Prevalence and Risk Factors for Overweight and Obesity among HIV-Infected Adults in Dar es Salaam,...
10
Article Prevalence and Risk Factors for Overweight and Obesity among HIV-Infected Adults in Dar es Salaam, Tanzania Helen Semu, MPH 1 , Rachel M. Zack, SM 2 , Enju Liu, MD, PhD 3 , Ellen Hertzmark, PhD 2,3,4 , Donna Spiegelman, SD 2,3,4 , Kevin Sztam, MD, MPH 5 , Claudia Hawkins, MD, MPH, DTM&H 6 , Guerino Chalamila, MD, PhD, MPH 7 , Aisa Muya, MD, SD 7 , Hellen Siril, MD, MPH 7 , Ramadhani Mwiru, MD, SD 7 , Deo Mtasiwa, MD 8 , and Wafaie Fawzi, MD, SD 2,3,9 Abstract Background: Overweight and obesity are increasingly prevalent among HIV-infected populations. We describe their prevalence and associated risk factors among HIV-infected adults in Dar es Salaam, Tanzania. Methods: A cross-sectional study was conducted to determine the proportion of patients who were overweight or obese at enrollment to care and treatment centres from 2004 to 2011. Multivariate relative risk regression models were fit to identify risk factors. Results: A total of 53 825 patients were included in the analysis. In all, 16% of women and 8% of men were overweight, while 7% and 2% were obese, respectively. In multivariate analyses, older age, higher CD4 count, higher hemoglobin levels, female sex, and being married were associated with obesity and overweight. World Health Organization HIV disease stage, tuberculosis history, and previous antiretroviral therapy were inversely associated with obesity and overweight. Conclusion: Overweight and obesity were highly prevalent among HIV-infected patients. Screening for overweight and obesity and focused interventions should be integrated into HIV care. Keywords obesity, overweight, HIV, AIDS, ART Introduction The prevalence of overweight (body mass index [BMI] 25 to <30 kg/m 2 ) and obesity (BMI 30kg/m 2 ) is an increasingly important public health concern in sub-Saharan Africa, espe- cially in urban areas. 1 In Tanzania, overweight and obesity were previously associated with persons with diabetes and high-ranking executives; however, these conditions are becoming more common in the general population. 2,3 In the decade from 1995 to 2004, the prevalence of obesity among women attending antenatal clinics in Dar es Salaam, an urban center, increased from 3.6% to 9.1%. 4 The Tanzania Demo- graphic and Health Surveys (TDHS) similarly show an increase in the nationwide prevalence of overweight and obe- sity, from 18% in 2004/2005 to 22% in 2010. 5,6 In 2010, the prevalence of overweight and obesity in Dar es Salaam was 28.1% and 16.4%, respectively, double and triple the national figures. 6 Recent changes in Tanzanians’ lifestyles, including migration to urban areas, an increasingly Western-style diet, and a shift away from manual work, are associated with over- weight and obesity. 7,8 Social perceptions, such as the belief that overweight is symbolic of health and beauty, also contrib- ute to the increasing prevalence of overweight and obesity. 1 Department of Preventive Services, Ministry of Health and Social Welfare, Dar es Salaam, Tanzania 2 Department of Epidemiology, Harvard School of Public Health, Boston, MA, USA 3 Department of Nutrition, Harvard School of Public Health, Boston, MA, USA 4 Department of Biostatistics, Harvard School of Public Health, Boston, MA, USA 5 Clinical Nutritional Service, Division of GI/Nutrition, Children’s Hospital, Boston, MA, USA 6 Northwestern University, Feinberg School of Medicine, Chicago, IL, USA 7 Management and Development for Health, Dar es Salaam, Tanzania 8 Prime Ministers’ Office, Regional Authority and Local Government, Dar es Salaam, Tanzania 9 Department of Global Health and Population, Harvard School of Public Health, Boston, MA, USA Corresponding Author: Helen Semu, Ministry of Health and Social Welfare, PO Box 9083, Dar es Salaam, Tanzania. Email: [email protected] Journal of the International Association of Providers of AIDS Care 1–10 ª The Author(s) 2014 Reprints and permission: sagepub.com/journalsPermissions.nav DOI: 10.1177/2325957414542574 jiapac.sagepub.com at Harvard Libraries on February 20, 2015 jia.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Prevalence and Risk Factors for Overweight and Obesity among HIV-Infected Adults in Dar es Salaam,...

Article
Prevalence and Risk Factorsfor Overweight and Obesity amongHIV-Infected Adults in Dar esSalaam, Tanzania
Helen Semu, MPH1, Rachel M. Zack, SM2, Enju Liu, MD, PhD3,Ellen Hertzmark, PhD2,3,4, Donna Spiegelman, SD2,3,4,Kevin Sztam, MD, MPH5, Claudia Hawkins, MD, MPH, DTM&H6,Guerino Chalamila, MD, PhD, MPH7, Aisa Muya, MD, SD7,Hellen Siril, MD, MPH7, Ramadhani Mwiru, MD, SD7,Deo Mtasiwa, MD8, and Wafaie Fawzi, MD, SD2,3,9
AbstractBackground: Overweight and obesity are increasingly prevalent among HIV-infected populations. We describe their prevalenceand associated risk factors among HIV-infected adults in Dar es Salaam, Tanzania. Methods: A cross-sectional study was conductedto determine the proportion of patients who were overweight or obese at enrollment to care and treatment centres from 2004to 2011. Multivariate relative risk regression models were fit to identify risk factors. Results: A total of 53 825 patients wereincluded in the analysis. In all, 16% of women and 8% of men were overweight, while 7% and 2% were obese, respectively. Inmultivariate analyses, older age, higher CD4 count, higher hemoglobin levels, female sex, and being married were associatedwith obesity and overweight. World Health Organization HIV disease stage, tuberculosis history, and previous antiretroviraltherapy were inversely associated with obesity and overweight. Conclusion: Overweight and obesity were highly prevalentamong HIV-infected patients. Screening for overweight and obesity and focused interventions should be integrated into HIV care.
