmaphaeresis in five dogs with systemic immune-mediated disease. J Am Vet MedAssoc 1985 Sep 15;187(6):595-9.
90

Review of Tests of Liver Function in Companion Animals Jana Gordon DVM, DACVIM
Introduction Liver disease is common in our companion animals, but the diagnosis is not always straight forward. As clinicians, we rely on information from our patient history and physical examination to determine if we should consider liver diseases as differentials and then utilize primary and secondary laboratory diagnostics to further our suspicions. In some instances, these laboratory tests can narrow the differential list down to a few diseases. This session will cover the use and limitations of laboratory tests in the diagnosis of liver disease.
The CBC The complete blood count does not provide any information specific for liver disease, but abnormalities can be found in red cell numbers and morphology with liver disease. Non-regenerative anemia (normocytic, normochromic) is uncommon but can occur as part of the ‘chronic disease’ phenomenon. A microcytic anemia can be seen with portosystemic vascular anomalies (PSVA), cirrhosis and hepatic lipidosis (cats) believed to be secondary to alterations in iron metabolism from decreases in hepatic blood and reduced hepatocyte function. Iron deficiency anemia may also be more of a ‘blood loss’ phenomenon from chronic bleeding into the GI tract as a result of portal hypertension. Poikilocytes are abnormally shaped red cells and include acanthocytes, elliptocytes, keratocytes, schistocytes, stomatocytes and target cells. Acanthocytes and keratocytes form from alterations in cholesterol in the red cell membrane and as a result of fragmentation injury, both of which can occur with liver diseases. Elliptocytes are elongated red blood cells and can occur in some feline liver diseases, particularly hepatic lipidosis. Target cells may be noted secondary to cell membrane abnormalities or iron deficiency.
Hepatobiliary Enzymes Hepatobiliary enzymes of interest in the dog and cat include alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP) and gamma glutamyl-transpeptidase (GGT). Liver enzymes are highly sensitive but carry a low specificity for liver disease. In other words, they often tell you that there is something wrong with the liver but not what is specifically wrong with the liver and may be abnormal in diseases that are not hepatic in origin but affect the liver. This is in part because the liver is a highly vascular organ and susceptible to the effects of diseases in other organ systems. Unfortunately, the degree of enzyme elevation does not correlate with severity of hepatobiliary damage, it is not specific for any disease process, or predictive of hepatobiliary function or return to function. One reason is that the liver has a remarkable regenerative capacity. In addition, in end stage liver disease, the functional mass of liver cells is reduced and so less enzymes are theoretically produced. This may, in part, be due to hepatocyte cellular senescence which occurs when there are fewer active cells to handle metabolic activity.
Increases in Liver Enzymes - not primary liver disease
Corticosteroids - D Systemic Infection Pregnancy - C Anticonvulsants Colostrum feeding - D Septic shock Hyperthyroidism – C Neoplasia CHF Diabetes mellitus Muscle injury Bone growth Hypothyroidism – D Shock Osteomyelitis Hypoadrenocorticism Seizure Osteosarcoma Hyperaldosteronism – D Hypotension Surgery Gastrointestinal disease Inflammation
ALT and AST are leakage enzymes which mean they suggest increased membrane permeability and cell damage. AST is more sensitive but less specific than ALT because large amounts of AST are found in the muscle so if the degree of AST elevation is much more significant than ALT (but ALT is increased) then muscle origin should be suspected. In acute liver injury, a drop in ALT of >/= 50% over 48 hours is considered a good prognostic indicator with acute liver disease.
ALP and GGT are associated with diseases that have a cholestatic component and, since they are membrane bound, may also be induced by certain drugs such as phenobarbital and glucocorticoids (dog). ALP has multiple
91

isoenzymes including liver, corticosteroid-induced, bone, kidney, intestine and placenta origin. Intestinal, kidney and placental ALP have short half-lives that don’t contribute to serum ALP except for pregnant females late in gestation. Bone ALP can contribute up to 1/3 of total serum ALP and can increase minimally in growing dogs, with osteomyelitis and in osteosarcoma. Liver (L-ALP) and corticosteroid ALP (C-ALP) are the largest contributors to increases in ALP in the dog. Cats do not have C-ALP which is why cats ALP does not increase with glucocorticoids. ALP may be elevated due to increased synthesis or release from the hepatocellular membrane, generally with diseases that have a cholestatic component. In cats, hepatobiliary disease is the most common cause of increased ALP. ALP increases in cats are often not as dramatic because of the shorter half-life and lower hepatic stores of this enzyme. In cats, cholangitis, cirrhosis and biliary obstruction are associated with increases of GGT that are usually more significant than ALP. With hepatic lipidosis in cats, ALP is more markedly elevated than GGT (e.g. ALP might be 10 times normal with a GGT twice normal).
Tests Assessing Liver Function Cholesterol - The liver is involved in cholesterol synthesis. Dietary cholesterol is solubilized by bile salts and lecithin forming micelles. These micelles aid digestion of fats as well as deliver cholesterol to the intestinal brush border where they more readily diffuse across the cell membrane. Within the enteric epithelial cells, cholesterol forms chylomicrons (along with triglycerides and phospholipids) that are excreted by exocytosis into the lacteals and then into venous circulation. These chylomicrons are extracted by the liver or other tissues where they are stored or used for energy. A small amount of cholesterol may be recovered from absorption of bile acids. Most circulating cholesterol is derived from synthesis by the liver with other tissues playing a minor role. Both increases and decreases in cholesterol can be seen in liver disease. Increased cholesterol can be seen with biliary obstruction or cholestasis primarily due to increased synthesis but back-diffusion from the biliary system also plays a role. Decreases are seen with acquired and congenital vascular diseases and cirrhosis as a result of synthetic failure. Cholesterol is necessary for synthesis of bile acids so cholesterol may decrease with increased production of bile acids (i.e. bile acids are a negative feedback for cholesterol).
Glucose - The liver is largely responsible for maintenance of euglycemia in the fasting state. Carbohydrates can be utilized immediately for an energy source, stored in the liver as glycogen or converted to lipids for storage or transportation. Stored glycogen can be broken down in the liver (glycogenolysis) for energy. Proteins and lipids can be utilized for energy production in the liver via gluconeogenesis as needed. Hypoglycemia can be seen with severe acute or chronic liver failure and in small breeds with vascular anomalies. Hypoglycemia may also be paraneoplastic with hepatomas and hepatocellular carcinoma. Glycogen storage diseases have also been associated with hypoglycemia due to their interference with glucose production in the liver and muscle.
BUN - Serum blood urea nitrogen (BUN) can be affected by liver disease because the liver detoxifies ammonia in the urea cycle and generates urea for excretion. BUN may decrease secondary to decreased production in a failing liver. An increase in glomerular filtration rate and fluid diuresis can also decrease BUN as a result of medullary washout as can a heavily protein restricted diet. The BUN may be increased by dehydration, increased dietary protein and GI hemorrhage.
Albumin & Globulin - The liver synthesizes proteins such as albumin, non-immunoglobulins (α-globulins and β-globulins) and coagulation proteins. Hypoalbuminemia can be seen with severe liver disease and is primarily due to synthetic failure, but portal hypertension and sodium/water retention may contribute. Albumin is also a negative acute phase protein so it may decrease with inflammatory conditions in and outside the liver. The non-immunoglobulins may be decreased in hepatic failure or increased with chronic inflammatory liver disease (some of these are acute phase proteins). Although immunoglobulins are not synthesized in the liver they may be increased in chronic inflammatory liver diseases in or outside the liver, especially in the cat.
Procoagulants - The liver is important to hemostasis. Hepatocytes synthesize all factors except VIII (von WIllebrands) so prothrombin time (factor VII, extrinsic pathway) and activated partial thromboplastin time (factors VIII, IX, XI, XII, intrinsic pathway) may be prolonged with severe liver disease. Diseases in which there is a decrease in functional mass (PSVS, cirrhosis, acute liver injury) may have prolonged bleeding due to decreased factor synthesis. The liver is the site of vitamin K-dependent activation of factors II, VII, IX and X as well. In animals with severe cholestasis, inhibition of bile flow may lead to impaired uptake of fat-soluble vitamins like vitamin K. Without adequate vitamin K, activation of factors II, VII, IX and X may not occur. This explains why we assess clotting times in dogs and cats with significant biliary disease (hepatic lipidosis, obstructive cholangitis).
92
Anticoagulants - Hepatocytes synthesize inhibitors of coagulation such as protein C and antithrombin III. Protein C is a vitamin-dependent proenzyme that is activated when thrombin binds thrombomodulin on endothelial cells. Protein C acts as an anticoagulant by cleaving factors Va and VIIIa thus down-regulating thrombin production. In dogs, protein C is decreased in many forms of liver disease so it is not a specific test for any particular type of liver disease. Its clinical utility is in differentiating two types of congenital vascular diseases. In dogs with congenital PSS, microvascular dysplasia has been associated with higher protein C levels (> 70% protein C activity) than those with a single PSVA (< 70% activity). In a study of 238 dog s, including 78 with PSVA and 39 with MVD, a protein C < 70% was found in 68/78 PSVA dogs and protein C > 70% in 37/38 MVD dogs. In addition, protein C has been used to monitor success in shunt ligation.1 In this same study 10 dogs with PSVA’s underwent ligation and although protein C increased in all, 5/10 dogs did not increase above 70%.
The liver also clears coagulation factors, plasminogen activators and products of fibrinolysis. Because of the role of the liver in production of anticoagulants and procoagulants, animals with severe liver disease may be in a hypo- or hypercoagulable state.
Bile acids - Bile is composed of > 90% bile acids kept in solution by the formation of micelles. Bile acids are formed from cholesterol in the liver. In the liver they are conjugated to glycine or taurine and excreted into the bile and stored in the gall bladder. Dietary fat and protein in the duodenum stimulate cholecystokinin, which causes contraction of the gall bladder and transport of bile to the duodenum. Bile acids solubilize fat in the intestinal tract to aid absorption. Once the conjugated bile acids reach the ileum, which contains the receptors for conjugated bile acids, they are absorbed into the portal circulation and are re-extracted by bile acid transporters in the hepatic sinusoids. In hepatobiliary disease, increases in bile acids are seen as a result of decreased extraction by the liver from the portal blood (shunting, hepatocellular failure) or reflux into the bloodstream (cholestasis). Bile acids can be artificially increased or decreased by inadequate fat or protein in the test meal, severe ileal disease, variations in gastrointestinal motility, and unpredictable gall bladder contraction.
Fasting and post-prandial bile acids have been used historically to evaluate liver function. There is a normal range established for fasting and post prandial bile acids with post prandial basically 2-to-3-fold baseline. A prolonged fast may not be necessary because, basically, no matter when you measure bile acids, they should never be above the reference range for post-prandial. However, I have seen a few dogs for shunt evaluation with increased bile acids that we repeat and are normal. Fasting bile acids may be normal in a small number of dogs with PSS likely because if fasted long enough, even a dysfunctional liver will be able to pull bile acids out of circulation. Post-prandial bile acids will increase the sensitivity for the diagnosis of liver shunts.2 The sensitivity of bile acids for diagnosis of PSS is reported at 64 – 100%.2,3,4,5,6
It seems intuitive you could use bile acids to follow up a successful shunt ligation. In a study looking at long term follow up of dogs after complete ligation of extrahepatic shunts, bile acids decreased in all dogs but did not normalize at 18 months in 64% of pre and 86% of post prandial samples.2
Mild to moderate increases in bile acids are also occasionally seen in animals with airway collapse syndrome.7 Maltese dogs may also have higher bile acids as a result of testing methodology.8 Interestingly, bile acids are less sensitive than serum ALT and ALP for detecting early acute and chronic hepatitis.9
Urine bile acids have also been evaluated in dogs and cats for diagnosis of hepatobiliary disease.10,11 The theory is that bile acids are excreted in increased amounts in the urine over time. A ratio of bile acids to creatinine is used much like other urinary excretion tests. Urine bile acids have the advantage of not requiring fasting, venipuncture or multiple samples. Despite the advantages of this test, serum bile acids are believed to be a more sensitive test for early liver disease.
Ammonia - The liver is responsible for most ammonia detoxification in the body. A minor source is production in the small intestine by bacterial degradation of purines, amino acids and amines producing ammonia. Bacterial ureases degrade urea in the colon and are responsible for the largest source of ammonia production. Glutamine catabolism in the small intestine also produces ammonia. Ammonia diffuses readily through the intestines and into portal circulation. Detoxification may occur via metabolism in the urea cycle or by consumption in the production
93

of glutamine in the liver. Kidneys, muscle, brain, and intestines are also capable of detoxification of ammonia via formation of glutamine. Animals with some forms of portosystemic shunting can have increased circulating ammonia levels as a result of failure to detoxify. Deficiencies in argininosuccinate synthetase (rare enzyme deficiency) in dogs and arginine (seen with prolonged anorexia) in cats have also been associated with hyperammonemia because both are necessary to complete the urea cycle. Fasting ammonia levels can be measured or, alternatively, an ammonia tolerance test performed. The ammonia tolerance test is typically done with rectal administration of ammonium chloride. Ammonia is measured in whole heparinized blood but must be measured shortly after sampling (within 20 minutes). Samples should be drawn and placed on an ice water bath until testing is performed to prevent errors secondary to cellular metabolism. In house laboratory tests are available but there are concerns regarding sensitivity of certain analyzers with some analyzers correlating well with laboratory analyzers and others not.12,13,14 With that said, there appears to be good correlation between laboratory methods and some point of care analyzers. Fasting ammonia has a reported sensitivity of 81 – 100% for diagnosing PSS.5,6,15 In a study of dogs with congenital portosystemic shunts, fasting ammonia levels were abnormal in 21 of 23 dogs and correlated well with degree of shunt closure at surgery.16 In this same study all dogs ammonia decreased to normal. Studies are conflicting that report fasting ammonia is more sensitive than bile acids for detecting PSS.5,17,18 Increased sensitivity for diagnosis of PSS is likely with combined fasting ammonia and bile acids.19
Bilirubin - Bilirubin is a breakdown product of heme that is derived from red blood cells. Bilirubin is produced as a result of red blood cell breakdown in the reticuloendothelial cell system of the spleen and liver and is called unconjugated bilirubin. The unconjugated bilirubin produced is bound to albumin to increase water solubility. The unconjugated bilirubin is extracted by the liver and conjugated with glucuronic acid. Conjugated bilirubin is secreted into the bile and into the intestinal tract. Bilirubin is then excreted in the feces or converted to urobilinogen by intestinal bacteria. Urobilinogen is converted to stercobolin (brown pigment of feces) or enters portal circulation where it is re-excreted into the bile (after hepatic extraction) or excreted in the urine. Icterus is the result of bilirubin retention and may be pre-hepatic (hemolysis), hepatic (impaired uptake, conjugation or excretion) or post-hepatic (biliary obstruction). Historically measures of direct (conjugated) and indirect (unconjugated) bilirubin had been used to differentiate prehepatic from hepatic or post hepatic causes of hyperbilirubinemia but there is significant overlap in the types of bilirubin produced in different disease states. There is no improved specificity in utilizing direct vs. indirect (conjugated vs. unconjugated) bilirubin. Bilirubin may be a normal finding in dog urine (dog kidneys can conjugate bilirubin and excrete it), but its presence in cat urine is suggestive of hemolysis or hepatic disease.
Uroliths - Ammonium biurate crystals are sometimes detected in the urine of animals with liver disease. Uric acid is a by-product of purine metabolism in the liver. In liver disease, a deficiency of hepatic urate oxidase (uricase) may cause hyperuricemia. Increased blood urate and ammonia (failure of the urea cycle) are excreted into the urine and ammonium urate crystals may form. Crystals and stones secondary to liver disease are most common with congenital portosystemic shunts. Remember crystal do not always mean stones but some dogs with PSVA will present with lower urinary tract signs because of calculi.
Conclusion Routine laboratory tests are often too poorly sensitive and specific to diagnose specific liver disease. This has led to the investigation of better biomarkers of liver disease. Bile acids, ammonia and protein C have been used to help further define whether liver disease is present and the type of disease. Unfortunately these tests also come with limitations. As practitioners we must know how to interpret these tests so we know when to incorporate additional tests such as abdominal ultrasonography, CT angiography or liver biopsy.
References 1.Toulza O, et al. Evaluation of plasma protein C activity for detection of hepatobiliary disease and portosystemicshunting in dogs. J AM Vet Med Assoc Dec1;229(1):1761-71.
2. Bristow P, et al. Long-term serum bile acid concentrations in 51 dogs after complete extrahepatic congenital shuntligation. J Small Anim Pract 2017 Aug;58(8):454-60.
3. Center SA, et al. Evaluation of serum bile acid concentrations for the diagnosis of venous anomalies in the dogand cat. J Am Vet Med Assoc 1985 May 15;186(10):1090-4.
94

4. Meyer DJ, et al. Liver function tests in dogs with portosystemic shunts: Measurement of serum bile acidconcentration. J Am Vet Med Assoc 1986 Jan 15;188(2):168-9.5. Ruland K, et al. Sensitivity and specificity of fasting ammonia and serum bile acids in the diagnosis ofportosystemic shunts in dogs and cats. Vet Clin Pathol 2010 Mar;39(1):57-64.6. D’ Anjou MA, et al. Ultrasonographic diagnosis of portosystemic shunting in dogs and cats. Vet Rad Ultra 2004Sep-Oct;45(5):424-37.7. Bauer NB, et al. Liver disease in dogs with tracheal collapse. J Vet Int Med 2006 Jul-Aug;20(4):845-9.8. Tisdall PL, et al. Post-prandial serum bile acid concentrations and ammonia tolerance in Maltese dogs with andwithout hepatic vascular anomalies. Aust Vet J 1995 Apr;72(4):121-6.9. Dirksen K, et al. Sensitivity and specificity of plasma ALT, ALP, and bile acids for hepatitis in Labradorretrievers. J Vet Int Med 2017 Jul;31(4):1017-27.
10. Trainor D, et al. Urine sulfated and nonsulfated bile acids as a diagnostic test for liver disease in cats. J Vet IntMed 2003 Mar-Apr;17(2):145-53.11. Balkman CE, et al. Evaluation of urine sulfated and nonsulfated bile acids as a diagnostic test for liver disease indogs. J Am Vet Med Assoc 2003 May 15;222(10):1368-75.12. Sterczer, et al. Evaluation of ammonia measurerments in dogs with two analysers for use in veterinary practice.Vet Rec 1999 May 8;144(19):523-6.13, Goggs R, et al. Clinical investigation of a point-of-care blood ammonia analyzer. Vet Clin Path 2008Jun;37(2):198-206.14. Funes S, et al. Clinical evaluation of a benchtop dry chemistry analyzer for measurement of ammoniumconcentrations in canine plasma samples. J Am Vet Med Assoc 2018 Jul 1;253(1):61-5.15. Tisdall PL, et al. Congenital portosystemic shunts in Maltese and Australian cattle dogs. Aus Vet J 1994Jun;71(6):174-8.16. Meyer HP, et al. Progressive remission of portosystemic shunting in 23 dogs after partial closure of congenitalportosystemic shunts. Vet Rec 1999 Mar 27;144(13):333-7.17. Gerritzen-Bruning MJ, et al. Diagnostic value of fasting plasma ammonia and bile acid concentrations in theidentification of portosystemic shunting in dogs. J Vet Int Med 2006 Jan-Feb;20(1):13-9.18. Vallarino N, et al. Diagnostic value of blood variables following attenuation of congenital extrahepaticportosystemic shunt in dogs. Vet Rec 2020 Oct;187(7):e48.19. Van Straten G, et al. Diagnostic value of rectal ammonia tolerance test, fasting plasma ammonia and fastingplasma bile acids for canine portosystemic shunting. The Vet J 2015 Jun;204(3):282-6.20. Johnson CA, et al. Congenital portosystemic shunts in dogs: 46 cases (1979-1986). J Am Vet Med Assoc 1987Dec 1;191(11):1478-83.
95

Bovine Anaplasmosis: A Blood Borne Disease in Cattle Lee Jones DVM, MS
UGA College of Veterinary Medicine Tifton Veterinary Diagnostic Lab, Tifton, GA
Bovine Anaplasmosis Bovine anaplasmosis (BA) is an infectious, non-contagious blood borne disease that affects cattle worldwide (Kocan et al., 2010) and one of the most prevalent tick borne diseases diagnosed around the world (Kocan and de la Fuente, 2003). It is endemic in the Southeast and West Central United States and has been reported in all US States except Hawaii. In Georgia, the incidence has been increasing since 2009 according to veterinary diagnostic lab data (Coarsey et al., 2018). It is estimated that the economic burden of anaplasmosis to the beef industry is more than $300 million per year (Reppert, 2019). The economic losses of anaplasmosis include decreased production and fertility, mortality, abortion and clinical treatment expense. In the US, the cost of a clinical case of anaplasmosis is conservatively estimated at >$400 per animal (Coetzee, 2017). In one Iowa dairy herd study, seropositive dairy cows produced significantly less milk than did seronegative herd mates (Curtis and Coetzee, 2021). If cattle recover from the disease, they become persistently infected carriers for life, which confers resistance to clinical disease but serves as a significant reservoir of Anaplasma marginale (A. marginale) to expose naïve cattle (Aubry and Geale, 2011). In North America, BA is caused by the rickettsial organism A. marginale, which lives in the red blood cells of cattle (Aubry and Geale, 2011). Anaplasmosis is not contagious but requires a vector to be transmitted from one animal to another. The primary method of transmission is by ticks (biological host) but transmission is strain dependent. Some strains of A. marginale are not transmissible by ticks (Kocan et al., 2004) and are more likely transmitted mechanically by blood feeding flies (Scoles et al., 2005). There are several species of ticks that can spread the disease including Rhipicephalus, Boophilus, (southern cattle ticks) and Dermacentor spp. including D andersoni and D variabilis. A. marginale may be transmitted transstadially throughout the tick’s life cycle. Mechanical vectors such as blood feeding flies and blood-contaminated fomites such as needles, ear-tagging instruments, castrating knives, de-horning tools and implant guns can also transfer infected erythrocytes to naïve cattle. Cattle of all ages are susceptible to infection but severity of disease increases with age of the animal. Calves less than one year of age may show no clinical signs following infection; animals 1-2 years of age may display mild illness; while animals over 2 years of age often experience the more severe clinical disease and animals over 3 years of age may experience 30-50% mortality (Kocan and de la Fuente, 2003; Richey, 1991). Once within the blood stream, A. marginale invades erythrocytes and replicates for about 15 to 30 days (incubation ranges from 7-60 days depending on exposure and strain) (Richey and Palmer, 1990). Clinical signs vary and commonly include fever, loss of appetite, pale or yellow mucous membranes (caused by anemia), poor body condition, abortion, weakness, and labored breathing. Animals may experience abnormal behavior signs such as increased aggression, excitability, or staggering due to effects of hypoxia. Abortions can occur when individuals are infected during late stage gestation and should be considered in herd abortion cases. Also, one study has demonstrated that 16% of pregnant carrier cows passed anaplasmosis in utero resulting in persistently infected offspring (Potgieter and Van Rensburg, 1987). Regardless of clinical signs, once animals become infected they are carriers for life and are a source of transmission to naïve members of the herd (Richey, 1991). Outbreaks of disease occur when susceptible, unexposed animals are exposed to infected vectors. Or when carriers (like a bull or replacement cows and heifers) are brought onto the farm. It is recommended to test all purchased cattle, including new yearling bulls, for anaplasmosis before commingling with the herd.
Diagnostics Anaplasmosis is usually diagnosed by clinical signs and physical exam findings. Laboratory methods for diagnosing A. marginale in cattle include stained blood smear for direct, microscopic detection of parasites in RBCs, competitive enzyme-linked immunosorbent assay (cELISA) for detection of antibodies for A. marginale and polymerase chain reaction (PCR) for detection of A. marginale DNA (Kocan et al., 2010). Blood smears are a quick, inexpensive method to diagnose A. marginale infection in clinically diseased cattle but the sensitivity is very low. The cELISA detects antibodies for A. marginale and is relatively inexpensive, so it is useful for seroprevalence screening of herds for A. marginale but it may give false negative results early in infection prior to development of an antibody response. PCR is the most sensitive of the tests and useful in detecting small amounts of A. marginale DNA in clinically normal cattle but it is more expensive than blood smear or cELISA. Additionally, persistently infected cattle do not always have detectable amounts of organisms in their blood because of the cyclical nature of the infection with the organism (Aubry and Geale, 2011).
96

Treatment Historically, treatment of anaplasmosis consisted of injectable oxytetracycline (OTC). However, injectable OTC has been shown to be ineffective in clearing A. marginale infections in carrier cattle (Coetzeea et al., 2005). On the other hand, the label dose of oral chlortetracycline (CTC) was shown to effectively chemosterilize persistently infected calves (Reinbold et al., 2010). Free choice oral CTC is approved for control of active infection of anaplasmosis at 0.5-2.0 mg/lb body per day. Control of active A. marginale infection is the only label approved free choice oral CTC indication in cattle. Therefore, in order to write a valid Veterinary Feed Directive (VFD) to feed CTC, veterinarians must have previously diagnosed A. marginale in the herd, have seropositive cattle or be aware of herds that have active infections or have had A. marginale diagnosed in the area. Imidocarb is also highly efficacious against A marginale as a single injection (as the dihydrochloride salt at 1.5 mg/kg, SC, or as imidocarb dipropionate at 3 mg/kg). Elimination of the carrier state requires the use of higher repeated doses of imidocarb (eg, 5 mg/kg, IM or SC, two injections of the dihydrochloride salt 2 wk apart). Imidocarb is a suspected carcinogen with long withholding periods and is not approved for use in the USA or Europe. (Merck Veterinary Manual, https://www.merckvetmanual.com/circulatory-system/blood-parasites/anaplasmosis) . Recently, enrofloxacin (Baytril® 100-CA1) has received conditional approval for treatment of clinical anaplasmosis. Enrofloxacin given SQ at 5.7mg/lb reduced mortality and anemia associated with clinical anaplasmosis in experimentally induced cases (Shane, et al., 2020).
Georgia Prevalence Study The objective of the study was to determine the seroprevalence of A. marginale infected beef herds in Georgia and to identify herd risk factors associated with A. marginale positive herds. In addition, we compared the cELISA serology and real-time PCR for determining the prevalence of A. marginale infected herds in Georgia. Moreover, herd information from the beef operations was collected from the sampled herds through a management survey questionnaire to determine factors or practices that may increase or decrease the risk of herd infections with A. marginale. Blood samples were collected from 1059 adult beef cattle (≥ 2 years) from 33 herds. The sera were screened with a commercial cELISA Anaplasma antibody test kit (VMRD). Samples were identified as seropositive to A. marginale with a 30% inhibition cutoff. Overall, 8.12% (86/1059) of cattle tested were ELISA positive as well as 42% of the herds (14/33). Plasma samples from a subset of corresponding seropositive samples (n=73) were tested by real-time PCR and 77% (56/73) were PCR positive. Out of the 406 sero-negative samples, none of those animals were found to be PCR positive for A. marginale DNA. There was almost perfect agreement by Cohen kappa statistics between PCR and cELISA (k= 0.85). Survey response rate was 100%. Surprisingly, 27% of the producer respondents had not heard of Anaplasmosis (9/33). About 18% of the respondents had operations where Anaplasmosis was diagnosed one year prior to this study and they had administered chlortetracycline for the control of anaplasmosis in their herds (6/33) either through free choice of loose minerals or mineral mixed in feed. Survey revealed that many producers had management procedures at their operations (dehorning, castration, tattooing, others) that could potentially cause mechanical transmission of A. marginale. Moreover, while 55% respondents did not always disinfect tools between animals, 88% of the operations used same needle to inject more than one animal. Over 80% of the producer respondents had brought in new cattle onto their operations in the last 3 years from the time of this study.
References Archer, K.J., Lemeshow, S., 2006. Goodness-of-fit test for a logistic regression model fitted using survey sample data. The Stata Journal 6, 97-105.
Aubry, P., Geale, D.W., 2011. A Review of Bovine Anaplasmosis. Transboundary and Emerging Diseases 58, 1-30. Carelli, G., Decaro, N., Lorusso, A., Elia, G., Lorusso, E., Mari, V., Ceci, L., Buonavoglia, C., 2007. Detection and quantification of Anaplasma marginale DNA in blood samples of cattle by real-time PCR. Veterinary microbiology 124, 107-114.
Coarsey, M.D., Wilkes, R.P., Jones, L., Naikare, H.K., 2018. A retrospective study of bovine anaplasmosis cases in Georgia: 2009-2017. In: AAVLD, Kansas City, MO, p. 36.
Coetzee, J.F., 2017. Bovine anaplasmosis. In: American Association of Bovine Practitioners Proceedings of the Annual Conference, pp. 28-31.
97
Coetzeea, J.F., Apleya, M.D., Kocanb, K.M., Rurangirwac, F.R., Van Donkersgoedd, J., 2005. Comparison of three oxytetracycline regimens for the treatment of persistent Anaplasma marginale infections in beef cattle. Veterinary parasitology 127, 61-73.
Curtis, A.K., Coetzee, J.F., 2021. Assessment of within-herd seroprevalence of Anaplasma marginale antibodies and associated decreased milk production in an Iowa dairy herd. Applied Animal Science 37, 126-131. Dean, N., Pagano, M., 2015. Evaluating confidence interval methods for binomial proportions in clustered surveys. Journal of Survey Statistics and Methodology 3, 484-503.
Durrani, A., Goyal, S., 2012. A retrospective study of Anaplasma in Minnesota cattle. Turkish Journal of Veterinary and Animal Sciences 36, 131-136.
Kocan, K.M., de la Fuente, J., 2003. Co-feeding studies of ticks infected with Anaplasma marginale. Veterinary Parasitology 112, 295-305.
Kocan, K.M., de la Fuente, J., Blouin, E.F., Coetzee, J.F., Ewing, S.A., 2010. The natural history of Anaplasma marginale. Veterinary Parasitology 167, 95-107.
Kocan, K.M., De La Fuente, J., Blouin, E.F., Garcia-Garcia, J.C., 2004. Anaplasma marginale (Rickettsiales: Anaplasmataceae): recent advances in defining host–pathogen adaptations of a tick-borne rickettsia. Parasitology 129, S285-S300.
Landis, J.R., Koch, G.G., 1977. An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics, 363-374. Okafor, C.C., Collins, S.L., Daniel, J.A., Coetzee, J.F., Whitlock, B.K., 2019a. Factors associated with seroprevalence of bovine anaplasmosis in Mississippi, USA. Veterinary Parasitology: Regional Studies and Reports 17, 100301.
Okafor, C.C., Collins, S.L., Daniel, J.A., Coetzee, J.F., Whitlock, B.K., 2019b. Seroprevalence of bovine anaplasmosis in Georgia. Veterinary Parasitology: Regional Studies and Reports 15, 100258. Potgieter, F., Van Rensburg, L., 1987. The persistence of colostral Anaplasma antibodies and incidence of in utero transmission of Anaplasma infections in calves under laboratory conditions. Onderstepoort Journal of Veterinary Research 54, 557-560.
Reinbold, J.B., Coetzee, J.F., Hollis, L.C., Nickell, J.S., Riegel, C., Olson, K., Ganta, R.R., 2010. The efficacy of three chlortetracycline regimens in the treatment of persistent Anaplasma marginale infection. Veterinary microbiology 145, 69-75.
Reppert, E.J., 2019. Review of current anaplasmosis control strategies and future directions. In: American Association of Bovine Practitioners Proceedings of the Annual Conference, pp. 71-72. Richey, E., 1991. Bovine anaplasmosis. In: American Association of Bovine Practitioners Proceedings of the Annual Conference, pp. 3-11.
Richey, E., Palmer, G., 1990. Bovine anaplasmosis. Compendium on Continuing Education for the Practicing Veterinarian 12, 1661-1668.
Rogan, W.J., Gladen, B., 1978. Estimating prevalence from the results of a screening test. American journal of epidemiology 107, 71-76.
Scoles, G.A., Broce, A.B., Lysyk, T.J., Palmer, G.H., 2005. Relative Efficiency of Biological Transmission of Anaplasma marginale (Rickettsiales: Anaplasmataceae) by Dermacentor andersoni (Acari: Ixodidae) Compared with Mechanical Transmission by Stomoxys calcitrans (Diptera: Muscidae). Journal of Medical Entomology 42, 668-675. Shane, DD, Lechtenberg, KF, Seagren J, Tessman RK, Singu VK, Wang Y, Coetzee J, Reif KE. 2020. Clinical effectiveness of enrofloxacin 100 mg/mL injectable solution for the treatment of acute anaplasmosis in cattle caused by Anaplasma marginale. Bovine Practitioner 54:51-57
98

Spare, M.R., Hanzlicek, G.A., Wootten, K.L., Anderson, G.A., Thomson, D.U., Sanderson, M.W., Ganta, R.R., Reif, K.E., Raghavan, R.K., 2020. Bovine anaplasmosis herd prevalence and management practices as risk-factors associated with herd disease status. Veterinary Parasitology: 2775,100021
Whitlock, B., Daniel, J., Harvey, B., Johnson, J., Coetzee, J., 2014. Seroprevalence of bovine anaplasmosis in the southern US. In: The AABP Proceedings.
99

Four Updates That Will Change Your Heartworm Strategies
Byron L. Blagburn University Distinguished Professor of Parasitology
College of Veterinary Medicine Auburn University, Alabama
To say that canine and feline heartworm diagnostic, treatment and prevention strategies are changing is the archetype of understatement. We are experiencing an extraordinary increase in the numbers and kinds of available preventives and diagnostic tests, and the capability to acquire and apply new information. This can be both beneficial and disadvantageous. Beneficial because pet owners have become more aware of the dangers of heartworm infections. Also, available treatment and prevention products have become more effective and convenient to use. That said, misinformation could be communicated through electronic mail, social media, and web sites dealing with heartworm. It is difficult to separate fact from opinion and to know and understand what is important. Among emerging issues are 1) resistance and its influence on our selection and use of products, 2) antigen blocking and the inclusion of heat andchemical treatment in our diagnostic strategies, 3) selection of treatment strategies and 4) Wohlbachia and its functionin heartworm infection and disease. All add complexities in dealing with heartworm infection. Discrepancies betweenmicrofilaria tests and antigen or antibody test results can lead to confusion regarding the actual infection status of pets.The availability of approved adulticide and experimental “slow-kill” strategies provide a landscape of options that canbe difficult to navigate. I will discuss some of these issues and try to identify what we know and what is important.
Diagnostic challenges
Widespread use of macrolide heartworm preventives such as ivermectin, milbemycin oxime, moxidectin, eprinomectin and selamectin has had a demonstrable effect on the numbers of heartworm-infected dogs seen by veterinarians. Reductions in the number of cases of clinical canine heartworm infections is even more dramatic. The excellent efficacies of the medications, together with the convenience of monthly or semi-annual administration has almost eliminated heartworm infection if some areas - or so it seems. With these enhanced efficacies come some additional problems. Failure to administer these medications regularly or at appropriate dosages can result in heartworm infections. However, these infections generally involve fewer numbers of worms - sometimes too few worms to detect. Fewer worms also means an increased possibility of single-sex infections and failure to produce detectable microfilaria. We also now know that most preventives will, to varying degrees, reduce or eliminate circulating microfilaria from infected dogs. Consequently, detection of microfilaria is no longer as reliable a confirmation of diagnosis as it once was. Although point-of-care heartworm antigen tests have become increasingly sensitive and rigorously specific, the lower worm burdens likely to occur in infected dogs seen by veterinarians can challenge the capabilities of these tests. Other phenomena such as fluctuating antigen levels and potentially conflicting antigen test results, antibody test results (for feline tests) and microfilaria test results can create diagnostic dilemmas for the veterinarian. In addition, concurrent infections in dogs with other parasites or presence of other diseases, or simply excess heartworm antibody compared to circulating antigen, could affect the detection of heartworm antigen (antigen blocking). Heat or chemical treatment of blocked samples may return a positive result. Currently marketed antigen tests approach 100% specificity. Specificity can be a more important test attribute than sensitivity, since most of the dogs seen by veterinarians in any region are negative. A test with limited specificity could result in a significant number of false-positive dogs. These dogs might then be treated unnecessarily with an organo-arsenical compound. Reduced sensitivity might fail to detect dogs with low worm burdens (false negatives - a possible occurrence anyway). These dogs are less likely than dogs with high worm burdens to develop severe heartworm disease. Research has shown that currently marketed tests do differ in their sensitivities, particularly in dogs with low worm burdens. In addition to sensitivity and specificity the following should also be considered in test selection: 1) need to process single vs. multiple simultaneous samples (batching), 2) ease of conduct of the test (i.e. number of steps, reagents etc.), 3) ease of visualization of results (brightness of line or dot, or liquid color change), 4) time required to conduct thetest, 5) cost per test and 6) other diagnostic capabilities of tests (i.e. detection of antibodies or antigens to other diseaseagents). Most of the immuno-ELISA and immuno-chromatographic tests that are currently marketed would score wellwhen these criteria are applied to them. An understanding of situations that current diagnosis and preventionenvironments can create is essential if veterinarians are to use these excellent products and diagnostic aids to their full
100

potential. An extensive array of point-of-care (POC) and reference laboratories test are available to veterinarians. I remain a strong supporter of in-clinic heartworm tests. Excellent POC tests include Snap® Heartworm RT, Snap® 4DX Plus, Dirochek®, Witness® Heartworm, VetScan® and Solostep®. Many tests are also available through commercial, state and academic laboratories. However, it is essential to inquire about their performance characteristics before deciding on a specific test.
Emerging issues
Heartworm infection can result in potentially serious and sometimes fatal diseases in both dogs and cats. Fortunately, numerous safe and effective monthly, semi-annual and annual heartworm preventives have been developed and delivered to the market in the last 30 years. All major heartworm preventives belong to the macrocyclic lactone (ML) class of endectocides. Current MLs approved for heartworm prevention in dogs and cats include ivermectin, milbemycin oxime, moxidectin, eprinomectin and selamectin. All approved MLs exert their effects by targeting a group of ligand-gated chloride ion channels unique to invertebrates. The L3 and L4 larval stages of D. immitis are exceptionally sensitive to the MLs. Recently, it seems that the frequency of lack of heartworm preventive efficacy (LOE) reports for the MLs in dogs has increased. In reality, failure of any of the preventives to prevent heartworm infection in dogs is extremely rare (estimated to be <0.1% - although it may be higher in certain regions). It is now known that certain LOE reports are the result of resistant heartworms. However, other factors such as improved tests, increased frequency of testing, clinic or client compliance, or a combination of these, can contribute to an increase in numbers of heartworm positive dogs.
Melarsomine dihydrochloride (Diroban™, Immiticide®) provides the veterinarian with a product with efficacy, safety and ease of administration when eliminating heartworms. Melarsomine was introduced with a flexible dosing regimen that was correlated to the clinical condition of the heartworm-infected dog and worm burden. Dogs that are asymptomatic or in the early symptomatic stages of heartworm disease may be treated with the standard two-dose regimen, with 24 hours intervening between each dose. Dogs with late stage heartworm disease (class III disease) or dogs with suggestion of high worm burdens (semi-quantitative antigen tests; historically high worm burdens in an area; radiographic lesions suggesting high worm burden [not always definitive]) can be given a single dose of melarsomine and subsequently released to the owners care and vigilance at home. The dog is returned one month later to receive the standard two-dose regimen. The rationale for the three-dose regimen is that a partial kill of the adult worms following the single treatment (approximately 50%) and the dog’s subsequent recuperation prior to the full regimen a month later would impose less stress and potential for serious post-treatment thromboembolic disease. The three-dose regimen is also more effective at eliminating adult heartworm. The safety appeal of the flexible dosing regimen has led many veterinarians to adopt this regimen as their only treatment protocol. Veterinarians must remember that the flexible dosing regimen increases the period of time that exercise restriction is required, since worms are killed over two treatment periods. In addition, the pet owner must bear the cost of an additional treatment and must be responsible enough to return for all scheduled treatments. The flexible dosing regimen is the treatment of choice of the Companion Animal Parasite Council (CAPC) and the American Heartworm Society (AHS). Treatment to remove adult heartworms is not always 100% effective. A positive heartworm test 7 months or more after treatment can be due to several factors that we will discuss. AHS now recommends the concurrent use of doxycycline (see below) together with placement of dogs on preventive for two or more months prior to initiation of the adulticide regimen. This delay is considered unnecessary by some, given the efficacy of the heartworm preventives and melarsomine dihydrochloride. Recent research also suggests that the delay can be reduced to one month based on the efficacy of the preventives and adulticide.
Another consequence of the improved performance of melarsomine is increased cost. In this case, it is undeniable that the excellent properties of melarsomine are well worth the increase in price. The cost of melarsomine therapy, particularly in large dogs, has resulted in some hesitation by pet owners to pursue adulticidal therapy. This and other issues such as how to deal with heartworm-infected geriatric patients, or patients suffering from other terminal conditions, has resulted in veterinarians considering other adulticidal options. The most popular of these options has been the slow adulticidal effects (often referred to as “slow kill”) of the macrolide preventives (i.e. ivermectin, milbemycin oxime, moxidectin and selamectin). These adulticidal properties are best known and characterized for ivermectin/pyrantel pamoate (Heartgard® Plus, Boerhinger Ingelheim). For example, if dogs harboring adult worms are given ivermectin using the dose band regimen (minimum target: dose 6 µg/kg) at monthly intervals for 1.5 to two years or more, many (in some cases most) of the heartworms will die during the regimen. Remaining worms appear structurally abnormal and will likely die. The prevailing mantra seems to be “the older the worms, the longer they will
101

require to kill”. It is important to note that the adult worms can induce a proliferative endarteritis in the cardiopulmonary vessels, and the longer that they are left in those vessels, the more severe that reaction is likely to be. It is also notable that the chronic effects of slow worm death have been the subject of a limited amount of research. Some research suggests that the “slow kill” approach should not be used in active dogs or dogs with clinical signs of heartworm disease. At this point it seems that the best advice is to recommend the use of melarsomine when adult infections are detected. If the approved adulticide is refused, then the use of macrolide preventives in heartworm positive dogs might be considered. Recent research indicates that concurrent use of doxycycline (for one month; see dosage and regimen below) and moxidectin (Advantage Multi®; monthly) results in demonstrable efficacy against adult heartworms. Additional research indicates that ProHeart 12 together with doxycycline may also be a useful alternative to melarsomine dihydrochloride.
I am asked about the need to remove microfilaria (mff) from heartworm-infected dogs. In the past, several of us have recommended placing microfilaremic dogs on prevention. If adult worms are removed, mff will eventually disappear. I now believe that active removal of mff after the use of melarsomine is necessary for two reasons. Persistent of mff exposed to heartworm preventives may increase the likelihood of resistance. Second, the continued presence of mff serves as a source of infection for mosquito vectors. We have encountered a few dogs whose mff persist with the repeated use of milbemycin oxime (0.5 mg/kg per os) or high dose ivermectin (50 µg/kg and higher either per os or by subcutaneous injection). These microfilariae were eliminated in some dogs by concurrent use of doxycycline and microfilaricides. With the approval of Advantage Multi® as a microfilaricide, it seems reasonable to take advantage of this claim. Benefits include the support of the product sponsor if adverse events occur or if mff cannot be eliminated.
Interest in mosquito control as an adjunct to heartworm preventives is increasing. Mosquito avoidance strategies such as use of screen barriers and restricting outdoor animal activity to times when mosquitoes are not likely to be present can be helpful in preventing heartworm transmission. A more achievable preventive goal is to utilize topical flea/tick products that also have claims against mosquitoes (e.g. Vectra 3D® CEVA).These products prevent mosquito feeding and block uptake of microfilaria and prevent transmission of infective larvae to recipient dogs. Research is now available to support this strategy.
Wolbachia pipientis: What is it and what do you need to know?
Wolbachia pipientis is an intracellular bacterium that infects numerous species of filarial worms including heartworms. Many contend that these friendly inhabitants (endosymbionts) play a role in the pathogenesis of diseases caused by heartworms and other filarids. Contention is that host immune responses directed at Wolbachia can actually go awry and enhance the disease process in heartworm infections. Some also contend that elimination of Wolbachia from heartworms may affect the survival of adult heartworms and microfilariae, the ability of microfilariae to infect and develop within mosquito vectors, and may decrease the host’s errant immunologic responses when adult worms are killed or die. At present, there appears to be evidence that pretreatment of heartworm infected dogs with doxycycline at the rate of 20 mg/kg per day (10 mg/kg BID) for one month prior to administration of melarsomine dihydrochloride may decrease the severity post-treatment thromboembolic and immunopathologic events. Data also suggest that administration of doxycycline (together with a microfilaricide) also can aid in the elimination of microfilariae from heartworm infected dogs and can render microfilariae noninfectious to mosquitoes. As mentioned above, concurrent administration of doxycycline and preventive may hasten the death and elimination of adult heartworms in dogs.
References available on request.
102
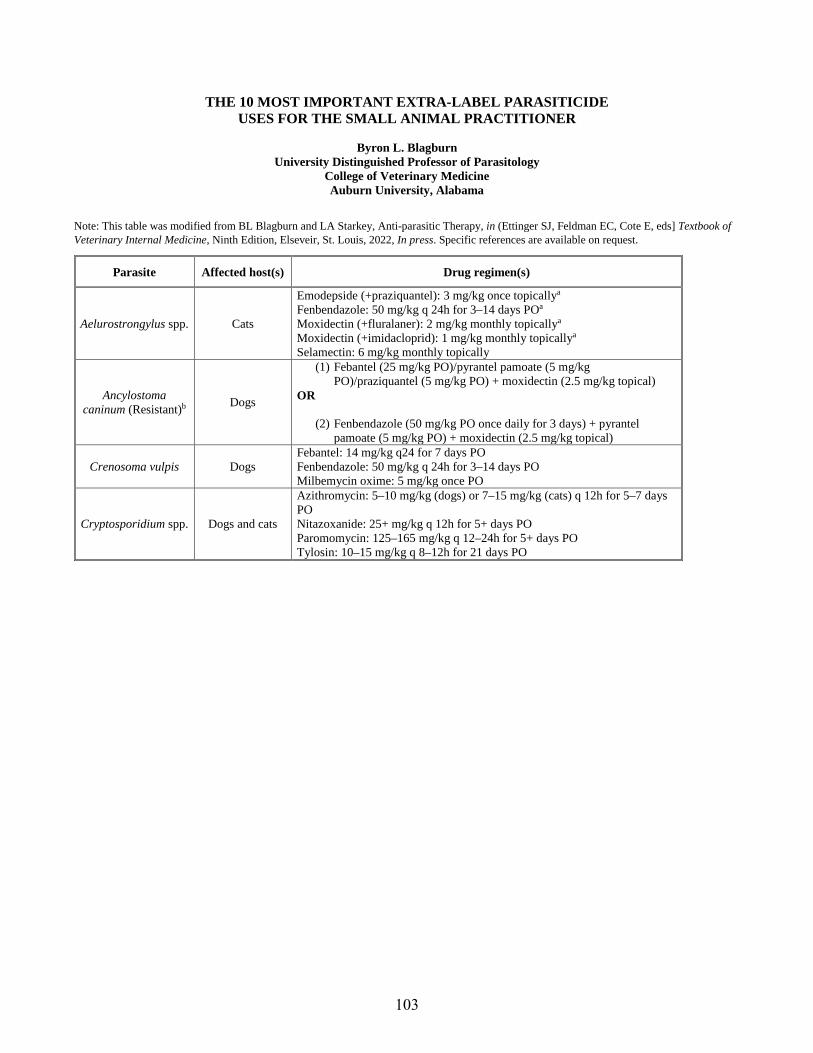
THE 10 MOST IMPORTANT EXTRA-LABEL PARASITICIDE USES FOR THE SMALL ANIMAL PRACTITIONER
Byron L. Blagburn University Distinguished Professor of Parasitology
College of Veterinary Medicine Auburn University, Alabama
Note: This table was modified from BL Blagburn and LA Starkey, Anti-parasitic Therapy, in (Ettinger SJ, Feldman EC, Cote E, eds] Textbook of Veterinary Internal Medicine, Ninth Edition, Elseveir, St. Louis, 2022, In press. Specific references are available on request.
Parasite Affected host(s) Drug regimen(s)
Aelurostrongylus spp. Cats
Emodepside (+praziquantel): 3 mg/kg once topicallya
Fenbendazole: 50 mg/kg q 24h for 3–14 days POa Moxidectin (+fluralaner): 2 mg/kg monthly topicallya Moxidectin (+imidacloprid): 1 mg/kg monthly topicallya Selamectin: 6 mg/kg monthly topically
Ancylostoma caninum (Resistant)b Dogs
(1) Febantel (25 mg/kg PO)/pyrantel pamoate (5 mg/kgPO)/praziquantel (5 mg/kg PO) + moxidectin (2.5 mg/kg topical)
OR
(2) Fenbendazole (50 mg/kg PO once daily for 3 days) + pyrantelpamoate (5 mg/kg PO) + moxidectin (2.5 mg/kg topical)
Crenosoma vulpis Dogs Febantel: 14 mg/kg q24 for 7 days PO Fenbendazole: 50 mg/kg q 24h for 3–14 days PO Milbemycin oxime: 5 mg/kg once PO
Cryptosporidium spp. Dogs and cats
Azithromycin: 5–10 mg/kg (dogs) or 7–15 mg/kg (cats) q 12h for 5–7 days PO Nitazoxanide: 25+ mg/kg q 12h for 5+ days PO Paromomycin: 125–165 mg/kg q 12–24h for 5+ days PO Tylosin: 10–15 mg/kg q 8–12h for 21 days PO
103
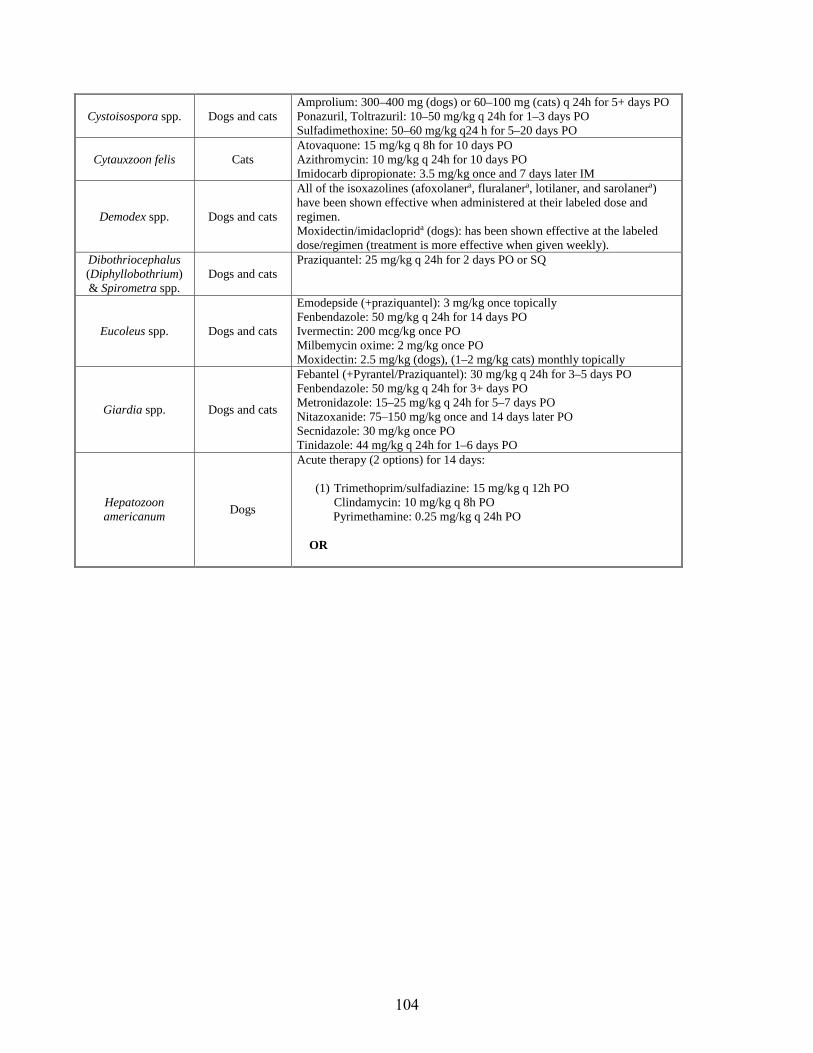
Cystoisospora spp. Dogs and cats Amprolium: 300–400 mg (dogs) or 60–100 mg (cats) q 24h for 5+ days PO Ponazuril, Toltrazuril: 10–50 mg/kg q 24h for 1–3 days PO Sulfadimethoxine: 50–60 mg/kg q24 h for 5–20 days PO
Cytauxzoon felis Cats Atovaquone: 15 mg/kg q 8h for 10 days PO Azithromycin: 10 mg/kg q 24h for 10 days PO Imidocarb dipropionate: 3.5 mg/kg once and 7 days later IM
Demodex spp. Dogs and cats
All of the isoxazolines (afoxolanera, fluralanera, lotilaner, and sarolanera) have been shown effective when administered at their labeled dose and regimen. Moxidectin/imidacloprida (dogs): has been shown effective at the labeled dose/regimen (treatment is more effective when given weekly).
Dibothriocephalus (Diphyllobothrium) & Spirometra spp.
Dogs and cats Praziquantel: 25 mg/kg q 24h for 2 days PO or SQ
Eucoleus spp. Dogs and cats
Emodepside (+praziquantel): 3 mg/kg once topically Fenbendazole: 50 mg/kg q 24h for 14 days PO Ivermectin: 200 mcg/kg once PO Milbemycin oxime: 2 mg/kg once PO Moxidectin: 2.5 mg/kg (dogs), (1–2 mg/kg cats) monthly topically
Giardia spp. Dogs and cats
Febantel (+Pyrantel/Praziquantel): 30 mg/kg q 24h for 3–5 days PO Fenbendazole: 50 mg/kg q 24h for 3+ days PO Metronidazole: 15–25 mg/kg q 24h for 5–7 days PO Nitazoxanide: 75–150 mg/kg once and 14 days later PO Secnidazole: 30 mg/kg once POTinidazole: 44 mg/kg q 24h for 1–6 days PO
Hepatozoon americanum Dogs
Acute therapy (2 options) for 14 days:
(1) Trimethoprim/sulfadiazine: 15 mg/kg q 12h POClindamycin: 10 mg/kg q 8h POPyrimethamine: 0.25 mg/kg q 24h PO
OR
104
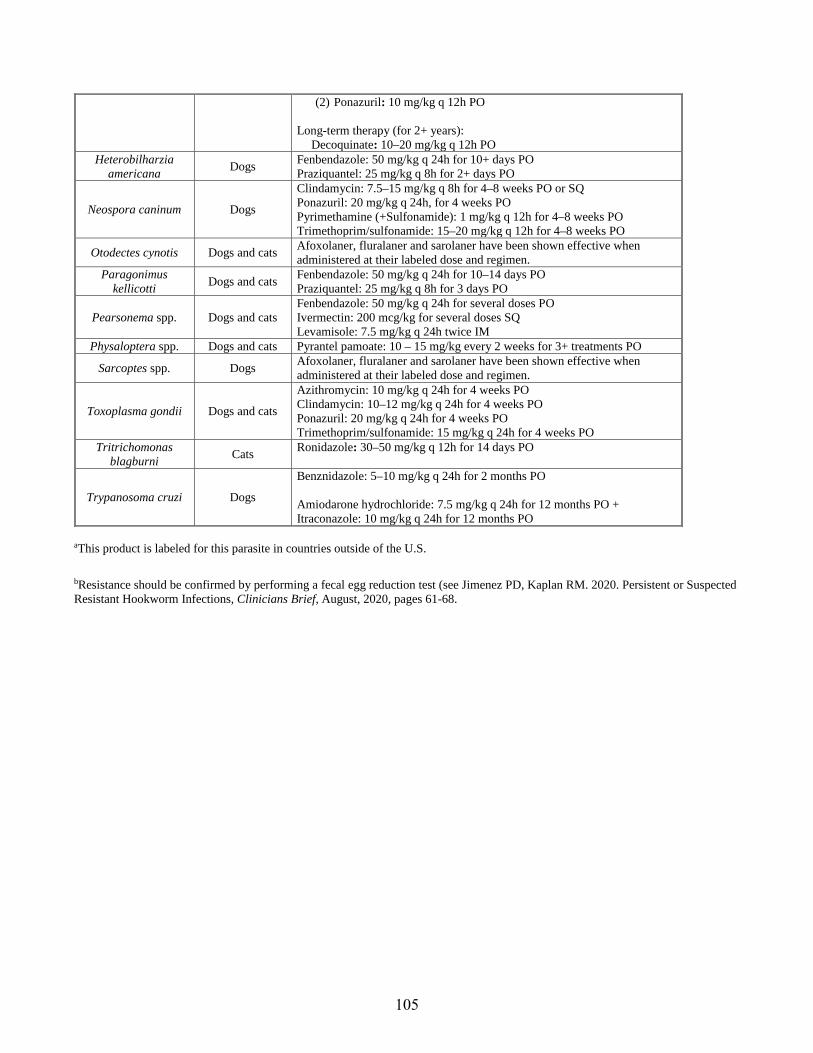
(2) Ponazuril: 10 mg/kg q 12h PO
Long-term therapy (for 2+ years): Decoquinate: 10–20 mg/kg q 12h PO
Heterobilharzia americana Dogs Fenbendazole: 50 mg/kg q 24h for 10+ days PO
Praziquantel: 25 mg/kg q 8h for 2+ days PO
Neospora caninum Dogs
Clindamycin: 7.5–15 mg/kg q 8h for 4–8 weeks PO or SQ Ponazuril: 20 mg/kg q 24h, for 4 weeks PO Pyrimethamine (+Sulfonamide): 1 mg/kg q 12h for 4–8 weeks PO Trimethoprim/sulfonamide: 15–20 mg/kg q 12h for 4–8 weeks PO
Otodectes cynotis Dogs and cats Afoxolaner, fluralaner and sarolaner have been shown effective when administered at their labeled dose and regimen.
Paragonimus kellicotti Dogs and cats Fenbendazole: 50 mg/kg q 24h for 10–14 days PO
Praziquantel: 25 mg/kg q 8h for 3 days PO
Pearsonema spp. Dogs and cats Fenbendazole: 50 mg/kg q 24h for several doses PO Ivermectin: 200 mcg/kg for several doses SQ Levamisole: 7.5 mg/kg q 24h twice IM
Physaloptera spp. Dogs and cats Pyrantel pamoate: 10 – 15 mg/kg every 2 weeks for 3+ treatments PO
Sarcoptes spp. Dogs Afoxolaner, fluralaner and sarolaner have been shown effective when administered at their labeled dose and regimen.
Toxoplasma gondii Dogs and cats
Azithromycin: 10 mg/kg q 24h for 4 weeks PO Clindamycin: 10–12 mg/kg q 24h for 4 weeks PO Ponazuril: 20 mg/kg q 24h for 4 weeks PO Trimethoprim/sulfonamide: 15 mg/kg q 24h for 4 weeks PO
Tritrichomonas blagburni Cats Ronidazole: 30–50 mg/kg q 12h for 14 days PO
Trypanosoma cruzi Dogs
Benznidazole: 5–10 mg/kg q 24h for 2 months PO
Amiodarone hydrochloride: 7.5 mg/kg q 24h for 12 months PO + Itraconazole: 10 mg/kg q 24h for 12 months PO
aThis product is labeled for this parasite in countries outside of the U.S.
bResistance should be confirmed by performing a fecal egg reduction test (see Jimenez PD, Kaplan RM. 2020. Persistent or Suspected Resistant Hookworm Infections, Clinicians Brief, August, 2020, pages 61-68.
105
Heartworm Testing: What to Do When Test Results and Experts Disagree
Byron L. Blagburn University Distinguished Professor of Parasitology
College of Veterinary Medicine Auburn University, Alabama
The following represent actual cases presented to the Auburn University Parasitology Diagnostic Laboratory. The author acknowledges Ms. Joy V. Bowles, Coordinator of Heartworm Diagnostics, for her assistance and input. In some cases, signalment was changed to preserve patient confidentiality.
1. “DISCREPANT ANTIGEN TEST RESULTS”
• 6 y/o canine F/S, South Alabama• No detailed information on prevention history• Clinically WNL; no coughing• Commercial antigen test: positive (borderline)• Patient-side antigen test: negative (twice)• No microfilariae (mff) on direct smear• Auburn University (AU) spec ELISA antigen test: positive (OD = 0.056; cutoff 0.004)
Comments: Illustrates differences in sensitivity of well ELISA and patient side tests and possibility of variation in circulating antigen.
Recommendation: Treat, place on preventive.
2. “PERSISTENT MICROFILARIAE; MIXED INFECTION”
• 4 y/o female Border Collie, unknown location• Treated with AHS (3-treatment) protocol in July/August 2018• Antigen positive on patient-side antigen test at 7 months post-tx (March 2019)• Antigen positive at pharmaceutical reference laboratory at 7 months post-tx• Mff positive at 7 months post-tx• Treated with milbemycin oxime April 2019• Treated with imidacloprid/moxidectin May 2019• Positive for mff on modified Knott’s test (MKT, ~1,075 D. immitis/mL) in AU lab June 2019• Negative for antigen at AU lab (June 2019)• Dog started on doxycycline (10mg/kg BID X 30), and continued on monthly
imidacloprid/moxidectin• Retested in AU lab October 2019; antigen negative; positive for A. reconditum (28 mff/mL)
Comment: Illustrates the importance of mixed mff infections and how persistence of mff can confound diagnosis. Antigen depletion can take longer than expected. Reinforces the need to conduct a modified Knott’s test (MKT) to confirm species of mff. Also illustrated how A. reconditum mff may take longer to clear than D. immitis and are more difficult to diagnose in a mixed infection.
Recommendation: Continue on preventive (imidacloprid/moxidectin should eventually eliminate A. reconditum mff).
106
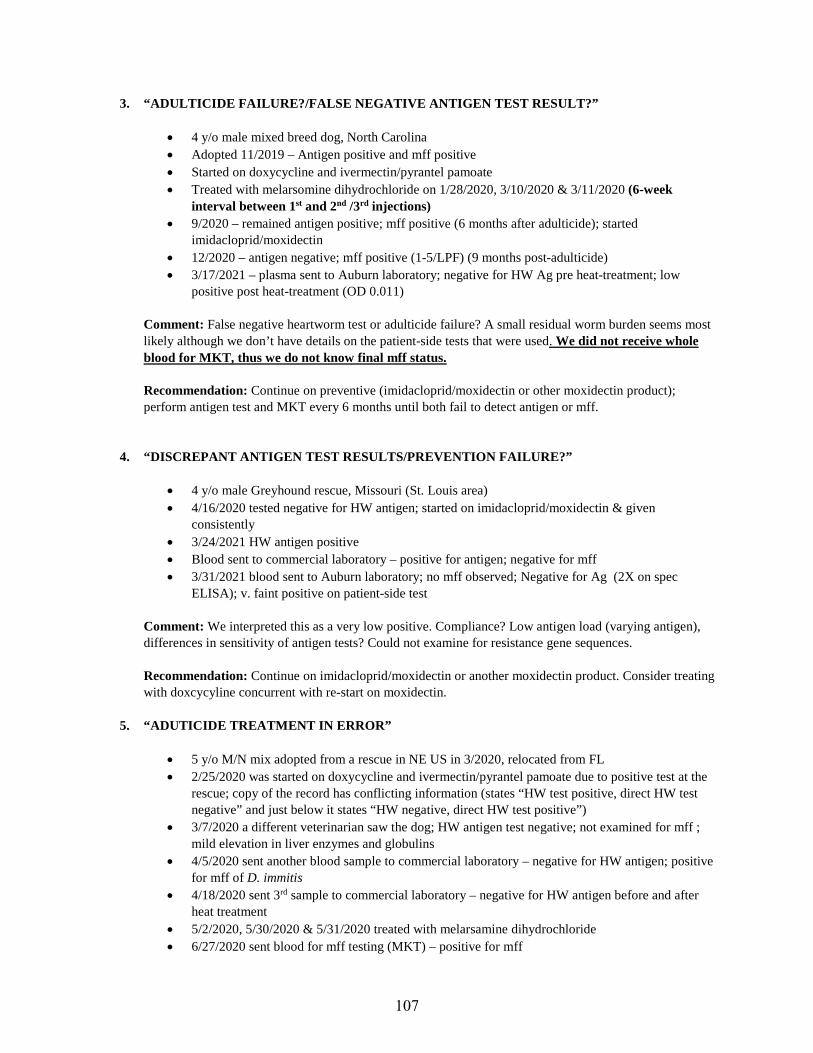
3. “ADULTICIDE FAILURE?/FALSE NEGATIVE ANTIGEN TEST RESULT?”
• 4 y/o male mixed breed dog, North Carolina• Adopted 11/2019 – Antigen positive and mff positive• Started on doxycycline and ivermectin/pyrantel pamoate• Treated with melarsomine dihydrochloride on 1/28/2020, 3/10/2020 & 3/11/2020 (6-week
interval between 1st and 2nd /3rd injections)• 9/2020 – remained antigen positive; mff positive (6 months after adulticide); started
imidacloprid/moxidectin• 12/2020 – antigen negative; mff positive (1-5/LPF) (9 months post-adulticide)• 3/17/2021 – plasma sent to Auburn laboratory; negative for HW Ag pre heat-treatment; low
positive post heat-treatment (OD 0.011)
Comment: False negative heartworm test or adulticide failure? A small residual worm burden seems most likely although we don’t have details on the patient-side tests that were used. We did not receive whole blood for MKT, thus we do not know final mff status.
Recommendation: Continue on preventive (imidacloprid/moxidectin or other moxidectin product); perform antigen test and MKT every 6 months until both fail to detect antigen or mff.
4. “DISCREPANT ANTIGEN TEST RESULTS/PREVENTION FAILURE?”
• 4 y/o male Greyhound rescue, Missouri (St. Louis area)• 4/16/2020 tested negative for HW antigen; started on imidacloprid/moxidectin & given
consistently• 3/24/2021 HW antigen positive• Blood sent to commercial laboratory – positive for antigen; negative for mff• 3/31/2021 blood sent to Auburn laboratory; no mff observed; Negative for Ag (2X on spec
ELISA); v. faint positive on patient-side test
Comment: We interpreted this as a very low positive. Compliance? Low antigen load (varying antigen), differences in sensitivity of antigen tests? Could not examine for resistance gene sequences.
Recommendation: Continue on imidacloprid/moxidectin or another moxidectin product. Consider treating with doxcycyline concurrent with re-start on moxidectin.
5. “ADUTICIDE TREATMENT IN ERROR”
• 5 y/o M/N mix adopted from a rescue in NE US in 3/2020, relocated from FL• 2/25/2020 was started on doxycycline and ivermectin/pyrantel pamoate due to positive test at the
rescue; copy of the record has conflicting information (states “HW test positive, direct HW testnegative” and just below it states “HW negative, direct HW test positive”)
• 3/7/2020 a different veterinarian saw the dog; HW antigen test negative; not examined for mff ;mild elevation in liver enzymes and globulins
• 4/5/2020 sent another blood sample to commercial laboratory – negative for HW antigen; positivefor mff of D. immitis
• 4/18/2020 sent 3rd sample to commercial laboratory – negative for HW antigen before and afterheat treatment
• 5/2/2020, 5/30/2020 & 5/31/2020 treated with melarsamine dihydrochloride• 6/27/2020 sent blood for mff testing (MKT) – positive for mff
107

• 7/1/2020 treated with ivermectin/pyrantel pamoate• 8/1/2020 switched to imidacloprid/moxidectin monthly• 1/16/2021 positive for mff (has received 6 monthly doses of imidacloprid/moxidectin)• 2/2021 blood was sent to AU lab for testing; there was insufficient volume for MKT; negative for
antigen; recommended sending more blood for MKT due to history• 2/2021 (3 weeks later) more blood was sent to our lab; negative for antigen; MKT – A. reconditum
(35 mff/mL); measured 26 of 35 mff (others were unable to be measured) and ALL wereconsistent with A. reconditum based on structure and measurements (Heat TX was NOTrequested; had been performed at a reference laboratory previously and was negative)
Comment: The presumption here was that mff present in a dog with a negative antigen test result must be infected with D. immitis. This is an example of how presumptions or incorrect conclusions can lead to unnecessary treatment.
Recommendation: Always confirm the species of mff prior to making treatment and prevention decisions.
6. “POSSIBLE RESISTANCE”
• 2 y/o F Black & Tan Coonhound• Heartworm Ag positive at a rescue in MS; now lives in TN• Feb 2020 treated with melarsomine dihydrochloride (regimen unknown)• Apr 2020 was started on imidacloprid/moxidectin• HW antigen negative, mff positive at the time of adoption (unknown date)• Dog tested HW Ag negative & mff positive multiple times and/with different platforms (patient
side and reference laboratory tests• 1/19/2021 started on doxycycline• 1/27/2021 blood sample sent to Auburn laboratory for heat treatment and MKT: HW Ag negative;
173mff/mL (D. immitis)• Recommended staying on imidacloprid/moxidectin with re-test for mff in approimately 6 months• 6/22/2021 received a blood sample: MKT – 1 mff seen in 1 mL blood (D. immitis); HW antigen
negative
Comment: This case has many of the elements of heartworm resistance. Most notable is geography and difficulty in clearing mff. It is important to remember that resistant heartworms are not resistant to melarsomine dihydrochloride. Mff reduction was aided by doxycycline and continued imidacloprid/moxidectin. Note that significant reduction in mff numbers required 6 months.
Recommendation: Continue on imidacloprid/moxidectin. Alternative moxidectin products could be considered.
108

