
Prevalence and variations of pneumatized articular eminence: A study from Turkey
6
Prevalence and variations of pneumatized articular eminence: A study from Turkey Kaan Orhan, DDS, PhD, a Cagri Delilbasi, DDS, PhD, b Ilker Cebeci, DDS, PhD, a and Candan Paksoy, DDS, PhD, c Ankara and Istanbul, Turkey ANKARA UNIVERSITY AND YEDITEPE UNIVERSITY Objectives. Pneumatized articular eminence or tubercule (PAT) is an air cell cavity in the zygomatic process of the temporal bone that is similar to air cells in the mastoid process and ethmoid bone. The purpose of this study was to determine the prevalence and variations of PAT among an outpatient dental clinic population at Ankara University, Turkey, to make a contribution to the few current studies about PAT. Study design. A total of 1006 panoramic radiographs were retrospectively investigated for the prevalence and radiographic features of PAT. Meta-analysis was done for 4 large case series in the literature and our case series. Furthermore, we performed Chi-square test to evaluate age, gender, localization, and prevalence differences among 5 case series including ours. Results. PATwas found in 19 (1.88%) patients with a mean age of 36.6 (SD 21.06) years. Twelve cases (63.1%) occurred in females and 7 cases (36.9%) occurred in males. Bilateral PAT was found in 7 patients (36.9%). Meta-analysis of 5 large case series revealed a total of 6669 patients, of whom 115 had PAT (1.76% prevalence) occurring over an age range of 7 to 90 years. Fifty (43.47%) occurred in males and 65 (56.53%) occurred in females. Bilateral PAT was found in 28 (24.34%) patients. The result of Chi-square test showed no statistically significant differences among the 5 studies with respect to age, gender, localization, and prevalence. Conclusions. Knowledge about these structures is helpful for the interpretation of imaging such as panoramic radiographs and provides valuable information to understand the spread and differential diagnosis of pathological entities in this region. Moreover, clinicians who are planning to perform temporomandibular joint surgery are advised to assess radiographic imaging thoroughly before the surgery to avoid intra-operative complications and reconstruction. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:349-54) There are many air-filled cavities (pneumatization) inside the skull. In addition to the major paranasal sinuses, accessory air cells may rise in numerous locations in the skull including the temporal bone. 1,2 Studies about the mastoid air cell system and temporal bone pneumatization have been discussed and the distribution of temporal bone pneumatization have pre- viously been described in the literature. 1-18 Tremble, 1 in 1934, reported 10 locations within the temporal bone where accessory air cells could be found, includ- ing 1 in the zygomatic process of the temporal bone. Pneumatization of the temporal bone can be divided into 5 regions, which in turn are subdivided into areas. The primary regions consist of the middle ear, mastoid (squamomastoid), perilabyrinthine, petrous apex, and accessory. The phrase PAT was coined by Tyndall and Matteson 9 to describe accessory air cells that occur in the root of the zygomatic arch and in the articular eminence of the temporal bone that is similar to air cells in the mastoid process and ethmoid bone. In 1976, Roser et al 13 noticed 1 case while examining the temporomandibular joint (TMJ) and termed his finding an ‘‘unusual bony lesion of the zygomatic arch.’’ Kulikowski et al, 14 in 1982, reported 1 patient who was undergoing surgical removal of the articular eminence. Yurosko, 15 in 1985, reported an 18-year-old female patient noticed at third molar examination. Tyndall and Matteson, 9 in 1985, identified for the first time the common characteristics of the pneumatized articular eminence of the temporal bone as (1) an asymptomatic radiolucent defect in the zygomatic process of the temporal bone with the appearance similar to mastoid air cells, (2) extension of the defect anteriorly as far as the articular eminence but not beyond the zygomaticotemporal suture, and (3) no enlargement or cortical destruction of the zygoma. The