
Treating Patients with Melioidosis
38
Treating Patients with Melioidosis Bart Currie Infectious Diseases Department, Royal Darwin Hospital Tropical and Emerging Infectious Diseases Division, MSHR Northern Territory Medical Program, Flinders University
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Treating Patients with Melioidosis

Treating Patients with Melioidosis
Bart Currie
Infectious Diseases Department, Royal Darwin Hospital
Tropical and Emerging Infectious Diseases Division, MSHR
Northern Territory Medical Program, Flinders University

Melioidosis
• Infection with Burkholderia pseudomallei
• Environmental bacterium – in soil and surface water in endemic areas
• Disease in infected humans and animals
• Strong association with rainfall and environmental damage

Burkholderia pseudomallei
Tier 1 Biothreat Select Agent USA CDC – high mortality – antibiotic resistant – no vaccine – aerosol transmission – potential for bioweoponisation

“The unknown infection in Rangoon”
..an infective disease somewhat resembling glanders..
..prevalent among the ill-nourished
neglected wastrels of the town.
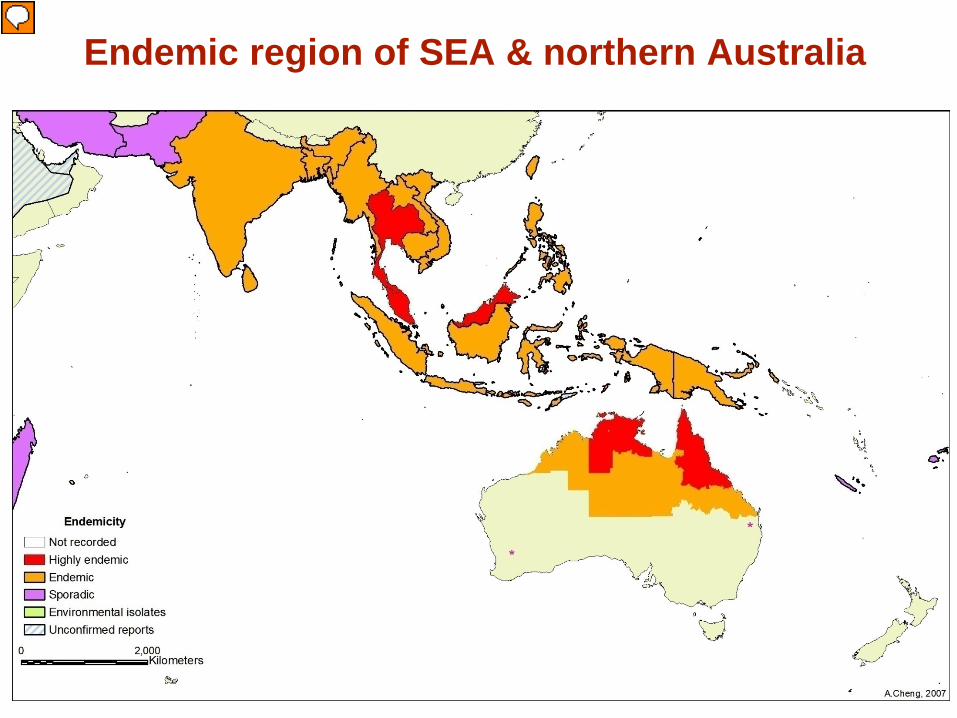
Endemic region of SEA & northern Australia
Presenter
Presentation Notes
Not recognised in Thailand until 1955

Melioidosis in Australia
1950 First Australian human case 32yo diabetic in Townsville Fatal septicemic melioidosis
Rimington Med J Aust 1962
1960 First case in the Northern Territory
Crotty Med J Aust 1962
1949 Outbreak in sheep
Winton Queensland (22.5oS) Cottew Aust J Exp Biol Med Sci 1950
Presenter
Presentation Notes
Not recognised in Thailand until 1955

The Darwin Prospective Melioidosis Study
Darwin
819 cases over 23.5 years 109 deaths (13%)
Melioidosis Clinical Presentations
• 85% acute illness, recent infection
– Incubation Period 1-21 days (median 9 days)
• 11% chronic illness, recent infection – Sick for > 2 months
• 4% reactivation from latent focus: up to 62 yrs

Melioidosis Clinical Presentations
• 55% blood culture +ve
• 22% present with septic shock
– 75% of these pneumonia is primary site – mortality 50-90% if septic shock

Chronic melioidosis Sick > 2 months
11% of cases Mis-diagnosed as TB

Skin 13%
Presenter
Presentation Notes
58 with primary 10 secondary of 486 total cases = 12% primary cutaneous

