Priceless Clinical Pearls in the Performance of Cardiac CT
11
VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE S3 OPTIMIZING OUTCOMES IN CT I MAGING Priceless Clinical Pearls in the Performance of Cardiac CT Norman E. Lepor, MD,* † Hooman Madyoon, MD,* † Gerald Friede, MS † *David Geffen School of Medicine at UCLA, Cedars-Sinai Medical Center, Los Angeles, CA; † Westside Medical Imaging, Beverly Hills, CA Cardiovascular CT represents an important innovation in cardiac imaging as a nonin- vasive modality for the diagnosis of coronary artery disease. As a screening examina- tion, coronary CT has the ability to identify the presence, extent, location, and severity of coronary artery disease in patients at risk. As a diagnostic examination in patients with chest discomfort and dyspnea, it can not only evaluate for the presence of coro- nary artery disease but also evaluate the pulmonary vasculature and aorta. The ability to perform high-quality cardiac CT requires a combination of technical expertise and knowledge of cardiac anatomy. From our experience having performed over 6000 cardiac CTs, we provide the reader with a number of clinical and technical pearls that will enhance his or her ability to perform high-quality studies even in the more challenging patient. [Rev Cardiovasc Med. 2008;9(suppl 1):S3-S13] © 2008 MedReviews, LLC Key words: 64-slice CT • Cardiac CT • CT coronary angiography T he emergence of 64-slice CT scanners and associated software capable of complex 3-dimensional image reconstruction of coronary arteries has revolutionized our approach to patients with cardiovascular disease. Ultrafast CT coronary angiography (CTCA) is capable of providing diagnostic- quality coronary images of soft noncalcified plaque and calcified plaque in the vast majority of patients evaluated with impressive sensitivity and specificity. With spatial resolution of 64-slice CT scanners as low as 0.4 mm, coupled with a positive predictive accuracy above 95% for the presence of coronary artery disease
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Priceless Clinical Pearls in the Performance of Cardiac CT
VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE S3
OPTIMIZING OUTCOMES IN CT IMAGING
Priceless Clinical Pearls in thePerformance of Cardiac CTNorman E. Lepor, MD,*† Hooman Madyoon, MD,*† Gerald Friede, MS†
*David Geffen School of Medicine at UCLA, Cedars-Sinai Medical Center, Los Angeles, CA; †Westside Medical Imaging, Beverly Hills, CA
Cardiovascular CT represents an important innovation in cardiac imaging as a nonin-vasive modality for the diagnosis of coronary artery disease. As a screening examina-tion, coronary CT has the ability to identify the presence, extent, location, and severityof coronary artery disease in patients at risk. As a diagnostic examination in patientswith chest discomfort and dyspnea, it can not only evaluate for the presence of coro-nary artery disease but also evaluate the pulmonary vasculature and aorta. The abilityto perform high-quality cardiac CT requires a combination of technical expertise andknowledge of cardiac anatomy. From our experience having performed over 6000cardiac CTs, we provide the reader with a number of clinical and technical pearls that will enhance his or her ability to perform high-quality studies even in the morechallenging patient.[Rev Cardiovasc Med. 2008;9(suppl 1):S3-S13]
© 2008 MedReviews, LLC
Key words: 64-slice CT • Cardiac CT • CT coronary angiography
The emergence of 64-slice CT scanners and associated software capable ofcomplex 3-dimensional image reconstruction of coronary arteries hasrevolutionized our approach to patients with cardiovascular disease.
Ultrafast CT coronary angiography (CTCA) is capable of providing diagnostic-quality coronary images of soft noncalcified plaque and calcified plaque in thevast majority of patients evaluated with impressive sensitivity and specificity.With spatial resolution of 64-slice CT scanners as low as 0.4 mm, coupled with apositive predictive accuracy above 95% for the presence of coronary artery disease
RICMS0002(GE)_03-14.qxd 3/14/08 3:25 PM Page S3

Priceless Clinical Pearls in the Performance of Cardiac CT continued
S4 VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE
(CAD), CTCA has emerged as a main-stream technology.1 This article pro-vides the most comprehensive practi-cal overview of the approach tocardiac and vascular CT-angiography(CTA) based on our experience withover 6000 patients at Westside Med-ical Imaging (Beverly Hills, CA). Weguide you through how to identify theappropriate patients who present forreferral for CTCA, review the benefitsand risks of CTCA, and share with youthe many valuable clinical pearls thatwe have accumulated by virtue of ourextensive experience pioneering thistechnology.
Screening for Coronary Artery DiseaseWhy Perform Screening CTCA? A total of 869,724 Americans diedfrom heart disease in 2004.2 Heartdisease kills more Americans thanthe 553,000 people who succumb toall cancers combined each year.However, although screening forsome cancers (including breast,colon, and prostate) in all risk groupshas become the norm and is coveredby most third-party payors, there isstill resistance from these payors tocover coronary artery screening. It isestimated that 770,000 Americanswill have a heart attack in 2008, withan additional 175,000 patients hav-ing their first heart attack in 2008.Adverse coronary heart disease mor-tality trends among young adults(aged 35-54 years), particularlyamong women, have recently beenobserved.3 Despite our best of inten-tions and the availability of medicaltherapies such as statins, we fail toidentify the presence of disease in at-risk populations in anything close toan adequate fashion, costing thou-sands of lives each year.
The most commonly appliedmodel for CAD risk assessment is theFramingham risk score (FRS), whichwas developed in 1948.4 This model
uses a point system for each risk fac-tor, including hypertension, totalcholesterol, high-density lipoprotein(HDL) cholesterol, tobacco use, pres-ence of diabetes, and age. The sumof these points is related to futurerisk of a cardiovascular event. TheFRS has come under fire recently fornot providing an accurate enoughassessment of cardiac risk for a vari-ety of reasons. About 40% of pa-tients in the fifth decade of life whohave documented CAD do not haveclassic risk factors and therefore aremistakenly categorized as low risk byFRS.5
A recent analysis of womenshowed that when FRS was used toassess cardiovascular risk, 95% ofwomen with no pre-existing CADbetween the ages of 45 and 79 yearswere defined as low risk (risk of acardiovascular event � 10% in 10years)6; 32% of these “low risk”women were found to have coronarycalcium, which increased their riskof a cardiovascular event by a factorof 5 over women with no coronarycalcium.7 Consider the hypotheticalcase of a 50-year-old woman withonly 1 major coronary heart disease(CHD) risk factor who, by FRS stan-dards, would be defined as low risk.In actuality, she has a 50% lifetimemortality risk from CHD and an esti-mated 8-year shorter medial survivalcompared with a woman with nomajor CHD risk factors.8
In a recently published assessmentof coronary risk factors and CAD de-fined by intravascular ultrasound inthe Reversal of Atherosclerosis withAggressive Lipid Lowering (REVER-SAL) study,9 there seemed to be a dis-connect between FRS and CAD bur-den. In an evaluation of patientspresenting with ST-elevation myocar-dial infarction, unstable angina, orfor percutaneous coronary interven-tion, over 50% of these patientswould have been categorized as low
risk by FRS.10 Some of the shortcom-ings of the FRS may be related to itsinability to account for the geneticaspects of cardiovascular disease bynot including family history, and thefailure to factor in specific low-density lipoprotein (LDL) cholesterollevels or duration of diabetes andsmoking. In addition, consideringtotal HDL cholesterol to be protectivemay be an oversimplification, assome HDL cholesterol molecules areactually proinflammatory andatherogenic.