Broad Spectrum Feline Parasite Control: The Time Has Come!
Byron L. Blagburn University Distinguished Professor of Parasitology
College of Veterinary Medicine Auburn University, Alabama
Background
Despite the increasing popularity of cats as pets, the importance of internal parasites as causes of disease and potential zoonoses is often ignored. Increasing evidence indicates that cats harbor internal parasites more frequently than previously thought (Table 1). The perception that cats have fewer internal parasites probably results from less frequent fecal examinations and the lower parasite burdens in adult cats. Lower parasite burdens require the use of more sensitive fecal examination procedures such as centrifugal fecal flotation. Other techniques like simple flotation or direct smear usually result in lower parasite recovery rates. Recommendations by the Centers for Disease Control and Prevention (CDC) and the Companion Animal Parasite Council (CAPC) strive to increase pet-owner compliance in parasite control and decrease the likelihood of human exposure to zoonotic parasites. I will discuss key internal parasites found in cats and emphasize the need for more effective parasite control. The latter is becoming more achievable with the introduction of newer broad-spectrum parasiticides. Certain of these products are effective beyond the traditional one-month efficacy period.
Heartworm Disease
Heartworm (Dirofilaria immitis) infection in cats was first reported more than 85 years ago. However, many pet owners are not aware that heartworms can cause serious and sometimes fatal disease in cats. Most of us understand the consequences of heartworm infections in dogs, but we may not be aware that heartworm infections in cats can result in different clinical responses (Table 2). Although the prevalence of heartworm in cats has been studied, distinctive features of feline infections make establishing the true prevalence difficult. Several techniques—including radiography, angiography, ultrasonography, necropsy, and detection of microfilariae, antibody, and antigen have been used. The different diagnostic methods makes comparison of studies difficult. Moreover, because many of these tests were developed for diagnosing adult heartworms in dogs, they may not be directly applicable in cats (see HARD below). The types of available tests and features of feline heartworm infections detailed in Table 3 probably result in underestimated prevalence of heartworm in cats. Most heartworm researchers agree that exposure of cats to heartworm-infected mosquitoes is surprisingly high and that the risk of feline heartworm infection remains a concern in most regions of the US.
Cats with clinical heartworm disease usually present with respiratory signs such as coughing, dyspnea or intermittent vomiting not associated with eating. Signs can be limited to weight loss or diarrhea accompanying respiratory signs. When present, the respiratory signs are similar to those observed with feline bronchial disease, which is frequently described as asthma by the owners. A small percentage of cats that develop clinical signs may die suddenly. This peracute presentation also mimics signs of acute dyspnea associated with feline asthma, cardiomyopathy, pleural diseases, or infections with other pulmonary parasites. Many of these cats are clinically normal before the acute event.
In the past, the signs of feline heartworm disease were usually attributed to the death of adult heartworms and the cat's unique pulmonary reaction to fragments of dead and dying adult worms. Continuing research suggests that early death of immature heartworms in cats can also evoke severe and potentially fatal pulmonary reactions. Moreover, these infections cannot be easily diagnosed using antigen tests, antibody tests, or radiography because of the absence of adult female heartworms, potentially waning antibody levels, and/or the similarity of lung lesions to those associated with other feline pulmonary diseases.
In cats, immature worms arrive in the lungs 70-90 days after infection. However, because of the cat’s unique pulmonary response, most of these worms are killed in the lungs and do not survive to the adult stage. The
109

intense inflammation caused by the death of these immature adult heartworms results in respiratory disease characterized by coughing and dyspnea. Because these signs correspond to the death of worms about 90 days after infection, disease was attributed to 3-month-old worms and was referred to as the 3-month disease cycle. Using a laboratory model of feline heartworm disease, we reproduced the 3-month-disease cycle by strategically treating experimentally infected cats to eliminate 70-90 day-old heartworms. Results demonstrated that experimentally induced death of immature heartworms in the lungs could cause clinical disease identical to the naturally occurring 3-month disease. This syndrome was named heartworm associated respiratory disease and given the acronymHARD to characterize the potential for cats to present with heartworm disease that is not caused by matureheartworms. Radiographs of the lungs of cats with abbreviated infections (HARD) were similar to radiographs ofcats with naturally occurring heartworm and other pulmonary diseases such as feline asthma. In support of naturallyoccurring HARD, other researchers demonstrated a correlation between antigen, antibody, and necropsy results thatwere similar to those of our HARD study. They also correlated these test results with lung lesions, concluding thatcats can have lesions consistent with heartworm infection, but without serologic or necropsy confirmation ofheartworm infection.
Our HARD studies, taken with the additional study mentioned above should alert veterinarians that heartworm disease in cats can be caused by immature heartworms and that diagnosis of these infections can be challenging. It is important to note that specific therapies for HARD are unknown at this time. Cats with HARD can only be treated symptomatically as described below. A comparison of HARD and feline heartworm disease caused by mature heartworms worm is presented in table 3.
Diagnosis of HARD and feline heartworm infection
Heartworm disease in cats is difficult to diagnose and is often mistaken for other diseases. Heartworm infected cats often are asymptomatic or present with a history of transient clinical signs. An array of tests can be employed when either HARD or heartworm disease caused by mature worms is suspected (Table 3). Serologic tests are available as both point-of-care and reference laboratory tests for detection of antigen or antibodies specific for D. immitis. A positive antigen test or a positive echocardiogram is diagnostic for heartworm in cats infected with mature worms. These tests are not helpful for confirming or ruling out HARD. Radiography may be helpful, although lesions are not specific for heartworm disease. Antibody tests are useful in confirming that infective larvae were introduced by mosquitoes and that sufficient development occurred to induce an antibody response. When used with presenting clinical signs, a positive antibody test raises the index of suspicion for heartworm. Other laboratory tests such as a CBC and chemistry panel can b provide marginally helpful ancillary data, but include no definitive test parameter that is diagnostic for heartworm. Necropsy examination is definitive of course but cannot be applied under ante-mortem circumstances. Necropsy examination is also useful in confirming that heartworms are the cause of lesions and/or disease due to aberrant heartworm migration.
A recently described phenomenon referred to as “antigen-blocking” has complicated our interpretation of a negative antigen tests in both dogs and cats. Under conditions of antibody excess, antibodies may bind to circulating heartworm antigen and prevent the capture of antigen by substrate-bound capture antibodies. This blocking phenomenon can be reversed by either heat or acid treatment of serum or plasma. These reversal procedures dissociate heartworm antigen and antibody complexes and allows the antigen to be captured by the substrate-bound antibody.
Because of the lack of specificity of clinical signs, it is likely that a combination of the tests and diagnostic methods mentioned above will be necessary to confirm heartworm disease in cats (Table 3). As with other diseases, a detailed history including travel, current geographic location and indoor/outdoor habits can be helpful in interpreting clinical signs and test results.
Treatment of HARD and feline heartworm infection
Treatment of mature heartworm infections and HARD is palliative at best. Strategies are either to reduce clinical signs until heartworms are eliminated by natural host mechanisms or a normal balance of the host-parasite relationship is re-established. Information on the use of melarsomine dihydrochloride to eliminate adult worms in cats is inadequate and inconsistent. Efficacy against transplanted worms using both standard 2-dose regimen and the alternative 3-dose regimen yielded reductions in worm burdens without severe adverse events. Assuming these results will be achieved under the spectrum of conditions that occurs in naturally infected cats is presumptive and potentially dangerous. Use of melarsomine in naturally infected cats often resulted in host mortality or unacceptable adverse events. Current thought leaders do not recommend the use of heartworm adulticides in cats.
110
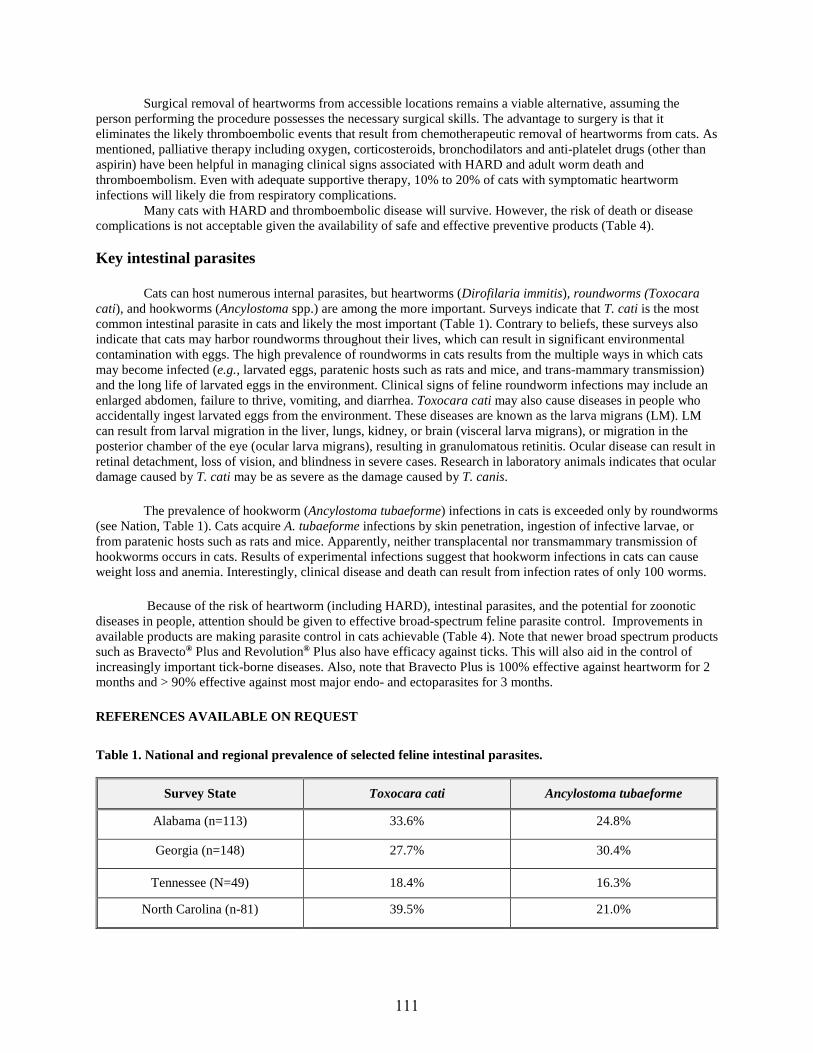
Surgical removal of heartworms from accessible locations remains a viable alternative, assuming the person performing the procedure possesses the necessary surgical skills. The advantage to surgery is that it eliminates the likely thromboembolic events that result from chemotherapeutic removal of heartworms from cats. As mentioned, palliative therapy including oxygen, corticosteroids, bronchodilators and anti-platelet drugs (other than aspirin) have been helpful in managing clinical signs associated with HARD and adult worm death and thromboembolism. Even with adequate supportive therapy, 10% to 20% of cats with symptomatic heartworm infections will likely die from respiratory complications.
Many cats with HARD and thromboembolic disease will survive. However, the risk of death or disease complications is not acceptable given the availability of safe and effective preventive products (Table 4).
Key intestinal parasites
Cats can host numerous internal parasites, but heartworms (Dirofilaria immitis), roundworms (Toxocara cati), and hookworms (Ancylostoma spp.) are among the more important. Surveys indicate that T. cati is the most common intestinal parasite in cats and likely the most important (Table 1). Contrary to beliefs, these surveys also indicate that cats may harbor roundworms throughout their lives, which can result in significant environmental contamination with eggs. The high prevalence of roundworms in cats results from the multiple ways in which cats may become infected (e.g., larvated eggs, paratenic hosts such as rats and mice, and trans-mammary transmission) and the long life of larvated eggs in the environment. Clinical signs of feline roundworm infections may include an enlarged abdomen, failure to thrive, vomiting, and diarrhea. Toxocara cati may also cause diseases in people who accidentally ingest larvated eggs from the environment. These diseases are known as the larva migrans (LM). LM can result from larval migration in the liver, lungs, kidney, or brain (visceral larva migrans), or migration in the posterior chamber of the eye (ocular larva migrans), resulting in granulomatous retinitis. Ocular disease can result in retinal detachment, loss of vision, and blindness in severe cases. Research in laboratory animals indicates that ocular damage caused by T. cati may be as severe as the damage caused by T. canis.
The prevalence of hookworm (Ancylostoma tubaeforme) infections in cats is exceeded only by roundworms (see Nation, Table 1). Cats acquire A. tubaeforme infections by skin penetration, ingestion of infective larvae, or from paratenic hosts such as rats and mice. Apparently, neither transplacental nor transmammary transmission of hookworms occurs in cats. Results of experimental infections suggest that hookworm infections in cats can cause weight loss and anemia. Interestingly, clinical disease and death can result from infection rates of only 100 worms.
Because of the risk of heartworm (including HARD), intestinal parasites, and the potential for zoonotic diseases in people, attention should be given to effective broad-spectrum feline parasite control. Improvements in available products are making parasite control in cats achievable (Table 4). Note that newer broad spectrum products such as Bravecto® Plus and Revolution® Plus also have efficacy against ticks. This will also aid in the control of increasingly important tick-borne diseases. Also, note that Bravecto Plus is 100% effective against heartworm for 2 months and > 90% effective against most major endo- and ectoparasites for 3 months.
REFERENCES AVAILABLE ON REQUEST
Table 1. National and regional prevalence of selected feline intestinal parasites.
Survey State Toxocara cati Ancylostoma tubaeforme
Alabama (n=113) 33.6% 24.8%
Georgia (n=148) 27.7% 30.4%
Tennessee (N=49) 18.4% 16.3%
North Carolina (n-81) 39.5% 21.0%
111
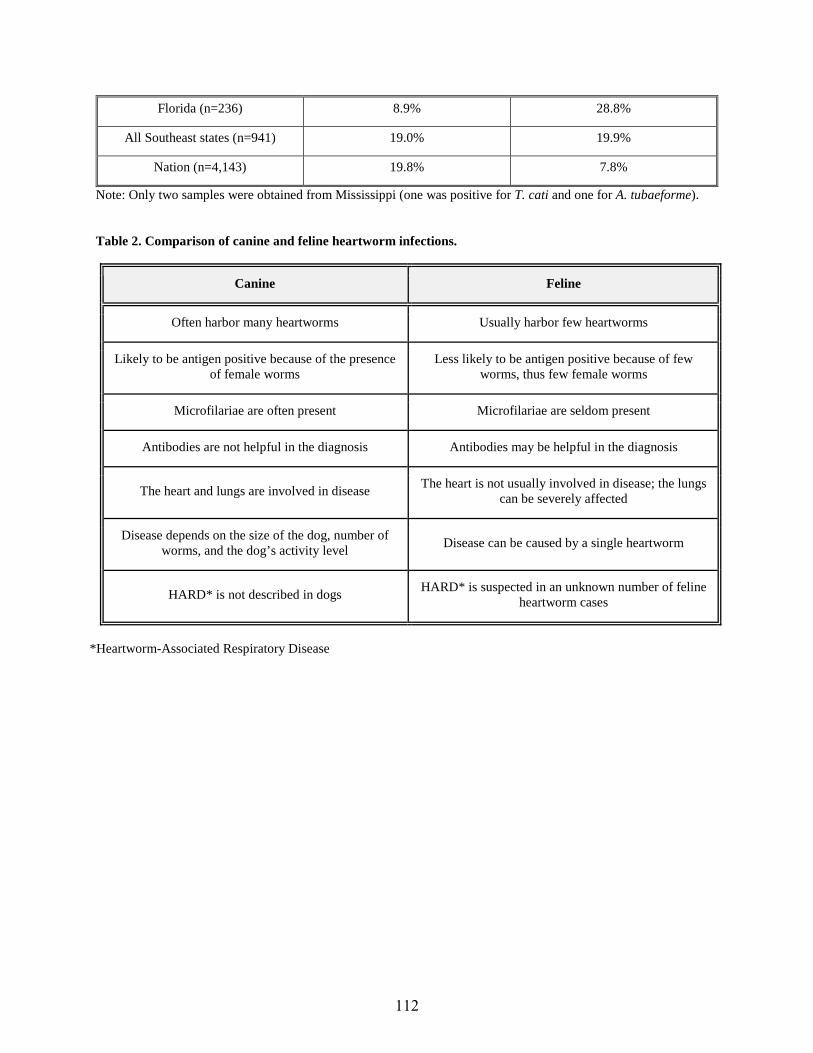
Florida (n=236) 8.9% 28.8%
All Southeast states (n=941) 19.0% 19.9%
Nation (n=4,143) 19.8% 7.8%
Note: Only two samples were obtained from Mississippi (one was positive for T. cati and one for A. tubaeforme).
Table 2. Comparison of canine and feline heartworm infections.
Canine Feline
Often harbor many heartworms Usually harbor few heartworms
Likely to be antigen positive because of the presence of female worms
Less likely to be antigen positive because of few worms, thus few female worms
Microfilariae are often present Microfilariae are seldom present
Antibodies are not helpful in the diagnosis Antibodies may be helpful in the diagnosis
The heart and lungs are involved in disease The heart is not usually involved in disease; the lungs can be severely affected
Disease depends on the size of the dog, number of worms, and the dog’s activity level Disease can be caused by a single heartworm
HARD* is not described in dogs HARD* is suspected in an unknown number of feline heartworm cases
*Heartworm-Associated Respiratory Disease
112
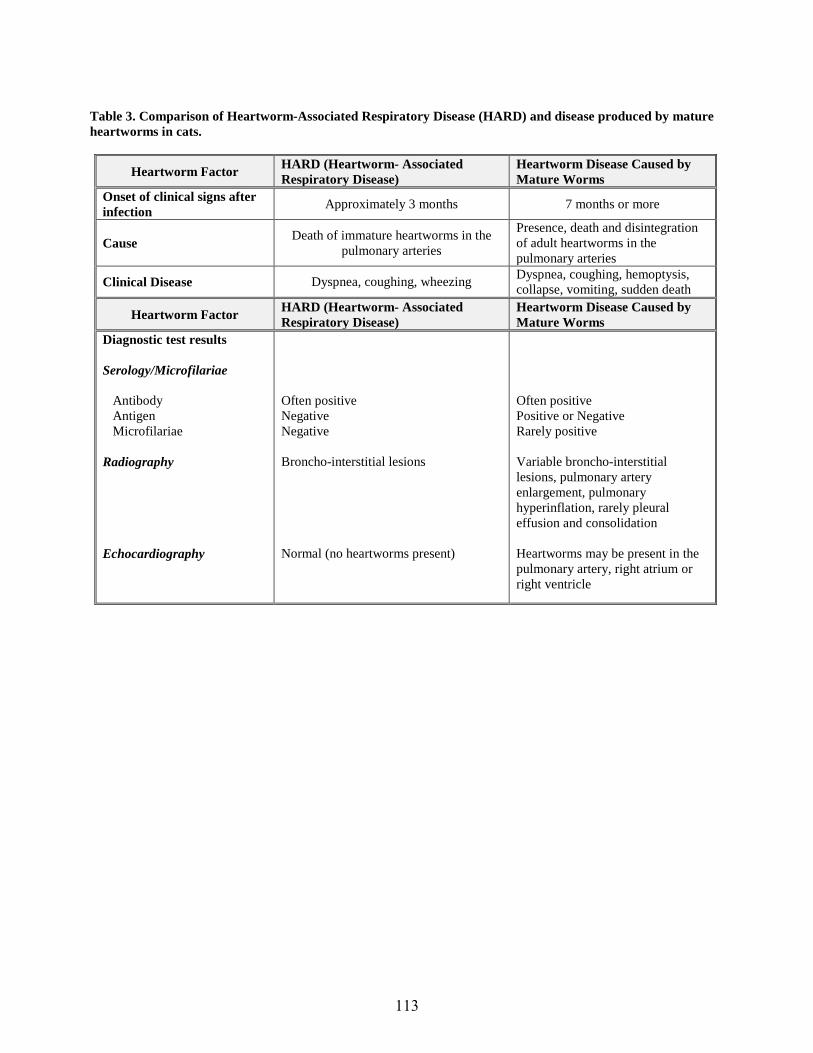
Table 3. Comparison of Heartworm-Associated Respiratory Disease (HARD) and disease produced by mature heartworms in cats.
Heartworm Factor HARD (Heartworm- Associated Respiratory Disease)
Heartworm Disease Caused by Mature Worms
Onset of clinical signs after infection Approximately 3 months 7 months or more
Cause Death of immature heartworms in the pulmonary arteries
Presence, death and disintegration of adult heartworms in the pulmonary arteries
Clinical Disease Dyspnea, coughing, wheezing Dyspnea, coughing, hemoptysis, collapse, vomiting, sudden death
Heartworm Factor HARD (Heartworm- Associated Respiratory Disease)
Heartworm Disease Caused by Mature Worms
Diagnostic test results
Serology/Microfilariae
Antibody Antigen Microfilariae
Radiography
Echocardiography
Often positive Negative Negative
Broncho-interstitial lesions
Normal (no heartworms present)
Often positive Positive or Negative Rarely positive
Variable broncho-interstitial lesions, pulmonary artery enlargement, pulmonary hyperinflation, rarely pleural effusion and consolidation
Heartworms may be present in the pulmonary artery, right atrium or right ventricle
113

Tabl
e 4.
Bro
ad-s
pect
rum
pro
duct
s fo
r cat
s.
Diro
filar
ia
imm
itis
Oth
er P
aras
ites
Trad
e N
ame
(Spo
nsor
) G
ener
ic A
ctiv
es
Dos
ing
Sche
dule
T =
Tabl
et
C =
Che
w
Tissue Larvae
Microfilariae
Fleas
Ticksa
Ear Mites
Hookwormsb
Roundwormsb
Tapeworms
Ora
l
Hea
rtGar
d®
(Boe
ringe
r Ing
elhe
im)
Iver
mec
tin
Mon
thly
, C
X X
Inte
rcep
tor®
(E
lanc
o)
Milb
emyc
in o
xim
e M
onth
ly, T
X
X X
Milb
egua
rd
(Cev
a)
Milb
emyc
in o
xim
e M
onth
ly, T
X
X X
Topi
cal (
Spot
-on)
Adva
ntag
e M
ulti®
(E
lanc
o)
Imox
i (V
etoq
uino
l)
Imid
aclo
prid
/mox
idec
tin
Mon
thly
X
X X
X X
Bra
vect
o® P
lus
(Mer
ck)
Flur
alan
er/m
oxid
ectin
Ev
ery
2 m
onth
s X
X X
X X
Cen
traga
rd®
(Boe
ringe
r Ing
elhe
im)
Eprin
omec
tin/p
razi
quan
tel
Mon
thly
X
X X
Xc
Rev
olut
ion®
(Zoe
tis)
Para
dyne
® (Z
oetis
) R
evol
t™ (A
uror
a)
Syne
rgy™
(Virb
ac)
Sela
rid™
(Nor
broo
k)
Sela
mec
tin
Mon
thly
X
X X
X X
Rev
olut
ion®
Plu
s (Z
oetis
) Se
lam
ectin
/sar
olan
er
Mon
thly
X
X X
X X
X
Not
e: T
his
tabl
e is
an
upda
te a
nd m
odifi
catio
n of
a s
imila
r tab
le th
at a
ppea
red
in A
mer
ican
Hea
rtwor
m S
ocie
ty B
ulle
tin, M
arch
, 202
0, V
ol 4
7 N
o.1,
Pa
ge 9
. a S
ee in
divi
dual
pro
duct
labe
ls fo
r spe
cies
of t
icks
that
are
rem
oved
. b S
ee in
divi
dual
pro
duct
labe
ls fo
r spe
cies
and
sta
ges
of h
ookw
orm
s an
d st
ages
of r
ound
wor
ms
that
are
rem
oved
. c D
ipyl
idiu
m c
anin
um, E
chin
ococ
cus
mul
tiloc
ular
is
114

These Parasites Won’t Take No for an Answer
Byron L. Blagburn University Distinguished Professor of Parasitology
College of Veterinary Medicine Auburn University, Alabama
Giardiasis
Giardia infections in dogs and cats are caused by Giardia duodenalis (G. intestinalis, G. lamblia). A number of variants of Giardia exist (called assemblages or genospecies). It now appears that dogs and cats are infected in most cases with host-specific Giardia. However, the potential does exist for pets to harbor isolates infective for humans and vice-versa. The parasite usually resides in the small intestine, although exceptional infections in the lower bowel cannot be ruled out. Giardia is a dimorphic parasite in that it exists as a fragile flagellated bi-nucleate trophozoite and a quadrinucleate cyst. The trophozoite attaches to the surface of epithelial cells in the small intestine; encystment (formation of cysts) occurs in the ileum, cecum or colon. Although the mechanism(s) of Giardia-induced disease remain unknown, evidence suggests that the disease is likely multifactorial involving inhibition of brush border enzymes or other factors such as altered immune responses, nutritional status of the hosts, presence of intercurrent disease agents, changes in the ecology of communal intestinal fauna (microbiome), and the strain of Giardia involved in the infection. Although many infected animals remain asymptomatic, the most common presenting sign is small bowel diarrhea. Feces are usually semi-formed, but may be liquid. Blood usually is not present. Feces have been described as pale (often gray or light brown), fetid and containing large amounts of fat. Dogs or cats with giardiasis may present with poor body condition, weight loss, and occasional vomiting. As mentioned previously, it is not unusual to find Giardia present with other parasites or other gastrointestinal diseases such as inflammatory bowel disease.
Giardiasis is best diagnosed by fecal flotation using zinc sulfate (specific gravity = 1.18) as the flotation solution. Centrifugation of the preparation increases the likelihood of recovering cysts. The addition of a small amount of Lugol’s iodine to the slide prior to placement of the coverslip containing the concentrated cysts may aid in visualizing the small (10-12 µm) cysts, although not all laboratories utilize or recommend the use of iodine. Use of barium sulfate, anti-diarrheals or enemas prior to sampling feces may interfere with detection of cysts and should be avoided if possible. Other diagnostic techniques that can be used to recover either trophozoites, cysts, or proteins produced by the parasite include direct examination of feces (wet-mount), immunofluorescent procedures, and ELISA techniques. A fecal ELISA test for Giardia (Snap® Giardia, Idexx, Westbrook, ME) will assist in ruling out Giardia as a cause of diarrhea in dogs and cats, but should not be used routinely in the asymptomatic patient. Many reference diagnostic laboratories also offer fecal ELISA tests for Giardia.
Some controversy surrounds the potential of animal strains of Giardia to infect humans. As mentioned above, it is likely that some host specificity among animal strains of Giardia does exist, My opinion is that all animals that are positive for cysts following fecal examination should be treated. Not only will treatment reduce the risk of zoonotic transmission, it will also help to control outbreaks in kennels, catteries and multiple pet households hosting susceptible species.
Several treatment options are available for treatment of Giardia infections in dogs or cats (Table 1). At present, I believe that the combined use of fenbendazole and metronidazole should be the first of the agents selected for treatment. Published data also indicates that a combination of pyrantel pamoate, febantel, and praziquantel (Drontal Plus®, Bayer Animal Health) can be effective against Giardia. Febantel, a prodrug, is metabolized to fenbendazole and oxfendazole once in the host. The activity of Drontal Plus®, some believe, results from this endogenous metabolic conversion. Fenbendazole and metronidazole can be used as single agents but usually with less efficacy, Many veterinarians combine their use in a 5- or 10-day regimen. Fenbendazole also is effective against other canine intestinal parasites that may be responsible for the observed signs. Cats may be treated with a combination of metronidazole and fenbendazole as indicated in Table 1. There also are human drugs available that may be helpful in the treatment of canine or feline giardiasis.
115

Coccidiosis
Coccidial infections in dogs and cats are caused by Cystoisospora. Our recent surveys indicated that about 5% of shelter dogs sampled were passing coccidial oocysts in their feces. The principal agents in the dog are C. canis and C. ohioensis. The principal agents in the cat are C. felis and C. rivolta. These parasites reside in the posterior smallintestine and in the large intestine for some species. Their life cycles are generally self-limiting, after which theinfection is terminated. The parasites replicate first asexually by schizogony resulting in destruction of many hostenterocytes in which they develop. Asexual development is followed by production of gametes that fuse to producenon-infective oocysts that are passed in feces. The developmental cycles in the canine or feline host require 5-9 daysdepending upon the species. Development to the infective stage (sporulation) requires 1-2 days in the animal’senvironment. Only sporulated oocysts are infective to susceptible hosts.
Clinical signs of coccidiosis include hemorrhagic or mucoid diarrhea, abdominal pain, dehydration, anemia, weight loss and emesis, as well as respiratory and neurologic signs. Death can ensue in extreme cases, particularly in young puppies and kittens. Nursing animals, recently weaned animals, or those that are immunocompromised are more likely to develop clinically apparent infections. There is some indication that stress that results from shipping can lead to outbreaks of coccidiosis in young dogs. It is my belief that clinical coccidiosis in adult animals reflects either underlying concomitant infection and/or immunosuppression. I base this on the self-limiting nature of the life cycle and on research that indicates that experimental reproduction of coccidiosis in adult dogs is difficult following inoculation with sporulated oocysts.
Diagnosis of coccidiosis is based on signalment (usually puppies and kittens), clinical signs, and recovery of oocysts in feces. Fecal flotation remains the most practical means of recovering oocysts. A point to remember is that recovery of oocysts alone in feces is not sufficient proof to implicate coccidia as the cause of clinical signs. I have observed coccidial oocysts in the feces of many animals without evidence of intestinal disease. Oocysts of the coccidia mentioned above are round to oblong and measure from 16-51 µm long, depending on the species. Oocysts of C. canis and C. felis are large (34-51 µm), while those of C. ohioensis and C. rivolta are smaller (16-28 µm). Sulfadimethoxine is the most commonly used medication in dogs or cats. Several other agents are likely more effective (Table 2). Recent research suggests that ponazuril (Boehringer Ingleheim) is very effective against coccidia (see Table 2) and has become my treatment of choice. Continuing research will likely provide more definitive data regarding its use in companion animals.
Many inquiries about outbreaks of coccidiosis that I have responded to involve young animals housed in groups such as in kennels or cages maintained by breeders or in pet stores. In most of these situations, treatment with amprolium or ponazuril has resolved the problem. Little can be done to disinfect environments because of the ability of the oocysts to withstand chemicals and adverse environmental conditions. Good sanitation, including prompt removal of feces to prevent development of oocysts to the infective stage, and treatment of dams and queens with anticoccidial agents prior to parturition, have been shown to reduce the occurrence of coccidiosis in young animals.
Ancylostoma spp. (“Hookworms”)
Canine and feline hookworms are small (up to about 0.75 inches) whitish or reddish-brown worms with a hooked anterior end (hence the name). As adults, they reside in the small intestine of dog, cats and rarely humans. Ancylostoma spp. include A. caninum (the universally distributed canine hookworm), and A. braziliense (found in both dogs and cats in the subtropical US). In national surveys conducted in 1996 and 2016, A. caninum eggs were recovered from 19.2% of 6,458 and 30% of 6,418 fecal samples from shelter dogs. These results support that hookworms remain common in dogs that are beyond the reach of veterinarians and remain a source of infection for pet dogs.
Developmental cycles of hookworms include a free living phase in which larvae hatch from eggs and develop through 3 distinct stages. The 3rd environmental larval stage (infective stage) enters the host either by oral ingestion or by skin penetration. Most (but not all) orally ingested larvae establish in the intestine without extraintestinal migration. Those that penetrate the skin follow a vascular/pulmonary migration prior to their establishment in the small intestine. In addition, both prenatal (transplacental) and transmammary modes of transmission can occur. The transmammary route appears to predominate in A caninum infections. The reservoir for such larvae is somatic as is
116

the case with Toxocara canis. This somatic reservoir (which is refractory to conventional treatment) can result in a “replenishment” of intestinal hookworms that are removed by routine deworming. This phenomenon (often referred to as “larval leak”) can confound fecal results after deworming. Unless the interval of post-treatment fecal examination is shorter than the parasite’s prepatent period, one might falsely assume that residual hookworms are resistant to the chosen therapy.
Hookworms may cause dermal disease, pulmonary disease and intestinal disease. The latter is the most common syndrome in the dog. Hemorrhagic enteritis caused by A. caninum can be a peracute, life-threatening disease in young dogs. In these animals, the transmammary route of infection can lead to the establishment of very high worm burdens in neonatal dogs in a short period of time. The remaining species are less significant pathogens, but not always innocuous. Ancylostoma caninum is a prolific egg producer. It is estimated that mature females of A. caninum can produce up to 20,000 eggs per day. This magnitude of fecundity can result in substantial environmental reservoirs of infective larvae in rather short periods of time.
Free-living infective larvae of some Ancylostoma spp. may penetrate the skin of humans and migrate subsequently for short periods of time. These dermal wonderings result in reddish, pruritic, serpentine lesions. This condition is referred to as cutaneous larva migrans (CLM) or “creeping eruption”. Although less significant than the larva migrans syndromes caused by the roundworms, the cutaneous syndrome caused by the hookworms remains a concern for veterinarians and pet owners. Larvae of Ancylostoma braziliense appear to be the most common cause, although cases of CLM caused by A. caninum have been documented. Recent evidence suggests that adults of A. caninum may also inhabit the intestines of humans. More than 200 such cases of “eosinophilic enteritis” have now been reported in the medical literature. Human infections with adult A. caninum can result in both acute and chronic signs. Clinical signs included recurrent abdominal pain, small bowel thickening, eosinophilia, increased levels of IgE and also inflammation of the distal ileum and colon.
Hookworm infections can be controlled either by strategic deworming with narrow spectrum or broad spectrum agents, or by repeated monthly administration of available broad spectrum heartworm preventives. Injectable moxidectin (ProHeart® 6/ProHeart® 12), administered at either 6 or 12-month intervals, is also effective against hookworms (Ancylostoma caninum, Uncinaria stenocephala) at the time of treatment.
It is now known that multi-drug hookworm resistance (MDHR) exists in certain sub-populations of Ancylostoma caninum. Although not proven, some researchers believe that MDHR developed because of repeated deworming of closed populations of infected dogs. Resistant hookworms may vary in their responses to individual products or combinations of products depending on the genetic characteristics of the hookworm population. A current strategy to eliminate resistant hookworms is to administer imidacloprid/moxidectin (Advantage Multi®) monthly with the addition of febantel/pyrantel pamoate/praziquantel (Drontal® Plus), alternating with imidacloprid/moxidectin at 2-week intervals. Alternatively, fenbendazole may be used in combination with imidacloprid/moxidectin. Additional research using emodepside appears promising.
Dipylidium caninum (“flea tapeworm”, “cucumber seed tapeworm”) and Taenia spp. (“dog-rabbit tapeworm”; “cat-rodent tapeworm”
Tapeworms are common intestinal parasites of pets in many regions of the US. Dipylidium caninum is the more common tapeworm of dogs and cats, especially in regions with a warm climate. It is transmitted by consumption of fleas, usually during the pet’s self-grooming. The consensus has been that tapeworm infections in dogs and cats do not result in clinical disease. However, recent research suggests that tapeworms may occasionally cause transient digestive problems. Human infections with D. caninum occur when small children inadvertently ingest fleas. Although not usually of pathogenic significance, infections in children are a cause of considerable alarm and distress among parents and caregivers when proglottids are passed in feces or are found in soiled diapers. Human infections are best prevented by controlling D. caninum in dog and cat hosts. Flea control is a must is complete elimination of D. caninum is to be expected. Both narrow spectrum, combination products and combination products withheartworm preventive capabilities are available for elimination of common tapeworms.
More importantly and similar to what we have observed for Ancylostoma caninum, there are increasing reports of failure to eliminate D. caninum infections from infected dogs and cats using either praziquantel or epsiprantel. Most
117
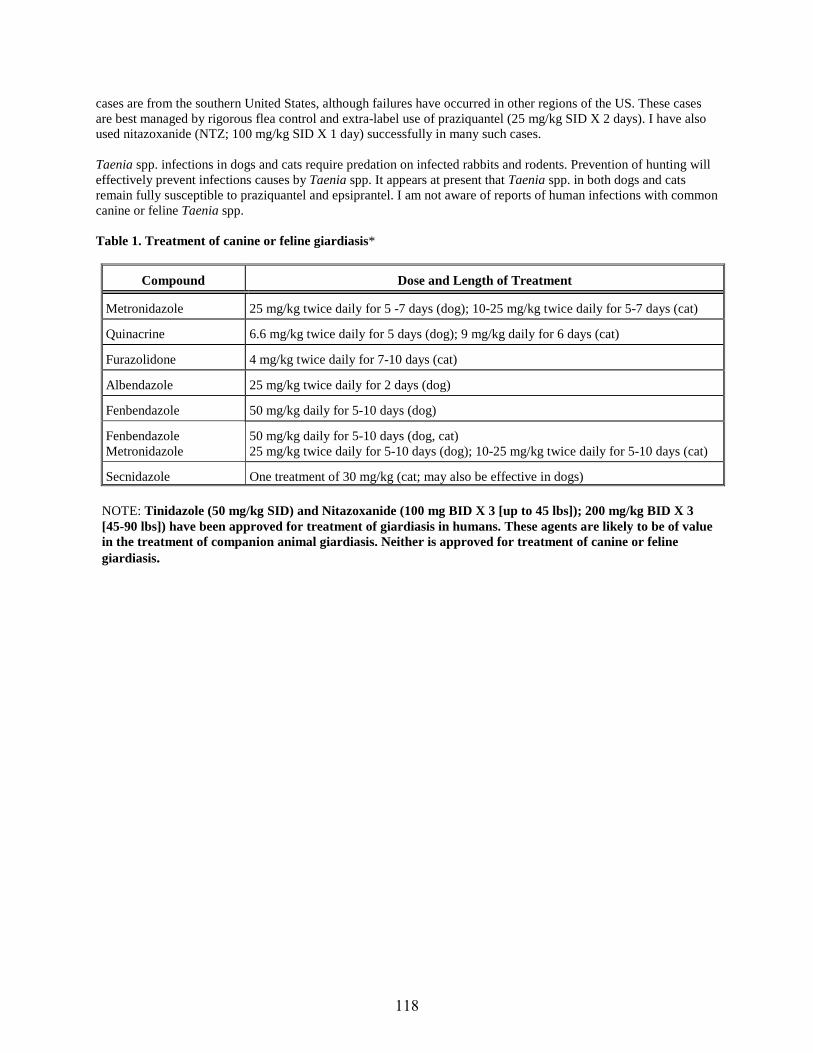
cases are from the southern United States, although failures have occurred in other regions of the US. These cases are best managed by rigorous flea control and extra-label use of praziquantel (25 mg/kg SID X 2 days). I have also used nitazoxanide (NTZ; 100 mg/kg SID X 1 day) successfully in many such cases.
Taenia spp. infections in dogs and cats require predation on infected rabbits and rodents. Prevention of hunting will effectively prevent infections causes by Taenia spp. It appears at present that Taenia spp. in both dogs and cats remain fully susceptible to praziquantel and epsiprantel. I am not aware of reports of human infections with common canine or feline Taenia spp.
Table 1. Treatment of canine or feline giardiasis*
Compound Dose and Length of Treatment
Metronidazole 25 mg/kg twice daily for 5 -7 days (dog); 10-25 mg/kg twice daily for 5-7 days (cat)
Quinacrine 6.6 mg/kg twice daily for 5 days (dog); 9 mg/kg daily for 6 days (cat)
Furazolidone 4 mg/kg twice daily for 7-10 days (cat)
Albendazole 25 mg/kg twice daily for 2 days (dog)
Fenbendazole 50 mg/kg daily for 5-10 days (dog)
Fenbendazole Metronidazole
50 mg/kg daily for 5-10 days (dog, cat) 25 mg/kg twice daily for 5-10 days (dog); 10-25 mg/kg twice daily for 5-10 days (cat)
Secnidazole One treatment of 30 mg/kg (cat; may also be effective in dogs)
NOTE: Tinidazole (50 mg/kg SID) and Nitazoxanide (100 mg BID X 3 [up to 45 lbs]); 200 mg/kg BID X 3 [45-90 lbs]) have been approved for treatment of giardiasis in humans. These agents are likely to be of value in the treatment of companion animal giardiasis. Neither is approved for treatment of canine or feline giardiasis.
118

Table 2. Treatment of canine and feline coccidiosis.
Compound Dose and Length of Treatment
Sulfadimethoxine 50-60 mg/kg daily for 5-20 days (dog and cat)
Sulfaguanidine 150 or 200 mg/kg daily for 6 days (dog and cat); or 100-200 mg/kg every 8 hours for 5 days (dog and cat)
Furazolidone 8-20 mg/kg once or twice daily for 5 days (dog and cat)
Trimethoprim/ Sulfonamides
Dose and length of treatment depends on type of sulfonamide; 30 - 60 mg/kg of trimethoprim daily for 6 days in animals 4 kg; or 15- 30 mg/kg trimethoprim daily for 6 days in animals < 4 kg
Sulfadimethoxine/
Ormetaprim
55 mg/kg of sulfadimethozine and 11 mg/kg of Ormetaprim for 7- 23 days (dog)
Quinacrine 10 mg/kg daily for 5 days (cat)
Ponazuril 20 mg/kg daily for 2 days; 50 mg/kg for 1 day
Retreatment may be necessary
Amprolium 300 to 400 mg (total) daily for 5 days (dog); 110-200 (total) daily for 7 to 12 days (dog); 60-100 mg total daily for 7 days (cat); 1.5 tbsp/gal (sole water source) not to exceed 10 days (dog)
Amprolium/ Sulfadimethoxine
150 mg/kg of amprolium and 25 mg/kg of sulfadimethoxine for 14 days (dog)
REFERENCES AVAILABLE ON REQUEST.
119
Fleas, Ticks and Vector-borne diseases: Bad Things Come in Threes
Byron L. Blagburn University Distinguished Professor of Parasitology
College of Veterinary Medicine Auburn University, Alabama
Importance of ticks
• Ticks are second only to mosquitoes in the number of diseases that they transmit.• Ticks feeding may cause irritation, anemia, hypersensitivity reactions, and toxicosis.• Ticks may transmit numerous pathogens including helminths, protozoa, viruses, bacteria (including
rickettsiae) and fungi.• Several pathogens transmitted by ticks are potential zoonotic agents.• Two families of ticks are important in veterinary medicine
Ixodidae (hard ticks)
• Environmental stages found in open areas on vegetation.• Mouthparts visible from dorsal surface.• Body capable of limited expansion (dorsal surface covered by leathery scutum [see
below]).• Balance water using salivary secretions.• Secrete cement from salivary glands for attachment.• Female hard ticks feed and engorge slowly over long periods.• Imbibe many times their body weight in host blood.• Females lay thousands of eggs per oviposition in environment.
Argasidae (soft ticks)
• Environmental stages live in nests and burrows of hosts.• Mouthparts not visible from dorsal surface.• Body is soft and easily expandable.• Life cycle consists of many nymphal stages.• Females feed intermittently and lay eggs in masses.• Soft ticks do not produce cement for attachment.
Important ixodid (hard) tick species found on companion animals
• Rhipicephalus sanguineus (Brown Dog Tick)• Dermacentor variabilis (American Dog Tick); Dermacentor andersoni (Rocky Mountain Wood Tick)• Ixodes scapularis (Black-legged Tick; Deer Tick); Ixodes pacificus (Western Black-legged Tick)• Amblyomma americanum (Lone Star Tick); Amblyomma maculatum (Gulf Coast Tick)• Haemaphysalis longicornis (Long-horned Tick)
Ixodid (hard) tick structure and function
• Body is divided into head (capitulum [contains mouthparts]), and body (idiosoma).• Mouthparts consist of structures that function in tactile sensing (palps), lacerating host skin (chelicerae),
and anchoring the tick to the host (hypostome).• Body is covered by a complex waxy somewhat inflexible exoskeleton (tegument) that protects the tick from
water loss and predators.
120

• A scutum (dorsal shield) covers the entire surface of adult male tick, but only a portion of the dorsal surfaceof females, nymphs, and larvae.
• The scutum is sometimes colored with iridescent white or yellow patches (ornate tick) or may be devoid ofsuch ornamentation (inornate ticks).
• Partial coverage of the dorsal surface of female ticks allow for enormous expansion during feeding andengorgement.
• Ticks have an excretory system (malpighian tubules), “liver” (fat body), an open circulatory system with ablood-like hemolymph, a respiratory system (net-like tracheae with openings called spiracles), a rathercomplex nervous system and a number of sensory structures that detect chemical, thermal, light andmechanical stimuli. A multifunctional organ located on the legs (Haller’s organ) receives stimuli usedduring questing (crawling on vegetation to gain entry onto a host) and host detection. Some ticks have eyes.
Ixodid tick developmental cycles
• Ticks develop through four distinct life cycle stages.• Egg, larva, nymph, adult• Larvae, nymphs, and adults are similar in appearance, but differ in size and numbers of legs
(larvae possess 6 legs; nymph and adults possess 8 legs).• Stages increase in size from larva to adult.• Larvae and nymphs are without features of sexual dimorphism.
• Ticks that infest companion animals are 3-host ticks.• Most species utilize a different species of host at each stage; R. sanguineus utilizes the dog during each
developmental phase.• Ixodes scapularis (Black-legged Tick; Deer Tick) may parasitize in excess of 100 host species representing
three vertebrate classes (mammals, birds, reptiles).• Certain ticks (i.e. R. sanguineus) can complete their life cycles in weeks, while others require two years or
more.• Eggs are laid by replete females in sheltered environments off the host.• Larvae and each subsequent stage seek a host, feed to repletion, drop from the host and either molt to next
stage or deposit eggs (replete females).• Adult females of H. longicornis may reproduce without male ticks (parthenogenesis).
Behavior of ticks in the environment
• Free-living ixodid ticks reside in numerous environments including forests, savannahs, fields, shrubs andbrush.
• They are capable of developmental arrest (diapause) to allow them to survive periods of environmentalstress• Diapause is triggered by environmental changes such as day length, temperature changes, changes
in humidity, and seasonal changes.• Ticks seek hosts by questing on vegetation; types and height of vegetation is determined by the host they
seek (lower vegetation for smaller hosts; higher vegetation for larger hosts)• Ticks utilize vibrations, shadows produced by changing light patterns, body heat, odors and chemicals as
host-seeking cues.• Ticks literally “grab” hosts as they pass in close proximity to questing sites.
Feeding habits, pathogen transmission, vector competence
• After gaining access to the host, ticks search for a desired attachment site.• Attachment occurs by cleaving the host skin with the chelicerae, insertion of the hypostome (anchor) and
production of adhesive cement and salivary secretions.• Tick saliva contains numerous moieties that inhibit immune responses, coagulation of blood, and exert anti-
inflammatory and early analgesic effects.• The tick body undergoes enlargement and expansion (greatest in female) during imbibition of blood.
121

• As ticks feed, they ingest pathogens that may be circulating in the host’s blood.• Pathogens undergo replication in tick gut cells and are disseminated to numerous tick organs (i.e. salivary
glands).• Pathogens gain entry into a new host when the next stage (after molting) feeds on susceptible hosts (trans-
stadial transmission; AKA horizontal or state to stage transmission) or by larvae that hatch from eggsthrough which the pathogen was passed (trans-ovarian transmission; AKA vertical transmission ).
• Successful transmission can occur via salivary secretions, coxal fluid, regurgitated gut contents,contaminated mouthparts, or a combination of these mechanisms.
• Whether a tick will serve as a successful vector depends on several factors• Size of blood meal ingested, virulence of pathogen, susceptibility of host.• Capability of pathogen to infect and replicate in the tick.• Successful dissemination of the pathogen throughout the tick’s body.• Trans-stadial or trans-ovarial habits of the pathogen.• Interactions between multiple microbes infecting the same tick.
Tick control
• Treatment of the animal (there are numerous available agents; the following are marketed by the veterinaryprofession)
• Afoxolaner• Fluralaner• Lotilaner• Sarolaner• Amitraz• Fipronil• Flumethrin• Selamectin• Deltamethrin• Cyphenothrin• Etofenprox• Isopropyl myristate
• Treatment of the environment
• Habitat modification• Host elimination• Targeted acaricides
• Integrated Tick Control
• Combination of animal treatment and environment treatment/management.
Vector-borne disease control
• Prevent tick infestation by using appropriate tick avoidance behavior (difficult).• Avoid tick infested areas• Wear light-colored clothing (allows you to see ticks crawling on clothing)• Use a chemical repellent such as DEETor Picaridin
• Prevent tick feeding (ticks may gain access to pet host, but do not attach or feed)• Use of products mentioned above can also aid in the prevention of vector transmission.
122

• Treat host with antimicrobial medications (therapeutic or prophylactic regimens).
Canine ehrlichiosis/anaplasmosis
Canine ehrlichiosis and anaplasmosis are multi-systemic diseases that may be caused by different genera and species of gram-negative obligate intracellular bacteria. The taxonomy of this group of organisms has undergone significant changes due to new information derived from molecular biological characterizations. Most ehrlichial species of importance to companion animal veterinarians use ixodid ticks as vectors. Some are transmitted by a single tick species; others may utilize multiple tick vectors. Ehrlichia canis, the principle cause of canine ehrlichiosis, is transmitted in salivary secretions by the ubiquitous brown dog tick (R. sanguineus). Infections are acquired by larvae and nymphs and are transmitted by the next life cycle stage after the molt and attachment to a new canine host (trans-stadial transmission). Transmission from adult female ticks to ova (trans-ovarial transmission) does not occur. Clinical canine ehrlichiosis occurs as three phases. The acute phase of infection persists for 1- 3 weeks. The hallmark of the acute phase is the development of vascular inflammation and subsequent thrombocytopenia. Thrombocytopathia and hyperglobulinemia also are characteristics of the acute phase of disease. Dogs either eliminate the organism or enter the subclinical phase. During this phase, the parasite is restricted to somewhat dormant occupation of visceral (predominantly splenic) macrophages. The subclinical phase may last only for weeks, but can persist for years. During this phase many dogs remain antibody positive and some retain abnormal hemograms. Mechanisms of disease during the final or chronic phase of ehrlichiosis is poorly understood, but probably results from immune events induced by the parasite. Features of this phase include bleeding tendencies (thrombocytopenia), non-regenerative anemia, pronounced hyperglobulinemia and thrombocytopathia. Clinical finding in dogs represent a wide array of abnormalities and presenting signs. These include lethargy, anorexia, weight loss, epistaxis, melena, petechial and echymotic hemorrhage, retinal hemorrhage and hematuria. Additional findings might include enlarged lymph nodes, pale mucus membranes (anemia), and splenomegaly. Occasionally ocular disease (anterior uveitis, retinal changes) and CNS signs such as ataxia, proprioceptive defects, head tilt, nystagmus and seizures have been reported. Diseases caused by Anaplasma phagocytophilum, Ehrlichia chaffeensis and Ehrlichia ewingii are similar to E. canis except that polyarthritis appears more common with E. ewingii. Diagnosis of canine ehrlichiosis/ anaplasmosis is based on history, clinical signs, hemogram and chemistries, and the results of immunologic and/or molecular biologic testing. Keep in mind that dogs can be infected with multiple vector-borne agents, given the wide geographic ranges of ixodid ticks and their capability to feed on multiple hosts. The availability of commercially available serological tests (some capable of detecting multiple pathogens) can greatly assist veterinarians in diagnosing ehrlichiosis. However, cross-reaction between the different species occurs only within genotypic groups. This can be a positive aspect of diagnosis if response to treatment is successful for all members of the group (not always the case). It can be a hindrance if infection is caused by a species not detected by the particular test employed. Specimens must be referred to specialty laboratories for molecular based tests. Some reference laboratories may also perform serologic tests for Ehrlichia species other than those caused by E. canis. Dogs are also host to E. ewingii, E. chaffeensis, Ehrlichia muris, Panola Mountain Ehrlichia, Anaplasma phagocytophilum and A. platys. The treatment of choice for Ehrlichiosis/Anaplasmosis is doxycycline (10-20 mg/kg per day [split if necessary] for 4-6 weeks). Other effective drugs include tetracycline, oxytetracycline, minocycline, and chloramphenicol. Only marginal success was achieved with imidocarb diproprionate. Ehrlichial infections in cats are considered uncommon. Cats are host to E. canis and A. phagocytophilum.
Canine borreliosis (Lyme disease)
Canine Lyme borreliosis (CLB) is an infectious vector borne (potentially zoonotic) arthropathy that is enzootic in the northeastern US. Other smaller foci of infection occur in the upper midwest and the west. CLB is transmitted in the US by two species of ixodid ticks. Ixodes scapularis is the primary vector in the northeastern, southern and midwestern US. Ixodes pacificus serves that same purpose in the west. The causative agent of CLB is Borrelia burgdorferi, one of more than 20 such small bacteria (spirochetes). Other species of Borrelia are responsible for the disease in other parts of the world. Differences in strains or species of the organisms can account for differences in the presentation and/or severity of resulting disease. Spirochetes gain entry into hosts (whether dog or human) in the saliva of the offending tick species. Severity of resulting disease is likely the result of the numbers of ticks that infest the host, as well as the number of organisms present and introduced by
123
the ticks. As was mentioned for other agents, the disease syndrome is generally the result of the infected host’s immune response. CLB is transmitted tran-stadially by nymphs and adults. Nymphs likely account for most human infections. The primary reservoir host in nature is the white-footed mouse. Clinical disease in dogs generally occurs 2-6 months after exposure to infected ticks. Signs include fever, shifting leg lameness, regional lymphadenopathy, and malaise. Polyarthritis is reported as the most common sign accompanying clinically significant canine infections. Glomerulopathy (azotemia, uremia, proteinuria, peripheral edema) has been observed occasionally. Diagnosis of CLB is based on history, clinical signs, laboratory findings, results of serologic tests (IFA, ELISA), and rarely, detection of organisms by culture. An available point of care ELISA test that detects the so-called C6 protein is helpful in differentiating true infection titers from those that are vaccine induced. This test also detects antibodies to Ehrlichia canis and Ehrlichia chaffeensis, Anaplasma phagocytophilum, Anaplasma platys and antigens produced by the canine heartworm, Dirofilaria immitis. Idexx Corporation can quantify antibodies to C6 protein. This quantitative test can be helpful in identifying a treatment strategy in an asymptomatic dog, monitoring responses to treatment, and monitoring antibody responses in an asymptomatic dog over time. Doxycyline and amoxicillin are the treatments of choice for Lyme borreliosis, although other agents such as cefovecin have proved effective.
Rocky mountain spotted fever (RMSP)
RMSF is a disease of man, dogs, cats, and horses caused by Rickettsia rickettsii, an organism related to Ehrlichia sp. Dogs are infected following infestation by and subsequent feeding of ixodid ticks of the genus Dermacentor (D. variabilis, D. andersoni). Recent reports indicate that Rhipicephalus sanguineus also can transmit RMSF. Ticks serve as both vectors and reservoirs for the disease, since the agent can persist and develop in successive generations of ticks without the necessity of infecting a vertebrate host. RMSF occurs throughout the United States but is seen with more frequency in the southeast in an area encompassing the Carolinas westward through Tennessee, Arkansas and Oklahoma. RMSF results from infection and replication of R. rickettsii in microvessels (arterioles and venules), causing disseminated vasculitis. Following an incubation period of 2 days to 2 weeks, the following clinical syndromes may result: lymphadenopathy, myalgia, cough, dyspnea, edema of face and extremities, congestion of vessels in the conjunctiva and sclera, abdominal pain, and petechiae/rash. Interestingly, rash, which is a principal presenting sign in humans, occurs only rarely in dogs. Diagnosis is based on history (including presence of ticks or exposure to ticks), clinical signs, laboratory data (thrombocytopenia), and serology. Effective treatments include doxycycline, other tetracyclines, chloramphenicol and drugs from the fluoroquinolone class.
Feline cytauxzoonosis
Cytauxzoonosis is a sometimes fatal tick-borne disease of rural outdoor cats caused by a dimorphic, biphasic protozoal parasite called Cytauxzoon felis. Cytauxzoonosis has been described in cats from many states in the southeastern US including Texas, Arkansas, Louisiana, Oklahoma, Missouri, Tennessee, Alabama, Georgia and Florida. Wild felids (e.g. bobcats) are natural hosts, from which the common name “Bobcat Fever” was derived. Stages of the parasite occur in erythrocytes (piroplasms) and in leukocytes (schizonts). Both intra-erythrocytic and leukocytic stages are structurally similar to parasites within the genus Theileria. Intra-erythrocytic piroplasms are ingested by American Dog Ticks (Dermacentor variabilis) or Lone Star Ticks (Amblyomma americanum). A complex developmental cycle occurs in the tick that culminates in the production of infectious zoites. These zoites are injected when infected ticks feed on a susceptible feline host. Infection of mononuclear cells (macrophages) leads to the development of intracellular schizonts. These so-called “foamy” macrophages are found in a variety of organs including lung, spleen, liver and lymph nodes. It is this tissue phase of parasite development that is responsible for the clinical syndrome. Affected cats often develop a rapid course of disease which includes anorexia, dyspnea, lethargy, dehydration, depression, icterus, pallor, and high fever. Regenerative anemia and thrombocytopenia also have been observed. Hemoglobinuria and bilirubinuria are rare sequelae. The period of clinical illness is extremely rapid. Death usually occurs less than a week after development of initial clinical signs. The pathogenesis of the disease is not known but probably results from a combination of the obstructive effects of the proliferative tissue schizonts, and perhaps their production of toxic, vasoactive, and pyrogenic byproducts. The intraerythrocytic piroplasms may destroy erythrocytes or enhance their destruction and phagocytosis. Some cats diagnosed with cytauxzoonosis survive infection. Survival in these cases is thought to be due to differences in pathogenicity of field strains of C. felis. Diagnosis of
124

cytauxzoonosis is based on recognition of the clinical syndrome in outdoor cats with a history of exposure to ticks. Intra-erythrocytic piroplasms are described as either “signet ring”-shaped bodies or bipolar “safety pin” forms that usually occur singly within infected erythrocytes. Necropsy usually reveals dehydration, pallor, icterus, and enlarged, edematous, and petechiated lymph nodes. The spleen and liver may be enlarged. The lungs are often congested and edematous. Hydropericardium is often observed. The lungs, liver, lymph nodes and spleen usually contain numerous schizont-infected (“foamy”) macrophages. Feline cytauxzoonosis has been treated successfully with imidocarb diproprionate as per babesiosis in dogs, however, the second treatment should be administered within one week. The combination of atovaquone and azithromycin mentioned below for treatment of babesiosis has also been used successfully to treat feline cytauxzoonosis. Tick control remains the best means of preventing the disease.
Canine babesiosis
Babesiosis is a tick borne disease of dogs caused by several different species or subspecies of Babesia. Taxonomy of organisms in this group is currently under intense study. Babesia spp. that infect dogs in the United States are all thought to be transmitted by Rhipicephalus sanguineus. The possibility also exists that certain species are transmitted horizontally between infected dogs. Babesia spp. produce large (B. vogeli, Babesis sp. [Coco]) or small (B. gibsoni, B. conradae, B. vulpes) intraerythrocytic piroplasms. Those of B. vogeli are usually 4-5 µm, often occur paired within erythrocytes, and usually are bilobed. Those of B. gibsoni are 1-2 um, occur individually in erythrocytes, and are usually round to oval, or ring-shaped. Piroplasms of B. conradae are also smaller than B. c. vogeli. These intraerythrocytic stages are the only stages that occur in dogs. Ticks ingest piroplasms during feeding. A sexual cycle of development in the tick vector culminates in the production of infective zoites. Feeding on susceptible hosts by infected tick vectors leads to injection of infectious zoites and subsequent parasitemia. Successful transmission usually requires lengthy (at least 2-3 days) feeding by ticks. The piroplasms reproduce by binary fission within infected vertebrate erythrocytes. Other means of transmission may include transplacental transmission, transfusion, use of contaminated vaccination needles or instruments used during wound repair or surgery, and bite wounds resulting from dog fights. The latter appear to be causes for enzootics of B. gibsoni in certain breeds in the United States. Clinical signs of babesiosis vary depending on the species or subspecies of Babesia involved. However, common features of the disease include hemolytic anemia, thrombocytopenia, lethargy, fever, anorexia and hemoglobinuria. Many infected dogs are either subclinical carriers or become carriers after brief bouts of disease. Diagnosis of canine babesiosis is based on recognition of intraerythrocytic piroplasms, positive serologic tests, or response to treatment. Molecular-based diagnostic tests are available in laboratories conducting specialized research on these agents. Babesiosis can be treated with imidocarb diproprionate (6.6 mg/kg IM; repeat in 2 weeks). Imidocarb appears to be effective against B. vogeli. Atovaquone (13.5 mg/kg PO TID) and azithromycin (10 mg/kg PO Q 24 hr) in combination for 10 days are more effective against the smaller piroplasms. Supportive care may be necessary in severe or complicated cases.
American hepatozoonosis
American hepatozoonosis is a canine disease caused by Hepatozoon americanum that is increasing in prevalence, particularly in the southeastern United States. It is a tick-transmitted hemosporazoon, distantly related to Babesia and the animal malaria-like organisms. The tick vector is Amblyomma maculatum. Transmission is unique for H. americanum in that the tick is ingested by the vertebrate host. Dogs suffering from hepatozoonosis present with a stiff gait, inactivity, weight loss, and myalgia. Other signs include bilateral ocular discharge and periosteal proliferations of the femur, pelvis and vertebrae. The latter sign appears to occur most commonly in young dogs. Other aids in diagnosis include profound leucocytosis (mature neutrophilia; 70,000-200,000 cells/µL), and elevated serum glucose and alkaline phosphatase. The disease is confirmed by demonstration of foci of pyogranulomatous inflammation in affected muscles. Also present are large cystic structures resembling onions, with a compact, often darkly staining center surrounded by concentric lamellar-like rings. These stages represent schizont-like structures present in the coccidia and coccidia-like organisms. Acute American hepatozoonosis is best treated with ponazuril at a dose of 10 mg/kg PO q12 h for 14 days. A combination of sulfadiazine/clindamycin/pyrimethamine is also effective. Long term (24 month) administration of decoquinate has proved helpful in preventing relapses.
125
Canine and feline bartonellosis
Principle Bartonella species infecting dogs and cats include Bartonella vinsonii subsp berkhoffi and B. henselae. Ticks have been implicated in the transmission of some Bartonella spp. Canine bartonellosis (Bv) may present as endocarditis and/or granulomatous hepatitis. Some reports indicate that polyarthritis and lameness are also common findings. Anemia and thrombocytopenia have been reported in approximately 50% of the canine cases. The pathogenetic potential of B. henselae is questioned by some. Some reports implicate B. henselae as a cause of lymphadenopathy and stomatitis in cats. However, cats in these reports were co-infected with feline immunodeficiency virus. Serologic positivity is indicative of exposure or active infection. PCR tests confirm active infection. Improved culture techniques will likely increase our capability to recover B. henselae from infected cats. Bartonellosis has been treated with azithromycin (5-10 mg/kg PO q24 hours for 5 days); recent studies indicate that enrofloxacin (22.7 mg PO p12 hours for 14 or 28 days) and pradofloxacin also possess excellent activity against B. henselae. Humans with particular immunodeficiencies have been infected with Bartonella spp.
Biology and behavior of fleas
Fleas are wingless insects that belong to the order Siphonaptera (named because of their siphon-like mouthparts). Of the approximately 2000 species of fleas, 95% are found on mammals; fewer species are found on birds and other hosts. The species that most commonly infests dogs and cats is Ctenocephalides felis; less common species include Ctenocephalides canis, Echidnophaga gallinacea and Pulex simulans. Occasionally, the odd rodent or rabbit flea will be found on pets that prey on or scavenge rodents or rabbits.
Fleas, like many insects, undergo a complex cycle of development. Adult fleas feed immediately after infesting dogs and cats. In fact, data indicates that host blood is demonstrable in both male and female fleas generally in less than 3 minutes after gaining access to a host. Egg production begins within 24 hours of the first acquisition of a blood meal. During feeding, the body weight of the adult female flea can increase by 140%. Female fleas are prolific egg layers and can produce an average of 27 eggs per day, totaling 1,350 eggs or more in 50 days. Eggs hatch in 1 to 10 days, depending on temperature and relative humidity (RH). At 95 F and 70% RH, 50% of eggs hatch in 1.5 days. At 70% RH and 55 F, 50% of eggs hatch in 6 days. Maggot-like larvae that hatch from eggs develop through 3 larval stages. Larvae are susceptible to heat and desiccation and cannot survive below 50% RH or above 90 F. At 75 F and 78% RH the larval stage develops to the cocoon (pupa) in about 11 days. Adults emerge from eggs in about 5 days when the temperature is 80 F and RH is 80%. However, the pre-emerged adult can remain in the pupa for up to 174 days (pupal window). Emergence of adults from cocoons in stimulated by heat, pressure, movement, and C02 produced by the host. During the warmer summer months, the entire flea life cycle can be completed in 2-3 weeks. Control of fleas and flea- induced diseases requires a thorough understanding of the life cycle of fleas and the attributes and efficacies of flea control agents. It is important to remember that most flea life stages (eggs, larvae and pupae) remain off the host and generally inaccessible to on-animal agents. Pre-emerged adult fleas in the cocoon can be especially difficult to control. As mentioned above, unstimulated adults can emerge over extended developmental periods, convincing the unknowing pet owner that control efforts are having little effect. This is particularly true when these stages are in locations where the pet spends time, unbeknownst to the pet owner (e.g. under the bed in the carpeted bedroom). Abiotic factors such as temperature and relative humidity drive the flea’s life cycle. Cooler, drier climates result in longer life cycles, causing adults to emerge over a longer period. Warmer, humid climates support shorter flea life cycles. A third flea biology characteristic that should guide our control efforts is the lack of C. felis host specificity. Cat fleas can infest various mammalian species, including some urban-adapted wildlife. These are sources of infestation that aren’t apparent to the pet owner. Finally, remember the female flea’s prolific egg-laying potential. A small residual population of surviving fleas can produce many eggs in a short time. We now know that fleas survive even the most effective control agents,
126

and these fleas can serve as a continuing environmental infestation source. If we communicate these points to pet owners, we can select and use products more effectively and eliminate many misperceptions about lack of efficacy of flea control agents.
Flea allergy dermatitis
Flea allergy dermatitis (FAD) is the most common allergic skin disease of dogs and cats in certain regions of the US. It is caused by an atypical and exaggerated immune response to antigens present in flea saliva. At present, at least 15 potentially allergenic components have been described. These are complete antigens and not haptens. Dogs with FAD can present with several types of hypersensitivity: Type 1 (immediate) hypersensitivity; Type IV delayed hypersensitivity; and cutaneous basophil hypersensitivity (CBH). Type I hypersensitivity is a humoral response which occurs in as little as a few minutes. It is triggered by immunoglobulin E (reaginic antibody) binding to mast cells resulting in the release of inflammatory mediators such as histamine, serotonin, and leukotrienes. Type IV reactions are cell-mediated and involve interactions of T lymphocytes. Production of numerous lymphokines results in the release of pruritogenic inflammatory mediators. CBH is a transient delayed type reaction in which basophils comprise the main cell population. Type 1 and Type IV reactions (particularly Type I) are the reactions sought in intradermal skin tests for flea allergy.
Flea bite dermatitis (FBD; the typical reaction to irritation caused by flea bites) and FAD are two distinctly different conditions. Some believe that all cases of flea bite dermatitis involve some degree of allergy. In my experience, non-allergic dogs usually present with fleas and demonstrate few signs of typical FAD. Normally, they have mild skin irritation, acute moist dermatitis (“hot spots”) or acral lick granulomas. Allergic dogs (many times between the ages of 3 and 5 years) usually present with one or more of the following: crusted papules with erythema, alopecia, and/or lichenification or hyperpigmentation - usually on the dorsal lumbosacral area, caudomedial thighs, or ventral abdomen. In many cases, atopic dogs also suffer concurrently from FAD. In true cases of FAD, the ears, feet and face are usually devoid of lesions. Dogs with FBD and FAD many times are infected with Dipylidium tapeworms. FAD in dogs must be differentiated from food and atopic allergies, other parasitic dermatoses such as lice and Cheyletiella, dermatophytosis, demodicosis, and superficial pyoderma. Dogs intermittently exposed to fleas are more likely to develop FAD than dogs that are exposed chronically to fleas. Consequently, if a dog is treated irregularly or flea control is discontinued until fleas reappear, this intermittent nature of flea challenge is more likely to result in the development of FAD. We have observed this in our colony of cats used for propagation of fleas. We infest them weekly with fleas. Since cats tend to groom many fleas from the hair coat we are, in essence, pulsing them with fleas at weekly intervals. This can lead to the frequent development of FAD in our colony.
Flea control
Successful control of pet flea infestations usually involves a combination of strategies. These include host-targeted and environmental insecticides, and mechanical means of reducing or eliminating environmental flea stages. Mechanical means of environmental control include washing of pet bedding or bed cloths in areas frequented by pets. Vacuuming of carpets, furniture cushions, rugs or other substrata with a vacuum machine containing a “beater bar” will reach deeper in carpet or furniture fabric, and the associated vibration will stimulate adult fleas to emerge from pupa. Assure that vacuum bags are disposed of properly to prevent recolonization of the home with flea stages previously removed by vacuuming. Treatment of indoor and outdoor environments with insecticides requires both a knowledge of what to use and where to use it. For this reason, I suggest that pet owners consult with a licensed pest control specialist for such applications.
Numerous safe and effective host-targeted flea control agents are available. Available agents include oral or topical adulticides (i.e. afoxolaner, fluralaner, lotilaner, sarolaner, imidacloprid, dinotefuran, fipronil, indoxacarb, deltamethrin, selamectin, spinetoram, spinosad, nitenpyram) adulticides. Products may also have activity against tick and mites, and can be combined with other products to yield broad spectrum parasite control. Some flea control formulations also combine adulticides with insect growth regulators (IGRs: methoprene, pyriproxyfen) or insect development inhibitors (IDIs: lufenuron). Combinations of adulticide/IGR or adulticide/IDI enhance flea control and are less likely to result in survival of resistant fleas. Many adulticides exert their effects quickly and may not allow fleas to survive long enough to lay viable eggs.
127
Fleas as vectors of disease
Fleas can be vectors for parasites and other disease agents. Among them are Bartonella spp. (see above also), hemoplasmas (previously Hemobartonella spp.), the plague bacillus, tularemia, cat flea typhus-like disease and murine typhus
Bartonella spp. are gram negative, hemotropic, aerobic bacteria that may cause infection in dogs, cats, humans and other animals. Bartonella hensalae, the causative agent of "cat scratch disease" is transmitted horizontally between cats and dogs via fleas or by blood transfusion, and to humans via cat bite or scratch and subsequent percutaneous inoculation of bacteria. Canine infection may result in granulomatous hepatitis and peliosis hepatitis. Cats are usually asymptomatic. However, infection has been associated with fever, endocarditis, uveitis, urinary tract disease and stomatitis. Cats that were infected experimentally developed lymphadenopathy and myalgia. Disease in humans may present in several ways: bacillary angiomatosis, peliosis, fever, optic neuritis, granulomatous disease, and osteomyelitis. Very severe or fatal disease can occur in humans that are immunocompromised. Diagnosis is based on clinical signs and specific serologic or PCR results. All dogs and cats should be on effective flea control regimens to decrease the likelihood of transmission. Treatment of dogs or cats consists of azithromycin (10 mg/kg PO q24 hr for 7days and every other day for 5 weeks) and doxycycline (10 mg/kg PO q12 hr for 2-4 weeks).
Bartonella vinsonii subsp berkhoffii is a cause of canine bartonellosis. Ticks are probably the principle vectors, although fleas may play a role in transmission. Wild canids (particularly coyotes) are likely reservoir hosts. Canine infections have been associated with granulomatous rhinitis, lymphadenopathy, endocarditis, myocarditis, cutaneous vasculitis, anterior uveitis, and polyarthritis. Bartonella vinsonii was recovered from a human with endocarditis. Diagnosis is via serology and/or PCR. Treatment includes either azithromycin or doxycycline.
Rickettsia felis is a small gram-negative, coccobacillus that may cause flea-born spotted fever, or cat flea typhus-like disease in humans. Infected cats are usually asymptomatic. Signs in humans may include: rash, headache, nausea, vomiting, diarrhea, myalgia, abdominal pain, conjunctivitis or CNS involvement. R. felis is transmitted via infected flea feces. Opossums are the usual reservoir hosts. Increasing numbers of reports of human infections suggest the R. felis-infected fleas are common. Certainly, use of effective flea control products can help reduce the prevalence of R. felis in the feline population.
Rickettsia typhi is the causative agent of murine or endemic typhus. Humans develop signs similar to those described above for R. felis. The pathogenicity of R. typhi in dogs and cats is not known. The route of infection is similar to R. felis. Rodents appear to be the usual reservoir hosts.
Feline infectious anemia, or more accurately feline hemotropic mycoplasmosis, is caused by Mycoplasma spp. (formerly Hemobartonella spp.). The causative agents are Mycoplasma haemofelis and/or Mycoplasma hemominutum. A third species, Mycoplasma turicensis was recently described from Swiss cats. Infected cats may be asymptomatic, they may have mild disease, or they may be severely infected in which case they are weak, anorexic, anemic, dehydrated and jaundiced. Transmission can occur via fleas, ticks, blood transfusion, and from queen to kittens. Signs are usually more severe in FeLV-infected cats. Diagnosis is achieved by observing intra-erythrocytic mycoplasmas in stained blood smears. Presence and numbers of organisms in circulating blood can vary. PCR is also used for diagnosis. Tetracycline, oxytetracycline and doxycycline are effective treatments for clinically ill cats. In severely affected cats, concurrent administration of corticosteroids may reduce host-mediated destruction of red blood cells. In the most severe of cases, blood transfusion may be necessary. Effective flea and tick control are the foundations of prevention.
Fleas may also transmit parasites such as Dipylidium caninum, Hymenolepis nana, and Dipetalonema (Acanthocheilonema) reconditum.
REFERENCES AVAILABLE ON REQUEST
128

Techniques and Strategies in Fecal Diagnosis
Byron L. Blagburn University Distinguished Professor of Parasitology
College of Veterinary Medicine Auburn University, Alabama
Fecal detection of internal parasites is an important component of veterinary practice as they remain prevalent and important disease agents in companion animals. Techniques include gross examination, fecal smear (wet mount), flotation (both centrifugal and standing, with or without quantification), Baermann procedure, sedimentation, fecal culture, fecal immunologic, fecal molecular biologic, and artificial intelligence imaging. Failure to employ “best practice” techniques when conducting fecal examination procedures can result in failure to detect parasite stages or components in fecal specimens. It is important to be reminded that feces should be fresh (to preserve motility if present) and an appropriate sample volume (≥1g formed feces) should be used for optimal parasite recovery.
It is also important to recall that microscope settings for fecal flotations are different from those used to examine blood smears, tissue sections, etc. Adjust the sub-stage condenser to provide better contrast for visualization of parasites. Furthermore, the entire area under the coverslip should be examined using the 10X objective (with use of the 40X objective for verification as needed).
Gross Examination
Take note of the color, consistency and look for the presence of blood, mucus or froth (air bubbles) as those are often indicators of gastrointestinal disease that may be caused by parasites. In addition, be sure to examine for any parasites that may be present (e.g. tapeworm proglottids).
Fecal Smear
The direct fecal smear or “wet mount” is the technique of choice for detection of motile parasites such as Giardia, Tritrichomonas, Pentatrichomonas, amoeba, or larvae that may be damaged by flotation solution. It is paramount that the sample be fresh if examining for motility.
Fecal Flotation Techniques
Fecal flotation continues to be the most common fecal procedure performed in veterinary clinics and laboratories. Fecal flotation is intended to separate parasites from other objects and debris based on their different densities, and that ability to separate is enhanced using centrifugation. Recall that there are a number of optional flotation solutions that can be used (e.g. Zinc Sulfate [ZnSO4], Magnesium Sulfate [MgSO4], Sodium Nitrate [NaNO3], Sodium Chloride [NaCl], Sheather’s Sucrose), and for majority of the parasites, flotation solution selection may not make much of a difference. However, recovery of certain parasites may be either enhanced (e.g. ZnSO4 & Giardia cysts; Sheather’s Sucrose & Trichuris, Taenia, & Physaloptera ova) or hindered (NaNO3 & Giardia cysts) by use of certain solutions. Furthermore, specific gravity of flotation solutions should be checked routinely with a hydrometer.
Although not historically performed in companion animal practice, egg quantification techniques should be considered when evaluating a patient for suspected drug-resistant intestinal parasites (e.g. hookworms). The ability to quantify eggs per gram of feces with something like a Modified Wisconsin technique is useful in determining an appropriate response to treatment. The only difference between a standard centrifugal flotation technique and a Modified Wisconsin is that the latter uses a known quantity of both feces and flotation solution, while the feces is typically not weighed with the former.
129

Baermann Procedure
The goal of the Baermann procedure is to recover motile larvae of parasites (e.g. Aelurostrongylus, Strongyloides, etc.) from fresh fecal specimens. Immobile ova or dead larvae cannot be recovered with this technique.
Fecal Sedimentation
Sedimentation is used to concentrate eggs or larvae that are too dense to float in flotation solutions or that might be distorted by the solutions. Keep in mind that most all parasites and debris will be present in the sediment. Sedimentation can be performed using either the standing or centrifugal procedure, but with water or saline in lieu of flotation solution. I prefer to use a centrifuge because it results in faster movement of parasites to the bottom of the tube.
Fecal Culture
Fecal culture techniques are rarely performed except perhaps to aid in the detection of Tritrichomonas blagburni in feline fecal samples. The In Pouch® TF-Feline (Biomed Diagnostics) can be inoculated and either incubated and examined in practice or sent to a referral laboratory for evaluation. Diamond’s media can also be used to culture trichomonads.
Fecal Immunologic
Fecal antigen-detection platforms are available for use either in-clinic or through veterinary diagnostic reference laboratories. Some reference laboratories offering additional immunologic techniques for fecal parasites (e.g. IFA).
In-clinic options include several commercially available Giardia antigen-detection platforms which can aid in the diagnosis as Giardia stages may be difficult to detect using the traditional aforementioned parasitological techniques. Use of these diagnostics as a screening tool for all fecal samples is not recommended, rather they can be used when a patient’s history and clinical signs are indicative of a Giardia infection. Using these tools in conjunction with ZnSO4 fecal flotation resulted in enhanced sensitivity of Giardia detection.
Antigens from Toxocara spp., Baylisascaris spp., Ancylostoma spp., Uncinaria spp., and Trichuris spp. in canine and feline feces can be detected in samples submitted to IDEXX reference laboratories. Benefits of antigen-based diagnostics include the ability to detect pre-patent infections 1–6 weeks before egg-shedding and environmental contamination can occur, as well as aiding in the determination of spurious versus real parasitism. Enhanced sensitivity has been reported by combining antigen-based diagnostics with traditional flotation techniques.
Fecal Molecular Biologic
Molecular biology continues to expand its presence in diagnostic parasitology. Polymerase chain reaction (PCR) techniques are now commonplace in many reference laboratories and can be important additions to other test methods. PCR is a technique that duplicates a specific segment of DNA when a known sequence (primer) is attached (annealed) to it. The duplicate DNA product (amplicon) is specific to the parasite DNA to which the primer is attached. The sequence of DNA subunits (nucleotides) in the DNA product is compared to known published sequences. This allows identification of the parasite with a high degree of accuracy.
PCR is a useful resource when other fecal examination methods fail or when additional diagnostic information is needed. Some parasites for which PCR is helpful either in diagnosis or for further taxonomic analysis include Giardia, Tritrichomonas blagburni, Cryptosporidium spp., Toxoplasma gondii and taeniid tapeworms including Echinococcus spp. PCR is usually combined with conventional fecal techniques such as flotation or direct smear. If these tests yield negative or questionable results, additional PCR testing might be warranted. PCR tests can provide helpful guidance when selecting appropriate treatments or counseling clients on prevention or zoonosis.
Fecal PCR tests can include either universal or species-specific primers. Universal PCR tests are helpful in identifying groups of parasites at a general level such as Giardia or Cryptosporidium. Species-specific PCR tests can
130

identify a particular parasite from a group of parasites. Species-specific tests can differentiate individual Giardia assemblages or specific species of Cryptosporidium such as C. hominis, C. parvum or C. bovis. Likewise, species-specific PCR tests could identify Tritrichomonas blagburni when similar parasites such as Giardia or Pentatrichomonas hominis might be present. All three of these parasites could be present in a pet with diarrhea and appear similar to persons not trained specifically to recognize them. Furthermore, tapeworm eggs of Taenia and Echinococcus spp. are difficult (if not impossible) to differentiate in a fecal flotation preparation. Species-specific PCR procedures can successfully identify parasites in the different genera and specific species such as E. granulosus and E. canadensis within a genus. Other examples include T. gondii oocysts in feline feces and their similarity to Hammondia spp., a parasite also found in feline feces but without the primary or zoonotic disease implications. Similarly, Neospora caninum and Hammondia spp. are identical in appearance and both can be present in the feces of dogs. Universal and species-specific PCR can also help identify gross parasites that are passed in feces. With all their advantages, molecular procedures are not without limits or liabilities. PCR procedures require meticulously clean laboratories, specialized equipment and extensive validation. Tests can take two or more days to perform, depending on the procedure. Fecal samples must be as fresh as possible and either kept refrigerated or fixed in 70% ethanol. Although formalin fixed samples can be processed and examined successfully, special procedures must be used for extracting DNA. If extraction procedures are not performed properly, the quality of the DNA sample and the accuracy of the result could be compromised. Also, be aware that a negative result does not necessarily mean that the target parasite is not present in the host nor the cause of disease. It could simply mean that parasites were not present in the sample that was analyzed. Sensitivity of PCR tests can be improved by increasing the amount of sample, or by submitting multiple samples collected at different time points. Molecular tests can be important adjuncts to other fecal procedures. If you are considering a PCR test, it is best to contact the receiving laboratory in advance. Laboratory personnel can then provide instruction on amount of sample required, fixation, storage and shipment. Artificial Intelligence Imaging (The author gratefully acknowledges Zoetis Inc, Parsippany, NJ USA for providing the following information). The utilization of machine learning artificial intelligence in veterinary medicine has historically focused on assisting medical decision-making using physical examinations and laboratory test findings. More recently, image-based recognition technology has been applied to in-hospital urine sediment analyzers. Additionally, use of image recognition to identify intestinal parasite eggs, cysts, and oocysts in veterinary medicine has been reported. The VETSCAN IMAYST (Zoetis Inc., Parsippany, New Jersey, USA) system is the first commercial diagnostic platform that uses a combination of image recognition technology and cloud based artificial intelligence algorithms to identify Ancylostoma spp., Toxocara spp., Trichuris vulpis, Cystoisospora canis, C. felis, C. ohioensis, C. rivolta, Taeniid, and Giardia spp. in dog and cat fecal flotations. To use the system, 1 gram of feces is prepared using a sample device of 33% zinc sulfate solution (specific gravity, 1.18) and/or sucrose solution (specific gravity, 1.28), centrifuged for 2 minutes, and transferred to a specialized coverslip that defines the scan area to ensure that a thorough, complete scan by a specialized microscope at optimal depths is completed for each sample tested. The scan and cloud-based analysis are controlled from a user software interface and/or the practice management software. Identified parasites are highlighted by a box and viewable at slide level with user-controlled zoom (Figure 1a), or in a summary results view (Figure 1b), which can be printed out to share with the pet owner or saved to the medical record. The system is integrated with a “deep learning” object detection algorithm, and with more training, the algorithm can improve its performance and functionality (e.g., additional parasites) over time. Compared to “shallow learning” systems, “deep learning” algorithms facilitate the system to continuously adapt to new data and apply it to new output classes with fewer examples. Artificial intelligence image recognition can provide a reliable and consistent approach to fecal examination for busy veterinary practices, while allowing veterinary professionals to review and confirm the identified parasite images. Since captured photographs are stored in the cloud or medical record, questionable results or suspicious objects can
131

be sent for expert evaluation and second opinion, and the parasite images can also be used for client education, teaching, or training materials.
REFERENCES AVAILABLE ON REQUEST
132

FLUTD: WHAT IS ALL THE STRESS? Kara M. Burns, MS, MEd, LVT,VTS (Nutrition)
Academy of Veterinary Nutrition Technicians [email protected]
Any condition affecting the urinary bladder or urethra of cats is known as feline lower urinary tract disease (FLUTD). FLUTD is a common reason for which cats present to the veterinary hospital. Regardless of underlying cause, FLUTD is characterized by the following signs: dysuria, pollakiuria, stranguria, hematuria, and/or periuria (urination in inappropriate places). It is vital that veterinary technicians are aware of signs and symptoms of FLUTD when talking with clients.
For a number of years, information regarding specific causes of FLUTD has increased in the veterinary profession, which allows for diagnostic and therapeutic efforts to be directed toward identification and elimination of specific underlying disorders. The most common cause of FLUTD in cats < 10 years of age is feline idiopathic cystitis (FIC). This is followed by uroliths, and urethral plugs. A diagnosis of FIC is made by excluding all other causes of FLUTD. In older cats (> 10 years), urinary tract infection and/or uroliths are the most common cause of FLUTD.
In 1981, 78% of feline uroliths were composed of struvite and only 2% were calcium oxalate. In the mid- to late-1980s, the occurrence of calcium oxalate uroliths began to increase. Between 1994 and 2002, approximately 55% of uroliths were calcium oxalate and only 33% were struvite. Since 2001, however, the number of struvite uroliths has continued to increase while occurrence of calcium oxalate uroliths has decreased. Based on 10,093 feline uroliths analyzed at the Minnesota Urolith Center in 2006, the most common mineral types were struvite (50%) and calcium oxalate (39%), followed by purine (5%). These trends have continued into 2011. In 2006, 88% of urethral plugs evaluated at the Minnesota Urolith Center were composed of struvite, 9% were matrix, < 1% were calcium oxalate, and 2% were of other mineral compositions.
Diagnostic Evaluation Veterinary nurses assisting with the diagnostic evaluation of cats with recurrent or persistent lower urinary tract signs should include a urinalysis and diagnostic imaging. A urine culture should be performed if there is a history of urinary tract manipulation (e.g., urethral catheterization), evidence of urinary tract infection (e.g., pyuria, bacteriuria, malodorous urine), or the cat is older (usually > 10 years). More advanced procedures (e.g., contrast radiography) may be appropriate in some cases.
When evaluating patients with signs of lower urinary tract disease, urinalysis is considered one of the most important parts of the evaluation. If possible, the veterinary technician should perform the urinalysis in-house since fresh urine samples analyzed within 30 minutes of collection are preferred. Urine specimens evaluated after this time may form crystals that are not in fact present in the patient. Samples may be refrigerated for up to 8 hours and then evaluated (after the sample has returned to room temperature). This method is not best for evaluating crystalluria and should be avoided as much as possible by the veterinary technician.
While it may be tempting to only perform dipstick analysis, measure urine specific gravity, and ignore urine sediment examination, it is crucial for the veterinary team to perform a complete urinalysis. The only way to accurately detect pyuria, hematuria, bacteriuria, and crystalluria is by sediment examination. Veterinary teams cannot rely solely on urine dipstick analysis because results for detection of pyuria are often false positive in cats and the occult blood reagent pad on the dipstick is not specific for hematuria (in addition to red blood cells, it also becomes positive with hemoglobin and myoglobin). Pyuria (> 5 WBCs/hpf) indicates inflammation and it may be caused by several disorders (urolithiasis, bacterial infection); it is less commonly observed in cats with FIC. If you see increased numbers of white cells, you should look carefully for bacteria. Take care not to misinterpret presence of cellular debris and Brownian motion as bacteriuria.
Several different types of crystals may be identified on urine sediment examination, although struvite (triple phosphate) and calcium oxalate are the most common. The presence of crystals indicates that the urine is supersaturated with that substance and the patient is at risk for forming uroliths. Remember that cats also may have crystals and never develop
133

uroliths. In the absence of other findings such as uroliths or urethral plugs, the presence of crystals alone is not diagnostic of urolithiasis or struvite disease. Struvite crystals may be present in normal cats and cats with struvite uroliths (sterile or infection-induced), non-struvite urolithis (including some cats with calcium oxalate uroliths), urethral plugs, or other urinary disorders such as FIC.
Survey radiographs are helpful for identifying radiopaque uroliths and crystalline-matrix urethral plugs. Remember during positioning to include the caudal abdomen (urethra) in the radiograph, or you risk missing potentially important information. Normal survey radiographs do not exclude FIC, radiolucent uroliths (urate/purine), small uroliths (< 2 mm), neoplasia, blood clots, or anatomic defects. Abdominal ultrasonography and/or contrast urethrocystography is helpful in these cases. If no cause is identified after thorough diagnostic evaluation, a diagnosis of FIC is very likely. Treatment of Cats with Feline Idiopathic Cystitis The goals of managing cats with FIC are to decrease severity of clinical signs and increase the interval between episodes of lower urinary tract disease. Over the past 40 years, many different treatments have been recommended to control signs in cats with FIC, yet only a few have been evaluated in clinical trials of cats with FIC. Nutritional Management It has been found that feeding moist food (>60% moisture) has been associated with a decreased recurrence of clinical signs in cats with FIC. During a 1-year study, clinical signs recurred less often in cats with FIC when fed a moist food compared with cats fed the dry formulation of the same food. Beneficial effects have been observed in cats with FIC when urine specific gravity values decrease from 1.050 to values between 1.032 and 1.041. Veterinary technicians should be aware of and discuss with clients, additional methods for increasing water intake (eg, adding broth to foods, placing ice cubes in the cat’s water, and providing water fountains) as these may be useful for some cats. A recent study shows that consistently feeding a therapeutic urinary food was associated with a reduction in recurrent episodes of FIC signs. This is the first study to definitively show that foods of different nutritional profiles impact the expression of acute episodes of FIC signs in cats. Likewise, the addition of L-tryptophan, a precursor of serotonin that inhibits neurotransmitters in the brain to balance mood, as well as hydrolyzed casein, a bioactive peptide that helps relieve anxiety in cats has been identified as nutrients that will aid in managing the stress component of FIC. Increasing salt content of food is an effective method of causing urine dilution in cats. However, the potential for adverse effects should be considered. At this time, there are differing opinions regarding role of sodium in cats with kidney disease. In a recent study, the effects of high-salt [1.2% sodium, dry matter basis (DMB)] intake for 3 months were evaluated in 6 cats with mild azotemia due to naturally occurring chronic kidney disease. These cats had progressive increases in BUN, serum creatinine, and serum phosphorus compared with consumption of food with 0.4% sodium (DMB). Based on all findings to date, further study is needed to better determine the role of sodium in healthy cats fed long-term as well as cats with hypertension, chronic kidney disease, and calcium oxalate uroliths. Pending further studies, it is sensible to avoid high-salt foods in cats with chronic kidney disease and monitor kidney function when high-salt foods are fed to cats at risk for kidney disease. Inflammation plays a role in many causes of FLUTD, especially FIC and urolithiasis. Therefore, a key nutritional factor for managing cats with FLUTD includes omega-3 fatty acids, which are known to have potent anti-inflammatory effects. In addition, vitamin E and beta-carotene are helpful for counteracting oxidative stress and reducing free radical damage, conditions that often accompany inflammation. Environmental Enrichment In addition to nutritional management, the currently recommended treatment for cats with FIC also includes environmental enrichment and stress reduction. This is crucial in a FIC treatment plan and the veterinary technician should be readily able to discuss environmental enrichment with the client.
134