Keywordsobesity, overweight, HIV, AIDS, ART
Introduction
The prevalence of overweight (body mass index [BMI] 25 to
<30 kg/m2) and obesity (BMI � 30kg/m2) is an increasingly
important public health concern in sub-Saharan Africa, espe-
cially in urban areas.1 In Tanzania, overweight and obesity
were previously associated with persons with diabetes and
high-ranking executives; however, these conditions are
becoming more common in the general population.2,3 In the
decade from 1995 to 2004, the prevalence of obesity among
women attending antenatal clinics in Dar es Salaam, an urban
center, increased from 3.6% to 9.1%.4 The Tanzania Demo-
graphic and Health Surveys (TDHS) similarly show an
increase in the nationwide prevalence of overweight and obe-
sity, from 18% in 2004/2005 to 22% in 2010.5,6 In 2010, the
prevalence of overweight and obesity in Dar es Salaam was
28.1% and 16.4%, respectively, double and triple the national
figures.6 Recent changes in Tanzanians’ lifestyles, including
migration to urban areas, an increasingly Western-style diet,
and a shift away from manual work, are associated with over-
weight and obesity.7,8 Social perceptions, such as the belief
that overweight is symbolic of health and beauty, also contrib-
ute to the increasing prevalence of overweight and obesity.
1 Department of Preventive Services, Ministry of Health and Social Welfare,
Dar es Salaam, Tanzania2 Department of Epidemiology, Harvard School of Public Health, Boston, MA,
USA3 Department of Nutrition, Harvard School of Public Health, Boston, MA, USA4 Department of Biostatistics, Harvard School of Public Health, Boston, MA,
USA5 Clinical Nutritional Service, Division of GI/Nutrition, Children’s Hospital,
Boston, MA, USA6 Northwestern University, Feinberg School of Medicine, Chicago, IL, USA7 Management and Development for Health, Dar es Salaam, Tanzania8 Prime Ministers’ Office, Regional Authority and Local Government, Dar es
Salaam, Tanzania9 Department of Global Health and Population, Harvard School of Public
Health, Boston, MA, USA
Corresponding Author:
Helen Semu, Ministry of Health and Social Welfare, PO Box 9083, Dar es
Salaam, Tanzania.
Email: [email protected]
Journal of the InternationalAssociation of Providers of AIDS Care1–10ª The Author(s) 2014Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/2325957414542574jiapac.sagepub.com
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from

Furthermore, some Tanzanians believe that overweight is a
sign of not being infected with HIV.9-11 Such beliefs contribute
to a preference of overweight and obesity over normal weight.
Obesity is associated with metabolic abnormalities includ-
ing insulin resistance,8 dyslipidemia,8,12 and kidney disease,13
which can lead to chronic diseases such as hypertension,14
diabetes,15 cardiovascular disease,16,17 and some cancers.18
Although obesity is the underlying cause of several chronic
diseases and imposes an economic burden to individuals and
to Tanzania as a whole,19 limited resources are available to
address the condition and associated consequences.
Obesity is relatively common among people infected
with HIV,20,21 a disease once defined by ‘‘wasting’’ and
‘‘slimming.’’22 Recent studies have reported a high preva-
lence of obesity among antiretroviral therapy (ART)-naive
populations23 in both developed24-26 and developing27 coun-
tries, including Tanzania.28 Some authors have projected
that the proportion of patients on ART who are overweight
or obese will soon be similar to or higher than that of the
general population.26,27 As in the general population, over-
weight and obesity have been found to be associated with
hypertension and dyslipidemia, risk factors for cardiovascu-
lar diseases.24,27,29
There are limited published studies on the prevalence
and predictors of overweight and obesity among HIV-infected
adults in Tanzania. Most previous studies were composed of
small samples and compared overweight and obese participants
to nonoverweight and nonobese participants, which included
underweight rather than only normal-weight partici-
pants.23,25,26,29,30 We conducted a study of participants in care
and treatment centres (CTCs) to describe the prevalence of over-
weight and obesity in HIV-infected patients and compared over-
weight and obese participants to normal-weight participants to
identify factors associated with overweight and obesity at CTC
enrollment.
Methods
Study Site and Population
This cross-sectional study uses data on HIV-infected patients
who enrolled in HIV/AIDS CTCs in Dar es Salaam, Tanzania,
between November 2004 and December 2011. These CTCs
were supported by Management and Development for Health
(MDH), one of the recipients of the US President’s Emergency
Plan for AIDS Relief. All nonpregnant patients aged 15 years
and older whose weight and height were recorded at program
enrollment were included.
Standard practice dictates that all patients attending MDH-
supported HIV CTCs receive comprehensive care and support
per Tanzanian national guidelines.31
Data Collection
Physicians and nurses at the CTCs complete standard forms to
record demographic, clinical, laboratory, and medication
information. Weight and height are measured using standar-
dized protocols, which include measuring height to the nearest
0.1 cm using a stadiometer and weight to the nearest 0.1 kg on a
calibrated scale.32 Clinical data collected include history of
tuberculosis (TB) and medication data collected include previ-
ous use of ART. Laboratory data collected include CD4 count
and hemoglobin. All patients are referred for general nutrition
education provided by a trained nurse counselor and nutrition
counseling provided by the nutritionist. Additional sessions
of nutrition counseling and therapeutic food are provided to
those undernourished until they graduate from malnutrition.
Clinical and laboratory data are entered into a national standard
case report form, reviewed at site level for accuracy and com-
pleteness, and then entered into a protected computerized data-
base which is updated daily and undergoes weekly quality
assurance audits.
The study protocol was approved by the Institutional
Review Boards of the National Institute of Medical Research,
Muhimbili University of Health and Allied Sciences, and the
Harvard School of Public Health.
