Prevalence, awareness, treatment and control of hypertension among slum dwellers in Nairobi, Kenya
8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Prevalence, awareness, treatment and control of hypertension in urban poor communities in Accra, Ghana Raphael B. Awuah a , John K. Anarfi a , Charles Agyemang b , Gbenga Ogedegbe c , and Ama de-Graft Aikins a Background: Hypertension is a major public health problem in many sub-Saharan African countries including Ghana, but data on urban poor communities are limited. The aim of this study was therefore to assess the prevalence, awareness, management and control of hypertension among a young adult population in their reproductive ages living in urban poor communities in Accra. Methods: Cross-sectional, population-based survey of 714 young adults in their reproductive ages (women aged 15–49 years, men aged 15–59 years) living in three urban poor suburbs of Accra, Ghana. Results: The overall prevalence of hypertension in all three communities was 28.3% (women 25.6% and men 31.0%). Among respondents who had hypertension, 7.4% were aware of their condition; 4% were on antihypertensive medication while only 3.5% of hypertensive individuals had adequate blood pressure (BP) control (BP <140/90 mmHg). The level of awareness and treatment was lower in men than in women (3.1 and 1.3% for men and 11.9 and 6.5% for women, respectively). Among individuals with hypertension, the rate of control was higher among women than among men (5.0 and 2.1%, respectively). Conclusion: Although about a quarter of the young adult population in these low-income communities of Accra have hypertension, the levels of awareness, treatment and control are abysmally low. We recommend community- specific primary and secondary prevention interventions that draw on existing resources, specifically implementing cardiovascular disease (CVD) interventions in faith-based organizations and task-shifting CVD care through the national Community-based Health Planning and Services (CHPS) programme. Keywords: Accra, awareness, control, hypertension, prevalence, treatment, urban poor Abbreviations: AMA, Accra Metropolitan Assembly; BP, blood pressure; CHPS, Community-based Health Planning and Services; CVD, cardiovascular disease; IRB, Institutional Review Board INTRODUCTION C ardiovascular diseases (CVDs) are a growing public health problem in low and middle-income countries (LMICs) [1]. It is estimated that by 2030, mortality due to CVD in the adult population will reach 23 million with about 85% of such deaths occurring in LMICs [2]. Hypertension is a major risk factor for CVD. It has been suggested that the prevalence of hypertension is increasing rapidly due to rising longevity and the increasing preva- lence of contributing factors such as unhealthy diet, obesity and physical inactivity [3]. In Ghana, hypertension prevalence has increased stead- ily over the last two decades with more than a 10-fold increase in the number of reported new cases of hyperten- sion [blood pressure (BP) 140/90 mmHg] in public health facilities from 49 087 in 1988 to 505 180 in 2007 [4]. Studies have indicated a prevalence between 25 and 48% with higher rates in urban populations than in rural populations [5]. Evidence also suggests that many Ghanaians living with hypertension are not aware of their condition [6]. In the Greater Accra Region of Ghana, hypertension moved from fourth to become second to malaria as the leading cause of outpatient morbidity in 2007 [7]. Although high rates of hypertension have been documented in urban areas of Accra [8], its prevalence, awareness, management and control in an urban poor context has not yet been fully assessed despite the fact that urban poor residents are disproportionately affected by the double burden of communicable and chronic noncommunicable diseases. Ghana’s epidemiological transition has been described in terms of a ‘protracted polarized model’, because there has Journal of Hypertension 2014, 32:000–000 a Regional Institute for Population Studies, University of Ghana, Accra, Ghana, b Department of Public Health, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands and c Center for Healthful Behavior Change, Division of Health and Behavior, New York University School of Medicine and NYU Global Institute of Public Health, New York, New York, USA Correspondence to Ama de-Graft Aikins, Regional Institute for Population Studies, University of Ghana, P.O. Box LG 96 Legon, Accra, Ghana. Tel: +233 302 500 274; fax: +233 302 500 273; e-mail: [email protected] Received 21 January 2014 Accepted 2 February 2014 J Hypertens 32:000–000 ß 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins. DOI:10.1097/HJH.0000000000000165 Journal of Hypertension www.jhypertension.com 1 Original Article
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Prevalence, awareness, treatment and control of hypertension among slum dwellers in Nairobi, Kenya
CE: Swati; JH-D-14-00085; Total nos of Pages: 8;
JH-D-14-00085
Original Article
Prevalence, awareness, treatment and control ofhypertension in urban poor communities in Accra,Ghana
Raphael B. Awuaha, John K. Anarfia, Charles Agyemangb, Gbenga Ogedegbec, andAma de-Graft Aikinsa
Journal of Hypertension 2014, 32:000–000aRegional Institute for Population Studies, University of Ghana, Accra, Ghana,bDepartment of Public Health, Academic Medical Centre, University of Amsterdam,Amsterdam, The Netherlands and cCenter for Healthful Behavior Change, Division ofHealth and Behavior, New York University School of Medicine and NYU GlobalInstitute of Public Health, New York, New York, USA
Correspondence to Ama de-Graft Aikins, Regional Institute for Population Studies,University of Ghana, P.O. Box LG 96 Legon, Accra, Ghana. Tel: +233 302 500 274; fax:+233 302 500 273; e-mail: [email protected]
Received 21 January 2014 Accepted 2 February 2014
Background: Hypertension is a major public healthproblem in many sub-Saharan African countries includingGhana, but data on urban poor communities are limited.The aim of this study was therefore to assess theprevalence, awareness, management and control ofhypertension among a young adult population in theirreproductive ages living in urban poor communities inAccra.
Methods: Cross-sectional, population-based survey of714 young adults in their reproductive ages (women aged15–49 years, men aged 15–59 years) living in three urbanpoor suburbs of Accra, Ghana.
Results: The overall prevalence of hypertension in all threecommunities was 28.3% (women 25.6% and men31.0%). Among respondents who had hypertension, 7.4%were aware of their condition; 4% were onantihypertensive medication while only 3.5% ofhypertensive individuals had adequate blood pressure (BP)control (BP <140/90 mmHg). The level of awareness andtreatment was lower in men than in women (3.1 and1.3% for men and 11.9 and 6.5% for women,respectively). Among individuals with hypertension, therate of control was higher among women than amongmen (5.0 and 2.1%, respectively).