A prospective study assessing effects of multimodal environmental modification was reported in 46 client-owned cats with FIC. The findings showed significant reductions in lower urinary tract signs, fearfulness, and nervousness after treatment for 10 months. With cats that are suffering with FIC, stressful situations (e.g., conflict with other cats in the home) should be avoided or minimized. Owners should provide opportunities for play/resting (horizontal and vertical surfaces for scratching, hiding places, and climbing platforms). Any changes (eg, switching to a new food) should be made gradually so the cat has adequate time to adapt and avoid becoming stressed.
Another critical component of managing cats with FLUTD, especially FIC, involves appropriate use and maintenance of litter boxes in the home. Most cats prefer clumping, unscented litter; however, it may be necessary to give cats several choices and let them select their preference. It may be possible to have cats within the home that prefer different types of litter or litter boxes. In general, uncovered litter boxes are recommended because they are less likely to trap odors inside. For older cats with mobility issues, the owner should select a litter box with low sides to facilitate the cat getting in and out of the box. Litter boxes should be scooped daily and washed every few weeks with warm, soapy water. Because plastic can absorb odors over time (months to years), owners should consider replacing litter boxes with new ones periodically. Finally, there should be an adequate number of litter boxes (the 1 + 1 rule = 1 more than the number of cats) in the home and they should be located on multiple floors where cats can enter and exit readily. More detailed information about environmental enrichment and litter box management is available in the suggested reading. It may be helpful to encourage owners to read this additional information as well because their involvement is critical for a successful outcome. Finally, health care team members, especially technicians, play a crucial role in educating cat owners about the importance of environmental enrichment and litter box management.
Summary Increased understanding of specific causes of FLUTD has allowed diagnostic and therapeutic efforts to be directed toward identification and elimination of specific underlying disorders. The most common cause of FLUTD in cats < 10 years of age is feline idiopathic cystitis (FIC), followed by uroliths, and urethral plugs. A diagnosis of FIC is made by excluding all other causes of FLUTD. In older cats (> 10 years), urinary tract infection and/or uroliths are the most common cause of FLUTD. It is imperative that veterinary technicians have a thorough understanding of FLUTD and the how the various treatments affect the different types of FLUTD. Veterinary nurses play a very important role in the treatment of FLUTD. The history obtained from discussions with the pet owner aids in the diagnosis of FLUTD. The veterinary nurses’ discussion of the treatment plan with the client is key to the client’s understanding and compliance with the veterinarian’s recommendation and ultimately the health of the pet.
References 1. Burns, KM. FLUTD – Using Nutrition to Go with the Flow. NAVTA Journal Convention Edition. 2014. Pp. 7-
122. Sparkes, A. Feline idiopathic cystitis: Epidemiology, risk factors, and pathogenesis. Hill’s Global Symposium on
Feline Lower Urinary Tract Health Proceedings. April, 2014. Prague3. Cameron ME, Casey RA, Bradshaw JW, Waran NK, Gunn-Moore DA. A study of environmental and
behavioural factors that may be associated with feline idiopathic cystitis. J Small Anim Pract 2004; 45: 144–147.
4. Defauw PA, Van de Maele I, Duchateau L, Polis IE,Saunders JH, Daminet S. Risk factors and clinicalpresentation of cats with feline idiopathic cystitis. JFeline Med Surg 2011; 13: 967–975.
5. Lulich JP. FLUTD: Are you missing the correct diagnosis? Proc 2007 Hill's FLUTD Symposium 2007:12-19(www.hillsvet.com/conferenceproceedings).
6. Forrester, SD. FLUTD: How Important is it? Proc 2007 Hill's FLUTD Symposium 2007:5-11(www.hillsvet.com/conferenceproceedings).
7. Burns KM, Forrester SD. Feline Lower Urinary Tract Disease. NAVTA Journal. July/August 2007.8. Markwell PJ, Buffington CA, Chew DJ, et al. Clinical evaluation of commercially available urinary acidification
diets in the management of idiopathic cystitis in cats. J Am Vet Med Assoc 1999;214:361.9. Kirk CA, Jewell DE, Lowry SR. Effects of sodium chloride on selected parameters in cats. Vet Ther
2006;7:333-346.
135

10. Kruger JM, Lulich JP, Merrills J, et al. A Year-Long prospective, randomized, Double-masked study of nutrition on Feline Idiopathic Cystitis.Proceedings. American College of Veterinary Internal Medicine Forum 2013.
11. Buffington CA, Westropp JL, Chew DJ, et al. Clinical evaluation of multimodal environmental modification (MEMO) in the management of cats with idiopathic cystitis. J Feline Med Surg 2006;8:261-268.
12. Westropp JL, Buffington CAT, Chew D. Feline lower urinary tract diseases In: Ettinger SJ, Feldman EC, eds. Textbook of Veterinary Internal Medicine, 6th ed. Philadelphia: Elsevier Saunders, 2005;1828-1850.
13. Neilson JC. FLUTD: When should you call the behaviorist? Proc 2007 Hill's FLUTD Symposium 2007:20-28 (www.hillsvet.com/conferenceproceedings).
14. The Indoor Cat Initiative (www.vet.osu.edu/indoorcat) 2007. 15. Bohnenkamp G. From the Cat's Point of View - The Complete Book on Cat Behavior, 1991. 16. Lulich JP, Osborne CA, Lekcharoensuk C, et al. Effects of diet on urine composition of cats with calcium
oxalate urolithiasis. J Am Anim Hosp Assoc 2004;40:185-191. 17. Grauer, G. Current Thoughts on Pathophysiology & Treatment of Feline Idiopathic Cystitis. Today’s Veterinary
Journal. Nov/Dec 2013, pp 38 – 41. 18. Osborne C, Lulich J, et al. Feline urolith epidemiology update: 1981 to 2011. Tracking the trends of mineral
composition in cats with urolithiasis. DVM360. June, 2013. 19. Pereira GG, Fragoso S, Pires E. Effect of dietary intake of l-tryptophan supplementation on multi-housed cats
presenting stress related behaviors. Proeedings, BSAVA 2010. 20. Beata C, Beaumont-Graff E, Coll V, et al. Effect of alpha-casozepine (Zylkene) on anxiety in cats. Journal of
Veterinary Behavior, 2007; 2(2):40-46.
136

FELINE NUTRITION – CATS ARE NOT SMALL DOGS! Kara M. Burns, MS, MEd, LVT, VTS (Nutrition)
Academy of Veterinary Nutrition Technicians Lafayette, IN
The order Carnivora includes canines and felines and consequently both species are classified as carnivores. However, when looking at cats and dogs from a dietary perspective, dogs are considered omnivores and domestic cats and other members of the superfamily Feloidea are strict or obligate carnivores. This difference is supported by specific behavioral, anatomic, physiologic, and metabolic adaptations of cats to a strictly carnivorous diet.
Domestic cats today display some feeding behaviors that are similar to felids in the wild. Cats naturally do not display a regular daily rhythmic sleep-wake cycle, or regular cycles of activity, feeding, and drinking. Cats are known to consume 10 to 20 small meals throughout the day and night, behavior that is believed to be reflective of the evolutionary relationship of cats and their prey. Cats are known to hunt alone. Feral cats typically catch prey/mice as their source of food. On average a mouse provides approximately 30 kcal (125 kJ) of metabolizable energy (ME). This amount is about 12 to 13% of a feral cat’s daily energy requirement. Therefore, we can see that hunting throughout the day and night is required to provide sufficient food for an average cat. Hence, recommendations of meal feeding, especially once per day, conflict with the natural behavior of cats. Conversely, we have also seen that free feeding has contributed to the obesity epidemic that is seen in cats, as well as other species.
The metabolism of cats is unique when compared to other species. Nutrition for felines must be closely monitored to ensure the specific nutritional requirements of a true carnivore are met. Some of these unique attributes include:
1. A limited ability to downregulate enzymes of nitrogen catabolism and urea cycle enzymes2. A strict requirement for the amino acid arginine,
Lack of arginine in the diet for longer than 24 hours, may have life-threatening concerns3. An inability to synthesize taurine from cysteine4. An inability to synthesize vitamin A from beta carotenes5. An inability to synthesize niacin from the amino acid tryptophan
Cats are very sensitive to food - the form, the odor, and the taste. The flavor and texture preferences of individual cats are frequently influenced by early experience that can affect preferences throughout life. Cats familiar with a certain texture or type of food (i.e., moist, dry, semi-moist) may refuse foods with different textures. Cats do have a preference for certain ‘flavors’ such as animal fat, protein hydrolysates (digests), meat extracts, and certain free amino acids found in animal muscle (i.e., alanine, proline, lysine, histidine and leucine). Food temperature also plays a role in acceptance of the food by the cat. When feeding canned/moist foods, the preference is for the moist food to be at, or near, body temperature (38.5ºC [101.5ºF]). These factors are critical to the proper nutrition of a cat, especially if seriously ill.
As determined, cats are carnivores with unique anatomic, physiologic, metabolic and behavioral adaptations that support eating foods higher in protein and lower in carbohydrates as compared to dogs. Cats are well adapted hunters with increased visual acuity, upright ears, sensitive facial whiskers, tactile hairs, retractable claws and conical, sharply pointed teeth. Cats have low liver glucokinase activity which limits the ability to metabolize large amounts of simple carbohydrates. Cats also demonstrate decreased intestinal and pancreatic amylase activity, the enzymes responsible for the digestion and uptake of starches and sugars. These adaptations support consumption of natural prey, such as small rodents which are estimated to contain around 55% protein, 45% fat and 1-2% carbohydrate on a dry matter basis. Despite these specific adaptations cats efficiently use carbohydrates and carbohydrates provide a good source of energy. Dry foods containing 40% or more dietary carbohydrates with an average digestibility of 85% are well tolerated by normal cats.
Unique Anatomic and Physiologic Features
Cat’s eyes are well adapted for hunting. Their visual acuity is greater than that of dogs because of their larger optic cortex. Cats’ ears are upright, face forward and have 20 associated muscles to provide the fine control needed to precisely locate sound. Cats also respond to high-pitched sounds, which represent the range of sound frequencies
137

emitted by typical prey. Facial whiskers and tactile hairs are very sensitive and are responsible for helping cats to hunt in dim light and to protect their eyes.
Cats and dogs have the same number of incisor, canine, and carnassial teeth but cats have fewer premolar and molar teeth. Additionally, cats do not possess fissured crowns, which are a hallmark of omnivorous animals. The jaws of cats have limited grinding ability. The scissors-like action of the carnassial teeth is ideal for delivering the cervical bite used to transect the spinal cord and immobilize or kill prey. It is important to note that cats lack salivary amylase which is used to initiate digestion of dietary starches. Cats have evolved to eat small frequent meals; thus the stomach is less important for storage as compared to dogs. Therefore, the stomach of domestic cats is simpler (i.e., relatively smaller with a smaller glandular fundus). Also, the length of the feline intestine is shorter as compared to omnivores and herbivores. A greater villus height in cats increases the absorptive surface area. The absorptive capacity is estimated to be 10% less as compared to canines. The sugar transport system of the small intestine is not adaptive to varying levels of dietary carbohydrate. Also, cats have low activities of intestinal disaccharidases (i.e., sucrase, maltase and isomaltase). Pancreatic amylase production is also reduced when compared to dogs. Pancreatic amylase production is relatively nonadaptive in cats, as would be expected in a species unaccustomed to significant changes in dietary carbohydrate levels. Cats have been found to harbor higher concentrations of bacteria in their small intestine versus omnivores. Remarkably, the numbers typical for cats would be diagnostic for small intestinal bacterial overgrowth in dogs. Certain amino acid transporters in the small intestines of cats are highly adaptable, particularly the transporter responsible for arginine uptake. This finding underscores the importance of the amount of protein and specific amino acids in foods for cats. Cats are unable to synthesize significant quantities of ornithine or citrulline within the intestine. Both are precursors to arginine synthesis. It is because of this inability that cats have an absolute requirement for arginine in cat foods.
KEY NUTRITIONAL FACTORS
Most animal’s livers have two enzyme systems for converting glucose to glucose-6-phosphate: hexokinase and glucokinase. This conversion must take place before the liver can use glucose. Adult cats have very low hepatic glucokinase activity and a limited ability to metabolize large amounts of simple carbohydrates. Kittens ingest digestible carbohydrates (i.e., lactose or milk sugar) before weaning. Adult cats must rely primarily on gluconeogenesis from glucogenic amino acids, lactic acid, and glycerol for maintenance of blood glucose concentration. In cats, immediately following a meal and during the absorptive phase, gluconeogenesis is maximal.
Protein Protein metabolism is unique in cats and cats have a higher maintenance requirement for protein versus dogs. Cats also are known for having a special need for four amino acids: arginine, taurine, methionine, and cystine. The protein requirement for growth in kittens is only 50% higher than that of puppies, whereas the protein requirement for feline maintenance is twice that of adult dogs. The higher protein requirement of cats is a result of high activity of hepatic enzymes (i.e., transaminases and deaminases) that remove amino groups from amino acids so the resulting ketoacids can be used for energy or glucose production. Felines have a limited ability to decrease the activity of these enzymes when fed low-protein foods. In cats, hepatic enzyme systems are constantly active. Consequently, specific amounts of dietary protein are always catabolized for energy.
Arginine Arginine deficiency in cats’ results in a dramatic response in cats; more so than any other nutrient deficiency. Cats cannot synthesize adequate ornithine or citrulline to convert to arginine, which is needed for the urea cycle. Deprived of arginine, the urea cycle cannot convert ammonia to urea resulting in ammonia toxicity. Even eating one meal devoid of arginine may result in hyperammonemia in less than one hour. These cats exhibit severe signs of ammonia toxicity (i.e., vocalization, emesis, ptyalism, hyper activity, hyperesthesia, ataxia, tetanic spasms, apnea, and cyanosis) and may die within two to five hours.
Taurine Taurine (a b-amino sulfonic acid), is abundant as a free amino acid in the natural food of cats, such as small rodents, birds and fish. Dietary taurine is essential in cats and clinical disease results if insufficient amounts are present. Many species can use either glycine or taurine to conjugate bile acids into bile salts before they are secreted into
138

bile. Cats need taurine to conjugate bile acids. The loss of taurine in bile coupled with a low rate of taurine synthesis contributes to the obligatory taurine requirement of cats. Methionine and Cystine Methionine and cystine are sulfur-containing amino acids which are required in higher amounts by cats, especially during growth. Methionine and cystine are considered together because cysteine can replace up to half of the methionine requirement of cats. Methionine serves as a precursor to cysteine; therefore, cysteine is not an essential amino acid. Cysteine cannot be converted to methionine; however, a minimal requirement for methionine must be met with methionine. The potential for nutritional deficiencies exist, especially in cats fed home-prepared or vegetable-based foods. Clinical signs of methionine deficiency include poor growth and a crusting dermatitis at the mucocutaneous junctions of the mouth and nose. To meet the requirement in kittens, approximately 19% of a food must be composed of animal protein. Foods that are higher in plant proteins will require additional methionine. Supplementation can be supplied as DLmethionine, a crystalline form of the amino acid.
Fat Metabolism Cats are able to digest and utilize high levels of dietary fat. Being a true carnivore, cats have a special need for arachidonic acid (AA) (20:4n6) because of their limited ability to synthesize AA from linoleic acid (18:2n6). An exogenous source of AA is especially important for more challenging lifestages, (gestation, lactation, growth). The basis for this additional requirement is the low hepatic delta-6 desaturase activity in cats.
Vitamin Metabolism The vitamin needs of cats are different than dogs in several ways. It is known that cats do not convert sufficient amounts of tryptophan to niacin. An animal tissue-based diet is well supplied with niacin from NAD and NADP (nicotinamideadenine dinucleotide phosphate) coenzymes; therefore, cats don’t need to produce niacin from tryptophan. The niacin requirement of cats is 2.4 times higher than that of dogs. Cats have high transaminase activities, which is consistent with consuming a diet high in energy from dietary protein. Therefore, it is logical to expect that their pyridoxine turnover and requirement would be higher than that of omnivores. The pyridoxine requirement of cats is estimated to be 1.7 times higher than that of dogs. Vitamin A occurs naturally only in animal tissue. Plants synthesize vitamin A precursors (e.g., b-carotene). Omnivorous and herbivorous animals can convert b-carotene to vitamin A; cats cannot because they lack intestinal dioxygenase that cleaves b-carotene to retinol. Inaddition, cats have insufficient 7-dehydrocholesterol in the skin to meet the metabolic need for vitamin Dphotosynthesis; therefore, they require a dietary source of vitamin D. Vitamin D is relatively abundant in animalliver; therefore, the need for dermal production is minimal and alternate pathways rapidly metabolize 7-dehydrocholesterol.
Water As we are aware, water is the most important nutrient. The water needs of cats differ from dogs, because of their ancestors’ adaptation to environmental extremes. Domestic cats are believed to have descended from the African wildcat (Felis silvestris libyca), known to be a desert dweller. Adaptation to a dry environment may explain a few special features of water balance in cats. Cats are able to survive on less water than dogs and may fail to increase water intake at minor levels of dehydration, up to 4% of body weight. Highly concentrated urine is formed in cats to compensate for reduced water intake. However, this strong concentrating ability in addition to a weak thirst drive may result in highly saturated urine. Highly saturated urine increases the risk of crystalluria or urolithiasis. Cats consume 1.5 to 2 ml of water/g of dry matter (DM). This 2:1 ratio of water to DM is similar to that of typical prey. This ratio represents approximately 0.5 ml water/kcal ME intake. Practical recommendations for water provision are somewhat higher at 1 ml water/kcal ME. Water ingested from moist foods containing 78 to 82% moisture will result in diuresis.
Cats are not small dogs! Cats have unique nutritional requirements, based on many factors; most important being the fact that cats are obligate carnivores. Proper nutrition and care throughout a cats’ life maximizes health, longevity and quality of life. For veterinary technicians, thorough understanding of the nutritional needs of cats will help maximize the care of that cat.
References/Suggested Reading
139

1 Armstrong PJ, Gross KL, et al. Introduction to Feeding Normal Cats. In Small Animal Clinical Nutrition, 5th ed. Hand M, Thatcher C, Remillard R, Roudebush P, Novotny B., eds. 2010. MMI, Topeka, KS.
2 Hamper B, Bartges J, Kirk C., et al. The Unique Nutritional Requirements of the Cat: A Strict Carnivore. Little, S.ed. The Cat. W.B. Saunders Company, 2012.
3 Bartges J, Raditic D, Kirk C, et al. Nutritional Management of Diseases. The Cat: Clinical Medicine and Management. Little S. ed. W.B. Saunders Company, 2012.
4 Wortinger A, Burns KM. Nutrition and Disease Management for Veterinary Technicians and Nurses. 2015. Wiley-Blackwell. Ames, IA.
5 Armstrong J. Nutrition. Augusts Consultations in Feline Internal Medicine, 7th ed. Little SE, ed. 2016. Elsevier, St. Louis
140

0101
0202
Heartworm Transmission Happens FAST.
Heartworm Damage Can Develop QUICKLY.
List in order the correct steps of heartworm disease transmission:
Microfilariae mature into infective larvae in the mosquito. Mosquito bites an infected dog and collects the microfilariae. The infected mosquito uses its stylet to puncture the dog’s skin and deposits hemolymph around the puncture site.L3 larvae develop into adult heartworm in the dog and reproduce.When the mosquito withdraws its stylet, the L3 larvae migrate into the puncture wound.
In the illustration below, draw a circle on the location where heartworms are commonly found in a living dog during early stages of infection. Then, draw a rectangle on the location where heartworms can be found during advanced stages of infection.
Circle the image that shows signs of a pulmonary artery infected with heartworm disease.
worksheet
4 REALITIES EXPOSED:A VISUAL TOUR OFHEARTWORM DISEASE
A B
Pulmonary arteries
Right atrium
Right ventricle
141
caused by (meashwrot).
03030404
Untreated Heartworm Disease Is PROGRESSIVE.
Heartworm Disease Damage Can Be PERMANENT.
Infected dogs with heartworm disease display pulmonary arterial thickening also called(borifssi), and rough, cobblestoned appearance. This vascular change is only
Unscramble the words to complete the sentence.
What aspect of heartworm disease causes pulmonary arterial thickening and what are the possible outcomes to this damage?
After heartworm disease treatment, there will be no signs of heartworm disease in the dog.
True/False
Circle true or false.
Heartworm disease, if untreated can become over time. Dogs may present symptoms of coughing, and if not properly treated, will result in congestive heart failure.
syndrome is when heartworms interfere with the tricuspid valve.
Fill in the blank.
Educate yourself and become a better patient advocate.
Teach pet owners how they can prevent heartworm disease.
Share your stories and share what you have learned with your peers below.
Prevent: AHS and CAPC recommend year-round heartworm disease prevention for all dogs in the US.
Write down additional key takeaways for each category of heartworm disease management:
P.E.T.S Key Takeaways on Heartworm Disease Management
©2020 Boehringer Ingelheim Animal Health USA Inc., Duluth, GA 30096. All rights reserved. US-PET-0038-2020-V2
142
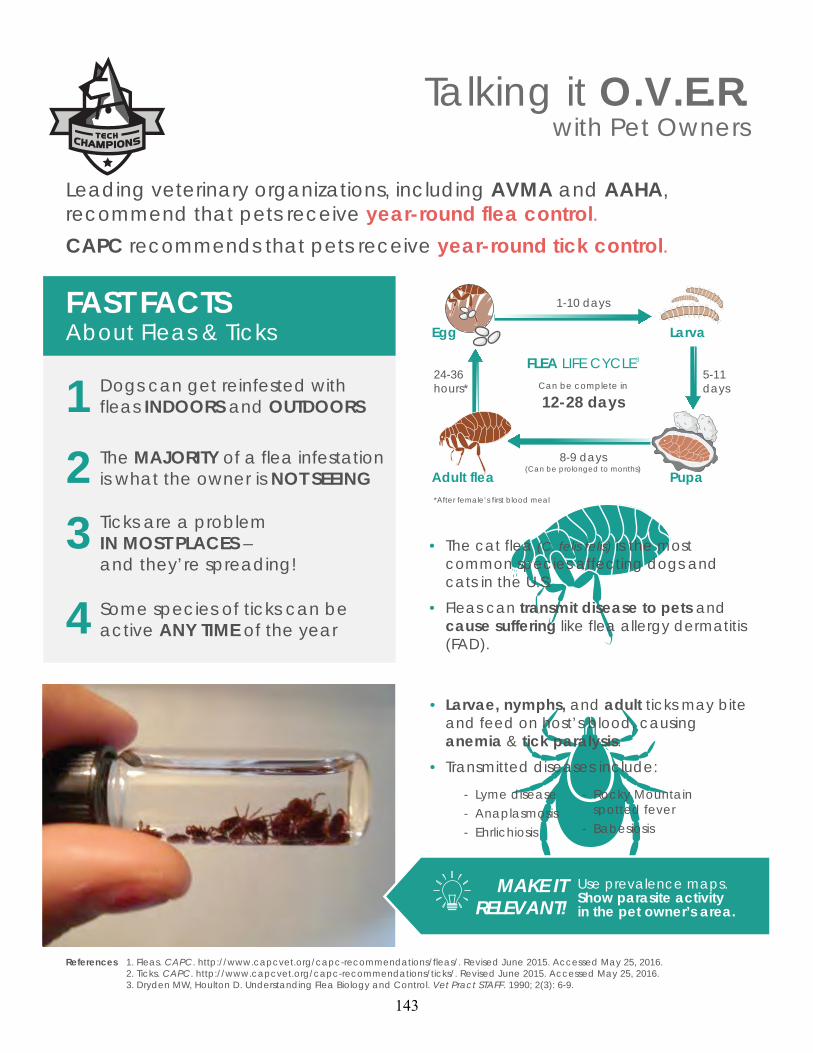
1.2. 3.
Fleas. CAPC. http://www.capcvet.org/capc-recommendations/fleas/. Revised June 2015. Accessed May 25, 2016.Ticks. CAPC. http://www.capcvet.org/capc-recommendations/ticks/. Revised June 2015. Accessed May 25, 2016.Dryden MW, Houlton D. Understanding Flea Biology and Control. Vet Pract STAFF. 1990; 2(3): 6-9.
References
Larvae, nymphs, and adult ticks may bite and feed on host’s blood, causing anemia & tick paralysis.
Transmitted diseases include:
Lyme disease
Anaplasmosis
Ehrlichiosis
-
-
-
-
-
Rocky Mountain spotted fever
Babesiosis
Use prevalence maps. Show parasite activity in the pet owner’s area.
MAKE IT RELEVANT!
•
•
•
•
The cat flea (C. felis felis) is the mostcommon species affecting dogs andcats in the U.S.
Fleas can transmit disease to pets andcause suffering like flea allergy dermatitis(FAD).
1-10 days
5-11days
8-9 days(Can be prolonged to months)
24-36hours*
*After female’s first blood meal
FLEA LIFE CYCLE3
Can be complete in
12-28 days
Larva
PupaAdult flea
Egg
Dogs can get reinfested with fleas INDOORS and OUTDOORS1
23
4
The MAJORITY of a flea infestation is what the owner is NOT SEEING
Ticks are a problemIN MOST PLACES – and they’re spreading!
Some species of ticks can be active ANY TIME of the year
FAST FACTSAbout Fleas & Ticks
Leading veterinary organizations, including AVMA and AAHA, recommend that pets receive year-round flea control.
CAPC recommends that pets receive year-round tick control.
Talking it O.V.E.R.with Pet Owners
143

NOTES
© 2021 Boehringer Ingelheim Animal Health USA Inc., Duluth GA. All Rights Reserved. US-PET-0105-2021
ADDITIONAL RESOURCESFLEA & TICK FACTS
VetFolio:www.vetfolio.com*
• What Do You Believe? Flea Control• What Do You Believe? Tick Control• The Science and Art of Flea Control
PREVALENCE MAPS
CAPC Disease Prevalence Maps: www.capcvet.org/parasite-prevalence-maps
CDC Tick Distribution Maps:www.cdc.gov/ticks/geographic_distribution.html
COMMUNICATION
VetFolio:www.vetfolio.com*
• Communication 101-104
1 2 3When your clients feel heard, they will listen, especially when they believe that they can benefit from what you have to tell them.
With fleas, what you don’t see is what you get, and what you get can be a horrible flea infestation on your pet and in your home!
There are more ticks in more places than ever before, and they can transmit diseases throughout the year.
The TAKEAWAYS
OPEN - Find out the pet owner’s perspective, questions and concerns
O
VALIDATE - Give their point of viewvalidityVEDUCATE - Provide information that is targeted to their needs and concerns
ERECOMMEND - Be sure that they receive a specific recommendationAND product to protect their pet
R
“Tell me about your experience using flea and tick control products on your dog, Sadie.”
“You’ve never observed fleas on Sadie, so you don’t see a reason to use flea control. I understand where you are coming from.”
“I would like to share some information with you about fleas living in your environment. Would you be open to chatting more about this?”
“We have products available for treating and controlling fleas and ticks that you can give orally or apply topically. Let’s discuss which one best suits your needs.”
Talking it O.V.E.R. KEYS TO SUCCESS
*Access to www.vetfolio.com requires a paid subscription
144

NUTRITIONAL MANAGEMENT OF PANCREATITIS Kara M. Burns, MS, MEd, LVT, VTS (Nutrition)
Academy of Veterinary Nutrition Technicians
One of the leading causes for which pets present to veterinary hospitals is gastrointestinal (GI) problems. However, we know the main challenge to the veterinary healthcare team presented with a pet that has GI dysfunction, is to determine whether this is an emergency or potentially serious problem versus a chronic or intermittent problem. The GI tract is known for its resiliency and the veterinary healthcare team has seen countless pets with clinical signs of acute vomiting and/or diarrhea resolve uneventfully, sometimes without any supportive care. However, this cannot be held to all acute GI events as some may be life-threatening disorders, which if not identified and treated, could lead to poor patient management and/or death of the pet.
Acute pancreatitis is an important differential diagnosis for vomiting and abdominal pain in canines. Pancreatitis is a less common diagnosis in cats because of the challenges in diagnosing pancreatitis in felines. However, over the last twenty years clinical and pathologic reports are finding an increase in the prevalence and subsequent diagnosis of pancreatitis in felines.
History and Physical Examination
Reportedly, 90% of dogs with pancreatitis present to the hospital with acute vomiting. Vomiting may be sporadic and mild or very severe. Other clinical signs include abdominal pain, depression, anorexia, fever, and diarrhea. Icterus and pale colored stools may be reported if pancreatic inflammation and edema are severe enough to result in common bile duct obstruction. If present, diarrhea is usually of large bowel origin because the transverse colon passes dorsal to the pancreas and is susceptible to local inflammation at that site. Often, an episode of dietary indiscretion has occurred during the 24 hours prior to the onset of vomiting. The owner commonly relates consumption of high-fat human food. Occasionally, the onset of clinical signs is preceded by administration of drugs associated with pancreatitis. Corticosteroids have been linked to pancreatitis in dogs. Cats with pancreatitis have highly variable clinical signs. Cats may present similarly to the aforementioned canine presentation - acute vomiting, lethargy, anorexia, diarrhea, and abdominal pain. However, in milder but more prolonged cases the presentation is more of a slow, smoldering course. The most common clinical signs in cats are anorexia, lethargy, dehydration, and weight loss.
A complete history is the first step, and a very crucial step, in trying to establish a cause for vomiting and diarrhea. The signalment and history, as well as a description of the vomiting episodes, are important. First, one must determine whether the animal truly is vomiting. The healthcare team should differentiate the owner's report of vomiting from gagging, coughing, dysphagia, or regurgitation. The description of retching is characteristic for vomiting. Signalment may also be helpful. For example, young, unvaccinated pets are more susceptible to infectious disease, such as parvovirus. Vaccination status, travel history, previous medical problems, and the medication history should be determined. Many drugs can result in vomiting, such as nonsteroidal anti-inflammatory drugs (NSAIDs), which are known to cause gastrointestinal ulceration and vomiting. The healthcare team member should also explore the possibility of toxin or foreign body ingestion and of other concurrent signs that often arise with systemic or metabolic disease. An example: polydipsia, polyuria, and weight loss are typical of vomiting associated with diabetic ketoacidosis or chronic kidney failure.
The history should then focus on the actual vomiting episodes. The duration, frequency, and relationship of the episodes to eating or drinking should be ascertained. A complete physical description of the vomited material should be documented. A dietary history, including the type of diet or recent dietary changes, is important because vomiting may be associated with an adverse reaction to food. Vomiting of an undigested or a partly digested meal more than 6 to 8 hours after eating, a time at which the stomach should normally be empty, suggests a gastric outflow obstruction or gastric hypomotility disorder. The description of the vomit should include the volume, color, consistency, odor, and the presence or absence of bile or blood. Undigested food suggests a gastric origin, whereas vomit-containing bile makes a gastric outflow obstruction unlikely. Vomit having a fecal odor is suggestive of a low-intestinal obstruction or bacterial overgrowth in the small intestine. Hematemesis, (either as fresh, bright-red blood or as digested blood with the appearance of coffee grounds), is indicative of gastrointestinal erosion or ulceration. Gastric
145

ulceration is caused by metabolic conditions such as hypoadrenocorticism, reaction to certain drugs, clotting abnormalities, gastritis, or neoplasia.
When performing a physical examination, the findings usually include depression, fever and dehydration, and stance indicating abdominal pain. Typically, the stance involves the patient in what appears to be a ‘downward dog’ position – the cranial portion is ‘down’ and the caudal portion ‘up’. This is indicative of the patient trying to find a body position that is less painful. Palpation of the abdomen may produce splinting and discomfort which is localized to the right cranial quadrant. Veterinary healthcare team members must be watching for icterus, shock, and coagulopathies, especially in more severe cases. Chronic pancreatitis may result in variable clinical signs. Felines may be limited in the signs they present with, and weight loss and poor body condition may be the only signs.
The laboratory diagnosis of acute and chronic pancreatitis can be very frustrating. Histopathology is considered the gold standard when diagnosing acute and chronic pancreatitis. However, pancreatic biopsies are rarely performed because the procedure is invasive and many patients with pancreatitis are poor anesthetic risks. However, laparoscopic techniques for the diagnosis of pancreatic disease in dogs and cats may be a viable alternative as these provide a minimally invasive method for collection of pancreatic biopsy specimens. One of the downsides to laparoscopy is the lack of good visualization of the entire pancreas, which may result in failure to biopsy affected areas of the organ.
KEY NUTRITIONAL FACTORS
Following the veterinarian’s diagnosis of pancreatitis, the vomiting and/or diarrhea signs along with the condition of pancreatitis overall, will need to be managed. The healthcare team should be knowledgeable of key nutritional factors and their impact when managing a patient nutritionally. This management of pancreatitis should consider the following nutritional factors:
Water - Water is extremely important when working with patients with acute vomiting and pancreatitis due to the potential for life-threatening dehydration from excess fluid loss and inability of the patient to replace the lost fluid. Patients with persistent nausea and vomiting should be supported with subcutaneous or intravenous rather than oral fluids. Where applicable, moderate to severe dehydration should be corrected with appropriate parenteral fluid therapy.
Electrolytes - Gastric and intestinal secretions differ from extracellular fluids in electrolyte composition, so their loss can result in systemic electrolyte abnormalities. Dogs and cats presenting with vomiting and diarrhea may have abnormal serum potassium, chloride, and sodium concentrations. Serum electrolyte concentrations are useful in tailoring appropriate fluid therapy and nutritional management of these patients. Mild hypokalemia, hypochloremia and either hypernatremia or hyponatremia are the electrolyte abnormalities most associated with acute vomiting (and diarrhea). Initially, electrolyte disorders should be addressed and corrected with appropriate parenteral fluid and electrolyte therapy. Patients experiencing vomiting and/or diarrhea should begin nutritional therapy ideally containing levels of potassium, chloride, and sodium above the minimum allowances for normal dogs and cats. Recommended levels of these nutrients are 0.8 to 1.1% potassium (dry matter [DM]), 0.5 to 1.3% DM chloride and 0.3% to 0.5% DM sodium).
Digestibility – In managing pancreatitis nutritionally, it is recommended that the diet be highly digestible or ≥ 85% digestible on a DMB.
Protein – Nutritional therapy for patients with pancreatitis should provide protein at levels of 15% - 30% for dogs and 30% - 40% for cats. In the duodenum, free amino acids (i.e., phenylalanine, tryptophan, and valine) are a strong stimulus for pancreatic secretion – even more than fat. Excess dietary protein should be avoided, while providing adequate protein for recovery and tissue repair.
Fat - Solids and liquids higher in fat empty more slowly from the stomach than comparable foods with less fat. Fat in the duodenum stimulates the release of cholecystokinin, which delays gastric emptying. Foods with less than 15% DM fat for dogs and less than 25% DM fat for cats are appropriate for dietary management. Obese and hypertriglyceridemic patients recovering from pancreatitis should receive low-fat foods (≤10 and ≤15% DM for dog and cat foods, respectively). This will help to reduce fasting serum triglycerides.
146

Fiber - Foods containing gel-forming soluble fibers should be avoided in vomiting and/or diarrhea patients as these fibers increase the viscosity of ingesta and slow gastric emptying. These fibers include pectins and gums (e.g., gum arabic, guar gum, carrageenan, psyllium gum, xanthan gum, carob gum, gum ghatti and gum tragacanth). Overall, the crude fiber content should not exceed more than 5% DM. Prebiotic fiber such as beet pulp and flax seed help to restore the balance of bacteria in the gut.
Food Form and Temperature - Moist foods are the best form since they reduce gastric retention time. For the same reason, the veterinary healthcare team should educate clients to warm foods to between room and body temperature (70 to 100°F [21 to 38°C]).
Additional Nutritional Factors in Pancreatitis
Ginger – Ginger has been associated with a reduction in nausea and vomiting. The University of Maryland Medical Center web site has information discussing ginger and its relation to less vomiting related to motion sickness in humans and may reduce the severity and duration of nausea during chemotherapy (in human patients). The UMMC web site also reports preliminary studies suggesting that ginger may lower cholesterol and help prevent blood from clotting. Ginger in nutritional management of canine patients is aimed at soothing and calming the GI tract of these patients.
Omega-3 fatty acids – Omega-3 fatty acids provide the benefit of helping to break the cycle of inflammation associated with pancreatitis.
Begin feeding sooner - Enteral nutrition is the most potent stimulator of intestinal mucosal regeneration. In addition, enteral nutrition may decrease cytokine production, modulate the acute phase response, decrease catabolism, and preserve protein. Experimental models of pancreatitis in dogs have shown a benefit of early enteral nutrition compared with parenteral nutrition in decreasing bacterial translocation and downregulating the severity of inflammation. More recent studies in people also suggest that gastric feeding (rather than jejunal) is well tolerated and safe, with no exacerbation of pain. The addition of anti-emetics should also aid in instituting enteral feeding as soon as possible.
GI signs are known to be a major reason for which owners bring their pets to the hospital. It is essential for veterinary technicians to identify these clinical signs and perform a complete history and evaluation regarding these signs and assist the veterinarian in their diagnosis of pancreatitis based on these signs. Nutritional management is a crucial part of therapy in the management of pancreatitis. Certain key nutritional factors play a role in managing vomiting and diarrhea in cats and dogs – through enteral and parenteral nutrition – and veterinary technicians should recognize the circumstances and reasoning for the KNF’s to insure a positive outcome for the pancreatitis patient.
REFERENCES
1. Davenport DJ, Remilliard RL, Simpson KW. (2010a) Acute and Chronic Pancreatitis. In Small Animal Clinical Nutrition 5th Ed. Hand MS, Thatcher CD, Remilliard RL, Roudebush P, Novotny BJ eds. 2010, pp 1143-1153. MMI, Topeka, KS;
2. Hall, EJ, German, AJ. 2010. Diseases of the small intestine. In Textbook of Veterinary Internal Medicine 7th edition. Ettinger, SJ and Feldman, EC, editors. Pp. 1526 – 1572. Elsevier: St. Loius, MO.
3. Burns, KM. Gastrointestinal Disorders. In Internal Medicine for Veterinary Technicians. Merrill L ed. 2012, Wiley-Blackwell, Ames, IA.
4. Willard, Michael D. 2009. Disorders of the Intestinal Tract. In Small Animal Internal Medicine 4th edition, pp. 441-476. Mosby: St. Louis, MO.
5. Tams, TR. 2003. Chronic Diseases of the Small Intestine. In Handbook of Small Animal Gastroenterology 2nd Edition. Tams, TR editor. Pp.211-250. Saunders: St. Louis, MO.
6. Allenspach, K, Gaschein, FP. 2008. Small Intestinal Disease. In Small Animal Gastroenterology. Steiner, JM editor. Pp. 187-202. Schlutersche: Germany.
7. Wortinger A, Burns KM. Nutrition and Disease Management for Veterinary Technicians and Nurses. 2nd ed. 2015. Wiley Blackwell. Ames, IA.
147

Keeping Pets Youthful with Senior Nutrition
Kara M. Burns, MS, MEd, LVT, VTS (Nutrition) Academy of Veterinary Nutrition Technicians
The age at which a pet enters their ‘senior years’ is variable and differs depending on species and breed. Assessment as a pet reaches middle age should be performed more frequently. Additionally, these assessments should be based on breed lifespan, with an appropriate senior wellness workup.1 The veterinary healthcare team should properly assess a pet to determine whether the feeding plan and nutritional needs of the patient. This includes a complete nutritional assessment, taking into account any medical conditions (eg, renal disease, diabetes) that require nutritional modification, and making a nutritional recommendation.2
Continued improvements in control of infection and nutrition in recent years has resulted in a gradual increase in the average lifespan of the companion cat and dog. The maximum lifespan of any given species has remained relatively fixed; the average lifespan within a given population can be affected by genetics, health care and nutrition.3 It is estimated that more than 40% of the dogs and 30% of the cats in the United States are at least 6 years old, and approximately 30% of these animals are older than 11 years. While we are seeing more and more older animals, it is important to remember that old age is not a disease, and if they are otherwise healthy, old age alone will not kill any animal.4
In the United States, older dogs reportedly make up a significant amount of the pet dog population. It is estimated that ~ 40% of the 78 million pet dogs in the United States are 7 years old4,5 with another survey suggesting the percentage of older dogs to be as high as 49%.6 37% of dogs and 44% of cats in Australia are over 7 years of age7. Around the world it has been reported that only 1 in 5 owners of older cats and 1 in 4 owners of older dogs are providing age appropriate nutrition.8
Senior or Mature Adult Dogs The senior, or geriatric, dog is approximately 7 years of age in an animal with an average life expectancy of approximately 13.5 years.9,10 This range varies widely, however; the figure given here is for medium-sized dogs. Smaller breeds tend to have longer life spans; larger-breed dogs tend to have shorter life spans. The nutritional goals for the senior dog are similar to those for the adult dog—optimize quality of life, increase longevity, and minimize disease. As the animal reaches the age of a senior pet, bodily changes occur. The senior dog has a diminished ability to hear, see, smell, and taste. The animal may not be able to readily adapt to stress, and its organs may not function at a normal level. As animals age, their organs lose the ability to compensate. Many older dogs and cats face chronic renal disease as they age. As the disease progresses, it affects the animal’s ability to eliminate waste products. It’s important not to feed a food that will create additional work for the kidneys or liver. The kidneys must work harder to excrete phosphorus, urea, and other metabolic waste by-products. The goals of feeding the senior patient are to decrease protein, phosphorus, and sodium. Every animal is an individual; the feeding regimen should take into account each animal’s specific needs. Some senior dogs have difficulty maintaining body weight, while others gain weight easily. It’s important not to make general recommendations for a subset of animals.
Nutritional management of mature adult dogs is focused upon: • Maintenance of optimal nutrition• Risk factor management• Disease management (i.e., slowing progression of certain chronic diseases)• Improvement in the quality and length of life.
Older dogs are more susceptible to dehydration especially if they are prescribed diuretics or have chronic renal disease. Access to fresh, clean water must be discussed with pet owners and water intake should be routinely monitored.10
As dogs age, they become slower and less active. Thus, it may be appropriate to feed a more energy-dense food to very old dogs. Because of the potential for mature dogs to have different energy needs, energy densities in foods
148
recommended for this age group may vary from 3.0 to 4.0 kcal/g dry matter (DM). Fat levels for the majority of mature dogs should fall between 7 and 15% DMB.9
Constipation is a common finding in mature dogs due to reduced water intake, limited activity and reduced motility in the colon. Fiber helps to combat these findings and normalize the GI tract. Also, fiber added to foods for obese-prone mature dogs dilutes calories. The recommended levels of crude fiber in foods to be fed to mature dogs are at least 2% (DMB). Healthy mature dogs should receive enough protein to insure protein-energy malnutrition does not occur. Older pets may begin to lose muscle mass and therefore increasing protein in the diet may be warranted. However, older pets are also at increased risk for renal disease in which case higher levels of protein are not recommended. Improving protein quality, rather than increasing the amount eaten, can provide sufficient protein for the older pet. Dietary protein should not be restricted in healthy mature adult cats. Adequate protein and energy intake are needed to sustain lean body mass, protein synthesis and immune function. For healthy mature dogs the protein percentage is recommended to be 15 to 23% protein DMB.
Senior or Mature Adult Cats Cats are considered senior at 10 to 12 years of age.10,11 Once a cat turns 7, there is an increased risk of age-related diseases. At 7 the cats’ nutritional needs are changing. As cats age, they become less active and may lose muscle mass or lean body mass. It’s important to feed the older cat to maintain body composition and weight. Remember to discuss fresh water with senior cat owners. Make yourself aware of the risks older cats may experience and provide food and an environment to decrease those risks, if possible. Many older cats face chronic renal disease as they age. The kidneys must work harder to excrete phosphorus, urea, and other metabolic waste by-products. Senior cats have an increased requirement for potassium during renal disease. Feeding a food lower in protein and phosphorus but higher in potassium will help meet the nutritional needs of the feline senior renal patient. Always have fresh water available to the pet. Nutritional management of mature adult cats should be focused on: • Maintenance of optimal nutrition • Risk factor management • Disease management (i.e., slowing progression of certain chronic diseases) • Improvement in the quality and length of life. Older cats are more susceptible to dehydration especially if they are prescribed diuretics or have chronic renal disease. In cats, aging impairs thirst sensitivity even further than previously known for cats. Access to fresh, clean water must be discussed with pet owners and water intake should be routinely monitored. Older cats begin to slow down and are less active. Thus, it may be appropriate to feed a more energy-dense food to senior pets. In mature cats, the energy density of foods should range from 3.5 to 4.5 kcal/g DMB.10,11
Fat levels for the majority of mature cats should range between 10 and 25% fat on a DMB.11 Essential fatty acid requirements should also be met as previously discussed with adult cats. Constipation is a more common in senior cats due to reduced water intake, limited activity and reduced motility in the colon. Fiber helps to combat these findings and normalize the GI tract. Also, fiber added to foods for obese-prone mature cats dilutes calories. The recommended levels of crude fiber in foods to be fed to mature cats ≤5% DMB. Healthy mature adult cats should receive enough protein to insure protein-energy malnutrition does not occur. Older pets may begin to lose muscle mass and therefore increasing protein in the diet may be warranted. However, older pets are also at increased risk for renal disease in which case higher levels of protein are not recommended. Improving protein quality, rather than increasing the amount eaten, can provide sufficient protein for the older pet. Dietary protein should not be restricted in healthy mature adult cats. Adequate protein and energy intake are needed to sustain lean body mass, protein synthesis and immune function. For healthy mature cats, moderate levels of dietary protein - 30 to 45% DMB are recommended.
149
Completing a Nutritional Evaluation for Senior Pets An in-depth nutritional history should be taken with every pet that presents to the hospital, every time they present. Veterinary technicians should ask questions of the owner in an open-ended questioning style. This allows for the owner to provide reliable and accurate information without feeling as though they are being judged by the veterinary team. The following are some questions to ask the client when completing a nutritional evaluation:
■ Tell me about the pet’s activity level? • Have you noticed any changes?
■ Tell me about where your pet spends his/her days and nights. ■ What changes in weight have you noticed?
• What’s the percentage of change of weight? • What’s the time frame of the change?
■ How often do you body condition score your pet? • Tell me the latest 3 scores that you have done
■ Tell me about your pets’ drinking habits? • Is water available at all times? • How is it offered?
■ What are your pet’s exercise habits? ■ Tell me what your pet eats over a 24 hour period
• What feeding method is used? • Does your pet have a good appetite? • How much food is offered at each feeding? • Have you noticed any difficulties when your pet eats? • Tell me of any recent changes in anything your pet eats.
■ What doesn’t your pet like to eat? ■ Does the pet have any adverse food reactions? ■ How is the food stored at home? ■ Tell me about the treats your pet receives? ■ Does your pet receive any medications?
• Supplements ■ Is the pet experiencing any vomiting or diarrhea? ■ Tell me about your pet’s sleeping habits ■ Tell me about your pet’s toileting habits
Answering these questions will help better identify problems and potential solutions in managing the senior patient, both in wellness and disease. Aging & Nutrition Science It is important for veterinary nurses to remember that although pets may not be showing outward signs of aging, every cell in the body does age. As pets age there is an increased risk of impact on the brain; effecting thinking, learning, memory, and social interactions. Ultimately, this may lead to behavioral changes in dogs and cats. Pet owners may notice these changes, but not attribute the behavior alterations to ageing. Cutting edge scientific tools such as predictive biology have been utilized to explore the effects of nutrition on cell function. Predictive Biology looks at what is occurring at the gene level. Each gene in the body contains the code to build a specific protein. Nutrients can influence genes to produce more or less of the protein for which they code. This is known as gene expression. It has been found that younger dogs and cats have very different gene expressions than older animals. These gene expression changes affect key metabolic pathways and body functions including oxidation, inflammation, and the immune system. The next step was to identify nutritional interventions which may positively impact the gene expression alterations in older pets. This, coupled with the scientific knowledge of taste preferences in older pets, resulted in age appropriate nutrition for older pets which helps to counter the free radicals that lead to aging in every cell.
Old age is not a disease. However, physiologic changes do occur, and the nutritional needs of senior pets differ from those of younger adult pets. It is important for veterinary technicians to understand these needs and educate pet
150
owners about them, and how nutrition plays a role in managing senior pets. Proper nutrition can help the pet live longer and with a better quality of life – and isn’t that why we all entered this field?
References
1. Linder DE. Diets for each life stage. Clinician’s Brief, January 2017, 77-80
2. Baldwin K, Bartges J, Buffington T, et al. AAHA nutritional assessment guidelines for dogs and cats. J Am AnimHosp Assoc. 2010;46(4):285-296.
3. Case LP, Carey DP, Hirakawa DA, Daristotle L (2000) Geriatrics. In Canine and Feline Nutrition (2nd ed), pp.275–86, St Louis MO:, Mosby.
4. AVMA. Total pet ownership and pet population. In: US pet ownership and demographics sourcebook.Schaumburg, Ill: AVMA, 2007;6–23.
5. Bellows J, Colitz CMH, Daristotle L, et al. Common physical and functional changes associated with aging indogs. JAVMA, Vol 246, No. 1, January 1, 2015. Pp. 67-75.
6. Delaney S, Fascetti A (2012) Feeding the healthy dog and cat. In S Delaney, A Fascetti (eds), Applied VeterinaryClinical Nutrition, pp. 85–6, Ames, IA: Wiley-Blackwell.
7. ACA Research 2016
8. Global statistics sourced from an average % of all dog/cat owners who have changed any of pets from adult tosenior food. The data was from 9 countries including the USA and EU from the TNS Pet Screener, 2011 &European Usage & Attitudinal Study, 2012
9. Debraekeleer J, Gross KL, Zicker S. Feeding mature adult dogs: Middle aged and older. In MS Hand, CDThatcher, RL Remillard et al. (eds), Small Animal Clinical Nutrition (5th ed), 2010, Topeka, KS; MMI.
10. Wortinger A, Burns KM. Feeding the Healthy Geriatric Dog and Cat. In Nutrition and Disease Management forVeterinary Technicians and Nurses, 2nd ed. 2015. Wiley Blackwell. Ames, IA.
11. Gross KL, Becvarova I, Debraekeleer J (2010) Feeding mature adult cats: Middle aged and older. In MS Hand,CD Thatcher, RL Remillard et al. (eds), Small Animal Clinical Nutrition (5th ed), Topeka, KS; MMI.
151

CANINE OSTEOARTHRITIS (OA)A PROACTIVE APPROACH TO
Watch for the early signs of OA in pets.
Exercise & physical therapystrengthening the muscles around the joints may improve function. Controlled physicaltherapy may be needed during OA flare-ups
Nutrition & weight controla healthy weight can prevent excessive joint stress, reduce pain and increase spine movement
Nutraceuticals/supplementsnutrients such as glucosamine/chondroitin or omega-3 fatty acid supplements
MedicationsNSAIDs can help
decrease pain and inflammation
while opioids such as tramadol can be used
to alleviate pain in dogs
Adjunct therapytreatments such as
cold or heat pad application or massage
MULTIMODALMANAGEMENT OF
OA
Management of OA should involve multiple therapies.
Multimodal Management of OA
Early indicators of OA in dogs
Abnormal gaitDecreased activityChange in temperamentDifficulty rising
152

Recognize the signs of OA and educate pet owners
Be the bridge between the veternarian and the pet owner
Use PROACTIVE OBSERVATION and CONVERSATION at every stage
The Role of the Vet Tech
Steps to increase success
©2021 Boehringer Ingelheim Animal Health USA Inc., Duluth, GA. All rights reserved. US-PET-0238-2021
1. ASSESSMENTLook for early signs of osteoarthritisin young, growing, and adult dogs.Continue to monitor over the dog’s life.
Observe mobility, activity, and temperament.
Watch for changes over time.
2. TREATMENT & MANAGEMENTRelay what you haveobserved to the veterinarian.
Educate the pet owner.
3. FOLLOW-UPFollow-up appointmentsare critical.
Contact the pet owner 2 days after initial visit to ensure owner is comfortable.
ASSESSMENTTREATMENT &MANAGEMENT
ASSESSMENTFOLLOW-UPASSESSMENTASSESSMENT
153

Tachyarrhythmias: diagnosis & treatment in general practice
Michael Aherne, MVB, GradDipVetStud, MS, MANZCVS (Small Animal Surgery), DACVIM (Cardiology)
Department of Small Animal Clinical Sciences
College of Veterinary Medicine
University of Florida, Gainesville, Florida
SUPRAVENTRICULAR TACHYARRHYTHMIAS
SINUS TACHYCARDIA
All the criteria for sinus rhythm are met, however the HR is too fast. This is usually a physiologic response to an
external stimulus. Specific treatment is not indicated but the underlying etiology should be addressed (e.g. pain).
Sinus tachycardia can result from excessive sympathetic nervous system stimulation (e.g. fear, excitement, pain,
fever, hyperthyroidism, hypovolemia, cardiac tamponade, heart failure, hypoxia) or certain drugs (e.g.
catecholamines, atropine, glycopyrrolate, terbutaline, aminophylline, theophylline).
SUPRAVENTRICULAR PREMATURE COMPLEXES (ATRIAL OR JUNCTIONAL)
Early depolarizations originating from an abnormal site anywhere above the ventricles (“supra-ventricular”). This
could include the atrial myocardium or junctional tissue (proximal AV bundle, AV node, bundle of His). These are
single premature (faster than the SA node) beats. Typically, a premature beat will fire faster than a rate of about 160
bpm (so a coupling interval faster than 375 msec). A QRS complex is present that is >90% like the normal QRS
complex in all leads (because the ventricular depolarization still uses the bundle of His, bundle branches and
Purkinje fibers). A P wave may or may not be present and if present, may or may not be normal in configuration and
timing, depending on the site of origin. When it is not be possible to distinguish a premature atrial beat from a
premature junctional beat, the term premature supraventricular beat is preferred.
Occasionally, a P wave may not be readily identified in association with a premature supraventricular complex and
there are several possible reasons for this. One reason is that it may be buried in the previous T wave if the beat is
very premature. Alternatively, if the premature complex originates in the junctional tissue, it may not retrogradely
penetrate the atria. Finally, if the premature complex originates in the junctional tissue and does retrogradely
penetrate the atria, this may occur coincident with the ventricular depolarization, thus the resultant P wave would be
buried in the QRS complex.
Single premature supraventricular complexes do not require treatment. This arrhythmia is uncommon in normal
dogs and therefore its recognition should prompt an investigation into the possibility of cardiac disease. Also,
remember that non-cardiac disease such as electrolyte abnormalities, ischemia, drug toxicities can also lead to
development of arrhythmias.
SUPRAVENTRICULAR TACHYCARDIA (ATRIAL OR JUNCTIONAL)
Supraventricular tachycardia (SVT) is when there are three or more consecutive premature supraventricular
complexes. As discussed above for premature supraventricular depolarizations, the origin of the SVT can be atrial or
junctional. The QRS configuration should be >90% like the normal QRS in all leads and a P wave may or may not
be present, may or may not be normal in configuration (positive or negative) and may occur before, simultaneous
with or after the QRS complex.
Reentry can be a mechanism and shows a rapid onset and rapid termination. Automatic SVTs may show a “wind up
and wind down” pattern where the rate slowly increases and slowly decreases. The rate for SVTs in dogs can range
from 170-350 bpm. SVT in dogs is usually associated with underlying cardiac disease and less commonly to severe
systemic disease.
154
The presence or absence of clinical signs depends on the presence of absence of severe underlying myocardial
disease and the rate. SVT with rates of 250-300 bpm usually causes weakness or collapse. Perfusion is poor at these
high rates because diastolic filling time is inadequate. Prolonged SVT can cause myocardial failure. Patients
presenting for weakness or collapse should be considered medical emergencies.
Acute Treatment of SVT:
Vagal maneuvers may be attempted to increase vagal tone with the intent of slowing conduction through the AV
node. These are often unsuccessful in veterinary medicine, possibly due to the high sympathetic tone of the patient
in this situation. They are worth attempting, however and will occasionally be successful.
a. Ocular pressure – gentle pressure on both eyes
b. Carotid sinus massage – gentle upper neck massage
Precordial thump – this is often successful for at least short-term conversion of the SVT but carries a risk of
inducing VT. With the dog in right lateral recumbancy, the apex beat is located on the left side of the chest and
thumped with the fist (strength dependent on the size of the patient). The intent is to produce a VPC to interrupt the
SVT.
Drugs:
Calcium channel blockers (e.g. diltiazem) block the slow inward calcium channel (ICa-L). Since this channel is
present in pacemaker cells (SA node and AV node), this class of drugs often is effective for SVT by slowing
conduction through the AV node. They work by prolonging the refractory period of the AV node and allowing less
of the impulses coming from an SVT to traverse the AV node. If conduction is slowed enough, the depolarization
will be blocked. If the SVT has a reentrant mechanism and the AV node is part of the circuit, a calcium channel
blocker should be effective by slowing conduction through the AV node to the point of breaking the SVT.
If the SVT originates in atrial tissue and does not use the AV node for its circuit, calcium channel blockers will not
break the SVT but may still be effective by slowing the ventricular response rate (i.e. the number of atrial impulses
traversing the AV node and causing a ventricular depolarization) by slowing AV node conduction and prolonging its
refractory period (i.e. causing AV block).
Beta blockers (e.g. esmolol, propranolol) antagonize the actions of sympathetic stimulation and therefore have
negative chronotropic effects (slowing of the heart rate) and negative inotropic effects (decreased contractile force
generation). Their negative chronotropic effects result in slowing of AV node conduction and prolonging the
refractory period of the AV node. Esmolol is short-lived, with a half-life of approximately 9 minutes. If a response
occurs, it can be given as a CRI. Moderate to severe myocardial failure is a relative contraindication to the
administration of beta-blockers due to their negative inotropic effects.
Lidocaine occasionally converts atrial fibrillation or some SVTs to sinus rhythm although it is predominately used in
the management of ventricular arrhythmias.
Chronic Treatment of SVT
1. Digoxin – digoxin has several pharmacologic effects. One of these is its effect on autonomic tone – it serves to
increase vagal tone and decrease sympathetic tone. This can prove effective for treatment of SVT by prolonging
conduction in the AV node.
2. Calcium channel blockers (diltiazem for long-term use)
3. Beta blockers (especially atenolol for long-term use)
4. Class I antiarrhythmics (e.g. procainamide, quinidine) – these agents block the fast sodium channel (INa) and
slow conduction velocity.
5. Class III antiarrhythmics (e.g. sotalol, amiodarone) – these agents block potassium channels and thus prolong
repolarization. They also block fast sodium channels and slow calcium channels as well as have anti-adrenergic
properties.
ATRIAL FLUTTER
Atrial flutter is an uncommon SVT. It is a very fast SVT with atrial rates between 350-450 bpm. The atrial rate is so
fast that some beats are blocked in the AV node because the depolarization rate exceeds the refractory period of the
155

AV node, producing functional 2nd degree AV block. This arrhythmia may also be seen in horses during conversion
of atrial fibrillation with quinidine.
Treatment
a. Digoxin
b. Calcium channel blockers
c. Beta blockers
d. Procainamide
ATRIAL FIBRILLATION (AF)
Atrial fibrillation is one of the most common supraventricular arrhythmias encountered in clinical small animal
practice. Initiation of atrial fibrillation requires a “critical mass”. Meaning, a large atrium is required to establish and
sustain atrial fibrillation. This is why it is seen commonly in large breed dogs and horses and uncommonly in small
breed dogs and cats. During this arrhythmia, the atria fibrillate at a rate of 500-600 bpm. Because the atrial
depolarization is chaotic, organized atrial contraction does not occur. The many depolarizations during AF
constantly bombard the AV node, which cannot conduct all of them to the ventricle. The pattern for which atrial
depolarizations are conducted through the AV node is irregular, resulting in an irregular ventricular response rate.
The number of impulses that reach the ventricle is dependent on the refractory period of the AV node, its conduction
characteristics and autonomic tone (high sympathetic tone will shorten the AV node refractory period and allow
more impulses to get through, high vagal tone will allow fewer impulses through).
Two factors predispose to the development of atrial fibrillation. These are large atrial mass and elevated vagal tone.
A large atrial mass is necessary to sustain AF; large hearts fibrillate more easily than small hearts. Horses can
develop AF in the absence of heart disease since their atrial mass is large normally. Giant and large breed dogs can
occasionally develop AF in the absence of heart disease (“lone AF”). Small and medium sized dogs require
significant cardiac disease (atrial enlargement due to pathology) to sustain AF. AF occurs in cats occasionally when
severe atrial enlargement is present.
Both sympathetic and vagal tone shorten the refractory period in the atria and the elevation of both simultaneously
may predispose to AF (e.g. pain and stress of a GDV with narcotic drugs, racing horses during cool down periods).
Vagal tone increases the heterogeneity of atrial refractoriness (allows for different refractory periods within the atria
by unequal shortening of the refractory period) which can predispose to multiple reentrant wavelets (atrial
fibrillation). Horses naturally have high resting vagal tone, which is another predisposing factor for the development
of AF in this species.
ECG diagnosis of Atrial Fibrillation
1. Rapid heart rate (usually greater than 200 bpm)
2. Supraventricular morphology to the QRS complexes (narrow and upright in lead II).
3. Chaotic rhythm (i.e. irregularly irregular – there is no identifiable pattern).
4. P waves cannot be identified.
5. The baseline may have irregular undulations (fibrillation or f-waves).
6. There may be variation in the height of the QRS complex.
***Note that when atrial fibrillation gets very fast (>250 bpm) it can be very difficult to pick out the irregularity of
it. You need to run lots of ECG to be able to pick up the irregularities. It is also helpful to run the ECG at 50
mm/sec.***
Primary “Lone” Atrial Fibrillation
In Lone AF, significant underlying cardiac disease is not present. Therefore, resting sympathetic tone is not elevated
and the heart rate is usually relatively normal (100-140 bpm in the large breed dogs in which this occurs). The
rhythm is still supraventricular, irregularly irregular and no P waves are identifiable. Lone AF could be a precursor
to the development of dilated cardiomyopathy in the future in these dogs.
HEMODYNAMIC CONSEQUENCES OF ATRIAL FIBRILLATION
The hemodynamic consequences of Lone AF are minimal since underlying heart disease is not present and the rate
is usually slow. Since atrial contraction contributes about 20-25% to the cardiac output (“atrial kick”), the loss of
atrial contraction in horses with AF and no underlying heart disease is usually only evident when exercised.
156
Decreased performance, usually in racehorses, is the typical chief complaint, with no signs evident at rest. The loss
of atrial contraction due to the development of AF in a dog with serious heart disease can be very detrimental.
Stroke volume and cardiac output decline and end diastolic pressure increases. Clinical deterioration occurs,
possibly with the development of congestive heart failure. The sustained increase in heart rate can induce further
myocardial systolic dysfunction over several weeks (tachycardia-induced cardiomyopathy).
CLINICAL FEATURES OF ATRIAL FIBRILLATION
On auscultation, atrial fibrillation is characterized by an erratic cardiac rhythm and varying intensity of the heart
sounds (i.e. “tennis shoes in a dryer”). Pulse deficits and variation in pulse quality (the strength of the pulse depends
on the preceding diastolic interval, which varies due to the irregular heart rate). Pulse deficits are common and a
heart rate based off pulse rate is inaccurate. It is difficult to count a heart rate by auscultation in AF due to the usual
rapid and irregular nature of the arrhythmia. It is best to determine heart rate off an ECG with AF.
TREATMENT OF ATRIAL FIBRILLATION
Conversion to sinus rhythm is often not a realistic goal in dogs. The presence of severe underlying heart disease
usually makes these dogs refractory to successful conversion. The need for conversion in Lone AF is controversial.
The ventricular response rate is slow in these dogs (or can be controlled with medication if it is rapid) and they are
asymptomatic, making the need for conversion debatable. In human medicine, rate control has been shown to be as
good as rhythm control.
Conversion is also difficult in long standing atrial fibrillation. The general dogma is that “Atrial fibrillation begets
atrial fibrillation” meaning the longer standing the AF is, the more likely this rhythm is to be sustained. Significant
electrical remodeling occurs within the atria during AF, which preclude their ability to convert to and sustain sinus
rhythm. In general, it is less likely that conversion will occur if AF has been present for 3 weeks or more. The less
time in AF, the more likely conversion will be possible.
Conversion is often attempted in horses if underlying disease is not present and the horse is used for performance
purposes. Horses are usually diagnosed early on because of poor performance and are therefore more likely to
convert. Conversion can be attempted with medical therapy (quinidine) or with electrical current (DC conversion to
deliver a low voltage current to the atrial myocardium).
Control of heart rate with medical therapy is usually the treatment for dogs and cats. Drugs that slow AV node
conduction are used to slow ventricular response rate to AF. These drugs increase the AV node refractory period and
therefore allow fewer impulses to traverse the AV node.
Digoxin
Digoxin increases vagal tone, thereby increasing the refractory period of the AV node and slowing conduction. This
decreases the number of depolarizations that are conducted to the ventricle. Digoxin is a weak positive inotrope (as
opposed to the remaining drugs which are negative inotropes) and this is beneficial for DCM It usually only slows
the HR 10-30 bpm and therefore often a second drug is needed to slow the heart rate further.
Diltiazem
Diltiazem is a calcium channel blocker that slows conduction through the AV node (see for SVT). Diltiazem appears
to be synergistic with digoxin for HR control in AF.
Beta blockers
Beta-blockers decrease sympathetic tone resulting in slowed conduction through the AV node (see for SVT).
Atenolol and propranolol are the most commonly used beta blockers. At higher doses, Sotalol has properties of both
beta-blockers and potassium channel blockers (Class II and III antiarrhythmic). Caution is used with beta-blockers
when myocardial failure is present. The dose must be started low and titrated to the lowest effective dose that can be
tolerated by the patient.
VENTRICULAR TACHYARRHYTHMIAS
Ventricular premature complexes (single, bigeminy, trigeminy)
Ventricular premature complexes (VPCs), Ventricular premature depolarizations (VPDs), and Premature ventricular
contractions (PVCs) are all synonyms that can be used to described premature ectopic beats arising from the
ventricles.
157

ECG characteristics
a. Premature (earlier than the sinus beat), wide and bizarre QRS (<90% like the normal beat). This is because the
VPC originates below the bundle of His and cannot take advantage of the specialized conduction system. It must
therefore depolarize the ventricles muscle cell to muscle cell. This is relatively slow and produces a wide bizarre
complex. QRS complexes can be positive or negative in lead II, depending on the site of origin.
b. No associated P wave
c. Large bizarre T wave. Because depolarization is abnormal, repolarization is also abnormal.
VPCs can occur in patterns (bigeminy – every other beat is a VPC, trigeminy – every 3rd beat is a VPC). If the VPC
fires rapidly and occurs on the downslope of the T wave of the sinus beat, it is called “R on T phenomenon”. The
downslope of the T wave is the vulnerable period and depolarization during this time may predispose to ventricular
fibrillation.
Causes of VPCs
a. Can be seen in normal animals in very low numbers (less than 24 per 24-hour period on a Holter monitor)
b. Commonly in association with non-cardiac disease. Possibly due to myocardial ischemia, electrolyte
abnormalities or other factors surrounding the underlying disease ( post-trauma [e.g. traumatic myocarditis], post-
surgery, GDV, splenic disease, infectious myocarditis, other systemic diseases)
c. Anesthesia
d. Primary myocardial diseases (especially Doberman pinschers with DCM and Boxers with ARVC)
e. Idiopathic
f. Parasystole (rare) - this describes a focus of ventricular discharge that is independent of and not influenced by the
normal sinus rhythm. It is protected from overdrive suppression and will produce a ventricular depolarization
whenever the myocardium is not refractory from sinus rhythm. This is uncommon, thought to be fairly benign, and
can be difficult to diagnose. The diagnosis is based on finding that the interectopic interval between VPCs are all
multiples of one shorter interval, finding fusion beats, and finding a variable coupling interval with the previous
normal beats.
Treatment
Clinical signs do not occur with single VPCs. Dogs with VPCs secondary to systemic disease often do not need to
be treated and the arrhythmias tend to be self-limiting if the underlying disease can be addressed. Dogs with single
VPCs and underlying myocardial disease may or may not need to be treated. Usually this indicates the need to
further investigate the arrhythmia (e.g. with Holter analysis) to determine if more serious arrhythmias are occurring
at other times. Since dogs with VPCs do not show clinical signs associated with only single premature beats,
alleviation of clinical signs is not a reasonable reason to treat. In this instance, the reason to treat is to attempt to
prevent sudden death. However, our ability to predict the likelihood of sudden death associated with VPCs is poor
and no antiarrhythmics have been proven to eliminate the risk of sudden death in animals with ventricular
arrhythmias. It appears that in dogs with VPCs and no underlying heart disease, the number of VPCs is not
predictive of the risk of sudden death, which appears to be low. Very high numbers of VPCs, however, may cause
reduced myocardial function. In the presence of myocardial disease, the presence of VPCs may indicate an increased
risk of sudden death or they may simply be a marker for the severity of the disease (e.g. Doberman pinschers with
dilated cardiomyopathy). The presence of VPCs in Boxers with familial ventricular arrhythmias may indicate an
increased risk of sudden death. If deemed necessary, the treatment is the same for ventricular tachycardias (see
below).
Ventricular Tachycardia (VT)
A ventricular couplet is two consecutive VPCs, a ventricular triplet is three consecutive VPCs and ventricular
tachycardia is >3 consecutive VPCs. Ventricular tachycardia is considered sustained if it lasts >30 seconds and
nonsustained if <30 seconds.
Ventricular tachycardia vs. accelerated idioventricular rhythm
A ventricular rhythm that is less than approximately 140-170 bpm is not truly a tachycardia, and is therefore best
termed an accelerated idioventricular rhythm (AIVR). A true ventricular tachycardia is a ventricular rhythm that is
fast (rate >170 bpm). Accelerated idioventricular rhythms (AIVR) are seen commonly in hospitalized patients in
association with non-cardiac diseases (e.g. GDV surgery, splenic disease, pancreatitis, prostatitis, post trauma and
neurologic disease). These are often benign, with a slow rate and they often do not require therapy.
158
ECG diagnosis of ventricular tachycardia
The morphology of the QRS complex is wide and bizarre as it is for VPCs. The shape and orientation depend on the
origin of the ectopic depolarization and the conduction pathway. Ventricular premature complexes can be
monomorphic (one shape) or polymorphic (several different shapes). The latter might imply multifocal origins for
the arrhythmias, however different pathways may also produce multiform complexes. Most VTs are regular,
however they may be irregular.
Clinical signs of VT
If the rate of the VT is slow, no clinical signs may be present. If the rate of the VT is rapid (greater than 250-300
bpm) signs of poor cardiac output may be present or syncope may occur. Clinical signs will be influenced by the
degree of underlying heart disease.
Treatment of VT
The goals of treatment for VT are to improve hemodynamics and to prevent sudden death When making the
decision to treat or not, one must consider if the arrhythmia causing hemodynamic compromise. A healthy heart can
tolerate more abuse than a diseased heart. Therefore, the presence or absence of underlying cardiac disease is an
important factor in this decision. The patient should be evaluated (peripheral pulse quality, mucous membrane color,
attitude, and arterial blood pressure). Sustained VT at a high rate is more likely to cause hemodynamic compromise
than VT at slower rates.
One must also consider if the arrhythmia likely to degenerate into ventricular fibrillation, which will cause sudden
death. Again, the presence or absence of underlying cardiac disease is important since a healthy heart can tolerate
more than a diseased heart. The faster the VT, the more likely that a beat will fall within the vulnerable period and
induce ventricular fibrillation (R on T phenomenon). Polymorphic VT is thought to be more dangerous than
monomorphic VT. Certain patient groups appear to have an increased risk of sudden death associated with
ventricular tachycardia (e.g. Doberman pinchers with DCM, boxers with ARVC, dogs with severe subaortic
stenosis, German shepherds with inherited ventricular arrhythmias).
Acute therapy of VT
• Lidocaine is the initial drug of choice (class IB antiarrhythmic - blocks fast sodium channels); only available for
intravenous use; given as a bolus (2 mg/kg) or as a CRI
• Reasons for lack of lidocaine efficacy include hypokalemia, incorrect diagnosis (e.g. AIVR), inappropriately
low dose, the patient’s VT may be refractory to lidocaine administration (rare).
• Lidocaine toxicity is associated with neurologic signs at high doses (cats are more sensitive)
• Procainamide can used as an alternative if lidocaine is ineffective
• Magnesium sulfate may be effective in some cases.
• Beta blockers can be attempted but should be used with caution since they are negative inotropes and so may
worsen cardiac output which may already be reduced due to the tachyarrhythmia.
• Ensure that the patient is hydrated, acid base status is normal, and electrolyte concentrations are normal.
Chronic therapy of VT
Class I Antiarrhythmics (sodium channel blockers) - Mexiletine is the most commonly used oral drug in this class
for ventricular arrhythmias and is considered an oral analogue of lidocaine. A combination of mexiletine and sotalol
has been shown to be effective for the reduction of ventricular ectopy in boxers with ARVC.
Class II Antiarrhythmics (beta-blockers) - These can be effective for ventricular arrhythmias but are usually used in
combination with other drugs. They are contraindicated in moderate to severe myocardial failure due to their
negative inotropic effects. Atenolol and propranolol are the most commonly used beta-blockers. Sotalol has part
beta-blocker and part Class III effects at higher doses.
Class III Antiarrhythmics (potassium channel blockers) - Sotalol has been shown to be extremely effective for the
reduction of ventricular tachycardia in Boxers with ARVC. Since sotalol also has some beta-blocking properties it
must be used with caution in dogs with myocardial failure. Amiodarone is very effective for refractory arrhythmias,
however can have significant, idiosyncratic side effects.
Ventricular fibrillation (VF)
Ventricular fibrillation is a pre-terminal event where ventricular electrical activity is chaotic and no organized
ventricular contractions occur. If untreated, ventricular fibrillation will result in death.
159

ECG Characteristics
• Irregular baseline undulations
• No discernable P, QRS or T waves
Treatment of VF
Although several medical therapies have been purported, the only effective method for treatment of VF is
cardioversion either by electrical defibrillation or by precordial thump. The chance of successful conversion depends
on the clinical situation. A healthy dog with an anesthetic complication causing VF stands a good chance of
successful defibrillation. A dog with severe systemic or cardiac disease has a very poor chance of conversion.
160