Outcomes and Risk Factors
The primary outcome in this cross-sectional study was the preva-
lence of overweight or obesity at enrollment. Normal weight was
defined as 18.5 to <25 kg/m2, overweight as 25 to <30 kg/m2,
and obese as �30 kg/m2. For each risk factor studied, two com-
parisons were made: overweight versus normal weight and obese
versus normal weight.32
We examined the following potential baseline risk factors
for overweight and obesity: age, sex, marital status, parity,
functional status (categorized as confined to bed, limited
ambulation, or able to work), CD4 count, World Health Orga-
nization (WHO) HIV staging, hemoglobin concentration, pre-
vious ART use, and history of TB at enrollment. We also
assessed the relationships between overweight or obesity and
opportunistic infections (diarrhea, oral candidiasis, and other
AIDS-defining illnesses).
Statistical Analyses
A total of 90 118 patients aged 15 years and older were
enrolled in the MDH program between 2004 and 2011. We
excluded 36 293 patients, because of pregnancy (11 674), miss-
ing height or weight (3998), or being underweight (20 621;
BMI < 18.5 kg/m2).
Chi-square tests were used to test for differences in the preva-
lence of obesity and overweight by potential risk factors. Uni-
variate and multivariate relative risk models were used
to assess the associations between overweight and obesity
compared to normal weight (18.5 kg/m2 � BMI < 25.0 kg/m2)
and baseline risk factors.33 Log-binomial regression was used
for all univariate regressions. Poisson regression was used for
the multivariate regressions because the multivariate log-
binomial regressions did not converge. All variables in the uni-
variate analyses were included in the multivariate models. We
2 Journal of the International Association of Providers of AIDS Care
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from

used the missing indicator method and set continuous variables
to the mean value for missing covariates. Wald tests were calcu-
lated for median scores of categorical variables and for binary
variables. Based on known differences in the proportion of and
risk factors for overweight and obesity between men and
women, we tested for an interaction between sex and each risk
factor associated with overweight and obesity.
We examined the possibly nonlinear relation between age
and CD4 count with the relative risks of obesity and overweight
nonparametrically with restricted cubic splines.34 All analyses
were performed using SAS software version 9.3 (SAS Institute,
Inc, Cary, North Carolina). P values less than .05 were consid-
ered statistically significant.
Results
Demographic characteristics of the 53 825 patients included in
the analyses are shown in Table 1. Among the patients, 69%were female, the median age was 35 years (interquartile range
[IQR], 30–42 years), and the median BMI was 22 (IQR 20–25
kg/m2). The female and male patients who were overweight
was 16% and 8% and obese was 7% and 2%, respectively.
Associations between individual risk factors and obesity
are reported in Table 2. Compared to the reference group
(<30 years), patients aged 30–40 years, 40–50 years, and those
aged 50 and older had 2.12 (95% confidence interval [CI],
1.93–2.32), 3.19 (95% CI, 2.90–3.51) and 3.62 (95% CI,
3.22–4.06) times the risk of being obese (trend test P value
<.001). The prevalence of obesity was 4-fold higher in women
than in men, that is, in women with no children, the prevalence
ratio (PR) was 4.39 (95% CI, 3.97–4.87); in women with 1
child the PR was 4.38 (95% CI, 3.93–4.88); in women with 2
children the PR was 4.20 (95% CI, 3.73–4.74); and in women
with 3 or more children the PR was 3.98 (95% CI, 3.50–4.51).
Relative to patients with CD4 counts greater than 200 cells/
mm3, patients with CD4 counts between 50 and 99 cells/mm3
had a reduced risk of obesity (PR, 0.64; 95% CI, 0.56–0.72).
Lower hemoglobin concentrations were associated with a
lower risk of obesity. Compared to patients with normal hemo-
globin concentrations (>11 g/dL), patients with hemoglobin
concentrations of <8.5 g/dL were less likely to be obese (PR,
0.32; 95% CI, 0.27–0.37). The risk of being obese was lower
in patients diagnosed with WHO stage IV compared to those
with stage I disease (PR, 0.28; 95% CI, 0.24–0.32). History
of TB was associated with a decreased risk of obesity (PR,
0.70; 95% CI, 0.62–0.78).
Older age, female sex, being married, higher CD4 count,
higher hemoglobin levels, lower WHO stage, no history of
TB at enrollment, and history of antiretroviral (ARV) drug use
were found to be risk factors for overweight after adjustment
for covariates (Table 3). Relative to patients aged <30, patients
aged 30–40, 40–50, and those aged 50 and older had 1.31 (95%CI, 1.25–1.38), 1.73 (95% CI, 1.64–1.82), and 1.86 (95% CI,
1.74–1.99) times the risk of being overweight. The prevalence
of overweight was twice as high in women compared to men:
2.05 (95% CI, 1.95–2.16) in women with no children, 2.13
(95% CI, 2.02–2.25) in women with 1 child, 2.07 (95% CI,
1.94–2.29) in women with 2 children, and 1.87 (95% CI,
1.73–2.01) in women with 3 or more children. High CD4
counts were associated with a high risk of overweight, while
lower hemoglobin concentrations were associated with a lower
risk of overweight. Compared to patients with CD4 counts
greater than 200 cells/mm3, patients with CD4 counts between
50 and 99 cells/mm3 had a reduced risk of overweight (PR,
0.84; 95% CI, 0.79–0.90). Compared to patients with normal
hemoglobin concentrations (>11 g/dL), patients with hemoglo-
bin concentrations of <8.5 g/dL were less likely to be over-
weight (PR, 0.53; 95% CI, 0.49–0.57). The risk of being
obese was lower in patients diagnosed with WHO stage IV than
in those with stage I disease (PR, 0.47; 95% CI, 0.43–0.51).
History of TB at enrollment was associated with a decreased
risk of overweight (PR, 0.82; 95% CI, 0.77–0.87) and history
of previous ARV medication use was associated with increased
risk of overweight (PR, 1.12; 95% CI, 1.06–1.18).
Sex modified the association between the following risk fac-
tors and overweight and obesity: age (obese, P ¼ .0002; over-
weight, P < .0001), marital status (obese, P < .0001;
overweight, P < .0001), and WHO stage (obese, P < .0001;
overweight, P ¼ .0001). Married men were more likely to be
obese (PR, 1.68; 95%CI, 1.37–2.05) and more likely to be over-
weight (PR, 1.47; 95% CI, 1.34–1.60) than men who were not
married. The association between marital status and weight
was weaker in women. Married women were more likely to
be obese (PR, 1.09; 95% CI, 1.02–1.16) and overweight (PR,
1.05; 95%CI, 1.01–1.10) than unmarried women.