Conclusion: Although about a quarter of the young adultpopulation in these low-income communities of Accrahave hypertension, the levels of awareness, treatment andcontrol are abysmally low. We recommend community-specific primary and secondary prevention interventionsthat draw on existing resources, specifically implementingcardiovascular disease (CVD) interventions in faith-basedorganizations and task-shifting CVD care through thenational Community-based Health Planning and Services(CHPS) programme.
Keywords: Accra, awareness, control, hypertension,prevalence, treatment, urban poor
Abbreviations: AMA, Accra Metropolitan Assembly; BP,blood pressure; CHPS, Community-based Health Planningand Services; CVD, cardiovascular disease; IRB, InstitutionalReview Board
Copyright © Lippincott Williams & Wilkins. UnauthJournal of Hypertension
INTRODUCTION
Cardiovascular diseases (CVDs) are a growing publichealth problem in low and middle-income countries(LMICs) [1]. It is estimated that by 2030, mortality
due to CVD in the adult population will reach 23 millionwith about 85% of such deaths occurring in LMICs [2].Hypertension is a major risk factor for CVD. It has beensuggested that the prevalence of hypertension is increasingrapidly due to rising longevity and the increasing preva-lence of contributing factors such as unhealthy diet, obesityand physical inactivity [3].
In Ghana, hypertension prevalence has increased stead-ily over the last two decades with more than a 10-foldincrease in the number of reported new cases of hyperten-sion [blood pressure (BP) �140/90 mmHg] in public healthfacilities from 49 087 in 1988 to 505 180 in 2007 [4]. Studieshave indicated a prevalence between 25 and 48% withhigher rates in urban populations than in rural populations[5]. Evidence also suggests that many Ghanaians living withhypertension are not aware of their condition [6].
In the Greater Accra Region of Ghana, hypertensionmoved from fourth to become second to malaria as theleading cause of outpatient morbidity in 2007 [7]. Althoughhigh rates of hypertension have been documented in urbanareas of Accra [8], its prevalence, awareness, managementand control in an urban poor context has not yet been fullyassessed despite the fact that urban poor residents aredisproportionately affected by the double burden ofcommunicable and chronic noncommunicable diseases.Ghana’s epidemiological transition has been described interms of a ‘protracted polarized model’, because there has
orized reproduction of this article is prohibited.
J Hypertens 32:000–000 � 2014 Wolters Kluwer Health | Lippincott Williams &Wilkins.
DOI:10.1097/HJH.0000000000000165
www.jhypertension.com 1

CE: Swati; JH-D-14-00085; Total nos of Pages: 8;
JH-D-14-00085
Awuah et al.
been a coexistence of communicable and noncommuni-cable diseases over a long period of time and the impact ofthe double disease burden has been polarized acrosssocioeconomic status. Therefore, although wealthy com-munities are predominantly affected by chronic noncom-municable diseases, poor communities are affected byboth noncommunicable and communicable diseases [9].This study aimed to assess the prevalence, levels of aware-ness, management and control of hypertension among theadult population in three urban poor communities inAccra.
MATERIALS ANDMETHODS
SettingThe study was conducted in three urban poor communitiesin Accra: James Town, Ussher Town and Agbogbloshie. Thecommunities are characterized by high population density,low socioeconomic status and a built-up environment withpoor sanitary conditions and poor housing structures. Theaverage monthly household income in all three commun-ities is only USD 78.83 [10]. About three-quarters of thepopulation have attained up to Junior High School (ormiddle school) education and above. James Town andUssher Town are indigenous communities inhabited mainlyby the Ga-Dangme ethnic group with fishing and pettytrading constituting their main economic activities, whileAgbogbloshie is a largely heterogeneous and migrantcommunity with most inhabitants working as traders andartisans.
The study was part of a broader longitudinal ‘UrbanPoverty and Health Survey’ conducted by the RegionalInstitute for Population Studies (RIPS). RIPS, with supportfrom the Secretariat of the African Caribbean and PacificGroup of States – ACP-EU Cooperation Programme inHigher Education (EDULINK) and IDRC, has establishedan active research field site in the three study communities.The aim of the Urban Poverty and Health Survey (UPHS) isto examine health, poverty and development indicators inthese settings over time and to provide vital data to localand regional stakeholders for the development of thecommunities. Two survey rounds were conducted at18-month intervals in 2010 (June) and 2011 (December),with households and individuals. The third survey roundis currently in progress. The study reported here wasconducted as part of the 2011 survey round (hereafterUPHS-II).
SamplingThe UPHS-II study sample was drawn from 29 enumerationareas, each with 40 households systematically chosen tomake up a total sample size of 1160 households distributedover the three localities. The number of enumeration areasand, therefore, households in each locality was propor-tionate to the population size of that locality. There werefive enumeration areas from Agbogbloshie, eight fromJames Town and 16 from Ussher Town. The aim of thissampling procedure was to arrive at a survey with 986households interviewed. Estimates from the Ghana Statisti-cal Service indicated that the nonresponse rate in theGreater Accra Region is about 15%. As such, adding an
Copyright © Lippincott Williams & Wilkins. Unaut2 www.jhypertension.com
extra 15% of households to 986 households led to a total of1160 households surveyed in this study. In each householdchosen, the head of the household responded to the house-hold questionnaire, although every woman between theages of 15 and 49 years and every man between the ages of15 and 59 years responded to the individual questionnaire.The data were collected using an interviewer-administeredquestionnaire.
Inclusion criteriaMen aged 15–59 and women aged 15–49 years (i.e. adultpopulation in their reproductive ages) were eligible toanswer the individual questionnaire in the survey and byextension had their BP measurements taken. Pregnantwomen and those who had given birth in the last 6 monthspreceding the study were excluded from the studybecause of the potential for pregnancy-induced hyper-tension [11].
In total, a representative sample of 974 individuals waseligible to be interviewed for the individual questionnaireout of which 714 individuals had their BP measurementstaken. Some respondents refused BP measurements eventhough they responded to the individual questionnaire. Ithas been determined that a sample size of 400 is adequateto detect prevalence of hypertension with 5% precision and95% confidence level [12].
