
Primary Healthcare Models: Evidence for a Sustainable Approach in Canada
61
Primary Healthcare Models Evidence for a Sustainable Approach in Canada Elizabeth A. Sajdak, Juergen Krause January 2014
Transcript of Primary Healthcare Models: Evidence for a Sustainable Approach in Canada

Primary Healthcare Models Evidence for a Sustainable Approach in Canada
Elizabeth A. Sajdak, Juergen Krause
January 2014
i
Abstract
Primary Healthcare Models: Evidence for a Sustainable Approach in Canada
By: Elizabeth A. Sajdak and Juergen Krause
Primary healthcare is a grave topic of conversation for all Canadians and is
particularly so for politicians given that in 2014 the health accord that sets the funding
and health service delivery agreement between the Federal and Provincial
Governments is due for renewal. This paper sets out to review the evidence for where
primary care should be positioned within the overall healthcare system, who should be
delivering services in primary healthcare and what needs to be achieved. The paper
discusses different models of care measured against what primary care should be
aiming to provide in an ideal state. Incentives and funding models are also considered
in this context and respective recommendations are outlined. Finally a primary
healthcare model that could potentially be applied to Canada is presented.
1
ABSTRACT .......................................................................................................................................................... I
LIST OF TABLES................................................................................................................................................ 2
LIST OF FIGURES ..................................................................................................................................................... 3
INTRODUCTION ................................................................................................................................................. 4
BACKGROUND ........................................................................................................................................................... 4
DEFINITIONS .............................................................................................................................................................. 6
RATIONALE FOR RESEARCH ..................................................................................................................................... 6
PURPOSE AND AIM OF RESEARCH............................................................................................................................ 7
RESEARCH STRATEGY ................................................................................................................................... 8
RESEARCH QUESTIONS AND ANALYTICAL FOCUS ................................................................................................... 8
LITERATURE REVIEW METHODOLOGY ...................................................................................................................... 9
Search Inclusion Terminology .......................................................................................................................... 9
Search Results ................................................................................................................................................. 10
STRENGTHS AND LIMITATIONS ................................................................................................................................ 11
PRIMARY HEALTHCARE ................................................................................................................................ 11
WHO SHOULD DELIVER PRIMARY HEALTHCARE?.................................................................................................. 13
PRIMARY HEALTHCARE GOALS .............................................................................................................................. 21
Managing Chronic Conditions ........................................................................................................................ 23
FUNDING AND INCENTIVES ...................................................................................................................................... 29
QUALITY .................................................................................................................................................................. 37
A POTENTIAL PRIMARY HEALTHCARE MODEL FOR CANADA’S FUTURE ........................................ 39
FUNDING MODEL ..................................................................................................................................................... 43
PRACTICE MANAGEMENT ........................................................................................................................................ 44
QUALITY MANAGEMENT .......................................................................................................................................... 44
THE INFORMATION SYSTEM .................................................................................................................................... 45
THE RECEPTION TEAM ............................................................................................................................................ 45
THE CLINICAL TEAM ................................................................................................................................................ 45
RECOMMENDATIONS ..................................................................................................................................... 47
CONCLUSION ................................................................................................................................................... 47
APPENDIX A: SUMMARY OF PROFESSIONAL MODELS REVIEWED ................................................... 54
APPENDIX B: PRIMARY CARE ACTIVITIES ................................................................................................ 55
APPENDIX C: FUNDING MODELS ................................................................................................................ 57
BIBLIOGRAPHY ..................................................................................................................................................... 58

2
List of Tables
Table 1: Breakdown of research sources by category ....................................................................... 10
Table 2: Characteristics of professional and practising managers (Gerst, 2011, p. 4) ................. 20
Table 3: Comparison of the Chronic Care Model and the Expanded Chronic Care Model (Barr,
et al., 2003, p. 79) .................................................................................................................................... 26
Table 4: Average and current GDP health expenditure comparisons (Pritchard & Wallace, 2011,
p. 4) ............................................................................................................................................................ 35
Table 5: Examples of the applications of the six characteristics of high performing primary
healthcare (Kates, et al., 2012, p. 12). .................................................................................................. 41

3
List of Figures
Figure 1: Total per capita health expenditures ($000’s), Canada, 2003-2013 (Canadian Institute
for Health Information, 2013) ...................................................................................................... 7
Figure 2: Primary care as a hub of coordination, adapted from “Primary Health Care Now More
Than Ever” (World Health Organisation, 2008, p. 55) ........................................................................ 12
Figure 3: Quality Improvement and Innovation Partnership Improvement Framework (Kates,
Hutchison, O'Brien, Fraser, Wheeler, & Chapman, 2012, p. 11) ...................................................... 40
Figure 4: Structural Domain (Hogg, Rowan, Russell, Geneau, & Muldoon, 2008, p. 311) .......... 42
Figure 5: Primary Care Practice Team Model ..................................................................................... 43

4
Introduction
Healthcare is an emotive subject for most people as at some point in their lives
they will have a need for healthcare services. Health related problems like long waiting
times in emergency rooms (ER), a lack of family physicians, nurses, specialists, no
available hospital beds, etc. are often documented in the press (Rachlis & Kushner,
1989; Simpson, 2012). Health systems have struggled to provide quality care while
managing their finances (Simpson, 2012). Recent developments suggests that strides
have been made in the United Kingdom (UK) to further develop preventative care and to
manage existing chronic conditions within primary care thus enabling people to stay out
of acute care services. This required services in primary care to be developed to
provide care closer to home but in a way that is cost effective and accountable to the
tax payer (Department of Health (UK), 2006).
Background
Healthcare in Canada evolved from the 1957 Hospital Insurance and Diagnostic
Services Act. This act offered provinces federal funding to establish a hospital insurance
program (Rachlis & Kushner, 1989). The act covered hospital services only and no
coverage was provided for care outside the hospital walls. At first the Federal
Government paid half of the resulting costs for each province; however this changed to
a block or lump sum through the Canada Health Act (1984). In 1966 the Hospital
Insurance and Diagnostic Services Act was passed into legislation federally and
became the National Medicare Insurance Act that covered the cost of some services
within a doctors’ office. The result of these Acts was that funding and provision of

5
services was concentrated within hospitals while the potential of primary prevention and
health promotion was neglected (Rachlis & Kushner, 1989; World Health Organisation,
2008). The focus on care within hospitals has led Canada to rank below other OECD
countries in terms of the quality of primary healthcare delivered (Dahrouge, et al., 2012).
In 1974 Marc Lalonde released his report ‘A new perspective on the Health of
Canadians’. This report contained a broader view on maintenance of health and on
causes of death and included the number of years lost for the principal causes of death
at the time. Marc Lalonde’s conclusion was that improving health requires improvement
in the environment to reduce accidents, as well as moderating self-imposed risks such
as smoking and obesity - in other words health promotion and disease prevention
(Lalonde, 1974). It is generally accepted that the improvement of people’s health is not
caused by health systems, but is the result of public health measures such as better
food, access to clean water and a healthier environment (Rachlis & Kushner, 1989;
World Health Organisation, 2008). However, a modern primary care system using
nurses and other health professionals as part of a collaborative team has been shown
to be effective in attaining significant improvements in preventative measures being
undertaken by patients (Hogg, Lemelin, Moroz, Soto, & Russell, 2008). The Lamarche
et al report (2003) suggested that there are six broad outcomes that primary healthcare
should strive for:
Effectiveness
Productivity
Accessibility
Continuity

6
Quality
Responsiveness
(Lamarche P. A., et al., 2003, p. 2)
Definitions
The term ‘primary healthcare’ means different things to different people. For the
present project the following definition of primary healthcare was adopted “a set of
universally accessible first-level services that promote health, prevent disease, and
provide diagnostic, curative, rehabilitative, supportive, and palliative services”
(Lamarche P. A., et al., 2003, p. 2). This definition takes originates from the 1978
Declaration of Alma Alta that stated that primary care “addresses the main health
problems in the community, providing promotive, preventive, curative and rehabilitative
services” (International Conference on Primary Health Care, 1978, p. 2).
Rationale for Research
It has been documented that Canada is lagging behind other developed
countries in the development of an adequate and fully functional primary healthcare
system (Canadian Institutes of Health Research, 2010).
The Canadian healthcare system faces significant challenges, both on the
federal level and provincially. These challenges consist of:
An increasing demand for services as an increasing number of Canadians are
facing chronic illness,
A shortage of healthcare professionals,

7
Growing costs for the provision of healthcare.
These challenges are faced by all jurisdictions in Canada and have nationally given rise
to concern in terms of access, coverage and quality of healthcare (Peckham, 2012).
Costs per capita have been growing nationally, though the forecast for 2012 and 2013
expects these costs to stabilize as can be seen in Figure 1 (Canadian Institute for
Health Information, 2013).
Figure 1: Total per capita health expenditures ($000’s), Canada, 2003-2013
Source: Canadian Institute for Health Information, National Health Expenditure Trends, 1975 to
2013 (Ottawa, Ont.: CIHI, 2013).
Note: 2012 and 2013 are forecast
Purpose and Aim of Research
The purpose and aim of the research presented in this contribution is to explore
different models of primary healthcare delivery described in literature to identify
3,000
3,100
3,200
3,300
3,400
3,500
3,600
3,700
3,800
3,900
4,000
4,100
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Total Health Expenditure in Constant 1997
Dollars per Capita
Year

8
successful models and their underlying approaches. Finally a conceptual model of care
is proposed based on the evidence collected.
Research strategy
Research Questions and Analytical Focus
The literature for this paper was reviewed analyzing the following dimensions:
System Perspective
Primary Healthcare Delivery
Chronic Care
Payment Models
Quality of Healthcare
Health Promotion
The research questions were developed keeping in mind the need to identify and
design a primary healthcare system that will meet the requirements of today’s patient
population. Many of the questions previously appeared in the media and have also been
asked by those working within the system. The research questions identified were
formulated to evaluate if a primary healthcare model could:
1. Assist in keeping individuals as healthy as possible
2. Be financially viable
3. Account for the increase in service required by the baby boomer generation while
remaining responsive to patient needs
4. Provide a high standard of care that is effective, efficient, accessible and
continuous

9
Literature Review Methodology
The research was qualitative in nature using a literature content analysis
approach. A systematic literature review was conducted to identify key published
material in English language that provided evidence on the present status of primary
healthcare delivery with a focus on Canadian, American and UK literature. Specific
areas of interest included:
Primary Healthcare Models
Health promotion and disease prevention
Collaborative healthcare
Financing of healthcare
Quality of healthcare
Chronic care service delivery
Peer reviewed papers and publications as well as books and published opinions
were identified by searching health related websites. One of the sources reviewed the
Cochrane database, which is part of the Cochrane Library, and constitutes an
international collection of systematic reviews of primary research of healthcare and
health policy. A limited number of relevant organizations such as the Canadian Health
Services Research Foundation were also searched.
Search Inclusion Terminology
Specific search parameters were developed for this review including time frame
and language of publication.

