2008 A singular beeswax representation of Namarrkon, the Lightning Man, from western Arnhem Land
Upload
independentCategory
view
1download
0
Journal of Feline Medicine and Surgery (2009) 11, 856e863doi:10.1016/j.jfms.2009.02.009
CASE REPORTPrimary ocular melioidosis due to a single genotype ofBurkholderia pseudomallei in two cats from ArnhemLand in the Northern Territory of Australia
Helen M Parkes BVSc, MSc, MACVSc1, Catherine M Shilton BSc, DVM, DVSc, MACVSc
2,Ian V Jerrett BVSc, MACVSc
2, Suresh Benedict BSc, MSc, MPhil, PhD2, Brian G Spratt CBE, FRS,
FMedSci3, Daniel Godoy BSc
3, Carolyn R O’Brien BVSc, MVetClinStud, FACVSc, MASM4,
Mark B Krockenberger BVSc, PhD, MACVSc, MASM5, Mark Mayo BSc
6,Bart J Currie MBBS, FRACP
6, Richard Malik DVSc, DipVetAn, MVetClinStud, PhD, FACVSc, FASM5,7*
1Gove Vet Clinic, PO Box 1030,Nhulunbuy, Northern Territory0881, Australia2Berrimah Veterinary Laboratories,Department of Primary Industryand Fisheries, Darwin, NorthernTerritory 0801, Australia3Department of Infectious DiseaseEpidemiology, Imperial CollegeLondon, England, UK4Faculty of Veterinary Science,University of Melbourne, Werribee,Victoria 3030, Australia5Faculty of Veterinary Science,Building B14, The University ofSydney, New South Wales 2006,Australia6Tropical and Emerging InfectiousDiseases Division, Menzies Schoolof Health Research, Charles DarwinUniversity, Northern Territory0811, Australia7Centre for Veterinary Education,Building B22, The University ofSydney, New South Wales 2006,Australia
*Corresponding author. Centre for Veteing B22, The University of Sydney, NAustralia. E-mail: [email protected]
1098-612X/09/100856+08 $36.00/0
Melioidosis was diagnosed in two domestic crossbred cats presented forunilateral ocular disease. One patient was born and bred in Nhulunbuy, ArnhemLand, while the other had moved there 6 months previously from Townsville,Queensland. Both patients were presented with sudden onset of a ‘red eye’ andblepharospasm, which progressed to an enlarged, painful, firm globe with loss ofpupillary light reflexes and vision. An obvious primary focus of infection outsidethe eye was not detected in either cat. In both patients, the affected eye wassurgically removed and vitreal culture revealed a pure growth of Burkholderiapseudomallei. In each instance, the infection had penetrated the sclera to produceretrobulbar cellulitis, and in one case frank retrobulbar abscessation.Histologically, there was a pyogranulomatous uveitis with extensive destructionof intraocular structures. The first case was still alive approximately 1 yearfollowing enucleation and limited antimicrobial therapy using amoxicillinclavulanate and doxycycline. The second was euthanased when a localisedabscess developed on the same side of the face as the healed surgical incision,despite appropriate antimicrobial therapy. Both cases were caused by the samemultilocus sequence type of B pseudomallei (ST 116), which had only beenisolated previously from two human patients, both living in the same isolatedgeographical area as the cats of this report. Apart from the geographicalclustering, no epidemiological links were evident between the two cats and/orthe two people. The presumptive pathogenesis of these infections is discussed inrelation to current knowledge about melioidosis in northern Australia.
Date accepted: 17 February 2009 � 2009 ESFM and AAFP. Published by Elsevier Ltd. All rights reserved.
Melioidosis is an infection caused by the aer-obic, Gram-negative bacillus Burkholderiapseudomallei. This bacterium is a soil and
water saprophyte endemic to Southeast Asia, tropical
rinary Education, Build-ew South Wales 2006,.au
� 2009 ESFM a
and subtropical Australia, Papua-New Guinea, theCaribbean, parts of South America and the SouthPacific.1e3 B pseudomallei has been isolated from moistsoil and waterholes in these areas and these environ-ments are thought to be the primary reservoirs fromwhich infections are acquired.3,4 In endemic locationsup to 85% of human cases occur during monsoonalwet seasons and it is postulated that rising water
nd AAFP. Published by Elsevier Ltd. All rights reserved.

857Primary ocular melioidosis due to a single genotype of Burkholderia pseudomallei
tables cause organisms to percolate up through soil,thereby increasing exposure of humans and animals.3
In mammals, the main modes of infection include:(1) inoculation via penetrating injuries, (2) inhalationof dust or aerosols containing organisms, (3) ingestionof soil or contaminated carcasses and (4) transmissionvia infected milk following mammary gland infec-tion.5,6 Melioidosis can affect virtually any organ sys-tem. The spectrum of disease ranges from mild orinapparent infection, localised skin ulceration, chronicabscessation and granuloma formation in subcutane-ous tissues or internal organs, chronic pneumonia toacute fulminant septicaemia.