Blood pressure measurementsField personnel received standard training on BP measure-ments, which were obtained on a single visit. Respondentswere made to sit on a chair with their back rested while theyrested their arm on a table at the level of the heart.Respondents’ arm circumferences were measured andthe appropriate cuff size was used to take the measure-ments [13]. At each examination, after a 5-min rest, BP wasmeasured on the seated participant’s right or left arm usinga validated automated BP monitoring device (MicrolifeWatch BP Home, Model BP3MX1-1; Microlife Corporation)[14]. Three measurements were taken at 1 to 2-min(s)intervals and the average of the three readings was usedfor the analysis. This is in line with the WHO’s recommen-dation of using the average of three BP readings at one visitin risk factor surveys [15].
MeasurementsSocio-demographic details, information on health con-ditions and behaviour, and use of medication was obtainedfrom the respondents [16]. Ages of respondents were reca-tegorized into younger adults (15–24 years), middle-agedadults (25–34 years) and older adults (�35 years). Edu-cational status referred to the highest level of formal school-ing attained by an individual. On this basis, five categorieswere obtained (no education, primary and middle/juniorhigh, secondary/senior high and tertiary education).Locality referred to the usual residence of respondents(James Town, Ussher Town or Agbogbloshie).
Physical activity was measured at the household level[17]. It was estimated by quantifying moderate-intensityactivities such as carrying light loads, washing clothes, briskwalking, scrubbing floors and sweeping inside or around
horized reproduction of this article is prohibited.Volume 32 � Number 1 � Month 2014

CE: Swati; JH-D-14-00085; Total nos of Pages: 8;
JH-D-14-00085
Prevalence of hypertension in Accra
their home for at least 20min daily [18]. Physical activity wasrecategorized as at least 3 days in a week and less than3 days in a week. Alcohol consumption was based onthe pattern of consumption [19] and was reclassified intothree categories: nondrinkers, occasional drinkers andregular drinkers. Weight was measured to the nearest0.1 kg with respondents wearing light clothing. Heightwas measured without shoes with a measuring tape tothe nearest 0.1 cm. BMI was calculated as weight (kg)divided by standing height (m2). BMI was then categorizedas normal (19–24.9 kg/m2), overweight (25–29.9 kg/m2)and obese (�30 kg/m2).
Hypertension was defined as a SBP at least 140 mmHgand/or a DBP at least 90 mmHg or the use of antihyper-tensive medication. Awareness was assessed amongindividuals with hypertension and was based on therespondents’ report of a prior diagnosis of hypertensionmade by a health professional [20]. Treatment of hyperten-sion was defined as self-reported use of antihypertensivemedication [16,20]. Hypertension control was defined as theproportion of hypertensive individuals with SBP of less than140 mmHg and DBP of less than 90mmHg.
Ethical informationEthical approval for the study was obtained from theInstitutional Review Board (IRB) of the Noguchi MemorialInstitute for Medical Research. Respondents were asked tosign or thumbprint a consent form read to them before theinterview and BP measurements proceeded.
Copyright © Lippincott Williams & Wilkins. Unauth
TABLE 1. Characteristics of respondents by sex
Characteristic Total sample (n¼714)
Mean age (years) 31.0 (�10.6)
SBP (mmHg) 121.6 (�.16.6)
DBP (mmHg) 76.5 (�11.9)
BMI (kg/m2) 25.0 (�6.8)
Age groups (years)Younger adults (15–24) 240 (33.6%)
Middle-aged adults (25–34) 222 (31.1%)
Older adults (�35) 252 (35.3%)
Highest level of educationNo education 39 (5.5%)
Primary 141 (19.7%)
Middle/Junior high school (JHS) 315 (44.1%)
Senior high school (SHS) 185 (25.9%)
Tertiary 34 (4.8%)
Locality of residenceJames Town 242 (33.9%)
Ussher Town 351 (49.2%)
Agbogbloshie 121 (16.9%)
EthnicityGa-Dangme 419 (58.7%)
Akan 188 (26.3%)
Ewe 35 (4.9%)
Northern ethnic groups 72 (10.1%)
Physical activity�3 days in a week 202 (28.3%)
<3 days in a week 512 (71.7%)
Alcohol consumptionNondrinkers 261 (36.6%)
Occasional drinkers 327 (45.8%)
Regular drinkers 126 (17.6%)
Values are mean� SD or n (%).
Journal of Hypertension
Statistical analysisResults were expressed as mean� standard deviation (forcontinuous variables) or as percentages. Bivariate compari-sons were performed using x2 test for categorical variables.Multivariate analysis was performed using the binary logis-tic regression and results were expressed as odds ratios with95% confidence intervals (CIs). The factors known to influ-ence BP in our data (i.e. alcohol consumption, BMI,physical activity, locality of residence, education, ethnicityand age) were evaluated in a logistic regression modelusing the enter method. All statistical analyses were per-formed using SPSS 19.0 for Windows (SPSS, Inc., an IBMCompany Copyright 2010).
RESULTS
Characteristics of study participantsThe characteristics of the study population are presented inTable 1. A total of 714 respondents were included in theanalysis with an almost equal proportion of men andwomen, and a mean age of 31 years (range 15–59 years).Majority of the sample were educated at the primary orsecondary education level; were either occasional orregular drinkers; and were engaged in a moderate physicalactivity less than 3 days a week. Of the three communities,Agbogbloshie had the highest proportion of residents withno formal education (41.0%) while Ussher Town had thehighest proportion of residents with higher or tertiaryeducation (58.8%). With regard to BMI, over one-third of
orized reproduction of this article is prohibited.