Two key questions that need to beanswered in the debate on the utilityand cost effectiveness of screeningexaminations are 1) whether theylead to changes in patient/physicianbehavior, and 2) whether thesebehavior changes lead to a reductionin cardiovascular events. A recentanalysis of the effects of carotid inti-mal-medial thickness (CIMT) screen-ing did show that physicians weremore likely to prescribe aspirin andlipid-lowering therapy and applymore stringent LDL cholesterol treat-ment goals in patients who had ab-normal examination results, and thatthese patients did perceive them-selves to be at a higher cardiovascularrisk.11 There were also trends in pa-tients making healthy lifestylechanges as a result of the screeningexamination. Whether those pa-tients who modify their behavioralrisk factors earlier because of the re-sults of a cardiovascular screening ex-amination will be less likely to sufferfrom a cardiovascular event is anunanswered question. However, onewould have to presume until provenotherwise by virtue of the plethora ofdata assessing cardiovascular risk re-duction with lipid lowering therapiesthat such would be the case.Whether imaging modalities such asCTCA will lead to even more impres-sive effects is currently under studyby our group.
RICMS0002(GE)_03-14.qxd 3/14/08 3:25 PM Page S4
Priceless Clinical Pearls in the Performance of Cardiac CT
VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE S5
Available Modalities for CardiovascularDisease ScreeningCurrently, the most commonly usedimaging modalities to help assesscardiovascular risk are coronaryartery calcium scoring (CCS), CIMT,and CTCA. CCS and CIMT examina-tions have been shown to enhancecardiovascular risk assessment byFRS and are simple to perform.11,12
Recently published data from theMultiEthnic Subclinical Atheroscle-rosis (MESA) investigators12 hasshown that CCS is a stronger predic-tor of cardiac events than FRS. Theshortcoming of CCS is that it pro-vides no anatomic information, suchas whether the coronary artery is lo-cated in the key higher-risk proximallocations such as the left main andproximal left anterior descendingartery (LAD), or indication of theseverity of disease.13 Anatomy doesmatter in defining mortality risk inpatients with known CAD. Even inthe lower-risk group of patients with“low CCS scores” (CCS � 100 inwomen and CCS � 50 in men), ourgroup has shown that the incidenceof hemodynamically significantCAD greater than 50% in asympto-matic patients was nearly 10%.14 Ul-trasound detection of carotid arteryplaque is a potent predictor of car-diovascular events.15 Recent datafrom our group call into question thesensitivity of CIMT as a screeningmodality that can define coronaryrisk.16 On CTCA, 25% of patientswith normal CIMT had hemody-namically significant CAD. Theankle-brachial index is also used toscreen for cardiovascular disease. It iseasy to perform, inexpensive, andhas a high specificity, but is not asensitive indicator for detecting dis-ease. Stress testing has also been usedin the past for disease screening de-spite the fact that a stress test doesnot become abnormal until the coro-nary artery develops a severe stenosis
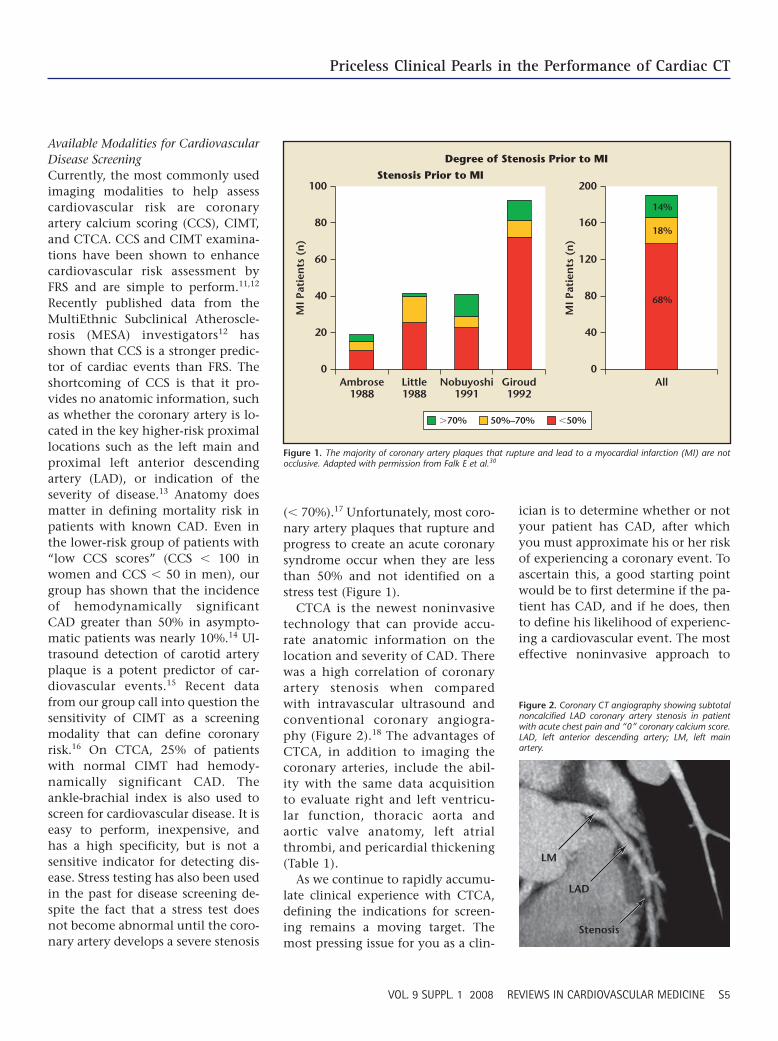
(� 70%).17 Unfortunately, most coro-nary artery plaques that rupture andprogress to create an acute coronarysyndrome occur when they are lessthan 50% and not identified on astress test (Figure 1).
CTCA is the newest noninvasivetechnology that can provide accu-rate anatomic information on thelocation and severity of CAD. Therewas a high correlation of coronaryartery stenosis when comparedwith intravascular ultrasound andconventional coronary angiogra-phy (Figure 2).18 The advantages ofCTCA, in addition to imaging thecoronary arteries, include the abil-ity with the same data acquisitionto evaluate right and left ventricu-lar function, thoracic aorta andaortic valve anatomy, left atrialthrombi, and pericardial thickening(Table 1).