What determines clinical nature and severity?
• Infecting dose
• Host risk factors
• B. pseudomallei strain virulence factors
• Mode of infection percutaneous vs inhalation vs ingestion

What determines clinical nature and severity?
• Infecting dose
• Host risk factors
• B. pseudomallei strain virulence factors
• Mode of infection percutaneous vs inhalation vs ingestion

What determines clinical nature and severity?
107/109 fatal cases in the Darwin study had at least one risk factor
esp. diabetes, hazardous alcohol use, chronic lung disease
the other two were elderly (aged 75yo and 82yo)
Independent predictors of mortality by multivariable analysis
Presence of ≥ 1 risk factor OR 9.4 (2.3-39.0) Age ≥ 50 y OR 2.0 (1.2-3.3)
PLoS NTD 2010;4:e900
What determines clinical nature and severity?
• Infecting dose
• Host risk factors
• B. pseudomallei strain virulence factors
• Mode of infection percutaneous vs inhalation vs ingestion

What % of cases overall are from inhalation?
Is it 10%??
Is it 50%??

B. pseudomallei: a dynamic pathogen
• 2 chromosomes and an “open” genome – 86% “core” and 14% “accessory” genome
• >15Mbp of accessory genome characterised to date
• Genomic heterogeneity from extensive horizontal gene
transfer of multiple genomic islands (GIs) occurring in the environment
• Also core genome recombination >> mutation
In-silico pan-genome from 11 Bps genomes Illumina reads aligned to K96243 type strain
Presenter
Presentation Notes
Open genome = substantial genomic variation between strains Accessory – ie variably present across diffferent strains – one of the largest of any known bacterium 16 GIs in type strain K69243 from Thailand. Now over 150 GIs characterised Core genes also recombine, with importation of environmental DNA from both conspecifics and other species22. We have estimated that 25 times more Multilocus Sequence Typing (MLST) allelic diversity is generated by recombination than by mutation9, the highest ratio documented in a bacterium to date. On MLST recombination 25 x mutation – conspecifics and other environ species In silico pan-genome reference from 11 Bps genomes, which spans >10Mbp (x-axis), including 128 GIs. Illumina reads are aligned to the pan-genome reference and show high coverage for the core genome and differential coverage of the accessory genome. 128GIs, >60,000 SNPs

B. pseudomallei: a dynamic pathogen
• Complex intrinsic antimicrobial resistance
BUT • Little diversity in susceptibility patterns of primary isolates
AND
• Acquired resistance is rare although well characterised
AND • No evidence of plasmid or transposon mediated acquired
resistance: acquired resistance is conferred by mutations and/or gene loss
Presenter
Presentation Notes
Bps plasmids described by Russians but only 1-3 found to date in over ?1000 genomes looked at – 1 from PNG and ?from B. multivorans - ?virulence related T6SS?? NOT AMR. 2 other strains have plamid sequences but unsure if true plasmids. So this is despite all the plasmids and AMR in near neighbour Burks eg cepacia complex - ?due to lack of porin channels in OMP??cant cross cell membrane

Intrinsic antimicrobial resistance in Bps
• Efflux pumps – aminoglycoside & macrolide resistance (AmrAB-OprB) – trimethoprim resistance (BpeEF-OprC)
• Outer membrane permeability
– polymyxins
• Enzymatic break-down – various β-lactamases: resistance to many β–lactams
eg; penicillin, amoxicillin, cephalexin; reversed by clavulanate
Presenter
Presentation Notes
Deletion of this efflux pump causes sensitivity in B. mallei and very few strains of b. pseudomallei in the Trunk study. In the phylogentically restricted Malaysian clade, aminoglycoside sensitivity is cuase by a non-synonomous SNP. While many resistant to trimethoprim, still sensit to sulfa and TMP/SMX Ambler class A,B,D β-lactamases. Most important of these is the Bush-Jacoby Class 2e β-lactamase which hydrolyses most cephalosporins but is inhibited by clavulanate. Encoded on bla-A gene.