Men (n¼329) Women (n¼385)
31.5 (�11.6) 30.6 (�9.6)
124.4 (�15.9) 119.4 (�16.7)
77.5 (�12.2) 75.4 (�11.5)
22.8 (�3.9) 26.9 (�8.1)
110 (33.4%) 130 (33.8%)
104 (31.6%) 118 (30.6%)
115 (35.0%) 137 (35.6%)
10 (3.0%) 29 (7.5%)
37 (11.2%) 104 (27.0%)
147 (44.7%) 168 (43.6%)
107 (32.5%) 78 (20.3%)
28 (8.5%) 6 (1.6%)
119 (36.2%) 123 (31.9%)
160 (48.6%) 191 (49.6%)
50 (15.2%) 71 (18.4%)
211 (64.1%) 208 (54.0%)
78 (23.7%) 110 (28.6%)
13 (4.0%) 22 (5.7%)
27 (8.2%) 45 (11.7%)
66 (20.1%) 136 (35.3%)
263 (79.9%) 249 (64.7%)
108 (32.8%) 153 (39.7%)
144 (43.8%) 183 (47.5%)
77 (23.4%) 49 (12.7%)
www.jhypertension.com 3

CE: Swati; JH-D-14-00085; Total nos of Pages: 8;
JH-D-14-00085
Agbogbloshie
James Town
Ussher Town
ACCRA
GA SOUTH
GA EAST
LEDZOKUKU KROWOR
N
LegendTransportation
Rail line1st class road2nd class road3rd class roadTrackFootpathHydroStudy areaBuilt up areaSeaAccra metropolitan area
1 : 4000
3000 0 3000 5000 MetersGulf of Guinea
STUDY AREA MAPACCRA METROPOLITAN MAP
FIGURE 1 Map of Accra showing the study areas (Colour version). Map of Accra showing the study areas (Noncolour version).
Awuah et al.
the study population were either overweight or obese withhigher rates in women than in men (P< 0.001).
SBP and DBP valuesSBP and DBP levels were higher in men than in women(P< 0.001 for systolic and P¼ 0.007 for diastolic). SBP andDBP increased progressively with age in men and inwomen (P< 0.001 for systolic and P< 0.001 for diastolic).However, no clear pattern was observed by educationallevel (Fig. 1).
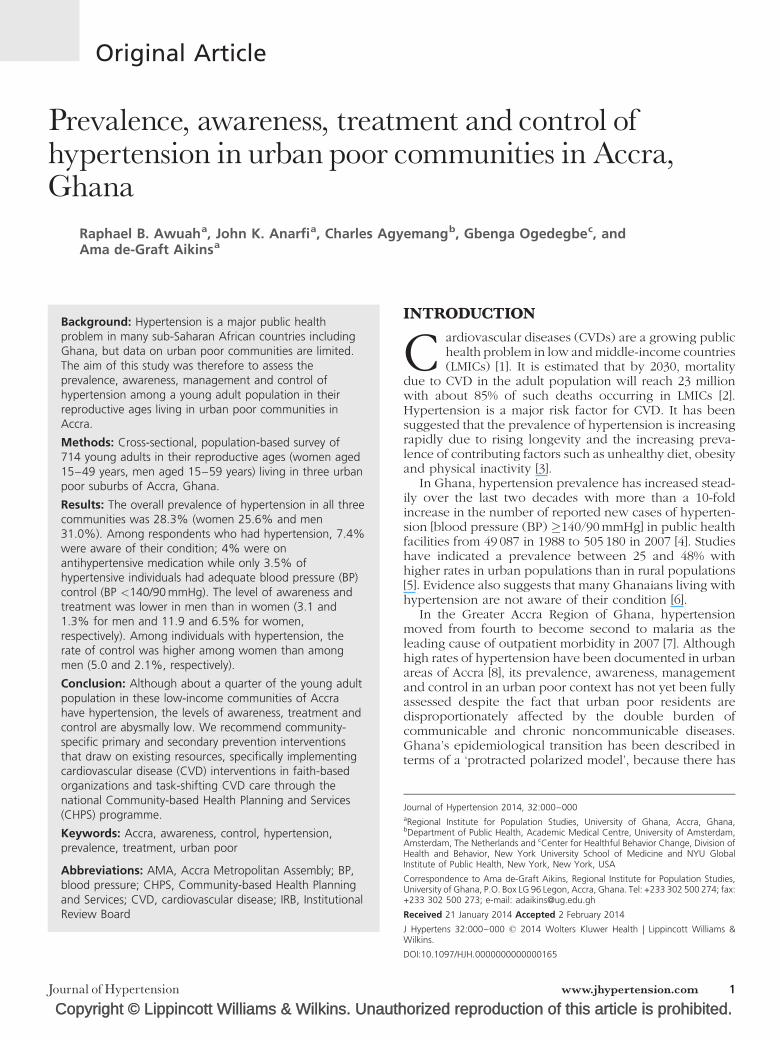
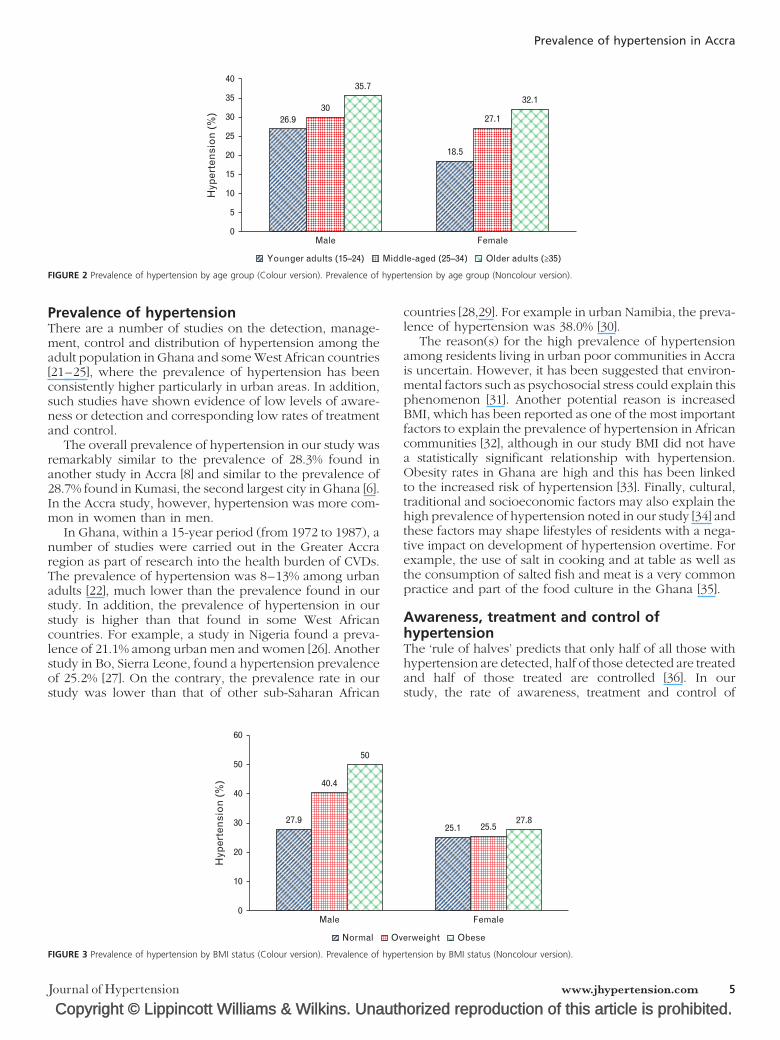
Prevalence, awareness, treatment and controlof hypertensionThe overall prevalence of hypertension was 28.3% (95% CI25.1–31.7) [women 25.6% (95% CI 21.5–30.2) and men31.0% (95% CI 26.3–36.2)] (Table 2). The prevalence ofhypertension increased with age in both men and womenin all three localities. In all the age categories, men had ahigher prevalence of hypertension than women (Fig. 2).Among the ethnic groups, Akans had the highest preva-lence (30.9%). Respondents with secondary education hadthe highest prevalence of hypertension than the othercategories of education (P¼ 0.018). The prevalence ofhypertension was higher among overweight and obeserespondents (31.0 and 30.3%, respectively) than inrespondents with normal weight (27.2%), although the
Copyright © Lippincott Williams & Wilkins. Unaut
TABLE 2. Prevalence, awareness, treatment and control of hypertens
All (n¼714)
Hypertension 202 (28.3%)
Awareness among hypertensive individuals 15 (7.4%)
Treatment among hypertensive individuals 8 (4.0%)
Control among hypertensive individuals 7 (3.5%)
Values are n (%).
4 www.jhypertension.com
difference was not statistically significant (P¼ 0.661)(Fig. 3).
Among respondents with a prior diagnosis of hyperten-sion, only 7.4% were aware of their condition; about 4%were on antihypertensive medications while 3.5% had theirBP controlled below 140/90mmHg. The level of awarenessand treatment was lower in men than in women (P¼ 0.035and P¼ 0.085, respectively), and similarly, the level of BPcontrol was higher among women than among men.
Correlates of hypertension prevalenceTable 3 shows correlates of hypertension among men andwomen. The factors related to awareness, treatment andcontrol of hypertension were not analysed due to thesmall proportions of respondents in these categories (7.4,4.0 and 3.5%, respectively). In the multivariate model,advancement in age, living in James Town and lowphysical activity were correlated to the prevalence ofhypertension.