As we continue to rapidly accumu-late clinical experience with CTCA,defining the indications for screen-ing remains a moving target. Themost pressing issue for you as a clin-
ician is to determine whether or notyour patient has CAD, after whichyou must approximate his or her riskof experiencing a coronary event. Toascertain this, a good starting pointwould be to first determine if the pa-tient has CAD, and if he does, thento define his likelihood of experienc-ing a cardiovascular event. The mosteffective noninvasive approach to
0Ambrose
1988
MI P
atie
nts
(n
)
Little1988
Nobuyoshi1991
Giroud1992
Stenosis Prior to MI
Degree of Stenosis Prior to MI
40
20
80
60
100
�70% 50%–70% �50%
MI P
atie
nts
(n
)
All0
80
40
160
120
200
14%
18%
68%
Figure 1. The majority of coronary artery plaques that rupture and lead to a myocardial infarction (MI) are notocclusive. Adapted with permission from Falk E et al.30
LM
LAD
Stenosis
Figure 2. Coronary CT angiography showing subtotalnoncalcified LAD coronary artery stenosis in patientwith acute chest pain and “0” coronary calcium score.LAD, left anterior descending artery; LM, left mainartery.
RICMS0002(GE)_03-14.qxd 3/14/08 3:25 PM Page S5

Priceless Clinical Pearls in the Performance of Cardiac CT continued
S6 VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE
define the presence or absence ofCAD is CTCA. Vulnerability may berelated to such factors as plaquecomposition—which can be assessedby CTCA—or inflammatory and ox-idative stress status—which can beassessed with high-sensitivity C-reac-tive protein, lipoprotein-associatedphospholipase A2, or myeloperoxi-dase. If the patient does not haveCAD, the issue of vulnerability be-comes moot. The most recent appro-priateness guidelines for CTCA werepublished in 2006 by the AmericanCollege of Cardiology Foundation(ACCF)/American College of Radiol-ogy (ACR)/Society of CardiovascularComputed Tomography (SCCT)/Society of Cardiovascular MagneticResonance (SCMR)/American Societyof Nephrology (ASN)/North Ameri-can Society for Cardiac Imaging(NASCI)/Society for CardiovascularAngiography and Interventions(SCAI)/Society of InterventionalRadiology (SIR) before there was the
LAD or greater than 60% stenosis ofthe left main coronary artery will betriaged to follow-up conventionalcoronary angiography. All other pa-tients with stenosis greater than 70%in other lower-risk coronary arterysegments will be referred for stresstesting (preferably to stress echocar-diography) to minimize radiation ex-posure or for nuclear myocardial per-fusion stress imaging (MPSI) ifacoustic windows are limited or thepatient is incapable of exercising. Ifthe stress examination result is ab-normal, consideration for referral toconventional angiography is made.All patients, unless there is a con-traindication, are started on aspirinand lipid-lowering therapies with agoal LDL cholesterol below 70 mg/dL.
Who Should Have a Diagnostic CTCA? In the symptomatic patient popula-tion, the 2006 ACCF/ACR/SCCT/SCMR/ASN/NASCI/SCAI/SIR guide-lines consider a variety of circum-stances acceptable for use of CTCA(Table 2). A recent report shows thatCTCA in symptomatic patients hadsensitivity, specificity, and positiveand negative predictive accuracy of95%, 95%, 75%, and 99%, respec-tively.21 In our own clinical practice,the cost saving and efficacy havebeen shown by significant reductionsin referral to the nuclear stress labo-ratory and for conventional coronaryangiography. These findings are con-sistent with those of Danciu and col-leagues,22 who found that multisliceCT (MSCT) was able to identify 80%of a cohort of patients with symp-toms suggestive of CAD and inter-mediate-risk MPSI who were at a lowrisk of events and in whom conven-tional coronary angiography couldbe avoided. The benefit of CTCA doesnot take into account the enhancedability to define the cardiac and non-cardiac (thoracic aortic aneurysm
Table 1Uses of CT in Cardiovascular Disorders
Identify noncalcified and calcified coronary plaque
Semiquantitatively estimate coronary artery stenosis severity
Define anomalous origins of coronary arteries
Evaluate pulmonary vein anatomy prior to and following atrial fibrillation ablation
Evaluate coronary sinus and anterolateral vein anatomy prior to placement of biventricular lead
Identify pericardial effusion and thickening
Identify myocardial infarct (transluminal and subendocardial)
Visualize patency of saphenous vein grafts and arterial bypass conduits
Quantitative assessment of the aortic valve area
Define the anatomy of aortic valves (bicuspid vs tricuspid)
Assess global and regional left and right ventricular function
Identify interarterial communications (atrial septal defects and patent foramen ovale)
Identify left atrial thrombi
Identify cardiac tumors
Identify thoracic aneurysms and dissections
Reprinted with permission from Lepor NE.31
depth of clinical experience that wenow have with regard to CTCA.19
Surprisingly, in these guidelinesthere was no asymptomatic popula-tion that was felt to be appropriatefor CTCA, even though the majorityof the 175,000 Americans who willexperience their first myocardial in-farction this year come from thelower- and intermediate-risk groupas defined by the FRS. An abnormalCTCA outcome in someone fromthese lower-risk patient groupsshould result in the patient beingtreated as high-risk. The recentlypublished Screening for Heart AttackPrevention and Education (SHAPE)20
classification recommends a proac-tive approach to “screening all appar-ently healthy (with no prior diagno-sis of CHD) men 45 to 75 years of ageand women 55 to 75 years of age whoare not considered very low risk.”
In our practice, patients who un-dergo screening CTCA and have se-vere (� 75%) stenosis of the proximal
RICMS0002(GE)_03-14.qxd 3/14/08 3:25 PM Page S6

Priceless Clinical Pearls in the Performance of Cardiac CT
VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE S7
and dissection, pulmonary emboli)causes of chest pain symptoms in anexpeditious fashion.
Utility of CTA in PeripheralArterial DiseaseCTCA virtually replaced conven-tional peripheral angiography for thediagnosis of peripheral vascular dis-ease years ago and the improvedresolution of the ultrafast CTA hasadded a new dimension to the diag-nosis and treatment of peripheral ar-terial disease (PAD). After the confir-mation of PAD by ankle-brachialindex and/or vascular ultrasound inpatients with symptoms of claudica-tion and resting foot pain or non-healing ulcers, CTA provides a non-invasive arterial luminogram, alongwith insights into the type of plaquein the vessel wall that can have impli-cations into the selection of devicesfor revascularization. For instance,the presence or absence of calcium as
well as accurate measurement of thevessel size are crucial in planning thenonsurgical treatment of PAD.