purpose of this study was to determine the prevalence and variations of pneumatized articular eminence among a general dental clinic population in Turkey, and to conduct meta-analysis and statistical a Senior Resident, Ankara University, Faculty of Dentistry, De- partment of Oral Diagnosis and Radiology, Ankara, Turkey. b Lecturer, Yeditepe University, Faculty of Dentistry, Department of Oral and Maxillofacial Surgery, Istanbul, Turkey. c Professor, Ankara University, Faculty of Dentistry, Department of Oral Diagnosis and Radiology, Ankara, Turkey. Received for publication Nov 1, 2003; returned for revision Jun 16, 2004; accepted for publication Aug 7, 2004. 1079-2104/$ - see front matter Ó 2005 Elsevier Inc. All rights reserved. doi:10.1016/j.tripleo.2004.08.005 349
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Prevalence and variations of pneumatized articular eminence: A study from Turkey

Prevalence and variations of pneumatized articular eminence: A study
from Turkey
Kaan Orhan, DDS, PhD,a Cagri Delilbasi, DDS, PhD,b Ilker Cebeci, DDS, PhD,a
and Candan Paksoy, DDS, PhD,c Ankara and Istanbul, TurkeyANKARA UNIVERSITY AND YEDITEPE UNIVERSITY
Objectives. Pneumatized articular eminence or tubercule (PAT) is an air cell cavity in the zygomatic process of the temporal
bone that is similar to air cells in the mastoid process and ethmoid bone. The purpose of this study was to determine the
prevalence and variations of PAT among an outpatient dental clinic population at Ankara University, Turkey, to make
a contribution to the few current studies about PAT.
Study design. A total of 1006 panoramic radiographs were retrospectively investigated for the prevalence and radiographic
features of PAT. Meta-analysis was done for 4 large case series in the literature and our case series. Furthermore, we performed
Chi-square test to evaluate age, gender, localization, and prevalence differences among 5 case series including ours.
Results. PAT was found in 19 (1.88%) patients with a mean age of 36.6 (SD 21.06) years. Twelve cases (63.1%) occurred in
females and 7 cases (36.9%) occurred in males. Bilateral PAT was found in 7 patients (36.9%). Meta-analysis of 5 large case
series revealed a total of 6669 patients, of whom 115 had PAT (1.76% prevalence) occurring over an age range of 7 to 90 years.
Fifty (43.47%) occurred in males and 65 (56.53%) occurred in females. Bilateral PAT was found in 28 (24.34%) patients. The
result of Chi-square test showed no statistically significant differences among the 5 studies with respect to age, gender,
localization, and prevalence.
Conclusions. Knowledge about these structures is helpful for the interpretation of imaging such as panoramic radiographs and
provides valuable information to understand the spread and differential diagnosis of pathological entities in this region.
Moreover, clinicians who are planning to perform temporomandibular joint surgery are advised to assess radiographic imaging
thoroughly before the surgery to avoid intra-operative complications and reconstruction.
(Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:349-54)
There are many air-filled cavities (pneumatization)inside the skull. In addition to the major paranasalsinuses, accessory air cells may rise in numerouslocations in the skull including the temporal bone.1,2
Studies about the mastoid air cell system and temporalbone pneumatization have been discussed and thedistribution of temporal bone pneumatization have pre-viously been described in the literature.1-18 Tremble,1
in 1934, reported 10 locations within the temporalbone where accessory air cells could be found, includ-ing 1 in the zygomatic process of the temporal bone.Pneumatization of the temporal bone can be dividedinto 5 regions, which in turn are subdivided into areas.The primary regions consist of the middle ear, mastoid
aSenior Resident, Ankara University, Faculty of Dentistry, De-
partment of Oral Diagnosis and Radiology, Ankara, Turkey.bLecturer, Yeditepe University, Faculty of Dentistry, Department of
Oral and Maxillofacial Surgery, Istanbul, Turkey.cProfessor, Ankara University, Faculty of Dentistry, Department of
Oral Diagnosis and Radiology, Ankara, Turkey.