10
Inclusion Criteria:
Systematic reviews, meta-analyses and other high level evidence-based
synthesis studies
Canadian primary healthcare studies
Studies of primary healthcare in OECD countries
Canadian expert opinion articles and documents
Publication in English
Published within the last 23 years (1989-2012), with priority given to more recent
work
Exclusion Criteria
Acute Healthcare reviews
Non-English language publications
Articles and documents covering lower and middle income countries
Acute healthcare reviews were excluded as the focus of this paper is primary
healthcare, only English publications were researched to avoid translation errors and
articles covering high income countries were selected in order to be more comparable
with Canada.
Search Results
From the research conducted articles and documentation from the eighty-six
sources, including books, were retrieved and analyzed. Table 1 shows the breakdown
of the research by category.
Table 1: Breakdown of research sources by category
Chronic
Care
Payment
Models
Health
Promotion
Primary
Healthcare
Quality System
based
15 18 4 28 8 13

11
Strengths and Limitations
Adding to the relevance of this research contribution is its timeliness as the
Canadian healthcare system has come under scrutiny in recent years because of the
upcoming renewal of the federal transfers to the provinces in 2014. This prompted the
Canadian Health Service Research Foundation to commission a series of papers
ranging from healthcare efficiency, to primary care delivery and collaborative teams.
A potential limitation of this research is the focus on primary care. Primary care is
only one segment of the overall healthcare system and changes to one part will
inevitably have an impact in other areas of the system, such as acute care.
Furthermore, healthcare constitutes only one pillar of the complete approach in terms of
the promotion of health and prevention of illness.
Primary Healthcare
Primary healthcare has been described as the foundation of the overall
healthcare system (Barrett, Curran, Glynn, & Godwin, 2007; Cook & Kachala, 2004;
Kates, et al., 2012; Canadian Institutes of Health Research, 2010; Scott & Lagendyk,
2012; Sutherland & Leatherman, 2012). It provides the first point of contact for patients
(Barrett, Curran, Glynn, & Godwin, 2007; Canadian Institutes of Health Research, 2010)
as well as the first level of care (Glazier, 2007) and acts as the gateway to further
services (Cook & Kachala, 2004). The World Health organisation (WHO) states that
primary care providers should have the responsibility for a well-defined patient
population, such a defined segment is described as a population that a specific
healthcare provider is responsible for, which could either be defined geographically or

12
resemble the patients registered with a family physician. This would strengthen primary
healthcare professionals role as coordinators of care in order to provide effective
healthcare as described by Lamarche et al (2003). Figure 2 shows primary care as the
hub of the healthcare system (World Health Organisation, 2008).
Figure 2: Primary care as a hub of coordination, adapted from “Primary Health Care Now More Than Ever” (World Health Organisation, 2008, p. 55)
(Reproduced, with the permission of the publisher from the World Health Report: Primary Care Now More Than Ever)
This view point was also discussed at a Healthcare Forum on Healthcare Innovation
resulting in an agreement that delivery and innovation should move from centralised
centres of expertise to the periphery, i.e. different healthcare professionals in the wider
primary healthcare setting (Chin, Hamermesh, Huckman, McNeil, & Newhouse, 2012).
Given the importance of primary healthcare for the whole of the healthcare
system it is vital to ensure that it is designed to function as effectively as possible for

13
those that need to rely on it. Indeed, evidence suggests that a strong provision of
primary healthcare improves the population health as a whole (Glazier, 2007).
Hogg et al suggest that primary care should be broader in its conceptual
apporach and focus on education, community empowerment and population health
(Hogg, Rowan, Russell, Geneau, & Muldoon, 2008). Other researchers describe
population health as having an emphasis on health promotion, early intervention and
self-management functions (Health Systems Research and Consulting Unit, 2009;
Rush, 2010; Sutherland & Leatherman, 2012), which certainly appears to link population
health back into primary healthcare. The population health approach is also seen as a
way to establish priorities and strategies and to make investments that will improve
general health (Enhancing Interdiscipinary Collaboration In Primary Health Care, 2006;
Jacobson & HDR, 2012).
Stephen Peckham in his commentary in the journal “Healthcare Papers” raises
questions about the effectiveness of primary care such as:
Who should deliver care
What services should be provided
Which skills are required
How should health professionals be incentivised, and
How should they be held accountable (Peckham, 2012).
Who Should Deliver Primary Healthcare?
The current evidence suggests that an inter-professional integrated and
collaborative model performs the best in terms of health outcomes (Browne, Birch, &

14
Thabane, 2012; Canadian Institutes of Health Research, 2010). The team can include
doctors, nurses or other healthcare professionals (Barrett, Curran, Glynn, & Godwin,
2007; The College of Family Physicians, 2011) such as midwives and dieticians (Mable,
Marriott, & Mable, 2012) or pharmacists (Scott & Lagendyk, 2012). Inter-professional
models are collaborative in nature working towards common goals, sharing information
to support each other’s work within their scope of practice (Virani, 2012) and have been
described as “…patient-centered. It involves the continuous interaction of two or more
professionals or disciplines, organized into a common effort to solve or explore common
issues, with the best possible participation of the patient.” (Barrett, Curran, Glynn, &
Godwin, 2007, p. 1). There is increasing evidence that the experience of individuals
working within an inter-professional and collaborative model is more positive compared
to those working in a unilateral professional model and that an inter-professional
approach enhances providers’ skills as a direct positive result of the inter-professional
model (Barrett, Curran, Glynn, & Godwin, 2007). In the UK physicians are increasingly
encouraged by their Colleges to actively learn from other healthcare professionals
(Quam & Smith, 2005). Interestingly there is some evidence to suggest that patients
knowledge of their conditions increases when they are cared for by a team (Health
Council of Canada, 2009). Moreover, health professionals’ satisfaction levels are also
enhanced when working in multi-professional teams (Canadian Institutes of Health
Research, 2010; Enhancing Interdiscipinary Collaboration In Primary Health Care,
2006; Health Canada, 2012; Barrett, Curran, Glynn, & Godwin, 2007). In addition the
levels of increased satisfaction and positive experience were not only confined to
healthcare professionals but also extended to the patients they served (Barrett, Curran,

15
Glynn, & Godwin, 2007; Canadian Institutes of Health Research, 2010; Health Canada,
2012). Collaborative care has been shown to improve the level of care patients receive
as measured by clinical outcomes in conditions such as depression, diabetes and in
processes, for example in medication reviews, resulting in fewer hospital and
emergency room visits (Barrett, Curran, Glynn, & Godwin, 2007). A medication review
looks at the patients' medications with the aim of reducing medication related side
effects or interactions, reducing waste and maximising the benefit of the medicines the
same time. The following examples illustrate different primary healthcare models:
1. One emerging model is the nurse led model in which the nurse works independently.
This model can be generic or customized for patients with a specific condition such
as cardiac problems or rheumatoid arthritis where the interventions are more holistic
in nature and include assessment, treatment, patient education, and self-care
supports, as well as outreach activities for hard-to-reach populations (Virani, 2012).
A model in this category is the Community Matron, which was developed in the UK
and is based on the Evercare model from the US. The concept involves assisting
patients suffering from long term and/or complex conditions to live at home with a
coordinated care package while gaining a better understanding of their condition. In
2006 the UK Department of Health described a Community Matron as “a qualified
nurse who can provide advanced nursing and clinical care, as well as effective case
management” (Lillyman, Saxon, & Treml, 2009, p. 3). However, the authors of the
literature review found that the Matrons had moved beyond this definition of
providing clinical care and care co-ordination to include education, advocacy and
psychological support. Some Matrons had expanded their scope of practice to take

16
on some clinical tasks previously performed by general practitioners. Ultimately the
results from the review revealed that there was no evidence to support the
continuance of the Community Matron role (Lillyman, Saxon, & Treml, 2009). In
contrast the Evercare model in the United States (US) was viewed as valuable and
successful and described as achieving:
A 50% reduction in unplanned hospital admissions, without detriment to
health
A significant reduction in medications, with benefits to health
97% family and care giver satisfaction and high physician satisfaction
rates (Department of Health (UK), 2004, p. 1)
On the whole, the existing evidence demonstrates that nurse-led models of care
provide services that are equal to or better than physician led models (Virani, 2012;
Jacobson & HDR, 2012). However, there are data to suggest that nurse leadership
roles which supplement physician roles rather than replace them are more effective in
terms of healthcare delivery and can potentially be less costly than models relying
exclusively on physicians (Browne, Birch, & Thabane, 2012).
2. An example of a physician-led model is shared care. In 1994 Hickman defined
shared care as ‘the joint participation of primary care physicians and specialist care
physicians in the planned delivery of care for patients with a chronic condition,
informed by an enhanced information exchange over and above routine discharge
and referral” (Smith, Allwright, & O’Dowd, 2009, p. 2). The authors of this systematic
review of the Cochrane database reason that this model of increasing engagement
in primary care could create further demand on specialist services as more patients

17
are found to have chronic conditions or more complications are diagnosed due to the
improvements in the quality of care (Smith, Allwright, & O’Dowd, 2009). In other
words the increase in the primary care physicians’ knowledge might lead to an
improvement in the diagnosis of chronic conditions or associated complications.
While the evidence to support shared care was not consistent across the studies
evaluated for this research, some relevant findings emerged. For example a number
of studies including patients with depression and chronic mental health issues and
those focussing on patients who had high levels of morbidity found shared care to be
more effective (Smith, Allwright, & O’Dowd, 2009). Furthermore, no study reported
the effectiveness of shared care to be less favourable compared to controls, i.e.
those medical practices that did not provide shared care. Areas which did
demonstrated an improvement as a result of shared care included “appropriate
prescribing” and medication compliance as well as the recording of risk factors, all of
which effect on health outcomes. The authors caution that their findings do not
advocate the scaling up of shared care into mainstream service delivery but only into
research settings for further study (Smith, Allwright, & O’Dowd, 2009).
If shared care does become a model of choice for primary healthcare then family
physicians will require the capacity and capability to take on and deliver this approach to
care. Such multi-disciplinary teams appear to allow physicians to do what they are best
at: medical diagnosis and management of diseases while allowing other healthcare
professionals to support the patients in improving their health and managing their
conditions (Health Council of Canada, 2009). A shared care model has been developed
in which care is shared between a family physician and a nurse. This model is