The 3-dimensional reconstitutionof the peripheral arterial tree thatcan be performed with CT providesuseful information that is unavail-able from conventional peripheralangiography. A 360° multiple projec-tion evaluation of peripheral vascu-lature is readily available usingsmaller volumes of radiocontrastthan the 1-dimensional conventionalangiography. Late-phase imaging foridentifying the target distal vessels inpatients with below-the-knee totalocclusions are more accurate and re-liable when done by CTA as com-pared with conventional angiogra-phy (Figure 3).
The treatment of carotid obstruc-tive disease has particularly bene-fited from the information derivedfrom the more advanced ultrafast CTscanning. Plaque composition and
calcification, as well as presence orabsence of thrombus, are much bet-ter defined by CTA and play an im-portant role in determining whethercarotid endarterectomy or carotidartery stenting are the treatment ofchoice (Figure 4).
CTA plays a key role in developingan approach to stent-graft endolumi-nal repair of abdominal and thoracicaortic aneurysms. CTA can be usedfor diagnosis, to provide critically ac-curate measurements for device siz-
Table 2Guideline-Supported Use of Cardiac CT
Intermediate pretest probability of CAD with an uninterpretable ECG or inability toexercise
Evaluation of suspected coronary anomalies
Evaluation of acute chest pain syndrome when there is intermediate pretest likeli-hood for CAD, no ECG changes, and serial negative cardiac enzymes
Evaluation of chest pain syndrome with an uninterpretable or equivocal stress test
Evaluation of coronary arteries in patients with new-onset heart failure to assess etiology
Evaluation of cardiac mass in patients with technically limited images from ECHO, MRI, or TEE
Evaluation of pericardial conditions with technically limited images from ECHO, MRI, or TEE
Evaluation of pulmonary vein anatomy prior to invasive radiofrequency ablation for atrial fibrillation
Noninvasive coronary vein mapping prior to placement of biventricular pacemakers
Noninvasive coronary arterial mapping, including internal mammary artery prior to repeat surgical revascularization
Evaluation of suspected aortic dissection or thoracic aortic aneurysm
Evaluation of suspected pulmonary embolism
CAD, coronary artery disease; ECG, electrocardiogram; ECHO, echocardiogram; TEE, transesophagealechocardiogram.
Severe StenosisProx R ATA
Occl R TP Trunk
Occl L PTA
Occl R Peroneal
Figure 3. Lower extremity CT angiography with arte-rial runoff showing severe disease in the anterior tibialartery (ATA), and occlusive disease in the tibial-peroneal (TP) trunk and peroneal and posterior tibialarteries (PTA). L, left; Occl, occlusion; Prox, proximal;R, right.
R Carotid
Figure 4. Carotid CT angiography showing a severelystenotic internal carotid stenosis in a patient who wasreferred to surgery because of the appearance ofcalcium and distal tortuosity that made placement ofa distal protection device problematic. R, right.
RICMS0002(GE)_03-14.qxd 3/14/08 3:26 PM Page S7

Priceless Clinical Pearls in the Performance of Cardiac CT continued
S8 VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE
ing, to assess the iliac artery tortuos-ity and calcification (which impactssuccessful device delivery), and toprovide short- and long-term follow-up for endoleaks. The unsurpassableresolution of the new generation ofMSCT is essential for planning thesurgical and nonsurgical treatment ofthoracic aortic aneurysms, particu-larly those that involve the arch andthe great vessels.
An evolving use of peripheral CTAis in the early detection of atheroscle-rosis, which may predate the devel-opment of coronary atherosclerosis.Even though the temporal relation-ship of peripheral arterial atheroscle-rosis and cardiac and cerebral athero-sclerosis is not well defined, theinformation provided by peripheralCTA may be important in determin-ing the aggressiveness of the treat-ment for atherosclerosis. Surrogatesof atherosclerosis, such as CIMT, havebeen used for risk stratification ofpatients with hyperlipidemia.
Imaging Difficult Cases There are many technical factors toconsider when imaging coronaryarteries. These are emphasized incourses on cardiac imaging that weteach at Westside Medical Imaging.Radiographic dose is an importantconsideration, but the most impor-tant goal is achieving a diagnosticstudy. Radiographic dose is analo-gous to the intensity of a flashlight;below a dose threshold the intensityof light does not allow enough illu-mination for the production of a di-agnostic-quality study. It is impor-tant that dose be minimized inyounger patients (particularly womenunder the age of 40 years who have asteady, low heart rate and normal orbelow normal body mass index), be-cause they are at the highest risk forcomplications of radiographic expo-sure. For these patients, the coronaryarteries can nearly always be inter-
preted in the diastolic phase of theheart cycle during diastases. Dosecan be reduced by lowering radiation(mAs) during systole and by reduc-ing peak mAs for patients with lowerbody mass index. Unfortunately thisstrategy will often result in a nondi-agnostic study when attempted inpatients with arrhythmias, elderly orobese patients, and in patients withcoronary stents or bypass grafts.Achieving a diagnostic study ondifficult patients often involves ex-perience-based preplanning, imagingin both systole and diastole, andextensive postprocessing reconstruc-tion strategies that cannot be substi-tuted for by imaging hardware with agreater number of detectors (slices).
Patients With Atrial FibrillationAtrial fibrillation (AF) is a commonarrhythmia in a cardiology practice.A large segment of these patients willbe excluded from being imaged withcoronary artery CTA if techniques forimaging are not optimized. Pre-AFablation pulmonary vein studiesfrequently include evaluation of thecoronary arteries when patients arein AF. When the ventricular responsein patients with AF is not controlledit is difficult to obtain a diagnostic-quality study. If the base heart ratecan be lowered to less than 80 beatsper minute (bpm), and ideally to near60 bpm, a diagnostic study is most al-ways achievable. In patients with AFit is important to image in both sys-tole and diastole. Frequently, atrialsegments that cannot be adequatelyvisualized in diastole will be visiblein systole between 20% and 45% ofthe R-R interval. Bolus timing is im-portant, as the left atrium and leftatrial appendage must be well en-hanced to allow for observation ofthrombus. Close reconstruction in-tervals of 1% or 2% are required inboth systole and diastole to obtainimages with minimal motion arti-
fact. The coronary arteries will fre-quently need to be analyzed by seg-ment as a continuous image fromthe proximal to distal segment israrely achieved in a single-phasereconstruction.