Melioidosis was previously considered an uncom-mon human condition resulting in severe and mostlyfatal disease. The current consensus is that most infec-tions in people living in endemic regions are probablyasymptomatic,1e3 with epidemiological studies dem-onstrating widespread occurrence of antibodies to Bpseudomallei in apparently healthy individuals.2,7,8
Chronic infections are characterised by the formationof single or multiple abscesses or granulomas in anyorgan, although liver, spleen and lungs tend to be in-volved preferentially in both animals and humans.3,5
A further characteristic feature of melioidosis is itspropensity for re-activation following long periodsof dormancy; in many of these cases the primary in-fection is inapparent.2,3
Melioidosis has been reported in many domesticand wild animal genera. Susceptibility to the infectionvaries between species, with sheep and goats beingparticularly susceptible.9,10 In Australia, melioidosismost commonly affects goats, sheep and pigs. Al-though infections can occur in dogs, cats and cattle,these species are considered to be relatively resistant.Melioidosis has also been recorded in rodents, camels,alpacas, horses, deer, laboratory animals, tree kanga-roos, wallabies, koalas, crocodiles, various birds5 andcaptive marine mammals.11 To the knowledge of theauthors, only three well documented case reports offeline infection have been published.12e14
Although a wide spectrum of signs can be seenamong individuals, it has been suggested there maybe a trend towards infection of particular organ sys-tems in given species. Mastitis, for example, is seenmore frequently in melioidosis of goats whereas therespiratory system is involved preferentially insheep.5 In horses, the disease usually takes the formof multifocal pneumonia with high fever and a shortclinical course, whereas the disease in pigs is usuallychronic and manifest as cervical lymphadenitis orasymptomatic liver abscesses. Multiple abscesses inmost organs, particularly the lungs, liver and spleen,but also the subcutis and sometimes associated lymphnodes, are characteristic of the disease in all specieswhen severe infection occurs.
The present report documents two cats with melioi-dosis which were presented for unilateral ocular dis-ease. Molecular typing using multilocus sequencetyping (MLST) demonstrated that both infections
were caused by the same sequence type (ST) of B pseu-domallei. Delay in making a definitive diagnosis com-promised case management, thus the purpose of thisreport is to alert veterinarians to the possibility of Bpseudomallei infection as a cause of uveitis or panoph-thalmitis in cats in endemic regions. In addition, wepresent molecular genotyping information on furtherfeline isolates referred to our reference laboratories,but for which detailed clinical data is lacking.
Case 1 was a 13-month-old female neutered domes-tic shorthair cat (3.5 kg) presented (2/9/2005) witha 2e3 day history of a painful eye. The cat was bornand lived in Nhulunbuy (north-east Arnhem Land)in the Northern Territory, Australia. There was no his-tory or physical findings indicative of ocular or con-junctival trauma. The cat was anorexic, and hadrecently lost weight. It was pyrexic (rectal temperature40.3�C). Examination showed a ‘red eye’, blepharo-spasm and partial prolapse of the nictitatingmembrane.
Topical chloramphenicol eye ointment and oraldoxycycline monohydrate paste (25 mg twice daily),plus a single injection of dexamethasone sodiumphosphate (1.4 mg) were prescribed, followed byprednisolone (5 mg orally once daily). Although thecat’s general condition and demeanor improved, theeye deteriorated becoming enlarged, firm and painful.It was enucleated under general anaesthesia 20 daysafter initial presentation. No pre-anaesthetic haema-tology or serum biochemistry, serology or otherwork-up was undertaken due to cost constraints. Sur-gery was uneventful. The cat was discharged onamoxicillin clavulanate (50 mg orally bid).
Following enucleation, an aseptic specimen of vitre-ous was collected by needle aspiration. Grossly, thiswas a thick, cloudy, grey, mucoid fluid. It was submit-ted to Berrimah Veterinary Laboratories for cytologi-cal examination and microbial culture. The rest ofthe eye was submitted in formalin, following injectionof formalin into the globe and making a small incisioninto the sclera to facilitate fixation.
Smears of intraocular fluid were stained with Diff-Quik, Geimsa and Bourke’s modification of theGram stain. Cytologically, there was high cellularitydominated by degenerate neutrophils, with rare lym-phocytes and macrophages. Moderate numbers ofGram-negative bacilli were evident extracellularlyand intracellularly within neutrophils. Culture onblood agar at 37�C resulted in a moderate puregrowth of B pseudomallei. The isolate was susceptibleto amoxicillin clavulanate, tetracycline and trimetho-prim/sulphonamide, but resistant to ampicillin andcephalothin with intermediate susceptibility to enro-floxacin. The isolate was sent to the laboratory of BGSpratt for MLST (Table 1).