18
described as being different from a multi-disciplinary team requiring formal agreements
and a division of duties between two healthcare professionals. Examples (Virani, 2012)
include:
The Family Practice Nurses in Nova Scotia
The Nurse Practitioner/Family Physician Primary Care model in British
Columbia
The Nurse-led weekly clinic with general physician (GP) support occurring
twice a year for patients with poor diabetic control in the UK
The Nurse/pharmacy-led capecitabine clinic for colorectal cancer
3. The integrated community model promotes the inclusion of primary healthcare into
other components of the healthcare system and focusses on cooperation and
interaction between healthcare professionals. Examples include healthcare centres
in Scandinavian countries and Primary Care Trusts in the UK (Lamarche P. , et al.,
2003). A summary of the different models included in this review is given in
Appendix A.
The evidence presented suggests that a team-based approach including different
healthcare professionals can provide a greater range of services which in turn utilizes
resources more efficiently resulting in improvements in terms of access to care, wait
times, care coordination as well as more comprehensive care compared to individual
healthcare professional models (Barrett, Curran, Glynn, & Godwin, 2007). The model at
the Southcentral Foundation in Alaska is an example of successful team work (Baker &
Denis, 2011) based on the following five key principles that appear to be aligned with
the outcomes described by Lamarche et al (Lamarche P. A., et al., 2003):

19
1. Patient driven care: Involving patients in the design and evaluation of care taking
into account patients` values, preferences and needs.
2. Team-based care: Using teams to make care more efficient and ensure that all
team members are practicing to the highest level of their credentials.
3. Proactive Panel Health Improvement: Assigning a panel of patients to a team of
providers who proactively determine and meet preventive care needs.
4. Integrated Behavioural Health: Incorporating a behavioural health practitioner
into the team to identify barriers to self-care as well as to screen for and treat
mood and behavioural issues.
5. Barrier-Free Access: Removing barriers that stand in the way of prompt and
appropriate care, such as language, culture, attitude, time and place (Baker &
Denis, 2011, p. 13).
However, no one organizational model in primary care is expected to meet all of
the six broad outcomes (Effectiveness, Productivity, Accessibility, Continuity, Quality
and Responsiveness) that have been suggested by Lamarche et al (Lamarche P. A., et
al., 2003; Cook & Kachala, 2004).
Whatever the configuration, a team requires a certain level of oversight and
management in order to be effective but there is little research relating to this aspect.
One study addressed the merits of ‘professional management’ over ‘practicing
management’, considering practicing management as “hands on” management, and
came to the conclusion that practicing management was more successful in supporting
change and improvement based on the various characteristics identified in Table 2
below (Gerst, 2011).

20
Table 2: Characteristics of professional and practising managers (Gerst, 2011, p. 4)
(Reproduced by kind permission of the author)
Comparing professional and practicing management characteristics
Characteristic Professional Management Practicing Management
Th
ink
ing
/ P
ers
pec
tive
Management Model/Thinking
Command and control Systems
Organizational Perspective
Top-down, hierarchy Outside-in, system
Role of Management
Act on the people Act on the system
Ethos
Ideological, rules, control Pragmatic, scientific, experiments, learning
Location 42th floor Gemba, heart and soul of the operation
Information processing / understanding
Enumerative, descriptive Analytic, explanatory/predictive
Acti
on
/ e
tho
ds
Primary activity Reading reports, writing directions
Running the business, meeting people
Measurement Targets, standards, related to budgets (enumerative)
Capability, variation, related to purpose (analytic)
Improvement Strategy
Focus on results Focus on causes
Change Is a project Is a process
Decision Making Separated from the work Integrated with the work
A study on the economic impact of improvements in primary healthcare found that the
quality of the primary healthcare system was related to how it is structured to meet the
individual and population needs, suggesting that practices that had at least one female
doctor, a panel size of 1600 patients per fulltime equivalent doctor and the presence of
electronic health records provided stronger predictors of performance than those
practices without (Dahrouge, et al., 2012). The study evaluated a comparison

21
conducted by the Commonwealth Fund which ranked Canada amongst the countries
with poor support and organization in primary healthcare leading to concerns of
accessibility as well as quality of primary healthcare provision (Dahrouge, et al., 2012).
Primary Healthcare Goals
In terms of goals for inter-professional teams in primary healthcare research
suggests, that a range of essential services that promote and preserve health as well as
provide care for illness and disability, need to be included in the primary healthcare
service. Primary healthcare should be well positioned to facilitate care coordination
across providers and systems in order to address the broader determinants of health
(Cook & Kachala, 2004). In the UK, for instance, the practice nurse role was enhanced
to assess patients’ cardiovascular risk factors and as a result patients identified as
exhibiting risk factors for preventable illnesses were referred to physicians. Furthermore
practice nurses were trained to perform health checks and to supervise the audit of
patient records and to add patients to a recall system for future review (Grumbach,
Bainbridge, & Bodenheimer, 2012). Health Canada states that inter-professional teams
in primary healthcare would be well suited for health promotion and for improving the
management of chronic diseases (Health Canada, 2012).
One report, which considered a number of systematic reviews, presented
evidence that nurses play an important role in primary healthcare, particularly in health
education and management of patients with chronic diseases, while at the same time
supporting the compliance with required treatments thereby leading to improved clinical
outcomes (Dahrouge, et al., 2012). This evidence is also supported by the view of the
WHO in their report “Primary Health Care: Now More Than Ever”. This report states that

22
the diversity of healthcare needs and the challenges patients face require a
comprehensive range of resources that should include health promotion and disease
prevention as well as the traditional diagnosis and treatment or referral for chronic or
long-term care (World Health Organisation, 2008).
Kates et al suggest that primary care should offer both, primary prevention
through early detection and secondary prevention to maintain and stabilize patients'
health (Kates, et al., 2012). This view was reinforced by Dr. Joshua Tepper at the
Canadian Institutes of Health Research Primary Healthcare Summit held in 2010
(Canadian Institutes of Health Research, 2010). The Corpus Sanchez report indicated
that primary healthcare activities could include prevention, assessment, observation,
treatment and rehabilitation (Corpus Sanchez International, 2008). Appendix B gives a
more detailed view of the activities that can be performed in primary care and by whom.
The available evidence reinforces the concept of re-aligning the healthcare system
around an interdisciplinary primary healthcare to enable chronic conditions to be
managed more effectively (World Health Organization, 2008).
Other healthcare professionals such as pharmacists could also have a role in
improving medication adherence and providing patient education (Dahrouge, et al.,
2012).
Published evidence suggests that primary healthcare in Canada is poorly
organized and supported in comparison to other OECD countries (Dahrouge, et al.,
2012). It is also obvious from the data provided by some sources used for this research,
that a shift is required in how services are provided and that a need exists to base the

23
focus on primary healthcare instead of on acute care. At the same time there is
pressure on the healthcare system to provide support for an increasing number of
people with chronic conditions, which is proving difficult for a system that is inherently
designed around acute care (Rand, Vilis, Dort, & White, 2006). Designing services
around primary healthcare instead would improve productivity in terms of cost versus
type and quantity of services as defined by Lamarche et al (2003). However funding
primary healthcare requires some thought as stated in one study conducted in Nova
Scotia by Nemis-White et al:
“Fee-For Service Physicians do not have any remuneration for the cost of a
nurse and as they cannot recoup their cost by bringing in additional income to the
practice the likelihood of extending team based care is low.” (Nemis-White, MacKillop, &
Montague, 2012, p. 56).
Managing Chronic Conditions
Chronic disease management has been defined Rand et al as “a clinical
management process of care. It spans the continuum of care from primary prevention to
ongoing long-term maintenance for individuals with chronic health conditions or
disease” (Rand, Vilis, Dort, & White, 2006, p. 58). It has also been described as a
proactive population based approach that seeks to address chronic diseases in the
prevention stage and early in the disease cycle in order to slow down or even prevent
disease progression and complications (Ontario Ministry of Health and Long-Term Care,
2005; Kates, et al., 2012).

24
These definitions are significant given that in 2005 the World Health Organization
(WHO) projected that chronic diseases would account for 89% of all deaths in Canada,
including cancer, cardiovascular disease, chronic respiratory disease, diabetes and
other chronic diseases and that this percentage was projected to rise over the next
decade, particularly based on deaths occurring from diabetes (World Health
Organization, 2005). Current evidence suggests that people from lower socio-economic
positions bear the brunt of suffering caused by chronic disease in that they get sicker
and die sooner than the segment of the population with a higher socio-economic
position (World Health Organization, 2010).
From the research literature reviewed for this paper it is evident that that chronic
diseases are on the rise and that optimized primary healthcare should be the foundation
of any healthcare system. As a result, any primary healthcare model should take into
account the management of chronic diseases (World Health Organization, 2008).
Successful chronic disease management programs share some common characteristics
such as:
Being evidence-based (Ontario Ministry of Health and Long-Term Care, 2005;
World Health Organization, 2008),
Empowering individuals to increase their control to improve their health
(Ontario Ministry of Health and Long-Term Care, 2005; UK Department of
Health, 2004; World Health Organization, 2008)
Being patient-centered (Ontario Ministry of Health and Long-Term Care,
2005; World Health Organisation, 2008; Brasset-Latulippe, Verma, Mulvale, &
Barclay, 2011)

25
Promoting collaboration among providers, organizations, individuals, families
and community groups to integrate care across organizational boundaries
(UK Department of Health, 2004; Ontario Ministry of Health and Long-Term
Care, 2005; Brasset-Latulippe, Verma, Mulvale, & Barclay, 2011)
Using multidisciplinary teams (Brasset-Latulippe, Verma, Mulvale, & Barclay,
2011; UK Department of Health, 2004; Rand, Vilis, Dort, & White, 2006)
One of the most well-known chronic care models is the Expanded Chronic Care
Model based on Wagner’s Chronic Care Model shown in Table 3. The development of
the expanded chronic care model in a region, province, or country would support the
attainment of the productivity, continuity, equity of access and responsiveness
outcomes as defined by Lamarche (Lamarche P. , et al., 2003).