Elderly PatientsEven without a prior history of heartdisease, elderly patients frequentlypresent with increased coronaryartery calcium and some degree ofdelayed left ventricular relaxation(diastolic dysfunction). Delayed re-laxation often results in left ventric-ular motion throughout the nor-mally imaged portion of the diastolicphase, in which diastasis occurs. Par-ticularly when combined with calci-fication, this diastolic motion arti-fact can create a false-positive severestenosis or obscure the presence of asignificant stenosis. Again, imagingduring systole and diastole is impor-tant as satisfactory images can oftenbe obtained between 25% and 40%of the R-R interval or even in late di-astole between 75% and 90% of theR-R interval. Close reconstructionintervals of 1% to 3% are often re-quired, particularly to obtain arti-fact-free images of the LAD, which ismost affected by diastolic dysfunc-tion. Complete cardiac CTA functionstudies are typically performed onelderly patients.
Patients With PacemakersPacemakers pose multiple challengeswhen performing cardiac CT imag-ing. The pacemaker wires themselvescause a metallic artifact on CT thatwill obscure adjacent structures. Thismetallic artifact is more of a prob-lem with biventricular pacemakersin which the third wire causes anartifact on left-side coronary arteriesas well as the distal right coronaryartery/posterior descending coronaryartery, which is typically affected bya 2-wire pacemaker. If the patient has
RICMS0002(GE)_03-14.qxd 3/14/08 3:26 PM Page S8

Priceless Clinical Pearls in the Performance of Cardiac CT
VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE S9
a demand pacemaker, it is importantto schedule the study so a pacemakerrepresentative can adjust the pace-maker rate to 60 bpm. Once the rateis reset, if the heart rate is too rapid,intravenous �-blockers can be ad-ministered until the pacing becomesactivated (of course the patientshould always be prescreened forcontraindications for �-blockers). Ifthe heart is paced and regular duringthe study, a diagnostic study is fre-quently obtainable. Reconstructionin both systole and diastole is impor-tant. Metallic wire artifact in diastolemay obscure a segment of a vessel indiastole but not systole, or vice versa.Also, many pacemaker patients havesome degree of either systolic or di-astolic heart failure and a slight tosignificant amount of dyssynchronycan be expected, necessitating 1% to2% reconstruction intervals.
Large PatientsLarge patients are a significant chal-lenge because thin slices are requiredto properly evaluate diseased coro-nary arteries. Radiographic tubes arelimited by the ability to provide therequired dose (mAs) to obtain imageswith an acceptable noise level. Whenpatients approach 300 pounds, havedense upper body musculature, or alarge amount of breast tissue, imagescannot be properly evaluated. Thepresence of an elevated heart rate orirregular heart rhythm, stents, orcoronary artery calcification furthercomplicates the study. Thicker slicesat 1.0 or 1.5 mm may be used to vi-sualize the coronary arteries if calcifi-cation is absent or minimal and nostents are present. In younger pa-tients in whom the clinical questionis whether the coronary arteries arediseased or healthy, the study can beperformed with thick slices and willusually determine if the arteries arehealthy or not. Large patients with acomplicated cardiac history or
known substantial coronary arterycalcification are best studied by con-ventional coronary angiography.
Patients With StentsExcellent image quality is required toevaluate coronary stents for resteno-sis or thrombosis. The heart rateshould ideally be below 65 bpm witha steady R-R interval. A sharp recon-struction kernel is also required;therefore, patients with a large bodyhabitus are not good candidates forstent evaluation. Dense calcificationin the stented segment can also pre-vent optimal evaluation of a stent.Reconstruction intervals of 1% to 2%are desired in these cases. Typically 5to 6 images at 1% intervals areviewed as a cine series. At least 2 con-tiguous phases should show nomovement in the stented segment toensure that any hypodensity seenwithin the stent or at the proximaland distal ends of the stent is not theresult of motion artifact inducedbeam hardening. Measuring stenosiswithin a stent is not possible, but hy-podensity within the stent is alwayssuspicious for in-stent restenosis.Even with good image quality andno motion, stents that are less than3.0 mm in diameter can only be eval-uated in patients with normal or lowbody mass index (Figure 5).
Coronary Artery Bypass SurgeryCoronary artery bypass graft (CABG)patients typically have at least 1 in-ternal mammary artery graft requir-ing coverage from the subclavianartery to the apex of the heart. Thescanning direction is reversed tocaudal-cranial in these patients and a2-phase bolus is used. It is crucial tohave good enhancement in the infe-rior portion of the heart to evaluatethe arteries distal to graft anastomo-sis. The majority of bypass patientsare elderly and there are frequentdysrhythmias and wall motionabnormalities. Pacemakers and auto-matic implantable cardioverter de-fibrillators are also frequently pre-sent in bypass patients. Ideally, apacemaker representative shouldbe present to reset the pacemaker to60 bpm for the study. Evaluation ofnative vessels typically requires re-construction in multiple phases ofsystole and diastole with close recon-struction intervals of 1% to 2%. It isnot unusual to find optimal phasesfor the grafts in diastole and optimalphases for the native vessels in sys-tole (Figure 6). Metallic surgical clipstypically will obscure short segmentsof the graft or the site of anastomo-sis with the native vessel. Fewer clipsare used in recently performed by-pass surgeries and do not typically
Figure 5. Coronary CT angiography showing norestenosis in the 2.5 mm stent in the mid rightcoronary artery.
Figure 6. Cardiac CT angiography showing patencyof the left internal mammary artery and 3 saphenousvein grafts.
RICMS0002(GE)_03-14.qxd 3/14/08 3:26 PM Page S9

Priceless Clinical Pearls in the Performance of Cardiac CT continued
S10 VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE
compromise the study. Large num-bers of metallic surgical clips oftenresult in a study that is limited toevaluation of graft patency and en-hancement in distal native vessels,but not a study that is able to evalu-ate the grafts for the presence ofstenosis or degradation.
Extrasystoles or Heart Rate InstabilityDuring Image AcquisitionBoth premature contractions and anincrease/decrease in heart rate causea change in stroke volume and thusa spatial change in the position ofthe coronary arteries. In the case of apremature contraction, a 64-slice–wide volume will be spatiallydisplaced and the affected coronarysegment will not be contiguous withthe preceding and following coro-nary artery segments. Multiple pre-mature contractions cause multipledisplaced segments. A prematurecontraction can be manually editedout using the scanner software, but ahazy band remains in the image atthe location where the prematurecontraction is removed. If the coro-nary arteries are normal or minimallydiseased, a premature contractiondoes not cause the affected segmentto be nondiagnostic; however, if thepremature contraction occurs in astented segment or a segment withheavy diffuse calcification, then ac-curate stenosis evaluation or quan-tification may not be possible. In thecase of a focal stenosis, evaluation inboth diastole and systole may solvethe problem as a focal stenosis willshift in a cranial caudal direction dur-ing the heart cycle and frequentlywill be clearly seen in either the sys-tolic or diastolic phase.
A steadily increasing or decreasingheart rate that exceeds 8 to 10 bpmfrom the start to end of the scancauses a continual change in strokevolume, and all 64-slice volume coro-nary segments will be discontinuous.