Histological examination of the eye showed severepyogranulomatous uveitis and panophthalmitis (Fig1B, D and F). The optic chambers contained an exu-date comprising large numbers of degenerate neutro-phils and eosinophilic material. The inflammatory

Table 1. Multilocus sequence type for B pseudo-mallei isolated from cats in the Northern Territory
Feline melioidosis cases MLST type
[A] Cases in this reportCase 1 (2005) ST 116*Case 2 (March 2007) ST 116*
[B] Nosocomial outbreak24
Cat 1 1992 ST 616yCat 2 1992 ST 616yCat 3 1992 ST 616yCat 4 1992 ST 616y
[C] Sporadic Darwin cases1996 ST 616y1997 ST 333z1998 ST 320z2002 ST 6122002 ST 612k
[D] Previous JFMS report13
Case 1 (Malaysian strain) ST 414{Case 2 (Darwin cat) ST 572x
*Isolated also from two human patients from Nhulun-buy; has not been isolated elsewhere from either hu-man or animal patients.yThis is a novel ST, a double locus variant of severalSTs, including the two most common causes of humaninfection (ST 109 and ST 132).zAssociated with local soil and human cases.xIsolated also from human patients.kA novel ST.{This ST confirms a Southeast Asian origin ratherthan Australian origin for the B pseudomallei.
858 HM Parkes et al
exudate extended from a severely inflamed uvealtract, with a loss of distinction between the vasculartunic and the optic chambers. The uvea was disruptedby a severe infiltrate of macrophages with moderate tolarge numbers of interspersed neutrophils and scat-tered plasma cells and lymphocytes. The retina wascompletely effaced by inflammatory exudate. A floridsuppurative perilimbal keratitis extended to a bulbarconjunctivitis. For most of its circumference, inflam-mation was constrained within the globe by the densefibrous connective tissue of the sclera; however, the in-flammatory exudate extended into the periocular con-nective tissue adjacent to the limbus.
The cat was treated with a combination of amoxicil-lin clavulanate (50 mg combined orally every 12 h)and doxycycline (25 mg every 12 h) starting on theday of suture removal, 10 days following the surgery.Although it was recommended that the patient shouldreceive a 3-months course of combination therapy us-ing amoxicillin clavulanate and doxycycline, the catwas not returned for follow-up treatment and only 2weeks of antimicrobials were dispensed. The cat re-mained well 12 months following surgery, the last
time that it was possible to obtain telephone follow-up from its owners.
Case 2 was a 7-year-old male neutered domesticshorthair cat presented (11/3/2007) following a 1e2day history of anorexia and lethargy. The cat was orig-inally from Townsville in north Queensland Australia,but had moved to Nhulunbuy approximately 6months prior to presentation. Physical findings in-cluded pyrexia (40.5�C), mild dehydration, tachyp-noea without dyspnoea and icterus. The left eye was‘red’, with mild blepharospasm and a dilated pupilthat did not respond to bright light. The iris wasslightly more yellow than the contralateral eye, witha cloudy aqueous. The cat’s serum was icteric. Serumbiochemistry showed mildly elevated alanine amino-transferase, normal alkaline phosphatase, elevatedtotal bilirubin (41 mg/l) and stress hyperglycaemia.Haematology demonstrated anaemia (haematocrit0.22 l/l) and leukocytosis (total white cell count18.8� 109/l). A blood smear showed a mature neutro-philia with toxic changes (granulation and Dohle bod-ies) and large numbers of the red blood cells infectedby haemotropic mycoplasmas. Urine (specific grav-ity> 1.050) collected by cystocentesis had high levelsof bilirubin, protein and haemolysed blood. The pre-sumptive diagnosis was a systemic infection with sec-ondary uveitis, possibly with concurrent felineinfectious anaemia and/or sepsis causing haemolysis,anaemia and icterus. An immunomigration test for fe-line immunodeficiency virus antibodies was negative.
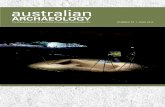
The cat was started on intravenous fluids and enro-floxacin (30 mg subcutaneously), which was laterchanged to doxycycline (25 mg orally twice daily).Chloramphenicol ointment was applied to the af-fected eye. The cat improved systemically over 2days and was discharged on doxycycline, with a nor-mal temperature (38.5�C). It ate well and appeared ini-tially to be improving, with the haematocrit increasingto 0.28 l/l over 13 days, lessening of jaundice and dis-appearance of haemoplasma forms from red cells instained blood smears. The eye, however, became en-larged, firm and painful, with bleeding into the ante-rior chamber and development of corneal oedema(Fig 2). The other eye remained unremarkable.
The affected eye was enucleated 5 weeks after ini-tial presentation. At surgery, retrobulbar abscessationand cellulitis was found in addition to an intact, en-larged globe containing thick, purulent fluid. Afterthe eye was removed the retrobulbar tissues were de-brided and flushed with sterile saline. Unfortunatelysome abnormal, soft, grey tissue remained deep inthe orbit. The cat was given amoxicillin clavulanate(0.3 ml subcutaneously) and enrofloxacin (30 mgsubcutaneously).