26
Table 3: Comparison of the Chronic Care Model and the Expanded Chronic Care Model (Barr, et al., 2003, p. 79)
(Reproduced by kind permission from Longwoods Publishing)
The respective research suggests that the Chronic Care Model provides a
practical and supportive evidence-based approach to link a patient suffering with a
chronic disease to a prepared, proactive practice team (Morgan, Zamora, & Hindmarsh,
2007). The practicality of this model includes: the use of information systems to access
key data on individuals and populations, identifying patients with chronic disease,
stratifying patients by risk, coordinating care, integrating generalist and specialist
expertise, integrating care across organisational boundaries, aiming to minimise
Examples
Health System-
Organization of
Healthcare
Program planning that
includes measurable
goals for better care of
chronic illness
Self-Management
Support
Emphasis on the
importance of the central
role that patients have in
managing their own care
Self-Management/
Develop Personal Skills
Enhancing skills and capacities
for personal health and wellness
Smoking prevention and
cessation programs
Seniors' walking programs
Decision Support Integration of evidence-
based guidelines into
daily clinical practice
Decision Support Integration of strategies for
facilitating the community's
abilities to stay healthy
Development of health
promotion and prevention
"best practice" guidelines
Delivery System DesignFocus on teamwork and
an expanded scope of
practice to support
chronic care
Delivery System Design/
Re-orient Health
Services
Expansion of mandate to support
individuals and communities in a
more holistic way
Advocacy on behalf of and
with vulnerable populations
Emphasis in quality
improvement on health and
quality of life outcomes, not
just clinical outcomes
Developing partnerships
with community
organizations that support
and meet patients' needs
Build Healthy Public
Policy
Development and implementation
of policies designed to improve
population health
Advocating for/ developing:
smoking bylaws
walking trails
reductions in the price of
whole wheat flour
Creative Supportive
Environments
Generating living and
employment conditions that are
safe, stimulating, satisfying and
enjoyable
Maintaining older people in
their homes for as long as
possible
Work towards the
development of well-lit
streets and bicycle paths
Strengthen Community
Action
Working with community groups
to set priorities and achieve
goals that enhance the health of
the community
Supporting the community in
addressing the need for safe,
affordable housing
Components of the Chronic Care Model Components of the Expanded Chronic Care Model
Community
Resources and
Policies

27
unnecessary visits and admissions and providing care in the least intensive setting (UK
Department of Health, 2004). Required structural supports for this model are adequate
administration and management systems (Morgan, Zamora, & Hindmarsh, 2007; World
Health Organization, 2008; Baker & Denis, 2011) as well as an information system
incorporating electronic records (Corpus Sanchez International, 2008; Lamarche P. , et
al., 2003; Canadian Institutes of Health Research, 2010; World Health Organisation,
2008; Cook & Kachala, 2004; Enhancing Interdiscipinary Collaboration In Primary
Health Care, 2006; Baker & Denis, 2011).
The UK developed a National Framework for the management of chronic
diseases, which was based on the Chronic Care Model developed by Wagner and
integrated health and social care. This framework also drew on the work of Kaiser
Permante in the US (Canadian Institutes of Health Research, 2010). Evidence of
reducing the utilization of emergency beds by patients with chronic diseases has been
presented using this model (Canadian Institutes of Health Research, 2010; Denis,
Davies, Ferlie, & Fitzgerald, 2011). Additional research also suggests that the
integration within the healthcare system (integrated community model) is an effective
approach for chronic disease management (Nasmith, et al., 2010). Studies conducted
reveal that an integrated health and social model of care can support seniors in their
own home with no reduction in the quality of care given or level of access to care
(Canadian Institute for Health Information, 2011) and that a shift away from just dealing
with the disease to understanding the patients’ environment and social circumstances is
required (Cohen, Hall, & Murphy, 2009).

28
Good evidence exists on successful approaches for treating chronic diseases
and symptoms as well as reducing risk factors; nonetheless this evidence does not
appear to drive clinical practice or to be translated into individual clinical care.
Furthermore, people with multiple chronic diseases (multi-morbidity) often are treated
for each disease separately rather than in a holistic or personalized approach (Brasset-
Latulippe, Verma, Mulvale, & Barclay, 2011).
The research performed to date has been in patients with co-morbidities (one or
more disease or pathological illness in addition to the primary diagnosis) rather than in
patients suffering from multi-morbidities, which require a more complex care approach
(Smith, Soubhi, Fortin, Hudon, & O’Dowd, 2012). The results obtained suggest that
interventions focussed on co-morbidities do appear to be effective (Smith, Soubhi,
Fortin, Hudon, & O’Dowd, 2012). Smith et al (2012) concluded from their systematic
review that although it was more challenging to design interventions for patients who
have a broad range of conditions (multi-morbidity), those healthcare professionals who
did focus their efforts on specific patients’ concerns, such as medicine management and
functionality appeared to be more effective (Smith, Soubhi, Fortin, Hudon, & O’Dowd,
2012). This is supported by the reflections of Michael Hindmarsh shared at a primary
healthcare summit in Toronto, where he advised that the single disease centred
approach does not work in primary healthcare (Canadian Institutes of Health Research,
2010). It also needs to be factored in, that recent studies in Scotland have confirmed
that people from lower socio-economic groups are more likely to develop multi-morbidity
at a younger age and as a consequence die younger (Smith, Soubhi, Fortin, Hudon, &
O’Dowd, 2012). These findings are corroborated by research which found that people

29
from lower socio-economic groups were twice as likely to be hospitalized for chronic
conditions that potentially could be treated in primary care (Cohen, Hall, & Murphy,
2009). This further supports the evidence suggesting that people from lower socio-
economic groups suffer more from chronic conditions than those who are wealthier that
was mentioned earlier in this review (World Health Organization, 2010).
It was further suggested that additional benefits may be attainable if primary care
programs also contain preventative population approaches in lifestyle management to
reduce chronic disease development and progression (Morgan, Zamora, & Hindmarsh,
2007; World Health Organization, 2008). This places the management of chronic care
firmly within the primary healthcare setting. In summary, the successful implementation
of a chronic disease model relies on integrated teams; proactive and planned population
based care, self-management, clinical practice guidelines, community partnership and
engaged leadership (Canadian Institutes of Health Research, 2010, p. 15). This
approach appears to fit with the desired continuity, responsiveness and quality
outcomes as described by Lamarche et al (2003).
From the evidence provided by the research conducted it is obvious that the full
utilization of other healthcare professionals within collaborative teams in primary
healthcare is required in order to make the best use of scarce physician resources. This
will, in turn, allow healthcare to be more cost effective while also providing a more
flexible approach (Jacobson & HDR, 2012; Health Canada, 2012).
Funding and Incentives
Currently the most dominant model for primary healthcare in Canada is the
professional contact model based on the physician fee-for-service funding approach,

30
which rewards volume rather than value (Rosenthal, 2008; Leger P. T., 2011). None of
the research reviewed presented evidence that the fee-for-service model is efficient in
terms of service delivery or cost savings as it does not support cost control and does
not provide any incentive to deliver high quality care (Leger P. , 2011; Park, Braun,
Carrin, & Evans, 2007). These findings are also supported by research conducted by
Lamarche et al in 2003, who concludes that the professional contact model was the
least desirable model Canada should aspire to (Lamarche P. , et al., 2003). In Germany
the model is predominantly fee-for-service, however there also appears to be some
budgetary control by physicians earning “points” for the provision of services, thus
encouraging physicians in primary care to treat patients instead of referring them to
secondary care. A physicians’ final remuneration depends on the number of points he
has earned (Park, Braun, Carrin, & Evans, 2007). However, one study found that
physicians funded through the Fee-for-service had 41% more hospitalizations than
physicians funded by a capitation method (Carrin & Hanvoravongchai, 2002).
One aspect that has been pointed out as an anomaly within the Canadian
healthcare system compared to other high-income countries is the fact that in some
provinces certain prescription drugs are available within hospitals and not in primary
care settings (Allin, Stabile, & Tuohy, 2010). This results in the fact that some
Canadians may end up with a medical bill that exceeds their income (Rachlis M. ,
2004).
However the evidence of certain models being more cost effective than others is not
that clear-cut. Some experts suggest that if the healthcare system is redesigned or
transformed to be more effective and efficient then not only is the burden of chronic

31
diseases reduced, but it can also potentially run at a lower cost (Brasset-Latulippe,
Verma, Mulvale, & Barclay, 2011). Further evidence demonstrates that early
interventions for individuals at high risk of developing chronic diseases can be very
effective as preventative measures supporting the cost effectiveness of healthcare
provision by lowering overall cost (World Health Organization, 2010). Yet other research
does suggest that cost savings can also be achieved through an effective and robust
primary healthcare approach which entails equitable access, quality improvement, more
direct management and the use of electronic health records (Canadian Institutes of
Health Research, 2010), a view that replicates Lamarche et al’s six outcomes of
effectiveness, productivity, accessibility, continuity, quality and responsiveness
(Lamarche P. , et al., 2003). Even for those models utilizing advanced nurse
practitioners it could not be definitely demonstrated that they can provide cost
advantages over existing models (Browne, Birch, & Thabane, 2012; Mable, Marriott, &
Mable, 2012). If primary healthcare professionals act as gate-keepers for healthcare
services, they can reduce costs by optimizing the quality of prevention, coordination and
the continuity of care, as well as through improved administration and support of
primary care delivery (Dahrouge, et al., 2012).
Capitation is a method of payment based on the number of patients belonging to
a physician’s practice where payments would cover the cost of multi-disciplinary clinical
team salaries, infrastructure costs and other required expenses based on the number of
patients registered to the practice (Rosenthal, 2008). One criticism of this approach is
that physicians are likely to select patients that will incur little cost in terms of care
provision (Leger P. T., 2011). Generally this would mean patients who have complex

32
care needs such as patients with chronic diseases would not be selected by the
physician, especially as hospital care is covered by the capitation payments made to the
primary care physician.
An alternative funding model to consider is paying physicians a salary. The
advantage of this method is that there is no incentive to provide services that may not
be of benefit to the patient and financial planning is made easier, however the
disadvantages are that doctors may reduce their productivity and it may lead to low
morale for those who feel they work hard but are not compensated for their efforts
(Carrin & Hanvoravongchai, 2002).
As described earlier, the UK fundholding model encompasses a framework that
gives primary care organizations responsibility for the provision of healthcare within a
defined population. In this model general practitioners receive funds, which cover the
costs of salaries of a multi-disciplinary team, the infrastructure such as electronic health
records, funding for service and quality improvements as well as drug costs. This has
increased the administration costs but has also improved communication, health
promotion and improved disease prevention (Cook & Kachala, 2004). Again, a criticism
of this model is that physicians can pick and choose their patients based on the level of
care they need (Leger P. T., 2011). However in the UK patients do have a right to a
general practitioner and can be allocated a physician by the Health Authority.
The mixed payment approach attempts to balance out the negatives of both the
fee-for-service and the capitation methods of funding by having a prospective payment
component and retrospective payments. The new General Medical Service (GMS)

33
contract in the UK is an example of this method and was implemented in April 2002.
The contract rests with a practice team, usually with the family physicians as the lead,
and operates on a mixed payment method of capitation, an overall service fee and an
activity level payment based on the number of patients treated. The benefit of the mixed
payment method is that it can provide both an incentive for both quality and a measure
of cost control (Leger P. T., 2011). Research conducted by Park et al (2007) shows that
OECD countries appear to be moving towards this type of payment approach. Another
country where this method is applied is Finland, where physicians receive a base salary
that constitutes 60% of their earnings supplemented with a capitation amount of 20%,
while fee-for-service and a local allowance account for another 15% and 5%
respectively. The rationale behind this model is to avoid the weaknesses of all the other
models described while incorporating all the positives (Park, Braun, Carrin, & Evans,
2007).
Pay-for-performance is another approach used: in the UK the Quality and
Outcomes Framework was developed as part of an incentive scheme that focuses on
organizational process as well as health outcomes for chronic diseases and was used
alongside the new GMS contract. Leger (2011) suggested using a pay-for-performance
model that could be employed with any form of funding to reward high quality care
based on health outcomes (Leger P. T., 2011). Other research suggests that a pay-for-
performance approach is not a good tool to use for improving the efficiency in the
delivery of care as it can focus attention and effort on the attainment of targets, which in
turn can lead to unwanted outcomes. For example in the UK a four hour wait time
national target for patients being seen in ER was instituted as a key performance