Normal or minimally diseased coro-nary arteries may be grossly inter-pretable by viewing each individualvolume segment of the arteries, but anondiagnostic scan will result in thecase of significant diffuse disease.
Minimizing Risk and Maximizing BenefitAs with any other examination thatexposes a patient to ionizing radia-tion ranging from a chest radiograph(CXR) routinely performed as part ofan annual physical examination, anuclear medicine scan, or a CTCA,both the benefits of obtaining the in-formation as well as the risk need tobe assessed. The often-used analogyto dissuade against the use of CTCA—one CTCA radiation exposure is equiva-lent to 100 CXRs—may be technicallycorrect; however, the benefit of the in-formation gleaned from 1 CTCA isprobably greater than 100 times thatobtained from a CXR. Unfortunately,most of the discussions in both thelay and medical press regarding ben-efit and risk have been unbalanced,focusing mostly on the later.
It is generally accepted in the sci-entific community that high doses ofradiation are linked to both short-and long-term effects.23 There is nosuch agreement among scientistswith regard to the risk associatedwith long-term exposure to the typesof low-level radiation used in medicaldiagnostic studies. Examples of cer-tain patient populations that are ex-posed to higher levels of backgroundradiation either in their living envi-ronment or their occupation (eg, air-line pilots) have not been found tohave increased incidence of can-cers.24,25 The lifetime risk of develop-ing a cancer is not fixed in thegeneral population. Because of therelatively long time it takes for radi-ographic exposure to induce a cancer(eg, at least 12 years in survivors ofthe nuclear blast in Hiroshima),
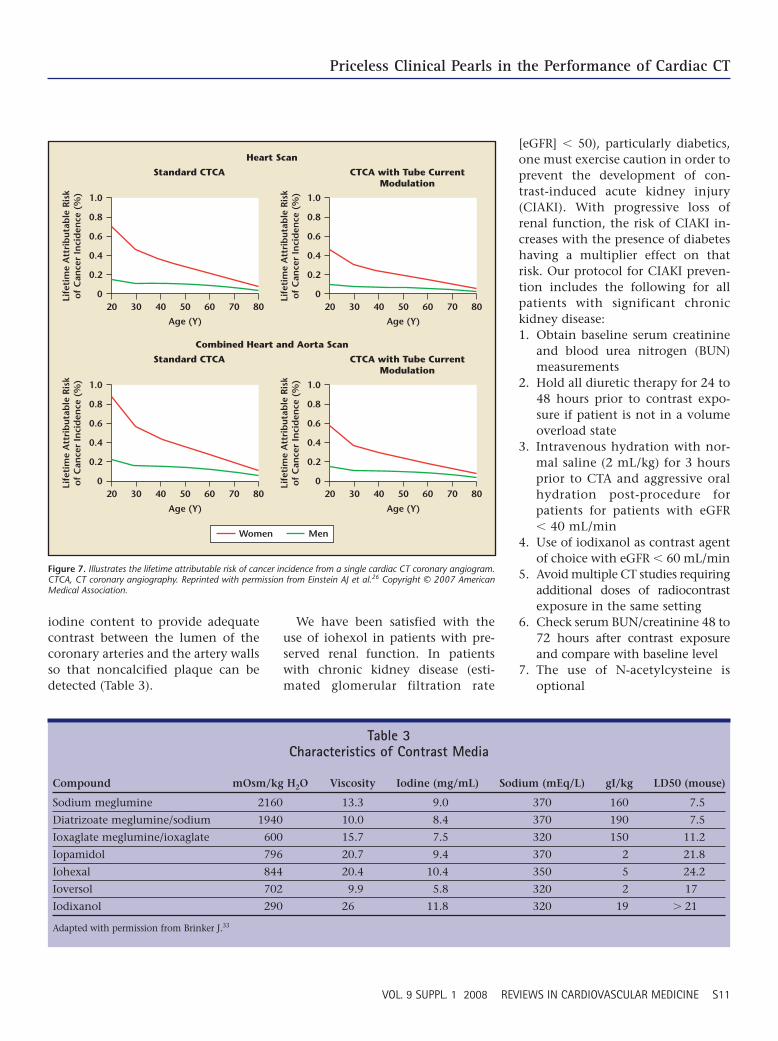
younger people who have longer lifespans would have a greater lifetimeattributable risk (LAR) of developinga cancer. Women are more radiosen-sitive than men, largely attributed tothe radiosensitivity of breast tissue.In a recent analysis estimating can-cer risk associated with exposurefrom a 64-slice CTCA, a 40-year-oldwoman’s LAR was 0.35%, droppingto 0.22% at the age of 60 years, andfurther to 0.075% at 80 years of age(Figure 7). For men, the LAR of cancerwas 0.099% at age 40 years, 0.081%at 60 years, and 0.44% at 80 years ofage.26 These estimates were based onthe effective dose of 14 mSv inwomen and 9 mSv in men usingelectrocardiographically controlledtube current modulation (ECTCM).At Westside Medical Imaging, insti-tuting low radiation protocols in2005 in nonobese patients (� 85 kg)by reducing the tube voltage has ledto significant reductions in effec-tive radiation doses on top of whatis achieved with ECTCM. This pro-tocol is simple to initiate andshould not lead to any degradationin the quality of the CT study. Fur-ther reductions in radiation dosingmay be achieved in the future withprospective gating, which reducesthe use of radiographic exposure toone-fifth of the cardiac cycle.27
SHAPE20 recommendations for car-diac screening suggest excludingwomen under 40 years who wouldhave the higher LAR of developingcancer. In the symptomatic patient,the advantage of CTCA over con-ventional coronary angiography isin being able to avoid the signifi-cant vascular risk associated withthe later, in particular vascularaccess site complications.
Contrast Agent Issues With CTCAThe optimal performance of CTCA re-quires a contrast agent with sufficient
RICMS0002(GE)_03-14.qxd 3/14/08 3:26 PM Page S10
Priceless Clinical Pearls in the Performance of Cardiac CT
VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE S11
iodine content to provide adequatecontrast between the lumen of thecoronary arteries and the artery wallsso that noncalcified plaque can bedetected (Table 3).