Received for publication Nov 1, 2003; returned for revision Jun 16,
2004; accepted for publication Aug 7, 2004.
1079-2104/$ - see front matter
� 2005 Elsevier Inc. All rights reserved.
doi:10.1016/j.tripleo.2004.08.005
(squamomastoid), perilabyrinthine, petrous apex, andaccessory.The phrase PATwas coined by Tyndall and Matteson9
to describe accessory air cells that occur in the root ofthe zygomatic arch and in the articular eminence of thetemporal bone that is similar to air cells in the mastoidprocess and ethmoid bone. In 1976, Roser et al13 noticed1 case while examining the temporomandibular joint(TMJ) and termed his finding an ‘‘unusual bony lesion ofthe zygomatic arch.’’ Kulikowski et al,14 in 1982,reported 1 patient whowas undergoing surgical removalof the articular eminence. Yurosko,15 in 1985, reportedan 18-year-old female patient noticed at third molarexamination. Tyndall and Matteson,9 in 1985, identifiedfor the first time the common characteristics of thepneumatized articular eminence of the temporal bone as(1) an asymptomatic radiolucent defect in the zygomaticprocess of the temporal bone with the appearancesimilar to mastoid air cells, (2) extension of the defectanteriorly as far as the articular eminence but not beyondthe zygomaticotemporal suture, and (3) no enlargementor cortical destruction of the zygoma.The purpose of this study was to determine the
prevalence and variations of pneumatized articulareminence among a general dental clinic population inTurkey, and to conduct meta-analysis and statistical
349
OOOOE
350 Orhan et al March 2005
comparison of 5 large case series of PAT including ourcases in order to better understand the nature of thesedefects and to contribute to the few current studies aboutPAT.
MATERIALS AND METHODSPanoramic radiographs of 1006 patients, who were
referred to the Oral Diagnosis and Radiology outpatientclinic at Ankara University Faculty of Dentistry, wereevaluated retrospectively from January 1997 to January2000 for the presence of PAT. Selection criteria for patientsincluded third molar evaluation, need for extensiverestorative dental procedures, extensive alveolar ridgeresorption, atypical pain in the dentomaxillofacial region,swelling, asymmetry, missing or supernumerary teeth,severe generalized caries, mixed dentition analysis, andexamination for TMJ disorders. Cases in which thezygomatic arch was not adequately seen for technical oranatomic reasons and the cases that had maxillofacialfracture history or having maxillofacial anomalies werenot included in the study.All scans were made on a 75-kVp, 10-mA film-based
Odontoma PC panoramic radiography imaging unit(Trophy Radiologie SA;Marne La Vallee, France) usinga T-Mat G/ Lanex medium film/screen combination(Eastman Kodak Co; Rochester, NY). Exposed filmswere processed according to manufacturer’s recom-mendations using an automatic film processor (XR 24,Durr Dental GmbH & Co KG; Bietigheim-Bissingen,Germany) with Kodak ReadyMatic chemistry. Blindedto the clinical status of the patient, an oral and maxillo-facial radiologist examined the radiographs on a standardviewing box in a darkened room. The age and sex wererecorded for all patients and for the cases of PAT;age, gender, location, and radiographic appear-ance were noted as well. Diagnosis of PAT on the ra-
Table I. The results of the survey of 1006 panoramicradiographs
Panoramic films surveyed 1006
Patients with PAT 19
Total number of PAT 26
Prevalence 1.88%
Patients with bilateral PAT 7
Female patients 12
Male patients 7
Mean age 36.6
Age Range 11-90
Unilocular PAT number 10
Multilocular PAT number 16
Unilateral PAT 12
Bilateral PAT 7
Right localization 18
Left localization 8
diographs was done only if unequivocal pneumatizationof the articular eminence could be seen or if thedefect was located in the articular eminence posteriorto the zygomaticotemporal suture as a well-defineduni- or multilocular radiolucency. PAT was classifiedas unilocular or multilocular as in the study by TyndallandMatteson.9 Unilocular PATwas identified as a singleradiolucent oval defect with well-defined bony borders.Multilocular PATwas identified as numerous radiolucentsmall cavities.A meta-analysis for PAT was done using a Medline
search for the English, French, and German literaturebetween the years 1966 and 2002. The keywords for thissearch were pneumatization, temporal bone, pneu-matized articular eminence, zygomatic air cell defect,articular eminence, air cells, mastoid process, zygomaticarch, and zygomatic process. Four case series werefound reported byKaugars et al,6 Tyndall andMatteson,9
Hofmann et al,11 and Carter et al.12 Besides this, we alsoperformed Chi-square test using SPSS 11.0 program(SPSS Inc, Chicago, Ill) for evaluating age, gender,localization, and prevalence differences among the 4large case series in the literature and our case series.