The eye was incised following its removal andfound to be filled with pus. A pure heavy growth ofB pseudomallei was cultured after 48 h incubation at37�C on blood agar from both the contents of theeye and a swab of the retrobulbar exudate. Both iso-lates were sensitive in vitro to amoxicillin clavulanate,

Fig 1. (A). Case 2. Low power image of the enucleated eye illustrates a markedly inflamed proliferative conjunctiva (*) withsuppurative exudate. The cornea (#) has a less florid suppurative infiltrate, difficult to appreciate at low power. Haematox-ylin and eosin (H&E). (B). Case 1. High power image illustrates a suppurative keratitis (#) in the region of the limbus withneutrophilic exudate in the anterior chamber (x) near the drainage angle. Descemet’s membrane can be seen as the eosino-philic band separating the cornea from the anterior chamber. H&E. (C). Case 2. Low power image. The photomicrographillustrates a markedly inflamed iris ({) and anterior chamber (x). The cornea (#) is less affected. H&E. (D). Case 1. Highpower image. The photomicrograph illustrates a markedly inflamed iris with mixed inflammatory exudate. H&E. (E).Case 2. Low power image. The photomicrograph illustrates an inflamed choroid (J), sclera and periscleral tissues (F). Athigher magnification the infiltrate is mixed in the scleral tissues and dominated by plasma cells in the choroid. The vitreouscontains large numbers of neutrophils. H&E. (F). Case 1. High power image. The photomicrograph illustrates the drainageangle with a markedly inflamed iris ({) and the anterior chamber (x) to contain large numbers of neutrophils. The cornea isjust evident in the image above Descemet’s membrane (#). H&E.
859Primary ocular melioidosis due to a single genotype of Burkholderia pseudomallei
tetracycline and trimethoprim/sulphonamide, but re-sistant to ampicillin, enrofloxacin and cephalothin.The cat was discharged on amoxicillin clavulanate(50 mg combined orally every 12 h). Histologically,retrobulbar tissue consisted of oedematous fibrovas-cular tissue infiltrated with large numbers of
neutrophils and macrophages. A florid panophthalmi-tis included a mixed but predominantly lymphocyticand plasmacytic infiltration of the uveal tract, withlarge numbers of neutrophils in the sclera, cornea,conjunctiva and subconjunctival connective tissue(Fig 1A, C and E). The posterior chamber was filled

Fig 2. The affected eye of case 2 immediately prior to enu-cleation. Note the increased size of the globe, the pupillarydilatation, cloudy cornea and hyphaema (blood clot in theanterior chamber). Note the contralateral eye appears com-pletely normal.
860 HM Parkes et al
with partially vascularised material containing aggre-gates of neutrophils and macrophages. At the caudalextent of the globe there was obliteration of the retinaand sclera with intense neutrophil and macrophageinfiltration extending from the posterior chamber tothe retrobulbar connective tissue. The histological di-agnosis was suppurative panophthalmitis with retro-bulbar abscessation.
Four weeks after surgery, and while still receivingamoxicillin clavulanate, the cat presented with an ab-scess on the left side of the face. The surgical incisionhad healed well and the abscess was some distanceaway. Pus was aspirated using a needle and syringe.Smears of the purulent exudate revealed macrophagesand neutrophils containing intracellular bacilli. Apure heavy growth of B pseudomallei was obtained.The cat was euthanased as the owner was pregnantand concerned about the possibility of zoonotic infec-tion. Necropsy examination revealed that the infectiveprocess was still active within the orbit, which wasfound to extend to the cheek abscess. No evidenceof dissemination was found elsewhere in the body, al-though the central nervous system was not examined.
The isolates from case 1 and 2 were compared withother feline isolates from 1990 to 2008 stored in theMenzies School of Health Research B pseudomallei iso-late collection and submitted for MLST analysis. Thismolecular technique characterises isolates of bacterialspecies using the sequences of internal fragments ofseven house-keeping genes.15 The MLST scheme forB pseudomallei was developed in the laboratory of DrBG Spratt and data on global B pseudomallei isolatesare accessible at http://bpseudomallei.mlst.net/ (as-sessed June 2008). For MLST, the alleles at each ofthe seven previously described loci are assigned foreach isolate by comparing the sequences to those atthe B pseudomallei MLST website.15 Following the stan-dard MLST protocol, each different DNA sequence at
a locus is assigned a different allele number and theallelic profile (string of seven integers) is used to de-fine the sequenced type (ST) for that isolate. Thereare now over 600 STs described for B pseudomallei,with extensive molecular diversity of B pseudomalleibeing seen especially from the Northern Territory ofAustralia, from where over 250 distinct STs havebeen identified.16
The additional feline B pseudomallei isolates ana-lysed by MLST included the cluster of iatrogenic casesattributed to use of a multi-dose vial of Saffan,14 spo-radic cases from veterinary practices in Darwin, andtwo previously reported cases from Australia.13 Bothisolates from cats with ocular melioidosis in this re-port were of the same MLST type, namely ST 116(Table 1 e [A]). This MLST type had only been iso-lated previously from two human patients, bothfrom the same small community of Nhulunbuy in re-mote Arnhem Land. One patient (seen in 2001) had se-vere non-fatal septicaemia, while the second (seen in2006) had a skin ulcer. We were unable, however, tofind any other epidemiological association between ei-ther of the cats and the two human cases, which were,therefore, linked only by geographical proximity.