We have been satisfied with theuse of iohexol in patients with pre-served renal function. In patientswith chronic kidney disease (esti-mated glomerular filtration rate
[eGFR] � 50), particularly diabetics,one must exercise caution in order toprevent the development of con-trast-induced acute kidney injury(CIAKI). With progressive loss ofrenal function, the risk of CIAKI in-creases with the presence of diabeteshaving a multiplier effect on thatrisk. Our protocol for CIAKI preven-tion includes the following for allpatients with significant chronickidney disease:1. Obtain baseline serum creatinine
and blood urea nitrogen (BUN)measurements
2. Hold all diuretic therapy for 24 to48 hours prior to contrast expo-sure if patient is not in a volumeoverload state
3. Intravenous hydration with nor-mal saline (2 mL/kg) for 3 hoursprior to CTA and aggressive oralhydration post-procedure forpatients for patients with eGFR� 40 mL/min
4. Use of iodixanol as contrast agentof choice with eGFR � 60 mL/min
5. Avoid multiple CT studies requiringadditional doses of radiocontrastexposure in the same setting
6. Check serum BUN/creatinine 48 to72 hours after contrast exposureand compare with baseline level
7. The use of N-acetylcysteine isoptional
1.0
0.8
0.6
Life
tim
e A
ttri
but
able
Ris
ko
f C
ance
r In
cid
ence
(%
)
0.4
0.2
020 30 40 50
Age (Y) Age (Y)
Age (Y) Age (Y)
60 70 80
1.0
0.8
0.6
Life
tim
e A
ttri
but
able
Ris
ko
f C
ance
r In
cid
ence
(%
)
0.4
0.2
020 30 40
Standard CTCA CTCA with Tube CurrentModulation
CTCA with Tube CurrentModulation
Combined Heart and Aorta Scan
Heart Scan
Standard CTCA
50 60 70 80
1.0
0.8
0.6
Life
tim
e A
ttri
but
able
Ris
ko
f C
ance
r In
cid
ence
(%
)
0.4
0.2
020 30 40 50 60 70 80
1.0
0.8
0.6
Life
tim
e A
ttri
but
able
Ris
ko
f C
ance
r In
cid
ence
(%
)
0.4
0.2
020 30 40 50 60 70 80
Women Men
Figure 7. Illustrates the lifetime attributable risk of cancer incidence from a single cardiac CT coronary angiogram.CTCA, CT coronary angiography. Reprinted with permission from Einstein AJ et al.26 Copyright © 2007 AmericanMedical Association.
Table 3Characteristics of Contrast Media
Compound mOsm/kg H2O Viscosity Iodine (mg/mL) Sodium (mEq/L) gI/kg LD50 (mouse)
Sodium meglumine 2160 13.3 9.0 370 160 7.5
Diatrizoate meglumine/sodium 1940 10.0 8.4 370 190 7.5
Ioxaglate meglumine/ioxaglate 600 15.7 7.5 320 150 11.2
Iopamidol 796 20.7 9.4 370 2 21.8
Iohexal 844 20.4 10.4 350 5 24.2
Ioversol 702 9.9 5.8 320 2 17
Iodixanol 290 26 11.8 320 19 � 21
Adapted with permission from Brinker J.33
RICMS0002(GE)_03-14.qxd 3/14/08 11:31 PM Page S11

Priceless Clinical Pearls in the Performance of Cardiac CT continued
S12 VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE
References1. Harmon M, Biondi-Zoccai GGL, Malagutti P, et al.
Diagnostic performance of multislice spiralcomputed tomography of coronary arteries ascompared with conventional invasive coronaryangiography: a meta analysis. J Am Coll Cardiol.2006;48:1896-1910.
2. Rosamond W, Flegal K, Furie K, et al. Heartdisease and stroke statistics—2008 update: areport from the American Heart AssociationStatistics Committee and Stroke Statistics Sub-committee. Circulation. 2008;117:e25-e146.
3. Ford ES, Capewell S. Coronary heart diseasemortality among young adults in the U.S. from1980 through 2002. J Am Coll Cardiol.2007;50:2128-2132.
4. Dawber TR, Meadors GF, Moore FEJ. Epidemio-logical approaches to heart disease: the Fram-ingham Study. Am J Public Health. 1951;41:279-286.
5. Khot UN, Khot MB, Bajzer CT, et al. Prevalence ofconventional risk factors in patients with coro-nary heart disease. JAMA. 2003;290:898-904.
6. Ford ES, Giles WH, Mokdad AH. The distribu-tion of 10-year risk for coronary heart diseaseamong U.S. adults: findings from the NationalHealth and Nutrition Examination Survey III. JAm Coll Cardiol. 2004;43:1791-1796.
7. Lakoski SG, Greenland P, Wong ND, et al.Coronary artery calcium scores and risk for car-diovascular events in women classified as “lowrisk” based on Framingham risk score. TheMulti-Ethnic Study of Atherosclerosis (MESA).Arch Intern Med. 2007;167:2437-2442.
8. Lloyd-Jones DM, Leip EP, Larson G, et al.Prediction of lifetime risk for cardiovasculardisease by risk factor burden at 50 years of age.Circulation. 2006;113:791-798.
9. Nissen S, Tuzcu E, Schoenhagen P, et al. Effectof intensive compared with moderate lipid-lowering therapy on progression of coronaryatherosclerosis: a randomized controlled trial.JAMA. 2004;291:1071-1080.
10. Khot U, Khot M, Bajzer C, et al. Prevalence ofconventional risk factors in patients with coro-nary heart disease. JAMA. 2003;290:898-904.
Main Points• Cardiovascular CT represents an important innovation in cardiac imaging as a noninvasive modality for the diagnosis
of coronary artery disease; the emergence of 64-slice CT scanners and associated software capable of complex 3-dimensional image reconstruction of coronary arteries has revolutionized the approach to patients with cardiovas-cular disease.
• In addition to imaging the coronary arteries, the advantages of CT coronary angiography (CTCA) include the abilitywith the same data acquisition to evaluate right and left ventricular function, thoracic aorta and aortic valve anatomy,left atrial thrombi, and pericardial thickening.
• The unsurpassable resolution of the new generation of multislice CT is essential for planning the surgical andnonsurgical treatment of thoracic aortic aneurysms, particularly those that involve the arch and the great vessels.
• The optimal performance of CTCA requires a contrast agent with sufficient iodine content to provide adequatecontrast between the lumen of the coronary arteries and the artery walls so that noncalcified plaque can be detected.
• The recently published Screening for Heart Attack Prevention and Education classification recommends a proactiveapproach to screening all apparently healthy (with no prior diagnosis of coronary heart disease) men 45 to 75 yearsof age and women 55 to 75 years of age who are not considered very low risk.
Contrast ReactionsAcute allergy-like hypersensitivity re-actions occur in 10% to 15% of pa-tients receiving contrast agents andseem to be more common with intra-venous administration.28 Pretreat-ment with steroids 12 and 2 hoursprior to contrast exposure seems toreduce the incidence of hypersensi-tivity reactions in patients at risk.Late reactions usually occur within 3days of exposure to contrast but canbe delayed for up to 1 week. It is im-portant that both clinicians and pa-tients alike be aware of these late re-actions, which can be confused withother conditions. The incidence ofdelayed reactions seems to be morecommon in patients with no previ-ous history of radiocontrast expo-sure, history of allergies, past adversecontrast reactions, and serum creati-nine above 2.0 mg/dL.29 A flu-likesyndrome with fever, malaise,arthralgias, and nausea can occur, aswell as vomiting, abdominal pain,diarrhea, dizziness. Rare symptomsinclude wheezing, parotitis, and hy-potension. The types of skin reac-tions vary from the most commonmeasles-like eruptions to erythemamultiforme, erythrodermia, eczema,and urticaria. Most delayed reactions
are mild and require no specifictreatment. If therapy is indicated,symptom-directed treatment withanalgesics, antipyretics, and antihist-amines is usually sufficient.