34
indicator that had to be met. This led to an increase in potentially unnecessary hospital
admissions as when patients in ER were nearing the 4 hour wait time they were
admitted rather than being seen. However paying for performance can have a positive
effect on the composition of primary care teams through the introduction of other
healthcare professionals, though this requires a governance framework for monitoring
and adjusting goals (Denis, Davies, Ferlie, & Fitzgerald, 2011; World Health
Organization, 2010). Based on their findings other researchers argue that financial
incentives tied to performance do change professional behaviour and that patients’ do
receive higher quality care (Campbell, et al., 2007). The pay-for-performance model is
seen as part of a general trend of European countries in moving away from implicit trust
in their healthcare professionals towards more active monitoring (Campbell, et al.,
2007). Interestingly it has been recorded that physicians react positively to incentives
such as pay-for-performance (Denis, Davies, Ferlie, & Fitzgerald, 2011). A pilot
approach to pay-for-performance is currently being developed in the US that is based
on a patient focused ‘medical home’ where accountability for the patient rests with the
medical team within the ‘medical home’ (Rosenthal, 2012), how similar this model will
be to the UK Clinical Outcomes Framework described earlier remains to be seen.
Another model that has been developed in the US is the shared savings model.
In this setting a group practice will take on the management of their patients’ healthcare
and up to 80% of the savings achieved are shared with the group or are allocated to the
group based on a point system relying on an index of their expected versus their actual
total of allowed charges and a set of three risk-adjusted measures of performance: use

35
of generic medications, emergency department use and the number of office visits
(Rosenthal, 2008).
However, funding models should be considered in terms of the health outcomes
that they deliver. Morgan et al (2007) compared seven countries concerning the impact
of their delivery on chronic care. They found that overall the UK performed the best with
Canada in 7th place behind Germany (2nd), New Zealand (3rd), Netherlands (4th),
Australia (5th) and the US (6th) (Morgan, Zamora, & Hindmarsh, 2007). In addition to
performing better in terms of health outcomes the UK also had a lower GDP health
expenditure (GDPHE) than most as can be seen in Table 4 below (Pritchard & Wallace,
2011).
Table 4: Average and current GDP health expenditure comparisons (Pritchard & Wallace, 2011, p. 4)
(Reproduced by kind permission of the authors)
Average and current percentage GDP health expenditure (ranked by average 1980–2005 GDPHE)
Country GDPHE 1980
Current GDPHE Public
Current GDPHE Private
Current Total GDPHE
Total GDPHE average 1980–2005
1 USA 8.8 6.9 8.4 15.3 12.2
2 Germany 8.7 8.2 2.5 10.7 9.7
3 Switzerland 7.4 6.9 4.0 11.6 9.3
4 Sweden 9.0 7.7 1.4 9.1 8.8
4 France 7.0 8.9 2.2 11.1 8.8
6 Canada 7.1 6.9 2.9 9.8 8.7
7 Netherlands 7.2 5.7 3.5 9.2 8.4
7 Greece 6.6 4.3 5.8 10.1 8.4
9 Australia 7.5 6.4 3.1 9.5 8.3
10 Italy 7.0 6.8 2.1 8.9 8.2
10 Norway 7.0 7.6 1.5 9.1 8.2
12 Austria 7.5 7.7 2.5 10.2 8.1
13 Portugal 5.6 7.4 2.8 10.2 7.7
14 New Zealand 5.9 7.0 2.0 9.0 7.2
15 UK 5.6 7.1 2.1 9.3 7.1

36
15 Ireland 8.3 5.8 1.7 7.5 7.1
15 Finland 6.3 5.9 1.6 7.5 7.1
18 Japan 6.5 6.6 1.4 8.0 7.0
19 Spain 5.3 5.9 2.3 8.2 6.8
Western countries average
7.1 6.9 2.8 9.7 7.4
Average GDPHE 1980, 7.0; 1 s.d. =1.1
Average [1980–2005] 8.3; 1 s.d. =1.5
Current GDPHE average 9.7; 1 s.d. = 1.7
There is no doubt that the costs generated by chronic diseases are set to rise
with significant expenditure to be borne by individuals, families, businesses,
governments and healthcare systems (World Health Organization, 2010). Costs are
increasing and researchers caution that improving the quality and delivery in primary
care will create a corresponding increase in cost (Smith, Allwright, & O’Dowd, 2009).
Evidence suggest that the rising costs are linked to inflation, the rise in the cost of
services, improved and greater access to technology and the use of new and more
expensive drugs as well as an increased number of medical interventions, in other
words providing more care at a higher level (Canadian Institute for Health Information,
2011; Husereau & Cameron, 2011; Canadian Institute for Health Information, 2010).
One aspect the studies did not relate to the climbing cost was the numerical increase
within the aging population.
One study suggested that the best primary healthcare model for potentially
containing costs is the integrated community model (Lamarche P. A., et al., 2003),
described earlier in this paper. With any of the methods described in this section (see
Appendix C for list of funding models) there are advantages and disadvantages and the

37
choice will depend on the framework within a country and the level of influence from
interested lobbying groups.
Throughout all the payment models there are some common themes:
Value-based payment
Cost control
Clinical guidelines
Quality measurement (Rosenthal, 2008, p. 1199)
However current research suggests that an optimal system would be a mixed payment
system with some regulatory commitment for cost containment aligned with a quality
management system (Park, Braun, Carrin, & Evans, 2007). Indeed focusing on value as
the central objective was one of the five imperatives agreed upon by the Forum on
Healthcare Innovation conference (Chin, Hamermesh, Huckman, McNeil, & Newhouse,
2012). This approach would be consistent with attaining the productivity, quality and
continuity outcomes as described by Lamarche et al (2003).
Quality
Quality is one of the desired outcomes emphasized by Lamarche et al (2003).
Quality in healthcare was stated by Dr. Rachlis at the ‘Better with Age’ series of round
tables hosted by the Canadian Health Services Research Foundation as containing the
following attributes: “safe, effective, patient-centred, accessible, efficient, equitable,
integrated, appropriately resourced and focused on population health” (Canadian Health
Services Research Foundation, 2011, p. 6). And yet a study by Nasmith suggests that
Canada’s primary care lags behind other countries with similar wealth and healthcare

38
systems “in after-hours care, wait times, chronic disease management, mental health,
quality improvement and electronic medical records. Moreover, Canada’s primary care
sectors are characterized by fragmentation, ineffective use of providers, and inefficient
use of resources”. This is not surprising as the study further notes that primary care
physicians in Canada report the lowest rate of quality training (Nasmith, et al., 2010).
Canada has very few nationally driven studies which measure the quality of care,
particularly with respect to patient outcomes and in the monitoring of adverse events
(Sutherland & Leatherman, 2012; Veillard, Gula, Huynh, & Klazinga, 2012) . This in turn
leaves Canada in the “middle of the pack” when compared with other countries in terms
of the quality of healthcare provision (Veillard, Gula, Huynh, & Klazinga, 2012;
Dahrouge, et al., 2012; Canadian Institutes of Health Research, 2010).
Evidence from research data suggests that Canada is facing a “Quality Chasm”,
which is defined as the gap between what has been recommended and the care
patients receive. Factors of a quality chasm have been documented as:
Hospital services designed around acute care
Fragmented care resulting in patients being lost in transition from one
sector of healthcare to another
Poor uptake of clinical decision support tools such as reminders, protocols
and guidelines
Reluctance to measure performance and quality improvement
Misalignment of incentives and re-imbursement strategies

39
Lack of patient, family and community involvement (Morgan, Zamora, &
Hindmarsh, 2007, p. 8)
The data further suggest that improvement in the quality of care and the uptake of
evidence-informed practices cannot be achieved without the support of standardized
performance measures (Brasset-Latulippe, Verma, Mulvale, & Barclay, 2011).
Other countries such as the UK have developed national frameworks (Veillard,
Gula, Huynh, & Klazinga, 2012) where the Royal College of Physicians has worked with
the National Institute for Health and Clinical Excellence (NICE) to produce clinical
guidelines (Sutherland & Leatherman, 2012). NICE has also been credited with
supporting the reduction of practice variation and ensuring more evidence-based
treatments in the UK (Denis, Davies, Ferlie, & Fitzgerald, 2011).
The results from the research also suggest that while pay-for-performance can
make a difference in improving the quality of care, this model is more effective as part of
a comprehensive program (Campbell, et al., 2007).
Focussing on improving quality can also be a way of managing costs as doing
something the right way the first time could be a cost effective approach (Rachlis M. ,
2004; Baker & Denis, 2011).
A Potential Primary Healthcare Model for Canada’s Future
It is suggested that Canada should aim to create an integrated primary
healthcare system as depicted by the WHO and mentioned earlier in this paper and
outlined in Figure 2 (World Health Organisation, 2008). This would further ensure that

40
any system to be designed for the future will strive towards the important outcome
parameters identified by Lamarche et al (2003).
But what does this mean for the primary healthcare team? In 2007 the World
Health Organization stated “The concept of integrated Primary Health Care is best
viewed from the perspective of the individual: the aim being to develop service delivery
mechanisms that encourage continuity of care for an individual across health conditions,
across levels of care, and over a lifetime.” (World Health Organization, 2007, p. 5).
Kates et al developed a framework for primary care in order to deliver better
health, better care and better value as can be seen in Figure 3 (Kates, et al., 2012).
Figure 3: Quality Improvement and Innovation Partnership Improvement Framework (Kates, et al., 2012, p. 11)
(Reproduced by kind permission of Longwoods Publishing)

41
The model contains six characteristics which the authors list as critical to the success of
a high performing primary healthcare model. The practical application of these six
characteristics are described in Table 5 below.
Table 5: Examples of the applications of the six characteristics of high performing primary healthcare (Kates, et al., 2012, p. 12).
(Reproduced by kind permission of Longwoods Publishing)
Critics of this framework argue that while it relies on the three precepts of better health,
better care and better value, based on the Institute of Healthcare Improvement, it
received mixed results because of a lack of authority and encouragement or support to
implement the framework in the face of potential opposition from physicians. This was