The likely nosocomial 1992 Saffan-associated felineoutbreak cluster in Darwin had previously beenshown to be clonal on random amplified polymorphicDNA analysis (RAPD).14 MLST confirmed the clonal-ity, with B pseudomallei isolates from this outbreak allbeing ST 616 (Table 1 e [B]). This is a novel ST, a dou-ble locus variant of several STs, including the twomost common STs (ST 109 and ST 132) isolated fromhuman patients in the Northern Territory. An addi-tional ST 616 strain was found from a cat with melioi-dosis in Darwin in 1996. Five additional isolates fromcats over the period 1997 to 2004 comprised five dif-ferent MLST types (Table 1 e [C] and [D]), includingone of the cats described previously.13
The ocular presentations of the two cases of thepresent report were remarkably similar. Both pre-sented with a unilateral red eye, which progressedto panophthalmitis with a subacute to chronic course.The clinical signs shown by the two cats describedmay prove to be characteristic of feline melioidosis.
Ocular manifestations of melioidosis in other spe-cies, including people, are rare. A human patientwith signs remarkably similar to our cats was pub-lished recently.18 Three human patients in Thailandwith corneal ulceration due to B pseudomallei havebeen reported19; extensive ulcers, subconjunctival ab-scesses and hypopyon were managed with topicaland intravenous ceftazidime, with good outcomes.Another report describes orbital cellulitis with contig-uous spread to the sinuses.20
Both cats were initially systemically unwell, with con-stitutional signs including anorexia, fever and in the sec-ond case, probably sepsis syndrome with icterus.31e33
Unfortunately, a diagnosis of ocular melioidosis wasnot initially considered in either case. The red eye was at-tributed to uveitis, which was thought possibly to be

861Primary ocular melioidosis due to a single genotype of Burkholderia pseudomallei
immune-mediated and secondary to a systemic infec-tion. As a result, corticosteroids were administered aspart of therapy, while antimicrobial doses were less ag-gressive than optimal. Both cats improved systemicallyafter commencing antimicrobial therapy, although theinfection within the globe progressed relentlessly. Thismay have been the result of suboptimal drug selection,and/or poor penetration of antimicrobials into the eye.
Treatment of melioidosis in human patients is pro-tracted, expensive and not always successful. Thereare very few reports of successfully managed veteri-nary patients.5 Acute severe melioidosis is particu-larly difficult to treat.21 B pseudomallei is generallyresistant in vitro to penicillin, amino-penicillins, firstand second-generation cephalosporins, most amino-glycosides including gentamicin, most macrolides,quinolones and rifampicin.21 Generally, it is suscepti-ble in vitro to some third generation cephalosporins,carbapenems, chloramphenicol, tetracyclines, trimeth-oprim/sulphonamide (TMP-SMX), amoxicillin clavu-lanate and ticarcillin clavulanate.21
Based on recent trials, the current recommendationfor initial therapy of acute melioidosis in humans isan intensive therapy phase with intravenous ceftazi-dime or a carbapenem (imipenem or meropenem),with or without TMP-SMX, given for at least 10days or until definite signs of a response.3,21 Bacterio-static antibiotics, including tetracyclines and chlor-amphenicol are inferior in acute cases. Intravenoustherapy is followed by an eradication regimen oforally administered TMP-SXT with or without doxy-cycline, given usually for 8e12 weeks to prevent re-lapse. Finally, granulocyte colony stimulating factortherapy may be helpful in the setting of melioidosisseptic shock.3
Such a regimen would be problematic in the cat be-cause of the need for prolonged and costly intrave-nous therapy (imipenem, ceftazidime) or toxicityissues (chloramphenicol, TMP-SMX). As amoxicillin/clavulanic acid has been shown to be an alternativetherapy for eradication treatment,22 it is possible thatit (or ticarcillin/clavulanate in countries where intra-venous formulations of amoxicillin/clavulanate arenot available, such as Australia) may be adequate infeline patients, possibly in combination with doxycy-cline, and at high doses. In critically ill cats, thismay be preceded by a short course of intravenous imi-penem. Although prolonged oral eradication therapyshould minimise the risk of relapse, it is recommen-ded that all human patients receive lifelong monitor-ing.21 This would seem appropriate for cats.