ConclusionsCardiac CT has changed the para-digm for evaluating the patient atrisk for developing CAD or symptomssuggestive of a cardiac or vasculardisorder. The information fromCTCA will often affect the approachof cardiologists in the care of theirpatients. The shortcomings of FRS toassess cardiac risk increases the im-portance of imaging to enhance car-diovascular disease risk assessment.To produce optimal CTCA images,the imaging center must be dedi-cated to the technical aspects of car-diac image reconstruction, which is alabor-intensive process that can attimes be tedious. To guarantee theproduction of high-quality coronarystudies, it is imperative that cardiolo-gists who are dedicated to imagingand who have expertise in coronaryanatomy and physiology assumeleadership roles in the field.
Dr. Lepor, Dr. Madyoon, and Mr. Friede have noreal or apparent conflicts of interest to report.
RICMS0002(GE)_03-14.qxd 3/14/08 3:26 PM Page S12
Priceless Clinical Pearls in the Performance of Cardiac CT
VOL. 9 SUPPL. 1 2008 REVIEWS IN CARDIOVASCULAR MEDICINE S13
11. Wyman RA, Gimelli G, McBride PE, et al. Doesdetection of carotid plaque affect physicianbehavior or motivate patients. Am Heart J.2007;154:1072-1077.
12. Detrano RC, Guerci A, Carr JJ, et al. Coronarycalcium predicts near-term coronary heart dis-ease events in major American ethnic groups:the multi-ethnic study of atherosclerosis[abstract]. J Am Coll Cardiol. 2007;49(Suppl A):101A.
13. Morrow DA, Gersh BJ, Braunwald, E. Chroniccoronary artery disease. In: Zipes DP, Libby P,Bonow R, eds. Braunwald’s Heart Disease: ATextbook of Cardiovascular Medicine. 7th ed.Philadelphia: WB Saunders; 2004.
14. Cheng VY, Lepor NE, Madyoon H, et al. Pres-ence and severity of noncalcified coronaryplaque on 64-slice computed tomographiccoronary angiography in patients with zeroand low coronary artery calcium. Am J Cardiol.2007;99:1183-1186.
15. Wyman RA, Mays ME. McBride ME, et al. Ul-trasound detected carotid plaque as a predictorof cardiovascular events. Vasc Med. 2006;31:123-130.
16. Lepor N, Madyoon H, Azmoon S, et al. Associa-tion of carotid disease using ultrasound to coro-nary artery stenosis and coronary calciumusing 64 slice cardiac CT angiography. Presentedat: 19th Annual Transcatheter CardiovascularTherapeutics Scientific Sessions; October 2007;Washington, DC.
17. Falk E, Shah PK, Fuster V. Coronary plaque dis-ruption. Circulation. 1995;92:657-671.
18. Van Mieghem C, McFadden E, deFeyter P, et al.Noninvasive detection of subclinical athero-
sclerosis coupled with assessment of changes inplaque characteristics using novel invasiveimaging modalities. The Integrated Biomarkerand Imaging Study (IBIS). J Am Coll Cardiol.2006;47:1134-1142.
19. Hendel RC, Patel MR, Kramer CM, et al.ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR2006 appropriateness criteria for cardiaccomputed tomography and cardiac magneticresonance imaging: a report of the AmericanCollege of Cardiology Foundation QualityStrategic Directions Committee Appropriate-ness Criteria Working Group, American Collegeof Radiology, Society of Cardiovascular Com-puted Tomography, Society for CardiovascularMagnetic Resonance, American Society ofNuclear Cardiology, North American Societyfor Cardiac Imaging, Society for CardiovascularAngiography and Interventions, and Society ofInterventional Radiology. J Am Coll Cardiol.2006;48:1475-1497.
20. Naghavi M, Falk E, Hecht HS, et al. From vul-nerable plaque to vulnerable patient—Part III:Executive summary of the Screening for HeartAttack Prevention and Education (SHAPE) TaskForce report. Am J Cardiol. 2006;98:2H-15H.
21. Weustink AC, Meijboom WB, Mollet NR, et al.Reliable high-speed coronary computed tomog-raphy in symptomatic patients. J Am Coll Cardiol.2007;50:786-794.
22. Danciu SC, Herrera CJ, Stecy PJ, et al. Usefull-ness of multislice computed tomographic coro-nary angiography to identify patients withabnormal myocardial perfusion stress in whomdiagnostic catheterization may be safelyavoided. Am J Cardiol. 2007;100:1605-1608.
23. Preston RJ. Radiation biology: concepts for radi-ation protection. Health Phys. 2005;88:545-556.
24. Wei L. Health survey in high background radia-tion areas in China. Science. 1980;209:877-880.
25. Langner I, Blettner, M. Gundestrup M, et al. Cos-mic radiation and cancer mortality among air-line pilots: results from a European cohortstudy (ESCAPE). Radiat Environ Biophys. 2004;42:247-256.
26. Einstein AJ, Henzlova MJ, Rajagopalan S. Esti-mating risk of cancer associated with radiationexposure from 64-slice computed tomographycoronary angiography. JAMA. 2007;298:317-323.
27. Earls J, Urban B, Berman E, et al. Prospectivegated coronary CT angiography: an evaluationof effective dose and reliability in large patientgroup [abstract]. J Comput Tomogr. 2007;1:S6-S7.
28. Shehadi WH, Toniolo G. Adverse reactions tocontrast material. Radiology. 1980;137:299-302.
29. Hosoya T, Yamaguchi K, Akutsu T, et al. De-layed adverse reactions to iodinated contrastmedia and their risk factors. Radiat Med.2000;18:39-45.
30. Falk E, Shah PK, Fuster V. Coronary plaquedisruption. Circulation. 1995;92:657-671.
31. Lepor NE. Screening CT-Coronary Angiogra-phy: Ready for Prime Time? Rev Cardiovasc Med.2006;7(4):198-204.
32. Einstein AJ, Henzlova MJ, Rajagopalan S. Esti-mating risk of cancer associated with radiationexposure from 64-slice computed tomographycoronary angiography. JAMA. 2007;298:317-323.
33. Brinker J. What Every Cardiology Should KnowAbout Intravascular Contrast. Rev CardiovascMed. 2003;4(suppl 5):S19-S27.
RICMS0002(GE)_03-14.qxd 3/14/08 3:26 PM Page S13