In both men and women, the risk of being overweight
decreased significantly with higher WHO stage. Compared to
men with WHO stage I, the risk of being overweight in men
with WHO stage II was lower (PR, 0.72; 95% CI, 0.65–0.80)
as was the risk in men with WHO stage IV (PR, 0.44; 95%CI, 0.37–0.53). Compared to women with WHO stage I,
women with WHO stage II were less likely to be overweight
(PR, 0.82; 95% CI, 0.78–0.87) as were women with WHO stage
IV (PR, 0.48; 95% CI, 0.43–0.52; P for trend<.0001).
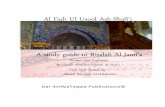
The relative risk curves for overweight and obesity by age
(Figure 1) show that the risks of both overweight and obesity
reach a maximum point in the mid-50s and then decline. The
curves for overweight and obesity by CD4 count (Figure 2)
show that the risks of both overweight and obesity increase rap-
idly up to approximately 500 cells/mm3 and then continue to
increase but at a lower rate.
Discussion
This article identifies risk factors for overweight and obesity
and describes their prevalence among adult HIV-infected
patients in Dar es Salaam. This is the first study to report on
overweight and obesity among people infected with HIV at
enrollment to CTCs in Tanzania. It is also the first study of this
population that excluded underweight participants from the ref-
erence group when looking at predictors of overweight and
obesity. Exclusion of underweight patients from the reference
Semu et al 3
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from

Table 1. Baseline characteristics of the study population.a
VariableNormal Weight
(18.5 � BMI < 25; N ¼ 40 143)b,cObese
(BMI � 30; N ¼ 3840)b,c P ValuecOverweight
(25 � BMI < 30; N ¼ 9809)b,c P Valued
Age category, years<30 8712 (21.7%) 556 (14.5%) <.0001 1919 (19.6%) <.000130–<40 17 483 (43.6%) 1699 (44.3%) 4122 (42.0%)40–<50 9684 (24.2%) 1109 (28.9%) 2616 (26.7%)�50 4220 (10.5%) 475 (12.4%) 1150 (11.7%)
SexFemale 26 006 (64.8%) 3383 (88.1%) <.0001 7777 (79.3%) <.0001Male 14 137 (35.2%) 457 (11.9%) 2032 (20.7%)
MarriedNo 21 577 (57.7%) 1951 (54.8%) 4967 (54.3%)Yes 15 805 (42.3%) 1608 (45.2%) .0008 4181 (45.7%) <.0001
CD4 count category, cells/mm3
<50 5536 (16.6%) 6441 (15.5%) <.0001 900 (11.0%) <.000150–99 4099 (12.3%) 4798 (11.5%) 697 (8.5%)100–199 7246 (21.7%) 8795 (21.1%) 1540 (18.8%)�200 16 478 (49.4%) 21 563 (51.8%) 5072 (61.8%)
Hgb Category, g/dL<8.5 4853 (17.0%) 161 (6.0%) <.0001 645 (9.3%) <.00018.5–10.9 10 836 (37.9%) 730 (27.2%) 2140 (30.9%)�11.0 12 907 (45.1%) 1797 (66.9%) 4146 (59.8%)
WHO stageI 6032 (15.6%) 1324 (36.7%) <.0001 2640 (28.2%) <.0001II 8316 (21.5%) 1075 (29.8%) 2566 (27.4%)III 18 556 (47.9%) 1010 (28.0%) 3430 (36.6%)IV 5799 (15.0%) 201 (5.6%) 730 (7.8%)
Oral candidiasisNo 36 852 (95.2%) 3597 (98.0%) <.0001 9149 (97.3%) <.0001Yes 1860 (4.8%) 75 (2.0%) 251 (2.7%)
TB history at enrollmentNo 29 339 (77.3%) 3271 (90.0%) <.0001 7948 (86.1%) <.0001Yes 8627 (22.7%) 363 (10.0%) 1282 (13.9%)
Previous ARV useNo 34 901 (88.4%) 3165 (84.1%) <.0001 8262 (86.1%) <.0001Yes 4571 (11.6%) 600 (15.9%) 1332 (13.9%)
AIDS-defining illnessNo 32 467 (82.5%) 3528 (94.2%) <.0001 8696 (90.9%) <.0001Yes 6906 (17.5%) 218 (5.8%) 867 (9.1%)
DiarrheaNo 37 275 (95.4%) 3642 (97.9%) <.0001 9202 (97.0%) <.0001Yes 1802 (4.6%) 79 (2.1%) 287 (3.0%)
Parity0 12 188 (46.9%) 1573 (46.5%) .05 3608 (46.4%) .841 7058 (27.1%) 887 (26.2%) 2140 (27.5%)2 4092 (15.7%) 525 (15.5%) 1240 (15.9%)3þ 2668 (10.3%) 398 (11.8%) 789 (10.2%)
Functional statusWorking 29 591 (94%) 2876 (97.5%) <.0001 7493 (96.7%) <.0001Ambulatory 1679 (5.3%) 59 (2.0%) 208 (2.7%)Bedridden 254 (0.8%) 15 (0.5%) 46 (0.6%)
Year2004–2005 7359 (18.3%) 814 (21.2%) .02 1924 (19.6%) .0022006 6575 (16.4%) 642 (16.7%) 1615 (16.5%)2007 7600 (18.9%) 680 (17.7%) 1833 (18.7%)2008 7610 (18.9%) 672 (17.5%) 1707 (17.4%)2009 6901 (17.2%) 649 (16.9%) 1734 (10.1%)2010–2011 4098 (10.2%) 383 (10.0%) 996 (10.2%)
Abbreviations: BMI, body mass index; Hgb, hemoglobin; TB, tuberculosis; WHO, World Health Organization.a N ¼ 53 825.b Except where otherwise noted, data represent n (%) of patients.c Not all numbers add up to 53 825 because of missing data.d Chi-square test.