Bradyarrhythmias & conduction disturbances: diagnosis & treatment in
general practice
Michael Aherne, MVB, GradDipVetStud, MS, MANZCVS (Small Animal Surgery), DACVIM (Cardiology)
Department of Small Animal Clinical Sciences
College of Veterinary Medicine
University of Florida, Gainesville, Florida
Conduction disturbances
For the ECG to appear normal, the impulse from the SA node must be conducted along normally throughout the
heart. This includes the high speed conduction pathways of the bundles and fascicles. From the AV node, the
impulse travels down the bundle of His before moving into the left and right bundles. Interruption of either of these,
left or right bundles, can change the shape of the ECG but in a predictable and consistent manner. As a result of the
block, the impulse has to spread muscle cell to muscle cell to reach the blocked region which is much slower and as
a result, the QRS is widened (usually over 0.08 s in the dog, 0.05 s in the cat). The left bundle further divides into
the anterior and posterior fascicles and left anterior fascicular block is recognized especially in cats. As the
conduction from the SA node to the AV node is not affected, the complexes are usually preceded by a P wave and
are said to be sinus in origin. The bundle branches have a refractory period and if the supraventricular rate exceeds this, the QRS can be conducted with a bundle block pattern which needs to be differentiated from ventricular
enlargement.
Left bundle branch block
The right ventricle is depolarized normally and the impulse spreads slowly to the left resulting in a complex
dominated by the left ventricle so the ECG orientation appears normal, i.e. positive in leads I, II, III and aVF but the
complex is wide. The T wave will also be large and opposite in polarity. Although it does not require specific
treatment, it is often associated with significant LV pathology
Right bundle branch block
In right bundle branch block, the left ventricle depolarizes normally and then the impulse travels slowly to the right
resulting in a late negative swing on the ECG with a wide complex. The ECG shows a small, narrow R wave
(normal LV depolarization) with deep negative S waves in lead I, II, III and aVF and the MEA is shifted to the right
similar to RV hypertrophy patterns. The right bundle is small and more susceptible to injury, so although I can be
associated with RV pathology, it is an incidental finding in about 50% of cases. Like left bundle branch block, it
does not require specific treatment.
Left anterior fascicular block
This causes slight prolongation of the QRS but a significant effect on the MEA. The QRS complexes in lead I is
positive with a prominent R wave while in leads II, III and aVF the QRS complexes are negative due to prominent S
waves. Although left anterior fascicular block is not associated with clinical signs, this pattern is commonly
associated with hypertrophic cardiomyopathy in cats and its find should prompt further evaluation with an
echocardiogram. There is debate as to whether left posterior fascicular block exists.
Bradyarrhythmias
To be classified as bradycardic or tachycardic, the heart rate must be outside the reference range for that animal.
Canine heart rates typically vary from 60 to 160 bpm in the clinic. However, Holter monitor studies suggest a more
variable range with heart rates as low as 40 bpm with a 4 second pause while sleeping and as high as 300 bpm when
excited/exercising. Cats are typically faster as they are more adrenergically driven in the clinic with rates of 140 to
220 bpm. Immature animals also have slightly faster heart rates than mature adults.
Examination of the ECG can reveal if the abnormal rhythm arises above the AV node and is supraventricular usually
similar in appearance to sinus complexes or is wide and bizarre often with no preceding P wave suggesting it is
161
ventricular in origin. Bradycardias may require treatment if they cause symptoms but underlying causes should be
investigated and treated first.
Sinus Bradycardia
This is a sinus rhythm that is slower than the normal for that species. It is important to rule out causes of high vagal
tone (e.g. GI, respiratory, ocular or CNS disease), hypothermia, drugs (beta blockers or anesthetics) and
hypothyroidism. If there are no clinical signs, patients with sinus bradycardia do not require treatment. If the patient
is symptomatic and responds to atropine, oral anticholinergics may be used. Rarely, if ever, do these patients require
pacemaker implantation.
Sinus Block or Sinus Arrest
Sinus arrest or sinus block are commonly encountered in brachycephalic breeds. In sinus block, the SA node
depolarizes but does not result in atrial activity. Sinus arrest is the intermittent cessation of atrial activity. It is
difficult to differentiate on a surface ECG between block and arrest. If there is a pause equal to two R – R intervals,
it suggests that the impulse formed in the SA node and did not escape i.e. was blocked. These typically do not
require treatment if infrequent and not resulting in clinical signs.
Atrial Standstill
There are no P waves visible on the surface ECG and the heart rate is slow. This can be the result of underlying
atrial myocardial disease but also hyperkalemia. Primary atrial myocardial disease is seen particular in springer
spaniels but also in other breeds as well as cats. A junctional escape rhythm is typically seen on the ECG. With the
exception of atrial standstill secondary to hyperkalemia, treatment requires pacemaker implantation which addresses
the bradycardia but not the underlying atrial disease which is usually progressive. Patients are usually symptomatic
however prognosis following pacemaker implantation is typically poor in those dogs with atrial myocardial disease
although some dogs can do well in the medium term.
Causes of hyperkalemia should be investigated and treated appropriately e.g. Addison’s disease or urethral
obstruction. Increased potassium concentrations make the resting membrane potential less negative. The difference
between the resting membrane potential and the threshold is decreased so the upstroke velocity is decreased and the
cell may not be able to be depolarized. Atrial tissue is especially sensitive to this. The SA node and internodal tracts
are more resistant resulting in a sinoatrial rhythm. In cases of potassium changes, causes of hyperkalemia should be
addressed.
Atrioventricular (AV) Blocks
1st degree AV Block
The P-R interval is prolonged but every P has a QRS so the rhythm is not affected. It can be associated with
increased vagal tone and drug therapy such as digoxin, beta blockers and calcium channel blockers. It is an
incidental ECG finding and does not require specific treatment.
2nd degree AV block
In 2nd degree AV block, some, but not all, P waves are conducted. Unconducted P waves are not followed by an
associated QRS complex. If there are two or more unconducted P waves for each QRS, the 2nd degree AV block is
considered to be “high grade” and patients are more likely to be symptomatic.
Furthermore, 2nd degree AV block can be subdivided into 2 types:
Mobitz Type 1 (Wenckebach phenomenon): There is gradual lengthening or variation in the PR interval before an
unconducted P wave. The subsequent conducted P wave has a short R-R interval and the cycle repeats itself. This is
a sign of high vagal tone. An atropine response test can help confirm this in small animals.
Mobitz Type 2: There is usually a fixed relationship between conducted P waves and QRS complexes (i.e. the PR
interval does not change) with some unconducted P waves. This typically indicates structural disease affecting
conduction tissues of the AV node. It may progress to 3rd degree AV block. If the disease becomes severe with
many unconducted P waves, the patient is likely to display clinical signs and require treatment.
3rd degree (Complete) AV block
In 3rd degree block, there complete dissociation between P waves and QRS complexes due to severe structural
disease of the conduction system. The SA node continues to drive the atrial rate and P waves are recognized but
162

there is no relationship to the QRS complexes. The atria and ventricles are functioning independently due to absence
of conduction through the AV node and thus the P waves and QRS complexes march back and forth across each
other at independent rates. The QRS complexes arise from the inherent pacemaker activity of the conduction tissues
of AV junction / Bundle of His or the Purkinje fibers of the ventricles, so they these QRS complexes are called
junctional or ventricular escape complexes, since they have escaped the control of the faster SA node. Junctional
escape rhythms start in the His bundle with a rate of approximately 40–80 bpm and the QRS will have a normal
appearance (i.e. supraventricular; narrow and upright in lead II). Ventricular escape complexes have different
morphologies depending on which ventricle they arise from (negative if from the left ventricle, positive if from the
right ventricle) with a slower rate of typically 20-40 bpm. They will also be wide as the wave of depolarization has
to travel from muscle cell to muscle cell, and is unable to utilize the normal conduction pathways. Although the
complexes are ventricular, the rate is slow and these cases must not be treated with antiarrhythmic drugs such as
lidocaine as there is a risk of sudden death if the escape rhythm is suppressed. The escape rhythm does not respond
to atropine administration. Care should be exercised in investigating these patients as sedation especially with an
opioid may generate a life-threatening bradycardia and necessitate emergency pacing.
The cause of 3rd degree AV block is often unknown in many cases but Lyme disease and myocarditis should be
excluded as potential causes. Clinical signs depend on the escape rate, the duration, and the activity level of the
patient however, weakness, exercise intolerance and syncope are common. Right sided congestive heart failure can
develop in chronic cases. There is always a risk of sudden death in patients with 3rd degree AV block and pacemaker
implantation is required to treat this condition. Cats with 3rd degree AV block often have faster escape rhythms (100-
120 bpm) and pacemaker implantation is usually only performed in this species if clinical signs are present.
Sick sinus syndrome (SSS) / Sinus Node Dysfunction
Although the name suggests this is a problem of the sinus node, all impulse generation and conduction at all levels
of the conduction pathway can also be affected. As a result, pronounced sinus arrhythmia with long pauses (6-8 s)
due to sinus arrest is often seen with absence of expected escape complexes. Following such pauses, ventricular or
supraventricular escape complexes may be apparent. Junctional rhythms may also be seen. Sick sinus syndrome is
frequently encountered in older West Highland white terriers, miniature schnauzers and Cairn terriers. These
patients may respond to an oral positive chronotrope drugs. In the miniature schnauzer, a form of SSS with periods
of bradycardia and tachycardia is occasionally seen. Dogs with this ‘brady-tachy’ syndrome may require pacemaker
implantation prior to treatment for their tachycardia. Care should be exercised in investigating these patients as
sedation especially with an opioid may generate a life-threatening bradycardia and necessitate emergency pacing.
Some but not all dogs respond to an atropine response test and this is typically a good indication whether they will
respond to medical management or not since vagal tone is an important determinant in most cases. If patients are
asymptomatic, the term ‘sinus node dysfunction’ is used. Similar to 3rd degree AV block clinical signs include
weakness and syncope. However, unlike 3rd degree AV block sudden death is rare with SSS / sinus node
dysfunction.
Treatment of Bradyarrhythmias
1. Assess if the bradyarrhythmia is vagally mediated (e.g. accentuated sinus arrhythmia, sinus arrest, Mobitz type II
2nd degree AV block). An atropine response test should be performed. Atropine 0.04 mg/kg may be given by IV, IM,
subcutaneous injection and the EGC is reassessed 5-10 mins later (IV injection) or 20-30 mins later (IM or
subcutaneous injection. A positive atropine response is typically characterized by an increase in heart rate > 50%
from baseline with a regular rhythm and a uniform appear to P waves. *Note – following IV administration a brief
reflex bradycardia may be encountered and the bradyarrhythmia may briefly worsen before a positive response is
noted*
2. Life threatening bradyarrhythmias require emergency treatment. Isoproterenol (aka. isoprenaline) infusion can be
administered if available but be aware this can be pro-arrhythmic. This is a beta-1 adrenergic agonist that works to
increase the ventricular escape rate in order to stabilize the patients in the short-term until pacemaker implantation
can be performed
3. Oral treatments often have limited efficacy. If the bradyarrhythmia suspected to be vagally mediated or responds
to atropine, oral anticholinergic drugs (e.g. propantheline bromide) can be used. These are only effective in dogs that
conduct through the AV node as there is no parasympathetic supply to the ventricles. The oral beta-1 adrenergic
agonist (e.g. isoprenaline) may be considered however this is pro-arrhythmic and so may carry increased risk of
163

complications. Therefore, a safer option is use of beta-2 adrenergic agonists (e.g. terbutaline) or xanthine derivatives
(theophylline, aminophylline).
4. Pacemaker implantation can be performed in referral settings. Ultimately many dogs with symptomatic
bradycardias require pacemaker implantation. A permanent pacemaker is the only treatment which is likely to
significantly reduce clinical signs and improve exercise tolerance in patients with significant bradyarrhythmias.
While over 90% of dogs would be expected to survive the procedure, long term survival is guarded as many dogs
are older at the time of diagnosis. Owners should be aware of possible complications which can occur in up to 30%
of dogs. Major complications include lead dislodgement which usually occurs within one month of implantation and
infection which requires replacement of the entire pacing system. Occasionally a seroma can develop over the
generator site and this should be treated with rest and light pressure bandage, not drainage. Lead perforation rarely
occurs. Owners and referring veterinarians should be advised that the dogs with permanent transvenous should never
have a blood samples collected from the jugular veins and they should not use neck leads or collars as these may
cause lead fracture. In cats and small dogs, endocardial leads may obstruct the entrance of the thoracic duct leading
to a chylothorax. As a result, an epicardial lead is sutured directly to the myocardium via a transdiaphragmatic
approach and the pacemaker secured in the abdomen. Patients are reevaluated after one month and the rate response
mode activated. Beyond that annual rechecks are recommended to ensure appropriate functioning of the device.
Effect of Electrolyte Abnormalities on the ECG
The depolarization of the heart is a result of potassium, sodium and calcium movements across the myocardial cell
membrane. Changes in the levels of potassium or calcium can cause changes to the surface ECG.
Potassium
Increased potassium concentrations cause ECG changes that increase with increasing concentrations although the
potassium concentration cannot be predicted accurately from the changes as other electrolytes or acid/base changes
play a role.
Typically, the following progression is observed:
• Mild hyperkalemia: Spiked tall T waves
• Moderate hyperkalemia: Small P waves, tall T waves and bradycardia
• Severe hyperkalemia: Loss of P waves (see atrial standstill) with a sinoventricular rhythm – the SA node still
depolarizes but the atria do not. The impulse is transmitted to the AV node via specialized atrial conduction
pathways. There is bradycardia and a wide QRS with right bundle branch block pattern eventually looking like
a sine wave.
Decreased potassium levels rarely cause ECG changes but could result in T prolongation, prominent U waves and
intermittent AV dissociation.
Calcium
Calcium is important for contraction of the cardiac myocyte. Increased levels shorten the duration of phase 2 of the
action potential shortening the QT interval while low levels prolong the QT interval. Hypocalcemia can also result
in tachycardia and tall R waves.
164

Identification & management of cardiac disease in cats
Michael Aherne, MVB, GradDipVetStud, MS, MANZCVS (Small Animal Surgery), DACVIM (Cardiology)
Department of Small Animal Clinical Sciences
College of Veterinary Medicine
University of Florida, Gainesville, Florida
Hypertrophic Cardiomyopathy
HCM is a primary myocardial disease characterized by concentric hypertrophy that is not due to a pressure overload
or hormonal stimulation and, therefore, it is a diagnosis of exclusion. HCM is typically confined to the left ventricle
although both ventricles may be affected. It is very common in cats and very rare in dogs. Concentric hypertrophy is
characterized by thickened walls with a normal chamber size or small chamber size. It can be classified as either
primary hypertrophy or secondary hypertrophy. Primary hypertrophy refers to HCM likely due to underlying genetic
mutation. Secondary hypertrophy occurs as a result of various conditions including hyperthyroidism, systemic
hypertension, aortic stenosis, hyperadrenocorticism, acromegaly and neoplastic infiltration.
There can be tremendous variation in the appearance of ventricular hypertrophy in cats with HCM. Some cats may
have classic diffuse hypertrophy, while others may have more segmental hypertrophy. HCM is often familial and
inherited in humans and in many cases has been shown to be due to a mutation of one or more sarcomeric genes
(genes that encode for the contractile apparatus in the myocardial cell). In cats, HCM has been shown to be familial
in the Maine Coon and Ragdoll breeds, inherited in an autosomal dominant manner. The genetic mutation has
recently been identified in Maine Coons and Ragdolls to be a missense mutation in myosin binding protein C.
Testing is now available through a cheek swab test kit through NC State Genetics Lab. Test kits can be ordered on
line and are able to detect both the heterozygote and homozygote state. HCM also appears to be inherited in an
autosomal dominant manner in American Shorthairs and British Shorthairs. Other predisposed breeds include
Persians, and Rex breeds. HCM is most commonly detected in the domestic shorthair with the cause unknown but
suspected to also be genetic in origin. Cats are usually middle aged to older; however, the disease may be diagnosed
at a young age especially in the purebreds.
Coronary flow and therefore myocardial perfusion occurs mostly during diastole. Because of the hypertrophy and
increased diastolic filling pressure, blood flow to the endocardium is diminished. Additionally, cats with HCM have
“small vessel disease” where the walls of the coronary arteries are thickened and the lumen of the vessel decreased
in size, decreasing blood flow even further. The major lesions of wall thickening included degeneration or
denudation of endothelium, subendothelial edema, proliferation of collagen fiber, and hyperplasia of smooth muscle
cells. This is yet another factor adding to the pathology and myocardial dysfunction in cats. These various factors
lead to a decrease in myocardial perfusion, ischemia and eventually fibrosis, thus adding to the disease process.
Pathophysiology of CHF with HCM
Concentric hypertrophy can result in increased ventricular stiffness and slow myocardial relaxation which are both
components of diastolic dysfunction, the major abnormality in this disease. Systolic function is normal. When the
heart relaxes incompletely and is stiff, intracardiac diastolic pressures rise. This increase in pressure is transferred to
the pulmonary vasculature and pulmonary edema can result. The concentric hypertrophy not only makes the
ventricle stiffer than normal, but it also can encroach on the LV chamber, making it smaller. This reduces end-
diastolic volume, which may reduce stroke volume. As with other diseases, a decrease in stroke volume translates to
decreased perfusion which stimulates the renin angiotensin aldosterone system to cause fluid retention.
Mitral valve systolic anterior motion (SAM) is present in many patients with HCM (but typically not in cats with
other cardiomyopathies). Abnormal papillary muscles and altered left ventricular geometry cause the septal leaflet of
the mitral valve to be flipped back towards the LV outflow tract during systole, and thus, two consequences occur:
1) mitral regurgitation and 2) obstruction of left ventricular outflow to the aorta. When left ventricular outflow tract
obstruction is identified in patients with HCM the term hypertrophic obstructive cardiomyopathy (HOCM) is
sometimes used. The degree to which these abnormalities contribute to increased intracardiac pressures and the
165
development of heart failure is debated, however they may worsen the situation. Additionally, reduced stroke
volume stimulates RAAS to cause volume expansion.
Restrictive Cardiomyopathy (RCM)
Restrictive cardiomyopathy (RCM) is a feline cardiac disease whereby endocardial or myocardial disease in the
absence of significant hypertrophy restricts ventricular filling. The major abnormality is diastolic dysfunction
(systolic function is normal or only mildly diminished). This is often diagnosed when the left ventricle appears
normal or only mildly hypertrophied on echocardiographic examination however the atria (one or both) are very
enlarged. Mild to moderate mitral insufficiency is usually present. Fractional shortening is usually normal or mildly
depressed. Doppler echocardiographic interrogation of mitral and pulmonary venous inflow is useful in diagnosing
restrictive physiology but can be time consuming and difficult to perform. Treatment and prognosis for RCM is
similar to HCM.
Pathophysiology of RCM
The hallmark of RCM is also diastolic dysfunction, but it is different from the diastolic dysfunction of HCM. Early
diastolic filling is impeded and slow in HCM. In RCM, early diastolic filling is rapid but is then suddenly restrained,
impeded by rigid ventricular walls or endocardium that impairs myocardial elasticity. The end result, elevated filling
pressures, is similar to HCM but the mechanism of how it occurs is different.
Regardless of stage, in addition to thorough physical examination, diagnosis generally necessitates
echocardiography to determine the presence, type, and severity of cardiomyopathy. Thoracic radiographs are
indicated in patients with stage C disease for detection and quantitation of pulmonary edema or pleural effusion, but
have poor sensitivity in stage B feline cardiomyopathy. Electrocardiography (ECG) is indicated if an arrhythmia is
auscultated. Biomarkers such as NT-proBNP may play a role in the detection of preclinical (stage B)
cardiomyopathy, or in the differentiation of cardiac from respiratory disease in cats presenting with respiratory
signs.
Arrhythmogenic Right Ventricular Cardiomyopathy
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is seen very infrequently in cats and there is no known
underlying genetic cause identified. It is characterized by atrophy and fibrofatty replacement of the right ventricular
free wall and rarely the left ventricle. Echocardiography shows a dilated RV with a thin wall. Tricuspid regurgitation
may also be present because of annular dilation. This has therefore led to the misdiagnosis of tricuspid dysplasia in
these cats. Some of these cats also have supraventricular and ventricular arrhythmias. Histologically, there is
myocardial degeneration and necrosis with fibrous and fatty infiltration of the myocardium. These changes tend to
be more severe in the right ventricular free wall, but may also involve the interventricular septum and left ventricular
free wall. Although ventricular arrhythmias are considered a hallmark of the disease, especially in dogs, progressive
myocardial failure appears to be the more predominant manifestation of this disease in cats. The prognosis for cats
with ARVC has not been well established but is typically considered to be guarded-to-poor since many cats present
in right-sided congestive heart failure.
Diagnosis
Cats with ARVC may present with signs of right-sided congestive heart failure. They may also present with syncope
or collapse secondary to ventricular arrhythmias or may be asymptomatic. On physical exam, many affected cats
will have auscultable arrhythmias with associated pulse deficits. This may be the only sign of ARVC, but some may
present in a sustained tachycardia with poor pulses and cardiogenic shock. There are no standardized
recommendations for the diagnosis of ARVC in cats. Echocardiographic findings are usually diagnostic for ARVC
in cats and consist of RV eccentric hypertrophy, pleural and/or pericardial effusion, septal flattening and LV volume
underload. It is often possible to identify ventricular premature complexes (VPCs) as singles, couplets, or runs on a
routine ECG. Most commonly the VPCs are of a left bundle branch block configuration which is consistent with a
right ventricular origin, but this is not always consistent.
Dilated Cardiomyopathy (DCM)
Historically feline DCM was the 2nd most commonly diagnosed feline cardiomyopathy. Two major forms of feline
DCM exist: 1) idiopathic DCM and 2) taurine deficient DCM. Since the late 1980s, following identification of the
166

link between taurine deficiency and development of DCM with subsequent taurine supplementation in commercial
cat foods, feline DCM is now uncommon and idiopathic DCM now accounts for the majority of cases identified.
The hallmark of dilated cardiomyopathy is systolic ventricular dysfunction with secondary eccentric hypertrophy of
the left ventricle. There is often no identifiable cause for feline DCM and the myocardium may be grossly normal on
echo, there are histological changes including muscle cell atrophy, wavy attenuated appearance of the myocytes, and
fibrous or fibro-fatty myocardial replacement. Additionally, there may be small areas of myocardial degeneration,
necrosis, and fibrosis.
In some cats, DCM is actually an end-stage progression of HCM. As HCM progresses, the myocardial hypertrophy
can result in myocardial ischemia (by outgrowing and/or compression its coronary blood supply). This then may
result on myocyte necrosis with replacement fibrosis. Since fibrous tissue does not have contractile function, systolic
myocardial dysfunction develops. As the myocardial failure progresses, the compensatory mechanisms are
overwhelmed and heart failure occurs. Most patients demonstrate predominant signs of left-sided heart congestive
heart failure, but right-sided or biventricular heart failure may also occur.
Arrhythmias may occur in feline patients with DCM however this appears to occur at a lower frequency than
observed in dogs with DCM. When present, these arrhythmias may contribute considerably to morbidity and
mortality. Ventricular arrhythmias appear to be more common although, rarely, atrial fibrillation may be
documented in some cats.
The prognosis for cats with DCM depends on the underlying cause. For cats with taurine deficient DCM, prognosis
is usually excellent with treatment however this cause is rarely seen nowadays. For idiopathic DCM, prognosis is
typically guarded-to-poor since many cats present in left-sided congestive heart failure. Prognosis is usually very
poor in those with DCM secondary to end-stage HCM with replacement fibrosis of the myocardium.
Non-specific Cardiomyopathy (Formerly Unclassified Cardiomyopathy [UCM])
Unless one can actually demonstrate this restrictive pattern of filling or endomyocardial fibrosis, the term non-
specific cardiomyopathy is used. This is just a “catch-all” term for those feline cardiac diseases which do not fit
perfectly into any other category and restrictive physiology cannot be diagnosed. These cats do not demonstrate
‘typical’ features of HCM but also do not fit ‘perfectly’ into any other category such as DCM. Non-specific
cardiomyopathy probably represents a variety of etiologies. Treatment and prognosis for non-specific
cardiomyopathy is similar to HCM.
TREATMENT
In comparison to canine cardiac disease, far less is known or established about the treatment of feline cardiac
disease. Treatment of feline cardiac disease is largely dictated by clinician preference and experience, more so than
evidence-based therapy.
Treatment of Stage B Feline Myocardial Disease (Preclinical)
The benefit of any therapy in stage B feline cardiomyopathy remains unsubstantiated and controversial. Therapies
that have been of interest, either in the past or presently, have included calcium channel blockers, beta blockers,
ACE-inhibitors (ACEi), aldosterone-antagonists such as spironolactone, and anti-thrombotic therapy. However, the
reality is that it is no therapy has been proven to delay the progression of disease, diminish risk of complications, or
improve survival in cats with stage B cardiomyopathies.
There is a lot of debate amongst veterinary cardiologists as to the use of beta blockers in feline myocardial disease.
Beta blockers (e.g. atenolol) may sometimes be used in cats with HOCM when there is evidence of moderate to
severe dynamic LV outflow obstruction, or significant ventricular arrhythmias. Again, they have not been proven to
improve survival in feline patients with HOCM. Beta blockers are used in humans with HOCM exhibiting exercise
intolerance, and symptomatic improvement is noted in 60-80%. They reduce heart rate, wall stress, myocardial
oxygen demand, and left ventricular outflow tract obstruction, and have anti-arrhythmic properties. Achieving an in-
hospital heart rate of 150-160 bpm is often used as a therapeutic target in cats, in addition to demonstrating a
reduction in dynamic LV outflow tract obstruction on echocardiography. Caution must always be used in using beta-
blockers in patients with systolic dysfunction.
167

The rationale for ACEi or spironolactone is their potential to decrease myocyte hypertrophy and fibrosis via
blockade of the renin-angiotensin-aldosterone system. This could in theory benefit cats with any type of primary
cardiomyopathy. While they have only been evaluated in few small studies in cats with HCM, and not in other forms
of feline cardiomyopathy, they have not been shown to be beneficial in stage B HCM. In one small study,
approximately 30% of cats taking spironolactone developed a severe ulcerative facial dermatitis that resolved with
drug discontinuation. Most veterinary cardiologists do not use spironolactone or other aldosterone antagonists in
stage B feline cardiomyopathy.
While calcium channel blockers (diltiazem) were used commonly in the past for their potential effects on heart rate,
ventricular relaxation and filling, they have fallen out of favor due to lack of evidence of efficacy. They are no
longer used in stage B feline HCM, with the rare exception being for treating some supraventricular
tachyarrhythmias.
Cats with left atrial dilation may be at increased risk for thromboembolic disease and thus may be candidates for
anti-thrombotic therapy, such as clopidogrel or aspirin, with the former often being favored. Cats that are difficult to
medicate may be candidates for aspirin since it is administered only once every 3 days as opposed to daily. It is
worth noting, however, that there are no studies evaluating the efficacy of drugs in primary prevention of feline
thromboembolic disease (prevention of a first occurrence of thromboembolism). It is also worth noting that, to date,
none of the commonly used anti-platelet drugs have ever been compared to placebo and so the utility of anti-platelet
therapy remains unclear.
Treatment of Stage C Feline Myocardial Disease (CHF)
Therapy in this stage is directed at minimizing of clinical signs related to pulmonary edema or pleural effusion while
maintaining adequate cardiac output, minimizing risk of thromboembolic disease, blocking deleterious effects of
RAAS activation known to contribute to progression of CHF, and improving survival. Most feline cardiomyopathies
result in CHF through progressive diastolic dysfunction, and systolic function may be preserved. Alternatively, some
cases may experience systolic dysfunction if there is profound ischemia, as may occur in HCM, or in the case of
DCM or ARVC.
Furosemide is indicated in CHF due to any feline cardiomyopathy. Oral dosing may be used immediately in stable
patients with mild heart failure, whereas parenteral dosing (IV or IM) may be required in more severe or unstable
cases. The goal is to eventually find the lowest effective dose to keep the patient free of clinical signs. Recognize
that doses are typically less than those used and required in dogs. Thoracocentesis should be performed to relieve
tachypnea or dyspnea due to substantial pleural effusion as diuretics will have no effect in resolving effusions that
are already present. Furosemide is then prescribed to delay the reaccumulation of effusion.
Angiotensin converting enzyme inhibitors are routinely used to counteract the RAAS activation that is inherent to
CHF and induced by diuretic administration. Nevertheless, evidence that ACEis improve morbidity or mortality
beyond furosemide alone in cats with CHF is lacking. Despite this, their use is advocated by most veterinary
cardiologists in stage C feline cardiomyopathy of any types once the patient is stable and eating, and assuming there
is not significant preexisting azotemia.
While beta blockers may have theoretic benefits in diseases characterized by diastolic dysfunction (reduction in
heart rate to aid ventricular filling and coronary perfusion, anti-arrhythmic properties), there are legitimate concerns
about the use of beta blockers in cats with active CHF. This coupled with the lack of evidence of impact on
morbidity and mortality have limited their use in these patients. They should not be used in cats with moderate to
severe edema or effusion. They may only be indicated and cautiously up-titrated in cats with significant LV outflow
obstruction (identified on echocardiography) who are stable and exhibiting only mild congestion. Heart rate and
blood pressure monitoring within 7-10 days is indicated, targeting an in-hospital heart rate of roughly 150-160 bpm.
Another indication may be significant supraventricular or ventricular tachyarrhythmias. In cats already on atenolol
(initiated in stage B), it does not necessarily need to be discontinued. If the cat is stable, does not have severe
pulmonary edema, has heart rate > 150 bpm, and normal blood pressure, then it is possible to continue beta blocker
therapy assuming it was initially initiated for LV outflow obstruction. If, however, there is relative bradycardia, low
blood pressure, development of systolic dysfunction, or severe pulmonary edema, then the dose should be at least
reduced by half if not discontinued.
The role of pimobendan in cats with CHF due to HCM is unclear and caution should be exerted, especially
considering the vastly different pharmacokinetics in cats relative to dogs despite similar doses. Recall that many
168

feline cardiomyopathies are characterized primarily by diastolic dysfunction and not systolic dysfunction, with
pimobendan being targeted at the latter since it is a positive inotrope, hence calling into question its therapeutic
rationale in most cases of HCM. Furthermore, it may be expected to exacerbate cases with LV outflow obstruction
(obstructive HCM). Surprisingly, two retrospective studies have suggested improved survival times in cats with
CHF treated with pimobendan, however a prospective study showed no survival benefit beyond furosemide when
compared to placebo in cats with CHF secondary to both non-obstructive and obstructive forms of HCM. Thus,
caution should still be exercised, particularly if it is uncertain whether LV outflow obstruction exists or not.
Cats with stage C cardiac disease will generally have marked left atrial dilation and often poor atrial contractile
function, rendering them at risk for thromboembolic disease. There are no studies evaluating the efficacy of primary
prevention of thromboembolic disease in cats, however the FATCAT trial evaluated the efficacy of clopidogrel vs
aspirin in secondary prevention (prevention of a secondary occurrence in cats that had survived a first occurrence).
Clopidogrel was associated with significantly reduced risk of thromboembolism recurrence, longer time to
recurrence, and longer time to composite endpoint of cardiac death or embolism recurrence. This has rendered
clopidogrel the favored anti-thrombotic drug for many clinicians.
Treatment of Stage D Feline Myocardial Disease (Refractory CHF)
The options for treating cats with heart failure refractory to therapy above are generally much more limited than for
dogs. Strategies may include:
Alternative approaches to furosemide administration
a. Increasing frequency of administration
b. SQ therapy – many owners can be taught how to administer
c. Short term IV therapy either by bolus or constant rate infusion in hospital to correct an acute-on-chronic crisis
Addition of adjunctive therapies
a. Spironolactone, particularly if hypokalemic
b. Pimobendan, while maintaining caution if using in HOCM patients
Sodium restriction
There is little data in cats as to the tolerability or efficacy of sodium restriction in patients with CHF.
Monitoring and Follow-up
For asymptomatic cats with stage B cardiomyopathy, monitoring cardiac structure and function with
echocardiography is suggested at roughly 6-12 months. More frequent evaluation may be indicated when reassessing
the effect of beta blocker therapy in obstructive HCM. Heart rate and blood pressure monitoring 1-2 weeks after beta
blocker initiation is recommended. Owners can be counseled on home respiratory rate monitoring for cats with left
atrial dilation in whom heart failure may be a foreseeable future outcome.
For cats with CHF, following the initiation of medication, reevaluation of renal biochemistry and electrolytes, blood
pressure, and thoracic radiography is indicated within 1-2 weeks. Thereafter, rechecks should be regularly scheduled
anywhere from weeks to months apart, dependent on the patient’s clinical status and any changes to therapy.
Echocardiography continues to be a useful means to monitor severity of disease, degree of outflow obstruction,
systolic function, and thromboembolic risk. One critical and ongoing goal is the balance of hydration/perfusion and
edema/effusion status. Diuretic doses are adjusted upwards or downwards based on patient need, and sometimes
other medication doses need to be optimized to improve perfusion. Additional means of increasing oral water intake
may be necessary in patients with pre-renal azotemia. Addition of a potassium supplement may be necessary in
hypokalemic patients.
169

Feline arterial thromboembolism
Michael Aherne, MVB, GradDipVetStud, MS, MANZCVS (Small Animal Surgery), DACVIM (Cardiology)
Department of Small Animal Clinical Sciences
College of Veterinary Medicine
University of Florida, Gainesville, Florida
Pathophysiology
According to Virchow’s triad there are 3 factors that predispose to thromboembolism, which are:
1) endothelial injury,
2) stasis of blood flow, and
3) hypercoagulability.
A common finding in cats with nearly all types of cardiac disease is left atrial enlargement. Blood flow can become
sluggish in the enlarged LA and predispose to thromboembolism (ATE). When blood flow slows, red cells, platelets
and factors clump together. Some studies have suggested that feline platelets are hypercoagulable. This may explain
why it is very uncommon for dogs with dilated cardiomyopathy to develop ATE even though blood flow stasis
probably occurs in their enlarged atria as well. Another study suggested that cats with thrombosis are
hypercoagulable due to high levels of homocysteine. The syndrome is not entirely understood; occasionally, cats
without any cardiac disease may develop ATE and conversely, not all cats with severe cardiac disease develop ATE.
Due to the factors described above, thrombus formation therefore most likely occurs in the left atrium and auricle of
cats with cardiac disease. The thrombus may then stay in the LA or it can dislodge and result in embolization of an
artery of smaller diameter than itself.
The most common sites of arterial thromboembolism are (in descending order of frequency):
1. Aortic trifurcation – this causes hind limb paralysis, AKA the “saddle thrombus”. This can be partial with only
one back leg affected or one leg affected worse than the other. Partial occlusion is due to smaller clots lodging more
distal in the aortic trifurcation.
2. Brachial arteries – this results in paralysis of a forelimb. Typically, the right forelimb is more commonly affected
than the left forelimb.
3. Cerebral, myocardial, renal, mesenteric arteries etc.
Studies have been performed showing that the distal aorta can be ligated in cats. These cats are not painful and can
walk after surgery because collateral vessels open up to carry arterial flow to distal sites. Therefore, obstruction to
flow does not explain clinical findings entirely. The clinical disease can be reproduced if a thrombus is placed in the
aorta, resulting in the release serotonin and thromboxane A2 which cause intense vasoconstriction of collateral
vessels. Once the vessel is embolized, the tissues distal to the embolism become hypoxic and significant damage
occurs to the muscles and nerves.
Natural thrombolysis can occur after the acute event, however the time is variable and depends on the size of the
embolus. Function of the limb may be regained within hours or never and complications are dependent on this time
frame.
Co-Morbidities
At presentation, some cats with ATE may have evidence of underlying cardiac disease (eg, murmur, gallop rhythm,
or arrhythmia). Nevertheless, in cats, absence of auscultation abnormalities does not preclude underlying cardiac
disease. Furthermore, the presence of a gallop sound in cats with ATE has been associated with reduced survival.
Concurrent CHF is present in approximately 40-65% of cats with ATE. Tachypnea and open-mouth breathing may
also be manifestations of acute pain as a result of ATE.
170

Many cats with ATE are hyperglycemic, due to epinephrine and cortisol release. Azotemia is also frequently
encountered, which may be prerenal or renal in etiology with BUN elevation typically encountered more frequently
and tends to be more severe than creatinine elevation. The BUN:Creatinine ratio may be elevated. Prerenal azotemia
in these cats occurs in response to poor systemic perfusion and shock. Renal azotemia occurs as a direct
consequence of renal ATE. Serum creatinine kinase is often severely elevated because of muscle ischemia.
Hyperphosphatemia is also frequently encountered. Hyperkalemia, which can be severe and life-threatening, may
result from reperfusion injury and is one of the most significant complications of ATE as perfusion to affected
tissues is restored and, although it is most often seen following treatment of the ATE, some cats may have this
abnormality at presentation.
Diagnosis
Appendicular ATE in cats can typically be diagnosed on the basis of physical examination alone. There are 5
cardinal signs that are associated with appendicular ATE (the 5 P’s), which are pain, paralysis/paresis, pulselessness,
pallor, and poikilothermy (cold extremities). Affected limbs are painful, and the muscles are often firm. Patients
display lower motor neuron signs in affected limbs with severity ranging from mild paresis to complete paralysis.
Up to 34% of cats with ATE will have some motor function in affected limbs with the likelihood of this being higher
for embolic events affecting the forelimbs or unilaterally affecting a single hindlimb. Doppler flow evaluation and
differential measurements of blood glucose and serum lactate between affected and unaffected limbs may also
provide supportive evidence of ATE. In peripheral venous blood samples from affected limbs, blood glucose is
lower and lactate is higher than that in venous samples from nonaffected limbs or central veins.
Treatment
Emergency Stabilization
Most cats with ATE are extremely painful and distressed. Supplemental oxygen should be provided to dyspneic
patients. Prompt and effective analgesia with full-mu opioids should be administered as soon as possible. Various
prognostic factors should be considered when deciding to proceed with treatment versus euthanasia, all of which
should be clearly discussed with clients. Factors associated with non-survival include rectal temperature < 98.6°F),
bradycardia, absent motor function, having more than 1 limb affected, and concurrent CHF.
Most cats with ATE will have signs of shock and poor systemic perfusion, which should be quickly addressed.
These signs may be the result of maldistributive shock secondary to tissue ischemia distal to the embolus and the
resultant release of vasoactive substances, cardiogenic shock secondary to significant cardiac disease, or a
combination of both and approaches for correcting systemic perfusion will therefore vary according to the
underlying cause. For dehydrated cats without CHF, fluid therapy may be considered, although great care must be
taken when administering IV fluids to any patient with cardiac disease. Positive inotropes such as pimobendan
(extra-label) 0.3 mg/kg PO may therefore be a better option for patients with cardiac compromise with or without
CHF. Although it may seem desirable to attempt to actively warm these hypothermic patients, warming should be
avoided until the patient’s systemic perfusion has been corrected because active warming results in peripheral
vasodilation, which will divert more blood away from the core organs and therefore worsens core perfusion and the
effects of shock.
Short-Term ATE Therapy
Once stabilized, antithrombotic therapy should be initiated. Antithrombotic therapies are given to prevent
propagation of existing thrombi and prevent development of new thrombi however these drugs do not cause lysis of
existing thrombi. Treatment with low–molecular weight heparin (e.g. dalteparin 75 to 150 U/kg SC q6h) or
unfractionated heparin (250 to 300 U/kg q6h) is recommended, although data regarding clinical outcomes with these
medications for acute ATE management are lacking. Heparin therapy is typically discontinued 2 to 3 days after the
patient has been stabilized and is receiving oral anti-thrombotics. Once oral medication is tolerated, clopidogrel
should be started. An initial loading dose of 75 mg PO per cat is recommended, followed by a maintenance dose of
18.75 mg PO per cat q 24h. Clopidogrel tablets are bitter-tasting to cats and it is recommended to administer this
drug in gelatin capsules although flavored oral liquid formulations appear to be well-tolerated.
Analgesia should be continued, and the patient should be regularly assessed for pain. For most cats, pain greatly
eases after the first 24 to 48 hours. At this time, buprenorphine (a partial mu opioid receptor agonist) may be
sufficient for analgesia; it can also be used for cats with only mild ATE signs at presentation. To minimize the risk
171

for muscle contracture, physiotherapy exercises such as passive manipulation of affected limbs should be started as
soon as the patient is stabilized and pain is well controlled.
Perhaps the most significant complications in cats receiving treatment for ATE are severe, life-threatening
hyperkalemia and acidosis as a result of reperfusion injury to the tissues. For the first 48 to 72 hours after
presentation, ATE patients should be closely monitored for these biochemical derangements, which should be
rapidly addressed with appropriate therapies (eg, administration of dextrose, insulin and dextrose, calcium
gluconate, or sodium bicarbonate, as indicated).
Long-Term ATE Therapy
Clopidogrel (18.75 mg/cat q 24h) should be continued because it has been shown to be clinically superior to aspirin
for the secondary prevention of ATE. For cats severely affected by ATE or those with recurrent episodes of ATE,
low–molecular weight heparin or unfractionated heparin therapy can be continued long-term at home however this
approach is limited by cost and compliance. Since most cats with ATE have underlying cardiac disease, appropriate
management of clinical consequences of heart disease is necessary.
Prognosis
Long-term prognosis for cats with ATE is generally guarded to poor but may vary, depending on the clinical
severity and the precise underlying cause. Overall survival rates of approximately 30% to 40% and even as high as
73% have been reported however, these higher survival rates were observed in referral practice settings, which may
introduce a referral bias. Nevertheless, survival rates in cats with only a single limb affected are as high as 70% to
80% and even up to 90% if some motor function remains at presentation. In many cases, the clinical signs of ATE
significantly improve after the first 24 to 48 hours of therapy. In particular, the need for analgesia often reduces
significantly after this initial period and underscores the need for effective analgesia from the time of presentation.
Of cats that survive the first 48 to 72 hours, many will regain some or even all motor function within 1 to 2 months.
For these reasons, it may be prudent to encourage clients to at least consider therapy for the initial 72 hours, in order
to better determine the patient’s prognosis. Negative prognostic indicators include presence of a gallop heart rhythm,
reduced heart rate, previous occurrence of ATE, having 2 or more limbs affected, and rectal temperature lower than
98.6°F.
Several long-term complications may result as a consequence of ATE. Muscle contracture can occur but may be
avoided by performing physiotherapy both during hospitalization and at home following discharge. Occasionally,
some patients may experience skin necrosis and skin sloughing on affected limbs as a result of ATE-induced
ischemia with lesions sometimes becoming apparent only after several days. These lesions may be localized (e.g.
digits) but may also affected larger portions of skin which may require surgical treatment. For some cats with ATE,
perfusion may be so poor that entire limb necrosis necessitates limb amputation. In cats with persistent neurologic
deficits, dragging of the limbs may lead to excoriations on the paws, and some cats may self-traumatize affected
limbs. For these cats, gabapentin may be of some use for managing neuropathic pain, although its role in the
management of cats with ATE has not been clinically investigated.
172

Non-inherited dilated cardiomyopathy phenotypes in dogs
Michael Aherne, MVB, GradDipVetStud, MS, MANZCVS (Small Animal Surgery), DACVIM (Cardiology)
Department of Small Animal Clinical Sciences
College of Veterinary Medicine
University of Florida, Gainesville, Florida
Causes of Secondary Myocardial Failure
The pathophysiology, diagnosis, and treatment for secondary causes of myocardial failure are similar to primary
DCM, except that treatment should involve correcting the underlying cause. Prognosis with adequate treatment is
often much improved. Some causes of secondary dilated cardiomyopathy phenotypes in dogs and cats are listed
below:
Nutritional / Diet-Associated
• Taurine deficiency
• Carnitine deficiency
• Possibly certain boutique, exotic-ingredient and/or grain-free (BEG) diets
Myocarditis
• Viral – parvovirus, distemper
• Bacterial – Lyme disease
• Protozoal – Trypanosoma cruzi
• Fungal
• Inflammatory
Toxic
• Doxorubicin
Metabolic
• Hypothyroidism
• Hyperthyroidism
Tachycardia induced
Ischemic / Myocardial Infarction
Infiltrative
• Neoplastic
• Glycogen storage diseases
Hypertensive
Nutritional / Diet Associated DCM Phenotypes
Recently, concerns for potential associations between boutique, exotic and/or grain-free (BEG) diets have been
raised however the nature of these associations are still unclear and definitive causative factors have not been
established. In the absence of firm data to confirm or refute such possible associations, it may be prudent to
recommend the feeding of scientifically-supported, nutritionally-balanced diets that meet AAFCO recommendations
in accordance with the guidelines of the WSAVA Global Nutrition Committee.
Taurine deficiency
Taurine is an amino acid with many functions in many tissues including the myocardium and retina. Taurine is not
an essential amino acid in dogs and is not a common cause of myocardial failure in most dog breeds. However, there
173

are a few breeds in which individuals have been identified as taurine deficient; in these individuals, taurine
supplementation reverses myocardial failure and heart failure.
Taurine is an essential amino acid in cats and prior to this recognition, DCM was commonly seen in cats. This has
become a very uncommon cause of feline cardiac disease since taurine deficiency was discovered to be the cause
and commercial cat foods have been supplemented with taurine since the late 1980s. DCM is still occasionally seen
in cats however, but is most often not the result of taurine deficiency
Some American cocker spaniels with myocardial failure were found to respond to a combination of taurine and
carnitine supplementation and at least some respond to taurine alone. Cardiac function may not entirely normalize,
but enough improvement typically occurs that cardiac medications may be discontinued. Some Golden retrievers
and Newfoundlands with myocardial failure have also been found to be taurine deficient. In the 1990’s, some
Dalmations being fed Hill’s u/d diet for urate stones developed taurine deficient myocardial failure. Since then, the
diet has been supplemented with taurine and the incidence has decreased in this breed. All dogs and cats with
myocardial failure of the above breeds in addition to breeds not predisposed to DCM should be tested for taurine
deficiency.
Whole blood and plasma taurine levels can be measured and are diagnostic for a deficiency. Since results may take
weeks to return and these patients are often in congestive heart failure, it is prudent to begin supplementation
immediately. Once taurine supplementation is implemented improvement in cardiac function occurs over several
months.
Carnitine deficiency
Carnitine is responsible for transporting fatty acids into the mitochondria and deficiency results in myocardial
energy depletion and myocardial failure. While decreased myocardial carnitine levels have been found in several
cardiac diseases including DCM, this is a secondary abnormality and supplementation typically causes little to no
improvement in myocardial function. Systemic carnitine deficiency is a cause of myocardial failure, but this is a
very rare in dogs. One family of boxers with carnitine deficiency has been identified. In American cocker spaniels
the role of carnitine has not been completely explained, but it appears that some need both taurine and carnitine to
reverse myocardial failure.
Carnitine testing is difficult since tissue and not blood levels are most important and this requires myocardial biopsy.
In the above breeds, a 3-month trial supplementation of L-carnitine may be recommended and then response is
assessed by echocardiography. If myocardial function improves, supplementation is continued, but if not, it is
discontinued. Since L-carnitine is expensive this trial is not generally recommended for other breeds.
***It is important to note that L-carnitine is the physiologically active isomer. D-carnitine is not safe as it may
interfere with physiologic processes. Therefore, only L-carnitine must be administered.***
Myocarditis
Myocarditis is characterized by the presence of myocardial necrosis or degeneration and inflammation. Various
physical, chemical, and infectious agents can damage the myocardium, causing an inflammatory response that can
result in chamber enlargement, myocardial systolic dysfunction, and a variety of tachyarrhythmias and
bradyarrhythmias. Plasma cardiac troponin I (cTnI) levels are often elevated early in the disease course, suggesting
myocardial injury. However, these elevated cTnI levels rapidly decline within days of the initial insult and may be
normal by the time clinical signs are noted and a DCM phenotype is identified. Thus, normal cTnI levels do not
preclude myocarditis as the cause of a DCM phenotype in an atypical breed. In the dog, protozoal and viral
organisms are reported most commonly.
Chaga’s disease
This form of myocarditis is caused by the protozoan parasite Trypanosoma cruzi after dogs ingest the insect vector
(Triatomine [aka ‘kissing’] bugs) or infected reservoir host (opossum, armadillo, raccoons, mice, squirrels). The
incidence is relatively low and infected dogs are usually from Texas or other regions of southern North America.
The parasite enters the myocardium and multiplies rapidly, resulting in biventricular dilation and dysfunction,
although often the right sided is more severely affected. Chaga’s disease is characterized by three separate phases:
acute phase, latent or indeterminate phase, and chronic phase. In the acute phase, adult dogs may present with mild
non-cardiac signs including: depression, fever, anorexia, or lymphadenopathy. However, young dogs (< 1 year) will
develop signs of acute myocardial failure including: arrhythmias, collapse, fulminant congestive heart failure, and
174

sudden death. Neurologic signs have also been rarely reported. Survivors of the acute phase will enter the latent
phase of the disease. Patients in the latent phase do not display clinical signs and have no evidence of the parasite in
their blood stream. Physical exam and echocardiographic findings are often normal however, these patients may
present with ventricular arrhythmias. The chronic phase is the end-stage manifestation of the infection and not all
dogs will progress into the chronic stage, which is characterized by biventricular myocardial dilation with or without
arrhythmias. Time to progression to this stage is variable and was reported to develop in 8-36 months in
experimental young dogs post-inoculation. Clinical signs in the chronic phase include: right sided and/or
biventricular heart failure, bradyarrhythmias often requiring permanent pacemaker therapy, and tachyarrhythmias
particularly ventricular tachycardia and occasionally atrial fibrillation. Diagnosis is based on appropriate clinical
signs, corroborating diagnostic tests (ECG, echo, cTnI), and immunofluorescence assay (IFA). IFA titers > 1:80
considered positive. Therapy for Chaga’s disease is symptomatic: controlling heart failure and systolic dysfunction,
antiarrhythmic medications, and pacemaker implantation.
Other Protozoal Organisms
Other reported protozoal organism known to cause myocarditis include: Leishmania in the Mediterranean basin,
Neospora caninum, and Toxoplasma gondii. These organisms infect the myocardium and cause an intense
inflammatory response with myocyte destruction and edema.
Parvovirus
This is an uncommon cause of myocarditis in dogs. There is a per-acute form that affects puppies between 3 and 8
weeks of age. Affected puppies present with acute fulminant heart failure and typically die within hours. A second
form of the disease affects juvenile dogs (< 1 year) and has a clinical presentation and diagnostic findings similar
that of classical DCM.
West Nile Virus
Another viral infection that uncommonly affects dogs. Clinical signs are often vague including lethargy,
inappetence, neurologic signs, arrhythmias, and fever. Severe lymphocytic, neutrophilic myocarditis and vasculitis
have been observed with focally extensive hemorrhage and myonecrosis.
Blastomycosis
This is a rare form of fungal myocarditis reported in dogs. Clinical signs include syncope, sudden death, and
arrhythmias. Severe granulomatous disease can cause severe myocarditis with myocardial dysfunction. The
granulomatous disease is often diffuse including the valves, epicardium, and pericardium.
Lyme myocarditis
A somewhat uncommon cause of myocarditis in dogs caused by the spirochete Borrelia burgdorferi. It is most
commonly encountered in the Northeast, Western Coastal, and Upper Midwestern USA. Severe multifocal
myocarditis and valvular endocarditis have both been observed with this infection. Clinical signs are variable and
arrhythmias are most commonly reported.
Tachycardia-induced Cardiomyopathy (TICM)
Chronic sustained tachycardias can induce myocardial failure in weeks to months depending on the severity of the
tachycardia. This results in dilation of all four chambers, with thinning of the walls. Myocardial failure in TICM is
believed to result from energy store depletion at the cellular level, abnormal calcium cycling, and loss of
sarcomeres. Signs of left-sided, right-sided, or biventricular heart failure may occur. Successful abolishment of the
tachycardia leads to improvement in myocardial function and signs of heart failure over weeks to months, although
complete normalization may not occur depending on the duration of TICM prior to treatment. In patients with
tachyarrhythmia and myocardial failure, it may be difficult to determine which is the primary abnormality.
Nevertheless, myocardial function and heart failure are likely to improve to some degree with adequate control of
the tachyarrhythmia.
Ischemic / Myocardial infarction
Myocardial infarction is an uncommon form of myocardial disease, not associated with an infectious etiology. It is
most often associated with a concurrent systemic or cardiac disease causing a thromboembolic state: endocarditis,
protein-losing enteropathy, protein-losing nephropathy, immune-mediated hemolytic anemia, Cushing’s disease,
sepsis, and systemic inflammatory response syndrome. Unlike humans, atherosclerosis is an uncommon cause of
myocardial infarction in dogs and has been rarely reported as a sequela of severe hypothyroidism. Myocardial
175

infarction can also be a rare complication of endovascular stent placement for the treatment of pulmonic stenosis
secondary to compression of the coronary blood supply to the surrounding myocardium.
Doxorubicin toxicity
Doxorubicin is an anthracycline antibiotic used commonly in many chemotherapy protocols. Cumulative doses >
200-240 mg/m2 are considered cardiotoxic and can result in myocardial damage, systolic dysfunction, dilated
cardiomyopathy, and congestive heart failure. Arrhythmias, typically ventricular, are common. Most institutions
avoid cumulative doses > 180 mg/m2. Dexrazoxane, which is a derivative EDTA and an iron chelator, protects
against cardiotoxicity likely by binding free radicals, but can be cost prohibitive.
Metabolic
Hypothyroidism
Untreated hypothyroidism may cause a mild to moderate reduction in systolic function, but this is unlikely be
clinically significant unless there are concurrent cardiac abnormalities.
Treatment of Non-Inherited DCM Phenotypes
Whenever possible, the underlying cause of the patient’s DCM phenotype should be addressed (i.e. taurine, thyroid,
infectious etiology, etc.). Dogs with malignant ventricular arrhythmias should be treated appropriately with sotalol,
mexiletine, or a combination of both. Dogs with rapid atrial fibrillation (> 160 bpm) should be treated with drugs
such as diltiazem, digoxin, or amiodarone. Some dogs with myocarditis present with bradyarrhythmias such as high-
grade 2nd degree AV block and 3rd degree AV block. Although there is a possibility that these bradyarrhythmias may
be transient and may resolve once the underlying cause is treated, permanent pacemaker implantation is typically
indicated for these patients due to the risk for sudden death.
Once heart failure develops, furosemide should be initiated to controls clinical signs, while avoiding dehydration,
azotemia, and electrolyte loss. In addition to furosemide, all dogs with DCM should receive pimobendan, an ACE
inhibitor (benazepril), and spironolactone.
There is little to no evidence that angiotensin-converting enzyme (ACE) inhibitors or pimobendan (Vetmedin®) are
beneficial in the occult stage of DCM in breeds other than Doberman Pinschers and Irish Wolfhounds. As such,
conclusions about their efficacy at delaying the progression disease cannot be made in dogs of other breeds or in
cases of secondary DCM. Use of these medications is on a case-by-case basis although the general consensus is that
pimobendan is beneficial in non-Doberman and non-Irish Wolfhound breeds of dogs with preclinical DCM
phenotypes.
176
Beyond furosemide: a guide to cardiac drugs for the general practitioner
Michael Aherne, MVB, GradDipVetStud, MS, MANZCVS (Small Animal Surgery), DACVIM (Cardiology)
Department of Small Animal Clinical Sciences
College of Veterinary Medicine
University of Florida, Gainesville, Florida
POSITIVE INOTROPIC AGENTS.
Digoxin
Mechanism of action: A cardia glycoside which inhibits the Na+/K+ ATPase at the membrane level such that more
Na+ is made available for exchange with extracellular Ca++. This results in increased intracellular Ca++ being
available to the contractile apparatus, causing in a positive inotropic effect.
Indications: Digitalization may be indicated in patients with documented systolic pump failure (e.g. DCM) although
its efficacy has been superseded by that of pimobendan.
Contraindications:
Pericardial disease, the obstructive form of HCM, or in patients with restrictive myocardial disease, unless these
disorders are accompanied by a supraventricular tachyarrhythmias such as atrial fibrillation.
Although it can have a narrow therapeutic margin, informed judicious use, can usually help avoid toxic side effects
Signs of digitalization include 1) slowing of the heart rate, 2) relief of clinical signs of heart failure, 3) increased PR
interval duration (unreliable), and 4) demonstration of therapeutic blood levels. The therapeutic serum concentration
is typically 1.0 to 2.0 ng/ml however this should not be considered a target range to reach and adequate clinical
response may be seen at lower serum levels.
Oral Dose:
DOGS: Generally, 0.003 to 0.004 mg/kg q12h. Ideally, serum digoxin levels should be measured 5 to 7 days after
initiation of therapy with dose adjusted accordingly.
CATS: Not routinely administered and dosing is highly variable in literature, approximately 0.008 mg/kg q24-48h.
Important factors:
Digoxin elixir is absorbed more completely than the tablet form, resulting in higher blood levels at a given dosage.
Avoid switching between from one form to the other in any given patient.
Hypokalemia and hypercalcemia often contribute to development of digitalis toxicity. Attempt to maintain normal
electrolyte status.
Hypothyroid animals may require less digoxin than euthyroid animals. Hyperthyroid animals may require an
increased dose.
Digoxin is primarily cleared from the body via the kidneys. The presence of renal dysfunction often necessitates a
reduction in digoxin dosage or frequency of administration.
Dosage should be based on lean body weight (digoxin). Fat animals, pregnant animals, and animals with ascites
should be dosed accordingly.
Adverse Effects:
Signs of toxicity are common due to the narrow therapeutic index. Clinical signs usually consist of anorexia, nausea,
vomiting, diarrhea, depression and weakness. In addition, a variety of arrhythmias may be observed, some of which
are quite dangerous. With oral administration, gastrointestinal signs almost always develop prior to arrhythmias and
so are important sentinel signs for owners to be aware of. Digoxin toxocity is potentiated by hypokalemia and
hypernatremia.
177
Treatment of Toxicity:
Stop digitalis and diuretic administration for 24 to 36 hours. Then reinstitute at lower dose. Check electrolyte status;
correct hypokalemia if present. Oral administration of potassium salt is recommended. Life-threatening arrhythmias
may be treated with atropine, lidocaine, or propranolol. A specific antidote (DIGIFab/DIGIBind) is also available
and consists of antibody fragments that scavenge the free drug from the body and hasten renal elimination.
CALCIUM SENSITIZERS AND INODILATORS
Pimobendan
Mechanism of action: Increases myocardial contractility via phosphodiesterase 3 (PDE3) inhibition and by
increasing the Ca2+ affinity of troponin C, the calcium-binding protein that plays a regulatory role in cardiac muscle
contraction.
Oral Dose: 0.25 to 0.3 mg/kg q12 h however extra-label doses of up to 0.6 mg/kg q 8 h may be used in some
patients with severe refractory CHF however the efficacy of higher doses has not been scientifically evaluated.
Adverse Effects:
At standard doses pimobendane is typically very well tolerated. Although uncommon, very mild and typically self-
limiting GI upset is the most commonly encountered side effect. At very high doses, anorexia, vomiting, myocardial
necrosis, hypotension, tachycardia and certain arrhythmias have been reported.
Treatment of toxicity:
Reduce dose or stop administration.
SYMPATHOMIMETIC AGENTS
Dobutamine, Dopamine, Isoproterenol
Mechanism of action: These catecholamines exert a positive inotropic effect by stimulating beta-1 adrenergic
receptors on the myocardium, resulting in a net increase in intracellular Ca2+ that can be made available to the
contractile apparatus. Ideally, a purely selective ß1 agonist lacking chronotropic effects is desirable in patients with
heart failure. All sympathomimetic agents are best suited to short-term intravenous use. They are arrhythmogenic
and tolerance to their effects develops quickly.
Of these sympathomimetic drugs, dobutamine is preferred for the treatment of acute heart failure. Dobutamine
stimulates beta-1 and beta-2 adrenergic receptors, but its beta-2 effects are much weaker than isoproterenol, and its
beta-1 effects are weaker than epinephrine. Thus, it increases contractility with little change in heart rate or
afterload. Dobutamine infusions are often helpful for maintaining contractility in patients with heart disease that
must be anesthetized.
Dopamine stimulates beta-1 receptors and releases norepinephrine from sympathetic nerve terminals. It increases
contractility at doses that cause minimal increases in heart rate. At low doses, dopamine causes selective dilatation
of arterioles in the renal, mesenteric, coronary and cerebral vascular beds. At high doses, dopamine cause
generalized systemic arteriolar vasoconstriction and so has more limited application in patients with heart disease.
Isoproterenol stimulates beta-1 and beta-2 receptors, resulting in increased myocardial contractility, increased heart
rate, and peripheral vasodilation. The marked chronotropic and arrhythmogenic effects of isoproterenol make it
unsuitable for the treatment patients with CHF and it is primarily used for the temporary control of heart rate in
patients with symptomatic bradycardia.
Dobutamine
Parenteral Dose: 2 to 15 μg/kg/minute IV, as a continuous infusion diluted in 5% dextrose - monitor closely for
arrhythmias and tachycardia
178
Dopamine
Parenteral Dose: 2 to 8 μg/kg/minute IV, continuous infusion diluted in 5% dextrose - monitor closely for
arrhythmias, tachycardia and hypertension
Isoproterenol
Parenteral Dose: 0.04 to 0.1 μg/kg/min, IV infusion diluted in 5% dextrose - monitor closely for arrhythmias,
tachycardia and hypotension
Adverse and toxic effects of all sympathomimetic agents:
1) Excessive heart rates, dose related: isoproterenol > dopamine > dobutamine.
2) Arrhythmias, dose related: all drugs in this class.
3) Phlebitis, ischemic necrosis if outside vein: all drugs in this class.
4) Nausea, anorexia.
5) Hypertension (dopamine), Hypotension (isoproterenol)
Treatment of catecholamine toxicity:
Stop or slow administration of drug.
LOOP DIURETICS
Mechanism of action: Inhibition of chloride transport in the ascending loop of Henle, resulting in obligatory loss of
sodium and water into the urine. The oral absorption of furosemide is only 60 to 70% in healthy dogs and probably
less in animals with heart failure. When poor absorption is suspected (e.g. ascites with right-sided CHF), consider
torsemide, which is better absorbed. Torsemide may also have some effects in blocking aldosterone and reduce
fibrosis in the process of cardiac remodeling.
Furosemide
Parenteral Dose:
DOGS: 2 to 4 mg/kg IV or IM, as needed to control edema.
CATS: 1 to 2 mg/kg IV or IM, as needed to control edema.
Oral Dose:
DOGS: 2 to 4 mg/kg q8-24 h, as needed. (Use lower doses with ACE inhibitors)
CATS: 1 to 2 mg/kg q 8-12 h, as needed. (Use lower doses with ACE inhibitors)
TORSEMIDE
Oral Dose: (10x to 20x more potent than furosemide)
DOGS: 0.05 to 0.2 mg/kg q12 h, as needed
Adverse effects of loop diuretics:
May cause serious electrolyte imbalance characterized by hypokalemia, hyponatremia and hypochloremia
(hypochloremic alkalosis) and requiring temporary withdrawal of the loop diuretic or reduction in dosage. Excessive
use can lead to dehydration, renal failure, low cardiac output, and circulatory collapse. All diuretics activate
systemic compensatory mechanisms, including the RAAS and sympathetic nervous system. Thus, while these agents
are the most effective drugs used in the short-term management of congestive heart failure, they have inherent
limitations and contribute to the overall maladaptive neurohormonal response that characterizes congestive heart
failure.
THIAZIDE DIURETICS
Hydrochlorothiazide
Mechanism of action: Thiazides inhibit electrolyte reabsorption in the distal tubule, resulting in loss of sodium,
chloride, potassium and bicarbonate. In dogs, hydrochlorothiazide is mainly used in combination with a loop
diuretic to treat refractory heart failure.
179
Oral Dose:
DOGS & CATS: 2.0 to 4.0 mg/kg q12-24h - sometimes only given every 2 to 3 days to dogs also treated with
furosemide
Adverse Effects: Hydrochlorothiazide is more likely than furosemide to cause hypokalemia. When used excessively,
they also may cause hypochloremic metabolic alkalosis.
Aldosterone Antagonists
Spironolactone
Although traditionally-referred to a potassium sparing diuretic, spironolactone is an aldosterone with negligible
diuretic effects. This aldosterone antagonism results in anti-remodeling effects that appear to be important in
improving the quality and duration of life in patients with CHF as well as resulting in reduced loss of potassium
through the renal tubules.
Oral Dose:
DOGS & CATS: 1 to 2 mg/kg q 12-24 h.
Adverse Effects: Hyperkalemia is the most important adverse side effect of aldosterone antagonism and is seen most
often when these drugs are given in combination with an ACE inhibitor. Potassium levels should therefore be
routinely monitored. Severe facial dermatitis has been reported in cats which resolves with removal of the drug.
VASODILATORS
Classification of vasodilators based on vessels dilated.
Arteriolar: hydralazine, amlodipine, sildenafil (pulmonary arterioles and corpus cavernosum).
Venous: nitroglycerin, isosorbide dinitrate, isosorbide mononitrate.
Mixed: nitroprusside, prazosin, ACE inhibitors (weak), combinations such as hydralazine or amlodipine plus a
nitrate.
Classification of vasodilating drugs based on mechanism of action:
Direct-Acting: nitroprusside, nitroglycerin, isosorbide dinitrate, hydralazine.
Alpha-adrenergic blocking drugs: prazosin.
Calcium channel blocking drugs: amlodipine
Angiotensin-converting enzyme inhibitors: enalapril, benazepril
Phosphodiesterase 5 inhibitors: sildenafil, tadalafil
Most CHF cases have both congestive and low output signs and would be expected to benefit from a mixed
(arteriolar and venous) vasodilator. Low output states require afterload reduction or positive inotropic support, and
the use of a pure venodilator in these cases may lead to a sharp decline in patient stability. Venous congestion will
be improved with either arterial or venous vasodilation but it will be more rapid and specific with a venodilator
however these are rarely used alone since they contribute little to increasing cardiac output. All vasodilators carry
the risk of inducing hypotension with the attendant problems of reduced perfusion such as weakness, fainting,
reduced kidney function, and reflex tachycardia.
Calcium Channel Blocking Drugs
Amlodipine.
Oral Dose:
DOGS & CATS: Start at 0.05 mg/kg q 24 hrs. Titrate up to desired effect or up to a maximum dose of 3.0 mg/kg
twice daily. Endpoints of titration are determined by monitoring blood pressure, the patient's clinical response, and
radiographic resolution of pulmonary edema.
180
Direct-Acting Vasodilators
Hydralazine
Hydralazine is a direct-acting vasodilator which acts independently of the calcium channel. Hydralazine provides
long-term clinical improvement and prolongs survival in humans with myocardial failure when used in combination
with diuretics and nitrates. While studies provide a reasonable basis for the short-term use of hydralazine in dogs
with left heart failure caused by MMVD, the usefulness of hydralazine for long-term therapy is limited by poor
patient tolerance and lack of owner compliance.
Oral Dose:
DOGS: Start at 0.5 to 1.0 mg/kg - titrate to desired effect or up to a maximum dose of 3.0 mg/kg twice daily.
Endpoints of titration are determined by monitoring blood pressure, the patient's clinical response, and radiographic
resolution of pulmonary edema. When administered orally in the dog, hydralazine's vasodilatory effect begins within
one hour, peaks within 3 hours, and remains stable for several hours, with a total duration of effect of about 12
hours.
CATS: Start at 2.5 mg per cat q12h – can titrate up to 10 mg total per day.
Adverse effects and toxicity:
Common adverse effects of hydralazine include hypotension and gastrointestinal upset. Hydralazine may cause
sodium and water retention and often a reflex tachycardia by activating the sympathetic nervous system and
stimulating the release of renin.
Sodium nitroprusside
Nitroprusside is the only direct acting mixed vasodilator available for extra-label use in dogs with congestive heart
failure. It is an extremely potent vasodilator that is primarily used to rescue dogs with severe, decompensated CHF
caused by MMVD or DCM. Sodium nitroprusside is indicated for the short-term treatment of refractory, life-
threatening CHF in dogs with MMVD or DCM. In this circumstance, it is much more effective than furosemide for
decreasing left ventricular filling pressures. Sodium nitroprusside is rarely used alone, but is usually administered in
combination with diuretics, pimobendan and dobutamine.
Parenteral Dose:
DOGS: Intravenous CRI at an initial rate of 1.0 μg/kg/minute, diluted in 5% dextrose. The rate of administration is
titrated to effect, by very close monitoring of blood pressure and pulmonary capillary wedge pressure, to a
maximum dose of 10 μg/kg/min. Sodium nitroprusside is very light-sensitive and the CRI syringe and tubing should
be covered in light-protective material.
Toxicity and adverse effects: Adverse effects of nitroprusside include hypotension, tachycardia, nausea, vomiting,
and, with chronic administration (i.e. > 48 hrs), cyanide poisoning can occur. Hypotension is easily managed by
slowing the rate of infusion, and because of its short half-life, the serious consequences of profound hypotension are
avoidable when patients are very carefully monitored.
Phosphodiesterase 5 (PDE5) Inhibitors
Sildenafil
Mechanism of Action: Sildenafil inhibits PDE5 and thus reduces the breakdown of cGMP which results in
vasodilation. It is unclear why the pulmonary vascular bed is more sensitive to PDE5 inhibition than others but one
theory is that it may be related to the availability of nitric oxide to encourage the formation of cGMP.
Indication:
Alleviation of clinical signs resulting from moderate to severe pulmonary hypertension.
Oral Dose:
DOGS: 1.0-3.0 mg/kg q8h
181
Toxicity and adverse effects: Adverse side effects include hypotension and visual disturbances.
ANGIOTENSIN CONVERTING ENZYME INHIBITORS (ACEIs)
Mechanism of Action: ACE inhibitors decreased formation of angiotensin II, resulting in decreased aldosterone
concentrations. Through these mechanisms ACE inhibiting drugs are believed to palliate the deleterious maladaptive
neurohormonal consequences of vasoconstriction and sodium retention in patients with CHF.
Enalapril
Oral Dose:
DOGS: 0.25-0.5 mg/kg q12-24h.
CATS (extra-label): 0.25-0.5 mg/kg q12-24h.
Benazepril
Oral Dose:
DOGS: 0.25-0.5 mg/kg q12-24h
CATS: 0.25 mg/kg q24h
Toxicity and adverse effects:
Most ACEIs are well tolerated however they frequently may be associated with anorexia. Other side effects may
include vomiting, diarrhea, and hypotension. ACEIs are known to decrease glomerular filtration pressure by virtue
of their vasodilating effects on the renal afferent and efferent arterioles and thus, treatment with an ACE inhibitor
often results in mild azotemia and mildly increased serum creatinine concentrations. Renal dysfunction, including
refractory renal failure can develop in dogs treated with any ACEI, therefore preexisting renal disease is a relative
contraindication to the use of any ACEI. Renal dysfunction is most likely to develop in patients with preexisting
renal disease receiving high doses of ACEI and high doses of diuretics or in dogs treated concurrently with NSAIDs.
In most dogs treated with an ACEI, renal function will soon normalize or stabilize at a new steady state. However, in
some circumstances, severe renal failure is observed shortly after initiating ACE inhibitor therapy. This consequence
may be more common in patients with serious preexisting renal disease, in dehydrated patients, and in patients with
systemic hypotension. Significant renal dysfunction typically occurs within the first week following the initiation of
treatment. This problem is best avoided by reducing the dose of furosemide to less than 4 mg/kg/day prior to
initiating the ACEI. It is recommended to always evaluate renal function prior to and about 5 to 7 days after
initiating an ACEI. Therapy should be altered if serum creatinine concentrations exceed 2.5 to 3.0 mg/dl and blood
urea nitrogen concentrations exceed 60 to 70 mg/100ml. Most dogs can be adequately managed by decreasing either
the dose of the ACE inhibitor or diuretic, or both. However, in certain cases, ACEI therapy may have to be
discontinued. When used together with an aldosterone antagonist, serum potassium levels should be routinely
monitored.
MISCELLANEOUS AGENTS
Bronchodilators
Theophylline
Oral Dose: 9 mg/kg q 6-8 h (Dogs); 4 mg/kg q 8 h (Cats)
Aminophylline
Oral Dose: 11 mg/kg q 6-8 h (Dogs); 5 mg/kg TID (Cats)
Cough Suppressants
Hydrocodone
Oral Dose: 0.5-4 mg/kg q 8-24 hrs
182

Sedatives and Tranquilizers
Butorphanol
Reduces anxiety, decreases sympathetic tone
Parenteral Dose: 0.1-0.3 mg/kg IV, IM
Acepromazine
Reduces anxiety, vasodilator
Parenteral Dose: 0.02 to 0.05 mg/kg IV, IM
183

Tips from the trenches: avoiding common mistakes in the management of
cardiac disease
Michael Aherne, MVB, GradDipVetStud, MS, MANZCVS (Small Animal Surgery), DACVIM (Cardiology)
Department of Small Animal Clinical Sciences
College of Veterinary Medicine
University of Florida, Gainesville, Florida
Assess the patient thoroughly and frequently.
Treat the patient not the test (e.g. NTpro-BNP).
Resting respiratory rate is the most sensitive indicator for the presence of pulmonary edema.
Crackles and cough are both unreliable indicators of CHF in both cats and dogs – don’t treat for CHF on the basis of
these signs alone.
The presence or absence of a murmur in a cat is unreliable for determining the presence or absence of heart disease
in this species.
Doppler-cuff systolic blood pressure measurement is very valuable in patients with cardiac disease. Perform prior to
physical exam if possible and ideally with owner present to minimize ‘white coat effect’.
Never place a patient with suspected CHF in dorsal recumbency.
Don’t sacrifice patient stability for the sake of acquiring radiographs - if your clinical suspicion is high then perform
initial stabilization with diuretics.
For radiographic evaluation of cardiac disease, a dorsoventral (DV) projection is preferred over a ventrodorsal (VD)
projection. In addition to the risk posed in placing a dyspneic patient on their back, the size and appearance of
various chambers may be altered by the position the heart falls into when a patient is laying in dorsal recumbency.
Beware of breed specific variations – e.g. vertebral heart scale.
Echocardiography cannot confirm the presence of pulmonary edema. It is not an appropriate test in dyspneic patients
with suspected CHF that have not yet been stabilized.
Don’t underestimate the utility of oxygen as a drug for stabilization of dyspneic patients.
Cats are not small dogs – beware of altered pharmacokinetics and contraindications for certain cardiac drugs.
Always ensure patients on diuretics have access to water at all times.
There is little rationale or benefit to co-administration of diuretics and parenteral fluids in patients with CHF.
AIVR is a hemodynamically stable rhythm - it does not require treatment and furthermore treatment is ineffective.
Check ECG settings when performing calculations from ECG recordings – paper speed and amplitude.
Don’t trust machines to always be accurate (e.g. heart rate on ECG monitor, oscillometric blood pressure).
184
Myths & Misperceptions:
Recognizing the Problems and Avoiding Common
Mistakes Andrew Specht, DVM, DACVIM (SAIM)
University of Florida
INTRODUCTION: In recent years, there has been a substantial shift in the way many of us think about the clinical management and
prognosis for dogs and cats with kidney disease. Despite the longer survivals and better quality of life we are able to
provide now, there are a number of misconceptions about kidney disease that persist in our profession. This session
will focus on exploring some of the most persistent kidney “myths” and the common clinical management mistakes
that arise from them in order to help practitioners avoid these in the future.
Myth #1 – “X” times “maintenance” is a lot of fluids.
The fluid calculations and planning principles are really not significantly different for patients with kidney disease
than for patients with any other diseases. Ideally, we should still be making decisions about fluid therapy based on
the individual patient’s circumstances. The main factors that go into decisions about fluid rate are 1) the patient’s
maintenance needs 2) the patient’s fluid deficit (% dehydration x body weight in kg), and 3) any excess fluid losses
(estimate based on consideration of GI losses, polyuria, other…).
Some AKI patients will present with significant dehydration (i.e. ~10%) and a history of GI fluid losses (from
vomiting and diarrhea) as well as polyuria. In these cases, calculations may reveal that to make a significant
difference in the patient’s hydrations status we have to give a “scary” amount of fluids.
I generally do not worry a lot about my fluid rate as long as it is based on a calculation rather than guesswork, but
there are a couple of situations in which I would be more cautious and may accept a longer time to re-hydrate a
patient. Some of these situations would include patients with known heart disease or uncertain cardiac function,
patients with pathologic oliguria, patients with severe electrolyte abnormalities (especially sodium), or feline
patients. In these cases I will definitely be a bit more conservative and monitor very closely (weights, respiratory
rate/sounds, nasal discharge, others…)
Myth #2 – I am (or can be) good at assessing the hydration status of my patients.1,2
Numerous studies in both human and veterinary medicine have revealed that doctors are not accurate when
attempting to estimate dehydration in our patients. Furthermore, doctors actually do not seem to be significantly
better or worse than trained nurses/technicians or students. The use of specific scoring systems may help slightly,
but there is still a great degree of inaccuracy. Finally, in most of these studies, the general trend is to underestimate
the percentage of dehydration in patients that are actually dehydrated.
185
Myth #3 – After being rehydrated, a patient should be kept on a high rate of fluids for diuresis or to “flush
out” the toxins.3
Once a patient is rehydrated (i.e. has a normal blood volume and presumably normal renal blood flow), further
delivery of “excess” fluid is very unlikely to significantly change the serum concentration of most uremic toxins.
The serum concentration of most of these substances will be most affected by changes in GFR, but elimination of
extra water by the kidneys primarily occurs at the level of the tubules (by sodium excretion) and collecting ducts (by
not resorbing water). This is definitely true in patients with normal kidneys, and although patients with kidney
disease may lack some of the autoregulatory mechanisms that account for this, that may actually lead to some
adverse effects of giving those patients extra fluids.
Many patients with kidney disease, especially AKI, may not have a normal capacity to manage excess fluids or
control electrolyte concentrations. Therefore, overhydration is a significant concern in these patients and this can
contribute to kidney damage as well. Similarly, there is significant evidence that continuing to administer
hyperchloremic fluids after restoring adequate hydration and normalizing serum electrolytes can be harmful to the
kidneys.
So… both dehydration and overhydration are potentially problematic. Monitoring and adjustment in fluid rates is
therefore critical.
***The basic principles of fluid therapy calculation for patients with kidney disease are not
substantially different than for most other sick patients.***
Myth #4a – A negative urine culture “rules out” infection.
There have been a few studies in which infection was diagnosed only with sampling from the renal pelvis and not
from the urinary bladder. It is still not clear whether this should prompt us to specifically sample the renal pelvis in
certain patient populations, but I consider it in cases with ultrasound abnormalities and negative cultures.
Myth(s) #4b – A negative test “rules out” leptospirosis. OR We don’t have lepto in .
Over the years I have seen leptospirosis diagnosed in a wide variety of dog breeds and home environments. This has
included large breed hunting/farm dogs, suburban dogs and small dogs that never left their urban high rise apartment
buildings. I would still recommend testing any patient with acute kidney injury (AKI) for leptospirosis as well as
providing empiric coverage (i.e. a penicillin or doxycycline) while waiting for results.
Myth #5 – Unilateral ureteral obstruction does not cause azotemia.4
A high percentage of patients with documented ureteral obstruction (unilateral or bilateral) will be azotemic at the
time of diagnosis. The specific reason for this is unclear. It is possible that many of these patients have some
degree of underlying kidney disease, but that may not always be apparent and azotemia at the time of diagnosis
should not be automatically assumed to imply as poorer prognosis.
Myth #6 – The degree of azotemia is important when considering the patient’s prognosis.
In many cases, there is a combination of pre-renal and renal azotemia and without serial monitoring it will be hard to
sort out the specific renal component. In addition, once there is a significant decrease in GFR (i.e. enough to get to a
creatinine of >3) there will be a relatively dramatic increase in creatinine concentration with even minimal
additional decreases in GFR. Finally, there is a significant difference between interpretation of azotemia in a stable
CKD patient compared with a patient with AKI or in a uremic crisis.
Myth #6a – Kidney tissue can’t regenerate.
While this is essentially true of most CKD lesions, there are a number of AKI lesions that can heal over time,
provided there is an intact basement membrane. Although this may take some time, there are patients that can return
to completely normal serum creatinine values even after extremely severe azotemia.
186
Myth #6b – That kidney that looks like a bag of fluid can’t be functional
No matter how bad the kidney looks, there is a chance that some nephrons remain functional, and some recovery
from acute/active injury is possible. Ideally a nephron sparing approach should be used when possible (i.e. don’t
remove the kidney unless you have to).
Myth #6c – The IRIS CKD staging system is directly/significantly related to prognosis.
Although it is very likely that patients with stage 4 CKD are likely to have shorter survival times than patients with
stage 2 CKD, there is still minimal evidence to back this up. In addition, the cut-off values for the different stages
are somewhat arbitrary and not all patients within a category are comparable.
Myth #7 – SDMA (or creatinine) concentration is the most important parameter/biomarker for CKD
treatment decisions.
While SDMA has some advantages when compared to creatinine as an indicator of decreased GFR, some of these
are overstated in the literature because the SDMA cutoff is based on GFR measurements in a colony of research
cats, while the creatinine cutoff is based on a reference range established from a population of “healthy” pet cats. If
the cutoff values for creatinine concentration utilized for staging of CKD are used instead of the creatinine reference
range, much of the advantage of SDMA disappears. SDMA can still be very useful though, especially in patients
with significant muscle wasting.
Some of the recent consensus statements have suggested that in patients with significant proteinuria we may actually
choose to treat the proteinuria at the expense of preserving GFR as completely as possible. From the most recent
IRIS consensus5, tolerable increases in serum creatinine for patients being treated with ACEi are:
• IRIS CKD stages 1 & 2 – up to 30% higher than baseline
• IRIS CKD stage 3 – up to 10% higher than baseline
• IRIS CKD stage 4 – no acceptable increase?
Similarly, there has been a shift in thinking about other diseases such as hyperthyroidism in cats. Although we still
discuss the possibility of “unmasking” CKD in those patients, we may still choose to treat their hyperthyroidism to
prevent the long-term consequences of hypertension even though their serum creatinine may look worse in the short
term.
Myth #8 – Cystocentesis is the best way to collect urine samples for accurate analysis
This depends a bit on what we are trying to test for. For urine cultures, it is clear that a cystocentesis sample is the
preferred method of collection. However, this may not be true for urine protein measurement. More research is
required, but there is some evidence to suggest that factors involved in the visit to a veterinary clinic may alter the
pH and/or protein content of the urine.6
Myth #9 – Kidney disease patients need to be started on a prescription diet right away.
There are two problems with this one: Dietary therapy is clearly one of the most important things we can
recommend for most of our CKD patients. However, most of the benefits of this therapy are likely to accumulate
over a long time course. Starting a renal diet too early may actually lead to food aversions if the patient is not stable
and feeling well when we try to initiate a diet change. In addition, we now know that protein restriction is probably
not the key part of an appropriate kidney diet, but rather is often unfortunately necessary to achieve the other
beneficial aspects of these diets.7
Myth #10 – Kidney patients are supposed to be thin and/or muscle wasted.
Although dietary therapy is an important long-term management consideration for patients with chronic kidney
disease, so is caloric intake.8-10 There are a number of factors that can cause these patients to eat less than
recommended and I am much more aggressive about appetite stimulation, supportive/symptomatic therapy for any
187

suspect GI signs, or even considering feeding tubes in CKD patients than I used to be. It can be hard to recover
body/muscle condition if we fall too far behind.
KEY POINTS
• Think about fluid therapy for kidney disease the same way you think about it for other diseases. The
components of calculation are maintenance, rehydration, and excess losses and the primary goal is to
maintain adequate hydration.
• Be very careful about “ruling out” infectious or obstructive causes of kidney disease.
• Be very careful about basing your prognosis on laboratory values or “stage” of disease.
• Appropriate nutrition is critical in managing CKD, but this does not just mean that kidney diets should be
started ASAP. Food aversions can be common when special diets are started prematurely. Caloric intake
is critical for maintaining an appropriate body/muscle condition and this often requires monitoring and
support.
REFERENCES AND SUGGESTED READINGS
1. Hardy RM, Osborne CA. Water deprivation test in the dog: maximum normal values. J Am Vet Med Assoc.
174(5):479-483, 1979.
2. Hansen B, DeFrancesco T. Relationship between hydration estimate and body weight change after fluid
therapy in critically ill dogs and cats. J Vet Emerg Crit Care. 12(4):235-243, 2002.
3. Langston C, Eatroff A. Less is more - fluid therapy for kidney disease. J Feline Med Surg. 14(11):773. 2012.
4. Kyles AE1, Hardie EM, Wooden BG, et al. Clinical, clinicopathologic, radiographic, and ultrasonographic
abnormalities in cats with ureteral calculi: 163 cases (1984-2002). J Am Vet Med Assoc. 226(6):932-6, 2005.
5. Brown S, Elliot J, Francey T. Consensus Recommendations for Standard Therapy of Glomerular Disease in
Dogs. J Vet Intern Med. 27(Issue Supplement s1):S27–S43, 2013
6. Duffy ME, Specht A, Hill RC. Comparison between Urine Protein: Creatinine Ratios of Samples Obtained
from Dogs in Home and Hospital Settings. J Vet Intern Med. 29(4):1029-1035, 2015.
7. Scherk MA, Laflamme DP. Controversies in Veterinary Nephrology: Renal Diets Are Indicated for Cats with
International Renal Interest Society Chronic Kidney Disease Stages 2 to 4: The Con View. Vet Clin North Am
Small Anim Pract. 46(6):1067-1094, 2016.
8. Freeman LM. Cachexia and sarcopenia: emerging syndromes of importance in dogs and cats. J Vet Intern Med.
26(1):3-17. 2012.
9. Ross S. Utilization of Feeding Tubes in the Management of Feline Chronic Kidney Disease. Vet Clin North
Am Small Anim Pract. 46(6):1099-1114, 2016.
10. Markovich JE, Freeman LM, Labato MA, et al. Survey of dietary and medication practices of owners of cats
with chronic kidney disease. J Feline Med Surg. 17(12):979-983. 2015.
188