42
particularly the case for physicians who see the Government as a payer and not a
partner and their professional bodies, who view themselves only as a licensing and
complaints body (Martin, 2012). However another group of researchers have
developed a different framework that consists of two domains: Performance and
Structure (Hogg, Rowan, Russell, Geneau, & Muldoon, 2008). The Performance domain
appears to be very similar to the practical application of the six characteristics in the
Kates et al framework, which relates to service delivery at the practice team level.
However the structural domain is different and addresses practice organization, as
outlined in Figure 4 below.
Figure 4: Structural Domain (Hogg, Rowan, Russell, Geneau, & Muldoon, 2008, p. 311)
(Reproduced by kind permission the Oxford University Press)
43
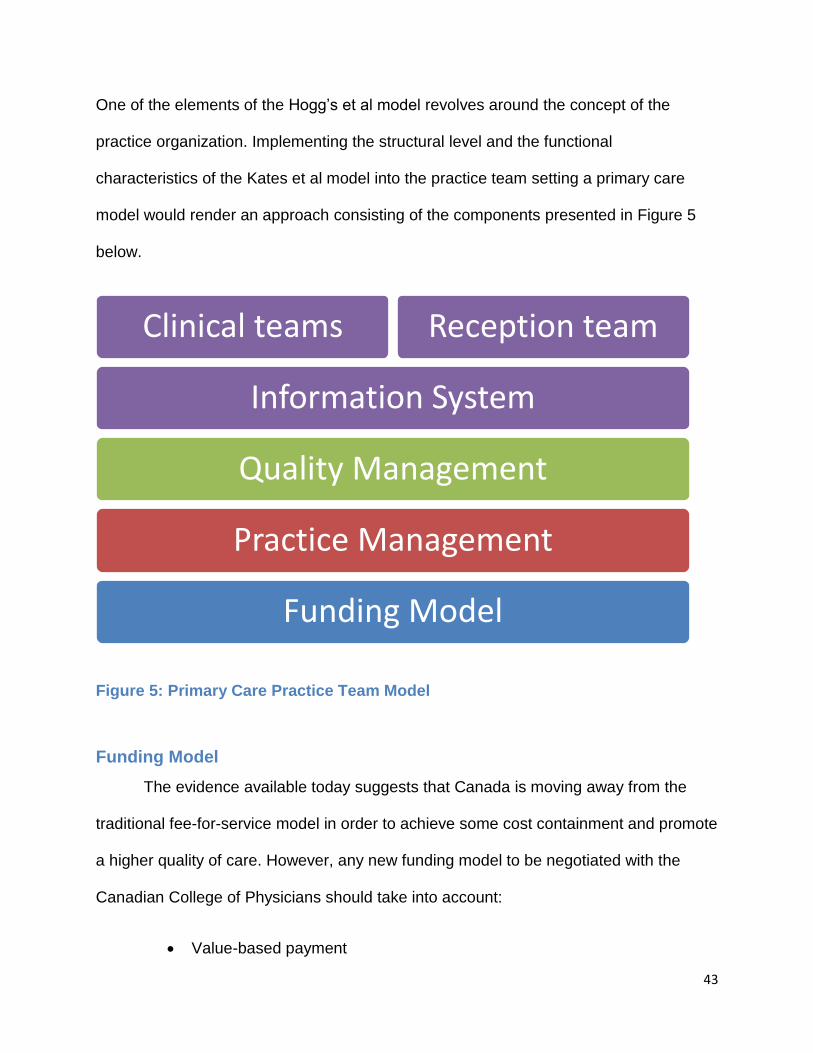
One of the elements of the Hogg’s et al model revolves around the concept of the
practice organization. Implementing the structural level and the functional
characteristics of the Kates et al model into the practice team setting a primary care
model would render an approach consisting of the components presented in Figure 5
below.
Figure 5: Primary Care Practice Team Model
Funding Model
The evidence available today suggests that Canada is moving away from the
traditional fee-for-service model in order to achieve some cost containment and promote
a higher quality of care. However, any new funding model to be negotiated with the
Canadian College of Physicians should take into account:
Value-based payment
Funding Model
Practice Management
Quality Management
Information System
Clinical teams Reception team

44
Cost control
Clinical guidelines
Quality measurement (Rosenthal, 2008, p. 1199)
The design of any future funding model under consideration will have consequences,
which need to be evaluated in advance. If, for example, a multi-disciplinary team is
desired then the funding model must reflect this composition. Furthermore the outcomes
and requirements for services can be flexible depending on the population needs, like
building flexible services for long term care into the model.
Practice Management
Gerst stated having managers working within the team is advantageous to
implement continuous improvements and the difficult business of managing pilots in
order to achieve some meaningful analysis (Gerst, 2011). To reduce the workload of the
physicians a group practice will require administrative support with responsibility for the
day to day management of the practice. This includes staffing levels, budget control,
staff development and oversight of premises, the latter addressing: facilities and
equipment management, maintenance of common parts, security and overall
operations. In addition the practice manager also needs be responsible for organising
the practice meetings, performance reports and support the improvement in quality of
clinical practice (Baker & Denis, 2011).
Quality Management
According to Kates et al providers have dual roles, to perform their clinical work
and to improve it (Kates, et al., 2012). Quality improvement needs to become part of the
culture of the primary care team and the surrounding organization. The UK Quality and

45
Outcomes Framework consists of two domains: Clinical and Organizational. The clinical
domain covers disease registries and chronic disease management, including mental
health, while the organizational domain covers:
Records and information storage
Information for patients
Education and training
Practice management
Medicines management
Quality and productivity (British Medical Association & NHS Employers,
2012)
The Information System
The majority of the research literature studied eluded to the fact that quality
management is not possible without robust information technology and information
management in place.
The Reception Team
For a group practice a team of receptionists is necessary which would provide
additional administrative support, such as scheduling and coordinating appointments,
filing, photocopying and completing patient registration.
The Clinical Team
The core clinical team should be comprised of physicians, nurses (including
Licensed Practical Nurses), a pharmacist, a pharmacy technician and a phlebotomist as
needed for a community. All members of the team would be expected to work to the full

46
scope of their practice. Other healthcare professionals, such as home care nurses,
nutritionists and physiotherapists not part of the core team would be assigned to work
with patients from the defined practice allowing the practice team healthcare
professionals to work collaboratively with them, as depicted in Figure 5. This view is
supported by the College of Family Physicians in their concept of a Patients’ Medical
Home that was outlined in 2011 (The College of Family Physicians, 2011). In order to
achieve advance access for patients, such as same day access (or access within 48
hours), the practice clinical team will be required to work with the reception team and
practice manager to ensure appropriate scheduling. Principles for effective teamwork
have been identified as:
patient engagement;
a population health approach;
a focus on the best possible care and services, using research to set
quality standards and make decisions about management of health
problems;
access to “the right service, provided at the right time, in the right place
and by the right health professional”;
trust and respect;
effective communication (Barrett, Curran, Glynn, & Godwin, 2007, p. 11)

47
Recommendations
Based on the research body analysed in this paper and when compared against
the wanted outcomes as outlined by Lamarche et al (2003) the following
recommendations are suggested:
1. To develop inter-disciplinary, collaborative primary healthcare teams
2. To strive towards an Integrated Community model of healthcare provision
within the health system
3. To establish links with social care when appropriate
4. To broaden the work of primary care to include a population approach,
prevention and health promotion as well as chronic disease management
5. To provide the supporting infrastructures of information systems and
practicing managers
6. To develop a mixed payment model with incentives and pay-for-
performance programs
7. To focus on quality
Conclusion
A quick and easy way to develop a cost effective, quality driven primary care
team is not apparent, especially not one that is designed to meet the six broad
outcomes described by Lamarche et al in 2003:
Effectiveness
Productivity
Accessibility

48
Continuity
Quality
Responsiveness
If a group practice model as depicted in Figure 5 is developed and appropriately funded
to deliver a high level of access providing coverage for a defined population, then some
savings could be realised in comparison to the cost of the many walk-in clinics currently
in operation. This approach would result in improvement of the quality of care,
especially in terms of continuity of care. This model could be extended to also cover out
of hours healthcare, thereby relieving the emergency room of primary care related
cases and further reducing costs, as emergency room expenses exceed those required
for a primary healthcare practice. Such a group practice model could be developed as a
pilot to create a centre of excellence for primary care.
Finally in the words of Amelia Earhart "The most effective way to do it is to do it."

54
Appendix A: Summary of Professional Models Reviewed
Inter-professional &
Collaborative Models
Nursing Models Physician Led Models
Integrated Community Model Community Matron (UK) Shared Care Models: Family Practice Nurse in Nova Scotia
Evercare (US) Nurse Practitioner/Family Physician
Primary Care model in British Columbia
Nurse-led weekly clinic with general
physician (GP) support
Nurse/pharmacy-led capecitabine clinic
Professional Contact Model

55
Appendix B: Primary Care Activities
Who provides care What care is delivered When care is delivered Where care is delivered
Family Physician, Nurses (including Family Practice Nurses, Public Health nurses, Nurse Practitioners, RN, LPN)
Youth clinic Depending on need: Daily, Weekly, Monthly, Quarterly e.g. for visiting consultants, specialist service like audiology
Buildings, GP premises, FHC, Open Access centers, Networks, Mobile facilities, Internet, Call lines
Minor Surgery- (no anesthesia required)
Child Health Surveillance (CHS)
GP and Nurse Practitioner consultations
Contraception and sexual health
Reproductive health, Pre-conceptual counseling
Family Physician, Midwives Pre-natal Clinic
Family Physician, Nurses (including Family Practice Nurses, Public Health nurses, Nurse Practitioners, RNs, LPNs), Dieticians, Social worker, Occupational therapist, Mental Health Counselors
Chronic disease management-Heart Disease, Diabetes Clinic, COPD, Asthma, Cardiac: stroke / chronic heart disease
Family Physician, Nurses (including Family Practice Nurses, Nurse Practitioners, RNs, LPNs), X-ray technicians
Minor fractures
Family Practice Nurse Flu vaccinations
Wound care
Cervical screening
Lifestyle advice- weight management
Ear syringing

56
Holiday vaccinations and travel health
Who provides care What care is delivered When care is delivered Where care is delivered
Family Practice Nurse, Technicians
Blood testing, INR Depending on need: Daily, Weekly, Monthly, Quarterly e.g. for visiting consultants, specialist service like audiology
Buildings, GP premises, FHC, Open Access centers, Networks, Mobile facilities, Internet, Call lines
Phlebotomy
Cholesterol testing
Nurses ( including Family Practice Nurses, Public Health nurses, Nurse Practitioners, RN, LPN), Smoking cessation advisors Pharmacist
Smoking cessation
Physiotherapist Physiotherapy
Consultants, Family Physician, Nurses (including Family Practice Nurses, Public Health nurses, Nurse Practitioners)
Chemotherapy
Outpatient clinics
Family Practice Nurses, Public Health nurses
Parenting support, including behavioral difficulties
Childhood immunizations
Well woman groups
Well baby groups
Fitness appraisal
Family Physician Medicals
Specialists Audiology
Podiatrists Foot care program
Home care Palliative care
Speech- Language Pathologist Speech therapy
Chiropractors Musculo-skeletal system disorders