DISCUSSIONIn this survey of urban poor communities in Accra, Ghana,the prevalence of hypertension was high with unacceptablylow levels of awareness, treatment and BP control amonghypertensive respondents.
horized reproduction of this article is prohibited.
ion
Men Women P
104 (31.0%) 98 (25.6%) 0.137
3 (3.1%) 12 (11.9%) 0.035
1 (1.3%) 7 (6.5%) 0.085
2 (2.1%) 5 (5.0%) 0.030
Volume 32 � Number 1 � Month 2014
CE: Swati; JH-D-14-00085; Total nos of Pages: 8;
JH-D-14-00085
0Male
26.930
35.7
18.5
27.1
32.1
Female
5
10
15
20
25
30
35
40
Younger adults (15–24) Middle-aged (25–34) Older adults (≥35)
Hyp
erte
nsi
on
(%
)
FIGURE 2 Prevalence of hypertension by age group (Colour version). Prevalence of hypertension by age group (Noncolour version).
Prevalence of hypertension in Accra
Prevalence of hypertensionThere are a number of studies on the detection, manage-ment, control and distribution of hypertension among theadult population in Ghana and some West African countries[21–25], where the prevalence of hypertension has beenconsistently higher particularly in urban areas. In addition,such studies have shown evidence of low levels of aware-ness or detection and corresponding low rates of treatmentand control.
The overall prevalence of hypertension in our study wasremarkably similar to the prevalence of 28.3% found inanother study in Accra [8] and similar to the prevalence of28.7% found in Kumasi, the second largest city in Ghana [6].In the Accra study, however, hypertension was more com-mon in women than in men.
In Ghana, within a 15-year period (from 1972 to 1987), anumber of studies were carried out in the Greater Accraregion as part of research into the health burden of CVDs.The prevalence of hypertension was 8–13% among urbanadults [22], much lower than the prevalence found in ourstudy. In addition, the prevalence of hypertension in ourstudy is higher than that found in some West Africancountries. For example, a study in Nigeria found a preva-lence of 21.1% among urban men and women [26]. Anotherstudy in Bo, Sierra Leone, found a hypertension prevalenceof 25.2% [27]. On the contrary, the prevalence rate in ourstudy was lower than that of other sub-Saharan African
Copyright © Lippincott Williams & Wilkins. Unauth
0
10
20
30 27.9
40.4
Male
50
40
50
60
Hyp
erte
nsi
on
(%
)
Normal Ov
FIGURE 3 Prevalence of hypertension by BMI status (Colour version). Prevalence of hype
Journal of Hypertension
countries [28,29]. For example in urban Namibia, the preva-lence of hypertension was 38.0% [30].
The reason(s) for the high prevalence of hypertensionamong residents living in urban poor communities in Accrais uncertain. However, it has been suggested that environ-mental factors such as psychosocial stress could explain thisphenomenon [31]. Another potential reason is increasedBMI, which has been reported as one of the most importantfactors to explain the prevalence of hypertension in Africancommunities [32], although in our study BMI did not havea statistically significant relationship with hypertension.Obesity rates in Ghana are high and this has been linkedto the increased risk of hypertension [33]. Finally, cultural,traditional and socioeconomic factors may also explain thehigh prevalence of hypertension noted in our study [34] andthese factors may shape lifestyles of residents with a nega-tive impact on development of hypertension overtime. Forexample, the use of salt in cooking and at table as well asthe consumption of salted fish and meat is a very commonpractice and part of the food culture in the Ghana [35].