4 Journal of the International Association of Providers of AIDS Care
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from

Table 2. Risk Factors for Obesity (BMI � 30) among Obese and Normal-Weight Patients Enrolled for Care and Monitoring at MDH-PEPFAR-Supported Facilities in Dar es Salaam, Tanzania.a
Characteristic
Univariate Multivariate
PR (95% CI) P Valueb PR (95% CI) P Valueb
Age category, years <.0001 <.0001<30 Reference Reference:30–<40 1.48 (1.35–1.62) 2.12 (1.93–2.32)40–<50 1.71 (1.55–1.89) 3.19 (2.90–3.51)50þ 1.69 (1.50–1.90) 3.62 (3.22–4.06)
Sex and Parity <.0001 <.0001Male Reference ReferenceFemale, no children 3.65 (3.30–4.04) 4.39 (3.97–4.87)Female, 1 child 3.57 (3.20–3.98) 4.38 (3.93–4.88)Female, 2 children 3.64 (3.23–4.11) 4.20 (3.73–4.74)Female, 3þ children 4.15 (3.65–4.72) 3.98 (3.50–4.51)
Married .0009 <.0001Yes 1.11 (1.05–1.19) 1.15 (1.08–1.22)No Reference Reference
CD4 category, cells/mm3 <.0001 <.0001<50 0.35 (0.31–0.40) 0.64 (0.56–0.72)50–99 0.40 (0.35–0.46) 0.63 (0.55–0.72)100–199 0.53 (0.48–0.58) 0.68 (0.62–0.74)200þ Reference Reference
Hemoglobin category, g/dL <.0001 <.0001<8.5 0.26 (0.22–0.31) 0.32 (0.27–0.37)8.5–10.9 0.52 (0.48–0.56) 0.53 (0.49–0.58)11þ Reference Reference
WHO stage <.0001 <.0001I Reference ReferenceII 0.64 (0.59–0.69) 0.67 (0.62–0.72)III 0.29 (0.27–0.31) 0.38 (0.35–0.41)IV 0.19 (0.16–0.22) 0.28 (0.24–0.32)
Oral candidiasis <.0001 .73No Reference ReferenceYes 0.44 (0.35–0.54) 0.96 (0.76–1.21)
History of TB at enrollment <.0001 <.0001No Reference ReferenceYes 0.40 (0.36–0.45) 0.70 (0.62–0.78)
Previous ARV drug use <.0001 <.0001No Reference ReferenceYes 1.40 (1.29–1.52) 1.22 (1.12–1.33)
AIDS-defining illness <.0001 .14No Reference ReferenceYes 0.31 (0.27–0.36) 0.89 (0.76–1.04)
Diarrhea <.0001 .07No Reference ReferenceYes 0.47 (0.38–0.59) 0.82 (0.67–1.02)
Functional status <.0001 .06Working Reference ReferenceAmbulatory 0.38 (0.30–0.50) 0.77 (0.60–0.99)Bedridden 0.63 (0.38–1.03) 0.85 (0.52–1.38)
Year <.0001 0.00012004–2005 Reference Reference2006 0.86 (0.75–0.98) 0.88 (0.77–1.00)2007 0.82 (0.73–0.92) 0.79 (0.70–0.90)2008 0.76 (0.67–0.85) 0.73 (0.64–0.83)2009 0.75 (0.66–0.84) 0.70 (0.61–0.80)2010–2011 0.79 (0.71–0.88) 0.74 (0.65–0.84)
Abbreviations: BMI, body mass index; CI, confidence interval; Hgb, hemoglobin; PR, prevalence ratio; TB, tuberculosis; WHO, World Health Organization; MDH,Management and Development for Health; PEPFAR, President’s Emergency Plan for AIDS Relief.a N ¼ 43 986.b Wald test for trend for median scores of categorical variables. Wald test for binary variables.
Semu et al 5
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from

Table 3. Risk Factors for Overweight (25� BMI < 30) among Overweight and Normal-Weight Patients Enrolled for Care and Monitoring atMDH-PEPFAR-Supported facilities in Dar es Salaam, Tanzania.a
Characteristic
Univariate Multivariate
RR (95% CI) P Valueb RR (95% CI) P Valueb
Age category <.0001 <.0001<30 Reference Reference:30–<40 1.06 (1.00–1.11) 1.31 (1.25–1.38)40–<50 1.18 (1.12–1.24) 1.73 (1.64–1.82)50þ 1.19 (1.11–1.27) 1.86 (1.74–1.99)
Sex and parity <.0001 <.0001Male Reference ReferenceFemale, no children 1.82 (1.73–1.91) 2.05 (1.95–2.16)Female, 1 child 1.85 (1.75–1.95) 2.13 (2.02–2.25)Female, 2 children 1.85 (1.73–1.97) 2.07 (1.94–2.20)Female, 3þ children 1.81 (1.68–1.95) 1.87 (1.73–2.01)
Married <.0001 <.0001Yes 1.12 (1.08–1.16) 1.14 (1.10–1.18)No Reference Reference
CD4 category, cells/mm3 <.0001 <.0001<50 0.60 (0.56–0.64) 0.84 (0.79–0.90)50–99 0.62 (0.58–0.67) 0.80 (0.75–0.86)100–199 0.75 (0.71–0.79) 0.87 (0.83–0.92)200þ Reference Reference
Hemoglobin category (g/dL) <.0001 <.0001<8.5 0.48 (0.45–0.52) 0.53 (0.49–0.57)8.5–10.9 0.68 (0.65–0.71) 0.68 (0.65–0.72)11þ Reference Reference:
WHO stage <.0001 <.0001I Reference ReferenceII 0.78 (0.74–0.81) 0.80 (0.76–0.84)III 0.51 (0.49–0.54) 0.60 (0.57–0.63)IV 0.37 (0.34–0.40) 0.47 (0.43–0.51)
Oral candidiasis <.0001 .05No Reference ReferenceYes 0.60 (0.53–0.67) 0.89 (0.79–1.00)
History of TB at enrollment <.0001 <.0001No Reference ReferenceYes 0.61 (0.58–0.64) 0.82 (0.77–0.87)
Previous ARV use <.0001 <.0001No Reference ReferenceYes 1.18 (1.12–1.24) 1.12 (1.06–1.18)
AIDS-defining illness <.0001 .03No Reference ReferenceYes 0.53 (0.49–0.56) 0.92 (0.85–0.99)
Diarrhea <.0001 .13No Reference ReferenceYes 0.70 (0.62–0.78) 0.93 (0.83–1.03)
Functional status <.0001 .006Working Reference ReferenceAmbulatory 0.54 (0.48–0.62) 0.82 (0.72–0.93)Bedridden 0.76 (0.58–0.99) 0.91 (0.71–1.18)
Year .02 <.00012004–2005 Reference Reference2006 0.92 (0.85–1.00) 0.90 (0.83–0.98)2007 0.91 (0.85–0.98) 0.85 (0.78–0.92)2008 0.90 (0.83–0.96) 0.83 (0.76–0.89)2009 0.85 (0.79–0.91) 0.78 (0.72–0.84)2010–2011 0.92 (0.86–0.98) 0.83 (0.77–0.90)
Abbreviations: BMI, body mass index; CI, confidence interval; Hgb, hemoglobin; RR, risk ratio; TB, tuberculosis; WHO, World Health Organization; MDH,Management and Development for Health; PEPFAR, President’s Emergency Plan for AIDS Relief.a N ¼ 49 982.b Wald test for trend for median scores of categorical variables. Wald test for binary variables.