Beyond Diet… What Else Should You Know about Treating Chronic Kidney
Disease? Andrew Specht, DVM, DACVIM (SAIM)
University of Florida
INTRODUCTION Chronic kidney disease (CKD) is defined as damage or dysfunction of one or both kidneys that has been present or persistent for >3 months. Note that this is not synonymous with, but also does not exclude conditions such as renal insufficiency or renal failure. Unlike acute kidney injury, CKD is characterized by irreversible structural lesions. Although the precipitating insult may no longer be present, CKD is typically progressive, even if progression is very slow.
CKD is common in both dogs and cats. It may be initiated by a variety of congenital or acquired conditions. Whenever possible the underlying etiology of CKD should be determined and treated if reasonable therapeutic options exist. In addition, other comorbid conditions or factors can promote progression of CKD even if they were not the inciting cause. Prognosis for patients with CKD is dependent upon the specific renal disease, the specific underlying cause, and the severity of disease, in addition to numerous other factors.
In order to make informed choices about treatment options, the veterinarian needs to have a certain amount of information about the patient. A diagnostic plan should be proposed that allows the clinician to determine the diagnosis, severity, current complications, comorbid conditions, and risk for progression. Some of the key information that might be a part of the information data base for a CKD patient is included in the table to the right. Not all of these tests should be performed right away, however. For example, the UPC should probably not be performed until there is some certainty that the patient has an inactive sediment, negative urine culture, and is not severely hypertensive. By gathering this information, treatment can be tailored to the specific circumstances of an individual patient. In addition, it is important to remember that CKD is a dynamic and progressive condition. Therefore, serial monitoring is an essential part of any individualized plan.
Data base for CKD patients: _________________________________________________________________________
• Thorough medical history• Complete physical examination• Serum biochemical values
- Creatinine- SDMA (?)- Urea nitrogen- Phosphorus- Albumin- Calcium- Sodium- Potassium- Chloride- TCO2 (or HCO3)- pH (?)
• Urinalysis (w/ sediment)• Urine culture (quantitati ve)• Urine protein-to-creatinine ratio• Blood pressure• Imaging (radiographs, ultrasound)
-kidneys (size, shape, morphology..)-bladder (size, shape, other..)-evidence of uroliths, obstruction
• Complete Blood Cell Count• Other considerations (the +/- ones):
- Additional imaging- contrast studies- skeletal radiographs
- GFR determination- plasma clearance (e.g. iohexol)- scintigraphy
- PTH and iCa++ levels- Infectious disease testing- Renal FNA or biopsy- Lipid levels (triglycerides)- Coagulation (TEG, ATIII levels,…)- SDS-PAGE
________________________________________________________________________
189

There are now numerous resources available to veterinary practitioners that offer guidelines for diagnosis and treatment of canine and feline CKD patients. Among these are some consensus guidelines published by the International Renal Interest Society (IRIS) in 2009, and updated regularly, most recently in 2019.1-3 If you are interested, a lot of information can be found on their website at http://www.iris-kidney.com. The primary IRIS recommendations will be related to their staging system which is primarily based on information about the serum creatinine concentration, blood pressure, and urine protein content. There is also a link at that site to a set of “consensus clinical practice guidelines” which offer recommendations for the diagnosis and treatment of persistent renal proteinuria in dogs.4 (http://onlinelibrary.wiley.com/doi/10.1111/jvim.2013.27.issue-s1/issuetoc)
While these guidelines/recommendations can be very helpful as a framework for decision making, it is still very important to individualize treatment plans to make sure they fit the needs of individual patients and clients. Although the underlying lesions in CKD are generally irreversible, there are many therapies that have been proposed for slowing progression of the disease. There are also numerous symptomatic and supportive strategies that should be considered in these patients. Some of the key factors that I consider when making treatment decisions in these cases are briefly described below.
Dietary Therapy First, despite the title of the talk, I do think it is critical to remember that there is very good evidence that dogs and cats with CKD which receive a specially formulated diet tend to have a longer time before they have episodes of felling sick from kidney disease and also live longer than dogs that receive regular dog food.5-7 While not every dog is willing or able to eat these diets, they should probably be an almost universal recommendation for CKD patients. The main current controversies about these diets are when to start them (as early as stage 1?) as well as whether they may cause some problems (such as hyperkalemia) in some patients with advanced, severe disease.
Hydration status / fluid therapy Patients with CKD often make more urine than normal and if they do not drink enough to counter-balance this, they can become dehydrated. I routinely recommend serial monitoring of body weight as a helpful tool for ass essing water losses and use these to help guide any recommendations about SQ fluid therapy or fluid administration through feeding tubes.
Serum Phosphorus Many patients with CKD eventually develop high serum phosphorus levels which can be detrimental for a number of reasons and can contribute to progression of their disease, can cause the patient to feel sick, and/or can participate in causing secondary problems including hormonal changes (such as renal secondary hyperparathyroidism). In many cases, simply eating a "kidney diet" can help keep serum phosphorus levels in a reasonable range for a long time. If/when the diet is no longer enough to keep the phosphorus levelin a desired range, additional medications such as phosphate binders can be added to the therapeutic regimen. There are several different types of medication that can help with this and which one we pick will be dependent on which other problems are present at the same time. This is one of the parameters that we recommend checking fairly frequently (typically, every 3-6 months depending on how stable the other renal values are)
Urine Protein Proteinuria may be present concurrently with or in the absence of azotemia, and can be a cause or result (or both) of ongoing/active problems in CKD. There is strong evidence to support an important role of proteinuria in renal- cause morbidity and mortality.8,9 Because of this, we try to control protein loss at a relatively early stage and to minimize the amount of protein being lost over time. Some key principles to consider when evaluating urine protein are verification, localization, magnitude, and persistence. For patients with convincing persistent renal proteinuria the most commonly used test for assessing or comparing urine protein loss over t ime is a urine protein/creatinine ratio. This will also be our standard test for monitoring progression and response to treatment. In general, the IRIS guidelines call for initiating treatment (diet modification if not already done and RAAS inhibition) for any patient with a ratio over 0.5. I am a bit more conservative and may start treatment only if the ratio is >1.0 or the patient has a low serum albumin. I also recommend checking this value at least a couple times a year for all CKD patients.
190

Key IRIS recommendations related to urine protein values are summarized below:
Dogs UPC 0.2-0.5 UPC >0.5 Stages 1-4 1, 2 1-6
Cats UPC 0.2-0.4 UPC >0.4 Stages 1-4 1, 2 1-5
1. Evaluate for underlying/concurrent disease2. Monitor for progression and/or response to treatment3. Consider kidney biopsy (sent to a specific renal pathology service)4. Renal diet therapy5. RAAS inhibition therapy (make sure patient is not dehydrated)
a. Standard has been to start with ACEib. Consider angiotensin receptor blocker (ARB)
i. instead of or in addition to ACEi6. Low dose acetylsalicylic acid (1-5 mg/kg q24hr) if serum Alb <2.0
There are still a couple of major controversies surrounding treatment of persistent renal proteinuria. One is how to evaluate the trade-off between the value of decreasing urine protein loss and increasing uremia when using medications that decrease GFR. The second major controversy is how and when to use immunosuppressive medications in these patients. Both of these are addressed in the IRIS consensus clinical practice guidelines for glomerular disease in Dogs.4
Blood Pressure High blood pressure can also be the cause of or result of progressive changes in CKD patients. Therefore, this is an important part of staging and monitoring CKD patients. There is good evidence to suggest that dogs and cats that are persistently hypertensive may benefit from anti-hypertensive medications.10,11 Because it is sometimes difficult to obtain accurate blood pressure readings in dogs due to the stress of visiting a veterinary hospital, we typically recommend that repeated tests be performed before starting or significantly changing therapy. I recommend monitoring BP fairly regularly even if it is initially within normal limits (every 3-6 months at on the same schedule the labwork rechecks are performed).
Key recommendations related to blood pressure values are summarized below: • Patients with moderate or severe risk of target organ damage from hypertension (systolic blood pressures >160
mmHg) should be treated if there is documentation of persistently high values.• Patients with evidence of extra-renal target organ damage (CNS, retinal, or cardiac effects) should be treated
without the need to document persistently high blood pressure values• The 2019 IRIS recommendations suggest the following stepwise approach for dogs:
1. Dietary sodium restriction (*There is minimal evidence for this and it is likely to be removed soon )2. Angiotensin converting enzyme inhibitor (ACEi) therapy at standard doses3. Double dose of ACEi4. Combination of ACEi and calcium channel blocker (CCB)5. Combination of ACEi, CCB, and hydralazine
• The 2019 IRIS recommendations suggest the following stepwise approach for cats:1. Dietary sodium restriction (*There is minimal evidence for this and it is likely to be removed soon )2. CCB therapy at standard doses3. Increased CCB dosing4. Combination of CCB and ACEi
Electrolyte Balance & Acid-Base Status The kidneys are responsible for much of the body's regulation of key electrolyte levels (including sodium, potassium, calcium, magnesium, etc...) and therefore patients with CKD are prone to electroly te imbalances. In particular, we are concerned about chronic losses of potassium and fee/ionized calcium (though the total calcium level may be high due to an inactive component called complexed calcium). In addition, some of the medications
191
commonly used to treat other problems that arise in CKD patients (such as ACEi for proteinuria) may cause electrolyte problems such as high potassiumlevels. The periodic labwork performed to evaluate kidney values and phosphorous levels can be used to make sure that patients are not having any issues with this. If a patient does develop electrolyte disturbances, there are various types of supplements or other treatment options that can be utilized to help correct any problems. At this time there is not a lot of specific evidence to support many of these treatments, but they make sense based on anecdotalexperience, theory, logic and intuition.
Similar to electrolytes, the kidneys are also responsible for helping to maintain and appropriate balance between metabolic acids and bases and keep the body's pH normalized. In some cases dogs and cats with CKD will accumulate acids which can also contribute to the progression of their condition. Although measurement of pH and bicarbonate concentrations is probably the best way to monitor this, the TCO2 on many serum chemistries can also be helpful. If this value starts to get very low (<16-18 persistently) it could indicate a metabolic acidosis and we may consider providing supplements to correct this. There is evidence for this treatment based on experimental models, but minimal specific/direct evidence for dogs and cats.
Anemia In advanced chronic kidney disease, anemia is quite common. This may be due to a relative lack of production of erythropoietin, a lack of appropriate response to erythropoietin, decreased red blood cell lifespan, or loss of blood through the kidneys or intestines. If GI bleeding is suspected, acid blocking medications such as H2 blockers or proton pump inhibitors may be helpful. I would use this type of medication in any CKD patient that I suspect of having GI signs related to their disease. If decreased RBC production is suspected, injections of synthetic erythropoietin analogues such as darbepoetin may be helpful. I typically only use these medications if the patient is clinical for anemia or the Hct is persistently < 20%.
Azodyl This medication has been marketed as “enteral dialysis” and there is evidence from the company to showthat it may reduce the concentration of BUN in patients with CKD. At this time there is minimal evidence to support an improvement in quality of life, increased time to uremic crisis, or longer survivals. Currently, I neither promote nor discourage its use in my CKD patients.
Secondary renal Hyperparathyroidism With CKD, excess amounts of the free form of calcium can be lost in the urine and there can be a decreased overall vitamin D activity which reduced absorption of calcium from the diet. To compensate for this, the body will sometimes produce extra amounts of parathyroid hormone which can help retrieve calcium from the bones, but this can cause a loss of bone density and it can also have further negative effects on kidney function as well. Some veterinarians do recommend monitoring for this problem (with periodic checks of ionized calcium and parathyroid hormone levels) and treatment with a vitamin D analogue called calcitriol. There is actually very good evidence for this type of treatment, but it does require careful and frequent monitoring that is often more than what clients are able/willing to pursue.
Urinary tract infections Patients with CKD have an increased susceptibility to urinary tract infections, but do not necessarily showoutwards signs when they do develop them. Therefore, I typically recommend performing a urinalysis with culture at least once every 6-12 months to make sure we do not miss an infection which could contribute to or accelerate the progression of the condition.
192

Key recommendations related to IRIS stage1-3 are summarized below:
Dogs hydration phosphorus Acidosis GI signs Anemia Nutrition &
Supplements Hypertension &
Proteinuria Stage 1 1 (a, b) See above Stage 2 1 (a, b) 2 (a,b) 3 See above Stage 3 1 (a, b, c) 2 (a, b, c) 3 4 (a, b) 5 (a) See above Stage 4 1 (a, b, c) 2 (a, b, c) 3 4 (a, b) 5 (a) 6 (a) See above
CatsStage 1 1 (a, b) See above Stage 2 1 (a, b) 2 (a,b) 3 7 See above Stage 3 1 (a, b, c) 2 (a, b) 3 4 (a, b) 5 (a) 7 See above Stage 4 1 (a, b, c) 2 (a, b) 3 4 (a, b) 5 (a) 6 (a), 7 See above
1. Maintain adequate hydration status / euvolemiaa. SQ or IV fluids to replace deficitsb. Fresh water available all the timec. Parenteral or enteral fluid support to maintain hydration
2. Maintain phosphate in target range: <4.6mg/dL for stage 2, <5.0 for stage 3, <6.0 for stage 4. (Never <2.7)a. Dietary restrictionb. Phosphate binders (aluminum-based, calcium-based, lanthanum, sevelamer)c. Calcitriol
3. Maintain blood bicarbonate / total CO2 in the range of 18-24 mmol/L (dog) or 16-24 mmol/L (cat)a. Sodium bicarbonate or Potassium citrate (if hypokalemic)
4. If decreased appetite, vomiting, nausea present, consider:a. Antiemeticsb. Proton pump inhibitors
5. Consider treatment for anemia if clinical effects or Hct <20%a. Darbopoetin
6. Prevent protein / calorie malnutritiona. Appetite stimulantsb. Feeding tube?
7. Avoid hypokalemiaa. Potassium gluconate or potassiumcitrate
KEY POINTS • Unfortunately, CKD is progressive and irreversible. However, early recognition and intervention may help to
prevent or minimize additional damage and slow the progression. This may involve the use of new biomarkers(i.e SDMA) or a “universal reference range” rather than laboratory specific reference ranges for creatinine.
• Therapy should be targeted to the specific problems identified in the patient, but general guidelines are availableto help guide treatment decisions.
• Key targets of therapy are phosphorus concentration, persistent renalproteinuria, and systemic hypertension.
193
REFERENCES AND SUGGESTED READINGS 1. IRIS staging of CKD. website: http://www.iris-kidney.com/pdf/3_staging-of-ckd.pdf. Updated 2016.2. IRIS Treatment Recommendations for CKD in Dogs. http://www.iris-kidney.com/pdf/003-5559.001-iris-
website-treatment-recommendation-pdfs-dogs_220116-final.pdf. Updated 2019.3. IRIS Treatment Recommendations for CKD in Cats. http://www.iris-kidney.com/pdf/002-5559-001-iris-
website-treatment-recommendation-pdfs-cats_070116-final.pdf. Updated 2019.4. Special Issue: International Renal Interest Society Consensus Clinical Practice Guidelines for Glomerular
Disease in Dogs. 27(Issue Supplement s1):S1–S75, 2013 (accessed via website at:http://onlinelibrary.wiley.com/doi/10.1111/jvim.2013.27.issue-s1/issuetoc.
5. Jacob F1, Polzin DJ, Osborne CA, et al. Clinical evaluation of dietary modification for treatment of spontaneouschronic renal failure in dogs. J Am Vet Med Assoc. 15;220(8):1163-1170, 2002.
6. Ross SJ, Osborne CA, Kirk CA, et al. Clinical evaluation of dietary modification for treatment of spontaneouschronic kidney disease in cats. J Am Vet Med Assoc. 229:949-957, 2006.
7. Elliott J1, Rawlings JM, Markwell PJ, et al. Survival of cats with naturally occurring chronic renal failure:effect of dietary management. J Small Anim Pract. 41(6):235-42, 2000.
8. Syme HM1, Markwell PJ, Pfeiffer D, et al. Survival of cats with naturally occurring chronic renal failure isrelated to severity of proteinuria. J Vet Intern Med. 20(3):528-35, 2006.
9. Grauer GF, Greco DS, Getzy DM, et al. Effects of enalapril versus placebo as a treatment for canine idiopathicglomerulonephritis. J Vet Intern Med. 14(5):526-33, 2000.
10. Jacob F, Polzin DJ, Osborne CA, et al. Association between initial systolic blood pressure and risk ofdeveloping a uremic crisis or of dying in dogs with chronic renal failure. J Am Vet Med Assoc. 222:322–329,2003.
11. Jepson RE, Elliott J, Brodbelt D, et al. Effect of control of systolic blood pressure on survival in cats withsystemic hypertension. J Vet Intern Med. 21:402-409, 2007.
12. Polzin DJ. Chronic Kidney Disease in Small Animals. Vet Clinics of N Am: Small Anim Pract. 41(1):15-30,2011.
13. Brown CA, Elliott J, Schmiedt CW, et al. Chronic Kidney Disease in Aged Cats: Clinical Features,Morphology, and Proposed Pathogeneses. Vet Pathol. 53(2):309-26, 2016.
194
Beyond Azotemia… What You Need to Know About Proteinuria in Dogs and
Cats Andrew Specht, DVM, DACVIM (SAIM)
University of Florida
INTRODUCTION In recent years there has been an increasing recognition of the importance of persistent renal proteinuria in our small animal patients. The emphasis on early and accurate detection of proteinuria is supported by a number of different studies that have demonstrated an association between proteinuria and renal-cause morbidity and mortality in both dogs and cats and evidence that the risk of adverse outcomes increases as the magnitude of proteinuria increases. There is additional evidence that some medications such as Angiotensin converting enzyme inhibitors (ACEi) also have reno-protective effects.
Assessment of urine protein is now considered an integral part of the diagnostic work-up for any patient with suspected renal disease. Published consensus recommendations from the American College of Veterinary Internal Medicine in 2005 and the International Renal Interest Society (IRIS) in 2009 and 2013 provide some useful guidelines for classification, diagnostic investigation, therapeutic intervention, and monitoring in our small animal patients. Unfortunately, however, there is still a relative paucity of convincing high quality evidence about whether many of these common diagnostic approaches or therapies really do improve our patients’ quality of life or survival times. While this may make some of the recommended guidelines a bit controversial, they can nonetheless serve as a valuable starting point or framework for addressing this challenging but important clinical problem. It is important to keep in mind that these are guidelines, not rules, and it is critical that veterinarians continue to use common sense and their best clinical judgment when determining how to best meet the needs of their individual patients and clients.
CLINICAL INVESTIGATION Among the most important principles when trying to determine the clinical importance of a finding of protein in the urine in any individual patient is to think about each of the following considerations:
1. Verification (Is it real?) - Know what your test really tells you and consider an additional method of testing ifyou are not sure about the result.
2. Localization – There are some classic broad categories to consider first (pre-renal, renal, post renal; or pre-glomerular, glomerular, post glomerular). However, most of the current literature used a slightly more nuancedversion of this that includes four categories:• Pre-renal – Technically this category only applies to dysproteinemias (multiple myeloma, inflammatory
proteins, heme pigments, other abnormal serum proteins…)• Transient Renal – this category incorporates many things previously considered pre-renal such as high
blood pressure, high dietary protein, stress, fever, exercise…• Pathologic renal – this category includes glomerular disease, amyloidosis, and tubular disease• Post-renal – This category includes conditions in which protein enters the urine after it enters the
collecting system such as UTIs, stones, masses, and bleeding.
195
3. Magnitude – While there are few ways to assess this, the Urine protein: creatinine ratio UPC) is the most widely used and forms the basis for most of the published consensus recommendations. The magnitude of proteinuria is only useful if you are confident that the proteinuria is glomerular in origin. Some other things to think about when interpreting UPC results include: o Day to day variation – There is substantial variation in the UPC from one day to the next. Variation is
highest when values are higher. o Method of collection – Although there seems to be a common perception that cystocentesis is better, this
does not actually seem to be particularly important. Urine can be collected by free catch or by cystocentesis for this test.
o Place of collection – Based on a recent study we did at UF, this may be important as we found that values may be higher in samples collected at our clinic compared to those from home samples. However, at this point we still do not know how to interpret this difference.
o Other variables – A number of other factors have also been evaluated such as container type, confinement, time of day, fasting, protein content of diet, etc… In addition, there are several medications such as steroids, ACEi, etc... which could affect the value so a thorough medical history is always important.
4. Persistence – Because there can be cases of transient proteinuria or substantial day-to-day variation, averaging
of UPC values from samples collected on several different day s over a 2-3 week period (or alternatively pooling equal volumes from these samples if they can be stored appropriately) is generally recommended before pursuing additional diagnostic testing or treatment for renal proteinuria.
Although renal proteinuria is not always glomerular in origin (renal tubular lesions can also lead to proteinuria), when serial UPCs reveal persistently high values, primary or secondary glomerular changes should be suspected. One key section in the new IRIS Consensus statements included recommendations for diagnostic investigation of dogs with suspected glomerular disease. Key recommendations from this paper are summarized in the table on the next page and include:
• It is recommended that a classification system involving tiers (based on clinical manifestations of disease -
+/- hypertension, +/- hypoalbuminemia, +/- azotemia) be used to facilitate making appropriate diagnostic testing recommendations.
• A hierarchy of importance (essential, recommended, or potentially helpful) is assigned to particular diagnostic tests based on contextual circumstances.
• Some tests are recommended for all cases of suspected glomerular disease, while others are recommended only when other criteria such as proteinuria of high magnitude or other clinical manifestations of disease (as reflected by tier groupings) are present.
When to Recommend a Kidney Biopsy There is still a fair amount of uncertainty in the veterinary community about the if/when to perform kidney biopsies. At this time, there is still no convincing evidence to support the utility of kidney biopsies in cases of CKD characterized primarily by azotemia. There is an emerging consensus among experts in the field that they may have value in some dogs with persistent renal proteinuria, especially if there is no response to standard therapy. Somewhat more controversial is the use in acute kidney injury cases.
Although there is no consensus about this, many clinicians believe that the following would each be a relative or absolute contraindication for kidney biopsy: 1) untreated/uncorrectable coagulopathy, 2) uncontrolled hypertension, 3) severe anemia, 4) large or multiple renal cysts, 5) hydronephrosis, 6) extensive pyelonephritis, 7) peri-renal abscess, and 8) end stage renal disease. There are a few risks of the procedure, which include damage to the remaining tissues, hemorrhage from the site, and urine leakage. Proper technique and monitoring as well as having an experienced person performing biopsy collection can minimize these risks.
There are several methods for procuring samples, but the most important consideration is to make sure that the sample contains adequate and appropriate tissue for evaluation. The sample(s) should be taken from the cortex and contain at least 5 glomeruli. Samples are divided and processed according to specific instructions provided by the pathology lab. Whenever possible, samples should be evaluated by pathologists with experience in nephropathology
196
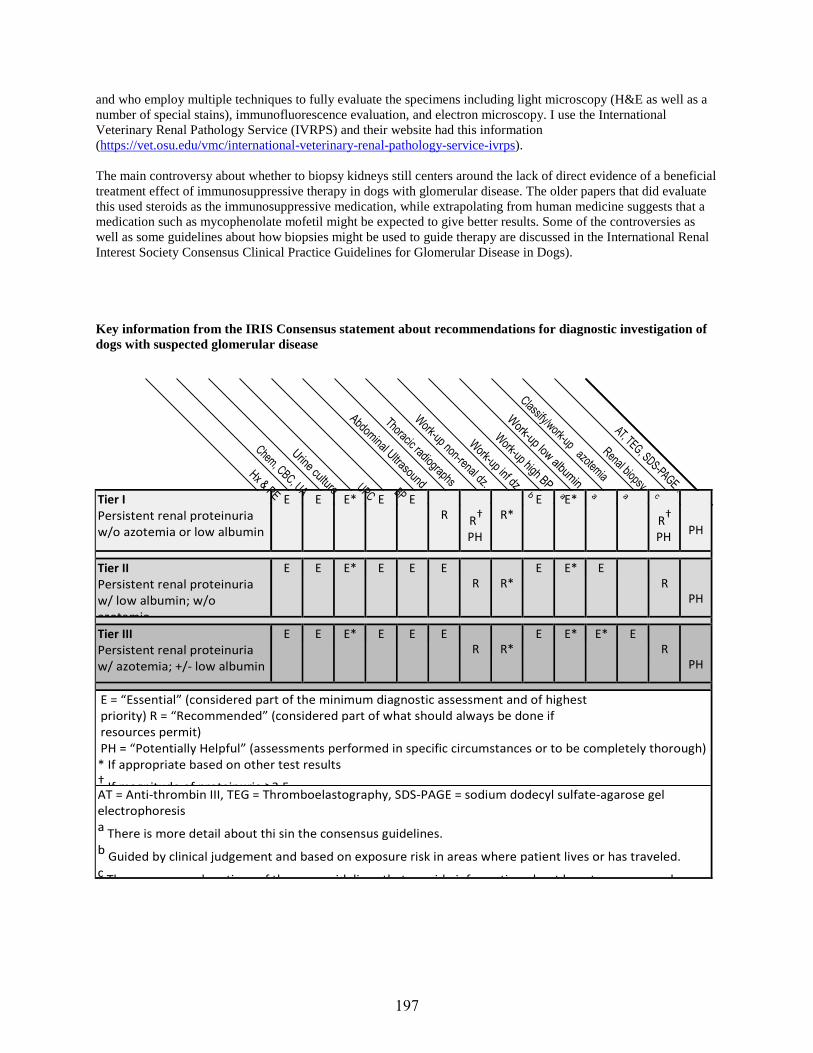
and who employ multiple techniques to fully evaluate the specimens including light microscopy (H&E as well as a number of special stains), immunofluorescence evaluation, and electron microscopy. I use the International Veterinary Renal Pathology Service (IVRPS) and their website had this information (https://vet.osu.edu/vmc/international-veterinary-renal-pathology-service-ivrps).
The main controversy about whether to biopsy kidneys still centers around the lack of direct evidence of a beneficial treatment effect of immunosuppressive therapy in dogs with glomerular disease. The older papers that did evaluate this used steroids as the immunosuppressive medication, while extrapolating from human medicine suggests that a medication such as mycophenolate mofetil might be expected to give better results. Some of the controversies as well as some guidelines about how biopsies might be used to guide therapy are discussed in the International Renal Interest Society Consensus Clinical Practice Guidelines for Glomerular Disease in Dogs).
Key information from the IRIS Consensus statement about recommendations for diagnostic investigation of dogs with suspected glomerular disease
Tier I Persistent renal proteinuria w/o azotemia or low albumin
E E E* E E R
R†
PH
R*
E E* R†
PH
PH
Tier II Persistent renal proteinuria w/ low albumin; w/o azotemia
E E E* E E E R
R*
E E* E R
PH
Tier III Persistent renal proteinuria w/ azotemia; +/- low albumin
E E E* E E E R
R*
E E* E* E R
PH
E = “Essential” (considered part of the minimum diagnostic assessment and of highest priority) R = “Recommended” (considered part of what should always be done if resources permit) PH = “Potentially Helpful” (assessments performed in specific circumstances or to be completely thorough) * If appropriate based on other test results † If magnitude of proteinuria ≥3 5 AT = Anti-thrombin III, TEG = Thromboelastography, SDS-PAGE = sodium dodecyl sulfate-agarose gel electrophoresis a There is more detail about thi sin the consensus guidelines. b Guided by clinical judgement and based on exposure risk in areas where patient lives or has traveled. c Th l ti f th id li th t id i f ti b t h t d
197
CLINICAL MANAGEMENT Another section of the most recent IRIS guidelines deals with recommendations for “standard therapy” of canine glomerular disease which are similar prior IRIS guidelines, but contain some new information/recommendations.
Some key recommendations include:
• Treatment should be considered in any canine patient with persistent renal proteinuria indicated by
repeated/average UPC values >0.5* (This is a bit different in that previously treatment was only recommended for non-azotemic patients when the UPC >1.0)
o Although the guidelines do not cover cats, there is a current IRIS recommendation to use a cutoff value of >0.4 for deciding when to treat proteinuria in cats.
• Serial UPC can be used to monitor response to therapy, with a reduction of UPC values to < 0.5 for dogs or 0.4 for cats (or by >50% from baseline for either species) considered evidence of success.
• Monitoring of patients treated for glomerular proteinuria should be performed at least once every 3 months and should include medical history, physical examination, UA, BP, and serum albumin, creatinine, and potassium concentrations.
• ACEi should be considered as the initial treatment for most patients o Discontinue or lower the dose of ACEi if:
▪ Serum creatinine increases by >30% in a patient with stage 1 or 2 CKD, by >10% in a patient with stage 3 CKD, or by any amount in a patient with stage 4 CKD
▪ Potassium increases to >6.0 mmol/L ▪ Systolic ABP decreases to <120 mmHg
• Dietary modification including reduced n-6: n-3 ratio of polyunsaturated fatty acids, reduced protein, and reduced sodium is recommended.
• Low dose aspirin (1-5mg/kg daily) is recommended for thromboprophylaxis if serum albumin is <2.0 mg/dL.
o Clopidogrel (1-3 mg/kg q24hr) can also be used • Anti-hypertensive therapy should be individualized, but is recommended for all patients with
reliable/repeatable systolic BP >160mmHg. • Careful, serial assessments of fluid status (hydration, vascular volume) are recommended and fluid therapy
should be used with great caution in nephrotic syndrome patients *Personally, I find that my patient population seems to have higher UPC than what is commonly reported in the literature, so I have continued to use a cutoff value of >1.0 UPC for dogs and >0.5 for cats when deciding whether to pursue treatment. I do not know if the difference is in the patients or the laboratory, but I suspect the former.
There are some additional recommendations for treatment with alternative medications if ACEi are not tolerated or target reduction in UPC is not achieved even after appropriate dose escalation. In these cases, addition of angiotensin-receptor blockers (ARBs) or aldosterone antagonists may be considered, but the veterinarian should be aware of and monitor for potential side-effects or consequences when using these medications. For many people a combination of anecdotal success and recent literature has prompted a change to using ARBs as a first-line treatment (in place of ACEi). There is now a licensed product and preliminary data from other clinical trials suggests that they may be more effective than ACEi without causing more side effects.
In addition, the most recently published guidelines do suggest that immunosuppressive medications may be indicated in a much higher proportion of patients than has been previously recommended, however this is still mostly dependent upon having kidney biopsy information, and even then, is among the most controversial of the new recommendations. Overall, unless you are very familiar with these medications or the medical literature related to the protein-losing nephropathies, I would suggest consultation with a specialist prior to instituting these additional treatments.
198
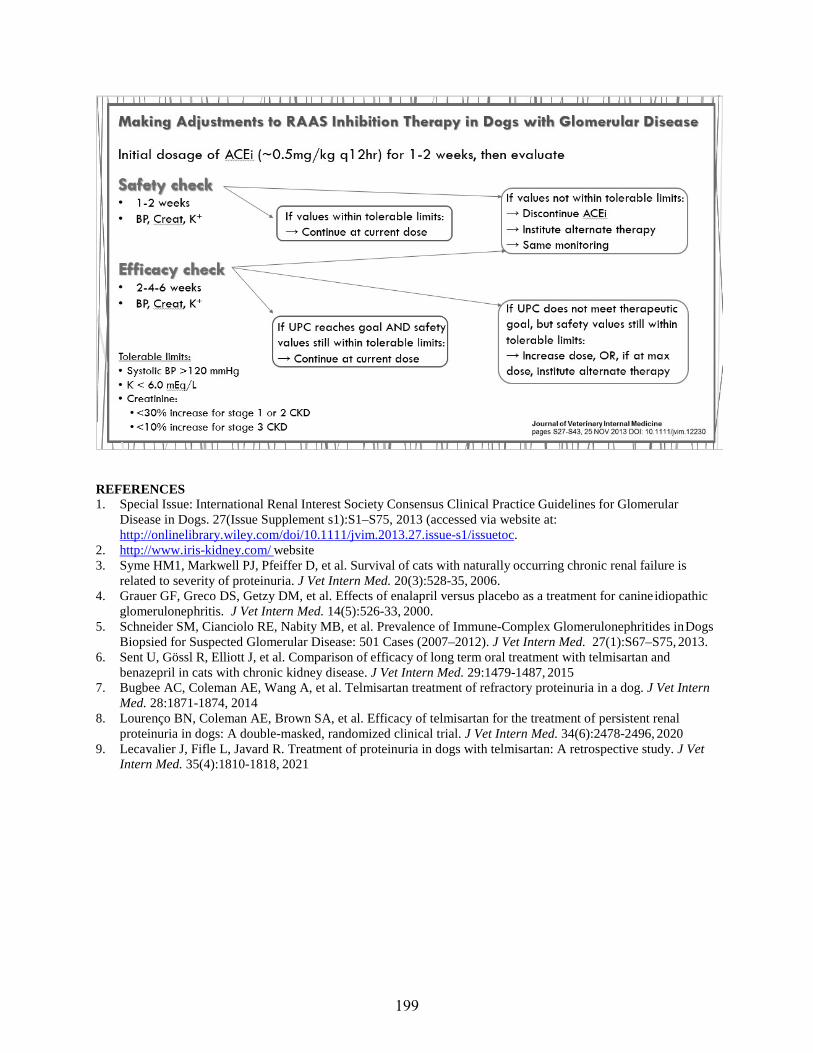
REFERENCES 1. Special Issue: International Renal Interest Society Consensus Clinical Practice Guidelines for Glomerular
Disease in Dogs. 27(Issue Supplement s1):S1–S75, 2013 (accessed via website at: http://onlinelibrary.wiley.com/doi/10.1111/jvim.2013.27.issue-s1/issuetoc.
2. http://www.iris-kidney.com/ website 3. Syme HM1, Markwell PJ, Pfeiffer D, et al. Survival of cats with naturally occurring chronic renal failure is
related to severity of proteinuria. J Vet Intern Med. 20(3):528-35, 2006. 4. Grauer GF, Greco DS, Getzy DM, et al. Effects of enalapril versus placebo as a treatment for canine idiopathic
glomerulonephritis. J Vet Intern Med. 14(5):526-33, 2000. 5. Schneider SM, Cianciolo RE, Nabity MB, et al. Prevalence of Immune-Complex Glomerulonephritides in Dogs
Biopsied for Suspected Glomerular Disease: 501 Cases (2007–2012). J Vet Intern Med. 27(1):S67–S75, 2013. 6. Sent U, Gössl R, Elliott J, et al. Comparison of efficacy of long term oral treatment with telmisartan and
benazepril in cats with chronic kidney disease. J Vet Intern Med. 29:1479-1487, 2015 7. Bugbee AC, Coleman AE, Wang A, et al. Telmisartan treatment of refractory proteinuria in a dog. J Vet Intern
Med. 28:1871-1874, 2014 8. Lourenço BN, Coleman AE, Brown SA, et al. Efficacy of telmisartan for the treatment of persistent renal
proteinuria in dogs: A double-masked, randomized clinical trial. J Vet Intern Med. 34(6):2478-2496, 2020 9. Lecavalier J, Fifle L, Javard R. Treatment of proteinuria in dogs with telmisartan: A retrospective study. J Vet
Intern Med. 35(4):1810-1818, 2021
199
Bothersome Bugs… How to Deal with Persistent or Recurrent UTIs
Andrew Specht, DVM, DACVIM (SAIM) University of Florida
INTRODUCTION Bacterial urinary tract infection (UTI) is a relatively frequent problem in small animal practice. It is estimated that up to 14% of dogs will have a UTI at some point during their life. Most of these are female dogs, but make dogs will also occasionally be affected. UTIs are much less common in cats, but the true incidence is unknown.
Most UTIs are classified as uncomplicated (or sporadic) and will respond to relatively short courses (~10-14 days) of an appropriate antibiotic. These are cases in which no underlying anatomic, structural, functional, neurologic, or mechanical abnormalities are identified. Clinical signs and laboratory abnormalities may improve within the first 24-48 hours in most cases.
Cases in which the patient has an intact reproductive tract, demonstrable predisposing systemic or local risk factors, or a recent history of UTI should be considered to be complicated UTI. There are also some people who argue that any UTI in a cat should be treated as a complicated UTI. When a patient has multiple UTI within a short time frame, we may classify that as a case of recurrent UTI (and this can be further subdivided into persistent UTI and reinfection)
Complicated UTIs should be treated differently than uncomplicated UTIs. An attempt should be made to identify where the host defenses failed. It is vitally important to know the specific pathogen involved in these cases. Multiple urine cultures and long-term antibiotic treatment are required to ensure successful outcomes.
The following text describes a plan for managing cases in which a patient appears to have a UTI that is refractory to treatment, or in which the patient appears to have recurrent UTIs.
DIAGNOSTIC CONSIDERATIONS Confirm the UTI and identify the agent. Confirmation of infection is important for all UTIs, but is essential for complicated UTIs. The only definitive test for UTI is urine culture. There are several situations in which a UTI may be suspected based upon clinical signs or laboratory analysis, but not confirmed with culture. Dysuria, strangury, hematuria, proteinuria, and pyuria are all common with UTI, but are also all non-specific signs. Likewise, a report of bacteriuria on a urinalysis report may be misleading. Many of the stains commonly used for in house analysis can harbor bacteria and urine that is shipped out may be contaminated and have time for even a small number of bacteria to multiply readily.
The distal portion of the urinary tract in normal animals has a resident population of bacteria. Ideally therefore, urine should be collected in a manner that bypasses this portion of the urinary tract (i.e. cystocentesis). Quantitative cultures are especially important if a sterile sample cannot be obtained by cystocentesis and catheterization or voided samples are used.
200
In addition to confirming the diagnosis, a urine culture with antibiotic sensitivity data allows for more rational and specific treatment decisions. This also serves as good baseline information if later testing to help differentiate between persistent infection, relapsing infection, or reinfection is necessary.
If the patient has a recent history of UTI, comparison of the organism species and/or sensitivity patterns can help provide insight into whether the previous treatment failed for some reason, or whether there is a new infection present
Distinguish between UTI and subclinical bacteriuria One paper found that about 9% of “healthy” dogs had subclinical bacteriuria and ~4-5% had the same bacteria present for at least 3 months. Other recent papers have identified bacteriuria in 12-25% of “healthy” older cats. For the most part, the organisms identified are typical for UTI. There is fairly good agreement that patients with no clinical signs and no evidence of urinary tract problems should probably not have cultures performed routinely.
*A good rule of thumb is to reserve urine cultures for situations in which you know in advance that you would treat the infection.
Differentiate between persistent or relapsing infection, and reinfection. Persistence or relapse is diagnosed when the same organism continues to infect the urinary tract despite attempted treatment. Essentially, this can be considered a treatment failure (although it doesn’t always mean that the therapy was inappropriate - just that it didn’t work for this particular case). There are numerous reasons for persistence. These might include iatrogenic factors (e.g. inappropriate dose or treatment duration…), microbial factors (e.g. development of antimicrobial resistance…), host factors (e.g. immunodeficiency…), or other factors (e.g. sequestration of infection within the matrix of a urolith). Recurrence or re-infection is diagnosed when an animal has multiple UTI. This may be due to the same bacterial species establishing a new infection after a period of time with documented clearance in between, or more commonly, a bacterial species identified as the cause of a UTI that is different from previously isolated species. Frequent re-infection typically implies compromise of host defenses.
A third possibility is superinfection. This is diagnosed when a patient that is currently receiving treatment for a UTI is found to have a different organism present in the face of treatment. Superinfections are typically highly resistant and often occur due to iatrogenic factors or compromised host defenses.
Make sure that treatment failure is not due to iatrogenic or microbial factors. A thorough review of the medical history, including initial diagnostic workup is warranted if treatment failure is suspected. In addition, drug choices, and drug doses should be recalculated and the duration of treatment reassessed. Other iatrogenic risk factors should be assessed (e.g. catheterization?...). The sensitivity of the organism should be reassessed to make sure that the resistance pattern has not changed over the course of treatment.
Evaluate the patient for compromise of systemic or local urinary tract defense mechanisms. This is also an important step for any UTI, but is especially important for a complicated UTI. Correction of any underlying disorder is crucial for effectively managing these cases. If the underlying defenses cannot be restored to normal, you may need to consider altering the therapeutic plan to account for this. Defense mechanisms that are at work in the urinary tract are listed in the box on this page.
These host defenses can be compromised by many different disease states or conditions. Some of these may be localized to the urinary tract, while others may de secondary to a distant or systemic process. Diagnostic tests must be chosen accordingly.
201
CURRENT GENERAL MANAGEMENT STRATEGIES General guidelines for uncomplicated/spontaneous/sporadic UTI
• Empiric treatment while pending culture results could include:o Amoxicillin, TMSo NSAIDs
• Antibiotics should not be started in cats until culture results are obtained.• Antibiotic treatment duration 3-5 days
General guidelines for complicated UTI • Choice of antibiotic should be based upon culture and sensitivity• Treatment duration:
o Consider short duration (~3-5 days) for re-infectiono Consider longer duration (~7-14 days) for persistent or relapsing infectiono Previously it was commonly argued that treatment should be continued for 4-8 weeks, and this
may still be required in some cases (see below)o If treating for a longer period, a culture should be performed during treatment
• Culture should be repeated 5-7 days after discontinuation of antibiotics
Additional guidelines for persistent or relapsing UTI • Confirm infection (urine culture)
o Identify organismo Localize source of infection
▪ Attempt to rule out deep tissue infection, uroliths, etc…• Review previous treatment
o Was infection treated as uncomplicated?o Was appropriate antibiotic used?o Were dose and frequency of administration appropriate?o Was duration of treatment appropriate?
o Even if yes, consider longer course this time.o Was owner compliance an issue?
• Review microbial factorso Is there evidence of acquired antimicrobial resistance?
• Review possible causes of compromise to host defenseso Thorough medical history and physical examinationo Minimum data base (Chem, CBC, UA)o Imaging tests
▪ Radiographs (+/- contrast)▪ Ultrasound▪ Endoscopy
o Urodynamic studies, residual volume measurements, etc…o Others as appropriate
▪ ACTH stim, evaluation for co-infections (e.g. mycoplasma), etc…• If no underlying risk factor or cause of treatment failure is identified, pick a new antibiotic and treat as
directed above for complicated UTI.o Consider tissue levels if applicable (i.e. suspected uropathogenic E. coli)
Additional Guidelines for Recurrent UTI or Reinfection • Confirm infection (urine culture) and review possible causes of compromise to host defenses as described
above.• If no underlying risk factor or cause of treatment failure is identified, pick a new antibiotic and treat as
directed above for complicated UTI.
202

OTHER CONSIDERATIONS & FUTURE DIRECTIONS If the approach described above does not result in successful resolution of the problem or if the patient continues to become re-infected on a frequent basis without any identifiable underlying cause (or with an untreatable cause), other therapeutic strategies may need to be employed.1
Urinary antiseptics1
Occasionally we may have some success with urinary antiseptic medications such as methenamine hippurate. This medication is converted to formaldehyde in acidic urine environments (usually <5.5-6.0). It will not be effective unless the urine is routinely acidic which often requires additional medications such as ammonium chloride or dl- methionine.
Prophylactic antibiotics1
We very rarely use this in cases of frequent recurrent UTI or re-infection (not for persistent or relapsing infections). The patient should be culture negative when this is started. Typically, I select a medication that is excreted in high concentration in urine and dose at a time when the urine is likely to be retained for a longer period. One example is to use amoxicillin once a day right before bedtime. This does obviously increase the risk that if another infection develops it will have some antibiotic resistance. This type of antibiotic use is discouraged in the current ISCAID guidelines.
Local infusions1,2
In some situations you might be able to use a medication locally that could not be used systemically. For example aminoglycosides can be infused into the bladder even in the presence of kidney dysfunction. Or an antiseptic such as chlorhexidine could be infused. There are also local medications such as Tris- or Tetra- EDTA that might help to disrupt biofilms. The obvious limitations of this is the short duration of the treatment and the need for an invasive procedure for installation. This technique is not recommended in the current ISCAID guidelines.
D-Mannose & Cranberry extracts1,3,4
D-Mannose sugar may bind to fimbriae of some E. coli strains to inhibit adherence to the urothelial surface.Similarly, proanthocyanidin is the ingredient in cranberry extracts may also inhibit E. coli adherence to theurothelium. There is some in vitro evidence for these, but clinical studies have shown limited or mixed results.
Probiotics & Bacterial interference5
Alterations in distal urogenital tract flora may have some role in establishing UTIs and probiotics have been recommended as a treatment strategy in women. So far, there has been no positive effect of systemic or local probiotic use in male or female dogs or cats that I am aware of, but there are some studies in progress.
There is some early data to suggest that it might be possible to displace a problematic UTI organism with a low- virulence non-pathogenic bacteria. This is still not widely studied and these strains are not available for patients yet, but this may be a future treatment for us.
KEY POINTS • Subclinical bacteriuria does not require treatment.• Patients with multiple UTI over time should be evaluated for underlying problems related to abnormal urinary
tract defenses or systemic immunocompromise.• Urine cultures are critical to classifying the infections in these patients and selecting the most appropriate
antibiotic therapy.• Although the success is variable, there are some options for preventing or managing recurrence or re-infection
in patients for which this is a frequent occurrence.
203
REFERENCES AND SUGGESTED READINGS 1. Olin SJ, Bartges JW. Urinary tract infections: treatment/comparative therapeutics. Vet Clin North Am Small
Anim Pract. 45(4):721-46, 2015. 2. Farca A, Piromalli G, Maffei F, et al. Potentiating effect of EDTA-Tris on the activity of antibiotics against
resistant bacteria associated with otitis, dermatitis and cystitis. J Small Anim Pract. 38:243-245, 1997. 3. Chou HI, Chen KS, Wang HC, et al. Effects of cranberry extract on prevention of urinary tract infection in
dogs and on adhesion of Escherichia coli to Madin-Darby canine kidney cells. Am J Vet Res. 77(4):421-7, 2016. 4. Olby NJ, Vaden SL, Williams K, et al. Effect of Cranberry Extract on the Frequency of Bacteriuria in Dogs
with Acute Thoracolumbar Disk Herniation: A Randomized Controlled Clinical Trial. J Vet Intern Med. 31(1):60-68, 2017.
5. M.F. Thompson, M.A. Schembri, P.C. Mills, et al. A modified three-dose protocol for colonization of the canine urinary tract with the asymptomatic bacteriuria Escherichia coli strain 83972. Vet Microbiol. 158:446- 450, 2012.
6. Byron JK. Urinary tract infection. Vet Clin N Amer Small Anim Pract. 49(2):211-221, 2019. 7. Wan SY, Hartmann FA, Jooss MK, et al. Prevalence and clinical outcome of subclinical bacteriuria in female
dogs. J Am Assoc Vet Med. 245(1);106-112, 2014. 8. Litster A1, Moss S, Platell J, et al. Occult bacterial lower urinary tract infections in cats-urinalysis and culture
findings. Vet Microbiol. 136(1-2):130-134, 2009. 9. Weese JS, Blondeau J, Boothe D, et al. International society for Companion Animal Infectious Diseases
(ISCAID) guidelines for the diagnosis and management of bacterial urinary tract infections in dogs and cats. Vet J. 247:8-25, 2019.
204

Trying Not To Let Cats Think Outside The Box: What We Know About Managing FIC
Andrew Specht, DVM, DACVIM (SAIM) University of Florida
INTRODUCTION Feline lower urinary tract diseases are characterized by hematuria, pollakiuria, and dysuria, and are common problems encountered in feline practice. It is estimated that they affect over one half million cats in the United States annually. Although there are numerous recognized causes of these signs, the exact cause is never identified in the majority of cases. These cases are classified as feline idiopathic cystitis (FIC) and may represent up to ~50-60% of non-obstructive lower urinary tract diseases.1 The biologic behavior of FIC is variable and may be complicated by urinary obstruction due to urethral plugs. Clinical signs in non-obstructed cats often resolve in 2-3 days without therapy, although in about 15% of cats signs may be frequently recurrent or may persist for longer than 3 weeks. The overall recurrence rate without any therapeutic intervention appears to be ~40-55%. Cats with persistent signs or frequent recurrence of signs are sometimes classified as having chronic FIC.
There are numerous theories regarding the etiopathogenesis of FIC. There are some suggestions that the problem is inherent to the urinary system either as a problem with urine, a problem with the urinary tract, or a problem with the urinary tract’s response to urine. Examples of these types of problems would include unrecognized uropathogens, urine toxins, increased permeability, alteration of urinary GAGs, etc… A second theory is that the problem has a more systemic origin, but that the bladder is one of the most commonly recognized sites of clinical problems. The specific systemic disorder(s) in this theory are not well understood but may include inappropriate neurological and hormonal responses to various stressors. This theory also suggests and is supported by the finding of an increased number of co-morbid conditions in cats with FIC. Unfortunately, identifying basic pathologic processes has been hindered by lack of comprehensive histopathologic descriptions of tissue samples (including urinary bladder and other organ systems) and the challenge of clearly establishing a progression or link between cystitis and con -morbid abnormalities in other systems.
Clinical features of FIC are similar to those observed in an idiopathic lower urinary tract disease of humans re ferred to as interstitial cystitis. Interstitial cystitis in humans is a chronic, persistent, and debilitating disorder characterize d by pollakiuria, dysuria, lower abdominal pain, normal urinalysis results and distinctive cystoscopic lesions called glomerulations. Similarities between the clinical features of idiopathic cystitis in cats and interstitial cystitis in humans have prompted speculation that these two conditions are analogous to one another. These similarities also seem to extend to underlying pathophysiologic disturbances and histopathologic lesions. For this reason, several studies have been performed in cats to try to identify beneficial effects for treatments that have shown promise in human medicine.
One of the primary difficulties in any clinical trial for this condition is identifying when a medication has a truly beneficial effect since the majority of cats will recover from their symptoms within 5-7 days without (or despite) therapy. Thus, it is exceptionally important to determine whether there was adequate placebo control and appropriate masking of investigators and clients when evaluating these studies.
DIAGNOSIS As the name implies, this is essentially a diagnosis of exclusion. All other reasonable differential diagnosis should be ruled out if possible. In a typical diagnostic plan for this condition, we would expect that the serum chemistry and CBC would be normal. Urinalysis often shows hematuria +/- pyuria. Urine cultures obviously have to be negative to make this diagnosis. Radiographs or ultrasound often reveal irregular thickening of the bladder wall which may be severe. Cystoscopy, if performed might reveal small hemorrhagic lesions called glomerulations.
It is always a bit challenging to decide how far to go with diagnostic testing of a cat that has previously been diagnosed with FIC, but has a relapse/recurrence at a later date. I do not have specific guidelines to offer, and I think you have to tailor your decisions to the individual patient’s circumstances. Ho wever, for cases in which signs
205
are very chronic or frequently recurrent, it would probably be excessive to perform a full diagnostic workup for each episode.
In addition, considering that one of the current theories about the etiology of this condition involves altered systemic neurologic and hormonal responses, there has been an emerging interest in evaluating patients for other comorbid conditions (e.g. chronic gastrointestinal, behavioral, endocrine, respiratory, or cardiovascular disorders).
TREATMENT OPTIONS At this time, because the underlying cause of FIC remains a mystery, current options for treatment are primarily based upon symptomatic relief, practice experience, and theoretical benefits. As we learn more about the disease, there may be more information available to allow identification of better options. Currently we do not expect that any treatment option will “cure” a cat of this condition. Many cats may not have more than one episode, and no treatment is recommended for these individuals. For those cats that have chronic symptoms or frequently recurrent episodes, some of the potential treatment options are listed below.
The primary goals of any treatment option are therefore aimed at minimizing risks and improving quality of life , by reducing the severity of the symptoms and/or increase the time between episodes . I typically consider four main questions when considering the goals for any therapeutic strategy for an FIC patient:
• Is it in keeping with the general principle of “do no harm”?• Could it reduce the risk of obstruction?• Could it reduce the severity of the clinical signs?• Could it decrease the frequency of clinically apparent episodes?
In all cases of FIC, client education is extremely important, both in terms of helping the clients understand the condition and helping them to understand why you might be choosing any particular strategy for managing the disease. There is even evidence suggesting that clients report improved clinical signs when trained veterinary personnelspend at least 20 minutes discussing the condition and management strategies.
Whatever strategy is chosen should be tailored to the circumstances of the specific patient.
Increase water intake The primary consideration here is to increase the overall water intake of the cat and by extension decrease the concentration of the urine. The primary means of accomplishing this in most cases is by using the canned food formulation of the cat’s normal diet. An early study demonstrated that this simple change decreased the recurrence rate from ~40% to ~10%.2 Latter studies have found similar recurrence rates when providing canned food. Any change of diet formulation should not be made suddenly, but rather gradually so that there is no added stress associated with the transition.
In addition to the increase water content of canned food, owners should be encouraged to try to increase their cat’s water intake in other ways. Consider follow up examinations to monitor the urine specific gravity to help determine if the clients are successfulin improving water intake.
Diet One study (with somewhat complicated data/results) showed fewer relapses and fewer days with clinical signs in cats that ate the test food (Hill’s c/d Multicare – now Metabolic urinary stress) compared with cats that ate the control food (manufactured to mimic common commercially available maintenance diets).3 It is still not clear if diet products marketed by other companies for this purpose would have similar benefits. There have also been anecdotalreports of improvement in some cats fed novel protein diets (as for food allergy), but no cause/effect relationship or objective data have been reported.
There does not appear to be any significant benefit to acidifying the urine or attempting to reduce struvite crystalluria in cats with non-obstructive FIC, but this may be critical in cats that have a history of urethral plugs.
206

Multimodal environmental enrichment (MMEE) or Multi-modal Environmental MOdification (MEMO) Whatever the true underlying disease may be, environmental stressors and indoor lifestyle factors do seem to have an association with the long term clinical picture of FIC. A multi-modal approach to improving the patient’s home environment and decreasing stressors as much as possible is typically recommended for almost all cats (especially if there is any recurrence of signs). This includes looking at a diverse array of factors including: litterboxes (number, cleaning protocol…), availability of food and water, social interactions (other animals and people), available activities/toys, and others. One study has identified that this type of MMEE approach seemed to have a positive effect (decreased severity and frequency of clinical episodes), however, the study did not have a control group. 4
One good source of information about environmental enrichment for cats is the website for the indoor pet initiative at http://indoorpet.osu.edu/. This site has information for veterinarians and pet owners.
Feline pheromone (Feliway®) There is one study that attempted to evaluate the efficacy of this product in cases of FIC. No significant difference was detected although there was a slight trend towards improvement.5 The study was likely underpowered and the methods would be difficult for the average cat owner to duplicate. Nonetheless, this is used by some veterinarians in an attempt to help minimize environmental stresses.
Tricyclic antidepressants (amitriptyline, clomipramine) and other antidepressants/anxiolytics There are conflicting reports about the efficacy of TCAs, and amitriptyline in particular, for cats with FIC. 6,7 There are several potential benefits including analgesia, anxiety reduction, mast cell stabilization, and antagonismof glutamate receptors and sodium channels. Even the proponents of TCA use do not recommend it for acute treatment, but rather for those cases that are severe and persistent or frequently recurrent and for which environmental enrichment, increased water intake and pheromones have not helped. Furthermore, if TCA are discontinued it must be done slowly as a taper over 2-3 weeks to avoid rebound withdrawal symptoms. Lastly, although there are no studies implicating specific drug interactions in cats, TCAs are metabolized b y the cytochrome P450 systemso caution is recommended when using them in conjunction with other medications.
Other antidepressants have also been recommended by some for cats with FIC, but there is even less evidence to support their use. This doesn’t mean that they would be ineffective, just that further study is needed.
GAGs (pentosan polysulfate, Cosequin®) There is some evidence in cats and humans that there are alterations in the GAGs in the urinary bladder. There are a few small reports of intravesical (infusions directly into the bladder) administration of a GAG called pentosan polysulfate helping a subset of human women with interstitial cystitis. There appear to be numerous potential reasons for this improvement, but the exact mechanism remains unknown. So far, studies in cats have not demonstrated significant improvements.8 I am not aware of any evidence of oral GAG (i.e. Cosequin™) supplementation being beneficial in humans or cats.9 However, many people feel that side effects are likely to be limited and minor, and therefore will recommend trying GAGs in refractory/severe FIC cases.
Analgesics & Anti-inflammatory medications There are no controlled studies of specifically analgesic medications in cats with FIC. It does appear that the condition is very uncomfortable and humans with interstitial cystitis report significant pain during symptomatic episodes. Therefore, it has been suggested that although these medications probably do not have an effect on the underlying pathology (still controversial and unproven), they may still be warranted as symptomatic therapy. There are multiple choices and no evidence to support on over the other, so it is probably best to use a medication that can be administered in a minimally stressfulmanner and will not adversely affect the cat’s quality of life at home (e.g. overly sedative).
207
There is no evidence at this time to support the potential benefit of steroids or NSAIDS in cases of FIC. Two small studies of NSAIDs and steroids did not identify significant clinical improvements or reduction in recurrence rates.10,11 In addition, no benefit has been identified in cases of interstitial cystitis in humans. Therefore, these are not generally recommended for cats.
Antibiotics There is no evidence to support the administration of antibiotics for FIC, but they are listed here because they are probably the most frequently administered medication for this condition (usually based upon a false assumption of urinary tract infection). However, because the cats typically get better in 2-3 days, it may appear that an antibiotic (or any other medication) is having a beneficial effect.
It is hard to overstate the importance of performing urine cultures when a UTI is really suspected. Cats actually have a very low incidence of infection (<1-5% of all lower urinary tract disease in youg cats; possibly up to 20% in older cats or cats with other diseases). Cats that do develop recurrent UTI (especially young cats) almost always have some important underlying medical problem.
KEY POINTS • FIC is the most common cause of lower urinary tract disease in cats. • Most cases are self-limiting and may not benefit from treatment. • Client communication is very important. • There are many options for treatment, but the primary ones with evidence of a positive effect are increasing
water consumption, utilizing urinary diets, and providing multi-modal environmental enrichment. • If you think a cat has a UTI, culture is indicated. If a cat has multiple UTIs, a search for underlying disease is
warranted. REFERENCES AND SUGGESTED READINGS 1. Forrester SD, Towell TL. Feline idiopathic cystitis. Vet Clin North Am Small Anim Pract. 45(4):783-806, 2015. 2. Markwell PJ1, Buffington CA, Chew DJ, et al. Clinical evaluation of commercially available urinary
acidification diets in the management of idiopathic cystitis in cats. J Am Vet Med Assoc. 214(3):361-365, 1999. 3. Kruger JM, Lulich JP, MacLeay J, et al. Comparison of foods with differing nutritional profiles for long -term
management of acute nonobstructive idiopathic cystitis in cats. J Am Assoc Vet Med. 247(5):508-517, 2015. 4. Buffington CA1, Westropp JL, Chew DJ, et al. Clinical evaluation of multimodal environmental modification
(MEMO) in the management of cats with idiopathic cystitis. J Feline Med Surg. 8(4):261-268, 2006. 5. Gunn-Moore DA1, Cameron ME. A pilot study using synthetic feline facial pheromone for the management of
feline idiopathic cystitis. J Feline Med Surg. 6(3):133-138, 2004. 6. Chew DJ1, Buffington CA, Kendall MS, et al. Amitriptyline treatment for severe recurrent idiopathic cystitis in
cats. J Am Vet Med Assoc. 213(9):1282-1286, 1998. 7. Kruger JM, Conway TS, Kaneene JB, et al. Randomized controlled trial of the efficacy of short-term
amitriptyline administration for treatment of acute, nonobstructive, idiopathic lower urinary tract disease in cats. J Am Vet Med Assoc. 222(6):749-758, 2003.
8. Wallius BM1, Tidholm AE. Use of pentosan polysulphate in cats with idiopathic, non -obstructive lower urinary tract disease: a double-blind, randomised, placebo-controlled trial. J Feline Med Surg. 11(6):409-412, 2009.
9. Gunn-Moore DA, Shenoy CM. Oral glucosamine and the management of feline idiopathic cystitis. J Feline Med Surg. 6(4):219-25, 2004.
10. Dorsch R, Zellner F, Schulz, et al. Evaluation of meloxicam for the treatment of obstructive idiopathic cystitis. J Feline Med Surg. 18(11):925-933, 2015.
11. Osborne CA1, Kruger JM, Lulich JP, et al. Prednisolone therapy of idiopathic feline lower urinary tract disease: a double-blind clinical study. Vet Clin North Am Small Anim Pract. 26(3):563-9, 1996
208
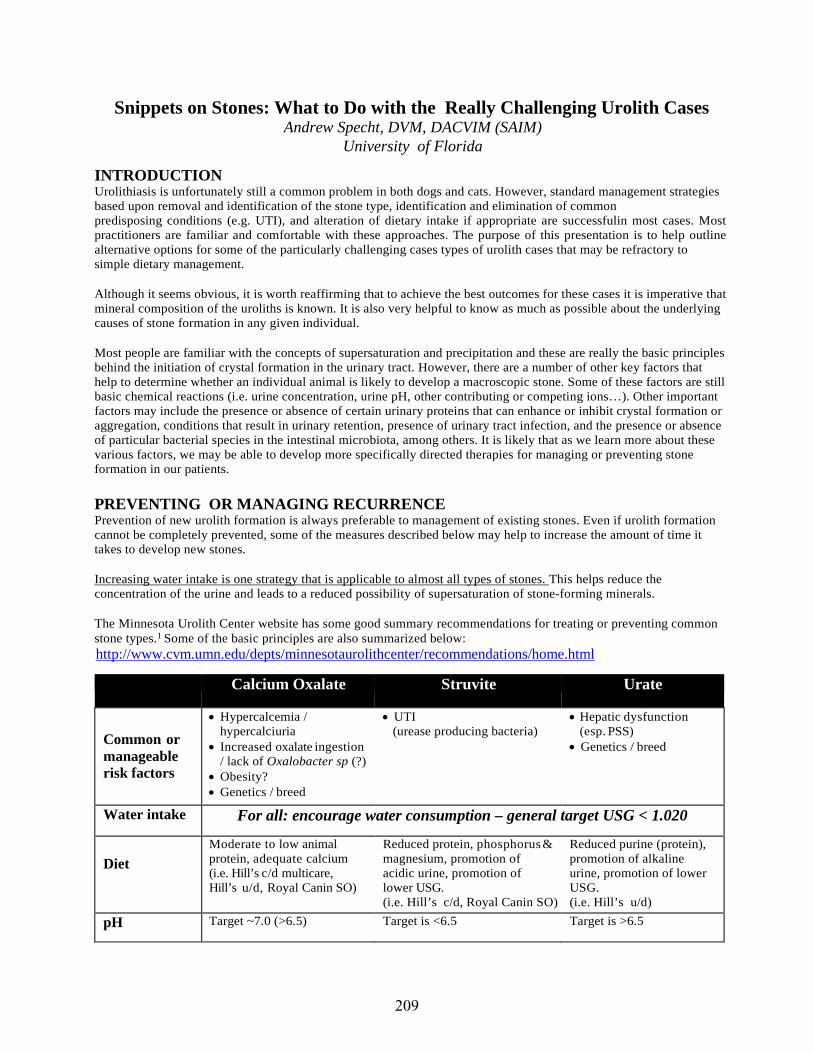
Snippets on Stones: What to Do with the Really Challenging Urolith Cases Andrew Specht, DVM, DACVIM (SAIM)
University of Florida
INTRODUCTION Urolithiasis is unfortunately still a common problem in both dogs and cats. However, standard management strategies based upon removal and identification of the stone type, identification and elimination of common predisposing conditions (e.g. UTI), and alteration of dietary intake if appropriate are successfulin most cases. Most practitioners are familiar and comfortable with these approaches. The purpose of this presentation is to help outline alternative options for some of the particularly challenging cases types of urolith cases that may be refractory to simple dietary management.
Although it seems obvious, it is worth reaffirming that to achieve the best outcomes for these cases it is imperative that mineral composition of the uroliths is known. It is also very helpful to know as much as possible about the underlying causes of stone formation in any given individual.
Most people are familiar with the concepts of supersaturation and precipitation and these are really the basic principles behind the initiation of crystal formation in the urinary tract. However, there are a number of other key factors that help to determine whether an individual animal is likely to develop a macroscopic stone. Some of these factors are still basic chemical reactions (i.e. urine concentration, urine pH, other contributing or competing ions…). Other important factors may include the presence or absence of certain urinary proteins that can enhance or inhibit crystal formation or aggregation, conditions that result in urinary retention, presence of urinary tract infection, and the presence or absence of particular bacterial species in the intestinal microbiota, among others. It is likely that as we learn more about these various factors, we may be able to develop more specifically directed therapies for managing or preventing stone formation in our patients.
PREVENTING OR MANAGING RECURRENCE Prevention of new urolith formation is always preferable to management of existing stones. Even if urolith formation cannot be completely prevented, some of the measures described below may help to increase the amount of time it takes to develop new stones.
Increasing water intake is one strategy that is applicable to almost all types of stones. This helps reduce the concentration of the urine and leads to a reduced possibility of supersaturation of stone-forming minerals.
The Minnesota Urolith Center website has some good summary recommendations for treating or preventing common stone types.1 Some of the basic principles are also summarized below: http://www.cvm.umn.edu/depts/minnesotaurolithcenter/recommendations/home.html
Calcium Oxalate Struvite Urate
Common or manageable risk factors
• Hypercalcemia /hypercalciuria
• Increased oxalate ingestion/ lack of Oxalobacter sp (?)
• Obesity?• Genetics / breed
• UTI(urease producing bacteria)
• Hepatic dysfunction(esp. PSS)
• Genetics / breed
Water intake For all: encourage water consumption – general target USG < 1.020
Diet Moderate to low animal protein, adequate calcium (i.e. Hill’s c/d multicare, Hill’s u/d, Royal Canin SO)
Reduced protein, phosphorus & magnesium, promotion of acidic urine, promotion of lower USG. (i.e. Hill’s c/d, Royal Canin SO)
Reduced purine (protein), promotion of alkaline urine, promotion of lower USG. (i.e. Hill’s u/d)
pH Target ~7.0 (>6.5) Target is <6.5 Target is >6.5
209
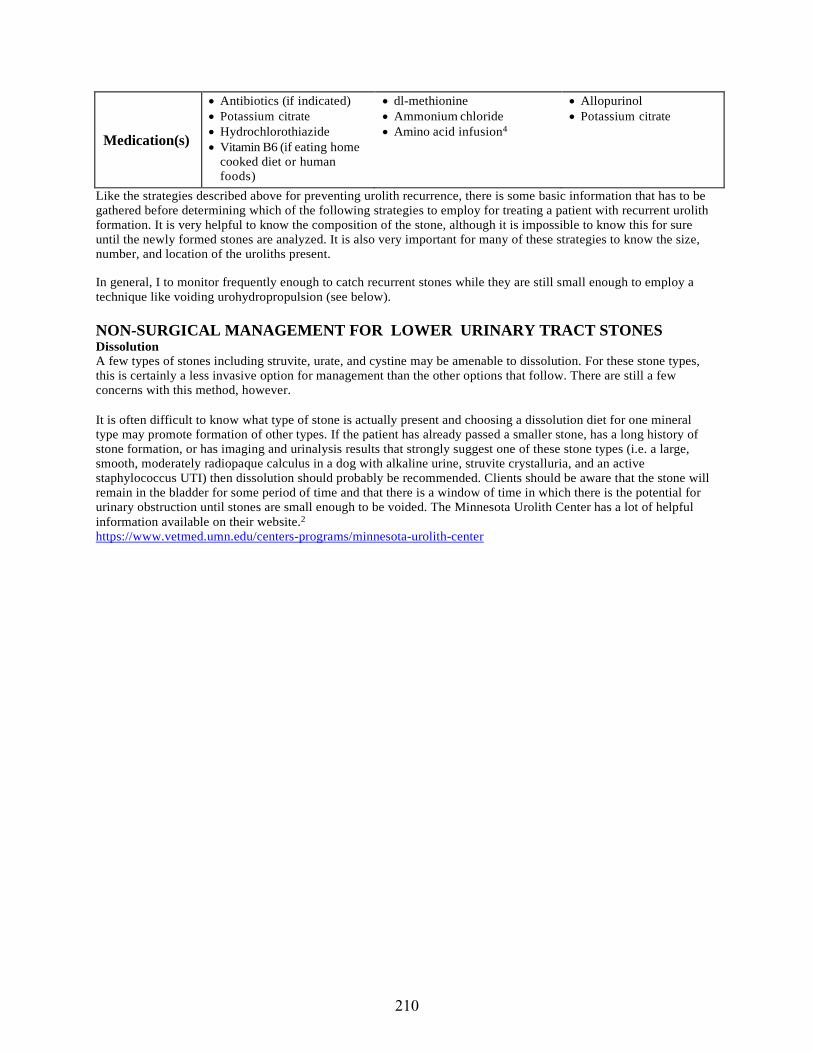
Medication(s)
• Antibiotics (if indicated) • Potassium citrate • Hydrochlorothiazide • Vitamin B6 (if eating home
cooked diet or human foods)
• dl-methionine • Ammonium chloride • Amino acid infusion4
• Allopurinol • Potassium citrate
Like the strategies described above for preventing urolith recurrence, there is some basic information that has to be gathered before determining which of the following strategies to employ for treating a patient with recurrent urolith formation. It is very helpful to know the composition of the stone, although it is impossible to know this for sure until the newly formed stones are analyzed. It is also very important for many of these strategies to know the size, number, and location of the uroliths present.
In general, I to monitor frequently enough to catch recurrent stones while they are still small enough to employ a technique like voiding urohydropropulsion (see below).
NON-SURGICAL MANAGEMENT FOR LOWER URINARY TRACT STONES Dissolution A few types of stones including struvite, urate, and cystine may be amenable to dissolution. For these stone types, this is certainly a less invasive option for management than the other options that follow. There are still a few concerns with this method, however.
It is often difficult to know what type of stone is actually present and choosing a dissolution diet for one mineral type may promote formation of other types. If the patient has already passed a smaller stone, has a long history of stone formation, or has imaging and urinalysis results that strongly suggest one of these stone types (i.e. a large, smooth, moderately radiopaque calculus in a dog with alkaline urine, struvite crystalluria, and an active staphylococcus UTI) then dissolution should probably be recommended. Clients should be aware that the stone will remain in the bladder for some period of time and that there is a window of time in which there is the potential for urinary obstruction until stones are small enough to be voided. The Minnesota Urolith Center has a lot of helpful information available on their website.2
https://www.vetmed.umn.edu/centers-programs/minnesota-urolith-center
210

Strategies for dissolution of different types of uroliths 3-5
Struvite Urate Cystine
Water For all: encourage water consumption – target USG of <1.020
Diet
Reduced protein, phosphorus & magnesium, promotion of acidic urine, promotion of lower USG. (i.e. Hill’s s/d, possibly c/d)
Reduced purine (protein), promotion of alkaline urine, promotion of lower USG. (i.e. Hill’s u/d)
Reduced protein, promotion of alkaline urine, promotion of lower USG. (i.e. Hill’s u/d)
Urine pH Target is <6.5 Target is >6.5 Target is ~7.5
Medications
• Antibiotics (if indicated) • dl-methionine • Ammonium chloride
• Allopurinol • Potassium citrate
• 2-mercaptopropionylglycine (Thiola)
• Potassium citrate
Situations in which I avoid offering dissolution (even if the suspected stone type is likely amenable) include: 1) obstruction, 2) patients with significant clinical signs related to the presence of the stones, 3) patients that cannot receive the appropriate diet or medications, 4) stones that are not able to sit in a pool of urine, and 5) infections that cannot be controlled with medical management.
Appropriate monitoring and follow-up is essentialin these cases. For struvite stones, a recent publication found that failure to document a reduction in urolith size after 2 weeks indicated misdiagnosis or client non -compliance.3
Catheter assisted removal This may work for very small uroliths or “sand”. A urinary catheter is placed with the tip located right at the level of the trigone. The bladder is distended with fluid and the animal positioned/held upright so that the neck and trigone point downward. The bladder is agitated to suspend the stone particles while urine is aspirated rapidly through the catheter. This is repeated until all fluid coming back is clear of stone particles. This can be performed in an awake animal if they tolerate catheterization, or the animal can be sedated if necessary. Voiding urohydropropulsion6
This technique involves expression of small uroliths through the urethra. The patient should be placed under general anesthesia to facilitate positioning and urethral relaxation. The patient is catheterized so that the bladder can be distended with fluid. The catheter is then removed and the animal positioned/held upright so that the neck and trigone point downward. The bladder is agitated to suspend the stone particles and then time is allowed to let the stones settle in the trigone. Next, the bladder is palpated with gradually increasing pressure until a forceful urine stream is created. Fluid and uroliths are collected in a container below the animal. The entire process is repeated until all fluid coming back is clear of stone particles.
This techniques requires that all stones be smaller than the diameter of the urethra (generally <5mm). It also works better for uroliths with a smooth surface rather than jagged stones. Possible complications include obstruction if a stone becomes lodged in the urethra, or rupture of the urinary bladder if excessive force is applied or the wall is unhealthy or damages (e.g. do not perform cystocentesis prior to doing this procedure). There should always be a contingency plan if this method of urolith removal fails or there is a major complication.
This method has worked very well for me in the long term management of patients that have recurrence of their uroliths despite appropriate medical therapy. Most of my monitoring schedules are designed to catch stones at a size <5mm so that this method can be employed if needed.
211
Cystoscopy6
A cystoscope can be used to visualize uroliths within the urinary tract and can be utilized to aid in management in several ways. This is a very quick way to facilitate voiding hydropropulsion. Other instrumentation can also be helpful however:
• Stone baskets can be passed through the channelof the scope and used to capture uroliths. If the stone is small enough it can be removed this way. Otherwise capture of uroliths with stone baskets can help aid the process of lithotripsy when a laser or electrohydraulic machine is used.
• An Ellik evacuator can also be attached to a cystoscope sheath to aid in removal of small uroliths or fragments created by lithotripsy. This process is similar to, but more efficient than, catheter-assisted retrieval as described above.
Lithotripsy6-10
Lithotripsy involves fragmentation of stones in vivo. Although this can be a less invasive procedure compared with surgery, it still requires general anesthesia. There are several methods, but two in particular are being used more frequently in clinical veterinary practice:
• Extracor poreal Shock Wave Lithotripsy (ESWL) utilizes shock waves that are generated outside the body, but focused precisely on a specific target within the body. ESWL is probably most applicable in cases where uroliths are fixed in location (e.g. nephroliths, ureteroliths), but is not currently available for most patients.
• Laser Lithotripsy is gaining popularity as a less invasive method for treating cystic calculi. It is currently only offered at a few referral institutions, but may become more available in the future. A holmium-YA G laser conducting fiber is passed through a cystoscope and a high energy laser is directed at a urolith causing fragmentation.
Surgery This is still the most common way to remove uroliths from the urinary bladder in veterinary patients. Although it is an invasive procedure, dogs and cats generally recover well. Interestingly, only ~0.3-0.4% of human patients with uroliths undergo a surgical procedure for removal, which suggests that it is worth considering the other optio ns listed above. However, for now it is still reasonable to perform surgery in our patients in cases where the above procedures are not appropriate or available. The most common surgical procedure is a laparotomy with cystotomy, however, laparoscopic-assisted cystotomy and percutaneous lithotomy procedures may be less invasive.11-12
MIXED OR COMPOUND UROLITHS Many uroliths are actually composed of more than one mineral type, but there is still typically a predominant (>70%) mineral. In cases in which a single mineral type does not comprise at least 70% of the stone, it is designated as a mixed urolith. Stones in which the different mineral types are separated into distinct layers are designated as compound uroliths. These mixed and compound uroliths comprise about 3-9% of all uroliths and it can sometimes be challenging to design effective medical protocols for managing these stones.
As a rule of thumb, if there is reason to suspect that a part of the stone is comprised of calcium oxalate mineral, there will need to be an interventional management approach at some point in plan. Otherwise, for medical management strategies, if the goal is treatment of existing stones, then the initial focus should be on the outer layer mineral first. If the goal is prevention, then the primary focus is on the core mineral, but also non-specific strategies.
Key highlights for management of some common compound stones include:
• CaOx core / Struvite shell – look for current infection, but focus long-term plan on CaOx prevention • Struvite core / CaPhos shell – Focus on dissolution/prevention of the struvite • Struvite core / CaOx shell – typically occur when efforts to prevent/dissolve struvites are not successful • Silica core – consider risk factor of plant material in diet • Purine core – Always evaluate for predisposing factors
o If shell is struvite – look for and treat infection o If CaOx shell, prevention strategies should be compatible.
212
NEPHROLITHS AND URETEROLITHS Another type of challenge is presented by stones that are identified in the upper urinary tract (i.e. kidneys or ureters). Many of the previous management strategies are not applicable for these stones and there may be very different assessments of the risk vs. benefit of interventions for these stones. Luckily these are much less common (~5-10% of all urinary tract calculi) than cystic calculi. Overall, however, there does seem to be a trend indicating an increase in the prevalence of ureteral calculi, especially in cats.
Some of the key questions to think about after diagnosing a nephrolith or ureterolith are:
1) Is it causing problems? a. Obstruction, infection, deteriorating renal function
2) What type of mineral is suspected? a. Unfortunately high likelihood of calcium oxalate (esp. for ureteroliths)
3) What is the benefit vs. risk of each management strategy?
Benign Neglect Stones that are not causing obstruction and are not associated with recurrent infection or declining kidney function are often simply left in place with a plan for monitoring over time. Many of the interventions mentioned below have at least some risk so it can sometimes be better to avoid them if possible.
Medical management Some kidney stones may still be amenable to dissolution therapy. This is most likely to be effective for struvite calculi. Typical struvite dissolution protocols (specially formulated diet and antibiotics) would be used. Another recent article described the use of intermittent intravenous amino acid administration to aid nephrolith dissolution.
In addition, some ureteral calculi will pass into the bladder if the patient can be supported during this period (analgesics, fluids, diuretics, +/- alpha adrenergic antagonists, +/- calcium channel blockers). This approach should only be used with caution and close monitoring and may not be appropriate if there is evidence of complete obstruction with progressive azotemia or ureteral / renal pelvic dilation, or pyelonephritis.
Extra-corporeal shockwave lithotripsy5
As described before, this is a minimally invasive procedure that has been used successfully in some veterinary patients. It tends to work better in dogs than cats and there are still some significant risks (damage to kidneys or surrounding tissues as well as possible ureteral obstruction from stone fragments). Furthermore, this requires very specialized and expensive equipment so it is not widely available.
Nephrotomy/Ureterotomy Some early research indicated that these procedures consistently resulted in a decrease in renal function (by as much as 20-50%), but more recent research indicated that this is may not always be the case. However, there is at least a risk of this in any case that undergoes surgery.
Percutaneous nephrolithotomy6-7
Although still surgical, this procedure offers a small incision and is considered more “nephron -sparing” than the other surgical approaches.
Ureteral stenting / Subcutaneous ureteral bypass (SUB) devices 8,9
These have recently become very popular in the US for treatment of ureteral calculi. Stents may be placed in a minimally invasive manner in many dogs, but this does require special equipment and expertise. SUBs can be used in dogs or cats, but typically require a surgical approach. The advantage of these procedures is that they reduce the risk of damage to the kidney and revision may be possible later if complications develop.
213
KEY POINTS • Prevention of stones is always preferable to managing recurrence, but is not always feasible (especially in
breeds or individuals with a genetic predisposition to stone formation). Identifying stones at the smallest size allows for less invasive methods of removal.
• Compound stones can be challenging to manage without removal, but once the core mineral type is identified, appropriate strategies for preventing recurrence can be identified.
• Nephroliths and ureteroliths do not always have to be addressed, but it they are obstructive, there are some minimally invasive treatment options available.
REFERENCES AND SUGGESTED READINGS 1. Web resource: https://www.vetmed.umn.edu/centers-programs/minnesota-urolith-center (accessed June 2017) 2. Lulich JP1, Kruger JM, Macleay JM, Merrills JM, Paetau-Robinson I, Albasan H, Osborne CA. Efficacy of two
commercially available, low-magnesium, urine-acidifying dry foods for the dissolution of struvite uroliths in cats. J Am Vet Med Assoc. 243(8):1147-1153, 2013.
3. Bartges JW, Osborne CA, Lulich JP, et al. Canine urate urolithiasis. Etiopathogenesis, diagnosis, and management. Vet Clin North Am Small Anim Pract 29:161–191, 1999.
4. Mishina M, Watanabe T, Fujii K, et al. Medical Dissolution of Struvite Nephrolithiasis Using Amino Acid Preparation in Dogs. J. Vet. Med. Sci. 62(8): 889-892, 2000.
5. Block G, Adams LG, Widmer WR, et al. Use of extracorporeal shock wave lithotripsy for treatment of spontaneous nephrolithiasis and ureterolithiasis in dogs. J Am Vet Med Assoc. 208:531–536, 1996.
6. Donner GS1, Ellison GW, Ackerman N, et al. Percutaneous nephrolithotomy in the dog. An experimental study. Vet Surg. 16(6):411-417, 1987.
7. Berent AC. Interventional Urology: Endourology in Small Animal Veterinary Medicine. Vet Clin N Amer: Sml Anim Pract. 45(4):825-855, 2015.
8. Kuntz JA1, Berent AC, Weisse CW, et al. Double pigtail ureteral stenting and renal pelvic lavage for renal- sparing treatment of obstructive pyonephrosis in dogs: 13 cases (2008-2012). J Am Vet Med Assoc. 246(2):216- 225, 2015.
9. Horowitz C1, Berent A, Weisse C, et al. Predictors of outcome for cats with ureteral obstructions after interventional management using ureteral stents or a s ubcutaneous ureteralbypass device. J Feline Med Surg. 15(12):1052-1062, 2013.
214