Awareness, treatment and control ofhypertensionThe ‘rule of halves’ predicts that only half of all those withhypertension are detected, half of those detected are treatedand half of those treated are controlled [36]. In ourstudy, the rate of awareness, treatment and control of
orized reproduction of this article is prohibited.
Female
25.1 25.527.8
erweight Obese
rtension by BMI status (Noncolour version).
www.jhypertension.com 5

CE: Swati; JH-D-14-00085; Total nos of Pages: 8;
JH-D-14-00085
TABLE 3. Factors related to hypertension prevalence
All Men Women
Odds ratio (95% CI) P Odds ratio (95% CI) P Odds ratio (95% CI) P
Alcohol consumptionNondrinkers (ref.) 1 (ref.) 1 (ref.) 1 (ref.)
Occasional drinkers 0.82 (0.53–1.29) 0.54 (0.27–1.10) 1.14 (0.61–2.13)
Regular drinkers 1.04 (0.58–1.86) 0.93 (0.40–2.13) 1.27 (0.50–3.20)
BMINormal 1 (ref.) 1 (ref.) 1 (ref.)
Overweight 1.18 (0.71–1.96) 2.17 (0.98–4.81) 0.88 (0.42–1.82)
Obese 1.06 (0.61–1.83) 0.27 (0.60–8.57) 0.82 (0.41–1.64)
Physical activity�3 days/week (ref.) 1 (ref.) 1 (ref.) 1 (ref.)
<3 days/week 1.60 (1.03–2.50) �� 2.17 (0.98–4.82) 1.50 (0.84–2.68)
LocalityAgbogbloshie (ref.) 1 (ref.) 1 (ref.) 1 (ref.)
James Town 18.07 (8.48–38.48) ��� 23.07 (6.13–86.82) ��� 16.10 (5.90–43.93) ���
Ussher Town 1.77 (0.80–3.88) 2.28 (0.57–9.12) 1.39 (0.50–3.85)
EducationNo education (ref.) 1 (ref.) 1 (ref.) 1 (ref.)
Primary 0.53 (0.21–1.34) 1.48 (0.15–14.33) 0.53 (0.18–1.59)
Middle/JHS 0.49 (0.20–1.19) 1.29 (0.15–10.81) 0.45 (0.15–1.31)
Secondary/SHS 0.73 (0.30–1.81) 2.10 (0.25–17.79) 0.66 (0.21–2.09)
Higher 0.35 (0.10–1.27) 0.79 (0.71–8.76) 0.65 (0.71–5.93)
EthnicityAkan (ref.) 1 (ref.) 1 (ref.) 1 (ref.)
Ga-Dangme 0.83 (0.51–1.35) 0.55 (0.26–1.14) 1.08 (0.54–2.16)
Ewe 0.90 (0.31–2.58) 0.32 (0.05–2.11) 1.55 (0.42–5.73)
Other 0.90 (0.42–1.93) 0.12 (0.24–0.61) �� 2.27 (0.88–5.91)
Age 1.45 (1.11–1.89) �� 1.12 (0.74–1.68) 1.84 (1.27–2.69) ���
Results are expressed as odds ratio and 95% confidence interval adjusted for locality, education, ethnicity and age. ref., reference group. ��P<0.01 and ���P< 0.001.
Awuah et al.
hypertension was alarmingly low at 7.4, 4.0 and 3.5%,respectively. These figures are lower than rates that havebeen reported in other studies in Ghana [8,21] and otherAfrican countries [37–39] in both rural and urban settings.The rate of awareness and treatment noted in our study waslower in men than in women. The reasons for the overalllow rate and sexual difference in the awareness and treat-ment of hypertension are being explored in an adjunctlongitudinal qualitative study of people living with hyper-tension and diabetes in the study communities, preliminaryaspects of which are reported elsewhere [40]. This qualita-tive study along with previous studies in other Ghanaiancommunities suggest that lay individuals are aware of theexistence of hypertension and other CVDs, but they havelimited knowledge of the risk factors and might not per-ceive themselves to be at risk [40–42]. The particularly lowrate of awareness may also be due to the fact that healthmessages are not having the desired impact in urban poorcommunities in Accra. A review of the literature on men’shealth in Africa suggests that the sexual differences mightbe attributable to the reluctance of men to report and treathealth problems [43]. The very low rate of BP control amonghypertensive individuals noted in our study may also bedue to poor access to medicines and healthcare and poormedication adherence [16]. Ghana has a National HealthInsurance Scheme that, in theory, offers exemptions forsome medications and treatments for all service users andcross-cutting medical support for particular vulnerablegroups such as the extremely poor and aged. In reality,however, means-testing for the deserving poor has notbeen robust and poor communities lack access to the full
Copyright © Lippincott Williams & Wilkins. Unaut6 www.jhypertension.com
range of health services, particularly complex servicesinvolving long-term chronic disease care [40]. Complexattitudes to medical adherence have been reported onGhanaians with hypertension. For example, Buene et al.[44] revealed that some Ghanaians altered or did not adhereto prescribed antihypertensive medications because of lackof money, fear of addiction and, for men, fear of negativeeffects of such medications on their sexual health. Thesestructural, cultural, gendered and psychological reasonscould explain the very low levels of control especiallyamong men in our study. Research shows that poor com-munities experience health disadvantage at multiple stages,from ‘the person’s beliefs about health and disease, andactual behaviour, to presentation, screening, risk assess-ment, negotiation, participation, programme persistenceand treatment adherence’ [45]. The multiple health dis-advantages of the urban poor will place a great toll onan already overburdened health infrastructure and under-mine development and poverty reduction strategy policies.It is imperative therefore to invest prevention and controlfor communities in hypertension that are disproportion-ately affected.