57
Appendix C: Funding Models
Funding Models Description
Physician Fee-for-service Payment by volume
Capitation Payment by number of patients physician responsible for
Mixed Payment Blended method of payments
Salary Physician paid a salary
Fund-holding GP holds the funds to spend on their patients
Pay-for-performance Usually used to reward quality of care delivered
Shared Savings Model A group practice shares up to 80% of savings they have made on the care of their patients

58
Bibliography
Allin, S., Stabile, M., & Tuohy, C. H. (2010). Financing Models for Non Canada Health Act Services in
Canada: Lessons from Local and International experiences with Social Insurance. Canadian
Health Services Research Foundation. Retrieved July 19, 2012, from http://www.cfhi-fcass.ca/sf-
docs/default-source/commissioned-research-reports/CHSRF_4FinancingModels_En-
final2.pdf?sfvrsn=0
Baker, G. R., & Denis, J.-L. (2011). A Comparative Study of Three Transformative Healthcare Systems:
Lessons for Canada. Canadian Health Service Research Foundation. Retrieved July 23, 2012,
from http://www.cfhi-fcass.ca/sf-docs/default-source/commissioned-research-reports/Baker-
Denis-EN.pdf?sfvrsn=0
Barr, V. J., Robinson, S., Marin-Link, B., Underhill, L., A. Dotts, D. R., & Salivaras, S. (2003). The Expanded
Chronic Care Model. Hospital Quarterly, 73-82.
Barrett, J., Curran, V., Glynn, L., & Godwin, M. (2007). CHSRF Synthesis: Interprofessional Collaboration
and Quality Primary Healthcare. Retrieved July 23, 2012, from
http://www.chsrf.org/Migrated/PDF/ResearchReports/CommissionedResearch/SynthesisReport
_E_rev4_FINAL.pdf
Brasset-Latulippe, A., Verma, J., Mulvale, G., & Barclay, K. (2011). Transformation Lessons from Disease
Based Strategies: An Environemental Scan Chronic disease: New Frontier of Healthcare.
Canadian Health Services Research Foundation. Retrieved July 23, 2012, from http://www.cfhi-
fcass.ca/sf-docs/default-source/commissioned-research-reports/EScanTransformationLessons-
EN.pdf?sfvrsn=0
British Medical Association & NHS Employers. (2012). Quality and Outcomes Framework for 2012/13:
Guidance for PCOs and practices. Retrieved July 19, 2012, from
http://www.nhsemployers.org/Aboutus/Publications/Documents/QOF_2012-13.pdf
Browne, D. G., Birch, S., & Thabane, L. (2012). Better Care: An Analysis of Nursing and Healthcare System
Outcomes. Canadian Health Services Research Foundation. Retrieved July 23, 2012, from
http://www.cfhi-fcass.ca/sf-docs/default-source/commissioned-research-reports/Browne-
BetterCare-EN.pdf?sfvrsn=0
Campbell, S., Reeves, D., Kontopantelis, E., Middleton, E., Sibbald, B., & Roland, M. (2007). Quality of
Primary Care in England with the Introduction of Pay-For-Performance. New England Journal of
Medicine, 181-191. Retrieved July 27, 2012, from
http://www.nejm.org/doi/pdf/10.1056/NEJMsr065990
Canadian Health Services Research Foundation. (2005). Myth: Managed care = mangled care. Canadian
Health Services Research Foundation.

59
Canadian Health Services Research Foundation. (2011). Better with Age: Health Systems Planning for the
Aging Population. Canadian Health Services Research Foundation. Retrieved July 19, 2012, from
http://www.cfhi-fcass.ca/sf-docs/default-source/aging-roundtable-reports/0604-
AGING_RNDTBLE-SNTHSS_FinalWEB.pdf?sfvrsn=0
Canadian Institute for Health Information. (2010). Health Care in Canada 2010. Canadian Institute for
Health Information. Retrieved July 19, 2012, from
https://secure.cihi.ca/free_products/HCIC_2010_Web_e.pdf
Canadian Institute for Health Information. (2011). Health Care in Canada, 2011: A Focus on Seniors and
Aging. Canadian Institute for Health Information. Retrieved September 28, 2012, from
https://secure.cihi.ca/free_products/HCIC_2011_seniors_report_en.pdf
Canadian Institute for Health Information. (2013, October 31). Natioanl Health Expenditure Trends 1975-
2013. Retrieved October 30, 2013, from Canadian Institute for Health Information:
https://secure.cihi.ca/estore/productFamily.htm?locale=en&pf=PFC2400
Canadian Institutes of Health Research. (2010). CIHR Primary Healthcare Summit: Patient Orientated
Primary Healthcare- Scaling Up Innovation. Retrieved July 27, 2012, from
http://www.f2fe.com/cihr/2010/postevent/CIHR%20PHC%20Summit%20Report_For%20Distrib
ution.pdf
Carrin, G., & Hanvoravongchai, P. (2002). Health care cost-containment policies in high-income countries:
how successful are monetary incentives? World Health Organization. Retrieved July 28, 2012,
from https://extranet.who.int/iris/restricted/bitstream/10665/69027/1/EIP_FER_DP_02.2.pdf
Chin, W., Hamermesh, R., Huckman, R., McNeil, B., & Newhouse, J. (2012). 5 Imperatives Addressing
Healthcare's Innovation Challenge. (pp. 1-26). Harvard Business School, Harvard Medical School.
Retrieved November 23, 2013, from http://www.hbs.edu/healthcare/pdf/Forum-on-Healthcare-
Innovation-5-Imperatives.pdf
Cohen, M., Hall, N., & Murphy, J. (2009). Innovations in Community Care: From Pilot Project to System
Change. Canadian Centre for Policy Alternatives. Retrieved July 19, 2012, from
http://www.policyalternatives.ca/sites/default/files/uploads/publications/BC_Office_Pubs/bc_2
009/CCPA_bc_innovations_web.pdf
Cook, R., & Kachala, E. (2004). Overview of Selected Primary Health Care Models. Retrieved July 28,
2012, from http://www.ontla.on.ca/library/repository/mon/10000/251131.pdf
Corpus Sanchez International. (2008). An Integrated Health System Review in PEI, A Call To Action: A
Plan For Change. Retrieved January 18, 2011, from PEI Department of Health:
http://www.gov.pe.ca/photos/original/doh_csi_report.pdf
Dahrouge, S., Devlin, R. A., Hogg, B., Russell, G., Coyle, D., & Fergusson, D. (2012). The Economic Impact
of Improvements in Primary Healthcare Performance. Canadian Health Sevices Research

60
Foundation. Retrieved July 21, 2012, from http://www.cfhi-fcass.ca/sf-docs/default-
source/commissioned-research-reports/Dahrouge-EconImpactPHC-E.pdf?sfvrsn=0
Denis, J.-L., Davies, H. T., Ferlie, E., & Fitzgerald, L. (2011). Assessing initiatives to transform healthcare
systems: lessons for the Canadian healthcare system. Canadian Health Services Research
Foundation. Retrieved July 23, 2012, from http://www.cfhi-fcass.ca/sf-docs/default-
source/commissioned-research-reports/JLD_REPORT.pdf?sfvrsn=0
Department of Finance and Municipal Affairs. (2011). Prince Edward Island Population Projections 2012
– 2052.
Department of Health (UK). (2004). Improving Chronic Disease Management.
Department of Health (UK). (2006). Our Health, our care, our say: a new direction for community
services.
Enhancing Interdiscipinary Collaboration In Primary Health Care. (2006). Interdisciplinary Primary Health
Care: Finding the Answers – A Case Study Report. Enhancing Interdiscipinary Collaboration In
Primary Health Care. Retrieved August 08, 2012, from
http://www.eicp.ca/en/resources/pdfs/enhancing-interdisciplinary-collaboration-in-primary-
health-care-in-canada.pdf
Gerst, R. M. (2011). The Decline of Health Services in Alberta: The triumph of 'professional' over 'real'
management. Converge Consulting Group Inc. Retrieved July 19, 2012, from
http://www.converge-group.net/wp-content/uploads/2011/07/Health-Services-in-Alberta.pdf
Glazier, R. H. (2007). Balancing Equity Issues in Health Systems: Perspectives of Primary Healthcare.
Healthcare Papers, 35-45.
Grumbach, K., Bainbridge, E., & Bodenheimer, T. (2012). Facilitating Improvement in Primary Care: The
Promise of Practice Coaching. The Commonwealth Fund. Retrieved July 19, 2012, from
http://www.commonwealthfund.org/~/media/Files/Publications/Issue%20Brief/2012/Jun/1605
_Grumbach_facilitating_improvement_primary_care_practice_coaching.pdf
Hay Group Health Care Consulting. (2010). Physician Humand Resource Report.
Health Canada. (2012, August 08). About Primary Care. Retrieved November 2012, from Health Canada:
http://www.hc-sc.gc.ca/hcs-sss/prim/about-apropos-eng.php#a1
Health Council of Canada. (2009). Teams in Action: Primary Health Care Teams for Canadians. Health
Council of Canada. Retrieved November 09, 2012, from http://www.hc-sc.gc.ca/hcs-
sss/prim/about-apropos-eng.php#a1
Health Systems Research and Consulting Unit. (2009). The Design of an Evidence-Informed Integrated
Mental Health, Substance Use and Problem Gambling Service System for Ontario. Health
Systems Research and Consulting Unit.