What’s New in Nephrology: Quick Hits and Hot Takes on a Variety of Topics
Andrew Specht, DVM, DACVIM (SAIM) University of Florida
INTRODUCTION This session will be broken into a few 2-5 short discussions about different topics in veterinary urology and nephrology. The audience will help me select the specific topics to be discussed from a list of things that small animal practitioners often ask about. These proceedings notes are not comprehensive, but cover some of the key points from each section.
Topics for this session might include any of the following: • Understanding and using SDMA• Asymptomatic/subclinical bacteriuria• When & how I use ARBs to treat proteinuria• When to recommend kidney biopsy• Phosphate binder choice / use in CKD• Stents and SUBs – why, when, what to do after• Updates on TCC• NSAIDS and CKD
SDMA1-4 This is a relatively new biomarker from IDEXX laboratories that had been heavily marketed in the last couple years. There are a few major claims that have been made about SDMA that will be examined if we choose this topic.
Claim #1 - SDMA is a biomarker for kidney disease. This is true and supported by evidence as SDMA is well correlated with GFR. However, this means that high SDMA could result from “pre-renal” causes of GFR decrease such as hypovolemia as well as kidney disease. Also, a normal SDMA does not rule out kidney disease (especially very early/mild changes, or changes to the glomeruli resulting in proteinuria.
Claim #2 - SDMA increases earlier than creatinine in chronic kidney disease. This is true and supported by evidence, but the degree to which it is true depends a lot on how you interpret both values. If you stage CKD according to IRIS guidelines and use a more “universal” cut-off for creatinine that is based on how it corresponds to GFR (like IDEXX suggests we do for SDMA), then the difference between the two values is probably dramatically less obvious.
Claim #3 – SDMA is specific for kidney function / GFR changes. There is not yet enough evidence to fully support this claim. There is very good evidence that SDMA is not affected by muscle mass in the same way that creatinine is. There are some conditions in people that can lead to increased SDMA measurements and these have not all been evaluated in veterinary patients.
Claim #4 – With SDMA, more patients could be diagnosed with CKD. This is true and supported by evidence, but requires clarification (especially if you utilize the laboratory specific cutoff and reference ranges for the key values).
215
Again, this difference is probably much less dramatic if we base our interpretations of both values on their relative correlation with GFR. It should also be noted that although regular monitoring is almost certainly a good practice, we do not have a lot of evidence to support making clinical decisions about treatments for patients diagnosed with CKD at a very early/mild stage.
ASYMPTOMATIC/SUBCLINICAL BACTERIURIA5,6 This is generally accepted to describe bacteria in urine (determined by culture) in the absence of other clinical and cytological evidence of infection. There seems to be an increasing level of interest in this in the veterinary community in recent years.
There is some evidence about the prevalence of this in dogs and cats. One paper found that about 9% of “healthy” dogs had subclinical bacteriuria and ~4-5% had the same bacteria present for at least 3 months. Other recent papers have identified bacteriuria in 12-25% of “healthy” older cats. For the most part, the organisms identified are typical for UTI.
The main controversy about this is whether/when to treat. There is wide agreement that any dog with clinical signs associated with a UTI should receive treatment. There is also a fairly good agreement that patients with no clinical signs and no evidence of urinary tract problems should probably not have cultures performed routinely. Areas of some controversy include cases where there is 1) evidence of a significant inflammatory response (i.e. hematuria, pyuria), 2) concurrent endocrine disease that could predispose the patient to infection or where the infection may affect medical management of other disorders (i.e. Cushing’s disease, diabetes mellitus), 3) patients with impaired urinary tract defenses, 4) patients with conditions that might make it difficult to recognize clinical signs (i.e. neurologic disease), and 5) those with risk of secondary medical problems (i.e. pyelonephritis).
A good rule of thumb is to reserve urine cultures for situations in which you know in advance that you would treat the infection.
WHEN & HOW I USE ARBS TO TREAT PROTEINURIA7,8 Essentially, I would consider using ARBs in any case that I thought might benefit from an ACEi, but especially those cases in which ACEi did not work or caused undesirable side effects. Angiotensin receptor blockers (ARBs) have similar effects to angiotensin converting enzyme inhibitors (ACEi) in terms of their effects on proteinuria, but there are some differences. When ACEi are effective they will have downstream effects on angiotensin receptors 1 & 2, while the commonly used are ARBs are specific for receptor 1 which may preserve some of the beneficial effects of ATR2 activation. Currently, I am still using ARBs as a second-line drug, but am leaning more and more towards using them as my first choice.
216
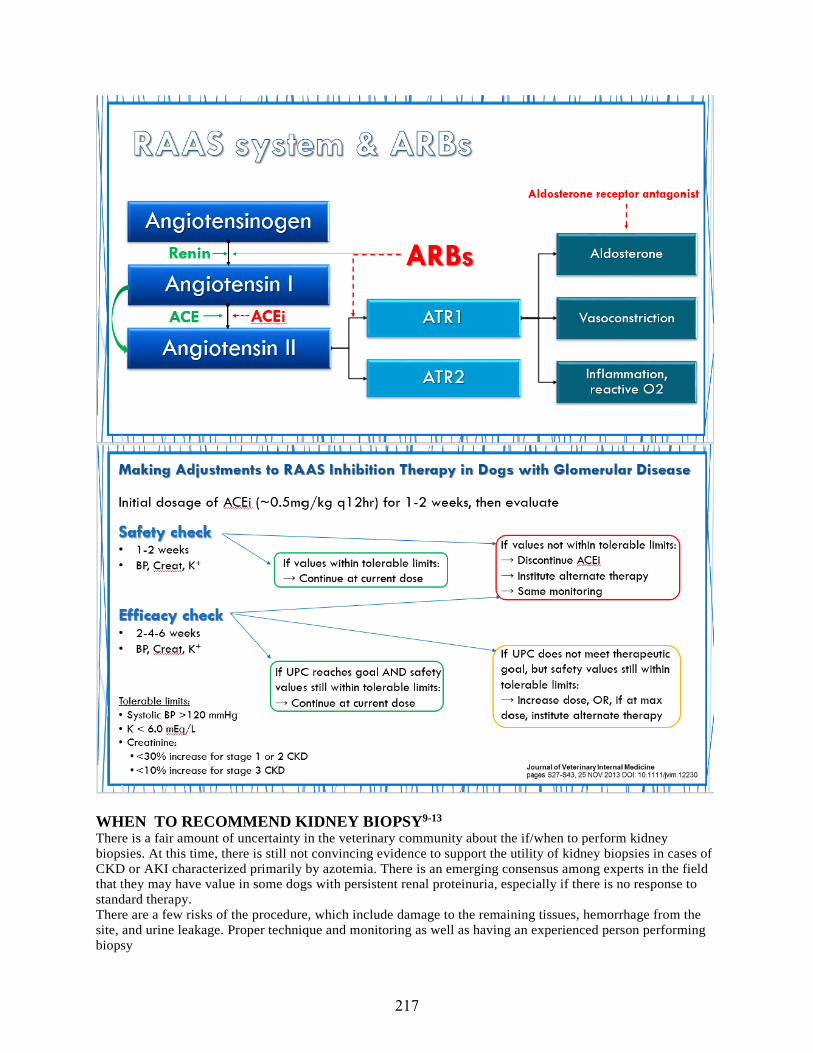
WHEN TO RECOMMEND KIDNEY BIOPSY9-13 There is a fair amount of uncertainty in the veterinary community about the if/when to perform kidney biopsies. At this time, there is still not convincing evidence to support the utility of kidney biopsies in cases of CKD or AKI characterized primarily by azotemia. There is an emerging consensus among experts in the field that they may have value in some dogs with persistent renal proteinuria, especially if there is no response to standard therapy. There are a few risks of the procedure, which include damage to the remaining tissues, hemorrhage from the site, and urine leakage. Proper technique and monitoring as well as having an experienced person performing biopsy
217

collection can minimize these risks. Although there is no consensus, many clinicians believe that the following would each be a relative or absolute contraindication for kidney biopsy: 1) untreated/uncorrectable coagulopathy, 2) uncontrolled hypertension, 3) severe anemia, 4) large or multiple renal cysts, 5) hydronephrosis, 6) extensive pyelonephritis, 7) peri-renal abscess, and 8) end stage renal disease.
There are several methods for procuring samples, but the most important consideration is to make sure that the sample contains adequate and appropriate tissue for evaluation. The sample(s) should be taken from the cortex and contain at least 5 glomeruli. Samples are processed according to specific instructions provided by the pathology lab. Whenever possible, samples should be evaluated by pathologists with experience in nephropathology and who employ multiple techniques to fully evaluate the specimens including light microscopy (H&E as well as a number of special stains), immunofluorescence evaluation, and electron microscopy. I use the International Veterinary Renal Pathology Service (IVRPS) and their website has this information (https://vet.osu.edu/vmc/international-veterinary- renal-pathology-service-ivrps).
The main controversy about whether to biops y kidneys still centers around the lack of direct evidence of a beneficial treatment effect of immunosuppressive therapy in dogs with glomerular disease. The older papers that did evaluate this used steroids as the immunosuppressive medication, while extrapolating from human medicine suggests that a medication such as mycophenolate mofetil might be expected to give better results. Some of the controversies as well as some guidelines about how biopsies might be used to guide therapy are discussed in the IRIS Consensus Clinical Practice Guidelines for Glomerular Disease in Dogs).
PHOSPHATE BINDER CHOICE / USE IN CKD There is good evidence that control of serum phosphorus levels is important in the management of chronic kidney disease. This can help to minimize ongoing tubular injury and slow progression of azotemia, prevent tissue mineralization, and help control the secondary hyperparathyroidism. However, there are variable recommendations about the target value and there are many different available t reatment options.
In many cases, especially with early/mild CKD, a specially formulated kidney diet may be enough to maintain adequate control of phosphorus levels. However, when patients refuse to eat these diets or when the disease progresses to later stages, medications are generally required.
Aluminum Calcium Chitosan Lanthanum Sevelamer
Form Complexed with hydroxide, carbonate,
Complexed with acetate, citrate, carbonate
i.e. Epakitin®Combinationproduct w/calcium carbonate
A rare earth metal complexed with carbonate One formulation i
An organic polymer resin complexed with carbonate or HCl
Toxicity / risks
-aluminum canbuild up overtime and causeneuromusculareffects,microcytosis-constipation
-hypercalcemia-tissuemineralization(if serum Phosvery high)-constipation
As for calcium- based products
Lower efficacy than other options
-vomiting, reducedappetence
-reduces vitaminabsorption?-may affectother electrolytes and acid-base balance -vomiting,
Drug interactions
-Many:-can decreaseabsorption ofothermedications -oftenrecommended to
-Several:-can decreaseabsorption ofothermedications-absorption maybe decreased if
As for calcium- based products
Unclear: -likely sensibleto assumesimilar effectsonabsorption ofmedications as
-Several:-can decreaseabsorption ofothermedications
218

calcium Phos binders (to improve efficacy and reduce toxicity)
-be aware ofcalcium effects-May havesynergism with aluminum Phos binders (to improve efficacy
-reduced effect ifstomach acidsecretionsuppressed?
Cost inexpensive inexpensive moderate expensive in US Very expensive in US
Other notes Powder or compounded capsules are often more palatable th fl d
May help minimize secondary hyper- parathyroidism
May reduce serum cholesterol Other beneficial effects reported in h di l i
Use with caution if GI tract not intact (i.e. ulcers, colitis…) as it may be absorbed.
May reduce serum cholesterol
NEPHROLITHS & URETEROLITHS14,15 Another type of challenge is presented by stones that are identified in the upper urinary tract (i.e. kidneys or ureters). Many of the previous management strategies are not applicable for these stones and there may be very different assessments of the risk vs. benefit of interventions for these stones. Luckily these are much less common (~5-10% of all urinary tract calculi) than cystic calculi. Overall, however, there does seem to be a recent trend indicating an increase in the prevalence of ureteral calculi, especially in cats.
Some of the key questions to think about after diagnosing a nephrolith or ureterolith are: 1. Is it causing problems?
a. Obstruction, infection, deteriorating renal function2. What type of mineral is suspected?
a. Unfortunately, high likelihood of calcium oxalate (esp. for ureteroliths)3. What is the benefit vs. risk of each management strategy?
Medical management Some kidney stones may still be amenable to dissolution therapy. This is most likely to be effective for struvite calculi. Typical struvite dissolution protocols (specially formulated diet and antibiotics) would be used. Another recent article described the use of intermittent intravenous amino acid administration to aid nephrolith dissolution.
In addition, some ureteral calculi will pass into the bladder if the patient can be supported during this period (analgesics, fluids, diuretics, +/- alpha adrenergic antagonists, +/- calcium channel blockers). This approach should only be used with caution and close monitoring and may not be appropriate if there is evidence of complete obstruction with progressive azotemia or ureteral / renal pelvic dilation, or pyelonephritis. Obstruction lasting greater than 4 days is likely associated with at least some degree of irreversible injury.
Lithotripsy As described before, extracorporeal shockwave lithotripsy is a minimally invasive procedure that has been used successfully in some veterinary patients. It tends to work better in dogs than cats and there are still some significant risks (damage to kidneys or surrounding tissues as well as possible ureteral obstruction from stone fragments). Furthermore, this requires very specialized and expensive equipment so it is not widely available. Endoscopic neprolithotomy has been used in a small number of cases so far and may provide another means for treatment, but this requires very specialized training and equipment, so it is also not widely available.
Nephrotomy / Ureterotomy Some early research indicated that these procedures consistently resulted in a decrease in renal function (by as much as 20-50%), but more recent research indicated that this is may not always be the case. However, there is at least a risk of this in any case that undergoes surgery.
219
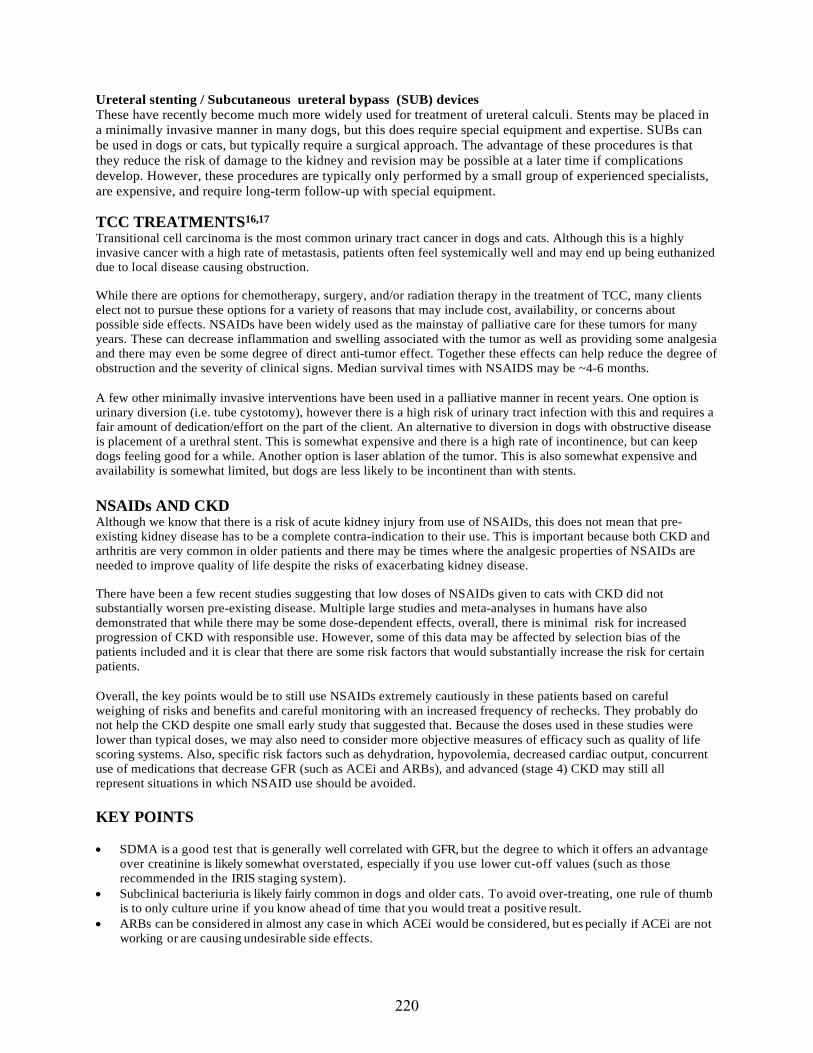
Ureteral stenting / Subcutaneous ureteral bypass (SUB) devices These have recently become much more widely used for treatment of ureteral calculi. Stents may be placed in a minimally invasive manner in many dogs, but this does require special equipment and expertise. SUBs can be used in dogs or cats, but typically require a surgical approach. The advantage of these procedures is that they reduce the risk of damage to the kidney and revision may be possible at a later time if complications develop. However, these procedures are typically only performed by a small group of experienced specialists, are expensive, and require long-term follow-up with special equipment.
TCC TREATMENTS16,17 Transitional cell carcinoma is the most common urinary tract cancer in dogs and cats. Although this is a highly invasive cancer with a high rate of metastasis, patients often feel systemically well and may end up being euthanized due to local disease causing obstruction.
While there are options for chemotherapy, surgery, and/or radiation therapy in the treatment of TCC, many clients elect not to pursue these options for a variety of reasons that may include cost, availability, or concerns about possible side effects. NSAIDs have been widely used as the mainstay of palliative care for these tumors for many years. These can decrease inflammation and swelling associated with the tumor as well as providing some analgesia and there may even be some degree of direct anti-tumor effect. Together these effects can help reduce the degree of obstruction and the severity of clinical signs. Median survival times with NSAIDS may be ~4-6 months.
A few other minimally invasive interventions have been used in a palliative manner in recent years. One option is urinary diversion (i.e. tube cystotomy), however there is a high risk of urinary tract infection with this and requires a fair amount of dedication/effort on the part of the client. An alternative to diversion in dogs with obstructive disease is placement of a urethral stent. This is somewhat expensive and there is a high rate of incontinence, but can keep dogs feeling good for a while. Another option is laser ablation of the tumor. This is also somewhat expensive and availability is somewhat limited, but dogs are less likely to be incontinent than with stents.
NSAIDs AND CKD Although we know that there is a risk of acute kidney injury from use of NSAIDs, this does not mean that pre- existing kidney disease has to be a complete contra-indication to their use. This is important because both CKD and arthritis are very common in older patients and there may be times where the analgesic properties of NSAIDs are needed to improve quality of life despite the risks of exacerbating kidney disease.
There have been a few recent studies suggesting that low doses of NSAIDs given to cats with CKD did not substantially worsen pre-existing disease. Multiple large studies and meta-analyses in humans have also demonstrated that while there may be some dose-dependent effects, overall, there is minimal risk for increased progression of CKD with responsible use. However, some of this data may be affected by selection bias of the patients included and it is clear that there are some risk factors that would substantially increase the risk for certain patients.
Overall, the key points would be to still use NSAIDs extremely cautiously in these patients based on careful weighing of risks and benefits and careful monitoring with an increased frequency of rechecks. They probably do not help the CKD despite one small early study that suggested that. Because the doses used in these studies were lower than typical doses, we may also need to consider more objective measures of efficacy such as quality of life scoring systems. Also, specific risk factors such as dehydration, hypovolemia, decreased cardiac output, concurrent use of medications that decrease GFR (such as ACEi and ARBs), and advanced (stage 4) CKD may still all represent situations in which NSAID use should be avoided.
KEY POINTS
• SDMA is a good test that is generally well correlated with GFR, but the degree to which it offers an advantageover creatinine is likely somewhat overstated, especially if you use lower cut-off values (such as thoserecommended in the IRIS staging system).
• Subclinical bacteriuria is likely fairly common in dogs and older cats. To avoid over-treating, one rule of thumbis to only culture urine if you know ahead of time that you would treat a positive result.
• ARBs can be considered in almost any case in which ACEi would be considered, but es pecially if ACEi are notworking or are causing undesirable side effects.
220
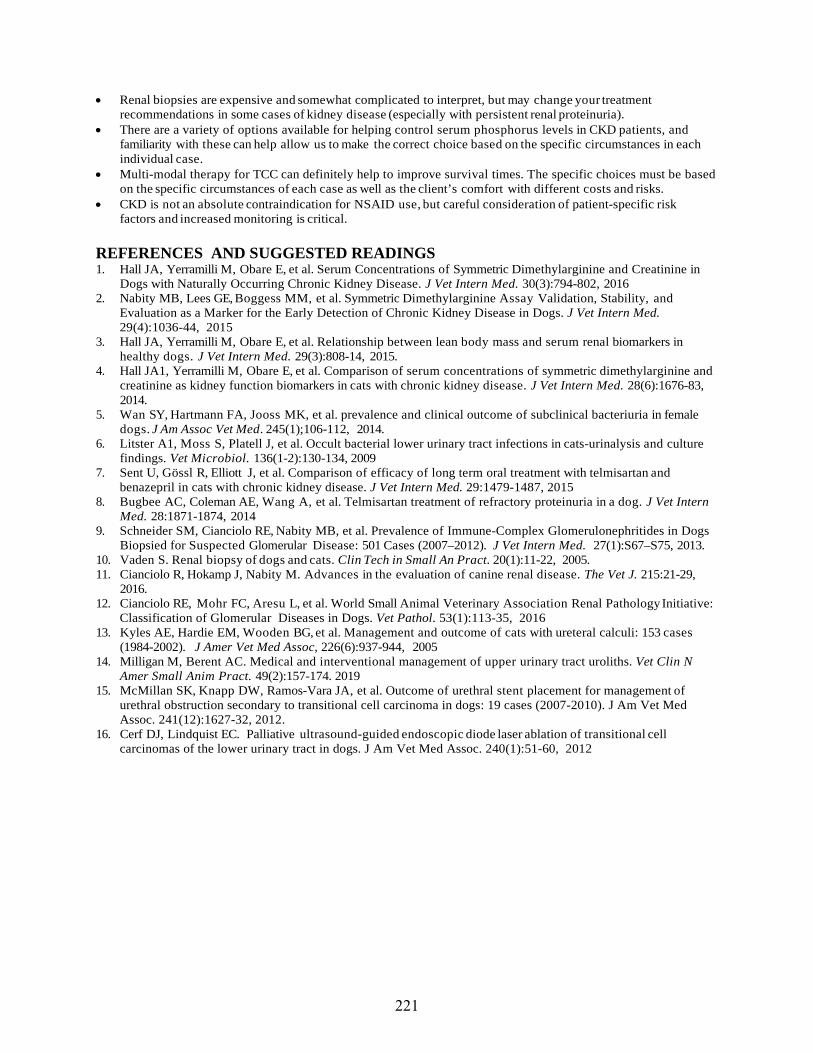
• Renal biopsies are expensive and somewhat complicated to interpret, but may change your treatmentrecommendations in some cases of kidney disease (especially with persistent renal proteinuria).
• There are a variety of options available for helping control serum phosphorus levels in CKD patients, andfamiliarity with these can help allow us to make the correct choice based on the specific circumstances in eachindividual case.
• Multi-modal therapy for TCC can definitely help to improve survival times. The specific choices must be basedon the specific circumstances of each case as well as the client’s comfort with different costs and risks.
• CKD is not an absolute contraindication for NSAID use, but careful consideration of patient-specific riskfactors and increased monitoring is critical.
REFERENCES AND SUGGESTED READINGS 1. Hall JA, Yerramilli M, Obare E, et al. Serum Concentrations of Symmetric Dimethylarginine and Creatinine in
Dogs with Naturally Occurring Chronic Kidney Disease. J Vet Intern Med. 30(3):794-802, 20162. Nabity MB, Lees GE, Boggess MM, et al. Symmetric Dimethylarginine Assay Validation, Stability, and
Evaluation as a Marker for the Early Detection of Chronic Kidney Disease in Dogs. J Vet Intern Med.29(4):1036-44, 2015
3. Hall JA, Yerramilli M, Obare E, et al. Relationship between lean body mass and serum renal biomarkers inhealthy dogs. J Vet Intern Med. 29(3):808-14, 2015.
4. Hall JA1, Yerramilli M, Obare E, et al. Comparison of serum concentrations of symmetric dimethylarginine andcreatinine as kidney function biomarkers in cats with chronic kidney disease. J Vet Intern Med. 28(6):1676-83,2014.
5. Wan SY, Hartmann FA, Jooss MK, et al. prevalence and clinical outcome of subclinical bacteriuria in femaledogs. J Am Assoc Vet Med. 245(1);106-112, 2014.
6. Litster A1, Moss S, Platell J, et al. Occult bacterial lower urinary tract infections in cats-urinalysis and culturefindings. Vet Microbiol. 136(1-2):130-134, 2009
7. Sent U, Gössl R, Elliott J, et al. Comparison of efficacy of long term oral treatment with telmisartan andbenazepril in cats with chronic kidney disease. J Vet Intern Med. 29:1479-1487, 2015
8. Bugbee AC, Coleman AE, Wang A, et al. Telmisartan treatment of refractory proteinuria in a dog. J Vet InternMed. 28:1871-1874, 2014
9. Schneider SM, Cianciolo RE, Nabity MB, et al. Prevalence of Immune-Complex Glomerulonephritides in DogsBiopsied for Suspected Glomerular Disease: 501 Cases (2007–2012). J Vet Intern Med. 27(1):S67–S75, 2013.
10. Vaden S. Renal biopsy of dogs and cats. Clin Tech in Small An Pract. 20(1):11-22, 2005.11. Cianciolo R, Hokamp J, Nabity M. Advances in the evaluation of canine renal disease. The Vet J. 215:21-29,
2016.12. Cianciolo RE, Mohr FC, Aresu L, et al. World Small Animal Veterinary Association Renal Pathology Initiative:
Classification of Glomerular Diseases in Dogs. Vet Pathol. 53(1):113-35, 201613. Kyles AE, Hardie EM, Wooden BG, et al. Management and outcome of cats with ureteral calculi: 153 cases
(1984-2002). J Amer Vet Med Assoc, 226(6):937-944, 200514. Milligan M, Berent AC. Medical and interventional management of upper urinary tract uroliths. Vet Clin N
Amer Small Anim Pract. 49(2):157-174. 201915. McMillan SK, Knapp DW, Ramos-Vara JA, et al. Outcome of urethral stent placement for management of
urethral obstruction secondary to transitional cell carcinoma in dogs: 19 cases (2007-2010). J Am Vet MedAssoc. 241(12):1627-32, 2012.
16. Cerf DJ, Lindquist EC. Palliative ultrasound-guided endoscopic diode laser ablation of transitional cellcarcinomas of the lower urinary tract in dogs. J Am Vet Med Assoc. 240(1):51-60, 2012
221

Urinalysis Tips and Tricks Heather L. Wamsley, BS, DVM, PhD, Dipl. ACVP-Clinical
Tampa, FL USA
OVERVIEW Urine samples are labile; components of the urine sample may change or may be lost during the delay between sample collection and sample analysis. Ideally, a trained individual should examine urine samples soon after collection. Routine urinalysis is a test that may be improved by performing it in-house.
INTRODUCTION Complete urinalysis includes assessment of several physical and chemical characteristics of urine. It is a simple, economical test that requires minimal specialized equipment and can be easily performed by trained staff in general veterinary practice. With proper sample handling and testing, data generated by urinalysis rapidly disclose vital information about the urinary tract and also provide a general screen of other body systems (e.g. endocrine, hepatic). Taking advantage of the full potential of in-house urinalysis can rapidly provide you with information that will benefit you and your patients.
ADDITIONAL DETAIL Urine Sample Collection Method, Timing, and Handling Prior to Analysis In addition to biologic variability of the patient, urinalysis results are influenced by the urine collection method, the timing of urine collection, administration of therapeutic or diagnostic agents prior to collection, and how the sample is handled prior to analysis. There are several methods of urine collection each with their own advantages and disadvantages. Ideally at least 6 mL of urine should be collected prior to the administration of therapeutic or diagnostic agents so that baseline information can be established. In most situations, either naturally voided urine, collected midstream into a sterile container or urine obtained by cystocentesis is preferred. Since urine collection method can have a significant effect upon urinalysis results, it is important to record the collection method in medical records. It should also be indicated whether or not therapeutic or diagnostic agents (e.g. parenteral fluids, antimicrobials, glucocorticoids, diuretics, antihypertensives, radiographic contrast) have been administered prior to urine collection. If so, the type of agent and timing and duration of administration relative to urine collection should be recorded.
Timing of collection during the day also influences results. First morning urine is maximally concentrated. This is good for USG monitoring. However, this urine is held in bladder for prolonged period, which may reduce viability of fastidious organisms and alter cell morphology due to cell degradation. First morning urine samples are also more likely to be acidic. Time of collection relative to a meal may influence biochemical tests. The effect of a pH modifying diet is maximal within 3-6 hours of a meal. Samples collected within 3-4 hours are helpful to detect hyperglycemic glucosuria. Samples collected within 1 hour of a meal are more likely to be alkaline due to postprandial alkaline tide. Randomly timed urine samples are held in bladder for less time. This may be good for cell morphology and culture of fastidious organisms. However, the USG value will not represent the maximal urine concentration ability of the renal tubules.
Ideally, urine should be collected into a sterile, opaque, sealable, labeled container and analyzed within 60 minutes of collection. If it is not possible to analyze the sample within 60 minutes, the sample should be preserved by refrigeration soon after collection for up to approximately 12 hours (i.e. overnight). Samples intended for routine urinalysis should not be frozen. Also, though numerous chemical preservatives of urine exist (e.g. boric acid,
222

formalin, Mucolexx™), routine use of these preservatives is not recommended, since each may affect differentcomponents of the urinalysis. It is important that sealed containers are used for urine sample storage since certain volatile compounds may evaporate (e.g. ketones), and samples should be protected from light since certain compounds may degrade due to light-exposure (e.g. bilirubin).
Refrigeration is considered the optimal preservation method since it prevents bacterial overgrowth, preserves cellular and cast morphology, and does not affect chemical testing as long as the sample is returned to room temperature prior to analysis. Cold urine may cause a false increase in urine specific gravity, and cold urine may inhibit the chemical reactions on the urine multitest dipstick. Refrigeration also promotes crystal formation (i.e. calcium oxalate dihydrate, magnesium ammonium phosphate) that becomes worse as the duration of storage increases (Albasan et al., 2003). To minimize refrigeration artifacts, samples should be allowed to warm to room temperature prior to urinalysis. Also, if crystalluria is observed in a sample that has been refrigerated or that has been stored for greater than 6 hours regardless of the storage temperature, the finding should be confirmed with a freshly obtained, nonrefrigerated urine sample that will be analyzed within 30 to 60 minutes of collection.
Urinalysis: wet-mount versus dry-mount Urinalysis performed in-house by a trained staff member, soon after urine sample collection is a great way to reduce or avoid artifacts that can arise during the delay between sample collection and sample analysis. Keeping such analysis in-house may increase productivity and potentially improve your urinalysis laboratory results. In addition to traditional wet-mount urinalysis, dry-mount cytology of urine samples can be very useful in suspected cases of urinary tract infection (Swenson et al., 2004) or urinary tract neoplasia. The method is described below here. Slides prepared using this method can be evaluated in-house, or they can be readily sent to an outside laboratory for review by a pathologist. The benefit is that diagnostic material on slides prepared this way will not degrade the same way that it would in a liquid urine sample during transport to an out-of-house, reference laboratory. Often when fluid urine samples are sent to a reference laboratory for pathologist review to diagnose neoplasia, cells deteriorate to the point where cytologic diagnosis no longer possible.
Method to prepare urine sediment for dry-mounting and routine cytologic examination 1) Centrifuge the urine as is done for wet-mounting.2) Use a transfer pipette to aspirate the pellet from the bottom of the conical centrifuge tube.3) Place a small drop of the aspirated material onto a clean, glass microscope slide.4) Use a second clean, glass microscope slide to spread the material in a monolayer.5) Allow the slide to air-dry. Heat fixation is not necessary and would alter cell morphology.6) Stain as a routine cytology using Diff Quik® or other similar stain. Alternatively, the slide can be stored in
a covered container at room temperature and sent to a outside diagnostic laboratory for evaluation by apathologist.
REFERENCES AND FURTHER READING 1. Albasan H, Lulich JP, Osborne CA, Lekcharoensuk C, Ulrich LK and Carpenter KA (2003) Effects of
storage time and temperature on pH, specific gravity, and crystal formation in urine samples from dogs andcats. Journal of the American Veterinary Medical Association 222, 176-179
2. Osborne CA and Stevens JB (1999) Urinalysis: A Clinical Guide to Compassionate Patient Care, 1stedn. Veterinary Learning Systems, Bayer Corporation, Shawnee Mission, Kansas
3. Swenson CL, Boisvert AM, Kruger JM and Gibbons-Burgener SN (2004) Evaluation of modified Wright-staining of urine sediment as a method for accurate detection of bacteriuria in dogs. Journal of theAmerican Veterinary Medical Association 224, 1282-1289
4. Wamsley HL (2019) Examination of Urine Sediment. In Valenciano AC, Cowell RL (ed): Cowell andTyler’s Diagnostic Cytology and Hematology of the Dog and Cat, 5th ed–St. Louis, MO: Elsevier, 2019,Chapter 23.
223

Urinalysis Sediment Microscopy Review Heather L. Wamsley, BS, DVM, PhD, Dipl. ACVP-Clinical
Tampa, FL USA
OVERVIEW Urine samples are labile; components of the urine sample may change or may be lost during the delay between sample collection and sample analysis. Ideally, urine samples should be examined soon after collection by a trained individual. Routine urinalysis is a test that may be improved by performing it in-house.
INTRODUCTION Complete urinalysis includes assessment of several physical and chemical characteristics of urine. It is a simple, economical test that requires minimal specialized equipment and can be easily performed by trained staff in general veterinary practice. With proper sample handling and testing, data generated by urinalysis rapidly disclose vital information about the urinary tract and also provide a general screen of other body systems (e.g. endocrine, hepatic). Taking advantage of the full potential of in-house urinalysis can rapidly provide you with information that will benefit you and your patients.
ADDITIONAL DETAIL Urine Sample Collection Method, Timing, and Handling Prior to Analysis In addition to biologic variability of the patient, urinalysis results are influenced by the urine collection method, the timing of urine collection, administration of therapeutic or diagnostic agents prior to collection, and how the sample is handled prior to analysis. There are several methods of urine collection each with their own advantages and disadvantages. Ideally at least 6 mL of urine should be collected prior to the administration of therapeutic or diagnostic agents so that baseline information can be established. In most situations, either naturally voided urine, collected midstream into a sterile container or urine obtained by cystocentesis is preferred. Since urine collection method can have a significant effect upon urinalysis results, it is important to record the collection method in medical records. It should also be indicated whether or not therapeutic or diagnostic agents (e.g. parenteral fluids, antimicrobials, glucocorticoids, diuretics, antihypertensives, radiographic contrast) have been administered prior to urine collection. If so, the type of agent and timing and duration of administration relative to urine collection should be recorded.
Ideally, urine should be collected into a sterile, opaque, sealable, labeled container and analyzed within 60 minutes of collection. If it is not possible to analyze the sample within 60 minutes, the sample should be preserved by refrigeration soon after collection for up to approximately 12 hours (i.e. overnight). Samples intended for routine urinalysis should not be frozen. Also, though numerous chemical preservatives of urine exist (e.g. boric acid, formalin, Mucolexx™), routine use of these preservatives is not recommended, since each may affect differentcomponents of the urinalysis. It is important that sealed containers are used for urine sample storage since certain volatile compounds may evaporate (e.g. ketones), and samples should be protected from light since certain compounds may degrade due to light-exposure (e.g. bilirubin).
Refrigeration is considered the optimal preservation method since it prevents bacterial overgrowth, preserves cellular and cast morphology, and does not affect chemical testing as long as the sample is returned to room temperature prior to analysis. Cold urine may cause a false increase in urine specific gravity, and cold urine may inhibit the chemical reactions on the urine multitest dipstick. Refrigeration also promotes crystal formation (i.e. calcium oxalate dihydrate, magnesium ammonium phosphate) that becomes worse as the duration of storage increases (Albasan et al., 2003). To minimize refrigeration artifacts, samples should be allowed to warm to room temperature prior to urinalysis. Also, if crystalluria is observed in a sample that has been refrigerated or that has been stored for greater than 6 hours regardless of the storage temperature, the finding should be confirmed with a freshly obtained, nonrefrigerated urine sample that will be analyzed within 30 to 60 minutes of collection.
Urine Sediment Wet-Mount Findings Crystalluria occurs when urine is saturated with dissolved minerals or other crystallogenic substances that precipitate out of solution to form crystals. Crystals may form in vivo for either pathologic or nonpathologic reasons, or crystals may precipitate in urine ex vivo due to cold temperature or prolonged storage, postcollection alterations of urine pH, or evaporation of water from the sample. To increase the likelihood that crystals present in the urine
224
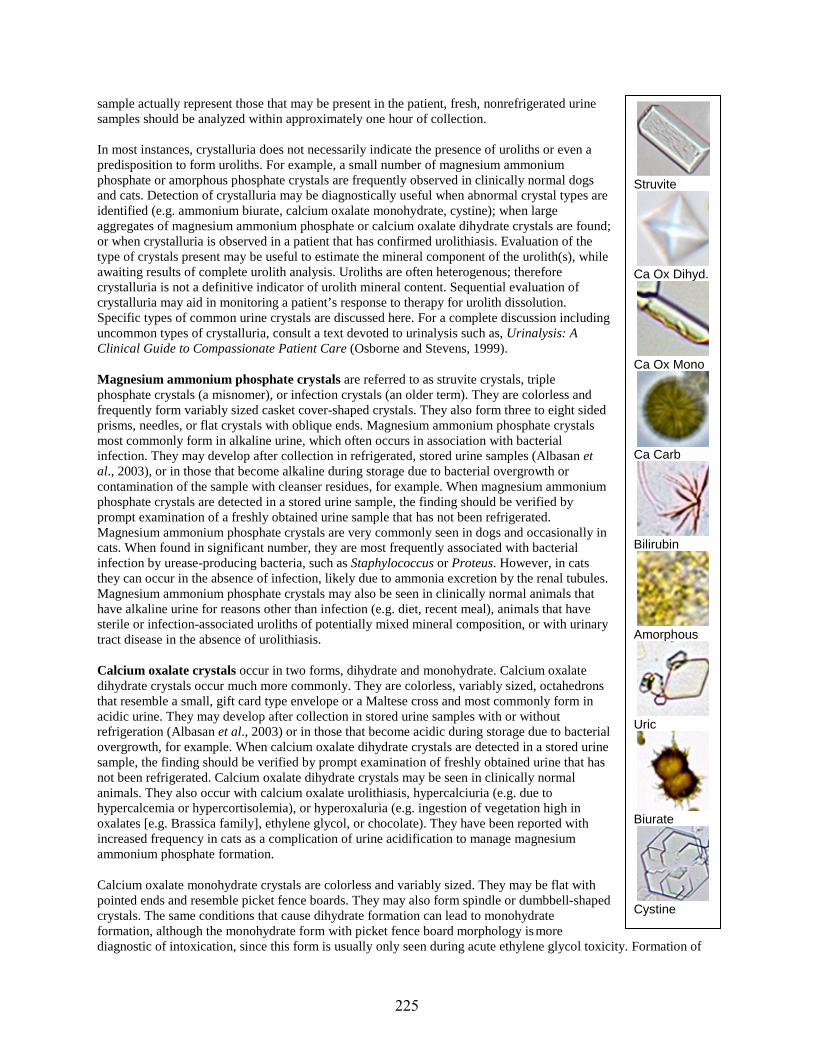
sample actually represent those that may be present in the patient, fresh, nonrefrigerated urine samples should be analyzed within approximately one hour of collection.
In most instances, crystalluria does not necessarily indicate the presence of uroliths or even a predisposition to form uroliths. For example, a small number of magnesium ammonium phosphate or amorphous phosphate crystals are frequently observed in clinically normal dogs and cats. Detection of crystalluria may be diagnostically useful when abnormal crystal types are identified (e.g. ammonium biurate, calcium oxalate monohydrate, cystine); when large aggregates of magnesium ammonium phosphate or calcium oxalate dihydrate crystals are found; or when crystalluria is observed in a patient that has confirmed urolithiasis. Evaluation of the type of crystals present may be useful to estimate the mineral component of the urolith(s), while awaiting results of complete urolith analysis. Uroliths are often heterogenous; therefore crystalluria is not a definitive indicator of urolith mineral content. Sequential evaluation of crystalluria may aid in monitoring a patient’s response to therapy for urolith dissolution. Specific types of common urine crystals are discussed here. For a complete discussion including uncommon types of crystalluria, consult a text devoted to urinalysis such as, Urinalysis: A Clinical Guide to Compassionate Patient Care (Osborne and Stevens, 1999).
Magnesium ammonium phosphate crystals are referred to as struvite crystals, triple phosphate crystals (a misnomer), or infection crystals (an older term). They are colorless and frequently form variably sized casket cover-shaped crystals. They also form three to eight sided prisms, needles, or flat crystals with oblique ends. Magnesium ammonium phosphate crystals most commonly form in alkaline urine, which often occurs in association with bacterial infection. They may develop after collection in refrigerated, stored urine samples (Albasan et al., 2003), or in those that become alkaline during storage due to bacterial overgrowth or contamination of the sample with cleanser residues, for example. When magnesium ammonium phosphate crystals are detected in a stored urine sample, the finding should be verified by prompt examination of a freshly obtained urine sample that has not been refrigerated. Magnesium ammonium phosphate crystals are very commonly seen in dogs and occasionally in cats. When found in significant number, they are most frequently associated with bacterial infection by urease-producing bacteria, such as Staphylococcus or Proteus. However, in cats they can occur in the absence of infection, likely due to ammonia excretion by the renal tubules. Magnesium ammonium phosphate crystals may also be seen in clinically normal animals that have alkaline urine for reasons other than infection (e.g. diet, recent meal), animals that have sterile or infection-associated uroliths of potentially mixed mineral composition, or with urinary tract disease in the absence of urolithiasis.
Calcium oxalate crystals occur in two forms, dihydrate and monohydrate. Calcium oxalate dihydrate crystals occur much more commonly. They are colorless, variably sized, octahedrons that resemble a small, gift card type envelope or a Maltese cross and most commonly form in acidic urine. They may develop after collection in stored urine samples with or without refrigeration (Albasan et al., 2003) or in those that become acidic during storage due to bacterial overgrowth, for example. When calcium oxalate dihydrate crystals are detected in a stored urine sample, the finding should be verified by prompt examination of freshly obtained urine that has not been refrigerated. Calcium oxalate dihydrate crystals may be seen in clinically normal animals. They also occur with calcium oxalate urolithiasis, hypercalciuria (e.g. due to hypercalcemia or hypercortisolemia), or hyperoxaluria (e.g. ingestion of vegetation high in oxalates [e.g. Brassica family], ethylene glycol, or chocolate). They have been reported with increased frequency in cats as a complication of urine acidification to manage magnesium ammonium phosphate formation.
Calcium oxalate monohydrate crystals are colorless and variably sized. They may be flat with pointed ends and resemble picket fence boards. They may also form spindle or dumbbell-shaped crystals. The same conditions that cause dihydrate formation can lead to monohydrate formation, although the monohydrate form with picket fence board morphology is more diagnostic of intoxication, since this form is usually only seen during acute ethylene glycol toxicity. Formation of
Struvite
Ca Ox Dihyd.
Ca Ox Mono
Ca Carb
Bilirubin
Amorphous
Uric
Biurate
Cystine
225
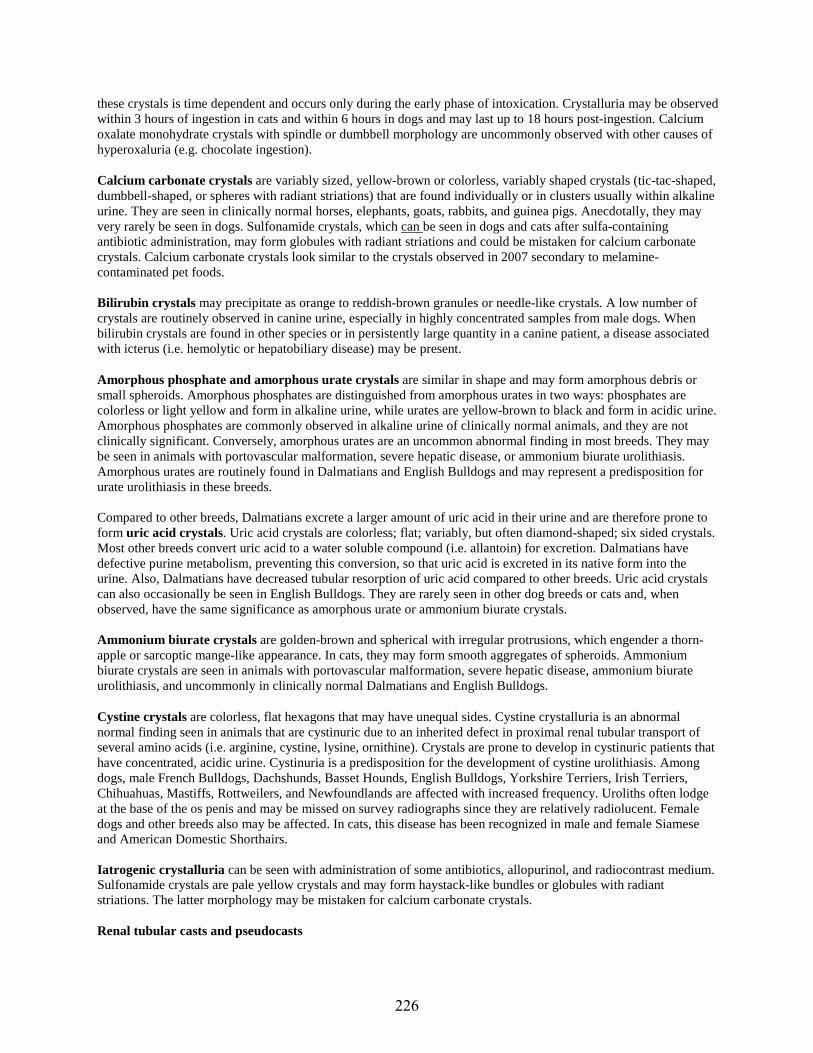
these crystals is time dependent and occurs only during the early phase of intoxication. Crystalluria may be observed within 3 hours of ingestion in cats and within 6 hours in dogs and may last up to 18 hours post-ingestion. Calcium oxalate monohydrate crystals with spindle or dumbbell morphology are uncommonly observed with other causes of hyperoxaluria (e.g. chocolate ingestion).
Calcium carbonate crystals are variably sized, yellow-brown or colorless, variably shaped crystals (tic-tac-shaped, dumbbell-shaped, or spheres with radiant striations) that are found individually or in clusters usually within alkaline urine. They are seen in clinically normal horses, elephants, goats, rabbits, and guinea pigs. Anecdotally, they may very rarely be seen in dogs. Sulfonamide crystals, which can be seen in dogs and cats after sulfa-containing antibiotic administration, may form globules with radiant striations and could be mistaken for calcium carbonate crystals. Calcium carbonate crystals look similar to the crystals observed in 2007 secondary to melamine- contaminated pet foods.
Bilirubin crystals may precipitate as orange to reddish-brown granules or needle-like crystals. A low number of crystals are routinely observed in canine urine, especially in highly concentrated samples from male dogs. When bilirubin crystals are found in other species or in persistently large quantity in a canine patient, a disease associated with icterus (i.e. hemolytic or hepatobiliary disease) may be present.
Amorphous phosphate and amorphous urate crystals are similar in shape and may form amorphous debris or small spheroids. Amorphous phosphates are distinguished from amorphous urates in two ways: phosphates are colorless or light yellow and form in alkaline urine, while urates are yellow-brown to black and form in acidic urine. Amorphous phosphates are commonly observed in alkaline urine of clinically normal animals, and they are not clinically significant. Conversely, amorphous urates are an uncommon abnormal finding in most breeds. They may be seen in animals with portovascular malformation, severe hepatic disease, or ammonium biurate urolithiasis. Amorphous urates are routinely found in Dalmatians and English Bulldogs and may represent a predisposition for urate urolithiasis in these breeds.
Compared to other breeds, Dalmatians excrete a larger amount of uric acid in their urine and are therefore prone to form uric acid crystals. Uric acid crystals are colorless; flat; variably, but often diamond-shaped; six sided crystals. Most other breeds convert uric acid to a water soluble compound (i.e. allantoin) for excretion. Dalmatians have defective purine metabolism, preventing this conversion, so that uric acid is excreted in its native form into the urine. Also, Dalmatians have decreased tubular resorption of uric acid compared to other breeds. Uric acid crystals can also occasionally be seen in English Bulldogs. They are rarely seen in other dog breeds or cats and, when observed, have the same significance as amorphous urate or ammonium biurate crystals.
Ammonium biurate crystals are golden-brown and spherical with irregular protrusions, which engender a thorn- apple or sarcoptic mange-like appearance. In cats, they may form smooth aggregates of spheroids. Ammonium biurate crystals are seen in animals with portovascular malformation, severe hepatic disease, ammonium biurate urolithiasis, and uncommonly in clinically normal Dalmatians and English Bulldogs.
Cystine crystals are colorless, flat hexagons that may have unequal sides. Cystine crystalluria is an abnormal normal finding seen in animals that are cystinuric due to an inherited defect in proximal renal tubular transport of several amino acids (i.e. arginine, cystine, lysine, ornithine). Crystals are prone to develop in cystinuric patients that have concentrated, acidic urine. Cystinuria is a predisposition for the development of cystine urolithiasis. Among dogs, male French Bulldogs, Dachshunds, Basset Hounds, English Bulldogs, Yorkshire Terriers, Irish Terriers, Chihuahuas, Mastiffs, Rottweilers, and Newfoundlands are affected with increased frequency. Uroliths often lodge at the base of the os penis and may be missed on survey radiographs since they are relatively radiolucent. Female dogs and other breeds also may be affected. In cats, this disease has been recognized in male and female Siamese and American Domestic Shorthairs.
Iatrogenic crystalluria can be seen with administration of some antibiotics, allopurinol, and radiocontrast medium. Sulfonamide crystals are pale yellow crystals and may form haystack-like bundles or globules with radiant striations. The latter morphology may be mistaken for calcium carbonate crystals.
Renal tubular casts and pseudocasts
226

Renal tubular casts are formed by proteinaceous plugs of dense, mesh-like mucoprotein (Tamm- Horsfall mucoprotein) that accumulate within the distal portion of the nephron. A low number (<2 per low power field) of these proteinaceous hyaline casts can occasionally be observed in urine of normal animals. Diuresis of dehydrated animals or proteinuria of preglomerular or renal etiology can cause an increased number of hyaline casts to be present in urine. Renal tubular epithelial cells that die and slough into the tubular lumen can be entrapped within this dense mucoprotein matrix. If present, inflammatory cells associated with renal tubulointerstitial inflammation may also be entrapped. During microscopic sediment evaluation, cellular casts are further classified as either epithelial, leukocyte, or erythrocyte casts, if the constituent cells can be discerned. Once locked within the proteinaceous matrix, cells continue to degenerate, progressing from intact cells, to granular cellular remnants, and finally to a waxy cholesterol- rich end product. A cast may dislodge from a given renal tubular lumen at any time during this degenerative process and may be observed in the urine sediment. However, in clinically normal animals only granular casts are rarely found (<2 per low power field). Other material can lodge within the proteinaceous matrix, such as lipid from degenerated renal tubular epithelial cells, hemoglobin during hemolytic disease, and bilirubin.
The number of casts observed in the sediment does not correlate with the severity of renal disease or its reversibility; and the absence of casts from urine sediment cannot be used to exclude the possibility of renal disease, especially since casts are fragile and prone to degeneration, particularly in alkaline urine. When hyaline or granular casts are present in increased numbers or when other cast types are observed, one can only conclude that the renal tubules are involved in an active disease process of unknown severity or reversibility. When present, the type of cast observed may provide additional information. Leukocyte casts indicate active renal tubulointerstitial inflammation. Waxy casts reflect a chronic tubular lesion. To recognize the onset of nephrotoxicity in patients receiving aminoglycoside antibiotic therapy, it is useful to monitor urine sediment for the appearance of tubular casts, which should prompt withdrawal of the antibiotic. Other abnormalities seen with aminoglycoside-induced nephrotoxicity include isosthenuria, proteinuria, glucosuria, aminoaciduria, all of which may precede the onset of azotemia.
Structures such as mucus threads or fibers may resemble casts and should not be mistaken for them during microscopic examination. Mucus threads are distinguished by their variable width and tapered ends. Fibers are typically much larger than the surrounding cells and may contain a repetitive internal structure, suggesting a synthetic origin.
Epithelial cells Epithelial surfaces along the length of the genitourinary tract undergo constant turnover, therefore it is routine to see a low number of epithelial cells (<5 per low power field) in normal urine samples. A greater number of epithelial cells are seen in urine samples collected by catheterization or in patients with inflamed, hyperplastic, or neoplastic mucosa. Using wet mount preparations, it can be challenging to distinguish the different types of epithelial cells, since transitional cells are highly pleomorphic and many types of epithelial cells will become rounded once sloughed into fluid and degenerate when exposed to urine. Cell morphology is best appreciated in freshly formed and collected urine that is promptly analyzed. When evaluation of cell morphology is critical, the sediment pellet can be evaluated by Diff Quik-stained, dry-mount cytology of the urine sediment pellet. Other methods to diagnose structural lesions within the urinary tract (e.g. ultrasonography, catheter biopsy) are often more reliable and conclusive than urinalysis.
Squamous epithelial cells line the distal third of the urethra, the vagina, and the prepuce. They are large, flat, or rolled cells that have angular sides and usually a single small, condensed nucleus or they may be anucleate. A variable number of squamous epithelial cells are most commonly observed with lower urinary tract contamination of voided or catheterized samples. Squamous epithelial cells should not be present in samples collected by cystocentesis. A significant number of squamous epithelial cells are very rarely seen in cystocentesis samples due to squamous cell carcinoma of the bladder or due to squamous metaplasia of the bladder, which can occur with transitional cell carcinoma or chronic bladder irritation. Squamous epithelial cells may also be found if the uterine body of an intact female was unintentionally penetrated during urine sample collection.
Hyaline cast
Cellular cast
Granular cst
Waxy cast
Mucus
Fiber
227
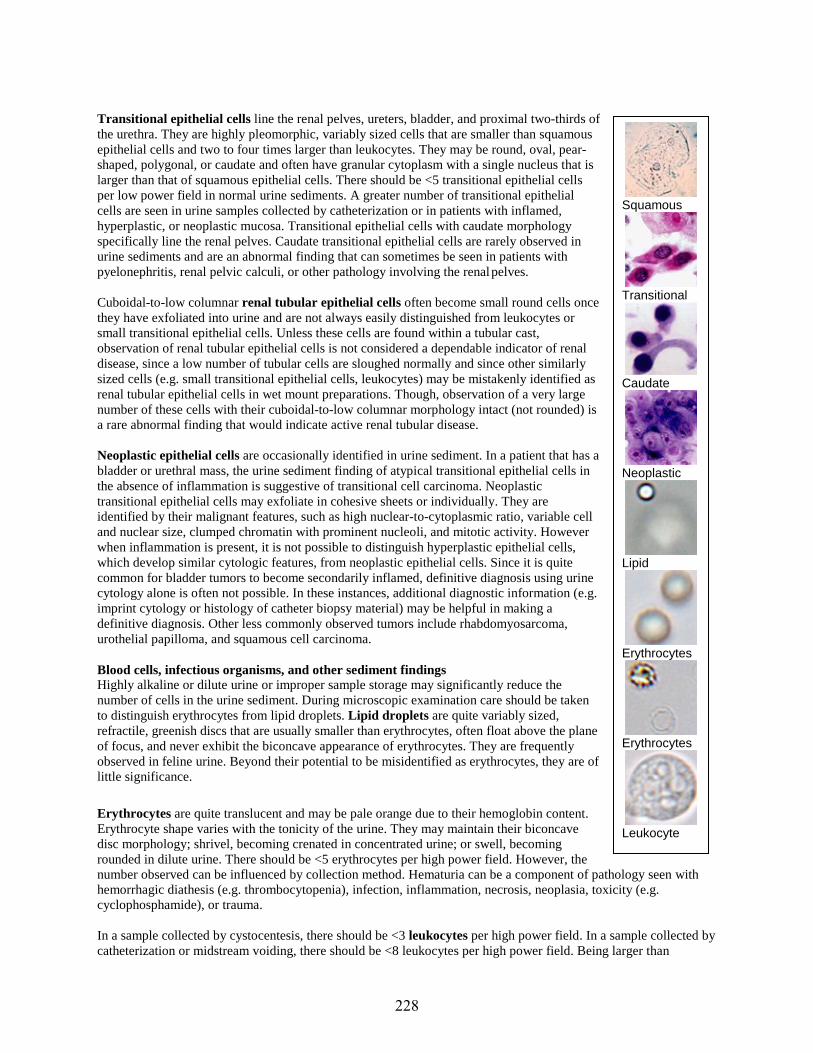
Transitional epithelial cells line the renal pelves, ureters, bladder, and proximal two-thirds of the urethra. They are highly pleomorphic, variably sized cells that are smaller than squamous epithelial cells and two to four times larger than leukocytes. They may be round, oval, pear- shaped, polygonal, or caudate and often have granular cytoplasm with a single nucleus that is larger than that of squamous epithelial cells. There should be <5 transitional epithelial cells per low power field in normal urine sediments. A greater number of transitional epithelial cells are seen in urine samples collected by catheterization or in patients with inflamed, hyperplastic, or neoplastic mucosa. Transitional epithelial cells with caudate morphology specifically line the renal pelves. Caudate transitional epithelial cells are rarely observed in urine sediments and are an abnormal finding that can sometimes be seen in patients with pyelonephritis, renal pelvic calculi, or other pathology involving the renal pelves.
Cuboidal-to-low columnar renal tubular epithelial cells often become small round cells once they have exfoliated into urine and are not always easily distinguished from leukocytes or small transitional epithelial cells. Unless these cells are found within a tubular cast, observation of renal tubular epithelial cells is not considered a dependable indicator of renal disease, since a low number of tubular cells are sloughed normally and since other similarly sized cells (e.g. small transitional epithelial cells, leukocytes) may be mistakenly identified as renal tubular epithelial cells in wet mount preparations. Though, observation of a very large number of these cells with their cuboidal-to-low columnar morphology intact (not rounded) is a rare abnormal finding that would indicate active renal tubular disease.
Neoplastic epithelial cells are occasionally identified in urine sediment. In a patient that has a bladder or urethral mass, the urine sediment finding of atypical transitional epithelial cells in the absence of inflammation is suggestive of transitional cell carcinoma. Neoplastic transitional epithelial cells may exfoliate in cohesive sheets or individually. They are identified by their malignant features, such as high nuclear-to-cytoplasmic ratio, variable cell and nuclear size, clumped chromatin with prominent nucleoli, and mitotic activity. However when inflammation is present, it is not possible to distinguish hyperplastic epithelial cells, which develop similar cytologic features, from neoplastic epithelial cells. Since it is quite common for bladder tumors to become secondarily inflamed, definitive diagnosis using urine cytology alone is often not possible. In these instances, additional diagnostic information (e.g. imprint cytology or histology of catheter biopsy material) may be helpful in making a definitive diagnosis. Other less commonly observed tumors include rhabdomyosarcoma, urothelial papilloma, and squamous cell carcinoma.
Blood cells, infectious organisms, and other sediment findings Highly alkaline or dilute urine or improper sample storage may significantly reduce the number of cells in the urine sediment. During microscopic examination care should be taken to distinguish erythrocytes from lipid droplets. Lipid droplets are quite variably sized, refractile, greenish discs that are usually smaller than erythrocytes, often float above the plane of focus, and never exhibit the biconcave appearance of erythrocytes. They are frequently observed in feline urine. Beyond their potential to be misidentified as erythrocytes, they are of little significance.
Erythrocytes are quite translucent and may be pale orange due to their hemoglobin content. Erythrocyte shape varies with the tonicity of the urine. They may maintain their biconcave disc morphology; shrivel, becoming crenated in concentrated urine; or swell, becoming rounded in dilute urine. There should be <5 erythrocytes per high power field. However, the number observed can be influenced by collection method. Hematuria can be a component of pathology seen with hemorrhagic diathesis (e.g. thrombocytopenia), infection, inflammation, necrosis, neoplasia, toxicity (e.g. cyclophosphamide), or trauma.
In a sample collected by cystocentesis, there should be <3 leukocytes per high power field. In a sample collected by catheterization or midstream voiding, there should be <8 leukocytes per high power field. Being larger than
Squamous
Transitional
Caudate
Neoplastic
Lipid
Erythrocytes
Erythrocytes
Leukocyte
228

erythrocytes and smaller than epithelial cells, leukocytes are intermediate in size compared to other cells that may be present in the sediment. They are usually round with a stippled appearance and greyish internal structure that transmits less light than erythrocytes; segmented nuclei are frequently visualized. Some leukocytes contain granules that are occasionally visible as refractile structures within the leukocyte. These cells may be referred to as glitter cells.
Observation of pyuria with concurrent bacteriuria indicates active urinary tract inflammation with either primary or secondary bacterial infection. Urine culture is useful to definitively identify microorganisms and to determine their antimicrobial sensitivities. Pyuria is also seen with other causes of genitourinary tract inflammation, such as urolithiasis, neoplasms, prostatitis, pyometra, and less common infections by viruses, mycoplasmas, or ureaplasmas. Cystocentesis may avoid contamination of the urine sample by leukocytes from the genital tract and aid in localizing the source of pyuria.
The absence of pyuria does not exclude the possibility of a urinary tract infection; therefore urine sediment evaluation alone cannot be used to definitively exclude the possibility of infectious urinary tract disease. Silent urinary tract infections (i.e. those lacking a detectable inflammatory response) can be seen with hyperadrenocorticism/hypercortisolemia, diabetes mellitus, and other immunosuppressed states. Also, leukocytes and bacteria may be diluted below the detection limit of light microscopy in polyuric conditions when large volumes of dilute urine are produced (e.g. pyelonephritis). At least 10,000 bacilli/mL or 100,000 cocci/mL are required for detection by light microscopy.
Bacteria may be observed in urine sediment for reasons other than urinary tract infection (e.g. normal finding in clinically normal animals, overgrowth after collection). When microorganisms are observed in stained wet mounts (e.g. sedi-stain, new methylene blue), it is necessary to distinguish them from contaminants by confirming their presence in unstained wet mounts or by cytologic examination of the dry-mount sediment pellet. The latter is a more sensitive and specific method to detect bacteria than wet mounting and permits more accurate identification of bacterial morphology (Swenson et al., 2004). Urine cultures can occasionally be negative, even though bacteria were presumptively detected during urinalysis. Reasons for this disparity include antimicrobial administration prior to sample collection, prolonged urine storage or extreme storage conditions prior to culture, improper culture technique, bacterial contamination of the sample during urinalysis, misidentification of nonbacterial structures as bacteria (common). Also, uncommon infections by viruses or highly fastidious microorganisms (e.g. Mycoplasma, Ureaplasma) may result in negative urine culture though a urinary tract infection is present.
Cystocentesis is the ideal collection method for urine culture, but take care to avoid incidental enterocentesis. The likelihood of representative culture results may be enhanced by collection of a randomly-timed urine sample (which will likely consist of freshly formed urine that has not stagnated within the bladder) along with inoculation of a Culturette™ tube immediately after collection. Afterward, the Culturette™ should be refrigerated to prevent overgrowth of robust bacteria.
With routine urine culture, results are reported that simply identify the bacteria present and their respective antimicrobial sensitivities. Quantitative urine culture is an alternative may be helpful to determine if the bacteria cultured from a urine sample likely represent a true infection or if they are likely contaminants of the sample. Some labs offer quantitative urine culture as the routine test. In addition to bacterial identification and elucidation of their antimicrobial sensitivities, quantitative culture enumerates the bacteria as colony forming units (CFU)/mL. Quantitative urine culture can be used even when the urine sample has been collected by transurethral catheterization or by collection of midstream voided urine, instead of cytocentesis. Quantitative urine culture results must be interpreted using published guidelines that are based upon the urine collection method.
Other sediment findings Dependent on geographic distribution, other infectious organisms are occasionally identified in urine sediment, such as fungi (e.g. Candida, Aspergillus, Blastomyces dermatitidis, Cryptococcus); algae (e.g. Prototheca); and nematode ova, larvae, or adults (e.g. Capillaria, Dirofilaria immitis, Dioctophyma renale). Trichuris (whipworm)
Bacteria
Bacteria
Fungus, RBCs
Capillaria
229
parasite eggs appear very similar to Capillaria parasite eggs. These two eggs can be distinguished by the positioning of their bipolar caps and the texture of their outer shells. The bipolar caps of Capillaria ova are slightly askew, rather than being perfectly bipolar as they are in Trichuris ova. And, the shells of Capillaria ova have a granular appearance, rather than perfectly smooth as they are in Trichuris ova. Capillaria are usually an incidental finding in the urine of asymptomatic cats. However, Capillaria eggs are rarely identified in cats that present with hematuria, which resolves after fenbendazole administration.
Common contaminants of urine samples include sperm, talc, glass chips, plant pollen, hair, and fibers. Aside from sperm, these contaminants can be mistaken for urine crystals (i.e. talc, glass chips), transitional epithelial cells (i.e. plant pollen), or casts (i.e. hair, fibers).
Urinalysis: wet-mount versus dry-mount Urinalysis performed in-house by a trained staff member, soon after urine sample collection is a great way to reduce or avoid artifacts that can arise during the delay between sample collection and sample analysis. Keeping such analysis in-house may increase productivity and potentially improve your urinalysis laboratory results.
In addition to traditional wet-mount urinalysis, dry-mount cytology of urine samples can be very useful in suspected cases of urinary tract infection (Swenson et al., 2004) or urinary tract neoplasia. The method is described below here. Slides prepared using this method can be evaluated in-house, or they can be readily sent to an outside laboratory for review by a pathologist. The benefit is that diagnostic material on slides prepared this way will not degrade the same way that it would in a liquid urine sample during transport to an out-of-house, reference laboratory. Often when fluid urine samples are sent to a reference laboratory for pathologist review to diagnose neoplasia, cells deteriorate to the point where cytologic diagnosis no longer possible.
REFERENCES 1. Albasan H, Lulich JP, Osborne CA, Lekcharoensuk C, Ulrich LK and Carpenter KA (2003) Effects of storage
time and temperature on pH, specific gravity, and crystal formation in urine samples from dogs and cats.Journal of the American Veterinary Medical Association 222, 176-179
2. Osborne CA and Stevens JB (1999) Urinalysis: A Clinical Guide to Compassionate Patient Care, 1st edn, pp. 1-214. Veterinary Learning Systems, Bayer Corporation, Shawnee Mission, Kansas
3. Swenson CL, Boisvert AM, Kruger JM and Gibbons-Burgener SN (2004) Evaluation of modified Wright-staining of urine sediment as a method for accurate detection of bacteriuria in dogs. Journal of the AmericanVeterinary Medical Association 224, 1282-1289
230

Cytology Submission and Review of Interpretation Heather L. Wamsley, BS, DVM, PhD, Dipl. ACVP-Clinical
Tampa, FL USA
KEY CLINICAL DIAGNOSTIC POINTS • Proper slide preparation is critical. Getting cellular material onto the slide in a thin-prep monolayer that is also
not lysed requires some practice, but is achievable.• Proper slide preparation and staining is even more pressing with increasing use of digital cytology and point of
care digital cytology.• Improve staining quality by placing slides in the stain fixative for at least two minutes. No heat-fixation is
needed for cytology. Heat fixation is for Gram stain, not cytology. If material tends to “fall off” in the quickstain, it is very likely because preps are too thick – too much material on the slide. Adipose tissue does actuallyadhere. Close the microscope condenser partially to see the free lipid.
• In-house quick stains create morphology artifacts usually due to inadequate fixation or under-staining. If futuresubmission to a pathologist is likely, try to reserve unstained at least one slide that is likely to be highly cellular.Do also submit the in-house quick-stained slides.
• Cells with intracytoplasmic granules, e.g., certain canine eosinophils, certain types of lymphocytes, and somemast cells, may not stain well with in-house quick stains. Approximately 20% of canine mast cell tumor cells donot stain with quick stain.
• For fluid preps, hunt for microorganisms at the feathered edges.• For fluid preps, prepare slides soon after collection. Use a microhematocrit tube to transfer a small drop of fluid
to the slide. Sediment pellet cytology is also useful.• For tissue aspirates, use a systematic approach and attempt to classify the lesion into one of the five diagnostic
categories.• Basic signalment – species, breed, age, and sex, is essential minimum information to include with submission to
pathologist.• Label individual cytology slides somehow – either indicate the mass sampled and/or the animal’s name/ID. If
non-frosted slides are used, label the slide somehow to indicate which side is up and, thereby, what part of theslide is safe to cover with an identifying sticker in the lab. Simply writing Top or Up or the animal’s name/ID isextremely useful.
• A brief description of the gross appearance of the lesion – size, shape, color, texture, superficial appearance, etc.is very helpful.
• If intra-cavitary (abdomen, thorax, etc.) lesions/organs are aspirated, it is valuable to include information aboutwhat was sampled – one lesion, two lesions, four lesions/nodes vs. general parenchyma etc., AND label theslides!! Is the organ enlarged, was a mass sampled, were masses sampled, was a node sampled, were nodessampled, was random parenchyma sampled, staging for metastasis – what neoplasm? If the ultrasound wasperformed outpatient by a specialist, then include the consult/ultrasound report with the cytology slides.
• “Don’t give any history – don’t want to bias the pathologist” is terrible advice.
ADDITIONAL DETAILS Cytology slide preparation – aspirates, fluids, biopsy imprints A 22- or 23-gauge needle is suitable for most subcutaneous aspirates. Imprinting an ulcerated mass does not yield the same diagnostic information as an aspirate. Aspirates may be obtained using a needle alone or with the needle attached to a syringe with negative pressure. Either method usually results in a diagnostic sample. Using the needle
231

alone without a syringe attached allows for better needle control, decreases hemorrhage, and allows a needle core- type sample.
When spreading an aspirate into thin film prep, quickly place the spreader slide over the aspirated material without additional downward pressure. This will usually cause the aspirated material to diffuse into a thin layer between the two slides. Then, gently slide the two glass slides apart to form a monolayer of aspirated cells. In some situations, surgical biopsies can also be imprinted for cytology.
Allow the slides to air-dry. Do not heat-fix or formalin-fix the slides. As an aside, also do not ship in the same bag or box cytology slides and surgical biopsies that are in formalin. If material seems to fall off of slides, the slide preps are very likely too thick. When using quick stain in-house, let slides site in fixative for at least two minutes. Try to reserve at least one cellular slide unstained for submission to a pathologist if desired. If using an outside lab, include basic signalment – species, breed, age, sex, and try to include a gross description of the lesion or diagnostic imaging results on the submission form. It may be faster to include a digital image of the lesion or the ultrasound/consult report with the request form.
For fluid cytology, EDTA tubes are preferred. Plain, red top tubes should be used for microbial culture. Thin film preparations of fluid samples should be made as soon as possible after collection and submitted along with the fluid if an outside lab will be used. It is helpful to use a microhematocrit tube to control the size of the fluid drop used to prepare the slide. The drop should be small, similar to preparing a blood film. Preps made using a transfer pipet usually have too much fluid, are too thick, partially detach in the stain, and limit ability to detect bacteria and other small structures. Cytology of the fluid sediment pellet is particularly useful to screen for microorganisms and to concentrate transudates/modified transudates. If this method is used, it is important to note it on the submission form and helpful to also include a smear of unconcentrated fluid.
Surgical biopsies can be used to prepare both cytology and histopathology samples. If the biopsy is sufficiently large, a portion of the biopsy can be imprinted onto glass slides before the sample is placed in formalin. The internal cut-surface of the biopsy should be imprinted; avoid imprinting the serosal surface or outer epithelium of tissues. Use a clean gauze or paper towel to gently dab away excess fluid prior to touching the tissue sample to the slide. As the tissue is repeatedly imprinted onto the slide, additional fluid may appear. Dab away excess fluid as it accumulates on the gauze or other absorbent material.
Very small pieces of soft tissue, e.g., liver, can simply be smeared into a thin film on the slide using a blade or a second spreader slide. Firm tissues, e.g., very firm tumors, like a sarcoma, may not exfoliate well. To promote exfoliation of cells, the surface area of the cut-surface of the tissue can be increased by scoring it using the point of an 11 blade or a needle, similar to what is done during a grid keratectomy. This gridding procedure and stronger pressure may be required to encourage exfoliation.
Surgical biopsies – small and large Biopsies or portions of biopsies that are intended for histopathology should not be macerated as above described. Small biopsy pieces are easily lost in jars of formalin. They should be placed in plastic cassettes or wrapped in formalin-soaked gauze and indicate such on the submission form. An adequate volume of formalin is 10 parts formalin to 1 part tissue for proper tissue preservation. To promote adequate fixation, organs with a lumen can be flushed with formalin, and large organs can be “loafed”. If necessary, very large samples can be formalin-fixed in- house and then shipped with a small volume of formalin in double-bagged zip closure bags. Inking of tissue edges can aid in measurement of surgical margins around neoplasms. Though it may seem obvious at the time of biopsy, along with a gross description of the lesion, it is helpful to indicate on the submission form exactly what has been submitted from a mass – specifically, if the excised tissue contains the whole mass (e.g., a skin biopsy with a small mass) or if the excised tissue is an incisional biopsy of the mass. It can be hard for technical staff in the laboratory to discern once the tissue is formalin-fixed.
Cytology interpretation overview When evaluating cytology, identify an area of the preparation that contains intact cells that are not lysed, distorted, or otherwise damaged. This is one of the hardest parts of cytology. If an area of intact cells within readable monolayer is found, then attempt to classify the lesion into one of five general categories. In many cases, more than
232

one pathologic process may be present in a single lesion. Real life cytology interpretation is typically not straightforward.
Five general lesion categories: • Inflammatory – leukocytes are increased above that which is subjectively expected to be caused by blood
contamination• Cystic – large number of mature, keratinized, squamous epithelial cells or abundant, amorphous, proteinaceous
material• Hemorrhagic – bloody and pink proteinaceous fluid with macrophages that contain phagocytosed erythrocytes or
erythrocyte breakdown pigments• Neoplastic – a monotypic cell population of one tissue origin• Mixed cell population – both inflammation and atypical-appearing monotypic cell population
Four neoplasm categories • Epithelial• Spindle cell/mesenchymal• Round• Neuroendocrine
Malignant criteria • Variation in size• High nucleus to cytoplasm ratio• Pleomorphism• Multinucleation• Nuclear molding• Coarse, open chromatin• Large, prominent nucleoli• Mitoses
ADDITIONAL READING Burton AG. Clinical Atlas of Small Animal Cytology. 1st ed. Hoboken, NJ: Wiley-Blackwell, 2017. Valenciano AC, Cowell RL, eds. Cowell and Tyler's Diagnostic Cytology and Hematology of the Dog and Cat. 5th ed. New York City, NY: Elsevier, 2019.
233