Community-based interventions that are cost-effectiveand sustainable will be highly relevant. There is evidence tosuggest the feasibility of developing and implementingCVD interventions in faith-based organizations in Accra[42]. An integral aspect of the primary healthcare systemin Ghana is the implementation of the Community-basedHealth Planning and Services (CHPS) programme [46]. TheCHPS programme uses community health nurses to deliverprimary care services at community health centres (CHCs)
horized reproduction of this article is prohibited.Volume 32 � Number 1 � Month 2014

CE: Swati; JH-D-14-00085; Total nos of Pages: 8;
JH-D-14-00085
Prevalence of hypertension in Accra
across the country. The current adaptation of the CHPSprogramme to urban poor communities, including theresearch communities, offers opportunities for developinga task-shifting approach to CVD interventions involvingtrained community health nurses. This approach hasworked in other resource-constrained African countries[47].
In conclusion, the high prevalence of hypertensionnoted in our study among urban poor communities iscomparable to rates recorded in other communities inGhana. However, a distinctive feature of these poor urbancommunities is the disproportionately low level of hyper-tension awareness, treatment and control. This suggeststhat they may run a disproportionately higher risk ofmorbidity and mortality than other communities. Further-more, hypertension and other prevalent chronic diseasesare likely to drive these communities further into poverty;this has been reported in studies on the household burdenof chronic disease in Ghana and other African countries[48,49]. There is a strong case to be made for target-specificprimary and secondary interventions for these poor urbancommunities. Community-based interventions that arecost-effective and sustainable will be important startingpoints.
ACKNOWLEDGEMENTSPoster presentation of parts of the work at the PopulationAssociation of America (PAA) conference 2013, NewOrleans, USA.
The study was supported by seed funding from theUniversity of Ghana-New York University Health Researchcollaborative project.
Conflicts of interestThe authors declare that there are no conflicts of interest.
REFERENCES1. Kearney PM, Whelton M, Reynolds K, Whelton PK, He J. Worldwide
prevalence of hypertension: a systematic review. J Hypertens 2004;22:11–19.
2. Mathers CD, Loncar D. Projections of global mortality and burden ofdisease from 2002 to 2030. PLoS Med 2006; 3:e442.
3. Seedat YK. Recommendations for hypertension in sub-Saharan Africa.Cardiovasc J S Afr 2004; 15:157–158.
4. Centre for Health Information Management. Outpatient morbidity inhealth facilities. Accra, Ghana: Ghana Health Service; 2008.
5. Addo J, Agyemang C, Smeeth L, de-Graft Aikins A, Edusei AK, Oge-degbe O. A review of population-based studies on hypertension inGhana. Ghana Med J 2012; 46:4–11.
6. Cappuccio FP, Micah FB, Emmett L, Kerry SM, Antwi S, Martin-PeprahR, et al. Prevalence, detection, management, and control of hyperten-sion in Ashanti, West Africa. Hypertension 2004; 43:1017–1022.
7. Greater Accra Regional Health Directorate. Annual report 2007. Accra:Ghana Health Service; 2008.
8. Amoah AGB. Hypertension in Ghana: a cross-sectional communityprevalence study in Greater Accra. Ethn Dis 2003; 13:310–315.
9. Agyei-Mensah S, de-Graft Aikins A. Epidemiological transition and thedouble burden of disease in Accra, Ghana. J Urban Health 2010;87:879–897.
10. Accra Metropolitan Assembly-UN Habitat. Participatory slum upgrad-ing and prevention millennium city of Accra. Nairobi, Kenya: AccraMetropolitan Assembly, Accra and UN-HABITAT. 2011.
11. Siddiqui Q, Anam M, Mahmood KT. Management of pregnancyinduced hypertension. J Pharm Sci Technol 2010; 2:421–426.
Copyright © Lippincott Williams & Wilkins. UnauthJournal of Hypertension
12. Addo J, Smeeth L, Leon DA. Hypertension in sub-Saharan Africa: asystematic review. Hypertension 2007; 50:1012–1018.
13. Chobanian AV, Bakris JL, Black HR, Cushman WC, Green LA, Izzo JL Jr,et al. Seventh report of the Joint National Committee on Prevention,Detection, Evaluation, and Treatment of High Blood Pressure: the JNC7 report. JAMA 2003; 289:2560–2572.
14. Stergiou GS, Tzamouranis D, Protogerou A, Nasothimiou E, Kapralos C.Validation of the Microlife Watch BP Office professional device foroffice blood pressure measurement according to the Internationalprotocol. Blood Press Monit 2008; 13:299–303.
15. World Health Organization. WHO STEPS surveillance manual. Gen-eva: WHO; 2008.
16. Agyemang C, Nicolaou M, Boateng L, Dijkshoorn H, van de Born BJ,Stronks K. Prevalence, awareness, treatment and control of hyperten-sion among Ghanaian population in Amsterdam, the Netherlands: theGHAIA study. Eur J Prev Cardiol 2012; 0:1–9.
17. Salmon J, Owen N, Bauman A, Schmitz MK, Booth M. Leisure-time,occupational, and household physical activity among professional,skilled, and less-skilled workers and homemakers. Prev Med 2000;30:191–199.
18. Pescatello LS, Franklin BA, Fagard R, Farquhar WB, Kelley GA, Ray CA,et al. American College of Sports Medicine position stand. Exercise andhypertension. Med Sci Sports Exerc 2004; 36:533–553.
19. Puddey IB, Rakic V, Dimmitt SB, Beilin LJ. Influence of pattern ofdrinking on cardiovascular disease and cardiovascular risk factors: areview. Addiction 1999; 94:649–663.
20. Burt VL, Cutler JA, Higgins M, Horan MJ, Labarthe D, Whelton P. Trendsin the prevalence, awareness, treatment and control of hypertension inthe adult US population. Data from the health examination surveys,1960 to 1991. Hypertension 1995; 26:60–69.
21. Agyemang C. Rural and urban differences in blood pressureand hypertension in Ghana, West Africa. Public Health 2006; 6:525–533.
22. Pobee JOM. Community-based high blood pressure programs in sub-Saharan Africa. Ethn Dis 1993; 3:S38–S45.
23. Oyati AI, Orogade AA, Danbauchi SS, Azuh PC. Awareness, treatmentand control of hypertension among hypertensives in Zaria. J Med Trop2011; 13:2.