A further problem in cases such as the two pre-sented here is the need to achieve high concentrationsof antibiotics in the eye. Although techniques such asintravitreal administration can be used in humans,this is unlikely to be applicable in a cat. If a diagnosis(or strong suspicion) of unilateral ocular melioidosiscould be made quickly (presumably by vitreocentesis,cytology and culture), it may be more prudent toremove the affected eye immediately and use
antimicrobials to eliminate residual infection in theretrobulbar tissues and at any potential unidentifiedprimary site of infection. In a veterinary setting,prompt enucleation prior to extension of infection tocontiguous tissues including the optic nerves andbrain offers the most definitive and cost-effectivechance of eliminating infection.
The cases outlined above suggest that the occur-rence of an acute red eye in a cat from an endemic re-gion should prompt a high index of suspicion formelioidosis, especially in the absence of a known pre-cipitating cause such as trauma, or where laboratoryfindings are not suggestive of known causes of uveitissuch as feline infectious peritonitis or toxoplasmosis.In such cases it may be appropriate to expeditiouslyobtain specimens such as blood cultures and aspiratesfrom the anterior or posterior chamber for cytologyand microbial culture.
Melioidosis is traditionally diagnosed by isolatingB pseudomallei from blood or lesions and this remainsthe diagnostic technique of choice.23 Although use ofselective media such as Ashdown’s agar may facili-tate diagnosis in samples from non-sterile sites suchas skin lesions and sputum, this is not essential andthe organism can be cultured on regular media. Forexperienced laboratory staff in melioidosis-endemiclocations, B pseudomallei is easy to identify, but thismay not be the case for those less familiar with theorganism.23 Under these circumstances, laboratorypersonnel may mistakenly identify isolates as a Pseu-domonas species. Careful examination of Gram-stained smears of purulent exudate from lesions cansometimes identify small numbers of bipolar‘safety-pin’ shaped, Gram-negative rods.1 The maindrawback of culture is that it may take as long as3e4 days to obtain definitive results; this may betoo slow for many patients, especially those withacute disease or when treating an organ such as theeye where restoration of function is critically depen-dent on timely therapy.23
Immunological assays for detecting Burkholderiaspecies antigen or antibodies have been developed.Such assays can provide a positive diagnosis muchfaster than culture. A number of readily performedantibody tests are available and used for screeningpurposes in both human and veterinary patients inendemic areas.10,23 They may have well have provenuseful in the cats of the present report. The main dis-advantage of antibody testing in highly melioidosis-endemic regions such as northern Australia andnortheast Thailand is that positive titres may reflectpast exposure rather than active disease, althougha single titre of �640 is highly suggestive of current in-fection in humans1 and may, therefore, be of value incats also. Antigen detection is potentially superior be-cause it indicates current infection, but to date suchtesting has mainly been used for confirmation of colo-nial identity on culture plates and not for direct test-ing on clinical samples such as blood or tissue.23
Polymerase chain reaction (PCR) tests that detect

862 HM Parkes et al
nucleic acid directly from clinical samples have beendeveloped and found to have varying sensitivityand specificity, with none as yet available commer-cially.24,25 Currently, culture of B pseudomallei froma clinical sample remains the gold standard for diag-nosis of melioidosis.
Both of the cats in this report spent time in endemicareas (Townsville, Queensland and Nhulunbuy,Northern Territory). However, the MLST data werestrongly supportive of both cats being infected inNhulunbuy by an endemic strain. Indeed, no ST hasbeen found to be common amongst isolates from theNorthern Territory and Queensland.26 It was of greatinterest that both isolates from the two cases of ocularmelioidosis of this report were of the same MLSTtype, namely ST 116. This MLST type had only beenisolated previously from two human patients fromNhulunbuy, ie, the same remote area. The two humancases were separated by 5 years in time. We were un-able to find any epidemiological associations betweenthe feline and human cases. It therefore seems likelythat ST 116 is present as a dominant ST in the Nhulun-buy environment and it is yet to be isolated from othersites.