FNA Cytology Interactive Case Session Heather L. Wamsley, BS, DVM, PhD, Dipl. ACVP-Clinical
Tampa, FL USA
OVERVIEW OBJECTIVES OF THE PRESENTATION During this interactive case session, we will evaluate photomicrograph cases and discuss cytodiagnosis of skin lesions, effusion fluid, and internal lesions, their biologic behavior and prognosis when applicable.
OBJECTIVES OF THE PRESENTATION • Apply systematic method to evaluate and interpret cytology in the context of clinical cases• Learn specific challenges and nuances for multiple neoplasms• Learn/review brief medical correlates for each case• Discuss preoperative predictors of canine mast cell tumor biologic behavior with brief comparison to melanoma
ADDITIONAL DETAILS Cytology interpretation overview When evaluating cytology, identify an area of the preparation that contains intact cells that are not lysed, distorted, or otherwise damaged. This is one of the hardest parts of cytology. If an area of intact cells within readable monolayer is found, then attempt to classify the lesion into one of five general categories. In many cases, more than one pathologic process may be present in a single lesion. Real life cytology interpretation is typically not straightforward.
Five general lesion categories: • Inflammatory – leukocytes are increased above that which is subjectively expected to be caused by blood
contamination• Cystic – large number of mature, keratinized, squamous epithelial cells or abundant, amorphous, proteinaceous
material• Hemorrhagic – bloody and pink proteinaceous fluid with macrophages that contain phagocytosed erythrocytes or
erythrocyte breakdown pigments• Neoplastic – a monotypic cell population of one tissue origin• Mixed cell population – both inflammation and atypical-appearing monotypic cell population
Four neoplasm categories • Epithelial• Spindle cell/mesenchymal• Round• Neuroendocrine
Malignant criteria • Variation in size• High nucleus to cytoplasm ratio• Pleomorphism• Multinucleation• Nuclear molding• Coarse, open chromatin• Large, prominent nucleoli• Mitoses
Case list Salivary mucocele, Cryptococcus, Pyothorax, Tooth root abscess, Basilar epithelial neoplasm, Inclusion cyst, Canine mast cell tumor well differentiated, Canine mast cell tumor poorly differentiated, Feline mast cell tumor, Thyroid neoplasms, Anal sac apocrine gland adenocarcinoma, Perianal gland neoplasms, Perineal soft tissue sarcoma, Cutaneous lymphoma, Plasmacytomas well differentiated, Plasmacytomas poorly differentiated, Histiocytoma, Soft tissue sarcoma and incidental heartworm, Lipoma and trick to see free lipid, Liposarcoma, Soft tissue sarcoma, Fibroadnexal hamartoma, Opportunistic fungal infection, Melanoma poorly differentiated,
234
Melanoma well differentiated with incidental oral bacteria, Transitional cell carcinoma, Viral papilloma, Squamous cell carcinoma, Mammary adenocarcinoma, Lung carcinoma and neoplastic pleural effusion, Leishmaniasis, Mediastinal lymphoma and neoplastic pleural effusion, Splenic lymphoma
ADDITIONAL READING
Burton AG. Clinical Atlas of Small Animal Cytology. 1st ed. Hoboken, NJ: Wiley-Blackwell, 2017. Valenciano AC, Cowell RL, eds. Cowell and Tyler's Diagnostic Cytology and Hematology of the Dog and Cat. 5th ed. New York City, NY: Elsevier, 2019.
235

RBC, PLT, and WBC Values Heather L. Wamsley, BS, DVM, PhD, Dipl. ACVP-Clinical
Tampa, FL USA
OVERVIEW CBC data and peripheral blood film evaluation are critical during evaluation and management of most patients. Abundant information is rapidly provided and may yield diagnosis of the case or, more commonly, guide decisions about future diagnostic testing and medical management. Clinical cases that focus on improved understanding of erythrocyte, platelet, and leukocyte data from CBCs will be presented and correlated with blood film and patient abnormalities. This presentation will review what the numeric parameters reported in a CBC mean.
KEY CLINICAL DIAGNOSTIC POINTS • CBC numeric data include multiple RBC and PLT parameters that may give clues about the cause of anemia,
conditions associated with thrombocytopenia, and response to treatment of anemia and thrombocytopenia. Bloodfilm evaluation enhances the value of these data and will detect abnormalities that hematology analyzers cannot,such as parasites, abnormal cell shapes, other.
• CBC data include information about WBC quantity and differential WBC count. All nucleated cells in thesample are counted and reported as WBC. Cells that are not actually WBCs, such as nucleated red blood cells(nRBC) or neoplastic cells, are included in this value. In order to fully interpret WBC data, a blood film mustalso be evaluated. A WBC correction formula may be needed if high nRBC is present.
• Important, clinically germane information may be missed if a well-prepared peripheral blood film is notevaluated as part of a complete CBC. This may lead to delayed case diagnosis or misdiagnosis with delayedtherapy or inappropriate therapy and diagnostic evaluation.
• Automated hematology analyzers may produce erroneous data; it is important to verify information fromautomated analyzers by peripheral blood film evaluation.
• Automated hematology analyzers are incapable of detecting clinically important changes, for example,neutrophil toxic change, blood-borne parasites, neoplastic cells, and others.
ADDITIONAL DETAIL RBC values Parameters in the CBC that provide information about red blood cell quantity include, RBC count (RBC), hemoglobin concentration (Hgb), and hematocrit (HCT). Some laboratories may also report a spun packed cell volume (PCV) based on the centrifugation of blood in a microhematocrit tube. The analyzer actually measures the RBC and the Hgb. The analyzer calculates the HCT based on the measured mean cell volume (MCV) and measured RBC. There are multiple parameters in the CBC that give information about red blood cell quantity. This is useful to help verify the information, especially since some conditions, such as, agglutination, can affect multiple parameters and cause false results. One way to verify the data is to multiply the Hgb value by 3. The product should be approximately equal to the calculated HCT or spun PCV.
Parameters in the CBC that provide information about red blood cell quality include, mean cell volume (MCV), red cell distribution width (RDW), mean cellular hemoglobin concentration (MCHC), mean cell hemoglobin (MCH). The analyzer actually measures the MCV. The RDW, MCHC, and MCH are calculated based on other data. The MCV indicates the average size of the red blood cells. The RDW describes variation in red blood cell size. Anisocytosis (unequal cell size) is a term used to describe variation in red blood cell size based on peripheral blood film evaluation. RDW conceptually is an electronic version of anisocytosis. The MCHC and MCH indicate how much hemoglobin there is in the red blood cells. Of the two values, MCHC is more useful. MCH is often ignored, particularly since other red blood cell features, not just the quantity of hemoglobin in the red blood cells, may affect it. The MCHC is a ratio of hemoglobin to the number of red blood cells. High values are typically false. There is no condition that causes the red blood cells to make extra hemoglobin. Conditions that cause elevated MCHC include
236

hemolysis, lipemia, Heinz bodies, and extremely increased WBC. Low values may be seen in anemia with very strong, marked regenerative response or with hemoglobin deficient RBCs – iron deficiency. Some laboratories may also report cellular hemoglobin concentration mean (CHCM). This value is conceptually similar to the MCHC - ratio of hemoglobin to the number of red blood cells; however, it is based on an actual measurement, rather than a calculation. The CHCM is typically not affected by the conditions that cause false increases in calculated MCHC.
PLT values Parameters in the CBC that provide information about platelets include, platelet count (PLT), mean platelet volume (MPV), platelet distribution width (PDW), and plateletcrit (PCT). The analyzer counts the platelets and determines the average size, which are reported as the platelet count, PLT, and mean platelet volume, MPV, respectively. Clumped platelets are not counted and included in the reported platelet count. Clumped platelets are common, particularly when the Vacutainer collection system is not use. Cats often form platelet clumps even with excellent venipuncture. A low automated platelet count should be confirmed by looking at a blood film since platelet clumping is very common. A normal platelet count should also be confirmed by blood film review since hemolysis and lipemia can both cause falsely increased automated counts.
Active platelet production can cause large platelets and high MPV. A mix of giant and large platelets with high MPV can also be seen with hereditary macrothrombocytopenia, which is production of large platelets in quantity that is lower than the general canine reference interval. This condition has been documented in the following breeds/mixes, Cavalier King Charles Spaniel, Chihuahua, English Toy Spaniel, Havanese, Parson Russell Terrier, Labradoodle, Labrador Retriever, Maltese, Poodle, Shih tzu. In the United States, 30-50% of CKCS are affected. Clinically normal dogs with this condition may have platelet counts between 30,000 to 200,000/uL. Affected dogs are sometimes misdiagnosed with immune-mediated thrombocytopenia. DNA testing is available to confirm this condition via Auburn, UPenn, and others.
The MPV may not be included with the reported CBC values from some laboratories. The platelet distribution width, PDW, describes variation in platelet size. It is conceptually similar to the red blood cell RDW. This value may not be included with the CBC from some laboratories. The plateletcrit, PCT, is a calculation based on the platelet count and the size of the platelets. It is conceptually similar to the red blood cell HCT. It gives an idea of overall platelet mass and accounts for both quantity and size of platelets. During treatment of immune-mediated thrombocytopenia, the PCT may become normal before the platelet count. The PCT can be used as an early indicator of positive response to treatment. The PCT may become normal before the platelet count normalizes because larger than normal platelets are released into circulation during active platelet production. With hereditary macrothrombocytopenia, the mean platelet volume (MPV) is typically very high with normal plateletcrit (PCT), though the platelet count is low. In affected dogs, the plateletcrit may be more useful than the traditional platelet count to evaluate the patient’s platelet mass.
WBC values CBC data include information about WBC quantity and differential WBC count. All nucleated cells in the sample are counted and reported as WBC. Cells that are not actually WBCs, such as nucleated red blood cells (nRBC) or neoplastic cells, are included in this value. A WBC correction formula may be needed with high nRBC:
uncorrected WBC count X 100 = corrected WBC count /µL number of nRBCs per 100 WBCs + 100
Blood film microscopy is required for full WBC evaluation. For example, when neutrophilia is present, considerations may include stress leukogram (glucocorticoid response), physiologic leukogram (epinephrine/excitement response), inflammation, or other less common causes. To distinguish between these possibilities, information about neutrophil morphology from the blood film is required – whether or not toxic change is present. When lymphocytosis is present, considerations may include physiologic leukogram (epinephrine/excitement response), response to antigenic stimulation, or lymphoid neoplasia. To help distinguish between these possibilities, information about lymphocyte morphology from the blood film is required, for example, whether or not large immature cells (blasts) or atypical lymphocytes are present. Most hematology analyzers provide a WBC differential. The automated WBC differential may not be accurate. Examples follow. When there is marked toxic change, the neutrophils may be counted as monocytes. Neutrophil left shift is not detected at all or is not definitively characterized by hematology analyzers, depending on the analyzer used. Eosinophils of some breeds are incorrectly counted as monocytes. Circulating neoplastic cells may be miscounted as any one of the WBCs,
237
depending on the condition, for example, a dog with marked mastocythemia had 60K WBCs reported by the automated analyzer. The hematology analyzer reported the WBCs as neutrophils. The clinical diagnosis was inflammation and infection. The dog arrested during biopsy of skin masses presumed to be infected. The skin masses were actually mast cell tumors. The diagnosis was missed prior to invasive testing because a properly made blood film was not examined.
Summary of WBC leukogram patterns Stress leukogram “Stress response” “Steroid response”
• The classic response is very common in dogs– Leukocytosis– Mature neutrophilia– Lymphopenia **most consistent change**– Eosinopenia– Monocytosis (dogs)
• Frequently observed; need to recognize and distinguish from inflammation– Hypercortisolemia (endogenous or exogenous): shipping, trauma, pain, hyperadrenocorticism,
chronic illness– But, often CONCURRENT with inflammation: animals have both “stress” and inflammation
• Changes in neutrophil pools due to glucocorticoids– Decrease the rate at which neutrophils leave blood and enter tissues
– Mature neutrophils stay in circulation longer; hypersegmentation common– Cause neutrophils in circulation to demarginate from vessel walls
– The number of mature neutrophils in the circulating neutrophil pool rises– Cause marrow to release segmented neutrophils at a faster rate
– The number of new mature neutrophils entering circulation is increased• Leukocytosis: due to neutrophilia, lymphopenia, eosinopenia, monocytosis• Neutrophilia without left shift & without hyperfibrinogenemia
– Occurs 4-8 hours after single episode of hypercortisolemia– Returns to normal within 24 hours after single episode– After long term hypercortisolemia, takes 2 to 3 days to return to normal
• Lymphopenia**most consistent change**– Due to sequestration in lymphoid tissue and cell death
– Long term can cause lymphoid involution– Stress OFTEN accompanies inflammatory disease
– Lymphopenia may be the only indication of steroid release– The clinical importance is to recognize the pattern
• Eosinopenia is often seen with stress leukogram, but eosinophils are already typically low in health– With hypoadrenocorticism, can have eosinophilia “reverse stress leukogram”
• Species differences: dogs and cats more responsive to this process than other domestic species
Physiologic leukogram “Physiologic neutrophilia” “Physiologic lymphocytosis” “Excitement response” • The classic response is common in young cats and horses
– Transient leukocytosis with or without concurrent erythrocytosis and thrombocytosis– Transient mature neutrophilia– Transient lymphocytosis– No bands, normal fibrinogen
• Endogenous epinephrine release– Increased capillary blood flow due to increased HR and BP
• Changes in neutrophils and lymphocytes due to epinephrine– High capillary blood flow demarginates mature neutrophils
– The number of mature neutrophils in the circulating neutrophil pool rises– Mature lymphocytes are flushed out of lymphoid organs and channels
– The number of mature lymphocytes in circulation is also increased• Occurrence
– Young, healthy animals– Occurs rapidly after epinephrine release and is transient
238

– Fear, strenuous exercise, restraint for blood draw, sudden seizures – Returns to normal within ~30 minutes – Species differences: more common in cats and horses – Cat: Mild neutrophilia and marked lymphocytosis (lymphocytes ≤ 20,000/µL) – Horse: Neutrophilia and lymphocytosis (lymphocytes 6000-14000/µL) – Bovine: Mild to mod. leukocytosis due to neutrophilia and lymphocytosis – Dog: Uncommon in dogs; mild leukocytosis due to mature neutrophilia +/- lymphs
Neutrophilia with regenerative left shift • There is a left shift • There is a neutrophilia • There are more mature segmented neutrophils than immature cells (e.g., band neutrophils, metamyelocytes) • At that time, marrow production is adequate
Neutropenia or normal neutrophil count with degenerative left shift
• There is a left shift • The total neutrophil count is normal or neutropenic • There are more immature cells (e.g., band neutrophils, metamyelocytes) than mature segmented neutrophils • At that time, tissue demands exceed marrow capacity to produce neutrophils • Close monitoring and intervention warranted
Leukemoid response
• A regenerative left shift with very high leukocyte counts, ~100K +/- 20K • Concurrent toxic change common. • Marked, established inflammation • Rarely, paraneoplastic; neoplasm makes compound that stimulates WBC production
Lymphocytosis
• The total lymphocyte count and the lymphocyte morphology are used to categorize lymphocytosis. • In dogs and cats, counts higher than 30 K/uL are usually considered neoplastic regardless of cell
morphology. • When counts are lower than 30 K/uL, the following are typically used to help classify a lymphocytosis -
cell morphology, concurrent disease and medications, whether or not the lymphocytosis is persistent, and other diagnostics tests, e.g., vector-borne infection screening, diagnostic imaging, advanced tests to characterize the lymphocytes (flow cytometry or PCR for antigen receptor rearrangement - PARR).
Blood collection & blood film preparation and evaluation Vacutainer tubes containing EDTA should be filled with the designated amount of blood. Partial filling of vacutainer tubes may cause false changes in cell morphology and numerical data. Over-filling of tubes may result in clotted blood samples. Blood films should be prepared soon after collection, preferably within 4 hours of collection, to minimize post-collection changes in erythrocytes and leukocytes such as echinocyte formation, leukocyte degradation, which can cause false differential counts and decrease accuracy of interpretation. In addition, prolonged exposure to EDTA may make it more difficult to identify blood-borne parasites, like haemoplasmas (formerly, hemobartonella), which may detach from the surfaces of erythrocytes due to the EDTA, or some Borrelia.
There are two commonly used techniques for blood film preparation, the push smear and the coverslip methods. Each has advantages and disadvantages. The push smear technique is easier to learn, and the slides that are produced are easier to stain in the Diff Quik jars (Coplin jars) used in most practices. The coverslip technique produces blood films that have a more even distribution of cells in the smear – there is no feathered edge with clumps of platelets and leukocytes, and the cells are less likely to lyse when blood films are prepared in this way. Using the coverslip technique permits more accurate estimation of leukocyte and platelet numbers and a better opportunity to evaluate cell morphology given the more even distribution of erythrocytes and fewer lysed cells. Blood films should be rapidly dried with a blow dryer to preserve optimal erythrocyte morphology. Instead, when blood films are permitted to air-dry on the lab bench top, refractile air-drying artifacts may occur and are more pronounced in humid environments. Refractile air-drying artifacts should be avoided since they severely impede one’s ability to identify red blood cell parasites and to evaluate red blood cell shape changes (poikilocytes). Tips for quick staining and a summary of one systematic approach to blood film evaluation are listed below here.
239

Tips for improved blood film staining • Control the amount of blood or fluid put on the slide.
o Use hematocrit tube to put blood on glass slide to control drop size. o Avoid applying too large of a drop or too much material to the slide. True for cytology and
hematology. Too much material will decrease ability to make diagnosis. • Rapidly air-dry blood film with heated air to avoid air-drying artifacts. • Fixative for 2 minutes
o Set slides in the fixative for at least 2 minutes. Improves staining quality of blood and cytology. • Rinse
o Distilled or deionized water is preferred. Tap water is usually used, though it may alter cell staining due to pH differences.
Low magnification examination (10X or 20X objective)
• Resist the urge to jump immediately to high magnification. • Find an area of the blood film where the erythrocytes are evenly distributed, neither too thick, nor too thin.
In this area, the erythrocytes are typically individual or only touching one or two other erythrocytes. • Form initial impressions about the leukocyte and erythrocyte counts. • Determine the predominant leukocyte, which should be the neutrophil in dogs and cats. • Screen for relatively large structures, like, clumped platelets, clumped leukocytes, large atypical cells,
microfilariae.
High magnification examination (50X or 100X objective) • Leukocytes
o Estimate the leukocyte count to validate automated data (detail how to is below). o Estimate the leukocyte differential to validate automated data, or perform a 100- or 200-cell
differential count. o Evaluate leukocyte morphology: look for left shifting, toxicity, altered morphology, infectious
organisms, other cellular inclusions, and atypical or neoplastic cells. • Erythrocytes
o Assess whether the density of the erythrocytes corresponds appropriately with RBC count data. o Evaluate the arrangement of erythrocytes: look for rouleaux, agglutination. o Evaluate erythrocyte morphology: look for changes in RBC size, shape, color, and inclusions.
• Platelets o Assess whether or not platelet clumps are present, which would cause automated hematology
analyzers to falsely report a low platelet count. o Estimate the platelet count to validate automated data (detail how to is below). o Evaluate platelet morphology: look for changes in platelet size and inclusions.
To estimate the total leukocyte count, determine the average number of leukocytes in at least ten microscopic fields in the monolayer portion of the blood film. Then, multiply the average number of leukocytes by the square of the objective that was used to perform the estimate. If the 50X objective was used, then multiply by 2,500. If the 100x objective was used, then multiply by 10,000. The product provides a rough estimate of the total leukocyte count per microliter. The 50X or 100X objective is typically preferred when performing leukocyte estimates, except when the patient is leukopenic – it may be better to use the 20X objective.
In dogs and cats, there should be a minimum of seven to ten platelets per 100X field. To estimate the total platelet count, determine the average number of platelets in at least ten representative 100X objective fields. For thrombocytopenic patients, determining the average number of platelets in thirty 100X objective fields may be necessary to obtain a more accurate estimate. Multiply the average number of platelets by 15,000. The product provides an estimate of the total platelet count per microliter. Some authors recommend multiplying by 20,000 for cats. Also, feline platelets are prone to clumping even with excellent venipuncture technique. When platelets are clumped, automated counts are unreliable, but a subjective assessment of whether or not the total number of platelets is adequate is typically possible.
240

Pet Food Labels – Demystifying the Package Kara M. Burns, MS, MEd, LVT, VTS (Nutrition)
Academy of Veterinary Nutrition Technicians
Proper nutrition is a critical component for maintaining the health of pets. Every patient, healthy or ill, that enters the veterinary hospital should have an evaluation of their nutritional status and healthcare team members should make a nutritional recommendation based on this evaluation. However, with the number of pet foods available it may be difficult for healthcare team members to make a nutritional recommendation and effectively communicate this recommendation to their clients. The purpose of this discussion is to review the role of nutrition in health maintenance and provide practical guidelines for evaluating the quality of pet foods.
Nutrition can be defined as the relationship of food and nutrients to health. Proper nutrient intake is essential to normal development, overall health, and disease management in companion animals. Nutrients have many metabolic roles essential to normal physiologic function that can be compromised by insufficient or irregular intake. Minimum requirements in dogs and cats have been determined to achieve optimal nutrition, focusing on the key nutrients for physical development, mobility, immune response, cognitive functions, disease prevention, or target treatment.
NUTRITIONAL EVALUATION Every animal that presents to the hospital should be assessed to establish nutritional needs and feeding goals, which depend on the pet’s physiology and/or disease condition. The role of the veterinary technician is to ascertain patient history, score the patient’s body condition, work with the veterinarian to determine the proper nutritional recommendation for the patient, and communicate this information to the pet owner.
The first step in evaluating a pet and determining its nutritional status is to obtain a complete history, including signalment (i.e., species, breed, age, gender, reproductive status, activity level, and environment). Next, a nutritional history should be taken to determine the quality and adequacy of the food being fed to the pet, the feeding protocol (e.g., whether the pet is fed at designated meals or has free choice, the amount of food given, the family member responsible for feeding the pet), and the type or types of food given to the pet. When evaluating a pet, the technician should ask the owner the following questions:
• What brand and type of food do you feed your pet?• What brand and type of snacks or treats do you give your pet?• Do you give your pet any supplements? If so, what kind?• Is your pet receiving any chewable medications? If so, what are they?• What type of chew toys does your pet play with?• What human foods does your pet consume?• Does your pet have access to other sources of food?
The technician should also ask the owner about the pet’s access to foods, supplements, and medications and how much of each substance the pet consumes each day. Pets also may be fed by more than one family member or receive numerous treats throughout the day. All these factors play a role in proper nutrition of pets.
All members of the health care team should be familiar with taking a nutritional history. Through this mechanism, the team can pinpoint a breakdown in owner compliance (e.g., are more than one person in the household feeding the pet, is the pet getting more calories than is being recommended, etc.) and begin to establish a feeding protocol to insure the pet’s proper calorie consumption.
ALL PET FOODS ARE EQUAL..RIGHT? Pet owners and healthcare team members today have access to a lot of information regarding pet nutrition via the internet, news sources, blogs, etc. However, with this wealth of information comes sometimes confusing and incorrect nutritional information. As veterinary technicians we need to educate ourselves on proper companion animal nutrition and sort through the minutiae to educate well intentioned owners on what constitutes proper nutrition for their beloved pet. There is a lot of misinformation regarding pet food; however, for the purpose of this discussion we will focus on pet food regulation and interpretation of pet food labels.
241

Pet Food Labels The pet food label is the primary means by which product information is communicated from the manufacturer or distributor to pet owners, veterinarians, health care team members, and regulatory officials. Reading and interpreting pet food labels is one method that healthcare team members and pet owners can obtain information about pet foods; however, labels do not necessarily provide information about food quality (e.g., digestibility and biological value). Owners and veterinary health care professionals should contact pet food manufacturers or nutrition experts for additional information that can be used to evaluate quality of various pet foods.
Pet food labels not only communicate information about the product, but also serve as a legal document. A number of agencies and organizations regulate production, marketing, and sales of pet foods in different countries. Each agency has different responsibilities with varying degrees of authority. Some of these agencies regulate information found on pet food labels whereas others influence the regulatory process. Pet foods are regulated at their point of sale (e.g., foods manufactured in the United States (US) but sold outside the US must meet labeling requirements of the country in which the food is sold). Pet foods sold in the US must conform to Food and Drug Administration (FDA), Association of American Feed Control Officials (AAFCO) and state pet food labeling requirements.
Pet food labels include two main parts: 1) the principal display panel and 2) the information panel. Certain pieces of information are required on each part of the label, whereas others are optional.
Principal display panel The principal display panel is defined by the FDA as “the part of a label that is most likely to be displayed, presented, shown or examined under customary conditions of display for retail sale.” It is the primary means of attracting the customer’s attention and should immediately communicate the product identity. The product identity must include a designator such as “dog food,” “cat food,” “for puppies,” or “for dogs and puppies.” The brand name is the name by which pet food products of a given company are identified. The product name is not essential and may be the same as the brand name; it is usually descriptive of the food and is subject to regulations dealing with composition of ingredients. The product vignette is a visual representation of the product and it must accurately depict the contents of the package (e.g., food pictured on the label cannot appear better that the actual product).
The amount of ingredients that must be present in order to use a certain product name are determined by percentage rules. For example, the term “chicken” requires that at least 70% of the product contain chicken; “chicken dinner/entrée,” etc must contain 10% chicken if moist and 25% chicken if dry; “with chicken” means that the product contains at least 3% chicken; “chicken flavor” means that chicken is recognizable by the pet (< 3% chicken). A nutrition statement may be provided on the display panel; it is usually brief and may include such terms as “complete and nutritious,” “100% nutritious,” or “100% complete nutrition.” The use of these terms implies that the product contains ingredients in quantities sufficient to provide the estimated nutrient requirements of a dog or cat or the product contains a combination of ingredients that when fed to a normal animal as the only source of nourishment will provide satisfactory results.
Information Panel The information panel is adjacent to the principal display panel and includes product information. The ingredient statement must be shown on the label and includes a list of ingredients (which must conform to AAFCO names), in descending order by weight. Ingredients are listed on an “as is” basis, which makes interpretation of ingredient lists difficult since many key ingredients are added with different moisture contents. Because meats contain more moisture, they may be listed first on the ingredient list, although the primary component of the food is a mixture of grains. This is often misleading to pet owners. In addition, the ingredient statement does not provide information about the quality of ingredients.
One limitation of the ingredient statement is that terms such as “meat by-products” are difficult to evaluate. Many owners are under the impression that ‘by-products’ are not healthy and maybe even harmful to their pets. However, the nutritive value of various meat by-products varies widely. It is often misinterpreted that foods containing meat by-products are inferior to foods containing whole meat. AAFCO defines meat on an ingredient label as any combination of skeletal, striated muscle or muscle found in the tongue, diaphragm, heart, and esophagus with or without the overlying fat and the portions of the skin, sinew, nerves, and blood vessels which normally accompany muscle. Meat must be suitable for use in animal foods and therefore excludes feathers, the head, feet, and entrails.
242

Meat by-products do not include hair, horns, teeth, or hooves. Nutritive values in meat by-products also vary greatly. For example, meat by-products such as liver, kidney, and lungs have excellent nutritive value, whereas udder, bone, and connective tissue have poor nutrient availability.
By-products are simply secondary products produced in addition to the principal product. Many human foods contain by-products, and the majority of pet foods contain by-products. For example, by-products of human milk production would be ice cream, cheese, and butter. Many by-products are excellent sources of nutrients for pets as well as people.
The guaranteed analysis includes crude protein (minimum), crude fat (minimum), crude fiber (maximum), and moisture (maximum). Additional guarantees are optional and may be included by the manufacturer. The guaranteed analysis is a general idea of the nutrient content of a food but is of little value in comparing foods because specific nutrient contents are not given and values are listed on an “as is” basis. While crude protein is an accurate index of protein quantity, it does not indicate protein quality. Crude fat may be used to estimate energy density of the food. Crude fiber is an estimate of the indigestible portion of the food; it usually underestimates the true level of fiber in the product. Foods that contain higher levels of fiber are generally lower in calories. The moisture content represents the water content in the food; it cannot exceed a maximum of 78% in the United States. Foods that are > 78% moisture must use a different name such as “in gravy,” “in sauce,” or “in aspic.” The dry matter contains all nutrients (except water) and subtle changes in moisture content may result in marked differences in dry matter, which subsequently affects amounts of nutrients in a food.
The nutritional adequacy statement on the information panel is often more detailed than the brief statements found on the principal display. Examples include “Complete and balanced nutrition for growth of kittens” and “meets…requirements for the entire life cycle of all dogs.” The nutrition statement will help you determine if the manufacturer is making claims for a specific purpose diet versus an all purpose diet. Pet foods with no statement of adequacy include snacks, treats, and some therapeutic foods. Therapeutic foods have a statement that they are to be used by or under the direction of a veterinarian. No further nutrition statement is required since the complete nutritional profile is usually available to the veterinarian.
The basis of the nutrition claim is documented on the pet food label by one of two methods: the formulation method or the feeding trial method. The formulation method is simply a laboratory nutrient profile analysis and does not require any feeding or digestibility trials to prove availability of the nutrients in the profile analysis. This method is recognized on a label by a statement such as “Meets or exceeds the minimal nutritional levels established by AAFCO” or “Formulated to meet the AAFCO dog nutrient profile for…” AAFCO nutrient profiles are published for two categories: 1) growth and reproduction and 2) adult maintenance. The feeding trial method is the preferred method for substantiating a claim. Feeding trials can results in adequacy claims for four categories including: 1) gestation and lactation, 2) growth, 3) maintenance, and 4) complete for all life stages. A food that has successfully completed a sequential growth and gestation/lactation trial can make a claim for all life stages. The required wording for labels that have passed these tests is: “Animal feeding tests using AAFCO procedures substantiate that (brand) provides complete and balanced nutrition for (lifestage).” Pet foods that do not meet AAFCO requirements by either of the standard methods will have a nutritional statement as follows: “this product is intended for intermittent or supplemental feeding only.”
Dog and cat foods labeled as complete and nutritious for any or all lifestages must list feeding directions on the product label. At a minimum, feeding directions should include the instructions “feed (weight/unit) per (weight) of dog or cat” and frequency of feeding. These feeding directions are general guidelines and should serve as a starting point; adjustments may be needed to maintain optimal body condition.
Summary Pet owners at present want and expect the very best for their pets. However, the information that pet owners are given is sometimes well-intentioned, but misleading. The veterinary healthcare team should focus on proper nutrition for every pet that presents to their hospital. To do this, the healthcare team must perform a complete nutritional history and patient assessment and be knowledgeable about the wide variety of foods that are on the market today. Not all foods are created equal and pet foods labels can be misleading and misinterpreted. Veterinary technicians must familiarize themselves with properly reading a pet food label and understanding how the pet food label can affect the nutritional recommendation being made.
243

References
1. Roudebush P, Dzanis D, Debraekeleer J, et al. Pet food labels. Small Animal Clinical Nutrition, 4th ed.Topeka: Mark Morris Institute, 2000;147-161.
2. Burns, KM. Managing Overweight or Obese Pets. Veterinary Technician, June 2006; 385-389.
3. Wortinger A. Nutritional myths. J Am Anim Hosp Assoc 2005;41:273-276.
4. Zicker SC. Evaluating pet foods: how confident are you when you recommend a commercial pet food? TopCompanion Anim Med 2008;23:121-126.
5. Crane SW, Griffin RW, Messent, PR: Introduction to commercial pet foods. Small Animal ClinicalNutrition, 4th ed. Topeka: Mark Morris Institute, 2000;111-126.
244

Busting Nutritional Myths
Kara M. Burns, MS, MEd, LVT, VTS (Nutrition) Academy of Veterinary Nutrition Technicians
Proper nutrition is essential to maintaining the health of pets and is one of the most important factors in managing disease in pets. As clients become more aware of the importance of nutrition in their own health, they will expect this same higher standard of nutritional care for their pets. The veterinary healthcare team should be the preferred, expert source of the best nutritional information for pets.1 Veterinary teams that understand and promote clinical nutrition and demonstrate in-clinic behaviors consistent with this conviction will benefit their patients, their clients, and their practices.2 Proper nutritional management is one of the most important factors in maximizing health, performance, and longevity in addition to managing disease conditions.
Pet owners and veterinary healthcare team members have access to a great deal of information regarding pet nutrition via the internet, news sources, blogs, etc. Along with this wealth of information comes confusing and often incorrect nutritional information. As veterinary nurses we need to educate ourselves on proper companion animal nutrition and sort through the minutiae to educate well intentioned owners on what constitutes proper nutrition for their pet. There is a lot of misinformation regarding pet food; veterinary teams should be viewed as the expert when it comes to veterinary medical questions, including proper nutrition.
Every patient that presents to the hospital should be assessed to establish nutritional needs and feeding goals, which are dependent upon the individual patient’s physiology and/or disease condition. This nutritional assessment should be performed every time the patient presents to the hospital. The role of the veterinary nurse is to ascertain patient history, score the patient’s body condition, work with the veterinarian to determine the proper nutritional recommendation for the patient, and communicate this information to the pet owner.
To discuss marketing gimmicks and pet food myths, we must begin with a basic understanding of the pet food label. The pet food label is the primary means by which product information is communicated from the manufacturer or distributor to pet owners, veterinarians, health care team members, and regulatory officials. Reading and interpreting pet food labels is one method that healthcare team members and pet owners can obtain information about pet foods; however, labels do not necessarily provide information about food quality (e.g., digestibility and biological value).
Pet food labels not only communicate information about the product, but also serve as a legal document. A number of agencies and organizations regulate production, marketing, and sales of pet foods in different countries. Each agency has different responsibilities with varying degrees of authority. Some of these agencies regulate information found on pet food labels whereas others influence the regulatory process. Pet foods are regulated at their point of sale (e.g., foods manufactured in the United States (US) but sold outside the US must meet labeling requirements of the country in which the food is sold). Pet foods sold in the US must conform to Food and Drug Administration (FDA), Association of American Feed Control Officials (AAFCO) and state pet food labeling requirements.
Pet food labels include two main parts: 1) the principal display panel and 2) the information panel. Understanding pet food labels is paramount to helping owners understand some of the marketing tactics as well as gaining clearer insight regarding many of the myths that are in the profession today. This presentation will review pet food labels and how misunderstandings result from the information that is found on (or is not found on) the pet food label.
Additionally, we will explore a number of long held beliefs which pet owners use in choosing the food that they believe to be appropriate for their pet. Grain Free, by-products, natural, human grade, etc., are all terms that are used by today’s pet owner. Do these terms hold true meaning?
By-Products
A byproduct is something produced from the making of another product. By-products are not by definition poor quality. For instance, Vitamin E is a by-product of soy. By-products are simply secondary products produced in addition to the principal product. Additionally, there are several human foods which contain by-products – so it is
245

not just something found in pet foods. For example, by-products of human milk production would be ice cream, cheese, and butter. Veterinary healthcare teams need to educate owners that by-products can be an excellent sources of nutrients for pets as well as people.
In relation to pet foods, by-products are generally parts of the animals that are not the muscle meat preferred by most American consumers. The term refers only to the anatomic parts included, not to the nutritional quality of the parts. AAFCO defines a meat by-product as “the non-rendered, clean parts, other than meat, derived from slaughtered mammals. It includes, but is not limited to, lungs, spleen, kidneys, brain, livers, …… and stomachs and intestines freed of their contents. It does not include hair, horns, teeth and hooves …” 3
Furthermore, it is important to note that many of the items included in “by-product” (e.g., organ meats) may be higher in nutrients essential to the pet such as amino acids, minerals, and vitamins. Also, pets find these to be more palatable than skeletal muscle meat. Interestingly, many popular dog treats (e.g., bully sticks [bull penis], lung, liver, pig ears, tendons, etc.) are actually items that would be appropriately classified under the label of “by-product”.
Grain Free
Pet parents believe that grain-free diets are better for their pets. Grain-free diets are assumed to be more natural, carbohydrate free, and less likely to result in health problems, especially allergies, in their pet. However, this is NOT the case.
To date, there has not been any credible evidence, nor any nutritional foundation supportive of grain free diets as being ‘better for pets’. Veterinary healthcare teams must educate pet owners regarding the difference between nutrients and ingredients. Pets need nutrients to maintain health. Ingredients are the vehicles that provide those nutrients. Nutrition can be defined as the relationship of food and nutrients to health. Proper nutrient intake is essential to normal development, overall health, and disease management in companion animals. Nutrients have numerous metabolic roles essential to normal physiologic function that can be compromised by insufficient or irregular intake.4
Pet owners are under the misperception that whole grains may be ‘fillers’ in pet foods. The term filler implies that the ingredient has little or no nutritional value.5,6 Whole grains do contribute vital nutrients such as vitamins, minerals, and essential fatty acids to pet foods. 7 Various grain products also provide protein which may be easier for the pet to digest versus certain protein from meat. Realistically, most dogs and cats are able to utilize and digest (>90%) nutrients from grains normally found in pet foods.5,6
Meat First
For dogs to reach their full growth potential they must have meat as the first ingredient, right? This is another long held myth - that foods listing meat first in the ingredient list are better foods. Healthy pets need nutrients and a complete balance of amino acids, and these may come from meat and non-meat sources.
There is a perception that “meat-first” foods are better. Healthy pets need nutrients and a complete balance of amino acids (proteins) from both meat and non-meat sources. Even in a “meat-first” food, meat is not the only source of protein available. Other ingredients, such as corn, can provide protein as well.
The veterinary healthcare team must also remember the fact that dogs and cats are unable to store protein. Consequently, excess dietary protein forces the liver to work harder metabolizing it and the kidneys to work harder when they must convert that protein into waste, which is then excreted in urine.
Carnivore or Omnivore?
Some pet owners believe that dogs are carnivores and as such must have a meat-first diet. However, dogs are actually omnivores, just as wolves are omnivores. Many owners will say that dogs descended from wolves and wolves eat meat only and that is what they would eat “naturally” or “in the wild.”
246

Dogs (and wolves) need a balanced diet of proteins, carbohydrates, and vitamins from a variety of sources including meats, vegetables and grains. Dogs and cats and humans require 6 basic nutrients – water, protein, fat, carbohydrates, vitamins and minerals.
Ingredient lists
Ingredient lists on packages are commonly used by pet owners to determine the quality of pet foods. However, going by the ingredients listed on the package label has many drawbacks. It also can be subject to intentional manipulation by the pet food manufacturer. The ingredient statement must be shown on the label and includes a list of ingredients (which must conform to AAFCO names), in descending order by weight. Ingredients are listed on an “as is” basis, which makes interpretation of ingredient lists difficult since many key ingredients are added with different moisture contents. Because meats contain more moisture, they may be listed first on the ingredient list, although the primary component of the food might be a mixture of grains. Thus for those owners wanting a meat first diet – they are getting one, although the complete diet may be made up of carbohydrates more so than meat. Additionally, the ingredient statement does not provide information about the quality of ingredients.
Ingredient splitting
Often what pet food manufacturers will do is split ingredients. Ingredient splitting is common in the pet food industry. By splitting an ingredient into several different forms, it allows a meat source to appear first or earlier on the ingredient panel. Obviously, meat can appear first due to its higher moisture content than other ingredients. Ingredients are listed on labels in order of weight, including water, thus ingredients with high water content (like fresh meats and vegetables) are listed before similar amounts of dry ingredients, even though they may contribute fewer nutrients overall.
Feeding a puppy a meat first diet will not guarantee a large adult dog. Genetics are already pre-determined and for a healthy dog, especially a large breed dog, feeding to maximal growth rate will put undue pressure on the puppy’s body and is more likely to result in obesity and skeletal growth disease. Free feeding is not recommended. Rather a controlled growth rate is what we are trying to achieve. A controlled growth feeds the correct amount of food and the proper nutrients to the puppy, to allow for growth at a controlled rate. This rate has NO effect on the ultimate size of the dog.
It is imperative that veterinary nurses remember that pets require nutrients, not ingredients. Pet owners do not like the name of certain ingredients and they do not know what some of the more technical sounding ingredients truly are. To pet owners, a food full of great-sounding ingredients can be less nutritious than one containing less appealing ingredients. Additionally, remember some manufacturers may add ingredients to products for the distinct purpose of marketing; in other words to increase the appeal of the food to consumers. The benefits of these particular ingredients may be unproven, be present in very small amounts, and provide nothing to the food but added expense. More is not always better! More ingredients also mean increased quality control measures – thus more time and expense - are necessary to ensure that the finished product adheres to the desired nutrient formulation. This aids in controlling excess nutrients that may be a risk for long-term health.
As veterinary technicians we need to educate ourselves on what is being discussed by pet owners in relation to pet foods and debunk any myths that are circulating on incorrect or unsubstantiated data.
Summary
Pet owners at present want and expect the very best for their pets. However, the information that pet owners are given is sometimes well-intentioned, but misleading. The veterinary healthcare team should focus on proper nutrition for every pet that presents to their hospital. To do this, the healthcare team must perform a complete nutritional history and patient assessment and be knowledgeable about the wide variety of foods that are on the market today. Not all foods are created equal and pet foods labels can be misleading and misinterpreted. It is important for the veterinary team to understand pet food labels, the evidence behind some of today’s beliefs, and not be afraid of the question – “what should I feed my pet?”
247
References
1. Burns KM. Nutrition: Is the new emphasis a fad? Veterinary Team Brief, 2014, 5:8-9.2. Burns KM. The Dreaded Question: What Should I Feed My Pet? Veterinary Team Brief. January 2015. Pp. 13-
14.3. Association of American Feed Control Officials. Feed Terms and Ingredient Definitions. 2017 AAFCO Official
Publication, page 359.4. Gross KL, Yamka RM, Choo C, Friesen KG, et al. Macronutrients. In Small Animal Clinical Nutrition 5th Ed.
Hand M, Thatcher, Remillard R, Roudebush P, Novotny B, eds. 2010, Mark Morris Institute, Topeka, KS. Pp.49-105.
5. Laflamme D, Izquierdo O, Eirmann L, Binder S. Myths and Misperceptions about ingredients used incommercial pet foods. In Veterinary Clinics of North America: Small Animal Practice; Clinical Nutrition.Laflamme D, Zoran DL, eds. July 2014, Pp 689-698. Elsevier, St. Louis.
6. Ograin VL, Burns KM. Nutritional Considerations in Allergic Skin Disease. The NAVTA Journal. 2016Convention Issue. Pp. 12 – 19.
7. http://vetnutrition.tufts.edu/2016/06/grain-free-diets-big-on-marketing-small-on-truth/Accessed 6-23-21.
Resources
www.wsava.net
www.petnutritionalliance.org
248
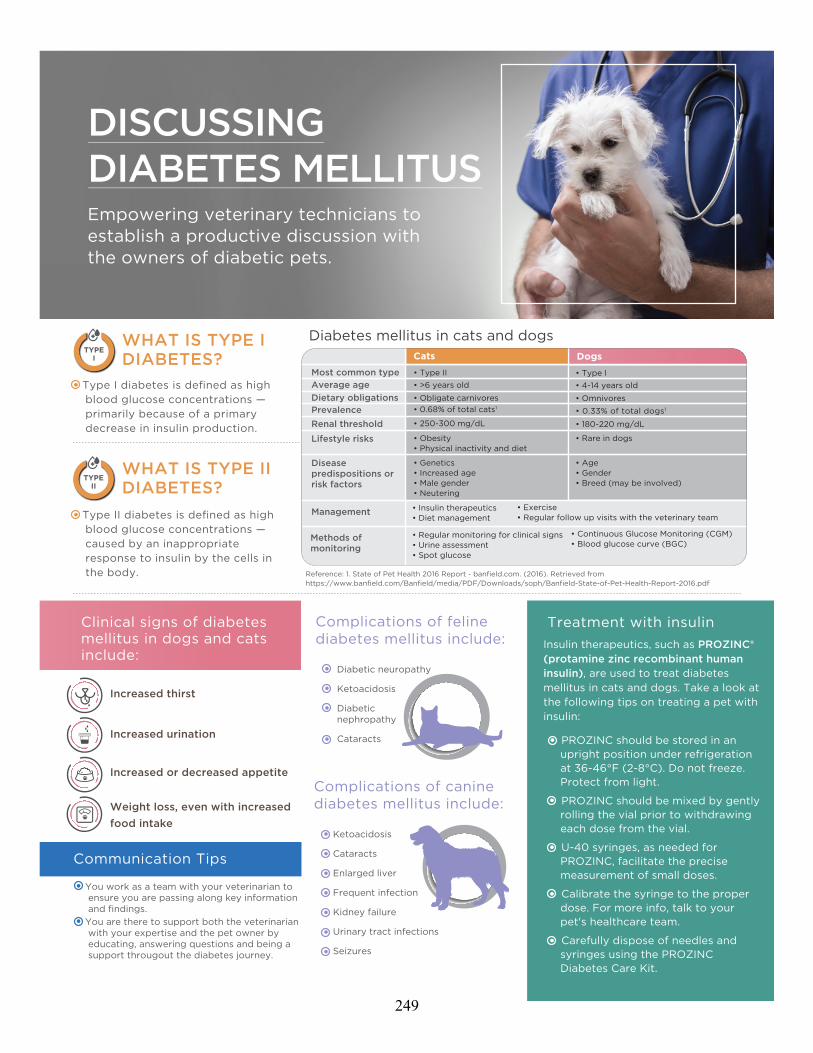
Communication Tips
DISCUSSING DIABETES MELLITUSEmpowering veterinary technicians to establish a productive discussion with the owners of diabetic pets.
Diabetes mellitus in cats and dogs
Clinical signs of diabetes mellitus in dogs and cats include:
Increased thirst
Increased urination
Increased or decreased appetite
Weight loss, even with increased food intake
Treatment with insulinInsulin therapeutics, such as PROZINC® (protamine zinc recombinant human insulin), are used to treat diabetes mellitus in cats and dogs. Take a look at the following tips on treating a pet with insulin:
• PROZINC should be stored in anupright position under refrigerationat 36-46°F (2-8°C). Do not freeze.Protect from light.
• PROZINC should be mixed by gentlyrolling the vial prior to withdrawingeach dose from the vial.
• U-40 syringes, as needed forPROZINC, facilitate the precisemeasurement of small doses.
• Calibrate the syringe to the properdose. For more info, talk to yourpet's healthcare team.
• Carefully dispose of needles andsyringes using the PROZINCDiabetes Care Kit.
Complications of feline diabetes mellitus include:
Diabetic neuropathy
Ketoacidosis
Diabetic nephropathy
Cataracts
WHAT IS TYPE I DIABETES?
TYPEI
WHAT IS TYPE II DIABETES?
TYPEII
• Type I diabetes is defined as highblood glucose concentrations —primarily because of a primarydecrease in insulin production.
• Type II diabetes is defined as highblood glucose concentrations —caused by an inappropriateresponse to insulin by the cells inthe body.
Disease predispositions or risk factors
Lifestyle risks
Renal thresholdPrevalenceDietary obligationsAverage ageMost common type
• Genetics • Increased age• Male gender• Neutering
• Obesity• Physical inactivity and diet
• 250-300 mg/dL
• 0.68% of total cats1
• Obligate carnivores
• >6 years old • Type II
Cats
Management • Insulin therapeutics • Diet management
• Exercise • Regular follow up visits with the veterinary team
Methods of monitoring
Dogs
• Age • Gender• Breed (may be involved)
• Rare in dogs
• 180-220 mg/dL
• 0.33% of total dogs1
• Omnivores
• 4-14 years old• Type I
• You work as a team with your veterinarian toensure you are passing along key informationand findings.
• You are there to support both the veterinarianwith your expertise and the pet owner byeducating, answering questions and being asupport througout the diabetes journey.
Complications of canine diabetes mellitus include:
Ketoacidosis
Cataracts
Enlarged liver
Frequent infection
Kidney failure
Urinary tract infections
Seizures
• Regular monitoring for clinical signs• Urine assessment• Spot glucose
• Continuous Glucose Monitoring (CGM)• Blood glucose curve (BGC)
Reference: 1. State of Pet Health 2016 Report - banfield.com. (2016). Retrieved from https://www.banfield.com/Banfield/media/PDF/Downloads/soph/Banfield-State-of-Pet-Health-Report-2016.pdf
249

*PR
OZ
INC
® fo
r d
og
s w
as n
ot
app
rove
d a
nd li
cens
ed f
or
use
in d
og
s at
the
tim
e o
f th
e 20
18 A
AH
A u
pd
ated
gui
del
ine
pub
licat
ion.
Ho
wev
er, i
t is
ant
icip
ated
to
be
AA
HA
rec
om
men
ded
in t
he n
ext
pub
licat
ion.
IMP
OR
TAN
T SA
FE
TY IN
FO
RM
ATI
ON
: P
RO
ZIN
C is
fo
r us
e in
do
gs
and
cat
s o
nly.
Kee
p o
ut o
f th
e re
ach
of
child
ren.
As
wit
h al
l ins
ulin
pro
duc
ts, c
aref
ul p
atie
nt
mo
nito
ring
fo
r hy
po
gly
cem
ia a
nd h
yper
gly
cem
ia is
ess
enti
al t
o a
ttai
n an
d m
aint
ain
adeq
uate
gly
cem
ic c
ont
rol a
nd t
o p
reve
nt
asso
ciat
ed c
om
plic
atio
ns. O
verd
ose
can
res
ult
in p
rofo
und
hyp
og
lyce
mia
and
dea
th. T
he m
ost
co
mm
on
adve
rse
reac
tio
ns w
ere
leth
arg
y, a
nore
xia,
hyp
og
lyce
mia
, vo
mit
ing
, sei
zure
s, s
haki
ng (
do
gs
onl
y), d
iarr
hea,
and
ata
xia.
Man
y o
f th
e ad
vers
e re
acti
ons
, su
ch a
s le
thar
gy,
sei
zure
s, s
haki
ng (
do
gs
onl
y), a
nd a
taxi
a, a
re a
sso
ciat
ed w
ith
hyp
og
lyce
mia
.G
luco
cort
ico
id a
nd
pro
ges
tog
en u
se s
ho
uld
be
avo
ided
. Th
e sa
fety
an
d e
�ec
tive
nes
s o
f P
RO
ZIN
C in
pu
pp
ies,
kit
ten
s, o
r b
reed
ing
, pre
gn
ant,
an
d la
ctat
ing
an
imal
s h
as n
ot
bee
n e
valu
ated
. PR
OZ
INC
is c
on
trai
nd
icat
ed d
uri
ng
ep
iso
des
of
hyp
og
lyce
mia
an
d in
an
imal
s se
nsi
tive
to
pro
tam
ine
zin
c re
com
bin
ant
hu
man
insu
lin o
r an
y o
ther
ing
red
ien
ts in
PR
OZ
INC
.F
or
mo
re in
form
atio
n, p
leas
e se
e th
e E
NC
LO
SE
D f
ull
pre
scri
bin
g in
form
atio
n.
Ref
eren
ce: 1
. Beh
ren
d E
, Ho
lfo
rd A
, Lat
han
P, R
uci
nsk
y R
, Sch
ulm
an R
. 20
18 A
AH
A D
iab
etes
Man
agem
ent
Gu
idel
ines
fo
r D
og
s an
d C
ats.
Jo
urn
al o
f th
e A
mer
ican
An
imal
Ho
spit
al A
sso
ciat
ion
. 20
18;5
4(1
):1-
21. d
oi:1
0.5
326
/jaa
ha-
ms-
68
22
PR
OZ
INC
® is
a r
egis
tere
d
trad
emar
k o
f B
oeh
ring
er
Ing
elhe
im A
nim
al H
ealt
h U
SA
Inc.
A
ll o
ther
tra
dem
arks
are
the
p
rop
erty
of
thei
r re
spec
tive
o
wne
rs.
©20
20 B
oeh
ring
er In
gel
heim
A
nim
al H
ealt
h U
SA
Inc.
, Dul
uth
GA
. All
Rig
hts
Res
erve
d.
US
-PE
T-0
452
-20
19-V
2
Lorem ipsum
AA
HA
rec
om
men
ded
fo
r d
og
s
AA
HA
rec
om
men
ded
fo
r ca
ts
FD
A-a
pp
rove
d
Insu
lin t
ype
Ind
icat
ion
Syri
nge
typ
e
Pea
k ac
tio
n (N
adir
)
VE
TSU
LIN
®
(Len
te)
NP
HLE
VE
MIR
®
(Det
emir
)LA
NTU
S®
(Gla
rgin
e)P
RO
ZIN
C®(P
ZI)
√ √√
√
*√
√
-P
rota
min
e zi
ncre
com
bin
ant
hum
an in
sulin
-R
eco
mb
inan
thu
man
insu
lin-
Rec
om
bin
ant
hum
an in
sulin
-R
eco
mb
inan
thu
man
insu
lin-
Pur
ified
po
rcin
ezi
nc in
sulin
susp
ensi
on
-In
dic
ated
fo
r us
e in
do
gs
and
cat
s-
No
t in
dic
ated
fo
rus
e in
do
gs
and
cats
—us
ed o
� la
bel
-F
elin
e: 5
-7 h
our
s
-C
anin
e: 1
8->
24ho
urs
-F
elin
e: 1
0-1
4 h
our
s
-C
anin
e: 0
.5-8
.5 h
our
s-
Can
ine:
1-1
0 h
our
s-
Fel
ine:
2-8
ho
urs
-F
elin
e: 1
2-24
ho
urs
Dur
atio
n-
Can
ine:
4-1
0 h
our
s-
Can
ine:
10
-24
ho
urs
-F
elin
e: 8
-14
ho
urs
-C
anin
e: 1
2-20
ho
urs
-F
elin
e: 1
2-24
ho
urs
-F
elin
e: 1
2-24
ho
urs
-N
ot
ind
icat
ed f
or
use
in d
og
s an
dca
ts—
used
o�
lab
el
-N
ot
ind
icat
ed f
or
use
in d
og
s an
dca
ts—
used
o�
lab
el
-In
dic
ated
fo
r us
ein
do
gs
and
cat
s
-U
-40
-U
-10
0-
U-
100
-U
- 10
0-
U-4
0-
Vet
Pen
®
INS
UL
IN T
HE
RA
PE
UT
ICS
Insu
lin t
her
apeu
tics
in a
dd
itio
n t
o P
RO
ZIN
C®
(pro
tam
ine
zin
c re
com
bin
ant
hu
man
insu
lin)1 :
250
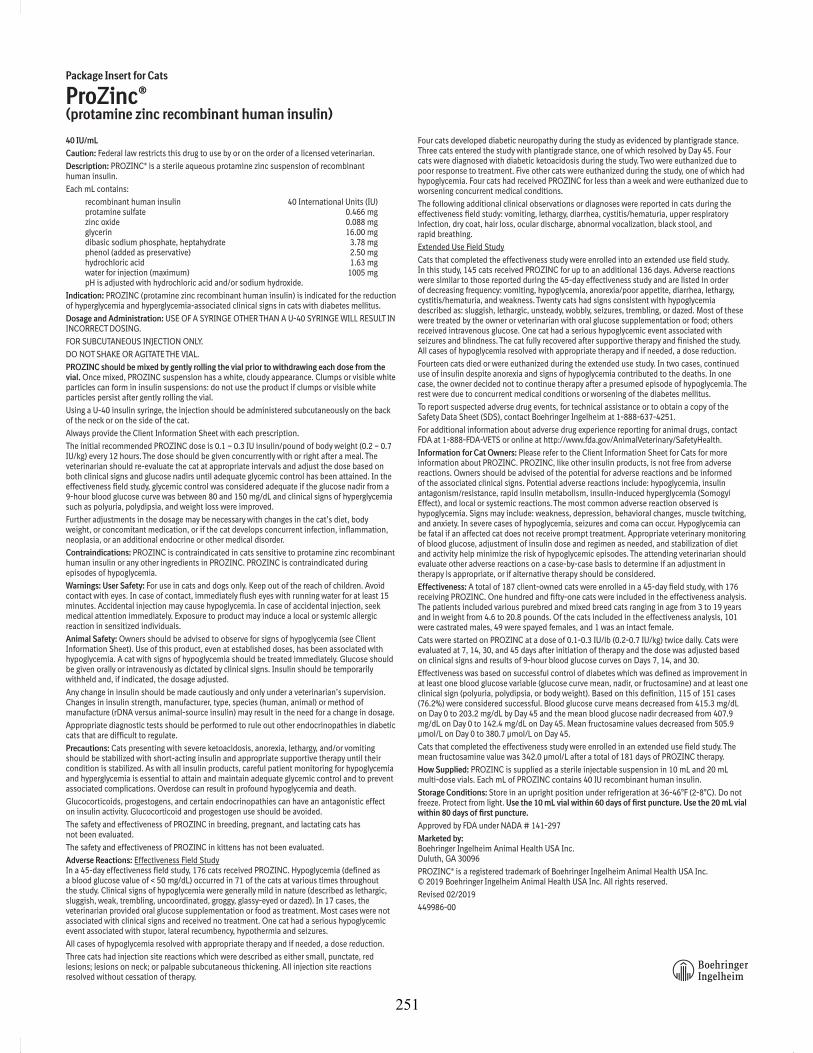
40 IU/mL
This summary contains important information about PROZINC. You should read this information before you start giving your cat PROZINC and review it each time the prescription is refilled. This sheet is provided only as a summary and does not take the place of instructions from your veterinarian. Talk to your veterinarian if you do not understand any of this information or if you want to know more about PROZINC.
What is PROZINC? PROZINC is an aqueous protamine zinc suspension of recombinant human insulin that is used to reduce high blood sugar (hyperglycemia) in cats with diabetes mellitus. A veterinarian must prescribe PROZINC for your cat. PROZINC should be given to cats only. Keep out of reach ofchildren. Seek medical attention immediately if you accidentally inject yourself with PROZINC.
What is diabetes mellitus? Diabetes mellitus occurs when a cat has insufficient levels of, or an abnormal response to, insulin. The low insulin levels may result in high blood sugar (hyperglycemia) that could produce the following changes in your cat:
• Increased thirst • Increased appetite
• High levels of sugar (glucose) in the urine (glucosuria) • Increased urination
• Weight loss • Weakness in the back legs
What kind of results can I expect when my cat is on PROZINC for diabetes mellitus?Although PROZINC is not a cure for diabetes mellitus, it can help reduce the levels of sugar (glucose) in the blood, which can help alleviate the clinical signs.
What should I discuss with my veterinarian before giving PROZINC?
Talk to your veterinarian about:
• The signs of diabetes mellitus you have observed in your cat (for example, increased thirst and urination).
• The importance of proper PROZINC storage, handling, and administration techniques (for example, how to gently roll the vial prior to each use, the proper appearance of productafter gently rolling, how to fill the U-40 syringe with the proper amount of insulin, and where and how to inject the insulin).
• The importance of maintaining your cat under the same conditions for diet, exercise, environment, etc.
• The importance of follow-up visits for testing to determine if dose adjustments of PROZINC are necessary.
Tell your veterinarian about:
• Any side effects your cat has had when receiving other insulin products.
• Any medical problems or allergies that your cat has now or has had in the past.
• All medications that you are giving your cat or plan to give your cat, including those you can get without a prescription.
• If your cat is pregnant, nursing, or if you plan to breed your cat.
What are the possible side effects that may occur in my cat during PROZINC therapy?PROZINC, like other drugs, may cause side effects. Serious side effects can occur with or without warning. Please contact your veterinarian immediately if you think your cat has a medical problem or side effect from PROZINC therapy. The most common insulin-related side effect is low blood sugar (hypoglycemia). Signs of low blood sugar (hypoglycemia) can occur suddenly and may include:
• Weakness • Staggering gait • Muscle twitching • Coma
• Depression, lethargy, sluggishness • Behavioral changes • Seizures, convulsions • Death
What actions do I take if my cat shows signs of low blood sugar (hypoglycemia)? • If your cat is unconscious or having a seizure, this is a medical emergency. Take your cat
to the veterinarian immediately.
• If your cat is conscious, rub approximately 1 tablespoon of corn syrup or honey on yourcat’s gums. When it is able to swallow, give corn syrup or honey by mouth until your cat is alert enough to eat. Feed the usual meal and contact your veterinarian.
When should my cat not be given PROZINC?Do not give your cat its prescribed dose of PROZINC if it: • Is experiencing an episode of low blood sugar (hypoglycemia). Common causes for low blood
sugar include excessive doses of insulin, failure to eat, strenuous exercise, changes in the body’s need for insulin, diabetes-inducing disease or drug effects.
• Is not eating or is vomiting.
• Is sensitive to protamine zinc recombinant human insulin or any other ingredients in PROZINC.
• Do not give your cat its prescribed dose of PROZINC if you see clumps or visible white particles in the vial after gently rolling.
How should I give PROZINC to my cat? PROZINC should be given with or right after a meal.
Give PROZINC with U-40 syringes only. Use of a syringe other than a U-40 syringe will result in incorrect dosing. Gently roll the vial until the PROZINC has a uniformly cloudy, white appearance. If there are clumps or visible white particles in the vial after gently rolling, do not use the PROZINC and call your veterinarian. PROZINC should be given according to your veterinarian’s instructions. Your veterinarian will tell you what amount of PROZINC is right for your cat and instruct you on techniques for administration.
Can PROZINC be given with other medications? PROZINC can be given with other medications, but the dose may need to be adjusted due to the medication resulting in either increased or decreased insulin requirements. Tell yourveterinarian about all medications you have given your cat in the past, and any medications that you are planning to give with PROZINC. This should include medications that you can getfor your cat without a prescription. Your veterinarian may want to ensure that all of your cat’s medications can be given together.
What should I do if I inject more than the prescribed amount of PROZINC? Contact your veterinarian immediately and, if your veterinarian is not available, seek otherveterinary advice at once.
What should I do if my cat receives less than the prescribed dose, or I miss an injection?
• Contact your veterinarian as soon as possible for advice on your cat’s next dose.
• If you cannot reach your veterinarian and your cat is eating and acting normally, give your cat the usual dose at the next regularly scheduled injection time.
How should I store PROZINC? PROZINC should be stored in an upright position under refrigeration at 36-46°F (2-8°C). Do notfreeze. Protect from light. Use the 10 mL vial within 60 days of first puncture. Use the 20 mL vial within 80 days of first puncture.
What else should I know about PROZINC? This sheet provides a summary of information about PROZINC. If you have any questions or concerns about the product or diabetes mellitus, talk to your veterinarian.
As with all prescribed medications, PROZINC should only be given to the cat for which it is prescribed and for the condition for which it was prescribed.
It is important to periodically discuss your cat’s response to PROZINC at regular checkups that may include blood glucose monitoring. Your veterinarian will best determine if your cat is responding as expected and should continue receiving PROZINC.
Approved by FDA under NADA # 141-297
PROZINC® is a registered trademark of Boehringer Ingelheim Animal Health USA Inc. © 2019 Boehringer Ingelheim Animal Health USA Inc. All rights reserved.
Revised 02/2019
Client Information Sheet for Cats
ProZinc®(protamine zinc recombinant human insulin)
40 IU/mL
Caution: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
Description: PROZINC® is a sterile aqueous protamine zinc suspension of recombinant human insulin.
Each mL contains:
recombinant human insulin 40 International Units (IU) protamine sulfate 0.466 mg zinc oxide 0.088 mg glycerin 16.00 mg dibasic sodium phosphate, heptahydrate 3.78 mg phenol (added as preservative) 2.50 mg hydrochloric acid 1.63 mg water for injection (maximum) 1005 mg pH is adjusted with hydrochloric acid and/or sodium hydroxide.
Indication: PROZINC (protamine zinc recombinant human insulin) is indicated for the reduction of hyperglycemia and hyperglycemia-associated clinical signs in cats with diabetes mellitus.
Dosage and Administration: USE OF A SYRINGE OTHER THAN A U-40 SYRINGE WILL RESULT IN INCORRECT DOSING.
FOR SUBCUTANEOUS INJECTION ONLY.
DO NOT SHAKE OR AGITATE THE VIAL.
PROZINC should be mixed by gently rolling the vial prior to withdrawing each dose from the vial. Once mixed, PROZINC suspension has a white, cloudy appearance. Clumps or visible white particles can form in insulin suspensions: do not use the product if clumps or visible white particles persist after gently rolling the vial.
Using a U-40 insulin syringe, the injection should be administered subcutaneously on the back of the neck or on the side of the cat.
Always provide the Client Information Sheet with each prescription.
The initial recommended PROZINC dose is 0.1 – 0.3 IU insulin/pound of body weight (0.2 – 0.7 IU/kg) every 12 hours. The dose should be given concurrently with or right after a meal. The veterinarian should re-evaluate the cat at appropriate intervals and adjust the dose based on both clinical signs and glucose nadirs until adequate glycemic control has been attained. In the effectiveness field study, glycemic control was considered adequate if the glucose nadir from a 9-hour blood glucose curve was between 80 and 150 mg/dL and clinical signs of hyperglycemia such as polyuria, polydipsia, and weight loss were improved.
Further adjustments in the dosage may be necessary with changes in the cat’s diet, body weight, or concomitant medication, or if the cat develops concurrent infection, inflammation, neoplasia, or an additional endocrine or other medical disorder.
Contraindications: PROZINC is contraindicated in cats sensitive to protamine zinc recombinant human insulin or any other ingredients in PROZINC. PROZINC is contraindicated during episodes of hypoglycemia.
Warnings: User Safety: For use in cats and dogs only. Keep out of the reach of children. Avoid contact with eyes. In case of contact, immediately flush eyes with running water for at least 15 minutes. Accidental injection may cause hypoglycemia. In case of accidental injection, seek medical attention immediately. Exposure to product may induce a local or systemic allergic reaction in sensitized individuals.
Animal Safety: Owners should be advised to observe for signs of hypoglycemia (see Client Information Sheet). Use of this product, even at established doses, has been associated with hypoglycemia. A cat with signs of hypoglycemia should be treated immediately. Glucose should be given orally or intravenously as dictated by clinical signs. Insulin should be temporarily withheld and, if indicated, the dosage adjusted.
Any change in insulin should be made cautiously and only under a veterinarian’s supervision. Changes in insulin strength, manufacturer, type, species (human, animal) or method of manufacture (rDNA versus animal-source insulin) may result in the need for a change in dosage.
Appropriate diagnostic tests should be performed to rule out other endocrinopathies in diabetic cats that are difficult to regulate.
Precautions: Cats presenting with severe ketoacidosis, anorexia, lethargy, and/or vomiting should be stabilized with short-acting insulin and appropriate supportive therapy until their condition is stabilized. As with all insulin products, careful patient monitoring for hypoglycemia and hyperglycemia is essential to attain and maintain adequate glycemic control and to prevent associated complications. Overdose can result in profound hypoglycemia and death.
Glucocorticoids, progestogens, and certain endocrinopathies can have an antagonistic effect on insulin activity. Glucocorticoid and progestogen use should be avoided.
The safety and effectiveness of PROZINC in breeding, pregnant, and lactating cats has not been evaluated.
The safety and effectiveness of PROZINC in kittens has not been evaluated.
Adverse Reactions: Effectiveness Field Study In a 45-day effectiveness field study, 176 cats received PROZINC. Hypoglycemia (defined as a blood glucose value of < 50 mg/dL) occurred in 71 of the cats at various times throughout the study. Clinical signs of hypoglycemia were generally mild in nature (described as lethargic, sluggish, weak, trembling, uncoordinated, groggy, glassy-eyed or dazed). In 17 cases, the veterinarian provided oral glucose supplementation or food as treatment. Most cases were not associated with clinical signs and received no treatment. One cat had a serious hypoglycemic event associated with stupor, lateral recumbency, hypothermia and seizures.
All cases of hypoglycemia resolved with appropriate therapy and if needed, a dose reduction.
Three cats had injection site reactions which were described as either small, punctate, red lesions; lesions on neck; or palpable subcutaneous thickening. All injection site reactions resolved without cessation of therapy.
Four cats developed diabetic neuropathy during the study as evidenced by plantigrade stance. Three cats entered the study with plantigrade stance, one of which resolved by Day 45. Four cats were diagnosed with diabetic ketoacidosis during the study. Two were euthanized due to poor response to treatment. Five other cats were euthanized during the study, one of which had hypoglycemia. Four cats had received PROZINC for less than a week and were euthanized due to worsening concurrent medical conditions.
The following additional clinical observations or diagnoses were reported in cats during the effectiveness field study: vomiting, lethargy, diarrhea, cystitis/hematuria, upper respiratory infection, dry coat, hair loss, ocular discharge, abnormal vocalization, black stool, and rapid breathing.
Extended Use Field Study
Cats that completed the effectiveness study were enrolled into an extended use field study. In this study, 145 cats received PROZINC for up to an additional 136 days. Adverse reactions were similar to those reported during the 45-day effectiveness study and are listed in order of decreasing frequency: vomiting, hypoglycemia, anorexia/poor appetite, diarrhea, lethargy, cystitis/hematuria, and weakness. Twenty cats had signs consistent with hypoglycemia described as: sluggish, lethargic, unsteady, wobbly, seizures, trembling, or dazed. Most of these were treated by the owner or veterinarian with oral glucose supplementation or food; others received intravenous glucose. One cat had a serious hypoglycemic event associated with seizures and blindness. The cat fully recovered after supportive therapy and finished the study. All cases of hypoglycemia resolved with appropriate therapy and if needed, a dose reduction.
Fourteen cats died or were euthanized during the extended use study. In two cases, continued use of insulin despite anorexia and signs of hypoglycemia contributed to the deaths. In one case, the owner decided not to continue therapy after a presumed episode of hypoglycemia. The rest were due to concurrent medical conditions or worsening of the diabetes mellitus.
To report suspected adverse drug events, for technical assistance or to obtain a copy of the Safety Data Sheet (SDS), contact Boehringer Ingelheim at 1-888-637-4251.
For additional information about adverse drug experience reporting for animal drugs, contact FDA at 1-888-FDA-VETS or online at http://www.fda.gov/AnimalVeterinary/SafetyHealth.
Information for Cat Owners: Please refer to the Client Information Sheet for Cats for more information about PROZINC. PROZINC, like other insulin products, is not free from adverse reactions. Owners should be advised of the potential for adverse reactions and be informed of the associated clinical signs. Potential adverse reactions include: hypoglycemia, insulin antagonism/resistance, rapid insulin metabolism, insulin-induced hyperglycemia (Somogyi Effect), and local or systemic reactions. The most common adverse reaction observed is hypoglycemia. Signs may include: weakness, depression, behavioral changes, muscle twitching, and anxiety. In severe cases of hypoglycemia, seizures and coma can occur. Hypoglycemia can be fatal if an affected cat does not receive prompt treatment. Appropriate veterinary monitoring of blood glucose, adjustment of insulin dose and regimen as needed, and stabilization of diet and activity help minimize the risk of hypoglycemic episodes. The attending veterinarian should evaluate other adverse reactions on a case-by-case basis to determine if an adjustment in therapy is appropriate, or if alternative therapy should be considered.
Effectiveness: A total of 187 client-owned cats were enrolled in a 45-day field study, with 176 receiving PROZINC. One hundred and fifty-one cats were included in the effectiveness analysis. The patients included various purebred and mixed breed cats ranging in age from 3 to 19 years and in weight from 4.6 to 20.8 pounds. Of the cats included in the effectiveness analysis, 101 were castrated males, 49 were spayed females, and 1 was an intact female.
Cats were started on PROZINC at a dose of 0.1-0.3 IU/lb (0.2-0.7 IU/kg) twice daily. Cats were evaluated at 7, 14, 30, and 45 days after initiation of therapy and the dose was adjusted based on clinical signs and results of 9-hour blood glucose curves on Days 7, 14, and 30.
Effectiveness was based on successful control of diabetes which was defined as improvement in at least one blood glucose variable (glucose curve mean, nadir, or fructosamine) and at least one clinical sign (polyuria, polydipsia, or body weight). Based on this definition, 115 of 151 cases (76.2%) were considered successful. Blood glucose curve means decreased from 415.3 mg/dL on Day 0 to 203.2 mg/dL by Day 45 and the mean blood glucose nadir decreased from 407.9 mg/dL on Day 0 to 142.4 mg/dL on Day 45. Mean fructosamine values decreased from 505.9 μmol/L on Day 0 to 380.7 μmol/L on Day 45.
Cats that completed the effectiveness study were enrolled in an extended use field study. The mean fructosamine value was 342.0 μmol/L after a total of 181 days of PROZINC therapy.
How Supplied: PROZINC is supplied as a sterile injectable suspension in 10 mL and 20 mL multi-dose vials. Each mL of PROZINC contains 40 IU recombinant human insulin.
Storage Conditions: Store in an upright position under refrigeration at 36-46°F (2-8°C). Do not freeze. Protect from light. Use the 10 mL vial within 60 days of first puncture. Use the 20 mL vial within 80 days of first puncture.
Approved by FDA under NADA # 141-297
Marketed by: Boehringer Ingelheim Animal Health USA Inc. Duluth, GA 30096
PROZINC® is a registered trademark of Boehringer Ingelheim Animal Health USA Inc. © 2019 Boehringer Ingelheim Animal Health USA Inc. All rights reserved.
Revised 02/2019
449986-00
Package Insert for Cats
ProZinc®(protamine zinc recombinant human insulin)
xtp320655_ProZincCatPI-Cnsmr-8.5x11_rsg.indd All Pages 11/11/19 4:39 PM
251