61
Hogg, W., Lemelin, J., Moroz, I., Soto, E., & Russell, G. (2008). Improving prevention in primary care:
Evaluating the sustainability of outreach facilitation. Canadian Family Physician, 712-720.
Retrieved July 19, 2012, from http://171.66.125.180/content/54/5/712.full.pdf
Hogg, W., Rowan, M., Russell, G., Geneau, R., & Muldoon, L. (2008). Framework for primary care
organizations: the importance of a structural domain. International Journal for Quality in Health
Care, 308-313. Retrieved September 16, 2012, from
http://intqhc.oxfordjournals.org/content/20/5/308.full.pdf+html
Husereau, D., & Cameron, C. G. (2011). The use of heath technology Assessment to Inform the value of
Provider Fees: Current Challenges and Future Opportunities. Canadian Health Services Research
Foundation. Retrieved July 23, 2012, from http://www.cfhi-fcass.ca/sf-docs/default-
source/commissioned-research-reports/Husereau-Fee-Schedule-E.pdf?sfvrsn=0
International Conference on Primary Health Care. (1978). International Conference on Primary Health
Care, Alma-Ata, USSR. Declaration of Alma-Ata. Retrieved July 19, 2012, from
http://www.who.int/publications/almaata_declaration_en.pdf
Jacobson, P. M., & HDR. (2012). Evidence Synthesis for the Effectiveness of Interprofessional Teams in
Primary Care. Canadian Health Services Research Foundation; Canadian Nurses Association.
Retrieved November 17, 2012, from http://www.cfhi-fcass.ca/sf-docs/default-
source/commissioned-research-reports/Jacobson-Interprofessional-EN.pdf?sfvrsn=0
Kates, N., Hutchison, B., O'Brien, P., Fraser, B., Wheeler, S., & Chapman, C. (2012). Framework for
Advancing Primary Care. Healthcare Papers, 8-21.
Lalonde, M. (1974). A New Perspective on the Health of Canadians. Governement of Canada.
Lamarche, P. A., Beaulieu, M., Pineault, R., Contandriopoulos, A., Denis, J., & Haggerty, J. (2003). Choices
for Change: The Path for Restructuring Primary Healthcare Services in Canada. Canadian Health
Services Research Foundation. Retrieved Juy 19, 2012, from http://www.cfhi-
fcass.ca/Migrated/PDF/ResearchReports/CommissionedResearch/choices_for_change_e.pdf
Leger, P. T. (2011). Physician Payment Mechanisms: An Overview of Policy options for Canada. Canadian
Health Services Research Foundation. Retrieved July 19, 2012, from http://www.cfhi-fcass.ca/sf-
docs/default-source/hospital-funding-docs/CHSRF-
LegerPhysicianRenumerationENG.pdf?sfvrsn=0
Lillyman, S., Saxon, A., & Treml, H. (2009). An evaluation of the role of the community matron: a
literature review. Journal of Health and Social Care Improvement, 1-11. Retrieved November 25,
2012, from http://www.wlv.ac.uk/pdf/nov2009_SLillyman.pdf
Mable, A., Marriott, J., & Mable, M. (2012). Canadian Primary Healthcare Policy. Canadian Health Servies
Research Foundation. Retrieved July 07, 2012, from http://www.cfhi-fcass.ca/sf-docs/default-
source/commissioned-research-reports/MariottMable-Jan2012-E.pdf?sfvrsn=0

62
Martin, D. (2012). Of Honey and Health Policy: The Limits of Sweet, Sticky Substances in Reforming
Primary Care. Healthcare Papers, 34-39.
Matteo, L. D., & Matteo, R. D. (2012). The Fiscal Sustainablity of Canadian Publicly Funded Healthcare
Systems and the Policy Response to the Fiscal Gap. Canadian Health Service Research
Foundation.
Morgan, M., Zamora, N., & Hindmarsh, M. (2007). An inconvenient Truth: A Sustainable Healthcare
System Requires Chronic Disease Prevention and Management Transformation. Healthcare
Papers, 6-23.
Nasmith, L., Ballem, P., Baxter, R., Bergman, H., Colin-Thomé, D., Herbert, C., . . . Zimmerman, B. (2010).
Transforming Care for Canadians with Chronic Health Conditions: Put People First, Expect the
Best, Manage for Results. Canadian Academy of Health Sciences. Retrieved December 17, 2012,
from http://www.cahs-acss.ca/wp-content/uploads/2011/09/cdm-final-English.pdf
Nemis-White, J., MacKillop, J., & Montague, T. (2012). Canada's Future Healthcare: Can It Be Better? Will
It Be Better? Healthcare Papers, 51-59.
Ontario Ministry of Health and Long-Term Care. (2005). Family Health Teams Advancing Primary Health
Care: Guide to Chronic Disease Management and Prevention. Retrieved July 19, 2012, from
http://www.health.gov.on.ca/en/pro/programs/fht/docs/fht_chronic_disease.pdf
Park, M., Braun, T., Carrin, G., & Evans, D. B. (2007). Provider Payments and cost-containment: Lessons
from OECD countries. World Health Organization. Retrieved July 28, 2012, from
http://www.who.int/health_financing/documents/pb_e_07_2-providerpay_oecd.pdf
Peckham, S. (2012). Now We Need a Framework for Action. Healthcare Papers, 60-64.
PEI Department of Health and Wellness. (2012). Promote, Prevent, Protect: Chief Public Health Officer's
Report and Health Trends 2012. Retrieved July 2012, from
http://www.gov.pe.ca/photos/original/hw_cphoar2012.pdf
PEI Department of Health and Wellness. (2012). Promote, Prevent, Protect: Chief Public Health Officer's
Report and Health Trends 2012.
Pritchard, C., & Wallace, M. S. (2011). Comparing the USA, UK and 17 Western countries’ efficiency and
effectiveness in reducing mortality. Journal of the Royal Society of Medicine Short Reports, 1-10.
Retrieved July 19, 2012, from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3147241/pdf/SHORTS-11-076.pdf
Quam, L., & Smith, R. (2005). Group US And UK Health Care: A Special Relationship? What Can The UK
And US Health SystemsLearn From Each Other? British Medical Journal, 530-533.
Rachlis, M. (2004). Prescription For Excellence: ow Innovation is Saving Canada's Health Care System.
HarperCollins.

63
Rachlis, M., & Kushner, C. (1989). Second Opinion. Toronto: Harper Collins.
Rand, C., Vilis, E., Dort, N., & White, H. (2006). Chapter 7: Chronic Disease Management. Guiding
Facilitation in the Canadian Context: Enhancing Primary Health Care. Department of Health and
Community Services, Government of Newfoundland and Labrador. Retrieved July 19, 2012, from
http://www.gnb.ca/0053/phc/pdf/Facilitation%20Guide%20-%20English.pdf
Rosenthal, M. B. (2008). Beyond Pay-For-Performance — Emerging Models of Provider-Payment Reform.
The New England Journal of Medicine, 1197-1200. Retrieved July 27, 2012, from
http://www.nejm.org/doi/full/10.1056/NEJMp0804658
Rosenthal, M. B. (2012). Meredith B. Rosenthal. Retrieved December 5, 2012, from Harvard School of
Public Health: http://www.hsph.harvard.edu/faculty/meredith-rosenthal/
Rush, B. (2010). Tiered frameworks for planning substance use service delivery systems: Origins and key
principles. Nordic Studies on Alcohol and Drugs, 27, 1-20. Retrieved July 23, 2012, from
http://www.nordicwelfare.org/PageFiles/4930/08_Rush.pdf
Scott, C., & Lagendyk, L. (2012). Contexts and Models in Primary Healthcare and their Impact on
Interprofessional Relationships. Canadian Health Services Reserch Foundation. Retrieved July 23,
2012, from http://www.cfhi-fcass.ca/sf-docs/default-source/commissioned-research-
reports/ScottLagendyk-April2012-E.pdf?sfvrsn=0
Simpson, J. (2012). Chronic Condition. Toronto: Penguin.
Smith, S., Allwright, S., & O’Dowd, T. (2009). Effectiveness of shared care across the interface between
primary and specialty care in chronic disease management. Cochrane Database of Systematic
Reviews 2007, Issue 3. Art. No.: CD004910. DOI:10.1002/14651858.CD004910.pub2. JohnWiley
& Sons, Ltd.
Smith, S., Soubhi, H., Fortin, M., Hudon, C., & O’Dowd, T. (2012). Interventions for improving outcomes in
patients with multimorbidity in primary care and community settings. Cochrane Database of
Systematic Reviews 2012, Issue 4. Art. No.: CD006560. DOI:10.1002/14651858.CD006560.pub2.
JohnWiley & Sons, Ltd.
Soroka, S. N., & Mahon, A. N. (2012). Better Value: An analysis of the impact of current healthcare
system funding and financing models and the value of health and healthcare in Canada.
Canadian Health Services Research Foundation.
Statistics Canada. (2010, July). Population Projections for Canada, Provinces and Territories 2009 to
2036. Retrieved December 2012, from Statistics Canada: http://www.statcan.gc.ca/pub/91-520-
x/2010001/part-partie4-eng.htm

64
Statistics Canada. (2012, September). Canada's population estimates: Age and sex, July 1, 2012.
Retrieved December 2012, from Statistics Canada: http://www.statcan.gc.ca/daily-
quotidien/120927/dq120927b-eng.htm
Sutherland, K., & Leatherman, S. (2012). Quality of Healthcare in Canada: A Chartbook. Canadian Health
Services Research Foundation. Retrieved July 23, 2012, from http://www.cfhi-
fcass.ca/migrated/pdf/chartbook/CHARTBOOK%20Eng_June_withdate.pdf
The College of Family Physicians. (2011). A Vision for Canada: Family Practice The Patient’s Medical
Home. The College of Family Physicians. Retrieved November 9, 2012, from
http://www.cfpc.ca/uploadedFiles/Resources/Resource_Items/PMH_A_Vision_for_Canada.pdf
UK Department of Health. (2004). Improving Chronic Disease Management.
Veillard, J., Gula, C., Huynh, T., & Klazinga, N. (2012). Measuring and Reporting on quality of Care and
Patient Safety in Canada: Focussing on What Matters. HealthCare Papers, 32-37.
Virani, T. (2012). Interprofessional Collaborative Teams. Canadian Helth Services Research Foundation.
Retrieved July 23, 2012, from http://www.cfhi-fcass.ca/sf-docs/default-source/commissioned-
research-reports/Virani-Interprofessional-EN.pdf?sfvrsn=0
World Health Organization. (2005). Facing the facts: The Impact of Chronic disease in Canada. World
Health Organzization. Retrieved July 19, 2012, from
http://www.who.int/chp/chronic_disease_report/media/CANADA.pdf
World Health Organization. (2007). Strengthening Health Systems to Improve Health Outcomes: WHO's
Framework for Action. World Health Organization. Retrieved July 19, 2012, from
http://www.who.int/healthsystems/strategy/everybodys_business.pdf
World Health Organization. (2008). 2008-2013 Action Plan for the Global Strategy for the Prevention and
Control of Noncommunicable Diseases. Retrieved July 19, 2013, from
http://whqlibdoc.who.int/publications/2009/9789241597418_eng.pdf
World Health Organisation. (2008). Primary Health Care: Now More Than Ever. WHO Press. Retrieved
July 19, 2012, from http://www.who.int/whr/2008/en/
World Health Organization. (2010). Global Status Report on noncommunicable diseases. World Health
Organization. Retrieved July 19, 2012, from
http://whqlibdoc.who.int/publications/2011/9789240686458_eng.pdf
World Health Organization. (2010). The World Health Report: Financing for Universal Coverage: Chapter
4 More Health for the Money. Retrieved July 28, 2012, from
http://www.who.int/whr/2010/10_chap04_en.pdf




