RESULTSThe findings of this survey are presented in Table I.
The average age of the 1006 patients was 36.7 (SD
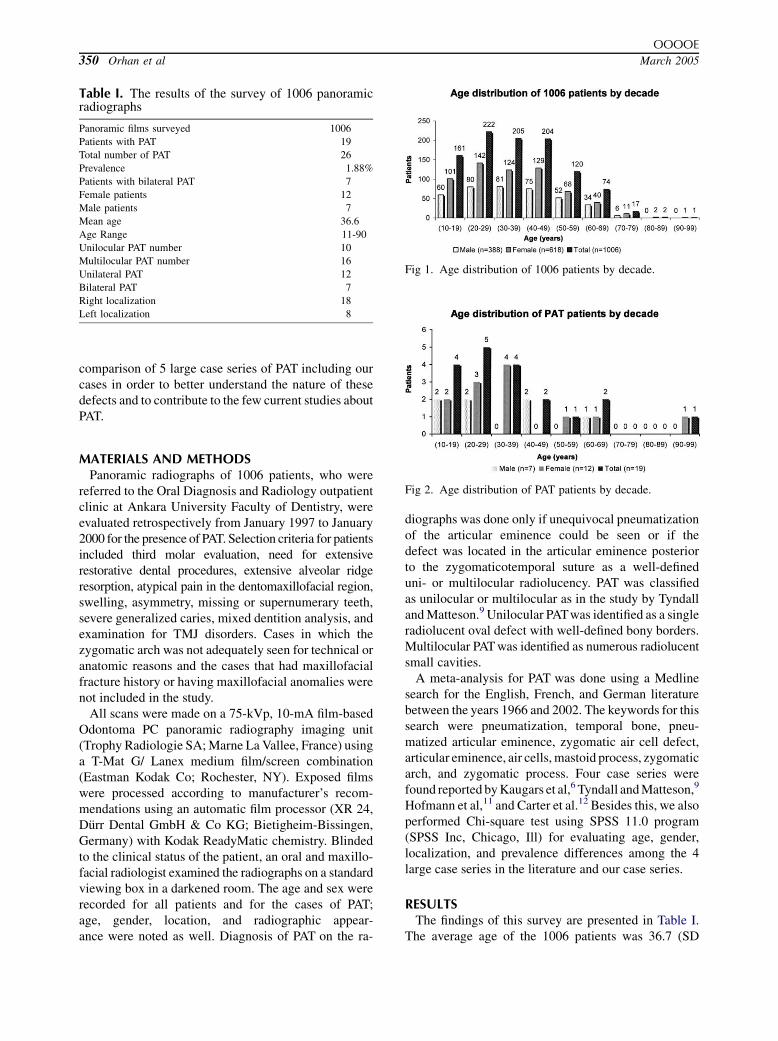
Fig 1. Age distribution of 1006 patients by decade.
Fig 2. Age distribution of PAT patients by decade.