It is now believed that inoculation is the major routeby which infections are acquired in human patients. Ina series of patients from Darwin, a quarter of patientsgave a history of a penetrating injury, and in suchpatients an incubation period of 1e21 days has beendefined.27 More chronic presentations are not uncom-mon, however, and incubation periods as long as 29years have been documented in human ex-servicepersonnel.3 The exact time course of the infections inthe cats reported above and the routes of entry ofthe bacteria cannot be determined with certainty. Weconsidered the pathogenesis in these cats may havehad two pathomechanisms: (i) traumatic introductionof organisms into the globe, eg, through a small pen-etrating injury through the sclera, possibly followinga cat-scratch injury, or following migration ofa grass-awn foreign body,28 (ii) haematogenousspread of infection from the primary site of inocula-tion to the tortuous vascular anatomy of the uvealtract, with subsequent extension of the infective pro-cess to structures within the globe and eventually toperiocular tissues. A primary site of infection fromwhence the infection disseminated, possibly the respi-ratory or gastrointestinal tract, was clinically inappar-ent in both cases, including case 2 in which a postmortem examination was undertaken. Both cats hadaccess to outdoors, but there was no recent historyor evidence of fights with other cats, and no signs oftrauma to the oculonasal region. Indeed, the infectionsmay have represented recrudescence of an infectiveprocess that had occurred sometime previously.3
In susceptible hosts, for example human patientswith predisposing conditions such as diabetes andrenal disease,3,29 B pseudomallei infections may dissem-inate widely, resulting in abscess formation in a varietyof organs.6 The presence of largely localised disease in
the two cats of this report, despite a protracted clinicalcourse, suggests both patients were likely to beimmune-competent.
Nosocomial transmission has been suspected insome scenarios. We further analysed by MLST a se-ries of feline cases thought attributable to infectionfrom a multi-dose vial of Saffan, although the clini-cal notes for these cats were irretrievable.14 Thesefour cases occurred in 1992: cats developed lesionsapproximately 7e10 days following intravenous ad-ministration of Saffan for a variety of routine proce-dures, and all had had surgery within about 48 h ofeach other. As the multi-dose vial had been dis-carded by the time the diagnoses were made, onlycircumstantial evidence implicated the vial as thesource of bacteria, which in all instances wereshown to be of the same MLST type (ST 616;Table 1). Affected patients developed large, ulcerat-ing lesions which eventually sloughed. Some weresituated on the cranial antebrachium (where thedrug had been injected into the cephalic vein), whileother lesions were in disparate regions including thetail in one case. The cats were apparently cured us-ing topical and systemic therapy, the details ofwhich were not obtainable. Subsequent studies dem-onstrated that B pseudomallei could survive in theintravenous anaesthetic agent under suspicion (al-phaxalone 9 mg/ml and alphadalone 3 mg/ml;Saffan, Schering-Plough Animal Health) and alsoan antiseptic/cleaning agent used for surgical sitepreparation (cetrimide 3% and chorhexidine 0.3%;Savlon, Novartis).5
Zoonotic transmission is thought to be extremelyuncommon, although there have been reports of pre-sumptive animal-to-human transmission in a meatworker, a veterinarian and a goat farmer, all ofwhom developed cutaneous lesions5 and one reportof transmission from a sheep.30 Recurrence of infec-tion in the second cat of this report on the same sideof the face as the surgical incision was likely attribut-able to amoxicillin/clavulanate therapy being insuffi-ciently effective at eliminating residual foci ofinfection in the retrobulbar tissues, with infection tak-ing the path of least resistance through fascial planes,giving rise to a subcutaneous abscess. We advised thatthe cat represented a potential source of infection tothe owner, who was pregnant.
AcknowledgementsMark Mayo, Bart Currie and the Menzies B pseudo-mallei collection are supported by a project grantfrom the Australian National Health and MedicalResearch Council. BG Spratt, SD Godoy and the Bpseudomallei MLST website, are supported by theWellcome Trust. We thank Linda Ward for databasesupport and analysis. Richard Malik is supportedby the Valentine Charlton Bequest of the Centrefor Veterinary Education of the University ofSydney.

863Primary ocular melioidosis due to a single genotype of Burkholderia pseudomallei
References1. Leelarasamee A, Bovornkitti S. Melioidosis: review and
update. Review Infect Dis 1989; 11: 413e25.2. White NJ. Melioidosis. Lancet 2003; 361: 1715e22.3. Cheng AC, Currie BJ. Melioidosis: epidemiology, patho-
physiology and management. Clin Microbiol Rev 2005; 18:383e416.
4. Brett PJ, Woods DE. Pathogenesis of and immunity tomelioidosis. Acta Tropica 2000; 74: 201e10.
5. Low Choy J, Mayo M, Janmaat A, Currie BJ. Animalmelioidosis in Australia. Acta Tropica 2000; 74: 153e8.
6. O’Brien CR, Greene CE. Melioidosis. In: Greene CE, ed.Infectious Diseases of the Dog and Cat. 3rd edn. Phila-delphia: WB Saunders, 2006: 436.
7. Ashdown LR, Guard RW. The prevalence of human me-lioidosis in northern Queensland. Am J Trop Med Hygiene1984; 33: 474e8.
8. Currie BJ, Fisher DA, Howard DM, et al. The epidemiol-ogy of melioidosis in Australia and Papua New Guinea.Acta Tropica 2000; 74: 121e7.
9. Thomas AD, Forbes-Faulkner JC, Norton JH, TruemanKF. Clinical and pathological observations on goats ex-perimentally infected with Pseudomonas pseudomallei.Austral Vet J 1988; 65: 43e6.