Summary of Current Melioidosis Treatment
ceftazidime or meropenem or imipenem +/- cotrimoxazole (TMP-SMX) (oral or IV)
– for at least 10 (Thailand) or 14 (Australia) days
cotrimoxazole (TMP-SMX) OR co-amoxyclav (Augmentin)
– for 12-20 weeks (Thai) or at least 3 months (Aust)
Initial IV Intensive Therapy
Subsequent Oral Eradication Therapy
Lipsitz et al. EID 2012;18 (12):e2 Wiersinga et al. NEJM 2012;367:1035
Presenter
Presentation Notes
White ceftaz study was Sept 86-July 88. Duration: IV at least 7d 86-93 then 10d minimum from 1994. Oral 86-89 4 drugs at least 6w then June 89 12-20 weeks

Acquired antimicrobial resistance in Bps 1. Ceftazidime
Mostly conferred by Ambler class A β-lactamase (penA) • Mutations lead to amino acid changes near active sites
resulting in increased ceftazidime hydrolysis – C69Y Sam et al., 2009 – P167S Tribuddharat et al., 2003 – S72F (also AMX-CLAV resistance)
• Upregulation of penA via SNP in promoter region Sarovich et al., 2012
Other mechanisms
• Target deletion – large scale genomic loss - (PBP3) Chantratita et al., 2011
Presenter
Presentation Notes
amino acid changes that alter substrate specificity in the highly conserved class A b-lactamase, PenA. SNPs that directly increased CAZ hydrolysis. Promoter SNP also seen in 1/2000 environ strains. P167F not seen in Australian ones yet. Large-scale genomic loss - 49 genes including penicillin binding protein 3 (BPSS1219)

Acquired antimicrobial resistance in Bps 2. Other antimicrobials
• No carbapenem resistance described to date
• Efflux pump over-expression?
– may account for doxycycline resistance
• TMP-SMX mechanism unclear but can be high level R
200kb duplication in a high level TMP-SMX resistant Bps Illumina reads aligned to K96243 type strain
Presenter
Presentation Notes
Shows a 200kb duplication in a TMP-SMX resistant strain (>32ug/mL), the only one we have ever seen – various mutations in this region also. We haven't been able to figure out the exact mechanism yet but we are looking at the WGS data. The reads have been mapped against a reference genome (K9) and you can see the increased coverage in the top genome cf. the bottom one.

Susceptibility profiles in 233 consecutive primary infection Bps: 2009-2012
Ceftazidime
Nicole McMahon, Amy Crowe, Rob Baird RDH
Presenter
Presentation Notes
Deletion of this efflux pump causes sensitivity in B. mallei and very few strains of b. pseudomallei in the Trunk study. In the phylogentically restricted Malaysian clade, aminoglycoside sensitivity is cuase by a non-synonomous SNP. While many resistant to trimethoprim, still sensit to sulfa and TMP/SMX Ambler class A,B,D β-lactamases. Most important of these is the Bush-Jacoby Class 2e β-lactamase which hydrolyses most cephalosporins but is inhibited by clavulanate. Encoded on bla-A gene.

Susceptibility profiles in 233 consecutive primary infection Bps: 2009-2012
Meropenem
Nicole McMahon, Amy Crowe, Rob Baird RDH
Presenter
Presentation Notes
Deletion of this efflux pump causes sensitivity in B. mallei and very few strains of b. pseudomallei in the Trunk study. In the phylogentically restricted Malaysian clade, aminoglycoside sensitivity is cuase by a non-synonomous SNP. While many resistant to trimethoprim, still sensit to sulfa and TMP/SMX Ambler class A,B,D β-lactamases. Most important of these is the Bush-Jacoby Class 2e β-lactamase which hydrolyses most cephalosporins but is inhibited by clavulanate. Encoded on bla-A gene.