OOOOE
Volume 99, Number 3 Orhan et al 351
15.63) years and ages ranged from 10 to 90 years. Therewere 388 (38.6%)male patients and 618 (61.4%) femalepatients. The mean age of the male patients was 37.1(SD 15.73) years with a range of 11 to 79 years whilemean age of the female patients was 36.4 (SD 15.57)years with a range of 10 to 90 years. Age distribution ofthe study population is presented in Figure 1.PAT was found in 19 (1.88%) patients. Patients with
PAT had a mean age of 36.6 (SD 21.06) years witha range of 11 to 90 years (Fig 2). All cases were locatedin the zygomatic process of the temporal bone, didnot extend anteriorly beyond the zygomaticotemporalsuture, and lacked expansile or destructive charac-teristics. Twelve (63.1%) cases occurred in females and7 (36.9%) cases occurred in males. The mean age ofmales was 32.1 (SD 20.39) years with a range of 11 to 66years while mean age of females was 39.2 (SD 21.88)years with a range of 16 to 90 years. Twelve cases of PATwere unilateral, with 10 on the right and 2 on the left.Bilateral PAT was found in 7 (36.9%) patients (Fig 3).Ten (38.5%) of the PATs were unilocular type (Fig 4).Sixteen (61.5%) of the PATs were multilocular type (Fig5). The youngest patient with PAT was an 11-year-oldboy (Fig 6).
Fig 3. The image of bilateral pneumatized articular emi-nence.
Fig 4. The appearance of unilocular pneumatized articulareminence.
In addition to the current series, we found in aMedlinesearch 4 large case series surveyed by Tyndall andMatteson in 1985,9 Kaugars et al in 1986,6 Carter et al in1998,12 and Hofmann et al in 2001.11 Total patientsample for these series (including current series) was6669 patients with a total of 115 cases of PAT (1.76%prevalence) occurring over an age range of 7 to 90. Fifty(43.47%) occurred inmales while 65 (56.53%) occurredin females (Table II).The Chi-square tests for evaluating a statistical
significance (P\ .05) between 4 large PAT case seriesand the current series showed no significant differencewith respect to age (P = .354), gender (P = .253),localization (P = .135), and prevalence (P = .941)among the studies.
DISCUSSIONMicroscopically a single flat layer of epithelium
separated from bone by subepithelial connective tissuelines an air cell. This subepithelial layer is largelyresponsible for air cell formation. The development of
Fig 5. The appearance of multilocular pneumatized articulareminence.
Fig 6. The panoramic image of PAT in an 11-year-old boy.

OOOOE
352 Orhan et al March 2005
Table II. Meta-analysis of PAT case steries
Series Patients (no) % PAT (no) Age range (yrs) % Male (no) %Female (no)
Tyndall & Matteson9 1061 2.6 (28) 15-74 46.4 (13) 53.6 (15)
Kaugars et al6 784 1.0 (8) 32-69 12.5 (1) 87.5 (7)
Carter et al12 2734 1.5 (40) 17-83 50.0 (20) 50.0 (20)
Hofmann et al11 1084 1.8 (20) 7-87 45.0 (9) 55.0 (11)
Present series 1006 1.88 (19) 11-90 36.9 (7) 63.1 (12)
Total 6669 1.76 (115) 7-90 43.47 (50) 56.53 (65)
air cells preceded by the formation of bone cavities isa normal physiologic process related to periostealactivity. The bone cavities contain primitive bonemarrow, which differentiates into a loose mesenchymalconnective tissue. After the epithelial mucous mem-brane has invaginated, it in turn undergoes atrophy,leaving a thin residual lining membrane and sub-epithelial bone resorption then further enlarges aircells.3,4,5,7,12 The development of complete adultpneumatization can be divided into 3 stages: theinfantile, from birth to 2 years of age; the transitional,from 2 to 5 years; and thereafter the adult. In theinfantile stage, the mastoid (squamomastoid) undergoesgradual enlargement, with migration of air cells towardperiphery. The air cells, which vary in size and shape,become more distinct with time because of progressivecalcification of their walls. Pneumatization ceasesduring the adult stage.3,6,12