40 IU/mL
This summary contains important information about PROZINC. You should read this information before you start giving your dog PROZINC and review it each time the prescription is refilled. This sheet is provided only as a summary and does not take the place of instructions from your veterinarian. Talk to your veterinarian if you do not understand any of this information or if you want to know more about PROZINC.
What is PROZINC? PROZINC is an aqueous protamine zinc suspension of recombinant human insulin that is used to reduce high blood sugar (hyperglycemia) in dogs with diabetes mellitus. A veterinarian must prescribe PROZINC for your dog. PROZINC should be given only to the dog for which it is prescribed. Keep out of reach of children. Seekmedical attention immediately if you accidentally inject yourself with PROZINC.
What is diabetes mellitus? Diabetes mellitus occurs when a dog has insufficient levels of, or an abnormal response to, insulin. The low insulinlevels may result in high blood sugar (hyperglycemia) that could produce the following changes in your dog:
What kind of results can I expect when my dog is on PROZINC for diabetes mellitus? Although PROZINC is not a cure for diabetes mellitus, it can help reduce the levels of sugar (glucose) in the blood, which can help alleviate the clinical signs.
What should I discuss with my veterinarian before giving PROZINC?
Talk to your veterinarian about:
• The signs of diabetes mellitus you have observed in your dog (for example, increased thirst and urination).
• The importance of proper PROZINC storage, handling, and administration techniques (for example, howto gently roll the vial prior to each use, the proper appearance of product after gently rolling, how to fill the U-40 syringe with the proper amount of insulin, and where and how to inject the insulin).
• The importance of maintaining your dog under the same conditions for diet, exercise, environment, etc.
• The importance of follow-up visits for testing to determine if dose adjustments of PROZINC are necessary.
Tell your veterinarian about:
• Any side effects your dog has had when receiving other insulin products.
• Any medical problems or allergies that your dog has now or has had in the past.
• All medications that you are giving your dog or plan to give your dog, including those you can getwithout a prescription.
• If your dog is pregnant, nursing, or if you plan to breed your dog.
What are the possible side effects that may occur in my dog during PROZINC therapy?PROZINC, like other drugs, may cause side effects. Serious side effects can occur with or without warning. Please contact your veterinarian immediately if you think your dog has a medical problem or side effect from PROZINC therapy. The most common insulin-related side effect is low blood sugar (hypoglycemia).
Signs of low blood sugar (hypoglycemia) can occur suddenly and may include:
• Weakness • Staggering gait • Muscle twitching • Coma
• Depression, lethargy, sluggishness • Behavioral changes • Seizures, convulsions • Death
What actions do I take if my dog shows signs of low blood sugar (hypoglycemia)?
• If your dog is unconscious or having a seizure, this is a medical emergency. Take your dog to the veterinarian immediately.
• If your dog is conscious, rub approximately 1 tablespoon of corn syrup or honey on your dog’s gums. When it can swallow, give corn syrup or honey by mouth until your dog is alert enough to eat. Feed the usual meal and contact your veterinarian.
When should my dog not be given PROZINC?
Do not give your dog its prescribed dose of PROZINC if it:
• Is experiencing an episode of low blood sugar (hypoglycemia). Common causes for low blood sugar include excessive doses of insulin, failure to eat, strenuous exercise, changes in the body’s need for insulin, diabetes-inducing disease or drug effects.
• Is not eating or is vomiting.
• Is sensitive to protamine zinc recombinant human insulin or any other ingredients in PROZINC.
• Do not give your dog its prescribed dose of PROZINC if you see clumps or visible white particles in the vial after gently rolling.
How should I give PROZINC to my dog?PROZINC should be given with or right after a meal.
Give PROZINC with U-40 syringes only. Use of a syringe other than a U-40 syringe will result in incorrect dosing. Gently roll the vial until the PROZINC has a uniformly cloudy, white appearance. If there are clumps or visible white particles in the vial after gently rolling, do not use the PROZINC and call your veterinarian. PROZINC should be given according to your veterinarian’s instructions. Your veterinarian will tell you what amount of PROZINC is right for your dog and instruct you on techniques for administration.
Can PROZINC be given with other medications? PROZINC can be given with other medications, but the dose may need to be adjusted due to the medication resulting in either increased or decreased insulin requirements. Tell your veterinarian about all medications you have given your dog in the past, and any medications that you are planning to give with PROZINC. This should include medications that you can get for your dog without a prescription. Your veterinarian may want to ensure that all your dog’s medications can be given together.
What should I do if I inject more than the prescribed amount of PROZINC? Contact your veterinarian immediately and, if your veterinarian is not available, seek other veterinary advice at once.
What should I do if my dog receives less than the prescribed dose, or I miss an injection?
• Contact your veterinarian as soon as possible for advice on your dog’s next dose.
• If you cannot reach your veterinarian and your dog is eating and acting normally, give your dog the usual dose at the next regularly scheduled injection time.
How should I store PROZINC? PROZINC should be stored in an upright position under refrigeration at 36-46°F (2-8°C). Do not freeze. Protect from light. Use the 10 mL vial within 60 days of first puncture. Use the 20 mL vial within 80 days of first puncture.
What else should I know about PROZINC? This sheet provides a summary of information about PROZINC. If you have any questions or concerns about the product or diabetes mellitus, talk to your veterinarian. As with all prescribed medications, PROZINC should onlybe given to the dog for which it is prescribed and for the condition for which it was prescribed.
It is important to periodically discuss your dog’s response to PROZINC at regular checkups that may include blood glucose monitoring. Your veterinarian will best determine if your dog is responding as expected and should continue receiving PROZINC.
Approved by FDA under NADA # 141-297
PROZINC® is a registered trademark of Boehringer Ingelheim Animal Health USA Inc. © 2019 Boehringer Ingelheim Animal Health USA Inc. All rights reserved.
Revised 02/2019
Client Information Sheet for Dogs
ProZinc®(protamine zinc recombinant human insulin)
40 IU/mL
Caution: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
Description: PROZINC® is a sterile aqueous protamine zinc suspension of recombinant human insulin.
Each mL contains:recombinant human insulin 40 International Units (IU)protamine sulfate 0.466 mgzinc oxide 0.088 mgglycerin 16.00 mgdibasic sodium phosphate, heptahydrate 3.78 mgphenol (added as preservative) 2.50 mghydrochloric acid 1.63 mgwater for injection (maximum) 1005 mgpH is adjusted with hydrochloric acid and/or sodium hydroxide.
Indication: PROZINC (protamine zinc recombinant human insulin) is indicated for the reduction of hyperglycemia and hyperglycemia-associated clinical signs in dogs with diabetes mellitus.
Dosage and Administration: USE OF A SYRINGE OTHER THAN A U-40 SYRINGE WILL RESULT IN INCORRECT DOSING.
FOR SUBCUTANEOUS INJECTION ONLY.
DO NOT SHAKE OR AGITATE THE VIAL.
PROZINC should be mixed by gently rolling the vial prior to withdrawing each dose from the vial. Once mixed, PROZINC suspension has a white, cloudy appearance. Clumps or visible white particles can form in insulin suspensions: do not use the product if clumps or visible white particles persist after gently rolling the vial.
Using a U-40 insulin syringe, the injection should be administered subcutaneously on the back of the neck or on the side of the dog.
Always provide the Client Information Sheet with each prescription.
Starting dose: The recommended starting dose for PROZINC is 0.2-0.5 IU insulin/pound of body weight (0.5-1.0 IU/kg) once daily. The recommended starting dose for naïve dogs is the lower end of the dose range. The recommended starting dose for dogs with poorly controlled diabetes mellitus and transitioning from another insulin product is the mid to higher end of the dose range based on the veterinarian’s experience with the dog’s medical history and previous insulin dose. When transitioning from another insulin, the dog’s blood glucose and general condition should be closely monitored. When transitioning from another insulin, PROZINC should be started once daily, regardless of the frequency of prior insulin use.
The dose should be given concurrently with or right after a meal. The veterinarian should re-evaluate the dog at appropriate intervals and adjust the dose and frequency based on both clinical signs and laboratory test results (the blood glucose curve values and shape, nadir, and fructosamine) until adequate glycemic control has been attained. In the effectiveness field study, glycemic control was considered adequate if the glucose nadir from a 9-hour blood glucose curve was between 80 and 125 mg/dL, the maximum blood glucose was < 300 mg/dL, and clinical signs of hyperglycemia such as polyuria, polydipsia, or weight loss were improved.
Changing to twice daily dosing: Twice daily dosing should be considered if the duration of insulin action is determined to be inadequate with once daily dosing. Use caution when adjusting from once daily to twice daily dosing because PROZINC may have prolonged duration of action in some dogs (see Clinical Pharmacology). The veterinarian should closely monitor the duration of action using blood glucose curves to avoid the increased risk of hypoglycemia. If twice daily dosing is initiated, the two doses should each be approximately 25% less than the once daily dose required to attain an acceptable glucose nadir. For example, if a dog receiving 10 units of PROZINC once daily has an acceptable nadir but inadequate duration of activity, the dose should be changed to 7 units twice daily (round down to the nearest whole unit).
Further adjustments in the dosage may be necessary with changes in the dog’s diet, body weight, or concomitant medication, or if the dog develops concurrent infection, inflammation, neoplasia, or an additional endocrine or other medical disorder.
Contraindications: PROZINC is contraindicated in dogs sensitive to protamine zinc recombinant human insulin or any other ingredients in PROZINC. PROZINC is contraindicated during episodes of hypoglycemia.
Warnings: User Safety: For use in dogs and cats. Keep out of the reach of children. Avoid contact with eyes. In case of contact, immediately flush eyes with running water for at least 15 minutes. Accidental injection may cause hypoglycemia. In case of accidental injection, seek medical attention immediately. Exposure to product may induce a local or systemic allergic reaction in sensitized individuals.
Animal Safety: Owners should be advised to observe for signs of hypoglycemia (see Client Information Sheet). Use of this product, even at established doses, has been associated with hypoglycemia. A dog with signs of hypoglycemia should be treated immediately. Glucose should be given orally or intravenously as dictated by clinical signs. Insulin should be temporarily withheld and, if indicated, the dosage adjusted.
Any change in insulin should be made cautiously and only under a veterinarian’s supervision. Changes in insulin strength, manufacturer, type, species (human, animal) or method of manufacture (rDNA versus animal-source insulin) may result in the need for a change in dosage.
Appropriate diagnostic tests should be performed to rule out other endocrinopathies in diabetic dogs that are difficult to regulate.
Precautions: Dogs presenting with severe ketoacidosis, anorexia, lethargy, and/or vomiting should be stabilized with short-acting insulin and appropriate supportive therapy until their condition is stabilized. As with all insulin products, careful patient monitoring for hypoglycemia and hyperglycemia is essential to attain and maintain adequate glycemic control and to prevent associated complications. Overdose can result in profound hypoglycemia and death.
Glucocorticoids, progestogens, and certain endocrinopathies can have an antagonistic effect on insulin activity. Glucocorticoid and progestogen use should be avoided.
The safety and effectiveness of PROZINC in breeding, pregnant, and lactating dogs has not been evaluated.
The safety and effectiveness of PROZINC in puppies has not been evaluated.
Adverse Reactions: In a 182-day field study, 276 dogs received PROZINC. The most common adverse reactions were lethargy, anorexia, hypoglycemia, vomiting, seizures, shaking, diarrhea, and ataxia.
Table 1 summarizes the adverse reactions reported in the study. Clinical signs of hypoglycemia varied and included seizure, collapse, ataxia, staggering, trembling, twitching, shaking, disorientation, lethargy, weakness, and vocalization. In Table 1, the individual clinical signs that were observed during the episodes of hypoglycemia are captured as separate adverse reactions and a single dog may have experienced more than one clinical sign of hypoglycemia.
Table 1. Adverse reactions seen in the safety population (276 dogs)
Adverse Reaction Number and Percentage
Lethargy (lethargy, depression, listless, and tiredness) 45 (16.3%)
Anorexia (anorexia, decreased appetite, inappetence, and not eating) 28 (10.1%)
Hypoglycemia with clinical signs 24 (8.9%)
Vomiting 21 (7.6%)
Seizures 16 (5.8%)
Shaking/trembling/twitching 13 (4.7%)
Ataxia (ataxia, balance problem, stumbling gait) 11 (4.0%)
Diarrhea (includes bloody diarrhea) 9 (3.3%)
Disorientation/confusion 9 (3.3%)
Weakness 8 (2.9%)
Restlessness/anxiety/agitation 6 (2.2%)
Cataract 6 (2.2%)
Panting (panting and tachypnea) 6 (2.2%)
Hematuria 4 (1.5%)
Clinical pathology: The only change seen in complete blood count, serum chemistry, and urinalysis results was an elevation in mean cholesterol at Day 182 (432.6 mg/dL, normal range 131-345 mg/dL) compared to Day -1 (333.7 mg/dL).)
Injection site reactions: Seven dogs had injection site reactions, including observations of thickened skin, swelling, bumps at the injection site, and redness. All injection site reactions resolved without cessation of PROZINC therapy. Reaction to the injection, including vocalization, was observed in four dogs.
Hypoglycemia: There were 80 hypoglycemic episodes recorded during the study with some dogs experiencing more than one episode; 37 episodes were associated with clinical signs in 24 dogs, 40 episodes were without clinical signs in 27 dogs, and 3 were with unknown signs in 2 dogs. Clinical signs of hypoglycemia varied and included seizure, collapse, ataxia, staggering, trembling, twitching, shaking, disorientation, lethargy, weakness, and vocalization. Some dogs required hospitalization and intravenous dextrose while most recovered after receiving oral supplementation with a meal and/or oral glucose such as syrup. Two dogs were euthanized when the hypoglycemia did not resolve with supportive care. Hypoglycemia without clinical signs was defined as two consecutive blood glucose curve values < 60 mg/dL unaccompanied by clinical signs.
Diabetic ketoacidosis and pancreatitis: Eleven dogs were diagnosed with diabetic ketoacidosis. Four of these 11 dogs died or were euthanized, one after one dose of PROZINC. Twenty-one dogs were diagnosed with pancreatitis. Seven of these 21 dogs died or were euthanized due to complications of pancreatitis. Four dogs had concurrent diabetic ketoacidosis and pancreatitis, three of which died or were euthanized. Not all the deaths were considered related to PROZINC.
Deaths: Thirty-six (36) dogs died or were euthanized, six of which were possibly related to PROZINC. One dog died from recurrent episodes of pancreatitis, and one died after developing severe vomiting and diarrhea followed by a seizure. Four dogs were euthanized: one developed severe pancreatitis and azotemia, one had recurrent episodes of pancreatitis and diabetic ketoacidosis, and two for lack of effectiveness.
To report suspected adverse drug events, for technical assistance or to obtain a copy of the Safety Data Sheet (SDS), contact Boehringer Ingelheim at 1-888-637-4251.
For additional information about adverse drug experience reporting for animal drugs, contact FDA at 1-888-FDA-VETS or online at http://www.fda.gov/AnimalVeterinary/ SafetyHealth.
Clinical Pharmacology: PROZINC was administered subcutaneously to 10 healthy Beagles using an incomplete crossover design at doses of 0.5 IU/kg (5 dogs), 0.8 IU/kg at a single site (10 dogs), or 0.8 IU/kg at three separate sites (6 dogs). Insulin and glucose concentrations were measured over 24 hours. The shapes of insulin and glucose curves were variable among dogs; and the relationship between insulin dose, concentration, and glucose-lowering effect was nonlinear (Table 2).
Table 2. Pharmacodynamics of three dosing groups
Dose group Onset of Action Time to nadir Duration of Action
0.5 IU/kg at a single site 1 to 14 hours 6 to 16 hours 16 to >24 hours
0.8 IU/kg at a single site 0.5 to 10 hours 5 to >24 hours 16 to >24 hours
0.8 IU/kg divided at three sites 1 to 10 hours 8 to 20 hours 18 to >24 hours
Information for Dog Owners: Please refer to the Client Information Sheet for Dogs for more information about PROZINC. PROZINC, like other insulin products, is not free from adverse reactions. Owners should be advised of the potential for adverse reactions and be informed of the associated clinical signs. Potential adverse reactions include hypoglycemia, insulin antagonism/resistance, rapid insulin metabolism, insulin-induced hyperglycemia (Somogyi Effect), and local or systemic reactions. The most common adverse reaction observed is hypoglycemia. Signs may include weakness, depression, behavioral changes, muscle twitching, and anxiety. In severe cases of hypoglycemia, seizures and coma can occur. Hypoglycemia can be fatal if an affected dog does not receive prompt treatment. Appropriate veterinary monitoring of blood glucose, adjustment of insulin dose and regimen as needed, and stabilization of diet and activity help minimize the risk of hypoglycemic episodes. The attending veterinarian should evaluate other adverse reactions on a case-by-case basis to determine if an adjustment in therapy is appropriate, or if alternative therapy should be considered.
Effectiveness: A total of 276 client-owned dogs were enrolled in an 84-day field study followed by a 98-day extended-use phase with 276 dogs receiving PROZINC. The dogs included various purebred and mixed breed dogs ranging in age from 2 to 16 years and in weight from 3.3 to 123 pounds. There were 128 neutered males, 8 intact males, 134 spayed females and 6 intact females. Two hundred twenty-four dogs (224) were included in the effectiveness analysis. Dogs were started on PROZINC at a dose of 0.2-0.5 IU/lb (0.5-1.0 IU/kg) once daily. Dogs were evaluated at 7, 14, 21, 28, 42, 63 and 84 days after initiation of therapy. The dose was adjusted based on clinical signs and results of 9-hour blood glucose curves on Days 7, 14, 21, 28, 42, 63 and 84.
Effectiveness was based on successful control of diabetes which was defined as improvement in at least one laboratory variable (blood glucose curve mean, blood glucose curve nadir, or fructosamine) and at least one clinical sign (polyuria, polydipsia, or weight loss). Based on this definition, 162 of 224 cases (72%) were considered successful.
How Supplied: PROZINC is supplied as a sterile injectable suspension in 10 mL and 20 mL multi-dose vials. Each mL of PROZINC contains 40 IU recombinant human insulin.
Storage Conditions: Store in an upright position under refrigeration at 36-46°F (2-8°C). Do not freeze. Protect from light. Use the 10 mL vial within 60 days of first puncture. Use the 20 mL vial within 80 days of first puncture.
Approved by FDA under NADA # 141-297
Marketed by: Boehringer Ingelheim Animal Health USA Inc. Duluth, GA 30096
PROZINC® is a registered trademark of Boehringer Ingelheim Animal Health USA Inc. © 2019 Boehringer Ingelheim Animal Health USA Inc. All rights reserved.
Revised 02/2019
449986-00
Package Insert for Dogs
ProZinc®(protamine zinc recombinant human insulin)
• Increased thirst
• Increased urination
• Increased appetite
• Weight loss
• High levels of sugar (glucose) in the urine (glucosuria)
xtp320655_ProZincDogPI-Cnsmr-8.5x11_rsg.indd All Pages 11/11/19 4:40 PM
252

40 IU/mL
This summary contains important information about PROZINC. You should read this information before you start giving your cat PROZINC and review it each time the prescription is refilled. This sheet is provided only as a summary and does not take the place of instructions from your veterinarian. Talk to your veterinarian if you do not understand any of this information or if you want to know more about PROZINC.
What is PROZINC? PROZINC is an aqueous protamine zinc suspension of recombinant human insulin that is used to reduce high blood sugar (hyperglycemia) in cats with diabetes mellitus. A veterinarian must prescribe PROZINC for your cat. PROZINC should be given to cats only. Keep out of reach of children. Seek medical attention immediately if you accidentally inject yourself with PROZINC.
What is diabetes mellitus? Diabetes mellitus occurs when a cat has insufficient levels of, or an abnormal response to, insulin. The low insulin levels may result in high blood sugar (hyperglycemia) that could produce the following changes in your cat:
• Increased thirst • Increased appetite
• High levels of sugar (glucose) in the urine (glucosuria) • Increased urination
• Weight loss • Weakness in the back legs
What kind of results can I expect when my cat is on PROZINC for diabetes mellitus? Although PROZINC is not a cure for diabetes mellitus, it can help reduce the levels of sugar (glucose) in the blood, which can help alleviate the clinical signs.
What should I discuss with my veterinarian before giving PROZINC?
Talk to your veterinarian about:
• The signs of diabetes mellitus you have observed in your cat (for example, increased thirst and urination).
• The importance of proper PROZINC storage, handling, and administration techniques (for example, how to gently roll the vial prior to each use, the proper appearance of product after gently rolling, how to fill the U-40 syringe with the proper amount of insulin, and where and how to inject the insulin).
• The importance of maintaining your cat under the same conditions for diet, exercise, environment, etc.
• The importance of follow-up visits for testing to determine if dose adjustments of PROZINC are necessary.
Tell your veterinarian about:
• Any side effects your cat has had when receiving other insulin products.
• Any medical problems or allergies that your cat has now or has had in the past.
• All medications that you are giving your cat or plan to give your cat, including those you can get without a prescription.
• If your cat is pregnant, nursing, or if you plan to breed your cat.
What are the possible side effects that may occur in my cat during PROZINC therapy? PROZINC, like other drugs, may cause side effects. Serious side effects can occur with or without warning. Please contact your veterinarian immediately if you think your cat has a medical problem or side effect from PROZINC therapy. The most common insulin-related side effect is low blood sugar (hypoglycemia). Signs of low blood sugar (hypoglycemia) can occur suddenly and may include:
• Weakness • Staggering gait • Muscle twitching • Coma
• Depression, lethargy, sluggishness • Behavioral changes • Seizures, convulsions • Death
What actions do I take if my cat shows signs of low blood sugar (hypoglycemia)? • If your cat is unconscious or having a seizure, this is a medical emergency. Take your cat
to the veterinarian immediately.
• If your cat is conscious, rub approximately 1 tablespoon of corn syrup or honey on your cat’s gums. When it is able to swallow, give corn syrup or honey by mouth until your cat is alert enough to eat. Feed the usual meal and contact your veterinarian.
When should my cat not be given PROZINC? Do not give your cat its prescribed dose of PROZINC if it: • Is experiencing an episode of low blood sugar (hypoglycemia). Common causes for low blood
sugar include excessive doses of insulin, failure to eat, strenuous exercise, changes in the body’s need for insulin, diabetes-inducing disease or drug effects.
• Is not eating or is vomiting.
• Is sensitive to protamine zinc recombinant human insulin or any other ingredients in PROZINC.
• Do not give your cat its prescribed dose of PROZINC if you see clumps or visible white particles in the vial after gently rolling.
How should I give PROZINC to my cat? PROZINC should be given with or right after a meal.
Give PROZINC with U-40 syringes only. Use of a syringe other than a U-40 syringe will result in incorrect dosing. Gently roll the vial until the PROZINC has a uniformly cloudy, white appearance. If there are clumps or visible white particles in the vial after gently rolling, do not use the PROZINC and call your veterinarian. PROZINC should be given according to your veterinarian’s instructions. Your veterinarian will tell you what amount of PROZINC is right for your cat and instruct you on techniques for administration.
Can PROZINC be given with other medications? PROZINC can be given with other medications, but the dose may need to be adjusted due to the medication resulting in either increased or decreased insulin requirements. Tell your veterinarian about all medications you have given your cat in the past, and any medications that you are planning to give with PROZINC. This should include medications that you can get for your cat without a prescription. Your veterinarian may want to ensure that all of your cat’s medications can be given together.
What should I do if I inject more than the prescribed amount of PROZINC? Contact your veterinarian immediately and, if your veterinarian is not available, seek other veterinary advice at once.
What should I do if my cat receives less than the prescribed dose, or I miss an injection?
• Contact your veterinarian as soon as possible for advice on your cat’s next dose.
• If you cannot reach your veterinarian and your cat is eating and acting normally, give your cat the usual dose at the next regularly scheduled injection time.
How should I store PROZINC? PROZINC should be stored in an upright position under refrigeration at 36-46°F (2-8°C). Do not freeze. Protect from light. Use the 10 mL vial within 60 days of first puncture. Use the 20 mL vial within 80 days of first puncture.
What else should I know about PROZINC? This sheet provides a summary of information about PROZINC. If you have any questions or concerns about the product or diabetes mellitus, talk to your veterinarian.
As with all prescribed medications, PROZINC should only be given to the cat for which it is prescribed and for the condition for which it was prescribed.
It is important to periodically discuss your cat’s response to PROZINC at regular checkups that may include blood glucose monitoring. Your veterinarian will best determine if your cat is responding as expected and should continue receiving PROZINC.
Approved by FDA under NADA # 141-297
PROZINC® is a registered trademark of Boehringer Ingelheim Animal Health USA Inc. © 2019 Boehringer Ingelheim Animal Health USA Inc. All rights reserved.
Revised 02/2019
Client Information Sheet for Cats
ProZinc®(protamine zinc recombinant human insulin)
40 IU/mL
Caution: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
Description: PROZINC® is a sterile aqueous protamine zinc suspension of recombinanthuman insulin.
Each mL contains:
recombinant human insulin 40 International Units (IU)protamine sulfate 0.466 mg zinc oxide 0.088 mg glycerin 16.00 mg dibasic sodium phosphate, heptahydrate 3.78 mg phenol (added as preservative) 2.50 mg hydrochloric acid 1.63 mg water for injection (maximum) 1005 mg pH is adjusted with hydrochloric acid and/or sodium hydroxide.
Indication: PROZINC (protamine zinc recombinant human insulin) is indicated for the reduction of hyperglycemia and hyperglycemia-associated clinical signs in cats with diabetes mellitus.
Dosage and Administration: USE OF A SYRINGE OTHER THAN A U-40 SYRINGE WILL RESULT IN INCORRECT DOSING.
FOR SUBCUTANEOUS INJECTION ONLY.
DO NOT SHAKE OR AGITATE THE VIAL.
PROZINC should be mixed by gently rolling the vial prior to withdrawing each dose from the vial. Once mixed, PROZINC suspension has a white, cloudy appearance. Clumps or visible white particles can form in insulin suspensions: do not use the product if clumps or visible white particles persist after gently rolling the vial.
Using a U-40 insulin syringe, the injection should be administered subcutaneously on the back of the neck or on the side of the cat.
Always provide the Client Information Sheet with each prescription.
The initial recommended PROZINC dose is 0.1 – 0.3 IU insulin/pound of body weight (0.2 – 0.7 IU/kg) every 12 hours. The dose should be given concurrently with or right after a meal. The veterinarian should re-evaluate the cat at appropriate intervals and adjust the dose based on both clinical signs and glucose nadirs until adequate glycemic control has been attained. In the effectiveness field study, glycemic control was considered adequate if the glucose nadir from a 9-hour blood glucose curve was between 80 and 150 mg/dL and clinical signs of hyperglycemia such as polyuria, polydipsia, and weight loss were improved.
Further adjustments in the dosage may be necessary with changes in the cat’s diet, bodyweight, or concomitant medication, or if the cat develops concurrent infection, inflammation, neoplasia, or an additional endocrine or other medical disorder.
Contraindications: PROZINC is contraindicated in cats sensitive to protamine zinc recombinant human insulin or any other ingredients in PROZINC. PROZINC is contraindicated during episodes of hypoglycemia.
Warnings: User Safety: For use in cats and dogs only. Keep out of the reach of children. Avoid contact with eyes. In case of contact, immediately flush eyes with running water for at least 15 minutes. Accidental injection may cause hypoglycemia. In case of accidental injection, seek medical attention immediately. Exposure to product may induce a local or systemic allergic reaction in sensitized individuals.
Animal Safety: Owners should be advised to observe for signs of hypoglycemia (see ClientInformation Sheet). Use of this product, even at established doses, has been associated with hypoglycemia. A cat with signs of hypoglycemia should be treated immediately. Glucose should be given orally or intravenously as dictated by clinical signs. Insulin should be temporarily withheld and, if indicated, the dosage adjusted.
Any change in insulin should be made cautiously and only under a veterinarian’s supervision. Changes in insulin strength, manufacturer, type, species (human, animal) or method of manufacture (rDNA versus animal-source insulin) may result in the need for a change in dosage.
Appropriate diagnostic tests should be performed to rule out other endocrinopathies in diabetic cats that are difficult to regulate.
Precautions: Cats presenting with severe ketoacidosis, anorexia, lethargy, and/or vomiting should be stabilized with short-acting insulin and appropriate supportive therapy until their condition is stabilized. As with all insulin products, careful patient monitoring for hypoglycemia and hyperglycemia is essential to attain and maintain adequate glycemic control and to prevent associated complications. Overdose can result in profound hypoglycemia and death.
Glucocorticoids, progestogens, and certain endocrinopathies can have an antagonistic effecton insulin activity. Glucocorticoid and progestogen use should be avoided.
The safety and effectiveness of PROZINC in breeding, pregnant, and lactating cats has not been evaluated.
The safety and effectiveness of PROZINC in kittens has not been evaluated.
Adverse Reactions: Effectiveness Field StudyIn a 45-day effectiveness field study, 176 cats received PROZINC. Hypoglycemia (defined as a blood glucose value of < 50 mg/dL) occurred in 71 of the cats at various times throughout the study. Clinical signs of hypoglycemia were generally mild in nature (described as lethargic, sluggish, weak, trembling, uncoordinated, groggy, glassy-eyed or dazed). In 17 cases, the veterinarian provided oral glucose supplementation or food as treatment. Most cases were notassociated with clinical signs and received no treatment. One cat had a serious hypoglycemic event associated with stupor, lateral recumbency, hypothermia and seizures.
All cases of hypoglycemia resolved with appropriate therapy and if needed, a dose reduction.
Three cats had injection site reactions which were described as either small, punctate, red lesions; lesions on neck; or palpable subcutaneous thickening. All injection site reactions resolved without cessation of therapy.
Four cats developed diabetic neuropathy during the study as evidenced by plantigrade stance. Three cats entered the study with plantigrade stance, one of which resolved by Day 45. Fourcats were diagnosed with diabetic ketoacidosis during the study. Two were euthanized due to poor response to treatment. Five other cats were euthanized during the study, one of which had hypoglycemia. Four cats had received PROZINC for less than a week and were euthanized due to worsening concurrent medical conditions.
The following additional clinical observations or diagnoses were reported in cats during the effectiveness field study: vomiting, lethargy, diarrhea, cystitis/hematuria, upper respiratory infection, dry coat, hair loss, ocular discharge, abnormal vocalization, black stool, and rapid breathing.
Extended Use Field Study
Cats that completed the effectiveness study were enrolled into an extended use field study. In this study, 145 cats received PROZINC for up to an additional 136 days. Adverse reactions were similar to those reported during the 45-day effectiveness study and are listed in orderof decreasing frequency: vomiting, hypoglycemia, anorexia/poor appetite, diarrhea, lethargy, cystitis/hematuria, and weakness. Twenty cats had signs consistent with hypoglycemia described as: sluggish, lethargic, unsteady, wobbly, seizures, trembling, or dazed. Most of these were treated by the owner or veterinarian with oral glucose supplementation or food; others received intravenous glucose. One cat had a serious hypoglycemic event associated with seizures and blindness. The cat fully recovered after supportive therapy and finished the study. All cases of hypoglycemia resolved with appropriate therapy and if needed, a dose reduction.
Fourteen cats died or were euthanized during the extended use study. In two cases, continued use of insulin despite anorexia and signs of hypoglycemia contributed to the deaths. In one case, the owner decided not to continue therapy after a presumed episode of hypoglycemia. The rest were due to concurrent medical conditions or worsening of the diabetes mellitus.
To report suspected adverse drug events, for technical assistance or to obtain a copy of the Safety Data Sheet (SDS), contact Boehringer Ingelheim at 1-888-637-4251.
For additional information about adverse drug experience reporting for animal drugs, contact FDA at 1-888-FDA-VETS or online at http://www.fda.gov/AnimalVeterinary/SafetyHealth.
Information for Cat Owners: Please refer to the Client Information Sheet for Cats for more information about PROZINC. PROZINC, like other insulin products, is not free from adverse reactions. Owners should be advised of the potential for adverse reactions and be informed of the associated clinical signs. Potential adverse reactions include: hypoglycemia, insulin antagonism/resistance, rapid insulin metabolism, insulin-induced hyperglycemia (Somogyi Effect), and local or systemic reactions. The most common adverse reaction observed is hypoglycemia. Signs may include: weakness, depression, behavioral changes, muscle twitching, and anxiety. In severe cases of hypoglycemia, seizures and coma can occur. Hypoglycemia can be fatal if an affected cat does not receive prompt treatment. Appropriate veterinary monitoring of blood glucose, adjustment of insulin dose and regimen as needed, and stabilization of dietand activity help minimize the risk of hypoglycemic episodes. The attending veterinarian should evaluate other adverse reactions on a case-by-case basis to determine if an adjustment in therapy is appropriate, or if alternative therapy should be considered.
Effectiveness: A total of 187 client-owned cats were enrolled in a 45-day field study, with 176 receiving PROZINC. One hundred and fifty-one cats were included in the effectiveness analysis. The patients included various purebred and mixed breed cats ranging in age from 3 to 19 years and in weight from 4.6 to 20.8 pounds. Of the cats included in the effectiveness analysis, 101 were castrated males, 49 were spayed females, and 1 was an intact female.
Cats were started on PROZINC at a dose of 0.1-0.3 IU/lb (0.2-0.7 IU/kg) twice daily. Cats were evaluated at 7, 14, 30, and 45 days after initiation of therapy and the dose was adjusted based on clinical signs and results of 9-hour blood glucose curves on Days 7, 14, and 30.
Effectiveness was based on successful control of diabetes which was defined as improvement in at least one blood glucose variable (glucose curve mean, nadir, or fructosamine) and at least one clinical sign (polyuria, polydipsia, or body weight). Based on this definition, 115 of 151 cases (76.2%) were considered successful. Blood glucose curve means decreased from 415.3 mg/dL on Day 0 to 203.2 mg/dL by Day 45 and the mean blood glucose nadir decreased from 407.9 mg/dL on Day 0 to 142.4 mg/dL on Day 45. Mean fructosamine values decreased from 505.9 μmol/L on Day 0 to 380.7 μmol/L on Day 45.
Cats that completed the effectiveness study were enrolled in an extended use field study. The mean fructosamine value was 342.0 μmol/L after a total of 181 days of PROZINC therapy.
How Supplied: PROZINC is supplied as a sterile injectable suspension in 10 mL and 20 mL multi-dose vials. Each mL of PROZINC contains 40 IU recombinant human insulin.
Storage Conditions: Store in an upright position under refrigeration at 36-46°F (2-8°C). Do notfreeze. Protect from light. Use the 10 mL vial within 60 days of first puncture. Use the 20 mL vial within 80 days of first puncture.
Approved by FDA under NADA # 141-297
Marketed by: Boehringer Ingelheim Animal Health USA Inc. Duluth, GA 30096
PROZINC® is a registered trademark of Boehringer Ingelheim Animal Health USA Inc. © 2019 Boehringer Ingelheim Animal Health USA Inc. All rights reserved.
Revised 02/2019
449986-00
Package Insert for Cats
ProZinc®(protamine zinc recombinant human insulin)
xtp320655_ProZincCatPI-Cnsmr-8.5x11_rsg.indd All Pages 11/11/19 4:39 PM
253

40 IU/mL
This summary contains important information about PROZINC. You should read this information before you start giving your dog PROZINC and review it each time the prescription is refilled. This sheet is provided only as a summary and does not take the place of instructions from your veterinarian. Talk to your veterinarian if you do not understand any of this information or if you want to know more about PROZINC.
What is PROZINC? PROZINC is an aqueous protamine zinc suspension of recombinant human insulin that is used to reduce high blood sugar (hyperglycemia) in dogs with diabetes mellitus. A veterinarian must prescribe PROZINC for your dog. PROZINC should be given only to the dog for which it is prescribed. Keep out of reach of children. Seek medical attention immediately if you accidentally inject yourself with PROZINC.
What is diabetes mellitus? Diabetes mellitus occurs when a dog has insufficient levels of, or an abnormal response to, insulin. The low insulin levels may result in high blood sugar (hyperglycemia) that could produce the following changes in your dog:
What kind of results can I expect when my dog is on PROZINC for diabetes mellitus? Although PROZINC is not a cure for diabetes mellitus, it can help reduce the levels of sugar (glucose) in the blood, which can help alleviate the clinical signs.
What should I discuss with my veterinarian before giving PROZINC?
Talk to your veterinarian about:
• The signs of diabetes mellitus you have observed in your dog (for example, increased thirst and urination).
• The importance of proper PROZINC storage, handling, and administration techniques (for example, how to gently roll the vial prior to each use, the proper appearance of product after gently rolling, how to fill the U-40 syringe with the proper amount of insulin, and where and how to inject the insulin).
• The importance of maintaining your dog under the same conditions for diet, exercise, environment, etc.
• The importance of follow-up visits for testing to determine if dose adjustments of PROZINC are necessary.
Tell your veterinarian about:
• Any side effects your dog has had when receiving other insulin products.
• Any medical problems or allergies that your dog has now or has had in the past.
• All medications that you are giving your dog or plan to give your dog, including those you can get without a prescription.
• If your dog is pregnant, nursing, or if you plan to breed your dog.
What are the possible side effects that may occur in my dog during PROZINC therapy? PROZINC, like other drugs, may cause side effects. Serious side effects can occur with or without warning. Please contact your veterinarian immediately if you think your dog has a medical problem or side effect from PROZINC therapy. The most common insulin-related side effect is low blood sugar (hypoglycemia).
Signs of low blood sugar (hypoglycemia) can occur suddenly and may include:
• Weakness • Staggering gait • Muscle twitching • Coma
• Depression, lethargy, sluggishness • Behavioral changes • Seizures, convulsions • Death
What actions do I take if my dog shows signs of low blood sugar (hypoglycemia)?
• If your dog is unconscious or having a seizure, this is a medical emergency. Take your dog to the veterinarian immediately.
• If your dog is conscious, rub approximately 1 tablespoon of corn syrup or honey on your dog’s gums. When it can swallow, give corn syrup or honey by mouth until your dog is alert enough to eat. Feed the usual meal and contact your veterinarian.
When should my dog not be given PROZINC?
Do not give your dog its prescribed dose of PROZINC if it:
• Is experiencing an episode of low blood sugar (hypoglycemia). Common causes for low blood sugar include excessive doses of insulin, failure to eat, strenuous exercise, changes in the body’s need for insulin, diabetes-inducing disease or drug effects.
• Is not eating or is vomiting.
• Is sensitive to protamine zinc recombinant human insulin or any other ingredients in PROZINC.
• Do not give your dog its prescribed dose of PROZINC if you see clumps or visible white particles in the vial after gently rolling.
How should I give PROZINC to my dog? PROZINC should be given with or right after a meal.
Give PROZINC with U-40 syringes only. Use of a syringe other than a U-40 syringe will result in incorrect dosing. Gently roll the vial until the PROZINC has a uniformly cloudy, white appearance. If there are clumps or visible white particles in the vial after gently rolling, do not use the PROZINC and call your veterinarian. PROZINC should be given according to your veterinarian’s instructions. Your veterinarian will tell you what amount of PROZINC is right for your dog and instruct you on techniques for administration.
Can PROZINC be given with other medications? PROZINC can be given with other medications, but the dose may need to be adjusted due to the medication resulting in either increased or decreased insulin requirements. Tell your veterinarian about all medications you have given your dog in the past, and any medications that you are planning to give with PROZINC. This should include medications that you can get for your dog without a prescription. Your veterinarian may want to ensure that all your dog’s medications can be given together.
What should I do if I inject more than the prescribed amount of PROZINC? Contact your veterinarian immediately and, if your veterinarian is not available, seek other veterinary advice at once.
What should I do if my dog receives less than the prescribed dose, or I miss an injection?
• Contact your veterinarian as soon as possible for advice on your dog’s next dose.
• If you cannot reach your veterinarian and your dog is eating and acting normally, give your dog the usual dose at the next regularly scheduled injection time.
How should I store PROZINC? PROZINC should be stored in an upright position under refrigeration at 36-46°F (2-8°C). Do not freeze. Protect from light. Use the 10 mL vial within 60 days of first puncture. Use the 20 mL vial within 80 days of first puncture.
What else should I know about PROZINC? This sheet provides a summary of information about PROZINC. If you have any questions or concerns about the product or diabetes mellitus, talk to your veterinarian. As with all prescribed medications, PROZINC should only be given to the dog for which it is prescribed and for the condition for which it was prescribed.
It is important to periodically discuss your dog’s response to PROZINC at regular checkups that may include blood glucose monitoring. Your veterinarian will best determine if your dog is responding as expected and should continue receiving PROZINC.
Approved by FDA under NADA # 141-297
PROZINC® is a registered trademark of Boehringer Ingelheim Animal Health USA Inc. © 2019 Boehringer Ingelheim Animal Health USA Inc. All rights reserved.
Revised 02/2019
Client Information Sheet for Dogs
ProZinc®(protamine zinc recombinant human insulin)
40 IU/mL
Caution: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
Description: PROZINC® is a sterile aqueous protamine zinc suspension of recombinant human insulin.
Each mL contains:recombinant human insulin 40 International Units (IU)protamine sulfate 0.466 mgzinc oxide 0.088 mgglycerin 16.00 mgdibasic sodium phosphate, heptahydrate 3.78 mgphenol (added as preservative) 2.50 mghydrochloric acid 1.63 mgwater for injection (maximum) 1005 mgpH is adjusted with hydrochloric acid and/or sodium hydroxide.
Indication: PROZINC (protamine zinc recombinant human insulin) is indicated for the reduction of hyperglycemia and hyperglycemia-associated clinical signs in dogs with diabetes mellitus.
Dosage and Administration: USE OF A SYRINGE OTHER THAN A U-40 SYRINGE WILL RESULT IN INCORRECT DOSING.
FOR SUBCUTANEOUS INJECTION ONLY.
DO NOT SHAKE OR AGITATE THE VIAL.
PROZINC should be mixed by gently rolling the vial prior to withdrawing each dose from the vial. Once mixed, PROZINC suspension has a white, cloudy appearance. Clumps or visible white particles can form in insulin suspensions: do not use the product if clumps or visible white particles persist after gently rolling the vial.
Using a U-40 insulin syringe, the injection should be administered subcutaneously on the back of the neck or on the side of the dog.
Always provide the Client Information Sheet with each prescription.
Starting dose: The recommended starting dose for PROZINC is 0.2-0.5 IU insulin/pound of body weight (0.5-1.0 IU/kg) once daily. The recommended starting dose for naïve dogs is the lower end of the dose range. The recommended starting dose for dogs with poorly controlled diabetes mellitus and transitioning from another insulin product is the mid to higher end of the dose range based on the veterinarian’s experience with the dog’s medical history and previous insulin dose. When transitioning from another insulin, the dog’s blood glucose and general condition should be closely monitored. When transitioning from another insulin, PROZINC should be started once daily, regardless of the frequency of prior insulin use.
The dose should be given concurrently with or right after a meal. The veterinarian should re-evaluate the dog atappropriate intervals and adjust the dose and frequency based on both clinical signs and laboratory test results (the blood glucose curve values and shape, nadir, and fructosamine) until adequate glycemic control has been attained. In the effectiveness field study, glycemic control was considered adequate if the glucose nadir from a 9-hour blood glucose curve was between 80 and 125 mg/dL, the maximum blood glucose was < 300 mg/dL, and clinical signs of hyperglycemia such as polyuria, polydipsia, or weight loss were improved.
Changing to twice daily dosing: Twice daily dosing should be considered if the duration of insulin action is determined to be inadequate with once daily dosing. Use caution when adjusting from once daily to twice dailydosing because PROZINC may have prolonged duration of action in some dogs (see Clinical Pharmacology). The veterinarian should closely monitor the duration of action using blood glucose curves to avoid the increased risk of hypoglycemia. If twice daily dosing is initiated, the two doses should each be approximately 25% less than the once daily dose required to attain an acceptable glucose nadir. For example, if a dog receiving 10 units of PROZINC once daily has an acceptable nadir but inadequate duration of activity, the dose should be changed to 7 units twice daily (round down to the nearest whole unit).
Further adjustments in the dosage may be necessary with changes in the dog’s diet, body weight, or concomitant medication, or if the dog develops concurrent infection, inflammation, neoplasia, or an additional endocrine or other medical disorder.
Contraindications: PROZINC is contraindicated in dogs sensitive to protamine zinc recombinant human insulin or any other ingredients in PROZINC. PROZINC is contraindicated during episodes of hypoglycemia.
Warnings: User Safety: For use in dogs and cats. Keep out of the reach of children. Avoid contact with eyes. In case ofcontact, immediately flush eyes with running water for at least 15 minutes. Accidental injection may cause hypoglycemia. In case of accidental injection, seek medical attention immediately. Exposure to product mayinduce a local or systemic allergic reaction in sensitized individuals.
Animal Safety: Owners should be advised to observe for signs of hypoglycemia (see Client Information Sheet). Use of this product, even at established doses, has been associated with hypoglycemia. A dog with signs of hypoglycemia should be treated immediately. Glucose should be given orally or intravenously as dictated by clinical signs. Insulin should be temporarily withheld and, if indicated, the dosage adjusted.
Any change in insulin should be made cautiously and only under a veterinarian’s supervision. Changes in insulin strength, manufacturer, type, species (human, animal) or method of manufacture (rDNA versus animal-source insulin) may result in the need for a change in dosage.
Appropriate diagnostic tests should be performed to rule out other endocrinopathies in diabetic dogs that are difficult to regulate.
Precautions: Dogs presenting with severe ketoacidosis, anorexia, lethargy, and/or vomiting should be stabilized with short-acting insulin and appropriate supportive therapy until their condition is stabilized. As with all insulin products, careful patient monitoring for hypoglycemia and hyperglycemia is essential to attain and maintain adequate glycemic control and to prevent associated complications. Overdose can result in profound hypoglycemia and death.
Glucocorticoids, progestogens, and certain endocrinopathies can have an antagonistic effect on insulin activity. Glucocorticoid and progestogen use should be avoided.
The safety and effectiveness of PROZINC in breeding, pregnant, and lactating dogs has not been evaluated.
The safety and effectiveness of PROZINC in puppies has not been evaluated.
Adverse Reactions: In a 182-day field study, 276 dogs received PROZINC. The most common adverse reactions were lethargy, anorexia, hypoglycemia, vomiting, seizures, shaking, diarrhea, and ataxia.
Table 1 summarizes the adverse reactions reported in the study. Clinical signs of hypoglycemia varied and included seizure, collapse, ataxia, staggering, trembling, twitching, shaking, disorientation, lethargy, weakness, and vocalization. In Table 1, the individual clinical signs that were observed during the episodes ofhypoglycemia are captured as separate adverse reactions and a single dog may have experienced more than one clinical sign of hypoglycemia.
Table 1. Adverse reactions seen in the safety population (276 dogs)
Adverse Reaction Number and Percentage
Lethargy (lethargy, depression, listless, and tiredness) 45 (16.3%)
Anorexia (anorexia, decreased appetite, inappetence, and not eating) 28 (10.1%)
Hypoglycemia with clinical signs 24 (8.9%)
Vomiting 21 (7.6%)
Seizures 16 (5.8%)
Shaking/trembling/twitching 13 (4.7%)
Ataxia (ataxia, balance problem, stumbling gait) 11 (4.0%)
Diarrhea (includes bloody diarrhea) 9 (3.3%)
Disorientation/confusion 9 (3.3%)
Weakness 8 (2.9%)
Restlessness/anxiety/agitation 6 (2.2%)
Cataract 6 (2.2%)
Panting (panting and tachypnea) 6 (2.2%)
Hematuria 4 (1.5%)
Clinical pathology: The only change seen in complete blood count, serum chemistry, and urinalysis results was an elevation in mean cholesterol at Day 182 (432.6 mg/dL, normal range 131-345 mg/dL) compared to Day -1 (333.7 mg/dL).)
Injection site reactions: Seven dogs had injection site reactions, including observations of thickened skin, swelling, bumps at the injection site, and redness. All injection site reactions resolved without cessation of PROZINC therapy. Reaction to the injection, including vocalization, was observed in four dogs.
Hypoglycemia: There were 80 hypoglycemic episodes recorded during the study with some dogs experiencing more than one episode; 37 episodes were associated with clinical signs in 24 dogs, 40 episodes were without clinical signs in 27 dogs, and 3 were with unknown signs in 2 dogs. Clinical signs of hypoglycemia varied and included seizure, collapse, ataxia, staggering, trembling, twitching, shaking, disorientation, lethargy, weakness, and vocalization. Some dogs required hospitalization and intravenous dextrose while most recovered afterreceiving oral supplementation with a meal and/or oral glucose such as syrup. Two dogs were euthanized when the hypoglycemia did not resolve with supportive care. Hypoglycemia without clinical signs was defined as two consecutive blood glucose curve values < 60 mg/dL unaccompanied by clinical signs.
Diabetic ketoacidosis and pancreatitis: Eleven dogs were diagnosed with diabetic ketoacidosis. Four of these 11 dogs died or were euthanized, one after one dose of PROZINC. Twenty-one dogs were diagnosed with pancreatitis. Seven of these 21 dogs died or were euthanized due to complications of pancreatitis. Four dogs had concurrent diabetic ketoacidosis and pancreatitis, three of which died or were euthanized. Not all the deaths were considered related to PROZINC.
Deaths: Thirty-six (36) dogs died or were euthanized, six of which were possibly related to PROZINC. One dog died from recurrent episodes of pancreatitis, and one died after developing severe vomiting and diarrhea followed by a seizure. Four dogs were euthanized: one developed severe pancreatitis and azotemia, one had recurrent episodes of pancreatitis and diabetic ketoacidosis, and two for lack of effectiveness.
To report suspected adverse drug events, for technical assistance or to obtain a copy of the Safety Data Sheet (SDS), contact Boehringer Ingelheim at 1-888-637-4251.
For additional information about adverse drug experience reporting for animal drugs, contact FDA at1-888-FDA-VETS or online at http://www.fda.gov/AnimalVeterinary/ SafetyHealth.
Clinical Pharmacology: PROZINC was administered subcutaneously to 10 healthy Beagles using an incomplete crossover design at doses of 0.5 IU/kg (5 dogs), 0.8 IU/kg at a single site (10 dogs), or 0.8 IU/kg at three separate sites (6 dogs). Insulin and glucose concentrations were measured over 24 hours. The shapes of insulin and glucose curves were variable among dogs; and the relationship between insulin dose, concentration, and glucose-lowering effect was nonlinear (Table 2).
Table 2. Pharmacodynamics of three dosing groups
Dose group Onset of Action Time to nadir Duration of Action
0.5 IU/kg at a single site 1 to 14 hours 6 to 16 hours 16 to >24 hours
0.8 IU/kg at a single site 0.5 to 10 hours 5 to >24 hours 16 to >24 hours
0.8 IU/kg divided at three sites 1 to 10 hours 8 to 20 hours 18 to >24 hours
Information for Dog Owners: Please refer to the Client Information Sheet for Dogs for more information about PROZINC. PROZINC, like other insulin products, is not free from adverse reactions. Owners should be advised of the potential for adverse reactions and be informed of the associated clinical signs. Potential adverse reactions include hypoglycemia, insulin antagonism/resistance, rapid insulin metabolism, insulin-induced hyperglycemia (Somogyi Effect), and local or systemic reactions. The most common adverse reaction observed is hypoglycemia. Signs may include weakness, depression, behavioral changes, muscle twitching, and anxiety. In severe cases of hypoglycemia, seizures and coma can occur. Hypoglycemia can be fatal if an affected dog does not receive prompt treatment. Appropriate veterinary monitoring of blood glucose, adjustment of insulin dose and regimen as needed, and stabilization of diet and activity help minimize the risk of hypoglycemic episodes. The attending veterinarian should evaluate other adverse reactions on a case-by-case basis to determine if an adjustment in therapy is appropriate, or if alternative therapy should be considered.
Effectiveness: A total of 276 client-owned dogs were enrolled in an 84-day field study followed by a 98-dayextended-use phase with 276 dogs receiving PROZINC. The dogs included various purebred and mixed breed dogs ranging in age from 2 to 16 years and in weight from 3.3 to 123 pounds. There were 128 neutered males, 8 intact males, 134 spayed females and 6 intact females. Two hundred twenty-four dogs (224) were included in the effectiveness analysis. Dogs were started on PROZINC at a dose of 0.2-0.5 IU/lb (0.5-1.0 IU/kg) once daily. Dogs were evaluated at 7, 14, 21, 28, 42, 63 and 84 days after initiation of therapy. The dose was adjusted based on clinical signs and results of 9-hour blood glucose curves on Days 7, 14, 21, 28, 42, 63 and 84.
Effectiveness was based on successful control of diabetes which was defined as improvement in at leastone laboratory variable (blood glucose curve mean, blood glucose curve nadir, or fructosamine) and at leastone clinical sign (polyuria, polydipsia, or weight loss). Based on this definition, 162 of 224 cases (72%) were considered successful.
How Supplied: PROZINC is supplied as a sterile injectable suspension in 10 mL and 20 mL multi-dose vials. Each mL of PROZINC contains 40 IU recombinant human insulin.
Storage Conditions: Store in an upright position under refrigeration at 36-46°F (2-8°C). Do not freeze. Protect from light. Use the 10 mL vial within 60 days of first puncture. Use the 20 mL vial within 80 days of first puncture.
Approved by FDA under NADA # 141-297
Marketed by:Boehringer Ingelheim Animal Health USA Inc. Duluth, GA 30096
PROZINC® is a registered trademark of Boehringer Ingelheim Animal Health USA Inc. © 2019 Boehringer Ingelheim Animal Health USA Inc. All rights reserved.
Revised 02/2019
449986-00
Package Insert for Dogs
ProZinc®(protamine zinc recombinant human insulin)
• Increased thirst
• Increased urination
• Increased appetite
• Weight loss
• High levels of sugar (glucose) in the urine (glucosuria)
xtp320655_ProZincDogPI-Cnsmr-8.5x11_rsg.indd All Pages 11/11/19 4:40 PM
254

CALM THE ANGRY GI TRACT: WHAT’S NEW IN NUTRITIONKara M. Burns, MS, MEd, LVT, VTS (Nutrition)
Academy of Veterinary Nutrition Technicians [email protected]
Throughout the United states and Canada, gastrointestinal (GI) problems are one of the most common reasons pet owners visit the veterinary hospital. The main challenge to the veterinary healthcare team presented with a pet that has GI dysfunction, is to determine whether this is an emergency or potentially serious problem versus a chronic or intermittent problem. The GI tract in veterinary patients is known for its resiliency and the veterinary healthcare team has seen many pets with clinical signs of acute vomiting and/or diarrhea resolve uneventfully, sometimes without any supportive care. However, this cannot be held to all acute GI events as some may be life-threatening disorders. These disorders if not identified and treated, could lead to poor patient management and/or death of the pet.
Vomiting is a clinical sign seen commonly in small animals and vomiting is associated with GI disorders; however, vomiting may occur with nongastrointestinal conditions as well. Consequently, it is difficult to identify the etiology of the vomiting and may require extensive diagnostic workup in some dogs and cats. The definition of vomiting is the forceful discharge of ingested material from the stomach and sometimes proximal small intestines. Vomiting truly consists of three stages: nausea, retching, and subsequently vomiting. Nausea is the first stage. Outward signs of nausea for which the healthcare team should be aware, may include depression, shivering, hiding, yawning, and licking of the lips. Increased salivation and swallowing occur, subsequently lubricating the esophagus. Retching often helps distinguish the episode from regurgitation, gagging, or coughing. Retching is the forceful contraction of the abdominal muscles and diaphragm. Negative intrathoracic pressure and positive abdominal pressure changes cause the movement of gastric contents into the esophagus and out the mouth. This vomiting process is initiated by the central nervous system. These stages are important to discuss with pet owners as often owners state the patient is vomiting when in fact it may be one of the stages. This may help to pinpoint the cause of GI distress in the pet.
Along with vomiting, diarrhea is one of the most common reasons pets are brought to the veterinary hospital. Diarrhea is the passage of feces containing an excessive amount of water thus resulting in an abnormal increase in stool liquidity and weight. Patients may also experience an increase in the frequency of their defecation. This would lead to the broad description of too rapid evacuation of too loose stools. It is important for the veterinary technician to gain a thorough understanding of the owner’s definition of diarrhea as it may not be as accurate as the healthcare team’s definition. This would incorporate a very involved discussion with the owner while gathering the history. Diarrhea is the trademark sign of intestinal dysfunction. It is important for healthcare team members to determine acute from chronic problems when assessing animals with diarrhea. Acute diarrhea is typically the result of diet, parasites, or infectious disease (e.g., parvovirus, coronavirus, etc.). Chronic diarrhea is termed as such when it has not responded to conventional therapy within a two to three-week time frame.
The next step is to determine the origination of the diarrhea – small intestine or large intestine. A thorough history by the veterinary technician is again the best tool. Increased frequency of
255

defecation resulting in larger than normal amounts of soft – to –watery stool is often seen in small bowel diarrhea. Failure to lose weight or body condition is typically indicative of large bowel disease. Weight loss usually indicates small bowel disease although severe large bowel diseases such as malignancy, histoplasmosis, and pythiosis may result in weight loss. Animals with weight loss from severe large bowel disease usually have signs associated with colonic involvement such as fecal mucus, marked tenesmus, and hematochezia. Fresh blood (bright red in color) in the stool or evidence that the pet is straining to defecate is indicative of a large bowel disorder. Hematochezia (bright-red blood) typically originates in the anus, rectum, or descending colon. Melena is described as coal tar black stools that result from digested blood. Melena may originate from the pharynx, lungs (coughed up and swallowed), esophagus, stomach, or upper small intestine. Tarry stools are the result of bacterial breakdown of hemoglobin. Dyschezia is difficult and/or painful defecation. Tenesmus refers to persistent and/or prolonged straining, typically with no effect. Owners may mistake tenesmus with constipation, so it is important to question the owner further to determine which clinical sign truly is manifesting in their pet. Dyschezia and tenesmus are most often associated with large bowel disorders.
DIAGNOSIS
A complete history is the first step (and a vital step) in trying to establish a cause for vomiting and diarrhea. The signalment and history, as well as a description of the vomiting episodes, are important. First, one must determine whether the animal truly is vomiting. The healthcare team should differentiate the owner's report of vomiting from gagging, coughing, dysphagia, or regurgitation. The description of retching is characteristic for vomiting. Signalment may also be helpful. For example, young, unvaccinated pets are more susceptible to infectious disease, such as parvovirus. Vaccination status, travel history, previous medical problems, and the medication history should be determined. Many drugs can result in vomiting, such as nonsteroidal anti-inflammatory drugs (NSAIDs), which are known to cause gastrointestinal ulceration and vomiting. The healthcare team member should also explore the possibility of toxin or foreign body ingestion and of other concurrent signs that often arise with systemic or metabolic disease. An example: polydipsia, polyuria, and weight loss are typical of vomiting associated with diabetic ketoacidosis or chronic kidney failure.
The history should then focus on the actual vomiting episodes. The duration, frequency, and relationship of the episodes to eating or drinking should be ascertained. A complete physical description of the vomited material should be documented. A dietary history, including the type of diet or recent dietary changes, is important because vomiting may be associated with an adverse reaction to food. Vomiting of an undigested or a partly digested meal more than 6 to 8 hours after eating, a time at which the stomach should normally be empty, suggests a gastric outflow obstruction or gastric hypomotility disorder. The description of the vomit should include the volume, color, consistency, odor, and the presence or absence of bile or blood. Undigested food suggests a gastric origin, whereas vomit-containing bile makes a gastric outflow obstruction unlikely. Vomit having a fecal odor is suggestive of a low-intestinal obstruction or bacterial overgrowth in the small intestine. Hematemesis, (either as fresh, bright-red blood or as digested blood with the appearance of coffee grounds), is indicative of gastrointestinal erosion or ulceration. Gastric ulceration is caused by metabolic conditions such as hypoadrenocorticism, reaction to certain drugs, clotting abnormalities, gastritis, or neoplasia.
256
A complete physical examination should begin with an evaluation of the mouth and oral cavity. The presence of a fever is suggestive of an infectious or inflammatory process. Bradycardia or cardiac arrhythmias in a vomiting animal may be a sign of a metabolic disturbance, such as hypoadrenocorticism. Careful palpation of the abdomen should be part of the physical examination to rule out; distention or tympany (e.g., gastric dilatation–volvulus [GDV] syndrome), effusion (e.g., peritonitis), masses or organomegaly (e.g., neoplasia, intussusception, or foreign body), and pain (e.g., peritonitis, pancreatitis, or intestinal obstruction). Obstruction is suggested when there are gas- and fluid-filled intestines, whereas bunching of the bowel is characteristic of intestinal plication from a linear foreign body obstruction. A rectal examination provides characteristics of colonic mucosa and feces. Melena suggests upper-gastrointestinal bleeding.
Performing a complete blood count (CBC) is extremely important for GI patients, especially in those animals at risk for neutropenia (e.g., parvoviral enteritis), infection, and anemia (e.g., melena, hemataemesis). Patients should also have a serum chemistry profile performed upon presentation. A serum biochemistry profile, especially in patients presenting with severe vomiting, diarrhea, ascites, unexplained weight loss, and/or anorexia should include alanine transaminase, alkaline phosphatase, blood urea nitrogen, creatinine, total protein, albumin, total CO2, cholesterol, calcium, phosphorous, magnesium, bilirubin, and glucose concentrations, along with electrolytes; sodium, chloride, and potassium.
Vomiting may result in significant fluid, electrolyte, and acid-base alterations. The most common electrolyte disturbance in vomiting cats and dogs is hypokalemia. Acid-base changes generally are minimal or, if abnormal, tend toward an acidosis. If metabolic alkalosis is identified and is associated with hyponatremia, hypochloremia, and hypokalemia, the most likely cause will be gastric outflow or high-duodenal obstruction. Rarely animals with gastrinomas or with frequent and unrelenting vomiting have a metabolic alkalosis. When routine diagnostic testing fails to identify an obvious etiology, additional tests may be necessary. Additional tests may include viral or heartworm serology, thyroid hormone testing, adrenocortical testing for hypoadrenocorticism, bile acid determination for liver disease, toxologic testing (e.g., lead poisoning), and a neurologic examination.
When testing fails to identify a nongastrointestinal cause for the vomiting, the focus should move to investigation of gastrointestinal disease as a possible etiology. The diagnostic approach includes contrast radiography, ultrasonography, endoscopy, or laparotomy. Frequently, inflammatory gastrointestinal lesions are a cause of chronic vomiting; these conditions include chronic gastritis, Helicobacter gastritis, inflammatory bowel disease (IBD), and chronic colitis. Cats with inflammatory bowel disease often have vomiting as the main clinical sign and diarrhea as a minor clinical component. Conditions such as gastric antral pyloric mucosal hypertrophy, antral polyps, foreign bodies, or neoplasia can cause gastric outflow obstruction. These conditions cause gastric retention and vomiting. Such gastric lesions can be easily identified endoscopically or using contrast radiography.
KEY NUTRITIONAL FACTORS
Following a diagnosis by the veterinarian, the vomiting and/or diarrhea will need to be managed. The healthcare team should be aware of key nutritional factors and their impact when managing
257
a patient nutritionally. Nutritional management of patients suffering with vomiting and/or diarrhea should consider the following nutritional factors:
Water - Water is extremely important when working with patients with acute vomiting due to the potential for life-threatening dehydration from excess fluid loss and inability of the patient to replace the lost fluid. Patients with persistent nausea and vomiting should be supported with subcutaneous or intravenous rather than oral fluids. Where applicable, moderate to severe dehydration should be corrected with appropriate parenteral fluid therapy.
Electrolytes - Gastric and intestinal secretions differ from extracellular fluids in electrolyte composition, so their loss can result in systemic electrolyte abnormalities. Dogs and cats presenting with vomiting and diarrhea may have abnormal serum potassium, chloride and sodium concentrations. Serum electrolyte concentrations are useful in tailoring appropriate fluid therapy and nutritional management of these patients. Mild hypokalemia, hypochloremia and either hypernatremia or hyponatremia are the electrolyte abnormalities most commonly associated with acute vomiting (and diarrhea). Initially, electrolyte disorders should be addressed and corrected with appropriate parenteral fluid and electrolyte therapy. Patients experiencing vomiting and/or diarrhea should begin nutritional therapy ideally containing levels of potassium, chloride and sodium above the minimum allowances for normal dogs and cats. Recommended levels of these nutrients are 0.8 to 1.1% potassium (dry matter [DM]), 0.5 to 1.3% DM chloride and 0.3% to 0.5% DM sodium).
Protein – Nutritional therapy for patients exhibiting vomiting and/or diarrhea should probably not provide excess protein (no more than 30% for dogs and 40% for cats). Products of protein digestion (peptides, amino acids and amines) increase gastrin and gastric acid secretion. “Hypoallergenic” or elimination foods for patients with vomiting/diarrhea have been recommended as dietary antigens are suspected to play a role in the etiopathogenesis.
Ideal elimination foods should: 1) avoid protein excess (16 to 26% for dogs; 30 to 40% for cats), 2) have high protein digestibility (≥ 87%) and 3) contain a limited number of novel protein sources to which the patient has never been exposed. On the other hand a food containing a protein hydrolysate may be utilized in nutritional management of the patient.
Fat - Solids and liquids higher in fat empty more slowly from the stomach than comparable foods with less fat. Fat in the duodenum stimulates the release of cholecystokinin, which delays gastric emptying. Foods with less than 15% DM fat for dogs and less than 25% DM fat for cats are appropriate for dietary management.
Fatty Acids - Ingestion of foods containing omega-3 fatty acids results in a decrease in membrane AA levels because omega-3 fatty acids replace AA in the substrate pool. This produces an accompanying decrease in the capacity to synthesize eicosanoids from AA. Inflammatory eicosanoids produced from AA are depressed when dogs consume foods with high levels of omega-3 fatty acids. In addition to their role in modulating the production of inflammatory eicosanoids, omega-3 fatty acids have a direct role in the resolution of inflammation.
258

Milk protein concentrate - a protein concentrate from the milk of hyperimmunized cows. containing hyperimmune milk factor (HIMF). HIMF is a protein concentrate of hyperimmunized milk in which the lactose and salts have been reduced and reduces inflammation by inhibiting neutrophil migration. Assays have shown that HIMF retains biologically active properties.
Fiber - Foods containing gel-forming soluble fibers should be avoided in vomiting and/or diarrhea patients as these fibers increase the viscosity of ingesta and slow gastric emptying. These fibers include pectins and gums (e.g., gum arabic, guar gum, carrageenan, psyllium gum, xanthan gum, carob gum, gum ghatti and gum tragacanth). Overall, the crude fiber content should not exceed more than 5% DM.
Food Form and Temperature - Moist foods are considered to be the best form since they reduce gastric retention time. For the same reason, the veterinary healthcare team should educate clients to warm foods to between room and body temperature (70 to 100°F [21 to 38°C]).
Vitamins and Trace Minerals - Iron, copper, and B vitamins may benefit patients with gastroduodenal ulceration and GI blood loss. Hematinics should be used in patients with nonregenerative, microcytic/hypochromic anemias attributable to iron deficiency. However, they probably are not necessary in most animals that have received a blood transfusion.
Acid Load - Alkalemia should be expected if vomiting patients lose hydrogen and chloride ions in excess of sodium and bicarbonate. Hypochloremia perpetuates the alkalosis by increasing renal bicarbonate reabsorption. A common finding is mild alkalemia in vomiting patients; however profound alkalemia is more likely to occur with pyloric or upper duodenal obstruction. Acidemia may occur in vomiting patients if the vomited gastric fluid is relatively low in hydrogen and chloride ion content (e.g., during fasting) or if concurrent loss of intestinal sodium and bicarbonate occurs. It is best to correct severe acid-base disorders with parenteral fluid and electrolyte therapy. Foods for patients with acute vomiting and diarrhea should avoid excess dietary acid load. Foods that normally produce alkaline urine are less likely to be associated with acidosis.
Digestive enzymes - work in the stomach and intestines to break down food ingested by the pet. Digestive enzymes help increase nutrient absorption and can be valuable in helping senior pets needing digestive system support. Absorption is increased in the GI tract when the nutrients are broken down to the building block level.
Vomiting and diarrhea are two of the main reasons pets present to the hospital. Veterinary technicians must be able to identify these clinical signs and perform a complete history and evaluation regarding these frequent signs in presenting pets. Nutritional management is a crucial part of therapy in the management of vomiting and/or diarrhea. Certain key nutritional factors play a role in managing vomiting and diarrhea in cats and dogs – through enteral and parenteral nutrition – and veterinary technicians should recognize the circumstances and reasoning for the KNF’s to insure a positive outcome for the vomiting and diarrheic patient.
259

REFERENCES – SUGGESTED READING • Allenspach, K, Gaschein, FP. 2008. Small Intestinal Disease. In Small Animal
Gastroenterology. Steiner, JM editor. Pp. 187-202. Schlutersche: Germany.• Burns, KM. Gastrointestinal Disorders. In Internal Medicine for Veterinary Technicians.
Merrill L ed. 2012, Wiley-Blackwell, Ames, IA.• Davenport DJ, Remilliard RL. (2010a) Introduction to Small Intestinal Disease. In Small
Animal Clinical Nutrition 5th Ed. Hand MS, Thatcher CD, Remilliard RL, Roudebush P,Novotny BJ eds. 2010, pp 1047-1049. MMI, Topeka, KS;
• Davenport, DJ, Remillard RL. (2010b)Acute Gastroenteritis and Enteritis. In SmallAnimal Clinical Nutrition 5th Ed. Hand MS, Thatcher CD, Remilliard RL, Roudebush P,Novotny BJ eds. 2010, pp 1053-1061. MMI, Topeka, KS;
• Hall, EJ, German, AJ. 2010. Diseases of the small intestine. In Textbook of VeterinaryInternal Medicine 7th edition. Ettinger, SJ and Feldman, EC, editors. Pp. 1526 – 1572.Elsevier: St. Loius, MO.
• Tams, TR. 2003. Chronic Diseases of the Small Intestine. In Handbook of Small AnimalGastroenterology 2nd Edition. Tams, TR editor. Pp.211-250. Saunders: St. Louis, MO.
• Willard, Michael D. 2009. Disorders of the Intestinal Tract. In Small Animal InternalMedicine 4th edition, pp. 441-476. Mosby: St. Louis, MO.
• Wortiner A, Burns KM. Nutrition and Disease Management for Veterinary Techniciansand Nurses. 2nd ed. 2015. Wiley-Blackwell, Ames, IA.
260
You Are What You Eat: Helping Clients with Diet Choices Kara M. Burns, MS, MED, LVT, VTS (Nutrition)
One of the most important factors in managing health and disease in pets is proper nutrition. As clients become more aware of the importance of nutrition in their own health, they are demanding the same high standard of nutritional care for their pets. The veterinary healthcare team should be the preferred, expert source of the best nutritional information for pets.1,2 Veterinary teams which understand and promote clinical nutrition and demonstrate in-clinic behaviors consistent with this conviction will benefit their clients, their practices, and most importantly their patients. Proper nutritional management is one of the most important factors in maximizing health, performance, and longevity in addition to managing disease conditions.
Veterinary health care teams recognize that nutrition is important to their patient’s health and want to make the best food recommendation. Clients want the best for their pets and for their pets to live long, healthy lives. This is the basic definition of communication, the interchange of thoughts, opinions, and information to reach a shared understanding.
Then why is communication around pet foods so difficult? The pet food category is a multi-billion dollar industry with an overwhelming selection of pet foods available. The healthcare team may feel uncomfortable or lack confidence having a conversation about specific pet food choices. Clients may have very strong emotions about the food they prefer to feed, and think is best for their pets. There are multiple pet food myths and nutrition trends that have muddied the world of pet food. The internet provides a vast amount of information on pet foods, and it can be very difficult to discern fact vs. myth vs. trends that can be dangerous to a pet’s health.
Making a pet food recommendation that best supports that pet’s health should not be a battle between what the veterinarian knows will support their patient’s health and what their client wants or believes is the best food for their beloved pet. Through consistent use of core communication skills and involvement of the entire healthcare team you can connect with your clients, overcome some of the more challenging pet food barriers, build nutritional confidence in your entire team and make the nutritional recommendation that you feel best supports that pet’s health and respects your client’s preferences.
From every media outlet, as well as family members, pet sores, etc., clients are inundated with information about foods for their pets. So, when they come to the veterinary healthcare team with the question—What should I feed my pet?—how does one answer?
Know Your Resources
The American Animal Hospital Association (AAHA) in 2021, published updated Nutritional Assessment Guidelines3 for veterinary practices. In 2011 the World Small Animal Veterinary Association (WSAVA) published Nutritional Guidelines.4 These guidelines were developed to support veterinary healthcare teams in the development and implementation of nutritional management protocols tailored to the individual needs of the patient. Both associations, with the assistance of veterinary nutritionists, veterinarians, and credentialed veterinary technicians, have developed tools to help healthcare teams educate clients on what they should feed their pet. These tools were developed to assist the veterinary team in determining what the pet should eat as well as offering a resource to help make a specific nutritional recommendation.
As with any recommendation, the veterinary healthcare team must do the research.2 When investigating the question “How do I distinguish one food from another?” look for answers to the following2:
• Is the pet food manufacturer’s contact information available on the product for the veterinary team and petowner?
• Does the pet food manufacturer employ full-time veterinary nutritionist(s), veterinarians, and credentialedveterinary technicians?
• Where are the foods produced and manufactured?• What are the specific quality control measures to guarantee product consistency and quality?
261
• Will the manufacturer provide a complete nutrient analysis for the pet food in question—above and beyondthe guaranteed analysis?
• Has the product undergone research? And are the results published in peer-reviewed journals?
These initial questions assist the team in determining if the product is made by a reputable and knowledgeable company. It also helps to determine if the manufacturer follows strict quality control measures.
Nutritional Adequacy Statement by AAFCO
In addition to researching the quality behind products, the team should research the Association of American Feed Control Officials (AAFCO) nutritional adequacy statement included on pet food labels to help determine the following important facts2,5:
1. Is the diet complete and balanced? All wellness foods should be complete and balanced.
2. If the food is complete and balanced, for which life stage is the food intended?
• Nutrient profiles and feeding trial requirements for growth, reproduction, and adultmaintenance are provided by AAFCO.
• The healthcare team should be aware that foods listed as formulated to meet the AAFCOprofiles for all life stages must meet the minimum nutrient levels for both growth and adultmaintenance.
3. What method was utilized to substantiate that the food is complete and balanced?
• AAFCO feeding trials:o Were the products fed to the intended species and intended life stage?o Does the product label state “Animal feeding tests using AAFCO procedures
substantiate [Product Name] provides complete and balanced nutrition for [lifestage(s)]”?
• AAFCO nutrient profiles:o Do the foods meet AAFCO nutrient profiles by formulation or by analysis of the
finished product?o Does the product label state “[Product Name] is formulated to meet the nutritional
levels established by the AAFCO (Dog or Cat) Food Nutrient Profiles for [lifestage(s)]”?
Formulated foods are manufactured so the ingredients meet specified levels, either based on the recipe or on analytical testing of the finished product, without testing via feeding trials.
The healthcare team should be educated and proactive when discussing nutrition with clients. There are differences amongst manufacturers, products, and lifestages, and veterinary team members should not be afraid to ask the questions. This will allow the team to present a researched and educated nutritional recommendation and preempt the ‘I read this on the internet response’.
References
1. Burns KM. Nutrition: Is the new emphasis a fad? Vet Team Brief 5:8-9, 2014.2. Burns KM. The Dreaded Question: What Should I Feed My Pet? Clinicians Brief. Febraury 2015. Pp. 13-
14.3. Cline M, Burns KM, Coe JB, et al. AAHA Nutrition and Weight Management Guidelines for Dogs and
Cats. JAAHA 57:4, 153-178, 2021.4. Nutritional Assessment Guidelines. WSAVA Nutritional Assessment Guidelines Task Force. J SMALL
ANIM PRACT 52:385-396, 2011.5. Association of American Feed Control Officers, AAFCO Official Publication 2020; accessed February
2020.
262
Resources
• www.petnutritionalliance. org• www.wsava.org/nutrition-toolkit• www.AAFCO.org
263

LIFEST YLE VACCINESHaving the conversation with pet owners
COMMON SIGNS2,3
• Polyuria/polydipsia
• Abdominal pain
• Vomiting
• Fever
• Anorexia
• Lethargy
DIRECT2,3 • Contact with infected animal
through - Bites, ingestion of contaminated urine, placental and venereal transfer
INDIRECT2,3
• Contact with water or soil containing contaminated urine
DISEASES CLINICAL SIGNS TRANSMISSION
RESPIRATORY SIGNS1
• Coughing (hacking, dry, or moist)
• Nasal or ocular discharge
• Sneezing
SYSTEMIC SIGNS1
• Anorexia• Fever• Lethargy
DIRECT1 • Contact with infected dogs
• Contact with aerosolized droplets from an infected dog (e.g., sneezing, coughing, nasal/ocular discharge)
INDIRECT1 • Contact with fomites (e.g.,
dog bowls, dog toys)
CANINE INFECTIOUS RESPIRATORY DISEASE COMPLEX (CIRDC)
LEPTOSPIROSIS
CANINE LYME DISEASE
COMMON SIGNS4,5
• Arthritis-like joint pain• Shifting-leg lameness • Anorexia• Swollen lymph nodes
LESS COMMON SIGNS4,5
• Renal disease (Lyme nephritis)
• Myocarditis-induced cardiac arrhythmia
• Neurologic disease
VECTOR-BORNE4,5
• Tick acquires the bacteria while feeding on an infected animal and then transmits to dog during its next blood meal
VECTORS IN THE US4,5 •East Coast: Black-legged
tick (Ixodes scapularis)
• West Coast: Western black-legged tick (Ixodes pacificus)
LET’S TALK
264
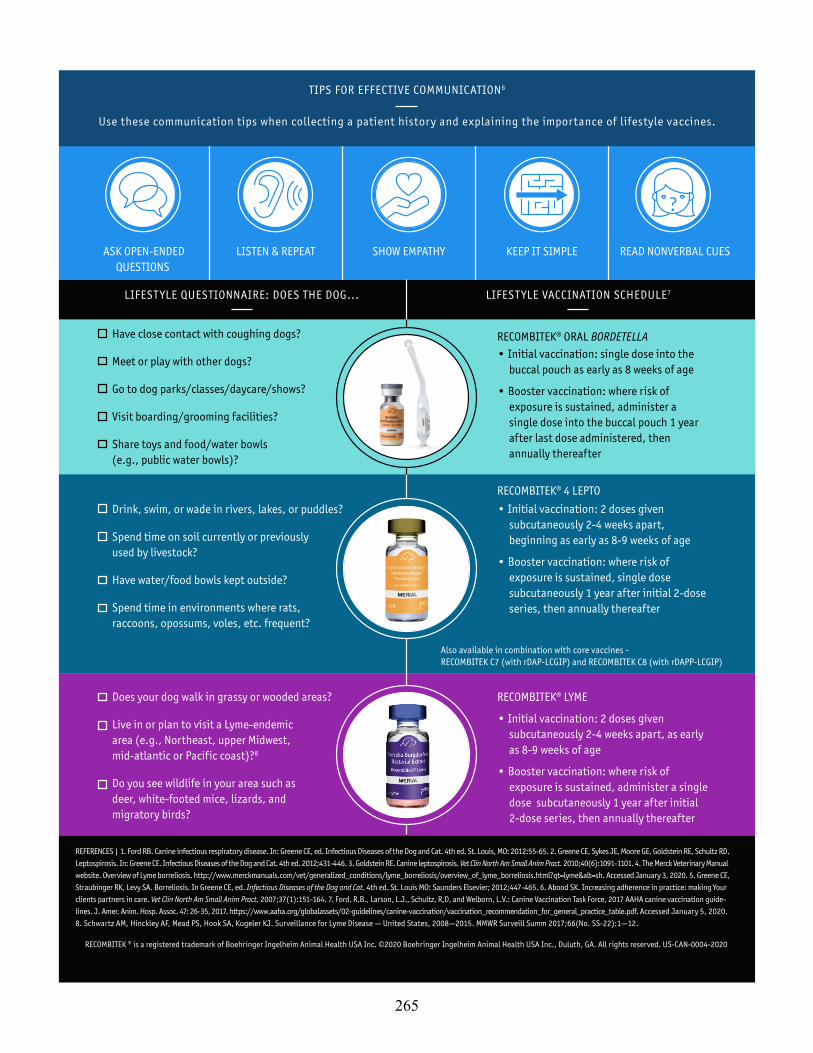
?
ASK OPEN-ENDED QUESTIONS
LISTEN & REPEAT KEEP IT SIMPLESHOW EMPATHY READ NONVERBAL CUES
RECOMBITEK® 4 LEPTO
RECOMBITEK® LYME
• Initial vaccination: 2 doses given subcutaneously 2-4 weeks apart, as early as 8-9 weeks of age
• Booster vaccination: where risk of exposure is sustained, administer a single dose subcutaneously 1 year after initial 2-dose series, then annually thereafter
TIPS FOR EFFECTIVE COMMUNICATION6
Use these communication tips when collecting a patient history and explaining the importance of lifestyle vaccines.
LIFEST YLE QUESTIONNAIRE: DOES THE DOG... LIFEST YLE VACCINATION SCHEDULE7
Have close contact with coughing dogs?
Meet or play with other dogs?
Go to dog parks/classes/daycare/shows?
Visit boarding/grooming facilities?
Share toys and food/water bowls (e.g., public water bowls)?
Drink, swim, or wade in rivers, lakes, or puddles?
Spend time on soil currently or previously used by livestock?
Have water/food bowls kept outside?
Spend time in environments where rats, raccoons, opossums, voles, etc. frequent?
Does your dog walk in grassy or wooded areas?
Live in or plan to visit a Lyme-endemic area (e.g., Northeast, upper Midwest, mid-atlantic or Pacific coast)?8
Do you see wildlife in your area such as deer, white-footed mice, lizards, and migratory birds?
REFERENCES | 1. Ford RB. Canine infectious respiratory disease. In: Greene CE, ed. Infectious Diseases of the Dog and Cat. 4th ed. St. Louis, MO: 2012:55-65. 2. Greene CE, Sykes JE, Moore GE, Goldstein RE, Schultz RD. Leptospirosis. In: Greene CE. Infectious Diseases of the Dog and Cat. 4th ed. 2012;431-446. 3. Goldstein RE. Canine leptospirosis. Vet Clin North Am Small Anim Pract. 2010;40(6):1091-1101. 4. The Merck Veterinary Manual website. Overview of Lyme borreliosis. http://www.merckmanuals.com/vet/generalized_conditions/lyme_borreliosis/overview_of_lyme_borreliosis.html?qt=lyme&alt=sh. Accessed January 3, 2020. 5. Greene CE, Straubinger RK, Levy SA. Borreliosis. In Greene CE, ed. Infectious Diseases of the Dog and Cat. 4th ed. St. Louis MO: Saunders Elsevier; 2012;447-465. 6. Abood SK. Increasing adherence in practice: making Your clients partners in care. Vet Clin North Am Small Anim Pract. 2007;37(1):151-164. 7. Ford, R.B., Larson, L.J., Schultz, R,D, and Welborn, L.V.: Canine Vaccination Task Force, 2017 AAHA canine vaccination guide- lines. J. Amer. Anim. Hosp. Assoc. 47: 26-35, 2017. https://www.aaha.org/globalassets/02-guidelines/canine-vaccination/vaccination_recommendation_for_general_practice_table.pdf. Accessed January 5, 2020. 8. Schwartz AM, Hinckley AF, Mead PS, Hook SA, Kugeler KJ. Surveillance for Lyme Disease — United States, 2008—2015. MMWR Surveill Summ 2017;66(No. SS-22):1—12.
RECOMBITEK® ORAL BORDETELLA
RECOMBITEK ® is a registered trademark of Boehringer Ingelheim Animal Health USA Inc. ©2020 Boehringer Ingelheim Animal Health USA Inc., Duluth, GA. All rights reserved. US-CAN-0004-2020
• Initial vaccination: single dose into the buccal pouch as early as 8 weeks of age
• Booster vaccination: where risk of exposure is sustained, administer a single dose into the buccal pouch 1 year after last dose administered, then annually thereafter
• Initial vaccination: 2 doses given subcutaneously 2-4 weeks apart, beginning as early as 8-9 weeks of age
• Booster vaccination: where risk of exposure is sustained, single dose subcutaneously 1 year after initial 2-dose series, then annually thereafter
Also available in combination with core vaccines - RECOMBITEK C7 (with rDAP-LCGIP) and RECOMBITEK C8 (with rDAPP-LCGIP)
265