Susceptibility profiles in 233 consecutive primary infection Bps: 2009-2012
Trimethoprim/sulfamethoxazole
Nicole McMahon, Amy Crowe, Rob Baird RDH
Presenter
Presentation Notes
Only 2/233 had MICs of 4 = low level resistance
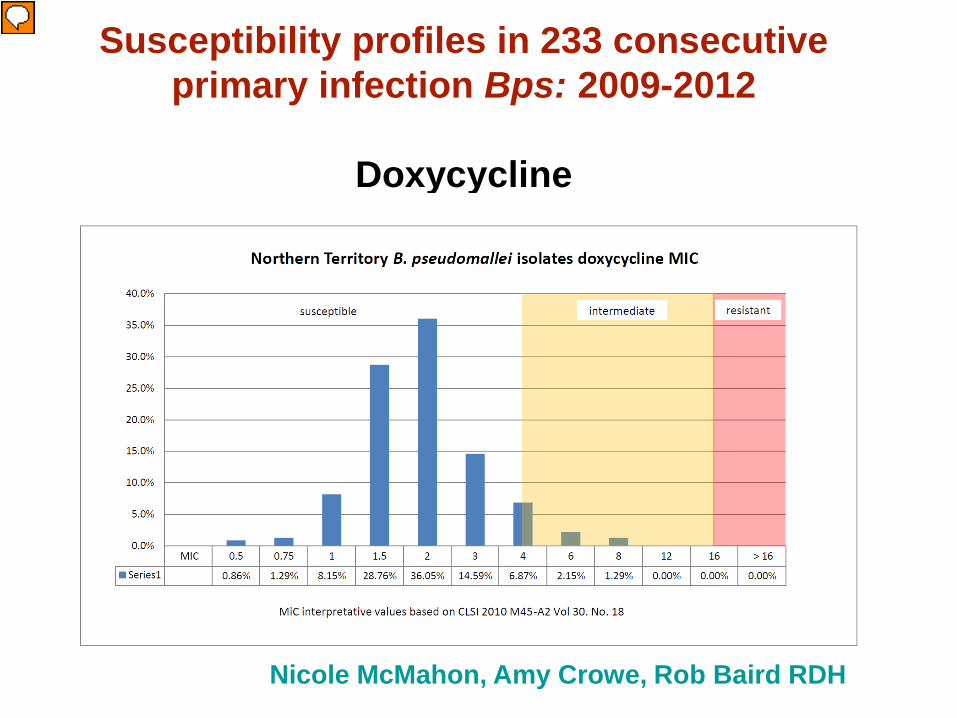
Susceptibility profiles in 233 consecutive primary infection Bps: 2009-2012
Doxycycline
Nicole McMahon, Amy Crowe, Rob Baird RDH
Presenter
Presentation Notes
Deletion of this efflux pump causes sensitivity in B. mallei and very few strains of b. pseudomallei in the Trunk study. In the phylogentically restricted Malaysian clade, aminoglycoside sensitivity is cuase by a non-synonomous SNP. While many resistant to trimethoprim, still sensit to sulfa and TMP/SMX Ambler class A,B,D β-lactamases. Most important of these is the Bush-Jacoby Class 2e β-lactamase which hydrolyses most cephalosporins but is inhibited by clavulanate. Encoded on bla-A gene.

Susceptibility profiles in 11 relapsed Bps
Doxycycline
Nicole McMahon, Amy Crowe, Rob Baird RDH See also Jenney et al. IJAA 2001;17:109
Doxycycline MIC's: Initial and recurrent B.pseudomallei isolates
0
5
10
15
20
25
30
35
40
0.5 0.75 1 1.5 2 3 4 6 8 12 16 >16
MIC μg/ml
Perc
enta
ge o
f iso
late
s
Initial isolates
Recurrent isolates
Susceptible Intermediate Resistant
Presenter
Presentation Notes
Deletion of this efflux pump causes sensitivity in B. mallei and very few strains of b. pseudomallei in the Trunk study. In the phylogentically restricted Malaysian clade, aminoglycoside sensitivity is cuase by a non-synonomous SNP. While many resistant to trimethoprim, still sensit to sulfa and TMP/SMX Ambler class A,B,D β-lactamases. Most important of these is the Bush-Jacoby Class 2e β-lactamase which hydrolyses most cephalosporins but is inhibited by clavulanate. Encoded on bla-A gene.

Summary of Current Melioidosis Treatment
ceftazidime or meropenem or imipenem +/- cotrimoxazole (TMP-SMX) (oral or IV)
– for at least 10 (Thailand) or 14 (Australia) days
cotrimoxazole (TMP-SMX) OR co-amoxyclav (Augmentin)
– for 12-20 weeks (Thai) or at least 3 months (Aust)
Initial IV Intensive Therapy
Subsequent Oral Eradication Therapy
Lipsitz et al. EID 2012;18 (12):e2 Wiersinga et al. NEJM 2012;367:1035
Presenter
Presentation Notes
White ceftaz study was Sept 86-July 88. Duration: IV at least 7d 86-93 then 10d minimum from 1994. Oral 86-89 4 drugs at least 6w then June 89 12-20 weeks

RCT ceftaz vs chloro/doxy/cotrimoxazole 161 patients
Mortality 37% vs 74% (p = 0.009)
Presenter
Presentation Notes
120 mg/kg/d in 3 doses minimum 7d. TMP-SMX 10-50mg/kg/d doxy 4mg/kg/d