After the first report of an extended large mastoid aircell by Roser et al13 in 1976, few cases have beenreported so far in the literature. Tyndall and Matteson9
reported the first detailed data on population distributionand radiographic appearance of pneumatized articulareminence. In their study, 1061 patients who admitted toa dental school outpatient clinic were examined for thepresence of PAT. PAT was found in 28 (2.6%) patientswith a mean age of 32.5 years and an age range of 15 to74 years. All cases were located in the zygomatic processof the temporal bone and did not extend anteriorlybeyond the zygomaticotemporal bone. There was nogender predilection and bilateral PAT was found in 5patients. There were 17 (53.1%) unilocular cases and 15(46.9%) multilocular cases. Tyndall and Matteson didnot give mean age, age range, or sex distribution of thetotal sample population.Kaugars et al6 in 1986 reported 8 (1%) cases of PAT in
784 patients with a mean age 45.9 years and an agerange of 32 to 69 years. All of the 8 patients were fromthe adult group. Four cases were unilateral and 4 werebilateral. Kaugars et al did not give a mean age for theirtotal same population but they provided a mean age foreach of the 3 subpopulations (children, adolescents,and adults). The average of their adult group,which comprised 61% of the total patients, was 41.2years.6
Carter et al12 in 1999 reported a detailed paper aboutpneumatized articular eminence. They examined 2734panoramic radiographs of the patients who admitted toa dental medicine school. The average age of the 2734patients was 41.4 years and an overall range of 4 to 93years. There were 1261 (46.1%) males and 1473(53.9%) females. The mean age of the males was 41.5years with a range of 4 to 91 years. The mean age of thefemales was 41.3 (SD 22.3) years with a range of 4 to 93years. PAT was found in 40 (1.5%) cases. Patients withPAT had amean age of 49.6 years and a range of 17 to 83years. Half of the patients weremales with amean age of45.8 years, and half of the patients were females witha mean age of 53.4 years. Thirty-two cases wereunilateral with 17 on the right side and 15 on the leftside. Bilateral PAT was found in 8 (20%) cases. Theyoungest patient with PAT was 17 years old. No overtgender predilection was detected.Hofmann et al11 in 2001 also reported a paper on
prevalence and characteristics of PAT. A total of 1084panoramic radiographs of the patients who admitted toa dental school in Germany were examined for thepresence of PAT. The average age of the 1084 patientswas 41.9 years with an overall range of 2 to 96 years.There were 628 (58%) males and 456 (42%) females.The mean age of the males was 40.3 years with a rangeof 3 to 89 years. The mean age of the females was 44years with a range of 2 to 96 years. PATwas found in 20(1.85%) cases. Patients with PAT had a mean age of 43.2years with a range of 7 to 87 years. Eleven (55%) of thepatients were males with a mean age of 34.4 years, and 9(45%) were females with a mean age of 50.4 years.Sixteen cases were unilateral with 7 on the right side and9 on the left side. Bilateral PAT was found in 4 (20%)cases. The youngest patient with PAT was 7 years old.No gender predilection was detected.11
Meta-analysis showed similarities for the prevalencein the 5 case series. The prevalences of PAT were2.6%, 1.0%, 1.5%, 1.85%, and 1.88% respectively foran average of 1.76% over 6669 patients. The mean ageof the present series (36.6 years) is similar to that ofTyndall and Matteson9 (32.5 years). Also age range ofpatients with PAT in the present series (11 to 90 years) issimilar to that in Hofmann et al11 (7 to 87 years). Meta-analysis showed similarities in age range of the patients.