6 Journal of the International Association of Providers of AIDS Care
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from

group was important to identify factors associated with being
overweight or obese compared to a healthy weight, and we did
not want our findings to be potentially distorted by underweight
caused by the HIV disease process itself.
Our data suggest 4 major findings. First, there was a sub-
stantial proportion of people infected with HIV who were over-
weight or obese at enrollment to the CTCs. We found that 8%of male patients and 16% of female patients were overweight,
while 2% of male patients and 7% of female patients were
obese. These numbers are approximately 10 percentage points
below the prevalence of overweight and obesity of the general
population, based on comparisons to data from the 2010 TDHS,
which reported a prevalence of 28% and 16% of overweight
and obesity, respectively, among women aged 15–49 years,
in Dar es Salaam.6 A comparison of our results with a study
conducted in the Kinondoni district, Dar es Salaam, in 2007–
2008 found that the prevalence of obesity in HIV-infected men
was 7.2 percentage points lower than that in the general popu-
lation (1.8% versus 9%).35
It is worth considering that the prevalence of overweight and
obesity among HIV-infected people in Dar es Salaam may be
higher than that observed by us. Our patients’ nutritional status
was measured at the time of enrollment to the CTC. We did not
have data on reasons for enrollment at that particular time.
Persistent and frequent sickness could have compromised indi-
viduals’ nutrition and weight and led to CTC enrollment. It is
important to monitor the BMI in patients after ART initiation,
as patients’ health hopefully improves and they potentially gain
weight. Furthermore, our study was limited to government-
supported facilities where the majority of patients were of low
socioeconomic status. In Dar es Salaam, the prevalence of
overweight and obesity is higher among the middle and upper
classes compared to the poor, and thus our population may have
reflected the lower weights among the poor.6,35
A high prevalence of obesity at the time of enrollment in
HIV clinics, at levels comparable to the general population, has
been noted in the United States.23-25,36 Our study adds evidence
that, in Tanzania where wasting and underweight remain
highly prevalent in the HIV-infected population, the prevalence
of obesity among people infected with HIV at CTC enrollment
is high but lower than that of general population.37,38
Second, we observed that overweight and obesity were more
prevalent in older patients, with the oldest age-group (>50 years)
having the highest burden. A similar trend has been observed in
the general Dar es Salaam population where the highest preva-
lence of obesity was among those aged 45–55 and slightly lower
in those aged 55þ.35 A study from the United States found a
similar relationship between age and weight at HIV diagnosis.24
Figure 1. Multivariate relative risks and 95% confidence intervals (CIs) of overweight (25 � BMI < 30) and obesity (BMI � 30) as a function ofage (years); 95% CIs are indicated by the gray area.
Semu et al 7
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from

The relative risk curves of overweight and obesity reache a max-
imum point in the mid-50s and then declines.
Third, this study builds on previous findings that, as in the
general population, overweight and obesity among people
infected with HIV is more prevalent in women than in
men.24-26,29,30 However, this result conflicts with other data
where no association was found between BMI and sex. A study
of HIV-infected US military personnel found no association
between sex and BMI, and a study of HIV-infected patients
in Philadelphia found that the prevalence of obesity, but not
overweight, was higher in women than in men.24,26 In our
study, the prevalence of overweight and obesity in women was
double and triple that of men at the time of enrollment in the
HIV CTC. A number of factors could contribute to these differ-
ences. In the general Dar es Salaam population, men are less
likely than women to be overweight and obese.35 Among those
infected with HIV in sub-Saharan Africa, men tend to begin
care later than women.39,40 This delay may mean that by the
time men begin care, they would have lost more weight than
have women. This weight loss could be due to inadequate
intake of food, malabsorption, frequent infection, or other, as
of yet unknown, biological or physiological factors. We found
that parity was inversely associated with overweight and
obesity in women. Similar findings have been observed in
the general population.41
As in the general population, we found that overweight
and obesity among people infected with HIV were signifi-
cantly more common among the married. Married men
were more likely to be overweight or obese than single
men, but the association with marital status was not signif-
icant in women. This could partly be explained by the cul-
tural differences in food consumption between men and
women; household food distribution often favors men, and
men are more likely to eat out regularly. It is also possible
that women are likely to take adequate care of themselves
whether they are married or not, while for men, marriage
makes more of a difference. Married men may receive
more care and food from their wives while unmarried men
don’t have this advantage.