24. Lisk DR, McEwen EK. The significance and trend of hypertensionrelated deaths in urban Sierra Leonean Africans. J Hum Hypertens1996; 10:215–218.
25. van der Sande MA, Milligan PJ, Walraven GE, Dolmans WM,Newport M, Nyan OA, et al. Geographical variation in prevalenceof hypertension within The Gambia. J Hum Hypertens 2001; 15:733–739.
26. Ekwunife O, Udeogaranya P, Nwatu I. Prevalence, awareness, treat-ment and control of hypertension in a Nigerian population. Health2010; 2:731–735.
27. Meehan KA, Bankoski AJ, Tejan E, Ansumana R, Bangura U, StengerDA, et al. Hypertension in Bo, Sierra Leone. Ethn Dis 2011; 21:237–242.
28. Goma FM, Nzala SH, Babaniyi O, Songolo P, Zyambo C, Rudatsikra E,et al. Prevalence of hypertension and its correlates in Lusaka urbandistrict of Zambia: a population based survey. Intl Arch Med 2011;4:34.
29. Jenson A, Omar AL, Omar MA, Rishad AS, Khoshnood K. Assessment ofhypertension control in a district of Mombasa, Kenya. Glob PublicHealth 2011; 6:293–306.
30. Hendriks ME, Wit FW, Roos MTL, Brewster LM, Akande TM, de Beer IH,et al. Hypertension in sub-Saharan Africa: cross-sectional surveys infour rural and urban communities. PLoS One 2012; 7:e32638.
31. Agyemang C, Addo J, Bhopal R, de-Graft Aikins A, Stronks K.Cardiovascular diseases, diabetes and established risk factors amongpopulations of sub-Saharan African descent in Europe: a literaturereview. Global Health 2009; 5:7.
32. Cooper R, Rotimi C, Ataman S, McGee D, Osotimehin B, Kadiri S, et al.The prevalence of hypertension in seven populations of West Africanorigin. Am J Public Health 1997; 87:160–168.
33. Escalona ALO, Sarfo M, Kudua L. Obesity and systematic hypertensionin Accra communities. Ghana Med J 2004; 38:4.
34. Agyemang C, Bhopal R, Bruijnzeels M. Negro, black, black African,African Caribbean, African American or what? Labelling African originpopulations in the health arena in the 21st century. J EpidemiolCommunity Health 2005; 59:1014–1018.
orized reproduction of this article is prohibited.www.jhypertension.com 7

CE: Swati; JH-D-14-00085; Total nos of Pages: 8;
JH-D-14-00085
Awuah et al.
35. Kerry SM, Emmett L, Micah FB, Martin-Peprah R, Antwi S, Phillips RO,et al. Rural and semi-urban differences in salt intake, and its dietarysources, in Ashanti, West Africa. Ethn Dis 2005; 15:33–39.
36. Smith WC, Lee AJ, Crombie IK, Tunstalll-Pedoe H. Control of bloodpressure in Scotland: the rule of halves. BMJ 1990; 300:981–983.
37. Dzudie A, Kengne AP, Muna WF, Ba H, Menanga A, Kouam Kouam C,et al. Prevalence, awareness, treatment and control of hypertension in aself-selected sub-Saharan African urban population: a cross-sectionalstudy. BMJ Open 2012; 2:1217.
38. Steyn K, Gaziano TA, Bradshaw D, Laubscher R, Fourie J, South AfricanDemographic, Health Coordinating Team. Hypertension in SouthAfrican adults: results from the Demographic and Health Survey,1998. J Hypertens 2001; 19:1717–1725.
39. Bovet P, Ross AG, Gervasoni JP, Mkamba M, Mtasiwa DM, Lengeler C,et al. Distribution of blood pressure, body mass index and smokinghabits in the urban population of Dar es Salaam, Tanzania, andassociations with socioeconomic status. Int J Epidemiol 2002; 31:240–247.
40. de-Graft Aikins A, Awuah RB, Pera T, Mendez M, Ogedegbe G.Explanatory models of diabetes in poor urban Ghanaian communities.Ethn Health (in press).
41. de-Graft Aikins A, Anum A, Agyemang C, Addo J, Ogedegbe O. Layrepresentations of chronic disease in Ghana: implications for primaryprevention. Ghana Med J 2012; 46 (Suppl):2.
Copyright © Lippincott Williams & Wilkins. Unaut8 www.jhypertension.com
42. Abanilla PKA, Huang K-Y, Shinners S, Levy A, Ayernor K, de-GraftAikins A, et al. Cardiovascular disease prevention in Ghana: feasibilityof a faith-based organizational approach to prevention. Bull WorldHealth Organ 2011; 89:648–656.
43. Heyns CF, Bornman MS. Men’s Health in Africa Part 1: reproductiveurogenital diseases and human immunodeficiency virus infection.J Men’s Health 2008; 5:66–72.
44. Beune EJ, Haafkens JA, Agyemang C, Schuster JS, Willems DL. HowGhanaian, African-Surinamese and Dutch patients perceive and man-age antihypertensive drug treatment: a qualitative study. J Hypertens2008; 26:648–656.
45. Capewell S, Graham H. Will cardiovascular disease prevention widenhealth inequalities? PLoS Med 2010; 7:e1000320.
46. Nyonator FK, Awoonor-Williams JK, Phillips JF. The Ghana Com-munity-based Health Planning and Services Initiative for scaling upservice delivery innovation. Health Policy Plan 2005; 20:25–34.
47. Lekoubou A, Awah P, Fezeu L, Sobngwi E, Kengne AP. Hypertension,diabetes mellitus and task shifting in their management in sub-SaharanAfrica. Int J Environ Res Public Health 2010; 7:353–363.
48. Tagoe HA. Household burden of chronic diseases in Ghana. GhanaMed J 2012; 46:54–58.
49. Tin Su T, Kouyate B, Flessa S. Catastrophic household expenditures forhealthcare in a low income society: a study from Nouna district,Burkina Faso. Bull World Health Organ 2006; 84:21–27.
horized reproduction of this article is prohibited.Volume 32 � Number 1 � Month 2014