OOOOE
Volume 99, Number 3 Orhan et al 353
In our study, the youngest patient with PATwas 11 yearsof age. It has been stated that the accessory air cellsbegin to pneumatize after puberty and achieve full sizeafter several years as with mastoid air cells proper.3,9,12
However, Hofmann et al’s11 and our findings detectedcases before the second half the second decade of life.We believe that further studies should be done aboutaccessory pneumatization in children to elucidate thisphenomenon.Panoramic radiograph is a useful technique to di-
agnose the PAT, since the posterior aspect of thezygomatic arch is usually displayed. Transorbital ortransmaxillary radiographs can also be adjunctiveprojections in visualization of PAT.6,9-12 Other radio-graphic projections such as transcranial view for TMJ,submentovertex view, Towne projection, orWater’s viewdo not provide adequate visualization of the posterioraspect of the zygomatic arch for this purpose.9,12
Computed tomography (CT) is also considered asa method of choice for the assessment of bony structuresand air spaces in the skull base. Since CT is not subjectto superimposition, it exceeds the diagnostic accuracy ofplain radiographs in the evaluation of temporal airspaces. Furthermore, less superficially located (such asmedial portion of the articular eminence) air cells,adjacent to the TMJ may only be visible on CT.3,5,6,9,10
Besides CT, magnetic resonance imaging (MRI) canalso be used to visualize the pneumatization of mastoidair cells. Although MRI is an excellent tool forevaluation of the soft tissues of the TMJ, high-resolutionCT remains the method of choice for the assessment ofbony structures and for pneumatized spaces.3,5 On theother hand, due to their low cost and widespreadavailability, panoramic radiographs and plain ra-diographs are considered the initial method for the di-agnosis of these defects.The differential diagnosis of radiolucencies within the
zygomatic arch includes aneurysmal bone cyst, osseoushemangioma, chondroblastoma, fibrous dysplasia, giantcell tumor, eosinophilic granuloma, metastatic tumor,and PAT. Only PAT can be visualized incidentally onradiograph without nonexpansile, nondestructivecharacteristics. The others would be characterized byenlarging and usually painful, bony expansions withcortical destruction.6,9,11,12 Temporal air spaces arepotential paths for the spread of various pathologicalprocesses. Tumors of the mastoid process and ear mayextend into the TMJ while otitis or mastoiditis mayinvolve the TMJ and can even result in ankylosis.11,19-22
Moreover, fractures of the skull base frequently extendthrough the pneumatized spaces of the temporal boneand may release air into the glenoid fossa.11,23
PAT requires no treatment but the presence of PAT canbe a contraindication for performing eminoplasty or
eminectomy to treat recurrent chronic mandibulardislocation.6,9,10,12 Some authors emphasized thatpanoramic radiographs are useful to eliminatepneumatization of those regions before surgical pro-cedure.6,9-12,16 Kaugars et al6 stated that PAT is notnecessarily a contraindication for performing emino-plasty or eminectomy unless the pneumatization islarge, but they did not mention a size. Lindenmuth andClark16 indicated that surgeons who are planning to dosuch surgical procedures should be aware of the detailsof pneumatized articular eminence. During the opera-tion, care must be taken while using osteotomes or bursto avoid sudden penetration through the defect. To besure that there is not an unrecognized dural tear, theanesthesiologist should perform a Valsalva manoeuvreon the patient when the procedure is completed, and thedefect should be observed for the presence of a cerebro-spinal fluid leak. If there is a small dural tear, it can beobdurated with muscle or fascia obtained from thealready exposed temporal region. The bony defect mustalso be obliterated.6,11 The use of methyl methacrylateand autogenous graft for this purpose can be useful.6,24
Because of potential problems, clinicians who areplanning to perform TMJ surgery should assess theradiographic imaging thoroughly before the surgery toavoid intraoperative reconstruction and complications.Such prevalence studies, particularly from developingcountries, will provide useful information to betterunderstand the nature and different clinical features ofuncommon entities.
REFERENCES1. Tremble GJ. Pneumatization of the temporal bone. Arch
Odontolaryngol 1934;19:172.2. Allam AF. Pneumatization of the temporal bone. Ann Otol
Rhinol Laryngol 1969;78:48-64.3. Virapongse C, Sarwar M, Bhimani S, Sasaki C, Shapiro R.