In Tanzania, excess weight continues to be perceived as a
status symbol, a sign of being HIV free, and an indicator of
good health.11 Unless countrywide interventions and educa-
tional campaigns on obesity and associated consequences are
implemented, overweight will continue to be perceived as a
symbol of a properly cared for family and of beauty, especially
among women.11,42
Figure 2. Multivariate relative risks and 95% confidence intervals (CIs) of overweight (25 � BMI < 30) and obesity (BMI � 30) as a function ofCD4 count (cells/mm3); 95% CIs are indicated by the gray area.
8 Journal of the International Association of Providers of AIDS Care
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from

Fourth, the prevalence of overweight and obesity at enroll-
ment was significantly higher among those with the highest
category of CD4 count. Similar to other studies in general and
in HIV-infected population prior to ART initiation, we found
that being overweight or obese was associated with higher
CD4 count.25,36,43 Our study found that overweight and obesity
were more prevalent among the patients with higher CD4
counts. Other studies have reported that higher baseline BMI
predicts greater gain in CD4 count, including maintenance of
immune status and better recovery when patients initiated
ART.25,36,44
Although higher enrollment weight is associated with
higher CD4 counts, this observation may be moderated by
known associations of excess weight and negative health con-
sequences.45,46 Excess weight in HIV-infected patients has
the potential to exacerbate higher rates of cardiovascular dis-
ease seen in HIV-infected patients who receive certain ART
medications.47 Thus, although nutritional status in HIV-
infected patients may reflect larger national secular trends
in obesity, specific obesity-related health issues require atten-
tion in HIV-infected patients.
Conclusion
The adverse health consequences of overweight and obesity are
well described in the general population.8,12-16,18 In this study,
we examined patients at enrollment to HIV CTCs in Dar es Sal-
aam, Tanzania, and found that overweight and obesity were
highly prevalent, although not as high as that found in the gen-
eral population. Targeted dietary counseling and weight man-
agement should be integral components of care given to
people infected with HIV.
Acknowledgement
We thank the Ministry of Health and Social Welfare (MOHSW) for
their support in integrating HIV CTCs in Dar es Salaam. We also
thank the MDH and all the patients and staff who have contributed
to these findings.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to
the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for
the research, authorship, and/or publication of this article: This HIV
intervention program in Dar es Salaam government facilities is funded
by United States President’s Emergency Plan for AIDS Relief through
Management and Development for Health in collaboration with the
Ministry of Health and Social Welfare and the Harvard School of Pub-
lic Health. RMZ is supported by a NIH T32 CA 09001 training grant.
References
1. Martorell R, Khan LK, Hughes ML, Grummer-Strawn LM. Obe-
sity in women from developing countries. 2000;54(3):247–252.
2. Lukmanji Z, Mrisho F, Moor S. 2003. The health status of mem-
bers of parliament in Tanzania. Unpublished.
3. McLarty DG, Pollitt C, Swai AB. Diabetes in Africa. Diabet Med.
1990;7(8):670–684.
4. Villamor E, Msamanga G, Urassa W, et al. Trends in obesity,
underweight, and wasting among women attending prenatal
clinics in urban Tanzania, 1995–2004. Am J Clin Nutr. 2006;
83(6):1387–1394.
5. Tanzania Demographic and Health Survey 2004-05. National
Bureau of Statistics and ICF Macro, 2005. http://www.dhspro
gram.com/pubs/pdf/FR173/FR173-TZ04-05.pdf. Accessed on 6
August 2013.
6. Tanzania Demographic and Health Survey 2010. National Bureau
of Statistics and ICF Macro, 2011. http://www.measuredhs.com/
pubs/pdf/FR243/FR243%5B24June2011%5D.pdf. Accessed on
6 August 2013.
7. Popkin BM. The nutrition transition and obesity in the developing
world. J Nutr. 2001;131(3):871S–873S.
8. Bonadonna RC, Groop L, Kraemer N, Ferrannini E, Del Prato S,
DeFronzo RA. Obesity and insulin resistance in humans: a dose-
response study. Metab Clin Exp. 1990;39(5):452–459.
9. Puoana T, Fourie JM, Shapiro M, Rosling L, Tsaka NC, Oelofse
A. ‘Big is beautiful’ - an exploration with urban black community
health workers in a South African township. S Afr J Clin Nutr.
2005;18(1):6–15.
10. Steyn NP. Editorial: ’Big is beautiful’ - and unhealthy and confus-
ing? S Afr J Clin Nutr. 2005;18(1):4–5.
11. Maletnlema T. A tanzanian perspective on the nutrition transition
and its implications for health. Public Health Nutr. 2002;5(1A):
163–168.
12. Franssen R, Monajemi H, Stroes ESG, Kastelein JJP. Obesity
and dyslipidemia. Endocrinol Metab Clin North Am. 2008;
37(3):623–633.
13. Fox CS, Larson MG, Leip EP, Culleton B, Wilson PW, Levy D.
PRedictors of new-onset kidney disease in a community-based
population. JAMA. 2004;291(7):844–850.
14. Dustan HP. Obesity and hypertension. Diabetes Care. 1991;
14(6):488–504.
15. Haffner SM, Mitchell BD, Hazuda HP, Stern MP. Greater influ-
ence of central distribution of adipose tissue on incidence of
non-insulin-dependent diabetes in women than men. Am J Clin
Nutr. 1991;53(5):1312–1317.
16. Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as
an independent risk factor for cardiovascular disease: a 26-year
follow-up of participants in the Framingham heart study. Circula-
tion. 1983;67(5):968–977.
17. Foster MC, Hwang SJ, Larson MG, et al. Overweight, obesity,
and the development of stage 3 CKD: the Framingham heart
study. Am J Kidney Dis. 2008;52(1):39–48.
18. Rapp K, Schroeder J, Klenk J, et al. Obesity and incidence of can-
cer: a large cohort study of over 145 000 adults in Austria. Br J
Cancer. 2005;93(9):1062–1067.
19. Ministry of Health and Social Welfare. National Strategy for Non
Communicable Diseases 2009 - 2015. Malaysia: Ministry of
Health and Social Welfare; 2009.