10. Thomas AD, Spinks GA, D’arcy TL, Norton JH, TruemanKF. Evaluation of four serological tests for the diagnosisof caprine melioidosis. Austral Vet J 1988; 65: 261e4.
11. Hicks CL, Kinoshita R, Ladds PW. Pathology of melioidosisin captive marine mammals. Austral Vet J 2000; 78: 193e5.
12. Toh I, Heng HG, Zamri-Saad M, Mutalib AR. Melioido-sis in a kitten. J Vet Malaysia 1998; 10: 73e6.
13. O’Brien CR, Krockenberger MB, Martin P, Parkes H,Kidd M, Malik R. Disseminated melioidosis in twocats. J Feline Med Surg 2003; 5: 83e9.
14. Haase A, Smith Vaughan H, Melder A, et al. Subdivisionof Burkholderia pseudomallei ribotypes into multiple typesby random amplified polymorphic DNA analysis pro-vides new insights into epidemiology. J Clin Microbiol1995; 33: 1687e90.
15. Godoy D, Randle G, Simpson AJ, et al. Multilocus se-quence typing and evolutionary relationships amongthe causative agents of melioidosis and glanders, Bur-kholderia pseudomallei and Burkholderia mallei. J Clin Micro-biol 2003; 41: 2068e79.
16. Cheng AC, Ward L, Godoy D, et al. Genetic Diversityof Burkholderia pseudomallei isolates in Australia. J ClinMicrobiol 2008; 46: 249e54.
18. Yang IH, Lee JJ, Liu JW, Teng MC. Melioidosis withendophthalmitis. Arch Ophthal 2007; 124: 1501e2.
19. Siripanthong S, Teerapantuwat S, Prugsanusak W, et al.Corneal ulcer caused by Pseudomonas pseudomallei: reportof three cases. Rev Infect Dis 1991; 13: 335e7.
20. Wong PK, Ng PH. Melioidosis presenting with orbitalcellulitis. Singapore Med J 1996; 37: 220e1.
21. Chaowagul W. Recent advances in the treatment ofsevere melioidosis. Acta Tropica 2000; 74: 133e7.
22. Rajchanuvong A, Chaowagul W, Suputtamonkol Y,Smith MD, Dance DAB, White NJ. A prospectivecomparison of co-amoxiclav and the combinationof chloramphenicol, doxycycline and co-trimoxazolefor the oral maintenance treatment of melioidosis.Transcripts Royal Soc Trop Med Hygiene 1995; 89:546e9.
23. Sirisinha S, Anuntagool N, Dharakul T, et al. Recentdevelopments in laboratory diagnosis of melioidosis.Acta Tropica 2000; 74: 235e45.
24. Haase A, Brennan M, Barrett S, et al. Evaluation of PCRfor diagnosis of melioidosis. J Clin Microbiol 1998; 36:1039e41.
25. Meumann EM, Novak RT, Gal D, et al. Clinical evalua-tion of a type III secretion system real-time PCR assayfor diagnosing melioidosis. J Clin Microbiol 2006; 44:3028e30.
26. Cheng AC, Godoy D, Mayo M, Gal D, Spratt BG, CurrieBJ. Isolates of Burkholderia pseudomallei from NorthernAustralia are distinct by multilocus sequence typing,but strain types do not correlate with clinical presenta-tion. J Clin Microbiol 2004; 42: 5477e83.
27. Currie BJ, Fisher DA, Anstey NM, Jacups SP. Melioido-sis: acute and chronic disease, relapse and re-activa-tion. Transact Royal Soc Trop Med Hygiene 2000; 94:301e4.
28. Malik R, Vogelnest L, O’Brien CR, et al. Infectionsand some other conditions affecting the skin andsubcutis of the naso-ocular region of cats e clinicalexperience 1987e2003. J Feline Med Surg 2004; 6:383e90.
29. Woods DE, DeShazer D, Moore RA, et al. Current stud-ies on the pathogenesis of melioidosis. Microbes Infect1999; 2: 157e62.
30. Idris A, Rachmat RFN, Ali SMM. Melioidosis: a case ofsheep to human transmission. J Vet Malaysia 1998; 10:77e9.
31. Brady CA, Otto CM, Van Winkle TJ, King LG. Severesepsis in cats: 29 cases (1986e1998). J Am Vet Med Assoc2000; 217: 531e5.
32. Weisse DJ, Krehbiel JD, Lund JE. Studies of the path-ogenesis of anaemia of inflammation: mechanisms ofimpaired erythropoiesis. Am J Vet Res 1983; 44:1832e5.
33. Weisse DJ, McClay CB. Studies on the pathogenesis ofthe erythrocyte destruction associated with the anae-mia of inflammatory disease. Vet Clin Pathol 1988; 17:90e3.
Available online at www.sciencedirect.com
Copyright © 2022 FDOKUMEN