Computed tomography of Temporal bone pneumatization: 1.Normal Pattern Morphology. AJNR 1995;6:551-9.
4. Ojala L. Pneumatization of the bone and environmental factors.Acta Otolaryngol 1950;86:1-134.
5. Groell R, Fleischmann B. The pneumatic spaces of the temporalbone: relationship to the temporomandibular joint. Dentomax-illofac Radiol 1999;28:69-72.
6. Kaugars G, Mercuri L, Laskin D. Pneumatization of the articulareminence of the temporal bone: prevalence, development andsurgical treatment. JADA 1986;113:55-7.
7. Tos M, Stangerup SE, Havid G. Mastoid pneumatization:evidence of the environmental theory. Arch Otolaryngol 1984;10:502-7.
8. Deluke MD. Pneumatization of the articular eminence of thetemporal bone. Oral Surg Oral Med Oral Pathol 1995;19:2-3.
9. Tyndall DA, Matteson RS. Radiographic appearance andpopulation distribution of the pneumatized articular eminenceof the temporal bone. J Oral Maxillofac Surg 1985;43:493-7.
10. Tyndall DA, Matteson RS. The appearance of the zygomatic aircell defect (ZACD) on panoramic radiographs. Oral Surg OralMed Oral Pathol 1987;64:373-6.
11. Hofmann T, Friedrich RE, Wedl JS, Schmelzle R. Pneumatiza-tion of the zygomatic arch on pantomography. Mund KieferGesichtschir 2001;5:173-9.

OOOOE
354 Orhan et al March 2005
12. Carter LC, Haller AD, Calamel AD, Pfaffenbach AC. Zygomaticair cell defect (ZACD). Prevalence and characteristics in a dentalclinic outpatient population. Dentomaxillofac Radiol 1999;28:116-22.
13. Roser SM, Rudin DE, Brady FA. Unusual bony lesion of thezygomatic arc. J Oral Med 1976;31:72-3.
14. Kulikowski BM, Schow SR, Kraut RA. Surgical management ofa pneumatized articular eminence of the temporal bone. J OralMaxillofac Surg 1982;40:311-3.
15. Yurosko JY. Pneumatized articular eminence. Oral Surg OralMed Oral Pathol 1985;60:346.
16. Lindenmuth JE, Clark MS. Pneumatization of the articulareminence. Cranio 1986;4:86-7.
17. Piette E. Pneumatization of the anterior zygomatic tubercle ofthe temporal bone. Rev Stomatol Chir Maxillofac 1986;87:223-6.
18. Hasnaini M. Extensive bone pneumatization: incidentalfinding in a patient with TMJ dysfunction. Dent Update 2000;27:187-9.
19. Faerber TH, Ennis RL, Allen GA. Temporomandibular jointankylosis following mastoiditis: report of a case. J OralMaxillofac Surg 1990;48:866-70.
20. Thomson HG. Septic. Septic arthritis of the temporomandibularjoint complicating otitis externa. J Otolaryngol 1989;103:319-21.
21. Hadlock T, Ferraro N, Rahbar R. Acute mastoiditis with temporo-mandibular joint. Otolaryngol Head Neck Surg 2001;125:111-2.
22. Dingle AF. Fistula between the external auditory canal and thetemporomandibular joint: a rare complication of otitis externa.J Laryngol Otol 1992;106:994-5.
23. Betz BW, Wiener MD. Air in the temporomandibular joint fossa:CT sign of temporal bone fracture. Radiology 1991;180:211-3.
24. Kraut R. Methyl methacrylate obturation of the temporal bone.J Maxillofac Surg 1985;43:554-5.
Reprint requests:
Cagri Delilbasi, DDS, PhD
Yeditepe University
Faculty of Dentistry
Department of Oral and Maxillofacial Surgery
Bagdat Caddesi No. 238
34728 Goztepe-Istanbul, Turkey




