Some Unanswered Therapeutic Questions
• Is IV intensive Tx with ceftazidime or meropenem really required in localised disease such as skin ulcers?
• Is eradication therapy always necessary – eg after 2 weeks IV intensive Tx for mild pneumonia or for bacteremia with no focus?
• Will longer IV intensive Tx alone be adequate for uncomplicated pneumonia – eg 4 weeks ceftazidime via PICC in HITH?
• Will TMP-SMX alone for eradication phase hold up?
• Role of co-amoxyclav vs TMP-SMX in eradication phase: children and pregnancy?
Initial "Intensive" Therapy
Ceftazidime dosing issues
Ceftazidime has no post-antibiotic effect
Walsh et al. AAC 1995;39:2356
• Area under drug level curve important
• Maintain drug level above MIC
• Aim for higher tissue levels - ? more frequent dosing - ? bigger total daily dose - ? longer duration of “intensive” therapy

Continuous infusion elastomeric infusers
via PICC line (Baxter, Sydney)
Hospital in the Home program 6g adult dose over 24 hours
Cost Aus$160/day Huffam et al.
Trop Med Int Health 2004;9:715

Initial "Intensive" Therapy
Carbapenems versus Ceftazidime ??
Carbapenems (imipenem, meropenem)
• RCT Thailand – imipenem at least as effective as ceftazidime - same mortality - fewer treatment failures Simpson et al. CID 1999;29:381
• Meropenem safer at high dose; seizures with imipenem
• Meropenem outcomes at least as good as ceftazidime
- 63 patients with severe melioidosis; mortality 19% Cheng et al. AAC 2004;48:1763
Presenter
Presentation Notes
Note lowish dose of imipenem? imipenem/cilastatin sodium (Tienam; MSD Asia, Hong Kong),at a dosage of 50 mg/kg/d) (usual adult dose, 1 g of imipenem three times daily by infusion), or iv ceftazidime (Fortum;Glaxo U.K., Greenford, U.K.), at a dosage of 120 mg/kg/d) (usual adult dose, 2 g three times daily by bolus injection).

Initial "Intensive" Therapy
Duration
Minimum 10d (Thailand) – 14d (Australia)
Australian Guidelines - 4 weeks or longer if: - septic shock - extensive lung disease - deep seated collections or organ abscesses - osteomyelitis and septic arthritis - neurological melioidosis Therapeutic Guidelines: Antibiotic 14th Ed 2010
Recurrent Melioidosis: Darwin, Australia
1989-2009: 30/465 (6.5%) survivors had recurrent melioidosis after completion of Tx
– 25 (5.4%) relapse & 5 (1.1%) new infection PLoS NTD 2010;4(11):e900
Oct 2009 - Aug 2013: 286 cases, 32 (11%) fatal Only 1/254 (0.4%) survivors has had relapsed
melioidosis after completion of Tx Despite often poor adherence to oral eradication Tx Is it the prolongation of IV therapy now occurring?
Presenter
Presentation Notes
Thai studies defined time as from when discharged once stable – ie still on oral Tx….

Presenter
Presentation Notes
A novel broad range monosulfactam antibiotic It was previously noted that the unique pattern of penicillin binding protein inhibition and bactericidal mode of action of BAL30072 confer potent in vitro activity against Gram-negativebacteria [5]. BAL30072 is a novel sulfactam antibiotic with potent antimicrobial activity against a broad range of Gram-negative bacteria, including clinically increasingly problematic multidrug-resistant pathogens such as Pseudomonas aeruginosa, Acinetobacter spp., Klebsiella spp. and Enterobacter spp. BAL30072 is stable towards many types of beta-lactamases that can deactivate most of the currently marketed beta-lactam antibiotics such as cephalosporins and carbapenems. The compound is taken up very readily into bacteria, exploiting essential nutrient uptake systems and is able to circumvent resistance caused by changes in the outer membrane of Gram-negative bacteria. The compound has shown to be highly compatible with agents used for treating Gram-positive infections and even works synergistically with some agents used for treating Gram-negative infections, such as carbapenems and aminoglycosides. hospital-acquired pneumonia (including ventilator-associated pneumonia), complicated intra-abdominal infections or complicated urinary tract infections.

Conclusions
• Lowering the bar for prolonging IV “intensive” therapy may account for the decreasing relapse rates in the Darwin Prospective Melioidosis Study
• Over half of patients now get at least 4 weeks of IV therapy (meropenem in ICU, ceftazidime in wards and then via elastomeric infuser in HITH)
• What about the role of the 3m+ oral “eradication” therapy? When is it not needed?
• Needs formal study: the next melioidosis RCT?

Acknowledgements RDH ID Registrars & Physicians
RDH Microbiology Lab Scientists
RDH ICU, ED, Ward and HITH Doctors & Nurses
NT CDC Staff
International Collaborators
Menzies Melioidosis Team
Funding: NHMRC, ARC, NIH, Aust PM+C & US DHS & DOD




