20. Carr A, Samaras K, Thorisdottir A, Kaufmann GR, Chisholm DJ,
Cooper DA. Diagnosis, prediction, and natural course of HIV-1
protease-inhibitor-associated lipodystrophy, hyperlipidaemia, and
Semu et al 9
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from

diabetes mellitus: acohort study. Lancet. 1999;353(9170):
2093–2099.
21. Grinspoon S. Insulin resistance in the HIV-lipodystrophy syn-
drome. Trends Endocrinol Metab. 2001;12(9):413–419.
22. Serwadda D, Mugerwa RD, Sewankambo NK, et al. Slim disease:
a new disease in Uganda and its association with HTLV-III infec-
tion. Lancet. 1985;2(8460):849–852.
23. Crum-Cianflone N, Tejidor R, Medina S, Barahona I, Ganesan A.
Obesity among patients with HIV: the latest epidemic. AIDS
Patient Care STDs. 2008;22(12):925–930.
24. Crum-Cianflone N, Roediger MP, Eberly L, et al. Increasing rates
of obesity among HIV-Infected persons during the HIV epidemic.
PLoS One. 2010;5(4):e10106.
25. Shuter J, Chang CJ, Klein RS. Prevalence and predictive value of
overweight in an urban HIV care clinic. J Acquir Immune Defic
Syndr. 2001;26(3):291–297.
26. Amorosa V, Synnestvedt M, Gross R, et al. A tale of 2 epi-
demics: the intersection between obesity and HIV infection in
Philadelphia. J Acquir Immune Defic Syndr. 2005;39(5):
557–561.
27. Maia Leite LH, De Mattos Marinho Sampaio AB. Progression
to overweight, obesity and associated factors after antiretro-
viral therapy initiation among Brazilian persons with HIV/
AIDS. Nutr Hosp. 2010;25(4):635–640.
28. Liu E, Spiegelman D, Semu H, et al. Nutritional status and mor-
tality among HIV-infected patients receiving antiretroviral ther-
apy in Tanzania. J Infect Dis. 2011;204(2):282–290.
29. Bloomfield GS, Hogan JW, Keter A, et al. Hypertension
and obesity as cardiovascular risk factors among HIV seropo-
sitive patients in Western Kenya. PLoS One. 2011;6(7):
e22288.
30. Kroll AF, Sprinz E, Leal SC, Labrea M, da G., Setubal, S. Preva-
lence of obesity and cardiovascular risk in patients with
HIV/AIDS in Porto Alegre, Brazil. Arq Bras Endocrinol Metabol.
2012;56(2):137–141.
31. National Guidelines for the management of HIV and AIDS. 2008
National AIDS Control Program, third edition. Dar es Salaam,
Tanzania: Ministry of Health; 2008.
32. WHO Expert Committee. Physical Status: the use and interpreta-
tion of anthropometry: report of the WHO expert committee.
World Health Organ Tech Rep Ser. 1995;854:1–452.
33. Spiegelman D, Hertzmark E. Easy SAS calculations for risk or
prevalence ratios and differences. Am J Epidemiol. 2005;162(3):
199–200.
34. Govindarajulu US, Spiegelman D, Thurston SW, Ganguli B,
Eisen EA. Comparing smoothing techniques in Cox models
for exposure-response relationships. Stat Med. 2007;26(20):
3735–3752.
35. Shayo GA, Mugusi FM. Prevalence of obesity and associated risk
factors among adults in Kinondoni municipal district, Dar es Sal-
aam Tanzania. BMC Public Health. 2011;11:365.
36. Shor-Posner G, Campa A, Zhang G, et al. When obesity is desir-
able: a longitudinal study of the Miami HIV-1-infected drug abu-
sers (MIDAS) cohort. J Acquir Immune Defic Syndr. 2000;23(1):
81–88.
37. Wanke CA, Silva M, Knox TA, Forrester J, Speigelman D, Gor-
bach SL. Weight loss and wasting remain common complications
in individuals infected with human immunodeficiency virus in the
era of highly active antiretroviral therapy. Clin Infect Dis. 2000;
31(3):803–805.
38. Tang AM, Jacobson DL, Spiegelman D, Knox TA, Wanke C.
Increasing risk of 5% or greater unintentional weight loss in a
cohort of HIV-infected patients, 1995 to 2003. J Acquir Immune
Defic Syndr. 2005;40(1):70–76.
39. Cornell M. Gender inequality: Bad for men’s health. South Afr J
HIV Med. 2013;14(1):12–14.
40. Braitstein P, Boulle A, Nash D, et al. Gender and the use of anti-
retroviral treatment in resource-constrained settings: findings
from a multicenter collaboration. J Womens Health (Larchmt).
2008;17(1):47–55.
41. Heliovaara M, Aromaa A. Parity and obesity. J Epidemiol Com-
mun Health. 1981;35(3):197.
42. Nyaruhucha CNM, Achen JH, Msuya JM, Shayo NB, Kulwa
KBM. Prevalence and awareness of obesity among people of dif-
ferent age groups in educational institutions in Morogoro, Tanza-
nia. East Afr Med J. 2003;80(2):68–72.
43. Womack J, Tien PC, Feldman J, et al. Obesity and immune cell
counts in women. Metab Clin Exp. 2007;56(7):998–1004.
44. Palermo B, Bosch RJ, Bennett K, Jacobson JM. Body mass index
and CD4þ T-lymphocyte recovery in HIV-infected men with
viral suppression on antiretroviral therapy. HIV Clin Trials.
2011;12(4):222–227.
45. Masters RK, Reither EN, Powers DA, Yang YC, Burger AE, Link
BG. The impact of obesity on US mortality levels: the importance
of age and cohort factors in population estimates. Am J Public
Health. 2013;103(10):1895–1901.
46. Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz
H, Kannel WB. Prediction of coronary heart disease using risk
factor categories. Circulation. 1998;97(18):1837–1847.
47. Islam FM, Wu J, Jansson J, Wilson DP. Relative risk of cardiovas-
cular disease among people living with HIV: a systematic review
and meta-analysis. HIV Med. 2012;13(8):453–468.
10 Journal of the International Association of Providers of AIDS Care
at Harvard Libraries on February 20, 2015jia.sagepub.comDownloaded from